الميسرات والعوائق أمام تنفيذ تقنيات الصحة الرقمية في المستشفيات في البلدان ذات الدخل المنخفض والمتوسط منذ بداية جائحة كوفيد-19: مراجعة شاملة Facilitators and Barriers to the Implementation of Digital Health Technologies in Hospital Settings in Lower- and Middle-Income Countries Since the Onset of the COVID-19 Pandemic: Scoping Review
الميسرات والعوائق أمام تنفيذ تقنيات الصحة الرقمية في المستشفيات في البلدان ذات الدخل المنخفض والمتوسط منذ بداية جائحة كوفيد-19: مراجعة شاملة
شينغ تشيان ييو, MBBS, BMedSci, MSc, MPH, PhD; داكشا تريفيتي, BSc, MSc, MPhil, PhD; نورول إيمان حفيظة أدانان, BSc, MSc; بون هاو تشيو, MD, MMED, PhD قسم طب الصحة العامة، كلية الطب، الجامعة الوطنية الماليزية، شيراس، ماليزيا مركز البحث في الصحة العامة ورعاية المجتمع، جامعة هيرتفوردشاير، هيرتفوردشاير، المملكة المتحدة وحدة البحث السريري، مستشفى سلطان عبد العزيز شاه، سيردانغ، ماليزيا كلية الطب وعلوم الصحة، قسم طب الأسرة، سيردانغ، ماليزياالمؤلف المراسل:داكشا تريفيتي، BSc, MSc, MPhil, PhDمركز البحث في الصحة العامة ورعاية المجتمعجامعة هيرتفوردشايركوليدج لين، هاتفيلدهيرتفوردشاير، AL10 9ABالمملكة المتحدةالهاتف: 4401707286389البريد الإلكتروني: d.trivedi@herts.ac.uk
الملخص
الخلفية: على الرغم من أن عملية تنفيذ تقنيات الصحة الرقمية (DHTs) قد تم توثيقها بشكل واسع في البلدان ذات الدخل المرتفع، إلا أن العوامل التي تسهل وتمنع تنفيذها في البلدان ذات الدخل المنخفض والمتوسط (LMICs) قد تختلف لأسباب متعددة. الهدف: لمعالجة هذه الفجوة في البحث، تهدف هذه المراجعة الشاملة إلى تحديد الميسرات والعوائق أمام تنفيذ تقنيات الصحة الرقمية في بيئات المستشفيات في LMICs بعد بداية جائحة COVID-19. بالإضافة إلى ذلك، حددت المراجعة أنواع تقنيات الصحة الرقمية التي تم تنفيذها في مستشفيات LMICs خلال هذه الجائحة وأخيرًا وضعت إطار تصنيف لتصنيف مشهد تقنيات الصحة الرقمية. الطرق: تم إجراء بحث منهجي على PubMed وScopus وWeb of Science وGoogle Scholar للدراسات المنشورة من مارس 2020 إلى ديسمبر 2023. قمنا باستخراج بيانات عن المؤلفين، سنوات النشر، أهداف الدراسة، دول الدراسة، حالات المرض، أنواع تقنيات الصحة الرقمية، مجالات الطب السريري التي يتم تطبيق تقنيات الصحة الرقمية فيها، تصاميم الدراسة، أحجام العينات، خصائص السكان المدروسين، موقع الدراسة، وطرق جمع البيانات للدراسات المشمولة. تم استخدام بيانات كمية ونوعية لإجراء تحليل موضوعي، باستخدام طريقة استنتاجية تعتمد على نموذج التنفيذ العملي والموثوقية والاستدامة (PRISM)، لتحديد الميسرات والعوائق أمام تنفيذ تقنيات الصحة الرقمية. أخيرًا، تم تحديد جميع تقنيات الصحة الرقمية المتاحة وتنظيمها لإنشاء إطار تصنيف جديد. النتائج: تم تضمين اثني عشر دراسة من 292 مقالة مسترجعة. كانت الطب عن بعد هو أكثر تقنيات الصحة الرقمية استخدامًا في مستشفيات LMICs، تليها أنظمة المعلومات المستشفوية (), السجلات الطبية الإلكترونية (), والصحة المتنقلة (). هذه الأربعة تقنيات، من بين تقنيات الصحة الرقمية الأخرى الموجودة، سمحت لنا بتطوير إطار تصنيف جديد لتقنيات الصحة الرقمية. استخدمت الدراسات المشمولة طرقًا نوعية ()، والتي شملت المقابلات ومجموعات التركيز، وطرقًا كمية ()، أو مزيجًا من الاثنين (). من بين 64 ميسرًا لتنفيذ تقنيات الصحة الرقمية، كانت توفر التدريب المستمر أثناء العمل ()، وقدرة تقنيات الصحة الرقمية على منع العدوى المتبادلة ()، والتجارب الإيجابية السابقة باستخدام تقنيات الصحة الرقمية () هي الثلاثة ميسرات الأكثر ذكرًا. ومع ذلك، من بين 44 عائقًا أمام تنفيذ تقنيات الصحة الرقمية، كان المرضى الذين يعانون من ضعف في المعرفة الرقمية والمهارات في تقنيات الصحة الرقمية ()، وعدم الوعي الكافي بشأن تقنيات الصحة الرقمية بين المهنيين الصحيين وأصحاب المصلحة ()، والقلق بشأن دقة تشخيص الأمراض وعلاجها من خلال تقنيات الصحة الرقمية () كانت من بين العوائق الأكثر ذكرًا.
الاستنتاجات: في عصر ما بعد الجائحة، شهدت الطب عن بعد، جنبًا إلى جنب مع تقنيات الصحة الرقمية الأخرى، زيادة في التنفيذ في المستشفيات داخل LMICs. يمكن تصنيف جميع الميسرات والعوائق إلى 6 مواضيع، وهي: (1) جوانب نظام الرعاية الصحية؛ (2) وجهات نظر المرضى؛ (3) البيئة الخارجية؛ (4) تنفيذ بنية تحتية مستدامة؛ (5) خصائص منظمة الرعاية الصحية؛ و(6) خصائص المرضى.
