DOI: https://doi.org/10.1186/s12944-024-02012-4
PMID: https://pubmed.ncbi.nlm.nih.gov/38218917
تاريخ النشر: 2024-01-13
العلاقة بين نسبة الكوليسترول غير مرتفع الكثافة إلى الكوليسترول مرتفع الكثافة (NHHR) والتفكير الانتحاري لدى البالغين: دراسة قائمة على السكان في الولايات المتحدة
الملخص
الخلفية: تعتبر نسبة الكوليسترول غير مرتفع الكثافة (non-HDL-C) إلى الكوليسترول مرتفع الكثافة (HDL-C) (NHHR) مؤشراً دهنياً موثوقاً مرتبطاً بخصائص تصلب الشرايين. وقد أظهرت الدراسات وجود ارتباط محتمل بين الانتحارية واستقلاب الدهون. تهدف هذه الدراسة إلى التحقيق في أي ارتباط محتمل بين NHHR وظهور الأفكار الانتحارية ضمن حدود الدراسة. الطرق: فحصت هذه الدراسة العلاقة بين مستويات NHHR والأفكار الانتحارية باستخدام بيانات من المسح الوطني لفحص الصحة والتغذية (NHANES)، الذي أُجري في الولايات المتحدة بين عامي 2005 و2016. يتوافق حساب NHHR مع نسبة HDL-C إلى Non-HDL-C. تم تنفيذ السؤال التاسع من استبيان صحة المرضى-9 لتقييم الأفكار الانتحارية. تم إجراء البحث باستخدام تحليل المجموعات الفرعية، وتناسب المنحنى السلس، وتحليل الانحدار اللوجستي المتعدد المتغيرات. النتائج: شملت مجموعة من 29,288 مشاركاً، وقد حدد التحليل أن 3.82% من الأفراد أبلغوا عن أفكار انتحارية. بعد استخدام الانحدار اللوجستي المتعدد المتغيرات والتعديلات الشاملة، كانت مستويات NHHR المرتفعة مرتبطة بشكل كبير وإيجابي بزيادة احتمال الأفكار الانتحارية، وفقاً للنتائج (نسبة الأرجحية
الكلمات الرئيسية: NHHR، نسبة الدهون، الأفكار الانتحارية، NHANES، دراسة مقطعية
الخلفية
المقارنة مع معايير الدهون القياسية في التنبؤ بخطر الأمراض الوعائية الدماغية، وأمراض الكبد، ومقاومة الأنسولين، ومتلازمة الأيض [13-15]. لذلك، قد يوفر استكشاف العلاقة بين NHHR والأفكار الانتحارية رؤى قيمة حول تقاطع استقلاب الدهون والصحة النفسية، مما يحفز المزيد من التحقيقات في استراتيجيات الوقاية والتدخلات.
الطرق
السكان المدروسون
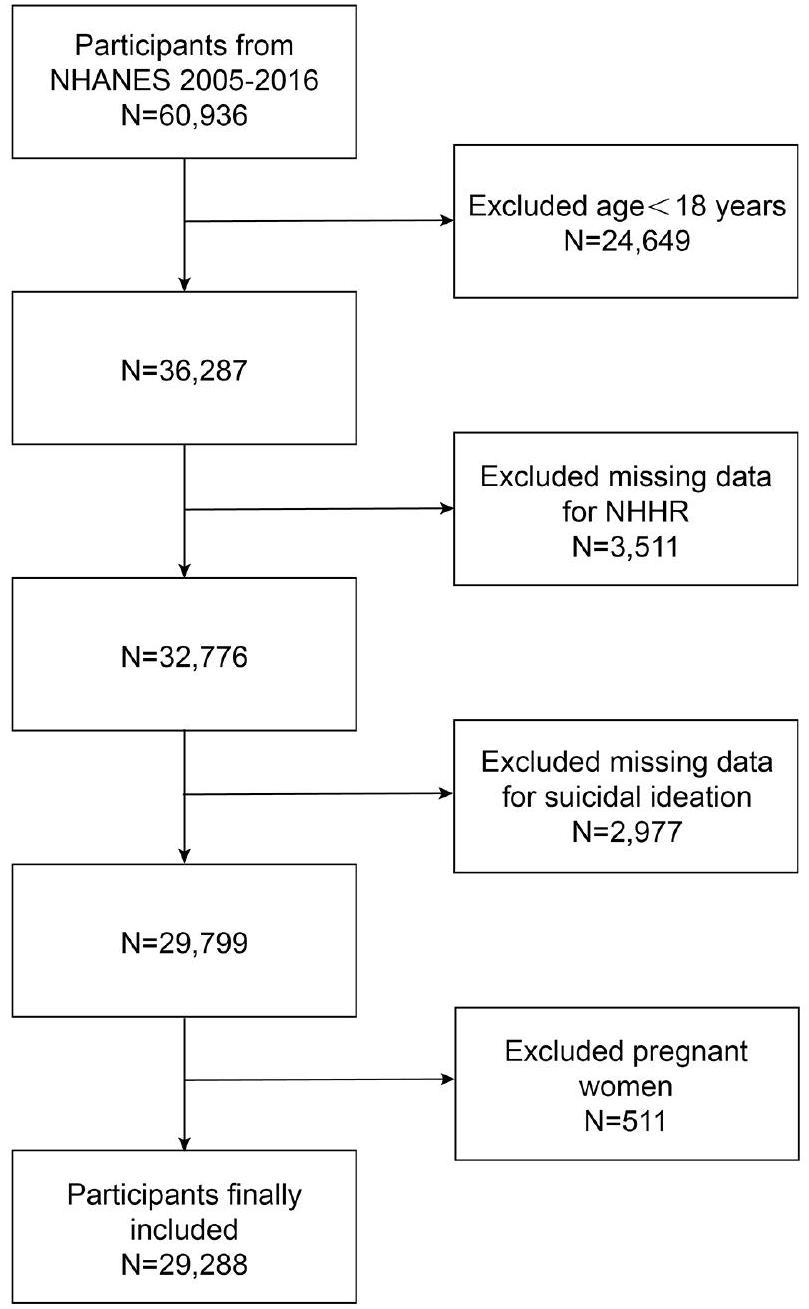
تم اختيار هذا الاختيار بناءً على توفر بيانات شاملة حول كل من NHHR والأفكار الانتحارية ضمن أربع دورات. في البداية، تم تسجيل 60,936 مشاركاً، مع استبعاد لاحق للأفراد الذين تقل أعمارهم عن 18 عاماً (
تقييم NHHR
تقييم الأفكار الانتحارية
المتغيرات المشتركة
باستخدام بيانات استهلاك المغذيات الشاملة. للحصول على معلومات مفصلة حول العمليات القابلة للقياس لمتغيرات الدراسة،www.cdc.gov/nchs/nhanes/هل الموقع الرسمي متاح للجمهور.
