المجلة: The Lancet، المجلد: 403، العدد: 10440
DOI: https://doi.org/10.1016/s0140-6736(24)00367-2
PMID: https://pubmed.ncbi.nlm.nih.gov/38582094
تاريخ النشر: 2024-04-03
DOI: https://doi.org/10.1016/s0140-6736(24)00367-2
PMID: https://pubmed.ncbi.nlm.nih.gov/38582094
تاريخ النشر: 2024-04-03
العبء العالمي لـ 288 سببًا للوفاة وتحليل العمر المتوقع في 204 دول وأقاليم و811 موقعًا دون وطني، 1990-2021: تحليل منهجي لدراسة العبء العالمي للأمراض 2021
811 موقعًا فرعيًا، 1990-2021: تحليل منهجي لدراسة عبء المرض العالمي 2021
متعاونون في أسباب الوفاة GBD 2021*
لانسيت 2024؛ 403: 2100-32
تم النشر على الإنترنت
3 أبريل 2024
https://doi.org/10.1016/
S0140-6736(24)00367-2
تم تصحيح هذه النشرة على الإنترنت. ظهرت النسخة المصححة لأول مرة فيthelancet.com في 19 أبريل 2024
انظر التعليق في الصفحة 1956
*المتعاونون مدرجون في نهاية المقال
تم النشر على الإنترنت
3 أبريل 2024
https://doi.org/10.1016/
S0140-6736(24)00367-2
تم تصحيح هذه النشرة على الإنترنت. ظهرت النسخة المصححة لأول مرة فيthelancet.com في 19 أبريل 2024
انظر التعليق في الصفحة 1956
*المتعاونون مدرجون في نهاية المقال
المراسلة إلى:
الأستاذ سيمون آي هاي، معهد قياسات الصحة والتقييم،
الأستاذ سيمون آي هاي، معهد قياسات الصحة والتقييم،
ملخص
الخلفية: يعد التقرير المنتظم والمفصل عن صحة السكان حسب سبب الوفاة أمرًا أساسيًا لاتخاذ قرارات الصحة العامة. تعتبر التقديرات الخاصة بالسبب لمعدلات الوفيات والآثار اللاحقة على العمر المتوقع عالميًا مقاييس قيمة لقياس التقدم في تقليل معدلات الوفيات. هذه التقديرات مهمة بشكل خاص بعد حدوث ارتفاعات كبيرة في الوفيات، مثل جائحة COVID-19. عند تحليلها بشكل منهجي، تسمح معدلات الوفيات والعمر المتوقع بمقارنات لنتائج أسباب الوفاة عالميًا وعلى مر الزمن، مما يوفر فهمًا دقيقًا لتأثير هذه الأسباب على السكان العالميين.
الطرق: تقدير تحليل أسباب الوفاة في دراسة عبء الأمراض والإصابات وعوامل الخطر (GBD) 2021 لمعدلات الوفيات وسنوات الحياة المفقودة (YLLs) من 288 سببًا للوفاة حسب العمر والجنس والموقع والسنة في 204 دول وأقاليم و811 موقعًا فرعيًا لكل سنة من 1990 حتى 2021. استخدم التحليل 56604 مصدر بيانات، بما في ذلك بيانات من التسجيل الحيوي والتشريح اللفظي بالإضافة إلى الاستطلاعات، والتعدادات، وأنظمة المراقبة، وسجلات السرطان، من بين أمور أخرى. كما هو الحال مع جولات GBD السابقة، تم تقدير معدلات الوفيات الخاصة بالسبب لمعظم الأسباب باستخدام نموذج مجموعة أسباب الوفاة – أداة نمذجة تم تطويرها لـ GBD لتقييم صلاحية التنبؤ خارج العينة لنماذج إحصائية مختلفة وتباديل المتغيرات المرافقة ودمج تلك النتائج لإنتاج تقديرات وفيات خاصة بالسبب مع استراتيجيات بديلة تم تكييفها لنمذجة الأسباب التي تفتقر إلى البيانات، أو التغيرات الكبيرة في الإبلاغ على مدار فترة الدراسة، أو علم الأوبئة غير العادي. تم حساب YLLs كمنتج لعدد الوفيات لكل سبب-عمر-جنس-موقع-سنة والعمر المتوقع القياسي عند كل عمر. كجزء من عملية النمذجة، تم توليد فترات عدم اليقين (UIs) باستخدام
النتائج: كانت الأسباب الرئيسية للوفيات الموحدة حسب العمر عالميًا هي نفسها في 2019 كما كانت في 1990؛ بالترتيب التنازلي، كانت هذه الأمراض القلبية الإقفارية، والسكتة الدماغية، ومرض الانسداد الرئوي المزمن، والتهابات الجهاز التنفسي السفلي. في 2021، ومع ذلك، حلت COVID-19 محل السكتة الدماغية كسبب الوفاة الثاني الموحد حسب العمر، مع
وأصبحت هذه الأسباب للوفاة تتركز بشكل متزايد منذ 1990، عندما أظهر 44 سببًا فقط هذا النمط. يتم مناقشة ظاهرة التركيز بشكل استدلالي فيما يتعلق بالعدوى المعوية والتهابات الجهاز التنفسي السفلي، والملاريا، وفيروس نقص المناعة البشرية/الإيدز، والاضطرابات حديثي الولادة، والسل، والحصبة.
وأصبحت هذه الأسباب للوفاة تتركز بشكل متزايد منذ 1990، عندما أظهر 44 سببًا فقط هذا النمط. يتم مناقشة ظاهرة التركيز بشكل استدلالي فيما يتعلق بالعدوى المعوية والتهابات الجهاز التنفسي السفلي، والملاريا، وفيروس نقص المناعة البشرية/الإيدز، والاضطرابات حديثي الولادة، والسل، والحصبة.
التفسير: تم تعطيل المكاسب المستمرة في العمر المتوقع وتقليل العديد من الأسباب الرئيسية للوفاة بسبب جائحة COVID-19، التي انتشرت آثارها السلبية بشكل غير متساوٍ بين السكان. على الرغم من الجائحة، كان هناك تقدم مستمر في مكافحة عدة أسباب ملحوظة للوفاة، مما أدى إلى تحسين العمر المتوقع العالمي على مدار فترة الدراسة. أظهرت كل من المناطق الفائقة السبع في GBD تحسنًا عامًا من 1990 إلى 2021، مما يخفي التأثير السلبي في سنوات الجائحة. بالإضافة إلى ذلك، فإن نتائجنا بشأن التباين الإقليمي في أسباب الوفاة التي تدفع الزيادات في العمر المتوقع تحمل فائدة واضحة للسياسات. تكشف تحليلات الاتجاهات المتغيرة في الوفيات أن عدة أسباب، كانت شائعة عالميًا، أصبحت الآن تتركز جغرافيًا بشكل متزايد. تقدم هذه التغييرات في تركيز الوفيات، جنبًا إلى جنب مع مزيد من التحقيق في المخاطر المتغيرة، والتدخلات، والسياسات ذات الصلة، فرصة مهمة لتعميق فهمنا لاستراتيجيات تقليل الوفيات. قد تكشف دراسة أنماط تركيز الوفيات عن مناطق تم تنفيذ تدخلات الصحة العامة الناجحة فيها. يمكن أن تساعد ترجمة هذه النجاحات إلى مواقع حيث تظل بعض أسباب الوفاة راسخة في إبلاغ السياسات التي تعمل على تحسين العمر المتوقع للناس في كل مكان.
التمويل: مؤسسة بيل وميليندا غيتس.
حقوق الطبع والنشر © 2024 المؤلفون. تم النشر بواسطة إلسفير المحدودة. هذه مقالة مفتوحة الوصول بموجب ترخيص CC BY 4.0.
حقوق الطبع والنشر © 2024 المؤلفون. تم النشر بواسطة إلسفير المحدودة. هذه مقالة مفتوحة الوصول بموجب ترخيص CC BY 4.0.
المقدمة
على مدى أكثر من ثلاثة عقود، كانت دراسة عبء الأمراض والإصابات وعوامل الخطر (GBD) تسجل وتحلل بشكل منهجي وشامل أسباب الوفاة البشرية مصنفة حسب العمر والجنس والزمن في جميع أنحاء العالم.
أسباب الوفاة ليست موزعة بشكل موحد بين السكان؛ بل إن التباين الكبير في الأسباب الرئيسية غالبًا ما يعكس اختلافات اجتماعية وجغرافية مهمة.
يوفر تحليلنا فرصة للإجابة على أسئلة وبائية مهمة كانت في طليعة النقاشات الصحية العالمية والعامة – مثل، ما هي الأسباب التي ساهمت في أكبر زيادة أو انخفاض في متوسط العمر المتوقع، وما هي المواقع التي تشهد تركيزات أكبر من أسباب الوفاة القابلة للتجنب، وكيف أثرت COVID-19 وغيرها من الوفيات المرتبطة بالجائحة (OPRM) على متوسط العمر المتوقع والعبء القاتل العام للأمراض؟ لا يزال التباين الإقليمي في العديد من الأسباب الرئيسية للوفاة واضحًا في هذه التقديرات الأخيرة، مما يمثل فرصًا مهمة لإنشاء سياسة صحية مصممة لتحسين الفجوات وتخفيف تركيزات الوفيات.
يوفر GBD 2021 مجموعة محدثة وشاملة من العبء القاتل للأمراض ملخصة بمقاييس الوفيات المحددة بسبب معين ومقاييس سنوات الحياة المفقودة (YLLs) لـ 288 سببًا حسب العمر والجنس عبر 204 دول وأقاليم من 1990 إلى 2021، وهو تحديث للتقديرات المنشورة سابقًا التي تغطي 1990-2019. في هذه الدراسة، نقدم تركيزات الوفيات وتحليل تفكيك متوسط العمر المتوقع بسبب أسباب الوفاة المختلفة ونوضح تأثير أسباب الوفاة على متوسط العمر المتوقع العالمي والإقليمي والخاص بالبلد، بالإضافة إلى تسليط الضوء على المواقع الأكثر تأثرًا بعبء الوفيات الجغرافية المركزة. كما هو الحال مع النسخ السابقة من GBD، يتضمن هذا الدورة مصادر بيانات جديدة متاحة وطرق منهجية محسنة لإعادة تقدير السلسلة الزمنية بالكامل، مما يوفر تقديرات محدثة تتجاوز جميع منشورات GBD السابقة حول أسباب الوفاة. يتضمن GBD 2021 تقديرًا لعدة نماذج مختلفة لنتائج الأمراض والإصابات. تم إنتاج هذه المخطوطة كجزء من شبكة المتعاونين في GBD ووفقًا لبروتوكول GBD.
أسباب الوفاة ليست موزعة بشكل موحد بين السكان؛ بل إن التباين الكبير في الأسباب الرئيسية غالبًا ما يعكس اختلافات اجتماعية وجغرافية مهمة.
يوفر تحليلنا فرصة للإجابة على أسئلة وبائية مهمة كانت في طليعة النقاشات الصحية العالمية والعامة – مثل، ما هي الأسباب التي ساهمت في أكبر زيادة أو انخفاض في متوسط العمر المتوقع، وما هي المواقع التي تشهد تركيزات أكبر من أسباب الوفاة القابلة للتجنب، وكيف أثرت COVID-19 وغيرها من الوفيات المرتبطة بالجائحة (OPRM) على متوسط العمر المتوقع والعبء القاتل العام للأمراض؟ لا يزال التباين الإقليمي في العديد من الأسباب الرئيسية للوفاة واضحًا في هذه التقديرات الأخيرة، مما يمثل فرصًا مهمة لإنشاء سياسة صحية مصممة لتحسين الفجوات وتخفيف تركيزات الوفيات.
يوفر GBD 2021 مجموعة محدثة وشاملة من العبء القاتل للأمراض ملخصة بمقاييس الوفيات المحددة بسبب معين ومقاييس سنوات الحياة المفقودة (YLLs) لـ 288 سببًا حسب العمر والجنس عبر 204 دول وأقاليم من 1990 إلى 2021، وهو تحديث للتقديرات المنشورة سابقًا التي تغطي 1990-2019. في هذه الدراسة، نقدم تركيزات الوفيات وتحليل تفكيك متوسط العمر المتوقع بسبب أسباب الوفاة المختلفة ونوضح تأثير أسباب الوفاة على متوسط العمر المتوقع العالمي والإقليمي والخاص بالبلد، بالإضافة إلى تسليط الضوء على المواقع الأكثر تأثرًا بعبء الوفيات الجغرافية المركزة. كما هو الحال مع النسخ السابقة من GBD، يتضمن هذا الدورة مصادر بيانات جديدة متاحة وطرق منهجية محسنة لإعادة تقدير السلسلة الزمنية بالكامل، مما يوفر تقديرات محدثة تتجاوز جميع منشورات GBD السابقة حول أسباب الوفاة. يتضمن GBD 2021 تقديرًا لعدة نماذج مختلفة لنتائج الأمراض والإصابات. تم إنتاج هذه المخطوطة كجزء من شبكة المتعاونين في GBD ووفقًا لبروتوكول GBD.
البحث في السياق
الأدلة قبل هذه الدراسة
قدمت دراسة العبء العالمي للأمراض والإصابات وعوامل الخطر (GBD) تحديثات منتظمة حول الأنماط المعقدة والاتجاهات في صحة السكان حول العالم منذ أول منشور لـ GBD في عام 1993. مع كل دورة تالية، كانت هناك تحديثات منهجية مهمة، ومجموعات بيانات جديدة مدرجة، وقائمة موسعة من الأسباب وعوامل الخطر والمواقع التي يتم إنتاج تقديرات عبء المرض لها. في عام 1993، تم الإبلاغ عن الوفيات وسنوات الحياة المفقودة (YLLs) لـ 107 فئات من الأمراض التي تغطي جميع أسباب الوفاة الممكنة، لثماني مناطق. في الدورة الأخيرة من GBD – GBD 2019 – تم إنتاج تقديرات الوفيات وYLLs لـ 286 سببًا للوفاة في 204 دول وأقاليم، بما في ذلك جميع الدول الأعضاء في منظمة الصحة العالمية، وللمواقع دون الوطنية في 21 دولة وإقليم، لكل عام من 1990 إلى 2019. على الرغم من أن العديد من المجموعات قد أبلغت عن الوفيات المحددة بسبب معين على المستوى الوطني، ومقاييس صحة السكان الأخرى، بما في ذلك تقارير إحصاءات الصحة العالمية لمنظمة الصحة العالمية، فإن GBD هو الجهد البحثي الأكثر تفصيلاً وشفافية حتى الآن. علاوة على ذلك، تم الإبلاغ عن تقديرات الوفيات المرتبطة بـ COVID-19 في 2020 و2021 من قبل عدة مصادر، بما في ذلك دراسات GBD التي قامت بتحديد الوفيات الزائدة بسبب الجائحة ضمن مجموعة من مواقع GBD. ومع ذلك، لم تقم أي منشورات سابقة بتحديد تأثير COVID-19 على متوسط العمر المتوقع، مع الأخذ في الاعتبار الطيف الكامل لوفيات الأمراض على مدى العقود الثلاثة الماضية، عبر جميع الدول والأقاليم. تقدم هذه الدراسة، للمرة الأولى، 288 سببًا للوفاة من 1990 إلى 2021، تكمل نتائج الوفيات لجميع الأسباب المقدمة في تحليل التركيبة السكانية لـ GBD 2021. مجتمعة، توفر هذه الدراسات رؤية شاملة لوفيات جميع الأسباب والوفيات المحددة بسبب معين من 1990 إلى 2021.
القيمة المضافة لهذه الدراسة
بالإضافة إلى تقييمات الوفيات لجميع الأسباب ومتوسط العمر المتوقع في المنشورات المرافقة لـ GBD 2021، توضح هذه التحليل الوفيات المحددة بسبب معين وتأثيرها على متوسط العمر المتوقع. تتضمن هذه الدراسة تحليل تفكيك شامل يوضح السبب الرئيسي للوفاة الذي يؤثر على متوسط العمر المتوقع على المستوى العالمي والإقليمي والوطني. بالإضافة إلى ذلك، نقدم أسباب الوفاة وYLLs لجميع الدول والأقاليم، مما يوفر لصانعي السياسات رؤى قيمة حول التباينات في الوفيات المحددة بسبب معين. هذه الدراسة هي أيضًا الأولى من نوعها التي تنشر تقديرات 2021 للوفيات المرتبطة بـ COVID-19 وYLLs لـ 204 دول وأقاليم في سياق العبء العالمي للأمراض. على الرغم من أن منشورات أخرى قد قدرت الوفيات بسبب COVID-19، إلا أن تلك الوفيات لم تتم مقارنتها سابقًا مع الوفيات من أسباب أخرى. من خلال نمذجة وفيات COVID-19 ضمن تسلسل هرمي
لأسباب وفاة متبادلة حصرية وشاملة، توفر هذه الدراسة لصانعي السياسات معلومات أساسية لوضع أولويات الصحة حول العالم. للحصول على رؤى أكثر شمولاً من متوسط العمر المتوقع، من الضروري تقسيمه إلى وفيات محددة حسب العمر، والتي تتأثر بمعدلات الوفيات المحددة بسبب معين. قمنا بفحص تأثير COVID-19 وأسباب الوفاة الأخرى على متوسط العمر المتوقع من خلال تفكيك أعداد الوفيات إلى معدلات الوفيات المحددة بسبب معين عبر أبعاد مختلفة، بما في ذلك الدولة أو الإقليم، المنطقة، السوبر-منطقة، وخمسة فترات زمنية متميزة: 1990-2000، 2000-2010، 2010-2019، 2019-2021، و1990-2021. وبالتالي، تمكنا من معايرة جائحة COVID-19 بشكل منهجي مقابل أسباب الوفيات الأخرى على مدى الفترة من 1990 إلى 2021. أخيرًا، حددت دراستنا عدة أسباب للوفاة التي أظهرت زيادة في التركيز الجغرافي بمرور الوقت – أي، أسباب لها تأثير غير متناسب ضمن منطقة جغرافية معينة مقارنة ببقية الملاحظات العالمية. يوفر هذا التحليل معلومات مهمة لصانعي السياسات حول التباين الإقليمي واللامساواة في الوفيات المحددة بسبب معين. أيضًا جديد في GBD 2021، نبلغ عن 12 سببًا إضافيًا للوفاة: COVID-19 والوفيات المرتبطة بالجائحة الأخرى، ارتفاع ضغط الدم الشرياني الرئوي، وتسعة أنواع من السرطان – ورم الكبد، لمفوما بوركيت، لمفوما غير هودجكين الأخرى، سرطان العين، ورم الشبكية، أنواع أخرى من سرطانات العين، الأنسجة الرخوة وساركوما أخرى خارج العظام، الورم الخبيث للعظام والغضاريف المفصلية، والورم العصبي والسرطانات الأخرى للخلايا العصبية المحيطية. تم تعزيز دقة تقدير الوفيات في الأطفال دون سن 5 سنوات من خلال إضافة أربع مجموعات عمرية جديدة: 1-5 أشهر، 6-11 شهرًا، 12-23 شهرًا، و2-4 سنوات.
لأسباب وفاة متبادلة حصرية وشاملة، توفر هذه الدراسة لصانعي السياسات معلومات أساسية لوضع أولويات الصحة حول العالم. للحصول على رؤى أكثر شمولاً من متوسط العمر المتوقع، من الضروري تقسيمه إلى وفيات محددة حسب العمر، والتي تتأثر بمعدلات الوفيات المحددة بسبب معين. قمنا بفحص تأثير COVID-19 وأسباب الوفاة الأخرى على متوسط العمر المتوقع من خلال تفكيك أعداد الوفيات إلى معدلات الوفيات المحددة بسبب معين عبر أبعاد مختلفة، بما في ذلك الدولة أو الإقليم، المنطقة، السوبر-منطقة، وخمسة فترات زمنية متميزة: 1990-2000، 2000-2010، 2010-2019، 2019-2021، و1990-2021. وبالتالي، تمكنا من معايرة جائحة COVID-19 بشكل منهجي مقابل أسباب الوفيات الأخرى على مدى الفترة من 1990 إلى 2021. أخيرًا، حددت دراستنا عدة أسباب للوفاة التي أظهرت زيادة في التركيز الجغرافي بمرور الوقت – أي، أسباب لها تأثير غير متناسب ضمن منطقة جغرافية معينة مقارنة ببقية الملاحظات العالمية. يوفر هذا التحليل معلومات مهمة لصانعي السياسات حول التباين الإقليمي واللامساواة في الوفيات المحددة بسبب معين. أيضًا جديد في GBD 2021، نبلغ عن 12 سببًا إضافيًا للوفاة: COVID-19 والوفيات المرتبطة بالجائحة الأخرى، ارتفاع ضغط الدم الشرياني الرئوي، وتسعة أنواع من السرطان – ورم الكبد، لمفوما بوركيت، لمفوما غير هودجكين الأخرى، سرطان العين، ورم الشبكية، أنواع أخرى من سرطانات العين، الأنسجة الرخوة وساركوما أخرى خارج العظام، الورم الخبيث للعظام والغضاريف المفصلية، والورم العصبي والسرطانات الأخرى للخلايا العصبية المحيطية. تم تعزيز دقة تقدير الوفيات في الأطفال دون سن 5 سنوات من خلال إضافة أربع مجموعات عمرية جديدة: 1-5 أشهر، 6-11 شهرًا، 12-23 شهرًا، و2-4 سنوات.
تداعيات جميع الأدلة المتاحة
تقدم دراستنا تحليلًا كاملًا لأسباب الوفاة في جميع أنحاء العالم وعلى مر الزمن، جنبًا إلى جنب مع الأنماط المتغيرة في متوسط العمر المتوقع الناتجة عن تلك الأسباب. لوحظ تزايد التركيز الجغرافي للوفيات للعديد من أسباب الوفاة، مما يبرز الفجوات بين المناطق والاختلافات الكبيرة في المساهمات المحددة لكل سبب في متوسط العمر المتوقع. على نطاق عالمي، توفر هذه المعلومات فرصة لفحص ما إذا كانت تخفيضات الوفيات كانت مرنة أمام ظهور جائحة جديدة. على المستوى الإقليمي، توفر التقديرات التي أنتجتها دراستنا تفاصيل مهمة حول التأثير المتطور لأسباب الوفاة بين الدول، مما يسمح برؤية حاسمة حول النجاح التفاضلي حسب الجغرافيا والوقت والسبب. الطبيعة الشاملة لتقدير أسباب الوفاة في GBD 2021 توفر فرصًا قيمة للتعلم من مكاسب وخسائر الوفيات، مما يساعد على تسريع التقدم في تقليل الوفيات.
الطرق
نظرة عامة
في GBD 2021، قمنا بإنتاج تقديرات لكل كمية وبائية ذات اهتمام لـ 288 سببًا للوفاة حسب العمر والجنس والموقع والسنة لـ 25 مجموعة عمرية من
الولادة حتى 95 عامًا وأكثر؛ للذكور والإناث وكلا الجنسين معًا؛ في 204 دول وأقاليم تم تجميعها في 21 منطقة وسبع مناطق عظمى؛ ولكل عام من 1990 إلى 2021. يتضمن GBD 2021 أيضًا تحليلات دون وطنية لـ 21 دولة وإقليم
(الملحق 1 القسم 2.1). توفر شبكة دولية من المتعاونين البيانات المتاحة وتراجعها وتحللها لتوليد هذه المقاييس؛ استند GBD 2021 إلى خبرة أكثر من 11000 متعاون من أكثر من 160 دولة وإقليم.
الولادة حتى 95 عامًا وأكثر؛ للذكور والإناث وكلا الجنسين معًا؛ في 204 دول وأقاليم تم تجميعها في 21 منطقة وسبع مناطق عظمى؛ ولكل عام من 1990 إلى 2021. يتضمن GBD 2021 أيضًا تحليلات دون وطنية لـ 21 دولة وإقليم
(الملحق 1 القسم 2.1). توفر شبكة دولية من المتعاونين البيانات المتاحة وتراجعها وتحللها لتوليد هذه المقاييس؛ استند GBD 2021 إلى خبرة أكثر من 11000 متعاون من أكثر من 160 دولة وإقليم.
اتبعت الطرق المستخدمة لتوليد هذه التقديرات عن كثب تلك المستخدمة في GBD 2019.
تشمل تقديرات أسباب الوفاة في GBD 2021 الموصوفة هنا الوفيات المحددة بالسبب ومقياس الوفاة المبكرة (YLLs). قمنا بحساب YLLs كعدد الوفيات لكل سبب-عمر-جنس-موقع-سنة مضروبًا في متوسط العمر المتوقع القياسي عند كل عمر (الملحق 1 القسم 6.3). يتم حساب متوسط العمر المتوقع القياسي من أدنى معدل وفيات محدد بالعمر بين الدول.
هرمية الأمراض والإصابات في GBD
يصنف GBD الأمراض والإصابات في هرمية تتكون من أربعة مستويات تشمل كل من الأسباب القاتلة وغير القاتلة. تشمل الأسباب في المستوى 1 ثلاث فئات واسعة
(الأمراض المعدية، والأمومية، والوليدية، والتغذوية [CMNN]؛ الأمراض غير المعدية [NCDs]؛ والإصابات) ويقوم المستوى 2 بتفكيك تلك الفئات إلى 22 مجموعة من الأسباب، والتي يتم تفكيكها بشكل أكبر إلى أسباب المستوى 3 والمستوى 4. على المستوى الأكثر تفصيلًا، يتم تقدير 288 سببًا قاتلًا. للحصول على قائمة كاملة بأسباب الوفاة حسب المستوى، انظر الملحق 1 (الجدول S2). بالنسبة لـ GBD 2021، نبلغ بشكل منفصل عن 12 سببًا للوفاة للمرة الأولى: COVID-19، OPRM، ارتفاع ضغط الدم الرئوي، وتسعة أنواع من السرطان: ورم الكبد، لمفوما بوركيت، لمفوما غير هودجكين الأخرى، سرطان العين، ورم الشبكية، سرطانات العين الأخرى، الأورام اللينة والأورام خارج العظام الأخرى، الورم الخبيث للعظام والغضاريف المفصلية، والورم العصبي والأورام الأخرى لخلايا الأعصاب الطرفية.
(الأمراض المعدية، والأمومية، والوليدية، والتغذوية [CMNN]؛ الأمراض غير المعدية [NCDs]؛ والإصابات) ويقوم المستوى 2 بتفكيك تلك الفئات إلى 22 مجموعة من الأسباب، والتي يتم تفكيكها بشكل أكبر إلى أسباب المستوى 3 والمستوى 4. على المستوى الأكثر تفصيلًا، يتم تقدير 288 سببًا قاتلًا. للحصول على قائمة كاملة بأسباب الوفاة حسب المستوى، انظر الملحق 1 (الجدول S2). بالنسبة لـ GBD 2021، نبلغ بشكل منفصل عن 12 سببًا للوفاة للمرة الأولى: COVID-19، OPRM، ارتفاع ضغط الدم الرئوي، وتسعة أنواع من السرطان: ورم الكبد، لمفوما بوركيت، لمفوما غير هودجكين الأخرى، سرطان العين، ورم الشبكية، سرطانات العين الأخرى، الأورام اللينة والأورام خارج العظام الأخرى، الورم الخبيث للعظام والغضاريف المفصلية، والورم العصبي والأورام الأخرى لخلايا الأعصاب الطرفية.
مصادر البيانات، المعالجة، والتقييم من أجل الاكتمال
تضمن قاعدة بيانات أسباب الوفاة في GBD 2021 مصادر البيانات التي تم تحديدها في الجولات السابقة من التقدير بالإضافة إلى 9248 مصدرًا جديدًا (الملحق 1 الجدول S5). قمنا بتضمين أنواع بيانات متعددة لالتقاط أوسع مجموعة من المعلومات، بما في ذلك تسجيل الوفيات والتشريح اللفظي لجميع الأسباب الـ 288 بالإضافة إلى الاستطلاعات، والتعداد، والمراقبة، وسجلات السرطان، وسجلات الشرطة، وقواعد البيانات مفتوحة المصدر، وأخذ عينات الأنسجة بشكل طفيف. لتوحيد هذه البيانات بحيث يمكن مقارنتها حسب السبب والعمر والجنس والموقع والوقت، قمنا بتطبيق مجموعة من تصحيحات معالجة البيانات. أولاً، تم تقسيم الوفيات التي تفتقر إلى بيانات عمر كافية لتقدير مجموعات أعمار GBD أو تفتقر إلى بيانات العمر والجنس لتعيين مجموعات أعمار GBD وكذلك الجنس (الملحق 1 القسم 3.5). بالإضافة إلى ذلك، تم إعادة توزيع الرموز غير المحددة، التي هي غير محددة، أو غير معقولة، أو متوسطة، بدلاً من رموز أسباب الوفاة الأساسية من التصنيف الدولي للأمراض، إلى أهداف مناسبة لتعيين السبب الأساسي للوفاة.
تقييم اكتمال البيانات يوضح التغطية من مصدر البيانات على الوفيات العامة للبلد. تم تقييم اكتمال بيانات تسجيل الوفيات والتشريح اللفظي – تقدير محدد لمصدر النسبة المئوية لإجمالي الوفيات المحددة بالسبب التي تم الإبلاغ عنها في موقع وسنة معينة – حسب سنة-موقع، وتم استبعاد المصادر التي كانت أقل من
انظر عبر الإنترنت للملحق 1
للحصول على مستودع قابل للبحث عن تفاصيل النموذج المحدد بالسبب انظرhttps://www.healthdata.org/gbd/methods-appendices-2021
للحصول على مستودع قابل للبحث عن تفاصيل النموذج المحدد بالسبب انظرhttps://www.healthdata.org/gbd/methods-appendices-2021
للحصول على مصادر بيانات GBD انظرhttps://ghdx.healthdata.org/gbd-2021/sources
تحسينات في معالجة وتقدير بيانات أسباب الوفاة في GBD 2021
تعديلات للتغير العشوائي
في GBD 2021، قمنا بإجراء تحسينين رئيسيين على الأساليب المستخدمة لتقليل التباين العشوائي، والتي تؤثر بشكل أكبر على أسباب الوفاة ذات أحجام العينات الصغيرة. أولاً، قمنا بتحديث الخوارزمية البايزية المستخدمة في تقليل الضوضاء لهذه البيانات لتحسين الحفاظ على الاتجاهات الحقيقية في البيانات ذات أحجام العينات الكبيرة، وأضفنا معلومات إضافية من الاتجاهات الإقليمية للبيانات ذات أحجام العينات الصغيرة. ثانياً، تم تحديث الحد الأدنى غير الصفري، وهو أسلوب يعالج أشكال البيانات المشوهة والاتجاهات غير المنطقية الناتجة عن الأعداد الصغيرة عند تحويلها إلى مساحة اللوغاريتم، ليكون غير متغير مع الزمن ومستقلاً عن المدخلات السكانية. يمكن العثور على التفاصيل الكاملة لهذين التحسينين الرئيسيين، بالإضافة إلى تحسينات أخرى تعالج التباين العشوائي، في الملحق 1 (القسم 3.14).
تقدير COVID-19 و OPRM
قمنا باشتقاق تقديرات COVID-19 و OPRM من تحليل إجمالي الوفيات الزائدة بسبب جائحة COVID-19 من 1 يناير 2020 إلى 31 ديسمبر 2021. يتم تقديم التفاصيل الكاملة لتقدير الوفيات الزائدة، وفيات COVID-19، و OPRM في الملحق 1 (القسم 5). لتقدير الوفيات الزائدة، قمنا أولاً بتطوير قاعدة بيانات للوفيات بسبب جميع الأسباب حسب الأسبوع والشهر بعد أخذ تأخيرات الإبلاغ، والظواهر الشاذة مثل موجات الحر، وتحت تسجيل الوفيات في الاعتبار. بعد ذلك، قمنا بتطوير نموذج جماعي للتنبؤ بالوفيات المتوقعة في غياب جائحة COVID-19 للسنوات 2020 و2021. في تركيبات المواقع والأوقات التي تم استخدام البيانات لها في هذه النماذج، قمنا بتقدير الوفيات الزائدة على أنها الوفيات الملاحظة ناقص الوفيات المتوقعة. لتقدير الوفيات الزائدة لمواقع-سنوات بدون بيانات، قمنا بتطوير نموذج إحصائي للتنبؤ مباشرة بالوفيات الزائدة بسبب COVID-19، باستخدام متغيرات تتعلق بكل من جائحة COVID-19 ومقاييس صحة السكان الخلفية على مستوى السكان قبل ظهور SARS-CoV-2. تم نقل عدم اليقين عبر كل خطوة من خطوات إجراء التقدير هذا.
لإنتاج التقديرات النهائية لوفيات COVID-19 المستخدمة في GBD 2021، استخدمنا نهجًا مضادًا للواقع.
لإنتاج التقديرات النهائية لوفيات COVID-19 المستخدمة في GBD 2021، استخدمنا نهجًا مضادًا للواقع.
تقدّر الفرضيات المضادة عدد الوفيات إذا كانت معدلات اكتشاف العدوى عند أعلى قيمة تم ملاحظتها لكل موقع-سنة. باستخدام نسبة الفرضيات المضادة إلى الوفيات الزائدة ونسبة الوفيات المبلغ عنها بسبب COVID-19 إلى الوفيات الزائدة، قمنا بحساب نسبة إجمالي وفيات COVID-19 إلى الوفيات المبلغ عنها بسبب COVID-19 وضربنا هذا الرقم بعدد الوفيات المبلغ عنها بسبب COVID-19 للحصول على تقديراتنا النهائية لوفيات COVID-19.
لتفسير الزيادات في الوفيات الزائدة في عامي 2020 و2021 التي لم يمكن نسبها إلى أسباب معينة، قدمنا سببًا متبقيًا، OPRM. حددنا أربعة أسباب للوفاة – التهابات الجهاز التنفسي السفلي، والحصبة، والملاريا، والسعال الديكي – على أنها مرتبطة بجائحة COVID-19 ولديها تقديرات موثوقة بما يكفي لعدم المساهمة في OPRM. وبالتالي، قمنا بحساب OPRM كالفارق بين الوفيات الزائدة ومجموع الوفيات الناتجة عن COVID-19 وهذه الأسباب الأربعة.
عرض تقديرات الوفيات حسب السبب
تُعطى تقديرات الوفيات المحددة بسبب في عام 2021 بعدد الوفيات ومعدلات موحدة العمر لكل 100000 نسمة، تم حسابها باستخدام هيكل السكان القياسي لمشروع عبء المرض.
تحليل متوسط العمر المتوقع
الهدف من تحليل تفكيك متوسط العمر المتوقع هو تحليل الفرق في متوسط العمر المتوقع حسب العمر والموقع، مع تحديد المساهمات من أسباب محددة (الملحق 1 القسم 7). قمنا بدراسة الاتجاهات الزمنية في الأسباب على مدى فترات زمنية مستمرة عبر مواقع مختلفة. كان هدفنا هو تحديد تأثير أسباب الوفاة على متوسط العمر المتوقع من خلال استخدام ثلاث خطوات رئيسية في التفكيك. في هذه الدراسة، بحثنا في أعلى 20 سببًا من المستوى 2 والمستوى 3 من أسباب الأمراض العالمية التي تساهم في تغيير متوسط العمر المتوقع. ثم تم دمج الأسباب المتبقية كـ “أخرى من الأمراض المعدية والأمومية” أو “أخرى من الأمراض غير المعدية”. كانت الخطوة الأولى تتعلق بتفكيك الفرق في متوسط العمر المتوقع حسب العمر. قمنا بحساب المساهمات الخاصة بالعمر لفهم التباين في متوسط العمر المتوقع عبر مجموعات عمرية مختلفة. في الخطوة الثانية، تم تفكيك كل مساهمة خاصة بالعمر إلى مساهمات خاصة بالأسباب والعمر. سمح هذا التحليل بتحديد الأسباب المحددة للوفاة التي ساهمت في الفروق في متوسط العمر المتوقع داخل كل مجموعة عمرية. أخيرًا، قمنا بتجميع المساهمات الخاصة بالأسباب والعمر عبر المجموعات العمرية لإنتاج مساهمات خاصة بالأسباب في الفرق العام.
في متوسط العمر المتوقع. قدمت هذه التجميعات فهماً شاملاً لكيفية مساهمة أسباب الوفاة المختلفة في التباينات الملحوظة في متوسط العمر المتوقع. من خلال تطبيق هذا النهج في التحليل، نحصل على رؤى حول التأثير النسبي لأسباب الوفاة المختلفة على التغيرات في متوسط العمر المتوقع حسب العمر والموقع.
في متوسط العمر المتوقع. قدمت هذه التجميعات فهماً شاملاً لكيفية مساهمة أسباب الوفاة المختلفة في التباينات الملحوظة في متوسط العمر المتوقع. من خلال تطبيق هذا النهج في التحليل، نحصل على رؤى حول التأثير النسبي لأسباب الوفاة المختلفة على التغيرات في متوسط العمر المتوقع حسب العمر والموقع.
حساب تركيز الوفيات
تشير الأسباب المركزة في GBD إلى الأسباب التي تظهر تأثيرًا غير متناسب في مجموعة جغرافية محددة من البيانات مقارنة ببقية الملاحظات العالمية. في GBD 2021، استخدمنا طريقتين مختلفتين لتحديد هذه الأسباب المركزة: معامل التباين وتركيز الوفيات.
معامل التباين
لكل سبب من أسباب GBD، قمنا بحساب معامل التباين باستخدام طرق إحصائية قياسية. يقيم هذا المقياس تباين السكان بالنسبة لمتوسطهم.
التباين لديه بيانات أقل تركيزًا حول المتوسط ويشير إلى احتمال أكبر لسبب مركّز.
التباين لديه بيانات أقل تركيزًا حول المتوسط ويشير إلى احتمال أكبر لسبب مركّز.
تركيز الوفيات
لتحديد تركيزات الوفيات – المواقع الجغرافية أو مجموعات المواقع ذات السكان المتأثرين بشكل غير متناسب بسبب معين، قمنا أولاً بحساب العدد الإجمالي للوفيات بجميع الأعمار ومن كلا الجنسين في عام 2021 حسب السبب في كل من المواقع الفرعية الـ 811، وقمنا بترتيب هذه المواقع حسب عدد الوفيات بترتيب تنازلي. ثم قمنا بحساب النسبة التراكمية للوفيات من خلال قسمة الوفيات التراكمية الخاصة بكل موقع على عدد الوفيات العالمية لكل سبب. عندما وصلت النسبة التراكمية إلى أو تجاوزت
| أسباب رئيسية 1990 | معدل الوفيات الموحد حسب العمر لكل 100000، 1990 | أسباب رئيسية 2019 | معدل الوفيات الموحد حسب العمر لكل 100000، 2019 | أسباب رئيسية 2021 | معدل الوفيات الموحد حسب العمر لكل 100000، 2021 |
| 1 مرض القلب الإقفاري | 158.9 (147.4 إلى 165.4) | 1 مرض القلب الإقفاري | 110.9 (102.5 إلى 116.9) | 1 مرض القلب الإقفاري | 108.7 (99.8 إلى 115.6) |
| دورة مزدوجة |
|
دورة مزدوجة | 89.3 (81.6 إلى 95.6) | 2 كوفيد-19 | 94.0 (89.2 إلى 100.0) |
| 3 مرض الانسداد الرئوي المزمن | 71.9 (64.6 إلى 77.5) | 3 مرض الانسداد الرئوي المزمن |
|
3 ضربة | 87.4 (79.5 إلى 94.4) |
| 4 التهابات الجهاز التنفسي السفلي | 61.8 (57.0 إلى 66.8) | 4 التهابات الجهاز التنفسي السفلي |
|
4 مرض الانسداد الرئوي المزمن | ٤٥.٢ (٤٠.٧ إلى ٤٩.٨) |
| 5 أمراض الإسهال | 60.6 (46.7 إلى 79.6) | 5 اضطرابات حديثي الولادة | 30.7 (26.8 إلى 35.3) | 5 وفيات أخرى مرتبطة بالوباء | 32.3 (24.8 إلى 43.3) |
| 6 اضطرابات حديثي الولادة | ٤٦.٠ (٤٣.٥ إلى ٤٨.٩) | 6 مرض الزهايمر وأنواع الخرف الأخرى | 25.0 (6.2 إلى 65.0) | 6 اضطرابات حديثي الولادة | 29.6 (25.3 إلى 34.4) |
| 7 السل | 40.0 (34.1 إلى 44.6) | 7 سرطان الرئة | 23.7 (21.8 إلى 25.8) | 7 التهابات الجهاز التنفسي السفلي | 28.7 (26.0 إلى 31.1) |
| 8 سرطان الرئة | 27.6 (26.1 إلى 29.0) | 8 داء السكري | 19.8 (18.5 إلى 20.8) | 8 مرض الزهايمر وأنواع الخرف الأخرى | 25.2 (6.4 إلى 65.6) |
| 9 مرض الزهايمر وأنواع الخرف الأخرى | 25.1 (6.0 إلى 66.1) | 9 مرض الكلى المزمن | 18.6 (16.9 إلى 19.8) | 9 سرطان الرئة |
|
| 10 تليف الكبد | ٢٤.٤ (٢٢.٣ إلى ٢٧.٥) | 10 أمراض الإسهال | 17.1 (12.4 إلى 23.2) | 10 داء السكري | 19.6 (18.2 إلى 20.8) |
| 11 سرطان المعدة |
|
11 تليف الكبد | 17.1 (15.9 إلى 18.5) | 11 مرض الكلى المزمن | 18.5 (16.7 إلى 19.9) |
| 12 إصابة على الطريق | 21.8 (20.9 إلى 22.8) | 12 مرض القلب الناتج عن ارتفاع ضغط الدم | 16.9 (14.1 إلى 18.6) | 12 تليف الكبد | 16.6 (15.2 إلى 18.2) |
| 13 مرض القلب الناتج عن ارتفاع ضغط الدم | 20.9 (17.1 إلى 23.3) | 13 إصابة على الطريق |
|
13 مرض القلب الناتج عن ارتفاع ضغط الدم | 16.3 (13.7 إلى 18.1) |
| 14 داء السكري | 18.2 (17.0 إلى 19.1) | 14 السل | 14.9 (13.7 إلى 16.4) | 14 أمراض الإسهال | 15.4 (10.9 إلى 20.9) |
| 15 سرطان القولون والمستقيم | 15.6 (14.5 إلى 16.3) | 15 سرطان القولون والمستقيم | 12.6 (11.6 إلى 13.4) | 15 إصابة على الطرق | 14.6 (13.6 إلى 15.6) |
| 16 عيوب خلقية | 15.2 (9.6 إلى 19.7) | 16 سرطان المعدة | 11.5 (9.9 إلى 12.9) | 16 السل | 14.0 (12.6 إلى 15.8) |
| 17 إيذاء النفس | 14.9 (12.8 إلى 15.8) | 17 شلال | 10.3 (8.8 إلى 11.2) | 17 سرطان القولون والمستقيم |
|
| 18 مرض الكلى المزمن | 14.9 (13.7 إلى 16.4) | 18 فيروس نقص المناعة البشرية/الإيدز | 9.8 (9.0 إلى 11.0) | 18 سرطان المعدة | 11.2 (9.6 إلى 12.6) |
| 19 ملاريا |
|
19 ملاريا | 9.3 (3.7 إلى 18.3) | 19 ملاريا | 10.5 (3.9 إلى 21.4) |
| 20 حصبة | 11.0 (3.9 إلى 22.6) | 20 إيذاء النفس | 9.2 (8.6 إلى 9.7) | 20 شلال | 9.9 (8.5 إلى 10.8) |
| 21 شلال | 10.9 (9.8 إلى 11.8) | 21 عيب خلقي | 8.9 (7.7 إلى 10.9) | 21 إيذاء النفس | 9.0 (8.3 إلى 9.6) |
| 34 فيروس نقص المناعة البشرية/الإيدز | 5.9 (4.5 إلى 7.8) | 67 حصبة | 1.4 (0.5 إلى 3.0) | 22 فيروس نقص المناعة البشرية/الإيدز | 8.7 (8.1 إلى 9.6) |
|
|
|
الشكل 1: الأسباب الرئيسية من المستوى 3 للوفيات العالمية ومعدل الوفيات المعدل حسب العمر لكل 100000 نسمة للذكور والإناث مجتمعة، 1990، 2019، و2021
يوضح الشكل 20 سببًا رئيسيًا للوفاة بترتيب تنازلي. الأسباب متصلة بخطوط بين الفترات الزمنية؛ تمثل الخطوط الصلبة زيادة أو تحول جانبي في الترتيب، بينما تمثل الخطوط المتقطعة انخفاضًا في الترتيب. COPD=مرض الانسداد الرئوي المزمن. سرطان الرئة=سرطان القصبة الهوائية والقصبات والرئة.
يوضح الشكل 20 سببًا رئيسيًا للوفاة بترتيب تنازلي. الأسباب متصلة بخطوط بين الفترات الزمنية؛ تمثل الخطوط الصلبة زيادة أو تحول جانبي في الترتيب، بينما تمثل الخطوط المتقطعة انخفاضًا في الترتيب. COPD=مرض الانسداد الرئوي المزمن. سرطان الرئة=سرطان القصبة الهوائية والقصبات والرئة.
انظر على الإنترنت للملحق 2
لرؤية وتنزيل التقديرات من أداة نتائج GBD، انظرhttps://www.vizhub. healthdata.org/gbd-results
لرؤية وتنزيل التقديرات من أداة نتائج GBD، انظرhttps://www.vizhub. healthdata.org/gbd-results
لاستكشاف تقديرات عبء الصحة باستخدام GBD Compare، انظرhttps://www.vizhub.healthdata. org/gbd-compare
لملخصات النتائج لكل سبب من أسباب الوفاة، انظر https:// www.healthdata.org/research-analysis/diseases-injuries-risks/نشرات المعلومات
لرمز الإحصائي انظرhttp://ghdx.healthdata.org/gbd2021/code
تكرار الوفيات بين المواقع والسكان. بالإضافة إلى تحديد هذه التركيزات من الوفيات في عام 2021، قمنا بإعادة نفس التحليل لعام 1990. من خلال مقارنة النسب المعنية من السكان العالميين في هذين العامين، تمكنا من تمييز الأسباب التي أظهرت زيادة أو نقصان أو عدم تغيير في تركيزات الوفيات. كانت الأسباب المميزة في هذه الدراسة هي تلك التي تتميز بمعدل وفيات موحد حسب العمر أكبر من 0.5 لكل 100000 نسمة. الغرض من تقديم تركيزات الوفيات هو توضيح الأسباب التي تؤثر بشكل غير متناسب على مجموعات سكانية معينة، عندما كانت تلك الأسباب تؤثر سابقًا على أجزاء كبيرة من السكان. وبالتالي، لم نحسب تركيز الوفيات للأسباب التي تتوطن في مناطق معينة، حيث إن معدل الوفيات معروف بالفعل بأنه مركز بين أجزاء معينة من السكان العالميين. استبعدنا سببين متوطنين، وهما مرض فيروس إيبولا ومرض شاغاس، من هذا الحساب.
تكرار الوفيات بين المواقع والسكان. بالإضافة إلى تحديد هذه التركيزات من الوفيات في عام 2021، قمنا بإعادة نفس التحليل لعام 1990. من خلال مقارنة النسب المعنية من السكان العالميين في هذين العامين، تمكنا من تمييز الأسباب التي أظهرت زيادة أو نقصان أو عدم تغيير في تركيزات الوفيات. كانت الأسباب المميزة في هذه الدراسة هي تلك التي تتميز بمعدل وفيات موحد حسب العمر أكبر من 0.5 لكل 100000 نسمة. الغرض من تقديم تركيزات الوفيات هو توضيح الأسباب التي تؤثر بشكل غير متناسب على مجموعات سكانية معينة، عندما كانت تلك الأسباب تؤثر سابقًا على أجزاء كبيرة من السكان. وبالتالي، لم نحسب تركيز الوفيات للأسباب التي تتوطن في مناطق معينة، حيث إن معدل الوفيات معروف بالفعل بأنه مركز بين أجزاء معينة من السكان العالميين. استبعدنا سببين متوطنين، وهما مرض فيروس إيبولا ومرض شاغاس، من هذا الحساب.
ممارسات البحث والتقارير في GBD
تتوافق هذه الدراسة مع توصيات إرشادات الإبلاغ عن تقديرات الصحة الدقيقة والشفافة (GATHER؛ الملحق 1 الجدول S4).
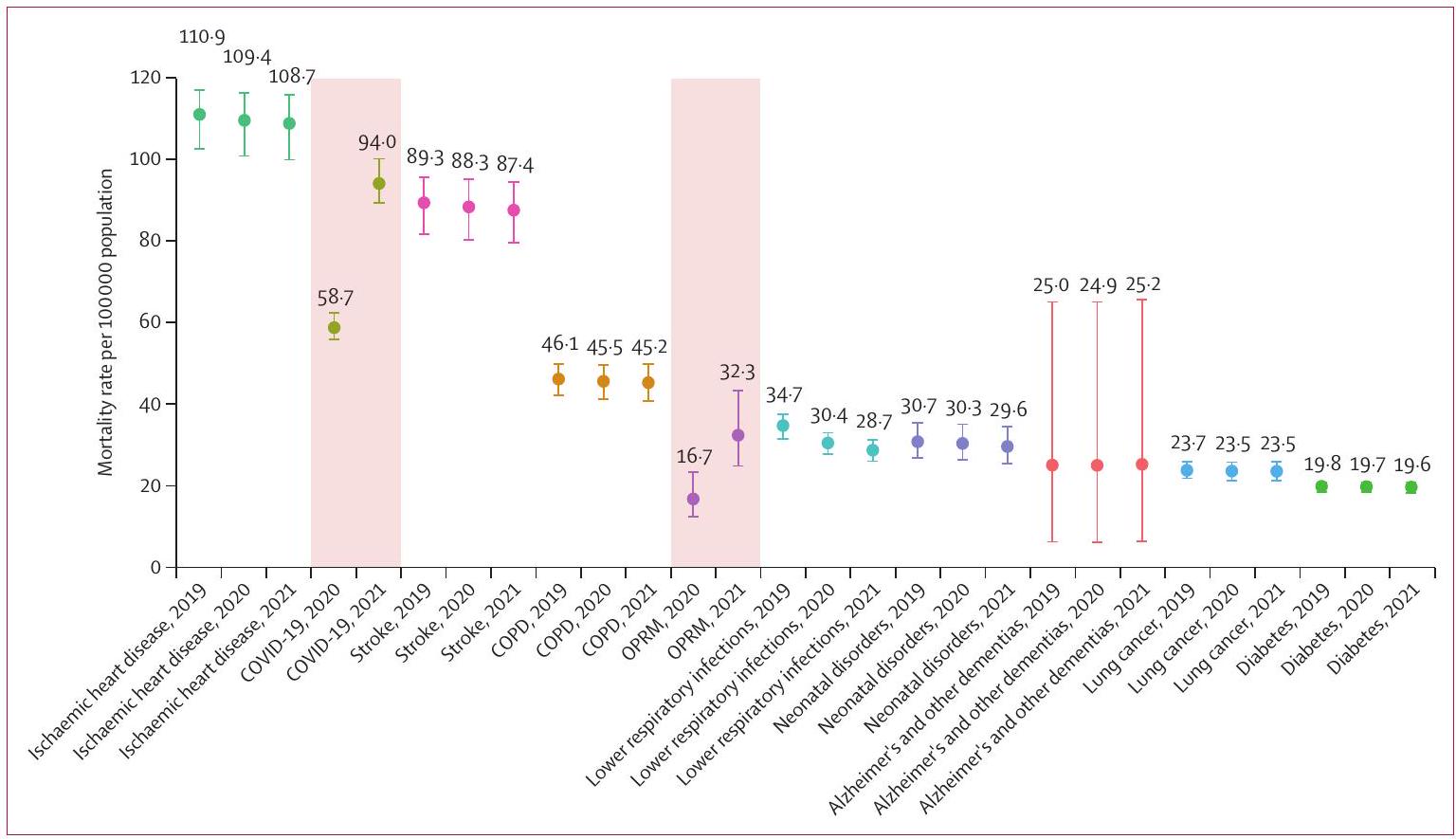
الشكل 2: معدل الوفيات الموحد حسب العمر لكل 100000 نسمة لأهم عشرة أسباب للوفاة من المستوى 3 على مستوى العالم، 2019-2021
مخطط الشوارب الذي فيه
مرض الانسداد الرئوي المزمن = COPD. وفيات أخرى مرتبطة بالوباء = OPRM.
مخطط الشوارب الذي فيه
مرض الانسداد الرئوي المزمن = COPD. وفيات أخرى مرتبطة بالوباء = OPRM.
دور مصدر التمويل
لم يكن للممول لهذه الدراسة أي دور في تصميم الدراسة، جمع البيانات، تحليل البيانات، تفسير البيانات، أو كتابة التقرير.
النتائج
يمكن الاطلاع على التقديرات الموضحة في المقال في الملحق 2. تتوفر النتائج التفصيلية لكل سبب من أسباب الوفاة في التحليل في شكل قابل للتنزيل من خلال أداة نتائج GBD ومن خلال الاستكشاف المرئي عبر الأداة الإلكترونية GBD Compare. تتوفر ملخصات النتائج لكل سبب من أسباب الوفاة المدرجة في التحليل عبر الإنترنت.
