DOI: https://doi.org/10.1038/s41591-024-03451-3
PMID: https://pubmed.ncbi.nlm.nih.gov/39775044
تاريخ النشر: 2025-01-07
الخلايا التائية CAR المستهدفة لبروتين B7-H3 داخل البطينات الدماغية لعلاج الورم الدبقي الجسري المنتشر في الجسر: تجربة المرحلة الأولى
تم القبول: 6 ديسمبر 2024
نُشر على الإنترنت: 7 يناير 2025
(أ) التحقق من التحديثات
تظهر قائمة بالمؤلفين وانتماءاتهم في نهاية الورقة.
خلايا CAR T المستهدفة لـ (HER2) (NCT03500991)
النتائج
تصميم الدراسة وخصائص المرضى
العلاج
| خصائص | قيمة |
| العمر الوسيط (بالسنوات (النطاق)) | 6 (2-22) |
| جنس
|
|
| ذكر | 9 (39) |
| أنثى | 14 (61) |
| درجة أداء لانسكي أو كارنوفسكي
|
|
| 90 | 12 (52) |
| ٨٠ | 7 (30) |
| 70 | 2 (9) |
| 60 | 2 (9) |
| متوسط الأشهر من التشخيص إلى التسجيل (النطاق) | 6 (3-22) |
| تأكيد هيستوباثولوجي أو جزيئي لـ DMG
|
18 (78) |
| تاريخ المرض عند التسجيل (
|
|
| التقدم السابق | 12 (52) |
| لا تقدم سابق | 11 (48) |
| تاريخ المرض عند الجرعة الأولى من CAR B7-H3
|
|
| التقدم السابق | 12 (57) |
| لا تقدم سابق | 9 (43) |
| العلاج الإشعاعي السابق
|
٢٣ (١٠٠) |
السلامة
النتائج السريرية
| حدث | الصف الأول-الثاني
|
الصف الثالث
|
الصف الرابع
|
| عصبي | |||
| صداع | 15 (71) | 2 (10) | 0 |
| ترنح | 3 (14) | 1 (5) | 0 |
| دوار | 2 (10) | 0 | 0 |
| عُسر الكلام | 1 (5) | 0 | 0 |
| عسر البلع | 1 (5) | 0 | 0 |
| اضطراب العصب الوجهي | 2 (10) | 0 | 0 |
| استسقاء الرأس | 0 | 1 (5) | 0 |
| ضعف عضلي أحادي الجانب | 2 (10) | 2 (10) | 0 |
| تنميل | 4 (19) | 0 | 0 |
| اعتلال الأعصاب الحسية الطرفية | 1 (5) | 0 | 0 |
| اهتزاز | 1 (5) | 0 | 0 |
| اضطراب العصب المائل | 1 (5) | 0 | 0 |
| عيني | |||
| ازدواج الرؤية | 1 (5) | 0 | 0 |
| رهاب الضوء | 2 (10) | 0 | 0 |
| جهاز الهضم | |||
| غثيان | 12 (57) | 1 (5) | 0 |
| التقيؤ | 15 (71) | 1 (5) | 0 |
| فقدان الشهية | 3 (14) | 0 | 0 |
| ألم بطني | 1 (5) | 0 | 0 |
| عسر البلع | 1 (5) | 0 | 0 |
| مرتبط بالورم | |||
| نزيف الورم | 0 | 0 | 1 (5) |
| دستوري | |||
| حمى | 11 (52) | 1 (5) | 0 |
| إرهاق | 13 (62) | 0 | 0 |
| malaise | 1 (5) | 0 | 0 |
| ألم | 2 (10) | 0 | 0 |
| تحريض | 1 (5) | 0 | 0 |
| تنفسي | |||
| ضيق التنفس | 1 (5) | 0 | 0 |
| زغطة | 6 (29) | 0 | 0 |
| القلب والأوعية الدموية | |||
| ارتفاع ضغط الدم | 1 (5) | 0 | 0 |
| انخفاض ضغط الدم | 1 (5) | 0 | 0 |
| عضلي هيكلي | |||
| ألم الظهر | 1 (5) | 0 | 0 |
| ألم الرقبة | 3 (14) | 1 (5) | 0 |
| بولية | |||
| سلس البول | 1 (5) | 0 | 0 |
| جلدي | |||
| حكة | 1 (5) | 0 | 0 |
| هيماتولوجي | |||
| نقص اللمفاويات | 1 (5) | 0 | 0 |
جزء من بقائهم العام. لذلك، بينما قمنا بحساب البقاء الوسيط من التشخيص الأولي، قمنا أيضًا بتقييم البقاء من تسجيل الدراسة (لجميع المرضى المسجلين) ومن حقن خلايا CAR T الأولية (لجميع المرضى المعالجين). تم متابعة المرضى من وقت التسجيل، الذي حدث بين أغسطس 2020 وأبريل 2023، حتى العلاج حتى الوفاة أو التوقف عند آخر زيارة متابعة لهم قبل 13 نوفمبر 2024.
كشف خلايا CAR T وتحليل السيتوكينات
قد انخفضت شدة الإشارة. ب، تصوير بالرنين المغناطيسي الطولي للآفة الجسيمية في SO53. صور الرنين المغناطيسي المحوري بتقنية T2 (الصف العلوي) وصور الرنين المغناطيسي المحوري بعد التباين بتقنية T1 (الصف السفلي)، تركزت على الآفة الجسيمية في نقاط زمنية مختلفة (انظر تسميات الأعمدة). عند التشخيص، كان الجسر متضخمًا (الأسهم) مع شدة إشارة T2 منتشرة، وتعزيز غير متجانس وتخفيف جزئي للبطين الرابع (النجوم). بعد الإشعاع (بعد العلاج الإشعاعي، شهرين قبل العلاج الداخلي)، كان هناك مزيد من توسع الجسر وزيادة في شذوذ إشارة T2 (الأسهم)، مع استمرار التعزيز. من قبل العلاج الداخلي إلى شهرين بعد العلاج الداخلي، كانت الآفة الجسيمية أصغر (الأسهم). ومع ذلك، بحلول 4 أشهر بعد العلاج الداخلي، كانت الآفة أكبر، مع منطقة جديدة من التعزيز (رؤوس الأسهم). عند 6 و 8 أشهر بعد العلاج الداخلي، تم تقليل حجم الآفة، وشذوذ إشارة T2 والتعزيز.
يدعم هذا الاكتشاف أنه بينما يتم الكشف عن خلايا CAR T B7-H3 التي تم توصيلها عبر ICV بشكل مستمر في السائل الدماغي الشوكي بعد الحقن، فإن الدورة الدموية الجهازية كانت نادرة وعابرة وبمستويات منخفضة.
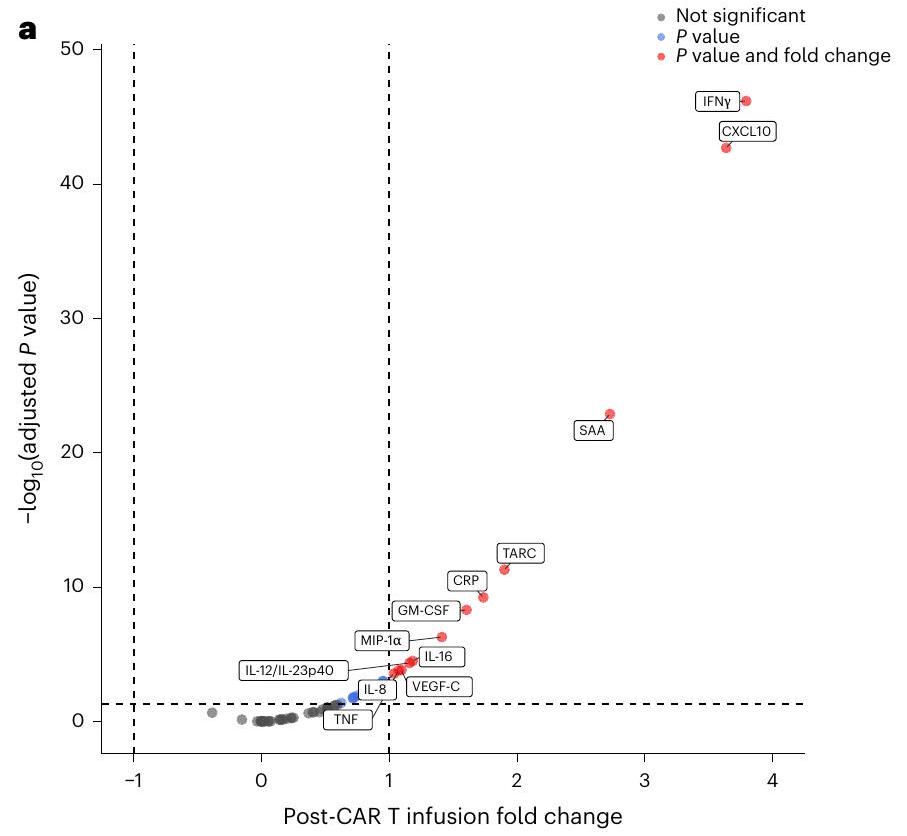
لم يزد مستوى بروتين الأميلويد A (SAA) بشكل ملحوظ بعد الحقنة الأولى، لكنه أظهر ارتفاعات ملحوظة بعد الحقنات اللاحقة (الشكل 4a، b). بينما أظهرت GM-CSF وTARC أكبر زيادات لها بعد الحقنة الأولى، أظهر CXCL10 وIFN
نقاش
مخطط بركان لجميع 53 سيتوكين تم اختبارها. تشير التسميات إلى السيتوكينات التي تظهر تغييرًا بمقدار الضعف على الأقل ومعدل اكتشاف خاطئ (FDR) معدل.
b
تم تضمين نفس المرضى. للتحليل المقدم في مخطط البركان، تم دمج بيانات من Cr1.W1 باستخدام النموذج الخطي المختلط.