التحليل الإحصائي
النتائج
ارتفاع ضغط الدم، النشاط البدني، أعراض الاكتئاب، والكوليسترول الغذائي ومحيط الخصر
العلاقة بين NHHR والتفكير الانتحاري
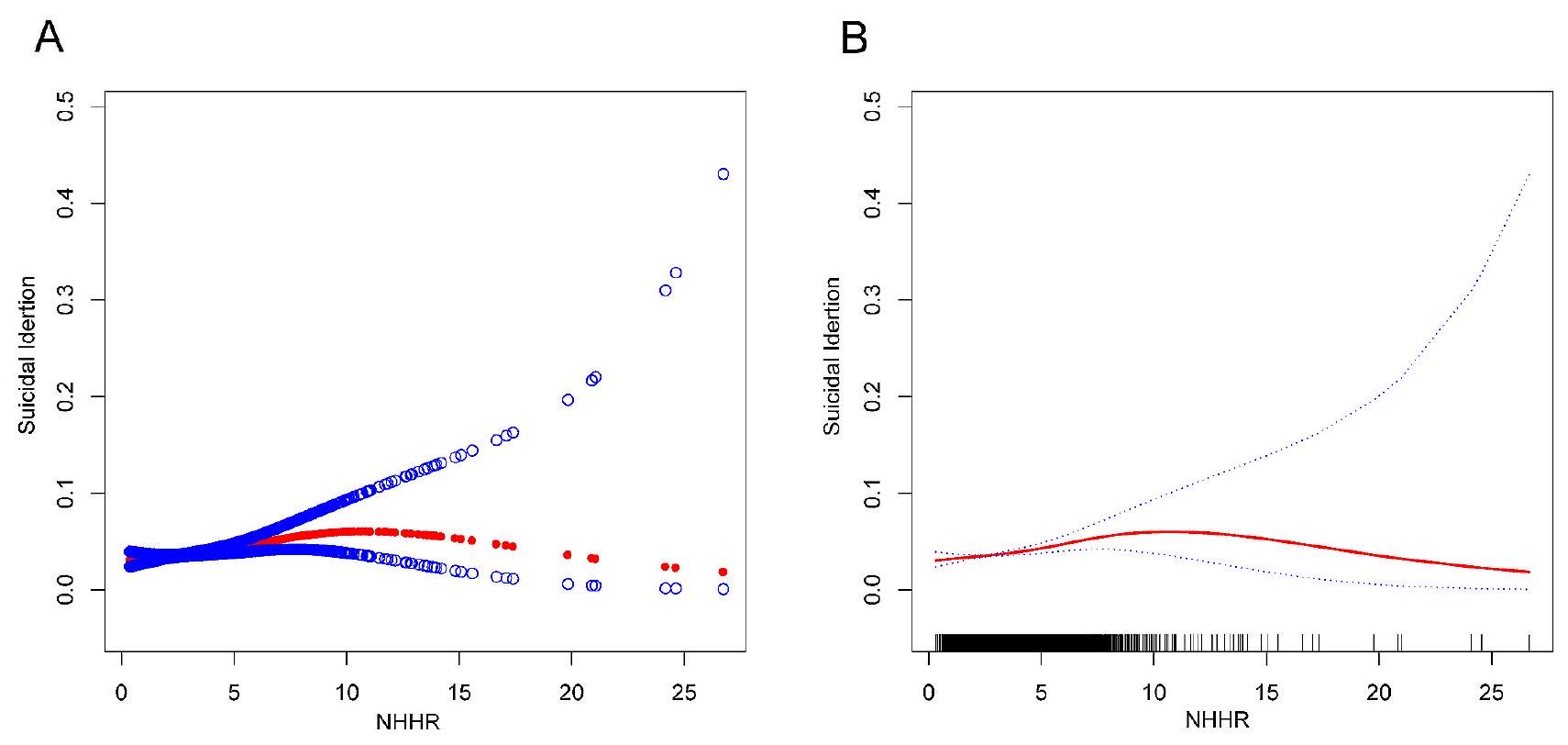
علاقة غير خطية بين NHHR والتفكير الانتحاري
| خاصية | الإجمالي (
|
دون أفكار انتحارية
|
مع أفكار انتحارية (
|
|
| العمر (سنة) |
|
|
|
0.793 |
| الجنس (%) | < 0.001 | |||
| ذكر | 17,360 (48.52%) | 14,421 (51.20%) | 668 (59.64%) | |
| أنثى | 18,416 (51.48%) | 13,747 (48.80%) | 452 (40.36%) | |
| العرق (%) | <0.001 | |||
| مكسيكي أمريكي | 4876 (16.65%) | 4655 (16.53%) | 221 (19.73%) | |
| هسبانيون آخرون | 2819 (9.63%) | 2642 (9.38%) | 177 (15.80%) | |
| الأبيض غير اللاتيني | 12,770 (43.60%) | 12,337 (43.80%) | 433 (38.66%) | |
| أسود غير هيسباني | 6124 (20.91%) | 5915 (21.00%) | 209 (18.66%) | |
| عرق آخر | 2699 (9.22%) | 2619 (9.30%) | 80 (7.14%) | |
| الحالة الاجتماعية (%) | <0.001 | |||
| متزوج أو يعيش مع شريك | 16,537 (59.02%) | 16,059 (59.59%) | 478 (44.67%) | |
| أرملة، مطلقة، منفصلة، ولم تتزوج أبداً | 11,483 (40.98%) | 10,891 (40.41%) | ٥٩٢ (٥٥.٣٣٪) | |
| مستوى التعليم (%) | <0.001 | |||
| أقل من الصف التاسع | 2919 (10.59%) | 2729 (10.30%) | 190 (18.08%) | |
| الصف التاسع إلى الحادي عشر | 4005 (14.53%) | 3783 (14.27%) | 222 (21.12%) | |
| خريج مدرسة ثانوية / شهادة GED أو ما يعادلها | 6310 (22.90%) | 6070 (22.90%) | 240 (22.84%) | |
| بعض الكلية أو درجة AA | 8045 (29.20%) | 7771 (29.32%) | 274 (26.07%) | |
| خريج كلية أو أعلى | 6276 (22.78%) | 6151 (23.21%) | 125 (11.89%) | |
| مؤشر كتلة الجسم
|
< 0.001 | |||
| <25 | 8767 (30.23%) | 8445 (30.27%) | 322 (29.30%) | |
| 25 إلى أقل من 30 | 9536 (32.88%) | 9220 (33.05%) | 316 (28.75%) | |
|
|
10,697 (36.89%) | 10,236 (36.69%) | 461 (41.95%) | |
| محيط الخصر (سم) |
|
|
|
<0.001 |
| نسبة الدخل إلى الفقر |
|
|
|
< 0.001 |
| حالة التدخين (%) | < 0.001 | |||
| نعم | 12,687 (45.21%) | 12,097 (44.82%) | 590 (55.09%) | |
| لا | 15,375 (54.79%) | 14,894 (55.18%) | 481 (44.91%) | |
| مرض السكري (%) | < 0.001 | |||
| نعم | 3522 (12.03%) | ٣٣١٧ (١١.٧٨٪) | 205 (18.30%) | |
| لا | 25,124 (85.85%) | 24,235 (86.10%) | 889 (79.38%) | |
| حدودي | 620 (2.12%) | 594 (2.11%) | ٢٦ (٢.٣٢٪) | |
| ارتفاع ضغط الدم (%) | <0.001 | |||
| نعم | 10,095 (34.52%) | 9618 (34.19%) | 477 (42.74%) | |
| لا | 19,153 (65.48%) | 18,514 (65.81%) | 639 (57.26%) | |
| النشاط البدني (%) | <0.001 | |||
| غير نشط | 12,151 (48.66%) | 11,832 (49.30%) | 319 (32.92%) | |
| نشط | 12,820 (51.34%) | 12,170 (50.70%) | 650 (67.08%) | |
| أعراض الاكتئاب (%) | < 0.001 | |||
| بدون اكتئاب | 26,282 (89.74%) | 25,947 (92.12%) | 335 (29.91%) | |
| مع الاكتئاب | 3006 (10.26%) | 2221 (7.88%) | 785 (70.09%) | |
| الكوليسترول الغذائي (ملغ) |
|
|
|
0.003 |
| TC (ملغ/دل) |
|
|
|
0.065 |
| HDL-C (ملغ/دل) |
|
|
|
< 0.001 |
| NHHR |
|
|
|
< 0.001 |
تحليل الفئات الفرعية
لم تؤثر العمر، الجنس، العرق، مؤشر كتلة الجسم، مستوى التعليم، الحالة الاجتماعية، ارتفاع ضغط الدم، السكري، وحالة التدخين على العلاقة. ومن الجدير بالذكر أن النتائج تشير باستمرار إلى وجود رابط كبير بين NHHR وأفكار الانتحار حتى عند التحكم في المتغيرات الديموغرافية الرئيسية التي تشمل العمر، الجنس، العرق، ومؤشر كتلة الجسم.
| نموذج خام (النموذج 1) | النموذج المعدل جزئيًا (النموذج 2) | النموذج المعدل بالكامل (النموذج 3) | |
| OR (فاصل الثقة 95%)
|
OR (فاصل الثقة 95%)
|
أو (
|
|
| NHHR | 1.09 (1.06, 1.13) < 0.0001 | 1.08 (1.04، 1.12) < 0.0001 | 1.06 (1.02, 1.11) 0.0048 |
| تيرتيلات NHHR | |||
| الثُلث الأول | مرجع | مرجع | مرجع |
| الثُلُث الثاني | 1.04 (0.90, 1.22) 0.5819 | 0.98 (0.84, 1.14) 0.7553 | 0.93 (0.76, 1.15) 0.5030 |
| الثلاثي الثالث | 1.30 (1.13، 1.51) 0.0004 | 1.20 (1.03, 1.39) 0.0179 | 1.15 (0.94, 1.41) 0.1751 |
| P للاتجاه | 1.12 (1.05, 1.19) 0.0002 | 1.08 (1.02, 1.15) 0.0083 | 1.07 (0.99, 1.17) 0.0857 |
نقاش
يمكن أن يقلل ما تحدده NHHR من الأفكار الانتحارية والسلوكيات المرتبطة بها.
