مع تقدم السكان في العمر على مستوى العالم، من الضروري تحديد الأنظمة الغذائية التي، بالإضافة إلى الوقاية من الأمراض غير المعدية، تعزز بشكل مثالي الشيخوخة الصحية. هنا، باستخدام بيانات استبيانات طولية من دراسة صحة الممرضات (1986-2016) ودراسة متابعة المهنيين الصحيين (1986-2016)، قمنا بفحص العلاقة بين الالتزام طويل الأمد بثمانية أنماط غذائية واستهلاك الأطعمة فائقة المعالجة مع الشيخوخة الصحية، كما تم تقييمه وفقًا لمقاييس الصحة العقلية والبدنية والنفسية، بالإضافة إلى العيش حتى سن 70 عامًا خاليًا من الأمراض المزمنة. بعد متابعة استمرت حتى 30 عامًا، بلغ عدد المشاركين 9,771 ( ) من 105,015 مشارك ( النساء، متوسط العمر سنوات (انحراف معياري )) حقق الشيخوخة الصحية. بالنسبة لكل نمط غذائي، كانت الالتزام الأعلى مرتبطًا بزيادة احتمالات الشيخوخة الصحية ومجالاتها. تراوحت نسب الأرجحية لأعلى خُمس مقابل الأدنى من فترة الثقةنظام غذائي نباتي صحي” إلى ; مؤشر النظام الغذائي الصحي البديل). عندما تم تغيير عتبة العمر للشيخوخة الصحية إلى 75 عامًا، أظهر نظام مؤشر النظام الغذائي الصحي البديل أقوى ارتباط بالشيخوخة الصحية، مع نسبة احتمالية من ارتبطت الكميات العالية من الفواكه والخضروات والحبوب الكاملة والدهون غير المشبعة والمكسرات والبقوليات ومنتجات الألبان قليلة الدسم بزيادة احتمالات الشيخوخة الصحية، في حين ارتبطت الكميات العالية من الدهون المتحولة والصوديوم والمشروبات السكرية واللحوم الحمراء أو المعالجة (أو كليهما) بعلاقة عكسية. تشير نتائجنا إلى أن الأنماط الغذائية الغنية بالأطعمة النباتية، مع تضمين معتدل للأطعمة الحيوانية الصحية، قد تعزز الشيخوخة الصحية بشكل عام، مما يوجه الإرشادات الغذائية المستقبلية.
لقد زاد عدد كبار السن في الولايات المتحدة بشكل مطرد في العقود القليلة الماضية؛ ومع ذلك،من كبار السن لديهم على الأقل حالة صحية مزمنة واحدة، مما يبرز التحديات الصحية المعقدة التي تواجه هذا التحول الديموغرافيتعزيز الشيخوخة الصحية هو أولوية عالميةهذا الالتزام مدفوع بهدف تعزيز جودة الحياة العالية، ودعم المساهمة المستمرة في المجتمع، وتقليل تكاليف الرعاية الصحية. النظام الغذائي هو أول عامل خطر سلوكي رئيسي للأمراض غير المعدية وعبء الوفيات على مستوى العالم.والثاني بعد استخدام التبغ بين كبار السن في الولايات المتحدة.
مؤخراً، اعترفت منظمة الصحة العالمية بأن إعطاء الأولوية للحفاظ على القدرة الوظيفية والوقاية من تدهور القدرة يجب أن يكون محورياً في نموذج الشيخوخة الصحية.. هذه التحول يبتعد عن النهج التقليدي الذي يركز على الأمراض في الشيخوخة، ويهدف إلى تقديم رعاية محسّنة لكبار السنلقد قدمت الدراسات التدخلية والدراسات الملاحظة أدلة قوية على أن النظام الغذائي عالي الجودة مفيد في الوقاية من أمراض القلب والأوعية الدموية.داء السكري من النوع 2والموت المبكرلقد قامت الدراسات أيضًا بتقييم تأثيرات أو ارتباطات الأطعمة والمغذيات
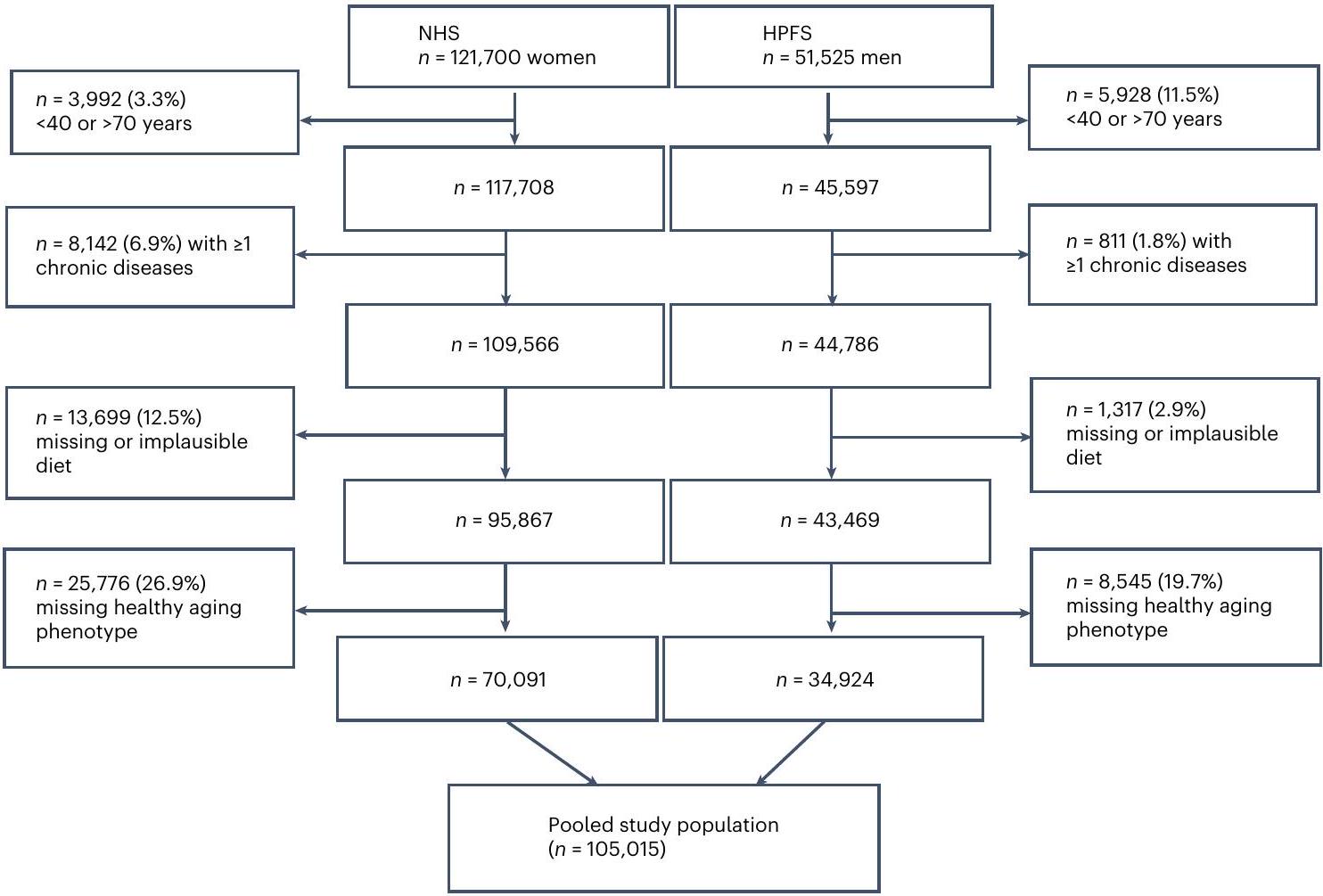
الشكل 1 | مخطط تدفق المشاركين في الدراسة. يوضح هذا المخطط التدريجي أحجام العينات الأولية في NHS و HPFS تليها تطبيق معايير الاستبعاد بشكل متسلسل لكل مجموعة. تشمل مجموعة الدراسة النهائية ما مجموعه 105,015 مشاركًا.
مع نتائج الأداء المعرفي والبدني المرتبطة بالعمروأعراض الاكتئاب. ومع ذلك، فإن القليل من الدراسات قد بحثت في العلاقة بين أنماط النظام الغذائي ونموذج متعدد الأبعاد للشيخوخة الصحيةستساعد دراسة ومقارنة أنماط التغذية فيما يتعلق بالشيخوخة الصحية في توجيه التوصيات الصحية العامة التي تهدف إلى تعزيز الصحة العامة ورفاهية كبار السن، بما في ذلك الصحة العقلية والبدنية والوقاية من الأمراض المزمنة.
في هذه الدراسة، قمنا بفحص العلاقة بين الالتزام طويل الأمد بثمانية أنماط غذائية صحية، بما في ذلك مؤشر النظام الغذائي الصحي البديل (AHEI)، ومؤشر البحر الأبيض المتوسط البديل (aMED)، والنهج الغذائية لوقف ارتفاع ضغط الدم (DASH)، وتدخل البحر الأبيض المتوسط-DASH لتأخير التنكس العصبي (MIND)، والنظام الغذائي النباتي الصحي (hPDI)، ومؤشر النظام الغذائي لصحة الكوكب (PHDI)، والنمط الغذائي الالتهابي التجريبي (EDIP)، ومؤشر النظام الغذائي التجريبي لفرط الأنسولين (EDIH) واستهلاك الأطعمة المعالجة بشكل مفرط (UPF)، والشيخوخة الصحية بعد 30 عامًا في مجموعتين كبيرتين من الدراسات المستقبلية في الولايات المتحدة. ثم قمنا بفحص هذه العلاقات في مجموعات فرعية محددة، بما في ذلك التقسيم وفقًا للجنس، والأصل، والحالة الاجتماعية والاقتصادية (SES) وعوامل نمط الحياة. كما قمنا بفحص علاقات الأطعمة الفردية والمغذيات التي تساهم في مثل هذه الأنماط الغذائية.
النتائج
من بين 105,015 مشاركًا، كانت 70,091 امرأة (NHS) و34,924 رجلًا (HPFS) (الشكل 1). بعد متابعة استمرت حتى 30 عامًا،حقق المشاركون شيخوخة صحية،في NHS و2,169 (6.2%) في HPFS. في المجموعات المجمعة، بلغ عدد الذين وصلوا إلى سن 70 عامًا 39,769 (37.9%)،ظل خالياً من 11 مرضاً مزمناً، 35,555 (33.9%) حافظوا على وظيفة إدراكية سليمة، 29,543 (28.1%) حافظوا على وظيفة جسدية سليمة و 27,842 (حافظت على صحة عقلية سليمة.
تظهر الخصائص الموحدة حسب العمر لسكان الدراسة في الجدول 1 (البيانات المجمعة) وفي الجداول الإضافية 1 و2 (حسب المجموعة). كان المشاركون في أعلى quintile لدرجة نمط النظام الغذائي المعدلة للطاقة أكثر عرضة لأن يكون لديهم مستوى اجتماعي اقتصادي أعلى، واستخدام الفيتامينات المتعددة، ومستوى أعلى من النشاط البدني ومؤشر كتلة الجسم (BMI) أقل قليلاً؛ كما كانوا أقل عرضة لوجود تاريخ من الاكتئاب مقارنة بأدنى quintile. استهلك المشاركون في أعلى quintile لـ AHEI وMIND وhPDI وPHDI وEDI العكسي (rEDIH) وEDIP العكسي (rEDIP) كميات أكبر من الكحول، بينما استهلك أولئك في أعلى quintile لـ DASH وaMED كميات أقل. بينما كانت نسبة أكبر من المشاركين من النساء في أعلى quintile لـ aMED وPHDI وrEDIH وrEDIP، كانت نسبة أكبر من الرجال في أعلى quintile لـ AHEI وDASH وMIND وhPDI. توضح الشكل الإضافي 1 ارتباطات سبيرمان بين جميع درجات أنماط النظام الغذائي واستهلاك الأطعمة المعالجة.
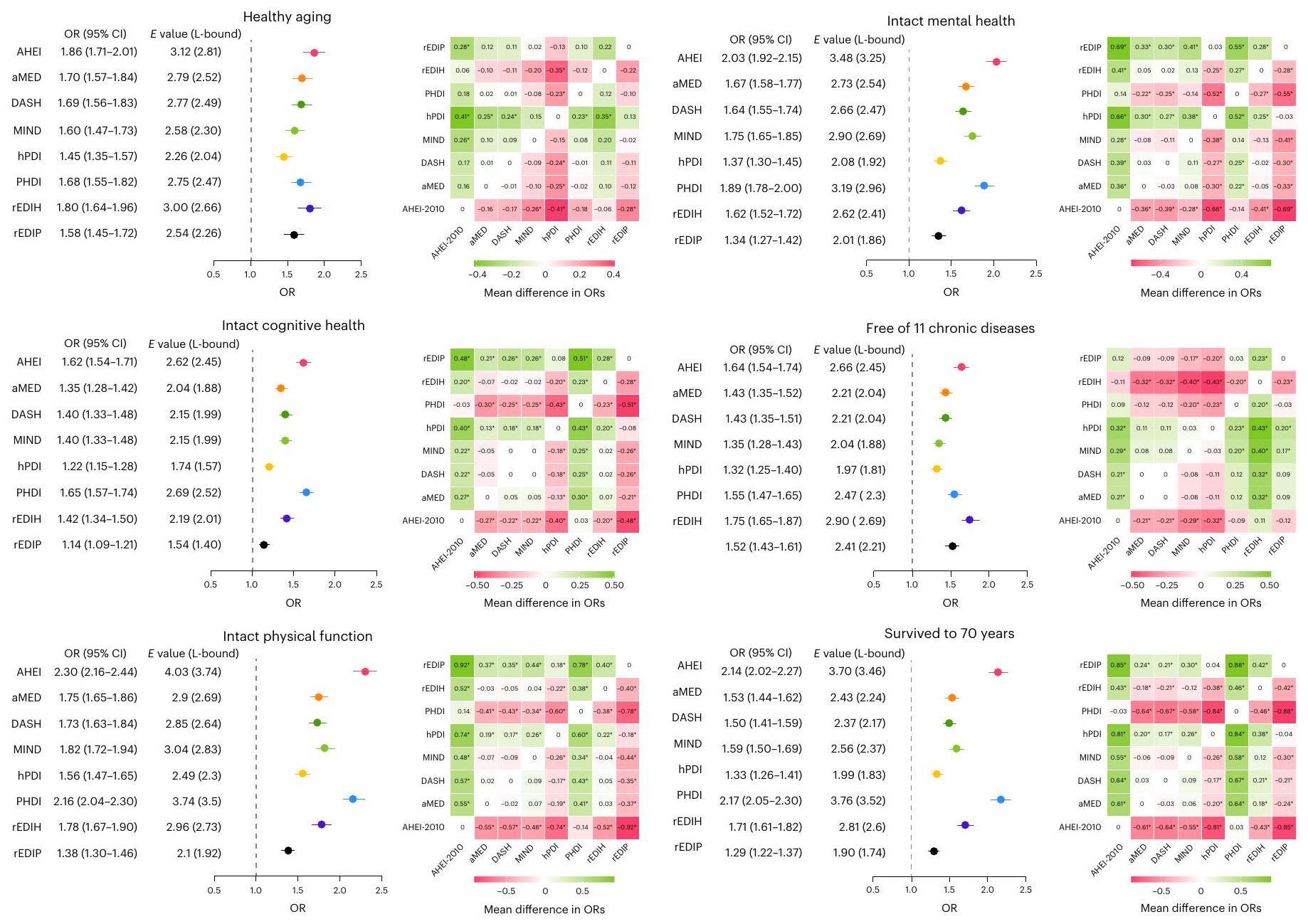
كان الالتزام الأعلى بجميع أنماط النظام الغذائي مرتبطًا بزيادة احتمالات الشيخوخة الصحية (الشكل 2 والجدول الإضافي 3)؛ مكونات أنماط النظام الغذائي موضحة في الشكل 3. تراوحت نسب الأرجحية المعدلة متعددة المتغيرات (ORs) (فترات الثقة (CIs) 95%) التي تقارن بين أعلى خُمس وأدنى خُمس من 1.45 (1.35-1.57؛ ) إلى أظهر AHEI أقوى ارتباط يليه rEDIH؛ بينما أظهر hPDI أضعف ارتباط. استنادًا إلى الفروق في ORs بين أزواج الدرجات والمقارنة المزدوجة.-الاختبارات، أظهرت AHEI احتمالات أعلى للشيخوخة الصحية مقارنةً بـ MIND و hPDI و rEDIP. كما أظهرت aMED و DASH و PHDI و rEDIH أيضًا احتمالات أعلى للشيخوخة الصحية مقارنةً بـ hPDI (الشكل 2). باستخدام درجات أنماط النظام الغذائي المودلة كمتغيرات مستمرة، كانت الارتباطات مع الشيخوخة الصحية أيضًا الأقوى لـ AHEI والأضعف لـ hPDI (البيانات الموسعة الجدول 3). كانت OR ( ) لكل زيادة موحدة معيارية (تمثل الزيادة بين النسبة المئوية العاشرة والتسعين) تراوحت من 1.40 (1.32-1.49) إلى 1.71 (1.60-1.82). المخاطر المطلقة، المحسوبة بناءً على الأصحاء
الجدول 1 | الخصائص المعيارية حسب العمر في أدنى وأعلى خمسيات درجات نمط النظام الغذائي المعدلة حسب الطاقة في المجموعات المجمعةبين عامي 1986 و 2010
خاصية
الربع الأول،
س5،
الربع الأول،
س5،
الربع الأول،
س5،
الربع الأول،
س5،
درجة النظام الغذائي
أهي-2010
أمد
داش
عقل
درجة معدلة للطاقة
٤١.٥ (٤.٢)
68.6 (4.6)
2.2 (0.6)
6.3 (0.6)
١٨.١ (١.٨)
٢٩.٥ (١.٧)
6.0 (0.6)
9.6 (0.6)
نساء
70.2
٥٩.٧
٥٧.٢
69.5
67.1
61.3
67.1
61.0
العمر عند البداية
٥٣.٥ (٧.٨)
٥٣.١ (٧.٧)
53.8 (7.6)
53.8 (7.5)
٥١.٦ (٧.٧)
٥٥.٣ (٧.٦)
54.4 (7.7)
٥٢.٨ (٧.٧)
الأنساب
أوروبي
95.2
94.1
95.6
94.1
94.5
94.8
95.5
93.5
آسيوي
0.6
1.4
0.7
1.3
1.1
0.9
0.6
1.7
أفريقي
1.1
1.4
0.8
1.5
1.4
1.2
0.8
1.6
آخر
3.1
3.0
3.0
3.1
3.0
3.1
3.1
3.1
درجة SES عند الخط الأساسي
-0.8 (3.3)
0.9 (4)
-0.6 (3.4)
-0.6 (3.4)
-0.6 (3.5)
0.5 (3.9)
-0.9 (3.3)
0.8 (3.9)
وحيد، إلى الأبد
٢٨.٠
٢٧.٧
٢٧.٢
٢٧.٢
٢٧.٢
٢٨.٩
30.2
25.4
تاريخ الاكتئاب، نعم
16.3
12.3
14.5
14.5
15.6
12.1
16.2
12.0
تاريخ السرطان، نعم
٤.٥
3.9
٤.١
٤.٢
3.8
٤.٣
٤.٣
3.8
تاريخ مرض السكري، نعم
3.3
2.7
٢.٧
2.8
1.9
٤.٠
3.2
2.9
تاريخ مرض القلب والأوعية الدموية، نعم
5.3
٥.٤
٤.٧
٥.٧
٤.٢
٦.٧
5.2
٥.٧
تاريخ عائلي للخرف، نعم
11.9
١٣.٢
10.8
13.8
12.1
12.2
11.7
12.5
استخدام متعدد الفيتامينات، في أي وقت
78.6
91.0
79.2
90.2
78.8
89.7
79.5
90.0
مؤشر كتلة الجسم
٢٦.٦ (٥.١)
25.2 (4)
٢٦.٦ (٤.٩)
٢٥.٢ (٤.١)
٢٦.٥ (٥)
٢٥.٢ (٤.٢)
٢٦.٥ (٥)
25.3 (4)
مدخن أبداً، %
71.4
60.2
67.2
63.9
63.4
69.3
69.8
٦٣.٥
النشاط البدني، MET-ساعة في الأسبوع
1.2 (2.1)
3.7 (3.7)
1.5 (2.5)
٣.٣ (٣.٥)
1.4 (2.2)
3.5 (3.6)
1.3 (2.3)
3.6 (3.7)
تناول الكحول، جرام في اليوم
7.4 (14.3)
8.1 (8.4)
8.4 (14.4)
٧.٥ (٨.٥)
8.8 (13.4)
6.3 (9.2)
6.2 (11.6)
8.4 (10.3)
مدخول الطاقة، كيلو كالوري
1804 (494)
1831 (493)
1839 (532)
1811 (445)
1819 (514)
1842 (468)
1815.1 (524.9)
1826.2 (476.5)
المعمرون الأصحاء، %
٥.٦
13.7
6.4
12.5
٧.٧
10.2
٥.٣
١٣.٠
درجة النظام الغذائي
hPDI
مؤشر التنمية البشرية المعدل
ريدِه
ريدب
درجة معدلة للطاقة
٤٧.٠ (٢.٤)
62.8 (2.9)
65.2 (5.1)
93.4 (5.1)
-0.6 (0.2)
أ (0.1)
-0.3 (0.2)
0.4 (0.2)
نساء
66.8
٦٣.٥
61.0
٦٣.٥
٣٤.١
٨٣.٩
٥٢.٩
٧١.٧
العمر عند البداية
٥٢.٥ (٧.٨)
٥٤.٢ (٧.٧)
٥٣.٥ (٨)
53 (7.6)
٥٢.٩ (٨.٤)
53.4 (7.4)
53.7 (8.1)
٥٢.٣ (٧.٥)
الأنساب
أوروبي
95.4
93.9
95.3
93.4
94.9
95.3
92.9
96.5
آسيوي
0.6
1.5
0.6
1.9
1.1
0.8
1.8
0.4
أفريقي
1.1
1.5
1.0
1.5
1.5
0.7
2.2
0.3
آخر
2.9
3.2
3.1
3.1
٢.٥
3.3
3.1
2.8
درجة SES عند خط الأساس
-0.2 (3.5)
0.3 (3.9)
-0.6 (3.5)
0.7 (3.9)
-0.6 (3.4)
0.7 (4)
-0.5 (3.5)
0.5 (3.9)
وحيد، إلى الأبد
٢٧.٩
٢٧.٦
27.5
٢٧.٠
٢٢.٣
31.5
٢٤.٨
٢٨.٥
تاريخ الاكتئاب، نعم
14.7
12.6
14.7
12.7
10.9
15.3
14.4
١٣.٦
تاريخ السرطان، نعم
٤.١
٤.٢
٤.٤
3.8
٤.١
٤.٠
٤.١
3.9
تاريخ مرض السكري، نعم
1.9
٤.١
3.2
2.6
5.3
1.4
٥.٤
1.5
تاريخ مرض القلب والأوعية الدموية، نعم
٤.٣
6.2
5.2
5.2
6.3
3.7
7.0
3.3
تاريخ عائلي من الخرف، نعم
12.5
12.5
10.5
13.7
7.3
١٦.٧
9.9
14.5
استخدام متعدد الفيتامينات، في أي وقت
81.1
٨٨.٦
78.2
91.3
78.8
89.8
80.8
87.6
مؤشر كتلة الجسم
٢٦.٥ (٤.٩)
٢٥.٤ (٤.٣)
٢٦.٤ (٤.٩)
25.3 (4)
٢٧.٤ (٤.٩)
٢٤.٤ (٣.٨)
٢٧.٥ (٥.٢)
٢٤.٨ (٣.٨)
مدخن أبداً، %
67.0
٦٤.٧
71.3
٥٩.٧
73.6
٥٦.٢
73.0
٥٦.٢
النشاط البدني، MET-ساعة في الأسبوع
1.5 (2.4)
3.3 (3.6)
1.5 (2.5)
3.5 (3.6)
2.2 (3.1)
2.8 (3.2)
2.0 (3.0)
٢.٧ (٣.١)
تناول الكحول، جرام في اليوم
6.7 (10.4)
8.1 (11.7)
7 (11.8)
8.3 (10.8)
7.2 (11.4)
١١.٣ (١٣.١)
٤.٦ (٩)
14.4 (14.8)
مدخول الطاقة، كيلو كالوري
1824 (474)
1824 (508)
1821 (543)
1814 (466)
1950 (543)
1849 (474)
1902 (535)
1853 (489)
المعمرون الأصحاء، %
٨.٠
11.2
5.8
13.6
٥.٥
13.5
٥.٥
١٣.١
القيم هي المتوسط (الانحراف المعياري) للمتغيرات المستمرة والنسبة المئوية للمتغيرات الفئوية. CVD، مرض القلب والأوعية الدموية؛ MET، مكافئ الأيض للمهام.
الشكل 2 | ارتباطات أنماط النظام الغذائي المتوسطة مع الشيخوخة الصحية ومجالاتها. في مجموعة البيانات المجمعة الرئيسية (تم حساب متوسط درجات نمط النظام الغذائي من 1986 إلى 2010. تُظهر الرسوم البيانية للغابات نسب الأرجحية (ORs) مقارنةً بالربع الخامس (Q5) بالربع الأول (Q1) لكل من أنماط النظام الغذائي (ممثلة بصريًا بمراكز أشرطة الخطأ)،فترات الثقة (الممثلة بصريًا بواسطة أشرطة الخطأ) والقيم وحدودها الدنيا. تم استخدام الانحدارات اللوجستية لتقدير نسب الأرجحية وتم تعديلها حسب العمر عند البداية (1986)، المجموعة (الجنس)، مؤشر كتلة الجسم (الأنساب (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، حالة التدخين (لم يدخن أبدًا، مدخن سابق، مدخن حالي): سجائر في اليوم، سجائر في اليوم و السجائر في اليوم)، استهلاك الكحول (غرام في اليوم) (لـ DASH، hPDI، PHDI)، النشاط البدني (ساعة MET في الأسبوعاستخدام الفيتامينات المتعددة على الإطلاق (نعم/لا)، التاريخ العائلي لـ
احتشاء عضلة القلب (نعم/لا)، تاريخ عائلي لمرض السكري من النوع 2، تاريخ عائلي للسرطان، تاريخ عائلي للخرف (نعم/لا)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام هرمونات انقطاع الطمث (لا، استخدام هرمونات سابق أو حالي؛ فقط للنساء)، الحالة الاجتماعية الاقتصادية في البداية، الحالة الزوجية (نعم/لا)، العيش بمفردك في أي وقت (نعم/لا) وتاريخ الاكتئاب (نعم/لا) في المجموعات المجمعة. rEDIH و rEDIP هما درجات معكوسة للسماح بالمقارنة مع درجات أخرى. جميع الجوانب الثنائيةتظهر خرائط الحرارة الفرق في نسبة الأرجحية بين جميع أزواج الدرجات. يتم الإشارة إلى الفروق الإيجابية باللون الأخضر والفروق السلبية باللون الوردي؛ كلما كان اللون أغمق، زادت الفروق. *ثنائي الاتجاهاستنادًا إلى زوج-اختبار مقارنة النسب (غير معدلة للمقارنات المتعددة). انتشار الشيخوخة و ORs المعدلة، تشير إلىإلىفرص تحقيق الشيخوخة الصحية بين الأفراد الذين يلتزمون بشكل أكبر بأنماط التغذية (البيانات الموسعة الجدول 4).
عند فحص الارتباطات مع كل مجال من مجالات الشيخوخة الصحية، كانت الالتزام الأعلى بجميع أنماط النظام الغذائي مرتبطًا بجميع المجالات الفردية (الشكل 2 والجدول الإضافي 3). تراوحت قيم النسب المئوية المعدلة المتعددة المهمة (فترات الثقة 95%) التي تقارن أعلى خُمس بأدنى خُمس منإلى 1.65 (1.57-1.74؛ ) لصحة عقلية سليمة، حيث أظهر مؤشر النظام الغذائي الصحي (PHDI) أقوى ارتباط، بينما أظهر مؤشر النظام الغذائي الصحي المعدل (hPDI) أضعف ارتباط. بالنسبة لوظيفة جسدية سليمة، فإن نسب الأرجحية (ORs) ( تراوحت CI من 1.38إلى، حيث أظهر AHEI أقوى ارتباط بينما أظهر rEDIP أضعف ارتباط. بالنسبة للصحة النفسية السليمة، كانت قيم ORs (تراوحت CI) منإلى“، حيث أظهر مؤشر AHEI أقوى ارتباط بينما أظهر مؤشر hPDI أضعف ارتباط. بالنسبة لكون الشخص خالياً من الأمراض المزمنة، فإن نسب الأرجحية (ORs) (تراوحت بينإلى، مع يظهر rEDIH أقوى ارتباط بينما يظهر hPDI أضعف ارتباط. بالنسبة للبقاء حتى سن السبعين، فإن ORsتراوح بينإلى )، حيث يظهر مؤشر التنمية البشرية المعدل (PHDI) أقوى ارتباط بينما يظهر مؤشر التنمية البشرية الصحي (hPDI) أضعف ارتباط.
