الجسيمات النانوية في إعادة تشكيل الميكروبيئة الورمية والعلاج المناعي للسرطان Nanoparticles in tumor microenvironment remodeling and cancer immunotherapy
لقد حسنت العلاجات المناعية ضد السرطان وتطوير اللقاحات بشكل كبير من مكافحة السرطانات. على الرغم من هذه التقدمات، لا تزال هناك تحديات، خاصة في تقديم المركبات المناعية في العيادات. يلعب الميكروبيئة الورمية (TME)، التي تتكون من البلعميات، والألياف، والخلايا المناعية، دورًا حاسمًا في تعديل الاستجابة المناعية. لقد أظهرت الجسيمات النانوية، التي تم تصميمها لإعادة تشكيل TME، نتائج واعدة في تعزيز العلاج المناعي من خلال تسهيل التوصيل المستهدف وتعديل المناعة. يمكن أن تثبط هذه الجسيمات النانوية تنشيط الألياف، وتعزز استقطاب البلعميات من النوع M1، وتساعد في نضوج الخلايا الشجرية، وتشجع على تسلل خلايا T. تعزز الجسيمات النانوية البيوميميتية العلاج المناعي من خلال زيادة إدخال العوامل المناعية في الخلايا المناعية مثل الخلايا الشجرية. علاوة على ذلك، تم استكشاف الإكسوزومات، سواء كانت تفرز بشكل طبيعي من الخلايا في الجسم أو تم هندستها حيويًا، لتنظيم TME والخلايا المرتبطة بالمناعة للتأثير على العلاج المناعي للسرطان. تظهر الناقلات النانوية المستجيبة للمؤثرات، التي يتم تنشيطها بواسطة درجة الحموضة، والأكسدة والاختزال، وظروف الضوء، القدرة على تسريع العلاج المناعي. إن التطبيق المشترك للجسيمات النانوية مع مثبطات نقاط التفتيش المناعية هو استراتيجية ناشئة لتعزيز المناعة المضادة للورم. بفضل قدرتها على تحفيز المناعة طويلة الأمد، تعتبر الهياكل النانوية هياكل واعدة في تطوير اللقاحات. تؤكد هذه المراجعة على الدور الحاسم للجسيمات النانوية في التغلب على التحديات الحالية ودفع تقدم العلاج المناعي للسرطان وتعديل TME.
الكلمات الرئيسية: الهياكل النانوية المهندسة بيولوجيًا؛ العلاج المناعي للسرطان، جزيئات النانو للهروب المناعي، البيئة الدقيقة للورم
مقدمة
تُعَاقَب خلايا السرطان بشكل رئيسي بواسطة الشبكات المعقدة في جهاز المناعة، ولكن الأورام تطور عدة آليات لتفادي المناعة المضادة للسرطان. ومن ثم، تم تقديم العلاج المناعي للسرطان كدعامة جديدة لاستغلال جهاز المناعة الخاص بالمريض في القضاء على خلايا السرطان. يمكن تصنيف مفهوم العلاج المناعي للسرطان إلى العلاج المستهدف لنقاط التفتيش المناعية ونقل الخلايا المناعية المعدلة. تساهم كل من هاتين الاستراتيجيتين في تحسين وظيفة جهاز المناعة في التعرف على خلايا السرطان والقضاء عليها. مثبطات نقاط التفتيش المناعية، بما في ذلك الأجسام المضادة لمستقبلات موت الخلايا المبرمج 1 (PD-L1) أو بروتين 4 المرتبط بالخلايا التائية السامة (CTLA-4) و المحفزات للجزيئات المساعدة، قد أظهرت نتائج مرضية في العيادات لعلاج مرضى السرطان، ومع ذلك، لا تزال تواجه عددًا من المشاكل المزعجة بما في ذلك انخفاض معدل الاستجابة، وارتفاع التكلفة، والسمية غير المحددة. طريقة أخرى هي النقل التبني للخلايا، التي تستخدم خلايا معدلة وراثيًا مثل خلايا CAR-T وغيرها مثل خلايا السلف الجذعية الوسيطة متعددة القدرات للتأثير على تعبير سيتوكين محدد وميزات أخرى للخلايا. منذ التطبيق الواعد لحجب نقاط التفتيش المناعية وعلاج خلايا CAR-T، شهدت المناعية ضد السرطان تقدمًا كبيرًا. تعتبر المناعية ضد السرطان الآن استراتيجية قوية ومبتكرة في العيادات مقارنة بالعلاجات التقليدية الأخرى مثل الجراحة، والعلاج الإشعاعي، والعلاج الكيميائي. استخدمت أحدث طرق العلاج المناعي خلايا T لتحفيز الاستجابات المناعية التكيفية. من ناحية أخرى، أظهرت الدراسات أن عددًا من نقاط التفتيش المناعية الفطرية التي تعبر عن نفسها على خلايا تقديم المستضد (APCs) تساهم في التهرب المناعي. هذه النقاط قادرة على اكتشاف وإبادة خلايا الورم من خلال البلعمة وكبح الاستجابة المناعية الفطرية. يتم توفير الخط الأول من نظام الدفاع المناعي بواسطة خلايا المناعة الفطرية مثل البلعميات، والوحيدات، والخلايا الشجرية التي تعمل كـ APCs. إنها تحفز ردود فعل التهابية تجاه الهجمات الخارجية وتساهم في إصلاح الأنسجة التالفة. تتمكن خلايا السرطان من التعبير عن عدد من الإشارات المعروفة باسم “لا تأكلني” من خلال التعبير عن CD47، CD24، PD-L1، والبيتا-2 ميكروغلوبيولين. ) وحدة فرعية من MHC-I [11]، ستانيكالكين 1 (STC-1) [12] و GD2 [13] لتجنب البلعمة التي تتوسطها البلعميات.
لقد كانت تطبيقات العلاج المناعي للسرطان مهمة في علاج كل من الأورام الدموية والأورام الصلبة. في الواقع، لقد أحدث العلاج المناعي ثورة في علاج السرطان، ويهدف إلى تطبيق مثبطات نقاط التفتيش المناعية، والعلاج الخلوي التبني، واللقاحات لاستهداف دورة المناعة الأورام في النهاية لتحسين نشاط الخلايا اللمفاوية التائية في قمع الورم. يجب تطبيق جميع هذه الأنظمة في دورة لتسريع تقديم مستضدات الورم بواسطة خلايا APC. خلايا APC هي الخلايا التي لديها القدرة على التقاط ومعالجة وتقديم المستضدات الخارجية إلى الخلايا التائية، وتُعرف بشكل أساسي من خلال تعبيرها عن MHCII وجزيئات التحفيز المساعدة الأخرى. تتكون خلايا APC بشكل رئيسي من الخلايا الشجرية، والبلعميات، وخلايا B. هناك أيضًا خلايا أخرى تعبر عن MHC-II مثل خلايا الظهارة التوتية. علاوة على ذلك، هناك أنواع أخرى من الخلايا، مثل الحمضات والقاعديات، التي لديها القدرة على التعبير عن MHC-II عند التحفيز. [16، 17]. فيما يتعلق بالأورام الصلبة، يتم امتصاص المستضدات وعرضها بشكل رئيسي بواسطة البلعميات والخلايا التغصنية [18]. على الرغم من أن البلعميات هي الخلايا البلعومية السائدة في السرطانات، إلا أنها تفتقر إلى القدرة على الهجرة إلى العقد اللمفاوية وتنشيط خلايا T [18]. ومن الجدير بالذكر أن البلعميات تعتبر عاملاً في إضعاف الاستجابات المعتمدة على خلايا T ضد الأورام، وتقلل من الاستجابة لحجب نقاط التفتيش المناعية، والعلاج الكيميائي، والعلاج الإشعاعي [19، 20]. من ناحية أخرى، تتمتع الخلايا التغصنية بقدرة كبيرة على الهجرة إلى العقد اللمفاوية لتحفيز خلايا T للمناعة [18، 21-24]. علاوة على ذلك، أظهرت الأدلة المتزايدة قدرة الخلايا التغصنية المقيمة في الورم على تحفيزاستجابة المناعة المضادة للسرطان المعتمدة على الخلايا [18، 24-28]. ومع ذلك، يجب ملاحظة أن البلعميات والخلايا الأخرى في البيئة المجهرية للورم، بما في ذلك الألياف، يمكن أن تمارس نشاطًا مسرطنًا عند التحفيز، وتنظيمها مهم لتعظيم العلاج المناعي للسرطان [19، 29-36]. يمثل تحفيز إعادة تشكيل البيئة المجهرية للورم استراتيجية مفيدة لعلاج السرطان والعلاج المناعي [37-43]. على الرغم من أن عددًا كبيرًا من الدراسات تدعم إمكانية العلاج المناعي في قمع السرطان [44-48]، إلا أن العلاج المناعي واجه مشاكله الخاصة، وأبرزها هو التهرب المناعي. فيما يتعلق بالطفرات وعدم تنظيم المسارات الجزيئية في الأورام البشرية، يتم تنشيط المسارات المسرطنة، مما يمكن أن يعزز في النهاية بقاء خلايا السرطان ويسهل هروبها من العلاج المناعي ومراقبة المناعة.
بالإضافة إلى مقاومة المناعة، تفتقر الأدوية الحالية المستخدمة في علاج السرطان المناعي وإعادة تشكيل بيئة الورم إلى ميزات الاستهداف. ونتيجة لذلك، تم تقديم الجسيمات النانوية لتسهيل المناعة المضادة للسرطان. يمكن أن تحسن الهياكل النانوية من وقت الاحتفاظ وتوفر التوصيل المستهدف. علاوة على ذلك، فإن الجسيمات النانوية قادرة على إعادة تشكيل بيئة الورم لتعطيل البيئة المثبطة للمناعة. إن تشوه الأوعية الدموية ومعدل النمو المرتفع لخلايا الورم يسبب نقص الأكسجين في بيئة الورم، مما يؤدي إلى بيئة مثبطة للمناعة، تتميز بزيادة تراكم الخلايا المثبطة للمناعة، بما في ذلك خلايا T التنظيمية (Tregs) وخلايا المثبطات المشتقة من النخاع (MDSCs)، بالإضافة إلى إفراز عدد من العوامل بما في ذلك عامل نمو بطانة الأوعية الدموية (VEGF) وعامل النمو المحول. (TGF- ). نتيجة لذلك، يتم قمع وظيفة الخلايا الشجرية ويتم استقطاب البلعميات إلى نمط M2. يمكن تطوير الجسيمات النانوية بشكل خاص لاستهداف مكونات البيئة الدقيقة للورم وتعطيل البيئة المناعية المثبطة لتحسين الوظيفة في العلاج المناعي للسرطان. علاوة على ذلك، يمكن اعتبار الجسيمات النانوية أنظمة توصيل على مقياس النانو للأدوية [50]. يمكن أن تتراكم بشكل انتقائي في أنسجة الورم وتعزز وقت الاحتفاظ بالأدوية. علاوة على ذلك، تظهر الهياكل النانوية تحسينًا
تأثير النفاذية والاحتفاظ (EPR)، مما يحسن تراكمها في مواقع الورم بسبب تسرب الأوعية الدموية الورمية وتضرر تصريف اللمف [51، 52]. علاوة على ذلك، يمكن تفعيل الهياكل النانوية باستخدام الروابط، لاستهداف الورم ومكونات البيئة الدقيقة للورم [53-55]. نتيجة لذلك، تم تقديم الجسيمات النانوية كتركيبات جديدة لتعزيز العلاج المناعي للسرطان والتغلب على التهرب المناعي [56-63].
في ظل التحديات الحالية في العلاج المناعي للسرطان، ظهرت الحاجة إلى تحسين العلاج المناعي للسرطان، ووعد الجسيمات النانوية، كاستراتيجية جديدة لتعزيز العلاج المناعي وإعادة تشكيل البيئة الدقيقة للورم. يمكن أن يعزز تطوير الجسيمات النانوية المستندة إلى استهداف البيئة الدقيقة للورم وتحسين العلاج المناعي للسرطان الإمكانية للقضاء على الورم. نظرًا لأن معدلات تعديل البيئة الدقيقة للورم تعاني من عمل مستهدف، يُفضل استخدام أنظمة توصيل غير مستهدفة على مقياس النانو لتنظيم البيئة الدقيقة للورم وتحسين العلاج المناعي للسرطان. تركز المراجعة الحالية
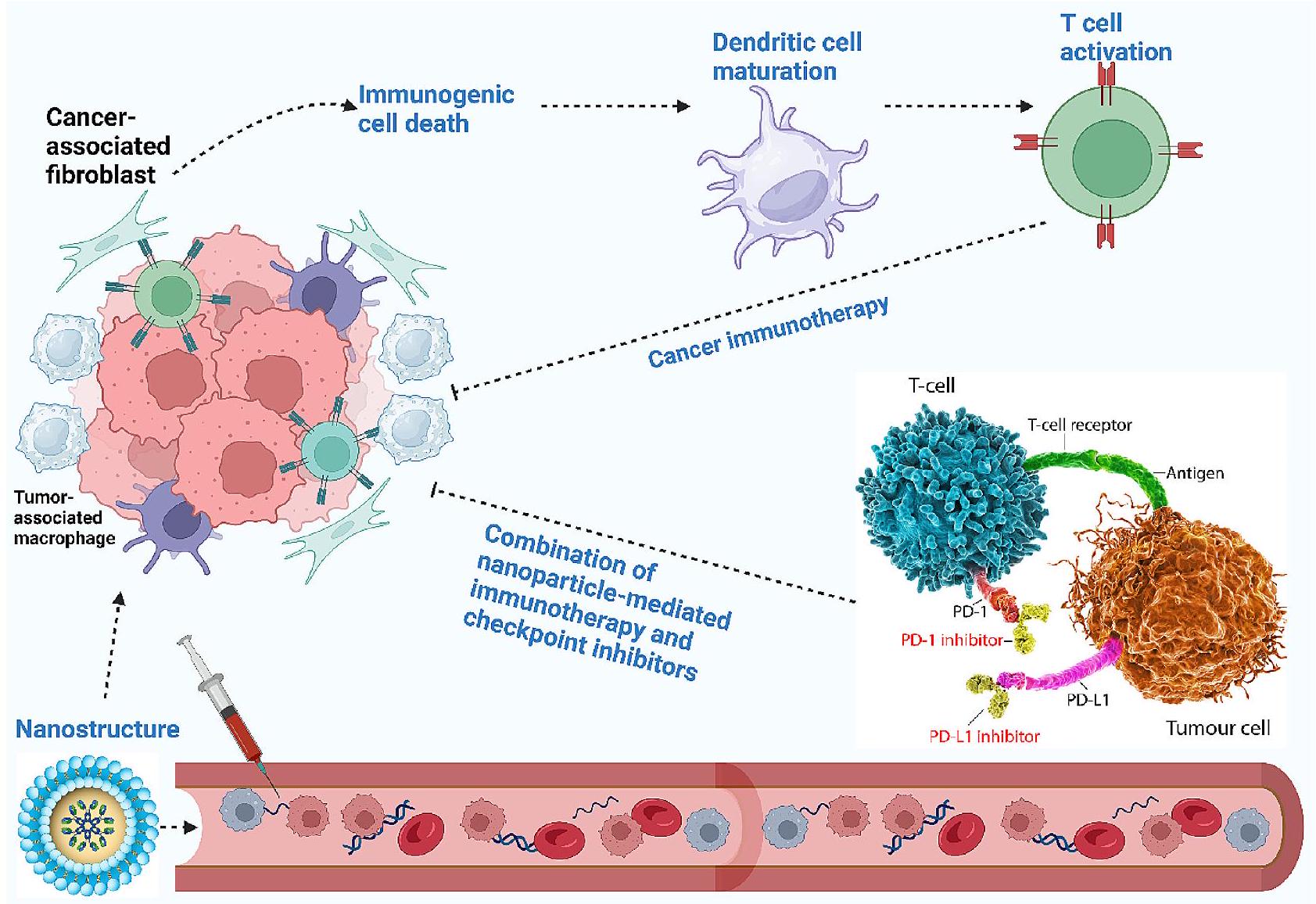
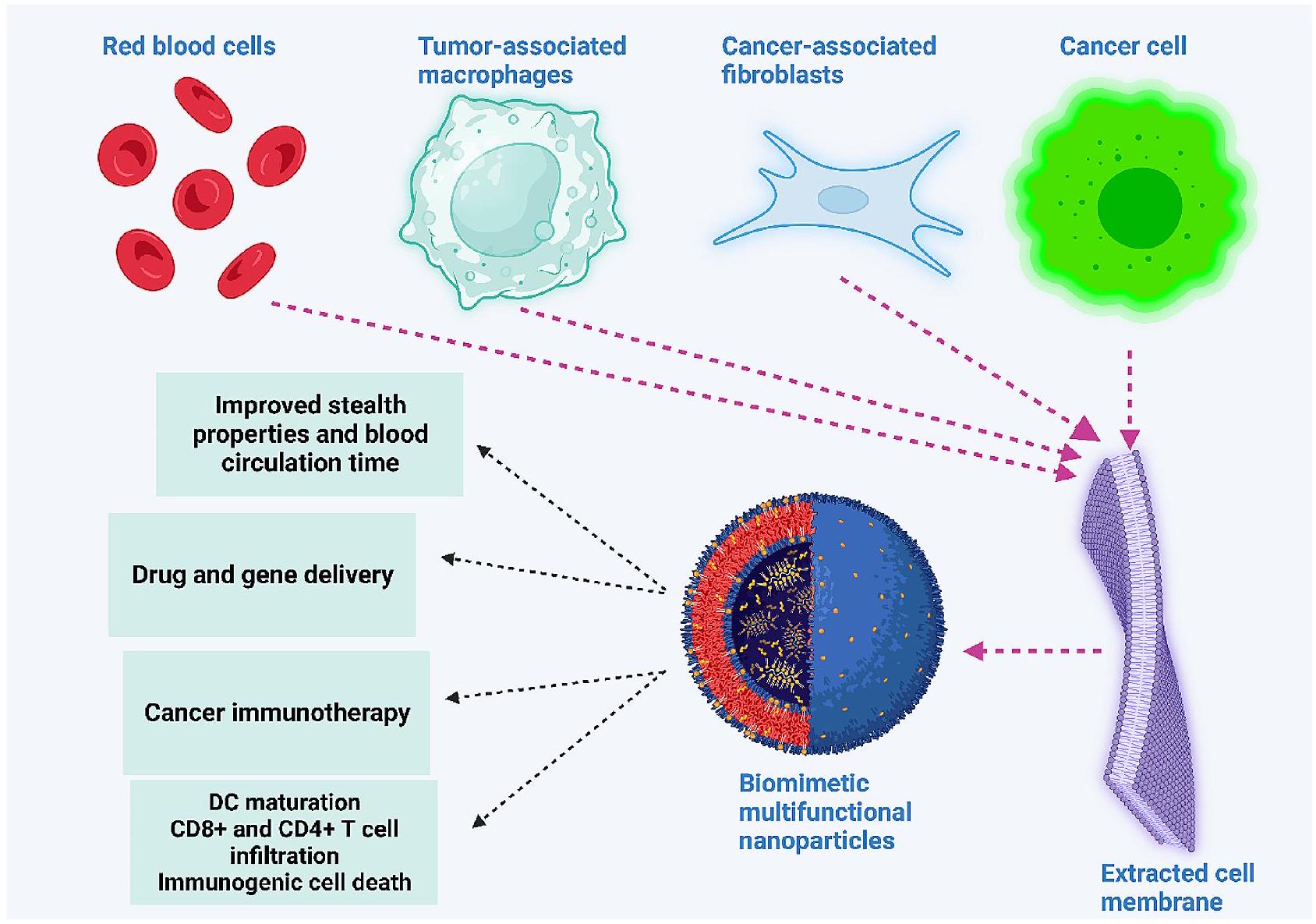
على تطبيق الجسيمات النانوية لإعادة تشكيل البيئة الدقيقة للورم وتعزيز العلاج المناعي للسرطان. ستقدم المراجعة الحالية أولاً مخططًا شاملاً بشأن مكونات البيئة الدقيقة للورم ثم يتم مناقشة التهرب المناعي. بعد ذلك، يتم وصف إمكانيات الجسيمات النانوية لإعادة تعليم البيئة الدقيقة للورم من خلال استهداف مكوناتها، بما في ذلك البلعميات. علاوة على ذلك، يتم وصف الجسيمات النانوية البيوميميتية وأنواعها المستجيبة للتحفيز لاستهداف الورم بشكل أفضل. نظرًا لأن الإكسوزومات ظهرت مؤخرًا في العلاج المناعي للسرطان، يتم مناقشة دور الإكسوزومات، سواء كانت داخلية أو مهندسة حيويًا، في تنظيم النظام المناعي لقمع الورم. توفر الشكل 1 نظرة عامة على استخدام الجسيمات النانوية في العلاج المناعي للسرطان.
مكونات البيئة الدقيقة للورم البلعميات
تعتبر البلعميات، المعروفة بطبيعتها البلعومية، تلعب دورًا حيويًا في النظام المناعي. تشارك في عمليات فسيولوجية متنوعة، بما في ذلك التطور
الشكل 1 نظرة عامة على استخدام الجسيمات النانوية في العلاج المناعي للسرطان. تتداول الجسيمات النانوية في الدم، وعند وصولها إلى موقع الورم، تعيد تعليم عدة مكونات من البيئة الدقيقة للورم، بما في ذلك الألياف المرتبطة بالسرطان والبلعميات المرتبطة بالورم، لتنشيط النظام المناعي في النهاية. علاوة على ذلك، يمكن أن تحفز الجسيمات النانوية موت الخلايا المناعية لتحسين نضوج الخلايا الشجرية لتنشيط خلايا المناعة، مثل خلايا T، لتعزيز العلاج المناعي للسرطان. يمكن أن يزيد التطبيق المشترك للجسيمات النانوية مع مثبطات نقاط التفتيش المناعية، مثل مثبطات PD-L1، من إمكانيات العلاج المناعي للسرطان
والتوازن. يتم تحديد نمط ووظيفة البلعميات بشكل معقد من خلال أصلها واستقطابها [64]. كان يُعتقد في البداية أنها تنشأ من خلايا جذعية دموية وحيدة الدوران [65]، لكن الدراسات الحديثة أفادت بأن البلعميات لها سلالة مشتقة من الأجنة، مع سلف مشتق من سلالات إريثرو-نخاعية في أكياس الصفار وكبد الجنين [65، 66]. الحفاظ على أو تعزيز عدد البلعميات أمر ضروري لعمل هذه الخلايا بشكل فعال [67،68]. هناك استراتيجيتان لتجديد البلعميات: تجنيد الخلايا الوحيدة وزيادة التكاثر في شكل بلعميات مقيمة في الأنسجة لرفع قدرة التجديد الذاتي [67، 69].
في البيئة الدقيقة للورم، تُعرف البلعميات باسم البلعميات المرتبطة بالورم (TAMs)، والتي تشكل من كتلة الورم [70]. تشارك TAMs في تفاعلات معقدة ليس فقط مع خلايا السرطان ولكن أيضًا مع خلايا القاتل الطبيعي (NK) وخلايا T والخلايا البطانية والألياف. تمتد أدوار TAMs إلى تنظيم تكاثر السرطان والغزو وتكوين الأوعية [71-73]. كما ارتبطت البلعميات بتطوير مقاومة للعلاجات السرطانية [74]. تنشأ TAMs بشكل أساسي من نخاع العظام أو كيس الصفار [75]. يمكن استقطابها إلى نمطين. البلعميات M1، المستحثة بواسطة الليبوساكاريد وسيتوكينات خلايا T المساعدة من النوع 1 (Th1)، تظهر وظائف مضادة للالتهابات ومضادة للسرطان [76]. البلعميات M2، المستحثة بواسطة سيتوكينات مشتقة من Th2 مثل إنترلوكين-4 (IL4) وIL-10 وIL-13، تعزز التكاثر والغزو وتكوين الأوعية [76]. يوجد توازن دقيق بين البلعميات M1 وM2 في الجسم، مما يؤثر على تكوين الأورام ونتائج العلاج [77، 78]. الطبيعة المضادة للالتهابات للبلعميات M2 تسرع تقدم السرطان. كانت تنظيم TAMs ذات أهمية للعلاج المناعي للسرطان. حاليًا، تستند الاستراتيجيات لاستهداف TMAs إلى التحكم في الأصل، الاستقطاب الوظيفي، ووظيفة البلعمة لـ TAMs. علاوة على ذلك، تم هندسة البلعميات والخلايا الوحيدة للتوسط في المناعة المضادة للسرطان. لهذا الغرض، تم استغلال أربع استراتيجيات متميزة، بما في ذلك تقليل عدد TAM، والتحول من استقطاب M2 إلى أنماط M1، والتحكم في إشارة البلعمة للبلعميات، والهندسة الحيوية للبلعميات لزيادة البلعمة [79]. حاليًا، تم تطبيق الهياكل النانوية على نطاق واسع لإعادة تعليم TAMs [80]، وتغيير قدرة البلعمة [81]، وقمع TAMs [82] وتوصيل الأدوية إلى TAMs [83] للعلاج المناعي للسرطان.
الألياف المرتبطة بالسرطان
تمثل الألياف المرتبطة بالسرطان (CAFs) مجموعة متنوعة من الخلايا التي تتسلل إلى البيئة الدقيقة للورم. تختلف CAFs عن الألياف الطبيعية [84]. تلعب هذه الخلايا دورًا محوريًا في تكوين الأورام من خلال تحفيز التغيرات الكيميائية الحيوية
والتغيرات في شبكة الإشارات التي تسرع من تطور الورم [85]. تحت ظروف معينة، قد تظهر CAFs أنشطة مضادة للسرطان، مما يساهم في قمع الورم [86].
تنشأ تباين CAFs من أصولها المتنوعة، بما في ذلك الألياف الطبيعية، والخلايا الظهارية، والخلايا البطانية، والخلايا الدهنية المحيطة بالورم، والخلايا المحيطية، والخلايا الجذعية الدموية، والخلايا الجذعية الوسيطة، وخلايا السرطان الجذعية [87]. بناءً على وظائفها، يمكن تصنيف CAFs إلى مجموعتين: CAFs مسرطنة وCAFs مضادة للسرطان [88، 89]. حدد أوهلوند وزملاؤه نوعين متميزين من CAFs في سرطان البنكرياس: الألياف العضلية (myCAFs) وCAFs الالتهابية (iCAFs) [90]. الألياف العضلية، الموجودة بالقرب من خلايا السرطان، يتم تحفيزها بواسطة عامل النمو المحول بيتا (TGF- ) وتظهر مستويات عالية من الأكتين العضلي الأملس (-SMA). في المقابل، تكون iCAFs موضوعة بعيدًا عن خلايا السرطان. تظهر مستويات مرتفعة من -SMA والقدرة على إفراز IL-6 وعامل تثبيط اللوكيميا [91].
فئة أخرى من CAFs، CAFs التي تقدم المستضدات (apCAFs)، تعبر عن علامات حيوية مرتبطة بفئة MHC-II وCD44، مما يمكنها من تحفيز خلايا CD بطريقة تعتمد على المستضد [92]. بالإضافة إلى ذلك، هناك نوع يعرف باسم CAFs المثبطة (rCAFs). تلعب كل من هذه الفئات الفرعية دورًا متميزًا في السرطان. على سبيل المثال، تساهم iCAFs وmyCAFs في إعادة برمجة التمثيل الغذائي وتكوين الأوعية في السرطان، على التوالي. يمكن أن تفرز iCAFs عوامل نمو وسيتوكينات وكيموكينات، بما في ذلك PD-L1/L2، وFas ligand، وغيرها، التي تؤثر على تنظيم النظام المناعي. من ناحية أخرى، تساهم myCAFs في إعادة تشكيل المصفوفة خارج الخلوية من خلال تعزيز تخليق الكولاجين. تشارك apCAFs في تحفيز الخلايا لتنظيم خلايا المناعة، بينما تظهر خلايا CAFs المعاد تشكيلها القدرة على قمع تكوين الأورام. فيما يتعلق بأهمية خلايا CAFs في تكوين الأورام، كان استهداف خلايا CAFs للعلاج المناعي للسرطان ذا أهمية. تُظهر الهياكل النانوية اختراقًا عاليًا ونفاذية في مواقع الأورام، ويمكن استخدامها لتنظيم خلايا CAFs. علاوة على ذلك، يمكن استخدام الجسيمات النانوية لتصميم خلايا CAFs لتعمل كخلايا تقديم المستضدات وتحفيز خلايا CD المحددة للمستضد.تعمل خلايا T في العلاج المناعي للسرطان [95]. يمكن أن تحفز الهياكل النانوية إزالة الخلايا الليفية المتفعلة والشيخوخة [96]، ويمكن أن تؤدي تنظيم الخلايا الليفية بواسطة الجسيمات النانوية إلى تعطيل انتشار السرطان وغزوه [97].
العدلات
حتىتشكل الخلايا البيضاء الدائرة نسبة من العدلات [98]، وتعتبر خط الدفاع الأول ضد مسببات الأمراض [99]. تتمتع العدلات بعمر قصير ويمكن أن تبقى في الدورة الدموية لمدة خمسة أيام [100]. عندما يحدث تلف في الأنسجة أو عدوى، تقوم الخلايا الظهارية بإفراز الكيموكينات لاستقطاب العدلات. بعد ذلك، تقوم العدلات بالخروج من الأوعية الدموية. تدخل الدورة الدموية الأنسجة التالفة لتفرز عددًا من السيتوكينات الالتهابية، وتحرر الفخاخ خارج الخلوية للعدلات (NETs)، وأخيرًا، تبتلع مسببات الأمراض أو الكائنات الدقيقة الغازية. تعتبر NETs وسائل للببتيدات السامة المضادة للميكروبات. في السرطان، هناك فئتان من العدلات المرتبطة بالأورام (TANs) مشابهتان لنمط Th1/Th2، بما في ذلك N1 وN2 مع وظيفة مثبطة للورم ووظيفة تعزز الورم، على التوالي. يحدد نوع الورم ومرحلته نمط العدلات في بيئة الورم. خلال المراحل الأولى من تكوين الورم، تظهر العدلات نمطًا التهابيًا، ومع تقدم السرطان، تحقق العدلات نمطًا مثبطًا للمناعة. تعتمد تنظيم الالتهاب الذي تسببه العدلات على إفراز ROS وRNS. علاوة على ذلك، يمكن إعادة تشكيل المصفوفة خارج الخلوية بواسطة العدلات من خلال إفراز الإيلاستاز العدلي وبروتينات المصفوفة المعدنية. تظهر العدلات القدرة على تحفيز تكوين الأوعية الدموية من خلال oncostatinM، وزيادة تكوين السرطان من خلال PGE2، وتعزيز انتشار السرطان من خلال إفراز ROS وRNS وNE وMMP-9. ومن الجدير بالذكر أن NETs تتكون من MMPs وcathepsin G وNE. وظيفة هذه البروتيازات هي الوساطة في تحلل السيتوكينات المؤيدة للالتهاب وإعادة تراكمها في بيئة الورم لتعزيز تكوين الورم والانتشار. في مرضى السرطان، تعتبر مرونة العدلات الدائرة مهمة، المعروفة باسم العدلات عالية الكثافة (HDNs) أو العدلات منخفضة الكثافة (LDNs)، والتي تت correspond إلى أنماط N1 وN2، على التوالي. تظهر LDNs التي لها نمط غير ناضج انتشارًا في الدورة الدموية للعديد من أنواع السرطان وتشارك في تكوين السرطان والانتشار. في مجال العلاج المناعي للسرطان، يمكن أن تحفز العدلات N1 تأثيرات سامة على خلايا السرطان. علاوة على ذلك، يمكن أن تعزز تحفيز العدلات Ly6Ehi من خلال مسار STING الحساسية للعلاج المضاد لـ PD-1، ويمكن استخدامها كمؤشرات للعلاج المناعي للسرطان. لذلك، فإن تطوير الجسيمات النانوية لاستهداف العدلات في العلاج المناعي للسرطان أمر مهم.
خلايا القاتل الطبيعي وخلايا T
كخلايا لمفاوية فطرية، تتمتع خلايا NK بعمر نصف أقصر مقارنة بخلايا B و T، مما يستلزم تجديدها من سلالات نخاع العظام. تمر خلايا NK بعملية تمايز خطي، حيث تتمايز خلايا NK غير الناضجة ذات التكاثر العالي إلى مؤثرات كاملة الوظيفة وغنية بالحبيبات. إن تعزيز تكرار خلايا NK، وتسللها، ووظيفتها يساهم في تحسين بقاء مرضى السرطان. وهذا يجعل خلايا NK ذات قيمة في العلاج المناعي للسرطان. يمكن لهذه الخلايا اللمفاوية الفطرية من المجموعة الأولى استهداف الخلايا بسرعة دون تحسس مسبق، وتعبر عن T-bet وسيتوكينات مرتبطة بـ Th1، بما في ذلك IFN- [119-121].
عند النضوج، تهاجر خلايا NK من نخاع العظام إلى الدم ثم تقيم في الأنسجة المحيطية. بسبب قدرتها على الانتقال بين الأنسجة اللمفاوية وغير اللمفاوية، تتوزع خلايا NK في العديد من الأعضاء والأنسجة. تكتسب خلايا NK الناضجة القدرة على exert تأثيرات سامة للخلايا على خلايا السرطان أو الخلايا المصابة بالفيروسات. كجزء من النظام المناعي التكيفي، تتفاعل خلايا NK مع خلايا المناعة الأخرى من خلال إفراز السيتوكينات وعوامل النمو والكيماويات. هذه التأثيرات تجعل خلايا NK فعالة في الأمراض مثل السرطان، والأمراض المعدية، والمناعة الذاتية، والالتهاب المزمن.
علاوة على ذلك، تلعب خلايا NK دورًا مهمًا في الجهاز المناعي الفطري، حيث توفر المراقبة في السرطانات الدموية وانتشار السرطان. يرتبط زيادة تسلل خلايا NK إلى بيئة الورم بشكل إيجابي مع توقعات الشفاء لمختلف أنواع السرطان، بما في ذلك الميلانوما، وسرطان الخلايا الكلوية، وأورام الكبد، وسرطان الثدي، من بين أمور أخرى.
يتم تشكيل الجهاز المناعي التكيفي بشكل أساسي بواسطة خلايا T، مما يوفر دفاعًا فعالًا ضد مسببات الأمراض والسرطانات. عند التعرض للسيتوكينات وإشارات التحفيز المساعدة، فإن الخلايا الساذجةت undergo الانقسام، متمايزة إلى خلايا فعالة. غير ناضجةيمكن للخلايا أن تتمايز إلى خلايا مساعدة T، بما في ذلك خلايا TH1 وTH2 وTH17 وTFH، لأداء وظائف مناعية. تمايز الخلايا الساذجةالخلايا إلى فعالةتُمكّن هذه الخلايا من محاربة العدوى والسرطانات من خلال إفراز IFN-TNF-وجزيئات سامة للخلايا [137].
تظهر التحديات في السرطان نتيجة للإرهاق في خلايا T. يتم تحفيز هذه الظاهرة بواسطة آليات مختلفة، حيث يُعتبر محور PD-1 الأكثر بروزًا. عند التعرض لمستضد، تتحول خلايا T الساذجة إلى خلايا T فعالة، حيث تموت بعض الخلايا بينما تشارك أخرى في القضاء على الورم. يمكن أن يؤدي تقديم المستضد إلى تكوين خلايا الذاكرة الجذعية T (TSCM)، التي تتحول إلى خلايا TCM وTEM وTRM. تقيم خلايا TRM في الأنسجة، جاهزة للاستجابة للتحفيز الثانوي، بينما تمتلك خلايا TSCM وTCM قدرة على التجديد الذاتي، مما ينتج عنه خلايا TEM وTE عند إعادة التحفيز.
تشمل علامات إرهاق خلايا T التعبير عن مستقبلات مثبطة، وانخفاض في وظيفة خلايا T، وانخفاض في التكاثر. تظهر خلايا T المرهقة ملفًا مميزًا من التغيرات الجينية قد يؤدي إلى استجابة متفاوتة أو ضعيفة للعلاج المناعي. بالإضافة إلى ذلك، تعاني خلايا T المرهقة من اختلال في الأيض، بما في ذلك كبت الميتوكوندريا وتثبيط التحلل السكري. يتجاوز التحدي في علاج السرطان إرهاق خلايا T، حيث يمكن أن تؤدي وفاتها وانخفاض تكاثرها إلى إضعاف التفاعلات المناعية. لقد عزز استهداف خلايا NK وT باستخدام الجسيمات النانوية العلاج المناعي للسرطان. الجسيمات النانوية ذات الامتصاص العالي يمكن استخدام الجسيمات النانوية المستندة إلى الدهون في خلايا NK، مثل الجسيمات النانوية المستندة إلى الدهون، لتعديل خلايا NK [140]. علاوة على ذلك، يمكن استخدام الهياكل النانوية لتتبع خلايا NK بشكل غير جراحي، بما في ذلك هجرتها وتوزيعها الحيوي في مناطق الورم [141]. يمكن تغيير مستويات التعبير عن CCR4 و CXCR4 على سطح خلايا NK بواسطة الجسيمات النانوية لتحسين تفاعلها مع خلايا السرطان [142]. ومن الجدير بالذكر أن الجسيمات النانوية يمكن تصميمها لتحفيز كل من خلايا NK والخلايا في العلاج المناعي للسرطان [143].
الخلايا البطانية والخلايا المحيطية
تشكل الخلايا البطانية البطانة الداخلية للأوعية الدموية. الوظائف البيولوجية للخلايا البطانية ضرورية للحفاظ على الظروف الفسيولوجية الطبيعية. تلعب هذه الخلايا أدوارًا مهمة في تنظيم تجلط الدم، وحجم الأوعية، والوظائف المناعية لتعزيز سيولة الدم، وتوزيع الأكسجين، ونقل الخلايا، وتوفير المغذيات. تقوم الخلايا البطانية باستمرار بإفراز بروتينات مضادة للتخثر لمنع التجلط في الأسرة الوعائية، مما يحافظ على التوازن الداخلي ويضمن تدفق الدم والضغط عند مستوى مناسب لتوصيل الأكسجين والمغذيات إلى الأنسجة.
على الرغم من وظائفها الفسيولوجية الأساسية، تم ربط الخلايا البطانية بتقدم السرطان. وقد سلطت المراجعات الأخيرة الضوء على دور الخلايا البطانية في نسيج الورم. في المراحل الأولية، تحفز الخلايا البطانية تكوين الأوعية الدموية لزيادة وجود الأوعية الدموية في الورم الأساسي. تعمل هذه الخلايا أيضًا كمنصة وموقع لعوامل وبروتينات مرتبطة بالغشاء، مما يخلق بيئة ميكروية مواتية لتقدم السرطان. تلعب هذه الوظائف الموضعية للخلايا البطانية أيضًا دورًا في تنظيم الإشارات الأنجيوكرينية في مواقع بعيدة، مما يؤثر على وظيفة الأعضاء. علاوة على ذلك، يمكن أن تمتد العوامل والبروتينات التي تفرزها خلايا الورم إلى ما وراء حدود الورم، مما يؤثر على الخلايا البطانية في مواقع بعيدة ويمارس وظائف منهجية.
فهم وظائف الأورام وتأثيراتها التنظيمية خارج مواقعها أمر بالغ الأهمية، نظرًا لأن معظم الوفيات المرتبطة بالسرطان ناتجة عن الغزو، والتخثر، والهزال [153-155]. يمكن أن تؤدي البروتينات والعوامل التي تفرزها خلايا الورم إلى تغييرات في خلايا البطانة في الموقع السابق للانتقال، مما يعزز انتشار خلايا السرطان ووساطة تكوين الأوعية الدموية. بالإضافة إلى ذلك، يمكن أن تؤدي هذه العوامل إلى التخثر في الأوعية الدموية البعيدة [156]. تم التعرف على الخلايا المحيطية الباطنية منذ أكثر من قرن كخلايا جدارية مرتبطة بالميكروأوعية [157]. هذه الخلايا الموجودة في محيط الأوعية [158-160] موزعة بشكل شائع في جميع الأنسجة المعرضة للأوعية الدموية [161، 162]. يتطلب تحديد الخلايا المحيطية استخدام الصبغات المناعية واستخدام العلامات الحيوية والمستضدات لتمييزها عن خلايا العضلات الملساء الوعائية، والأرومات الليفية، والخلايا الجذعية المتوسطة [157]. كانت تُعتبر في البداية خلايا خاملة تساهم في الاستقرار الفيزيائي للأوعية الدموية. [163، 164]، لقد أظهرت التقدمات الحديثة أدوارها في كل من الحالات الفسيولوجية والمرضية.
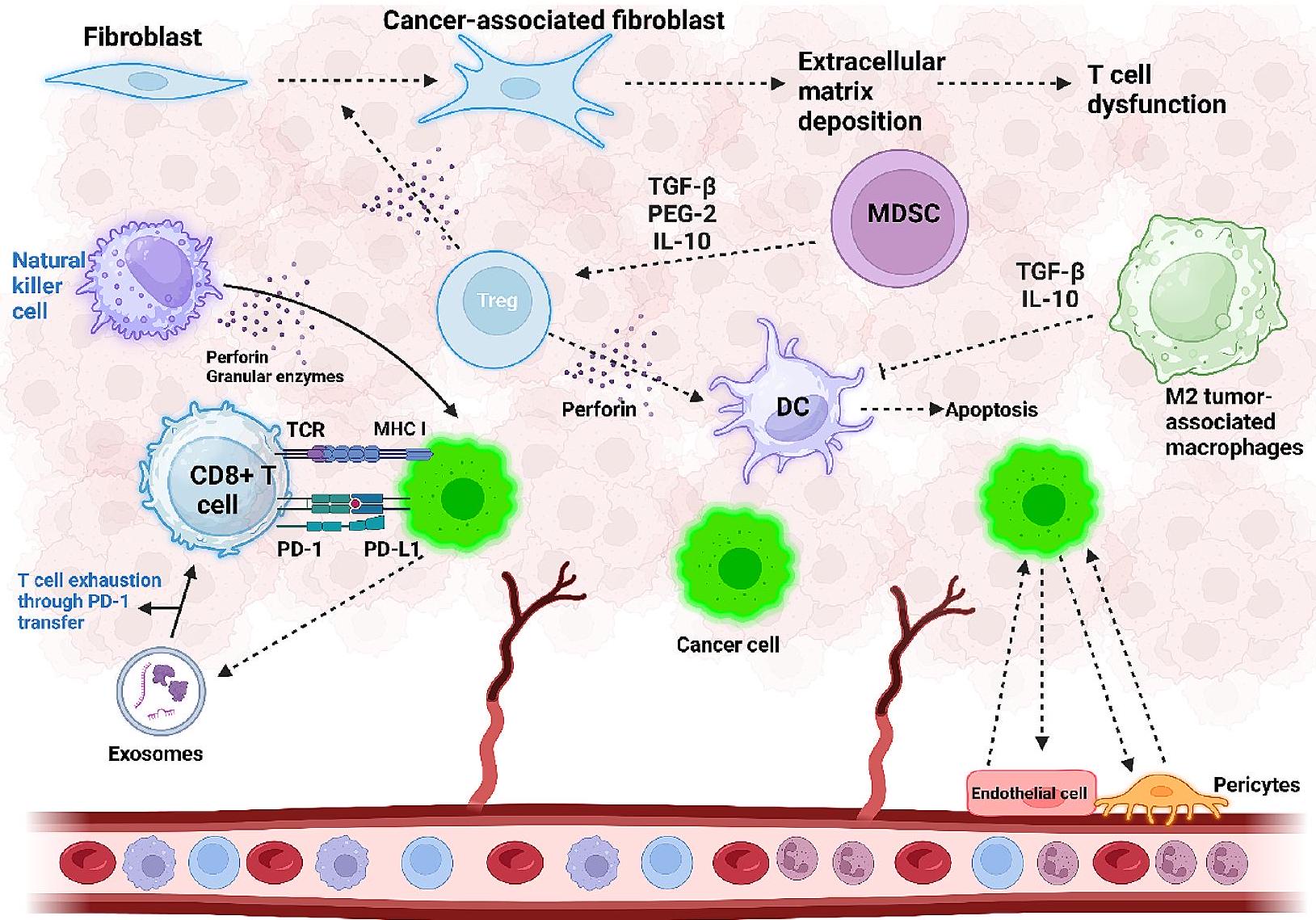
تلعب الخلايا المحيطية دورًا حاسمًا في تنظيم تطور الأوعية الدموية وتعديل تدفق الدم، والتخثر، ونفاذية الأوعية الدموية. تشمل بنية الشعيرات الدموية خلايا بطانية، وخلايا محيطية، والغشاء القاعدي، وخلايا العضلات الملساء الوعائية. الوظيفة الأساسية للخلايا المحيطية في تقدم السرطان هي تحفيز تكوين الأوعية الدموية في البيئة المجهرية للورم. يمكن أن يؤدي CD248 إلى زيادة تنظيم Wnt وزيادة مستويات OPN وSERPINE1 في الخلايا المحيطية مما يسبب تكوين الأوعية الدموية وتسريع تقدم السرطان. بالإضافة إلى ذلك، يمكن أن يتم تحفيز انقباض الخلايا المحيطية بواسطة إنزيم هيكسوكيناز 2 في عملية التحلل السكري، مما يؤدي إلى تشوهات في الأوعية الدموية للورم. عندما تكون موجودة في موقع الورم، RGS5-TGF.-سماديخلق بيئة مضادة للموت الخلوي تسارع نمو خلايا السرطان [170]. الشكل 2 هو تمثيل تخطيطي لمكونات البيئة المجاورة للورم.
خلايا مثبطة مشتقة من النخاع الشوكي
تعتبر خلايا المثبطات المشتقة من النخاع (MDSCs) نوعًا آخر من الخلايا الموجودة في بيئة الورم المجاورة (TME). هناك عدد من الحجج التي تشير إلى أن MDSCs هي نوع فرعي من العدلات [104] بسبب وجود علامات متداخلة بين MDSCs وTANs، مما يجعل من الصعب والمشكلة تمييزها. لا يزال هناك جدل حول ما إذا كانت MDSCs تمثل سلالة منفصلة من الخلايا أو أنها عدلات غير ناضجة مستقطبة [171]. بشكل عام، تعتبر MDSCs مجموعة غير متجانسة من الخلايا ذات الأصل النخاعي [172]. على الرغم من أنها تنشأ من خلايا سلف نخاعية، إلا أن MDSCs وTANs تعتبر أنواع خلايا مختلفة. علاوة على ذلك، تظهر MDSCs عدة ميزات مميزة عن العدلات، بما في ذلك تقليل تعبير CD16 وCD62L وزيادة تعبير Arg1 وCD66B وCD11b [173، 174]. بالإضافة إلى ذلك، أظهرت الدراسات أنواعًا فرعية أخرى من MDSCs بما في ذلك MDSCs أحادية النواة (M-MDSCs)، التي تميزت بظاهرة CD11b hi وLY6C hi وLY6G lo، وMDSCs متعددة النوى (PMN-MDSCs)، التي تظهر ظاهرة CD11b hi وLY6C lo وLY6G hi، وMDSCs في المرحلة المبكرة (eMDSCs) التي تكون CD13- وCD14- وCD33+ في البشر [175، 176]. في TME، من الممكن ملاحظة كل من M-MDSCs وPMN-MDSCs، وبالمقارنة مع MDSCs، تظهر نمطًا مثبطًا [177]. تقوم MDSCs بتثبيط خلايا T ونظام المناعة الفطري لخلق نمط مثبط للمناعة في TME [177]. تساهم MDSCs أيضًا في تشكيل مواقع ما قبل النقائل، ويمكن أن تعزز خصائص الخلايا الجذعية وتكوين الأوعية الدموية، وتعزز النقائل من خلال تحفيز EMT وزيادة إفراز IL-6 [178، 179]. هناك أيضًا عوامل أخرى في TME يمكن أن تؤثر على MDSCs. HIF-1، علامة على البيئة المجهرية منخفضة الأكسجين، تحفز تمايز خلايا MDSCs إلى
الشكل 2 المكونات الخلوية التي تؤثر على بيئة الورم الدقيقة (TME). تلعب التفاعلات داخل TME دورًا حاسمًا في تسريع تقدم السرطان. تقوم خلايا السرطان بتنشيط محور PD-L1/PD-1، مما يؤدي إلى استنفاد خلايا T وضعف وظيفة خلايا T. بالإضافة إلى ذلك، تساهم الإكسوزومات التي تفرزها خلايا السرطان وتحمل PD-1 في خلل وظيفة خلايا T، مما يقلل من التكاثر ويعيق الوظيفة السليمة. تتصدى خلايا القاتل الطبيعي لتكون الورم من خلال إفراز البيرفورين والإنزيمات الحبيبية. يؤدي زيادة تسلل خلايا Treg في TME إلى إفراز TGF-، مما يؤدي إلى تحويل الخلايا الليفية إلى الخلايا الليفية المرتبطة بالسرطان (CAFs)، وتعزيز ترسيب المصفوفة خارج الخلية، والتسبب في خلل وظيفة خلايا T. تقوم خلايا المثبطة المشتقة من النخاع (MDSCs) بتحفيز تكوين خلايا Treg في بيئة الورم من خلال إفراز PGE-2 و IL-10 و TGF-تقوم خلايا T التنظيمية (Treg) بدورها بقمع وظيفة الخلايا الشجرية (DCs) عن طريق إفراز البيرفورين، مما يؤدي إلى موت خلايا DC. تقوم البلعميات المستقطبة من النوع M2 بإفراز TGF-و IL-10، مما يعطل وظيفة خلايا DC. التفاعل بين الخلايا البطانية وخلايا السرطان يؤدي إلى تكوين الأوعية الدموية، مما يعزز تقدم السرطان بشكل أكبر (تم إنشاؤه بواسطة Biorender.com)
الخلايا المناعية المرتبطة بالورم (TAMs) ذات الوظيفة المسرطنة [180]. يمكن أن يتغير استقلاب الخلايا المناعية المثبطة للورم (MDSCs) في بيئة الورم (TME) نحو تحفيز أكسدة الأحماض الدهنية لزيادة مستويات Arg1 وNOS2 [181]. بالنسبة لعلاج السرطان المناعي، يمكن أن يوفر تنظيم MDSCs رؤى جديدة، مثل تقليل CCRK الذي يعطل نشاط تثبيط المناعة لـ MDSCs ويعزز إمكانيات علاج حجب نقاط التفتيش المناعية [182]. الهياكل النانوية قادرة على تقليل عدد ووظيفة MDSCs، وإضعاف تثبيط المناعة الذي تسببه MDSCs، والتسبب في إعادة قطبية MDSC [183-185].
السيتوكينات، الكيموكينات وعوامل أخرى
تستخدم الخلايا المناعية الموجودة في البيئة المجهرية للورم السيتوكينات لإرسال رسائل إلى خلايا أخرى بطريقة صماء أو جارية أو ذاتية وتوفر التواصل بين الخلايا. تُعرف السيتوكينات أيضًا بالعوامل المناعية المعدلة، ويمكن إنتاجها في الظروف الفسيولوجية. وحالة مرضية، ويمكن أن تفرزها فئات مختلفة من الخلايا، بما في ذلك الخلايا الدهنية وخلايا الورم. تساهم السيتوكينات في المناعة الخلوية (النوع 1) والمناعة المعتمدة على الأجسام المضادة (النوع 2) كعوامل مضادة/التهابية وعوامل مؤيدة/مضادة للورم تعتمد أيضًا على البيئة المجهرية للورم. يمكن أن ترتبط السيتوكينات بمستقبلات على سطح خلايا أخرى لتنظيم عملها وتغيير المسارات الجزيئية. هناك أنواع مختلفة من السيتوكينات في البيئة المجهرية للورم، بما في ذلك الكيموكينات، والإنترلوكينات، والأديبوكينات، وعوامل النمو المحولة (TGFs)، وعامل نخر الورم (TNF)، وعوامل تحفيز المستعمرات (CSFs)، والإنترفيرونات (IFN) التي يمكن أن تعمل بمفردها أو بطريقة تآزرية للتأثير على جهاز المناعة. تعتبر الكيموكينات سيتوكينات جاذبة كيميائيًا لتجنيد الخلايا الالتهابية، بما في ذلك الكريات البيضاء (المونوسيتات، العدلات)، إلى جانب أنواع أخرى من الخلايا، مثل الخلايا البطانية والخلايا الظهارية. اعتمادًا على موضع بقايا السيستين المحفوظة، هناك
فئات مختلفة من السيتوكينات بما في ذلك CX3C و CXC و CC أو C الكيميائية [189]. علاوة على ذلك، يمكن للسيتوكينات التفاعل مع مستقبلات الغشاء المرتبطة بالبروتين G المعروفة بمستقبلات السيتوكين [190]. عدد من السيتوكينات، مثل CXCL8 و CCL3، لها وظيفة التهابية، وتقوم بتجنيد الخلايا عبر العلامات الالتهابية أو/و التوازن الداخلي [191]. تمتلك الإنترلوكينات (ILs) وزن جزيئي منخفض وتظهر وظائف التهابية ومضادة للالتهابات. يمكن للخلايا المناعية، بما في ذلك خلايا T، والعدلات، والوحيدات، والبلاعم، والخلايا الدهنية، والخلايا البطانية، إفراز ILs [192]. تلعب ILs دورًا حاسمًا في تطوير وتمايز وتحفيز ونضوج وهجرة والتصاق الخلايا المناعية [193]. السيتوكينات الدهنية (المعروفة أيضًا بالسيتوكينات الدهنية) هي سيتوكينات يمكن إفرازها بواسطة الأنسجة الدهنية وتتكون من الخلايا الدهنية، والخلايا الدهنية السابقة، والبلاعم، والخلايا الداعمة، والألياف، والخلايا البطانية [194]. تتكون السيتوكينات الدهنية من سيتوكينات محددة للأنسجة الدهنية (الأديبونيكتين، اللبتين) وفئات أخرى، بما في ذلك ILs و TNFs و السيتوكينات الكيميائية. علاوة على ذلك، يمكن التحكم في الالتهاب، وعمليات الأيض للطاقة، وتوزيع الدهون بواسطة السيتوكينات الدهنية [195]. تساهم السيتوكينات الدهنية أيضًا في الالتهاب المرتبط بالسمنة لتنظيم الأمراض الأيضية [196]. تعتبر الخلايا الدهنية من المنظمين الرئيسيين لتكون الأورام والنقائل [197]. وفقًا لتأثير السيتوكينات الدهنية على الجهاز المناعي، هناك نوعان، بما في ذلك الالتهابية، مثل اللبتين و TNF و الإنترلوكين- (IL-1 )، والإنترلوكين-6 (IL-6) والإنترلوكين-8 (IL-8)، التي تربط بين السمنة والالتهاب، والمضادة للالتهابات، مثل الإنترلوكين-10 (IL-10) والأديبونيكتين [197، 198]. تظهر عدد من السيتوكينات الدهنية، مثل الأديبونيكتين، وظيفة مضادة للسرطان [198]، بينما تظهر أخرى، مثل اللبتين، وظيفة مسرطنة [199]. TGFs هي عدد من هرمونات البروتين التي يتم التعبير عنها بشكل مفرط في سرطانات البشر ويمكن أن تعدل تكون الأورام ونمو السرطان. TGFa هو عضو في عائلة EGF مع القدرة على تنظيم تطور الظهارة وتكاثر الخلايا ويمكن أن يعدل السرطنة وتكوين الأوعية [200]. يمكن للبلاعم M2 وأنواع أخرى من الخلايا، بما في ذلك خلايا السرطان، إفراز TGF- لتعديل وظيفة خلايا T و NK والخلايا البلاعم الموجودة في TME، مما يعطل المناعة المضادة للسرطان ويعزز السرطنة [201]. تم اكتشاف IFN عند وظيفته في التدخل في نمو الفيروسات [202]. تفرز خلايا المضيف IFNs، ويمكنها تنظيم الجهاز المناعي. يمكن للألياف والوحيدات إفراز نوع I IFNs مثل IFN- و IFN- أثناء الهجوم الفيروسي. ثم، يتم تنظيم التعبير عن البروتينات القادرة على إعاقة تكرار RNA و DNA. يمكن إطلاق IFNs من النوع II، بما في ذلك IFN- بواسطة وخلايا Th1 لتحفيز عدد من الخلايا، بما في ذلك خلايا NK و البلاعم M1 و الخلايا لتعزيز
تقديم MHC I و II، وتعزيز المناعة المضادة للسرطان [203].
الإنزيمات
تعتبر التغيرات في مستوى التعبير عن الإنزيمات سمة من سمات TME، ويمكن استغلالها بطريقة عقلانية لعلاج السرطان [204]. الإنزيمات هي نوع من البروتين أو RNA يمكن أن تسهل التفاعلات الكيميائية [205]. الإنزيمات التي تحفز التفاعلات هي انتقائية للغاية وتظهر تحت ظروف معتدلة الركائز المحددة لتعديل الآليات البيولوجية والأيضية [206]. تظهر الإنزيمات عددًا من التغيرات في التعبير في الأمراض مثل TME [207]. يظهر TME عدة إفرازات إنزيمية تتكون من MMPs و الهيالورونيداز و -غليتاميلي ترانسبيبتيداز و الإستراز مع تعبير أعلى في الأورام مقارنة بالأنسجة الطبيعية [208، 209]. تساهم البروتيازات في تحلل البروتينات أو الركائز الببتيدية. يمكن للأكسيدوريدوكتاز أن يتوسط في تحفيز نقل الإلكترون من المختزل إلى المؤكسد. توفر الكينازات الفسفرة للتأثير على نشاط البروتينات وتقوم الفوسفاتازات بوساطة إزالة الفسفرة. تظهر عدد من الإنزيمات زيادة في التعبير مثل MMP-2 [210]. في أورام المثانة، يتم تعزيز تعبير HAse مقارنة بالأنسجة الطبيعية [211].
مكونات المصفوفة خارج الخلوية
تتكون المصفوفة خارج الخلوية (ECM) من الكولاجين، والفبرونيكتين، واللامينين، والفيترونيكتين، والإيلاستين، وعوامل أخرى بما في ذلك عوامل النمو، والسيتوكينات، والميتالوبروتينازات المصفوفة التي تساهم في دعم هيكل الخلايا الظهارية [212،213]. تمتلك خلايا مختلفة القدرة على إفراز مكونات ECM ولكن يتم إفرازها بشكل رئيسي بواسطة الألياف [214]. خلال تقدم السرطان، يمكن اعتبار ECM كعامل بدء. يمكن أن يختلف تكوين ECM بناءً على نوع السرطان، مثل أورام المعدة، حيث يحسن انخفاض درجة التمايز وفرة مكونات ECM، ويزيد من الأيض الخلوي، ويزيد من إعادة برمجة الأيض [215]. وفقًا للتحليل البروتيني، لا يوجد فرق بين مكونات ECM في الأورام والأنسجة الطبيعية، بينما تظهر مستوياتها تغييرات تتجلى من خلال زيادة بروتينات ECM وتقليل مكونات الغشاء القاعدي التي تعدل تكوين الأوعية، والنقائل، والغزو [216]. تزداد كثافة مكونات ECM خلال تقدم الورم، وتظهر عدد من العوامل، مثل E-cadherin/ -catenin، تقليلًا، مما يعزز تكاثر ونقائل خلايا السرطان [217]. يمكن أن يؤدي زيادة كثافة المصفوفة إلى نوع من الضغط البيئي لتعزيز السرطنة. يمكن أن تحفز ECM عالية القوة EMT لزيادة تقدم السرطان وتعزيز تسلل البلاعم M2
المستقطبة بينما تقمع وظيفة الخلايا [218،219].
نقص الأكسجين
وجود نقص الأكسجين هو سمة أخرى من سمات TME الناتجة عن التكاثر العالي لخلايا الورم. يمكن أن تؤدي التغيرات في ضغط السائل بين الأنسجة، وانخفاض في pH، وزيادة في توليد ROS إلى نقص الأكسجين [220]. في المناطق التي تعاني من نقص الأكسجين، يكون هناك ضغط سائل بين الأنسجة مرتفع بسبب الأوعية الدموية المتسربة وتصريف اللمف غير الطبيعي في الورم [221]. علاوة على ذلك، يمكن أن يعزز نقص الأكسجين في TME توليد حمض اللبنيك وحمض الكربونيك من خلال تحفيز التحلل السكري، مما يوفر pH حمضي. يمكن لعامل نقص الأكسجين (HIF) أن يحفز الكربونيك أنهيدراز IX أو XII لتحويل ثاني أكسيد الكربون والماء إلى HCO 3 – الذي، عند الانتشار خارج غشاء الخلية، يعزز المستويات في TME. علاوة على ذلك، تظهر الحويصلات الإندوسومية والليزوزومية في خلايا الورم pH أكثر حمضية مقارنة بـ pH السيتوسولية [222]. يظهر TME نقص الأكسجين فرقًا في الجهد الأكسدي بين الفضاء داخل الخلوي (مخفض) والفضاء خارج الخلوي (مؤكسد). مثل هذا الجهد الأكسدي حيوي لتطوير توصيل ذكي وانتقائي للعلاجات [223]. يمكن أن يؤدي الاختزال الإنزيمي خلال نقص الأكسجين في TME إلى استقلاب العوامل الكيميائية، بما في ذلك النيترو، والكينونات، وأكاسيد N العطرية، وأكاسيد N الأليفاتية، والمعادن الانتقالية [224]. يمكن استغلال هذه السمة لتطوير هياكل استجابة لنقص الأكسجين لاستغلال المناطق التي تعاني من نقص الأكسجين [225].
آليات التهرب المناعي في السرطان والأسئلة غير المجابة في العلاج المناعي للسرطان
خضع الجهاز المناعي لتطور تحويلي لمكافحة تقدم السرطان. ومع ذلك، يمكن قمع الاستجابات المناعية، وغالبًا ما تستخدم خلايا الورم آليات للتهرب من هذه الاستجابات، وهو مفهوم يعرف بالتهرب المناعي. سلطت الدراسات الحديثة الضوء على الآليات الرئيسية التي تساهم في التهرب المناعي لخلايا السرطان.
يمكن أن تسهل الطفرات داخل خلايا الورم التهرب المناعي. يتضح ذلك من خلال عدم تنظيم الخلايا التي لوحظت في العينات السريرية المأخوذة من مرضى سرطان المبيض، مصحوبة بتنشيط الإشارات المثبطة للمناعة من خلال TGF- [226]. آلية معروفة لتحفيز التهرب المناعي هي زيادة التعبير عن PD-L1. في سرطان الكبد، يزداد تعبير USP22 عبر PRDM1، مما يؤدي إلى تقليل تحلل SPI1 من خلال زيادة التعبير عن USP22. وهذا بدوره يؤدي إلى زيادة تعبير PD-L1، مما يعزز التهرب المناعي [227].
أظهرت الجهود الرامية إلى قمع PD-L1 وعودًا في تعطيل التهرب المناعي. RNF31، بقدرته على تقليل PD-L1 من خلال تعزيز اليوبكويتين والتدهور لـ YAP، يحسن وظيفة الخلايا، مما يوفر إمكانيات في العلاج المناعي للسرطان [228]. بينما حسنت مثبطات نقاط التفتيش المناعية بشكل كبير من كبح الورم وإمكانيات العلاج المناعي، فإن فعالية هذه العلاجات تتعرض للخطر بسبب آليات تتعلق بالتهرب المناعي.
بالإضافة إلى الآليات التي تم مناقشتها سابقًا، اقترح تشوي وزملاؤه [229] أن حمض اللبنيك، وهو ناتج ثانوي لتمثيل الخلايا السرطانية، يلعب دورًا حاسمًا في قمع المناعة المضادة للسرطان. وقد تم دعم هذه الفرضية من خلال أبحاث إضافية، لا سيما في المراجعة الشاملة التي أجراها وانغ وزملاؤه [230]. تشير نتائجهم إلى أن تراكم حمض اللبنيك والبيئة الحمضية الناتجة في الميكروبيئة الورمية (TME) تعيق بشكل كبير الاستجابات المناعية المضادة للسرطان. ومن الجدير بالذكر أنه تم إثبات أن وجود حمض اللبنيك والظروف الحمضية داخل TME تعيق وظيفة خلايا المناعة المختلفة، بما في ذلك خلايا T والخلايا الشجرية. وهذا يؤدي إلى بيئة مثبطة للمناعة تعزز نمو الورم وانتشاره. تسلط هذه الرؤى الضوء على التفاعل المعقد بين تمثيل الخلايا السرطانية والهروب المناعي، مما يبرز الدور المحوري لحمض اللبنيك وTME الحمضية كعوامل رئيسية في تقدم السرطان.
تمت الإشارة إلى زيادة تنظيم المثبطات مثل SUSD6 وTMEM127 وWWP2 في MHC-I في التهرب المناعي. إن تقليل تنظيم SUSD6 يزيد من تقديم مستضد MHC-I، مما يثبط تقدم السرطان في بطريقة تعتمد على خلايا T. تتضمن الآلية تشكيل SUSD6 معقدًا مع TMEM127 وMHC-I لاستقطاب WWP2 من أجل التحلل الليزوزومي لـ MHC-I، مما يسهل التهرب المناعي [231].
MHC-I، وهو عامل رئيسي في التهرب المناعي، يخضع للداخلية والتحلل بواسطة CEMIP، مما يقلل من المراقبة المناعية [232]. بالإضافة إلى ذلك، فإن استنفاد خلايا T الناتج عن SOX4 يساهم في التهرب المناعي. التفاعل بين خلايا السرطان والخلايا، التي تسهلها ميدكين، تغير استجابات جهاز المناعة [233]. في نماذج الحيوانات التي تفتقر إلى PTEN، PI3Kيؤدي تقليل التعبير إلى قمع STAT3، مما يسرع الاستجابات المناعية ويكشف عن إمكانيات PI3K.في التسبب في تحمل المناعة والتجنب [234].
تؤدي التغيرات الكروموسومية والحذف أيضًا دورًا في التهرب المناعي. تؤثر الحذوف المتماثلة التي تؤثر على الكروموسوم 9 q 21.3 على وظيفة، مما يسرع من تكوين السرطان. تؤثر نصف هذه الحذف على مجموعة جينات IFN على الكروموسوم 9 q 21.3، مما يزيد من هروب خلايا الورم من مراقبة الخلايا [235].
الحفاظ على توازن استجابات الإنترفيرون أمر حيوي لعلاج السرطان المناعي، حيث يمكن أن تؤدي التغيرات في مستويات الإنترفيرون وخلايا T إلى تحفيز التهرب المناعي. يعزز mTORC1 تعبير B7-H3، مما يقلل من وظيفة خلايا T وIFN-الاستجابات مع زيادة تعبير MHC-II [236]. إحدى الآليات التي تسبب الهروب المناعي تتضمن تقليل عدد خلايا T، الذي يتم بوساطة تحفيز الاستماتة. يحفز الجاليكتين 4 خارج الخلية استماتة خلايا T، مما يقلل من المراقبة المناعية. على العكس، فإن تقليل الجاليكتين 4 يعزز استقطاب M1 للبلاعم ويزيد من خلايا T والخلايا التغصنية، مما يعطل الهروب المناعي.
لقد أظهرت خلايا المناعة إمكانيات في تحديد والتعرف على الخلايا الورمية التي تمتلك طفرات ابتدائية لقمع تكوين الأورام. على الرغم من أن نشوء الورم يأتي من خلية واحدة متحولة، فإن وجود عدم استقرار جيني يمكن أن يؤدي إلى توليد خلايا سرطانية تتسم بالتنوع الجيني مع خصائص مورفولوجية وفسيولوجية فريدة. علاوة على ذلك، أظهرت خلايا الورم ميزات ملحوظة من حيث تعبير جزيئات السطح، والتكاثر، وتكوين الأوعية الدموية، الناتجة عن اللدونة المورفولوجية والإبيجينية. وبالتالي، تظهر خلايا السرطان تعبيرًا عن مستضدات مختلفة قد تكون محددة للورم أو مرتبطة به، ومستضدات تمايز، ومواقع ربط اللكتين. تعرض هذه المستضدات توزيعًا غير متساوٍ على تحت مجموعات الورم ويمكن أن تحفز استجابات مناعية متنوعة. يمكن أن تؤثر هذه التغايرية الورمية بشكل كبير على النمط الجيني، وتعبير الجينات، والمورفولوجيا الخلوية، والنشاط الأيضي، والحركة، والسلوكيات، بما في ذلك التكاثر، وعرض المستضدات، واستجابة الأدوية، والأيض. علاوة على ذلك، يمكن الاستفادة من هذه التغايرية في التشخيص، وفعالية العلاج، والتعرف على الأهداف الواعدة. يمكن أن توفر هذه الطبيعة المتغايرة لخلايا السرطان فرصًا كبيرة للهروب من وظيفة خلايا المناعة. تتكاثر خلايا الورم بشكل كبير في البيئة المجهرية للورم، مما يمكن أن يسبب نقص الأكسجة. إن وجود نقص الأكسجة في البيئة المجهرية للورم يجذب خلايا MDSC ويضعف وظيفة خلايا NK لتوفير مكان مسبق للنقائل، مما يظهر أن خلايا السرطان تنتشر من خلال قمع المراقبة المناعية. عند الاستئصال الجراحي، تتعرض خلايا السرطان لصدمة، ويمكن أن تعزز هذه الخلايا الورمية إنتاج السيتوكينات وعوامل أخرى، بما في ذلك IL-6، وبروتين سي التفاعلي (CRP)، وTNF-، إيل- لتأثير على الجهاز المناعي [244]. لذلك، يجب أخذ تطبيق العلاجات التقليدية والطبيعة غير المتجانسة لخلايا السرطان في الاعتبار في التهرب المناعي. تتمكن خلايا المناعة من قمع خلايا السرطان الضعيفة التي تقدم مستضدات الورم [245]، بينما تسمح الطبيعة غير المتجانسة لخلايا السرطان لها بالهروب من مثل هذا العمل للجهاز المناعي. علاوة على ذلك، أظهرت خلايا الورم القدرة على تحفيز موت الخلايا المبرمج في الخلايا اللمفاوية التائية السامة الخاصة بالورم [246].
لذلك، نظرًا لأن التهرب المناعي يحدث بشكل شائع في السرطان، تم تقديم العلاج المناعي للسرطان. فيما يتعلق بالعلاج المناعي للسرطان، هناك عدد من التحديات التي يجب معالجتها. التحدي الأول والأهم يتعلق بحقيقة أن الهيمنة يجب تسليط الضوء على محركات مناعة السرطان. علاوة على ذلك، يجب توجيه المزيد من التحقيقات نحو فهم وظيفة السياق المناعي للأورام المحددة بالأعضاء. تُستخدم مثبطات نقاط التفتيش عادةً لعلاج السرطانات البشرية، ولكن لا يزال هناك طريق طويل لفهم المشهد الجزيئي للعوامل التي تنظم الهروب المناعي الأولي مقابل الثانوي. هناك سؤال كبير حول ما إذا كان من الأفضل استخدام المناعة الذاتية أو الاصطناعية لعلاج السرطانات البشرية. علاوة على ذلك، منذ أن تم تطبيق العلاج المناعي للسرطان في العيادات، هناك أيضًا أسئلة تتعلق بالتقييم الفعال للعلاج المناعي للسرطان في الدراسات السريرية. واحدة من الآمال هي التقدم في مجال البيولوجيا الذي يسلط الضوء على تطبيق العلامات الحيوية والتوقيعات لعلاج السرطان المناعي. لذلك، يمكن أن تستفيد الطب الدقيق بشكل كبير من تسليط الضوء على التوقيعات وتطوير استراتيجيات تستند إلى استهداف توقيعات دقيقة وفعالة لعلاج السرطان المناعي. سؤال آخر هو أنه تم تطوير أنواع مختلفة من الأنظمة لعلاج السرطان المناعي، وهناك حاجة لإجراء دراسات شاملة لتحسين البقاء على المدى الطويل من خلال الجمع بين مثل هذه الأنظمة. من أجل تحسين عملية العلاج المناعي للسرطان، يمكن أن يؤدي الاستجابة لمثل هذه المخاوف والأسئلة إلى تحسين الإمكانية لعلاج مرضى السرطان.