من أقصى ما يمكن فهمه حاليًا، تشير هذه الدراسة إلى التحقيق الأساسي في العلاقة بين NHHR والتفكير الانتحاري. تدعم الأدلة المتزايدة فكرة أن NHHR هو مؤشر متفوق على خطر الاضطرابات المتعلقة بالدهون [23-25]. بينما تفتقر الأبحاث التجريبية التي تفحص العلاقة بين مستويات NHHR والتفكير الانتحاري، توجد ثروة من الأدبيات التي تستكشف الروابط بين التفكير الانتحاري وعوامل مختلفة متعلقة بالدهون. في دراسة مقطعية شملت 13,772 بالغًا في كوريا، حددت هانا وآخرون ارتباطًا كبيرًا، مما يشير إلى أن انخفاض مستويات LDL-C كان مرتبطًا بزيادة احتمال التفكير الانتحاري لدى الأفراد الذكور الذين تزيد أعمارهم عن 19 عامًا [5]. تم تحديد ارتباط محتمل من قبل بلاشاي وآخرون بين زيادة مستويات TC وLDL وحدوث الأفكار الانتحارية لدى الإناث اللاتي كن يخضعن لepisode الأول من الفصام [26].
| حالة التدخين | ||
| نعم | لا | |
| التناسب بواسطة النموذج الخطي القياسي | ||
| OR (فاصل الثقة 95%) | 1.10 (0.96، 1.26) | 1.08 (1.00، 1.16) |
|
|
0.1596 | 0.0502 |
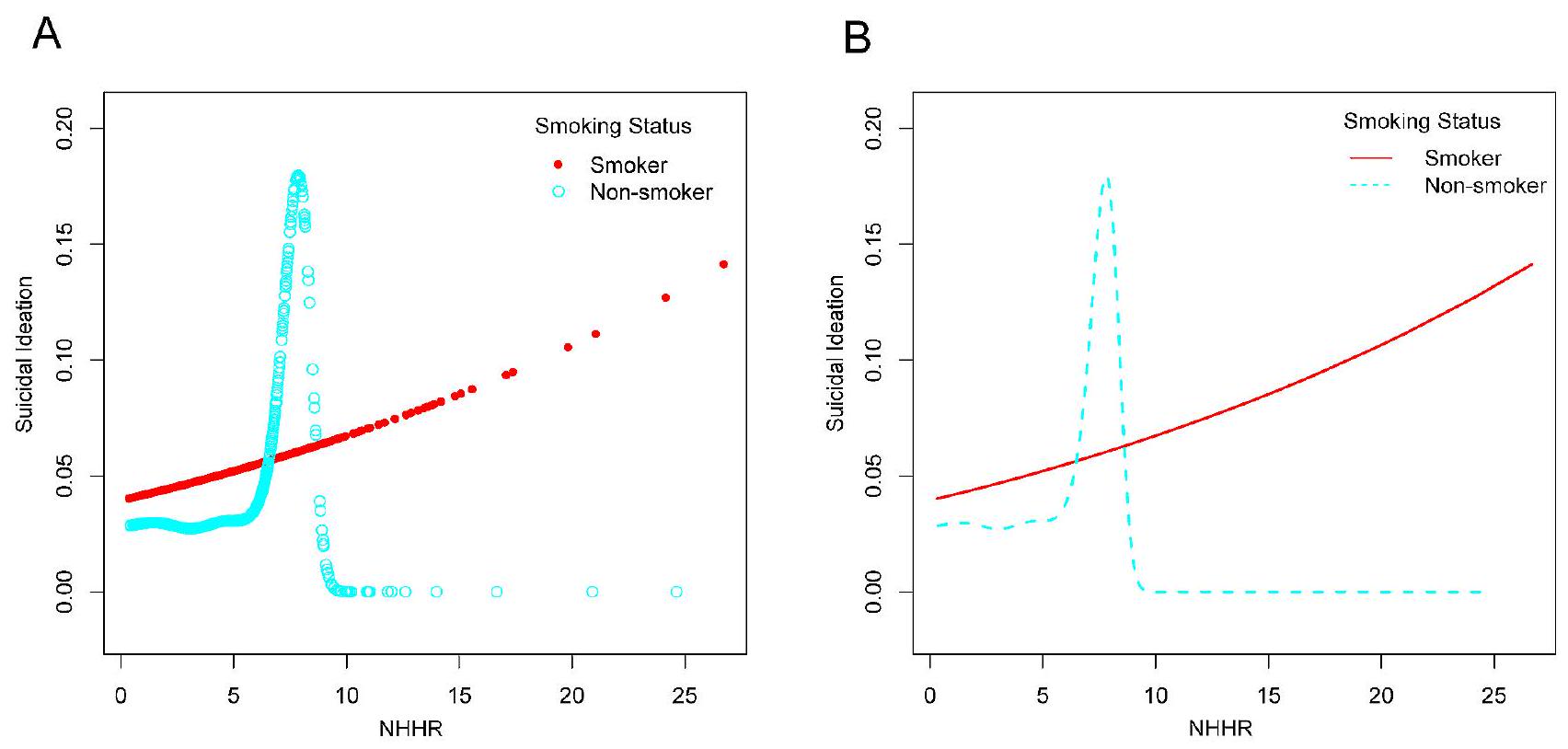
| توافق بواسطة نموذج خطي مقطعي ثنائي | ||
| نقطة التوقف (K) | 2.42 | ٧.٨٠ |
| OR1 (<K) | 2.03 (0.83, 4.97) 0.1211 | 1.14 (1.04, 1.25) 0.0054 |
| OR2(>K) | 1.04 (0.87, 1.24) 0.6749 | 0.47 (0.11, 2.09) 0.3236 |
| اختبار نسبة الاحتمالية اللوغاريتمية
|
0.150 | 0.028 |
أظهرت المرضى الخارجيين الذين تم تشخيصهم باضطراب الاكتئاب الشديد انخفاضًا ملحوظًا في مستويات TG ضمن المجموعة التي تظهر أفكار انتحارية، مقارنةً بالأفراد الذين لا يملكون مثل هذه الأفكار [27]. ترتبط الأفكار الانتحارية والانتحارات المكتملة بانخفاض مستويات الدهون في الدم، وخاصة TC، كما ذكر شونكوان وآخرون في تحليل تلوي شمل 65 دراسة وبائية [28]. بينما لا تقدم هذه النتائج دليلًا مباشرًا، إلا أنها تدعم بشكل غير مباشر أن مستويات NHHR مرتبطة إيجابيًا بالأفكار الانتحارية، مما يساهم في زيادة الأدبيات التي تفحص العلاقة بين ملفات الدهون والميول الانتحارية من خلال استخدام خصائص الدهون الجديدة.
