الرعاية الصحية على حافة الهاوية: مواجهة تحديات المجتمع المتقدم في السن في الولايات المتحدة Healthcare on the brink: navigating the challenges of an aging society in the United States
نظام الرعاية الصحية في الولايات المتحدة عند مفترق طرق. مع تزايد عدد السكان المسنين الذين يحتاجون إلى رعاية أكبر ونظام متوتر يواجه نقصًا في القوى العاملة، ومشكلات في القدرة، والتجزئة، هناك حاجة إلى حلول مبتكرة وإصلاحات سياسية. يهدف هذا البحث إلى إشعال الحوار والتعاون بين أصحاب المصلحة في الرعاية الصحية وإلهام العمل لتلبية احتياجات السكان المسنين. من خلال تحليل شامل لتأثير المجتمع المتقدم في السن، يبرز هذا العمل ضرورة معالجة هذه القضية وأهمية إعادة هيكلة نظام الرعاية الصحية ليكون أكثر كفاءة وعدلاً واستجابة.
تخضع الولايات المتحدة لتحول ديموغرافي وصحي سيكون له آثار عميقة على نظام الرعاية الصحية والمجتمع. تتقدم الفئة السكانية في العمر بمعدل غير مسبوق، حيث تصل جيل مواليد فترة الطفرة السكانية، المعروف بأنه أولئك الذين وُلدوا بين عامي 1946 و1964، إلى سن التقاعد ويعيشون لفترة أطول من أي وقت مضى. وفقًا لمكتب التعداد الأمريكي، بحلول عام 2030، سيكون جميع مواليد فترة الطفرة السكانية أكبر من 65 عامًا، مما يؤدي إلى أن يكون واحد من كل خمسة مقيمين في سن التقاعد.يمثل هذا التحول تحديًا مزدوجًا لنظام الرعاية الصحية: كيفية تلبية الاحتياجات الصحية المتزايدة والمعقدة لكبار السن، وكيفية ضمان استعداد النظام وتجهيزه لتقديم رعاية ذات جودة وعدالة لهذه الفئة المتزايدة من السكان.
تداعيات هذا التحول الديموغرافي بعيدة المدى. نظام الرعاية الصحية، كما هو مُهيكل حاليًا، غير مُستعد لمواجهة الطلبات المتزايدة التي ستفرضها هذه الفئة السكانية المتقدمة في السن.النظام أيضًا مجزأ وغير فعال ومكلف، مع وجود فجوات في التنسيق والجودة والوصول. علاوة على ذلك، لا يعالج النظام بشكل كافٍ المحددات الاجتماعية للصحة، مثل الدخل والتعليم والإسكان والنقل والدعم الاجتماعي، التي تؤثر على نتائج الصحة وسلوكيات الصحة لدى كبار السن.كما أنه لا يشارك بشكل كافٍ كبار السن ومقدمي الرعاية لهم في تخطيط وتقديم الرعاية، ولا يستفيد من إمكانيات نماذج الرعاية المجتمعية والرعاية المنزلية، التي يمكن أن تحسن من الوصول إلى الرعاية وجودتها وتكلفتها بالنسبة لكبار السن..
ومع ذلك، لا تنتهي التحديات هنا. هناك نقص متزايد في مقدمي الرعاية الصحية، مما يعني أن العرض وتوافر المهنيين المؤهلين والمهرة في مجال الرعاية الصحية، مثل الأطباء والممرضين والصيادلة والعاملين الاجتماعيين السريريين والفنيين، غير كافٍ وغير ملائم لتلبية الطلب واحتياجات السكان. هذه الظاهرة أكثر وضوحًا في البلدان ذات الدخل المنخفض والمتوسط، وكذلك في المناطق الريفية والنائية داخل الولايات المتحدة. وفقًا لمنظمة الصحة العالمية، كان عدد القوى العاملة الصحية العالمية 43.5 مليون في عام 2018، ومن المتوقع أن ينمو إلى 53.9 مليون بحلول عام 2030، لكنه لا يزال أقل من الطلب المقدر البالغ 80 مليون بحلول عام 2030، مما يؤدي إلى نقص عالمي. نقص قدره 18 مليون عامل صحي، معظمهم في البلدان ذات الدخل المنخفض والمتوسط. في الولايات المتحدة، تتوقع دراسة أجرتها جمعية كليات الطب الأمريكية (AAMC) نقصًا يصل إلى 139,000 طبيب بحلول إن نقص مقدمي الرعاية الصحية له تداعيات كبيرة على قطاع الصحة، حيث يؤثر على الوصول إلى الرعاية الصحية وجودتها وتكلفتها، بالإضافة إلى النتائج الصحية ورضا السكان.
وبالتالي، تواجه الولايات المتحدة مفارقة في الرعاية الصحيةمن جهة، هناك سكان مسنون يحتاجون إلى رعاية صحية متزايدة، ومن جهة أخرى، هناك نظام رعاية صحية متوتر يواجه نقصًا في القوى العاملة، وتحديات في القدرة الاستيعابية، وتفكك. يتطلب معالجة هذه المفارقة حلولًا مبتكرة، وإصلاحات سياسية، والتزامًا بإعادة هيكلة نظام الرعاية الصحية ليكون أكثر كفاءة، وعدلاً، واستجابة لاحتياجات مواطنيه المسنين.
على الرغم من أن العديد من هذه القضايا قد تكون في مقدمة اهتمامات متخصصي طب الشيخوخة، إلا أن العديد من أصحاب المصلحة الآخرين في نظام رعاية المسنين قد لا يفهمون الحجم الكامل للتحديات التي تسببت بها الزيادة السريعة في عدد المسنين أو قد يبالغون في تقدير استعدادهم للتغييرات الناتجة. وقد تم ملاحظة ذلك في استطلاع حديث لأصحاب المصلحة في سوق لقاحات البالغين، والذي يمثل قطاعًا حيويًا في صناعة رعاية المسنين.عند تقديم الزيادة المتوقعة في لقاحات البالغين، وهي اتجاه مدفوع إلى حد كبير باحتياجات السكان المسنين، لم يكن أصحاب المصلحة في السوق على دراية بالتعقيدات المرتبطة بذلك وتوقعوا تحديات بسيطة في اعتماد جداول اللقاحات الموسعة.بينما تمثل اللقاحات جزءًا فقط من سوق رعاية المسنين، من المعقول أن نعتقد أن هذا النقص في الفهم الشامل ينطبق على جميع القطاعات في صناعة رعاية المسنين.
تهدف هذه الورقة إلى تحفيز الحوار والتعاون بين أصحاب المصلحة في الرعاية الصحية، وإلهام العمل والابتكار لتلبية احتياجات وتطلعات السكان المسنين. لتحقيق ذلك، ستقدم هذه الدراسة تحليلاً شاملاً ونقدياً لتأثيرات وآثار المجتمع المتقدم في السن لتسليط الضوء على أهمية واستعجال هذه القضية.
ارتفاع موج احتياجات الرعاية الصحية: زيادة الطلب وتعقيد الرعاية
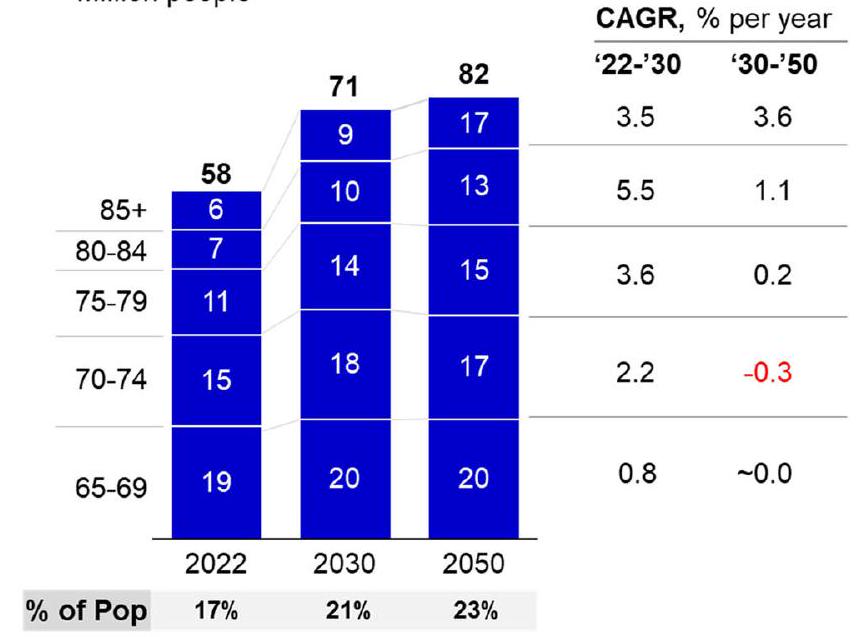
يشيخ السكان في الولايات المتحدة بسرعة بسبب عاملين مترابطين: شيخوخة جيل مواليد فترة الطفرة السكانية، وزيادة متوسط العمر المتوقع. يشكل جيل مواليد فترة الطفرة السكانية أكبر مجموعة في تاريخ الولايات المتحدة، حيث يضم حوالي 73 مليون عضو.مع وصول هذه الفئة إلى سن التقاعد، ستزداد نسبة السكان الذين تبلغ أعمارهم 65 عامًا فأكثر بشكل كبير، من 17% في عام 2022 إلى 21% في عام 2030، وإلى 23% في عام 2050 (الشكل 1A).بحلول عام 2050، سيزداد عدد الأمريكيين الذين تتراوح أعمارهم بين 65 عامًا وما فوقمن 58 مليون في 2022 إلى 82 مليون في 2050.
تقدم الفئة العمرية المتقدمة، وخاصة أولئك الذين تزيد أعمارهم عن 85 عامًا، تحديات جديدة للنظام الطبي. ستكون هذه الفئة هي الأسرع نموًا، حيث ستتضاعف من 6.5 مليون في عام 2022 إلى 17.3 مليون في عام 2050، وهو عدد يمكن مقارنته بعدد سكان ولاية نيويورك الحالي.غالبًا ما يعاني هؤلاء البالغون المسنون من حالات صحية متعددة ومعقدة، بما في ذلك الأمراض المرتبطة بالعمر التي تؤثر على قلوبهم وأدمغتهم وجهازهم المناعي. ومع ذلك، يفتقر النظام الطبي إلى الخبرة والمهارة لعلاج هذه الأمراض بفعالية وتقديم رعاية متخصصة وشخصية لهذه الفئة الضعيفة. سيؤدي زيادة حصة وحجم السكان المسنين إلى تأثيرات على الطلب والعرض في خدمات الرعاية الصحية والاجتماعية، فضلاً عن الاستقرار الاقتصادي والمالي للأمة.
أحد العوامل الرئيسية لزيادة الطلب على الرعاية الصحية واستخدامها بين كبار السن هو الانتشار العالي للحالات المزمنة المتعددة (MCCs)، والتي تُعرف بأنها وجود مرضين مزمنين أو أكثر يستمران لمدة عام على الأقل ويتطلبان رعاية طبية مستمرة أو يحدان من الأنشطة اليومية.وفقًا لمراكز السيطرة على الأمراض والوقاية منها (CDC)،من كبار السن لديهم على الأقل حالة مرضية مزمنة واحدة، ويجب أن يكون لدى المرضى على الأقل حالتين (الشكل 1B). تشمل هذه الحالات الشائعة مثل ارتفاع ضغط الدم، التهاب المفاصل، أمراض القلب، السرطان، السكري، وأمراض الكلى المزمنة. ترتبط الحالات المزمنة المتعددة بزيادة الوفيات، والعجز، وتدهور الوظائف، وانخفاض جودة الحياة. علاوة على ذلك، فإنها تشكل تحديات كبيرة لتقديم الرعاية الصحية وإدارتها، حيث تتطلب رعاية معقدة ومنسقة عبر عدة بيئات ومقدمي خدمات. وجدت دراسة أجراها ماكلين وآخرون (2019) أنه من بين المستفيدين من برنامج ميديكير الذين تتراوح أعمارهم بين 65 عامًا وما فوق، كان أولئك الذين يعانون من حالات مزمنة متعددة يمثلونمن إجمالي نفقات الرعاية الصحية في عام 2010، مقارنةً بـلمن لا يملكونكان متوسط الإنفاق السنوي لكل شخصلأولئك الذين لديهم أربعة أو أكثر من MCCs،لمن لديهم ثلاث MCCs،لأولئك الذين لديهم MCCs اثنين، ولأولئك
أ) تقديرات عدد السكان المسنين في الولايات المتحدة، حسب الفئة العمرية، مليون شخص
الشكل 1 | نمو عدد السكان المسنين وعبء الأمراض المزمنة. هذا الشكل
يوضح النمو المتوقع للسكان المسنين والزيادة المرتبطة في عبء الأمراض المزمنة. البيانات الخام مأخوذة من “2023 التعداد السكاني الوطني
جداول التوقعات: السلسلة الرئيسية”، التي تستخدم التقديرات الرسمية للسكان المقيمين
مع حالة MCC واحدة. تتناقض هذه الأرقام بشكل حاد مع الإنفاق على أولئك الذين ليس لديهم أي MCC.
من المتوقع أن تستمر أو حتى تزداد نسبة انتشار MCCs بين كبار السن في المستقبل، حيث ترتبط ارتباطًا وثيقًا بزيادة متوسط العمر المتوقع. مع عيش الناس لفترة أطول، فإنهم أكثر عرضة لتطوير وتراكم الأمراض المزمنة مع مرور الوقت، خاصة إذا كان لديهم عوامل خطر مثل التغيرات الفسيولوجية المرتبطة بالعمر، والتعرضات البيئية، وسلوكيات نمط الحياة، والاستعدادات الوراثية، والعوامل الاجتماعية المحددة للصحة. على سبيل المثال، وجدت دراسة أجراها كريمنز وبلتران-سانشيز أن الزيادة في متوسط العمر المتوقع في الولايات المتحدة بين عامي 1998 و2008 كانت مصحوبة بزيادة في عدد السنوات التي قضيت مع MCCs، خاصة بين كبار السن . قدرت الدراسة أن متوسط عدد السنوات التي قضيت مع MCCs زاد من 7.2 إلى 8.6 للرجال الذين تتراوح أعمارهم بين 65 عامًا وما فوق، ومن 10.0 إلى 11.3 للنساء اللواتي تتراوح أعمارهن بين 65 عامًا وما فوق. لذلك، سيواجه السكان المسنون عبئًا أكبر من الأمراض المزمنة وجودة حياة أقل في العقود القادمة. مما يزيد الأمور سوءًا، قد تتأثر صحة وطول عمر الجيل القادم من كبار السن أيضًا بعوامل خارجية جديدة، مثل السمنة، وتناول الأطعمة المعالجة، وتغيرات الميكروبيوم، وتغير المناخ، والأوبئة، والتلوث، التي يمكن أن يكون لها تأثيرات متنوعة وغير متوقعة على الأفراد المختلفين. يمكن أن تغير هذه العوامل أيضًا سلوكيات الصحة والوصول إلى الرعاية الصحية لكبار السن.