الجسيمات النانوية المستهدفة لمكونات الميكروبيئة الورمية في علاج السرطان المناعي
لمعالجة الدور المثبط للمناعة الذي تلعبه البلعميات المستقطبة من النوع M2، تظهر تحفيز الاستقطاب من النوع M1 من خلال الهياكل النانوية كمسار واعد لتعزيز العلاج المناعي. تتضمن آلية محورية تطوير خلايا نقية معدلة وراثيًا، حيث يتم استخدام غشاء الخلية المستخرج لتغطية وتفعيل الجسيمات النانوية في علاج السرطان. تظهر الجسيمات النانوية المغناطيسية المقلدة حيويًا التي تحتوي على أغشية خلايا معدلة وراثيًا القدرة على استهداف مسارات متعددة، مما ينظم استقطاب البلعميات ويثبط تكوين الأورام. على وجه التحديد، فإن وجود أغشية خلايا معدلة وراثيًا يثبط CD44/SIRP.محور عن طريق زيادة تنظيم SIRPالمتغيرات. تلعب الجسيمات النانوية المغناطيسية، التي تشكل النواة، دورًا حاسمًا في إعادة تعليم وإعادة برمجة البلعميات، مما يسرع من العلاج المناعي للسرطان [248]. تتجاوز التغيرات في البلعميات الاستقطاب، ودورها في تنظيم معالجة المستضدات أيضًا مهم. تشكل بعض المسارات السريرية المهمة، مثل STING، تحديًا لاستهدافها على المستوى السريري بسبب نقص التوصيل المستهدف. من خلال عملها كمنشط لـ STING، يقوم ZnCDA بتغليف CDA ويعطل الحاجز البطاني في الأوعية الدموية السرطانية، مما يسهل الاختراق إلى البيئة المجهرية للورم وموقع الورم.
تستهدف هذه الجسيمات النانوية البلعميات، مما يعزز معالجة المستضدات ويسرع الاستجابات المرتبطة بالخلايا التائية في العلاج المناعي للسرطان [249]. أظهرت عدد من الجسيمات النانوية إمكانيات في تغيير استقطاب البلعميات المرتبطة بالورم. في سياق استقطاب M1 للبلعميات، تتوفر آليات مختلفة لتحفيز استقطاب البلعميات إلى النمط الظاهري M1. يمكن أن تحفز الهياكل النانوية المستمدة من الجينسنغ المحاور TLR4/MyD88، مما يؤدي إلى زيادة استقطاب M1 للبلعميات، وارتفاع مستويات ROS، وتحفيز موت الخلايا المبرمج في الميلانوما [250]. في الواقع، تم ملاحظة أن استقطاب M1 للبلعميات قد صاحبته تحفيز لموت الخلايا المبرمج.
على الرغم من أن التركيز الأساسي في هذا القسم هو تقييم دور الجسيمات النانوية في إعادة تعليم البلعميات، فقد أظهرت الدراسات أنه يمكن استخراج الأغشية من البلعميات لتغطية الجسيمات النانوية وتفعيلها. تؤدي هذه الطريقة إلى تطوير هياكل متوافقة حيوياً ذات خصائص خفية. يمكن استخدام هذه الطريقة بشكل متبادل حيث يتم تفعيل الجسيمات النانوية بغشاء البلعميات لتحسين قدرتها على الاستهداف نحو البلعميات وبيئة الورم المجاورة، ومن ناحية أخرى، يمكن تصميمها لإعادة تعليم البلعميات إلى نمط M1.
استهداف البلعميات في علاج السرطان مدفوع أساسًا بوظيفتها المثبطة للمناعة. على الرغم من تطوير استراتيجيات مختلفة لتنظيم الاستجابة المناعية، مثل العلاج المناعي المستحث بالضوء، لا تزال المخاوف قائمة بشأن المناعية وتحفيز الالتهاب. لذلك، من الضروري أن تستخدم الجسيمات النانوية آليات آمنة ومتوافقة حيويًا لمواجهة تثبيط المناعة الذي تسببه البلعميات. -هياكل نانوية من نوع SAS@PLT، مشتقة من هياكل نانوية مغناطيسية مسامية محملة بالسلفاسالازين ومفعلّة بالصفيحات، تم تصميمها لقمع نظام ناقل الجلوتامات-سيستين Xc-pathway في تحفيز الفيروبتوز. يظهر هذا التحفيز للفيروبتوز تأثيرات تآزرية مع العلاج المناعي لنقطة التفتيش PD-L1، كما لوحظ في نماذج حيوانية. ومن الجدير بالذكر أن هذه الهياكل النانوية البيوميميتية تحفز الفيروبتوز، مما يعزز استقطاب M1 للبلاعم ويعطل البيئة المجهرية المثبطة للمناعة [252].
عند النظر في استخدام الجسيمات النانوية لتعديل البلعميات، خاصة للاستخدام المحتمل في العلاج المناعي للسرطان على المستوى السريري، فإن التوافق الحيوي مهم بقدر الوظائف. لقد أظهرت الجسيمات النانوية الدهنية ذات الخصائص الكاتيونية وعدًا كحاملات، حيث تقوم بتوصيل الرنا المرسال إلى المواقع المستهدفة. تحميل الرنا المرسال لإعادة تعليم استقطاب البلعميات على الجسيمات النانوية الدهنية يخلق هياكل نانوية آمنة ومتوافقة حيويًا للعلاج المناعي للسرطان. يعد هذا تقدمًا كبيرًا في استخدام الجسيمات النانوية لإعادة تعليم البلعميات. يتضمن ذلك تفعيلها بأغشية البلعميات لتعزيز الفعالية. تم اختبار هذه الفرضية في تجارب، مما يظهر إمكانيات الأغشية المستمدة من البلعميات المرتبطة بالأورام مع وظائف تعديل المناعة و affinity لاستهداف المستضدات. تم استخدام هذه الأغشية لتفعيل الهياكل النانوية التي تعيد التحويل المحملة بالمواد الحساسة للضوء. ومن الجدير بالذكر أن الجسيمات النانوية المفعلة بأغشية البلعميات المرتبطة بالأورام تثبط CSF1 والتفاعلات بين خلايا السرطان والبيئة الدقيقة للورم، مما يعيق تكوين الأورام. علاوة على ذلك، تحفز هذه الجسيمات النانوية العلاج الضوئي الديناميكي من خلال تثبيط النمط الظاهري M2، وتعزيز استقطاب البلعميات M1، وتحفيز موت الخلايا المناعية، وتحسين إنتاج خلايا T من خلال تعزيز تقديم المستضدات.
إعادة توجيه البلعميات نحو النمط الظاهري M2 يمثل عقبة في تحقيق العلاج المناعي الناجح. يتم تحفيز هذا الاستقطاب بشكل رئيسي بواسطة MCSF الذي تفرزه خلايا الورم، مما يؤدي إلى زيادة مستوى CSF1-R. علاوة على ذلك، فإن التعبير المرتفع عن SIRPعلى أسطح الخلايا النخاعية، ينشط SHP-1 وSHP-2 في البلعميات، مما يعيق العلاج المناعي عن طريق عرقلة البلعمة. وبالانتقال إلى ما هو أبعد من استقطاب البلعميات، يتم توجيه الجهود لمعالجة فشل نشاط البلعميات. لتعزيز بلعمة البلعميات، تتضمن الاستراتيجيات الواعدة تنظيم CSF1R وSHP2. الجسيمات النانوية المحملة بمثبطات CSF1R وSHP2 تحفز استقطاب البلعميات من النوع M1، مما يعزز البلعمة لعرقلة تكوين الأورام.
بعد توضيح الآليات الرئيسية التي تحكم استقطاب ونشاط البلعميات، يتمثل التركيز التالي في استكشاف الجسيمات النانوية ذات التطبيقات السريرية المحتملة. يُعتبر الفيروموكسيترول، وهو مكمل للحديد وهيكل نانوي من أكسيد الحديد، معتمدًا من إدارة الغذاء والدواء الأمريكية، ويؤدي دورين كونه نظام توصيل دوائي ووكيل تصوير. عند زراعته مع البلعميات لعلاج انتشار سرطان الرئة، يقوم الفيروموكسيترول بزيادة التعبير عن الكاسبيز-3، مما يحفز البلعميات على التعبير عن الرنا المرسال للاستجابات الالتهابية المرتبطة بـ Th1. يُثبط الفيروموكسيترول بشكل فعال انتشار الورم وتكاثره بينما يعزز استقطاب البلعميات من النوع M1 لتحسين جودة العلاج المناعي للسرطان.
يدعم عدد متزايد من الأدلة المشاركة المحتملة للبلاعم المرتبطة بالأورام في تطوير مقاومة الأدوية [257، 258]. تلعب هذه البلاعم دورًا يتجاوز تنظيم جهاز المناعة، حيث تؤثر على الاستجابة للعلاج الكيميائي. تستفيد الهياكل النانوية الذهبية المجمعة المعتمدة على الفورين من تأثير “النفاذية المعززة والاحتفاظ”، حيث تتجمع في سرطان الثدي بسبب زيادة تنظيم الفورين. تؤدي هذه العملية إلى قمع الإخراج الخلوي، مما يؤدي إلى زيادة التراكم التفضيلي في موقع الورم. كما أن هذه الجسيمات النانوية تثبط البلعمة الذاتية، مما يعزز تعليم البلاعم من النوع M1. لمواجهة مقاومة الأدوية [259]. توفر الجدول 1 نظرة عامة مختصرة عن تطبيقات الجسيمات النانوية في إعادة تعليم البلعميات لعلاج السرطان المناعي. توفر الشكل 3 نظرة عامة عن تنظيم البلعميات المرتبطة بالورم بواسطة الجسيمات النانوية في علاج السرطان المناعي.
تلعب الجسيمات النانوية دورًا حاسمًا في التأثير على الألياف المرتبطة بالسرطان (CAFs) ضمن مشهد علاج السرطان. تسهم التفاعلات بين خلايا السرطان وCAFs في البيئة المجهرية للورم (TME) في تكوين الأورام، مما يجعل من الضروري استكشاف تطبيقات الجسيمات النانوية في قمع هذه التفاعلات وإعاقة تقدم السرطان. في سرطان المبيض، تعزز خلايا سرطان المبيض وخلايا TME تنشيط CAFs المبيضية. وقد أدت الجسيمات النانوية الذهبية بحجم 20 نانومتر إلى تعطيل هذا التفاعل بشكل فعال، مما يمنع تنشيط CAF ويقدم إمكانيات في علاج سرطان المبيض.
تلعب الخلايا الليفية المرتبطة بالسرطان (CAFs) دورًا داعمًا في انتشار الأورام. كانت الجسيمات النانوية ذات النواة والقشرة، التي تحتوي على الذهب كنواة والفضة كقشرة، فعالة في قمع تعبير الأوستيو بونتين في CAFs، مما يعيق تقدم السرطان دون التأثير على تعبير علامات CAF [276]. بالإضافة إلى تعديل تنشيط CAFs وإفرازاتها، يمكن أيضًا استخدام الهياكل النانوية لتدمير CAFs المستهدف. تؤدي الناقلات النانوية من أكسيد الحديد فائقة الصغر (6 نانومتر في القطر) المدمجة مع مجالات مغناطيسية دوارة منخفضة التردد إلى تحفيز قوى ميكانيكية، مما يؤدي إلى موت CAFs وتفكيك الليزوزومات [277]. يستهدف تدمير CAFs تعزيز امتصاص الجسيمات النانوية. تعالج هذه الاستراتيجية تحدي البيئة المجهرية الكثيفة التي تعيق اختراق الجسيمات النانوية. ساعدت أقفاص الفيريتين المحملة بالمواد الحساسة للضوء ZnF16Pc والمعدلة بقطعة متغيرة ذات سلسلة واحدة تستهدف بروتين تنشيط الألياف، في تسهيل العلاج الضوئي لتقليل CAFs وتحسين اختراق الجسيمات النانوية إلى موقع الورم [278].
يمكن أن تعمل الجسيمات النانوية بوظائف مزدوجة في تنظيم الخلايا الليفية السرطانية وتعديل الاستجابات المناعية. الجسيمات النانوية من حمض البولي (لاكتيد-كو-جليكوليد) (PLGA) المجهزة بغشاء الخلايا السرطانية لم تعزز فقط تفاعلات الخلايا السرطانية مع الخلايا الليفية السرطانية، بل زادت أيضًا من امتصاص المستضد، مما يحفز و تعمل خلايا T من خلال MHC-I وMHC-II، مما يعزز العلاج المناعي للسرطان [279]. يمثل بروتين تنشيط الألياف، الذي يتم تنظيمه بشكل زائد على أسطح خلايا الألياف السرطانية، هدفًا واعدًا في العلاج المناعي للسرطان. كانت الجسيمات النانوية المجهزة بشظية متغيرة أحادية السلسلة لتوصيل ZnF16Pc في العلاج الضوئي للسرطان تفتقر إلى السمية الجهازية. قامت هذه الجسيمات النانوية المجهزة بتقليل تقدم السرطان في كل من المواقع الأولية والبعيدة من خلال تسريع الاستجابات المناعية وتعزيز المناعة المضادة لخلايا الألياف السرطانية [280].
تم تصميم بعض الجسيمات النانوية للاستجابة لبروتين تنشيط الألياف كعلامة حيوية لخلايا الأنسجة الليفية. أظهرت الهياكل النانوية للألبومين التي تحتوي على باكليتاكسيل والمفعلّة بـ CAP وعدًا في استهداف بروتين تنشيط الألياف في خلايا الأنسجة الليفية. كما أن دمج المركب الحسّاس للضوء IR-780 مكّن من استخدام إشعاع الليزر بالأشعة تحت الحمراء القريبة للعلاج الضوئي الحراري، مما أدى إلى كبح الورم وتحسين اختراق الورم العميق. إن مفهوم استهداف خلايا الأنسجة الليفية بشكل محدد باستخدام علاماتها الحيوية لديه إمكانيات كبيرة في تعزيز مكافحة السرطان.
جزيئات نانوية تستهدف خلايا T
الجسيمات النانوية، من خلال التنظيم المستهدف لخلايا T، ظهرت كمسار واعد لعلاج السرطان المناعي الفعال [282-288]. زيادة تسللالخلايا وخلايا T المساعدة في البيئة المجهرية للورم (TME) أمر حاسم لإعادة تشكيل TME وتنشيط الجهاز المناعي ضد تقدم السرطان. تلعب الجسيمات النانوية مثل هياكل كبريتيد الزنك والمنغنيز النانوية دورًا محوريًا في وساطة هذا التأثير [289]. تتضمن الاتجاهات الملحوظة في السنوات الأخيرة دمج العلاج المناعي مع أساليب علاجية أخرى مثل العلاج الكيميائي أو العلاج الضوئي. تحفز حوامل الأدوية الهجينة التي تحمل سيسبلاتين وكامبتوثيسين محور cGAS/STING وتسبب تلفًا في الحمض النووي. بالإضافة إلى ذلك، تعزز هذه الحوامل للأدوية الهجينةتسلل الخلايا في البيئة المجهرية للورم، مما يحسن نتائج العلاج المناعي لسرطان القولون والمستقيم. تمتلك هذه الحاملات النانوية الهجينة خاصية استجابة للجذور الحرة للأكسجين (ROS) وهي مصنوعة من mPEG2k-DSPE ومواد بوليمرية أخرى [290]. يمكن لحاملات النانو mPEG/PLGA/PLL، التي توصل CD155-siRNA والمعدلة بأجسام مضادة لـ PD-L1، أن تثبط في الوقت نفسه CD155 وPD-L1، مما يتجنب التهرب المناعي. إنها تعززتسلل الخلايا وتحفيز موت الخلايا المناعية في علاج سرطان الثدي [291].
يتطلب تطوير لقاح فعال ضد السرطان جزيئات نانوية يمكن أن تحفز المناعة النظامية.تعمل الهياكل النانوية لميلتين، المستجيبة للتغيرات في البيئة المجهرية للورم، كلقاحات واعدة من خلال تحفيز الاستجابات المناعية النظامية. تقوم هذه الهياكل النانوية بتحفيز موت خلايا السرطان من خلال تفاعل فينتون في البيئة المجهرية للورم، وتفعيل محور cGAS/STING، وتعزيز نضوج خلايا تقديم المستضدات. علاوة على ذلك،تحفز جزيئات الميلتين الاستجابات المناعية الجهازية، بما في ذلك تعزيز خلايا T وزيادة مستويات السيتوكينات والكيماوكينات المؤيدة للالتهابات [292].
دمج العلاج الكيميائي مع العلاج الضوئي هو استراتيجية أخرى لتسريع قمع الورم. حوامل الأدوية النانوية، التي تم تطويرها من حمض الهيالورونيك وثنائيات الهيدروكربون المرتبطة بالأدامانتين من PPa و JQ1، تستهدف خلايا سرطان البنكرياس التي تعبر عن CD44 بشكل مفرط.
الجدول 1 العلاج المناعي للسرطان المستحث بواسطة الجسيمات النانوية من خلال استهداف البلعميات
التوليف مع العلاج الإشعاعي يعيق استقطاب M2 للبلاعم ويزيد من الاستجابات المناعية
[260]
جزيئات الدواء المسبق
سرطان القولون والمستقيم / خلايا MC38 سرطان الثدي / خلايا MCF-7
أقل من
التوصيل المشترك للدكسوروبيسين وR848 تعديل الجسيمات النانوية باستخدام مضاد الببتيد ثنائي الوظيفة PD-1/PD-L1 PCP قطع الجسيمات النانوية باستخدام FAP-a في نسيج الورم إطلاق الحمولة في موقع الورم يحفز موت الخلايا المناعية ويؤدي إلى إعادة برمجة البلعميات
[261]
جزيئات الدهون النانوية
سرطان البنكرياس / خلايا KPC
ملي فولت
تحميل جزيئات الدهون النانوية في الهلاميات القابلة للحقن توصيل CCL5-siRNA بواسطة جزيئات الدهون النانوية لتحفيز استقطاب M1 للبلاعم وتعزيز الاستجابات المناعية المستحثة بواسطة خلايا T
[262]
الهياكل النانوية لتحويل الطاقة
سرطان الثدي/خلايا 4T1
و مللي فولت و -4.1 مللي فولت
مقدمة عن جزيئات النانو ذات التحويل العلوي المدعمة بمركبات الكربون الفلوري (PFC)/كلورين e6 (Ce6)
التوصيل المستهدف للباكليتاكسيل كدواء كيميائي زيادة إنتاج الأكسجين الأحادي تحفيز استقطاب M1 للبلعميات في تسريع إفراز السيتوكينات المؤيدة للالتهابات لإعاقة تقدم سرطان الثدي
[263]
ناقلات نانوية تشبه الميلانين مخلبية للحديد
سرطانات القولون والثدي / خلايا CT26 و 4T1
150 نانومتر
تحفيز استقطاب M1 للبلاعم وتوفير العلاج الضوئي الحراري، تسارعوا في إطلاق المستضدات المرتبطة بالورم لتحسين العلاج المناعي للسرطان
[264]
الجزيئات النانوية فوق الجزيئية
سرطان الثدي/خلايا 4T1
قمع CSF1R و MAPK لتحفيز استقطاب M1 للبلاعم
[265]
MIP-3بلازميد
سرطان الثدي/خلايا 4T1
زيادة نضوج الخلايا الشجرية وكبح استقطاب M2 للبلاعم
[266]
حاملات نانوية Au@PG
سرطان الرئة / خلايا سرطان الرئة لويس
32.2 نانومتر عند 2.5 مللي مولار ONPG، 29.8 نانومتر عندعند 50 مللي مولار، و18.3 نانومتر عند 75 مللي مولار
تكثيف الجليكول القائم على البوليمر في الهياكل النانوية تحويل البلعميات المستقطبة M2 إلى بلعميات مستقطبة M1 تظهر الجسيمات النانوية ذات الأحجام الأصغر فعالية أعلى في إعادة تعليم البلعميات
[267]
هياكل نانوية من الذهب محملة بـ CaCO3
البلاعم / خلايا RAW 264.7
32 نانومتر
إطالة شكل خلايا البلعميات تحفيز علامة M1 الحيوية والسيتوكينات الالتهابية تحفيز استقطاب M2 للبلعميات
[268]
حاملات نانوية بوليمرية
سرطان العظام / خلايا K7M2
جزيئات نانوية قابلة للتحلل الحيوي لتوصيل الريجورافينب كمركب لتطبيع الأوعية الدموية. إطلاق الحمولة عند تعرضها لأشعة الليزر بزاوية 808 نانومتر وزيادة نقص الأكسجين في بيئة الورم. تحفيز إطلاق أنواع الأكسجين التفاعلية والتوسط في موت الخلايا المناعية. تحفيز استقطاب M1 للبلاعم.
[269]
ناقلات نانو غادوفوليرين
سرطان الثدي/خلايا 4T1
استقطاب M1 للبلاعم وزيادة تسلل اللمفاويات التائية في البيئة المجهرية للورم لقمع السرطان
[270]
جزيئات النانو DGL-ZA
سرطان الثدي/خلايا 4T1
توزيع محتمل للسرطان، تسرب، واختراق عالٍ للورم ربط بوليمرات دندريغرافت من بولي-ل-لايسين كمنشطات للاوتوفاجي تنظيم البلعميات وزيادة نشاط مثبط الورم
[271]
الجدول 1 (مستمر)
جزيئات نانوية
نوع السرطان/خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
نتيجة
مرجع
جزيئات نانوية معدلة بالفوسفاتيديل سيرين
خلايا الميلانوما/B16F10
على مدى
يحدث خارجية الهياكل النانوية عندما تتعرض للبيئة المجهرية للورم مع زيادة تنظيم MMP2 وزيادة استنفاد البلعميات المرتبطة بالورم في البيئة المجهرية للورم.
[272]
جزيئات نانوية مفعلة بحمض الهيالورونيك
سرطان الرئة غير صغير الخلايا
التوصيل المستهدف لـ miR-125b وزيادة نقله أكثر من 6 مرات لتحفيز استقطاب M1 وزيادة مستويات iNOS
[273]
جزيئات الكيتوزان ثلاثي الميثيل
سرطان الثدي/خلايا 4T1
ملي فولت
تFunctionalization مع المانوز وحمض الجليكوكوليك
توصيل SIRPa-siRNA و MUC1 pDNA
توصيل الحمولة عن طريق الفم
pMUC1 يزيد من قدرة البلعمة لدى البلعميات واستقطابها نحو النوع M1
زيادة المناعة بواسطة SIRPa-siRNA
[274]
يجمع هذا المزيج من العلاج الضوئي والعلاج المناعي بين زيادة تسلل الخلايا اللمفاوية التائية. علاوة على ذلك، يقوم JQ1 بتثبيط التهرب المناعي الناتج عن العلاج الضوئي من خلال تقليل c-Myc وPD-L1، مما يؤدي إلى تثبيط كبير للورم [293]. نظرًا لأن تطور السرطان هو عملية تدريجية، يجب أن تركز العلاجات الفعالة على توفير مناعة طويلة الأمد. لقد زاد استخدام لقاحات السرطان بشكل كبير في السنوات الأخيرة؛ ومع ذلك، لا يزال هناك تحدٍ رئيسي في توصيل الحمولة المستهدفة، بما في ذلك المستضدات والمساعدات المناعية. لمعالجة هذه المشكلة، تم تطوير ناقلات نانوية من حمض البولي (لاكتيد-كو-جليكوليد) (PLGA) لتوصيل مستضد البيض البيضاوي وCpG كمساعد في تطعيم السرطان. يتم تعديل سطح الهياكل النانوية بالغالكتوز أو المانوز. تمتلك هذه الجسيمات النانوية قدرة تحميل عالية وإطلاق مستدام، وهي ميزات رئيسية لتطوير لقاحات السرطان. إنها تحفز نضوج الخلايا الشجرية، وتعزز امتصاص المستضد، وتزيد منمستويات الخلايا، مما يؤدي إلى زيادة التسلل منالخلايا في العلاج المناعي للسرطان [294]. نهج مبتكر في علاج السرطان يتضمن تطوير جزيئات نانوية تحاكي مسببات الأمراض لتحفيز استجابة مناعية قوية. تعمل الناقلات النانوية المستندة إلى خميرة Saccharomyces cerevisiae كأنماط جزيئية مرتبطة بمسببات الأمراض (nano-PAMPs) ومن خلال تحفيز Dectin-2 و TLR-4، تعزز استجابات TH17، مما يساهم في المناعة المضادة للسرطان. لقد أثبت تحفيز خلايا T المساعدة فعاليته في العلاج المناعي للسرطان. يمكن أن تحفز الهياكل النانوية المعدلة بالكوندرويتين الكبريتي المرتبطة بحمض الجليكوليك أو المانوز، إلى جانب الحويصلات الدهنية الكاتيونية المحملة بالألبومين البيض، نضوج خلايا التغصن وتثير استجابات خلايا T المساعدة من النوع الأول والثاني. في العديد من الحالات، لا تحفز الجزيئات النانوية فقط تسلل خلايا T، بل تسرع أيضًا نضوج خلايا التغصن، مما يساهم في العلاج المناعي للسرطان. مع الاعتراف بدور التغيرات الوراثية في خلل المناعة، تم استكشاف توصيل miRNAs في العلاج المناعي للسرطان. لقد أظهرت الجزيئات النانوية الدهنية التي توصل anti-miR-21 القدرة على تحفيز استقطاب M1 للبلاعم وتعزيز التسلل.الخلايا [298]. تم استخدام الجسيمات النانوية لتنظيم مستهدف لخلايا Treg المثبطة للمناعة في علاج السرطان، بهدف تعزيز إمكانيات العلاج المناعي. على سبيل المثال، تم تطوير جسيمات نانوية من PLGA تتمتع بقدرات التقاط المستضدات لهذا الغرض. هذه الجسيمات النانوية تعزز بشكل أساسي عدد الخلايا، مما يزيد بالتالي من نسبة خلايا T السامة للخلايا إلى خلايا Treg [299]. من خلال زيادة هذه النسبة، يمكن تخفيف التأثير السلبي لخلايا Treg على الاستجابات المناعية. من أجل تحسين توصيل الحمولة، تم تصميم هياكل نانوية بطبقات، تتكون من GITR/PLGA ومعدلة بـ
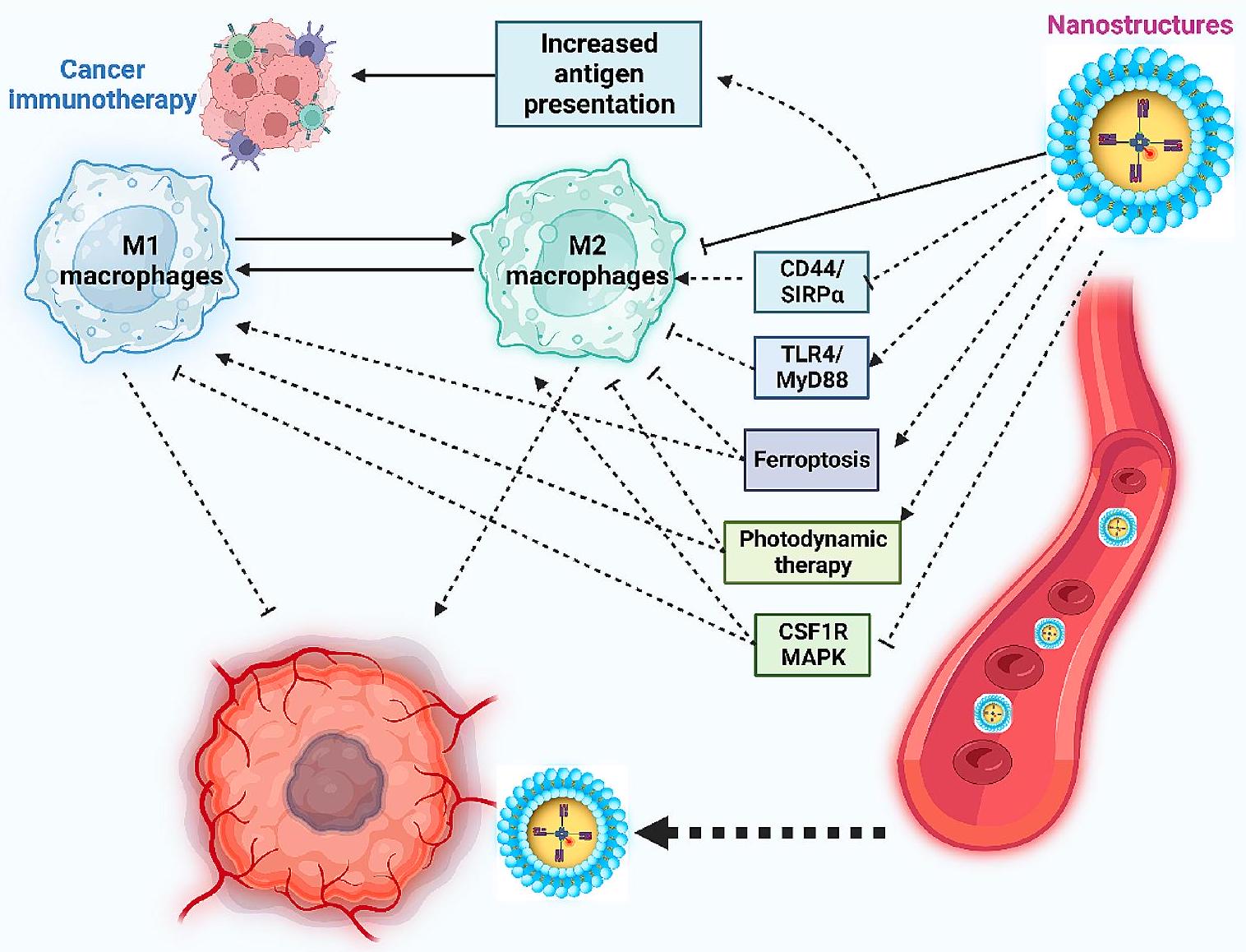
الشكل 3 تأثير الجسيمات النانوية على البلعميات، مما يبرز قدرتها على إعادة تعليمها وإعاقة تقدم السرطان. تستهدف هذه الجسيمات النانوية بفعالية الآليات الرئيسية المرتبطة بالاستقطاب M2 للبلعميات المرتبطة بالورم. إنها تثبط CD44/SIRPa وCS1R وMAPK، مما يدفع إلى الاستقطاب M1 للبلعميات. بالإضافة إلى ذلك، تنشط الحوامل النانوية محور TLR4/MyD88، مما يساهم في زيادة الاستقطاب M1 للبلعميات المرتبطة بالورم. كما أن الجسيمات النانوية تحفز الفيروبتوز والعلاج الضوئي الديناميكي، مما يعطل استقطاب هذه البلعميات إلى النمط الظاهري M2 (تم إنشاؤه بواسطة Biorender.com)
تم تصميم PLG و PLH اللذان يستجيبان لرقم الحموضة TME لتوصيل صبغة IR780. إن التعرض اللاحق لأشعة الليزر بزاوية 808 نانومتر يعزز نضوج الخلايا الشجرية، مما يزيد من النشاط. و الخلايا في العلاج المناعي للسرطان. من الجدير بالذكر أن هذه الجسيمات النانوية تظهر تأثيرًا مثبطًا على وظيفة خلايا Treg، مما يساهم بشكل إيجابي في التفاعلات المناعية [300].
تواجه العديد من الأدوية الكيميائية المستخدمة على نطاق واسع، بما في ذلك دوكسوروبيسين، قيودًا مثل انخفاض تراكمها في موقع الورم وتطور مقاومة الأدوية. تم تطوير ناقلات نانوية من الأدوية القائمة على دوكسوروبيسين وإندوكسيمود لقمع مسار IDO. تحفز هذه الناقلات النانوية من الأدوية موت الخلايا المناعية، وتعزز تسلل الخلايا السامة. خلايا ( خلايا T)، وتثبط خلايا Treg، وMDSCs، وTAMs في بيئة الورم، مما يعزز بشكل فعال نسبة خلايا T إلى خلايا Treg للعلاج المناعي للسرطان [301].
تم استخدام استراتيجيات التوصيل المشترك لتحسين العلاج المناعي للسرطان. الميتفورمين، مركب يُستخدم لـ العلاج المناعي للسرطان، أظهر وعدًا في إعادة تعليم البيئة المجهرية للورم وتعزيز نشاط البلعمة لدى البلعميات. تم تصميم جزيئات النانو المسببة للأدوية المشتركة، المصممة بحمض الهيالورونيك-سيسبلاتين/بوليمر بولي ميتفورمين، لتوصيل الميتفورمين والسيسبلاتين بشكل فعال. بحجم 166.5 نانومتر وجهد زتا -17.4 مللي فولت، تظهر هذه الجزيئات النانوية إمكانيات عالية في العلاج المناعي للسرطان. إنها تحفز موت الخلايا المبرمج من خلال زيادة تنظيم PARP، وتعزز حساسية السيسبلاتين من خلال قمع ERCC1، وتعدل AMPK.طرق لزيادة و الخلايا، وتقليل أعداد خلايا Treg [302].
تظهر الجسيمات النانوية غير المعدلة استهدافًا ضعيفًا لخلايا Treg. وقد دفع ذلك إلى استخدام تفعيل الناقلات النانوية. تم تطوير ناقلات نانوية هجينة مفعلة بببتيد tLyp1 لقمع STAT3 وSTAT5، مما يقلل من أعداد خلايا Treg ويزيد من تسللالخلايا في البيئة المجهرية للورم [303]. تساهم الجسيمات النانوية المفعلة في كبح الورم من خلال زيادة تسلل الخلايا الشجرية،، وخلايا القاتل الطبيعي، مع تقليل خلايا Treg وMDSC [304]. علاوة على ذلك، أظهرت البوليميروسومات أنها تحفز محور STING وتعزز تسلل وتكاثر خلايا T في العلاج المناعي للسرطان [57]. تلخص الجدول 2 تطبيق الجسيمات النانوية لتنظيم خلايا T في علاج السرطان. توضح الشكل 4 دور الجسيمات النانوية في تنظيم خلايا CAFs، وخلايا T، وخلايا Treg.
الجسيمات النانوية التي تنظم نقص الأكسجين
في كل ورم، تختلف مستويات الأكسجين [318]. عمومًا، تتراوح نقص الأكسجين في نسيج الورم من حالة شبه انعدام الأكسجين (تقريبًا لا يوجد أكسجين) إلى 60 مم زئبقي.الأكسجين). على الرغم من ذلك، تظهر خلايا الورم حالة محددة تعرف باسم نقص الأكسجة حيث تتقلب مستويات الأكسجين من انعدام الأكسجين إلى 7.5 مم زئبقي (حواليالأكسجين) [319]. يمكن اعتبار نقص الأكسجين علامة حيوية موثوقة، حيث يعزز تقدم خلايا الورم ويمكن أن يسبب مقاومة للعلاج [320]. إلى جانب تكوين الأورام، يعزز نقص الأكسجين في السرطان، ويظهر بعض التنسيق مع تكوين الأوعية الدموية، والتكاثر، والنقائل. نقص الأكسجين قادر على تعزيز مستويات CCL22 وCCL28 ويزيد من تراكم MDSCs وTregs للتوسط في بيئة الورم المثبطة للمناعة [321-323]. علاوة على ذلك، تم إظهار أن نقص الأكسجين هو عامل مشارك في مقاومة المناعة [324]. يمكن أن يحسن الميتفورمين من العلاج المناعي للسرطان من خلال إضعاف وظيفة نقص الأكسجين في إضعافلقد أظهرت الدراسات أن التمارين الرياضية تعمل كآلية لتحفيز الموت الخلوي (الموت المبرمج) وتقليل تكاثر خلايا السرطان. علاوة على ذلك، يمكن أن تحسن التمارين الرياضية من نقص الأكسجة، وتعزز وظيفة خلايا T وتقلل من مستويات خلايا Treg في علاج السرطان المناعي. كما أظهرت نقص الأكسجة كآلية في زيادة استقطاب M2 للخلايا البلعمية وإفراز عوامل ذات وظيفة مثبطة للمناعة، بما في ذلك VEGF وTGF-علاوة على ذلك، تم اقتراح أن نقص الأكسجين قد يسبب مقاومة للعلاج، خاصة خلال العلاج الضوئي والعلاج الإشعاعي حيث تتطلب جزيئات الأكسجين قمع السرطان.
لذلك، فإن وظيفة نقص الأكسجين في العلاج المناعي للسرطان تعتبر مهمة [329]. يمكن استغلال نقص الأكسجين بواسطة الجسيمات النانوية لتحسين خصوصيتها، ومؤخراً، تم تصميم الهياكل النانوية المستجيبة لنقص الأكسجين للعلاج المناعي للسرطان [330-332]. ومع ذلك، تم توجيه معظم الاهتمام نحو تنظيم نقص الأكسجين في العلاج المناعي للسرطان. يمكن للهياكل النانوية البوليمرية القابلة للتحلل الحيوي من نوع NIR-II أن تنظم نقص الأكسجين في العلاج المناعي للسرطان. يمكن لهذه الهياكل النانوية توصيل الريجورافينيب والاستجابة لإشعاع الليزر عند 808 نانومتر لإطلاق الأدوية من أجل تقليل نقص الأكسجين في السرطان من خلال تطبيع الأوعية الدموية، مما يسمح بدخول الأكسجين إلى الأورام. لزيادة إنتاج ROS، مما يسهم في الموت الخلوي المناعي (ICD) لعلاج السرطان المناعي. علاوة على ذلك، تعيد هذه الجسيمات النانوية برمجة البلعميات من M2 إلى M1. في جهد آخر، تم تطوير هياكل نانوية قائمة على الألبومين للتوصيل المشترك لـ IR780 وNLG919 والعقار النشط في نقص الأكسجة تيرابازامين (TPZ) في كبت الورم التآزري. التعرض للجسيمات النانوية مع إشعاع NIR يسهم في إنتاجلتحفيز إطلاق رابط مستجيب لجذور الأكسجين التفاعلية لإطلاق TPZ، مما يسبب العلاج الكيميائي من خلال تعزيز نقص الأكسجة في الورم. علاوة على ذلك، فإن هذه الهياكل النانوية تحفز ICD لتعزيز نشاط السمية الخلوية للخلايا اللمفاوية T [333]. إضافة المواد المخدرة إلى الجسيمات النانوية معيمكن أن يخفف من نقص الأكسجين ويزيد من حساسية cGAS، مما يحفز مسار cGAS/STING، مما يؤدي إلى إعادة تعليم البلعميات وزيادة نضوج الخلايا الجذعية [334]. في عدد من الحالات، يتم تعزيز نقص الأكسجين في بيئة الورم لتحفيز إطلاق الأدوية من الجسيمات النانوية لعلاج السرطان المناعي [335]. علاوة على ذلك، تم دمج الطحالب الدقيقة المقلدة للبلعميات والليبوزومات لقمع الالتهام الذاتي وتقليل نقص الأكسجين في علاج السرطان المناعي [336]. فيما يتعلق بتنظيم الالتهام الذاتي، يجب أن نبرز أن الالتهام الذاتي له وظيفة مزدوجة في السرطان ويمكن أن يمارس وظائف مسرطنة ومضادة للمسرطنات، مما يعقد تنظيمه في علاج السرطان [337، 338]. وفقًا لهذه الدراسات، يمكن أن يمهد تنظيم نقص الأكسجين بواسطة الجسيمات النانوية الطريق الجديد لعلاج السرطان المناعي [339-342].
الجسيمات النانوية المستهدفة لخلايا الكبت المشتقة من النخاع
تعتبر اختراق خلايا MDSCs ضد المناعة المضادة للسرطان لأنها تعيق تكاثر خلايا T وتعزز تمايز خلايا Treg. تُعتبر خلايا MDSCs خلايا نقي غير ناضجة ذات طبيعة غير متجانسة توفر بيئة ميكروية مثبطة للمناعة. بشكل عام، تستخدم خلايا MDSCs ثلاث آليات متميزة للتسبب في تثبيط المناعة. في الطريقة الأولى، يتم زيادة تنظيم الأرجيناز 1 و iNOS في خلايا MDSCs، ويمكنها استنفاد-أرجينين الذي يعد حيوياً لتكاثر خلايا T و CD3-تشكيل سلسلة TCR. ومع ذلك، يمكن أن يؤدي تعزيز نشاط الأرجيناز 1 و iNOS إلى قمع تكاثر ووظيفة خلايا T [344-347]. في الطريقة الثانية، يمكن أن تعزز MDSCs توليد ROS و RNS للتوسط في خلل وظائف خلايا T [348-350]. يمكن أن تسبب ROS والبيروكسينيتريت المشتقة من MDSCs تغييرات ما بعد النسخ في TCR و CD8 للتداخل مع وظيفة المحيط.الخلايا وتسبب التسامح المحدد للمستضد في هذه الخلايا من خلال إضعاف affinity الربط لجزيئات MHC الفسفورية [348]. في الطريقة الثالثة والأخيرة، تستطيع MDSCs تعزيز تمايز خلايا Treg لتعطيل المناعة المضادة للسرطان [172، 351]. بعد ذلك، تفرز خلايا Treg عددًا من السيتوكينات المثبطة مثل IL-10 وIL-35 وTGF-للتدخل في الصحيح
الجدول 2 تنظيم خلايا T بواسطة الجسيمات النانوية في علاج السرطان
جزيئات نانوية
نوع السرطان/خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
أبرز النقاط
مرجع
جزيئات نانوية بوليمرية
سرطان الرئة / خلايا LLC
نقل
ناقلات نانوية استجابة لـ ROS للتوصيل المشترك لـ FGL1 و PD-L1-siRNA
تطوير جزيئات نانوية من بولي-ل-لايسين-ثيوكيتال وcis-أكونيتات المعدلة لتسهيل الهروب من الحويصلات الداخلية
تفعيل الجسيمات النانوية باستخدام ببتيد iRGD
تعزيز التسلل من و الخلايا في العلاج المناعي للسرطان
[305]
جزيئات نانوية كيرالية
خلايا لمفوما/EG7.OVA
–
تحفيز خلايا NK وخلايا
[306]
جزيئات نانوية محاكاة حيوية
سرطان القولون / خلايا CT26
–
يمكن لجزيئات الفوسفوليبيد النانوية (PL1) توفير توصيل مستهدف للـ mRNA (CD137 أو OX40) في تحفيز خلايا T.
[307]
جزيئات سيسبلاتين
سرطان الرئة/سرطان الرئة ذو الخلايا الكبيرة
تعزيزتنشيط الخلايا من خلال تعزيز عرض المستضدات وتوفيرتداخل الخلايا
[308]
جزيئات الدهون النانوية
سرطان القولون/خلايا MC38
–
تحفيزالخلايا وإعادة برمجة البيئة المجهرية للورم لتعطيل تكاثر خلايا السرطان
[309]
جزيئات نانوية حاملة لمستضدات داخلية
سرطان الثدي/خلايا 4T1
زيادة انتشار و الخلايا وتعزيز نسبة خلايا T السامة للخلايا مقارنة بخلايا T التنظيمية
[310]
الهياكل النانوية البوليمرية الكاتيونية
خلايا الميلانوما/B16F10
، و
أقل من 60 مللي فولت
تطوير ناقلات نانوية تعتمد على دندريميرات بولي أميدو أمين وبولي (حمض اللاكتيك-حمض الجليكوليك)
تطوير لقاح السرطان
زيادة عدد خلايا T في الدم المحيطي
[311]
صفائح دموية
سرطان الثدي/خلايا 4T1
التوصيل المشترك للأجسام المضادة المضادة لـ PD-L1 وجزيئات أكسيد الحديد كعوامل ضوئية حرارية في علاج السرطان تحفيز النخر من خلال العلاج الضوئي
تحفيز الاستجابات المناعية الفطرية
تعزيز التسلل و خلايا
[312]
جزيئات نانوية مغطاة بغشاء بكتيري
خلايا الميلانوما/B78
يتكون من نواة PC7A/CpG مع قدرة على تحفيز جهاز المناعة
يمكن أن تزيد وجود أغشية بكتيرية ومجموعات إيميد من استرجاع المستضد
التقاط النيوأنتيجينات وعرضها على الخلايا الشجرية
تحفيز استجابات خلايا T
[313]
جزيئات نانوية مسببة للأدوية تستجيب للضوء
سرطان القولون / خلايا CT26
تسليم VPF كعامل حساس للضوء، FRRG ودوكسوروبيسين
تحفيز موت الخلايا المناعية
أثر نظام تخطيط موارد المؤسسة
نضوج الخلايا الشجرية لتقديم المستضدات بشكل متقاطع إلى خلايا T
[314]
ناقلات نانوية لتحويل الطاقة K3ZrF7:Yb/Er
سرطان الثدي/خلايا 4T1
20 نانومتر
زيادة مستويات ROS
زيادة تنظيم كاسبيز-1
تقطيع غازدرمين D
IL-1نضج
تحفيز التحلل الخلوي
زيادة نضوج خلايا الدندريت ورفع عدد خلايا T الذاكرة الفعالة
[315]
جزيئات الدواء المسبق
سرطان القولون / خلايا CT26
التوصيل المستهدف للكامبتوثيسين والتجميع مع الدهون المشتقة من PEG
زيادة نصف العمر ودورة الدم
تعزيز التسلل منخلايا
[316]
جزيئات نانوية
نوع السرطان/خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
أبرز النقاط
مرجع
جزيئات نانوية من فوسفات الكالسيوم المغلفة بالدهون
خلايا الميلانوما/B16F10
تحفيز الموت الخلوي
تسريع تثبيط المناعة
استقطاب البلعميات إلى نمط M1
زيادةخلايا
[317]
وظيفة الجهاز المناعي [352، 353]. لذلك، فإن استهداف خلايا النخاع العظمي المثبطة (MDSCs) أمر حيوي للغاية لمناعة مكافحة السرطان. يمكن أن يؤدي الإعطاء الوريدي للدهون المحملة بالثيوأبتامير DNA إلى استهداف محدد للبيئة المجهرية للورم (TME)، وخاصة خلايا النخاع العظمي المثبطة. علاوة على ذلك، قدمت هذه الدهون توصيلًا مستهدفًا للدكسوروبيسين في نماذج حيوانية لسرطان الثدي لتعزيز التسلل منالخلايا وتقليل MDSCs [354]. من الجدير بالذكر أن هناك أنواعًا مختلفة من الجزيئات المرتبطة بالاستجابة المناعية في TME، بما في ذلك IL-1 [355، 356]، IL-6 [357]، بروستاجلاندين E2 [358]، VEGF [359]، و IFN-[351] التي تعطل إجراء التمايز لزيادة تراكم الخلايا المياليد غير الناضجة [360]. ونتيجة لذلك، يمكن أن تكون إحدى الاستراتيجيات الواعدة هي استهداف MDSCs لتسهيل تمايزها إلى أنواع أخرى من الخلايا المناعية. وفي هذا السياق، تم تقديم هياكل نانوية مسامية مجوفة قابلة للتحلل ومغطاة بالدهون لتنظيم تمايز MDSC. هذه الهياكل النانوية قادرة على توصيل IL-2 وحمض الريتينويك الشامل لتحفيز تمايز MDSC إلى خلايا دندريتية ناضجة، وبلعميات، وحبيبات. أظهرت هذه الجسيمات النانوية قدرة كبيرة في تعزيز عدد الخلايا الدندريتية الناضجة وتقليل MDSCs. علاوة على ذلك، حفزت هذه الجسيمات النانوية و خلايا T وزيادة إفراز IL-12 و TNF-كعوامل سيتوكينية مضادة للأورام [361].
الجسيمات النانوية لتوصيل الحمولة إلى خلايا تقديم المستضدات والعقد اللمفاوية
تُعتبر واحدة من المشاكل البارزة في القضاء على السرطان باستخدام العلاج المناعي هي نقص التوصيل الفعال والصحيح إلى خلايا العرض المناعي (APCs) والعقد اللمفاوية. لقد فتحت الجسيمات النانوية بابًا جديدًا لتوصيل العلاجات المناعية إلى خلايا العرض المناعي والعقد اللمفاوية. ومن الجدير بالذكر أن عددًا من الهياكل النانوية، بناءً على تصميمها، تُظهر تأثيرًا مناعيًّا، وحتى في حالة عدم توصيل الحمولة، يمكنها تحفيز استجابات خلايا T وB. تم ربط مستضدات الورم بالهياكل النانوية، وعند حقنها في فئران تحمل الميلانوما أو الثيموما أو اللمفوما التي تعبر عن OVA، تسببت في مناعة مضادة للسرطان ملحوظة. علاوة على ذلك، فإن مثل هذه المستضدات النموذجية المرتبطة بالهياكل النانوية أثارت استجابات خلايا T والأجسام المضادة ضد اللمفوما أو أورام القولون مما أدى إلى إعاقة نمو السرطان وزيادة بقاء نماذج الحيوانات. وقد اعتُبر حجم الجسيمات عاملًا مهمًا في هذه الحالة، حيث أن الجسيمات الصغيرة بحجم الفيروس…يمكن أن تصل إلى العقد اللمفاوية وتظهر امتصاصًا خلويًا عاليًا بواسطة خلايا التغصن. ثم يحدث عرض الببتيد من المستضد المغلف بواسطة جزيئات MHC من الفئة الأولى المرتبطة بخلايا التغصن وتحفيزيتم ملاحظة الخلايا [369، 370]. يمكن أن يحفز ابتلاع مثل هذه الهياكل النانوية بواسطة الخلايا الشجرية مسار استشعار الخطر في الخلايا الشجرية.
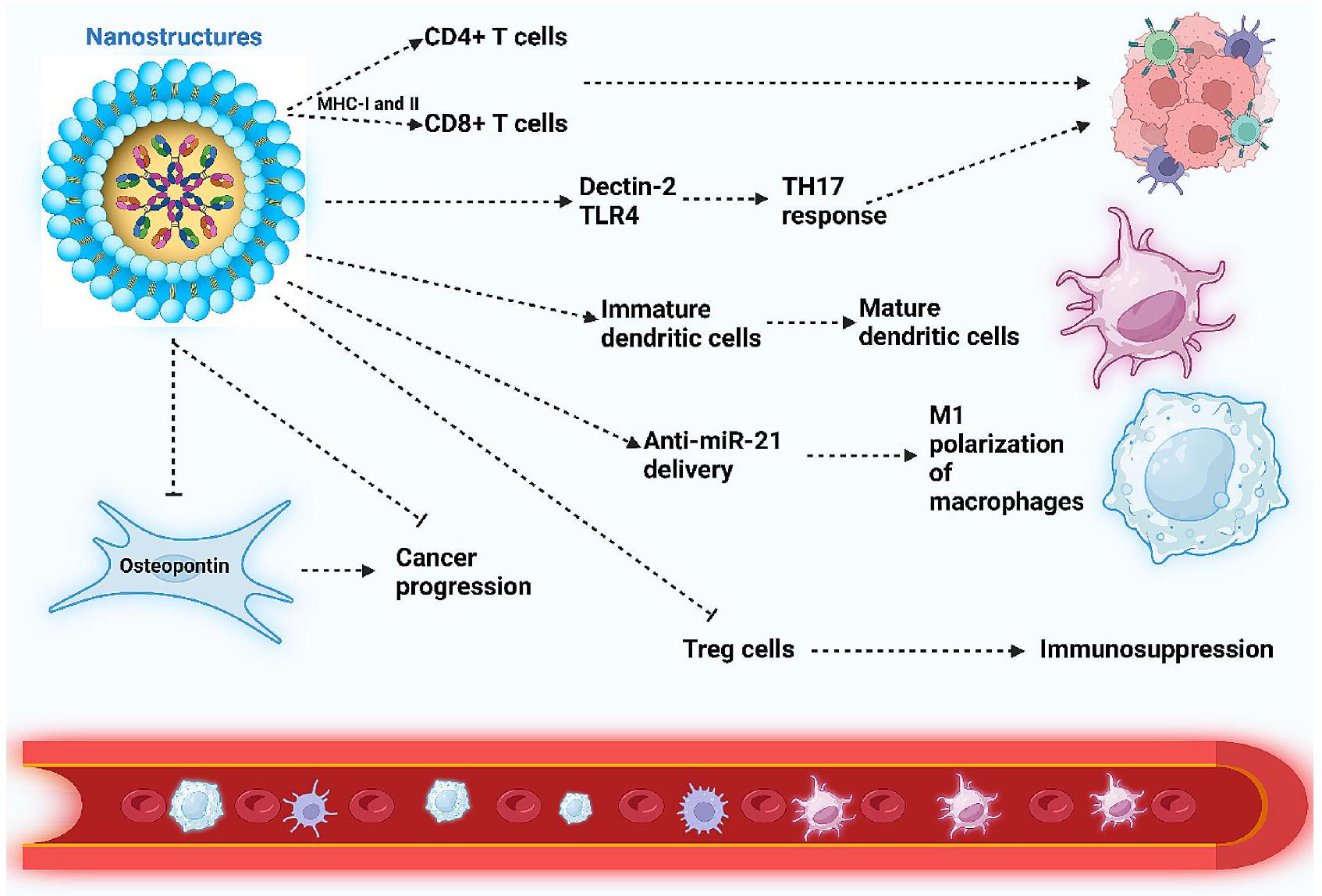
الشكل 4 الجسيمات النانوية تنظم خلايا المناعة والألياف المرتبطة بالسرطان (CAFs). ترفع الجسيمات النانوية تقديم المستضدات عبر MHC-I وMHC-II، مما يحفز و تساعد خلايا T، مما يسهل العلاج المناعي للسرطان. تعزز الهياكل النانوية مستويات Dectin-2 و TLR-4، مما يعزز استجابات TH17 لعلاج السرطان الفعال. بالإضافة إلى ذلك، تعزز نضوج الخلايا التغصنية، ومن خلال توصيل anti-miR-21، تحفز استقطاب البلعميات إلى النمط الظاهري M1. إن تقليل الجزيئات النانوية لمستوى الأوستيو بونتين في خلايا CAFs يعطل تقدم السرطان. علاوة على ذلك، تقوم هذه الجزيئات النانوية بتثبيط خلايا Treg، مما يمنع التثبيط المناعي (تم إنشاؤه بواسطة Biorender.com)
الخلايا وتنضيجها لتصبح خلايا APC المناعية [371]. يجب أن يصل مستضد الورم إلى العقد اللمفاوية التي تصرف الورم ليتم امتصاصه بواسطة خلايا APC المحترفة مثل الخلايا الشجرية، ثم تقديمه إلىتحدث الخلايا. الورم المحددتم العثور على خلايا في العقد اللمفاوية. ومع ذلك، فإن الخلايا الشجرية في العقد اللمفاوية التي تصرف الأورام تظهر شكلًا غير ناضج/غير نشط مما يضعف قدرتها على تحفيز الاستجابة المناعية ضد الورم.تم إثبات أن أوليغونوكليوتيدات السيتوزين-فوسفات-الغانين (CpG) المرتبطة بالجسيمات النانوية (مساعد) تتجمع في العقد اللمفاوية التي تصرف الورم في الميلانوما لتحفيز الخلايا الشجرية.
الجسيمات النانوية المستهدفة لخلايا الورم
عدد كبير من الطرق المعتمدة على النانوهياكل يحتاج إلى تسلل الورم بواسطة الجسيمات النانوية. لا تزال الأهمية السريرية لتأثير التوصيل المعتمد على الطيف (EPR) قيد التساؤل ونقاش مثير للجدل، وهناك مناقشة تشير إلى أن نسبة صغيرة فقط من النانوهياكل المعطاة يمكن أن تصل الجسيمات النانوية إلى أنسجة الورم، ولكنها تفتقر إلى الأهمية السريرية والقيمة العلاجية في الإعداد السريري. لذلك، تم بذل جهود كبيرة لتحسين قدرة الجسيمات النانوية على الوصول إلى أنسجة الورم وتحسين الهياكل النانوية بطريقة للتحكم في التفاعلات البيولوجية بسبب الطبيعة المعقدة للبيئة المجهرية للورم الناتجة عن التوزيع الوعائي غير المنتظم، وارتفاع ضغط السوائل بين الأنسجة الورمية، وانخفاض تدفق الدم، وكثافة الأنسجة المحيطة، وعدد كبير من خلايا السدى. لذلك، يجب توجيه الاستراتيجيات نحو تعزيز دخول الهياكل النانوية إلى أنسجة الورم، والتي يمكن الحصول عليها من خلال تحسين تدفق الدم إلى الورم، وزيادة نفاذية الأوعية الدموية للورم، وتعديل هيكل المصفوفة خارج الخلوية. كمثال، يمكن أن تعمل الهياكل النانوية المستخدمة في تدهور المصفوفة خارج الخلوية أو استعادة الأوعية الدموية للورم إلى الحالة الطبيعية على تحفيز البيئة المجهرية للورم لتوفير ردود فعل مناعية مرغوبة، مما يعكس البيئة المجهرية المثبطة للمناعة ويعزز المناعة المضادة للسرطان. في الحالات التي تكون فيها الأورام قابلة للوصول، يُفضل إعطاء الجسيمات النانوية داخل الورم بدلاً من النظامي. حقن لتعزيز التراكم في منطقة الورم. يمكن أن يعزز التراكم المناسب للجزيئات النانوية في البيئة المجهرية للورم وإطلاق الحمولة العلاجية من قمع الورم، بينما يقلل من الآثار السلبية. وقد اقترحت عدد من الدراسات السريرية حقن المركبات المناعية داخل الورم [387، 388]، وهو ما تم تأكيده أيضًا في الدراسات ما قبل السريرية عند حقن مثبطات نقاط التفتيش المناعية داخل الورم [389]. يمكن أن تعزز الجزيئات النانوية المحسّنة للارتباط مع المصفوفة خارج الخلوية أو خلايا السرطان تراكم هذه الهياكل في منطقة الورم [390] وتوفر رؤية جديدة حول التوصيل الفعال للعلاجات إلى خلايا الورم أو البيئة المجهرية للورم.
الجسيمات النانوية في موت الخلايا المناعية: طريقة عقلانية في علاج السرطان المناعي
في السنوات الأخيرة، تم اعتبار ICD استراتيجية واعدة في علاج السرطان [391]. تقوم الخلايا المتوترة والمحتضرة بإطلاق أنماط جزيئية مرتبطة بالضرر (DAMPs) للتوسط في الاستجابة المناعية الفطرية المضادة للسرطان وزيادة مناعة الورم المستحثة بواسطة الخلايا التائية [392]. إن ICD قادر على التوسط في الاستجابات المناعية المضادة للسرطان المستحثة بواسطة الخلايا التائية ضد مستضدات الورم [393]. في السنوات الأخيرة، تم اقتراح تحفيز ICD بواسطة الجسيمات النانوية كاستراتيجية واعدة في العلاج المناعي للسرطان. تم تحميل الهياكل النانوية PLGA بجسيمات نانوية من كلوريد البوتاسيوم ثم تم تفعيلها بغشاء خلايا السرطان لإطلاقوالأيونات عند التحلل الليزوزومي. ثم، تتسبب هذه الأيونات في موت خلايا السرطان من خلال التوسط في حالة فرط التوتر حيث تفرز الخلايا الأدينوزين ثلاثي الفوسفات (ATP) وصندوق المجموعة عالية الحركة 1 (HMGB-1) لتحفيز ICD [394].يمكن أن تطلق الهياكل النانوية الفضية المخفضة بواسطة -D-جلوكوز الكالريتولكين وتزيد من إفراز HSP70 وHSP90 وHMGGB1 وATP [395]. هذه العوامل هي متطلبات أساسية لتحفيز ICD. في استراتيجية جديدة، تم تحميل جزيئات النانو المغلفة بالكيتوزان من PLGA بـ HPV16 E7.تمت معالجة الببتيدات ثم تم تفعيلها مع غشاء خلايا الورم ICD لتعزيز نضوج الخلايا الشجرية لعلاج السرطان المناعي [396]. علاوة على ذلك،تم تعديل النانوهياكل باستخدام بكتيريا حية وأغشية خلايا سرطانية للتسبب في الفيروبتوزيس وإثارة الاستجابة المناعية المضادة للسرطان [397]. لذلك، تبرز الأدلة المتزايدة تطبيق النانوهياكل لتحفيز ICD في العلاج المناعي للسرطان [304، 398-403]. في محاولة، تم تطوير نانوهياكل الألبومين حيث تم تحميل IR780، كعامل حساس للضوء، في النواة وتم تحميل منبهات cGAS-STING/منتج H2S-ZnS في الغلاف لوساطة العلاج الضوئي والعلاج الحراري الضوئي. هذه النانوهياكل وسّعت الفيروبتوزيس من خلال محور الكاسبيز-3/GSDME في وساطة نضوج خلايا الدندريت. ثم، يتم تنشيط خلايا T و تحسين حجب PD-L1 المحتمل في العلاج المناعي للسرطان [404]. من أجل تحفيز ICD، تم تقديم أنواع مختلفة من الجسيمات النانوية بما في ذلك الهياكل النانوية البوليمرية [405، 406]، هياكل البوليسوبامين المعدلة بالليبوزوم [407]، الجسيمات النانوية TPGS المفعلة بـ cRGD [408]، الجسيمات النانوية من الحديد (II)-سيتوزين-فوسفات-غوانين [297] وهياكل أكسيد الحديد النانوية [409] لتعزيز العلاج المناعي للسرطان. لذلك، يمكن أن يؤدي ICD المعتمد على الجسيمات النانوية إلى تحفيز الخلايا الشجرية لتنشيط خلايا T في العقد اللمفاوية لزيادة العلاج المناعي للسرطان.
هياكل نانوية مقلدة مغطاة بغشاء الخلية جزيئات نانوية مفعلة بغشاء خلايا السرطان
تتميز الجسيمات النانوية البيوميميتية بهياكل تكون أسطحها معدلة أو مغطاة بأغشية من خلايا أخرى. يهدف تطوير الجسيمات النانوية البيوميميتية إلى تعزيز خصائص التخفي، مما يمنع تحديدها بواسطة النظام الشبكي البطاني. تظهر الجسيمات النانوية البيوميميتية توافقًا حيويًا جيدًا، مما يجعلها قابلة للتطبيق على نطاق واسع في علاج السرطان. استكشفت الدراسات الحديثة إمكانيات الجسيمات النانوية البيوميميتية في علاج السرطان، موضحة تنوعها عند تعديلها بالأبتامرات [410]، مما يسهل العلاج الكيميائي من خلال التوصيل المشترك لأدوية العلاج الكيميائي والمنتجات الطبيعية [411]، ويظهر ميزات اختراق واستهداف عالية [412]. كما تم استخدامها في التصوير الحيوي والعلاج المناعي [413، 414]، متجنبة نظام البلعميات أحادية النواة [415] وتحسين وقت دوران الدم [416].
لقد أظهرت تطبيقات الجسيمات النانوية البيوميميتية في العلاج المناعي للسرطان نتائج واعدة في كبح الأورام. في بعض الحالات، يمكن أن تنشط العلاج الكيميائي باستخدام الجسيمات النانوية البيوميميتية الجهاز المناعي. على سبيل المثال، معقدات الفوسفور دندريمر-نحاس(II) المفعلة بغشاء خلايا السرطانيمكن أن يتم قطع الناقلات النانوية البوليمرية المحملة بالتويوكاميسين (Toy) بحجم 210 نانومتر في البيئة المجهرية للورم (TME) لإطلاق الحمولة وتقليل مستويات الجلوتاثيون. من خلال التسبب في خلل وظيفي في الميتوكوندريا وإجهاد الشبكة الإندوبلازمية، تحفز هذه الناقلات النانوية موت الخلايا المبرمج وموت الخلايا المناعي. كما أنها تسرع نضوج الخلايا الشجرية وتزيد من تسلل الخلايا اللمفاوية التائية. مع تطبيق أجسام مضادة لـ PD-L1، يمكن أن تعزز الجسيمات النانوية العلاج الكيميائي، وتعيق الانتكاس، وتمنع غزو السرطان.
تعمل الجسيمات النانوية البيوميميتية أيضًا كحاملات فعالة لتوصيل siRNA. من خلال التعرف على PD-L1 كعامل هروب من المناعة، يمكن أن يسرع تقليل تعبيره بواسطة siRNA من العلاج المناعي للسرطان ويمنع إرهاق خلايا T. تظهر هذه الجسيمات النانوية القدرة على كبح تقدم السرطان بشكل فعال في الجسم الحي، مما يجعلها مرشحة واعدة لتطوير لقاحات السرطان.
لقد شهد مجال علاج السرطان تحولاً ثورياً مع تطبيق النانو هلام كحاملات للأدوية. تُظهر النانو هلام ميزات فيزيائية كيميائية ملائمة. إنها حاملات محتملة لتوصيل الأدوية الكارهة للماء والمحبّة للماء، والبروتينات المؤتلفة، والمواد الوراثية.
لقد أثبتت العلاجات المناعية المستحثة بواسطة النانو هلام فعاليتها في إعاقة تقدم السرطان. تم تطوير النانو هلام البوليمري من PDEA-co-HP--سيكلوديكسترين-بلاورونيك F127 وبوليمر قابل للعكس في الشحنة يُدعى أنهدريد ثنائي ميثيل مالئيك المعدل مع بولي إيثيلين أمين، تتعرض للتحلل في البيئة المجهرية للورم. هذه النانو هلامات، المفعلة بأغشية خلايا السرطان، تقوم بتوصيل كل من باكليتاكسيل وIL-2، مما يحفز نضوج خلايا الدندريت ويعزز تسلل خلايا التأثير.
تم تصميم ناقلات نانوية تحاكي الطبيعة تستجيب للمؤثرات لتحسين العلاج المناعي للسرطان. بوليدوبامين-النانو حوامل، المفعلة بأغشية خلايا السرطان وتتميز بخصائص استجابة للرقم الهيدروجيني، تمكّن من العلاج الضوئي والتصوير الحيوي. يؤدي التعرض للبيئة المجهرية للورم إلى تحلل النانو حوامل، مما يحررفقاعات تعزز العلاج المناعي المعتمد على العلاج الضوئي. الجمع بين هذا ومثبطات نقاط التفتيش يعزز العلاج المناعي للأورام بشكل أكبر [426].
في مجال اللقاحات النانوية البيوميميتية، تركزت الدراسات بشكل أساسي على توصيل العلاجات أو المحفزات إلى الخلايا الشجرية. ومع ذلك، يمكن أن تعيق وجود نظام الإندوسيتوز وعمليات التحلل داخل الحويصلات فعالية هذه اللقاحات النانوية. لمعالجة هذه المشكلة، تم تطوير منصات نانوية بيوميميتية لتسريع عملية إدخال الجسيمات النانوية في الخلايا الشجرية. من خلال استخدام نوى جزيئية نانوية تستجيب للجذور الحرة مرتبطة بالببتيدات وأغشية الخلايا، تحفز هذه اللقاحات النانوية عملية الميكروبينوسيتوز، مما يسهل التوصيل المباشر لمستحثات جينات الإنترفيرون (STING) إلى السيتوسول. هذا يعزز نضوج الخلايا الشجرية وتفعيل خلايا T من خلال زيادة تنظيم STING في العلاج المناعي للسرطان [427].
تحفيز موت الخلايا المناعية وتعزيز نضوج الخلايا الشجريةتسلل الخلايا يمثل الاستراتيجية الأساسية التي تستخدمها الناقلات النانوية البيوميميتية في علاج السرطان المناعي. تنظيم المستقلبات أمر حاسم لتحقيق استجابات أفضل للعلاج المناعي وموت الخلايا المناعية. تم تقديم أطر ZIF-8 المرتبطة بأيونات الزنك مع نقاط نانوية من CuS، المفعلة بأغشية خلايا السرطان، لتعزيز العلاج المناعي المعتمد على الحرارة الضوئية من خلالتعديل الأيض. هذه الأطر تحفز موت الخلايا المناعية، تعزز نضوج الخلايا التغصنية، وتزيدتسلل الخلايا [428]. على الرغم من أنه تم استكشافه بشكل أقل مقارنة بالأغشية المشتقة من البلعميات والسرطان، فإن أغشية الخلايا الحمراء يمكن أيضًا استخدام خلايا الدم لتطوير ناقلات نانوية تحاكي الطبيعة.
أحد الأسباب الرئيسية لتعديل الجسيمات النانوية مع غشاء خلايا السرطان هو توفير مصدر لمولدات المضادات [431، 432]. تم تعديل هياكل PLGA مع غشاء خلايا الميلانوما، ثم تم تضمين الليبيد أحادي الفوسفات A (MPLA) كعامل مساعد في الجسيمات النانوية لتحفيز نضوج الخلايا الشجرية لتعزيز استجابة خلايا T المحددة لمولد المضاد [433]. نظرًا لأن تعبير MHC-I يمكن أن يوجد في جميع الخلايا، مثل خلايا الورم، يمكن اعتبار الهياكل النانوية المعدلة بغشاء خلايا السرطان APC جديدة لتحفيز خلايا T، حتى في غياب APCs المحترفة. تم استخدام خلايا السرطان التي تعبر عن CD80 لاشتقاق أغشية الخلايا لتغطية الجسيمات النانوية. يمكن أن تحفز هذه الهياكل النانوية مباشرة استجابة محددة لمولد المضاد.الخلايا من خلال تفاعل CD28 مع مستقبلات خلايا T المتوافقة، مما يثبط تكوين الأورام في نماذج الأورام الوقائية والعلاجية [288]. علاوة على ذلك، يمكن اعتبار الجسيمات النانوية المخصصة لغشاء الخلايا السرطانية بمثابة لقاحات. على الرغم من الجهود الكبيرة لتسليط الضوء على إمكانيات الجسيمات النانوية المخصصة لغشاء الخلايا السرطانية في العلاج المناعي للسرطان، هناك العديد من القيود التي يجب أخذها بعين الاعتبار للدراسات المستقبلية. وقد سلطت الدراسات الحديثة الضوء على إمكانيات الفيروبتوز في العلاج المناعي للسرطان [434-436]. يجب بذل المزيد من الجهود فيما يتعلق بتطبيق المنصات النانوية البيوميميتية في تنظيم الفيروبتوز والمسارات ذات الصلة لتسهيل العلاج المناعي للسرطان. علاوة على ذلك، فإن الالتهام الذاتي هو عامل آخر في تنظيم العلاج المناعي للسرطان [437-440]. يجب تصميم الجسيمات النانوية البيوميميتية بطريقة عقلانية لتعديل الالتهام الذاتي من أجل تنظيم خلايا T ومكونات أخرى من أنظمة المناعة بالإضافة إلى إعادة برمجة البلعميات لتحقيق علاج مناعي فعال للسرطان.
جزيئات نانوية مُفَعَّلة بخلايا الدم الحمراء
لقد حصلت كريات الدم الحمراء (RBCs) على اهتمام كبير لغرض توصيل الأدوية بسبب عدد من الخصائص، بما في ذلك التوافق الحيوي، القابلية للتحلل الحيوي، العمر الطويل، والقدرة المرغوبة على الاحتواء. كريات الدم الحمراء المحاطة بمستضد OVA قادرة على تحفيز و الخلايا التائية بعد الحقن الوريدي في الفئران [442]. هناك أيضًا نهج واعد يتم فيه استخدام غشاء كريات الدم الحمراء لتغطية الهياكل النانوية من أجل تطوير لقاحات ذات قدرة على الدوران لفترة طويلة [443]. في محاولة، تم تصميم جزيئات نانوية من PLGA مفعلة بغشاء كريات الدم الحمراء لتوصيل كل من المستضد hgp10025-33 والمساعد MPLA. من أجل استهداف الخلايا الشجرية بشكل انتقائي، تم تضمين المانوز في غشاء كريات الدم الحمراء، وأظهرت هذه الهياكل إمكانيات عالية في قمع الميلانوما [444]. ومع ذلك، فإن الدراسات محدودة، وهناك حاجة إلى المزيد من التجارب. يجب إجراء تطبيقات لأنواع أخرى من الهياكل النانوية، مثل المواد النانوية المعدنية والكربونية، وتعديلها بغشاء كريات الدم الحمراء لتحسين الإمكانيات في علاج السرطان.