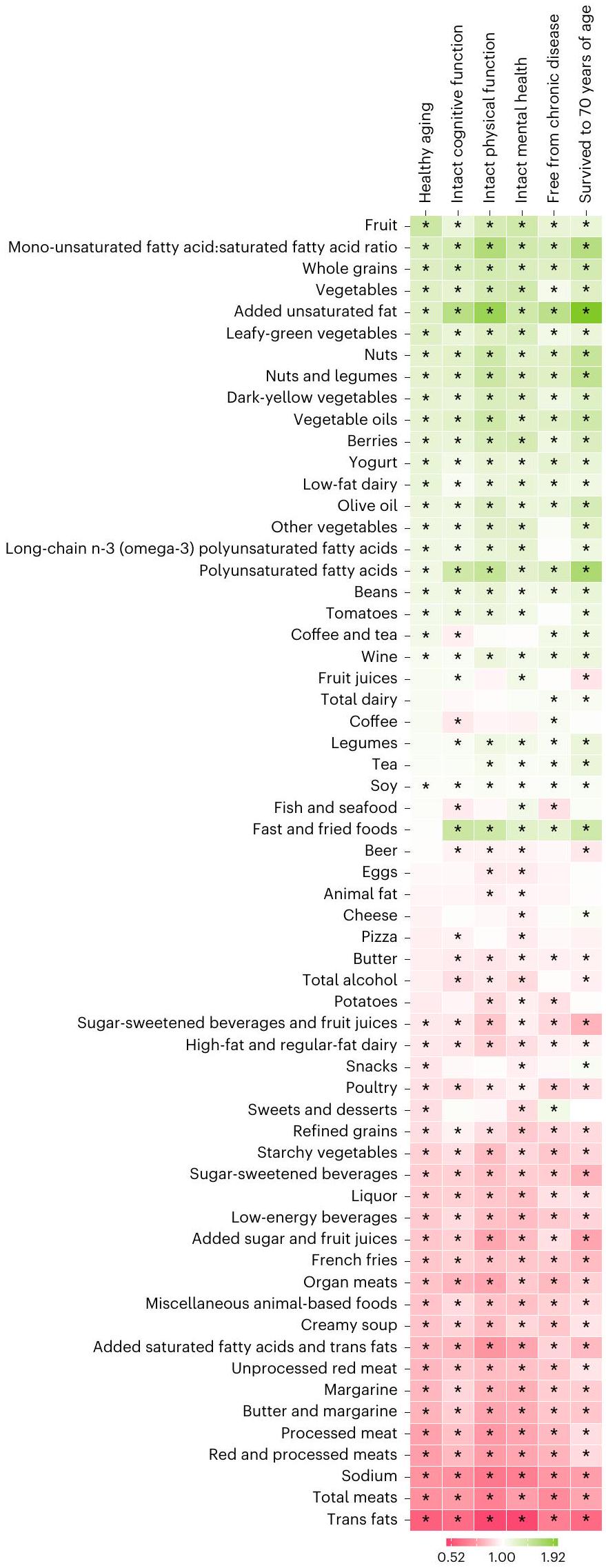
توضح الشكل 4 العلاقات بين العوامل الغذائية الفردية والشيخوخة الصحية ومجالاتها الفردية. بينما كانت الكميات الأعلى من الفواكه والحبوب الكاملة والخضروات والدهون غير المشبعة المضافة والمكسرات والبقوليات ومنتجات الألبان قليلة الدسم مرتبطة بزيادة احتمالات الشيخوخة الصحية، كانت الكميات الأعلى من الدهون المتحولة والصوديوم واللحوم الكلية واللحوم الحمراء والمعالجة مرتبطة بانخفاض الاحتمالات. كانت هذه الأطعمة أو العناصر الغذائية مرتبطة أيضًا بشكل متسق مع كل مجال من مجالات الشيخوخة الصحية. كانت كمية الدهون غير المشبعة المضافة، بما في ذلك الأحماض الدهنية المتعددة غير المشبعة، مرتبطة بشكل خاص بالنجاة حتى سن 70 عامًا، والاحتفاظ بالوظائف البدنية والمعرفية السليمة.
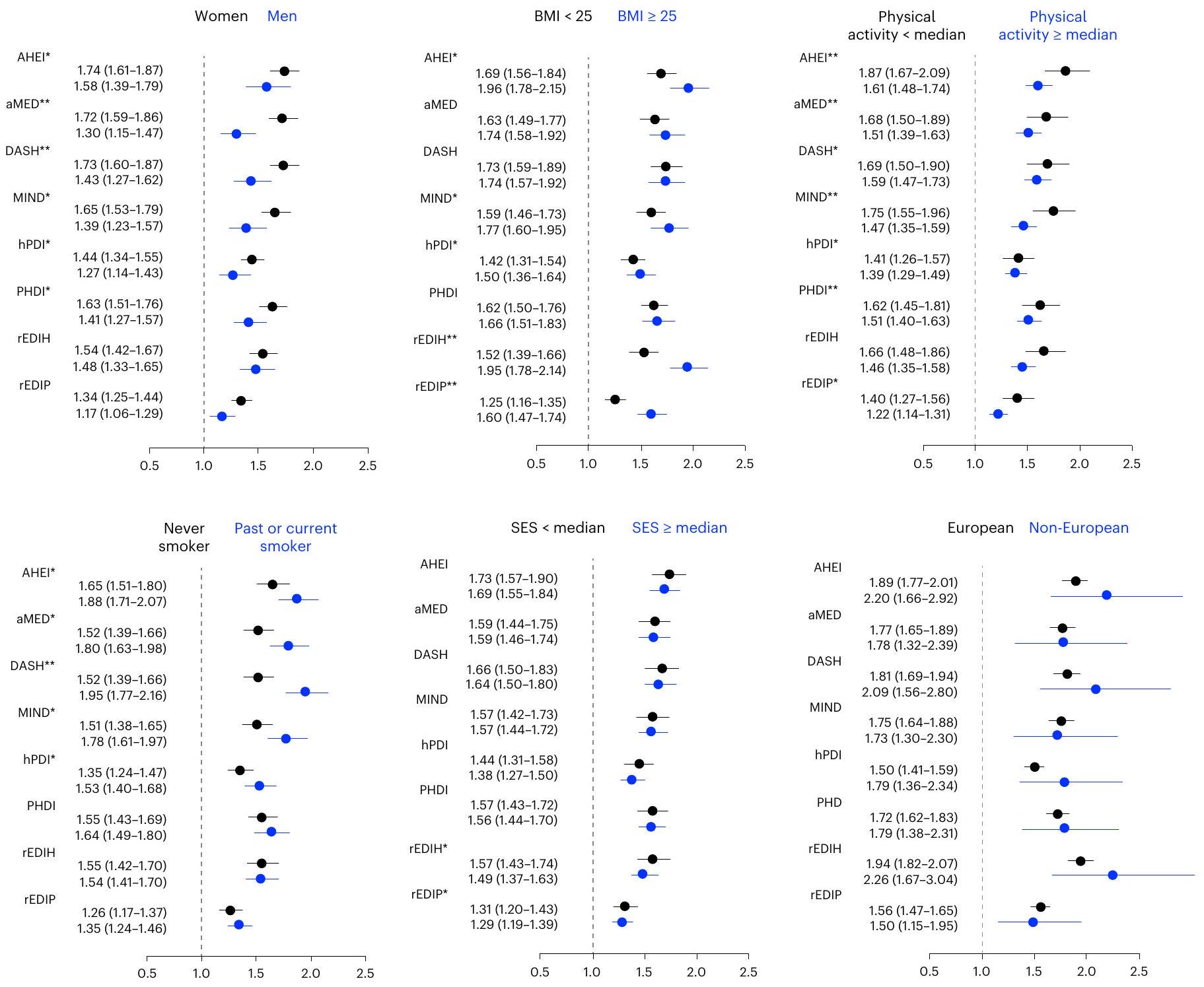
بينما كانت الالتزام بجميع أنماط النظام الغذائي مرتبطًا بشكل كبير بالشيخوخة الصحية لدى كل من الرجال والنساء، كانت الروابط أقوى لدى النساء.التفاعل: 0.0226 إلى <0.0001؛ الشكل 5)
العوامل الغذائية
أهي 2010
أمد
داش
عقل
hPDI
مؤشر التنمية البشرية المعدل
ريد
ريدب
فواكه
التوت
طماطم
خضروات
الخضروات النشوية
الخضروات الورقية الخضراء
خضروات صفراء داكنة
خضروات أخرى
بطاطس
الحبوب الكاملة
الحبوب المكررة
المكسرات والبقوليات
مكسرات
البقوليات
فاصوليا
فول الصويا
اللحوم الكلية
اللحوم الحمراء والمعالجة
اللحم الأحمر
اللحوم المعالجة
أعضاء داخلية
الدواجن
بيض
الأسماك والمأكولات البحرية
أسماك أخرى
أطعمة متنوعة قائمة على الحيوانات
الحلويات والحلويات
الأطعمة السريعة والمقلية
بطاطس مقلية
وجبات خفيفة
بيتزا
دهون حيوانية
زبدة وزبدة نباتية
زبدة
مارجرين
زيوت نباتية
شوربة كريمية
زيت الزيتون
المشروبات المحلاة بالسكر وعصائر الفواكه
المشروبات المحلاة بالسكر
مشروبات منخفضة الطاقة
عصائر الفواكه
إجمالي الكحول
نبيذ
بيرة
الشاي والقهوة
شاي
قهوة
الحليب الكامل
منتجات الألبان قليلة الدسم
منتجات الألبان عالية الدهون
جبن
الدهون المتحولة
الأحماض الدهنية طويلة السلسلة n-3 (أوميغا-3)
الأحماض الدهنية المتعددة غير المشبعة
حمض دهني أحادي غير مشبع: حمض دهني مشبع
تمت إضافة الدهون غير المشبعة
الدهون المشبعة والدهون المتحولة المضافة
السكر المضاف وعصائر الفواكه
صوديوم
الشكل 3 | العوامل الغذائية لأنماط النظام الغذائي. الوردي: تم تخصيص نقاط أقل أو أوزان سلبية للاستهلاك الأعلى لهذا العامل الغذائي؛ الأخضر: تم تخصيص نقاط أعلى أو أوزان إيجابية للاستهلاك الأعلى لهذا العامل الغذائي؛ تم تخصيص نقاط أعلى أو أوزان إيجابية للاستهلاك المعتدل. يتم تقديم EDIH و EDIP كدرجات معكوسة للسماح بالمقارنة مع درجات غذائية أخرى. باستثناء rEDIH و rEDIP (لا تفاعل). كانت الروابط أيضًا أقوى لدى المدخنين (بالنسبة لـ AHEI و aMED و DASH و MIND و hPDI؛التفاعل 0.047 إلى )، في المشاركين الذين لديهم مؤشر كتلة جسم أكبر من (لـ AHEI، MIND، hPDI، rEDIH، rEDIP؛ التفاعل 0.042 إلى <0.0001) وفي المشاركين الذين لديهم مستوى نشاط بدني أقل من الوسيط (لـ AHEI، aMED، DASH، MIND، hPDI، PHDI، rEDIP؛تفاعل 0.038 إلى <0.0001؛ الشكل 5). تفاعل كبير بين SES و rEDIH (تفاعل ) و rEDIP ( تفاعلتمت ملاحظة ذلك. لم يتم العثور على أي تفاعل بالنسبة للأصل (الأوروبي مقابل غير الأوروبي).
أظهرت التحليلات الثانوية اتساقًا مع النتائج الرئيسية. عند استخدام حد عمري أعلى يبلغ 75 عامًا، أظهر مؤشر النظام الغذائي الصحي المعدل (AHEI) أيضًا أقوى ارتباط (البيانات الموسعة الجدول 5). عند تطبيق الأوزان الخطية على درجات نمط النظام الغذائي، كانت النتائج متسقة مع التحليل الرئيسي (البيانات الموسعة الجدول 6).
كان استهلاك UPF الأعلى (مقارنة بأعلى خُمس مع أدنى خُمس) مرتبطًا بـاحتمالات أقل للشيخوخة الصحيةسي آي; جدول البيانات الموسع 7). كان الاستهلاك الأعلى للأغذية المعالجة بشكل كبير مرتبطًا أيضًا بانخفاض احتمالات الحفاظ على الوظائف الإدراكية السليمة الوظيفة، الوظيفة البدنية والصحة النفسية، العيش خالياً من الأمراض المزمنة والوصول إلى سن السبعين (الجدول البياني الموسع 7).
نقاش
في مجموعتين كبيرتين من النساء والرجال في الولايات المتحدة، وجدنا أن الالتزام الأعلى بأنماط النظام الغذائي، وهي AHEI و aMED و DASH و MIND و hPDI و PHDI و rEDIP و rEDIH، خلال منتصف العمر كان مرتبطًا بزيادة احتمالات الشيخوخة الصحية بعد متابعة لمدة 30 عامًا. من بين أنماط النظام الغذائي، كانت AHEI الأكثر ارتباطًا بالشيخوخة الصحية، بينما كانت hPDI الأقل ارتباطًا. مقارنة بالمشاركين في أدنى خُمس، كان أولئك الذين في أعلى خُمس من AHEI (متوسط الدرجة المعدلة للطاقةكاناحتمالات أكبر لتحقيق الشيخوخة الصحية باستخدام حد عمري يبلغ 70 عامًا و 2.24 مرة احتمالات أكبر باستخدام حد عمري يبلغ 75 عامًا. كان مؤشر النظام الغذائي الصحي (AHEI) يتبعه عن كثب مؤشر النظام الغذائي الصحي المعدل (rEDIH) و مؤشر النظام الغذائي المتوسطي (aMED) و نظام داش الغذائي (DASH) و مؤشر النظام الغذائي النباتي (PHDI) و مؤشر النظام الغذائي المعرفي (MIND) وأخيرًا مؤشر النظام الغذائي الصحي (hPDI). كانت الارتباطات مستقلة عن عوامل نمط الحياة الأخرى، بما في ذلك مستوى النشاط البدني، والتدخين ومؤشر كتلة الجسم (BMI). كان مؤشر النظام الغذائي الصحي (AHEI) أيضًا الأكثر ارتباطًا بالحفاظ على الوظيفة البدنية السليمة والصحة العقلية بين مجالات الشيخوخة الصحية الفردية. كان مؤشر النظام الغذائي النباتي (PHDI) الأكثر ارتباطًا بالحفاظ على الصحة المعرفية السليمة والبقاء على قيد الحياة حتى سن 70 عامًا. كان مؤشر النظام الغذائي الصحي المعدل (rEDIH) الأكثر ارتباطًا بالتحرر من الأمراض المزمنة. كان تناول أعلى من الأطعمة المعالجة مرتبطًا بشكل عكسي مع درجات جودة النظام الغذائي الأعلى وكان أيضًا مرتبطًا باحتمالات أقل للشيخوخة الصحية. تقدم نتائجنا دليلًا يدعم أن الالتزام بأنماط غذائية صحية يمثل استراتيجية محتملة للشيخوخة الصحية، وأنماطًا تكون غنية بشكل خاص بالفواكه والخضروات والحبوب الكاملة والدهون غير المشبعة والمكسرات والبقوليات، التي تشمل بعض منتجات الألبان، والتي تكون أقل في الدهون المتحولة والصوديوم واللحوم الحمراء والمعالجة.
بينما تشترك جميع أنماط الحمية في تشابهات مثل تعزيز تناول الفواكه والخضروات والحبوب الكاملة، مع تقليل كمية اللحوم الحمراء والمعالجة، يركز كل نمط على مكونات محددة. على سبيل المثال، بينما تركز حمية aMED على الأساسيات المتوسطية مثل زيت الزيتون والأسماك والمكسرات.تسلط MIND الضوء أيضًا على الفوائد المعرفية للتوتتُعطي حمية داش الأولوية لتقييد الصوديوم من أجل التحكم في ضغط الدم.يؤكد مؤشر التنمية البشرية على الأغذية الصحية ذات انبعاثات غازات دفيئة منخفضة، مثل الأطعمة البروتينية المستمدة من النباتاتوتنسب hPDI بشكل فريد درجات إيجابية للأطعمة النباتية الصحية ودرجات سلبية للأطعمة المشتقة من الحيوانات.في تقرير سابق، كانت الالتزام بمؤشر AHEI و aMED، الذي تم تقييمه في 1984-1986، مرتبطًا بـ و ) احتمالات أكبر للشيخوخة الصحية، على التوالي، في NHS . وقد فحصت هذه التحليل نمطين غذائيين مع الشيخوخة الصحية في عام 2000 باستخدام نفس التعريف كما في الدراسة الحالية، ولكن تم استخدام مقابلة الهاتف لحالة الإدراك لتقييم مجال الصحة الإدراكية. شمل تحليلنا، الذي تضمن كل من NHS وHPFS، تقييمًا غذائيًا طويل الأمد لثمانية أنماط غذائية على مدى 14 عامًا، مع تقييم لـ الشيخوخة الصحية التي أجريت بعد 30 عامًا من خط الأساس. أظهرت النتائج ارتباطات متسقة وأقوى لهذين الدرجتيناحتمالات أكبر لـ AHEI ولـ aMED). العلاقة بين النظام الغذائي
الشكل 4 | العلاقات المعدلة متعددة المتغيرات بين العوامل الغذائية والشيخوخة الصحية ومجالاتها في مجموعة البيانات الرئيسية المجمعة. يمثل كل مربع في خريطة الحرارة نسبة الأرجحية (OR) مقارنة بين النسبة المئوية 90 والنسبة المئوية 10 لكل من العوامل الغذائية. تم استخدام الانحدارات اللوجستية لتقدير نسب الأرجحية وتم تعديلها حسب العمر عند البداية (1986) ، المجموعة (الجنس) ، مؤشر كتلة الجسم (BMI) (الأنساب (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، حالة التدخين (لم يدخن أبدًا، مدخن سابق، مدخن حالي: 1-14 سيجارة في اليوم، 15-24 سيجارة في اليوم والسجائر في اليوم)، استهلاك الكحول (غرام في اليوم)، النشاط البدني (ساعة مكافئة للتمرين في الأسبوعاستخدام الفيتامينات المتعددة على الإطلاق (نعم/لا)، التاريخ العائلي لنوبة قلبية (نعم/لا)، التاريخ العائلي لمرض السكري من النوع 2، التاريخ العائلي للسرطان، التاريخ العائلي للخرف (نعم/لا)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام هرمونات انقطاع الطمث (لا، استخدام هرمونات سابق، أو استخدام هرمونات حالي؛ للنساء فقط)، الحالة الاجتماعية الاقتصادية في البداية، الحالة الزوجية (نعم/لا)، العيش بمفردك على الإطلاق (نعم/لا) وتاريخ الاكتئاب (نعم/لا) في المجموعات المجمعة. يتم الإشارة إلى ORs التي تزيد عن 1.0 باللون الأخضر؛ بينما يتم الإشارة إلى ORs التي تقل عن 1.0 باللون الوردي؛ لون أغمق يدل على ارتباط أقوى.* ذو جانبينالقيم المصححة للمقارنات المتعددة باستخدام معدل الاكتشاف الكاذب.
الشكل 5 | تحليل الفئات الفرعية للعلاقات بين درجات نمط النظام الغذائي المتوسط والشيخوخة الصحية في مجموعة البيانات الرئيسية المجمعةتظهر الرسوم البيانية للغابات نسب الأرجحية مقارنةً بين النسبة المئوية 90 والنسبة المئوية 10 لكل من أنماط النظام الغذائي (ممثلة بصريًا بمراكز أشرطة الخطأ) وفواصل الثقة 95% (ممثلة بصريًا بأشرطة الخطأ). تم استخدام الانحدارات اللوجستية لتقدير نسب الأرجحية وتم تعديلها حسب العمر عند البداية (1986) ، والفوج (الجنس) ، ومؤشر كتلة الجسم (الأنساب (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، حالة التدخين (لم يدخن أبدًا، مدخن سابق، مدخن حالي):السجائر في اليوم، 15-24 سجائر في اليوم والسجائر في اليوم)، استهلاك الكحول (غرام في اليوم)، النشاط البدني (ساعة مكافئة للتمرين في الأسبوعاستخدام الفيتامينات المتعددة على الإطلاق (نعم/لا)، تاريخ عائلي من احتشاء عضلة القلب (نعم/لا)، تاريخ عائلي من داء السكري من النوع 2، تاريخ عائلي من السرطان، تاريخ العائلة من الخرف (نعم/لا)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام هرمونات انقطاع الطمث (لا، سابق، أو استخدام هرموني حالي؛ للنساء فقط)، الحالة الاجتماعية والاقتصادية عند البداية، الحالة الزوجية (نعم/لا)، العيش بمفردك في أي وقت (نعم/لا) وتاريخ الاكتئاب (نعم/لا)، مع استبعاد المتغيرات المصنفة حيثما كان ذلك مناسبًا، في المجموعات المجمعة. ** ذو جانبينالتفاعل <0.0001 (غير معدّل للمقارنات المتعددة). *ذو جانبينالتفاعل < 0.05 (غير مُعدل للمقارنات المتعددة)؛ الجنس،; عقل ; hPDI ; PHDI ; مؤشر كتلة الجسم، مؤشر النظام الغذائي الصحي الأمريكي; عقل ; و . للنشاط البدني، نظام داش; hPDI ; rEDIP . للتدخين، AHEIأمدعقل hPDI . لSES، rEDIH; rEDIP . تمت دراسة الأنماط والشيخوخة الصحية أيضًا في مجموعات سكانية أخرى، وهي فرنساأسترالياالصينوإسرائيل، وأكدت نتائجنا. في دراسة المكملات بالفيتامينات والمعادن المضادة للأكسدة (المسنون الأصحاء، متابعة لمدة 13 عامًا) ودراسة صحة الصينيين في سنغافورة (SCHS) (الأشخاص الذين يتقدمون في السن بشكل صحي، متابعة لمدة 20 عامًا)، كانت الالتزام الأعلى بنظام غذائي على الطراز المتوسطي مرتبطًا بـ; الثلث 3 مقابل الثلث 1) و; الربع الرابع مقابل الربع الأول) احتمال أكبر لتحقيق الشيخوخة الصحية، على التوالي. كانت AHEI و HEI 2015 والالتزام بالإرشادات الغذائية الوطنية الأسترالية مرتبطة بشكل مشابه بالشيخوخة الصحية مع نسب الأرجحية تتراوح من 1.34 إلى 1.73 في SCHS، والمسح الوطني الإسرائيلي للصحة والتغذية لكبار السن. (المسنون الأصحاء؛باستثناء الوفيات؛ متوسط المتابعة 12.6 سنة) ودراسة عيون جبال بلو (المسنين الأصحاء، متابعة لمدة 10 سنوات). من بين الأنماط الغذائية التي تم فحصها أيضًا في مجموعات أخرى، وجدنا تفاعلات كبيرة بين الجنس وDASH، aMED، AHEI وhPDI؛ بين مستوى النشاط البدني وAHEI، aMED وhPDI؛ بين التدخين وAHEI، aMED، DASH وhPDI؛ وبين مؤشر كتلة الجسم وAHEI وhPDI. قد تفسر الاختلافات في مجموعات الدراسة فيما يتعلق بالجنس، وعوامل نمط الحياة ومؤشر كتلة الجسم التباينات الملحوظة في ORs عبر الدراسات. اختلفت طرق تقييم النظام الغذائي عبر الدراسات، كما اختلفت تعريفات الشيخوخة الصحية. شملت الاختلافات حدود العمر، والاستبيانات أو المقاييس المستخدمة لتقييم المجالات، وأخذ الأمراض المزمنة بعين الاعتبار و
شمول أو استبعاد مقاييس سريرية إضافية. علاوة على ذلك، استبعدت بعض الدراسات الأفراد المتوفين من عينة السكان، مما قد يؤدي إلى تفاوت في نسبة الأشخاص الأصحاء واختلافات في تصنيف الأشخاص الأصحاء. من الضروري توحيد نتيجة الشيخوخة الصحية المركبة للسماح بمقارنة صحيحة للدراسات البحثية؛ يجب اعتبار الوفيات كأشخاص عاديين ويجب تضمينها في التحليلات لتجنب التحيز في الاختيار.
باستخدام نهج مدفوع بالبيانات، قام هودج وآخرون.حددوا أربعة أنماط غذائية كانت مرتبطة بالشيخوخة الصحية في دراسة مجموعة ملبورن التعاونية (الأشخاص الأصحاء؛ متوسط المتابعة 11.7 سنة للناجين). كان نمط الغذاء الذي أظهر أقوى ارتباط إيجابي بالشيخوخة الصحية يتكون بشكل أساسي من الفواكه، بينما كان النمط المرتبط عكسياً بالشيخوخة الصحية يركز بشكل أساسي على اللحوم الحمراء. قام أسمان وآخرون.بدراسة العوامل الغذائية الفردية لنظام البحر الأبيض المتوسط الغذائي وارتباطها بالشيخوخة الصحية في مجموعة مكملات الفيتامينات والمعادن المضادة للأكسدة ووجدوا أن تناول الفواكه والخضروات بكميات أكبر كان مرتبطًا بشكل إيجابي بالشيخوخة الصحية، بينما كانت اللحوم والكحول مرتبطة بشكل سلبي.تتفق هذه النتائج مع نتائجنا التي تظهر أن تناول الفواكه (بشكل عام والتوت) والخضروات (بشكل عام، والخضروات الورقية والخضروات الصفراء الداكنة) كان مرتبطًا بفرص أكبر للشيخوخة الصحية، بينما كان تناول الدهون المتحولة والصوديوم واللحوم (الإجمالية، الحمراء والمعالجة وغير المعالجة) والمشروبات الكحولية مرتبطًا بفرص أقل للشيخوخة الصحية. في دراسة عيون جبال بلو، وجد جوبيناث وآخرون.وجدوا فقط ارتباطًا للفواكه (الشيخوخة الصحية; الأرباعمقابل الربع 1؛ غير دال للربع 4 مقابل الربع 1) بين العوامل الغذائية الفردية التي تم فحصها. في الدراسة الحالية، كانت معظم الأطعمة الفردية المرتبطة بالشيخوخة الصحية مرتبطة باستمرار بمجالات الشيخوخة الصحية بشكل فردي، باستثناء عدد قليل بما في ذلك الأطعمة السريعة والمقلية خارج المنزل، والوجبات الخفيفة، التي كانت مرتبطة بشكل إيجابي بالنجاة حتى سن 70 عامًا. على الرغم من أن استهلاك الأطعمة المقلية قد ارتبط بزيادة خطر الأحداث القلبية الوعائية، تشير الأدلة إلى عدم وجود ارتباط مع خطر الوفاة بسبب جميع الأسباب. قد يفسر الجانب الاجتماعي المرتبط بتناول الطعام خارج المنزل جزءًا من الارتباط بالعيش حتى سن 70 عامًاعلى الرغم من أن المزيد من البحث في هذا المجال مطلوب لشرح هذه الارتباطات.
أظهرت نتائجنا أن كل نمط غذائي تم فحصه كان مرتبطًا بكل مكون فردي محدد من الشيخوخة الصحية. كما فحصت دراسة مستقبلية أيضًا ارتباطات أنماط الغذاء، وبشكل خاص aMED وDASH وAHEI وPDI وhPDI، مع مجالات الشيخوخة الصحية.متسقة مع نتائجنا، وجد زو وآخرون.ارتباطات كبيرة بين aMED وDASH وAHEI وhPDI، والحفاظ على الوظيفة الإدراكية السليمة؛ AHEI وDASH للبقاء خاليًا من الأمراض المزمنة؛ aMED وDASH وAHEI وhPDI وPDI للحفاظ على الوظيفة البدنية والصحة العقلية (عدم وجود اكتئاب سريري) في دراسة SCHS. ومع ذلك، لم يتم العثور على ارتباط بين aMED وPDI وhPDI ومكون الأمراض المزمنة، وPDI ومكون الوظيفة الإدراكية. تدعم الأدلة الواسعة من الدراسات التدخلية والملاحظة أن الالتزام الأعلى بأنماط الغذاء الصحية يحمي أو يرتبط بانخفاض خطر الأمراض المزمنة.هناك أيضًا أدلة متزايدة تدعم ارتباط أنماط الغذاء والعوامل الغذائية بالصحة العقلية والبدنية والإدراكية (تمت مراجعتها في المراجع 29،30). بالإضافة إلى المقاييس التقليدية للعمر الزمني أو عبء المرض، فإن الشيخوخة الصحية متعددة الأبعاد كما اعترفت بها منظمة الصحة العالمية في تقريرها العالمي الأول عن الشيخوخة والصحة.بينما يوفر فحص المجالات بشكل منفصل رؤى أكثر استهدافًا حول الآليات المحتملة، قد يساعد التحقيق في الشيخوخة الصحية كنتيجة متعددة المكونات في إبلاغ استراتيجيات الصحة الشاملة.تسمح لنا نتائجنا بالتقاط الطبيعة متعددة الأبعاد للشيخوخة وتقييم أنماط الغذاء وارتباطات تناول الطعام بشكل شامل.
تشمل نقاط القوة في هذه الدراسة التصميم المستقبلي وحجم السكان الكبير لتحليلات قوية. سمحت القياسات المتكررة
للنظام الغذائي ووزن الجسم ومتغيرات نمط الحياة بأن نأخذ في الاعتبار الالتزام طويل الأمد بأنماط الغذاء الصحية والعوامل المربكة المحتملة، وتقليل أخطاء القياس العشوائية. سمح المتابعة الطويلة لمدة 30 عامًا بفحص النظام الغذائي في منتصف العمر وارتباطه بالشيخوخة الصحية في الحياة اللاحقة. ومع ذلك، يجب تفسير نتائج هذه الدراسة في سياق قيودها. أولاً، على الرغم من أنه تم اعتبار فترة تأخير مدتها 6 سنوات بين آخر تحديث للنظام الغذائي وتقييم الشيخوخة الصحية، لا يمكن استبعاد السبب العكسي تمامًا. بينما من المحتمل أن يكون الالتزام الأعلى بالأنظمة الغذائية الصحية مؤشرًا على مستوى اجتماعي واقتصادي أعلى ونمط حياة صحي بشكل عام، ظلت نتائجنا متسقة بعد الأخذ في الاعتبار مثل هذه العوامل. ومع ذلك، قد لا يزال هناك تداخل غير مقاس بسبب عوامل أخرى غير مقاسة، مثل التأثيرات البيئية، على الرغم من أن قيم E تشير إلى أن نتائجنا قوية أمام التداخل المحتمل. أيضًا، تم تقييم مجالات الوظيفة الإدراكية والبدنية باستخدام استبيانات موثوقة تم الإبلاغ عنها ذاتيًا بدلاً من القياسات الموضوعية، مما يحد من التقييم العميق والتصنيف. أخيرًا، شمل سكاننا محترفي الصحة، مما قد يحد من تعميم نتائجنا. سيوفر تكرار التحليلات في مجموعات سكانية ذات مستويات اجتماعية واقتصادية وأصول متنوعة رؤى إضافية حول تعميمها.