تشير مؤشرات الدهون إلى أن نسبة الدهون إلى الهيموجلوبين (NHHR) لديها قدرة تنبؤية أكثر قوة لمرض الكبد الدهني غير الكحولي (NAFLD) [31]. وفقًا لدراسة لين دي، تعتبر NHHR أداة تشخيصية موثوقة لتقييم مقاومة الأنسولين. مقارنةً بفحوصات الدهون العادية، أظهرت هذه المقياس دقة متفوقة في التنبؤ بالحالات المرتبطة بتطور مرض السكري [32]. باختصار، أثبتت NHHR فعالية تنبؤية استثنائية في مجموعة متنوعة من الدراسات. علاوة على ذلك، تعتبر NHHR طريقة متاحة على نطاق واسع تتميز بطبيعتها غير الغازية وسهولة الوصول إليها وفعاليتها من حيث التكلفة، مما يقدم آفاقًا واعدة للتطبيق السريري.
| مجموعة فرعية | OR (فاصل الثقة 95%) | P للتفاعل | |
| العمر (سنة) | 0.4618 | ||
| <50 |
|
1.05 (0.98, 1.12) | |
|
|
|
1.08 (1.02, 1.15) | |
| جنس | 0.3642 | ||
| ذكر |
|
1.05 (0.99، 1.11) | |
| أنثى |
|
1.09 (1.02, 1.17) | |
| سباق | 0.5036 | ||
| مكسيكي أمريكي |
|
1.08 (0.97، 1.20) | |
| هسبانيون آخرون |
|
1.16 (1.02، 1.32) | |
| الأبيض غير اللاتيني |
|
1.06 (1.00, 1.13) | |
| أسود غير هيسباني |
|
1.06 (0.93، 1.22) | |
| عرق آخر |
|
0.94 (0.76, 1.16) | |
| مؤشر كتلة الجسم (كجم/م²) | 0.5389 | ||
| <25 |
|
1.09 (0.96, 1.24) | |
| 25-30 |
|
1.10 (1.01, 1.20) | |
| >30 |
|
1.04 (0.98, 1.11) | |
| مستوى التعليم | |||
| أقل من الصف التاسع |
|
1.07 (0.95, 1.22) | |
| الصفوف 9-11 |
|
1.03 (0.93، 1.13) | |
| خريج مدرسة ثانوية / شهادة GED أو ما يعادلها |
|
1.08 (0.99, 1.18) | |
| بعض الكلية أو درجة AA |
|
1.02 (0.92, 1.12) | |
| خريج كلية أو أعلى |
|
1.21 (1.06, 1.38) | |
| الحالة الاجتماعية | 0.5930 | ||
| متزوج/يعيش مع شريك | ن=11,162 | 1.05 (0.99، 1.12) | |
| أرملة/مطلقة/مفصولة/لم تتزوج أبداً |
|
1.08 (1.01، 1.15) | |
| ارتفاع ضغط الدم | 0.9299 | ||
| نعم |
|
1.06 (1.00, 1.13) | |
| لا |
|
1.06 (0.99, 1.13) | |
| السكري | 0.1128 | ||
| نعم |
|
1.03 (0.93، 1.13) | |
| لا |
|
1.09 (1.03، 1.15) | |
| حدودي |
|
0.80 (0.55، 1.15) | |
| حالة التدخين | 0.7194 | ||
| نعم |
|
1.06 (1.00, 1.12) | |
| لا |
|
1.08 (1.00، 1.16) | |
تؤثر على نشاط السيروتونين وتساهم في السلوكيات الاندفاعية والانتحارية [33]. زيادة في نسبة
الفئة المستهدفة، إحدى التفسيرات المحتملة هي أن استهلاك الأحماض الدهنية المتعددة غير المشبعة يرتبط بانخفاض مستويات الدهون الثلاثية، مما قد يقلل من خطر الأفكار الانتحارية. لذلك، يمكن أن يكون استخدام نسبة الدهون غير HDL-C كوسيلة لتقييم النسبة في المرضى أداة أكثر فعالية لتقييم تأثير استقلاب الدهون على حدوث الأفكار الانتحارية.
نقاط القوة والقيود
بين الأفكار الانتحارية ومجموعة متنوعة من متغيرات التعرض. تم اتخاذ هذا النهج لتعزيز موثوقية وصدق النتائج. ومع ذلك، من الضروري الاعتراف بالحدود الكامنة في هذا البحث. أولاً، اعتمد تقييم الأفكار الانتحارية على المقابلات الشخصية، مما أدخل تحيزًا لا مفر منه في الاسترجاع. ثانيًا، على الرغم من أن العنصر التاسع من PHQ-9 قد تم استخدامه في أبحاث سابقة لقياس الأفكار الانتحارية، فإن تعريفه الواسع – الذي يشمل الأذى الذاتي غير الانتحاري – قد يؤثر على كيفية تقييم الدراسة لارتباط العنصر بالأفكار الانتحارية. ثالثًا، تفتقر الدراسة إلى التحقق الشامل من فائدة PHQ-9 في تقييم الأفكار الانتحارية بين الجمهور العام. ومع ذلك، عندما يتعلق الأمر بالرعاية الأولية في الطب الداخلي الأساسي، فإن PHQ-9 يتمتع بخصوصية وحساسية معززة. رابعًا، كانت بيانات الكوليسترول التي تم تحليلها في هذه الدراسة مستمدة من أفراد صائمين، بينما ظلت البيانات غير الصائمة غير مستكشفة. قد تؤدي التباينات في بروتوكولات الاختبار المعملية إلى إدخال تحيزات محتملة. خامسًا، كانت إمكانية العكس السببي قائمة نظرًا لأن الدراسة استخدمت تصميمًا ذا نهج مقطعي، مما يعيق القدرة على إقامة علاقة سببية. وبالتالي، لا يزال هناك ضرورة لإجراء تحقيقات مستقبلية تشمل أحجام عينات أكبر لتوضيح العلاقة السببية. في الوقت نفسه، على الرغم من تعديل بعض المتغيرات المحتملة، فإن التخفيف الكامل من العوامل المربكة المحتملة التي تتجاوز تلك المعدلة لا يزال بعيد المنال ضمن نطاق البحث.
الخاتمة
الاختصارات
| الكوليسترول غير HDL | الكوليسترول غير عالي الكثافة |
| كوليسترول HDL | كوليسترول البروتين الدهني عالي الكثافة |
| NHHR | نسبة الكوليسترول غير HDL إلى HDL |
| بي آي آر | نسبة الفقر إلى الدخل |
| مؤشر كتلة الجسم | مؤشر كتلة الجسم |
| تي سي | كوليسترول |
شكر وتقدير
مساهمات المؤلفين
تمويل
توفر البيانات
الإعلانات
موافقة الأخلاقيات والموافقة على المشاركة
موافقة على النشر
بيان لجنة المراجعة المؤسسية
المصالح المتنافسة
تفاصيل المؤلف
نُشر على الإنترنت: 13 يناير 2024
References
- Naghavi M. Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the global burden of Disease Study 2016. BMJ. 2019;364:194.
- Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227-39.
- Hubers AAM, Moaddine S, Peersmann SHM, Stijnen T, van Duijn E, van der Mast RC, Dekkers OM, Giltay EJ. Suicidal ideation and subsequent completed suicide in both psychiatric and non-psychiatric populations: a meta-analysis. Epidemiol Psychiatr Sci. 2018;27(2):186-98.
- Nuij C, van Ballegooijen W, de Beurs D, Juniar D, Erlangsen A, Portzky G, O’Connor RC, Smit JH, Kerkhof A, Riper H. Safety planning-type interventions for suicide prevention: meta-analysis. Br J Psychiatry. 2021;219(2):419-26.
- Cho H, Shin J, Choi JK. Serum lipid levels and suicidal ideation of adults: a cross-sectional study using the Korea National Health and Nutrition Examination Survey. J Clin Med 2023, 12(13).
- Lee YJ, Lee S, Hwang IC, Ahn HY. Association between the triglyceride-glucose index and suicidal ideation: a nationwide cross-sectional survey. J Affect Disord. 2024;344:100-3.
