العلاج النيوأدجوفانت باستخدام نيفولوماب والعلاج الكيميائي في سرطان الثدي المبكر الإيجابي لمستقبلات الإستروجين: تجربة عشوائية من المرحلة الثالثة Neoadjuvant nivolumab and chemotherapy in early estrogen receptor-positive breast cancer: a randomized phase 3 trial
العلاج النيوأدجوفانت باستخدام نيفولوماب والعلاج الكيميائي في سرطان الثدي المبكر الإيجابي لمستقبلات الإستروجين: تجربة عشوائية من المرحلة الثالثة
تاريخ الاستلام: 5 يوليو 2024 مقبول: نوفمبر 2024 نُشر على الإنترنت: 21 يناير 2025 تحقق من التحديثات
تظهر قائمة بالمؤلفين وانتماءاتهم في نهاية الورقة.
المرضى الذين يعانون من سرطان الثدي الأولي الإيجابي لمستقبلات الاستروجين (ER+)، السلبي لمستقبلات عامل نمو البشرة البشري 2 (HER2-) لديهم معدلات استجابة كاملة مرضية منخفضة (pCR) مع العلاج الكيميائي المساعد. تحتوي مجموعة فرعية من سرطان الثدي ER+/HER2- على تسلل لمفاوي كثيف. افترضنا أن إضافة عامل مضاد للبرامج الميتة 1 قد تزيد من معدلات pCR في هذا النوع الفرعي من سرطان الثدي. أجرينا تجربة عشوائية متعددة المراكز مزدوجة التعمية من المرحلة 3 للتحقيق في فائدة إضافة نيفولوماب إلى العلاج الكيميائي المساعد في المرضى الذين تم تشخيصهم حديثًا، والذين يعانون من مخاطر عالية، من الدرجة 3 أو 2 (ER 1 إلى ) سرطان الثدي الأولي ER+/HER2-. تم توزيع 510 مريضًا عشوائيًا لتلقي العلاج الكيميائي القائم على الأنثراسيكلين والتابوكسين مع إما نيفولوماب عن طريق الوريد أو دواء وهمي. كانت النتيجة الأساسية لـ pCR أعلى بشكل ملحوظ في مجموعة نيفولوماب مقارنةً بالدواء الوهمي ( ضد )، مع ملاحظة فائدة أكبر في المرضى الذين لديهم أورام إيجابية لمستقبلات ligand 1 المبرمجة للموت (VENTANA SP142 ضد على التوالي). لم يتم تحديد أي إشارات أمان جديدة. من بين خمس وفيات حدثت في مجموعة نيفولوماب، كانت حالتان مرتبطتين بسمية الدواء المدروس؛ ولم تحدث أي وفيات في مجموعة الدواء الوهمي. أدى إضافة نيفولوماب إلى العلاج الكيميائي المساعد إلى زيادة كبيرة في معدلات الاستجابة الكاملة النسيجية (pCR) في حالات سرطان الثدي المبكر عالية المخاطر ER+/HER2-، لا سيما بين المرضى الذين لديهم مستويات أعلى من الخلايا اللمفاوية المتسللة إلى الورم أو تعبير ligand 1 المبرمج للموت، مما يشير إلى نموذج علاج جديد يركز على دور العلاج المناعي ومراقبة المناعة بواسطة خلايا T في الأمراض اللمعية. السريريةtrials.govمعرف: NCT04109066
تم تشخيص حوالي 2.3 مليون حالة من سرطان الثدي على مستوى العالم في عام 2020، من بينهاكانت نوعية ER+/HER2-يظهر سرطان الثدي ER+/HER2- تباينًا كبيرًا في استجاباته للعلاج والنتائج السريرية، مما يطرح تحديات كبيرة للإدارة الفعالة. قد يكون هذا التباين ناتجًا عن اختلافات مميزة في الأنماط الجزيئية لسرطان الثدي ER+/HER2-، بما في ذلك الأنماط التي تعبر عن مستقبلات الاستروجين والبروجستيرون بشكل متنوع، وتلك التي تكون مناعية، متكاثرة، ومدفوعة بمستقبلات التيروزين كيناز، والتي تتطلب علاجات محددة..
تشمل الاستراتيجيات العلاجية النظامية الحالية لسرطان الثدي الإيجابي لمستقبلات هرمون الاستروجين/سلبي لمستقبلات HER2 في المراحل المبكرة وعالية المخاطر: العلاج الكيميائي المساعد أو المساعد (CT)؛ العلاج الهرموني المساعد المطول (ET) مع أو بدون العلاجات المستهدفة المساعدة، بما في ذلك مثبطات كيناز السيكلين المعتمد على 4/6؛ ومثبطات بوليميراز (ADP-ribose) للمرضى الذين يحملون طفرات جينية ضارة.تعديلات.
تعمل العوامل المضادة لبروتين الموت المبرمج 1 (PD-L1) على تحسين النتائج السريرية بشكل كبير في سرطان الثدي الثلاثي السلبي في مراحله المبكرة وسرطان الثدي الثلاثي السلبي النقيلي الإيجابي لـ PD-L1.تحتوي مجموعة فرعية من سرطان الثدي الإيجابي لمستقبلات هرمون الاستروجين/سلبي لمستقبلات HER2 على كثافة
infiltrate اللمفاوي، مشابه لما يُرى في TNBC؛ ومع ذلك، فإنه غير واضح كيف يرتبط ذلك بالاستجابة لمثبطات نقاط التفتيش المناعية في سرطان الثدي الإيجابي لمستقبلات هرمون الاستروجين/سلبي لمستقبلات HER2تشير نتائج دراسة I-SPY2 العشوائية التكيفية إلى أن العوامل المضادة لـ PD-(L)1 لديها القدرة على زيادة نسبة المرضى الذين يعانون من سرطان الثدي عالي المخاطر ER+/HER2- والذين يحققون استجابة كاملة (pCR) أو مرض متبقي ضئيل (درجة عبء السرطان المتبقي (RCB) تساوي 0 أو I) بعد العلاج المساعد.هدفت دراسة CheckMate 7FL (NCT04109066) إلى التحقيق في فائدة إضافة نيفولوماب إلى العلاج الكيميائي المساعد متبوعًا بالعلاج الهرموني المساعد لدى المرضى الذين تم تشخيصهم حديثًا بسرطان الثدي في مراحله المبكرة وعالي المخاطر ER+/HER2-. كما سعينا أيضًا لتحديد الفئات الفرعية من المرضى الأكثر احتمالًا للاستجابة لنيفولوماب بالاشتراك مع العلاج الكيميائي المساعد.
النتائج
السكان المدروسون والخصائص الديموغرافية
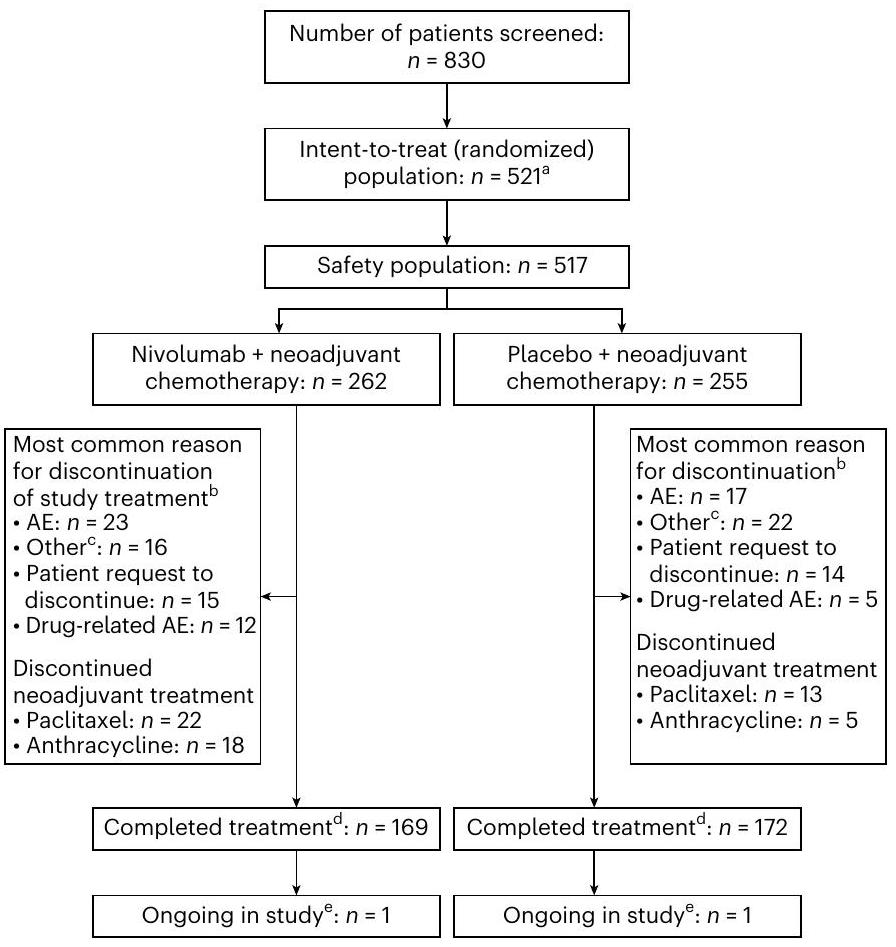
من 20 نوفمبر 2019 إلى 7 أبريل 2022، تم فحص 830 مريضًا في 221 موقعًا في 31 دولة. من بين 830 مريضًا تم فحصهم، تم توزيع 521 مريضًا عشوائيًا. بسبب قرار الراعي بإغلاق جميع المواقع في روسيا بعد بدء الصراع الجيوسياسي بين أوكرانيا وروسيا، تم استبعاد 11 مريضًا من مجموعة التحليل بسبب عدم كفاية المتابعة لتقييم pCR. شكلت المجموعة الناتجة مجموعة النية المعدلة للعلاج (mITT)، والتي تضم 510 مرضى تلقوا علاجًا كيميائيًا مساعدًا إما مع نيفولوماب ( ) أو دواء وهمي تكونت مجموعة السلامة من 517 مريضًا تلقوا العلاج الكيميائي المساعد باستخدام إما نيفولوماب ( ) أو دواء وهمي ( ) (الشكل 1). كانت الخصائص السكانية والسريرية للمرضى متوازنة بين ذراعي العلاج (الجدول 1).
في مجموعة السلامة، كانت مدة العلاج المتوسطة (الحد الأدنى، الحد الأقصى) خلال مرحلة العلاج المساعد بالباسيتاكسيل هيأسابيع للمرضى الذين يتلقون نيفولوماب وأسابيع للمرضى الذين يتلقون العلاج الوهمي. كانت مدة العلاج المتوسطة (الحد الأدنى، الحد الأقصى) خلال مرحلة العلاج المساعد بالأنتراسيكلين هيأسابيع للمرضى الذين يتلقون نيفولوماب و 7.7 (0.1، 15.1) أسابيع للمرضى الذين يتلقون الدواء الوهمي. من المرضى الذين تم توزيعهم عشوائيًا إلى نيفولوماب والدواء الوهمي، على التوالي، ( 233 من 263 ) و ( 236 من 258 ) خضعوا لعملية جراحية (الجدول التكميلي 1).
فعالية
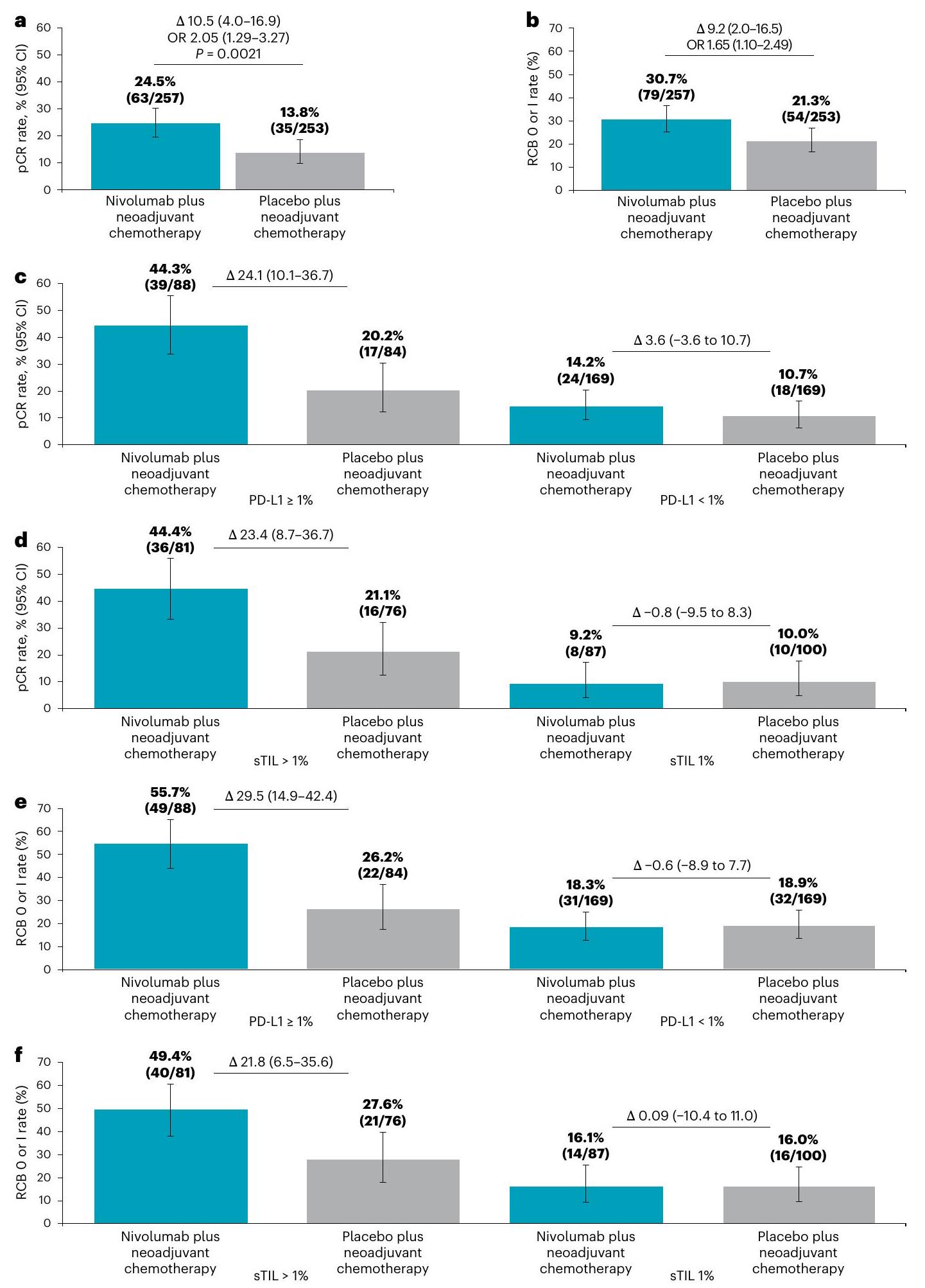
نسبة أكبر بشكل ملحوظ إحصائيًا من المرضى الذين تلقوا نيفولوماب حققوا pCR (ypT0/is، ypN0؛ من 257 ) مقابل الدواء الوهمي ( من 253؛ نسبة الأرجحية (OR) 2.05 (فترة الثقة (CI) من 1.29 إلى 3.27،بالإضافة إلى العلاج الكيميائي المساعد (الشكل 2أ).
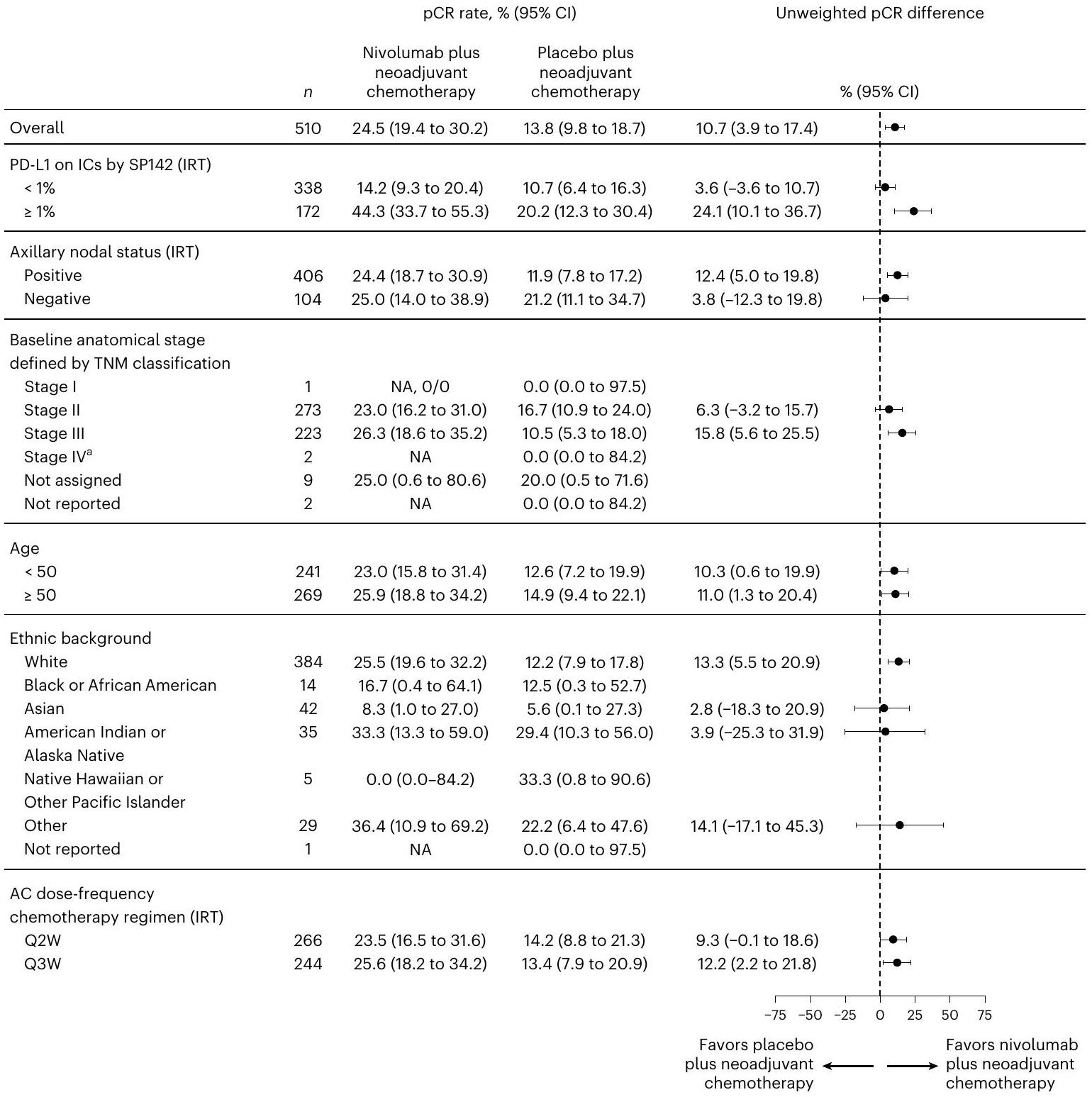
كانت نسبة المرضى الذين عانوا من الاستجابة الكاملة (pCR) أعلى عددياً بين أولئك الذين لديهم أورام إيجابية لمستقبل PD-L1 (خلايا المناعة المتسللة إلى الورم التي تعبر عن PD-L1). IC، ) مقابل أولئك الذين لديهم أورام PD-L1- ( IC، ). الفرق في معدلات pCR ( بين مجموعة نيفولوماب ومجموعة الدواء الوهمي كان (10.1 إلى 36.7) و 3.6 % (-3.6 إلى 10.7) للأورام الإيجابية لـ PD-L1 والأورام السلبية لـ PD-L1، على التوالي (الشكل 2c). كانت تحليلات المجموعات الفرعية لمعدلات pCR متوافقة مع هذه النتائج (الشكل 3).
كانت معدلات RCB 0 أو I في مجموعة المITT وحسب حالة PD-L1، بالإضافة إلى تحليلات المجموعات الفرعية، متوافقة مع النتائج التي لوحظت بالنسبة لـ pCR (الشكل 2b، e والشكل التوضيحي 1). لقد أمال نيفولوماب توزيع RCB نحو الفئات الأدنى مقارنةً بالعلاج الوهمي (الشكل التوضيحي 2).