تحدٍ آخر ينشأ من متطلبات الأدوية للسكان المسنين هو تعدد الأدوية، والذي يُعرف بأنه الاستخدام المتزامن لخمس أدوية أو أكثر . يمثل الأفراد الذين تتراوح أعمارهم بين 65 عامًا وما فوق أكثر من ثلث جميع الأدوية الموصوفة في الولايات المتحدة . ومع ذلك، يمكن أن يكون لتعدد الأدوية عواقب سلبية، مثل زيادة خطر تفاعلات الأدوية، والأحداث السلبية للأدوية، وعدم الالتزام بالعلاج، وأخطاء الأدوية. يمكن أن تؤدي هذه إلى نتائج سيئة، مثل تقليل الفعالية، وزيادة المراضة والوفيات، وانخفاض جودة الحياة. لذلك، يتطلب تعدد الأدوية إدارة دقيقة للأدوية ومراقبة، بالإضافة إلى مراجعات منتظمة للأدوية وإيقافها عند الاقتضاء. وجدت دراسة أجراها قاتو وآخرون أن بين البالغين في الولايات المتحدة الذين تتراوح أعمارهم بين 65 عامًا وما فوق، زادت نسبة تعدد الأدوية من في 1999-2000 إلى في 2011-2012، وزادت نسبة استخدام الأدوية غير المناسبة المحتملة من إلى . كما وجدت الدراسة أن تعدد الأدوية كان مرتبطًا بزيادة معدلات زيارات قسم الطوارئ والدخول إلى المستشفى .
تداعيات الاقتصادية للسكان المسنين على قطاع الرعاية الصحية عميقة، حيث تؤثر ليس فقط على الإنفاق على الرعاية الصحية و
ب) البالغين في الولايات المتحدة الذين يعانون من حالات مزمنة، حسب الفئة العمرية، %
السكان في 1 يوليو 2022 كأساس لتوقع السكان في الولايات المتحدة من 2023 إلى 2100 (اللوحة أ) وبورسم، وآخرون، “نسبة انتشار الحالات المزمنة المتعددة بين البالغين في الولايات المتحدة، 2018” (اللوحة ب).
الجدول 1 | التحديات وتأثيرات ديناميات القوى العاملة في الرعاية الصحية
العامل
التداعيات
إحصائيات ملحوظة
شيخوخة القوى العاملة في الرعاية الصحية نفسها، مما يؤدي إلى زيادة التقاعد وتقليل ساعات العمل.
– سيواجه النظام فقدانًا كبيرًا في الخبرة والمهارة، بالإضافة إلى تقليل توفر العمال.
– وفقًا لإدارة الموارد والخدمات الصحية، فإن حوالي ثلث الممرضات المسجلات الحاليين تزيد أعمارهن عن 50 عامًا، وحوالي نصف الأطباء الحاليين تزيد أعمارهم عن 55 عامًا .
العرض غير الكافي من الوافدين الجدد إلى مهن الرعاية الصحية، بسبب القدرة التعليمية المحدودة، ومعدلات التسرب العالية، ومعدلات الاحتفاظ المنخفضة.
– سيواجه النظام نقصًا في العمال المؤهلين والمهرة، بالإضافة إلى نقص التنوع والتمثيل في القوى العاملة.
– سيستمر عرض خريجي الرعاية الصحية الجدد في التقييد بسبب القدرة المحدودة للمؤسسات التعليمية، والتكاليف العالية والديون التعليمية، وطبيعة المهن التنافسية والم demanding .
– وفقًا للرابطة الأمريكية لكليات التمريض، رفضت مدارس التمريض الأمريكية أكثر من 75,000 متقدم مؤهل في عام 2018 بسبب نقص أعضاء هيئة التدريس، ومواقع سريرية غير كافية، وقيود الميزانية .
– وفقًا لـ AAMC، زادت كليات الطب الأمريكية من تسجيلها بنسبة منذ عام 2002، لكن هذا لا يزال غير كافٍ لتلبية الطلب المتوقع على الأطباء .
التوزيع غير المتكافئ للقوى العاملة في الرعاية الصحية عبر المناطق الجغرافية، والتخصصات، والإعدادات، مما يؤدي إلى نقص في المناطق الريفية والنائية، والرعاية الأولية ورعاية المسنين، والرعاية المجتمعية والرعاية المنزلية.
– سيواجه النظام تفاوتات وفجوات في الوصول وجودة الرعاية لمجموعات سكانية مختلفة، خاصة كبار السن، الذين غالبًا ما يكون لديهم احتياجات متعددة ومعقدة.
– سيصبح توزيع العاملين في الرعاية الصحية أكثر انحرافًا نحو المناطق الحضرية والغنية، مما يترك المناطق الريفية والنائية مع عدد أقل من مقدمي الخدمات وأقل وصولًا .
– وفقًا لإدارة الموارد والخدمات الصحية، يعيش حوالي 60 مليون أمريكي في مناطق تعاني من نقص في مقدمي الرعاية الأولية، وحوالي 77 مليون أمريكي يعيشون في مناطق تعاني من نقص في مقدمي الرعاية الصحية النفسية .
– وفقًا للجمعية الأمريكية لطب المسنين، هناك حوالي 7,300 طبيب مسن معتمد في الولايات المتحدة، وهو أقل بكثير من الحاجة المقدرة البالغة 30,000 بحلول .
زيادة عبء العمل والضغط على العاملين في الرعاية الصحية، مما يؤدي إلى الإرهاق، وعدم الرضا، والتقلب
– قد يؤدي تسرب مقدمي الرعاية الصحية إلى زيادة مما يؤدي إلى تقليل إجمالي عدد الموظفين المتاحين.
– وفقًا لاستطلاع أجرته الرابطة الأمريكية للممرضات، أفاد أكثر من نصف الممرضات بأنهن يشعرن بالإرهاق من عملهن، وأفاد أكثر من ثلثهن بأنهن يشعرن بالإرهاق العاطفي .
– وفقًا لاستطلاع أجرته ميدسكيب، أفاد أكثر من من الأطباء بأنهم يشعرون بالإرهاق، وأفاد أكثر من بأنهم يشعرون بالاكتئاب .
استخدام الموارد، ولكن أيضًا القوى العاملة في الرعاية الصحية، وجودة الرعاية الصحية، وابتكار الرعاية الصحية. وفقًا لمكتب الميزانية في الكونغرس، من المتوقع أن يزيد الإنفاق الفيدرالي على برامج الصحة الرئيسية لكبار السن، مثل ميديكير وميديكيد، من من الناتج المحلي الإجمالي (GDP) في عام 2020 إلى من الناتج المحلي الإجمالي في . من المتوقع أن يقود هذا النمو الفئات العمرية الأكبر اختلافات في أنماط استخدام الرعاية الصحية وزيادة تعقيد الرعاية. على وجه التحديد، يُقدر أن البالغين الذين تتراوح أعمارهم بين يزورون الأطباء بشكل متكرر أكثر من البالغين الأصغر سنًا ويشهدون زيادة ثلاثية في معدلات الاستشفاء . يدفع هذا الاستخدام المتزايد وتعقيد الرعاية إلى زيادة الإنفاق كما ورد في دراسة مؤسسة كايزر للعائلة لعام 2019 التي وجدت أن إنفاق ميديكير للمستفيدين الذين تتراوح أعمارهم بين 65 إلى 74 عامًا يبلغ متوسطه ، والذي يتضاعف تقريبًا إلى لأولئك الذين تتراوح أعمارهم بين 85 عامًا وما فوق .
تتعدد احتياجات الرعاية الصحية بسبب شيخوخة السكان، وتشمل زيادة استخدام الخدمات، وزيادة انتشار الأمراض المزمنة، وزيادة الإنفاق على الرعاية الصحية، وإدارة الأدوية المعقدة. تضع هذه السيناريوهات مطالب غير مسبوقة على نظام الرعاية الصحية، مما يتطلب أساليب مبتكرة في تقديم الرعاية، والتخطيط المالي، وتخصيص الموارد. يتطلب التكيف مع هذه التغييرات جهدًا منسقًا من مقدمي الرعاية الصحية، وصانعي السياسات، وأصحاب المصلحة لضمان أن يكون النظام ليس فقط استجابة ولكن أيضًا مستدامًا في تلبية الاحتياجات المتطورة لمجتمع مسن. لذلك، من الضروري الاعتراف ومناقشة التأثير الذي ستحدثه هذه التطورات على الطلب على المهنيين في الرعاية الصحية، مثل الأطباء، والممرضات، والصيادلة، والمتخصصين في طب المسنين، الذين سيكونون حاسمين في تقديم الرعاية الكافية والمناسبة لكبار السن ذوي الاحتياجات الطبية المعقدة.
المشهد الصحي المثقل: تحديات تقديم الرعاية الصحية
من المتوقع أن يتجاوز الطلب على العاملين في الرعاية الصحية العرض، مما يؤدي إلى عجز متوقع قدره 1.2 مليون ممرض مسجل و121,900 طبيب بحلول . إن نقص القوى العاملة في الرعاية الصحية مدفوع بعدة عوامل، مثل شيخوخة القوى العاملة نفسها، وعدم كفاية العرض من الداخلين الجدد، والتوزيع غير المتكافئ عبر المناطق والتخصصات، وزيادة عبء العمل والضغط على العاملين. هذه العوامل
ملخصة في الجدول 1، مع آثارها وإحصائياتها الملحوظة.
سيكون لنقص مقدمي الرعاية الصحية تأثير متسلسل على النظام الصحي بأكمله، مما يؤثر على الجودة، والوصول، وتكلفة الرعاية. يؤدي نقص الأطباء إلى زيادة الوفيات، وتقليل الرعاية الوقائية، وزيادة الإنفاق على الرعاية الصحية . علاوة على ذلك، فإن نقص الأطباء يخلق بيئة تنافسية للمواهب، حيث تتنافس مقدمو الرعاية الصحية على مجموعة محدودة من المهنيين المتاحين. قد تؤدي هذه المنافسة إلى دمج القطاع، حيث تستحوذ مقدمو الرعاية الأكبر والأكثر ثراءً على أو تندمج مع مقدمي الرعاية الأصغر والأقل ربحية، مما يخلق اقتصاديات الحجم والنطاق. ومع ذلك، قد يكون لهذا الدمج أيضًا عواقب سلبية، مثل تقليل المنافسة، وزيادة القوة السوقية، وارتفاع الأسعار .
تعتبر التوظيف المناسب وتوفير العمالة ضروريين لتقديم الرعاية، لكنهما ليسا كافيين دون موارد وبنية تحتية كافية. ومع ذلك، فإن النظام الحالي ليس مستعدًا جيدًا للتعامل مع الزيادة في حجم وتعقيد الرعاية، مما يؤدي إلى الازدحام، وأوقات الانتظار، والتأخيرات، والإلغاءات، وتوزيع الرعاية. بعض العوامل التي تسهم في هذه الفجوة في الموارد تشمل:
حالة وأداء تقديم الرعاية. إن البنية التحتية في الولايات المتحدة في حالة سيئة وتحتاج إلى مزيد من الاستثمار والتحسين، حيث أعطى تقرير عام 2017 من الجمعية الأمريكية للمهندسين المدنيين لها درجة D+ . يهدر النظام حوالي مليار، أو من إنفاقه، كل عام على تكاليف غير ضرورية أو مفرطة، والاحتيال، وغيرها من عدم الكفاءة . كما أن هناك تباينًا كبيرًا في جودة ونتائج الرعاية عبر مقدمي الرعاية المختلفين، والأماكن، والمناطق، مما يمكن أن يؤدي إلى استخدام مفرط، أو غير كافٍ، أو غير صحيح للخدمات . على سبيل المثال، أظهر تقرير من مشروع أطلس دارتموث أن إنفاق Medicare لكل مستفيد تراوح بأكثر من ثلاثة أضعاف عبر المناطق، وأن المزيد من الإنفاق لم يعني جودة أو رضا أفضل .
نقص وعدم توازن الأسرة. شهدت الولايات المتحدة انخفاضًا في عدد أسرة المستشفيات لكل شخص من 4.5 في عام 1980 إلى 2.4 في عام 2018، مما يعكس الانتقال من الرعاية الداخلية إلى الرعاية الخارجية ومحاولات توفير التكاليف وتعزيز الكفاءة. ومع ذلك، فإن هذا الاتجاه يعني أيضًا أن هناك قدرة زائدة أقل للتعامل مع تقلبات الطلب، مثل خلال الأوبئة، والكوارث، أو التغيرات الموسمية.
علاوة على ذلك، فإن تخصيص الأسرة عبر الولايات والمناطق غير متساوٍ، مما يخلق اختلافات في الوصول وجودة الرعاية لمجموعات سكانية مختلفة . على سبيل المثال، فإن الولايات التي لديها أقل عدد من الأسرة لكل شخص هي نيفادا (1.8)، وأوريغون (1.8)، وواشنطن (1.9)، بينما الولايات التي لديها أعلى عدد من الأسرة لكل شخص هي ساوث داكوتا (4.1)، ونورث داكوتا (4.0)، وويست فيرجينيا .
عدم كفاية وعدم كفاءة التكنولوجيا. يتخلف نظام الرعاية الصحية في الولايات المتحدة عن الركب في اعتماد واستخدام تكنولوجيا المعلومات والاتصالات (ICT)، مثل السجلات الصحية الإلكترونية (EHRs)، والطب عن بُعد، وتبادل المعلومات الصحية (HIE)، والتي يمكن أن تحسن الجودة، والسلامة، وتنسيق الرعاية، فضلاً عن تقليل التكاليف والأخطاء في الرعاية . وفقًا لتقرير عام 2023 من منظمة التعاون والتنمية الاقتصادية (OECD)، وصلت الولايات المتحدة فقط إلى عتبة استخدام السجلات الصحية الإلكترونية في من مكاتب الأطباء، ومكاتب الأطباء المتخصصين، والمستشفيات، وغرف الطوارئ في . على الرغم من أن الولايات المتحدة تنضم إلى 17-21 دولة أخرى، اعتمادًا على الإعداد، التي حققت هذا الإنجاز، إلا أنها واحدة من الدول الأربع التي لم تبلغ عن وجود نظام ملزم في مكانه . نتيجة لذلك، فإن الوصول إلى السجلات غير متسق وقد يتطلب استخدام عدة بوابات لعرض جميع بيانات المريض الطبية، مما يعيق الفوائد التي قد تُلاحظ من خلال البيانات الطبية المشتركة عبر الممارسات . على سبيل المثال، دعمت تحليلات السجلات الصحية الإلكترونية الجهود للتنبؤ بمخاطر حالات مثل سكري الحمل والاكتئاب بعد الولادة بالإضافة إلى تقييم الاتجاهات الطبية خلال جائحة COVID-19 . لقد أدى الحجم الكبير من البيانات المستخدمة في مثل هذه الجهود إلى إثارة الاهتمام بتطبيق التعلم الآلي، وخاصة التعلم العميق، لتحليل العلاقات المعقدة والمتعددة المتغيرات القابلة للتحديد ضمن سجلات المرضى . على الرغم من الإمكانيات، هناك مخاوف متنوعة تنشأ مع رقمنة وتوافر مثل هذه السجلات، مثل الانتهاكات من خلال الهجمات الإلكترونية . سيكون إيجاد سبل لمعالجة هذه المخاوف المتعلقة بخصوصية المرضى خطوة مهمة نحو تحقيق الفوائد من التقدم في السجلات الصحية الإلكترونية وتحليلها لتحديد الاتجاهات الصحية.
ستكون الفجوة في الموارد في نظام الرعاية الصحية في الولايات المتحدة لها عواقب وخيمة على صحة ورفاهية السكان، وخاصة كبار السن، الذين هم أكثر عرضة للخطر ويعتمدون على توفر وجودة الرعاية. وجدت دراسة من صندوق الكومنولث أن الولايات المتحدة احتلت المرتبة الأخيرة بين 11 دولة ذات دخل مرتفع في نتائج الصحة وتجارب كبار السن، مع أعلى معدلات للوفيات، والإعاقة، والدخول إلى المستشفيات، والاحتياجات غير الملباة . علاوة على ذلك، ستؤثر الفجوة في الموارد على الابتكار والتنافسية في قطاع الرعاية الصحية في الولايات المتحدة، حيث ستحد من القدرة والفرصة لتطوير وتنفيذ طرق جديدة وأفضل لتقديم وتحسين الرعاية، مثل الصحة الرقمية، والطب الدقيق، والذكاء الاصطناعي (AI) .