أسباب الوفاة العالمية
من 1990 إلى 2019، تراوحت نسبة التغير السنوي في الوفيات العالمية من جميع الأسباب بين
| عالمي | أوروبا الوسطى، أوروبا الشرقية، وآسيا الوسطى | دخل مرتفع | أمريكا اللاتينية ومنطقة البحر الكاريبي | شمال أفريقيا والشرق الأوسط | جنوب آسيا | جنوب شرق آسيا، شرق آسيا، وأوقيانوسيا | أفريقيا جنوب الصحراء | |
| ٢٠٢٠ | ||||||||
| 1 | ||||||||
| سبب | مرض القلب الإقفاري | مرض القلب الإقفاري | مرض القلب الإقفاري | كوفيد-19 | مرض القلب الإقفاري | مرض القلب الإقفاري | جلطة | كوفيد-19 |
| معدل موحد العمر (لكل 100000 نسمة) | ١٠٩.٤ (١٠٠.٧-١١٦.١) |
|
51.4 (45.1-54.6) | ١٣٣.٧ (
|
205.2 (182.7-225.6) |
|
|
158.9 (
|
| رقم | 8840000 (81800009360000) | ١٤١٠٠٠٠ (١٣١٠٠٠٠١٤٨٠٠٠) | ١٢٩٠٠٠٠ (١١١٠٠٠٠١٣٩٠٠٠) | 799000 (725 000869000) | 760000 (681000838000 | ١٩٦٠٠٠٠ (١٨٢٠٠٠٠٢١١٠٠٠) | ٣٤٦٠٠٠٠ (٣٠٣٠ ٠٠٠٣٨٨٠٠٠) | 659000 (615000706000) |
| 2 | سكتة دماغية | سكتة دماغية | كوفيد-19 | مرض القلب الإقفاري | كوفيد-19 | مرض الانسداد الرئوي المزمن | مرض القلب الإقفاري | جلطة |
| معدل موحد العمر (لكل 100000 نسمة) | ٨٨.٣ (٨٠.٢-٩٥.٠) |
|
41.8 (40.8-42.8) | 84.3 (77.2-89.4) |
|
١٠٤.١ (٩٢•٣-١١٧.٠) | 110.8 (97.3-124.6) | 126.2 (113.4-140.4) |
| رقم | 7140000 (6500 0007680000) | 726000 (675 000758000) | 930000 (908000952000) | 496000 (454000525000) | ٤٨٣٠٠٠ (٤١٥٠٠٠٥٣٧٠٠٠) | ١٢٣٠٠٠٠ (١٠٩٠ ٠٠٠١٣٧٠٠٠) | 2570000 (22600002880000) | 481000 (432000
|
| ٣ | ||||||||
| سبب | كوفيد-19 | كوفيد-19 | جلطة | سكتة دماغية | سكتة دماغية | كوفيد-19 | مرض الانسداد الرئوي المزمن | مرض القلب الإقفاري |
| معدل موحد العمر (لكل 100000 نسمة) | 58.7 (55.8-62.4) | 72.9 (64.1-81.7) | ٢٩.٠ (٢٤.٧-٣١.٢) | ٤٧.٥ (
|
١٠٣.٨ (٩٢•٠-١١٥•٦) |
|
66.9 (57.4-77.0) | 92.9 (83.1-103.0) |
| رقم | ٤٨٠٠٠٠٠ (٤٥٦٠٠٠٠٥١١٠٠٠) | 467000 (411000523000) | 764000 (636000830000) | 278000 (255000296000) | 370000 (329 000414000) | ١٣٢٠٠٠٠ (١٢٣٠ ٠٠٠
|
١٥٠٠٠٠٠ (١٢٩٠٠٠٠١٧٣٠٠٠) | 346000 (309 000388000) |
| ٤ | ||||||||
| سبب | مرض الانسداد الرئوي المزمن | نتائج أخرى متعلقة بجائحة كوفيد-19 | مرض الزهايمر وأنواع الخرف الأخرى | داء السكري | مرض القلب الناتج عن ارتفاع ضغط الدم | سكتة دماغية | سرطان القصبة الهوائية والشعب الهوائية والرئة | التهابات الجهاز التنفسي السفلي |
| معدل موحد العمر (لكل 100000 نسمة) |
|
41.0 (
|
|
|
40.2 (
|
٨٣.٣ (٧٥.٧-٩٠.٤) | ٣٤.٨ (
|
٨٨.٥ (٧٧.٨-٩٨.٢) |
| رقم | ٣٦٥٠٠٠٠ (٣٣٢٠٠٠٠٣٩٧٠٠٠ | 264000 (212 000333000) | 774000 (1980001900000) | 217000 (202000231000) | 138000 (110 000160000) | ١٠٦٠٠٠٠ (٩٦٩ ٠٠٠١١٥٠٠٠) | 938000 (7830001110000) | 588000 (494000686000) |
| ٥ | ||||||||
| سبب | التهابات الجهاز التنفسي السفلي | سرطان القصبة الهوائية والشعب الهوائية والرئة | سرطان القصبة الهوائية والشعب الهوائية والرئة | التهابات الجهاز التنفسي السفلي | مرض الكلى المزمن | أمراض الإسهال | مرض الزهايمر وأنواع الخرف الأخرى | الملاريا |
| معدل موحد العمر (لكل 100000 نسمة) | 30.4 (27.7-32.9) |
|
25.9 (23.8-27.0) | 32.8 (
|
37.9 (
|
|
27.9 (6.76-74.8) | 67.9 (
|
| رقم | ٢٢٨٠٠٠٠ (٢٠٨٠٠٠٠٢٤٦٠٠٠) | 168000 (161000174000) | 581000 (526 000610000) | 187000 (169000200000) | 142000 (125000159000) | 591000 (381000
|
562000 (136000
|
713000 (2510001480000) |
| ٦ | ||||||||
| سبب | اضطرابات حديثي الولادة | تليف الكبد وأمراض الكبد المزمنة الأخرى | مرض الانسداد الرئوي المزمن | مرض الكلى المزمن | نتائج أخرى متعلقة بجائحة كوفيد-19 | اضطرابات حديثي الولادة | التهابات الجهاز التنفسي السفلي | السل |
| معدل موحد العمر (لكل 100000 نسمة) |
|
|
19.2 (16.9-20.3) | 30.9 (28.3-33.1) | 30.4 (
|
43.8 (
|
|
67.3 (56.7-77.8) |
| رقم | 1910000 (1650 0002200000 ) | 131000 (127000136000) | ٤٩٠٠٠٠ (٤٢٤٠٠٠٥٢٢٠٠٠) | 184000 (169000197000) | 121000 (46500207000) | 672000 (571000792000) | 424000 (378000469000) | 378000 (313000442000) |
| (الجدول 1 يستمر في الصفحة التالية) | ||||||||
مقالات
| عالمي | أوروبا الوسطى، أوروبا الشرقية، وآسيا الوسطى | دخل مرتفع | أمريكا اللاتينية ومنطقة البحر الكاريبي | شمال أفريقيا والشرق الأوسط | جنوب آسيا | جنوب شرق آسيا، شرق آسيا، وأوقيانوسيا | أفريقيا جنوب الصحراء | |
| (مستمر من الصفحة السابقة) | ||||||||
| ٧ | ||||||||
| سبب | مرض الزهايمر وأنواع الخرف الأخرى | مرض الزهايمر وأنواع الخرف الأخرى | سرطان القولون والمستقيم | مرض الانسداد الرئوي المزمن | داء السكري | التهابات الجهاز التنفسي السفلي | مرض القلب الناتج عن ارتفاع ضغط الدم | فيروس نقص المناعة البشرية/الإيدز |
| معدل موحد العمر (لكل 100000 نسمة) | 24.9 (6.16-65.0) | 20.8 (4.88-55.3) |
|
25.0 (
|
٢٩.٤ (٢٦.٤-٣٢.٣) | 40.0 (
|
|
65.8 (59.9-73.2) |
| ٨ | ||||||||
| سبب | سرطان القصبة الهوائية والشعب الهوائية والرئة | التهابات الجهاز التنفسي السفلي | مرض الكلى المزمن | العنف بين الأفراد | مرض الانسداد الرئوي المزمن | السل | سرطان المعدة | أمراض الإسهال |
| معدل موحد العمر (لكل 100000 نسمة) |
|
|
14.0 (
|
|
٢٦.٩ (٢٣.٩-٢٩.٧) |
|
18.4 (14•2-22•0) | 57.0 (
|
| رقم | 1970000 (17800002160000) | 96200 (91200101000) | 364000 (307000
|
147000 (140000 155000) | 92400 (82500102000) | ٥٠٩٠٠٠ (٤٥٠ ٠٠٠ ٥٩٧٠٠٠) | 491000 (380 000589000) | ٤٥٢٠٠٠ (٣٢٤٠٠٠
|
|
|
داء السكري | اعتلال عضلة القلب والتهاب عضلة القلب | التهابات الجهاز التنفسي السفلي | نتائج أخرى متعلقة بجائحة كوفيد-19 | مرض الزهايمر وأنواع الخرف الأخرى | داء السكري | إصابات الطرق | نتائج أخرى متعلقة بجائحة كوفيد-19 |
| معدل موحد العمر (لكل 100000 نسمة) |
|
19.2 (17.9-20.4) |
|
20.9 (10•3-33:3) | 25.7 (6.30-67.6) | 33.1 (29.8-36.0) | 15.7 (13.9-17.6) |
|
| رقم | 1630000 (15200001720000) | ١١٣٠٠٠ (١٠٥٠٠٠١٢١٠٠٠) | ٣٦١٠٠٠ (٣٠٦٠٠٠٣٩٠٠٠٠) | 125000 (59 600199000) | 73600 (17900198000) | ٤١٩٠٠٠ (٣٧٨ ٠٠٠٤٥٧٠٠٠) | ٣٨٠٠٠٠ (٣٣٥٠٠٠٤٢٩٠٠٠) | 245000 (159000339000) |
| 10 | ||||||||
| سبب | مرض الكلى المزمن | سرطان القولون والمستقيم | إيذاء النفس | مرض الزهايمر وأنواع الخرف الأخرى | التهابات الجهاز التنفسي السفلي | نتائج أخرى متعلقة بجائحة كوفيد-19 | مرض الكلى المزمن | اضطرابات حديثي الولادة |
| معدل موحد العمر (لكل 100000 نسمة) | 18.6 (16.9-19.9) | 18.6 (17.6-19.4) | 10.9 (
|
20.8 (5.14-53.8) | 25.4 (
|
28.2 (
|
|
50.0 (
|
| رقم | ١٥٠٠٠٠٠ (١٣٦٠٠٠٠١٦١٠٠٠) | ١٢٢٠٠٠ (١١٥٠٠٠١٢٧٠٠٠) | 149000 (142000 153000) | 119000 (29200308000) | ١٠٣٠٠٠ (٩١٠٠٠١١٦٠٠٠) | 370000 (246 000514000) | ٣٧٦٠٠٠ (٣٣٣٠٠٠٤٢٠٠٠) | 889000 (749 0001050000 ) |
| 2021 | ||||||||
| 1 | ||||||||
| سبب | مرض القلب الإقفاري | مرض القلب الإقفاري | مرض القلب الإقفاري | كوفيد-19 | مرض القلب الإقفاري | كوفيد-19 | سكتة دماغية | كوفيد-19 |
| معدل موحد العمر (لكل 100000 نسمة) | ١٠٨.٧ (٩٩•٨-١١٥•٦) | 213.6 (196•1-229•1) | 51.0 (44.9-54.2) | 195.4 (182.1-211.4) |
|
|
|
٢٧١.٠ (٢٥٠.١-٢٩٠.٧) |
| رقم | 8990000 (82900009550000) | ١٤١٠٠٠٠ (١٢٩٠ ٠٠٠١٥١٠٠٠) | ١٣١٠٠٠٠ (١١٢٠٠٠٠١٤٠٠٠٠) | ١٢٠٠٠٠٠ (١١١٠٠٠٠
|
769000 (679 000863000) | 2060000 (19800002170000) | ٣٥٥٠٠٠٠ (٣١٠٠ ٠٠٠٤٠٢٠٠٠) | ١١٥٠٠٠٠ (١٠٦٠٠٠٠١٢٤٠٠٠) |
|
|
كوفيد-19 | كوفيد-19 | كوفيد-19 | مرض القلب الإقفاري | كوفيد-19 | مرض القلب الإقفاري | مرض القلب الإقفاري | جلطة |
| معدل موحد العمر (لكل 100000 نسمة) | 94.0 (89.2-100)
|
168.8 (150.6-186.1) | ٤٨.١ (٤٧.٤-٤٨.٨) | ٨٣.٨ (٧٥.٩-٩٠.٦) |
|
149.1 (
|
110.4 (94.9-124.6) |
|
| رقم | 7890000 (7490 0008400000) | ١١٠٠٠٠٠ (٩٨٢٠٠٠١٢١٠٠٠) | ١٠٧٠٠٠٠ (١٠٦٠٠٠٠١٠٩٠٠٠٠) | 504000 (457000545000) | 698000 (608000
|
١٩٩٠٠٠٠ (١٨٢٠٠٠٠٢١٦٠٠٠) | ٢٦٦٠٠٠٠ (٢٢٩٠٠٠٠٣٠٠٠٠٠) | 484000 (432000544000) |
| (الجدول 1 يستمر في الصفحة التالية) | ||||||||
| عالمي | أوروبا الوسطى، أوروبا الشرقية، وآسيا الوسطى | دخل مرتفع | أمريكا اللاتينية ومنطقة الكاريبي | شمال أفريقيا والشرق الأوسط | جنوب آسيا | جنوب شرق آسيا، شرق آسيا، وأوقيانوسيا | أفريقيا جنوب الصحراء | ||||||||||
| (مستمر من الصفحة السابقة) | |||||||||||||||||
| ٣ | |||||||||||||||||
| معدل موحد العمر (لكل 100000 نسمة) | 87.4 (
|
١٠٩.٨ (
|
28.8 (
|
|
|
101.6 (90.3-114.2) | 66.6 (56.2-77.7) | 123.9 (87.7-159.5) | |||||||||
| رقم | 7250000 (66000007820000) | 725000 (671000770000) | 771000 (641000838000) | 279000 (254000301000) | 372000 (325000421000) | ١٢٣٠٠٠٠ (١١٠٠ ٠٠٠١٣٨٠٠٠) | ١٥٦٠٠٠٠ (١٣١٠٠٠٠١٨٢٠٠٠) | 584000 (418 000757000) | |||||||||
| ٤ | |||||||||||||||||
| معدل موحد العمر (لكل 100000 نسمة) |
|
50.0 (
|
|
|
|
81.8 (
|
٣٤.٨ (٢٨.٨-٤١.١) | 92.8 (83.3-103.5) | |||||||||
| ٥ | ٣٧٢٠٠٠٠ (٣٣٦٠٠٠٠٤٠٩٠٠٠) | ٣٢١٠٠٠ (٢٢٣٠٠٠
|
792000 (2030001940000) | 236000 (135000355000) | 265000 (139 000414000) | ١٠٧٠٠٠٠ (٩٦٨٠٠٠١١٧٠٠٠) | 970000 (800 0001150000) | ٣٥٢٠٠٠ (٣١٦٠٠٠
|
|||||||||
| سبب | نتائج أخرى متعلقة بجائحة كوفيد-19 | سرطان القصبة الهوائية والشعب الهوائية والرئة | سرطان القصبة الهوائية والشعب الهوائية والرئة | داء السكري | مرض القلب الناتج عن ارتفاع ضغط الدم | نتائج أخرى متعلقة بجائحة كوفيد-19 | مرض الزهايمر وأنواع الخرف الأخرى | التهابات الجهاز التنفسي السفلي | |||||||||
| معدل موحد العمر (لكل 100000 نسمة) |
|
|
25.9 (23.8-27.0) | ٣٦.٣ (
|
|
|
28.9 (7.41-78.6) | 85.4 (75.3-95.0) | |||||||||
| ٦ | 2690000 (20600003610000) | 167000 (157000176000) | 591000 (537000620000) | ٢٢١٠٠٠ (٢٠٢٠٠٠٢٣٩٠٠٠) | 138000 (109 000162000) | ٨٣٨٠٠٠ (٦٧٤٠٠٠١٠٢٠٠٠) | 608000 (1550001670000) | 563000 (472 000655000) | |||||||||
| سبب | اضطرابات حديثي الولادة | تليف الكبد وأمراض الكبد المزمنة الأخرى | مرض الانسداد الرئوي المزمن | مرض الكلى المزمن | مرض الكلى المزمن | أمراض الإسهال | كوفيد-19 | الملاريا | |||||||||
| معدل موحد العمر (لكل 100000 نسمة) |
|
|
|
30.7 (27.8-33.5) | 37.7 (
|
٤٧.٨ (
|
|
65.9 (
|
|||||||||
| رقم | ١٨٣٠٠٠٠ (١٥٧٠ ٠٠٠٢١٣٠٠٠) | 131000 (123 000138000) | 495000 (428 000527000) | 187000 (170 000204000) | 145000 (126000164000) | 573000 (372 000908000 ) | 606000 (425000974000) | 704000 (2650001400000) | |||||||||
|
|||||||||||||||||
| معدل موحد العمر (لكل 100000 نسمة) | 28.7 (26.0-31.1) | 20.8 (4.94-55.6) | 14.7 (13.1-15.5) | 30.4 (27.0-33.3) |
|
|
|
65.8 (
|
|||||||||
| ٨ | 2180000 (19800002360000) | 137000 (32 500370000) | 348000 (304000372000) | 177000 (157000194000) | 116000 (102000129000) | 636000 (538000760000) | 431000 (384000482000) | ٣٧٣٠٠٠ (٣١٣٠٠٠
|
|||||||||
| سبب | مرض الزهايمر وأنواع الخرف الأخرى | اعتلال عضلة القلب والتهاب عضلة القلب | مرض الكلى المزمن | مرض الانسداد الرئوي المزمن | مرض الانسداد الرئوي المزمن | التهابات الجهاز التنفسي السفلي | مرض القلب الناتج عن ارتفاع ضغط الدم | فيروس نقص المناعة البشرية/الإيدز | |||||||||
| معدل موحد العمر (لكل 100000 نسمة) |
|
|
13.9 (
|
|
٢٦.٤ (
|
|
19.8 (
|
61.4 (
|
|||||||||
| رقم | 1960000 (499 0005120000) | ١١٢٠٠٠ (١٠٣٠٠٠١٢٢٠٠٠) | 368000 (310 000402000) | 145000 (130000156000) | 92700 (82000104000) | 516000 (451000584000) | ٤٧٠٠٠٠ (٣٣٣٠٠٠٥٧٥٠٠٠) | 515000 (467000583000) | |||||||||
| (الجدول 1 يستمر في الصفحة التالية) | |||||||||||||||||
مقالات
| عالمي | أوروبا الوسطى، أوروبا الشرقية، وآسيا الوسطى | دخل مرتفع | أمريكا اللاتينية ومنطقة الكاريبي | شمال أفريقيا والشرق الأوسط | جنوب آسيا | جنوب شرق آسيا، شرق آسيا، وأوقيانوسيا | أفريقيا جنوب الصحراء | |
| (مستمر من الصفحة السابقة) | ||||||||
| 9 | ||||||||
| معدل موحد العمر (لكل 100000 نسمة) |
|
|
11.9 (10.2-12.7) |
|
25.7 (6.22-66.8) |
|
18.1 (
|
54.4 (
|
| 10 | ||||||||
| سبب | داء السكري | التهابات الجهاز التنفسي السفلي | إيذاء النفس | مرض الزهايمر وأنواع الخرف الأخرى | تليف الكبد وأمراض الكبد المزمنة الأخرى | داء السكري | إصابات الطرق | اضطرابات حديثي الولادة |
| معدل موحد العمر (لكل 100000 نسمة) |
|
|
10.8 (
|
20.8 (5•18-54•3) | 23.2 (20.2-26.8) | 32.8 (
|
|
٤٨.٦ (٤٠.٣-٥٨.١) |
| رقم | ١٦٦٠٠٠٠ (١٥٤٠٠٠٠١٧٦٠٠٠) | 82800 (77800-87500) | 148000 (141000152000) | 121000 (30300317000) | 99600 (86100116000) | 426000 (383000468000) | ٣٧٩٠٠٠ (٣٣١٠٠٠٤٣٠٠٠٠) | 873000 (724000
|
| الجدول 1: عدد الوفيات ومعدلات الوفيات المعدلة حسب العمر لأهم عشرة أسباب للوفاة من المستوى 3 في عامي 2020 و2021، على مستوى العالم وحسب المناطق الكبرى، لجميع الأعمار وللذكور والإناث معًا | ||||||||
إضافي
كوفيد-19 و OPRM
تظهر تقديراتنا أن 4.80 مليون
كانت معدلات الوفيات بسبب COVID-19 متغيرة بشكل كبير بين المناطق الكبرى في GBD (الجدول 1). في عام 2021، كانت الترتيبات من الأعلى إلى الأدنى هي: أفريقيا جنوب الصحراء (271.0 وفاة [250.1-290.7] لكل 100000 نسمة)؛ أمريكا اللاتينية ومنطقة البحر الكاريبي (195.4 وفاة [182.1-211.4] لكل 100000 نسمة)؛ شمال أفريقيا والشرق الأوسط (172.4 وفاة
كانت معدلات الوفيات بسبب COVID-19 متغيرة بشكل كبير بين المناطق الكبرى في GBD (الجدول 1). في عام 2021، كانت الترتيبات من الأعلى إلى الأدنى هي: أفريقيا جنوب الصحراء (271.0 وفاة [250.1-290.7] لكل 100000 نسمة)؛ أمريكا اللاتينية ومنطقة البحر الكاريبي (195.4 وفاة [182.1-211.4] لكل 100000 نسمة)؛ شمال أفريقيا والشرق الأوسط (172.4 وفاة
تفاوتت الوفيات الناتجة عن كل من COVID-19 و OPRM بشكل كبير حسب العمر، حيث تأثرت الفئات العمرية الأكبر بشكل غير متناسب (الجدول 2). كان لدى الأفراد الذين تتراوح أعمارهم بين 70-74 عامًا أعلى عدد من الوفيات الناتجة عن كل من COVID-19 و OPRM في عام 2020 ومرة أخرى في عام 2021. كانت أعلى نسبة من إجمالي الوفيات الناتجة عن COVID-19 موجودة في الفئة العمرية 40-44 عامًا، بينما حدثت أعلى معدل للوفيات في الفئة العمرية 95 عامًا وما فوق. كانت معدلات الوفيات الناتجة عن OPRM مرتفعة بين الفئات العمرية الأكبر وبين أصغر الفئات العمرية، مع معدل من
| الوفيات | الوفيات لكل 100000 نسمة | نسبة إجمالي الوفيات | |||||||||||||||||||
| كوفيد-19 2020 | كوفيد-19 2021 |
|
|
|
كوفيد-19 2021 |
|
|
كوفيد-19 2020 | كوفيد-19 2021 | نتائج أخرى متعلقة بجائحة كوفيد-19 2020 | نتائج أخرى متعلقة بجائحة كوفيد-19 2021 | ||||||||||
| حديثي الولادة المبكر | 0 | 1 | ٣٥١٨ | ٣٤٦٢ | 0.0 | <0.1 | 141.4 | 141.2 | 0.0% | <0.1٪ | 0.2% | 0.2% | |||||||||
| حديث الولادة المتأخر | ٣ | ٥ | 5069 | 5641 | <0.1 | 0.1 |
|
77.3 | <0.1٪ | <0.1٪ | 1.1٪ | 1.3% | |||||||||
| 1-5 أشهر | 170 | 287 | 24269 | ٢٦٦٤٧ | 0.3 | 0.5 | ٤٤.٤ | ٤٩.٦ | <0.1٪ | <0.1٪ | 3.1% | ٣.٦٪ | |||||||||
| 6-11 شهر | 234 | 394 | 20478 | ٣٠٨٨٣ | 0.4 | 0.6 | 31.7 | ٤٨.٩ | <0.1٪ | 0.1% | 3.5% |
|
|||||||||
| 12-23 شهر | 998 | 1644 | 19042 | ٣٠٥٥٠ | 0.8 | 1.3 | 14.5 | ٢٣.٨ | 0.2% | 0.3% | 3.7% | 6.2% | |||||||||
| 2-4 سنوات | ٨٥٠٠ | 14386 | 14730 | 23574 | 2.1 | 3.6 | 3.6 | 5.8 | 1.2٪ | ٢.١٪ | 2.0% | 3.4٪ | |||||||||
| 5-9 سنوات | 7052 | 11393 | ٥٣٧٧ | 8196 | 1.0 | 1.7 | 0.8 | 1.2 | 1.9% | 3.2% | 1.5% | ٢.٣٪ | |||||||||
| 10-14 سنة | 8553 | 14405 | 1588 | ٢٧١٥ | 1.3 | 2.2 | 0.2 | 0.4 | 2.8٪ | ٤.٨٪ | 0.5% | 0.9% | |||||||||
| 15-19 سنة | 17032 | ٢٦٨٥٢ | 5932 | 12576 | 2.8 |
|
1.0 | 2.0 | ٣.١٪ | ٤.٨٪ | 1.1٪ | ٢.٢٪ | |||||||||
| 20-24 سنة | 25528 | ٤٠٧٤٣ | 8219 | 17453 |
|
6.8 | 1.4 | 2.9 | 3.6% | ٥.٥٪ | 1.2٪ | ٢.٤٪ | |||||||||
| 25-29 سنة | 47857 | 78496 | 12581 | 28816 | 8.1 | 13.3 | 2.1 | ٤.٩ | 5.9% | 9.2% | 1.6% | 3.4% | |||||||||
| 30-34 سنة | 81232 | 137979 | 21625 | 49808 | 13.4 | 22.8 | 3.6 | 8.2 | ٧.٩٪ | 12.3% | ٢.١٪ |
|
|||||||||
| 35-39 سنة | ١١٢٢٢٨ | 195380 | 29877 | 69402 |
|
٣٤.٨ |
|
12.4 | 9.0% | 14.1٪ | ٢.٤٪ | ٥٫٠٪ | |||||||||
| 40-44 سنة | 165337 | 287099 | ٤٤٣٩١ | ١٠٢٠٤١ |
|
٥٧.٤ | 9.0 | ٢٠.٤ | 10.3% | 16.0% | 2.8% | 5.7% | |||||||||
| 45-49 سنة | ٢٠٧٩٤٠ | 355388 | 55989 | ١٢٤٨٩٩ | ٤٤.٠ | 75.1 | 11.8 | ٢٦.٤ | 10.1٪ | 15.7% | ٢.٧٪ | 5.5٪ | |||||||||
| 50-54 سنة | 253491 | 426785 | 67629 | 147651 | ٥٧.٧ | 95.9 | 15.4 | ٣٣.٢ | 9.1% | 14.0% | ٢.٤٪ | ٤.٨٪ | |||||||||
| 55-59 سنة | 336162 | 564508 | 90815 | 191441 | 87.5 |
|
٢٣.٦ | ٤٨.٤ | 9.0% | 13.8% | ٢.٤٪ | ٤.٧٪ | |||||||||
| 60-64 سنة | 460769 | 774879 | ١٢٥٤٣٣ | 262008 | ١٤٦.١ | 242.1 | ٣٩.٨ | 81.9 | 9.8% | 15.0% | ٢.٧٪ | 5•1% | |||||||||
| 65-69 سنة | 564371 | 957557 | 155431 | 321301 | ٢٠٩.٤ | ٣٤٧.١ | ٥٧.٧ | ١١٦.٥ | 9.4% | 14.5% | 2.6% | ٤.٩٪ | |||||||||
| 70-74 سنة | 585549 | 989888 | 156931 | ٣٢٥٢٩٥ | 298.7 | ٤٨٠.٩ | 80.1 | 158.0 | 8.8٪ | 13.2% | ٢.٤٪ | ٤.٣٪ | |||||||||
| 75-79 سنة | 539515 | 861796 | 135849 | 276402 | ٤١٧.١ | 653.4 | ١٠٥.٠ | ٢٠٩.٦ | ٧.٩٪ | 11.8% | 2.0% | 3.8٪ | |||||||||
| 80-84 سنة | ٥٥١٠١٤ | 888813 | 146084 | 277786 | ٦٣٨.٩ | ١٠١٤.٨ | ١٦٩.٤ | 317.2 | ٧.٥٪ | 11.3٪ | 2.0% | 3.5% | |||||||||
| 85-89 سنة | 427770 | 658875 | 106842 | 191824 | 959.3 |
|
239.6 | ٤١٩.٥ | 6.9% | 10.0% | 1.7% | 2.9% | |||||||||
| 90-94 سنة | 280605 | 426185 | 67297 | ١١٤٤٤٩ | ١٦٠٨.٩ | ٢٣٨٢.٣ | ٣٨٥.٩ | 639.8 | ٧.٥٪ | 10.8٪ | 1.8٪ | 2.9% | |||||||||
|
|
١٢٠١٧٣ | 174390 | 24074 | 42104 | ٢٢٩٨.٦ | ٣١٩٩.٦ |
|
٧٧٢.٥ | ٧.٨٪ | 10.7% | 1.6٪ | 2.6% | |||||||||
الجدول 2: عدد الوفيات، معدلات الوفيات المعدلة حسب العمر، ونسبة إجمالي الوفيات بسبب COVID-19 وغيرها من الوفيات المرتبطة بالوباء حسب العمر، على مستوى العالم
الأسباب الرئيسية لفقدان سنوات الحياة المعدلة حسب الإعاقة على مستوى العالم
تظهر أسباب الوفاة التي تتمتع بأعلى معدلات سنوات الحياة المفقودة المعدلة حسب العمر تحولًا في الاتجاهات الوبائية من الأمراض المعدية إلى الأمراض غير المعدية في المستوى الثالث من تسلسل الأسباب (الملحق 2 الشكل S2). على مستوى العالم، كانت الأسباب الثلاثة الرئيسية لسنوات الحياة المفقودة المعدلة حسب العمر في عام 1990 جميعها من الأمراض المعدية. مرتبة بترتيب تنازلي، كانت هذه الأسباب هي الاضطرابات الوليدية، والتهابات الجهاز التنفسي السفلي، وأمراض الإسهال. في عام 2019، ظلت الاضطرابات الوليدية السبب الرئيسي لسنوات الحياة المفقودة المعدلة حسب العمر، لكن السبب الثاني والثالث تم استبدالهما بالأمراض غير المعدية: مرض القلب الإقفاري (المصنف في المرتبة الثانية) والسكتة الدماغية (المصنفة في المرتبة الثالثة). في عام 2021، كان COVID-19 السبب الثاني الرئيسي لسنوات الحياة المفقودة المعدلة حسب العمر على مستوى العالم، مما جعل السببين الرئيسيين من الأمراض المعدية (مع الاضطرابات الوليدية في المرتبة الأولى)، بينما كان مرض القلب الإقفاري في المرتبة الثالثة. من بين الأسباب الرئيسية لسنوات الحياة المفقودة المعدلة حسب العمر، كانت الملاريا السبب الوحيد الذي أظهر زيادة في معدلات سنوات الحياة المفقودة المعدلة حسب العمر بين عامي 2019 و2021 (حيث كانت في المرتبة التاسعة في عام 2019 والسابعة في عام 2021).
تحليل متوسط العمر المتوقع العالمي
لقد وجدنا اتجاهات إيجابية طويلة الأمد في متوسط العمر المتوقع العالمي منذ أوائل التسعينيات، مع زيادات ثابتة تحدث في كل عقد بين عامي 1990 و2019 (الملحق 2 الجدول S4). إجمالاً، بلغ الزيادة العالمية في متوسط العمر المتوقع من 1990 إلى 2019
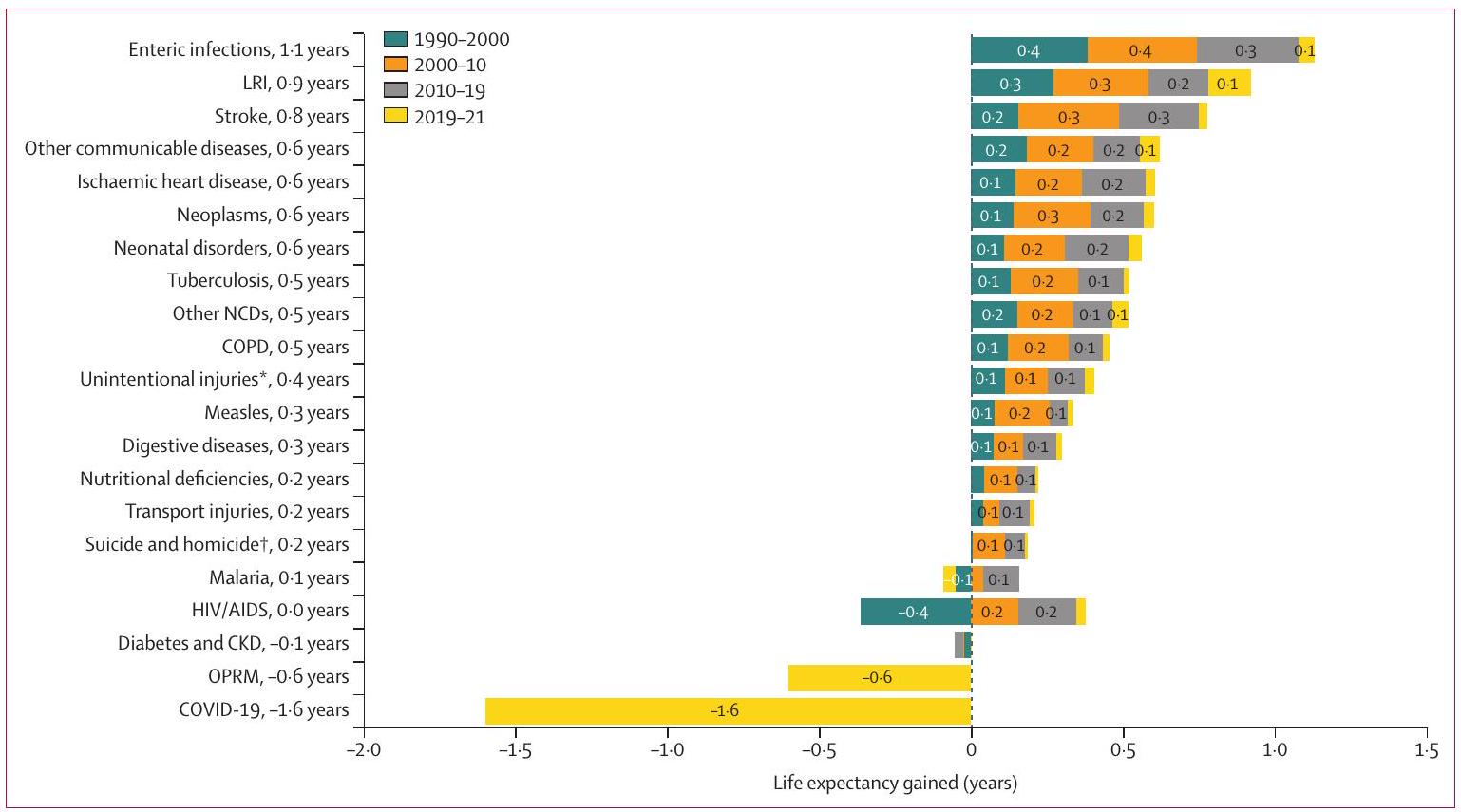
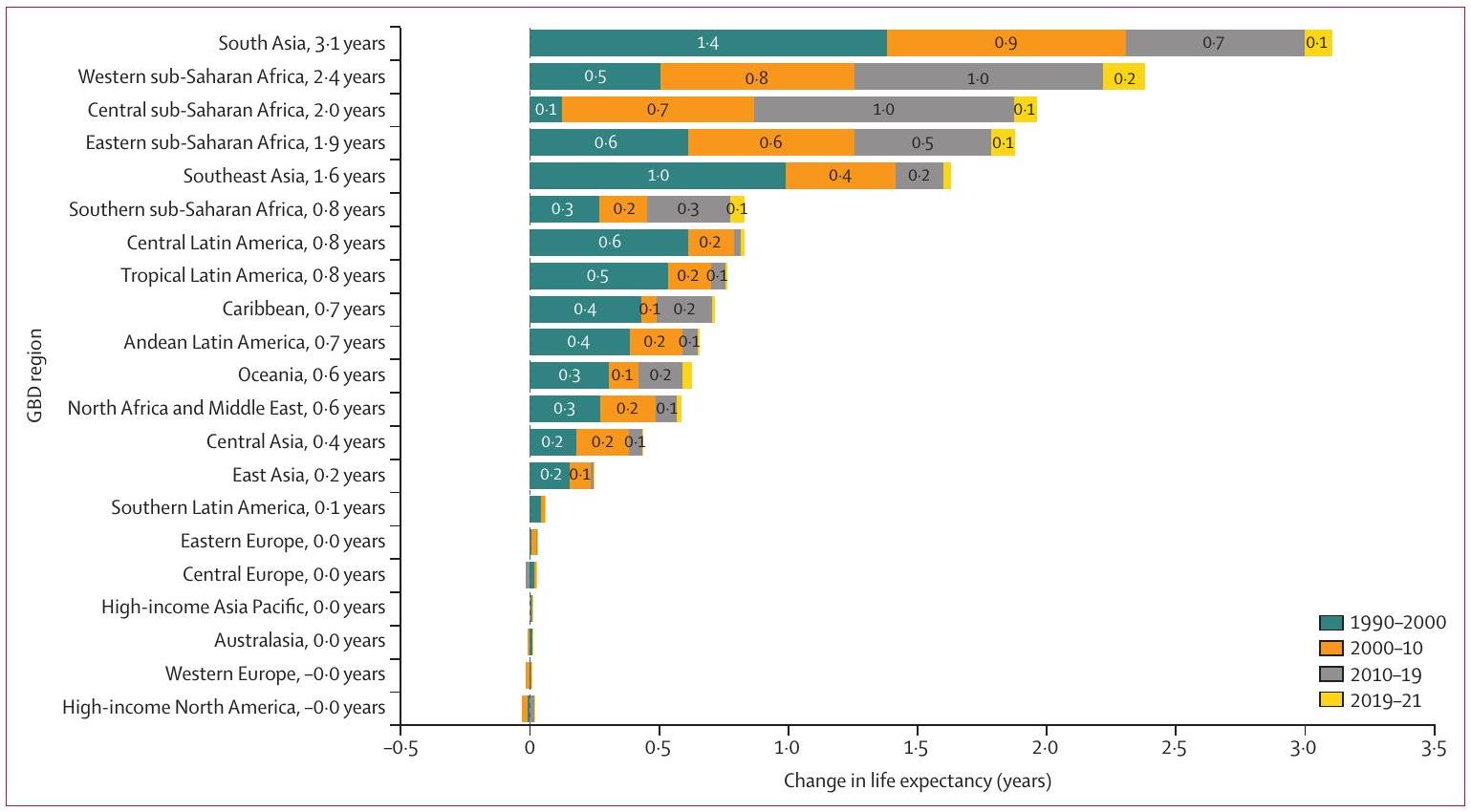
الشكل 3: التغير في متوسط العمر المتوقع الناتج عن الأسباب الرئيسية للوفاة للذكور والإناث معًا، 1990-2000، 2000-2010، 2010-2019، و2019-2021، على مستوى العالم
تمثل كل صف التغير في متوسط العمر المتوقع العالمي من 1990 إلى 2021 بسبب سبب معين. يتم تقسيم التغير الكلي في متوسط العمر المتوقع بشكل أكبر بواسطة ألوان مختلفة لتمثيل التغيرات على مر الفترات الزمنية. يمثل الشريط إلى يمين 0 زيادة في متوسط العمر المتوقع بسبب التغيرات في الفترة الزمنية المعطاة، ويمثل الشريط إلى يسار 0 انخفاضًا في متوسط العمر المتوقع بسبب فترة زمنية معينة. لأغراض القراءة، لا يتم عرض التسميات التي تشير إلى تغير في متوسط العمر المتوقع أقل من 0.05 سنوات. CKD=مرض الكلى المزمن. COPD=مرض الانسداد الرئوي المزمن. LRI=عدوى الجهاز التنفسي السفلي. NCD=مرض غير معدي. OPRM=وفيات أخرى مرتبطة بالوباء. *لا تشمل الكوارث الطبيعية. †لا تشمل الحرب والإرهاب.
تمثل كل صف التغير في متوسط العمر المتوقع العالمي من 1990 إلى 2021 بسبب سبب معين. يتم تقسيم التغير الكلي في متوسط العمر المتوقع بشكل أكبر بواسطة ألوان مختلفة لتمثيل التغيرات على مر الفترات الزمنية. يمثل الشريط إلى يمين 0 زيادة في متوسط العمر المتوقع بسبب التغيرات في الفترة الزمنية المعطاة، ويمثل الشريط إلى يسار 0 انخفاضًا في متوسط العمر المتوقع بسبب فترة زمنية معينة. لأغراض القراءة، لا يتم عرض التسميات التي تشير إلى تغير في متوسط العمر المتوقع أقل من 0.05 سنوات. CKD=مرض الكلى المزمن. COPD=مرض الانسداد الرئوي المزمن. LRI=عدوى الجهاز التنفسي السفلي. NCD=مرض غير معدي. OPRM=وفيات أخرى مرتبطة بالوباء. *لا تشمل الكوارث الطبيعية. †لا تشمل الحرب والإرهاب.
في الوفيات الناتجة عن هذه الأمراض مسؤول عن زيادة كبيرة في متوسط العمر المتوقع بمقدار 1.1 سنة خلال 1990-2021، لكن هذه الزيادة كانت أكثر وضوحًا بين 1990 و2000 مقارنة بالفترات الزمنية الأخرى. التأثير الثاني الأكبر على زيادة متوسط العمر المتوقع يُعزى إلى تقليل الوفيات الناتجة عن عدوى الجهاز التنفسي السفلي، مما ساهم في زيادة قدرها 0.9 سنوات من متوسط العمر المتوقع من 1990 إلى 2021. تشمل العوامل الرائدة الأخرى انخفاض الوفيات الناتجة عن السكتة الدماغية، وأمراض CMNN، والوفيات حديثي الولادة، وأمراض القلب الإقفارية، والأورام، وكل منها زاد متوسط العمر المتوقع العالمي بمقدار
تحليل متوسط العمر المتوقع على مستوى السوبر-منطقة، الإقليم، والدولة
شهدت كل من السبع سوبر-مناطق زيادة عامة في متوسط العمر المتوقع بين 1990 و2021، على الرغم من
أن التقدم في كل منها تأثر بشكل مختلف بـ COVID-19 (الأرقام 4، 5). أظهرت جنوب شرق آسيا، شرق آسيا، وأوقيانوسيا أعلى زيادة، مع تحسن صافي قدره 8.3 سنوات (
أن التقدم في كل منها تأثر بشكل مختلف بـ COVID-19 (الأرقام 4، 5). أظهرت جنوب شرق آسيا، شرق آسيا، وأوقيانوسيا أعلى زيادة، مع تحسن صافي قدره 8.3 سنوات (
تمت ملاحظة التأثير المختلف لـ COVID-19 على انخفاض متوسط العمر المتوقع عبر مناطق GBD (الشكل 6). على الرغم من أن معظم المناطق شهدت تحسينات عامة في متوسط العمر المتوقع بين 1990 و2021، حدث انخفاض في جنوب أفريقيا جنوب الصحراء الكبرى، التي واجهت أكبر تأثير لفيروس نقص المناعة البشرية وكانت أيضًا
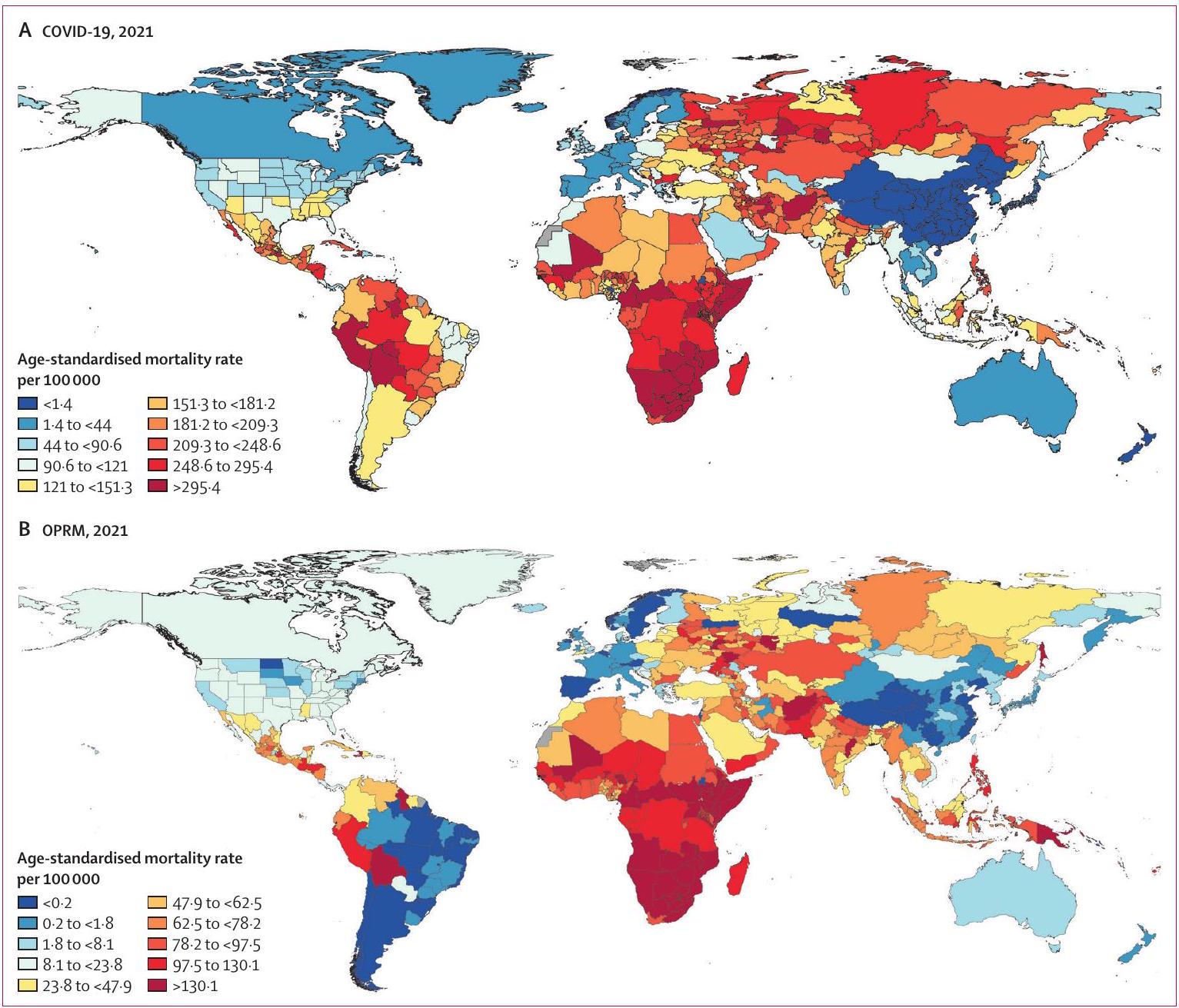
الشكل 4: معدل الوفيات المعدل حسب العمر بسبب COVID-19 وOPRM، 2021
خرائط الكوروبليث العالمية لـ COVID-19 (A) وOPRM (B) لعام 2021 التي تظهر تفاصيل دون الوطنية حيثما كان ذلك متاحًا. OPRM=وفيات أخرى مرتبطة بالوباء.
خرائط الكوروبليث العالمية لـ COVID-19 (A) وOPRM (B) لعام 2021 التي تظهر تفاصيل دون الوطنية حيثما كان ذلك متاحًا. OPRM=وفيات أخرى مرتبطة بالوباء.
الشكل 5: التغير في متوسط العمر المتوقع الناتج عن الأسباب الرئيسية للوفاة بين السوبر-مناطق، 1990-2021
تمثل كل صف التغير في متوسط العمر المتوقع من 1990 إلى 2021 لسوبر-منطقة معينة. يمثل الشريط إلى يمين 0 زيادة في متوسط العمر المتوقع بسبب التغيرات في السبب المعطى، ويمثل الشريط إلى يسار 0 انخفاضًا في متوسط العمر المتوقع بسبب سبب معين. لأغراض القراءة، لا يتم عرض التسميات التي تشير إلى تغير في متوسط العمر المتوقع أقل من
تمثل كل صف التغير في متوسط العمر المتوقع من 1990 إلى 2021 لسوبر-منطقة معينة. يمثل الشريط إلى يمين 0 زيادة في متوسط العمر المتوقع بسبب التغيرات في السبب المعطى، ويمثل الشريط إلى يسار 0 انخفاضًا في متوسط العمر المتوقع بسبب سبب معين. لأغراض القراءة، لا يتم عرض التسميات التي تشير إلى تغير في متوسط العمر المتوقع أقل من
مقالات
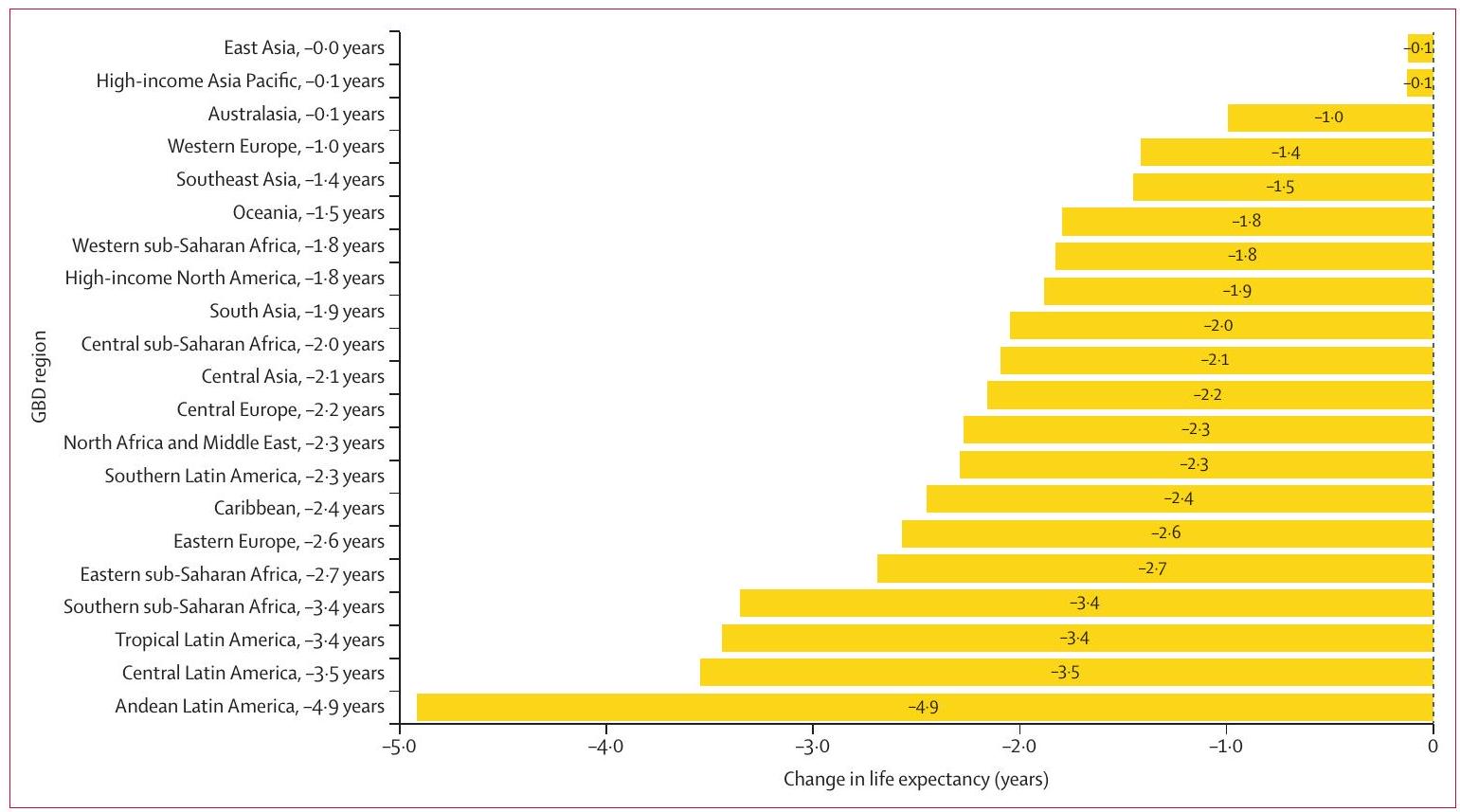
الشكل 6: تأثير COVID-19 على متوسط العمر المتوقع حسب منطقة GBD، 2019-21
لأغراض القراءة، لا يتم عرض التسميات التي تشير إلى تغير في متوسط العمر المتوقع أقل من 0.05 سنوات. GBD=دراسة العبء العالمي للأمراض والإصابات وعوامل الخطر.
تأثرت بشدة بـ COVID-19. شمل الانخفاض العام في متوسط العمر المتوقع 4.3 سنوات (
كان لفيروس نقص المناعة البشرية/الإيدز تأثير سلبي كبير على اتجاهات متوسط العمر المتوقع في جنوب أفريقيا جنوب الصحراء الكبرى من 1990 إلى 2021 (الملحق 2 الشكل S27). على الرغم من التحسينات في كل من الفترات الزمنية 2000-2010، 2010-2019، و2019-2021، لم تتمكن هذه المنطقة من استعادة 9.0 سنوات التي فقدت خلال 1990-2000. على الرغم من أننا وجدنا انخفاضًا صافيًا في الوفيات بسبب فيروس نقص المناعة البشرية/الإيدز بين 2000 و2019، إلا أن التحسينات تباطأت بشكل كبير من 2019 إلى 2021، عندما تم الحصول على 0.2 سنوات فقط في متوسط العمر المتوقع نتيجة لتقليل وفيات فيروس نقص المناعة البشرية/الإيدز. على العكس من ذلك،
كانت أفريقيا جنوب الصحراء الشرقية لديها أعلى مستوى من التعافي في متوسط العمر المتوقع بين المناطق، حيث زادت بمقدار 1.5 سنوات من متوسط العمر المتوقع على مدار فترة الدراسة بأكملها.
في عام 1990، كانت الوفيات المرتبطة بالملاريا لها تأثير ضئيل على متوسط العمر المتوقع في ثمانية من 21 منطقة GBD (الملحق 2 الشكل S13). بحلول عام 2021، ومع ذلك،
على المستوى الوطني، حدثت بعض من أعلى المكاسب في متوسط العمر المتوقع بين 1990 و2021 في المنطقة الشرقية من أفريقيا جنوب الصحراء الكبرى (الملحق 2 الشكل S12). زاد متوسط العمر المتوقع في إثيوبيا بمقدار
تأثرت بشدة بـ COVID-19. شمل الانخفاض العام في متوسط العمر المتوقع 4.3 سنوات (
كان لفيروس نقص المناعة البشرية/الإيدز تأثير سلبي كبير على اتجاهات متوسط العمر المتوقع في جنوب أفريقيا جنوب الصحراء الكبرى من 1990 إلى 2021 (الملحق 2 الشكل S27). على الرغم من التحسينات في كل من الفترات الزمنية 2000-2010، 2010-2019، و2019-2021، لم تتمكن هذه المنطقة من استعادة 9.0 سنوات التي فقدت خلال 1990-2000. على الرغم من أننا وجدنا انخفاضًا صافيًا في الوفيات بسبب فيروس نقص المناعة البشرية/الإيدز بين 2000 و2019، إلا أن التحسينات تباطأت بشكل كبير من 2019 إلى 2021، عندما تم الحصول على 0.2 سنوات فقط في متوسط العمر المتوقع نتيجة لتقليل وفيات فيروس نقص المناعة البشرية/الإيدز. على العكس من ذلك،
كانت أفريقيا جنوب الصحراء الشرقية لديها أعلى مستوى من التعافي في متوسط العمر المتوقع بين المناطق، حيث زادت بمقدار 1.5 سنوات من متوسط العمر المتوقع على مدار فترة الدراسة بأكملها.
في عام 1990، كانت الوفيات المرتبطة بالملاريا لها تأثير ضئيل على متوسط العمر المتوقع في ثمانية من 21 منطقة GBD (الملحق 2 الشكل S13). بحلول عام 2021، ومع ذلك،
على المستوى الوطني، حدثت بعض من أعلى المكاسب في متوسط العمر المتوقع بين 1990 و2021 في المنطقة الشرقية من أفريقيا جنوب الصحراء الكبرى (الملحق 2 الشكل S12). زاد متوسط العمر المتوقع في إثيوبيا بمقدار
الشكل 7: تأثير الأمراض المعدية المعوية على متوسط العمر المتوقع حسب الفترة الزمنية ومنطقة GBD، 1990-2021
لتحسين القراءة، لا تظهر التسميات التي تشير إلى تغيير في متوسط العمر المتوقع أقل من 0.05 سنة. GBD=عبء الأمراض العالمية، والإصابات، ودراسة عوامل الخطر.
لتحسين القراءة، لا تظهر التسميات التي تشير إلى تغيير في متوسط العمر المتوقع أقل من 0.05 سنة. GBD=عبء الأمراض العالمية، والإصابات، ودراسة عوامل الخطر.
تأثير أمراض CMNN على متوسط العمر المتوقع واتجاهات تركيز الوفيات
بين أسباب CMNN، ظهرت عدة اتجاهات رئيسية في تأثيرها على متوسط العمر المتوقع العالمي وتوزيع الوفيات مع مرور الوقت. أولاً، كان لانخفاض الوفيات بسبب الأمراض المعوية تأثير كبير على متوسط العمر المتوقع العالمي، مع تباينات إقليمية ملحوظة (الشكل 7). مع تقدم 160 دولة وإقليم في تقليل الوفيات المرتبطة بأمراض CMNN، ظهر تركيز الوفيات. أصبحت الوفيات أكثر تركيزًا في دول أو مناطق معينة، واستمرت جنبًا إلى جنب مع التقدم المحرز في أجزاء أخرى من العالم. مثال توضيحي هو التحول في الوفيات بسبب الأمراض المعوية لدى الأطفال دون سن 5 سنوات، حيث
على اتجاهات متوسط العمر المتوقع، خاصة في جنوب الصحراء الأفريقية، ومع
ساهمت الانخفاضات في وفيات حديثي الولادة في زيادة قدرها
على اتجاهات متوسط العمر المتوقع، خاصة في جنوب الصحراء الأفريقية، ومع
ساهمت الانخفاضات في وفيات حديثي الولادة في زيادة قدرها
الشكل 8: تأثير العدوى التنفسية السفلية على متوسط العمر المتوقع حسب الفترة الزمنية ومنطقة GBD، 1990-2021
لتحسين القراءة، لا تظهر التسميات التي تشير إلى تغيير في متوسط العمر المتوقع أقل من 0.05 سنة. GBD=عبء الأمراض العالمية، والإصابات، ودراسة عوامل الخطر.
لتحسين القراءة، لا تظهر التسميات التي تشير إلى تغيير في متوسط العمر المتوقع أقل من 0.05 سنة. GBD=عبء الأمراض العالمية، والإصابات، ودراسة عوامل الخطر.
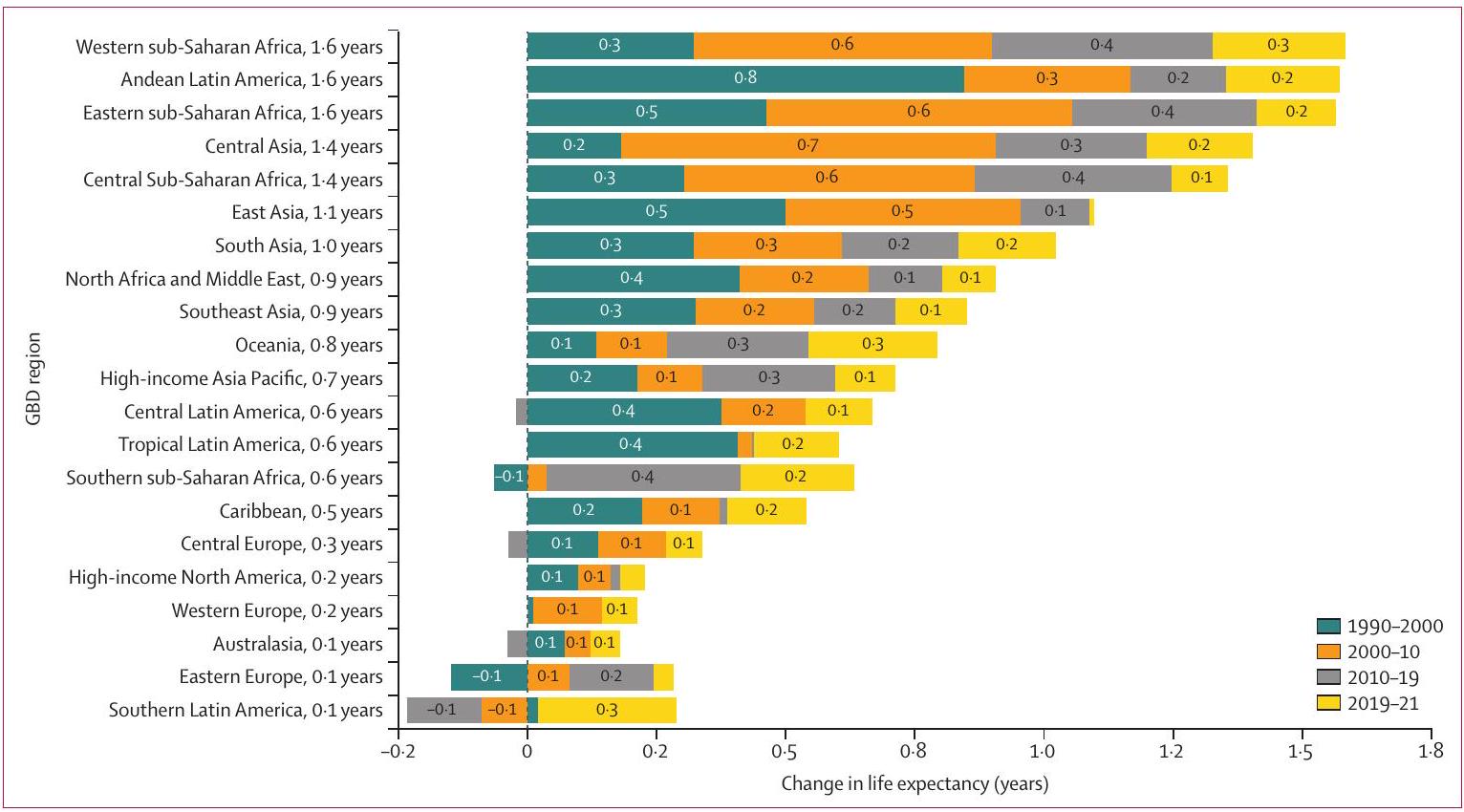
الشكل 9: التغيير في متوسط العمر المتوقع الناتج عن الأسباب الرئيسية للوفاة بين مناطق GBD، 1990-2021
تمثل كل صف التغيير في متوسط العمر المتوقع من 1990 إلى 2021 لمنطقة GBD معينة. يمثل شريط إلى يمين 0 زيادة في متوسط العمر المتوقع بسبب التغيرات في السبب المعطى، ويمثل شريط إلى يسار 0 انخفاضًا في متوسط العمر المتوقع لسبب معين. لتحسين القراءة، لا تظهر التسميات التي تشير إلى تغيير في متوسط العمر المتوقع أقل من 0.3 سنة. CKD=مرض الكلى المزمن. COPD=مرض الرئة الانسدادي المزمن. GBD=عبء الأمراض العالمية، والإصابات، ودراسة عوامل الخطر. LRI=العدوى التنفسية السفلية. NCD=مرض غير معدي. OPRM=وفيات أخرى مرتبطة بالوباء. *لا تشمل الحرب والإرهاب. †لا تشمل الكوارث الطبيعية.
تمثل كل صف التغيير في متوسط العمر المتوقع من 1990 إلى 2021 لمنطقة GBD معينة. يمثل شريط إلى يمين 0 زيادة في متوسط العمر المتوقع بسبب التغيرات في السبب المعطى، ويمثل شريط إلى يسار 0 انخفاضًا في متوسط العمر المتوقع لسبب معين. لتحسين القراءة، لا تظهر التسميات التي تشير إلى تغيير في متوسط العمر المتوقع أقل من 0.3 سنة. CKD=مرض الكلى المزمن. COPD=مرض الرئة الانسدادي المزمن. GBD=عبء الأمراض العالمية، والإصابات، ودراسة عوامل الخطر. LRI=العدوى التنفسية السفلية. NCD=مرض غير معدي. OPRM=وفيات أخرى مرتبطة بالوباء. *لا تشمل الحرب والإرهاب. †لا تشمل الكوارث الطبيعية.
شهدت أفريقيا جنوب الصحراء وآسيا الجنوبية زيادات ملحوظة. وجدنا تحولًا نحو تركيز الوفيات، مع
تأثير الأمراض غير المعدية على متوسط العمر المتوقع واتجاهات تركيز الوفيات
بين الأمراض غير المعدية، تعكس عدة نتائج تأثيرها على متوسط العمر المتوقع العالمي وتركيز الوفيات. أدت الانخفاضات في السكتة الدماغية إلى مكسب ملحوظ في متوسط العمر المتوقع قدره 0.8 سنة، لكن وفيات السكتة الدماغية لم تكن مركزة، مع
تأثير الإصابات على متوسط العمر المتوقع واتجاهات تركيز الوفيات
كان لانخفاض إصابات النقل تأثير إيجابي على متوسط العمر المتوقع، مما ساهم في زيادة قدرها 0.2 سنة. ومع ذلك، كما هو الحال مع الأمراض غير المعدية، لم يكن تركيز وفيات إصابات النقل مرتفعًا، مع
تركيزًا قليلًا للوفيات، مع
تركيزًا قليلًا للوفيات، مع
المناقشة النتائج الرئيسية
لقد ظهرت جائحة COVID-19 كواحدة من أكثر الأحداث الصحية العالمية تحديدًا في التاريخ الحديث. تقدم تقديراتنا الشاملة الأخيرة للوفيات حسب السبب نظرة ثاقبة على المشهد العالمي للأمراض قبل وخلال العامين الأولين من الجائحة، كاشفة عن التغيرات المهمة في أنماط عبء المرض التي تلت ذلك. بعد أكثر من ثلاثة عقود من التحسينات المستمرة في متوسط العمر المتوقع العالمي وانخفاض معدلات الوفيات المعدلة حسب العمر، عكست COVID-19 التقدم المستمر وأعاقت الاتجاهات في الانتقال الوبائي. باعتبارها السبب الثاني الرئيسي للوفيات المعدلة حسب العمر في عام 2021، كان لـ COVID-19 تأثير بارز على الانخفاض في متوسط العمر المتوقع العالمي الذي حدث. يوفر التأثير غير المتجانس للمرض عبر العالم رؤى مهمة لتحسين الاستعداد للجائحات المستقبلية وضمان تجهيز الدول بشكل عادل للاستجابة لتفشي الأمراض الجديدة. بالإضافة إلى ذلك، تمكننا تحليلاتنا للاتجاهات الجغرافية والزمنية في الوفيات من ملاحظة الأنماط المتغيرة في أسباب الوفاة على مستوى العالم. لقد أظهرت العديد من الأسباب نطاقًا جغرافيًا أقل – وهو انعكاس للجهود المخصصة والمستمرة للتخفيف من عبء بعض الأسباب، فضلاً عن التغيرات المحتملة في التعرض لعوامل الخطر.
جائحة كوفيد-19
ظهور وانتشار COVID-19 يتبع نمطًا مشابهًا من التباين الإقليمي الذي هو شائع بين العديد من الأسباب الرئيسية للوفاة القابلة للاكتساب، حيث تحدث معدلات إصابة أعلى وزيادة في الوفيات في البيئات ذات الموارد المحدودة.
تؤكد المواقع على تعقيد الجائحة. ساهمت التأثيرات الاجتماعية والاقتصادية والسياسية المتنوعة في الاختلافات في معدلات الوفيات التي لوحظت بين المواقع. بشكل عام، كانت المناطق التي تتمتع بأنظمة رعاية صحية متقدمة ومرافق طبية قوية أكثر قدرة على إدارة الزيادات المفاجئة في عدد حالات COVID-19. بالمقابل، كانت المواقع التي تعاني من بنية تحتية صحية ضعيفة أقل تجهيزًا للتعامل مع الزيادة في الإصابات التي حدثت.
تظهر دراستنا أن COVID-19 كان واحدًا من الأسباب الرئيسية للوفاة على مستوى العالم خلال العامين الأولين من الجائحة وتوفر فرصة لتحديد الفروق بين آثار المرض المباشرة وغير المباشرة على الوفيات بالإضافة إلى تأثيره على متوسط العمر المتوقع. كما تم التنبؤ به سابقًا،
تؤكد المواقع على تعقيد الجائحة. ساهمت التأثيرات الاجتماعية والاقتصادية والسياسية المتنوعة في الاختلافات في معدلات الوفيات التي لوحظت بين المواقع. بشكل عام، كانت المناطق التي تتمتع بأنظمة رعاية صحية متقدمة ومرافق طبية قوية أكثر قدرة على إدارة الزيادات المفاجئة في عدد حالات COVID-19. بالمقابل، كانت المواقع التي تعاني من بنية تحتية صحية ضعيفة أقل تجهيزًا للتعامل مع الزيادة في الإصابات التي حدثت.
تظهر دراستنا أن COVID-19 كان واحدًا من الأسباب الرئيسية للوفاة على مستوى العالم خلال العامين الأولين من الجائحة وتوفر فرصة لتحديد الفروق بين آثار المرض المباشرة وغير المباشرة على الوفيات بالإضافة إلى تأثيره على متوسط العمر المتوقع. كما تم التنبؤ به سابقًا،
اتجاهات مهمة في متوسط العمر المتوقع
لقد ساهمت التقدمات على مدى العقود الثلاثة الماضية في الوقاية من الأمراض المعدية ومكافحتها في زيادة متوسط العمر المتوقع في العديد من الأماكن، مما زاد الحاجة إلى دعم السكان الذين يعيشون مع الأمراض غير المعدية.
لقد عوض فيروس نقص المناعة البشرية/الإيدز والعدوى التنفسية السفلية والعدوى المعوية بشكل ما عن الانخفاض، كما أن انخفاض متوسط العمر المتوقع قد تفاقم أيضًا بسبب زيادة معدلات الوفيات من أسباب أخرى، مثل مرض السكري وأمراض الكلى.
أظهر تأثير COVID-19 على متوسط العمر المتوقع درجات متفاوتة من الشدة، تتراوح من فقدان كبير قدره 4.9 سنوات في أمريكا اللاتينية الأنديزية إلى تغير طفيف تقريبًا في شرق آسيا. من 1990 إلى 2021، أدت التخفيضات في العديد من الأسباب الرئيسية للوفاة إلى زيادات عامة في متوسط العمر المتوقع عبر معظم المناطق، على الرغم من الانتكاسات الكبيرة للعديد بسبب جائحة COVID-19. وجدنا أنه على الرغم من أن أمريكا اللاتينية الأنديزية شهدت أكبر انخفاض إقليمي في متوسط العمر المتوقع بسبب الجائحة، إلا أن التخفيضات العامة في متوسط العمر المتوقع عبر المنطقة تم تخفيفها من خلال التحسينات في أسباب أخرى، حيث كانت التخفيضات في معدلات الوفاة بسبب التهابات الجهاز التنفسي السفلي والاضطرابات الوليدية مسؤولة عن زيادة في متوسط العمر المتوقع قدرها 2.6 سنوات بشكل عام بين 1990 و2021. وقد تم نسب التخفيضات الملحوظة في الاضطرابات الوليدية في العديد من دول أمريكا اللاتينية الأنديزية إلى التحسينات التي تم تحقيقها في تنفيذ استراتيجيات التدخل الفعالة في صحة الأم والوليد.
لقد تجاوزت نسبة الانخفاض في متوسط العمر المتوقع في جنوب الصحراء الكبرى الأفريقية المتوسط العالمي بفارق كبير، حيث انخفض بمقدار 3.4 سنوات بسبب COVID-19. على الرغم من أن متوسط العمر المتوقع في المنطقة تأثر بشكل كبير بجائحة COVID-19، إلا أن الانخفاض كان أيضًا ناتجًا عن معدلات الوفيات العالية بسبب فيروس نقص المناعة البشرية/الإيدز. كانت بعض الدول التي شهدت أعدادًا مرتفعة من الوفيات المرتبطة بالجائحة من بين تلك التي كانت تعاني بالفعل من معدلات مرتفعة من الأمراض المعدية الأخرى. navigated العديد من الدول في جنوب الصحراء الكبرى الأفريقية التحديات التي فرضتها الجائحة، إلى جانب تاريخ طويل من مكافحة بعض من أعلى معدلات انتشار فيروس نقص المناعة البشرية/الإيدز في العالم.
أظهر تأثير COVID-19 على متوسط العمر المتوقع درجات متفاوتة من الشدة، تتراوح من فقدان كبير قدره 4.9 سنوات في أمريكا اللاتينية الأنديزية إلى تغير طفيف تقريبًا في شرق آسيا. من 1990 إلى 2021، أدت التخفيضات في العديد من الأسباب الرئيسية للوفاة إلى زيادات عامة في متوسط العمر المتوقع عبر معظم المناطق، على الرغم من الانتكاسات الكبيرة للعديد بسبب جائحة COVID-19. وجدنا أنه على الرغم من أن أمريكا اللاتينية الأنديزية شهدت أكبر انخفاض إقليمي في متوسط العمر المتوقع بسبب الجائحة، إلا أن التخفيضات العامة في متوسط العمر المتوقع عبر المنطقة تم تخفيفها من خلال التحسينات في أسباب أخرى، حيث كانت التخفيضات في معدلات الوفاة بسبب التهابات الجهاز التنفسي السفلي والاضطرابات الوليدية مسؤولة عن زيادة في متوسط العمر المتوقع قدرها 2.6 سنوات بشكل عام بين 1990 و2021. وقد تم نسب التخفيضات الملحوظة في الاضطرابات الوليدية في العديد من دول أمريكا اللاتينية الأنديزية إلى التحسينات التي تم تحقيقها في تنفيذ استراتيجيات التدخل الفعالة في صحة الأم والوليد.
لقد تجاوزت نسبة الانخفاض في متوسط العمر المتوقع في جنوب الصحراء الكبرى الأفريقية المتوسط العالمي بفارق كبير، حيث انخفض بمقدار 3.4 سنوات بسبب COVID-19. على الرغم من أن متوسط العمر المتوقع في المنطقة تأثر بشكل كبير بجائحة COVID-19، إلا أن الانخفاض كان أيضًا ناتجًا عن معدلات الوفيات العالية بسبب فيروس نقص المناعة البشرية/الإيدز. كانت بعض الدول التي شهدت أعدادًا مرتفعة من الوفيات المرتبطة بالجائحة من بين تلك التي كانت تعاني بالفعل من معدلات مرتفعة من الأمراض المعدية الأخرى. navigated العديد من الدول في جنوب الصحراء الكبرى الأفريقية التحديات التي فرضتها الجائحة، إلى جانب تاريخ طويل من مكافحة بعض من أعلى معدلات انتشار فيروس نقص المناعة البشرية/الإيدز في العالم.
أنماط تركيز الوفيات حسب السبب
تقديرات تركيز الوفيات تعكس أنماط الأمراض المتغيرة بمرور الوقت، من الأمراض التي لها انتشار واسع إلى مجموعات جغرافية أكثر تقليصًا من السكان العالميين. تسلط هذه التغييرات الضوء على الفروق بين السكان وتقدمهم نحو تقليل الوفيات الناتجة عن الأمراض والإصابات. كما توفر هذه النتائج فرصة مهمة لتحسين كيفية تطبيق أفضل الممارسات الصحية العامة لتحقيق مزيد من تقليل الأمراض. بشكل عام، أدت الانخفاضات الواسعة في العديد من الأمراض المعدية إلى ظهور الوفيات الناتجة عن هذه الأسباب بشكل أكثر
توزيعات جغرافية مركزة في عام 2021 مقارنة بالأنماط التي لوحظت في عام 1990. إن درجة تركيز الوفيات التي قدرتها هذه الدراسة بسبب العدوى المعوية والالتهابات التنفسية السفلية والملاريا وفيروس نقص المناعة البشرية/الإيدز والاضطرابات الوليدية والسل تعكس تقدمًا عالميًا كبيرًا في تقليل الوفيات الناتجة عن هذه الأسباب خلال فترة الدراسة، مما يبرز نجاح العديد من الحملات الصحية العامة والالتزامات العالمية والتحسينات في برامج الأمراض المعدية.
