الكشف عن ctDNA فائق الحساسية لتصنيف المرض قبل العملية في سرطان الرئة الغدي في مراحله المبكرة Ultrasensitive ctDNA detection for preoperative disease stratification in early-stage lung adenocarcinoma
يمكن أن يتنبأ اكتشاف الحمض النووي الورمي المتداول (ctDNA) بالمخاطر السريرية في الأورام في مراحلها المبكرة. ومع ذلك، فإن التطبيقات السريرية مقيدة بحساسية طرق اكتشاف ctDNA المعتمدة سريرياً. NeXT Personal هو منصة تعتمد على الجينوم الكامل ومعلومات الورم وقد تم التحقق من صحتها تحليلياً لاكتشاف ctDNA بحساسية فائقة عند من ctDNA مع الخصوصية. من خلال تحليل 171 مريضًا مصابًا بسرطان الرئة في مراحله المبكرة من دراسة TRACERx، اكتشفنا ctDNA قبل العملية ضمنمرضى سرطان الغدة الرئوية (LUAD)، بما في ذلك 53% من أولئك الذين يعانون من مرض المرحلة الأولى وفقًا لنظام TNM المرضي (pTNM). توقعت ctDNA نتائج سريرية أسوأ، وكان المرضى الذين يعانون من LUAD معمستويات ctDNA قبل العملية (الـحد الكشف عن نهج الكشف عن ctDNA الذي تم نشره سابقًا في TRACERx) شهد انخفاضًا في البقاء العام مقارنةً بالمرضى السلبيين لـ ctDNA المصابين بـ LUAD. على الرغم من الحاجة إلى دراسات مستقبلية لتأكيد الفائدة السريرية للاختبار، فإن هذه البيانات تظهر أن نهجنا لديه القدرة على تحسين تصنيف المرض في مراحل LUAD المبكرة.
تعتبر الخزعة السائلة للكشف عن الحمض النووي الورمي المتداول (ctDNA، وهو الحمض النووي الخالي من الخلايا المستمد من ورم) واعدة كاستراتيجية للإدارة السريرية المخصصة لسرطانات المرحلة المبكرة.لقد أظهر حالة ctDNA قبل العملية إمكانيات كعلامة حيوية، بينما يمكن أن توجيه اكتشاف ctDNA بعد العملية أنظمة العلاج المساعد.والمراقبة لوجود المرض الجزيئي المتبقي (MRD) خلال المتابعة لديها القدرة على تحديد الانتكاسة في وقت أبكر مما يمكن اكتشافه من خلال المراقبة السريرية الروتينية.. يمكن أن يكون اكتشاف ctDNA مستندًا إلى الورم أو غير مستند إلى الورم. تستفيد الأساليب المستندة إلى الورم من المعلومات المستمدة من التحليل الجيني لعينة نسيج الورم، مما يسمح بتتبع الطفرات المحددة للورم داخل البلازما وعادة ما يحسن الحساسية مقارنة بالأساليب غير المستندة إلى الورم. في عام 2020، تم استخدام التحليل الشخصي للسرطان عن طريق التسلسل العميق (CAPP-seq) في نهج مستند إلى الورم لإظهار أن اكتشاف ctDNA قبل العملية في سرطان الرئة غير صغير الخلايا (NSCLC) يمكن استخدامه لـ
تحديد المرضى الذين يعانون من المرحلة الأولى من المرض مع نتائج سريرية سيئة. العمل اللاحق ضمن الأورام الغدية الرئوية (LUADs) من مجموعة LUNGCA-1تجربة ناديمودراسة TRACERxأكدت دراسة سرطان الرئة غير صغير الخلايا (NSCLC) القدرة التنبؤية لاكتشاف الحمض النووي الخلوي الحر (ctDNA) قبل العملية الجراحية بالنسبة للبقاء على قيد الحياة بشكل عام (OS) والبقاء بدون انتكاسة (RFS) في سرطان الرئة ذو الخلايا الكبيرة (LUADs).
كشف ctDNA قبل العملية في مراحل مبكرة من LUAD يمثل تحديًا كبيرًا بسبب المستويات المنخفضة من ctDNA في البلازما، والتي غالبًا ما تكون أقل منبالإضافة إلى ذلك، يمكن أن تتأثر حساسية اكتشاف ctDNA بالتغيرات في إنتاج الحمض النووي الخالي من الخلايا (cfDNA) بواسطة خلايا غير خبيثة.خطأ في التسلسل والأنماط المتغيرة الناتجة عن تكوين الدم الخلوي غير المحدد (CHIP)، والتي يمكن أن تكون موجودة بمستويات منخفضة في البلازمايجب أن تحتوي منصة الكشف عن ctDNA عالية الجودة على عدد من الخصائص لتحقيق الفائدة السريرية المثلى: يجب أن تكون حساسة للغاية، وذات دقة عالية، وقابلة للتطبيق على طيف واسع من الأورام، ويجب أن تقدم نتائج مع كميات صغيرة من مدخلات الحمض النووي. ولهذا الغرض، كان هناك تركيز كبير مؤخرًا على البحث في تطوير أساليب للتغلب على هذه المشكلة..
على الرغم من أن العلاقة بين اكتشاف ctDNA والبقاء على قيد الحياة مستقلة عن مرحلة الورم والعقد والانتشار المرضي (pTNM) في هذا السياق، إلا أن الدرجة التي يؤثر بها حد الكشف (LOD) لاختبارات ctDNA على الحساسية السريرية لـ ctDNA كعلامة حيوية للمرض العدواني ليست مفهومة جيدًا.
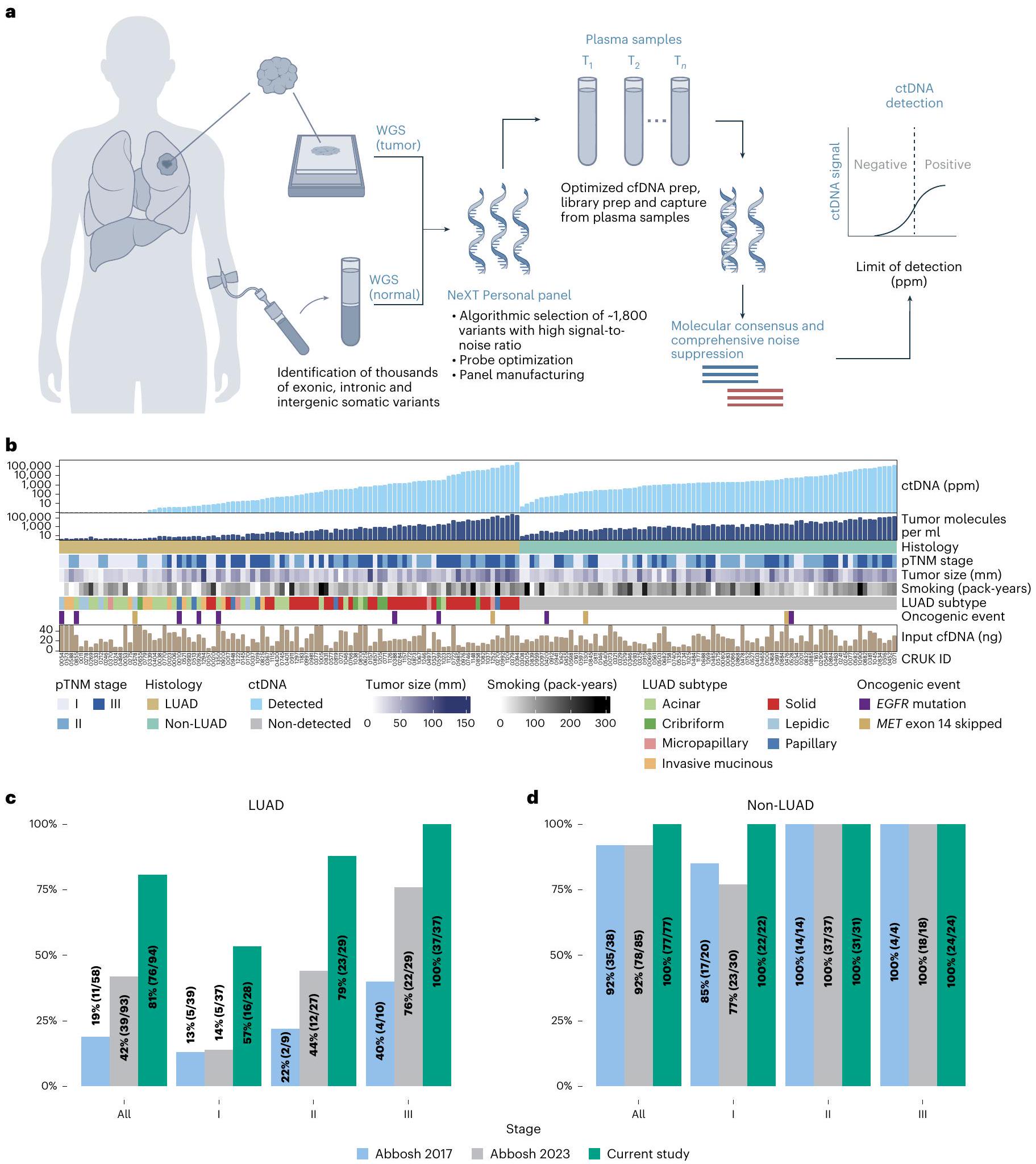
هنا، استخدمنا منصة NeXT Personal، وهي منصة سائلة للتشخيص الحيوي حساسة للغاية ومبنية على معلومات الأورام، لتوصيف ctDNA قبل العملية في 171 مريضًا في دراسة TRACERx.NeXT Personal هو منصة تحليل سائل مستنيرة بالأورام تستفيد من اختيار الأهداف ذات الأولوية من تسلسل الجينوم الكامل للورم وDNA الطبيعي المتطابق.تم توضيح تطوير والتحقق التحليلي لهذه الطريقة في الأساليب وفي المرجع 23. باختصار، تهدف الطريقة إلى تحقيق حد الكشف (LOD) يقترب من 1 جزء في المليون من خلال تجميع الإشارة من عدد أكبر من أهداف المتغيرات الجسدية مما يمكن اكتشافه من الإكسوم. لتجنب الانغماس في الإشارات الكاذبة الناجمة عن العدد الكبير من المتغيرات، يجب تقليل الضوضاء إلى مستويات منخفضة جداً، وهو ما يتحقق إلى حد كبير من خلال التوافق الجزيئي، الذي يسمح بتحديد قراءات التسلسل المستقلة الناشئة عن مؤسس مشترك، ويجمع هذه القراءات في عائلات جزيئية فريدة لمزيد من التحليل. تم تصميم لوحات NeXT Personal المخصصة باستخدام أفضلتم تصنيف المتغيرات الجسدية بناءً على نسبة الإشارة إلى الضوضاء لاكتشاف ctDNA من البلازما (أي، المجموعة الفرعية من cfDNA التي تحتوي على الطفرات المحددة للورم في اللوحة). يتبع ذلك تعزيز الأهداف الجينومية المعتمد على التهجين باستخدام اللوحة، ثم يتم إجراء تسلسل عميق للغاية لعينات البلازما. بعد ذلك، يقوم NeXT Personal بتجميع الإشارة المستمدة من الورم من الأهداف الجسدية. تتيح هذه العملية، جنبًا إلى جنب مع طرق شاملة لتقليل الضوضاء، لـ NeXT Personal تحقيق اكتشاف ctDNA فائق الحساسية لتصنيف الأمراض، ومراقبة العلاج، واكتشاف MRD (الطرق والشكل 1a).
تمت دراسة اختبارات الكشف عن ctDNA المستندة إلى الأورام الشخصية التي تستفيد من الطفرات الإكسونية في مجموعة TRACERx.لقد درسنا سابقًا قدرة ctDNA، المكتشف في عينة دم محيطي قبل العملية، على التنبؤ بالنتيجة السريرية في LUAD.تضمن ذلك اختبارًا مستندًا إلى الورم يحقق في المتغيرات الجسدية في متوسط 200 موقع لكل عينة، مما كشف أن المرضى الذين يعانون من سرطان الرئة ذو الخلايا غير الصغيرة (LUAD) والذين تم الكشف عن الحمض النووي الخلوي (ctDNA) في دمهم في وقت الجراحة كان لديهم توقعات سريرية أسوأ.. ومع ذلك، كان يمكن الكشف عن ctDNA فقط في للمرضى الذين يعانون من المرحلة المرضية الأولى من سرطان الرئة ذو الخلايا غير الصغيرة في هذه النقطة الزمنية. لذلك، قمنا بتقييم الدرجة التي يمكن أن تزيد بها اختبار أكثر حساسية وخصوصية من القيمة التنبؤية في مجموعة ذات خصائص سريرية مماثلة (البيانات الموسعة الجدول 1).
قمنا بتحليل عينات بلازما الدم التي تم جمعها قبل إزالة سرطان الرئة جراحيًا من 171 مريضًا في دراسة TRACERx، بما في ذلك 94 مريضًا مصابًا بسرطان الرئة ذو الخلايا الكبيرة (LUAD).المرحلة الأولىالمرحلة الثانيةالمرحلة الثالثة) و77 مع سرطان الرئة غير ذي الخلايا الصغيرة (28.6% المرحلة الأولى، 40.3% المرحلة الثانية، 31.2% المرحلة الثالثة) باستخدام NeXT Personal (البيانات الموسعة الجدول 2 والشكل 1b). من بين هؤلاء المرضى، كان لدى 160 ورم رئيسي واحد من سرطان الرئة غير ذي الخلايا الصغيرة و11 كان لديهم ورمين رئيسيين متزامنين.
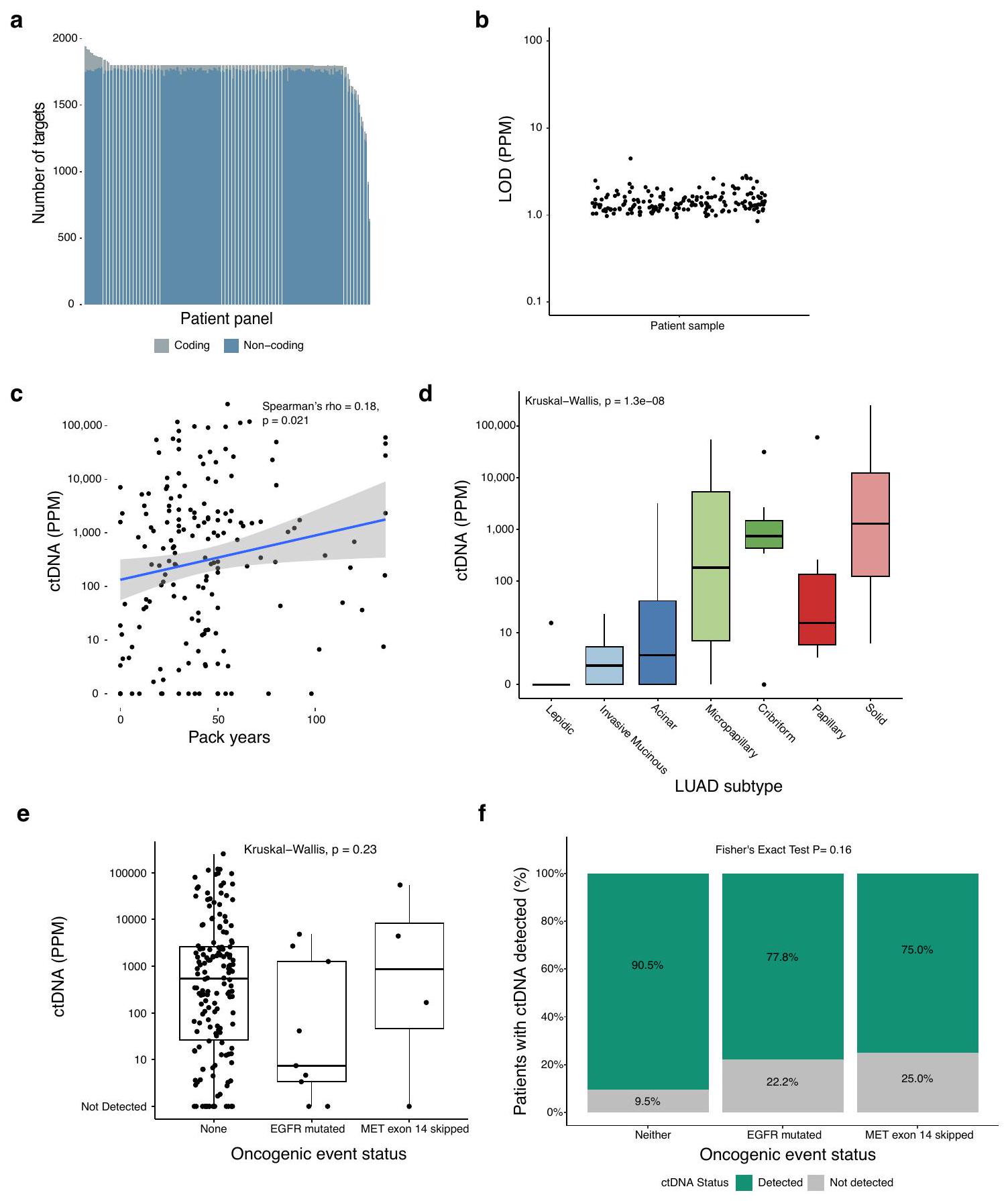
أورام NSCLC. تم تضمين متوسط 1,800 متغير جسمي محدد لكل مريض في تصميم لوحة NeXT Personal (النطاق، 646-1,942)، من بينها متوسطكانت من مناطق غير مشفرة (الشكل البياني الممتد 1a). وقد أسفر ذلك عن مجموعة من الألواح المخصصة بوسيط LOD متوقع قدره 1.33 جزء في المليون ونطاق من (الشكل البياني الممتد 1ب). كانت الكمية المتوسطة من الحمض النووي المدخل 23.5 نانوغرام (الشكل 1ب؛ النطاق، ). تم الكشف عن ctDNA في عينة بلازما قبل العملية فيمن المرضى الذين يعانون من LUAD (الشكل 1c، 76/94) و 100% من المرضى الذين يعانون من غير LUAD (الشكل 1d، 77/77) من NSCLCs عبر مجموعة واسعة من كسور الورم (نطاق اكتشاف ctDNA الإيجابي، ). وقد شمل ذلك 32 حالة من سرطان الرئة ذو الخلايا غير الصغيرة (LUAD) (من جميع حالات LUAD) التي تم فيها اكتشاف ctDNA، ولكن بمعدل أقل من 80 جزء في المليون،LOD في نهجنا السابقيمكننا اكتشاف ctDNA في دممن المرضى الذين يعانون من مرحلة pTNM ILUADs (16/28): كان من الصعب اكتشاف ctDNA من هذه الأورام في عينات الدم (فقطتم تحديد مثل هذه الأورام في أبوش وآخرون. و في أبوش وآخرون ). وبالمثل، تم الكشف عن ctDNA في من المرحلة الثانية من سرطان الرئة غير صغير الخلايا (LUAD)، مقارنة بـفي أبوش وآخرونتم الإبلاغ سابقًا عن أن تسرب ctDNA مرتبط بحالة التدخين (تاريخ عدد علب السجائر في السنة) (سبيرمان); الشكل البياني الموسع 1c) ومع الأنماط الفرعية السائدة عالية الدرجة من LUAD، لا سيما الأنماط الفرعية الصلبة والشبكية (اختبار كروسكال-واليس؛ الشكل البياني الممتد 1d)الأحداث المسرطنة، التي شملت في هذه المجموعةلم تكن الطفرات وتخطي إكسون 14 من MET (لم يتم الكشف عن أي اندماجات سرطانية RET-ROS1-ALK) مرتبطة بفارق كبير في مستوى ctDNA ppm.اختبار كروسكال-واليس؛ الشكل البياني الممتد 1e) أو معدل اكتشاف ctDNA قبل العملية (اختبار فيشر الدقيق؛ الشكل التوضيحي الممتد 1f)، على الرغم من أن هذه التحليل من المحتمل أن يكون ضعيف القوة نظرًا لعدد المرضى القليل الذين يحملون هذه الأحداث.
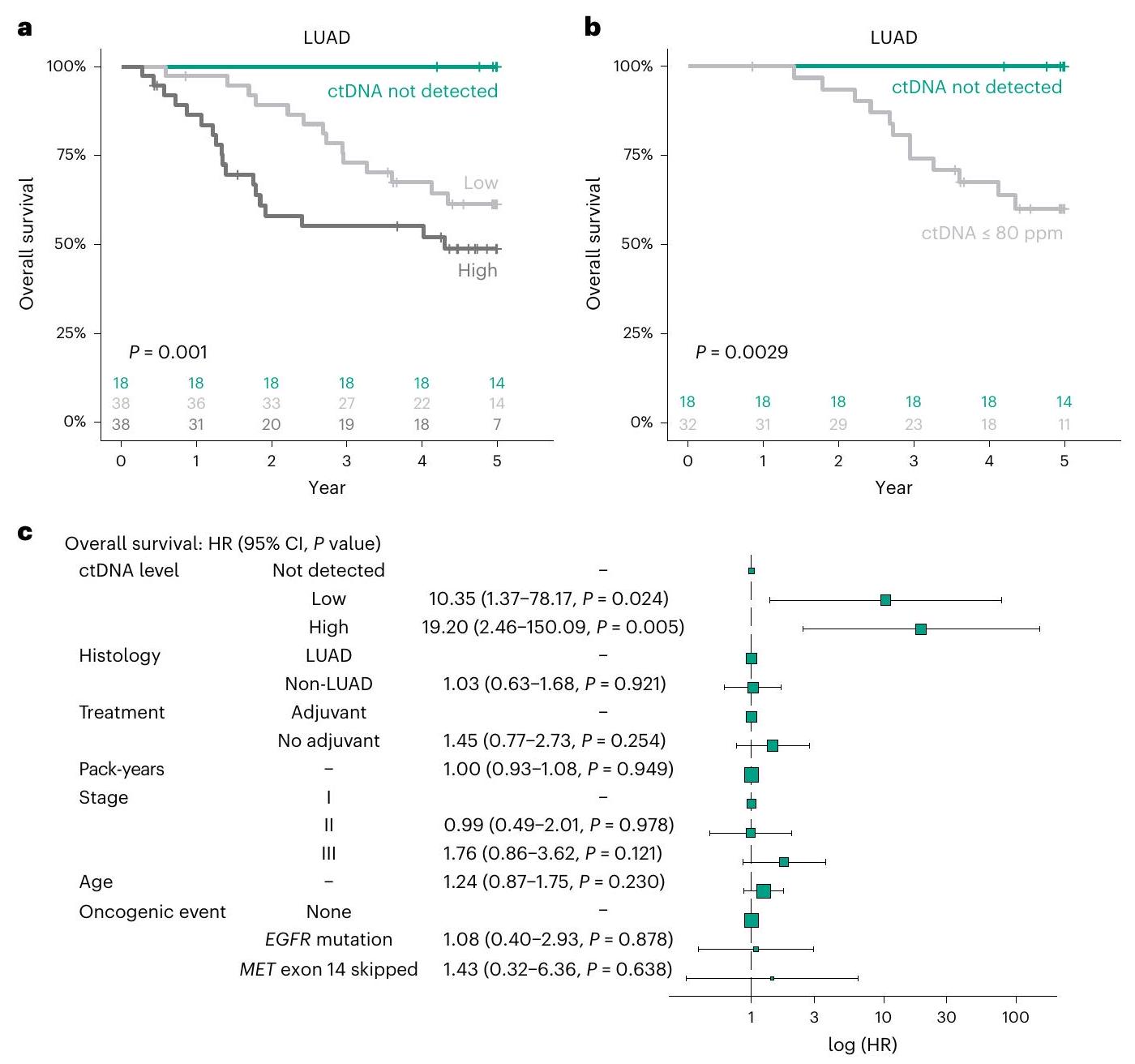
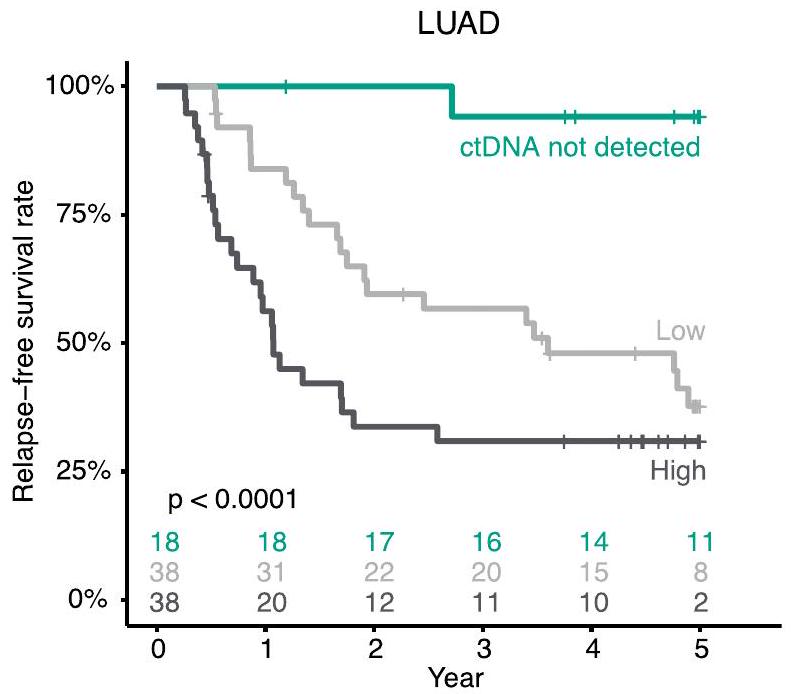
قمنا بعد ذلك بتقييم الدرجة التي حسنت بها هذه الحساسية الإضافية قدرتنا على تصنيف هؤلاء المرضى وفقًا للنتيجة السريرية. تم مقارنة المرضى الذين كانت نتائج ctDNA لديهم سلبية قبل العملية مع المرضى الذين كانت مستويات ctDNA لديهم أقل من الوسيط لتلك المكتشفة (ctDNA منخفض) وأولئك الذين كانت مستويات ctDNA لديهم أعلى من الوسيط لتلك المكتشفة (ctDNA مرتفع). توقعت حالة ctDNA البقاء على قيد الحياة في حالات LUAD (الشكل 2a، منخفض: نسبة المخاطرفترة الثقة1.48-83.2؛ مرتفع: ) و RFS (الشكل البياني الموسع 2a، منخفض: HR، ; مرتفع، كان لدى المرضى الذين لديهم حالة سلبية لـ ctDNA قبل العملية تحسن كبير في البقاء على قيد الحياة (البقاء على قيد الحياة لمدة 5 سنوات،; ; ) مقارنة مع مرضى ctDNA المنخفض ( 5 سنوات ) ، ومرضى ctDNA-high ( 5 سنوات OS، . ومن الجدير بالذكر أنه عندما تم تقييد التحليل ليشمل فقط المرضى الذين لم يكن من الممكن الكشف عن ctDNA لديهم بشكل موثوق باستخدام النهج في أبوش وآخرون.، كانت وجود ctDNA بمستويات أقل من 80 جزء في المليون لا يزال تنبؤيًا لضعف البقاء على قيد الحياة (الشكل 2ب، ) و RFS (الشكل البياني الموسع 2b، هذا يشير إلى أنه يتم الكشف عن إشارة ذات دلالة سريرية بواسطة الفحوصات التي تتمتع بحساسية عند نسب الأورام أقل من 80 جزء في المليون، وأن الفحص عالي الحساسية المقدم هنا يمكّن من تحديد مجموعة من المرضى ذوي المخاطر المنخفضة جداً المصابين بسرطان الرئة ذو الخلايا غير الصغيرة.
كما أبلغنا سابقًا، كانت العلاقة بين النتائج ومستويات ctDNA المرتفعة قبل العملية في غير LUADs أقل بكثير مقارنة بتلك الموجودة في LUADs؛ وقد وجدت الأعمال السابقة عدم وجود تأثير ملحوظ لمستويات ctDNA على النتائج السريرية في غير LUADs.. في هذا التحليل، لم يكن مستوى ctDNA الذي يزيد عن الوسيط في غير حالات LUAD مرتبطًا بتقليل فترة البقاء الخالية من المرض (الشكل 2c من البيانات الموسعة؛هذا يبرز علاقة مختلفة جوهريًا بين ctDNA وبيولوجيا المرض في غير LUADs مقارنة بتلك الموجودة في LUADs.