نظرًا لإنهائه المبكر، كانت الدراسة ضعيفة القوة بشكل كبير بالنسبة للبقاء بدون أحداث (EFS)، وكان متوسط المتابعة للبقاء بدون أحداث في مجموعة التحليل العشوائي المعدلة (mITT) عند الإبلاغ مبكرًا عند 19 شهرًا، مع عدد قليل من الأحداث التي تم ملاحظتها. أظهرت نتائج تحليل استكشافي وصفي أن البقاء بدون أحداث كان مشابهًا بين ذراعي العلاج، مع معدل لمدة 18 شهرًا من ( إلى 92.7) في مجموعة نيفولوماب وإلى 94.8) في مجموعة الدواء الوهمي (الشكل التوضيحي 3).
الفعالية وفقًا لمؤشرات المناعة
كانت نسبة السكان الإيجابيين لـ PD-L1 في الذراعين متوازنة، كما تم تقييمها من خلال حالة التعبير عن PD-L1 في البداية، المحددة بواسطة إما
الشكل 1 | مخطط تدفق يوضح توزيع المرضى. تلقى خمسة وعشرون مريضًا العلاج بالأبماسيكلب، وقد يكونوا قد تلقوه بعد العلاج المساعد أو أوقفوا العلاج المساعد لتلقي الأبماسيكلب.تكونت مجموعة المITT من 510 مرضى (257 مريضًا في مجموعة نيفولوماب و253 مريضًا في مجموعة الدواء الوهمي). بسبب قرار الراعي بإغلاق المواقع الروسية، تم استبعاد 11 مريضًا بسبب عدم كفاية المتابعة لتقييم الاستجابة الكاملة (pCR).توقف العلاج الدراسي شمل توقف العلاج خلال المرحلة المساعدة.أكثر الأسباب شيوعًا لوقف العلاج التي تم تسجيلها تحت ‘أخرى’ كانت تقدم المرض، تقدير الباحث الرئيسي، الأحداث الضائرة الخطيرة أو الأحداث الضائرة وسحب الموافقة.المكتملون هم المرضى الذين أتموا الجراحة ومرحلة العلاج المساعد.تم الإبلاغ عن المرضى على أنهم مستمرون في الوقت الذي تم فيه الإغلاق المبكر للمواقع الروسية.
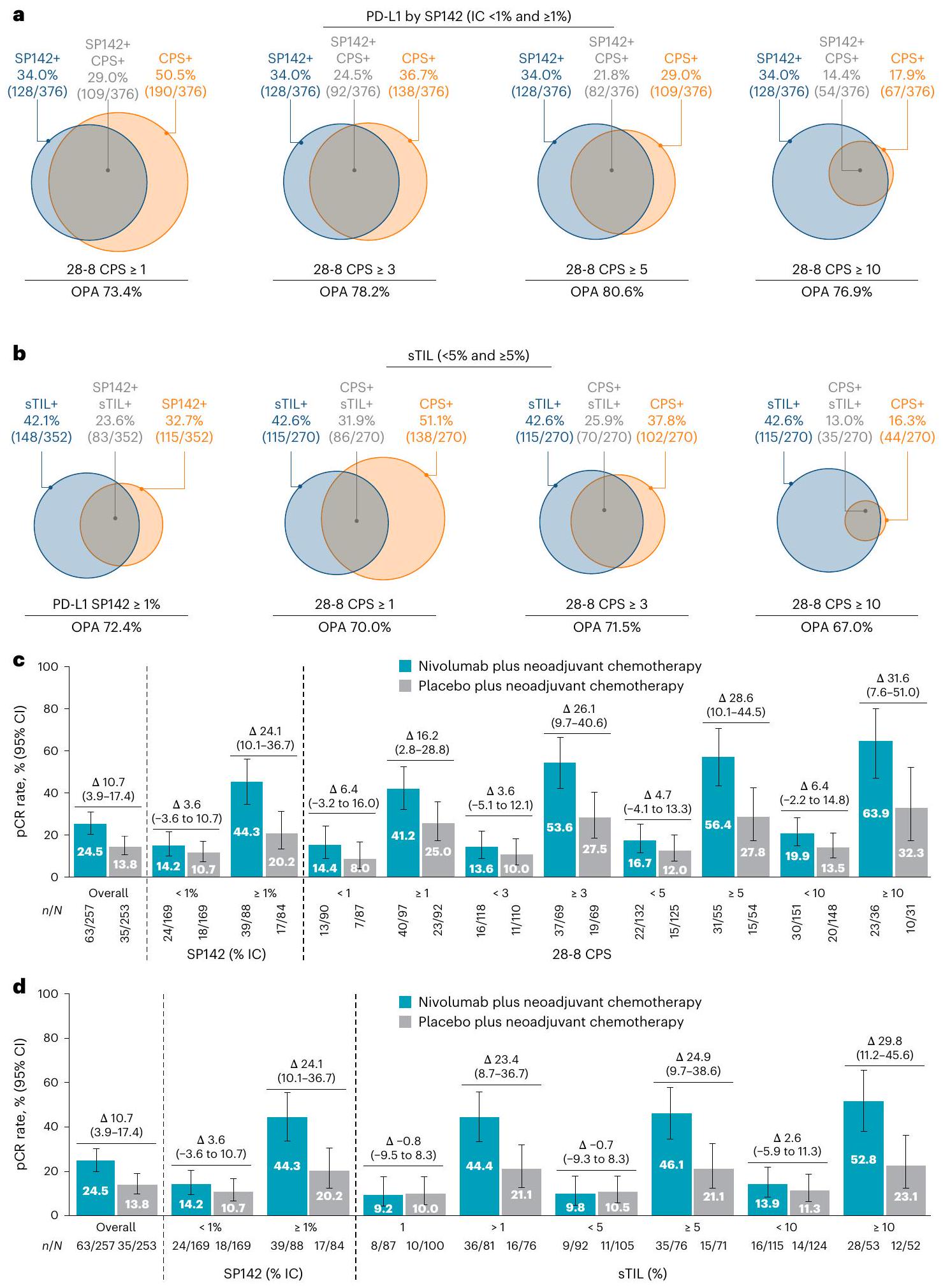
اختبار VENTANA SP142 IC) أو اختبار Dako 28-8 (درجة إيجابية مركبة لـ PD-L1 (CPS) و ) (الشكل التوضيحي الإضافي 4). أعلى نسبة اتفاق عامة تمت ملاحظته بين SP142 IC و 28-8 CPS (الشكل 4أ). زادت معدلات pCR و RCB 0 أو I في المرضى الذين لديهم أورام PD-L1+ كما تم قياسها بواسطة SP142 و ؛ كانت الفائدة أكبر مع زيادة حدود قطع CPS (الشكل 4c والأشكال التكميلية 5 و 6).
تظهر انتشار الفئات الإيجابية للعلامات البيولوجية في البداية مقسمة حسب نسبة الخلايا اللمفاوية المتسللة إلى الورم (sTILs) عند نقاط قطع مختلفة، مقارنة بتلك التي تم قياسها بواسطة PD-L1 SP142 عند 1% من الخلايا المناعية، في الشكل التوضيحي 7. كانت مستويات sTIL المتوسطة والوسطية و (s.d., 24.16 )، على التوالي، وكانت نسبة إيجابية السTIL متوازنة عبر مجموعات العلاج. تعريف المرضى الإيجابيين للسTIL على أنهم أولئك الذين لديهم مستويات قابلة للاكتشاف من السTIL (>1%)، كانت نسبة الاتفاق العامة بين اكتشاف السTIL وقطع PD-L1 المختلفة بواسطة الخلايا المناعية أو CPS تتراوح بين و (الشكل 4ب). زادت معدلات pCR و RCB 0 أو I مع نيفولوماب مقابل الدواء الوهمي في المرضى الذين لديهم مستويات أعلى من sTIL (الأشكال 2د، ف و 4د). عندما تم استخدام كل من اختبارات sTIL و PD-L1، لوحظت أعلى معدلات pCR في المرضى الذين اعتُبرت فيهما كل من تعبير sTIL و PD-L1 إيجابياً، ولكن من الجدير بالذكر أنه كان هناك أيضاً فائدة من نيفولوماب للمرضى الذين لديهم عدم تطابق بين PD-L1 <1% IC و sTIL+ (الشكل التكميلية 8). كانت معدلات pCR و RCB 0 أو I أعلى في المرضى الذين كانت أورامهم تحتوي على تعبير أقل لمستقبلات هرمون الاستروجين (<50%) و/أو مستقبلات البروجستيرون. ) من المرضى الذين كانت أورامهم تحتوي على مستويات أعلى من مستقبلات الاستروجين أو البروجستيرون
جميع القيم مقدمة كـ (%)، ما لم يُذكر خلاف ذلك.نسبة الخلايا المناعية المتسللة التي تعبر عن PD-L1 من مساحة الورم (PD-L1 يُعرف بأنه PD-L1 IC <1%; PD-L1+ يُعرف بأنه PD-L1 IC ) باستخدام اختبار VENTANA SP142، وفقًا للتقييم المركزي. تم تقييمه محليًا.شملت المجموعة ب مريضًا واحدًا مصابًا بمرض المرحلة الأولى واثنين من المرضى المصابين بمرض المرحلة الرابعة، الذين تم اعتبارهم مؤهلين وتم إعادة تصنيفهم لاحقًا على أنهم مصابون بمرض المرحلة الثانية.دليل تصنيف السرطان للجنة الأمريكية المشتركة لمكافحة السرطان، الطبعة الثامنة.تم السماح بالعلاج بم agonist هرمون إفراز الغدد التناسلية للحفاظ على المبيض. AC، أنثراسيكلين + سيكلوفوسفاميد؛ cTNM، نظام تصنيف TNM السريري (حجم T ومدى الورم الأولي؛ N مدى الانتشار إلى العقد اللمفاوية؛ M وجود النقائل)؛ ECOG PS، حالة الأداء لمجموعة التعاون الشرقي لعلم الأورام؛ QXW، كل X أسابيع. تعبير المستقبلات (الأشكال التكميلية 9 و 10). لم يُلاحظ أي ارتباط بين فائدة نيفولوماب ومؤشر Ki67 (الشكل التكميلية 11).
في تحليل متعدد المتغيرات لـ pCR حسب مجموعات العلامات الحيوية، بما في ذلك الميزات السريرية المرضية التنبؤية والعلامات الحيوية الرئيسية، نسبة sTIL ( أو ) و PD-L1 (المعرف كـ ICأو CPSكانت مرتبطة بشكل مستقل بفعالية نيفولوماب (الأشكال التكميلية 12a، b و 13a، b).
السلامة
تحليل السلامة يعتمد على مجموعة السلامة“; 262 مريضًا في مجموعة نيفولوماب و255 مريضًا في مجموعة الدواء الوهمي). في مرحلة العلاج المساعد، عانى نسبة مماثلة من المرضى في مجموعتي نيفولوماب مقابل الدواء الوهمي من أحداث سلبية (AEs) ( ضد ) وآثار جانبية مرتبطة بالعلاج من أي درجة ( ضد ” ). كانت الآثار الجانبية المرتبطة بالعلاج الأكثر شيوعًا هي تساقط الشعر ( ضد غثيان ضد فقر الدم ( ضد ) والإرهاق ( ضد ) في ذراعي نيفولوماب مقابل الدواء الوهمي، على التوالي. تم الإبلاغ عن آثار جانبية من الدرجة 3 أو 4 في ضد من المرضى في ذراع نيفولوماب مقابل الدواء الوهمي، على التوالي. تم الإبلاغ عن آثار جانبية مرتبطة بالعلاج من الدرجة 3 أو 4 في ضد من المرضى في ذراعي نيفولوماب مقابل الدواء الوهمي، على التوالي (الجدول 2). الأحداث الضائرة الخطيرة (22.9% مقابل 12.9%) والأحداث الضائرة الخطيرة المرتبطة بالعلاج ( ضد )، بالإضافة إلى الأحداث السلبية التي تؤدي إلى التوقف ( ضد ) وآثار جانبية مرتبطة بالعلاج أدت إلى التوقف ( ضد )، تم الإبلاغ عنها بشكل أكثر تكرارًا مع نيفولوماب مقارنةً بالعلاج الوهمي.
في مرحلة العلاج المساعد قبل الجراحة، كان هناك ثلاثة (أحداث غير مرتبطة بالعلاج من الدرجة 5 في مجموعة نيفولوماب (واحدة بسبب COVID-19؛ اثنتان بسبب انسداد رئوي، حدثت واحدة منهما خلال أسبوع من التعافي من COVID-19) ولم يتم الإبلاغ عن أي منها في مجموعة الدواء الوهمي. بالإضافة إلى ذلك، تم اعتبار حالتي وفاة إضافيتين في مجموعة نيفولوماب مرتبطة بسمية الدواء المستخدم في الدراسة، على الرغم من عدم الإبلاغ عنهما كحالة من الدرجة 5 (بسبب الفاصل الزمني الطويل بين بداية الأحداث السلبية والوفاة): التهاب رئوي (61 يومًا بعد الجرعة النهائية من العلاج المساعد) والتهاب الكبد (51 يومًا بعد الجرعة النهائية من العلاج المساعد)؛ ولم يتم الإبلاغ عن أي وفيات بسبب سمية الدواء في مجموعة الدواء الوهمي.
الأحداث السلبية خلال مرحلة العلاج المساعد التي تطلبت أدوية تعديل المناعة حدثت في و المرضى في ذراعي نيفولوماب والدواء الوهمي، على التوالي. حدثت آثار جانبية ذات اهتمام خاص في ثلاثة (1.1%) من المرضى في ذراع نيفولوماب ولم تحدث في أي من المرضى في ذراع الدواء الوهمي؛ كانت هذه الأحداث من الدرجة 3 أو 4 من متلازمة غيلان باري.التهاب عضلة القلب من الدرجة 3 أو 4 ) ودرجة التهاب الأعصاب المناعي الذاتي ).
كانت الجرعة التراكمية المتوسطة وشدة الجرعة النسبية لكل دواء من أدوية العلاج الكيميائي مشابهة في كلا ذراعي العلاج.
نقاش
في دراسة CheckMate 7FL، بحثنا فيما إذا كان إضافة نيفولوماب إلى العلاج الكيميائي المساعد باستخدام الأنثراسيكلين والتاكسين يمكن أن يزيد بشكل كبير من معدلات الاستجابة الكاملة (pCR) في حالات سرطان الثدي الإيجابي لمستقبلات هرمون الاستروجين (ER+) والسلبية لمستقبلات HER2 (HER2-) في مراحلها المبكرة وعالية المخاطر وعالية الدرجة. حققت الدراسة هدفها الأساسي، حيث كانت هناك زيادة ملحوظة في معدل الاستجابة الكاملة (pCR) في مجموعة نيفولوماب مقارنةً بالدواء الوهمي. كما تحسنت معدلات RCB 0 أو I في مجموعة نيفولوماب مقارنةً بالدواء الوهمي.
الشكل 2 | نقاط فعالية العلاج للسكان بشكل عام وحسب المجموعات الفرعية. أ، ب، نسبة المرضى الذين لديهم و RCB 0 أو I (ب) لعلاج النيفولوماب بالإضافة إلى العلاج الكيميائي المساعد ( ) والعلاج الوهمي بالإضافة إلى العلاج الكيميائي المساعد ( ) الأسلحة في مجموعة المITT. ج، د، نسبة المرضى الذين حققوا pCR في ذراع نيفولوماب بالإضافة إلى العلاج الكيميائي المساعد وذراع الدواء الوهمي بالإضافة إلى العلاج الكيميائي المساعد حسب حالة PD-L1 أو (ج) وحالة الخلايا اللمفاوية المتسللة إلى الورم الداعم (sTIL) أو نسبة المرضى الذين لديهم معدل RCB 0 أو I حسب حالة PD-L1 أو وحالة sTIL أو ، ) (ف). تُعرض البيانات كنسب مئوية مع أشرطة خطأ تُظهر فترة الثقة حول النسبة الملحوظة للمرضى في مجموعة العلاج. فترات الثقة تم حسابها لكل ذراع علاج باستخدام طريقة كلوبير-بيرسون وفترات الثقة للاختلافات (تم حساب الفروق بين مجموعات العلاج باستخدام طريقة نيوكومب دون تصحيح الاستمرارية. تم تحليل الفرق المعدل حسب الطبقات في معدل الاستجابة الكاملة للعلاج (pCR) بين المجموعتين باستخدام طريقة كوشران-مانتل-هانزل الموزونة مع مستوى ألفا ثنائي الجانب منتم تقييم OR المعدل حسب الطبقات باستخدام طريقة مانتل-هانزل (أ، ب). عدد المرضى الذين لديهم pCR أو RCB 0 أووإجمالي عدد المرضى في كل مجموعة فرعيةمبين فوق كل شريط. قفل قاعدة البيانات: 14 أبريل20 مارس 2024 (د-ف). ن، عدد المرضى الذين حققوا استجابة كاملة (pCR) أو تصنيف RCB 0/I؛ ن، عدد المرضى في كل مجموعة علاجية.
الشكل 3 | رسم بياني للغابات يوضح نسبة المرضى الذين حققوا استجابة كاملة (pCR) في ذراعي نيفولوماب مع العلاج الكيميائي المساعد ودواء وهمي مع العلاج الكيميائي المساعد حسب تحليلات المجموعات الفرعية. تُعرض البيانات كنسب مئوية مع أشرطة خطأ تظهر فترات الثقة 95% حول النسبة الملاحظة للمرضى في ذراع العلاج. تم حساب فترات الثقة لكل ذراع علاج باستخدام طريقة كلوبير-بيرسون، وتم حساب فترات الثقة للاختلافات بين أذرع العلاج باستخدام نيوكومب.
طريقة بدون تصحيح الاستمرارية. لم يتم حساب فرق معدل pCR للفئات الفرعية التي تحتوي على أقل من 10 مرضى لكل ذراع علاج.تم اعتبار المريضين اللذين تم تصنيفهما في البداية على أنهما يعانيان من مرض المرحلة الرابعة مؤهلين، وتم إعادة تصنيفه لاحقًا على أنهما يعانيان من مرض المرحلة الثانية. AC، أنثراسيكلين؛ IRT، تقنية الاستجابة التفاعلية؛، العدد الإجمالي للمرضى في المجموعة الفرعية؛ غير متوفر؛ كل أسبوعين؛ كل ثلاثة أسابيع. قفل قاعدة البيانات: 14 أبريل 2023. كانت هذه النتائج مدفوعة بشكل أساسي من قبل مجموعة فرعية من PD-L1+، حيث كانت هناك اختلاف مطلق يزيد عنتمت ملاحظته مع إضافة نيفولوماب إلى العلاج الكيميائي المساعد. كانت هذه الملاحظة مختلفة عن تلك في سرطان الثدي الثلاثي السلبي في مراحله المبكرة، حيث كان التأثير مستقلاً عن تعبير PD-L1.على الرغم من أن الأسباب وراء ذلك غير واضحة، إلا أن سرطان الثدي الثلاثي السلبي معروف بأنه أكثر تنوعًا من الناحية الجزيئية مقارنة بسرطان الثدي الإيجابي لمستقبلات هرمون الاستروجين، مما قد يؤدي إلى أن خزعة نسيجية واحدة غير مرجحة لاحتواء تعبير PD-L1 المتنوع.لا يزال متوسط المتابعة قصيرًا جدًا في هذا التحليل لاستنتاج أي استنتاجات حول EFS، على الرغم من أنه من الجدير بالذكر أنه لم تكن هناك وفيات مبكرة غير مرتبطة بسرطان الثدي. ومع ذلك، فإن تحقيق pCR و/أو RCB من 0 أو I مرتبط بتحسين النتائج على المدى الطويل في سرطان الثدي ER+/HER2-.تختلف ترجمة التحسينات في معدلات الاستجابة الكاملة (pCR) إلى تحسينات في فترة البقاء الخالية من الأحداث (EFS) عبر تجارب سريرية مختلفة. كانت هناك عدد قليل جداً من التجارب المبكرة التي كانت لديها قوة كافية لتقييم كلا النقطتين؛ ومع ذلك، بشكل عام، فإن تقريباً جميع العلاجات الكيميائية المركبة التي حسنت معدلات الاستجابة الكاملة. (من خلال دمج علاج قائم على التاكسين، وعلاج قائم على الكاربوبلاتين، وعلاج مستهدف لـ HER2 أو بيمبروليزوماب) أيضًا حسن من فترة البقاء خالية من الأحداث في دراسات سرطان الثديكما أنه من الواضح بشكل متزايد أن أنظمة العلاج المساعد المختلفة تؤدي إلى توزيعات مختلفة من RCB، وأن العلاجات التي تنقل الطيف الكامل لـ RCB إلى قيم أصغر قد يكون لها تأثير أكبر على EFS مقارنة بالعلاجات التي تحسن معدلات pCR من خلال نقل الأورام المتبقية الدنيا إلى فئة pCR..