التعقيد بالنسبة لـ DIPG حيث يمكن أن ينخفض الجسر نفسه في الحجم إلى حد معين وقياسات فرط شدة T2 تخضع لعيوب التصوير وتحامل المراسل. لذلك، يتم إجراء تحقيقات متقدمة في التصوير الحجمي القائم على التعلم الآلي والتصوير المنتشر لمعالجة هذه القيود
المحتوى عبر الإنترنت
References
- Cooney, T. et al. Contemporary survival endpoints: an International Diffuse Intrinsic Pontine Glioma Registry study. Neuro. Oncol. 19, 1279-1280 (2017).
- Vitanza, N. A. & Monje, M. Diffuse intrinsic pontine glioma: from diagnosis to next-generation clinical trials. Curr. Treat. Options Neurol. 21, 37 (2019).
- Gardner, R. A. et al. Intent-to-treat leukemia remission by CD19 CAR T cells of defined formulation and dose in children and young adults. Blood 129, 3322-3331 (2017).
- Maude, S. L. et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N. Engl. J. Med. 371, 1507-1517 (2014).
- Vitanza, N. A. et al. Locoregional CAR T cells for children with CNS tumors: clinical procedure and catheter safety. Neoplasia 36, 100870 (2023).
- Vitanza, N. A. et al. Intraventricular B7-H3 CAR T cells for diffuse intrinsic pontine glioma: preliminary first-in-human bioactivity and safety. Cancer Discov. 13, 114-131 (2023).
- Vitanza, N. A. et al. Locoregional CAR T cells for the treatment of CNS tumors in children: investigational drug service pharmacy activities. J. Hematol. Oncol. Pharm. 14, 148-154 (2024).
- Lin, F. Y. et al. Phase I trial of GD2.CART cells augmented with constitutive interleukin-7 receptor for treatment of high-grade pediatric CNS tumors. J. Clin. Oncol. 42, 2769-2779 (2024).
- Monje, M. et al. Intravenous and intracranial GD2-CAR T cells for H3K27M
diffuse midline gliomas. Nature https://doi.org/10.1038/ s41586-024-08171-9 (2024). - Wang, L. et al. Expansion of endogenous T cells in CSF of pediatric CNS tumor patients undergoing locoregional delivery of IL13Ra2-targeting CAR T cells: an interim analysis. Preprint at Research Square https://doi.org/10.21203/rs.3.rs-3454977/v1 (2023).
- Vitanza, N. A. et al. Locoregional infusion of HER2-specific CAR T cells in children and young adults with recurrent or refractory CNS tumors: an interim analysis. Nat. Med. 27, 1544-1552 (2021).
- Ravanpay, A. C. et al. EGFR806-CAR T cells selectively target a tumor-restricted EGFR epitope in glioblastoma. Oncotarget 10, 7080-7095 (2019).
- Haydar, D. et al. Cell-surface antigen profiling of pediatric brain tumors: B7-H3 is consistently expressed and can be targeted via local or systemic CAR T-cell delivery. Neuro. Oncol. 23, 999-1011 (2021).
- Majzner, R. G. et al. CAR T cells targeting B7-H3, a pan-cancer antigen, demonstrate potent preclinical activity against pediatric solid tumors and brain tumors. Clin. Cancer Res. 25, 2560-2574 (2019).
- Zhou, Z. et al. B7-H3, a potential therapeutic target, is expressed in diffuse intrinsic pontine glioma. J. Neurooncol. 111, 257-264 (2013).
- Maachani, U. B. et al. B7-H3 as a prognostic biomarker and therapeutic target in pediatric central nervous system tumors. Transl. Oncol. 13, 365-371 (2020).
- Du, H. et al. Antitumor responses in the absence of toxicity in solid tumors by targeting B7-H3 via chimeric antigen receptor T cells. Cancer Cell 35, 221-237.e8 (2019).
- Nehama, D. et al. B7-H3-redirected chimeric antigen receptor T cells target glioblastoma and neurospheres. EBioMedicine 47, 33-43 (2019).
- Talbot, L. J. et al. A novel orthotopic implantation technique for osteosarcoma produces spontaneous metastases and illustrates dose-dependent efficacy of B7-H3-CAR T cells. Front. Immunol. 12, 691741 (2021).
- Zhang, Z. et al. B7-H3-targeted CAR-T cells exhibit potent antitumor effects on hematologic and solid tumors. Mol. Ther. Oncolytics 17, 180-189 (2020).
- Tang, X. et al. Bioactivity and safety of B7-H3-targeted chimeric antigen receptor T cells against anaplastic meningioma. Clin. Transl. Immunol. 9, e1137 (2020).
- Tang, X. et al. Administration of B7-H3 targeted chimeric antigen receptor-T cells induce regression of glioblastoma. Signal Transduct. Target Ther. 6, 125 (2021).
- Pinto, N. et al. STRIvE-O2: A first-in-human phase I study of systemically administered B7-H3 chimeric antigen receptor T cells for patients with relapsed/refractory solid tumors. J. Clin. Oncol. 42, 4163-4172 (2024).
- Broniscer, A. et al. Intratumoral hemorrhage among children with newly diagnosed, diffuse brainstem glioma. Cancer 106, 1364-1371 (2006).
- Mahdi, J. et al. Tumor inflammation-associated neurotoxicity. Nat. Med. 29, 803-810 (2023).
- Morales La Madrid, A. et al. Second re-irradiation for DIPG progression, re-considering “old strategies” with new approaches. Childs Nerv. Syst. 33, 849-852 (2017).
- Gupta, N. et al. Prospective feasibility and safety assessment of surgical biopsy for patients with newly diagnosed diffuse intrinsic pontine glioma. Neuro. Oncol. 20, 1547-1555 (2018).
- Williams, J. R. et al. Progress in diffuse intrinsic pontine glioma: advocating for stereotactic biopsy in the standard of care. Neurosurg. Focus 48, E4 (2020).
- Aquino, D., Gioppo, A., Finocchiaro, G., Bruzzone, M. G. & Cuccarini, V. MRI in glioma immunotherapy: evidence, pitfalls, and perspectives. J. Immunol. Res. 2017, 5813951 (2017).
- Tam, L. T. et al. MRI-based radiomics for prognosis of pediatric diffuse intrinsic pontine glioma: an international study. Neurooncol. Adv. 3, vdab042 (2021).
- Mackay, A. et al. Integrated molecular meta-analysis of 1,000 pediatric high-grade and diffuse intrinsic pontine glioma. Cancer Cell 32, 520-537.e5 (2017).
(c) The Author(s) 2025
Nicholas A. Vitanza (IP)

طرق
منتج خلايا CAR T
الأهداف
المرضى
تصميم الدراسة والعلاج
في أبريل 2023. تم إجراء هذه الدراسة وفقًا لإرشادات إدارة الغذاء والدواء الأمريكية وإرشادات المؤتمر الدولي للتنظيم المتناغم لممارسات البحث السريري الجيدة، وإعلان هلسنكي ومتطلبات مجلس المراجعة المؤسسية المعمول بها، بما في ذلك الموافقة على بروتوكول الدراسة من قبل مجلس المراجعة المؤسسية لمستشفى الأطفال في سياتل. خضع مرضى BrainChild-03 الذراع C لعملية فصل الكريات البيضاء، وتصنيع خلايا CAR T، والتسريب من خلال قسطرة الجهاز العصبي المركزي الخاصة بهم. تم استخدام مستويات الجرعة داخل المريض (الشكل 1) في DRs بخلاف DR1 (الذي كانت فيه جميع الجرعات DL1). تم اتخاذ قرارات تصعيد الجرعة وتخفيضها باستخدام
التحليل الإحصائي
تحليل السائل الدماغي الشوكي
كشف خلايا CAR T في الدم المحيطي
ملخص التقرير
توفر البيانات
References
- Ceppi, F. et al. Modified manufacturing process modulates CD19CAR T-cell engraftment fitness and leukemia-free survival in pediatric and young adult subjects. Cancer Immunol. Res. 10, 856-870 (2022).
- Jonnalagadda, M. et al. Efficient selection of genetically modified human T cells using methotrexate-resistant human dihydrofolate reductase. Gene Ther. 20, 853-860 (2013).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Springer, 2016).
- Blighe, K., Rana, S. & Lewis, M. EnhancedVolcano: Publicationready volcano plots with enhanced colouring and labeling. GitHub https://github.com/kevinblighe/EnhancedVolcano (2024).
شكر وتقدير
مساهمات المؤلفين
المصالح المتنافسة
ن.أ.ف، ج.أ.ج، ج.ب.ف، ج.ر.ب و م.س.ج هم مخترعون في براءات اختراع صادرة ومعلقة تتعلق بعلاجات خلايا CAR T. المؤلفون الآخرون يعلنون عدم وجود مصالح متنافسة.