كان الالتزام الأكبر على المدى الطويل بنظام غذائي صحي خلال منتصف العمر مرتبطًا بفرص أكبر للشيخوخة الصحية ومجالاتها الفردية لدى البالغين في الولايات المتحدة. من بين ثمانية أنماط غذائية تم فحصها في هذه الدراسة، قد يوفر نظام غذائي تم تطويره للتنبؤ بخطر الأمراض المزمنة كما تم قياسه بواسطة AHEI أعلى فائدة للشيخوخة الصحية لكل من الرجال والنساء. بالإضافة إلى الوقاية من الأمراض المزمنة، تمتد توصياتنا لتعزيز الشيخوخة الصحية بشكل عام، بما في ذلك الصحة العقلية والبدنية والإدراكية.
المحتوى عبر الإنترنت
أي طرق، مراجع إضافية، ملخصات تقارير Nature Portfolio، بيانات المصدر، بيانات موسعة، معلومات إضافية، شكر وتقدير، معلومات مراجعة الأقران؛ تفاصيل مساهمات المؤلفين والمصالح المتنافسة؛ وبيانات توفر البيانات والرموز متاحة علىhttps://doi.org/10.1038/s41591-025-03570-5.
References
Centers for Disease Control and Prevention. Healthy Aging at a Glance, 2015: Helping People to Live Long and Productive Lives and Enjoy a Good Quality of Life https://stacks.cdc.gov/view/cdc/43961 (National Center for Chronic Disease Prevention and Health Promotion (U.S.) & Division of Adult and Community Health, 2015).
Office of Disease Prevention and Health Promotion. Healthy Aging https://health.gov/our-work/national-health-initiatives/ healthy-aging#:~:text=Promoting%20health%20and%20 preventing%2Odisease,live%20longer%20and%20stay%20 healthy (OASH, 2023).
Afshin, A. et al. Health effects of dietary risks in 195 countries, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 393, 1958-1972 (2019).
Mokdad, A. H. et al. The state of US health, 1990-2016: burden of diseases, injuries, and risk factors among US states. JAMA 319, 1444-1472 (2018).
Bautmans, I. et al. WHO working definition of vitality capacity for healthy longevity monitoring. Lancet Healthy Longev. 3, e789-e796 (2022).
Shan, Z. et al. Association between healthy eating patterns and risk of cardiovascular disease. JAMA Intern. Med. 180, 1090-1100 (2020).
Guasch-Ferré, M. & Willett, W. C. The Mediterranean diet and health: a comprehensive overview. J. Intern. Med. 290, 549-566 (2021).
Forouhi, N. G., Misra, A., Mohan, V., Taylor, R. & Yancy, W. Dietary and nutritional approaches for prevention and management of type 2 diabetes. BMJ 361, k2234-k2241 (2018).
English, L. K. et al. Evaluation of dietary patterns and all-cause mortality: a systematic review. JAMA Netw. Open 4, e2122277-e21222295 (2021).
Scarmeas, N., Anastasiou, C. A. & Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 17, 1006-1015 (2018).
Tessier, A.-J. & Chevalier, S. An update on protein, leucine, omega-3 fatty acids, and vitamin D in the prevention and treatment of sarcopenia and functional decline. Nutrients 10, 1099-1115 (2018).
Nicolaou, M. et al. Association of a priori dietary patterns with depressive symptoms: a harmonised meta-analysis of observational studies. Psychol. Med. 50, 1872-1883 (2020).
Okereke, O. I. et al. Effect of long-term vitamin D3 supplementation vs placebo on risk of depression or clinically relevant depressive symptoms and on change in mood scores: a randomized clinical trial. JAMA 324, 471-480 (2020).
Okereke, O. I. et al. Effect of long-term supplementation with marine omega-3 fatty acids vs placebo on risk of depression or clinically relevant depressive symptoms and on change in mood scores: a randomized clinical trial. JAMA 326, 2385-2394 (2021).
Zhou, Y.-F. et al. Association between dietary patterns in midlife and healthy ageing in Chinese adults: the Singapore Chinese Health Study. J. Am. Med. Dir. Assoc. 22, 1279-1286 (2021).
Assmann, K. E. et al. Association between adherence to the Mediterranean diet at midlife and healthy aging in a cohort of French adults. J. Gerontol. A Biol. Sci. Med. Sci. 73, 347-354 (2018).
Gopinath, B., Russell, J., Kifley, A., Flood, V. M. & Mitchell, P. Adherence to dietary guidelines and successful aging over 10 years. J. Gerontol. A Biol. Sci. Med. Sci. 71, 349-355 (2016).
Hodge, A. M., O’Dea, K., English, D. R., Giles, G. G. & Flicker, L. Dietary patterns as predictors of successful ageing. J. Nutr. Health Aging 18, 221-227 (2014).
Samieri, C. et al. The association between dietary patterns at midlife and health in aging: an observational study. Ann. Intern. Med. 159, 584-591 (2013).
Goshen, A. et al. Association of diet quality with longevity and successful aging in Israeli adults 65 years or older. JAMA Netw. Open 5, e2214916-e2214927 (2022).
Trichopoulou, A., Costacou, T., Bamia, C. & Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 348, 2599-2608 (2003).
Morris, M. C. et al. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement. 11, 1007-1014 (2015).
Karanja, N. M. et al. Descriptive characteristics of the dietary patterns used in the Dietary Approaches to Stop Hypertension Trial. J. Am. Diet. Soc. 99, S19-S27 (1999).
Bui, L. P. et al. Planetary Health Diet Index and risk of total and cause-specific mortality in three prospective cohorts. Am. J. Clin. Nutr. 120, 80-91 (2024).
Satija, A. et al. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J. Am. Coll. Cardiol. 70, 411-422 (2017).
Qin, P. et al. Fried-food consumption and risk of cardiovascular disease and all-cause mortality: a meta-analysis of observational studies. Heart 107, 1567-1575 (2021).
Björnwall, A., Mattsson Sydner, Y., Koochek, A. & Neuman, N. Eating alone or together among community-living older people-a scoping review. Int. J. Environ. Res. Public Health 18, 3495-3536 (2021).
Wang, P. et al. Optimal dietary patterns for prevention of chronic disease. Nat. Med. 29, 719-728 (2023).
Milte, C. M. & McNaughton, S. A. Dietary patterns and successful ageing: a systematic review. Eur. J. Nutr. 55, 423-450 (2016).
Yeung, S. S. Y., Kwan, M. & Woo, J. Healthy diet for healthy aging. Nutrients 13, 4310-4326 (2021).
Beard, J. R. et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet 387, 2145-2154 (2016).
Langevin, H. M., Weber, W. & Chen, W. Integrated multicomponent interventions to support healthy aging of the whole person. Aging Cell 23, e14001-e14045 (2024).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
تم إجراء التحليلات في NHS وHPFS. تم تأسيس NHS في عام 1976 وشملت 121,700 ممرضة مسجلة في الولايات المتحدة تتراوح أعمارهن بين 30-55 عامًا.تم بدء HPFS في عام 1986 وجند 51,525 من محترفي الصحة الذكور الذين تتراوح أعمارهم بينسنوات.تم نشر تفاصيل حول المجموعات سابقًا.تم إجراء تقييمات ثنائية سنوية لعوامل نمط الحياة والتاريخ الطبي من خلال استبيانات مرسلة، مع الحفاظ على معدل متابعة يتجاوز.تم الإبلاغ سابقًا عن صلاحية عالية وقابلية إعادة إنتاج المعلومات الصحية المبلغ عنها ذاتيًا في المجموعات.بالنسبة لكلا المجموعتين، كانت نقطة البداية لهذه التحليل هي عام 1986، أي عندما سمحت استبيانات تكرار الطعام (FFQ) بحساب جميع درجات أنماط الغذاء.
تظهر الشكل 1 مخطط تدفق الدراسة. شمل المشاركون في هذا التحليل الذين أجابوا على استبيانات عام 1986 وكان لديهم فرصة للوصول إلى 70 عامًا في نهاية المتابعة (تتراوح أعمارهم بين 39 و69 عامًا عند البداية؛تم استبعاد). المشاركون الذين لديهم تاريخ من واحد أو أكثر من 11 مرضًا مزمنًا رئيسيًا، بما في ذلك السرطان (باستثناء سرطانات الجلد غير الميلانينية)، السكري، احتشاء عضلة القلب، مرض الشريان التاجي، فشل القلب الاحتقاني، السكتة الدماغية، فشل الكلى، مرض الرئة الانسدادي المزمن، مرض باركنسون، التصلب المتعدد ومرض التصلب الجانبي الضموري، عند البداية ( )، مع بيانات مفقودة لواحد أو أكثر من درجات أنماط النظام الغذائي بين عامي 1986 و2010، أو الذين أبلغوا عن استهلاك إجمالي للطاقة غير معقول (<500 أو للنساء و أو للرجال) ) ومع وجود نقص في نمط الشيخوخة الصحية ( ) تم استبعادها.
تمت الموافقة على بروتوكول الدراسة من قبل لجان المراجعة المؤسسية (IRBs) في مستشفى بريغهام والنساء (BWH) ومدرسة هارفارد تي. إتش. تشان للصحة العامة (HSPH) والسجلات المشاركة (أرقام بروتوكول IRB 2001P001945/BWH و10372) كما هو مطلوب. وفقًا للإجراءات المعتمدة من قبل IRB في BWH وHSPH، فإن إكمال وإرجاع استبيانات الأساس والمتابعات اللاحقة يعني الموافقة. قبل عام 2006، كانت ممارسات الموافقة تختلف وتم إجراء العديد من الجمعيات بموافقة ضمنية. تم منح إعفاء من توثيق الموافقة المستنيرة لهذه الدراسات. كانت الموافقة المستنيرة المكتوبة مطلوبة للحصول على السجلات الطبية.
تقييم النظام الغذائي
تم قياس المدخول الغذائي باستخدام استبيان تكرار الطعام المعتمد (FFQ) الذي يحتوي على أكثر من 130 عنصرًا، وتم إدارته في عام 1986 وكل 4 سنوات بعد ذلك. وقد تم الإبلاغ سابقًا عن صلاحية وموثوقية استبيان تكرار الطعام في قياس المدخول من العناصر الغذائية والأطعمة ومجموعات الطعام.طُلب من المشاركين توضيح مدى تكرار استهلاكهم لأطعمة معينة في الاثني عشر شهرًا الماضية. تم حساب العناصر الغذائية باستخدام قواعد بيانات تكوين الأغذية التابعة لوزارة الزراعة الأمريكية (USDA) وجامعة هارفارد.، وتمت إضافتها مع تحليلات كيميائية حيوية. استنادًا إلى المدخولات الغذائية والمغذيات المبلغ عنها، تم حساب ثمانية درجات لنمط النظام الغذائي، بما في ذلك AHEI و aMED و DASH و MIND و hPDI و PHDI و EDIP و EDIH، بالإضافة إلى استهلاك الأطعمة المعالجة. تم تطوير درجات AHEI و aMED و DASH و MIND و hPDI و PHDI، واستهلاك الأطعمة المعالجة، استنادًا إلى التوصيات الغذائية والأدلة المتاحة. أظهرت الدرجات صلاحية وقابلية تكرار متوسطة إلى عالية.وكانت مرتبطة بمخاطر النتائج الصحيةتم اشتقاق EDIP و EDIH تجريبيًا باستخدام مؤشرات حيوية للالتهاب المزمن.وارتفاع مستوى الأنسولينعلى التوالي.
تم حساب درجة AHEI بناءً على استهلاك 11 نوعًا من الأطعمة والمغذيات التي تم ربطها بشكل إيجابي أو سلبي بمخاطر الأمراض المزمنة، بما في ذلك الفواكه، والخضروات، والمكسرات، والبقوليات، والكحول، واللحوم الحمراء والمعالجة، والحبوب الكاملة، والصوديوم، والدهون المتحولة والسلسلة الطويلة.أحماض دهنية (أوميغا-3)تم تقييم كل مكون على مقياس من 0 إلى 10، وكان نطاق AHEI من 0 إلى 110، حيث يشير الدرجة الأعلى إلى جودة نظام غذائي أفضل. تم تقييم الالتزام بالنظام الغذائي المتوسطي باستخدام نسخة معدلة من درجة aMED المكونة من 9 نقاط.. تم حساب الدرجة بناءً على الالتزام بتسعة عناصر غذائية (مع إما تناول أعلى أو أقل) التي تميز النظام الغذائي المتوسطي: الخضروات؛ البقوليات؛ الفواكه؛ المكسرات؛ الحبوب الكاملة؛ الأسماك؛ استهلاك الكحول بشكل معتدل؛ تناول أقل من اللحوم الحمراء والمعالجة؛ والأحماض الدهنية الأحادية غير المشبعة إلى المشبعة.تراوح معدل درجة aMED المعدلة من 0 إلى 9، حيث تشير الدرجة الأعلى إلى التزام أكبر بالنظام الغذائي المتوسطي.تم تصميم درجة DASH، التي تهدف إلى المساعدة في الوقاية من ارتفاع ضغط الدم أو علاجه، استنادًا إلى ثمانية عوامل غذائية، بما في ذلك تناول الفواكه والخضروات والمكسرات والبقوليات بكميات كبيرة، ومنتجات الألبان قليلة الدسم، وتناول الحبوب الكاملة، وانخفاض الصوديوم، والمشروبات المحلاة، واللحوم الحمراء المعالجة وغير المعالجة.تم تخصيص درجة لكل مكون تتراوح بين 0 و 5 بناءً على توزيعات الاستهلاك في الخمس. تراوحت الدرجة الإجمالية من ثمانية (أدنى مستوى من الالتزام) إلى 40 (أعلى مستوى من الالتزام). شملت درجة MIND عشرة عوامل غذائية صحية للدماغ، بما في ذلك الخضروات الورقية، والخضروات الأخرى، والتوت، والمكسرات، والحبوب الكاملة، والأسماك، والفاصوليا، والدواجن، والنبيذ (بكميات محدودة) وزيت الزيتون، وخمسة عوامل أقل صحة، بما في ذلك الزبدة والسمن، والجبن، واللحوم الحمراء، والأطعمة السريعة/المقلية، والمعجنات والحلويات.. نقاط من أو تم نسب 1 لكل منهما وكان مجموع درجة MIND يتراوح من 0 إلى 15، حيث تشير الدرجة الأعلى إلى التزام أعلى. تم تصميم hPDI ليعكس الالتزام بنظام غذائي صحي قائم على النباتات.؛ وقد شمل 18 عاملاً غذائياً وتراوح من 18 (أدنى مستوى من الالتزام) إلى 90 (أعلى مستوى من الالتزام). تم اشتقاق PHDI بناءً على الالتزام بالنظام الغذائي المرجعي المضمن في تقرير EAT-Lancet.. كانت الحمية المرجعية مبنية على أدلة تتعلق بالنتائج الصحية والبقاء ضمن الحدود الكوكبية لانبعاثات غازات الدفيئة ومعايير بيئية أخرى. شملت معايير التقييم 15 عاملًا غذائيًا. بالنسبة لكل عامل غذائي، تراوحت الدرجات من 0 إلى 10، باستثناء البقوليات غير الصويا وأطعمة الصويا، التي ساهمت بحد أقصى قدره 5. تراوحت الدرجة الإجمالية لمؤشر النظام الغذائي الصحي من 0 (عدم الالتزام) إلى 140 (الالتزام التام). تم تقييم مؤشر النظام الغذائي المضاد للالتهابات بناءً على 18 عاملًا غذائيًا مرتبطًا بالالتهاب.شملت EDIH 18 عاملًا غذائيًا مرتبطًا بفرط الأنسولين.نظرًا لأن درجات EDIH وEDIP الأعلى تشير إلى ارتفاع مستويات الأنسولين ووجود أنماط غذائية التهابية على التوالي، تم عكس اتجاه الدرجات لتسهيل المقارنة مع درجات غذائية أخرى وتم الإشارة إليها كـ rEDIH وrEDIP. الشكل 3 هو تمثيل بصري للأنماط الغذائية وعواملها الغذائية.
تم تصنيف المواد الغذائية أيضًا وفقًا لنظام تصنيف نوفاتم حساب متوسط مدخول الطاقة اليومي من الأطعمة المعالجة بشكل كبير، وتم تحديد نسبة إجمالي الطاقة اليومية من الأطعمة المعالجة بشكل كبير بناءً على متوسط إجمالي مدخول الطاقة.
تقييم الشيخوخة الصحية
استنادًا إلى مفهوم ‘الشيخوخة الناجحة’ الذي وصفه رو و كان والتقارير السابقة تم تعريف نمط الشيخوخة الصحية على أنه البقاء على قيد الحياة حتى سن 70 عامًا دون وجود 11 مرضًا مزمنًا رئيسيًا ودون أي ضعف في الوظيفة الإدراكية أو الوظيفة البدنية أو الصحة النفسية. تم اعتبار المشاركين الذين لم يستوفوا معايير النمط أو الذين توفوا قبل عام 2016 كشيخوخة عادية. أولئك الذين توفوا بعد عام 2016، ولكن كانت لديهم تقييم كامل للنمط، تم تضمينهم في التحليلات. تم تقييم الوظيفة الإدراكية باستخدام استبيان موثق لتراجع الإدراك الذاتي.حيث تم اعتبار الإبلاغ عن واحد أو أقل من سبعة (NHS) أو ستة (HPFS) مخاوف معرفية كوظيفة معرفية سليمة. تم تقييم الوظيفة البدنية باستخدام استبيان الشكل القصير المكون من 36 عنصرًا.قسم فرعي عن القيود البدنية يتضمن عشرة أسئلة. المشاركون الذين أبلغوا عن عدم وجود قيود في صعود طابق واحد من السلالم، المشي لمسافة كتلة واحدة، المشي لأكثر من ميل، استخدام المكنسة الكهربائية، تحريك طاولة، المشي لعدة كتل، الاستحمام أو ارتداء الملابس، وكانوا قليلي أو غير محدودين في صعود عدة طوابق من السلالم، الجري، الرفع، الانحناء، الركوع، والانحناء ورفع حمل البقالة، اعتُبروا كأن لديهم وظيفة بدنية سليمة. تم تقييم الصحة النفسية باستخدام مقياس الاكتئاب لدى المسنين المكون من 15 عنصرًا، والذي يتراوح من 0 إلى 15، حيث يشير انخفاض الدرجة إلى عدد أقل من أعراض الاكتئاب.تم اعتبار الإبلاغ عن 1 أو أقل من أعراض الاكتئاب (القيمة المتوسطة لكلتا المجموعتين) كدليل على صحة نفسية سليمة. تم اختيار 11 مرضًا مزمنًا رئيسيًا لأنها الأسباب الرئيسية لـ المعدل الوفيات في الولايات المتحدةأو تعتبر شديدة الإعاقة. كما تم تحديدها في البداية وعلى مدار المتابعات. تم الإبلاغ عن التشخيصات السريرية للأمراض المزمنة الرئيسية من قبل المشاركين أو الأقارب للمتوفين، ثم تم التأكد منها من قبل طبيب من خلال السجلات الطبية، تقارير علم الأمراض أو استفسارات استبيانات إضافية، والتي تعتبر ذات مصداقية عالية في هذه المجموعات.في NHS، تم تقييم الوظيفة الإدراكية في عام 2014؛ وتم تقييم وجود الأمراض المزمنة، والوظيفة البدنية، والصحة النفسية في عام 2016. في HPFS، تم تقييم جميع المجالات في عام 2016.
تقييم المتغيرات المشتركة
كل عامين، أكمل المشاركون استبيانًا يستفسر عن وزن الجسم، الأنساب، حالة التدخين، النشاط البدني، استخدام الفيتامينات المتعددة، التاريخ العائلي للأمراض المزمنة، بما في ذلك احتشاء عضلة القلب، السكري من النوع 2، السرطان والخرف، حالة ما بعد انقطاع الطمث واستخدام الهرمونات لدى النساء، الحالة الزوجية، العيش بمفردهم وتاريخ الاكتئاب (استنادًا إلى استخدام أدوية مضادة للاكتئاب والتقرير الذاتي عن الاكتئاب). الاستبيانات متاحة على الإنترنت على https:// nurseshealthstudy.org/participants/questionnaires لدراسة NHS وعلى https://www.hsph.harvard.edu/hpfs/hpfs-questionnaires/ لدراسة HPFS. تم حساب مؤشر كتلة الجسم من خلال قسمة الوزن (كجم) على الطول ( ). تم حساب الحالة الاجتماعية الاقتصادية كدرجة مركبة باستخدام عنوان المشاركين الجغرافي، مع دمج دخل الأسرة من التعداد الأمريكي، قيمة المنزل، درجة الكلية، الأنساب، وحدات السكن المشغولة والبطالة، وما إذا كانت الأسر تتلقى فوائد أو توزيعات .
التحليل الإحصائي
تم حساب مدة المتابعة من التاريخ الذي تم فيه إرجاع أول استبيان غذائي حتى تاريخ وفاة المشارك أو تاريخ التقييم للشيخوخة الصحية في عام 2016، أيهما حدث أولاً. استخدم التحليل الرئيسي متوسط درجات نمط النظام الغذائي المتاحة بين عامي 1986 و2010 كتعرض لالتقاط المدخول طويل الأمد والسماح بفترة تأخير مدتها 6 سنوات بين التعرضات والنتائج. تم استخدام الطريقة المتبقية لضبط درجات نمط النظام الغذائي لإجمالي المدخول من الطاقة، بما في ذلك الطاقة من الكحول ، وتم حساب الكوانتيلات. تم استبدال القيم المفقودة للمتغيرات المرافقة بالقيمة المتوسطة الخاصة بالكوهو. نظرًا لأن النتائج ثنائية وتقاس في نقطة زمنية واحدة، تم استخدام نماذج الانحدار اللوجستي لتقدير ORs و 95% CIs للشيخوخة الصحية ومجالاتها الفردية وفقًا لكوانتيلات درجات نمط النظام الغذائي المعدلة للطاقة، مع العمر عند خط الأساس في عام 1986 كمتغير مرافق (نموذج أساسي). تم ضبط النموذج المعدل متعدد المتغيرات بشكل إضافي لتاريخ الأنساب المبلغ عنه عند خط الأساس (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، SES (درجة مركبة) والحالة الزوجية (نعم/لا)، استخدام الفيتامينات المتعددة (نعم/لا)، العيش بمفردهم (نعم/لا)، التاريخ العائلي للخرف (نعم/لا)، احتشاء عضلة القلب، السرطان، والسكري (نعم/لا)، والتاريخ الطبي للاكتئاب (نعم/لا)، السكري وأمراض القلب والأوعية الدموية (نعم/لا)، حالة التدخين في عام 2010 (لم يدخن أبدًا، مدخن سابق، مدخن حالي: 1-14 سيجارة في اليوم، 15-24 سيجارة في اليوم و سيجارة في اليوم)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام الهرمونات بعد انقطاع الطمث (لا، سابق، أو استخدام هرمونات حالية؛ للنساء فقط)، ومتوسط (1986-2010) BMI ( )، النشاط البدني (MET-h أسبوع ) ومدخول الكحول (غرام في اليوم) لدراسة DASH و hPDI و PHDI. تشير قيمة OR فوق 1 إلى احتمال أعلى للشيخوخة الصحية. تم أيضًا فحص الارتباطات باستخدام الأنماط كمتغيرات مستمرة، موحدة وفقًا لزيادتها من النسبة المئوية العاشرة إلى التسعين. تم إجراء التحليلات في كل مجموعة وفي المجموعات المجمعة. تم ضبط التحليلات في المجموعات المجمعة بشكل إضافي لمجموعة (جنس). تم حساب المخاطر المطلقة في كلا الكوانتيلين باستخدام نسبة الأشخاص الذين يتمتعون بصحة جيدة في Q1 و OR المعدل متعدد المتغيرات مقارنةً بـ Q5 مقابل Q1. تم حساب قيم E والحد الأدنى أو الأقصى لـ ORs لتقييم التأثير المحتمل للاختلاط غير المقاس على الارتباطات الملاحظة. تشير قيمة E الأعلى إلى دليل أقوى على أن الاختلاط غير المقاس سيكون مطلوبًا لشرح الارتباط الملاحظ بالكامل. تم إجراء تحليلات فرعية محددة مسبقًا وفقًا لمجموعة (جنس)، BMI (<25 مقابل )، النشاط البدني (أعلى/أقل من الوسيط)، التدخين (نعم/لا)، SES (أعلى/أقل من الوسيط) والأنساب (أوروبي/غير أوروبي). تم تقييم التفاعلات الفرعية المحتملة باستخدام نماذج التفاعل، بما في ذلك حاصل ضرب المجموعة الفرعية والتعرض. كتحليلات ثانوية، تم تقييم ارتباط درجات نمط النظام الغذائي بالشيخوخة الصحية باستخدام حد عمري يبلغ 75 عامًا، وارتباط استهلاك UPF بالشيخوخة الصحية (>70 عامًا). كتحليل حساسية، قمنا بتطبيق أوزان خطية على درجات نمط النظام الغذائي عبر سبع نقاط زمنية، تتراوح من 1986 إلى 2010، مع تعيين أعلى وزن للسنة الأقرب إلى تقييم الشيخوخة الصحية (2010) وأدنى وزن لعام 1986.
تم ضبط المدخول في مجموعات الطعام الفردية والمغذيات التي تعكس درجات نمط النظام الغذائي أيضًا وفقًا للطاقة ومعيارها وفقًا لزيادتها من النسبة المئوية العاشرة إلى التسعين. تم فحص ارتباطات المدخول من مجموعات الطعام والمغذيات المعدلة للطاقة مع الشيخوخة الصحية ومجالاتها باستخدام الانحدارات اللوجستية، مع الأخذ في الاعتبار المتغيرات المرافقة الموصوفة في النموذج المعدل متعدد المتغيرات. نظرًا لأن جميع العوامل الغذائية موجودة أيضًا في درجات النمط، لم يتم ضبط النماذج لأي مقياس لجودة النظام الغذائي.تم تصحيح القيم لـ FDR باستخدام طريقة بنجاميني-هوشبرغ؛ وتم اعتبار FDR المصحح دلالة إحصائية.
تم إجراء التحليلات باستخدام SAS v.9.4 (معهد SAS) و R v.4.2.0. كانت الاختبارات الإحصائية ثنائية الجانب و اعتبرت دلالة إحصائية.
ملخص التقرير
معلومات إضافية حول تصميم البحث متاحة في ملخص تقرير Nature Portfolio المرتبط بهذه المقالة.
توفر البيانات
نظرًا لسرية المشاركين واهتمامات الخصوصية، تتوفر البيانات فقط عند الطلب الكتابي. وفقًا لإجراءات الوصول المنضبط القياسية، ستتم مراجعة الطلبات لاستخدام موارد NHS و HPFS من قبل لجنة المتعاونين الخارجيين لدينا لأغراض علمية، وتقييم ملاءمة البيانات للمنهجية المقترحة والتحقق من أن الاستخدام المقترح يتماشى مع إرشادات إطار الأخلاقيات والحوكمة والموافقة التي قدمها المشاركون. يمكن للباحثين توقع استجابات أولية خلال 4 أسابيع من تقديم الطلب. تتوفر معلومات إضافية، بما في ذلك إجراءات الحصول على البيانات والوصول إليها من NHS و HPSF، على https://www.nurseshealthstudy.org/researchers (nhsaccess@channing.harvard.edu) و https://hsph.harvard.edu/research/health-professionals/resources/ للمتعاونين الخارجيين/. قواعد بيانات تكوين الأغذية التابعة لوزارة الزراعة الأمريكية وجامعة هارفارد متاحة للجمهور على https://www.fns. usda.gov/usda-fis/usda-foods-database و https://hsph.harvard. edu/department/nutrition/nutrition-questionnaire-service-center /#nutrient-data.
توفر الشيفرة
الشيفرة التحليلية متاحة للجمهور عبر GitHub (https://github. com/DrTessier/diets_healthyaging/).
References
Bao, Y. et al. Origin, methods, and evolution of the three Nurses’ Health Studies. Am. J. Public Health 106, 1573-1581 (2016).
Rimm, E. B. et al. Prospective study of alcohol consumption and risk of coronary disease in men. Lancet 338, 464-468 (1991).
Colditz, G. A. et al. Validation of questionnaire information on risk factors and disease outcomes in a prospective cohort study of women. Am. J. Epidemiol. 123, 894-900 (1986).
Rimm, E. B. et al. Validity of self-reported waist and hip circumferences in men and women. Epidemiology 1, 466-473 (1990).
Wolf, A. M. et al. Reproducibility and validity of a self-administered physical activity questionnaire. Int. J. Epidemiol. 23, 991-999 (1994).
Gu, X. et al. Validity and reproducibility of a semiquantitative food frequency questionnaire for measuring intakes of foods and food groups. Am. J. Epidemiol. 193, 170-179 (2024).
Yuan, C. et al. Relative validity of nutrient intakes assessed by questionnaire, 24 -hour recalls, and diet records as compared with urinary recovery and plasma concentration biomarkers: findings for women. Am. J. Epidemiol. 187, 1051-1063 (2018).
Yue, Y. et al. Reproducibility and validity of diet quality scores derived from food-frequency questionnaires. Am. J. Clin. Nutr. 115, 843-853 (2022).
Berendsen, A. M. et al. Association of long-term adherence to the MIND diet with cognitive function and cognitive decline in American women. J. Nutr. Health Aging 22, 222-229 (2018).
Shan, Z. et al. Healthy eating patterns and risk of total and cause-specific mortality. JAMA Intern. Med. 183, 142-153 (2023).
Fung, T. T. et al. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 168, 713-720 (2008).
Tabung, F. K. et al. An empirical dietary inflammatory pattern score enhances prediction of circulating inflammatory biomarkers in adults. J. Nutr. 147, 1567-1577 (2017).
