آثار التجارب المرتبطة بالحرب على أعراض الصحة النفسية للأفراد الذين يعيشون في مناطق النزاع: دراسة طولية The effects of war-related experiences on mental health symptoms of individuals living in conflict zones: a longitudinal study
في 7 أكتوبر 2023، أدى هجوم واسع النطاق في جنوب إسرائيل والحرب اللاحقة إلى فقدان كبير في الأرواح وإصابات، حيث عانى العديد من الأفراد من خسائر صادمة، مثل قتل أو اختطاف أفراد من العائلة أو أصدقاء مقربين. تهدف هذه الدراسة إلى فحص آثارها على الصحة النفسية على المدى الطويل، وبشكل خاص، الأعراض السريرية للقلق والاكتئاب واضطراب ما بعد الصدمة (PTSD). توقعنا أن تكون شدة الأعراض أكبر بين الأفراد الذين عانوا من خسارة صادمة، أو تم تهجيرهم قسراً، أو عانوا من فقدان الدخل، وكذلك بين النساء وأعضاء الأقليات العرقية. قامت هذه الدراسة التي شملت ثلاث موجات من الاستطلاعات عبر الإنترنت بتقييم أعراض الصحة النفسية في عينة من 1052 فردًا، تتراوح أعمارهم بين 18-40، يقيمون في مناطق النزاع في إسرائيل من فبراير 2024 (اليوم 1) حتى مارس 2024 (اليوم 30) وحتى مايو 2024 (اليوم 90). تم قياس أعراض القلق والاكتئاب وPTSD باستخدام مقياس اضطراب القلق العام-7 (GAD-7)، واستبيان صحة المريض-9 (PHQ-9)، ومقياس PTSD للرعاية الأولية (PC-PTSD). أظهر الأفراد الذين يعانون من خسائر صادمة، أو تهجير قسري، أو صعوبات اقتصادية، وكذلك الإناث، باستمرار معدلات أعلى من أعراض القلق والاكتئاب وPTSD مقارنةً بأولئك الذين لم يعانوا من مثل هذه التجارب أو مقارنةً بالذكور، عبر جميع النقاط الزمنية (تراوحت قيم F من 17.7 إلى ). بالنسبة للأقليات العرقية (العرب وغيرهم)، مقارنةً باليهود، كانت أعراض القلق والاكتئاب أعلى في كل نقطة زمنية ( إلى <.001). تسلط هذه الدراسة الضوء على الحاجة الملحة للتدخلات المستهدفة في الصحة النفسية في مناطق النزاع، وخاصة للأفراد المتأثرين. يجب أن توسع الأبحاث المستقبلية هذه النتائج لتشمل مجموعات سكانية أوسع.
الكلمات الرئيسية: الحرب، الهجوم الإرهابي، القلق، الاكتئاب، PTSD، الجنس، التهجير
في 7 أكتوبر 2023، أدت سلسلة من الأحداث العنيفة إلى وقوع إصابات كبيرة وتهجير في إسرائيل، مع الإبلاغ عن وفاة أكثر من 1000 فرد و251 تم أسرهم. ساهمت الحوادث اللاحقة على الحدود الشمالية في مزيد من التهجير المدني، مما أثر على حوالي 100,000 فرد. بشكل عام، أدى النزاع إلى تهجير ما بين 200,000 و500,000 شخص داخل إسرائيل، مما أدى إلى عدم الاستقرار وصعوبات في العودة إلى الوطن. أدت هذه الأحداث أيضًا إلى تحديات اقتصادية، بما في ذلك فقدان الوظائف وزيادة نفقات المعيشة لأولئك المتأثرين. تهدف هذه الدراسة إلى تقييم العواقب النفسية والاجتماعية لأولئك الذين يقيمون في المناطق المتأثرة بالنزاع. بينما تركز هذه الدراسة حصريًا على آثار الصحة النفسية والآثار الاجتماعية والاقتصادية التي يعاني منها الأفراد في إسرائيل، فإنها تعترف بأن هذه هي مجرد جانب واحد من نزاع أوسع متعدد الأبعاد.
ركزت الدراسات السابقة حول آثار الصحة النفسية للهجمات الإرهابية على الأفراد المعرضين مباشرة، وخاصة أولئك القريبين من الأحداث، مثل سكان نيويورك خلال هجوم 11 سبتمبر الإرهابي. تزيد القرب الفوري من الأحداث الصادمة بشكل كبير من خطر تطوير حالات الصحة النفسية الخطيرة، بما في ذلك اضطراب ما بعد الصدمة (PTSD)، والاكتئاب، والقلق. يمكن أن تسهم الخسارة الصادمة والمفاجئة لشخص محبوب في فترات طويلة من الحزن، وأعراض الاكتئاب الشديد، والحزن البسيط أو المعقد. غالبًا ما يؤدي التهجير القسري إلى إجهاد حاد وقلق، ومشاعر انعدام الأمن وعدم الاستقرار، مما قد يؤدي إلى تفاقم أو تسريع مشاكل الصحة النفسية. يمكن أن تؤدي الأعباء المالية بسبب فقدان الوظيفة أو الدخل إلى مشاعر العجز. مثل هذا الضغط المستمر يزيد من خطر تطوير حالات مثل الاكتئاب والقلق. يمكن أن تضخم كل من هذه الضغوط شدة الاضطرابات النفسية الموجودة وتزيد من احتمالية ظهور حالات جديدة، مما يؤثر سلبًا على الصحة النفسية والرفاهية.
لقد زادت انتشار القلق والاكتئاب وPTSD عالميًا ببطء ولكن بشكل ملحوظ بين البالغين، وخاصة البالغين الأصغر سنًا. على سبيل المثال، أظهرت دراسة حديثة معدلات من للقلق و للاكتئاب، أكثر من ضعف معدلات البالغين الأكبر سنًا. على وجه التحديد، أظهرت الدراسات أن الأفراد الأصغر سنًا، بما في ذلك أولئك المعرضين لمناطق النزاع، هم في خطر أعلى للإصابة باضطرابات الصحة النفسية مثل PTSD، واضطراب الاكتئاب الشديد، واضطراب القلق العام. هذه المجموعة معرضة بشكل خاص للتأثيرات النفسية للهجمات الإرهابية أو الحرب، بما في ذلك فقدان الوظيفة أو تقليل ساعات العمل، والضغوط المالية، والانفصال عن الأحباء. لذلك، تركز هذه الدراسة على الأفراد الذين تتراوح أعمارهم بين 18-40، بناءً على أدلة تشير إلى زيادة تعرض البالغين الأصغر سنًا في هذه السياقات.
يؤثر الجنس والعرق أيضًا على نتائج الصحة النفسية. أظهرت مراجعة منهجية وتحليل تلوي أن النساء أكثر عرضة لتطوير الاكتئاب وPTSD في المناطق المتأثرة بالحرب. أظهرت النساء الإسرائيليات تعرضًا أكبر لأعراض الإجهاد الصادمة بعد الهجمات الإرهابية على المجتمع الإسرائيلي في أوائل. وبالمثل، من المعروف أن المجموعات العرقية الأقلية تواجه مخاطر أعلى لنتائج الصحة النفسية السلبية بعد التعرض لأحداث صادمة كبيرة. على وجه التحديد، وُجد أن العرب الإسرائيليين، الذين يشكلون من سكان إسرائيل (مقارنةً ب لليهود)، يحملون مخاطر متزايدة لعدة اضطرابات نفسية، بما في ذلك دراسة أجريت بعد هجوم 7 أكتوبر. بينما يتمتع العرب الإسرائيليون بنفس الحقوق القانونية للوصول إلى الرعاية، بما في ذلك الرعاية النفسية، مثل المواطنين الآخرين، مثل العديد من السكان المهمشين عالميًا، فإنهم يعانون من التحيز، والوصم، والتمييز الذي يؤثر بشكل كبير على وصولهم وجودة الرعاية. غالبًا ما يؤدي ذلك إلى إعطاء السلطات الحكومية أولوية أقل لاحتياجات الأقليات، مما يؤدي إلى استراتيجيات تكيف أسوأ وأعباء نفسية أكبر للعرب الإسرائيليين مقارنةً باليهود الإسرائيليين.
الدراسة الحالية
تهدف هذه الدراسة إلى تعميق الفهم حول الضغوط المختلفة المتعلقة بالحرب والعوامل الاجتماعية المحددة للصحة التي تؤثر على الصحة النفسية للمدنيين في مناطق النزاع. بشكل خاص، تفحص آثار الخسارة الصادمة، والتهجير القسري، وفقدان الدخل، والتي نتوقع أن تكون لها معدلات انتشار مرتفعة نسبيًا، بين عينة كبيرة من الأفراد الذين يعيشون في المناطق المتأثرة بالحرب في إسرائيل. بالإضافة إلى ذلك، تهدف الدراسة إلى تقييم دور الجنس والعرق في شدة أعراض الصحة النفسية في هذه الفئات. أجرينا دراسة طولية مع تقييمات تبدأ في فبراير 2024 (اليوم 1)، حتى مارس 2024 (اليوم 30)، وحتى مايو 2024 (اليوم 90). افترضنا أن (1) الأفراد الذين عانوا من خسارة صادمة، أو تم تهجيرهم قسراً، أو عانوا من فقدان الدخل سيظهرون اضطرابات نفسية أكبر، كما سيكون (2) النساء وأعضاء الأقليات العرقية.
الطرق
التوظيف والمشاركون
تمت عملية التوظيف بين فبراير ومايو 2024. قامت الدراسة بتجنيد مدنيين يتحدثون العبرية تتراوح أعمارهم بين 18 و40 عامًا يعيشون في مناطق النزاع الإسرائيلية الشمالية والجنوبية. كان التركيز على الأفراد (اليهود والعرب) من هذه المناطق لأنهم كانوا الأكثر تأثراً بهجمات 7 أكتوبر والحرب اللاحقة. استخدمت الدراسة Panel4all، وهي أداة تجميع جماهيري إسرائيلية تُستخدم عادة في الأبحاث الطبية والنفسية، والتي توفر الوصول إلى مجموعة عشوائية قائمة على الاحتمالات تضم حوالي 100,000 إسرائيلي، مما يضمن تمثيلًا دقيقًا للسكان الوطنيين. تؤكد المنصة على اتساق الخصائص الديموغرافية بمرور الوقت، وتمنع المشاركين الذين يستخدمون أدوات إخفاء الموقع، وتقوم بإجراء اختبارات لتحديد الروبوتات. لتعزيز صحة النتائج، استبعدنا الأفراد الذين حاولوا إكمال الاستبيان عدة مرات. كانت التعويضات للمشاركين تشمل قسائم نقدية مقدمة من خلال المنصة بناءً على متوسط طول الاستبيان. كان الميزانية لكل مشارك هيوافقت لجنة الأخلاقيات في كلية العلوم النفسية بجامعة تل أبيب على الدراسة وتنازلت عن الحاجة للحصول على موافقة مستنيرة. تم إجراء جميع الأبحاث وفقًا للإرشادات واللوائح ذات الصلة. قبل الدراسة، تلقى المشاركون ورقة معلومات/نموذج موافقة توضح الغرض منها وتؤكد لهم على السرية، وعدم الكشف عن الهوية، وخيار الانسحاب في أي مرحلة. قدم المشاركون الذين راجعوا ووافقوا على النموذج موافقتهم من خلال المتابعة لإكمال الدراسة عبر المنصة الإلكترونية.كوالتريكس.كوم. تم تسجيل الدراسة مسبقًا على منصة As Predicted في 2 فبراير 2024 (https://aspredicted.org/T2K_T53).