معلومات إضافية
| موضوع | مصدر | التشخيص المرضي | تشوهات جزيئية |
| S005 | نسيج الورم | دي إم جي | H3F3A، ATRX |
| S006 | نسيج الورم | دي إم جي | H3F3A، ATM، FGFR1 |
| سُو7
|
نسيج الورم | دي إم جي | H3F3A، TP53، PDGFRA مضاعف، FANCM |
| S008 | نسيج الورم | HGG | TP53، IDH-1، MGMT غير ميثيلated |
| S012 | غير متوفر | غير متوفر | غير متوفر |
| S014 | بلازما | دي إم جي | H3F3A |
| S018 | نسيج الورم | دي إم جي | HIST1H3B، ACVR1، NRAS |
| S021 | نسيج الورم | دي إم جي | H3F3A |
| S023 | نسيج الورم | دي إم جي | H3F3A، ACVR1 |
| S024 | غير متوفر | غير متوفر | غير متوفر |
| S027
|
نسيج الورم | غير متوفر | غير متوفر |
| S031 | نسيج الورم | دي إم جي | فقدان H3K27me3، فرط تعبير EZHIP، PPM1D، FGFR1 |
| S033 | نسيج الورم | دي إم جي | H3F3A، TP53 |
| S034 | نسيج الورم | دي إم جي | H3K27M IHC، TP53 |
| S036 | نسيج الورم والسائل الدماغي الشوكي | دي إم جي | H3K27M، TP53 |
| S039 | نسيج الورم | دي إم جي | H3K27M IHC |
| S041 | نسيج الورم | دي إم جي | فقدان H3K27me3 IHC |
| S044 | نسيج الورم | دي إم جي | H3F3A، TP53 |
| S045 | نسيج الورم | دي إم جي | H3F3A، BRAF V600E، KMT2D، MAP2K3 |
| S049 | السائل الدماغي الشوكي | دي إم جي | H3F3A، TP53 |
| S053 | نسيج الورم | دي إم جي | H3K27M IHC |
| S054
|
غير متوفر | غير متوفر | غير متوفر |
| S057 | غير متوفر | غير متوفر | غير متوفر |
الشكل 1 من البيانات الموسعة | المعلومات التشخيصية المرضية لجميع المرضى.
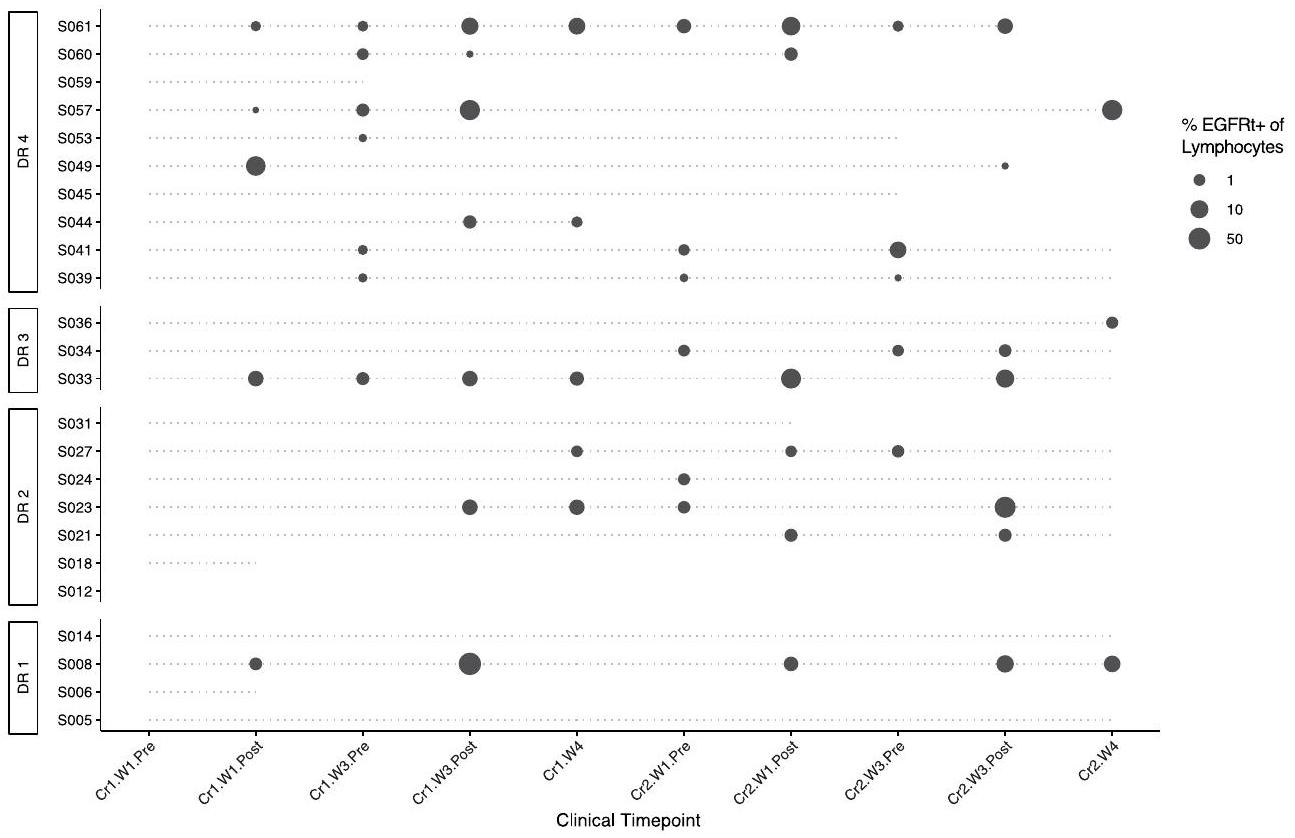
تمثل الدوائر عينات تم الكشف فيها عن خلايا CAR T B7-H3، والتي تم تعريفها بمستويات اللمفاويات/EGFRt+% التي تتجاوز حد الكشف (LOD) وعدد أدنى (>1) من خلايا EGFRt+ المكتشفة. حجم الدوائر يدل على نسبة اللمفاويات EGFRt+ (Lymph/EGFRt+%) المكتشفة في العينة. ومن الجدير بالذكر أن S014 لم يتم جمع أي عينة بسبب وضع التحويلة، وS018 تلقت جرعة واحدة فقط، وS045 فاتتها جميع عمليات الجمع بعد الحقن.
| جميع المرضى | الوسيط | الحد الأقصى | الحد الأدنى |
| Cr1.W1.Pre | 0 | 0 | 0 |
| كر1.و1.بريد | 0.2395 | 18.908 | 0 |
| Cr1.W3.Pre | 0.517 | 1.609 | 0 |
| Cr1.W3.Post | 0.598 | ٦٤.٤٣٥ | 0.008 |
| Cr1.W4 | 0.39 | ٣.٧٨٧ | 0 |
| Cr2.W1.Pre | 0.273 | 1.326 | 0 |
| Cr2.W1.Post | 0.337 | 21.901 | 0 |
| Cr2.W3.Pre | 0.3795 | 6.045 | 0 |
| Cr2.W3.Post | 1.416 | ٣٤.٩٦٧ | 0.079 |
| Cr2.W4 | 0.718 | 25.401 | 0 |
| المحلل | متوسط تركيز Cr1 – Cr2 (بيكوجرام/مل) (النطاق) | بعد-قبل FC (P.adj) Cr1-Cr2 | Cr1.W1 ما بعد-ما قبل FC (P.adj) | Cr1-W3 بعد-قبل FC (P.adj) | Cr2-W1 بوست-بري FC (P.adj) | Cr2-W3 بعد-قبل FC (P.adj) |
| CRP | 1508.04 (0.00 – 962046.22) |
|
1.2 (0.9) | 3.6 (8.9e-3) | 4.6 (8.0e
|
|
| س.ا.ع | ١٣٦٣.٠٧ (٠.٠٠ – ٨٤٩٣٢٠.٧١) |
|
2.3 (0.1) |
|
|
15.1 (2.6e-11) |
| CXCL10 | 408.85 (1.09 108926.77) | 12.4 (1.7e-42) |
|
8.1 (1.5e-7) |
|
9.6 (5.8e-8) |
| ICAM-1 | ١٤٤٢٫٨١ (٠٫٨٦ – ٨٤٩٧٩٫٦٦) | 1.6 (0.02) | 0.9 (0.99) | 1.4 (0.8) | 1.9 (0.3) | 3.3 (0.02) |
| MCP-1 | 199.63 (54.55 – 1409.79) | 0.98 (0.99) | 1.0 (0.99) | 0.9 (0.99) | 1.1 (0.9) | 0.9 (0.9) |
| إنترفيرون غاما | 4.55 (0.03 3388.64) |
|
|
11.3 (5.2e-10) | 19.8 (1.0e-14) |
|
| تارك | 15.51 (0.33 787.98) |
|
|
2.9 (3.8e-2) |
|
3.2 (
|
| GM-CSF | 1.38 (0.01 70.64) |
|
4.1 (7.6e
|
2.4 (0.09) | 3.3 (0.01) | 2.6 (0.07) |
| IL-16 | 6.89 (0.01 99.04) |
|
2.0 (0.2) | 2.0 (0.2) | 2.5 (0.07) | 2.6 (0.07) |
| MIP-1b | 21.87 (5.08 412.17) |
|
3.1 (0.01) | 2.1 (0.2) | 2.8 (0.03) | 2.7 (0.07) |
| TNFa | 0.66 (0.07 36.61) |
|
2.4 (0.08) | 1.7 (0.4) | 2.1 (0.1) | ٢.٣ (٠.١) |
| IL-8 | 30.89 (0.85 857.75) | 2.1 (
|
1.8 (0.03) | 1.3 (0.8) | 2.6 (0.05) | 3.1 (0.02) |
| VEGF-C | 31.80 (0.00 22287.80) |
|
2.9 (0.02) | 1.3 (0.8) | 2.4 (0.08) | 2.2 (0.2) |
| IL-12/IL23p40 | 17.61 (1.79 301.97) |
|
2.7 (0.03) | 2.2 (0.1) | 2.2 (0.1) | 1.8 (0.04) |
محفظة الطبيعة
نيكولاس فيتانزا
آخر تحديث بواسطة المؤلفين:
ملخص التقرير
الإحصائيات
غير متوفر
□ X
□

□
يجب أن تُوصف الاختبارات الشائعة فقط بالاسم؛ واصفًا التقنيات الأكثر تعقيدًا في قسم الطرق.