(J Med Internet Res 2025;27:e63482) doi: 10.2196/63482
الكلمات الرئيسية
تنفيذ الصحة الرقمية؛ الميسرات؛ العوائق؛ إطار تصنيف الصحة الرقمية؛ البلدان ذات الدخل المنخفض والمتوسط
المقدمة
تواجه السكان المقيمين في البلدان ذات الدخل المنخفض والمتوسط (LMICs) العديد من الاحتياجات الصحية غير الملباة بسبب عوامل متعددة [1]، بما في ذلك شيخوخة السكان [2]، تصاعد تكاليف الرعاية الصحية [3]، اتساع الفجوات في الدخل [4]، زيادة مرض وموت الأطفال [5]، ظهور أوبئة وجائحات جديدة [6]، وزيادة التمييز العنصري في الوصول إلى الرعاية الصحية [7]. لقد زادت جائحة COVID-19 من تفاقم الفجوات والقيود الموجودة في أنظمة الرعاية الصحية في LMICs، مما كشف عن مشاكل نقص الموظفين، نقص التمويل، البنية التحتية غير الكافية، الوصول المحدود للاختبارات والعلاج، والضعف أمام الطوارئ الصحية [8]. استجابةً لهذه الجائحة غير المسبوقة، حاولت العديد من المستشفيات في LMICs الاستفادة من تقنيات الصحة الرقمية (DHTs) كنهج مبتكر للحد من انتشار SARS-CoV-2، وتحسين تقديم الرعاية الصحية، وتعزيز جهود الاستجابة للجائحة [9].
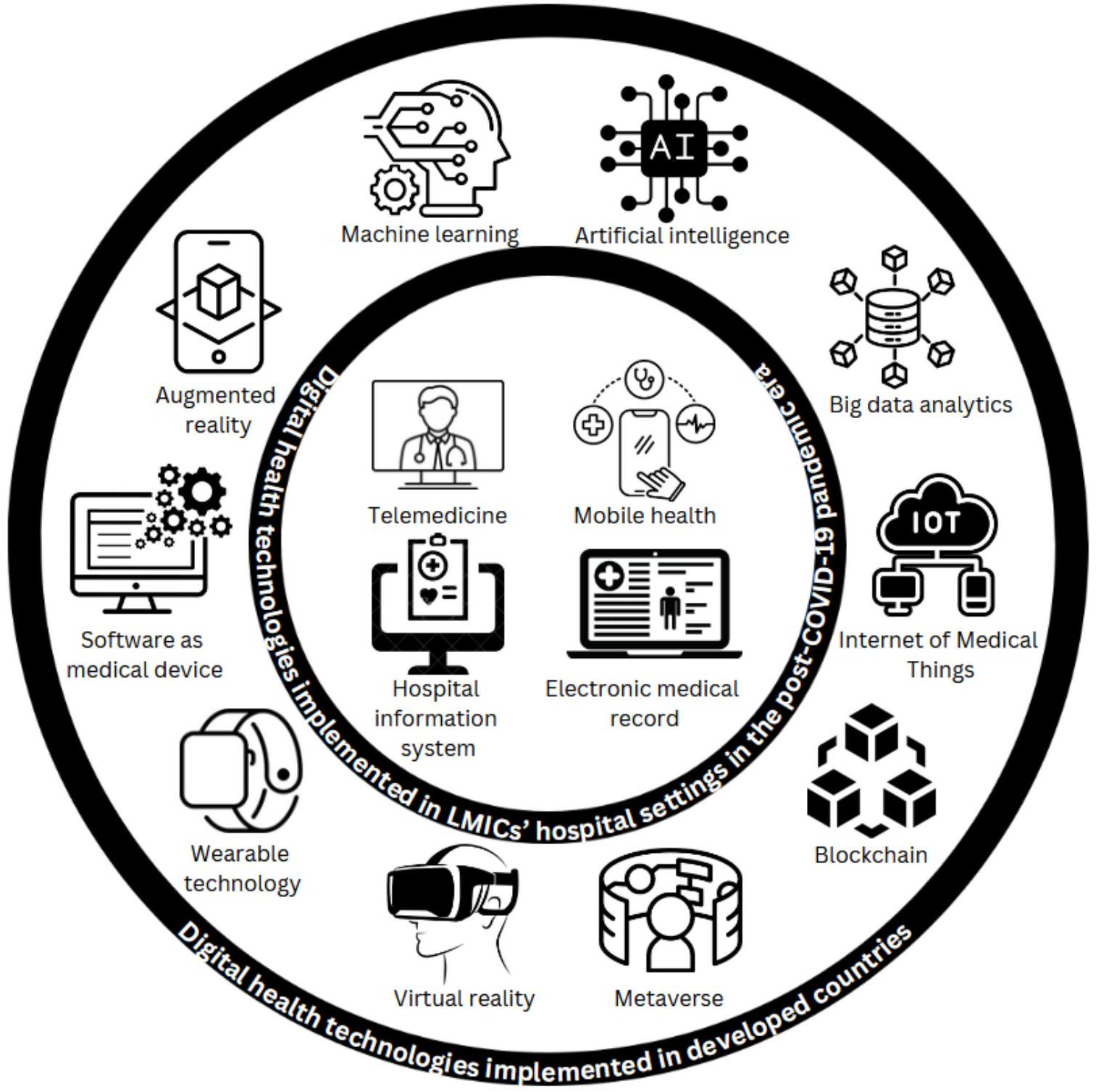
بشكل عام، تُعرف تقنيات الصحة الرقمية بأنها مجموعة من تكنولوجيا المعلومات والاتصالات المستخدمة في الطب والرعاية الصحية لإدارة الأمراض وتعزيز الصحة [10]. لقد توسعت هذه التقنيات كقوة تحويلية في الرعاية الصحية منذ بداية عصر جائحة COVID-19، مما يوفر مجموعة متنوعة من الفوائد التي تحدث ثورة في تقديم الرعاية الصحية وتحسين نتائج المرضى. تشمل هذه التقنيات مجموعة واسعة من الأدوات الرقمية، بما في ذلك الصحة المتنقلة (mHealth) [11]، الطب عن بعد [12]، التقنيات القابلة للارتداء [13]، السجلات الطبية الإلكترونية [14]، تحليلات البيانات الكبيرة [15]، إنترنت الأشياء الطبية [16]، البلوكشين في الرعاية الصحية [17]، الميتافيرس [18]، البرمجيات كجهاز طبي [19]، الواقع المعزز [20]، والواقع الافتراضي [21]. مع زيادة قوة الحوسبة وتقدير الذكاء الاصطناعي [22] وتعلم الآلة [23] في الصحة والطب، تظهر العديد من هذه الأدوات الذكية في جوانب مختلفة من رعاية المستشفيات [24،25].