يواجه نظام الرعاية الصحية في الولايات المتحدة أزمة في العرض، حيث إنه غير قادر على تلبية الاحتياجات المتزايدة والمعقدة للسكان المسنين. يعاني النظام من نقص في العمالة وقيود في الموارد، مما يؤدي إلى فجوة في القدرة تؤثر على الكفاءة، والعدالة، وجودة الرعاية. يتطلب معالجة هذه الأزمة نهجًا استراتيجيًا وشاملاً يتضمن زيادة كمية وجودة القوى العاملة في الرعاية الصحية، وتعزيز توفر وإمكانية الوصول إلى موارد الرعاية الصحية، وتحسين أداء وإنتاجية تقديم الرعاية الصحية. يتطلب تحقيق هذه الأهداف التعاون والتنسيق بين مقدمي الرعاية الصحية، وصانعي السياسات، وأصحاب المصلحة، فضلاً عن الالتزام والاستثمار في قطاع الرعاية الصحية.
التجزئة والفجوة في تقديم الرعاية الصحية: تحديات الوصول و”فجوة الأغنياء والفقراء”
يواجه نظام الرعاية الصحية في الولايات المتحدة تحديًا ليس فقط في تلبية الطلب والعرض على الرعاية الصحية، ولكن أيضًا في ضمان أن تكون الرعاية الصحية متاحة وميسورة التكلفة لجميع شرائح السكان، وخاصة كبار السن، الذين غالبًا ما يواجهون حواجز وصعوبات في الحصول على الرعاية التي يحتاجونها واستخدامها. يتميز النظام بالتجزئة والفجوة، مما يعني أن تقديم الرعاية الصحية مقسم وغير متصل عبر
مقدمي الرعاية المختلفين، والدافعين، والإعدادات، وأن نتائج وتجارب الرعاية الصحية تختلف على نطاق واسع عبر مجموعات، ومناطق، وظروف مختلفة. تخلق هذه الميزات من النظام عدم كفاءة، وعدم عدالة، وعدم اتساق في الوصول وجودة الرعاية، مما يمكن أن يكون له تأثيرات سلبية على صحة ورفاهية السكان.
ت stems from the lack of a universal and integrated system of healthcare coverage and delivery, which leads to gaps and overlaps in the coordination, continuity, and comprehensiveness of care . يتكون النظام من عدة دافعين متنافسين، مثل شركات التأمين الخاصة، والبرامج العامة، والأفراد الذين يدفعون من جيوبهم، كل منهم لديه معايير الأهلية الخاصة به، وحزم الفوائد، وآليات الدفع، والقواعد الإدارية. وهذا يخلق مشهداً معقداً ومربكاً للمستهلكين والمقدمي الرعاية، الذين يتعين عليهم التنقل عبر سياسات وإجراءات ومتطلبات مختلفة وغالباً ما تكون متعارضة. علاوة على ذلك، يتكون النظام من مقدمي رعاية مستقلين ومتعددين، مثل المستشفيات، والعيادات، والأطباء، والممرضات، والصيادلة، وغيرهم، كل منهم لديه أنماط ممارسة ومعايير جودة وأنظمة معلومات خاصة به. وهذا يخلق مشهداً معزولاً ومفككاً لتقديم وإدارة الرعاية، مما يمكن أن يؤدي إلى التكرار، والتجزئة، والفجوات في عملية الرعاية.
تجزئة نظام الرعاية الصحية في الولايات المتحدة لها آثار كبيرة على الوصول وجودة الرعاية، خاصة بالنسبة لكبار السن، الذين غالباً ما لديهم احتياجات متعددة ومعقدة تتطلب رعاية منسقة وشاملة عبر بيئات ومقدمي رعاية مختلفين. يمكن أن تؤدي التجزئة إلى نتائج سيئة، مثل زيادة الأخطاء، والمضاعفات، وإعادة الدخول إلى المستشفى، والتكاليف، فضلاً عن تقليل الرضا والثقة والالتزام.. على سبيل المثال، أظهرت دراسة أجراها فام وآخرون أن بين المستفيدين من ميديكير الذين تتراوح أعمارهم بين 65 عاماً وما فوق، أولئك الذين لديهم أربع حالات مزمنة أو أكثر وزاروا 10 أطباء أو أكثر كانت لديهم ضعف معدل دخول المستشفى القابلة للتجنب مقارنة بأولئك الذين زاروا طبيبين أو أقل . علاوة على ذلك، يمكن أن تؤدي التجزئة إلى احتياجات غير ملباة، مثل تأخير أو تفويت الرعاية، فضلاً عن زيادة الأعباء، مثل النفقات من الجيب، وصعوبات النقل، ومسؤوليات الرعاية . على سبيل المثال، بين المستفيدين من ميديكير الذين تتراوح أعمارهم بين 65 عاماً وما فوق، أفادوا بأنهم واجهوا صعوبة في الحصول على مواعيد في الوقت المناسب، أفادوا بأنهم واجهوا صعوبة في الحصول على الفحوصات أو العلاجات اللازمة، و9% أفادوا بأنهم واجهوا صعوبة في الحصول على الأدوية اللازمة .
تنبع الفجوة في نظام الرعاية الصحية في الولايات المتحدة من التوزيع غير المتكافئ وغير العادل لموارد الرعاية الصحية، والفرص، والنتائج عبر مجموعات ومناطق وظروف مختلفة، مما يؤدي إلى فجوات واختلافات في الوصول، وجودة، وقابلية تحمل الرعاية . يتأثر النظام بعوامل مختلفة، مثل الدخل، والتعليم، والعرق، والاثنية، والجنس، والعمر، والجغرافيا، والإعاقة، التي تؤثر على الحالة الصحية وسلوكيات الصحة للسكان، فضلاً عن توفر واستخدام خدمات الرعاية الصحية. هذه العوامل تخلق مشهداً متنوعاً وغير متجانس للمستهلكين والمقدمي الرعاية، الذين يواجهون تحديات وحواجز مختلفة وغالباً ما تكون غير متناسبة في الحصول على الرعاية وتقديمها. علاوة على ذلك، يتأثر النظام بسياسات وبرامج وممارسات مختلفة، مثل معدلات التعويض، ومعايير الجودة، والحوافز، التي تؤثر على تخصيص وتوزيع موارد الرعاية الصحية، مثل القوى العاملة، والمرافق، والمعدات، والتكنولوجيا. هذه السياسات والبرامج والممارسات تخلق مشهداً ديناميكياً ومعقداً للدافعين وصانعي السياسات، الذين يجب عليهم موازنة وتنسيق المصالح والأهداف المتنافسة والمتعارضة لأصحاب المصلحة في الرعاية الصحية.
مع زيادة الطلب على خدمات الرعاية الصحية بسبب شيخوخة السكان، وبقاء عرض العاملين في الرعاية الصحية والموارد غير كافٍ وغير ملائم، يظهر شكل جديد من التجزئة والفجوة في نظام الرعاية الصحية في الولايات المتحدة: الفجوة بين الأغنياء والفقراء. يشير هذا إلى الظاهرة التي تجذب فيها المناطق الغنية والحضرية المزيد من المهنيين والمرافق الصحية الأفضل، بينما تُترك المناطق الفقيرة والريفية مع خيارات رعاية صحية أقل وأدنى. وهذا يخلق دورة مفرغة، حيث تتمتع المناطق الغنية بمزيد من الوصول وجودة الرعاية، بينما تعاني المناطق الفقيرة من قلة الوصول وجودة الرعاية، مما يؤدي إلى اتساع الفجوات الصحية والاقتصادية بينهما.
أحد العوامل التي تسهم في هذا الشكل الجديد من التجزئة والفجوة هو الطبيعة المدفوعة بالسوق والتنافسية لقطاع الرعاية الصحية في الولايات المتحدة، حيث يتم تحفيز مقدمي الرعاية الصحية من خلال الحوافز والمكافآت المالية للعمل في المناطق والتخصصات التي تقدم تعويضات واعترافات أعلى. وهذا يخلق وضعاً حيث يكون عرض العاملين في الرعاية الصحية مائلاً نحو المناطق والتخصصات التي لديها طلب وموارد أكبر، مثل المناطق الحضرية والغنية، ورعاية التخصصات والفرعية. على العكس، يكون عرض العاملين في الرعاية الصحية نادراً في المناطق والتخصصات التي لديها طلب وموارد أقل، مثل المناطق الريفية والنائية، ورعاية الرعاية الأولية وكبار السن. وهذا يؤدي إلى عدم تطابق بين الاحتياجات وتوفر القوى العاملة في الرعاية الصحية، مما يؤثر على الوصول وجودة الرعاية للسكان المختلفين.
أحد الأمثلة التي توضح هذا الشكل الجديد من التجزئة والفجوة هو ارتفاع عدد الممرضات المتنقلات، اللواتي هن ممرضات مسجلات مع تدريب متقدم وشهادات في تخصصات مختلفة، ويعملن على أساس مؤقت أو تعاقدي في مواقع وإعدادات مختلفة. هذه الممرضات مطلوبة بشدة، حيث يمكنهن سد الفجوات والنقص في أطباء التخدير (أي، مربية تخدير متنقلة) أو غيرهن من الممرضات المتخصصات، اللواتي غالباً ما يتركزن في المراكز الحضرية والأكاديمية. علاوة على ذلك، يتم تعويض هؤلاء الممرضات بشكل جيد، حيث يمكنهن كسب رواتب ومزايا أعلى بكثير من الممرضات العاديات ولديهن مزيد من المرونة والاستقلالية في اختيار مهامهن وجداولهن. ومع ذلك، تساهم هؤلاء الممرضات أيضاً في تجزئة وفجوة نظام الرعاية الصحية، حيث يميلن للعمل في المناطق والإعدادات التي تقدم المزيد من الفرص والمكافآت، مثل المناطق الغنية والحضرية، والمستشفيات الخاصة والمتخصصة. وهذا يترك المناطق والإعدادات التي لديها فرص ومكافآت أقل، مثل المناطق الفقيرة والريفية، والمرافق العامة والرعاية الأولية، مع عدد أقل من العاملين في الرعاية الصحية المؤهلين، مما يؤثر على الوصول وجودة الرعاية للسكان الذين يخدمونهم.
يتطلب معالجة تحدي التجزئة والفجوة في نظام الرعاية الصحية في الولايات المتحدة نهجاً شمولياً ومتكاملاً يتضمن تحسين التنسيق واستمرارية الرعاية، وتعزيز العدالة والشمولية في الرعاية، وضمان قابلية تحمل واستدامة الرعاية. يتطلب تحقيق هذه الأهداف التعاون والتنسيق بين مقدمي الرعاية الصحية، والدافعين، وصانعي السياسات، وأصحاب المصلحة، فضلاً عن الالتزام والاستثمار في قطاع الرعاية الصحية.
التدخلات، إصلاح السياسات، والمقارنة العالمية
مع زيادة عدد الأفراد الذين يعيشون في الثمانينيات والتسعينيات وما بعدها بشكل كبير، تحول التركيز من إطالة العمر إلى تعزيز جودة هذه السنوات الإضافية. يُعرف هذا النهج باسم ‘تأخير الشيخوخة’، وقد شمل استثمارات في التكنولوجيا والسياسات التي تزيد من عدد السنوات التي تُعاش دون تراكم الحالات المزمنة وغيرها من الآثار الجانبية للشيخوخة. سيؤدي تحقيق ذلك إلى ضغط الأمراض، مما يعني أن الأمراض المزمنة ستتركز في فترة أقصر نحو نهاية الحياة. لن يكون لهذا التحول تأثير على الصحة العامة للسكان فحسب، بل سيكون له أيضاً تأثير مالي إيجابي. على سبيل المثال، قدرت دراسة أجراها غولدمان وآخرون في عام 2013 أن تأخير الشيخوخة على نطاق واسع سيوفر للولايات المتحدة تريليون دولار بحلول عام 2060.
يعتبر مجال علم الشيخوخة الناشئ مركزياً لزيادة عدد السنوات الصحية في السكان الأكبر سناً. يسعى هذا التخصص لفهم العلاقة بين الشيخوخة والأمراض المرتبطة بالعمر، بهدف التخفيف من الأخيرة من خلال استهداف العمليات البيولوجية للشيخوخة نفسها.تتضمن استراتيجية رئيسية تحديد العلامات الحيوية وعوامل الخطر، مثل الخيارات الاجتماعية والاقتصادية ونمط الحياة، التي تتنبأ بتطور المرض في مراحل الحياة اللاحقة (الجدول 2). لقد مكنت التقدمات التكنولوجية من تجميع مجموعات بيانات متعددة الأوميات الكبيرة والسجلات الطبية الطولية من مجموعات مرضى متنوعة وأنسجة متقدمة في العمر.. تشمل هذه الدم، الدماغ، العضلات، القلب، الكبد، المفاصل، الهيكل العظمي، الدهون، من بين أمور أخرى. على سبيل المثال، شراكة تسريع الأدوية ‘s (AMP برنامج مرض الزهايمر قد استخدم تحليلات متعددة الأوميات للبيانات الجزيئية من عينات الدماغ البشري لتحديد أكثر من 500 هدف فريد لمرشحات الأدوية.. توفر هذه الثروة من المعلومات فرصة غير مسبوقة للاستفادة من منهجيات الذكاء الاصطناعي لفك رموز العلامات الفريدة للمرضى وتحديد التدخلات المحتملة.
بمجرد تحديد هذه العوامل المسببة للمخاطر، يمكن للباحثين تطوير تدخلات تصحح أو تخفف منها. وتشمل هذه معالجة قضايا مثل شيخوخة المناعة، الالتهاب النسيجي المزمن منخفض الدرجة، السمنة، نقص الميتوكوندريا المرتبط بالعمر، وأمراض البروتينات الدماغية.على سبيل المثال، تهدف الدراسات السريرية مع العوامل المناعية المستهدفة الجديدة إلى تجديد نظام المناعة المتقدم في السن باستخدام مؤشرات الشيخوخة المناعية كنقاط نهاية بديلة.الأمل هو أن استعادة صحة المناعة يمكن أن تترجم إلى آثار مفيدة على الأنظمة الوعائية والقلبية والدماغية والكلوية. إن ظهور فئة أدوية GLP-1 (مثل سيماجلوتيد وتيرزيباتيد)، التي لا تملك فقط القدرة على منع الأمراض المرتبطة بالسمنة في وقت لاحق من الحياة، بل تقدم أيضًا طريقًا واعدًا لعكس الشيخوخة الأيضية وقد تعزز حتى إصلاح الحمض النووي في الأمراض التنكسية العصبية.الحفاظ على وظيفة العضلات أمر بالغ الأهمية أيضًا، خاصة في سياق الشيخوخة أو الحالات المزمنة مثل الساركوبينيا.تقدم الرؤى حول عوامل تعزيز العضلات والقدرة على تحريك وتمايز خلايا جذع العضلات مجالات حاسمة لتعزيز الشيخوخة الصحية.الهندسة الحيوية، بما في ذلك تطوير الهياكل الخارجية لمرضى إصابات العمود الفقري، تقدم حلولاً محتملة للحفاظ على القدرة على المشي خلال الشيخوخة..
قد تشمل التدخلات المستقبلية تحليلات طولية لسلامة الجينوم والحفاظ على أنظمة دقة الحمض النووي. تقليل تراكم الطفرات الجسدية، التي ترتبط بتقدم العمر في نخاع العظام.خلل في خلايا النخاع (تكون الدم النسلي)خلل في جدار الأوعية الدمويةوأورام الدمقد يكون ذلك ممكنًا. لقد أظهرت التجارب الناجحة الأولى في العلاج الجيني وتحرير الجينات ضوءًا جديدًا ووعدًا في الأمراض البشرية، مما يشير إلى أن استعادة سلامة الجينوم البشري وأنظمة الخلايا قد تكون في متناول تقنيتنا بشكل متزايد. يمكن أن يمتد ذلك لاستعادة الوظيفة في الأمراض المناعية الذاتية والأمراض الليفية، مما يبرز المزيد من الإمكانيات التحولية لعلم الشيخوخة والتكنولوجيا في تحسين الرعاية الصحية لكبار السن.