□
□
□
□
□ لتحليل بايزي، معلومات حول اختيار القيم الأولية وإعدادات سلسلة ماركوف مونت كارلو
□ لتصميمات هرمية ومعقدة، تحديد المستوى المناسب للاختبارات والتقارير الكاملة عن النتائج
□ تقديرات أحجام التأثير (مثل حجم تأثير كوهين)
تحتوي مجموعتنا على الويب حول الإحصائيات لعلماء الأحياء على مقالات تتناول العديد من النقاط المذكورة أعلاه.
تم التأكيد
حجم العينة بالضبط
حجم العينة بالضبط
بيان حول ما إذا كانت القياسات قد أُخذت من عينات متميزة أو ما إذا كانت نفس العينة قد تم قياسها عدة مرات
اختبار(ات) الإحصاء المستخدمة وما إذا كانت أحادية الجانب أو ثنائية الجانب
وصف جميع المتغيرات المرافقة التي تم اختبارها
ن
وصف كامل للمعلمات الإحصائية بما في ذلك الاتجاه المركزي (مثل المتوسطات) أو تقديرات أساسية أخرى (مثل معامل الانحدار) والتباين (مثل الانحراف المعياري) أو التقديرات المرتبطة بعدم اليقين (مثل فترات الثقة)
في اختبار فرضية العدم، إحصائية الاختبار (على سبيل المثال،
تحليل ساني، إعلام
أمة
اختيار القيم الأولية وإعدادات سلسلة ماركوف مونت كارلو
علماء الأحياء
” “” “” “
البرمجيات والشيفرة
معلومات السياسة حول توفر كود الكمبيوتر
بيانات
معلومات السياسة حول توفر البيانات
- رموز الانضمام، معرفات فريدة، أو روابط ويب لمجموعات البيانات المتاحة للجمهور
- وصف لأي قيود على توفر البيانات
- بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتماشى مع سياستنا
البحث الذي يتضمن مشاركين بشريين، بياناتهم، أو مواد بيولوجية
| التقارير عن الجنس والنوع الاجتماعي | كان المرضى مؤهلين بغض النظر عن الجنس والنوع. |
| التقارير عن العرق أو الإثنية أو غيرها من المجموعات الاجتماعية ذات الصلة | كان المرضى مؤهلين بغض النظر عن العرق والإثنية. |
| خصائص السكان | الخصائص مدرجة في الجدول 1 |
| التوظيف | تم تجنيد المرضى من خلال إحالة الأطباء والإحالة الذاتية. تم تجنيد المرضى من كل من المراكز الصحية الأكاديمية ومراكز الصحة المجتمعية. لم يتلق المرضى أي تعويض مالي للتسجيل، على الرغم من أنه قد يوجد تحيز في حقيقة أن العائلات كانت بحاجة إلى وسائل للسفر إلى سياتل والإقامة محليًا خلال جزء من العلاج. |
| رقابة الأخلاقيات | تم إجراء هذه الدراسة وفقًا لإرشادات إدارة الغذاء والدواء الأمريكية ومؤتمر التوافق الدولي لممارسات البحث السريري الجيدة، وإعلان هلسنكي، ومتطلبات مجلس المراجعة المؤسسية المعمول بها، بما في ذلك الموافقة على بروتوكول الدراسة من قبل مجلس المراجعة المؤسسية لمستشفى الأطفال في سياتل. |
التقارير الخاصة بالمجال
علوم الحياة
العلوم السلوكية والاجتماعية □ العلوم البيئية والتطورية والبيئية
لنسخة مرجعية من الوثيقة مع جميع الأقسام، انظرnature.com/documents/nr-reporting-summary-flat.pdf
تصميم دراسة العلوم الحياتية
| حجم العينة | تم تحديد حجم العينة بناءً على المرحلة
|
| استثناءات البيانات | لم يكن هناك بيانات مستبعدة. |
| التكرار | تم إجراء اختبارات السيتوكين بشكل مزدوج |
| التوزيع العشوائي | لم يتم إجراء أي عشوائية حيث كانت هذه تجربة سريرية من المرحلة الأولى غير عشوائية. |
| عمى | لم يتم إجراء أي تعمية حيث كانت هذه تجربة سريرية من المرحلة الأولى غير معمية. |
التقارير عن مواد وأنظمة وطرق محددة
|
|
مشارك في الدراسة |
|
|
الأجسام المضادة |
|
|
|
|
|
|
|
|
الحيوانات وغيرها من الكائنات الحية |
|
|
|
|
|
|
محفظة الطبيعة | ملخص التقرير أبريل 2023
الأجسام المضادة
| الأجسام المضادة المستخدمة | مادة حجب FcR البشرية (Miltenyi، رقم الكات#130-059-901، RRID:AB_2892112)؛ محلول صبغة برايلانت (BD، رقم الكات#563794، RRID:AB_2869750)؛ FVS520 (FITC، BD، رقم الكات#564407، RRID:AB_2869573)؛ FVS510 (FVS510، BD، رقم الكات#564406، RRID:AB_2869572)؛ CD36 (FITC، BD، رقم الكات#555454، RRID:AB_2291112)؛ CD3 (V450، BD، رقم الكات#652356، RRID:AB_2868395)؛ CD3 (FITC، BD، رقم الكات#555332، RRID:AB_395739)؛ CD4 (BV605، BD، رقم الكات#562658، RRID:AB_2744420)؛ CD4 (R718، BD، رقم الكات#567092، RRID:AB_2916435)؛ CD8 (PerCPCy5.5، BD، رقم الكات#560662، RRID:AB_1727513)؛ CD8 (BV605، BD، رقم الكات#564116، RRID:AB_2869551)؛ سيتوكسيماب (APC، BD، مخصص، RRID:AB_2459632). |
التحقق
البيانات السريرية
معلومات السياسة حول الدراسات السريرية
نباتات
غير متوفر
غير متوفر
غير متوفر
تدفق الخلايا
المؤامرات
أكد أن:
المقاييس على المحاور واضحة تمامًا. قم بتضمين الأرقام على المحاور فقط للرسم البياني في أسفل اليسار من المجموعة (المجموعة هي تحليل للعلامات المتطابقة).
جميع الرسوم البيانية هي رسوم بيانية متساوية الارتفاع مع نقاط شاذة أو رسوم بيانية بالألوان الزائفة.
تم توفير قيمة عددية لعدد الخلايا أو النسبة المئوية (مع الإحصائيات).