على الرغم من فوائد تقنيات الصحة الرقمية، مثل تحسين الوصول إلى الرعاية الصحية، وتعزيز مشاركة المرضى وتمكينهم، وتقديم الرعاية الصحية بكفاءة، والرعاية الشخصية في الوقت المناسب، والمراقبة عن بُعد، واتخاذ القرارات المستندة إلى البيانات، إلا أن عملية تنفيذ تقنيات الصحة الرقمية في بيئات المستشفيات،
بما في ذلك ميسراتها وعوائقها، توصف في الغالب في سياق البلدان ذات الدخل المرتفع [26،27]. نظرًا للاختلافات في الموارد، والبنية التحتية، وأنظمة الرعاية الصحية، والوضع الاجتماعي والاقتصادي، ومستوى الفجوة الرقمية، والأطر التنظيمية في LMICs مقارنة بالبلدان ذات الدخل المرتفع، قد لا تنطبق الأدلة حول الميسرات والعوائق أمام تنفيذ تقنيات الصحة الرقمية المبلغ عنها في الأدبيات السابقة على LMICs [28]. لمعالجة هذه الفجوات البحثية، تهدف هذه المراجعة الشاملة إلى:
تقديم نظرة عامة على الميسرات والعوائق في تنفيذ تقنيات الصحة الرقمية داخل بيئات المستشفيات في LMICs منذ بداية جائحة COVID-19.
تحديد ووصف أنواع تقنيات الصحة الرقمية التي تم تطبيقها في المستشفيات داخل LMICs منذ بداية جائحة COVID-19.
تطوير إطار تصنيف لتعريف مشهد تقنيات الصحة الرقمية بشكل أفضل، مما يوفر فهمًا أكثر شمولاً وعمليًا.
الطرق
التصميم
تم إجراء المراجعة الشاملة باستخدام الإطار المنهجي الذي طوره أركسي وأومايلي [29]. تم تسجيل البروتوكول في إطار العلوم المفتوحة وتم نشره سابقًا [30]. تم استخدام PRISMA-ScR (عناصر التقرير المفضلة للمراجعات المنهجية والتحليلات التلوية الممتدة للمراجعات الشاملة) [27،31] لإجراء والإبلاغ عن نتائجنا.
تحديد الأدبيات ذات الصلة
لتحديد الأدبيات المتعلقة بالتقنيات الصحية الرقمية (DHTs) بشكل شامل، تم تطبيق استراتيجية بحث واسعة وحساسة ودقيقة لالتقاط جميع الأدبيات المتعلقة بالتقنيات الصحية الرقمية. بمساعدة متخصص في تكنولوجيا المعلومات، تم تحديد قائمة شاملة من الأدبيات ذات الصلة بالتقنيات الصحية الرقمية وفقًا للمعايير أدناه. تصف المربعات النصية 1 و 2 معايير الإدراج والاستبعاد المعتمدة لهذه المراجعة الاستكشافية. كان التركيز على الفترة بين مارس 2020 وديسمبر 2023، حيث أعلنت منظمة الصحة العالمية (WHO) رسميًا عن COVID-19 كجائحة في مارس 2020.
المربع النصي 1. معايير الإدراج.
الدراسات التي أجريت في البلدان ذات الدخل المنخفض والمتوسط (LMICs). (تصنف البنك الدولي البلدان حسب الدخل كل عام، تغطي جميع الدول التي يزيد عدد سكانها عن 30,000. في عام 2023، تم تقسيم البلدان إلى 4 فئات دخل بناءً على دخلها القومي الإجمالي (GNI) للفرد. تُعرف البلدان ذات الدخل المنخفض بأنها تلك التي لديها GNI للفرد أقل من US أو أقل. البلدان ذات الدخل المنخفض والمتوسط لديها GNI للفرد بين 1146 دولارًا أمريكيًا و 4515 دولارًا أمريكيًا، بينما تقع البلدان ذات الدخل المتوسط الأعلى بين 4516 دولارًا أمريكيًا و 14,005 دولارًا أمريكيًا. البلدان ذات الدخل المرتفع هي تلك التي لديها GNI للفرد يتجاوز US . بناءً على هذا التصنيف، تُعرف البلدان ذات الدخل المنخفض والمتوسط في المراجعة الحالية بأنها البلدان التي لديها GNI أقل من 14,005 دولارًا أمريكيًا للفرد.)
الدراسات التي أفادت بتنفيذ التقنيات الصحية الرقمية في بيئات المستشفيات (لكلا الحالتين الحادة والمزمنة).
الدراسات التي تم الإبلاغ عنها بين مارس 2020 وديسمبر 2023.
الدراسات التي تم الإبلاغ عنها باللغة الإنجليزية.
الدراسات النوعية (الفينومينولوجيا، الإثنوغرافيا، النظرية المستندة، دراسة الحالة، إلخ)، الدراسات الكمية (دراسات الحالة الضابطة، دراسة المجموعة، الدراسات المقطعية، التجارب العشوائية المضبوطة، إلخ)، الدراسات المختلطة، والمراجعات (المراجعة السردية، المراجعة الاستكشافية، المراجعة المنهجية، التحليل التلوي، إلخ).
الأدبيات الرمادية ذات الصلة (مثل، Google Scholar).
المربع النصي 2. معايير الاستبعاد.
الدراسات التي لم تكن قائمة على الرقمية (أي، الدراسات التي لم تحقق في فعالية التدخلات الرقمية، مثل الدراسات الورقية واستطلاعات البريد).
الدراسات التي نفذت التقنيات الصحية الرقمية (DHTs) في الرعاية الأولية أو بيئات المجتمع فقط. ومع ذلك، ستظل الدراسات التي أفادت في الوقت نفسه بتنفيذ DHTs في بيئات المستشفيات مشمولة.
الدراسات التي استخدمت DHTs في طب الأسنان ومجالات الطب غير السريرية (مثل، طب الأسنان، العلوم الأساسية، التعليم الطبي، الهندسة الطبية، التغذية، الحمية، العلوم البيطرية، التجارب المخبرية، والأنثروبولوجيا الطبية).
تم إجراء عمليات بحث منهجية في قواعد بيانات PubMed وScopus وWeb of Science. تم البحث عن الأدبيات الرمادية المحتملة ذات الصلة من خلال عمليات بحث مستهدفة في Google Scholar. شمل البحث الجانبي فحص قوائم المراجع في الدراسات أو المراجعات المحددة للمنشورات ذات الصلة. تم استرجاع المقالات المنشورة باللغة الإنجليزية بين مارس 2020 وديسمبر 2023. قام محققان (SQY وNIHA) بإجراء عمليات بحث أدبية بشكل مستقل في قواعد البيانات الإلكترونية المذكورة أعلاه.
تم تطوير استراتيجية البحث بناءً على إطار “السكان-المفهوم-السياق” (PCC) كما أوصى به معهد جوانا بريجز للمراجعات الاستكشافية [32] (الجدول 1). كان الهدف هو تحديد التقاطع بين “السكان” و”المفهوم” و”السياق”. بناءً على إطار PCC، كانت استراتيجية البحث هي “السكان مجتمعة” و”المفهوم” و”السياق”. تم جدول تفاصيل استراتيجية البحث وعبارات البحث في الملحق المتعدد الوسائط 1.