مع تقدم مجال علم الشيخوخة، هناك خطر كبير من أن هذه الابتكارات قد تفيد بشكل أساسي أولئك الذين يمتلكون موارد كبيرة، مما يزيد من الفجوة بين الأغنياء والفقراء في رعاية المسنين ويبرز نوعًا من عدم المساواة التي قد يواجهها كبار السن في المستقبل. هناك بالفعل أدلة على أن تقليص الأمراض قد يكون ناتجًا أكثر عن العوامل الاجتماعية والاقتصادية من العوامل البيولوجية.. ومع ذلك، لا نزال لا نعرف ما هي التحديات الأخرى التي قد تواجهها هذه الأجيال المستقبلية. ستؤثر العوامل الاجتماعية والاقتصادية الجديدة والناشئة والعوامل المرتبطة بالمجموعات المهمشة في الفئات الشابة على كبار السن في المستقبل بشكل غير معروف حتى الآن. من المحتمل أن تؤثر المتطلبات الصحية المتغيرة للفئات السكانية الشابة، التي تتميز بعوامل مثل زيادة الرعاية المعززة للجنس، وتصاعد مشكلات الصحة النفسية، وسوء استخدام المواد، بما في ذلك المواد الأفيونية، على مشهد رعاية كبار السن في المستقبل بطرق غير معروفة حاليًا. تعتبر أزمة المواد الأفيونية، كما تم توضيحها في رواية باربرا كينغسولفر “ديمون كوبرهيد”، مثالًا على كيفية تأثير التحديات الصحية والاجتماعية السائدة على الصحة العامة وأنظمة الرعاية الصحية على المدى الطويل بشكل كبير.. هذه السردية، التي تعكس المشكلة الاجتماعية الأوسع المتعلقة بإساءة استخدام المواد، تؤكد على أهمية دمج العدالة كعامل أساسي في قرارات سياسة الرعاية الصحية. إن ضمان أن تكون تحسينات الرعاية الصحية، بما في ذلك تلك التي تنشأ من علم الشيخوخة، متاحة للجميع، بغض النظر عن وضعهم الاجتماعي والاقتصادي، أمر حيوي لمنع تفاقم الفجوة الاقتصادية في رعاية المسنين.
لهذا الغرض، أطلقت الولايات المتحدة إصلاحات سياسية على مدى العقدين الماضيين تهدف إلى تأمين الرعاية الصحية العادلة لمواطنيها المسنين. تسعى هذه التدابير إلى مواجهة التحديات البارزة في إمكانية الوصول إلى الخدمات وجودتها والجدوى المالية للخدمات التي تلبي احتياجات كبار السن. يعتبر توسيع برنامج Medicaid بموجب قانون الرعاية الميسورة (ACA)، الذي تم إقراره في عام 2010، حجر الزاوية لهذه المبادرات، حيث يعزز نطاق Medicaid ليشمل مزايا أفضل، وتخفيضات في التكاليف، وتحسين رعاية المسنين.. بشكل ملحوظ، قام قانون الرعاية الميسرة (ACA) بتقليل فجوة تغطية الأدوية في الجزء D من ميديكير، أو ما يُعرف بـ “فجوة الدواء”، مما يحسن الرعاية الوقائية دون مشاركة في التكاليف. تهدف مبادرات إضافية، مثل ميديكير أدفانتج، إلى تحسين تنسيق رعاية المسنين من خلال السماح لمستفيدي ميديكير بالتسجيل في خطط الرعاية المدارة (ميديكير أدفانتج). على سبيل المثال، سجلت ميديكير أدفانتج أكثر من 30.8 مليون فرد في عام 2023 وحده، وتمثل الآن أكثر من من جميع كبار السن الذين يتلقون ميديكير.
الجدول 2 | المؤشرات الحيوية التشخيصية للأمراض المرتبطة بالعمر وآثارها على الممارسة السريرية
عوامل الخطر التشخيصية
اختيار العلامات الحيوية
التغيير مع العمر
الأثر الفسيولوجي
الأمراض المرتبطة
اختبار
الاستخدام في الطب
مرجع
التهاب مزمن. (شيخوخة الالتهاب)
CRP؛ IL-6؛ TNF-; IL-1
زيادة
يؤدي إلى التهاب النظام مما يسبب تلف الأنسجة، استجابة مناعية متغيرة، وزيادة خطر الإصابة بأمراض القلب والأوعية الدموية المرتبطة بالشرايين.
أمراض القلب والأوعية الدموية؛
هشاشة
الخرف
مرض الكلى المزمن
DM؛
سرطان
الاكتئاب
ساركوبينيا
اختبارات الدم؛ اختبار بروتين سي التفاعلي عالي الحساسية
مستخدم حاليًا
90
الصحة الأيضية (أيض الجلوكوز، فرط سكر الدم)
الجلوكوز الصائم؛ HbA1c؛
مستويات الأنسولين
اضطراب
يؤثر سلبًا على استخدام الجلوكوز، مما يؤدي إلى ارتفاع مستوى السكر في الدم ويساهم في تلف الأوعية الدموية ومقاومة الأنسولين.
أمراض القلب والأوعية الدموية؛ تدهور إدراكي؛ السكري من النوع الثاني؛
متلازمة الأيض
اختبارات الدم (HbA1c، اختبار الجلوكوز، تحليل الأنسولين)
مستخدم حاليًا
91
وظيفة العضلات (الساركوبينيا)
كتلة العضلات؛ قوة القبضة؛ سرعة المشي؛ DEXA
انخفاض
يقلل من قوة ووظيفة العضلات الهيكلية، يعيق الحركة ويزيد من خطر السقوط
الساركوبينيا؛ الهشاشة؛ زيادة خطر السقوط والدخول إلى المستشفى؛ انخفاض الحركة والاستقلالية
التقييمات البدنية؛ DXA؛ CT؛ MRI؛ BIA
مستخدم حاليًا
92
هزال/سمنة
مؤشر كتلة الجسم؛ محيط الخصر؛ تكوين الجسم.
يختلف
يغير تنظيم الأيض، يزيد من الحمل الميكانيكي على المفاصل، ويساهم في الالتهاب الجهازي.
مرض السكري؛ أمراض القلب والأوعية الدموية؛
التهاب المفاصل العظمي
انقطاع النفس أثناء النوم
بعض أنواع السرطان (مثل: الثدي، القولون)؛ المخاطر والمضاعفات الجراحية
القياس البدني؛ DXA؛ BIA
مستخدم حاليًا
93
بصمة شيخوخة المناعة
تحديد المناعة الخلوية؛ علامات الخلايا المتقدمة في السن؛ خلايا T خالية من CD28
خلل المناعة
يؤدي إلى انخفاض المراقبة المناعية وزيادة انتشار الخلايا الشيخوخة مما يساهم في خلل الأنسجة.
زيادة القابلية للإصابات؛ اضطرابات المناعة الذاتية؛
سرطان
خفض VE
تدفق الخلايا؛ SA--تلوين الجال; تصنيف المناعة
قريبًا سيكون تشخيصيًا
94
عوامل الخطر الوراثية
تعدد الأشكال الجينية؛ SNPs
مستقر ولكن يؤثر على خطر المرض
تؤثر على المسارات الأيضية والاستجابات المناعية، مما يعرض الأفراد لمجموعة متنوعة من الحالات المزمنة.
متلازمة الأيض
أمراض القلب والأوعية الدموية؛
مرض الزهايمر
بعض أنواع السرطان؛
استجابة للأدوية
علم الوراثة الدوائية
الفحص الجيني؛ مصفوفات SNP
استكشافي
95,96
الميكروبيوم
تركيبات الميكروبات؛ ملفات الأحماض الدهنية قصيرة السلسلة
التغييرات مع النظام الغذائي، استخدام المضادات الحيوية
يؤثر على وظيفة حاجز الأمعاء، والالتهاب الجهازي، واستقلاب المغذيات.
اضطرابات الجهاز الهضمي؛ اختلال التمثيل الغذائي (مثل السمنة، السكري);
أمراض المناعة الذاتية؛
اضطرابات المزاج
تسلسل جين الرنا الريبوسومي 16S؛ تسلسل الميتاجينوم
استكشافي
90
طول التيلومير
طول التيلومير
يختصر
تقصر التيلوميرات مرتبط بالشيخوخة الخلوية وزيادة خطر الأمراض المرتبطة بالعمر.
أمراض القلب والأوعية الدموية، أنواع مختلفة من السرطان؛
OP;
السكري;
زيادة خطر الوفاة
PCR الكمي؛ تحليل طول التيلومير
استكشافي
97
علامات الإجهاد التأكسدي
MDA؛ 8-OHdG؛ القدرة المضادة للأكسدة
يزيد
يسبب ضررًا خلويًا ويساهم في عملية الشيخوخة وتطور الأمراض المرتبطة بالعمر.
الأمراض العصبية التنكسية؛ أمراض القلب والأوعية الدموية؛
السرطان؛ التنكس البقعي المرتبط بالعمر
اختبارات الدم؛ ELISA؛ الطيف الضوئي
استكشافي
98
مستويات فيتامين د
25-هيدروكسي فيتامين د
تختلف مع التعرض والتناول
تؤثر على صحة العظام، وظيفة المناعة، وقد ارتبطت بانخفاض خطر العديد من الأمراض المزمنة.
OP؛ أمراض القلب والأوعية الدموية؛
T2D؛
MS؛
الاكتئاب؛
بعض أنواع السرطان
اختبارات الدم (اختبار 25-هيدروكسي فيتامين د)
استكشافي
99
8-OHdG 8-هيدروكسي-2′-ديوكسي جوانوزين، AMD التنكس البقعي المرتبط بالعمر، ASCVD مرض القلب والأوعية الدموية التصلبي، BIA تحليل مقاومة الكهرباء الحيوية، BMI مؤشر كتلة الجسم، CIR محيط، CKD مرض الكلى المزمن، comp. التركيب، CPR بروتين سي التفاعلي، CT التصوير المقطعي المحوسب، CV مرض القلب والأوعية الدموية، DEXA قياس كثافة العظام بالأشعة السينية ثنائية الطاقة، DM السكري، Dysreg. عدم التنظيم، ELISA اختبار الامتزاز المناعي المرتبط بالإنزيم، GI مرض الجهاز الهضمي، HDA1c الهيموغلوبين A1C، IL إنترلوكين، MDA مالونديالديهايد، MRI التصوير بالرنين المغناطيسي، MS التصلب المتعدد، NDDs الأمراض العصبية التنكسية، OP هشاشة العظام، PCR تفاعل البوليميراز المتسلسل، Ref المراجع، SA--غال المرتبط بالشيخوخة -غالكتوزيداز، SCFA الأحماض الدهنية قصيرة السلسلة، SNPs تعدد أشكال النوكليوتيد المفرد، T2D السكري من النوع 2، TNF- عامل نخر الورم- , VE فعالية اللقاح.
كجزء من نماذج حماية المرضى، أظهرت منظمات الرعاية المسؤولة (ACOs) أيضًا فعالية في تحسين تنسيق الرعاية، مما أدى إلى تحسين نتائج المرضى وتقليل التكاليف. تقرير عام 2021 من مراكز خدمات Medicare و Medicaid (CMS) يؤكد أن ACOs حققت مليار في المدخرات الإجمالية و مليار في المدخرات الصافية لميديكير بين 2021 و 2022، بينما حسنت أيضًا جودة الرعاية . جنبًا إلى جنب مع هذه النماذج، أدت التحسينات في خدمات الرعاية والدعم طويلة الأجل من خلال توسيع خدمات المنزل والمجتمع (HCBS) عبر Medicaid إلى توسيع الوصول بشكل كبير إلى الرعاية طويلة الأجل المخصصة . تهدف هذه الخدمات إلى تسهيل كبار السن ‘للشيخوخة في مكانهم . في عام 2019 وحده، بلغت نفقات Medicaid HCBS حوالي مليار، مما يبرز اتجاهًا مستمرًا نحو زيادة الاستثمار في الخدمات التي تعزز الاستقلال والكرامة لكبار السن . بالإضافة إلى ذلك، يمثل هذا نهجًا فعالًا من حيث التكلفة للرعاية طويلة الأجل من خلال تقليل الاعتماد على بيئات الرعاية المؤسسية الأكثر تكلفة.
على الصعيد الدولي، اعتمدت الدول استراتيجيات متنوعة لتلبية احتياجات الرعاية الصحية لسكانها المتقدمين في السن. تركز اليابان وألمانيا، على سبيل المثال، على نماذج الرعاية المتكاملة والحلول المعتمدة على التأمين، مثل التأمين الصحي القانوني في ألمانيا المدعوم بتأمين الرعاية طويلة الأجل وتأمين الرعاية طويلة الأجل في اليابان . ومع ذلك، تواجه اليابان، كواحدة من أقدم السكان في العالم، تحديات فريدة في الحفاظ على قوة العمل في مجال الرعاية الصحية . في محاولة لتعويض ذلك، وضعت هذه الدولة نفسها في طليعة أتمتة رعاية المسنين بما في ذلك تطوير تقنيات مثل ‘روبوتات الرعاية’، لتحسين جودة الرعاية في دور رعاية المسنين . على غرار اليابان، نفذت سنغافورة أيضًا حلول الرعاية الصحية التكنولوجية لسكانها المتقدمين في السن، مستثمرة في تحسين الطب عن بُعد، وتطبيقات مراقبة الصحة عن بُعد، وتقنيات الرفاهية القابلة للارتداء، وحلول المنازل الذكية (مثل أجهزة استشعار اكتشاف السقوط) لتسهيل العيش المستقل وتقليل العبء على نظام الرعاية الصحية . هذه الدولة حاليًا في المرتبة الثانية في العالم من حيث أعلى متوسط عمر متوقع، مقارنة بالولايات المتحدة عند . السويد، رقم 20 في تلك القائمة ، معترف بها دوليًا كنموذج لرعاية المسنين. إنها دولة أخرى تركز بشدة على ‘الشيخوخة في المكان’ من خلال توفير رعاية ممولة بشكل كبير من خلال الضرائب البلدية والمنح الحكومية .
الخاتمة
غالبًا ما يقال إنه دائمًا هناك غد، مما يعني أنه يمكننا تأجيل أفعالنا وقراراتنا إلى تاريخ لاحق. ومع ذلك، لا يمكن أن يكون هذا الشعور صحيحًا بعد الآن عندما يتعلق الأمر برعاية السكان المتقدمين في السن. لكي يكون لدينا غد مزدهر، يجب أن نبدأ التخطيط والعمل اليوم. إن شيخوخة السكان ليست سيناريو بعيد أو افتراضي، بل هي واقع حاضر وحتمي. لا يمكننا تحمل الانتظار ورؤية ما يحدث. يجب أن نتصرف ونغير ما يحدث اليوم. لدينا القدرة والمسؤولية لخلق مستقبل أفضل وأكثر إشراقًا لكبار السن ولأنفسنا. السؤال هو: هل سنفعل؟
توفر البيانات
لم يتم إنشاء أو تحليل أي مجموعات بيانات لهذه المخطوطة.
تاريخ الاستلام: 24 يناير 2024؛ تاريخ القبول: 21 مارس 2024؛ تاريخ النشر على الإنترنت: 06 أبريل 2024
Chamie, J., Berkman, L., Hayutin, A. M., Smith, J. P. & Hoeksema, M. J. Why Population Ageing Matters: A Global Perspectives (Center for Migration Studies, 2007).