من الجدير بالذكر أن تقديراتنا تدعم النتائج السابقة
أظهرت العدوى المعوية تركيزًا كبيرًا للأمراض. كانت وفيات الأطفال دون سن الخامسة بسبب العدوى المعوية مركزة بشكل كبير في أفريقيا جنوب الصحراء وآسيا الجنوبية. كانت الدول في أفريقيا جنوب الصحراء وآسيا الجنوبية التي سجلت أعلى معدلات وفيات الأطفال دون سن الخامسة بسبب العدوى المعوية في عام 2021 تشمل تشاد وجنوب السودان وجمهورية إفريقيا الوسطى. هناك العديد من العوامل المساهمة التي يجب أخذها في الاعتبار عند دراسة كيفية تقليل العدوى المعوية في المواقع المتبقية المركزة. إلى جانب توفير محلول الإماهة الفموية ولقاحات الروتا فيروس، قد تكون التحسينات الحيوية في الصحة العامة مثل المياه والصرف الصحي والنظافة قد ساهمت في تقليل وفيات العدوى المعوية.
توزيعات جغرافية مركزة في عام 2021 مقارنة بالأنماط التي لوحظت في عام 1990. إن درجة تركيز الوفيات التي قدرتها هذه الدراسة بسبب العدوى المعوية والالتهابات التنفسية السفلية والملاريا وفيروس نقص المناعة البشرية/الإيدز والاضطرابات الوليدية والسل تعكس تقدمًا عالميًا كبيرًا في تقليل الوفيات الناتجة عن هذه الأسباب خلال فترة الدراسة، مما يبرز نجاح العديد من الحملات الصحية العامة والالتزامات العالمية والتحسينات في برامج الأمراض المعدية.
من الجدير بالذكر أن تقديراتنا تدعم النتائج السابقة
أظهرت العدوى المعوية تركيزًا كبيرًا للأمراض. كانت وفيات الأطفال دون سن الخامسة بسبب العدوى المعوية مركزة بشكل كبير في أفريقيا جنوب الصحراء وآسيا الجنوبية. كانت الدول في أفريقيا جنوب الصحراء وآسيا الجنوبية التي سجلت أعلى معدلات وفيات الأطفال دون سن الخامسة بسبب العدوى المعوية في عام 2021 تشمل تشاد وجنوب السودان وجمهورية إفريقيا الوسطى. هناك العديد من العوامل المساهمة التي يجب أخذها في الاعتبار عند دراسة كيفية تقليل العدوى المعوية في المواقع المتبقية المركزة. إلى جانب توفير محلول الإماهة الفموية ولقاحات الروتا فيروس، قد تكون التحسينات الحيوية في الصحة العامة مثل المياه والصرف الصحي والنظافة قد ساهمت في تقليل وفيات العدوى المعوية.
موضوع واسع ومتكرر من هذه الدراسة هو أن تقليل العدوى المعوية ساهم في تحسين متوسط العمر المتوقع على مدى العقود القليلة الماضية. وقد حدثت الانخفاضات في وفيات الأطفال المرتبطة بأمراض الإسهال في العديد من مناطق أفريقيا.
لقد وجدت دراستنا أيضًا أن بعض الأمراض التي يمكن الوقاية منها باللقاحات، مثل الحصبة، قد أظهرت انخفاضات واسعة في معدلات الوفيات وكانت مركزة جغرافيًا. كانت وفيات الأطفال دون سن الخامسة بسبب الحصبة مركزة في غرب وشرق أفريقيا جنوب الصحراء الكبرى. على الرغم من أن هناك عوامل متعددة تساهم في انخفاض عبء الأمراض المعدية، فإن التحسينات في وفيات الحصبة تعود إلى حد كبير إلى التوافر العالمي للقاح آمن وفعال ضد الحصبة، مما يوفر مناعة تدوم مدى الحياة، مع فعالية الجرعتين التي تتجاوز
بعض الأمراض المعدية، مثل فيروس نقص المناعة البشرية/الإيدز، أظهرت أيضًا تركيزًا في الوفيات. الوفيات الناتجة عن فيروس نقص المناعة البشرية/الإيدز
كانت تتركز بشكل كبير داخل منطقة جنوب الصحراء الكبرى في إفريقيا، وخاصة في جنوب منطقة جنوب الصحراء الكبرى. كانت الدول في منطقة جنوب الصحراء الكبرى التي سجلت أعلى معدل وفيات معيار العمر في عام 2021 تشمل ليسوتو، وإسواتيني، وبوتسوانا. وكانت الدول في منطقة جنوب الصحراء الكبرى التي سجلت أعلى معدلات وفيات الأطفال دون سن الخامسة بسبب فيروس نقص المناعة البشرية (HIV) في عام 2021 تشمل ليسوتو، وغينيا الاستوائية، وغينيا بيساو. تسلط هذه التركيزات الضوء على كيفية حملات السيطرة على فيروس نقص المناعة البشرية، والتدابير الوقائية،
لقد وجدت دراستنا أيضًا أن بعض الأمراض التي يمكن الوقاية منها باللقاحات، مثل الحصبة، قد أظهرت انخفاضات واسعة في معدلات الوفيات وكانت مركزة جغرافيًا. كانت وفيات الأطفال دون سن الخامسة بسبب الحصبة مركزة في غرب وشرق أفريقيا جنوب الصحراء الكبرى. على الرغم من أن هناك عوامل متعددة تساهم في انخفاض عبء الأمراض المعدية، فإن التحسينات في وفيات الحصبة تعود إلى حد كبير إلى التوافر العالمي للقاح آمن وفعال ضد الحصبة، مما يوفر مناعة تدوم مدى الحياة، مع فعالية الجرعتين التي تتجاوز
بعض الأمراض المعدية، مثل فيروس نقص المناعة البشرية/الإيدز، أظهرت أيضًا تركيزًا في الوفيات. الوفيات الناتجة عن فيروس نقص المناعة البشرية/الإيدز
كانت تتركز بشكل كبير داخل منطقة جنوب الصحراء الكبرى في إفريقيا، وخاصة في جنوب منطقة جنوب الصحراء الكبرى. كانت الدول في منطقة جنوب الصحراء الكبرى التي سجلت أعلى معدل وفيات معيار العمر في عام 2021 تشمل ليسوتو، وإسواتيني، وبوتسوانا. وكانت الدول في منطقة جنوب الصحراء الكبرى التي سجلت أعلى معدلات وفيات الأطفال دون سن الخامسة بسبب فيروس نقص المناعة البشرية (HIV) في عام 2021 تشمل ليسوتو، وغينيا الاستوائية، وغينيا بيساو. تسلط هذه التركيزات الضوء على كيفية حملات السيطرة على فيروس نقص المناعة البشرية، والتدابير الوقائية،
في العديد من الدول ذات الدخل المرتفع، انخفض معدل وفيات حديثي الولادة بشكل عام بين عامي 1990 و2021، وأصبح أكثر تركيزًا مع مرور الوقت. كانت وفيات الاضطرابات حديثي الولادة في عام 2021 مركزة في منطقة جنوب الصحراء الكبرى في أفريقيا وجنوب آسيا.
على العكس، على الرغم من أن عبء العديد من الأمراض غير السارية قد انخفض أيضًا، إلا أن هذه الأسباب عادةً لم تتبع نفس نمط تركيز الوفيات الذي لوحظ في الأمراض المعدية. تؤكد هذه الاتجاهات على تمييز رئيسي في الديناميات المكانية للأمراض غير السارية مقارنة بالعديد من الأمراض المعدية. على الرغم من أن الأسباب غير السارية قد لا تظهر نفس درجة التركيز مثل الأسباب المعدية، إلا أن عبء الوفيات قد تغير في التوزيع، حيث انخفض مع مرور الوقت في البلدان والمناطق ذات الدخل المرتفع، بينما استمر في البلدان والمناطق ذات الدخل المنخفض. انخفضت معدلات الوفيات المعدلة حسب العمر بسبب الأمراض غير السارية في معظم المواقع داخل البلدان ذات الدخل المرتفع؛ أمريكا اللاتينية ومنطقة البحر الكاريبي؛ شمال أفريقيا والشرق الأوسط؛ وأوروبا الوسطى وأوروبا الشرقية وآسيا الوسطى بين عامي 1990 و2021. ومع ذلك، فإن الأمراض غير السارية في جنوب آسيا؛ أفريقيا جنوب الصحراء الكبرى؛ ومنطقة جنوب شرق آسيا وشرق آسيا وأوقيانوسيا قد زادت أو
انخفضت بمستويات أقل بشكل ملحوظ في عام 2021 مقارنة بعام 1990. تشمل أمثلة على هذا الاتجاه مرض القلب الإقفاري، والأورام، والسكتة الدماغية، والتي انخفضت جميعها بشكل كبير خلال فترة الدراسة – على الرغم من أن تخفيضاتها كانت موزعة على نطاق واسع وليست مستهدفة مثل أسباب الأمراض غير السارية. تظهر هذه النتائج أن الأمراض غير السارية لا تبدو أنها تتحرك نحو مواقع جغرافية أكثر تركيزًا بمرور الوقت بنفس الطريقة التي تتحرك بها العديد من الأمراض السارية، مما قد يجعل التدخلات والسياسات أكثر تعقيدًا في التنفيذ.
انخفضت بمستويات أقل بشكل ملحوظ في عام 2021 مقارنة بعام 1990. تشمل أمثلة على هذا الاتجاه مرض القلب الإقفاري، والأورام، والسكتة الدماغية، والتي انخفضت جميعها بشكل كبير خلال فترة الدراسة – على الرغم من أن تخفيضاتها كانت موزعة على نطاق واسع وليست مستهدفة مثل أسباب الأمراض غير السارية. تظهر هذه النتائج أن الأمراض غير السارية لا تبدو أنها تتحرك نحو مواقع جغرافية أكثر تركيزًا بمرور الوقت بنفس الطريقة التي تتحرك بها العديد من الأمراض السارية، مما قد يجعل التدخلات والسياسات أكثر تعقيدًا في التنفيذ.
في النهاية، تعكس درجة تركيز الوفيات كل من التقدم المحرز في تقدم الرعاية الصحية والنقائص التي لا تزال قائمة في تنفيذها بشكل عادل. إن تركيز الأمراض هو دليل على وجود تدخلات وسياسات فعالة نجحت في تقليل عبء المرض في العديد من المواقع، ولكن لم يتم توزيع هذه الابتكارات بشكل عادل في جميع أنحاء العالم أو كانت غير فعالة في معالجة التحديات المحددة التي تواجهها بعض الفئات السكانية. لا يزال هناك حاجة عالمية لتحسين الوصول إلى التدخلات الجديدة واللقاحات، والاستثمار في تنفيذ السياسات الصحية العامة المعتمدة، ووضع استراتيجيات مع مراعاة المصادر الجغرافية للأمراض. يجب أن تستمر الجهود المستقبلية في التخفيف المستمر من الأمراض المعدية، مع التركيز على المواقع التي أصبحت فيها هذه الأسباب أكثر تركيزًا جغرافيًا، بينما يجب أيضًا بدء جهود لمكافحة الأسباب المزمنة في البيئات ذات الموارد المنخفضة. بالإضافة إلى ذلك، تعكس أنماط التركيز الجغرافي العالي بين الأسباب المعدية والتركيز الجغرافي المنخفض بين الأسباب المزمنة الانتقال الوبائي العالمي، حيث انخفضت معدلات الوفيات الناتجة عن الأمراض المعدية على مدار معظم سنوات دراستنا. إن زيادة تركيز سبب الوفاة، وخاصة الأمراض المعدية، توضح النجاح في التخفيف الذي يمكن تكييفه داخل البلدان والمناطق التي تم تحديد تركيز الوفيات فيها في دراستنا، مع إمكانية تقليل الوفيات بشكل كبير من تلك الأسباب.
القيود
لقد مكنت التقدمات المنهجية GBD 2021 من إنتاج تقديرات محددة للوفيات بشكل أسهل من النسخ السابقة؛ ومع ذلك، كما هو الحال مع أي دراسة من هذا النطاق، هناك عدة قيود مهمة يجب الاعتراف بها. يتم تفصيل القيود المحددة لكل سبب من أسباب الوفاة في GBD في الملحق 1 (القسم 3). هنا، نصف القيود المشتركة التي تنطبق عبر العديد من الأسباب. أولاً، يمكن أن تؤثر ندرة البيانات أو عدم موثوقية البيانات من مناطق معينة أو فترات زمنية أو مجموعات عمرية على دقة تقديراتنا، وخاصة جودة البيانات الضعيفة والتغطية من غرب وشرق وجنوب ووسط أفريقيا جنوب الصحراء وآسيا الجنوبية. ثانياً، تعتمد جودة بيانات أسباب الوفاة وبيانات التشريح اللفظي على شهادات الوفاة المرمزة بدقة وفقًا للمعايير الدولية التي وضعتها التصنيف الدولي للأمراض وهي
خاضع لممارسة الطبيب الذي يكمل شهادة الوفاة، والذي قد يكون قد تلقى تدريبًا لتسهيل قابلية المقارنة في الإبلاغ عن الأسباب الكامنة للوفاة أو لا. تتعقد هذه العملية أكثر بسبب الأمراض المصاحبة في وقت الوفاة، والتي قد تؤثر على دقة كل من مصادر تسجيل vital-registration و verbal-autopsy. إحدى الطرق الرئيسية لمعالجة البيانات في GBD هي إعادة تخصيص الوفيات التي تم تعيينها بشكل غير صحيح أو غير واضح – والتي تُعرف باسم النفايات.
تم توضيح الطرق المستخدمة لحساب COVID-19 بالكامل في المنشورات السابقة،
خاضع لممارسة الطبيب الذي يكمل شهادة الوفاة، والذي قد يكون قد تلقى تدريبًا لتسهيل قابلية المقارنة في الإبلاغ عن الأسباب الكامنة للوفاة أو لا. تتعقد هذه العملية أكثر بسبب الأمراض المصاحبة في وقت الوفاة، والتي قد تؤثر على دقة كل من مصادر تسجيل vital-registration و verbal-autopsy. إحدى الطرق الرئيسية لمعالجة البيانات في GBD هي إعادة تخصيص الوفيات التي تم تعيينها بشكل غير صحيح أو غير واضح – والتي تُعرف باسم النفايات.
تم توضيح الطرق المستخدمة لحساب COVID-19 بالكامل في المنشورات السابقة،
الاتجاهات المستقبلية
في النسخة القادمة من GBD، سنقوم بتضمين أكثر من 100 سنة موقعية من التسجيل الحيوي وأنواع بيانات أخرى تم الإبلاغ عنها منذ إنتاج تقديرات GBD 2021. بالإضافة إلى ذلك، سنواصل توسيع تقدير أسباب الوفاة من خلال تفكيك الفئات العامة لأسباب الوفاة إلى أسباب أكثر تفصيلاً حيثما كان ذلك متاحًا. تهدف هذه التحسينات إلى تعزيز دقة وتوقيت تقديرات الوفيات المرتبطة بـ COVID-19 وأسباب الوفاة الأخرى. كما نخطط لتبسيط نهجنا في تقدير الوفيات المرتبطة بـ COVID-19. بدلاً من فئة OPRM المتبقية المبلغ عنها في GBD 2021، سنستخدم جميع سنوات الموقع المتاحة من بيانات أسباب الوفاة لنسب الوفيات إلى أسباب محددة، مما يزيل هذه الفئة المتبقية. نتوقع أن تسهل هذه الطريقة الحصول على رؤى أكثر توقيتًا وقابلة للتنفيذ للتخطيط الصحي العام وصنع السياسات، خاصةً مع توقعنا لرؤية أنماط وفيات أكثر انتظامًا وقابلة للنمذجة في السنوات التي تلي الجائحة. من خلال هذه التقدمات، سنحسن من فائدة ودقة دراسة GBD كأداة لاستراتيجيات عامة فعالة.
الخاتمة
تقدم نتائج GBD 2021 نظرة شاملة على اتجاهات الوفيات على المدى الطويل مع رؤى مهمة حول سنوات جائحة COVID-19. لقد غيرت جائحة COVID-19 بشكل جذري مشهد الصحة العالمية والوفيات. كأحد الأسباب الرئيسية للوفاة، قلل COVID-19 من متوسط العمر المتوقع في عامين تقريبًا بقدر ما حسنت التخفيضات في الأمراض المعدية وغير المعدية على مدى عقود. لم تكن التغيرات في الوفيات الناتجة عن الجائحة قابلة للتنبؤ من خلال طرق تقدير GBD القياسية، وكانت تتطلب تطوير وتطبيق طرق تقدير جديدة مع ظهور الجائحة في الوقت الحقيقي. تعتبر هذه التحديثات في الوقت المناسب حول أسباب الوفاة ضرورية لمراقبة التقدم، وتحديد القضايا الصحية السائدة، وتوجيه التدخلات المستهدفة، وتحسين تخصيص الموارد. تظهر GBD 2021 أنه يمكن تحقيق نتائج أفضل في متوسط العمر المتوقع من خلال الاستفادة من النجاحات السابقة في تقليل الوفيات. إذا كانت جهود السياسات المستقبلية موجهة من خلال النجاحات التي تحققت في البلدان والمناطق التي لديها استراتيجيات فعالة لمكافحة الأمراض،
يمكن تكرار مثل هذه الإنجازات في المواقع التي تستمر فيها معدلات الوفيات العالية. بينما تستمر COVID-19 وغيرها من التحديات الصحية، يمكن أن تقدم GBD 2021 توجيهات قيمة للاستثمار في الصحة العامة وصنع السياسات.
يمكن تكرار مثل هذه الإنجازات في المواقع التي تستمر فيها معدلات الوفيات العالية. بينما تستمر COVID-19 وغيرها من التحديات الصحية، يمكن أن تقدم GBD 2021 توجيهات قيمة للاستثمار في الصحة العامة وصنع السياسات.
متعاونون في أسباب الوفاة GBD 2021
محسن نغافي*، كانيين ليان أونغ*، أمير علي عالي، حازم س. عبابنة، يوهانس حبتجيورجيس أباتي، كريستيانا أبافاتي، روزبه عباسغوليزاده، محمد رضا عباسيان، محسن عباسي-كانجيفاري، هداية عبستبار، سمر عبد الحفيظ، مايكل عبدالمسح، شريف عبد السلام، أحمد عبد الوهاب، محمد عبد اللهي، محمد أمين عبد اللهيفار، مريم عبدون، ديلدار مراد عبد الله، أولا عبد اللهي، ميسفين أبيبي، سمراويت شاول أبيبي، عيدين أبيدي، كدير حسين أبيغاز، إي. إس. أبهلاش، حسن عبيدي، أولوميد أبدون، ريتشارد جيان أبواغي، حسن أبو الحسن، ميسام أبو المعالي، محمد أبو زيد، جيرما بيريسا أبو ي، لوكاس غيمارايش أبريو، وولدو أبره أبرها، داريوش أبتاهي، سمير أبو رميليه، حسن أبو العروز، بيليامينو أبو بكر، إيمان أبو غربية، نيفين م. إي. أبو رميليه، صلاح الدين أبو رُز، أحمد أبو زيد، مانفريد ماريو كوكو أكومبسي، تادله جيروم أدار، عبدو أ. أدامو، إسحاق يبوah أدو، جيوفاني أديولوراتو، أكينديلي أولوبيلومي أديبي، فيكتور أديكانمبي، أبيولا فيكتور أديبويو، تشارلز أولواسون أديتونجي، جوليانا بونمي أديتونجي، تيميتايو إستر أدييولووا، دانيال أدي ديو أديينكا، أولورونسولا إسرائيل أديوموي، بيروك أدي أدي أدمس، قورينا إستي نينغتياس ساكيلا أدياني، ساريا أدرى، أنوالو أوبو أدييمكا أفولابي، محمد سهيل أفزال، سيرا أفزال، سونيث بوديكا أغامبودي، براديومنا أغاستي، مانك أغاروال، شاهين أغا ميري، فليك دوير أغييد، أنتونلا أغودي، أنوراغ أغراوال، ويليامز أجييمانغ-دواه، برايت أوبوكو أهيكورا، عقيل أحمد، دانيش أحمد، فيردوس أحمد، مؤيد م أحمد، سجاد أحمد، شاهزايب أحمد، توسييف أحمد، كيفان أحمدي، أمير محمود أحمد زاده، علي أحمد، أيمن أحمد، هارون أحمد، لؤي أ أحمد، مهرونيشا شريف أحمد، مقداد صالح أحمد، مختار بشير أحمد، سيد أنيس أحمد، مرجان عجمي، بودي أجي، إيسونا ماتاتوم أكارا، حسين أكبر علي آباد، كارولينا أكينوسوغلو، تومي أكينييميجو، محمد أحمد أككاف، صموئيل أكيريم، هنادي الحماد، سيد محفوظ الحسن، فارس العهدب، سامر ع. العلالمة، طارق أ. العلوان، زياد العلي، خورشيد عالم، منجورول عالم، نور عالم، رسمية مصطفى العامر، فهد مشهور العنزي، تركي م العنزي، ساير العزام، المازا البكري، محمد البشتي، محمد ت. البطاينة، جاكلين إليزابيث ألكالد-رابانال، خليفة أ. الدوسري، وفاء أ. الدحليقي، روبرت و. ألدريدج، هايليسيلاسي برهان أليما، ملوبيرهان أسيفا أليمايو، شريف الله ألمي، يهون مولوجيتا أليمو، عادل علي سعيد الغيثي، خالد ف. الحبيب، فدوى الحلايقة ناجي الحلايقة،
محمد خالد الحناوي، عبيد علي، أمجد علي، ليقات علي، محمد عثمان علي، رفعت علي، شهيد علي، سيد شجاعت شجاعت علي، جيانفرانكو أليكاندرو، الشيخ محمد ألف، ريحانة عليخاني، يوسف علي محمدي، أحمد نور أدم عليي، محمد أ. م الجاسر، سيد محمد الجونيد، فرانسوا ألا، بيتر أليبيك، صباح المرواني، صادق علي علي الماوري، جوزيف أوي المازان، هشام م المخلافي، لؤي الميداني، عمر الميداني، محمود أ. العماري، باسم العُماري، جوردي ألونسو، جابر س القحطاني، شهاب الدين القليوبي، أحمد ياسين القتيبي، سلمان خليفة الصباح، زيد الطني، أوايس الطاف، جعفر أ. التوفيق، خالد أ التيركاوي، ديبورا أويين ألوه، نيلسون ألويس-غوزمان، حسن الوافي، ياسر محمد الوارفي، هاني علي، صفوت علي، كرم ح الزعبي، رضا أماني، أزمروا ت أمار، برنس م أميغبور، إدوارد كوابينا أميyaw، طارق توفيق أمين، ألي رضا أميندارولزربي، سهراب أميري، محمد حسين أمير زاده-إيرانق، هوبيرت أمو، ديكسون أ أموغسي، غانييو أديني أموسا، روبرت أنكوسيان، ديانا أندرليني، ديفيد ب أندرسون، بيدرو براتا أندرادي، كاتالينا ليليانا أندري، تودوريل أندري، كولين أنغوس، أبهيسك أنيل، سنيها أنيل، أمير أنوشيرفاني، حسين أنصاري، أنصاريادي أنصاريادي، ألي رضا أنصاري-مغداد، كاثرين م أنطوني، إيرنويز أنترينديارتي، داود أنفاري، سعيد أنفاري، ساليها أنور، سوماتي لوكمان أنور، رزيق أنور، أنايوتشوكو إدوارد أنياسودور، محمد عقيل
محمد خالد الحناوي، عبيد علي، أمجد علي، ليقات علي، محمد عثمان علي، رفعت علي، شهيد علي، سيد شجاعت شجاعت علي، جيانفرانكو أليكاندرو، الشيخ محمد ألف، ريحانة عليخاني، يوسف علي محمدي، أحمد نور أدم عليي، محمد أ. م الجاسر، سيد محمد الجونيد، فرانسوا ألا، بيتر أليبيك، صباح المرواني، صادق علي علي الماوري، جوزيف أوي المازان، هشام م المخلافي، لؤي الميداني، عمر الميداني، محمود أ. العماري، باسم العُماري، جوردي ألونسو، جابر س القحطاني، شهاب الدين القليوبي، أحمد ياسين القتيبي، سلمان خليفة الصباح، زيد الطني، أوايس الطاف، جعفر أ. التوفيق، خالد أ التيركاوي، ديبورا أويين ألوه، نيلسون ألويس-غوزمان، حسن الوافي، ياسر محمد الوارفي، هاني علي، صفوت علي، كرم ح الزعبي، رضا أماني، أزمروا ت أمار، برنس م أميغبور، إدوارد كوابينا أميyaw، طارق توفيق أمين، ألي رضا أميندارولزربي، سهراب أميري، محمد حسين أمير زاده-إيرانق، هوبيرت أمو، ديكسون أ أموغسي، غانييو أديني أموسا، روبرت أنكوسيان، ديانا أندرليني، ديفيد ب أندرسون، بيدرو براتا أندرادي، كاتالينا ليليانا أندري، تودوريل أندري، كولين أنغوس، أبهيسك أنيل، سنيها أنيل، أمير أنوشيرفاني، حسين أنصاري، أنصاريادي أنصاريادي، ألي رضا أنصاري-مغداد، كاثرين م أنطوني، إيرنويز أنترينديارتي، داود أنفاري، سعيد أنفاري، ساليها أنور، سوماتي لوكمان أنور، رزيق أنور، أنايوتشوكو إدوارد أنياسودور، محمد عقيل
“خوان بابلو عرب، جلال عربلو، مصعب عرفات، ألكسندر ي أرافكين، ديملاش أريدا، عبد الفتاح أريمو، أولاتوندي أريمو، هاني عارفين، ميساي أركيو، بينيديتا أرموكيدا، مايكل بنجامين أرندت، يوهان أرنلوف، محوش أروج، أنطون أ آرتامونوف، جودي أرولابان، رافائيل تايوو أروليبا، أشوكان أروماغام، مالكي أسعد، محسن أسدي-لاري، أكيزا أويالوم أسجدوم، مونا أسغاري أحمد آباد، محمد أسغاري-جعفر آبادي، محمد أشرف، أرمين أسلاني، توماس أستيل-بيرت، محمد أثار، سيد شمس الدين أثاري، بانطاليم تيلاي تيلاي أتينافو، حبتامو ووندماجن أطلوا، برنس أتوركي، مها محمد وهبي أتوت، ألوك أترية، أفيناش أوجايب، مارسيل أوسلوس، أبولفازل أبان، أتاليل فنتاهون أوديو، أملكو مولات أويكي، بياتريز بولينا أيا لا كوينتانيللا، هاله آيات اللهي، خوسيه ل أياسو-ماتيوس، سيد محمد أيوب زاده، سينا آزاد نجف آباد، روي م س أزيفيدو، أحمد ي أزلام، دارشان ب ب، إبراهيم صموئيل بابو، محمد بدر، أشيش د بادي، سروش بغداد، ناصر باقري، سارة باقريه، سليمان باه، سعيد باهدر خاليلي، نجمة بهمن زيار، روحاي باي، عاطف أمين بايغ، جينيفر ل بيكر، عبد العزيز ت باكو، رافلين كاور باكشي، سينثيل كومار بالاكريشنان، مادن بالاسوبرا مانين، أوفيديو كونستانتين بالتاتو، كيران بام، ماتسيي باناش، سوهام بانديوبادياي، بالاش تشاندرا بانك، هانسي بانسال، كانو بانسال، فرانكا باربيك، مارتينا بارشيتا، ميناك باردهان، إرفان باردي، سوزان لين باركر-كولو، تيل وينفريد بارنيغهاوزن، فرانشيسكو باروني-أديسي، هبة جودات برقوي، لوبي إتش باريرو، أمدو بارو، ساندرا بارتيت، لينغكان باروا، زارين بشارات، آزاده بشيري، أفيسو باسيرو، بريتيش باسكاران، بوذا باسنيت، كيك باسات، جواو ديوغو باسو، آن في إل باستينغ، سانجاي باسو، كافيتا باترا، برنارد ت باون، محسن بياتي، نبيو سيمغنو بايليغن، توماس بيني، نيراج بيدي، ماسيميليانو بيغي، عماد بهبودي، بريامادهبا بيهرا، أمير حسين بهنوش، مسعود بهزاديفار، مريم بيراند، ديانا فرنندا بيخارانو راميريز، يانيك بيجو، سيفاليم أسيفا بيلاي، تشالي مولو بيليت، ميشيل ل بيل، محمد بشير بيلو، أولورونجوجون أومولايا بيلو، لويس بيلو، أبستولوس بيلوكاس، روز غريس بيندر، إيزابيلا م بنسينور، عزيز الله بيران، زومبور بيريزفاي، أليمشيت ييرغا برهي، بيتينا ن بريريس، روبرت س برنشتاين، غريغوري ج برتولاكي، باولو ج ج بيتينكورت، كيبيدي أ بيين، ديفيداس س بهاغات، أكشايا سريكانث بهاغافاتولا، نيراج بهالا، أشيش بهالا، دينيش بهانداري، كايلي بهانغديا، نيكها بهاردواج، بانكاج بهاردواج، براثنا ف بهاردواج، أشيش بهارجافا، سونو بهاسكار، فيفيك بهات، غورجيت كاور بهاتي، جاسويندر سينغ بهاتي، مانبريت س بهاتي، راجبير بهاتي، زلفقار أ بهوتا، بوريس بيكوف، جيسيكا ديفين بيشاي، كاثرين بيسيجنانو، فرانشيسكا بيسولي، أتانوا بيسواس، بيجيت بيسواس، سعيد بيطاراف، بيكيس ديستاو بيتي، فيرا ر بيتر، تون بيورغ، ميشيل كوفي بواشي، ماري سيفا بوامبونغ، أنكا فاسيليكا بوبيركا، فيرجينيا بودوليكا، آدام أولاليكان بودنرين، أيوب كيتما بوجالي، كاساومار أنجاو بوجالي، سميه بوهلولي، أوباسانجو أفولابي بولارينوا، أرتشيث بولور، ميلاد بونقدار هاشمي، إيم بوني، كاوتسوبه بورا، بيرراك بورا باسارا، حامد برهاني، أرتورو بورزوتسكي، سعاد بوعود، أنطوان بوسطن، كريستوفر بوكس، إدوارد ج بويكو، أوليفر ج برادي، ديجانا برايثويت، لويسا سي برانت، مايكل براور، ألكسندرا برازينوفا، خافيير برازو-سايافيرا، نيكولاس ج ك بريت بورد، سوزان بريتنر، هيرمان برينر، أندري نيكولايفيتش بريكو، نيكولاي إيفانوفيتش بريكو، غابرييل بريتون، ج
“إيشوار ك تشاندراسيكار، تشين-كواو تشانغ، جونغ-تشين تشانغ، غاشاو سيساي تشاني، بيريكلس شارالامبوس، فيجاي كومار شاتو، بانكاج تشاتورفيدي، فيكتوريا شاتزيمافريدou-غريغوريادو، أخيلا ناند تشوراسيا، أنجيلا و تشين، أن-تيان تشين، كاثرين س تشين، هاوي تشين، منغ شوان تشين، سيمياء تشين، تشينغ-يو تشينغ، إستر تي دبليو تشينغ، نيكولاس تشيربوا، وونديميي آشنفي تشير، جو-هوي تشين، أودجيريل تشيميد-أوشير، ريتشيس تشيموريا، باتريك آر تشينغ، خيسوس لورينزو تشيرينوس-كاسيريس، عبد العال شيثير، ويليام سي إس تشو، برايان تشونغ، هيتش تشوبرا، سونالي غاجانان تشوداري، راجيف تشودري، ديفاساهيام ج كريستوفر، إسحاق سونداي تشوكو، إريك تشونغ، إيرين تشونغ، يونس تشونغ، شينغ-شيا تشونغ، محمد شوتيامي، زينهل سيندي، يولاندا تشيوفي، ماريلي م كلاسنز، رافائيل م كلارو، كاليب كوبرلي، ريبيكا م كوجن، أليسا كولومبوس، هايلي كومفورت، جواو كوندي، سامويل كورتيسي، باولو أنجيلو كورتيسي، فيرا ماريسا كوستا، سيمونا كوستانزو، إيفرتون كوزين، روزا أ س كوتو، ريتشارد جي كاودن، كينيث مايكل كرامر، مايكل إتش كريكي، ناتاليا كروز-مارتينز، سيلفيا ماجالي كوادرا-هيرنانديز، غارلاند تي كولبريث، باتريشيا كولين، ماثيو كونينغهام، ماريا باولا كورادو، سريهارشا دادانا، أوميد دادراس، سييو داي، شياوشين داي، زهاولي داي، لاكلان إل دالي، جيوفاني دامياتي، جيريجنا دارغا جيلا، جاي ك داس، ساسواتي داس، سوباسيش داس، آنا ماريا داسكال، نيهار رانجان داش، محسن دشت، آنا داستيريدو، غايل ديفي، كلاوديو ألبرتو دافيلّا-سيرفانتس، نيكول ديفيس ويفر، كايرات دافليتوف، دييغو دي ليو، كاتي دي لوكا، أكليلو تامير ديبلي، شايوم ديبوبادهايا، لويزا ديغنهاردت، عزيز الله دهقان، لي ديتسفيلد، كريستيان ديل بو، إيفان ديلغادو-إنسيسو، بيريكا هونديسا ديميسا، أندرياس ك ديميتريادس، كي دينغ، شينلي دينغ، إدغار دينوفا-غوتيريز، نيلوفر ديرافي، نبييو ديريج، نيكولاوس ديرفينيس، إيمينا ديرفيشيفيتش، دون سي ديس جارلايس، هاردك دينشبهات ديساي، روباك ديساي، فينوت غنانا تشيلاييان ديفانبو، سيد مسعودور رحمن ديوان، أركاديب دالي، كولديب داما، ميغناث ديمال، سمير دينغرا، فيشال آر ذوليبالا، ديانا دياز دا سيلفا، دانيال دياز، مايكل ج دياز، أدريانا ديما، ديلاني د دينغ، هوانغهي دينغ، ريكاردو خورخي دينيس-أوليفيرا، م أشورث ديراك، شيرين جلالينيا، ثاو هوانغ فوانغ دو، كاميلا برونيلي دو برادو، سعيد دواع، مسعود دودانجه، ميلاد دودانجه، سوشيل دوهاري، كلارا جورجييفا دوكوفا، كريستيان دوليك، ريجينا ماي فيلانويفا دومينغيز، وانيوي دونغ، ديبا دونغاروار، ماريو دوريا، فاريبا دوروستكار، إي راي دورسي، ويندل مومباكي دوس سانتوس، راجكومار دوشي، ليلى دوشمغير، روبرت كوكو دوو، تيم روبرت دريسكول، هانييل لارسون ديسوزا، فيولا ديسوزا، مي دو، جون دوب، بروس ب دانيال، أندريه رودريغيز دورايس، سينباغام دورايسامي، أويول كريستوفر دوروجاي، لورا دوايرلينغرين، بولينا أغنيشكا دزياناخ، أركاديوس ماريان دزييدزيتش، عبد الرحمن إمار، إيجيماي إيبوريم، ألي رضا إيراهيمي، تشيديبيري بيتر إشيه، هشام أتان إدينور، ديفيد إدفاردسون، كريستينا إدفاردسون، ديفي إيفندي، فيري إيفندي، ديان إيرماوان إيفندي، تيرجي أندرياس إيكيمو، إبراهيم إيني، مايكل إيكهولونيتالي، تيميتوب كايروس إكوندايو، إيمان السعيد، إيفات إلبرازي، تيسوم بيكلي إليم
“أرتيم أليكسييفيتش فومينكوف، بهزاد فوروتان، مسعود فوروتان، إنغيبورغ فورتون، دانييلا فورتونا، ماتيو فوشي، كايويد رافائيل فوباجي، كيت لويز فرانسيس، ريتشارد تشارلز فرانكلين، ألبرتو فريتاس، جوزيف فريدمان، سارة د فريدمان، تاكيشي فوكوموتو، جون إي فولر، بليما فوك، بيتر أندراس غال، مختار أ. غادانيا، أبهى موتيرامجي غايداني، سانتوش غايره، إيمانويل غاكيدو، ياسين جلالي، ناتالي سي غاليس، سيلفانو غالوس، ماندوخاي غانبات، أرافيند ب. غاندي، بالاسانكار غانيسان، محمد عارف غانياني، م. أ. غارسيا-غورديلو، ويليام م. غاردنر، جلال جارج، نافال جارج، روبيش ك. غاوتام، سيمي أولاتوندي غباداموسي، تيلاي غيبرو غيبي، ميغلاس و. غبريغريغيس، ميسفين غبريهيوت، تيفيري غيبرو غبريمسكل، سيمونا روكسانا جورجيسكو، تاميرات غيتاشيو، بيتر و. غيثينغ، مولا غيتي، كيغوباد غاديري، سولماز غهراماني، خالد ياسر غيلان، محمد رضا قاسمي، غزال قاسمي بور داباغي، أفسانه قاسمي زاده، أحمد قاشغائي، فاريبا قاسمي، رامي محمد غازي، أجنش غيمير، سما غوبا، مريم غلاملي زاده، أسد الله غلاميان، علي غلامرضا نژاد، نسيم غوليزاده، مهسا غورباني، بويا غورباني واجارگاه، ألوك غوبال غوشال، بارامجيت سينغ غيل، تيفاني ك. غيل، ريتشارد ف. غيلوم، ثيمبا ج. غينيندزا، ألييم جيرماي، جيمس سي غلاسبي، إيلينا ف. غنيدوفسكايا، لازلو غوبولوس، مايرون أنطوني غودينيو، أميت غويل، علي غولتشين، محمد غولدست، مهافير غوليشا، بويا غوليج، نيلسون ج. م. غوميس، فيليمون ن. غونا، سمير فالي غوبالاني، جوزيبي غوريني، هومان غودارزي، أليساندرا سي غولارت، باربرا نيجيا غارسيا غولارت، أنمول غويال، أيمن غرايدا، سايمون ماثيو غراهام، ميشال غريفنا، جوزيبي غروسو، شي-يانغ جوان، جيوفاني غواردوكي، محمد إبراهيم محي الدين غباري، ميساي ديشاسا غوديتا، أفيروب غوه، ستيفانو غويتشياردي، رافائيل ألفيس غيمارايش، سنغده غولاتي، داميثا أسانغا غونارواداني، ساسيدار غونتورو، تسوي قوه، أنيش كومار غوبتا، بهونا غوبتا، مانوج كومار غوبتا، موهاك غوبتا، راجات داس غوبتا، راجييف غوبتا، سابنا غوبتا، فير بالا غوبتا، فيجاي كومار غوبتا، فيفيك كومار غوبتا، لامي غورميسا، رينا ألما غوتيريز، فاروق حبيب زاده، برهام حبيب زاده، رسول حدادي، مصطفى هادي، نجاح ر. هادي، نيلس هايب، نيماء حفيزي نژاد، أليمايهو هايلو، أرفين حاج ميرزايان، إسام س. هالبوب، بريان ج. هول، سيباستيان هالر، ربيع حلواني، رندة ر. حمادة، ساجد حميد، سامر حميدي، إيرين ب. هاملتون، تشييه هان، تشيوشيا هان، آصف حنيف، نسرين حنفي، غرايم ج. هانكي، فهد حنا، م. عبد الحنان، م. نوروز زمان هاك، هارابان هارابان، أريف هارجونو، جوزيب ماريا هارو، أحمد I حسيب الله، إكرامول حسن، م. تصديق حسن، حميد رضا حسني، محمد حسنيان، عبد الوهاب هاشي، م. سكيب حسنين، إكرامة حسن، سهيل حسني بور، هادي حسن خاني، يوهانس هاوبولد، راسموس ج. هافمولر، سايمون I هاي، جياوي هي، جيفري ج. هيبرت، عمر إ. هجازي، غولناز حيدري، محمد حيدري، مهسا حيدري-فروزان، بارتوش هيلفر، دليا هندري، بريندا يوليانا هيريرا-سيرنا، كلاوديو هيرتيليو، حامد حسامي، كمال هزام، كاثرين ل. هيل، يوتا هيرايكي، راميش هولا، نوبويكي هوريتا، م. محبوب حسين، سهادات حسين، محمد-سالم حسيني، حسن حسيني زاده، مهدي حسيني زاده، أحمد حسيني زاده عدلي، ميهايلا هوست
“هيثم جهرمي، نيتيا ناند جاين، عمار عبد الرحمن جيرون، أبهيسيك جايسوال، إلهام جمشيدي، مارك م جانو، أبو بكر إبراهيم جاتاو، سبزالي جافادوف، طاهرة جافاهري، ساتيش كومار جايابال، شوبا جايرام، ريمي جباي، سون ها جي، جاياكومار جيغاناثان، أنيل ك جها، رافي براكاش جها، هينغ جيانغ، ينغ زهاو جين، أولاتونجي جونسون، محمد جوكار، جوست ب جوناس، تاماس جو، أبيل جوزيف، نيتين جوزيف، تشاريتي إهيموينما جوشوا، غريس جوشي، ياتسيك جيرزي يوزويك، ميك جوريشون، فايشالي ك، بيلينغسلي كامبوا، علي كبير، زبير كبير، فيديا كاداشيتي، دler حسين قدير، رضوان كالاني، لاله ر كالانكيش، ليلى ر كالانكيش، فيروز كاليادان، سانجاي كالرا، فينيت كومار كمال، سيفيش كاثير كاماراجاه، راجيش كامات، زهراء كمياب، ناصر كمياري، ثانيغايفيلان كاناغاساباي، تانوج كانشان، هيمال كاندل، أرون ر كانمانثاريدي، إدموند ويدام كانميكي، كيهيندي كازيم كانمودي، سوتانثيرا كانان س، سوشيل كومار كانسال، رامي س كانتر، نيتى كابور، مهرداد كراجيزاده، شاما د كارانت، ريمة أ كاراسنه، إبراهيم م كراي، أندريه كارتش، أسيمة كاري، صلاح الدين كريمي، أرمان كريمي بهناج، فايزان زافر كاشو، قلندر حسين عبد الكريم كاسنازاني، هينغامه كسرائي، نيكولاس ج كاسيبوم، مولي ب كاسل، جوناس إتش كاوبلا، نافجوت كاور، نوريتو كاواكامي، غبنجا أ كايويدي، فؤاد كازمي، سينا كازميان، تحسین حيدر كازمي، غيتو موسيسا كيببيو، أدييرا ديبيلا كيبيدي، فاسيكاو كيبيدي، تيبيبسلاسي س كفل، بيتر نجنغا كييورو، كاثلين كيلر، جايمون تيرينس كيلي، جون إتش كيمبين، جيسيكا أ كير، إيمانويل كيس-غيو، هيمنشو خاجوريا، أمير محمد خلاج، نعمان خالد، أنيس أحمد خليل، علي رضا خليلان، فهم خامس بور، أجمل خان، أسعدوزمان خان، غلفراز خان، إكرام الله خان، امتياز أ خان، م نور الزمان خان، ماسير خان، محمد جوبر خان، موين أ ب خان، زيشان علي خان، محمد زيا الدين خان سوهب، شغايغ خانمحمّدي، خالد خطاب، فاطمة خاتمي، هيثم خطاب، معاوية محمد خطاب، أرمن خافنديجار، حميد رضا خياط كاشاني، فريحة فاطمة خضري، إلهه خدا دوست، محمد خورغامفر، معين خورمالي، زهراء خورامي، أحمد خسروي، محمد علي خسروي، زيميني ديملاش كيفلي، غريس كيم، جيهي كيم، كوانغهيون كيم، مين سيو كيم، يون جين كيم، روث و كيموكوتي، كاسي إي كينزل، عدنان كيسا، سيزر كيسا، ديسموند كلوي، آن كريستين سكريندو كنودسن، جوناثان م كوكارنيك، سونالي كوتشار، تيميا كوكسي، ديفيد س كوه، علي أصغر كولاهي، كايري كولفيس، فرزاد كومباني، جيربراند كورين، سيوارتا كوسن، كاريل كوستيف، بارفايز أ كول، سندهرا لاكشمي كولمان لاكشمنارايانا، كوال كريشان، هاري كريشنا، فارون كريشنا، فيجاي كريشنامورثي، يوفراج كريشنامورثي، كريس ج كروهن، بارتيلمي كواتي ديفو، بورجو كوجوك بيشر، م د عبد القدوس، محمد قدوس، إيلاري كويتونن، مختار كوليمبت، فيشنوتيرثا كولكارني، أكشاي كومار، أشيش كومار، هاريش كومار، ماناسي كومار، راكيش كومار، مدهولاتا كوماري، فانتاهون تاركيغن كومي، ساتياجيت كوندو، أوم ب كورمي، أسيب كوسنالي، ديان كوسوما، ألكسندر كوارتيغ، إلياس كيريوبولوس، هموي هموي كيو، كارلو لا فيكيا، بن لايسي، محمد أول لادن، لوسي لافلام، أبراهام ك لاغات، أنطون سي ج لاجر، عبد الإله الأحمر، دافني تيك تشينغ لاي، دارميش كومار لال، راتيلال لالو، تي لالوككا، هيلتون لام، جوديت لام، كيلسي ر لاندريم، فرانشيسكو لامفرانشي، جاستين ج لانغ، برثولد لانغغوث، فان تشارلز لانسينغ، أرياني لابلانت-ليفيسك، باgher لاريجاني، أندرس أ لارسون، سافيتا لاسرادو، زهراء س لاسي، كمال الدين لطيف، كافيه لطيف
عزام أ. مغزاتشي، سانديب ب. مهراج، سليمان محجوب، منصور آدم محمود، ألي رضا محمودي، إلهام محمودي، رزاق محمودي، عظيم مجيد، إيرسا فاطمة مخدوم، إلهه مالكان راد، فينكاتيش ماليد، رضا ملك زاده، أarman ك. مالهوتر، كاشيش مالهوتر، أحمد عزام مالك، إيرام مالك، ديبورا كارفالو مالطا، عبد الله أ. مامون، بيجمان منصوري، محمد علي منصورنيا، لورنزو جيوفاني مانتوفاني، ساجد مقصود، بيشنو ب. ماراسيني، حميد رضا مراتب، جومر سي. مارافيلا، أوغستينا م. ماركوني، بارهام مردي، ميركو مارينو، عبد الجليل مرجاني، غابرييل مارتينيز، برناردو ألفونسو مارتينيز-غويرا، رامون مارتينيز-بييدرا، دانييلا مارتيني، سانتي مارتيني، فرانسيسكو روجرلانديوم مارتينز-ميلو، ميكيل مارتوريل، وولفغانغ ماركس، شارمين مريم، روي ريليرا مارزو، أنطوني ماساكا، أويك ماسري، ستيفاني ماثيسون، ألكسندر ج. ماثيوداكيس، مانو راج ماثور، جيشانث ماثومبورام، ريتشارد ماتزوبولوس، ريتشارد جيمس مود، أندريا ماوجيري، بالاب ك. ماوليك، مهسا ماييلي، مريم مزاهري، محسن مزيدي، جون ج. مكغراث، مارتن مككي، آنا لورا و. مكوان، سوزان أ. مكلاكلين، ستيفن م. مكفيل، إنكيلينت أ. ميشيلي، جون روبرت كارابيو ميدينا، ريشى ب. ميديراتا، جيتيندرا كومار مينا، راهول مهرا، كمران مهراباني-زين آباد، انتظار مهربي نسب، تسفاهون ميكني ميتو، جبريكيوروس جبريميخايل ميلس، ماكس ألبرتو مينديز مينديز-لوبيز، والتر ميندوزا، ريتشارد ج. مينيزيس، بيليناه منغست، أليكسيوس-فوتيوس أ. مينتيس، سلطان أيوب ميو، هافتو أسميروم مريسا، أتي ميريتوجا، توومو ج. ميريتوجا، أبره م. مرشا، بيزاويت أفيوورك ميسفين، توميسلاف ميستروفيتش، كوكوليج تشاميلا دينوشي ميتاناندا، ساشيث ميتاناندا، بيتر ميلاخس، أدكوات مهلانغا، لوريت مهلانغا، تيانيي مي، توماسز ميازغوفسكي، جورجيا ميخا، إيرمينا ماريا ميشالك، تيد ر. ميلر، إدوارد ج. ميلز، لي هوو نات مين، جي كيه ميني، بويا مير محمد صادقي، أندريا ميريكا، أنطونيو ميريجييلو، إركين م. ميراخي موف، ميزان كيروس ميروست، مريم ميرزائي، أويك ميسغناو، أشييم ميشرا، سانجيف ميسرا، فيليب ب. ميتشل، براسانا ميثرا، شيتانيا ميتال، محمد رضا مبين، مادلين إ. موبرغ، أشرف محمدخاني، جما محمد، مهند ف. ح. محمد، نوح سعد محمد، ساكينة محمد علي زاده-شارندابي، سهيل محمدي، عبد الله محمدي-حفظجاني، نوشين محمديفارد، حسن محمد، حسين محمد، مصطفى محمد، صلاح الدين محمد، شفيع محمد، فيسواناث موهان، هدى مجيري-فروشاني، أمين مكاري، علي ح. مقداد، سابرينا مولينارو، مريم مولوخيا، سارة مومتازمانش، لورنزو موناستا، ستيفانيا مونديلو، محمد علي موني، أمير علي مودي غاليباف، مريم مرادي، يوسف مرادي، مازيار مرادي-لاكه، مليحة مراد زاده، باولا موراكا، ليديا موراوسكا، رافائيل سيلفيرا مورييرا، نغار مرواتدار، شين دوغلاس موريسون، ياكوب مورتزه، جوناثان ف. موسر، روهيث موتابا، فينسنت موغين، سيمين موودي، بارسا موسوي، سيد إحسان موسوي، أمين موسوي خانقاه، إيمانويل أ. مبوليا، ماتيوس مريجن، سميارة مبارك، لورنزو موكيولي، أولريش أوتو مولر، فراز مغل، سُموني موكيرجي، فرانسيسك موليتا، كافيتا منجال، إيفرين مورييلو-زامورا، فنجاي موسايغوا، خالد م. مسلّم، أحمد مصطفى، غلام مصطفى، سارافانان موثوبانديان، رامان موثوسامي، محمد مظفر، ووجاي ميونغ، أحمراشان جايرامان ناغراجان، غابرييل ناغل، بيروز نغافي، عليا ناهيد، غانيش ر. نايك، غورداتا نايك، فيرزان نينيو، سانجيف ناير، هستيار حما رشيد نجم الدين، نور الدين نكهوستين أنصاري
“Dina نور أنغرايني نينغرم، تشوكودي أ نناجي، لورانس أتشيلس ننيانزي، إيفاق علي نعمان، شهي نومورا، مامونة نورين، نافيسة نوروزي، بو نورفينغ، جان جاك نوبيا، أماندا نوفوتني، تشيسوم أداوبي نري-إزيدي، جورج نتايوس، مبيكو نيتسيكه، فيرجينيا نونيز-ساميوديو، دييتا نورريكا، جيري جون نوتور، بوغدان أونتسيا، كيهيندي أ أوباميرو، ماري أيغبيريمو أوبوه، إسماعيل أ أوديتوكُن، نكيشي مارتينا أودوغو، مارتن جيمس أودونيل، مايكل سافو أودورو، أكينييمي أ د أوفاكونرين، أبيولا أوغونكوي، أيوديبو سكيرو أوغونتادي، إن-هوان أوه، حسن أوكاتي-علياباد، سيلفستر روبن أوكيكي، أكينكونمي بول أوكيكونلي، أوساريتين كريستابل أوكونجي، أندرو ت أولاكونجو، ميدين تونبوسون أولايا، ماثيو إيدوو أولاتوبي، غلاوسيا ماريا مورايس أوليفيرا، إسحاق إيينولووا أولوفاديو، بولايوكو أولوبوكُنولا أولوسانيا، جاكوب أولوسيجون أولوسانيا، ينكا دوريس أولوافيمي، هاني أ عمر، أحمد عمر بالي، غوران لطيف عمر، موريين أومة أونديو، سوكينغ أونغ، أوبينا إ أونوجيكوي، كينيث إكيننا أونييديب، ميشال أوردك، أوريش إيبيري أوريساكو، فيرنر ن أوريش، دوريس ف أورتيغا-ألتاميرانو، ألبرتو أورتيز، وائل م س عثمان، صموئيل م أوستروف، أوشيتشوكوو ليفي أوسواجwu، أدريان أوتويو، نيكيتا أوتستافنوف، ستانيسلاف س أوتستافنوف، أمل أويحيا، قوقينغ أويانغ، مايوة أ أولا بي، ياز أوزتين، ماهيش بادوكودرو ب أ، أليثيا باديرون-مونييديرو، جاجاديش راو بادوبيدري، برامود كومار بال، تاماس باليتس، كلوديا بالادينو، رافاييل بالادينو، راؤول فيليبي بالما-ألفاريز، فنغ بان، هاي-فنغ بان، أدريان بان، بارامجوت باندا، سونغوميترا باندا-جوناس، سيثيكورببو ر باندى-برومال، هيلينا أوليارثا بانغاريبوان، جورجيوس د بانوس، ليونيداس د بانوس، إيوانيس بانتا زوبولوس، أنكا ميهايلا بانتي ستويان، باراسكيفي بابادوبولو، روميل ر بارخ، سيويون بارك، أشواجوشا بارثاساراثي، آفا باشايي، ماجا باسوفيتش، روبرتو باسيرا، ديباك كومار باسوبولا، هيمال م باتيل، جاي باتيل، سانغرام كيشور باتيل، شانكارغودا باتيل، ديميتريوس باتوليوس، فينكاتا سورش باتثيباتي، أوتام باوديل، حميد رضا بازوكي تورودي، سبنسر أ بيز، آمي إ بيدن، باولو بيديرسيني، أمبرتو بنساتو، فينسنت كريستيان فيليبنو بيبيتو، إيمانويل ك بيبرا، برينس بيبرا، جواو بيرديغاو، ماركوس بيريرا، ماريو ف ب بيريس، أروكيا سامي بيرياناياجام، نوربيرتو بيريكو، ريتشارد ج بيستيل، كونراد بيسودوف، فاني إميلي بيترمان-روتشا، ويليام أ بيتر، هوانغ تران فام، أنيل ك فيليب، مايكل ر فيليبس، دانييلا بييرانونزيو، مانون بيجوليه، ديفيد م بيغوت، توماس بيلغريم، زهراء زاهد بيراشا، مايكل أ بيرادوف، سعيد بيروزباناه، نيشاد بلاكال، يفغيني بلوتنيكوف، فيفيك بودر، ديمتري بوديغه، سوزان بوليندر، كيفان ر بولكينهورن، راميش بولورو، فيل تي بونكيلاين، فابيو بورّو، مارتن ج بوستما، غوفيندا راج باوديل، أكرم بورشامس، نعيمة بورطاهيري، سيرجيو أ برادا، برانيل مان سينغ برادهان، تيجسوار ن بركاشام، مانيا براساد، أكيلا براشانت، إلتون جونيور سادي براتيس، دانيال بريتو ألهامبرا، تينا بريسكيلا، ناتالي بريتشيت، بهاراتي م بوروهيت، جاجاديش بوفولا، نمير هاشم قاسم، إبراهيم قتيعة، أسماء سليم قاضي، غانغزين تشيان، سولي تشيو، مريم فايز قريشي، مهرداد ربيعي راد، أمير رادفار، راغو أنيكال رادهاكريشنان، فينكاترامان رادهاكريشنان
“أنطونيو لويس بيه ريبيرو، جينيفر ريكارد، هانا آر ريفا، هانا إليزابيث روبنسون-أودن، سيلفيا فورتونا رودريغيز، مونيكا رودريغيز، ليوناردو روفر، إيما لين بيست روجوفسكي، بيتر روهلوف، ديبي سياهر رومادلون، إسبيرانزا روميرو-رودريغيز، ميشيل رومولي، لوكا رونفاني، غلام رضا روشندل، غريغوري أ. روث، هيمنشو سيخار روت، نيتاي روي، بريانكا روي، إنريكو روباغوتي، غيليرمي دي أندرادي رويلا، سوزان فريد روميشا، تيليي رنغين، غودفري م. رويغيرا، أندريه رينكيفيتش، تشاندان إس. ن، علي م. أ. سعد، زهراء ساداتيان، كوروش صابر، مها محمد صابر-أياد، مرتضى صابري كمرپوشتي، سياماك صبور، سيمونا ساكو، بيرميندر إس. ساشديف، راجيش ساشديفا، بسيمة صادق، آدم سادلر، بشدار أبو زيد سادي، إحسان صادقي، عرفان صادقي، فريدة صادقيان، محمد رضا ساب، عمر سعيد، فهيمة صفاينجاد، شير زمان صافي، راجيش ساغار، أمينة ساغازاده، دومينيك ساغو، فاطمة صاحب شريف-أسكري، نارجيز صاحب شريف-أسكري، أمير حسين صاحبكار، سوميا سواروب ساهو، أومكانتا ساهو، مونا ليشا ساهو، زهراء سيف، ميرزا رضوان ساجد، جوزيف و. ساكشاوغ، ناصر سلام، بايمان سلامتي، أفيس أبولارينوا سلامي، لوسياني ب. سالارولي، محمد أ. صالح، سنا صالح، مروة رشاد سالم، محمد ز. ي. سالم، سهراب سليمي، حسين سمدي كافيل، سارة سمدزاده، سعد سمارغندي، يوسيف ليوناردو سامودرا، عبد الله م. سامي، خوان سانابريا، فرانشيسكا سانا، داميان فرانشيسكو سانتومارو، إيتامار س. سانتوس، ميلينا م. سانتريك-ميليتشيفيتش، برونو بياسي ساو خوسيه، مادي أري ساراسميتا، سيفان يجننارايانا آير ساراسواتي، أشفيني سارافانان، باباك سارافي، ياسر ساريخاني، تانماي ساركار، رودريغو سارمينتو-سواريز، غارغي ساشين سارودي، ساشين سي. سارودي، أراش سارفيزاد، بريجيش ساتيان، ثيرونافوكاراسو ساتيش، ماهيشوار ساتباتي، أبو سعيد، م. د. أبو سعيد، ميت سيلان، مهدي سيّاح، نيكولاوس سكارميا، بينيدكت ميخائيل شارسشميت، ماركوس ب. شلايش، وينفريد شلي، ماريا إينيس شميت، إيون جيس سيولا شنايدر، آرت شيرمانس، أوستن إ. شومخر، أليتا إليزابيث شوت، ميشائيل شوارزينغر، ديفيد سي. شويبيل، فالك شفينديك، ماريو شكرية، سيدهارثان سيلفاراج، سابياشاتشي سينا باتي، سوبرا مانيان سينثيل كوماران، سدف ج. سبانلو، دراغوس سيربان، ياشيندرا سيتي، فنغ شا، مريم شاباني، أمير شفاعت، ماهان شفي، نيلاي إس. شاه، بريتيك أ. شاه، سيد محبوب شاه، سعيد شهابي، عطا الله شاهبندي، عزة شهيد، سامية شهيد، وجيحة شهيد، حميد ر. شاهسافاري، مويد جمال شاهوان، أحمد شيخ، مسعود علي شيخ، علي رضا شاكري، علي س. شلاش، سوندر شام، محمد عاقب شميم، مهران شمس-بيراندفاند، هينا شمشاد، محمد أنس شمسي، محمد شانواز، أبهيسك شانكار، سدف شرفائي، أمين شريفان، جواد شريفي-راد، راجيش شارما، سوراب شارما، أوجوال شارما، فيشال شارما، راجيش ب. شاستري، أمين شافاندي، مريم شايان، عمرو محمد السيد شهاب الدين، عزيز شيخ، رحيم علي شيخي، جيابين شين، أديتي شتي، ب. سورش كومار شتي، بافانشاند إتش شتي، بيلين شي، كينجي شيمويا، ديسالين شيفيراو، ميكا شيغيماتسو، مين-جونغ شين، يون هو شين، رحمن شيري، رضا شيركوهي، نبييو أنيلي شيتاي، أمينو شيتو، آيفي شيو، ك. م. شيفاكومار، فيليزار شيفاروف، فرهاد شكرانه، آزاد شكري، سينا شول، سيد أفشين شرفي، سونيل شريستا، كيريم شوفال، إيمانويل إدوار سيديد، جوان بيدرو سيلفا، لويس مانويل لوبيز رودريغيز سيلفا، سورايا سيلفا، كولين ر. سيمبسون، أنجالي سينغال، أبهيناف سينغ، بالبیر باغيشا سينغ، غاريما سينغ، جسبير سينغ، ناريندر بال سينغ، بارامديب سينغ، سورجيت سينغ، ديريند
مقالات
انظر على الإنترنت للملحق 3
“هايتونغ زهي سون، جينغ سون، يوهان سوندستروم، ديفيد سنكرسينغ، كاثارينا س سونرهاغن، تشاندان كومار سوين، لوكاز شاربك، ميندي د سيتو، ميكلوش سوزوكا، بايام تابائي دامافاندي، رافائيل تاباريس-سيزديدوس، سيد محمد تاباطبائي، أوزرا تاباطبائي مالازي، سيد أمير تاباطبائي زاده، شيمة تاباطبائي، محمد تابيش، جيوثي تادكامادلا، سانتوش كومار تادكامادلا، ياسمين طاهري أبكنار، مسلم طاهري سوديجاني، جابين طيبة، كين تاكاهashi، إيمان م طلعت، أشيش تالوكدر، ميرسيا تامبا، جاك لوكنزي تاموزي، كير-كان تان، سارميلا تاندوكار، هاوسو تانغ، هونغ ك تانغ، إنغان أوكور تارغان، منغستي كاساهون تاركو، محمد طارق الجمان، إلفيس إينوبيانغ تاركانغ، رازيه توكولي أولياي، سيد محمد توانغار، نونو تافيرا، يبيكال ماناي تيfera، محمد-هاني تمساح، ريم محمد هاني تمساح، ماسايوكي تيراموتو، ريكي تسلر، إينوخ تيي-كوادجو، ريشو ثاكور، بوغازينثان ثانغاراجو، كافومبوراثو رامان ثانكابان، سمر ثروات، راسية ثايكاران، نيهال توماس، نيكيل كيني توماس، أزاليا م تومسون، أماندا ج ثريفت، تشيرن تشونغ تشيرن ثوم، لاو كاسبار ثيغسن، جينغ تيان، أليس تيشوباد، يانسي هيني فيرا تيكوالو، تالا تلاوي، تيناو ييمر تيروي، ماريا فلاديميروفنا تيتوفا، مارشيلو تونيللي، رومان توبور-مادري، أديتونجي ت توريولا، آنا إ تور، ماثيلد توفييه، ماركوس روبرتو توفاني-بالوني، ياسمين ت تران، نغيا مين تران، دومينيكو تريكو، صموئيل جوزيف ترومان، ثين تان تري تاي ترواين، أريستيديس تساتساكيس، غويش ميبراحتوم تسغاي، إيفانجيليا إيريني تسيرمبيني، مونختويا تومورخوو، كانغ تونغ، ستيفانوس تيروفولاس، سيد محمد ناظم الدين، أنيفيوك جون أودوكينغ، أريت أودوه، عطاء الله، إيرفان الله، سعيد الله، سنا الله، سريكانث أومكانثان، تشوكوما ديفيد أوميوكونكوا، بريغيد أونيم، بهسكا ران أونيكريشنان، كارولين آن أونسورث، إيرا أوبادياي، دانييل أورسو، جبريل سمّاني عثمان، سيد محمد وهبي، أوسوكن غوفينداراج فايثيناثان، روح الله فاليزاده، سارة م فان دي فيلدي، جف فان دن إيندي، أورسوليا فارجا، بريا فارت، شوبان بابو فارتيا، تومي جوهاني فاسانكاري، ميلينا فاسيك، سيافاش فازيري، بالاشاندر فيلينغيري، ناراياناسوامي فينكاتاسوبراهمانيان، نيكولاس ألكسندر فيرغيس، مدهور فيرما، ماسيميليانو فيروكس، جورجيوس-إيوانيس فيراس، دومينيك فيرفورت، خورخي هوغو فيلافاني، غابرييلا إينيس فيلانويفا، مانش فيناياك، فرانشيسكو س فيولانتي، ماريا فيسكادور، سيرجي كونستانتينوفيتش فلاديميروف، فاسيلي فلاسوف، باي فو، شتاين إميل فولست، أفينا فونغبراديث، ثيو فوس، إيسيدورا س فويكيتش، رادي فوكوفيتش، حاتم أ وفا، ياسر وحيد، ريتشارد ج واماي، كونغ وانغ، نينغ وانغ، شو وانغ، سونغ وانغ، يانزجونغ وانغ، يوان-بانغ وانغ، محمد وقاص، بول وارد، إيمبت غاشاو واسي، ستيفاني واتسون، ستيفاني لويز واتسون واتسون، كوسالا غايان ويراكوان، ميليسا واي وي، روبرت ج وينتراب، دانيال ج وايس، روني ويستمان، جوانا ل ويزنانت، تاويوات ويانغخام، داكشيثا برانيث ويكراماسينغ، نوان دارشانا ويكراماسينغ، أنغا ويلاندكا، كارولين ويلكيرسون، بيتر ويليت، شادرخ ويلسون، مارتشين و ووجوودزيتش، ديميووز هـ وولديغيبريال، أكسل والتر وولف، تشارلز د أ وولف، يوهانس أديشو وونديميجين، ين جون وونغ، أوتومبورن وونغسين، آي-مين وو، تشينكاي وو، فيليسيا وو، شينغشينغ وو، زينغهونغ وو، جوان شيا،
إلريك زويك، سامر ح. زيوود، إيف إي وول†، وكريستوفر ج. ل. موراي
*المؤلفون الأوائل المشتركين.