- Shin HY, Kang G, Kang HJ, Kim SW, Shin IS, Yoon JS, Kim JM. Associations between serum lipid levels and suicidal ideation among Korean older people. J Affect Disord. 2016;189:192-8.
- Su M, Li E, Tang C, Zhao Y, Liu R, Gao K. Comparison of blood lipid profile/ thyroid function markers between unipolar and bipolar depressed patients
and in depressed patients with anhedonia or suicidal thoughts. Mol Med. 2019;25(1):51. - Qi X, Wang S, Huang Q, Chen X, Qiu L, Ouyang K, Chen Y. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and risk of depression among US adults: a cross-sectional NHANES study. J Affect Disord. 2024;344:451-7.
- Cavanagh JT, Carson AJ, Sharpe M, Lawrie SM. Psychological autopsy studies of suicide: a systematic review. Psychol Med. 2003;33(3):395-405.
- Zhu L, Lu Z, Zhu L, Ouyang X, Yang Y, He W, Feng Y, Yi F, Song Y. Lipoprotein ratios are better than conventional lipid parameters in predicting coronary heart disease in Chinese Han people. Kardiol Pol. 2015;73(10):931-8.
- Liu Z, Lin X, Zeng L, Zhang H, Guo W, Lu Q, Huang C, Wang J, Liu P, Chang Q, et al. Elevated non-HDL-C/HDL-C ratio increases the 1-year risk of recurrent stroke in older patients with non-disabling ischemic cerebrovascular events: results from the Xi’an Stroke Registry Study of China. BMC Geriatr. 2023;23(1):410.
- Iannuzzi A, Giallauria F, Gentile M, Rubba P, Covetti G, Bresciani A, Aliberti E, Cuomo G, Panico C, Tripaldella M et al. Association between Non-HDL-C/ HDL-C ratio and carotid intima-media thickness in Post-menopausal Women. J Clin Med 2021, 11 (1).
- Yang S, Zhong J, Ye M, Miao L, Lu G, Xu C, Xue Z, Zhou X. Association between the non-HDL-cholesterol to HDL-cholesterol ratio and non-alcoholic fatty liver disease in Chinese children and adolescents: a large singlecenter cross-sectional study. Lipids Health Dis. 2020;19(1):242.
- Kim SW, Jee JH, Kim HJ, Jin SM, Suh S, Bae JC, Kim SW, Chung JH, Min YK, Lee MS, et al. Non-HDL-cholesterol/HDL-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int J Cardiol. 2013;168(3):2678-83.
- Curtin LR, Mohadjer LK, Dohrmann SM, Kruszon-Moran D, Mirel LB, Carroll MD, Hirsch R, Burt VL, Johnson CL. National Health and Nutrition Examination Survey: sample design, 2007-2010. Vital Health Stat 2 2013(160):1-23.
- Wang A, Li Y, Zhou L, Liu K, Li S, Zong C, Song B, Gao Y, Li Y, Tian C, et al. Non-HDL-C/HDL-C ratio is associated with carotid plaque stability in general population: a cross-sectional study. Front Neurol. 2022;13:875134.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-13.
- Costantini L, Pasquarella C, Odone A, Colucci ME, Costanza A, Serafini G, Aguglia A, Belvederi Murri M, Brakoulias V, Amore M, et al. Screening for depression in primary care with Patient Health Questionnaire-9 (PHQ-9): a systematic review. J Affect Disord. 2021;279:473-83.
- Levis B, Benedetti A, Thombs BD. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:11476.
- Han KM, Ko YH, Shin C, Lee JH, Choi J, Kwon DY, Yoon HK, Han C, Kim YK. Tinnitus, depression, and suicidal ideation in adults: a nationally representative general population sample. J Psychiatr Res. 2018;98:124-32.
- Vásquez E, Batsis JA, Germain CM, Shaw BA. Impact of obesity and physical activity on functional outcomes in the elderly: data from NHANES 20052010. J Aging Health. 2014;26(6):1032-46.
- Zhao X, Zheng H, Shan S, Wang K, Zhang M, Xie S, Liu C. Association between the non-HDL-cholesterol-to-HDL-cholesterol ratio and the risk of gallbladder polyp formation among men: a retrospective cohort study. Lipids Health Dis. 2020;19(1):146.
- Eliasson B, Cederholm J, Eeg-Olofsson K, Svensson AM, Zethelius B, Gudbjörnsdottir S. Clinical usefulness of different lipid measures for prediction of coronary heart disease in type 2 diabetes: a report from the Swedish National Diabetes Register. Diabetes Care. 2011;34(9):2095-100.
- Holman RR, Coleman RL, Shine BS, Stevens RJ. Non-HDL cholesterol is less informative than the total-to-HDL cholesterol ratio in predicting cardiovascular risk in type 2 diabetes. Diabetes Care. 2005;28(7):1796-7.
- Misiak B, Kiejna A, Frydecka D. Higher total cholesterol level is associated with suicidal ideation in first-episode schizophrenia females. Psychiatry Res. 2015;226(1):383-8.
- Park YM, Lee BH, Lee SH. The association between serum lipid levels, suicide ideation, and central serotonergic activity in patients with major depressive disorder. J Affect Disord. 2014;159:62-5.
- Wu S, Ding Y, Wu F, Xie G, Hou J, Mao P. Serum lipid levels and suicidality: a meta-analysis of 65 epidemiological studies. J Psychiatry Neurosci. 2016;41(1):56-69.
- Sheng G, Liu D, Kuang M, Zhong Y, Zhang S, Zou Y. Utility of Non-high-density Lipoprotein Cholesterol to high-density lipoprotein cholesterol ratio in evaluating Incident Diabetes Risk. Diabetes Metab Syndr Obes. 2022;15:1677-86.
- Zhao W, Gong W, Wu N, Li Y, Ye K, Lu B, Zhang Z, Qu S, Li Y, Yang Y, et al. Association of lipid profiles and the ratios with arterial stiffness in middle-aged and elderly Chinese. Lipids Health Dis. 2014;13:37.
- Kwok RM, Torres DM, Harrison SA. Vitamin D and nonalcoholic fatty liver disease (NAFLD): is it more than just an association? Hepatology. 2013;58(3):1166-74.
- Lin D, Qi Y, Huang C, Wu M, Wang C, Li F, Yang C, Yan L, Ren M, Sun K. Associations of lipid parameters with insulin resistance and diabetes: a populationbased study. Clin Nutr. 2018;37(4):1423-9.
- Mann JJ. Neurobiology of suicidal behaviour. Nat Rev Neurosci. 2003;4(10):819-28.
- Daray FM, Mann JJ, Sublette ME. How lipids may affect risk for suicidal behavior. J Psychiatr Res. 2018;104:16-23.
- Ganança L, Oquendo MA, Tyrka AR, Cisneros-Trujillo S, Mann JJ, Sublette ME. The role of cytokines in the pathophysiology of suicidal behavior. Psychoneuroendocrinology. 2016;63:296-310.
- Penttinen J. Hypothesis: low serum cholesterol, suicide, and interleukin-2. Am J Epidemiol. 1995;141(8):716-8.
- Lee K, Kim S, Jo JK. The relationships between abnormal serum lipid levels, Depression, and suicidal ideation according to sex. J Clin Med 2022, 11 (8).
- Delarue J, LeFoll C, Corporeau C, Lucas D. N-3 long chain polyunsaturated fatty acids: a nutritional tool to prevent insulin resistance associated to type 2 diabetes and obesity? Reprod Nutr Dev. 2004;44(3):289-99.
- Tanskanen A, Hibbeln JR, Hintikka J, Haatainen K, Honkalampi K, Viinamäki H. Fish consumption, depression, and suicidality in a general population. Arch Gen Psychiatry. 2001;58(5):512-3.
- Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical considerations, and uses to inform Public Policy. Adv Nutr. 2016;7(1):121-34.