شملت التقييمات في اليوم الأول من الدراسة معلومات ديموغرافية مثل العمر، الجنس، المستوى التعليمي، الحالة الاجتماعية والاقتصادية، وعوامل متعلقة بالحرب تقيم فقدان الأحباء، التهجير القسري، وفقدان الدخل. تلا ذلك قياسات للأعراض السريرية. وشملت التقييمات اللاحقة، التي أجريت بعد 30 و90 يومًا، نفس القياسات السريرية.
الأدوات
يقيّم مقياس اضطراب القلق العام-7 (GAD-7) سبعة عناصر لتقييم احتمال ظهور أعراض القلق العام خلال الأسبوعين الماضيين. يتم تسجيل كل عنصر من 0 (“ليس على الإطلاق”) إلى 3 (“تقريبًا كل يوم”)، مع مجموع ممكن يتراوح من 0 إلىدرجات GAD-7 منتقترح قلقًا خفيفًا،قلق معتدل و 15-21 قلق شديد. أظهرت الأبحاث السابقة أن درجة العتبة 10 تتمتع بحساسية عالية ( ) وخصوصية في الدراسة الحالية، كانت قيمة ألفا كرونباخ للتقييم الأول 0.94.
استبيان صحة المريض-9 (PHQ-9) هو أداة تقرير ذاتي للاكتئاب الشديد المحتمل بناءً على معايير DSM-5، تقيم الأعراض خلال الأسبوعين الماضيين.. يتراوح نظام الدرجات من 0 (“ليس على الإطلاق”) إلى 3 (“تقريبًا كل يوم”)، بمجموع يتراوح بين 0 و 27. يتم تفسير الدرجات على مقياس PHQ-9 على أنها اكتئاب محتمل خفيف (5-9)، معتدل (10-14)، معتدل إلى شديد (15-19)، وشديد (20-27). حساسية عالية ( ) وخصوصية ( تم الإبلاغ عن درجة القطع لـكان ألفا كرونباخ للتقييم الأول 0.91.
أداة PC-PTSD-5 المكونة من خمسة عناصر هي أداة سريعة للتقارير الذاتية تُستخدم للكشف عن اضطراب ما بعد الصدمة وفقًا لدليل التشخيص والإحصاء DSM-5.استجابة إيجابية لثلاثة عناصر أو أكثر تشير إلى احتمال وجود اضطراب ما بعد الصدمة. لقد أظهر اختبار PC-PTSD-5 أداءً موثوقًا به مقارنةً بمقابلات اضطراب ما بعد الصدمة التي يديرها الأطباء.لهذه الدراسة، تم تعديل العناصر لتتناول بشكل خاص أحداث 7 أكتوبر والحرب اللاحقة (على سبيل المثال، “في الشهر الماضي، هل حلمت كوابيس عن حدث 7 أكتوبر/الحرب أو فكرت في هذه الأحداث ذات الصلة عندما لم تكن ترغب في ذلك؟”). كانت قيمة ألفا كرونباخ للتقييم الأول 0.75.
لتقييم آثار أحداث 7 أكتوبر وتجارب الحرب ذات الصلة، قمنا بتضمين أسئلة لتحديد ما إذا كان المشاركون قد تعرضوا لفقدان صادم، مثل مقتل أو إصابة أو اختطاف أحد أفراد الأسرة أو صديق مقرب إلى غزة. كما أضفنا أسئلة لاستكشاف التهجير القسري المؤقت أو المستمر، واستفسارات حول الآثار الاقتصادية، بما في ذلك فقدان الدخل أو الوظيفة وزيادة النفقات.
تحليل البيانات
استخدمنا اختبار كاي تربيع لبييرسون والاستقلالية-اختبارات لمقارنة الخصائص الديموغرافية (العمر، الجنس، العرق، التعليم، الدخل، الإقامة) والخصائص المتعلقة بالحرب (فقدان صادم، تهجير قسري، وفقدان الدخل) بين الذين أكملوا الدراسة والذين لم يكملوها لتحديد التحيزات المحتملة وضمان تمثيل عينتنا وقابلية تعميم النتائج الناشئة.
تم قياس الفروق بين المجموعات في الأعراض السريرية على مر الزمن باستخدام نماذج مختلطة خطية. قمنا بتطبيق نموذج كامل العوامل عبر النقاط الزمنية الثلاث (اليوم 1، اليوم 30، واليوم 90) لفقدان الصدمة (نعم/لا)، التهجير القسري (نعم/لا)، فقدان الدخل (نعم/لا)، الجنس (أنثى/ذكر)، والعرق (يهودي مقابل عربي وآخر، والذي شمل الدروز، غير اليهود، وغير المحدد). تم تضمين تقاطعات عشوائية للمشاركين لأخذ تصميم القياسات المتكررة في الاعتبار. كانت جميع الاختبارات الإحصائية ثنائية الجانب، مع تحديد مستوى ألفا عندلتعديل المقارنات المتعددة باستخدام تصحيح بونفيروني (0.05 مقسومًا على 5). تم إجراء تحليل البيانات باستخدام IBM SPSS Statistics 29.
النتائج
خصائص العينة
بعد إزالة 196 مشاركاً (بسبب فشل اختبارات الصلاحية، تألفت عيّنتنا النهائية من 1052 فردًا أكملوا المجموعة الأولى من التقييمات. من بين هؤلاء،أكمل التقييم المتابع لمدة 30 يومًا وأكمل التقييم المتابع لمدة 90 يومًا. لم تختلف الخصائص الأساسية بين المنتهين وغير المنتهين. كان متوسط عمر المستجيبين ± الانحراف المعياري هو (النطاق 18-40). كان أكثر من نصف المشاركين بقليل من الإناث ( ” ); لم يتم تحديد أي شخص على أنه متحول جنسياً أو غير ثنائي. الجدول 1 يعرض أعراق العينة، التعليم، الدخل، الإقامة، الفقدان الصادم (أي، قتل أو إصابة أو اختطاف أفراد الأسرة أو الأصدقاء المقربين إلى غزة) (التهجير القسري منذ 7 أكتوبر ) ، وفقدان الدخل بسبب الحرب ( ).
آثار السابع من أكتوبر والحرب التي تلت ذلك على الأعراض السريرية
تقدم الجدول 2 الأعراض السريرية عبر نقاط زمنية. من بين 1052 فردًا،أبلغوا عن أعراض القلق أو الاكتئاب أو اضطراب ما بعد الصدمة فوق العتبة في اليومأبلغ عن هذه الأعراض في اليوم 30، وفي اليوم 90. على شاشة GAD-7،تجاوزت العتبة المتوسطة (درجات GAD-7 ) في اليوم في اليوم الثلاثين، وفي اليوم 90. بالنسبة لأعراض الاكتئاب،تجاوزت العتبة المتوسطة (درجات PHQ-9 من 10 إلى 27) في اليومفي اليوم الثلاثين، و ( ) في اليوم 90. بشكل عام، من المستجيبين أبلغوا عن أعراض تشير إلى احتمال الإصابة باضطراب ما بعد الصدمة (درجة PCPTSD ) في اليوم في اليوم الثلاثين، وفي اليوم التسعين.
تقدم الشكل 1 متوسط درجات GAD-7 و PHQ-9 و PC-PTSD حسب الخسارة الصادمة، والنزوح القسري، وفقدان الدخل. في كل نقطة زمنية، كانت متوسط درجات GAD-7 أعلى باستمرار بين الأفراد الذين يعانون من خسارة صادمة.التهجير القسريوخسارة الدخل. بينما وجدنا تأثيرًا زمنيًا فقط لفقدان الصدمة، مما يعكس انخفاضًا ذا دلالة إحصائية في درجات GAD-7، لم نلاحظ مثل هذا التأثير لفقدان التهجير القسري أو فقدان الدخل، كما لم نجد تأثيرًا تفاعليًا لأي من الظروف. وبالمثل، كانت متوسطات درجات PHQ-9 أعلى باستمرار بين الأفراد الذين يعانون من فقدان الصدمة (التهجير القسري، وفقدان الدخللم نجد أي تأثير زمني أو تفاعلي لأي من هذه الضغوط. كانت متوسط درجات PC-PTSD أعلى في كل نقطة زمنية بين الأفراد الذين يعانون من فقدان صادم.التهجير القسري، ، وفقدان الدخل (كما هو الحال مع درجات PHQ-9، لم نجد أي تأثير زمني أو تفاعل لأي من الظروف.
تقدم الشكل 2 متوسط درجات GAD-7 و PHQ-9 و PC-PTSD حسب الجنس والعرق. بالنسبة للجنس، في كل نقطة زمنية، كانت النساء لديهن درجات GAD-7 متوسطة أعلى باستمرار. )، متوسط درجات PHQ-9 ( )، ومتوسط درجات PC-PTSD ( أظهرت درجات GAD-7 و PHQ-9 تأثيرًا زمنيًا، مما يعكس انخفاضًا ذا دلالة إحصائية مع مرور الوقت. ومع ذلك، لم تُظهر أي من مقاييس القياس تأثيرًا تفاعليًا. قمنا بإجراء تحليلات إضافية لاستكشاف التفاعلات المحتملة بين العمر والجنس؛ ومع ذلك، لم تُلاحظ أي نتائج ذات دلالة، ربما بسبب
عناصر
الإجمالي ( )
المكملون )
غير المكتملين )
إحصائية
معنى
SD
معنى
SD
معنى
SD
اختبارات t
عمر
31.3
٥.٦
٢٨.٧
6.1
30.4
٥.٩
6.86
<. 001
ن
%
ن
%
ن
%
جنس
6.97
. 008
نساء
566
٥٤
٣٩١
٥٧
١٧٥
٤٨
رجال
٤٨٦
٤٦
298
43
188
52
ترانسجندر/غير ثنائي/آخر
0
0
0
0
0
0
العرق
٤.٦٥
. 098
يهودي
٩٦٩
92
642
93
٣٢٧
90
عربي
64
٦
٣٤
٥
30
٨
آخر
19
2
١٣
2
٦
2
التعليم
٢٩.٥
<. 001
لم يكمل المدرسة الثانوية أبداً
11
1
٥
1
٦
2
خريج مدرسة ثانوية
318
30
172
٢٥
146
40
بعض الساعات المعتمدة في الكلية
231
٢٢
161
23
70
19
درجة البكالوريوس
٣٨٨
37
277
40
111
31
درجة الماجستير
100
10
71
10
٢٩
٨
درجة الدكتوراه
٤
0
٣
0
1
0
دخل
7.65
. ١٠٥
أقل بكثير من المتوسط
246
23
153
٢٢
93
٢٦
دون المتوسط
٢٨٣
27
١٧٩
26
١٠٤
٢٩
متوسط
٢٨٢
27
٢٠٠
٢٩
82
23
فوق المتوسط
204
19
١٢٩
19
75
21
أعلى بكثير من المتوسط
37
٤
٢٨
٤
9
٣
الإقامة
٢.٧٥
. ٠٩٧
شمال إسرائيل
٥٥٠
52
316
٤٦
186
51
جنوب إسرائيل
٥٠٢
٤٨
373
٥٤
١٧٧
٤٩
7 أكتوبر والأحداث المتعلقة بالحرب
فقدان صادم: تم قتل أو إصابة أو اختطاف أحد أفراد الأسرة أو صديق مقرب إلى غزة
٢٦٨
٢٦
158
23
١١٠
30
٦.٨٠
. 009
التهجير القسري
243
23
١٦٠
23
83
23
0.01
. 896
فقدان الدخل
479
٤٥
302
٤٤
١٧٧
٤٩
2.32
. 127
الجدول 1. الخصائص الديموغرافية. اختبار كاي تربيع لبييرسون؛اختبارات t المستقلة؛آخر: دروز ) ، الروسية ( )، مسيحي ( )، لا دين ( )، غير محدد ( ).