الانتماءات
للاطلاع على قائمة انتماءات المتعاونين، يرجى مراجعة الملحق 3
المساهمون
يرجى مراجعة الملحق 1 القسم 10 للحصول على معلومات أكثر تفصيلاً حول مساهمات المؤلفين الفردية في البحث، مقسمة إلى الفئات التالية: إدارة المشروع البحثي بشكل عام؛ كتابة المسودة الأولى من المخطوطة؛ المسؤولية الرئيسية عن تطبيق الأساليب التحليلية لإنتاج التقديرات؛ المسؤولية الرئيسية عن البحث، وتوثيق، واستخراج، أو تنظيف البيانات؛ تصميم أو ترميز الأشكال والجداول؛ تقديم البيانات أو التعليقات النقدية على مصادر البيانات؛ تطوير الأساليب أو الآلات الحاسوبية؛ تقديم تعليقات نقدية على الأساليب أو النتائج؛ صياغة المخطوطة أو مراجعتها بشكل نقدي للمحتوى الفكري المهم؛ وإدارة عملية التقدير أو النشر. كان للمؤلفين الرئيسيين والمراسلين وكبار المؤلفين وصول كامل إلى البيانات في الدراسة وكان لديهم المسؤولية النهائية عن القرار بتقديمها للنشر.
*المؤلفون الأوائل المشتركين.
الانتماءات
للاطلاع على قائمة انتماءات المتعاونين، يرجى مراجعة الملحق 3
المساهمون
يرجى مراجعة الملحق 1 القسم 10 للحصول على معلومات أكثر تفصيلاً حول مساهمات المؤلفين الفردية في البحث، مقسمة إلى الفئات التالية: إدارة المشروع البحثي بشكل عام؛ كتابة المسودة الأولى من المخطوطة؛ المسؤولية الرئيسية عن تطبيق الأساليب التحليلية لإنتاج التقديرات؛ المسؤولية الرئيسية عن البحث، وتوثيق، واستخراج، أو تنظيف البيانات؛ تصميم أو ترميز الأشكال والجداول؛ تقديم البيانات أو التعليقات النقدية على مصادر البيانات؛ تطوير الأساليب أو الآلات الحاسوبية؛ تقديم تعليقات نقدية على الأساليب أو النتائج؛ صياغة المخطوطة أو مراجعتها بشكل نقدي للمحتوى الفكري المهم؛ وإدارة عملية التقدير أو النشر. كان للمؤلفين الرئيسيين والمراسلين وكبار المؤلفين وصول كامل إلى البيانات في الدراسة وكان لديهم المسؤولية النهائية عن القرار بتقديمها للنشر.
إعلان المصالح
S Afzal يُبلغ عن دعم للمخطوطة الحالية من جامعة الملك إدوارد الطبية بما في ذلك مواد الدراسة، مقالات البحث، مصادر البيانات الصالحة والمعلومات الحقيقية الموثوقة لهذه المخطوطة؛ الدفع أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من جامعة الملك إدوارد الطبية والشركاء المتعاونين بما في ذلك جامعة جونز هوبكنز، جامعة كاليفورنيا، جامعة ماساتشوستس، KEMCAANA، مؤتمرات وندوات KEMCA-UK العلمية؛ الدعم لحضور الاجتماعات و/أو السفر من جامعة الملك إدوارد الطبية لحضور الاجتماعات؛ المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري مع اللجنة الوطنية للأخلاقيات الحيوية في باكستان، مجلس المراجعة الأخلاقية بجامعة الملك إدوارد الطبية، بالإضافة إلى مجلس المراجعة الأخلاقية بجامعة فاطمة جناح ومستشفى سير غانغا رام؛ الأدوار القيادية أو الائتمانية في مجلس أو جمعية أو لجنة أو مجموعات مناصرة، مدفوعة أو غير مدفوعة مع جمعية محرري الطب في باكستان، زميل في كلية الصحة العامة بالكلية الملكية في المملكة المتحدة (FFPH)، ومجتمع الوقاية والمناصرة والبحث، جامعة الملك إدوارد الطبية (SPARK)؛ ودعم آخر كعميد للصحة العامة والطب الوقائي في جامعة الملك إدوارد الطبية، كمحرر رئيسي لمجلة جامعة الملك إدوارد الطبية، كمدير لخلايا تعزيز الجودة بجامعة الملك إدوارد الطبية، كزميل على مستوى دولي في كلية الصحة العامة في المملكة المتحدة، كعضو في المجلس الاستشاري ورئيس الجلسة العلمية KEMCA-UK، كرئيسة لـ KEMCAANA (المؤتمر العلمي الدولي)، كعضو على المستوى الوطني في لجنة البحث والنشر بالهيئة العليا للتعليم (HEC باكستان)، كعضو في لجنة البحث والمجلات (باكستان) لمجلس الطب والأسنان (باكستان)، اللجنة الوطنية للأخلاقيات الحيوية (باكستان)، مجموعة الخبراء الاستشارية لكورونا (البنجاب)، رئيس مجموعة الخبراء الاستشارية للدينغ، وعضو في لجنة بحث برنامج الإقامة في البنجاب؛ كل ذلك خارج العمل المقدم. R Ancuceanu يُبلغ عن رسوم استشارية من Abbvie؛ الدفع أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من Abbvie، Sandoz، B. Braun، Laropharm، وMagnaPharm؛ كل ذلك خارج العمل المقدم. J Ärnlöv يُبلغ عن الدفع أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من AstraZeneca وNovartis مقابل رسوم المحاضرات؛ المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري مع AstraZeneca، Astella، Boehringer Ingelheim؛ كل ذلك خارج العمل المقدم. O C Baltatu يُبلغ عن دعم للمخطوطة الحالية من المجلس الوطني للتنمية العلمية والتكنولوجية (CNPq، 304224/2022-7) ومعهد أنيما (زمالة أستاذ بحث AI)؛ دور قيادي أو ائتماني في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوعة أو غير مدفوعة، كعضو مؤسس في المجلس الاستشاري للصحة والتكنولوجيا الحيوية في حديقة التكنولوجيا في ساو جوزيه دوس كامبوس – مركز الابتكار في تكنولوجيا الصحة (CITS)، خارج العمل المقدم. T W Bärnighausen يُبلغ عن منح أو عقود من المعاهد الوطنية للصحة، مؤسسة ألكسندر فون هومبولت، المؤسسة الوطنية للبحث العلمي الألمانية (DFG)، الأوروبية
الاتحاد، وزارة التعليم والبحث الألمانية، وزارة البيئة الألمانية، ويلكوم، وKfW، جميعها كمدفوعات لمؤسستهم؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري في مجلسين استشاريين علميين لمشاريع بحثية ممولة من NIH في أفريقيا حول تغير المناخ والصحة؛ الأسهم أو خيارات الأسهم في CHEERS، وهي شركة صغيرة متوسطة تركز على أساليب قياس تغير المناخ والمتغيرات المتعلقة بالصحة في مجموعات سكانية؛ جميعها خارج العمل المقدم. S Barteit يذكر منحًا من مؤسسة كارل زيس ومؤسسة البحث الألمانية (DFG)؛ الأسهم أو خيارات الأسهم في CHEERS، وهي شركة ربحية تركز على تقييم تغير المناخ وأنظمة الاستجابة للصحة؛ جميعها خارج العمل المقدم. M Beghi يذكر رسوم استشارية من Lundbeck وAngelini، جميعها خارج العمل المقدم. Y Bejot يذكر رسوم استشارية من Medtronic وNovartis؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب متحدثين، كتابة مخطوطات أو أحداث تعليمية من BMS وPfizer وMedtronic وAmgen وNovoNordisk وServier؛ دعم لحضور الاجتماعات و/أو السفر من Medtronic؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوع، مع الجمعية الفرنسية للأعصاب الوعائية؛ جميعها خارج العمل المقدم. M Bell يذكر منحًا أو عقودًا من وكالة حماية البيئة الأمريكية، NIH، مؤسسة High Tide، معهد آثار الصحة، منتدى النساء في جامعة ييل، صندوق الدفاع البيئي، مركز ييل لتغير المناخ والصحة، مؤسسة ويلكوم، مؤسسة روبرت وود جونسون، وزمالة هاتشينسون لما بعد الدكتوراه (جميعها مدفوعة لمؤسستهم)؛ رسوم استشارية من Clinique؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب متحدثين، كتابة مخطوطات أو أحداث تعليمية من كلية الصحة العامة بجامعة كولورادو، جامعة ديوك، جامعة تكساس، Data4Justice، جامعة كوريا، منظمة متخصصي معلومات التشوهات، جامعة بنسلفانيا، جامعة بوسطن، IOP Publishing، NIH، صحة كندا، PAC-10، UKRI، زمالة صندوق أبحاث AXA، جامعة هارفارد وجامعة مونتانا؛ دعم لحضور الاجتماعات و/أو السفر من كلية الصحة العامة بجامعة كولورادو، جامعة تكساس، جامعة ديوك، جامعة بوسطن، جامعة بنسلفانيا، جامعة هارفارد، المجلة الأمريكية للصحة العامة، جامعة كولومبيا وجامعة هارفارد؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوع مع التقييم الوطني الخامس لتغير المناخ وLancet Countdown، مجلس استشاري جونز هوبكنز، اللجنة الاستشارية الخارجية لجامعة هارفارد لمنحة التدريب، مجموعة الاستشارات الفنية لمنظمة الصحة العالمية حول تلوث الهواء والصحة ولجان الأكاديميات الوطنية؛ ومدفوع مع اللجنة الاستشارية العلمية للهواء النظيف التابعة لوكالة حماية البيئة الأمريكية (CASAC)؛ خارج العمل المقدم. L Belo يذكر مصالح مالية أو غير مالية أخرى مع UCIBIO – FFUP من خلال الدعم من FCT في نطاق المشروع UIDP/04378/2020 وUIDB/04378/2020 من UCIBIO ومشروع LA/P/0140/2020 من i4HB، جميعها خارج العمل المقدم. R S Bernstein يذكر دعمًا ماليًا أو غير مالي آخر كموظف استشاري طبي بدوام كامل في وزارة الصحة العامة في كاليفورنيا في مركز جودة الرعاية الصحية؛ خارج العمل المقدم. P J G Bettencourt يذكر براءات اختراع مخطط لها، صادرة، أو قيد الانتظار (WO2020229805A1، BR112021022592A2، EP3965809A1، OA1202100511، US2023173050A1، EP4265271A2، وEP4275700A2)؛ مصالح مالية أو غير مالية أخرى مع مؤسسة Botnar كمراجع مشروع، خارج العمل المقدم. S Bhaskar يذكر منحًا أو عقودًا من جمعية اليابان لتعزيز العلوم (JSPS)، وزارة التعليم والثقافة والرياضة والعلوم والتكنولوجيا اليابانية (MEXT) وJSPS والأكاديمية الأسترالية للعلوم؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة مع منطقة الروتاري 9675 كرئيس المنطقة، مجتمع الصحة العالمية والهجرة كرئيس ومدير (برلين، ألمانيا)، PLOS One، BMC Neurology، Frontiers in Neurology، Frontiers in Stroke، Frontiers in Public Health وBMC Medical Research Methodology كعضو في هيئة التحرير، وكم عضو في كلية المراجعين (المعاهد الكندية للأبحاث الصحية، كندا)؛ خارج العمل المقدم. B Bikbov يذكر منحًا أو عقودًا من المفوضية الأوروبية وجامعة روما؛ دعم لحضور الاجتماعات/السفر من الجمعية الأوروبية للكلى؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوع في مجموعة مناصرة مع الجمعية الدولية لأمراض الكلى وغير مدفوع في المجلس الإقليمي لأوروبا الغربية للجمعية الدولية لأمراض الكلى؛ دعم مالي أو غير مالي آخر من Scientific-Tools.org؛ خارج ال
العمل المقدم. يذكر A Biswas رسوم استشارية من شركة INTAS Pharmaceuticals Ltd، الهند، وشركة Lupin Pharmaceuticals، Ltd، الهند، وشركة Alkem Laboratories، الهند كمدفوعات شخصية؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من Roche Diagnostics، الهند، كمدفوعات شخصية؛ جميعها خارج العمل المقدم. يذكر E J Boyko مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من الجمعية الكورية للسكري، جمعية السكري في جمهورية الصين (تايوان)، الجمعية الأمريكية للسكري، والجمعية الدولية للقدم السكري؛ دعم لحضور الاجتماعات و/أو السفر من الجمعية الكورية للسكري؛ جمعية السكري في جمهورية الصين (تايوان)، الجمعية الدولية للقدم السكري؛ خارج العمل المقدم. يذكر M Carvalho مصالح مالية أو غير مالية أخرى من LAQV/ REQUIMTE، جامعة بورتو (بورتو، البرتغال) ويعترف بالدعم من FCT في إطار مشروع UIDP/50006/2020؛ خارج العمل المقدم. يذكر E Chung الدعم للمخطوطة الحالية من المعهد الوطني للصحة NICHD T32HD007233. يذكر J Conde منح أو عقود من مجلس البحث الأوروبي منحة بدء ERC-StG-2019-848325 (تمويل 1.5 مليون يورو)، خارج العمل المقدم. يذكر S Cortese منح أو عقود من المعهد الوطني للصحة والبحث والرعاية (NIHR) والوكالة التنفيذية الأوروبية للبحث؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من جمعية الصحة النفسية للأطفال والمراهقين، الجمعية البريطانية للطب النفسي الدوائي، Medice، وتحالف موارد ADHD الكندي؛ دعم لحضور الاجتماعات و/أو السفر من جمعية الصحة النفسية للأطفال والمراهقين، الجمعية البريطانية للطب النفسي الدوائي، Medice، وتحالف موارد ADHD الكندي؛ قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع مجموعة إرشادات ADHD الأوروبية والشبكة الأوروبية للاضطرابات الحركية المفرطة؛ جميعها خارج العمل المقدم. يذكر Sa Das قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع جمعية التشخيص والطب المختبري كرئيس برنامج، وفصل النساء في الصحة العالمية في الهند، خارج العمل المقدم. يذكر A Dastiridou الدعم لحضور الاجتماعات و/أو السفر من THEA وABBVIE، خارج العمل المقدم. يذكر L Degenhardt منح تعليمية غير مقيدة من Indivior وSeqirus لفحص أدوية الأفيون الجديدة في أستراليا، خارج العمل المقدم. يذكر A K Demetriades قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع لجنة التوجيه للمنتدى المعرفي AO، مجلس مؤسسة الأعصاب العالمية، ومجلس ضباط الجمعية الأوروبية للجمعيات العصبية، جميعها خارج العمل المقدم. يذكر A Faro الدعم للمخطوطة الحالية من المجلس الوطني للتنمية العلمية والتكنولوجية، CNPq، البرازيل كباحث CNPq (منحة دراسية). يذكر I Filip الدعم للمخطوطة الحالية من معهد أفيسينا للبحوث الطبية والسريرية. يذكر D Flood منح أو عقود من NHLBI (رقم الجائزة K23HL161271)، جامعة ميتشيغان مركز استقلال الأمريكيين الأكبر سناً (رقم الجائزة 5P30AG024824)، وبرنامج علماء البحث السريري في معهد كاسويل للسكري بجامعة ميتشيغان؛ رسوم استشارية من منظمة الصحة العالمية كمدفوعات لمؤسستهم؛ قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، كطبيب موظف في Maya Health Alliance، منظمة صحية غير حكومية في غواتيمالا؛ جميعها خارج العمل المقدم. يذكر A A Fomenkov الدعم للمخطوطة الحالية من تطوير تقنيات حيوية فعالة تعتمد على زراعة الخلايا، الأنسجة والأعضاء من النباتات العليا، الطحالب الدقيقة والزرنيخيات. البحث الذي تم إجراؤه ضمن التكليف الحكومي لوزارة العلوم والتعليم العالي في الاتحاد الروسي (الموضوع رقم 1220426000867). يذكر M Foschi رسوم استشارية من Roche وNovartis؛ دعم لحضور الاجتماعات و/أو السفر من Biogen، Roche، Novartis، Sanofi، Bristol، وMerck؛ قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع مؤسسة MBase؛ جميعها خارج العمل المقدم. يذكر R Franklin منح أو عقود من Heatwaves (حكومة كوينزلاند، كوينزلاند، أستراليا) وArc Flash (العوامل البشرية، حكومة كوينزلاند، كوينزلاند، أستراليا)، وMobile Plant Safety (Agrifutures)؛ دعم لحضور
اجتماعات و/أو سفر من مؤتمر ACTM للطب الاستوائي وطب السفر 2022 و2023، ومؤتمر ISTM لطب السفر في بازل 2023؛ دور قيادي أو ائتماني في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، كرئيس/مدير لـ Kidsafe، ومدير لـ Auschem، وعضو في لجنة الحوكمة لـ ISASH، ومدير لـ Farmsafe، ونائب رئيس ACTM، وكمنسق لمجموعة SIG للوقاية من الإصابات في PHAA؛ خارج العمل المقدم. P S Gill يذكر دعمًا للمخطوطة الحالية من المعهد الوطني للبحوث الصحية والرعاية (NIHR) كمحقق رئيسي مع مدفوعات لمؤسستهم؛ الآراء المعبر عنها في هذا المنشور هي آراء المؤلفين وليست بالضرورة آراء NIHR أو وزارة الصحة والرعاية الاجتماعية في المملكة المتحدة. A Guha يذكر منحًا أو عقودًا من جمعية القلب الأمريكية ووزارة الدفاع؛ رسوم استشارية من Pfizer وNovartis وMyovant؛ دور قيادي أو ائتماني في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع مجموعة العمل ZERO Prostate Cancer Health Equity وDoctopedia كشريك طبي مؤسس؛ جميعها خارج العمل المقدم. C Herteliu يذكر منحًا أو عقودًا من وزارة البحث والابتكار والرقمنة الرومانية، MCID، رقم المشروع ID-585-CTR-42-PFE-2021؛ منحة من المفوضية الأوروبية Horizon 4P-CAN (البحث في الوقاية الأولية من السرطان المخصص من خلال مشاركة المواطنين والابتكار الاجتماعي المدعوم رقميًا)؛ مشروع “المرونة الاجتماعية والاقتصادية في بيئة متعددة المخاطر في رومانيا” الممول من الاتحاد الأوروبي – NextgenerationEU والحكومة الرومانية، بموجب خطة التعافي والمرونة الوطنية لرومانيا، العقد رقم 760050/ 23.05.2023، رمز PNRR-C9-I8-CF 267/29.11.2022، من خلال وزارة البحث والابتكار والرقمنة الرومانية، ضمن المكون 9، الاستثمار I8؛ مشروع “فهم أفضل للأنظمة الاجتماعية والاقتصادية باستخدام طرق كمية من الفيزياء” الممول من الاتحاد الأوروبي-NextgenerationEU والحكومة الرومانية، بموجب خطة التعافي والمرونة الوطنية لرومانيا، رقم العقد 760034/ 23.05.2023، رمز PNRR-C9-I8-CF 255/ 29.11.2022، من خلال وزارة البحث والابتكار والرقمنة الرومانية، ضمن المكون 9، الاستثمار I8؛ خارج العمل المقدم. M Hultström يذكر دعمًا للمخطوطة الحالية من مؤسسة Knut och Alice Wallenberg ومؤسسة القلب والرئة السويدية، جميعها كمدفوعات لمؤسستهم؛ دعم لحضور الاجتماعات و/أو السفر من الجمعية الفيزيولوجية الأمريكية والجمعية السويدية للتخدير والرعاية المركزة؛ دور قيادي أو ائتماني في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع الجمعية الفيزيولوجية الأمريكية، قسم الماء والإلكتروليت؛ جميعها خارج العمل المقدم. I Ilic وM Ilic يذكران دعمًا للمخطوطة الحالية من وزارة العلوم والتنمية التكنولوجية والابتكار في جمهورية صربيا. S M Islam يذكر دعمًا للمخطوطة الحالية من NHMRC ومؤسسة القلب، N E Ismail يذكر دورًا قياديًا أو ائتمانيًا في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، غير مدفوعة، كأمين (عضو مجلس) من الأكاديمية الماليزية للصيدلة، خارج العمل المقدم. T Joo يذكر دعمًا للمخطوطة الحالية من المكتب الوطني للبحث والتطوير والابتكار في المجر (RRF-2.3.1-21-2022-00006)، قسم الصحة المدفوعة بالبيانات من المختبر الوطني للأمن الصحي. G Joshy يذكر منحًا أو عقودًا من وزارة الصحة والرعاية المسنّة 2023 (فهم العبء القاتل لـ COVID-19 في مرافق الرعاية المسنّة السكنية)؛ دعم لحضور الاجتماعات و/أو السفر من منحة الجمعية الإحصائية الأسترالية 2023 لدعم تسجيل المؤتمر؛ المشاركة في مجلس مراقبة سلامة البيانات مع معهد العلوم الرياضية الأسترالي (AMSI) والجمعية الإحصائية الأسترالية (SSA) لمشروع برنامج التغذية ونمط الحياة الذي يقوده المجتمع لفقدان الوزن والصحة الأيضية: تجربة عشوائية محكومة (ELCHO)، 2022؛ جميعها خارج العمل المقدم. J Jozwiak يذكر مدفوعات أو أتعاب لمحاضرات، عروض، مكاتب المتحدثين، كتابة مخطوطات أو أحداث تعليمية من Novartis وAdamed وAmgen؛ خارج العمل المقدم. N Kawakami يذكر منحًا أو عقودًا من مؤسسة Junpukai ووزارة الصحة العقلية الرقمية كقسم مخصص، مدعومًا بمنحة غير مقيدة من 15 مؤسسة.https://dmh.m.u-tokyo.ac.jp/cرسوم الاستشارات من معهد ريكن، وكالة استكشاف الفضاء اليابانية (JAXA)، شركة سيكي سوي للكيماويات، وSB@WORK؛ دور قيادي أو وصائي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع الجمعية اليابانية للصحة المهنية؛
كل ما يتعلق بالعمل المقدم. يذكر ج. ه. كيمبين منحًا أو عقودًا من برنامج جراحة العين والأذن في ماساتشوستس وSight for Souls من خلال المدفوعات لمؤسستهم؛ دور قيادي أو وصائي في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوعة أو غير مدفوعة، كرئيس لـSight for Souls؛ أسهم أو خيارات أسهم مع Betaliq وTarsier؛ كل ما يتعلق بالعمل المقدم. يذكر ت. كوكسي منحًا أو عقودًا من Novartis Magyarország Ltd من خلال الدفع لأنشطة الوصول إلى السوق، خارج العمل المقدم. يذكر ك. كريشان مصالح غير مالية أخرى من مركز UGC للدراسات المتقدمة، CAS II، الممنوحة لقسم الأنثروبولوجيا، جامعة بنجاب (تشاندigarh، الهند)؛ خارج العمل المقدم. يذكر ب. لايسي دعمًا للمخطوطة الحالية من بنك المملكة المتحدة الحيوي، الممول بشكل كبير من مجلس البحوث الطبية في المملكة المتحدة وWellcome، من خلال عملهم في جامعة أكسفورد. يذكر م. لي دعمًا للمخطوطة الحالية من وزارة التعليم في جمهورية كوريا ومؤسسة البحث الوطنية في كوريا (NRF-2021R1I1A4A01057428) وبرنامج التعليم في تكنولوجيا التوافق الحيوي من خلال معهد كوريا للتقدم التكنولوجي (KIAT) الممول من وزارة التجارة والصناعة والطاقة (رقم P0017805). يذكر م-ج. لي منحًا أو عقودًا من المجلس الوطني للعلوم والتكنولوجيا في تايوان (NSTC 112-2410-H-003-031؛ دور قيادي أو وصائي في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوعة أو غير مدفوعة، كمحرر تقني لمجلة جمعية القلب الأمريكية؛ خارج العمل المقدم. يذكر ج. ليو دعمًا للمخطوطة الحالية من المؤسسة الوطنية للعلوم الطبيعية في الصين (رقم المنحة: 72122001؛ 72211540398). يذكر س. لوركوفسكي منحًا أو عقودًا من Akcea Therapeutics ألمانيا من خلال المدفوعات لمؤسستهم؛ رسوم استشارية من دانون، نوفارتس فارما، سويديش أورفان بيوفيتروم (SOBI)، وأبفيلد؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب متحدثين، كتابة مخطوطات أو أحداث تعليمية من Akcea Therapeutics ألمانيا، AMARIN ألمانيا، Amedes Holding، AMGEN، برلين-كيمي، بوهيرنجر إنجلهايم فارما، داييتشي سانكيو ألمانيا، دانون، هوبيرت بوردا ميديا هولدينغ، جانسن-سيلاج، ليلي ألمانيا، نوفارتس فارما، نوفو نورديسك فارما، روش فارما، سانوفي-أفنتيس، وSYNLAB هولدينغ ألمانيا وSYNLAB أكاديمية؛ دعم لحضور الاجتماعات و/أو السفر من AMGEN؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري مع Akcea Therapeutics ألمانيا، AMGEN، داييتشي سانكيو ألمانيا، نوفارتس فارما، وسانوفي-أفنتيس؛ كل ذلك خارج العمل المقدم. يذكر م. أ. محمود تمويل منحة أو عقد من وكالة البحث والابتكار، وزارة التعليم في المملكة العربية السعودية (رقم المشروع 445-5-748). يذكر ل. ج. مانتوفاني دعمًا للمخطوطة الحالية من وزارة الصحة الإيطالية. يذكر ح. ر. مراتب دعمًا للمخطوطة الحالية من برنامج بياتريو دي بينوس لما بعد الدكتوراه من مكتب سكرتير الجامعات والبحث من وزارة الأعمال والمعرفة في حكومة كاتالونيا: 2020 BP 00261. يذكر ر. ماتزوبولوس رسوم استشارية من جامعة نيويورك وDG موري ترست؛ دعم لحضور الاجتماعات/السفر مدفوع من SA MRC وجامعة كيب تاون؛ دور قيادي أو وصائي في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، غير مدفوعة، كعضو مجلس في Gun Free South Africa؛ أسهم أو خيارات أسهم مع Sanlam؛ خارج العمل المقدم. يذكر ر. ج. مود دعمًا للمخطوطة الحالية من Wellcome Trust [رقم المنحة 220211] حيث يوفر تمويلًا أساسيًا لبحوث الطب الاستوائي في ماهيدول أكسفورد ويساهم في راتبه. يذكر أ-ف. أ. مينتيس منحًا أو تمويل عقود من ‘MilkSafe: خط أنابيب جديد لتغذية حليب الأطفال باستخدام تقنيات الأوميكس’، وهو بحث ممول جزئيًا من صندوق التنمية الإقليمية الأوروبية للاتحاد الأوروبي والأموال الوطنية اليونانية من خلال البرنامج التشغيلي للتنافسية، ريادة الأعمال والابتكار، تحت دعوة البحث – الإنشاء – الابتكار (رمز المشروع: T2EDK-02222)، بالإضافة إلى ELIDEK (المؤسسة اليونانية للبحث والابتكار، MIMS-860) (كلاهما خارج المخطوطة الحالية)؛ مدفوعات لشهادة خبير من العمل كمراجع خارجي لـFONDAZIONE CARIPLO، إيطاليا؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري كعضو في هيئة التحرير لـ”المراجعات المنهجية”، و”سنوات الوبائيات”، وكمدير مساعد لـ”الطب التحويلي”؛ أسهم أو خيارات أسهم من مصنع نبيذ عائلي؛ ومصالح مالية أخرى كمسؤول علمي حالي لمجموعة BGI؛ خارج العمل المقدم. يذكر س. أ. ميو
الدعم من جامعة الملك سعود، الرياض، المملكة العربية السعودية (RSP-2024 R47). T R Miller يذكر منحًا أو عقودًا من مؤسسة AB InBev، والمعهد الوطني للصحة النفسية (مقاطعة سانتا كلارا، كاليفورنيا)، وEverytown من أجل سلامة الأسلحة؛ دفع مقابل الشهادة كخبير في ولايات ميشيغان، نيفادا ونيو مكسيكو، مجلس الصحة في مقاطعة موبايل؛ خارج العمل المقدم. P B Mitchell يذكر دفعًا أو أتعابًا للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية، من Janssen (أستراليا)، خارج العمل المقدم. L Monasta يذكر دعمًا للمخطوطة الحالية من وزارة الصحة (Ricerca Corrente 34/2017) من خلال المدفوعات المقدمة إلى معهد صحة الأم والطفل IRCCS Burlo Garofolo. R S Moreira يذكر منحًا أو عقودًا من منحة إنتاجية البحث CNPq (المجلس الوطني للتنمية العلمية والتكنولوجية) رقم تسجيل المنحة 316607/2021-5؛ خارج العمل المقدم. J Mosser يذكر دعمًا للمخطوطة الحالية من مؤسسة بيل وميليندا غيتس؛ منح أو عقود من Gavi؛ دعم لحضور الاجتماعات و/أو السفر من مؤسسة بيل وميليندا غيتس؛ خارج العمل المقدم. S Nomura يذكر دعمًا للمخطوطة الحالية من وزارة التعليم والثقافة والرياضة والعلوم والتكنولوجيا في اليابان (21H03203) والبحث الاستباقي للعلوم والتكنولوجيا الجنينية من وكالة العلوم والتكنولوجيا اليابانية (JPMJPR22R8). B Norrving يذكر المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري مع Simbec Orion، خارج العمل المقدم. A P Okekunle يذكر دعمًا للمخطوطة الحالية من مؤسسة البحث الوطنية في كوريا الممولة من وزارة العلوم وتكنولوجيا المعلومات والاتصالات (2020H1D3A1A04081265). A Ortiz يذكر منحًا أو عقودًا من Sanofi كمدفوعات لمؤسستهم؛ أتعاب استشارية، أتعاب متحدثين أو دعم للسفر من Advicciene، Astellas، Astrazeneca، Amicus، Amgen، Boehringer Ingelheim، Fresenius Medical، Care، GSK، Bayer، Sanofi-Genzyme، Menarini، Mundipharma، Kyowa Kirin، Lilly، Alexion، Freeline، Idorsia، Chiesi، Otsuka، Novo-Nordisk، Sysmex وVifor Fresenius Medical Care Renal، Pharma وهو مدير كاتدرائية، Mundipharma-UAM لمرض الكلى السكري، وكاتدرائية Astrazeneca-UAM لمرض الكلى المزمن والإلكتروليتات؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع الجمعية الأوروبية للكلى؛ أسهم أو خيارات أسهم مع Telara Farma؛ جميعها خارج العمل المقدم. P K Pal يذكر منحًا أو عقودًا مدفوعة لمؤسستهم من المجلس الهندي للبحوث الطبية (ICMR)، وزارة العلوم والتكنولوجيا (DST)-مجلس أبحاث العلوم والهندسة، وزارة التكنولوجيا الحيوية (DBT)، مبادرة أبحاث العلوم المعرفية DST، تحالف Wellcome Trust UK-India DBT، خطة PACE من BIRAC، مؤسسة Michael J. Fox، وSKAN (المعرفة العلمية للشيخوخة والأمراض العصبية)-صندوق البحث؛ دفع وأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية كأعضاء هيئة تدريس/متحدثين/مؤلفين من الجمعية الدولية لمرض باركنسون واضطرابات الحركة، وجمعيات اضطرابات الحركة في كوريا، تايوان وبنغلاديش؛ دعم لحضور الاجتماعات و/أو السفر من المعهد الوطني للصحة النفسية والأعصاب (NIMHANS)، الجمعية الدولية لمرض باركنسون واضطرابات الحركة، وجمعيات اضطرابات الحركة في كوريا، تايوان وبنغلاديش؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، كرئيس سابق للأكاديمية الهندية للأعصاب، السكرتير السابق للفرع الآسيوي والأوقياني من الجمعية الدولية لمرض باركنسون واضطرابات الحركة (MDS-AOS)، رئيس تحرير مجلة Annals of Movement Disorders، رئيس لجنة التعليم في الجمعية الدولية لمرض باركنسون واضطرابات الحركة (IPMDS)، رئيس جمعية باركنسون في كارناتاكا، رئيس مجموعة دراسة اضطرابات الحركة المتعلقة بالعدوى من MDS، عضو مجموعة دراسة اضطرابات الحركة النادرة من الجمعية الدولية لمرض باركنسون واضطرابات الحركة (IPMDS)، عضو لجنة التعليم من IAPRD، عضو لجنة برنامج التعليم والتدريب لمقاييس التقييم من IPMDS، عضو فريق عمل علم الأعصاب من IPMDS، عضو مجموعة دراسة اضطرابات الحركة في آسيا، عضو اضطرابات الحركة بعد السكتة الدماغية، عضو مجموعة دراسة التأتأة من IPMDS، وعضو المبادرة العالمية للتأتأة؛ جميعها خارج العمل المقدم. C Palladino يذكر منحًا أو عقودًا من FCT Fundação para a Ciência e a Tecnologia، I.P. (تمويل وطني)، بموجب برنامج عقد كما هو محدد في DL No. 57/2016 وقانون No. 57/2017 (DL57/2016/CP1376/CT0004). DOI 10.54499/DL57/2016/CP1376/CT0004
(https://doi.org/10.54499/DL57/2016/CP1376/CT0004). R F بالما-ألفاريز يذكر المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من أنجليني، لوندبيك، كاسين ريكورداتي وتاكيدا؛ الدعم لحضور الاجتماعات و/أو السفر من جانسن ولوندبيك؛ جميعها خارج العمل المقدم. A M بانتيا ستويان يذكر رسوم استشارية من أسترازينيكا، بويرنجر إنجلهايم، إيلي ليلي، نوفو نورديسك، نوفارتس، ساندوز، وسانوفي؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من أسترازينيكا، بويرنجر إنجلهايم، إيلي ليلي، نوفو نورديسك، نوفارتس، ساندوز، ميدوكيمي، سيرفيير، وسانوفي؛ الدعم لحضور الاجتماعات و/أو السفر من سانوفي، نوفو نورديسك، وميدوكيمي؛ المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري مع أسترازينيكا، إيلي ليلي، نوفو نورديسك، وسانوفي؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوع، مع الجمعية الأوروبية الوسطى للسكري وجمعية الدراسات الكلوية-التمثيلية والتغذوية (ASRMN)؛ خارج العمل المقدم. R باسيرا يذكر المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري مع التجربة السريرية غير الربحية “التوحيد مع ADCT-402 (لونكاستوكسيماب تيسيرين) بعد العلاج المناعي الكيميائي: دراسة المرحلة الثانية في مرضى ليمفوما الخلايا الجدارية (MCL) المعالجين بـ BTKi/غير المؤهلين” – الراعي FIL، مؤسسة ليمفوما إيطالية، أليساندريا-آي (دور غير مدفوع)؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوع أو غير مدفوع، عضو في اللجنة الإحصائية لجمعية EBMT الأوروبية لزراعة العظام ونخاع العظام، باريس-ف (دور غير مدفوع)؛ خارج العمل المقدم. A E بيدن يذكر الدعم للمخطوطة الحالية من [المجلس الوطني الأسترالي للصحة والبحوث الطبية (رقم المنحة: APP2009306)]. V C F بيبيتو يذكر المنح أو العقود من سانوفي للرعاية الصحية الاستهلاكية والمبادرة الدولية لتقييم الأثر؛ خارج العمل المقدم. M بيجوليه يذكر منحة من صندوق الأطفال البلجيكي للبحوث pediatrics، خارج العمل المقدم. T بيلغريم يذكر المنح المدفوعة للمؤسسة دون تعويض شخصي من بيترونيك، إدواردز لايفساينس، وATSens؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من بيترونيك، بوسطن ساينتيفيك، إدواردز لايفساينس، أبوت، ميدترونيك، بيوسينسورز، وهايلايف؛ المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري لدراسة EMPIRE برعاية بيوسينسورز؛ واستلام المعدات (AT-Patches) من ATSens؛ خارج العمل المقدم. D بريتو-ألهامبرا يذكر الدعم للمخطوطة الحالية من وكالة الأدوية الأوروبية ومبادرة الأدوية المبتكرة، من خلال مؤسستهم؛ المنح أو العقود من أميجن، تشيزي-تايلور، ليلي، جانسن، نوفارتس، وUCB بيوفارما من خلال مؤسستهم؛ رسوم استشارية من أسترازينيكا وUCB بيوفارما؛ مصلحة مالية أو غير مالية أخرى في أميجن، أستيللاس، جانسن، شراكة إدارة سينابس وUCB بيوفارما لبرامج التدريب المدعومة؛ خارج العمل المقدم. A رادفار يذكر الدعم للمخطوطة الحالية من معهد أفيكينا للبحوث الطبية والسريرية. A راني يذكر الأسهم أو خيارات الأسهم كموظف بدوام كامل في أجياس فارما. L F ريس يذكر المنح أو العقود من MSD وفايزر؛ رسوم استشارية من GSK، MSD، وفايزر؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من GSK وفايزر؛ المدفوعات لشهادة الخبراء من GSK وMSD؛ الدعم لحضور الاجتماعات و/أو السفر من GSK؛ خارج العمل المقدم. T G ريه يذكر المنح أو العقود من NIH (R21AG070666؛ R21DA057540؛ R21AG078972؛ R01MH131528؛ R01AG080647)؛ خارج العمل المقدم. S ساكو يذكر المنح أو العقود من نوفارتس وأورياش؛ رسوم استشارية من نوفارتس، أليغران-أبفبي، تيفا، ليلي، لوندبيك، فايزر، نوفو نورديسك، أبوت، أسترازينيكا؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من نوفارتس، أليغران-أبفبي، تيفا، ليلي، لوندبيك، فايزر، نوفو نورديسك، أبوت، أسترازينيكا؛ الدعم لحضور الاجتماعات و/أو السفر من ليلي، نوفارتس، تيفا، لوندبيك؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوع أو غير مدفوع، كرئيس منتخب لجمعية السكتة الدماغية الأوروبية، ونائب الرئيس الثاني للاتحاد الأوروبي للصداع؛ استلام المعدات، المواد، الأدوية، الكتابة الطبية، الهدايا أو خدمات أخرى من أليغران-أبفبي، نوفو نورديسك؛ جميعها خارج العمل المقدم. P ساكديف يذكر المنح أو العقود من الصحة الوطنية والبحوث الطبية
العمل المقدم. يذكر A Biswas رسوم استشارية من شركة INTAS Pharmaceuticals Ltd، الهند، وشركة Lupin Pharmaceuticals، Ltd، الهند، وشركة Alkem Laboratories، الهند كمدفوعات شخصية؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من Roche Diagnostics، الهند، كمدفوعات شخصية؛ جميعها خارج العمل المقدم. يذكر E J Boyko مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من الجمعية الكورية للسكري، جمعية السكري في جمهورية الصين (تايوان)، الجمعية الأمريكية للسكري، والجمعية الدولية للقدم السكري؛ دعم لحضور الاجتماعات و/أو السفر من الجمعية الكورية للسكري؛ جمعية السكري في جمهورية الصين (تايوان)، الجمعية الدولية للقدم السكري؛ خارج العمل المقدم. يذكر M Carvalho مصالح مالية أو غير مالية أخرى من LAQV/ REQUIMTE، جامعة بورتو (بورتو، البرتغال) ويعترف بالدعم من FCT في إطار مشروع UIDP/50006/2020؛ خارج العمل المقدم. يذكر E Chung الدعم للمخطوطة الحالية من المعهد الوطني للصحة NICHD T32HD007233. يذكر J Conde منح أو عقود من مجلس البحث الأوروبي منحة بدء ERC-StG-2019-848325 (تمويل 1.5 مليون يورو)، خارج العمل المقدم. يذكر S Cortese منح أو عقود من المعهد الوطني للصحة والبحث والرعاية (NIHR) والوكالة التنفيذية الأوروبية للبحث؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من جمعية الصحة النفسية للأطفال والمراهقين، الجمعية البريطانية للطب النفسي الدوائي، Medice، وتحالف موارد ADHD الكندي؛ دعم لحضور الاجتماعات و/أو السفر من جمعية الصحة النفسية للأطفال والمراهقين، الجمعية البريطانية للطب النفسي الدوائي، Medice، وتحالف موارد ADHD الكندي؛ قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع مجموعة إرشادات ADHD الأوروبية والشبكة الأوروبية للاضطرابات الحركية المفرطة؛ جميعها خارج العمل المقدم. يذكر Sa Das قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع جمعية التشخيص والطب المختبري كرئيس برنامج، وفصل النساء في الصحة العالمية في الهند، خارج العمل المقدم. يذكر A Dastiridou الدعم لحضور الاجتماعات و/أو السفر من THEA وABBVIE، خارج العمل المقدم. يذكر L Degenhardt منح تعليمية غير مقيدة من Indivior وSeqirus لفحص أدوية الأفيون الجديدة في أستراليا، خارج العمل المقدم. يذكر A K Demetriades قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع لجنة التوجيه للمنتدى المعرفي AO، مجلس مؤسسة الأعصاب العالمية، ومجلس ضباط الجمعية الأوروبية للجمعيات العصبية، جميعها خارج العمل المقدم. يذكر A Faro الدعم للمخطوطة الحالية من المجلس الوطني للتنمية العلمية والتكنولوجية، CNPq، البرازيل كباحث CNPq (منحة دراسية). يذكر I Filip الدعم للمخطوطة الحالية من معهد أفيسينا للبحوث الطبية والسريرية. يذكر D Flood منح أو عقود من NHLBI (رقم الجائزة K23HL161271)، جامعة ميتشيغان مركز استقلال الأمريكيين الأكبر سناً (رقم الجائزة 5P30AG024824)، وبرنامج علماء البحث السريري في معهد كاسويل للسكري بجامعة ميتشيغان؛ رسوم استشارية من منظمة الصحة العالمية كمدفوعات لمؤسستهم؛ قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، كطبيب موظف في Maya Health Alliance، منظمة صحية غير حكومية في غواتيمالا؛ جميعها خارج العمل المقدم. يذكر A A Fomenkov الدعم للمخطوطة الحالية من تطوير تقنيات حيوية فعالة تعتمد على زراعة الخلايا، الأنسجة والأعضاء من النباتات العليا، الطحالب الدقيقة والزرنيخيات. البحث الذي تم إجراؤه ضمن التكليف الحكومي لوزارة العلوم والتعليم العالي في الاتحاد الروسي (الموضوع رقم 1220426000867). يذكر M Foschi رسوم استشارية من Roche وNovartis؛ دعم لحضور الاجتماعات و/أو السفر من Biogen، Roche، Novartis، Sanofi، Bristol، وMerck؛ قيادة أو دور وصي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، مع مؤسسة MBase؛ جميعها خارج العمل المقدم. يذكر R Franklin منح أو عقود من Heatwaves (حكومة كوينزلاند، كوينزلاند، أستراليا) وArc Flash (العوامل البشرية، حكومة كوينزلاند، كوينزلاند، أستراليا)، وMobile Plant Safety (Agrifutures)؛ دعم لحضور
اجتماعات و/أو سفر من مؤتمر ACTM للطب الاستوائي وطب السفر 2022 و2023، ومؤتمر ISTM لطب السفر في بازل 2023؛ دور قيادي أو ائتماني في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، كرئيس/مدير لـ Kidsafe، ومدير لـ Auschem، وعضو في لجنة الحوكمة لـ ISASH، ومدير لـ Farmsafe، ونائب رئيس ACTM، وكمنسق لمجموعة SIG للوقاية من الإصابات في PHAA؛ خارج العمل المقدم. P S Gill يذكر دعمًا للمخطوطة الحالية من المعهد الوطني للبحوث الصحية والرعاية (NIHR) كمحقق رئيسي مع مدفوعات لمؤسستهم؛ الآراء المعبر عنها في هذا المنشور هي آراء المؤلفين وليست بالضرورة آراء NIHR أو وزارة الصحة والرعاية الاجتماعية في المملكة المتحدة. A Guha يذكر منحًا أو عقودًا من جمعية القلب الأمريكية ووزارة الدفاع؛ رسوم استشارية من Pfizer وNovartis وMyovant؛ دور قيادي أو ائتماني في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع مجموعة العمل ZERO Prostate Cancer Health Equity وDoctopedia كشريك طبي مؤسس؛ جميعها خارج العمل المقدم. C Herteliu يذكر منحًا أو عقودًا من وزارة البحث والابتكار والرقمنة الرومانية، MCID، رقم المشروع ID-585-CTR-42-PFE-2021؛ منحة من المفوضية الأوروبية Horizon 4P-CAN (البحث في الوقاية الأولية من السرطان المخصص من خلال مشاركة المواطنين والابتكار الاجتماعي المدعوم رقميًا)؛ مشروع “المرونة الاجتماعية والاقتصادية في بيئة متعددة المخاطر في رومانيا” الممول من الاتحاد الأوروبي – NextgenerationEU والحكومة الرومانية، بموجب خطة التعافي والمرونة الوطنية لرومانيا، العقد رقم 760050/ 23.05.2023، رمز PNRR-C9-I8-CF 267/29.11.2022، من خلال وزارة البحث والابتكار والرقمنة الرومانية، ضمن المكون 9، الاستثمار I8؛ مشروع “فهم أفضل للأنظمة الاجتماعية والاقتصادية باستخدام طرق كمية من الفيزياء” الممول من الاتحاد الأوروبي-NextgenerationEU والحكومة الرومانية، بموجب خطة التعافي والمرونة الوطنية لرومانيا، رقم العقد 760034/ 23.05.2023، رمز PNRR-C9-I8-CF 255/ 29.11.2022، من خلال وزارة البحث والابتكار والرقمنة الرومانية، ضمن المكون 9، الاستثمار I8؛ خارج العمل المقدم. M Hultström يذكر دعمًا للمخطوطة الحالية من مؤسسة Knut och Alice Wallenberg ومؤسسة القلب والرئة السويدية، جميعها كمدفوعات لمؤسستهم؛ دعم لحضور الاجتماعات و/أو السفر من الجمعية الفيزيولوجية الأمريكية والجمعية السويدية للتخدير والرعاية المركزة؛ دور قيادي أو ائتماني في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع الجمعية الفيزيولوجية الأمريكية، قسم الماء والإلكتروليت؛ جميعها خارج العمل المقدم. I Ilic وM Ilic يذكران دعمًا للمخطوطة الحالية من وزارة العلوم والتنمية التكنولوجية والابتكار في جمهورية صربيا. S M Islam يذكر دعمًا للمخطوطة الحالية من NHMRC ومؤسسة القلب، N E Ismail يذكر دورًا قياديًا أو ائتمانيًا في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، غير مدفوعة، كأمين (عضو مجلس) من الأكاديمية الماليزية للصيدلة، خارج العمل المقدم. T Joo يذكر دعمًا للمخطوطة الحالية من المكتب الوطني للبحث والتطوير والابتكار في المجر (RRF-2.3.1-21-2022-00006)، قسم الصحة المدفوعة بالبيانات من المختبر الوطني للأمن الصحي. G Joshy يذكر منحًا أو عقودًا من وزارة الصحة والرعاية المسنّة 2023 (فهم العبء القاتل لـ COVID-19 في مرافق الرعاية المسنّة السكنية)؛ دعم لحضور الاجتماعات و/أو السفر من منحة الجمعية الإحصائية الأسترالية 2023 لدعم تسجيل المؤتمر؛ المشاركة في مجلس مراقبة سلامة البيانات مع معهد العلوم الرياضية الأسترالي (AMSI) والجمعية الإحصائية الأسترالية (SSA) لمشروع برنامج التغذية ونمط الحياة الذي يقوده المجتمع لفقدان الوزن والصحة الأيضية: تجربة عشوائية محكومة (ELCHO)، 2022؛ جميعها خارج العمل المقدم. J Jozwiak يذكر مدفوعات أو أتعاب لمحاضرات، عروض، مكاتب المتحدثين، كتابة مخطوطات أو أحداث تعليمية من Novartis وAdamed وAmgen؛ خارج العمل المقدم. N Kawakami يذكر منحًا أو عقودًا من مؤسسة Junpukai ووزارة الصحة العقلية الرقمية كقسم مخصص، مدعومًا بمنحة غير مقيدة من 15 مؤسسة.https://dmh.m.u-tokyo.ac.jp/cرسوم الاستشارات من معهد ريكن، وكالة استكشاف الفضاء اليابانية (JAXA)، شركة سيكي سوي للكيماويات، وSB@WORK؛ دور قيادي أو وصائي في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع الجمعية اليابانية للصحة المهنية؛
كل ما يتعلق بالعمل المقدم. يذكر ج. ه. كيمبين منحًا أو عقودًا من برنامج جراحة العين والأذن في ماساتشوستس وSight for Souls من خلال المدفوعات لمؤسستهم؛ دور قيادي أو وصائي في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوعة أو غير مدفوعة، كرئيس لـSight for Souls؛ أسهم أو خيارات أسهم مع Betaliq وTarsier؛ كل ما يتعلق بالعمل المقدم. يذكر ت. كوكسي منحًا أو عقودًا من Novartis Magyarország Ltd من خلال الدفع لأنشطة الوصول إلى السوق، خارج العمل المقدم. يذكر ك. كريشان مصالح غير مالية أخرى من مركز UGC للدراسات المتقدمة، CAS II، الممنوحة لقسم الأنثروبولوجيا، جامعة بنجاب (تشاندigarh، الهند)؛ خارج العمل المقدم. يذكر ب. لايسي دعمًا للمخطوطة الحالية من بنك المملكة المتحدة الحيوي، الممول بشكل كبير من مجلس البحوث الطبية في المملكة المتحدة وWellcome، من خلال عملهم في جامعة أكسفورد. يذكر م. لي دعمًا للمخطوطة الحالية من وزارة التعليم في جمهورية كوريا ومؤسسة البحث الوطنية في كوريا (NRF-2021R1I1A4A01057428) وبرنامج التعليم في تكنولوجيا التوافق الحيوي من خلال معهد كوريا للتقدم التكنولوجي (KIAT) الممول من وزارة التجارة والصناعة والطاقة (رقم P0017805). يذكر م-ج. لي منحًا أو عقودًا من المجلس الوطني للعلوم والتكنولوجيا في تايوان (NSTC 112-2410-H-003-031؛ دور قيادي أو وصائي في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوعة أو غير مدفوعة، كمحرر تقني لمجلة جمعية القلب الأمريكية؛ خارج العمل المقدم. يذكر ج. ليو دعمًا للمخطوطة الحالية من المؤسسة الوطنية للعلوم الطبيعية في الصين (رقم المنحة: 72122001؛ 72211540398). يذكر س. لوركوفسكي منحًا أو عقودًا من Akcea Therapeutics ألمانيا من خلال المدفوعات لمؤسستهم؛ رسوم استشارية من دانون، نوفارتس فارما، سويديش أورفان بيوفيتروم (SOBI)، وأبفيلد؛ مدفوعات أو أتعاب لمحاضرات، عروض تقديمية، مكاتب متحدثين، كتابة مخطوطات أو أحداث تعليمية من Akcea Therapeutics ألمانيا، AMARIN ألمانيا، Amedes Holding، AMGEN، برلين-كيمي، بوهيرنجر إنجلهايم فارما، داييتشي سانكيو ألمانيا، دانون، هوبيرت بوردا ميديا هولدينغ، جانسن-سيلاج، ليلي ألمانيا، نوفارتس فارما، نوفو نورديسك فارما، روش فارما، سانوفي-أفنتيس، وSYNLAB هولدينغ ألمانيا وSYNLAB أكاديمية؛ دعم لحضور الاجتماعات و/أو السفر من AMGEN؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري مع Akcea Therapeutics ألمانيا، AMGEN، داييتشي سانكيو ألمانيا، نوفارتس فارما، وسانوفي-أفنتيس؛ كل ذلك خارج العمل المقدم. يذكر م. أ. محمود تمويل منحة أو عقد من وكالة البحث والابتكار، وزارة التعليم في المملكة العربية السعودية (رقم المشروع 445-5-748). يذكر ل. ج. مانتوفاني دعمًا للمخطوطة الحالية من وزارة الصحة الإيطالية. يذكر ح. ر. مراتب دعمًا للمخطوطة الحالية من برنامج بياتريو دي بينوس لما بعد الدكتوراه من مكتب سكرتير الجامعات والبحث من وزارة الأعمال والمعرفة في حكومة كاتالونيا: 2020 BP 00261. يذكر ر. ماتزوبولوس رسوم استشارية من جامعة نيويورك وDG موري ترست؛ دعم لحضور الاجتماعات/السفر مدفوع من SA MRC وجامعة كيب تاون؛ دور قيادي أو وصائي في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، غير مدفوعة، كعضو مجلس في Gun Free South Africa؛ أسهم أو خيارات أسهم مع Sanlam؛ خارج العمل المقدم. يذكر ر. ج. مود دعمًا للمخطوطة الحالية من Wellcome Trust [رقم المنحة 220211] حيث يوفر تمويلًا أساسيًا لبحوث الطب الاستوائي في ماهيدول أكسفورد ويساهم في راتبه. يذكر أ-ف. أ. مينتيس منحًا أو تمويل عقود من ‘MilkSafe: خط أنابيب جديد لتغذية حليب الأطفال باستخدام تقنيات الأوميكس’، وهو بحث ممول جزئيًا من صندوق التنمية الإقليمية الأوروبية للاتحاد الأوروبي والأموال الوطنية اليونانية من خلال البرنامج التشغيلي للتنافسية، ريادة الأعمال والابتكار، تحت دعوة البحث – الإنشاء – الابتكار (رمز المشروع: T2EDK-02222)، بالإضافة إلى ELIDEK (المؤسسة اليونانية للبحث والابتكار، MIMS-860) (كلاهما خارج المخطوطة الحالية)؛ مدفوعات لشهادة خبير من العمل كمراجع خارجي لـFONDAZIONE CARIPLO، إيطاليا؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري كعضو في هيئة التحرير لـ”المراجعات المنهجية”، و”سنوات الوبائيات”، وكمدير مساعد لـ”الطب التحويلي”؛ أسهم أو خيارات أسهم من مصنع نبيذ عائلي؛ ومصالح مالية أخرى كمسؤول علمي حالي لمجموعة BGI؛ خارج العمل المقدم. يذكر س. أ. ميو
الدعم من جامعة الملك سعود، الرياض، المملكة العربية السعودية (RSP-2024 R47). T R Miller يذكر منحًا أو عقودًا من مؤسسة AB InBev، والمعهد الوطني للصحة النفسية (مقاطعة سانتا كلارا، كاليفورنيا)، وEverytown من أجل سلامة الأسلحة؛ دفع مقابل الشهادة كخبير في ولايات ميشيغان، نيفادا ونيو مكسيكو، مجلس الصحة في مقاطعة موبايل؛ خارج العمل المقدم. P B Mitchell يذكر دفعًا أو أتعابًا للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية، من Janssen (أستراليا)، خارج العمل المقدم. L Monasta يذكر دعمًا للمخطوطة الحالية من وزارة الصحة (Ricerca Corrente 34/2017) من خلال المدفوعات المقدمة إلى معهد صحة الأم والطفل IRCCS Burlo Garofolo. R S Moreira يذكر منحًا أو عقودًا من منحة إنتاجية البحث CNPq (المجلس الوطني للتنمية العلمية والتكنولوجية) رقم تسجيل المنحة 316607/2021-5؛ خارج العمل المقدم. J Mosser يذكر دعمًا للمخطوطة الحالية من مؤسسة بيل وميليندا غيتس؛ منح أو عقود من Gavi؛ دعم لحضور الاجتماعات و/أو السفر من مؤسسة بيل وميليندا غيتس؛ خارج العمل المقدم. S Nomura يذكر دعمًا للمخطوطة الحالية من وزارة التعليم والثقافة والرياضة والعلوم والتكنولوجيا في اليابان (21H03203) والبحث الاستباقي للعلوم والتكنولوجيا الجنينية من وكالة العلوم والتكنولوجيا اليابانية (JPMJPR22R8). B Norrving يذكر المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري مع Simbec Orion، خارج العمل المقدم. A P Okekunle يذكر دعمًا للمخطوطة الحالية من مؤسسة البحث الوطنية في كوريا الممولة من وزارة العلوم وتكنولوجيا المعلومات والاتصالات (2020H1D3A1A04081265). A Ortiz يذكر منحًا أو عقودًا من Sanofi كمدفوعات لمؤسستهم؛ أتعاب استشارية، أتعاب متحدثين أو دعم للسفر من Advicciene، Astellas، Astrazeneca، Amicus، Amgen، Boehringer Ingelheim، Fresenius Medical، Care، GSK، Bayer، Sanofi-Genzyme، Menarini، Mundipharma، Kyowa Kirin، Lilly، Alexion، Freeline، Idorsia، Chiesi، Otsuka، Novo-Nordisk، Sysmex وVifor Fresenius Medical Care Renal، Pharma وهو مدير كاتدرائية، Mundipharma-UAM لمرض الكلى السكري، وكاتدرائية Astrazeneca-UAM لمرض الكلى المزمن والإلكتروليتات؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع الجمعية الأوروبية للكلى؛ أسهم أو خيارات أسهم مع Telara Farma؛ جميعها خارج العمل المقدم. P K Pal يذكر منحًا أو عقودًا مدفوعة لمؤسستهم من المجلس الهندي للبحوث الطبية (ICMR)، وزارة العلوم والتكنولوجيا (DST)-مجلس أبحاث العلوم والهندسة، وزارة التكنولوجيا الحيوية (DBT)، مبادرة أبحاث العلوم المعرفية DST، تحالف Wellcome Trust UK-India DBT، خطة PACE من BIRAC، مؤسسة Michael J. Fox، وSKAN (المعرفة العلمية للشيخوخة والأمراض العصبية)-صندوق البحث؛ دفع وأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية كأعضاء هيئة تدريس/متحدثين/مؤلفين من الجمعية الدولية لمرض باركنسون واضطرابات الحركة، وجمعيات اضطرابات الحركة في كوريا، تايوان وبنغلاديش؛ دعم لحضور الاجتماعات و/أو السفر من المعهد الوطني للصحة النفسية والأعصاب (NIMHANS)، الجمعية الدولية لمرض باركنسون واضطرابات الحركة، وجمعيات اضطرابات الحركة في كوريا، تايوان وبنغلاديش؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوعة، كرئيس سابق للأكاديمية الهندية للأعصاب، السكرتير السابق للفرع الآسيوي والأوقياني من الجمعية الدولية لمرض باركنسون واضطرابات الحركة (MDS-AOS)، رئيس تحرير مجلة Annals of Movement Disorders، رئيس لجنة التعليم في الجمعية الدولية لمرض باركنسون واضطرابات الحركة (IPMDS)، رئيس جمعية باركنسون في كارناتاكا، رئيس مجموعة دراسة اضطرابات الحركة المتعلقة بالعدوى من MDS، عضو مجموعة دراسة اضطرابات الحركة النادرة من الجمعية الدولية لمرض باركنسون واضطرابات الحركة (IPMDS)، عضو لجنة التعليم من IAPRD، عضو لجنة برنامج التعليم والتدريب لمقاييس التقييم من IPMDS، عضو فريق عمل علم الأعصاب من IPMDS، عضو مجموعة دراسة اضطرابات الحركة في آسيا، عضو اضطرابات الحركة بعد السكتة الدماغية، عضو مجموعة دراسة التأتأة من IPMDS، وعضو المبادرة العالمية للتأتأة؛ جميعها خارج العمل المقدم. C Palladino يذكر منحًا أو عقودًا من FCT Fundação para a Ciência e a Tecnologia، I.P. (تمويل وطني)، بموجب برنامج عقد كما هو محدد في DL No. 57/2016 وقانون No. 57/2017 (DL57/2016/CP1376/CT0004). DOI 10.54499/DL57/2016/CP1376/CT0004
(https://doi.org/10.54499/DL57/2016/CP1376/CT0004). R F بالما-ألفاريز يذكر المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من أنجليني، لوندبيك، كاسين ريكورداتي وتاكيدا؛ الدعم لحضور الاجتماعات و/أو السفر من جانسن ولوندبيك؛ جميعها خارج العمل المقدم. A M بانتيا ستويان يذكر رسوم استشارية من أسترازينيكا، بويرنجر إنجلهايم، إيلي ليلي، نوفو نورديسك، نوفارتس، ساندوز، وسانوفي؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من أسترازينيكا، بويرنجر إنجلهايم، إيلي ليلي، نوفو نورديسك، نوفارتس، ساندوز، ميدوكيمي، سيرفيير، وسانوفي؛ الدعم لحضور الاجتماعات و/أو السفر من سانوفي، نوفو نورديسك، وميدوكيمي؛ المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري مع أسترازينيكا، إيلي ليلي، نوفو نورديسك، وسانوفي؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، غير مدفوع، مع الجمعية الأوروبية الوسطى للسكري وجمعية الدراسات الكلوية-التمثيلية والتغذوية (ASRMN)؛ خارج العمل المقدم. R باسيرا يذكر المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري مع التجربة السريرية غير الربحية “التوحيد مع ADCT-402 (لونكاستوكسيماب تيسيرين) بعد العلاج المناعي الكيميائي: دراسة المرحلة الثانية في مرضى ليمفوما الخلايا الجدارية (MCL) المعالجين بـ BTKi/غير المؤهلين” – الراعي FIL، مؤسسة ليمفوما إيطالية، أليساندريا-آي (دور غير مدفوع)؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوع أو غير مدفوع، عضو في اللجنة الإحصائية لجمعية EBMT الأوروبية لزراعة العظام ونخاع العظام، باريس-ف (دور غير مدفوع)؛ خارج العمل المقدم. A E بيدن يذكر الدعم للمخطوطة الحالية من [المجلس الوطني الأسترالي للصحة والبحوث الطبية (رقم المنحة: APP2009306)]. V C F بيبيتو يذكر المنح أو العقود من سانوفي للرعاية الصحية الاستهلاكية والمبادرة الدولية لتقييم الأثر؛ خارج العمل المقدم. M بيجوليه يذكر منحة من صندوق الأطفال البلجيكي للبحوث pediatrics، خارج العمل المقدم. T بيلغريم يذكر المنح المدفوعة للمؤسسة دون تعويض شخصي من بيترونيك، إدواردز لايفساينس، وATSens؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من بيترونيك، بوسطن ساينتيفيك، إدواردز لايفساينس، أبوت، ميدترونيك، بيوسينسورز، وهايلايف؛ المشاركة في مجلس مراقبة سلامة البيانات أو المجلس الاستشاري لدراسة EMPIRE برعاية بيوسينسورز؛ واستلام المعدات (AT-Patches) من ATSens؛ خارج العمل المقدم. D بريتو-ألهامبرا يذكر الدعم للمخطوطة الحالية من وكالة الأدوية الأوروبية ومبادرة الأدوية المبتكرة، من خلال مؤسستهم؛ المنح أو العقود من أميجن، تشيزي-تايلور، ليلي، جانسن، نوفارتس، وUCB بيوفارما من خلال مؤسستهم؛ رسوم استشارية من أسترازينيكا وUCB بيوفارما؛ مصلحة مالية أو غير مالية أخرى في أميجن، أستيللاس، جانسن، شراكة إدارة سينابس وUCB بيوفارما لبرامج التدريب المدعومة؛ خارج العمل المقدم. A رادفار يذكر الدعم للمخطوطة الحالية من معهد أفيكينا للبحوث الطبية والسريرية. A راني يذكر الأسهم أو خيارات الأسهم كموظف بدوام كامل في أجياس فارما. L F ريس يذكر المنح أو العقود من MSD وفايزر؛ رسوم استشارية من GSK، MSD، وفايزر؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من GSK وفايزر؛ المدفوعات لشهادة الخبراء من GSK وMSD؛ الدعم لحضور الاجتماعات و/أو السفر من GSK؛ خارج العمل المقدم. T G ريه يذكر المنح أو العقود من NIH (R21AG070666؛ R21DA057540؛ R21AG078972؛ R01MH131528؛ R01AG080647)؛ خارج العمل المقدم. S ساكو يذكر المنح أو العقود من نوفارتس وأورياش؛ رسوم استشارية من نوفارتس، أليغران-أبفبي، تيفا، ليلي، لوندبيك، فايزر، نوفو نورديسك، أبوت، أسترازينيكا؛ المدفوعات أو الأتعاب للمحاضرات، العروض التقديمية، مكاتب المتحدثين، كتابة المخطوطات أو الفعاليات التعليمية من نوفارتس، أليغران-أبفبي، تيفا، ليلي، لوندبيك، فايزر، نوفو نورديسك، أبوت، أسترازينيكا؛ الدعم لحضور الاجتماعات و/أو السفر من ليلي، نوفارتس، تيفا، لوندبيك؛ دور قيادي أو ائتماني في مجلس آخر، جمعية، لجنة أو مجموعة مناصرة، مدفوع أو غير مدفوع، كرئيس منتخب لجمعية السكتة الدماغية الأوروبية، ونائب الرئيس الثاني للاتحاد الأوروبي للصداع؛ استلام المعدات، المواد، الأدوية، الكتابة الطبية، الهدايا أو خدمات أخرى من أليغران-أبفبي، نوفو نورديسك؛ جميعها خارج العمل المقدم. P ساكديف يذكر المنح أو العقود من الصحة الوطنية والبحوث الطبية
مجلس الأبحاث الأسترالي والمعاهد الوطنية للصحة في الولايات المتحدة؛ دفع أو مكافآت لمحاضرات من مختبرات ألكيم لندوة حدود الطب النفسي في يونيو 2023، مومباي، الهند؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري مع بيجن أستراليا وروش أستراليا؛ دور قيادي أو ائتماني في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، غير مدفوع، مع جمعية فاسكوج والجمعية العالمية للطب النفسي؛ جميعها خارج العمل المقدم. ي. ل. سامودرا يذكر منحًا أو عقودًا من جامعة تايبيه الطبية؛ دور قيادي أو ائتماني في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوع أو غير مدفوع، مع مركز بنانغ ميرا للبحوث؛ جميعها خارج العمل المقدم. ج. سانابريا يذكر دعمًا لحضور الاجتماعات و/أو السفر من قسم الجراحة، كلية الطب بجامعة مارشال؛ ثلاثة براءات اختراع قيد الانتظار؛ المشاركة في تقييم الجودة وضمانها لعمليات قسم الجراحة؛ دور قيادي أو ائتماني في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوع أو غير مدفوع مع SSAT وASTS وAHPBA وIHPBA وAASLD؛ جميعها خارج العمل المقدم. ن. سكارميا يذكر منحًا أو عقودًا مع نوفو نورديسك كمدير محلي لموقع التجنيد لتجربة علاجية متعددة الجنسيات ومتعددة المراكز من المرحلة الثالثة لمرض الزهايمر مع تمويل مدفوع للمؤسسة؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري مع كلية الطب ألبرت أينشتاين (دراسة ممولة من NIH) كرئيس لمجلس مراقبة سلامة البيانات؛ جميعها خارج العمل المقدم. أ. إ. شوت يذكر مكافآت المتحدثين من سيرفييه ونوفارتس وسانوفي ومدترونيك وأبوت وأومرون وأكتييا؛ دعم لحضور الاجتماعات و/أو السفر من سيرفييه ومدترونيك وأبوت؛ المشاركة في مجلس مراقبة سلامة البيانات أو مجلس استشاري مع مجلس استشاري لشركة أبوت للأدوية، ومجلس استشاري لأجهزة سكاي لاب؛ دور قيادي أو ائتماني في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، مدفوع أو غير مدفوع، مع نائب رئيس: مجموعة العمل الوطنية لارتفاع ضغط الدم في أستراليا، عضو مجلس إدارة: ارتفاع ضغط الدم أستراليا، سكرتير الشركة: التحالف الأسترالي للقلب والأوعية الدموية؛ جميعها خارج العمل المقدم. ب. م. شارسشميت يذكر منح بحثية من مؤسسة إلس كروينر-فريزينيوس وDFG وفارماسيبت؛ دفع أو مكافآت لمحاضرات وعروض ومكاتب المتحدثين وكتابة المخطوطات أو الفعاليات التعليمية من أسترازينيكا؛ دعم لحضور الاجتماعات و/أو السفر من باير AG؛ جميعها خارج العمل المقدم. م. شكرية يذكر رسوم استشارية من روش؛ دفع أو مكافآت لمحاضرات وعروض ومكاتب المتحدثين وكتابة المخطوطات أو الفعاليات التعليمية من جونسون وجونسون وأستيللاس؛ خارج العمل المقدم. أ. شريفان يذكر دورًا قياديًا أو ائتمانيًا في مجلس أو جمعية أو لجنة أو مجموعة مناصرة أخرى، غير مدفوع مع كوكراين كعضو توجيهي في شبكة المحترفين في بداية حياتهم المهنية؛ واستلام ثلاثين يومًا من الوصول المجاني إلى ساينس دايركت وسكوبس ورياكسيز وجيوفاسيتس بعد مراجعة المخطوطات لمجلتين تنشرهما إلسفير؛ خارج العمل المقدم. س. شارما يذكر دعمًا للمخطوطة الحالية من زمالة جون ج. بونيكا ما بعد الدكتوراه من الجمعية الدولية لدراسة الألم (IASP؛ 2021-2023)؛ دفع أو مكافآت لمحاضرات وعروض ومكاتب المتحدثين وكتابة المخطوطات أو الفعاليات التعليمية ومنحة سفر لتقديم حديث حول “التقنيات لتعليم الألم في البلدان النامية” التي نظمتها مجموعة تعليم الألم SIG من IASP في المؤتمر العالمي للألم في تورونتو (2022)؛ خارج العمل المقدم. ف. شارما يذكر دعمًا ماليًا أو غير مالي آخر من مشروع البحث DFSS (MHA) (DFSS28(1)2019/EMR/6) في معهد العلوم الجنائية والطب الشرعي، جامعة بنجاب، تشانديغار، الهند، خارج العمل المقدم. ك. شيبويا يذكر دعمًا للمخطوطة الحالية من مؤسسة طوكيو للبحوث السياسية. ف. شيفاروف يذكر براءة اختراع واحدة ونموذج منفعة واحد مع مكتب براءات الاختراع البلغاري؛ أسهم أو خيارات أسهم من ICONplc (RSUs)؛ ومصالح مالية أخرى من راتب ICONplc؛ جميعها خارج العمل المقدم. س. شريستا يذكر مصالح مالية أخرى من منحة البحث المتميزة من مدرسة الصيدلة في جامعة موناش ماليزيا، خارج العمل المقدم. ج. ب. سيلفا يذكر دعمًا للمخطوطة الحالية من المؤسسة البرتغالية للعلوم والتكنولوجيا من خلال دفع راتبهم (عقد بالمرجع 2021.01789.CEECIND/CP1662/CT0014). ل. م. ل. ر. سيلفا يذكر منحًا أو عقودًا من CENTRO-04-3559-FSE-000162، صندوق التضامن الأوروبي (FSE)، خارج العمل المقدم. ج. ر. سيمبسون يذكر منحًا أو عقودًا من MBIE (NZ) وHRC (NZ) ووزارة الصحة (NZ) وMRC (UK) وCSO (UK)؛ دور قيادي أو
دور الائتمان في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة مع مجموعة استشارية أخلاقية للبيانات الحكومية في نيوزيلندا كرئيس؛ خارج العمل المقدم. يذكر د. ج. شتاين أنه يتلقى رسوم استشارية من ديسكفري فيتاليتي، وجونسون آند جونسون، وكانا، ولوريال، ولوندبيك، وأوريون، وسانوفي، وسيرفييه، وتاكد، وفيستاجين، خارج العمل المقدم. يذكر ك. ستبرانت سونرهاغن أنه يتولى دور القيادة أو الائتمان في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة كرئيس للجنة العلمية لمؤسسة السكتة الدماغية السويدية؛ خارج العمل المقدم. يذكر س. ستورتكي أنه يتلقى منحًا أو عقودًا مدفوعة لمؤسسته من إدواردز لايفساينس، وميدترونيك، وأبوت، وبوسطن ساينتيفيك؛ رسوم استشارية من تيليفليكس؛ مدفوعات أو مكافآت لمحاضرات أو عروض تقديمية أو مكاتب متحدثين أو كتابة مخطوطات أو أحداث تعليمية من بوسطن ساينتيفيك/بي تي جي؛ خارج العمل المقدم. يذكر أ. ج. ثريفت أنه يتلقى منحًا أو عقودًا مدفوعة لمؤسسته من المجلس الوطني للصحة والبحوث الطبية (أستراليا) (أرقام المنح 1171966، 1182071)، ومؤسسة القلب (أستراليا) ومؤسسة السكتة الدماغية (أستراليا)؛ خارج العمل المقدم. يذكر ج. هـ. ف. تيكوالو أنه يتولى دور القيادة أو الائتمان في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع مركز بنانغ ميرا للبحوث كمؤسس مشارك، خارج العمل المقدم. يذكر م. ف. تيتوفا أنه يتلقى دعمًا للمخطوطة الحالية من وزارة العلوم والتعليم العالي في الاتحاد الروسي (الموضوع رقم 122042600086-7). يذكر س. ج. ترومانز أنه يتلقى منحًا أو عقودًا من فريق مسح الأمراض النفسية للبالغين لعام 2023، الذي يجمع بيانات وبائية عن البالغين المقيمين في إنجلترا. هذه دراسة متعاقد عليها من NHS Digital، عبر وزارة الصحة والرعاية الاجتماعية؛ خارج العمل المقدم. يذكر ب. ويليت أنه يتلقى رسوم استشارية من نوفارتس؛ خارج العمل المقدم. تذكر م. زيلينسكا اهتمامًا ماليًا آخر كموظفة في أسترازينيكا، خارج العمل المقدم. يذكر أ. زوملا أنه يتلقى منحًا أو عقودًا من الشبكة الأفريقية حول العدوى الناشئة والمتجددة (PANDORA-ID-NET، CANTAM-3، وEACCR-3) الممولة من شراكة التجارب السريرية للدول الأوروبية والنامية، وبرنامج هورايزون 2020 للاتحاد الأوروبي، والمعهد الوطني للصحة والرعاية في المملكة المتحدة، وجائزة مهاتير للعلوم وجائزة باسكوال موكومبي من الاتحاد الأوروبي؛ المشاركة في مجلس مراقبة سلامة البيانات أو كعضو في المجلس الاستشاري لمجموعة خبراء التجمعات الكبيرة التابعة لمنظمة الصحة العالمية وبرنامج الطوارئ الصحية لمنظمة الصحة العالمية في جنيف، وعضو في اللجنة العلمية للاتحاد الأوروبي-EDCTP3-الصحة العالمية (بروكسل)؛ جميعها خارج العمل المقدم.