ملاحظة الناشر
DOI: https://doi.org/10.1186/s12944-024-02012-4
PMID: https://pubmed.ncbi.nlm.nih.gov/38218917
Publication Date: 2024-01-13
The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and suicidal ideation in adults: a populationbased study in the United States
Abstract
Background The ratio of non-high-density lipoprotein cholesterol (non-HDL-C) to high-density lipoprotein cholesterol (HDL-C) (NHHR) serves as a reliable lipid indicator associated with atherogenic characteristics. Studies have indicated a potential connection between suicidality and lipid metabolism. This research aims to investigate any possible association between the NHHR and the emergence of suicidal ideation within the confines of the study. Methods This study examined the association between NHHR levels and suicidal ideation using data from the National Health and Nutrition Examination Survey (NHANES), conducted in the United States spanning 2005 and 2016. Calculation of the NHHR corresponds to the proportion of HDL-C to Non-HDL-C. The Patient Health Questionnaire-9’s ninth question was implemented for assessing suicidal ideation. Using subgroup analysis, smooth curve fitting, and multivariate logistic regression analysis, the research was conducted. Results Encompassing a cohort of 29,288 participants, the analysis identified that 3.82% of individuals reported suicidal ideation. After using multivariable logistic regression and thorough adjustments, elevated NHHR levels were significantly and positively associated with a heightened likelihood of suicidal ideation, according to the findings (odds ratio
Keywords NHHR, Lipid ratio, Suicidal ideation, NHANES, Cross-sectional study
Background
comparison with standard lipid parameters in predicting the risk of cerebrovascular diseases, liver disease, insulin resistance, and metabolic syndrome [13-15]. Therefore, exploring the relationship between the NHHR and suicidal ideation may provide valuable insights into the intersection between lipid metabolism and mental health, prompting further investigation into preventive strategies and interventions.
Methods
Study population
ideation. This selection was based on the availability of comprehensive data on both the NHHR and suicidal ideation within four cycles. Initially, 60,936 participants were enrolled, with subsequent exclusions for individuals under 18 years of age (
Assessment of NHHR
Assessment of suicidal ideation
Covariates
utilizing comprehensive nutrient consumption data. For detailed information on the quantifiable processes of the study variables, www.cdc.gov/nchs/nhanes/ is the official website accessible to the public.
Statistical analysis
Results
hypertension, physical activity, depressive symptoms, and dietary cholesterol and waist circumference (
The association between NHHR and suicidal ideation
A nonlinear relationship between NHHR and suicidal ideation
| Characteristic | Total (
|
Without suicidal ideation (
|
With suicidal ideation (
|
|
| Age(year) |
|
|
|
0.793 |
| Gender (%) | < 0.001 | |||
| Male | 17,360 (48.52%) | 14,421 (51.20%) | 668 (59.64%) | |
| Female | 18,416 (51.48%) | 13,747 (48.80%) | 452 (40.36%) | |
| Race(%) | <0.001 | |||
| Mexican American | 4876 (16.65%) | 4655 (16.53%) | 221 (19.73%) | |
| Other Hispanic | 2819 (9.63%) | 2642 (9.38%) | 177 (15.80%) | |
| Non-Hispanic White | 12,770 (43.60%) | 12,337 (43.80%) | 433 (38.66%) | |
| Non-Hispanic Black | 6124 (20.91%) | 5915 (21.00%) | 209 (18.66%) | |
| Other Race | 2699 (9.22%) | 2619 (9.30%) | 80 (7.14%) | |
| Marital status(%) | <0.001 | |||
| Married or Living with Partner | 16,537 (59.02%) | 16,059 (59.59%) | 478 (44.67%) | |
| Widowed, divorced, separated, and never married | 11,483 (40.98%) | 10,891 (40.41%) | 592 (55.33%) | |
| Education level(%) | <0.001 | |||
| Less Than 9th Grade | 2919 (10.59%) | 2729 (10.30%) | 190 (18.08%) | |
| 9-11th Grade | 4005 (14.53%) | 3783 (14.27%) | 222 (21.12%) | |
| High School Grad/GED or Equivalent | 6310 (22.90%) | 6070 (22.90%) | 240 (22.84%) | |
| Some College or AA degree | 8045 (29.20%) | 7771 (29.32%) | 274 (26.07%) | |
| College Graduate or above | 6276 (22.78%) | 6151 (23.21%) | 125 (11.89%) | |
| Body mass index(
|
< 0.001 | |||
| <25 | 8767 (30.23%) | 8445 (30.27%) | 322 (29.30%) | |
| 25 to < 30 | 9536 (32.88%) | 9220 (33.05%) | 316 (28.75%) | |
|
|
10,697 (36.89%) | 10,236 (36.69%) | 461 (41.95%) | |
| Waist circumference(cm) |
|
|
|
<0.001 |
| Income to poverty ratio |
|
|
|
< 0.001 |
| Smoking status(%) | < 0.001 | |||
| Yes | 12,687 (45.21%) | 12,097 (44.82%) | 590 (55.09%) | |
| No | 15,375 (54.79%) | 14,894 (55.18%) | 481 (44.91%) | |
| Diabetes(%) | < 0.001 | |||
| Yes | 3522 (12.03%) | 3317 (11.78%) | 205 (18.30%) | |
| No | 25,124 (85.85%) | 24,235 (86.10%) | 889 (79.38%) | |
| Borderline | 620 (2.12%) | 594 (2.11%) | 26 (2.32%) | |
| Hypertension(%) | <0.001 | |||
| Yes | 10,095 (34.52%) | 9618 (34.19%) | 477 (42.74%) | |
| No | 19,153 (65.48%) | 18,514 (65.81%) | 639 (57.26%) | |
| Physical activity(%) | <0.001 | |||
| Inactive | 12,151 (48.66%) | 11,832 (49.30%) | 319 (32.92%) | |
| active | 12,820 (51.34%) | 12,170 (50.70%) | 650 (67.08%) | |
| Depressive symptom(%) | < 0.001 | |||
| Without depression | 26,282 (89.74%) | 25,947 (92.12%) | 335 (29.91%) | |
| With depression | 3006 (10.26%) | 2221 (7.88%) | 785 (70.09%) | |
| Dietary cholesterol (mg) |
|
|
|
0.003 |
| TC (mg/dL) |
|
|
|
0.065 |
| HDL-C (mg/dL) |
|
|
|
< 0.001 |
| NHHR |
|
|
|
< 0.001 |
Subgroup analysis
age, gender, race, BMI, education level, marital status, hypertension, diabetes, and smoking status did not influence the association. Notably, the findings continuously indicate a significant link between NHHR and suicidal ideation even controlling for major demographic variables comprising age, sex, race, BMI,
| Crude Model (Model 1) | Partially Adjusted Model (Model 2) | Fully Adjusted Model (Model 3) | |
| OR (95% CI)
|
OR (95% CI)
|
OR (
|
|
| NHHR | 1.09 (1.06, 1.13) < 0.0001 | 1.08 (1.04, 1.12) < 0.0001 | 1.06 (1.02, 1.11) 0.0048 |
| NHHR Tertiles | |||
| Tertile 1 | Reference | Reference | Reference |
| Tertile 2 | 1.04 (0.90, 1.22) 0.5819 | 0.98 (0.84, 1.14) 0.7553 | 0.93 (0.76, 1.15) 0.5030 |
| Tertile 3 | 1.30 (1.13, 1.51) 0.0004 | 1.20 (1.03, 1.39) 0.0179 | 1.15 (0.94, 1.41) 0.1751 |
| P for trend | 1.12 (1.05, 1.19) 0.0002 | 1.08 (1.02, 1.15) 0.0083 | 1.07 (0.99, 1.17) 0.0857 |
Discussion
determined by NHHR could reduce suicidal ideation and associated behaviors.