جزيئات نانوية مفعلة بالصفائح الدموية
تُطلق الصفائح الدموية بواسطة الخلايا العملاقة، ويمكنها التحكم في التوازن الداخلي، وغزو الأورام، والأحداث الفسيولوجية والمرضية بشكل عام. نظرًا لأن الصفائح الدموية أظهرت تعبيرًا عن بروتينات معترف بها ذاتيًا، بما في ذلك CD47، فإنها مفيدة في تقليل الإزالة وتحفيز نظام المتممات لتعزيز وقت دوران الدم للهياكل النانوية. تم استغلال الجسيمات النانوية المفعلة بغشاء الصفائح الدموية لتوصيل R848 كمنبه لـ TLR7/8 في تعزيز التراكم في منطقة الورم وتعزيز التفاعل مع مكونات البيئة المجاورة للورم. علاوة على ذلك، حتى عند الجرعات المنخفضة (لقاح لكل فأر)، كانوا قادرين على قمع الأورام فيمن الفئران [447]. علاوة على ذلك، هناك إمكانية تضمين الميتفورمين وIR780 كمواد حساسة للضوء في أغشية الصفائح الدموية لتحفيز ICD وتحسين الإمكانية في العلاج المناعي للسرطان من خلال قمع خلايا MDSCs وTreg [448]. ومع ذلك، يجب تسليط الضوء على إمكانيات هذه الناقلات النانوية في تنظيم TAMs وCAFs للعلاج المناعي للسرطان.
جزيئات نانوية مفعلة بغشاء البلعميات
تكمن ميزة الجسيمات النانوية البيوميميتية الحساسة لدرجة الحموضة في قدرتها على تحفيز العلاج المناعي للسرطان بطريقة أكثر تحديدًا بسبب التحلل المستهدف في البيئة المجهرية للورم. يمكن تعزيز العلاج المناعي باستخدام الناقلات النانوية البيوميميتية من خلال العلاج الضوئي. تعمل الناقلات النانوية المستجيبة للضوء، من خلال تسريع إنتاج أنواع الأكسجين التفاعلية، على الوساطة في العلاج المناعي. تعمل الحويصلات المستندة إلى غشاء البلعميات، التي تعمل كجسيمات نانوية، على توصيل الأدوية والمستشعرات الضوئية (TAPP) لتحفيز البيروبتوز. هذه الحويصلات البيوميميتية، التي تطلق أيونات النحاس، تعمل على الوساطة في البيروبتوز الناتج عن أنواع الأكسجين التفاعلية. عند استخدامها كجسيمات نانوية، تزيد من مستويات أنواع الأكسجين التفاعلية، مما يحفز البيروبتوز من خلال زيادة تنظيم الكاسبيز-3 الذي يحفز الغازدرمين E، مما يؤدي إلى العلاج المناعي الناتج عن البيروبتوز.
لقد أظهرت الهياكل النانوية المغلفة بغشاء البلعميات إمكانيات عالية في استهداف الأورام بشكل محدد. تم استخدام الجسيمات النانوية المغلفة بغشاء البلعميات لتوصيل سايكوبسابونين D، وتمت هجنتهما بإضافة ببتيد T7 لتوفير قدرة التوجه نحو البلعميات للهياكل النانوية واستهداف خلايا الورم التي تزيد من تعبير مستقبل ترانسفيرين. تتجمع هذه الجسيمات النانوية بشكل محدد في موقع الورم ويمكنها الهروب من البلعمة بواسطة النظام الشبكي البطاني. إن تفعيل الكربون المسامي المشتق من MOF. تم إجراء دراسات على النانوهياكل مع أغشية البلعميات لزيادة قدرتها على الهروب من البلعمة وتحسين إمكانياتها في علاج السرطان. بالإضافة إلى التخصص العالي في استهداف الأورام، تُظهر الجسيمات النانوية المفعلة بأغشية البلعميات توافقًا حيويًا عاليًا، مما يجعلها مرشحة واعدة للقضاء على الأورام، جنبًا إلى جنب مع نشاطها المضاد للسرطان. لذلك، تبرز الأدلة المتزايدة تطبيق الجسيمات النانوية المفعلة بأغشية البلعميات في علاج السرطان. من أجل تسليط الضوء بشكل أفضل على إمكانياتها، يُقترح تطوير جسيمات نانوية تحاكي البيولوجيا مفعلة بأغشية السرطان والبلعميات لتحسين الإمكانيات في العلاج المناعي للسرطان.
تعتبر المنصات النانوية البيوميميتية مثيرة للاهتمام أيضًا لتنظيم آليات محددة مثل نقص الأكسجين وعمليات الأيض الدهني في بيئة الورم. يمكن تصميم الجسيمات النانوية البيوميميتية لتقديم مستضدات الورم وجزيئات التحفيز المساعدة في نفس الوقت للعلاج المناعي للسرطان. حتى الآن، تركز الاستراتيجية الأكثر فعالية على تطوير الجسيمات النانوية البيوميميتية ذات الميزات الشبيهة بالعوامل الممرضة. يمكن أن تثير هذه الجسيمات النانوية البيوميميتية استجابات مناعية كبيرة وطويلة الأمد في علاج السرطان. واحدة من الأسباب الرئيسية لتطبيق الجسيمات النانوية البيوميميتية هي قدرتها على تعزيز وقت دوران الدم للشحنات. إن تقليل الكوليسترول في الغشاء المستخدم لتفعيل الجسيمات النانوية يحسن من وقت دوران الدم وفعاليته في تحفيز العلاج المناعي للسرطان. بسبب التكاثر السريع لخلايا السرطان، فإن الظروف الناقصة من الأكسجين والمغذيات داخل بيئة الورم تعيق الوظيفة السليمة للخلايا المناعية. يمكن أن يؤدي تطوير منصة بيوميميتية لزيادة مستويات الجلوكوز والجلوتامين المطلوبة من قبل خلايا T إلى إعادة برمجة بيئة الورم وتسريع العلاج المناعي للسرطان. تلخص الجدول 3؛ الشكل 5 تطبيق الجسيمات النانوية البيوميميتية في العلاج المناعي للسرطان.
الإكسوزومات، التي يتراوح قطرها من 30 إلى 150 نانومتر، هي حويصلات خارج خلوية تفرزها الخلايا حقيقية النواة. تلعب دورًا حاسمًا في التواصل بين الخلايا من خلال حمل الدهون والبروتينات والأحماض النووية. بعد إفرازها في المصفوفة خارج الخلوية، يمكن العثور على الإكسوزومات في سوائل بيولوجية متنوعة مثل السائل الأمنيوسي، واللعاب، والبول، وحليب الثدي، من بين أمور أخرى.
في السنوات الأخيرة، كان هناك زيادة ملحوظة في تطبيق الإكسوزومات في مجال علاج السرطان، مع تركيز متزايد على الحمولة المتنوعة التي يمكن أن تنقلها. تظهر الإكسوزومات القدرة على استهداف أنواع مختلفة من الخلايا داخل الجسم وتعمل كعلامات حيوية موثوقة للسرطان. لقد مكنت التقدمات في تقنيات الهندسة الحيوية من التوصيل الفعال للحمولة باستخدام
الجدول 3 تطبيق الهياكل النانوية المستوحاة من الطبيعة لتعزيز العلاج المناعي للسرطان
مركبة
نوع السرطان / خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
أبرز النقاط
مرجع
نانوزيكلات بيوميميتية
سرطان الثدي/خلايا 4T1
500 نانومتر
تحميل هيدروكلوريد 5-أمينوليفولينيك (HAL) و3-ميثيل أدينين (3MA) في جزيئات دقيقة مشتقة من خلايا السرطان
زيادة تخليق PpIX في الميتوكوندريا، مما يسبب توليد ROS بعد الإشعاع وزيادة خلل الميتوكوندريا وكبح الميتوفاجي.
تنظيم خفض PD-L1 للتوسط في موت الخلايا المناعية
[463]
جزيئات نانوية هجينة
سرطان الثدي/خلايا 4T1
و -26.4 مللي فولت
تطوير جزيئات نانوية هجينة من GTe وتعديلها بغشاء خلايا السرطان والغشاء الخارجي للبكتيريا
تعمل GTe كعامل حساسية للإشعاع ويمكن أن تزيد الأغشية من الاستجابات المناعية المضادة للسرطان.
زيادة إنتاج أنواع الأكسجين التفاعلية
تحفيز موت الخلايا المناعية
[464]
اللقاح النانوي البيوميميتي
–
–
تفعيل الجسيمات النانوية بغشاء خلايا السرطان
التوصيل المشترك لـ CpG وبروبرانولول
تراكم عالي في العقد اللمفاوية وإطلاق كاف للدواء
زيادة نضوج الخلايا الشجرية وعرض المستضدات
تعزيزتنشيط الخلايا و
تعزيز تسلل خلايا B وخلايا NK
تثبيط البيئة المجهرية المثبطة للمناعة
[465]
جزيئات نانوية من PLGA تحاكي الطبيعة
توصيل 2-برومو-بالميتات بواسطة جزيئات نانوية من PLGA لزيادة إمكانيته في علاج سرطان الثدي
تFunctionalization للجزيئات النانوية مع غشاء خلايا السرطان
خفض تنظيم PD-1/PD-L1
[466]
ناقلات نانوية من السيليكون المسامي@ذهب
سرطان الثدي/خلايا 4T1
حتى 243.30 نانومتر
تفعيل النانو مركبات بغشاء خلايا السرطان
تحفيز الاستجابات المناعية المضادة للسرطان وتخفيف البيئة الميكروية المثبطة للمناعة
كبح انتشار وغزو السرطانات
[467]
الجنز
سرطان الثدي/خلايا 4T1
تعديل باستخدام غشاء مشتق من الخلايا التغصنية
تراكم في قطرات الدهون لخلايا السرطان
وجود غشاء الخلية يسمح بتسريع عملية ركوب AIEdots إلى خلايا T ويحفزها في العلاج المناعي للسرطان
[468]
أوراق نانوية
سرطان القولون / خلايا CT26
، و +0.2 مللي فولت
تعديل الجسيمات النانوية بغشاء خلايا السرطان
تحميل ببتيد مضاد PD-1 في الجسيمات النانوية
الاستجابات المناعية الناتجة عن العلاج الضوئي واستئصال الورم
قمع محور PD-1/PD-L1 لتحفيز خلايا T
[469]
الشكل 5 يمكن تطوير الجسيمات النانوية البيوميميتية من خلال استخراج الأغشية من خلايا الدم الحمراء، خلايا السرطان، الخلايا المناعية المرتبطة بالورم (TAMs) والخلايا الليفية المرتبطة بالسرطان (CAFs). هذه التعديلات تحسن من قدرة الجسيمات النانوية في العلاج المناعي للسرطان. يمكن استخدام الجسيمات النانوية البيوميميتية في توصيل الأدوية والحمض النووي من خلال تحسين خصائص التخفي. إنها تظهر دوراناً طويلاً في الدم ويمكن أن تحفز نضوج الخلايا الشجرية، وتزيد من تسلل و خلايا T، وتسبب موت الخلايا المناعي. (تم إنشاؤه بواسطة Biorender.com)
الإكسوزومات في علاج السرطان. تتناول الفقرات التالية استكشاف إمكانيات الإكسوزومات الذاتية التي تفرزها الخلايا بشكل طبيعي في الجسم، بالإضافة إلى الإكسوزومات المهندسة حيوياً التي تم إنشاؤها في المختبر لعلاج السرطان.
الإكسوزومات الذاتية المنشأ
المصدر الرئيسي لإفراز الإكسوزومات يشمل الخلايا الطبيعية، خلايا السدى، خلايا السرطان، والخلايا المناعية. على سبيل المثال، تلعب الإكسوزومات التي تفرزها خلايا سرطان الثدي دورًا في تحفيز العلاج المناعي من خلال إعادة برمجة استقطاب البلعميات. تحمل هذه الإكسوزومات PEDF، مما يعزز استقطاب البلعميات من النوع M1 عن طريق زيادة CD80 وIRF5 وMCP1 وIL-1.المستويات، مع تقليل CD206 وArg وTGM2 وTGF-المستويات [473].
على الرغم من الإمكانيات المناعية للعلاج باستخدام الإكسوزومات، هناك إكسوزومات تُفرز بشكل داخلي تعزز من نشاط البلعميات M2، مما يساهم في تقدم السرطان. يمكن أن تؤدي الالتهابات، التي تُعتبر عامل خطر للسرطان، إلى بدء تطور السرطان، ويمكن أن تؤثر الوظائف التنظيمية للبلعميات في الالتهابات على مسببات المرض. خلايا المثبطات المشتقة من النخاع (MDSCs) في بيئة الورم تفرز الإكسوزومات، مما ينقل miR-93-5p لقمع محور STAT3. يؤدي تراكم miR-93-5p في هذه الإكسوزومات، الذي تحفزه IL-6، إلى تمايز MDSC إلى البلعميات M2، مما يسهل تطور السرطان الناتج عن التهاب القولون.
عندما تت polarize البلعميات إلى النمط الظاهري M2، فإنها تطلق حويصلات غنية بالبروتين الدهني E الذي يقلل من تعبير MHC-I، مما يؤدي إلى انخفاض المناعية وزيادة المقاومة المناعية. يتطلب اكتشاف الحويصلات ذات الوظائف المثبطة/التحريضية التعرف على العلامات الحيوية السطحية لها. الحويصلات الإيجابية لـ PD-L1 مرتبطة بقمع التفاعلات المناعية خلال تقدم السرطان. تحفز الحويصلات الإيجابية لـ PD-L1استنفاد الخلايا، مما يعزز تكوين الأورام خلال انتشار السرطان [476]. تتضمن إفراز الحويصلات الإكزوسومية الموجبة لـ PD-L1 مسارات جزيئية معقدة، حيث يقوم HMGB1 بزيادة مستويات mRNA لـ RICTOR من خلال تقليل miR-200، وخاصة miR-429. هذه التفاعلات بين HMGB1 وRICTOR تزيد من إنتاج PD-L1، مما يعزز نشاط PD-L1 + الإكسوزومات في العلاج المناعي للسرطان [477].
على الرغم من أن الإكسوزومات الموجبة لـ PD-L1 لها وظائف مسرطنة، إلا أن إكسوزومات أخرى يمكن أن تثبط تعبير PD-L1. بالنظر إلى قدرة الإكسوزومات على تحفيز العلاج المناعي للسرطان، يمكن استخدامها كلقاحات محتملة في المستقبل. تظهر الإكسوزومات المستمدة من السرطان قدرات متفوقة في نضوج الخلايا الشجرية وعرض مستضدات MHC، مقارنة بالخلايا اللمفاوية التائية السامة. علاوة على ذلك، يمكن أن تقلل الإكسوزومات من أعداد خلايا Treg في العلاج المناعي للسرطان من خلال تثبيط تعبير PD-L1. تشير هذه الرؤية إلى أن الإكسوزومات المهندسة حيوياً، المصممة خصيصاً لاستهداف الخلايا الشجرية، قد تعمل كلقاحات فعالة في علاج السرطان. على الرغم من أن المناقشة حول الإكسوزومات المهندسة حيوياً محفوظة للقسم التالي، إلا أنه من الجدير بالذكر أن الخلايا يمكن هندستها لإفراز الإكسوزومات لعلاج السرطان. على سبيل المثال، يمكن أن تؤدي نوى خلايا السرطان المقدمة إلى البلعميات M1 إلى إفراز إكسوزومات هجينة، تتجمع بشكل انتقائي في العقد اللمفاوية وتقوم بتحفيز الخلايا التائية لتحفيز ردود فعل مناعية ضد خلايا السرطان. لذلك، تعتبر الإكسوزومات منظمين محتملين للجهاز المناعي في السرطان. إن استكشاف تنظيم إفراز الإكسوزومات وتكوينها من الخلايا يفتح آفاقاً جديدة للتحكم في العلاج المناعي للسرطان.
الإكسوزومات المهندسة حيوياً
تُستخدم الإكسوزومات في علاج السرطان لأنها موجودة بشكل طبيعي في الجسم، مما يجعل من غير المحتمل أن يتم التعرف عليها كأجسام غريبة وإزالتها. إن توافقها الحيوي العالي يسمح بتوصيل فعال للحمولة واختبارها في التجارب السريرية. الإكسوزومات المستمدة من خلايا السرطان الميتة، المعدلة بببتيد MART-1 و CCL22-siRNA، تحفز استجابات تعتمد على خلايا T وتثبط توسع خلايا Treg. يمكن أن تنتج الإكسوزومات المهندسة حيوياً مناعة مستمرة ضد خلايا السرطان، وهذا يمهد الطريق لتطوير لقاحات قائمة على البيولوجيا. الإكسوزومات المهندسة حيوياً، المطلية بـ HMGB1، تحفز الخلايا الشجرية، وتعزز المناعية، وتسبب مناعة طويلة الأمد ضد السرطان. تتراكم هذه الإكسوزومات في الأنسجة اللمفاوية وتعززوظيفة الخلايا، مما يحفز المناعة طويلة الأمد ويكبح تقدم السرطان [482]. تتضمن نهجًا آخر يتمثل في تفعيل الإكسوزومات عبر الحمض النووي CpG لتحفيز الخلايا الجذعية وتعزيز تقديم المستضدات، مما يظهر قدرتها على التوصيل المشترك في العلاج المناعي التآزري للسرطان [483، 484].
تم تصنيع الإكسوزومات الفوسونية لمعالجة هروب خلايا السرطان من نظام المناعة بسبب التعرف الذاتي. تقوم هذه الإكسوزومات بإدخال مستضدات فيروسية، وتحفيز الخلايا الشجرية، وتقديم المستضدات إلى الخلايا اللمفاوية التائية من أجلتحفيز خلايا T المتقاطعة [485]. الإكسوزومات من خلايا جذعية مسننة من نخاع العظم، محملة بـ الـ siRNA الخاص بـ galectin-9 و oxaliplatin، يحفزان موت الخلايا المناعية، يجذبان الخلايا اللمفاوية T، يقللان من خلايا Treg، ويعززان استقطاب M1 للبلاعم، مما يساهم في علاج السرطان المناعي [486]. الإكسوزومات المستمدة من البلاعم M1 المهندسة، التي تستهدف TAMs باستخدام IL4RPep-1، وNF-кВ p50 siRNA، وmiR-511-3p، تحفز علاج السرطان المناعي من خلال إعادة برمجة البلاعم وتقييد تكاثر السرطان [487]. تعتبر الإكسوزومات حوامل متوافقة حيوياً، ويمكن استخدامها لتعديل جزيئات نانوية أخرى. إن الجمع بين الإكسوزومات والليبوزومات يعزز توصيل الجينات، ويكبح إشارة CD47، ويزيد منجهد الخلية. هذه الاستراتيجية لديها القدرة على التطبيقات السريرية في علاج السرطان المناعي [488]. الجدول 4 هو ملخص لاستخدام الإكسوزومات في علاج السرطان المناعي.
يمكن استخدام الجسيمات النانوية الذكية المستجيبة لمحفزات البيئة المجهرية للورم (TME) لإنشاء أنظمة توصيل مستهدفة. تنبع تعددية وظائفها من تغيير الهياكل استجابةً لمحفزات TME، مما يسهل إطلاق الحمولة في موقع الورم. تعتبر البيئة المجهرية للورم، بسبب درجة حموضتها، مميزة عن الخلايا الطبيعية، مما يجعل الجسيمات النانوية الحساسة لدرجة الحموضة مثالية لعلاج السرطان المناعي. تم تصنيع الجسيمات النانوية باستخدام نواة من PLA-b-PEG وسطح غني بالسايتوزين (C) من الحمض النووي i-motif لإنتاج ما يسمى باللقاحات النانوية. تُستخدم لتوصيل الديوكليوتيدات الحلقية مثل أحادي فوسفات الجوانوزين الديميري (CDG) إلى الحويصلات، مما يسرع من المناعة المضادة للورم ويمنع تثبيط المناعة في TME. في درجة الحموضة الحمضية الخفيفة لـ TME، يحرر تبديل تكويني الحمولة، بينما تزيد درجة الحموضة الفسيولوجية بشكل طفيف من إطلاق CDG. تحمي هذه الجسيمات النانوية الحساسة لدرجة الحموضة CDG من التحلل الإنزيمي، مما يحرر الحمولة إلى السيتوبلازم، ويحفز استقطاب البلعميات إلى النمط الظاهري M1.
إنجاز رائد في علاج السرطان المناعي يتضمن إنشاء جزيئات نانوية من الأدوية المسبقة لتوصيل الحمولة. تطلق هذه الجزيئات الحمولة استجابةً لدرجة حموضة البيئة المجهرية للورم. تم تصميم دواء مسبق مبتكر ذاتي التسلسل يتكون من دوكسوروبيسين قابل للتفعيل عند درجة حموضة حمضية، ومادة مضيئة مستحثة بالتجمع (AIEgen) مرتبطة بببتيد يستجيب لإنزيم الكاسبيز-3. يظهر هذا الدواء المسبق المصمم وظائف مزدوجة – يمكنه إطلاق دوكسوروبيسين بنشاط في البيئة الحمضية للورم وبدء تفعيل الكاسبيز-3 المرتبط بالاستماتة. علاوة على ذلك، يمكن أن يؤدي الكاسبيز-3 المفعل إلى إطلاق وتجمع موضعي لمواد حساسة للضوء. تعزز هذه العملية نضوج الخلايا الشجرية، وتزيد منأرقام الخلايا، ويمنع انتشارها إلى نسيج الرئة [505].
الجدول 4 تطبيق الإكسوزومات في علاج السرطان المناعي
مصدر الإكسوزوم
شحنة
نوع السرطان
خط الخلية
ملاحظة
مرجع
خلية شجرية
النيوانتجينات
الميلانوما
خلايا B16F10
توصيل الشحنات إلى العقد اللمفاوية وتحفيز استجابات المناعة من خلايا T و B توافق حيوي عالي
تحسين بقاء نموذج الحيوان
قمع الانتشار وتأخير عودة الورم
[489]
ورم دبقي متعدد الأشكال
الحمض النووي الريبي غير المشفر الطويل
ورم دبقي متعدد الأشكال
خط الخلايا البشرية للورم الدبقي LN229، خط الخلايا الورمية الدبقية للفئران GL261، خط الخلايا المجهرية البشرية HMC3، وخط الخلايا المجهرية للفئران BV-2
تحفيز الخلايا الدبقية الصغيرة لإنتاج وإفراز المكمل C5 في تطوير مقاومة العلاج الكيميائي
[490]
ماكروفاج M1
هوتيب
سرطان الرأس والعنق
خلايا هب-2
زيادة التعبير عن TLR5/NF-kB لتعطيل تقدم سرطان الرأس والعنق
[491]
CD45RO- CDخلايا T
–
سرطان بطانة الرحم
خلايا إشيكاوا و RL95-2 و KLE
تقوم الإكسوزومات بتثبيط تقدم سرطان بطانة الرحم الناتج عن الإستروجين من خلال إفراز miR-765
[492]
ماكروفاج M1
SN38
سرطان الثدي
خلايا 4T1
قدرة استهداف السرطان وإطالة الدورة الدموية
تحفيز استقطاب M1 للبلاعم
زيادة تجنيد خلايا NK
[493]
خلايا
–
سرطان البلعوم الأنفي
خلايا NP69 و HK-1 و NPC43
القضاء على خلايا الورم وقتلها
تحفيز محور FasL و DR5/TRAIL
كبح نمو السرطان
زيادة بقاء نموذج الحيوان
تحفيز الموت الخلوي
زيادة هجرة خلايا T إلى موقع الورم من خلال زيادة تنظيم CCR5
[494]
–
–
سرطان الثدي
خلايا 4T1
الإكسوزومات الذكية والمصممة بيولوجيًا مع CD62L و OX40L يمكن أن تحفز خلايا T وتثبط وظيفة خلايا Treg.
[495]
الخلايا الشجرية
–
الميلانوما
خلايا B16-OVA
تفعيل الإكسوزومات باستخدام مضادات CD3 ومضادات EGFR للارتباط بخلايا T
[496]
الخلايا الجذعية المستحثة (iPSCs) وإكسوزومات الخلايا الشجرية
دوكسوروبيسين
سرطان المعدة
خط الخلايا MFC
توصيل دواء العلاج الكيميائي
قدرة استهداف الورم
تجنيد خلايا المناعة إلى البيئة المجهرية للورم
[497]
خلايا السرطان
باكليتاكسيل
سرطان الثدي
خلايا 4T1
تطوير مركب ليفوزوم-إكسوزوم ذو توافق حيوي عالي لزيادة العدد منخلايا
[498]
خلايا السرطان
–
سرطان الثدي
خلايا 4T1
تركيبة من الماء المؤكسج والإكسوزومات التي تفرزها السرطانات تحفز استجابات مضادة للأورام وتثبط تكوين الأوعية الدموية والغزو.
[499]
خلايا السرطان
–
سرطان البنكرياس
خلايا PANC-1
تقلل الإكسوزومات من مستويات HLA-DR على سطح وحيدات النواة CD14 + مما يسبب تثبيط المناعة من خلال تنظيم STAT3، وتحفيز تعبير الأرجيناز وROS.
[500]
البلاعم M1
دوستكسل
سرطان الثدي
خلايا 4T1
تقوم الإكسوزومات المحملة بالدوستكسل بتحفيز العلاج المناعي للسرطان من خلال استقطاب M1 للبلاعم
[501]
الخلايا الشجرية
siRNA
الميلانوما
خلايا B16-F10
توصيل siRNA الخاص بـ BRAF بواسطة الإكسوزومات لتحفيز الخلايا اللمفاوية T
[502]
خلايا HEK 293T
كلورين e6 (Ce6) ومحفز المناعة R848
سرطان البروستاتا
خلايا RM-1
تتراكم الإكسوزومات بشكل تفضيلي في موقع الورم وتحث على نضوج خلايا الدندريت. مما يزيد من مستويات CD80 وCD86 كعلامات حيوية لخلايا الدندريت.
تحفيز استقطاب M1 للبلاعم
[503]
تدعم الأدلة المتزايدة الجمع بين العلاج الكيميائي والعلاج المناعي باستخدام جزيئات نانوية حساسة للرقم الهيدروجيني لقمع السرطان. على سبيل المثال، تم استخدام بولي (L-هيستيدين) (PHIS) لتغليف R848، مما يشكل نواة نانوية حساسة للرقم الهيدروجيني PHIS/R848. يؤدي ربط دوكسوروبيسين بحمض الهيالورونيك إلى إنشاء جزيئات نانوية من الأدوية التي تغلف PHIS/R848. تخضع هذه الحاملات النانوية لتغيير من حالة كارهة للماء إلى حالة محبة للماء استجابةً لتغير الرقم الهيدروجيني، مما يؤدي إلى إطلاق R848 لتعديل الجهاز المناعي. عند الرقم الهيدروجيني 5.5، ينفصل رابط الهيدرازون، مما يؤدي إلى إطلاق دوكسوروبيسين. يتم إدخال الأخير إلى خلايا الورم عبر البلعمة. هذا ينشط الجهاز المناعي ويقمع تكاثر السرطان [506].
يمكن أيضًا تصميم الجسيمات النانوية المعتمدة على المعادن لتتحلل استجابةً لدرجة حموضة البيئة الورمية. تم تطوير إطار زيوتيك مغطى بألبومين مصل الإنسان (HSA) لتوصيل مادة حساسة للضوء (HPZ) للتعرف الانتقائي على البيئة الورمية. يتيح هذا الإطار زيادة سريعة في تركيزات أيونات الزنك مع ضمان إطلاق محكوم للمادة الحساسة للضوء المحصورة. تحت درجة حموضة فسيولوجية (7.4)، يظهر HPZ بحجم يقارب 170 نانومتر، وينخفض بشكل كبير إلى أقل من 10 نانومتر في الظروف الحمضية (درجة حموضة 6.5). تؤدي التحلل الناتج عن الحمض لـ HPZ إلى زيادة سريعة في تركيز أيونات الزنك، مما يسبب تأثيرات سامة خلوية قوية ضد سرطانات القولون والثدي والبنكرياس. تؤدي الإدارة الوريدية لـ HPZ في نموذج فأر يحمل ورم CT26 إلى توسيع خلايا T المساعدة والخلايا التائية السامة، وتقليل عدد خلايا Treg. تؤدي هذه التغيرات إلى تثبيط كبير لنمو الورم.
بينما يركز هذا القسم بشكل أساسي على تقييم دور الجسيمات النانوية في العلاج المناعي للسرطان، يجدر بالذكر أن مصفوفات الإبر الدقيقة، المكونة من إبر صغيرة، يمكن استخدامها أيضًا لتوصيل الحمولة بشكل مستدام. يمكن دمج الجسيمات النانوية الحساسة للرقم الهيدروجيني في الإبر الدقيقة، مما يسهل الإفراج المستدام لتحفيز الجهاز المناعي وإنشاء اللقاحات النانوية. كما تتوفر الهلاميات المائية لتوصيل الحمولة بشكل مستدام. على سبيل المثال، يمكن تضمين الجسيمات النانوية في هلاميات مائية حساسة للرقم الهيدروجيني لتوصيل دوكسوروبيسين وJQ1 (مثبط جزيئي صغير) لتحفيز موت الخلايا المناعية. ومن الجدير بالذكر أن الناقلات النانوية البيوميميتية الحساسة للرقم الهيدروجيني، المصنوعة من PLGA والمغطاة بأغشية من البلعميات وخلايا السرطان، يمكن أن توصل FGL1-siRNA والميتفورمين للعلاج المناعي للسرطان. تعزز هذه الجسيمات النانوية البيوميميتية هروب الحمولة من الحويصلات، حيث يقوم الميتفورمين بتثبيط PD-L1 من خلال زيادة تنظيم AMPK، ويقلل siRNA من تعبير FGL1 لتعزيز المناعة المضادة للسرطان من خلال تحفيز خلايا T. نظرًا لتأثير الرقم الهيدروجيني للبيئة المجهرية للورم على تكوين الأورام، تم تطوير منظمات الرقم الهيدروجيني. تقوم الهياكل النانوية لكربونات الكالسيوم بتحييد الرقم الهيدروجيني للبيئة المجهرية للورم من خلال استهلاك اللاكتات، مما يعزز استقطاب البلعميات من النوع M1. تسلل خلايا المناعة، تحفيز الخلايا الشجرية، وتجنيد الخلايا لعلاج السرطان المناعي [511]. تلخص الجدول 5 تطبيق الجسيمات النانوية الحساسة لدرجة الحموضة في علاج السرطان المناعي.
جزيئات نانوية حساسة للأكسدة والاختزال
الجسيمات النانوية الحساسة للأكسدة والاختزال هي حوامل تطلق الحمولة استجابةً للاختلالات الأكسدة والاختزال في البيئة المجهرية للورم. يتضمن تطوير هذه الجسيمات النانوية إدخال روابط حساسة للأكسدة والاختزال، مثل الروابط ثنائية الكبريتيد. وقد وجدت تطبيقات في العلاج المناعي للسرطان، قادرة على تحفيز خلايا المناعة المختلفة.
تم تصميم ناقلات نانوية متعددة الوظائف ذات ميزات حساسة للأكسدة والاختزال، تتضمن منبهات مستقبلات مثل Toll، وكاتالاز، وPD-L1-siRNA، لعلاج السرطان. هذه الجسيمات النانوية تحفز استقطاب M1 للبلاعم، وتزيد من إنتاج ROS، وتقلل من تعبير PD-L1، وتعززتعمل الخلايا عن طريق قمع خلايا Treg [525].
التطبيق السريري للعلاج المناعي يعتمد على استخدام هياكل نانوية متوافقة حيوياً وآمنة على المدى الطويل مثل الميسيلات. تم استخدام ميسيلات تحتوي على دوكسوروبيسين وR848، وهو منبه TLR7/8، تجريبياً كلقاحات نانوية. مستويات الجلوتاثيون المرتفعة في بيئة الورم تحفز تحلل الميسيلات، مما يؤدي إلى إطلاق الحمولة وتحفيز موت الخلايا المناعية، وتحفيز خلايا التغصن، وتسريع الاستجابات المناعية. بالإضافة إلى ذلك، فإن البوليمرات المستجيبة للأكسدة ومضاد A2AR داخل الميسيلات تقمع الإشارات الأدينوسينية لتنشيط خلايا NK والخلايا في العلاج المناعي للسرطان [526].
نقاط البوليمر الكاتيونية، المعروفة بحجم جزيئاتها الصغيرة، وقدرات التصوير، وإمكانات توصيل الأدوية، قد شهدت استخدامًا واسعًا في الطب الحيوي. تم استخدام هياكل نانوية من بوليمر (الأمينات الأميدية) المتفرعة الحساسة للأكسدة والمعدلة بـ PEI600، والتي تم كربنتها جزئيًا مع نقاط البوليمر، لحمل الألبومين البيضاوي. تعزز هذه الهياكل تكاثر الخلايا الطحالية، وترفع مستويات السيتوكينات (بما في ذلك IL-12 و IFN- )، تعزيز نضوج الخلايا الشجرية، وزيادة و عدد الخلايا، بالإضافة إلى الخلايا اللمفاوية التائية. إطلاق الألبومين البيضاوي من هذه الهياكل يستجيب للتأكسد والاختزال [527].
نظرًا لأن كلاً من الرقم الهيدروجيني والاختزال يعملان كمنبهات داخلية، تم تطوير ناقلات نانوية جديدة تظهر استجابة مزدوجة. يتم استخدام الميسيلات الحساسة للرقم الهيدروجيني والاختزال التي تحتوي على الألبومين البيضاوي، المعدلة بـ PLH-PEG، كلقاحات ضد السرطان. تمكّن هذه الهياكل النانوية الميسيلية من توصيل الألبومين البيضاوي إلى السيتوسول من خلال إطلاق الاختزال، وتدفق البروتونات، وتفكيك الميسيل، وفي النهاية، تأثير إسفنجة البروتون وكسر الليزوزوم. تعزز هذه الميسيلات معدلات MHC-I، وعرض المستضد، وتراكم العقد اللمفاوية، وتحسن التفاعلات المناعية [528].
جزيئات نانوية حساسة للضوء والعلاج بالضوء
يعمل الضوء كمنبه خارجي في تطوير الجسيمات النانوية، حيث يؤدي إشعاع الليزر إلى كسر الروابط لإطلاق الحمولة المحملة. يشكل هذا أساس العلاج الضوئي الديناميكي (PDT) والعلاج الضوئي الحراري (PTT) لاستئصال السرطان. في PDT، يؤدي إنتاج أنواع الأكسجين التفاعلية (ROS) إلى موت الخلايا، بينما يسبب PTT موت الخلايا من خلال فرط الحرارة. يمكن أن يعزز دمج العلاج الضوئي مع العلاج المناعي من قمع السرطان. يتم استخدام طريقتين، بما في ذلك الجمع بين العلاج الضوئي والعلاج المناعي أو تحفيز العلاج المناعي المدعوم بالعلاج الضوئي. كلا الطريقتين توفران احتمالية عالية لقمع الورم، مما يحسن من مكافحة السرطان. تُستخدم الجسيمات النانوية PLGA المحملة بـ R837، دوكسيتاكسل، وعوامل PB للعلاج المناعي و PTT. يتم تعديل هذه الجسيمات النانوية مع أغشية خلايا السرطان لزيادة الفعالية. يحفز R837 نضوج الخلايا الشجرية، ويزيد دوكسيتاكسل من استقطاب M1 للبلعميات، مما يعيق البيئة المجهرية المثبطة للمناعة (TME). يؤدي ذلك إلى زيادة تسلل الخلايا اللمفاوية التائية السامة للخلايا في TME لعلاج السرطان المناعي الفعال.
على غرار الدوكسوروبيسين، الذي يحفز موت الخلايا المناعية، أظهر الدوكيتاكسيل إمكانيات في علاج السرطان المناعي من خلال تنظيم استقطاب الخلايا المناعية المرتبطة بالورم. جزيئات CuS النانوية معالمجموعات الوظيفية، المفعلة بحمض الفوليك والمربوطة بـ PEI-PpIX لزيادة الذوبانية، توصل دوستكسل وCpG، مما يحفز العلاج الحراري والعلاج المناعي. تظهر هذه الجسيمات النانوية قدرة ممتازة على التحويل الضوئي الحراري عند التعرض لأشعة الليزر بطول موجي 650 و808 نانومتر وتسبب استقطاب M1 للبلاعم من خلال وظيفة دوستكسل في العلاج المناعي للسرطان [530].
بالإضافة إلى دمج العلاج المناعي والعلاج الضوئي الحراري، من الممكن تحفيز ردود فعل مناعية ناتجة عن العلاج الضوئي الحراري. يمكن أن يؤدي قتل خلايا الورم وإطلاق المستضدات إلى تسريع ردود الفعل المناعية. تم تطوير مركب ببتيد-عامل حساس للضوء، مستمد من ببتيد مضاد PD-L1، قابل للتفكيك بواسطة MMP2، وبورفيرين 18 كعامل حساس للضوء، ويتجمع في موقع الورم. يؤدي تحلل إنزيم MMP-2 إلى إطلاق الببتيد، مما يسبب إطلاق المستضد. التحريض بالإشعاع يحفز نضوج الخلايا الشجرية، مما يؤدي إلى هجرتها إلى العقد اللمفاوية، مما يزيد منتسلل الخلايا، وكبح انتشار السرطان إلى نسيج الرئة، وتحفيز استجابات المناعة المضادة للورم [531].
يمكن أن تعمل الهياكل المستجيبة للضوء أيضًا كلقاحات. الت Chelation لـالأيونات مع الألبومين البيضاوي تؤدي إلى التمعدن الحيوي إلى نانو لقاحات، embedding IR820 كعامل حساس للضوء من خلال الإدماج الكهروستاتيكي. وجود الحديد يحفز الموت الخلوي الفيروبتي، مما يتوسط الموت الخلوي المناعي. الموت الخلوي المناعي يحفز النيوانتجينات وDAMPs، مما يتعاون مع الألبومين البيضاوي في علاج السرطان المناعي. الإشعاع تحت الأحمر القريب يحفز PTT، مما يعزز العلاج المناعي. هذه تعزز الهياكل النانويةتسلل الخلايا، تثبيط الورم الأساسي، وإظهار تأثيرات واعدة عند الجمع مع مثبطات نقاط التفتيش [532].
لقد أظهرت مجموعة العلاج الضوئي الديناميكي والعلاج المناعي نتائج واعدة في علاج السرطان المناعي. على الرغم من أن العلاج الضوئي الديناميكي والعلاج الحراري بالليزر لهما آليات عمل مختلفة، إلا أنه يمكن دمجهما مع العلاج المناعي لتسريع العملية المناعية من خلال تعريض المستضدات أو تحفيز موت الخلايا لتحفيز الاستجابات المناعية. يُفضل العلاج الضوئي الديناميكي على العلاج الحراري بالليزر بسبب التأثيرات المحتملة لفرط الحرارة على الأنسجة الطبيعية. ومع ذلك، عندما يتم تطوير جزيئات نانوية مستهدفة للأورام، يمكنها تنفيذ العلاج الضوئي الديناميكي بدقة في موقع الورم، مما يؤدي إلى قتل خلايا السرطان بشكل فعال. يمكن تطوير إنزيمات نانوية متنوعة مع تراكم خلايا السرطان لتحفيز العلاج الضوئي الديناميكي وتعزيز العلاج المناعي للسرطان.
تم إنشاء نواة نانوية من خلال ربط أدوية باكليتاكسيل عبر رابطة ثنائية الكبريتيد (PTX-SS-PTX)، مع P18 كعامل حساس للضوء مرتبط بـ MPEG-CPPA-b-P(M4). استجابةً للجلوتاثيون، تتحلل الرابطة الثنائية الكبريتيد، ويؤدي الإشعاع بالليزر استجابةً لجذور الأكسجين التفاعلية إلى زيادة إنتاج الأكسجين المفرد، مما يؤدي إلى إطلاق مجموعة البروتينات عالية الحركة 1 (HMGB1) بسبب تنشيط GSDME. يؤدي إطلاق HMGB1 وتحفيز البيروبتوز إلى نضوج الخلايا الشجرية، مما يثقف الخلايا التائية الساذجة.الخلايا في العقد اللمفاوية، وتوسيع خلايا T، وتطوير خلايا T الذاكرة لعلاج السرطان المناعي [533].
لتحفيز العلاج الضوئي الديناميكي، يتم تحميل المادة الحساسة للضوء في الجسيمات النانوية. أظهرت الدراسات الحديثة إمكانيات الطب العشبي في علاج السرطان. يمكن للجسيمات النانوية السيليكا المسامية المعدلة بـ PEG أن تحمل كل من الكلورين e6 والأستراجالوسيد III، مما يحفز خلايا NK ويكبح نمو خلايا السرطان. تتجمع هذه الجسيمات النانوية في موقع الورم، مما يزيد من تسلل خلايا المناعة، ويعزز النشاط والسمية الخلوية.الخلايا وخلايا NK، وإعاقة تكوين الأورام [534].
الليبوسومات هي أيضًا ناقلات نانوية محتملة في علاج السرطان المناعي. الليبوسومات التي تحمل IPI-549 كـ PI3Kالمثبط والكلورين E6 كعامل حساس للضوء يحفزان توليد ROS بعد الإشعاع، مما يسهل موت الخلايا المناعية ويعزز قدرة الخلايا اللمفاوية T على القضاء على خلايا السرطان. يمكن أن يقلل توصيل IPI-549 بواسطة الجسيمات النانوية من مستويات الأرجيناز-1 (Arg-1) وROS، مما يزيد من موت الخلايا المبرمج في MDSCs، ويمنع وظيفتها المثبطة على خلايا T. بالإضافة إلى ذلك، تقلل هذه الجسيمات النانوية من تسلل البلعميات المستقطبة من النوع M2 والخلايا الجذعية الناضجة في العلاج المناعي للسرطان.
في كل من العلاج الضوئي والعلاج الحراري المعتمدين على الجسيمات النانوية، الآلية الأكثر بروزًا هي تحفيز موت الخلايا المناعية لتسريع العلاج المناعي للسرطان. تبرز الأدلة المتزايدة تطبيق العلاج الضوئي والعلاج المناعي المعتمدين على الجسيمات النانوية في قمع السرطان [536-540]. الجدول 6 يلخص
الجدول 5: الجسيمات النانوية الحساسة لدرجة الحموضة في علاج السرطان المناعي
جزيئات نانوية
نوع السرطان / خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
أبرز النقاط
مرجع
جزيئات نانوية من PEG/PEI/CAD
سرطان الثدي/خلايا 4T1
على مدىمجموعة من
توصيل الدوكسوروبيسين وإطلاقه بطريقة حساسة لدرجة الحموضة
تحفيز موت الخلايا المناعي
حمضية الإندوسوم تحفز انقسام السيز-أكونيتيل
تجنيد الخلايا الشجرية
[512]
الهياكل النانوية السيليكا المجوفة
سرطان الثدي/خلايا 4T1
زيادة الاحتفاظ استجابةً لمستوى pH المنخفض في TME
استهداف الميتوكوندريا وزيادة مستويات الجذور الحرة للأكسجين
تحفيز العلاج الضوئي الديناميكي
التوليف مع مثبطات نقاط التفتيش يساهم في المناعة المضادة للورم
[513]
ناقلات نانوية معدلة بالدكستران BLZ-945
سرطان الثدي/خلايا 4T1
11.35، 112.4، و
وجود رابطة استر البورات كرابطة حساسة لدرجة الحموضة
تحفيز موت الخلايا المناعي
نضوج الخلايا الشجرية، استنفاد خلايا المناعة المرتبطة بالورم وتسلل خلايا T
[514]
جزيئات نانوية من المنغنيز
خلايا الميلانوما/B16OVA
130 نانومتر
وقد تم استخدام 2-ميثيل إيميدازول (2-MI) لتغليف الألبومين البيضاوي بخصائص حساسة لدرجة الحموضة وقدرة على نضوج الخلايا الشجرية في العلاج المناعي للسرطان.
[515]
الهياكل النانوية من السيليكا المسامية المتوسطة
–
146 نانومتر
خاصية حساسة لدرجة الحموضة وتوصيل R848
امتصاص الجسيمات النانوية بواسطة خلايا تقديم المستضد
تحفيز الخلايا الشجرية وتعزيزهااستجابات المناعة المعتمدة على الخلايا
[516]
فقاعات نانوية مفعلة بالببتيد
سرطان الثدي/خلايا 4T1
تفعيل النانو فقاعات باستخدام ببتيد مضاد PD-L1
تحميل Ce6، ميتفورمين و بيرفلوروهيكسان في فقاعات نانوية
تراكم الجسيمات النانوية في درجة حموضة حمضية يؤدي إلى انفصال ربيطات PEG ومن ثم، تعرض الببتيد لقمع PD-L1
تخفيف نقص الأكسجين بواسطة الميتفورمين وزيادة فعالية Ce6 في علاج السرطان
زيادة المناعة المضادة للأورام والوقاية من تثبيط المناعة
[517]
معقدات البوليمر والدهون
ليمفوما / خلايا E. G7-OVA
–
تطلق الحويصلات المدمجة بالبوليمر والدهون الألبومين البيض استجابةً لدرجة الحموضة وتحفز المناعة المضادة للسرطان من خلال إطلاق الألبومين البيض في السيتوبلازم للخلايا الشجيرية.
تم تطوير الغشاء من غشاء الخلايا الجذعية الميزانشيمية والليبوبروتينات الحساسة لدرجة الحموضة.
التوصيل المستهدف لـ BPTES
تحفيز مسار STNG واستقطاب M1 للبلاعم
تخفيف تثبيط المناعة TME
[522]
الجدول 5 (مستمر)
جزيئات نانوية
نوع السرطان / خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
أبرز النقاط
مرجع
بوليمرات قائمة على البوليسكاريد
ليمفوما / خلايا E. G7-OVA
تحفيز الخلايا الشجرية
توصيل المستضد إلى السيتوبلازم
إنتاج السيتوكينات Th1 بواسطة الخلايا التغصنية
[523]
الحويصلات الدهنية
خلايا الميلانوما/B16OVA
401، 754، 636 و 674 نانومتر
الحويصلات الدهنية الحساسة لدرجة الحموضة توصل منبهات STING و TLR9 مما يزيد من استجابات المناعة Th1 في قمع الورم
[524]
الجزيئات النانوية التي تسبب العلاج الضوئي الديناميكي والعلاج الحراري الديناميكي، وعلاقتها مع العلاج المناعي. توضح الشكل 6 تطبيق الحوامل النانوية المستجيبة للمؤثرات في علاج السرطان المناعي. نظرًا لأن الدراسات ما قبل السريرية تظهر وظيفة الجزيئات النانوية في علاج السرطان المناعي وكبح الورم، فقد تم تنفيذ التطبيق السريري للهياكل النانوية في علاج السرطان المناعي لتقييم إمكانياتها [541]. تلخص الجدول 7 والجدول 8 التطبيق السريري للجزيئات النانوية في علاج السرطان المناعي.
نظرة عامة على فئات مختلفة من الجسيمات النانوية في علاج السرطان المناعي جزيئات نانوية بوليمرية
تعتبر الجسيمات النانوية البوليمرية من بين الهياكل الأكثر استخدامًا في علاج السرطان المناعي نظرًا لتوافقها الحيوي، وقابليتها للتحلل البيولوجي، واستقرارها الكيميائي، وقابليتها للذوبان في الماء، وقدرتها العالية على تحميل الأدوية. لقد تم استخدام جسيمات نانوية من PLGA وPGA وPLG وPEG وPEI والكيتوزان على نطاق واسع في علاج السرطان المناعي. علاوة على ذلك، أظهرت هذه الهياكل النانوية إمكانيات كمنشطات مناعية في علاج السرطان المناعي. إن تحميل المحفزات TLR7/8 في الهياكل النانوية من PLGA زاد من مستويات CD40 وCD80 وCD86 من خلال تحفيز خلايا الدبقية المستمدة من نخاع العظام، كما أن الإدارة تحت الجلد لهذه الجسيمات النانوية حفزت خلايا الدبقية.الخلايا [570].
جزيئات الدهون النانوية
تعتبر الليبوسومات من الحوامل النانوية الواعدة للأدوية والحمض النووي واللقاحات [571]. حتى الآن، تم تطوير أنواع متعددة من الهياكل النانوية الليبوسومية بما في ذلك 1،2-ديوليويل-3-تريميثيل أمونيوم-بروبان (DOTAP)، – ( الكوليسترول (DC-Chol) ودي ميثيل ديوكتيل أمونيوم (DDA) [572، 573] تم تطبيقهما بشكل كبير لتعرض المستضدات على خلايا APCs وتوفير معززات اللقاح لزيادة التفاعلات المناعية المحددة للمستضد [574، 575]. أظهرت الحويصلات الدهنية المفعلة بالدكستران ذات النشاط الحساس للرقم الهيدروجيني امتصاصًا عاليًا بواسطة الخلايا الشجرية، ويمكنها توفير توصيل السيتوسول للألبومين البيضوي لتسريع التفاعلات المناعية المحددة للمستضد وإعاقة تقدم السرطان [576]. علاوة على ذلك، يمكن أن يعزز تحميل CpG-ODNs كمنبه TLR9 و3،5-ديدوديسيلوكسي بنزاميدين كمعزز داخل الحويصلات الدهنية إنتاج السيتوكينات التي تتوسطها الخلايا الشجرية لتعزيز المناعة المحددة للمستضد [521]. الميسيلات هي نوع آخر من الجسيمات النانوية الدهنية التي يمكن أن تعمل كنظم توصيل للمستضد/المعزز لتحسين إمكانيات اللقاحات. تم استخدام الميسيلات الهجينة البوليمرية لتوصيل CpG-ODN وTrp2 لإنشاء لقاح نانوي يستهدف العقد اللمفاوية ويعزز تراكم الحمولة في الخلايا الشجرية، مما يؤدي إلى تفعيل استجابات المناعة المعتمدة على الخلايا وتعزيز قمع السرطان (الميلانوما) [577].
جزيئات الكربون النانوية
لقد أظهرت الأنابيب النانوية الكربونية (CNTs) قدرتها على التوسط في التأثيرات المناعية المحفزة في المختبر وفي الكائنات الحية. وقد أظهرت الأنابيب النانوية الكربونية متعددة الجدران المؤكسدة (MWCNT) القدرة على توصيل مستضدات السرطان المرتبطة بالخصية، المعروف باسم NY-ESO-1 و CpG-ODNs. وقد أظهرت هذه الهياكل امتصاصًا بواسطة الخلايا الشجرية وتوسطت في تأثيرات قوية. و ردود الفعل المناعية المعتمدة على الخلايا لتقليل تقدم الميلانوما [578]. علاوة على ذلك، أظهرت التوصيل المشترك للألبومين وCpG-ODN، بالإضافة إلى Ig المضاد لـ CD40 كمواد مساعدة مناعية بواسطة MWCNTs، إمكانيات في تسريعاستجابات الخلايا وكبح تقدم الميلانوما [579].
جزيئات النانو المعدنية
تعتبر الهياكل النانوية الذهبية عوامل واعدة في علاج السرطان المناعي بفضل خصائصها، بما في ذلك التوافق الحيوي، كيمياء السطح القابلة للتعديل، وسهولة التحكم في الحجم والشكل. لقد أظهرت الهياكل النانوية الذهبية إمكانيات في تحفيز تمايز البلعميات إلى خلايا شبيهة بالخلايا الشجيرية لتعزيز تكاثر خلايا T وتعزيز إفراز السيتوكينات. علاوة على ذلك، أظهرت الهياكل النانوية الذهبية إمكانيات مذهلة للعمل كمعززات لتعزيز إنتاج الأجسام المضادة. تم الكشف عن إمكانيات جزيئات الذهب النانوية في علاج السرطان من خلال تعديل البيئة المجهرية للورم. تم تعديل سطح الهياكل النانوية الذهبية المجوفة باستخدام CpG-ODNs لتعزيز امتصاصها الخلوي وتعزيز وظيفتها في تحفيز الاستجابات المناعية، بما في ذلك تعزيز TNF-الإفراز [585]. تم استخدام جزيئات السيليكا النانوية على نطاق واسع في الطب الحيوي للتصوير [586]، واستهداف السرطان بشكل محدد [587]، وتوصيل الأدوية والحمض النووي [588]. تم استخدام جزيئات السيليكا النانوية المسامية لتوصيل المستضدات وعملت كلقاحات لتحفيز ردود فعل مناعية تعتمد على الأجسام المضادة والخلايا، مع وجود توافق حيوي عالي وغياب السمية [589]. وقد أظهرت جزيئات السيليكا النانوية المسامية المجوفة أنها قابلة للتحلل البيولوجي وقادرة على إعادة تشكيل البيئة المجهرية للورم في علاج السرطان المناعي [361]. وفقًا لهذه الدراسات، تظهر فئات مختلفة من الهياكل النانوية خصائص واعدة في علاج السرطان المناعي، وقد أظهرت جميعها إمكانيات في إعادة تشكيل البيئة المجهرية للورم. الخطوة التالية للتطبيق السريري لهذه الحاملات النانوية تعتمد على توافقها الحيوي وسلامتها على المدى الطويل، حيث تعتبر جزيئات الدهون النانوية في المقدمة.
الخاتمة والتحديات
لقد أدت العلاجات المناعية للسرطان وتطوير اللقاحات إلى ushered in a new era in cancer treatment, instilling hope in patients and significantly enhancing prognosis. ومعدلات البقاء. ومع ذلك، لا تزال التحديات قائمة في استخدام المواد المساعدة والعوامل المناعية. وقد دفع ذلك إلى استكشاف حلول جديدة، لا سيما من خلال تطبيق الجسيمات النانوية. تلعب التفاعلات المعقدة داخل بيئة الورم دورًا حيويًا في التأثير على استجابة خلايا السرطان للعلاج المناعي. في هذا السياق، ظهرت الجسيمات النانوية المصممة للتوصيل المستهدف للمركبات المناعية وإعادة تشكيل بيئة الورم كأدوات واعدة في العلاج المناعي للسرطان.
تتناول الجسيمات النانوية التحديات الحالية في العلاج المناعي للسرطان من خلال إظهار القدرة على تنظيم مكونات بيئة الورم، وتغيير مسار تقدم خلايا الورم، وتخفيف البيئة المثبطة للمناعة في السرطان. يمكن أن تزيد الهياكل النانوية المصممة لإعادة تشكيل بيئة الورم من تسلل الخلايا السامة.الخلايا، تحفيز الخلايا الشجيرية، تحفيز استقطاب البلعميات M1، وتثبيط MDSCs. علاوة على ذلك، تعمل الجسيمات النانوية كحاملات فعالة لتوصيل المحفزات ومركبات تعديل المناعة الأخرى، مثل الأدوية أو الجينات، في علاج السرطان المناعي.
تتمثل خطوة هامة في تطوير الجسيمات النانوية لعلاج السرطان المناعي في إنشاء ناقلات نانوية تحاكي البيولوجيا، تتضمن أغشية وظيفية مستمدة من خلايا الدم الحمراء، والبلعميات المرتبطة بالأورام، والألياف المرتبطة بالسرطان، وخلايا الأورام. بالإضافة إلى ذلك، فإن استخدام الإكسوزومات، سواء كانت تفرز بشكل طبيعي من الخلايا أو تم هندستها حيوياً في المختبر، يحمل وعداً في تنظيم الجهاز المناعي في علاج السرطان. تظهر الجسيمات النانوية القدرة على تقليل عدد خلايا Treg وMDSCs، مما يمنع تثبيط المناعة. علاوة على ذلك، فإن الموت الخلوي المناعي الناتج عن الجسيمات النانوية يعزز تنشيط الخلايا الشجرية، مما يسهل هجرتها إلى العقد اللمفاوية لتحفيز خلايا T لعلاج السرطان المناعي.
تزيد الناقلات النانوية المستجيبة للمؤثرات، وخاصة الجسيمات النانوية الحساسة للرقم الهيدروجيني والأكسدة والاختزال، من إمكانيات العلاج المناعي للسرطان. تساهم الجسيمات النانوية المستجيبة للضوء، من خلال العلاج الحراري الضوئي والعلاج الديناميكي الضوئي، في تعزيز العلاج المناعي للسرطان من خلال تحفيز موت الخلايا المناعية، وتنظيم الخلايا الشجرية والخلايا التائية، وتعزيز استقطاب M1 للبلاعم. يبرز هذا النهج المتعدد الأوجه مرونة ووعد الجسيمات النانوية في تقدم العلاج المناعي للسرطان.
يتضمن التطبيق السريري للجزيئات النانوية عدة اعتبارات حاسمة [590]. بمجرد أن نفهم إمكانيات الجزيئات النانوية في علاج السرطان المناعي، يصبح من الضروري نقل هذه التقنيات والتطورات والنتائج إلى الإعداد السريري. تجري بالفعل تجارب سريرية تتعلق بالعلاج المناعي لمرضى السرطان. في سياق الأورام الصلبة وعلاجها السريري، يتم الاستفادة من تأثير الجزيئات النانوية.
الجدول 6 العلاج الضوئي الديناميكي والعلاج الحراري باستخدام الجسيمات النانوية وعلاقتهما بالعلاج المناعي للسرطان
جزيئات نانوية
نوع السرطان / خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
نتيجة
مرجع
نانوبروتكس
سرطان الثدي/خلايا 4T1
40 و
تتكون الجسيمات النانوية من PpIX كعامل حساس للضوء وببتيد PROTAC المستهدف لـ SHP2 (aPRO)
يحدث تحفيز aPRO استجابةً لزيادة تنظيم الكاسبيز-3
التحلل المستهدف لـ SHP2 من خلال نظام اليوبكويتين-البروتيازوم
نقص SHP2 يثبط المسارات المثبطة للمناعة، بما في ذلك CD47/SIRPa و PD-1/PD-L1، لتحسين وظائف مكافحة السرطان للبلاعم وخلايا T.
[542]
جزيئات MRC
سرطان الثدي/خلايا 4T1
التوصيل المشترك لـ RGX-104 كمنشط مناعي وكلورين e6
تحفيز ApoE بواسطة RGX-104 لإضعاف وظيفة MDSCs وتسريع البيروبتوز
العلاج الضوئي المحفز بواسطة الكلورين e6 لتسهيل الضرر التأكسدي وزيادة المناعية
[543]
معدل بواسطة Ru(II)حاملات نانوية
4NQO – سرطان الفم
و
تحميل HIF-1a-siRNA في الجسيمات النانوية
تحفيز العلاج الضوئي وإحداث ضرر في الجسيمات الحالة
خفض تنظيم HIF-1 ألفا وزيادة قتل سرطان الفم
تحفيز و خلايا
[544]
جزيئات نانوية PDA-FA
سرطان القولون / خلايا CT26
توصيل CpG كعامل مناعي لتحفيز نضوج الخلايا الشجرية وزيادة نشاط خلايا T
قمع خلايا Treg وMDSCs
تحفيز PTT
[545]
منصات نانوية من كبريتيد النحاس
ميلانوما / خلايا B16F10
توصيل بروتين ريبونوكليوبروتين Cas9 إلى الهدف PTPN2
خفض تنظيم PTPN2 لزيادة تسللخلايا
زيادة مستويات IFN-و TNF-α
تحسين حساسية المناعة
[546]
المساعدات النانوية البوليمرية
سرطان الثدي/خلايا 4T1
التعاطي مع المحفزات TLR كعامل مساعد مناعي
وجود غلاف دهني استجابةً لدرجة الحرارة
إمكانات PTT استجابةً لـ NIR-II
تحفيز موت الخلايا المناعية وإطلاق منبهات مستقبلات المناعة
زيادة تنظيم TLR7/TLR8 وتحفيز موت الخلايا المناعية يعززان نضوج الخلايا الجذعية وزيادة الاستجابة المناعية المضادة للسرطان
[547]
الإنزيمات النانوية
سرطان الثدي/خلايا 4T1
100 نانومتر
النانوزيم المكون من MoOx المدعوم بالنحاس (CMO) يتكون من نواة مغطاة بغشاء خلايا السرطان.
زيادة تراكم الورم والنانوزيمات تسبب ضررًا أكسديًا من خلال زيادة إنتاج أنواع الأكسجين التفاعلية.
يسبب PTT موت الخلايا المناعية لتنشيط الجهاز المناعي
[548]
الأسطوانة النانوية الذهبية
سرطان القولون / خلايا CT26
، ، و ملي فولت
إشعاع الليزر بزاوية 808 نانومتر يسبب العلاج الحراري بالليزر
تحفيز خلايا المناعة في العقد اللمفاوية
[549]
إيه
سرطان الثدي/خلايا 4T1
تعديل مع غشاء خلايا السرطان
تحفيز موت الخلايا المناعية
زيادة إنتاج أنواع الأكسجين التفاعلية من خلال العلاج الضوئي
[550]
ناهض بوليمري نانوي
سرطان الثدي/خلايا 4T1
42 وملي فولت
تحفيز PTT
زيادة العلاج المناعي وتحفيز موت الخلايا المناعية
[551]
جزيئات نانوية لالتقاط المستضدات
سرطان الثدي/خلايا 4T1
41.1 نانومتر
تحفيز العلاج بالضوء تحت إشعاع NIR
زيادة امتصاص المستضدات وعرضها
كبح تقدم السرطان
[552]
جزيئات نانوية
نوع السرطان / خط الخلايا
الحجم (نانومتر)/إمكانات زيتا (ملي فولت)
نتيجة
مرجع
نانوحويصلات نقاط الكم من الفوسفور الأسود
سرطان الثدي/خلايا 4T1
تحميلها في الهلاميات الهيدروجينية الحساسة للحرارة
يؤدي إشعاع NIR إلى زيادة تنشيط الخلايا الشجرية، ثم تهاجر إلى العقد اللمفاوية لتحفيزخلايا
[553]
أقفاص نانوية من الذهب
سرطان القولون / خلايا CT26
توصيل مضاد PD-L1 وجالونيسيرتيب بواسطة الأقفاص النانوية
تحفيز PTT للتسبب في العلاج المناعي
[554]
يوصى بالعلاج الضوئي لتعزيز الاستجابات المناعية وتحفيز الخلايا الشجرية بالإضافة إلى نضوجها. وأخيرًا، ولكن ليس آخرًا، من الضروري تقييم التوافق الحيوي للاستجابات المناعية الناتجة عن الجسيمات النانوية لمنع التفاعلات المناعية النظامية ضد الخلايا الطبيعية. يجب إجراء تقييم لتوصيل العوامل المناعية المعدلة جنبًا إلى جنب مع أدوية العلاج الكيميائي لتحديد التأثير التآزري على علاج السرطان. ومع ذلك، يجب أن يؤخذ بعين الاعتبار بعناية ما إذا كانت الآثار الجانبية المرتبطة قابلة للتحمل بالنسبة للمرضى. لذلك، فإن تقييم التوافق الحيوي وملف السمية للجسيمات النانوية يبرز كجانب حاسم من تطبيقها السريري.
حالياً، ركز عدد كبير من الدراسات على الاستخدام السريري للهياكل النانوية لتعزيز العلاج المناعي [591]. واحدة من أبرز العيوب هي أن المنصات النانوية المطورة حالياً في المرحلة الأولى أو الثانية. قدمت المراجعة الحالية التفاعل المحتمل ووظيفة الجسيمات النانوية مع مكونات البيئة المجهرية للورم والخلايا المناعية لتحفيز العلاج المناعي للسرطان الذي يمكن استخدامه في العيادات. في معظم الحالات، تم استخدام نماذج حيوانية لتقييم إمكانيات الجسيمات النانوية في العلاج المناعي للسرطان، مما يجعل من الصعب ترجمتها إلى البشر. يمكن أن يحسن اختيار نماذج حيوانية مخصصة للبشر من فرصة الترجمة إلى العيادة. علاوة على ذلك، يجب اختيار الجسيمات النانوية المناسبة للعلاج المناعي للسرطان. بهذه الطريقة، يُقترح استخدام عوامل معتمدة من إدارة الغذاء والدواء مثل البوليمرات أو الجسيمات النانوية الدهنية لتسريع وتيرة الترجمة السريرية وتنظيم المناعة. يجب أيضاً مراعاة السلامة الحيوية، وقابلية التحمل، وإمكانية التكرار لحاملات النانو للاستخدام السريري. في السنوات الأخيرة، تم إدخال عدد كبير من الجسيمات النانوية إلى العيادات لعلاج السرطانات، بما في ذلك الجسيمات النانوية القائمة على الدهون (الاسم العام: JVRS-100) لعلاج اللوكيميا (NCT00860522)، والليبوسومات لعلاج اللمفوما، والميلانوما، وسرطان الثدي، وسرطان المبيض وسرطان البروستاتا (NCT03349450، NCT01052142، NCT01095848)، وجسيمات PLGA لعلاج الميلانوما النقيلي (NCT01753089) وهياكل الذهب الغرواني لعلاج الأورام الصلبة المتقدمة [592]. ومع ذلك، تم تقييم جميع هذه الجسيمات النانوية في الدراسات من المرحلة الأولى والثانية.
عند أخذ كل شيء في الاعتبار، هناك عدد من النقاط التي يجب النظر فيها لتطبيق الجسيمات النانوية في العلاج المناعي للسرطان. في الوقت الحالي، يعتمد العلاج المناعي للسرطان بشكل أساسي على تطبيق أنظمة توصيل على نطاق النانو للمواد المناعية التقليدية، بما في ذلك الأجسام المضادة، والبروتينات المؤتلفة، والعوامل المناعية الصغيرة القائمة على الجزيئات، سواء كانت منشطة أو مساعدة أو مثبطة. السبب وراء تطبيق الجسيمات النانوية هو تحسين الملف الدوائي للعلاج المناعي.
الشكل 6: الناقلات النانوية المستجيبة للمؤثرات في العلاج المناعي للسرطان. يمكن للجزيئات النانوية التي تستجيب للرقم الهيدروجيني أو الأكسدة والاختزال أو الضوء أن تطلق الحمولة لتحفيز موت الخلايا المبرمج، وإحداث تلف في الحمض النووي، وتنظيم المسارات الجزيئية. علاوة على ذلك، تحفز الناقلات النانوية المستجيبة للمؤثرات موت الخلايا المناعية لزيادة نضوج الخلايا الجذعية. تهاجر إلى العقد اللمفاوية وتزيد من تنشيط خلايا T.
الجدول 7 تطبيق العلاج المناعي القائم على الجسيمات النانوية في الدراسات السريرية [541،555-557]
تحفيز موت الخلايا المناعية المثيرة لقمع إشارات نمو مستحثة بواسطة EGFR
NCT02833766
ليبوبروتينات كاتيونية محملة بمركب الحمض النووي البلازميدي
المرحلة الأولى
تحفيز جهاز المناعة
NCT00860522
تركيبة من مضادات PD-1 وهياكل نانوية من أكسيد الهفنيوم
المرحلة الأولى
زيادة في موت خلايا الورم، تعزيز موت الخلايا المناعية، وتحفيز الجهاز المناعي
NCT03589339 [563]
العوامل، تقلل من الآثار الجانبية، تمنع عاصفة السيتوكينات الناتجة عن فرط تنشيط المناعة، وتحسن نقص الاستجابة المناعية. علاوة على ذلك، فإن الجسيمات النانوية واعدة في عكس تثبيط المناعة ومنع التهرب المناعي. على الرغم من أن هذا مجال متعدد التخصصات يجمع بين البيولوجيا والهندسة، يجب دراسة عدد من العوامل بعناية. بما في ذلك المناعية المتوسطة بواسطة الجسيمات النانوية، والتوافق الحيوي، والجوانب الهندسية المتعلقة بتحميل المركبات العلاجية في الهياكل النانوية. علاوة على ذلك، تمتلك العديد من الجسيمات النانوية نشاطًا مضادًا للسرطان، مما يسبب تأثيرًا تآزريًا مع العلاجات المناعية. واحدة من أهم ميزات الجسيمات النانوية هي قدرتها على الإفراج المنضبط عن العلاجات.
الجدول 8 التحديات المتعلقة بتطبيق الجسيمات النانوية في العلاج المناعي للسرطان
– الإمكانية في توصيل شحنات متنوعة بما في ذلك الأدوية الصغيرة الجزيئات، البروتينات، الببتيدات، والأحماض النووية
– زيادة استقرار الأدوية ومنع التحلل
– تحفيز جهاز المناعة
– التوافق الحيوي والقابلية للتحلل البيولوجي
– تطوير الجسيمات النانوية بحجم وشحنة وقدرة استهداف مرغوبة يعد تحديًا
– قواعد صارمة بشأن التطبيق السريري
– تفاعلات غير متوقعة مع جهاز المناعة
– التحديات في توسيع نطاق التوليد والتخزين والاستقرار
جزيئات الدهون النانوية
– توصيل فعال للأدوات الجينية بما في ذلك mRNA وsiRNA وDNA
– توصيل مستهدف
– حماية الشحن
– التوافق الحيوي والسلامة على المدى الطويل
– التأثير المساعد الذي يمكن أن تعمل به عدد من مكونات الدهون كمساعدات وزيادة الاستجابات المناعية المضادة للسرطان
– إنتاج معقد من الشركات المصنعة، خاصة تطوير الجسيمات النانوية لتوصيل الجينات
– يحتاجون إلى درجات حرارة منخفضة للغاية للحفاظ على استقرارهم
– المناعية التي يمكن أن تؤدي إلى الالتهاب وآثار جانبية أخرى
– سعة تحميل منخفضة
جزيئات النانو المعدنية
– توصيل مستهدف للأدوية وكفاءات تحميل وتغليف عالية
– تطبيق للعلاج الضوئي الحراري، حيث يمكن لعدد من الهياكل النانوية مثل الناقلات النانوية الذهبية امتصاص الضوء والتسبب في تدمير الورم بواسطة الحرارة الناتجة عن الضوء.
– توصيل العوامل المناعية لعلاج السرطان المناعي
– العلاج التآزري من خلال مزيج من توصيل الأدوية والعلاج الضوئي الحراري
– التصوير والاستشعار الحيوي
– توزيع المعادن النانوية في الجسم يمثل تحديًا إلى جانب التخلص منها من الجسم
– تمتلك الهياكل النانوية المعدنية سمية خلوية عالية وتوافق حيوي ضعيف
– فرصة حدوث الالتهابات والتفاعلات المناعية
– الاستقرار والسمية تجاه الخلايا الطبيعية
جزيئات الكربون النانوية
– إمكانيات تحميل عالية للأدوية لتوصيل الأدوية والبروتينات والأدوات الجينية
– التطبيق في العلاج الضوئي الحراري والعلاج الضوئي الديناميكي
– تصوير واستشعار البيولوجيا لعلامات السرطان
-السُمية وسوء التوافق الحيوي
– التغيرات في التحلل الحيوي لجزيئات الكربون النانوية، مما يؤدي إلى تراكمها على المدى الطويل
– التعقيد في إنتاج الجسيمات النانوية على نطاق واسع وتحقيق الخصائص الفيزيائية والكيميائية المرغوبة بما في ذلك الحجم، والجهد الكهربائي الساكن، وغيرها
– وظائف بيولوجية غير متجانسة بين الفئات المختلفة من المواد النانوية الكربونية بما في ذلك الأنابيب والنقاط والأوراق
فرط تنشيط أنظمة المناعة باستخدام المحفزات المناعية أو المعززات يمكن أن يؤثر على الخلايا والأنسجة الطبيعية. لذلك، يجب أن يتم توصيل العلاجات بطريقة محكومة ويجب أن يتم توصيل مستويات آمنة. علاوة على ذلك، فإن الإفراج السريع أو المفاجئ عن مركبات العلاج المناعي ليس فعالاً في توفير مناعة مضادة للسرطان على المدى الطويل. عدد من الجسيمات النانوية واعدة للإفراج المحكوم عن المركبات العلاجية، بما في ذلك هياكل PLGA النانوية التي، عند تحلل البوليمر، يحدث الإفراج عن المركب المناعي [594، 595]. كانت التوافق الحيوي عاملاً مهماً آخر في الدراسات ما قبل السريرية والسريرية [596]. بالإضافة إلى التحكم في سمية العوامل المناعية، بما في ذلك السيتوكينات المؤتلفة [597-599]، يجب تعديل الخصائص الفيزيائية والكيميائية للهياكل النانوية بما في ذلك الحجم والشكل وقدرة التحويل الحراري، من بين أمور أخرى، بطريقة تقلل من الآثار الجانبية للجسيمات النانوية [600، 601]. بهذه الطريقة، يجب التحقيق في سمية الجسيمات النانوية في المختبر وفي الجسم، والتوافق مع الدم، وتأثيرها على الأعضاء الرئيسية بما في ذلك الكبد والكلى، والمسارات الأيضية [602]. يعتبر تفعيل سطح الجسيمات النانوية عاملاً مهماً آخر في العلاج المناعي للسرطان. يمكن أن يؤثر تفعيل السطح على امتصاص الهياكل النانوية داخل الخلايا وحتى معالجتها [603]. علاوة على ذلك، نظرًا لأن الجسيمات النانوية قد تم تطبيقها لالتقاط المستضدات، يمكن أن تؤثر الشحنة السطحية، والخصائص الكارهة للماء، والمحبة للماء على وظيفة الهياكل النانوية في العلاج المناعي للسرطان [299]. عامل آخر هو أن الهياكل النانوية يمكن أن تستهدف بشكل محدد الأنسجة اللمفاوية أو خلايا المناعة لتعزيز قدرة الأدوية في العلاج المناعي للسرطان [604]. أظهرت الجسيمات النانوية البوليمرية إمكانيات عالية في الهروب الوعائي، والتسلل إلى الأنسجة واللمفاويات واستهداف اللمفاويات، بينما تظهر الحويصلات الدهنية امتصاصًا عاليًا بواسطة الخلايا البلعومية، بما في ذلك البلعميات [603]. بالإضافة إلى ذلك، تظهر هذه الجسيمات النانوية أمانًا عاليًا مع قدرة في العلاج المناعي للسرطان [605608]. من الجدير بالذكر أن الجسيمات النانوية يمكن اعتبارها معززات مناعية حيث يمكن للجسيمات النانوية المعدنية، والهياكل النانوية الشبيهة بالفيروسات وفئات أخرى أن تحفز الاستجابات المناعية من خلال تحفيز و الخلايا [603، 609] التي تعتمد بشكل كبير على حجم وشحنة السطح للهياكل النانوية [366، 610، 611]. ومع ذلك، فقد أظهرت الهياكل النانوية الكربونية تأثيرات مثبطة للمناعة في بعض الحالات [612، 613]. لذلك، فإن إدخال الجسيمات النانوية لغرض العلاج المناعي للسرطان هو أمر مهم.