عند التعديل وفقًا للهستولوجيا، مرحلة pTNM، حالة التدخين، العمر، ووجود حدث ورمي (مثل طفرة محرك EGFR أو تخطي الإكسون 14 في ) وإضافة العلاج المساعد،
الشكل 1| الكشف عالي الحساسية عن ctDNA قبل العملية. أ، تعتمد منصة NeXT Personal على المعلومات المستندة إلى الورم لتحقيق الكشف عن السرطان المتبقي والمتكرر بدقة فائقة وحساسية عالية، والمراقبة الطولية ومراقبة العلاج من عينات خزعة سائلة. ب، المتغيرات السريرية والمرضية المتعلقة بكشف ctDNA قبل العملية في المرضى الذين يعانون من NSCLC في دراسة TRACERx: مستوى ctDNA (جزء في المليون من كتلة الورم)؛ عدد جزيئات الورم لكل مل من البلازما؛ مرحلة العقدة الورمية المرضية (pTNM)؛ علم الأنسجة لسرطان الرئة غير صغير الخلايا (NSCLC)؛ حجم الورم (حجم الورم المستند إلى علم الأمراض (مم))؛ تدخين السجائر (سنوات علبة)؛ النوع الفرعي المرضي لسرطان الرئة ذو الخلايا غير الصغيرة (LUAD)؛ وجود حدث ورمي (ضمن هذه المجموعة، إما وجود طفرة في EGFR أو تخطي إكسون 14 من MET)؛ وكمية إدخال cfDNA (نانوجرام). الأورام LUAD (د) التي تم اكتشافها قبل العملية. الألوان تمثل دراسات مختلفة: الأزرق، أبوش وآخرون.;رمادي، أبوش وآخرون; الأخضر، هذه الدراسة. لوادغير LUAD.
الشكل 2 | مستوى ctDNA الأساسي هو مؤشر للتنبؤ بالبقاء على قيد الحياة. أ، منحنى كابلان-ماير (KM) للبقاء على قيد الحياة في المرضى ذوي مستويات ctDNA العالية (رمادي داكن)، ctDNA المنخفضة (رمادي فاتح) وctDNA السلبية (أخضر) المصابين بسرطان الرئة ذو الخلايا غير الصغيرة. تم تعريف مجموعات ctDNA العالية والمنخفضة وفقًا لمستويات ctDNA المتوسطة عبر حالات سرطان الرئة ذو الخلايا غير الصغيرة الإيجابية لـ ctDNA.تم حساب القيم باستخدام اختبارات لوغ-رانك. ب، منحنى كابلان-ماير يوضح البقاء على قيد الحياة في المرضى الذين يحملون ctDNA عند نسبة ورم مقدرة أقل من حد الكشف الموثوق به كما هو موصوف في أبوش وآخرون. (رمادي فاتح) والمرضى السلبيين لـ ctDNA (أخضر). تم حساب القيم باستخدام اختبارات لوغ-رانك. ج، نتائج التحليل المتعدد المتغيرات
تحليل الانحدار كوكس بما في ذلك مستوى ctDNA (ctDNA-high، ctDNA-low، ctDNA-negative)؛ علم الأنسجة؛ ما إذا كان المريض قد تلقى العلاج الكيميائي المساعد؛ تاريخ تدخين السجائر (بزيادات قدرها 10 سنوات علبة)؛ مرحلة pTNM؛ العمر (بزيادات قدرها 10 سنوات)؛ ووجود حدث ورمي (إما طفرة أوتخطي الإكسون 14).تمثل أشرطة الخطأفترات الثقة. تمثل أحجام الصناديق عدد المرضى في كل فئة. وجود ctDNA – سواء اعتُبر كمقياس مستمر أو تم تقسيمه إلى مجموعات كما هو محدد أعلاه – كان مرتبطًا بشكل مستقل بانخفاض البقاء على قيد الحياة (OS) (الشكل 2c والشكل الإضافي 3a) ومدة البقاء الخالية من المرض (RFS) (الشكل الإضافي 3b,c) في مجموعة مجمعة من المرضى الذين يعانون من LUADs وغير LUADs. ومن الجدير بالذكر أن مستوى ctDNA لم يكن ذا دلالة كعامل تنبؤي مستقل لمدى البقاء الخالية من المرض في مجموعة غير LUAD (الشكل الإضافي 3d,e). لم يكن التأثير التنبؤي لـ ctDNA كمتغير مستمر على كل من RFS وOS ذا دلالة عند التعديل لعوامل النسيجية (نوع حرشفي مقابل غير حرشفي) وعوامل سريرية مرضية أخرى (الشكل الإضافي 3f,g).
لقد استفاد هذا العمل من NeXT Personal، وهو اختبار مستند إلى الورم قادر على الكشف بشكل موثوق عن ctDNA في الدم عند ( نسبة الورم). من الجدير بالذكر أن هذه الحساسية العالية للغاية يمكن تحقيقها مع تقدير للخصوصية بـحتى من أحجام إدخال الحمض النووي غير المثلى. قد يكون هذا مهمًا في العديد من الإعدادات السريرية، ويمكن تطبيقه على أحجام إدخال الحمض النووي غير المثلى.
يظل المرضى الذين يعانون من سرطان الرئة غير صغير الخلايا في مراحله المبكرة معرضين لخطر عالٍ من الانتكاس، على الرغم من العلاج العدواني الذي يهدف إلى الشفاء. لذلك، من الأهمية القصوى تصنيف المرضى بدقة لزيادة احتمالية الشفاء من المرض بعد الجراحة والعلاج المساعد و تقليل خطر العلاج المفرط لدى المرضى الذين يُتوقع أن تكون نتائجهم جيدة. تم ربط وجود ctDNA القابل للكشف قبل العملية بتدهور البقاء على قيد الحياة بدون تكرار وتقليلوقد تم اقتراحه كعلامة محتملة لاختيار العلاج المساعد قبل الجراحةلقد أظهرنا أن الاختبارات التي لا تستطيع الكشف عن ctDNA عند نسب الأورام أقل من 80 جزء في المليون تفشل في التقاط إشارة ذات تأثير سريري تنشأ من مجموعة كبيرة من المرضى الذين يعانون من LUAD.في هذه الدراسة، عانى هؤلاء المرضى الذين لديهم مستويات قابلة للكشف ولكن منخفضة للغاية من ctDNA من نتائج سريرية أسوأ من أولئك الذين لم نكتشف لديهم دليل على ctDNA. وهذا يشير إلى أن هناك مجموعة فرعية من المرضى ذوي المخاطر المنخفضة جداً المصابين بسرطان الرئة ذو الخلايا غير الصغيرة (LUAD) يمكن تحديدها بشكل قاطع فقط باستخدام اختبار ctDNA فائق الحساسية، مما يرفع من إمكانية استخدام اختبار فائق الحساسية ودقيق للتنبؤ بتصعيد العلاج في مراحل LUADs التي تظهر إفراز ctDNA.
على الرغم من أن هذه الدراسة تقدم نتائج من عينات البلازما قبل العملية، إلا أن الحساسية العالية لاختبار NeXT Personal تشير إلى إمكانية تحقيق فائدة سريرية كبيرة في حالة وجود مرض متبقي ضئيل لتتبع استجابة العلاج واكتشاف الانتكاسة.
من الجدير بالذكر أن هناك عددًا من التقنيات في هذا المجال تهدف إلى تحقيق الكشف عن ctDNA المستند إلى الأورام بحساسية فائقة، مثل تلك تم تطويره بواسطة Foresight Diagnostics (PhasED-seq)سي2آي جينوميكسوإنيفاتا (رادار).
هذا العمل له قيود. تم تحليل البيانات من TRACERx بأثر رجعي، على الرغم من أنها كانت بطريقة معمية. ستكون هناك حاجة إلى بيانات مستقبلية من مجموعات مستقبلية لتقييم الفائدة السريرية لهذا الاختبار. على الرغم من أن NeXT Personal قيد الاستخدام بالفعل كاختبار تشخيصي سريري، إلا أنه، مثل اختبارات الكشف عن ctDNA المستندة إلى الأورام الأخرى، يتمتع بتعقيد أعلى، ويمكن أن يكون أكثر تكلفة للإنتاج ويتطلب فترة زمنية أطول لتطوير اللوحة والحصول على نتيجة قابلة للتنفيذ سريرياً، مقارنة بالأساليب غير المستندة إلى الأورام.
إذا كان من المقرر استخدام ctDNA في التنبؤ بالمخاطر السريرية، فإن تصميم أنظمة العلاج المساعد الشخصية والكشف المبكر عن الانتكاس ودمجها في الرعاية السريرية الروتينية، يجب أن تتمتع اختبارات ctDNA بدرجة عالية من الحساسية. بهذه الطريقة، فإنها تحمل وعدًا بتحويل تصميم التجارب السريرية المساعدة والممارسة السريرية.
المحتوى عبر الإنترنت
أي طرق، مراجع إضافية، ملخصات تقارير Nature Portfolio، بيانات المصدر، بيانات موسعة، معلومات تكميلية، شكر وتقدير، معلومات مراجعة الأقران؛ تفاصيل مساهمات المؤلفين والمصالح المتنافسة؛ وبيانات توفر البيانات والرموز متاحة علىhttps://doi.org/10.1038/s41591-024-03216-y.
References
Abbosh, C. et al. Phylogenetic ctDNA analysis depicts early stage lung cancer evolution. Nature 545, 446-451 (2017).
Abbosh, C. et al. Tracking early lung cancer metastatic dissemination in TRACERx using ctDNA. Nature 616, 553-562 (2023).
Pascual, J. et al. ESMO recommendations on the use of circulating tumour DNA assays for patients with cancer: a report from the ESMO Precision Medicine Working Group. Ann. Oncol. 33, 750-768 (2022).
Garcia-Murillas, I. et al. Mutation tracking in circulating tumor DNA predicts relapse in early breast cancer. Sci. Transl. Med. 7, 302ra133 (2015).
Reinert, T. et al. Analysis of plasma cell-free DNA by ultradeep sequencing in patients with stages I to III colorectal cancer. JAMA Oncol. 5, 1124-1131 (2019).
Gale, D. et al. Residual ctDNA after treatment predicts early relapse in patients with early-stage non-small cell lung cancer. Ann. Oncol. 33, 500-510 (2022).
Kotani, D. et al. Molecular residual disease and efficacy of adjuvant chemotherapy in patients with colorectal cancer. Nat. Med. 29, 127-134 (2023).
Powles, T. et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature 595, 432-437 (2021).
Tie, J. et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage II colon cancer. N. Engl. J. Med. 386, 2261-2272 (2022).
Chaudhuri, A. A. et al. Early detection of molecular residual disease in localized lung cancer by circulating tumor DNA profiling. Cancer Discov. 7, 1394-1403 (2017).
Chabon, J. J. et al. Integrating genomic features for non-invasive early lung cancer detection. Nature 580, 245-251 (2020).
Xia, L. et al. Perioperative ctDNA-based molecular residual disease detection for non-small cell lung cancer: a prospective multicenter cohort study (LUNGCA-1). Clin. Cancer Res. 28, 3308-3317 (2022).
Provencio, M. et al. Overall survival and biomarker analysis of neoadjuvant nivolumab plus chemotherapy in operable stage IIIA non-small-cell lung cancer (NADIM phase II trial). J. Clin. Oncol. 40, 2924 (2022).
Chin, R.-I. et al. Detection of solid tumor molecular residual disease (MRD) using circulating tumor DNA (ctDNA). Mol. Diagn. Ther. 23, 311-331 (2019).
Mattox, A. K. et al. The origin of highly elevated cell-free DNA in healthy individuals and patients with pancreatic, colorectal, lung, or ovarian cancer. Cancer Discov. 13, 2166-2179 (2023).
Hu, Y. et al. False-positive plasma genotyping due to clonal hematopoiesis. Clin. Cancer Res. 24, 4437-4443 (2018).
Cohen, J. D. et al. Detection of low-frequency DNA variants by targeted sequencing of the Watson and Crick strands. Nat. Biotechnol. 39, 1220-1227 (2021).
Kurtz, D. M. et al. Enhanced detection of minimal residual disease by targeted sequencing of phased variants in circulating tumor DNA. Nat. Biotechnol. 39, 1537-1547 (2021).
Zviran, A. et al. Genome-wide cell-free DNA mutational integration enables ultra-sensitive cancer monitoring. Nat. Med. 26, 1114-1124 (2020).
Cohen, J. D. et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 359, 926-930 (2018).
Jamal-Hanjani, M. et al. Tracking the evolution of non-small-cell lung cancer. N. Engl. J. Med. 376, 2109-2121 (2017).
Martínez-Ruiz, C. et al. Genomic-transcriptomic evolution in lung cancer and metastasis. Nature 616, 543-555 (2023).
Northcott, J. et al. Analytical validation of NeXT Personal , an ultra-sensitive personalized circulating tumor DNA assay. Oncotarget 15, 200-218 (2024).
Zhao, J. et al. Personalized cancer monitoring assay for the detection of ctDNA in patients with solid tumors. Mol. Diagn. Ther. 27, 753-768 (2023).
Karasaki, T. et al. Evolutionary characterization of lung adenocarcinoma morphology in TRACERx. Nat. Med. 29, 833-845 (2023).
Jung, H.-A. et al. Longitudinal monitoring of circulating tumor DNA from plasma in patients with curative resected stages I to IIIA EGFR-mutant non-small cell lung cancer. J. Thorac. Oncol. 18, 1199-1208 (2023).
Li, N. et al. Perioperative circulating tumor DNA as a potential prognostic marker for operable stage I to IIIA non-small cell lung cancer. Cancer 128, 708-718 (2022).
Isbell, J. M. et al. Abstract 3375: ultrasensitive ctDNA minimal residual disease monitoring in early NSCLC with PhasED-Seq. Cancer Res. 83, 3375 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
¹Cancer Research UK Lung Cancer Centre of Excellence, University College London Cancer Institute, London, UK. ²Cancer Evolution and Genome Instability Laboratory., The Francis Crick Institute, London, UK. Personalis Inc., Fremont, CA, USA. Cancer Metastasis Laboratory, University College London Cancer Institute, London, UK. Department of Thoracic Surgery, Respiratory Center, Toranomon Hospital, Tokyo, Japan. Cancer Genome Evolution Research Group, Cancer Research UK Lung Cancer Centre of Excellence, University College London Cancer Institute, London, UK. Department of Cellular Pathology, University College London Hospitals, London, UK. Department of Experimental Medicine, Sapienza University, Rome, Italy. Leicester NIHR BRC & University of Leicester, Leicester, UK. Cancer Research UK & UCL Cancer Trials Centre, London, UK. Department of Oncology, University College London Hospitals, London, UK. These authors contributed equally: James R. M. Black, Gabor Bartha. These authors jointly supervised this work: Richard O. Chen, Charles Swanton. e-mail: Charles.swanton@crick.ac.uk
اتحاد TRACERx
تشارلز سوانتونألكسندر م. فرانكلمريم جمال-هانجانينيكولاس مكغرانهانألان هاكشوجاكي أ. شاوجيمس ر. م. بلاكتاكاهيرو كاراساكيسيلفاراجو فيريامايسة البكيروينغ كين ليومارك س. هيلكيرستين ثولأريانا هوبنركريس بيليإيما سي. كوليفركارلوس مارتينيز-رويزكريستيانا غريغورياديسبيوتر باوليكديفيد أ. مورمونيكا سيفاكومارجيسون ف. ليسترأمريتا باجاجأبولس ناكاسأزميـنـا سودهـا-رامدينمحمد طفيلمولي اسكتلنداريبيكا بويلزسريدhar راثينامكلير ويلسوندومينيك مارونشون دولودين أ. فينيلغورديف ماثاروإيكاتريني بوليتيهيذر شينمحمد خليلشيرلي ريتشاردسونتريسي كروكشانكجيليان برايسكيث م. كيرسارة بنفيفجاك فرينشكيلي غيلبرتبابو نايدوأكشاي ج. باتيلآية عثمانكارول إنستونجيرالد لانغمانهيلين شاكلفوردمدافا جيرامانسلمى قديريغاري ميدلتونأنجيلا ليكجاك ديفيز هودجكينسوننيكولا توتونأنجيليس مونتيروإلين سميثيوستاس فونتينفليتشي جراناتوأنتونيو بايفا-كوريياجولييت نوفاسيوكيندادي رامموهانلينا جوزيفبول بيشوبراجش شاهستيوارت موسفيجاي جوشيفيليب أ. ج. كروسبيكاثرين د. براونماثيو كارترأنشومان شاتورفيديبيدرو أوليفيراكولين ر. ليندسيفيونا إتش. بلاكهولماثيو ج. كريبسإيفون سامرزألكسندرا كليبسنجوناثان توغوودألاستير كيردومينيك جي. روثويلكارولين ديفهوجو جي دبليو إل آرتسرولاند ف. شوارزتوم ل. كوفمانغاريث أ. ويلسونراشيل روزنثالبيتر فان لونيكولاي ج. بيركباكزولتان ساللاسيجوديت كيسستوكماتيو سوكروبرتو سالغادوميكلوش ديوسيجوناس ديمولميسترأبيجيل بانكومأنجيلا دورنكألاستير ماغنيسأندرو ج. روانأنجيليكي كارامانيأنتونيا تونشيفابيني تشينكارلا كاستيجنانيكريستوفر أبوشكلير باتيككلير إي. ويدنكلوديا ليكورنتين ريتشاردكريسبين ت. هايليكريستينا ناصر-لومبارديليديفيد ر. بيرسديسبينا كاراجيانيذروبا بيسواسدينا ليفيإليزابيث لاروز كاديهإميليا ل. ليمإيما نايإيفا غرونروسفيلب غالفز-كانسينوفرانسيسكو خيمينيو-فالينتيجورج كاسيوتيسجورجيا ستافروجيراسيموس-ثيودوروس ماستروكالوسهيلين ل. لوإغناسيو غارسيا ماتوسعمران نورانيجاكي جولدمانجيمس ل. ريدينغجايانت ك. رانيجيروم نيكودجون أ. هارتليكارل س. بيغزكايتي إس. إس. إنفيلدكايلفيزي سيلفاراجوكيفن ليتشفيلدكيفن و. نجكيزونغ تشينكراين ديكستراكروبا ثاكرليا إنسيلمانسي شاهماريا ليتوفيتشينكومارينا ويرنر سندرلاندماثيو ر. هوسكاميشيل ديتزنميشيل م. ليونغميكائيل إسكوديروميهلا أنجيلوفاميلجانا تانيćنينانيا كانوأولغا تشيرفوفاأوليفيا لوكاسأوريول بيتشعثمان السوافبولينا بريماسفيليب هوبسونريتشارد كيفن ستونروبرت بينثامروبرت إي. هايندسروبرتو فيندرامينصادق صغافينياصموئيل غامبلسنغ كونغ أناكين أونغسيرجيو أ. كيزاداشارون فانلوسيمون زاكارياسونيا هيسيصوفيا ووردسيان هاريسستيفان بوينغستيفان بيكسوبريت كور بولاتمارا دينرتيريزا مارافيوتيتوماس ب. ك. واتكينزتوماس باتريك جونزفيكتوريا سبانزويكفيتوريو باربيوي-تينغ لوويليام هيلين وويوتاكا نايتوزوي رامسدنكاتارينا فيغاغاري رويالتشارلز-أنتوان كولينز-فيكيتفرانشيسكو فريوليبول آشوردمارتن د. فورسترسيو مينغ ليإلين بورغماري فالزونديونيسيوس باباداتوس-باستوسجيمس ويلسونتانيا أحمدألكسندر جيمس بروكترآسيا أحمدماجالي ن. تايلورأرجون نايرديفيد لورانسدافيد باترينينيل نافانيريكي م. ثاكراسام م. جاينزإميلي مارتينوني هوغنبوومفلور مونكجيمس و. هولدينجونيد شودريكونال باخريماركو سكارشيبات غورمانرينا خيروياروبرت سي إم ستيفنزيين نينغ صوفيا وونغزولتان كابلارستيف باندولاآن ماري هاكرأبيجيل شاربشون سميثهارجوت كور دهانداكاميللا بيلوتيراشيل ليزليأنكا غراپاهانيون زانغخالد عبدالجبارشياو شي بانين يين يوانديفيد تشوترمايريد ماكنزيسيرينا تشيأيمن الزتانيجوديث كافجينيفر ريتشاردزإريك ليمباولو دي سوزاسيمون جوردانألكسندرا رايسهيلغاردت راوبنهايمرهارشيل بهيانيلين أمبروزأناند ديفاراجهيما تشافانصوفينا بيغومسيلفيو I. بوديريدانيال كانيومفهو ماليمسارة بوثأندرو جي. نيكولسونناديا فرنانديزبراتيبا شاهكيارا بروليمادلين هيويشسارة دانسونمايكل ج. شاكلاوثليلي روبنسونبيتر راسلكيفن جي. بلايثأندرو كيدكريغ ديكجون لو كوينآلان كيركمو أسيفروكو بيليانشيانيكوس كوستولاسوماثيو توماس مستشفى سينجلتون، مجلس صحة جامعة سوانسي باي، سوانسي، المملكة المتحدة.مستشفيات جامعة ليستر NHS Trust، ليستر، المملكة المتحدة.كلية الطب في ليستر، جامعة ليستر، ليستر، المملكة المتحدة.جامعة ليستر، ليستر، المملكة المتحدة.مركز أبحاث السرطان، جامعة ليستر، ليستر، المملكة المتحدة.مؤسسة رويال فري لندن NHS، لندن، المملكة المتحدة.مستشفى أبردين الملكي NHS غرامبيان، أبردين، المملكة المتحدة.قسم الأورام الطبية، مستشفى أبردين الملكي NHS غرامبيان، أبردين، المملكة المتحدة.جامعة أبردين، أبردين، المملكة المتحدة.قسم الأمراض، مستشفى أبردين الملكي NHS غرامبيان، أبردين، المملكة المتحدة.مستشفى ويتينغتون NHS، لندن، المملكة المتحدة.مجموعة أبحاث الرعاية الحادة في برمنغهام، معهد الالتهاب والشيخوخة، جامعة برمنغهام، برمنغهام، المملكة المتحدة.مؤسسة غايز وسانت توماس NHS، لندن، المملكة المتحدة.مستشفى جامعة برمنغهام NHS Foundation Trust، برمنغهام، المملكة المتحدة.معهد المناعة والعلاج المناعي، جامعة برمنغهام، برمنغهام، المملكة المتحدة. بنك الأنسجة لمركز أبحاث السرطان في مانشستر، مانشستر، المملكة المتحدة.مستشفى ويذنشو، مؤسسة مانشستر الجامعية NHS، ويذنشو، المملكة المتحدة.مؤسسة مانشستر الجامعية NHS، مانشستر، المملكة المتحدة.قسم العدوى والمناعة وطب الجهاز التنفسي، جامعة مانشستر، مانشستر، المملكة المتحدة.مركز التميز لأبحاث سرطان الرئة في المملكة المتحدة، جامعة مانشستر، مانشستر، المملكة المتحدة.مؤسسة كريستي NHS، مانشستر، المملكة المتحدة.قسم علوم السرطان، جامعة مانشستر ومؤسسة كريستي NHS، مانشستر، المملكة المتحدة.مركز مؤشرات السرطان، معهد أبحاث السرطان في المملكة المتحدة، جامعة مانشستر، مانشستر، المملكة المتحدة.برنامج الذكاء الاصطناعي في الطب (AIM)، ماس جنرال بريغهام، كلية هارفارد الطبية، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية.قسم علاج الأورام بالإشعاع، مستشفى بريغهام والنساء، معهد دانا فاربر للسرطان، كلية هارفارد الطبية، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية.الأشعة والطب النووي، كاريم وغرو، جامعة ماستريخت، ماستريخت، هولندا.معهد بيولوجيا السرطان الحاسوبية، مركز الأورام المتكاملة (CIO)، مركز أبحاث السرطان كولونيا إيسن (CCCE)، كلية الطب ومستشفى جامعة كولونيا، جامعة كولونيا، كولونيا، ألمانيا.معهد برلين لأسس التعلم والبيانات (BIFOLD)، برلين، ألمانيا.معهد برلين لبيولوجيا الأنظمة الطبية، مركز ماكس ديلبروك للطب الجزيئي في جمعية هيلمهولتز (MDC)، برلين، ألمانيا.قسم الوراثة، مركز أندرسون للسرطان بجامعة تكساس، هيوستن، تكساس، الولايات المتحدة الأمريكية.قسم الطب الجينومي، مركز أندرسون للسرطان بجامعة تكساس، هيوستن، تكساس، الولايات المتحدة الأمريكية.مختبر جينوميات السرطان، معهد فرانسيس كريك، لندن، المملكة المتحدة.قسم الطب الجزيئي، مستشفى جامعة آرهوس، آرهوس، الدنمارك.قسم الطب السريري، جامعة آرهوس، آرهوس، الدنمارك.مركز أبحاث المعلوماتية الحيوية، جامعة آرهوس، آرهوس، الدنمارك.مركز أبحاث جمعية السرطان الدنماركية، كوبنهاغن، الدنمارك.برنامج المعلوماتية الصحية الحاسوبية، مستشفى الأطفال في بوسطن، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية.قسم المعلوماتية الحيوية، جامعة سملويس، بودابست، المجر.قسم علم الأمراض، مستشفيات زاس، أنتويرب، بلجيكا.قسم الأبحاث، مركز بيتر ماكولوم للسرطان، ملبورن، أستراليا.قسم فيزياء الأنظمة المعقدة، جامعة إلت إيوتفوس لوراند، بودابست، المجر.مختبر جينوميات السرطان التكاملية، مركز VIB لبيولوجيا السرطان، لوفين، بلجيكا.مركز VIB للذكاء الاصطناعي وعلم الأحياء الحاسوبي، لوفين، بلجيكا.قسم الأورام، جامعة KU لوفين، لوفين، بلجيكا.مجموعة أبحاث جينوميات السرطان الحاسوبية، معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.معهد فرانسيس كريك، لندن، المملكة المتحدة.الطب الجينومي، معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.مركز معلومات بيل ليونز، معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.علم الأمراض التجريبي، معهد فرانسيس كريك، لندن، المملكة المتحدة.قسم الأمراض المعدية، كلية الطب، إمبريال كوليدج لندن، لندن، المملكة المتحدة.مرافق التسلسل المتقدم، معهد فرانسيس كريك، لندن، المملكة المتحدة.قسم أمراض الدم، مستشفيات جامعة كوليدج لندن، لندن، المملكة المتحدة.وحدة مناعة السرطان، قسم أبحاث أمراض الدم، معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.مختبر جينوميات المناعة الورمية والمراقبة المناعية، معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.مجموعة المناعة الفيروسية العكسية، معهد فرانسيس كريك، لندن، المملكة المتحدة.المعلوماتية الحيوية وعلم الأحياء النظامية، تطوير المنهج والبنية التحتية للبحث، معهد روبرت كوخ، برلين، ألمانيا.علم الأورام التجريبي، معهد الأورام والأشعة في صربيا، بلغراد، صربيا.قسم علم الأوبئة والرعاية الصحية بجامعة كوليدج لندن، لندن، المملكة المتحدة.مستشفيات جامعة كوليدج لندن، لندن، المملكة المتحدة.قسم الطب الباطني الأول، مستشفى جامعة كولونيا، كولونيا، ألمانيا.مجموعة تنظيم المناعة والعلاج المناعي للورم، وحدة مناعة السرطان، قسم أبحاث أمراض الدم، معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.مختبر تطور السرطان وعدم استقرار الجينوم، معهد فرانسيس كريك، لندن، المملكة المتحدة.مركز حسابات الصور الطبية، قسم الفيزياء الطبية والهندسة الطبية الحيوية، جامعة كوليدج لندن، لندن، المملكة المتحدة.قسم الفيزياء الطبية والهندسة الحيوية، معهد السرطان بجامعة كوليدج لندن، لندن، المملكة المتحدة.قسم الفيزياء الطبية والهندسة الطبية الحيوية، جامعة كوليدج لندن، لندن، المملكة المتحدة.معهد الطب النووي، قسم الطب، جامعة كوليدج لندن، لندن، المملكة المتحدة.معهد البيولوجيا الهيكلية والجزيئية، جامعة كوليدج لندن، لندن، المملكة المتحدة.قسم الأشعة، مستشفيات جامعة كوليدج لندن، لندن، المملكة المتحدة.قسم التنفس، قسم الطب، جامعة كوليدج لندن، لندن، المملكة المتحدة.قسم جراحة الصدر، مستشفى جامعة كوليدج لندن NHS Trust، لندن، المملكة المتحدة.مركز أبحاث الرئة للحياة، قسم التنفس، جامعة كوليدج لندن، لندن، المملكة المتحدة.قسم الطب الصدري، مستشفيات جامعة كوليدج لندن، لندن، المملكة المتحدة.مركز أبحاث الرئة للحياة، قسم التنفس، قسم الطب، جامعة كوليدج لندن، لندن، المملكة المتحدة.قسم الأشعة المتكاملة، مستشفى سانت جون المركزي، شمال بودا، بودابست، المجر.معهد الطب النووي، مستشفيات جامعة كوليدج لندن، لندن، المملكة المتحدة.معهد أبحاث السرطان، لندن، المملكة المتحدة.Case45، لندن، المملكة المتحدة.مركز أندرسون للسرطان بجامعة تكساس، هيوستن، الولايات المتحدة الأمريكية.صوت مرضى السرطان المستقل، لندن، المملكة المتحدة.مستشفى جامعة ساوثهامبتون NHS Foundation Trust، ساوثهامبتون، المملكة المتحدة.قسم الأورام، مستشفى جامعة ساوثهامبتون NHS Foundation Trust، ساوثهامبتون، المملكة المتحدة.القسم الأكاديمي لجراحة الصدر، إمبريال كوليدج لندن، لندن، المملكة المتحدة.مستشفيات رويال برومبتون وهارفيلد، جزء من NHS Foundation Trust لغي وسانت توماس، لندن، المملكة المتحدة.المعهد الوطني للقلب والرئة، إمبريال كوليدج، لندن، المملكة المتحدة.مستشفى رويال ساري، NHS Foundation Trust لمستشفيات رويال ساري، غيلدفورد، المملكة المتحدة.جامعة ساري، غيلدفورد، المملكة المتحدة.جامعة شيفيلد، شيفيلد، المملكة المتحدة.مستشفيات شيفيلد التعليمية NHS Foundation Trust، شيفيلد، المملكة المتحدة.مستشفى ليفربول للقلب والصدر، ليفربول، المملكة المتحدة.مستشفى الأميرة ألكسندرا، NHS Trust لمستشفى الأميرة ألكسندرا، هارلو، المملكة المتحدة.مدرسة علوم السرطان، جامعة غلاسكو، غلاسكو، المملكة المتحدة.معهد بيتسون لأبحاث السرطان، جامعة غلاسكو، غلاسكو، المملكة المتحدة.مستشفى الملكة إليزابيث الجامعي، غلاسكو، المملكة المتحدة.معهد العدوى والمناعة والالتهاب، جامعة غلاسكو، غلاسكو، المملكة المتحدة.NHS غلاسكو الكبرى وكلايد، غلاسكو، المملكة المتحدة.معهد أبحاث السرطان في اسكتلندا، غلاسكو، المملكة المتحدة.معهد علوم السرطان، جامعة غلاسكو، غلاسكو، المملكة المتحدة.قسم علم الأمراض في NHS غلاسكو الكبرى وكلايد، مستشفى الملكة إليزابيث الجامعي، غلاسكو، المملكة المتحدة.مستشفى الذكرى الذهبية الوطنية، كلايدبانك، المملكة المتحدة.