خاصية
يوم
يوم
اليوم 90 ( )
الدرجة الإجمالية لمقياس القلق GAD-7 (النطاق من 0 إلى 21؛ المتوسط والانحراف المعياري)
7.6
5.8
7.1
٥.٩
٦.٥
٥.٥
ن
%
ن
%
ن
%
مقياس القلق العام-7
678
64
٤٨٤
61
٤٠٠
٥٩
مقياس القلق العام-7
٣٣٢
32
228
٢٩
162
٢٤
الدرجة الإجمالية لـ PHQ-9 (النطاق 0-27؛ المتوسط والانحراف المعياري)
8.2
8.1
٧.٦
6.6
7.3
6.4
ن
%
ن
%
PHQ-9
653
62
٤٧٠
٥٩
395
٥٨
PHQ-9
374
٣٦
255
32
٢١٢
31
الدرجة الإجمالية لـ PC-PTSD (النطاق 0-5؛ المتوسط والانحراف المعياري)
2.2
2.2
2.1
1.7
1.9
1.7
ن
%
ن
%
ن
%
٤٦٥
٤٤
313
40
٢٥٠
37
الجدول 2. الأعراض السريرية على مر الزمن. GAD-7، اضطراب القلق العام؛ PHQ-9، استبيان صحة المريض؛ PC-PTSD، فحص PTSD للرعاية الأولية لـ DSM-5.
جيد-7 (القلق) 10 8 6 4
فقدان صادم (TL)
التهجير القسري (FD)
فقدان الدخل (IL)
اليوم 1 اليوم 30 اليوم 90
⟶ بدون ترجمة
اليوم 1 اليوم 30 اليوم 90
-FD-لا FD
اليوم 1 اليوم 30 اليوم 90
-IL-No IL
اليوم 1 اليوم 30 اليوم 90
-TL – لا TL
اليوم 1 اليوم 30 اليوم 90
-FD-لا FD
اليوم 1 اليوم 30 اليوم 90
-IL-No IL
٣
2
اليوم 1 اليوم 30 اليوم 90
اليوم 1 اليوم 30 اليوم 90
-FD – لا FD
اليوم 1 اليوم 30 اليوم 90
-IL -لا IL
الشكل 1. درجات اضطراب القلق العام-7 (GAD-7)، استبيان صحة المريض-9 (PHQ-9)، ومقياس PTSD للرعاية الأولية (PC-PTSD) حسب الخسارة الصادمة (TL)، التهجير القسري (FD)، وفقدان الدخل (IL). ملاحظات: TL، الخسارة الصادمة؛ FD، التهجير القسري؛ IL، فقدان الدخل؛ GAD-7، اضطراب القلق العام؛ PHQ-9، استبيان صحة المريض؛ PC-PTSD، مقياس PTSD للرعاية الأولية لـ DSM-5. النماذج الخطية المختلطة: تراوحت قيم F من 26.7 إلى 215.3، مع جميع.
حجم العينة يحد من القدرة على اكتشاف مثل هذه التأثيرات. بالنسبة للعرق، كانت متوسط درجات GAD-7 في كل نقطة زمنية أعلى باستمرار بين المستجيبين العرب وغيرهم.. وجدنا نتائج مشابهة لدرجات PHQ-9 المتوسطة (لم نجد أي تأثير من هذا القبيل على درجات PC-PTSD، ولا تأثير زمني أو تأثير تفاعلي لأي مقياس قياس.
نقاش
دراستنا قيمت الأعراض الذاتية المبلغ عنها للقلق والاكتئاب واضطراب ما بعد الصدمة على مدى 90 يومًا بين 1052 فردًا يعيشون في مناطق النزاع. وجدنا أعراض صحة نفسية تتجاوز العتبة فيمن المشاركين، الذين انخفض عددهم قليلاً على مدى ثلاثة أشهر. كما تم الافتراض، أظهر الأفراد الذين يعانون من خسائر صادمة، أو تهجير قسري، أو صعوبات اقتصادية معدلات أعراض أعلى عبر جميع المقاييس (GAD-7، PHQ9، PC-PTSD). كان هذا واضحًا في الدرجات المتوسطة المرتفعة باستمرار بين هذه المجموعات، مقارنةً بأولئك الذين لم يمروا بتجارب مماثلة، عبر جميع النقاط الزمنية. بالإضافة إلى ذلك، كانت النساء وأعضاء الأقليات العرقية يبلّغون باستمرار عن مستويات ضيق أعلى من الرجال والأفراد اليهود. هذه الأنماط من الضيق المرتفع تتطلب اهتمامًا فوريًا بالاحتياجات الصحية النفسية لأولئك الذين يتحملون أكبر الأعباء في المناطق المتأثرة بالنزاع.
بشكل عام،، و من المشاركين أبلغوا عن أعراض القلق والاكتئاب و/أو اضطراب ما بعد الصدمة في اليوم الأول، اليوم 30، واليوم 90، على التوالي. الأبحاث حول المناطق المتأثرة بالحرب والنتائج النفسية في السكان العامين محدودة. مراجعة منهجية وتحليل تلوي حدّث تقديرات منظمة الصحة العالمية ووجدت أن انتشار الاضطرابات النفسية مثل الاكتئاب، القلق، اضطراب ما بعد الصدمة، الاضطراب ثنائي القطب، والفصام في السكان المتأثرين بالنزاع هوفي أي وقت معين. دراسة مماثلة للمهاجرين المعرضين للصراعات المسلحة
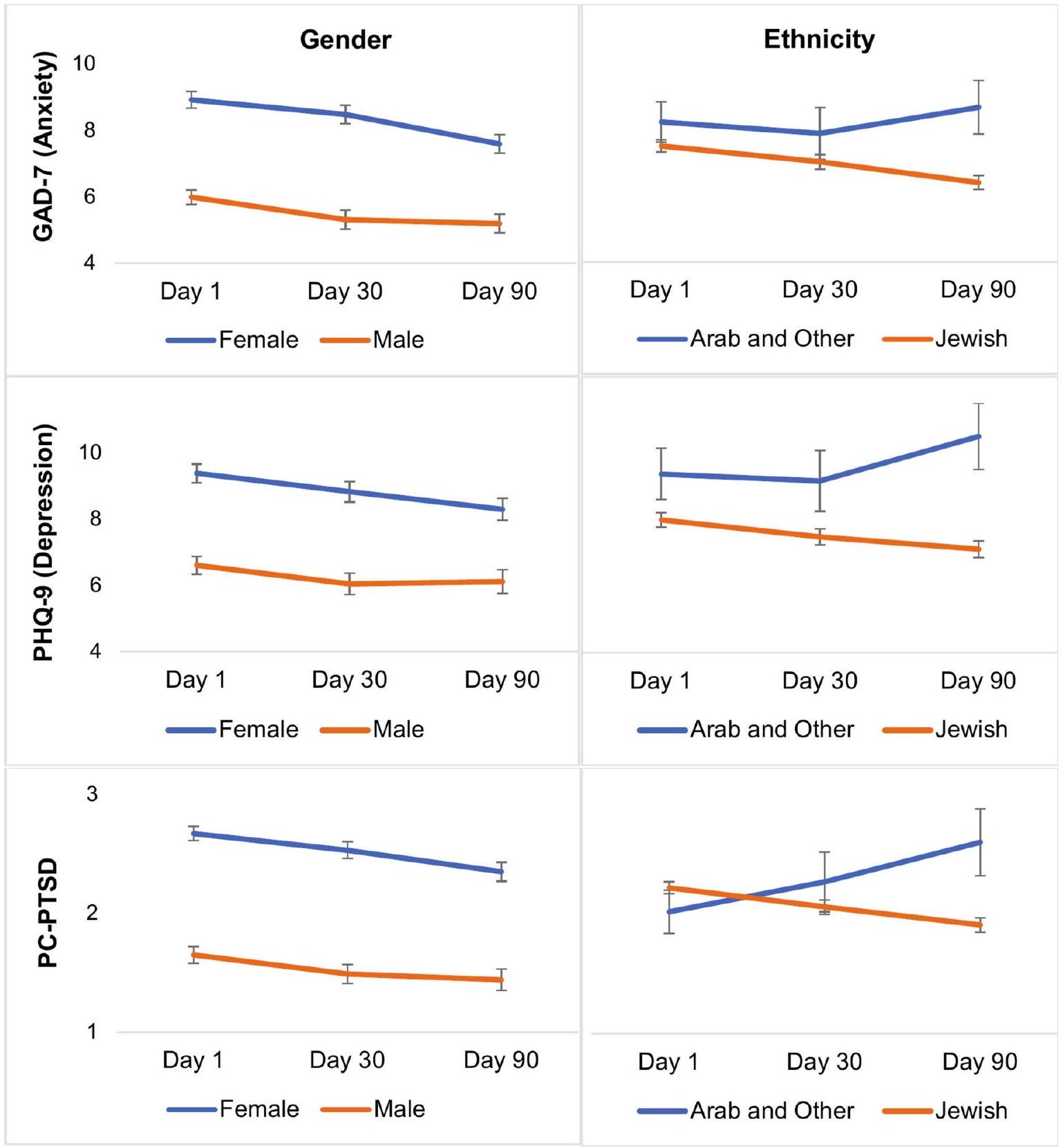
الشكل 2. درجات اضطراب القلق العام-7 (GAD-7)، استبيان صحة المريض-9 (PHQ-9)، ودرجات اضطراب ما بعد الصدمة في الرعاية الأولية (PC-PTSD) حسب الجنس والعرق. ملاحظات: عربي ( ) وأخرى: دروز ( ) ، الروسية ( )، مسيحي ( )، لا دين ( )، غير محدد ( ); GAD-7، اضطراب القلق المعمم؛ PHQ9، استبيان صحة المريض؛ PC-PTSD، فحص اضطراب ما بعد الصدمة للرعاية الأولية وفقًا لـ DSM-5. النماذج الخطية المختلطة: تراوحت قيم F من 8.3 إلى 213.9، مع p تتراوح من .004 إلى أقل من .001.