نتائجنا تتماشى مع نتائج دراسة KEYNOTE-756، الذي بحث في البمبروليزوماب في نفس مجموعة المرضى. في KEYNOTE-756، تم أيضًا رؤية معدلات pCR المحسنة في سياق زيادة تعبير PD-L1 ولكن فقط عند المستويات الأعلى باستخدام 22 C3 pharmDx CPS (CPSتؤكد نتائج CheckMate 7FL فائدة إضافة مثبط نقطة تفتيش مناعية إلى العلاج الكيميائي المساعد في هذا النوع من سرطان الثدي والسياق، وسيوضح المتابعة الأطول ما إذا كانت هذه الاستجابات الكاملة (pCRs) تترجم إلى فائدة أكبر في فترة البقاء خالية من الأحداث (EFS) لـ
الشكل 4 | فعالية نيفولوماب حسب المجموعات الفرعية. أ، التوافق بين اختبارات PD-L1 SP142 و28-8 CPS. ب، sTIL وتعبير PD-L1 في المرضى الذين لديهم sTIL وPD-L1 قابلين للقياس بواسطة SP142 أو 28-8 CPS. ج، معدلات pCR في ذراعي نيفولوماب بالإضافة إلى العلاج الكيميائي المساعد ودواء وهمي بالإضافة إلى العلاج الكيميائي المساعد حسب حالة PD-L1 كما تحددها اختبارات SP142 (IC%) و28-8 CPS (الحدود 1-20). د، حالة PD-L1 كما تحددها اختبار SP142 (IC%) ونسبة sTIL (الحدود ). عدد المرضى الذين لديهم بيانات مؤهلة ( ) وإجمالي عدد المرضى في كل مجموعة فرعية موجودة فوق كل دائرة ) أو أسفل كل شريط ( ). تُعرض البيانات كنسب مئوية. كانت فترات الثقة للنسبة الملاحظة من المرضى في مجموعة العلاج هي تم حسابها باستخدام طريقة كلوبير-بيرسون وتم حساب فترات الثقة للاختلافات بين أذرع العلاج باستخدام طريقة نيوكومب دون تصحيح الاستمرارية (ج، د). الخطوط العمودية المتقطعة تهدف إلى التمييز بصريًا بين الإجمالي، SP142 و 28-8 في (ج)، والإجمالي، SP142 و sTIL في (د). 28-8 CPS، اختبار Dako 28-8 باستخدام خوارزمية CPS؛ OPA، النسبة المئوية العامة للاتفاق؛ SP142 VENTANA، اختبار PD-L1SP142. قاعدة البيانات السريرية؛ نقطة قطع SP142 عند ضد نظرًا لصغر حجم العينة، لم يتم حساب نسبة الاتفاق لـ CPS. ). قفل قاعدة البيانات: 20 مارس 2024. تم تضمين مرضى إضافيين في مجموعة CPSevaluable في هذا القفل النهائي لقاعدة البيانات.
قفل قاعدة البيانات: 20 مارس 2024.الأحداث المبلغ عنها بين الجرعة الأولى و30 يومًا بعد الجرعة الأخيرة من العلاج المساعد للمرضى الذين لم يتلقوا العلاج المساعد أو قبل العلاج المساعد للمرضى الذين بدأوا العلاج المساعد. الأحداث المعروضة هي العشرة الأكثر شيوعًا في مجموعة نيفولوماب.من المحتمل أن يكون تساقط الشعر قد تم الإبلاغ عنه بشكل ناقص. تتكون معايير السمية الشائعة لتصنيف الأحداث الضارة لتساقط الشعر من الدرجة 1 أو 2 فقط؛ وقد تم الإبلاغ عن تساقط الشعر من الدرجة 3 أو 4 في هذه الدراسة بشكل غير صحيح.الأحداث المبلغ عنها بين الجرعة الأولى و100 يوم بعد الجرعة الأخيرة من العلاج المساعد للمرضى الذين لم يتلقوا العلاج المساعد أو قبل العلاج المساعد للمرضى الذين بدأوا العلاج المساعد.الأحداث السلبية المرتبطة بالمناعة (IMAEs) هي أحداث محددة، بغض النظر عن السبب، اعتبرها الباحث محتملة الارتباط بالمناعة دون وجود سبب بديل واضح، حدثت خلال 100 يوم من الجرعة النهائية، وتم علاجها بأدوية معدلة للمناعة (باستثناء IMAEs الغدد الصماء، التي لا تتطلب استخدام أدوية معدلة للمناعة). ALT، إنزيم الألانين ترانس أميناز؛ AST، إنزيم الأسبارتات ترانس أميناز؛ SAE، حدث سلبي خطير؛ TRAE، حدث سلبي مرتبط بالعلاج؛ TRSAE، حدث سلبي خطير مرتبط بالعلاج. سواء للجميع أو فقط للمرضى الذين يعانون من أورام إيجابية PD-L1. ومن الجدير بالذكر أنه بينما أظهرت الدراسات السابقة أن إضافة تثبيط بروتين الموت المبرمج 1 في سرطان الثدي الثلاثي السلبي أدى إلى زيادات صغيرة في معدلات الاستجابة الكاملة (pCR)، بما في ذلك في المرضى الذين لديهم تعبير منخفض عن PD-L1، تم ملاحظة فائدة كبيرة في فترة البقاء خالية من الأحداث (EFS).. بشكل عام، تمثل هذه النتائج علامة فارقة جديدة في العلاج المساعد لسرطان الثدي ER+/HER2-، لأنه كانت هناك جهود مكثفة ولكنها لم تنجح حتى الآن في تحسين معدلات الاستجابة الكاملة المرضية في هذه الفئة من المرضى.
تتمثل إحدى نقاط القوة المهمة في CheckMate 7FL في أنه تم تقييم ثلاثة اختبارات مناعية في مجموعة تجريبية من المرحلة الثالثة. كما لوحظت زيادات في معدلات الاستجابة الكاملة النسيجية مع إضافة نيفولوماب لزيادات sTIL من القليل.، والذي كان مستوى sTIL الوسيط في هذه الفئة من المرضى. لوحظ توافق معتدل بين اختبارات SP142 و28-8 pharmDx CPS وsTIL. ومن المثير للاهتمام، على الرغم من كانت معدلات pCR الأعلى مع إضافة نيفولوماب عندما اتفقت الفحوصات على إيجابية sTIL و PD-L1، ومع ذلك فإن المرضى الذين كانت نتائج فحوصاتهم متناقضة لا يزالون يستفيدون. هذه البيانات لها تداعيات مهمة للمرضى الذين يعانون من سرطان الثدي، وتقترح أن استخدام فحوصات متعددة قد يكون الأفضل لتحديد جميع المرضى الذين يمكن أن يستفيدوا من العلاج المناعي المساعد في هذا النوع الفرعي، على الرغم من أن sTIL قد يكون العلامة الحيوية الأكثر عملية وقابلية للوصول عالميًا لأنه يمكن تقييمه على الشرائح الملونة بالهيماتوكسيليين والإيوزين القياسية.تحليل مؤشرات حيوية استكشافية أخرى لتصنيف المرضى جارٍ.
تحليلات معدلات pCR حسب مستويات مستقبلات الاستروجين والبروجستيرون تؤكد أن المرضى الذين لديهم مستويات من مستقبلات الاستروجين و/أو البروجستيرونتحقق فائدة أكبر مع إضافة نيفولوماب من المرضى الذين لديهم مستويات من مستقبلات الاستروجين و/أو البروجستيرونمن الجدير بالذكر أننا لاحظنا هذا التأثير أيضًا في سياق. على الرغم من أن هذا لا يزال بحاجة إلى مزيد من التحقق، إلا أنه يشير إلى أن المرضى الذين لديهم مستويات منخفضة من مستقبلات الاستروجين والبروجستيرون قد يتم علاجهم بشكل مشابه للمرضى الذين يعانون من سرطان الثدي الثلاثي السلبي المبكر. أظهرت الأبحاث السابقة أن الأورام ذات مستويات الاستروجين المنخفضة تحتوي على المزيد من الخلايا اللمفاوية التائية المتسللة (sTILs) وCD8.خلايا T، التي تعبر عن PD-L1 بمستويات أعلى، وتتشابه أكثر مع سرطان الثدي الثلاثي السلبي من حيث التوقيعات المتعلقة بالمناعة.
كانت السلامة متوافقة مع ملفات السلامة المعروفة، دون تغيير في جدوى الجراحة بعد إضافة نيفولوماب إلى العلاج الكيميائي. ومع ذلك، من المهم ملاحظة أنه تم رصد حالتي وفاة مرتبطتين بالعلاج في مجموعة نيفولوماب.
القوة الرئيسية لهذه الدراسة هي: تضمينها لسكان عالي المخاطر، حيث كان الغالبية منهم إيجابيين للعقدة وذوي درجة 3؛ تقييم الاستجابة في مجموعة سكانية إيجابية PD-L1 كهدف ثانوي رئيسي؛ وبيانات شاملة عن العلامات البيولوجية، بما في ذلك تقييم الاستجابة في مجموعة سكانية ذات مستوى عالٍ من السTIL، المقدمة في سياق سرطان الثدي المبكر. تشمل القيود التعديل الكبير في البروتوكول الذي قلل بشكل كبير من حجم العينة و/أو عدد الأحداث ومدة المتابعة مما أدى إلى تصنيف EFS كهدف استكشافي.
في الختام، أدى إضافة نيفولوماب إلى العلاج الكيميائي القائم على الأنثراسيكلين والتاكسين في حالات سرطان الثدي المبكر عالي المخاطر ER+/HER2- إلى زيادة كبيرة في معدل الاستجابة الكاملة. تعيد هذه النتائج تشكيل فهمنا لهذا المرض في سياق مراقبة المناعة بواسطة خلايا T واستجابة العلاج المناعي في المرض اللمعي. عانى المرضى الذين لديهم مستويات أعلى من sTIL أو تعبير PD-L1 من معدلات استجابة كاملة أعلى، مما قد يضع معيارًا جديدًا لدراسات العلاج المساعد المستقبلية في هذه الفئة. تهدف تحليلات العلامات البيولوجية إلى كشف المحركات البيولوجية وراء الاستجابات المناعية القوية الناتجة عن إضافة العلاج المناعي إلى العلاج الكيميائي الذي لوحظ في سرطان الثدي ER+، مما قد يساعد في تحسين وتخصيص الأساليب العلاجية المناعية لهذا المرض.
المحتوى عبر الإنترنت
أي طرق، مراجع إضافية، ملخصات تقارير Nature Portfolio، بيانات المصدر، بيانات موسعة، معلومات تكميلية، شكر وتقدير، معلومات مراجعة الأقران؛ تفاصيل مساهمات المؤلفين والمصالح المتنافسة؛ وبيانات توفر البيانات والرموز متاحة علىhttps://doi.org/10.1038/s41591-024-03414-8.
References
Arnold, M. et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast 66, 15-23 (2022).
Clusan, L., Ferriere, F., Flouriot, G. & Pakdel, F. A basic review on estrogen receptor signaling pathways in breast cancer. Int. J. Mol. Sci. 24, 6834 (2023).
Jin, X. et al. Molecular classification of hormone receptor-positive HER2-negative breast cancer. Nat. Genet. 55, 1696-1708 (2023).
Loibl, S. et al. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 35, 159-182 (2024).
Burstein, H. J., Lacchetti, C. & Griggs, J. J. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update. J. Oncol. Pract. 15, 106-107 (2019).
Johnston, S. R. D. et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. 24, 77-90 (2023).
Korde, L. A. et al. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO Guideline. J. Clin. Oncol. 39, 1485-1505 (2021).
Freedman, R. A. et al. Optimal adjuvant chemotherapy and targeted therapy for early breast cancer-cyclin-dependent kinase 4 and 6 inhibitors: ASCO guideline rapid recommendation update. J. Clin. Oncol. 42, 2233-2235 (2024).
Cortes, J. et al. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N. Engl. J. Med. 387, 217-226 (2022).
Nanda, R. et al. Effect of pembrolizumab plus neoadjuvant chemotherapy on pathologic complete response in women with early-stage breast cancer: an analysis of the ongoing phase 2 adaptively randomized I-SPY2 trial. JAMA Oncol. 6, 676-684 (2020).
Schmid, P. et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N. Engl. J. Med. 386, 556-567(2022).
O’Meara, T. et al. Immunological differences between immune-rich estrogen receptor-positive and immune-rich triple-negative breast cancers. JCO Precis. Oncol. 4, 767-779 (2020).
Wolf, D. M. et al. Immune signatures and MammaPrint (ultra) high risk class (MP2) as predictors of response to pembrolizumab combined with the TLR9 agonist SD101 in the neoadjuvant I-SPY 2 TRIAL. Cancer Res. 82, P5-13-12 (2022).
Dieci, M. V. et al. Neoadjuvant chemotherapy and immunotherapy in luminal B-like breast cancer: results of the phase II GIADA trial. Clin. Cancer Res. 28, 308-317 (2022).
Loi, S. Tumor-infiltrating lymphocytes, breast cancer subtypes and therapeutic efficacy. Oncoimmunology 2, e24720 (2013).
Rios-Hoyo, A. et al. Correlation of hormone receptor positive HER2-negative/MammaPrint high-2 breast cancer with triple negative breast cancer: Results from gene expression data from the ISPY2 trial. J. Clin. Oncol. 573, abstract 573 (2024).
Symmans, W. F. et al. Assessment of residual cancer burden and event-free survival in neoadjuvant treatment for high-risk breast cancer: an analysis of data from the I-SPY2 randomized clinical trial. JAMA Oncol. 7, 1654-1663 (2021).
Schmid, P., Cortes, J. & Dent, R. Pembrolizumab in early triple-negative breast cancer. Reply. N. Engl. J. Med. 386, 1771-1772 (2022).
Pareja, F. et al. Triple-negative breast cancer: the importance of molecular and histologic subtyping, and recognition of low-grade variants. NPJ Breast Cancer 2, 16036 (2016).
Kahn, A. M., Golestani, R., Harigopal, M. & Pusztai, L. Intratumor spatial heterogeneity in programmed death-ligand 1 (PD-L1) protein expression in early-stage breast cancer. Breast Cancer Res. Treat. 201, 289-298 (2023).
Cortazar, P. et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 384, 164-172 (2014).
Symmans, W. F. et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J. Clin. Oncol. 25, 4414-4422 (2007).
Pusztai, L. et al. Event-free survival by residual cancer burden with pembrolizumab in early-stage TNBC: exploratory analysis from KEYNOTE-522. Ann. Oncol. 35, 429-436 (2024).
I-SPY2 Trial Consortium et al.Association of event-free and distant recurrence-free survival with individual-level pathologic complete response in neoadjuvant treatment of stages 2 and 3 breast cancer: three-year follow-up analysis for the I-SPY2 adaptively randomized clinical trial. JAMA Oncol. 6, 1355-1362 (2020).
Marczyk, M. et al. Treatment Efficacy Score-continuous residual cancer burden-based metric to compare neoadjuvant chemotherapy efficacy between randomized trial arms in breast cancer trials. Ann. Oncol. 33, 814-823 (2022).
Symmans, W. F. et al. Assessment of residual cancer burden and event-free survival in neoadjuvant treatment for high-risk breast cancer: an analysis of data from the I-SPY2 randomized clinical trial. JAMA Oncol. 7, 1654-1663 (2021).
Cardoso, F. et al. LBA21 KEYNOTE-756: phase III study of neoadjuvant pembrolizumab (pembro) or placebo (pbo) + chemotherapy (chemo), followed by adjuvant pembro or pbo + endocrine therapy (ET) for early-stage high-risk ER+/HER2- breast cancer. Ann. Oncol. 34, S1260-S1261 (2023).
Cardoso, F. et al. Phase 3 study of neoadjuvant pembrolizumab or placebo plus chemotherapy, followed by adjuvant pembrolizumab or placebo plus endocrine therapy for early-stage high-risk ER+/HER2- breast cancer: KEYNOTE-756. Cancer Res. 84, abstract GSO1-02 (2023).
Schmid, P. et al. Pembrolizumab for early triple-negative breast cancer. N. Engl. J. Med. 382, 810-821(2020).
Salgado, R. et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann. Oncol. 26, 259-271 (2015).
Loi, S. et al. The journey of tumor-infiltrating lymphocytes as a biomarker in breast cancer: clinical utility in an era of checkpoint inhibition. Ann. Oncol. 32, 1236-1244 (2021).
Voorwerk, L. et al. Immune landscape of breast tumors with low and intermediate estrogen receptor expression. NPJ Breast Cancer 9, 39 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons. org/licenses/by/4.0/.
(c) Crown 2025
¹مركز بيتر ماكالوم للسرطان، ملبورن، فيكتوريا، أستراليا. ²جامعة ملبورن، باركفيل، فيكتوريا، أستراليا. ³قسم علم الأمراض، مستشفيات زاس، أنتويرب، بلجيكا.المعهد الأوروبي للسرطان، IRCCS، ميلانو، إيطاليا.جامعة ميلانو، ميلانو، إيطاليا.عيادة أخصائي الأورام، أوكساكا، المكسيك.مستشفى غاستاف روسي للسرطان، فيليجويف، فرنسا.برادفورد هيل البحث السريري، المنطقة الحضرية، سانتياغو، تشيلي.معهد السرطان الهولندي، أمستردام، هولندا.مستشفى جامعة فال د’هيبرون، معهد فال د’هيبرون للأورام (VHIO)، برشلونة، إسبانيا.مركز الثدي، قسم التوليد وأمراض النساء ومركز السرطان في ميونيخ، مستشفى جامعة لودفيغ ماكسيميليان، ميونيخ، ألمانيا.مركز دانا-فاربر بريغهام للسرطان، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية.معهد سارة كانون للأبحاث، ناشفيل، تينيسي، الولايات المتحدة الأمريكية.سينيت أونكولوجيكوس، مكسيكو سيتي، المكسيك.المستشفى الإيطالي في قرطبة، قرطبة، الأرجنتين.مركز العلاج الإشعاعي كلوج ش.م.م، فلوريستي، رومانيا.عيادة الدكتور خواكين غابرييل رينوسو توليدو، مونتيري، المكسيك.معهد أونكولوجيا فينيتو IRCCS، بادوفا، إيطاليا.قسم الجراحة، الأورام وأمراض الجهاز الهضمي، جامعة بادوفا، بادوفا، إيطاليا.قسم أمراض النساء، جامعة إنسبروك الطبية، إنسبروك، النمسا.ABCSG – مجموعة دراسة سرطان الثدي والقولون النمساوية، فيينا، النمسا.بريستول مايرز سكويب، برينستون، نيو جيرسي، الولايات المتحدة الأمريكية.مستشفى سميلو للسرطان في ييل، نيو هافن، كونيتيكت، الولايات المتحدة الأمريكية.مركز جامعة تكساس Southwestern الطبي، دالاس، تكساس، الولايات المتحدة الأمريكية. البريد الإلكتروني: sherene.loi@petermac.org
طرق
المرضى
كان المرضى المؤهلون قد تم تشخيصهم حديثًا بسرطان الثدي الإيجابي لمستقبلات هرمون الاستروجين/سلبي لمستقبلات HER2، مع وجود ورم أولي مؤكد وفئات العقد اللمفاوية لأحجام الأورام و cN2 أو cT3-cT4 و cNO-cN2؛ مرض من الدرجة 3 أو مرض من الدرجة 2 مع تعبير عن مستقبلات هرمون الاستروجين من 1 إلى؛ وظيفة الأعضاء الكافية؛ الأنسجة المتاحة لتقييم المؤشرات الحيوية؛ وحالة الأداء وفقًا لمجموعة التعاون الشرقي لعلم الأورام 0-1. كان المرضى مؤهلين بغض النظر عن حالة PD-L1. كانت الأورام متعددة البؤر (بؤرتان أو أكثر من السرطان في نفس ربع الثدي) مسموح بها إذا كانت أكبر آفة لا تقل عن 2 سم وتم تحديدها كآفة مستهدفة. كان المرضى الذين يعانون من سرطان القنوات المختلط والسرطان الغدي مؤهلين. تم استبعاد المرضى إذا كان لديهم سرطان ثدي متعدد المراكز، أو تاريخ من سرطان الثدي الغازي في نفس الجانب، أو دليل على وجود مرض نقيل، أو تلقوا أي علاج سابق لسرطان الثدي المشخص حاليًا أو تلقوا العلاج المناعي سابقًا.