الجدول 1. إطار PCC المستخدم لتوليد عبارات البحث.
الإطار
عبارات البحث
السكان
– السكان 1: بيئات المستشفيات (عبارات البحث كما في الملحق المتعدد الوسائط 1).
– السكان 2: LMICs (عبارات البحث كما في الملحق المتعدد الوسائط 1).
– السكان مجتمعة: السكان 1 و السكان 2.
المفهوم
– التقنيات الصحية الرقمية (عبارات البحث كما في الملحق المتعدد الوسائط 1).
السياق
– الميسرات، الحواجز، والتنفيذ.
PCC: السكان-المفهوم-السياق. LMICs: البلدان ذات الدخل المنخفض والمتوسط
اختيار الدراسة
تم تنزيل السجلات في برنامج Rayyan (برنامج فرز المقالات المدعوم بالذكاء الاصطناعي) [24] وبعد إزالة التكرارات، تم فحص جميع العناوين والملخصات بشكل مستقل وفقًا لمعايير الإدراج من قبل 2 من المراجعين (SQY وNIHA). من بين جميع العناوين والملخصات الموجودة، تم اختيار 70 من 279 بشكل عشوائي وفحصها لتحديد موثوقية المراجعين. كانت موثوقية المراجعين (K) 0.63، مما يدل على موثوقية جيدة. تم فحص المقالات الكاملة للأوراق المحتملة ذات الصلة بشكل مستقل من قبل SQY وNIHA. تم حل الخلافات من خلال المناقشة، مع استشارة من مراجعة ثالثة (BHC) إذا لزم الأمر للتوصل إلى توافق. قمنا بتضمين الدراسات التي استوفت معايير المراجعة وأفادت عن الحواجز والميسرات لتنفيذ DHT. بالنسبة لهذه المراجعة، تم تعريف DHTs على أنها مجموعة من تكنولوجيا المعلومات والاتصالات المستخدمة في الطب والرعاية الصحية لإدارة الأمراض وتعزيز الصحة [10].
رسم البيانات
استخرج مؤلفان (SQY وNIHA) بشكل مستقل البيانات التالية من الأوراق المدرجة: المؤلفون، سنوات النشر، أهداف الدراسة، دول الدراسة، حالات الأمراض، أنواع DHTs، مجالات الطب السريري التي يتم تطبيق DHTs فيها، تصاميم الدراسة، أحجام العينات، خصائص السكان المدروسة، موقع الدراسة، وطرق جمع البيانات للتدخل أو البرنامج. قمنا بتصنيف DHTs وفقًا لأنواع المعدات وطريقة التشغيل. تم حل أي خلافات من خلال المناقشة واستشارة مؤلف ثالث (BHC).
تجميع، تلخيص، وتقرير النتائج
تم الإبلاغ عن أوصاف الدراسات المدرجة، مثل دول الدراسة، أنواع DHTs، مجالات الطب السريري التي يتم تطبيق DHTs فيها، وتصاميم الدراسة باستخدام إحصائيات وصفية (مثل، توزيع التكرار). تم تحليل الميسرات والحواجز لتنفيذ DHT، والتي كانت في شكل بيانات كمية ونوعية، بشكل موضوعي باستخدام نهج استنتاجي. لتوجيه التحليل الموضوعي، تم تنظيم الميسرات والحواجز لتنفيذ DHT باستخدام نموذج التنفيذ العملي والموثوقية والاستدامة (PRISM) [33].
خلال عملية الترميز، حدد مؤلفان (SQY وNIHA) المكونات الرئيسية لنموذج PRISM ذات الصلة بتنفيذ DHT. قاموا برسم الميسرات والحواجز المبلغ عنها في الدراسات المدرجة إلى الفئات المحددة مسبقًا ومن ثم تجميع الفئات المماثلة تحت مواضيع شاملة. من خلال تنظيم الميسرات والحواجز في مواضيع وفئات، يمكن تحديد الأنماط والاتجاهات والعلاقات بين العوامل المؤثرة على تنفيذ DHT، مما يوفر إطارًا منظمًا لفهم تعقيدات تنفيذ DHTs في بيئات المستشفيات في البلدان ذات الدخل المنخفض والمتوسط [34].
التشاور مع أصحاب المصلحة
تم دعوة الأطباء وخبراء تكنولوجيا المعلومات من مستشفى تعليمي محلي للمساعدة في تفسير وتحديد سياق النتائج. من خلال المناقشات التفاعلية والجلسات التعاونية، قدم أصحاب المصلحة مدخلات قيمة حول تصنيف الميسرات والحواجز وكذلك آثار تنفيذ DHTs في سياقاتهم الخاصة. للمضي قدمًا، يخطط المؤلفون لمواصلة التواصل مع هؤلاء أصحاب المصلحة لنشر نتائج المراجعة الاستكشافية من خلال العروض التقديمية، والموجزات السياسية، والمنشورات التي تمت مراجعتها من قبل الأقران.