الاختصارات
ICLs
مثبطات نقاط التفتيش المناعية
تي إم إي
بيئة الورم الدقيقة
NFAT
عامل النووي للخلايا التائية المنشطة
توكس
اختيار الخلايا التائية المرتبط بالحركة العالية
بروتين مجموعة الصندوق
NR4A
مجموعة فرعية 4 من مستقبلات النووية A
إدارة الغذاء والدواء
إدارة الغذاء والدواء الأمريكية
CTLA4
مستضد اللمفاويات التائية السامة للخلايا 4
PD-1
بروتين موت الخلايا المبرمج 1
PD-L1
الليغاند المبرمج للموت 1
تام
البلاعم المرتبطة بالورم
ث1
خلايا المساعدة من النوع 1
IL-4، IL-10، IL-13
إنترلوكين-4، إنترلوكين-10، إنترلوكين-13
M1
البلاعم M1
M2
البلاعم M2
TGF-
عامل نمو بيتا
-SMA
ألفا-أكتين العضلي الأملس
خلايا NK
خلايا القاتل الطبيعي
إنترفيرون-
إنترفيرون غاما
خلايا ب
الخلايا اللمفاوية ب
خلايا T
الخلايا اللمفاوية التائية
PD-1
بروتين موت الخلايا المبرمج 1
TCM
خلايا الذاكرة المركزية
تم
خلايا الذاكرة الفعالة T
TRM
خلايا الذاكرة المقيمة
TSCM
خلايا الذاكرة التائية الجذعية
تي إي
خلايا T الفعالة
ث1
خلايا المساعدة من النوع 1
إنترفيرون-
إنترفيرون غاما
TCM
خلايا الذاكرة المركزية
سيميب
هيالورونيداز 1 المحفز لهجرة الخلايا
يو إس بي 22
ببتيداز يوبكويتين المحدد 22
RNF31
بروتين إصبع الخاتم 31
ياب
بروتين مرتبط بـ Yes
سي دي كيه إن 2 إيه / بي
مثبط كيناز المعتمد على السيكلين 2 A/B
SUSD6
مجال السوشي يحتوي على 6
TMEM127
بروتين عبر الغشاء 127
WWP2
الليزاز البروتيني يوبكويتين E3 2 المحتوي على نطاق WW
mTORC1
المركب الآلي لهدف الراباميسين 1
CD248
مجموعة التمايز 248
أوبن
أوستيو بونتين
سيربين1
عضو 1 من عائلة سيربين
RGS5
منظم إشارات بروتين G 5
apCAFs
الخلايا الليفية المرتبطة بالسرطان التي تقدم المستضدات
مستقبل عامل نخر الورم، عائلة السوبر، العضو 4 (TNFRSF4)
سي بي جي
سيتوزين-فوسفات-غوانين
PL1
جزيئات الفوسفوليبيد النانوية 1
جيتير
مستقبل عامل نخر الورم الناتج عن الجلوكوكورتيكويد
PLG
بوليمر (لاكتيد-كوجلايكوليد)
PLH
بولى-إل-هيستيدين
إيدو
إندولامين 2,3-دي أوكسيجيناز
mPEG2k-DSPE
ميثوكسي بولي إيثيلين غليكول
2000-ديستيارويلفوسفاتيديل إيثانول أمين
mPEG2k
ERCC1
مجموعة التكامل المتقاطع لإصلاح الاستئصال 1
سي بي جي
سيتوزين-فوسفات-غوانين
PL1
جزيئات الفوسفوليبيد النانوية 1
نقاط الذكاء الاصطناعي
نقاط الانبعاث الناتجة عن التجميع
HMGB1
مجموعة الصناديق عالية الحركة 1
مارت-1
ميلان-أ
CCL22
الليغاند 22 لمولد الكيموكين من نوع C-C
الحمض النووي الريبي غير المشفر الطويل
RNA غير المشفر الطويل
شكر وتقدير
نود أن نعبر عن امتناننا للدكتورة روباينجي فيرما من وحدة الاتصالات الطبية والعلمية، دعم البحث في نظام الصحة الوطني، سنغافورة، على مراجعتها الدقيقة وتحريرها لمخطوطتنا من حيث دقة اللغة الإنجليزية.
مساهمات المؤلفين
كتب Q.L و D.K و S.L و M.A المسودة الأولى من الورقة (كتابة المسودة الأصلية). قام A.R.A و I.C و Y.T و X.N و Y.W و P.T و L.W بمراجعة الورقة بشكل نقدي والإشراف عليها. طور G.S و V.T و F.T و Z.Y و P.H الفكرة والمفهوم وقاموا بمراجعة الورقة (كتابة-مراجعة-تحرير).
تمويل
تم دعم هذا العمل من قبل البرنامج العام لمؤسسة العلوم الطبيعية الوطنية في الصين (82072640)، ومشروع الشباب المتميز لمؤسسة العلوم الطبيعية في هيلونغجيانغ (YQ2021H023)، والمشاريع الرئيسية الخاصة لتوجيه الابتكار التكنولوجي في مقاطعة شنشي (2021QFY01-03) ومشروع البحث السريري الرئيسي لمستشفى تانغدو (2021LCYJ008). كما تم دعم هذا العمل من قبل منحة المستوى 1 من وزارة التعليم في سنغافورة للدكتور غوتام سيثي.
توفر البيانات
لم يتم إنشاء أو تحليل أي مجموعات بيانات خلال الدراسة الحالية.
الإعلانات
موافقة الأخلاقيات والموافقة على المشاركة
غير قابل للتطبيق.
موافقة على النشر
غير قابل للتطبيق.
المصالح المتنافسة
يعلن المؤلفون عدم وجود مصالح متنافسة.
تفاصيل المؤلف
¹قسم جراحة الصدر، مستشفى تانغدو، جامعة الطب الجوية، 569 طريق شينسي، شيآن 710038، الصين قسم الطب التأهيلي، مركز تشونغتشينغ للصحة العامة، تشونغتشينغ، الصين قسم جراحة القولون والمستقيم، مستشفى هاربين الطبي الجامعي للسرطان، هاربين، الصين قسم الجراحة العامة، معهد التشخيص الدقيق وعلاج أورام الجهاز الهضمي، مركز كارسن الدولي للسرطان، مستشفى جامعة شنتشن العامة، جامعة شنتشن، شنتشن 518055، قوانغدونغ، الصين معهد شنغهاي لأمراض القلب، مستشفى تشونغشان، جامعة فودان، شنغهاي 200032، الصين قسم علاج الأورام بالإشعاع، مستشفى ومعهد شاندونغ للسرطان، جامعة شاندونغ الطبية الأولى، أكاديمية شاندونغ للعلوم الطبية، جينان 250000، شاندونغ، الصين إكسفيرا بيوساينسز، مجموعة الطب الانتقالي، 6 شارع تايد، بوسطن، MA 02210، الولايات المتحدة الأمريكية قسم الأورام الطبية، معهد دانا فاربر للسرطان، كلية هارفارد الطبية، بوسطن، MA 02115، الولايات المتحدة الأمريكية برنامج تطوير ووظيفة خلايا الدم، مركز فوكس تشيس للسرطان، فيلادلفيا، بنسلفانيا، الولايات المتحدة الأمريكية كلية الصحة العامة، جامعة بنديكتين، ليسل، الولايات المتحدة الأمريكية قسم علوم المسالك البولية ومركز فانكوفر للبروستاتا، جامعة كولومبيا البريطانية، فانكوفر، كولومبيا البريطانية V6H3Z6، كندا كلية كامينغ للطب، معهد أرني شاربونو لأبحاث السرطان، جامعة كالغاري، كالغاري، ألبرتا T2N 4Z6، كندا قسم العلوم الطبية، جامعة كالغاري، كالغاري، ألبرتا T2N 4Z6، كندا العنوان الحالي: مركز أبحاث السرطان بجامعة نانيانغ التكنولوجية (N2CR)، كلية يونغ لوو لين للطب، الجامعة الوطنية في سنغافورة، سنغافورة 117599، سنغافورة العنوان الحالي: قسم علم الأدوية، مدرسة يونغ لوو لين للطب، الجامعة الوطنية في سنغافورة، 16 طريق الطب، سنغافورة 117600، سنغافورة مختبر إشارات NF-kB، معهد البيولوجيا الجزيئية والخلوية (IMCB)، وكالة العلوم والتكنولوجيا والبحث (A*STAR)، 61 شارع بيوبوليس، بروتيوس، 138673 سنغافورة، جمهورية سنغافورة مدرسة الدراسات العليا، جامعة أوغوستا، 30912 أوغوستا، جورجيا، الولايات المتحدة الأمريكية قسم جراحة الأورام، مستشفى هاربين الطبي الجامعي للسرطان، هاربين، الصين المختبر الرئيسي لعلم المناعة الورمي في هيلونغجيانغ، هاربين، الصين
تاريخ الاستلام: 30 ديسمبر 2023 / تاريخ القبول: 15 مارس 2024 نُشر على الإنترنت: 02 أبريل 2024
References
Liu Y, et al. Emerging phagocytosis checkpoints in cancer immunotherapy. Signal Transduct Target Ther. 2023;8(1):104.
Kennedy LB, Salama AKS. A review of cancer immunotherapy toxicity. CA Cancer J Clin. 2020;70(2):86-104.
Mahoney KM, Rennert PD, Freeman GJ. Combination cancer immunotherapy and new immunomodulatory targets. Nat Rev Drug Discov. 2015;14(8):561-84.
Webster RM. The immune checkpoint inhibitors: where are we now? Nat Rev Drug Discov. 2014;13(12):883-4.
Zhang Q, et al. Immune and Clinical features of CD96 expression in Glioma by in silico analysis. Front Bioeng Biotechnol. 2020;8:592.
Galipeau J, Sensébé L. Mesenchymal stromal cells: Clinical challenges and Therapeutic opportunities. Cell Stem Cell. 2018;22(6):824-33.
Liotta F, et al. Toll-like receptors 3 and 4 are expressed by human bone marrow-derived mesenchymal stem cells and can inhibit their T-cell modulatory activity by impairing notch signaling. Stem Cells. 2008;26(1):279-89.
Majeti R, et al. CD47 is an adverse prognostic factor and therapeutic antibody target on human acute myeloid leukemia stem cells. Cell. 2009;138(2):286-99.
Barkal AA, et al. CD24 signalling through macrophage Siglec-10 is a target for cancer immunotherapy. Nature. 2019;572(7769):392-6.
Gordon SR, et al. PD-1 expression by tumour-associated macrophages inhibits phagocytosis and tumour immunity. Nature. 2017;545(7655):495-9.
Barkal AA, et al. Engagement of MHC class I by the inhibitory receptor LILRB1 suppresses macrophages and is a target of cancer immunotherapy. Nat Immunol. 2018;19(1):76-84.
Lin H, et al. Stanniocalcin 1 is a phagocytosis checkpoint driving tumor immune resistance. Cancer Cell. 2021;39(4):480-e4936.
Theruvath J, et al. Anti-GD2 synergizes with CD47 blockade to mediate tumor eradication. Nat Med. 2022;28(2):333-44.
Gardner A, de Mingo Á, Pulido, Ruffell B. Dendritic cells and their role in Immunotherapy. Front Immunol. 2020;11:924.
Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39(1):1-10.
Nakayama M. Antigen Presentation by MHC-Dressed cells. Front Immunol. 2014;5:672.
Lin A, Loré K. Granulocytes: New members of the Antigen-presenting cell family. Front Immunol. 2017;8:1781.
Broz ML, et al. Dissecting the tumor myeloid compartment reveals rare activating antigen-presenting cells critical for T cell immunity. Cancer Cell. 2014;26(5):638-52.
DeNardo DG, Ruffell B. Macrophages as regulators of tumour immunity and immunotherapy. Nat Rev Immunol. 2019;19(6):369-82.
Ruffell B, Coussens LM. Macrophages and therapeutic resistance in cancer. Cancer Cell. 2015;27(4):462-72.
Sánchez-Paulete AR, et al. Cancer Immunotherapy with Immunomodulatory Anti-CD137 and Anti-PD-1 monoclonal antibodies requires BATF3-Dependent dendritic cells. Cancer Discov. 2016;6(1):71-9.
Hildner K, et al. Batf3 deficiency reveals a critical role for CD8alpha + dendritic cells in cytotoxic T cell immunity. Science. 2008;322(5904):1097-100.
Roberts EW, et al. Critical role for CD103(+)/CD141(+) dendritic cells bearing CCR7 for Tumor Antigen Trafficking and priming of T cell immunity in Melanoma. Cancer Cell. 2016;30(2):324-36.
Salmon H, et al. Expansion and activation of CD103(+) dendritic cell progenitors at the Tumor Site enhances tumor responses to therapeutic PD-L1 and BRAF inhibition. Immunity. 2016;44(4):924-38.
de Pulido M. TIM-3 regulates CD103(+) dendritic cell function and response to chemotherapy in breast Cancer. Cancer Cell. 2018;33(1):60-74.e6.
Garris CS, et al. Successful Anti-PD-1 Cancer Immunotherapy requires T cell-dendritic cell crosstalk involving the cytokines IFN- and IL-12. Immunity. 2018;49(6):1148-e11617.
Spranger S, et al. Tumor-residing Batf3 dendritic cells are required for effector cell trafficking and adoptive cell therapy. Cancer Cell. 2017;31(5):711-e7234.
Chow MT, et al. Intratumoral Activity of the CXCR3 chemokine system is required for the efficacy of Anti-PD-1 therapy. Immunity. 2019;50(6):1498-e15125.
Xia Y, et al. Engineering macrophages for Cancer Immunotherapy and Drug Delivery. Adv Mater. 2020;32(40):e2002054.
Gao J, Liang Y, Wang L. Shap Polarization Tumor-Associated Macrophages Cancer Immunotherapy Front Immunol. 2022;13:888713.
Kumari N, Choi SH. Tumor-associated macrophages in cancer: recent advancements in cancer nanoimmunotherapies. J Exp Clin Cancer Res. 2022;41(1):68.
Li L, Ma SR, Yu ZL. Targeting the lipid metabolic reprogramming of tumorassociated macrophages: a novel insight into cancer immunotherapy. Cell Oncol (Dordr); 2023.
Pei L, et al. Roles of cancer-associated fibroblasts (CAFs) in anti- PD-1/PD-L1 immunotherapy for solid cancers. Mol Cancer. 2023;22(1):29.
Zhang H, et al. Define cancer-associated fibroblasts (CAFs) in the tumor microenvironment: new opportunities in cancer immunotherapy and advances in clinical trials. Mol Cancer. 2023;22(1):159.
Raskov H, et al. Cancer-Associated fibroblasts and Tumor-Associated macrophages in Cancer and Cancer Immunotherapy. Front Oncol. 2021;11:668731.
Thiery J. Modulation of the antitumor immune response by cancer-associated fibroblasts: mechanisms and targeting strategies to hamper their immunosuppressive functions. Explor Target Antitumor Ther. 2022;3(5):598-629.
Wang Q, et al. Role of tumor microenvironment in cancer progression and therapeutic strategy. Cancer Med. 2023;12(10):11149-65.
Han S et al. Tumor Microenvironment Regulation and Cancer Targeting Therapy based on nanoparticles. J Funct Biomater, 2023. 14(3).
Li Z, Yin P. Tumor microenvironment diversity and plasticity in cancer multidrug resistance. Biochim Biophys Acta Rev Cancer. 2023;1878(6):188997.
Yang R, et al. Tumor microenvironment responsive metal nanoparticles in cancer immunotherapy. Front Immunol. 2023;14:1237361.
Zhang Z, et al. Involvement of inflammasomes in tumor microenvironment and tumor therapies. J Hematol Oncol. 2023;16(1):24.
Jin HR, et al. Lipid metabolic reprogramming in tumor microenvironment: from mechanisms to therapeutics. J Hematol Oncol. 2023;16(1):103.
Arner EN, Rathmell JC. Metabolic programming and immune suppression in the tumor microenvironment. Cancer Cell. 2023;41(3):421-33.
Lin MJ, et al. Cancer vaccines: the next immunotherapy frontier. Nat Cancer. 2022;3(8):911-26.
Beck JD, et al. mRNA therapeutics in cancer immunotherapy. Mol Cancer. 2021;20(1):69.
Siminiak N, et al. Immunotherapy in Ovarian Cancer. Arch Immunol Ther Exp (Warsz). 2022;70(1):19.
Mauricio D, et al. Immunotherapy in Cervical Cancer. Curr Oncol Rep. 2021;23(6):61.
Bockorny B, Grossman JE, Hidalgo M. Facts and hopes in Immunotherapy of Pancreatic Cancer. Clin Cancer Res. 2022;28(21):4606-17.
Yang M, et al. The application of nanoparticles in cancer immunotherapy: targeting tumor microenvironment. Bioact Mater. 2021;6(7):1973-87.
Overchuk M, Zheng G. Overcoming obstacles in the tumor microenvironment: recent advancements in nanoparticle delivery for cancer theranostics. Biomaterials. 2018;156:217-37.
Matsumura Y, Maeda H. A new concept for macromolecular therapeutics in cancer chemotherapy: mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res. 1986;46(12 Pt 1):6387-92.
Prabhakar U, et al. Challenges and key considerations of the enhanced permeability and retention effect for nanomedicine drug delivery in oncology. Cancer Res. 2013;73(8):2412-7.
Yang S, Gao H. Nanoparticles for modulating tumor microenvironment to improve drug delivery and tumor therapy. Pharmacol Res. 2017;126:97-108.
Chen Q , et al. Remodeling the Tumor Microenvironment with Emerging Nanotherapeutics. Trends Pharmacol Sci. 2018;39(1):59-74.
Li M, et al. Nanoparticles designed to regulate tumor microenvironment for cancer therapy. Life Sci. 2018;201:37-44.
Guo B, et al. Cuproptosis Induced by ROS responsive nanoparticles with Elesclomol and Copper Combined with APD-L1 for enhanced Cancer Immunotherapy. Adv Mater. 2023;35(22):e2212267.
Wang-Bishop L, et al. STING-activating nanoparticles normalize the vascularimmune interface to potentiate cancer immunotherapy. Sci Immunol. 2023;8(83):eadd1153.
Ding , et al. ZIF-8 nanoparticles evoke pyroptosis for high-efficiency Cancer Immunotherapy. Angew Chem Int Ed Engl. 2023;62(10):e202215307.
Liu J et al. Ultrathin clay nanoparticles-mediated mutual reinforcement of ferroptosis and Cancer immunotherapy. Adv Mater, 2023: p. e2309562.
Huang A, et al. Engineered apoptosis-bioinspired nanoparticles initiate Immune Cascade for Cancer Immunotherapy of Malignant ascites. ACS Appl Mater Interfaces. 2023;15(8):10371-82.
Liu D et al. Tumor Microenvironment-Responsive nanoparticles amplifying STING Signaling Pathway for Cancer Immunotherapy. Adv Mater, 2023: p. e2304845.
Sun Y, et al. Sialic acid-targeted cyclodextrin-based nanoparticles deliver CSF-1R siRNA and reprogram tumour-associated macrophages for immunotherapy of prostate cancer. Eur J Pharm Sci. 2023;185:106427.
Liu C, et al. Microfluidic sonication to assemble Exosome membranecoated nanoparticles for Immune evasion-mediated targeting. Nano Lett. 2019;19(11):7836-44.
Li M et al. Signaling pathways in macrophages: molecular mechanisms and therapeutic targets MedComm (2020), 2023;4(5):e349.
Ginhoux F, Guilliams M. Tissue-Resident Macrophage Ontogeny and Homeostasis. Immunity. 2016;44(3):439-49.
Epelman S, Lavine KJ, Randolph GJ. Origin and functions of tissue macrophages. Immunity. 2014;41(1):21-35.
Italiani P, Boraschi D. From monocytes to M1/M2 macrophages: phenotypical vs. functional differentiation. Front Immunol. 2014;5:514.
Schulz , et al. A lineage of myeloid cells independent of myb and hematopoietic stem cells. Science. 2012;336(6077):86-90.
Sieweke MH, Allen JE. Beyond stem cells: self-renewal of differentiated macrophages. Science. 2013;342(6161):1242974.
Zhan C et al. Antitumor therapy for breast cancer: focus on tumor-associated macrophages and nanosized drug delivery systems. Cancer Med, 2023.
Wang N, et al. Research trends in pharmacological modulation of tumorassociated macrophages. Clin Transl Med. 2021;11(1):e288.
Vitale I, et al. Macrophages and metabolism in the Tumor Microenvironment. Cell Metab. 2019;30(1):36-50.
Wang J, et al. Crosstalk between cancer and immune cells: role of tumorassociated macrophages in the tumor microenvironment. Cancer Med. 2019;8(10):4709-21.
Wu T, Dai Y. Tumor microenvironment and therapeutic response. Cancer Lett. 2017;387:61-8.
Munir MT et al. Tumor-Associated macrophages as multifaceted regulators of breast tumor growth. Int J Mol Sci, 2021. 22(12).
Qiu SQ, et al. Tumor-associated macrophages in breast cancer: innocent bystander or important player? Cancer Treat Rev. 2018;70:178-89.
Wang C, et al. Macrophage balance fraction determines the degree of immunosuppression and metastatic ability of breast cancer. Int Immunopharmacol. 2021;97:107682.
Steenbrugge J, et al. Anti-inflammatory signaling by mammary tumor cells mediates prometastatic macrophage polarization in an innovative intraductal mouse model for triple-negative breast cancer. J Exp Clin Cancer Res. 2018;37(1):191.
Shu Y, Cheng P. Targeting tumor-associated macrophages for cancer immunotherapy Biochimica et Biophysica Acta (BBA) – Reviews on Cancer, 2020;1874(2):188434.
Nascimento C, et al. Reprogramming of tumor-associated macrophages by polyaniline-coated iron oxide nanoparticles applied to treatment of breast cancer. Int J Pharm. 2023;636:122866.
Shang Y, et al. Bioengineered Nanospores selectively blocking LC3-Associated phagocytosis in Tumor-Associated macrophages Potentiate Antitumor Immunity. ACS Nano. 2023;17(11):10872-87.
Liu Y, et al. Multifunctional nanoparticles inhibit tumor and tumor-associated macrophages for triple-negative breast cancer therapy. J Colloid Interface Sci. 2024;657:598-610.
Liang DS, et al. Targeted delivery of pexidartinib to tumor-associated macrophages via legumain-sensitive dual-coating nanoparticles for cancer immunotherapy. Colloids Surf B Biointerfaces. 2023;226:113283.
Sun , et al. The role of cancer-associated fibroblasts in tumorigenesis of gastric cancer. Cell Death Dis. 2022;13(10):874.
Gu J, et al. The role of PKM2 nuclear translocation in the constant activation of the NF-kB signaling pathway in cancer-associated fibroblasts. Cell Death Dis. 2021;12(4):291.
Bu L, et al. Biological heterogeneity and versatility of cancer-associated fibroblasts in the tumor microenvironment. Oncogene. 2019;38(25):4887-901.
Kalluri R. The biology and function of fibroblasts in cancer. Nat Rev Cancer. 2016;16(9):582-98.
Kobayashi H, et al. Cancer-associated fibroblasts in gastrointestinal cancer. Nat Rev Gastroenterol Hepatol. 2019;16(5):282-95.
Zhang T, et al. Cancer-associated fibroblasts in pancreatic ductal adenocarcinoma. Cell Death Dis. 2022;13(10):897.
Öhlund D , et al. Distinct populations of inflammatory fibroblasts and myofibroblasts in pancreatic cancer. J Exp Med. 2017;214(3):579-96.
Biffi G, et al. IL1-Induced JAK/STAT signaling is antagonized by TGF to shape CAF heterogeneity in pancreatic ductal adenocarcinoma. Cancer Discov. 2019;9(2):282-301.
Elyada E, et al. Cross-species single-cell analysis of pancreatic ductal adenocarcinoma reveals Antigen-Presenting Cancer-Associated fibroblasts. Cancer Discov. 2019;9(8):1102-23.
Fang Z, et al. Signaling pathways in cancer-associated fibroblasts: recent advances and future perspectives. Cancer Commun. 2023;43(1):3-41.
Ai W, et al. Modulation of cancer-associated fibroblasts by nanodelivery system to enhance efficacy of tumor therapy. Nanomed (Lond). 2023;18(15):1025-39.
Geng , et al. Safe engineering of cancer-associated fibroblasts enhances checkpoint blockade immunotherapy. J Control Release. 2023;356:272-87.
Jian C et al. Biomimetic Nanoplatform for Dual-Targeted Clearance of Activated and Senescent Cancer-Associated Fibroblasts to Improve Radiation Resistance in Breast Cancer Small, 2024: p. e2309279.
Hu M, et al. Salvianolic acid B-loaded polydopamine-modified hollow mesoporous organic silica nanoparticles for treatment of breast cancer metastasis via suppressing cancer-associated fibroblasts. Eur J Pharm Sci. 2024;192:106641.
Hinshaw DC, Shevde LA. The Tumor Microenvironment innately modulates Cancer Progression. Cancer Res. 2019;79(18):4557-66.
Wang J, et al. The clinical significance of tumor-infiltrating neutrophils and neutrophil-to-CD8 + lymphocyte ratio in patients with resectable esophageal squamous cell carcinoma. J Transl Med. 2014;12:7.
Deniset JF, Kubes P. Recent Adv Underst Neutrophils F1000Res. 2016;5:2912.
Uribe-Querol E, Rosales C. Neutrophils in Cancer: two sides of the same Coin. J Immunol Res. 2015;2015:983698.
Cools-Lartigue J, et al. Neutrophil extracellular traps in cancer progression. Cell Mol Life Sci. 2014;71(21):4179-94.
Jin W, et al. Tumor-infiltrating NETs predict postsurgical survival in patients with pancreatic ductal adenocarcinoma. Ann Surg Oncol. 2019;26(2):635-43.
Fridlender ZG, Albelda SM. Tumor-associated neutrophils: friend or foe? Carcinogenesis. 2012;33(5):949-55.
Demers M, et al. Priming of neutrophils toward NETosis promotes tumor growth. Oncoimmunology. 2016;5(5):e1134073.
He M, et al. Peritumoral stromal neutrophils are essential for c-Met-elicited metastasis in human hepatocellular carcinoma. Oncoimmunology. 2016;5(10):e1219828.
Schauer C, et al. Aggregated neutrophil extracellular traps limit inflammation by degrading cytokines and chemokines. Nat Med. 2014;20(5):511-7.
Ralph SJ, Reynolds MJ. Intratumoral pro-oxidants promote cancer immunotherapy by recruiting and reprogramming neutrophils to eliminate tumors. Cancer Immunol Immunother. 2023;72(3):527-42.
Benguigui et al. Interferon-stimulated neutrophils as a predictor of immunotherapy response. Cancer Cell, 2024.
Huntington ND, Cursons J, Rautela J. The cancer-natural killer cell immunity cycle. Nat Rev Cancer. 2020;20(8):437-54.
Huntington ND, Vosshenrich CA, Di Santo JP. Developmental pathways that generate natural-killer-cell diversity in mice and humans. Nat Rev Immunol. 2007;7(9):703-14.
Pfefferle , et al. Intra-lineage plasticity and functional reprogramming maintain natural killer cell repertoire diversity. Cell Rep. 2019;29(8):2284-e22944.
Gil M, Kim KE. Interleukin-18 is a prognostic biomarker correlated with CD8+T cell and natural killer cell infiltration in skin cutaneous melanoma Journal of clinical medicine, 2019;8(11):1993.
Cursons J, et al. A gene signature Predicting Natural Killer Cell Infiltration and Improved Survival in Melanoma patients. Cancer Immunol Res. 2019;7(7):1162-74.
Lee H, et al. Integrated molecular and immunophenotypic analysis of NK cells in anti-PD-1 treated metastatic melanoma patients. Oncoimmunology. 2019;8(2):e1537581.
Li B et al. Natural killer cell and stroma abundance are independently prognostic and predict gastric cancer chemotherapy benefit. JCl Insight, 2020. 5(9).
Ran GH, et al. Natural killer cell homing and trafficking in tissues and tumors: from biology to application. Signal Transduct Target Therapy. 2022;7(1):205.
Scoville SD, Freud AG, Caligiuri MA. Model Hum Nat Killer Cell Dev Era Innate Lymphoid Cells Front Immunol. 2017;8:360.
Stokic-Trtica V, Diefenbach A, Klose CSN. NK Cell Dev Times Innate Lymphoid Cell Divers Front Immunol. 2020;11:813.
Vivier E, et al. Innate lymphoid cells: 10 years on. Cell. 2018;174(5):1054-66.
Freud AG, et al. The Broad Spectrum of Human Natural Killer Cell Diversity. Immunity. 2017;47(5):820-33.
Björkström NK, Ljunggren HG, Michaëlsson J. Emerging insights into natural killer cells in human peripheral tissues. Nat Rev Immunol. 2016;16(5):310-20.
Yu J, Freud AG, Caligiuri MA. Location and cellular stages of natural killer cell development. Trends Immunol. 2013;34(12):573-82.
Vivier E, et al. Functions of natural killer cells. Nat Immunol. 2008;9(5):503-10.
Fang F, Xiao W, Tian Z. NK cell-based immunotherapy for cancer. Semin Immunol. 2017;31:37-54.
Li Y, et al. Natural killer cells: friend or foe in metabolic diseases? Front Immunol. 2021;12:614429.
Shimasaki N, Jain A, Campana D. NK cells for cancer immunotherapy. Nat Rev Drug Discov. 2020;19(3):200-18.
Maskalenko NA, Zhigarev D, Campbell KS. Harnessing natural killer cells for cancer immunotherapy: dispatching the first responders. Nat Rev Drug Discov. 2022;21(8):559-77.
Pockley AG, Vaupel P, Multhoff G. NK cell-based therapeutics for lung cancer. Expert Opin Biol Ther. 2020;20(1):23-33.
Muntasell A, et al. NK Cell infiltrates and HLA Class I expression in primary HER2(+) breast Cancer Predict and Uncouple Pathological Response and Disease-free survival. Clin Cancer Res. 2019;25(5):1535-45.
Liu P, Chen L, Zhang H. Natural killer cells in Liver Disease and HepatocelIular Carcinoma and the NK cell-based immunotherapy. J Immunol Res. 2018;2018:p1206737.
Ali TH, et al. Enrichment of CD56(dim)KIR + CD57 + highly cytotoxic NK cells in tumour-infiltrated lymph nodes of melanoma patients. Nat Commun. 2014;5:5639.
Terrén I et al. NK Cell-based immunotherapy in renal cell carcinoma. Cancers (Basel), 2020. 12(2).
Lim SA, et al. Lipid metabolism in T cell signaling and function. Nat Chem Biol. 2022;18(5):470-81.
Ando M , et al. Memory T cell, exhaustion, and tumor immunity. Immunological Med. 2020;43(1):1-9.
Franco F, et al. Metabolic and epigenetic regulation of T-cell exhaustion. Nat Metabolism. 2020;2(10):1001-12.
Douka S, et al. Lipid nanoparticle-mediated messenger RNA delivery for ex vivo engineering of natural killer cells. J Control Release. 2023;361:455-69.
Shamalov K, et al. Noninvasive Tracking of Natural Killer cells using gold nanoparticles. ACS Omega. 2021;6(43):28507-14.
Kim KS, et al. Cationic nanoparticle-mediated activation of natural killer cells for Effective Cancer Immunotherapy. ACS Appl Mater Interfaces. 2020;12(51):56731-40.
Sun , et al. Acid-switchable nanoparticles induce self-adaptive aggregation for enhancing antitumor immunity of natural killer cells. Acta Pharm Sin B. 2023;13(7):3093-105.
Liu GW, et al. Lipid nanoparticles for nucleic acid delivery to endothelial cells. Pharm Res. 2023;40(1):3-25.
Stoltz JF, et al. Introduction to endothelial cell biology. Clin Hemorheol Microcirc. 2007;37(1-2):5-8.
Martin FA, Murphy RP, Cummins PM. Thrombomodulin and the vascular endothelium: insights into functional, regulatory, and therapeutic aspects. Am J Physiol Heart Circ Physiol. 2013;304(12):H1585-97.
Maroney SA, Mast AE. Expression of tissue factor pathway inhibitor by endothelial cells and platelets. Transfus Apher Sci. 2008;38(1):9-14.
Mohan Rao LV, Esmon CT, Pendurthi UR. Endothelial cell protein C receptor: a multiliganded and multifunctional receptor. Blood. 2014;124(10):1553-62.
Bremnes RM, et al. The role of tumor stroma in cancer progression and prognosis: emphasis on carcinoma-associated fibroblasts and non-small cell lung cancer. J Thorac Oncol. 2011;6(1):209-17.
Pietras K, Ostman A. Hallmarks of cancer: interactions with the tumor stroma. Exp Cell Res. 2010;316(8):1324-31.
McAllister SS, Weinberg RA. The tumour-induced systemic environment as a critical regulator of cancer progression and metastasis. Nat Cell Biol. 2014;16(8):717-27.
Dillekås H, Rogers MS, Straume O. Are of deaths from cancer caused by metastases? Cancer Med. 2019;8(12):5574-6.
Khorana AA, et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-4.
Tisdale MJ. Cachexia in cancer patients. Nat Rev Cancer. 2002;2(11):862-71.
Eilken HM, et al. Pericytes regulate VEGF-induced endothelial sprouting through VEGFR1. Nat Commun. 2017;8(1):1574.
Rouget C. Memoire sur les development, la structure et la proprietes physiologiques des capillaires sanguines et lymphatiques. Arch Physiol, 1873: p. 603-63.
Zimmermann KW. Der Feinere Bau Der Blutcapillaren. Z für Anatomie und Entwicklungsgeschichte. 1923;68:29-109.
Schrimpf C, et al. The role of pericyte detachment in vascular rarefaction. J Vasc Res. 2014;51(4):247-58.
Hirschi KK, D’Amore PA. Pericytes in the microvasculature. Cardiovascular Res. 1996;32(4):687-98.
Díaz-Flores L, et al. Microvascular pericytes, a review of their morphological and functional characteristics. Histology and histopathology; 1991.
Birbrair A, et al. How plastic are pericytes? Stem Cells Dev. 2017;26(14):1013-9.
Birbrair A, et al. Pericytes at the intersection between tissue regeneration and pathology. Clin Sci. 2015;128(2):81-93.
Picoli CC et al. Pericytes cross-talks within the tumor microenvironment Biochimica et Biophysica Acta (BBA)-Reviews on Cancer, 2021;1876(2):188608.
Jiang Z et al. Pericytes in the tumor microenvironment. Cancer Lett, 2023: p. 216074.
Chen Z, Xu XH, Hu J. Role of pericytes in angiogenesis: focus on cancer angiogenesis and anti-angiogenic therapy. Neoplasma. 2016;63(2):173-82.
Hong CL, et al. CD248 regulates wnt signaling in Pericytes to Promote Angiogenesis and Tumor Growth in Lung Cancer. Cancer Res. 2022;82(20):3734-50.
Meng YM, et al. Hexokinase 2-driven glycolysis in pericytes activates their contractility leading to tumor blood vessel abnormalities. Nat Commun. 2021;12(1):6011.
Dasgupta S, et al. RGS5-TGF -Smad axis switches pro- to anti-apoptotic signaling in tumor-residing pericytes, assisting tumor growth. Cell Death Differ. 2021;28(11):3052-76.
Pillay J, et al. Immune suppression by neutrophils and granulocytic myeloidderived suppressor cells: similarities and differences. Cell Mol Life Sci. 2013;70(20):3813-27.
Gabrilovich DI, Nagaraj S. Myeloid-derived suppressor cells as regulators of the immune system. Nat Rev Immunol. 2009;9(3):162-74.
Rodriguez PC, et al. Arginase I-producing myeloid-derived suppressor cells in renal cell carcinoma are a subpopulation of activated granulocytes. Cancer Res. 2009;69(4):1553-60.
Youn JI, et al. Characterization of the nature of granulocytic myeloid-derived suppressor cells in tumor-bearing mice. J Leukoc Biol. 2012;91(1):167-81.
Gabrilovich DI, Ostrand-Rosenberg S, Bronte V. Coordinated regulation of myeloid cells by tumours. Nat Rev Immunol. 2012;12(4):253-68.
Bronte V, et al. Recommendations for myeloid-derived suppressor cell nomenclature and characterization standards. Nat Commun. 2016;7:12150.
Kumar V, et al. The nature of myeloid-derived suppressor cells in the Tumor Microenvironment. Trends Immunol. 2016;37(3):208-20.
Condamine T, et al. Regulation of tumor metastasis by myeloid-derived suppressor cells. Annu Rev Med. 2015;66:97-110.
Condamine T et al. Lectin-type oxidized LDL receptor-1 distinguishes population of human polymorphonuclear myeloid-derived suppressor cells in cancer patients. Sci Immunol, 2016. 1(2).
Corzo CA, et al. HIF-1a regulates function and differentiation of myeloidderived suppressor cells in the tumor microenvironment. J Exp Med. 2010;207(11):2439-53.
Hossain F, et al. Inhibition of fatty acid oxidation modulates immunosuppressive functions of myeloid-derived suppressor cells and enhances Cancer therapies. Cancer Immunol Res. 2015;3(11):1236-47.
Zhou J, et al. Hepatoma-intrinsic CCRK inhibition diminishes myeloid-derived suppressor cell immunosuppression and enhances immune-checkpoint blockade efficacy. Gut. 2018;67(5):931-44.
Wu C, et al. Repolarization of myeloid derived suppressor cells via magnetic nanoparticles to promote radiotherapy for glioma treatment. Nanomedicine. 2019;16:126-37.
Ding , et al. Augmenting immunogenic cell death and alleviating myeloidderived suppressor cells by Sono-Activatable Semiconducting Polymer Nanopartners for Immunotherapy. Adv Mater. 2023;35(33):e2302508.
Zuo H, et al. Circumventing myeloid-derived suppressor cell-mediated immunosuppression using an oxygen-generated and -economized nanoplatform. ACS Appl Mater Interfaces. 2020;12(50):55723-36.
Habanjar O et al. Crosstalk of inflammatory cytokines within the breast Tumor Microenvironment. Int J Mol Sci, 2023. 24(4).
Zhang JM, An J. Cytokines, inflammation, and pain. Int Anesthesiol Clin. 2007;45(2):27-37.
Raman D, Sobolik-Delmaire T, Richmond A. Chemokines in health and disease. Exp Cell Res. 2011;317(5):575-89.
Bachelerie F, et al. International Union of Basic and Clinical Pharmacology. [corrected]. LXXXIX. Update on the extended family of chemokine receptors
and introducing a new nomenclature for atypical chemokine receptors. Pharmacol Rev. 2014;66(1):1-79.
Mélik-Parsadaniantz S, Rostène W. Chemokines and neuromodulation. J Neuroimmunol. 2008;198(1-2):62-8.
Zlotnik A, Yoshie O. The chemokine superfamily revisited. Immunity. 2012;36(5):705-16.
Kaneko N, et al. The role of interleukin-1 in general pathology. Inflamm Regen. 2019;39:12.
Akdis et al. Interleukins, from 1 to 37 , and interferon- : receptors, functions, and roles in diseases J Allergy Clin Immunol, 2011;127(3):701-21.e1-70.
Shin E, Koo JS. The role of Adipokines and bone marrow adipocytes in breast Cancer bone metastasis. Int J Mol Sci, 2020. 21(14).
Blüher M, Mantzoros CS. From leptin to other adipokines in health and disease: facts and expectations at the beginning of the 21st century. Metabolism. 2015;64(1):131-45.
Mancuso P. The role of adipokines in chronic inflammation. Immunotargets Ther. 2016;5:47-56.
Barchetta I, et al. Sick fat: the good and the bad of old and new circulating markers of adipose tissue inflammation. J Endocrinol Invest. 2019;42(11):1257-72.
Nehme R et al. Targeting adiponectin in breast Cancer. Biomedicines, 2022. 10(11).
Artac M, Altundag K. Leptin and breast cancer: an overview. Med Oncol. 2012;29(3):1510-4.
Ferrer I, et al. Transforming growth factor-alpha (TGF-alpha) and epidermal growth factor-receptor (EGF-R) immunoreactivity in normal and pathologic brain. Prog Neurobiol. 1996;49(2):99-123.
MaruYama T, Chen W, Shibata H. TGF- Cancer Immunotherapy Biol Pharm Bull. 2022;45(2):155-61.
Isaacs A, Lindenmann J. Virus interference. I. The interferon. Proc R Soc Lond B Biol Sci. 1957;147(927):258-67.
Schroder K, et al. Interferon-gamma: an overview of signals, mechanisms and functions. J Leukoc Biol. 2004;75(2):163-89.
Peng S, et al. Tumor-microenvironment-responsive nanomedicine for enhanced Cancer Immunotherapy. Adv Sci (Weinh). 2022;9(1):e2103836.
Mu J, et al. Development of endogenous enzyme-responsive nanomaterials for theranostics. Chem Soc Rev. 2018;47(15):5554-73.
Hu J, Zhang G, Liu S. Enzyme-responsive polymeric assemblies, nanoparticles and hydrogels. Chem Soc Rev. 2012;41(18):5933-49.
Shahriari M, et al. Enzyme responsive drug delivery systems in cancer treatment. J Control Release. 2019;308:172-89.
Qiu N, et al. Esterase-activated charge-reversal polymer for fibroblast-exempt Cancer Gene Therapy. Adv Mater. 2016;28(48):10613-22.
Luo Z, Dai Y, Gao H. Development and application of hyaluronic acid in tumor targeting drug delivery. Acta Pharm Sin B. 2019;9(6):1099-112.
Li H, et al. The relationship between MMP-2 and MMP-9 expression levels with breast cancer incidence and prognosis. Oncol Lett. 2017;14(5):5865-70.
Pham HT, Block NL, Lokeshwar VB. Tumor-derived hyaluronidase: a diagnostic urine marker for high-grade bladder cancer. Cancer Res. 1997;57(4):778-83.
Moreira AM et al. The Extracellular Matrix: an accomplice in gastric Cancer Development and Progression. Cells, 2020. 9(2).
Liu Y, et al. Tumor microenvironment-mediated immune tolerance in development and treatment of gastric cancer. Front Immunol. 2022;13:1016817.
Mohan V, Das A, Sagi I. Emerging roles of ECM remodeling processes in cancer. Semin Cancer Biol. 2020;62:192-200.
Sung JY, Cheong JH. The Matrisome is Associated with metabolic reprograming in stem-like phenotypes of gastric Cancer. Cancers (Basel), 2022. 14(6).
Moreira AM, et al. Proteomic identification of a gastric tumor ECM signature Associated with Cancer Progression. Front Mol Biosci. 2022;9:818552.
Jang , et al. Increased extracellular matrix density disrupts E-cadherin/ catenin complex in gastric cancer cells. Biomater Sci. 2018;6(10):2704-13.
Acerbi I, et al. Human breast cancer invasion and aggression correlates with ECM stiffening and immune cell infiltration. Integr Biol (Camb). 2015;7(10):1120-34.
Kuczek DE, et al. Collagen density regulates the activity of tumor-infiltrating cells. J Immunother Cancer. 2019;7(1):68.
Patel A, Sant S. Hypoxic tumor microenvironment: opportunities to develop targeted therapies. Biotechnol Adv. 2016;34(5):803-12.
Nelson DA, et al. Hypoxia and defective apoptosis drive genomic instability and tumorigenesis. Genes Dev. 2004;18(17):2095-107.
Saito G, Swanson JA, Lee K-D. Drug delivery strategy utilizing conjugation via reversible disulfide linkages: role and site of cellular reducing activities. Adv Drug Deliv Rev. 2003;55(2):199-215.
Wilson WR, Hay MP. Targeting hypoxia in cancer therapy. Nat Rev Cancer. 2011;11(6):393-410.
Naughton D. Drug targeting to hypoxic tissue using self-inactivating bioreductive delivery systems. Adv Drug Deliv Rev. 2001;53(2):229-33.
Vázquez-García I, et al. Ovarian cancer mutational processes drive sitespecific immune evasion. Nature. 2022;612(7941):778-86.
Li Q, et al. PRDM1/BLIMP1 induces cancer immune evasion by modulating the USP22-SPI1-PD-L1 axis in hepatocellular carcinoma cells. Nat Commun. 2022;13(1):7677.
Yang H, et al. RNF31 represses cell progression and immune evasion via YAP/ PD-L1 suppression in triple negative breast Cancer. J Exp Clin Cancer Res. 2022;41(1):364.
Choi SY, et al. Cancer-generated lactic acid: a regulatory, immunosuppressive metabolite? J Pathol. 2013;230(4):350-5.
Wang JX et al. Lactic acid and an acidic Tumor Microenvironment suppress Anticancer Immunity. Int J Mol Sci, 2020. 21(21).
Chen X, et al. A membrane-associated MHC-I inhibitory axis for cancer immune evasion. Cell. 2023;186(18):3903-e392021.
Zhang B et al. Tumor CEMIP drives immune evasion of colorectal cancer via MHC-I internalization and degradation. J Immunother Cancer, 2023. 11(1).
Quah HS, et al. Single cell analysis in head and neck cancer reveals potential immune evasion mechanisms during early metastasis. Nat Commun. 2023;14(1):1680.
Bergholz JS, et al. PI3Kß controls immune evasion in PTEN-deficient breast tumours. Nature. 2023;617(7959):139-46.
Barriga FM, et al. MACHETE identifies interferon-encompassing chromosome 9p21.3 deletions as mediators of immune evasion and metastasis. Nat Cancer. 2022;3(11):1367-85.
Liu HJ, et al. mTORC1 upregulates B7-H3/CD276 to inhibit antitumor T cells and drive tumor immune evasion. Nat Commun. 2023;14(1):1214.
Lidström T, et al. Extracellular galectin 4 drives Immune Evasion and promotes T-cell apoptosis in pancreatic Cancer. Cancer Immunol Res. 2023;11(1):72-92.
Vinay DS, et al. Immune evasion in cancer: mechanistic basis and therapeutic strategies. Sem Cancer Biol. 2015;35:S185-98.
Polyak K, et al. Breast tumor heterogeneity: causes and consequences. Breast Cancer Res. 2009;11:1-1.
Miller FR. Intratumor immunologic heterogeneity. Cancer Metastasis Rev. 1982;1:319-34.
Nicolson GL. Generation of phenotypic diversity and progression in metastatic tumor cells. Cancer Metastasis Rev. 1984;3:25-42.
Merlo LM, et al. Cancer as an evolutionary and ecological process. Nat Rev Cancer. 2006;6(12):924-35.
Sceneay J, et al. Primary tumor hypoxia recruits CD11b+/Ly6Cmed/ Ly6G + immune suppressor cells and compromises NK cell cytotoxicity in the premetastatic niche. Cancer Res. 2012;72(16):3906-11.
Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340(6):448-54.
Dunn GP, Old U, Schreiber RD. The three Es of cancer immunoediting. Annu Rev Immunol. 2004;22:329-60.
Lauritzsen GF, et al. Clonal deletion of thymocytes as a tumor escape mechanism. Int J Cancer. 1998;78(2):216-22.
Hegde PS, Chen DS. Top 10 challenges in cancer immunotherapy. Immunity. 2020;52(1):17-35.
Rao L, et al. Activating macrophage-mediated Cancer Immunotherapy by genetically edited nanoparticles. Adv Mater. 2020;32(47):e2004853.
Yang K, et al. Zinc cyclic di-AMP nanoparticles target and suppress tumours via endothelial STING activation and tumour-associated macrophage reinvigoration. Nat Nanotechnol. 2022;17(12):1322-31.
Cao M, et al. Ginseng-derived nanoparticles alter macrophage polarization to inhibit melanoma growth. J Immunother Cancer. 2019;7(1):326.
Zhang Y, et al. Macrophage-membrane-coated nanoparticles for Tumortargeted chemotherapy. Nano Lett. 2018;18(3):1908-15.
Jiang Q, et al. Platelet membrane-camouflaged magnetic nanoparticles for ferroptosis-enhanced Cancer Immunotherapy. Small. 2020;16(22):e2001704.
Melamed JR, et al. Ionizable lipid nanoparticles deliver mRNA to pancreatic cells via macrophage-mediated gene transfer. Sci Adv. 2023;9(4):eade1444.
Chen C, et al. Tumor-Associated-Macrophage-membrane-coated nanoparticles for improved photodynamic immunotherapy. Nano Lett. 2021;21(13):5522-31.
Ramesh A, et al. CSF1R- and SHP2-Inhibitor-loaded nanoparticles enhance cytotoxic activity and phagocytosis in Tumor-Associated macrophages. Adv Mater. 2019;31(51):e1904364.
Zanganeh S, et al. Iron oxide nanoparticles inhibit tumour growth by inducing pro-inflammatory macrophage polarization in tumour tissues. Nat Nanotechnol. 2016;11(11):986-94.
Chim LK, et al. Tumor-associated macrophages induce inflammation and drug resistance in a mechanically tunable engineered model of osteosarcoma. Biomaterials. 2023;296:122076.
Rohila D, et al. Syk Inhibition reprograms Tumor-Associated macrophages and overcomes Gemcitabine-Induced Immunosuppression in Pancreatic Ductal Adenocarcinoma. Cancer Res. 2023;83(16):2675-89
Xie R, et al. Furin-instructed aggregated gold nanoparticles for re-educating tumor associated macrophages and overcoming breast cancer chemoresistance. Biomaterials. 2021;275:120891.
Shen W, et al. Metabolic homeostasis-regulated nanoparticles for antibody-independent Cancer Radio-Immunotherapy. Adv Mater. 2022;34(51):e2207343.
Sun M, et al. Fibroblast activation Protein-a responsive peptide assembling Prodrug nanoparticles for Remodeling the Immunosuppressive Microenvironment and Boosting Cancer Immunotherapy. Small. 2022;18(9):e2106296.
Gao C, et al. Injectable Immunotherapeutic Hydrogel containing RNA-Loaded lipid nanoparticles reshapes Tumor Microenvironment for Pancreatic Cancer Therapy. Nano Lett. 2022;22(22):8801-9.
Yoon J, et al. Macrophage-reprogramming upconverting nanoparticles for enhanced TAM-mediated antitumor therapy of hypoxic breast cancer. J Control Release. 2023;360:482-95.
Rong , et al. Iron chelated melanin-like nanoparticles for tumorassociated macrophage repolarization and cancer therapy. Biomaterials. 2019;225:119515.
Ramesh A, et al. Dual inhibition of CSF1R and MAPK pathways using supramolecular nanoparticles enhances macrophage immunotherapy. Biomaterials. 2020;227:119559.
He Y, et al. Targeted MIP-3 plasmid nanoparticles induce dendritic cell maturation and inhibit M2 macrophage polarisation to suppress cancer growth. Biomaterials. 2020;249:120046.
Su WP, et al. Polyaniline-based glyco-condensation on au nanoparticles enhances Immunotherapy in Lung Cancer. ACS Appl Mater Interfaces. 2022;14(21):24144-59.
Yang S, et al. CaCO(3)-Encapsulated au nanoparticles modulate macrophages toward M1-like phenotype. ACS Appl Bio Mater. 2021;4(4):3214-23.
Wan J, et al. Biodegradable NIR-II Pseudo Conjugate Polymeric nanoparticles amplify photodynamic immunotherapy via alleviation of Tumor Hypoxia and Tumor-Associated Macrophage Reprogramming. Adv Mater. 2023;35(31):e2209799.
Li L, et al. Functional Gadofullerene nanoparticles trigger Robust Cancer Immunotherapy based on rebuilding an immunosuppressive Tumor Microenvironment. Nano Lett. 2020;20(6):4487-96.
Guo Q, et al. Dandelion-Like Tailorable nanoparticles for Tumor Microenvironment Modulation. Adv Sci (Weinh). 2019;6(21):1901430.
Liu Y, et al. Targeting Tumor-Associated macrophages by MMP2-Sensitive apoptotic body-mimicking nanoparticles. ACS Appl Mater Interfaces. 2020;12(47):52402-14.
Parayath NN, Parikh A, Amiji MM. Repolarization of Tumor-Associated macrophages in a genetically Engineered Nonsmall Cell Lung Cancer Model by Intraperitoneal Administration of Hyaluronic Acid-based nanoparticles encapsulating MicroRNA-125b. Nano Lett. 2018;18(6):3571-9.
Xu L, et al. Engineering the Intestinal Lymphatic Transport of oral nanoparticles to Educate macrophages for Cancer Combined Immunotherapy. ACS Nano. 2023;17(12):11817-37.
Zhang Y, et al. Gold nanoparticles inhibit activation of cancer-associated fibroblasts by disrupting communication from tumor and microenvironmental cells. Bioact Mater. 2021;6(2):326-32.
Kovács D, et al. Core-shell nanoparticles suppress metastasis and modify the tumour-supportive activity of cancer-associated fibroblasts. J Nanobiotechnol. 2020;18(1):18.
Lopez S, et al. Magneto-mechanical destruction of cancer-associated fibroblasts using ultra-small iron oxide nanoparticles and low frequency rotating magnetic fields. Nanoscale Adv. 2022;4(2):421-36.
Li L, et al. Photosensitizer-encapsulated ferritins mediate photodynamic therapy against Cancer-Associated fibroblasts and improve Tumor Accumulation of nanoparticles. Mol Pharm. 2018;15(8):3595-9.
Jin J, et al. Human Cancer Cell membrane-coated biomimetic nanoparticles reduce fibroblast-mediated Invasion and Metastasis and induce T-Cells. ACS Appl Mater Interfaces. 2019;11(8):7850-61.
Zhou S et al. FAP-Targeted photodynamic therapy mediated by Ferritin nanoparticles elicits an Immune response against Cancer cells and Cancer Associated fibroblasts. Adv Funct Mater, 2021. 31(7).
Yu Q, et al. Targeting cancer-associated fibroblasts by dual-responsive lipid-albumin nanoparticles to enhance drug perfusion for pancreatic tumor therapy. J Control Release. 2020;321:564-75.
Liu JQ, et al. Intratumoral delivery of IL-12 and IL-27 mRNA using lipid nanoparticles for cancer immunotherapy. J Control Release. 2022;345:306-13.
Huang KW, et al. Highly efficient and tumor-selective nanoparticles for dualtargeted immunogene therapy against cancer. Sci Adv. 2020;6(3):eaax5032.
Xiong J, et al. Cancer-Erythrocyte Hybrid membrane-camouflaged magnetic nanoparticles with enhanced photothermal-immunotherapy for ovarian Cancer. ACS Nano. 2021;15(12):19756-70.
Patel SK, et al. Hydroxycholesterol substitution in ionizable lipid nanoparticles for mRNA delivery to T cells. J Control Release. 2022;347:521-32.
Billingsley MM, et al. Orthogonal Design of experiments for optimization of lipid nanoparticles for mRNA Engineering of CART cells. Nano Lett. 2022;22(1):533-42.
Lin YX et al. Reactivation of the tumor suppressor PTEN by mRNA nanoparticles enhances antitumor immunity in preclinical models Sci Transl Med, 2021. 13(599).
Jiang Y, et al. Engineered cell-membrane-coated nanoparticles directly Present Tumor antigens to promote anticancer immunity. Adv Mater. 2020;32(30):e2001808.
Li Z, et al. Immunogenic cell death augmented by Manganese Zinc Sulfide nanoparticles for metastatic Melanoma Immunotherapy. ACS Nano. 2022;16(9):15471-83.
Cao L, et al. Activating cGAS-STING pathway with ROS-responsive nanoparticles delivering a hybrid prodrug for enhanced chemo-immunotherapy. Biomaterials. 2022;290:121856.
Chen C, et al. Asynchronous blockade of PD-L1 and CD155 by polymeric nanoparticles inhibits triple-negative breast cancer progression and metastasis. Biomaterials. 2021;275:p120988.
Tang S, et al. MnO(2)-melittin nanoparticles serve as an effective anti-tumor immunotherapy by enhancing systemic immune response. Biomaterials. 2022;288:121706.
Sun F, et al. Regulating glucose metabolism with Prodrug nanoparticles for promoting photoimmunotherapy of pancreatic Cancer. Adv Sci (Weinh). 2021;8(4):2002746.
Chou PY, et al. Glycosylation of OVA antigen-loaded PLGA nanoparticles enhances DC-targeting for cancer vaccination. J Control Release. 2022;351:970-88.
Son S, et al. Induction of T-helper-17-cell-mediated anti-tumour immunity by pathogen-mimicking polymer nanoparticles. Nat Biomed Eng. 2023;7(1):72-84.
Kim KS, et al. Ovalbumin and poly(i:c) encapsulated dendritic cell-targeted nanoparticles for Immune activation in the small intestinal lymphatic system. Adv Healthc Mater. 2022;11(21):e2200909.
Li S, et al. Pre-induced ICD membrane-coated carrier-free nanoparticles for the personalized Lung Cancer Immunotherapy. Small Methods. 2023;7(5):e2201569.
Zhang Z, et al. Antitumor Activity of Anti-mir-21 delivered through lipid nanoparticles. Adv Healthc Mater. 2023;12(6):e2202412.
Min Y, et al. Antigen-capturing nanoparticles improve the abscopal effect and cancer immunotherapy. Nat Nanotechnol. 2017;12(9):877-82.
Ou W, et al. Combination of NIR therapy and regulatory T cell modulation using layer-by-layer hybrid nanoparticles for effective cancer photoimmunotherapy. Theranostics. 2018;8(17):4574-90.
Zang , et al. Polymeric indoximod based prodrug nanoparticles with doxorubicin entrapment for inducing immunogenic cell death and improving the immunotherapy of breast cancer. J Mater Chem B. 2022;10(12):2019-27.
Yang T, et al. Dual polymeric prodrug co-assembled nanoparticles with precise ratiometric co-delivery of cisplatin and metformin for lung cancer chemoimmunotherapy. Biomater Sci. 2020;8(20):5698-714.
Ou W, et al. Regulatory T cell-targeted hybrid nanoparticles combined with immuno-checkpoint blockage for cancer immunotherapy. J Control Release. 2018;281:84-96.
He Y, et al. Remodeling tumor immunosuppression with molecularly imprinted nanoparticles to enhance immunogenic cell death for cancer immunotherapy. J Control Release. 2023;362:44-57.
Wan WJ, et al. Coadministration of iRGD peptide with ROS-sensitive nanoparticles co-delivering siFGL1 and siPD-L1 enhanced tumor immunotherapy. Acta Biomater. 2021;136:473-84.
Wang W, et al. The development of Chiral nanoparticles to target NK cells and CD8(+) T cells for Cancer Immunotherapy. Adv Mater. 2022;34(16):e2109354.
Wang B, et al. Liposomes co-loaded with ursolic acid and ginsenoside Rg3 in the treatment of hepatocellular carcinoma. Acta Biochim Pol. 2021;68(4):711-5.
Yao H, et al. Cisplatin nanoparticles promote Intratumoral CD8(+) T cell priming via Antigen Presentation and T cell receptor crosstalk. Nano Lett. 2022;22(8):3328-39.
Munakata L, et al. Lipid nanoparticles of Type-A CpG D35 suppress tumor growth by changing tumor immune-microenvironment and activate CD8 T cells in mice. J Control Release. 2019;313:106-19.
Chang HC, et al. Targeting and specific activation of Antigen-presenting cells by endogenous Antigen-Loaded nanoparticles elicits tumor-specific immunity. Adv Sci (Weinh). 2020;7(1):1900069.
Smith R, et al. Cationic nanoparticles enhance cell tumor infiltration and antitumor immune responses to a melanoma vaccine. Sci Adv. 2022;8(29):eabk3150.
Gao Y, et al. Engineering platelets with PDL1 antibodies and Iron oxide nanoparticles for Postsurgical Cancer Immunotherapy. ACS Appl Bio Mater. 2023;6(1):257-66.
Patel RB, et al. Development of an in situ Cancer vaccine via Combinational Radiation and bacterial-membrane-coated nanoparticles. Adv Mater. 2019;31(43):e1902626.
Choi J, et al. Visible-light-triggered Prodrug nanoparticles combine chemotherapy and photodynamic therapy to Potentiate Checkpoint Blockade Cancer Immunotherapy. ACS Nano. 2021;15(7):12086-98.
Ding B, et al. Biodegradable Upconversion nanoparticles induce pyroptosis for Cancer Immunotherapy. Nano Lett. 2021;21(19):8281-9.
Zhang , et al. Glutathione-responsive nanoparticles of Camptothecin Prodrug for Cancer Therapy. Adv Sci (Weinh). 2023;10(3):e2205246.
Zhang Y, et al. Gemcitabine nanoparticles promote antitumor immunity against melanoma. Biomaterials. 2019;189:48-59.
Gowd V, et al. Advancement of cancer immunotherapy using nanoparticlesbased nanomedicine. Sem Cancer Biol. 2022;86:624-44.
Casazza A, et al. Tumor stroma: a complexity dictated by the hypoxic tumor microenvironment. Oncogene. 2014;33(14):1743-54.
Yu JL, et al. Effect of p53 status on tumor response to antiangiogenic therapy. Science. 2002;295(5559):1526-8.
Taylor CT, Colgan SP. Regulation of immunity and inflammation by hypoxia in immunological niches. Nat Rev Immunol. 2017;17(12):774-85.
Facciabene A, et al. Tumour hypoxia promotes tolerance and angiogenesis via CCL28 and Treg cells. Nature. 2011;475(7355):226-30.
Doedens AL, et al. Macrophage expression of hypoxia-inducible factor-1a suppresses T-cell function and promotes tumor progression. Cancer Res. 2010;70(19):7465-75.
Abou Khouzam R, et al. Hypoxia as a potential inducer of immune tolerance, tumor plasticity and a driver of tumor mutational burden: impact on cancer immunotherapy. Semin Cancer Biol. 2023;97:104-23.
Finisguerra V et al. Metformin improves cancer immunotherapy by directly rescuing tumor-infiltrating CD8 T lymphocytes from hypoxia-induced immunosuppression. J Immunother Cancer, 2023. 11(5).
Yan H, et al. Exercise sensitizes PD-1/PD-L1 immunotherapy as a hypoxia modulator in the tumor microenvironment of melanoma. Front Immunol. 2023;14:1265914.
Barsoum IB, et al. A mechanism of hypoxia-mediated escape from adaptive immunity in cancer cells. Cancer Res. 2014;74(3):665-74.
Silva VL. Exploiting the cancer niche: tumor-associated macrophages and hypoxia as promising synergistic targets for nano-based therapy. J Controlled Release. 2017;253:82-96.
Jiang T et al. TAM-Hijacked Immunoreaction Rescued by Hypoxia-PathwayIntervened Strategy for Enhanced Metastatic Cancer Immunotherapy Small, 2023: p. e2305728.
Qu S et al. Light-enhanced hypoxia-responsive gene editing for Hypoxiaresistant photodynamic and Immunotherapy. Adv Healthc Mater, 2023: p. e2302615.
Sun T et al. Metal-Organic Framework-Mediated Synergistic HypoxiaActivated Chemo-Immunotherapy Induced by High Intensity Focused Ultrasound for Enhanced Cancer Theranostics Small, 2023: p. e2306338.
Luo W et al. Strengthening the Combinational Immunotherapy from modulating the Tumor Inflammatory Environment via Hypoxia-Responsive Nanogels. Adv Healthc Mater, 2023: p. e2302865.
Wang M, et al. Controllable hypoxia-activated chemotherapy as a dual enhancer for synergistic cancer photodynamic immunotherapy. Biomaterials. 2023;301:122257.
Luo G, et al. Multifunctional calcium-manganese Nanomodulator provides Antitumor Treatment and Improved Immunotherapy via Reprogramming of the Tumor Microenvironment. ACS Nano. 2023;17(16):15449-65.
Kang , et al. A photo-triggered self-accelerated nanoplatform for multifunctional image-guided combination cancer immunotherapy. Nat Commun. 2023;14(1):5216.
Gao C, et al. Conjugation of macrophage-mimetic Microalgae and Liposome for Antitumor Sonodynamic Immunotherapy via Hypoxia Alleviation and Autophagy Inhibition. ACS Nano. 2023;17(4):4034-49.
Qin Y, et al. Autophagy and cancer drug resistance in dialogue: pre-clinical and clinical evidence. Cancer Lett. 2023;570:216307.
Ashrafizadeh M, et al. A bioinformatics analysis, pre-clinical and clinical conception of autophagy in pancreatic cancer: complexity and simplicity in crosstalk. Pharmacol Res. 2023;194:106822.
Wang S, et al. Metabolic intervention Liposome boosted Lung Cancer Radio-Immunotherapy via Hypoxia Amelioration and PD-L1 Restraint. Adv Sci (Weinh). 2023;10(18):e2207608.
Liu Y et al. An Injectable puerarin depot can potentiate chimeric antigen receptor natural killer cell immunotherapy against targeted solid tumors by reversing tumor immunosuppression Small, 2024: p. e2307521.
Jiang , et al. Mitochondrial disruption Nanosystem simultaneously depressed programmed death Ligand-1 and transforming growth Factor- to overcome photodynamic immunotherapy resistance. ACS Nano; 2024.
Li M, et al. Sono-activatable semiconducting polymer nanoreshapers multiply remodel tumor microenvironment for potent immunotherapy of orthotopic pancreatic cancer. Adv Sci (Weinh). 2023;10(35):e2305150.
Jang H et al. Nanoparticles targeting innate immune cells in tumor microenvironment. Int J Mol Sci, 2021. 22(18).
Bronte V, Zanovello P. Regulation of immune responses by L-arginine metabolism. Nat Rev Immunol. 2005;5(8):641-54.
Rodriguez PC, et al. Arginase I in myeloid suppressor cells is induced by COX-2 in lung carcinoma. J Exp Med. 2005;202(7):931-9.
Rodríguez PC, Ochoa AC. Arginine regulation by myeloid derived suppressor cells and tolerance in cancer: mechanisms and therapeutic perspectives. Immunol Rev. 2008;222:180-91.
Rodriguez PC, et al. Regulation of T cell receptor CD3zeta chain expression by L-arginine. J Biol Chem. 2002;277(24):21123-9.
Nagaraj , et al. Altered recognition of antigen is a mechanism of cell tolerance in cancer. Nat Med. 2007;13(7):828-35.
Kusmartsev S, et al. Antigen-specific inhibition of CD8 + T cell response by immature myeloid cells in cancer is mediated by reactive oxygen species. J Immunol. 2004;172(2):989-99.
Kusmartsev S, Nagaraj S, Gabrilovich DI. Tumor-associated CD8+T cell tolerance induced by bone marrow-derived immature myeloid cells. J Immunol. 2005;175(7):4583-92.
Huang B, et al. Gr-1 + CD115 + immature myeloid suppressor cells mediate the development of tumor-induced T regulatory cells and T-cell anergy in tumor-bearing host. Cancer Res. 2006;66(2):1123-31.
Sawant DV, et al. Adaptive plasticity of IL-10(+) and IL-35(+) T(reg) cells cooperatively promotes tumor T cell exhaustion. Nat Immunol. 2019;20(6):724-35.
Liu H, et al. A novel DNA aptamer for dual targeting of Polymorphonuclear myeloid-derived suppressor cells and Tumor cells. Theranostics. 2018;8(1):31-44.
Song X , et al. CD11b+/Gr-1 + immature myeloid cells mediate suppression of T cells in mice bearing tumors of IL-1 beta-secreting cells. J Immunol. 2005;175(12):8200-8.
Bunt SK, et al. Inflammation induces myeloid-derived suppressor cells that facilitate tumor progression. J Immunol. 2006;176(1):284-90.
Jiang M, et al. Interleukin-6 trans-signaling pathway promotes immunosuppressive myeloid-derived suppressor cells via Suppression of Suppressor of Cytokine Signaling 3 in breast Cancer. Front Immunol. 2017;8:1840.
Sinha P, et al. Prostaglandin E2 promotes tumor progression by inducing myeloid-derived suppressor cells. Cancer Res. 2007;67(9):4507-13.
Gabrilovich DI, et al. Production of vascular endothelial growth factor by human tumors inhibits the functional maturation of dendritic cells. Nat Med. 1996;2(10):1096-103.
Groth C, et al. Immunosuppression mediated by myeloid-derived suppressor cells (MDSCs) during tumour progression. Br J Cancer. 2019;120(1):16-25.
Kong M, et al. Biodegradable Hollow Mesoporous silica nanoparticles for regulating Tumor Microenvironment and Enhancing Antitumor Efficiency. Theranostics. 2017;7(13):3276-92.
Shao K, et al. Nanoparticle-based immunotherapy for cancer. ACS Nano. 2015;9(1):16-30.
Zolnik BS, et al. Minireview: nanoparticles and the immune system. Endocrinology. 2010;151(2):458-65.
Dwivedi PD, et al. Impact of nanoparticles on the immune system. J Biomed Nanotechnol. 2011;7(1):193-4.
Falo L Jr, et al. Targeting antigen into the phagocytic pathway in vivo induces protective tumour immunity. Nat Med. 1995;1(7):649-53.
Fifis T, et al. Size-dependent immunogenicity: therapeutic and protective properties of nano-vaccines against tumors. J Immunol. 2004;173(5):3148-54.
Uto T, et al. Targeting of antigen to dendritic cells with poly ( -glutamic acid) nanoparticles induces antigen-specific humoral and cellular immunity. J Immunol. 2007;178(5):2979-86.
Cho N-H, et al. A multifunctional core-shell nanoparticle for dendritic cellbased cancer immunotherapy. Nat Nanotechnol. 2011;6(10):675-82.
Bourquin C, et al. Targeting CpG oligonucleotides to the lymph node by nanoparticles elicits efficient antitumoral immunity. J Immunol. 2008;181(5):2990-8.
Zwiorek K, et al. Delivery by cationic gelatin nanoparticles strongly increases the immunostimulatory effects of CpG oligonucleotides. Pharm Res. 2008;25:551-62.
Romero P, et al. Ex vivo staining of metastatic lymph nodes by class I major histocompatibility complex tetramers reveals high numbers of antigen-experienced tumor-specific cytolytic T lymphocytes. J Exp Med. 1998;188(9):1641-50.
Cochran AJ, et al. Sentinel lymph nodes show profound downregulation of antigen-presenting cells of the paracortex: implications for tumor biology and treatment. Mod Pathol. 2001;14(6):604-8.