تصميم التجربة والعلاجات
كانت دراسة CheckMate 7FL تجربة عشوائية متعددة المراكز مزدوجة التعمية خاضعة للتحكم الوهمي من المرحلة الثالثةClinicalTrials.govالمعرف: NCT04109066)، الذي كان لديه في الأصل نقاط نهاية رئيسية مشتركة من pCR وEFS، والتي تم تقييمها مركزيًا. بعد الموافقة على الأبيماسيكلب كعلاج مساعد لسرطان الثدي الإيجابي لمستقبلات هرمون الاستروجين/سلبي HER2 عالي المخاطر، تم تعديل نقطة النهاية الرئيسية لتكون pCR فقط، مما جعل التسجيل وتقييم EFS تحديًا لإكماله. كان من المتوقع أن يؤدي الجمع بين الأبيماسيكلب والنيوفولوماب إلى معدل مرتفع من الانسحابات بسبب المخاوف المتعلقة بالسلامة حول الجمع بين مثبط CDK4/6 ووكيل مضاد الموت المبرمج 1.في المرحلة المساعدة، تم توزيع المرضى عشوائيًا بنسبة 1:1 لتلقي إما نيفولوماب 360 ملغ أو دواء وهمي كل 3 أسابيع مع باكليتاكسيل أسبوعيًا لمدة 12 أسبوعًا. تلا ذلك نيفولوماب (إما 360 ملغ كل 3 أسابيع أو 240 ملغ كل 2 أسبوع) بالاشتراك مع الأنثراسيكلين والسيكلوفوسفاميد، أو دواء وهمي بالاشتراك مع الأنثراسيكلين والسيكلوفوسفاميد؛ تم تحديد تكرار جرعات الأنثراسيكلين والسيكلوفوسفاميد من قبل الباحث. جميع المرضى الذين ظلوا مرشحين للجراحة خضعوا لجراحة الثدي والإبط (وفقًا للمعايير المحلية) خلال 4 أسابيع من الانتهاء من مرحلة العلاج المساعد. وفقًا لتعديل البروتوكول، تم الكشف عن الدراسة في المرحلة المساعدة، وتلقى المرضى نيفولوماب 480 ملغ مع اختيار الباحث للعلاج الهرموني (تاموكسيفين، ليتروزول، أنستروزول أو إكسمستين، مع أو بدون قمع وظيفة المبيض) لمدة تصل إلى سبع دورات.
تم تقسيم العشوائية حسب تقنية الاستجابة التفاعلية وفقًا لنسبة الخلايا المناعية التي تعبر عن PD-L1 (نسبة الخلايا المناعية بواسطة صبغة VENTANA PD-L1 SP142 المناعية، الحد الأدنى عنددرجة الورم (2 أو 3)، الحالة العقدية الإبطية المؤكدة مرضيًا (إيجابية في المراجعة المرضية أو سلبية في المراجعة الشعاعية و/أو المرضية) وتكرار جرعات الأنثراسيكلين (كل 3 أسابيع أو كل 2 أسبوع). قبل بدء الدراسة، تلقى كل مشارك معلومات تسجيل الدخول وإرشادات حول كيفية الوصول إلى تقنية الاستجابة التفاعلية. تم تخصيص رقم فريد لكل مشارك بعد توقيع نموذج الموافقة المستنيرة. تم استخدام أرقام المشاركين في جميع معلومات دراسة المشاركين. لم يتم إعادة تخصيص أرقام المشاركين. تم استخدام تقنية الاستجابة التفاعلية لإدارة عشوائية المشاركين. قام الباحث أو المفوض بتسجيل المشارك للتسجيل من خلال اتباع إجراءات التسجيل التي وضعتها الجهة الراعية.
نقاط النهاية
النقطة النهائية الرئيسية كانتفي مجموعة المITT. في البداية، كانت EFS نقطة نهاية مشتركة؛ ومع ذلك، بعد القرار بوقف التسجيل في الدراسة في أبريل 2022 بسبب تغير مشهد العلاج بسرعة، تم تحديث نقطة النهاية الأساسية للتجربة للتركيز فقط على pCR، وتم تغيير EFS إلى نقطة نهاية استكشافية لأن العدد الإجمالي للمرضى المسجلين والأحداث كان منخفضًا جدًا ومدة المتابعة المحدثة كانت قصيرة جدًا لتوفير قوة كافية للمقارنة. وبالتالي، تم تقليل المتابعة
إلى سنة واحدة بعد الجراحة لجميع المرضى، وأصبح المرحلة المساعدة مفتوحة.
تغيير رئيسي آخر في الدراسة بعد وقف التسجيل في أبريل 2022 كان تقييم pCR في مجموعة PD-L1+ بواسطة VENTANA SP142 % IC كنقطة نهاية ثانوية. شملت نقاط النهاية الثانوية الأخرى معدلات RCB 0 أو I في مجموعات المITT وPD-L1+. تم تقييم الاستجابة المرضية، وتم حساب درجة RCB بواسطة أطباء الأمراض المحليين. جمعت درجة RCB حجم الورم، وكثافة الورم، ووجود العقد اللمفاوية في درجة واحدة مستمرة تم تقسيمها إلى أربع فئات، وهي درجة RCB 0 (أي، pCR)، وI، II وIII، والتي تت correspond إلى سرطان متبقي أكبر بشكل متزايد وبقاء خالٍ من الانتكاسة أسوأ.. تم تقييم السلامة والتحمل خلال المراحل المساعدة والمساعدة في جميع المرضى الذين تلقوا على الأقل جرعة واحدة من دواء الدراسة. شملت نقاط النهاية الاستكشافية المحددة مسبقًا ارتباط نتائج الفعالية بحالة العلامات الحيوية بناءً على PD-L1 CPS، وsTILs، ومستويات مستقبلات الاستروجين / البروجستيرون ومؤشر Ki67.
تقييمات الدراسة
تم تقييم pCR بعد العلاج المساعد (yp) وتم تعريفه على أنه عدم وجود مرض متبقي غازي في الثدي والعقد اللمفاوية (ypT0/is، ypNO) بواسطة طبيب أمراض محلي. تم مراقبة الأحداث الضائرة طوال التجربة ولمدة 30 يومًا بعد وقف علاج الدراسة (90 يومًا للأحداث الضائرة الخطيرة) وتم تصنيفها وفقًا لمعايير السمية الشائعة للأحداث الضائرة v.5.0 من المعهد الوطني للسرطان. تم تقييم السلامة بعد 30 يومًا و100 يوم بعد الجرعة النهائية، وكانت المتابعة طويلة الأمد تصل إلى 12 شهرًا بعد الجراحة. شملت تحليلات العلامات الحيوية تقييم تعبير PD-L1 ومعدل sTILs بشكل مركزي. تم تقييم PD-L1 بواسطة المناعية النسيجية النوعية على الخلايا المناعية باستخدام اختبار VENTANA SP142 (روشي دياغنوستكس) وPD-L1 CPS باستخدام اختبارpharmDx (أجليت). تم تحديد نسبة sTILs على شريحة ملونة بالهيماتوكسيلين والإيوزين وفقًا للإرشادات المعمول بها.. في هذه الدراسة، كانت sTIL بمعدلأقل قيمة ممكنة وأشارت إلى عدم وجود sTILs قابلة للاكتشاف. تم استخدام اختبار SP142% IC وpharmDx CPS لتقييم التباين بين الاختبارات، وكذلك لتحديد تعبير PD-L1 في الخلايا المناعية المتسللة للورم مقابل كل من الخلايا المناعية وخلايا الورم. تم تقييم تعبير ER وKi 67 مركزيًا باستخدام المناعية النسيجية Agilent MIB-Dako pharmDx. تم تقييم مستويات المناعية النسيجية لمستقبلات البروجستيرون من اختبارات الأمراض المحلية. شملت الخصائص الأخرى المسجلة للمرضى والمرض درجة الورم، حالة العقد الإبطية، مرحلة المرض، مؤشر Ki67، حالة انقطاع الطمث والعمر.
التحليلات الإحصائية
استنادًا إلى التقريب الطبيعي للثنائي، فإن حجم العينة المكون من 521 مريضًا في مجموعة النية للعلاج سيعطي تقريبًاقوة (ألفا ثنائية الجانب 0.05) لاكتشاف فرق فيمعدلات pCR بين ذراعي العلاج، بافتراض معدلفي ذراع التحكم. بسبب قرار الراعي بإغلاق جميع المواقع في روسيا بعد بدء الصراع الجيوسياسي بين أوكرانيا وروسيا، تم استبعاد 11 مريضًا بسبب عدم كفاية المتابعة لتقييم pCR، مما أثر بشكل طفيف على قوة الدراسة (). أدى ذلك إلى حجم مجموعة المITT المكونة من 510 مرضى. تم تحليل الفرق المعدل حسب الطبقات في معدل pCR بين الذراعين باستخدام طريقة كوكراين-مانتل-هانزل المعدلة بالطبقات مع مستوى ألفا ثنائي الجانب 0.05. تم تقييم OR المعدل حسب الطبقات باستخدام طريقة مانتل-هانزل. كانت الحدود المستخدمة لـ sTIL وتعبير PD-L1 بواسطة SP142 أوpharmDx CPS محددة مسبقًا لهذه الدراسة.
تم تقييم قيم CI لمعدلات pCR وRCB 0 أو I باستخدام طريقة كلوبير-بيرسون. تم حساب الفروق غير الموزونة في معدلات pCR وRCB 0 أو I بين ذراعي العلاج في مجموعات فرعية مختلفة من المرضى مع CI ثنائي الجانب 95% المقابلة باستخدام طريقة نيوكومب دون تصحيح الاستمرارية. تم إجراء تحليلات متعددة المتغيرات الاستكشافية باستخدام الانحدار اللوجستي لتقييم ارتباط العلامات الحيوية وغيرها من الخصائص الأساسية مع
pCR. تم حساب العلامات الحيوية المدرجة في التحليلات متعددة المتغيرات كإما متغيرات فئوية (تعبير PD-L1بواسطة SP142 أو 28-8 pharmDx CPSمع حدود sTIL منأو) أو متغيرات مستمرة. كانت الخصائص الأساسية الأخرى في التحليلات متعددة المتغيرات هي مرض المرحلة III، حالة العقد السلبية، تعبير ER, حالة ما بعد انقطاع الطمث والعمرسنوات. كانت CI للتحليلات الثانوية والاستكشافية لأغراض وصفية، وبالتالي، لم يتم إجراء أي تعديلات على التعددية.
كان جنس المرضى المسجلين في التجربة موثقًا ذاتيًا ولم يتم جمع بيانات عن الجنس. لم يتم تقديم أي تحليلات حسب الجنس أو بيانات مفككة لأن القيام بذلك سيؤدي إلى تقديم معلومات قد تحدد الهوية.
إشراف التجربة
تم تطوير هذه التجربة والإشراف عليها من قبل لجنة توجيه أكاديمية وموظفي الراعي (بريستول مايرز سكويب). قدمت لجنة مراقبة البيانات المستقلة الخارجية إشرافًا على اعتبارات السلامة والفعالية خلال الدراسة. تم اعتماد بروتوكول التجربة والتعديلات من قبل الهيئة الأخلاقية المناسبة في كل موقع مشارك. قدم جميع المرضى موافقة مستنيرة مكتوبة. يؤكد جميع المؤلفين أن التجربة أجريت باحترام لمعايير الممارسات السريرية الجيدة. كان لجميع المؤلفين الوصول إلى البيانات وشاركوا في كتابة ومراجعة هذه المخطوطة. تم كتابة المسودة الأولى من المخطوطة بواسطة المؤلف الأول مع المساعدة التحريرية المقدمة من كاتب طبي يعمل لدى الراعي. راجع جميع المؤلفين وشاركوا في صياغة المخطوطة ووافق جميع المؤلفين على المسودة المقدمة ويمكنهم الشهادة على دقة واكتمال البيانات.
ملخص التقرير
معلومات إضافية حول تصميم البحث متاحة في ملخص تقرير Nature Portfolio المرتبط بهذه المقالة.
توفر البيانات
ستقوم بريستول مايرز سكويب بتلبية الطلبات المشروعة لبيانات التجارب السريرية من الباحثين المؤهلين الذين لديهم هدف علمي محدد بوضوح. ستنظر بريستول مايرز سكويب في طلبات مشاركة البيانات للتجارب السريرية التدخلية من المرحلة II-IV التي اكتملت في أو بعد 1 يناير 2008. بالإضافة إلى ذلك، يجب أن تكون النتائج الأولية من هذه التجارب قد نُشرت في مجلات محكمة وأن تكون الأدوية أو المؤشرات قد تم الموافقة عليها في الولايات المتحدة، والاتحاد الأوروبي والأسواق المحددة الأخرى. المشاركة تخضع أيضًا لحماية خصوصية المرضى واحترام موافقة المرضى المستنيرة. قد تشمل البيانات التي تعتبر للمشاركة بيانات سريرية على مستوى المرضى والدراسة غير القابلة للتحديد، وتقارير دراسات سريرية كاملة وبروتوكولات.
References
Masuda, J. et al. Efficacy, safety, and biomarker analysis of nivolumab in combination with abemaciclib plus endocrine therapy in patients with HR-positive HER2-negative metastatic breast cancer: a phase II study (WJOG11418B NEWFLAME trial). J. Immunother. Cancer 11, e007126 (2023).
Rugo, H. S. et al. Abemaciclib in combination with pembrolizumab for HR+, HER2- metastatic breast cancer: phase 1b study. NPJ Breast Cancer 8, 118 (2022).
الشكر
نشكر المرضى وعائلاتهم وجميع الباحثين المشاركين في هذه الدراسة. بالإضافة إلى ذلك، نشكر C. Jeyamohan (رائد العلوم السريرية)، A. Demeaux (مدير البروتوكول)، R. Soomro (طبيب التجارب السريرية) وD. Jiang (محلل العلامات الحيوية) من بريستول مايرز سكويب على مساهماتهم في الدراسة. يتم دعم S.L. من قبل مؤسسة سرطان الثدي الوطنية في أستراليا ومؤسسة أبحاث سرطان الثدي، نيويورك، الولايات المتحدة الأمريكية. يتم دعم R.S. من قبل مؤسسة أبحاث سرطان الثدي. تم رعاية هذه الدراسة وتمويلها من قبل بريستول
كانت شركة مايرز سكويب هي المسؤولة النهائية عن تصور وتصميم وإجراء التجربة، وجمع البيانات وتحليلها. إلى جانب المؤلفين، كانت الجهة الراعية أيضًا متورطة في قرار النشر وإعداد المخطوطة. تم تقديم الكتابة الطبية والمساعدة التحريرية، بما في ذلك مساعدة المؤلفين في تطوير المخطط، وصياغة ودمج التعليقات، والتحقق من الحقائق، والإشارة، وإعداد الأشكال، والتنسيق، والتدقيق اللغوي، والتقديم من قبل E. Haygreen وK. Wellington وC. Charles وL. McArdle، جميعهم من Spark (قسم من Prime، نيويورك، الولايات المتحدة الأمريكية)، بدعم من Bristol Myers Squibb وفقًا لإرشادات الممارسات الجيدة للنشر.https://www.acpjournals.org/doi/abs/10.7326/ M22-1460?journalCode=aim).
مساهمات المؤلفين
S.L.، R.S.، G.C.، R.I.R.D.، S.D.، C.I.R.G.، M.K.، C.S.، N.H.، F.A.، R.C.، T.S. و H.M. كان لهم دور رئيسي في تصميم أو تخطيط الدراسة. S.L.، R.I.R.D.، S.D.، C.I.R.G.، M.K.، C.S.، N.H.، A.E.M.، D.A.Y.، L.P.، A.S.Z.، F.R.C.، A.U.، J.G.R.-T.، V.G. و D.E. كان لهم دور كبير في جمع البيانات. S.D.، C.I.R.G.، M.K.، C.S.، N.H.، F.A.، M.P.، A.C.، R.C.، R.N.، T.S. و J.Q.W. كان لهم دور رئيسي في تحليل البيانات. S.L.، R.S.، G.C.، R.I.R.D.، S.D.، C.I.R.G.، M.K.، C.S.، N.H.، A.E.M.، D.A.Y.، L.P.، A.S.Z.، F.R.C.، A.U.، J.G.R.-T.، V.G.، D.E.، F.A.، R.N.، T.S.، J.Q.W. و H.M. كان لهم دور رئيسي في تفسير البيانات. جميع المؤلفين كان لديهم وصول إلى البيانات وشاركوا في كتابة ومراجعة وتنقيح المخطوطة. جميع المؤلفين وافقوا على المخطوطة النهائية للنشر. جميع المؤلفين يتحملون المسؤولية عن دقة وسلامة جميع جوانب البحث.