المنهجية
| تحضير العينة | تم جمع عينات السائل الدماغي الشوكي (CSF) من المرضى عن طريق البزل القطني أو القسطرة البطينية وتم الاحتفاظ بها في
|
| آلة | حدد الأداة المستخدمة لجمع البيانات، مع تحديد العلامة التجارية ورقم الطراز. |
| برمجيات | فلو جو |
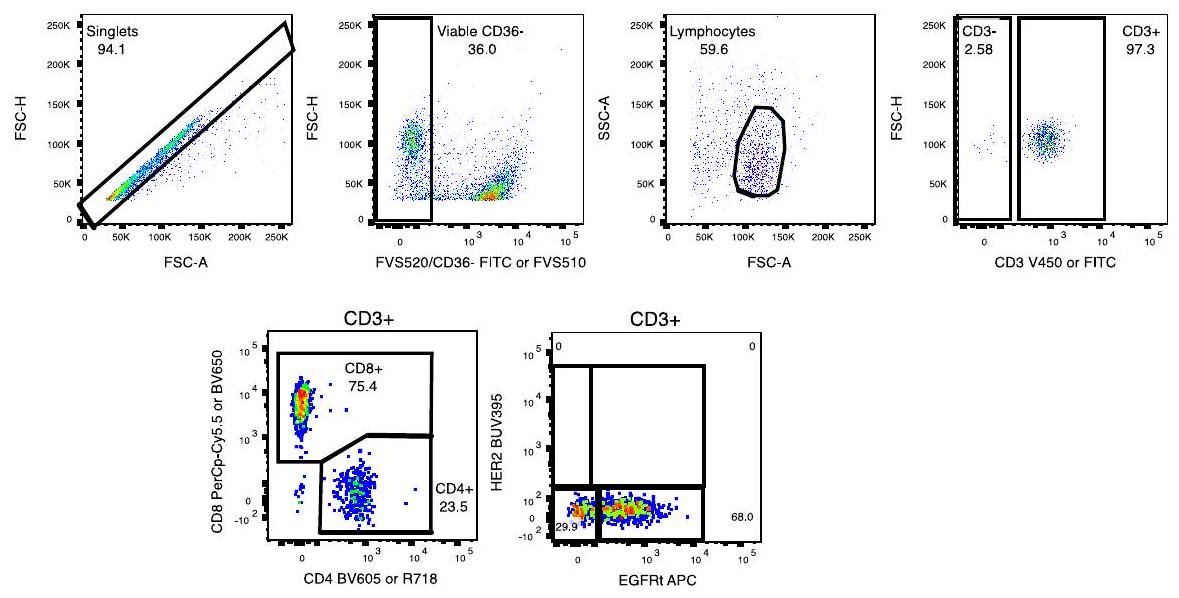
| وفرة تجمع الخلايا | تم استبعاد العينات التي تحتوي على عدد اللمفاويات أقل من حد الكمية المطلوب (LOQ) للاختبار من التقرير. يتم تحديد حالة اكتشاف خلايا CART من خلال مجموعة من عدد خلايا EGFRt+ القابلة للاكتشاف في العينة، بالإضافة إلى مستوى خلايا اللمفاويات/نسبة EGFRt+ في العينة ليكون فوق الحد المحدد مسبقًا للكشف (LOD) للاختبار. |
| استراتيجية البوابة | استراتيجية التصفية المستخدمة للكشف عن CAR المعتمد على التدفق في السائل الدماغي الشوكي. تم اختيار مجموعة اللمفاويات الفردية القابلة للحياة [CD36-] قبل تصفية خلايا T وفحص خلايا CART الإيجابية لـ EGFRt وتعبير CD4/CD8. |
التصوير بالرنين المغناطيسي
تصميم تجريبي
| نوع التصميم | الدراسات السريرية |
| مواصفات التصميم | الدراسات السريرية |
| مقاييس الأداء السلوكي | غير متوفر |
| نوع (أنواع) تصوير الاستحواذ | الدراسات السريرية |
| شدة المجال | 1.5T و 3T |
| معلمات التسلسل والتصوير | تصوير بالرنين المغناطيسي الروتيني يتكون من الدماغ = تصوير T1 MPRAGE في الوضع السهمي بدقة 1 مم مع إعادة تشكيل متعددة المستويات بدون وبتباين؛ تصوير T2 في الوضع المحوري والجبهي؛ تصوير FLAIR في الوضع المحوري؛ تصوير DWI في الوضع المحوري مع خرائط ADC؛ تصوير SWI في الوضع المحوري. العمود الفقري = تصوير T1 في الوضع المحوري والسهمي بعد التباين. |
| مجال الاستحواذ | الدماغ والحبل الشوكي |
| الرنين المغناطيسي الانتشاري | غير مستخدم |
| معايير التصوير بالرنين المغناطيسي الانتشاري السريري الروتيني |
التحضير المسبق
| برمجيات المعالجة المسبقة | غير متوفر |
| التطبيع | غير متوفر |
| قالب التطبيع | غير متوفر |
| إزالة الضوضاء والعيوب | غير متوفر |
| تصفية الحجم | غير متوفر |
النمذجة الإحصائية والاستدلال
| نوع النموذج والإعدادات | غير متوفر | ||||
| التأثيرات المختبرة |
|
||||
| حدد نوع التحليل: | □ | □ قائم على العائد على الاستثمار | □ كلاهما | ||
(انظر إكلوند وآخرون 2016)
- □ الاتصال الوظيفي و/أو الفعال
نموذج متعدد المتغيرات أو التحليل التنبؤي
محفظة الطبيعة | ملخص التقرير
- ®البريد الإلكتروني: nicholas.vitanza@seattlechildrens.org
DOI: https://doi.org/10.1038/s41591-024-03451-3
PMID: https://pubmed.ncbi.nlm.nih.gov/39775044
Publication Date: 2025-01-07
Intracerebroventricular B7-H3-targeting CART cells for diffuse intrinsic pontine glioma: a phase 1 trial
Accepted: 6 December 2024
Published online: 7 January 2025
(A) Check for updates
A list of authors and their affiliations appears at the end of the paper
(HER2)-specific CAR T cells (NCT03500991)
Results
Study design and patient characteristics
Treatment
| Characteristics | Value |
| Median age (years (range)) | 6 (2-22) |
| Sex (
|
|
| Male | 9 (39) |
| Female | 14 (61) |
| Lansky or Karnofsky performance status score (
|
|
| 90 | 12 (52) |
| 80 | 7 (30) |
| 70 | 2 (9) |
| 60 | 2 (9) |
| Median months from diagnosis to enrollment (range) | 6 (3-22) |
| Histopathologic or molecular confirmation of DMG (
|
18 (78) |
| Disease history at enrollment (
|
|
| Previous progression | 12 (52) |
| No previous progression | 11 (48) |
| Disease history at first dose of B7-H3 CAR (
|
|
| Previous progression | 12 (57) |
| No previous progression | 9 (43) |
| Previous radiation therapy (
|
23 (100) |
Safety
Clinical outcomes
| Event | Grade 1-2,
|
Grade 3,
|
Grade 4,
|
| Neurologic | |||
| Headache | 15 (71) | 2 (10) | 0 |
| Ataxia | 3 (14) | 1 (5) | 0 |
| Dizziness | 2 (10) | 0 | 0 |
| Dysarthria | 1 (5) | 0 | 0 |
| Dysphagia | 1 (5) | 0 | 0 |
| Facial nerve disorder | 2 (10) | 0 | 0 |
| Hydrocephalus | 0 | 1 (5) | 0 |
| Unilateral muscle weakness | 2 (10) | 2 (10) | 0 |
| Paresthesia | 4 (19) | 0 | 0 |
| Peripheral sensory neuropathy | 1 (5) | 0 | 0 |
| Tremor | 1 (5) | 0 | 0 |
| Trochlear nerve disorder | 1 (5) | 0 | 0 |
| Ophthalmic | |||
| Diplopia | 1 (5) | 0 | 0 |
| Photophobia | 2 (10) | 0 | 0 |
| Gastrointestinal | |||
| Nausea | 12 (57) | 1 (5) | 0 |
| Vomiting | 15 (71) | 1 (5) | 0 |
| Anorexia | 3 (14) | 0 | 0 |
| Abdominal pain | 1 (5) | 0 | 0 |
| Dysphagia | 1 (5) | 0 | 0 |
| Tumor related | |||
| Tumor hemorrhage | 0 | 0 | 1 (5) |
| Constitutional | |||
| Fever | 11 (52) | 1 (5) | 0 |
| Fatigue | 13 (62) | 0 | 0 |
| Malaise | 1 (5) | 0 | 0 |
| Pain | 2 (10) | 0 | 0 |
| Agitation | 1 (5) | 0 | 0 |
| Respiratory | |||
| Dyspnea | 1 (5) | 0 | 0 |
| Hiccups | 6 (29) | 0 | 0 |
| Cardiovascular | |||
| Hypertension | 1 (5) | 0 | 0 |
| Hypotension | 1 (5) | 0 | 0 |
| Musculoskeletal | |||
| Back pain | 1 (5) | 0 | 0 |
| Neck pain | 3 (14) | 1 (5) | 0 |
| Urinary | |||
| Incontinence | 1 (5) | 0 | 0 |
| Dermatologic | |||
| Pruritus | 1 (5) | 0 | 0 |
| Hematologic | |||
| Lymphocytopenia | 1 (5) | 0 | 0 |
portion of their overall survival. Therefore, while we calculated the median survival from initial diagnosis, we also evaluated the survival from study enrollment (for all enrolled patients) and from initial CAR T cell infusion (for all treated patients). Patients were followed from the time of enrollment, which occurred between August 2020 and April 2023, through treatment until death or censoring at their last follow-up visit before 13 November 2024.