وجدت انتشاراً لـلـ PTSD الحالي،للاكتئاب الشديد، ولاضطراب القلق العام، استنادًا إلى المقابلات النفسية القياسيةأظهر المهاجرون الأصغر سناً معدلات أعلى من اضطراب ما بعد الصدمة والقلق، في حين أن مرور وقت أطول منذ التهجير ارتبط بانخفاض انتشار اضطراب ما بعد الصدمة والاكتئاب على مدى الحياة.أظهرت دراسة مستقبلية على مستوى البلاد أجريت في إسرائيل بعد 7 أكتوبر مستويات عالية من القلق والاكتئاب واضطراب ما بعد الصدمة مقارنة بالمستويات قبل أكتوبر.. ومع ذلك، لم تركز هذه الدراسة الوطنية على مناطق النزاع، ولا على الضغوط المرتبطة بالحرب. من المهم أنه على الرغم من أننا لا نستطيع مقارنة عيّنتنا بعينات تمثيلية قائمة على السكان، إلا أن عينات الفرص الذاتية المبلغ عنها عبر الإنترنت أظهرت معدلات مرتفعة مماثلة في المناطق المتأثرة بالحرب..
تحديدًا، تتماشى نتائجنا حول ارتفاع درجات GAD-7 وPHQ-9 وPC-PTSD بين الأفراد الذين يعيشون في مناطق متأثرة بالحرب في إسرائيل والذين عانوا من فقدان صادم أو تهجير قسري أو فقدان الدخل مع الأدبيات الموجودة.تعكس هذه الأعراض المرتفعة التحديات العميقة في الصحة النفسية التي يواجهها الأفراد في التعامل مع الآثار الفورية للصعوبات المرتبطة بالحرب. المعنى السريري تسلط الأعراض المرتبطة بهذه الحالات الضوء على دورها كعوامل حاسمة في تفاقم مشكلات الصحة النفسية، مما يستدعي تدخلات عاجلة ومتخصصة تعالج هذه المصادر المحددة للضغط النفسي.يجب أن تصمم مثل هذه التدخلات لتلبية الاحتياجات المحددة لأولئك الأكثر تأثراً، مع الأخذ في الاعتبار عوامل مثل مدة وشدة التعرض، والعمر، وطبيعة الصعوبات التي تم مواجهتها. هذه المقاربة المستهدفة ضرورية للتخفيف من الأثر الشديد والمستمر على الرفاهية النفسية في بيئات النزاع.
تؤكد نتائجنا المتعلقة بزيادة الأعراض بين النساء الأدبيات الموجودة.على سبيل المثال، حددت مراجعة منهجية للتأثيرات النفسية لـ COVID-19 على السكان العامين انتشارًا أعلى لمشاكل الصحة النفسية بين النساء وأشارت إلى الجنس كعامل خطر.؛ ومع ذلك، تشير الأبحاث أيضًا إلى أن الفروق بين الجنسين تختفي مع مرور الوقتتشير هذه النتائج مجتمعة إلى وجود ضعف فوري متزايد أو استعداد بين النساء لتجربة والإبلاغ عن أعراض القلق والاكتئاب واضطراب ما بعد الصدمة في البيئات المتأثرة بالنزاع. تؤكد هذه النتائج على الفرصة لتدخلات الصحة النفسية المستهدفة المستندة إلى الأدلة التي تأخذ في الاعتبار الضعف الفوري المحدد وعوامل المرونة الموجودة في الفئات النسائية في هذه البيئات عالية الضغط. على سبيل المثال، يمكن أن تكون العلاج النفسي بين الأشخاص (IPT) وسيلة فعالة، تركز على العلاقات الشخصية والاستجابات العاطفية للأحداث الحياتية التي قد تكون ساحقة أحيانًا.. قد يكون من الممكن أيضًا أن تكون الإناث أكثر استعدادًا لتأييد أعراض الضيق المرتبطة بالنزاعات المسلحة، أو أن الأعراض بين الذكور ستظهر لاحقًا. تم تحديد ظهور الأعراض على مسارات زمنية مختلفة بين مجموعات المحاربين القدامى. هناك حاجة إلى جهود طولية مستمرة لاستكشاف مثل هذه الاحتمالات.
تكشف نتائجنا عن تفاوتات عرقية مستمرة في أعراض الصحة النفسية، حيث يظهر أعضاء من المجتمعات العربية وغيرها من الأقليات المقيمة في مناطق النزاع باستمرار درجات أعلى من GAD-7 و PHQ-9. على الرغم من حجم العينة المحدود ()، فإن الفروق الكبيرة تبرز الضعف المتزايد للأفراد من هذه المجموعات مقارنة باليهود الإسرائيليين. بينما يتمتع العرب الإسرائيليون بنفس الحقوق القانونية للوصول إلى الرعاية الصحية النفسية مثل المواطنين الآخرين، فإن هذا التفاوت من المحتمل أن يكون بسبب الوصول المحدود إلى الموارد، والضغط الاجتماعي، والتمييز. علاوة على ذلك، قد تسهم الوضع الاجتماعي والسياسي للعرب الإسرائيليين، بما في ذلك التحديات المتعلقة بالولاء المزدوج المدرك (إسرائيل مقابل الفلسطينيين) والخوف من أن يتم تصنيفهم كأعداء من قبل اليهود، في هذه التفاوتات. هذه العوامل، التي تتفاقم بسبب الموارد المحدودة، تبرز الحاجة الملحة إلى تدخلات صحية نفسية مستهدفة مستندة إلى الأدلة وحساسة ثقافيًا. بالإضافة إلى ذلك، تشير الاتجاهات الملاحظة في الأرقام إلى مسارات أعراض متعارضة بمرور الوقت للمشاركين اليهود والعرب، مما يعكس على الأرجح ضعفًا متباينًا وفقدانًا للموارد بين الأفراد العرب.
لمعالجة المخاوف المتعلقة بالصحة النفسية التي تم تحديدها في دراستنا بشكل فعال، يجب تنفيذ تدابير استباقية لدعم الأفراد الأكثر عرضة للخطر. على وجه التحديد، يجب على مقدمي الرعاية الصحية إعطاء الأولوية لأولئك الذين عانوا من فقدان صادم، وأولئك الذين تم تهجيرهم قسراً، وأولئك الذين يعانون من انعدام الأمن الاقتصادي المرتبط بالحرب، حيث يمكن أن تؤدي كل من هذه التجارب إلى عدم الاستقرار وردود فعل إجهاد حادة. يجب أن تكون هذه الضغوط بمثابة علامات حاسمة لمساعدة مقدمي الرعاية الصحية على تحديد الأولويات وتخصيص جهود العلاج، مما يضمن أن أولئك الذين في أمس الحاجة يتلقون رعاية مركزة مستندة إلى الأدلة ومتاحة. تعتبر مثل هذه التدخلات المستهدفة ضرورية ليس فقط لرفاهية الأفراد المتأثرين مباشرة ولكن أيضًا للصحة المجتمعية الأوسع، مما يساهم في الاستقرار العام ومرونة المجتمعات التي تعيش في مناطق النزاع.
تحتوي دراستنا على عدة قيود. أولاً، قد يختلف مستخدمو جمع البيانات الناطقون بالعبرية من الناحية الاجتماعية والديموغرافية عن السكان في جنوب وشمال إسرائيل، مما يحد من إمكانية تعميم النتائج، بما في ذلك انخفاض معدلات العرب الإسرائيليين مقارنة بالسكان العام. يجب أن تهدف الدراسات المستقبلية إلى تجنيد عينة أكبر وأكثر تمثيلاً من الأقليات غير اليهودية، بما في ذلك العرب الإسرائيليين ومجموعات فرعية أخرى. بالإضافة إلى ذلك، قد تكون طريقة التجنيد قد أدت إلى إدخال تحيزات، مثل نقص تمثيل الأفراد الذين ليس لديهم وصول إلى الإنترنت أو أولئك الأقل احتمالًا للمشاركة في الاستطلاعات عبر الإنترنت. ثانيًا، استهدفنا الفئة العمرية من عامًا، مستبعدين الأفراد الأكبر سنًا، بسبب ارتفاع معدل حدوث الأمراض النفسية في الفئة العمرية الأصغر؛ كما أن التأثيرات على الفئات الأكبر (والأصغر) تستحق الاستكشاف. ثالثًا، من القيود الملحوظة في الدراسة هو غياب بيانات خط الأساس التي تسبق أحداث أكتوبر، وهي مشكلة شائعة في الأبحاث التي ت triggered by crises مفاجئة وغير متوقعة. كما أننا لم نستفسر عن الصدمات غير المتعلقة بالحرب منذ 7 أكتوبر. رابعًا، التقييمات السريرية المستندة إلى استبيانات ذاتية بدلاً من مقابلات تشخيصية رسمية عرضة للإبلاغ المفرط أو الناقص. أخيرًا، بينما توفر هذه الدراسة رؤى قيمة حول تصورات المدنيين الإسرائيليين، من المهم أن نلاحظ أنها لا تتناول التأثيرات على الفلسطينيين، مما يمثل قيدًا كبيرًا في فهم النطاق الكامل لعواقب النزاع.
الاستنتاجات
تؤكد هذه الدراسة على الحاجة الملحة لأنظمة دعم الصحة النفسية الشاملة في مناطق النزاع. يجب أن تكون الخدمات المستندة إلى الأدلة مصممة لتلبية احتياجات أولئك الأكثر عرضة للخطر بشكل فوري، بما في ذلك النساء، وأعضاء الأقليات العرقية، والأفراد الذين يواجهون خسائر صادمة، أو تهجير، أو صعوبات اقتصادية، بهدف التخفيف من تطور الأعراض المستمرة و/أو الاضطرابات النفسية. من خلال تسليط الضوء على الانتشار الكبير لأعراض القلق والاكتئاب واضطراب ما بعد الصدمة داخل هذه المجموعات، تؤكد أبحاثنا على ضرورة التدخلات المستهدفة المستندة إلى الأدلة المصممة خصيصًا لدعم الأفراد الذين يتمتعون بهذه الخصائص الديموغرافية، أو أولئك الذين يواجهون مثل هذه الضغوط. هناك حاجة إلى مزيد من البحث لتوسيع هذه النتائج لتشمل مجموعات سكانية أخرى ولتشمل أولئك الذين تزيد أعمارهم عن 40 أو أقل من 18.
توفر البيانات
تتوفر مجموعات البيانات المستخدمة و/أو التي تم تحليلها خلال الدراسة الحالية من المؤلف المقابل عند الطلب المعقول.
تاريخ الاستلام: 2 نوفمبر 2024؛ تاريخ القبول: 23 ديسمبر 2024
تم النشر عبر الإنترنت: 06 يناير 2025
References
Vinograd, C. & Kershner, I. Israel’s Attackers Took Over 200 Hostages. Here’s What to Know About Them. The New York Times (2023).
Around Half a Million Israelis Displaced Inside Israel: Military. Barron’s. 16 October 2023. Retrieved 18 November 2023.
Israel sharpens warning to Lebanon as cross-border hostilities spike. Reuters. 13 November 2023. Archived from the original on 13 November 2023. Retrieved 30 January 2024.
Lowell, A. et al. 9/11-related PTSD among highly exposed populations: A systematic review 15 years after the attack. Psychol. Med. 48, 537-553 (2018).
Bonanno, G. A., Galea, S., Bucciarelli, A. & Vlahov, D. Psychological resilience after disaster: New York City in the aftermath of the September 11th terrorist attack. Psychol. Sci. 17, 181-186 (2006).
Garfin, D. R., Poulin, M. J., Blum, S. & Silver, R. C. Aftermath of terror: a nationwide longitudinal study of posttraumatic stress and worry across the decade following the September 11, 2001 terrorist at- tacks. J. Trauma Stress 31(1), 146-156 (2018).