المصالح المتنافسة
“S.L. يُبلغ عن تمويل بحثي مؤسسي من أسترازينيكا/ داييتشي سانكيو، بريستول مايرز سكويب، نوفارتس، بومه بيولوجي، روش-جينينتيك وسياتل جينتيكس؛ رسوم استشارية من أماروك ثيرابيوتيكس، أسترازينيكا/ داييتشي سانكيو، بريستول مايرز سكويب، دومين ثيرابيوتيكس، جلعاد، ليلي، ميرسانا ثيرابيوتيكس، MSD، روش-جينينتيك ونوفارتس؛ مكافآت من أماروك ثيرابيوتيكس، أسترازينيكا/ داييتشي سانكيو، بايونتيك، بريستول مايرز سكويب، دومين ثيرابيوتيكس، جلعاد ساينس، ليلي، ميرسانا ثيرابيوتيكس، MSD، نوفارتس وروش-جينينتيك؛ دعم للاجتماعات/ السفر من بريستول مايرز سكويب وليلي. R.S. يُبلغ عن رسوم استشارية من أوكين؛ مكافآت من أسترازينيكا، داييتشي سانكيو وعلوم إكزاكت؛ دعم للاجتماعات/ السفر من أسترازينيكا وداييتشي سانكيو؛ منصب قيادي في مجموعة العمل الدولية لعلامات المناعة والعلاج المناعي؛ دعم بحثي من بريستول مايرز سكويب وتقديم نصائح غير مدفوعة لـ Case 45. G.C. يُبلغ عن المشاركة في مجالس استشارية لأسترازينيكا، بريستول مايرز سكويب، داييتشي سانكيو، سيلكيوتي، إليبسيس، علوم إكزاكت، جلعاد، ليلي، ميناريني، ميرك، نوفارتس، فايزر، روش، سانوفي وفيراسيتي. S.D. يُبلغ عن تمويل بحثي مؤسسي من أميجن، أسترازينيكا، بريستول مايرز سكويب، المفوضية الأوروبية، الحكومة الفرنسية، ليلي، نوفارتس، أوريون، بيير فابر، فايزر، روش-جينينتيك، سانوفي وتايو؛ دعم للاجتماعات/ السفر من نوفارتس، روش وسياغن؛ المشاركة في مجالس استشارية لأسترازينيكا، بيسينز، ديسيبيو، إلسان، جلعاد وسانوفي؛ المشاركة في نشاط لجنة مراقبة البيانات المستقلة لمجموعة الثدي الدولية وفايزر. C.I.R.G. يُبلغ عن مكافآت من أسترازينيكا، بريستول مايرز سكويب، نايت، MSD، فايزر، روش وتكنوفارما؛ المشاركة في مجالس مراقبة سلامة البيانات/ الاستشارية لبريستول مايرز سكويب، فايزر وسانوفي. M.K. يُبلغ عن تمويل بحثي مؤسسي من أسترازينيكا، بريستول مايرز سكويب وروش؛ مكافآت من بريستول مايرز سكويب وجلعاد؛ المشاركة في مجالس استشارية لأسترازينيكا، بايونتيك، بريستول مايرز سكويب، MSD وروش. C.S. يُبلغ عن تمويل بحثي من أسترازينيكا، بوهينجر إنجلهايم، بريستول مايرز سكويب، بايونديس BV، داييتشي سانكيو “رسوم من أسترازينيكا، داييتشي سانكيو، إيساي، جلعاد، ليلي، ميديتيك، نوفارتس، فايزر، فيليبس هيلث كير، فارمالكس، بيير فابر، بومة بيولوجيا، روش، سيجن، سينثون وزايم ووركس؛ أتعاب من أسترازينيكا، داييتشي سانكيو، إكستر فارماسيتيكالز، ليلي، فايزر، بيير فابر، بومة بيولوجيا وسيجن؛ مدفوعات لشهادة الخبراء من AX’s Consulting SARL، بوهينجر إنجلهايم، بريستول مايرز سكويب، جينينتيك، إينوب، MSD إسبانيا، نوفارتس وسانوفي؛ دعم للاجتماعات/السفر من أسترازينيكا، داييتشي سانكيو، إيساي أوروبا، جلعاد، ليلي، نوفارتس، فايزر، بيير فابر، بومة بيولوجيا، روش وسيجن؛ المشاركة في مجالس مراقبة سلامة البيانات/المشورة لأسترازينيكا، داييتشي سانكيو، إيساي أوروبا، جلعاد، ليلي، ميناريني، MSD، نوفارتس، فايزر، فيليبس، بيير فابر، روش وسيجن. ن.هـ. يذكر أنه يتلقى رسوم استشارية من داييتشي سانكيو، جلعاد، نوفارتس، فايزر، روش، سيجن وفياتريس؛ أتعاب من أسترازينيكا، داييتشي سانكيو، جلعاد، ليلي، MSD، نوفارتس، بيير فابر، فايزر، روش، سيجن، فياتريس وزويليغ فارما؛ المشاركة في مجالس مراقبة سلامة البيانات/المشورة لجلياد، روش وسيجن؛ منصب قيادي في مجموعة الدراسات الغربية الألمانية. إ.أ.م. يذكر أنه يتلقى تمويل بحثي من جينينتيك، جلعاد وروش؛ رسوم استشارية من أسترازينيكا، بايونتيك، موديرنا وMSD؛ أتعاب من MSD؛ دعم للاجتماعات/السفر من MSD؛ مناصب قيادية في مجلس إدارة الجمعية الأمريكية لعلم الأورام السريري 2019-2023 ومستشار علمي لصندوق سوزان ج. كومن. د.أ.ي. يذكر أنه يتلقى تمويل بحثي مؤسسي من أبفي، أمبريكس، أسترازينيكا، معهد دانا فاربر للسرطان، ليلي، روش-جينينتيك، G1 ثيرابيوتيكس، جلعاد، إنسايت، إنوكراين فارماسيتيكالز، ميرك، نوفارتس، بوليفور، ستيملاين ثيرابيوتيكس، يو إس أونكولوجي وUT Southwestern؛ ورسوم استشارية مدفوعة للمؤسسة من أسترازينيكا، داييتشي سانكيو، جلعاد، إنتيغرا كونكت، نوفارتس وستيملاين ثيرابيوتيكس. ف.ج. يذكر أنه يتلقى أتعاب من أسترازينيكا، داييتشي سانكيو، إكزاكت ساينسز، جلعاد، غلاكسو سميث كلاين، ليلي، ميناريني ستيملاين، نوفارتس، روش وزينتيفا؛ مدفوعات لشهادة الخبراء من ليلي؛ دعم للاجتماعات/السفر من أسترازينيكا وجلعاد؛ براءة اختراع مؤسسية لـ Her2DX؛ والمشاركة في مجالس مراقبة سلامة البيانات/المشورة لأسترازينيكا، داييتشي سانكيو، إكزا
سيجن و سيريوس ميديكال؛ دعم الاجتماعات/السفر من داييتشي سانكيو و فايزر؛ وتلقي دعم الكتابة الطبية من سيريوس ميديكال. أف.أ. يذكر أنه موظف في بريستول مايرز سكويب. إم.بي. يذكر أنه موظف ومساهم في بريستول مايرز سكويب. أي.سي. يذكر أنه موظف في بريستول مايرز سكويب ومساهم في ميرك. آر.سي. يذكر أنه موظف في بريستول مايرز سكويب. آر.إن. يذكر أنه موظف ومساهم في بريستول مايرز سكويب. تي.إس. يذكر أنه موظف ومساهم في بريستول مايرز سكويب. جي.كيو.دبليو. يذكر أنه موظف ومساهم في بريستول مايرز سكويب. إل.بي. يذكر تمويل بحثي مؤسسي من أسترازينيكا، بريستول مايرز سكويب، غلاكسو سميث كلاين، ميرك، فايزر و سيجن؛ رسوم استشارية من أسترازينيكا، بريستول مايرز سكويب، داييتشي، إكزاكت ساينس، جينينتيك-روش، غلاكسو سميث كلاين، ميرك، ناتيرا، نوفارتس، بيرسوناليس، فايزر و ستيملاين-ميناريني؛ وأتعاب للمشاركة في مجلس استشاري من أسترازينيكا، بريستول مايرز سكويب، داييتشي، إكزاكت ساينس، جينينتيك-روش، غلاكسو سميث كلاين، ميرك، ناتيرا، نوفارتس، بيرسوناليس، فايزر و ستيملاين-ميناريني. إتش.إم. يذكر رسوم استشارية من أميجن، أسترازينيكا، بريستول مايرز سكويب، كاليثيرا، سيلجين، كراون بايوساينس داييتشي سانكيو، ليلي، جينينتيك-روش، جلياد، إيمونوميدكس، ميرك، أوبى فارما، بيريجراين، فايزر، بومة، سبكتروم فارماسيتيكالز، سندكس فارماسيتيكالز، سياتل جينيتكس و تابليمون؛ وتمويل بحثي من بريستول مايرز سكويب، بي تي جي، ذ.م.م/أسترازينيكا، ميد إيميون و ميرك. آر.آي.آر.دي، أي.إس.زد، إف.آر.سي، أي.يو و جي.جي.آر.-تي. يعلنون عدم وجود مصالح متنافسة.
معلومات مراجعة الأقران تشكر مجلة ناتشر ميديسين كارين جيلمون، بينغهي شيو و المراجعين الآخرين المجهولين على مساهمتهم في مراجعة الأقران لهذا العمل. المحرر الرئيسي: أولريكه هارجيس، بالتعاون مع فريق ناتشر ميديسين.
المؤلف(ون) المراسل(ون):
شيرين لوى
آخر تحديث من المؤلف(ين): 17 أكتوبر 2024
ملخص التقرير
تسعى ناتشر بورتفوليو لتحسين قابلية إعادة إنتاج العمل الذي ننشره. يوفر هذا النموذج هيكلًا للاتساق والشفافية في التقرير. لمزيد من المعلومات حول سياسات ناتشر بورتفوليو، انظر سياسات التحرير وقائمة مراجعة سياسة التحرير.
إحصائيات
لجميع التحليلات الإحصائية، تأكد من أن العناصر التالية موجودة في أسطورة الشكل، أسطورة الجدول، النص الرئيسي، أو قسم الطرق.
n/a
□ X
حجم العينة الدقيقة لكل مجموعة/شرط تجريبي، معطاة كرقم منفصل ووحدة قياس
□ بيان حول ما إذا كانت القياسات قد أُخذت من عينات متميزة أو ما إذا كانت نفس العينة قد تم قياسها عدة مرات
□ X
اختبار(ات) إحصائية مستخدمة وما إذا كانت أحادية أو ثنائية الجانب
يجب وصف الاختبارات الشائعة فقط بالاسم؛ وصف تقنيات أكثر تعقيدًا في قسم الطرق.
□
□ وصف لجميع المتغيرات التي تم اختبارها
□
وصف لأي افتراضات أو تصحيحات، مثل اختبارات الطبيعية والتعديل للمقارنات المتعددة
□
وصف كامل للمعلمات الإحصائية بما في ذلك الاتجاه المركزي (مثل المتوسطات) أو تقديرات أساسية أخرى (مثل معامل الانحدار) و التباين (مثل الانحراف المعياري) أو تقديرات عدم اليقين المرتبطة (مثل فترات الثقة)
□ X
لاختبار الفرضية الصفرية، إحصائية الاختبار (مثل ) مع فترات الثقة، أحجام التأثير، درجات الحرية و القيمة المذكورة أعطِ القيم كقيم دقيقة كلما كان ذلك مناسبًا.
□ لتحليل بايزي، معلومات حول اختيار الأوليات وإعدادات سلسلة ماركوف مونت كارلو
□ للتصاميم الهرمية والمعقدة، تحديد المستوى المناسب للاختبارات والتقارير الكاملة للنتائج
□ تقديرات أحجام التأثير (مثل حجم كوهين , حجم بيرسون )، مع الإشارة إلى كيفية حسابها
تحتوي مجموعتنا على الإنترنت حول الإحصائيات لعلماء الأحياء على مقالات حول العديد من النقاط أعلاه.
البرمجيات والرموز
معلومات السياسة حول توفر كود الكمبيوتر
جمع البيانات
لم يتم استخدام أي برمجيات
تحليل البيانات
لم يتم استخدام أي برمجيات
بالنسبة للمخطوطات التي تستخدم خوارزميات أو برمجيات مخصصة تكون مركزية للبحث ولكن لم يتم وصفها بعد في الأدبيات المنشورة، يجب أن تكون البرمجيات متاحة للمحررين والمراجعين. نشجع بشدة على إيداع الكود في مستودع مجتمعي (مثل GitHub). انظر إرشادات ناتشر بورتفوليو لتقديم الكود والبرمجيات لمزيد من المعلومات.
البيانات
معلومات السياسة حول توفر البيانات
يجب أن تتضمن جميع المخطوطات بيانًا حول توفر البيانات. يجب أن يوفر هذا البيان المعلومات التالية، حيثما ينطبق:
رموز الوصول، معرفات فريدة، أو روابط ويب لمجموعات البيانات المتاحة للجمهور
وصف لأي قيود على توفر البيانات
بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتماشى مع سياستنا
ستقوم بريستول مايرز سكويب بتلبية الطلبات المشروعة لبيانات التجارب السريرية من الباحثين المؤهلين الذين لديهم هدف علمي محدد بوضوح. ستنظر بريستول مايرز سكويب في طلبات مشاركة البيانات للتجارب السريرية التدخلية من المرحلة الثانية إلى الرابعة التي اكتملت في أو بعد 1 يناير 2008. بالإضافة إلى ذلك، يجب أن تكون النتائج الأولية من هذه التجارب قد نُشرت في مجلات مراجعة الأقران وأن تكون الأدوية أو المؤشرات قد تم الموافقة عليها في الولايات المتحدة، الاتحاد الأوروبي، والأسواق المحددة الأخرى. المشاركة تخضع أيضًا
لحماية خصوصية المرضى واحترام موافقة المريض المستنيرة. قد تشمل البيانات التي تعتبر للمشاركة بيانات تجريبية سريرية على مستوى المرضى وغير قابلة للتعريف، تقارير دراسات سريرية كاملة وبروتوكولات.
البحث الذي يشمل المشاركين البشريين، بياناتهم، أو المواد البيولوجية
معلومات السياسة حول الدراسات التي تشمل المشاركين البشريين أو البيانات البشرية. انظر أيضًا معلومات السياسة حول الجنس، الهوية/العرض، والتوجه الجنسي والعرق، الإثنية والعنصرية.
التقرير عن الجنس والهوية
التقرير عن العرق، الإثنية، أو مجموعات اجتماعية أخرى ذات صلة
خصائص السكان
التجنيد
الإشراف الأخلاقي
كان جنس المرضى المسجلين في التجربة مُبلغًا عنه ذاتيًا ولم يتم جمع بيانات حول الجنس. كانت مجموعة المرضى المؤهلين في الغالب من الإناث، وسجلت التجربة مريضًا واحدًا ذكرًا؛ لم يتم تقديم أي تحليلات حسب الجنس أو بيانات مفككة لأن القيام بذلك قد يؤدي إلى تقديم معلومات قد تحدد الهوية.
مقدم في الجدول 1
مقدم في الجدول 1
من 20 نوفمبر 2019 حتى 7 أبريل 2022، تم فحص 830 مريضًا في 221 موقعًا سريريًا في 31 دولة. من بين 830 مريضًا تم فحصهم، تم توزيع 521. كان المرضى المؤهلون قد تم تشخيصهم حديثًا بسرطان الثدي ER+/HER2-، مع ورم أولي مؤكد وفئات العقد من الأورام بحجم و أو و ; مرض من الدرجة 3 أو مرض من الدرجة 2 مع تعبير ER من 1 إلى ; وظيفة عضوية كافية؛ نسيج متاح لتقييم العلامات البيولوجية؛ وحالة أداء مجموعة التعاون الشرقي للسرطان 0-1. كان المرضى مؤهلين بغض النظر عن حالة PD-L1. كانت الأورام متعددة البؤر (بؤرتان أو أكثر من السرطان داخل نفس ربع الثدي) مسموح بها إذا كان أكبر آفة لا تقل عن 2 سم وتم تعيينها كآفة مستهدفة. تم استبعاد المرضى إذا كان لديهم سرطان ثدي متعدد المراكز، تاريخ من سرطان الثدي الغازي في نفس الجانب، دليل على مرض نقيل، قد تلقوا أي علاج سابق لسرطان الثدي المشخص حاليًا، أو قد تلقوا علاجًا مناعي سابقًا.
تم تطوير هذه التجربة والإشراف عليها من قبل لجنة توجيه أكاديمية وموظفين من الراعي (بريستول مايرز سكويب). وقدمت لجنة مراقبة البيانات الخارجية المستقلة إشرافًا على اعتبارات السلامة والفعالية خلال الدراسة. تم اعتماد بروتوكول التجربة والتعديلات من قبل الهيئة الأخلاقية المناسبة في كل موقع مشارك. قدم جميع المرضى موافقة خطية مستنيرة. يؤكد جميع المؤلفين أن التجربة أجريت مع احترام معايير الممارسات السريرية الجيدة.
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة حول اعتماد بروتوكول الدراسة في المخطوطة.
التقارير الخاصة بالمجالات
يرجى اختيار الخيار أدناه الذي يناسب بحثك بشكل أفضل. إذا لم تكن متأكدًا، اقرأ الأقسام المناسبة قبل اتخاذ قرارك.
علوم الحياة □ العلوم السلوكية والاجتماعية □ العلوم البيئية والتطورية والبيئية
لنسخة مرجعية من الوثيقة بجميع الأقسام، انظر nature.com/documents/nr-reporting-summary-flat.pdf
تصميم دراسة علوم الحياة
يجب على جميع الدراسات الإفصاح عن هذه النقاط حتى عندما يكون الإفصاح سلبيًا.
حجم العينة
سيؤدي حجم عينة مكونة من 521 مريضًا في مجموعة النية للعلاج إلى قوة (ألفا ثنائية الجانب 0.05) لاكتشاف فرق في معدلات pCR بين أذرع العلاج، بافتراض معدل في الذراع الضابطة. نظرًا لقرار الراعي بإغلاق جميع المواقع في روسيا، تم استبعاد 11 مريضًا بسبب عدم كفاية المتابعة لتقييم pCR، مع تأثير ضئيل على قوة الدراسة ( ).
استبعاد البيانات
نظرًا لقرار الراعي بإغلاق جميع المواقع في روسيا، تم استبعاد 11 مريضًا بسبب عدم كفاية المتابعة لتقييم pCR.
التكرار
بدأت الدراسة في تسجيل المرضى من 31 دولة في نوفمبر 2019 وانتهت في ديسمبر 2023. تم متابعة كل مريض مشارك من وقت التسجيل حتى توقف الدراسة أو الوفاة. وبالتالي، لم يكن من الممكن تكرار الدراسة.
العشوائية
تمت العشوائية وفقًا لتقنية الاستجابة التفاعلية حسب نسبة خلايا المناعة المعبرة عن PD-L1 (نسبة خلايا المناعة حسب VENTANA PD-L1 SP142 المناعية، الحد الأدنى عند 1%)، درجة الورم (2 أو 3)، حالة العقدة الإبطية المؤكدة مرضيًا (إيجابية في المراجعة المرضية أو سلبية في المراجعة الشعاعية و/أو المرضية) وتكرار جرعات الأنثراسيكلين (كل 3 أسابيع أو كل أسبوعين).
التعمية
تم تعمية المرضى، والأشخاص المعنيين بإدارتهم، والأشخاص الذين يجمعون البيانات ويحللونها؛ ومع ذلك، وفقًا لتعديل البروتوكول، تم فك تعمية الدراسة في المرحلة المساعدة بعد اعتماد الأبيماسيكلب لعلاج ER+/HER2 عالي الخطورة. كان من المتوقع أن يؤدي الجمع بين الأبيماسيكلب والنفولوماب إلى معدل مرتفع من الانسحابات بسبب مخاوف السلامة حول الجمع بين مثبط CDK4/6 ووكيل مضاد PD-1. وفقًا لتعديل البروتوكول، في المرحلة المساعدة، تلقى المرضى نفولوماب 480 ملغ مع اختيار المحقق للعلاج الهرموني (تاموكسيفين، ليتروزول، أنستروزول، أو إكسمستين، مع أو بدون قمع وظيفة المبيض) لمدة تصل إلى سبع دورات.
nature portfolio | ملخص التقرير أبريل 2023
التقارير للمواد والأنظمة والأساليب المحددة
نحتاج إلى معلومات من المؤلفين حول بعض أنواع المواد والأنظمة التجريبية والأساليب المستخدمة في العديد من الدراسات. هنا، حدد ما إذا كانت كل مادة أو نظام أو طريقة مدرجة ذات صلة بدراستك. إذا لم تكن متأكدًا مما إذا كان عنصر القائمة ينطبق على بحثك، اقرأ القسم المناسب قبل اختيار رد.
المواد والأنظمة التجريبية
غير متاح
المعنيون بالدراسة
□
Xالأجسام المضادة
□ خطوط خلايا حقيقية النواة
□ علم الحفريات وعلم الآثار
X
□ الحيوانات وغيرها من الكائنات الحية
□
X البيانات السريرية
X
□
X
□
الأساليب
المعنيون بالدراسة
ChIP-seq
تدفق الخلايا
التصوير العصبي القائم على الرنين المغناطيسي
الأجسام المضادة
الأجسام المضادة المستخدمة
التحقق
تم تقييم PD-L1 بواسطة المناعية النوعية على خلايا المناعة باستخدام اختبار VENTANA SP142 (روشي دياغنوستكس) ودرجة PD-L1 الإيجابية المجمعة مع اختبار pharmDx (أجيلة).
صف تحقق كل جسم مضاد رئيسي للنوع والتطبيق، مع الإشارة إلى أي بيانات تحقق على موقع الشركة المصنعة، والاستشهادات ذات الصلة، وملفات تعريف الأجسام المضادة في قواعد البيانات عبر الإنترنت، أو البيانات المقدمة في المخطوطة.
البيانات السريرية
معلومات السياسة حول الدراسات السريرية
يجب أن تمتثل جميع المخطوطات لإرشادات ICMJE لنشر الأبحاث السريرية ويجب تضمين قائمة مراجعة CONSORT المكتملة مع جميع التقديمات.
تسجيل التجارب السريرية
بروتوكول الدراسة
جمع البيانات
النتائج
NCT04109066
البروتوكول متاح كمكمل لهذا المنشور.
تم جمع البيانات السريرية في المواقع المشاركة (معاهد الأبحاث السريرية والمستشفيات) من 20 نوفمبر 2019 إلى 07 أبريل 2022. تم إجراء الدراسة في 221 موقعًا في 31 دولة (الأرجنتين، أستراليا، النمسا، بلجيكا، البرازيل، كندا، تشيلي، الصين، كولومبيا، جمهورية التشيك، الدنمارك، فنلندا، فرنسا، ألمانيا، هونغ كونغ، أيرلندا، إيطاليا، جمهورية كوريا، المكسيك، هولندا، بولندا، البرتغال، رومانيا، الاتحاد الروسي [أوقفت BMS جميع الأنشطة في روسيا في يونيو 2022]، سنغافورة، إسبانيا، سويسرا، تايوان، تركيا، المملكة المتحدة، والولايات المتحدة الأمريكية)
كانت النقطة النهائية الأولية هي في مجموعة النية المعدلة للعلاج. بعد القرار بوقف التسجيل في الدراسة في أبريل 2022 بسبب تغير مشهد العلاج، تم تغيير البقاء خاليًا من الأحداث من نقطة نهائية مشتركة إلى نقطة نهائية استكشافية، حيث كان العدد الإجمالي للمرضى المسجلين منخفضًا جدًا لتوفير قوة كافية للمقارنة. وبالتالي، تم تقليل المتابعة إلى سنة واحدة بعد الجراحة لجميع المرضى، وأصبحت المرحلة المساعدة مفتوحة. تضمنت النقاط النهائية الثانوية pCR في مجموعة PD-L1+، ومعدل RCB 0/I في المجموعات المعدلة للنية PD-L1+. تم تقييم الاستجابة المرضية، وتم حساب درجة RCB بواسطة أطباء الأمراض المحليين. جمعت درجة RCB حجم الورم، وكثافة الورم، ومشاركة العقدة في درجة واحدة مستمرة تم تقسيمها إلى أربع فئات، وهي درجة RCB 0 (أي استجابة مرضية كاملة)، وI، II، وIII. تم تقييم السلامة والقبول خلال المرحلتين المساعدة والنيودجية في جميع المرضى الذين تلقوا جرعة واحدة على الأقل من دواء الدراسة. تضمنت النقاط النهائية الاستكشافية المحددة مسبقًا ارتباط نتائج الفعالية بحالة العلامة الحيوية بناءً على درجة PD-L1 الإيجابية المجمعة، وخلايا اللمف المتسللة في الورم (sTILs)، ومستويات مستقبلات الاستروجين/البروجستيرون، ومؤشر Ki67.