Curiel TJ, et al. Blockade of B7-H1 improves myeloid dendritic cell-mediated antitumor immunity. Nat Med. 2003;9(5):562-7.
Munn DH, et al. Expression of indoleamine 2, 3-dioxygenase by plasmacytoid dendritic cells in tumor-draining lymph nodes. J Clin Investig. 2004;114(2):280-90.
Gabrilovich D. Mechanisms and functional significance of tumour-induced dendritic-cell defects. Nat Rev Immunol. 2004;4(12):941-52.
Pinzon-Charry A, Maxwell T, López JA. Dendritic cell dysfunction in cancer: a mechanism for immunosuppression. Immunol Cell Biol. 2005;83(5):451-61.
Vicari AP, et al. Reversal of tumor-induced dendritic cell paralysis by CpG immunostimulatory oligonucleotide and anti-interleukin 10 receptor antibody. J Exp Med. 2002;196(4):541-9.
van Mierlo GJ, et al. Activation of dendritic cells that cross-present tumorderived antigen licenses CD8 + CTL to cause tumor eradication. J Immunol. 2004;173(11):6753-9.
Munn DH, Mellor AL. The tumor-draining lymph node as an immune-privileged site. Immunol Rev. 2006;213(1):146-58.
Jeanbart L, et al. Enhancing efficacy of anticancer vaccines by targeted delivery to tumor-draining lymph nodes. Cancer Immunol Res. 2014;2(5):436-47.
Nam J, et al. Cancer nanomedicine for combination cancer immunotherapy. Nat Reviews Mater. 2019;4(6):398-414.
Shi J, et al. Cancer nanomedicine: progress, challenges and opportunities. Nat Rev Cancer. 2017;17(1):20-37.
Ojha T, et al. Pharmacological and physical vessel modulation strategies to improve EPR-mediated drug targeting to tumors. Adv Drug Deliv Rev. 2017;119:44-60.
Wilhelm S, et al. Analysis of nanoparticle delivery to tumours. Nat Reviews Mater. 2016;1(5):1-12.
Siegler EL, Kim YJ, Wang P. Nanomedicine targeting the tumor microenvironment: therapeutic strategies to inhibit angiogenesis, remodel matrix, and modulate immune responses. J Cell Immunotherapy. 2016;2(2):69-78.
Shi K, Haynes M, Huang L. Nanovaccines for remodeling the suppressive tumor microenvironment: new horizons in cancer immunotherapy. Front Chem Sci Eng. 2017;11:676-84.
Marabelle A, et al. Intratumoral immunotherapy: using the tumor as the remedy. Ann Oncol. 2017;28:xii33-43.
Aznar MA, et al. Intratumoral delivery of immunotherapy—act locally, think globally. J Immunol. 2017;198(1):31-9.
Ishihara J, et al. Matrix-binding checkpoint immunotherapies enhance antitumor efficacy and reduce adverse events. Sci Transl Med. 2017;9(415):eaan0401.
Raavé R, van Kuppevelt TH, Daamen WF. Chemotherapeutic drug delivery by tumoral extracellular matrix targeting. J Controlled Release. 2018;274:1-8.
Yu S et al. Reinforcing the immunogenic cell death to enhance cancer immunotherapy efficacy Biochimica et Biophysica Acta (BBA) – Reviews on Cancer, 2023;1878(5):188946.
Wu Q, et al. Autophagy induction by IGF1R inhibition with picropodophyllin and linsitinib. Autophagy. 2021;17(8):2046-7.
Petroni G, et al. Immunomodulation by targeted anticancer agents. Cancer Cell. 2021;39(3):310-45.
Huang Z, et al. KCI nanoparticles as potential inducer of immunogenic cell death for Cancer Immunotherapy. ACS Appl Bio Mater. 2023;6(6):2404-14.
Félix-Piña P et al. Antitumoral and Immunogenic Capacity of -D-Glucosereduced silver nanoparticles in breast Cancer. Int J Mol Sci, 2023. 24(10).
Liu Q, et al. Exploiting immunostimulatory mechanisms of immunogenic cell death to develop membrane-encapsulated nanoparticles as a potent tumor vaccine. J Nanobiotechnol. 2023;21(1):326.
Xie B, et al. Supramolecularly Engineered Conjugate of Bacteria and cell membrane-coated magnetic nanoparticles for enhanced ferroptosis and immunotherapy of tumors. Adv Sci (Weinh). 2023;10(34):e2304407.
Lu Y, et al. Self-driven bioactive hybrids co-deliver doxorubicin and indocyanine green nanoparticles for chemo/photothermal therapy of breast cancer. Biomed Pharmacother. 2023;169:115846.
Wang H et al. Near-Infrared Light-Driven Nanoparticles for Cancer Photoimmunotherapy by Synergizing Immune Cell Death and Epigenetic Regulation Small, 2023: p. e2309202.
Wu Q et al. Photothermal ferrotherapy – induced immunogenic cell death via iron-based ternary chalcogenide nanoparticles against triple-negative breast cancer Small, 2023: p. e2306766.
Song S, et al. All-in-one glycol chitosan nanoparticles for co-delivery of doxorubicin and anti-PD-L1 peptide in cancer immunotherapy. Bioact Mater. 2023;28:358-75.
Wang R, et al. Hydroxyapatite nanoparticles promote TLR4 agonist-mediated anti-tumor immunity through synergically enhanced macrophage polarization. Acta Biomater. 2023;164:626-40.
Wang Y, et al. Docetaxel-loaded ROS dual-responsive nanoparticles with self-supplied ROS for inhibiting metastasis and enhancing immunotherapy of breast cancer. J Nanobiotechnol. 2023;21(1):286.
Yang J, et al. Self-assembled albumin nanoparticles induce pyroptosis for photodynamic/photothermal/immuno synergistic therapies in triple-negative breast cancer. Front Immunol. 2023;14:1173487.
Xu X, et al. Guanidine-modified nanoparticles as robust BTZ delivery carriers and activators of immune responses. J Control Release. 2023;357:310-8.
Chen W, et al. PEI-Based nanoparticles for Tumor Immunotherapy via in situ Antigen-capture triggered by Photothermal Therapy. ACS Appl Mater Interfaces. 2023;15(48):55433-46.
Li Y, et al. Antigen-capturing dendritic-cell-targeting nanoparticles for enhanced Tumor Immunotherapy based on Photothermal-Therapy-Induced in situ vaccination. Adv Healthc Mater. 2023;12(22):e2202871.
Zou C, et al. cRGD-modified nanoparticles of multi-bioactive agent conjugate with pH-sensitive linkers and PD-L1 antagonist for integrative collaborative treatment of breast cancer. Nanoscale Horiz. 2023;8(7):870-86.
Chen S, et al. Tumor Acidic Microenvironment-Responsive Promodulator Iron Oxide nanoparticles for Photothermal-enhanced Chemodynamic Immunotherapy of Cancer. ACS Biomater Sci Eng. 2023;9(2):773-83.
Ma W, et al. Biomimetic nanoerythrosome-coated Aptamer-DNA Tetrahedron/Maytansine conjugates: pH-Responsive and targeted cytotoxicity for HER2-Positive breast Cancer. Adv Mater. 2022;34(46):e2109609.
Zheng , et al. Biomimetic co-assembled nanodrug of doxorubicin and berberine suppresses chemotherapy-exacerbated breast cancer metastasis. Biomaterials. 2021;271:120716.
Liu XL, et al. Biomimetic liposomal nanoplatinum for targeted Cancer Chemophototherapy. Adv Sci (Weinh). 2021;8(8):2003679.
Zhao Y, et al. Biomimetic manganese-based theranostic nanoplatform for cancer multimodal imaging and twofold immunotherapy. Bioact Mater. 2023;19:237-50.
Zhao P, et al. Programming cell pyroptosis with biomimetic nanoparticles for solid tumor immunotherapy. Biomaterials. 2020;254:120142.
Ying K, et al. Macrophage membrane-biomimetic adhesive polycaprolactone nanocamptothecin for improving cancer-targeting efficiency and impairing metastasis. Bioact Mater. 2023;20:449-62.
Miao Y, et al. Cell membrane-camouflaged nanocarriers with Biomimetic Deformability of erythrocytes for Ultralong circulation and enhanced Cancer Therapy. ACS Nano. 2022;16(4):6527-40.
Guo Y, et al. Chemotherapy mediated by Biomimetic Polymeric Nanoparticles Potentiates Enhanced Tumor Immunotherapy via Amplification of Endoplasmic Reticulum Stress and mitochondrial dysfunction. Adv Mater. 2022;34(47):e2206861.
Wu P, et al. Engineered EGCG-Containing Biomimetic nanoassemblies as effective delivery platform for enhanced Cancer Therapy. Adv Sci (Weinh). 2022;9(15):e2105894.
Reuven EM, et al. Biomimetic Glyconanoparticle Vaccine for Cancer Immunotherapy. ACS Nano. 2019;13(3):2936-47.
Molina M, et al. Stimuli-responsive nanogel composites and their application in nanomedicine. Chem Soc Rev. 2015;44(17):6161-86.
Chuard N, et al. Strain-promoted thiol-mediated Cellular Uptake of Giant substrates: liposomes and polymersomes. Angew Chem Int Ed Engl. 2017;56(11):2947-50.
Wang , et al. A cooperative dimensional strategy for enhanced nucleustargeted delivery of anticancer drugs. Adv Funct Mater. 2017;27(24):1700339.
Tang , et al. Enhancing cell therapy through TCR-signaling-responsive nanoparticle drug delivery. Nat Biotechnol. 2018;36(8):707-16.
Sun CY, et al. Tumor acidity-sensitive polymeric vector for active targeted siRNA delivery. J Am Chem Soc. 2015;137(48):15217-24.
Shang , et al. Enhancing cancer chemo-immunotherapy by biomimetic nanogel with tumor targeting capacity and rapid drug-releasing in tumor microenvironment. Acta Pharm Sin B. 2022;12(5):2550-67.
Wan L, et al. Biomimetic, pH-Responsive nanoplatforms for Cancer Multimodal Imaging and Photothermal Immunotherapy. ACS Appl Mater Interfaces. 2023;15(1):1784-97.
Yang , et al. Biomimetic nanovaccines potentiating dendritic cell internalization via CXCR4-Mediated macropinocytosis. Adv Healthc Mater. 2023;12(5):e2202064.
Wei X et al. Biomimetic nano-immunoactivator via ionic metabolic modulation for strengthened nir-ii photothermal immunotherapy small, 2023: p. e2304370.
Wang Y, et al. Engineering Endogenous Tumor-Associated macrophagetargeted biomimetic Nano-RBC to Reprogram Tumor Immunosuppressive Microenvironment for enhanced chemo-immunotherapy. Adv Mater. 2021;33(39):e2103497.
Zhao H, et al. Biomimetic Decoy inhibits Tumor Growth and Lung Metastasis by reversing the drawbacks of Sonodynamic Therapy. Adv Healthc Mater. 2020;9(1):e1901335.
Feng , et al. Biomimetic and bioinspired nano-platforms for cancer vaccine development. Explor (Beijing). 2023;3(3):20210263.
Fang RH, et al. Cancer cell membrane-coated nanoparticles for anticancer vaccination and drug delivery. Nano Lett. 2014;14(4):2181-8.
Zheng S, Guan XY. Ferroptosis: promising approach for cancer and cancer immunotherapy. Cancer Lett. 2023;561:216152.
Yin J, et al. Ferroptosis and Cancer immunotherapy. Curr Mol Med. 2023;23(5):401-9.
Xu H, et al. Ferroptosis in the tumor microenvironment: perspectives for immunotherapy. Trends Mol Med. 2021;27(9):856-67.
Gao W, et al. Autophagy, ferroptosis, pyroptosis, and necroptosis in tumor immunotherapy. Signal Transduct Target Ther. 2022;7(1):196.
Lei Y et al. Autophagy in cancer immunotherapy cells, 2022. 11(19).
Pan H, et al. Autophagy-associated immune responses and cancer immunotherapy. Oncotarget. 2016;7(16):21235-46.
Jin Z, et al. Regulation of autophagy fires up the cold tumor microenvironment to improve cancer immunotherapy. Front Immunol. 2022;13:1018903.
Hamidi M, et al. Applications of carrier erythrocytes in delivery of biopharmaceuticals. J Control Release. 2007;118(2):145-60.
Banz A, et al. In situ targeting of dendritic cells by antigen-loaded red blood cells: a novel approach to cancer immunotherapy. Vaccine. 2010;28(17):2965-72.
Hu CMJ, Fang RH, Zhang L. Erythrocyte-inspired delivery systems. Adv Healthc Mater. 2012;1(5):537-47.
Guo Y, et al. Erythrocyte membrane-enveloped polymeric nanoparticles as Nanovaccine for induction of Antitumor immunity against Melanoma. ACS Nano. 2015;9(7):6918-33.
Hu Q, et al. Anticancer Platelet-Mimicking Nanovehicles. Adv Mater. 2015;27(44):7043-50.
Hu CM, et al. Nanoparticle biointerfacing by platelet membrane cloaking. Nature. 2015;526(7571):118-21.
Bahmani B et al. Intratumoral immunotherapy using platelet-cloaked nanoparticles enhances antitumor immunity in solid tumors Nat Commun, 2021;12(1):1999.
Mai X , et al. Integration of immunogenic activation and immunosuppressive reversion using mitochondrial-respiration-inhibited platelet-mimicking nanoparticles. Biomaterials. 2020;232:119699.
Wang Q et al. Biomimetic Nanophotosensitizer amplifies immunogenic pyroptosis and triggers synergistic Cancer Therapy. Adv Healthc Mater, 2023: p. e2301641.
Gong P et al. Immunocyte membrane-coated nanoparticles for Cancer Immunotherapy. Cancers (Basel), 2020. 13(1).
Sun K, et al. Saikosaponin D loaded macrophage membrane-biomimetic nanoparticles target angiogenic signaling for breast cancer therapy. Appl Mater Today. 2020;18:100505.
Chen LJ, et al. Macrophage membrane coated persistent luminescence nanoparticle@MOF-derived mesoporous carbon core-shell nanocomposites for autofluorescence-free imaging-guided chemotherapy. J Mater Chem B. 2020;8(35):8071-83.
Cao H, et al. Liposomes coated with isolated macrophage membrane can target lung metastasis of breast Cancer. ACS Nano. 2016;10(8):7738-48.
Meng QF, et al. Macrophage membrane-coated iron oxide nanoparticles for enhanced photothermal tumor therapy. Nanotechnology. 2018;29(13):134004.
Zhao H, et al. C-C Chemokine Ligand 2 (CCL2) recruits macrophage-mem-brane-camouflaged Hollow Bismuth Selenide nanoparticles to facilitate Photothermal Sensitivity and inhibit lung metastasis of breast Cancer. ACS Appl Mater Interfaces. 2018;10(37):31124-35.
Liang , et al. Biomimetic theranostic strategy for anti-metastasis therapy of breast cancer via the macrophage membrane camouflaged superparticles. Mater Sci Eng C Mater Biol Appl. 2020;115:111097.
Xuan M, et al. Macrophage cell membrane camouflaged mesoporous silica nanocapsules for in vivo Cancer therapy. Adv Healthc Mater. 2015;4(11):1645-52.
Rao L , et al. Effective cancer targeting and imaging using macrophage membrane-camouflaged upconversion nanoparticles. J Biomed Mater Res A. 2017;105(2):521-30.
Cao X, et al. Paclitaxel-loaded macrophage membrane camouflaged Albumin nanoparticles for targeted Cancer Therapy. Int J Nanomed. 2020;15:1915-28.
Ma J, et al. Copresentation of Tumor antigens and Costimulatory molecules via Biomimetic nanoparticles for Effective Cancer Immunotherapy. Nano Lett. 2020;20(6):4084-94.
Li L, et al. Cholesterol removal improves performance of a model biomimetic system to co-deliver a photothermal agent and a STING agonist for cancer immunotherapy. Nat Commun. 2023;14(1):5111.
Xie W, et al. Biomimetic nanoplatform loading type I Aggregation-Induced Emission Photosensitizer and glutamine blockade to regulate nutrient partitioning for enhancing Antitumor Immunotherapy. ACS Nano. 2022;16(7):10742-53.
Zuo L, et al. Biomimetic nanovesicle with Mitochondria-Synthesized Sonosensitizer and Mitophagy Inhibition for Cancer Sono-Immunotherapy. Nano Lett. 2023;23(7):3005-13.
Pan P, et al. A heterogenic membrane-based biomimetic hybrid nanoplatform for combining radiotherapy and immunotherapy against breast cancer. Biomaterials. 2022;289:121810.
Yang , et al. Leveraging -Adrenergic receptor signaling blockade for Improved Cancer Immunotherapy through Biomimetic Nanovaccine. Small. 2023;19(14):e2207029.
Wang , et al. Intelligent Biomimetic Nanoplatform for systemic treatment of metastatic triple-negative breast Cancer via enhanced EGFR-Targeted therapy and immunotherapy. ACS Appl Mater Interfaces; 2022.
Li J, et al. Multifunctional biomimetic nanovaccines based on Photothermal and weak-immunostimulatory Nanoparticulate cores for the immunotherapy of solid tumors. Adv Mater. 2022;34(9):e2108012.
Xu X, et al. A Biomimetic Aggregation-Induced Emission Photosensitizer with Antigen-presenting and hitchhiking function for lipid droplet targeted photodynamic immunotherapy. Adv Mater. 2021;33(33):e2102322.
Fang , et al. Biomimetic Anti-PD-1 peptide-loaded 2D FePSe(3) nanosheets for efficient photothermal and enhanced Immune Therapy with Multimodal MR/PA/Thermal Imaging. Adv Sci (Weinh). 2021;8(2):2003041.
Liu Z, et al. Exosomes in HBV infection. Clin Chim Acta. 2023;538:65-9.
Zhang F, et al. Janus nanocarrier-based co-delivery of doxorubicin and berberine weakens chemotherapy-exacerbated hepatocellular carcinoma recurrence. Acta Biomater. 2019;100:352-64.
Chen G , et al. Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response. Nature. 2018;560(7718):382-6.
Moradi-Chaleshtori M, et al. Overexpression of pigment epithelium-derived factor in breast cancer cell-derived exosomes induces M1 polarization in macrophages. Immunol Lett. 2022;248:31-6.
Wang Y et al. G-MDSC-derived exosomes mediate the differentiation of M-MDSC into M2 macrophages promoting colitis-to-cancer transition. J Immunother Cancer, 2023. 11(6).
Zheng N, et al. M2 macrophage-derived exosomes suppress tumor intrinsic immunogenicity to confer immunotherapy resistance. Oncoimmunology. 2023;12(1):2210959.
Chen J, et al. PDL1-positive exosomes suppress antitumor immunity by inducing tumor-specific CD8(+) T cell exhaustion during metastasis. Cancer Sci. 2021;112(9):3437-54.
Wei Y, et al. An RNA-RNA crosstalk network involving HMGB1 and RICTOR facilitates hepatocellular carcinoma tumorigenesis by promoting glutamine metabolism and impedes immunotherapy by PD-L1 + exosomes activity. Signal Transduct Target Ther. 2021;6(1):421.
Wang C, et al. Tumor Cell-associated exosomes robustly elicit anti-tumor Immune responses through modulating dendritic cell vaccines in Lung Tumor. Int J Biol Sci. 2020;16(4):633-43.
Wang S, et al. Macrophage-tumor chimeric exosomes accumulate in lymph node and tumor to activate the immune response and the tumor microenvironment. Sci Transl Med. 2021;13(615):eabb6981.
Lu Z, et al. Dendritic cell-derived exosomes elicit tumor regression in autochthonous hepatocellular carcinoma mouse models. J Hepatol. 2017;67(4):739-48.
Zhou W, et al. Exosomes derived from immunogenically dying tumor cells as a versatile tool for vaccination against pancreatic cancer. Biomaterials. 2022;280:121306.
Zuo B, et al. Alarmin-painted exosomes elicit persistent antitumor immunity in large established tumors in mice. Nat Commun. 2020;11(1):1790.
Morishita M , et al. Exosome-based tumor antigens-adjuvant co-delivery utilizing genetically engineered tumor cell-derived exosomes with immunostimulatory CpG DNA. Biomaterials. 2016;111:55-65.
Gehrmann U, et al. Synergistic induction of adaptive antitumor immunity by codelivery of antigen with a-galactosylceramide on exosomes. Cancer Res. 2013;73(13):3865-76.
Kim GB et al. Xenogenization of tumor cells by fusogenic exosomes in tumor microenvironment ignites and propagates antitumor immunity. Sci Adv, 2020. 6(27).
Zhou W, et al. Pancreatic cancer-targeting exosomes for enhancing immunotherapy and reprogramming tumor microenvironment. Biomaterials. 2021;268:120546.
Gunassekaran GR, et al. M1 macrophage exosomes engineered to foster M1 polarization and target the IL-4 receptor inhibit tumor growth by reprogramming tumor-associated macrophages into M1-like macrophages. Biomaterials. 2021;278:121137.
Cheng L, et al. Gene-engineered exosomes-thermosensitive liposomes hybrid nanovesicles by the blockade of CD47 signal for combined photothermal therapy and cancer immunotherapy. Biomaterials. 2021;275:120964.
Li J, et al. Dendritic cell derived exosomes loaded neoantigens for personalized cancer immunotherapies. J Control Release. 2023;353:423-33.
Xu J, et al. Enhanced penetrative siRNA delivery by a nanodiamond drug delivery platform against hepatocellular carcinoma 3D models. Nanoscale. 2021;13(38):16131-45.
Jiang H, et al. M1 macrophage-derived exosomes and their key molecule IncRNA HOTTIP suppress head and neck squamous cell carcinoma progression by upregulating the TLR5/NF-kB pathway. Cell Death Dis. 2022;13(2):183.
Zhou WJ, et al. CD45RO(-)CD8(+) T cell-derived exosomes restrict estrogendriven endometrial cancer development via the ERß/miR-765/PLP2/Notch axis. Theranostics. 2021;11(11):5330-45.
Cheng L, et al. Multifunctional hybrid exosomes enhanced cancer chemo-immunotherapy by activating the STING pathway. Biomaterials. 2023;301:122259.
Wang et al. Exosomes derived from T cells synergize with radiotherapy and preserve antitumor activities against nasopharyngeal carcinoma in immunosuppressive microenvironment. J Immunother Cancer, 2022. 10(2).
Ji P, et al. Smart exosomes with lymph node homing and immune-amplifying capacities for enhanced immunotherapy of metastatic breast cancer. Mol Ther Nucleic Acids. 2021;26:987-96.
Fan M, et al. A CAR T-inspiring platform based on antibody-engineered exosomes from antigen-feeding dendritic cells for precise solid tumor therapy. Biomaterials. 2022;282:121424.
Li Y, et al. A nanotherapeutic system for gastric cancer suppression by synergistic chemotherapy and immunotherapy based on iPSCs and DCs exosomes. Cancer Immunol Immunother. 2023;72(6):1673-83.
Huang H, et al. Synergistic strategy with hyperthermia therapy based immunotherapy and engineered exosomes-liposomes targeted chemotherapy prevents tumor recurrence and metastasis in advanced breast cancer. Bioeng Transl Med. 2022;7(2):e10284.
Pakravan N, Abbasi A, Hassan ZM. Immunotherapy using oxygenated water and tumor-derived exosomes potentiates antitumor immune response and attenuates malignancy tendency in mice model of breast cancer oxid med cell longev, 2021;2021:5529484.
Javeed N, et al. Immunosuppressive CD14(+)HLA-DR(lo/neg) monocytes are elevated in pancreatic cancer and primed by tumor-derived exosomes. Oncoimmunology. 2017;6(1):e1252013.
Zhao Y, et al. Docetaxel-loaded M1 macrophage-derived exosomes for a safe and efficient chemoimmunotherapy of breast cancer. J Nanobiotechnol. 2022;20(1):359.
Lin J, et al. Dendritic cell-derived exosomes Driven Drug Co-delivery Biomimetic Nanosystem for Effective Combination of Malignant Melanoma Immunotherapy and Gene Therapy. Drug Des Devel Ther. 2023;17:2087-106.
Wang D, et al. Sonodynamical reversion of immunosuppressive microenvironment in prostate cancer via engineered exosomes. Drug Deliv. 2022;29(1):702-13.
Zhang Y et al. pH-Responsive STING-Activating DNA nanovaccines for Cancer Immunotherapy. Adv Ther (Weinh), 2020. 3(9).
Yao D, et al. A self-cascaded unimolecular prodrug for pH -responsive chemotherapy and tumor-detained photodynamic-immunotherapy of triple-negative breast cancer. Biomaterials. 2023;292:121920.
Liu Y, et al. Dual pH-responsive multifunctional nanoparticles for targeted treatment of breast cancer by combining immunotherapy and chemotherapy. Acta Biomater. 2018;66:310-24.
Lim B, Kim KS, Na K. pH-Responsive zinc lon regulating Immunomodulatory nanoparticles for Effective Cancer Immunotherapy. Biomacromolecules. 2023;24(9):4263-73.
Duong HTT, et al. Smart vaccine delivery based on microneedle arrays decorated with ultra-ph-responsive copolymers for cancer immunotherapy. Biomaterials. 2018;185:13-24.
Gu J, et al. Injectable pH-responsive hydrogel for combinatorial chemoimmunotherapy tailored to the tumor microenvironment. J Nanobiotechnol. 2022;20(1):372.
Gong C, et al. Regulating the immunosuppressive tumor microenvironment to enhance breast cancer immunotherapy using pH-responsive hybrid membrane-coated nanoparticles. J Nanobiotechnol. 2021;19(1):58.
Ding Y, et al. Construction of pH-Sensitive nanovaccines encapsulating tumor cell lysates and Immune adjuvants for breast Cancer therapy. Small. 2023;19(37):e2301420.
Jiang M, et al. Sequentially pH-Responsive drug-delivery Nanosystem for Tumor Immunogenic Cell Death and cooperating with Immune checkpoint blockade for efficient Cancer Chemoimmunotherapy. ACS Appl Mater Interfaces. 2021;13(37):43963-74.
Yang G, et al. Smart Nanoreactors for pH-Responsive Tumor Homing, Mitochondria-Targeting, and enhanced photodynamic-immunotherapy of Cancer. Nano Lett. 2018;18(4):2475-84.
Sun , et al. Binary regulation of the tumor microenvironment by a responsive reversible shielding nanoplatform for improved tumor chemoimmunotherapy. Acta Biomater. 2022;138:505-17.
Lv X, et al. Multi-signaling pathway activation by pH responsive manganese particles for enhanced vaccination. J Control Release. 2023;357:109-19.
Wagner J, et al. Mesoporous silica nanoparticles as pH-Responsive carrier for the Immune-Activating Drug Resiquimod enhance the local Immune response in mice. ACS Nano. 2021;15(3):4450-66.
Zhao M, et al. Immune/Hypoxic Tumor Microenvironment Regulationenhanced photodynamic treatment realized by pH -Responsive phase Transition-Targeting Nanobubbles. ACS Appl Mater Interfaces. 2021;13(28):32763-79.
Yuba E, et al. The application of pH-sensitive polymer-lipids to antigen delivery for cancer immunotherapy. Biomaterials. 2013;34(22):5711-21.
Yoshizaki Y, et al. Potentiation of pH-sensitive polymer-modified liposomes with cationic lipid inclusion as antigen delivery carriers for cancer immunotherapy. Biomaterials. 2014;35(28):8186-96.
Yuba E, et al. A liposome-based antigen delivery system using pHsensitive fusogenic polymers for cancer immunotherapy. Biomaterials. 2013;34(12):3042-52.
Yoshizaki Y, et al. pH-sensitive polymer-modified liposome-based immunityinducing system: effects of inclusion of cationic lipid and CpG-DNA. Biomaterials. 2017;141:272-83.
Zhang J, et al. pH-sensitive tumor-tropism hybrid membrane-coated nanoparticles for reprogramming the tumor microenvironment and boosting the antitumor immunity. Acta Biomater. 2023;166:470-84.
Yuba E, et al. Bioactive polysaccharide-based pH-sensitive polymers for cytoplasmic delivery of antigen and activation of antigen-specific immunity. Biomaterials. 2017;120:32-45.
Kocabas BB, et al. Dual-adjuvant effect of pH-sensitive liposomes loaded with STING and TLR9 agonists regress tumor development by enhancing Th1 immune response. J Control Release. 2020;328:587-95.
Zhang W, et al. Multifunctional redox-responsive nanoplatform with Dual Activation of Macrophages and T Cells for Antitumor Immunotherapy. ACS Nano. 2023;17(15):14424-41.
Yan P, et al. A redox-responsive Nanovaccine combined with A2A receptor antagonist for Cancer Immunotherapy. Adv Healthc Mater. 2021;10(21):e2101222.
Lv M, et al. Redox-responsive hyperbranched poly(amido amine) and polymer dots as a vaccine delivery system for cancer immunotherapy. J Mater Chem B. 2017;5(48):9532-45.
Jiang D, et al. Cascade Cytosol Delivery of Dual-Sensitive Micelle-tailored vaccine for Enhancing Cancer Immunotherapy. ACS Appl Mater Interfaces. 2018;10(44):37797-811.
Chen Q, et al. Cancer cell membrane-coated nanoparticles for bimodal imaging-guided photothermal therapy and docetaxel-enhanced immunotherapy against cancer. J Nanobiotechnol. 2021;19(1):449.
Chen L , et al. Tumor-targeted drug and CpG delivery system for Phototherapy and Docetaxel-enhanced immunotherapy with polarization toward M1-Type macrophages on Triple negative breast cancers. Adv Mater. 2019;31(52):e1904997.
Sun Y, et al. An enzyme-responsive and transformable PD-L1 blocking peptide-photosensitizer conjugate enables efficient photothermal immunotherapy for breast cancer. Bioact Mater. 2023;22:47-59.
Ma S, et al. Boosting cancer immunotherapy by biomineralized nanovaccine with ferroptosis-inducing and photothermal properties. Biomater Sci. 2023;11(2):518-32.
Xiao Y, et al. Microenvironment-responsive prodrug-induced pyroptosis boosts cancer immunotherapy. Adv Sci (Weinh). 2021;8(24):e2101840.
Wu X, et al. Nano-herb medicine and PDT induced synergistic immunotherapy for colon cancer treatment. Biomaterials. 2021;269:120654.
Ding D, et al. Multifunctional Nanodrug mediates synergistic photodynamic therapy and MDSCs-Targeting immunotherapy of Colon cancer. Adv Sci (Weinh). 2021;8(14):e2100712.
Zhou H, et al. A tumor-microenvironment-activatable Molecular Pro-theranostic Agent for Photodynamic and Immunotherapy of Cancer. Adv Mater. 2023;35(30):e2211485.
Yu Y, et al. Polymeric PD-L1 blockade nanoparticles for cancer photothermalimmunotherapy. Biomaterials. 2022;280:121312.
Liang , et al. Photothermal cancer immunotherapy by erythrocyte membrane-coated black phosphorus formulation. J Control Release. 2019;296:150-61.
Zhang R, et al. Chemodynamic/Photothermal synergistic Cancer immunotherapy based on yeast microcapsule-derived Au/Pt nanoparticles. ACS Appl Mater Interfaces. 2023;15(20):24134-48.
Wang M, et al. Synergistic interventional photothermal therapy and immunotherapy using an iron oxide nanoplatform for the treatment of pancreatic cancer. Acta Biomater. 2022;138:453-62.
Debele TA, Yeh C-F, Su W-P. Cancer immunotherapy and application of nanoparticles in cancers immunotherapy as the delivery of immunotherapeutic agents and as the immunomodulators. Cancers. 2020;12(12):3773.
Zhang C, et al. Checkpoint Nano-PROTACs for Activatable Cancer PhotoImmunotherapy. Adv Mater. 2023;35(6):e2208553.
Qiu W, et al. Immunomodulatory-photodynamic nanostimulators for invoking pyroptosis to augment Tumor Immunotherapy. Adv Healthc Mater. 2022;11(21):e2201233.
Zhou JY, et al. Ru(II)-modified TiO(2) nanoparticles for hypoxia-adaptive photo-immunotherapy of oral squamous cell carcinoma. Biomaterials. 2022;289:121757.
Duan Y, et al. Immune Modulator and Low-Temperature PTT-Induced Synergistic Immunotherapy for Cancer Treatment. ACS Appl Bio Mater. 2021;4(2):1524-35.
Yan T, et al. Synergistic photothermal cancer immunotherapy by Cas9 ribonucleoprotein-based copper sulfide nanotherapeutic platform targeting PTPN2. Biomaterials. 2021;279:121233.
Li J, et al. Second Near-Infrared Photothermal Semiconducting polymer nanoadjuvant for enhanced Cancer Immunotherapy. Adv Mater. 2021;33(4):e2003458.
Jana D et al. A defect-Engineered Nanozyme for targeted NIR-II Photothermal Immunotherapy of Cancer. Adv Mater, 2022: p. e2206401.
Hwang J, et al. Escherichia coli Mimetic Gold nanorod-mediated photoand immunotherapy for Treating Cancer and its metastasis. ACS Nano. 2022;16(5):8472-83.
Tang Y, et al. Pyroptosis-mediated synergistic photodynamic and photothermal immunotherapy enabled by a tumor-membrane-targeted photosensitive dimer. Adv Mater. 2023;35(25):e2300232.
Xu M, et al. Activatable Immunoprotease Nanorestimulator for Second Near-Infrared Photothermal Immunotherapy of Cancer. ACS Nano. 2023;17(9):8183-94.
Wang M, et al. NIR-Triggered Phototherapy and Immunotherapy via an Antigen-capturing nanoplatform for metastatic Cancer treatment. Adv Sci (Weinh). 2019;6(10):1802157.
Ye X, et al. Surgical Tumor-Derived Personalized Photothermal Vaccine Formulation for Cancer Immunotherapy. ACS Nano. 2019;13(3):2956-68.
Wang S, et al. Photothermal therapy mediated by gold nanocages composed of anti-PDL1 and galunisertib for improved synergistic immunotherapy in colorectal cancer. Acta Biomater. 2021;134:621-32.
Mikelez-Alonso I, Aires A, Cortajarena AL. Cancer nano-immunotherapy from the injection to the target: the role of protein corona. Int J Mol Sci. 2020;21(2):519.
Yetisgin AA et al. Therapeutic nanoparticles and their targeted delivery applications. Molecules, 2020. 25(9).
Anselmo AC, Mitragotri S. Nanoparticles in the clinic: an update. Bioeng Transl Med. 2019;4(3):e10143.
Kranz LM, et al. Systemic RNA delivery to dendritic cells exploits antiviral defence for cancer immunotherapy. Nature. 2016;534(7607):396-401.
Beg MS, et al. Phase I study of MRX34, a liposomal miR-34a mimic, administered twice weekly in patients with advanced solid tumors. Invest New Drugs. 2017;35(2):180-8.
Burris III et al. H.A., A phase 1, open-label, multicenter study to assess the safety, tolerability, and immunogenicity of mRNA-4157 alone in subjects with resected solid tumors and in combination with pembrolizumab in subjects with unresectable solid tumors (Keynote-603). 2019, American Society of Clinical Oncology.
Pfannenstiel LW, et al. Paclitaxel enhances early dendritic cell maturation and function through TLR4 signaling in mice. Cell Immunol. 2010;263(1):79-87.
Graziani SR, et al. Phase II study of paclitaxel associated with lipid core nanoparticles (LDE) as third-line treatment of patients with epithelial ovarian carcinoma. Med Oncol. 2017;34:1-7.
Shen C, et al. Phase I study of NBTXR3 activated by radiotherapy in patients with advanced cancers treated with an anti-PD-1 therapy. American Society of Clinical Oncology; 2020.
Li S, et al. Polymer nanoparticles as adjuvants in cancer immunotherapy. Nano Res. 2018;11:5769-86.
Thakur N, et al. Nanoparticles as smart carriers for enhanced Cancer Immunotherapy. Front Chem. 2020;8:597806.
Zhao L, et al. Nanoparticle vaccines. Vaccine. 2014;32(3):327-37.
Chen P-G, et al. Chitosan nanoparticles based nanovaccines for cancer immunotherapy. Pure Appl Chem. 2017;89(7):931-9.
Shi GN, et al. Enhanced antitumor immunity by targeting dendritic cells with tumor cell lysate-loaded chitosan nanoparticles vaccine. Biomaterials. 2017;113:191-202.
Yang R, et al. Cancer Cell membrane-coated adjuvant nanoparticles with mannose modification for effective anticancer vaccination. ACS Nano. 2018;12(6):5121-9.
Kim H, et al. Polymeric nanoparticles encapsulating novel TLR7/8 agonists as immunostimulatory adjuvants for enhanced cancer immunotherapy. Biomaterials. 2018;164:38-53.
Banerjee R. Liposomes: applications in medicine. J Biomater Appl. 2001;16(1):3-21.
Klinguer-Hamour C, et al. DDA adjuvant induces a mixed Th1/Th2 immune response when associated with BBG2Na, a respiratory syncytial virus potential vaccine. Vaccine. 2002;20(21-22):2743-51.
Christensen D, et al. Cationic liposomes as vaccine adjuvants. Expert Rev Vaccines. 2011;10(4):513-21.
Korsholm KS, et al. The adjuvant mechanism of cationic dimethyldioctadecylammonium liposomes. Immunology. 2007;121(2):216-26.
Zamani P, et al. Nanoliposomes as the adjuvant delivery systems in cancer immunotherapy. J Cell Physiol. 2018;233(7):5189-99.
Yuba E, et al. Dextran derivative-based pH-sensitive liposomes for cancer immunotherapy. Biomaterials. 2014;35(9):3091-101.
Zeng Q, et al. Tailoring polymeric hybrid micelles with lymph node targeting ability to improve the potency of cancer vaccines. Biomaterials. 2017;122:105-13.
de Faria PC, et al. Oxidized multiwalled carbon nanotubes as antigen delivery system to promote superior CD8(+) T cell response and protection against cancer. Nano Lett. 2014;14(9):5458-70.
Hassan HA, et al. Dual stimulation of antigen presenting cells using carbon nanotube-based vaccine delivery system for cancer immunotherapy. Biomaterials. 2016;104:310-22.
Zhou Q, et al. Different-sized gold nanoparticle Activator/Antigen increases dendritic cells Accumulation in Liver-Draining Lymph Nodes and CD8 + T cell responses. ACS Nano. 2016;10(2):2678-92.
Fallarini S, et al. Factors affecting T cell responses induced by fully synthetic glyco-gold-nanoparticles. Nanoscale. 2013;5(1):390-400.
Dykman LA, et al. Gold nanoparticles as an adjuvant: influence of size, shape, and technique of combination with CpG on antibody production. Int Immunopharmacol. 2018;54:163-8.
Melamed JR, et al. Using gold nanoparticles to disrupt the Tumor Microenvironment: an emerging therapeutic strategy. ACS Nano. 2016;10(12):10631-5.
Saha S, et al. Gold nanoparticle reprograms pancreatic Tumor Microenvironment and inhibits Tumor Growth. ACS Nano. 2016;10(12):10636-51.
Luo J, et al. Self-assembled CpG oligodeoxynucleotides conjugated hollow gold nanospheres to enhance cancer-associated immunostimulation. Colloids Surf B Biointerfaces. 2019;175:248-55.
Ow H, et al. Bright and stable core-shell fluorescent silica nanoparticles. Nano Lett. 2005;5(1):113-7.
Benezra M, et al. Multimodal silica nanoparticles are effective cancer-targeted probes in a model of human melanoma. J Clin Invest. 2011;121(7):2768-80.
Chattopadhyay S, et al. Nanoparticle vaccines adopting virus-like features for enhanced Immune Potentiation. Nanotheranostics. 2017;1(3):244-60.
Mahony D, et al. Mesoporous silica nanoparticles act as a self-adjuvant for ovalbumin model antigen in mice. Small. 2013;9(18):3138-46.
Selvaraja VK, Gudipudi DK. Fundamentals to clinical application of nanoparticles in cancer immunotherapy and radiotherapy. Ecancermedicalscience. 2020;14:1095.
Saeed M, et al. Engineering nanoparticles to reprogram the Tumor Immune Microenvironment for Improved Cancer Immunotherapy. Theranostics. 2019;9(26):7981-8000.
Libutti SK, et al. Phase I and pharmacokinetic studies of CYT-6091, a novel PEGylated colloidal gold-rhTNF nanomedicine. Clin Cancer Res. 2010;16(24):6139-49.
Wang S, Sun Z, Hou Y. Engineering nanoparticles toward the modulation of emerging cancer immunotherapy. Adv Healthc Mater. 2021;10(5):2000845.
Chiang CL-L, Coukos G, Kandalaft LE. Whole tumor antigen vaccines: where are we? Vaccines. 2015;3(2):344-72.
Prasad S, et al. Polymer nanoparticles containing tumor lysates as antigen delivery vehicles for dendritic cell-based antitumor immunotherapy. Nanomed Nanotechnol Biol Med. 2011;7(1):1-10.
Higashisaka K, et al. Nano-safety research: examining the associations among the biological effects of nanoparticles and their physicochemical properties and kinetics. Biol Pharm Bull. 2017;40(3):243-8.
Niu L, et al. Cytokine-mediated disruption of lymphocyte trafficking, hemopoiesis, and induction of lymphopenia, anemia, and thrombocytopenia in anti-CD137-treated mice. J Immunol. 2007;178(7):4194-213.
Leonard JP, et al. Effects of single-dose interleukin-12 exposure on interleukin-12-associated toxicity and interferon-gamma production. Blood. 1997;90(7):2541-8.
Di Giacomo AM, Biagioli M, Maio M. The emerging toxicity profiles of anti-CTLA-4 antibodies across clinical indications. Semin Oncol. 2010;37(5):499-507.
Xia Q et al. Size-and cell type-dependent cellular uptake, cytotoxicity and in vivo distribution of gold nanoparticles. Int J Nanomed, 2019: p. 6957-70.
Bekić , et al. The effect of stabilisation agents on the immunomodulatory properties of gold nanoparticles obtained by ultrasonic spray pyrolysis. Materials. 2019;12(24):4121.
Zhong Y, et al. In vivo molecular imaging for immunotherapy using ultra-bright near-infrared-llb rare-earth nanoparticles. Nat Biotechnol. 2019;37(11):1322-31.
Smith DM, Simon JK, Baker JR Jr. Applications of nanotechnology for immunology. Nat Rev Immunol. 2013;13(8):592-605.
Irvine DJ, Swartz MA, Szeto GL. Engineering synthetic vaccines using cues from natural immunity. Nat Mater. 2013;12(11):978-90.
Kwong B, et al. Localized immunotherapy via liposome-anchored AntiCD137 + IL-2 prevents lethal toxicity and elicits local and systemic antitumor immunity. Cancer Res. 2013;73(5):1547-58.
Kwong B, Liu H, Irvine DJ. Induction of potent anti-tumor responses while eliminating systemic side effects via liposome-anchored combinatorial immunotherapy. Biomaterials. 2011;32(22):5134-47.
Liu H, et al. Structure-based programming of lymph-node targeting in molecular vaccines. Nature. 2014;507(7493):519-22.
Wu TY-H et al. Rational design of small molecules as vaccine adjuvants. Sci Transl Med, 2014. 6(263): p. 263ra160-263ra160.
Zolnik BS, et al. Nanoparticles and the immune system. Endocrinology. 2010;151(2):458-65.
Manolova V, et al. Nanoparticles target distinct dendritic cell populations according to their size. Eur J Immunol. 2008;38(5):1404-13.
Reddy ST, et al. Exploiting lymphatic transport and complement activation in nanoparticle vaccines. Nat Biotechnol. 2007;25(10):1159-64.
Tkach AV, et al. Direct effects of carbon nanotubes on dendritic cells induce immune suppression upon pulmonary exposure. ACS Nano. 2011;5(7):5755-62.
Ryan JJ, et al. Fullerene nanomaterials inhibit the allergic response. J Immunol. 2007;179(1):665-72.
ملاحظة الناشر
تظل شركة سبرينجر ناتشر محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
Nanoparticles in tumor microenvironment remodeling and cancer immunotherapy
Qiang , Dongquan , Shenghan , Milad Ashrafizadeh , Amir Reza Aref , Israel Canadas , Yu Tian , Xiaojia Niu , Yuzhuo Wang , Pedram Torabian , Lingzhi Wang , Gautam Sethi , Vinay Tergaonkar , Franklin Tay , Zhennan Yuan and Peng Han
Abstract
Cancer immunotherapy and vaccine development have significantly improved the fight against cancers. Despite these advancements, challenges remain, particularly in the clinical delivery of immunomodulatory compounds. The tumor microenvironment (TME), comprising macrophages, fibroblasts, and immune cells, plays a crucial role in immune response modulation. Nanoparticles, engineered to reshape the TME, have shown promising results in enhancing immunotherapy by facilitating targeted delivery and immune modulation. These nanoparticles can suppress fibroblast activation, promote M1 macrophage polarization, aid dendritic cell maturation, and encourage T cell infiltration. Biomimetic nanoparticles further enhance immunotherapy by increasing the internalization of immunomodulatory agents in immune cells such as dendritic cells. Moreover, exosomes, whether naturally secreted by cells in the body or bioengineered, have been explored to regulate the TME and immune-related cells to affect cancer immunotherapy. Stimuli-responsive nanocarriers, activated by pH , redox, and light conditions, exhibit the potential to accelerate immunotherapy. The co-application of nanoparticles with immune checkpoint inhibitors is an emerging strategy to boost anti-tumor immunity. With their ability to induce long-term immunity, nanoarchitectures are promising structures in vaccine development. This review underscores the critical role of nanoparticles in overcoming current challenges and driving the advancement of cancer immunotherapy and TME modification.
Keywords Bioengineered nanostructures; cancer immunotherapy, Immune evasion nanoparticles, Tumor microenvironment
Introduction
Cancer cells are mainly suppressed by the complicated networks in the immune system, but tumors develop several mechanisms to evade anti-cancer immunity [1]. Hence, cancer immunotherapy has been introduced as a new mainstay to utilize the patient’s own immune system in cancer cell eradication. The cancer immunotherapy concept can be categorized into immune checkpointstargeted therapy and the adoptive transfer of manipulated immune cells. Both of these strategies contribute to improving the immune system’s function in the identification and eradication of cancer cells [2]. A number of
immune checkpoint inhibitors, including programmed cell death ligand 1 (PD-L1) or cytotoxic T-lymphocyteassociated protein 4 (CTLA-4) antibodies and agonists of costimulatory molecules have shown satisfactory results in clinics for the treatment of cancer patients, however, they still have a number of troublesome problems including low response rate, high cost and non-specific toxicity [3-5]. Another method is the adoptive transfer of cells, which uses genetically engineered cells such as chimeric antigen receptor (CAR)-T cells and others such as multipotent mesenchymal stem cells to affect the expression of a specific cytokine and other features of cells [6, 7]. Since the promising application of immune checkpoint blockade and CAR-T cell therapy, cancer immunotherapy has undergone significant advances. Cancer immunotherapy is now considered a powerful and innovative strategy in clinics compared to other conventional treatments such as surgery, radiotherapy, and chemotherapy. The most recent immunotherapeutic methods have utilized T cells for the induction of adaptive immune responses. On the other hand, studies have shown that a number of innate immune checkpoints with expression on the antigenpresenting cells (APCs) contribute to immune evasion. These checkpoints are capable of detecting and eradicating tumor cells through phagocytosis and suppressing innate immune response. The first line of the immune defense system is provided by innate immune cells such as macrophages, monocytes, and dendritic cells that act as APCs. They induce pro-inflammatory reactions to foreign attacks and contribute to the repair of damaged tissues. The cancer cells are able to express a number of signals known as “do not eat me” signals through expression of CD47 [8], CD24 [9], PD-L1 [10], the beta-2 microglobulin ( ) subunit of MHC-I [11], stanniocalcin 1 (STC-1) [12] and GD2 [13] to evade the macrophagemediated phagocytosis.
The application of cancer immunotherapy has been of importance in the treatment of both hematological and solid tumors [14]. In fact, immunotherapy has revolutionized cancer therapy, and it aims to apply immune checkpoint inhibitors, adoptive cell therapy, and vaccines to finally target the immune-oncology cycle for improving the activity of T lymphocytes in tumor suppression. All of these regimens should be applied in a cycle to accelerate the tumor antigen presentation by APCs [15]. APCs are the cells with the ability to capture, process, and present the exogenous antigens to T cells, and are primarily recognized through the expression of MHCII and other co-stimulatory molecules. APCs are mainly comprised of dendritic cells, macrophages, and B cells. There are also other cells with expression of MHC-II such as thymic epithelial cells. Moreover, there are also other kinds of cells, such as eosinophils and basophils, with the ability of MHC-II expression upon stimulation
[16, 17]. Regarding solid tumors, antigen uptake and presentation are mainly performed by macrophages and dendritic cells [18]. Although macrophages are the prevalent phagocytic cells in cancers, they lack the ability to migrate into lymph nodes and activate T cells [18]. Noteworthy, macrophages are considered a factor in impairing the T cell-mediated responses against tumors, and they reduce the response to immune checkpoint blockade, chemotherapy, and radiotherapy [19, 20]. On the other hand, the dendritic cells have a significant ability in lymph node migration to induce T cells for immunity [18, 21-24]. Moreover, increasing evidence has shown the ability of tumor-resident dendritic cells to stimulate cell-mediated anti-cancer immune response [18, 24-28]. However, it should be noted that macrophages and other cells in the TME, including fibroblasts, can exert carcinogenic activity upon induction and their regulation is of importance for maximizing cancer immunotherapy [19, 29-36]. Stimulation of TME remodeling represents a beneficial strategy for cancer treatment and immunotherapy [37-43]. Although a significant number of studies advocate the potential of immunotherapy in cancer suppression [44-48], immunotherapy has faced its own problems, and the most prominent one is immune evasion. Regarding the mutations and dysregulation of molecular pathways in human tumors, the oncogenic pathways are activated, which can finally promote the survival of cancer cells and mediate their escape from cancer immunotherapy and immune surveillance.
In addition to immune resistance, current drugs used for cancer immunotherapy and TME remodeling lack targeting features. As a result, the nanoparticles have been introduced to facilitate anti-cancer immunity. Nanostructures can improve the retention time and provide the targeted delivery [49]. Furthermore, nanoparticles are capable of TME remodeling to disrupt an immunosuppressive environment. The distortion of blood vessels and high growth rate of tumor cells cause hypoxia in TME that mediates an immunosuppressive environment, characterized by an increase in the accumulation of immunosuppressive cells, including regulatory T cells (Tregs) and myeloid-derived suppressor cells (MDSCs), as well as secretion of a number of factors including vascular endothelial growth factor (VEGF) and transforming growth factor (TGF- ). As a result, the function of dendritic cells is suppressed and macrophages are polarized into M2 phenotype. The nanoparticles can be specifically developed to target TME components and disrupt the immunosuppressive TME to improve the function in cancer immunotherapy. Moreover, nanoparticles can be considered as nano-scale delivery systems for drugs [50]. They can selectively accumulate in tumor tissue and enhance the retention time of drugs. Moreover, nanostructures demonstrate enhanced
permeability and retention (EPR) effect, improving their accumulation in tumor sites because of leaky tumor vasculature and damaged lymphatic drainage [51, 52]. Furthermore, nanostructures can be functionalized with ligands, to specifically target the tumor and even the TME components [53-55]. As a result, nanoparticles have been introduced as new structures for potentiating cancer immunotherapy and overcoming immune evasion [56-63].
Amidst the current challenges in cancer immunotherapy, the need for improving cancer immunotherapy, and the promise of nanoparticles, the use of targeting systems has emerged as a novel strategy for immunotherapy enhancement and TME remodeling. The development of nanoparticles based on targeting TME and improving cancer immunotherapy can strengthen the potential for tumor eradication. Since the TME modulators suffer from targeted action, it is preferred to use targeted non-scale delivery systems for the regulation of TME and improving cancer immunotherapy. The present review
focuses on the application of nanoparticles for TME remodeling and boosting cancer immunotherapy. The current review will first provide a comprehensive outline regarding TME components and then, immune evasion is discussed. Then, the potential of nanoparticles for TME re-education through targeting its components, including macrophages, is described. Moreover, biomimetic nanoparticles and their stimuli-responsive kinds for better tumor targeting are described. Since exosomes have emerged recently in cancer immunotherapy, the role of exosomes, both endogenous and bioengineered, in the regulation of the immune system for tumor suppression is discussed. Figure 1 provides an overview of using nanoparticles for cancer immunotherapy.
Tumor microenvironment components Macrophages
Macrophages, renowned for their phagocytic nature, play a crucial role in the immune system. They participate in various physiological processes, including development
Fig. 1 An overview of using nanoparticles in cancer immunotherapy. The nanoparticles circulate in blood, and upon reaching the tumor site, they reeducate several tumor microenvironment components, including cancer-associated fibroblasts and tumor-associated macrophages, to finally activate the immune system. Moreover, nanoparticles can stimulate immunogenic cell death to enhance the maturation of dendritic cells for the activation of immune cells, such as T cells, to enhance cancer immunotherapy. The co-application of nanoparticles with immune checkpoint inhibitors, such as PD-L1 blockers, can augment the potential of cancer immunotherapy
and homeostasis. The phenotype and function of macrophages are intricately determined by their origin and polarization [64]. Initially believed to originate from hematopoietic stem cells and circulating monocytes [65], the recent studies reported that macrophages have an embryo-derived lineage, with precursors derived from erythro-myeloid progenitors in yolk sacs and fetal liver [65, 66]. Maintaining or enhancing the macrophage population is essential for these cells to function effectively [67,68]. There are two strategies for the replenishment of macrophages: monocyte recruitment and increased proliferation in the form of tissue-resident macrophages for elevating self-renewal ability [67, 69].
In the TME, macrophages are referred to as tumorassociated macrophages (TAMs), constituting of the tumor mass [70]. The TAMs engage in intricate interactions not only with cancer cells but also with natural killer (NK) cells, T cells, endothelial cells, and fibroblasts. The roles of TAMs extend to the regulation of cancer proliferation, invasion, and angiogenesis [71-73]. Macrophages have also been associated with the development of resistance to cancer therapies [74]. The TAMs primarily originate from the bone marrow or the yolk sac [75]. They can be polarized into two phenotypes. The M1 macrophages, induced by lipopolysaccharide and type 1 T helper cell (Th1)-derived cytokines, exhibit pro-inflammatory and anti-cancer functions [76]. The M2 macrophages, induced by Th2-derived cytokines like interleukin-4 (IL4), IL-10, and IL-13, promote proliferation, invasion, and angiogenesis [76]. A delicate balance exists between M1 and M2 macrophages in vivo, influencing tumorigenesis and treatment outcomes [77, 78]. The anti-inflammatory nature of M2 macrophages accelerates cancer progression. The regulation of TAMs has been of importance for cancer immunotherapy. Currently, the strategies for targeting TMAs are based on controlling the origin, functional polarization, and phagocytic function of TAMs. Moreover, macrophages and monocytes have been engineered to mediate anti-cancer immunity. For this purpose, four distinct strategies have been exploited, including a decrease in TAM population, switching from M2 polarization into M1 phenotypes, controlling macrophage phagocytic signal, and bioengineering of macrophages for increasing phagocytosis [79]. Currently, the nanostructures have been widely applied to re-educate TAMs [80], change phagocytosis ability [81], suppress TAMs [82] and deliver drugs to TAMs [83] for cancer immunotherapy.
Cancer-associated fibroblasts
Cancer-associated fibroblasts (CAFs) represent a diverse group of cells that infiltrate the TME. The CAFs are distinct from normal fibroblasts [84]. These cells play a pivotal role in tumorigenesis by inducing biochemical
alterations and signaling network changes that accelerate tumor development [85]. Under specific conditions, CAFs may exhibit anti-cancer activities, contributing to tumor suppression [86].
The heterogeneity of CAFs arises from their diverse origins, including normal fibroblasts, epithelial cells, endothelial cells, peritumoral adipocytes, pericytes, hematopoietic stem cells, mesenchymal stem cells, and cancer stem cells [87]. Based on their functions, CAFs may be categorized into two groups: carcinogenic and anti-carcinogenic CAFs [88, 89]. Ohlund and colleagues identified two distinct subtypes of CAFs in pancreatic cancer: myofibroblasts (myCAFs) and inflammatory CAFs (iCAFs) [90]. The myCAFs, located near cancer cells, are stimulated by transforming growth factor-beta (TGF- ) and exhibit high levels of alpha-smooth muscle actin ( -SMA). In contrast, iCAFs are positioned further away from cancer cells. They demonstrate elevated -SMA levels and the ability to secrete IL-6 and leukemia inhibitory factor [91].
Another subclass of CAFs, antigen-presenting CAFs (apCAFs), express biomarkers related to the MHC-II class and CD44, enabling them to stimulate CD cells in an antigen-dependent manner [92]. Additionally, there is a subtype known as restraining CAFs (rCAFs). Each of these subpopulations plays a distinct role in cancer. For example, iCAFs and myCAFs contribute to metabolic reprogramming and angiogenesis in cancer, respectively. The iCAFs can secrete growth factors, cytokines, and chemokines, including PD-L1/L2, Fas ligand, and others, that influence the regulation of the immune system. The myCAFs, on the other hand, contribute to extracellular matrix remodeling by enhancing collagen synthesis. The apCAFs are involved in stimulating cells for immune cell regulation, while rCAFs exhibit the ability to suppress tumorigenesis [93]. Regarding the importance of CAFs in tumorigenesis, targeting CAFs for cancer immunotherapy has been of importance. The nanostructures demonstrate high penetration and permeability in tumor sites, and can be utilized to regulate CAFs [94]. Moreover, nanoparticles can be utilized to engineer CAFs to act as APCs and stimulate antigen-specific CD T cells in cancer immunotherapy [95]. Nanostructures can trigger clearance of activated and senescent CAFs [96], and regulation of CAFs by nanoparticles can disrupt cancer metastasis and invasion [97].
Neutrophils
Up to of circulating leukocytes are comprised of neutrophils [98], and are considered a first-line against pathogens [99]. Neutrophils have a short life and can persist in circulation for five days [100]. When there is tissue damage or infection, the epithelial cells secrete chemokines to recruit neutrophils. Upon this, neutrophils extravasate
the blood circulation, enter damaged tissue to secrete a number of inflammatory cytokines, release neutrophil extracellular traps (NETs), and finally, phagocytose the pathogens or invading microorganisms [101]. NETs are vehicles for anti-microbial peptides and toxins [102, 103]. In cancer, there are two categories of tumor-associated neutrophils (TANs) similar to the Th1/Th2 pattern, including N1 and N2 with tumor-suppressor and tumorpromoting function, respectively. Tumor type and stage determine the phenotype of neutrophils in TME. During the first stages of tumorigenesis, neutrophils demonstrate an inflammatory phenotype, and as the cancer advances, the neutrophils achieve an immunosuppression phenotype [104]. Neutrophil-mediated inflammation regulation relies on the secretion of ROS and RNS. Moreover, the extracellular matrix can be re-configured by the neutrophils through the secretion of neutrophil elastase and matrix metalloproteinases. The neutrophils display the ability to stimulate angiogenesis through oncostatinM, increase carcinogenesis through PGE2, and enhance metastasis of cancer through the release of ROS, RNS, NE and MMP-9. Noteworthy, the NETs have consisted of MMPs, cathepsin G, and NE [105, 106]. The function of these proteases is to mediate pro-inflammatory cytokine degradation and re-accumulate in TME for enhancement in tumorigenesis and metastasis [107]. In cancer patients, the plasticity of circulating neutrophils is of importance, known as high-density neutrophils (HDNs) or low-density neutrophils (LDNs), corresponding to N1 and N2 phenotypes, respectively. LDNs that have an immature phenotype, show prevalence in the circulation of many cancers and participate in carcinogenesis and metastasis [100]. In the field of cancer immunotherapy, the stimulation of N1 neutrophils can mediate toxic impacts on cancer cells [108]. Furthermore, the stimulation of Ly6Ehi neutrophils through the STING pathway can enhance sensitivity to anti-PD-1 therapy, and they can be utilized as predictors of cancer immunotherapy [109]. Therefore, the development of nanoparticles for targeting neutrophils in cancer immunotherapy is important.
Natural killer cells and T cells
As innate lymphocytes, NK cells exhibit a shorter half-life compared to B and T cells, necessitating their replenishment from bone marrow progenitors [110]. The NK cells undergo linear differentiation, with highly proliferative immature NK cells differentiating into fully functional and granular effectors [111-113]. Enhancing the frequency, infiltration, and function of NK cells contributes to the improved survival of cancer patients [114-117]. This renders NK cells valuable in cancer immunotherapy. These group I innate lymphoid cells can rapidly target cells without prior sensitization [118], and express T-bet and Th1-related cytokines, including IFN- [119-121].
Upon maturation, NK cells migrate from the bone marrow to the blood and subsequently reside in peripheral tissues. Because of their capacity to move between lymphatic and non-lymphatic tissues, NK cells are distributed in numerous organs and tissues [122-124]. Mature NK cells acquire the capability to exert cytotoxic impacts on cancer cells or virus-infected cells [125]. Serving as contributors to the adaptive immune system, NK cells interact with other immune cells through the secretion of cytokines, growth factors, and chemokines [125]. These effects position NK cells as effective effectors in diseases such as cancer, infectious diseases, autoimmunity, and chronic inflammation [126-129].
Moreover, NK cells play a significant role in the innate immune system, providing surveillance in hematological cancers and cancer metastasis [110, 130, 131]. The increased infiltration of NK cells into the TME is positively associated with the prognosis of various cancer types, including melanoma, renal cell cancer, liver tumors, and breast cancer, among others [132-136].
The adaptive immune system is primarily shaped by T cells, providing effective defense against pathogens and cancers. Upon exposure to cytokines and co-stimulatory signals, naïve cells undergo proliferation, differentiating into effector cells. Naïve cells can differentiate into T helper cells, including TH1, TH2, TH17, and TFH cells, to exert immune functions. The differentiation of naïve cells into effective cells enables these cells to combat infections and cancers through the release of IFN- , TNF- , and cytotoxic molecules [137].
A challenge in cancer arises from T cell exhaustion. This phenomenon is mediated by various mechanisms, with the PD-1 axis being the most prominent. Upon antigen exposure, naïve T cells transform into effector T cells, with some undergoing cell death and others participating in tumor elimination. Antigen presentation can lead to the formation of stem cell memory T (TSCM) cells, which convert into TCM, TEM, and TRM. The TRM cells reside in the tissue, ready to respond to secondary stimulation, while TSCM and TCM possess self-renewal capacity, generating TEM and TE upon re-stimulation [138].
Signs of T cell exhaustion include the expression of inhibitory receptors, reduction in T cell function, and decreased proliferation. Exhausted T cells exhibit a unique epigenetic profile that may result in a differential or poor response to immunotherapy. Additionally, exhausted T cells experience metabolic dysregulation, including mitochondrial suppression and glycolysis inhibition [139]. The challenge in cancer therapy extends beyond T cell exhaustion, as their death and reduced proliferation can impair immune reactions. Targeting NK and T cells with nanoparticles has strengthened cancer immunotherapy. The nanoparticles with high uptake
in NK cells, such as lipid-based nanoparticles, can be utilized to engineer NK cells [140]. Furthermore, nanostructures can be utilized for non-invasive tracking of NK cells, including their migration and biodistribution in tumor regions [141]. The expression levels of CCR4 and CXCR4 on the surface of NK cells can be changed by nanoparticles to improve their interaction with cancer cells [142]. Noteworthy, the nanoparticles can be designed to stimulate both NK and cells in cancer immunotherapy [143].
Endothelial cells and pericytes
Endothelial cells form the inner lining of blood vessels. The biological functions of endothelial cells are crucial for preserving normal physiological conditions [144]. These cells play important roles in regulating blood clotting, vessel size, and immune functions to enhance blood fluidity, oxygen distribution, cell transport, and nutrient supply. Endothelial cells continuously secrete anticoagulant proteins to prevent clotting in vascular beds, maintaining homeostasis and ensuring blood flow and pressure at an appropriate level to deliver oxygen and nutrients to tissues [145-149].
Despite their essential physiological functions, endothelial cells have been implicated in cancer progression. Recent reviews have highlighted the role of endothelial cells in the tumor stroma [150, 151]. In the initial stages, endothelial cells induce angiogenesis to increase the presence of blood vessels in the primary tumor. These cells also function as a platform and site for membrane-bound factors and proteins, creating a TME conducive to cancer progression. These localized functions of endothelial cells also play a role in regulating angiocrine signaling at distant sites, influencing organ function. Furthermore, factors and proteins secreted by tumor cells can extend beyond tumor boundaries, affecting endothelial cells at distant sites and exerting systematic functions [152].
Understanding the functions and regulatory impacts of tumors beyond their sites is crucial, given that most cancer-related deaths result from invasion, thrombosis, and cachexia [153-155]. Proteins and factors secreted by tumor cells can induce changes in endothelial cells in the pre-metastatic niche, enhancing the dissemination of cancer cells and mediating angiogenesis. Additionally, these factors can lead to thrombosis in distant vasculature [156]. Endothelial pericytes have been recognized more than a century ago as microvasculature-associated mural cells [157]. These perivascularly positioned cells [158-160] are ubiquitously distributed in all vascularized tissues [161, 162]. Identification of pericytes requires immunostaining and the use of biomarkers and antigens to differentiate them from vascular smooth muscle cells, fibroblasts, and mesenchymal cells [157]. Initially considered inert cells contributing to physical vascular stability
[163, 164], recent advances have illuminated their roles in both physiological and pathological conditions.
Pericytes play a crucial role in regulating blood vessel development and modulating blood flow, coagulation, and vascular permeability [165]. The structure of capillaries includes endothelial cells, pericytes, the basement membrane, and vascular smooth muscle cells [166]. The primary function of pericyte function in cancer progression is stimulating angiogenesis in the TME [167]. The CD248 is capable of Wnt upregulation and increasing the levels of OPN and SERPINE1 in pericytes to cause angiogenesis and expedite cancer progression [168]. Additionally, pericyte contractility can be induced by the enzyme hexokinase 2 in glycolysis, leading to abnormalities in tumor blood vessels [169]. When present in the tumor site, RGS5-TGF -Smad creates an anti-apoptotic environment that accelerates cancer cell growth [170]. Figure 2 is a schematic representation of TME components.
Myeloid-derived suppressor cells
The Myeloid-derived suppressor cells (MDSCs) are another type of cell present in TME. There are a number of arguments that MDSCs are a subtype of neutrophils [104] due to the presence of overlapping markers among MDSCs and TANs, making it challenging and problematic to distinguish them. There is still controversy regarding whether MDSCs represent a separate lineage of cells or are polarized immature neutrophils [171]. Overall, MDSCs are considered a heterogeneous population of cells with myeloid origin [172]. In spite of origination from myeloid progenitor cells, MDSCs and TANs are considered different cell types. Furthermore, MDSCs demonstrate several distinct features from neutrophils, including downregulation of CD16 and CD621 and upregulation of Arg1, CD66B, and CD11b [173, 174]. Furthermore, the studies have shown other subtypes of MDSCs including monocytic MDSCs (M-MDSCs), which are distinguished by a CD11b hi, LY6C hi, and LY6G lo phenotype, polymorphonuclear MDSCs (PMNMDSCs), which display a CD11b hi, LY6C lo, and LY6G hi phenotype, and early stage MDSCs (eMDSCs) which are CD13- and CD14-, and CD33+in humans [175, 176]. In TME, it is possible to observe both M-MDSCs and PMN-MDSCs, and compared to MDSCs, they demonstrate a suppressive phenotype [177]. The MDSCs suppress T cells and the innate immune system to create an immunosuppressive phenotype in TME [177]. MDSCs also contribute to the formation of pre-metastatic niches, can elevate stemness and angiogenesis, and promote metastasis through EMT induction and enhancing IL-6 secretion [178, 179]. There are also other factors in TME that can affect MDSCs. The HIF-1 , a marker of hypoxic TME, stimulates the differentiation of MDSCs into
Fig. 2 Cellular components that influence the tumor microenvironment (TME). Interactions within the TME play a crucial role in accelerating cancer progression. Cancer cells activate the PD-L1/PD-1 axis, leading to T cell exhaustion and impairment of T cell function. In addition, cancer cell-secreted exosomes that carry PD-1 contribute to T cell dysfunction, reducing proliferation and hindering proper function. Natural killer cells counteract tumorigenesis by secreting perforin and granular enzymes. Increased infiltration of Treg cells in the TME secretes TGF- , inducing fibroblast transformation into cancerassociated fibroblasts (CAFs), promoting extracellular matrix deposition, and causing T cell dysfunction. Myeloid-derived suppressor cells (MDSCs) induce Treg cell formation in the TME through the secretion of PGE-2, IL-10, and TGF- . Regulatory T cells (Treg), in turn, suppress the function of dendritic cells (DCs) by secreting perforin, leading to DC cell apoptosis. M2-polarized macrophages secrete TGF- and IL-10, disrupting DC cell function. The interaction between endothelial cells and cancer cells results in angiogenesis, further enhancing cancer progression (created by Biorender.com)
TAMs with carcinogenic function [180]. The metabolism of MDSCs in TME can be changed towards stimulation of fatty acid oxidation to enhance levels of Arg1 and NOS2 [181]. For cancer immunotherapy, the regulation of MDSCs can provide new insights, such as the downregulation of CCRK that disrupts the immunosuppression activity of MDSCs and promotes the potential of immune-checkpoint blockade therapy [182]. The nanostructures are able to reduce the population and function of MDSCs, impair MDSC-mediated immunosuppression and cause MDSC repolarization [183-185].
Cytokines, chemokines and other factors
The immune cells present in the TME use the cytokines to send messages to other cells in an endocrine, paracrine or autocrine manner and provide intercellular communication [186]. Cytokines, also known as immunomodulatory agents, can be produced in physiological
and pathological status, and various classes of cells, including adipocytes and tumor cells, can secrete them. The cytokines contribute to the cellular (type 1) and antibody-mediated (type 2) immunity as anti/proinflammatory and pro/anti-tumorigenic effectors that also rely on the TME. Cytokines can bind to the receptor on the surface of other cells to regulate their action and change the molecular pathways. There are different kinds of cytokines in TME, including chemokines, interleukins, adipokines, transforming growth factors (TGFs), tumor necrosis factor (TNF), colony-stimulating factors (CSFs), and interferons (IFN) that can act alone or in a synergistic way to affect immune system [187]. Chemokines are considered as chemoattractant cytokines for the recruitment of inflammatory cells, including leukocytes (monocytes, neutrophils), along with other kinds of cells, such as endothelial and epithelial cells [188]. Depending on the position of conserved cysteine residues, there are
various classes of cytokines including CX3C, CXC, CC, or C chemokines [189]. Moreover, chemokines are able to interact with the G protein-linked transmembrane receptors known as chemokine receptors [190]. A number of chemokines, such as CXCL8 and CCL3, have an inflammatory function, and they recruit the cells via the inflammatory signs or/and homeostatic [191]. Interleukins (ILs) possess a low molecular weight and demonstrate proand anti-inflammatory functions. The immunocompetent cells, including T cells, granulocytes, monocytes, macrophages, adipocytes, and endothelial cells, can secrete ILs [192]. The ILs play a critical role in the development, differentiation, induction, maturation, migration, and adhesion of immune cells [193]. Adipokines (also known as adipocytokines) are cytokines that can be secreted by adipose tissue and consist of adipocytes, pre-adipocytes, macrophages, stromal cells, fibroblasts, and endothelial cells [194]. The adipokines are comprised of adipose tissue-specific cytokines (adiponectin, leptin) and other categories, including ILs, TNFs, and chemokines. Moreover, inflammation, energy metabolism, and fat distribution can be controlled by adipokines [195]. The adipokines also contribute to obesity-related inflammation to regulate metabolic diseases [196]. Adipocytes are critical regulators of tumorigenesis and metastasis [197]. According to the impact of adipokines on the immune system, there are two kinds, including pro-inflammatory, such as leptin, TNF , interleukin- (IL-1 ), interleu-kin-6 (IL-6), and interleukin-8 (IL-8), potentially linking adiposity and inflammation, and anti-inflammatory, such as interleukin-10 (IL-10) and adiponectin [197, 198]. A number of adipokines, such as adiponectin, demonstrate anti-carcinogenic function [198], while others, such as leptin, demonstrate carcinogenic function [199]. TGFs are a number of protein hormones that are overexpressed in human cancers and can modulate tumorigenesis and cancer growth. TGFa is a member of the EGF family with the potential to regulate epithelial development and cell proliferation and can modulate carcinogenesis and angiogenesis [200]. M2 macrophages and other kinds of cells, including cancer cells, can secrete TGF- to modulate the function of T cells, NK cells, and macrophages present in TME, disrupting anti-cancer immunity and enhancing carcinogenesis [201]. IFN was discovered upon its function to interfere with viral growth [202]. The host cells secret IFNs, and they can regulate the immune system. The fibroblasts and monocytes are able to secrete type I IFNs such as IFN- and IFN- during the viral attack. Then, the expression of proteins with the ability to impair RNA and DNA replication is upregulated. The type II IFNs, including IFN- can be released by and Th1 cells to induce a number of cells, including NK cells, M1 macrophages, and cells for enhancing
MHC I and II presentation, promoting the anti-cancer immunity [203].