دور الائتمان في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة مع مجموعة استشارية أخلاقية للبيانات الحكومية في نيوزيلندا كرئيس؛ خارج العمل المقدم. يذكر د. ج. شتاين أنه يتلقى رسوم استشارية من ديسكفري فيتاليتي، وجونسون آند جونسون، وكانا، ولوريال، ولوندبيك، وأوريون، وسانوفي، وسيرفييه، وتاكد، وفيستاجين، خارج العمل المقدم. يذكر ك. ستبرانت سونرهاغن أنه يتولى دور القيادة أو الائتمان في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة كرئيس للجنة العلمية لمؤسسة السكتة الدماغية السويدية؛ خارج العمل المقدم. يذكر س. ستورتكي أنه يتلقى منحًا أو عقودًا مدفوعة لمؤسسته من إدواردز لايفساينس، وميدترونيك، وأبوت، وبوسطن ساينتيفيك؛ رسوم استشارية من تيليفليكس؛ مدفوعات أو مكافآت لمحاضرات أو عروض تقديمية أو مكاتب متحدثين أو كتابة مخطوطات أو أحداث تعليمية من بوسطن ساينتيفيك/بي تي جي؛ خارج العمل المقدم. يذكر أ. ج. ثريفت أنه يتلقى منحًا أو عقودًا مدفوعة لمؤسسته من المجلس الوطني للصحة والبحوث الطبية (أستراليا) (أرقام المنح 1171966، 1182071)، ومؤسسة القلب (أستراليا) ومؤسسة السكتة الدماغية (أستراليا)؛ خارج العمل المقدم. يذكر ج. هـ. ف. تيكوالو أنه يتولى دور القيادة أو الائتمان في مجلس آخر أو جمعية أو لجنة أو مجموعة مناصرة، مدفوعة أو غير مدفوعة، مع مركز بنانغ ميرا للبحوث كمؤسس مشارك، خارج العمل المقدم. يذكر م. ف. تيتوفا أنه يتلقى دعمًا للمخطوطة الحالية من وزارة العلوم والتعليم العالي في الاتحاد الروسي (الموضوع رقم 122042600086-7). يذكر س. ج. ترومانز أنه يتلقى منحًا أو عقودًا من فريق مسح الأمراض النفسية للبالغين لعام 2023، الذي يجمع بيانات وبائية عن البالغين المقيمين في إنجلترا. هذه دراسة متعاقد عليها من NHS Digital، عبر وزارة الصحة والرعاية الاجتماعية؛ خارج العمل المقدم. يذكر ب. ويليت أنه يتلقى رسوم استشارية من نوفارتس؛ خارج العمل المقدم. تذكر م. زيلينسكا اهتمامًا ماليًا آخر كموظفة في أسترازينيكا، خارج العمل المقدم. يذكر أ. زوملا أنه يتلقى منحًا أو عقودًا من الشبكة الأفريقية حول العدوى الناشئة والمتجددة (PANDORA-ID-NET، CANTAM-3، وEACCR-3) الممولة من شراكة التجارب السريرية للدول الأوروبية والنامية، وبرنامج هورايزون 2020 للاتحاد الأوروبي، والمعهد الوطني للصحة والرعاية في المملكة المتحدة، وجائزة مهاتير للعلوم وجائزة باسكوال موكومبي من الاتحاد الأوروبي؛ المشاركة في مجلس مراقبة سلامة البيانات أو كعضو في المجلس الاستشاري لمجموعة خبراء التجمعات الكبيرة التابعة لمنظمة الصحة العالمية وبرنامج الطوارئ الصحية لمنظمة الصحة العالمية في جنيف، وعضو في اللجنة العلمية للاتحاد الأوروبي-EDCTP3-الصحة العالمية (بروكسل)؛ جميعها خارج العمل المقدم.
مشاركة البيانات
لتحميل البيانات المستخدمة في هذه التحليلات، يرجى زيارة موقع تبادل بيانات الصحة العالمية GBD 2021 (https://ghdx.healthdata.org/gbd-2021/المصادر).
شكر وتقدير
البحث الذي تم الإبلاغ عنه في هذه المنشورة تم دعمه من قبل مؤسسة بيل وميليندا غيتس؛ وزارة الصحة في كوينزلاند، أستراليا؛ وزارة الصحة والرعاية الاجتماعية في المملكة المتحدة؛ المعهد النرويجي للصحة العامة؛ مستشفى سانت جود لأبحاث الأطفال؛ ووزارة الصحة في نيوزيلندا. المحتوى هو مسؤولية المؤلفين فقط ولا يمثل بالضرورة الآراء الرسمية للجهات الممولة. منح المكتب المركزي للإحصاء الفلسطيني الباحثين الوصول إلى البيانات ذات الصلة وفقًا لرقم الترخيص SLN2014-3-170، بعد إخضاع البيانات للمعالجة بهدف الحفاظ على سرية البيانات الفردية وفقًا لقانون الإحصاءات العامة-2000. المؤلفون مسؤولون وحدهم عن الاستنتاجات والاستدلالات المستندة إلى البيانات المتاحة. تم جمع هذه البيانات بفضل الوكالة الأمريكية للتنمية الدولية (USAID) بموجب شروط الاتفاق التعاوني GPO-A-00-08-000_D3-00. الآراء المعبر عنها هي آراء المؤلفين ولا تعكس بالضرورة آراء الوكالة الأمريكية للتنمية الدولية أو الحكومة الأمريكية. تم توفير البيانات لهذا البحث من قبل MEASURE Evaluation، الممولة من قبل الوكالة الأمريكية للتنمية الدولية (USAID). الآراء المعبر عنها لا تعكس بالضرورة آراء الوكالة الأمريكية للتنمية الدولية أو الحكومة الأمريكية أو MEASURE Evaluation. البيانات المبلغ عنها هنا تم تزويدها من قبل نظام بيانات الكلى الأمريكي (USRDS). تفسير هذه البيانات والإبلاغ عنها هو مسؤولية المؤلفين ولا ينبغي بأي حال من الأحوال أن يُنظر إليها على أنها سياسة رسمية أو تفسير للحكومة الأمريكية. هذه المخطوطة تستند إلى بيانات تم جمعها ومشاركتها من قبل المعهد الدولي للقاحات (IVI) من دراسة أصلية أجراها. لم يتم إعداد هذه المخطوطة بالتعاون مع الباحثين في IVI ولا تعكس بالضرورة آراء أو وجهات نظر IVI.
تم توفير بيانات هذا البحث من قبل سجل السرطان في جمهورية سلوفينيا. تفسير هذه البيانات والإبلاغ عنها هو مسؤولية المؤلفين ولا ينبغي بأي حال من الأحوال أن يُنظر إليها على أنها سياسة رسمية أو تفسير للمكتب الإحصائي لجمهورية سلوفينيا. تم توفير مجموعات البيانات من قبل المركز الأوروبي للوقاية من الأمراض ومكافحتها (ECDC) استنادًا إلى البيانات المقدمة من منظمة الصحة العالمية ووزارات الصحة من الدول المتأثرة. الآراء والأفكار التي يعبر عنها المؤلفون هنا لا تعبر بالضرورة عن تلك الخاصة بـ ECDC. دقة التحليل الإحصائي للمؤلفين والنتائج التي يبلغون عنها ليست مسؤولية ECDC. ECDC ليست مسؤولة عن الاستنتاجات أو الآراء المستخلصة من البيانات المقدمة. ECDC ليست مسؤولة عن صحة البيانات وإدارة البيانات ودمج البيانات وتجميع البيانات بعد تقديم البيانات. لا يجوز تحميل ECDC المسؤولية عن الاستخدام غير الصحيح أو غير الدقيق للبيانات.
تم توفير بيانات هذا البحث من قبل سجل السرطان في جمهورية سلوفينيا. تفسير هذه البيانات والإبلاغ عنها هو مسؤولية المؤلفين ولا ينبغي بأي حال من الأحوال أن يُنظر إليها على أنها سياسة رسمية أو تفسير للمكتب الإحصائي لجمهورية سلوفينيا. تم توفير مجموعات البيانات من قبل المركز الأوروبي للوقاية من الأمراض ومكافحتها (ECDC) استنادًا إلى البيانات المقدمة من منظمة الصحة العالمية ووزارات الصحة من الدول المتأثرة. الآراء والأفكار التي يعبر عنها المؤلفون هنا لا تعبر بالضرورة عن تلك الخاصة بـ ECDC. دقة التحليل الإحصائي للمؤلفين والنتائج التي يبلغون عنها ليست مسؤولية ECDC. ECDC ليست مسؤولة عن الاستنتاجات أو الآراء المستخلصة من البيانات المقدمة. ECDC ليست مسؤولة عن صحة البيانات وإدارة البيانات ودمج البيانات وتجميع البيانات بعد تقديم البيانات. لا يجوز تحميل ECDC المسؤولية عن الاستخدام غير الصحيح أو غير الدقيق للبيانات.
ملاحظة تحريرية: تتخذ مجموعة لانسيت موقفًا محايدًا فيما يتعلق بالمطالبات الإقليمية في الخرائط المنشورة والانتماءات المؤسسية.
References
1 Murray CJL. The Global Burden of Disease Study at 30 years. Nat Med 2022; 28: 2019-26.
2 World Bank. World development report 1993: investing in health. Washington, DC: Oxford University Press, 1993.
3 Wang H, Paulson KR, Pease SA, et al. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19related mortality, 2020-21. Lancet 2022; 399: 1513-36.
4 Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1736-88.
5 Institute for Health Metrics and Evaluation. Protocol for the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD). Version 4.0. March, 2020. https://www.healthdata.org/sites/default/ files/files/Projects/GBD/March2020_GBD%20Protocol_v4.pdf (accessed March 15, 2023).
6 Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1204-22.
7 GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 385: 117-71.
8 Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388: 1459-544.
9 Naghavi M, Abajobir AA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017; 390: 1151-210.
10 Wang H, Abbas KM, Abbasifard M, et al. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1160-203.
11 Johnson SC, Cunningham M, Dippenaar IN, et al. Public health utility of cause of death data: applying empirical algorithms to improve data quality. BMC Med Inform Decis Mak 2021; 21: 175.
12 GBD 2021 Demographics Collaborators. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950-2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet 2024; published online March 11. https://doi.org/10.1016/S0140-6736(24)00476-8.
13 Doi SAR, Williams GM, eds. Methods of clinical epidemiology. Berlin, Heidelberg: Springer, 2013.
14 Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet 2016; 388: e19-23.
2 World Bank. World development report 1993: investing in health. Washington, DC: Oxford University Press, 1993.
3 Wang H, Paulson KR, Pease SA, et al. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19related mortality, 2020-21. Lancet 2022; 399: 1513-36.
4 Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1736-88.
5 Institute for Health Metrics and Evaluation. Protocol for the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD). Version 4.0. March, 2020. https://www.healthdata.org/sites/default/ files/files/Projects/GBD/March2020_GBD%20Protocol_v4.pdf (accessed March 15, 2023).
6 Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1204-22.
7 GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 385: 117-71.
8 Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388: 1459-544.
9 Naghavi M, Abajobir AA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017; 390: 1151-210.
10 Wang H, Abbas KM, Abbasifard M, et al. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1160-203.
11 Johnson SC, Cunningham M, Dippenaar IN, et al. Public health utility of cause of death data: applying empirical algorithms to improve data quality. BMC Med Inform Decis Mak 2021; 21: 175.
12 GBD 2021 Demographics Collaborators. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950-2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet 2024; published online March 11. https://doi.org/10.1016/S0140-6736(24)00476-8.
13 Doi SAR, Williams GM, eds. Methods of clinical epidemiology. Berlin, Heidelberg: Springer, 2013.
14 Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet 2016; 388: e19-23.
15 Murray CJL, Aravkin AY, Zheng P, et al. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1223-49.
16 Levin AT, Owusu-Boaitey N, Pugh S, et al. Assessing the burden of COVID-19 in developing countries: systematic review, metaanalysis and public policy implications. BMJ Glob Health 2022; 7: e008477.
17 Barber RM, Sorensen RJD, Pigott DM, et al. Estimating global, regional, and national daily and cumulative infections with SARS-CoV-2 through Nov 14, 2021: a statistical analysis. Lancet 2022; 399: 2351-80.
18 Telles CR, Roy A, Ajmal MR, et al. The impact of COVID-19 management policies tailored to airborne SARS-CoV-2 transmission: policy analysis. JMIR Public Health Surveill 2021; 7: e20699.
19 Bollyky TJ, Hulland EN, Barber RM, et al. Pandemic preparedness and COVID-19: an exploratory analysis of infection and fatality rates, and contextual factors associated with preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021. Lancet 2022; 399: 1489-512.
20 Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global challenges to public health care systems during the COVID-19 pandemic: a review of pandemic measures and problems. J Pers Med 2022; 12: 1295.
21 The Independent Panel for Pandemic Preparedness and Response. COVID-19: make it the last pandemic. May 21, 2021. https:// theindependentpanel.org/wp-content/uploads/2021/05/COVID-19-Make-it-the-Last-Pandemic_final.pdf (accessed Nov 9, 2023).
22 Lazarus JV, Romero D, Kopka CJ, et al. A multinational Delphi consensus to end the COVID-19 public health threat. Nature 2022; 611: 332-45.
23 Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1859-922.
24 Haws R, Winch PJ, Castillo J. Innovative community-based interventions to improve newborn health in Latin America and the Caribbean. Johns Hopkins University, CORE Group, 2004. https:// coregroup.org/wp-content/uploads/2020/03/LAC-Neonatalenglish_final_pdf.pdf (accessed Nov 3, 2023).
25 Whiteside A, Henry FE. The impact of HIV and AIDS research: a case study from Swaziland. Health Res Policy Syst 2011; 9 (suppl 1): S9.
26 Dwyer-Lindgren L, Cork MA, Sligar A, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature 2019; 570: 189-93.
27 Nachega JB, Kapata N, Sam-Agudu NA, et al. Minimizing the impact of the triple burden of COVID-19, tuberculosis and HIV on health services in sub-Saharan Africa. Int J Infect Dis 2021; 113 (suppl 1): S16-21.
28 Duarte R, Silva DR, Rendon A, et al. Eliminating tuberculosis in Latin America: making it the point. J Bras Pneumol 2018; 44: 73-76.
29 WHO. World health statistics 2022: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2022. https://www.who.int/data/gho/publications/ world-health-statistics (accessed Sept 16, 2022).
30 WHO. World health statistics 2023: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2023. https://www.who.int/publications-detailredirect/9789240074323 (accessed Oct 27, 2023).
31 Rosenthal PJ, John CC, Rabinovich NR. Malaria: how are we doing and how can we do better? Am J Trop Med Hyg 2019; 100: 239-41.
32 Bhatt S, Weiss DJ, Cameron E, et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015; 526: 207-11.
33 WHO. WHO recommends R21/Matrix-M vaccine for malaria prevention in updated advice on immunization. Geneva: World Health Organization, 2023. https://www.who.int/news/item/02-10-2023-who-recommends-r21-matrix-m-vaccine-for-malaria-prevention-in-updated-advice-on-immunization (accessed Oct 24, 2023).
34 Naddaf M. Second malaria vaccine to win global approval is cheaper and easier to make. Nature 2023; published online Oct 3. https:// doi.org/10.1038/d41586-023-03115-1.
16 Levin AT, Owusu-Boaitey N, Pugh S, et al. Assessing the burden of COVID-19 in developing countries: systematic review, metaanalysis and public policy implications. BMJ Glob Health 2022; 7: e008477.
17 Barber RM, Sorensen RJD, Pigott DM, et al. Estimating global, regional, and national daily and cumulative infections with SARS-CoV-2 through Nov 14, 2021: a statistical analysis. Lancet 2022; 399: 2351-80.
18 Telles CR, Roy A, Ajmal MR, et al. The impact of COVID-19 management policies tailored to airborne SARS-CoV-2 transmission: policy analysis. JMIR Public Health Surveill 2021; 7: e20699.
19 Bollyky TJ, Hulland EN, Barber RM, et al. Pandemic preparedness and COVID-19: an exploratory analysis of infection and fatality rates, and contextual factors associated with preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021. Lancet 2022; 399: 1489-512.
20 Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global challenges to public health care systems during the COVID-19 pandemic: a review of pandemic measures and problems. J Pers Med 2022; 12: 1295.
21 The Independent Panel for Pandemic Preparedness and Response. COVID-19: make it the last pandemic. May 21, 2021. https:// theindependentpanel.org/wp-content/uploads/2021/05/COVID-19-Make-it-the-Last-Pandemic_final.pdf (accessed Nov 9, 2023).
22 Lazarus JV, Romero D, Kopka CJ, et al. A multinational Delphi consensus to end the COVID-19 public health threat. Nature 2022; 611: 332-45.
23 Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1859-922.
24 Haws R, Winch PJ, Castillo J. Innovative community-based interventions to improve newborn health in Latin America and the Caribbean. Johns Hopkins University, CORE Group, 2004. https:// coregroup.org/wp-content/uploads/2020/03/LAC-Neonatalenglish_final_pdf.pdf (accessed Nov 3, 2023).
25 Whiteside A, Henry FE. The impact of HIV and AIDS research: a case study from Swaziland. Health Res Policy Syst 2011; 9 (suppl 1): S9.
26 Dwyer-Lindgren L, Cork MA, Sligar A, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature 2019; 570: 189-93.
27 Nachega JB, Kapata N, Sam-Agudu NA, et al. Minimizing the impact of the triple burden of COVID-19, tuberculosis and HIV on health services in sub-Saharan Africa. Int J Infect Dis 2021; 113 (suppl 1): S16-21.
28 Duarte R, Silva DR, Rendon A, et al. Eliminating tuberculosis in Latin America: making it the point. J Bras Pneumol 2018; 44: 73-76.
29 WHO. World health statistics 2022: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2022. https://www.who.int/data/gho/publications/ world-health-statistics (accessed Sept 16, 2022).
30 WHO. World health statistics 2023: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2023. https://www.who.int/publications-detailredirect/9789240074323 (accessed Oct 27, 2023).
31 Rosenthal PJ, John CC, Rabinovich NR. Malaria: how are we doing and how can we do better? Am J Trop Med Hyg 2019; 100: 239-41.
32 Bhatt S, Weiss DJ, Cameron E, et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015; 526: 207-11.
33 WHO. WHO recommends R21/Matrix-M vaccine for malaria prevention in updated advice on immunization. Geneva: World Health Organization, 2023. https://www.who.int/news/item/02-10-2023-who-recommends-r21-matrix-m-vaccine-for-malaria-prevention-in-updated-advice-on-immunization (accessed Oct 24, 2023).
34 Naddaf M. Second malaria vaccine to win global approval is cheaper and easier to make. Nature 2023; published online Oct 3. https:// doi.org/10.1038/d41586-023-03115-1.
35 Black R, Fontaine O, Lamberti L, et al. Drivers of the reduction in childhood diarrhea mortality 1980-2015 and interventions to eliminate preventable diarrhea deaths by 2030. J Glob Health 2019; 9: 020801.
36 Troeger CE, Khalil IA, Blacker BF, et al. Quantifying risks and interventions that have affected the burden of lower respiratory infections among children younger than 5 years: an analysis for the Global Burden of Disease Study 2017. Lancet Infect Dis 2020; 20: 60-79.
37 Das JK, Salam RA, Saeed M, Kazmi FA, Bhutta ZA. Effectiveness of interventions for managing acute malnutrition in children under five years of age in low-income and middle-income countries: a systematic review and meta-analysis. Nutrients 2020; 12: 116.
38 Mertens A, Benjamin-Chung J, Colford JM Jr, et al. Causes and consequences of child growth faltering in low-resource settings. Nature 2023; 621: 568-76.
39 Reiner RC Jr, Hay SI. The overlapping burden of the three leading causes of disability and death in sub-Saharan African children. Nat Commun 2022; 13: 7457.
40 Shah MP, Tate JE, Mwenda JM, Steele AD, Parashar UD. Estimated reductions in hospitalizations and deaths from childhood diarrhea following implementation of rotavirus vaccination in Africa. Expert Rev Vaccines 2017; 16: 987-95.
41 Reiner RC Jr, Graetz N, Casey DC, et al. Variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
42 Burstein R, Henry NJ, Collison ML, et al. Mapping 123 million neonatal, infant and child deaths between 2000 and 2017. Nature 2019; 574: 353-58.
43 Galles NC, Liu PY, Updike RL, et al. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980-2019: a systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021; 398: 503-21.
44 Deshpande A, Miller-Petrie MK, Lindstedt PA, et al. Mapping geographical inequalities in access to drinking water and sanitation facilities in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1162-85.
45 Bhattacharjee NV, Schaeffer LE, Hay SI, et al. Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000-2018. Nat Hum Behav 2021; 5: 1027-45.
46 Wiens KE, Lindstedt PA, Blacker BF, et al. Mapping geographical inequalities in oral rehydration therapy coverage in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1038-60.
47 Reiner RC Jr, Graetz N, Casey DC, et al. Local variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
48 GBD 2015 Healthcare Access and Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet 2017; 390: 231-66.
49 Bill & Melinda Gates Foundation. Enteric and diarrheal diseases. https://www.gatesfoundation.org/our-work/programs/global-health/enteric-and-diarrheal-diseases (accessed Oct 26, 2023).
50 Troeger C, Khalil IA, Rao PC, et al. Rotavirus vaccination and the global burden of rotavirus diarrhea among children younger than 5 years. JAMA Pediatr 2018; 172: 958-65.
51 Causey K, Fullman N, Sorensen RJD, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. Lancet 2021; 398: 522-34.
52 Barros LL, Barros LL, do Carmo RF, et al. Change in rotavirus vaccine coverage in Brazil from before (2015-2019) through the COVID-19 pandemic period (2020-2021). Viruses 2023; 15: 292.
53 DeSilva MB, Haapala J, Vazquez-Benitez G, et al. Association of the COVID-19 pandemic with routine childhood vaccination rates and proportion up to date with vaccinations across 8 US health systems in the Vaccine Safety Datalink. JAMA Pediatr 2022; 176: 68-77.
54 WHO. Vaccine-preventable diseases. Geneva: World Health Organization, 2023. https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases (accessed Nov 12, 2023).
55 WHO. The big catch-up: an essential immunization recovery plan for 2023 and beyond. Geneva: World Health Organization, 2023. https://www.who.int/publications-detail-redirect/9789240075511 (accessed Nov 12, 2023).
36 Troeger CE, Khalil IA, Blacker BF, et al. Quantifying risks and interventions that have affected the burden of lower respiratory infections among children younger than 5 years: an analysis for the Global Burden of Disease Study 2017. Lancet Infect Dis 2020; 20: 60-79.
37 Das JK, Salam RA, Saeed M, Kazmi FA, Bhutta ZA. Effectiveness of interventions for managing acute malnutrition in children under five years of age in low-income and middle-income countries: a systematic review and meta-analysis. Nutrients 2020; 12: 116.
38 Mertens A, Benjamin-Chung J, Colford JM Jr, et al. Causes and consequences of child growth faltering in low-resource settings. Nature 2023; 621: 568-76.
39 Reiner RC Jr, Hay SI. The overlapping burden of the three leading causes of disability and death in sub-Saharan African children. Nat Commun 2022; 13: 7457.
40 Shah MP, Tate JE, Mwenda JM, Steele AD, Parashar UD. Estimated reductions in hospitalizations and deaths from childhood diarrhea following implementation of rotavirus vaccination in Africa. Expert Rev Vaccines 2017; 16: 987-95.
41 Reiner RC Jr, Graetz N, Casey DC, et al. Variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
42 Burstein R, Henry NJ, Collison ML, et al. Mapping 123 million neonatal, infant and child deaths between 2000 and 2017. Nature 2019; 574: 353-58.
43 Galles NC, Liu PY, Updike RL, et al. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980-2019: a systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021; 398: 503-21.
44 Deshpande A, Miller-Petrie MK, Lindstedt PA, et al. Mapping geographical inequalities in access to drinking water and sanitation facilities in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1162-85.
45 Bhattacharjee NV, Schaeffer LE, Hay SI, et al. Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000-2018. Nat Hum Behav 2021; 5: 1027-45.
46 Wiens KE, Lindstedt PA, Blacker BF, et al. Mapping geographical inequalities in oral rehydration therapy coverage in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1038-60.
47 Reiner RC Jr, Graetz N, Casey DC, et al. Local variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
48 GBD 2015 Healthcare Access and Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet 2017; 390: 231-66.
49 Bill & Melinda Gates Foundation. Enteric and diarrheal diseases. https://www.gatesfoundation.org/our-work/programs/global-health/enteric-and-diarrheal-diseases (accessed Oct 26, 2023).
50 Troeger C, Khalil IA, Rao PC, et al. Rotavirus vaccination and the global burden of rotavirus diarrhea among children younger than 5 years. JAMA Pediatr 2018; 172: 958-65.
51 Causey K, Fullman N, Sorensen RJD, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. Lancet 2021; 398: 522-34.
52 Barros LL, Barros LL, do Carmo RF, et al. Change in rotavirus vaccine coverage in Brazil from before (2015-2019) through the COVID-19 pandemic period (2020-2021). Viruses 2023; 15: 292.
53 DeSilva MB, Haapala J, Vazquez-Benitez G, et al. Association of the COVID-19 pandemic with routine childhood vaccination rates and proportion up to date with vaccinations across 8 US health systems in the Vaccine Safety Datalink. JAMA Pediatr 2022; 176: 68-77.
54 WHO. Vaccine-preventable diseases. Geneva: World Health Organization, 2023. https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases (accessed Nov 12, 2023).
55 WHO. The big catch-up: an essential immunization recovery plan for 2023 and beyond. Geneva: World Health Organization, 2023. https://www.who.int/publications-detail-redirect/9789240075511 (accessed Nov 12, 2023).
56 Moss WJ, Strebel PM. Chapter 38 measles vaccines. In: Plotkin’s Vaccines, 8th edn. Philadelphia, PA: Elsevier, 2023: 629-63.
57 PAHO, WHO. Measles elimination in the Americas. Sept 27, 2016. https://www3.paho.org/hq/index.php?option=com_content&view= article&id=12526:measles-elimination-in-the-americas (accessed Nov 8, 2023).
58 Gidding HF, Martin NV, Stambos V, et al. Verification of measles elimination in Australia: application of World Health Organization regional guidelines. J Epidemiol Glob Health 2016; 6: 197-209.
59 WHO. Tenth meeting of the European Regional Verification Commission for Measles and Rubella Elimination: summary of virtual sessions held on Oct 6, 2021, Nov 2, 2021, Dec 8, 2021, and Feb 16, 2022. https://www.who.int/europe/publications/i/item/ WHO-EURO-2022-6093-45858-66035 (accessed Nov 8, 2023).
60 Sbarra AN, Rolfe S, Nguyen JQ, et al. Mapping routine measles vaccination in low- and middle-income countries. Nature 2021; 589: 415-19.
61 Minta AA, Ferrari M, Antoni S, et al. Progress toward regional measles elimination-worldwide, 2000-2021. MMWR Morb Mortal Wkly Rep 2022; 71: 1489-95.
62 Majekodunmi OB, Oladele EA, Greenwood B. Factors affecting poor measles vaccination coverage in sub-Saharan Africa with a special focus on Nigeria: a narrative review. Trans
63 National Institute of Allergy and Infectious Diseases. Condom use for preventing HIV infection. 2018. https://www.niaid.nih.gov/ diseases-conditions/condom-use (accessed Nov 6, 2023).
64 National Institute of Allergy and Infectious Diseases. HIV prevention. 2020. https://www.niaid.nih.gov/diseases-conditions/ hiv-prevention (accessed Nov 6, 2023).
65 Granich R, Gupta S, Hersh B, et al. Trends in AIDS deaths, new infections and ART coverage in the top 30 countries with the highest AIDS mortality burden; 1990-2013. PLoS One 2015; 10: e0131353.
66 National Institute of Allergy and Infectious Diseases. HIV undetectable=untransmittable (
67 Akpa OM, Adeolu-Olaiya V, Olusegun-Odebiri CA, Aganaba D. HIV/AIDS-related stigma and access to HIV treatments by people living with HIV/AIDS: a case study of selected states in north-west Nigeria. HIV AIDS Rev 2011; 10: 19-25.
68 Oturu K. Stigma in access to HIV treatment in African countries: the importance of social connections. Grounded Theory Rev 2011; 10: 63-90.
69 Rosen S, Fox MP, Gill CJ. Patient retention in antiretroviral therapy programs in sub-Saharan Africa: a systematic review. PLoS Med 2007; 4: e298.
70 Global HIV Prevention Working Group. Access to HIV prevention: closing the gap. Foreign Aff 2003; 82: 1-42.
71 Ford N, Boulle A, Egger M. Accounting for and responding to HIVassociated mortality. AIDS 2016; 30: 521-23.
72 Straetemans M, Bierrenbach AL, Nagelkerke N, Glaziou P, van der Werf MJ. The effect of tuberculosis on mortality in HIV positive people: a meta-analysis. PLoS One 2010; 5: e15241.
73 Piot P, Bartos M, Larson H, Zewdie D, Mane P. Coming to terms with complexity: a call to action for HIV prevention. Lancet 2008; 372: 845-59.
74 Gupta GR, Parkhurst JO, Ogden JA, Aggleton P, Mahal A. Structural approaches to HIV prevention. Lancet 2008; 372: 764-75.
75 Paulson KR, Kamath AM, Alam T, et al. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet 2021; 398: 870-905.
76 Saugstad OD. Reducing global neonatal mortality is possible. Neonatology 2011; 99: 250-57.
77 Tura G, Fantahun M, Worku A. The effect of health facility delivery on neonatal mortality: systematic review and meta-analysis. BMC Pregnancy Childbirth 2013; 13: 18.
78 Bill & Melinda Gates Foundation. Exemplars in global health. July 25, 2020. https://www.gatesfoundation.org/ideas/articles/ exemplars-global-health-niranjan-bose (accessed Nov 12, 2023).
57 PAHO, WHO. Measles elimination in the Americas. Sept 27, 2016. https://www3.paho.org/hq/index.php?option=com_content&view= article&id=12526:measles-elimination-in-the-americas (accessed Nov 8, 2023).
58 Gidding HF, Martin NV, Stambos V, et al. Verification of measles elimination in Australia: application of World Health Organization regional guidelines. J Epidemiol Glob Health 2016; 6: 197-209.
59 WHO. Tenth meeting of the European Regional Verification Commission for Measles and Rubella Elimination: summary of virtual sessions held on Oct 6, 2021, Nov 2, 2021, Dec 8, 2021, and Feb 16, 2022. https://www.who.int/europe/publications/i/item/ WHO-EURO-2022-6093-45858-66035 (accessed Nov 8, 2023).
60 Sbarra AN, Rolfe S, Nguyen JQ, et al. Mapping routine measles vaccination in low- and middle-income countries. Nature 2021; 589: 415-19.
61 Minta AA, Ferrari M, Antoni S, et al. Progress toward regional measles elimination-worldwide, 2000-2021. MMWR Morb Mortal Wkly Rep 2022; 71: 1489-95.
62 Majekodunmi OB, Oladele EA, Greenwood B. Factors affecting poor measles vaccination coverage in sub-Saharan Africa with a special focus on Nigeria: a narrative review. Trans
63 National Institute of Allergy and Infectious Diseases. Condom use for preventing HIV infection. 2018. https://www.niaid.nih.gov/ diseases-conditions/condom-use (accessed Nov 6, 2023).
64 National Institute of Allergy and Infectious Diseases. HIV prevention. 2020. https://www.niaid.nih.gov/diseases-conditions/ hiv-prevention (accessed Nov 6, 2023).
65 Granich R, Gupta S, Hersh B, et al. Trends in AIDS deaths, new infections and ART coverage in the top 30 countries with the highest AIDS mortality burden; 1990-2013. PLoS One 2015; 10: e0131353.
66 National Institute of Allergy and Infectious Diseases. HIV undetectable=untransmittable (
67 Akpa OM, Adeolu-Olaiya V, Olusegun-Odebiri CA, Aganaba D. HIV/AIDS-related stigma and access to HIV treatments by people living with HIV/AIDS: a case study of selected states in north-west Nigeria. HIV AIDS Rev 2011; 10: 19-25.
68 Oturu K. Stigma in access to HIV treatment in African countries: the importance of social connections. Grounded Theory Rev 2011; 10: 63-90.
69 Rosen S, Fox MP, Gill CJ. Patient retention in antiretroviral therapy programs in sub-Saharan Africa: a systematic review. PLoS Med 2007; 4: e298.
70 Global HIV Prevention Working Group. Access to HIV prevention: closing the gap. Foreign Aff 2003; 82: 1-42.
71 Ford N, Boulle A, Egger M. Accounting for and responding to HIVassociated mortality. AIDS 2016; 30: 521-23.
72 Straetemans M, Bierrenbach AL, Nagelkerke N, Glaziou P, van der Werf MJ. The effect of tuberculosis on mortality in HIV positive people: a meta-analysis. PLoS One 2010; 5: e15241.
73 Piot P, Bartos M, Larson H, Zewdie D, Mane P. Coming to terms with complexity: a call to action for HIV prevention. Lancet 2008; 372: 845-59.
74 Gupta GR, Parkhurst JO, Ogden JA, Aggleton P, Mahal A. Structural approaches to HIV prevention. Lancet 2008; 372: 764-75.
75 Paulson KR, Kamath AM, Alam T, et al. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet 2021; 398: 870-905.
76 Saugstad OD. Reducing global neonatal mortality is possible. Neonatology 2011; 99: 250-57.
77 Tura G, Fantahun M, Worku A. The effect of health facility delivery on neonatal mortality: systematic review and meta-analysis. BMC Pregnancy Childbirth 2013; 13: 18.
78 Bill & Melinda Gates Foundation. Exemplars in global health. July 25, 2020. https://www.gatesfoundation.org/ideas/articles/ exemplars-global-health-niranjan-bose (accessed Nov 12, 2023).
Journal: The Lancet, Volume: 403, Issue: 10440
DOI: https://doi.org/10.1016/s0140-6736(24)00367-2
PMID: https://pubmed.ncbi.nlm.nih.gov/38582094
Publication Date: 2024-04-03
DOI: https://doi.org/10.1016/s0140-6736(24)00367-2
PMID: https://pubmed.ncbi.nlm.nih.gov/38582094
Publication Date: 2024-04-03
Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and
811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021
GBD 2021 Causes of Death Collaborators*
Lancet 2024; 403: 2100-32
Published Online
April 3, 2024
https://doi.org/10.1016/
S0140-6736(24)00367-2
This online publication has been corrected. The corrected version first appeared at thelancet.com on April 19, 2024
See Comment page 1956
*Collaborators are listed at the end of the Article
Published Online
April 3, 2024
https://doi.org/10.1016/
S0140-6736(24)00367-2
This online publication has been corrected. The corrected version first appeared at thelancet.com on April 19, 2024
See Comment page 1956
*Collaborators are listed at the end of the Article
Correspondence to:
Prof Simon I Hay, Institute for Health Metrics and Evaluation,
Prof Simon I Hay, Institute for Health Metrics and Evaluation,
Summary
Background Regular, detailed reporting on population health by underlying cause of death is fundamental for public health decision making. Cause-specific estimates of mortality and the subsequent effects on life expectancy worldwide are valuable metrics to gauge progress in reducing mortality rates. These estimates are particularly important following large-scale mortality spikes, such as the COVID-19 pandemic. When systematically analysed, mortality rates and life expectancy allow comparisons of the consequences of causes of death globally and over time, providing a nuanced understanding of the effect of these causes on global populations.
Methods The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021 cause-of-death analysis estimated mortality and years of life lost (YLLs) from 288 causes of death by age-sex-location-year in 204 countries and territories and 811 subnational locations for each year from 1990 until 2021. The analysis used 56604 data sources, including data from vital registration and verbal autopsy as well as surveys, censuses, surveillance systems, and cancer registries, among others. As with previous GBD rounds, cause-specific death rates for most causes were estimated using the Cause of Death Ensemble model-a modelling tool developed for GBD to assess the out-of-sample predictive validity of different statistical models and covariate permutations and combine those results to produce cause-specific mortality estimateswith alternative strategies adapted to model causes with insufficient data, substantial changes in reporting over the study period, or unusual epidemiology. YLLs were computed as the product of the number of deaths for each cause-age-sex-location-year and the standard life expectancy at each age. As part of the modelling process, uncertainty intervals (UIs) were generated using the
Findings The leading causes of age-standardised deaths globally were the same in 2019 as they were in 1990; in descending order, these were, ischaemic heart disease, stroke, chronic obstructive pulmonary disease, and lower respiratory infections. In 2021, however, COVID-19 replaced stroke as the second-leading age-standardised cause of death, with
and these causes of death became progressively more concentrated since 1990, when only 44 causes showed this pattern. The concentration phenomenon is discussed heuristically with respect to enteric and lower respiratory infections, malaria, HIV/AIDS, neonatal disorders, tuberculosis, and measles.
and these causes of death became progressively more concentrated since 1990, when only 44 causes showed this pattern. The concentration phenomenon is discussed heuristically with respect to enteric and lower respiratory infections, malaria, HIV/AIDS, neonatal disorders, tuberculosis, and measles.
Interpretation Long-standing gains in life expectancy and reductions in many of the leading causes of death have been disrupted by the COVID-19 pandemic, the adverse effects of which were spread unevenly among populations. Despite the pandemic, there has been continued progress in combatting several notable causes of death, leading to improved global life expectancy over the study period. Each of the seven GBD super-regions showed an overall improvement from 1990 and 2021, obscuring the negative effect in the years of the pandemic. Additionally, our findings regarding regional variation in causes of death driving increases in life expectancy hold clear policy utility. Analyses of shifting mortality trends reveal that several causes, once widespread globally, are now increasingly concentrated geographically. These changes in mortality concentration, alongside further investigation of changing risks, interventions, and relevant policy, present an important opportunity to deepen our understanding of mortality-reduction strategies. Examining patterns in mortality concentration might reveal areas where successful public health interventions have been implemented. Translating these successes to locations where certain causes of death remain entrenched can inform policies that work to improve life expectancy for people everywhere.
Funding Bill & Melinda Gates Foundation.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
Introduction
For more than three decades, the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) has been systematically and comprehensively recording and analysing causes of human death stratified by age, sex, and time across the world.
Causes of death are not uniformly distributed between populations; rather, large variability in the leading causes often reflects important social and geographical differences.
a limited subset of the global population. Our analysis provides an opportunity to answer important epidemiological questions that have been at the forefront of global and public health discourse-eg, which causes have contributed to the largest increase or decrease in life expectancy, which locations are experiencing greater concentrations of preventable causes of death, and how has COVID-19 and other pandemic-related mortality (OPRM) affected life expectancy and the overall fatal burden of diseases? Regional variation in many of the leading causes of death remains evident in these most recent estimates, representing important opportunities for creating tailored health policy to improve disparities and alleviate concentrations of mortality.
GBD 2021 provides an updated, comprehensive set of the fatal burden of disease summarised with causespecific mortality metrics and years-of-life-lost (YLLs) metrics for 288 causes by age and sex across 204 countries and territories from 1990 to 2021, an update from the previously published estimates covering 1990-2019. In this study, we present mortality concentrations and a decomposition analysis of life expectancy due to different causes of death and illustrate the impact of causes of death on global, regional, and country-specific life expectancy, as well as highlighting locations that are most affected by concentrated geographical mortality burden. As with previous iterations of GBD, this cycle incorporates newly available data sources and improved methodological approaches to re-estimate the entire time series, providing updated estimates that supersede all previous GBD cause-of-death publications. GBD 2021 includes an estimation of several different models for disease and injury outcomes. This manuscript was produced as part of the GBD Collaborator Network and in accordance with the GBD Protocol.
Causes of death are not uniformly distributed between populations; rather, large variability in the leading causes often reflects important social and geographical differences.
a limited subset of the global population. Our analysis provides an opportunity to answer important epidemiological questions that have been at the forefront of global and public health discourse-eg, which causes have contributed to the largest increase or decrease in life expectancy, which locations are experiencing greater concentrations of preventable causes of death, and how has COVID-19 and other pandemic-related mortality (OPRM) affected life expectancy and the overall fatal burden of diseases? Regional variation in many of the leading causes of death remains evident in these most recent estimates, representing important opportunities for creating tailored health policy to improve disparities and alleviate concentrations of mortality.
GBD 2021 provides an updated, comprehensive set of the fatal burden of disease summarised with causespecific mortality metrics and years-of-life-lost (YLLs) metrics for 288 causes by age and sex across 204 countries and territories from 1990 to 2021, an update from the previously published estimates covering 1990-2019. In this study, we present mortality concentrations and a decomposition analysis of life expectancy due to different causes of death and illustrate the impact of causes of death on global, regional, and country-specific life expectancy, as well as highlighting locations that are most affected by concentrated geographical mortality burden. As with previous iterations of GBD, this cycle incorporates newly available data sources and improved methodological approaches to re-estimate the entire time series, providing updated estimates that supersede all previous GBD cause-of-death publications. GBD 2021 includes an estimation of several different models for disease and injury outcomes. This manuscript was produced as part of the GBD Collaborator Network and in accordance with the GBD Protocol.
Research in context
Evidence before this study
The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) has provided regular updates on the complex patterns and trends in population health around the world since the first GBD publication in 1993. With each subsequent iteration, there have been important methodological updates, new datasets included, and an expanded list of causes, risk factors, and locations for which estimates of the burden of disease are produced. In 1993, mortality and years of life lost (YLLs) were reported for 107 categories of diseases that covered all possible causes of death, for eight regions. In the last GBD cycle-GBD 2019—estimates of mortality and YLLs were produced for 286 causes of death in 204 countries and territories, including all WHO member states, and for subnational locations in 21 countries and territories, for every year from 1990 to 2019. Although many groups have reported on national-level, causespecific mortality and other population-health metrics, including the WHO World Health Statistics reports, GBD is the most detailed and transparent research effort to date. Further, estimates of COVID-19-related deaths in 2020 and 2021 have been reported by several sources, including GBD studies that have quantified excess mortality due to the pandemic within a subset of GBD locations. However, no previous publications have quantified the effect of COVID-19 on life expectancy, while considering the full spectrum of disease mortality over the past three decades, across all countries and territories. This study presents, for the first time, 288 causes of death from 1990 to 2021, complementary to the all-cause mortality findings presented in the GBD 2021 Demographics analysis. Combined, these studies provide a comprehensive view of all-cause and cause-specific mortality from 1990 to 2021.
Added value of this study
Alongside the all-cause mortality and life-expectancy assessments in companion publications for GBD 2021, this analysis delineates cause-specific mortality and its effect on life expectancy. This study includes a comprehensive decomposition analysis elucidating the primary cause of death influencing life expectancy on a global, regional, and national level. Additionally, we present causes of death and YLLs for all countries and territories, providing policy makers with valuable insights into variations in cause-specific mortality. This study is also the first of its kind to publish 2021 estimates of COVID-19related deaths and YLLs for 204 countries and territories in the context of the global burden of disease. Although other publications have estimated deaths due to COVID-19, those deaths have not previously been compared with deaths from other causes. By modelling COVID-19 deaths within a hierarchy
of mutually exclusive and collectively exhaustive causes of death, this study provides policy makers with information that is essential for setting health priorities around the world. To obtain more comprehensive insights from life expectancy, it is necessary to break it down into age-specific mortality, which is influenced by cause-specific mortality rates. We examined the effect of COVID-19 and other causes of death on life expectancy by decomposing death counts into different cause-specific mortality rates across various dimensions, including country or territory, region, super-region, and five distinct time periods: 1990-2000, 2000-2010, 2010-2019, 2019-2021, and 1990-2021. We could therefore systematically calibrate the COVID-19 pandemic against other causes of mortality over the period 1990-2021. Finally, our study identified several causes of death that exhibited increased geographical concentration over time-ie, causes with a disproportionate impact within a specific geographical area compared with the rest of the global observations. This analysis provides policy makers important information on regional variation and inequalities in causespecific mortality. Also new to GBD 2021, we report on 12 additional causes of death: COVID-19 and other pandemicrelated mortality, pulmonary arterial hypertension, and nine cancer types-hepatoblastoma, Burkitt lymphoma, other non-Hodgkin lymphoma, eye cancer, retinoblastoma, other eye cancers, soft tissue and other extraosseous sarcomas, malignant neoplasm of bone and articular cartilage, and neuroblastoma and other peripheral nervous-cell tumours. Granularity of the estimation of deaths in children younger than 5 years was enhanced by the addition of four new age groups: 1-5 months, 6-11 months, 12-23 months, and 2-4 years.
of mutually exclusive and collectively exhaustive causes of death, this study provides policy makers with information that is essential for setting health priorities around the world. To obtain more comprehensive insights from life expectancy, it is necessary to break it down into age-specific mortality, which is influenced by cause-specific mortality rates. We examined the effect of COVID-19 and other causes of death on life expectancy by decomposing death counts into different cause-specific mortality rates across various dimensions, including country or territory, region, super-region, and five distinct time periods: 1990-2000, 2000-2010, 2010-2019, 2019-2021, and 1990-2021. We could therefore systematically calibrate the COVID-19 pandemic against other causes of mortality over the period 1990-2021. Finally, our study identified several causes of death that exhibited increased geographical concentration over time-ie, causes with a disproportionate impact within a specific geographical area compared with the rest of the global observations. This analysis provides policy makers important information on regional variation and inequalities in causespecific mortality. Also new to GBD 2021, we report on 12 additional causes of death: COVID-19 and other pandemicrelated mortality, pulmonary arterial hypertension, and nine cancer types-hepatoblastoma, Burkitt lymphoma, other non-Hodgkin lymphoma, eye cancer, retinoblastoma, other eye cancers, soft tissue and other extraosseous sarcomas, malignant neoplasm of bone and articular cartilage, and neuroblastoma and other peripheral nervous-cell tumours. Granularity of the estimation of deaths in children younger than 5 years was enhanced by the addition of four new age groups: 1-5 months, 6-11 months, 12-23 months, and 2-4 years.
Implications of all the available evidence
Our study provides a full analysis of causes of death worldwide and across time, alongside the changing patterns in life expectancy precipitated by those causes. Increasing geographical concentration of mortality was observed for many causes of death, highlighting disparities between regions and substantial differences in cause-specific contributions to life expectancy. On a global scale, this information provides an opportunity to examine whether reductions in mortality were resilient to the onset of a novel pandemic. On a regional level, the estimates generated by our study provide important detail on the evolving impact of causes of death among countries, allowing crucial insight into differential success by geography, time, and cause. The comprehensive nature of GBD 2021 cause-of-death estimation provides valuable opportunities to learn from mortality gains and losses, helping to accelerate progress in reducing mortality.
Methods
Overview
In GBD 2021, we produced estimates for each epidemiological quantity of interest for 288 causes of death by age-sex-location-year for 25 age groups from
birth to 95 years and older; for males, females, and both sexes combined; in 204 countries and territories grouped into 21 regions and seven super-regions; and for every year from 1990 to 2021. GBD 2021 also includes subnational analyses for 21 countries and territories
(appendix 1 section 2.1). An international network of collaborators provides, reviews, and analyses the available data to generate these metrics; GBD 2021 drew on the expertise of more than 11000 collaborators from more than 160 countries and territories.
birth to 95 years and older; for males, females, and both sexes combined; in 204 countries and territories grouped into 21 regions and seven super-regions; and for every year from 1990 to 2021. GBD 2021 also includes subnational analyses for 21 countries and territories
(appendix 1 section 2.1). An international network of collaborators provides, reviews, and analyses the available data to generate these metrics; GBD 2021 drew on the expertise of more than 11000 collaborators from more than 160 countries and territories.
The methods used to generate these estimates closely followed those for GBD 2019.
The GBD 2021 cause-of-death estimates described here include cause-specific mortality and the premature death metric (YLLs). We calculated YLLs as the number of deaths for each cause-age-sex-location-year multiplied by the standard life expectancy at each age (appendix 1 section 6.3). Standard life expectancy is calculated from the lowest age-specific mortality rate between countries.
The GBD disease and injury hierarchy
GBD classifies diseases and injuries into a hierarchy with four levels that include both fatal and non-fatal causes. Level 1 causes include three broad aggregate categories
(communicable, maternal, neonatal, and nutritional [CMNN] diseases; non-communicable diseases [NCDs]; and injuries) and Level 2 disaggregates those categories into 22 clusters of causes, which are further disaggregated into Level 3 and Level 4 causes. At the most detailed level, 288 fatal causes are estimated. For a full list of causes of death by level, see appendix 1 (table S2). For GBD 2021, we separately report on 12 causes of death for the first time: COVID-19, OPRM, pulmonary arterial hypertension, and nine cancer types: hepatoblastoma, Burkitt lymphoma, other non-Hodgkin lymphoma, eye cancer, retinoblastoma, other eye cancers, soft tissue and other extraosseous sarcomas, malignant neoplasm of bone and articular cartilage, and neuroblastoma and other peripheral nervous cell tumours.
(communicable, maternal, neonatal, and nutritional [CMNN] diseases; non-communicable diseases [NCDs]; and injuries) and Level 2 disaggregates those categories into 22 clusters of causes, which are further disaggregated into Level 3 and Level 4 causes. At the most detailed level, 288 fatal causes are estimated. For a full list of causes of death by level, see appendix 1 (table S2). For GBD 2021, we separately report on 12 causes of death for the first time: COVID-19, OPRM, pulmonary arterial hypertension, and nine cancer types: hepatoblastoma, Burkitt lymphoma, other non-Hodgkin lymphoma, eye cancer, retinoblastoma, other eye cancers, soft tissue and other extraosseous sarcomas, malignant neoplasm of bone and articular cartilage, and neuroblastoma and other peripheral nervous cell tumours.
Data sources, processing, and assessing for completeness
The GBD 2021 cause-of-death database included data sources identified in previous rounds of estimation in addition to 9248 new sources (appendix 1 table S5). We included multiple data types to capture the widest array of information, including vital registration and verbal autopsy for all 288 causes as well as survey, census, surveillance, cancer registry, police records, open-source databases, and minimally invasive tissue sampling. To standardise these data so that they can be compared by cause, age, sex, location, and time, we applied a set of data processing corrections. First, deaths with insufficient age data to estimate the GBD age groups or missing age and sex data underwent age and sex splitting to assign GBD age groups as well as sex (appendix 1 section 3.5). Additionally, garbage codes, which are non-specific, implausible, or intermediate, rather than underlying cause of death codes from the International Classification of Diseases, were redistributed to appropriate targets to assign the underlying cause of death.
Assessing data completeness illustrates the coverage from a data source on overall mortality for the country. Vital registration and verbal autopsy data completeness-a source-specific estimate of the percentage of total cause-specific deaths that are reported in a given location and year-was assessed by locationyear, and sources with less than
See Online for appendix 1
For a searchable repository of cause-specific model details see https://www.healthdata.org/ gbd/methods-appendices-2021
For a searchable repository of cause-specific model details see https://www.healthdata.org/ gbd/methods-appendices-2021
For the GBD data sources see https://ghdx.healthdata.org/ gbd-2021/sources
Improvements in GBD 2021 to cause of death data processing and estimation
Adjustments for stochastic variation
In GBD 2021, we made two primary improvements to the methods used to reduce stochastic variation, most affecting causes of death with small sample sizes. First, we updated the Bayesian algorithm used in the noise reduction of these data to improve the preservation of real trends in data with large sample sizes, and imparted additional information from regional trends for data with small sample sizes. Second, the non-zero floor, a method that addresses distorted data shapes and nonsensical trends caused by small numbers when transformed to log space, was updated to be time-invariant and independent of demographic inputs. The full details of these two key improvements, as well as other improvements that address stochastic variation, can be found in appendix 1 (section 3.14).
COVID-19 and OPRM estimation
We derived COVID-19 and OPRM estimates from an analysis of the overall excess mortality due to the COVID-19 pandemic from January 1, 2020, to December 31, 2021. Full details of the estimation of excess mortality, COVID-19 deaths, and OPRM are provided in appendix 1 (section 5). To estimate excess mortality, we first developed a database of all-cause mortality by week and month after accounting for reporting lags, anomalies such as heat waves, and underregistration of deaths. Next, we developed an ensemble model to predict expected deaths in the absence of the COVID-19 pandemic for the years 2020 and 2021. In location and time combinations with data used for these models, we estimated excess mortality as observed mortality minus expected mortality. To estimate excess mortality for location-years without data, we developed a statistical model to directly predict the excess mortality due to COVID-19, using covariates that pertained to both the COVID-19 pandemic and background population-health-related metrics at the population level before SARS-CoV-2 emerged. Uncertainty was propagated through each step of this estimation procedure.
To produce the final estimates of COVID-19 deaths used in GBD 2021, we used a counterfactual approach.
To produce the final estimates of COVID-19 deaths used in GBD 2021, we used a counterfactual approach.
The counterfactual estimates the number of deaths if infection detection rates were at the highest observed value for each location-year. Using the ratio of counterfactual over estimated excess deaths and the ratio of reported COVID-19 deaths over excess deaths, we calculated the ratio of total COVID-19 deaths over reported COVID-19 deaths and multiplied this figure by the number of reported COVID-19 deaths for our final estimates of COVID-19 deaths.
To account for increases in excess mortality in 2020 and 2021 that could not be attributed to particular causes, we introduced a residual cause, OPRM. We identified four causes of death-lower respiratory infections, measles, malaria, and pertussis-as related to the COVID-19 pandemic and having reliable enough estimates to not contribute to OPRM. Thus, we calculated OPRM as the difference between excess mortality and the sum of deaths due to COVID-19 and these four causes.
Presentation of cause-specific mortality estimates
Cause-specific mortality estimates for 2021 are given in death counts and age-standardised rates per 100000 population, calculated using the GBD standardpopulation structure.
Life-expectancy decomposition
The objective of life-expectancy decomposition is to analyse the difference in life expectancy by age and location, quantifying contributions from specific causes (appendix 1 section 7). We examined temporal trends in causes over continuous time periods across different locations. We aimed to identify the effect of causes of death on life expectancy by using three main decomposition steps. For this study, we investigated the top-20 Level 2 and Level 3 GBD causes contributing to change in life expectancy. The remaining causes were then combined as “other communicable and maternal disorders” or “other NCDs”. The first step involved decomposing the difference in life expectancy by age. We calculated age-specific contributions to understand the variation in life expectancy across different age groups. In the second step, each age-specific contribution was further decomposed into cause-agespecific contributions. This analysis allowed for the identification of the specific causes of death that contributed to the differences in life expectancy within each age group. Finally, we aggregated the cause-agespecific contributions across age groups to produce cause-specific contributions to the overall difference
in life expectancy. This aggregation provided a comprehensive understanding of how different causes of death contributed to the observed variations in life expectancy. By applying this decomposition approach, we gain insights into the relative effect of different causes of death on changes in life expectancy by age and location.
in life expectancy. This aggregation provided a comprehensive understanding of how different causes of death contributed to the observed variations in life expectancy. By applying this decomposition approach, we gain insights into the relative effect of different causes of death on changes in life expectancy by age and location.