النباتات
مخزونات البذور
أبلغ عن مصدر جميع مخزونات البذور أو المواد النباتية الأخرى المستخدمة. إذا كان ذلك ممكنًا، اذكر مركز مخزون البذور ورقم الكتالوج. إذا تم جمع عينات نباتية من الحقل، صف موقع الجمع، التاريخ وإجراءات أخذ العينات.
أنماط نباتية جديدة
صف الطرق التي تم من خلالها إنتاج جميع الأنماط النباتية الجديدة. يشمل ذلك تلك التي تم إنشاؤها بواسطة طرق نقل الجينات، وتحرير الجينات، والطفرات الكيميائية/الإشعاعية والتهجين. بالنسبة لخطوط النقل الجيني، صف طريقة التحويل، وعدد الخطوط المستقلة التي تم تحليلها والجيل الذي أجريت عليه التجارب. بالنسبة لخطوط التحرير الجيني، صف المحرر المستخدم، والتسلسل الداخلي المستهدف للتحرير، وتسلسل RNA الدليل المستهدف (إذا كان ذلك ممكنًا) وكيف تم توفير المحرر.
التحقق
تم توفيره.
صف أي إجراءات تحقق لكل مخزون بذور مستخدم أو نمط جديد تم إنتاجه. صف أي تجارب استخدمت لتقييم تأثير الطفرة، وأينما كان ذلك ممكنًا، كيف تم فحص التأثيرات الثانوية المحتملة (مثل إدخالات T-DNA في الموقع الثاني، التباين، تحرير الجينات خارج الهدف).
Neoadjuvant nivolumab and chemotherapy in early estrogen receptor-positive breast cancer: a randomized phase 3trial
Received: 5 July 2024
Accepted: November 2024
Published online: 21 January 2025
Check for updates
A list of authors and their affiliations appears at the end of the paper
Patients with estrogen receptor-positive (ER+), human epidermal growth factor receptor 2-negative (HER2-) primary breast cancer (BC) have low pathological complete response (pCR) rates with neoadjuvant chemotherapy. A subset of ER+/HER2-BC contains dense lymphocytic infiltration. We hypothesized that addition of an anti-programmed death1 agent may increase pCR rates in this BC subtype. We conducted a randomized, multicenter, double-blind phase 3 trial to investigate the benefit of adding nivolumab to neoadjuvant chemotherapy in patients with newly diagnosed, high-risk, grade 3 or 2 (ER 1 to ) ER+/HER2- primary BC. In total, 510 patients were randomized to receive anthracycline and taxane-based chemotherapy with either intravenous nivolumab or placebo. The primary endpoint of pCR was significantly higher in the nivolumab arm compared with placebo ( versus ), with greater benefit observed in patients with programmed death ligand 1-positive tumors (VENTANA SP142 versus respectively). There were no new safety signals identified. Of the five deaths that occurred in the nivolumab arm, two were related to study drug toxicity; no deaths occurred in the placebo arm. Adding nivolumab to neoadjuvant chemotherapy significantly increased pCR rates in high-risk, early-stage ER+/HER2-BC, particularly among patients with higher stromal tumor-infiltrating lymphocyte levels or programmed death ligand 1 expression, suggesting a new treatment paradigm that emphasizes the role of immunotherapy and T cell immunosurveillance in luminal disease. Clinical trials.gov identifier: NCT04109066
Approximately 2.3 million cases of BC were diagnosed globally in 2020, of which were the ER+/HER2- subtype . ER+/HER2- BC exhibits significant heterogeneity in its responses to treatment and clinical outcomes, posing substantial challenges for effective management. This heterogeneity may be caused by distinct differences in the molecular subtypes of ER+/HER2-BC, including subtypes with varying estrogen and progesterone receptor expression, and those that are immunogenic, proliferative and receptor tyrosine kinase-driven, which require specific treatments .
Current systemic therapeutic strategies for high-risk, early-stage ER+/HER2-BC include: neoadjuvant or adjuvant chemotherapy (CT); prolonged adjuvant endocrine therapy (ET) with or without adjuvant targeted therapies, including cyclin-dependent kinase 4/6 inhibitors; and poly(ADP-ribose) polymerase inhibitors for patients carrying germline pathogenic alterations .
Anti-programmed death ligand 1 (PD-L1) agents significantly improve clinical outcomes in early-stage triple-negative BC (TNBC) and PD-L1+ metastatic TNBC .A subset of ER+/HER2-BC contains a dense
lymphocytic infiltration, similar to that seen in TNBC ; however, it is unclear how this relates to the response to immune checkpoint inhibitors in ER+/HER2- BC . Results from the adaptively randomized I-SPY2 study suggest that anti-PD-(L)1 agents have the potential to increase the proportion of patients with high-risk ER+/HER2-BC who achieve pCR or minimal residual disease (residual cancer burden (RCB) score of 0 or I) following neoadjuvant treatment . The CheckMate 7FL (NCT04109066) study aimed to investigate the benefit of adding nivolumab to neoadjuvant CT followed by adjuvant ET in patients with newly diagnosed early-stage high-risk ER+/HER2-BC. We also sought to define patient subpopulations most likely to respond to nivolumab in combination with neoadjuvant CT.
Results
Study population and demographics
From 20 November 2019 to 7 April 2022, 830 patients were screened at 221 sites in 31 countries. Of the 830 patients screened, 521 were randomized. Because of the sponsor’s decision to close all sites in Russia after the Ukraine-Russia geopolitical conflict began, 11 patients were excluded from the analysis population because of insufficient follow-up for pCR assessment. The resulting population formed the modified intent-to-treat population (mITT), which comprised 510 patients who received neoadjuvant CT with either nivolumab ( ) or placebo . The safety population consisted of the 517 patients who received neoadjuvant CT with either nivolumab ( ) or placebo ( ) (Fig.1). Patient demographic and clinical characteristics were balanced between the two treatment arms (Table 1).
In the safety population, the mean (min, max) treatment duration during the paclitaxel neoadjuvant phase was weeks for patients receiving nivolumab and weeks for patients receiving placebo. The mean (min, max) treatment duration during the anthracycline neoadjuvant phase was weeks for patients receiving nivolumab and 7.7 (0.1,15.1) weeks for patients receiving placebo. Of patients randomized to nivolumab and placebo, respectively, ( 233 of 263 ) and ( 236 of 258 ) underwent surgery (Supplementary Table 1).
Efficacy
A statistically significantly higher proportion of patients who received nivolumab achieved pCR (ypT0/is, ypN0; of 257 ) versus placebo ( of 253; odds ratio (OR) 2.05 ( confidence interval (CI) 1.29 to 3.27, ) in addition to neoadjuvant CT (Fig. 2a).
The proportion of patients who experienced pCR was numerically higher among those who had PD-L1+ tumors (PD-L1-expressing tumor-infiltrating immune cells (IC) IC, ) versus those with PD-L1- tumors ( IC, ). The difference in pCR rates ( ) between the nivolumab arm and placebo arm was (10.1 to 36.7) and 3.6 % (-3.6 to 10.7) for PD-L1+ and PD-L1- tumors, respectively (Fig. 2c). Subgroup analyses of pCR rates were consistent with these results (Fig.3).
RCB 0 or I rates in the mITT population and by PD-L1 status, as well as subgroup analyses, were consistent with the findings observed for pCR (Fig. 2b,e and Supplementary Fig. 1). Nivolumab skewed the distribution of RCB toward the lower classes versus placebo (Supplementary Fig. 2).
Because of its early termination, the study was significantly underpowered for event-free survival (EFS), and median follow-up for EFS in the mITT population at reporting was premature at 19 months, with a low number of events observed. Results of a descriptive exploratory analysis showed that EFS was similar between the two treatment arms, with an 18 -month rate of ( to 92.7) in the nivolumab arm and to 94.8) in the placebo arm (Supplementary Fig. 3).
Efficacy according to immune biomarkers
The prevalence of the PD-L1+ population in the two arms was balanced, as evaluated by baseline PD-L1 expression status, defined by either
Fig. 1 | Flow chart showing patient disposition. Twenty-five patients received abemaciclib, and may have received it after neoadjuvant treatment or discontinued adjuvant treatment to receive abemaciclib. The mITT population comprised 510 patients ( 257 patients in the nivolumab arm and 253 patients in the placebo arm). Because of the sponsor’s decision to close Russian sites, 11 patients were excluded owing to insufficient follow-up for pCR. Discontinuation of study treatment included treatment discontinuation during the adjuvant phase. Most common reasons for discontinuation of treatment captured by ‘Other’ were disease progression, principal investigator discretion, serious AEs or AEs and withdrawal of consent. Completers were patients who completed surgery and the adjuvant phase. Patients were reported as ongoing at the time of the premature closure of Russian sites.
VENTANA SP142 assay ( IC) or Dako 28-8 assay (PD-L1 combined positive score (CPS) and ) (Supplementary Fig. 4). The highest overall percentage agreement of was observed between SP142 IC and 28-8 CPS (Fig. 4a). pCR and RCB 0 or I rates were increased in patients with PD-L1+ tumors as measured by both SP142 and ; the benefit was greater with increasing CPS cutoffs (Fig. 4c and Supplementary Figs. 5 and 6).
The prevalence of biomarker-positive populations at baseline stratified by percentage of stromal tumor-infiltrating lymphocytes (sTILs) at various cutoffs, compared with those by PD-L1 SP142 at 1% IC, is shown in Supplementary Fig. 7. Median and mean sTIL levels were and (s.d., 24.16 ), respectively, and the prevalence of sTIL positivity was balanced across the treatment groups. Defining sTIL-positive patients as those with detectable sTILs (>1%), the overall percentage agreement between sTIL detection and various PD-L1 by immune cell or CPS cutoffs ranged between and (Fig. 4b). pCR and RCB 0 or I rates with nivolumab versus placebo increased in patients with higher sTIL levels (Figs. 2d,f and 4d). When both sTIL and PD-L1 assays were used, the highest pCR rates were observed in patients in whom both sTIL and PD-L1 expression were considered positive, but notably, there was also nivolumab benefit seen for patients with discordance between PD-L1 <1% IC and sTIL+ (Supplementary Fig. 8).
pCR and RCB 0 or I rates were higher in patients whose tumors had lower ER (<50%) and/or progesterone receptor expression ( ) than in patients whose tumors had higher ER or progesterone
All values are given as (%), unless stated otherwise. PD-L1-expressing tumor-infiltrating IC as percentage of tumor area (PD-L1- defined as PD-L1 IC <1%; PD-L1+ defined as PD-L1 IC ) using the VENTANA SP142 assay, per central assessment. Locally assessed. Arm B included one patient with stage I disease and two patients with stage IV disease, who were deemed eligible and later recategorized as having stage II disease. American Joint Committee on Cancer Cancer Staging Manual, 8th edition. Gonadotropin-releasing hormone agonist therapy was allowed for ovarian preservation. AC, anthracycline + cyclophosphamide; cTNM, clinical TNM staging system (T size and extent of primary tumor; N extent of spread to the lymph nodes; M presence of metastasis); ECOG PS, Eastern Cooperative Oncology Group performance status; QXW, every X weeks.
receptor expression (Supplementary Figs. 9 and 10). No association between nivolumab benefit and the Ki67 index was observed (Supplementary Fig. 11).
In a multivariable analysis of pCR by biomarker subgroups, including prognostic clinicopathological features and key biomarkers, sTIL percentage ( or ) and PD-L1 (defined as IC or CPS ) were independently associated with nivolumab efficacy (Supplementary Figs. 12a,b and 13a,b).
Safety
The safety analysis is based on the safety population ( ; 262 patients in the nivolumab arm and 255 patients in the placebo arm). In the neoadjuvant treatment phase, a similar proportion of patients in the nivolumab versus placebo arms experienced adverse events (AEs) ( versus ) and treatment-related AEs of any grade ( versus ). The most frequently reported treatment-related AEs were alopecia ( versus ), nausea ( versus ), anemia ( versus ) and fatigue ( versus ) in the nivolumab versus placebo arms, respectively. Grade 3 or 4 AEs were reported in versus of patients in the nivolumab versus placebo arm, respectively. Grade 3 or 4 treatment-related AEs were reported in versus of patients in the nivolumab versus placebo arms, respectively (Table 2). Serious AEs (22.9% versus 12.9%) and treatment-related serious AEs ( versus ), as well as AEs leading to discontinuation ( versus ) and treatment-related AEs leading to discontinuation ( versus ), were reported more frequently with nivolumab than with placebo.
In the neoadjuvant treatment phase, there were three ( ) grade 5 treatment-unrelated events in the nivolumab arm (one due to COVID19; two due to pulmonary embolism, of which one occurred within a week postrecovery from COVID-19) and none in the placebo arm. In addition, two further deaths in the nivolumab arm were deemed related to study drug toxicity, although not reported as grade 5 (because of the extended time interval between AE onset and death): pneumonitis (61 days after final dose of neoadjuvant treatment) and hepatitis (51 days after final dose of neoadjuvant treatment); no deaths due to study drug toxicity were reported with placebo.
AEs during the neoadjuvant treatment phase that required immune-modulating medication occurred in and patients in the nivolumab and placebo arms, respectively. AEs of special interest occurred in three (1.1%) patients in the nivolumab arm and no patients in the placebo arm; these events were grade 3 or 4 GuillainBarré syndrome ( ), grade 3 or 4 myocarditis ( ) and grade autoimmune neuropathy ( ).
The mean cumulative dose and relative dose intensity of each CT drug were similar in both treatment arms.
Discussion
In the CheckMate 7FL study, we investigated whether the addition of nivolumab to anthracycline and taxane neoadjuvant CT could significantly increase pCR rates in newly diagnosed early-stage, high-risk, high-grade ER+/HER2-BC. The study met its primary endpoint, with a significantly higher rate of pCR in the nivolumab arm versus placebo. RCB 0 or I rates were also improved in the nivolumab versus placebo
Fig. 2 | Efficacy endpoints for the overall population and by subgroups. a,b, Proportion of patients with and RCB 0 or I (b) for the nivolumab plus neoadjuvant CT ( ) and placebo plus neoadjuvant CT ( ) arms in the mITT population. c,d, Proportion of patients with pCR in the nivolumab plus neoadjuvant CT and placebo plus neoadjuvant CT arms by PD-L1 status or (c) and stromal tumor infiltrating lymphocyte (sTIL) status or . e,f, Proportion of patients with RCB 0 or I rate by PD-L1 status or and sTIL status or , ) (f). Data are presented as percentages with error bars showing the CI around the observed proportion of patients in the treatment arm. The CIs
for each treatment arm were calculated using the Clopper-Pearson method and CIs for differences ( ) between treatment arms were calculated using the Newcombe method without continuity correction. Strata-adjusted difference in pCR rate between the two arms was analyzed with the stratified Cochran-Mantel-Haenszel method of weighting with a two-sided alpha level of . Strata-adjusted OR was assessed with the Mantel-Haenszel method (a,b). The number of patients with pCR or RCB 0 or and the total number of patients in each subgroup are shown above each bar. Database lock: 14 April and 20 March 2024 (d-f). n, number of patients with pCR or RCB 0/I; N, number of patients in each treatment group.
Fig. 3 | Forest plot of proportion of patients with pCR in the nivolumab plus neoadjuvant CT and placebo plus neoadjuvant CT arms by subgroup analyses. Data are presented as percentages with error bars showing the 95% CIs around the observed proportion of patients in the treatment arm. The CIs for each treatment arm were calculated using the Clopper-Pearson method and CIs for differences between treatment arms were calculated using the Newcombe
method without continuity correction. pCR rate difference was not computed for subsets with fewer than 10 patients per treatment arms. The two patients who were initially categorized as having stage IV disease were deemed eligible and later recategorized as having stage II disease. AC, anthracycline; IRT, interactive response technology; , total number of patients in subgroup; NA, not available; Q2W, every 2 weeks; Q3W every 3 weeks. Database lock: 14 April 2023.
arm. These findings were predominantly driven by the PD-L1+ subpopulation, in which an absolute difference of more than was seen with the addition of nivolumab to the neoadjuvant CT. This observation differed from that in early-stage TNBC, where the effect was independent of PD-L1 expression . Although the reasons for this are unclear, TNBC is known to be more molecularly heterogeneous than ER+BC, potentially resulting in a single core biopsy unlikely to encapsulate heterogenous PD-L1 expression . The median follow-up remains too short in this analysis to make any conclusions about EFS, although notably there were no early non-BC-related deaths. However, achievement of a pCR and/or a RCB of 0 or I is associated with improved long-term outcomes in ER+/HER2-BC . Translation of improvements in pCR rates into EFS improvements varies across different clinical trials. Very few early trials were adequately powered to assess both endpoints; however, overall, almost all combination chemotherapies that improved pCR rates
(by incorporating a taxane-based, carboplatin-based, HER2-targeted therapy or pembrolizumab) also improved EFS in BC studies . It is also becoming increasingly clear that different neoadjuvant regimens result in different distributions of RCB, and therapies that shift the entire spectrum of RCB to smaller values may have a greater impact on EFS than therapies that improve pCR rates by moving minimal residual cancers to the pCR category .
Our results are consistent with those of the KEYNOTE-756 study , which investigated pembrolizumab in the same patient setting. In KEYNOTE-756, improved pCR rates were also seen in the setting of increasing PD-L1 expression but only at the higher levels using the 22 C3 pharmDx CPS (CPS ) assay. Results from CheckMate 7FL consolidate the benefit of adding an immune checkpoint inhibitor to neoadjuvant CT in this BC subtype and context, and longer follow-up will indicate whether these pCRs translate into greater EFS benefit for
Fig. 4 |Efficacy of nivolumab by subgroups. a, Concordance between PD-L1 assays SP142 and 28-8 CPS.b, sTIL and PD-L1 expression in patients with quantifiable sTIL and PD-L1 by SP142 or 28-8 CPS. c, pCR rates in the nivolumab plus neoadjuvant CT and placebo plus neoadjuvant CT arms by PD-L1 status as determined by the SP142 (IC%) and 28-8 CPS (cutoffs 1-20) assays. d, PD-L1 status as determined by the SP142 (IC%) assay and percentage of sTIL (cutoffs ). The number of patients with qualifying data ( ) and the total number of patients in each subgroup are shown above each circle ( ) or below each bar ( ). Data are presented as percentages. CIs for the observed proportion of patients in the treatment arm were
calculated using the Clopper-Pearson method and CIs for differences between treatment arms were calculated using the Newcombe method without continuity correction (c,d). Vertical dashed lines are to visually distinguish between Overall, SP142 and 28-8 in c, and Overall, SP142 and sTIL in d. 28-8 CPS, Dako 28-8 assay using the CPS algorithm; OPA, overall percentage agreement; SP142 VENTANA, PD-L1SP142 assay. Clinical database;SP142 cutoff at versus . Because of the small sample size, the percent agreement was not calculated for CPS ). Database lock: 20 March 2024. Additional patients were included in the CPSevaluable group at this final database lock.
Nonendocrine IMAEs where immunomodulation was initiated
Rash
15 (5.7)
4 (1.5)
12 (4.7)
1 (0.4)
Hepatitis
13 (5.0)
8 (3.1)
3 (1.2)
2 (0.8)
Pneumonitis
8 (3.1)
4 (1.5)
2 (0.8)
0
Hypersensitivity
10 (3.8)
0
3 (1.2)
0
Nephritis/renal dysfunction
2 (0.8)
1 (0.4)
0
0
Diarrhea/colitis
1 (0.4)
0
1 (0.4)
1 (0.4)
Database lock: 20 March 2024 . Events reported between the first dose and 30 days after the last dose of neoadjuvant therapy for patients who did not go on to adjuvant therapy or before adjuvant therapy for patients who started adjuvant therapy. The events shown are the 10 most frequent in the nivolumab arm. Alopecia is likely to have been under-reported. Common Toxicity Criteria for Adverse Events grading for alopecia consists of only grade 1 or 2 ; the grade 3 or 4 alopecia reported in this study was reported incorrectly. Events reported between the first dose and 100 days after the last dose of neoadjuvant therapy for patients who did not go on to adjuvant therapy or before adjuvant therapy for patients who started adjuvant therapy. Immune-mediated adverse events (IMAEs) are specific events, regardless of causality, that were considered as potentially immune-mediated by the investigator with no clear alternate etiology, occurred within 100 days of the final dose, and were treated with immune-modulating medication (except for endocrine IMAEs, which do not require immune-modulating medication use). ALT, alanine transaminase; AST, aspartate transaminase; SAE, serious adverse event; TRAE, treatment-related adverse event; TRSAE, treatment-related serious adverse event.
all or just for patients with PD-L1+ tumors. Notably, whereas previous studies have shown that addition of programmed death 1 inhibition in TNBC led to small increases in pCR rates, including in patients with low PD-L1 expression, significant EFS benefit was observed . Overall, these results represent a new milestone in the neoadjuvant treatment of ER+/HER2-BC, because there have been intensive but thus far unsuccessful efforts to improve pCR rates in this patient population.