Tabung, F. K. et al. Development and validation of empirical indices to assess the insulinaemic potential of diet and lifestyle. Br. J. Nutr. 116, 1787-1798 (2016).
Chiuve, S. E. et al. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 142, 1009-1018 (2012).
Satija, A. & Hu, F. B. Plant-based diets and cardiovascular health. Trends Cardiovasc. Med. 28, 437-441 (2018).
Willett, W. et al. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 393, 447-492 (2019).
Tabung, F. K. et al. Development and validation of an empirical dietary inflammatory index. J. Nutr. 146, 1560-1570 (2016).
Khandpur, N. et al. Categorising ultra-processed foods in large-scale cohort studies: evidence from the Nurses’ Health Studies, the Health Professionals Follow-up Study, and the Growing Up Today Study. J. Nutr. Sci. 10, e77-e91 (2021).
Rowe, J. W. & Kahn, R. L. Human aging: usual and successful. Science 237, 143-149 (1987).
Sun, Q. et al. Alcohol consumption at midlife and successful ageing in women: a prospective cohort analysis in the nurses’ health study. PLoS Med. 8, e1001090-e1001099 (2011).
Shi, H. et al. Sleep duration and snoring at midlife in relation to healthy aging in women 70 years of age or older. Nat. Sci. Sleep 13, 411-422 (2021).
Shi, H., Huang, T., Schernhammer, E. S., Sun, Q. & Wang, M. Rotating night shift work and healthy aging after 24 years of follow-up in the Nurses’ Health Study. JAMA Netw. Open 5, e2210450-e2210464 (2022).
Ardisson Korat, A. V. et al. Dietary protein intake in midlife in relation to healthy aging—results from the prospective Nurses’ Health Study cohort. Am. J. Clin. Nutr. 119, 271-282 (2024).
Molinuevo, J. L. et al. Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement. 13, 296-311 (2017).
Ware, J. E. & Sherbourne, C. D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 30, 473-483 (1992).
de Craen, A. J. M., Heeren, T. J. & Gussekloo, J. Accuracy of the 15 -item geriatric depression scale (GDS-15) in a community sample of the oldest old. Int. J. Geriatr. Psychiatry 18, 63-66 (2003).
Xu, J., Murphy, S. L., Kochanek, K. D. & Arias, E. Mortality in the United States, 2021. NCHS Data Brief www.cdc.gov/nchs/products/ databriefs/db456.htm (US Department of Health and Human Services, CDC & National Center for Health Statistics, 2022).
Sun, Q. et al. Physical activity at midlife in relation to successful survival in women at age 70 years or older. Arch. Intern. Med. 170, 194-201 (2010).
DeVille, N. V. et al. Neighborhood socioeconomic status and mortality in the Nurses’ Health Study (NHS) and the Nurses’ Health Study II (NHSII). Environ. Epidemiol. 7, e235-e241 (2022).
Willett, W. & Stampfer, M. J. Total energy intake: implications for epidemiologic analyses. Am. J. Epidemiol. 124, 17-27 (1986).
الشكر والتقدير
تحظى NHS و HPFS بدعم من منح من المعاهد الوطنية للصحة (الأرقام: UM1 CA186107، P01 CA87969، RO1 HL034594، R01 HL088521، U01 CA167552 و R01 HL35464). المحتوى هو مسؤولية المؤلفين فقط ولا يمثل بالضرورة الآراء الرسمية للمعاهد الوطنية للصحة. تم دعم A.-J.T. من خلال منحة زمالة ما بعد الدكتوراه من معاهد الصحة الكندية. تم دعم A.A.K. من خلال اتفاقية تعاونية مع وزارة الزراعة الأمريكية رقم 58-8050-3-003 ومركز العلوم لترقية العلوم الانتقالية (رقم 1K12TROO4384). تم دعم J.L. من قبل المعهد الوطني للسكري وأمراض الجهاز الهضمي والكلى (الأرقام: ROODK122128 و RO1AG087356). تم دعم M.G.-F. من خلال منحة مؤسسة نوفو نورديسك رقم NNF23SA0084103. لم يكن للممولين أي دور في تصميم وإجراء الدراسة، جمع البيانات، إدارتها، تحليلها وتفسيرها، إعدادها، مراجعتها أو الموافقة على المخطوطة، وقرار تقديم المخطوطة للنشر.
مساهمات المؤلفين
كان لدى أ.-ج.ت. و م.ج.-ف. وصول كامل إلى جميع بيانات الدراسة ويتحملان مسؤولية سلامة البيانات ودقة تحليل البيانات. صمم أ.-ج.ت. و م.ج.-ف. و ف.ب.هـ. البحث. أجرى أ.-ج.ت. التحليلات، وأعد الجداول والأشكال، وكتب المخطوطة. ساهم جميع المؤلفين في تفسير النتائج والمراجعة النقدية للمخطوطة من حيث المحتوى الفكري الهام. وافق جميع المؤلفين على النسخة النهائية من المخطوطة. يؤكد المؤلف المراسل أن جميع المؤلفين المدرجين يستوفون معايير التأليف وأنه لم يتم استبعاد أي شخص آخر يستوفي المعايير.
المصالح المتنافسة
M.G.-F. هو الباحث الرئيسي في منحة ممولة من المجلس الدولي للمكسرات. المؤلفون الآخرون يعلنون عدم وجود مصالح متنافسة.
يجب توجيه المراسلات والطلبات للحصول على المواد إلى آن-جولي تيييه، فرانك ب. هو أو مارتا غواسخ-فير.
معلومات مراجعة الأقران تشكر مجلة ناتشر ميديسين إيريني تريشيا والمراجعين الآخرين المجهولين على مساهمتهم في مراجعة هذا العمل. المحرر الرئيسي: مايكل باسان، بالتعاون مع فريق ناتشر ميديسين.
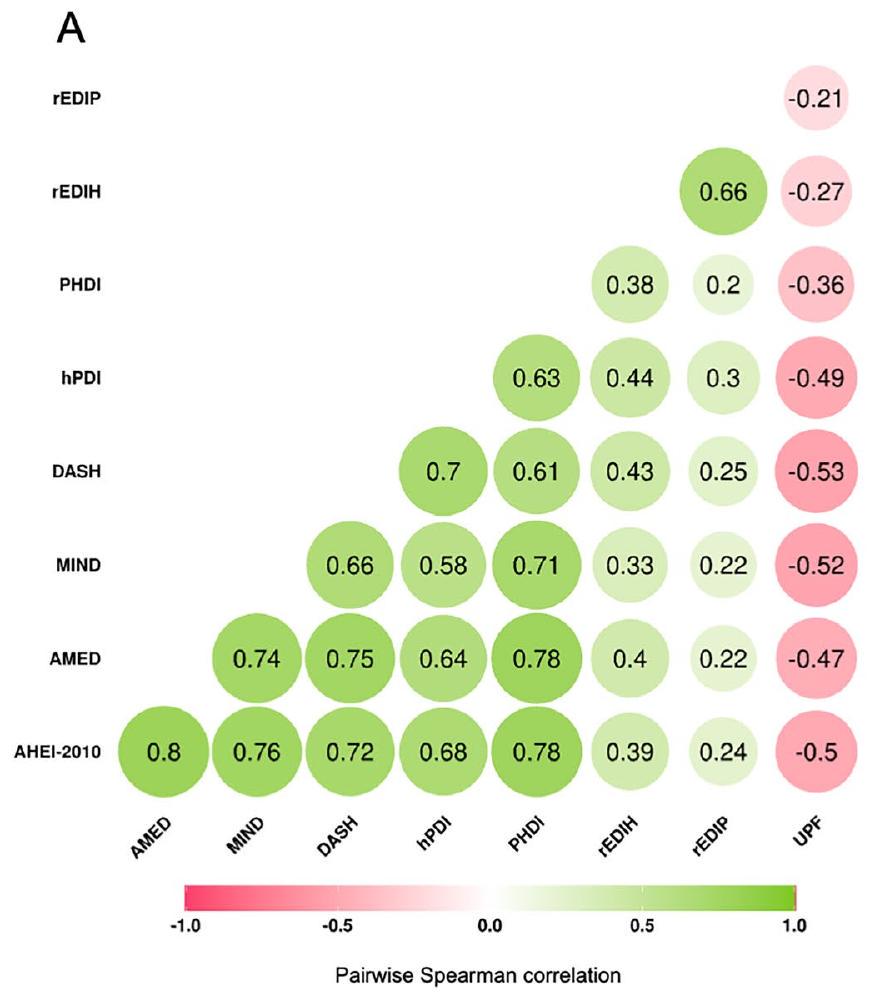
الشكل البياني الممتد 1| ارتباطات سبيرمان الزوجية بين درجات نمط النظام الغذائي المعدلة للطاقة (1986-2010). أ. تم تطبيق ارتباطات سبيرمان الزوجية في مجموعة البيانات الرئيسية المجمعة. ). قيم P لجميع الارتباطات ثنائية الجانب وأقل من 0.0001 (غير معدلة للمقارنات المتعددة)؛ ب. تم تطبيق ارتباطات سبيرمان الزوجية في مجموعة البيانات المجمعة التي استبعدت المشاركين الذين لديهم بيانات UPF مفقودة ( ). قيم P لجميع الارتباطات ثنائية الجانب و (غير معدلة للمقارنات المتعددة). AHEI,
ب
مؤشر تناول الطعام الصحي البديل؛ AMED، مؤشر النظام الغذائي المتوسطي البديل؛ DASH، أساليب غذائية لوقف ارتفاع ضغط الدم؛ MIND، تدخل النظام الغذائي المتوسطي-DASH لتأخير الأمراض العصبية؛ hPDI، مؤشر النظام الغذائي النباتي الصحي؛ PHDI، مؤشر النظام الغذائي لصحة الكوكب؛ EDIH، المؤشر الغذائي التجريبي لفرط الأنسولين؛ EDIP، نمط الالتهاب الغذائي التجريبي. تعتبر rEDIH و rEDIP درجات معكوسة للسماح بالمقارنة مع درجات غذائية أخرى.
البيانات الموسعة الجدول 1 | الخصائص المعيارية للعمر لسكان الدراسة في أدنى وأعلى خمسيات درجات نمط النظام الغذائي المعدلة للطاقة في NHS بين عامي 1986 و2010
كوانتيل
الربع الأول
Q5
الربع الأول
Q5
الربع الأول
Q5
الربع الأول
Q5
١٤,٠١٨
١٤,٠١٨
١٤٠١٨
١٤٠١٨
١٤,٠١٨
١٤,٠١٨
١٤,٠١٨
١٤,٠١٨
درجة النظام الغذائي
أهي-2010
أَمِيد
داش
عقل
درجة معدلة حسب الطاقة
٤١.٥ (٣.٩)
67.9 (4.7)
٢.٤ (٠.٦)
6.3 (0.6)
18.3 (1.8)
٢٩.٣ (١.٧)
6.0 (0.6)
9.5 (0.6)
العمر، عند البداية
53.0 (7.3)
٥٢.٢ (٧.١)
٥٢.٣ (٧.٤)
53.2 (7.0)
٥١.٢ (٧.٢)
٥٤.٤ (٧.٠)
٥٤.٠ (٧.٢)
52.0 (7.1)
الأنساب
أوروبي
95.0
93.5
95.1
93.8
94.3
94.2
95.2
93.2
آسيوي
0.3
1.3
0.4
1.1
0.7
0.9
0.3
1.4
أفريقي
1.0
1.6
0.8
1.7
1.4
1.4
0.8
2.0
آخر
3.7
٣.٥
3.8
3.4
3.6
3.6
3.7
٣.٥
درجة SES، عند الخط الأساسي
-0.9 (3.3)
1.0 (4.1)
-0.6 (3.4)
0.7 (4)
-0.6 (3.5)
0.6 (3.9)
-0.9 (3.3)
0.9 (4)
وحيد، دائمًا
30.7
٣٢.٦
٣١.٧
31.4
٢٩.٨
٣٥.٠
٣٤.٤
٢٩.٨
تاريخ الاكتئاب، نعم
21.4
18.2
٢٢.٣
17.4
21.0
17.9
٢٢.١
17.8
تاريخ السرطان، نعم
٤.٣
٤.٠
٤.٠
٤.٣
3.7
٤.٣
٤.٣
٤.٠
تاريخ مرض السكري، نعم
3.0
2.3
2.5
٢.٤
1.9
3.1
2.9
2.5
تاريخ أمراض القلب والأوعية الدموية، نعم
٤.٨
3.5
٤.٢
3.8
3.8
٤.٤
٤.٨
3.7
تاريخ عائلي من الخرف، نعم
15.5
19.8
16.2
18.4
16.4
17.9
15.9
18.6
استخدام متعدد الفيتامينات، في أي وقت
81.1
92.8
82.1
91.9
81.0
92.0
82.6
91.7
مؤشر كتلة الجسم، كجم/م²
٢٦.٦ (٥.٥)
٢٥.٣ (٤.٤)
٢٦.٧ (٥.٥)
٢٥.٣ (٤.٤)
٢٦.٥ (٥.٤)
٢٥.٣ (٤.٦)
٢٦.٦ (٥.٥)
٢٥.٤ (٤.٥)
مدخن أبداً، %
67.5
52.8
62.0
٥٨.٤
٥٩.٠
63.1
65.4
٥٧.١
النشاط البدني، مهام MET/الأسبوع
0.9 (1.4)
2.7 (2.7)
0.9 (1.5)
2.6 (2.7)
0.9 (1.5)
٢.٦ (٢.٧)
0.9 (1.5)
2.7 (2.7)
تناول الكحول، غرام/يوم
5.1 (11.1)
6.3 (7.1)
٥.٣ (١٠.٩)
5.9 (7)
6.3 (10.7)
٤.٥ (٧)
4 (8.7)
6.4 (8.1)
مدخول الطاقة، كيلو كالوري
1726 (456)
1725 (449)
1714 (485)
1723 (396)
١٧٢٨ (٤٧٢)
1737 (420)
1724 (484)
1722 (433)
درجة النظام الغذائي
hPDI
مؤشر التنمية البشرية المعدل
ريد
ريدب
درجة معدلة للطاقة
٤٧.٠ (٢.٤)
62.5 (2.8)
66.4 (4.6)
92.9 (5.0)
-0.5 (0.1)
0.0 (0.1)
-0.3 (0.1)
0.4 (0.2)
العمر، عند الأساس النسب
52.2 (7.3)
53.4 (7.1)
٥٣.١ (٧.٤)
52.2 (7.0)
٥١.٤ (٧.٣)
٥٣.١ (٧.١)
٥٢.٦ (٧.٣)
52.0 (7.1)
أوروبي
95.3
93.3
95.1
92.8
94.5
95.3
92.6
96.3
آسيوي
0.4
1.3
0.3
1.8
0.5
0.7
1.3
0.3
أفريقي
1.1
1.7
0.8
1.9
1.6
0.6
2.5
0.3
آخر
٣.٣
3.7
3.7
3.6
3.4
3.4
3.7
3.1
درجة SES، عند الخط الأساسي
-0.3 (3.5)
0.4 (4)
-0.6 (3.4)
0.8 (4)
-0.6 (3.4)
0.8 (4)
-0.6 (3.5)
0.7 (3.9)
وحيد، دائماً
٣١.٧
٣٢.٣
31.9
31.3
٢٨.٨
٣٣.١
٢٩.٧
31.3
تاريخ الاكتئاب، نعم
19.9
18.0
21.5
18.1
٢٣.٠
17.5
٢٣.٣
17.5
تاريخ السرطان، نعم
٤.٠
٤.٣
٤.٥
3.8
٤.٠
٤.١
٤.٣
٤.٠
تاريخ مرض السكري، نعم
1.9
3.6
2.8
2.3
٤.٨
1.2
٥.١
1.2
تاريخ مرض القلب والأوعية الدموية، نعم
٤.٠
٤.٣
٤.٧
3.4
5.1
3.2
5.8
2.6
تاريخ عائلي للخرف، نعم
17.1
17.8
15.0
19.6
15.9
19.3
15.9
18.9
استخدام متعدد الفيتامينات، في أي وقت
٨٣.٧
90.6
81.2
92.9
82.9
90.6
٨٣.٧
89.5
مؤشر كتلة الجسم، كجم/م²
٢٦.٧ (٥.٤)
٢٥.٣ (٤.٦)
٢٦.٤ (٥.٤)
٢٥.٣ (٤.٥)
٢٨.٣ (٥.٩)
٢٤.٢ (٣.٨)
٢٨.١ (٥.٨)
٢٤.٥ (٤)
مدخن غير مدخن، %
62.6
٥٩.٣
66.5
53.7
65.8
53.2
67.4
٥١.٢
النشاط البدني، مهام MET/الأسبوع
1.0 (1.6)
2.5 (2.8)
0.9 (1.6)
٢.٦ (٢.٧)
1.1 (1.7)
٢.٤ (٢.٦)
1.2 (1.8)
2.2 (2.5)
تناول الكحول، غرام/يوم
5 (8.7)
5.7 (9)
٤.٧ (٩.١)
٦.٢ (٨.٦)
3.5 (7.5)
10.4 (11.7)
2.8 (6.7)
11.5 (12.2)
مدخول الطاقة، كيلو كالوري
1731 (430)
1722 (464)
1714 (485)
1716 (434)
1781 (490)
1806 (434)
1769 (481)
١٧٦٩ (٤٤٩)
البيانات الموسعة الجدول 2 | الخصائص المعيارية للعمر لسكان الدراسة في أدنى وأعلى خمسيات درجات نمط النظام الغذائي المعدلة للطاقة في دراسة HPFS بين عامي 1986 و2010
كوانتيل
الربع الأول
Q5
الربع الأول
Q5
الربع الأول
Q5
الربع الأول
Q5
6,984
6,984
٦,٩٨٤
٦,٩٨٤
6,984
6,984
6,984
6,984
درجة النظام الغذائي
أهي-2010
أَمِيد
داش
عقل
درجة معدلة حسب الطاقة
٤١.٩ (٤.٤)
69.9 (4.5)
1.9 (0.6)
6.2 (0.6)
١٨.١ (١.٩)
30.1 (1.8)
6.0 (0.6)
9.8 (0.6)
العمر، عند البداية
٥٤.٥ (٨.٧)
٥٤.٥ (٨.٥)
٥٣.٢ (٨.٧)
٥٥.٤ (٨.٤)
٥٢.٣ (٨.٥)
٥٦.٧ (٨.٤)
٥٥.٣ (٨.٧)
53.8 (8.5)
الأنساب
أوروبي
95.7
95.1
96.3
94.8
94.9
95.8
96.1
94.5
آسيوي
1.1
1.5
1.0
1.6
2.0
1.0
1.1
1.9
أفريقي
1.2
1.0
0.9
1.2
1.3
0.9
0.7
1.1
آخر
2.0
٢.٤
1.7
٢.٤
1.8
2.3
2.1
2.5
درجة SES، في البداية
-0.7 (3.4)
0.7 (3.9)
-0.6 (3.4)
0.6 (3.9)
-0.6 (3.5)
0.5 (3.8)
-0.8 (3.4)
0.7 (3.8)
وحيد، إلى الأبد
٢٠.٧
٢٠.٣
21.7
18.9
٢٢.٠
18.9
21.6
18.9
تاريخ الاكتئاب، نعم
٤.١
3.4
٤.٥
3.1
٤.٥
2.8
٤.١
3.2
تاريخ السرطان، نعم
٤.٨
3.7
٤.٢
٤.٣
٤.١
٤.١
٤.٥
3.4
تاريخ مرض السكري، نعم
3.9
3.4
2.9
3.7
1.8
٥.٤
3.8
3.4
تاريخ مرض القلب والأوعية الدموية، نعم
6.3
8.1
٥.٣
9.8
٤.٩
10.6
6.2
8.9
تاريخ عائلي من الخرف، نعم
3.3
3.3
٣.٥
3.3
3.4
٣.٣
3.0
3.6
استخدام متعدد الفيتامينات، في أي وقت
72.4
٨٨.٧
75.4
86.3
74.3
85.4
73.0
٨٨.٢
مؤشر كتلة الجسم،
٢٦.٤ (٣.٩)
٢٥.٢ (٣.٣)
٢٦.٥ (٣.٩)
٢٥.١ (٣.٣)
٢٦.٣ (٣.٨)
٢٥.١ (٣.٤)
٢٦.٤ (٤)
٢٥.٢ (٣.٢)
مدخن أبداً، %
80.9
71.3
74.1
76.0
72.4
80.0
78.9
72.7
النشاط البدني، مهام MET/الأسبوع
2.1 (2.9)
٥.١ (٤.٤)
٢.٣ (٣.١)
٤.٩ (٤.٤)
2.3 (3)
٤.٨ (٤.٥)
2.2 (3.2)
٥.١ (٤.٤)
تناول الكحول، غرام/يوم
12.9 (18.6)
10.7 (9.6)
12.9 (17.6)
10.9 (10.4)
١٣.٧ (١٦.٥)
9.1 (11.4)
10.7 (15.1)
11.6 (12.2)
مدخول الطاقة، كيلو كالوري
1987 (528)
1990 (511)
2013 (554)
2012 (485)
2006 (543)
2008 (489)
1999 (555)
1994 (502)
درجة النظام الغذائي
hPDI
مؤشر التنمية البشرية المعدل
ريدِه
ريدب
درجة معدلة للطاقة
٤٦.٨ (٢.٥)
63.4 (3.1)
63.0 (5.5)
94.4 (5.2)
-0.7 (0.2)
-0.1 (0.1)
-0.4 (0.2)
0.4 (0.2)
العمر، عند البداية
٥٣.١ (٨.٧)
٥٥.٦ (٨.٤)
54.0 (8.8)
٥٤.٤ (٨.٣)
53.3 (8.8)
٥٤.٦ (٨.٥)
55.0 (8.7)
53.1 (8.4)
الأنساب
أوروبي
95.6
94.8
95.5
94.6
95.0
٩٦.١
93.0
97.0
آسيوي
1.2
1.8
1.3
2.1
1.3
1.1
2.5
0.6
أفريقي
1.0
1.2
1.2
1.0
1.6
0.7
2.1
0.4
آخر
2.2
2.3
2.0
2.3
2.0
2.2
٢.٤
2.0
درجة SES، عند الخط الأساسي
-0.1 (3.6)
0.1 (3.8)
-0.6 (3.5)
0.6 (3.8)
-0.8 (3.4)
0.7 (3.9)
-0.4 (3.6)
0.2 (3.7)
وحيد، إلى الأبد
٢٠.١
19.3
٢٠.٦
19.7
19.8
٢٠.٤
٢٠.١
٢٠.٧
تاريخ الاكتئاب، نعم
٤.٣
3.3
٤.٠
٣.٤
٤.٥
3.4
٤.٣
3.4
تاريخ السرطان، نعم
٤.٤
٤.١
٤.١
3.8
٤.٣
3.7
٤.٤
3.7
تاريخ مرض السكري، نعم
1.9
5.1
3.8
٣.٥
٥.٩
1.7
٥.٧
2.0
تاريخ مرض القلب والأوعية الدموية، نعم
5.0
9.5
5.8
8.3
٦.٧
6.8
8.4
5.2
تاريخ عائلي من الخرف، نعم
3.2
3.3
3.1
3.3
3.0
٣.٥
3.2
3.1
استخدام متعدد الفيتامينات، في أي وقت
76.0
85.1
73.0
٨٨.٥
٧٤.٩
85.7
77.6
٨٣.١
مؤشر كتلة الجسم
٢٦.٢ (٣.٧)
25.4 (3.6)
٢٦.٤ (٤)
٢٥.١ (٣.١)
٢٧.١ (٤.٢)
٢٤.٩ (٣.١)
٢٦.٨ (٤.١)
25.5 (3.2)
مدخن أبداً، %
75.9
74.1
78.5
70.2
78.2
69.9
79.3
67.9
النشاط البدني، مهام MET/الأسبوع
٢.٦ (٣.٣)
٤.٧ (٤.٥)
٢.٤ (٣.٣)
5 (4.4)
2.5 (3.4)
٤.٧ (٤.٣)
2.9 (3.7)
٤.١ (٤.١)
تناول الكحول، غرام/يوم
10.1 (12.6)
١٢.٣ (١٤.٥)
10.5 (14.6)
١٢.١ (١٣.١)
8.8 (12.5)
17.2 (16.3)
6.5 (10.7)
٢١.٤ (١٧.٣)
مدخول الطاقة، كيلو كالوري
2008 (502)
1999 (531)
1985 (592)
1982 (470)
٢٠٨٦ (٥٧٤)
2105 (510)
٢٠٦٨ (٥٧٢)
٢٠٦٢ (٥١٣)
البيانات الموسعة الجدول 3 | ارتباطات درجات نمط النظام الغذائي المتوسط (1986-2010) مع الشيخوخة الصحية ومجالاتها في المجموعات المجمعة
نتيجة
الشيخوخة الصحية
الشيخوخة الصحية
الإدراك السليم
وظيفة جسدية سليمة
صحة نفسية سليمة
لا مرض مزمن
عاش حتى 70 عامًا
درجة النظام الغذائي للحالات
نموذج
9,771 أو (95% فترة الثقة) (Q5 مقابل Q1)
9,771 أو (95% فترة الثقة) (مستمرة)
29,543 أو (95% فترة الثقة) (Q5 مقابل Q1)
27,842 أو (95%CI) (Q5 مقابل Q1)
27,842 أو (95% فترة الثقة) (Q5 مقابل Q1)
23,908 أو (95% فترة الثقة) (Q5 مقابل Q1)
39,769 أو (95%CI) (Q5 مقابل Q1)
أهي-2010
عمر
3.06 (2.84, 3.30)
2.71 (2.56، 2.87)
2.46 (2.34, 2.57)
4.03 (3.82، 4.26)
3.27 (3.10, 3.44)
2.57 (2.44، 2.71)
3.38 (3.21, 3.55)
MV
1.86 (1.71، 2.01)
1.71 (1.60، 1.82)
1.62 (1.54، 1.71)
2.30 (2.16، 2.44)
2.03 (1.92, 2.15)
1.64 (1.54، 1.74)
2.14 (2.02, 2.27)
أَمِيد
عمر
2.67 (2.48، 2.87)
2.43 (2.29، 2.58)
1.82 (1.74، 1.91)
2.91 (2.76، 3.07)
2.50 (2.37، 2.63)
2.06 (1.96, 2.17)
2.16 (2.05, 2.26)
MV
1.70 (1.57، 1.84)
1.59 (1.49، 1.70)
1.35 (1.28، 1.42)
1.75 (1.65, 1.86)
1.67 (1.58, 1.77)
1.43 (1.35، 1.52)
1.53 (1.44، 1.62)
داش
عمر
2.62 (2.43، 2.81)
2.48 (2.34, 2.64)
1.85 (1.77, 1.94)
2.79 (2.64, 2.94)
2.42 (2.30، 2.55)
2.01 (1.91, 2.12)
2.10 (1.99, 2.20)
MV
1.69 (1.56, 1.83)
1.65 (1.54, 1.76)
1.40 (1.33، 1.48)
1.73 (1.63، 1.84)
1.64 (1.55، 1.74)
1.43 (1.35، 1.51)
1.50 (1.41، 1.59)
عقل
عمر
2.47 (2.29, 2.67)
2.36 (2.22, 2.50)
1.82 (1.74، 1.91)
2.93 (2.78, 3.09)
2.50 (2.37، 2.63)
1.91 (1.81، 2.01)
2.12 (2.02، 2.22)
MV
1.60 (1.47، 1.73)
1.57 (1.47، 1.68)
1.40 (1.33، 1.48)
1.82 (1.72، 1.94)
1.75 (1.65, 1.85)
1.35 (1.28، 1.43)
1.59 (1.50، 1.69)
hPDI
عمر
2.00 (1.87, 2.15)
1.88 (1.78، 1.99)
1.44 (1.38، 1.51)
2.18 (2.07, 2.29)
1.78 (1.69, 1.87)
1.64 (1.56, 1.72)
1.60 (1.52، 1.68)
MV
1.45 (1.35, 1.57)
1.40 (1.32، 1.49)
1.21 (1.15, 1.28)
1.56 (1.47، 1.65)
1.37 (1.30، 1.45)
1.32 (1.25، 1.40)
1.33 (1.26، 1.41)
مؤشر التنمية البشرية المعدل
عمر
2.75 (2.55, 2.96)
2.44 (2.31, 2.59)
2.45 (2.34, 2.56)
3.73 (3.54, 3.93)
3.01 (2.86، 3.17)
2.43 (2.31، 2.57)
3.35 (3.19, 3.52)
MV
1.68 (1.55، 1.82)
1.56 (1.47، 1.66)
1.65 (1.57, 1.74)
2.16 (2.04, 2.30)
1.89 (1.78, 2.00)
1.55 (1.47، 1.65)
2.17 (2.05, 2.30)
ريدِه
عمر
3.20 (2.96, 3.46)
2.60 (2.45، 2.76)
2.15 (2.05, 2.26)
3.89 (3.68, 4.11)
2.79 (2.64، 2.95)
2.89 (2.73, 3.06)
2.87 (2.72, 3.02)
MV
1.80 (1.64، 1.96)
1.53 (1.43، 1.63)
1.42 (1.34، 1.50)
1.78 (1.67, 1.90)
1.62 (1.52, 1.72)
1.75 (1.65, 1.87)
1.71 (1.61, 1.82)
ريدب
عمر
2.34 (2.17, 2.53)
1.84 (1.75، 1.94)
1.57 (1.50، 1.64)
2.45 (2.33, 2.58)
1.98 (1.88، 2.09)
2.20 (2.09, 2.32)
1.90 (1.81، 2.00)
MV
1.58 (1.45، 1.72)
1.29 (1.22, 1.37)
1.14 (1.09, 1.21)
1.38 (1.30، 1.46)
1.34 (1.27، 1.42)
1.52 (1.43، 1.61)
1.29 (1.22، 1.37)
حجم العينة منتم تعديل نماذج الانحدار اللوجستي المعدلة حسب العمر لعمر الأساس (1986) والفوج (الجنس). تم تعديل نماذج الانحدار اللوجستي المعدلة حسب المتغيرات المتعددة لعمر الأساس (1986)، الفوج (الجنس)، مؤشر كتلة الجسم (كجم/م²)، السلالة (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، حالة التدخين (لم يدخن أبدًا، مدخن سابق، مدخن حالي: 1-14 سيجارة في اليوم، 15-24 سيجارة في اليوم، وعدد السجائر في اليوم)، استهلاك الكحول (غرام/يوم)، النشاط البدني (ساعات مكافئة للتمثيل الغذائي/أسبوع)، استخدام الفيتامينات المتعددة (نعم/لا)، التاريخ العائلي لنوبة قلبية (نعم/لا)، التاريخ العائلي لمرض السكري من النوع 2، التاريخ العائلي للسرطان، التاريخ العائلي للخرف (نعم/لا)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام هرمونات انقطاع الطمث (لا، استخدام هرمونات سابق، أو حالي) (فقط للنساء)، الحالة الاجتماعية والاقتصادية عند البداية، الحالة الاجتماعية (نعم/لا)، العيش بمفرد (نعم/لا)، تاريخ الاكتئاب (نعم/لا). MV، متعدد المتغيرات؛ OR، نسبة الأرجحية؛ CI، فترة الثقة؛ AHEI، مؤشر النظام الغذائي الصحي البديل؛ AMED، مؤشر النظام الغذائي المتوسطي البديل؛ DASH، الأساليب الغذائية لوقف ارتفاع ضغط الدم؛ MIND، تدخل النظام الغذائي المتوسطي-DASH لتأخير الأمراض التنكسية؛ hPDI، مؤشر النظام الغذائي النباتي الصحي؛ PHDI، مؤشر النظام الغذائي لصحة الكوكب؛ EDIH، المؤشر الغذائي التجريبي لفرط الأنسولين؛ EDIP، النمط الغذائي الالتهابي التجريبي. EDIH وEDIP هما درجات معكوسة للسماح بالمقارنة مع درجات غذائية أخرى.