CAR T cell detection and cytokine analysis
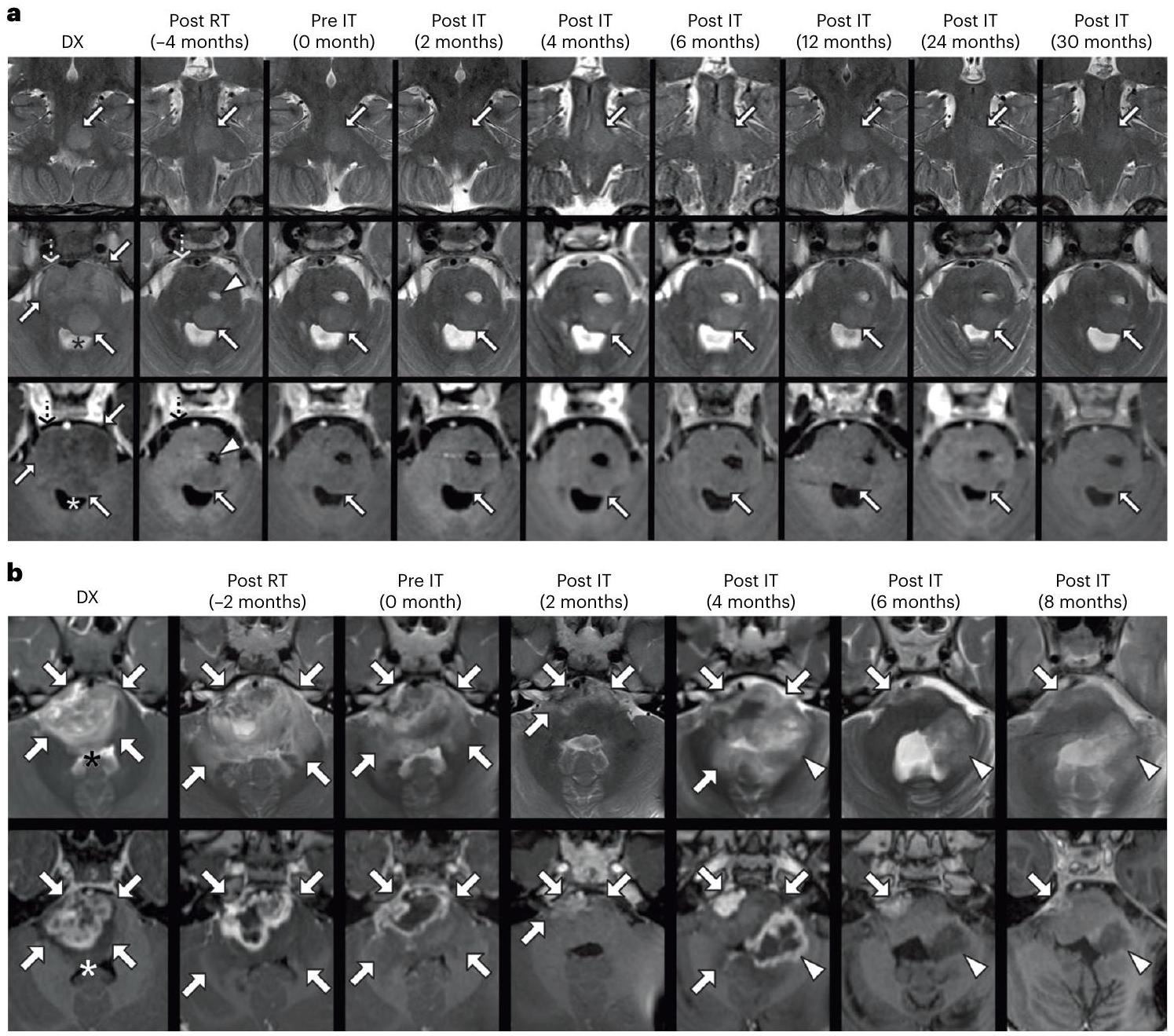
hyperintensity has decreased. b, Longitudinal MRI of the pontine lesion of SO53. Axial T2-weighted (top row) and axial post-contrast T1-weighted (bottom row) MRI images, focused on the pontine lesion at various timepoints (see column labels). At DX, the pons is enlarged (arrows) with diffuse T2 hyperintensity, heterogeneous enhancement and partial effacement of the fourth ventricle (asterisks). Following radiation (Post RT, 2 months before IT), there is further expansion of the pons and increased T2 signal abnormality (arrows), with persistent enhancement. From Pre IT to 2 months Post IT, the pontine lesion is smaller (arrows). However, by 4 months Post IT, the lesion is larger, with a new region of enhancement (arrowheads). At 6 and 8 months Post IT, the lesion size, T2 signal abnormality and enhancement are reduced.
supports the finding that while ICV delivered B7-H3 CAR T cells are consistently detected in CSF after infusion, systemic circulation was rare, transient and at low levels.
serum amyloid A (SAA) did not significantly increase after the first infusion but showed notable elevations following subsequent infusions (Fig. 4a,b). While GM-CSF and TARC showed their most pronounced increases after the first infusion, CXCL10 and IFN
Discussion
a, A volcano plot of all 53 cytokines tested. The labels indicate cytokines showing at least a twofold change and a false discovery rate (FDR)-adjusted
b
same patient were included. For the analysis presented in the volcano plot, the linear mixed model combined data from Cr1.W1
complexity for DIPG as the pons itself can only decrease in size to a certain extent and T2 hyperintensity measurements are subject to imaging artifact and reporter bias. Therefore, advanced machine-learning volumetric and diffuse based imaging investigations are ongoing to address these limitations
Online content
References
- Cooney, T. et al. Contemporary survival endpoints: an International Diffuse Intrinsic Pontine Glioma Registry study. Neuro. Oncol. 19, 1279-1280 (2017).
- Vitanza, N. A. & Monje, M. Diffuse intrinsic pontine glioma: from diagnosis to next-generation clinical trials. Curr. Treat. Options Neurol. 21, 37 (2019).
- Gardner, R. A. et al. Intent-to-treat leukemia remission by CD19 CAR T cells of defined formulation and dose in children and young adults. Blood 129, 3322-3331 (2017).
- Maude, S. L. et al. Chimeric antigen receptor T cells for sustained remissions in leukemia. N. Engl. J. Med. 371, 1507-1517 (2014).
- Vitanza, N. A. et al. Locoregional CAR T cells for children with CNS tumors: clinical procedure and catheter safety. Neoplasia 36, 100870 (2023).
- Vitanza, N. A. et al. Intraventricular B7-H3 CAR T cells for diffuse intrinsic pontine glioma: preliminary first-in-human bioactivity and safety. Cancer Discov. 13, 114-131 (2023).
- Vitanza, N. A. et al. Locoregional CAR T cells for the treatment of CNS tumors in children: investigational drug service pharmacy activities. J. Hematol. Oncol. Pharm. 14, 148-154 (2024).
- Lin, F. Y. et al. Phase I trial of GD2.CART cells augmented with constitutive interleukin-7 receptor for treatment of high-grade pediatric CNS tumors. J. Clin. Oncol. 42, 2769-2779 (2024).
- Monje, M. et al. Intravenous and intracranial GD2-CAR T cells for H3K27M
diffuse midline gliomas. Nature https://doi.org/10.1038/ s41586-024-08171-9 (2024). - Wang, L. et al. Expansion of endogenous T cells in CSF of pediatric CNS tumor patients undergoing locoregional delivery of IL13Ra2-targeting CAR T cells: an interim analysis. Preprint at Research Square https://doi.org/10.21203/rs.3.rs-3454977/v1 (2023).
- Vitanza, N. A. et al. Locoregional infusion of HER2-specific CAR T cells in children and young adults with recurrent or refractory CNS tumors: an interim analysis. Nat. Med. 27, 1544-1552 (2021).
- Ravanpay, A. C. et al. EGFR806-CAR T cells selectively target a tumor-restricted EGFR epitope in glioblastoma. Oncotarget 10, 7080-7095 (2019).
- Haydar, D. et al. Cell-surface antigen profiling of pediatric brain tumors: B7-H3 is consistently expressed and can be targeted via local or systemic CAR T-cell delivery. Neuro. Oncol. 23, 999-1011 (2021).
- Majzner, R. G. et al. CAR T cells targeting B7-H3, a pan-cancer antigen, demonstrate potent preclinical activity against pediatric solid tumors and brain tumors. Clin. Cancer Res. 25, 2560-2574 (2019).
- Zhou, Z. et al. B7-H3, a potential therapeutic target, is expressed in diffuse intrinsic pontine glioma. J. Neurooncol. 111, 257-264 (2013).
- Maachani, U. B. et al. B7-H3 as a prognostic biomarker and therapeutic target in pediatric central nervous system tumors. Transl. Oncol. 13, 365-371 (2020).
- Du, H. et al. Antitumor responses in the absence of toxicity in solid tumors by targeting B7-H3 via chimeric antigen receptor T cells. Cancer Cell 35, 221-237.e8 (2019).
- Nehama, D. et al. B7-H3-redirected chimeric antigen receptor T cells target glioblastoma and neurospheres. EBioMedicine 47, 33-43 (2019).
- Talbot, L. J. et al. A novel orthotopic implantation technique for osteosarcoma produces spontaneous metastases and illustrates dose-dependent efficacy of B7-H3-CAR T cells. Front. Immunol. 12, 691741 (2021).
- Zhang, Z. et al. B7-H3-targeted CAR-T cells exhibit potent antitumor effects on hematologic and solid tumors. Mol. Ther. Oncolytics 17, 180-189 (2020).
- Tang, X. et al. Bioactivity and safety of B7-H3-targeted chimeric antigen receptor T cells against anaplastic meningioma. Clin. Transl. Immunol. 9, e1137 (2020).
- Tang, X. et al. Administration of B7-H3 targeted chimeric antigen receptor-T cells induce regression of glioblastoma. Signal Transduct. Target Ther. 6, 125 (2021).
- Pinto, N. et al. STRIvE-O2: A first-in-human phase I study of systemically administered B7-H3 chimeric antigen receptor T cells for patients with relapsed/refractory solid tumors. J. Clin. Oncol. 42, 4163-4172 (2024).
- Broniscer, A. et al. Intratumoral hemorrhage among children with newly diagnosed, diffuse brainstem glioma. Cancer 106, 1364-1371 (2006).
- Mahdi, J. et al. Tumor inflammation-associated neurotoxicity. Nat. Med. 29, 803-810 (2023).