From the utmost of present understanding, this research signifies the relationship’s primary investigation between NHHR and suicidal ideation. Growing evidence supports the notion that NHHR is a superior indicator of lipid-related disorder risk [23-25]. While empirical research examining the relationship between NHHR levels and ideation of suicide is lacking, a wealth of literature exists exploring the links between suicidal ideation and various lipid-related factors. In a crosssectional investigation involving 13,772 adults in Korea, Hana et al. identified a significant association, indicating that reduced levels of LDL-C were linked to an elevated likelihood of suicidal thoughts for male individuals above the age of 19 [5]. A potential association was identified by Bałażej et al. between increased levels of TC and LDL and the occurrence of suicidal thoughts in females who were undergoing their initial episode of schizophrenia [26]. A retrospective cohort investigation involving 73
| Smoking status | ||
| Yes | No | |
| Fitting by standard linear model | ||
| OR (95% CI) | 1.10 (0.96, 1.26) | 1.08 (1.00, 1.16) |
|
|
0.1596 | 0.0502 |
| Fitting by two-piecewise linear model | ||
| Breakpoint (K) | 2.42 | 7.80 |
| OR1 (<K) | 2.03 (0.83, 4.97) 0.1211 | 1.14 (1.04, 1.25) 0.0054 |
| OR2(>K) | 1.04 (0.87, 1.24) 0.6749 | 0.47 (0.11, 2.09) 0.3236 |
| Logarithmic likelihood ratio test
|
0.150 | 0.028 |
outpatients diagnosed with major depressive disorder suggested a noteworthy reduction in TG levels within the cohort exhibiting suicidal ideation, contrasting with individuals lacking such notions [27]. Suicidal ideation and completed suicides are associated with decreased blood lipid levels, particularly TC, as stated by Shunquan et al. in a meta-analysis involving 65 epidemiological studies [28]. While these findings do not directly present evidence, they indirectly support that NHHR levels are positively associated with suicidal ideation, contributing to the growing body of literature examining the association between profiles of lipids and suicidal tendencies through the use of novel lipid characteristics.
lipid indicators, the NHHR has a more robust predictive ability for non-alcoholic fatty liver disease (NAFLD) [31]. According to Lin D’s study, the NHHR is a reliable diagnostic instrument for assessing insulin resistance. Compared to normal lipid inspections, this metric demonstrated superior accuracy in predicting conditions associated with the development of diabetes [32]. In summary, the NHHR has demonstrated exceptional predictive efficacy in a variety of studies. Furthermore, the NHHR is a widely accessible method distinguished by its noninvasive nature, ease of accessibility, and costeffectiveness, presenting promising prospects for clinical implementation.
| Subgroup | OR(95%CI) | P for interaction | |
| Age(year) | 0.4618 | ||
| <50 |
|
1.05 (0.98, 1.12) | |
|
|
|
1.08 (1.02, 1.15) | |
| Gender | 0.3642 | ||
| Male |
|
1.05 (0.99, 1.11) | |
| Female |
|
1.09 (1.02, 1.17) | |
| Race | 0.5036 | ||
| Mexican American |
|
1.08 (0.97, 1.20) | |
| Other Hispanic |
|
1.16 (1.02, 1.32) | |
| Non-Hispanic White |
|
1.06 (1.00, 1.13) | |
| Non-Hispanic Black |
|
1.06 (0.93, 1.22) | |
| Other Race |
|
0.94 (0.76, 1.16) | |
| BMI(kg/m2) | 0.5389 | ||
| <25 |
|
1.09 (0.96, 1.24) | |
| 25-30 |
|
1.10 (1.01, 1.20) | |
| >30 |
|
1.04 (0.98, 1.11) | |
| Education level | |||
| Less Than 9th Grade |
|
1.07 (0.95, 1.22) | |
| 9-11th Grade |
|
1.03 (0.93, 1.13) | |
| High School Grad/GED or Equivalent |
|
1.08 (0.99, 1.18) | |
| Some College or AA degree |
|
1.02 (0.92, 1.12) | |
| College Graduate or above |
|
1.21 (1.06, 1.38) | |
| Marital status | 0.5930 | ||
| Married/living with partner | N=11,162 | 1.05 (0.99, 1.12) | |
| Widowed/divorced/separated/ Never married |
|
1.08 (1.01, 1.15) | |
| Hypertension | 0.9299 | ||
| Yes |
|
1.06 (1.00, 1.13) | |
| No |
|
1.06 (0.99, 1.13) | |
| Diabetes | 0.1128 | ||
| Yes |
|
1.03 (0.93, 1.13) | |
| No |
|
1.09 (1.03, 1.15) | |
| Borderline |
|
0.80 (0.55, 1.15) | |
| Smoking status | 0.7194 | ||
| Yes |
|
1.06 (1.00, 1.12) | |
| No |
|
1.08 (1.00, 1.16) | |
impacting serotonin activity and contributing to impulsive and suicidal behaviors [33]. An elevation in the ratio of
target demographic, one plausible interpretation is that PUFA consumption correlates with reduced TG levels, potentially mitigating the risk of suicidal ideation [38, 39]. Therefore, employing the NHHR as a means to assess the non-HDL-C proportion in patients could serve as a more effective tool for evaluating the impact that lipid metabolism has on the occurrence of suicidal ideation.
Strengths and limitations
between suicidal ideation and various exposure variables. This approach was undertaken to enhance the reliability and validity of the results. However, it’s essential to acknowledge the inherent limits of this research. First, the assessment of suicidal ideation relied on personal interviews, introducing an inevitable recall bias. Second, though the PHQ-9’s ninth item has been used in prior research to measure suicide ideation, its extensive definition-which includes non-suicidal self-harm-may affect how the study evaluates the item’s association with suicidal ideation. Third, comprehensive validation of the PHQ-9’s utility in assessing suicidal ideation among the general public is lacking. Nonetheless, when it comes to basic internal medicine primary care, PHQ-9 possesses strengthened specificity and sensitivity. Fourth, the cholesterol data analyzed in this study were derived from fasting individuals, with non-fasting data remaining unexplored. Discrepancies in the laboratory testing protocols may introduce potential biases. Fifth, reverse causality was a possibility since the study employed a design with a cross-sectional approach, which hinders the ability to establish a causal relationship. Hence, there remains a necessity for prospective investigations encompassing larger sample sizes to elucidate the causative relationship. Meanwhile, despite adjusting for certain potential covariates, fully mitigating potential confounding factors beyond those adjusted remains elusive within the scope of the research.
Conclusion
Abbreviations
| non-HDL-C | Non-high-density lipoprotein cholesterol |
| HDL-C | High-density lipoprotein cholesterol |
| NHHR | Non-HDL-C and HDL-C ratio |
| PIR | Poverty-to-income ratio |
| BMI | Body mass index |
| TC | Cholesterol |
Acknowledgements
Author contributions
Funding
Data availability
Declarations
Ethics approval and consent to participate
Consent for publication
Institutional Review Board Statement
Competing interests
Author details
Published online: 13 January 2024
References
- Naghavi M. Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the global burden of Disease Study 2016. BMJ. 2019;364:194.
- Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227-39.
- Hubers AAM, Moaddine S, Peersmann SHM, Stijnen T, van Duijn E, van der Mast RC, Dekkers OM, Giltay EJ. Suicidal ideation and subsequent completed suicide in both psychiatric and non-psychiatric populations: a meta-analysis. Epidemiol Psychiatr Sci. 2018;27(2):186-98.
- Nuij C, van Ballegooijen W, de Beurs D, Juniar D, Erlangsen A, Portzky G, O’Connor RC, Smit JH, Kerkhof A, Riper H. Safety planning-type interventions for suicide prevention: meta-analysis. Br J Psychiatry. 2021;219(2):419-26.
- Cho H, Shin J, Choi JK. Serum lipid levels and suicidal ideation of adults: a cross-sectional study using the Korea National Health and Nutrition Examination Survey. J Clin Med 2023, 12(13).
- Lee YJ, Lee S, Hwang IC, Ahn HY. Association between the triglyceride-glucose index and suicidal ideation: a nationwide cross-sectional survey. J Affect Disord. 2024;344:100-3.
- Shin HY, Kang G, Kang HJ, Kim SW, Shin IS, Yoon JS, Kim JM. Associations between serum lipid levels and suicidal ideation among Korean older people. J Affect Disord. 2016;189:192-8.