Enzymes
The changes in the expression level of enzymes are a feature of TME, and it can be exploited in a rational way to treat cancer [204]. Enzymes are a kind of protein or RNA that can facilitate chemical reactions [205]. The enzymes for catalyzing reactions are highly selective and under mild conditions, demonstrate the specific substrates to modulate biological and metabolic mechanisms [206]. The enzymes display a number of changes in expression in diseases such as TME [207]. The TME shows several enzyme secretions consisting of MMPs, hyaluronidase, -glutamyl transpeptidase, and esterase with higher expression in tumors compared to normal tissues [208, 209]. The proteases contribute to the degradation of proteins or peptide substrates. The oxidoreductases can mediate the catalysis of electron transfer from the reductant to the oxidant. Kinases provide phosphorylation to affect protein activity and phosphatases mediate dephosphorylation. A number of enzymes demonstrate upregulation such as MMP-2 [210]. In bladder tumors, the expression of HAse is enhanced compared to the normal tissues [211].
Extracellular matrix components
The extracellular matrix (ECM) is comprised of collagen, fibronection, laminin, vitronectin, elastin, and other factors including growth factors, cytokines, and matrix metalloproteinases that contribute to the support of the epithelial cell structure [212,213]. Various cells have the ability to secrete ECM components but they are mainly secreted by fibroblasts [214]. During cancer progression, ECM can be considered as an initiation factor. The composition of ECM can be different based on the type of cancer, such as gastric tumors, in which a lower degree of differentiation improves the abundance of ECM components, heightens cell metabolism, and increases metabolic reprogramming [215]. According to the proteomic analysis, there is no difference between ECM components in tumor and normal tissues, while their levels demonstrate changes that are manifested by enhancement in ECM proteins and reduction in basement membrane components modulating tumor angiogenesis, metastasis, and invasion [216]. The density of ECM components increases during tumor progression, and a number of factors, such as E-cadherin/ -catenin, demonstrate reduction, enhancing proliferation and metastasis of cancer cells [217]. The increase in matrix density can cause a kind of environmental stress to enhance carcinogenesis. The high-strength ECM can stimulate EMT to increase cancer progression and promote the infiltration of M2
polarized macrophages while it suppresses the function of cells [218,219].
Hypoxia
The presence of hypoxia is another feature of TME resulting from the high proliferation of tumor cells. The alterations in interstitial fluid pressure, decrease in pH , and enhancement in ROS generation can result from hypoxia [220]. In regions with hypoxia, there is high interstitial fluid pressure due to leaky vasculature and abnormal lymphatic drainage in the tumor [221]. Moreover, the hypoxia in TME can enhance the generation of lactic acid and carbonic acid through glycolysis induction, providing an acidic pH . The hypoxia-inducible factor (HIF) can induce carbonic anhydrase IX or XII to transform carbon dioxide and water into HCO 3 – that, upon diffusion out of the cell membrane, it enhances levels in TME. Furthermore, the endosomal and lysosomal vesicles in tumor cells demonstrate more acidic pH compared to cytosolic pH [222]. The hypoxia TME displays a redox potential difference between intracellular space (reducing) and extracellular space (oxidizing). Such redox potential is vital for the development of smart and selective delivery of therapeutics [223]. The enzymatic reduction during hypoxia in TME can cause the metabolism of chemical factors, including nitro, quinones, aromatic N -oxides, aliphatic N -oxides, and transition metals [224]. Such a feature can be utilized to develop hypoxia-responsive structures for exploiting the hypoxic regions [225].
Mechanisms of immune evasion in cancer and unanswered questions in cancer immunotherapy
The immune system has undergone a transformative evolution to combat cancer progression. However, immune responses can be suppressed, and tumor cells often employ mechanisms to evade these responses, a concept known as immune evasion. Recent studies have shed light on the major mechanisms contributing to the immune evasion of cancer cells.
Mutations within tumor cells can facilitate immune evasion. This is evidenced by the dysregulation of cells observed in clinical specimens harvested from ovarian cancer patients, accompanied by the activation of immunosuppressive signaling through TGF- [226]. A well-known mechanism for inducing immune evasion is the upregulation of PD-L1. In hepatocellular carcinoma, USP22 expression increases via PRDM1, leading to diminished SPI1 degradation through USP22 upregulation. This, in turn, results in increased PD-L1 expression, promoting immune evasion [227].
Efforts to suppress PD-L1 have shown promise in disrupting immune evasion. RNF31, with its ability to downregulate PD-L1 by enhancing ubiquitination and degradation of YAP, improves the function of
cells, offering potential in cancer immunotherapy [228]. While immune checkpoint inhibitors have significantly improved tumor suppression and immunotherapy potential, the efficacy of these treatments is compromised by mechanisms related to immune evasion.
In addition to the previously discussed mechanisms, Choi and colleagues [229] proposed that lactic acid, a byproduct of cancer cell metabolism, plays a crucial role in suppressing anti-cancer immunity. This hypothesis has been substantiated by further research, notably in the comprehensive review by Wang and colleagues [230]. Their findings indicate that the accumulation of lactic acid and the resulting acidic tumor microenvironment (TME) significantly impair anti-cancer immune responses. Notably, it has been demonstrated that the presence of lactic acid and the acidic conditions within the TME inhibit the function of various immune cells, including T cells and dendritic cells. This leads to an immunosuppressive environment that promotes tumor growth and metastasis. Such insights underscore the complex interplay between cancer cell metabolism and immune evasion, emphasizing the pivotal role of lactic acid and the acidic TME as key contributors to cancer progression.
Upregulation of inhibitors such as SUSD6, TMEM127, and WWP2 in MHC-I has been implicated in immune evasion. Downregulation of SUSD6 increases MHC-I antigen presentation, suppressing cancer progression in a T cell-dependent manner. The mechanism involves SUSD6 forming a complex with TMEM127 and MHC-I to recruit WWP2 for lysosomal degradation of MHC-I, facilitating immune evasion [231].
MHC-I, a key factor in immune evasion, undergoes internalization and degradation by CEMIP, further reducing immune surveillance [232]. In addition, SOX4induced T cell exhaustion mediated immune evasion. The interaction between cancer cells and cells, facilitated by Midkine, alters immune system responses [233]. In PTEN-deficient animal models, PI3K downregulation results in STAT3 suppression, accelerating immune responses and revealing the potential of PI3K in causing immune tolerance and evasion [234].
Chromosomal changes and deletions also play a role in immune evasion. Homozygous deletions affecting chromosome 9 q 21.3 impair the function of , hastening carcinogenesis. Half of these deletions affect the IFN gene cluster on chromosome 9 q 21.3 , increasing the escape of tumor cells from cell surveillance [235].
Maintaining the balance of interferon responses is vital for cancer immunotherapy, as alterations in interferon and T cell levels can induce immune evasion. mTORC1 enhances B7-H3 expression, reducing T cell function and IFN- responses while increasing MHC-II expression [236]. One mechanism causing immune escape involves
reducing the number of T cells, mediated by apoptosis induction. Extracellular galectin 4 stimulates T cell apoptosis, diminishing immune surveillance. Conversely, the downregulation of galectin 4 promotes M1 polarization of macrophages and enhances T cells and dendritic cells, disrupting immune escape [237].
The immune cells have shown potential in the identification and recognition of neoplastic cells possessing initiation mutations to suppress tumorigenesis [238]. Although the origination of a tumor is from a single transformed cell, the presence of genomic instability can cause the generation of cancer cells that are genetically heterogeneous with unique morphological and physiological characteristics. Moreover, the tumor cells have shown significant features in terms of surface molecule expression, proliferation and angiogenesis [239] resulting from the morphological and epigenetic plasticity. Hence, the cancer cells demonstrate expression of different antigens that may be tumor-specific or tumor-associated, differentiation antigens, and lectin-binding sites. Such antigens display uneven distribution on tumor subpopulations and can stimulate various immune responses [240]. Such tumor heterogeneity can significantly affect the genotype, gene expression, cellular morphology, metabolic activity, motility, and behaviors, including proliferation, antigen presentation, drug response, and metabolism [241]. Furthermore, this heterogeneity can be utilized for the diagnosis, therapeutic efficacy, and recognition of promising targets [242]. Such a heterogeneous nature of cancer cells can provide significant opportunities to escape from the function of immune cells. The tumor cells significantly proliferate in TME, which can cause hypoxia. The presence of hypoxia in TME recruits MDSCs and impairs the function of NK cells to provide a pre-metastatic niche [243], showing that cancer cells metastasize through suppressing immune surveillance. Upon surgical resection, the cancer cells undergo trauma, and such tumor cells can enhance the generation of cytokines and other factors, including IL-6, C-reactive protein (CRP), TNF- , IL- to affect the immune system [244]. Therefore, the application of conventional therapies and the heterogeneous nature of cancer cells should be considered in immune evasion. The immune cells are able to suppress vulnerable cancer cells presenting tumor antigens [245], while the heterogeneous nature of cancer cells allows them to escape such action of the immune system. Furthermore, the tumor cells have shown capacity to induce apoptosis in tumor-specific cytotoxic T lymphocytes [246].
Therefore, since immune evasion commonly occurs in cancer, cancer immunotherapy has been introduced. Regarding cancer immunotherapy, there are a number of challenges that should be addressed. The first and most important challenge is regarding the fact that dominant
drivers of cancer immunity should be highlighted. Moreover, more investigation should be directed towards understanding the function of organ-specific tumor immune context. Checkpoint inhibitors are commonly utilized for the treatment of human cancers, but there is still a long way towards understanding the molecular landscape of factors regulating primary versus secondary immune escape. There is a big question about whether it is better to use endogenous or synthetic immunity for the treatment of human cancers. Moreover, since cancer immunotherapy has been applied in clinics, there are also questions regarding the effective evaluation of cancer immunotherapy in clinical studies. One of the hopes is the advances in the field of biology highlighting the application of biomarkers and signatures for cancer immunotherapy. Therefore, precision medicine can significantly benefit by highlighting the signatures and developing strategies based on targeting accurate and efficient signatures for cancer immunotherapy. Another question is that various types of regimens for cancer immunotherapy have been developed, and comprehensive studies are required to be performed in improving long-term survival through a combination of such regimens. In order to optimize the process of cancer immunotherapy, responding to such concerns and questions can improve the potential for the treatment of cancer patients [247].
Nanoparticles targeting tumor microenvironment components in cancer immunotherapy
To address the immunosuppressive role played by M2-polarized macrophages, the stimulation of M1 polarization through nanostructures emerges as a promising avenue for enhancing immunotherapy. A pivotal mechanism involves the development of genetically modified pristine cells, whose extracted cell membrane is utilized to coat and functionalize nanoparticles in cancer therapy. Biomimetic magnetic nanoparticles featuring gene-edited cell membranes demonstrate the capacity to target multiple pathways, thereby regulating macrophage polarization and suppressing tumorigenesis. Specifically, the presence of gene-edited cell membranes suppresses the CD44/SIRP axis by upregulating SIRP variants. Magnetic nanoparticles, forming the core, play a crucial role in re-educating and reprogramming macrophages, thereby accelerating cancer immunotherapy [248].
Changes in macrophages extend beyond polarization, and their role in regulating antigen processing is also significant. Certain clinically important pathways, such as STING, pose a challenge for targeting at the clinical level due to a lack of targeted delivery. By functioning as a STING agonist, ZnCDA encapsulates CDA and disrupts the endothelial barrier in cancer vasculature, facilitating penetration into the TME and tumor site.
These nanoparticles target macrophages, enhancing antigen processing and expediting T-cell-related responses in cancer immunotherapy [249]. A number of nanoparticles have shown potential in changing the polarization of TAMs. In the context of M1 polarization of macrophages, different mechanisms are available for the induction of polarization of macrophages into the M1 phenotype. Ginseng-derived nanostructures with extracellular vesi-cle-like properties can stimulate the TLR4/MyD88 axis, resulting in increased M1 polarization of macrophages, elevated ROS levels, and induction of apoptosis in melanoma [250]. In fact, the M1 polarization of macrophages has been accompanied by apoptosis induction.
Although the primary focus of this section is to evaluate the role of nanoparticles in macrophage re-education, studies have demonstrated that membranes can be extracted from macrophages to coat and functionalize nanoparticles. This approach results in the development of biocompatible structures with stealth properties [251]. Such an approach can be used mutually in which nanoparticles are functionalized with macrophage membrane to improve their targeting ability towards macrophages and TME, and on the other hand, they can be designed for re-education of macrophages into M1 phenotype.
Targeting macrophages in cancer treatment is primarily driven by their immunosuppressive function. Despite the development of various immune response regulation strategies, such as phototherapy-induced immunotherapy, concerns persist regarding immunogenicity and inflammation induction. Therefore, it is crucial for nanoparticles to employ safe and biocompatible mechanisms to counteract macrophage-mediated immunosuppression. The biomimetic -SAS@PLT nanostructures, derived from sulfasalazine-loaded mesoporous magnetic nanostructures and functionalized with platelets, have been designed to suppress the glutamatecystine antiporter system Xc-pathway in ferroptosis induction. This ferroptosis induction demonstrates synergistic effects with PD-L1 immune checkpoint immunotherapy, as observed in animal models. Notably, these biomimetic nanostructures induce ferroptosis, promoting M1 polarization of macrophages and disrupting the immunosuppressive TME [252].
When considering nanoparticles for modulating macrophages, especially for potential use in cancer immunotherapy at the clinical level, biocompatibility is as important as functionality. Lipid nanoparticles with cationic features have shown promise as carriers, delivering mRNA to targeted sites. Loading mRNA for re-educating macrophage polarization onto lipid nanoparticles creates safe and biocompatible nanostructures for cancer immunotherapy [253]. A significant advancement in utilizing nanoparticles for macrophage re-education
involves functionalizing them with macrophage membranes to enhance efficacy. This hypothesis has been tested in experiments, demonstrating the potential of membranes derived from tumor-associated macrophages with immunomodulatory functions and anti-gen-homing affinity. These membranes were employed to functionalize upconversion nanostructures loaded with photosensitizers. Notably, tumor-associated macrophage membrane-functionalized nanoparticles suppress CSF1 and interactions between cancer cells and the tumor microenvironment, impairing tumorigenesis. Moreover, these nanoparticles stimulate photodynamic therapy by suppressing the M2 phenotype, enhancing M1 macrophage polarization, inducing immunogenic cell death, and improving the generation of T cells through enhanced antigen presentation [254].
Reorienting macrophages toward the M2 phenotype presents a hurdle in achieving successful immunotherapy. This polarization is chiefly instigated by tumor cell-secreted MCSF, resulting in the elevation of CSF1-R. Moreover, the heightened expression of SIRP on myeloid cell surfaces activates SHP-1 and SHP-2 in macrophages, impeding immunotherapy by hampering phagocytosis. Moving beyond macrophage polarization, efforts are redirected to address macrophage activity failure. To augment macrophage phagocytosis, promising strategies involve the regulation of CSF1R and SHP2. Nanoparticles laden with CSF1R and SHP2 suppressors induce M1 macrophage polarization, boosting phagocytosis to impede tumorigenesis [255].
After elucidating the key mechanisms governing macrophage polarization and activity, the subsequent focus involves exploring nanoparticles with potential clinical applications. The FDA-approved ferumoxytol, an iron supplement and iron oxide nanostructure, serves dual roles as a drug delivery system and imaging agent. When co-cultured with macrophages for treating lung cancer metastasis, ferumoxytol upregulates caspase-3, inducing macrophages to express mRNAs for pro-inflammatory Th1-related responses. Ferumoxytol effectively suppresses tumor metastasis and proliferation while promoting M1 macrophage polarization to enhance the quality of cancer immunotherapy [256].
A growing body of evidence supports the potential involvement of tumor-associated macrophages in the development of drug resistance [257, 258]. These macrophages play a role beyond immune system regulation, influencing the response to chemotherapy. Furinbased aggregated gold nanostructures capitalize on the “enhanced permeability and retention” effect, aggregating in breast cancer due to furin upregulation. This process suppresses exocytosis, leading to increased preferential accumulation at the tumor site. These nanoparticles also inhibit autophagy, promoting M1 macrophage education
to counteract drug resistance [259]. Table 1 provides a concise overview of the applications of nanoparticles in macrophage re-education for cancer immunotherapy. Figure 3 provides an overview of the regulation of tumorassociated macrophages by nanoparticles in cancer immunotherapy.
Nanoparticles play a crucial role in influencing cancerassociated fibroblasts (CAFs) within the cancer treatment landscape. Interactions between cancer cells and CAFs in the TME contribute to tumorigenesis, making it essential to explore nanoparticle applications in suppressing these interactions and impeding cancer progression. In ovarian cancer, ovarian cancer cells and TME cells promote the activation of ovarian CAFs. Gold nanoparticles with a size of 20 nm effectively disrupted this interaction, inhibiting CAF activation and offering potential in the treatment of ovarian cancer [275].
CAFs play a supportive role in tumor metastasis. Core-shell nanoparticles, with gold as the core and silver as the shell, were effective in suppressing osteopontin expression in CAFs, hindering cancer progression without impacting CAF biomarker expression [276]. Besides modulating CAF activation and secretions, nanostructures may also be used for targeted CAF destruction. Ultra-small iron oxide nanocarriers ( 6 nm in diameter) combined with low-frequency rotating magnetic fields induce mechanical forces, leading to CAF death and lysosomal disruption [277]. Targeting CAFs for destruction enhances nanoparticle internalization. Such a strategy addresses the challenge of a dense TME that hinders nanoparticle penetration. Ferritin nanocages loaded with the photosensitizer ZnF16Pc and modified with a singlechain variable fragment that targeted fibroblast activation protein, facilitated phototherapy to reduce CAFs and improve nanoparticle penetration into the tumor site [278].
Nanoparticles can serve dual functions in regulating CAFs and modulating immune responses. Poly(lactic-co-glycolic acid) (PLGA) nanoparticles functionalized with cancer cell membrane not only enhanced cancer cell-CAF interactions, but also increased antigen uptake, stimulating and T cells through MHC-I and MHC-II, thus promoting cancer immunotherapy [279]. The fibroblast activation protein, upregulated on CAF surfaces, represents a promising target in cancer immunotherapy. Nanoparticles functionalized with a singlechain variable fragment for ZnF16Pc delivery in cancer phototherapy lacked systemic toxicity. These functionalized nanoparticles suppressed cancer progression in both primary and distant sites by accelerating immune responses and promoting anti-CAF immunity [280].
Some nanoparticles are designed to respond to fibroblast activation protein as a CAF biomarker. Albumin nanostructures encapsulating paclitaxel and functionalized with CAP showed promise in targeting fibroblast activation protein in CAFs. Incorporation of the photosensitive compound IR-780 further enabled near-infrared laser irradiation for photothermal therapy, resulting in tumor suppression and improved deep tumor penetration [281]. The concept of specifically targeting CAFs using their biomarkers has significant potential in enhancing the fight against cancer.
Nanoparticles targeting T cells
Nanoparticles, through targeted regulation of T cells, have emerged as a promising avenue for effective cancer immunotherapy [282-288]. Increasing the infiltration of cells and T helper cells in the TME is crucial for TME remodeling and activating the immune system against cancer progression. Nanoparticles such as manganese zinc sulfide nanostructures play a pivotal role in mediating this effect [289]. A noteworthy trend in recent years involves the integration of immunotherapy with other therapeutic modalities like chemotherapy or phototherapy. Hybrid prodrug nanocarriers carrying cisplatin and camptothecin, stimulate the cGAS/STING axis and induce DNA damage. Additionally, these prodrug nanocarriers enhance cell infiltration in the TME, improving immunotherapy outcomes for colorectal cancer. These hybrid nanocarriers possess a responsive feature to reactive oxygen species (ROS) and are constructed from mPEG2k-DSPE and other polymers [290]. The mPEG/PLGA/PLL nanocarriers, delivering CD155-siRNA and modified with PD-L1 antibodies, can simultaneously suppress CD155 and PD-L1, avoiding immune evasion. They enhance cell infiltration and induce immunogenic cell death in breast cancer therapy [291].
Developing an effective anti-cancer vaccine requires nanoparticles that can induce systemic immunity. melittin nanostructures, responsive to changes in the TME, serve as promising vaccines by triggering systemic immune responses. These nanostructures induce cancer cell death through the Fenton reaction in the TME, activate the cGAS/STING axis, and enhance antigen-presenting cell maturation. Furthermore, melittin nanoparticles stimulate systemic immune reactions, including the promotion of T cells and increased levels of pro-inflammatory cytokines and chemokines [292].
Combining chemotherapy with phototherapy is another strategy to expedite tumor suppression. Prodrug nanocarriers, developed from hyaluronic acid and adamantine-conjugated heterodimers of PPa and JQ1, target CD44-overexpressed pancreatic cancer cells.
Table 1 Nanoparticle-induced cancer immunotherapy through targeting macrophages
Nanoparticle
Cancer type/Cell line
Size (nm)/Zeta potential (mV)
Outcome
Reference
PEGylated liposomes
Breast cancer/4T1 cells
Pancreatic cancer/ murine KPC1245 and KPC1242 cells
75 nm
Delivery of mannose and levamisole hydrochloride for glycolysis suppression and reducing mitochondrial energy metabolism Suppression of cancer proliferation
Combination with radiotherapy impairs M2 polarization of macrophages and increases immune responses
[260]
Prodrug nanoparticles
Colorectal cancer/ MC38 cells Breast cancer/ MCF-7 cells
less than
Co-delivery of doxorubicin and R848 Modification of nanoparticles with bifunctional PD-1/PD-L1 peptide antagonist PCP Cleavage of nanoparticles with FAP-a in the tumor stroma Release of cargo in the tumor site stimulates immunogenic cell death and causes macrophage reprogramming
[261]
Lipid nanoparticles
Pancreatic cancer/ KPC cells
mV
Loading lipid nanoparticles in injectable hydrogels Delivery of CCL5-siRNA by lipid nanoparticles to induce M1 polarization of macrophages and enhance T cell-induced immune responses
[262]
Upconversion nanostructures
Breast cancer/4T1 cells
and mV and -4.1 mV
Introduction of upconversion nanoparticles co-doped with perfluorocarbon (PFC)/chlorin e6 (Ce6)
Targeted delivery of paclitaxel as a chemotherapy drug Increasing singlet oxygen production Stimulating M1 polarization of macrophage in accelerating pro-inflammatory cytokine release to impair breast cancer progression
[263]
Iron-chelated melanin-like nanocarriers
Colon and breast cancers/ CT26 and 4T1 cells
150 nm
Stimulating M1 polarization of macrophages and providing photothermal therapy, they accelerated tumor-associated antigen release to improve cancer immunotherapy
[264]
Supramolecular nanoparticles
Breast cancer/4T1 cells
Suppression of CSF1R and MAPK to stimulate M1 polarization of macrophages
[265]
MIP-3 plasmid
Breast cancer/4T1 cells
Increasing dendritic cell maturation and suppressing M2 polarization of macrophages
[266]
Au@PG nanocarriers
Lung cancer/ Lewis lung carcinoma cells
32.2 nm at 2.5 mM ONPG, 29.8 nm at at 50 mM , and 18.3 nm at 75 mM
Polyaniline-based glycol-condensation on the nanostructures Switching M2 polarized macrophages into M1 polarized macrophages Nanoparticles with smaller sizes demonstrate higher efficacy in the macrophage re-education
[267]
CaCO3-loaded Au nanostructures
Macrophages/ RAW 264.7 cells
32 nm
Elongating macrophage cell morphology Stimulation of M1 biomarker and inflammatory cytokines Inducing M2 polarization of macrophages
[268]
Polymeric nanocarriers
Osteosarcoma/ K7M2 cells
Biodegradable nanoparticles for delivery of regorafenib as vascular normalization compound Release of cargo upon laser irradiation of 808 nm and increasing hypoxia in TME Induction of the release of reactive oxygen species and mediation of immunogenic cell death Stimulation of M1 polarization of macrophages
[269]
Gadofullerene nanocarriers
Breast cancer/4T1 cells
M1 polarization of macrophages and increasing infiltration of T lymphocytes in the TME for cancer suppression
[270]
DGL-ZA nanoparticles
Breast cancer/4T1 cells
Potential cancer biodistribution, extravasation, and high tumor penetration Conjugation of dendrigraft poly-L-lysines as inducers of autophagy Macrophage regulation and increasing tumor-suppressor activity
[271]
Table 1 (continued)
Nanoparticle
Cancer type/Cell line
Size (nm)/Zeta potential (mV)
Outcome
Reference
Phosphatidyl-serine-modified nanoparticles
Melanoma/B16F10 cells
at a range of
Externalization of nanostructures occurs when they are exposed to the TME with upregulation of MMP2 Increasing depletion of tumular-associated macrophages in TME
[272]
Hyaluronic acidfunctionalized nanoparticles
Non-small cell lung cancer
Targeted delivery of miR-125b and increasing its transfection more than 6 times to induce M1 polarization and enhance iNOS levels
[273]
Trimethyl chitosan nanoparticles
Breast cancer/4T1 cells
mV
Functionalization with mannose and glycocholic acid
Delivery of SIRPa-siRNA and MUC1 pDNA
Oral delivery of cargo
pMUC1 increases macrophage phagocytosis ability and M1 polarization
Increasing immunity by the SIRPa-siRNA
[274]
This combination of phototherapy and immunotherapy increases T lymphocyte infiltration. Moreover, JQ1 suppresses phototherapy-induced immune evasion by downregulating c-Myc and PD-L1, resulting in significant tumor suppression [293].
As cancer development is a gradual process, effective treatment should focus on providing long-term immunity. The use of cancer vaccines has significantly increased in recent years; however, a major challenge remains in the targeted delivery of cargo, including antigens and adjuvants. To address this issue, glycosylated poly(lactic-co-glycolic acid) (PLGA) nanocarriers have been developed for the delivery of the ovalbumin antigen and CpG as an adjuvant in cancer vaccination. The surface of the nanostructures is modified with galactose or mannose. These nanoparticles possess high loading ability and sustained release, which are key features for the development of cancer vaccines. They stimulate dendritic cell maturation, promote antigen uptake, and enhance cell levels, leading to increased infiltration of cells in cancer immunotherapy [294].
An innovative approach in cancer therapy involves developing nanoparticles that mimic pathogens to induce a robust immune response. Saccharomyces cerevisiae (yeast)-based nanocarriers function as nano-patho-gen-associated molecular patterns (nano-PAMPs) and, through the induction of Dectin-2 and TLR-4, enhance TH17 responses, contributing to anti-cancer immunity [295]. Stimulation of T helper cells has proven effective in cancer immunotherapy. Chondroitin sulfate-modified nanostructures conjugated with glycolic acid or mannose, along with cationic liposomes loaded with ovalbumin , can stimulate the maturation of dendritic cells and evoke T helper type I and II responses [296]. In many cases, nanoparticles not only stimulate T cell infiltration, but also accelerate the maturation of dendritic cells, contributing to cancer immunotherapy [297]. Recognizing the role of epigenetic changes in immune dysfunction, the delivery of miRNAs has been explored in cancer immunotherapy. Lipid nanoparticles delivering anti-miR-21 have demonstrated the ability to stimulate M1 polarization of macrophages and enhance the infiltration of cells [298].
Nanoparticles have been employed for targeted regulation of immunosuppressive Treg cells in cancer treatment, aiming to enhance immunotherapy potential. For example, PLGA nanoparticles with antigen-capturing capabilities have been developed for this purpose. These nanoparticles primarily elevate the cell count, consequently increasing the ratio of cytotoxic T cells to Treg cells [299]. By augmenting this ratio, the negative impact of Treg cells on immune responses can be alleviated. For enhanced cargo delivery, layer-by-layer nanostructures, composed of GITR/PLGA and modified with
Fig. 3 The impact of nanoparticles on macrophages, showcasing their potential to re-educate and impede cancer progression. These nanoparticles effectively target key mechanisms associated with the M2 polarization of tumor-associated macrophages. They inhibit CD44/SIRPa, CS1R, and MAPK, prompting the M1 polarization of macrophages. Additionally, nanocarriers activate the TLR4/MyD88 axis, contributing to increased M1 polarization of the tumor-associated macrophages. The nanoparticles further induce ferroptosis and photodynamic therapy, disrupting the polarization of these macrophages into the M2 phenotype (Created by Biorender.com)
PLG and PLH that are responsive to the TME pH, have been designed to deliver IR780 dye. Subsequent irradiation with a 808 nm laser promotes the maturation of dendritic cells, thereby increasing the activity of and cells in cancer immunotherapy. Notably, these nanoparticles exhibit a suppressive effect on Treg cell function, contributing positively to immune reactions [300].
Several widely used chemotherapeutic drugs, including doxorubicin, face limitations such as low tumor site accumulation and the development of drug resistance. Prodrug nanocarriers based on doxorubicin and indoximod have been developed to suppress the IDO pathway. These prodrug nanocarriers induce immunogenic cell death, enhance the infiltration of cytotoxic cells ( T cells), and suppress Treg cells, MDSCs, and TAMs in the TME, thereby effectively promoting T cell/Treg cell ratio for cancer immunotherapy [301].
Co-delivery strategies have been used to improve cancer immunotherapy. Metformin, a compound utilized for
cancer immunotherapy, has shown promise in re-educating the TME and enhancing macrophage phagocytosis activity. Co-assembled prodrug nanoparticles, designed with hyaluronic acid-cisplatin/polystyrene-polymetformin , effectively co-deliver metformin and cisplatin. With a size of 166.5 nm and a zeta potential of -17.4 mV , these nanoparticles exhibit high potential in cancer immunotherapy. They induce apoptosis through PARP upregulation, enhance cisplatin sensitivity by suppressing ERCC1, and modulate AMPK pathways to increase and cells, and reduce Treg cell numbers [302].
Unmodified nanoparticles exhibit poor specific targeting of Treg cells. This prompted the use of nanocarrier functionalization. Hybrid nanocarriers functionalized with tLyp1 peptide have been developed to suppress STAT3 and STAT5, reducing Treg cell numbers and increasing the infiltration of cells in the TME [303]. The functionalized nanoparticles contribute to tumor suppression by increasing the infiltration of
dendritic cells, , and natural killer cells, while reducing Treg and MDSC cells [304]. Furthermore, polymerosomes have been shown to stimulate the STING axis and enhance the infiltration and proliferation of T cells in cancer immunotherapy [57]. Table 2 summarizes the application of nanoparticles for the regulation of T cells in cancer therapy. Figure 4 demonstrates the role of nanoparticles in the regulation of CAFs, T cells, and Treg cells.
Nanoparticles regulating hypoxia
In each tumor, the levels of oxygen are different [318]. The oxygen insufficiency in tumor tissue generally ranges from more or less anoxic state (almost no oxygen) to 60 mm Hg ( oxygen). In spite of this, the tumor cells demonstrate a specific condition known as hypoxia in which oxygen levels fluctuate from anoxia to 7.5 mm Hg (about oxygen) [319]. Hypoxia can be considered a reliable biomarker, since it promotes the progression of tumor cells and can cause therapy resistance [320]. Along with tumorigenesis, the hypoxia in cancer enhances, and it shows some coordination with angiogenesis, proliferation, and metastasis. Hypoxia is able to enhance the levels of CCL22, CCL28 and increases the accumulation of MDSCs and Tregs to mediate immunosuppressive TME [321-323]. Furthermore, hypoxia has been shown to be a factor involved in immune resistance [324]. Metformin is able to improve cancer immunotherapy by impairing the function of hypoxia in impairing cells [325]. Exercise has been shown as a mechanism for apoptosis induction and decreasing the proliferation of cancer cells. Moreover, exercise can ameliorate hypoxia, and enhance the function of T cells and reduces levels of Treg cells in cancer immunotherapy [326]. Hypoxia has been also shown as a mechanism in increasing M2 polarization of macrophages and secretion of factors with immunosuppressive function, including VEGF and TGF- . Moreover, hypoxia has been suggested to cause therapy resistance, especially during photodynamic therapy and radiation in which oxygen molecules are required for cancer suppression [180, 327, 328].
Therefore, the function of hypoxia in cancer immunotherapy is of importance [329]. Hypoxia can be exploited by the nanoparticles for improving their specificity and recently, the hypoxia-responsive nanostructures have been designed for cancer immunotherapy [330-332]. However, most of the attention has been paid to the regulation of hypoxia in cancer immunotherapy. The biodegradable NIR-II pseudo conjugate polymeric nanostructures can regulate hypoxia in cancer immunotherapy. These nanostructures can deliver regorafenib and respond to 808 nm laser irradiation to release drugs for the reduction of cancer hypoxia through vascular normalization, allowing for oxygen entrance into tumors
to increase ROS generation, mediating immunogenic cell death (ICD) for cancer immunotherapy. Moreover, these nanoparticles reprogram macrophages from M2 to M1 [269]. In another effort, albumin-based nanostructures have been developed for the co-delivery of IR780, NLG919, and hypoxia-activated prodrug tirapazamine (TPZ) in synergistic tumor suppression. Exposure to nanoparticles to NIR irradiation mediates the generation of to trigger the release of ROS-responsive linker for TPZ release, causing chemotherapy through enhancing tumor hypoxia. Moreover, these nanostructures stimulate ICD to enhance the activity of cytotoxicity of T lymphocytes [333]. Doping the nanoparticles with can alleviate hypoxia and increase cGAS sensitivity, inducing the cGAS/STING pathway, causing macrophage re-education, and increasing the maturation of dendritic cells [334]. In a number of cases, the hypoxia is boosted in the TME to promote the release of drugs from nanoparticles for cancer immunotherapy [335]. Furthermore, mac-rophage-mimetic microalgae and liposomes have been conjugated to suppress autophagy and reduce hypoxia in cancer immunotherapy [336]. Regarding autophagy regulation, it should be highlighted that autophagy has a dual function in cancer and can exert carcinogenic and anticarcinogenic functions, complicating its regulation in cancer therapy [337, 338]. According to these studies, the regulation of hypoxia by nanoparticles can pave the new gate for cancer immunotherapy [339-342].
The infiltration of MDSCs is against anti-cancer immunity since it impairs T-cell proliferation and enhances the differentiation of Treg cells [343]. MDSCs are consideredimmature myeloid cells with a heterogeneous nature providing, an immunosuppressive TME [172]. Overall, MDSCs utilize three distinct mechanisms to cause immunosuppression. In the first method, the arginase 1 and iNOS undergo upregulation in MDSCs, and they can deplete -arginine which is vital for the proliferation of T cells and CD3 -chain formation of TCR. However, enhancement in arginase 1 activity and iNOS can suppress the proliferation and function of T cells [344-347]. In the second method, the MDSCs can enhance the generation of ROS and RNS to mediate dysfunction in T cells [348-350]. The ROS and peroxynitrite derived from MDSCs can cause post-transcriptional alterations in TCR and CD8 to interfere with the function of peripheral cells and cause antigen-specific tolerance in these cells through impairing binding affinity to phosphorylated MHC molecules [348]. In the third and final way, MDSCs are able to enhance Treg cell differentiation to disrupt anti-cancer immunity [172, 351]. Upon that, Treg cells secrete a number of inhibitory cytokines such as IL-10, IL-35, and TGF- to interfere with the proper
Table 2 Nanoparticle-mediated T cell regulation in cancer therapy
Nanoparticle
Cancer type/Cell line
Size (nm)/Zeta potential (mV)
Highlights
Reference
Polymeric nanoparticles
Lung cancer/LLC cells
mv
ROS-responsive nanocarriers for the co-delivery of FGL1- and PD-L1-siRNA
Development of nanoparticles from poly-l-lysine-thioketal and modified cis-aconitate to facilitate endosomal escape
Functionalization of nanoparticles with iRGD peptide
Enhancing infiltration of and cells in cancer immunotherapy
[305]
Chiral nanoparticles
Lymphoma/EG7.OVA cells
–
Stimulation of NK and cells
[306]
Biomimetic nanoparticles
Colon cancer/CT26 cells
–
The phospholipid nanoparticles (PL1) can provide targeted delivery of mRNA (CD137 or OX40) in the stimulation ofT cells
[307]
Cisplatin nanoparticles
Lung cancer/LLC
Enhancing cell priming through elevating antigen presentation and providing cell crosstalk
[308]
Lipid nanoparticles
Colon cancer/MC38 cells
–
Stimulation of cells and reprogramming TME to disrupt the proliferation of cancer cells
[309]
Endogenous antigen-carrying nanoparticles
Breast cancer/4T1 cells
Increasing proliferation of and cells and promoting the ratio of cytotoxic T cells compared to Treg cells
[310]
Cationic polymeric nanostructures
Melanoma/B16F10 cells
, and
less than 60 mV
Development of nanocarriers based on polyadmidoamine dendrimers and poly(d,I-lactic-co-glycolic acid)
Development of cancer vaccine
Enhancing the number of T cells in the peripheral blood
[311]
Platelet
Breast cancer/4T1 cells
Co-delivery of anti-PD-L1 antibodies and iron oxide nanoparticles as photothermal agents in cancer therapy Stimulation of necrosis through phototherapy
Stimulation of innate immune responses
Promoting infiltration of and cells
[312]
Bacterial mem-brane-coated nanoparticles
Melanoma/B78 cells
Comprised of PC7A/CpG core with immune system induction ability
The presence of bacterial membrane and imide groups can increase antigen retrieval
Capturing neoantigens and their presentation to dendritic cells
Stimulation of T cell responses
[313]
Photo-responsive prodrug nanoparticles
Colon cancer/CT26 cells
Delivery of VPF as photosensitizer, FRRG and doxorubicin
Stimulation of immunogenic cell death
ERP effect
Maturation of dendritic cells for cross-presenting of antigens to T cells
[314]
K3ZrF7:Yb/Er upconversion nanocarriers
Breast cancer/4T1 cells
20 nm
Increasing ROS levels
Capase-1 upregulation
Gasdermin D cleavage
IL-1 maturity
Cytolysis induction
Increasing dendritic cell maturation and promoting number of effector-memory T cells
[315]
Prodrug nanoparticles
Colon cancer/CT26 cells
Targeted delivery of camptothecin and assembling with PEGylated lipids
Increasing half-life and blood circulation
Enhancing infiltration of cells
[316]
Nanoparticle
Cancer type/Cell line
Size (nm)/Zeta potential (mV)
Highlights
Reference
Lipid-coated calcium phosphate nanoparticles
Melanoma/B16F10 cells
Apoptosis induction
Acceleration of immunosuppression
Polarization of macrophages into M1 phenotype
Increasing cells
[317]
function of the immune system [352, 353]. Therefore, targeting MDSCs is critically vital for anti-cancer immunity. The intravenous administration of DNA thioaptamerfunctionalized liposomes can cause specific targeting of TME, particularly MDSCs. Moreover, such liposomes provided targeted delivery of doxorubicin in breast cancer animal models to enhance infiltration of cells and diminish MDSCs [354]. Notably, there are different kinds of immune response-related molecules in TME, including IL-1 [355, 356], IL-6 [357], prostaglandin E2 [358], VEGF [359], and IFN- [351] that disrupt the differentiation procedure to increase the accumulation of immature myeloid cells [360]. As a result, one of the promising strategies can be targeting MDSCs for mediating their differentiation into other kinds of immune cells. In line with this, the lipid-coated biodegradable hollow mesoporous silica nanostructures have been introduced to regulate MDSC differentiation. Such nanostructures are able to co-deliver IL-2 and all-trans retinoic acid to trigger the MDSC differentiation into mature dendritic cells, macrophages and granulocytes. These nanoparticles showed significant capacity in enhancing the number of mature dendritic cells and decreasing MDSCs. Furthermore, these nanoparticles stimulated and T cells and increased the secretion of IL-12 and TNF- as anti-tumor cytokines [361].
Nanoparticles for delivery of cargo into antigen-presenting cells and lymph nodes
One of the prominent problems in cancer eradication using immunotherapy is the lack of effective and proper delivery into APCs and lymph nodes. The nanoparticles have opened a new gate for the delivery of immunotherapeutics into APCs and lymph nodes [362]. Noteworthy, a number of nanostructures based on their design, demonstrate the immunostimulatory impact, and even in lack of delivery of cargo, they can stimulate T and B cell responses [363, 364]. The tumor antigens have been conjugated into nanostructures, and upon injection into OVA-expressing melanoma, thymoma, or lymphoma-bearing mice, they caused significant anticancer immunity [365, 366]. Furthermore, such model antigens conjugated into nanostructures triggered T cell and antibody responses against lymphoma or colon tumors to impair cancer growth and enhance the survival of animal models [366-368]. The particle size has been considered an important factor in this case, as small virus-size particles ( ) can reach the lymph nodes and demonstrate high cellular uptake by dendritic cells. Then, the peptide presentation from coated antigen by dendritic cell-related MHC class I molecules occurs and the stimulation of cells is observed [369, 370]. The endocytosis of such nanostructures by dendritic cells can stimulate the danger-sensing pathway in dendritic
Fig. 4 Nanoparticles orchestrating immune cells and cancer-associated fibroblasts (CAFs). Nanoparticles elevate antigen presentation via MHC-I and MHC-II, stimulating and T cells, thereby facilitating cancer immunotherapy. The nanostructures amplify Dectin-2 and TLR-4 levels, fostering TH17 responses for effective cancer immunotherapy. Additionally, they boost dendritic cell maturation and, through the delivery of anti-miR-21, induce polarization of macrophages into the M1 phenotype. The nanoparticles’ downregulation of osteopontin in CAFs disrupts cancer progression. Moreover, these nanoparticles suppress Treg cells, preventing immunosuppression (Created by Biorender.com)
cells and mature them for immunogenic APCs [371]. The tumor antigen should reach the tumor-draining lymph nodes to be absorbed by professional APC cells such as dendritic cells, and then, their presentation to cells occurs. The tumor-specific cells have been found in lymph nodes. However, the dendritic cells in tumordraining lymph nodes demonstrate an immature/inactive form that compromises their ability to induce anti-tumor cell responses [372-379]. The nanoparticle-bound cytosine-phosphate-guanine ( CpG ) oligonucleotides (an adjuvant) have been shown to accumulate in tumordraining lymph nodes in melanoma to induce dendritic cells [380].
Nanoparticles targeting tumor cells
A high number of nanostructure-based methods need tumor infiltration by nanoparticles [381]. The clinical implication of EPR [382, 383] is still under question and a controversial debate, and there is a discussion in which only a small proportion of administered nanostructures
can reach the tumor tissues, lacking clinical importance and therapeutic value in the clinical setting [384]. Therefore, significant efforts have been made to improve the ability of nanoparticles to reach tumor tissues and optimize the nanostructures in a way to control biological interactions due to the complicated nature of TME resulting from irregular vascular distribution, high tumor interstitial fluid pressure, low blood flow, dense EZN and high number of stroma cells. Therefore, the strategies should be directed towards enhancing the entry of nanostructures into tumor tissue that can be obtained through improving tumor perfusion, elevating tumor vasculature permeability, and mediating ECM remodeling. As an example, the nanostructures applied for ECM degradation or restoring tumor vasculature into normal condition [385] can mediate TME priming to provide desirable immune reactions, reversing immunosuppressive TME and enhancing anti-cancer immunity [386]. In cases where tumors are accessible, the intratumoral administration of nanoparticles is preferred into systemic
injection to enhance accumulation at the tumor region. The proper accumulation of nanoparticles in TME and the release of therapeutic cargo can enhance tumor suppression, while it reduces the adverse impacts. A number of clinical studies have suggested the intratumoral injection of immunotherapeutic compounds [387, 388] which has also been confirmed in pre-clinical studies upon intratumoral injection of immune checkpoint inhibitors [389]. The nanoparticles optimized to bind into ECM or cancer cells can enhance the accumulation of these structures in the tumor region [390] and provide a new insight into the effective delivery of therapeutics into tumor cells or TME.
Nanoparticles in immunogenic cell death: a rational way in cancer immunotherapy
In recent years, ICD has been considered a promising strategy in cancer therapy [391]. The stressed and dying cells release damage-associated molecular patterns (DAMPs) to mediate innate anti-cancer immune response and increase T lymphocyte-induced tumor immunity [392]. The ICD is capable of mediating T cellinduced anti-cancer immune responses against tumor antigens [393]. In recent years, the stimulation of ICD by nanoparticles has been suggested as a promising strategy in cancer immunotherapy. The PLGA nanostructures have been loaded with potassium chloride nanoparticles and then, functionalized with the cancer cell membrane to release and ions upon lysosomal degradation. Then, these ions cause cancer cell death by mediating a hypertonic state in which cells secrete adenosine triphosphate (ATP) and high mobility group box 1 (HMGB-1) for stimulation of ICD [394]. The -D-Glucose-reduced silver nanostructures can release calreticulin and increase the release of HSP70, HSP90, HMGGB1, and ATP [395]. These factors are prerequisites for the induction of ICD. In a novel strategy, the chitosan-coated PLGA nanoparticles have been loaded with HPV16 E7 peptides and then, their functionalization with ICD tumor cell membrane has been performed to enhance the maturation of dendritic cells for cancer immunotherapy [396]. Furthermore, the nanostructures have been modified with living bacteria and cancer cell membranes to cause ferroptosis and ICD for enhancing anti-cancer immune responses [397]. Therefore, the increasing evidence highlight the application of nanostructures for the stimulation of ICD in cancer immunotherapy [304, 398-403]. In an effort, albumin nanostructures have been developed in which IR780, as photosensitizer was loaded in core and cGAS-STING agonists/H2S producer-ZnS was loaded in shell to mediate photodynamic and photothermal therapy. These nanostructures mediated pyroptosis through the caspase-3/GSDME axis in mediating dendritic cell maturation. Then, T cells are activated and
improve the potential PD-L1 blockade in cancer immunotherapy [404]. For stimulation of ICD, various kinds of nanoparticles including polymeric nanostructures [405, 406], liposome-modified polysopamine structures [407], cRGD-functionalized TPGS nanoparticles [408], iron (II)-cytosine-phosphate-guanine nanoparticles [297] and iron oxide nanostructures [409] have been introduced to enhance cancer immunotherapy. Therefore, nanoparti-cle-mediated ICD can cause stimulation of dendritic cells to activate T cells in lymph nodes for increasing cancer immunotherapy.
Cell membrane-coated biomimetic nanostructures Cancer cell membrane-functionalized nanoparticles
Biomimetic nanoparticles are characterized by structures whose surfaces are modified or coated with membranes from other cells. The development of biomimetic nanoparticles aims to enhance stealth properties, preventing their identification by the reticuloendothelial system. Biomimetic nanoparticles exhibit good biocompatibility, making them widely applicable in cancer treatment. Recent studies have explored the potential of biomimetic nanoparticles in cancer therapy, demonstrating their versatility when modified with aptamers [410], facilitating chemotherapy through co-delivery of chemotherapy drugs and natural products [411], and showcasing high penetration and targeting features [412]. They have also been utilized for bioimaging and immunotherapy [413, 414], evading the mononuclear phagocyte system [415] and improving blood circulation time [416].
The application of biomimetic nanoparticles in cancer immunotherapy has shown promising results in tumor suppression. In some cases, chemotherapy using biomimetic nanoparticles can activate the immune system. For instance, cancer cell membrane-functionalized phosphorus dendrimer-copper(II) complexes ( ) and toyocamycin (Toy)-loaded polymeric nanocarriers with a size of 210 nm can be cleaved in the TME to release cargo and reduce glutathione levels. By causing mitochondrial dysfunction and endoplasmic reticulum stress, these nanocarriers trigger apoptosis and immunogenic cell death. They accelerate the maturation of dendritic cells and increase T lymphocyte infiltration. With the application of PD-L1 antibodies, the nanoparticles can enhance chemotherapy, impair relapse, and prevent the invasion of cancer [417].
Biomimetic nanoparticles also serve as effective carriers for delivering siRNA. Recognizing PD-L1 as an immune evasion factor, its downregulation by siRNA can expedite cancer immunotherapy and prevent T cell exhaustion [418]. These nanoparticles exhibit the capability to effectively suppress cancer progression in vivo, making them promising candidates for the development of cancer vaccines [419].
The field of cancer therapy has undergone a revolutionary transformation with the application of nanogels as drug carriers [420, 421]. Nanogels exhibit favorable physicochemical features. They are potential carriers for delivering both hydrophobic and hydrophilic drugs [422], recombinant proteins [423], and genetic materials [424].
Nanogel-induced immunotherapy has proven effective in impeding cancer progression. Polymeric nanogels, developed from PDEA-co-HP- -cyclodextrin-co-Pluronic F127 and a charge-reversible polymer named dimethylmaleic anhydride-modified polyethyleneimine, undergo degradation in the TME. These nanogels, functionalized with cancer cell membranes, co-deliver paclitaxel and IL-2, inducing the maturation of dendritic cells and enhancing the infiltration of effector cells [425].
Stimuli-responsive biomimetic nanocarriers have been engineered to optimize cancer immunotherapy. Polydopamine- nanocarriers, functionalized with cancer cell membranes and featuring pH -responsive characteristics, enable phototherapy and bioimaging. Exposure to the TME triggers the degradation of nanocarriers, releasing bubbles that promote photo-therapy-mediated immunotherapy. Combining this with checkpoint inhibitors further enhances tumor immunotherapy [426].
In the realm of biomimetic nanovaccines, studies have primarily focused on delivering therapeutics or stimulators to dendritic cells. However, the presence of the endocytosis system and endosomal degradation can hinder the effectiveness of these nanovaccines. To address this issue, biomimetic nanoplatforms have been developed to accelerate the internalization of nanoparticles in dendritic cells. Utilizing ROS-responsive nanoparticulate cores fused with peptides and cell membranes, these nanovaccines induce micropinocytosis, facilitating direct cytosolic delivery of Stimulator of Interferon Genes (STING) agonists. This enhances dendritic cell maturation and T cell priming through STING upregulation in cancer immunotherapy [427].
The stimulation of immunogenic cell death and the promotion of dendritic cell maturation and cell infiltration represents the primary strategy utilized by biomimetic nanocarriers in cancer immunotherapy. Regulation of metabolites is crucial for achieving better immunotherapy responses and immunogenic cell death. Zinc ions-bonded ZIF-8 frameworks with CuS nanodots, functionalized with cancer cell membranes, have been introduced to amplify photothermal-mediated immunotherapy through metabolic modulation. These frameworks induce immunogenic cell death, enhance dendritic cell maturation, and increase cell infiltration [428]. Although less explored compared to macrophageand cancer-derived membranes, the membranes of red
blood cells may also be utilized for the development of biomimetic nanocarriers [429, 430].
One of the main reasons for the modification of nanoparticles with the cancer cell membrane is to provide an antigen resource [431, 432]. The PLGA structures have been functionalized with the membrane of melanoma cells and then, monophosphoryl lipid A (MPLA) as an adjuvant was embedded into nanoparticles to stimulate the maturation of dendritic cells for enhancing anti-gen-specific T cell response [433]. Since the expression of MHC-I can be found in all cells, such as tumor cells, the cancer cell membrane-functionalized nanostructures can be considered novel APC to induce T cells, even in the absence of professional APCs. The CD80-expressing cancer cells were utilized to derive cell membranes for coating nanoparticles. These nanostructures can directly induce antigen-specific cells through the interaction of CD28 with cognate T cell receptors, suppressing tumorigenesis in prophylactic and therapeutic tumor models [288]. Furthermore, the cancer cell-membrane functionalized nanoparticles could be considered as vaccines. Despite significant efforts to highlight the potential of cancer cell membrane-functionalized nanoparticles in cancer immunotherapy, there are several limitations to be considered for future studies. Recent studies have highlighted the potential of ferroptosis in cancer immunotherapy [434-436]. More effort regarding the application of biomimetic nanoplatforms in the regulation of ferroptosis and related pathways should be performed to facilitate cancer immunotherapy. Moreover, autophagy is another factor in the regulation of cancer immunotherapy [437-440]. The biomimetic nanoparticles should be designed in a rational way to modulate autophagy for the regulation of T cells and other components of immune systems as well as reprogramming macrophages for effective cancer immunotherapy.
Red blood cell-functionalized nanoparticles
Red blood cells (RBCs) have obtained much attention for the purpose of drug delivery due to a number of characteristics, including biocompatibility, biodegradability, long lifespan, and desirable encapsulation capacity [441]. The OVA-encapsulated RBCs are able to stimulate and T cells after intravenous injection in mice [442]. There is also a promising approach in which RBC membrane is utilized to coat the nanostructures for the development of vaccines with long circulation ability [443]. In an attempt, RBC membrane-functionalized PLGA nanoparticles were designed to deliver both antigen hgp10025-33 and adjuvant MPLA. In order to selectively target the dendritic cells, mannose was included in the RBC membrane, and these structures demonstrated high potential in suppression of melanoma [444]. However, the studies are limited, and more experiments
regarding the application of other kinds of nanostructures, such as metal and carbon nanomaterials, and their modification with RBC membrane should be performed to improve the potential in cancer therapy.
Platelet-functionalized nanoparticles
Platelets are released by megakaryocytes, and they can control homeostasis, tumor invasion, and overall physiological and pathological events. Since the platelets have shown expression of self-recognized proteins, including CD47, they are beneficial for reducing clearance and stimulation of the complement system to enhance the blood circulation time of nanostructures [445, 446]. The platelet membrane-functionalized nanoparticles have been exploited to deliver R848 as a TLR7/8 agonist in enhancing accumulation at the tumor region and promoting the interaction with TME components. Moreover, even at low doses ( vaccine per mouse), they could suppress tumors in of mice [447]. Moreover, there is the possibility of embedding metformin and IR780 as photosensitizers in platelet membranes to stimulate ICD and improve the potential in cancer immunotherapy through suppressing MDSCs and Treg cells [448]. However, the potential of these nanocarriers in the regulation of TAMs and CAFs for cancer immunotherapy should be highlighted.
Macrophage membrane-functionalized nanoparticles
The advantage of pH -sensitive biomimetic nanoparticles lies in their ability to induce cancer immunotherapy in a more specific manner due to targeted decomposition in the TME. Immunotherapy with the use of biomimetic nanocarriers may be enhanced through phototherapy. Photo-responsive nanocarriers, through the acceleration of ROS generation, mediate immunotherapy. Macrophage membrane-based vesicles, functioning as nanoparticles, deliver drugs and photosensitizers (TAPP) to induce pyroptosis. These biomimetic vesicles, releasing copper ions, mediate ROS-induced pyroptosis. Utilized as nanoparticles, they increase ROS levels, inducing pyroptosis through the upregulation of caspase-3-induced gasdermin E, resulting in pyroptosis-induced immunotherapy [449].
The macrophage membrane-functionalized nanostructures have shown high potential in specific tumor targeting [450]. The macrophage membrane-coated nanoparticles have been utilized for the delivery of saikopsaponin D, and the surface has been hybridized by adding T7 peptide to provide macrophage-homing capacity for nanostructures and target the tumor cells upregulating transferrin receptor. These nanoparticles specifically accumulate at the tumor site and can escape phagocytosis by the reticuloendothelial system [451]. The functionalization of MOF-derived mesoporous carbon
nanostructures with macrophage membranes has been performed to increase their escape from phagocytosis and improve the potential in cancer therapy [452]. In addition to high specificity in tumor targeting, the macrophage membrane-functionalized nanoparticles demonstrate high biocompatibility that, along with their anti-cancer activity, are promising candidates for tumor eradication [251, 453]. Therefore, increasing evidences highlight the application of macrophage membrane-functionalized nanoparticles in cancer therapy [454-459]. In order to better highlight their potential, it is suggested to develop biomimetic nanoparticles functionalized with cancer and macrophage membranes to improve potential in cancer immunotherapy.
The biomimetic nanoplatforms are also interesting for the regulation of specific mechanisms such as hypoxia and lipid metabolism in TME. Biomimetic nanoparticles may be designed to present tumor antigens and co-stimulatory molecules simultaneously for cancer immunotherapy [460]. The most effective strategy thus far is centered around the development of biomimetic nanoparticles with pathogen-like features. These biomimetic nanoparticles can elicit significant and long-term immune responses in cancer therapy. One of the key reasons for the application of biomimetic nanoparticles is their ability to enhance the blood circulation time of cargo. Cholesterol reduction in the membrane used for nanoparticle functionalization improves blood circulation time and its effectiveness in inducing cancer immunotherapy [461]. Because of rapid cancer cell proliferation, the hypoxic and nutrient-deficient conditions within the TME hinder the proper functioning of immune cells. The development of a biomimetic platform to increase glucose and glutamine levels required by T cells can reprogram the TME, and accelerate cancer immunotherapy [462]. Table 3; Fig. 5 summarize the application of biomimetic nanoparticles in cancer immunotherapy.
Exosomes as emerging nanostructures for cancer immunotherapy
Exosomes, ranging in diameter from 30 to 150 nm , are extracellular vesicles secreted by eukaryotic cells [470]. They play a crucial role in intercellular communication by carrying lipids, proteins, and nucleic acids. After their secretion into the extracellular matrix, exosomes can be found in various biological fluids such as amniotic fluid, saliva, urine, and breast milk, among others [471, 472].
In recent years, there has been a significant increase in the application of exosomes in the field of cancer therapy, with a heightened focus on the diverse cargo they can transport. Exosomes exhibit the ability to target various cell types within the body and serve as reliable biomarkers for cancer. Advancements in bioengineering techniques have enabled the effective delivery of cargo using
Table 3 Application of biomimetic nanostructures for enhancement of cancer immunotherapy
Vehicle
Cancer type/ Cell line
Size (nm)/zeta potential (mV)
Highlights
Ref-erence
Biomimetic nanovesicles
Breast cancer/4T1 cells
500 nm
Loading 5-aminolevulinate hydrochloride (HAL) and 3-methyladenine (3MA) into cancer cell-derived microparticles
Increasing biosynthesis of PpIX in mitochondria, causing ROS generation after irradiation and increasing mitochondrial dysfunction Suppression of mitophagy
PD-L1 downregulation to mediate immunogenic cell death
[463]
Hybrid nanoparticles
Breast cancer/4T1 cells
and -26.4 mV
Development of hybrid nanoparticles from GTe and modification with cancer cell membrane and bacterial outer membrane
GTe functions as a radiosensitizer and the membranes can increase anti-cancer immune responses
Increasing ROS generation
Stimulation of immunogenic cell death
[464]
Biomimetic nanovaccine
–
–
Functionalization of nanoparticles with cancer cell membrane
Co-delivery of CpG and propranolol
High accumulation in lymph nodes and enough drug release
Increasing dendritic cell maturation and antigen presentation
Enhancing cell priming and
Promoting infiltration of B and NK cells
Inhibiting the immunosuppressive TME
[465]
Biomimetic PLGA nanoparticles
Delivery of 2-bromo-palmitate by PLGA nanoparticles to increase its potential in breast cancer therapy
Functionalization of nanoparticles with cancer cell membrane
Downregulation of PD-1/PD-L1
[466]
Porous silicon@Au nanocarriers
Breast cancer/4T1 cells
Up to 243.30 nm
Functionalization of nanocomposites with cancer cell membrane
Stimulation of anti-cancer immune responses and relieving immunosuppressive microenvironment
Suppressing the proliferation and invasion of cancers
[467]
AlEgens
Breast cancer/4T1 cells
Modification with dendritic cell-derived membrane
Accumulation in lipid droplets of cancer cells
The presence of cell membrane allows to accelerate hitchhiking of AIEdots into T cells and stimulates them in cancer immunotherapy
[468]
nanosheets
Colon cancer/ CT26 cells
, and +0.2 mV
Modification of nanoparticles with cancer cell membrane
Loading anti-PD-1 peptide in the nanoparticles
Phototherapy-induced immune responses and tumor ablation
Suppression of PD-1/PD-L1 axis to stimulate T cells
[469]
Fig. 5 Biomimetic nanoparticles may be developed by the extraction of membranes from red blood cells, cancer cells, TAMs and CAFs. These modifications improve the potential of nanoparticles in cancer immunotherapy. Biomimetic nanoparticles may be utilized for drug and gene delivery by improving stealth properties. They demonstrate prolonged blood circulation and can induce maturation of dendritic cells, increase infiltration of and T cells, and cause immunogenic cell death. (Created by Biorender.com)
exosomes in cancer treatment. The following subsections delve into the exploration of the potential of endogenous exosomes that are naturally secreted by cells in the body, as well as bioengineered exosomes created in the laboratory for the treatment of cancer.
Endogenous exosomes
The primary source of exosome secretion includes normal cells, stromal cells, cancer cells, and immune cells. Exosomes secreted by breast cancer cells, for example, play a role in inducing immunotherapy by reprogramming macrophage polarization. These exosomes carry PEDF, promoting M1 macrophage polarization by increasing CD80, IRF5, MCP1, and IL-1 levels, while reducing CD206, Arg, TGM2, and TGF- levels [473].
Despite the immunotherapeutic potential of exosomes, there are endogenously-secreted exosomes that enhance M2 macrophages, thereby contributing to cancer progression. Inflammation, a risk factor for cancer, can initiate cancer development, and the regulatory functions of macrophages in inflammation can alter the pathogenesis
of cancer. Myeloid-derived suppressor cells (MDSCs) in the TME secrete exosomes, transferring miR-93-5p to suppress the STAT3 axis. Enrichment of miR-93-5p in these exosomes, induced by IL-6, leads to MDSC differentiation into M2 macrophages, facilitating colitisinduced cancer development [474].
When macrophages polarize into the M2 phenotype, they release exosomes enriched with apolipoprotein E that reduces MHC-I expression, resulting in decreased immunogenicity and induced immune resistance [475]. Detecting exosomes with immunosuppressive/inductive functions involves recognizing their surface biomarkers. Exosomes positive for PD-L1 are implicated in suppressing immune reactions during cancer progression. PD-L1+exosomes stimulate cell exhaustion, enhancing tumorigenesis during cancer metastasis [476]. The secretion of PD-L1 + exosomes involves intricate molecular pathways, where HMGB1 upregulates RICTOR mRNA levels through miR-200 family downregulation, particularly miR-429. This HMGB1 and RICTOR crosstalk increases PD-L1 generation, promoting the
activity of PD-L1 + exosomes in cancer immunotherapy [477].
Although PD-L1 + exosomes have carcinogenic functions, other exosomes can suppress PD-L1 expression. Considering the ability of exosomes to induce cancer immunotherapy, they may be utilized as potential vaccines in the future. Cancer-derived exosomes exhibit superior capabilities in dendritic cell maturation and MHC cross-presentation, compared to cytotoxic T lymphocytes. Furthermore, exosomes can reduce Treg cell numbers in cancer immunotherapy by suppressing PD-L1 expression [478]. This insight suggests that bioengineered exosomes, specifically designed to target dendritic cells, may serve as effective vaccines in cancer therapy. Although the discussion on bioengineered exosomes is reserved for the next section, it is noteworthy that cells can be engineered to secrete exosomes for cancer immunotherapy. For example, the nuclei of cancer cells introduced to M1 macrophages can lead to the secretion of chimeric exosomes, selectively accumulating in lymph nodes and priming T cells to stimulate immune reactions against cancer cells [479]. Therefore, exosomes are potential regulators of the immune system in cancer [480]. Exploring the regulation of exosome secretion and biogenesis from cells opens new avenues for controlling cancer immunotherapy.
Bioengineered exosomes
Exosomes are used in cancer therapy because they are naturally present in the body, making it less likely for them to be identified as foreign and cleared. Their high biocompatibility allows effective cargo delivery and testing in clinical trials. Dying cancer cell-derived exosomes, modified with MART-1 peptide and CCL22-siRNA, induce T cell-mediated responses and suppress Treg expansion [481]. Bioengineered exosomes can produce persistent immunity against cancer cells, and this paves the way for the development of bio-based vaccines. Bioengineered exosomes, painted with HMGB1, stimulate dendritic cells, enhance immunogenicity, and induce long-term immunity against cancer. These exosomes accumulate in lymphoid tissues and enhance cell function, inducing long-term immunity and suppressing cancer progression [482]. Another approach involves functionalizing exosomes via CpG DNA to stimulate dendritic cells and enhance antigen presentation, showcasing their co-delivery ability in synergistic cancer immunotherapy [483, 484].
Fusogenic exosomes have been synthesized to address cancer cells escaping the immune system due to selfrecognition. These exosomes introduce viral antigens, stimulate dendritic cells, and present antigens to T lymphocytes for T cell cross-priming [485]. Exosomes from bone marrow-mesenchymal stem cells, loaded with
galectin-9 siRNA and oxaliplatin, induce immunogenic cell death, recruit T lymphocytes, reduce Treg cells, and promote M1 polarization of macrophages, contributing to cancer immunotherapy [486]. Engineered M1 macrophage-derived exosomes, targeting TAMs with IL4RPep-1, NF-кВ p50 siRNA, and miR-511-3p, induce cancer immunotherapy by reprogramming macrophages and restricting cancer proliferation [487]. Considered as biocompatible carriers, exosomes may be used to modify other nanoparticles. Combining exosomes and liposomes enhances gene delivery, suppresses CD47 signal, and increases cell potential. This strategy has the potential for clinical applications in cancer immunotherapy [488]. Table 4 is a summary of the use of exosomes in cancer immunotherapy.
Stimuli-responsive nanostructures for cancer immunotherapy
pH-sensitive nanostructures
Smart nanoparticles responsive to TME stimuli may be used to generate targeted delivery systems. Their multifunctionality stems from changing structures in response to TME stimuli, facilitating cargo release at the tumor site. The TME, because of its acidic pH , is distinctive from normal cells, making pH -sensitive nanoparticles ideal for cancer immunotherapy. Nanoparticles have been synthesized using a PLA-b-PEG core and a cytosine (C)-rich i-motif DNA surface to produce the so-called nanovaccines. They are used to deliver cyclic dinucleotides such as cyclic dimeric guanosine monophosphate (CDG) to endosomes, accelerating anti-tumor immunity and preventing TME immunosuppression. In TME’s mild acidic pH , a conformational switch releases cargo, while physiological pH minimally increases CDG release. These pH -sensitive nanoparticles protect CDG from enzymatic degradation, releasing the cargo into the cytoplasm, and stimulating polarization of macrophages into the M1 phenotype [504].
A groundbreaking achievement in cancer immunotherapy involves the creation of prodrug nanoparticles for cargo delivery. These nanoparticles release cargo in response to the pH of the TME. An innovative selfcascaded unimolecular prodrug was designed, comprising an acidic pH -activatable doxorubicin, and an aggregation-induced emission luminogen (AIEgen) photosensitizer linked to a caspase-3-responsive peptide. This engineered prodrug exhibits dual functionality- it can actively release doxorubicin in the acidic TME and initiate apoptosis-related caspase-3 activation. Furthermore, the activated caspase-3 can induce the release and in-situ aggregation of photosensitizers. This process enhances dendritic cell maturation, increases cell numbers, and prevents metastasis to lung tissue [505].
Table 4 Application of exosomes in cancer immunotherapy
Exosome source
Cargo
Cancer type
Cell line
Remark
Reference
Dendritic cell
Neoantigens
Melanoma
B16F10 cells
Delivery of cargo to the lymph nodes and stimulation of T- and B-cell immune responses High biocompatibility
Improving survival of animal model
Suppressing proliferation and delayed tumor relapse
[489]
Glioblastoma
LncRNA
Glioblastoma
Human glioma cell line LN229, mouse glioma cell line GL261, human microglial cell line HMC3, and mouse microglial cell line BV-2
Stimulation of microglia to generate and secrete complement C5 in chemotherapy resistance development
[490]
M1 macrophage
HOTTIP
Head and neck cancer
Hep-2 cells
TLR5/NF-kB overexpression to impair progression of head and neck cancer
[491]
CD45RO- CD T cell
–
Endometrial cancer
Ishikawa, RL95-2 and KLE cells
The exosomes suppress estrogen-induced endometrial cancer progression through miR-765 release
[492]
M1 macrophage
SN38
Breast cancer
4T1 cells
Cancer-targeting ability and prolonging blood circulation
Stimulating M1 polarization of macrophages
Increasing recruitment of NK cells
[493]
cells
–
Nasopharyngeal cancer
NP69, HK-1 and NPC43 cells
Elimination and killing tumor cells
Stimulation of FasL and DR5/TRAIL axis
Suppressing cancer growth
Increasing survival of animal model
Apoptosis induction
Increasing migration of T cells to the tumor site through CCR5 upregulation
[494]
–
–
Breast cancer
4T1 cells
The smart and bioengineered exosomes with CD62L and OX40L can induce T cells and suppress Treg cell function
[495]
Dendritic cells
–
Melanoma
B16-OVA cells
Functionalization of exosomes with anti-CD3 and anti-EGFR to bind to T cells
[496]
iPSCs and dendritic cells exosomes
Doxorubicin
Gastric cancer
MFC cell line
Delivery of chemotherapy drug
Tumor-targeting ability
Recruitment of immune cells to the TME
[497]
Cancer cells
Paclitaxel
Breast cancer
4T1 cells
Development of liposome-exosome conjugate with high biocompatibility to increase the number of cells
[498]
Cancer cells
–
Breast cancer
4T1 cells
A combination of oxygenated water and cancer-secreted exosomes induce anti-tumor responses and suppress angiogenesis and invasion
[499]
Cancer cells
–
Pancreatic cancer
PANC-1 cells
Exosomes reduce the levels of HLA-DR on the surface of CD14 + monocytes to cause immunosuppression through regulation of STAT3, stimulation of arginase expression and ROS
[500]
M1 macrophages
Docetaxel
Breast cancer
4T1 cells
The docetaxel-loaded exosomes stimulate cancer immunotherapy through M1 polarization of macrophages
[501]
Dendritic cells
siRNA
Melanoma
B16-F10 cells
BRAF siRNA delivery by exosomes to induce T lymphocytes
[502]
HEK 293T cell
Chlorin e6 (Ce6) and immune adjuvant R848
Prostate cancer
RM-1 cells
The exosomes preferentially accumulate in the tumor site and induce dendritic cell maturation Increasing levels of CD80 and CD86 as biomarkers of dendritic cells
Inducing M1 polarization of macrophages
[503]
Mounting evidence supports the combination of chemotherapy and immunotherapy using pH -sensitive nanoparticles for cancer suppression. For example, poly(L-histidine) (PHIS) has been used to encapsulate R848, forming pH-sensitive PHIS/R848 nanocores. Conjugating doxorubicin to hyaluronic acid creates prodrug nanoparticles that coat PHIS/R848. These nanocarriers undergo a switch from hydrophobic to hydrophilic in response to pH change, releasing R 848 to modulate the immune system. At pH 5.5 , the hydrazone bond cleaves, releasing doxorubicin. The latter is internalized into tumor cells via endocytosis. This activates the immune system and suppresses cancer proliferation [506].
Metal-based nanoparticles can also be designed to decompose in response to TME pH . A human serum albumin-coated zeolite imidazolate framework-8 has been developed for the delivery of a photosensitizer (HPZ), for selective recognition of the TME [507]. This framework enables rapid elevation of zinc ion concentrations while ensuring controlled release of the encapsulated photosensitizer. Under physiological pH (7.4), HPZ exhibits a size of approximately 170 nm , decreasing significantly to less than 10 nm in acidic conditions ( pH 6.5 ). The acid-induced decomposition of HPZ prompts a swift increase in zinc ion concentration, exerting potent cytotoxic effects against colorectal, breast, and pancreatic cancers. Intravenous administration of HPZ in a CT26 tumor-bearing mouse model results in the expansion of T helper and cytotoxic T cells, and reduction in the Treg cell population. These changes lead to a significant inhibition of tumor growth.