- Morales La Madrid, A. et al. Second re-irradiation for DIPG progression, re-considering “old strategies” with new approaches. Childs Nerv. Syst. 33, 849-852 (2017).
- Gupta, N. et al. Prospective feasibility and safety assessment of surgical biopsy for patients with newly diagnosed diffuse intrinsic pontine glioma. Neuro. Oncol. 20, 1547-1555 (2018).
- Williams, J. R. et al. Progress in diffuse intrinsic pontine glioma: advocating for stereotactic biopsy in the standard of care. Neurosurg. Focus 48, E4 (2020).
- Aquino, D., Gioppo, A., Finocchiaro, G., Bruzzone, M. G. & Cuccarini, V. MRI in glioma immunotherapy: evidence, pitfalls, and perspectives. J. Immunol. Res. 2017, 5813951 (2017).
- Tam, L. T. et al. MRI-based radiomics for prognosis of pediatric diffuse intrinsic pontine glioma: an international study. Neurooncol. Adv. 3, vdab042 (2021).
- Mackay, A. et al. Integrated molecular meta-analysis of 1,000 pediatric high-grade and diffuse intrinsic pontine glioma. Cancer Cell 32, 520-537.e5 (2017).
(c) The Author(s) 2025
Nicholas A. Vitanza (IP)
Methods
CAR T cell product
Objectives
Patients
Study design and treatment
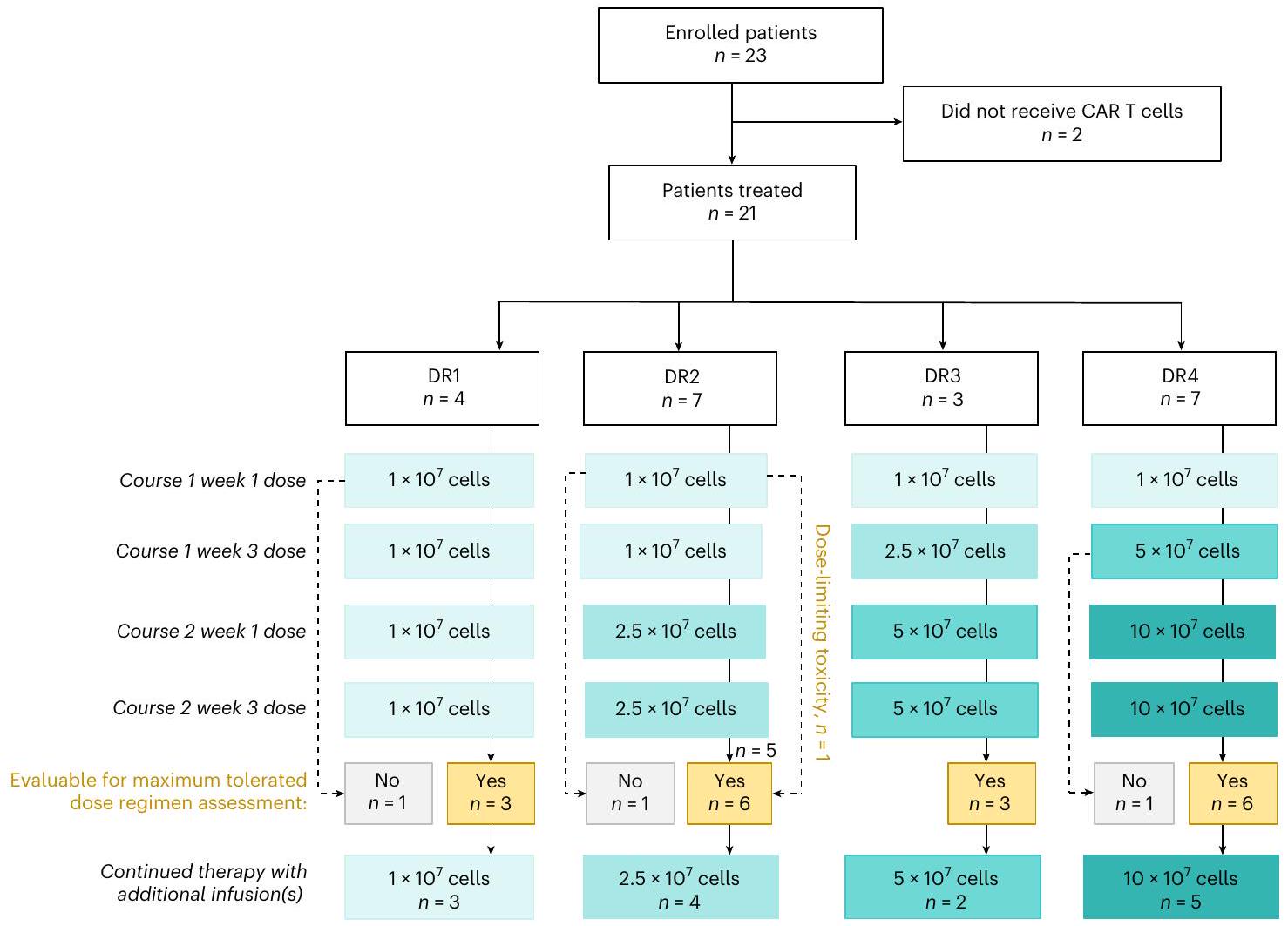
in April 2023. This study was conducted in accordance with FDA and International Conference on Harmonisation Guidelines for Good Clinical Practice, the Declaration of Helsinki and applicable institutional review board requirements, including study protocol approval by the Seattle Children’s Institutional Review Board. BrainChild-03 Arm C patients underwent leukopheresis, CAR T cell manufacture and infusions through their CNS catheter. DRs other than DR1 (in which all doses were DL1) used an intra-patient DL (Fig. 1). Dose escalation and de-escalation decisions were made using a modified
Statistical analysis
CSF analysis
Peripheral blood CAR T cell detection
Reporting summary
Data availability
References
- Ceppi, F. et al. Modified manufacturing process modulates CD19CAR T-cell engraftment fitness and leukemia-free survival in pediatric and young adult subjects. Cancer Immunol. Res. 10, 856-870 (2022).
- Jonnalagadda, M. et al. Efficient selection of genetically modified human T cells using methotrexate-resistant human dihydrofolate reductase. Gene Ther. 20, 853-860 (2013).
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis (Springer, 2016).
- Blighe, K., Rana, S. & Lewis, M. EnhancedVolcano: Publicationready volcano plots with enhanced colouring and labeling. GitHub https://github.com/kevinblighe/EnhancedVolcano (2024).
Acknowledgements
Author contributions
Competing interests
N.A.V., J.A.G., J.B.F., J.R.P. and M.C.J. are inventors on issued and pending patents related to CAR T cell therapies. The other authors declare no competing interests.
Additional information
| Subject | Source | Pathologic Diagnosis | Molecular Aberrations |
| S005 | tumor tissue | DMG | H3F3A, ATRX |
| S006 | tumor tissue | DMG | H3F3A, ATM, FGFR1 |
| SOO7
|
tumor tissue | DMG | H3F3A, TP53, PDGFRA amp, FANCM |
| S008 | tumor tissue | HGG | TP53, IDH-1, MGMT unmethylated |
| S012 | N/A | N/A | N/A |
| S014 | plasma | DMG | H3F3A |
| S018 | tumor tissue | DMG | HIST1H3B, ACVR1, NRAS |
| S021 | tumor tissue | DMG | H3F3A |
| S023 | tumor tissue | DMG | H3F3A, ACVR1 |
| S024 | N/A | N/A | N/A |
| S027
|
tumor tissue | N/A | N/A |
| S031 | tumor tissue | DMG | H3K27me3 loss, EZHIP over-expression, PPM1D, FGFR1 |
| S033 | tumor tissue | DMG | H3F3A, TP53 |
| S034 | tumor tissue | DMG | H3K27M IHC, TP53 |
| S036 | tumor tissue and CSF | DMG | H3K27M, TP53 |
| S039 | tumor tissue | DMG | H3K27M IHC |
| S041 | tumor tissue | DMG | H3K27me3 loss IHC |
| S044 | tumor tissue | DMG | H3F3A, TP53 |
| S045 | tumor tissue | DMG | H3F3A, BRAF V600E, KMT2D, MAP2K3 |
| S049 | CSF | DMG | H3F3A, TP53 |
| S053 | tumor tissue | DMG | H3K27M IHC |
| S054
|
N/A | N/A | N/A |
| S057 | N/A | N/A | N/A |
Extended Data Fig. 1| Pathologic diagnostic information for all patients.
circles represent samples where B7-H3 CAR T cells were detected, defined by lymphocyte/EGFRt+% levels above the limit of detection (LOD) and a minimal count (>1) of detected EGFRt+ cells. The size of the circles denotes the percentage of EGFRt+lymphocytes (Lymph/EGFRt+%) detected in the sample. Notably, S014 had no sample collected due to the placement of the shunt, S018 only received one dose, and S045 missed all post-infusion collection.