One important strength of CheckMate 7FL is that three immune assays were evaluated in a phase III trial population. Increases in pCR rates with the addition of nivolumab were also observed for sTIL increases from as little , which was the median sTIL level in this patient population. Moderate concordance between the SP142, 28-8 pharmDx CPS and sTIL assays was observed. Interestingly, although
pCR rates were highest with the addition of nivolumab when the assays agreed on sTIL and PD-L1 positivity, patients with discordant assay results still derived benefit. These data have important implications for patients with BC, and suggest that the use of multiple assays may be best to identify all patients who could benefit from neoadjuvant immunotherapy in this subtype, although sTIL may be the most pragmatic and globally accessible biomarker because it can be evaluated on standard hematoxylin and eosin-stained slides . Analysis of other exploratory biomarkers for patient stratification is ongoing.
Analyses of pCR rates by ER and progesterone receptor levels confirm that patients with ER and/or progesterone receptor levels have greater benefit with the addition of nivolumab than
patients with ER and/or progesterone receptor levels . Notably, we observed this effect also in the setting of . Although this remains to be further validated, it suggests that patients with lower ER and progesterone receptor levels may be treated similarly to patients with early TNBC. Previous research has shown that tumors with lower ER levels harbor more sTILs and CD8 T cells, with higher PD-L1 expression, and are more similar to TNBC with regard to immune-related signatures .
Safety was consistent with the known safety profiles, with no change in the feasibility of surgery following the addition of nivolumab to CT. However, it is important to note that two treatment-related deaths were observed in the nivolumab arm.
The key strengths of this study are: its inclusion of a high-risk population, the majority of whom were node-positive and grade 3; evaluation of response in a PD-L1+ population as a key secondary endpoint; and comprehensive biomarker data, including evaluation of response in a sTIL-high population, presented in the early BC setting. Limitations include the major protocol amendment that significantly reduced the sample size and/or number of events and follow-up time resulting in EFS being designated as an exploratory endpoint.
In conclusion, adding nivolumab to neoadjuvant anthracycline and taxane-based CT in high-risk, early-stage ER+/HER2- BC significantly increased the pCR rate. These findings reshape our understanding of this disease in the context of T cell immunosurveillance and immunotherapy response in luminal disease. Patients with higher levels of sTIL or PD-L1 expression experienced higher pCR rates, potentially setting a new standard for future neoadjuvant treatment studies in this subset. Biomarker analyses aim to uncover the biological drivers behind the robust immune responses to the addition of immunotherapy to CT observed in ER+ BC, which could help further refine and personalize immunotherapeutic approaches for this disease.
Online content
Any methods, additional references, Nature Portfolio reporting summaries, source data, extended data, supplementary information, acknowledgements, peer review information; details of author contributions and competing interests; and statements of data and code availability are available at https://doi.org/10.1038/s41591-024-03414-8.
References
Arnold, M. et al. Current and future burden of breast cancer: global statistics for 2020 and 2040. Breast 66, 15-23 (2022).
Clusan, L., Ferriere, F., Flouriot, G. & Pakdel, F. A basic review on estrogen receptor signaling pathways in breast cancer. Int. J. Mol. Sci. 24, 6834 (2023).
Jin, X. et al. Molecular classification of hormone receptor-positive HER2-negative breast cancer. Nat. Genet. 55, 1696-1708 (2023).
Loibl, S. et al. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 35, 159-182 (2024).
Burstein, H. J., Lacchetti, C. & Griggs, J. J. Adjuvant endocrine therapy for women with hormone receptor-positive breast cancer: ASCO clinical practice guideline focused update. J. Oncol. Pract. 15, 106-107 (2019).
Johnston, S. R. D. et al. Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol. 24, 77-90 (2023).
Korde, L. A. et al. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO Guideline. J. Clin. Oncol. 39, 1485-1505 (2021).
Freedman, R. A. et al. Optimal adjuvant chemotherapy and targeted therapy for early breast cancer-cyclin-dependent kinase 4 and 6 inhibitors: ASCO guideline rapid recommendation update. J. Clin. Oncol. 42, 2233-2235 (2024).
Cortes, J. et al. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N. Engl. J. Med. 387, 217-226 (2022).
Nanda, R. et al. Effect of pembrolizumab plus neoadjuvant chemotherapy on pathologic complete response in women with early-stage breast cancer: an analysis of the ongoing phase 2 adaptively randomized I-SPY2 trial. JAMA Oncol. 6, 676-684 (2020).
Schmid, P. et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N. Engl. J. Med. 386, 556-567(2022).
O’Meara, T. et al. Immunological differences between immune-rich estrogen receptor-positive and immune-rich triple-negative breast cancers. JCO Precis. Oncol. 4, 767-779 (2020).
Wolf, D. M. et al. Immune signatures and MammaPrint (ultra) high risk class (MP2) as predictors of response to pembrolizumab combined with the TLR9 agonist SD101 in the neoadjuvant I-SPY 2 TRIAL. Cancer Res. 82, P5-13-12 (2022).
Dieci, M. V. et al. Neoadjuvant chemotherapy and immunotherapy in luminal B-like breast cancer: results of the phase II GIADA trial. Clin. Cancer Res. 28, 308-317 (2022).
Loi, S. Tumor-infiltrating lymphocytes, breast cancer subtypes and therapeutic efficacy. Oncoimmunology 2, e24720 (2013).
Rios-Hoyo, A. et al. Correlation of hormone receptor positive HER2-negative/MammaPrint high-2 breast cancer with triple negative breast cancer: Results from gene expression data from the ISPY2 trial. J. Clin. Oncol. 573, abstract 573 (2024).
Symmans, W. F. et al. Assessment of residual cancer burden and event-free survival in neoadjuvant treatment for high-risk breast cancer: an analysis of data from the I-SPY2 randomized clinical trial. JAMA Oncol. 7, 1654-1663 (2021).
Schmid, P., Cortes, J. & Dent, R. Pembrolizumab in early triple-negative breast cancer. Reply. N. Engl. J. Med. 386, 1771-1772 (2022).
Pareja, F. et al. Triple-negative breast cancer: the importance of molecular and histologic subtyping, and recognition of low-grade variants. NPJ Breast Cancer 2, 16036 (2016).
Kahn, A. M., Golestani, R., Harigopal, M. & Pusztai, L. Intratumor spatial heterogeneity in programmed death-ligand 1 (PD-L1) protein expression in early-stage breast cancer. Breast Cancer Res. Treat. 201, 289-298 (2023).
Cortazar, P. et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 384, 164-172 (2014).
Symmans, W. F. et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J. Clin. Oncol. 25, 4414-4422 (2007).
Pusztai, L. et al. Event-free survival by residual cancer burden with pembrolizumab in early-stage TNBC: exploratory analysis from KEYNOTE-522. Ann. Oncol. 35, 429-436 (2024).
I-SPY2 Trial Consortium et al.Association of event-free and distant recurrence-free survival with individual-level pathologic complete response in neoadjuvant treatment of stages 2 and 3 breast cancer: three-year follow-up analysis for the I-SPY2 adaptively randomized clinical trial. JAMA Oncol. 6, 1355-1362 (2020).
Marczyk, M. et al. Treatment Efficacy Score-continuous residual cancer burden-based metric to compare neoadjuvant chemotherapy efficacy between randomized trial arms in breast cancer trials. Ann. Oncol. 33, 814-823 (2022).
Symmans, W. F. et al. Assessment of residual cancer burden and event-free survival in neoadjuvant treatment for high-risk breast cancer: an analysis of data from the I-SPY2 randomized clinical trial. JAMA Oncol. 7, 1654-1663 (2021).
Cardoso, F. et al. LBA21 KEYNOTE-756: phase III study of neoadjuvant pembrolizumab (pembro) or placebo (pbo) + chemotherapy (chemo), followed by adjuvant pembro or pbo + endocrine therapy (ET) for early-stage high-risk ER+/HER2- breast cancer. Ann. Oncol. 34, S1260-S1261 (2023).
Cardoso, F. et al. Phase 3 study of neoadjuvant pembrolizumab or placebo plus chemotherapy, followed by adjuvant pembrolizumab or placebo plus endocrine therapy for early-stage high-risk ER+/HER2- breast cancer: KEYNOTE-756. Cancer Res. 84, abstract GSO1-02 (2023).
Schmid, P. et al. Pembrolizumab for early triple-negative breast cancer. N. Engl. J. Med. 382, 810-821(2020).
Salgado, R. et al. The evaluation of tumor-infiltrating lymphocytes (TILs) in breast cancer: recommendations by an International TILs Working Group 2014. Ann. Oncol. 26, 259-271 (2015).
Loi, S. et al. The journey of tumor-infiltrating lymphocytes as a biomarker in breast cancer: clinical utility in an era of checkpoint inhibition. Ann. Oncol. 32, 1236-1244 (2021).
Voorwerk, L. et al. Immune landscape of breast tumors with low and intermediate estrogen receptor expression. NPJ Breast Cancer 9, 39 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons. org/licenses/by/4.0/.
(c) Crown 2025
¹Peter MacCallum Cancer Centre, Melbourne, Victoria, Australia. ²University of Melbourne, Parkville, Victoria, Australia. ³Department of Pathology, ZAS Hospitals, Antwerp, Belgium. European Institute of Oncology, IRCCS, Milan, Italy. University of Milan, Milan, Italy. Consultorio de Oncólogo Médico, Oaxaca, Mexico. Gustave Roussy Cancer Campus, Villejuif, France. Bradford Hill Investigación Clinica, Región Metropolitana, Santiago, Chile. Netherlands Cancer Institute, Amsterdam, the Netherlands. Vall d’Hebron University Hospital, Vall d’Hebron Institute of Oncology (VHIO), Barcelona, Spain. Breast Center, Department of Obstetrics and Gynecology and CCC Munich, Ludwig Maximilians University Hospital, Munich, Germany. Dana-Farber Brigham Cancer Center, Boston, MA, USA. Sarah Cannon Research Institute, Nashville, TN, USA. CENEIT Oncológicos, Mexico City, Mexico. Hospital Italiano De Córdoba, Córdoba, Argentina. Radiotherapy Center CLUJ S.R.L., Florești, Romania. Consultorio del Dr. Joaquin Gabriel Reinoso Toledo, Monterrey, Mexico. Istituto Oncologico Veneto IRCCS, Padua, Italy. Department of Surgery, Oncology and Gastroenterology, University of Padova, Padova, Italy. Department of Gynecology, Medical University of Innsbruck, Innsbruck, Austria. ABCSG – Austrian Breast & Colorectal Cancer Study Group, Vienna, Austria. Bristol Myers Squibb, Princeton, NJ, USA. Smilow Cancer Hospital at Yale, New Haven, CT, USA. University of Texas Southwestern Medical Center, Dallas, TX, USA. e-mail: sherene.loi@petermac.org
Methods
Patients
Eligible patients had newly diagnosed ER+/HER2-BC, with a confirmed primary tumor and node categories of tumors sized and cN 2 or cT3-cT4 and cNO-cN2; grade 3 disease or grade 2 disease with ER expression of 1 to ; adequate organ function; tissue available for biomarker assessment; and Eastern Cooperative Oncology Group performance status 0-1. Patients were eligible irrespective of PD-L1 status. Multifocal tumors (two or more foci of cancer in the same breast quadrant) were permitted if the largest lesion was at least 2 cm and designated as the target lesion. Patients with mixed ductal and lobular carcinoma were eligible. Patients were excluded if they had multicentric BC, a history of ipsilateral invasive BC, evidence of metastatic disease, had received any previous treatment for the currently diagnosed BC or had received immunotherapy previously.
Trial design and treatments
CheckMate 7FL was a prospective, randomized, multicenter, double-blind, placebo-controlled phase 3 trial (ClinicalTrials.gov identifier: NCT04109066), originally with co-primary endpoints of pCR and EFS, which were centrally assessed. Following the approval of adjuvant abemaciclib for high-risk primary ER+/HER2, the primary endpoint was amended to pCR alone, making enrollment and assessment of EFS challenging to complete. The combination of abemaciclib with nivolumab was expected to result in a high rate of withdrawals because of safety concerns around combining a CDK4/6 inhibitor with an anti-programmed death 1 agent . In the neoadjuvant phase, patients were randomized 1:1 to receive either nivolumab 360 mg or placebo every 3 weeks with weekly paclitaxel for 12 weeks. This was followed by nivolumab (either 360 mg every 3 weeks or 240 mg every 2 weeks) in combination with anthracycline and cyclophosphamide, or placebo in combination with anthracycline and cyclophosphamide; the anthracycline and cyclophosphamide dosing frequency was determined by the investigator. All patients who remained operative candidates underwent surgery of the breast and axilla (per local standards) within 4 weeks of completing the neoadjuvant treatment phase. Per the protocol amendment, the study was unblinded in the adjuvant phase, and patients received nivolumab 480 mg with investigator’s choice of ET (tamoxifen, letrozole, anastrozole or exemestane, with or without ovarian function suppression) for up to seven cycles.
Randomization was stratified per interactive response technology by the proportion of PD-L1-expressing immune cells (percentage of immune cells by VENTANA PD-L1 SP142 immunohistochemistry, cutoff at ), tumor grade (2 or 3), pathologically confirmed axillary nodal status (positive on pathological review or negative on radiographic and/or pathologic review) and anthracycline dosing frequency (every 3 weeks or every 2 weeks). Before the study was initiated, each participant received log-in information and directions on accessing the interactive response technology. Each participant was assigned a unique number after signing the informed consent form. Participant numbers were used on all participants’ study information. Participant numbers were not reassigned. An interactive response technology was used to manage participant randomization. The investigator or designee registered the participant for enrollment by following the enrollment procedures established by the sponsor.
Endpoints
The primary endpoint was in the mITT population. Initially, EFS was a co-primary endpoint; however, following the decision to discontinue enrollment in the study in April 2022 because of the rapidly changing treatment landscape, the primary endpoint of the trial was updated to focus solely on pCR , and EFS was changed to an exploratory endpoint because the total number of enrolled patients and events was too low and updated follow-up time was too short to provide sufficient power for comparison. Consequently, follow-up
was reduced to 1 year post-surgery for all patients, and the adjuvant phase became open label.
Another key change to the study after discontinuation of enrollment in April 2022 was the evaluation of pCR in the PD-L1+ population by VENTANA SP142 % IC as a secondary endpoint. Other secondary endpoint included RCB 0 or I rates in the mITT and PD-L1+ populations. Pathological response was assessed, and RCB score calculated by local pathologists. The RCB score combined tumor size, tumor cellularity and nodal involvement into a single continuous score that was grouped into four classes, namely, RCB score of 0 (that is, pCR), and I, II and III, which corresponded to increasingly larger residual cancer and worse recurrence-free survival . Safety and tolerability were assessed during the neoadjuvant and adjuvant phases in all patients who received at least one dose of study drug. Prespecified exploratory endpoints included association of efficacy outcomes with biomarker status based on PD-L1 CPS, sTILs, levels of estrogen/progesterone receptors and Ki67 index.
Study assessments
pCR was assessed post-neoadjuvant (yp) treatment and was defined as no invasive residual disease in breast and lymph nodes (ypT0/is, ypNO) by a local pathologist. AEs were monitored throughout the trial and for 30 days after the discontinuation of study treatment ( 90 days for serious AEs) and graded according to Common Toxicity Criteria for Adverse Events v.5.0 of the National Cancer Institute. Safety was assessed at 30 days and 100 days after the final dose, and long-term follow-up was up to 12 months after surgery. Biomarker analyses included centrally reviewed PD-L1 expression and percentage of sTILs. PD-L1 was evaluated by qualitative immunohistochemistry on immune cells with the VENTANA SP142 assay (Roche Diagnostics) and PD-L1 CPS with the pharmDx assay (Agilent). The percentage of sTILs was quantified on a hematoxylin and eosin-stained slide according to established guidelines . In this study, an sTIL of was the lowest possible value and indicated a lack of detectable sTILs. The SP142% IC assay and the pharmDx CPS were used to evaluate the variation between assays, as well as to determine PD-L1 expression in tumor-infiltrating ICs versus both immune and tumor cells. ER and Ki 67 expression were centrally evaluated using Agilent MIB-Dako pharmDx immunohistochemistry. Progesterone receptor immunohistochemistry levels were evaluated from local pathology testing. Other recorded patient and disease characteristics included tumor grade, axillary nodal status, disease stage, Ki67 index, menopausal status and age.
Statistical analyses
Based on the normal approximation to the binomial, a sample size of 521 patients in the intent-to-treat population would yield approximately power (two-sided alpha of 0.05 ) to detect a difference of in pCR rates between treatment arms, assuming a rate in the control arm. Because of the sponsor’s decision to close all sites in Russia after the Ukraine-Russia geopolitical conflict began, 11 patients were excluded owing to insufficient follow-up for pCR assessment, with a small impact on the study power ( ). This resulted in a mITT population size of 510 patients. Strata-adjusted difference in pCR rate between the two arms was analyzed with the stratified Cochran-Mantel-Haenszel method of weighting with a two-sided alpha level of 0.05. Strata-adjusted OR was assessed with the Mantel-Haenszel method. The cutoffs used for sTIL and PD-L1 expression by SP142 or pharmDx CPS were predefined for this study.
CI values for pCR and RCB 0 or I rates were evaluated using the Clopper-Pearson method. The unweighted differences in pCR and RCB 0 or I rates between treatment arms in different patient subgroups were calculated along with the corresponding 95% two-sided CIs using the Newcombe method without continuity correction. Exploratory multivariable analyses were conducted using logistic regression to evaluate the association of biomarkers and other baseline characteristics with
pCR. Biomarkers included in the multivariable analyses were calculated as either categorical (PD-L1 expression by SP142 or 28-8 pharmDx CPS with sTIL cutoffs of or ) or continuous variables. Other baseline characteristics in the multivariable analyses were stage III disease, negative nodal status, ER expression , postmenopausal status and age years. The CIs for the secondary and exploratory analyses were for descriptive purposes and, therefore, no adjustments were made for multiplicity.
The sex of patients enrolled in the trial was self-reported and data for gender were not collected. No analyses by sex or disaggregated data are presented because doing so would result in the presentation of potentially identifying information.
Trial oversight
This trial was developed and overseen by an academic steering committee and employees of the sponsor (Bristol Myers Squibb). An external, independent data monitoring committee provided oversight of safety and efficacy considerations during the study. The trial protocol and amendments were approved by the appropriate ethics body at each participating site. All patients provided written informed consent. All authors confirm that the trial was conducted with respect to the standards of Good Clinical Practice. All authors had access to the data and participated in the writing and reviewing of this manuscript. The first draft of the manuscript was written by the first author with editorial assistance provided by a medical writer employed by the sponsor. All authors reviewed and participated in drafting the manuscript and all authors approved the submitted draft and can vouch for the accuracy and completeness of the data.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Bristol Myers Squibb will honor legitimate requests for clinical trial data from qualified researchers with a clearly defined scientific objective. Bristol Myers Squibb will consider data sharing requests for Phase II-IV interventional clinical trials that completed on or after 1 January 2008. In addition, primary results from these trials must have been published in peer-reviewed journals and the medicines or indications approved in the US, EU and other designated markets. Sharing is also subject to protection of patient privacy and respect for the patient’s informed consent. Data considered for sharing may include nonidentifiable patient-level and study-level clinical trial data, full clinical study reports and protocols.
References
Masuda, J. et al. Efficacy, safety, and biomarker analysis of nivolumab in combination with abemaciclib plus endocrine therapy in patients with HR-positive HER2-negative metastatic breast cancer: a phase II study (WJOG11418B NEWFLAME trial). J. Immunother. Cancer 11, e007126 (2023).