CDC. Equitably Addressing Social Determinants of Health and Chronic Diseases, CDC https://www.cdc.gov/chronicdisease/ healthequity/social-determinants-of-health-and-chronic-disease. html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov% 2Fchronicdisease%2Fprograms-impact%2Fsdoh.htm (2022).
Chetty, R. et al. The association between income and life expectancy in the United States, 2001-2014. JAMA 315, 1750-1766 (2016).
He, Y., Wei, B. & Li, Y. The impact of using community home-based elderly care services on older adults’ self-reported health: fresh evidence from China. Front. Public Health 11, 1257463 (2023).
WHO. Global Health Workforce statistics database. WHO https://www. who.int/data/gho/data/themes/topics/health-workforce (2023).
Dall, T. et al. The Complexities of Physician Supply and Demand: Projections From 2018 to 2033. AAMC https://www.aamc.org/ system/files/2020-06/stratcomm-aamc-physician-workforce-projections-june-2020.pdf (2020).
Gurwitz, J. H. The paradoxical decline of geriatric medicine as a profession. JAMA 330, 693-694 (2023).
Jones, C. H., Jenkins, M. P., Adam Williams, B., Welch, V. L. & True, J. M. Exploring the future adult vaccine landscape-crowded schedules and new dynamics. npj Vaccines 9, 27 (2024).
2023 National Population Projections Tables: Main Series. United States Census Bureau https://www.census.gov/data/tables/2023/ demo/popproj/2023-summary-tables.html (2023).
Davis-Ajami, M. L., Lu, Z. K. & Wu, J. Multiple chronic conditions and associated health care expenses in US adults with cancer: a 2010-2015 Medical Expenditure Panel Survey study. BMC Health Serv. Res. 19, 1-10 (2019).
Goodman, R. A., Posner, S. F., Huang, E. S., Parekh, A. K. & Koh, H. K. Peer reviewed: defining and measuring chronic conditions: imperatives for research, policy, program, and practice. Prev. Chronic Dis. 10, E66 (2013).
Machlin, S. R. & Soni, A. Health care expenditures for adults with multiple treated chronic conditions: estimates from the Medical Expenditure Panel Survey, 2009. Prev. Chronic Dis. 10, E63 (2013).
Crimmins, E. M. & Beltrán-Sánchez, H. Mortality and morbidity trends: is there compression of morbidity? J. Gerontol. B: Psychol. Sci. Soc. Sci. 66, 75-86 (2011).
Masnoon, N., Shakib, S., Kalisch-Ellett, L. & Caughey, G. E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 17, 1-10 (2017).
Cohen, R. A. & Boersma, P. Strategies used by adults aged 65 and over to reduce their prescription drug costs, 2016-2017. NCHS Data Brief 335, 1-8 (2019).
Qato, D. M., Wilder, J., Schumm, L. P., Gillet, V. & Alexander, G. C. Changes in prescription and over-the-counter medication and dietary supplement use among older adults in the United States, 2005 vs 2011. JAMA Intern. Med. 176, 473-482 (2016).
Health, United States, 2014: With Special Feature on Adults Aged 55-64. National Center for Health Statistics https://www.cdc.gov/ nchs/data/hus/hus14.pdf (2015).
Cubanski, J., Neuman T., Griffin, S., and Damico, A. Medicare Spending at the End of Life: A Snapshot of Beneficiaries Who Died in 2014 and the Cost of Their Care. KFF https://www.kff.org/medicare/ issue-brief/medicare-spending-at-the-end-of-life/ (2016).
Zhang, X., Lin, D., Pforsich, H. & Lin, V. W. Physician workforce in the United States of America: forecasting nationwide shortages. Hum Resour Health 18, 8 (2020).
Gaynor, M. & Town, R. the Impact of Hospital Consolidationupdate (The Synthesis Project, Robert Wood Johnson Foundation, 2012).
McGinnis, J. M., Stuckhardt, L., Saunders, R. & Smith, M. Best care at lower cost: the path to continuously learning health care in America (National Academies Press, 2013).
Wennberg, J. E., Fisher, E. S. & Skinner, J. S. Geography and the debate over medicare reform: A reform proposal that addresses some underlying causes of Medicare funding woes: geographic variation and lack of incentive for efficient medical practices. Health Affairs 21, W96-W112 (2002).
Hospital Beds per 1,000 Population by Ownership Type. KFF https:// www.kff.org/other/state-indicator/beds-by-ownership/? currentTimeframe=0&sortModel=%7B%22colld%22:%22Location %22,%22sort%22:%22asc%22%7D (2022).
Health Care Resources: Hospital Beds. OECD https://data.oecd.org/ healtheqt/hospital-beds.htm (2020).
Adler-Milstein, J. & Jha, A. K. HITECH Act drove large gains in hospital electronic health record adoption. Health Aff 36, 1416-1422 (2017).
Slawomirski, L. et al. Progress on implementing and using electronic health record systems. OECD https://www.oecd.org/publications/ progress-on-implementing-and-using-electronic-health-record-systems-4f4ce846-en.htm (2023).
Artzi, N. S. et al. Prediction of gestational diabetes based on nationwide electronic health records. Nat. Med. 26, 71-76 (2020).
Amit, G. et al. Estimation of postpartum depression risk from electronic health records using machine learning. BMC Pregnancy Childbirth 21, 630 (2021).
Wood, A. et al. Linked electronic health records for research on a nationwide cohort of more than 54 million people in England: data resource. BMJ 373 (2021).
Wang, Q. Q., Kaelber, D. C., Xu, R. & Volkow, N. D. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol. Psychiatry 26, 30-39 (2021).
Collaborative, O. et al. OpenSAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients. MedRxiv https://doi.org/10.1101/2020.05. 06.20092999 (2020).
Ayala Solares, J. R. et al. Deep learning for electronic health records: a comparative review of multiple deep neural architectures. J. Biomed. Inform. 101, 103337 (2020).
Li, Y. et al. BEHRT: transformer for electronic health records. Sci. Rep. 10, 7155 (2020).
Huang, S.-C., Pareek, A., Seyyedi, S., Banerjee, I. & Lungren, M. P. Fusion of medical imaging and electronic health records using deep learning: a systematic review and implementation guidelines. NPJ Digit Med. 3, 136 (2020).
Keshta, I. & Odeh, A. Security and privacy of electronic health records: Concerns and challenges. Egypt Inform. J. 22, 177-183 (2021).
Osborn, R., Doty, M. M., Moulds, D., Sarnak, D. O. & Shah, A. Older Americans were sicker and faced more financial barriers to health care than counterparts in other countries. Health Aff. 36, 2123-2132 (2017).
Topol, E. J. High-performance medicine: the convergence of human and artificial intelligence. Nat. Med. 25, 44-56 (2019).
Shortell, S. M. & McCurdy, R. K. Integrated health systems. IKMS 8, 369-382 (2009).
O’Malley, A. S. & Rich, E. C. Measuring comprehensiveness of primary care: challenges and opportunities. J. Gen. Intern. Med. 30, 568-575 (2015).
Pham, H. H., Schrag, D., O’Malley, A. S., Wu, B. & Bach, P. B. Care patterns in Medicare and their implications for pay for performance. NEJM 356, 1130-1139 (2007).
Komisar, H. The Effects of Rising Health Care Costs on Middle-Class Economic Security, https://www.aarp.org/pri/topics/health/ coverage-access/impacts-of-rising-healthcare-costs-AARP-ppisec.html (2013).
Shi, L., Regan, J., Politzer, R. M. & Luo, J. Community Health Centers and racial/ethnic disparities in healthy life. Int J Health Serv 31, 567-582 (2001).
Braveman, P. & Gruskin, S. Defining equity in health. JECH 57, 254 (2003).
Kennedy, B. K. et al. Geroscience: linking aging to chronic disease. Cell 159, 709-713 (2014).
Babu, M. & Snyder, M. Multi-omics profiling for health. Mol Cell Proteomics 22, 100561 (2023).
Tenchov, R., Sasso, J. M., Wang, X. & Zhou, Q. A. Aging Hallmarks and progression and age-related diseases: a landscape view of research advancement. ACS Chem Neurosci 15, 1-30 (2024).
Tran Van Hoi, E. et al. Biomarkers of the ageing immune system and their association with frailty-a systematic review.Exp. Gerontol. 176, 112163 (2023).
Wilbon, S. S. & Kolonin, M. G. GLP1 receptor Agonists-effects beyond obesity and diabetes. Cells 13, 65 (2024).
Grevendonk, L. et al. Impact of aging and exercise on skeletal muscle mitochondrial capacity, energy metabolism, and physical function. Nat. Commun. 12, 4773 (2021).
Sousa-Victor, P., García-Prat, L. & Muñoz-Cánoves, P. Control of satellite cell function in muscle regeneration and its disruption in ageing. Nat. Rev. Mol. Cell Biol. 23, 204-226 (2022).
Kapsalyamov, A., Hussain, S. & Jamwal, P. K. State-of-the-art assistive powered upper limb exoskeletons for elderly. IEEE Access 8, 178991-179001 (2020).
Patel, N., Dulau-Florea, A. & Calvo, K. R. Characteristic bone marrow findings in patients with UBA1 somatic mutations and VEXAS syndrome. Semin. Hematol. 58, 204-211 (2021).
Park, S. J. & Bejar, R. Clonal hematopoiesis in cancer. Exp. Hematol. 83, 105-112 (2020).
Revêchon, G., Merino, L. G., Machtel, P. & Eriksson, M. Somatic mutations in vascular wall function and age-associated disease. Eur. Heart J. 44, 4208-4210 (2023).
Feusier, J. E. et al. Large-scale identification of clonal hematopoiesis and mutations recurrent in blood cancers. Blood Cancer Discov. 2, 226-237 (2021).
House, J. S., Kessler, R. C. & Herzog, A. R. Age, socioeconomic status, and health. Milbank Q. 68, 383-411 (1990).
Rowe, J. W. & Berkman, L. Decompression of morbidity and the workforce. Nat. Aging 2, 3-4 (2022).
Chidambaram, P., Burns, A., Rudowitz, R. Who Uses Medicaid LongTerm Services and Supports? KFF https://www.kff.org/medicaid/ issue-brief/who-uses-medicaid-long-term-services-and-supports/ (2023).
Aging in Place: Growing Older at Home. NIH https://www.nia.nih.gov/ health/aging-place/aging-place-growing-older-home#resources (2023).
Burns, A., Mohamed, M., Watts, M. O. M. Pandemic-Era Changes to Medicaid Home- and Community-Based Services (HCBS): A Closer Look at Family Caregiver Policies. KFF https://www.kff.org/ medicaid/issue-brief/pandemic-era-changes-to-medicaid-home-and-community-based-services-hcbs-a-closer-look-at-family-caregiver-policies/ (2023).
Busse, R., Blümel, M., Knieps, F. & Bärnighausen, T. Statutory health insurance in Germany: a health system shaped by 135 years of solidarity, self-governance, and competition. Lancet 390, 882-897 (2017).
Yamada, M. & Arai, H. Long-term care system in Japan. Ann. Geriatr. Med. Res. 24, 174-180 (2020).
Okamoto, S. & Komamura, K. Towards universal health coverage in the context of population ageing: a narrative review on the implications from the long-term care system in Japan. Arch. Pub. Health 80, 210 (2022).
Wright, J. Inside Japan’s long experiment in automating elder care. Technology Review https://www.technologyreview.com/2023/01/ 09/1065135/japan-automating-eldercare-robots/ (2023).
Lorenzoni, L. Case Study—Sweden. Organization for Economic Cooperation and Development https://extranet.who.int/kobe_centre/ sites/default/files/pdf/Sweden_draft_rev-2.pdf (2021).
Auerbach, D. I. & Staiger, D. O. How fast will the registered nurse workforce grow through 2030? Projections in nine regions of the country. Nurs. Outlook 65, 116-122 (2017).
Supply and Demand Projections of the Nursing Workforce: 20142030. National Center for Health Workforce Analysis https://bhw.hrsa. gov/sites/default/files/bhw/nchwa/projections/NCHWA_HRSA_ Nursing_Report.pdf (2017).
State Physician Workforce Data Report. AAMC https://www.aamc. org/data-reports/workforce/report/state-physician-workforce-datareport (2019).
Medscape National Physician Burnout & Suicide Report 2020: The Generational Divide. Medscape https://www.medscape.com/ slideshow/2020-lifestyle-burnout-6012460 (2020).
Ferrucci, L. & Fabbri, E. Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 15, 505-522 (2018).
Chia, C. W., Egan, J. M. & Ferrucci, L. Age-related changes in glucose metabolism, hyperglycemia, and cardiovascular risk. Circ. Res. 123, 886-904 (2018).
Lena, A., Coats, A. J. S. & Anker, M. S. Metabolic disorders in heart failure and cancer. ESC Heart Fail 5, 1092-1098 (2018).
Martin, L. et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 31, 1539-1547 (2013).
Tchkonia, T., Zhu, Y., Van Deursen, J., Campisi, J. & Kirkland, J. L. Cellular senescence and the senescent secretory phenotype: therapeutic opportunities. JCI 123, 966-972 (2013).
Dominguez, L. J. & Barbagallo, M. The biology of the metabolic syndrome and aging. Curr. Opin. Clin. Nutr. Metab. Care 19, 5-11 (2016).
Guo, Y. et al. Plasma proteomic profiles predict future dementia in healthy adults. Nat. Aging 4, 247-260 (2024).
Rizvi, S., Raza, S. T. & Mahdi, F. Telomere length variations in aging and age-related diseases. Curr. Aging Sci. 7, 161-167 (2014).
Liguori, I. et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 13, 757-772 (2018).
Meehan, M. & Penckofer, S. The role of vitamin D in the aging adult. J. Aging Gerontol. 2, 60-71 (2014).
الشكر والتقدير
يشكر المؤلفون أندرو هيل وماري بيتيلشيس (بلومور للاستشارات، لوك بورت، نيويورك، الولايات المتحدة الأمريكية) على رؤاهم الاستراتيجية، والدعم التحريري، والمراجعة في إعداد هذه المقالة. تم تمويل هذا العمل من قبل فايزر. كما نشكر كريستين برينتس على مساهماتها في الرؤى الاستراتيجية. تم تمويل هذا العمل من قبل فايزر.
مساهمات المؤلفين
C.H.J. تصور النشر، طور المخطط، بحث عن المصادر، كتب وحرر المخطوطة، وقدم مدخلات استراتيجية. M.D. قدم رؤى استراتيجية، حرر المخطوطة، وقدم مواد بحثية.
المصالح المتنافسة
يعلن المؤلفون عدم وجود مصالح غير مالية متنافسة ولكن يعلنون عن المصالح المالية المتنافسة التالية: C.H.J. وD.M. يبلغان أنهما موظفان في شركة فايزر وقد يمتلكان أسهمًا أو خيارات أسهم في الشركة.
معلومات إضافية
يجب توجيه المراسلات وطلبات المواد إلى تشارلز إتش. جونز أو ميكائيل دولستين.
The US healthcare system is at a crossroads. With an aging population requiring more care and a strained system facing workforce shortages, capacity issues, and fragmentation, innovative solutions and policy reforms are needed. This paper aims to spark dialogue and collaboration among healthcare stakeholders and inspire action to meet the needs of the aging population. Through a comprehensive analysis of the impact of an aging society, this work highlights the urgency of addressing this issue and the importance of restructuring the healthcare system to be more efficient, equitable, and responsive.
The United States is undergoing a demographic and health transformation that will have profound implications for its healthcare system and society. The population is aging at an unprecedented rate, with the baby boomer generation, defined as those born between 1946 and 1964, reaching retirement age and living longer than ever before. According to the U.S. Census Bureau, by 2030, all baby boomers will be older than 65, leading to about one in every five residents being retirement age . This shift poses a dual challenge for the healthcare system: how to meet the increasing and complex healthcare needs of the elderly, and how to ensure that the system is prepared and equipped to provide quality and equitable care for this growing segment of the population.