طرق
توصيف خط الأساس لعينات سرطان الرئة
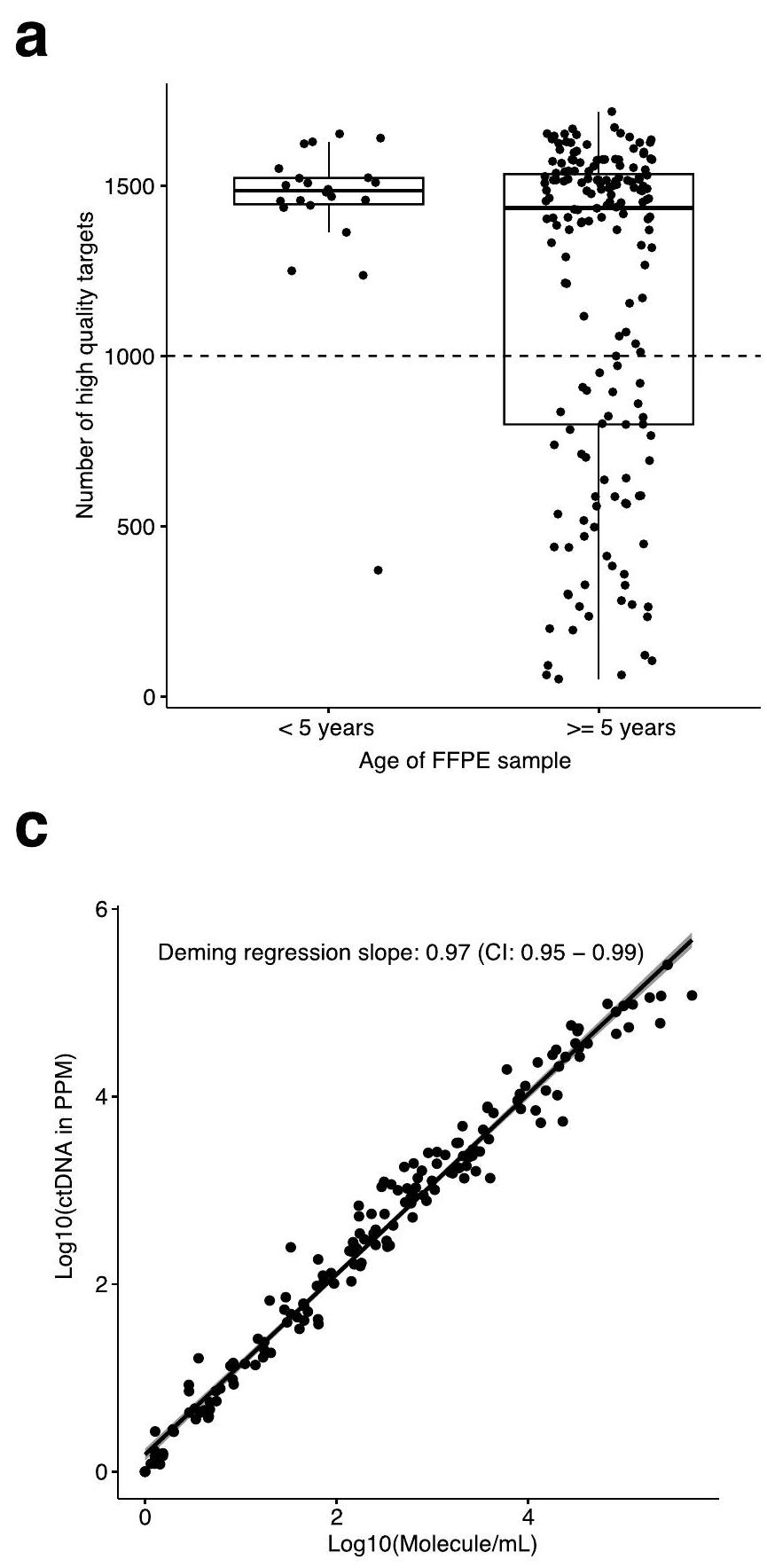
تمت مراعاة جميع اللوائح الأخلاقية ذات الصلة في تجنيد المرضى وجمع العينات في دراسة TRACERx كما تم وصفها سابقًا.. تم وصف معايير الأهلية سابقًا.. من الجدير بالذكر أنه تم استخدام النسخة الثامنة من تصنيف pTNM في هذا التحليل. تم تسجيل المرضى الذين تم تأكيد إصابتهم بالمرحلة I-IIIB من سرطان الرئة غير صغير الخلايا والذين كانوا مؤهلين للجراحة الأولية في دراسة TRACERx المراقبة الاستباقية (ClinicalTrials.gov المعرف: NCT01888601). تم الموافقة على تصميم الدراسة من قبل لجنة أخلاقيات البحث المستقلة (لجنة NRES لندن، مرجع REC 13/ LO/1546)، وتم الحصول على موافقة مستنيرة من جميع المرضى قبل دخول الدراسة. تم إخفاء هوية معرفات عينات المرضى وتم تتبعها في قاعدة بيانات مركزية تحت سيطرة راعي الدراسة. يمكن أن تؤثر تدهور الحمض النووي للعينات المحفوظة في الفورمالين والمثبتة بالشمع (FFPE) مع مرور الوقت على جودة اللوحة لاكتشاف ctDNA، وقد لا تعكس العينات المتدهورة بدقة جودة العينة النموذجية في بيئة سريرية حيث تم جمع عينات FFPE مؤخرًا (الشكل الممتد 4a). حصلنا على أنسجة FFPE لـ 204 مرضى. من بين هؤلاء، كان لدى 62 عدد غير عادي من أهداف اللوحة عالية الجودة ( )، على الأرجح بسبب العمر و/أو جودة عينات FFPE الضعيفة، واثنان لم يجتازا تصميم اللوحة. بالنسبة لـ 31 من 64 مريضًا، كانت هناك عينات من الحمض النووي المستخرج من الأنسجة المجمدة الطازجة (FF) متاحة بحلول سبتمبر 2023. لهذه العينات، تم إنشاء مجموعة محدثة من اللوحات، كانت جودتها أكثر اتساقًا مع عينات FFPE التي تقل أعمارها عن 5 سنوات (الشكل البياني الممتد 4b). تم بناء لوحة واحدة من عينة ورم FF وفشلت في تحقيق 1000 هدف عالي الجودة؛ ومع ذلك، تم تضمينها لضمان أن تكون المجموعة تمثل مجموعة TRACERx الأوسع. تم بناء لوحتين FF حيث فشل بناء لوحة FFPE تمامًا. كانت المجموعة النهائية في دراستنا تتكون من عينات ما قبل الجراحة من 171 مريضًا تم تجنيدهم بشكل متتابع في دراسة TRACERx الأكبر، حيث كانت هناك بلازما كافية متاحة لتحليل ctDNA الذي اكتمل بحلول سبتمبر 2023، بالإضافة إلى بيانات النتائج السريرية المؤكدة حتى فبراير 2024. تم إجراء تحليل ctDNA بأثر رجعي باستخدام عينات تم جمعها بشكل استباقي وأثناء المتابعة السريرية. في هذه المجموعة، أظهرنا أن قياسنا لإشارة ctDNA (ppm) كان متوافقًا بشدة مع جزيئات الورم لكل مل من البلازما، والتي تأخذ في الاعتبار حجم البلازما الذي يتم استخراج cfDNA منه (انحدار ديمينغ؛ الميل الملائم=0.97، CI= 0.95-0.99؛ الشكل البياني الممتد 4c). كان الباحثون في Personalised معزولين تمامًا عن نتائج المرضى السريرية وخصائصهم السريرية المرضية أثناء معالجة العينات وتحليل ctDNA. وبالمثل، كان الباحثون في TRACERx معزولين عن حالة ctDNA للمرضى أثناء جمع البيانات السريرية وعينات المرضى. تم توثيق طفرات EGFR، وأشكال الاندماج السرطانية، وحالات تخطي إكسون 14 من MET من مرضى مجموعة TRACERx كما تم وصفه سابقًا..
تسلسل الجينوم الكامل للورم والطبيعي
تمت إزالة أقسام الورم بشكل ماكرو لتحسين محتوى الورم وكان من الضروري أن تلبي عتبة كثافة الخلايا الورمية، كما تحدده المراجعة المرضية، لتكون مؤهلة لاستخراج الحمض النووي والمعالجة اللاحقة. عند هذا العتبة، (2/171) من العينات اعتُبرت غير مؤهلة للتحليل واحتاجت إلى استبدالها بعينات مختلفة. في اختيارنا عند عتبة القطع، لم نلاحظ أي ارتباط كبير بين نقاء الورم وحدود الكشف (LOD) للاختبار (الشكل التوضيحي 1). تم عزل الحمض النووي الجينومي من عينات الورم والعينات الطبيعية المتطابقة باستخدام مجموعة Qiagen AllPrep DNA/RNA FFPE Tissue Kit أو مجموعة QIAamp DNA Mini Kit (Qiagen) باستخدام سير عمل محسن داخليًا. تم إعداد مكتبات تسلسل الجينوم الكامل (WGS) باستخدام 100-500 نانوغرام من الحمض النووي الجينومي المقطوع صوتيًا (Covaris) باستخدام مجموعة KAPA HyperPrep Kit (Roche Sequencing Solutions) وطرق مخصصة. تم تنظيف المكتبات باستخدام كرات AMPure XP ثم تم قياس كميتها باستخدام مجموعة KAPA Library Quantification Kit (Roche Sequencing Solutions)، قبل أن يتم تسلسلها إلىعمق التغطية باستخدام جهاز NovaSeq 6000 (إيلومينا). التأثير تم تقييم تأثير كميات مدخلات الحمض النووي المتغيرة خلال تسلسل الجينوم الكامل للأورام على تصميم اللوحة باستخدام 19 زوجًا من الأنسجة الطبيعية والأورام. بالنسبة لكل زوج، تم إعداد مكتبات الأنسجة الطبيعية باستخدام 550 نانوغرام من الحمض النووي المدخل، ومكتبات الأورام باستخدام، أو 550 نانوغرام من الحمض النووي المدخل. لاحظنا حجم اللوحة المتسق إلى حد كبير والتشابه عبر نطاق كميات الحمض النووي المدخل (الشكل التكميلية 2أ، ب). قائمة شاملة بالمواد المستخدمة في هذه الدراسة متاحة في الجدول التكميلية 1.
محاذاة واستدعاء المتغيرات من تسلسل الجينوم الكامل للورم والطبيعي
تقوم الأنبوبة بأداء المحاذاة، وإزالة التكرارات، وإعادة معايرة جودة درجات القاعدة (BQSR) لعينات تسلسل الجينوم الكامل (WGS) المتطابقة من الورم والطبيعي باستخدام إرشادات الممارسات الأفضل الموصى بها من معهد برود.باختصار، تم أولاً تعيين أزواج القراءة الفردية إلى بناء الجينوم المرجعي hs37d5 باستخدام محاذي BWA-MEM. ثم استخدمنا مجموعة أدوات Picard (RRID: SCR_006525) لتحديد القراءات المكررة من خلال مقارنة تمت إزالة القراءات المكررة بعد ذلك. تم استخدام مجموعة أدوات تحليل الجينوم (GATK، RRID: SCR_001876) لإعادة محاذاة التسلسل وتطبيق درجات جودة القاعدة (BQSR): تستخدم أداة BaseRecalibrator البيانات التي تم إزالة التكرار منها ومجموعة من المتغيرات المعروفة لبناء نموذج للتغاير، والذي يستخدم بعد ذلك لإنشاء ملف إعادة المعايرة. ثم تستخدم أداة ApplyBQSR هذا النموذج لضبط درجات جودة القاعدة في البيانات، مما ينتج عنه ملف BAM جديد. يتم كتابة بيانات التسلسل المحاذاة بتنسيق BAM وفقًا لمواصفات SAM (RRID: SCR_01095). تم استخدام MuTect (RRID: SCR_000559) لتحليل ملفات BAM الخاصة بالورم والطبيعي معًا لاكتشاف المتغيرات الأحادية النوكليوتيدية الجسدية (SNV). تم تصفية استدعاءات SNV الجسدية بناءً على مجموعة واسعة من مقاييس مراقبة الجودة، مثل تغطية التسلسل المحلية وجودة القراءة، والانحياز الاتجاهي والاحتمالية الإحصائية لوجود الأليل في العينة الطبيعية.
تصميم لوحة استكشاف شخصية NeXT
تم تصميم لوحات مجسات الالتقاط الهجينة المستخدمة في هذه الدراسة باستخدام خوارزميات منصة NeXT Personal المملوكة، كما هو محدد في إجراءات التشغيل القياسية في شركة Personalis. في عملية تصميم اللوحة المخصصة، تم اختيار أهداف ctDNA لكل لوحة مريض من المتغيرات الجسدية الموجودة في المناطق الإكسونية، والداخلية، وبين الجينية التي تم تحديدها من خلال تسلسل الجينوم الكامل لعينة الورم والعينة الطبيعية المتطابقة، كما هو موضح أعلاه. تم اختيار المتغيرات الجسدية التي تم تحديدها باستخدام Mutect (الإصدار 1.1.6، مع المعلمات الافتراضية) وتم تعيين معدل خطأ لها وفقًا للاستبدال الملحوظ في الورم الصلب. على وجه التحديد، تم تقدير معدل خطأ الاستبدال من خلال نسبة الكمية المجمعة من الإشارة إلى العدد الإجمالي للجزيئات التي تم ملاحظتها في كل استبدال محتمل في أكثر من 200 عينة بلازما صحية.تم اختيار أهداف MRD بعد ذلك من المتغيرات الجسدية ذات تردد الأليل فوق. تم تصفية المتغيرات بشكل إضافي من خلال استبعاد تلك الموجودة في مناطق معينة من الجينوم. شملت معايير الاستبعاد المناطق التي تحتوي على SNPs معروفة في الخط الجرثومي، ومتغيرات CHIP المعروفة، ومحتوى GC العالي (نسب تعدد الأشكال العالية، صعوبات في التحديد، انحياز منهجي، تكرارات قصيرة متجاورة، وانخفاض تعقيد التسلسل.
تم تصنيف استدعاءات المتغيرات الجسدية بناءً على حاصل ضرب تردد الأليل في الورم الصلب ومعدل الخطأ القائم على الاستبدال لاستبدالات الورم الصلب. حتىتم اختيار أعلى المتغيرات الجسدية تصنيفًا على مستوى الجينوم لإدراجها في اللوحة من قبل منصة NeXT Personal. كما شملت اللوحة النهائية 43 متغيرًا أحادي النوكليوتيد سكانيًا لأغراض ضمان الجودة (أي للكشف عن أي عدم تطابق محتمل بين العينة واللوحة أو التلوث). تم استخدام عدة معايير لتحسين اختيار الـ 43 متغيرًا أحادي النوكليوتيد، بما في ذلك وجود تردد سكاني لا يقل عن، كونها في توازن هاردي-واينبرغ وخارج منطقة HLA. تم إعطاء الأولوية لـ SNPs لتكون لها تمثيل متساوٍ تقريبًا عبر المجموعات السكانية الفرعية. تم تصميم تسلسلات البروب بواسطة خوارزمية خاصة بمنصة NeXT Personal قبل أن يتم معالجتها للتصنيع. عند استلام كواشف اللوحة، تم استخدام اللوحة الجديدة للتسلسل المستهدف للدم. البلازما من متبرع صحي غير مرتبط. وقد خدم هذا غرضين: تم استخدام اختبارات مراقبة الجودة على بيانات التسلسل لتأهيل اللوحة لاستخدامها على عينات بلازما المريض، وأي أهداف لمستويات المرض الدقيقة (MRD) تم ملاحظة أي إشارة غير مرجعية لها تم تعطيلها في تصميم اللوحة المنطقي، لتقليل خطر أن يتم تعزيز تلك الأهداف بالضوضاء.
تحضير مكتبة cfDNA الشخصية من NeXT، إثراء الهدف والتسلسل
تم إعداد مكتبات التسلسل، وإثراء الأهداف، وتسلسل عينات cfDNA في مختبرات معتمدة من CLIA وCAP، وفقًا لإجراءات التشغيل القياسية في شركة Personalis. باختصار، تم إعداد مكتبات التسلسل منمدخل cfDNA (الوسيط، 15 نانوغرام)، باستخدام مجموعة KAPA HyperPrep (حلول تسلسل روش) وطرق مخصصة. قمنا بتقييم تأثير كمية المدخل الكلي لـ cfDNA على اكتشاف MRD وحمولة ctDNA ولاحظنا عدم وجود ارتباطات ذات دلالة إحصائية بين كمية مدخل cfDNA وحالة اكتشاف ctDNA (الشكل التكميلي 3). بشكل متسق، لم يكن هناك ارتباط ذو دلالة إحصائية بين كمية cfDNA المدخلة وحمولة ctDNA أو بين حمولة ctDNA وحدود الكشف للاختبار (الشكل التكميلي 3ب، ج). معًا، تشير هذه الأدلة إلى أن حمولة ctDNA وحالة الاكتشاف لم تتأثر بكمية الحمض النووي الدائري الكلي في المجموعة. تدعم هذه النتائج دراسة تحقق تحليلية منفصلة.تم قياس المكتبات قبل الالتقاط باستخدام مقياس الطيف الضوئي Lunatic (Unchained Labs)، وحتىتم إثراءه بألواح مجسات NeXT الشخصية المحددة للمرضى باستخدام تعديلات خاصة على مجموعة التهجين السريع والغسل (Twist Bioscience) وسير العمل. ثم تم تضخيم المكتبات بعد الالتقاط بواسطة PCR (تسع دورات)، وتم إجراء تقييم للجودة باستخدام نظام TapeStation (Agilent Technologies). تم تنظيف المكتبات النهائية باستخدام كرات AMPure XP ثم تم قياس كميتها باستخدام مجموعة قياس المكتبات KAPA (Roche Sequencing Solutions) قبل أن يتم تسلسلها على جهاز NovaSeq 6000 (Illumina). تم تسلسل المكتبات بعمق لتحسين عدد الجزيئات الفريدة الملاحظة. لاحظنا ارتباطًا ضعيفًا بين عمق التسلسل وحدود الكشف (LOD) لكل اختبار مخصص، وكذلك بين عمق التسلسل وقوة إشارة ctDNA المكتشفة (مستوى ppm)؛ ومع ذلك، لم يكن وضع اكتشاف ctDNA (مكتشف أو غير مكتشف) متأثرًا بتقلب عمق التسلسل، مع عدم وجود فرق كبير في عمق التسلسل بين المجموعتين (الشكل التوضيحي التكميلي 4a-c).
تحليل cfDNA الشخصي من NeXT
تم إجراء تحليل جميع بيانات NeXT Personal في هذه الدراسة باستخدام نسخة ثابتة ومتسقة من خط الإنتاج الذي طورته شركة Personalis. باختصار، تم محاذاة بيانات تسلسل cfDNA إلى الجينوم البشري المرجعي (الإصدار hs37d5)، تلاها تقليل الضوضاء واكتشاف ctDNA. بشكل أكثر تحديدًا، قمنا ببناء وتصنيف الإجماع الجزيئي على النحو التالي. أولاً، قمنا بمحاذاة جميع القراءات إلى المرجع البشري باستخدام BWA-MEM (محاذي باروز-ويلر، الإصدار 1.0.2). ثانيًا، قمنا بتجميع أزواج القراءات وفقًا لمواقعها المرسومة المزدوجة لتشكيل مجموعات الإجماع الأولية. مع وجود نهج موضعي مثل هذا، هناك خطر من تجميع جزيئات متعددة معًا تشترك في مواقع مرسومة مزدوجة. لقد خففنا من هذا الخطر من خلال اكتشاف وجود أليلات غير مرجعية كانت موجودة ليس فقط في مجموعة فرعية من قراءات مجموعة الإجماع، ولكن أيضًا في مجموعتين أخريين على الأقل من مجموعات الإجماع. عندما كان هناك أليل موجود في مجموعة فرعية من القراءات مع دعم إضافي من مجموعات إجماع أخرى، قمنا بتقسيم مجموعة الإجماع لعزل القراءات التي تحتوي على الأليل في مجموعتها الجديدة الخاصة. بالنسبة لكل مجموعة، تطلبنا ملاحظة ما لا يقل عن جزيء واحد من كل شريط DNA. كانت القراءات الخام التي تختلف بأكثر منلم يتم تضمين الجزيئات المتسقة عبر الجزيء المتسق. تم إخفاء القواعد ذات الجودة الأقل من 29. بمجرد أن حددنا مجموعات التوافق، قمنا بتشكيل جزيء متسق واحد من القراءات في كل مجموعة بناءً على تحديد قاعدة التوافق في كل موضع على طول مجموعة أزواج القراءة. القواعد التي تحتوي على أقل منتم إخفاء الاتفاق في المجموعة الجزيئية. تمت إزالة القراءات التي تحتوي على أكثر من 20% من قواعدها مخفية. ثم، قمنا بإعادة رسم هذه القراءات التوافقية مرة أخرى باستخدام BWA-MEM لتجنب أي محاذاة خاطئة ناجمة عن أخطاء التسلسل. بعد تقليل الضوضاء، تم تجميع الإشارة المستمدة من الورم في عينة مختبرة عبر أهداف ctDNA في كل لوحة خاصة بالمريض لحساب مستوى ctDNA (المقاس بوحدات ppm، بناءً على إجمالي عدد الجزيئات الفريدة). ثم تم إجراء اختبار بواسون أحادي الجانب لتحديد حالة اكتشاف ctDNA لكل عينة مختبرة. تعتبر الإشارة المستمدة من الورم المجمعة الملحوظة عبر كل لوحة هي القيمة المختبرة، مع تعيين الضوضاء المتوقعة الناجمة عن تراكم الأخطاء الخلفية كمتوسط توزيع بواسون.تم تحديد عتبة القيمة كما تم وصفها سابقًا. باختصار، الـتم تعيين عتبة القيمة عند <0.001 لضمان تلبية متطلبات الخصوصية التحليلية لـتمت مقابلته. لذلك، الـتم تحديد عتبة القيمة عند 0.001 لهذه الدراسة لضمان دقة أعلى. إذا كان إشارة الورم بشكل ملحوظفوق الضوضاء المتوقعة، تم تصنيف العينة على أنها إيجابية لـ ctDNA (أي ‘تم الكشف عنها’)؛ وإلا، تم تصنيفها على أنها سلبية لـ ctDNA (أي ‘لم يتم الكشف عنها’). نظرًا لأن القيمة هي احتمال أن الإشارة المرصودة تأتي من الضوضاء، ويتم ضبط عتبة الكشف لفرض متطلبات الخصوصية وهي مستقلة عن العوامل التي تؤثر على المستويات المرصودة. قد تؤثر التغيرات في عوامل الاختبار والعوامل المحددة للموقع على كفاءة الكشف عن تغيير جيني معين. قد تكون التغيرات الجينية المختلفة موجودة أيضًا بترددات مختلفة في الدم. المستوى الفعلي للجزء في المليون (تردد الأليل) المقاس هو دالة لمجموعة الأهداف المختارة. ومع ذلك، بعد التجميع عبر العديد من المواقع، تميل الكفاءة المتوسطة لكل موقع في الكشف نحو المتوسط السكاني لكفاءة الكشف عن تغيير جيني معين. يتم توضيح ذلك في الشكل التوضيحي 5a، الذي يظهر أنه مع اقتراب حجم اللوحة من 1,800 هدف، فإن معامل التباين (CV) لمستوى الجزء في المليون المرصود يضيف القليل إلى التباين العام للاختبار. يعتمد وضع الكشف على القيمة، بدلاً من عتبة تردد الأليل، سمحت لطريقتنا بتطبيع كفاءة الكشف عن طفرات محددة من خلال جمع الإشارة عبر ما يصل إلى 1,800 موقع متغير تم اختيارها بناءً على معدلات الخطأ المحددة للموقع، والضوضاء الفطرية، والتعقيد.
تكوين الدم النسلي ذو الإمكانية غير المحددة
قمنا بتصميم اختبارنا لمنع تضمين طفرات CHIP في اللوحة المخصصة من خلال اتباع نهج مطابق للورم-الطبيعي لاستدعاء المتغيرات الجسدية لإبلاغ تصميم اللوحة. هذه طريقة فعالة لأن إشارة CHIP تكون أعلى في خلايا الدم الطبيعية مقارنةً بأنسجة الورم، وبالتالي سيتم تصفيتها في المقارنة الخوارزمية بين الورم والطبيعي. كما استبعدنا أكثر مناطق CHIP شيوعًا من تصميم لوحتنا.
استخراج وقياس cfDNA في TRACERx
تم جمع عينات الدم في-أنابيب EDTA. تم معالجة العينات خلال ساعتين من الجمع عن طريق الطرد المركزي المزدوج للدم، أولاً لمدة 10 دقائق عندثم البلازما لمدة 10 دقائق فيتم تخزين البلازما فيعينات عند. بعد العزل، تم شحن البلازما على الثلج الجاف. في وقت التحليل، كانت عينات بلازما TRACERx تتراوح أعمارها بين 2 و 9 سنوات. قبل 24 ساعة من استخراج cfDNA، تم إذابة البلازما وتم دمج عينات من نفس نقطة زمنية لبلازما المريض ثم تم تخزينها في. مباشرة قبل استخراج cfDNA باستخدام مجموعات QIAamp Circulating Nucleic Acid أو QIAsymphony Circulating DNA (Qiagen)، تم توضيح البلازما المجمعة عند لإزالة الكريوبريسيبيتيت.