النتائج
بحث الأدبيات
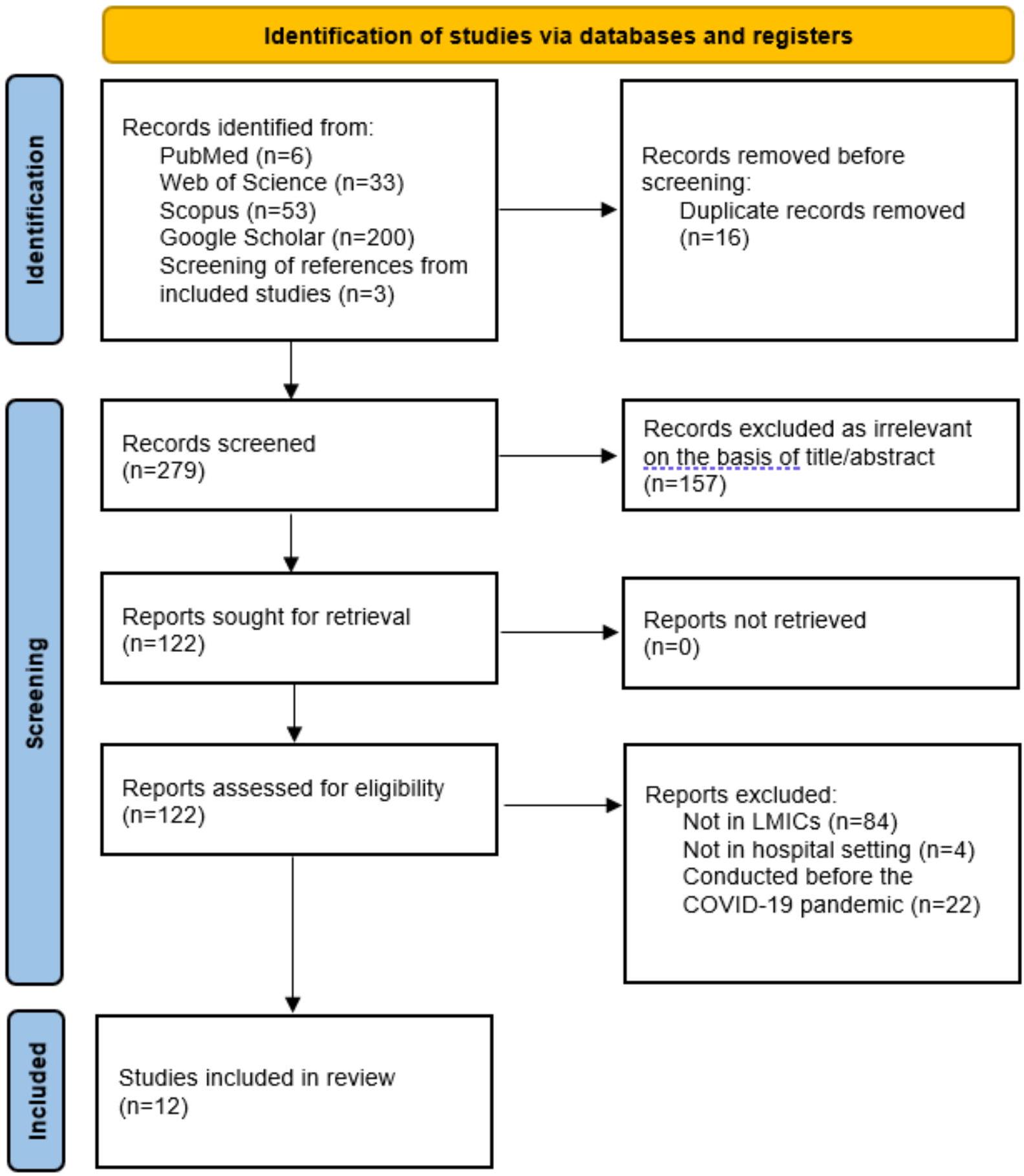
أسفر البحث المنهجي عن 295 عنوانًا وملخصًا. بعد إزالة 16 تكرارًا، تبقى 279 مقالة فريدة. من بين هذه، تم استبعاد 157 بناءً على مراجعة العنوان أو الملخص. قمنا بتقييم 122 مقالة نص كامل بدقة، وفي النهاية، استوفت 12 المعايير الأهلية. تم استخدام مخطط تدفق PRISMA لتوضيح عملية اتخاذ قرار البحث في المراجعة الاستكشافية [35] (الشكل 1 والملحق المتعدد الوسائط 2).
الشكل 1. مخطط PRISMA (عناصر التقرير المفضلة للمراجعات المنهجية والتحليلات التلوية). LMIC: بلد ذو دخل منخفض ومتوسط.
خصائص الدراسات المدرجة
من بين 12 مقالة، تم إجراء 4 (33%) في أفريقيا [42-45]، 1 (8%) في الشرق الأوسط [46]، و1 (8%) في أمريكا الجنوبية [47]. لم تحدد معظم الدراسات (10/12، 83%) [36،37،40-47] المجال المحدد للطب السريري الذي تم تطبيق DHTs فيه. ومع ذلك، أبلغت بعض الدراسات عن التنفيذ في طب الجهاز التنفسي (1/12، 8%) [38] والسرطان (1/12، 8%) [39]. الطب عن بُعد (5/12، 42%) [37،38،40،41،46] كانت التكنولوجيا الأكثر شيوعًا المبلغ عنها، تليها أنظمة معلومات المستشفيات (4/12، 33%) [36،42،45،47]، والسجلات الطبية الإلكترونية (2/12، 17%) [43،44]، وmHealth (1/12، 8%) [39]. من حيث تصميم الدراسة، كان هناك 5 (42%) دراسات مقطعية [37،41،42،44،46]، و4 (33%) دراسات نوعية [38-40،43]،دراسات الطرق المختلطة [45،47]، ودراسة حالة [36]. تراوحت أعداد المشاركين من 12 إلى 3386 فردًا (الجدول 2).
الجدول 2. نظرة عامة على خصائص الدراسات المشمولة.
المؤلفون وسنوات النشر
تفاصيل الدراسة
الهدف (الأهداف)
بلد
حالة مرضية
أنواع DHTs
مجال الطب السريري
تصميم
أحجام العينات وخصائص السكان
الموقع
طريقة جمع البيانات
عبد الله وآخرون [36]
لتحقيق في المواقف والفرص والتحديات في استخدام نظام المعلومات الصحية.
الهند
عام
نظام معلومات الصحة
عام
دراسة حالة
20 مقدمي الرعاية الصحية والمديرين
مستشفى أبولو ومستشفى ميدنتا
استبيان ذاتي الإدارة
البورعي وآخرون [37]
لتقييم فائدة الطب عن بُعد والحواجز المختلفة التي تعيق استخدامه.
مصر
عام
الطب عن بُعد
الطب العام، الجراحة، والأشعة
دراسة مقطعية
642 مزود خدمة صحية
جميع المستشفيات في مصر
استبيان ذاتي الإدارة عبر الإنترنت
بارادوان والحنوي [46]
للحصول على فهم شامل لتصورات وحواجز المستخدمين النهائيين (المشاركين) تجاه فائدة الطب عن بُعد.
المملكة العربية السعودية
عام
الطب عن بُعد
عام
دراسة مقطعية
1024 فرداً
على مستوى البلاد
استبيان ذاتي الإدارة
جيانغ وآخرون [38]
لاستكشاف تصورات وتجارب المرضى المسنين ومقدمي الرعاية الصحية في تطبيق الرعاية الصحية عن بُعد والمعلومات الصحية عبر الإنترنت في إدارة الأمراض المزمنة لمرض الانسداد الرئوي المزمن.
الصين
مرض الانسداد الرئوي المزمن
الطب عن بُعد
طب الجهاز التنفسي
نوعي
31 مريضًا مسنًا يعانون من مرض الانسداد الرئوي المزمن و23 مقدم رعاية صحية
مستشفى مجتمعي في جيانغنان، الصين
مقابلات معمقة
مكريا وآخرون [42]
لتقييم مستوى استخدام نظام المعلومات الصحية بين المهنيين الصحيين في المرافق الصحية العامة.