The implications of this demographic shift are far-reaching. The healthcare system, as currently structured, is underprepared for the onslaught of demands this aging population will impose . The system is also fragmented, inefficient, and costly, with gaps in coordination, quality, and access. Moreover, the system does not adequately address the social determinants of health, such as income, education, housing, transportation, and social support, that impact the health outcomes and health behaviors of the older adults . Nor does it sufficiently engage the older adults and their caregivers in the planning and delivery of care or leverage the potential of community-based and home-based care models, which can improve the access, quality, and affordability of care for the elderly .
However, the challenge does not end there. There is a growing shortage of healthcare providers, which means that the supply and availability of qualified and skilled healthcare professionals, such as physicians, nurses, pharmacists, clinical social workers and technicians, is insufficient and inadequate to meet the demand and need of the population. This phenomenon is even more pronounced in low- and middle-income countries, as well as in the rural and remote areas within the U.S. According to the World Health Organization (WHO), the global health workforce was 43.5 million in 2018, and is projected to grow to 53.9 million by 2030 , but still falls short of the estimated demand of 80 million by 2030 , resulting in a global
shortfall of 18 million health workers, mostly in low- and middle-income countries . In the U.S., a study by the Association of American Medical Colleges (AAMC) predicts a shortage of up to 139,000 physicians by . The shortage of healthcare providers has significant implications for the health sector, as it affects the access, quality, and cost of healthcare, as well as the health outcomes and satisfaction of the population.
As such, the U.S. is facing a healthcare paradox . On one side, there is an aging population with increasing healthcare needs, and on the other, there is a strained healthcare system grappling with workforce shortages, capacity challenges, and fragmentation. Addressing this paradox requires innovative solutions, policy reforms, and a commitment to restructuring the healthcare system to be more efficient, equitable, and responsive to the needs of its aging citizens.
Although many of these issues may be front-of-mind for geriatrics specialists, many other stakeholders in the eldercare system likely do not understand the full scale of challenges brought on by a rapidly aging populace or may underestimate their preparedness for the resulting changes. This was seen in a recent survey of stakeholders in adult vaccine market, which represents a sector critical in the eldercare industry . When presented with the projected rise of adult vaccines, a trend driven largely by the needs of the aging population, stakeholders across the market were unaware of the associated complexities and anticipated minimal challenges in adopting expanded vaccine schedules . While vaccines represent only a portion of the eldercare market, it is reasonable to believe that this lack of a holistic understanding applies to all sectors in the eldercare industry.
This paper aims to stimulate dialogue and collaboration among the healthcare stakeholders, and to inspire action and innovation to address the needs and aspirations of the aging population. To accomplish this, this work will provide a comprehensive and critical analysis of the impact and implications of an aging society to highlight the importance and urgency of this issue.
Rising tide of healthcare needs: increasing demand and complexity of care
The U.S. population is aging rapidly because of two interrelated factors: the aging of the baby boomer generation, and the increase in life expectancy. The baby boomer generation constitutes the largest cohort in the U.S. history, with about 73 million members . As this cohort reaches retirement age, the share of the population that is 65 and older will increase significantly, from 17% in 2022 to 21% in 2030, and to 23% in 2050 (Fig. 1A) . By 2050, the number of Americans aged 65 and older will increase by , from 58 million in 2022 to 82 million in 2050.
The aging population, particularly those over 85 years old, presents new challenges for the medical system. This will be the fastest growing segment, tripling in size from 6.5 million in 2022 to 17.3 million in 2050, a number comparable to the current population of New York state . These elderly adults often suffer from multiple and complex health conditions, including age-related diseases that affect their heart, brain, and immune system. However, the medical system lacks the experience and expertise to effectively treat these diseases and provide specialized, personalized care for this vulnerable group. The increase in the share and size of the older population will have implications for the demand and supply of healthcare and social services, as well as for the economic and fiscal stability of the nation.
One of the main drivers of the increased healthcare demand and utilization among the elderly is the high prevalence of multiple chronic conditions (MCCs), which are defined as having two or more chronic diseases that last at least a year and require ongoing medical attention or limit activities of daily living . According to the Centers for Disease Control and Prevention (CDC), of older adults have at least one MCC, and have at least two (Fig. 1B). These include common conditions such as hypertension, arthritis, heart disease, cancer, diabetes, and chronic kidney disease. MCCs are associated with increased mortality, disability, functional decline, and reduced quality of life. Moreover, they pose significant challenges to healthcare provision and management, as they require complex and coordinated care across multiple settings and providers. A study by Machlin et al. (2019) found that among Medicare beneficiaries aged 65 and older, those with MCCs accounted for of total healthcare expenditures in 2010, compared to for those without . The average annual expenditure per person was for those with four or more MCCs, for those with three MCCs, for those with two MCCs, and for those
a) U.S. senior population estimates, by age group, Million people
Fig. 1 | Growth of senior population and chronic disease burden. This figure
illustrates the expected growth of the senior population and the associated increase in chronic disease burden. Raw data sourced from “2023 National Population
Projections Tables: Main Series”, which utilizes official estimates of resident
with one MCC. These figures contrast sharply with the spent for those without any MCC.
The high prevalence of MCCs among the elderly is expected to persist or even increase in the future, as it is closely linked to the increase in life expectancy. As people live longer, they are more likely to develop and accumulate chronic diseases over time, especially if they have risk factors such as age-related physiological changes, environmental exposures, lifestyle behaviors, genetic predispositions, and social determinants of health. For example, a study by Crimmins and Beltrán-Sánchez found that the increase in life expectancy in the U.S. between 1998 and 2008 was accompanied by an increase in the number of years spent with MCCs, especially among the elderly . The study estimated that the average number of years spent with MCCs increased from 7.2 to 8.6 for men aged 65 and older, and from 10.0 to 11.3 for women aged 65 and older. Therefore, the aging population will face a higher burden of chronic diseases and a lower quality of life in the coming decades. Making matters worse, the health and longevity of the next wave of aging people may also be affected by new external triggers, such as obesity, processed food intake, microbiome changes, climate change, pandemics, and pollution, which can have diverse and unpredictable impacts on different individuals. These triggers can also change the health behaviors and healthcare access of the elderly.
Another challenge that arises from the medication requirements of the aging population is polypharmacy, which is defined as the concurrent use of five or more medications . Individuals aged 65 and over account for over a third of all prescribed medications in the U.S. . However, polypharmacy can have negative consequences, such as increased risk of drug interactions, adverse drug events, medication non-adherence, and medication errors. These can lead to poor outcomes, such as reduced effectiveness, increased morbidity and mortality, and decreased quality of life. Therefore, polypharmacy necessitates careful medication management and monitoring, as well as regular medication reviews and deprescribing when appropriate. A study by Qato et al. found that among U.S. adults aged 65 and older, the prevalence of polypharmacy increased from in 1999-2000 to in 2011-2012, and the prevalence of potentially inappropriate medication use increased from to . The study also found that polypharmacy was associated with higher rates of emergency department visits and hospitalizations .
The economic implications of the aging population for the healthcare sector are profound, as they affect not only the healthcare spending and
b) U.S. adults with chronic conditions, by age group, %
population on July 1, 2022 as the base for projecting the U.S. population from 2023 to 2100 (panel a) and Boersma, et al., “Prevalence of Multiple Chronic Conditions Among U.S. Adults, 2018” (panel b).
Table 1 | Challenges and impacts of workforce dynamics in healthcare
Factor
Implication
Notable Statistics
The aging of the healthcare workforce itself, leading to increased retirements and reduced working hours.
– The system will face a significant loss of experience and expertise, as well as a reduced availability of workers.
– According to the Health Resources and Services Administration, about a third of the current registered nurses are over 50 years old, and about half of the current physicians are over 55 years old .
The insufficient supply of new entrants into the healthcare professions, due to limited educational capacity, high attrition rates, and low retention rates.
– The system will face a shortage of qualified and skilled workers, as well as a lack of diversity and representation in the workforce.
– The supply of new healthcare graduates will continue to be constrained by the limited capacity of educational institutions, the high costs and debts of education, and the competitive and demanding nature of the professions .
– According to the American Association of Colleges of Nursing, U.S. nursing schools turned away more than 75,000 qualified applicants in 2018 due to faculty shortages, insufficient clinical sites, and budget constraints .
– According to the AAMC, U.S. medical schools have increased their enrollment by since 2002, but this is still not enough to meet the projected demand for physicians .
The uneven distribution of the healthcare workforce across geographic regions, specialties, and settings, resulting in shortages in rural and remote areas, primary care and geriatric care, and community-based and home-based care.
– The system will face disparities and gaps in access and quality of care for different populations, especially the elderly, who often have multiple and complex needs.
– The distribution of healthcare workers will become even more skewed towards urban and affluent areas, leaving rural and remote areas with fewer and less accessible providers .
– According to the Health Resources and Services Administration, about 60 million Americans live in areas with a shortage of primary care providers, and about 77 million Americans live in areas with a shortage of mental health providers .
– According to the American Geriatrics Society, there are only about 7,300 certified geriatricians in the U.S., which is far below the estimated need of 30,000 by .
The increased workload and stress of the healthcare workers, leading to burnout, dissatisfaction, and turnover
– Attrition of healthcare provider could increase leading to overall reduction in available staff.
– According to a survey by the American Nurses Association, more than half of the nurses reported feeling overwhelmed by their work, and more than a third reported feeling emotionally exhausted .
– According to a survey by the Medscape, more than of the physicians reported feeling burned out, and more than reported feeling depressed .
resource utilization, but also the healthcare workforce, the healthcare quality, and the healthcare innovation. According to the Congressional Budget Office, the federal spending on major health programs for the elderly, such as Medicare and Medicaid, will increase from of gross domestic product (GDP) in 2020 to of GDP in . This projected growth is presumably driven by the older age segments differing healthcare utilization patterns and the increasing complexity of care. Specifically, it is estimated that adults aged visits doctors more frequently than younger adults and experience a threefold increase in hospitalization rates . This increased utilization and complexity of care drives increased spending as reported in a 2019 Kaiser Family Foundation study that found Medicare spending for beneficiaries aged 65 to 74 averages , which nearly doubles to for those aged 85 and older .
The rising tide of healthcare needs due to an aging population is multifaceted, encompassing increased service utilization, higher prevalence of chronic diseases, escalated healthcare spending, and complex medication management. This scenario places unprecedented demands on the healthcare system, calling for innovative approaches in care delivery, financial planning, and resource allocation. Adapting to these changes requires a concerted effort from healthcare providers, policymakers, and stakeholders to ensure that the system is not only responsive but also sustainable in meeting the evolving needs of an aging society. Therefore, it is imperative to recognize and discuss the impact this evolution will have on the demand for healthcare professionals, such as physicians, nurses, pharmacists, and specialists in geriatrics, who will be the critical in providing adequate and appropriate care for the elderly with complex medical needs.
The overburdened healthcare landscape: healthcare delivery challenges
The demand for healthcare workers is expected to outpace the supply, resulting in a projected deficit of 1.2 million registered nurses and 121,900 physicians by . The healthcare workforce shortage is driven by several factors, such as the aging of the workforce itself, the insufficient supply of new entrants, the uneven distribution across regions and specialties, and the increased workload and stress of the workers. These factors
are summarized in Table 1, along with their implications and notable statistics.
The shortage of healthcare providers will have a ripple effect on the entire healthcare system, affecting the quality, accessibility, and affordability of care. Physician shortages lead to increased mortality, reduced preventive care, and higher healthcare spending . Moreover, the shortage of physicians creates a competitive environment for talent, where healthcare providers vie for the limited pool of available professionals. This competition may result in sector consolidation, where larger and more affluent providers acquire or merge with smaller and less profitable ones, creating economies of scale and scope. However, this consolidation may also have negative consequences, such as reduced competition, increased market power, and higher prices .
Appropriate staffing and labor supply are necessary for delivering care, but they are not sufficient without adequate resources and infrastructure. However, the current system is not well prepared to handle the increase in volume and complexity of care, resulting in overcrowding, wait times, delays, cancellations, and rationing of care. Some of the factors that contribute to this resource gap include:
The state and performance of care delivery. The U.S. infrastructure is in bad shape and needs more investment and improvement, as a 2017 report by the American Society of Civil Engineers gave it a D+ grade . The system wastes about billion, or of its spending, every year on unnecessary or excessive costs, fraud, and other inefficiencies . It also has high variation in the quality and results of care across different providers, places, and regions, which can lead to too much, too little, or improper use of services . For instance, a report by the Dartmouth Atlas Project showed that Medicare spending per beneficiary ranged by more than three times across regions, and that more spending did not mean better quality or satisfaction .
The lack and imbalance of beds. The U.S. has seen a decline in the number of hospital beds per person from 4.5 in 1980 to 2.4 in 2018, reflecting the move from inpatient to outpatient care and the attempts to save costs and enhance efficiency. However, this trend also implies that there is less excess capacity to cope with fluctuations in demand, such as during pandemics, disasters, or seasonal variations.
Furthermore, the allocation of beds across states and regions is unequal, creating differences in access and quality of care for various populations . For example, the states with the lowest number of beds per person are Nevada (1.8), Oregon (1.8), and Washington (1.9), while the states with the highest number of beds per person are South Dakota (4.1), North Dakota (4.0), and West Virginia .
The inadequacy and inefficiency of technology. The U.S. healthcare system is lagging behind in the adoption and use of information and communication technology (ICT), such as electronic health records (EHRs), telemedicine, and health information exchange (HIE), which can improve the quality, safety, and coordination of care, as well as reduce the costs and errors of care . According to a 2023 report by the Organisation for Economic Co-operation and Development (OECD), the U.S. only hit the threshold of EHR use in of physician offices, medical specialist offices, hospitals, and emergency rooms in . Although the U.S. joins 17-21 other countries that, depending on the setting, have achieved this milestone, it is one of the four countries that did not report having a mandated system in place . As a result, access to records is inconsistent and may require use of multiple portals to view all of a patient’s medical data, impeding benefits that may be observed through shared medial data across practices . For example, analysis of EHRs have supported efforts to predict risk of conditions such as gestational diabetes and postpartum depression as well as to evaluate medical trends during the COVID-19 pandemic . The large volume of data used in such efforts has generated interest for the application of machine-learning, particularly deep learning, to parse through complex and multivariate relationships identifiable within patient records . Despite the potential, there are various concerns that arise with the digitization and availability of such records, such as breaches through cyber-attacks . Finding avenues to address such concerns regarding patient privacy will be an important step towards realizing the benefits from advances in EHRs and their analysis to identify health trends.
The resource gap in the U.S. healthcare system will have serious consequences for the health and well-being of the population, especially the elderly, who are more vulnerable and dependent on the availability and quality of care. A study by the Commonwealth Fund found that the U.S. ranked last among 11 high-income countries in the health outcomes and experiences of older adults, with the highest rates of mortality, disability, hospitalizations, and unmet needs . Moreover, the resource gap will have implications for the innovation and competitiveness of the U.S. healthcare sector, as it will limit the ability and opportunity to develop and implement new and better ways of delivering and improving care, such as digital health, precision medicine, and artificial intelligence (AI) .
The U.S. healthcare system is facing a supply crisis, as it is unable to meet the rising and complex needs of the aging population. The system is suffering from a shortage of labor and a constraint of resources, resulting in a capacity gap that affects the efficiency, equity, and quality of care. Addressing this crisis requires a strategic and comprehensive approach that involves increasing the quantity and quality of the healthcare workforce, enhancing the availability and accessibility of the healthcare resources, and improving the performance and productivity of the healthcare delivery. Achieving these goals requires collaboration and coordination among the healthcare providers, policymakers, and stakeholders, as well as a commitment and investment in the healthcare sector.