While the primary focus of this section is to assess the role of nanoparticles in cancer immunotherapy, it is worth mentioning that microneedle arrays, composed of tiny needles, can also be used for sustained cargo delivery. pH -sensitive nanoparticles can be incorporated into microneedles, facilitating sustained release for hyperactivating the immune system and creating nanovaccines [508]. Hydrogels are also available for sustained cargo delivery. For example, nanoparticles can be embedded in pH -sensitive hydrogels for delivering doxorubicin and JQ1 (a small molecular inhibitor) to induce immunogenic cell death [509]. Of note, pH -sensitive biomimetic nanocarriers, crafted from PLGA and coated with membranes from macrophages and cancer cells, can deliver FGL1-siRNA and metformin for cancer immunotherapy. These biomimetic nanoparticles enhance cargo endosomal escape, with metformin suppressing PD-L1 through AMPK upregulation, and siRNA reducing FGL1 expression to boost anti-cancer immunity through T cell induction [510]. Given the impact of TME pH on tumorigenesis, pH regulators have been developed. Calcium carbonate nanostructures neutralize TME pH by consuming lactate, promoting M1 macrophage polarization,
immune cell infiltration, dendritic cell stimulation, and cell recruitment for cancer immunotherapy [511]. Table 5 summarizes the application of pH -sensitive nanoparticles in cancer immunotherapy.
Redox-sensitive nanoparticles
Redox-sensitive nanoparticles are carriers that release cargo in response to redox imbalances in the TME. The development of these nanoparticles involves introducing redox-sensitive bonds, such as disulfide bonds. They have found application in cancer immunotherapy, capable of stimulating various immune cells.
Multifunctional nanocarriers with redox-sensitive features, comprising toll-like receptor agonists, catalase, and PD-L1-siRNA, have been designed for cancer therapy. These nanoparticles induce M1 polarization of macrophages, increase ROS production, downregulate PD-L1 expression, and enhance cell functions by suppressing Treg cells [525].
Clinical application of immunotherapy hinges on using biocompatible and long-term safe nanostructures like micelles. Micelles containing doxorubicin and R848, a TLR7/8 agonist, were experimentally used as nanovaccines. Elevated glutathione levels in the TME trigger micelle decomposition, releasing cargo and inducing immunogenic cell death, dendritic cell stimulation, and accelerated immune responses. Additionally, redoxresponsive polymers and an A2AR antagonist within micelles suppress adenosinergic signaling to activate NK and cells in cancer immunotherapy [526].
Cationic polymer dots, known for their small particle size, imaging capabilities, and drug delivery potential, have seen extensive use in biomedicine. PEI600-modified redox-sensitive hyperbranched poly(amido amine) nanostructures, partially carbonized with polymer dots, were used for carrying ovalbumin. These structures enhance splenocyte proliferation, elevate cytokine levels (including IL-12 and IFN- ), promote dendritic cell maturation, and increase and cell counts, as well as T lymphocytes. Ovalbumin release from these structures is redox-responsive [527].
Given that both pH and redox serve as endogenous stimuli, new nanocarriers have been developed that exhibit dual responsiveness. pH – and redox-sensitive micelles containing ovalbumin, modified with PLH-PEG, are used as cancer vaccines. These micellar nanostructures enable cytosolic delivery of ovalbumin through redox release, proton influx, micelle disassembly, and ultimately, a proton sponge effect and lysosome break. These micelles enhance MHC-I rates, antigen presentation, lymph node accumulation, and improve immune reactions [528].
Photo-responsive nanoparticles and phototherapy
Light serves as an exogenous stimulus in nanoparticle development, where laser irradiation induces bond cleavage to release the loaded cargo. This forms the basis of photodynamic therapy (PDT) and photothermal therapy (PTT) for cancer ablation. In PDT, ROS production induces cell death, while PTT causes cell death through hyperthermia. Combining phototherapy with immunotherapy can enhance cancer suppression. Two methods are utilized, including a combination of phototherapy and immunotherapy or stimulation of phototherapymediated immunotherapy. Both methods offer a high likelihood of tumor suppression, improving the fight against cancer. PLGA nanoparticles loaded with R837, docetaxel, and PB agents are used for immunotherapy and PTT. These nanoparticles are modified with cancer cell membranes for enhanced effectiveness. R837 stimulates dendritic cell maturation, and docetaxel increases M1 polarization of macrophages, impairing the immunosuppressive TME. This leads to increased infiltration of cytotoxic T lymphocytes in the TME for effective cancer immunotherapy [529].
Similar to doxorubicin, which induces immunogenic cell death, docetaxel has shown potential in cancer immunotherapy by regulating TAM polarization. CuS nanoparticles with functional groups, functionalized with folic acid and conjugated to PEI-PpIX for enhanced solubility, deliver docetaxel and CpG , inducing PTT and immunotherapy. These nanoparticles exhibit excellent photothermal conversion ability upon exposure to 650 and 808 nm laser irradiation and induce M1 polarization of macrophages through the function of docetaxel in cancer immunotherapy [530].
Beyond combining immunotherapy and PTT, it is possible to induce immune reactions resulting from PTT. Tumor cell killing and antigen release can accelerate immune reactions. A peptide-photosensitizer conjugate, developed from anti-PD-L1 peptide, cleavable by MMP2 , and purpurin 18 as a photosensitizer, accumulates in the tumor site. MMP-2 enzyme degradation releases the peptide, causing antigen release. Irradiation induces dendritic cell maturation, migrating into lymph nodes, increasing cell infiltration, suppressing metastasis to lung tissue, and eliciting anti-tumor immune responses [531].
Photo-responsive structures can also function as vaccines. Chelation of ions with ovalbumin leads to biomineralization into nanovaccines, embedding IR820 as a photosensitizer through electrostatic incorporation. The presence of iron induces ferroptosis, mediating immunogenic cell death. Immunogenic cell death stimulates neoantigens and DAMPs, synergizing with ovalbumin in cancer immunotherapy. Near-infrared irradiation induces PTT, enhancing immunotherapy. These
nanostructures enhance cell infiltration, inhibit the primary tumor, and show promising impacts in combination with checkpoint inhibitors [532].
The combination of PDT and immunotherapy has shown promising results in cancer immunotherapy. Although PDT and PTT have different mechanisms of action, both can be combined with immunotherapy to expedite the immunotherapeutic process by exposing antigens or inducing cell death to stimulate immune responses. Photodynamic therapy is preferred over PTT due to potential hyperthermia effects on normal tissues. However, when tumor-targeted nanoparticles are developed, they can precisely execute PDT in the tumor site, effectively killing cancer cells. Various nanoenzymes with cancer cell accumulation can be developed to induce PDT and enhance cancer immunotherapy.
A nanoparticle core was created by connecting paclitaxel drugs through a disulfide bond (PTX-SS-PTX), with P18 as a photosensitizer connected to MPEG-CPPA-b-P(M4). In response to glutathione, the disulfide bond degrades, and laser irradiation in response to ROS increases singlet oxygen generation, releasing high mobility group box 1 (HMGB1) due to GSDME activation. HMGB1 releases and pyroptosis induction leads to dendritic cell maturation, educating naïve cells in lymph nodes, expanding T cells, and developing memory T cells for cancer immunotherapy [533].
For PDT stimulation, the photosensitizer is loaded into nanoparticles. Recent studies have shown the potential of herbal medicine in cancer treatment. Mesoporous silica nanoparticles modified with PEG can carry both chlorin e6 and astragaloside III, stimulating NK cells and suppressing cancer cell growth. These nanoparticles accumulate in the tumor site, increasing immune cell infiltration, promoting the activity and cytotoxicity of cells and NK cells, and impairing tumorigenesis [534].
Liposomes are also potential nanocarriers in cancer immunotherapy. Liposomes carrying IPI-549 as a PI3K inhibitor and chlorin e6 as a photosensitizer induce ROS generation after irradiation, facilitating immunogenic cell death and improving the potential of T lymphocytes in eliminating cancer cells. IPI-549 delivery by nanoparticles can decrease arginase-1 (Arg-1) and ROS levels, increasing apoptosis in MDSCs, and preventing their suppressive function on T cells. In addition, these nanoparticles decrease the infiltration of M2-polarized macrophages and mature dendritic cells in cancer immunotherapy [535].
In both nanoparticle-mediated PDT and PTT, the most prominent mechanism is the stimulation of immunogenic cell death to accelerate cancer immunotherapy. Increasing evidence highlights the application of nanoparticle-mediated phototherapy and immunotherapy in cancer suppression [536-540]. Table 6 summarizes
Table 5 pH -sensitive nanoparticles in cancer immunotherapy
Nanoparticle
Cancer type/ cell line
Size (nm)/zeta potential (mV)
Highlights
Reference
PEG/PEI/CAD nanoparticles
Breast cancer/4T1 cells
At a range of a range of
Delivery of doxorubicin and its release in a pH -sensitive manner
Immunogenic cell death induction
The acidity of the endosome induces cleavage of cis-aconityl
Recruitment of dendritic cells
[512]
Hollow silica nanostructures
Breast cancer/4T1 cells
Increased retention in response to low pH level of TME
Targeting mitochondria and increasing ROS levels
Stimulation of photodynamic therapy
Combination with checkpoint inhibitors mediates anti-tumor immunity
[513]
Dextran-modified BLZ-945 nanocarriers
Breast cancer/4T1 cells
11.35, 112.4, and
Presence of a borate ester bond as a pH-sensitive bond
Immunogenic cell death induction
Dendritic cell maturation, TAM depletion and T cell infiltration
[514]
Manganese nanoparticles
Melanoma/B16OVA cells
130 nm
and 2-methylimidazole (2-MI) have been used to encapsulate ovalbumin with pH-sensitive features and the ability of dendritic cell maturation in cancer immunotherapy
[515]
Mesoporous silica nanostructures
–
146 nm
pH-sensitive feature and delivery of R848
Uptake of nanoparticles by antigen-presenting cells
Stimulation of dendritic cells and boosting cell-mediated immune responses
[516]
Peptidefunctionalized nanobubbles
Breast cancer/4T1 cells
Functionalization of nanobubbles with anti-PD-L1 peptide
Loading Ce6, metformin and perfluorohexane in nanobubbles
Accumulation of nanoparticles in acidic pH causes detachment of PEG ligands and then, exposure of peptide to suppress PD-L1
Hypoxia relief by metformin and increasing potential of Ce6 in cancer therapy
Increasing anti-tumor immunity and prevention of immunosuppression
[517]
Polymer-lipid complexes
Lymphoma/E. G7-OVA cells
–
The polymer-lipid-embedded liposomes release ovalbumin in response to pH and stimulate anti-cancer immunity by releasing ovalbumin in the cytoplasm of dendritic cells
[518]
Polymer-modified liposomes
Lymphoma/E. G7-OVA cells
and 1.3 mV at pH 7.4 and pH 5.5
pH -responsive feature and cationic lipid inclusion
Delivery of ovalbumin
Increasing cytokine generation
Antigen presentation through MHC-I and MHC-II
[519]
Liposome
Lymphoma/E. G7-OVA cells
136, 108 and and -6.1 mV
Modification of liposomes with polymer
Destabilization of liposomes in pH 6
Uptake of liposomes by dendritic cells
Delivery of ovalbumin to cytosol
Tumor growth suppression
[520]
Polymer-modified liposomes
Lymphoma/E. G7-OVA cells
97, 100, 88, 110, 108 and ,
and
Inclusion of cationic lipid and CpG-DNA
Inducing dendritic cells to secrete cytokines
Stimulation of antigen-specific immune responses
pH-sensitive feature
[521]
Biomimetic nanoparticles
Breast cancer/4T1 cells
102.86 nm
Coating manganese nanoparticles with hybrid membranes
Membrane is developed from mesenchymal stem cell membrane and pH-sensitive liposomes
Targeted delivery of BPTES
Inducing STNG pathway and M1 polarization of macrophages
Relief of immunosuppression TME
[522]
Table 5 (continued)
Nanoparticle
Cancer type/ cell line
Size (nm)/zeta potential (mV)
Highlights
Reference
Polysaccharidebased polymers
Lymphoma/E. G7-OVA cells
Stimulation of dendritic cells
Cytoplasmic delivery of antigen
Th1 cytokine production by dendritic cells
[523]
Liposomes
Melanoma/B16OVA cells
401, 754, 636 and 674 nm
pH-sensitive liposomes deliver STING and TLR9 agonist Increasing Th1 immune responses in tumor suppression
[524]
the nanoparticles causing PDT and PTT, and their combination and relationship with immunotherapy. Figure 6 shows the application of stimuli-responsive nanocarriers in cancer immunotherapy. Since the pre-clinical studies demonstrate the function of nanoparticles for cancer immunotherapy and tumor suppression, the clinical application of nanostructures in cancer immunotherapy has been performed to evaluate their potential [541]. Table 7 and table 8 summarize the clinical application of nanoparticles in cancer immunotherapy.
An overview of various classes of nanoparticles in cancer immunotherapy
Polymeric nanoparticles
Polymeric nanoparticles are among the most commonly applied structures in cancer immunotherapy owing to their biocompatibility, biodegradability, chemical stability, water solubility, and high drug loading [564, 565]. The PLGA, PGA, PLG, PEG, PEI and chitosan nanoparticles have been widely used in cancer immunotherapy [566]. Moreover, such nanostructures have shown potential as immunostimulatory adjuvants in cancer immunotherapy [567-569]. Loading TLR7/8 agonists in PLGA nanostructures enhanced levels of CD40, CD80, and CD86 through stimulation of bone marrow-derived dendritic cells and subcutaneous administration of such nanoparticles stimulated dendritic cells and cells [570].
Lipid nanoparticles
Liposomes are among the promising nanocarriers for drugs, genes and vaccines [571]. Until now, multiple kinds of liposomal nanostructures including 1,2-dioleoyl3 -trimethylammonium-propane (DOTAP), – ( , N’-dimethyl aminoethane] – carbamoyl) cholesterol (DC-Chol), and dimethyl diocta decylammonium (DDA) [572, 573] have been significantly applied for the antigen exposure to APCs and providing vaccine adjuvants to increase antigen-specific immune reactions [574, 575]. The dextran-functionalized liposomes with pH -sensitivity activity have shown high uptake by dendritic cells and they can provide cytosol delivery of ovalbumin to accelerate antigen-specific immune reactions and impair cancer progression [576]. Furthermore, loading CpG-ODNs as TLR9 agonist and 3,5-didodecyloxybenzamidine as an adjuvant into liposomes can enhance dendritic cellmediated cytokine production to enhance antigen-specific immunity [521]. Micelles are among another kind of lipid nanoparticles that can function as delivery systems for antigen/adjuvant to improve potential of vaccines. The polymeric hybrid micelles have been utilized for the delivery of CpG-ODN and Trp2 to create a nanovaccine for targeting lymph nodes and enhancing the accumulation of cargo in dendritic cells, triggering
cell-mediated immune responses and enhancing cancer suppression (melanoma) [577].
Carbon nanoparticles
Carbon nanotubes (CNTs) have been shown to mediate immunostimulatory impacts in vitro and in vivo. The oxidized multiwalled carbon nanotubes (MWCNT) have shown the ability for the delivery of cancer-testis antigen, known as NY-ESO-1 and CpG-ODNs. These structures showed uptake by dendritic cells and mediated powerful and cell-driven immune reactions to impair melanoma progression [578]. Furthermore, the co-delivery of ovalbumin and CpG-ODN, as well as antiCD40 Ig as immunoadjuvants by MWCNTs has shown potential in accelerating cell responses and suppressing melanoma progression [579].,
Metal nanoparticles
Gold nanostructures are promising factors in cancer immunotherapy owing to their characteristics, including biocompatibility, adjustable surface chemistry, and ease of controlling size and shape [580]. The gold nanostructures have shown potential in inducing differentiation of macrophages into dendritic-like cells to enhance T cell proliferation and promote cytokine release [581]. Furthermore, the gold nanostructures have shown incredible potential to act as adjuvants for enhancing antibody generation [582]. The potential of gold nanoparticles in cancer therapy via TME modulation has been revealed [583, 584]. The surface of hollow gold nanostructures has been functionalized with CpG-ODNs to enhance their cellular uptake and enhance function in the induction of immune responses, including enhancing TNF- secretion [585]. The silica nanoparticles have also been applied widely in biomedicine for imaging [586], specific targeting of cancer [587], and delivery of drugs and genes [588]. The mesoporous silica nanoparticles have been applied for antigen delivery and acted as vaccines to induce humoral- and cell-driven immune reactions while having high biocompatibility and lacking toxicity [589]. The hollow mesoporous silica nanoparticles have been shown to be biodegradable and are capable of TME remodeling in cancer immunotherapy [361]. According to these studies, various categories of nanostructures demonstrate promising characteristics in cancer immunotherapy, and all of them have shown potential in TME remodeling. The next step for the clinical application of these nanocarriers depends on their biocompatibility and long-term safety that lipid nanoparticles are at the front line.
Conclusion and challenges
Cancer immunotherapy and the development of vaccines have ushered in a new era in cancer treatment, instilling hope in patients and significantly enhancing prognosis
and survival rates. However, challenges persist in the utilization of adjuvants and immunomodulatory agents. This prompted the exploration of novel solutions, particularly through the application of nanoparticles. The intricate interactions within the TME play a pivotal role in influencing cancer cell responses to immunotherapy. In this context, nanoparticles designed for targeted delivery of immunomodulatory compounds and TME remodeling have emerged as promising tools in cancer immunotherapy.
Nanoparticles address the current challenges in cancer immunotherapy by demonstrating the capability to regulate TME components, altering the trajectory of tumor cell progression, and mitigating the immunosuppressive milieu in cancer. Nanostructures designed for TME remodeling can increase the infiltration of cytotoxic cells, stimulate dendritic cells, induce M1 macrophage polarization, and inhibit MDSCs. Furthermore, nanoparticles serve as effective carriers for delivering adjuvants and other immunomodulatory compounds, such as drugs or genes, in cancer immunotherapy.
A significant breakthrough in nanoparticle development for cancer immunotherapy lies in the creation of biomimetic nanocarriers, incorporating functionalized membranes derived from red blood cells, tumorassociated macrophages, cancer-associated fibroblasts, and tumor cells. In addition, the utilization of exosomes, whether naturally secreted by cells or bioengineered in the laboratory, holds promise in regulating the immune system in cancer therapy. Nanoparticles exhibit the capacity to diminish the number of Treg cells and MDSCs, preventing immunosuppression. Moreover, nanoparticle-induced immunogenic cell death promotes the activation of dendritic cells, facilitating their migration into lymph nodes to stimulate T cells for cancer immunotherapy.
Stimuli-responsive nanocarriers, particularly pH – and redox-sensitive nanoparticles, enhance the potential of cancer immunotherapy. Photo-responsive nanoparticles, through photothermal and photodynamic therapy, contribute to the augmentation of cancer immunotherapy by inducing immunogenic cell death, regulating dendritic cells and T cells, and promoting M1 polarization of macrophages. This multifaceted approach highlights the versatility and promise of nanoparticles in advancing cancer immunotherapy.
The clinical application of nanoparticles involves several crucial considerations [590]. Once we comprehend the potential of nanoparticles in cancer immunotherapy, translation of these technologies, advancements, and findings to the clinical setting becomes imperative. Clinical trials involving immunotherapy for cancer patients are already underway. In the context of solid tumors and their clinical treatment, leveraging nanoparticle-induced
Table 6 Nanoparticle-mediated PDT and PTT and their relationship with cancer immunotherapy
Nanoparticle
Cancer type/ Cell line
Size (nm)/zeta potential (mV)
Outcome
Ref-erence
Nano-PROTACs
Breast cancer/4T1 cells
40 and
The nanoparticles have been comprised of PpIX as photosensitizer and SHP2-targeting PROTAC peptide (aPRO)
The stimulation of aPRO occurs as a response to upregulation of caspase-3
Targeted degradation of SHP2 through ubiquitin-proteasome system
SHP2 depletion suppresses immunosuppressive pathways, including CD47/SIRPa and PD-1/PD-L1, to improve anti-cancer functions of macrophages and T cells
[542]
MRC nanoparticles
Breast cancer/4T1 cells
Co-delivery of RGX-104 as an immune agonist and chlorin e6
Stimulation of ApoE by RGX-104 to impair the function of MDSCs and accelerate pyroptosis
Chlorin e6-induced PDT to facilitate oxidative damage and enhance immunogenicity
[543]
Ru(II)-modified nanocarriers
4NQO-Oral cancer
and
Loading HIF-1a-siRNA in nanoparticles
Stimulation of PDT and inducing lysosomal damage
Downregulation of HIF-1 a and enhancing killing of oral cancer
Stimulation of and cells
[544]
PDA-FA nanoparticles
Colon cancer/ CT26 cells
Delivery of CpG as immunomodulatory to induce dendritic cell maturation and increase T cell activity
Suppressing Treg cells and MDSCs
PTT induction
[545]
Copper sulphide nanoplatforms
Melanoma/ B16F10 cells
Delivery of Cas9 ribonucleoprotein to target PTPN2
Downregulation of PTPN2 to increase infiltration of cells
Increasing levels of IFN- and TNF-a
Improving immune-sensitivity
[546]
Polymer nanoadjuvants
Breast cancer/4T1 cells
Doping with TLR agonist as an immunomodulatory adjuvant
Presence of lipid shell response to temperature
The PTT potential in response to NIR-II
Immunogenic cell death induction and release of TLR agonist
Upregulation of TLR7/TLR8 and stimulation of immunogenic cell death enhance dendritic cell maturation and amplification of anticancer immune responses
[547]
Nanoenzymes
Breast cancer/4T1 cells
100 nm
Cu-doped MoOx (CMO) nanozyme comprises the core that is coated with cancer cell membrane
Increasing the tumor accumulation and nanozymes causes oxidative damage through increasing ROS generation
PTT causes immunogenic cell death to activate the immune system
[548]
Gold nanorod
Colon cancer/ CT26 cells
, , and mV
The 808 nm laser irradiation causes PTT
Stimulation of immune cells in the lymph nodes
[549]
AIE
Breast cancer/4T1 cells
Modification with cancer cell membrane
Stimulation of immunogenic cell death
Increasing ROS generation through PDT
[550]
Polymer nanoagonist
Breast cancer/4T1 cells
42 and mV
Stimulation of PTT
Increasing immunotherapy and induction of immunogenic cell death
[551]
Antigen-capturing nanoparticles
Breast cancer/4T1 cells
41.1 nm
Stimulation of phototherapy under NIR irradiation
Increasing antigen uptake and presentation
Suppressing cancer progression
[552]
Nanoparticle
Cancer type/ Cell line
Size (nm)/zeta potential (mV)
Outcome
Ref-erence
Black phosphorus quantum dot nanovesicles
Breast cancer/4T1 cells
Loading them into thermosensitive hydrogels
NIR irradiation increases dendritic cell activation and then, they migrate into lymph nodes for the stimulation of cells
[553]
Gold nanocages
Colon cancer/ CT26 cells
Delivery of anti-PD-L1 and galunisertib by nanocages
Stimulation of PTT to cause immunotherapy
[554]
phototherapy is recommended to enhance immune responses and stimulate dendritic cells along with their maturation.
Last, but not least, it is essential to assess the biocompatibility of nanoparticle-induced immune responses to prevent systemic immune reactions against normal cells. Evaluation of delivering immunomodulatory agents alongside chemotherapy drugs should be conducted to determine the synergistic impact on cancer therapy. However, careful consideration must be given to whether the associated side effects are tolerable for patients. Therefore, assessing the biocompatibility and toxicity profile of nanoparticles stands out as a critical aspect of their clinical application.
Currently, a high number of studies have focused on the clinical utilization of nanostructures for boosting immunotherapy [591]. One of the most prominent drawbacks is that currently developed nanoplatforms are in phase I or II. The present review provided the possible interaction and function of nanoparticles with TME components and immune cells to induce cancer immunotherapy that can be used in clinics. In most cases, animal models have been utilized to evaluate the potential of nanoparticles in cancer immunotherapy, making it hard to translate to humans. The selection of humanized animal models can improve the chance of translation into the clinic. Moreover, the appropriate nanoparticles should be chosen for cancer immunotherapy. In this way, it is suggested to use FDA-approved agents such as polymers or lipid nanoparticles to accelerate the pace of clinical translation and immune regulation. The biosafety, tolerability, and reproducibility of nanocarriers should also be considered for clinical application. In recent years, a high number of nanoparticles have been introduced into clinics for the treatment of cancers, including lipid-based nanoparticles (generic name: JVRS-100) for the treatment of leukemia (NCT00860522), liposomes for the treatment of lymphoma, melanoma, breast, ovarian and prostate cancers (NCT03349450, NCT01052142, NCT01095848), PLGA nanoparticles for the treatment of metastatic melanoma (NCT01753089) and colloidal gold structures for the treatment of advanced solid tumors [592]. However, all of these nanoparticles have been evaluated in phase I and II studies.
Taking everything together, there are a number of points that should be considered for the application of nanoparticles in cancer immunotherapy [593]. Currently, cancer immunotherapy is mainly based on the application of nano-scale delivery systems for conventional immunotherapeutic compounds, including antibodies, recombinant proteins, and small molecularbased immune agonist, adjuvant, or inhibitor. The rationale for the application of nanoparticles is to improve the pharmacokinetic profile of immunotherapeutic
Fig. 6 Stimuli-responsive nanocarriers in cancer immunotherapy. Nanoparticles that respond to pH , redox, or light can release cargo to induce apoptosis, DNA damage, and regulation of molecular pathways. Moreover, stimuli-responsive nanocarriers stimulate immunogenic cell death to increase dendritic cell maturation. They migrate into lymph nodes and increase activation of T cells
Table 7 The application of nanoparticle-based immunotherapy in clinical studies [541,555-557]
Nanoparticle
Phase
Remark
Reference
RNA-lipoplexes
Phase I
Increasing maturation of dendritic cells and increasing T cell response
[558]
miR-34a-loaded liposomes
Phase I
Reduction in the expression of immune evasion genes
[559]
miR-4157-loaded lipids
Phase I
Stimulation of neoantigen-specific cells and increasing anticancer immune responses
[560]
Iron oxide nanostructures
Not applicable
Increasing M1 polarization of macrophages from M2 phenotype
[256]
Paclitaxel-loaded lipid core nanostructures
Phase II
Enhancing dendritic cell maturation
[561, 562]
Doxorubicin-loaded anti-EGFR immunoliposomes
Phase II
Stimulation of immunogenic cell death Suppressing EGFR-induced growth signaling
NCT02833766
Plasmid DNA complex-loaded cationic liposomes
Phase I
Stimulation of the immune system
NCT00860522
Combination of anti-PD-1 and hafnium oxide nanostructures
Phase I
Increase in tumor cell death, promotion of immunogenic cell death, and induction of the immune system
NCT03589339 [563]
agents, diminish the side impacts, prevent the cytokine storm by immune hyperactivation, and ameliorate deficiency in immune responses. Moreover, nanoparticles are promising for reversing immunosuppression and preventing immune evasion. Although this is an interdisciplinary field combining biology and engineering, a number of factors should be carefully investigated,
including nanoparticle-mediated immunogenicity, biocompatibility and engineering aspects regarding therapeutic compound loading in nanostructures. Moreover, several nanoparticles have anti-cancer activity, causing synergistic impact with immunotherapeutics. One of the most important features of nanoparticles is their ability for controlled release of therapeutics. The
Table 8 The challenges regarding the application of nanoparticles in cancer immunotherapy
Nanoparticles
Benefits
Challenges
Polymeric nanoparticles
– Targeted delivery of cargo to improve the therapeutic index and reduce the systemic side effects
– Prolonged release of drugs
– Potential in the delivery of various cargoes including small molecule drugs, proteins, peptides, and nucleic acids
– Increased stability of drugs and preventing degradation
– Stimulation of the immune system
– Biocompatibility and biodegradability
– The development of nanoparticles with desirable size, charge, and targeting capacity is challenging
– Strict rules regarding clinical application
– Unexpected interactions with the immune system
– Challenges in the scale-up generation, storage and stability
Lipid nanoparticles
– Efficient delivery of genetic tools including mRNA, siRNA, and DNA
– Targeted delivery
– Protection of cargo
– Long-term biocompatibility and safety
– Adjuvant impact that a number of lipid components can function as adjuvants and increase anticancer immune responses
– Complex manufacturer production, especially the development of nanoparticles for gene delivery
– They require ultra-low temperatures to preserve their stability
– Immunogenicity that can lead to inflammation and other side effects
– Low loading capacity
Metal nanoparticles
– Targeted delivery of drugs and high loading and encapsulation efficiencies
– Application for photothermal therapy, since a number of nanostructures such as gold nanocarriers can absorb light and cause photothermal-mediated tumor ablation
– Delivery of immunomodulatory agents for cancer immunotherapy
– Synergistic therapy through a combination of drug delivery and photothermal therapy
– Imaging and biosensing
– The biodistribution of metal nanostructures is challenging along with their clearance from the body
– The metal nanostructures possess high cytotoxicity and poor biocompatibility
– The chance of inflammation and immune reactions
– Stability and toxicity towards normal cells
Carbon nanoparticles
– High drug-loading potential for the delivery of drugs, proteins, and genetic tools
– Application in photothermal and photodynamic therapy
– Imaging and biosensing of cancer biomarkers
-The toxicity and poor biocompatibility
– The changes in the biodegradation of carbon nanoparticles, leading to their long-term accumulation
– Complexity in the generation of nanoparticles at a large scale and achieving the desirable physicochemical properties including size, zeta potential and others
– Heterogeneous biological functions among the various classes of carbon nanomaterials including tubes, dots and sheets
hyperactivation of immune systems using immune agonists or adjuvants can affect normal cells and tissues. Therefore, the delivery of therapeutics should be performed in a controlled manner and safe levels should be delivered. Moreover, the rapid or burst release of immunotherapy compounds is not effective in providing longterm anti-cancer immunity. A number of nanoparticles are promising for the controlled release of therapeutic compounds, including PLGA nanostructures that, upon degradation of the polymer, the release of the immunotherapeutic compound occurs [594, 595]. Biocompatibility has been another important factor in pre-clinical and clinical studies [596]. Along with controlling the toxicity of immunomodulatory factors, including recombinant cytokines [597-599], the physicochemical characteristics of nanostructures including size, shape and thermal conversion ability, among others, should be adjusted in a manner to reduce the side effects of nanoparticles [600, 601]. In this way, the toxicity of nanoparticles in vitro and in vivo, hemocompatibility, effect on major organs including liver and kidney, and metabolic pathways should be investigated [602]. The surface functionalization of nanoparticles is another important factor in cancer immunotherapy. The surface functionalization can affect the intracellular uptake of nanostructures and even their processing [603]. Furthermore, since nanoparticles have been applied for antigen capture, the surface charge, hydrophobicity and hydrophobicity can change the function of nanostructures in cancer immunotherapy [299]. Another factor is that the nanostructures can specifically target the lymphoid tissues or immune cells to enhance the potential of drugs in cancer immunotherapy [604]. Polymeric nanoparticles have shown high potential in vascular escape, infiltration into tissues and lymphatics and targeting lymphocytes, while liposomes show high uptake by phagocytic cells, including macrophages [603]. In addition, these nanoparticles demonstrate high safety along with capacity in cancer immunotherapy [605608]. Notably, the nanoparticles can be considered as immune potentiates in which metal nanoparticles, viruslike nanostructures and other categories can stimulate immune responses through induction of and cells [603, 609] that is highly dependent on the size and surface charge of nanostructures [366, 610, 611]. However, carbon nanostructures have shown immunosuppressive impacts in some cases [612, 613]. Therefore, the introduction of nanoparticles for thr purpose of cancer immunotherapy is of importance.
Abbreviations
ICls
Immune Checkpoint Inhibitors
TME
Tumor Microenvironment
NFAT
Nuclear Factor of Activated T Cells
TOX
Thymocyte Selection-Associated High Mobility
Group Box Protein
NR4A
Nuclear Receptor Subfamily 4 Group A
FDA
U.S. Food and Drug Administration
CTLA4
Cytotoxic T-Lymphocyte Antigen 4
PD-1
Programmed Cell Death Protein 1
PD-L1
Programmed Death-Ligand 1
TAMs
Tumor-Associated Macrophages
Th1
Type 1 T Helper Cell
IL-4, IL-10, IL-13
Interleukin-4, Interleukin-10, Interleukin-13
M1
M1 Macrophages
M2
M2 Macrophages
TGF-
Transforming Growth Factor-Beta
-SMA
Alpha-Smooth Muscle Actin
NK cells
Natural Killer Cells
IFN-
Interferon-Gamma
B cells
B Lymphocytes
T cells
T Lymphocytes
PD-1
Programmed Cell Death Protein 1
TCM
Central Memory T Cells
TEM
Effector Memory T Cells
TRM
Resident Memory T Cells
TSCM
Stem Cell Memory T Cells
TE
Effector T Cells
Th1
Type 1 T Helper Cell
IFN-
Interferon-Gamma
TCM
Central Memory T Cells
CEMIP
Cell Migration-Inducing Hyaluronidase 1
USP22
Ubiquitin-Specific Peptidase 22
RNF31
Ring Finger Protein 31
YAP
Yes-Associated Protein
CDKN2A/B
Cyclin-Dependent Kinase Inhibitor 2 A/B
SUSD6
Sushi Domain Containing 6
TMEM127
Transmembrane Protein 127
WWP2
WW Domain Containing E3 Ubiquitin Protein Ligase 2
mTORC1
Mechanistic Target of Rapamycin Complex 1
CD248
Cluster of Differentiation 248
OPN
Osteopontin
SERPINE1
Serpin Family E Member 1
RGS5
Regulator of G Protein Signaling 5
apCAFs
Antigen-Presenting Cancer-Associated Fibroblasts
rCAFs
Restraining Cancer-Associated Fibroblasts
iCAFs
Inflammatory Cancer-Associated Fibroblasts
PRDM1
PR Domain Zinc Finger Protein 1
ZnCDA
Zinc Chlorodipyridine Acetate
STING
Stimulator of Interferon Genes
ROS
Reactive Oxygen Species
TLR4
Toll-Like Receptor 4
MyD88
Myeloid Differentiation Primary Response 88
Fe3O4-SAS@PLT
Ferrimagnetic Mesoporous Silica Nanoparticles Loaded with Sulfasalazine and Functionalized with Platelets
CSF1
Colony Stimulating Factor 1
CSF1-R
Colony Stimulating Factor 1 Receptor
SIRPa
Signal Regulatory Protein Alpha
MCSF
Macrophage Colony-Stimulating Factor
MAPK
Mitogen-Activated Protein Kinase
PEGylated liposomes
Polyethylene Glycol-coated Liposomes
R848
Imiquimod analog
CCL5-siRNA
Chemokine (C-C motif) Ligand 5 Small Interfering RNA
Ce6
Chlorin e6
PFC
Perfluorocarbon
MIP-3
Macrophage Inflammatory Protein-3
Au@PG
Gold Nanoparticles coated with Polyaniline-Glucose
CaCO3
Calcium Carbonate
DGL-ZA
Dendrigraft Poly-L-Lysines-Zoledronate
MMP2
Matrix Metalloproteinase 2
cGAS/STING
Cyclic GMP-AMP Synthase/Stimulator of Interferon Genes
PLGA
Poly(lactic-co-glycolic acid)
CTL
Cytotoxic T Lymphocyte
MDSCs
Myeloid-Derived Suppressor Cells
Treg cells
Regulatory T cells
PARP
Poly(ADP-ribose) Polymerase
AMPKa/mTOR
AMP-Activated Protein Kinase Alpha/Mammalian Target of Rapamycin
We would like to express our gratitude to Dr. Rupangi Verma from the Medical and Scientific Communication, Research Support Unit at the National University Health System, Singapore for her meticulous review and editing of our manuscript for English language accuracy.
Author contributions
Q.L, D.K, S.L and M.A wrote the first draft of paper (Writing original draft). A.R.A, I.C, Y.T, X.N, Y.W, P.T and L.W critically revised and supervised the paper. G.S, V.T, F.T, Z.Y and P.H developed the idea and concept and revised the paper (Writing-review-editing).
Funding
This work was supported by National Natural Science Foundation of China’s General Program (82072640), Outstanding Youth Project of Heilongjiang Natural Science Foundation (YQ2021H023), Special Key Projects of Guiding Technological Innovation in Shaanxi Province(2021QFY01-03) and Major clinical research project of Tangdu Hospital(2021LCYJ008). This work was also supported by Singapore Ministry of Education Tier 1 grant to Dr. Gautam Sethi.
Data availability
No datasets were generated or analysed during the current study.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Author details
¹Department of Thoracic Surgery, Tangdu Hospital, Air Force Medical University, 569 Xinsi Road, Xi’an 710038, China Department of Rehabilitation Medicine, Chongqing Public Health Medical Center, Chongqing, China Department of Colorectal Surgery, Harbin Medical University Cancer Hospital, Harbin, China Department of General Surgery, Institute of Precision Diagnosis and Treatment of Digestive System Tumors, Carson International Cancer Center, Shenzhen University General Hospital, Shenzhen University, Shenzhen 518055, Guangdong, China Shanghai Institute of Cardiovascular Diseases, Zhongshan Hospital, Fudan University, Shanghai 200032, China Department of Radiation Oncology, Shandong Cancer Hospital and Institute, Shandong First Medical University, Shandong Academy of Medical Sciences, Jinan 250000, Shandong, China Xsphera Biosciences, Translational Medicine Group, 6 Tide Street, Boston, MA 02210, USA Department of Medical Oncology, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA 02115, USA Blood Cell Development and Function Program, Fox Chase Cancer Center, Philadelphia, PA, USA School of Public Health, Benedictine University, Lisle, USA Department of Urologic Sciences and Vancouver Prostate Centre, University of British Columbia, Vancouver, BC V6H3Z6, Canada Cumming School of Medicine, Arnie Charbonneau Cancer Research Institute, University of Calgary, Calgary, AB T2N 4Z6, Canada Department of Medical Sciences, University of Calgary, Calgary, AB T2N 4Z6, Canada Present address: NUS Center for Cancer Research (N2CR), Yong Loo Lin School of Medicine, National University of Singapore, Singapore 117599, Singapore Present address: Department of Pharmacology, Yong Loo Lin School of Medicine, National University of Singapore, 16 Medical Drive, Singapore 117600, Singapore Laboratory of NF-kB Signalling, Institute of Molecular and Cell Biology (IMCB), Agency for Science, Technology and Research (A*STAR), 61 Biopolis Drive, Proteos, 138673 Singapore, Republic of Singapore The Graduate School, Augusta University, 30912 Augusta, GA, USA Department of Oncology Surgery, Harbin Medical University Cancer Hospital, Harbin, China Key Laboratory of Tumor Immunology in Heilongjiang, Harbin, China
Received: 30 December 2023 / Accepted: 15 March 2024
Published online: 02 April 2024
References
Liu Y, et al. Emerging phagocytosis checkpoints in cancer immunotherapy. Signal Transduct Target Ther. 2023;8(1):104.
Kennedy LB, Salama AKS. A review of cancer immunotherapy toxicity. CA Cancer J Clin. 2020;70(2):86-104.
Mahoney KM, Rennert PD, Freeman GJ. Combination cancer immunotherapy and new immunomodulatory targets. Nat Rev Drug Discov. 2015;14(8):561-84.
Webster RM. The immune checkpoint inhibitors: where are we now? Nat Rev Drug Discov. 2014;13(12):883-4.
Zhang Q, et al. Immune and Clinical features of CD96 expression in Glioma by in silico analysis. Front Bioeng Biotechnol. 2020;8:592.
Galipeau J, Sensébé L. Mesenchymal stromal cells: Clinical challenges and Therapeutic opportunities. Cell Stem Cell. 2018;22(6):824-33.
Liotta F, et al. Toll-like receptors 3 and 4 are expressed by human bone marrow-derived mesenchymal stem cells and can inhibit their T-cell modulatory activity by impairing notch signaling. Stem Cells. 2008;26(1):279-89.
Majeti R, et al. CD47 is an adverse prognostic factor and therapeutic antibody target on human acute myeloid leukemia stem cells. Cell. 2009;138(2):286-99.
Barkal AA, et al. CD24 signalling through macrophage Siglec-10 is a target for cancer immunotherapy. Nature. 2019;572(7769):392-6.
Gordon SR, et al. PD-1 expression by tumour-associated macrophages inhibits phagocytosis and tumour immunity. Nature. 2017;545(7655):495-9.
Barkal AA, et al. Engagement of MHC class I by the inhibitory receptor LILRB1 suppresses macrophages and is a target of cancer immunotherapy. Nat Immunol. 2018;19(1):76-84.
Lin H, et al. Stanniocalcin 1 is a phagocytosis checkpoint driving tumor immune resistance. Cancer Cell. 2021;39(4):480-e4936.
Theruvath J, et al. Anti-GD2 synergizes with CD47 blockade to mediate tumor eradication. Nat Med. 2022;28(2):333-44.
Gardner A, de Mingo Á, Pulido, Ruffell B. Dendritic cells and their role in Immunotherapy. Front Immunol. 2020;11:924.
Chen DS, Mellman I. Oncology meets immunology: the cancer-immunity cycle. Immunity. 2013;39(1):1-10.
Nakayama M. Antigen Presentation by MHC-Dressed cells. Front Immunol. 2014;5:672.
Lin A, Loré K. Granulocytes: New members of the Antigen-presenting cell family. Front Immunol. 2017;8:1781.
Broz ML, et al. Dissecting the tumor myeloid compartment reveals rare activating antigen-presenting cells critical for T cell immunity. Cancer Cell. 2014;26(5):638-52.
DeNardo DG, Ruffell B. Macrophages as regulators of tumour immunity and immunotherapy. Nat Rev Immunol. 2019;19(6):369-82.
Ruffell B, Coussens LM. Macrophages and therapeutic resistance in cancer. Cancer Cell. 2015;27(4):462-72.
Sánchez-Paulete AR, et al. Cancer Immunotherapy with Immunomodulatory Anti-CD137 and Anti-PD-1 monoclonal antibodies requires BATF3-Dependent dendritic cells. Cancer Discov. 2016;6(1):71-9.
Hildner K, et al. Batf3 deficiency reveals a critical role for CD8alpha + dendritic cells in cytotoxic T cell immunity. Science. 2008;322(5904):1097-100.
Roberts EW, et al. Critical role for CD103(+)/CD141(+) dendritic cells bearing CCR7 for Tumor Antigen Trafficking and priming of T cell immunity in Melanoma. Cancer Cell. 2016;30(2):324-36.
Salmon H, et al. Expansion and activation of CD103(+) dendritic cell progenitors at the Tumor Site enhances tumor responses to therapeutic PD-L1 and BRAF inhibition. Immunity. 2016;44(4):924-38.
de Pulido M. TIM-3 regulates CD103(+) dendritic cell function and response to chemotherapy in breast Cancer. Cancer Cell. 2018;33(1):60-74.e6.
Garris CS, et al. Successful Anti-PD-1 Cancer Immunotherapy requires T cell-dendritic cell crosstalk involving the cytokines IFN- and IL-12. Immunity. 2018;49(6):1148-e11617.
Spranger S, et al. Tumor-residing Batf3 dendritic cells are required for effector cell trafficking and adoptive cell therapy. Cancer Cell. 2017;31(5):711-e7234.
Chow MT, et al. Intratumoral Activity of the CXCR3 chemokine system is required for the efficacy of Anti-PD-1 therapy. Immunity. 2019;50(6):1498-e15125.
Xia Y, et al. Engineering macrophages for Cancer Immunotherapy and Drug Delivery. Adv Mater. 2020;32(40):e2002054.
Gao J, Liang Y, Wang L. Shap Polarization Tumor-Associated Macrophages Cancer Immunotherapy Front Immunol. 2022;13:888713.
Kumari N, Choi SH. Tumor-associated macrophages in cancer: recent advancements in cancer nanoimmunotherapies. J Exp Clin Cancer Res. 2022;41(1):68.
Li L, Ma SR, Yu ZL. Targeting the lipid metabolic reprogramming of tumorassociated macrophages: a novel insight into cancer immunotherapy. Cell Oncol (Dordr); 2023.
Pei L, et al. Roles of cancer-associated fibroblasts (CAFs) in anti- PD-1/PD-L1 immunotherapy for solid cancers. Mol Cancer. 2023;22(1):29.
Zhang H, et al. Define cancer-associated fibroblasts (CAFs) in the tumor microenvironment: new opportunities in cancer immunotherapy and advances in clinical trials. Mol Cancer. 2023;22(1):159.
Raskov H, et al. Cancer-Associated fibroblasts and Tumor-Associated macrophages in Cancer and Cancer Immunotherapy. Front Oncol. 2021;11:668731.
Thiery J. Modulation of the antitumor immune response by cancer-associated fibroblasts: mechanisms and targeting strategies to hamper their immunosuppressive functions. Explor Target Antitumor Ther. 2022;3(5):598-629.
Wang Q, et al. Role of tumor microenvironment in cancer progression and therapeutic strategy. Cancer Med. 2023;12(10):11149-65.
Han S et al. Tumor Microenvironment Regulation and Cancer Targeting Therapy based on nanoparticles. J Funct Biomater, 2023. 14(3).
Li Z, Yin P. Tumor microenvironment diversity and plasticity in cancer multidrug resistance. Biochim Biophys Acta Rev Cancer. 2023;1878(6):188997.
Yang R, et al. Tumor microenvironment responsive metal nanoparticles in cancer immunotherapy. Front Immunol. 2023;14:1237361.
Zhang Z, et al. Involvement of inflammasomes in tumor microenvironment and tumor therapies. J Hematol Oncol. 2023;16(1):24.
Jin HR, et al. Lipid metabolic reprogramming in tumor microenvironment: from mechanisms to therapeutics. J Hematol Oncol. 2023;16(1):103.
Arner EN, Rathmell JC. Metabolic programming and immune suppression in the tumor microenvironment. Cancer Cell. 2023;41(3):421-33.
Lin MJ, et al. Cancer vaccines: the next immunotherapy frontier. Nat Cancer. 2022;3(8):911-26.
Beck JD, et al. mRNA therapeutics in cancer immunotherapy. Mol Cancer. 2021;20(1):69.
Siminiak N, et al. Immunotherapy in Ovarian Cancer. Arch Immunol Ther Exp (Warsz). 2022;70(1):19.
Mauricio D, et al. Immunotherapy in Cervical Cancer. Curr Oncol Rep. 2021;23(6):61.
Bockorny B, Grossman JE, Hidalgo M. Facts and hopes in Immunotherapy of Pancreatic Cancer. Clin Cancer Res. 2022;28(21):4606-17.
Yang M, et al. The application of nanoparticles in cancer immunotherapy: targeting tumor microenvironment. Bioact Mater. 2021;6(7):1973-87.
Overchuk M, Zheng G. Overcoming obstacles in the tumor microenvironment: recent advancements in nanoparticle delivery for cancer theranostics. Biomaterials. 2018;156:217-37.
Matsumura Y, Maeda H. A new concept for macromolecular therapeutics in cancer chemotherapy: mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res. 1986;46(12 Pt 1):6387-92.
Prabhakar U, et al. Challenges and key considerations of the enhanced permeability and retention effect for nanomedicine drug delivery in oncology. Cancer Res. 2013;73(8):2412-7.
Yang S, Gao H. Nanoparticles for modulating tumor microenvironment to improve drug delivery and tumor therapy. Pharmacol Res. 2017;126:97-108.
Chen Q , et al. Remodeling the Tumor Microenvironment with Emerging Nanotherapeutics. Trends Pharmacol Sci. 2018;39(1):59-74.
Li M, et al. Nanoparticles designed to regulate tumor microenvironment for cancer therapy. Life Sci. 2018;201:37-44.
Guo B, et al. Cuproptosis Induced by ROS responsive nanoparticles with Elesclomol and Copper Combined with APD-L1 for enhanced Cancer Immunotherapy. Adv Mater. 2023;35(22):e2212267.
Wang-Bishop L, et al. STING-activating nanoparticles normalize the vascularimmune interface to potentiate cancer immunotherapy. Sci Immunol. 2023;8(83):eadd1153.
Ding , et al. ZIF-8 nanoparticles evoke pyroptosis for high-efficiency Cancer Immunotherapy. Angew Chem Int Ed Engl. 2023;62(10):e202215307.
Liu J et al. Ultrathin clay nanoparticles-mediated mutual reinforcement of ferroptosis and Cancer immunotherapy. Adv Mater, 2023: p. e2309562.
Huang A, et al. Engineered apoptosis-bioinspired nanoparticles initiate Immune Cascade for Cancer Immunotherapy of Malignant ascites. ACS Appl Mater Interfaces. 2023;15(8):10371-82.
Liu D et al. Tumor Microenvironment-Responsive nanoparticles amplifying STING Signaling Pathway for Cancer Immunotherapy. Adv Mater, 2023: p. e2304845.
Sun Y, et al. Sialic acid-targeted cyclodextrin-based nanoparticles deliver CSF-1R siRNA and reprogram tumour-associated macrophages for immunotherapy of prostate cancer. Eur J Pharm Sci. 2023;185:106427.
Liu C, et al. Microfluidic sonication to assemble Exosome membranecoated nanoparticles for Immune evasion-mediated targeting. Nano Lett. 2019;19(11):7836-44.
Li M et al. Signaling pathways in macrophages: molecular mechanisms and therapeutic targets MedComm (2020), 2023;4(5):e349.
Ginhoux F, Guilliams M. Tissue-Resident Macrophage Ontogeny and Homeostasis. Immunity. 2016;44(3):439-49.
Epelman S, Lavine KJ, Randolph GJ. Origin and functions of tissue macrophages. Immunity. 2014;41(1):21-35.
Italiani P, Boraschi D. From monocytes to M1/M2 macrophages: phenotypical vs. functional differentiation. Front Immunol. 2014;5:514.
Schulz , et al. A lineage of myeloid cells independent of myb and hematopoietic stem cells. Science. 2012;336(6077):86-90.
Sieweke MH, Allen JE. Beyond stem cells: self-renewal of differentiated macrophages. Science. 2013;342(6161):1242974.
Zhan C et al. Antitumor therapy for breast cancer: focus on tumor-associated macrophages and nanosized drug delivery systems. Cancer Med, 2023.
Wang N, et al. Research trends in pharmacological modulation of tumorassociated macrophages. Clin Transl Med. 2021;11(1):e288.
Vitale I, et al. Macrophages and metabolism in the Tumor Microenvironment. Cell Metab. 2019;30(1):36-50.
Wang J, et al. Crosstalk between cancer and immune cells: role of tumorassociated macrophages in the tumor microenvironment. Cancer Med. 2019;8(10):4709-21.
Wu T, Dai Y. Tumor microenvironment and therapeutic response. Cancer Lett. 2017;387:61-8.
Munir MT et al. Tumor-Associated macrophages as multifaceted regulators of breast tumor growth. Int J Mol Sci, 2021. 22(12).
Qiu SQ, et al. Tumor-associated macrophages in breast cancer: innocent bystander or important player? Cancer Treat Rev. 2018;70:178-89.
Wang C, et al. Macrophage balance fraction determines the degree of immunosuppression and metastatic ability of breast cancer. Int Immunopharmacol. 2021;97:107682.
Steenbrugge J, et al. Anti-inflammatory signaling by mammary tumor cells mediates prometastatic macrophage polarization in an innovative intraductal mouse model for triple-negative breast cancer. J Exp Clin Cancer Res. 2018;37(1):191.
Shu Y, Cheng P. Targeting tumor-associated macrophages for cancer immunotherapy Biochimica et Biophysica Acta (BBA) – Reviews on Cancer, 2020;1874(2):188434.
Nascimento C, et al. Reprogramming of tumor-associated macrophages by polyaniline-coated iron oxide nanoparticles applied to treatment of breast cancer. Int J Pharm. 2023;636:122866.
Shang Y, et al. Bioengineered Nanospores selectively blocking LC3-Associated phagocytosis in Tumor-Associated macrophages Potentiate Antitumor Immunity. ACS Nano. 2023;17(11):10872-87.
Liu Y, et al. Multifunctional nanoparticles inhibit tumor and tumor-associated macrophages for triple-negative breast cancer therapy. J Colloid Interface Sci. 2024;657:598-610.
Liang DS, et al. Targeted delivery of pexidartinib to tumor-associated macrophages via legumain-sensitive dual-coating nanoparticles for cancer immunotherapy. Colloids Surf B Biointerfaces. 2023;226:113283.
Sun , et al. The role of cancer-associated fibroblasts in tumorigenesis of gastric cancer. Cell Death Dis. 2022;13(10):874.
Gu J, et al. The role of PKM2 nuclear translocation in the constant activation of the NF-kB signaling pathway in cancer-associated fibroblasts. Cell Death Dis. 2021;12(4):291.
Bu L, et al. Biological heterogeneity and versatility of cancer-associated fibroblasts in the tumor microenvironment. Oncogene. 2019;38(25):4887-901.
Kalluri R. The biology and function of fibroblasts in cancer. Nat Rev Cancer. 2016;16(9):582-98.
Kobayashi H, et al. Cancer-associated fibroblasts in gastrointestinal cancer. Nat Rev Gastroenterol Hepatol. 2019;16(5):282-95.
Zhang T, et al. Cancer-associated fibroblasts in pancreatic ductal adenocarcinoma. Cell Death Dis. 2022;13(10):897.
Öhlund D , et al. Distinct populations of inflammatory fibroblasts and myofibroblasts in pancreatic cancer. J Exp Med. 2017;214(3):579-96.
Biffi G, et al. IL1-Induced JAK/STAT signaling is antagonized by TGF to shape CAF heterogeneity in pancreatic ductal adenocarcinoma. Cancer Discov. 2019;9(2):282-301.
Elyada E, et al. Cross-species single-cell analysis of pancreatic ductal adenocarcinoma reveals Antigen-Presenting Cancer-Associated fibroblasts. Cancer Discov. 2019;9(8):1102-23.
Fang Z, et al. Signaling pathways in cancer-associated fibroblasts: recent advances and future perspectives. Cancer Commun. 2023;43(1):3-41.
Ai W, et al. Modulation of cancer-associated fibroblasts by nanodelivery system to enhance efficacy of tumor therapy. Nanomed (Lond). 2023;18(15):1025-39.
Geng , et al. Safe engineering of cancer-associated fibroblasts enhances checkpoint blockade immunotherapy. J Control Release. 2023;356:272-87.
Jian C et al. Biomimetic Nanoplatform for Dual-Targeted Clearance of Activated and Senescent Cancer-Associated Fibroblasts to Improve Radiation Resistance in Breast Cancer Small, 2024: p. e2309279.
Hu M, et al. Salvianolic acid B-loaded polydopamine-modified hollow mesoporous organic silica nanoparticles for treatment of breast cancer metastasis via suppressing cancer-associated fibroblasts. Eur J Pharm Sci. 2024;192:106641.
Hinshaw DC, Shevde LA. The Tumor Microenvironment innately modulates Cancer Progression. Cancer Res. 2019;79(18):4557-66.
Wang J, et al. The clinical significance of tumor-infiltrating neutrophils and neutrophil-to-CD8 + lymphocyte ratio in patients with resectable esophageal squamous cell carcinoma. J Transl Med. 2014;12:7.
Deniset JF, Kubes P. Recent Adv Underst Neutrophils F1000Res. 2016;5:2912.
Uribe-Querol E, Rosales C. Neutrophils in Cancer: two sides of the same Coin. J Immunol Res. 2015;2015:983698.
Cools-Lartigue J, et al. Neutrophil extracellular traps in cancer progression. Cell Mol Life Sci. 2014;71(21):4179-94.
Jin W, et al. Tumor-infiltrating NETs predict postsurgical survival in patients with pancreatic ductal adenocarcinoma. Ann Surg Oncol. 2019;26(2):635-43.
Fridlender ZG, Albelda SM. Tumor-associated neutrophils: friend or foe? Carcinogenesis. 2012;33(5):949-55.
Demers M, et al. Priming of neutrophils toward NETosis promotes tumor growth. Oncoimmunology. 2016;5(5):e1134073.
He M, et al. Peritumoral stromal neutrophils are essential for c-Met-elicited metastasis in human hepatocellular carcinoma. Oncoimmunology. 2016;5(10):e1219828.
Schauer C, et al. Aggregated neutrophil extracellular traps limit inflammation by degrading cytokines and chemokines. Nat Med. 2014;20(5):511-7.
Ralph SJ, Reynolds MJ. Intratumoral pro-oxidants promote cancer immunotherapy by recruiting and reprogramming neutrophils to eliminate tumors. Cancer Immunol Immunother. 2023;72(3):527-42.
Benguigui et al. Interferon-stimulated neutrophils as a predictor of immunotherapy response. Cancer Cell, 2024.
Huntington ND, Cursons J, Rautela J. The cancer-natural killer cell immunity cycle. Nat Rev Cancer. 2020;20(8):437-54.
Huntington ND, Vosshenrich CA, Di Santo JP. Developmental pathways that generate natural-killer-cell diversity in mice and humans. Nat Rev Immunol. 2007;7(9):703-14.
Pfefferle , et al. Intra-lineage plasticity and functional reprogramming maintain natural killer cell repertoire diversity. Cell Rep. 2019;29(8):2284-e22944.
Gil M, Kim KE. Interleukin-18 is a prognostic biomarker correlated with CD8+T cell and natural killer cell infiltration in skin cutaneous melanoma Journal of clinical medicine, 2019;8(11):1993.
Cursons J, et al. A gene signature Predicting Natural Killer Cell Infiltration and Improved Survival in Melanoma patients. Cancer Immunol Res. 2019;7(7):1162-74.
Lee H, et al. Integrated molecular and immunophenotypic analysis of NK cells in anti-PD-1 treated metastatic melanoma patients. Oncoimmunology. 2019;8(2):e1537581.
Li B et al. Natural killer cell and stroma abundance are independently prognostic and predict gastric cancer chemotherapy benefit. JCl Insight, 2020. 5(9).
Ran GH, et al. Natural killer cell homing and trafficking in tissues and tumors: from biology to application. Signal Transduct Target Therapy. 2022;7(1):205.
Scoville SD, Freud AG, Caligiuri MA. Model Hum Nat Killer Cell Dev Era Innate Lymphoid Cells Front Immunol. 2017;8:360.
Stokic-Trtica V, Diefenbach A, Klose CSN. NK Cell Dev Times Innate Lymphoid Cell Divers Front Immunol. 2020;11:813.
Vivier E, et al. Innate lymphoid cells: 10 years on. Cell. 2018;174(5):1054-66.
Freud AG, et al. The Broad Spectrum of Human Natural Killer Cell Diversity. Immunity. 2017;47(5):820-33.
Björkström NK, Ljunggren HG, Michaëlsson J. Emerging insights into natural killer cells in human peripheral tissues. Nat Rev Immunol. 2016;16(5):310-20.
Yu J, Freud AG, Caligiuri MA. Location and cellular stages of natural killer cell development. Trends Immunol. 2013;34(12):573-82.
Vivier E, et al. Functions of natural killer cells. Nat Immunol. 2008;9(5):503-10.
Fang F, Xiao W, Tian Z. NK cell-based immunotherapy for cancer. Semin Immunol. 2017;31:37-54.
Li Y, et al. Natural killer cells: friend or foe in metabolic diseases? Front Immunol. 2021;12:614429.
Shimasaki N, Jain A, Campana D. NK cells for cancer immunotherapy. Nat Rev Drug Discov. 2020;19(3):200-18.
Maskalenko NA, Zhigarev D, Campbell KS. Harnessing natural killer cells for cancer immunotherapy: dispatching the first responders. Nat Rev Drug Discov. 2022;21(8):559-77.
Pockley AG, Vaupel P, Multhoff G. NK cell-based therapeutics for lung cancer. Expert Opin Biol Ther. 2020;20(1):23-33.
Muntasell A, et al. NK Cell infiltrates and HLA Class I expression in primary HER2(+) breast Cancer Predict and Uncouple Pathological Response and Disease-free survival. Clin Cancer Res. 2019;25(5):1535-45.
Liu P, Chen L, Zhang H. Natural killer cells in Liver Disease and HepatocelIular Carcinoma and the NK cell-based immunotherapy. J Immunol Res. 2018;2018:p1206737.
Ali TH, et al. Enrichment of CD56(dim)KIR + CD57 + highly cytotoxic NK cells in tumour-infiltrated lymph nodes of melanoma patients. Nat Commun. 2014;5:5639.
Terrén I et al. NK Cell-based immunotherapy in renal cell carcinoma. Cancers (Basel), 2020. 12(2).
Lim SA, et al. Lipid metabolism in T cell signaling and function. Nat Chem Biol. 2022;18(5):470-81.
Ando M , et al. Memory T cell, exhaustion, and tumor immunity. Immunological Med. 2020;43(1):1-9.
Franco F, et al. Metabolic and epigenetic regulation of T-cell exhaustion. Nat Metabolism. 2020;2(10):1001-12.
Douka S, et al. Lipid nanoparticle-mediated messenger RNA delivery for ex vivo engineering of natural killer cells. J Control Release. 2023;361:455-69.
Shamalov K, et al. Noninvasive Tracking of Natural Killer cells using gold nanoparticles. ACS Omega. 2021;6(43):28507-14.
Kim KS, et al. Cationic nanoparticle-mediated activation of natural killer cells for Effective Cancer Immunotherapy. ACS Appl Mater Interfaces. 2020;12(51):56731-40.
Sun , et al. Acid-switchable nanoparticles induce self-adaptive aggregation for enhancing antitumor immunity of natural killer cells. Acta Pharm Sin B. 2023;13(7):3093-105.
Liu GW, et al. Lipid nanoparticles for nucleic acid delivery to endothelial cells. Pharm Res. 2023;40(1):3-25.
Stoltz JF, et al. Introduction to endothelial cell biology. Clin Hemorheol Microcirc. 2007;37(1-2):5-8.
Martin FA, Murphy RP, Cummins PM. Thrombomodulin and the vascular endothelium: insights into functional, regulatory, and therapeutic aspects. Am J Physiol Heart Circ Physiol. 2013;304(12):H1585-97.
Maroney SA, Mast AE. Expression of tissue factor pathway inhibitor by endothelial cells and platelets. Transfus Apher Sci. 2008;38(1):9-14.
Mohan Rao LV, Esmon CT, Pendurthi UR. Endothelial cell protein C receptor: a multiliganded and multifunctional receptor. Blood. 2014;124(10):1553-62.
Bremnes RM, et al. The role of tumor stroma in cancer progression and prognosis: emphasis on carcinoma-associated fibroblasts and non-small cell lung cancer. J Thorac Oncol. 2011;6(1):209-17.
Pietras K, Ostman A. Hallmarks of cancer: interactions with the tumor stroma. Exp Cell Res. 2010;316(8):1324-31.
McAllister SS, Weinberg RA. The tumour-induced systemic environment as a critical regulator of cancer progression and metastasis. Nat Cell Biol. 2014;16(8):717-27.
Dillekås H, Rogers MS, Straume O. Are of deaths from cancer caused by metastases? Cancer Med. 2019;8(12):5574-6.
Khorana AA, et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632-4.
Tisdale MJ. Cachexia in cancer patients. Nat Rev Cancer. 2002;2(11):862-71.
Eilken HM, et al. Pericytes regulate VEGF-induced endothelial sprouting through VEGFR1. Nat Commun. 2017;8(1):1574.
Rouget C. Memoire sur les development, la structure et la proprietes physiologiques des capillaires sanguines et lymphatiques. Arch Physiol, 1873: p. 603-63.
Zimmermann KW. Der Feinere Bau Der Blutcapillaren. Z für Anatomie und Entwicklungsgeschichte. 1923;68:29-109.
Schrimpf C, et al. The role of pericyte detachment in vascular rarefaction. J Vasc Res. 2014;51(4):247-58.
Hirschi KK, D’Amore PA. Pericytes in the microvasculature. Cardiovascular Res. 1996;32(4):687-98.
Díaz-Flores L, et al. Microvascular pericytes, a review of their morphological and functional characteristics. Histology and histopathology; 1991.
Birbrair A, et al. How plastic are pericytes? Stem Cells Dev. 2017;26(14):1013-9.
Birbrair A, et al. Pericytes at the intersection between tissue regeneration and pathology. Clin Sci. 2015;128(2):81-93.
Picoli CC et al. Pericytes cross-talks within the tumor microenvironment Biochimica et Biophysica Acta (BBA)-Reviews on Cancer, 2021;1876(2):188608.
Jiang Z et al. Pericytes in the tumor microenvironment. Cancer Lett, 2023: p. 216074.
Chen Z, Xu XH, Hu J. Role of pericytes in angiogenesis: focus on cancer angiogenesis and anti-angiogenic therapy. Neoplasma. 2016;63(2):173-82.
Hong CL, et al. CD248 regulates wnt signaling in Pericytes to Promote Angiogenesis and Tumor Growth in Lung Cancer. Cancer Res. 2022;82(20):3734-50.
Meng YM, et al. Hexokinase 2-driven glycolysis in pericytes activates their contractility leading to tumor blood vessel abnormalities. Nat Commun. 2021;12(1):6011.
Dasgupta S, et al. RGS5-TGF -Smad axis switches pro- to anti-apoptotic signaling in tumor-residing pericytes, assisting tumor growth. Cell Death Differ. 2021;28(11):3052-76.
Pillay J, et al. Immune suppression by neutrophils and granulocytic myeloidderived suppressor cells: similarities and differences. Cell Mol Life Sci. 2013;70(20):3813-27.
Gabrilovich DI, Nagaraj S. Myeloid-derived suppressor cells as regulators of the immune system. Nat Rev Immunol. 2009;9(3):162-74.
Rodriguez PC, et al. Arginase I-producing myeloid-derived suppressor cells in renal cell carcinoma are a subpopulation of activated granulocytes. Cancer Res. 2009;69(4):1553-60.
Youn JI, et al. Characterization of the nature of granulocytic myeloid-derived suppressor cells in tumor-bearing mice. J Leukoc Biol. 2012;91(1):167-81.
Gabrilovich DI, Ostrand-Rosenberg S, Bronte V. Coordinated regulation of myeloid cells by tumours. Nat Rev Immunol. 2012;12(4):253-68.
Bronte V, et al. Recommendations for myeloid-derived suppressor cell nomenclature and characterization standards. Nat Commun. 2016;7:12150.
Kumar V, et al. The nature of myeloid-derived suppressor cells in the Tumor Microenvironment. Trends Immunol. 2016;37(3):208-20.
Condamine T, et al. Regulation of tumor metastasis by myeloid-derived suppressor cells. Annu Rev Med. 2015;66:97-110.
Condamine T et al. Lectin-type oxidized LDL receptor-1 distinguishes population of human polymorphonuclear myeloid-derived suppressor cells in cancer patients. Sci Immunol, 2016. 1(2).
Corzo CA, et al. HIF-1a regulates function and differentiation of myeloidderived suppressor cells in the tumor microenvironment. J Exp Med. 2010;207(11):2439-53.
Hossain F, et al. Inhibition of fatty acid oxidation modulates immunosuppressive functions of myeloid-derived suppressor cells and enhances Cancer therapies. Cancer Immunol Res. 2015;3(11):1236-47.
Zhou J, et al. Hepatoma-intrinsic CCRK inhibition diminishes myeloid-derived suppressor cell immunosuppression and enhances immune-checkpoint blockade efficacy. Gut. 2018;67(5):931-44.
Wu C, et al. Repolarization of myeloid derived suppressor cells via magnetic nanoparticles to promote radiotherapy for glioma treatment. Nanomedicine. 2019;16:126-37.
Ding , et al. Augmenting immunogenic cell death and alleviating myeloidderived suppressor cells by Sono-Activatable Semiconducting Polymer Nanopartners for Immunotherapy. Adv Mater. 2023;35(33):e2302508.
Zuo H, et al. Circumventing myeloid-derived suppressor cell-mediated immunosuppression using an oxygen-generated and -economized nanoplatform. ACS Appl Mater Interfaces. 2020;12(50):55723-36.
Habanjar O et al. Crosstalk of inflammatory cytokines within the breast Tumor Microenvironment. Int J Mol Sci, 2023. 24(4).
Zhang JM, An J. Cytokines, inflammation, and pain. Int Anesthesiol Clin. 2007;45(2):27-37.
Raman D, Sobolik-Delmaire T, Richmond A. Chemokines in health and disease. Exp Cell Res. 2011;317(5):575-89.
Bachelerie F, et al. International Union of Basic and Clinical Pharmacology. [corrected]. LXXXIX. Update on the extended family of chemokine receptors
and introducing a new nomenclature for atypical chemokine receptors. Pharmacol Rev. 2014;66(1):1-79.
Mélik-Parsadaniantz S, Rostène W. Chemokines and neuromodulation. J Neuroimmunol. 2008;198(1-2):62-8.
Zlotnik A, Yoshie O. The chemokine superfamily revisited. Immunity. 2012;36(5):705-16.
Kaneko N, et al. The role of interleukin-1 in general pathology. Inflamm Regen. 2019;39:12.
Akdis et al. Interleukins, from 1 to 37 , and interferon- : receptors, functions, and roles in diseases J Allergy Clin Immunol, 2011;127(3):701-21.e1-70.
Shin E, Koo JS. The role of Adipokines and bone marrow adipocytes in breast Cancer bone metastasis. Int J Mol Sci, 2020. 21(14).
Blüher M, Mantzoros CS. From leptin to other adipokines in health and disease: facts and expectations at the beginning of the 21st century. Metabolism. 2015;64(1):131-45.
Mancuso P. The role of adipokines in chronic inflammation. Immunotargets Ther. 2016;5:47-56.
Barchetta I, et al. Sick fat: the good and the bad of old and new circulating markers of adipose tissue inflammation. J Endocrinol Invest. 2019;42(11):1257-72.
Nehme R et al. Targeting adiponectin in breast Cancer. Biomedicines, 2022. 10(11).
Artac M, Altundag K. Leptin and breast cancer: an overview. Med Oncol. 2012;29(3):1510-4.
Ferrer I, et al. Transforming growth factor-alpha (TGF-alpha) and epidermal growth factor-receptor (EGF-R) immunoreactivity in normal and pathologic brain. Prog Neurobiol. 1996;49(2):99-123.
MaruYama T, Chen W, Shibata H. TGF- Cancer Immunotherapy Biol Pharm Bull. 2022;45(2):155-61.
Isaacs A, Lindenmann J. Virus interference. I. The interferon. Proc R Soc Lond B Biol Sci. 1957;147(927):258-67.
Schroder K, et al. Interferon-gamma: an overview of signals, mechanisms and functions. J Leukoc Biol. 2004;75(2):163-89.
Peng S, et al. Tumor-microenvironment-responsive nanomedicine for enhanced Cancer Immunotherapy. Adv Sci (Weinh). 2022;9(1):e2103836.
Mu J, et al. Development of endogenous enzyme-responsive nanomaterials for theranostics. Chem Soc Rev. 2018;47(15):5554-73.
Hu J, Zhang G, Liu S. Enzyme-responsive polymeric assemblies, nanoparticles and hydrogels. Chem Soc Rev. 2012;41(18):5933-49.
Shahriari M, et al. Enzyme responsive drug delivery systems in cancer treatment. J Control Release. 2019;308:172-89.
Qiu N, et al. Esterase-activated charge-reversal polymer for fibroblast-exempt Cancer Gene Therapy. Adv Mater. 2016;28(48):10613-22.
Luo Z, Dai Y, Gao H. Development and application of hyaluronic acid in tumor targeting drug delivery. Acta Pharm Sin B. 2019;9(6):1099-112.
Li H, et al. The relationship between MMP-2 and MMP-9 expression levels with breast cancer incidence and prognosis. Oncol Lett. 2017;14(5):5865-70.
Pham HT, Block NL, Lokeshwar VB. Tumor-derived hyaluronidase: a diagnostic urine marker for high-grade bladder cancer. Cancer Res. 1997;57(4):778-83.
Moreira AM et al. The Extracellular Matrix: an accomplice in gastric Cancer Development and Progression. Cells, 2020. 9(2).
Liu Y, et al. Tumor microenvironment-mediated immune tolerance in development and treatment of gastric cancer. Front Immunol. 2022;13:1016817.