Boudoukha, A. H., Ouagazzal, O. & Goutaudier, N. When traumatic event exposure characteristics matter: impact of traumatic event exposure characteristics on posttraumatic and dissociative symptoms. Psychol. Trauma 9(5), 561 (2017).
Rigutto, C., Sapara, A. O. & Agyapong, V. I. Anxiety, depression and posttraumatic stress disorder after terrorist attacks: A general review of the literature. Behav. Sci. 11(10), 140 (2021).
Ozbay, F., der Heyde, T. A., Reissman, D. & Sharma, V. The enduring mental health impact of the September 11th terrorist attacks: Challenges and lessons learned. Psychiatr. Clin. 36(3), 417-429 (2013).
Donoho, C. J., Bonanno, G. A., Porter, B., Kearney, L. & Powell, T. M. A decade of war: Prospective trajectories of PTSD symptoms among deployed US military personnel and the influence of combat exposure. Am. J. Epidemiol. 186(12), 1310-1318 (2017).
Kristensen, P., Weisæth, L. & Heir, T. Bereavement and mental health after sudden and violent losses: A review. Psychiatry 75(1), 76-97. https://doi.org/10.1521/psyc.2012.75.1.76 (2012).
Porter, M. & Haslam, N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: a meta-analysis. JAMA 294(5), 602-612. https://doi.org/10.1001/jama.294.5.602 (2005).
Ruengorn, C., Awiphan, R., Wongpakaran, N., Wongpakaran, T., Nochaiwong, S., Health Outcomes and Mental Health Care Evaluation Survey Research Group (HOME-Survey). Association of job loss, income loss, and financial burden with adverse mental health outcomes during coronavirus disease 2019 pandemic in Thailand: A nationwide cross-sectional study. Depress. Anxiety 38(6), 648-660 (2021).
Kujawa, A., Green, H., Compas, B. E., Dickey, L. & Pegg, S. Exposure to COVID-19 pandemic stress: Associations with depression and anxiety in emerging adults in the United States. Depress. Anxiety. 37(12), 1280-1288 (2020).
Hawes, M. T., Szenczy, A. K., Klein, D. N., Hajcak, G. & Nelson, B. D. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol. Med. 52, 1-9 (2021).
Amsalem, D. et al. Anxiety and depression symptoms among young US essential workers during the COVID-19 pandemic. Psychiatric Serv. 74(10), 1010-1018 (2023).
Zhang, W., Walkover, M. & Wu, Y. Y. The challenge of COVID-19 for adult men and women in the United States: Disparities of psychological distress by gender and age. Public Health 198, 218-222 (2021).
Mesa-Vieira, C. et al. Mental health of migrants with pre-migration exposure to armed conflict: A systematic review and metaanalysis. Lancet Public Health 7(5), e469-e481 (2022).
Newnham, E. A., Pearson, R. M., Stein, A. & Betancourt, T. S. Youth mental health after civil war: The importance of daily stressors. Br. J. Psychiatry 206(2), 116-121. https://doi.org/10.1192/bjp.bp.114.146324 (2015).
Morina, N., Stam, K., Pollet, T. V. & Priebe, S. Prevalence of depression and posttraumatic stress disorder in adult civilian survivors of war who stay in war-afflicted regions. A systematic review and meta-analysis of epidemiological studies. J. Affect. Disord. 239, 328-338 (2018).
Bleich, A., Gelkopf, M. & Solomon, Z. Exposure to terrorism, stress-related mental health symptoms, and coping behaviors among a nationally representative sample in Israel. JAMA 290(5), 612-620. https://doi.org/10.1001/jama.290.5.612 (2003).
Brewin, C. R., Andrews, B. & Valentine, J. D. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J. Consult. Clin. Psychol. 68(5), 748 (2000).
Groweiss, Y., Blank, C., Hamdan, S., Neria, Y. & Levi-Belz, Y. The mental health impact of the October 7th terror attack on Jews and Arabs in Israel: A nationwide prospective study. Psychiatry Res. 337, 115973 (2024).
Pearlin, L. I., Schieman, S., Fazio, E. M. & Meersman, S. C. Stress, health, and the life course: Some conceptual perspectives. J. Health Soc. Behav. 46(2), 205-219 (2005).
Achdut, N. Ethnic inequality between Arabs and Jews in Israel in global life satisfaction: A social determinants examination among young adults. Am. J. Orthopsychiatry (2024).
Hobfoll, S. E., Canetti-Nisim, D. & Johnson, R. J. Exposure to terrorism, stress-related mental health symptoms, and defensive coping among Jews and Arabs in Israel. J. Consult. Clin. Psychol. 74(2), 207 (2006).
Marciano, H., Kimhi, S. & Eshel, Y. Predictors of individual, community and national resiliencies of Israeli Jews and Arabs. Int. J. Psychol. 55(4), 553-561 (2020).
Spitzer, R. L., Kroenke, K., Williams, J. B. W. & Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166(10), 1092-1097. https://doi.org/10.1001/archinte.166.10.1092 (2006).
Levis, B., Benedetti, A. & Thombs, B. D. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ 365, I1476. https://doi.org/10.1136/bmj.l1476 (2019).
Prins, A. et al. The primary care PTSD screen for DSM-5 (PC-PTSD-5): Development and evaluation within a veteran primary care sample. J. Gen. Intern Med. 31(10), 1206-1211. https://doi.org/10.1007/s11606-016-3703-5 (2016).
Ouimette, P., Wade, M., Prins, A. & Schohn, M. Identifying PTSD in primary care: Comparison of the Primary Care-PTSD Screen (PC-PTSD) and the General Health Questionnaire-12 (GHQ). J. Anxiety Disord. 22(2), 337-343. https://doi.org/10.1016/j.janxdis .2007.02.010 (2008).
Charlson, F. et al. New WHO prevalence estimates of mental disorders in conflict settings: A systematic review and meta-analysis. Lancet 394(10194), 240-248 (2019).
Levi-Belz, Y., Groweiss, Y., Blank, C. & Neria, Y. PTSD, depression, and anxiety after the October 7, 2023 attack in Israel: A nationwide prospective study. EClinicalMedicine 68, 102418 (2024).
Zasiekina, L., Zasiekin, S. & Kuperman, V. Post-traumatic stress disorder and moral injury among Ukrainian civilians during the ongoing war. J. Community Health 48(5), 784-792. https://doi.org/10.1007/s10900-023-01225-5 (2023).
Scholte, W. F. et al. Mental health symptoms following war and repression in eastern Afghanistan. JAMA 292(5), 585-593 (2004).
Priebe, S. et al. Psychological symptoms as long-term consequences of war experiences. Psychopathology 46(1), 45-54. https://doi. org/10.1159/000338640 (2013).
Mollica, R. F. et al. Longitudinal study of psychiatric symptoms, disability, mortality, and emigration among Bosnian refugees. JAMA 286(5), 546-554. https://doi.org/10.1001/jama.286.5.546 (2001).
Miller, K. E. & Rasmussen, A. The mental health of civilians displaced by armed conflict: an ecological model of refugee distress. Epidemiol. Psychiatr. Sci. 26(2), 129-138. https://doi.org/10.1017/S2045796016000172 (2017).
Siriwardhana, C., Ali, S. S., Roberts, B. & Stewart, R. A systematic review of resilience and mental health outcomes of conflictdriven adult forced migrants. Conflict Health 8, 1-4 (2014).
Xiong, J. et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 277, 55-64 (2020).
Fenollar-Cortés, J., Jiménez, Ó., Ruiz-García, A. & Resurrección, D. M. Gender differences in psychological impact of the confinement during the COVID-19 outbreak in Spain: A longitudinal study. Front Psychol. 12, 682860. https://doi.org/10.3389/fp syg. 2021.682860 (2021).
Markowitz, J. C. In the Aftermath of the Pandemic: Interpersonal psychotherapy for Anxiety, Depression, and PTSD (Oxford University Press, 2021).
Boerma, T., Hosseinpoor, A. R., Verdes, E. & Chatterji, S. A global assessment of the gender gap in self-reported health with survey data from 59 countries. BMC Public Health 16, 1-9. https://doi.org/10.1186/s12889-016-2767-x (2016).
الشكر والتقدير
نشكر المدنيين الذين شاركوا في الدراسة.
مساهمات المؤلف
كتب د.أ. المسودة الأولى من هذه المخطوطة. قام د.أ.، س.هـ.ن، أ.ل، ي.ل.ب، و ي.ن. بتنسيق التجربة، والمساهمة في تصميم وتنفيذ التجربة، وجمع البيانات. قام د.أ.، س.هـ.ن، و أ.ل. بإجراء التحليلات الإحصائية. راجع جميع المؤلفين ووافقوا على المخطوطة.
التمويل
تم توفير التمويل من قبل HOMIYAH.
الإعلانات
المصالح المتنافسة
يعلن المؤلفون عدم وجود مصالح متنافسة.
معلومات إضافية
يجب توجيه المراسلات وطلبات المواد إلى د.أ.
معلومات إعادة الطبع والتصاريح متاحة علىwww.nature.com/reprints.
ملاحظة الناشر تظل Springer Nature محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
قسم الطب النفسي، معهد الطب النفسي بولاية نيويورك، نيويورك، نيويورك، الولايات المتحدة الأمريكية.كلية الأطباء والجراحين بجامعة كولومبيا، مركز جامعة كولومبيا الطبي إيرفينغ، 1051 شارع ريفرسايد، نيويورك، نيويورك 10032، الولايات المتحدة الأمريكية.كلية العمل الاجتماعي، جامعة تل أبيب، تل أبيب، إسرائيل.كلية العلوم النفسية، جامعة تل أبيب، تل أبيب، إسرائيل.مركز لior تسفاتي لدراسات الانتحار والألم النفسي، مركز روبيين الأكاديمي، إيمك هيفر، إسرائيل.الخدمات النفسية، جامعة بن غوريون في النقب، بئر السبع، إسرائيل.أقسام الطب الفيزيائي وإعادة التأهيل، الطب النفسي، وعلوم الأعصاب، جامعة كولورادو، حرم أنشوتز الطبي، أورا، كولورادو، الولايات المتحدة الأمريكية.قسم الطب النفسي، مركز حايم شبا الطبي، تل هشومر، إسرائيل.مركز شالڤاتا للصحة النفسية، هود هشارون، إسرائيل.كلية الطب، جامعة تل أبيب، تل أبيب، إسرائيل. ® البريد الإلكتروني:doron.amsalem@nyspi.columbia.edu
The effects of war-related experiences on mental health symptoms of individuals living in conflict zones: a longitudinal study
Doron Amsalem , Shilat Haim-Nachum , Amit Lazarov , Yossi Levi-Belz , John C. Markowitz , Maja Bergman , Alexandra Klein Rafaeli , Lisa A. Brenner , Nitsa Nacasch , Milton L. Wainberg , Ido Lurie , Shlomo Mendlovic & Yuval Neria
Abstract
On October 7, 2023, a large-scale attack in southern Israel and the subsequent war resulted in extensive loss of life and injuries, with many individuals experiencing traumatic losses, such as family members or close friends being killed or kidnapped. This study aims to longitudinally examine its effects on mental health, specifically, clinical symptoms of anxiety, depression, and posttraumatic stress disorder (PTSD). We anticipated greater symptom severity among individuals who experienced traumatic loss, were forcibly displaced, or suffered income loss, as well as among women and members of ethnic minorities. This three-wave online survey study assessed mental health symptoms in a sample of 1052 individuals, aged 18-40, residing in conflict zones in Israel from February 2024 (day 1), through March 2024 (day 30), to May 2024 (day 90). Symptoms of anxiety, depression, and PTSD were measured using the Generalized Anxiety Disorder-7 (GAD-7), Patient Health Questionnaire-9 (PHQ-9), and Primary Care PTSD Screen (PC-PTSD). Individuals experiencing traumatic losses, forced displacement, or economic hardships, as well as females, consistently demonstrated higher rates of anxiety, depression, and PTSD symptoms compared to those without such experiences or to males, across all time points (F values ranged from 17.7 to ). For ethnic minorities (Arab and other), as compared to Jewish, anxiety and depression symptoms were higher at every time point ( to <.001). This study highlights the urgent need for targeted mental health interventions in conflict zones, particularly for affected individuals. Further research should expand these findings to broader populations.