| All Patients | Median | Upper Limit | Lower Limit |
| Cr1.W1.Pre | 0 | 0 | 0 |
| Cr1.W1.Post | 0.2395 | 18.908 | 0 |
| Cr1.W3.Pre | 0.517 | 1.609 | 0 |
| Cr1.W3.Post | 0.598 | 64.435 | 0.008 |
| Cr1.W4 | 0.39 | 3.787 | 0 |
| Cr2.W1.Pre | 0.273 | 1.326 | 0 |
| Cr2.W1.Post | 0.337 | 21.901 | 0 |
| Cr2.W3.Pre | 0.3795 | 6.045 | 0 |
| Cr2.W3.Post | 1.416 | 34.967 | 0.079 |
| Cr2.W4 | 0.718 | 25.401 | 0 |
| Analyte | Cr1 – Cr2 Median Conc (pg/mL) (Range) | Cr1-Cr2 Post-Pre FC (P.adj) | Cr1.W1 Post-Pre FC (P.adj) | Cr1-W3 Post-Pre FC (P.adj) | Cr2-W1 Post-Pre FC (P.adj) | Cr2-W3 Post-Pre FC (P.adj) |
| CRP | 1508.04 (0.00 – 962046.22) |
|
1.2 (0.9) | 3.6 (8.9e-3) | 4.6 (8.0e
|
|
| SAA | 1363.07 (0.00 – 849320.71) |
|
2.3 (0.1) |
|
|
15.1 (2.6e-11) |
| CXCL10 | 408.85 (1.09 108926.77) | 12.4 (1.7e-42) |
|
8.1 (1.5e-7 ) |
|
9.6 (5.8e-8) |
| ICAM-1 | 1442.81 (0.86 – 84979.66) | 1.6 (0.02) | 0.9 (0.99) | 1.4 (0.8) | 1.9 (0.3) | 3.3 (0.02) |
| MCP-1 | 199.63 (54.55 – 1409.79) | 0.98 (0.99) | 1.0 (0.99) | 0.9 (0.99) | 1.1 (0.9) | 0.9 (0.9) |
| IFNg | 4.55 (0.03 3388.64) |
|
|
11.3 (5.2e-10) | 19.8 (1.0e-14) |
|
| TARC | 15.51 (0.33 787.98) |
|
|
2.9 (3.8e-2) |
|
3.2 (
|
| GM-CSF | 1.38 (0.01 70.64) |
|
4.1 (7.6e
|
2.4 (0.09) | 3.3 (0.01) | 2.6 (0.07) |
| IL-16 | 6.89 (0.01 99.04) |
|
2.0 (0.2) | 2.0 (0.2) | 2.5 (0.07) | 2.6 (0.07) |
| MIP-1b | 21.87 (5.08 412.17) |
|
3.1 (0.01) | 2.1 (0.2) | 2.8 (0.03) | 2.7 (0.07) |
| TNFa | 0.66 (0.07 36.61) |
|
2.4 (0.08) | 1.7 (0.4) | 2.1 (0.1) | 2.3 (0.1) |
| IL-8 | 30.89 (0.85 857.75) | 2.1 (
|
1.8 (0.03) | 1.3 (0.8) | 2.6 (0.05) | 3.1 (0.02) |
| VEGF-C | 31.80 (0.00 22287.80) |
|
2.9 (0.02) | 1.3 (0.8) | 2.4 (0.08) | 2.2 (0.2) |
| IL-12/IL23p40 | 17.61 (1.79 301.97) |
|
2.7 (0.03) | 2.2 (0.1) | 2.2 (0.1) | 1.8 (0.04) |
natureportfolio
Nicholas Vitanza
Last updated by author(s):
Reporting Summary
Statistics
n/a
□ X
□
□
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
□
□
□
□
□ For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
□ For hierarchical and complex designs, identification of the appropriate level for tests and full reporting of outcomes
□ Estimates of effect sizes (e.g. Cohen’s
Our web collection on statistics for biologists contains articles on many of the points above.
Confirmed
The exact sample size
the exact sample size
statement on whether measurements were taken from distinct samples or whether the same sample was measured repeatedly
he statistical test(s) used AND whether they are one- or two-sided
description of all covariates tested
a
full description of the statistical parameters including central tendency (e.g. means) or other basic estimates (e.g. regression coefficient) ND variation (e.g. standard deviation) or associated estimates of uncertainty (e.g. confidence intervals)
r null hypothesis testing, the test statistic (e.g.
sian analysis, inform
ation
the choice of priors and Markov chain Monte Carlo settings
biologists
” ” ” ” “
Software and code
Policy information about availability of computer code
Data
Policy information about availability of data
- Accession codes, unique identifiers, or web links for publicly available datasets
- A description of any restrictions on data availability
- For clinical datasets or third party data, please ensure that the statement adheres to our policy
Research involving human participants, their data, or biological material
| Reporting on sex and gender | Patients were eligible regardless of sex and gender. |
| Reporting on race, ethnicity, or other socially relevant groupings | Patients were eligible regardless of race and ethnicity. |
| Population characteristics | Characteristics are listed in Table 1 |
| Recruitment | Patients were recruited through physician and self-referral. Patients were recruited from both academic and community health centers. Patients received no financial compensation to enroll though bias may exist in the fact families required the means to travel to Seattle and stay locally during a portion of therapy. |
| Ethics oversight | This study was conducted in accordance with FDA and International Conference on Harmonisation Guidelines for Good Clinical Practice, the Declaration of Helsinki, and applicable institutional review board requirements, including study protocol approval by the Seattle Children’s Institutional Review Board. |
Field-specific reporting
Life sciences
Behavioural & social sciences □ Ecological, evolutionary & environmental sciences
For a reference copy of the document with all sections, see nature.com/documents/nr-reporting-summary-flat.pdf
Life sciences study design
| Sample size | Sample size was based on the phase
|
| Data exclusions | There was no excluded data. |
| Replication | Cytokine assays were performed in duplicate |
| Randomization | No randomization was performed as this was a non-randomized phase 1 clinical trial. |
| Blinding | No blinding was performed as this was a non-blinded phase 1 clinical trial. |
Reporting for specific materials, systems and methods
|
|
Involved in the study |
|
|
Antibodies |
|
|
|
|
|
|
|
|
Animals and other organisms |
|
|
|
|
|
|
nature portfolio | reporting summary April2023
Antibodies
| Antibodies used | FcR Blocking Reagent human (Miltenyi, cat#130-059-901, RRID:AB_2892112); Brilliant Stain Buffer (BD, cat#563794, RRID:AB_2869750); FVS520 (FITC, BD, cat#564407, RRID:AB_2869573); FVS510 (FVS510, BD, cat#564406, RRID:AB_2869572); CD36 (FITC, BD, cat#555454, RRID:AB_2291112); CD3 (V450, BD, cat#652356,RRID:AB_2868395); CD3 (FITC, BD, cat#555332, RRID:AB_395739); CD4 (BV605, BD, cat#562658, RRID:AB_2744420); CD4 (R718, BD, cat#567092, RRID:AB_2916435); CD8 (PerCPCy5.5, BD, cat#560662, RRID:AB_1727513); CD8 (BV605, BD, cat#564116, RRID:AB_2869551); Cetuximab (APC, BD, custom, RRID:AB_2459632). |
Validation
Clinical data
Policy information about clinical studies
Plants
n/a
n/a
n/a
Flow Cytometry
Plots
Confirm that:
The axis scales are clearly visible. Include numbers along axes only for bottom left plot of group (a ‘group’ is an analysis of identical markers).
All plots are contour plots with outliers or pseudocolor plots.
A numerical value for number of cells or percentage (with statistics) is provided.
Methodology
| Sample preparation | Patient cerebrospinal fluid (CSF) samples were collected via lumbar puncture or ventricular catheter and kept at
|
| Instrument | Identify the instrument used for data collection, specifying make and model number. |
| Software | FlowJo |
| Cell population abundance | Samples with lymphocytes count under the limit of quantitation (LOQ) requirement for the assay were excluded from reporting. CART cell detection status is determined by a combination of at least one detectable EGFRt+ cell count in the sample, as well as the level of Lymphocytes/EGFRt+% cell in the sample to be above the pre-defined limit of detection (LOD) for the assay. |
| Gating strategy | Gating strategy used for flow-based CAR detection in CSF. Selection of the singlet, viable [CD36-] lymphocyte population was performed prior to T cell gating and examination of the EGFRt+ CART cells and CD4/CD8 expression. |
Magnetic resonance imaging
Experimental design
| Design type | Clinical studies |
| Design specifications | Clinical studies |
| Behavioral performance measures | n/a |
| Acquisition Imaging type(s) | clinical studies |
| Field strength | 1.5T and 3T |
| Sequence & imaging parameters | Routine clinical MRI consisting of Brain = sagittal T1 MPRAGE at 1 mm with multiplanar reformats without and with contrast; axial and coronal T2; axial FLAIR; axial DWI with ADC maps; axial SWI. Spine = post-contrast axial and sagittal T1 |
| Area of acquisition | Brain and spinal cord |
| Diffusion MRI | Not used |
| Parameters Routine clinical DWI |
Preprocessing
| Preprocessing software | n/a |
| Normalization | n/a |
| Normalization template | n/a |
| Noise and artifact removal | n/a |
| Volume censoring | n/a |
Statistical modeling & inference
| Model type and settings | n/a | ||||
| Effect(s) tested |
|
||||
| Specify type of analysis: | □ | □ ROI-based | □ Both | ||
(See Eklund et al. 2016)
- □ Functional and/or effective connectivity
X □ Multivariate modeling or predictive analysis
nature portfolio | reporting summary