عينات مستخدمة لتوصيف أداء إدخال الحمض النووي
تم إجراء جميع التجارب في مختبرات معتمدة من تعديلات تحسين المختبرات السريرية (CLIA) ومعتمدة من كلية أطباء الأمراض الأمريكية (CAP) في شركة بيرسوناليس، كما هو موضح بواسطة
توصيات الجمعية الأمريكية لعلم الأمراض الجزيئي (AMP) وCAP المشتركةتم الحصول على أنسجة المتبرعين والمرضى الصحية وعينات البوفيه والبلasma المطابقة المستخدمة في الأشكال التكميلية 2 و 5 من Boca Biolistics أو Cureline أو iProcess. تم جمع عينات المرضى في هذه الدراسة من بائعين تجاريين من مرضى مطلعين بعد استلام موافقتهم الخطية وفقًا لبروتوكولات الدراسة المعتمدة من لجنة أخلاقيات مستقلة أو مجلس مراجعة مؤسسي (أرقام البروتوكول: PG-ONC 2003/1؛ IRB7 – التسجيل 5136؛ IRB 800959).
تحليلات البقاء
تم تعريف OS على أنه الأيام من التسجيل حتى الوفاة أو فقدان المتابعة. تم تعريف RFS على أنه الأيام من التسجيل حتى أي تكرار للمرض، أو أحداث ورم أولي جديد، أو الوفاة. تم إجراء تحليل استكشافي يقارن بين OS و RFS عند مستويات مختلفة من ctDNA لعدد إجمالي من 171 مريضًا كما هو موضح في الشكل 2 والشكل الإضافي 3. تم استخدام حزم R مثل survival (3.3-1) و survminer (0.4.9) و finalfit (1.0.4) لتوليد نسب المخاطر، وفترات الثقة، واحتمالية البقاء لمدة عامين، ومخططات الغابات، ومخططات KM، ونماذج الانحدار Cox. تم تقييم الفروق في OS أو RFS بين مجموعات مختلفة من المرضى باستخدام اختبارات log-rank. تم تقييم ارتباط OS أو RFS بالمتغيرات المستمرة، مثل مستوى ctDNA، من خلال نمذجة الانحدار Cox. تم تقييم القيمة التنبؤية المستقلة لـ ctDNA سواء في الشكل المستمر أو الفئوي من خلال نماذج الانحدار المتعددة المتغيرات التي شملت علم الأنسجة، وحالة العلاج المساعد، وحالة التدخين، والمرحلة المرضية، والعمر.
التحليل الإحصائي ومعالجة البيانات
لم يتم استخدام أي طرق إحصائية لتحديد حجم العينة مسبقًا. تم إجراء التحليل في البيئة الإحصائية (4.1.3). كانت جميع الاختبارات الإحصائية ثنائية الاتجاه، ما لم يُذكر خلاف ذلك. بالنسبة لتحليلات أداء الاختبار، تم حساب القيمة التنبؤية الإيجابية على أنها جميع النتائج الإيجابية الحقيقية مقسومة على مجموع النتائج الإيجابية الحقيقية والنتائج الإيجابية الكاذبة؛ وتم حساب القيمة التنبؤية السلبية على أنها جميع النتائج السلبية الحقيقية مقسومة على مجموع النتائج السلبية الكاذبة بالإضافة إلى النتائج السلبية الحقيقية؛ وتم حساب الحساسية على أنها النتائج الإيجابية الحقيقية مقسومة على مجموع النتائج الإيجابية الحقيقية والنتائج السلبية الكاذبة؛ وتم حساب الخصوصية على أنها النتائج السلبية الحقيقية مقسومة على مجموع النتائج السلبية الحقيقية والنتائج الإيجابية الكاذبة. بالنسبة لعمليات الإدخال والإخراج ومعالجة البيانات العامة، تم استخدام حزم R tidyverse (v1.3.2) و lubridate (v1.9.2). بالنسبة للتصور العام، تم استخدام حزم R ggplot2 (v.3.4.2) و ggpubr (v.0.4.0) و scales (v.1.2.1.) و ggnewscale (v.0.4.9). بالنسبة للتحليلات الإحصائية والتصورات ذات الصلة، تم استخدام حزم R survival (v.3.3-1) و survminer (v.0.4.9) و finalfit (v.1.0.4) و gt (v.0.10.1) و mcr (v.1.2.2).
ملخص التقرير
معلومات إضافية حول تصميم البحث متاحة في ملخص تقرير Nature Portfolio المرتبط بهذه المقالة.
توفر البيانات
تم إيداع بيانات مرضى TRACERx المعالجة على Zenodo في https://doi.org/10.5281/zenodo. 8400837 (مرجع 34). تتضمن البيانات الداعمة من تجارب التحقق كجدول بيانات إضافي 1. تم إيداع البيانات الخام من مرضى TRACERx الذين تم تحليلهم في هذه الدراسة، بما في ذلك ملفات fastq و bam من ورم و WGS طبيعي، بالإضافة إلى ملفات fastq من cfDNA، في أرشيف الجينوم والظاهرة الأوروبي (EGA)، الذي يستضيفه المعهد الأوروبي للمعلوماتية الحيوية (EBI) ومركز تنظيم الجينوم (CRG) تحت رموز الوصول EGAS00001006494، تحت وصول محكوم.
توفر الشيفرة
الشيفرة الداعمة المطلوبة لإعادة إنتاج جميع التحليلات والأشكال المدرجة في هذه الورقة متاحة على Zenodo في https://doi.org/ 10.5281/zenodo. 8400837 (مرجع 34).
References
Frankell, A. M. et al. The evolution of lung cancer and impact of subclonal selection in TRACERx. Nature 616, 525-533 (2023).
Van der Auwera, G. A. & O’Connor, B. D. Genomics in the Cloud: Using Docker, GATK, and WDL in Terra (O’Reilly Media, 2020).
DePristo, M. A. et al. A framework for variation discovery and genotyping using next-generation DNA sequencing data. Nat. Genet. 43, 491-498 (2011).
Freeman, T. M. et al. Genomic loci susceptible to systematic sequencing bias in clinical whole genomes. Genome Res. 30, 415-426 (2020).
Jennings, L. J. et al. Guidelines for validation of next-generation sequencing-based oncology panels: a joint consensus recommendation of the Association for Molecular Pathology and College of American Pathologists. J. Mol. Diagn. 19, 341-365 (2017).
Black, J. An ultra-sensitive and specific ctDNA assay provides novel pre-operative disease stratification in early stage lung adenocarcinoma. Zenodo https://doi.org/10.5281/zenodo. 8400837 (2024).
الشكر والتقدير
نشكر موظفي مرفق التسلسل المتقدم في معهد فرانسيس كريك، بالإضافة إلى أعضاء اتحاد TRACERx على مساهماتهم في هذه الدراسة. TRACERx (ClinicalTrials.gov رقم: NCTO1888601) برعاية كلية لندن الجامعية (UCL/12/0279) وتمت الموافقة عليه من قبل لجنة أخلاقيات البحث المستقلة (REC 13/LO/1546). يتم تمويل TRACERx من قبل أبحاث السرطان في المملكة المتحدة (CRUK؛ C11496/A17786) ويتم تنسيقه من قبل CRUK ومركز تجارب السرطان في UCL، الذي لديه منحة أساسية من CRUK (C444/ A15953). نحن نقدر بامتنان المرضى والأقارب الذين شاركوا في دراسة TRACERx؛ جميع موظفي الموقع، والمحققين، والممولين، وشركاء الصناعة الذين دعموا توليد البيانات ضمن هذه الدراسة. تم دعم هذا العمل أيضًا من قبل مركز تميز سرطان الرئة CRUK وجائزة مركز مدينة لندن CRUK (C7893/A26233) بالإضافة إلى مركز أبحاث السرطان التجريبية في UCL. نحن نقدر فريق البحث والتطوير في Personalis لعملهم في تطوير والتحقق من صحة منصة NeXT Personal، بما في ذلك المساهمات الرئيسية من J. Li و A. Stram. نحن نقدر أيضًا فريق عمليات Personalis لمساعدتهم في معالجة العينات باستخدام NeXT Personal. T.K. مدعوم من قبل برنامج زمالات البحث الخارجي لجمعية اليابان لتعزيز العلوم (JSPS) (202060447). M.J.-H. هو زميل CRUK وقد حصل على تمويل من CRUK و NIHR و Rosetrees Trust و UKI NETs ومركز أبحاث جامعة لندن الجامعية. N.M. هو زميل سير هنري ديل، ممول بشكل مشترك من قبل مؤسسة ويلكوم والجمعية الملكية (211179/Z/18/Z)، ويتلقى أيضًا تمويلًا من CRUK و Rosetrees Trust و NIHR BRC في مستشفيات جامعة لندن الجامعية و CRUK مركز أبحاث السرطان التجريبية في جامعة لندن. C.S. هو أستاذ أبحاث الجمعية الملكية نابير (RSRPR210001). يتم دعم عمله من قبل معهد فرانسيس كريك، الذي يتلقى تمويله الأساسي من أبحاث السرطان في المملكة المتحدة (CC2041)، ومجلس الأبحاث الطبية في المملكة المتحدة (CC2041) ومؤسسة ويلكوم (CC2041). لغرض الوصول المفتوح، قام المؤلف بتطبيق ترخيص حقوق الطبع والنشر CC BY العامة على أي نسخة مخطوطة مقبولة من المؤلف ناتجة عن هذا التقديم. يتم تمويل C.S. من قبل أبحاث السرطان في المملكة المتحدة (TRACERx (C11496/A17786)، PEACE (C416/A21999) وشبكة CRUK لعلاج السرطان المناعي)؛ مركز تميز سرطان الرئة CRUK (C11496/ A30025)؛ Rosetrees Trust و Butterfield و Stoneygate Trusts؛ مؤسسة NovoNordisk (ID16584)؛ جائزة تعزيز أستاذية الجمعية الملكية (RP/EA/180007 و RFERE231118))؛ المعهد الوطني للبحوث الصحية (NIHR) مركز أبحاث جامعة لندن الجامعية؛ مركز أبحاث السرطان في المملكة المتحدة – جامعة لندن الجامعية؛ مركز أبحاث السرطان التجريبية
؛ مركز أبحاث سرطان الثدي (الولايات المتحدة) (BCRF-22-157)؛ جائزة أبحاث الكشف المبكر والتشخيص من أبحاث السرطان في المملكة المتحدة (منحة EDDPMA-Nov21/100034)؛ وجائزة Aspire من مؤسسة مارك لأبحاث السرطان (منحة 21-029-ASP) وجائزة ASPIRE Phase II (منحة 23-034-ASP). حصل C.S. على منحة متقدمة من ERC (PROTEUS) من المجلس الأوروبي للبحث بموجب برنامج أفق 2020 للبحث والابتكار التابع للاتحاد الأوروبي (رقم اتفاقية المنحة 835297).
مساهمات المؤلفين
صمم J.R.M.B. و C.S. الجزء السريري من الدراسة. قام S.V. و M.C. بتنسيق التعامل مع العينات السريرية. قام J.R.M.B. و M.S.H. و K.T. و A.H. و C.B. و E.C.C. و C.M.R. و K.G. و P.P. بإجراء مراقبة الجودة للبيانات الجينومية. قام T.K. و M.A.B. و W.K.L. و D.A.M. و D.M. و O.G.S. و C.M. و M.S. و J.R.M.B. بإجراء مراقبة الجودة على البيانات السريرية. قام M.A.B. و D.A.M. و J.A.S. و A.H. و M.J.-H. و C.S. بتنسيق تجربة TRACERx السريرية. قام R.O.C. و G.B. بتصور منصة NeXT Personal. قام G.B. بإنشاء تصميم اللوحة وخوارزميات اكتشاف ctDNA. قام G.B. و R.M.P. و F.C.P.N. بتطوير طرق تقليل الضوضاء. قام J.L. و J.N. و G.B. بتصميم الدراسة التحليلية وتحليل البيانات المرتبطة. قاد J.N. و J.L. تطوير الاختبار والتجارب الدراسية التحليلية. قاد J.H. تطوير خط الأنابيب. تم تحليل البيانات السريرية بواسطة J.R.M.B.، ثم تم تحليلها بشكل منفصل بواسطة C.W.A. و B.L. أعد J.R.M.B. و A.M.F. و N.M. و C.W.A. و R.O.C. و J.L. و G.B. و J.H. و R.C. و J.N. و R.P. و S.B. و C.S. المخطوطة. أشرف R.O.C. و C.S. بشكل مشترك على الدراسة.
التمويل
تم توفير تمويل الوصول المفتوح من قبل معهد فرانسيس كريك.
المصالح المتنافسة
استشار M.A.B. شركة Achilles Therapeutics. يُفيد D.A.M. بأنه تلقى أتعاب متحدث من AstraZeneca وEli Lilly وBristol Myers Squibb وTakeda، وأتعاب استشارية من AstraZeneca وThermo Fisher وTakeda وAmgen وJanssen وMIM Software وBristol Myers Squibb وEli Lilly، وقد حصل على دعم تعليمي من Takeda وAmgen. استشار M.J.-H. شركة Achilles Therapeutics، وهو عضو في المجلس الاستشاري العلمي (SAB) ولجنة التوجيه، وقد حصل على أتعاب متحدث من Pfizer وAstex Pharmaceuticals وOslo Cancer Cluster. حصل N.M. على أتعاب استشارية ولديه خيارات أسهم في Achilles Therapeutics. يُقر C.S. بالحصول على منح من AstraZeneca وBoehringer-Ingelheim وBristol Myers Squibb وPfizer وRoche-Ventana وInvitae (سابقًا Archer Dx Inc، تعاون في تقنيات تسلسل المرض المتبقي الأدنى) وOno Pharmaceutical وPersonalis. هو المحقق الرئيسي في التجارب السريرية AZ MeRmaiD 1 و2 ورئيس لجنة التوجيه. كما أنه المحقق الرئيسي المشارك في تجربة NHS Galleri الممولة من GRAIL وعضو مدفوع في SAB الخاص بـ GRAIL. يتلقى أتعاب استشارية من Achilles Therapeutics (وهو عضو في SAB) وBicycle Therapeutics (وهو عضو في SAB) وGenentech وMedicxi وChina Innovation Centre of Roche (سابقًا Roche Innovation Centre – Shanghai وMetabomed حتى يوليو 2022) وRelay Therapeutics (وهو عضو في SAB) وSaga Diagnostics (وهو عضو في SAB) ومعهد سارة كانون للبحوث. حصل C.S. على أتعاب من Amgen وAstraZeneca وBristol Myers Squibb وGSK.
إيلومينا، MSD، نوفارتس، فايزر وروش-فينتانا. كان لدى C.S. سابقًا خيارات أسهم في Apogen Biotechnologies وGRAIL، ولديه حاليًا خيارات أسهم في Bicycle Therapeutics وRelay Therapeutics، وهو يمتلك أسهمًا وهو أحد مؤسسي Achilles Therapeutics. G.B. وC.W.A. وS.M.B وR.C. وJ.H. وB.L. وJ.L. وF.C.P.N. وJ.N. وR.M.P. وR.O.C. هم موظفون ومساهمون في Personalis. A.M.F. مدرج كمخترع مشارك في طلب براءة اختراع لتحديد طرق وأنظمة لمراقبة الأورام (PCT/EP2022/077987؛ ‘طرق وأنظمة لمراقبة الأورام’). S.V. هو مخترع مشارك في براءة اختراع لطرق اكتشاف الجزيئات في عينة (رقم براءة اختراع الولايات المتحدة 10578620؛ ‘طرق لاكتشاف الجزيئات في عينة’). M.J.-H. مدرج كمخترع مشارك في طلب براءة اختراع أوروبية تتعلق بطرق اكتشاف سرطان الرئة (PCT/US2017/O28013؛ ‘طرق لاكتشاف سرطان الرئة’)؛ وقد تم ترخيص هذه البراءة للكيانات التجارية، ووفقًا لشروط العمل، يحق لـ M.J.-H. الحصول على حصة من أي إيرادات يتم توليدها من هذه الترخيصات. N.M. يحمل براءات اختراع أوروبية تتعلق باستهداف النيوأنتيجينات (PCT/EP2016/059401؛ ‘طريقة لعلاج السرطان’)، وتحديد استجابة المرضى لحجب نقاط التفتيش المناعية (PCT/EP2016/071471؛ ‘تدخل نقاط التفتيش المناعية’ في السرطان)، وتحديد HLA LOH (PCT/GB2018/052004؛ ‘تحليل أليلات HLA في الأورام واستخداماتها’)، وتوقع معدلات البقاء للمرضى المصابين بالسرطان (PCT/GB2020/050221؛ ‘طريقة لتوقع معدلات البقاء للمرضى المصابين بالسرطان’). يعلن C.S. عن طلب براءة اختراع لطرق لاكتشاف سرطان الرئة (PCT/US2017/O28013)؛ واستهداف النيوأنتيجينات (PCT/EP2016/059401)؛ وتحديد استجابة المرضى لحجب نقاط التفتيش المناعية (PCT/EP2016/071471)؛ وطرق لاكتشاف سرطان الرئة (US20190106751A1)؛ وتحديد المرضى الذين يستجيبون لعلاج السرطان (PCT/GB2018/051912)؛ وتحديد HLA LOH (PCT/GB2018/052004)؛ وتوقع معدلات البقاء للمرضى المصابين بالسرطان (PCT/GB2020/050221)؛ وطرق وأنظمة لمراقبة الأورام (PCT/EP2022/O77987). C.S. هو مخترع في طلب براءة اختراع أوروبية (PCT/GB2017/053289) تتعلق بتقنية الفحص لاكتشاف تكرار الأورام. وقد تم ترخيص هذه البراءة لجهة تجارية، ووفقًا لشروط عملهم، يحق لـ C.S. الحصول على حصة من أي إيرادات يتم توليدها من هذه الترخيصات. المؤلفون الآخرون يعلنون عدم وجود مصالح متنافسة.
يجب توجيه المراسلات والطلبات للحصول على المواد إلى تشارلز سوانتون.
معلومات مراجعة الأقران تشكر مجلة ناتشر ميديسين ألان تييري، وبنجامين بيس، والمراجعين الآخرين المجهولين على مساهمتهم في مراجعة هذا العمل. المحرر الرئيسي: آنا ماريا رانزوني، بالتعاون مع فريق ناتشر ميديسين.
البيانات الموسعة الجدول 1 | الخصائص الديموغرافية الأساسية وخصائص الورم للسكان المدروسين مقسمة حسب سرطان الرئة الغدي والسكان غير الغديين. البيانات هيما لم يُذكر خلاف ذلك. قد لا تصل النسب المئوية إلى 100% بسبب التقريب.
خاصية
مستويات
لواد
غير LUAD
ب
ن
–
94
77
غير متوفر
العمر (بالسنوات)
المتوسط (الانحراف المعياري)
67.2 (8.9)
70.1 (8.0)
0.028
جنس
أنثى
٤٠ (٤٢.٦)
٢٩ (٣٧.٧)
0.623
ذكر
٥٤ (٥٧.٤)
٤٨ (٦٢.٣)
TNM المرضي
1أ
11 (11.7)
6 (7.8)
0.718
1ب
17 (18.1)
16 (20.8)
2أ
٤ (٤.٣)
٤ (٥.٢)
2ب
٢٥ (٢٦.٦)
٢٧ (٣٥.١)
3a
٣٥ (٣٧.٢)
22 (28.6)
3ب
2 (2.1)
2 (2.6)
حالة التدخين
مدخن سابق
41 (43.6)
٤٦ (٥٩.٧)
0.086
لم يدخن أبداً
6 (6.4)
2 (2.6)
مدخن
٤٧ (٥٠.٠)
٢٩ (٣٧.٧)
العلاج المساعد
مساعد
٤٦ (٤٨.٩)
٣٦ (٤٦.٨)
0.896
لا مساعد
٤٨ (٥١.١)
41 (53.2)
نوع LUAD
ليبدك
6 (6.4)
حليمي
6 (6.4)
غدي
٢٣ (٢٤.٥)
مصفوف
7 (7.4)
ميكروببلي
٤ (٤.٣)
صلب
٣٨ (٤٠.٤)
مخاطي غزوي
10 (10.6)
حدث سرطاني
لا شيء
85 (90.4)
73 (94.8)
0.364
متحور EGFR
7 (7.4)
2 (2.6)
تخطي إكسون 14 في جين MET
2 (2.1)
2 (2.6)
متابعة (أيام؛ OS)
الوسيط (عدد الأحداث)
1839 (39)
1862 (38)
0.84
متابعة (الأيام؛ RFS)
الوسيط (عدد الأحداث)
1821 (49)
1849 (40)
0.58
تم حساب القيم باستخدام اختبارات كاي تربيع للمتغيرات الفئوية واختبارات للمتغيرات المستمرة.
البيانات الموسعة الجدول 2 | الخصائص الديموغرافية الأساسية وخصائص الورم للدراسة الحالية المقدمة جنبًا إلى جنب مع الخصائص العامة للمرضى المدرجين في العمل المفصل في المراجع 1، 2. البيانات هيما لم يُذكر خلاف ذلك. قد لا تتجمع النسب المئوية إلىبسبب التقريب
خاصية
مستويات
عبوش وآخرون 2023
عبوش وآخرون 2017
نظام نيكست الشخصي
العمر (بالسنوات)
المتوسط (الانحراف المعياري)
68.8 (9.4)
68.4 (9.3)
68.5 (8.6)
جنس
أنثى
79 (40.9)
٣٦ (٣٧.٥)
69 (40.4)
ذكر
114 (59.1)
60 (62.5)
١٠٢ (٥٩.٦)
العلاج المساعد
مساعد
77 (39.9)
٢٨ (٢٩.٢)
82 (48.0)
لا مساعد
116 (60.1)
68 (70.8)
89 (52.0)
علم الأنسجة
سرطان الغدد
١٠١ (٥٢.٣)
٥٧ (٥٩.٤)
94 (55.0)
آخر
25 (13.0)
8 (8.3)
20 (11.7)
سرطان الخلايا الحرشفية
67 (34.7)
31 (32.3)
57 (33.3)
نوع LUAD
ليبدك
٤ (٤.٢)
10 (17.9)
6 (6.4)
حليمي
11 (11.5)
4 (7.1)
6 (6.4)
غدي
٣٣ (٣٤.٤)
21 (37.5)
٢٣ (٢٤.٥)
مصفوف
9 (9.4)
1 (1.8)
7 (7.4)
ميكروببلي
٤ (٤.٢)
٤ (٤.٣)
صلب
٢٤ (٢٥.٠)
14 (25.0)
٣٨ (٤٠.٤)
مخاطي غازي
11 (11.5)
6 (10.7)
10 (10.6)
TNM مرضي
الذكاء الاصطناعي
37 (19.2)
٢٦ (٢٧.١)
17 (9.9)
IB
37 (19.2)
٣٢ (٣٣.٣)
33 (19.3)
IIA
40 (20.7)
14 (14.6)
8 (4.7)
آي آي بي
30 (15.5)
10 (10.4)
52 (30.4)
IIIأ
٤٩ (٢٥.٤)
١٣ (١٣.٥)
٥٧ (٣٣.٣)
III ب
1 (1.0)
4 (2.3)
حالة التدخين
مدخن سابق
١٠٣ (٥٣.٤)
٤٩ (٥١.٠)
87 (50.9)
لم يدخن أبدًا
10 (5.2)
11 (11.5)
8 (4.7)
مدخن
80 (41.5)
٣٦ (٣٧.٥)
76 (44.4)
الشكل البياني الممتد 1| العلاقة بين ctDNA وميزات العيادة الجينومية لسرطان الرئة غير صغير الخلايا. أ. رسم بياني عمودي مكدس لعدد الأهداف المستمدة من المناطق المشفرة (رمادي) وغير المشفرة (أزرق) من الجينوم لكل لوحة. ب. رسم بياني نقطي يوضح حد الكشف الخاص باللوحة (LOD) بوحدات ppm في جميع عينات البلازما قبل العملية. ج. رسم بياني مبعثر يوضح العلاقة بين مستوى ctDNA وعدد سنوات التدخين لعينة ما قبل العملية. الخط المنحني يمثل نموذجًا خطيًا، والمنطقة المظللة تمثلفترة الثقة. د. مخطط الصندوق لمستوى ctDNA قبل العملية لكل نوع مرضي من سرطان الرئة الغدي. تُظهر مخططات الصندوق الوسيط في الخط الأوسط، وتمثل الحواف السفلية والعلوية الربع الأول والربع الثالث، على التوالي، وتظهر الشعيرات القيم الدنيا إلى القصوى التي لا تتجاوزنطاق الربيع الربعي (IQR)، مع المتبقي نقاط البيانات الشاذة مرسومة بشكل فردي. حجم العينة هوالمرضى.تم حساب القيمة باستخدام اختبار كروسكال-واليس للرتب ذو الجانبين. ج. مخطط الصندوق لمستوى ctDNA قبل العملية حسب حالة الحدث الورمي. تُظهر مخططات الصندوق الوسيط في الخط الأوسط، بينما تمثل الأجزاء السفلية والعلوية الربع الأول والربع الثالث، على التوالي، وتظهر الشعيرات القيم الدنيا إلى القصوى التي لا تتجاوزالمدى بين الربيعي، مع رسم النقاط البيانية المتبقية بشكل فردي. حجم العينة هوالمرضى.تم حساب القيمة باستخدام اختبار كروسكال واليس للرتب ذو الجانبين. ف. رسم بياني عمودي لحالة الحدث الورمي للمرضى ملونًا حسب حالة اكتشاف ctDNA قبل العملية.تم حساب القيمة باستخدام اختبار فيشر الدقيق ذو الجانبين. ن b LUAD
ج غير LUAD
الشكل البياني الممتد 2 | انظر الصفحة التالية للتعليق.
الشكل البياني الممتد 2 | زيادة حساسية الاختبار تحسن تصنيف البقاء بدون انتكاسة. أ. منحنى كابلان-ماير (KM) يوضح البقاء بدون انتكاسة (RFS) بين مرضى سرطان الرئة الغدي الذين لديهم مستويات عالية من ctDNA (رمادي داكن)، ومستويات منخفضة من ctDNA (رمادي فاتح) ومرضى ctDNA-negative (أخضر). تم تعريف مجموعات ctDNA العالية والمنخفضة وفقًا لمستويات ctDNA المتوسطة عبر حالات LUAD الإيجابية لـ ctDNA. تم حساب قيم P باستخدام اختبارات لوغ-رانك. ب. منحنى KM يوضح
RFS داخل المرضى الذين يحملون ctDNA بمعدل تقديري أقل من الحد الأدنى للكشف الموثوق الذي تم وصفه في أبوش وآخرون. (رمادي فاتح)، ومرضى سلبية ctDNA (أخضر). تم حساب قيم P باستخدام اختبارات لوغ-رانك. ج. منحنى KM يوضح الفرق في فترة البقاء الخالية من المرض بين مرضى ctDNA العالي ومرضى ctDNA المنخفض مع غير LUAD. تم حساب قيم P باستخدام اختبارات لوغ-رانك.
ن
البقاء العام: نسبة المخاطر (95% فترة الثقة، قيمة p)
حمض نووي خالٍ من الخلايا
–
1.51 (1.22-1.86، ص<0.001)
علم الأنسجة
لواد
–
غير LUAD
0.86 (0.50-1.47، )
علاج
مساعد
–
لا مساعد
1.28 (0.67-2.45، )
سنوات التعبئة
–
0.97 (0.90-1.04، ص=0.420)
مرحلة
أنا
–
الثاني
0.92 (0.45-1.89، ص=0.818)
ثالث
1.68 (0.81-3.50، ص=0.167)
عمر
–
1.37 (0.94-1.99، ص=0.100)
حدث سرطاني
لا شيء
–
متحور EGFR
1.12 (0.42-3.02، ص=0.816)
تخطي إكسون 14 في جين MET
1.34 (0.31-5.83، ص=0.700)
لوغ (HR)
ج
البقاء بدون انتكاسة: HR (95% CI، قيمة p)
مستوى ctDNA
لم يتم الكشف
–
منخفض
14.94 (1.99-112.33، ص=0.009)
عالي
27.18 (3.51-210.26، ص=0.002)
علم الأنسجة
لواد
–
غير LUAD
0.73 (0.47-1.15، ص=0.180)
علاج
مساعد
–
لا مساعد
1.23 (0.70-2.19، ص=0.472)
سنوات التعبئة
–
0.97 (0.91-1.05، )
مرحلة
أنا
–
الثاني
0.96 (0.50-1.87، ص=0.909)
ثالث
1.35 (0.68-2.66، )
عمر
–
1.15 (0.85-1.56، )
حدث سرطاني
لا شيء
–
متحور EGFR
1.65 (0.72-3.79، ص=0.239)
تخطي إكسون 14 في جين MET
ن
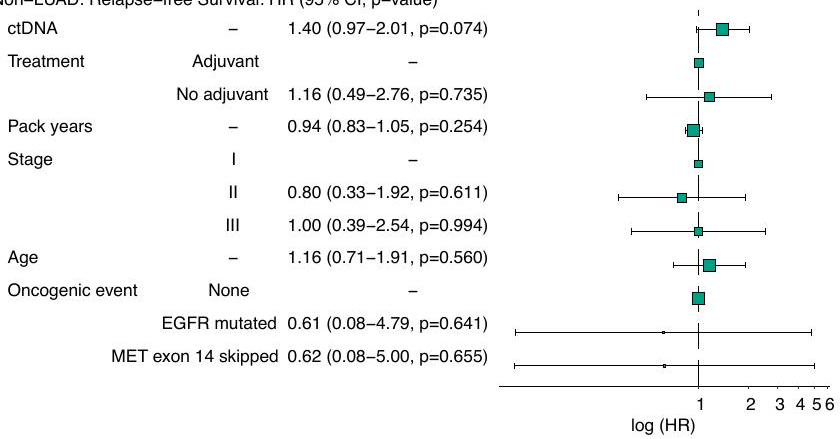
غير LUAD: البقاء بدون انتكاسة: HR (قيمة p) g
الشكل 3 من البيانات الموسعة | انظر الصفحة التالية للتعليق.