Calculation of mortality concentration
Concentrated causes in GBD refer to causes that exhibit a disproportionate impact in a specific geographical subset of the data compared with the rest of the global observations. In GBD 2021, we used two different methods to identify these concentrated causes: coefficient of variation and mortality concentration.
Coefficient of variation
For each GBD cause, we calculated a coefficient of variation using standard statistical methods. This measure assesses the variability of a population relative to its mean.
variation have data that are less centred around the mean and indicate a greater likelihood of a concentrated cause.
variation have data that are less centred around the mean and indicate a greater likelihood of a concentrated cause.
Mortality concentration
To identify concentrations of mortality-geographical locations or groups of locations with populations that are disproportionately affected by a particular causewe first calculated the total number of all-age, both-sex deaths in 2021 by cause in each of the 811 subnational locations and sorted these locations by number of deaths in descending order. We then calculated the cumulative percentage of deaths by dividing locationspecific cumulative deaths by the number of global deaths for each cause. When the cumulative percentage reached or exceeded
| Leading causes 1990 | Age-standardised rate of deaths per 100000, 1990 | Leading causes 2019 | Age-standardised rate of deaths per 100000, 2019 | Leading causes 2021 | Age-standardised rate of deaths per 100000, 2021 |
| 1 Ischaemic heart disease | 158.9 (147.4 to 165.4) | 1 Ischaemic heart disease | 110.9 (102.5 to 116.9) | 1 Ischaemic heart disease | 108.7 (99.8 to 115.6) |
| 2 Stroke |
|
2 Stroke | 89.3 (81.6 to 95.6) | 2 COVID-19 | 94.0 (89.2 to 100.0) |
| 3 COPD | 71.9 (64.6 to 77.5) | 3 COPD |
|
3 Stroke | 87.4 (79.5 to 94.4) |
| 4 Lower respiratory infections | 61.8 (57.0 to 66.8) | 4 Lower respiratory infections |
|
4 COPD | 45.2 (40.7 to 49.8) |
| 5 Diarrhoeal diseases | 60.6 (46.7 to 79.6) | 5 Neonatal disorders | 30.7 (26.8 to 35.3) | 5 Other pandemic-related death | 32.3 (24.8 to 43.3) |
| 6 Neonatal disorders | 46.0 (43.5 to 48.9) | 6 Alzheimer’s and other dementias | 25.0 (6.2 to 65.0) | 6 Neonatal disorders | 29.6 (25.3 to 34.4) |
| 7 Tuberculosis | 40.0 (34.1 to 44.6) | 7 Lung cancer | 23.7 (21.8 to 25.8) | 7 Lower respiratory infections | 28.7 (26.0 to 31.1) |
| 8 Lung cancer | 27.6 (26.1 to 29.0) | 8 Diabetes | 19.8 (18.5 to 20.8) | 8 Alzheimer’s and other dementias | 25.2 (6.4 to 65.6) |
| 9 Alzheimer’s and other dementias | 25.1 (6.0 to 66.1) | 9 Chronic kidney disease | 18.6 (16.9 to 19.8) | 9 Lung cancer |
|
| 10 Cirrhosis | 24.4 (22.3 to 27.5) | 10 Diarrhoeal diseases | 17.1 (12.4 to 23.2) | 10 Diabetes | 19.6 (18.2 to 20.8) |
| 11 Stomach cancer |
|
11 Cirrhosis | 17.1 (15.9 to 18.5) | 11 Chronic kidney disease | 18.5 (16.7 to 19.9) |
| 12 Road injuries | 21.8 (20.9 to 22.8) | 12 Hypertensive heart disease | 16.9 (14.1 to 18.6) | 12 Cirrhosis liver | 16.6 (15.2 to 18.2) |
| 13 Hypertensive heart disease | 20.9 (17.1 to 23.3) | 13 Road injuries |
|
13 Hypertensive heart disease | 16.3 (13.7 to 18.1) |
| 14 Diabetes | 18.2 (17.0 to 19.1) | 14 Tuberculosis | 14.9 (13.7 to 16.4) | 14 Diarrheal diseases | 15.4 (10.9 to 20.9) |
| 15 Colorectal cancer | 15.6 (14.5 to 16.3) | 15 Colorectal cancer | 12.6 (11.6 to 13.4) | 15 Road injuries | 14.6 (13.6 to 15.6) |
| 16 Congenital defects | 15.2 (9.6 to 19.7) | 16 Stomach cancer | 11.5 (9.9 to 12.9) | 16 Tuberculosis | 14.0 (12.6 to 15.8) |
| 17 Self-harm | 14.9 (12.8 to 15.8) | 17 Falls | 10.3 (8.8 to 11.2) | 17 Colorectal cancer |
|
| 18 Chronic kidney disease | 14.9 (13.7 to 16.4) | 18 HIV/AIDS | 9.8 (9.0 to 11.0) | 18 Stomach cancer | 11.2 (9.6 to 12.6) |
| 19 Malaria |
|
19 Malaria | 9.3 (3.7 to 18.3) | 19 Malaria | 10.5 (3.9 to 21.4) |
| 20 Measles | 11.0 (3.9 to 22.6) | 20 Self-harm | 9.2 (8.6 to 9.7) | 20 Falls | 9.9 (8.5 to 10.8) |
| 21 Falls | 10.9 (9.8 to 11.8) | 21 Congenital defects | 8.9 (7.7 to 10.9) | 21 Self-harm | 9.0 (8.3 to 9.6) |
| 34 HIV/AIDS | 5.9 (4.5 to 7.8) | 67 Measles | 1.4 (0.5 to 3.0) | 22 HIV/AIDS | 8.7 (8.1 to 9.6) |
|
|
|
Figure 1: Leading Level 3 causes of global deaths and age-standardised death rate per 100000 population for males and females combined, 1990, 2019, and 2021
Figure shows the 20 leading causes of death in descending order. Causes are connected by lines between time periods; solid lines represent an increase or lateral shift in ranking and dashed lines are decreases in rank. COPD=chronic obstructive pulmonary disease. Lung cancer=tracheal, bronchus, and lung cancer.
Figure shows the 20 leading causes of death in descending order. Causes are connected by lines between time periods; solid lines represent an increase or lateral shift in ranking and dashed lines are decreases in rank. COPD=chronic obstructive pulmonary disease. Lung cancer=tracheal, bronchus, and lung cancer.
See Online for appendix 2
To view and download estimates from the GBD Results tool see https://www.vizhub. healthdata.org/gbd-results
To view and download estimates from the GBD Results tool see https://www.vizhub. healthdata.org/gbd-results
To explore estimates of health burden using GBD Compare see https://www.vizhub.healthdata. org/gbd-compare
For summaries of results for each cause of death see https:// www.healthdata.org/research-analysis/diseases-injuries-risks/ factsheets
For the statistical code see http://ghdx.healthdata.org/gbd2021/code
incidence of mortality between locations and populations. In addition to identifying these concentrations of mortality in 2021, we repeated this same analysis for 1990. By comparing the respective proportions of affected global population in these two years, we were able to differentiate causes that showed increased, decreased, or unchanged concentrations of mortality. The causes highlighted in this study were those characterised by an age-standardised mortality rate greater than 0.5 per 100000 population. The purpose of presenting mortality concentrations is to illustrate causes that are disproportionately affecting specific populations, when previously that cause affected large swaths of the population. Thus, we did not calculate the mortality concentration for causes that are endemic to certain regions, as the mortality rate is already known to be concentrated among specific parts of the global population. We excluded two endemic causes, Ebola virus disease and Chagas disease, from this calculation.
incidence of mortality between locations and populations. In addition to identifying these concentrations of mortality in 2021, we repeated this same analysis for 1990. By comparing the respective proportions of affected global population in these two years, we were able to differentiate causes that showed increased, decreased, or unchanged concentrations of mortality. The causes highlighted in this study were those characterised by an age-standardised mortality rate greater than 0.5 per 100000 population. The purpose of presenting mortality concentrations is to illustrate causes that are disproportionately affecting specific populations, when previously that cause affected large swaths of the population. Thus, we did not calculate the mortality concentration for causes that are endemic to certain regions, as the mortality rate is already known to be concentrated among specific parts of the global population. We excluded two endemic causes, Ebola virus disease and Chagas disease, from this calculation.
GBD research and reporting practices
This research is compliant with the Guidelines for Accurate and Transparent Health Estimates Reporting recommendations (GATHER; appendix 1 table S4).
Figure 2: Age-standardised mortality rate per 100000 population for the ten leading Level 3 causes of death globally, 2019-21
Whisker plot in which the
COPD=chronic obstructive pulmonary disease. OPRM=other pandemic-related mortality.
Whisker plot in which the
COPD=chronic obstructive pulmonary disease. OPRM=other pandemic-related mortality.
Role of the funding source
The funder of this study had no role in study design, data collection, data analysis, data interpretation, or the writing of the report.
Results
Estimates described in the Article are viewable in appendix 2. Detailed results for each cause of death in the analysis are available in downloadable form through the GBD Results tool and via visual exploration through the online tool GBD Compare. Summaries of results for each cause of death included in the analysis are available online.
Global causes of death
From 1990 to 2019, the annual rate of change in global deaths from all causes ranged from
| Global | Central Europe, eastern Europe, and central Asia | High income | Latin America and Caribbean | North Africa and Middle East | South Asia | Southeast Asia, east Asia, and Oceania | Sub-Saharan Africa | |
| 2020 | ||||||||
| 1 | ||||||||
| Cause | Ischaemic heart disease | Ischaemic heart disease | Ischaemic heart disease | COVID-19 | Ischaemic heart disease | Ischaemic heart disease | Stroke | COVID-19 |
| Age-standardised rate (per 100000 population) | 109.4 (100.7-116.1) |
|
51.4 (45•1-54•6) | 133.7 (
|
205.2 (182•7-225•6) |
|
|
158.9 (
|
| Number | 8840000 (81800009360000 ) | 1410000 (13100001480000) | 1290000 (11100001390000 ) | 799000 (725 000869000) | 760000 (681000838000 | 1960000 (18200002110000) | 3460000 (3030 0003880000 ) | 659000 (615000706000) |
| 2 | Stroke | Stroke | COVID-19 | Ischaemic heart disease | COVID-19 | Chronic obstructive pulmonary disease | Ischaemic heart disease | Stroke |
| Age-standardised rate (per 100000 population) | 88.3 (80.2-95.0) |
|
41.8 (40•8-42•8) | 84.3 (77.2-89.4) |
|
104.1 (92•3-117.0) | 110.8 (97.3-124.6) | 126.2 (113•4-140•4) |
| Number | 7140000 (6500 0007680000) | 726000 (675 000758000) | 930000 (908000952000 ) | 496000 (454000525000) | 483000 (415000537000) | 1230000 (1090 0001370000) | 2570000 (22600002880000 ) | 481000 (432000
|
| 3 | ||||||||
| Cause | COVID-19 | COVID-19 | Stroke | Stroke | Stroke | COVID-19 | Chronic obstructive pulmonary disease | Ischaemic heart disease |
| Age-standardised rate (per 100000 population) | 58.7 (55.8-62.4) | 72.9 (64.1-81.7) | 29.0 (24.7-31.2) | 47.5 (
|
103.8 (92•0-115•6) |
|
66.9 (57.4-77.0) | 92.9 (83.1-103.0) |
| Number | 4800000 (45600005110000) | 467000 (411000523000) | 764000 (636000830000) | 278000 (255000296000) | 370000 (329 000414000) | 1320000 (1230 000
|
1500000 (12900001730000) | 346000 (309 000388000 ) |
| 4 | ||||||||
| Cause | Chronic obstructive pulmonary disease | Other COVID-19 pandemic-related outcomes | Alzheimer’s disease and other dementias | Diabetes mellitus | Hypertensive heart disease | Stroke | Tracheal, bronchus, and lung cancer | Lower respiratory infections |
| Age-standardised rate (per 100000 population) |
|
41.0 (
|
|
|
40.2 (
|
83.3 (75.7-90.4) | 34.8 (
|
88.5 (77.8-98.2) |
| Number | 3650000 (33200003970000 | 264000 (212 000333000 ) | 774000 (1980001900000) | 217000 (202000231000) | 138000 (110 000160000) | 1060000 (969 0001150000) | 938000 (7830001110000 ) | 588000 (494000686000) |
| 5 | ||||||||
| Cause | Lower respiratory infections | Tracheal, bronchus, and lung cancer | Tracheal, bronchus, and lung cancer | Lower respiratory infections | Chronic kidney disease | Diarrhoeal diseases | Alzheimer’s disease and other dementias | Malaria |
| Age-standardised rate (per 100000 population) | 30.4 (27.7-32.9) |
|
25.9 (23.8-27.0) | 32.8 (
|
37.9 (
|
|
27.9 (6.76-74.8) | 67.9 (
|
| Number | 2280000 (20800002460000) | 168000 (161000174000) | 581000 (526 000610000) | 187000 (169000200000 ) | 142000 (125000159000) | 591000 (381000
|
562000 (136000
|
713000 (2510001480000) |
| 6 | ||||||||
| Cause | Neonatal disorders | Cirrhosis and other chronic liver diseases | Chronic obstructive pulmonary disease | Chronic kidney disease | Other COVID-19 pandemicrelated outcomes | Neonatal disorders | Lower respiratory infections | Tuberculosis |
| Age-standardised rate (per 100000 population) |
|
|
19.2 (16.9-20.3) | 30.9 (28.3-33.1) | 30.4 (
|
43.8 (
|
|
67.3 (56.7-77.8) |
| Number | 1910000 (1650 0002200000 ) | 131000 (127000136000) | 490000 (424000522000) | 184000 (169000197000) | 121000 (46500207000) | 672000 (571000792000) | 424000 (378000469000 ) | 378000 (313000442000 ) |
| (Table 1 continues on next page) | ||||||||
Articles
| Global | Central Europe, eastern Europe, and central Asia | High income | Latin America and Caribbean | North Africa and Middle East | South Asia | Southeast Asia, east Asia, and Oceania | Sub-Saharan Africa | |
| (Continued from previous page) | ||||||||
| 7 | ||||||||
| Cause | Alzheimer’s disease and other dementias | Alzheimer’s disease and other dementias | Colon and rectum cancer | Chronic obstructive pulmonary disease | Diabetes mellitus | Lower respiratory infections | Hypertensive heart disease | HIV/AIDS |
| Age-standardised rate (per 100000 population) | 24.9 (6.16-65.0) | 20.8 (4.88-55.3) |
|
25.0 (
|
29.4 (26.4-32.3) | 40.0 (
|
|
65.8 (59.9-73.2) |
| 8 | ||||||||
| Cause | Tracheal, bronchus, and lung cancer | Lower respiratory infections | Chronic kidney disease | Interpersonal violence | Chronic obstructive pulmonary disease | Tuberculosis | Stomach cancer | Diarrhoeal diseases |
| Age-standardised rate (per 100000 population) |
|
|
14.0 (
|
|
26.9 (23.9-29.7) |
|
18.4 (14•2-22•0) | 57.0 (
|
| Number | 1970000 (17800002160000 ) | 96200 (91200101000) | 364000 (307000
|
147000 (140 000155000) | 92400 (82500102000) | 509000 (450 000597000) | 491000 (380 000589000) | 452000 (324000
|
|
|
Diabetes mellitus | Cardiomyopathy and myocarditis | Lower respiratory infections | Other COVID-19 pandemicrelated outcomes | Alzheimer’s disease and other dementias | Diabetes mellitus | Road injuries | Other COVID-19 pandemicrelated outcomes |
| Age-standardised rate (per 100000 population) |
|
19.2 (17.9-20.4) |
|
20.9 (10•3-33:3) | 25.7 (6.30-67.6) | 33.1 (29•8-36.0) | 15.7 (13.9-17.6) |
|
| Number | 1630000 (15200001720000) | 113000 (105000121000) | 361000 (306000390000 ) | 125000 (59 600199000) | 73600 (17900198000) | 419000 (378 000457000) | 380000 (335000429000) | 245000 (159000339000 ) |
| 10 | ||||||||
| Cause | Chronic kidney disease | Colon and rectum cancer | Self-harm | Alzheimer’s disease and other dementias | Lower respiratory infections | Other COVID-19 pandemic-related outcomes | Chronic kidney disease | Neonatal disorders |
| Age-standardised rate (per 100000 population) | 18.6 (16.9-19.9) | 18.6 (17.6-19.4) | 10.9 (
|
20.8 (5.14-53.8) | 25.4 (
|
28.2 (
|
|
50.0 (
|
| Number | 1500000 (13600001610000) | 122000 (115000127000) | 149000 (142 000153000) | 119000 (29200308000 ) | 103000 (91000116000) | 370000 (246 000514000) | 376000 (333000420000) | 889000 (749 0001050000 ) |
| 2021 | ||||||||
| 1 | ||||||||
| Cause | Ischaemic heart disease | Ischaemic heart disease | Ischaemic heart disease | COVID-19 | Ischaemic heart disease | COVID-19 | Stroke | COVID-19 |
| Age-standardised rate (per 100000 population) | 108.7 (99•8-115•6) | 213.6 (196•1-229•1) | 51.0 (44.9-54.2) | 195.4 (182•1-211•4) |
|
|
|
271.0 (250.1-290.7) |
| Number | 8990000 (82900009550000 ) | 1410000 (1290 0001510000) | 1310000 (11200001400000) | 1200000 (1110000
|
769000 (679 000863000) | 2060000 (19800002170000) | 3550000 (3100 0004020000) | 1150000 (10600001240000 ) |
|
|
COVID-19 | COVID-19 | COVID-19 | Ischaemic heart disease | COVID-19 | Ischaemic heart disease | Ischaemic heart disease | Stroke |
| Age-standardised rate (per 100000 population) | 94.0 (89•2-100
|
168.8 (150.6-186.1) | 48.1 (47.4-48.8) | 83.8 (75.9-90.6) |
|
149.1 (
|
110.4 (94•9-124•6) |
|
| Number | 7890000 (7490 0008400000) | 1100000 (9820001210000) | 1070000 (10600001090000 ) | 504000 (457000545000) | 698000 (608 000
|
1990000 (18200002160000) | 2660000 (22900003000000 ) | 484000 (432000544000) |
| (Table 1 continues on next page) | ||||||||
| Global | Central Europe, eastern Europe, and central Asia | High income | Latin America and Caribbean | North Africa and Middle East | South Asia | Southeast Asia, east Asia, and Oceania | Sub-Saharan Africa | ||||||||||
| (Continued from previous page) | |||||||||||||||||
| 3 | |||||||||||||||||
| Age-standardised rate (per 100000 population) | 87.4 (
|
109.8 (
|
28.8 (
|
|
|
101.6 (90•3-114•2) | 66.6 (56.2-77.7) | 123.9 (87.7-159.5) | |||||||||
| Number | 7250000 (66000007820000) | 725000 (671000770000) | 771000 (641000838000 ) | 279000 (254000301000) | 372000 (325000421000) | 1230000 (1100 0001380000) | 1560000 (13100001820000) | 584000 (418 000757000) | |||||||||
| 4 | |||||||||||||||||
| Age-standardised rate (per 100000 population) |
|
50.0 (
|
|
|
|
81.8 (
|
34.8 (28.8-41.1) | 92.8 (83.3-103.5) | |||||||||
| 5 | 3720000 (33600004090000) | 321000 (223 000
|
792000 (2030001940000) | 236000 (135000355000) | 265000 (139 000414000) | 1070000 (9680001170000) | 970000 (800 0001150000) | 352000 (316000
|
|||||||||
| Cause | Other COVID-19 pandemicrelated outcomes | Tracheal, bronchus, and lung cancer | Tracheal, bronchus, and lung cancer | Diabetes mellitus | Hypertensive heart disease | Other COVID-19 pandemic-related outcomes | Alzheimer’s disease and other dementias | Lower respiratory infections | |||||||||
| Age-standardised rate (per 100000 population) |
|
|
25.9 (23.8-27.0) | 36.3 (
|
|
|
28.9 (7.41-78.6) | 85.4 (75.3-95.0) | |||||||||
| 6 | 2690000 (20600003610000 ) | 167000 (157000176000) | 591000 (537000620000) | 221000 (202000239000) | 138000 (109 000162000) | 838000 (6740001020000) | 608000 (1550001670000) | 563000 (472 000655000) | |||||||||
| Cause | Neonatal disorders | Cirrhosis and other chronic liver diseases | Chronic obstructive pulmonary disease | Chronic kidney disease | Chronic kidney disease | Diarrhoeal diseases | COVID-19 | Malaria | |||||||||
| Age-standardised rate (per 100000 population) |
|
|
|
30.7 (27.8-33.5) | 37.7 (
|
47.8 (
|
|
65.9 (
|
|||||||||
| Number | 1830000 (1570 0002130000 ) | 131000 (123 000138000) | 495000 (428 000527000) | 187000 (170 000204000) | 145000 (126000164000) | 573000 (372 000908000 ) | 606000 (425000974000) | 704000 (2650001400000) | |||||||||
|
|||||||||||||||||
| Age-standardised rate (per 100000 population) | 28.7 (26.0-31.1) | 20.8 (4.94-55.6) | 14.7 (13.1-15.5) | 30.4 (27.0-33.3) |
|
|
|
65.8 (
|
|||||||||
| 8 | 2180000 (19800002360000) | 137000 (32 500370000) | 348000 (304000372000) | 177000 (157000194000) | 116000 (102000129000) | 636000 (538000760000) | 431000 (384000482000) | 373000 (313000
|
|||||||||
| Cause | Alzheimer’s disease and other dementias | Cardiomyopathy and myocarditis | Chronic kidney disease | Chronic obstructive pulmonary disease | Chronic obstructive pulmonary disease | Lower respiratory infections | Hypertensive heart disease | HIV/AIDS | |||||||||
| Age-standardised rate (per 100000 population) |
|
|
13.9 (
|
|
26.4 (
|
|
19.8 (
|
61.4 (
|
|||||||||
| Number | 1960000 (499 0005120000) | 112000 (103000122000) | 368000 (310 000402000) | 145000 (130000156000) | 92700 (82000104000) | 516000 (451000584000) | 470000 (333000575000) | 515000 (467000583000) | |||||||||
| (Table 1 continues on next page) | |||||||||||||||||
Articles
| Global | Central Europe, eastern Europe, and central Asia | High income | Latin America and Caribbean | North Africa and Middle East | South Asia | Southeast Asia, east Asia, and Oceania | Sub-Saharan Africa | |
| (Continued from previous page) | ||||||||
| 9 | ||||||||
| Age-standardised rate (per 100000 population) |
|
|
11.9 (10.2-12.7) |
|
25.7 (6.22-66.8) |
|
18.1 (
|
54.4 (
|
| 10 | ||||||||
| Cause | Diabetes mellitus | Lower respiratory infections | Self-harm | Alzheimer’s disease and other dementias | Cirrhosis and other chronic liver diseases | Diabetes mellitus | Road injuries | Neonatal disorders |
| Age-standardised rate (per 100000 population) |
|
|
10.8 (
|
20.8 (5•18-54•3) | 23.2 (20.2-26.8) | 32.8 (
|
|
48.6 (40.3-58.1) |
| Number | 1660000 (15400001760000) | 82800 (77800-87500) | 148000 (141000152000) | 121000 (30300317000) | 99600 (86100116000) | 426000 (383000468000) | 379000 (331000430000 ) | 873000 (724000
|
| Table 1: Number of deaths and age-standardised mortality rates for ten leading Level 3 causes of death in 2020 and 2021, globally and by super-region, for all ages and males and females combined | ||||||||
an additional
COVID-19 and OPRM
Our estimates show that 4.80 million (
of death due to COVID-19 were highly variable among GBD super-regions (table 1). In 2021, the rankings from highest to lowest were sub-Saharan Africa ( 271.0 deaths [250.1-290.7] per 100000 population); Latin America and the Caribbean ( 195.4 deaths [182.1-211.4] per 100000 population); north Africa and the Middle East ( 172.4 deaths
of death due to COVID-19 were highly variable among GBD super-regions (table 1). In 2021, the rankings from highest to lowest were sub-Saharan Africa ( 271.0 deaths [250.1-290.7] per 100000 population); Latin America and the Caribbean ( 195.4 deaths [182.1-211.4] per 100000 population); north Africa and the Middle East ( 172.4 deaths
Deaths from both COVID-19 and OPRM also varied substantially by age, with older ages being disproportionately affected (table 2). Individuals aged 70-74 years had the highest number of deaths from both COVID-19 and OPRM in 2020 and again in 2021. The highest percentage of total deaths from COVID-19 was found in those aged 40-44 years, whereas the highest mortality rate occurred in those aged 95 years and older. Death rates from OPRM were high among older age groups and among the youngest ages, with a rate of
| Deaths | Deaths per 100000 population | Percentage of total deaths | |||||||||||||||||||
| COVID-19 2020 | COVID-19 2021 |
|
|
|
COVID-19 2021 |
|
|
COVID-19 2020 | COVID-19 2021 | Other COVID-19 pandemicrelated outcomes 2020 | Other COVID-19 pandemicrelated outcomes 2021 | ||||||||||
| Early neonatal | 0 | 1 | 3518 | 3462 | 0.0 | <0.1 | 141.4 | 141.2 | 0.0% | <0.1% | 0.2% | 0.2% | |||||||||
| Late neonatal | 3 | 5 | 5069 | 5641 | <0.1 | 0.1 |
|
77.3 | <0.1% | <0.1% | 1.1% | 1.3% | |||||||||
| 1-5 months | 170 | 287 | 24269 | 26647 | 0.3 | 0.5 | 44.4 | 49.6 | <0.1% | <0.1% | 3.1% | 3.6% | |||||||||
| 6-11 months | 234 | 394 | 20478 | 30883 | 0.4 | 0.6 | 31.7 | 48.9 | <0.1% | 0.1% | 3.5% |
|
|||||||||
| 12-23 months | 998 | 1644 | 19042 | 30550 | 0.8 | 1.3 | 14.5 | 23.8 | 0.2% | 0.3% | 3.7% | 6.2% | |||||||||
| 2-4 years | 8500 | 14386 | 14730 | 23574 | 2.1 | 3.6 | 3.6 | 5.8 | 1.2% | 2.1% | 2.0% | 3.4% | |||||||||
| 5-9 years | 7052 | 11393 | 5377 | 8196 | 1.0 | 1.7 | 0.8 | 1.2 | 1.9% | 3.2% | 1.5% | 2.3% | |||||||||
| 10-14 years | 8553 | 14405 | 1588 | 2715 | 1.3 | 2.2 | 0.2 | 0.4 | 2.8% | 4.8% | 0.5% | 0.9% | |||||||||
| 15-19 years | 17032 | 26852 | 5932 | 12576 | 2.8 |
|
1.0 | 2.0 | 3.1% | 4.8% | 1.1% | 2.2% | |||||||||
| 20-24 years | 25528 | 40743 | 8219 | 17453 |
|
6.8 | 1.4 | 2.9 | 3.6% | 5.5% | 1.2% | 2.4% | |||||||||
| 25-29 years | 47857 | 78496 | 12581 | 28816 | 8.1 | 13.3 | 2.1 | 4.9 | 5.9% | 9.2% | 1.6% | 3.4% | |||||||||
| 30-34 years | 81232 | 137979 | 21625 | 49808 | 13.4 | 22.8 | 3.6 | 8.2 | 7.9% | 12.3% | 2.1% |
|
|||||||||
| 35-39 years | 112228 | 195380 | 29877 | 69402 |
|
34.8 |
|
12.4 | 9.0% | 14.1% | 2.4% | 5.0% | |||||||||
| 40-44 years | 165337 | 287099 | 44391 | 102041 |
|
57.4 | 9.0 | 20.4 | 10.3% | 16.0% | 2.8% | 5.7% | |||||||||
| 45-49 years | 207940 | 355388 | 55989 | 124899 | 44.0 | 75.1 | 11.8 | 26.4 | 10.1% | 15.7% | 2.7% | 5.5% | |||||||||
| 50-54 years | 253491 | 426785 | 67629 | 147651 | 57.7 | 95.9 | 15.4 | 33.2 | 9•1% | 14.0% | 2.4% | 4.8% | |||||||||
| 55-59 years | 336162 | 564508 | 90815 | 191441 | 87.5 |
|
23.6 | 48.4 | 9.0% | 13.8% | 2.4% | 4.7% | |||||||||
| 60-64 years | 460769 | 774879 | 125433 | 262008 | 146.1 | 242.1 | 39.8 | 81.9 | 9.8% | 15.0% | 2.7% | 5•1% | |||||||||
| 65-69 years | 564371 | 957557 | 155431 | 321301 | 209.4 | 347.1 | 57.7 | 116.5 | 9.4% | 14.5% | 2.6% | 4.9% | |||||||||
| 70-74 years | 585549 | 989888 | 156931 | 325295 | 298.7 | 480.9 | 80.1 | 158.0 | 8.8% | 13.2% | 2.4% | 4.3% | |||||||||
| 75-79 years | 539515 | 861796 | 135849 | 276402 | 417.1 | 653.4 | 105.0 | 209.6 | 7.9% | 11.8% | 2.0% | 3.8% | |||||||||
| 80-84 years | 551014 | 888813 | 146084 | 277786 | 638.9 | 1014.8 | 169.4 | 317.2 | 7.5% | 11.3% | 2.0% | 3.5% | |||||||||
| 85-89 years | 427770 | 658875 | 106842 | 191824 | 959.3 |
|
239.6 | 419.5 | 6.9% | 10.0% | 1.7% | 2.9% | |||||||||
| 90-94 years | 280605 | 426185 | 67297 | 114449 | 1608.9 | 2382.3 | 385.9 | 639.8 | 7.5% | 10.8% | 1.8% | 2.9% | |||||||||
|
|
120173 | 174390 | 24074 | 42104 | 2298.6 | 3199.6 |
|
772.5 | 7.8% | 10.7% | 1.6% | 2.6% | |||||||||
Table 2: Number of deaths, age-standardised mortality rates, and percentage of total deaths due to COVID-19 and other pandemic-related mortality by age, globally
Leading causes of global YLLs
The causes of death with the highest age-standardised YLL rates show shifting epidemiological trends from CMNN diseases to NCDs at Level 3 of the cause hierarchy (appendix 2 figure S2). Globally, the leading three causes of age-standardised YLLs in 1990 were all CMNN diseases. Ranked in descending order, these causes were neonatal disorders, lower respiratory infections, and diarrhoeal diseases. In 2019, neonatal disorders remained the leading cause of agestandardised YLLs, but the second and third leading causes were replaced by NCDs: ischaemic heart disease (ranked second) and stroke (ranked third). In 2021, COVID-19 was the second-leading cause of global agestandardised YLLs, making the leading two causes CMNN diseases (with neonatal disorders ranked first), with ischaemic heart disease ranked third. Among the leading causes of age-standardised YLLs, malaria was the only cause to show an increase in age-standardised YLL rates between 2019 and 2021 (ranking ninth in 2019 and seventh in 2021).
Decomposition of global life expectancy
We found long-standing positive trends in global life expectancy since the early 1990s, with steady increases occurring across each decade between 1990 and 2019 (appendix 2 table S4). Altogether, the global increase in life expectancy from 1990 to 2019 totalled
Figure 3: Change in life expectancy attributable to leading causes of death for males and females combined, 1990-2000, 2000-10, 2010-19, and 2019-21, globally
Each row represents the change in global life expectancy from 1990 to 2021 for a given cause. The total change in life expectancy is further broken down by different colours to represent changes over time periods. A bar to the right of 0 represents an increase in life expectancy due to changes in the given time period, and a bar to the left of 0 represents a decrease in life expectancy due to a given time period. For readability, labels indicating a change in life expectancy of less than 0.05 years are not shown. CKD=chronic kidney disease. COPD=chronic obstructive pulmonary disease. LRI=lower respiratory infection. NCD=non-communicable disease. OPRM=other pandemic-related mortality. *Does not include natural disasters. †Does not include war and terrorism.
Each row represents the change in global life expectancy from 1990 to 2021 for a given cause. The total change in life expectancy is further broken down by different colours to represent changes over time periods. A bar to the right of 0 represents an increase in life expectancy due to changes in the given time period, and a bar to the left of 0 represents a decrease in life expectancy due to a given time period. For readability, labels indicating a change in life expectancy of less than 0.05 years are not shown. CKD=chronic kidney disease. COPD=chronic obstructive pulmonary disease. LRI=lower respiratory infection. NCD=non-communicable disease. OPRM=other pandemic-related mortality. *Does not include natural disasters. †Does not include war and terrorism.
in deaths from these diseases is responsible for a substantial increase in life expectancy of 1.1 years during 1990-2021, but this increase was most pronounced between 1990 and 2000 compared with other time periods. The second-largest effect on increasing life expectancy is attributed to the reduction in deaths from lower respiratory infection, contributing 0.9 years of gained life expectancy from 1990 to 2021. Other leading factors include reduced mortality from stroke, CMNN diseases, neonatal deaths, ischaemic heart disease, and neoplasms, each of which increased global life expectancy by
Decomposition of super-region, regional, and countrylevel life expectancy
Each of the seven super-regions experienced an overall increase in life expectancy between 1990 and 2021, despite
progress in each being differentially affected by COVID-19 (figures 4, 5). Southeast Asia, east Asia, and Oceania showed the highest gain, with a net improvement of 8.3 years (
progress in each being differentially affected by COVID-19 (figures 4, 5). Southeast Asia, east Asia, and Oceania showed the highest gain, with a net improvement of 8.3 years (
The differential effect of COVID-19 on reduced life expectancy was observed across GBD regions (figure 6). Although most regions experienced overall improvements in life expectancy between 1990 and 2021, a reduction occurred in southern sub-Saharan Africa, which faced the greatest impact of HIV and was also
Figure 4: Age-standardised mortality rate of COVID-19 and OPRM, 2021
Global choropleth maps of COVID-19 (A) and OPRM (B) for 2021 that show sub-national detail where available. OPRM=other pandemic-related mortality.
Global choropleth maps of COVID-19 (A) and OPRM (B) for 2021 that show sub-national detail where available. OPRM=other pandemic-related mortality.
Figure 5: Change in life expectancy attributable to leading causes of death among super-regions, 1990-2021
Each row represents the change in life expectancy from 1990 to 2021 for a given super-region. A bar to the right of 0 represents an increase in life expectancy due to changes in the given cause, and a bar to the left of 0 represents a decrease in life expectancy for a given cause. For readability, labels indicating a change in life expectancy of less than
Each row represents the change in life expectancy from 1990 to 2021 for a given super-region. A bar to the right of 0 represents an increase in life expectancy due to changes in the given cause, and a bar to the left of 0 represents a decrease in life expectancy for a given cause. For readability, labels indicating a change in life expectancy of less than
Articles
Figure 6: Effect of COVID-19 on life expectancy by GBD region, 2019-21
For readability, labels indicating a change in life expectancy of less than 0.05 years are not shown. GBD=Global Burden of Diseases, Injuries, and Risk Factors Study.
heavily affected by COVID-19. The overall decrease in life expectancy of 4.3 years (
HIV/AIDS had a substantial negative effect on lifeexpectancy trends in southern sub-Saharan Africa from 1990 to 2021 (appendix 2 figure S27). Despite improvements in each of the time periods 2000-2010, 2010-2019, and 2019-2021, this region was unable to recover the 9.0 years lost during 1990-2000. Although we found a net decline in deaths due to HIV/AIDS between 2000 and 2019, improvements slowed substantially from 2019 to 2021, when only 0.2 years in life expectancy were gained as a result of reduced HIV/AIDS mortality. Conversely, eastern
sub-Saharan Africa had the highest level of recovery to their life expectancy among the regions, gaining 1.5 years of life expectancy over the entire study period.
In 1990, malaria-related deaths had almost no effect on life expectancy in eight of the 21 GBD regions (appendix 2 figure S13). By 2021, however,
At the national level, some of the highest gains in life expectancy between 1990 and 2021 occurred in the eastern region of sub-Saharan Africa (appendix 2 figure S12). Life expectancy in Ethiopia increased by
heavily affected by COVID-19. The overall decrease in life expectancy of 4.3 years (
HIV/AIDS had a substantial negative effect on lifeexpectancy trends in southern sub-Saharan Africa from 1990 to 2021 (appendix 2 figure S27). Despite improvements in each of the time periods 2000-2010, 2010-2019, and 2019-2021, this region was unable to recover the 9.0 years lost during 1990-2000. Although we found a net decline in deaths due to HIV/AIDS between 2000 and 2019, improvements slowed substantially from 2019 to 2021, when only 0.2 years in life expectancy were gained as a result of reduced HIV/AIDS mortality. Conversely, eastern
sub-Saharan Africa had the highest level of recovery to their life expectancy among the regions, gaining 1.5 years of life expectancy over the entire study period.
In 1990, malaria-related deaths had almost no effect on life expectancy in eight of the 21 GBD regions (appendix 2 figure S13). By 2021, however,
At the national level, some of the highest gains in life expectancy between 1990 and 2021 occurred in the eastern region of sub-Saharan Africa (appendix 2 figure S12). Life expectancy in Ethiopia increased by
Figure 7: Effect of enteric infectious diseases on life expectancy by time period and GBD region, 1990-2021
For readability, labels indicating a change in life expectancy of less than 0.05 years are not shown. GBD=Global Burden of Diseases, Injuries, and Risk Factors Study.
For readability, labels indicating a change in life expectancy of less than 0.05 years are not shown. GBD=Global Burden of Diseases, Injuries, and Risk Factors Study.
Effect of CMNN diseases on life expectancy and trends in mortality concentration
Among CMNN causes, several key trends emerged in their effect on global life expectancy and the localisation of deaths over time. First, the reduction of deaths due to enteric disease had a substantial impact on global life expectancy, with notable regional variations (figure 7). As 160 countries and territories made progress in reducing CMNN disease-related mortality, mortality concentration emerged. Deaths became more concentrated into certain countries or regions, persisting alongside advancements made in other parts of the world. An illustrative example is the shift in deaths due to enteric diseases in children younger than 5 years, with
impact on life-expectancy trends, particularly in southern sub-Saharan Africa, and with
Reductions in neonatal deaths contributed to a
impact on life-expectancy trends, particularly in southern sub-Saharan Africa, and with
Reductions in neonatal deaths contributed to a
Figure 8: Effect of lower respiratory infections on life expectancy by time period and GBD region, 1990-2021
For readability, labels indicating a change in life expectancy of less than 0.05 years are not shown. GBD=Global Burden of Diseases, Injuries, and Risk Factors Study.
For readability, labels indicating a change in life expectancy of less than 0.05 years are not shown. GBD=Global Burden of Diseases, Injuries, and Risk Factors Study.
Figure 9: Change in life expectancy attributable to leading causes of death among GBD regions, 1990-2021
Each row represents the change in life expectancy from 1990 to 2021 for a given GBD region. A bar to the right of 0 represents an increase in life expectancy due to changes in the given cause, and a bar to the left of 0 represents a decrease in life expectancy for a given cause. For readability, labels indicating a change in life expectancy of less than 0.3 years are not shown. CKD=chronic kidney disease. COPD=chronic obstructive pulmonary disease. GBD=Global Burden of Diseases, Injuries, and Risk Factors Study. LRI=lower respiratory infection. NCD=non-communicable disease. OPRM=other pandemic-related mortality. *Does not include war and terrorism. †Does not include natural disasters.
Each row represents the change in life expectancy from 1990 to 2021 for a given GBD region. A bar to the right of 0 represents an increase in life expectancy due to changes in the given cause, and a bar to the left of 0 represents a decrease in life expectancy for a given cause. For readability, labels indicating a change in life expectancy of less than 0.3 years are not shown. CKD=chronic kidney disease. COPD=chronic obstructive pulmonary disease. GBD=Global Burden of Diseases, Injuries, and Risk Factors Study. LRI=lower respiratory infection. NCD=non-communicable disease. OPRM=other pandemic-related mortality. *Does not include war and terrorism. †Does not include natural disasters.
sub-Saharan Africa, and south Asia saw notable increases. We found a shift towards mortality concentration, with
Effect of NCDs on life expectancy and trends in mortality concentration
Among NCDs, several findings reflect their effect on global life expectancy and death concentration. Reductions in stroke led to a notable gain in life expectancy of 0.8 years, but stroke deaths were not concentrated, with
Effect of injuries on life expectancy and trends in mortality concentration
The reduction in transport injuries had a positive effect on life expectancy, contributing to a gain of 0.2 years. However, as with NCDs, transport injury-related mortality was not concentrated, with
showed little mortality concentration, with
showed little mortality concentration, with
Discussion Main findings
The COVID-19 pandemic has emerged as one of the most defining global health events of recent history. Our latest comprehensive estimates of cause-specific mortality give insight into the global landscape of disease before and during the first 2 years of the pandemic, revealing the important changes in disease-burden patterns that followed. After more than three decades of consistent improvements in global life expectancy and declining agestandardised death rates, COVID-19 reversed longstanding progress and disrupted trends in the epidemiological transition. As the second leading cause of age-standardised deaths in 2021, COVID-19 had a pronounced influence on the reduction in global life expectancy that occurred. The heterogeneous influence of the disease across the globe provides important insights for improving future pandemic preparedness and ensuring that nations are equitably equipped to respond to new outbreaks. Additionally, our analysis of geographical and temporal trends in mortality enables us to observe the changing patterns in causes of death worldwide. Many causes have exhibited a reduced geographical reach-a reflection of dedicated and persistent mitigation efforts to reduce the burden of certain causes, as well as potential changes to risk-factor exposure.
The COVID-19 pandemic
The emergence and spread of COVID-19 follows a similar pattern of regional heterogeneity that is common among many leading communicable causes of death, with higher rates of infection and increased fatalities occurring in lower-resource settings.
locations emphasises the complexity of the pandemic. Diverse social, economic, and political influences contributed to the variations in death rates observed between locations. In general, areas with advanced healthcare systems and robust medical facilities were better able to manage abrupt increases in the number of COVID-19 cases. By contrast, locations with poorer health-care infrastructure were less equipped to handle the surge in infections that occurred,
Our study shows that COVID-19 was one of the leading global causes of death during the first 2 years of the pandemic and provides an opportunity to delineate between the disease’s direct and indirect mortality effects as well as its effect on life expectancy. As previously predicted,
locations emphasises the complexity of the pandemic. Diverse social, economic, and political influences contributed to the variations in death rates observed between locations. In general, areas with advanced healthcare systems and robust medical facilities were better able to manage abrupt increases in the number of COVID-19 cases. By contrast, locations with poorer health-care infrastructure were less equipped to handle the surge in infections that occurred,
Our study shows that COVID-19 was one of the leading global causes of death during the first 2 years of the pandemic and provides an opportunity to delineate between the disease’s direct and indirect mortality effects as well as its effect on life expectancy. As previously predicted,
Important trends in life expectancy
Advancements over the past three decades in the prevention and control of infectious diseases have contributed to increases in life expectancy in many locations, increasing the need to support populations living with NCDs.
HIV/AIDS and lower respiratory and enteric infectionssomewhat counterbalanced the decline, the decrease in life expectancy was also compounded by increasing rates of mortality from other causes, such as diabetes and kidney diseases.
The effect of COVID-19 on life expectancy showed varying degrees of severity, ranging from a large loss of 4.9 years in Andean Latin America to almost no change in east Asia. From 1990 to 2021, reductions in many of the leading causes of death resulted in overall lifeexpectancy increases across most regions, despite heavy setbacks for many because of the COVID-19 pandemic. We found that despite Andean Latin America having the largest regional reduction in life expectancy due to the pandemic, overall life-expectancy reductions across the region were tempered by improvements in other causes, with reductions in rates of death from lower respiratory infections and neonatal disorders responsible for an increase in life expectancy of 2.6 years overall between 1990 and 2021. The impressive reductions in neonatal disorders throughout many countries in Andean Latin America have been attributed to the improvements made in implementing effective maternal and neonatal health intervention strategies.
The reduction in life expectancy in southern subSaharan Africa also exceeded the global average by a substantial margin, with a reduction of 3.4 years due to COVID-19. Although life expectancy in the region was substantially affected by the COVID-19 pandemic, the reduction was also attributable to high mortality rates from HIV/AIDS. Some nations with high pandemicrelated death tolls were among those already burdened by high rates of other infectious diseases. Several countries in southern sub-Saharan Africa navigated the challenges of the pandemic, alongside long histories of combatting some of the highest HIV/AIDS prevalence rates in the world.
The effect of COVID-19 on life expectancy showed varying degrees of severity, ranging from a large loss of 4.9 years in Andean Latin America to almost no change in east Asia. From 1990 to 2021, reductions in many of the leading causes of death resulted in overall lifeexpectancy increases across most regions, despite heavy setbacks for many because of the COVID-19 pandemic. We found that despite Andean Latin America having the largest regional reduction in life expectancy due to the pandemic, overall life-expectancy reductions across the region were tempered by improvements in other causes, with reductions in rates of death from lower respiratory infections and neonatal disorders responsible for an increase in life expectancy of 2.6 years overall between 1990 and 2021. The impressive reductions in neonatal disorders throughout many countries in Andean Latin America have been attributed to the improvements made in implementing effective maternal and neonatal health intervention strategies.
The reduction in life expectancy in southern subSaharan Africa also exceeded the global average by a substantial margin, with a reduction of 3.4 years due to COVID-19. Although life expectancy in the region was substantially affected by the COVID-19 pandemic, the reduction was also attributable to high mortality rates from HIV/AIDS. Some nations with high pandemicrelated death tolls were among those already burdened by high rates of other infectious diseases. Several countries in southern sub-Saharan Africa navigated the challenges of the pandemic, alongside long histories of combatting some of the highest HIV/AIDS prevalence rates in the world.
Cause-specific patterns of mortality concentration
Estimates of mortality concentration reflect shifting patterns of disease over time, from diseases that have a widespread presence moving to more geographically reduced subsets of the global population. These changes highlight differences between populations and their progress towards reducing mortality due to diseases and injuries. These findings also provide an important opportunity to improve how best public health practices are applied to further disease reduction. Broadly, widespread declines in many communicable diseases resulted in mortality from these causes exhibiting more
concentrated geographical distributions in 2021 relative to patterns seen in 1990. The degree of mortality concentration estimated by this study for enteric and lower respiratory infections, malaria, HIV/AIDS, neonatal disorders, and tuberculosis reflects substantial global progress in reducing mortality from these causes over the study period, underscoring the success of several public health campaigns, global commitments, and improvements in communicable-disease programmes.
Notably, our estimates support previous findings
Enteric infections showed large disease concentration. Under-5 deaths from enteric infections were largely concentrated within sub-Saharan Africa and south Asia. Countries in sub-Saharan Africa and south Asia with the highest under-5 death rates from enteric infections in 2021 included Chad, South Sudan, and the Central African Republic. There are many contributing factors that should be considered when examining how to reduce enteric infections in the remaining concentrated locations. Alongside the provision of oral rehydration solution and rotavirus vaccines, critical public health improvements such as in water, sanitation, and hygiene might have contributed to decreases in enteric deaths.
concentrated geographical distributions in 2021 relative to patterns seen in 1990. The degree of mortality concentration estimated by this study for enteric and lower respiratory infections, malaria, HIV/AIDS, neonatal disorders, and tuberculosis reflects substantial global progress in reducing mortality from these causes over the study period, underscoring the success of several public health campaigns, global commitments, and improvements in communicable-disease programmes.
Notably, our estimates support previous findings
Enteric infections showed large disease concentration. Under-5 deaths from enteric infections were largely concentrated within sub-Saharan Africa and south Asia. Countries in sub-Saharan Africa and south Asia with the highest under-5 death rates from enteric infections in 2021 included Chad, South Sudan, and the Central African Republic. There are many contributing factors that should be considered when examining how to reduce enteric infections in the remaining concentrated locations. Alongside the provision of oral rehydration solution and rotavirus vaccines, critical public health improvements such as in water, sanitation, and hygiene might have contributed to decreases in enteric deaths.
A broad and recurring theme from this study is that reductions in enteric infections contributed to improved life expectancies over the past several decades. The reductions in childhood mortality associated with diarrhoeal diseases that have occurred across many parts of Africa
Our study also found that some vaccine-preventable diseases, such as measles, have shown widespread reductions in mortality rates and were geographically concentrated. Under-5 deaths from measles were concentrated within western and eastern sub-Saharan Africa. Although multiple factors contribute to decreases in infectious disease burden, improvements in measles mortality have largely been attributable to the global availability of a safe and effective vaccine against measles, producing life-long immunity, with two-dose efficacy exceeding
Some infectious diseases, such as HIV/AIDS, also showed mortality concentration. Deaths from HIV/AIDS
were largely concentrated within sub-Saharan Africa, most notably southern sub-Saharan Africa. Countries in subSaharan Africa with the highest age-standardised mortality rate in 2021 included Lesotho, Eswatini, and Botswana. Countries in sub-Saharan Africa with the highest under-5 death rates from HIV in 2021 included Lesotho, Equatorial Guinea, and Guinea-Bissau. This concentration highlights how HIV-control campaigns, preventative measures,
Our study also found that some vaccine-preventable diseases, such as measles, have shown widespread reductions in mortality rates and were geographically concentrated. Under-5 deaths from measles were concentrated within western and eastern sub-Saharan Africa. Although multiple factors contribute to decreases in infectious disease burden, improvements in measles mortality have largely been attributable to the global availability of a safe and effective vaccine against measles, producing life-long immunity, with two-dose efficacy exceeding
Some infectious diseases, such as HIV/AIDS, also showed mortality concentration. Deaths from HIV/AIDS
were largely concentrated within sub-Saharan Africa, most notably southern sub-Saharan Africa. Countries in subSaharan Africa with the highest age-standardised mortality rate in 2021 included Lesotho, Eswatini, and Botswana. Countries in sub-Saharan Africa with the highest under-5 death rates from HIV in 2021 included Lesotho, Equatorial Guinea, and Guinea-Bissau. This concentration highlights how HIV-control campaigns, preventative measures,
In many high-income nations, the overall rate of neonatal deaths decreased between 1990 and 2021, becoming more concentrated over time. Deaths from neonatal disorders in 2021 were concentrated within subSaharan Africa and south Asia.
Conversely, although the burden of many NCDs has also been reducing, these causes have typically not followed the same pattern of mortality concentration seen in CMNN diseases. These trends emphasise a key distinction in the spatial dynamics of NCDs compared with many communicable diseases. Although noncommunicable causes might not exhibit the same degree of concentration as communicable causes, the mortality burden has changed in distribution, reducing over time in high-income countries and regions, while persisting in low-income countries and regions. Age-standardised mortality rates due to NCDs decreased in most locations within the high-income; Latin America and the Caribbean; north Africa and the Middle east; and central Europe, eastern Europe, and central Asia super-regions between 1990 and 2021. However, NCDs in the south Asia; sub-Saharan Africa; and southeast Asia, east Asia, and Oceania super-regions have either increased or
decreased at notably lower levels in 2021 compared with in 1990. Examples of this trend include ischaemic heart disease, neoplasms, and stroke, all of which largely declined over the study period-although their reductions have been widely dispersed and not as targeted as the CMNN causes. These findings show that NCDs do not appear to be moving towards more condensed geographical locations over time in the same way that many CMNN diseases are, which could make interventions and policies more complex to implement.
decreased at notably lower levels in 2021 compared with in 1990. Examples of this trend include ischaemic heart disease, neoplasms, and stroke, all of which largely declined over the study period-although their reductions have been widely dispersed and not as targeted as the CMNN causes. These findings show that NCDs do not appear to be moving towards more condensed geographical locations over time in the same way that many CMNN diseases are, which could make interventions and policies more complex to implement.
Ultimately, the extent of mortality concentration reflects both the progress achieved in health-care advancements and the shortcomings that persist in their equitable implementation. Disease concentration is evidence that there are effective interventions and policies that have successfully reduced disease burden in many locations, but these innovations have not been equitably distributed throughout the world or have been ineffective at addressing the specific challenges certain populations face. There remains a global need to improve access to new interventions and vaccines, to invest in the implementation of validated public health policies, and to strategise with geographical sources of disease in mind. Future efforts should continue the ongoing mitigation of communicable diseases, focusing on locations where these causes have become more geographically concentrated, while also initiating efforts to combat chronic causes within low-resourced settings. Additionally, patterns of high geographical concentration among infectious causes and low geographical concentration among chronic causes reflect the global epidemiological transition, wherein mortality rates of infectious deaths declined throughout most years of our study. The increased concentration of a cause of death, particularly communicable diseases, illustrates success in mitigation that can be adapted within the countries and regions with mortality concentration identified in our study, with the potential to greatly reduce mortality from those causes of death.
Limitations
Methodological advancements have enabled GBD 2021 to produce cause-specific estimates of mortality more easily than in previous iterations; however, as with any study of this scope, there are several important limitations to acknowledge. Cause-specific limitations for every cause of death in GBD are detailed in appendix 1 (section 3). Here, we describe cross-cutting limitations with applicability across many causes. First, sparsity of data or unreliability of data from specific regions, time periods, or age groups can influence the accuracy of our estimates, particularly poor data quality and coverage from western, eastern, southern, and central subSaharan Africa and south Asia. Second, the quality of cause-of-death and verbal-autopsy data rely on accurately coded death certificates to the international standards set by the International Classification of Diseases and are
subject to the practice of the doctor completing the death certificate, who may or may not have received training to facilitate comparability of reporting underlying causes of death. This process is further complicated by comorbidities at the time of death, which might affect the accuracy of both vital-registration and verbal-autopsy data sources. A key data-processing method for GBD is the re-allocation of incorrectly or vaguely assigned deaths-referred to as garbage
used to calculate COVID-19 have been fully outlined in previous publications,
subject to the practice of the doctor completing the death certificate, who may or may not have received training to facilitate comparability of reporting underlying causes of death. This process is further complicated by comorbidities at the time of death, which might affect the accuracy of both vital-registration and verbal-autopsy data sources. A key data-processing method for GBD is the re-allocation of incorrectly or vaguely assigned deaths-referred to as garbage
used to calculate COVID-19 have been fully outlined in previous publications,
Future directions
In the next iteration of GBD, we will include over 100 location-years of vital registration and other data types that have been reported since GBD 2021 estimates were produced. Additionally, we will continue to expand the estimation of causes of death by disaggregating broad categories of causes of death into more detailed causes where available. These improvements aim to enhance precision and timeliness of estimates of COVID-19related deaths and other cause of death. We also plan to simplify our approach to estimating COVID-19-related deaths. In lieu of the residual OPRM category reported in GBD 2021, we will use all available location-years of cause-of-death data to attribute mortality to specific causes, removing this residual category. We anticipate that this method will facilitate more timely and actionable insights for public health planning and policy making, especially as we expect to observe more regular and modellable mortality patterns in the post-pandemic years. Through these advancements, we will improve the utility and accuracy of the GBD study as a tool for effective public strategies.
Conclusion
Findings from GBD 2021 provide a comprehensive overview of long-term mortality trends along with important insights into the COVID-19 pandemic years. The COVID-19 pandemic fundamentally changed the landscape of global health and mortality. As a leading cause of death, COVID-19 reduced life expectancy in 2 years nearly as much as reductions in communicable and NCDs have improved it over decades. The changes in mortality caused by the pandemic were not predictable through the standard GBD estimation methods and required the development and application of novel estimation methods as the pandemic emerged in real time. These timely updates on causes of death are essential for monitoring progress, identifying prevailing health concerns, guiding targeted interventions, and optimising resource allocation. GBD 2021 shows that better life expectancy outcomes might be achieved by leveraging past successes in mortality reduction. If future policy efforts are guided by the successes made in countries and regions with effective disease-mitigation
programmes, such achievements might be replicated in locations where high mortality persists. While COVID-19 and other health challenges continue, GBD 2021 can offer valuable guidance for public health investment and policy making.
programmes, such achievements might be replicated in locations where high mortality persists. While COVID-19 and other health challenges continue, GBD 2021 can offer valuable guidance for public health investment and policy making.