Keywords War, Terrorist attack, Anxiety, Depression, PTSD, Gender, Displacement
On October 7, 2023, a series of violent events led to significant casualties and displacement in Israel, with over 1000 individuals reported deceased and 251 taken captive . Subsequent incidents along the northern border contributed to further civilian displacement, affecting approximately 100,000 individuals. Overall, the conflict has displaced between 200,000 and 500,000 people within Israel, leading to instability and difficulties in returning home . These events have also resulted in economic challenges, including job losses and increased living expenses for those impacted. This study aims to assess the psychological and social consequences for those residing in conflict-affected areas. While this study focuses exclusively on the mental health and socioeconomic effects experienced by individuals in Israel, it acknowledges that this is only one aspect of a broader, multifaceted conflict.
Previous studies on the mental health effects of terrorist attacks have focused on directly exposed individuals, particularly those close to the events, such as New Yorkers during the September 11 terrorist attack . Immediate proximity to traumatic events significantly increases the risk of developing serious mental health conditions, including posttraumatic stress disorder (PTSD), depression, and anxiety . Traumatic and sudden loss of a loved one can contribute to prolonged periods of sorrow, symptoms of major depression, and uncomplicated or complicated grief . Forced displacement often induces acute stress and anxiety, and feelings of insecurity and instability, which may worsen or precipitate mental health issues . Financial burdens due to job or income loss can produce feelings of helplessness. Such ongoing stress exacerbates the risk of developing conditions such as depression and anxiety . Each of these stressors can amplify the severity of existing psychopathology and increase the likelihood of new conditions, impairing mental health and well-being.
The global prevalence of anxiety, depression, and PTSD has already been slowly but significantly increasing among adults, especially younger adults . For example, a recent study showed rates of for anxiety and for depression, more than twice the rates of older adults . Specifically, studies have shown that younger individuals, including those exposed to conflict zones, are at higher risk for mental health disorders such as PTSD, major depressive disorder, and generalized anxiety disorder . This group is particularly vulnerable to the psychological effects of terrorist attacks or war, including job loss or reduced hours, financial strains, and separation from loved ones. Therefore, this study focuses on individuals aged 18-40, based on evidence indicating the heightened vulnerability of younger adults in these contexts.
Gender and ethnicity also influence mental health outcomes. A systematic review and meta-analysis showed that women are more likely to develop depression and PTSD in war-afflicted regions . Israeli women demonstrated higher vulnerability to traumatic stress-related symptoms following terrorist attacks on Israeli society in the early . Similarly, minority ethnic groups are known to face higher risks for adverse mental health outcomes after exposure to major traumatic events . Specifically, Israeli Arabs, who comprise of Israel’s population (compared to for Jews), were found in studies, including one conducted following the October 7 attack, to carry increased risks for several psychopathologies . While Israeli Arabs have the same legal rights to access care, including mental health care, as other citizens, like many minoritized populations globally, they experience bias, stigmatization, and discrimination that significantly impact their access and quality of care . This often results in state authorities giving less priority to minority needs, leading to poorer coping strategies and greater psychological burdens for Israeli Arabs compared to Israeli Jews .
The current study
This study seeks to deepen understanding of the various war-related stressors and social determinants of health that affect the mental health of civilians in conflict zones. Specifically, it examines the impacts of traumatic loss, forced displacement, and income loss, which we anticipate having relatively high prevalence rates, among a substantial sample of individuals living in war-affected areas in Israel. Additionally, the study aims to assess the role of gender and ethnicity on the severity of mental health symptoms in these populations. We conducted a longitudinal study with assessments starting in February 2024 (day 1), through March 2024 (day 30), to May 2024 (day 90). We hypothesized that (1) individuals who experienced traumatic loss, were forcibly displaced, or suffered income loss would exhibit greater psychopathology, as would (2) women and members of ethnic minorities.
Methods
Recruitment and participants
Recruitment occurred between February and May 2024. The study recruited Hebrew-speaking civilians aged 18 to 40 living in northern and southern Israeli conflict areas. The focus was on individuals (both Jewish and Arabs) from these regions because they were the ones most directly affected by the October 7 attacks and subsequent war. The study used Panel4all, an Israeli crowdsourcing tool commonly employed in medical and psychological research, which provides access to a probability-based pool panel of approximately 100,000 Israelis, thus ensuring representative sampling of the national population. The platform confirms consistency in demographic characteristics over time, blocks participants who use location masking tools, and runs tests to identify bots. To enhance the validity of results, we excluded individuals who attempted multiple survey completions. Compensation for participants included monetary vouchers provided through the platform based on the average length of the survey. The budget per participant was . The Ethics Committee of the School of Psychological Sciences at Tel Aviv University approved the study and waived the need to obtain informed consent. All research was performed in accordance with relevant guidelines and regulations. Before the study, participants received an information sheet/consent form outlining its purpose and assuring them of confidentiality, anonymity, and the option to withdraw at any stage. Participants who reviewed and agreed to the form provided their consent by proceeding to complete the study via the online platform, Qualtrics.com. The study was registered in advance on the As Predicted platform on February 2, 2024 (https://aspredicted.org/T2K_T53).
Assessments on study day 1 included demographic information such as age, gender, educational level, socioeconomic status, and war-related factors assessing loss of loved ones, forced displacement, and income loss. This was followed by measurements of clinical symptoms. Follow-up assessments, conducted 30 and 90 days later, included the same clinical measurements.
Instruments
The Generalized Anxiety Disorder-7 (GAD-7) assesses seven items to evaluate the likelihood of generalized anxiety symptoms over the previous two weeks. Each item is scored from 0 (“not at all”) to 3 (“nearly every day”), with a possible total ranging from 0 to . GAD-7 scores of suggest mild anxiety, moderate anxiety,
and 15-21 severe anxiety. Previous research has shown a threshold score of 10 has high sensitivity ( ) and specificity . In the current study, Cronbach’s alpha for the first assessment was 0.94 .
The Patient Health Questionnaire-9 (PHQ-9) is a self-report tool for probable major depression based on DSM-5 criteria, assessing symptoms over the last two weeks . Its scoring system ranges from 0 (“not at all”) to 3 (“nearly every day”), totaling between 0 and 27 . Scores on the PHQ-9 are interpreted as probable mild (5-9), moderate (10-14), moderate-to-severe (15-19), and severe (20-27) depression. High sensitivity ( ) and specificity ( ) have been reported for the cut-off score of . Cronbach’s alpha for the first assessment was 0.91 .
The five-item PC-PTSD-5 is a brief self-report tool used to screen for DSM-5 PTSD . A positive response to three or more items indicates possible PTSD. The PC-PTSD-5 has demonstrated reliable performance in comparison to clinician-administered PTSD interviews . For this study, items were modified to specifically address the events of October 7th and the subsequent war (e.g., “In the past month, had nightmares about the October 7 event(s)/the war or thought about these related events when you did not want to?”). Cronbach’s alpha for the first assessment was 0.75 .
To assess the effects of the October 7 events and related war experiences, we included questions to determine if participants had experienced traumatic losses, such as a family member or close friend being killed, injured, or kidnapped to Gaza. We also added questions to explore temporary or ongoing forced displacement, and inquiries about economic impacts, including loss of income or job and increased expenses.
Data analysis
We used Pearson’s chi-square and independent -tests to compare demographic (age, gender, ethnicity, education, income, residency) and war-related characteristics (traumatic loss, forced displacement, and income loss) between those who completed the study and those who did not to identify potential biases and ensure the representativeness of our sample and the generalizability of emerging findings.
Group differences in clinical symptoms over time were measured using Linear Mixed Models. We applied a full factorial model across the three time points (day 1 , day 30 , and day 90 ) for traumatic loss (yes/no), forced displacement (yes/no), income loss (yes/no), gender (female/male), and ethnicity (Jewish versus Arab and Other, which included Druze, non-Jewish, and unspecified). Random intercepts for participants were included to account for repeated measures design. All statistical tests were two-sided, with the alpha level set at to adjust for multiple comparisons using the Bonferroni correction (0.05 divided by 5). Data analysis was performed using IBM SPSS Statistics 29.
Results
Sample characteristics
Following the removal of 196 participants ( ) due to failed validity tests, our final sample comprised 1052 individuals who completed the first set of assessments. Of those, completed the 30 -day follow-up assessment and completed the 90 -day follow-up assessment. Baseline characteristics did not differ between completers and non-completers. Mean ± SD respondent age was (range 18-40). Slightly more than half of participants were female ( ); none identified as transgender or non-binary. Table 1 presents the sample’s ethnicities, education, income, residency, traumatic loss (i.e., family members or close friends being killed, injured, or kidnapped to Gaza) ( ), forced displacement since October 7 ( ), and income loss due to the war ( ).
Effects of October 7th and the ensuing war on clinical symptoms
Table 2 presents the clinical symptoms across time points. Of the 1052 individuals, reported above threshold anxiety, depression, or PTSD symptoms at day reported these symptoms at day 30 , and at day 90 . On the GAD-7 screen, exceeded the moderate threshold (GAD-7 scores ) at day on day 30 , and on day 90 . For depressive symptoms, exceeded the moderate threshold (PHQ-9 scores 10-27) at day on day 30 , and ( ) on day 90 . Overall, of respondents reported symptoms suggesting probable PTSD (PCPTSD score ) at day at day 30 , and at day 90 .
Figure 1 presents the mean GAD-7, PHQ-9, and PC-PTSD scores by traumatic loss, forced displacement, and income loss. At every time point, mean GAD-7 scores were consistently higher among individuals experiencing traumatic loss , forced displacement , and income loss . While we found a time effect only for traumatic loss, reflecting a statistically significant reduction in GAD-7 scores, we did not observe such an effect for forced displacement or income loss, nor did we find an interaction effect for any of the conditions. Similarly, mean PHQ-9 scores were consistently higher among individuals experiencing traumatic loss ( ), forced displacement , and income loss . We found no time or interaction effect for any of these stressors. Mean PC-PTSD scores were higher at every time point among individuals experiencing traumatic loss ( ), forced displacement ( , , and income loss ( ). As with the PHQ-9 scores, we found no time or interaction effect for any of the conditions.