البيانات الموسعة الجدول 4 | المخاطر المطلقة للربع الأول والربع الخامس عبر جميع درجات أنماط النظام الغذائي
نمط غذائي
المخاطر المطلقة، %
الربع الأول
Q5
أهي
5.3 (5.4، 5.3)
9.9 (9.2، 10.7)
أَمِيد
6.1 (6.2، 6.1)
10.4 (9.7, 11.2)
داش
7.3 (7.4، 7.2)
12.4 (11.5, 13.2)
عقل
5.1 (5.2، 5.1)
8.2 (7.6، 8.8)
hPDI
7.7 (7.8، 7.7)
11.2 (10.5, 12.0)
مؤشر التنمية البشرية المعدل
5.6 (5.6، 5.5)
9.4 (8.7، 10.1)
ريد
5.3 (5.3، 5.2)
9.5 (8.7، 10.2)
ريدب
5.3 (5.4، 5.3)
8.4 (7.8، 9.1)
تم استخدام نسبة الأشخاص الذين يتقدمون في السن بصحة جيدة في الربع الأول ونسبة الأرجحية المعدلة متعددة المتغيرات لمقارنة الربع الخامس مقابل الربع الأول لحساب المخاطر المطلقة في كلا الربعين.
البيانات الموسعة الجدول 5 | ارتباطات درجات نمط النظام الغذائي المتوسط (1986-2010) مع الشيخوخة الصحية باستخدام حد عمري يبلغ 75 عامًا
نتيجة
الشيخوخة الصحية
الشيخوخة الصحية
حالات
الإجمالي 89,755
٥٤٤٥
٥٤٤٥
درجة النظام الغذائي
نموذج
OR (95%CI) (Q5 مقابل Q1)
OR (95%CI) (مستمر)
أهي-2010
عمر
٤.٣٦ (٣.٩٤، ٤.٨٣)
3.46 (3.21, 3.73)
MV
2.24 (2.01, 2.50)
1.91 (1.76، 2.08)
أَمِيد
عمر
3.25 (2.95, 3.58)
2.89 (2.67, 3.12)
MV
1.86 (1.67، 2.06)
1.71 (1.58، 1.86)
داش
عمر
3.16 (2.87, 3.48)
2.89 (2.68, 3.13)
MV
1.84 (1.66, 2.04)
1.77 (1.62، 1.92)
عقل
عمر
3.02 (2.73, 3.34)
٢.٧٤ (٢.٥٤، ٢.٩٦)
MV
1.78 (1.60، 1.98)
1.70 (1.56، 1.85)
hPDI
عمر
2.36 (2.15, 2.59)
2.18 (2.03, 2.34)
MV
1.61 (1.46، 1.77)
1.53 (1.42، 1.66)
مؤشر التنمية البشرية المعدل
عمر
3.70 (3.35, 4.09)
3.12 (2.90، 3.36)
MV
1.94 (1.74, 2.16)
1.77 (1.63، 1.91)
ريد
عمر
4.23 (3.79, 4.72)
3.17 (2.94, 3.41)
MV
2.03 (1.80، 2.30)
1.68 (1.54، 1.83)
ريدب
عمر
2.85 (2.57, 3.15)
2.04 (1.91, 2.17)
MV
1.68 (1.50، 1.88)
1.34 (1.24, 1.44)
حجم العينة منتم تعديل نماذج الانحدار اللوجستي المعدلة حسب العمر لعمر الأساس (1986) والفوج (الجنس). تم تعديل نماذج الانحدار اللوجستي المعدلة حسب المتغيرات المتعددة لعمر الأساس (1986)، الفوج (الجنس)، مؤشر كتلة الجسم (كجم/م²)، السلالة (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، حالة التدخين (لم يدخن أبدًا، مدخن سابق، مدخن حالي: 1-14 سيجارة في اليوم، 15-24 سيجارة في اليوم، وعدد السجائر في اليوم)، استهلاك الكحول (غرام/يوم)، النشاط البدني (ساعات مكافئة للتمثيل الغذائي/أسبوع)، استخدام الفيتامينات المتعددة (نعم/لا)، تاريخ العائلة في الإصابة بالنوبات القلبية (نعم/لا)، تاريخ العائلة في الإصابة بمرض السكري من النوع 2، تاريخ العائلة في الإصابة بالسرطان، تاريخ العائلة في الإصابة بالخرف (نعم/لا)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام هرمونات انقطاع الطمث (لا، استخدام هرمونات سابق، أو حالي) (فقط للنساء)، الحالة الاجتماعية والاقتصادية عند البداية، الحالة الزوجية (نعم/لا)، العيش بمفردك في أي وقت (نعم/لا)، تاريخ الاكتئاب (نعم/لا)، في المجموعات المجمعة. MV، متعدد المتغيرات؛ OR، نسبة الأرجحية؛ CI، فترة الثقة؛ AHEI، مؤشر التغذية الصحية البديلة؛ AMED، مؤشر النظام الغذائي المتوسطي البديل؛ DASH، أساليب غذائية لوقف ارتفاع ضغط الدم؛ MIND، تدخل النظام الغذائي المتوسطي-DASH لتأخير الأمراض التنكسية؛ hPDI، مؤشر النظام الغذائي النباتي الصحي؛ PHDI، مؤشر النظام الغذائي لصحة الكوكب؛ EDIH، المؤشر الغذائي التجريبي لفرط الأنسولين؛ EDIP، نمط الالتهاب الغذائي التجريبي. تعتبر درجات EDIH وEDIP درجات معكوسة للسماح بالمقارنة مع درجات غذائية أخرى.
البيانات الموسعة الجدول 6 | ارتباطات درجات نمط النظام الغذائي المتوسط المرجح (1986-2010) مع الشيخوخة الصحية
نتيجة
الشيخوخة الصحية
الشيخوخة الصحية
حالات
الإجمالي 105,015
9,771
9,771
درجة النظام الغذائي
نموذج
OR (95%CI) (Q5 مقابل Q1)
OR (95%CI) (مستمر)
أهي-2010
عمر
3.22 (2.92, 3.54)
2.87 (2.66, 3.09)
MV
1.97 (1.77, 2.19)
1.82 (1.67, 1.97)
أَمِيد
عمر
2.52 (2.30، 2.77)
2.34 (2.17, 2.53)
MV
1.63 (1.48، 1.81)
1.54 (1.42، 1.67)
داش
عمر
2.59 (2.36, 2.84)
2.41 (2.23, 2.60)
MV
1.67 (1.51، 1.85)
1.61 (1.48، 1.76)
عقل
عمر
2.42 (2.20، 2.67)
2.30 (2.13, 2.49)
MV
1.61 (1.45، 1.78)
1.56 (1.43، 1.69)
hPDI
عمر
1.94 (1.77، 2.12)
1.86 (1.73، 2.00)
MV
1.43 (1.30، 1.57)
1.41 (1.31, 1.52)
مؤشر التنمية البشرية المعدل
عمر
2.62 (2.38, 2.88)
2.41 (2.24، 2.60)
MV
1.64 (1.48، 1.81)
1.56 (1.44، 1.68)
ريد
عمر
3.06 (2.76, 3.38)
2.56 (2.37، 2.76)
MV
1.79 (1.60، 2.01)
1.57 (1.44، 1.70)
ريدب
عمر
2.28 (2.07, 2.52)
1.72 (1.61, 1.83)
MV
1.60 (1.43, 1.79)
1.26 (1.17, 1.35)
حجم العينة منتم تعديل نماذج الانحدار اللوجستي المعدلة حسب العمر لعمر الأساس (1986) والفوج (الجنس). تم تعديل نماذج الانحدار اللوجستي المعدلة حسب MV لعمر الأساس (1986)، الفوج (الجنس)، مؤشر كتلة الجسم (كجم/م²)، السلالة (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، حالة التدخين (لم يدخن أبدًا، مدخن سابق، مدخن حالي: 1-14 سيجارة في اليوم، 15-24 سيجارة في اليوم، وعدد السجائر في اليوم)، استهلاك الكحول (غرام/يوم)، النشاط البدني (ساعات مكافئة للتمثيل الغذائي/أسبوع)، استخدام الفيتامينات المتعددة (نعم/لا)، التاريخ العائلي لنوبة قلبية (نعم/لا)، التاريخ العائلي لمرض السكري من النوع 2، التاريخ العائلي للسرطان، التاريخ العائلي للخرف (نعم/لا)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام هرمونات انقطاع الطمث (لا، استخدام هرمونات سابق، أو حالي) (فقط للنساء)، الحالة الاجتماعية والاقتصادية في البداية، الحالة الزوجية (نعم/لا)، العيش بمفرد (نعم/لا)، تاريخ الاكتئاب (نعم/لا)، في المجموعات المجمعة. MV، متعددة المتغيرات؛ OR، نسبة الأرجحية؛ CI، فترة الثقة؛ AHEI، مؤشر النظام الغذائي الصحي البديل؛ AMED، مؤشر النظام الغذائي المتوسطي البديل؛ DASH، الأساليب الغذائية لوقف ارتفاع ضغط الدم؛ MIND، تدخل النظام الغذائي المتوسطي-DASH لتأخير الأمراض العصبية؛ hPDI، مؤشر النظام الغذائي النباتي الصحي؛ PHDI، مؤشر النظام الغذائي لصحة الكوكب؛ EDIH، المؤشر الغذائي التجريبي لفرط الأنسولين؛ EDIP، النمط الغذائي الالتهابي التجريبي. تعتبر EDIH وEDIP درجات معكوسة للسماح بالمقارنة مع درجات غذائية أخرى. تم تطبيق أوزان خطية كما يلي: 1986=1، 1990=2، 1994=3،.
البيانات الموسعة الجدول 7 | ارتباطات استهلاك الأغذية فائقة المعالجة المتوسطة (1986-2010) مع الشيخوخة الصحية ومجالاتها في المجموعات المجمعة
نتيجة
الشيخوخة الصحية
الشيخوخة الصحية
الإدراك السليم
وظيفة جسدية سليمة
صحة نفسية سليمة
لا مرض مزمن
عاش حتى 70 عامًا
حالات
9,768
9,768
٣٥,٥٤١
٢٩,٥٢٦
27,828
٢٣,٨٩٨
٣٩,٧٥٧
درجة النظام الغذائي
نموذج
OR (95%CI) (Q5 مقابل Q1)
قيم E (الحد الأعلى)
OR (95%CI) (مستمر)
OR (95%CI) (Q5 مقابل Q1)
OR (95%CI) (Q5 مقابل Q1)
OR (95%CI) (Q5 مقابل Q1)
OR (95%CI) (Q5 مقابل Q1)
OR (95%CI) (Q5 مقابل Q1)
UPF
عمر
0.50 (0.47، 0.54)
3.41 (3.11)
0.54 (0.51، 0.57)
0.79 (0.75، 0.83)
0.54 (0.51، 0.57)
0.57 (0.54، 0.60)
0.69 (0.65، 0.73)
0.75 (0.72، 0.79)
MV
0.68 (0.63، 0.73)
2.30 (2.08)
0.72 (0.67، 0.76)
0.89 (0.84، 0.94)
0.73 (0.69، 0.78)
0.71 (0.67، 0.75)
0.85 (0.80، 0.90)
0.83 (0.79، 0.88)
حجم العينة مندون فقدان تناول UPF. تم تعديل نماذج الانحدار اللوجستي المعدلة حسب العمر لعمر الأساس (1986) والفوج (الجنس). تم تعديل نماذج الانحدار اللوجستي المعدلة حسب MV لعمر الأساس (1986)، الفوج (الجنس)، مؤشر كتلة الجسم (كجم/م²)، السلالة (أوروبي، آسيوي، أمريكي من أصل أفريقي، آخر)، حالة التدخين (لم يدخن أبدًا، مدخن سابق، مدخن حالي: 1-14 سيجارة في اليوم، 15-24 سيجارة في اليوم، وعدد السجائر في اليوم)، استهلاك الكحول (غرام/يوم)، النشاط البدني (ساعات مكافئ الأيض/أسبوع)، استخدام الفيتامينات المتعددة (نعم/لا)، تاريخ العائلة في الإصابة بالنوبة القلبية (نعم/لا)، تاريخ العائلة في الإصابة بمرض السكري من النوع 2، تاريخ العائلة في الإصابة بالسرطان، تاريخ العائلة في الإصابة بالخرف (نعم/لا)، حالة ما بعد انقطاع الطمث (نعم/لا) واستخدام هرمونات انقطاع الطمث (لا، استخدام هرمونات سابق، أو استخدام هرمونات حالي) (للنساء فقط)، الحالة الاجتماعية والاقتصادية عند البداية، الحالة الزوجية (نعم/لا)، العيش بمفرد (نعم/لا)، تاريخ الاكتئاب (نعم/لا)، في المجموعات المجمعة. MV، متعدد المتغيرات؛ OR، نسبة الأرجحية؛ CI، فترة الثقة؛ UPF، الأطعمة فائقة المعالجة (نوفا 4)؛ Q1: أقل استهلاك للأطعمة فائقة المعالجة؛ Q5: أعلى استهلاك للأطعمة فائقة المعالجة. تم استخدام استهلاك الأطعمة فائقة المعالجة كنسبة مئوية من إجمالي الطاقة.
محفظة الطبيعة
المؤلف (المؤلفون) المراسلون:
آخر تحديث من المؤلف(ين): 23 يناير 2025
ملخص التقرير
تسعى Nature Portfolio إلى تحسين إمكانية تكرار العمل الذي ننشره. يوفر هذا النموذج هيكلًا للاتساق والشفافية في التقرير. لمزيد من المعلومات حول سياسات Nature Portfolio، يرجى الاطلاع على سياسات التحرير وقائمة مراجعة سياسة التحرير.
الإحصائيات
لجميع التحليلات الإحصائية، تأكد من أن العناصر التالية موجودة في أسطورة الشكل، أسطورة الجدول، النص الرئيسي، أو قسم الطرق. غير متوفر تم التأكيد □ X حجم العينة بالضبطلكل مجموعة/شرط تجريبي، معطاة كرقم منفصل ووحدة قياس □
بيان حول ما إذا كانت القياسات قد أُخذت من عينات متميزة أو ما إذا كانت نفس العينة قد تم قياسها عدة مرات □
اختبار(ات) الإحصاء المستخدمة وما إذا كانت أحادية الجانب أو ثنائية الجانب يجب أن تُوصف الاختبارات الشائعة فقط بالاسم؛ واصفًا التقنيات الأكثر تعقيدًا في قسم الطرق. □
وصف لجميع المتغيرات المشتركة التي تم اختبارها □
وصف لأي افتراضات أو تصحيحات، مثل اختبارات الطبيعية والتعديل للمقارنات المتعددة □
وصف كامل للمعلمات الإحصائية بما في ذلك الاتجاه المركزي (مثل المتوسطات) أو تقديرات أساسية أخرى (مثل معامل الانحدار) و التباين (مثل الانحراف المعياري) أو تقديرات مرتبطة بعدم اليقين (مثل فترات الثقة) □ X لاختبار الفرضية الصفرية، يتم استخدام إحصائية الاختبار (مثل F، t، r) مع فترات الثقة، وأحجام التأثير، ودرجات الحرية وقيمة ملحوظة أعطِالقيم كقيم دقيقة كلما كان ذلك مناسبًا. □ لتحليل بايزي، معلومات حول اختيار القيم الأولية وإعدادات سلسلة ماركوف مونت كارلو □ لتصميمات هرمية ومعقدة، تحديد المستوى المناسب للاختبارات والتقارير الكاملة للنتائج □ تقديرات أحجام التأثير (مثل حجم تأثير كوهين)بيرسون )، مما يشير إلى كيفية حسابها
تحتوي مجموعتنا على الويب حول الإحصائيات لعلماء الأحياء على مقالات تتناول العديد من النقاط المذكورة أعلاه.
البرمجيات والشيفرة
معلومات السياسة حول توفر كود الكمبيوتر جمع البيانات لم يتم استخدام أي برنامج لجمع البيانات.
تحليل البيانات تم إجراء التحليلات الرئيسية باستخدام برنامج SAS الإصدار 9.4 وتم إجراء تحليلات لعوامل النظام الغذائي الفردية باستخدام برنامج R الإصدار 4.2.0. برامج التحليل متاحة للجمهور علىhttps://github.com/DrTessier/diets_healthyaging.
بالنسبة للمخطوطات التي تستخدم خوارزميات أو برامج مخصصة تكون مركزية في البحث ولكن لم يتم وصفها بعد في الأدبيات المنشورة، يجب أن تكون البرمجيات متاحة للمحررين والمراجعين. نحن نشجع بشدة على إيداع الشيفرة في مستودع مجتمعي (مثل GitHub). راجع إرشادات مجموعة Nature لتقديم الشيفرة والبرمجيات لمزيد من المعلومات.
بيانات
معلومات السياسة حول توفر البيانات
يجب أن تتضمن جميع المخطوطات بيانًا حول توفر البيانات. يجب أن يتضمن هذا البيان المعلومات التالية، حيثما ينطبق:
رموز الانضمام، معرفات فريدة، أو روابط ويب لمجموعات البيانات المتاحة للجمهور
وصف لأي قيود على توفر البيانات
بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتماشى مع سياستنا
البحث الذي يتضمن مشاركين بشريين، بياناتهم، أو مواد بيولوجية
معلومات السياسة حول الدراسات التي تشمل مشاركين بشريين أو بيانات بشرية. انظر أيضًا معلومات السياسة حول الجنس، الهوية/التقديم الجنسي، والتوجه الجنسي والعرق، والاثنية والعنصرية.
التقارير عن الجنس والنوع الاجتماعي
التقارير عن العرق أو الإثنية أو غيرها من التجمعات الاجتماعية ذات الصلة
خصائص السكان
تم تضمين كلا الجنسين (المبلغ عنه ذاتيًا) في هذه الدراسة. تظهر الخصائص التفصيلية للمشاركين حسب الجنس في الجدول الإضافي 1 و 2. قمنا بتضمين الجنس كمتغير مصاحب في تحليلاتنا الرئيسية. بالإضافة إلى ذلك، أجرينا تحليلات فرعية حسب الجنس وتم الإبلاغ عن تقديرات التأثير في الشكل 2. كانت النتائج متسقة في كلا المجموعتين.
مُبلغ عنه في الجدول 1.
شملت الدراسة 70,091 امرأة من دراسة صحة الممرضات و34,924 رجلًا من دراسة متابعة المهنيين الصحيين خالية من 11 مرضًا مزمنًا في البداية ومع تقييم غذائي مفصل. يمكن العثور على وصف تفصيلي لخصائص السكان في أقسام النتائج والأساليب وكذلك في الجدول 1 والبيانات الموسعة 1 و2 من المخطوطة.
التوظيف
تشمل دراسات صحة الممرضات (NHS) وNHSII ممرضات مسجلات. تشمل دراسة متابعة المهنيين الصحيين (HPFS) رجال المهنيين الصحيين (الأطباء البيطريين، أطباء الأسنان، الصيادلة، أطباء العيون، أطباء العظام، الأطباء، وأطباء القدم). تم إرسال استبيانات إلى المشاركين في هذه المجموعات لجمع وتحديث نمط حياتهم وتاريخهم الطبي كل عامين. قدم المشاركون بيانات عن تناولهم الغذائي خلال السنة السابقة باستخدام استبيان تكرار الطعام شبه الكمي المعتمد بشكل موسع كل أربع سنوات. كانت معدلات المتابعة تقريبًا في جميع المجموعات.
الإشراف الأخلاقي
هذه دراسة رصدية. تم الموافقة على بروتوكول الدراسة من قبل مجلس المراجعة المؤسسية (IRBs) في مستشفى بريغهام والنساء، كلية هارفارد تي. إتش. تشان للصحة العامة، والسجلات المشاركة (رقم بروتوكول IRB: 2001P001945/BWH و10372. سمحت IRBs بإكمال المشاركين للاستبيانات ليعتبر بمثابة موافقة ضمنية للمشاركة في هذه الدراسات للمهنيين الصحيين. كانت الموافقة المستنيرة المكتوبة مطلوبة لجمع المؤشرات الحيوية وللحصول على السجلات الطبية. تم إجراء الدراسة وفقًا لإعلان هلسنكي.
لاحظ أنه يجب أيضًا تقديم معلومات كاملة عن الموافقة على بروتوكول الدراسة في المخطوطة.
التقارير الخاصة بالمجال
يرجى اختيار الخيار أدناه الذي يناسب بحثك بشكل أفضل. إذا لم تكن متأكدًا، اقرأ الأقسام المناسبة قبل اتخاذ اختيارك.
علوم الحياة □ العلوم السلوكية والاجتماعية □ العلوم البيئية والتطورية والبيئية
لنسخة مرجعية من الوثيقة مع جميع الأقسام، انظر nature.com/documents/nr-reporting-summary-flat.pdf
تصميم دراسة علوم الحياة
يجب على جميع الدراسات الإفصاح عن هذه النقاط حتى عندما يكون الإفصاح سلبيًا.
حجم العينة
السكان في الدراسة موجودون مسبقًا. وثقنا 9,771 حالة من كبار السن الأصحاء، مما سمح لنا بالكشف عن النتائج الرئيسية للدراسة الحالية بقوة إحصائية قدرها من تحليل لاحق
استبعاد البيانات
استبعدنا المشاركين الذين لم يعودوا استبيان تكرار الطعام بين 1986-2010، أولئك الذين لديهم تناول طاقة غير معقول، أولئك الذين لديهم واحد أو أكثر من 11 مرضًا مزمنًا، وأولئك الذين لديهم نمط شيخوخة صحي مفقود في 2016.
التكرار
تم الإبلاغ عن صلاحية واستنساخ الاستبيانات وتحديد النتائج سابقًا ووصفها في الأساليب. لوحظت علاقات معتدلة للأطعمة والمغذيات وأنماط النظام الغذائي عند مقارنة التقديرات من استبيانات تكرار الطعام مع تلك من سجلات النظام الغذائي لمدة أسبوع واحد. طُلب من المشاركين الذين أبلغوا عن تشخيص جديد لمرض مزمن رئيسي الحصول على إذن للحصول على سجلاتهم الطبية والتقارير المرضية. أظهرت الانحدارات المعرفية الذاتية (SCD)، نموذج 36 القصير ومقياس الاكتئاب لدى المسنين جميعها صلاحية جيدة في قياس الانحدار المعرفي المدرك ذاتيًا، والقيود البدنية، وأعراض الاكتئاب، على التوالي. تم تحديد الوفيات من خلال الأقارب أو مكتب البريد عندما تم إرسال الاستبيانات ومن خلال البحث في السجل الوطني للوفيات. تم الإبلاغ عن تحديد الوفيات باستخدام السجل الوطني للوفيات بأنه ذو حساسية عالية (98%) وخصوصية .لم يكن تكرار هذه التحليلات قابلاً للتطبيق وبالتالي لم يتم إجراؤه.
العشوائية
غير قابل للتطبيق. هذه الدراسة هي دراسة رصدية بدون تدخل.
التعمية
غير قابلة للتطبيق. هذه الدراسة هي دراسة رصدية بدون تدخل.
التقارير للمواد والأنظمة والأساليب المحددة
نحتاج إلى معلومات من المؤلفين حول بعض أنواع المواد والأنظمة التجريبية والأساليب المستخدمة في العديد من الدراسات. هنا، حدد ما إذا كانت كل مادة أو نظام أو طريقة مدرجة ذات صلة بدراستك. إذا لم تكن متأكدًا مما إذا كان عنصر القائمة ينطبق على بحثك، اقرأ القسم المناسب قبل اختيار رد.
¹قسم التغذية، كلية هارفارد تي. إتش. تشان للصحة العامة، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية. ²قسم التغذية، كلية الطب، جامعة مونتريال، مونتريال، كيبيك، كندا. مركز EPIC لمعهد القلب في مونتريال، مونتريال، كيبيك، كندا. معهد تعزيز البيانات (IVADO)، مونتريال، كيبيك، كندا. مركز أبحاث التغذية البشرية في وزارة الزراعة الأمريكية، جامعة تافتس، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية. كلية الطب بجامعة تافتس، جامعة تافتس، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية. قسم الوبائيات، كلية هارفارد تي. إتش. تشان للصحة العامة، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية. قسم تشانينغ للطب الشبكي، قسم الطب، مستشفى بريغهام والنساء وكلية الطب بجامعة هارفارد، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية. مركز مرض الزهايمر في راش، مركز راش الطبي، شيكاغو، إلينوي، الولايات المتحدة الأمريكية. قسم الطب الوقائي، قسم الطب، مستشفى بريغهام والنساء وكلية الطب بجامعة هارفارد، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية. قسم الإحصاء الحيوي، كلية هارفارد تي. إتش. تشان للصحة العامة، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية. قسم الصحة العامة، كلية الصحة والعلوم الطبية، جامعة كوبنهاغن، كوبنهاغن، الدنمارك. مركز مؤسسة نوفو نورديسك للبحث الأساسي في التمثيل الغذائي، كلية الصحة والعلوم الطبية، جامعة كوبنهاغن، كوبنهاغن، الدنمارك.
↩البريد الإلكتروني: anne-julie.tessier@umontreal.ca; fhu@hsph.harvard.edu; marta.guasch@sund.ku.dk
حجم العينة من . القيم هي المتوسط (الانحراف المعياري) للمتغيرات المستمرة و% للمتغيرات الفئوية. مؤشر كتلة الجسم، مؤشر كتلة الجسم؛ AHEI، مؤشر الأكل الصحي البديل؛ AMED، مؤشر النظام الغذائي المتوسطي البديل؛ DASH، أساليب النظام الغذائي لوقف ارتفاع ضغط الدم؛ MIND، تدخل النظام الغذائي المتوسطي-DASH لتأخير الأمراض التنكسية؛ hPDI، مؤشر النظام الغذائي النباتي الصحي؛ PHDI، مؤشر النظام الغذائي الصحي الكوكبي؛ EDIH، المؤشر الغذائي التجريبي لفرط الأنسولين؛ EDIP، نمط النظام الغذائي الالتهابي التجريبي؛ SES، الحالة الاجتماعية والاقتصادية؛ MET، مكافئ التمثيل الغذائي للمهام. تعتبر EDIH وEDIP درجات معكوسة للسماح بالمقارنة مع درجات النظام الغذائي الأخرى.
حجم العينة من . القيم هي المتوسط (الانحراف المعياري) للمتغيرات المستمرة و% للمتغيرات الفئوية. مؤشر كتلة الجسم، مؤشر كتلة الجسم؛ AHEI، مؤشر الأكل الصحي البديل؛ AMED، مؤشر النظام الغذائي المتوسطي البديل؛ DASH، أساليب النظام الغذائي لوقف ارتفاع ضغط الدم؛ MIND، تدخل النظام الغذائي المتوسطي-DASH لتأخير الأمراض التنكسية؛ hPDI، مؤشر النظام الغذائي النباتي الصحي؛ PHDI، مؤشر النظام الغذائي الصحي الكوكبي؛ EDIH، المؤشر الغذائي التجريبي لفرط الأنسولين؛ EDIP، نمط النظام الغذائي الالتهابي التجريبي. تعتبر EDIH وEDIP درجات معكوسة للسماح بالمقارنة مع درجات النظام الغذائي الأخرى.
Anne-Julie Tessier , Fenglei Wang , Andres Ardisson Korat , A. Heather Eliassen (1) , Jorge Chavarro , Francine Grodstein , Jun Li , Liming Liang , Walter C. Willett , Qi Sun , Meir J. Stampfer , Frank B. Hu & Marta Guasch-Ferré .