GBD 2021 Causes of Death Collaborators
Mohsen Naghavi*, Kanyin Liane Ong*, Amirali Aali, Hazim S Ababneh, Yohannes Habtegiorgis Abate, Cristiana Abbafati, Rouzbeh Abbasgholizadeh, Mohammadreza Abbasian, Mohsen Abbasi-Kangevari, Hedayat Abbastabar, Samar Abd ElHafeez, Michael Abdelmasseh, Sherief Abd-Elsalam, Ahmed Abdelwahab, Mohammad Abdollahi, Mohammad-Amin Abdollahifar, Meriem Abdoun, Deldar Morad Abdulah, Auwal Abdullahi, Mesfin Abebe, Samrawit Shawel Abebe, Aidin Abedi, Kedir Hussein Abegaz, E S Abhilash, Hassan Abidi, Olumide Abiodun, Richard Gyan Aboagye, Hassan Abolhassani, Meysam Abolmaali, Mohamed Abouzid, Girma Beressa Aboye, Lucas Guimarães Abreu, Woldu Aberhe Abrha, Dariush Abtahi, Samir Abu Rumeileh, Hasan Abualruz, Bilyaminu Abubakar, Eman Abu-Gharbieh, Niveen ME Abu-Rmeileh, Salahdein Aburuz, Ahmed Abu-Zaid, Manfred Mario Kokou Accrombessi, Tadele Girum Adal, Abdu A Adamu, Isaac Yeboah Addo, Giovanni Addolorato, Akindele Olupelumi Adebiyi, Victor Adekanmbi, Abiola Victor Adepoju, Charles Oluwaseun Adetunji, Juliana Bunmi Adetunji, Temitayo Esther Adeyeoluwa, Daniel Adedayo Adeyinka, Olorunsola Israel Adeyomoye, Biruk Adie Adie Admass, Qorinah Estiningtyas Sakilah Adnani, Saryia Adra, Aanuoluwapo Adeyimika Afolabi, Muhammad Sohail Afzal, Saira Afzal, Suneth Buddhika Agampodi, Pradyumna Agasthi, Manik Aggarwal, Shahin Aghamiri, Feleke Doyore Agide, Antonella Agodi, Anurag Agrawal, Williams Agyemang-Duah, Bright Opoku Ahinkorah, Aqeel Ahmad, Danish Ahmad, Firdos Ahmad, Muayyad M Ahmad, Sajjad Ahmad, Shahzaib Ahmad, Tauseef Ahmad, Keivan Ahmadi, Amir Mahmoud Ahmadzade, Ali Ahmed, Ayman Ahmed, Haroon Ahmed, Luai A Ahmed, Mehrunnisha Sharif Ahmed, Meqdad Saleh Ahmed, Muktar Beshir Ahmed, Syed Anees Ahmed, Marjan Ajami, Budi Aji, Essona Matatom Akara, Hossein Akbarialiabad, Karolina Akinosoglou, Tomi Akinyemiju, Mohammed Ahmed Akkaif, Samuel Akyirem, Hanadi Al Hamad, Syed Mahfuz Al Hasan, Fares Alahdab, Samer O Alalalmeh, Tariq A Alalwan, Ziyad Al-Aly, Khurshid Alam, Manjurul Alam, Noore Alam, Rasmieh Mustafa Al-amer, Fahad Mashhour Alanezi, Turki M Alanzi, Sayer Al-Azzam, Almaza Albakri, Mohammed Albashtawy, Mohammad T AlBataineh, Jacqueline Elizabeth Alcalde-Rabanal, Khalifah A Aldawsari, Wafa A Aldhaleei, Robert W Aldridge, Haileselasie Berhane Alema, Mulubirhan Assefa Alemayohu, Sharifullah Alemi, Yihun Mulugeta Alemu, Adel Ali Saeed Al-Gheethi, Khalid F Alhabib, Fadwa Alhalaiqa Naji Alhalaiqa,
Mohammed Khaled Al-Hanawi, Abid Ali, Amjad Ali, Liaqat Ali, Mohammed Usman Ali, Rafat Ali, Shahid Ali, Syed Shujait Shujait Ali, Gianfranco Alicandro, Sheikh Mohammad Alif, Reyhaneh Alikhani, Yousef Alimohamadi, Ahmednur Adem Aliyi, Mohammad A M Aljasir, Syed Mohamed Aljunid, François Alla, Peter Allebeck, Sabah Al-Marwani, Sadeq Ali Ali Al-Maweri, Joseph Uy Almazan, Hesham M Al-Mekhlafi, Louay Almidani, Omar Almidani, Mahmoud A Alomari, Basem Al-Omari, Jordi Alonso, Jaber S Alqahtani, Shehabaldin Alqalyoobi, Ahmed Yaseen Alqutaibi, Salman Khalifah Al-Sabah, Zaid Altaany, Awais Altaf, Jaffar A Al-Tawfiq, Khalid A Altirkawi, Deborah Oyine Aluh, Nelson Alvis-Guzman, Hassan Alwafi, Yaser Mohammed Al-Worafi, Hany Aly, Safwat Aly, Karem H Alzoubi, Reza Amani, Azmeraw T Amare, Prince M Amegbor, Edward Kwabena Ameyaw, Tarek Tawfik Amin, Alireza Amindarolzarbi, Sohrab Amiri, Mohammad Hosein Amirzade-Iranaq, Hubert Amu, Dickson A Amugsi, Ganiyu Adeniyi Amusa, Robert Ancuceanu, Deanna Anderlini, David B Anderson, Pedro Prata Andrade, Catalina Liliana Andrei, Tudorel Andrei, Colin Angus, Abhishek Anil, Sneha Anil, Amir Anoushiravani, Hossein Ansari, Ansariadi Ansariadi, Alireza Ansari-Moghaddam, Catherine M Antony, Ernoiz Antriyandarti, Davood Anvari, Saeid Anvari, Saleha Anwar, Sumadi Lukman Anwar, Razique Anwer, Anayochukwu Edward Anyasodor, Muhammad Aqeel,
Mohammed Khaled Al-Hanawi, Abid Ali, Amjad Ali, Liaqat Ali, Mohammed Usman Ali, Rafat Ali, Shahid Ali, Syed Shujait Shujait Ali, Gianfranco Alicandro, Sheikh Mohammad Alif, Reyhaneh Alikhani, Yousef Alimohamadi, Ahmednur Adem Aliyi, Mohammad A M Aljasir, Syed Mohamed Aljunid, François Alla, Peter Allebeck, Sabah Al-Marwani, Sadeq Ali Ali Al-Maweri, Joseph Uy Almazan, Hesham M Al-Mekhlafi, Louay Almidani, Omar Almidani, Mahmoud A Alomari, Basem Al-Omari, Jordi Alonso, Jaber S Alqahtani, Shehabaldin Alqalyoobi, Ahmed Yaseen Alqutaibi, Salman Khalifah Al-Sabah, Zaid Altaany, Awais Altaf, Jaffar A Al-Tawfiq, Khalid A Altirkawi, Deborah Oyine Aluh, Nelson Alvis-Guzman, Hassan Alwafi, Yaser Mohammed Al-Worafi, Hany Aly, Safwat Aly, Karem H Alzoubi, Reza Amani, Azmeraw T Amare, Prince M Amegbor, Edward Kwabena Ameyaw, Tarek Tawfik Amin, Alireza Amindarolzarbi, Sohrab Amiri, Mohammad Hosein Amirzade-Iranaq, Hubert Amu, Dickson A Amugsi, Ganiyu Adeniyi Amusa, Robert Ancuceanu, Deanna Anderlini, David B Anderson, Pedro Prata Andrade, Catalina Liliana Andrei, Tudorel Andrei, Colin Angus, Abhishek Anil, Sneha Anil, Amir Anoushiravani, Hossein Ansari, Ansariadi Ansariadi, Alireza Ansari-Moghaddam, Catherine M Antony, Ernoiz Antriyandarti, Davood Anvari, Saeid Anvari, Saleha Anwar, Sumadi Lukman Anwar, Razique Anwer, Anayochukwu Edward Anyasodor, Muhammad Aqeel,
Juan Pablo Arab, Jalal Arabloo, Mosab Arafat, Aleksandr Y Aravkin, Demelash Areda, Abdulfatai Aremu, Olatunde Aremu, Hany Ariffin, Mesay Arkew, Benedetta Armocida, Michael Benjamin Arndt, Johan Ärnlöv, Mahwish Arooj, Anton A Artamonov, Judie Arulappan, Raphael Taiwo Aruleba, Ashokan Arumugam, Malke Asaad, Mohsen Asadi-Lari, Akeza Awealom Asgedom, Mona Asghariahmadabad, Mohammad Asghari-Jafarabadi, Muhammad Ashraf, Armin Aslani, Thomas Astell-Burt, Mohammad Athar, Seyyed Shamsadin Athari, Bantalem Tilaye Tilaye Atinafu, Habtamu Wondmagegn Atlaw, Prince Atorkey, Maha Moh’d Wahbi Atout, Alok Atreya, Avinash Aujayeb, Marcel Ausloos, Abolfazl Avan, Atalel Fentahun Awedew, Amlaku Mulat Aweke, Beatriz Paulina Ayala Quintanilla, Haleh Ayatollahi, Jose L Ayuso-Mateos, Seyed Mohammad Ayyoubzadeh, Sina Azadnajafabad, Rui M S Azevedo, Ahmed Y Azzam, Darshan B B, Abraham Samuel Babu, Muhammad Badar, Ashish D Badiye, Soroush Baghdadi, Nasser Bagheri, Sara Bagherieh, Sulaiman Bah, Saeed Bahadorikhalili, Najmeh Bahmanziari, Ruhai Bai, Atif Amin Baig, Jennifer L Baker, Abdulaziz T Bako, Ravleen Kaur Bakshi, Senthilkumar Balakrishnan, Madhan Balasubramanian, Ovidiu Constantin Baltatu, Kiran Bam, Maciej Banach, Soham Bandyopadhyay, Palash Chandra Banik, Hansi Bansal, Kannu Bansal, Franca Barbic, Martina Barchitta, Mainak Bardhan, Erfan Bardideh, Suzanne Lyn Barker-Collo, Till Winfried Bärnighausen, Francesco Barone-Adesi, Hiba Jawdat Barqawi, Lope H Barrero, Amadou Barrow, Sandra Barteit, Lingkan Barua, Zarrin Basharat, Azadeh Bashiri, Afisu Basiru, Pritish Baskaran, Buddha Basnyat, Quique Bassat, João Diogo Basso, Ann V L Basting, Sanjay Basu, Kavita Batra, Bernhard T Baune, Mohsen Bayati, Nebiyou Simegnew Bayileyegn, Thomas Beaney, Neeraj Bedi, Massimiliano Beghi, Emad Behboudi, Priyamadhaba Behera, Amir Hossein Behnoush, Masoud Behzadifar, Maryam Beiranvand, Diana Fernanda Bejarano Ramirez, Yannick Béjot, Sefealem Assefa Belay, Chalie Mulu Belete, Michelle L Bell, Muhammad Bashir Bello, Olorunjuwon Omolaja Bello, Luis Belo, Apostolos Beloukas, Rose Grace Bender, Isabela M Bensenor, Azizullah Beran, Zombor Berezvai, Alemshet Yirga Berhie, Betyna N Berice, Robert S Bernstein, Gregory J Bertolacci, Paulo J G Bettencourt, Kebede A Beyene, Devidas S Bhagat, Akshaya Srikanth Bhagavathula, Neeraj Bhala, Ashish Bhalla, Dinesh Bhandari, Kayleigh Bhangdia, Nikha Bhardwaj, Pankaj Bhardwaj, Prarthna V Bhardwaj, Ashish Bhargava, Sonu Bhaskar, Vivek Bhat, Gurjit Kaur Bhatti, Jasvinder Singh Bhatti, Manpreet S Bhatti, Rajbir Bhatti, Zulfiqar A Bhutta, Boris Bikbov, Jessica Devin Bishai, Catherine Bisignano, Francesca Bisulli, Atanu Biswas, Bijit Biswas, Saeid Bitaraf, Bikes Destaw Bitew, Veera R Bitra, Tone Bjørge, Micheal Kofi Boachie, Mary Sefa Boampong, Anca Vasilica Bobirca, Virginia Bodolica, Aadam Olalekan Bodunrin, Eyob Ketema Bogale, Kassawmar Angaw Bogale, Somayeh Bohlouli, Obasanjo Afolabi Bolarinwa, Archith Boloor, Milad Bonakdar Hashemi, Aime Bonny, Kaustubh Bora, Berrak Bora Basara, Hamed Borhany, Arturo Borzutzky, Souad Bouaoud, Antoine Boustany, Christopher Boxe, Edward J Boyko, Oliver J Brady, Dejana Braithwaite, Luisa C Brant, Michael Brauer, Alexandra Brazinova, Javier Brazo-Sayavera, Nicholas J K Breitborde, Susanne Breitner, Hermann Brenner, Andrey Nikolaevich Briko, Nikolay Ivanovich Briko, Gabrielle Britton, Julie Brown, Traolach Brugha, Norma B Bulamu, Lemma N Bulto, Danilo Buonsenso, Richard A Burns, Reinhard Busse, Yasser Bustanji, Nadeem Shafique Butt, Zahid A Butt, Florentino Luciano Caetano dos Santos, Daniela Calina, Luis Alberto Cámera, Luciana Aparecida Campos, Ismael R Campos-Nonato, Chao Cao, Yin Cao, Angelo Capodici, Rosario Cárdenas, Sinclair Carr, Giulia Carreras, Juan J Carrero, Andrea Carugno, Cristina G Carvalheiro, Felix Carvalho, Márcia Carvalho, Joao Mauricio Castaldelli-Maia, Carlos A Castañeda-Orjuela, Giulio Castelpietra, Ferrán Catalá-López, Alberico L Catapano, Maria Sofia Cattaruzza, Christopher R Cederroth, Luca Cegolon, Francieli Cembranel, Muthia Cenderadewi, Kelly M Cercy, Ester Cerin, Muge Cevik, Joshua Chadwick, Yaacoub Chahine, Chiranjib Chakraborty, Promit Ananyo Chakraborty, Jeffrey Shi Kai Chan, Raymond N C Chan, Rama Mohan Chandika,
Eeshwar K Chandrasekar, Chin-Kuo Chang, Jung-Chen Chang, Gashaw Sisay Chanie, Periklis Charalampous, Vijay Kumar Chattu, Pankaj Chaturvedi, Victoria Chatzimavridou-Grigoriadou, Akhilanand Chaurasia, Angela W Chen, An-Tian Chen, Catherine S Chen, Haowei Chen, Meng Xuan Chen, Simiao Chen, Ching-Yu Cheng, Esther T W Cheng, Nicolas Cherbuin, Wondimye Ashenafi Cheru, Ju-Huei Chien, Odgerel Chimed-Ochir, Ritesh Chimoriya, Patrick R Ching, Jesus Lorenzo Chirinos-Caceres, Abdulaal Chitheer, William C S Cho, Bryan Chong, Hitesh Chopra, Sonali Gajanan Choudhari, Rajiv Chowdhury, Devasahayam J Christopher, Isaac Sunday Chukwu, Eric Chung, Erin Chung, Eunice Chung, Sheng-Chia Chung, Muhammad Chutiyami, Zinhle Cindi, Iolanda Cioffi, Mareli M Claassens, Rafael M Claro, Kaleb Coberly, Rebecca M Cogen, Alyssa Columbus, Haley Comfort, Joao Conde, Samuele Cortese, Paolo Angelo Cortesi, Vera Marisa Costa, Simona Costanzo, Ewerton Cousin, Rosa A S Couto, Richard G Cowden, Kenneth Michael Cramer, Michael H Criqui, Natália Cruz-Martins, Silvia Magali Cuadra-Hernández, Garland T Culbreth, Patricia Cullen, Matthew Cunningham, Maria paula Curado, Sriharsha Dadana, Omid Dadras, Siyu Dai, Xiaochen Dai, Zhaoli Dai, Lachlan L Dalli, Giovanni Damiani, Jiregna Darega Gela, Jai K Das, Saswati Das, Subasish Das, Ana Maria Dascalu, Nihar Ranjan Dash, Mohsen Dashti, Anna Dastiridou, Gail Davey, Claudio Alberto Dávila-Cervantes, Nicole Davis Weaver, Kairat Davletov, Diego De Leo, Katie de Luca, Aklilu Tamire Debele, Shayom Debopadhaya, Louisa Degenhardt, Azizallah Dehghan, Lee Deitesfeld, Cristian Del Bo’, Ivan Delgado-Enciso, Berecha Hundessa Demessa, Andreas K Demetriades, Ke Deng, Xinlei Deng, Edgar Denova-Gutiérrez, Niloofar Deravi, Nebiyu Dereje, Nikolaos Dervenis, Emina Dervišević, Don C Des Jarlais, Hardik Dineshbhai Desai, Rupak Desai, Vinoth Gnana Chellaiyan Devanbu, Syed Masudur Rahman Dewan, Arkadeep Dhali, Kuldeep Dhama, Meghnath Dhimal, Sameer Dhingra, Vishal R Dhulipala, Diana Dias da Silva, Daniel Diaz, Michael J Diaz, Adriana Dima, Delaney D Ding, Huanghe Ding, Ricardo Jorge Dinis-Oliveira, M Ashworth Dirac, Shirin Djalalinia, Thao Huynh Phuong Do, Camila Bruneli do Prado, Saeid Doaei, Masoud Dodangeh, Milad Dodangeh, Sushil Dohare, Klara Georgieva Dokova, Christiane Dolecek, ReginaMae Villanueva Dominguez, Wanyue Dong, Deepa Dongarwar, Mario D’Oria, Fariba Dorostkar, E Ray Dorsey, Wendel Mombaque dos Santos, Rajkumar Doshi, Leila Doshmangir, Robert Kokou Dowou, Tim Robert Driscoll, Haneil Larson Dsouza, Viola Dsouza, Mi Du, John Dube, Bruce B Duncan, Andre Rodrigues Duraes, Senbagam Duraisamy, Oyewole Christopher Durojaiye, Laura DwyerLindgren, Paulina Agnieszka Dzianach, Arkadiusz Marian Dziedzic, Abdel Rahman E’mar, Ejemai Eboreime, Alireza Ebrahimi, Chidiebere Peter Echieh, Hisham Atan Edinur, David Edvardsson, Kristina Edvardsson, Defi Efendi, Ferry Efendi, Diyan Ermawan Effendi, Terje Andreas Eikemo, Ebrahim Eini, Michael Ekholuenetale, Temitope Cyrus Ekundayo, Iman El Sayed, Iffat Elbarazi, Teshome Bekele Elema, Noha Mousaad Elemam, Frank J Elgar, Islam Y Elgendy, Ghada Metwally Tawfik ElGohary, Hala Rashad Elhabashy, Muhammed Elhadi, Waseem El-Huneidi, Legesse Tesfaye Elilo, Omar Abdelsadek Abdou Elmeligy, Mohamed A Elmonem, Mohammed Elshaer, Ibrahim Elsohaby, Theophilus I Emeto, Luchuo Engelbert Bain, Ryenchindorj Erkhembayar, Christopher Imokhuede Esezobor, Babak Eshrati, Sharareh Eskandarieh, Juan Espinosa-Montero, Habtamu Esubalew, Farshid Etaee, Natalia Fabin, Adewale Oluwaseun Fadaka, Adeniyi Francis Fagbamigbe, Ayesha Fahim, Saman Fahimi, Aliasghar Fakhri-Demeshghieh, Luca Falzone, Mohammad Fareed, Carla Sofia e Sá Farinha, MoezAlIslam Ezzat Mahmoud Faris, Pawan Sirwan Faris, Andre Faro, Abidemi Omolara Fasanmi, Ali Fatehizadeh, Hamed Fattahi, Nelsensius Klau Fauk, Pooria Fazeli, Valery L Feigin, Alireza Feizkhah, Ginenus Fekadu, Xiaoru Feng, Seyed-Mohammad Fereshtehnejad, Abdullah Hamid Feroze, Daniela Ferrante, Alize J Ferrari, Nuno Ferreira, Getahun Fetensa, Bikila Regassa Feyisa, Irina Filip, Florian Fischer, Joanne Flavel, David Flood, Bobirca Teodor Florin, Nataliya A Foigt, Morenike Oluwatoyin Folayan,
Artem Alekseevich Fomenkov, Behzad Foroutan, Masoud Foroutan, Ingeborg Forthun, Daniela Fortuna, Matteo Foschi, Kayode Raphael Fowobaje, Kate Louise Francis, Richard Charles Franklin, Alberto Freitas, Joseph Friedman, Sara D Friedman, Takeshi Fukumoto, John E Fuller, Blima Fux, Peter Andras Gaal, Muktar A Gadanya, Abhay Motiramji Gaidhane, Santosh Gaihre, Emmanuela Gakidou, Yaseen Galali, Natalie C Galles, Silvano Gallus, Mandukhai Ganbat, Aravind P Gandhi, Balasankar Ganesan, Mohammad Arfat Ganiyani, MA Garcia-Gordillo, William M Gardner, Jalaj Garg, Naval Garg, Rupesh K Gautam, Semiu Olatunde Gbadamosi, Tilaye Gebru Gebi, Miglas W Gebregergis, Mesfin Gebrehiwot, Teferi Gebru Gebremeskel, Simona Roxana Georgescu, Tamirat Getachew, Peter W Gething, Molla Getie, Keyghobad Ghadiri, Sulmaz Ghahramani, Khalid Yaser Ghailan, Mohammad-Reza Ghasemi, Ghazal Ghasempour Dabaghi, Afsaneh Ghasemzadeh, Ahmad Ghashghaee, Fariba Ghassemi, Ramy Mohamed Ghazy, Ajnish Ghimire, Sama Ghoba, Maryam Gholamalizadeh, Asadollah Gholamian, Ali Gholamrezanezhad, Nasim Gholizadeh, Mahsa Ghorbani, Pooyan Ghorbani Vajargah, Aloke Gopal Ghoshal, Paramjit Singh Gill, Tiffany K Gill, Richard F Gillum, Themba G Ginindza, Alem Girmay, James C Glasbey, Elena V Gnedovskaya, Laszlo Göbölös, Myron Anthony Godinho, Amit Goel, Ali Golchin, Mohamad Goldust, Mahaveer Golechha, Pouya Goleij, Nelson G M Gomes, Philimon N Gona, Sameer Vali Gopalani, Giuseppe Gorini, Houman Goudarzi, Alessandra C Goulart, Bárbara Niegia Garcia Goulart, Anmol Goyal, Ayman Grada, Simon Matthew Graham, Michal Grivna, Giuseppe Grosso, Shi-Yang Guan, Giovanni Guarducci, Mohammed Ibrahim Mohialdeen Gubari, Mesay Dechasa Gudeta, Avirup Guha, Stefano Guicciardi, Rafael Alves Guimarães, Snigdha Gulati, Damitha Asanga Gunawardane, Sasidhar Gunturu, Cui Guo, Anish Kumar Gupta, Bhawna Gupta, Manoj Kumar Gupta, Mohak Gupta, Rajat Das Gupta, Rajeev Gupta, Sapna Gupta, Veer Bala Gupta, Vijai Kumar Gupta, Vivek Kumar Gupta, Lami Gurmessa, Reyna Alma Gutiérrez, Farrokh Habibzadeh, Parham Habibzadeh, Rasool Haddadi, Mostafa Hadei, Najah R Hadi, Nils Haep, Nima Hafezi-Nejad, Alemayehu Hailu, Arvin Haj-Mirzaian, Esam S Halboub, Brian J Hall, Sebastian Haller, Rabih Halwani, Randah R Hamadeh, Sajid Hameed, Samer Hamidi, Erin B Hamilton, Chieh Han, Qiuxia Han, Asif Hanif, Nasrin Hanifi, Graeme J Hankey, Fahad Hanna, Md Abdul Hannan, Md Nuruzzaman Haque, Harapan Harapan, Arief Hargono, Josep Maria Haro, Ahmed I Hasaballah, Ikramul Hasan, M Tasdik Hasan, Hamidreza Hasani, Mohammad Hasanian, Abdiwahab Hashi, Md Saquib Hasnain, Ikrama Hassan, Soheil Hassanipour, Hadi Hassankhani, Johannes Haubold, Rasmus J Havmoeller, Simon I Hay, Jiawei He, Jeffrey J Hebert, Omar E Hegazi, Golnaz Heidari, Mohammad Heidari, Mahsa Heidari-Foroozan, Bartosz Helfer, Delia Hendrie, Brenda Yuliana Herrera-Serna, Claudiu Herteliu, Hamed Hesami, Kamal Hezam, Catherine L Hill, Yuta Hiraike, Ramesh Holla, Nobuyuki Horita, Md Mahbub Hossain, Sahadat Hossain, Mohammad-Salar Hosseini, Hassan Hosseinzadeh, Mehdi Hosseinzadeh, Ahmad Hosseinzadeh Adli, Mihaela Hostiuc, Sorin Hostiuc, Mohamed Hsairi, Vivian Chia-rong Hsieh, Rebecca L Hsu, Chengxi Hu, Junjie Huang, Michael Hultström, Ayesha Humayun, Tsegaye Gebreyes Hundie, Javid Hussain, M Azhar Hussain, Nawfal R Hussein, Foziya Mohammed Hussien, Hong-Han Huynh, Bing-Fang Hwang, Segun Emmanuel Ibitoye, Khalid S Ibrahim, Pulwasha Maria Iftikhar, Desta Ijo, Adalia I Ikiroma, Kevin S Ikuta, Paul Chukwudi Ikwegbue, Olayinka Stephen Ilesanmi, Irena M Ilic, Milena D Ilic, Mohammad Tarique Imam, Mustapha Immurana, Sumant Inamdar, Endang Indriasih, Muhammad Iqhrammullah, Arnaud Iradukunda, Kenneth Chukwuemeka Iregbu, Md Rabiul Islam, Sheikh Mohammed Shariful Islam, Farhad Islami, Faisal Ismail, Nahlah Elkudssiah Ismail, Hiroyasu Iso, Gaetano Isola, Masao Iwagami, Chidozie C D Iwu, Ihoghosa Osamuyi Iyamu, Mahalaxmi Iyer, Linda Merin J, Jalil Jaafari, Louis Jacob, Kathryn H Jacobsen, Farhad Jadidi-Niaragh, Morteza Jafarinia, Abdollah Jafarzadeh, Khushleen Jaggi, Kasra Jahankhani, Nader Jahanmehr,
Haitham Jahrami, Nityanand Jain, Ammar Abdulrahman Jairoun, Abhishek Jaiswal, Elham Jamshidi, Mark M Janko, Abubakar Ibrahim Jatau, Sabzali Javadov, Tahereh Javaheri, Sathish Kumar Jayapal, Shubha Jayaram, Rime Jebai, Sun Ha Jee, Jayakumar Jeganathan, Anil K Jha, Ravi Prakash Jha, Heng Jiang, Yingzhao Jin, Olatunji Johnson, Mohammad Jokar, Jost B Jonas, Tamas Joo, Abel Joseph, Nitin Joseph, Charity Ehimwenma Joshua, Grace Joshy, Jacek Jerzy Jozwiak, Mikk Jürisson, Vaishali K, Billingsley Kaambwa, Ali Kabir, Zubair Kabir, Vidya Kadashetti, Dler Hussein Kadir, Rizwan Kalani, Laleh R Kalankesh, Leila R Kalankesh, Feroze Kaliyadan, Sanjay Kalra, Vineet Kumar Kamal, Sivesh Kathir Kamarajah, Rajesh Kamath, Zahra Kamiab, Naser Kamyari, Thanigaivelan Kanagasabai, Tanuj Kanchan, Himal Kandel, Arun R Kanmanthareddy, Edmund Wedam Kanmiki, Kehinde Kazeem Kanmodi, Suthanthira Kannan S, Sushil Kumar Kansal, Rami S Kantar, Neeti Kapoor, Mehrdad Karajizadeh, Shama D Karanth, Reema A Karasneh, Ibraheem M Karaye, André Karch, Asima Karim, Salah Eddin Karimi, Arman Karimi Behnagh, Faizan Zaffar Kashoo, Qalandar Hussein Abdulkarim Kasnazani, Hengameh Kasraei, Nicholas J Kassebaum, Molly B Kassel, Joonas H Kauppila, Navjot Kaur, Norito Kawakami, Gbenga A Kayode, Foad Kazemi, Sina Kazemian, Tahseen Haider Kazmi, Getu Mosisa Kebebew, Adera Debella Kebede, Fassikaw Kebede, Tibebeselassie S Keflie, Peter Njenga Keiyoro, Cathleen Keller, Jaimon Terence Kelly, John H Kempen, Jessica A Kerr, Emmanuelle Kesse-Guyot, Himanshu Khajuria, Amirmohammad Khalaji, Nauman Khalid, Anees Ahmed Khalil, Alireza Khalilian, Faham Khamesipour, Ajmal Khan, Asaduzzaman Khan, Gulfaraz Khan, Ikramullah Khan, Imteyaz A Khan, M Nuruzzaman Khan, Maseer Khan, Mohammad Jobair Khan, Moien AB Khan, Zeeshan Ali Khan, Mahammed Ziauddin Khan suheb, Shaghayegh Khanmohammadi, Khaled Khatab, Fatemeh Khatami, Haitham Khatatbeh, Moawiah Mohammad Khatatbeh, Armin Khavandegar, Hamid Reza Khayat Kashani, Feriha Fatima Khidri, Elaheh Khodadoust, Mohammad Khorgamphar, Moein Khormali, Zahra Khorrami, Ahmad Khosravi, Mohammad Ali Khosravi, Zemene Demelash Kifle, Grace Kim, Jihee Kim, Kwanghyun Kim, Min Seo Kim, Yun Jin Kim, Ruth W Kimokoti, Kasey E Kinzel, Adnan Kisa, Sezer Kisa, Desmond Klu, Ann Kristin Skrindo Knudsen, Jonathan M Kocarnik, Sonali Kochhar, Timea Kocsis, David S Q Koh, Ali-Asghar Kolahi, Kairi Kolves, Farzad Kompani, Gerbrand Koren, Soewarta Kosen, Karel Kostev, Parvaiz A Koul, Sindhura Lakshmi Koulmane Laxminarayana, Kewal Krishan, Hare Krishna, Varun Krishna, Vijay Krishnamoorthy, Yuvaraj Krishnamoorthy, Kris J Krohn, Barthelemy Kuate Defo, Burcu Kucuk Bicer, Md Abdul Kuddus, Mohammed Kuddus, Ilari Kuitunen, Mukhtar Kulimbet, Vishnutheertha Kulkarni, Akshay Kumar, Ashish Kumar, Harish Kumar, Manasi Kumar, Rakesh Kumar, Madhulata Kumari, Fantahun Tarekegn Kumie, Satyajit Kundu, Om P Kurmi, Asep Kusnali, Dian Kusuma, Alexander Kwarteng, Ilias Kyriopoulos, Hmwe Hmwe Kyu, Carlo La Vecchia, Ben Lacey, Muhammad Awwal Ladan, Lucie Laflamme, Abraham K Lagat, Anton C J Lager, Abdelilah Lahmar, Daphne Teck Ching Lai, Dharmesh Kumar Lal, Ratilal Lalloo, Tea Lallukka, Hilton Lam, Judit Lám, Kelsey R Landrum, Francesco Lanfranchi, Justin J Lang, Berthold Langguth, Van Charles Lansingh, Ariane Laplante-Lévesque, Bagher Larijani, Anders O Larsson, Savita Lasrado, Zohra S Lassi, Kamaluddin Latief, Kaveh Latifinaibin, Paolo Lauriola, Nhi Huu Hanh Le, Thao Thi Thu Le, Trang Diep Thanh Le, Caterina Ledda, Jorge R Ledesma, Munjae Lee, Paul H Lee, Seung Won Lee, Shaun Wen Huey Lee, Wei-Chen Lee, Yo Han Lee, Kate E LeGrand, James Leigh, Elvynna Leong, Temesgen L Lerango, Ming-Chieh Li, Wei Li, Xiaopan Li, Yichong Li, Zhihui Li, Virendra S Ligade, Andrew Tiyamike Makhiringa Likaka, Lee-Ling Lim, Stephen S Lim, Megan Lindstrom, Christine Linehan, Chaojie Liu, Gang Liu, Jue Liu, Runben Liu, Shiwei Liu, Xiaofeng Liu, Xuefeng Liu, Erand Llanaj, Michael J Loftus, Rubén López-Bueno, Platon D Lopukhov, Arianna Maever Loreche, Stefan Lorkowski, Paulo A Lotufo, Rafael Lozano, Jailos Lubinda, Giancarlo Lucchetti, Alessandra Lugo, Raimundas Lunevicius, Zheng Feei Ma, Kelsey Lynn Maass, Nikolaos Machairas, Monika Machoy, Farzan Madadizadeh, Christian Madsen, Áurea M Madureira-Carvalho,
Azzam A Maghazachi, Sandeep B Maharaj, Soleiman Mahjoub, Mansour Adam Mahmoud, Alireza Mahmoudi, Elham Mahmoudi, Razzagh Mahmoudi, Azeem Majeed, Irsa Fatima Makhdoom, Elaheh Malakan Rad, Venkatesh Maled, Reza Malekzadeh, Armaan K Malhotra, Kashish Malhotra, Ahmad Azam Malik, Iram Malik, Deborah Carvalho Malta, Abdullah A Mamun, Pejman Mansouri, Mohammad Ali Mansournia, Lorenzo Giovanni Mantovani, Sajid Maqsood, Bishnu P Marasini, Hamid Reza Marateb, Joemer C Maravilla, Agustina M Marconi, Parham Mardi, Mirko Marino, Abdoljalal Marjani, Gabriel Martinez, Bernardo Alfonso Martinez-Guerra, Ramon Martinez-Piedra, Daniela Martini, Santi Martini, Francisco Rogerlândio Martins-Melo, Miquel Martorell, Wolfgang Marx, Sharmeen Maryam, Roy Rillera Marzo, Anthony Masaka, Awoke Masrie, Stephanie Mathieson, Alexander G Mathioudakis, Manu Raj Mathur, Jishanth Mattumpuram, Richard Matzopoulos, Richard James Maude, Andrea Maugeri, Pallab K Maulik, Mahsa Mayeli, Maryam Mazaheri, Mohsen Mazidi, John J McGrath, Martin McKee, Anna Laura W McKowen, Susan A McLaughlin, Steven M McPhail, Enkeleint A Mechili, John Robert Carabeo Medina, Rishi P Mediratta, Jitendra Kumar Meena, Rahul Mehra, Kamran Mehrabani-Zeinabad, Entezar Mehrabi Nasab, Tesfahun Mekene Meto, Gebrekiros Gebremichael Meles, Max Alberto Mendez Mendez-Lopez, Walter Mendoza, Ritesh G Menezes, Belayneh Mengist, Alexios-Fotios A Mentis, Sultan Ayoub Meo, Haftu Asmerom Meresa, Atte Meretoja, Tuomo J Meretoja, Abera M Mersha, Bezawit Afework Mesfin, Tomislav Mestrovic, Kukulege Chamila Dinushi Mettananda, Sachith Mettananda, Peter Meylakhs, Adquate Mhlanga, Laurette Mhlanga, Tianyue Mi, Tomasz Miazgowski, Georgia Micha, Irmina Maria Michalek, Ted R Miller, Edward J Mills, Le Huu Nhat Minh, GK Mini, Pouya Mir Mohammad Sadeghi, Andreea Mirica, Antonio Mirijello, Erkin M Mirrakhimov, Mizan Kiros Mirutse, Maryam Mirzaei, Awoke Misganaw, Ashim Mishra, Sanjeev Misra, Philip B Mitchell, Prasanna Mithra, Chaitanya Mittal, Mohammadreza Mobayen, Madeline E Moberg, Ashraf Mohamadkhani, Jama Mohamed, Mouhand F H Mohamed, Nouh Saad Mohamed, Sakineh Mohammad-Alizadeh-Charandabi, Soheil Mohammadi, Abdollah Mohammadian-Hafshejani, Noushin Mohammadifard, Hassen Mohammed, Hussen Mohammed, Mustapha Mohammed, Salahuddin Mohammed, Shafiu Mohammed, Viswanathan Mohan, Hoda Mojiri-Forushani, Amin Mokari, Ali H Mokdad, Sabrina Molinaro, Mariam Molokhia, Sara Momtazmanesh, Lorenzo Monasta, Stefania Mondello, Mohammad Ali Moni, AmirAli Moodi Ghalibaf, Maryam Moradi, Yousef Moradi, Maziar Moradi-Lakeh, Maliheh Moradzadeh, Paula Moraga, Lidia Morawska, Rafael Silveira Moreira, Negar Morovatdar, Shane Douglas Morrison, Jakub Morze, Jonathan F Mosser, Rohith Motappa, Vincent Mougin, Simin Mouodi, Parsa Mousavi, Seyed Ehsan Mousavi, Amin Mousavi Khaneghah, Emmanuel A Mpolya, Matías Mrejen, Sumaira Mubarik, Lorenzo Muccioli, Ulrich Otto Mueller, Faraz Mughal, Sumoni Mukherjee, Francesk Mulita, Kavita Munjal, Efrén Murillo-Zamora, Fungai Musaigwa, Khaled M Musallam, Ahmad Mustafa, Ghulam Mustafa, Saravanan Muthupandian, Raman Muthusamy, Muhammad Muzaffar, Woojae Myung, Ahamarshan Jayaraman Nagarajan, Gabriele Nagel, Pirouz Naghavi, Aliya Naheed, Ganesh R Naik, Gurudatta Naik, Firzan Nainu, Sanjeev Nair, Hastyar Hama Rashid Najmuldeen, Noureddin Nakhostin Ansari, Vinay Nangia, Atta Abbas Naqvi, Sreenivas Narasimha Swamy, Aparna Ichalangod Narayana, Shumaila Nargus, Bruno Ramos Nascimento, Gustavo G Nascimento, Samar Nasehi, Abdulqadir J Nashwan, Zuhair S Natto, Javaid Nauman, Muhammad Naveed, Biswa Prakash Nayak, Vinod C Nayak, Athare Nazri-Panjaki, Rawlance Ndejjo, Sabina Onyinye Nduaguba, Hadush Negash, Ionut Negoi, Ruxandra Irina Negoi, Serban Mircea Negru, Seyed Aria Nejadghaderi, Chakib Nejjari, Evangelia Nena, Samata Nepal, Marie Ng, Haruna Asura Nggada, Georges Nguefack-Tsague, Josephine W Ngunjiri, Anh Hoang Nguyen, Dang H Nguyen, Hau Thi Hien Nguyen, Phat Tuan Nguyen, Van Thanh Nguyen, Robina Khan Niazi, Katie R Nielsen, Yeshambel T Nigatu, Taxiarchis Konstantinos Nikolouzakis, Ali Nikoobar, Fatemeh Nikoomanesh, Amin Reza Nikpoor,
Dina Nur Anggraini Ningrum, Chukwudi A Nnaji, Lawrence Achilles Nnyanzi, Efaq Ali Noman, Shuhei Nomura, Mamoona Noreen, Nafise Noroozi, Bo Norrving, Jean Jacques Noubiap, Amanda Novotney, Chisom Adaobi Nri-Ezedi, George Ntaios, Mpiko Ntsekhe, Virginia Nuñez-Samudio, Dieta Nurrika, Jerry John Nutor, Bogdan Oancea, Kehinde O Obamiro, Mary Aigbiremo Oboh, Ismail A Odetokun, Nkechi Martina Odogwu, Martin James O’Donnell, Michael Safo Oduro, Akinyemi O D Ofakunrin, Abiola Ogunkoya, Ayodipupo Sikiru Oguntade, In-Hwan Oh, Hassan Okati-Aliabad, Sylvester Reuben Okeke, Akinkunmi Paul Okekunle, Osaretin Christabel Okonji, Andrew T Olagunju, Muideen Tunbosun Olaiya, Matthew Idowu Olatubi, Gláucia Maria Moraes Oliveira, Isaac Iyinoluwa Olufadewa, Bolajoko Olubukunola Olusanya, Jacob Olusegun Olusanya, Yinka Doris Oluwafemi, Hany A Omar, Ahmed Omar Bali, Goran Latif Omer, Maureene Auma Ondayo, Sokking Ong, Obinna E Onwujekwe, Kenneth Ikenna Onyedibe, Michal Ordak, Orish Ebere Orisakwe, Verner N Orish, Doris V Ortega-Altamirano, Alberto Ortiz, Wael M S Osman, Samuel M Ostroff, Uchechukwu Levi Osuagwu, Adrian Otoiu, Nikita Otstavnov, Stanislav S Otstavnov, Amel Ouyahia, Guoqing Ouyang, Mayowa O Owolabi, Yaz Ozten, Mahesh Padukudru P A, Alicia Padron-Monedero, Jagadish Rao Padubidri, Pramod Kumar Pal, Tamás Palicz, Claudia Palladino, Raffaele Palladino, Raul Felipe Palma-Alvarez, Feng Pan, Hai-Feng Pan, Adrian Pana, Paramjot Panda, Songhomitra Panda-Jonas, Seithikurippu R Pandi-Perumal, Helena Ullyartha Pangaribuan, Georgios D Panos, Leonidas D Panos, Ioannis Pantazopoulos, Anca Mihaela Pantea Stoian, Paraskevi Papadopoulou, Romil R Parikh, Seoyeon Park, Ashwaghosha Parthasarathi, Ava Pashaei, Maja Pasovic, Roberto Passera, Deepak Kumar Pasupula, Hemal M Patel, Jay Patel, Sangram Kishor Patel, Shankargouda Patil, Dimitrios Patoulias, Venkata Suresh Patthipati, Uttam Paudel, Hamidreza Pazoki Toroudi, Spencer A Pease, Amy E Peden, Paolo Pedersini, Umberto Pensato, Veincent Christian Filipino Pepito, Emmanuel K Peprah, Prince Peprah, João Perdigão, Marcos Pereira, Mario F P Peres, Arokiasamy Perianayagam, Norberto Perico, Richard G Pestell, Konrad Pesudovs, Fanny Emily Petermann-Rocha, William A Petri, Hoang Tran Pham, Anil K Philip, Michael R Phillips, Daniela Pierannunzio, Manon Pigeolet, David M Pigott, Thomas Pilgrim, Zahra Zahid Piracha, Michael A Piradov, Saeed Pirouzpanah, Nishad Plakkal, Evgenii Plotnikov, Vivek Podder, Dimitri Poddighe, Suzanne Polinder, Kevan R Polkinghorne, Ramesh Poluru, Ville T Ponkilainen, Fabio Porru, Maarten J Postma, Govinda Raj Poudel, Akram Pourshams, Naeimeh Pourtaheri, Sergio I Prada, Pranil Man Singh Pradhan, Thejeswar N Prakasham, Manya Prasad, Akila Prashant, Elton Junio Sady Prates, Daniel Prieto Alhambra, TINA PRISCILLA, Natalie Pritchett, Bharathi M Purohit, Jagadeesh Puvvula, Nameer Hashim Qasim, Ibrahim Qattea, Asma Saleem Qazi, Gangzhen Qian, Suli Qiu, Maryam Faiz Qureshi, Mehrdad Rabiee Rad, Amir Radfar, Raghu Anekal Radhakrishnan, Venkatraman Radhakrishnan, Hadi Raeisi Shahraki, Quinn Rafferty, Alberto Raggi, Pankaja Raghav Raghav, Nasiru Raheem, Fakher Rahim, Md Jillur Rahim, Vafa Rahimi-Movaghar, Md Mosfequr Rahman, Mohammad Hifz Ur Rahman, Mosiur Rahman, Muhammad Aziz Rahman, Amir Masoud Rahmani, Shayan Rahmani, Vahid Rahmanian, Sathish Rajaa, Prashant Rajput, Ivo Rakovac, Shakthi Kumaran Ramasamy, Sheena Ramazanu, Kritika Rana, Chhabi Lal Ranabhat, Nemanja Rancic, Amey Rane, Chythra R Rao, Indu Ramachandra Rao, Mithun Rao, Sowmya J Rao, Drona Prakash Rasali, Davide Rasella, Sina Rashedi, Vahid Rashedi, Mohammad-Mahdi Rashidi, Ashkan Rasouli-Saravani, Azad Rasul, Giridhara Rathnaiah Babu, Santosh Kumar Rauniyar, Ramin Ravangard, Nakul Ravikumar, David Laith Rawaf, Salman Rawaf, Lal Rawal, Reza Rawassizadeh, Bharat Rawlley, Rabail Zehra Raza, Christian Razo, Elrashdy Moustafa Mohamed Redwan, Faizan Ur Rehman, Lennart Reifels, Robert C Reiner Jr, Giuseppe Remuzzi, Luis Felipe Reyes, Maryam Rezaei, Nazila Rezaei, Negar Rezaei, Mohsen Rezaeian, Taeho Gregory Rhee, Mavra A Riaz,
Antonio Luiz P Ribeiro, Jennifer Rickard, Hannah R Riva, Hannah Elizabeth Robinson-Oden, Célia Fortuna Rodrigues, Mónica Rodrigues, Leonardo Roever, Emma Lynn Best Rogowski, Peter Rohloff, Debby Syahru Romadlon, Esperanza Romero-Rodríguez, Michele Romoli, Luca Ronfani, Gholamreza Roshandel, Gregory A Roth, Himanshu Sekhar Rout, Nitai Roy, Priyanka Roy, Enrico Rubagotti, Guilherme de Andrade Ruela, Susan Fred Rumisha, Tilleye Runghien, Godfrey M Rwegerera, Andrzej Rynkiewicz, Chandan S N, Aly M A Saad, Zahra Saadatian, Korosh Saber, Maha Mohamed Saber-Ayad, Morteza SaberiKamarposhti, Siamak Sabour, Simona Sacco, Perminder S Sachdev, Rajesh Sachdeva, Basema Saddik, Adam Saddler, Bashdar Abuzed Sadee, Ehsan Sadeghi, Erfan Sadeghi, Farideh Sadeghian, Mohammad Reza Saeb, Umar Saeed, Fahimeh Safaeinejad, Sher Zaman Safi, Rajesh Sagar, Amene Saghazadeh, Dominic Sagoe, Fatemeh Saheb Sharif-Askari, Narjes Saheb Sharif-Askari, Amirhossein Sahebkar, Soumya Swaroop Sahoo, Umakanta Sahoo, Monalisha Sahu, Zahra Saif, Mirza Rizwan Sajid, Joseph W Sakshaug, Nasir Salam, Payman Salamati, Afeez Abolarinwa Salami, Luciane B Salaroli, Mohamed A Saleh, Sana Salehi, Marwa Rashad Salem, Mohammed Z Y Salem, Sohrab Salimi, Hossein Samadi Kafil, Sara Samadzadeh, Saad Samargandy, Yoseph Leonardo Samodra, Abdallah M Samy, Juan Sanabria, Francesca Sanna, Damian Francesco Santomauro, Itamar S Santos, Milena M Santric-Milicevic, Bruno Piassi Sao Jose, Made Ary Sarasmita, Sivan Yegnanarayana Iyer Saraswathy, Aswini Saravanan, Babak Saravi, Yaser Sarikhani, Tanmay Sarkar, Rodrigo Sarmiento-Suárez, Gargi Sachin Sarode, Sachin C Sarode, Arash Sarveazad, Brijesh Sathian, Thirunavukkarasu Sathish, Maheswar Satpathy, Abu Sayeed, Md Abu Sayeed, Mete Saylan, Mehdi Sayyah, Nikolaos Scarmeas, Benedikt Michael Schaarschmidt, Markus P Schlaich, Winfried Schlee, Maria Inês Schmidt, Ione Jayce Ceola Schneider, Art Schuermans, Austin E Schumacher, Aletta Elisabeth Schutte, Michaël Schwarzinger, David C Schwebel, Falk Schwendicke, Mario Šekerija, Siddharthan Selvaraj, Sabyasachi Senapati, Subramanian Senthilkumaran, Sadaf G Sepanlou, Dragos Serban, Yashendra Sethi, Feng Sha, Maryam Shabany, Amir Shafaat, Mahan Shafie, Nilay S Shah, Pritik A Shah, Syed Mahboob Shah, Saeed Shahabi, Ataollah Shahbandi, Izza Shahid, Samiah Shahid, Wajeehah Shahid, Hamid R Shahsavari, Moyad Jamal Shahwan, Ahmed Shaikh, Masood Ali Shaikh, Alireza Shakeri, Ali S Shalash, Sunder Sham, Muhammad Aaqib Shamim, Mehran Shams-Beyranvand, Hina Shamshad, Mohammad Anas Shamsi, Mohd Shanawaz, Abhishek Shankar, Sadaf Sharfaei, Amin Sharifan, Javad Sharifi-Rad, Rajesh Sharma, Saurab Sharma, Ujjawal Sharma, Vishal Sharma, Rajesh P Shastry, Amin Shavandi, Maryam Shayan, Amr Mohamed Elsayed Shehabeldine, Aziz Sheikh, Rahim Ali Sheikhi, Jiabin Shen, Adithi Shetty, B Suresh Kumar Shetty, Pavanchand H Shetty, Peilin Shi, Kenji Shibuya, Desalegn Shiferaw, Mika Shigematsu, Min-Jeong Shin, Youn Ho Shin, Rahman Shiri, Reza Shirkoohi, Nebiyu Aniley Shitaye, Aminu Shittu, Ivy Shiue, K M Shivakumar, Velizar Shivarov, Farhad Shokraneh, Azad Shokri, Sina Shool, Seyed Afshin Shorofi, Sunil Shrestha, Kerem Shuval, Emmanuel Edwar Siddig, João Pedro Silva, Luís Manuel Lopes Rodrigues Silva, Soraia Silva, Colin R Simpson, Anjali Singal, Abhinav Singh, Balbir Bagicha Singh, Garima Singh, Jasbir Singh, Narinder Pal Singh, Paramdeep Singh, Surjit Singh, Dhirendra Narain Sinha, Robert Sinto, Md Shahjahan Siraj, Sarah Brooke Sirota, Freddy Sitas, Shravan Sivakumar, Valentin Yurievich Skryabin, Anna Aleksandrovna Skryabina, David A Sleet, Bogdan Socea, Anton Sokhan, Ranjan Solanki, Shipra Solanki, Hamidreza Soleimani, Sameh S M Soliman, Suhang Song, Yimeng Song, Reed J D Sorensen, Joan B Soriano, Ireneous N Soyiri, Michael Spartalis, Sandra Spearman, Chandrashekhar T Sreeramareddy, Vijay Kumar Srivastava, Jeffrey D Stanaway, Muhammad Haroon Stanikzai, Benjamin A Stark, Joseph R Starnes, Antonina V Starodubova, Caroline Stein, Dan J Stein, Fridolin Steinbeis, Caitlyn Steiner, Jaimie D Steinmetz, Paschalis Steiropoulos, Aleksandar Stevanović, Leo Stockfelt, Mark A Stokes, Stefan Stortecky, Vetriselvan Subramaniyan, Muhammad Suleman, Rizwan Suliankatchi Abdulkader, Abida Sultana,
Articles
See Online for appendix 3
Haitong Zhe Sun, Jing Sun, Johan Sundström, David Sunkersing, Katharina S Sunnerhagen, Chandan Kumar Swain, Lukasz Szarpak, Mindy D Szeto, Miklós Szócska, Payam Tabaee Damavandi, Rafael Tabarés-Seisdedos, Seyyed Mohammad Tabatabaei, Ozra Tabatabaei Malazy, Seyed-Amir Tabatabaeizadeh, Shima Tabatabai, Mohammad Tabish, Jyothi Tadkamadla, Santosh Kumar Tadakamadla, Yasaman Taheri Abkenar, Moslem Taheri Soodejani, Jabeen Taiba, Ken Takahashi, Iman M Talaat, Ashis Talukder, Mircea Tampa, Jacques Lukenze Tamuzi, Ker-Kan Tan, Sarmila Tandukar, Haosu Tang, Hong K Tang, Ingan Ukur Tarigan, Mengistie Kassahun Tariku, Md Tariqujjaman, Elvis Enowbeyang Tarkang, Razieh Tavakoli Oliaee, Seyed Mohammad Tavangar, Nuno Taveira, Yibekal Manaye Tefera, Mohamad-Hani Temsah, Reem Mohamad Hani Temsah, Masayuki Teramoto, Riki Tesler, Enoch Teye-Kwadjo, Rishu Thakur, Pugazhenthan Thangaraju, Kavumpurathu Raman Thankappan, Samar Tharwat, Rasiah Thayakaran, Nihal Thomas, Nikhil Kenny Thomas, Azalea M Thomson, Amanda G Thrift, Chern Choong Chern Thum, Lau Caspar Thygesen, Jing Tian, Ales Tichopad, Jansje Henny Vera Ticoalu, Tala Tillawi, Tenaw Yimer Tiruye, Mariya Vladimirovna Titova, Marcello Tonelli, Roman Topor-Madry, Adetunji T Toriola, Anna E Torre, Mathilde Touvier, Marcos Roberto Tovani-Palone, Jasmine T Tran, Nghia Minh Tran, Domenico Trico, Samuel Joseph Tromans, Thien Tan Tri Tai Truyen, Aristidis Tsatsakis, Guesh Mebrahtom Tsegay, Evangelia Eirini Tsermpini, Munkhtuya Tumurkhuu, Kang Tung, Stefanos Tyrovolas, Sayed Mohammad Nazim Uddin, Aniefiok John Udoakang, Arit Udoh, Atta Ullah, Irfan Ullah, Saeed Ullah, Sana Ullah, Srikanth Umakanthan, Chukwuma David Umeokonkwo, Brigid Unim, Bhaskaran Unnikrishnan, Carolyn Anne Unsworth, Era Upadhyay, Daniele Urso, Jibrin Sammani Usman, Seyed Mohammad Vahabi, Asokan Govindaraj Vaithinathan, Rohollah Valizadeh, Sarah M Van de Velde, Jef Van den Eynde, Orsolya Varga, Priya Vart, Shoban Babu Varthya, Tommi Juhani Vasankari, Milena Vasic, Siavash Vaziri, Balachandar Vellingiri, Narayanaswamy Venketasubramanian, Nicholas Alexander Verghese, Madhur Verma, Massimiliano Veroux, Georgios-Ioannis Verras, Dominique Vervoort, Jorge Hugo Villafañe, Gabriela Ines Villanueva, Manish Vinayak, Francesco S Violante, Maria Viskadourou, Sergey Konstantinovitch Vladimirov, Vasily Vlassov, Bay Vo, Stein Emil Vollset, Avina Vongpradith, Theo Vos, Isidora S Vujcic, Rade Vukovic, Hatem A Wafa, Yasir Waheed, Richard G Wamai, Cong Wang, Ning Wang, Shu Wang, Song Wang, Yanzhong Wang, Yuan-Pang Wang, Muhammad Waqas, Paul Ward, Emebet Gashaw Wassie, Stefanie Watson, Stephanie Louise Watson Watson, Kosala Gayan Weerakoon, Melissa Y Wei, Robert G Weintraub, Daniel J Weiss, Ronny Westerman, Joanna L Whisnant, Taweewat Wiangkham, Dakshitha Praneeth Wickramasinghe, Nuwan Darshana Wickramasinghe, Angga Wilandika, Caroline Wilkerson, Peter Willeit, Shadrach Wilson, Marcin W Wojewodzic, Demewoz H Woldegebreal, Axel Walter Wolf, Charles D A Wolfe, Yohannes Addisu Wondimagegene, Yen Jun Wong, Utoomporn Wongsin, Ai-Min Wu, Chenkai Wu, Felicia Wu, Xinsheng Wu, Zenghong Wu, Juan Xia, Hong Xiao, Yang Xie, Suowen Xu, Wang-Dong Xu, Xiaoyue Xu, Yvonne Yiru Xu, Ali Yadollahpour, Kazumasa Yamagishi, Danting Yang, Lin Yang, Yuichiro Yano, Yao Yao, Habib Yaribeygi, Pengpeng Ye, Sisay Shewasinad Yehualashet, Metin Yesiltepe, Subah Abderehim Yesuf, Saber Yezli, Siyan Yi, Amanuel Yigezu, Arzu Yiğit, Vahit Yiğit, Paul Yip, Malede Berihun Yismaw, Yazachew Yismaw, Dong Keon Yon, Naohiro Yonemoto, Seok-Jun Yoon, Yuyi You, Mustafa Z Younis, Zabihollah Yousefi, Chuanhua Yu, Yong Yu, Faith H Yuh, Siddhesh Zadey, Vesna Zadnik, Nima Zafari, Fathiah Zakham, Nazar Zaki, Sojib Bin Zaman, Nelson Zamora, Ramin Zand, Moein Zangiabadian, Heather J Zar, Iman Zare, Armin Zarrintan, Mohammed G M Zeariya, Zahra Zeinali, Haijun Zhang, Jianrong Zhang, Jingya Zhang, Liqun Zhang, Yunquan Zhang, ZhiJiang Zhang, Hanqing Zhao, Chenwen Zhong, Juexiao Zhou, Bin Zhu, Lei Zhu, Makan Ziafati, Magdalena Zielińska, Osama A Zitoun, Mohammad Zoladl, Zhiyong Zou, Liesl J Zuhlke, Alimuddin Zumla,
Elric Zweck, Samer H Zyoud, Eve E Wool†, and Christopher J L Murray
*Joint first authors.
Affiliations
For list of collaborator affiliations see appendix 3
Contributors
Please see appendix 1 section 10 for more detailed information about individual author contributions to the research, divided into the following categories: managing the overall research enterprise; writing the first draft of the manuscript; primary responsibility for applying analytical methods to produce estimates; primary responsibility for seeking, cataloguing, extracting, or cleaning data; designing or coding figures and tables; providing data or critical feedback on data sources; developing methods or computational machinery; providing critical feedback on methods or results; drafting the manuscript or revising it critically for important intellectual content; and managing the estimation or publications process. The lead, corresponding, and senior authors had full access to the data in the study and had final responsibility for the decision to submit for publication.
*Joint first authors.
Affiliations
For list of collaborator affiliations see appendix 3
Contributors
Please see appendix 1 section 10 for more detailed information about individual author contributions to the research, divided into the following categories: managing the overall research enterprise; writing the first draft of the manuscript; primary responsibility for applying analytical methods to produce estimates; primary responsibility for seeking, cataloguing, extracting, or cleaning data; designing or coding figures and tables; providing data or critical feedback on data sources; developing methods or computational machinery; providing critical feedback on methods or results; drafting the manuscript or revising it critically for important intellectual content; and managing the estimation or publications process. The lead, corresponding, and senior authors had full access to the data in the study and had final responsibility for the decision to submit for publication.