Figure 2 presents the mean GAD-7, PHQ-9, and PC-PTSD scores by gender and ethnicity. For gender, at every time point, women had consistently higher mean GAD-7 scores ( ), mean PHQ-9 scores ( ), and mean PC-PTSD scores ( ). GAD-7 and PHQ-9 scores showed a temporal effect, reflecting a statistically significant reduction over time. However, none of the measurement scales showed an interaction effect. We conducted additional analyses to explore potential age-by-gender interactions; however, no significant results were observed, possibly due to the
Items
Total ( )
Completers ( )
Noncompleters ( )
Statistic
Mean
SD
Mean
SD
Mean
SD
t-tests
Age
31.3
5.6
28.7
6.1
30.4
5.9
6.86
<. 001
n
%
n
%
n
%
Gender
6.97
. 008
Women
566
54
391
57
175
48
Men
486
46
298
43
188
52
Transgender/non-binary/other
0
0
0
0
0
0
Ethnicity
4.65
. 098
Jewish
969
92
642
93
327
90
Arab
64
6
34
5
30
8
Other
19
2
13
2
6
2
Education
29.5
<. 001
Never completed high school
11
1
5
1
6
2
High school graduate
318
30
172
25
146
40
Some college credit
231
22
161
23
70
19
Bachelor’s degree
388
37
277
40
111
31
Master’s degree
100
10
71
10
29
8
Doctorate degree
4
0
3
0
1
0
Income
7.65
. 105
Significantly below average
246
23
153
22
93
26
Below average
283
27
179
26
104
29
Average
282
27
200
29
82
23
Above average
204
19
129
19
75
21
Significantly above average
37
4
28
4
9
3
Residency
2.75
. 097
Northern Israel
550
52
316
46
186
51
Southern Israel
502
48
373
54
177
49
October 7 and war-related events
Traumatic loss: A family member or close friend was killed, injured, or kidnapped to Gaza
268
26
158
23
110
30
6.80
. 009
Forced displacement
243
23
160
23
83
23
0.01
. 896
Income loss
479
45
302
44
177
49
2.32
. 127
Table 1. Demographic characteristics. Pearson Chi-square; Independent t -tests; Other: Druze ( ), Russian ( ), Christian ( ), no religion ( ), unspecified ( ).
Characteristic
Day
Day
Day 90 ( )
GAD-7 total score (range 0-21; Mean and SD)
7.6
5.8
7.1
5.9
6.5
5.5
n
%
n
%
n
%
GAD-7
678
64
484
61
400
59
GAD-7
332
32
228
29
162
24
PHQ-9 total score (range 0-27; Mean and SD)
8.2
8.1
7.6
6.6
7.3
6.4
n
%
n
%
PHQ-9
653
62
470
59
395
58
PHQ-9
374
36
255
32
212
31
PC-PTSD total score (range 0-5; Mean and SD)
2.2
2.2
2.1
1.7
1.9
1.7
n
%
n
%
n
%
465
44
313
40
250
37
Table 2. Clinical symptoms over time. GAD-7, Generalized Anxiety Disorder; PHQ-9, Patient Health Questionnaire; PC-PTSD, Primary Care PTSD Screen for DSM-5.
GAD-7 (Anxiety) 10 8 6 4
Traumatic Loss (TL)
Forced Displacement (FD)
Income Loss (IL)
Day 1 Day 30 Day 90
⟶ TL – No TL
Day 1 Day 30 Day 90
-FD-No FD
Day 1 Day 30 Day 90
-IL-No IL
Day 1 Day 30 Day 90
-TL – No TL
Day 1 Day 30 Day 90
-FD-No FD
Day 1 Day 30 Day 90
-IL-No IL
3
2
Day 1 Day 30 Day 90
Day 1 Day 30 Day 90
-FD – No FD
Day 1 Day 30 Day 90
-IL -No IL
Fig. 1. Generalized Anxiety Disorder-7 (GAD-7), Patient Health Questionnaire-9 (PHQ-9), and the Primary Care PTSD (PC-PTSD) Scores by Traumatic Loss (TL), Forced Displacement (FD), and Income Loss (IL). Notes: TL, Traumatic Loss; FD, Forced Displacement; IL, Income Loss; GAD-7, Generalized Anxiety Disorder; PHQ-9, Patient Health Questionnaire; PC-PTSD, Primary Care PTSD Screen for DSM-5. Linear Mixed Models: F values ranged from 26.7 to 215.3 , with all .
sample size limiting the ability to detect such effects. For ethnicity, at every time point mean GAD-7 scores were consistently higher among Arab and Other respondents . We found similar findings for mean PHQ-9 scores ( ). We found no such effect for PC-PTSD scores, nor a time effect or interaction effect for any measurement scale.
Discussion
Our study assessed self-reported symptoms of anxiety, depression, and PTSD over 90 days among 1052 individuals living in conflict zones. We found above-threshold mental health symptoms in of participants, which slightly decreased over three months. As hypothesized, individuals experiencing traumatic losses, forced displacement, or economic hardships demonstrated higher symptom rates across all measures (GAD-7, PHQ9, PC-PTSD). This was evident in the consistently elevated mean scores among these groups, compared to those without such experiences, across all time points. In addition, women and members of ethnic minorities consistently reported higher distress levels than men and Jewish individuals. These patterns of elevated distress call for immediate attention to the mental health needs of those bearing the greatest burdens in conflict-affected regions.
Overall, , and of the participants reported symptoms of anxiety, depression, and/or PTSD on day 1 , day 30 , and day 90 , respectively. Research on war-affected zones and psychological outcomes in the general population is limited. A systematic review and meta-analysis updated WHO estimates and found that the prevalence of mental disorders such as depression, anxiety, PTSD, bipolar disorder, and schizophrenia in conflict-affected populations is at any given time . A similar study of migrants exposed to armed conflicts
Fig. 2. Generalized Anxiety Disorder-7 (GAD-7), Patient Health Questionnaire-9 (PHQ-9), and the Primary Care PTSD (PC-PTSD) Scores by Gender and Ethnicity. Notes: Arab ( ) and Other: Druze ( ), Russian ( ), Christian ( ), no religion ( ), unspecified ( ); GAD-7, Generalized Anxiety Disorder; PHQ9, Patient Health Questionnaire; PC-PTSD, Primary Care PTSD Screen for DSM-5. Linear Mixed Models: F values ranged from 8.3 to 213.9, with p ranging from .004 to < . 001 .
found prevalences of for current PTSD, for major depressive disorder, and for generalized anxiety disorder, based on standardized psychiatric interviews . Younger migrants displayed higher incidences of PTSD and anxiety, while longer time since displacement correlated with lower lifetime prevalences of PTSD and depression . A nationwide prospective study conducted in Israel after October 7 showed high levels of anxiety, depression, and PTSD compared to levels before October . However, this national study did not focus on conflict zones, nor on war-related stressors. Importantly, although we cannot compare our sample to population-based representative samples, other web-based self-reported opportunity samples have shown similarly high rates in war-affected zones .
Specifically, our findings on elevated GAD-7, PHQ-9, and PC-PTSD scores among individuals living in war-affected areas in Israel who have experienced traumatic loss, forced displacement, or income loss align with existing literature . These elevated symptoms reflect the profound mental health challenges individuals face in grappling with the immediate effects of war-related adversities. The clinically meaningful
symptoms associated with these conditions highlight their role as critical factors in the exacerbation of mental health issues, calling for urgent and specialized interventions that address these specific sources of psychological strain . Such interventions should be designed to address the specific needs of those most affected, considering factors such as the duration and intensity of exposure, age, and the nature of the adversity experienced. This targeted approach is crucial for mitigating the severe and prolonged impact on mental well-being in conflict settings.
Our findings of higher symptomatology among women corroborate extant literature . For example, a systematic review of the psychological effects of COVID-19 on the general population identified a higher prevalence of mental health issues among women and pointed to gender as a risk factor ; however, research also suggests that gender differences disappear over time . In combination these results suggest a heightened immediate vulnerability or willingness among women to experience and report symptoms of anxiety, depression, and PTSD in conflict-affected settings. These findings emphasize the opportunity for targeted evidenceinformed mental health interventions that consider the specific immediate vulnerabilities and resilience factors present in female populations in these high-stress environments. For example, Interpersonal Psychotherapy (IPT) could be one effective method, focusing on interpersonal relationships and emotional responses to sometimes overwhelming life events . It may also be that females are more willing to endorse symptoms of distress associated with armed conflicts, or that symptoms among males will emerge later . The emergence of symptoms along different time-based trajectories has been identified among Veteran cohorts . Continued longitudinal efforts are required to explore such possibilities.
Our findings reveal persistent ethnic disparities in mental health symptoms, with members of Arab and other minority communities residing in conflict zones consistently showing higher GAD-7 and PHQ-9 scores. Despite a limited sample size ( ), the significant differences underscore the enhanced vulnerability of individuals from these groups compared to Israeli Jews. While Israeli Arabs have the same legal rights to access mental health care, as other citizens, this disparity is likely due to restricted access to resources, social strain, and discrimination . Moreover, the sociopolitical situation of Israeli Arabs, including challenges related to perceived double allegiance (Israel vs. fellow Palestinians) and fear of being branded as enemies by Jews, may contribute to these disparities. These factors, compounded by limited resources, highlight the urgent need for targeted evidence-informed, culturally sensitive mental health interventions. Additionally, trends observed in the figures suggest opposing symptom trajectories over time for Jewish and Arab participants, potentially reflecting divergent vulnerabilities and a loss of resources among Arab individuals .
To effectively address the mental health concerns identified in our study, proactive measures must be implemented to support individuals most at risk. Specifically, healthcare providers should prioritize those who have endured traumatic loss, those who have been forcibly displaced, and those suffering from war-related economic insecurity, as each of these experiences can lead to instability and acute stress reactions. These stressors should serve as critical markers to help healthcare providers prioritize and tailor treatment efforts, ensuring that those in greatest need receive focused evidence-informed and accessible care. Such targeted interventions are essential not only for the well-being of the individuals directly affected but also for the broader societal health, contributing to the overall stability and resilience of communities living in conflict-affected areas.
Our study has several limitations. First, Hebrew-speaking crowdsourcing users may differ sociodemographically from the population in southern and northern Israel, thus limiting generalizability, specifically including lower rates of Israeli Arabs compared to the general population. Future studies should aim to recruit a larger and more representative sample of non-Jewish minorities, including Israeli Arabs and other subgroups. Additionally, the recruitment method may have introduced biases, such as underrepresentation of individuals without internet access or those less likely to participate in online surveys. Second, we targeted the age range of years, excluding older individuals, due to the higher incidence of psychopathology in the younger demographic; effects on older (and younger) populations also warrant exploration. Third, a notable study limitation is the absence of baseline data predating the October events, a common issue in research triggered by sudden, unexpected crises. We also did not inquire about non-war-related trauma since October 7. Fourth, clinical assessments based on self-report questionnaires rather than formal diagnostic interviews are subject to over- or underreporting. Lastly, while this study provides valuable insights into the perceptions of Israeli civilians, it is important to note that it does not address the effects on Palestinians, which represents a significant limitation in understanding the full scope of the conflict’s consequences.