The fragmentation and disparity in healthcare provision: access challenges and the “rich-poor divide”
The U.S. healthcare system is facing a challenge not only in meeting the demand and supply of healthcare, but also in ensuring that the healthcare is accessible and affordable for all segments of the population, especially the elderly, who often face barriers and difficulties in obtaining and utilizing the care they need. The system is characterized by fragmentation and disparity, meaning that the healthcare provision is divided and disconnected across
different providers, payers, and settings, and that the healthcare outcomes and experiences vary widely across different groups, regions, and conditions. These features of the system create inefficiencies, inequities, and inconsistencies in the access and quality of care, which can have negative impacts on the health and well-being of the population.
The fragmentation of the U.S. healthcare system stems from the lack of a universal and integrated system of healthcare coverage and delivery, which leads to gaps and overlaps in the coordination, continuity, and comprehensiveness of care . The system is composed of multiple and competing payers, such as private insurers, public programs, and self-pay individuals, each with their own eligibility criteria, benefit packages, payment mechanisms, and administrative rules. This creates a complex and confusing landscape for the consumers and the providers, who have to navigate through different and often conflicting policies, procedures, and requirements. Moreover, the system is composed of multiple and independent providers, such as hospitals, clinics, physicians, nurses, pharmacists, and others, each with their own practice patterns, quality standards, and information systems. This creates a siloed and disjointed landscape for the delivery and management of care, which can result in duplication, fragmentation, and gaps in the care process.
The fragmentation of the U.S. healthcare system has significant implications for the access and quality of care, especially for the elderly, who often have multiple and complex needs that require coordinated and comprehensive care across different settings and providers. The fragmentation can lead to poor outcomes, such as increased errors, complications, readmissions, and costs, as well as reduced satisfaction, trust, and adherence . For example, a study by Pham et al. found that among Medicare beneficiaries aged 65 and older, those who had four or more chronic conditions and saw 10 or more physicians had twice the rate of preventable hospitalizations than those who saw two or fewer physicians . Moreover, the fragmentation can lead to unmet needs, such as delayed or foregone care, as well as increased burden, such as out-of-pocket expenses, transportation difficulties, and caregiving responsibilities . For example, among Medicare beneficiaries aged 65 and older, reported having trouble getting timely appointments, reported having trouble getting needed tests or treatments, and 9% reported having trouble getting needed medications .
The disparity in the U.S. healthcare system stems from the unequal and unfair distribution of healthcare resources, opportunities, and outcomes across different groups, regions, and conditions, which leads to gaps and differences in the access, quality, and affordability of care . The system is influenced by various factors, such as income, education, race, ethnicity, gender, age, geography, and disability, that affect the health status and health behaviors of the population, as well as the availability and utilization of healthcare services. These factors create a diverse and heterogeneous landscape for the consumers and the providers, who face different and often disproportionate challenges and barriers in obtaining and delivering care. Moreover, the system is influenced by various policies, programs, and practices, such as reimbursement rates, quality measures, and incentives, that affect the allocation and distribution of healthcare resources, such as workforce, facilities, equipment, and technology. These policies, programs, and practices create a dynamic and complex landscape for the payers and the policymakers, who must balance and align the competing and conflicting interests and objectives of the healthcare stakeholders.
As the demand for healthcare services increases due to the aging population, and the supply of healthcare workers and resources remains insufficient and inadequate, a new form of fragmentation and disparity is emerging in the U.S. healthcare system: the rich-poor divide. This refers to the phenomenon where the affluent and urban areas attract and retain more and better healthcare professionals and facilities, while the poor and rural areas are left with fewer and worse healthcare options. This creates a vicious cycle, where the rich areas have more access and quality of care, and the poor areas have less access and quality of care, leading to further widening of the health and economic gaps between them.
One of the factors that contributes to this new form of fragmentation and disparity is the market-driven and competitive nature of the U.S. healthcare sector, where healthcare providers are motivated by financial incentives and rewards to work in areas and specialties that offer higher compensation and recognition. This creates a situation where the supply of healthcare workers is skewed towards the areas and specialties that have more demand and resources, such as urban and affluent areas, and specialty and subspecialty care. Conversely, the supply of healthcare workers is scarce in the areas and specialties that have less demand and resources, such as rural and remote areas, and primary and geriatric care. This results in a mismatch between the needs and the availability of the healthcare workforce, which affects the access and quality of care for different populations.
One of the examples that illustrates this new form of fragmentation and disparity is the rise of travel nurses, who are registered nurses with advanced training and certification in various specialties, and work on a temporary or contract basis in different locations and settings. These nurses are in high demand, as they can fill the gaps and shortages of anesthesiologists (i.e., travel nurse anesthetist) or other nurse specialists, who are often concentrated in urban and academic centers. Moreover, these nurses are well compensated, as they can earn significantly higher salaries and benefits than regular nurses and have more flexibility and autonomy in choosing their assignments and schedules. However, these nurses also contribute to the fragmentation and disparity of the healthcare system, as they tend to work in areas and settings that offer more opportunities and rewards, such as affluent and urban areas, and private and specialty hospitals. This leaves the areas and settings that have less opportunities and rewards, such as poor and rural areas, and public and primary care facilities, with fewer and less qualified healthcare workers, which affects the access and quality of care for the populations they serve.
Addressing the challenge of fragmentation and disparity in the U.S. healthcare system requires a holistic and integrated approach that involves improving the coordination and continuity of care, enhancing the equity and inclusivity of care, and ensuring the affordability and sustainability of care. Achieving these goals requires collaboration and coordination among the healthcare providers, payers, policymakers, and stakeholders, as well as a commitment and investment in the healthcare sector.
Interventions, policy reform, and global comparison
As the number of individuals living into their 80 s, 90 s and beyond increases dramatically, focus has shifted from extending lifespan to enhancing the quality of these additional years. This approach, known as ‘delayed aging,’ has encompassed investments in technology and policies that increase the number of years lived without the accumulation of chronic conditions and other side effects of aging. Achieving this would result in the compression of morbidity, meaning that chronic illnesses would be concentrated into a shorter period towards the end of life. This shift would not only have an impact on the general health of the population, would also have a positive financial impact. For example, a 2013 study conducted by Goldman et al. estimated that wide-spread delayed aging would save the U.S. trillion by 2060 .
The emerging field of geroscience is central to increasing the number of healthy years in older populations. This discipline seeks to understand the relationship between aging and age-related diseases, aiming to mitigate the latter by targeting the biological processes of aging itself . A key strategy involves identifying biomarkers and risk factors, such as socioeconomic and lifestyle choices, that predict disease development in later life (Table 2). Technological advancements have enabled the aggregation of large multiOmics datasets and longitudinal medical records from diverse patient groups and different aging tissues . These include blood, brain, muscle, heart, liver, joint, skeleton, fat, among others. For example, the Accelerating Medicines Partnership ‘s (AMP ‘s) Alzheimer’s Disease program has used a multi-omic analyses of molecular data from human brain samples to identify over 500 unique drug candidate targets . This wealth of information offers an unprecedented opportunity to leverage AI methodologies to decipher unique patient markers and identify potential interventions.
Once these risk factors are identified, researchers can develop interventions that correct or mitigate them. These include addressing issues such as immune aging, chronic low-grade tissue inflammation, obesity, mitochondrial age-related insufficiency, and brain proteinopathies . For instance, clinical studies with new targeted immune agents aim to rejuvenate the aging immune system using immune aging biomarkers as surrogate endpoints . The hope is that restoring immune health could translate to beneficial downstream effects on the vascular, heart, brain, and kidney systems. The advent of the GLP-1 drug class (e.g., Semaglutide and Tirzepatide), which not only have the potential to prevent obesity-related diseases later in life, also offers a promising avenue for the reversal of metabolic aging and may even promote DNA repair in neurodegenerative diseases . Maintaining muscle function is also crucial, particularly in the context of aging or chronic conditions like sarcopenia . Insights into muscle augmenting factors and the ability to mobilize and differentiate muscle stem cells present critical areas for promoting healthy aging . Bioengineering, including the development of exoskeletons for spinal injury patients, offers potential solutions for maintaining ambulation during aging .
Future interventions may include longitudinal analyses of genome integrity and maintaining DNA fidelity systems. Reducing the accumulation of somatic mutations, which correlate with aging of bone marrow , myeloid cell dysplasia (clonal hematopoiesis) , vascular wall dysfunction , and blood cancers , could be possible. The first successful trials in gene therapy and gene editing have shed new light and promise on human disease, suggesting that restoring the integrity of the human genome and cell systems may increasingly be within our technological reach. This could expand to restore function in autoimmune and fibrotic diseases, further underscoring the transformative potential of geroscience and technology in improving healthcare for the elderly.
As the field of geroscience advances, there is a significant risk that these innovations may predominantly benefit those with substantial resources, further exacerbating the ‘rich-poor’ divide in eldercare and highlighting one type of inequity that tomorrow’s elderly may face. There is already evidence that compression of morbidity may be due more to socioeconomic factors than biological determinants . However, we do not yet know what other challenges these future generations may face. New and emerging socioeconomic factors and factors associated with marginalized groups in younger populations will have a yet unknown impact on tomorrow’s elderly. The shifting healthcare requirements of younger demographics, characterized by factors such as the increase in gender-affirming care, escalating mental health issues, and substance misuse, including opioids, are likely to affect the future landscape of elderly care in ways that are currently unknown. The opioid crisis, as elaborated in Barbara Kingsolver’s Demon Copperhead, serves as an illustration of how prevalent health and societal challenges can have significant long-term impacts on public health and healthcare systems . This narrative, which mirrors the broader societal problem of substance abuse, underscores the importance of incorporating equity as a fundamental factor in healthcare policy decisions. Ensuring that healthcare improvements, including those emerging from geroscience, are accessible to all, irrespective of their socioeconomic status, is vital to prevent further exacerbation of the economic disparity in eldercare.
To this end, the U.S. has launched policy reforms over the last two decades aimed at securing equitable healthcare for its senior citizens. These measures seek to confront salient challenges in the accessibility, quality, and financial viability of services catering to the elderly. The expansion of Medicaid under the Affordable Care Act (ACA), enacted in 2010, serves as a cornerstone of these initiatives, enhancing Medicaid’s scope to encompass superior benefits, cost reductions, and improved eldercare . Significantly, the ACA reducing the Medicare Part D prescription drug “donut hole,” or drug coverage gaps, improving preventive care with no cost-sharing. Additional initiatives, such as Medicare Advantage, aim to improve eldercare coordination by allowing Medicare beneficiaries to enroll in managed care plans (Medicare Advantage). Medicare Advantage, for example, enrolled over 30.8 million individuals in 2023 alone, and now represent over of all seniors on Medicare .
Table 2 | Diagnostic biomarkers for age-related diseases and their implications for clinical practice
Diagnostic Risk Factor(s)
Select Biomarkers
Change with Age
Physiological Impact
Associated Diseases
Testing
Use in Medicine
Ref
Chronic Inflamm. (Inflamm-ageing)
CRP; IL-6; TNF- ; IL-1
Increase
Leads to system inflamm. causing tissue damage, altered immune response, and increase risk of ASCVD.
CV diseases;
Frailty;
Dementia;
CKD;
DM;
Cancer;
Depression;
Sacropenia
Blood tests; High Sensitivity CRP Test
Utilized currently
90
Metabolic Health (Glucose Metabolism, Hyperglycemia)
Fasting glucose; HbA1c;
Insulin levels
Dysreg.
Impairs glucose utilization, leading to hyperglycemia and contributing to vascular damage and insulin resistance.
Influences metabolic pathways and immune responses, predisposing individuals to various chronic conditions.
Metabolic syndrome;
CV diseases;
Alzheimer’s disease;
Certain cancers;
Response to medications
(pharmacogenomics)
Genetic screening; SNP arrays
Exploratory
95,96
Microbiome
Microbial comp.; SCFA profiles
Changes with diet, antibiotic usage
Affects gut barrier function, systemic inflamm., and nutrient metabolism.
GI disorders; Metabolic dysregulation (e.g., obesity, diabetes);
Autoimmune diseases;
Mood disorders
16 S rRNA gene sequencing; Metagenomic sequencing
Exploratory
90
Telomere Length
Telomere length
Shortens
Shortening of telomeres is associated with cellular aging and increased risk of age-related diseases.
CV diseases, various cancers;
OP;
Diabetes;
Increased risk of mortality
Quantitative PCR; Telomere length analysis
Exploratory
97
Oxidative Stress Markers
MDA; 8-OHdG; Antioxidant capacity
Increases
Causes cellular damage and contributes to the aging process and development of age-related diseases.
NDDs; CV diseases;
Cancer; AMD
Blood tests; ELISA; Spectro-photometry
Exploratory
98
Vitamin D Levels
25-hydroxyvitamin D
Varies with exposure and intake
Influences bone health, immune function, and has been linked to a lower risk of several chronic diseases.
OP; CV diseases;
T2D;
MS;
Depression;
Certain Cancers
Blood tests (25-hydroxyvitamin D assay)
Exploratory
99
8-OHdG 8-hydroxy-2′-deoxyguanosine, AMD age-related macular degeneration, ASCVD atherosclerotic cardiovascular disease, BIA bioelectrical impedance analysis, BMI body mass index, CIR circumference, CKD chronic kidney disease, comp. composition, CPR C-reactive protein, CT computed tomography, CV cardiovascular disease, DEXA dual-energy x-ray absorptiometry, DM diabetes mellitus, Dysreg. dysregulation, ELISA enzyme-linked immunosorbent assay, GI gastrointestinal disease, HDA1c hemoglobin A1C, IL interleukin, MDA malondialdehyde, MRI magnetic resonance imaging, MS multiple sclerosis, NDDs neurodegenerative diseases, OP osteoporosis, PCR polymerase chain reaction, Ref references, SA- -gal senescence-associated -galactosidase, SCFA short chain fatty acids, SNPs single nucleotide polymorphisms, T2D Type 2 diabetes, TNF- tumor necrosis factor- , VE vaccine efficacy.
As components of the patient protection models, accountable care organizations (ACOs) have also exhibited efficacy in enhancing care coordination, leading to improved patient outcomes and decreased costs. A 2021 report from the Centers for Medicare & Medicaid Services (CMS) asserts that ACOs yielded billion in gross savings and billion in net savings for Medicare between 2021 and 2022, while also improving the quality of care . Alongside these models, enhancements in Long-Term Care and Support Services through the expansion of home and community-based services (HCBS) via Medicaid have substantially widened access to personalized longterm care . These services are aimed at facilitating elderly individuals to ‘age in place . In 2019 alone, Medicaid HCBS expenditures amounted to billion, highlighting a sustained trend towards increased investment in services that promote autonomy and dignity for the elderly . Additionally, this represents a cost-effective approach to long-term care by minimizing dependence on more costly institutional care settings.
Internationally, countries have adopted diverse strategies to address the healthcare needs of their aging populations. Japan and Germany, for example, both emphasize integrated care models and insurance-based solutions, like Germany’s statutory health insurance complemented by long-term care insurance and Japan’s Long-Term Care Insurance . However, Japan, as one of the world’s oldest populations, faces unique challenges in sustaining its healthcare workforce . In an attempt to compensate for this, this country has positioned itself at the forefront of automating elder care including the development of technologies such as ‘care robots,’ to improve the quality of care in nursing homes . Similar to Japan, Singapore has also implemented technological healthcare solutions for its aging population, investing in improving telemedicine, remote health monitoring apps, wearable wellness technology, and smart home solutions (e.g., fall detect sensors) to facilitate independent living and reduce the burden on the healthcare system . This country is currently second in the word in terms of highest life expectancy, compared with the U.S. at . Sweden, number 20 on that list , is internationally recognized as a model for eldercare. It is another country that heavily focuses on ‘aging in place’ by providing heavily funded care through municipal taxes and government grants .