Mohan V, Das A, Sagi I. Emerging roles of ECM remodeling processes in cancer. Semin Cancer Biol. 2020;62:192-200.
Sung JY, Cheong JH. The Matrisome is Associated with metabolic reprograming in stem-like phenotypes of gastric Cancer. Cancers (Basel), 2022. 14(6).
Moreira AM, et al. Proteomic identification of a gastric tumor ECM signature Associated with Cancer Progression. Front Mol Biosci. 2022;9:818552.
Jang , et al. Increased extracellular matrix density disrupts E-cadherin/ catenin complex in gastric cancer cells. Biomater Sci. 2018;6(10):2704-13.
Acerbi I, et al. Human breast cancer invasion and aggression correlates with ECM stiffening and immune cell infiltration. Integr Biol (Camb). 2015;7(10):1120-34.
Kuczek DE, et al. Collagen density regulates the activity of tumor-infiltrating cells. J Immunother Cancer. 2019;7(1):68.
Patel A, Sant S. Hypoxic tumor microenvironment: opportunities to develop targeted therapies. Biotechnol Adv. 2016;34(5):803-12.
Nelson DA, et al. Hypoxia and defective apoptosis drive genomic instability and tumorigenesis. Genes Dev. 2004;18(17):2095-107.
Saito G, Swanson JA, Lee K-D. Drug delivery strategy utilizing conjugation via reversible disulfide linkages: role and site of cellular reducing activities. Adv Drug Deliv Rev. 2003;55(2):199-215.
Wilson WR, Hay MP. Targeting hypoxia in cancer therapy. Nat Rev Cancer. 2011;11(6):393-410.
Naughton D. Drug targeting to hypoxic tissue using self-inactivating bioreductive delivery systems. Adv Drug Deliv Rev. 2001;53(2):229-33.
Vázquez-García I, et al. Ovarian cancer mutational processes drive sitespecific immune evasion. Nature. 2022;612(7941):778-86.
Li Q, et al. PRDM1/BLIMP1 induces cancer immune evasion by modulating the USP22-SPI1-PD-L1 axis in hepatocellular carcinoma cells. Nat Commun. 2022;13(1):7677.
Yang H, et al. RNF31 represses cell progression and immune evasion via YAP/ PD-L1 suppression in triple negative breast Cancer. J Exp Clin Cancer Res. 2022;41(1):364.
Choi SY, et al. Cancer-generated lactic acid: a regulatory, immunosuppressive metabolite? J Pathol. 2013;230(4):350-5.
Wang JX et al. Lactic acid and an acidic Tumor Microenvironment suppress Anticancer Immunity. Int J Mol Sci, 2020. 21(21).
Chen X, et al. A membrane-associated MHC-I inhibitory axis for cancer immune evasion. Cell. 2023;186(18):3903-e392021.
Zhang B et al. Tumor CEMIP drives immune evasion of colorectal cancer via MHC-I internalization and degradation. J Immunother Cancer, 2023. 11(1).
Quah HS, et al. Single cell analysis in head and neck cancer reveals potential immune evasion mechanisms during early metastasis. Nat Commun. 2023;14(1):1680.
Bergholz JS, et al. PI3Kß controls immune evasion in PTEN-deficient breast tumours. Nature. 2023;617(7959):139-46.
Barriga FM, et al. MACHETE identifies interferon-encompassing chromosome 9p21.3 deletions as mediators of immune evasion and metastasis. Nat Cancer. 2022;3(11):1367-85.
Liu HJ, et al. mTORC1 upregulates B7-H3/CD276 to inhibit antitumor T cells and drive tumor immune evasion. Nat Commun. 2023;14(1):1214.
Lidström T, et al. Extracellular galectin 4 drives Immune Evasion and promotes T-cell apoptosis in pancreatic Cancer. Cancer Immunol Res. 2023;11(1):72-92.
Vinay DS, et al. Immune evasion in cancer: mechanistic basis and therapeutic strategies. Sem Cancer Biol. 2015;35:S185-98.
Polyak K, et al. Breast tumor heterogeneity: causes and consequences. Breast Cancer Res. 2009;11:1-1.
Miller FR. Intratumor immunologic heterogeneity. Cancer Metastasis Rev. 1982;1:319-34.
Nicolson GL. Generation of phenotypic diversity and progression in metastatic tumor cells. Cancer Metastasis Rev. 1984;3:25-42.
Merlo LM, et al. Cancer as an evolutionary and ecological process. Nat Rev Cancer. 2006;6(12):924-35.
Sceneay J, et al. Primary tumor hypoxia recruits CD11b+/Ly6Cmed/ Ly6G + immune suppressor cells and compromises NK cell cytotoxicity in the premetastatic niche. Cancer Res. 2012;72(16):3906-11.
Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340(6):448-54.
Dunn GP, Old U, Schreiber RD. The three Es of cancer immunoediting. Annu Rev Immunol. 2004;22:329-60.
Lauritzsen GF, et al. Clonal deletion of thymocytes as a tumor escape mechanism. Int J Cancer. 1998;78(2):216-22.
Hegde PS, Chen DS. Top 10 challenges in cancer immunotherapy. Immunity. 2020;52(1):17-35.
Rao L, et al. Activating macrophage-mediated Cancer Immunotherapy by genetically edited nanoparticles. Adv Mater. 2020;32(47):e2004853.
Yang K, et al. Zinc cyclic di-AMP nanoparticles target and suppress tumours via endothelial STING activation and tumour-associated macrophage reinvigoration. Nat Nanotechnol. 2022;17(12):1322-31.
Cao M, et al. Ginseng-derived nanoparticles alter macrophage polarization to inhibit melanoma growth. J Immunother Cancer. 2019;7(1):326.
Zhang Y, et al. Macrophage-membrane-coated nanoparticles for Tumortargeted chemotherapy. Nano Lett. 2018;18(3):1908-15.
Jiang Q, et al. Platelet membrane-camouflaged magnetic nanoparticles for ferroptosis-enhanced Cancer Immunotherapy. Small. 2020;16(22):e2001704.
Melamed JR, et al. Ionizable lipid nanoparticles deliver mRNA to pancreatic cells via macrophage-mediated gene transfer. Sci Adv. 2023;9(4):eade1444.
Chen C, et al. Tumor-Associated-Macrophage-membrane-coated nanoparticles for improved photodynamic immunotherapy. Nano Lett. 2021;21(13):5522-31.
Ramesh A, et al. CSF1R- and SHP2-Inhibitor-loaded nanoparticles enhance cytotoxic activity and phagocytosis in Tumor-Associated macrophages. Adv Mater. 2019;31(51):e1904364.
Zanganeh S, et al. Iron oxide nanoparticles inhibit tumour growth by inducing pro-inflammatory macrophage polarization in tumour tissues. Nat Nanotechnol. 2016;11(11):986-94.
Chim LK, et al. Tumor-associated macrophages induce inflammation and drug resistance in a mechanically tunable engineered model of osteosarcoma. Biomaterials. 2023;296:122076.
Rohila D, et al. Syk Inhibition reprograms Tumor-Associated macrophages and overcomes Gemcitabine-Induced Immunosuppression in Pancreatic Ductal Adenocarcinoma. Cancer Res. 2023;83(16):2675-89
Xie R, et al. Furin-instructed aggregated gold nanoparticles for re-educating tumor associated macrophages and overcoming breast cancer chemoresistance. Biomaterials. 2021;275:120891.
Shen W, et al. Metabolic homeostasis-regulated nanoparticles for antibody-independent Cancer Radio-Immunotherapy. Adv Mater. 2022;34(51):e2207343.
Sun M, et al. Fibroblast activation Protein-a responsive peptide assembling Prodrug nanoparticles for Remodeling the Immunosuppressive Microenvironment and Boosting Cancer Immunotherapy. Small. 2022;18(9):e2106296.
Gao C, et al. Injectable Immunotherapeutic Hydrogel containing RNA-Loaded lipid nanoparticles reshapes Tumor Microenvironment for Pancreatic Cancer Therapy. Nano Lett. 2022;22(22):8801-9.
Yoon J, et al. Macrophage-reprogramming upconverting nanoparticles for enhanced TAM-mediated antitumor therapy of hypoxic breast cancer. J Control Release. 2023;360:482-95.
Rong , et al. Iron chelated melanin-like nanoparticles for tumorassociated macrophage repolarization and cancer therapy. Biomaterials. 2019;225:119515.
Ramesh A, et al. Dual inhibition of CSF1R and MAPK pathways using supramolecular nanoparticles enhances macrophage immunotherapy. Biomaterials. 2020;227:119559.
He Y, et al. Targeted MIP-3 plasmid nanoparticles induce dendritic cell maturation and inhibit M2 macrophage polarisation to suppress cancer growth. Biomaterials. 2020;249:120046.
Su WP, et al. Polyaniline-based glyco-condensation on au nanoparticles enhances Immunotherapy in Lung Cancer. ACS Appl Mater Interfaces. 2022;14(21):24144-59.
Yang S, et al. CaCO(3)-Encapsulated au nanoparticles modulate macrophages toward M1-like phenotype. ACS Appl Bio Mater. 2021;4(4):3214-23.
Wan J, et al. Biodegradable NIR-II Pseudo Conjugate Polymeric nanoparticles amplify photodynamic immunotherapy via alleviation of Tumor Hypoxia and Tumor-Associated Macrophage Reprogramming. Adv Mater. 2023;35(31):e2209799.
Li L, et al. Functional Gadofullerene nanoparticles trigger Robust Cancer Immunotherapy based on rebuilding an immunosuppressive Tumor Microenvironment. Nano Lett. 2020;20(6):4487-96.
Guo Q, et al. Dandelion-Like Tailorable nanoparticles for Tumor Microenvironment Modulation. Adv Sci (Weinh). 2019;6(21):1901430.
Liu Y, et al. Targeting Tumor-Associated macrophages by MMP2-Sensitive apoptotic body-mimicking nanoparticles. ACS Appl Mater Interfaces. 2020;12(47):52402-14.
Parayath NN, Parikh A, Amiji MM. Repolarization of Tumor-Associated macrophages in a genetically Engineered Nonsmall Cell Lung Cancer Model by Intraperitoneal Administration of Hyaluronic Acid-based nanoparticles encapsulating MicroRNA-125b. Nano Lett. 2018;18(6):3571-9.
Xu L, et al. Engineering the Intestinal Lymphatic Transport of oral nanoparticles to Educate macrophages for Cancer Combined Immunotherapy. ACS Nano. 2023;17(12):11817-37.
Zhang Y, et al. Gold nanoparticles inhibit activation of cancer-associated fibroblasts by disrupting communication from tumor and microenvironmental cells. Bioact Mater. 2021;6(2):326-32.
Kovács D, et al. Core-shell nanoparticles suppress metastasis and modify the tumour-supportive activity of cancer-associated fibroblasts. J Nanobiotechnol. 2020;18(1):18.
Lopez S, et al. Magneto-mechanical destruction of cancer-associated fibroblasts using ultra-small iron oxide nanoparticles and low frequency rotating magnetic fields. Nanoscale Adv. 2022;4(2):421-36.
Li L, et al. Photosensitizer-encapsulated ferritins mediate photodynamic therapy against Cancer-Associated fibroblasts and improve Tumor Accumulation of nanoparticles. Mol Pharm. 2018;15(8):3595-9.
Jin J, et al. Human Cancer Cell membrane-coated biomimetic nanoparticles reduce fibroblast-mediated Invasion and Metastasis and induce T-Cells. ACS Appl Mater Interfaces. 2019;11(8):7850-61.
Zhou S et al. FAP-Targeted photodynamic therapy mediated by Ferritin nanoparticles elicits an Immune response against Cancer cells and Cancer Associated fibroblasts. Adv Funct Mater, 2021. 31(7).
Yu Q, et al. Targeting cancer-associated fibroblasts by dual-responsive lipid-albumin nanoparticles to enhance drug perfusion for pancreatic tumor therapy. J Control Release. 2020;321:564-75.
Liu JQ, et al. Intratumoral delivery of IL-12 and IL-27 mRNA using lipid nanoparticles for cancer immunotherapy. J Control Release. 2022;345:306-13.
Huang KW, et al. Highly efficient and tumor-selective nanoparticles for dualtargeted immunogene therapy against cancer. Sci Adv. 2020;6(3):eaax5032.
Xiong J, et al. Cancer-Erythrocyte Hybrid membrane-camouflaged magnetic nanoparticles with enhanced photothermal-immunotherapy for ovarian Cancer. ACS Nano. 2021;15(12):19756-70.
Patel SK, et al. Hydroxycholesterol substitution in ionizable lipid nanoparticles for mRNA delivery to T cells. J Control Release. 2022;347:521-32.
Billingsley MM, et al. Orthogonal Design of experiments for optimization of lipid nanoparticles for mRNA Engineering of CART cells. Nano Lett. 2022;22(1):533-42.
Lin YX et al. Reactivation of the tumor suppressor PTEN by mRNA nanoparticles enhances antitumor immunity in preclinical models Sci Transl Med, 2021. 13(599).
Jiang Y, et al. Engineered cell-membrane-coated nanoparticles directly Present Tumor antigens to promote anticancer immunity. Adv Mater. 2020;32(30):e2001808.
Li Z, et al. Immunogenic cell death augmented by Manganese Zinc Sulfide nanoparticles for metastatic Melanoma Immunotherapy. ACS Nano. 2022;16(9):15471-83.
Cao L, et al. Activating cGAS-STING pathway with ROS-responsive nanoparticles delivering a hybrid prodrug for enhanced chemo-immunotherapy. Biomaterials. 2022;290:121856.
Chen C, et al. Asynchronous blockade of PD-L1 and CD155 by polymeric nanoparticles inhibits triple-negative breast cancer progression and metastasis. Biomaterials. 2021;275:p120988.
Tang S, et al. MnO(2)-melittin nanoparticles serve as an effective anti-tumor immunotherapy by enhancing systemic immune response. Biomaterials. 2022;288:121706.
Sun F, et al. Regulating glucose metabolism with Prodrug nanoparticles for promoting photoimmunotherapy of pancreatic Cancer. Adv Sci (Weinh). 2021;8(4):2002746.
Chou PY, et al. Glycosylation of OVA antigen-loaded PLGA nanoparticles enhances DC-targeting for cancer vaccination. J Control Release. 2022;351:970-88.
Son S, et al. Induction of T-helper-17-cell-mediated anti-tumour immunity by pathogen-mimicking polymer nanoparticles. Nat Biomed Eng. 2023;7(1):72-84.
Kim KS, et al. Ovalbumin and poly(i:c) encapsulated dendritic cell-targeted nanoparticles for Immune activation in the small intestinal lymphatic system. Adv Healthc Mater. 2022;11(21):e2200909.
Li S, et al. Pre-induced ICD membrane-coated carrier-free nanoparticles for the personalized Lung Cancer Immunotherapy. Small Methods. 2023;7(5):e2201569.
Zhang Z, et al. Antitumor Activity of Anti-mir-21 delivered through lipid nanoparticles. Adv Healthc Mater. 2023;12(6):e2202412.
Min Y, et al. Antigen-capturing nanoparticles improve the abscopal effect and cancer immunotherapy. Nat Nanotechnol. 2017;12(9):877-82.
Ou W, et al. Combination of NIR therapy and regulatory T cell modulation using layer-by-layer hybrid nanoparticles for effective cancer photoimmunotherapy. Theranostics. 2018;8(17):4574-90.
Zang , et al. Polymeric indoximod based prodrug nanoparticles with doxorubicin entrapment for inducing immunogenic cell death and improving the immunotherapy of breast cancer. J Mater Chem B. 2022;10(12):2019-27.
Yang T, et al. Dual polymeric prodrug co-assembled nanoparticles with precise ratiometric co-delivery of cisplatin and metformin for lung cancer chemoimmunotherapy. Biomater Sci. 2020;8(20):5698-714.
Ou W, et al. Regulatory T cell-targeted hybrid nanoparticles combined with immuno-checkpoint blockage for cancer immunotherapy. J Control Release. 2018;281:84-96.
He Y, et al. Remodeling tumor immunosuppression with molecularly imprinted nanoparticles to enhance immunogenic cell death for cancer immunotherapy. J Control Release. 2023;362:44-57.
Wan WJ, et al. Coadministration of iRGD peptide with ROS-sensitive nanoparticles co-delivering siFGL1 and siPD-L1 enhanced tumor immunotherapy. Acta Biomater. 2021;136:473-84.
Wang W, et al. The development of Chiral nanoparticles to target NK cells and CD8(+) T cells for Cancer Immunotherapy. Adv Mater. 2022;34(16):e2109354.
Wang B, et al. Liposomes co-loaded with ursolic acid and ginsenoside Rg3 in the treatment of hepatocellular carcinoma. Acta Biochim Pol. 2021;68(4):711-5.
Yao H, et al. Cisplatin nanoparticles promote Intratumoral CD8(+) T cell priming via Antigen Presentation and T cell receptor crosstalk. Nano Lett. 2022;22(8):3328-39.
Munakata L, et al. Lipid nanoparticles of Type-A CpG D35 suppress tumor growth by changing tumor immune-microenvironment and activate CD8 T cells in mice. J Control Release. 2019;313:106-19.
Chang HC, et al. Targeting and specific activation of Antigen-presenting cells by endogenous Antigen-Loaded nanoparticles elicits tumor-specific immunity. Adv Sci (Weinh). 2020;7(1):1900069.
Smith R, et al. Cationic nanoparticles enhance cell tumor infiltration and antitumor immune responses to a melanoma vaccine. Sci Adv. 2022;8(29):eabk3150.
Gao Y, et al. Engineering platelets with PDL1 antibodies and Iron oxide nanoparticles for Postsurgical Cancer Immunotherapy. ACS Appl Bio Mater. 2023;6(1):257-66.
Patel RB, et al. Development of an in situ Cancer vaccine via Combinational Radiation and bacterial-membrane-coated nanoparticles. Adv Mater. 2019;31(43):e1902626.
Choi J, et al. Visible-light-triggered Prodrug nanoparticles combine chemotherapy and photodynamic therapy to Potentiate Checkpoint Blockade Cancer Immunotherapy. ACS Nano. 2021;15(7):12086-98.
Ding B, et al. Biodegradable Upconversion nanoparticles induce pyroptosis for Cancer Immunotherapy. Nano Lett. 2021;21(19):8281-9.
Zhang , et al. Glutathione-responsive nanoparticles of Camptothecin Prodrug for Cancer Therapy. Adv Sci (Weinh). 2023;10(3):e2205246.
Zhang Y, et al. Gemcitabine nanoparticles promote antitumor immunity against melanoma. Biomaterials. 2019;189:48-59.
Gowd V, et al. Advancement of cancer immunotherapy using nanoparticlesbased nanomedicine. Sem Cancer Biol. 2022;86:624-44.
Casazza A, et al. Tumor stroma: a complexity dictated by the hypoxic tumor microenvironment. Oncogene. 2014;33(14):1743-54.
Yu JL, et al. Effect of p53 status on tumor response to antiangiogenic therapy. Science. 2002;295(5559):1526-8.
Taylor CT, Colgan SP. Regulation of immunity and inflammation by hypoxia in immunological niches. Nat Rev Immunol. 2017;17(12):774-85.
Facciabene A, et al. Tumour hypoxia promotes tolerance and angiogenesis via CCL28 and Treg cells. Nature. 2011;475(7355):226-30.
Doedens AL, et al. Macrophage expression of hypoxia-inducible factor-1a suppresses T-cell function and promotes tumor progression. Cancer Res. 2010;70(19):7465-75.
Abou Khouzam R, et al. Hypoxia as a potential inducer of immune tolerance, tumor plasticity and a driver of tumor mutational burden: impact on cancer immunotherapy. Semin Cancer Biol. 2023;97:104-23.
Finisguerra V et al. Metformin improves cancer immunotherapy by directly rescuing tumor-infiltrating CD8 T lymphocytes from hypoxia-induced immunosuppression. J Immunother Cancer, 2023. 11(5).
Yan H, et al. Exercise sensitizes PD-1/PD-L1 immunotherapy as a hypoxia modulator in the tumor microenvironment of melanoma. Front Immunol. 2023;14:1265914.
Barsoum IB, et al. A mechanism of hypoxia-mediated escape from adaptive immunity in cancer cells. Cancer Res. 2014;74(3):665-74.
Silva VL. Exploiting the cancer niche: tumor-associated macrophages and hypoxia as promising synergistic targets for nano-based therapy. J Controlled Release. 2017;253:82-96.
Jiang T et al. TAM-Hijacked Immunoreaction Rescued by Hypoxia-PathwayIntervened Strategy for Enhanced Metastatic Cancer Immunotherapy Small, 2023: p. e2305728.
Qu S et al. Light-enhanced hypoxia-responsive gene editing for Hypoxiaresistant photodynamic and Immunotherapy. Adv Healthc Mater, 2023: p. e2302615.
Sun T et al. Metal-Organic Framework-Mediated Synergistic HypoxiaActivated Chemo-Immunotherapy Induced by High Intensity Focused Ultrasound for Enhanced Cancer Theranostics Small, 2023: p. e2306338.
Luo W et al. Strengthening the Combinational Immunotherapy from modulating the Tumor Inflammatory Environment via Hypoxia-Responsive Nanogels. Adv Healthc Mater, 2023: p. e2302865.
Wang M, et al. Controllable hypoxia-activated chemotherapy as a dual enhancer for synergistic cancer photodynamic immunotherapy. Biomaterials. 2023;301:122257.
Luo G, et al. Multifunctional calcium-manganese Nanomodulator provides Antitumor Treatment and Improved Immunotherapy via Reprogramming of the Tumor Microenvironment. ACS Nano. 2023;17(16):15449-65.
Kang , et al. A photo-triggered self-accelerated nanoplatform for multifunctional image-guided combination cancer immunotherapy. Nat Commun. 2023;14(1):5216.
Gao C, et al. Conjugation of macrophage-mimetic Microalgae and Liposome for Antitumor Sonodynamic Immunotherapy via Hypoxia Alleviation and Autophagy Inhibition. ACS Nano. 2023;17(4):4034-49.
Qin Y, et al. Autophagy and cancer drug resistance in dialogue: pre-clinical and clinical evidence. Cancer Lett. 2023;570:216307.
Ashrafizadeh M, et al. A bioinformatics analysis, pre-clinical and clinical conception of autophagy in pancreatic cancer: complexity and simplicity in crosstalk. Pharmacol Res. 2023;194:106822.
Wang S, et al. Metabolic intervention Liposome boosted Lung Cancer Radio-Immunotherapy via Hypoxia Amelioration and PD-L1 Restraint. Adv Sci (Weinh). 2023;10(18):e2207608.
Liu Y et al. An Injectable puerarin depot can potentiate chimeric antigen receptor natural killer cell immunotherapy against targeted solid tumors by reversing tumor immunosuppression Small, 2024: p. e2307521.
Jiang , et al. Mitochondrial disruption Nanosystem simultaneously depressed programmed death Ligand-1 and transforming growth Factor- to overcome photodynamic immunotherapy resistance. ACS Nano; 2024.
Li M, et al. Sono-activatable semiconducting polymer nanoreshapers multiply remodel tumor microenvironment for potent immunotherapy of orthotopic pancreatic cancer. Adv Sci (Weinh). 2023;10(35):e2305150.
Jang H et al. Nanoparticles targeting innate immune cells in tumor microenvironment. Int J Mol Sci, 2021. 22(18).
Bronte V, Zanovello P. Regulation of immune responses by L-arginine metabolism. Nat Rev Immunol. 2005;5(8):641-54.
Rodriguez PC, et al. Arginase I in myeloid suppressor cells is induced by COX-2 in lung carcinoma. J Exp Med. 2005;202(7):931-9.
Rodríguez PC, Ochoa AC. Arginine regulation by myeloid derived suppressor cells and tolerance in cancer: mechanisms and therapeutic perspectives. Immunol Rev. 2008;222:180-91.
Rodriguez PC, et al. Regulation of T cell receptor CD3zeta chain expression by L-arginine. J Biol Chem. 2002;277(24):21123-9.
Nagaraj , et al. Altered recognition of antigen is a mechanism of cell tolerance in cancer. Nat Med. 2007;13(7):828-35.
Kusmartsev S, et al. Antigen-specific inhibition of CD8 + T cell response by immature myeloid cells in cancer is mediated by reactive oxygen species. J Immunol. 2004;172(2):989-99.
Kusmartsev S, Nagaraj S, Gabrilovich DI. Tumor-associated CD8+T cell tolerance induced by bone marrow-derived immature myeloid cells. J Immunol. 2005;175(7):4583-92.
Huang B, et al. Gr-1 + CD115 + immature myeloid suppressor cells mediate the development of tumor-induced T regulatory cells and T-cell anergy in tumor-bearing host. Cancer Res. 2006;66(2):1123-31.
Sawant DV, et al. Adaptive plasticity of IL-10(+) and IL-35(+) T(reg) cells cooperatively promotes tumor T cell exhaustion. Nat Immunol. 2019;20(6):724-35.
Liu H, et al. A novel DNA aptamer for dual targeting of Polymorphonuclear myeloid-derived suppressor cells and Tumor cells. Theranostics. 2018;8(1):31-44.
Song X , et al. CD11b+/Gr-1 + immature myeloid cells mediate suppression of T cells in mice bearing tumors of IL-1 beta-secreting cells. J Immunol. 2005;175(12):8200-8.
Bunt SK, et al. Inflammation induces myeloid-derived suppressor cells that facilitate tumor progression. J Immunol. 2006;176(1):284-90.
Jiang M, et al. Interleukin-6 trans-signaling pathway promotes immunosuppressive myeloid-derived suppressor cells via Suppression of Suppressor of Cytokine Signaling 3 in breast Cancer. Front Immunol. 2017;8:1840.
Sinha P, et al. Prostaglandin E2 promotes tumor progression by inducing myeloid-derived suppressor cells. Cancer Res. 2007;67(9):4507-13.
Gabrilovich DI, et al. Production of vascular endothelial growth factor by human tumors inhibits the functional maturation of dendritic cells. Nat Med. 1996;2(10):1096-103.
Groth C, et al. Immunosuppression mediated by myeloid-derived suppressor cells (MDSCs) during tumour progression. Br J Cancer. 2019;120(1):16-25.
Kong M, et al. Biodegradable Hollow Mesoporous silica nanoparticles for regulating Tumor Microenvironment and Enhancing Antitumor Efficiency. Theranostics. 2017;7(13):3276-92.
Shao K, et al. Nanoparticle-based immunotherapy for cancer. ACS Nano. 2015;9(1):16-30.
Zolnik BS, et al. Minireview: nanoparticles and the immune system. Endocrinology. 2010;151(2):458-65.
Dwivedi PD, et al. Impact of nanoparticles on the immune system. J Biomed Nanotechnol. 2011;7(1):193-4.
Falo L Jr, et al. Targeting antigen into the phagocytic pathway in vivo induces protective tumour immunity. Nat Med. 1995;1(7):649-53.
Fifis T, et al. Size-dependent immunogenicity: therapeutic and protective properties of nano-vaccines against tumors. J Immunol. 2004;173(5):3148-54.
Uto T, et al. Targeting of antigen to dendritic cells with poly ( -glutamic acid) nanoparticles induces antigen-specific humoral and cellular immunity. J Immunol. 2007;178(5):2979-86.
Cho N-H, et al. A multifunctional core-shell nanoparticle for dendritic cellbased cancer immunotherapy. Nat Nanotechnol. 2011;6(10):675-82.
Bourquin C, et al. Targeting CpG oligonucleotides to the lymph node by nanoparticles elicits efficient antitumoral immunity. J Immunol. 2008;181(5):2990-8.
Zwiorek K, et al. Delivery by cationic gelatin nanoparticles strongly increases the immunostimulatory effects of CpG oligonucleotides. Pharm Res. 2008;25:551-62.
Romero P, et al. Ex vivo staining of metastatic lymph nodes by class I major histocompatibility complex tetramers reveals high numbers of antigen-experienced tumor-specific cytolytic T lymphocytes. J Exp Med. 1998;188(9):1641-50.
Cochran AJ, et al. Sentinel lymph nodes show profound downregulation of antigen-presenting cells of the paracortex: implications for tumor biology and treatment. Mod Pathol. 2001;14(6):604-8.
Curiel TJ, et al. Blockade of B7-H1 improves myeloid dendritic cell-mediated antitumor immunity. Nat Med. 2003;9(5):562-7.
Munn DH, et al. Expression of indoleamine 2, 3-dioxygenase by plasmacytoid dendritic cells in tumor-draining lymph nodes. J Clin Investig. 2004;114(2):280-90.
Gabrilovich D. Mechanisms and functional significance of tumour-induced dendritic-cell defects. Nat Rev Immunol. 2004;4(12):941-52.
Pinzon-Charry A, Maxwell T, López JA. Dendritic cell dysfunction in cancer: a mechanism for immunosuppression. Immunol Cell Biol. 2005;83(5):451-61.
Vicari AP, et al. Reversal of tumor-induced dendritic cell paralysis by CpG immunostimulatory oligonucleotide and anti-interleukin 10 receptor antibody. J Exp Med. 2002;196(4):541-9.
van Mierlo GJ, et al. Activation of dendritic cells that cross-present tumorderived antigen licenses CD8 + CTL to cause tumor eradication. J Immunol. 2004;173(11):6753-9.
Munn DH, Mellor AL. The tumor-draining lymph node as an immune-privileged site. Immunol Rev. 2006;213(1):146-58.
Jeanbart L, et al. Enhancing efficacy of anticancer vaccines by targeted delivery to tumor-draining lymph nodes. Cancer Immunol Res. 2014;2(5):436-47.
Nam J, et al. Cancer nanomedicine for combination cancer immunotherapy. Nat Reviews Mater. 2019;4(6):398-414.
Shi J, et al. Cancer nanomedicine: progress, challenges and opportunities. Nat Rev Cancer. 2017;17(1):20-37.
Ojha T, et al. Pharmacological and physical vessel modulation strategies to improve EPR-mediated drug targeting to tumors. Adv Drug Deliv Rev. 2017;119:44-60.
Wilhelm S, et al. Analysis of nanoparticle delivery to tumours. Nat Reviews Mater. 2016;1(5):1-12.
Siegler EL, Kim YJ, Wang P. Nanomedicine targeting the tumor microenvironment: therapeutic strategies to inhibit angiogenesis, remodel matrix, and modulate immune responses. J Cell Immunotherapy. 2016;2(2):69-78.
Shi K, Haynes M, Huang L. Nanovaccines for remodeling the suppressive tumor microenvironment: new horizons in cancer immunotherapy. Front Chem Sci Eng. 2017;11:676-84.
Marabelle A, et al. Intratumoral immunotherapy: using the tumor as the remedy. Ann Oncol. 2017;28:xii33-43.
Aznar MA, et al. Intratumoral delivery of immunotherapy—act locally, think globally. J Immunol. 2017;198(1):31-9.
Ishihara J, et al. Matrix-binding checkpoint immunotherapies enhance antitumor efficacy and reduce adverse events. Sci Transl Med. 2017;9(415):eaan0401.
Raavé R, van Kuppevelt TH, Daamen WF. Chemotherapeutic drug delivery by tumoral extracellular matrix targeting. J Controlled Release. 2018;274:1-8.
Yu S et al. Reinforcing the immunogenic cell death to enhance cancer immunotherapy efficacy Biochimica et Biophysica Acta (BBA) – Reviews on Cancer, 2023;1878(5):188946.
Wu Q, et al. Autophagy induction by IGF1R inhibition with picropodophyllin and linsitinib. Autophagy. 2021;17(8):2046-7.
Petroni G, et al. Immunomodulation by targeted anticancer agents. Cancer Cell. 2021;39(3):310-45.
Huang Z, et al. KCI nanoparticles as potential inducer of immunogenic cell death for Cancer Immunotherapy. ACS Appl Bio Mater. 2023;6(6):2404-14.
Félix-Piña P et al. Antitumoral and Immunogenic Capacity of -D-Glucosereduced silver nanoparticles in breast Cancer. Int J Mol Sci, 2023. 24(10).
Liu Q, et al. Exploiting immunostimulatory mechanisms of immunogenic cell death to develop membrane-encapsulated nanoparticles as a potent tumor vaccine. J Nanobiotechnol. 2023;21(1):326.
Xie B, et al. Supramolecularly Engineered Conjugate of Bacteria and cell membrane-coated magnetic nanoparticles for enhanced ferroptosis and immunotherapy of tumors. Adv Sci (Weinh). 2023;10(34):e2304407.
Lu Y, et al. Self-driven bioactive hybrids co-deliver doxorubicin and indocyanine green nanoparticles for chemo/photothermal therapy of breast cancer. Biomed Pharmacother. 2023;169:115846.
Wang H et al. Near-Infrared Light-Driven Nanoparticles for Cancer Photoimmunotherapy by Synergizing Immune Cell Death and Epigenetic Regulation Small, 2023: p. e2309202.
Wu Q et al. Photothermal ferrotherapy – induced immunogenic cell death via iron-based ternary chalcogenide nanoparticles against triple-negative breast cancer Small, 2023: p. e2306766.
Song S, et al. All-in-one glycol chitosan nanoparticles for co-delivery of doxorubicin and anti-PD-L1 peptide in cancer immunotherapy. Bioact Mater. 2023;28:358-75.
Wang R, et al. Hydroxyapatite nanoparticles promote TLR4 agonist-mediated anti-tumor immunity through synergically enhanced macrophage polarization. Acta Biomater. 2023;164:626-40.
Wang Y, et al. Docetaxel-loaded ROS dual-responsive nanoparticles with self-supplied ROS for inhibiting metastasis and enhancing immunotherapy of breast cancer. J Nanobiotechnol. 2023;21(1):286.
Yang J, et al. Self-assembled albumin nanoparticles induce pyroptosis for photodynamic/photothermal/immuno synergistic therapies in triple-negative breast cancer. Front Immunol. 2023;14:1173487.
Xu X, et al. Guanidine-modified nanoparticles as robust BTZ delivery carriers and activators of immune responses. J Control Release. 2023;357:310-8.
Chen W, et al. PEI-Based nanoparticles for Tumor Immunotherapy via in situ Antigen-capture triggered by Photothermal Therapy. ACS Appl Mater Interfaces. 2023;15(48):55433-46.
Li Y, et al. Antigen-capturing dendritic-cell-targeting nanoparticles for enhanced Tumor Immunotherapy based on Photothermal-Therapy-Induced in situ vaccination. Adv Healthc Mater. 2023;12(22):e2202871.
Zou C, et al. cRGD-modified nanoparticles of multi-bioactive agent conjugate with pH-sensitive linkers and PD-L1 antagonist for integrative collaborative treatment of breast cancer. Nanoscale Horiz. 2023;8(7):870-86.
Chen S, et al. Tumor Acidic Microenvironment-Responsive Promodulator Iron Oxide nanoparticles for Photothermal-enhanced Chemodynamic Immunotherapy of Cancer. ACS Biomater Sci Eng. 2023;9(2):773-83.
Ma W, et al. Biomimetic nanoerythrosome-coated Aptamer-DNA Tetrahedron/Maytansine conjugates: pH-Responsive and targeted cytotoxicity for HER2-Positive breast Cancer. Adv Mater. 2022;34(46):e2109609.
Zheng , et al. Biomimetic co-assembled nanodrug of doxorubicin and berberine suppresses chemotherapy-exacerbated breast cancer metastasis. Biomaterials. 2021;271:120716.
Liu XL, et al. Biomimetic liposomal nanoplatinum for targeted Cancer Chemophototherapy. Adv Sci (Weinh). 2021;8(8):2003679.
Zhao Y, et al. Biomimetic manganese-based theranostic nanoplatform for cancer multimodal imaging and twofold immunotherapy. Bioact Mater. 2023;19:237-50.
Zhao P, et al. Programming cell pyroptosis with biomimetic nanoparticles for solid tumor immunotherapy. Biomaterials. 2020;254:120142.
Ying K, et al. Macrophage membrane-biomimetic adhesive polycaprolactone nanocamptothecin for improving cancer-targeting efficiency and impairing metastasis. Bioact Mater. 2023;20:449-62.
Miao Y, et al. Cell membrane-camouflaged nanocarriers with Biomimetic Deformability of erythrocytes for Ultralong circulation and enhanced Cancer Therapy. ACS Nano. 2022;16(4):6527-40.
Guo Y, et al. Chemotherapy mediated by Biomimetic Polymeric Nanoparticles Potentiates Enhanced Tumor Immunotherapy via Amplification of Endoplasmic Reticulum Stress and mitochondrial dysfunction. Adv Mater. 2022;34(47):e2206861.
Wu P, et al. Engineered EGCG-Containing Biomimetic nanoassemblies as effective delivery platform for enhanced Cancer Therapy. Adv Sci (Weinh). 2022;9(15):e2105894.
Reuven EM, et al. Biomimetic Glyconanoparticle Vaccine for Cancer Immunotherapy. ACS Nano. 2019;13(3):2936-47.
Molina M, et al. Stimuli-responsive nanogel composites and their application in nanomedicine. Chem Soc Rev. 2015;44(17):6161-86.
Chuard N, et al. Strain-promoted thiol-mediated Cellular Uptake of Giant substrates: liposomes and polymersomes. Angew Chem Int Ed Engl. 2017;56(11):2947-50.
Wang , et al. A cooperative dimensional strategy for enhanced nucleustargeted delivery of anticancer drugs. Adv Funct Mater. 2017;27(24):1700339.
Tang , et al. Enhancing cell therapy through TCR-signaling-responsive nanoparticle drug delivery. Nat Biotechnol. 2018;36(8):707-16.
Sun CY, et al. Tumor acidity-sensitive polymeric vector for active targeted siRNA delivery. J Am Chem Soc. 2015;137(48):15217-24.
Shang , et al. Enhancing cancer chemo-immunotherapy by biomimetic nanogel with tumor targeting capacity and rapid drug-releasing in tumor microenvironment. Acta Pharm Sin B. 2022;12(5):2550-67.
Wan L, et al. Biomimetic, pH-Responsive nanoplatforms for Cancer Multimodal Imaging and Photothermal Immunotherapy. ACS Appl Mater Interfaces. 2023;15(1):1784-97.
Yang , et al. Biomimetic nanovaccines potentiating dendritic cell internalization via CXCR4-Mediated macropinocytosis. Adv Healthc Mater. 2023;12(5):e2202064.
Wei X et al. Biomimetic nano-immunoactivator via ionic metabolic modulation for strengthened nir-ii photothermal immunotherapy small, 2023: p. e2304370.
Wang Y, et al. Engineering Endogenous Tumor-Associated macrophagetargeted biomimetic Nano-RBC to Reprogram Tumor Immunosuppressive Microenvironment for enhanced chemo-immunotherapy. Adv Mater. 2021;33(39):e2103497.
Zhao H, et al. Biomimetic Decoy inhibits Tumor Growth and Lung Metastasis by reversing the drawbacks of Sonodynamic Therapy. Adv Healthc Mater. 2020;9(1):e1901335.
Feng , et al. Biomimetic and bioinspired nano-platforms for cancer vaccine development. Explor (Beijing). 2023;3(3):20210263.
Fang RH, et al. Cancer cell membrane-coated nanoparticles for anticancer vaccination and drug delivery. Nano Lett. 2014;14(4):2181-8.
Zheng S, Guan XY. Ferroptosis: promising approach for cancer and cancer immunotherapy. Cancer Lett. 2023;561:216152.
Yin J, et al. Ferroptosis and Cancer immunotherapy. Curr Mol Med. 2023;23(5):401-9.
Xu H, et al. Ferroptosis in the tumor microenvironment: perspectives for immunotherapy. Trends Mol Med. 2021;27(9):856-67.
Gao W, et al. Autophagy, ferroptosis, pyroptosis, and necroptosis in tumor immunotherapy. Signal Transduct Target Ther. 2022;7(1):196.
Lei Y et al. Autophagy in cancer immunotherapy cells, 2022. 11(19).
Pan H, et al. Autophagy-associated immune responses and cancer immunotherapy. Oncotarget. 2016;7(16):21235-46.
Jin Z, et al. Regulation of autophagy fires up the cold tumor microenvironment to improve cancer immunotherapy. Front Immunol. 2022;13:1018903.
Hamidi M, et al. Applications of carrier erythrocytes in delivery of biopharmaceuticals. J Control Release. 2007;118(2):145-60.
Banz A, et al. In situ targeting of dendritic cells by antigen-loaded red blood cells: a novel approach to cancer immunotherapy. Vaccine. 2010;28(17):2965-72.
Hu CMJ, Fang RH, Zhang L. Erythrocyte-inspired delivery systems. Adv Healthc Mater. 2012;1(5):537-47.
Guo Y, et al. Erythrocyte membrane-enveloped polymeric nanoparticles as Nanovaccine for induction of Antitumor immunity against Melanoma. ACS Nano. 2015;9(7):6918-33.
Hu Q, et al. Anticancer Platelet-Mimicking Nanovehicles. Adv Mater. 2015;27(44):7043-50.
Hu CM, et al. Nanoparticle biointerfacing by platelet membrane cloaking. Nature. 2015;526(7571):118-21.
Bahmani B et al. Intratumoral immunotherapy using platelet-cloaked nanoparticles enhances antitumor immunity in solid tumors Nat Commun, 2021;12(1):1999.
Mai X , et al. Integration of immunogenic activation and immunosuppressive reversion using mitochondrial-respiration-inhibited platelet-mimicking nanoparticles. Biomaterials. 2020;232:119699.
Wang Q et al. Biomimetic Nanophotosensitizer amplifies immunogenic pyroptosis and triggers synergistic Cancer Therapy. Adv Healthc Mater, 2023: p. e2301641.
Gong P et al. Immunocyte membrane-coated nanoparticles for Cancer Immunotherapy. Cancers (Basel), 2020. 13(1).
Sun K, et al. Saikosaponin D loaded macrophage membrane-biomimetic nanoparticles target angiogenic signaling for breast cancer therapy. Appl Mater Today. 2020;18:100505.
Chen LJ, et al. Macrophage membrane coated persistent luminescence nanoparticle@MOF-derived mesoporous carbon core-shell nanocomposites for autofluorescence-free imaging-guided chemotherapy. J Mater Chem B. 2020;8(35):8071-83.
Cao H, et al. Liposomes coated with isolated macrophage membrane can target lung metastasis of breast Cancer. ACS Nano. 2016;10(8):7738-48.
Meng QF, et al. Macrophage membrane-coated iron oxide nanoparticles for enhanced photothermal tumor therapy. Nanotechnology. 2018;29(13):134004.
Zhao H, et al. C-C Chemokine Ligand 2 (CCL2) recruits macrophage-mem-brane-camouflaged Hollow Bismuth Selenide nanoparticles to facilitate Photothermal Sensitivity and inhibit lung metastasis of breast Cancer. ACS Appl Mater Interfaces. 2018;10(37):31124-35.
Liang , et al. Biomimetic theranostic strategy for anti-metastasis therapy of breast cancer via the macrophage membrane camouflaged superparticles. Mater Sci Eng C Mater Biol Appl. 2020;115:111097.
Xuan M, et al. Macrophage cell membrane camouflaged mesoporous silica nanocapsules for in vivo Cancer therapy. Adv Healthc Mater. 2015;4(11):1645-52.
Rao L , et al. Effective cancer targeting and imaging using macrophage membrane-camouflaged upconversion nanoparticles. J Biomed Mater Res A. 2017;105(2):521-30.
Cao X, et al. Paclitaxel-loaded macrophage membrane camouflaged Albumin nanoparticles for targeted Cancer Therapy. Int J Nanomed. 2020;15:1915-28.
Ma J, et al. Copresentation of Tumor antigens and Costimulatory molecules via Biomimetic nanoparticles for Effective Cancer Immunotherapy. Nano Lett. 2020;20(6):4084-94.
Li L, et al. Cholesterol removal improves performance of a model biomimetic system to co-deliver a photothermal agent and a STING agonist for cancer immunotherapy. Nat Commun. 2023;14(1):5111.
Xie W, et al. Biomimetic nanoplatform loading type I Aggregation-Induced Emission Photosensitizer and glutamine blockade to regulate nutrient partitioning for enhancing Antitumor Immunotherapy. ACS Nano. 2022;16(7):10742-53.
Zuo L, et al. Biomimetic nanovesicle with Mitochondria-Synthesized Sonosensitizer and Mitophagy Inhibition for Cancer Sono-Immunotherapy. Nano Lett. 2023;23(7):3005-13.
Pan P, et al. A heterogenic membrane-based biomimetic hybrid nanoplatform for combining radiotherapy and immunotherapy against breast cancer. Biomaterials. 2022;289:121810.
Yang , et al. Leveraging -Adrenergic receptor signaling blockade for Improved Cancer Immunotherapy through Biomimetic Nanovaccine. Small. 2023;19(14):e2207029.
Wang , et al. Intelligent Biomimetic Nanoplatform for systemic treatment of metastatic triple-negative breast Cancer via enhanced EGFR-Targeted therapy and immunotherapy. ACS Appl Mater Interfaces; 2022.
Li J, et al. Multifunctional biomimetic nanovaccines based on Photothermal and weak-immunostimulatory Nanoparticulate cores for the immunotherapy of solid tumors. Adv Mater. 2022;34(9):e2108012.
Xu X, et al. A Biomimetic Aggregation-Induced Emission Photosensitizer with Antigen-presenting and hitchhiking function for lipid droplet targeted photodynamic immunotherapy. Adv Mater. 2021;33(33):e2102322.
Fang , et al. Biomimetic Anti-PD-1 peptide-loaded 2D FePSe(3) nanosheets for efficient photothermal and enhanced Immune Therapy with Multimodal MR/PA/Thermal Imaging. Adv Sci (Weinh). 2021;8(2):2003041.
Liu Z, et al. Exosomes in HBV infection. Clin Chim Acta. 2023;538:65-9.
Zhang F, et al. Janus nanocarrier-based co-delivery of doxorubicin and berberine weakens chemotherapy-exacerbated hepatocellular carcinoma recurrence. Acta Biomater. 2019;100:352-64.
Chen G , et al. Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response. Nature. 2018;560(7718):382-6.
Moradi-Chaleshtori M, et al. Overexpression of pigment epithelium-derived factor in breast cancer cell-derived exosomes induces M1 polarization in macrophages. Immunol Lett. 2022;248:31-6.
Wang Y et al. G-MDSC-derived exosomes mediate the differentiation of M-MDSC into M2 macrophages promoting colitis-to-cancer transition. J Immunother Cancer, 2023. 11(6).
Zheng N, et al. M2 macrophage-derived exosomes suppress tumor intrinsic immunogenicity to confer immunotherapy resistance. Oncoimmunology. 2023;12(1):2210959.
Chen J, et al. PDL1-positive exosomes suppress antitumor immunity by inducing tumor-specific CD8(+) T cell exhaustion during metastasis. Cancer Sci. 2021;112(9):3437-54.
Wei Y, et al. An RNA-RNA crosstalk network involving HMGB1 and RICTOR facilitates hepatocellular carcinoma tumorigenesis by promoting glutamine metabolism and impedes immunotherapy by PD-L1 + exosomes activity. Signal Transduct Target Ther. 2021;6(1):421.
Wang C, et al. Tumor Cell-associated exosomes robustly elicit anti-tumor Immune responses through modulating dendritic cell vaccines in Lung Tumor. Int J Biol Sci. 2020;16(4):633-43.
Wang S, et al. Macrophage-tumor chimeric exosomes accumulate in lymph node and tumor to activate the immune response and the tumor microenvironment. Sci Transl Med. 2021;13(615):eabb6981.
Lu Z, et al. Dendritic cell-derived exosomes elicit tumor regression in autochthonous hepatocellular carcinoma mouse models. J Hepatol. 2017;67(4):739-48.
Zhou W, et al. Exosomes derived from immunogenically dying tumor cells as a versatile tool for vaccination against pancreatic cancer. Biomaterials. 2022;280:121306.
Zuo B, et al. Alarmin-painted exosomes elicit persistent antitumor immunity in large established tumors in mice. Nat Commun. 2020;11(1):1790.
Morishita M , et al. Exosome-based tumor antigens-adjuvant co-delivery utilizing genetically engineered tumor cell-derived exosomes with immunostimulatory CpG DNA. Biomaterials. 2016;111:55-65.
Gehrmann U, et al. Synergistic induction of adaptive antitumor immunity by codelivery of antigen with a-galactosylceramide on exosomes. Cancer Res. 2013;73(13):3865-76.
Kim GB et al. Xenogenization of tumor cells by fusogenic exosomes in tumor microenvironment ignites and propagates antitumor immunity. Sci Adv, 2020. 6(27).
Zhou W, et al. Pancreatic cancer-targeting exosomes for enhancing immunotherapy and reprogramming tumor microenvironment. Biomaterials. 2021;268:120546.
Gunassekaran GR, et al. M1 macrophage exosomes engineered to foster M1 polarization and target the IL-4 receptor inhibit tumor growth by reprogramming tumor-associated macrophages into M1-like macrophages. Biomaterials. 2021;278:121137.
Cheng L, et al. Gene-engineered exosomes-thermosensitive liposomes hybrid nanovesicles by the blockade of CD47 signal for combined photothermal therapy and cancer immunotherapy. Biomaterials. 2021;275:120964.
Li J, et al. Dendritic cell derived exosomes loaded neoantigens for personalized cancer immunotherapies. J Control Release. 2023;353:423-33.
Xu J, et al. Enhanced penetrative siRNA delivery by a nanodiamond drug delivery platform against hepatocellular carcinoma 3D models. Nanoscale. 2021;13(38):16131-45.
Jiang H, et al. M1 macrophage-derived exosomes and their key molecule IncRNA HOTTIP suppress head and neck squamous cell carcinoma progression by upregulating the TLR5/NF-kB pathway. Cell Death Dis. 2022;13(2):183.
Zhou WJ, et al. CD45RO(-)CD8(+) T cell-derived exosomes restrict estrogendriven endometrial cancer development via the ERß/miR-765/PLP2/Notch axis. Theranostics. 2021;11(11):5330-45.
Cheng L, et al. Multifunctional hybrid exosomes enhanced cancer chemo-immunotherapy by activating the STING pathway. Biomaterials. 2023;301:122259.
Wang et al. Exosomes derived from T cells synergize with radiotherapy and preserve antitumor activities against nasopharyngeal carcinoma in immunosuppressive microenvironment. J Immunother Cancer, 2022. 10(2).
Ji P, et al. Smart exosomes with lymph node homing and immune-amplifying capacities for enhanced immunotherapy of metastatic breast cancer. Mol Ther Nucleic Acids. 2021;26:987-96.
Fan M, et al. A CAR T-inspiring platform based on antibody-engineered exosomes from antigen-feeding dendritic cells for precise solid tumor therapy. Biomaterials. 2022;282:121424.
Li Y, et al. A nanotherapeutic system for gastric cancer suppression by synergistic chemotherapy and immunotherapy based on iPSCs and DCs exosomes. Cancer Immunol Immunother. 2023;72(6):1673-83.
Huang H, et al. Synergistic strategy with hyperthermia therapy based immunotherapy and engineered exosomes-liposomes targeted chemotherapy prevents tumor recurrence and metastasis in advanced breast cancer. Bioeng Transl Med. 2022;7(2):e10284.
Pakravan N, Abbasi A, Hassan ZM. Immunotherapy using oxygenated water and tumor-derived exosomes potentiates antitumor immune response and attenuates malignancy tendency in mice model of breast cancer oxid med cell longev, 2021;2021:5529484.
Javeed N, et al. Immunosuppressive CD14(+)HLA-DR(lo/neg) monocytes are elevated in pancreatic cancer and primed by tumor-derived exosomes. Oncoimmunology. 2017;6(1):e1252013.
Zhao Y, et al. Docetaxel-loaded M1 macrophage-derived exosomes for a safe and efficient chemoimmunotherapy of breast cancer. J Nanobiotechnol. 2022;20(1):359.
Lin J, et al. Dendritic cell-derived exosomes Driven Drug Co-delivery Biomimetic Nanosystem for Effective Combination of Malignant Melanoma Immunotherapy and Gene Therapy. Drug Des Devel Ther. 2023;17:2087-106.
Wang D, et al. Sonodynamical reversion of immunosuppressive microenvironment in prostate cancer via engineered exosomes. Drug Deliv. 2022;29(1):702-13.
Zhang Y et al. pH-Responsive STING-Activating DNA nanovaccines for Cancer Immunotherapy. Adv Ther (Weinh), 2020. 3(9).
Yao D, et al. A self-cascaded unimolecular prodrug for pH -responsive chemotherapy and tumor-detained photodynamic-immunotherapy of triple-negative breast cancer. Biomaterials. 2023;292:121920.
Liu Y, et al. Dual pH-responsive multifunctional nanoparticles for targeted treatment of breast cancer by combining immunotherapy and chemotherapy. Acta Biomater. 2018;66:310-24.
Lim B, Kim KS, Na K. pH-Responsive zinc lon regulating Immunomodulatory nanoparticles for Effective Cancer Immunotherapy. Biomacromolecules. 2023;24(9):4263-73.
Duong HTT, et al. Smart vaccine delivery based on microneedle arrays decorated with ultra-ph-responsive copolymers for cancer immunotherapy. Biomaterials. 2018;185:13-24.
Gu J, et al. Injectable pH-responsive hydrogel for combinatorial chemoimmunotherapy tailored to the tumor microenvironment. J Nanobiotechnol. 2022;20(1):372.
Gong C, et al. Regulating the immunosuppressive tumor microenvironment to enhance breast cancer immunotherapy using pH-responsive hybrid membrane-coated nanoparticles. J Nanobiotechnol. 2021;19(1):58.
Ding Y, et al. Construction of pH-Sensitive nanovaccines encapsulating tumor cell lysates and Immune adjuvants for breast Cancer therapy. Small. 2023;19(37):e2301420.
Jiang M, et al. Sequentially pH-Responsive drug-delivery Nanosystem for Tumor Immunogenic Cell Death and cooperating with Immune checkpoint blockade for efficient Cancer Chemoimmunotherapy. ACS Appl Mater Interfaces. 2021;13(37):43963-74.
Yang G, et al. Smart Nanoreactors for pH-Responsive Tumor Homing, Mitochondria-Targeting, and enhanced photodynamic-immunotherapy of Cancer. Nano Lett. 2018;18(4):2475-84.
Sun , et al. Binary regulation of the tumor microenvironment by a responsive reversible shielding nanoplatform for improved tumor chemoimmunotherapy. Acta Biomater. 2022;138:505-17.
Lv X, et al. Multi-signaling pathway activation by pH responsive manganese particles for enhanced vaccination. J Control Release. 2023;357:109-19.
Wagner J, et al. Mesoporous silica nanoparticles as pH-Responsive carrier for the Immune-Activating Drug Resiquimod enhance the local Immune response in mice. ACS Nano. 2021;15(3):4450-66.
Zhao M, et al. Immune/Hypoxic Tumor Microenvironment Regulationenhanced photodynamic treatment realized by pH -Responsive phase Transition-Targeting Nanobubbles. ACS Appl Mater Interfaces. 2021;13(28):32763-79.
Yuba E, et al. The application of pH-sensitive polymer-lipids to antigen delivery for cancer immunotherapy. Biomaterials. 2013;34(22):5711-21.
Yoshizaki Y, et al. Potentiation of pH-sensitive polymer-modified liposomes with cationic lipid inclusion as antigen delivery carriers for cancer immunotherapy. Biomaterials. 2014;35(28):8186-96.
Yuba E, et al. A liposome-based antigen delivery system using pHsensitive fusogenic polymers for cancer immunotherapy. Biomaterials. 2013;34(12):3042-52.
Yoshizaki Y, et al. pH-sensitive polymer-modified liposome-based immunityinducing system: effects of inclusion of cationic lipid and CpG-DNA. Biomaterials. 2017;141:272-83.
Zhang J, et al. pH-sensitive tumor-tropism hybrid membrane-coated nanoparticles for reprogramming the tumor microenvironment and boosting the antitumor immunity. Acta Biomater. 2023;166:470-84.
Yuba E, et al. Bioactive polysaccharide-based pH-sensitive polymers for cytoplasmic delivery of antigen and activation of antigen-specific immunity. Biomaterials. 2017;120:32-45.
Kocabas BB, et al. Dual-adjuvant effect of pH-sensitive liposomes loaded with STING and TLR9 agonists regress tumor development by enhancing Th1 immune response. J Control Release. 2020;328:587-95.
Zhang W, et al. Multifunctional redox-responsive nanoplatform with Dual Activation of Macrophages and T Cells for Antitumor Immunotherapy. ACS Nano. 2023;17(15):14424-41.
Yan P, et al. A redox-responsive Nanovaccine combined with A2A receptor antagonist for Cancer Immunotherapy. Adv Healthc Mater. 2021;10(21):e2101222.
Lv M, et al. Redox-responsive hyperbranched poly(amido amine) and polymer dots as a vaccine delivery system for cancer immunotherapy. J Mater Chem B. 2017;5(48):9532-45.
Jiang D, et al. Cascade Cytosol Delivery of Dual-Sensitive Micelle-tailored vaccine for Enhancing Cancer Immunotherapy. ACS Appl Mater Interfaces. 2018;10(44):37797-811.
Chen Q, et al. Cancer cell membrane-coated nanoparticles for bimodal imaging-guided photothermal therapy and docetaxel-enhanced immunotherapy against cancer. J Nanobiotechnol. 2021;19(1):449.
Chen L , et al. Tumor-targeted drug and CpG delivery system for Phototherapy and Docetaxel-enhanced immunotherapy with polarization toward M1-Type macrophages on Triple negative breast cancers. Adv Mater. 2019;31(52):e1904997.
Sun Y, et al. An enzyme-responsive and transformable PD-L1 blocking peptide-photosensitizer conjugate enables efficient photothermal immunotherapy for breast cancer. Bioact Mater. 2023;22:47-59.
Ma S, et al. Boosting cancer immunotherapy by biomineralized nanovaccine with ferroptosis-inducing and photothermal properties. Biomater Sci. 2023;11(2):518-32.
Xiao Y, et al. Microenvironment-responsive prodrug-induced pyroptosis boosts cancer immunotherapy. Adv Sci (Weinh). 2021;8(24):e2101840.
Wu X, et al. Nano-herb medicine and PDT induced synergistic immunotherapy for colon cancer treatment. Biomaterials. 2021;269:120654.
Ding D, et al. Multifunctional Nanodrug mediates synergistic photodynamic therapy and MDSCs-Targeting immunotherapy of Colon cancer. Adv Sci (Weinh). 2021;8(14):e2100712.
Zhou H, et al. A tumor-microenvironment-activatable Molecular Pro-theranostic Agent for Photodynamic and Immunotherapy of Cancer. Adv Mater. 2023;35(30):e2211485.
Yu Y, et al. Polymeric PD-L1 blockade nanoparticles for cancer photothermalimmunotherapy. Biomaterials. 2022;280:121312.
Liang , et al. Photothermal cancer immunotherapy by erythrocyte membrane-coated black phosphorus formulation. J Control Release. 2019;296:150-61.
Zhang R, et al. Chemodynamic/Photothermal synergistic Cancer immunotherapy based on yeast microcapsule-derived Au/Pt nanoparticles. ACS Appl Mater Interfaces. 2023;15(20):24134-48.
Wang M, et al. Synergistic interventional photothermal therapy and immunotherapy using an iron oxide nanoplatform for the treatment of pancreatic cancer. Acta Biomater. 2022;138:453-62.
Debele TA, Yeh C-F, Su W-P. Cancer immunotherapy and application of nanoparticles in cancers immunotherapy as the delivery of immunotherapeutic agents and as the immunomodulators. Cancers. 2020;12(12):3773.
Zhang C, et al. Checkpoint Nano-PROTACs for Activatable Cancer PhotoImmunotherapy. Adv Mater. 2023;35(6):e2208553.
Qiu W, et al. Immunomodulatory-photodynamic nanostimulators for invoking pyroptosis to augment Tumor Immunotherapy. Adv Healthc Mater. 2022;11(21):e2201233.
Zhou JY, et al. Ru(II)-modified TiO(2) nanoparticles for hypoxia-adaptive photo-immunotherapy of oral squamous cell carcinoma. Biomaterials. 2022;289:121757.
Duan Y, et al. Immune Modulator and Low-Temperature PTT-Induced Synergistic Immunotherapy for Cancer Treatment. ACS Appl Bio Mater. 2021;4(2):1524-35.
Yan T, et al. Synergistic photothermal cancer immunotherapy by Cas9 ribonucleoprotein-based copper sulfide nanotherapeutic platform targeting PTPN2. Biomaterials. 2021;279:121233.
Li J, et al. Second Near-Infrared Photothermal Semiconducting polymer nanoadjuvant for enhanced Cancer Immunotherapy. Adv Mater. 2021;33(4):e2003458.
Jana D et al. A defect-Engineered Nanozyme for targeted NIR-II Photothermal Immunotherapy of Cancer. Adv Mater, 2022: p. e2206401.
Hwang J, et al. Escherichia coli Mimetic Gold nanorod-mediated photoand immunotherapy for Treating Cancer and its metastasis. ACS Nano. 2022;16(5):8472-83.
Tang Y, et al. Pyroptosis-mediated synergistic photodynamic and photothermal immunotherapy enabled by a tumor-membrane-targeted photosensitive dimer. Adv Mater. 2023;35(25):e2300232.
Xu M, et al. Activatable Immunoprotease Nanorestimulator for Second Near-Infrared Photothermal Immunotherapy of Cancer. ACS Nano. 2023;17(9):8183-94.
Wang M, et al. NIR-Triggered Phototherapy and Immunotherapy via an Antigen-capturing nanoplatform for metastatic Cancer treatment. Adv Sci (Weinh). 2019;6(10):1802157.
Ye X, et al. Surgical Tumor-Derived Personalized Photothermal Vaccine Formulation for Cancer Immunotherapy. ACS Nano. 2019;13(3):2956-68.
Wang S, et al. Photothermal therapy mediated by gold nanocages composed of anti-PDL1 and galunisertib for improved synergistic immunotherapy in colorectal cancer. Acta Biomater. 2021;134:621-32.
Mikelez-Alonso I, Aires A, Cortajarena AL. Cancer nano-immunotherapy from the injection to the target: the role of protein corona. Int J Mol Sci. 2020;21(2):519.
Yetisgin AA et al. Therapeutic nanoparticles and their targeted delivery applications. Molecules, 2020. 25(9).
Anselmo AC, Mitragotri S. Nanoparticles in the clinic: an update. Bioeng Transl Med. 2019;4(3):e10143.
Kranz LM, et al. Systemic RNA delivery to dendritic cells exploits antiviral defence for cancer immunotherapy. Nature. 2016;534(7607):396-401.
Beg MS, et al. Phase I study of MRX34, a liposomal miR-34a mimic, administered twice weekly in patients with advanced solid tumors. Invest New Drugs. 2017;35(2):180-8.
Burris III et al. H.A., A phase 1, open-label, multicenter study to assess the safety, tolerability, and immunogenicity of mRNA-4157 alone in subjects with resected solid tumors and in combination with pembrolizumab in subjects with unresectable solid tumors (Keynote-603). 2019, American Society of Clinical Oncology.
Pfannenstiel LW, et al. Paclitaxel enhances early dendritic cell maturation and function through TLR4 signaling in mice. Cell Immunol. 2010;263(1):79-87.
Graziani SR, et al. Phase II study of paclitaxel associated with lipid core nanoparticles (LDE) as third-line treatment of patients with epithelial ovarian carcinoma. Med Oncol. 2017;34:1-7.
Shen C, et al. Phase I study of NBTXR3 activated by radiotherapy in patients with advanced cancers treated with an anti-PD-1 therapy. American Society of Clinical Oncology; 2020.
Li S, et al. Polymer nanoparticles as adjuvants in cancer immunotherapy. Nano Res. 2018;11:5769-86.
Thakur N, et al. Nanoparticles as smart carriers for enhanced Cancer Immunotherapy. Front Chem. 2020;8:597806.
Zhao L, et al. Nanoparticle vaccines. Vaccine. 2014;32(3):327-37.
Chen P-G, et al. Chitosan nanoparticles based nanovaccines for cancer immunotherapy. Pure Appl Chem. 2017;89(7):931-9.
Shi GN, et al. Enhanced antitumor immunity by targeting dendritic cells with tumor cell lysate-loaded chitosan nanoparticles vaccine. Biomaterials. 2017;113:191-202.
Yang R, et al. Cancer Cell membrane-coated adjuvant nanoparticles with mannose modification for effective anticancer vaccination. ACS Nano. 2018;12(6):5121-9.
Kim H, et al. Polymeric nanoparticles encapsulating novel TLR7/8 agonists as immunostimulatory adjuvants for enhanced cancer immunotherapy. Biomaterials. 2018;164:38-53.
Banerjee R. Liposomes: applications in medicine. J Biomater Appl. 2001;16(1):3-21.
Klinguer-Hamour C, et al. DDA adjuvant induces a mixed Th1/Th2 immune response when associated with BBG2Na, a respiratory syncytial virus potential vaccine. Vaccine. 2002;20(21-22):2743-51.
Christensen D, et al. Cationic liposomes as vaccine adjuvants. Expert Rev Vaccines. 2011;10(4):513-21.
Korsholm KS, et al. The adjuvant mechanism of cationic dimethyldioctadecylammonium liposomes. Immunology. 2007;121(2):216-26.
Zamani P, et al. Nanoliposomes as the adjuvant delivery systems in cancer immunotherapy. J Cell Physiol. 2018;233(7):5189-99.
Yuba E, et al. Dextran derivative-based pH-sensitive liposomes for cancer immunotherapy. Biomaterials. 2014;35(9):3091-101.
Zeng Q, et al. Tailoring polymeric hybrid micelles with lymph node targeting ability to improve the potency of cancer vaccines. Biomaterials. 2017;122:105-13.
de Faria PC, et al. Oxidized multiwalled carbon nanotubes as antigen delivery system to promote superior CD8(+) T cell response and protection against cancer. Nano Lett. 2014;14(9):5458-70.
Hassan HA, et al. Dual stimulation of antigen presenting cells using carbon nanotube-based vaccine delivery system for cancer immunotherapy. Biomaterials. 2016;104:310-22.
Zhou Q, et al. Different-sized gold nanoparticle Activator/Antigen increases dendritic cells Accumulation in Liver-Draining Lymph Nodes and CD8 + T cell responses. ACS Nano. 2016;10(2):2678-92.
Fallarini S, et al. Factors affecting T cell responses induced by fully synthetic glyco-gold-nanoparticles. Nanoscale. 2013;5(1):390-400.
Dykman LA, et al. Gold nanoparticles as an adjuvant: influence of size, shape, and technique of combination with CpG on antibody production. Int Immunopharmacol. 2018;54:163-8.
Melamed JR, et al. Using gold nanoparticles to disrupt the Tumor Microenvironment: an emerging therapeutic strategy. ACS Nano. 2016;10(12):10631-5.
Saha S, et al. Gold nanoparticle reprograms pancreatic Tumor Microenvironment and inhibits Tumor Growth. ACS Nano. 2016;10(12):10636-51.
Luo J, et al. Self-assembled CpG oligodeoxynucleotides conjugated hollow gold nanospheres to enhance cancer-associated immunostimulation. Colloids Surf B Biointerfaces. 2019;175:248-55.
Ow H, et al. Bright and stable core-shell fluorescent silica nanoparticles. Nano Lett. 2005;5(1):113-7.
Benezra M, et al. Multimodal silica nanoparticles are effective cancer-targeted probes in a model of human melanoma. J Clin Invest. 2011;121(7):2768-80.
Chattopadhyay S, et al. Nanoparticle vaccines adopting virus-like features for enhanced Immune Potentiation. Nanotheranostics. 2017;1(3):244-60.
Mahony D, et al. Mesoporous silica nanoparticles act as a self-adjuvant for ovalbumin model antigen in mice. Small. 2013;9(18):3138-46.
Selvaraja VK, Gudipudi DK. Fundamentals to clinical application of nanoparticles in cancer immunotherapy and radiotherapy. Ecancermedicalscience. 2020;14:1095.
Saeed M, et al. Engineering nanoparticles to reprogram the Tumor Immune Microenvironment for Improved Cancer Immunotherapy. Theranostics. 2019;9(26):7981-8000.
Libutti SK, et al. Phase I and pharmacokinetic studies of CYT-6091, a novel PEGylated colloidal gold-rhTNF nanomedicine. Clin Cancer Res. 2010;16(24):6139-49.
Wang S, Sun Z, Hou Y. Engineering nanoparticles toward the modulation of emerging cancer immunotherapy. Adv Healthc Mater. 2021;10(5):2000845.
Chiang CL-L, Coukos G, Kandalaft LE. Whole tumor antigen vaccines: where are we? Vaccines. 2015;3(2):344-72.
Prasad S, et al. Polymer nanoparticles containing tumor lysates as antigen delivery vehicles for dendritic cell-based antitumor immunotherapy. Nanomed Nanotechnol Biol Med. 2011;7(1):1-10.
Higashisaka K, et al. Nano-safety research: examining the associations among the biological effects of nanoparticles and their physicochemical properties and kinetics. Biol Pharm Bull. 2017;40(3):243-8.
Niu L, et al. Cytokine-mediated disruption of lymphocyte trafficking, hemopoiesis, and induction of lymphopenia, anemia, and thrombocytopenia in anti-CD137-treated mice. J Immunol. 2007;178(7):4194-213.
Leonard JP, et al. Effects of single-dose interleukin-12 exposure on interleukin-12-associated toxicity and interferon-gamma production. Blood. 1997;90(7):2541-8.
Di Giacomo AM, Biagioli M, Maio M. The emerging toxicity profiles of anti-CTLA-4 antibodies across clinical indications. Semin Oncol. 2010;37(5):499-507.
Xia Q et al. Size-and cell type-dependent cellular uptake, cytotoxicity and in vivo distribution of gold nanoparticles. Int J Nanomed, 2019: p. 6957-70.
Bekić , et al. The effect of stabilisation agents on the immunomodulatory properties of gold nanoparticles obtained by ultrasonic spray pyrolysis. Materials. 2019;12(24):4121.
Zhong Y, et al. In vivo molecular imaging for immunotherapy using ultra-bright near-infrared-llb rare-earth nanoparticles. Nat Biotechnol. 2019;37(11):1322-31.
Smith DM, Simon JK, Baker JR Jr. Applications of nanotechnology for immunology. Nat Rev Immunol. 2013;13(8):592-605.
Irvine DJ, Swartz MA, Szeto GL. Engineering synthetic vaccines using cues from natural immunity. Nat Mater. 2013;12(11):978-90.
Kwong B, et al. Localized immunotherapy via liposome-anchored AntiCD137 + IL-2 prevents lethal toxicity and elicits local and systemic antitumor immunity. Cancer Res. 2013;73(5):1547-58.
Kwong B, Liu H, Irvine DJ. Induction of potent anti-tumor responses while eliminating systemic side effects via liposome-anchored combinatorial immunotherapy. Biomaterials. 2011;32(22):5134-47.
Liu H, et al. Structure-based programming of lymph-node targeting in molecular vaccines. Nature. 2014;507(7493):519-22.
Wu TY-H et al. Rational design of small molecules as vaccine adjuvants. Sci Transl Med, 2014. 6(263): p. 263ra160-263ra160.
Zolnik BS, et al. Nanoparticles and the immune system. Endocrinology. 2010;151(2):458-65.
Manolova V, et al. Nanoparticles target distinct dendritic cell populations according to their size. Eur J Immunol. 2008;38(5):1404-13.
Reddy ST, et al. Exploiting lymphatic transport and complement activation in nanoparticle vaccines. Nat Biotechnol. 2007;25(10):1159-64.
Tkach AV, et al. Direct effects of carbon nanotubes on dendritic cells induce immune suppression upon pulmonary exposure. ACS Nano. 2011;5(7):5755-62.
Ryan JJ, et al. Fullerene nanomaterials inhibit the allergic response. J Immunol. 2007;179(1):665-72.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Qiang Lu, Dongquan Kou and Shenghan Lou contributed equally to this work.
*Correspondence:
Gautam Sethi phcgs@nus.edu.sg
Zhennan Yuan yuanzhennan123@hrbmu.edu.cn
Peng Han leospiv@hrbmu.edu.cn
Full list of author information is available at the end of the article