- Su M, Li E, Tang C, Zhao Y, Liu R, Gao K. Comparison of blood lipid profile/ thyroid function markers between unipolar and bipolar depressed patients
and in depressed patients with anhedonia or suicidal thoughts. Mol Med. 2019;25(1):51. - Qi X, Wang S, Huang Q, Chen X, Qiu L, Ouyang K, Chen Y. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and risk of depression among US adults: a cross-sectional NHANES study. J Affect Disord. 2024;344:451-7.
- Cavanagh JT, Carson AJ, Sharpe M, Lawrie SM. Psychological autopsy studies of suicide: a systematic review. Psychol Med. 2003;33(3):395-405.
- Zhu L, Lu Z, Zhu L, Ouyang X, Yang Y, He W, Feng Y, Yi F, Song Y. Lipoprotein ratios are better than conventional lipid parameters in predicting coronary heart disease in Chinese Han people. Kardiol Pol. 2015;73(10):931-8.
- Liu Z, Lin X, Zeng L, Zhang H, Guo W, Lu Q, Huang C, Wang J, Liu P, Chang Q, et al. Elevated non-HDL-C/HDL-C ratio increases the 1-year risk of recurrent stroke in older patients with non-disabling ischemic cerebrovascular events: results from the Xi’an Stroke Registry Study of China. BMC Geriatr. 2023;23(1):410.
- Iannuzzi A, Giallauria F, Gentile M, Rubba P, Covetti G, Bresciani A, Aliberti E, Cuomo G, Panico C, Tripaldella M et al. Association between Non-HDL-C/ HDL-C ratio and carotid intima-media thickness in Post-menopausal Women. J Clin Med 2021, 11 (1).
- Yang S, Zhong J, Ye M, Miao L, Lu G, Xu C, Xue Z, Zhou X. Association between the non-HDL-cholesterol to HDL-cholesterol ratio and non-alcoholic fatty liver disease in Chinese children and adolescents: a large singlecenter cross-sectional study. Lipids Health Dis. 2020;19(1):242.
- Kim SW, Jee JH, Kim HJ, Jin SM, Suh S, Bae JC, Kim SW, Chung JH, Min YK, Lee MS, et al. Non-HDL-cholesterol/HDL-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int J Cardiol. 2013;168(3):2678-83.
- Curtin LR, Mohadjer LK, Dohrmann SM, Kruszon-Moran D, Mirel LB, Carroll MD, Hirsch R, Burt VL, Johnson CL. National Health and Nutrition Examination Survey: sample design, 2007-2010. Vital Health Stat 2 2013(160):1-23.
- Wang A, Li Y, Zhou L, Liu K, Li S, Zong C, Song B, Gao Y, Li Y, Tian C, et al. Non-HDL-C/HDL-C ratio is associated with carotid plaque stability in general population: a cross-sectional study. Front Neurol. 2022;13:875134.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606-13.
- Costantini L, Pasquarella C, Odone A, Colucci ME, Costanza A, Serafini G, Aguglia A, Belvederi Murri M, Brakoulias V, Amore M, et al. Screening for depression in primary care with Patient Health Questionnaire-9 (PHQ-9): a systematic review. J Affect Disord. 2021;279:473-83.
- Levis B, Benedetti A, Thombs BD. Accuracy of Patient Health Questionnaire-9 (PHQ-9) for screening to detect major depression: individual participant data meta-analysis. BMJ. 2019;365:11476.
- Han KM, Ko YH, Shin C, Lee JH, Choi J, Kwon DY, Yoon HK, Han C, Kim YK. Tinnitus, depression, and suicidal ideation in adults: a nationally representative general population sample. J Psychiatr Res. 2018;98:124-32.
- Vásquez E, Batsis JA, Germain CM, Shaw BA. Impact of obesity and physical activity on functional outcomes in the elderly: data from NHANES 20052010. J Aging Health. 2014;26(6):1032-46.
- Zhao X, Zheng H, Shan S, Wang K, Zhang M, Xie S, Liu C. Association between the non-HDL-cholesterol-to-HDL-cholesterol ratio and the risk of gallbladder polyp formation among men: a retrospective cohort study. Lipids Health Dis. 2020;19(1):146.
- Eliasson B, Cederholm J, Eeg-Olofsson K, Svensson AM, Zethelius B, Gudbjörnsdottir S. Clinical usefulness of different lipid measures for prediction of coronary heart disease in type 2 diabetes: a report from the Swedish National Diabetes Register. Diabetes Care. 2011;34(9):2095-100.
- Holman RR, Coleman RL, Shine BS, Stevens RJ. Non-HDL cholesterol is less informative than the total-to-HDL cholesterol ratio in predicting cardiovascular risk in type 2 diabetes. Diabetes Care. 2005;28(7):1796-7.
- Misiak B, Kiejna A, Frydecka D. Higher total cholesterol level is associated with suicidal ideation in first-episode schizophrenia females. Psychiatry Res. 2015;226(1):383-8.
- Park YM, Lee BH, Lee SH. The association between serum lipid levels, suicide ideation, and central serotonergic activity in patients with major depressive disorder. J Affect Disord. 2014;159:62-5.
- Wu S, Ding Y, Wu F, Xie G, Hou J, Mao P. Serum lipid levels and suicidality: a meta-analysis of 65 epidemiological studies. J Psychiatry Neurosci. 2016;41(1):56-69.
- Sheng G, Liu D, Kuang M, Zhong Y, Zhang S, Zou Y. Utility of Non-high-density Lipoprotein Cholesterol to high-density lipoprotein cholesterol ratio in evaluating Incident Diabetes Risk. Diabetes Metab Syndr Obes. 2022;15:1677-86.
- Zhao W, Gong W, Wu N, Li Y, Ye K, Lu B, Zhang Z, Qu S, Li Y, Yang Y, et al. Association of lipid profiles and the ratios with arterial stiffness in middle-aged and elderly Chinese. Lipids Health Dis. 2014;13:37.
- Kwok RM, Torres DM, Harrison SA. Vitamin D and nonalcoholic fatty liver disease (NAFLD): is it more than just an association? Hepatology. 2013;58(3):1166-74.
- Lin D, Qi Y, Huang C, Wu M, Wang C, Li F, Yang C, Yan L, Ren M, Sun K. Associations of lipid parameters with insulin resistance and diabetes: a populationbased study. Clin Nutr. 2018;37(4):1423-9.
- Mann JJ. Neurobiology of suicidal behaviour. Nat Rev Neurosci. 2003;4(10):819-28.
- Daray FM, Mann JJ, Sublette ME. How lipids may affect risk for suicidal behavior. J Psychiatr Res. 2018;104:16-23.
- Ganança L, Oquendo MA, Tyrka AR, Cisneros-Trujillo S, Mann JJ, Sublette ME. The role of cytokines in the pathophysiology of suicidal behavior. Psychoneuroendocrinology. 2016;63:296-310.
- Penttinen J. Hypothesis: low serum cholesterol, suicide, and interleukin-2. Am J Epidemiol. 1995;141(8):716-8.
- Lee K, Kim S, Jo JK. The relationships between abnormal serum lipid levels, Depression, and suicidal ideation according to sex. J Clin Med 2022, 11 (8).
- Delarue J, LeFoll C, Corporeau C, Lucas D. N-3 long chain polyunsaturated fatty acids: a nutritional tool to prevent insulin resistance associated to type 2 diabetes and obesity? Reprod Nutr Dev. 2004;44(3):289-99.
- Tanskanen A, Hibbeln JR, Hintikka J, Haatainen K, Honkalampi K, Viinamäki H. Fish consumption, depression, and suicidality in a general population. Arch Gen Psychiatry. 2001;58(5):512-3.
- Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES Dietary Data: Focus on Collection, Release, Analytical considerations, and uses to inform Public Policy. Adv Nutr. 2016;7(1):121-34.
Publisher’s Note
- *Correspondence:
Bo Wei
weibo0806@163.com
Full list of author information is available at the end of the article