Conclusion
It is often said that there is always tomorrow, implying that we can postpone our actions and decisions to a later date. However, this sentiment cannot hold true anymore when it comes to the care of the aging population. For us to have a prosperous tomorrow, we must begin planning and actioning today. The aging of the population is not a distant or hypothetical scenario, but a present and inevitable reality. We cannot afford to wait and see what happens. We must act and change what happens today. We have the potential and the responsibility to create a better and brighter future for the elderly and for ourselves. The question is: will we?
Data availability
No datasets were generated or analyzed for this manuscript.
Received: 24 January 2024; Accepted: 21 March 2024; Published online: 06 April 2024
Chamie, J., Berkman, L., Hayutin, A. M., Smith, J. P. & Hoeksema, M. J. Why Population Ageing Matters: A Global Perspectives (Center for Migration Studies, 2007).
CDC. Equitably Addressing Social Determinants of Health and Chronic Diseases, CDC https://www.cdc.gov/chronicdisease/ healthequity/social-determinants-of-health-and-chronic-disease. html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov% 2Fchronicdisease%2Fprograms-impact%2Fsdoh.htm (2022).
Chetty, R. et al. The association between income and life expectancy in the United States, 2001-2014. JAMA 315, 1750-1766 (2016).
He, Y., Wei, B. & Li, Y. The impact of using community home-based elderly care services on older adults’ self-reported health: fresh evidence from China. Front. Public Health 11, 1257463 (2023).
WHO. Global Health Workforce statistics database. WHO https://www. who.int/data/gho/data/themes/topics/health-workforce (2023).
Dall, T. et al. The Complexities of Physician Supply and Demand: Projections From 2018 to 2033. AAMC https://www.aamc.org/ system/files/2020-06/stratcomm-aamc-physician-workforce-projections-june-2020.pdf (2020).
Gurwitz, J. H. The paradoxical decline of geriatric medicine as a profession. JAMA 330, 693-694 (2023).
Jones, C. H., Jenkins, M. P., Adam Williams, B., Welch, V. L. & True, J. M. Exploring the future adult vaccine landscape-crowded schedules and new dynamics. npj Vaccines 9, 27 (2024).
2023 National Population Projections Tables: Main Series. United States Census Bureau https://www.census.gov/data/tables/2023/ demo/popproj/2023-summary-tables.html (2023).
Davis-Ajami, M. L., Lu, Z. K. & Wu, J. Multiple chronic conditions and associated health care expenses in US adults with cancer: a 2010-2015 Medical Expenditure Panel Survey study. BMC Health Serv. Res. 19, 1-10 (2019).
Goodman, R. A., Posner, S. F., Huang, E. S., Parekh, A. K. & Koh, H. K. Peer reviewed: defining and measuring chronic conditions: imperatives for research, policy, program, and practice. Prev. Chronic Dis. 10, E66 (2013).
Machlin, S. R. & Soni, A. Health care expenditures for adults with multiple treated chronic conditions: estimates from the Medical Expenditure Panel Survey, 2009. Prev. Chronic Dis. 10, E63 (2013).
Crimmins, E. M. & Beltrán-Sánchez, H. Mortality and morbidity trends: is there compression of morbidity? J. Gerontol. B: Psychol. Sci. Soc. Sci. 66, 75-86 (2011).
Masnoon, N., Shakib, S., Kalisch-Ellett, L. & Caughey, G. E. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 17, 1-10 (2017).
Cohen, R. A. & Boersma, P. Strategies used by adults aged 65 and over to reduce their prescription drug costs, 2016-2017. NCHS Data Brief 335, 1-8 (2019).
Qato, D. M., Wilder, J., Schumm, L. P., Gillet, V. & Alexander, G. C. Changes in prescription and over-the-counter medication and dietary supplement use among older adults in the United States, 2005 vs 2011. JAMA Intern. Med. 176, 473-482 (2016).
Health, United States, 2014: With Special Feature on Adults Aged 55-64. National Center for Health Statistics https://www.cdc.gov/ nchs/data/hus/hus14.pdf (2015).
Cubanski, J., Neuman T., Griffin, S., and Damico, A. Medicare Spending at the End of Life: A Snapshot of Beneficiaries Who Died in 2014 and the Cost of Their Care. KFF https://www.kff.org/medicare/ issue-brief/medicare-spending-at-the-end-of-life/ (2016).
Zhang, X., Lin, D., Pforsich, H. & Lin, V. W. Physician workforce in the United States of America: forecasting nationwide shortages. Hum Resour Health 18, 8 (2020).
Gaynor, M. & Town, R. the Impact of Hospital Consolidationupdate (The Synthesis Project, Robert Wood Johnson Foundation, 2012).
McGinnis, J. M., Stuckhardt, L., Saunders, R. & Smith, M. Best care at lower cost: the path to continuously learning health care in America (National Academies Press, 2013).
Wennberg, J. E., Fisher, E. S. & Skinner, J. S. Geography and the debate over medicare reform: A reform proposal that addresses some underlying causes of Medicare funding woes: geographic variation and lack of incentive for efficient medical practices. Health Affairs 21, W96-W112 (2002).
Hospital Beds per 1,000 Population by Ownership Type. KFF https:// www.kff.org/other/state-indicator/beds-by-ownership/? currentTimeframe=0&sortModel=%7B%22colld%22:%22Location %22,%22sort%22:%22asc%22%7D (2022).
Health Care Resources: Hospital Beds. OECD https://data.oecd.org/ healtheqt/hospital-beds.htm (2020).
Adler-Milstein, J. & Jha, A. K. HITECH Act drove large gains in hospital electronic health record adoption. Health Aff 36, 1416-1422 (2017).
Slawomirski, L. et al. Progress on implementing and using electronic health record systems. OECD https://www.oecd.org/publications/ progress-on-implementing-and-using-electronic-health-record-systems-4f4ce846-en.htm (2023).
Artzi, N. S. et al. Prediction of gestational diabetes based on nationwide electronic health records. Nat. Med. 26, 71-76 (2020).
Amit, G. et al. Estimation of postpartum depression risk from electronic health records using machine learning. BMC Pregnancy Childbirth 21, 630 (2021).
Wood, A. et al. Linked electronic health records for research on a nationwide cohort of more than 54 million people in England: data resource. BMJ 373 (2021).
Wang, Q. Q., Kaelber, D. C., Xu, R. & Volkow, N. D. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol. Psychiatry 26, 30-39 (2021).
Collaborative, O. et al. OpenSAFELY: factors associated with COVID-19-related hospital death in the linked electronic health records of 17 million adult NHS patients. MedRxiv https://doi.org/10.1101/2020.05. 06.20092999 (2020).
Ayala Solares, J. R. et al. Deep learning for electronic health records: a comparative review of multiple deep neural architectures. J. Biomed. Inform. 101, 103337 (2020).
Li, Y. et al. BEHRT: transformer for electronic health records. Sci. Rep. 10, 7155 (2020).
Huang, S.-C., Pareek, A., Seyyedi, S., Banerjee, I. & Lungren, M. P. Fusion of medical imaging and electronic health records using deep learning: a systematic review and implementation guidelines. NPJ Digit Med. 3, 136 (2020).
Keshta, I. & Odeh, A. Security and privacy of electronic health records: Concerns and challenges. Egypt Inform. J. 22, 177-183 (2021).
Osborn, R., Doty, M. M., Moulds, D., Sarnak, D. O. & Shah, A. Older Americans were sicker and faced more financial barriers to health care than counterparts in other countries. Health Aff. 36, 2123-2132 (2017).
Topol, E. J. High-performance medicine: the convergence of human and artificial intelligence. Nat. Med. 25, 44-56 (2019).
Shortell, S. M. & McCurdy, R. K. Integrated health systems. IKMS 8, 369-382 (2009).
O’Malley, A. S. & Rich, E. C. Measuring comprehensiveness of primary care: challenges and opportunities. J. Gen. Intern. Med. 30, 568-575 (2015).
Pham, H. H., Schrag, D., O’Malley, A. S., Wu, B. & Bach, P. B. Care patterns in Medicare and their implications for pay for performance. NEJM 356, 1130-1139 (2007).
Komisar, H. The Effects of Rising Health Care Costs on Middle-Class Economic Security, https://www.aarp.org/pri/topics/health/ coverage-access/impacts-of-rising-healthcare-costs-AARP-ppisec.html (2013).
Shi, L., Regan, J., Politzer, R. M. & Luo, J. Community Health Centers and racial/ethnic disparities in healthy life. Int J Health Serv 31, 567-582 (2001).
Braveman, P. & Gruskin, S. Defining equity in health. JECH 57, 254 (2003).
Kennedy, B. K. et al. Geroscience: linking aging to chronic disease. Cell 159, 709-713 (2014).
Babu, M. & Snyder, M. Multi-omics profiling for health. Mol Cell Proteomics 22, 100561 (2023).
Tenchov, R., Sasso, J. M., Wang, X. & Zhou, Q. A. Aging Hallmarks and progression and age-related diseases: a landscape view of research advancement. ACS Chem Neurosci 15, 1-30 (2024).
Tran Van Hoi, E. et al. Biomarkers of the ageing immune system and their association with frailty-a systematic review.Exp. Gerontol. 176, 112163 (2023).
Wilbon, S. S. & Kolonin, M. G. GLP1 receptor Agonists-effects beyond obesity and diabetes. Cells 13, 65 (2024).
Grevendonk, L. et al. Impact of aging and exercise on skeletal muscle mitochondrial capacity, energy metabolism, and physical function. Nat. Commun. 12, 4773 (2021).
Sousa-Victor, P., García-Prat, L. & Muñoz-Cánoves, P. Control of satellite cell function in muscle regeneration and its disruption in ageing. Nat. Rev. Mol. Cell Biol. 23, 204-226 (2022).
Kapsalyamov, A., Hussain, S. & Jamwal, P. K. State-of-the-art assistive powered upper limb exoskeletons for elderly. IEEE Access 8, 178991-179001 (2020).
Patel, N., Dulau-Florea, A. & Calvo, K. R. Characteristic bone marrow findings in patients with UBA1 somatic mutations and VEXAS syndrome. Semin. Hematol. 58, 204-211 (2021).
Park, S. J. & Bejar, R. Clonal hematopoiesis in cancer. Exp. Hematol. 83, 105-112 (2020).
Revêchon, G., Merino, L. G., Machtel, P. & Eriksson, M. Somatic mutations in vascular wall function and age-associated disease. Eur. Heart J. 44, 4208-4210 (2023).
Feusier, J. E. et al. Large-scale identification of clonal hematopoiesis and mutations recurrent in blood cancers. Blood Cancer Discov. 2, 226-237 (2021).
House, J. S., Kessler, R. C. & Herzog, A. R. Age, socioeconomic status, and health. Milbank Q. 68, 383-411 (1990).
Rowe, J. W. & Berkman, L. Decompression of morbidity and the workforce. Nat. Aging 2, 3-4 (2022).
Chidambaram, P., Burns, A., Rudowitz, R. Who Uses Medicaid LongTerm Services and Supports? KFF https://www.kff.org/medicaid/ issue-brief/who-uses-medicaid-long-term-services-and-supports/ (2023).
Aging in Place: Growing Older at Home. NIH https://www.nia.nih.gov/ health/aging-place/aging-place-growing-older-home#resources (2023).
Burns, A., Mohamed, M., Watts, M. O. M. Pandemic-Era Changes to Medicaid Home- and Community-Based Services (HCBS): A Closer Look at Family Caregiver Policies. KFF https://www.kff.org/ medicaid/issue-brief/pandemic-era-changes-to-medicaid-home-and-community-based-services-hcbs-a-closer-look-at-family-caregiver-policies/ (2023).
Busse, R., Blümel, M., Knieps, F. & Bärnighausen, T. Statutory health insurance in Germany: a health system shaped by 135 years of solidarity, self-governance, and competition. Lancet 390, 882-897 (2017).
Yamada, M. & Arai, H. Long-term care system in Japan. Ann. Geriatr. Med. Res. 24, 174-180 (2020).
Okamoto, S. & Komamura, K. Towards universal health coverage in the context of population ageing: a narrative review on the implications from the long-term care system in Japan. Arch. Pub. Health 80, 210 (2022).
Wright, J. Inside Japan’s long experiment in automating elder care. Technology Review https://www.technologyreview.com/2023/01/ 09/1065135/japan-automating-eldercare-robots/ (2023).
Lorenzoni, L. Case Study—Sweden. Organization for Economic Cooperation and Development https://extranet.who.int/kobe_centre/ sites/default/files/pdf/Sweden_draft_rev-2.pdf (2021).
Auerbach, D. I. & Staiger, D. O. How fast will the registered nurse workforce grow through 2030? Projections in nine regions of the country. Nurs. Outlook 65, 116-122 (2017).
Supply and Demand Projections of the Nursing Workforce: 20142030. National Center for Health Workforce Analysis https://bhw.hrsa. gov/sites/default/files/bhw/nchwa/projections/NCHWA_HRSA_ Nursing_Report.pdf (2017).
State Physician Workforce Data Report. AAMC https://www.aamc. org/data-reports/workforce/report/state-physician-workforce-datareport (2019).
Medscape National Physician Burnout & Suicide Report 2020: The Generational Divide. Medscape https://www.medscape.com/ slideshow/2020-lifestyle-burnout-6012460 (2020).
Ferrucci, L. & Fabbri, E. Inflammageing: chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 15, 505-522 (2018).
Chia, C. W., Egan, J. M. & Ferrucci, L. Age-related changes in glucose metabolism, hyperglycemia, and cardiovascular risk. Circ. Res. 123, 886-904 (2018).
Lena, A., Coats, A. J. S. & Anker, M. S. Metabolic disorders in heart failure and cancer. ESC Heart Fail 5, 1092-1098 (2018).
Martin, L. et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 31, 1539-1547 (2013).
Tchkonia, T., Zhu, Y., Van Deursen, J., Campisi, J. & Kirkland, J. L. Cellular senescence and the senescent secretory phenotype: therapeutic opportunities. JCI 123, 966-972 (2013).
Dominguez, L. J. & Barbagallo, M. The biology of the metabolic syndrome and aging. Curr. Opin. Clin. Nutr. Metab. Care 19, 5-11 (2016).
Guo, Y. et al. Plasma proteomic profiles predict future dementia in healthy adults. Nat. Aging 4, 247-260 (2024).
Rizvi, S., Raza, S. T. & Mahdi, F. Telomere length variations in aging and age-related diseases. Curr. Aging Sci. 7, 161-167 (2014).
Liguori, I. et al. Oxidative stress, aging, and diseases. Clin. Interv. Aging 13, 757-772 (2018).
Meehan, M. & Penckofer, S. The role of vitamin D in the aging adult. J. Aging Gerontol. 2, 60-71 (2014).
Acknowledgements
The authors thank Andrew Hill and Marie Beitelshees (Bulmore Consulting, Lockport, NY, USA) for their strategic insights, editorial support, and review in preparing this article. This work was funded by Pfizer. We also thank Kristen Prentice for her strategic insight contributions. This work was funded by Pfizer.
Author contributions
C.H.J. conceptualized the publication, developed the outline, researched sources, drafted and edited the manuscript, and provided strategic input. M.D. provided strategic insights, edited the manuscript, and provided research source material.
Competing interests
The authors declare no competing non-financial but declare the following Competing Financial Interests: C.H.J. and D.M. report that they are employees of Pfizer Inc. and may hold stock or stock options in the company.
Additional information
Correspondence and requests for materials should be addressed to Charles H. Jones or Mikael Dolsten.