Rugo, H. S. et al. Abemaciclib in combination with pembrolizumab for HR+, HER2- metastatic breast cancer: phase 1b study. NPJ Breast Cancer 8, 118 (2022).
Acknowledgements
We thank the patients, their families and all investigators involved in this study. In addition, we thank C. Jeyamohan (Clinical Science Lead), A. Demeaux (Protocol Manager), R. Soomro (Clinical Trial Physician) and D. Jiang (Biomarker Analyst) of Bristol Myers Squibb for their contributions to the study. S.L. is supported by the National Breast Cancer Foundation of Australia and the Breast Cancer Research Foundation, New York, USA. R.S. is supported by the Breast Cancer Research Foundation. This study was sponsored and funded by Bristol
Myers Squibb who had final responsibility for the conceptualization, design and conduct of the trial, data collection and analysis. Alongside the authors, the sponsor was also involved with the decision to publish and preparation of the manuscript. Medical writing and editorial assistance, including assisting authors with development of the outline, drafting and incorporation of comments, fact checking, referencing, figure preparation, formatting, proofreading and submission were provided by E. Haygreen, K. Wellington, C. Charles and L. McArdle, all of Spark (a division of Prime, New York, USA), supported by Bristol Myers Squibb according to Good Publication Practice guidelines (https://www.acpjournals.org/doi/abs/10.7326/ M22-1460?journalCode=aim).
Author contributions
S.L., R.S., G.C., R.I.R.D., S.D., C.I.R.G., M.K., C.S., N.H., F.A., R.C., T.S. and H.M. had major involvement in study conception or design. S.L., R.I.R.D., S.D., C.I.R.G., M.K., C.S., N.H., A.E.M., D.A.Y., L.P., A.S.Z., F.R.C., A.U., J.G.R.-T., V.G. and D.E. had substantial involvement in data acquisition. S.D., C.I.R.G., M.K., C.S., N.H., F.A., M.P., A.C., R.C., R.N., T.S. and J.Q.W. had major involvement in data analysis. S.L., R.S., G.C., R.I.R.D., S.D., C.I.R.G., M.K., C.S., N.H., A.E.M., D.A.Y., L.P., A.S.Z., F.R.C., A.U., J.G.R.-T., V.G., D.E., F.A., R.N., T.S., J.Q.W. and H.M. had major involvement in data interpretation. All authors had access to the data and participated in writing, reviewing, and revising the manuscript. All authors approved the final manuscript for publication. All authors accept responsibility for the accuracy and integrity of all aspects of the research.
Competing interests
S.L. reports institutional research funding from AstraZeneca/ Daiichi Sankyo, Bristol Myers Squibb, Novartis, Puma Biotechnology, Roche-Genentech and Seattle Genetics; consulting fees from Amaroq Therapeutics, Astra Zeneca/Daiichi Sankyo, Bristol Myers Squibb, Domain Therapeutics Gilead, Lilly, Mersana Therapeutics, MSD, Roche-Genentech and Novartis; honoraria from Amaroq Therapeutics, AstraZeneca/Daiichi Sankyo, BioNTech, Bristol Myers Squibb, Domain Therapeutics, Gilead Sciences, Lilly, Mersana Therapeutics, MSD, Novartis and Roche-Genentech; meeting/ travel support from Bristol Myers Squibb and Lilly. R.S. reports consulting fees from Owkin; honoraria from AstraZeneca, Daiichi Sankyo and Exact Sciences; meeting/travel support from AstraZeneca and Daichii Sankyo; leadership position at The International Immuno-Oncology Biomarker Working Group; research support from Bristol Myers Squibb and providing unpaid advice to Case 45. G.C. reports participation on advisory boards for AstraZeneca, Bristol Myers Squibb, Daichii Sankyo, Celcuity, Ellipsis, Exact Science, Gilead, Lilly, Menarini, Merck, Novartis, Pfizer, Roche, Sanofi and Veracyte. S.D. reports institutional research funding from Amgen, AstraZeneca, Bristol Myers Squibb, European Commission, the French government, Lilly, Novartis, Orion, Pierre Fabre, Pfizer, Roche-Genentech, Sanofi and Taiho; meeting/ travel support from Novartis, Roche and Seagen; participation on advisory boards for AstraZeneca, Besins, Decibio, Elsan, Gilead and Sanofi; participation on independent data monitoring committee activity for Breast International Group and Pfizer. C.I.R.G. reports honoraria from AstraZeneca, Bristol Myers Squibb, Knight, MSD, Pfizer, Roche and Tecnofarma; participation on data safety monitoring/ advisory boards for Bristol Myers Squibb, Pfizer and Sanofi. M.K. reports institutional research funding from AstraZeneca, Bristol Myers Squibb and Roche; honoraria from Bristol Myers Squibb and Gilead; participation on advisory boards for AstraZeneca, BioNTech, Bristol Myers Squibb, MSD and Roche. C.S. reports research funding from AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Byondis BV, Daiichi Sankyo, Eisai, Genentech, Gilead, Glaxo, Menarini, Merus, MSD, Novartis, Pfizer, Philips Healthcare, Piere Fabre, Puma Biotechnology, Roche, Sanofi Aventis, Seagen, Synthon and Zymeworks; consulting
fees from AstraZeneca, Daiichi Sankyo, Eisai, Gilead, Lilly, MediTech, Novartis, Pfizer, Philips Healthcare, Pharmalex, Piere Fabre, Puma Biotechnology, Roche, Seagen, Synthon and Zymeworks; honoraria from AstraZeneca, Daiichi Sankyo, Exeter Pharmaceuticals, Lilly, Pfizer, Pierre Fabre, Puma Biotechnology and Seagen; payment for expert testimony from AX’s Consulting SARL, Boehringer Ingelheim, Bristol Myers Squibb, Genentech, Innoup, MSD España, Novartis and Sanofi; meeting/travel support from AstraZeneca, Daiichi Sankyo, Eisai Europe, Gilead, Lilly, Novartis, Pfizer, Pierre Fabre, Puma Biotechnology, Roche and Seagen; participation on data safety monitoring/advisory boards for AstraZeneca, Daiichi Sankyo, Eisai Europe, Gilead, Lilly, Menarini, MSD, Novartis, Pfizer, Philips, Pierre Fabre, Roche and Seagen. N.H. reports consulting fees from Daiichi Sankyo, Gilead, Novartis, Pfizer, Roche, Seagen and Viatris; honoraria from AstraZeneca, Daiichi Sankyo, Gilead, Lilly, MSD, Novartis, Pierre Fabre, Pfizer, Roche, Seagen, Viatris and Zuelligpharma; participation on data safety monitoring/advisory boards for Gilead, Roche and Seagen; leadership position at the West German Study Group. E.A.M. reports research funding from Genentech, Gilead and Roche; consulting fees from AstraZeneca, BioNTech, Moderna and MSD; honoraria from MSD; meeting/travel support from MSD; leadership positions at the American Society of Clinical Oncology Board of Directors 2019-2023 and Scientific Advisor for Susan G. Komen. D.A.Y. reports institutional research funding from AbbVie, Ambrx, AstraZeneca, Dana Farber Cancer Institute, Lilly, Roche-Genentech, G1 Therapeutics, Gilead, Incyte, Innocrin Pharmaceuticals, Merck, Novartis, Polyphor, Stemline Therapeutics, US Oncology and UT Southwestern; and consulting fees paid to institution from AstraZeneca, Daiichi Sankyo, Gilead, Integra Connect, Novartis and Stemline Therapeutics. V.G. reports honoraria from AstraZeneca, Daiichi Sankyo, Exact Sciences, Gilead, GlaxoSmithKline, Lilly, Menarini Stemline, Novartis, Roche, and Zentiva; payment for expert testimony from Lilly; meeting/travel support from AstraZeneca and Gilead; institutional patent for Her2DX; and participation on data safety monitoring/advisory boards for AstraZeneca, Daiichi Sankyo, Exact Sciences, Gilead, Lilly, MSD, Novartis, Olema Oncology, Pierre Fabre, Pfizer-Seagen and Roche. D.E. reports consulting fees from AstraZeneca, Daiichi Sankyo, Gilead, Lilly, Menarini, MSD, Novartis, Pfizer, Roche, Seagen and Sirius Medical; honoraria from AstraZeneca, Daiichi Sankyo, Gilead, Lilly, Menarini, MSD, Novartis, Pfizer, Roche,
Seagen and Sirius Medical; meeting/travel support from Daiichi Sankyo and Pfizer; and receipt of medical writing support from Sirius Medical. F.A. reports being an employee of Bristol Myers Squibb. M.P. reports being an employee and shareholder of Bristol Myers Squibb. A.C. reports being an employee of Bristol Myers Squibb and shareholder of Merck. R.C. reports being an employee of Bristol Myers Squibb. R.N. reports being an employee and shareholder of Bristol Myers Squibb. T.S. reports being an employee and shareholder of Bristol Myers Squibb. J.Q.W. reports being an employee and shareholder of Bristol Myers Squibb. L.P. reports institutional research funding from AstraZeneca, Bristol Myers Squibb, GlaxoSmithKline, Merck, Pfizer and Seagen; consulting fees from AstraZeneca, Bristol Myers Squibb, Daiichi, Exact Sciences, Genentech-Roche, GlaxoSmithKline, Merck, Natera, Novartis, Personalis, Pfizer and Stemline-Menarini; and honoraria for advisory board participation from AstraZeneca, Bristol Myers Squibb, Daiichi, Exact Sciences, Genentech-Roche, GlaxoSmithKline, Merck, Natera, Novartis, Personalis, Pfizer and Stemline-Menarini. H.M. reports consulting fees from Amgen, AstraZeneca, Bristol Myers Squibb, Calithera, Celgene, Crown Bioscience Daiichi Sankyo, Lilly, Genentech-Roche, Gilead, Immunomedics, Merck, OBI Pharma, Peregrine, Pfizer, Puma, Spectrum Pharmaceuticals, Syndax Pharmaceuticals, Seattle Genetics and Taplmmune; and research funding from Bristol Myers Squibb, BTG, LLC/AstraZeneca, MedImmune and Merck. R.I.R.D., A.S.Z., F.R.C., A.U. and J.G.R.-T. declare no competing interests.
Correspondence and requests for materials should be addressed to Sherene Loi.
Peer review information Nature Medicine thanks Karen Gelmon, Binghe Xu and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Ulrike Harjes, in collaboration with the Nature Medicine team.
Corresponding author(s):
Sherene Loi
Last updated by author(s): Oct 17, 2024
Reporting Summary
Nature Portfolio wishes to improve the reproducibility of the work that we publish. This form provides structure for consistency and transparency in reporting. For further information on Nature Portfolio policies, see our Editorial Policies and the Editorial Policy Checklist.
Statistics
For all statistical analyses, confirm that the following items are present in the figure legend, table legend, main text, or Methods section.
n/a
□ X
The exact sample size for each experimental group/condition, given as a discrete number and unit of measurement
□ A statement on whether measurements were taken from distinct samples or whether the same sample was measured repeatedly
□ X
The statistical test(s) used AND whether they are one- or two-sided
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
□
□ A description of all covariates tested
□
A description of any assumptions or corrections, such as tests of normality and adjustment for multiple comparisons
□
A full description of the statistical parameters including central tendency (e.g. means) or other basic estimates (e.g. regression coefficient) AND variation (e.g. standard deviation) or associated estimates of uncertainty (e.g. confidence intervals)
□ X
For null hypothesis testing, the test statistic (e.g. ) with confidence intervals, effect sizes, degrees of freedom and value noted Give values as exact values whenever suitable.
□ For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
□ For hierarchical and complex designs, identification of the appropriate level for tests and full reporting of outcomes
□ Estimates of effect sizes (e.g. Cohen’s , Pearson’s ), indicating how they were calculated
Our web collection on statistics for biologists contains articles on many of the points above.
Software and code
Policy information about availability of computer code
Data collection
No software was used
Data analysis
No software was used
For manuscripts utilizing custom algorithms or software that are central to the research but not yet described in published literature, software must be made available to editors and reviewers. We strongly encourage code deposition in a community repository (e.g. GitHub). See the Nature Portfolio guidelines for submitting code & software for further information.
Data
Policy information about availability of data
All manuscripts must include a data availability statement. This statement should provide the following information, where applicable:
Accession codes, unique identifiers, or web links for publicly available datasets
A description of any restrictions on data availability
For clinical datasets or third party data, please ensure that the statement adheres to our policy
Bristol Myers Squibb will honor legitimate requests for clinical trial data from qualified researchers with a clearly defined scientific objective. Bristol Myers Squibb will consider data sharing requests for Phase II-IV interventional clinical trials that completed on or after January 1, 2008. In addition, primary results from these trials must have been published in peer-reviewed journals and the medicines or indications approved in the U.S., EU, and other designated markets. Sharing is also
subject to protection of patient privacy and respect for the patient’s informed consent. Data considered for sharing may include non-identifiable patient-level and study-level clinical trial data, full clinical study reports and protocols.
Research involving human participants, their data, or biological material
Policy information about studies with human participants or human data. See also policy information about sex, gender (identity/presentation), and sexual orientation and race, ethnicity and racism.
Reporting on sex and gender
Reporting on race, ethnicity, or other socially relevant groupings
Population characteristics
Recruitment
Ethics oversight
The sex of patients enrolled in the trial was self-reported and data for gender were not collected. The eligible patient population was predominantly female, and the trial enrolled a single male patient; no analyses by sex or disaggregated data were presented because doing so would result in presentation of potentially identifying information.
Provided in Table 1
Provided in Table 1
From November 20, 2019 through April 07, 2022, 830 patients were screened at 221 clinical sites in 31 countries. Of the 830 patients screened, 521 were randomized. Eligible patients had newly diagnosed ER+/HER2- breast cancer, with a confirmed primary tumor and node categories of tumors sized and or and ; grade 3 disease or grade 2 disease with ER expression of 1 to ; adequate organ function; tissue available for biomarker assessment; and Eastern Cooperative Oncology Group performance status 0-1. Patients were eligible irrespective of PD-L1 status. Multifocal tumors (two or more foci of cancer within the same breast quadrant) were permitted if the largest lesion was at least 2 cm and designated as the target lesion. Patients were excluded if they had multicentric breast cancer, a history of ipsilateral invasive breast cancer, evidence of metastatic disease, had received any prior treatment for the currently diagnosed breast cancer, or had received prior immunotherapy.
This trial was developed and overseen by an academic steering committee and employees of the sponsor (Bristol Myers Squibb). An external, independent data monitoring committee provided oversight of safety and efficacy considerations during the study. The trial protocol and amendments were approved by the appropriate ethics body at each participating site. All patients provided written informed consent. All authors confirm that the trial was conducted with respect to the standards of Good Clinical Practice.
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Field-specific reporting
Please select the one below that is the best fit for your research. If you are not sure, read the appropriate sections before making your selection.
Life sciences □ Behavioural & social sciences □ Ecological, evolutionary & environmental sciences
For a reference copy of the document with all sections, see nature.com/documents/nr-reporting-summary-flat.pdf
Life sciences study design
All studies must disclose on these points even when the disclosure is negative.
Sample size
A sample size of 521 patients in the intent-to-treat population would yield power (two-sided alpha 0.05 ) to detect a difference of in pCR rates between treatment arms, assuming a rate in the control arm. Due to the sponsor’s decision to close all sites in Russia, 11 patients were excluded due to insufficient follow-up for pCR assessment, with a small impact on the study power ( ).
Data exclusions
Due to the sponsor’s decision to close all sites in Russia, 11 patients were excluded due to insufficient follow-up for pCR assessment.
Replication
The study started enrolling patients from 31 countries in November 2019 and completed in December 2023. Each participating patient was followed from the time of enrollment until study discontinuation or death. As such, replication of the study was not possible.
Randomization
Randomization was stratified per interactive response technology by the proportion of PD-L1-expressing immune cells (percentage of immune cells by VENTANA PD-L1 SP142 immunohistochemistry, cut-off at 1%), tumor grade (2 or 3), pathologically confirmed axillary nodal status (positive on pathological review or negative on radiographic and/or pathologic review) and anthracycline dosing frequency (every 3 weeks or every 2 weeks).
Blinding
Patients, those involved with their management and those collecting and analyzing the data were blinded; however, as per the protocol amendment, the study was unblinded in the adjuvant phase following the approval of adjuvant abemaciclib for high-risk primary ER+/HER2. The combination of abemaciclib with nivolumab was expected to result in a high rate of withdrawals due to safety concerns around combining a CDK4/6 inhibitor with an anti-PD-1 agent. Per the protocol amendment, in the adjuvant phase, patients received nivolumab 480 mg with investigator’s choice of ET (tamoxifen, letrozole, anastrozole, or exemestane, with or without ovarian function suppression) for up to seven cycles.
nature portfolio | reporting summary April 2023
Reporting for specific materials, systems and methods
We require information from authors about some types of materials, experimental systems and methods used in many studies. Here, indicate whether each material, system or method listed is relevant to your study. If you are not sure if a list item applies to your research, read the appropriate section before selecting a response.
Materials & experimental systems
n/a
Involved in the study
□
XAntibodies
□ Eukaryotic cell lines
□ Palaeontology and archaeology
X
□ Animals and other organisms
□
X Clinical data
X
□
X
□
Methods
Involved in the study
ChIP-seq
Flow cytometry
MRI-based neuroimaging
Antibodies
Antibodies used
Validation
PD-L1 was evaluated by qualitative immunohistochemistry on immune cells with the VENTANA SP142 assay (Roche Diagnostics) and PD-L1 combined positive score with the pharmDx assay (Agilent).
Describe the validation of each primary antibody for the species and application, noting any validation statements on the manufacturer’s website, relevant citations, antibody profiles in online databases, or data provided in the manuscript.
Clinical data
Policy information about clinical studies
All manuscripts should comply with the ICMJE guidelines for publication of clinical research and a completed CONSORT checklist must be included with all submissions.
Clinical trial registration
Study protocol
Data collection
Outcomes
NCT04109066
The protocol is available as a supplement to this publication.
Clinical data was collected at participating sites (clinical research institutes and hospitals) from November 20, 2019 to April 07, 2022. The study was conducted at 221 sites in 31 countries (Argentina, Australia, Austria, Belgium, Brazil, Canada, Chile, China, Colombia, Czech Republic, Denmark, Finland, France, Germany, Hong Kong, Ireland, Italy, Republic of Korea, Mexico, Netherlands, Poland, Portugal, Romania, Russian Federation [BMS terminated all activities in Russia on June 2022], Singapore, Spain, Switzerland, Taiwan, Turkey, United Kingdom, and USA)
The primary endpoint was in the modified intent-to-treat population. Following the decision to discontinue enrollment in the study in April 2022 due to the changing treatment landscape, event-free survival was changed from a co-primary endpoint to an exploratory endpoint, as the total number of enrolled patients was too low to provide sufficient power for comparison. Consequently, the follow-up was reduced to 1 year post-surgery for all patients, and the adjuvant phase became openlabel. Secondary endpoints included pCR in the PD-L1+ population, and RCB 0/I rate in the modified intent-to-treat and PD-L1+ populations. Pathological response was assessed, and RCB score calculated by local pathologists. The RCB score combined tumor size, tumor cellularity, and nodal involvement into a single continuous score that was grouped into four classes, namely, RCB score of 0 (i.e. pathologic complete response ), and I, II, and III. Safety and tolerability were assessed during the neoadjuvant and adjuvant phases in all patients who received at least one dose of study drug. Prespecified exploratory endpoints included association of efficacy outcomes by biomarker status based on PD-L1 combined positive score, stromal tumor-infiltrating lymphocytes (sTILs), levels of estrogen/progesterone receptors, and Ki67 index.
Plants
Seed stocks
Report on the source of all seed stocks or other plant material used. If applicable, state the seed stock centre and catalogue number. If plant specimens were collected from the field, describe the collection location, date and sampling procedures.
Novel plant genotypes
Describe the methods by which all novel plant genotypes were produced. This includes those generated by transgenic approaches, gene editing, chemical/radiation-based mutagenesis and hybridization. For transgenic lines, describe the transformation method, the number of independent lines analyzed and the generation upon which experiments were performed. For gene-edited lines, describe the editor used, the endogenous sequence targeted for editing, the targeting guide RNA sequence (if applicable) and how the editor
Authentication
was upplied.
Describe any authentication procedures for each seed stock used or novel genotype generated. Describe any experiments used to assess the effect of a mutation and, where applicable, how potential secondary effects (e.g. second site T-DNA insertions, mosiacism, off-target gene editing) were examined.