As the global population ages, it is critical to identify diets that, beyond preventing noncommunicable diseases, optimally promote healthy aging. Here, using longitudinal questionnaire data from the Nurses’ Health Study (1986-2016) and the Health Professionals Follow-Up Study (1986-2016), we examined the association of long-term adherence to eight dietary patterns and ultraprocessed food consumption with healthy aging, as assessed according to measures of cognitive, physical and mental health, as well as living to 70 years of age free of chronic diseases. After up to 30 years of follow-up, 9,771 ( ) of 105,015 participants ( women, mean age years (s.d. )) achieved healthy aging. For each dietary pattern, higher adherence was associated with greater odds of healthy aging and its domains. The odds ratios for the highest quintile versus the lowest ranged from confidence interval ; healthful plant-based diet) to ; Alternative Healthy Eating Index). When the age threshold for healthy aging was shifted to 75 years, the Alternative Healthy Eating Index diet showed the strongest association with healthy aging, with an odds ratio of . Higher intakes of fruits, vegetables, whole grains, unsaturated fats, nuts, legumes and low-fat dairy products were linked to greater odds of healthy aging, whereas higher intakes of trans fats, sodium, sugary beverages and red or processed meats (or both) were inversely associated. Our findings suggest that dietary patterns rich in plant-based foods, with moderate inclusion of healthy animal-based foods, may enhance overall healthy aging, guiding future dietary guidelines.
The US population of older adults has steadily increased in the past few decades; however, of older adults have at least one chronic health condition, highlighting the complex health challenges facing this demographic shift . Promoting healthy aging is a global priority . This commitment is driven by the goal of promoting a high quality of life, supporting continued contribution to society and reducing healthcare costs. Diet is the first leading behavioral risk factor for noncommunicable diseases and mortality burden globally , and the second after tobacco use in US older adults .
Recently, the World Health Organization acknowledged that prioritizing the preservation of functional ability and the prevention of capacity decline should be central to the model of healthy aging . This shift moves away from the traditional disease-centric approach to aging, aiming to offer older adults enhanced care . Intervention and observational studies have provided compelling evidence that a better-quality diet is beneficial for the prevention of cardiovascular disease , type 2 diabetes and premature mortality . Studies have also evaluated the effects or the associations of foods and nutrients
Fig. 1 | Flow diagram of the study participants. This flow diagram shows the initial sample sizes in the NHS and HPFS followed by the sequential application of exclusion criteria for each cohort. The final study population includes a total of 105,015 participants.
with age-related cognitive and physical performance outcomes and depressive symptoms . However, few studies have examined the association of dietary patterns with a multidimensional model of healthy aging . Examining and contrasting dietary patterns in relation to healthy aging will inform public health recommendations aimed at fostering the overall health and well-being of older adults, encompassing cognitive, physical and mental health, and the prevention of chronic diseases.
In this study, we examined the association between long-term adherence to eight healthy dietary patterns, including the Alternative Healthy Eating Index (AHEI), Alternative Mediterranean Index (aMED), the Dietary Approaches to Stop Hypertension (DASH), the Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND), the healthful plant-based diet (hPDI), the Planetary Health Diet Index (PHDI), the empirically inflammatory dietary pattern (EDIP), the empirical dietary index for hyperinsulinemia (EDIH) and ultraprocessed food (UPF) consumption, and healthy aging after 30 years in two large prospective US cohorts. We then examined these associations in specific subgroups, including stratification according to sex, ancestry, socioeconomic status (SES) and lifestyle factors. We also examined the associations of individual foods and nutrients contributing to such dietary patterns.
Results
Of 105,015 participants, 70,091 were women (NHS) and 34,924 were men (HPFS) (Fig. 1). After a follow-up of up to 30 years, participants achieved healthy aging, in the NHS and 2,169 (6.2%) in the HPFS. In the pooled cohorts, 39,769 (37.9%) reached the age of 70 years, remained free of 11 chronic diseases, 35,555 (33.9%) maintained intact cognitive function, 29,543 (28.1%) maintained intact physical function and 27,842 ( ) maintained intact mental health.
The age-standardized characteristics of the study population are shown in Table 1 (pooled data) and in Extended Data Tables 1 and 2 (according to cohort). Participants in the highest energy-adjusted dietary pattern score quintile were more likely to have a higher SES, use multivitamins, have a higher level of physical activity and slightly lower body mass index (BMI); they were also less likely to have a history of depression compared to the lowest quintile. Participants in the highest quintile for the AHEI, MIND, hPDI, PHDI, reverse EDIH (rEDIH) and reverse EDIP (rEDIP) consumed more alcohol, while those in the highest quintile for DASH and aMED consumed less. While a higher proportion of participants were women in the highest quintile for aMED, PHDI, rEDIH and rEDIP, a higher proportion were men in the highest quintile for AHEI, DASH, MIND and hPDI. Extended Data Fig. 1 shows the Spearman correlations between all dietary pattern scores and UPF consumption.
Higher adherence to all dietary patterns was associated with greater odds of healthy aging (Fig. 2 and Extended Data Table 3); components of the dietary patterns are shown in Fig. 3. The multivariableadjusted odds ratios (ORs) (95% confidence intervals (CIs)) comparing the highest quintile to the lowest ranged from 1.45 (1.35-1.57; ) to . The AHEI showed the strongest association followed by the rEDIH; the hPDI showed the weakest association. Based on the differences in ORs between pairs of scores and paired -tests, the AHEI showed higher odds of healthy aging compared to the MIND, hPDI and rEDIP. The aMED, DASH, PHDI and rEDIH also demonstrated higher odds of healthy aging compared to the hPDI (Fig. 2). Using dietary pattern scores modeled as continuous variables, the associations with healthy aging were also the strongest for the AHEI and the weakest for the hPDI (Extended Data Table 3). The OR ( ) per standardized unit increase (representing the increment between the 10th and 90th percentiles) ranged from 1.40 (1.32-1.49) to 1.71 (1.60-1.82). Absolute risks, calculated based on the healthy
Table 1 | Age-standardized characteristics in the lowest and highest quintiles of energy-adjusted dietary pattern scores in the pooled cohorts ( ) between 1986 and 2010
Characteristic
Q1,
Q5,
Q1,
Q5,
Q1,
Q5,
Q1,
Q5,
Dietary score
AHEI-2010
aMED
DASH
MIND
Energy-adjusted score
41.5 (4.2)
68.6 (4.6)
2.2 (0.6)
6.3 (0.6)
18.1 (1.8)
29.5 (1.7)
6.0 (0.6)
9.6 (0.6)
Women
70.2
59.7
57.2
69.5
67.1
61.3
67.1
61.0
Age at baseline
53.5 (7.8)
53.1 (7.7)
53.8 (7.6)
53.8 (7.5)
51.6 (7.7)
55.3 (7.6)
54.4 (7.7)
52.8 (7.7)
Ancestry
European
95.2
94.1
95.6
94.1
94.5
94.8
95.5
93.5
Asian
0.6
1.4
0.7
1.3
1.1
0.9
0.6
1.7
African
1.1
1.4
0.8
1.5
1.4
1.2
0.8
1.6
Other
3.1
3.0
3.0
3.1
3.0
3.1
3.1
3.1
SES score at baseline
-0.8 (3.3)
0.9 (4)
-0.6 (3.4)
-0.6 (3.4)
-0.6 (3.5)
0.5 (3.9)
-0.9 (3.3)
0.8 (3.9)
Alone, ever
28.0
27.7
27.2
27.2
27.2
28.9
30.2
25.4
History of depression, yes
16.3
12.3
14.5
14.5
15.6
12.1
16.2
12.0
History of cancer, yes
4.5
3.9
4.1
4.2
3.8
4.3
4.3
3.8
History of diabetes, yes
3.3
2.7
2.7
2.8
1.9
4.0
3.2
2.9
History of CVD, yes
5.3
5.4
4.7
5.7
4.2
6.7
5.2
5.7
Family history of dementia, yes
11.9
13.2
10.8
13.8
12.1
12.2
11.7
12.5
Multivitamin use, ever
78.6
91.0
79.2
90.2
78.8
89.7
79.5
90.0
BMI,
26.6 (5.1)
25.2 (4)
26.6 (4.9)
25.2 (4.1)
26.5 (5)
25.2 (4.2)
26.5 (5)
25.3 (4)
Never smoker, %
71.4
60.2
67.2
63.9
63.4
69.3
69.8
63.5
Physical activity, MET-hweek
1.2 (2.1)
3.7 (3.7)
1.5 (2.5)
3.3 (3.5)
1.4 (2.2)
3.5 (3.6)
1.3 (2.3)
3.6 (3.7)
Alcohol intake, g per day
7.4 (14.3)
8.1 (8.4)
8.4 (14.4)
7.5 (8.5)
8.8 (13.4)
6.3 (9.2)
6.2 (11.6)
8.4 (10.3)
Energy intake, kcal
1804 (494)
1831 (493)
1839 (532)
1811 (445)
1819 (514)
1842 (468)
1815.1 (524.9)
1826.2 (476.5)
Healthy agers, %
5.6
13.7
6.4
12.5
7.7
10.2
5.3
13.0
Dietary score
hPDI
PHDI
rEDIH
rEDIP
Energy-adjusted score
47.0 (2.4)
62.8 (2.9)
65.2 (5.1)
93.4 (5.1)
-0.6 (0.2)
O (0.1)
-0.3 (0.2)
0.4 (0.2)
Women
66.8
63.5
61.0
63.5
34.1
83.9
52.9
71.7
Age at baseline
52.5 (7.8)
54.2 (7.7)
53.5 (8)
53 (7.6)
52.9 (8.4)
53.4 (7.4)
53.7 (8.1)
52.3 (7.5)
Ancestry
European
95.4
93.9
95.3
93.4
94.9
95.3
92.9
96.5
Asian
0.6
1.5
0.6
1.9
1.1
0.8
1.8
0.4
African
1.1
1.5
1.0
1.5
1.5
0.7
2.2
0.3
Other
2.9
3.2
3.1
3.1
2.5
3.3
3.1
2.8
SES score at baseline
-0.2 (3.5)
0.3 (3.9)
-0.6 (3.5)
0.7 (3.9)
-0.6 (3.4)
0.7 (4)
-0.5 (3.5)
0.5 (3.9)
Alone, ever
27.9
27.6
27.5
27.0
22.3
31.5
24.8
28.5
History of depression, yes
14.7
12.6
14.7
12.7
10.9
15.3
14.4
13.6
History of cancer, yes
4.1
4.2
4.4
3.8
4.1
4.0
4.1
3.9
History of diabetes, yes
1.9
4.1
3.2
2.6
5.3
1.4
5.4
1.5
History of CVD, yes
4.3
6.2
5.2
5.2
6.3
3.7
7.0
3.3
Family history of dementia, yes
12.5
12.5
10.5
13.7
7.3
16.7
9.9
14.5
Multivitamin use, ever
81.1
88.6
78.2
91.3
78.8
89.8
80.8
87.6
BMI,
26.5 (4.9)
25.4 (4.3)
26.4 (4.9)
25.3 (4)
27.4 (4.9)
24.4 (3.8)
27.5 (5.2)
24.8 (3.8)
Never smoker, %
67.0
64.7
71.3
59.7
73.6
56.2
73.0
56.2
Physical activity, MET-hweek
1.5 (2.4)
3.3 (3.6)
1.5 (2.5)
3.5 (3.6)
2.2 (3.1)
2.8 (3.2)
2.0 (3.0)
2.7 (3.1)
Alcohol intake, g per day
6.7 (10.4)
8.1 (11.7)
7 (11.8)
8.3 (10.8)
7.2 (11.4)
11.3 (13.1)
4.6 (9)
14.4 (14.8)
Energy intake, kcal
1824 (474)
1824 (508)
1821 (543)
1814 (466)
1950 (543)
1849 (474)
1902 (535)
1853 (489)
Healthy agers, %
8.0
11.2
5.8
13.6
5.5
13.5
5.5
13.1
Values are the mean (s.d.) for continuous variables and % for categorical variables. CVD, cardiovascular disease; MET, metabolic equivalent of task.
Fig. 2 | Associations of average dietary patterns with healthy aging and its domains. In the main pooled dataset ( ), the average dietary pattern scores were calculated from 1986 to 2010. The forest plots show the ORs comparing Q5 to Q1 for each of the dietary patterns (visually represented by the centers of the error bars), the CIs (visually represented by the error bars) and values and their lower bound. Logistic regressions were used to estimate ORs and were adjusted for age at baseline (1986), cohort (sex), BMI ( ), ancestry (European, Asian, African-American, Other), smoking status (never, former, current smoker: cigarettes per day, cigarettes per day and cigarettes per day), alcohol intake (g per day) (for DASH, hPDI, PHDI), physical activity (MET-h week ), multivitamin use ever (yes/no), family history of
myocardial infarction (yes/no), family history of type 2 diabetes, family history of cancer, family history of dementia (yes/no), postmenopausal status (yes/no) and menopausal hormone use (no, past or current hormone use; only women), SES at baseline, marital status (yes/no), living alone ever (yes/no) and history of depression (yes/no) in the pooled cohorts. rEDIH and rEDIP are reversed scores to allow comparison with other scores. All two-sided . The heatmaps show the OR difference between all pairs of scores. Positive differences are denoted in green and negative differences in pink; a darker color indicates a greater difference. *Two-sided based on a paired -test comparing ORs (not adjusted for multiple comparisons).
aging prevalence and adjusted ORs, indicated to chances of achieving healthy aging among individuals with higher adherence to the dietary patterns (Extended Data Table 4).
When examining associations with each healthy aging domain, higher adherence to all dietary patterns was associated with all individual domains (Fig. 2 and Extended Data Table 3). The significant multivariable-adjusted ORs (95% CIs) comparing the highest quintile to the lowest ranged from to 1.65 (1.57-1.74; ) for intact cognitive health, with the PHDI showing the strongest association and the hPDI showing the weakest association. For intact physical function, the ORs ( CIs) ranged from 1.38 to , with the AHEI showing the strongest association and the rEDIP showing the weakest association. For intact mental health, the ORs ( CIs) ranged from to , with the AHEI showing the strongest association and the hPDI showing the weakest association. For being free of chronic diseases, the ORs ( ) ranged from to , with
the rEDIH showing the strongest association and the hPDI showing the weakest association. For surviving to the age of 70 years, the ORs ranged from to ), with the PHDI showing the strongest association and the hPDI showing the weakest association.
Figure 4 illustrates the associations between individual dietary factors and healthy aging and its individual domains. While higher intakes of fruits, whole grains, vegetables, added unsaturated fats, nuts, legumes and low-fat dairy were associated with greater odds of healthy aging, higher intakes of trans fats, sodium, total meats, and red and processed meats were associated with lower odds. These foods or nutrients were also consistently associated with each healthy aging domain. Added unsaturated fat intake, including polyunsaturated fatty acids, was particularly associated with surviving to the age of 70 years, and intact physical and cognitive functions.
While adherence to all dietary patterns was significantly associated with healthy aging in both men and women, the associations were stronger in women ( interaction: 0.0226 to <0.0001; Fig. 5)
Dietary factors
AHEI2010
aMED
DASH
MIND
hPDI
PHDI
rEDIH
rEDIP
Fruits
Berries
Tomatoes
Vegetables
Starchy vegetables
Leafy-green vegetables
Dark-yellow vegetables
Other vegetables
Potatoes
Whole grains
Refined grains
Nuts and legumes
Nuts
Legumes
Beans
Soybean
Total meats
Red and processed meats
Red meat
Processed meats
Organ meats
Poultry
Eggs
Fish and seafood
Other fish
Miscellaneous animal-based foods
Sweets and desserts
Fast and fried foods
French fries
Snacks
Pizza
Animal fat
Butter and margarine
Butter
Margarine
Vegetable oils
Creamy soup
Olive oil
Sugar-sweetened beverages and fruit juices
Sugar-sweetened beverages
Low-energy beverages
Fruit juices
Total alcohol
Wine
Beer
Tea and coffee
Tea
Coffee
Total dairy
Low-fat dairy
High-fat dairy
Cheese
Trans fats
Long-chain n-3 (omega-3) fatty acids
Polyunsaturated fatty acids
Mono-unsaturated fatty acid:saturated fatty acid
Added unsaturated fats
Added saturated fat and trans fats
Added sugar and fruit juices
Sodium
Fig. 3 | Dietary factors of dietary patterns. Pink: lower points or negative weights were assigned to higher intakes for this dietary factor;green: higher points or positive weights were assigned to higher intakes for this dietary factor;
gray: higher points or positive weights were assigned to moderate intake. The EDIH and EDIP are presented as reversed scores to allow for comparison with other dietary scores.
except for rEDIH and rEDIP (no interaction). The associations were also stronger in smokers (for AHEI, aMED, DASH, MIND, hPDI; interaction 0.047 to ), in participants with a BMI greater than (for AHEI, MIND, hPDI, rEDIH, rEDIP; interaction 0.042 to <0.0001) and in participants with a physical activity level below the median (for AHEI, aMED, DASH, MIND, hPDI, PHDI, rEDIP; interaction 0.038 to <0.0001; Fig. 5). A significant interaction between SES and rEDIH ( interaction ) and rEDIP ( interaction ) was observed. No interaction was found for ancestry (European versus non-European).
Secondary analyses showed consistency with the main results. When using a higher age cutoff of 75 years, the AHEI also showed the strongest association (Extended Data Table 5). When applying linear weights to dietary pattern scores, results were consistent with the main analysis (Extended Data Table 6).
Higher UPF consumption (comparing the highest quintile to the lowest) was associated with lower odds of healthy aging ( CI ; Extended Data Table 7). Higher consumption of UPFs was also associated with lower odds of maintaining intact cognitive
function, physical function and mental health, living free of chronic diseases and reaching the age of 70 years (Extended Data Table 7).
Discussion
In two large prospective cohorts of US women and men, we found that higher adherence to dietary patterns, namely the AHEI, aMED, DASH, MIND, hPDI, PHDI, rEDIP and rEDIH, during mid-life was associated with greater odds of healthy aging after a 30 -year follow-up. Among dietary patterns, AHEI was the most strongly associated with healthy aging and hPDI was the least associated. Compared to participants in the lowest quintile, those who were in the highest AHEI quintile (energy-adjusted mean score ) had greater odds of achieving healthy aging using an age cutoff of 70 years and 2.24 times greater odds using an age cutoff of 75 years. The AHEI was closely followed by the rEDIH, aMED, DASH, PHDI, MIND, rEDIP and lastly the hPDI. Associations were independent of other lifestyle factors, including physical activity level, smoking and BMI. The AHEI was also the most strongly associated with maintaining intact physical function and mental health among individual healthy aging domains. The PHDI was most strongly associated with maintaining intact cognitive health and surviving to the age of 70 years. The rEDIH was the most strongly associated with being free of chronic diseases. A higher intake of UPFs was inversely correlated with higher diet quality scores and was also associated with lower odds of healthy aging. Our findings provide evidence to support that adherence to healthy dietary patterns represents a potential strategy for healthy aging, patterns that particularly are richer in fruits, vegetables, whole grains, unsaturated fats, nuts and legumes, that include some dairy products, and that are lower in trans fats, sodium, and red and processed meats.
While all dietary patterns share similarities such as promoting an intake of fruits, vegetables and whole grains, while reducing the amount of red and processed meats, each pattern emphasizes specific components. For instance, while the aMED diet focuses on the Mediterranean staples of olive oil, fish and nuts , MIND further highlights the cognitive benefits of berries . The DASH diet prioritizes sodium restriction for blood pressure control , the PHDI emphasizes healthy low greenhouse gas emission foods, such as plant-sourced protein food , and the hPDI uniquely attributes positive scoring to healthy plant-based foods and negative scoring to animal-derived foods . In a previous report, adherence to the AHEI and aMED, assessed in 1984-1986, was associated with and ) greater odds of healthy aging, respectively, in the NHS . This analysis examined two dietary patterns with healthy aging in 2000 using the same definition as in the current study, but the Telephone Interview for Cognitive Status was used to assess the cognitive health domain. Our analysis, which included both the NHS and HPFS, involved long-term dietary assessment of eight dietary patterns over a period of 14 years, with an assessment of
healthy aging conducted 30 years after baseline. The results showed consistent and stronger associations for these two scores ( greater odds for AHEI and for aMED). The association between dietary
Fig. 4 | Multivariable-adjusted associations between dietary factors and healthy aging and its domains in the main pooled dataset . Each heatmap square represent the OR comparing the 90th to the 10th percentile for each of the dietary factors. Logistic regressions were used to estimate ORs and were adjusted for age at baseline (1986), cohort ( sex ), BMI ( ), ancestry (European, Asian, African-American, Other), smoking status (never, former, current smoker: 1-14 cigarettes per day, 15-24 cigarettes per day and cigarettes per day), alcohol intake (g per day), physical activity (MET-h week ), multivitamin use ever (yes/no), family history of myocardial infarction (yes/ no), family history of type 2 diabetes, family history of cancer, family history of dementia (yes/no), postmenopausal status (yes/no) and menopausal hormone use (no, past, or current hormone use; women only), SES at baseline, marital status (yes/no), living alone ever (yes/no) and history of depression (yes/no) in the pooled cohorts. ORs greater than 1.0 are denoted in green; ORs below 1.0 are denoted in pink; a darker color indicates a stronger association.*Two-sided values corrected for multiple comparisons using a false discovery rate .
Fig. 5 | Subgroup analysis of the associations between average dietary pattern scores and healthy aging in the main pooled dataset . The forest plots show the ORs comparing the 90th to the 10th percentile for each of the dietary patterns (visually represented by the centers of the error bars) and 95% CIs (visually represented by error bars). Logistic regressions were used to estimate the ORs and were adjusted for age at baseline (1986), cohort (sex), BMI ( ), ancestry (European, Asian, African-American, Other), smoking status (never, former, current smoker: cigarettes per day, 15-24 cigarettes per day and cigarettes per day), alcohol intake (g per day), physical activity (MET-h week ), multivitamin use ever (yes/no), family history of myocardial infarction (yes/no), family history of type 2 diabetes, family history of cancer,
family history of dementia (yes/no), postmenopausal status (yes/no) and menopausal hormone use (no, past, or current hormone use; women only), SES at baseline, marital status (yes/no), living alone ever (yes/no) and history of depression (yes/no), excluding the stratified variable where applicable, in the pooled cohorts.** two-sided interaction <0.0001 (not adjusted for multiple comparisons). *Two-sided interaction < 0.05 (not adjusted for multiple comparisons); sex, ; MIND ; hPDI ; PHDI ; BMI, AHEI ; MIND ; and . For physical activity, DASH ; hPDI ; rEDIP . For smoking, AHEI aMED MIND hPDI . For SES, rEDIH ; rEDIP .
patterns and healthy aging was also examined in other populations, namely in France , Australia , China and Israel , and corroborated our findings. In the SUpplementation en VItamines et Minéraux AntioXydants study ( healthy agers, 13-year follow-up) and Singapore Chinese Health Study (SCHS) ( healthy agers, 20-year follow-up), higher adherence to a Mediterranean-style diet was associated with ; tertile 3 versus tertile 1) and ; quartile 4 versus quartile 1) greater likelihood of achieving healthy aging, respectively. The AHEI, HEI 2015 and adherence to the Australian National Dietary Guidelines were similarly associated with healthy aging with ORs ranging from 1.34 to 1.73 in the SCHS, the Israeli National Health and Nutrition Survey of Older Adults
( healthy agers; excluding deaths; median follow-up of 12.6 years) and the Blue Mountains Eye Study ( healthy agers, 10 -year follow-up). Among the dietary patterns also examined in other cohorts, we found significant interactions between sex and DASH, aMED, AHEI and hPDI; between physical activity level and the AHEI, aMED and hPDI; between smoking and the AHEI, aMED, DASH and hPDI; and between BMI and the AHEI and hPDI. Differences in the study populations regarding sex, lifestyle factors and BMI may explain the variations observed in the ORs across studies. The methods for assessing diet varied across studies, as did the definitions of healthy aging. Differences included age cutoffs, questionnaires or measures used for assessing domains, consideration of chronic diseases and
the inclusion or exclusion of additional clinical measures. Moreover, some studies excluded deceased individuals from the sample population, potentially resulting in varying proportion of healthy agers and discrepancies in the classification of healthy agers. Standardization of a composite healthy aging outcome is warranted to allow proper comparison of research studies; deaths should be considered as usual agers and be included in the analyses to avoid selection bias.
Using a data-driven approach, Hodge et al. discerned four dietary patterns that were associated with healthy aging in the Melbourne Collaborative Cohort Study ( healthy agers; median follow-up of 11.7 years for survivors). The dietary pattern that showed the strongest positive association with healthy aging predominantly consisted of fruits, whereas the pattern inversely associated with healthy aging primarily featured red meat. Assman et al. examined the individual dietary factors of the Mediterranean-style diet and their association with healthy aging in the SUpplementation en VItamines et Minéraux AntioXydants cohort and found a higher intake of fruits and vegetables to be favorably associated with healthy aging, and meat and alcohol to be unfavorably associated . These findings agree with our results showing that a higher intake of fruits (overall and berries) and vegetables (overall, leafy green and dark yellow) was associated with greater odds of healthy aging, whereas a higher intake in trans fats, sodium, meats (total, red and processed and unprocessed) and liquor was associated with lower odds of healthy aging. In the Blue Mountains Eye Study, Gopinath et al. only found an association for fruits (healthy aging ; quartiles versus quartile 1; not significant for quartile 4 versus quartile 1) among the individual dietary factors examined. In the current study, most of the individual foods associated with healthy aging were consistently associated with the healthy aging domains individually, except for a few including fast and fried foods away from home, and snacks, which were positively associated with surviving to the age of 70 years. Although the consumption of fried food has been associated with an increased risk of cardiovascular events, evidence suggests no association with an all-cause mortality risk. The social aspect related to eating away from home may explain part of the association with living to the age of 70 years , although more research in this area is needed to explain these associations.
Our findings showed that each dietary pattern examined was associated with each specific individual component of healthy aging. One prospective study also examined associations of dietary patterns, specifically the aMED, DASH, AHEI, PDI and hPDI, with the healthy aging domains . Consistent with our results, Zhou et al. found significant associations between the aMED, DASH, AHEI and hPDI, and maintaining intact cognitive function; AHEI and DASH for staying free of chronic diseases; aMED, DASH, AHEI, hPDI and PDI for maintaining physical function and mental health (no clinical depression) in the SCHS study. However, no association was found between aMED, PDI and hPDI and the chronic disease component, and the PDI and the cognitive function component. Extensive evidence from intervention and observational studies supports that higher adherence to healthy dietary patterns is protective or associated with a lower risk of chronic diseases . There is also accumulating evidence supporting the association of dietary patterns and dietary factors with mental, physical and cognitive health (reviewed in refs. 29,30). Beyond traditional measures of chronological age or disease burden, healthy aging is multifaceted as recognized by the World Health Organization in their first World report on ageing and health . While examining domains in isolation provides more targeted insights into the potential mechanisms, investigating healthy aging as a multi-component outcome may inform holistic health strategies . Our findings allow us to capture the multidimensional nature of aging and evaluate dietary patterns and food intake associations comprehensively.
Strengths of this study include the prospective design and large population size for robustly powered analyses. Repeated
measurements of diet, body weight and lifestyle variables enabled us to consider long-term adherence to healthy dietary patterns and potential confounding factors, and mitigate random measurement errors. The long 30-year follow-up allowed the examination of the mid-life diet and its association with healthy aging in later life. Nevertheless, the results of this study need to be interpreted in the context of its limitations. First, although a lag of 6 years between the last diet update and healthy aging assessment was considered, reverse causation cannot be completely excluded. While it is plausible that higher adherence to healthy diets could be indicative of a higher SES and overall healthy lifestyle, our results remained consistent after accounting for such factors. However, residual confounding may still exist because of other unmeasured factors, such as environmental influences, although the E values indicate that our results are robust to potential confounding. Also, the cognitive and physical function domains were assessed using validated self-reported questionnaires instead of objective measurements, which limits in-depth assessment and classification. Lastly, our population included health professionals, which may limit the generalizability of our results. Replicating the analyses in populations with diverse SES and ancestries would offer further insights into their generalizability.
Greater long-term adherence to a healthy diet during mid-life was associated with greater odds of healthy aging and of its individual domains in US adults. Among the eight dietary patterns examined in this study, a diet that was developed to predict chronic disease risk as measured by the AHEI may confer the highest benefit for healthy aging in both men and women. Beyond the prevention of chronic disease, our findings extend recommendations to promote overall healthy aging, encompassing cognitive, physical and mental health.
Online content
Any methods, additional references, Nature Portfolio reporting summaries, source data, extended data, supplementary information, acknowledgements, peer review information; details of author contributions and competing interests; and statements of data and code availability are available at https://doi.org/10.1038/s41591-025-03570-5.
References
Centers for Disease Control and Prevention. Healthy Aging at a Glance, 2015: Helping People to Live Long and Productive Lives and Enjoy a Good Quality of Life https://stacks.cdc.gov/view/cdc/43961 (National Center for Chronic Disease Prevention and Health Promotion (U.S.) & Division of Adult and Community Health, 2015).
Office of Disease Prevention and Health Promotion. Healthy Aging https://health.gov/our-work/national-health-initiatives/ healthy-aging#:~:text=Promoting%20health%20and%20 preventing%2Odisease,live%20longer%20and%20stay%20 healthy (OASH, 2023).
Afshin, A. et al. Health effects of dietary risks in 195 countries, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 393, 1958-1972 (2019).
Mokdad, A. H. et al. The state of US health, 1990-2016: burden of diseases, injuries, and risk factors among US states. JAMA 319, 1444-1472 (2018).
Bautmans, I. et al. WHO working definition of vitality capacity for healthy longevity monitoring. Lancet Healthy Longev. 3, e789-e796 (2022).
Shan, Z. et al. Association between healthy eating patterns and risk of cardiovascular disease. JAMA Intern. Med. 180, 1090-1100 (2020).
Guasch-Ferré, M. & Willett, W. C. The Mediterranean diet and health: a comprehensive overview. J. Intern. Med. 290, 549-566 (2021).
Forouhi, N. G., Misra, A., Mohan, V., Taylor, R. & Yancy, W. Dietary and nutritional approaches for prevention and management of type 2 diabetes. BMJ 361, k2234-k2241 (2018).