ب
البقاء بدون انتكاسة: HR ( Cl، قيمة p)
حمض نووي خالٍ من الخلايا
–
1.43 (1.19-1.73، ص<0.001)
علم الأنسجة
لواد
–
غير LUAD
0.67 (0.41-1.10، ص=0.114)
علاج
مساعد
–
لا مساعد
1.12 (0.62-2.03، ص=0.701)
سنوات التعبئة
–
0.95 (0.88-1.02، ص=0.181)
مرحلة
1
–
الثانية
1.01 (0.52-1.96، ص=0.986)
ثالث
1.46 (0.73-2.92، ص=0.289)
عمر
–
1.25 (0.90-1.73، ص=0.192)
حدث ورمي
لا شيء
–
متحور EGFR
1.56 (0.68-3.60، ص=0.293)
تخطي إكسون 14 في جين MET
0.90 (0.21-3.87، ص=0.891)
غير LUAD: البقاء بدون انتكاسة: HR (قيمة p)
الشكل 3 من البيانات الموسعة | تؤكد التحليلات المتعددة المتغيرة مع تعديل عوامل الخطر المعروفة القيمة التنبؤية المستقلة لـ ctDNA قبل العملية. أ. تحليل الانحدار المتعدد المتغيرات باستخدام نموذج كوكس للبقاء العام (OS) الذي يحتوي على ctDNA (مستمر، لكل زيادة بمقدار 10 أضعاف)؛ النسيج؛ ما إذا كان المريض قد تلقى العلاج الكيميائي المساعد؛ حالة تدخين السجائر (بزيادات 10 علب سنويًا)؛ مرحلة pTNM؛ العمر (بزيادات 10 سنوات)؛ ووجود حدث ورمي. عدد المرضى = 171. ب. تحليل الانحدار المتعدد المتغيرات باستخدام نموذج كوكس للبقاء بدون انتكاسة (RFS) الذي يحتوي على ctDNA (مستمر، لكل زيادة بمقدار 10 أضعاف)؛ النسيج؛ ما إذا كان المريض قد تلقى العلاج الكيميائي المساعد؛ تاريخ تدخين السجائر؛ مرحلة pTNM؛ العمر؛ ووجود حدث ورمي.المرضى. ج. تحليل الانحدار المتعدد المتغيرات لكوكسي لفترة البقاء خالية من المرض (RFS) يحتوي على مستوى ctDNA (ctDNA-high، ctDNA-low، ctDNA-negative)؛ النسيج؛ ما إذا كان المريض قد تلقى العلاج الكيميائي المساعد؛ تاريخ تدخين السجائر؛ مرحلة pTNM؛ العمر؛ ووجود حدث ورمي. ن = 171 مريض. د. تحليل الانحدار المتعدد المتغيرات لكوكسي لفترة البقاء خالية من المرض (RFS) في غير LUADs يحتوي على مستوى ctDNA (ctDNA مرتفع، ctDNA منخفض)؛ ما إذا كان المريض قد تلقى علاجًا كيميائيًا مساعدًا؛ تاريخ تدخين السجائر؛ مرحلة pTNM؛ العمر؛ والأحداث الورمية.المرضى. هـ. تحليل الانحدار المتعدد المتغيرات لكسر البقاء على قيد الحياة الخالي من المرض في حالات غير سرطان الرئة ذو الخلايا غير الصغيرة (nonLUADs) التي تحتوي على ctDNA (مستمر)؛ ما إذا كان المريض قد تلقى العلاج الكيميائي المساعد؛ تاريخ تدخين السجائر؛ مرحلة pTNM؛ العمر؛ والأحداث الورمية.المرضى. ف. تحليل الانحدار المتعدد المتغيرات لعمر البقاء في غير LUADs التي تحتوي على ctDNA (مستمر، لكل زيادة بمقدار 10 أضعاف)؛ تحت النسيج؛ ما إذا كان المريض قد تلقى العلاج الكيميائي المساعد؛ تاريخ تدخين السجائر؛ مرحلة pTNM؛ العمر والأحداث المسرطنة. ن = 77 مريضًا. ج. تحليل متعدد المتغيرات لفترة البقاء الخالية من المرض في غير LUADs التي تحتوي على ctDNA (مستمر، لكل زيادة بمقدار 10 أضعاف)؛ تحت النسيج؛ ما إذا كان المريض قد تلقى العلاج الكيميائي المساعد؛ تاريخ تدخين السجائر؛ مرحلة pTNM؛ العمر؛ والأحداث المسرطنة. ن = 77 مريضًا. بالنسبة لجميع الرسوم البيانية في هذه الشكل، تمثل أشرطة الخطأفترات الثقة. حجم الصناديق يمثل عدد المرضى في كل فئة.
الشكل الممتد 4 | تأثير عمر العينة وصيغة الحفظ على أهداف اللوحة. أ. رسم بياني مربع ونقطي يقارن عدد الأهداف عالية الجودة لكل لوحة من عينات محفوظة في الفورمالين ومغلفة بالشمع (FFPE) التي تزيد عن 5 سنوات مقابل تلك التي تقل عن 5 سنوات. الخط الأفقي المتقطع عند 1000 يشير إلى عتبة جودة التحكم. الخط المركزي يمثل الوسيط. الشعيرات العليا تمثل القيمة القصوى للبيانات التي تقع ضمن 1.5 مرة من النطاق الربعي فوق النسبة المئوية 75. الشعيرات السفلية تمثل القيمة الدنيا للبيانات التي تقع ضمن 1.5 مرة من النطاق الربعي تحت النسبة المئوية 25. حجم العينة هو. ب. تم إعادة إنتاج اللوحات التي فشلت في الحصول على 1000 هدف عالي الجودة أو أقل من ذلك باستخدام أنسجة مجمدة طازجة (FF) حيثما كان ذلك متاحًا. تشير النقاط الخضراء إلى العينات المضمنة في تحليلنا، بينما تشير النقاط الرمادية إلى تلك التي فشلت في تحقيق أهداف عالية الجودة كافية لمزيد من المعالجة. حيثما كان ذلك ممكنًا، تم استبدال هذه اللوحات بأخرى مستمدة من الأنسجة المجمدة.
ب تشير إلى لوحات المرضى المزدوجة المصممة من عينة ورم FF أو FFPE. يمثل الخط الأوسط الوسيط. الشعيرات العلوية هي القيمة القصوى للبيانات التي تقع ضمن 1.5 مرة من النطاق الربعي فوق النسبة المئوية 75. الشعيرات السفلية هي القيمة الدنيا للبيانات التي تقع ضمن 1.5 مرة من النطاق الربعي تحت النسبة المئوية 25. حجم العينة هوالألواح. فشل أحد الألواح المكونة من عينة ورم FF في تحقيق 1,000 هدف عالي الجودة ولكنه تم تضمينه لضمان أن تكون المجموعة تمثل مجموعة TRACERx الأوسع. تم إنشاء لوحين FF حيث فشلت الألواح FFPE تمامًا؛ وهذه ممثلة بالنقاط الخضراء على جانب FF غير المتصلة بنقطة FFPE. ج. انحدار ديمينغ يوضح الاتفاق بين قياس ctDNA PPM وجزيئات الورم لكل مليلتر من البلازما. يمثل الخط الملائم نموذجًا خطيًا، والمنطقة المظللة تمثل فترة الثقة
محفظة الطبيعة
المؤلف (المؤلفون) المراسلون: جيمس بلاك
آخر تحديث بواسطة المؤلف(ين):16 مايو 2024
ملخص التقرير
تسعى Nature Portfolio إلى تحسين إمكانية تكرار العمل الذي ننشره. يوفر هذا النموذج هيكلًا للاتساق والشفافية في الإبلاغ. لمزيد من المعلومات حول سياسات Nature Portfolio، يرجى الاطلاع على سياسات التحرير وقائمة مراجعة سياسة التحرير.
الإحصائيات
لجميع التحليلات الإحصائية، تأكد من أن العناصر التالية موجودة في أسطورة الشكل، أسطورة الجدول، النص الرئيسي، أو قسم الطرق.
غير متوفر
□ □ تم التأكيد
حجم العينة بالضبطلكل مجموعة/شرط تجريبي، معطاة كرقم منفصل ووحدة قياس □ □
اختبار(ات) الإحصاء المستخدمة وما إذا كانت أحادية الجانب أو ثنائية الجانب يجب أن تُوصف الاختبارات الشائعة فقط بالاسم؛ واصفًا التقنيات الأكثر تعقيدًا في قسم الطرق. □
وصف لجميع المتغيرات المشتركة التي تم اختبارها □ □ وصف لأي افتراضات أو تصحيحات، مثل اختبارات الطبيعية والتعديل للمقارنات المتعددة وصف كامل للمعلمات الإحصائية بما في ذلك الاتجاه المركزي (مثل المتوسطات) أو تقديرات أساسية أخرى (مثل معامل الانحدار) والتباين (مثل الانحراف المعياري) أو تقديرات عدم اليقين المرتبطة (مثل فترات الثقة) □
لاختبار الفرضية الصفرية، فإن إحصائية الاختبار (على سبيل المثال ) مع فترات الثقة، وأحجام التأثير، ودرجات الحرية و القيمة المذكورة أعطِ القيم كقيم دقيقة كلما كان ذلك مناسبًا.
□
□
□
لتحليل بايزي، معلومات حول اختيار الأوليات وإعدادات سلسلة ماركوف مونت كارلو
للتصاميم الهرمية والمعقدة، تحديد المستوى المناسب للاختبارات والتقارير الكاملة عن النتائج
تقديرات أحجام التأثير (مثل حجم تأثير كوهين، , معامل بيرسون r)، موضحًا كيف تم حسابها
تحتوي مجموعتنا على الإنترنت حول الإحصائيات لعلماء الأحياء على مقالات حول العديد من النقاط المذكورة أعلاه.
بيان حول ما إذا كانت القياسات قد أُخذت من عينات متميزة أو ما إذا كانت نفس العينة قد تم قياسها عدة مرات
اختبار(ات) إحصائي(ة) مستخدمة وما إذا كانت أحادية أو ثنائية الجانب
يجب وصف الاختبارات الشائعة فقط بالاسم؛ وصف تقنيات أكثر تعقيدًا في قسم الطرق.
□
□
تحتوي مجموعتنا على الإنترنت حول الإحصائيات لعلماء الأحياء على مقالات حول العديد من النقاط المذكورة أعلاه.
البرمجيات والشيفرة
معلومات السياسة حول توفر الشيفرة الحاسوبية
جمع البيانات
تحليل البيانات
لم يتم استخدام أي برمجيات لجمع البيانات.
Personalis NeXT Personal Platform (v1.8)
R version 4.1.3
R packages:
tidyverse (version 1.3.2)
lubridate (version 1.9.2)
ComplexHeatmap (version 2.15.4)
ggplot2 (version 3.4.2)
ggpubr (version 0.4.0)
scales (version 1.2.1)
wesanderson (version 0.3.6)
ggnewscale (version 0.4.9)
survival (version 3.3-1)
survminer (version 0.4.9)
finalfit (version 1.0.4)
gt (version 0.10.1)
mcr (version 1.2.2)
□
□
تم استخدام
ستكون جميع الشيفرات اللازمة لإعادة إنتاج الأشكال متاحة عند الطلب.
بالنسبة للمخطوطات التي تستخدم خوارزميات أو برمجيات مخصصة والتي تعتبر مركزية للبحث ولكن لم يتم وصفها بعد في الأدبيات المنشورة، يجب أن تكون البرمجيات متاحة للمحررين والمراجعين. نشجع بشدة على إيداع الشيفرة في مستودع مجتمعي (مثل GitHub). انظر إرشادات Nature Portfolio لتقديم الشيفرة والبرمجيات لمزيد من المعلومات.
البيانات
البيانات
معلومات السياسة حول توفر البيانات
يجب أن تتضمن جميع المخطوطات بيانًا حول توفر البيانات. يجب أن يوفر هذا البيان المعلومات التالية، حيثما كان ذلك مناسبًا:
رموز الوصول، معرفات فريدة، أو روابط ويب لمجموعات البيانات المتاحة للجمهور
وصف لأي قيود على توفر البيانات
بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتماشى مع سياستنا
تم إيداع بيانات مرضى TRACERx المعالجة في Zenodo على الرابط: 10.5281/zenodo.10689003. تم إيداع البيانات الخام من مرضى TRACERx الذين تم تحليلهم في هذه الدراسة بما في ذلك ملفات fastq وbam من WGS الورمي والطبيعي، بالإضافة إلى ملفات fastq من cfDNA في أرشيف الجينوم-الظاهرة الأوروبي (EGA)، الذي يستضيفه المعهد الأوروبي للمعلوماتية الحيوية (EBI) ومركز تنظيم الجينوم (CRG) تحت رموز الوصول (EGAS00001006494) تحت الوصول المنظم.
البحث الذي يشمل المشاركين البشريين، بياناتهم، أو المواد البيولوجية
معلومات السياسة حول الدراسات التي تشمل المشاركين البشريين أو البيانات البشرية. انظر أيضًا معلومات السياسة حول الجنس، الهوية/العرض، والتوجه الجنسي والعرق، والاثنية والعنصرية.
التقارير حول الجنس
التقارير حول العرق، الاثنية، أو مجموعات اجتماعية ذات صلة
خصائص السكان
تم تضمين معلومات الجنس في البيانات المشتركة عبر الإنترنت. لم يتم جمع معلومات عن جنس المرضى كجزء من الدراسة.
لم يتم تضمين معلومات عن العرق، الاثنية أو مجموعات اجتماعية ذات صلة في المخطوطة.
الخصائص الديموغرافية للكوهو ( ) مدرجة في جدول البيانات الموسع 1، وتفاصيل إضافية على مستوى المرضى متاحة مع بيانات جزيئية داعمة على Zenodo (الرابط: 10.5281/zenodo.10689003). معايير الإدراج والاستبعاد لدراسة TRACERx (رقم التجربة السريرية: NCT01888601) هي كما يلي:
معايير الإدراج:
موافقة مستنيرة مكتوبة
المرضى سنوات، مع مرض في المرحلة المبكرة IIA-IIIB (وفقًا للإصدار الثامن من TNM) الذين هم مؤهلون للجراحة الأولية. يمكن أيضًا تضمين المرضى الذين لديهم تصنيف إشعاعي من IB (NO) والذين يمكن أن يتم تصنيفهم إلى IA-IIIB بعد الجراحة (بسبب وجود احتمال لتورط العقدة في الفحص قبل الجراحة)، ولكن سيتم سحبهم إذا ظل التصنيف بعد الجراحة IB.
سرطان الرئة غير صغير الخلايا المؤكد نسيجيًا، أو اشتباه قوي في السرطان على تصوير الرئة يتطلب جراحة (مثل التشخيص المحدد من القسم المجمد في غرفة العمليات)
الجراحة الأولية وفقًا لإرشادات NICE المخطط لها (انظر القسم 9.3)
الاتفاق على المتابعة في موقع TRACERx
حالة الأداء 0 أو 1
قطر الورم الأدنى لا يقل عن 15 مم للسماح بأخذ عينات من منطقتين على الأقل من الورم (إذا كان 15 مم، هناك احتمال كبير لتورط العقدة في التصوير قبل الجراحة المطلوب لتلبية الأهلية وفقًا للمرحلة، أي T1N1-3)
معايير الاستبعاد:
أي سرطان آخر* تم تشخيصه أو انتكس في أي وقت، والذي يتم علاجه حاليًا (بما في ذلك العلاج الهرموني). أي سرطان آخر* حالي أو سرطان تم تشخيصه أو انتكس خلال السنوات الثلاث الماضية**.
*الاستثناءات هي: سرطان الجلد غير الميلانيني، الميلانوما في المرحلة 0، وسرطان عنق الرحم في الموقع
**سيتم عمل استثناء للسرطانات التي تم تشخيصها أو انتكست منذ أكثر من 2، ولكن أقل من 3، سنوات فقط إذا أكدت خزعة قبل الجراحة من الآفة الرئوية تشخيص سرطان الرئة غير صغير الخلايا.
حالة نفسية قد تمنع الموافقة المستنيرة
العلاج بالعلاج المساعد الجديد لسرطان الرئة الحالي يعتبر ضروريًا
التصنيف بعد الجراحة ليس IIA-IIIB
معرفة فيروس نقص المناعة البشرية (HIV)، فيروس التهاب الكبد B (HBV)، فيروس التهاب الكبد C (HCV) أو عدوى الزهري.
من غير المحتمل الحصول على نسيج كافٍ، أي حد أدنى من منطقتين من الورم، للدراسة بناءً على التصوير قبل الجراحة
عندما يتم تشخيص المرضى في البداية بمرحلة I-III من سرطان الرئة ثم يتم إحالتهم لإجراء استئصال جراحي، يقوم ممرض بحثي بتحديدهم في قائمة العيادة/العمليات. يتم إجراء تقييم أولي للأهلية للمريض ثم يتم تزويده بمعلومات مكتوبة حول دراسة TRACERx ويمكنه/يمكنها طرح أي أسئلة على الممرض البحثي.
يجب على المرضى الموافقة على تقديم عينات دم متسلسلة كلما حضروا العيادة لأخذ عينات الدم الروتينية، لذا فإن هذا يمثل فقط التحيز الذاتي المحتمل الرئيسي (أي أن المرضى المستعدين للقيام بذلك فقط هم من سيشاركون). ومع ذلك، ليس من الواضح كيف سيؤثر ذلك على تحليلات العلامات الحيوية. أيضًا، خصائص الجنس والعرق تتماشى مع المرضى الذين يتم رؤيتهم في الممارسة الروتينية.
تمت الموافقة على هذه الدراسة من قبل لجنة NRES لندن مع التفاصيل التالية:
عنوان الدراسة: تتبع تطور سرطان الرئة غير صغير الخلايا من خلال العلاج (Rx)
التجنيد
الإشراف الأخلاقي
مرجع REC: 13/LO/1546
رقم البروتوكول: UCL/12/0279
معرف مشروع IRAS: 138871
تم الحصول على موافقة مستنيرة مكتوبة من جميع المشاركين.
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة حول الموافقة على بروتوكول الدراسة في المخطوطة.
التقارير الخاصة بالمجال
يرجى اختيار الخيار أدناه الذي يناسب بحثك بشكل أفضل. إذا لم تكن متأكدًا، اقرأ الأقسام المناسبة قبل اتخاذ اختيارك.
علوم الحياة
علوم السلوك والاجتماع
علوم البيئة، التطور والبيئة
لنسخة مرجعية من الوثيقة مع جميع الأقسام، انظر nature.com/documents/nr-reporting-summary-flat.pdf
تصميم دراسة علوم الحياة
يجب على جميع الدراسات الإفصاح عن هذه النقاط حتى عندما يكون الإفصاح سلبيًا.
حجم العينة
هنا، نبلغ عن تحليلات من 204 مريضًا من TRACERx. لم يتم إجراء حسابات حجم العينة للدراسة الفرعية للـ ctDNA قبل الجراحة؛ تم تحديد حجم العينة بناءً على توفر العينة، ويشمل 18 مريضًا من دراسة Abbosh وآخرون، 2017 و43 مريضًا من دراسة Abbosh وآخرون، 2023. أدت WGS الورمي/الطبيعي لـ 171 مريضًا إلى لوحات ctDNA ناجحة تم تضمينها لمزيد من التحليل. كان لدى 171 مريضًا بلازما قبل الجراحة متاحة، بما في ذلك 89 مريضًا انتكسوا.
استثناءات البيانات
تم استبعاد المرضى إذا لم يكن لديهم بلازما أساسية. تم تضمين البلازما المتاحة التي تم جمعها عند أو الأقرب إلى الجراحة في التحليلات للمرضى الذين لديهم بلازما متعددة قبل الجراحة. حصلنا على نسيج FFPE لـ 204 مريضًا. من بين هؤلاء، كان لدى 62 عدد غير عادي من أهداف اللوحة عالية الجودة من المحتمل أن يكون بسبب العمر و/أو ضعف جودة عينات FFPE، و2 لم ينجحوا في تصميم اللوحة. بالنسبة لـ 31 من هؤلاء الـ 64 مريضًا، كانت الحمض النووي المستخرج من نسيج مجمد طازج متاحة وتم استبعاد الـ 33 مريضًا المتبقيين من التحليل.
تكرار
تم استخدام النسخ التقنية والنسخ الحاسوبية للتحقق من صحة منصة NeXT الشخصية. تم وصف التجارب الداعمة في كل من النص الرئيسي للمخطوطة وكذلك في الأساليب، وتم تصورها في الشكل 1 والشكل الممتد 1.
العشوائية
لم يتم إجراء أي عشوائية في هذه الدراسة حيث لم يتم اختبار أي تدخلات علاجية.
التعمية
تم إجراء تحليل ctDNA بأثر رجعي باستخدام عينات تم جمعها بشكل استباقي ومتابعة سريرية. كان الباحثون في Personalise معزولين تمامًا عن نتائج المرضى السريرية وخصائصهم السريرية المرضية أثناء معالجة العينات وتحليل ctDNA. وبالمثل، كان الباحثون في TRACERx معزولين عن حالة ctDNA للمرضى أثناء جمع البيانات السريرية وعينات المرضى.
التقارير عن مواد وأنظمة وأساليب محددة
نحتاج إلى معلومات من المؤلفين حول بعض أنواع المواد والأنظمة التجريبية والأساليب المستخدمة في العديد من الدراسات. هنا، حدد ما إذا كانت كل مادة أو نظام أو طريقة مدرجة ذات صلة بدراستك. إذا لم تكن متأكدًا مما إذا كان عنصر القائمة ينطبق على بحثك، اقرأ القسم المناسب قبل اختيار رد.
المواد والأنظمة التجريبية
الأساليب
غير متاح
مشارك في الدراسة
غير متاح
مشارك في الدراسة
X
□
X
□
□
X
□
V
□
□
□
□
خطوط الخلايا حقيقية النواة
معلومات السياسة حول خطوط الخلايا والجنس في البحث
مصدر خط الخلية (خطوط الخلايا)
التحقق من الهوية
تلوث الميكوبلازما
خطوط تم التعرف عليها بشكل خاطئ بشكل شائع (انظر سجل ICLAC)
غير متاح
كما قدمته ATCC (تحليل STR).
تم فحصه بواسطة ATCC وتأكيد عدم اكتشافه.
لا توجد أي من هذه خطوط الخلايا التي تم التعرف عليها بشكل خاطئ بشكل شائع كما هو مذكور في سجل ICLAC.
البيانات السريرية
معلومات السياسة حول الدراسات السريرية
يجب أن تمتثل جميع المخطوطات لإرشادات ICMJE لنشر الأبحاث السريرية ويجب تضمين قائمة مراجعة CONSORT مكتملة مع جميع التقديمات.
يتم جمع البيانات السريرية والمرضية من المرضى خلال متابعة الدراسة – هذه الفترة لا تقل عن خمس سنوات. يتم الإشراف على جمع البيانات من قبل راعي الدراسة (أبحاث السرطان في المملكة المتحدة ومركز تجارب السرطان في UCL) وتتم في المستشفيات في جميع أنحاء المملكة المتحدة. يتم استخدام قاعدة بيانات مركزية تسمى MACRO لهذا الغرض. بدأ تجنيد TRACERx في أبريل 2014 وما زال مستمرًا.
النتائج
النتيجة السريرية المحددة مسبقًا التي تم تحليلها في هذه المخطوطة هي البقاء العام (OS) المقاس من وقت تسجيل الدراسة حتى تاريخ الوفاة لأي سبب. تم تعريف هذه النتيجة سابقًا في بروتوكول TRACERx (الموصوف في Jamal-Hanjani et al.، 2017 NEJM). تم تضمين تحليل إضافي للبقاء بدون انتكاسة أيضًا في هذه المخطوطة، ويتم تعريفه على أنه الأيام من التسجيل إلى أي تكرار للمرض أو أحداث ورم أولي جديدة. كانت النتائج الأولية والثانوية محددة مسبقًا بناءً على الأهداف الأولية والثانوية للدراسة التالية:
الأهداف الأولية:
تحديد العلاقة بين التباين داخل الورم والنتيجة السريرية (البقاء بدون مرض والبقاء العام) بعد الجراحة والعلاج المساعد (بما في ذلك العلاقات بين التباين داخل الورم ومرحلة المرض السريرية وأنماط الأنسجة المرضية لسرطان الرئة غير صغير الخلايا).
تحديد تأثير أنظمة العلاج المساعد المحتوية على البلاتين على التباين داخل الورم في المرض المتكرر مقارنة بالورم الأولي المستأصل.
الأهداف الثانوية:
تطوير والتحقق من صحة مؤشر نسبة التباين داخل الورم كعلامة حيوية تنبؤية أو تنبؤية فيما يتعلق بارتباطه بالبقاء بدون مرض والبقاء العام
استنتاج صورة كاملة لديناميات تطور سرطان الرئة غير صغير الخلايا: تحديد محركات عدم الاستقرار الجيني، والتقدم النقيلي ومقاومة الأدوية من خلال تحديد وتتبع ديناميات التباين الطفري الجسدي، وعدم الاستقرار الهيكلي والعددي الكروموسومي الموجود في الورم الأولي وفي المواقع النقيلي. ستحلل شجرة النسب الورمي الفردية:
a) تحديد ترتيب الأحداث الجسدية فيما يتعلق ببدء عدم الاستقرار الجيني والتقدم النقيلي
b) فك شفرة أحداث “اختناق” الجينات بعد النقائل والعلاج الدوائي
c) تحديد ديناميات تطور الورم خلال مسار المرض من المرحلة المبكرة إلى المرحلة المتأخرة من سرطان الرئة غير صغير الخلايا.
بدء بنك حيوي للخلية الورمية الدائرة (CTC) وcfDNA غير الغازية على المدى الطويل لتطوير طرق تحليلية للكشف المبكر ومراقبة تطور الورم مع مرور الوقت.
تطوير مورد نسيجي طويل الأمد ليكون بمثابة منصة لتقييم العلاقة بين التباين الجيني داخل الورم واستجابة الجهاز المناعي للمضيف.
عزل العدلات واللمفاويات لتوليد خلايا T المتفاعلة مع النيوأنتيجين في المختبر لاختبار استجابتها المناعية لعينات الورم المتطابقة
تطوير مستودع لخطوط خلايا سرطان الرئة، والأورغانويد ونماذج الفئران الحية لسرطانات الرئة المستمدة من المرضى التي يمكن استخدامها كنماذج في المختبر وفي الجسم الحي لدراسة أسباب أمراض الرئة، بما في ذلك سرطان الرئة وتوقع الاستجابة للعلاج والمقاومة في سرطان الرئة.
تحديد العلاقات بين التباين داخل الورم ونتيجة العلاج المستهدف/السامة.
من خلال لوحة جينات UCL-GCLP في بيئة مختبر معتمدة، ستحدد TRACERx محركات المرض السائدة من الناحية الكلونية (مقارنات المواقع الأولية والنقيلي في ما لا يقل عن 270 مريضًا يعانون من مرض متكرر) لمعالجة دور هيمنة المحرك الكلوني في الاستجابة للعلاج المستهدف، ولتوجيه تصنيف علاج سرطان الرئة وإدراج الدراسات السريرية المستقبلية بالتعاون مع برنامج CRUK للأدوية المصنفة المرحلة الثانية.