إثيوبيا
عام
نظام معلومات الصحة
عام
دراسة مقطعية
378 مزود خدمة صحية
إدارة دير داوا في شرق إثيوبيا
استبيان ذاتي الإدارة
المؤلفون وسنوات النشر
تفاصيل الدراسة
الهدف (الأهداف)
بلد
حالة مرضية
أنواع DHTs
مجال الطب السريري
تصميم
أحجام العينات وخصائص السكان
الموقع
طريقة جمع البيانات
موسي وآخرون [47]
لفهم تنفيذ نظام معلومات المستشفيات في المستشفيات الجامعية.
البرازيل
عام
نظام معلومات الصحة
عام
طرق مختلطة استكشافية
770 مديرًا صحيًا (24 في مقابلات معمقة، 10 في مناقشات مجموعات التركيز، و736 في دراسة مقطعية)
5 مستشفيات جامعية في البرازيل
المقابلات، مناقشات مجموعات التركيز، الاستبيانات، والبحث الوثائقي
نجوجي وآخرون [43]
لاستكشاف تصورات وتجارب المستخدمين النهائيين حول العوامل التي تسهل وتعيق استخدام السجلات الطبية الإلكترونية في مرافق الرعاية الصحية.
كينيا
عام
السجل الطبي الإلكتروني
عام
نوعي
20 مزودًا للرعاية الصحية
20 منشأة صحية في كينيا
مناقشة مجموعة التركيز
نينغ وآخرون [39]
لاستكشاف احتياجات وتصورات المرضى المصابين بسرطان الرأس والعنق بشأن برامج النشاط البدني المعتمدة على الصحة المتنقلة.
الصين
سرطان الرأس والعنق
الصحة المتنقلة
أذن أنف حنجرة
نوعي
17 مريضًا تم تشخيصهم بسرطان الرأس والعنق
المستشفى الأول لجامعة شانشي الطبية، تاييوان، الصين
مقابلات معمقة
شاردها وآخرون [40]
لاستكشاف وجهة نظر المتخصصين في الرعاية الصحية بشأن الفوائد والتحديات وآفاق الطب عن بُعد لمعالجة الفجوة التي تعيق استخدامه الفعال في المناطق الريفية.
باكستان
عام
الطب عن بُعد
التخصصات غير الجراحية
نوعي (سردي)
12 مزود خدمة صحية
مستشفيان ثالثيان في السند، باكستان
مقابلات معمقة
تسفا وآخرون [44]
لتقييم مستوى استخدام السجلات الصحية الإلكترونية والعوامل المرتبطة بها بين المهنيين الصحيين في المستشفيات التعليمية.
إثيوبيا
عام
السجل الطبي الإلكتروني
عام
دراسة مقطعية
383 مزودًا للرعاية الصحية
مستشفى جامعة غوندار التعليمي المتخصص ومستشفى تيبيبي غيون التعليمي المتخصص
استبيان ذاتي الإدارة
المؤلفون وسنوات النشر
تفاصيل الدراسة
الهدف (الأهداف)
بلد
حالة مرضية
أنواع DHTs
مجال الطب السريري
تصميم
أحجام العينات وخصائص السكان
الموقع
طريقة جمع البيانات
تيلاهون وآخرون [45]
لتقييم النتائج ومشاركة التجارب في العمل مع الجامعات لتعزيز نظام المعلومات الصحية الوطني.
إثيوبيا
عام
نظام معلومات الصحة
عام
دراسة بأساليب مختلطة
23 مزود خدمة صحية
47 منظمة صحية في إثيوبيا
مقابلات معمقة
يو-تونغ وآخرون [41]
لتقييم جاهزية التمريض السريري للتكنولوجيا الصحية عن بُعد واستكشاف العوامل التي تؤثر على جاهزيتهم لهذه التكنولوجيا.
الصين
عام
الطب عن بُعد
عام
دراسة مقطعية
3386 ممرضة
19 مستشفى في الصين
استبيان يتم إدارته ذاتيًا
دي إتش تي: تكنولوجيا الصحة الرقمية. أذن، أنف، وحنجرة.
الميسرات والعوائق لتنفيذ تقنية DHT
من بين الدراسات الاثني عشر، استكشفت 9 دراسات كل من العوامل الميسرة والعوائق لتنفيذ تقنيات الصحة الرقمية في بيئات المستشفيات في البلدان ذات الدخل المنخفض والمتوسط منذ بداية جائحة كوفيد-19 [36-40، 43-45، 47]. ركزت دراستان فقط على العوامل الميسرة [41، 42]، بينما تناولت دراسة واحدة فقط العوائق [46]. بلغ إجمالي العوامل الميسرة 63 وعائقًا 44. تم التعرف عليها. بعد ذلك، تم تنظيم هذه الميسرات والعوائق بشكل منهجي في 6 مواضيع وفقًا لنموذج PRISM، والتي تشمل ما يلي: (1) جوانب نظام الرعاية الصحية؛ (2) وجهات نظر المرضى؛ (3) البيئة الخارجية؛ (4) تنفيذ البنية التحتية المستدامة؛ (5) خصائص منظمة الرعاية الصحية؛ و(6) خصائص المرضى. تم توضيح ذلك في الجدول 3.
الجدول 3. العوامل الميسرة والعوائق لاستخدام التكنولوجيا الرقمية للصحةالتنفيذ في المستشفيات في البلدان ذات الدخل المنخفض والمتوسط بعد جائحة COVID-19.