English, L. K. et al. Evaluation of dietary patterns and all-cause mortality: a systematic review. JAMA Netw. Open 4, e2122277-e21222295 (2021).
Scarmeas, N., Anastasiou, C. A. & Yannakoulia, M. Nutrition and prevention of cognitive impairment. Lancet Neurol. 17, 1006-1015 (2018).
Tessier, A.-J. & Chevalier, S. An update on protein, leucine, omega-3 fatty acids, and vitamin D in the prevention and treatment of sarcopenia and functional decline. Nutrients 10, 1099-1115 (2018).
Nicolaou, M. et al. Association of a priori dietary patterns with depressive symptoms: a harmonised meta-analysis of observational studies. Psychol. Med. 50, 1872-1883 (2020).
Okereke, O. I. et al. Effect of long-term vitamin D3 supplementation vs placebo on risk of depression or clinically relevant depressive symptoms and on change in mood scores: a randomized clinical trial. JAMA 324, 471-480 (2020).
Okereke, O. I. et al. Effect of long-term supplementation with marine omega-3 fatty acids vs placebo on risk of depression or clinically relevant depressive symptoms and on change in mood scores: a randomized clinical trial. JAMA 326, 2385-2394 (2021).
Zhou, Y.-F. et al. Association between dietary patterns in midlife and healthy ageing in Chinese adults: the Singapore Chinese Health Study. J. Am. Med. Dir. Assoc. 22, 1279-1286 (2021).
Assmann, K. E. et al. Association between adherence to the Mediterranean diet at midlife and healthy aging in a cohort of French adults. J. Gerontol. A Biol. Sci. Med. Sci. 73, 347-354 (2018).
Gopinath, B., Russell, J., Kifley, A., Flood, V. M. & Mitchell, P. Adherence to dietary guidelines and successful aging over 10 years. J. Gerontol. A Biol. Sci. Med. Sci. 71, 349-355 (2016).
Hodge, A. M., O’Dea, K., English, D. R., Giles, G. G. & Flicker, L. Dietary patterns as predictors of successful ageing. J. Nutr. Health Aging 18, 221-227 (2014).
Samieri, C. et al. The association between dietary patterns at midlife and health in aging: an observational study. Ann. Intern. Med. 159, 584-591 (2013).
Goshen, A. et al. Association of diet quality with longevity and successful aging in Israeli adults 65 years or older. JAMA Netw. Open 5, e2214916-e2214927 (2022).
Trichopoulou, A., Costacou, T., Bamia, C. & Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 348, 2599-2608 (2003).
Morris, M. C. et al. MIND diet associated with reduced incidence of Alzheimer’s disease. Alzheimers Dement. 11, 1007-1014 (2015).
Karanja, N. M. et al. Descriptive characteristics of the dietary patterns used in the Dietary Approaches to Stop Hypertension Trial. J. Am. Diet. Soc. 99, S19-S27 (1999).
Bui, L. P. et al. Planetary Health Diet Index and risk of total and cause-specific mortality in three prospective cohorts. Am. J. Clin. Nutr. 120, 80-91 (2024).
Satija, A. et al. Healthful and unhealthful plant-based diets and the risk of coronary heart disease in U.S. adults. J. Am. Coll. Cardiol. 70, 411-422 (2017).
Qin, P. et al. Fried-food consumption and risk of cardiovascular disease and all-cause mortality: a meta-analysis of observational studies. Heart 107, 1567-1575 (2021).
Björnwall, A., Mattsson Sydner, Y., Koochek, A. & Neuman, N. Eating alone or together among community-living older people-a scoping review. Int. J. Environ. Res. Public Health 18, 3495-3536 (2021).
Wang, P. et al. Optimal dietary patterns for prevention of chronic disease. Nat. Med. 29, 719-728 (2023).
Milte, C. M. & McNaughton, S. A. Dietary patterns and successful ageing: a systematic review. Eur. J. Nutr. 55, 423-450 (2016).
Yeung, S. S. Y., Kwan, M. & Woo, J. Healthy diet for healthy aging. Nutrients 13, 4310-4326 (2021).
Beard, J. R. et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet 387, 2145-2154 (2016).
Langevin, H. M., Weber, W. & Chen, W. Integrated multicomponent interventions to support healthy aging of the whole person. Aging Cell 23, e14001-e14045 (2024).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Analyses were performed in the NHS and HPFS. The NHS was established in 1976 and included 121,700 US female registered nurses aged 30-55 years . The HPFS was initiated in 1986 and recruited 51,525 male health professionals aged years . Details about the cohorts were published previously . Biennial assessments of lifestyle factors and medical history were conducted through mailed questionnaires, maintaining a follow-up rate exceeding . High validity and reproducibility of self-reported health information in the cohorts has been reported previously . For both cohorts, the baseline for this analysis was 1986, that is, when the food frequency questionnaires (FFQ) allowed for computing all dietary pattern scores.
Figure 1 shows the flow diagram of the study. Participants included in this analysis had answered the 1986 questionnaires and had a chance of attaining 70 years at the end of the follow-up (aged between 39 and 69 years at baseline; excluded). Participants with a history of one or more of 11 major chronic diseases, including cancer (except for non-melanoma skin cancers), diabetes, myocardial infarction, coronary artery disease, congestive heart failure, stroke, kidney failure, chronic obstructive pulmonary disease, Parkinson disease, multiple sclerosis and amyotrophic lateral sclerosis, at baseline ( ), with missing data for one or more dietary pattern scores between 1986 and 2010, or who reported implausible total energy intakes (<500 or for women and or for men) ( ) and with missing healthy aging phenotype ( ) were excluded.
The study protocol was approved by the institutional review boards (IRBs) of the Brigham and Women’s Hospital (BWH), Harvard T.H. Chan School of Public Health (HSPH) and participating registries (IRB protocol nos. 2001P001945/BWH and 10372) as required. Per long-standing IRB-approved procedures at BWH and HSPH, the completion and return of the baseline and subsequent follow-up questionnaires implies consent. Before 2006, consenting practices varied and many collections were conducted with implied consent. A waiver of documentation for informed consent was granted for these studies. Written informed consent was required for medical record acquisition.
Dietary assessment
Dietary intake was measured using a validated FFQ with more than 130 items administered in 1986 and every 4 years thereafter. The validity and reliability of the FFQ for measuring nutrient, food and food group intakes have been reported previously . Participants were asked how frequently they consumed specific foods in the past 12 months. Nutrients were calculated using the United States Department of Agriculture (USDA) and Harvard University Food Composition Databases , and supplemented with biochemical analyses. Based on the reported nutrient and food intakes, eight dietary pattern scores were computed, including the AHEI, aMED, DASH, MIND, hPDI, PHDI, EDIP and EDIH, as well as UPF consumption. The AHEI, aMED, DASH, MIND, hPDI, and PHDI scores, and UPF consumption, have been developed based on dietary recommendations and available evidence. The scores showed moderate-to-high validity and reproducibility and were associated with risk of health outcomes . The EDIP and EDIH were empirically derived using biomarkers of chronic inflammation and hyperinsulinemia , respectively.
The AHEI score was computed based on the intake of 11 foods and nutrients that have been positively or inversely associated with chronic disease risk, including fruits, vegetables, nuts and legumes, alcohol, red and processed meat, whole grains, sodium, trans fats and long-chain (omega-3) fatty acids . Each component was scored on a scale from 0 to 10 and the AHEI ranged from 0 to 110, a higher score indicating better overall diet quality. Adherence to the Mediterranean diet was assessed using a modified version of the 9-point aMED score . The score was calculated based on adherence to nine food items (with
either higher or lower intake) that characterize the Mediterranean diet: vegetables; legumes; fruits; nuts; whole grains; fish; moderate alcohol consumption; lower intake of red and processed meat; and monounsaturated to saturated fatty acids . The modified aMED score ranged from 0 to 9, a higher score denoting a higher adherence to the Mediterranean diet . The DASH score, designed to help prevent or treat hypertension, was based on eight dietary factors, including intake of high fruits, vegetables, nuts and legumes, low-fat dairy products, whole grain intake, low sodium, sweetened beverages and processed and unprocessed red meats . Each component was attributed a score between 0 and 5 based on intake distribution quintiles. The overall score ranged from eight (lowest adherence) to 40 (highest adherence). The MIND score included ten brain-healthy dietary factors, including leafy-green vegetables, other vegetables, berries, nuts, whole grains, fish, beans, poultry, wine (in limited amounts) and olive oil, and five less healthy factors, including butter and margarine, cheese, red meat, fast/fried foods, and pastries and sweets . Points of or 1 were attributed to each and the total MIND score ranged from 0 to 15 , a higher score indicating a higher adherence. The hPDI was designed to reflect adherence to a healthy plant-based diet ; it included 18 dietary factors and ranged from 18 (lowest adherence) to 90 (highest adherence). The PHDI was derived based on the adherence to the reference diet included in the EAT-Lancet report . The reference diet was based on evidence for health outcomes and staying within planetary boundaries for greenhouse gas emissions and other environmental parameters . The scoring criteria included 15 dietary factors. For each dietary factor, the score ranged from 0 to 10 , except for non-soy legumes and soy foods, which contributed a maximum score of 5 . The total PHDI score ranged from 0 (non-adherence) to 140 (perfect adherence). The EDIP was scored based on 18 dietary factors related to inflammation . The EDIH included 18 dietary factors related to hyperinsulinemia . Given that higher EDIH and EDIP scores denote higher hyperinsulinemia and inflammatory dietary patterns, respectively, the orientation of the scores were reversed to ease comparison with other dietary scores and were denoted as rEDIH and rEDIP. Figure 3 is a visual representation of the dietary patterns and their dietary factors.
Food items were also categorized according to the NOVA classification system . The average daily energy intake from UPFs was calculated, and the percentage of total daily energy from UPFs was determined based on the average total energy intake.
Assessment of healthy aging
Based on the construct of ‘successful aging’ described by Rowe & Kahn and previous reports , a healthy aging phenotype was defined as surviving to the age of 70 years without the presence of 11 major chronic diseases and with no impairment in cognitive function, physical function or mental health. Participants who did not meet the phenotype criteria or who died before 2016 were considered as usual agers. Those who died after 2016, but had a complete assessment of the phenotype were included in the analyses. Cognitive function was assessed using a validated Subjective Cognitive Decline questionnaire in which reporting one or fewer of seven (NHS) or six (HPFS) cognitive concerns was considered as intact cognitive function. Physical function was assessed using the 36 -item Short Form survey subsection on physical limitations that includes ten questions. Participants who reported not being limited in climbing one flight of stairs, walking one block, walking more than a mile, vacuuming, moving a table, walking several blocks, bathing or dressing, and being a little or not limited in climbing several flights of stairs, running lifting, bending, kneeling stooping and lifting carrying groceries, were considered as having intact physical function. Mental health was evaluated using the 15-item Geriatric Depression Scale, which ranges from 0 to 15 with a lower score indicating fewer depressive symptoms . Reporting 1 or fewer depressive symptom (median value of both cohorts) was considered as having intact mental health. The 11 major chronic diseases were selected as they are the primary causes of
mortality in the United States or are considered to be highly debilitating. They were also those ascertained at baseline and throughout the follow-ups. Clinical diagnoses of the major chronic diseases were reported by participants or next of kin for the deceased and were then ascertained by a physician through medical records, pathology reports or supplemental questionnaire inquiries, which are highly valid in these cohorts . In the NHS, cognitive function was assessed in 2014; the presence of chronic diseases, physical function and mental health were assessed in 2016. In the HPFS, all domains were assessed in 2016.
Assessment of covariates
Every 2 years, participants completed a questionnaire that queried on body weight, ancestry, smoking status, physical activity, multivitamin use ever, family history of chronic diseases, including myocardial infarction, type 2 diabetes, cancer and dementia, postmenopausal status and hormone use in women, marital status, living alone and history of depression (based on antidepressant medication use and self-report of depression). The questionnaires are available online at https:// nurseshealthstudy.org/participants/questionnaires for the NHS and at https://www.hsph.harvard.edu/hpfs/hpfs-questionnaires/ for the HPFS. BMI was calculated by dividing the weight (kg) by the height ( ). SES was calculated as a composite score using the participant’s geocoded address, combining US census household income, home value, college degree, ancestry, occupied housing units and unemployment, and whether families were receiving interest or dividends .
Statistical analysis
The follow-up duration was calculated from the date when the first FFQ was returned until the date of the participant’s death or the date of assessment for healthy aging in 2016, whichever occurred first. The main analysis used the average of available dietary pattern scores between 1986 and 2010 as the exposure to capture long-term intake and allow a lag of 6 years between exposures and outcomes. The residual method was used to adjust dietary pattern scores for total energy intake, including energy from alcohol , and quintiles were calculated. Missing values for covariates were replaced with the cohort-specific median value. As outcomes are binary and measured at one time point, logistic regression models were used to estimate the ORs and 95% CIs of healthy aging and its individual domains according to quintiles of energy-adjusted dietary pattern scores, with age at baseline in 1986 as a covariate (base model). The multivariable-adjusted model was further adjusted for baseline-reported ancestry (European, Asian, African-American, Other), SES (composite score) and marital status (yes/no), ever used multivitamins (yes/no), ever lived alone (yes/no), family history of dementia (yes/no), myocardial infarction, cancer, and diabetes (yes/no), and medical history of depression (yes/no), diabetes and CVD (yes/no), smoking status in 2010 (never, former, current smoker: 1-14 cigarettes per day, 15-24 cigarettes per day and cigarettes per day), postmenopausal status (yes/no) and menopausal hormone use (no, past, or current hormone use; women only), and mean (1986-2010) BMI ( ), physical activity (MET-h week ) and alcohol intake (g per day) for DASH, hPDI and PHDI. An OR above 1 indicated a higher likelihood of healthy aging. Associations using the patterns as continuous variables, standardized according to their respective increment from the 10th to the 90th percentiles, were also examined. Analyses were performed in each cohort and in the pooled cohorts. The analyses in the pooled cohorts were further adjusted for cohort(sex). Absolute risks in both quintiles were calculated using the proportion of healthy agers in Q1 and the multivariable-adjusted OR comparing Q5 versus Q1. E values and the lower or upper bound were calculated for the ORs to assess the potential impact of unmeasured confounding on the observed associations. A higher E value denotes stronger evidence that unmeasured confounding would be required to fully explain away the observed association. Prespecified subgroup analyses were conducted according to cohort (sex), BMI (<25 versus ), physical activity (above/below median), smoking (yes/no), SES (above/below median) and ancestry (European/non-European). Potential subgroup interactions were evaluated using interaction models, including the product of the subgroup and the exposure. As secondary analyses, the association of dietary patterns scores with healthy aging using an age cutoff of 75 years, and the association of UPF consumption with healthy aging (>70 years) were assessed. As a sensitivity analysis, we applied linear weights to dietary pattern scores across seven time points, ranging from 1986 to 2010, assigning the highest weight to the year closest to the healthy aging assessment (2010) and the lowest weight to 1986.
Intake in the individual food groups and nutrients that reflect the dietary pattern scores were also energy-adjusted and standardized according to their respective increment from the 10th to the 90th percentiles. The associations of energy-adjusted food group and nutrient intakes with healthy aging and its domains were examined using logistic regressions, accounting for the covariates described in the multivariable-adjusted model. Given that all dietary factors are also found in the pattern scores, the models were not adjusted for any measure of diet quality. values were corrected for FDR using the Ben-jamini-Hochberg method; an FDR-corrected was considered statistically significant.
Analyses were performed with SAS v.9.4 (SAS Institute) and R v.4.2.0. Statistical tests were two-sided and was considered statistically significant.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Because of participant confidentiality and privacy concerns, data are available only upon written request. According to standard controlled access procedures, applications to use the NHS and HPFS resources will be reviewed by our External Collaborators Committee for scientific aims, evaluation of the fit of the data for the proposed methodology and verification that the proposed use meets the guidelines of the Ethics and Governance Framework and the consent that was provided by the participants. Investigators can expect initial responses within 4 weeks of request submission. Further information, including the procedures for obtaining and accessing data from the NHS and HPSF is described at https://www.nurseshealthstudy.org/researchers (nhsaccess@channing.harvard.edu) and https://hsph.harvard.edu/research/health-professionals/resources/ for-external-collaborators/. The USDA and Harvard University food composition databases are publicly available at https://www.fns. usda.gov/usda-fis/usda-foods-database and https://hsph.harvard. edu/department/nutrition/nutrition-questionnaire-service-center /#nutrient-data.
Code availability
The analysis code is publicly available through GitHub (https://github. com/DrTessier/diets_healthyaging/).
References
Bao, Y. et al. Origin, methods, and evolution of the three Nurses’ Health Studies. Am. J. Public Health 106, 1573-1581 (2016).
Rimm, E. B. et al. Prospective study of alcohol consumption and risk of coronary disease in men. Lancet 338, 464-468 (1991).
Colditz, G. A. et al. Validation of questionnaire information on risk factors and disease outcomes in a prospective cohort study of women. Am. J. Epidemiol. 123, 894-900 (1986).
Rimm, E. B. et al. Validity of self-reported waist and hip circumferences in men and women. Epidemiology 1, 466-473 (1990).
Wolf, A. M. et al. Reproducibility and validity of a self-administered physical activity questionnaire. Int. J. Epidemiol. 23, 991-999 (1994).
Gu, X. et al. Validity and reproducibility of a semiquantitative food frequency questionnaire for measuring intakes of foods and food groups. Am. J. Epidemiol. 193, 170-179 (2024).
Yuan, C. et al. Relative validity of nutrient intakes assessed by questionnaire, 24 -hour recalls, and diet records as compared with urinary recovery and plasma concentration biomarkers: findings for women. Am. J. Epidemiol. 187, 1051-1063 (2018).
Yue, Y. et al. Reproducibility and validity of diet quality scores derived from food-frequency questionnaires. Am. J. Clin. Nutr. 115, 843-853 (2022).
Berendsen, A. M. et al. Association of long-term adherence to the MIND diet with cognitive function and cognitive decline in American women. J. Nutr. Health Aging 22, 222-229 (2018).
Shan, Z. et al. Healthy eating patterns and risk of total and cause-specific mortality. JAMA Intern. Med. 183, 142-153 (2023).
Fung, T. T. et al. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch. Intern. Med. 168, 713-720 (2008).
Tabung, F. K. et al. An empirical dietary inflammatory pattern score enhances prediction of circulating inflammatory biomarkers in adults. J. Nutr. 147, 1567-1577 (2017).
Tabung, F. K. et al. Development and validation of empirical indices to assess the insulinaemic potential of diet and lifestyle. Br. J. Nutr. 116, 1787-1798 (2016).
Chiuve, S. E. et al. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 142, 1009-1018 (2012).
Satija, A. & Hu, F. B. Plant-based diets and cardiovascular health. Trends Cardiovasc. Med. 28, 437-441 (2018).
Willett, W. et al. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 393, 447-492 (2019).
Tabung, F. K. et al. Development and validation of an empirical dietary inflammatory index. J. Nutr. 146, 1560-1570 (2016).
Khandpur, N. et al. Categorising ultra-processed foods in large-scale cohort studies: evidence from the Nurses’ Health Studies, the Health Professionals Follow-up Study, and the Growing Up Today Study. J. Nutr. Sci. 10, e77-e91 (2021).
Rowe, J. W. & Kahn, R. L. Human aging: usual and successful. Science 237, 143-149 (1987).
Sun, Q. et al. Alcohol consumption at midlife and successful ageing in women: a prospective cohort analysis in the nurses’ health study. PLoS Med. 8, e1001090-e1001099 (2011).
Shi, H. et al. Sleep duration and snoring at midlife in relation to healthy aging in women 70 years of age or older. Nat. Sci. Sleep 13, 411-422 (2021).
Shi, H., Huang, T., Schernhammer, E. S., Sun, Q. & Wang, M. Rotating night shift work and healthy aging after 24 years of follow-up in the Nurses’ Health Study. JAMA Netw. Open 5, e2210450-e2210464 (2022).
Ardisson Korat, A. V. et al. Dietary protein intake in midlife in relation to healthy aging—results from the prospective Nurses’ Health Study cohort. Am. J. Clin. Nutr. 119, 271-282 (2024).
Molinuevo, J. L. et al. Implementation of subjective cognitive decline criteria in research studies. Alzheimers Dement. 13, 296-311 (2017).
Ware, J. E. & Sherbourne, C. D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 30, 473-483 (1992).
de Craen, A. J. M., Heeren, T. J. & Gussekloo, J. Accuracy of the 15 -item geriatric depression scale (GDS-15) in a community sample of the oldest old. Int. J. Geriatr. Psychiatry 18, 63-66 (2003).
Xu, J., Murphy, S. L., Kochanek, K. D. & Arias, E. Mortality in the United States, 2021. NCHS Data Brief www.cdc.gov/nchs/products/ databriefs/db456.htm (US Department of Health and Human Services, CDC & National Center for Health Statistics, 2022).
Sun, Q. et al. Physical activity at midlife in relation to successful survival in women at age 70 years or older. Arch. Intern. Med. 170, 194-201 (2010).
DeVille, N. V. et al. Neighborhood socioeconomic status and mortality in the Nurses’ Health Study (NHS) and the Nurses’ Health Study II (NHSII). Environ. Epidemiol. 7, e235-e241 (2022).
Willett, W. & Stampfer, M. J. Total energy intake: implications for epidemiologic analyses. Am. J. Epidemiol. 124, 17-27 (1986).
Acknowledgements
The NHS and HPFS are supported by grants from the National Institutes of Health (nos. UM1 CA186107, P01 CA87969, RO1 HL034594, R01 HL088521, U01 CA167552 and R01 HL35464). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. A.-J.T. was supported by a Canadian Institutes of Health Research Postdoctoral Fellowship Award. A.A.K. was supported by a USDA Cooperative Agreement no. 58-8050-3-003 and the National Center for Advancing Translational Sciences (no. 1K12TROO4384). J.L. was supported by National Institute of Diabetes and Digestive and Kidney Diseases (nos. ROODK122128 and RO1AG087356). M.G.-F. was supported by a Novo Nordisk Foundation grant no. NNF23SA0084103. The funders had no role in the design and conduct of the study, data collection, management, analysis and interpretation, preparation, review or approval of the manuscript, and decision to submit the manuscript for publication.
Author contributions
A.-J.T. and M.G.-F. had full access to all the study data and take responsibility for the integrity of the data and the accuracy of the data analysis. A.-J.T., M.G.-F. and F.B.H. designed the research. A.-J.T. conducted the analyses, prepared the tables and figures, and wrote the manuscript. All authors contributed to the interpretation of the results and critical revision of the manuscript for important intellectual content. All authors approved the final version of the manuscript. The corresponding author attests that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted.
Competing interests
M.G.-F. is the principal investigator of a grant funded by the International Nut Council. The other authors declare no competing interests.
Correspondence and requests for materials should be addressed to Anne-Julie Tessier, Frank B. Hu or Marta Guasch-Ferré.
Peer review information Nature Medicine thanks Eirini Trichia and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Michael Basson, in collaboration with the Nature Medicine team.
Extended Data Fig. 1| Pairwise Spearman correlations between energyadjusted average (1986-2010) dietary pattern scores. A. Pairwise Spearman correlations were applied in the pooled main dataset ( ). P values for all correlations are two-sided and <0.0001 (not adjusted for multiple comparisons); B. Pairwise Spearman correlations were applied in the pooled dataset excluded participants with missing UPF data ( ). P values for all correlations are two-sided and (not adjusted for multiple comparisons). AHEI,
B
alternative healthy eating index; AMED, alternative Mediterranean diet index; DASH, Dietary approaches to stop hypertension; MIND, Mediterranean-DASH intervention for neurodegenerative delay diet; hPDI, healthful plant-based diet index; PHDI, planetary health diet index; EDIH, empirical dietary index for hyperinsulinemia; EDIP, empirical dietary inflammatory pattern. The rEDIH and rEDIP are reversed scores to allow for comparison with other dietary scores.