تطوير طرق تحليلية لتحديد التباين الشكلي داخل مناطق الورم المنفصلة.
مجموعة الطبيعة | ملخص التقرير
سيتم تحليل عينات الأنسجة المأخوذة من استئصال الرئة، سواء كانت ورمية أو طبيعية، باستخدام المجهر عالي القوة، مثل المجهر الإلكتروني، من أجل الحصول على معلومات حول الهياكل الخلوية.
تقييم العمل المقدم في هذه المخطوطة تأثير ctDNA على بقاء المرضى عبر تحليل الانحدار Cox وطريقة Kaplan Meier.
Ultrasensitive ctDNA detection for preoperative disease stratification in early-stage lung adenocarcinoma
Received: 21 September 2023
Accepted: 29 July 2024
Published online: 13 January 2025
Check for updates
James R. M. Black , Gabor Bartha , Charles W. Abbott , Sean M. Boyle , Takahiro Karasaki , Bailiang Li , Rui Chen , Jason Harris , Selvaraju Veeriah , Martina Colopi , Maise Al Bakir , Wing Kin Liu , John Lyle , Fábio C. P. Navarro , Josette Northcott , Rachel Marty Pyke , Mark S. Hill , Kerstin Thol , Ariana Huebner , Chris Bailey , Emma C. Colliver , Carlos Martínez-Ruiz , Kristiana Grigoriadis , Piotr Pawlik , David A. Moore , Daniele Marinelli , Oliver G. Shutkever , Cian Murphy Monica Sivakumar¹, TRACERx consortium*, Jacqui A. Shaw , Allan Hackshaw , Nicholas McGranahan , Mariam Jamal-Hanjani 14,11 , Alexander M. Frankell , Richard O. Chen Charles Swanton
Circulating tumor DNA (ctDNA) detection can predict clinical risk in early-stage tumors. However, clinical applications are constrained by the sensitivity of clinically validated ctDNA detection approaches. NeXT Personal is a whole-genome-based, tumor-informed platform that has been analytically validated for ultrasensitive ctDNA detection at of ctDNA with specificity. Through an analysis of 171 patients with early-stage lung cancer from the TRACERx study, we detected ctDNA pre-operatively within of patients with lung adenocarcinoma (LUAD), including 53% of those with pathological TNM (pTNM) stage I disease. ctDNA predicted worse clinical outcome, and patients with LUAD with preoperative ctDNA levels (the limit of detection of a ctDNA detection approach previously published in TRACERx) experienced reduced overall survival compared with ctDNA-negative patients with LUAD. Although prospective studies are needed to confirm the clinical utility of the assay, these data show that our approach has the potential to improve disease stratification in early-stage LUADs.
Liquid biopsy for detecting circulating tumor DNA (ctDNA, namely cell-free DNA derived from a tumor) holds promise as a strategy for personalized clinical management of early-stage cancers .Preoperative ctDNA status has shown potential as a biomarker, while postoperative ctDNA detection can direct adjuvant therapy regimens , and monitoring for molecular residual disease (MRD) during follow-up has the potential to identify relapse earlier than would be detected with routine clinical surveillance .
ctDNA detection can be tumor-informed or tumor-agnostic. Tumor-informed approaches leverage information from genomic profiling of a tumor tissue specimen, allowing for tracking of tumor-specific mutations within plasma and typically improving sensitivity relative to tumor-agnostic approaches. In 2020, cancer personalized profiling by deep sequencing (CAPP-seq), was used in a tumor-informed approach to demonstrate that preoperative ctDNA detection in non-small-cell lung cancer (NSCLC) could be used to
identify patients with stage I disease with poor clinical outcome . Subsequent work within lung adenocarcinomas (LUADs) from the LUNGCA-1 cohort , the NADIM trial and the TRACERx study of NSCLC confirmed the prognostic capacity of preoperative ctDNA detection for overall survival (OS) and relapse-free survival (RFS) in LUADs.
Detection of preoperative ctDNA in early-stage LUAD is a considerable challenge owing to the low levels of ctDNA in plasma, which are frequently below . Additionally, the sensitivity of ctDNA detection can be impaired by variations in the production of cell-free DNA (cfDNA) by non-malignant cells , sequencing error and variants arising from clonal hematopoiesis of indeterminate potential (CHIP), which can be present at low levels in plasma . A high-quality ctDNA detection platform must have a number of attributes for optimal clinical utility: it must be extremely sensitive, highly specific and applicable to a broad spectrum of tumors, and it must deliver results with small amounts of DNA input. To that end, there has recently been significant focus on research into developing approaches to overcome this problem .
Although the relationship between ctDNA detection and survival is independent of pathological tumor-node-metastasis (pTNM) stage in this setting, the degree to which the limit of detection (LOD) of ctDNA assays affects the clinical sensitivity of ctDNA as a biomarker for aggressive disease is not well understood.
Here, we used NeXT Personal, an ultrasensitive, tumor-informed liquid-biopsy platform to characterize preoperative ctDNA in 171 patients in the TRACERx study . NeXT Personal is a tumor-informed liquid-biopsy platform that leverages prioritized target selection from whole-genome sequencing of tumor and matched normal DNA . The development and analytical validation of this assay is outlined in Methods and in ref. 23 . In brief, the method aims to achieve a LOD approaching 1 ppm by aggregating the signal from a larger number of somatic variant targets than can be detected from an exome. To avoid being overwhelmed by false signals arising from the large number of variants, noise must be suppressed to very low levels, which is largely accomplished by molecular consensus, which allows identification of independent sequence reads arising from a common founder, and groups these reads into unique molecule families for further analysis. NeXT Personal bespoke panels are designed using the top signal-to-noise ranked somatic variants for ctDNA detection from plasma (that is, the subset of cfDNA that contains the tumor-specific mutations in the panel). Hybridization-based genomic-target enrichment using the panel is followed by ultradeep sequencing of the plasma samples. NeXT Personal then aggregates the tumor-derived signal from the somatic targets. This process, combined with comprehensive noise-suppression methods, enables NeXT Personal to achieve ultrasensitive ctDNA detection for disease stratification, therapy monitoring and MRD detection (Methods and Fig. 1a).
Personalized tumor-informed ctDNA-detection assays that leverage exonic mutations have been investigated in the TRACERx cohort . We have previously studied the ability of ctDNA, detected in a preoperative peripheral blood sample, to predict clinical outcome in LUAD . This involved a tumor-informed assay investigating somatic variants at an average of 200 positions per sample, revealing that patients with LUAD who had ctDNA detected in their blood at the time of surgery had a worse clinical prognosis . However, ctDNA was detectable in only of patients with pathological stage I LUAD at this time point. We therefore set out to assess the degree to which a more sensitive and specific assay would increase prognostic value in a cohort with comparable clinical demographics (Extended Data Table 1).
We analyzed blood plasma samples collected before the surgical removal of lung cancer from 171 TRACERx patients, including 94 with LUAD ( stage I, stage II, stage III) and 77 with nonLUAD (28.6% stage I, 40.3% stage II, 31.2% stage III) NSCLC, using NeXT Personal (Extended Data Table 2 and Fig. 1b). Of these patients, 160 had one primary NSCLC tumor and 11 had two synchronous primary
NSCLC tumors. A median of 1,800 patient-specific somatic variants were included in the NeXT Personal panel design (range, 646-1,942), of which a median of were from non-coding regions (Extended Data Fig. 1a). This resulted in a set of bespoke panels with a median predicted LOD of 1.33 ppm and a range of (Extended Data Fig. 1b). The median DNA input quantity was 23.5 ng (Fig 1b; range, ).
ctDNA was detected in a preoperative plasma sample in of patients with LUAD (Fig. 1c, 76/94) and 100% of patients with non-LUAD (Fig.1d,77/77) NSCLCs across a broad range of tumor fractions (positive ctDNA detection range, ). This included 32 LUADs ( of all LUADs) in which ctDNA was detected, but at below 80 ppm , the LOD in our previous approach . We could detect ctDNA in the blood of of patients with pTNM stage ILUADs (16/28): ctDNA from these tumors has been difficult to detect in blood samples (only of such tumors were identified in Abbosh et al. and in Abbosh et al. ). Similarly, ctDNA was detected in of pTNM stage II LUADs ( , compared to in Abbosh et al. ). ctDNA shedding, as previously reported, was associated with smoking status (pack-year history) (Spearman’s ; Extended Data Fig. 1c) and with the high-grade predominant subtypes of LUAD, in particular the solid and cribriform subtypes ( , Kruskal-Wallis test; Extended Data Fig. 1d) . Oncogenic events, which in this cohort comprised mutations and skipping of MET exon 14 (no RET-ROS1-ALK oncogenic fusions were detected), were not associated with a significant difference in ctDNA ppm level ( , Kruskal-Wallis test; Extended Data Fig. 1e) or rate of preoperative ctDNA detection ( , Fisher’s exact test; Extended Data Fig. 1f), although this analysis is likely to have been underpowered given the small numbers of patients harboring these events.
We next assessed the degree to which this additional sensitivity improved our ability to stratify these patients according to clinical outcome. Preoperative ctDNA-negative patients were compared with patients whose ctDNA levels were below the median of those detected (ctDNA-low) and those with ctDNA levels above the median of those detected (ctDNA high). ctDNA status predicted OS in LUADs (Fig. 2a, low: hazard ratio confidence interval 1.48-83.2; high: ) and RFS (Extended Data Fig. 2a, low: HR, ; high, . Patients with a preoperative ctDNA-negative status had significantly improved OS ( 5 -year OS, ; ; ) compared with ctDNA-low patients ( 5 -year ), and ctDNA-high patients ( 5 -year OS, ). Notably, when analysis was restricted to include only patients in whom ctDNA would not have been reliably detected using the approach in Abbosh et al. , the presence of ctDNA at levels below 80 ppm remained prognostic for poor OS (Fig. 2b, ) and RFS (Extended Data Fig. 2b, ) in LUAD. This suggests that clinically meaningful signal is detected by assays with sensitivity at tumor fractions below 80 ppm , and that the ultra-high-sensitivity assay presented here enables identification of a group of very-lowrisk patients with LUAD.
As we have previously reported, the association between outcomes and elevated preoperative ctDNA levels in non-LUADs was substantially reduced compared with that in LUADs; previous work has found no discernible impact of ctDNA levels on clinical outcome in non-LUADs . In this analysis, a ctDNA level greater than the median in non-LUADs was not associated with reduced RFS (Extended Data Fig. 2c; ). This highlights a fundamentally different relationship between ctDNA and disease biology in non-LUADs compared with that in LUADs.
When adjusted for histology, pTNM stage, smoking status, age, the presence of an oncogenic event (such as an EGFR driver mutation or the skipping of exon 14 in ) and the addition of adjuvant therapy,
Fig. 1| Highly sensitive detection of preoperative ctDNA. a, The NeXT Personal platform leverages tumor-informed information to achieve ultrasensitive and specific residual and recurrent cancer detection, longitudinal monitoring and therapy monitoring from liquid-biopsy samples. b, Clinicopathological variables relating to preoperative ctDNA detection in patients with NSCLC in the TRACERx study: ctDNA level (ppm tumor fraction); number of tumor molecules per ml plasma; pathological tumor node metastasis (pTNM) stage; NSCLC histology;
tumor size (pathology-based tumor size (mm)); cigarette smoking (pack-years); pathological subtype of LUAD; presence of an oncogenic event (within this cohort, either the presence of an EGFR mutation or skipping of MET exon 14); and cfDNA input amount (ng). LUAD (d) tumors detected pre-operatively. Colors represent different studies: blue, Abbosh et al. ;gray, Abbosh et al. ; green, this study. LUAD, non-LUAD.
Fig. 2 | Baseline ctDNA level is prognostic of OS. a, Kaplan-Meier (KM) curve of OS in ctDNA-high (dark gray), ctDNA-low (light gray) and ctDNA-negative (green) patients with LUAD. ctDNA-high and ctDNA-low groups were defined according to the median ctDNA levels across ctDNA-positive LUADs. values were calculated using log-rank tests. b, KM curve demonstrating OS in patients harboring ctDNA at an estimated tumor fraction below the limit of reliable detection described in Abbosh et al. (light gray) and ctDNA-negative patients (green). values were calculated using log-rank tests. c, Results of multivariable
Cox regression analysis including ctDNA level (ctDNA-high, ctDNA-low, ctDNAnegative); histology; whether the patient received adjuvant chemotherapy; cigarette smoking history (in increments of 10 pack-years); pTNM stage; age (in increments of 10 years); and the presence of an oncogenic event (either an mutation or exon 14 skipping). . Error bars represent confidence intervals. The size of the boxes represent the number of patients within each category.
the presence of ctDNA-whether considered either as a continuous metric or stratified into groups as specified above-was independently associated with reduced OS (Fig. 2c and Extended Data Fig. 3a) and RFS (Extended Data Fig. 3b,c) in a pooled cohort of patients with LUADs and non-LUADs. Of note, the ctDNA level was not significant as an independent prognostic factor for RFS in the non-LUAD group (Extended Data Fig. 3d,e). The prognostic effect of ctDNA as a continuous variable on both RFS and OS was not significant when adjusting for histological (squamous versus non-squamous) subtype and other clinicopathological factors (Extended Data Fig. 3f,g).
This work has leveraged NeXT Personal, a tumor-informed assay that is capable of reliably detecting ctDNA in blood at ( tumor fraction). Notably, this ultra-high sensitivity can be achieved with an estimated specificity of and even from suboptimal DNA input volumes. This could be important in many clinical settings, and can be applied to suboptimal DNA input volumes.
Patients with early-stage NSCLC remain at high risk of relapse, despite aggressive curative-intent treatment. Thus, it is of critical importance to accurately stratify patients to both maximize the likelihood of disease cure following surgery and adjuvant therapy and
minimize risk of overtreatment in those patients predicted to have good outcome. Detectable preoperative ctDNA has been associated with worsened recurrence-free survival and reduced , and has been suggested as a potential marker for neoadjuvant treatment selection . We have demonstrated that assays that cannot detect ctDNA at tumor fractions below 80 ppm fail to capture a clinically impactful signal arising from a significant subset of patients with LUAD . In this study, these patients with detectable but extremely low levels of ctDNA experienced a worse clinical outcome than those in whom we did not detect evidence of ctDNA. This suggests that there is a subset of very-low-risk patients with LUADs who can be definitively identified only by using an ultrasensitive ctDNA assay, raising the potential for an ultrasensitive and specific assay to be used prognostically for escalation of therapy in stage ILUADs exhibiting ctDNA release.
Although this study presents results from preoperative plasma samples, the high sensitivity of the NeXT Personal assay suggests the potential for significant clinical benefit in the setting of minimal residual disease for tracking treatment response and detecting recurrence.
Of note, there are a number of technologies in the field aiming to achieve ultrasensitive tumor-informed ctDNA detection, such those
developed by Foresight Diagnostics (PhasED-seq) , C2i Genomics and Inivata (RaDaR) .
This work has limitations. The data from TRACERx was analyzed retrospectively, although in a blinded fashion. Future data from prospective cohorts will be needed to evaluate the clinical utility of this assay. Although NeXT Personal is already in use as a clinical diagnostic test, it, like other tumor-informed ctDNA detection assays, is of higher complexity, can be more costly to produce and requires a longer turnaround period to develop the panel and obtain a clinically actionable result, compared with non-tumor-informed approaches.
If ctDNA is to be used for clinical risk prediction, the design of personalized adjuvant treatment regimens and early detection of recurrence and integrated into routine clinical care, ctDNA assays should have a high degree of sensitivity. In this way, they hold promise to transform adjuvant clinical trial design and clinical practice.
Online content
Any methods, additional references, Nature Portfolio reporting summaries, source data, extended data, supplementary information, acknowledgements, peer review information; details of author contributions and competing interests; and statements of data and code availability are available at https://doi.org/10.1038/s41591-024-03216-y.
References
Abbosh, C. et al. Phylogenetic ctDNA analysis depicts early stage lung cancer evolution. Nature 545, 446-451 (2017).
Abbosh, C. et al. Tracking early lung cancer metastatic dissemination in TRACERx using ctDNA. Nature 616, 553-562 (2023).
Pascual, J. et al. ESMO recommendations on the use of circulating tumour DNA assays for patients with cancer: a report from the ESMO Precision Medicine Working Group. Ann. Oncol. 33, 750-768 (2022).
Garcia-Murillas, I. et al. Mutation tracking in circulating tumor DNA predicts relapse in early breast cancer. Sci. Transl. Med. 7, 302ra133 (2015).
Reinert, T. et al. Analysis of plasma cell-free DNA by ultradeep sequencing in patients with stages I to III colorectal cancer. JAMA Oncol. 5, 1124-1131 (2019).
Gale, D. et al. Residual ctDNA after treatment predicts early relapse in patients with early-stage non-small cell lung cancer. Ann. Oncol. 33, 500-510 (2022).
Kotani, D. et al. Molecular residual disease and efficacy of adjuvant chemotherapy in patients with colorectal cancer. Nat. Med. 29, 127-134 (2023).
Powles, T. et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature 595, 432-437 (2021).
Tie, J. et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage II colon cancer. N. Engl. J. Med. 386, 2261-2272 (2022).
Chaudhuri, A. A. et al. Early detection of molecular residual disease in localized lung cancer by circulating tumor DNA profiling. Cancer Discov. 7, 1394-1403 (2017).
Chabon, J. J. et al. Integrating genomic features for non-invasive early lung cancer detection. Nature 580, 245-251 (2020).
Xia, L. et al. Perioperative ctDNA-based molecular residual disease detection for non-small cell lung cancer: a prospective multicenter cohort study (LUNGCA-1). Clin. Cancer Res. 28, 3308-3317 (2022).
Provencio, M. et al. Overall survival and biomarker analysis of neoadjuvant nivolumab plus chemotherapy in operable stage IIIA non-small-cell lung cancer (NADIM phase II trial). J. Clin. Oncol. 40, 2924 (2022).
Chin, R.-I. et al. Detection of solid tumor molecular residual disease (MRD) using circulating tumor DNA (ctDNA). Mol. Diagn. Ther. 23, 311-331 (2019).
Mattox, A. K. et al. The origin of highly elevated cell-free DNA in healthy individuals and patients with pancreatic, colorectal, lung, or ovarian cancer. Cancer Discov. 13, 2166-2179 (2023).
Hu, Y. et al. False-positive plasma genotyping due to clonal hematopoiesis. Clin. Cancer Res. 24, 4437-4443 (2018).
Cohen, J. D. et al. Detection of low-frequency DNA variants by targeted sequencing of the Watson and Crick strands. Nat. Biotechnol. 39, 1220-1227 (2021).
Kurtz, D. M. et al. Enhanced detection of minimal residual disease by targeted sequencing of phased variants in circulating tumor DNA. Nat. Biotechnol. 39, 1537-1547 (2021).
Zviran, A. et al. Genome-wide cell-free DNA mutational integration enables ultra-sensitive cancer monitoring. Nat. Med. 26, 1114-1124 (2020).
Cohen, J. D. et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 359, 926-930 (2018).
Jamal-Hanjani, M. et al. Tracking the evolution of non-small-cell lung cancer. N. Engl. J. Med. 376, 2109-2121 (2017).
Martínez-Ruiz, C. et al. Genomic-transcriptomic evolution in lung cancer and metastasis. Nature 616, 543-555 (2023).
Northcott, J. et al. Analytical validation of NeXT Personal , an ultra-sensitive personalized circulating tumor DNA assay. Oncotarget 15, 200-218 (2024).
Zhao, J. et al. Personalized cancer monitoring assay for the detection of ctDNA in patients with solid tumors. Mol. Diagn. Ther. 27, 753-768 (2023).
Karasaki, T. et al. Evolutionary characterization of lung adenocarcinoma morphology in TRACERx. Nat. Med. 29, 833-845 (2023).
Jung, H.-A. et al. Longitudinal monitoring of circulating tumor DNA from plasma in patients with curative resected stages I to IIIA EGFR-mutant non-small cell lung cancer. J. Thorac. Oncol. 18, 1199-1208 (2023).
Li, N. et al. Perioperative circulating tumor DNA as a potential prognostic marker for operable stage I to IIIA non-small cell lung cancer. Cancer 128, 708-718 (2022).
Isbell, J. M. et al. Abstract 3375: ultrasensitive ctDNA minimal residual disease monitoring in early NSCLC with PhasED-Seq. Cancer Res. 83, 3375 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
¹Cancer Research UK Lung Cancer Centre of Excellence, University College London Cancer Institute, London, UK. ²Cancer Evolution and Genome Instability Laboratory., The Francis Crick Institute, London, UK. Personalis Inc., Fremont, CA, USA. Cancer Metastasis Laboratory, University College London Cancer Institute, London, UK. Department of Thoracic Surgery, Respiratory Center, Toranomon Hospital, Tokyo, Japan. Cancer Genome Evolution Research Group, Cancer Research UK Lung Cancer Centre of Excellence, University College London Cancer Institute, London, UK. Department of Cellular Pathology, University College London Hospitals, London, UK. Department of Experimental Medicine, Sapienza University, Rome, Italy. Leicester NIHR BRC & University of Leicester, Leicester, UK. Cancer Research UK & UCL Cancer Trials Centre, London, UK. Department of Oncology, University College London Hospitals, London, UK. These authors contributed equally: James R. M. Black, Gabor Bartha. These authors jointly supervised this work: Richard O. Chen, Charles Swanton. e-mail: Charles.swanton@crick.ac.uk
TRACERx consortium
Charles Swanton , Alexander M. Frankell , Mariam Jamal-Hanjani , Nicholas McGranahan , Allan Hackshaw , Jacqui A. Shaw , James R. M. Black , Takahiro Karasaki , Selvaraju Veeriah , Maise Al Bakir , Wing Kin Liu , Mark S. Hill , Kerstin Thol , Ariana Huebner , Chris Bailey , Emma C. Colliver , Carlos Martínez-Ruiz , Kristiana Grigoriadis , Piotr Pawlik , David A. Moore , Monica Sivakumar , Jason F. Lester , Amrita Bajaj , Apostolos Nakas , Azmina Sodha-Ramdeen , Mohamad Tufail , Molly Scotland , Rebecca Boyles , Sridhar Rathinam , Claire Wilson , Domenic Marrone , Sean Dulloo , Dean A. Fennell , Gurdeep Matharu , Ekaterini Boleti , Heather Cheyne , Mohammed Khalil , Shirley Richardson , Tracey Cruickshank , Gillian Price , Keith M. Kerr , Sarah Benafif , Jack French , Kayleigh Gilbert , Babu Naidu , Akshay J. Patel , Aya Osman , Carol Enstone , Gerald Langman , Helen Shackleford , Madava Djearaman , Salma Kadiri , Gary Middleton , Angela Leek , Jack Davies Hodgkinson , Nicola Totton , Angeles Montero , Elaine Smith , Eustace Fontaine , Felice Granato , Antonio Paiva-Correia , Juliette Novasio , Kendadai Rammohan , Leena Joseph , Paul Bishop , Rajesh Shah , Stuart Moss , Vijay Joshi , Philip A. J. Crosbie , Katherine D. Brown , Mathew Carter , Anshuman Chaturvedi , Pedro Oliveira , Colin R. Lindsay , Fiona H. Blackhall , Matthew G. Krebs , Yvonne Summers , Alexandra Clipson , Jonathan Tugwood , Alastair Kerr , Dominic G. Rothwell , Caroline Dive , Hugo JWL Aerts , Roland F. Schwarz , Tom L. Kaufmann , Gareth A. Wilson , Rachel Rosenthal , Peter Van Loo , Nicolai J. Birkbak , Zoltan Szallasi , Judit Kisistok , Mateo Sokac , Roberto Salgado , Miklos Diossy , Jonas Demeulemeester , Abigail Bunkum , Angela Dwornik , Alastair Magness , Andrew J. Rowan , Angeliki Karamani , Antonia Toncheva , Benny Chain , Carla Castignani , Christopher Abbosh , Clare Puttick , Clare E. Weeden , Claudia Lee , Corentin Richard , Crispin T. Hiley , Cristina Naceur-Lombardelli , David R. Pearce , Despoina Karagianni , Dhruva Biswas , Dina Levi , Elizabeth Larose Cadieux , Emilia L. Lim , Emma Nye , Eva Grönroos , Felip Gálvez-Cancino , Francisco Gimeno-Valiente , George Kassiotis , Georgia Stavrou , Gerasimos-Theodoros Mastrokalos , Helen L. Lowe , Ignacio Garcia Matos , Imran Noorani , Jacki Goldman , James L. Reading , Jayant K. Rane , Jerome Nicod , John A. Hartley , Karl S. Peggs , Katey S. S. Enfield , Kayalvizhi Selvaraju , Kevin Litchfield , Kevin W. Ng , Kezhong Chen , Krijn Dijkstra , Krupa Thakkar , Leah Ensell , Mansi Shah , Maria Litovchenko , Mariana Werner Sunderland , Matthew R. Huska , Michelle Dietzen , Michelle M. Leung , Mickael Escudero , Mihaela Angelova , Miljana Tanić , Nnennaya Kanu , Olga Chervova , Olivia Lucas , Oriol Pich , Othman Al-Sawaf , Paulina Prymas , Philip Hobson , Richard Kevin Stone , Robert Bentham , Robert E. Hynds , Roberto Vendramin , Sadegh Saghafinia , Samuel Gamble , Seng Kuong Anakin Ung , Sergio A. Quezada , Sharon Vanloo , Simone Zaccaria , Sonya Hessey , Sophia Ward , Sian Harries , Stefan Boeing , Stephan Beck , Supreet Kaur Bola , Tamara Denner , Teresa Marafioti , Thomas B. K. Watkins , Thomas Patrick Jones , Victoria Spanswick , Vittorio Barbè , Wei-Ting Lu , William Hill , Yin Wu , Yutaka Naito , Zoe Ramsden , Catarina Veiga , Gary Royle , Charles-Antoine Collins-Fekete , Francesco Fraioli , Paul Ashford , Martin D. Forster , Siow Ming Lee , Elaine Borg , Mary Falzon , Dionysis Papadatos-Pastos , James Wilson , Tanya Ahmad , Alexander James Procter , Asia Ahmed , Magali N. Taylor , Arjun Nair , David Lawrence , Davide Patrini , Neal Navani , Ricky M. Thakrar , Sam M. Janes , Emilie Martinoni Hoogenboom , Fleur Monk , James W. Holding , Junaid Choudhary , Kunal Bhakhri , Marco Scarci , Pat Gorman , Reena Khiroya , Robert CM Stephens , Yien Ning Sophia Wong , Zoltan Kaplar , Steve Bandula , Anne-Marie Hacker , Abigail Sharp , Sean Smith , Harjot Kaur Dhanda , Camilla Pilotti , Rachel Leslie , Anca Grapa , Hanyun Zhang , Khalid AbdulJabbar , Xiaoxi Pan , Yinyin Yuan , David Chuter , Mairead MacKenzie , Serena Chee , Aiman Alzetani , Judith Cave , Jennifer Richards , Eric Lim , Paulo De Sousa , Simon Jordan , Alexandra Rice , Hilgardt Raubenheimer , Harshil Bhayani , Lyn Ambrose , Anand Devaraj , Hema Chavan , Sofina Begum , Silviu I. Buderi , Daniel Kaniu , Mpho Malima , Sarah Booth , Andrew G. Nicholson , Nadia Fernandes , Pratibha Shah , Chiara Proli , Madeleine Hewish , Sarah Danson , Michael J. Shackcloth , Lily Robinson , Peter Russell , Kevin G. Blyth , Andrew Kidd , Craig Dick , John Le Quesne , Alan Kirk , Mo Asif , Rocco Bilancia , Nikos Kostoulas & Mathew Thomas Singleton Hospital, Swansea Bay University Health Board, Swansea, UK. University Hospitals of Leicester NHS Trust, Leicester, UK. Leicester Medical School, University of Leicester, Leicester, UK. University of Leicester, Leicester, UK. Cancer Research Centre, University of Leicester, Leicester, UK. Royal Free London NHS Foundation Trust, London, UK. Aberdeen Royal Infirmary NHS Grampian, Aberdeen, UK. Department of Medical Oncology, Aberdeen Royal Infirmary NHS Grampian, Aberdeen, UK. University of Aberdeen, Aberdeen, UK. Department of Pathology, Aberdeen Royal Infirmary NHS Grampian, Aberdeen, UK. The Whittington Hospital NHS Trust, London, UK. Birmingham Acute Care Research Group, Institute of Inflammation and Ageing, University of Birmingham, Birmingham, UK. Guy’s and St Thomas’ NHS Foundation Trust, London, UK. University Hospital Birmingham NHS Foundation Trust, Birmingham, UK. Institute of Immunology and Immunotherapy, University of Birmingham, Birmingham, UK. Manchester Cancer Research Centre Biobank, Manchester, UK. Wythenshawe Hospital, Manchester University NHS Foundation Trust, Wythenshawe, UK. Manchester University NHS Foundation Trust, Manchester, UK. Division of Infection, Immunity and Respiratory Medicine, University of Manchester, Manchester, UK. Cancer Research UK Lung Cancer Centre of Excellence, University of Manchester, Manchester, UK. The Christie NHS Foundation Trust, Manchester, UK. Division of Cancer Sciences, The University of Manchester and The Christie NHS Foundation Trust, Manchester, UK. Cancer Research UK Manchester Institute Cancer Biomarker Centre, University of Manchester, Manchester, UK. Artificial Intelligence in Medicine (AIM) Program, Mass General Brigham, Harvard Medical School, Boston, MA, USA. Department of Radiation Oncology, Brigham and Women’s Hospital, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA, USA. Radiology and Nuclear Medicine, CARIM & GROW, Maastricht University, Maastricht, The Netherlands. Institute for Computational Cancer Biology, Center for Integrated Oncology (CIO), Cancer Research Center Cologne Essen (CCCE), Faculty of Medicine and University Hospital Cologne, University of Cologne, Cologne, Germany. Berlin Institute for the Foundations of Learning and Data (BIFOLD), Berlin, Germany. Berlin Institute for Medical Systems Biology, Max Delbrück Center for Molecular Medicine in the Helmholtz Association (MDC), Berlin, Germany. Department of Genetics, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA. Department of Genomic Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas, USA. Cancer Genomics Laboratory, The Francis Crick Institute, London, UK. Department of Molecular Medicine, Aarhus University Hospital, Aarhus, Denmark. Department of Clinical Medicine, Aarhus University, Aarhus, Denmark. Bioinformatics Research Centre, Aarhus University, Aarhus, Denmark. Danish Cancer Society Research Center, Copenhagen, Denmark. Computational Health Informatics Program, Boston Children’s Hospital, Boston, MA, USA. Department of Bioinformatics, Semmelweis University, Budapest, Hungary. Department of Pathology, ZAS Hospitals, Antwerp, Belgium. Division of Research, Peter MacCallum Cancer Centre, Melbourne, Australia. Department of Physics of Complex Systems, ELTE Eötvös Loránd University, Budapest, Hungary. Integrative Cancer Genomics Laboratory, VIB Center for Cancer Biology, Leuven, Belgium. VIB Center for AI & Computational Biology, Leuven, Belgium. Department of Oncology, KU Leuven, Leuven, Belgium. Computational Cancer Genomics Research Group, University College London Cancer Institute, London, UK. University College London Cancer Institute, London, UK. The Francis Crick Institute, London, UK. Medical Genomics, University College London Cancer Institute, London, UK. Bill Lyons Informatics Centre, University College London Cancer Institute, London, UK. Experimental Histopathology, The Francis Crick Institute, London, UK. Department of Infectious Disease, Faculty of Medicine, Imperial College London, London, UK. Advanced Sequencing Facility, The Francis Crick Institute, London, UK. Department of Haematology, University College London Hospitals, London, UK. Cancer Immunology Unit, Research Department of Haematology, University College London Cancer Institute, London, UK. Tumour Immunogenomics and Immunosurveillance Laboratory, University College London Cancer Institute, London, UK. Retroviral Immunology Group, The Francis Crick Institute, London, UK. Bioinformatics and Systems Biology, Method Development and Research Infrastructure, Robert Koch Institute, Berlin, Germany. Experimental Oncology, Institute for Oncology and Radiology of Serbia, Belgrade, Serbia. University College London Department of Epidemiology and Health Care, London, UK. University College London Hospitals, London, UK. Department I of Internal Medicine, University Hospital of Cologne, Cologne, Germany. Immune Regulation and Tumour Immunotherapy Group, Cancer Immunology Unit, Research Department of Haematology, University College London Cancer Institute, London, UK. Cancer Evolution and Genome Instability Laboratory, The Francis Crick Institute, London, UK. Centre for Medical Image Computing, Department of Medical Physics and Biomedical Engineering, University College London, London, UK. Department of Medical Physics and Bioengineering, University College London Cancer Institute, London, UK. Department of Medical Physics and Biomedical Engineering, University College London, London, UK. Institute of Nuclear Medicine, Division of Medicine, University College London, London, UK. Institute of Structural and Molecular Biology, University College London, London, UK. Department of Radiology, University College London Hospitals, London, UK. UCL Respiratory, Department of Medicine, University College London, London, UK. Department of Thoracic Surgery, University College London Hospital NHS Trust, London, UK. Lungs for Living Research Centre, UCL Respiratory, University College London, London, UK. Department of Thoracic Medicine, University College London Hospitals, London, UK. Lungs for Living Research Centre, UCL Respiratory, Department of Medicine, University College London, London, UK. Integrated Radiology Department, North-buda St. John’s Central Hospital, Budapest, Hungary. Institute of Nuclear Medicine, University College London Hospitals, London, UK. The Institute of Cancer Research, London, UK. Case45, London, UK. The University of Texas MD Anderson Cancer Center, Houston, USA. Independent Cancer Patients’ Voice, London, UK. University Hospital Southampton NHS Foundation Trust, Southampton, UK. Department of Oncology, University Hospital Southampton NHS Foundation Trust, Southampton, UK. Academic Division of Thoracic Surgery, Imperial College London, London, UK. Royal Brompton and Harefield Hospitals, part of Guy’s and St Thomas’ NHS Foundation Trust, London, UK. National Heart and Lung Institute, Imperial College, London, UK. Royal Surrey Hospital, Royal Surrey Hospitals NHS Foundation Trust, Guildford, UK. University of Surrey, Guildford, UK. University of Sheffield, Sheffield, UK. Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK. Liverpool Heart and Chest Hospital, Liverpool, UK. Princess Alexandra Hospital, The Princess Alexandra Hospital NHS Trust, Harlow, UK. School of Cancer Sciences, University of Glasgow, Glasgow, UK. Beatson Institute for Cancer Research, University of Glasgow, Glasgow, UK. Queen Elizabeth University Hospital, Glasgow, UK. Institute of Infection, Immunity & Inflammation, University of Glasgow, Glasgow, UK. NHS Greater Glasgow and Clyde, Glasgow, UK. Cancer Research UK Scotland Institute, Glasgow, UK. Institute of Cancer Sciences, University of Glasgow, Glasgow, UK. NHS Greater Glasgow and Clyde Pathology Department, Queen Elizabeth University Hospital, Glasgow, UK. Golden Jubilee National Hospital, Clydebank, UK.