Conclusions
This study underscores the urgent need for comprehensive mental health support systems in conflict zones. Evidence-informed services should be tailored to engage and address the needs of those at greatest immediate reported risk including women, members of ethnic minorities, and individuals facing traumatic losses, displacement, or economic hardship, with the goal of mitigating the development of persistent symptoms and/ or psychiatric disorders. By highlighting the significant prevalence of anxiety, depression, and PTSD symptoms within these groups, our research reaffirms the necessity for targeted evidence-informed interventions specifically designed to support individuals with these demographic characteristics, or those who are facing such stressors. Further research is required to extend these findings to other populations and to include those older than 40 or younger than 18 .
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Received: 2 November 2024; Accepted: 23 December 2024
Published online: 06 January 2025
References
Vinograd, C. & Kershner, I. Israel’s Attackers Took Over 200 Hostages. Here’s What to Know About Them. The New York Times (2023).
Around Half a Million Israelis Displaced Inside Israel: Military. Barron’s. 16 October 2023. Retrieved 18 November 2023.
Israel sharpens warning to Lebanon as cross-border hostilities spike. Reuters. 13 November 2023. Archived from the original on 13 November 2023. Retrieved 30 January 2024.
Lowell, A. et al. 9/11-related PTSD among highly exposed populations: A systematic review 15 years after the attack. Psychol. Med. 48, 537-553 (2018).
Bonanno, G. A., Galea, S., Bucciarelli, A. & Vlahov, D. Psychological resilience after disaster: New York City in the aftermath of the September 11th terrorist attack. Psychol. Sci. 17, 181-186 (2006).
Garfin, D. R., Poulin, M. J., Blum, S. & Silver, R. C. Aftermath of terror: a nationwide longitudinal study of posttraumatic stress and worry across the decade following the September 11, 2001 terrorist at- tacks. J. Trauma Stress 31(1), 146-156 (2018).
Boudoukha, A. H., Ouagazzal, O. & Goutaudier, N. When traumatic event exposure characteristics matter: impact of traumatic event exposure characteristics on posttraumatic and dissociative symptoms. Psychol. Trauma 9(5), 561 (2017).
Rigutto, C., Sapara, A. O. & Agyapong, V. I. Anxiety, depression and posttraumatic stress disorder after terrorist attacks: A general review of the literature. Behav. Sci. 11(10), 140 (2021).
Ozbay, F., der Heyde, T. A., Reissman, D. & Sharma, V. The enduring mental health impact of the September 11th terrorist attacks: Challenges and lessons learned. Psychiatr. Clin. 36(3), 417-429 (2013).
Donoho, C. J., Bonanno, G. A., Porter, B., Kearney, L. & Powell, T. M. A decade of war: Prospective trajectories of PTSD symptoms among deployed US military personnel and the influence of combat exposure. Am. J. Epidemiol. 186(12), 1310-1318 (2017).
Kristensen, P., Weisæth, L. & Heir, T. Bereavement and mental health after sudden and violent losses: A review. Psychiatry 75(1), 76-97. https://doi.org/10.1521/psyc.2012.75.1.76 (2012).
Porter, M. & Haslam, N. Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: a meta-analysis. JAMA 294(5), 602-612. https://doi.org/10.1001/jama.294.5.602 (2005).
Ruengorn, C., Awiphan, R., Wongpakaran, N., Wongpakaran, T., Nochaiwong, S., Health Outcomes and Mental Health Care Evaluation Survey Research Group (HOME-Survey). Association of job loss, income loss, and financial burden with adverse mental health outcomes during coronavirus disease 2019 pandemic in Thailand: A nationwide cross-sectional study. Depress. Anxiety 38(6), 648-660 (2021).
Kujawa, A., Green, H., Compas, B. E., Dickey, L. & Pegg, S. Exposure to COVID-19 pandemic stress: Associations with depression and anxiety in emerging adults in the United States. Depress. Anxiety. 37(12), 1280-1288 (2020).
Hawes, M. T., Szenczy, A. K., Klein, D. N., Hajcak, G. & Nelson, B. D. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol. Med. 52, 1-9 (2021).
Amsalem, D. et al. Anxiety and depression symptoms among young US essential workers during the COVID-19 pandemic. Psychiatric Serv. 74(10), 1010-1018 (2023).
Zhang, W., Walkover, M. & Wu, Y. Y. The challenge of COVID-19 for adult men and women in the United States: Disparities of psychological distress by gender and age. Public Health 198, 218-222 (2021).
Mesa-Vieira, C. et al. Mental health of migrants with pre-migration exposure to armed conflict: A systematic review and metaanalysis. Lancet Public Health 7(5), e469-e481 (2022).
Newnham, E. A., Pearson, R. M., Stein, A. & Betancourt, T. S. Youth mental health after civil war: The importance of daily stressors. Br. J. Psychiatry 206(2), 116-121. https://doi.org/10.1192/bjp.bp.114.146324 (2015).
Morina, N., Stam, K., Pollet, T. V. & Priebe, S. Prevalence of depression and posttraumatic stress disorder in adult civilian survivors of war who stay in war-afflicted regions. A systematic review and meta-analysis of epidemiological studies. J. Affect. Disord. 239, 328-338 (2018).
Bleich, A., Gelkopf, M. & Solomon, Z. Exposure to terrorism, stress-related mental health symptoms, and coping behaviors among a nationally representative sample in Israel. JAMA 290(5), 612-620. https://doi.org/10.1001/jama.290.5.612 (2003).
Brewin, C. R., Andrews, B. & Valentine, J. D. Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. J. Consult. Clin. Psychol. 68(5), 748 (2000).
Groweiss, Y., Blank, C., Hamdan, S., Neria, Y. & Levi-Belz, Y. The mental health impact of the October 7th terror attack on Jews and Arabs in Israel: A nationwide prospective study. Psychiatry Res. 337, 115973 (2024).
Pearlin, L. I., Schieman, S., Fazio, E. M. & Meersman, S. C. Stress, health, and the life course: Some conceptual perspectives. J. Health Soc. Behav. 46(2), 205-219 (2005).
Achdut, N. Ethnic inequality between Arabs and Jews in Israel in global life satisfaction: A social determinants examination among young adults. Am. J. Orthopsychiatry (2024).
Hobfoll, S. E., Canetti-Nisim, D. & Johnson, R. J. Exposure to terrorism, stress-related mental health symptoms, and defensive coping among Jews and Arabs in Israel. J. Consult. Clin. Psychol. 74(2), 207 (2006).
Marciano, H., Kimhi, S. & Eshel, Y. Predictors of individual, community and national resiliencies of Israeli Jews and Arabs. Int. J. Psychol. 55(4), 553-561 (2020).
Spitzer, R. L., Kroenke, K., Williams, J. B. W. & Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166(10), 1092-1097. https://doi.org/10.1001/archinte.166.10.1092 (2006).
Levis, B., Benedetti, A. & Thombs, B. D. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: Individual participant data meta-analysis. BMJ 365, I1476. https://doi.org/10.1136/bmj.l1476 (2019).
Prins, A. et al. The primary care PTSD screen for DSM-5 (PC-PTSD-5): Development and evaluation within a veteran primary care sample. J. Gen. Intern Med. 31(10), 1206-1211. https://doi.org/10.1007/s11606-016-3703-5 (2016).
Ouimette, P., Wade, M., Prins, A. & Schohn, M. Identifying PTSD in primary care: Comparison of the Primary Care-PTSD Screen (PC-PTSD) and the General Health Questionnaire-12 (GHQ). J. Anxiety Disord. 22(2), 337-343. https://doi.org/10.1016/j.janxdis .2007.02.010 (2008).
Charlson, F. et al. New WHO prevalence estimates of mental disorders in conflict settings: A systematic review and meta-analysis. Lancet 394(10194), 240-248 (2019).
Levi-Belz, Y., Groweiss, Y., Blank, C. & Neria, Y. PTSD, depression, and anxiety after the October 7, 2023 attack in Israel: A nationwide prospective study. EClinicalMedicine 68, 102418 (2024).
Zasiekina, L., Zasiekin, S. & Kuperman, V. Post-traumatic stress disorder and moral injury among Ukrainian civilians during the ongoing war. J. Community Health 48(5), 784-792. https://doi.org/10.1007/s10900-023-01225-5 (2023).
Scholte, W. F. et al. Mental health symptoms following war and repression in eastern Afghanistan. JAMA 292(5), 585-593 (2004).
Priebe, S. et al. Psychological symptoms as long-term consequences of war experiences. Psychopathology 46(1), 45-54. https://doi. org/10.1159/000338640 (2013).
Mollica, R. F. et al. Longitudinal study of psychiatric symptoms, disability, mortality, and emigration among Bosnian refugees. JAMA 286(5), 546-554. https://doi.org/10.1001/jama.286.5.546 (2001).
Miller, K. E. & Rasmussen, A. The mental health of civilians displaced by armed conflict: an ecological model of refugee distress. Epidemiol. Psychiatr. Sci. 26(2), 129-138. https://doi.org/10.1017/S2045796016000172 (2017).
Siriwardhana, C., Ali, S. S., Roberts, B. & Stewart, R. A systematic review of resilience and mental health outcomes of conflictdriven adult forced migrants. Conflict Health 8, 1-4 (2014).
Xiong, J. et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 277, 55-64 (2020).
Fenollar-Cortés, J., Jiménez, Ó., Ruiz-García, A. & Resurrección, D. M. Gender differences in psychological impact of the confinement during the COVID-19 outbreak in Spain: A longitudinal study. Front Psychol. 12, 682860. https://doi.org/10.3389/fp syg. 2021.682860 (2021).
Markowitz, J. C. In the Aftermath of the Pandemic: Interpersonal psychotherapy for Anxiety, Depression, and PTSD (Oxford University Press, 2021).
Boerma, T., Hosseinpoor, A. R., Verdes, E. & Chatterji, S. A global assessment of the gender gap in self-reported health with survey data from 59 countries. BMC Public Health 16, 1-9. https://doi.org/10.1186/s12889-016-2767-x (2016).
Acknowledgements
We thank the civilians who participated in the study.
Author contributions
D.A. wrote the first draft of this manuscript. D.A., S.H.N., A.L., Y.L.B., and Y.N. coordinated the trial, contributed to the design and implementation of the trial, and collected the data. D.A., S.H.N., and A.L. performed the statistical analyses. All authors reviewed and approved the manuscript.
Funding
Funding was provided by the HOMIYAH.
Declarations
Competing interests
The authors declare no competing interests.
Additional information
Correspondence and requests for materials should be addressed to D.A.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Department of Psychiatry, New York State Psychiatric Institute, New York, NY, USA. Columbia University Vagelos College of Physicians and Surgeons, Columbia University Irving Medical Center, 1051 Riverside Drive, New York, NY 10032, USA. School of Social Work, Tel Aviv University, Tel Aviv, Israel. School of Psychological Sciences, Tel Aviv University, Tel Aviv, Israel. The Lior Tsfaty Center for Suicide and Mental Pain Studies, Ruppin Academic Center, Emek Hefer, Israel. Psychological Services, Ben Gurion University of the Negev, Be’er Sheva, Israel. Departments of Physical Medicine and Rehabilitation, Psychiatry, and Neurology, University of Colorado, Anschutz Medical Campus, Aurora, CO, USA. Division of Psychiatry, Chaim Sheba Medical Center, Tel Hashomer, Israel. Shalvata Mental Health Center, Hod Hasharon, Israel. School of Medicine, Tel Aviv University, Tel Aviv, Israel. ® email: doron.amsalem@nyspi.columbia.edu