المواضيع والفئات
رموز للميسرين
رموز الحواجز
جوانب نظام الرعاية الصحية )
الاستعداد
– فهم أساسيات تكنولوجيا المعلومات [37]
– المعرفة في حماية سرية البيانات [37]
– مستوى عالٍ من الكفاءة الذاتية [42]
– موقف جيد تجاه DHTs [42]
– وعي عالٍ بشأن تنفيذ تقنيات DHTs [47]
– اهتمام شخصي عالٍ ودافع [47]
– الرغبة العالية لمقدمي الرعاية الصحية في تقديم العلاجات الرقمية للمرضى [41]
– الوعي غير الكافي بشأن DHTs [40،44]
– الشعور بأن التقنيات الصحية الرقمية (DHTs) هي فقط مكملة للرعاية الصحية التقليدية [38]
– تفضيل بعض مقدمي الرعاية الصحية للمواد المطبوعة [44]
قوة قاعدة الأدلة; )
– قدرة تقنيات DHTs على تقديم التحليل الإحصائي والتقارير لدعم اتخاذ القرار [36]
– قدرة تقنيات الصحة الرقمية على تقديم معلومات محدثة وفي الوقت المناسب عن المرضى [36]
– مخاوف بشأن الدقة في تشخيص الأمراض وعلاجها [40،46]
يتناول الحواجز التي تواجه الموظفين في الخط الأمامي )
– سهولة الوصول إلى أجهزة الكمبيوتر في منطقة العمل [44]
– الخوف من حماية البيانات غير المناسبة قد ينتهك خصوصية المريض [37]
– عدم كفاية أجهزة الكمبيوتر في مكان العمل ونقطة الخدمة لشبكة المنطقة المحلية في مكان العمل [43]
التنسيق بين الأقسام والتخصصات )
– استخدام سياسة تكنولوجيا المعلومات الموحدة ونظام المعلومات الصحية الموحد [47]
– نقص معايير التوافقية بين الأنظمة [47]
عبء (تعقيد وتكلفة؛; )
– إدراك أن عمليات DHTs ليست معقدة [42]
– توفر ميزانية تكنولوجيا المعلومات [47]
– ترقيات منتظمة على أجهزة DHT [43]
– دعم التمويل الذي يركز على البحث وفرص التعلم حول تقنيات التوزيع اللامركزي [45]
– الحاجة إلى إدخال البيانات بأثر رجعي في الأنظمة [43]
قابلية الاستخدام والتكيف; )
– قدرة DHTs على منع العدوى المتبادلة [38،40]
– القدرة على تقديم الرعاية الصحية في المناطق النائية [40]
– تتوافق وظائف تقنيات الصحة الرقمية مع ممارسات المستشفيات [47]
– سهولة استخدام تقنيات الصحة الرقمية [43]
– صعوبة إجراء الفحص البدني باستخدام تقنيات الصحة الرقمية [40]
– نقص الالتزام بين المهنيين الصحيين والمرضى [40]
– قد تقلل تقنيات الصحة الرقمية من جودة الخدمات الطبية من خلال زيادة احتمال الأخطاء الطبية [37]
– يُنظر إلى تقنيات الصحة الرقمية كجدول أعمال بحثي فقط [45]
– بعض تقنيات الصحة الرقمية ليست سهلة الاستخدام [36]
قابلية التجربة والرجوع ( ; )
– إجراء اختبارات تجريبية واختبارات تجريبية قبل تنفيذ تقنيات الصحة الرقمية [47]
– غير متاح
القدرة على ملاحظة النتائج ( ; )
– تجارب إيجابية سابقة باستخدام تقنيات الصحة الرقمية [41,47]
– قدرة تقنيات الصحة الرقمية على زيادة الكفاءة الإدارية والرعاية الصحية [36]
– قدرة تقنيات الصحة الرقمية على تقليل أخطاء الأدوية [36]
– غير متاح
وجهات نظر المرضى ( )
المواضيع والفئات
رموز الميسرين
رموز الحواجز
تركيز المريض ( )
– استخدام التكنولوجيا يعطي شعورًا متفوقًا [38]
– الكلمات التحفيزية أو المدحية المتكررة تزيد من استخدام المرضى لتقنيات الصحة الرقمية [38]
– شعور المسافة بين المريض ومقدمي الرعاية الصحية أثناء التفاعل عن بُعد [38]
– شعور بالإجبار على استخدام تقنيات الصحة الرقمية [38]
معالجة حواجز المرضى ( ; )
– يمكن أن يُحسن إشراك أطفال المرضى من كفاءة وفعالية تقنيات الصحة الرقمية [38]
– مقاومة المرضى لتغيير الممارسات [46]
سلاسة الانتقال بين عناصر البرنامج ( )
– توحيد المستشفيات في شبكة واحدة وإدارة مركزية [47]
– غير متاح
الخدمة والوصول ( )
– سهولة الوصول إلى المعلومات الصحية عبر الإنترنت وتطبيق المعرفة [38]
– غير متاح
العبء (التعقيد والتكلفة؛ ; )
– قدرة تقنيات الصحة الرقمية على تقليل التوتر بين المرضى [40]
– تقنيات الصحة الرقمية فعالة من حيث التكلفة [38]
– غير متاح
تغذية راجعة للنتائج (
– تقنيات الصحة الرقمية سهلة ومريحة للاستخدام
– تقنيات الصحة الرقمية قادرة على تحسين مستوى راحة المرضى [39]
– غير متاح
البيئة الخارجية ( )
المنافسة
– غير متاح
– المنافسة على الموارد بين معدات تكنولوجيا المعلومات ومعدات الرعاية الصحية الأخرى [45,47]
البيئة التنظيمية ( ; )
– وجود عملية تواصل جيدة بين الهيئة التنظيمية والمستشفيات [47]
– عدم الاستقرار السياسي والاقتصادي [45,47]
موارد المجتمع ( )
– توفر وصول جيد إلى الإنترنت بين مستخدمي تقنيات الصحة الرقمية [44]
– غير متاح
تنفيذ بنية تحتية مستدامة ( )
تدريب ودعم المتبنين ( ; )
– الإلمام بالتعامل مع أدوات تقنيات الصحة الرقمية [40]
– غير متاح
العلاقة والتواصل مع المتبنين ( )
– غير متاح
– فجوة التواصل بين المشرفين والمشرفين [45]
بروتوكولات وإجراءات قابلة للتكيف ( )
– يمكن تقديم خدمات الصحة عن بُعد بسهولة بين الأطباء [37]
– غير متاح
تسهيل تبادل أفضل الممارسات ( )
– تبادل الخبرات بين المستشفيات المتقدمة والمبتدئة [47]
– غير متاح
خطة للاستدامة ( )
– تعطي مرافق الرعاية الصحية الأولوية لتنفيذ واستدامة تقنيات الصحة الرقمية [47]
– انتهاء جائحة كوفيد-19 قلل من الطلب على تقنيات الصحة الرقمية [46]
خصائص منظمة الرعاية الصحية ( )
المواضيع والفئات
رموز الميسرين
رموز الحواجز
الصحة والثقافة التنظيمية ( )
– توفر دعم تنظيمي عادل إلى جيد [42]