Declaration of interests
S Afzal reports support for the present manuscript from King Edward Medical University including study material, research articles, valid data sources and authentic real time information for this manuscript; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from King Edward Medical University and collaborative partners including University of Johns Hopkins, University of California, University of Massachusetts, KEMCAANA, KEMCA-UK Scientific Conferences and Webinars; support for attending meetings and/or travel from King Edward Medical University to attend meetings; participation on a Data Safety Monitoring Board or Advisory Board with National Bioethics Committee Pakistan, King Edward Medical University Ethical Review Board, as well as Ethical Review Board Fatima Jinnah Medical University and Sir Ganga Ram Hospital; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with Pakistan Association of Medical Editors, Fellow of Faculty of Public Health Royal Colleges UK (FFPH), and Society of Prevention, Advocacy And Research, King Edward Medical University (SPARK); and other support as Dean of Public Health and Preventive Medicine at King Edward Medical University, as the Chief Editor Annals of King Edward Medical University, as the Director of Quality Enhancement Cell King Edward Medical University, as an international-level Fellow of Faculty of Public Health United Kingdom, as an Advisory Board Member and Chair Scientific Session KEMCA-UK, as a Chairperson of KEMCAANA (the International Scientific Conference), as a national-level member on the Research and Publications Higher Education Commission (HEC Pakistan), as a member of the Research and Journals Committee (Pakistan) the Medical and Dental Council (Pakistan), the National Bioethics Committee (Pakistan), the Corona Experts Advisory Group (Punjab), the Chair of the Dengue Experts Advisory Group, and a member of the Punjab Residency Program Research Committee; all outside the submitted work. R Ancuceanu reports consulting fees from Abbvie; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Abbvie, Sandoz, B. Braun, Laropharm, and MagnaPharm; all outside the submitted work. J Ärnlöv reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from AstraZeneca and Novartis for lecture fees; participation on a Data Safety Monitoring Board or Advisory Board with AstraZeneca, Astella, Boehringer Ingelheim; all outside the submitted work. O C Baltatu reports support for the present manuscript from National Council for Scientific and Technological Development (CNPq, 304224/2022-7) and Anima Institute (AI research professor fellowship); Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, as Founding Member of the Health and Biotechnology Advisory Board at Technology Park São José dos Campos-Center for Innovation in Health Technologies (CITS), outside the submitted work. T W Bärnighausen reports grants or contracts from National Institutes of Health, Alexander von Humboldt Foundation, German National Research Foundation (DFG), European
Union, German Ministry of Education and Research, German Ministry of the Environment, Wellcome, and KfW, all as payments to their institution; participation on a Data Safety Monitoring Board or Advisory Board on two Scientific Advisory Boards for NIH-funded research projects in Africa on Climate Change and Health; stock or stock options in CHEERS, an SME focusing on approaches to measure climate change and health-related variables in population cohorts; all outside the submitted work. S Barteit reports grants from Carl-Zeiss Foundation and the German research foundation (DFG); stock or stock options in CHEERS, a for-profit company focusing on climate change and health evaluation and response systems; all outside the submitted work. M Beghi reports consulting fees from Lundbeck and Angelini, all outside the submitted work. Y Bejot reports consulting fees from Medtronic and Novartis; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from BMS, Pfizer, Medtronic, Amgen, NovoNordisk, and Servier; support for attending meetings and/or travel from Medtronic; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the French Neurovascular Society; all outside the submitted work. M Bell reports grants or contracts from US EPA, NIH, High Tide Foundation, Health Effects Institute, Yale Women Faculty Forum, Environmental Defense Fund, Yale Climate Change and Health Center, Wellcome Trust Foundation, Robert Wood Johnson Foundation, and the Hutchinson Postdoctoral Fellowship (all paid to their institution); Consulting fees from Clinique; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or education events from Colorado School of Public Health, Duke University, University of Texas, Data4Justice, Korea University, Organization of Teratology Information Specialists, University of Pennsylvania, Boston University, IOP Publishing, NIH, Health Canada, PAC-10, UKRI, AXA Research Fund Fellowship, Harvard University and the University of Montana; Support for attending meeting and/or travel from Colorado School of Public Health, University of Texas, Duke University, Boston University, University of Pennsylvania, Harvard University, American Journal of Public Health, Columbia University and Harvard University; Leadership or fiduciary role in other board, society, committee or advocacy group, unpaid with Fifth National Climate Assessment and Lancet Countdown, Johns Hopkins Advisory Board, Harvard external advisory committee for training grant, WHO Global Air Pollution and Health Technical Advisory group and the National Academies Panels and Committee; and paid with the US EPA Clean Air Scientific Advisory Committee (CASAC); outside the submitted work. L Belo reports other financial or non-financial interests with UCIBIO – FFUP through support from FCT in the scope of the project UIDP/04378/2020 and UIDB/04378/2020 of UCIBIO and the project LA/P/0140/2020 of i4HB, all outside the submitted work. R S Bernstein reports other financial or non-financial support as a full-time Medical Consultant employee of the California Department of Public Health in the Center for Heal Care Quality; outside the submitted work. P J G Bettencourt reports patents planned, issued, or pending (WO2020229805A1, BR112021022592A2, EP3965809A1, OA1202100511, US2023173050A1, EP4265271A2, and EP4275700A2); other financial or non-financial interests with the Botnar Foundation as project reviewer, outside the submitted work. S Bhaskar reports grants or contracts from the Japan Society for the Promotion of Science (JSPS), Japanese Ministry of Education, Culture, Sports, Science and Technology (MEXT) and JSPS and the Australian Academy of Science; Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid with Rotary District 9675 as the district chair, Global Health & Migration Hub Community as Chair and Manager (Berlin, Germany), PLOS One, BMC Neurology, Frontiers in Neurology, Frontiers in Stroke, Frontiers in Public Health and the BMC Medical Research Methodology as an Editorial Board Member, and as a Member of the College of Reviewers (Canadian Institutes of Health Research, Canada); outside the submitted work. B Bikbov reports grants or contracts from the European Commission and The University of Rome; Support for attending meetings/travel from the European Renal Association; Leadership or fiduciary role in other board, society, committee or advocacy group, unpaid in an advocacy group with the International Society of Nephrology and unpaid on the Western Europe Regional Board of the International Society of Nephrology; Other financial or non-financial support from Scientific-Tools.org; outside the
submitted work. A Biswas reports consulting fees from INTAS Pharmaceuticals Ltd, India, Lupin Pharmaceuticals, Ltd, India, and Alkem Laboratories, India as personal payments; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Roche Diagnostics, India, as personal payments; all outside the submitted work. E J Boyko reports payment or Honoria for lectures, presentations, speakers bureaus, manuscript writing or education events from the Korean Diabetes Association, Diabetes Association of the R.O.C (Taiwan), the American Diabetes Association, and the International Society for the Diabetic Foot; Support for attending meetings and/or travel from the Korean Diabetes Association; Diabetes Association of the R.O.C (Taiwan), International Society for the Diabetic Foot; outside the submitted work. M Carvalho reports other financial or non-financial interests from LAQV/ REQUIMTE, University of Porto (Porto, Portugal) and acknowledges the support from FCT under the scope of the project UIDP/50006/2020; outside the submitted work. E Chung reports support for the present manuscript from the National Institute of Health NICHD T32HD007233. J Conde reports grants or contracts form the European Research Council Starting Grant ERC-StG-2019-848325 (funding 1.5M Euro), outside the submitted work. S Cortese reports grants or contracts from National Institute for Health and Care Research (NIHR) and the European Research Executive Agency; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from the Association of Child and Adolescent Mental Health, British Association of Psychopharmacology, Medice, and Canadian ADHD Resource Alliance; support for attending meetings and/or travel the Association of Child and Adolescent Mental Health, British Association of Psychopharmacology, Medice, and Canadian ADHD Resource Alliance; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the European ADHD Guidelines Group and the European Network for Hyperkinetic Disorders; all outside the submitted work. Sa Das reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the Association for Diagnostics and Laboratory Medicine as program chair, and the Women in Global Health India Chapter, outside the submitted work. A Dastiridou reports support for attending meetings and/or travel from THEA and ABBVIE, outside the submitted work. L Degenhardt reports untied educational grants from Indivior and Seqirus to examine new opioid medications in Australia, outside the submitted work. A K Demetriades reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the AO Knowledge Forum Degenerative Steering Committee, Global Neuro Foundation Board, and the European Association of Neurological Societies Board of Officers, all outside the submitted work. A Faro reports support for the present manuscript from National Council for Scientific and Technological Development, CNPq, Brazil as CNPq Researcher (scholarship). I Filip reports support for the present manuscript from Avicenna Medical and Clinical Research Institute. D Flood reports grants or contracts from NHLBI (award number K23HL161271), the University of Michigan Claude D. Pepper Older Americans Independence Center (award number 5P30AG024824), and the University of Michigan Caswell Diabetes Institute Clinical Translational Research Scholars Program; consulting fees from the World Health Organization as payments to their institution; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as Staff Physician for Maya Health Alliance, a non-governmental health organization in Guatemala; all outside the submitted work. A A Fomenkov reports support for the present manuscript from Development of effective biotechnologies based on cell cultures, tissues and organs of higher plants, microalgae and cyanobacteria. The research carried out within the state assignment of Ministry of Science and Higher Education of the Russian Federation (theme No. 1220426000867). M Foschi reports consulting fees from Roche and Novartis; support for attending meetings and/or travel from Biogen, Roche, Novartis, Sanofi, Bristol, and Merck; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with MBase Foundation; all outside the submitted work. R Franklin reports grants or contracts from Heatwaves (Queensland Government, Queensland, Australia) and Arc Flash (Human Factors, Queensland Government, Queensland, Australia), and Mobile Plant Safety (Agrifutures); Support for attending
meetings and/or travel from ACTM Tropical Medicine and Travel Medicine Conference 2022 and 2023, and ISTM Travel Medicine Conference in Basel 2023; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as the president/ director of Kidsafe, the director of Auschem, a member of the governance committee of ISASH, the director of Farmsafe, the Vice President of ACTM, and as a PHAA Injury Prevention SIG Convenor; outside the submitted work. P S Gill reports support for the present manuscript from the National Institute for Health and Care Research (NIHR) as Senior Investigator with payments to their institution; the views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care. A Guha reports grants or contracts from the American Heart Association and Department of Defense; consulting fees from Pfizer, Novartis, and Myovant; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with ZERO Prostate Cancer Health Equity Task Force and Doctopedia as a founding medical partner; all outside the submitted work. C Herteliu reports grants or contracts from the Romanian Ministry of Research Innovation and Digitalization, MCID, project number ID-585-CTR-42-PFE-2021; grant of the European Commission Horizon 4P-CAN (Personalised Cancer Primary Prevention Research through Citizen Participation and Digitally Enabled Social Innovation); Project “Societal and Economic Resilience within multi-hazards environment in Romania” funded by European Union – NextgenerationEU and Romanian Government, under National Recovery and Resilience Plan for Romania, contract no.760050/ 23.05.2023, cod PNRR-C9-I8-CF 267/29.11.2022, through the Romanian Ministry of Research, Innovation and Digitalization, within Component 9, Investment I8; Project “A better understanding of socioeconomic systems using quantitative methods from Physics” funded by European Union-NextgenerationEU and Romanian Government, under National Recovery and Resilience Plan for Romania, contract number 760034/ 23.05.2023, cod PNRR-C9-I8-CF 255/ 29.11.2022, through the Romanian Ministry of Research, Innovation and Digitalization, within Component 9, Investment I8; outside the submitted work. M Hultström reports support for the present manuscript from Knut och Alice Wallenberg Foundation and the Swedish Heart-Lung Foundation, all as payments to their institution; Support for attending meetings and/or travel from the American Physiological Society and the Swedish Society for Anaesthesiology and Intensive Care; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the American Physiological Society, Water and Electrolyte Section; all outside the submitted work. I Ilic and M Ilic report support for the present manuscript from Ministry of Science, Technological Development and Innovation of the Republic of Serbia. S M Islam reports support for the present manuscript from NHMRC and Heart Foundation, N E Ismail reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as Bursar (Council Member) of the Malaysian Academy of Pharmacy, outside the submitted work. T Joo reports support for the present manuscript from National Research, Development, and Innovation Office in Hungary (RRF-2.3.1-21-2022-00006), Data-Driven Health Division of National Laboratory for Health Security. G Joshy reports grants or contracts from the Department of Health and Aged Care 2023 (Understanding the fatal burden of COVID-19 in residential aged care facilities); support for attending meetings and/or travel from the Statistical Society of Australia Grant 2023 supporting conference registration; participation on a Data Safety Monitoring Board with the Australian Mathematical Sciences Institute (AMSI) and the Statistical Society of Australia (SSA) for the project Community-led nutrition and Lifestyle program for weight loss and metabolic Health: a randomised Controlled trial (ELCHO), 2022; all outside the submitted work. J Jozwiak reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Novartis, Adamed, and Amgen; outside the submitted work. N Kawakami reports grants or contracts from the Junpukai Foundation and the Department of Digital Mental Health is an endowment department, supported with an unrestricted grant from 15 enterprises (https://dmh.m.u-tokyo.ac.jp/c); consulting fees from Riken Institute, JAXA, Sekisui Chemicals, and SB@WORK; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the Japan Society for Occupational Health;
all outside the submitted work. J H Kempen reports grants or contracts from the Massachusetts Eye and Ear Surgery Program and Sight for Souls through payments to their institution; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, as President of Sight for Souls; stock or stock options with Betaliq and Tarsier; all outside the submitted work. T Kocsis reports grants or contracts from Novartis Magyarország Ltd through payment for market access activities, outside the submitted work. K Krishan reports other non-financial interests from the UGC Centre of Advanced Study, CAS II, awarded to the Department of Anthropology, Panjab University (Chandigarh, India); outside the submitted work. B Lacey reports support for the present manuscript from the UK Biobank, funded largely by the UK Medical Research Council and Wellcome, through their employment at the University of Oxford. M Lee reports support for the present manuscript from the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2021R1I1A4A01057428) and Bio-convergence Technology Education Program through the Korea Institute for Advancement Technology (KIAT) funded by the Ministry of Trade, Industry and Energy (No. P0017805). M-C Li reports grants or contracts from The National Science and Technology Council in Taiwan (NSTC 112-2410-H-003-031; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, as the technical editor of the Journal of the American Heart Association; outside the submitted work. J Liu reports support for the present manuscript from the National Natural Science Foundation of China (grant number: 72122001; 72211540398). S Lorkowski reports grants or contracts from Akcea Therapeutics Germany through payments to their institution; consulting fees from Danone, Novartis Pharma, Swedish Orphan Biovitrum (SOBI), and Upfield; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Akcea Therapeutics Germany, AMARIN Germany, Amedes Holding, AMGEN, Berlin-Chemie, Boehringer Ingelheim Pharma, Daiichi Sankyo Deutschland, Danone, Hubert Burda Media Holding, Janssen-Cilag, Lilly Deutschland, Novartis Pharma, Novo Nordisk Pharma, Roche Pharma, Sanofi-Aventis, and SYNLAB Holding Deutschland & SYNLAB Akademie; support for attending meetings and/or travel from AMGEN; participation on a Data Safety Monitoring Board or Advisory Board with Akcea Therapeutics Germany, AMGEN, Daiichi Sankyo Deutschland, Novartis Pharma, and Sanofi-Aventis; all outside the submitted work. M A Mahmoud reports grant or contract funding from the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia (project number 445-5-748). L G Mantovani reports support for the present manuscript from the Italian Ministry of Health. H R Marateb reports support for the present manuscript from The Beatriu de Pinós post-doctoral programme from the Office of the Secretary of Universities and Research from the Ministry of Business and Knowledge of the Government of Catalonia programme: 2020 BP 00261. R Matzopoulos reports consulting fees from New York University and DG Murray Trust; Support for attending meetings/travel paid by SA MRC and University of Cape Town; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as a Board member of Gun Free South Africa; Stock or Stock options with Sanlam; outside the submitted work. R J Maude reports support for the present manuscript from Wellcome Trust [Grant number 220211] as it provides core funding for Mahidol Oxford Tropical Medicine Research and contributes to his salary. A-F A Mentis reports grants or contract funding from ‘MilkSafe: A novel pipeline to enrich formula milk using omics technologies’, a research co financed by the European Regional Development Fund of the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship and Innovation, under the call RESEARCH – CREATE – INNOVATE (project code: T2EDK-02222), as well as from ELIDEK (Hellenic Foundation for Research and Innovation, MIMS-860) (both outside of the present manuscript); payment for expert testimony from serving as external peer-reviewer for FONDAZIONE CARIPLO, ITALY; participation in a Data Safety Monitoring or Advisory Board as Editorial Board Member for “Systematic Reviews”, for “Annals of Epidemiology”, and as Associate Editor for “Translational Psychiatry”; stock or stock options from a family winery; and other financial interests as the current scientific officer for BGI Group; outside the submitted work. S A Meo reports
support from King Saud University, Riyadh, Saudi Arabia (RSP-2024 R47). T R Miller reports grants or contracts from AB InBev Foundation, National Institute for Mental Health (Santa Clara County, CA), and Everytown for Gun Safety; payment for expert testimony in the states of Michigan, Nevada & New Mexico Mobile County Board of Health; outside the submitted work. P B Mitchell reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events, from Janssen (Australia), outside the submitted work. L Monasta reports support for the present manuscript from the Ministry of Health (Ricerca Corrente 34/2017) through payments made to the Institute for Maternal and Child Health IRCCS Burlo Garofolo. R S Moreira reports grants or contracts from CNPq Research Productivity Scholarship (National Council for Scientific and Technological Development) scholarship registration number 316607/2021-5; outside the submitted work. J Mosser reports support for the present manuscript from the Bill and Melinda Gates Foundation; grants or contractions from Gavi; Support for attending meetings and/or travel from the Bill and Melinda Gates Foundation; outside the submitted work. S Nomura reports support for the present manuscript from Ministry of Education, Culture, Sports, Science and Technology of Japan (21H03203) and Precursory Research for Embryonic Science and Technology from the Japan Science and Technology Agency (JPMJPR22R8). B Norrving reports participation on a Data Safety Monitoring Board or Advisory Board with Simbec Orion, outside the submitted work. A P Okekunle reports support for the present manuscript from the National Research Foundation of Korea funded by the Ministry of Science and ICT (2020H1D3A1A04081265). A Ortiz reports grants or contracts from Sanofi as payments to their institution; consulting fees, speaker fees or support for travel from, Advicciene, Astellas, Astrazeneca, Amicus, Amgen, Boehringer Ingelheim, Fresenius Medical, Care, GSK, Bayer, Sanofi-Genzyme, Menarini, Mundipharma, Kyowa Kirin, Lilly, Alexion, Freeline, Idorsia, Chiesi, Otsuka, Novo-Nordisk, Sysmex and Vifor Fresenius Medical Care Renal, Pharma and is Director of the Catedra, Mundipharma-UAM of diabetic kidney disease, and the Catedra Astrazeneca-UAM of chronic, kidney disease and electrolytes; Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the European Renal Association; stock or stock options with Telara Farma; all outside the submitted work. P K Pal reports grants or contracts paid to their institution from the Indian Council of Medical Research (ICMR), the Department of Science & Technology (DST)-Science and Engineering Research Board, the Department of Biotechnology (DBT), DST-Cognitive Science Research Initiative, Wellcome Trust UK-India Alliance DBT, PACE scheme of BIRAC, Michael J. Fox Foundation, and SKAN (Scientific Knowledge for Ageing and Neurological ailments)-Research Trust; Payment and honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events as Faculty/Speaker/ Author from the International Parkinson and Movement Disorder Society, and Movement Disorder Societies of Korea, Taiwan and Bangladesh; support for attending meetings and/or travel from the National Institute of Mental Health and Neurosciences (NIMHANS), International Parkinson and Movement Disorder Society, and Movement Disorder Societies of Korea, Taiwan and Bangladesh; Leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as the Past President of Indian Academy of Neurology, Past Secretary of Asian and Oceanian subsection of International Parkinson and Movement Disorder Society (MDS-AOS), Editor-in-Chief of Annals of Movement Disorders, Chair of the Education Committee of International Parkinson and Movement Disorder Society (IPMDS), President of the Parkinson Society of Karnataka, Chair of Infection Related Movement Disorders Study Group of MDS, Member of Rare Movement Disorders Study Group of International Parkinson and Movement Disorder Society (IPMDS), Member of Education Committee of IAPRD, Member of Rating Scales Education and Training Program Committee of IPMDS, Member of Neurophysiology Task Force of IPMDS, Member of Movement Disorders in Asia Study Group, Member of Post-Stroke Movement Disorders, Member of Ataxia Study Group of IPMDS, and as a Member of Ataxia Global Initiative; all outside the submitted work. C Palladino reports grants or contracts from FCT Fundação para a Ciência e a Tecnologia, I.P. (national funding), under a contract-programme as defined by DL No. 57/2016 and Law No. 57/2017 (DL57/2016/CP1376/CT0004). DOI 10.54499/DL57/2016/CP1376/CT0004
(https://doi.org/10.54499/DL57/2016/CP1376/CT0004). R F Palma-Alvarez reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Angelini, Lundbeck, Casen Recordati and Takeda; support for attending meetings and/or travel from Janssen and Lundbeck; all outside the submitted work. A M Pantea Stoian reports consulting fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Novartis, Sandoz, and Sanofi; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Astra Zeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Novartis, Sandoz, Medochemie, Servier, and Sanofi; support for attending meetings and/or travel from Sanofi, Novo Nordisk, and Medochemie; Participation on a Data Safety Monitoring Board or Advisory Board with Astra Zeneca, Eli Lilly, Novo Nordisk, and Sanofi; Leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the Central European Diabetes Association and the Association for Renal-Metabolic & Nutritional Studies (ASRMN); outside the submitted work. R Passera reports Participation on a Data Safety Monitoring Board or Advisory Board with the non-profit clinical trial “Consolidation with ADCT-402 (loncastuximab tesirine) after immunochemotherapy: a phase II study in BTKi-treated/ineligible Relapse/Refractory Mantle Cell Lymphoma (MCL) patients” – sponsor FIL, Fondazione Italiana Linfomi, Alessandria-I (unpaid role); leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, Member of the Statistical Committee of the EBMT European Society for Bone and Marrow Transplantation, Paris-F (unpaid role); outside the submitted work. A E Peden reports support for the present manuscript from the [Australian] National Health and Medical Research Council (Grant Number: APP2009306). V C F Pepito reports grants or contracts from Sanofi Consumer Healthcare and the International Initiative for Impact Evaluation; outside the submitted work. M Pigeolet reports a grant from the Belgian Kids’ Fund for Pediatric Research, outside the submitted work. T Pilgrim reports grants paid to the institution without personal remuneration from Biotronik, Edwards Lifesciences, and ATSens; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Biotronik, Boston Scientific, Edwards Lifesciences, Abbott, Medtronic, Biosensors, and Highlife; Participation on a Data Safety Monitoring Board or Advisory Board for EMPIRE study sponsored by Biosensors; and receipt of equipment (AT-Patches) from ATSens; outside the submitted work. D Prieto-Alhambra reports support for the present manuscript from European Medicines Agency and Innovative Medicines Initiative, through their institution; grants or contracts from Amgen, Chiesi-Taylor, Lilly, Janssen, Novartis, and UCB Biopharma through their institution; consulting fees from Astra Zeneca and UCB Biopharma; other financial or non-financial interest in Amgen, Astellas, Janssen, Synapse Management Partners and UCB Biopharma for supported training programmes; outside the submitted work. A Radfar reports support for the present manuscript from Avicenna Medical and Clinical Research Institute. A Rane reports stock or stock options as a full-time employee at Agios Pharmaceuticals; outside the submitted work. L F Reyes reports grants or contracts form MSD and Pfizer; consulting fees from GSK, MSD, and Pfizer; Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from GSK and Pfizer; payment for expert testimony from GSK and MSD; support for attending meetings and/or travel from GSK; outside the submitted work. T G Rhee reports grants or contracts from the NIH (R21AG070666; R21DA057540; R21AG078972; R01MH131528; R01AG080647); outside the submitted work. S Sacco reports grants or contracts from Novartis and Uriach; consulting fees from Novartis, Allergan-Abbvie, Teva, Lilly, Lundbeck, Pfizer, Novo Nordisk, Abbott, AstraZeneca; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Novartis, Allergan-Abbvie, Teva, Lilly, Lundbeck, Pfizer, Novo Nordisk, Abbott, AstraZeneca; support for attending meetings and/or travel from Lilly, Novartis, Teva, Lundbeck; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, as the President elect of the European Stroke Organization, and the Second vice-president of the European Headache Federation; receipt of equipment, materials, drugs, medical writing, gifts or other services from Allergan-Abbvie, Novo Nordisk; all outside the submitted work. P Sachdev reports grants or contracts from national Health and Medical
submitted work. A Biswas reports consulting fees from INTAS Pharmaceuticals Ltd, India, Lupin Pharmaceuticals, Ltd, India, and Alkem Laboratories, India as personal payments; payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from Roche Diagnostics, India, as personal payments; all outside the submitted work. E J Boyko reports payment or Honoria for lectures, presentations, speakers bureaus, manuscript writing or education events from the Korean Diabetes Association, Diabetes Association of the R.O.C (Taiwan), the American Diabetes Association, and the International Society for the Diabetic Foot; Support for attending meetings and/or travel from the Korean Diabetes Association; Diabetes Association of the R.O.C (Taiwan), International Society for the Diabetic Foot; outside the submitted work. M Carvalho reports other financial or non-financial interests from LAQV/ REQUIMTE, University of Porto (Porto, Portugal) and acknowledges the support from FCT under the scope of the project UIDP/50006/2020; outside the submitted work. E Chung reports support for the present manuscript from the National Institute of Health NICHD T32HD007233. J Conde reports grants or contracts form the European Research Council Starting Grant ERC-StG-2019-848325 (funding 1.5M Euro), outside the submitted work. S Cortese reports grants or contracts from National Institute for Health and Care Research (NIHR) and the European Research Executive Agency; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from the Association of Child and Adolescent Mental Health, British Association of Psychopharmacology, Medice, and Canadian ADHD Resource Alliance; support for attending meetings and/or travel the Association of Child and Adolescent Mental Health, British Association of Psychopharmacology, Medice, and Canadian ADHD Resource Alliance; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the European ADHD Guidelines Group and the European Network for Hyperkinetic Disorders; all outside the submitted work. Sa Das reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the Association for Diagnostics and Laboratory Medicine as program chair, and the Women in Global Health India Chapter, outside the submitted work. A Dastiridou reports support for attending meetings and/or travel from THEA and ABBVIE, outside the submitted work. L Degenhardt reports untied educational grants from Indivior and Seqirus to examine new opioid medications in Australia, outside the submitted work. A K Demetriades reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the AO Knowledge Forum Degenerative Steering Committee, Global Neuro Foundation Board, and the European Association of Neurological Societies Board of Officers, all outside the submitted work. A Faro reports support for the present manuscript from National Council for Scientific and Technological Development, CNPq, Brazil as CNPq Researcher (scholarship). I Filip reports support for the present manuscript from Avicenna Medical and Clinical Research Institute. D Flood reports grants or contracts from NHLBI (award number K23HL161271), the University of Michigan Claude D. Pepper Older Americans Independence Center (award number 5P30AG024824), and the University of Michigan Caswell Diabetes Institute Clinical Translational Research Scholars Program; consulting fees from the World Health Organization as payments to their institution; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as Staff Physician for Maya Health Alliance, a non-governmental health organization in Guatemala; all outside the submitted work. A A Fomenkov reports support for the present manuscript from Development of effective biotechnologies based on cell cultures, tissues and organs of higher plants, microalgae and cyanobacteria. The research carried out within the state assignment of Ministry of Science and Higher Education of the Russian Federation (theme No. 1220426000867). M Foschi reports consulting fees from Roche and Novartis; support for attending meetings and/or travel from Biogen, Roche, Novartis, Sanofi, Bristol, and Merck; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with MBase Foundation; all outside the submitted work. R Franklin reports grants or contracts from Heatwaves (Queensland Government, Queensland, Australia) and Arc Flash (Human Factors, Queensland Government, Queensland, Australia), and Mobile Plant Safety (Agrifutures); Support for attending
meetings and/or travel from ACTM Tropical Medicine and Travel Medicine Conference 2022 and 2023, and ISTM Travel Medicine Conference in Basel 2023; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as the president/ director of Kidsafe, the director of Auschem, a member of the governance committee of ISASH, the director of Farmsafe, the Vice President of ACTM, and as a PHAA Injury Prevention SIG Convenor; outside the submitted work. P S Gill reports support for the present manuscript from the National Institute for Health and Care Research (NIHR) as Senior Investigator with payments to their institution; the views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care. A Guha reports grants or contracts from the American Heart Association and Department of Defense; consulting fees from Pfizer, Novartis, and Myovant; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with ZERO Prostate Cancer Health Equity Task Force and Doctopedia as a founding medical partner; all outside the submitted work. C Herteliu reports grants or contracts from the Romanian Ministry of Research Innovation and Digitalization, MCID, project number ID-585-CTR-42-PFE-2021; grant of the European Commission Horizon 4P-CAN (Personalised Cancer Primary Prevention Research through Citizen Participation and Digitally Enabled Social Innovation); Project “Societal and Economic Resilience within multi-hazards environment in Romania” funded by European Union – NextgenerationEU and Romanian Government, under National Recovery and Resilience Plan for Romania, contract no.760050/ 23.05.2023, cod PNRR-C9-I8-CF 267/29.11.2022, through the Romanian Ministry of Research, Innovation and Digitalization, within Component 9, Investment I8; Project “A better understanding of socioeconomic systems using quantitative methods from Physics” funded by European Union-NextgenerationEU and Romanian Government, under National Recovery and Resilience Plan for Romania, contract number 760034/ 23.05.2023, cod PNRR-C9-I8-CF 255/ 29.11.2022, through the Romanian Ministry of Research, Innovation and Digitalization, within Component 9, Investment I8; outside the submitted work. M Hultström reports support for the present manuscript from Knut och Alice Wallenberg Foundation and the Swedish Heart-Lung Foundation, all as payments to their institution; Support for attending meetings and/or travel from the American Physiological Society and the Swedish Society for Anaesthesiology and Intensive Care; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the American Physiological Society, Water and Electrolyte Section; all outside the submitted work. I Ilic and M Ilic report support for the present manuscript from Ministry of Science, Technological Development and Innovation of the Republic of Serbia. S M Islam reports support for the present manuscript from NHMRC and Heart Foundation, N E Ismail reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as Bursar (Council Member) of the Malaysian Academy of Pharmacy, outside the submitted work. T Joo reports support for the present manuscript from National Research, Development, and Innovation Office in Hungary (RRF-2.3.1-21-2022-00006), Data-Driven Health Division of National Laboratory for Health Security. G Joshy reports grants or contracts from the Department of Health and Aged Care 2023 (Understanding the fatal burden of COVID-19 in residential aged care facilities); support for attending meetings and/or travel from the Statistical Society of Australia Grant 2023 supporting conference registration; participation on a Data Safety Monitoring Board with the Australian Mathematical Sciences Institute (AMSI) and the Statistical Society of Australia (SSA) for the project Community-led nutrition and Lifestyle program for weight loss and metabolic Health: a randomised Controlled trial (ELCHO), 2022; all outside the submitted work. J Jozwiak reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Novartis, Adamed, and Amgen; outside the submitted work. N Kawakami reports grants or contracts from the Junpukai Foundation and the Department of Digital Mental Health is an endowment department, supported with an unrestricted grant from 15 enterprises (https://dmh.m.u-tokyo.ac.jp/c); consulting fees from Riken Institute, JAXA, Sekisui Chemicals, and SB@WORK; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the Japan Society for Occupational Health;
all outside the submitted work. J H Kempen reports grants or contracts from the Massachusetts Eye and Ear Surgery Program and Sight for Souls through payments to their institution; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, as President of Sight for Souls; stock or stock options with Betaliq and Tarsier; all outside the submitted work. T Kocsis reports grants or contracts from Novartis Magyarország Ltd through payment for market access activities, outside the submitted work. K Krishan reports other non-financial interests from the UGC Centre of Advanced Study, CAS II, awarded to the Department of Anthropology, Panjab University (Chandigarh, India); outside the submitted work. B Lacey reports support for the present manuscript from the UK Biobank, funded largely by the UK Medical Research Council and Wellcome, through their employment at the University of Oxford. M Lee reports support for the present manuscript from the Ministry of Education of the Republic of Korea and the National Research Foundation of Korea (NRF-2021R1I1A4A01057428) and Bio-convergence Technology Education Program through the Korea Institute for Advancement Technology (KIAT) funded by the Ministry of Trade, Industry and Energy (No. P0017805). M-C Li reports grants or contracts from The National Science and Technology Council in Taiwan (NSTC 112-2410-H-003-031; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, as the technical editor of the Journal of the American Heart Association; outside the submitted work. J Liu reports support for the present manuscript from the National Natural Science Foundation of China (grant number: 72122001; 72211540398). S Lorkowski reports grants or contracts from Akcea Therapeutics Germany through payments to their institution; consulting fees from Danone, Novartis Pharma, Swedish Orphan Biovitrum (SOBI), and Upfield; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Akcea Therapeutics Germany, AMARIN Germany, Amedes Holding, AMGEN, Berlin-Chemie, Boehringer Ingelheim Pharma, Daiichi Sankyo Deutschland, Danone, Hubert Burda Media Holding, Janssen-Cilag, Lilly Deutschland, Novartis Pharma, Novo Nordisk Pharma, Roche Pharma, Sanofi-Aventis, and SYNLAB Holding Deutschland & SYNLAB Akademie; support for attending meetings and/or travel from AMGEN; participation on a Data Safety Monitoring Board or Advisory Board with Akcea Therapeutics Germany, AMGEN, Daiichi Sankyo Deutschland, Novartis Pharma, and Sanofi-Aventis; all outside the submitted work. M A Mahmoud reports grant or contract funding from the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia (project number 445-5-748). L G Mantovani reports support for the present manuscript from the Italian Ministry of Health. H R Marateb reports support for the present manuscript from The Beatriu de Pinós post-doctoral programme from the Office of the Secretary of Universities and Research from the Ministry of Business and Knowledge of the Government of Catalonia programme: 2020 BP 00261. R Matzopoulos reports consulting fees from New York University and DG Murray Trust; Support for attending meetings/travel paid by SA MRC and University of Cape Town; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as a Board member of Gun Free South Africa; Stock or Stock options with Sanlam; outside the submitted work. R J Maude reports support for the present manuscript from Wellcome Trust [Grant number 220211] as it provides core funding for Mahidol Oxford Tropical Medicine Research and contributes to his salary. A-F A Mentis reports grants or contract funding from ‘MilkSafe: A novel pipeline to enrich formula milk using omics technologies’, a research co financed by the European Regional Development Fund of the European Union and Greek national funds through the Operational Program Competitiveness, Entrepreneurship and Innovation, under the call RESEARCH – CREATE – INNOVATE (project code: T2EDK-02222), as well as from ELIDEK (Hellenic Foundation for Research and Innovation, MIMS-860) (both outside of the present manuscript); payment for expert testimony from serving as external peer-reviewer for FONDAZIONE CARIPLO, ITALY; participation in a Data Safety Monitoring or Advisory Board as Editorial Board Member for “Systematic Reviews”, for “Annals of Epidemiology”, and as Associate Editor for “Translational Psychiatry”; stock or stock options from a family winery; and other financial interests as the current scientific officer for BGI Group; outside the submitted work. S A Meo reports
support from King Saud University, Riyadh, Saudi Arabia (RSP-2024 R47). T R Miller reports grants or contracts from AB InBev Foundation, National Institute for Mental Health (Santa Clara County, CA), and Everytown for Gun Safety; payment for expert testimony in the states of Michigan, Nevada & New Mexico Mobile County Board of Health; outside the submitted work. P B Mitchell reports payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events, from Janssen (Australia), outside the submitted work. L Monasta reports support for the present manuscript from the Ministry of Health (Ricerca Corrente 34/2017) through payments made to the Institute for Maternal and Child Health IRCCS Burlo Garofolo. R S Moreira reports grants or contracts from CNPq Research Productivity Scholarship (National Council for Scientific and Technological Development) scholarship registration number 316607/2021-5; outside the submitted work. J Mosser reports support for the present manuscript from the Bill and Melinda Gates Foundation; grants or contractions from Gavi; Support for attending meetings and/or travel from the Bill and Melinda Gates Foundation; outside the submitted work. S Nomura reports support for the present manuscript from Ministry of Education, Culture, Sports, Science and Technology of Japan (21H03203) and Precursory Research for Embryonic Science and Technology from the Japan Science and Technology Agency (JPMJPR22R8). B Norrving reports participation on a Data Safety Monitoring Board or Advisory Board with Simbec Orion, outside the submitted work. A P Okekunle reports support for the present manuscript from the National Research Foundation of Korea funded by the Ministry of Science and ICT (2020H1D3A1A04081265). A Ortiz reports grants or contracts from Sanofi as payments to their institution; consulting fees, speaker fees or support for travel from, Advicciene, Astellas, Astrazeneca, Amicus, Amgen, Boehringer Ingelheim, Fresenius Medical, Care, GSK, Bayer, Sanofi-Genzyme, Menarini, Mundipharma, Kyowa Kirin, Lilly, Alexion, Freeline, Idorsia, Chiesi, Otsuka, Novo-Nordisk, Sysmex and Vifor Fresenius Medical Care Renal, Pharma and is Director of the Catedra, Mundipharma-UAM of diabetic kidney disease, and the Catedra Astrazeneca-UAM of chronic, kidney disease and electrolytes; Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the European Renal Association; stock or stock options with Telara Farma; all outside the submitted work. P K Pal reports grants or contracts paid to their institution from the Indian Council of Medical Research (ICMR), the Department of Science & Technology (DST)-Science and Engineering Research Board, the Department of Biotechnology (DBT), DST-Cognitive Science Research Initiative, Wellcome Trust UK-India Alliance DBT, PACE scheme of BIRAC, Michael J. Fox Foundation, and SKAN (Scientific Knowledge for Ageing and Neurological ailments)-Research Trust; Payment and honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events as Faculty/Speaker/ Author from the International Parkinson and Movement Disorder Society, and Movement Disorder Societies of Korea, Taiwan and Bangladesh; support for attending meetings and/or travel from the National Institute of Mental Health and Neurosciences (NIMHANS), International Parkinson and Movement Disorder Society, and Movement Disorder Societies of Korea, Taiwan and Bangladesh; Leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, as the Past President of Indian Academy of Neurology, Past Secretary of Asian and Oceanian subsection of International Parkinson and Movement Disorder Society (MDS-AOS), Editor-in-Chief of Annals of Movement Disorders, Chair of the Education Committee of International Parkinson and Movement Disorder Society (IPMDS), President of the Parkinson Society of Karnataka, Chair of Infection Related Movement Disorders Study Group of MDS, Member of Rare Movement Disorders Study Group of International Parkinson and Movement Disorder Society (IPMDS), Member of Education Committee of IAPRD, Member of Rating Scales Education and Training Program Committee of IPMDS, Member of Neurophysiology Task Force of IPMDS, Member of Movement Disorders in Asia Study Group, Member of Post-Stroke Movement Disorders, Member of Ataxia Study Group of IPMDS, and as a Member of Ataxia Global Initiative; all outside the submitted work. C Palladino reports grants or contracts from FCT Fundação para a Ciência e a Tecnologia, I.P. (national funding), under a contract-programme as defined by DL No. 57/2016 and Law No. 57/2017 (DL57/2016/CP1376/CT0004). DOI 10.54499/DL57/2016/CP1376/CT0004
(https://doi.org/10.54499/DL57/2016/CP1376/CT0004). R F Palma-Alvarez reports payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Angelini, Lundbeck, Casen Recordati and Takeda; support for attending meetings and/or travel from Janssen and Lundbeck; all outside the submitted work. A M Pantea Stoian reports consulting fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Novartis, Sandoz, and Sanofi; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Astra Zeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, Novartis, Sandoz, Medochemie, Servier, and Sanofi; support for attending meetings and/or travel from Sanofi, Novo Nordisk, and Medochemie; Participation on a Data Safety Monitoring Board or Advisory Board with Astra Zeneca, Eli Lilly, Novo Nordisk, and Sanofi; Leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the Central European Diabetes Association and the Association for Renal-Metabolic & Nutritional Studies (ASRMN); outside the submitted work. R Passera reports Participation on a Data Safety Monitoring Board or Advisory Board with the non-profit clinical trial “Consolidation with ADCT-402 (loncastuximab tesirine) after immunochemotherapy: a phase II study in BTKi-treated/ineligible Relapse/Refractory Mantle Cell Lymphoma (MCL) patients” – sponsor FIL, Fondazione Italiana Linfomi, Alessandria-I (unpaid role); leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, Member of the Statistical Committee of the EBMT European Society for Bone and Marrow Transplantation, Paris-F (unpaid role); outside the submitted work. A E Peden reports support for the present manuscript from the [Australian] National Health and Medical Research Council (Grant Number: APP2009306). V C F Pepito reports grants or contracts from Sanofi Consumer Healthcare and the International Initiative for Impact Evaluation; outside the submitted work. M Pigeolet reports a grant from the Belgian Kids’ Fund for Pediatric Research, outside the submitted work. T Pilgrim reports grants paid to the institution without personal remuneration from Biotronik, Edwards Lifesciences, and ATSens; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Biotronik, Boston Scientific, Edwards Lifesciences, Abbott, Medtronic, Biosensors, and Highlife; Participation on a Data Safety Monitoring Board or Advisory Board for EMPIRE study sponsored by Biosensors; and receipt of equipment (AT-Patches) from ATSens; outside the submitted work. D Prieto-Alhambra reports support for the present manuscript from European Medicines Agency and Innovative Medicines Initiative, through their institution; grants or contracts from Amgen, Chiesi-Taylor, Lilly, Janssen, Novartis, and UCB Biopharma through their institution; consulting fees from Astra Zeneca and UCB Biopharma; other financial or non-financial interest in Amgen, Astellas, Janssen, Synapse Management Partners and UCB Biopharma for supported training programmes; outside the submitted work. A Radfar reports support for the present manuscript from Avicenna Medical and Clinical Research Institute. A Rane reports stock or stock options as a full-time employee at Agios Pharmaceuticals; outside the submitted work. L F Reyes reports grants or contracts form MSD and Pfizer; consulting fees from GSK, MSD, and Pfizer; Payment or honoraria for lectures, presentations, speakers’ bureaus, manuscript writing or educational events from GSK and Pfizer; payment for expert testimony from GSK and MSD; support for attending meetings and/or travel from GSK; outside the submitted work. T G Rhee reports grants or contracts from the NIH (R21AG070666; R21DA057540; R21AG078972; R01MH131528; R01AG080647); outside the submitted work. S Sacco reports grants or contracts from Novartis and Uriach; consulting fees from Novartis, Allergan-Abbvie, Teva, Lilly, Lundbeck, Pfizer, Novo Nordisk, Abbott, AstraZeneca; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Novartis, Allergan-Abbvie, Teva, Lilly, Lundbeck, Pfizer, Novo Nordisk, Abbott, AstraZeneca; support for attending meetings and/or travel from Lilly, Novartis, Teva, Lundbeck; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, as the President elect of the European Stroke Organization, and the Second vice-president of the European Headache Federation; receipt of equipment, materials, drugs, medical writing, gifts or other services from Allergan-Abbvie, Novo Nordisk; all outside the submitted work. P Sachdev reports grants or contracts from national Health and Medical
Research Council of Australia and the US National Institutes of Health; Payment or honoraria for lectures from Alkem Labs for the Frontiers of Psychiatry June 2023 Seminar, Mumbai, India; Participation on a Data Safety Monitoring Board or Advisory Board with Biogen Australia and Roche Australia; leadership or fiduciary role in other board, society, committee or advocacy group, unpaid, with the VASCOG Society and the World Psychiatric Association; all outside the submitted work. Y L Samodra reports grants or contracts from Taipei Medical University; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the Benang Merah Research Center; all outside the submitted work. J Sanabria reports support for attending meetings and/or travel from the Department of Surgery, Marshall University School of Medicine; three patents pending; participation in quality assessment and assurance for surgeries of the Department of Surgery; leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid with SSAT, ASTS, AHPBA, IHPBA, and AASLD; all outside the submitted work. N Scarmeas reports grants or contracts with Novo Nordisk as the Local PI of recruiting site for multinational, multicenter industry sponsored phase III treatment trial for Alzheimer’s disease with funding paid to the institution; Participation on a Data Safety Monitoring Board or Advisory Board with Albert Einstein College of Medicine (NIH funded study) as the Chair of Data Safety Monitoring Board; all outside the submitted work. A E Schutte reports Speaker Honoraria from Servier, Novartis, Sanofi, Medtronic, Abbott, Omron, Aktiia; Support for attending meetings and/or travel from Servier, Medtronic, and Abbott; Participation on a Data Safety Monitoring Board or Advisory Board with Abbott Pharmaceuticals Advisory Board, Skylabs devices Advisory Board; Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with Co-Chair: National Hypertension Taskforce of Australia, Board Member: Hypertension Australia, Company Secretary: Australian Cardiovascular Alliance; all outside the submitted work. B M Schaarschmidt reports research grants from Else Kröner-Fresenius Foundatuin, DFG, and PharmaCept; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AstraZeneca; support for attending meetings and/or travel from Bayer AG; all outside the submitted work. M Šekerija reports consulting fees from Roche; Payment or Honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Johnson and Johnson, and Astellas; outside the submitted work. A Sharifan reports leadership or fiduciary role in other board, society, committee or advocacy group, unpaid with Cochrane as a steering member of the Cochrane Early Career Professionals Network; and receipt of thirty days of complimentary access to ScienceDirect, Scopus, Reaxys, and Geofacets after reviewing manuscripts for two journals published by Elsevier; outside the submitted work. S Sharma reports support for the present manuscript from the John J. Bonica Postdoctoral Fellowship from the International Association for the Study of Pain (IASP; 2021-2023); Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events and a travel grant for delivering a talk on “Technologies for pain education in developing countries” conducted by the Pain Education SIG of the IASP at the World Pain Congress in Toronto (2022); outside the submitted work. V Sharma reports other financial or non-financial support from DFSS (MHA)’s research project (DFSS28(1)2019/EMR/6) at Institute of Forensic Science & Criminology, Panjab University, Chandigarh, India, outside the submitted work. K Shibuya reports support for the present manuscript from Tokyo Foundation for Policy Research. V Shivarov reports one patent and one utility model with the Bulgarian Patent Office; stock or stock options from ICONplc (RSUs); and other financial interests from an ICONplc salary; all outside the submitted work. S Shrestha reports other financial interests from the Graduate Research Merit Scholarship from the School of Pharmacy at Monash University Malaysia, outside the submitted work. J P Silva reports support for the present manuscript from the Portuguese Foundation for Science and Technology through payment of their salary (contract with reference 2021.01789.CEECIND/CP1662/CT0014). L M L R Silva reports grants or contracts from CENTRO-04-3559-FSE-000162, Fundo Social Europeu (FSE), outside the submitted work. C R Simpson reports grants or contracts from MBIE (NZ), HRC (NZ), Ministry of Health (NZ), MRC (UK), and CSO (UK); Leadership or
fiduciary role in other board, society, committee or advocacy group, paid or unpaid with the New Zealand Government Data Ethics Advisory Group as the Chair; outside the submitted work. D J Stein reports consulting fees from Discovery Vitality, Johnson & Johnson, Kanna, L’Oreal, Lundbeck, Orion, Sanofi, Servier, Takeda, and Vistagen, outside the submitted work. K Stibrant Sunnerhagen reports Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as the head of the scientific committee of the Sweidhs Stroke Foundation; outside the submitted work. S Stortecky reports grants or contracts paid to their institution from Edwards Lifesciences, Medtronic, Abbott, and Boston Scientific; consulting fees from Teleflex; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Boston Scientific/BTG; outside the submitted work. A G Thrift reports grants or contracts paid to their institution from the National Health & Medical Research Council (Australia) (grant numbers 1171966, 1182071), Heart Foundation (Aus) and the Stroke Foundation (Australia); outside the submitted work. J H V Ticoalu reports Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with Benang Merah Research Center as co-founder, outside the submitted work. M V Titova reports support for the present manuscript from the Ministry of Science and Higher Education of the Russian Federation (theme No. 122042600086-7). S J Tromans reports grants or contracts from the 2023 Adult Psychiatric Morbidity Survey team, collecting epidemiological data on community-based adults living in England. This is a contracted study from NHS Digital, via the Department of Health and Social Care; outside the submitted work. P Willeit reports consulting fees from Novartis; outside the submitted work. M Zielińska reports other financial interest as an AstraZeneca employee, outside the submitted work. A Zumla reports grants or contracts from The Pan-African Network on Emerging and Re-Emerging Infections (PANDORA-ID-NET, CANTAM-3, and EACCR-3) funded by the European and Developing Countries Clinical Trials Partnership, the EU Horizon 2020 Framework Programme, UK National Institute for Health and Care Research Senior Investigator, and Mahathir Science Award and EU-EDCTP Pascoal Mocumbi Prize Laureate; Participation on a Data Safety Monitoring Board or Advisory Board member of the WHO Mass Gatherings Expert Group and WHO Health Emergencies Programme in Geneva, a member of the EU-EDCTP3-Global Health (Brussels) Scientific Committee; all outside the submitted work.
fiduciary role in other board, society, committee or advocacy group, paid or unpaid with the New Zealand Government Data Ethics Advisory Group as the Chair; outside the submitted work. D J Stein reports consulting fees from Discovery Vitality, Johnson & Johnson, Kanna, L’Oreal, Lundbeck, Orion, Sanofi, Servier, Takeda, and Vistagen, outside the submitted work. K Stibrant Sunnerhagen reports Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid as the head of the scientific committee of the Sweidhs Stroke Foundation; outside the submitted work. S Stortecky reports grants or contracts paid to their institution from Edwards Lifesciences, Medtronic, Abbott, and Boston Scientific; consulting fees from Teleflex; Payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from Boston Scientific/BTG; outside the submitted work. A G Thrift reports grants or contracts paid to their institution from the National Health & Medical Research Council (Australia) (grant numbers 1171966, 1182071), Heart Foundation (Aus) and the Stroke Foundation (Australia); outside the submitted work. J H V Ticoalu reports Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with Benang Merah Research Center as co-founder, outside the submitted work. M V Titova reports support for the present manuscript from the Ministry of Science and Higher Education of the Russian Federation (theme No. 122042600086-7). S J Tromans reports grants or contracts from the 2023 Adult Psychiatric Morbidity Survey team, collecting epidemiological data on community-based adults living in England. This is a contracted study from NHS Digital, via the Department of Health and Social Care; outside the submitted work. P Willeit reports consulting fees from Novartis; outside the submitted work. M Zielińska reports other financial interest as an AstraZeneca employee, outside the submitted work. A Zumla reports grants or contracts from The Pan-African Network on Emerging and Re-Emerging Infections (PANDORA-ID-NET, CANTAM-3, and EACCR-3) funded by the European and Developing Countries Clinical Trials Partnership, the EU Horizon 2020 Framework Programme, UK National Institute for Health and Care Research Senior Investigator, and Mahathir Science Award and EU-EDCTP Pascoal Mocumbi Prize Laureate; Participation on a Data Safety Monitoring Board or Advisory Board member of the WHO Mass Gatherings Expert Group and WHO Health Emergencies Programme in Geneva, a member of the EU-EDCTP3-Global Health (Brussels) Scientific Committee; all outside the submitted work.
Data sharing
To download the data used in these analyses, please visit the Global health Data Exchange GBD 2021 website (https://ghdx.healthdata.org/ gbd-2021/sources).
Acknowledgments
Research reported in this publication was supported by the Bill & Melinda Gates Foundation; Queensland Department of Health, Australia; UK Department of Health and Social Care; the Norwegian Institute of Public Health; St Jude Children’s Research Hospital; and the New Zealand Ministry of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders. The Palestinian Central Bureau of Statistics granted the researchers access to relevant data in accordance with license number SLN2014-3-170, after subjecting data to processing aiming to preserve the confidentiality of individual data in accordance with the General Statistics Law-2000. The researchers are solely responsible for the conclusions and inferences drawn upon available data. Collection of these data was made possible by USAID under the terms of cooperative agreement GPO-A-00-08-000_D3-00. The opinions expressed are those of the authors and do not necessarily reflect the views of USAID or the US Government. Data for this research were provided by MEASURE Evaluation, funded by the US Agency for International Development (USAID). Views expressed do not necessarily reflect those of USAID, the US Government, or MEASURE Evaluation. The data reported here have been supplied by the US Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the US Government. This manuscript is based on data collected and shared by the International Vaccine Institute (IVI) from an original study it conducted. This manuscript was not prepared in
collaboration with investigators of IVI and does not necessarily reflect the opinions or views of IVI. Data for this research were provided by the Cancer Registry of the Republic of Slovenia. The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the Statistical Office of the Republic of Slovenia. Datasets were provided by the European Centre for Disease Prevention and Control (ECDC) based on data provided by WHO and Ministries of Health from the affected countries. The views and opinions of the authors expressed herein do not necessarily state or reflect those of the ECDC. The accuracy of the authors’ statistical analysis and the findings they report are not the responsibility of the ECDC. The ECDC is not responsible for conclusions or opinions drawn from the data provided. The ECDC is not responsible for the correctness of the data and for data management, data merging, and data collation after provision of the data. The ECDC shall not be held liable for improper or incorrect use of the data.
collaboration with investigators of IVI and does not necessarily reflect the opinions or views of IVI. Data for this research were provided by the Cancer Registry of the Republic of Slovenia. The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the Statistical Office of the Republic of Slovenia. Datasets were provided by the European Centre for Disease Prevention and Control (ECDC) based on data provided by WHO and Ministries of Health from the affected countries. The views and opinions of the authors expressed herein do not necessarily state or reflect those of the ECDC. The accuracy of the authors’ statistical analysis and the findings they report are not the responsibility of the ECDC. The ECDC is not responsible for conclusions or opinions drawn from the data provided. The ECDC is not responsible for the correctness of the data and for data management, data merging, and data collation after provision of the data. The ECDC shall not be held liable for improper or incorrect use of the data.
Editorial note: The Lancet Group takes a neutral position with respect to territorial claims in published maps and institutional affiliations.
References
1 Murray CJL. The Global Burden of Disease Study at 30 years. Nat Med 2022; 28: 2019-26.
2 World Bank. World development report 1993: investing in health. Washington, DC: Oxford University Press, 1993.
3 Wang H, Paulson KR, Pease SA, et al. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19related mortality, 2020-21. Lancet 2022; 399: 1513-36.
4 Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1736-88.
5 Institute for Health Metrics and Evaluation. Protocol for the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD). Version 4.0. March, 2020. https://www.healthdata.org/sites/default/ files/files/Projects/GBD/March2020_GBD%20Protocol_v4.pdf (accessed March 15, 2023).
6 Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1204-22.
7 GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 385: 117-71.
8 Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388: 1459-544.
9 Naghavi M, Abajobir AA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017; 390: 1151-210.
10 Wang H, Abbas KM, Abbasifard M, et al. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1160-203.
11 Johnson SC, Cunningham M, Dippenaar IN, et al. Public health utility of cause of death data: applying empirical algorithms to improve data quality. BMC Med Inform Decis Mak 2021; 21: 175.
12 GBD 2021 Demographics Collaborators. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950-2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet 2024; published online March 11. https://doi.org/10.1016/S0140-6736(24)00476-8.
13 Doi SAR, Williams GM, eds. Methods of clinical epidemiology. Berlin, Heidelberg: Springer, 2013.
14 Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet 2016; 388: e19-23.
2 World Bank. World development report 1993: investing in health. Washington, DC: Oxford University Press, 1993.
3 Wang H, Paulson KR, Pease SA, et al. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19related mortality, 2020-21. Lancet 2022; 399: 1513-36.
4 Roth GA, Abate D, Abate KH, et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1736-88.
5 Institute for Health Metrics and Evaluation. Protocol for the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD). Version 4.0. March, 2020. https://www.healthdata.org/sites/default/ files/files/Projects/GBD/March2020_GBD%20Protocol_v4.pdf (accessed March 15, 2023).
6 Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1204-22.
7 GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 385: 117-71.
8 Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016; 388: 1459-544.
9 Naghavi M, Abajobir AA, Abbafati C, et al. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017; 390: 1151-210.
10 Wang H, Abbas KM, Abbasifard M, et al. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950-2019: a comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1160-203.
11 Johnson SC, Cunningham M, Dippenaar IN, et al. Public health utility of cause of death data: applying empirical algorithms to improve data quality. BMC Med Inform Decis Mak 2021; 21: 175.
12 GBD 2021 Demographics Collaborators. Global age-sex-specific mortality, life expectancy, and population estimates in 204 countries and territories and 811 subnational locations, 1950-2021, and the impact of the COVID-19 pandemic: a comprehensive demographic analysis for the Global Burden of Disease Study 2021. Lancet 2024; published online March 11. https://doi.org/10.1016/S0140-6736(24)00476-8.
13 Doi SAR, Williams GM, eds. Methods of clinical epidemiology. Berlin, Heidelberg: Springer, 2013.
14 Stevens GA, Alkema L, Black RE, et al. Guidelines for accurate and transparent health estimates reporting: the GATHER statement. Lancet 2016; 388: e19-23.
15 Murray CJL, Aravkin AY, Zheng P, et al. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020; 396: 1223-49.
16 Levin AT, Owusu-Boaitey N, Pugh S, et al. Assessing the burden of COVID-19 in developing countries: systematic review, metaanalysis and public policy implications. BMJ Glob Health 2022; 7: e008477.
17 Barber RM, Sorensen RJD, Pigott DM, et al. Estimating global, regional, and national daily and cumulative infections with SARS-CoV-2 through Nov 14, 2021: a statistical analysis. Lancet 2022; 399: 2351-80.
18 Telles CR, Roy A, Ajmal MR, et al. The impact of COVID-19 management policies tailored to airborne SARS-CoV-2 transmission: policy analysis. JMIR Public Health Surveill 2021; 7: e20699.
19 Bollyky TJ, Hulland EN, Barber RM, et al. Pandemic preparedness and COVID-19: an exploratory analysis of infection and fatality rates, and contextual factors associated with preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021. Lancet 2022; 399: 1489-512.
20 Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global challenges to public health care systems during the COVID-19 pandemic: a review of pandemic measures and problems. J Pers Med 2022; 12: 1295.
21 The Independent Panel for Pandemic Preparedness and Response. COVID-19: make it the last pandemic. May 21, 2021. https:// theindependentpanel.org/wp-content/uploads/2021/05/COVID-19-Make-it-the-Last-Pandemic_final.pdf (accessed Nov 9, 2023).
22 Lazarus JV, Romero D, Kopka CJ, et al. A multinational Delphi consensus to end the COVID-19 public health threat. Nature 2022; 611: 332-45.
23 Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1859-922.
24 Haws R, Winch PJ, Castillo J. Innovative community-based interventions to improve newborn health in Latin America and the Caribbean. Johns Hopkins University, CORE Group, 2004. https:// coregroup.org/wp-content/uploads/2020/03/LAC-Neonatalenglish_final_pdf.pdf (accessed Nov 3, 2023).
25 Whiteside A, Henry FE. The impact of HIV and AIDS research: a case study from Swaziland. Health Res Policy Syst 2011; 9 (suppl 1): S9.
26 Dwyer-Lindgren L, Cork MA, Sligar A, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature 2019; 570: 189-93.
27 Nachega JB, Kapata N, Sam-Agudu NA, et al. Minimizing the impact of the triple burden of COVID-19, tuberculosis and HIV on health services in sub-Saharan Africa. Int J Infect Dis 2021; 113 (suppl 1): S16-21.
28 Duarte R, Silva DR, Rendon A, et al. Eliminating tuberculosis in Latin America: making it the point. J Bras Pneumol 2018; 44: 73-76.
29 WHO. World health statistics 2022: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2022. https://www.who.int/data/gho/publications/ world-health-statistics (accessed Sept 16, 2022).
30 WHO. World health statistics 2023: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2023. https://www.who.int/publications-detailredirect/9789240074323 (accessed Oct 27, 2023).
31 Rosenthal PJ, John CC, Rabinovich NR. Malaria: how are we doing and how can we do better? Am J Trop Med Hyg 2019; 100: 239-41.
32 Bhatt S, Weiss DJ, Cameron E, et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015; 526: 207-11.
33 WHO. WHO recommends R21/Matrix-M vaccine for malaria prevention in updated advice on immunization. Geneva: World Health Organization, 2023. https://www.who.int/news/item/02-10-2023-who-recommends-r21-matrix-m-vaccine-for-malaria-prevention-in-updated-advice-on-immunization (accessed Oct 24, 2023).
34 Naddaf M. Second malaria vaccine to win global approval is cheaper and easier to make. Nature 2023; published online Oct 3. https:// doi.org/10.1038/d41586-023-03115-1.
16 Levin AT, Owusu-Boaitey N, Pugh S, et al. Assessing the burden of COVID-19 in developing countries: systematic review, metaanalysis and public policy implications. BMJ Glob Health 2022; 7: e008477.
17 Barber RM, Sorensen RJD, Pigott DM, et al. Estimating global, regional, and national daily and cumulative infections with SARS-CoV-2 through Nov 14, 2021: a statistical analysis. Lancet 2022; 399: 2351-80.
18 Telles CR, Roy A, Ajmal MR, et al. The impact of COVID-19 management policies tailored to airborne SARS-CoV-2 transmission: policy analysis. JMIR Public Health Surveill 2021; 7: e20699.
19 Bollyky TJ, Hulland EN, Barber RM, et al. Pandemic preparedness and COVID-19: an exploratory analysis of infection and fatality rates, and contextual factors associated with preparedness in 177 countries, from Jan 1, 2020, to Sept 30, 2021. Lancet 2022; 399: 1489-512.
20 Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global challenges to public health care systems during the COVID-19 pandemic: a review of pandemic measures and problems. J Pers Med 2022; 12: 1295.
21 The Independent Panel for Pandemic Preparedness and Response. COVID-19: make it the last pandemic. May 21, 2021. https:// theindependentpanel.org/wp-content/uploads/2021/05/COVID-19-Make-it-the-Last-Pandemic_final.pdf (accessed Nov 9, 2023).
22 Lazarus JV, Romero D, Kopka CJ, et al. A multinational Delphi consensus to end the COVID-19 public health threat. Nature 2022; 611: 332-45.
23 Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392: 1859-922.
24 Haws R, Winch PJ, Castillo J. Innovative community-based interventions to improve newborn health in Latin America and the Caribbean. Johns Hopkins University, CORE Group, 2004. https:// coregroup.org/wp-content/uploads/2020/03/LAC-Neonatalenglish_final_pdf.pdf (accessed Nov 3, 2023).
25 Whiteside A, Henry FE. The impact of HIV and AIDS research: a case study from Swaziland. Health Res Policy Syst 2011; 9 (suppl 1): S9.
26 Dwyer-Lindgren L, Cork MA, Sligar A, et al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature 2019; 570: 189-93.
27 Nachega JB, Kapata N, Sam-Agudu NA, et al. Minimizing the impact of the triple burden of COVID-19, tuberculosis and HIV on health services in sub-Saharan Africa. Int J Infect Dis 2021; 113 (suppl 1): S16-21.
28 Duarte R, Silva DR, Rendon A, et al. Eliminating tuberculosis in Latin America: making it the point. J Bras Pneumol 2018; 44: 73-76.
29 WHO. World health statistics 2022: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2022. https://www.who.int/data/gho/publications/ world-health-statistics (accessed Sept 16, 2022).
30 WHO. World health statistics 2023: monitoring health for the SDGs, sustainable development goals. Geneva: World Health Organization, 2023. https://www.who.int/publications-detailredirect/9789240074323 (accessed Oct 27, 2023).
31 Rosenthal PJ, John CC, Rabinovich NR. Malaria: how are we doing and how can we do better? Am J Trop Med Hyg 2019; 100: 239-41.
32 Bhatt S, Weiss DJ, Cameron E, et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015; 526: 207-11.
33 WHO. WHO recommends R21/Matrix-M vaccine for malaria prevention in updated advice on immunization. Geneva: World Health Organization, 2023. https://www.who.int/news/item/02-10-2023-who-recommends-r21-matrix-m-vaccine-for-malaria-prevention-in-updated-advice-on-immunization (accessed Oct 24, 2023).
34 Naddaf M. Second malaria vaccine to win global approval is cheaper and easier to make. Nature 2023; published online Oct 3. https:// doi.org/10.1038/d41586-023-03115-1.
35 Black R, Fontaine O, Lamberti L, et al. Drivers of the reduction in childhood diarrhea mortality 1980-2015 and interventions to eliminate preventable diarrhea deaths by 2030. J Glob Health 2019; 9: 020801.
36 Troeger CE, Khalil IA, Blacker BF, et al. Quantifying risks and interventions that have affected the burden of lower respiratory infections among children younger than 5 years: an analysis for the Global Burden of Disease Study 2017. Lancet Infect Dis 2020; 20: 60-79.
37 Das JK, Salam RA, Saeed M, Kazmi FA, Bhutta ZA. Effectiveness of interventions for managing acute malnutrition in children under five years of age in low-income and middle-income countries: a systematic review and meta-analysis. Nutrients 2020; 12: 116.
38 Mertens A, Benjamin-Chung J, Colford JM Jr, et al. Causes and consequences of child growth faltering in low-resource settings. Nature 2023; 621: 568-76.
39 Reiner RC Jr, Hay SI. The overlapping burden of the three leading causes of disability and death in sub-Saharan African children. Nat Commun 2022; 13: 7457.
40 Shah MP, Tate JE, Mwenda JM, Steele AD, Parashar UD. Estimated reductions in hospitalizations and deaths from childhood diarrhea following implementation of rotavirus vaccination in Africa. Expert Rev Vaccines 2017; 16: 987-95.
41 Reiner RC Jr, Graetz N, Casey DC, et al. Variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
42 Burstein R, Henry NJ, Collison ML, et al. Mapping 123 million neonatal, infant and child deaths between 2000 and 2017. Nature 2019; 574: 353-58.
43 Galles NC, Liu PY, Updike RL, et al. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980-2019: a systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021; 398: 503-21.
44 Deshpande A, Miller-Petrie MK, Lindstedt PA, et al. Mapping geographical inequalities in access to drinking water and sanitation facilities in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1162-85.
45 Bhattacharjee NV, Schaeffer LE, Hay SI, et al. Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000-2018. Nat Hum Behav 2021; 5: 1027-45.
46 Wiens KE, Lindstedt PA, Blacker BF, et al. Mapping geographical inequalities in oral rehydration therapy coverage in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1038-60.
47 Reiner RC Jr, Graetz N, Casey DC, et al. Local variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
48 GBD 2015 Healthcare Access and Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet 2017; 390: 231-66.
49 Bill & Melinda Gates Foundation. Enteric and diarrheal diseases. https://www.gatesfoundation.org/our-work/programs/global-health/enteric-and-diarrheal-diseases (accessed Oct 26, 2023).
50 Troeger C, Khalil IA, Rao PC, et al. Rotavirus vaccination and the global burden of rotavirus diarrhea among children younger than 5 years. JAMA Pediatr 2018; 172: 958-65.
51 Causey K, Fullman N, Sorensen RJD, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. Lancet 2021; 398: 522-34.
52 Barros LL, Barros LL, do Carmo RF, et al. Change in rotavirus vaccine coverage in Brazil from before (2015-2019) through the COVID-19 pandemic period (2020-2021). Viruses 2023; 15: 292.
53 DeSilva MB, Haapala J, Vazquez-Benitez G, et al. Association of the COVID-19 pandemic with routine childhood vaccination rates and proportion up to date with vaccinations across 8 US health systems in the Vaccine Safety Datalink. JAMA Pediatr 2022; 176: 68-77.
54 WHO. Vaccine-preventable diseases. Geneva: World Health Organization, 2023. https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases (accessed Nov 12, 2023).
55 WHO. The big catch-up: an essential immunization recovery plan for 2023 and beyond. Geneva: World Health Organization, 2023. https://www.who.int/publications-detail-redirect/9789240075511 (accessed Nov 12, 2023).
36 Troeger CE, Khalil IA, Blacker BF, et al. Quantifying risks and interventions that have affected the burden of lower respiratory infections among children younger than 5 years: an analysis for the Global Burden of Disease Study 2017. Lancet Infect Dis 2020; 20: 60-79.
37 Das JK, Salam RA, Saeed M, Kazmi FA, Bhutta ZA. Effectiveness of interventions for managing acute malnutrition in children under five years of age in low-income and middle-income countries: a systematic review and meta-analysis. Nutrients 2020; 12: 116.
38 Mertens A, Benjamin-Chung J, Colford JM Jr, et al. Causes and consequences of child growth faltering in low-resource settings. Nature 2023; 621: 568-76.
39 Reiner RC Jr, Hay SI. The overlapping burden of the three leading causes of disability and death in sub-Saharan African children. Nat Commun 2022; 13: 7457.
40 Shah MP, Tate JE, Mwenda JM, Steele AD, Parashar UD. Estimated reductions in hospitalizations and deaths from childhood diarrhea following implementation of rotavirus vaccination in Africa. Expert Rev Vaccines 2017; 16: 987-95.
41 Reiner RC Jr, Graetz N, Casey DC, et al. Variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
42 Burstein R, Henry NJ, Collison ML, et al. Mapping 123 million neonatal, infant and child deaths between 2000 and 2017. Nature 2019; 574: 353-58.
43 Galles NC, Liu PY, Updike RL, et al. Measuring routine childhood vaccination coverage in 204 countries and territories, 1980-2019: a systematic analysis for the Global Burden of Disease Study 2020, Release 1. Lancet 2021; 398: 503-21.
44 Deshpande A, Miller-Petrie MK, Lindstedt PA, et al. Mapping geographical inequalities in access to drinking water and sanitation facilities in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1162-85.
45 Bhattacharjee NV, Schaeffer LE, Hay SI, et al. Mapping inequalities in exclusive breastfeeding in low- and middle-income countries, 2000-2018. Nat Hum Behav 2021; 5: 1027-45.
46 Wiens KE, Lindstedt PA, Blacker BF, et al. Mapping geographical inequalities in oral rehydration therapy coverage in low-income and middle-income countries, 2000-17. Lancet Glob Health 2020; 8: e1038-60.
47 Reiner RC Jr, Graetz N, Casey DC, et al. Local variation in childhood diarrheal morbidity and mortality in Africa, 2000-2015. N Engl J Med 2018; 379: 1128-38.
48 GBD 2015 Healthcare Access and Quality Collaborators. Healthcare Access and Quality Index based on mortality from causes amenable to personal health care in 195 countries and territories, 1990-2015: a novel analysis from the Global Burden of Disease Study 2015. Lancet 2017; 390: 231-66.
49 Bill & Melinda Gates Foundation. Enteric and diarrheal diseases. https://www.gatesfoundation.org/our-work/programs/global-health/enteric-and-diarrheal-diseases (accessed Oct 26, 2023).
50 Troeger C, Khalil IA, Rao PC, et al. Rotavirus vaccination and the global burden of rotavirus diarrhea among children younger than 5 years. JAMA Pediatr 2018; 172: 958-65.
51 Causey K, Fullman N, Sorensen RJD, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. Lancet 2021; 398: 522-34.
52 Barros LL, Barros LL, do Carmo RF, et al. Change in rotavirus vaccine coverage in Brazil from before (2015-2019) through the COVID-19 pandemic period (2020-2021). Viruses 2023; 15: 292.
53 DeSilva MB, Haapala J, Vazquez-Benitez G, et al. Association of the COVID-19 pandemic with routine childhood vaccination rates and proportion up to date with vaccinations across 8 US health systems in the Vaccine Safety Datalink. JAMA Pediatr 2022; 176: 68-77.
54 WHO. Vaccine-preventable diseases. Geneva: World Health Organization, 2023. https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases (accessed Nov 12, 2023).
55 WHO. The big catch-up: an essential immunization recovery plan for 2023 and beyond. Geneva: World Health Organization, 2023. https://www.who.int/publications-detail-redirect/9789240075511 (accessed Nov 12, 2023).
56 Moss WJ, Strebel PM. Chapter 38 measles vaccines. In: Plotkin’s Vaccines, 8th edn. Philadelphia, PA: Elsevier, 2023: 629-63.
57 PAHO, WHO. Measles elimination in the Americas. Sept 27, 2016. https://www3.paho.org/hq/index.php?option=com_content&view= article&id=12526:measles-elimination-in-the-americas (accessed Nov 8, 2023).
58 Gidding HF, Martin NV, Stambos V, et al. Verification of measles elimination in Australia: application of World Health Organization regional guidelines. J Epidemiol Glob Health 2016; 6: 197-209.
59 WHO. Tenth meeting of the European Regional Verification Commission for Measles and Rubella Elimination: summary of virtual sessions held on Oct 6, 2021, Nov 2, 2021, Dec 8, 2021, and Feb 16, 2022. https://www.who.int/europe/publications/i/item/ WHO-EURO-2022-6093-45858-66035 (accessed Nov 8, 2023).
60 Sbarra AN, Rolfe S, Nguyen JQ, et al. Mapping routine measles vaccination in low- and middle-income countries. Nature 2021; 589: 415-19.
61 Minta AA, Ferrari M, Antoni S, et al. Progress toward regional measles elimination-worldwide, 2000-2021. MMWR Morb Mortal Wkly Rep 2022; 71: 1489-95.
62 Majekodunmi OB, Oladele EA, Greenwood B. Factors affecting poor measles vaccination coverage in sub-Saharan Africa with a special focus on Nigeria: a narrative review. Trans
63 National Institute of Allergy and Infectious Diseases. Condom use for preventing HIV infection. 2018. https://www.niaid.nih.gov/ diseases-conditions/condom-use (accessed Nov 6, 2023).
64 National Institute of Allergy and Infectious Diseases. HIV prevention. 2020. https://www.niaid.nih.gov/diseases-conditions/ hiv-prevention (accessed Nov 6, 2023).
65 Granich R, Gupta S, Hersh B, et al. Trends in AIDS deaths, new infections and ART coverage in the top 30 countries with the highest AIDS mortality burden; 1990-2013. PLoS One 2015; 10: e0131353.
66 National Institute of Allergy and Infectious Diseases. HIV undetectable=untransmittable (
67 Akpa OM, Adeolu-Olaiya V, Olusegun-Odebiri CA, Aganaba D. HIV/AIDS-related stigma and access to HIV treatments by people living with HIV/AIDS: a case study of selected states in north-west Nigeria. HIV AIDS Rev 2011; 10: 19-25.
68 Oturu K. Stigma in access to HIV treatment in African countries: the importance of social connections. Grounded Theory Rev 2011; 10: 63-90.
69 Rosen S, Fox MP, Gill CJ. Patient retention in antiretroviral therapy programs in sub-Saharan Africa: a systematic review. PLoS Med 2007; 4: e298.
70 Global HIV Prevention Working Group. Access to HIV prevention: closing the gap. Foreign Aff 2003; 82: 1-42.
71 Ford N, Boulle A, Egger M. Accounting for and responding to HIVassociated mortality. AIDS 2016; 30: 521-23.
72 Straetemans M, Bierrenbach AL, Nagelkerke N, Glaziou P, van der Werf MJ. The effect of tuberculosis on mortality in HIV positive people: a meta-analysis. PLoS One 2010; 5: e15241.
73 Piot P, Bartos M, Larson H, Zewdie D, Mane P. Coming to terms with complexity: a call to action for HIV prevention. Lancet 2008; 372: 845-59.
74 Gupta GR, Parkhurst JO, Ogden JA, Aggleton P, Mahal A. Structural approaches to HIV prevention. Lancet 2008; 372: 764-75.
75 Paulson KR, Kamath AM, Alam T, et al. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet 2021; 398: 870-905.
76 Saugstad OD. Reducing global neonatal mortality is possible. Neonatology 2011; 99: 250-57.
77 Tura G, Fantahun M, Worku A. The effect of health facility delivery on neonatal mortality: systematic review and meta-analysis. BMC Pregnancy Childbirth 2013; 13: 18.
78 Bill & Melinda Gates Foundation. Exemplars in global health. July 25, 2020. https://www.gatesfoundation.org/ideas/articles/ exemplars-global-health-niranjan-bose (accessed Nov 12, 2023).
57 PAHO, WHO. Measles elimination in the Americas. Sept 27, 2016. https://www3.paho.org/hq/index.php?option=com_content&view= article&id=12526:measles-elimination-in-the-americas (accessed Nov 8, 2023).
58 Gidding HF, Martin NV, Stambos V, et al. Verification of measles elimination in Australia: application of World Health Organization regional guidelines. J Epidemiol Glob Health 2016; 6: 197-209.
59 WHO. Tenth meeting of the European Regional Verification Commission for Measles and Rubella Elimination: summary of virtual sessions held on Oct 6, 2021, Nov 2, 2021, Dec 8, 2021, and Feb 16, 2022. https://www.who.int/europe/publications/i/item/ WHO-EURO-2022-6093-45858-66035 (accessed Nov 8, 2023).
60 Sbarra AN, Rolfe S, Nguyen JQ, et al. Mapping routine measles vaccination in low- and middle-income countries. Nature 2021; 589: 415-19.
61 Minta AA, Ferrari M, Antoni S, et al. Progress toward regional measles elimination-worldwide, 2000-2021. MMWR Morb Mortal Wkly Rep 2022; 71: 1489-95.
62 Majekodunmi OB, Oladele EA, Greenwood B. Factors affecting poor measles vaccination coverage in sub-Saharan Africa with a special focus on Nigeria: a narrative review. Trans
63 National Institute of Allergy and Infectious Diseases. Condom use for preventing HIV infection. 2018. https://www.niaid.nih.gov/ diseases-conditions/condom-use (accessed Nov 6, 2023).
64 National Institute of Allergy and Infectious Diseases. HIV prevention. 2020. https://www.niaid.nih.gov/diseases-conditions/ hiv-prevention (accessed Nov 6, 2023).
65 Granich R, Gupta S, Hersh B, et al. Trends in AIDS deaths, new infections and ART coverage in the top 30 countries with the highest AIDS mortality burden; 1990-2013. PLoS One 2015; 10: e0131353.
66 National Institute of Allergy and Infectious Diseases. HIV undetectable=untransmittable (
67 Akpa OM, Adeolu-Olaiya V, Olusegun-Odebiri CA, Aganaba D. HIV/AIDS-related stigma and access to HIV treatments by people living with HIV/AIDS: a case study of selected states in north-west Nigeria. HIV AIDS Rev 2011; 10: 19-25.
68 Oturu K. Stigma in access to HIV treatment in African countries: the importance of social connections. Grounded Theory Rev 2011; 10: 63-90.
69 Rosen S, Fox MP, Gill CJ. Patient retention in antiretroviral therapy programs in sub-Saharan Africa: a systematic review. PLoS Med 2007; 4: e298.
70 Global HIV Prevention Working Group. Access to HIV prevention: closing the gap. Foreign Aff 2003; 82: 1-42.
71 Ford N, Boulle A, Egger M. Accounting for and responding to HIVassociated mortality. AIDS 2016; 30: 521-23.
72 Straetemans M, Bierrenbach AL, Nagelkerke N, Glaziou P, van der Werf MJ. The effect of tuberculosis on mortality in HIV positive people: a meta-analysis. PLoS One 2010; 5: e15241.
73 Piot P, Bartos M, Larson H, Zewdie D, Mane P. Coming to terms with complexity: a call to action for HIV prevention. Lancet 2008; 372: 845-59.
74 Gupta GR, Parkhurst JO, Ogden JA, Aggleton P, Mahal A. Structural approaches to HIV prevention. Lancet 2008; 372: 764-75.
75 Paulson KR, Kamath AM, Alam T, et al. Global, regional, and national progress towards Sustainable Development Goal 3.2 for neonatal and child health: all-cause and cause-specific mortality findings from the Global Burden of Disease Study 2019. Lancet 2021; 398: 870-905.
76 Saugstad OD. Reducing global neonatal mortality is possible. Neonatology 2011; 99: 250-57.
77 Tura G, Fantahun M, Worku A. The effect of health facility delivery on neonatal mortality: systematic review and meta-analysis. BMC Pregnancy Childbirth 2013; 13: 18.
78 Bill & Melinda Gates Foundation. Exemplars in global health. July 25, 2020. https://www.gatesfoundation.org/ideas/articles/ exemplars-global-health-niranjan-bose (accessed Nov 12, 2023).