Methods
Baseline characterization of lung cancer samples
TRACERx patient recruitment and sample collection complied with all relevant ethical regulations and were carried out as previously described . The eligibility criteria have been previously described . Of note, the eighth version of pTNM staging was used in this analysis. Patients with histopathologically confirmed stage I-IIIB NSCLC who were eligible for primary surgery were enrolled in the prospective observational TRACERx study (ClinicalTrials.gov identifier: NCT01888601). The study design was approved by an independent research ethics committee (NRES Committee London, REC ref. 13/ LO/1546), and informed consent was obtained from all patients before study admittance. Patient sample identifiers were anonymized and tracked in a centralized database controlled by the study sponsor. DNA degradation of archived formalin-fixed paraffin-embedded (FFPE) samples over time can affect panel quality for ctDNA detection, and degraded samples might not accurately reflect the typical sample quality in a clinical setting in which FFPE samples were recently collected (Extended Data Fig. 4a). We obtained FFPE tissue for 204 patients. Of these, 62 had atypically low counts of high-quality panel targets ( ), likely owing to age and/or poor quality of the FFPE samples, and 2 did not pass panel design. For 31 of the 64 patients, DNA extracted from fresh frozen (FF) tissue was available by September 2023. For these samples, an updated set of panels was generated, the quality of which was more consistent with <5-year-old FFPE samples (Extended Data Fig. 4b). One panel was constructed from an FF tumor sample and failed to attain 1,000 high-quality targets; however, this was included to ensure that the cohort was representative of the wider TRACERx cohort. Two FF panels were constructed where FFPE panel construction had failed entirely. The final cohort in our study consisted of preoperative samples from 171 consecutively recruited patients in the larger TRACERx study in whom adequate plasma was available for the ctDNA analysis completed by September 2023, in addition to confirmed clinical outcome data as of February 2024. Retrospective ctDNA analysis was conducted using prospectively collected specimens and during clinical follow-up. In this cohort, we demonstrated that our measure of ctDNA signal (ppm) was in strong agreement with tumor molecules per ml plasma, which accounts for the volume of plasma from which input cfDNA is extracted (Demming regression; fitted slope=0.97, CI= 0.95-0.99; Extended Data Fig. 4c). Personalis investigators were fully blinded to patient clinical outcome and clinical pathological characteristics during sample processing and ctDNA analysis. Likewise, TRACERx investigators were blinded to patient ctDNA status during clinical data and patient specimen collection. EGFR mutations, oncogenic fusion isoforms and instances of MET exon 14 skipping from patients in the TRACERx cohort were annotated as previously described .
Tumor and normal whole-genome sequencing
Tumor sections were macrodissected to improve tumor content and were required to meet a tumor cellularity threshold of , as determined by pathological review, to be eligible for DNA extraction and further processing. At this threshold, (2/171) of samples were considered ineligible for analysis and required replacement with different specimens. At our chosen cut-off threshold, we observed no significant correlation between tumor purity and the LOD of the assay (Supplementary Fig. 1). Genomic DNA was isolated from matched tumor and normal samples using the Qiagen AllPrep DNA/RNA FFPE Tissue Kit or the QIAamp DNA Mini Kit (Qiagen) using internally optimized workflows. Whole-genome sequencing (WGS) libraries were prepared with 100-500 ng of acoustically sheared genomic DNA (Covaris) using the KAPA HyperPrep Kit (Roche Sequencing Solutions) and customized methods. Libraries were cleaned up using AMPure XP beads and then quantified using the KAPA Library Quantification Kit (Roche Sequencing Solutions), before being sequenced to depth of coverage using a NovaSeq 6000 instrument (Illumina). The impact
of varying DNA input amounts during tumor WGS on panel design was assessed using 19 normal-tumor pairs. For each pair, normal libraries were made using 550 ng input DNA, and tumor libraries with , or 550 ng of input DNA. We observed largely consistent panel size and similarity across the range of input DNA amounts (Supplementary Fig. 2a,b). A comprehensive list of reagents used in this study is provided in Supplementary Table 1.
Alignment and variant calling from tumor and normal whole-genome sequencing
The pipeline performs alignment, duplicate removal and base quality-score recalibration (BQSR) of the matched tumor and normal WGS samples using best-practice guidelines recommended by the Broad Institute . In brief, individual read-pairs were first mapped to the hs37d5 reference genome build using the BWA-MEM aligner. We then used the Picard toolkit (RRID: SCR_006525) to identify duplicate reads through comparison of the position of reads and read-pairs. Duplicate reads were then removed. The Genome Analysis Toolkit (GATK, RRID: SCR_001876) was then used for sequence realignment and to apply base quality scores (BQSR): the BaseRecalibrator tool uses the deduplicated data and a set of known variants to construct a model of covariation, which is the used to generate a recalibration file. The ApplyBQSR tool then uses this model to adjust base quality scores in the data, yielding a new BAM file. Aligned sequence data are written in BAM format according to SAM (RRID: SCR_01095) specification. MuTect (RRID: SCR_000559) was used to co-analyze the tumor and normal BAM files for somatic single-nucleotide variant (SNV) detection. Somatic SNV calls were filtered on the basis of a broad set of quality-control metrics, such as local sequence coverage and read quality, strand bias and the statistical likelihood that the allele is present in the normal sample.
NeXT personal probe panel design
Hybrid capture probe panels used in this study were designed with the NeXT Personal platform’s proprietary algorithms, as governed by the standard operating procedures at Personalis. In the design process for the bespoke panel, for each patient’s panel, the ctDNA targets were selected from exonic, intronic and intergenic somatic variants identified through WGS of matched tumor and normal samples, as described above. Somatic variants identified using Mutect (v1.1.6, default parameters) were selected and assigned an error rate according to the observed substitution in the solid tumor. Namely, the substitution error rate was estimated by the ratio of the aggregated amount of signal and the total number of molecules observed in each possible substitution in more than 200 healthy plasma samples . The MRD targets were then selected from somatic variants with an allele frequency above . Variants were further filtered by excluding those found in particular regions of the genome. Exclusion criteria included regions containing known germline SNPs, known CHIP variants, high GC content ( ), high polymorphism rates, mapping difficulties, systematic bias, short tandem repeats and low sequence complexity .
Somatic variant calls were ranked by the product of allele frequency in solid tumor and the substitution-based error rate of solid tumor substitutions. Up to top ranked somatic variants were selected genome-wide for panel inclusion by the NeXT Personal platform. The final panel also included 43 population SNVs for quality-assurance purposes (that is, to detect potential sample-panel mismatch or contamination). Several criteria were used to optimize the selection of the 43 SNVs, including having a population frequency of at least , being in Hardy-Weinberg equilibrium and being outside of the HLA region. The SNPs were prioritized to have roughly equivalent representation across subpopulations. Probe sequences were designed by the NeXT Personal platform’s proprietary algorithm before being processed for manufacturing. Upon receiving panel reagents, the new panel was used for targeted sequencing of blood
plasma from an unrelated healthy donor. This served two purposes: quality-control tests on the sequencing data were used to qualify the panel for use on the patient’s plasma samples, and any MRD targets for which any non-reference signal was observed were deactivated in the logical panel design, to mitigate the risk that those targets could be enriched for noise.
NeXT Personal cfDNA library preparation, target enrichment and sequencing
Library preparation, target enrichment and sequencing of the cfDNA samples were performed in CLIA-certified and CAP-accredited laboratories, as governed by the standard operating procedures at Personalis. In brief, sequencing libraries were prepared from cfDNA input (median, 15 ng ), using the KAPA HyperPrep Kit (Roche Sequencing Solutions) and customized methods. We assessed the effect of the quantity of total input cfDNA on MRD detection and ctDNA burden and observed no significant associations between the amount of cfDNA input and ctDNA detection status (Supplementary Fig. 3). Consistently, there was no significant correlation between the quantity of input cfDNA and ctDNA burden or ctDNA burden and the LOD of the assay (Supplementary Fig. 3b,c). Together, this evidence suggests that ctDNA burden and detection status were not confounded by the quantity of total circulating DNA in the cohort. These findings are supported by a separate analytical validation study . The pre-capture libraries were quantified using a Lunatic spectrophotometer (Unchained Labs), and up to was enriched with patient-specific NeXT Personal probe panels using proprietary modifications to the Fast Hybridization and Wash Kit (Twist Bioscience) and workflow. The postcapture libraries were then amplified by PCR (nine cycles), and a quality assessment was performed using the TapeStation system (Agilent Technologies). The final libraries were cleaned up using AMPure XP beads and then quantified using the KAPA Library Quantification Kit (Roche Sequencing Solutions) before being sequenced on a NovaSeq 6000 instrument (Illumina). The libraries were deeply sequenced to optimize the number of unique observed molecules. We observed a weak correlation between sequencing depth and the LOD for each custom assay, as well as between sequencing depth and the strength of ctDNA signal detected (ppm level); however, the ctDNA detection status (detected or not detected) was not confounded by the variability of sequencing depth, with no significant difference in sequencing depth observed between the two groups (Supplementary Fig. 4a-c).
NeXT Personal cfDNA analysis
Analysis of all NeXT Personal data in this study was performed using a consistent, locked version of the production pipeline developed by Personalis. In summary, the cfDNA sequencing data were aligned to the human reference genome (version hs37d5), followed by noise suppression and ctDNA detection. More specifically, we built and filtered the molecular consensus as follows. First, we aligned all reads to the human reference using BWA-MEM (Burrows-Wheeler Aligner, v1.0.2). Second, we grouped read-pairs according to their paired mapped positions to form initial consensus groups. With a positional approach like this, there is a risk of grouping multiple molecules together that share paired mapped positions. We mitigated this risk by detecting the presence of non-reference alleles that were present in not only a subset of the consensus-group reads, but also at least two other consensus groups. When there was an allele present in a subset of reads with additional support from other consensus groups, we split the consensus group to isolate the allele-containing reads in their own new group. For each group, we required observation of at least one molecule from each DNA strand. Raw reads that differed by more than across the consensus molecule were not included. Bases with a quality of less than 29 were masked. Once we defined the consensus groups, we formed a single consensus molecule from the reads in each group on the basis of identification of the consensus basecall at
each position along the group of read-pairs. Bases with less than agreement in the molecular group were masked. Reads with more than 20% of their bases masked were removed. Then, we re-mapped these consensus reads again using BWA-MEM to avoid any erroneous alignment caused by sequencing errors. Following noise suppression, tumor-derived signal was aggregated in a tested sample across ctDNA targets in each patient-specific panel to calculate the ctDNA level (measured in ppm, based on the total unique molecule count). A one-tailed Poisson test was then performed to determine ctDNA detection status for each tested sample. The observed aggregate tumor-derived signal across each panel serves as the tested value, with the expected noise arising from accumulated background error being set as the mean of the Poisson distribution. The value threshold was established as previously described . In brief, the value threshold is set at <0.001 to ensure that an analytical specificity requirement of was met. Therefore, the value threshold was set to 0.001 for this study to ensure higher specificity. If the tumor signal was significantly above the expected noise, the sample was classified as ctDNA-positive (that is ‘detected’); otherwise, it was classified as ctDNA-negative (that is ‘not detected’). Given that the value is the probability that the observed signal comes from noise, the detection threshold is set to enforce a specificity requirement and is independent of factors that affect observed levels. Variations in assay and locus-specific factors might affect the efficiency of detection of a specific genetic alteration. Different genetic alterations could also be present at different frequencies in the blood. The actual ppm level (allele frequency) measured is a function of the set of targets selected. After aggregation across many loci, however, the average per-locus efficiency of detection tends toward the population mean of the efficiency of detecting a specific genetic alteration. This is demonstrated in Supplementary Figure 5a, which shows that, as the panel size approaches 1,800 targets, the coefficient of variation (CV) of the observed ppm level adds little to the overall variability of the assay. Basing detection status on a value, rather than an allele frequency threshold, allowed our approach to normalize detection efficiency for specific mutations through the summation of signal across up to 1,800 variant loci that have been selected on the basis of their site-specific error rates, inherent noise and complexity.
Clonal hematopoiesis of indeterminate potential
We designed our assay to prevent CHIP mutations from being included in the bespoke panel by taking a tumor-matched-normal approach for somatic variant calling to inform panel design. This is an effective approach because the CHIP signal is higher in the normal blood cells than in tumor tissue, and thus will be filtered out in the tumor normal algorithmic comparison. We also excluded the most common CHIP regions from our panel design.
TRACERx cfDNA extraction and quantification
Blood samples were collected in -EDTA tubes. Samples were processed within 2 h of collection by double centrifugation of the blood, first for 10 min at , then the plasma for 10 min at . Plasma was stored in aliquots at . Following isolation, plasma was shipped on dry ice. At the time of analysis, TRACERx plasma samples were between 2 and 9 years old. Up to 24 h before cfDNA extraction, the plasma was thawed and aliquots from the same patient plasma time point were consolidated and then stored at . Immediately before cfDNA extraction using QIAamp Circulating Nucleic Acid or QIAsymphony Circulating DNA kits (Qiagen), consolidated plasma was clarified at to remove cryoprecipitates.
Samples used for DNA input performance characterization
All experiments were performed in the Clinical Laboratory Improvement Amendments (CLIA)-certified and College of American Pathologists (CAP)-accredited laboratories at Personalis, as guided by the
Association for Molecular Pathology (AMP) and CAP’s joint recommendations . Healthy donor and patient tissue and matched buffy-coat and plasma samples used in Supplementary Figures 2 and 5 were sourced from either Boca Biolistics, Cureline or iProcess. Patient samples in this study obtained from commercial vendors were collected from informed patients following receipt of their written consent under study protocols approved by an Independent Ethical Committee or Institutional Review Board (Protocol numbers: PG-ONC 2003/1; IRB7 – Registration 5136; IRB 800959).
Survival analyses
OS was defined as the days from registration to death or loss of follow-up. RFS was defined as the days from registration to any disease recurrence, new primary tumor events or death. Exploratory analysis comparing OS and RFS at different ctDNA levels was performed for a total 171 patients shown in Figure 2 and Extended Data Figure 3. Survival (3.3-1), survminer (0.4.9) and finalfit (1.0.4) R packages were used to generate hazard ratios, CIs, 2-year survival probability, forest plots, KM plots and Cox regression models. Differences in OS or RFS between different groups of patients were assessed using log-rank tests. The association of OS or RFS with continuous variables, such as ctDNA level, was assessed through Cox regression modeling. The independent prognostic value of ctDNA in either the continuous or categorical form was assessed by multivariable Cox regression models that included histology, adjuvant treatment status, smoking status, pathological stage and age.
Statistical analysis and data handling
No statistical methods were used to predetermine sample size. Analysis was performed in the statistical environment (4.1.3). All statistical tests were two-sided, unless stated otherwise. For assay-performance analyses, positive predictive value was calculated as all true-positive results divided by the sum of true-positive and false-positive results; negative predictive value was calculated as all true-negative results divided by the sum of false-negative plus true-negative results; sensitivity was calculated as true-positive results divided by the sum of true-positive and false-negative results; and specificity was calculated as true negatives divided by the sum of true negatives and false positives. For input and output operations and general data manipulation, the R packages tidyverse (v1.3.2) and lubridate were used (v1.9.2). For general visualization, the R packages ggplot2 (v.3.4.2), ggpubr (v.0.4.0), scales (v.1.2.1.) and ggnewscale (v.0.4.9) were used. For statistical analyses and related visualization, R packages survival (v.3.3-1), survminer (v.0.4.9), finalfit (v.1.0.4), gt (v.0.10.1) and mcr (v.1.2.2) were used.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Processed TRACERx patient data have been deposited on Zenodo at https://doi.org/10.5281/zenodo. 8400837 (ref. 34). Supporting data from validation experiments are included as Extended Data Table 1. Raw data from TRACERx patients analyzed in this study, including fastq and bam files from tumor and normal WGS, as well as fastq files from cfDNA, have been deposited at the European Genome-phenome Archive (EGA), hosted by The European Bioinformatics Institute (EBI) and the Centre for Genomic Regulation (CRG) under the accession codes EGAS00001006494, under controlled access.
Code availability
Supporting code required to reproduce all analyses and figures included in this paper are available on Zenodo at https://doi.org/ 10.5281/zenodo. 8400837 (ref. 34).
References
Frankell, A. M. et al. The evolution of lung cancer and impact of subclonal selection in TRACERx. Nature 616, 525-533 (2023).
Van der Auwera, G. A. & O’Connor, B. D. Genomics in the Cloud: Using Docker, GATK, and WDL in Terra (O’Reilly Media, 2020).
DePristo, M. A. et al. A framework for variation discovery and genotyping using next-generation DNA sequencing data. Nat. Genet. 43, 491-498 (2011).
Freeman, T. M. et al. Genomic loci susceptible to systematic sequencing bias in clinical whole genomes. Genome Res. 30, 415-426 (2020).
Jennings, L. J. et al. Guidelines for validation of next-generation sequencing-based oncology panels: a joint consensus recommendation of the Association for Molecular Pathology and College of American Pathologists. J. Mol. Diagn. 19, 341-365 (2017).
Black, J. An ultra-sensitive and specific ctDNA assay provides novel pre-operative disease stratification in early stage lung adenocarcinoma. Zenodo https://doi.org/10.5281/zenodo. 8400837 (2024).
Acknowledgements
We thank the staff of the Advanced Sequencing Facility at The Francis Crick Institute, as well as the members of the TRACERx consortium for their contributions to this study. TRACERx (ClinicalTrials.gov no.: NCTO1888601) is sponsored by University College London (UCL/12/0279) and was approved by an independent research ethics committee (REC 13/LO/1546). TRACERx is funded by Cancer Research UK (CRUK; C11496/A17786) and is coordinated by CRUK and the UCL Cancer Trials Centre, which has a core grant from CRUK (C444/ A15953). We gratefully acknowledge the patients and relatives who participated in the TRACERx study; all site personnel, investigators, funders and industry partners that supported the generation of the data within this study. This work was also supported by the CRUK Lung Cancer Centre of Excellence and the CRUK City of London Centre Award (C7893/A26233) as well as theUCL Experimental Cancer Medicine Centre. We acknowledge the Personalis research and development team for their work in developing and validating the NeXT Personal platform, including major contributions from J. Li and A. Stram. We also acknowledge the Personalis operations team for helping to process the samples using NeXT Personal. T.K. is supported by the Japan Society for the Promotion of Science (JSPS) overseas research fellowships program (202060447). M.J.-H. is a CRUK Fellow and has received funding from CRUK, NIHR, the Rosetrees Trust, UKI NETs and the NIHR University College London Hospitals Biomedical Research Centre. N.M. is a Sir Henry Dale Fellow, jointly funded by the Wellcome Trust and the Royal Society (211179/Z/18/Z), and also receives funding from CRUK, the Rosetrees Trust, the NIHR BRC at University College London Hospitals and the CRUK University College London Experimental Cancer Medicine Centre. C.S. is a Royal Society Napier Research Professor (RSRPR210001). His work is supported by the Francis Crick Institute, which receives its core funding from Cancer Research UK (CC2041), the UK Medical Research Council (CC2041) and the Wellcome Trust (CC2041). For the purpose of Open Access, the author has applied a CC BY public copyright licence to any author accepted manuscript version arising from this submission. C.S. is funded by Cancer Research UK (TRACERx (C11496/A17786), PEACE (C416/A21999) and CRUK Cancer Immunotherapy Catalyst Network); Cancer Research UK Lung Cancer Centre of Excellence (C11496/ A30025); the Rosetrees Trust, Butterfield and Stoneygate Trusts; NovoNordisk Foundation (ID16584); Royal Society Professorship Enhancement Award (RP/EA/180007 and RFERE231118)); National Institute for Health Research (NIHR) University College London Hospitals Biomedical Research Centre; the Cancer Research UK-University College London Centre; Experimental Cancer Medicine
Centre; the Breast Cancer Research Foundation (US) (BCRF-22-157); Cancer Research UK Early Detection an Diagnosis Primer Award (Grant EDDPMA-Nov21/100034); and The Mark Foundation for Cancer Research Aspire Award (Grant 21-029-ASP) and ASPIRE Phase II award (Grant 23-034-ASP). C.S. received an ERC Advanced Grant (PROTEUS) from the European Research Council under the European Union’s Horizon 2020 research and innovation program (grant agreement no. 835297).
Author contributions
J.R.M.B. and C.S. designed the clinical portion of the study. S.V. and M.C. coordinated handling of clinical specimens. J.R.M.B., M.S.H., K.T., A.H., C.B., E.C.C., C.M.R., K.G. and P.P. performed quality control of genomic data. T.K., M.A.B., W.K.L., D.A.M., D.M., O.G.S., C.M., M.S. and J.R.M.B. performed quality control on clinical data. M.A.B., D.A.M., J.A.S., A.H., M.J.-H. and C.S. coordinated the TRACERx clinical trial. R.O.C. and G.B. conceived the NeXT Personal platform. G.B. created the panel design and ctDNA-detection algorithms. G.B., R.M.P. and F.C.P.N. developed the noise-suppression methods. J.L., J.N. and G.B. designed the analytical study and analyzed the associated data. J.N. and J.L. led the assay development and analytical study experiments. J.H. led the pipeline development. Clinical data were analyzed by J.R.M.B., and then analyzed separately by C.W.A. and B.L. J.R.M.B., A.M.F., N.M., C.W.A., R.O.C., J.L., G.B., J.H., R.C., J.N., R.P., S.B. and C.S. prepared the manuscript. R.O.C. and C.S. jointly supervised the study.
Funding
Open Access funding provided by The Francis Crick Institute.