Extended Data Table 1 | Age-standardized characteristics of the study population in the lowest and highest quintiles of energy-adjusted dietary pattern scores in the NHS between 1986 and 2010
Quintile
Q1
Q5
Q1
Q5
Q1
Q5
Q1
Q5
14,018
14,018
14,018
14,018
14,018
14,018
14,018
14,018
Dietary score
AHEI-2010
AMED
DASH
MIND
Energy-adjusted score
41.5 (3.9)
67.9 (4.7)
2.4 (0.6)
6.3 (0.6)
18.3 (1.8)
29.3 (1.7)
6.0 (0.6)
9.5 (0.6)
Age, at baseline
53.0 (7.3)
52.2 (7.1)
52.3 (7.4)
53.2 (7.0)
51.2 (7.2)
54.4 (7.0)
54.0 (7.2)
52.0 (7.1)
Ancestry
European
95.0
93.5
95.1
93.8
94.3
94.2
95.2
93.2
Asian
0.3
1.3
0.4
1.1
0.7
0.9
0.3
1.4
African
1.0
1.6
0.8
1.7
1.4
1.4
0.8
2.0
Other
3.7
3.5
3.8
3.4
3.6
3.6
3.7
3.5
SES score, at baseline
-0.9 (3.3)
1.0 (4.1)
-0.6 (3.4)
0.7 (4)
-0.6 (3.5)
0.6 (3.9)
-0.9 (3.3)
0.9 (4)
Alone, ever
30.7
32.6
31.7
31.4
29.8
35.0
34.4
29.8
History of depression, yes
21.4
18.2
22.3
17.4
21.0
17.9
22.1
17.8
History of cancer, yes
4.3
4.0
4.0
4.3
3.7
4.3
4.3
4.0
History of diabetes, yes
3.0
2.3
2.5
2.4
1.9
3.1
2.9
2.5
History of CVD, yes
4.8
3.5
4.2
3.8
3.8
4.4
4.8
3.7
Family history of dementia, yes
15.5
19.8
16.2
18.4
16.4
17.9
15.9
18.6
Multivitamin use, ever
81.1
92.8
82.1
91.9
81.0
92.0
82.6
91.7
BMI, kg/m2
26.6 (5.5)
25.3 (4.4)
26.7 (5.5)
25.3 (4.4)
26.5 (5.4)
25.3 (4.6)
26.6 (5.5)
25.4 (4.5)
Never smoker, %
67.5
52.8
62.0
58.4
59.0
63.1
65.4
57.1
Physical activity, MET task-h/wk
0.9 (1.4)
2.7 (2.7)
0.9 (1.5)
2.6 (2.7)
0.9 (1.5)
2.6 (2.7)
0.9 (1.5)
2.7 (2.7)
Alcohol intake, g/d
5.1 (11.1)
6.3 (7.1)
5.3 (10.9)
5.9 (7)
6.3 (10.7)
4.5 (7)
4 (8.7)
6.4 (8.1)
Energy intake, kcal
1726 (456)
1725 (449)
1714 (485)
1723 (396)
1728 (472)
1737 (420)
1724 (484)
1722 (433)
Dietary score
hPDI
PHDI
rEDIH
rEDIP
Energy-adjusted score
47.0 (2.4)
62.5 (2.8)
66.4 (4.6)
92.9 (5.0)
-0.5 (0.1)
0.0 (0.1)
-0.3 (0.1)
0.4 (0.2)
Age, at baseline Ancestry
52.2 (7.3)
53.4 (7.1)
53.1 (7.4)
52.2 (7.0)
51.4 (7.3)
53.1 (7.1)
52.6 (7.3)
52.0 (7.1)
European
95.3
93.3
95.1
92.8
94.5
95.3
92.6
96.3
Asian
0.4
1.3
0.3
1.8
0.5
0.7
1.3
0.3
African
1.1
1.7
0.8
1.9
1.6
0.6
2.5
0.3
Other
3.3
3.7
3.7
3.6
3.4
3.4
3.7
3.1
SES score, at baseline
-0.3 (3.5)
0.4 (4)
-0.6 (3.4)
0.8 (4)
-0.6 (3.4)
0.8 (4)
-0.6 (3.5)
0.7 (3.9)
Alone, ever
31.7
32.3
31.9
31.3
28.8
33.1
29.7
31.3
History of depression, yes
19.9
18.0
21.5
18.1
23.0
17.5
23.3
17.5
History of cancer, yes
4.0
4.3
4.5
3.8
4.0
4.1
4.3
4.0
History of diabetes, yes
1.9
3.6
2.8
2.3
4.8
1.2
5.1
1.2
History of CVD, yes
4.0
4.3
4.7
3.4
5.1
3.2
5.8
2.6
Family history of dementia, yes
17.1
17.8
15.0
19.6
15.9
19.3
15.9
18.9
Multivitamin use, ever
83.7
90.6
81.2
92.9
82.9
90.6
83.7
89.5
BMI, kg/m2
26.7 (5.4)
25.3 (4.6)
26.4 (5.4)
25.3 (4.5)
28.3 (5.9)
24.2 (3.8)
28.1 (5.8)
24.5 (4)
Never smoker, %
62.6
59.3
66.5
53.7
65.8
53.2
67.4
51.2
Physical activity, MET task-h/wk
1.0 (1.6)
2.5 (2.8)
0.9 (1.6)
2.6 (2.7)
1.1 (1.7)
2.4 (2.6)
1.2 (1.8)
2.2 (2.5)
Alcohol intake, g/d
5 (8.7)
5.7 (9)
4.7 (9.1)
6.2 (8.6)
3.5 (7.5)
10.4 (11.7)
2.8 (6.7)
11.5 (12.2)
Energy intake, kcal
1731 (430)
1722 (464)
1714 (485)
1716 (434)
1781 (490)
1806 (434)
1769 (481)
1769 (449)
Extended Data Table 2 | Age-standardized characteristics of the study population in the lowest and highest quintiles of energy-adjusted dietary pattern scores in the HPFS between 1986 and 2010
Quintile
Q1
Q5
Q1
Q5
Q1
Q5
Q1
Q5
6,984
6,984
6,984
6,984
6,984
6,984
6,984
6,984
Dietary score
AHEI-2010
AMED
DASH
MIND
Energy-adjusted score
41.9 (4.4)
69.9 (4.5)
1.9 (0.6)
6.2 (0.6)
18.1 (1.9)
30.1 (1.8)
6.0 (0.6)
9.8 (0.6)
Age, at baseline
54.5 (8.7)
54.5 (8.5)
53.2 (8.7)
55.4 (8.4)
52.3 (8.5)
56.7 (8.4)
55.3 (8.7)
53.8 (8.5)
Ancestry
European
95.7
95.1
96.3
94.8
94.9
95.8
96.1
94.5
Asian
1.1
1.5
1.0
1.6
2.0
1.0
1.1
1.9
African
1.2
1.0
0.9
1.2
1.3
0.9
0.7
1.1
Other
2.0
2.4
1.7
2.4
1.8
2.3
2.1
2.5
SES score, at baseline
-0.7 (3.4)
0.7 (3.9)
-0.6 (3.4)
0.6 (3.9)
-0.6 (3.5)
0.5 (3.8)
-0.8 (3.4)
0.7 (3.8)
Alone, ever
20.7
20.3
21.7
18.9
22.0
18.9
21.6
18.9
History of depression, yes
4.1
3.4
4.5
3.1
4.5
2.8
4.1
3.2
History of cancer, yes
4.8
3.7
4.2
4.3
4.1
4.1
4.5
3.4
History of diabetes, yes
3.9
3.4
2.9
3.7
1.8
5.4
3.8
3.4
History of CVD, yes
6.3
8.1
5.3
9.8
4.9
10.6
6.2
8.9
Family history of dementia, yes
3.3
3.3
3.5
3.3
3.4
3.3
3.0
3.6
Multivitamin use, ever
72.4
88.7
75.4
86.3
74.3
85.4
73.0
88.2
BMI,
26.4 (3.9)
25.2 (3.3)
26.5 (3.9)
25.1 (3.3)
26.3 (3.8)
25.1 (3.4)
26.4 (4)
25.2 (3.2)
Never smoker, %
80.9
71.3
74.1
76.0
72.4
80.0
78.9
72.7
Physical activity, MET task-h/wk
2.1 (2.9)
5.1 (4.4)
2.3 (3.1)
4.9 (4.4)
2.3 (3)
4.8 (4.5)
2.2 (3.2)
5.1 (4.4)
Alcohol intake, g/d
12.9 (18.6)
10.7 (9.6)
12.9 (17.6)
10.9 (10.4)
13.7 (16.5)
9.1 (11.4)
10.7 (15.1)
11.6 (12.2)
Energy intake, kcal
1987 (528)
1990 (511)
2013 (554)
2012 (485)
2006 (543)
2008 (489)
1999 (555)
1994 (502)
Dietary score
hPDI
PHDI
rEDIH
rEDIP
Energy-adjusted score
46.8 (2.5)
63.4 (3.1)
63.0 (5.5)
94.4 (5.2)
-0.7 (0.2)
-0.1 (0.1)
-0.4 (0.2)
0.4 (0.2)
Age, at baseline
53.1 (8.7)
55.6 (8.4)
54.0 (8.8)
54.4 (8.3)
53.3 (8.8)
54.6 (8.5)
55.0 (8.7)
53.1 (8.4)
Ancestry
European
95.6
94.8
95.5
94.6
95.0
96.1
93.0
97.0
Asian
1.2
1.8
1.3
2.1
1.3
1.1
2.5
0.6
African
1.0
1.2
1.2
1.0
1.6
0.7
2.1
0.4
Other
2.2
2.3
2.0
2.3
2.0
2.2
2.4
2.0
SES score, at baseline
-0.1 (3.6)
0.1 (3.8)
-0.6 (3.5)
0.6 (3.8)
-0.8 (3.4)
0.7 (3.9)
-0.4 (3.6)
0.2 (3.7)
Alone, ever
20.1
19.3
20.6
19.7
19.8
20.4
20.1
20.7
History of depression, yes
4.3
3.3
4.0
3.4
4.5
3.4
4.3
3.4
History of cancer, yes
4.4
4.1
4.1
3.8
4.3
3.7
4.4
3.7
History of diabetes, yes
1.9
5.1
3.8
3.5
5.9
1.7
5.7
2.0
History of CVD, yes
5.0
9.5
5.8
8.3
6.7
6.8
8.4
5.2
Family history of dementia, yes
3.2
3.3
3.1
3.3
3.0
3.5
3.2
3.1
Multivitamin use, ever
76.0
85.1
73.0
88.5
74.9
85.7
77.6
83.1
BMI,
26.2 (3.7)
25.4 (3.6)
26.4 (4)
25.1 (3.1)
27.1 (4.2)
24.9 (3.1)
26.8 (4.1)
25.5 (3.2)
Never smoker, %
75.9
74.1
78.5
70.2
78.2
69.9
79.3
67.9
Physical activity, MET task-h/wk
2.6 (3.3)
4.7 (4.5)
2.4 (3.3)
5 (4.4)
2.5 (3.4)
4.7 (4.3)
2.9 (3.7)
4.1 (4.1)
Alcohol intake, g/d
10.1 (12.6)
12.3 (14.5)
10.5 (14.6)
12.1 (13.1)
8.8 (12.5)
17.2 (16.3)
6.5 (10.7)
21.4 (17.3)
Energy intake, kcal
2008 (502)
1999 (531)
1985 (592)
1982 (470)
2086 (574)
2105 (510)
2068 (572)
2062 (513)
Extended Data Table 3 | Associations of average dietary pattern scores (1986-2010) with healthy aging and its domains in the pooled cohorts
Outcome
Healthy aging
Healthy aging
Intact cognition
Intact physical function
Intact mental health
No chronic disease
Survived to 70 years
Cases Dietary score
Model
9,771 OR (95%CI) (Q5 vs. Q1)
9,771 OR (95%CI) (continuous)
29,543 OR (95%CI) (Q5 vs. Q1)
27,842 OR (95%CI) (Q5 vs. Q1)
27,842 OR (95%CI) (Q5 vs. Q1)
23,908 OR (95%CI) (Q5 vs. Q1)
39,769 OR (95%CI) (Q5 vs. Q1)
AHEI-2010
Age
3.06 (2.84, 3.30)
2.71 (2.56, 2.87)
2.46 (2.34, 2.57)
4.03 (3.82, 4.26)
3.27 (3.10, 3.44)
2.57 (2.44, 2.71)
3.38 (3.21, 3.55)
MV
1.86 (1.71, 2.01)
1.71 (1.60, 1.82)
1.62 (1.54, 1.71)
2.30 (2.16, 2.44)
2.03 (1.92, 2.15)
1.64 (1.54, 1.74)
2.14 (2.02, 2.27)
AMED
Age
2.67 (2.48, 2.87)
2.43 (2.29, 2.58)
1.82 (1.74, 1.91)
2.91 (2.76, 3.07)
2.50 (2.37, 2.63)
2.06 (1.96, 2.17)
2.16 (2.05, 2.26)
MV
1.70 (1.57, 1.84)
1.59 (1.49, 1.70)
1.35 (1.28, 1.42)
1.75 (1.65, 1.86)
1.67 (1.58, 1.77)
1.43 (1.35, 1.52)
1.53 (1.44, 1.62)
DASH
Age
2.62 (2.43, 2.81)
2.48 (2.34, 2.64)
1.85 (1.77, 1.94)
2.79 (2.64, 2.94)
2.42 (2.30, 2.55)
2.01 (1.91, 2.12)
2.10 (1.99, 2.20)
MV
1.69 (1.56, 1.83)
1.65 (1.54, 1.76)
1.40 (1.33, 1.48)
1.73 (1.63, 1.84)
1.64 (1.55, 1.74)
1.43 (1.35, 1.51)
1.50 (1.41, 1.59)
MIND
Age
2.47 (2.29, 2.67)
2.36 (2.22, 2.50)
1.82 (1.74, 1.91)
2.93 (2.78, 3.09)
2.50 (2.37, 2.63)
1.91 (1.81, 2.01)
2.12 (2.02, 2.22)
MV
1.60 (1.47, 1.73)
1.57 (1.47, 1.68)
1.40 (1.33, 1.48)
1.82 (1.72, 1.94)
1.75 (1.65, 1.85)
1.35 (1.28, 1.43)
1.59 (1.50, 1.69)
hPDI
Age
2.00 (1.87, 2.15)
1.88 (1.78, 1.99)
1.44 (1.38, 1.51)
2.18 (2.07, 2.29)
1.78 (1.69, 1.87)
1.64 (1.56, 1.72)
1.60 (1.52, 1.68)
MV
1.45 (1.35, 1.57)
1.40 (1.32, 1.49)
1.21 (1.15, 1.28)
1.56 (1.47, 1.65)
1.37 (1.30, 1.45)
1.32 (1.25, 1.40)
1.33 (1.26, 1.41)
PHDI
Age
2.75 (2.55, 2.96)
2.44 (2.31, 2.59)
2.45 (2.34, 2.56)
3.73 (3.54, 3.93)
3.01 (2.86, 3.17)
2.43 (2.31, 2.57)
3.35 (3.19, 3.52)
MV
1.68 (1.55, 1.82)
1.56 (1.47, 1.66)
1.65 (1.57, 1.74)
2.16 (2.04, 2.30)
1.89 (1.78, 2.00)
1.55 (1.47, 1.65)
2.17 (2.05, 2.30)
rEDIH
Age
3.20 (2.96, 3.46)
2.60 (2.45, 2.76)
2.15 (2.05, 2.26)
3.89 (3.68, 4.11)
2.79 (2.64, 2.95)
2.89 (2.73, 3.06)
2.87 (2.72, 3.02)
MV
1.80 (1.64, 1.96)
1.53 (1.43, 1.63)
1.42 (1.34, 1.50)
1.78 (1.67, 1.90)
1.62 (1.52, 1.72)
1.75 (1.65, 1.87)
1.71 (1.61, 1.82)
rEDIP
Age
2.34 (2.17, 2.53)
1.84 (1.75, 1.94)
1.57 (1.50, 1.64)
2.45 (2.33, 2.58)
1.98 (1.88, 2.09)
2.20 (2.09, 2.32)
1.90 (1.81, 2.00)
MV
1.58 (1.45, 1.72)
1.29 (1.22, 1.37)
1.14 (1.09, 1.21)
1.38 (1.30, 1.46)
1.34 (1.27, 1.42)
1.52 (1.43, 1.61)
1.29 (1.22, 1.37)
Sample size of . The age-adjusted logistic regression models are adjusted for age at baseline (1986) and cohort (sex). The MV-adjusted logistic regression models are adjusted for age at baseline (1986), cohort (sex), BMI (kg/m²), ancestry (European, Asian, African-American, other), smoking status (never, former, current smoker: 1-14 cigarettes per day, 15-24 cigarettes per day, and cigarettes per day), alcohol intake (g/d), physical activity (metabolic equivalent task-hours/week), multivitamin use ever (yes/no), family history of myocardial infarction (yes/ no), family history of type 2 diabetes, family history of cancer, family history of dementia (yes/no), postmenopausal status (yes/no) and menopausal hormone use (no, past, or current hormone use) (only women), socio-economic status at baseline, marital status (yes/no), living alone ever (yes/no), history of depression (yes/no). MV, multivariable; OR, odds ratio; CI, confidence interval; AHEI, alternative healthy eating index; AMED, alternative Mediterranean diet index; DASH, Dietary approaches to stop hypertension; MIND, Mediterranean-DASH intervention for neurodegenerative delay diet; hPDI, healthful plant-based diet index; PHDI, planetary health diet index; EDIH, empirical dietary index for hyperinsulinemia; EDIP, empirical dietary inflammatory pattern. The EDIH and EDIP are reversed scores to allow for comparison with other dietary scores.
Extended Data Table 4 | Absolute risks for Q1 and Q5 across all dietary pattern scores
Dietary pattern
Absolute risks, %
Q1
Q5
AHEI
5.3 (5.4, 5.3)
9.9 (9.2, 10.7)
AMED
6.1 (6.2, 6.1)
10.4 (9.7, 11.2)
DASH
7.3 (7.4, 7.2)
12.4 (11.5, 13.2)
MIND
5.1 (5.2, 5.1)
8.2 (7.6, 8.8)
hPDI
7.7 (7.8, 7.7)
11.2 (10.5, 12.0)
PHDI
5.6 (5.6, 5.5)
9.4 (8.7, 10.1)
rEDIH
5.3 (5.3, 5.2)
9.5 (8.7, 10.2)
rEDIP
5.3 (5.4, 5.3)
8.4 (7.8, 9.1)
The proportion of healthy agers in Q1 and the multivariable-adjusted OR comparing Q5 versus Q1 was used to calculate the absolute risks in both quintiles.
Extended Data Table 5 | Associations of average dietary pattern scores (1986-2010) with healthy aging using an age cutoff of 75 years
Outcome
Healthy aging
Healthy aging
Cases
Total 89,755
5,445
5,445
Dietary score
Model
OR (95%CI) (Q5 vs. Q1)
OR (95%CI) (continuous)
AHEI-2010
Age
4.36 (3.94, 4.83)
3.46 (3.21, 3.73)
MV
2.24 (2.01, 2.50)
1.91 (1.76, 2.08)
AMED
Age
3.25 (2.95, 3.58)
2.89 (2.67, 3.12)
MV
1.86 (1.67, 2.06)
1.71 (1.58, 1.86)
DASH
Age
3.16 (2.87, 3.48)
2.89 (2.68, 3.13)
MV
1.84 (1.66, 2.04)
1.77 (1.62, 1.92)
MIND
Age
3.02 (2.73, 3.34)
2.74 (2.54, 2.96)
MV
1.78 (1.60, 1.98)
1.70 (1.56, 1.85)
hPDI
Age
2.36 (2.15, 2.59)
2.18 (2.03, 2.34)
MV
1.61 (1.46, 1.77)
1.53 (1.42, 1.66)
PHDI
Age
3.70 (3.35, 4.09)
3.12 (2.90, 3.36)
MV
1.94 (1.74, 2.16)
1.77 (1.63, 1.91)
rEDIH
Age
4.23 (3.79, 4.72)
3.17 (2.94, 3.41)
MV
2.03 (1.80, 2.30)
1.68 (1.54, 1.83)
rEDIP
Age
2.85 (2.57, 3.15)
2.04 (1.91, 2.17)
MV
1.68 (1.50, 1.88)
1.34 (1.24, 1.44)
Sample size of . The age-adjusted logistic regression models are adjusted for age at baseline (1986) and cohort (sex). The MV-adjusted logistic regression models are adjusted for age at baseline (1986), cohort (sex), BMI (kg/m²), ancestry (European, Asian, African-American, other), smoking status (never, former, current smoker: 1-14 cigarettes per day, 15-24 cigarettes per day, and cigarettes per day), alcohol intake (g/d), physical activity (metabolic equivalent task-hours/week), multivitamin use ever (yes/no), family history of myocardial infarction (yes/ no), family history of type 2 diabetes, family history of cancer, family history of dementia (yes/no), postmenopausal status (yes/no) and menopausal hormone use (no, past, or current hormone use) (only women), socio-economic status at baseline, marital status (yes/no), living alone ever (yes/no), history of depression (yes/no), in the pooled cohorts. MV, multivariable; OR, odds ratio; CI , confidence interval; AHEI, alternative healthy eating index; AMED, alternative Mediterranean diet index; DASH, Dietary approaches to stop hypertension; MIND, Mediterranean-DASH intervention for neurodegenerative delay diet; hPDI, healthful plant-based diet index; PHDI, planetary health diet index; EDIH, empirical dietary index for hyperinsulinemia; EDIP, empirical dietary inflammatory pattern. The EDIH and EDIP are reversed scores to allow for comparison with other dietary scores.
Extended Data Table 6 | Associations of weighted average dietary pattern scores (1986-2010) with healthy aging
Outcome
Healthy aging
Healthy aging
Cases
Total 105,015
9,771
9,771
Dietary score
Model
OR (95%CI) (Q5 vs. Q1)
OR (95%CI) (continuous)
AHEI-2010
Age
3.22 (2.92, 3.54)
2.87 (2.66, 3.09)
MV
1.97 (1.77, 2.19)
1.82 (1.67, 1.97)
AMED
Age
2.52 (2.30, 2.77)
2.34 (2.17, 2.53)
MV
1.63 (1.48, 1.81)
1.54 (1.42, 1.67)
DASH
Age
2.59 (2.36, 2.84)
2.41 (2.23, 2.60)
MV
1.67 (1.51, 1.85)
1.61 (1.48, 1.76)
MIND
Age
2.42 (2.20, 2.67)
2.30 (2.13, 2.49)
MV
1.61 (1.45, 1.78)
1.56 (1.43, 1.69)
hPDI
Age
1.94 (1.77, 2.12)
1.86 (1.73, 2.00)
MV
1.43 (1.30, 1.57)
1.41 (1.31, 1.52)
PHDI
Age
2.62 (2.38, 2.88)
2.41 (2.24, 2.60)
MV
1.64 (1.48, 1.81)
1.56 (1.44, 1.68)
rEDIH
Age
3.06 (2.76, 3.38)
2.56 (2.37, 2.76)
MV
1.79 (1.60, 2.01)
1.57 (1.44, 1.70)
rEDIP
Age
2.28 (2.07, 2.52)
1.72 (1.61, 1.83)
MV
1.60 (1.43, 1.79)
1.26 (1.17, 1.35)
Sample size of . The age-adjusted logistic regression models are adjusted for age at baseline (1986) and cohort (sex). The MV-adjusted logistic regression models are adjusted for age at baseline (1986), cohort (sex), BMI (kg/m²), ancestry (European, Asian, African-American, other), smoking status (never, former, current smoker: 1-14 cigarettes per day, 15-24 cigarettes per day, and cigarettes per day), alcohol intake (g/d), physical activity (metabolic equivalent task-hours/week), multivitamin use ever (yes/no), family history of myocardial infarction (yes/ no), family history of type 2 diabetes, family history of cancer, family history of dementia (yes/no), postmenopausal status (yes/no) and menopausal hormone use (no, past, or current hormone use) (only women), socio-economic status at baseline, marital status (yes/no), living alone ever (yes/no), history of depression (yes/no), in the pooled cohorts. MV, multivariable; OR, odds ratio; CI, confidence interval; AHEI, alternative healthy eating index; AMED, alternative Mediterranean diet index; DASH, Dietary approaches to stop hypertension; MIND, Mediterranean-DASH intervention for neurodegenerative delay diet; hPDI, healthful plant-based diet index; PHDI, planetary health diet index; EDIH, empirical dietary index for hyperinsulinemia; EDIP, empirical dietary inflammatory pattern. The EDIH and EDIP are reversed scores to allow for comparison with other dietary scores. Linear weights were applied as follows: 1986=1,1990=2,1994=3, .
Extended Data Table 7 | Associations of average ultraprocessed food consumption (1986-2010) with healthy aging and its domains in the pooled cohorts
Outcome
Healthy aging
Healthy aging
Intact cognition
Intact physical function
Intact mental health
No chronic disease
Survived to 70 years
Cases
9,768
9,768
35,541
29,526
27,828
23,898
39,757
Dietary score
Model
OR (95%CI) (Q5 vs. Q1)
E-values (Upper bound)
OR (95%CI) (continuous)
OR (95%CI) (Q5 vs. Q1)
OR (95%CI) (Q5 vs. Q1)
OR (95%CI) (Q5 vs. Q1)
OR (95%CI) (Q5 vs. Q1)
OR (95%CI) (Q5 vs. Q1)
UPF
Age
0.50 (0.47, 0.54)
3.41 ( 3.11)
0.54 (0.51, 0.57)
0.79 (0.75, 0.83)
0.54 (0.51, 0.57)
0.57 (0.54, 0.60)
0.69 (0.65, 0.73)
0.75 (0.72, 0.79)
MV
0.68 (0.63, 0.73)
2.30 (2.08)
0.72 (0.67, 0.76)
0.89 (0.84, 0.94)
0.73 (0.69, 0.78)
0.71 (0.67, 0.75)
0.85 (0.80, 0.90)
0.83 (0.79, 0.88)
Sample size of without missing UPF intake. The age-adjusted logistic regression models are adjusted for age at baseline (1986) and cohort (sex). The MV-adjusted logistic regression models are adjusted for age at baseline (1986), cohort (sex), BMI (kg/m²), ancestry (European, Asian, African-American, other), smoking status (never, former, current smoker: 1-14 cigarettes per day, 15-24 cigarettes per day, and cigarettes per day), alcohol intake (g/d), physical activity (metabolic equivalent task-hours/week), multivitamin use ever (yes/no), family history of myocardial infarction (yes/no), family history of type 2 diabetes, family history of cancer, family history of dementia (yes/no), postmenopausal status (yes/no) and menopausal hormone use (no, past, or current hormone use) (only women), socio-economic status at baseline, marital status (yes/no), living alone ever (yes/no), history of depression (yes/no), in the pooled cohorts. MV, multivariable; OR, odds ratio; CI, confidence interval; UPF, ultraprocessed foods (nova 4); Q1: lowest UPF intake; Q5: highest UPF intake. UPF intake as % of total energy was used.
natureportfolio
Corresponding author(s):
Last updated by author(s): January 23, 2025
Reporting Summary
Nature Portfolio wishes to improve the reproducibility of the work that we publish. This form provides structure for consistency and transparency in reporting. For further information on Nature Portfolio policies, see our Editorial Policies and the Editorial Policy Checklist.
Statistics
For all statistical analyses, confirm that the following items are present in the figure legend, table legend, main text, or Methods section.
n/a
Confirmed
□ X
The exact sample size for each experimental group/condition, given as a discrete number and unit of measurement
□
A statement on whether measurements were taken from distinct samples or whether the same sample was measured repeatedly
□
The statistical test(s) used AND whether they are one- or two-sided
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
□
A description of all covariates tested
□
A description of any assumptions or corrections, such as tests of normality and adjustment for multiple comparisons
□
A full description of the statistical parameters including central tendency (e.g. means) or other basic estimates (e.g. regression coefficient) AND variation (e.g. standard deviation) or associated estimates of uncertainty (e.g. confidence intervals)
□ X
For null hypothesis testing, the test statistic (e.g. F, t, r) with confidence intervals, effect sizes, degrees of freedom and value noted Give values as exact values whenever suitable.
□ For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
□ For hierarchical and complex designs, identification of the appropriate level for tests and full reporting of outcomes
□ Estimates of effect sizes (e.g. Cohen’s , Pearson’s ), indicating how they were calculated
Our web collection on statistics for biologists contains articles on many of the points above.
Software and code
Policy information about availability of computer code
Data collection
No software was used for data collection.
Data analysis
Main analyses were performed using SAS version 9.4 and analyses for individual dietary factors were performed using R versions 4.2.0.The analysis programs are publicly available at https://github.com/DrTessier/diets_healthyaging.
For manuscripts utilizing custom algorithms or software that are central to the research but not yet described in published literature, software must be made available to editors and reviewers. We strongly encourage code deposition in a community repository (e.g. GitHub). See the Nature Portfolio guidelines for submitting code & software for further information.
Data
Policy information about availability of data
All manuscripts must include a data availability statement. This statement should provide the following information, where applicable:
Accession codes, unique identifiers, or web links for publicly available datasets
A description of any restrictions on data availability
For clinical datasets or third party data, please ensure that the statement adheres to our policy
Because of participant confidentiality and privacy concerns, data are available upon written request. According to standard controlled access procedure, applications to use NHS/HPFS resources will be reviewed by our External Collaborators Committee for scientific aims, evaluation of the fit of the data for the proposed methodology, and verification that the proposed use meets the guidelines of the Ethics and Governance Framework and the consent that was provided
by the participants. Investigators can expect initial responses within 4 weeks of request submission. Further information including the procedures for obtaining and accessing data from the Nurses’ Health Studies and Health Professionals’ Follow-up Study is described at https://www.nurseshealthstudy.org/researchers (email: nhsaccess@channing.harvard.edu) and https://sites.sph.harvard.edu/hpfs/for-collaborators.The Harvard University Food Composition tables are publicly available at https://hsph.harvard.edu/department/nutrition/nutrition-questionnaire-service-center/#nutrient-data.
Research involving human participants, their data, or biological material
Policy information about studies with human participants or human data. See also policy information about sex, gender (identity/presentation), and sexual orientation and race, ethnicity and racism.
Reporting on sex and gender
Reporting on race, ethnicity, or other socially relevant groupings
Population characteristics
Both sexes (self-reported) are included in this study. Detailed participants’ characteristics by sex are shown in Extended Data Table 1 and 2. We included sex as a covariate in our main analyses. Additionally, we conducted subgroup analyses by sex and effect estimate are reported in Figure 2. The results were consistent in both groups.
Reported in Table 1.
he study included 70,091 women from the Nurses’ Health Study and 34,924 men from the Health Professionals Follow-up Study free of 11 chronic diseases at baseline and with detailed dietary assessment. A detailed description of the population characteristics can be found in the Results and Methods sections as well as in Table 1 and Extended Data Tables 1 and 2 of the manuscript.
Recruitment
The Nurses health studies (NHS) and NHSII include registered women nurses. The Health Professionals Follow-up study (HPFS) includes men health professionals (veterinarians, dentists, pharmacists, optometrists, osteopath, physicians, and podiatrists). Questionnaires were sent to participants in these cohorts to collect and update their lifestyle and medical history every two years. Participants provided data on their dietary intake during the preceding year using an extensively validated semi-quantitative food frequency questionnaire every four years. The follow-up rates were approximately in all cohorts.
Ethics oversight
This is an observational study. The study protocol was approved by the Institutional Review Board (IRBs) of the Brigham and Women’s Hospital, Harvard T.H. Chan School of Public Health, and participating registries (IRB Protocol number: 2001P001945/BWH and 10372. The IRBs allowed participants’ completion of questionnaires to be considered as implied consent for participation in these studies of health professionals. Written informed consent was required for biomarkers collection and for medical record acquisition. The study was performed in accordance with the Declaration of Helsinki.
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Field-specific reporting
Please select the one below that is the best fit for your research. If you are not sure, read the appropriate sections before making your selection.
Life sciences □ Behavioural & social sciences □ Ecological, evolutionary & environmental sciences
For a reference copy of the document with all sections, see nature.com/documents/nr-reporting-summary-flat.pdf
Life sciences study design
All studies must disclose on these points even when the disclosure is negative.
Sample size
The study population is preexisting. We documented 9,771 cases of healthy agers, allowing us to detect the major findings of the present study with statistical power of from a post hoc analysis
Data exclusions
We excluded participants who had not returned a food frequency questionnaire between 1986-2010, those with implausible energy intake, those with one or more of the 11 chronic diseases, those with missing healthy aging phenotype in 2016.
Replication
The validity and reproducibility of questionnaires and outcome ascertainment have been reported previously and described in the Methods. Moderate correlations were observed for foods, nutrients, and dietary patterns comparing the estimates from food frequency questionnaires with those from multiple one-week diet records. Participants who reported a new diagnosis of major chronic disease were asked for permission to obtain their medical records and pathological reported. The Subjective Cognitive Decline (SCD), Short-Form 36 and the Geriatric Depression Scale have all shown good validity at measuring self-perceived cognitive decline, physical limitations, and depressive symptoms, respectively. Deaths were identified through the next-of-kin or portal office when questionnaires were mailed and through searches of the National Death Index. Death ascertainment using National Death Index was reported to have a high sensitivity (98%) and specificity .Replication of these analyses was not applicable and therefore not conducted.
Randomization
Not applicable. This study is an observational study without an intervention.
Blinding
Not applicable. This study is an observational study without an intervention.
Reporting for specific materials, systems and methods
We require information from authors about some types of materials, experimental systems and methods used in many studies. Here, indicate whether each material, system or method listed is relevant to your study. If you are not sure if a list item applies to your research, read the appropriate section before selecting a response.
¹Department of Nutrition, Harvard T.H. Chan School of Public Health, Boston, MA, USA. ²Department of Nutrition, Faculty of Medicine, Université de Montréal, Montreal, Quebec, Canada. EPIC Center of the Montreal Heart Institute, Montreal, Quebec, Canada. Institut de Valorisation des Données (IVADO), Montreal, Quebec, Canada. USDA Human Nutrition Research Center on Aging, Tufts University, Boston, MA, USA. Tufts University School of Medicine, Tufts University, Boston, MA, USA. Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, MA, USA. Channing Division of Network Medicine, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, USA. Rush Alzheimer’s Disease Center, Rush University Medical Center, Chicago, IL, USA. Division of Preventive Medicine, Department of Medicine, Brigham and Women’s Hospital and Harvard Medical School, Boston, MA, USA. Department of Biostatistics, Harvard T.H. Chan School of Public Health, Boston, MA, USA. Department of Public Health, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark. Novo Nordisk Foundation Center for Basic Metabolic Research, Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark.
↩e-mail: anne-julie.tessier@umontreal.ca; fhu@hsph.harvard.edu; marta.guasch@sund.ku.dk
Sample size of . Values are the mean (s.d.) for continuous variables and % for categorical variables. BMI, body mass index; AHEI, alternative healthy eating index; AMED, alternative Mediterranean diet index; DASH, Dietary approaches to stop hypertension; MIND, Mediterranean-DASH intervention for neurodegenerative delay diet; hPDI, healthful plant-based diet index; PHDI, planetary health diet index; EDIH, empirical dietary index for hyperinsulinemia; EDIP, empirical dietary inflammatory pattern; SES, socio-economic status; MET, metabolic equivalent of task. The EDIH and EDIP are reversed scores to allow for comparison with other dietary scores.
Sample size of . Values are the mean (s.d.) for continuous variables and % for categorical variables. BMI, body mass index; AHEI, alternative healthy eating index; AMED, alternative Mediterranean diet index; DASH, Dietary approaches to stop hypertension; MIND, Mediterranean-DASH intervention for neurodegenerative delay diet; hPDI, healthful plant-based diet index; PHDI, planetary health diet index; EDIH, empirical dietary index for hyperinsulinemia; EDIP, empirical dietary inflammatory pattern. The EDIH and EDIP are reversed scores to allow for comparison with other dietary scores.