Competing interests
M.A.B. has consulted for Achilles Therapeutics. D.A.M. reports receiving speaker fees from AstraZeneca, Eli Lilly, Bristol Myers Squibb and Takeda, consultancy fees from AstraZeneca, Thermo Fisher, Takeda, Amgen, Janssen, MIM Software, Bristol Myers Squibb and Eli Lilly and has received educational support from Takeda and Amgen. M.J.-H. has consulted for, and is a member of, the Achilles Therapeutics scientific advisory board (SAB) and steering committee, and has received speaker honoraria from Pfizer, Astex Pharmaceuticals and the Oslo Cancer Cluster. N.M. has received consultancy fees and has stock options in Achilles Therapeutics. C.S. acknowledges grants from AstraZeneca, Boehringer-Ingelheim, Bristol Myers Squibb, Pfizer, Roche-Ventana, Invitae (previously Archer Dx Inc, collaboration in minimal residual disease sequencing technologies), Ono Pharmaceutical and Personalis. He is chief investigator for the AZ MeRmaiD 1 and 2 clinical trials and is the steering committee chair. He is also co-chief investigator of the NHS Galleri trial funded by GRAIL and a paid member of GRAIL’s SAB. He receives consultant fees from Achilles Therapeutics (and is a SAB member), Bicycle Therapeutics (and is a SAB member), Genentech, Medicxi, China Innovation Centre of Roche (formerly Roche Innovation Centre – Shanghai, Metabomed (until July 2022)), Relay Therapeutics (and is a SAB member), Saga Diagnostics (and is a SAB member) and the Sarah Cannon Research Institute. C.S has received honoraria from Amgen, AstraZeneca, Bristol Myers Squibb, GSK,
Illumina, MSD, Novartis, Pfizer and Roche-Ventana. C.S. has previously held stock options in Apogen Biotechnologies and GRAIL, and currently has stock options in Bicycle Therapeutics and Relay Therapeutics, and has stock and is a co-founder of Achilles Therapeutics. G.B., C.W.A., S.M.B, R.C., J.H., B.L., J.L., F.C.P.N., J.N., R.M.P. and R.O.C. are employees and stockholders of Personalis. A.M.F. is listed as a co-inventor on a patent application to determine methods and systems for tumor monitoring (PCT/EP2022/077987; ‘Methods and systems for tumour monitoring’). S.V. is a co-inventor on a patent for methods for detecting molecules in a sample (US patent no. 10578620; ‘Methods for detecting molecules in a sample’). M.J.-H. is listed as a co-inventor on a European patent application related to methods to detect lung cancer (PCT/US2017/O28013; ‘Methods for lung cancer detection’); this patent has been licensed to commercial entities and, under terms of employment, M.J.-H. is due a share of any revenue generated from such license(s). N.M. holds European patents related to targeting neoantigens (PCT/EP2016/059401; ‘Method for treating cancer’), identifying patient response to immune checkpoint blockade (PCT/EP2016/071471; “Immune checkpoint intervention” in cancer’), determining HLA LOH (PCT/GB2018/052004; ‘Analysis of HLA alleles in tumours and the uses thereof’), and predicting survival rates of patients with cancer (PCT/GB2020/050221; ‘Method of predicting survival rates for cancer patients’). C.S declares a patent application for methods to lung cancer (PCT/US2017/O28013); targeting neoantigens (PCT/EP2016/059401); identifying patent response to immune checkpoint blockade (PCT/EP2016/071471); methods for lung cancer detection (US20190106751A1); identifying patients who respond to cancer treatment (PCT/GB2018/051912); determining HLA LOH (PCT/GB2018/052004); predicting survival rates of patients with cancer (PCT/GB2020/050221); and methods and systems for tumor monitoring (PCT/EP2O22/O77987). C.S. is an inventor on a European patent application (PCT/GB2017/053289) related to assay technology to detect tumor recurrence. This patent has been licensed to a commercial entity, and under their terms of employment, C.S is due a revenue share of any revenue generated from such license(s). The other authors declare no competing interests.
Correspondence and requests for materials should be addressed to Charles Swanton.
Peer review information Nature Medicine thanks Alain Thierry, Benjamin Besse and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Anna Maria Ranzoni, in collaboration with the Nature Medicine team.
Extended Data Table 1 | Baseline demographic and tumor characteristics for the study population split by lung adenocarcinoma and non-adenocarcinoma populations. Data are , unless otherwise stated. Percentages may not sum to 100% due to rounding
Characteristic
levels
LUAD
Non-LUAD
p
n
–
94
77
NA
Age (years)
Mean (SD)
67.2 (8.9)
70.1 (8.0)
0.028
Sex
Female
40 (42.6)
29 (37.7)
0.623
Male
54 (57.4)
48 (62.3)
Pathological TNM
1a
11 (11.7)
6 (7.8)
0.718
1b
17 (18.1)
16 (20.8)
2a
4 (4.3)
4 (5.2)
2b
25 (26.6)
27 (35.1)
3a
35 (37.2)
22 (28.6)
3b
2 (2.1)
2 (2.6)
Smoking status
Ex-Smoker
41 (43.6)
46 (59.7)
0.086
Never Smoked
6 (6.4)
2 (2.6)
Smoker
47 (50.0)
29 (37.7)
Adjuvant treatment
Adjuvant
46 (48.9)
36 (46.8)
0.896
No adjuvant
48 (51.1)
41 (53.2)
LUAD subtype
Lepidic
6 (6.4)
Papillary
6 (6.4)
Acinar
23 (24.5)
Cribriform
7 (7.4)
Micropapillary
4 (4.3)
Solid
38 (40.4)
Invasive mucinous
10 (10.6)
Oncogenic event
None
85 (90.4)
73 (94.8)
0.364
EGFR mutated
7 (7.4)
2 (2.6)
MET exon 14 skipped
2 (2.1)
2 (2.6)
Follow up (days; OS)
Median (# of events)
1839 (39)
1862 (38)
0.84
Follow up (days; RFS)
Median (# of events)
1821 (49)
1849 (40)
0.58
values were calculated using chi-squared tests for categorical variables and tests for continuous variables.
Extended Data Table 2 | Baseline demographic and tumor characteristics for the current study presented alongside general characteristics of patients included in the work detailed in refs. 1,2. Data are , unless otherwise stated. Percentages may not sum to due to rounding
Characteristic
levels
Abbosh et al. 2023
Abbosh et al. 2017
NeXT Personal
Age (years)
Mean (SD)
68.8 (9.4)
68.4 (9.3)
68.5 (8.6)
Sex
Female
79 (40.9)
36 (37.5)
69 (40.4)
Male
114 (59.1)
60 (62.5)
102 (59.6)
Adjuvant treatment
Adjuvant
77 (39.9)
28 (29.2)
82 (48.0)
No adjuvant
116 (60.1)
68 (70.8)
89 (52.0)
Histology
Adenocarcinoma
101 (52.3)
57 (59.4)
94 (55.0)
Other
25 (13.0)
8 (8.3)
20 (11.7)
Squamous cell carcinoma
67 (34.7)
31 (32.3)
57 (33.3)
LUAD subtype
Lepidic
4 (4.2)
10 (17.9)
6 (6.4)
Papillary
11 (11.5)
4 (7.1)
6 (6.4)
Acinar
33 (34.4)
21 (37.5)
23 (24.5)
Cribriform
9 (9.4)
1 (1.8)
7 (7.4)
Micropapillary
4 (4.2)
4 (4.3)
Solid
24 (25.0)
14 (25.0)
38 (40.4)
Invasive Mucinous
11 (11.5)
6 (10.7)
10 (10.6)
Pathological TNM
IA
37 (19.2)
26 (27.1)
17 (9.9)
IB
37 (19.2)
32 (33.3)
33 (19.3)
IIA
40 (20.7)
14 (14.6)
8 (4.7)
IIB
30 (15.5)
10 (10.4)
52 (30.4)
IIIA
49 (25.4)
13 (13.5)
57 (33.3)
IIIB
1 (1.0)
4 (2.3)
Smoking status
Ex-Smoker
103 (53.4)
49 (51.0)
87 (50.9)
Never Smoked
10 (5.2)
11 (11.5)
8 (4.7)
Smoker
80 (41.5)
36 (37.5)
76 (44.4)
Extended Data Fig. 1| Association between ctDNA and clinicogenomic features of NSCLC. a. Stacked barplot of the number of targets obtained from coding (grey) and noncoding (blue) regions of the genome for each panel. b. Dot plot depicting panel-specific limit of detection (LOD) in ppm in all pre-operative plasma samples. c. Scatterplot demonstrating the association of ctDNA level with pack years of smoking for preoperative samples. Fitted line represents a linear model, and the shaded area represents the confidence interval. d. Boxplot of preoperative ctDNA level for each pathological subtype of lung adenocarcinoma. The boxplots depict the median at the middle line, the lower and upper hinges represent the first and third quartiles, respectively, the whiskers show minima to maxima no greater than the interquartile range (IQR), with the remaining
outlying data points plotted individually. Sample size is patients. value was calculated using two-sided Kruskal-Wallis rank sum test.e. Boxplot of preoperative ctDNA level by oncogenic event status. The boxplots depict the median at the middle line, the lower and upper hinges represent the first and third quartiles, respectively, the whiskers show minima to maxima no greater than the IQR, with the remaining outlying data points plotted individually. Sample size is patients. value was calculated using two-sided KruskalWallis rank sum test.f. Barplot of patient oncogenic event status colored by preoperative ctDNA detection status. value was calculated using two-sided Fisher’s exact test.
a
b
LUAD
C
Non-LUAD
Extended Data Fig. 2 | See next page for caption.
Extended Data Fig. 2 | Increased assay sensitivity improves stratification of relapse-free survival. a. Kaplan-Meier (KM) curve demonstrating relapsefree survival (RFS) within ctDNA-high (dark grey), ctDNA-low (light grey) and ctDNA-negative (green) patients with lung adenocarcinoma. ctDNA high and low groups were defined according to the median ctDNA levels across ctDNA-positive LUADs. P values were calculated using log-rank tests. b. KM curve demonstrating
RFS within patients harbouring ctDNA at an estimated ppm below the limit of reliable detection described in Abbosh et al. (light grey), and ctDNA negative patients (green). P values were calculated using log-rank tests. c. KM curve illustrating difference in RFS between ctDNA-high and ctDNA-low patients with non-LUAD. P values were calculated using log-rank tests.
a
Overall Survival: HR (95% Cl, p-value)
ctDNA
–
1.51 (1.22-1.86, p<0.001)
Histology
LUAD
–
Non-LUAD
0.86 (0.50-1.47, )
Treatment
Adjuvant
–
No adjuvant
1.28 (0.67-2.45, )
Pack years
–
0.97 (0.90-1.04, p=0.420)
Stage
I
–
II
0.92 (0.45-1.89, p=0.818)
III
1.68 (0.81-3.50, p=0.167)
Age
–
1.37 (0.94-1.99, p=0.100)
Oncogenic event
None
–
EGFR mutated
1.12 (0.42-3.02, p=0.816)
MET exon 14 skipped
1.34 (0.31-5.83, p=0.700)
log (HR)
C
Relapse-free Survival: HR (95% Cl, p-value)
ctDNA level
Not Detected
–
Low
14.94 (1.99-112.33, p=0.009)
High
27.18 (3.51-210.26, p=0.002)
Histology
LUAD
–
Non-LUAD
0.73 (0.47-1.15, p=0.180)
Treatment
Adjuvant
–
No adjuvant
1.23 (0.70-2.19, p=0.472)
Pack years
–
0.97 (0.91-1.05, )
Stage
I
–
II
0.96 (0.50-1.87, p=0.909)
III
1.35 (0.68-2.66, )
Age
–
1.15 (0.85-1.56, )
Oncogenic_Event
None
–
EGFR mutated
1.65 (0.72-3.79, p=0.239)
MET exon 14 skipped
e
Non-LUAD: Relapse-free Survival: HR ( , p-value)
g
Extended Data Fig. 3 | See next page for caption.
b
Relapse-free Survival: HR ( Cl, p-value)
ctDNA
–
1.43 (1.19-1.73, p<0.001)
Histology
LUAD
–
Non-LUAD
0.67 (0.41-1.10, p=0.114)
Treatment
Adjuvant
–
No adjuvant
1.12 (0.62-2.03, p=0.701)
Pack years
–
0.95 (0.88-1.02, p=0.181)
Stage
1
–
II
1.01 (0.52-1.96, p=0.986)
III
1.46 (0.73-2.92, p=0.289)
Age
–
1.25 (0.90-1.73, p=0.192)
Oncogenic event
None
–
EGFR mutated
1.56 (0.68-3.60, p=0.293)
MET exon 14 skipped
0.90 (0.21-3.87, p=0.891)
d
Non-LUAD: Relapse-free Survival: HR ( , p-value)
Extended Data Fig. 3 | Multivariable analyses adjusting for known risk factors confirms independent prognostic value of pre-operative ctDNA.
a. Multivariable Cox regression analysis for overall survival (OS) containing ctDNA (continuous, per 10-fold increase); histology; whether the patient received adjuvant chemotherapy; cigarette smoking status (in 10 pack year increments); pTNM stage; age (in 10 year increments); and the presence of an oncogenic event. n = 171 patients. b. Multivariable Cox regression analysis for relapse-free survival (RFS) containing ctDNA (continuous, per 10-fold increase); histology; whether the patient received adjuvant chemotherapy; cigarette smoking history; pTNM stage; age; and the presence of an oncogenic event. patients. c. Multivariable Cox regression analysis for RFS containing ctDNA level (ctDNA-high, ctDNA-low, ctDNA-negative); histology; whether the patient received adjuvant chemotherapy; cigarette smoking history; pTNM stage; age.; and the presence of an oncogenic event. n = 171 patients. d. Multivariable Cox regression analysis for RFS in non-LUADs containing
ctDNA level (ctDNA-high, ctDNA-low); whether the patient received adjuvant chemotherapy; cigarette smoking history;pTNM stage; age; and oncogenic events. patients. e. Multivariable Cox regression analysis for RFS in nonLUADs containing ctDNA (continuous); whether the patient received adjuvant chemotherapy; cigarette smoking history;pTNM stage; age; and oncogenic events. patients. f. Multivariable Cox regression analysis for OS in nonLUADs containing ctDNA (continuous, per 10-fold increase); sub-histology; whether the patient received adjuvant chemotherapy; cigarette smoking history; pTNM stage; age and oncogenic events. n = 77 patients. g. Multivariable analysis for RFS in non-LUADs containing ctDNA (continuous, per 10-fold increase); sub-histology; whether the patient received adjuvant chemotherapy; cigarette smoking history; pTNM stage; age; and oncogenic events. n= 77 patients. For all plots in this figure, error bars represent confidence intervals. The size of the boxes represents the number of patients within each category.
Extended Data Fig. 4 | The impact of sample age and preservation format on panel targets. a. Box and dot plot comparing number of high quality targets per panel from formalin-fixed paraffin embedded (FFPE) samples greater than 5 years vs less than 5 years old. Horizontal dashed line at 1000 indicates QC threshold. Center line represents the median. The upper whisker is the maximum value of the data that is within 1.5 times the interquartile range over the 75th percentile. The lower whisker is the minimum value of the data that is within 1.5 times the interquartile range under the 25th percentile. Sample size is . b. Failed FFPE or FFPE-derived panels which yielded fewer than 1000 high quality targets were re-generated using fresh frozen (FF) tissue where available. Green dots indicate samples included in our analysis, grey dots indicate those that failed to attain sufficient high quality targets for further processing. Where possible these panels were replaced with FF-derived panels. Connecting lines
b
indicate paired patient panels designed from either FF or FFPE tumor sample. Center line represents the median. The upper whisker is the maximum value of the data that is within 1.5 times the interquartile range over the 75th percentile. The lower whisker is the minimum value of the data that is within 1.5 times the interquartile range under the 25th percentile. Sample size is panels. One panel constructed from an FF tumor sample failed to attain 1,000 high-quality targets but was included to ensure that the cohort was representative of the wider TRACERx cohort. Two FF panels were constructed where FFPE panels had failed altogether; these are represented by green dots on the FF side not connected to an FFPE dot.c. Deming regression demonstrating agreement between measured ctDNA PPM and tumor molecules per milliliter of plasma. Fitted line represents a linear model, and the shaded area represents the confidence interval.
natureportfolio
Corresponding author(s): James Black
Last updated by author(s): May 16, 2024
Reporting Summary
Nature Portfolio wishes to improve the reproducibility of the work that we publish. This form provides structure for consistency and transparency in reporting. For further information on Nature Portfolio policies, see our Editorial Policies and the Editorial Policy Checklist.
Statistics
For all statistical analyses, confirm that the following items are present in the figure legend, table legend, main text, or Methods section.
n/a
□
□
Confirmed
The exact sample size for each experimental group/condition, given as a discrete number and unit of measurement
□
□
The statistical test(s) used AND whether they are one- or two-sided
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
□
A description of all covariates tested
□
□
A description of any assumptions or corrections, such as tests of normality and adjustment for multiple comparisons
A full description of the statistical parameters including central tendency (e.g. means) or other basic estimates (e.g. regression coefficient) AND variation (e.g. standard deviation) or associated estimates of uncertainty (e.g. confidence intervals)
□
For null hypothesis testing, the test statistic (e.g. ) with confidence intervals, effect sizes, degrees of freedom and value noted Give values as exact values whenever suitable.
□
□
□
For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
For hierarchical and complex designs, identification of the appropriate level for tests and full reporting of outcomes
Estimates of effect sizes (e.g. Cohen’s , Pearson’s r), indicating how they were calculated
Our web collection on statistics for biologists contains articles on many of the points above.
A statement on whether measurements were taken from distinct samples or whether the same sample was measured repeatedly
The statistical test(s) used AND whether they are one- or two-sided
nly common tests should be described solely by name; describe more complex techniques in the Methods section.
□
□
Our web collection on statistics for biologists contains articles on many of the points above.
Software and code
Policy information about availability of computer code
Data collection
Data analysis
No software was used to collect data.
Personalis NeXT Personal Platform (v1.8)
R version 4.1.3
R packages:
tidyverse (version 1.3.2)
lubridate (version 1.9.2)
ComplexHeatmap (version 2.15.4)
ggplot2 (version 3.4.2)
ggpubr (version 0.4.0)
scales (version 1.2.1)
wesanderson (version 0.3.6)
ggnewscale (version 0.4.9)
survival (version 3.3-1)
survminer (version 0.4.9)
finalfit (version 1.0.4)
gt (version 0.10.1)
mcr (version 1.2.2)
□
□
are was use
All code needed to reproduce figures will be available on request.
For manuscripts utilizing custom algorithms or software that are central to the research but not yet described in published literature, software must be made available to editors and reviewers. We strongly encourage code deposition in a community repository (e.g. GitHub). See the Nature Portfolio guidelines for submitting code & software for further information.
Data
Data
Policy information about availability of data
All manuscripts must include a data availability statement. This statement should provide the following information, where applicable:
Accession codes, unique identifiers, or web links for publicly available datasets
A description of any restrictions on data availability
For clinical datasets or third party data, please ensure that the statement adheres to our policy
Processed TRACERx patient data has been deposited at Zenodo at the link: 10.5281/zenodo.10689003. Raw data from TRACERx patients analyzed in this study including fastq and bam files from tumour and normal WGS, as well as fastq files from cfDNA have been deposited at the European Genome-phenome Archive (EGA), hosted by The European Bioinformatics Institute (EBI) and the Centre for Genomic Regulation (CRG) under accession codes (EGAS00001006494) under controlled access.
Research involving human participants, their data, or biological material
Policy information about studies with human participants or human data. See also policy information about sex, gender (identity/presentation), and sexual orientation and race, ethnicity and racism.
Reporting on sex and gender
Reporting on race, ethnicity, or other socially relevant groupings
Population characteristics
Sex information has been included in the data shared online. Information on patients’ gender was not collected as part of the study.
Information on race, ethicity or other socially relevant groupings was not included in the manuscript.
Cohort demographics ( ) are included in Extended Data Table 1, and further patient-level details are available with supporting molecular data on Zenodo (link: 10.5281/zenodo.10689003). Inclusion and exclusion criteria for the TRACERx study (Clinical trial number: NCT01888601) are as follows:
Inclusion Criteria:
Written Informed consent
Patients years of age, with early stage IIA-IIIB disease (according to TNM 8th edition) who are eligible for primary surgery. Patients with a radiological staging of IB (NO) who could be upstaged to IA-IIIB following surgery (due to the presence of possible nodal involvement on the pre-operative scan) may also be included, but will be withdrawn if post-surgical staging remains IB.
Histopathologically confirmed NSCLC, or a strong suspicion of cancer on lung imaging necessitating surgery (e.g. diagnosis determined from frozen section in theatre)
Primary surgery in keeping with NICE guidelines planned (see section 9.3)
Agreement to be followed up at a TRACERx site
Performance status 0 or 1
Minimum tumour diameter at least 15 mm to allow for sampling of at least two tumour regions (if 15 mm , a high likelihood of nodal involvement on pre-operative imaging required to meet eligibility according to stage, i.e. T1N1-3)
Exclusion Criteria:
Any other* malignancy diagnosed or relapsed at any time, which is currently being treated (including by hormonal therapy). Any other* current malignancy or malignancy diagnosed or relapsed within the past 3 years**.
*Exceptions are: non-melanomatous skin cancer, stage 0 melanoma in situ, and in situ cervical cancer
**An exception will be made for malignancies diagnosed or relapsed more than 2 , but less than 3 , years ago only if a preoperative biopsy of the lung lesion has confirmed a diagnosis of NSCLC.
Psychological condition that would preclude informed consent
Treatment with neo-adjuvant therapy for current lung malignancy deemed necessary
Post-surgery staging is not IIA-IIIB
Known Human Immunodeficiency Virus (HIV), Hepatitis B Virus (HBV), Hepatitis C Virus (HCV) or syphilis infection.
Sufficient tissue, i.e. a minimum of two tumour regions, is unlikely to be obtained for the study based on pre-operative imaging
When patients are initially diagnosed with stage I-III lung cancer and then referred for surgical resection, a research nurse identifies them on a clinic/operating list. The patient has an initial eligibility assessment and is then provided with written information about the TRACERx study and he/she can ask the research nurse any questions.
Patients have to agree to provide serial blood samples whenever they attend clinic for routine blood sampling, so this represents the only main potential self-selecting bias (i.e. only patients willing to do this would participate). However, it is unclear how this would affect the biomarker analyses. Also, the gender and ethnicity characteristics are in line with patients seen in routine practice.
This study was approved by the NRES Committee London with the following details:
Study title: TRAcking non small cell lung Cancer Evolution through therapy (Rx)
Recruitment
Ethics oversight
REC reference: 13/LO/1546
Protocol number: UCL/12/0279
IRAS project ID: 138871
Written informed consent was obtained from all participants.
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Field-specific reporting
Please select the one below that is the best fit for your research. If you are not sure, read the appropriate sections before making your selection.
Life sciences
Behavioural & social sciences
Ecological, evolutionary & environmental sciences
For a reference copy of the document with all sections, see nature.com/documents/nr-reporting-summary-flat.pdf
Life sciences study design
All studies must disclose on these points even when the disclosure is negative.
Sample size
Here, we report analyses from 204 TRACERx patients. No sample size calculations were performed for the preoperative ctDNA substudy; sample size was determined by sample availability, and includes 18 patients from the Abbosh et al., 2017 study and 43 patients from the Abbosh et al., 2023 study. Tumor / normal WGS for 171 patients yielded passing ctDNA panels that were included for further analysis. 171 patients had preoperative plasma available, including 89 patients who had disease relapse.
Data exclusions
Patients were excluded if they did not have baseline plasma. The available plasma collected at or closest to surgery was included in the analyses for patients with multiple pre-surgical plasma. We obtained FFPE tissue for 204 patients. Of these, 62 had atypically low counts of high quality panel targets likely due to age and/or poor quality of the FFPE samples, and 2 did not pass panel design. For 31 of these 64 patients, DNA extracted from fresh frozen tissue was available and the remaining 33 patients were excluded from analysis.
Replication
In-silico and technical replicates were used for analytical validation of the NeXT Personal Platform. Supporting experiments are described in both the main body of the manuscript as well as in the methods, and are visualized in Figure 1 and Extended Data Figure 1.
Randomization
No randomization was performed in the this study as no therapeutic interventions are tested.
Blinding
Retrospective ctDNA analysis was conducted using prospectively collected specimens and clinical follow up. Personalis investigators were fully blinded to patient clinical outcome and clinical pathological characteristics during sample processing and ctDNA analysis. Likewise, TRACERx investigators were blinded to patient ctDNA status during clinical data and patient specimen collection.
Reporting for specific materials, systems and methods
We require information from authors about some types of materials, experimental systems and methods used in many studies. Here, indicate whether each material, system or method listed is relevant to your study. If you are not sure if a list item applies to your research, read the appropriate section before selecting a response.
Materials & experimental systems
Methods
n/a
Involved in the study
n/a
Involved in the study
X
□
X
□
□
X
□
V
□
□
□
□
Eukaryotic cell lines
Policy information about cell lines and Sex and Gender in Research
Cell line source(s)
Authentication
Mycoplasma contamination
Commonly misidentified lines (See ICLAC register)
NA
As provided by ATCC (STR profiling).
Examined by ATCC and confirmed as not detected.
None of these are commonly misidentified cell lines as reported by the ICLAC register.
Clinical data
Policy information about clinical studies
All manuscripts should comply with the ICMJE guidelines for publication of clinical research and a completed CONSORT checklist must be included with all submissions.
Clinical and pathological data is collected from patients during study follow up – this period is a minimum of five years. Data collection is overseen by the sponsor of the study (Cancer Research UK & UCL Cancer Trials Centre) and takes place in hospitals across the United Kingdom. A centralised database called MACRO is used for this purpose. Recruitment to TRACERx started in April 2014 and is ongoing.
Outcomes
The pre-defined clinical outcome analysed in this manuscript is overall survival (OS) measured from the time of study registration to date of death from any cause. This outcome was previously defined in the TRACERx protocol (described in Jamal-Hanjani et al., 2017 NEJM). Additional analyis of relapse-free survival is also included in this manuscript, and is defined as the days from registration to any disease recurrence or new primary tumor events. The primary and secondary outcomes were pre-defined based on the following primary and secondary study objectives:
Primary objectives:
Define the relationship between intratumour heterogeneity and clinical outcome (disease-free survival and overall survival) following surgery and adjuvant therapy (including relationships between intratumour heterogeneity and clinical disease stage and histological subtypes of NSCLC).
Establish the impact of adjuvant platinum-containing regimens upon intratumour heterogeneity in relapsed disease compared to primary resected tumour.
Secondary objectives:
Development and validation of an intratumour heterogeneity ratio index as a prognostic or predictive biomarker in relation to its association with DFS and OS
Infer a complete picture of NSCLC evolutionary dynamics: Define drivers of genomic instability, metastatic progression and drug resistance by identifying and tracking the dynamics of somatic mutational heterogeneity, and chromosomal structural and numerical instability present in the primary tumour and at metastatic sites. Individual tumour phylogenetic tree analysis will:
a) Establish the order of somatic events in relation to genomic instability onset and metastatic progression
b) Decipher genetic “bottlenecking” events following metastasis and drug therapy
c) Establish dynamics of tumour evolution during the disease course from early to late stage NSCLC.
Initiate a longitudinal minimally-invasive circulating tumour cells (CTC) and cfDNA biobank to develop analytical methods for the early detection and monitoring of tumour evolution over time.
Develop a longitudinal tissue resource to serve as a platform to assess the relationship between genetic intratumour heterogeneity and the host immune response.
Isolate monocytes and lymphocytes for the in vitro generation of neoantigen-reactive T cells to be tested for immunoreactivity to matched tumour samples
Develop a repository of lung cancer cell lines, organoids and in vivo mouse models of patient- derived lung cancers that can be used as in vitro and in vivo models to study the aetiology of lung diseases, including lung cancer and predict response to therapeutics and resistance in lung cancer.
Define relationships between intratumour heterogeneity and targeted/cytotoxic therapeutic outcome.
Through UCL-GCLP gene panel in a certified laboratory environment, TRACERx will define clonally dominant disease drivers (paired primary-metastatic site comparisons in at least 270 patients with relapsed disease) to address the role of clonal driver dominance in targeted therapeutic response, and to guide stratification of lung cancer treatment and future clinical study inclusion in collaboration with the CRUK Stratified Medicines Phase II program.
Develop analytical methods for determining morphological heterogeneity within separate tumour regions.
nature portfolio | reporting summary
Tissue samples obtained from lung resections, both tumour and normal, will be analysed using high-power microscopy, such as electron microscopy, in order to obtain information regarding cellular structures.
The work presented in this manuscript assessed the impact of ctDNA on patient survival via Cox regression analysis and the Kaplan Meier method.