– الالتزام من الإدارة العليا أو المديرين [47]
– الإدارة العليا تفرض اعتماد تقنيات الصحة الرقمية [47]
– تعزيز تبادل الخبرات والمعرفة بين شبكات المستشفيات [47]
– ثقافة مكان العمل التي تتقبل التغيير [47]
– فهم السياسات التي وضعتها الحكومة [41]
– تغييرات متكررة في فريق إدارة المستشفى [47]
– نقص التخطيط لسياسات تكنولوجيا المعلومات على المدى المتوسط والطويل [47]
دعم الإدارة والتواصل ( )
– وجود إشراف في مكان العمل [42]
– توفر دعم تقني عادل إلى جيد [42]
– توفير الدعم للمجموعات ذات المعرفة القليلة بالتكنولوجيا [47]
– نقص التخطيط وتنفيذ تصميم النظام [47]
الأهداف المشتركة والتعاون ( ; )
– قسم تكنولوجيا المعلومات في المستشفى مرتبط مباشرة بالقطاعات المحلية لتكنولوجيا المعلومات [47]
– إنشاء لجنة إدارة متعددة التخصصات [47]
– شراكة مع الجامعات لتطوير تقنيات الصحة الرقمية [45]
– مقاومة مقدمي الرعاية الصحية لتغيير الممارسات [46]
القيادة السريرية ( )
– مستوى عالٍ من الاستقلالية في اتخاذ القرار في مكان العمل [42]
– ضعف القيادة وقلة الالتزام على مستوى المستشفى [45]
الأنظمة والتدريب ( )
– يحتوي مكان العمل على مرافق كافية [37]
– توفر تدريب مستمر أثناء العمل [37,43,47]
– تحديثات منتظمة للنظام [43]
– توفر مساعدة تقنية سريعة من دعم المكتب [43]
– نقص التدريب في التقنيات المتقدمة [36,40]
– تأخيرات في تطوير النظام وتنفيذه وتحديثاته [43,47]
– انقطاع متكرر في التيار الكهربائي [43]
– ضعف الطاقة الكهربائية ومرافق النسخ الاحتياطي [36]
– نقص المهارات بين مقدمي الرعاية الصحية في الوصول إلى تقنيات الصحة الرقمية واستخدامها [44]
البيانات ودعم القرار ( ; )
– توفر خدمات الدعم الفني على مدار 24 ساعة في مكان العمل [37]
– مركزية تطوير النظام والدعم الفني [47]
– نقص خطة الطوارئ لتقنيات الصحة الرقمية [47]
– تأخر الدعم الفني لتكنولوجيا المعلومات [43]
التوظيف والحوافز (
– يحتوي مكان العمل على عدد كافٍ من الأفراد المدربين في تقنيات الصحة الرقمية [37]
– تحسين تمويل الموارد البشرية والمادية [47]
– تخصيص كافٍ للموارد البشرية [41]
– نقص الحوافز لمقدمي الرعاية الصحية لاستخدام تقنيات الصحة الرقمية [38]
– معدل دوران الموظفين المرتفع، والعبء الزائد في العمل، وتقليل التوظيف [43,47]
– مقدمو الرعاية الصحية الذين هم من كبار السن [43]
توقعات الاستدامة ; )
– غير متاح
– مقدمو الرعاية الصحية ليس لديهم وقت وطاقة كافيين للمشاركة وتقديم تغذية راجعة في الوقت المناسب أثناء استخدام تقنيات الصحة الرقمية [38,44]
– توقعات غير واقعية تجاه تقنيات الصحة الرقمية [47]
خصائص المرضى ( )
المواضيع والفئات
رموز الميسرين
رموز الحواجز
التركيبة السكانية ( )
– غير متاح
– المرضى الأكبر سنًا يفكرون في استخدام تقنيات الصحة الرقمية ولديهم ثقة منخفضة فيها [38]
– الجمود الشخصي والعقلية المحافظة للجيل الأكبر [38]
– تكاليف الوصول إلى الإنترنت تتجاوز القدرة المالية للمرضى من ذوي الوضع الاجتماعي والاقتصادي المنخفض [39]
– ضعف الاتصال بشبكة الهاتف المحمول والوصول إلى الإنترنت في بعض المناطق الجغرافية [39]
المعرفة والمعتقدات (
– الثقة في التعلم والمشاركة والمشاركة المستدامة في تقنيات الصحة الرقمية [38]
– مستوى عالٍ من معرفة الصحة الإلكترونية ومهارات الكمبيوتر بين المرضى [38,44]
– مهارات عالية في البحث عن المعلومات بين المرضى [44]
– المرضى لديهم معرفة رقمية ومهارات ضعيفة في تقنيات الصحة الرقمية [36,38,39]
– المرضى لديهم شكوك حول دقة التشخيص عن بُعد [38]
– التحيز الاجتماعي ضد تقنيات الصحة الرقمية [38]
تقنية الصحة الرقمية: التكنولوجيا الصحية الرقمية. : عدد الدراسات بشكل عام. : عدد الدراسات التي أبلغت عن الميسرين. : عدد الدراسات التي أبلغت عن الحواجز. غير متاح: غير قابل للتطبيق.
بشكل خاص، شمل موضوع جوانب نظام الرعاية الصحية 23 ميسرًا و13 حاجزًا ( دراسات). من بين الميسرين البارزين كانت قدرة تقنيات الصحة الرقمية على منع العدوى المتبادلة ( ) وتجارب إيجابية سابقة باستخدام تقنيات الصحة الرقمية ( ). بالمقابل، كانت الوعي غير الكافي بشأن تقنيات الصحة الرقمية ( ) والقلق بشأن الدقة في تشخيص الأمراض وعلاجها ( ) هي الحواجز الرئيسية المميزة.
فيما يتعلق بموضوع وجهات نظر المرضى، تم الإبلاغ عن 9 ميسرين و3 حواجز ( دراسات). من بين هذه، كانت سهولة وراحة استخدام تقنيات الصحة الرقمية ( ) هي الميسر الرئيسي. ومع ذلك، فإن شعور المسافة بين المريض ومقدمي الرعاية الصحية أثناء التفاعل عن بُعد ، وشعور بالإجبار على استخدام تقنيات الصحة الرقمية ( )، ومقاومة المرضى لتغيير الممارسات قد تشكل تحديات لتنفيذ تقنيات الصحة الرقمية في بيئات المستشفيات ضمن البلدان ذات الدخل المنخفض والمتوسط.
تعتمد نجاح تنفيذ تقنيات الصحة الرقمية أيضًا على موضوع البيئة الخارجية ( دراسات). في هذا السياق، هناك ميسرَين يساعدان في التنفيذ، وهما وجود عملية تواصل جيدة بين الهيئة التنظيمية والمستشفيات ( ) وتوفر وصول جيد إلى الإنترنت بين مستخدمي تقنيات الصحة الرقمية ( ). من بين الحواجز التي تم تحديدها في هذا السياق، تبرز المنافسة على الموارد بين معدات تكنولوجيا المعلومات ومعدات الرعاية الصحية الأخرى ( ) كأكثر الحواجز انتشارًا.
يتضمن موضوع تنفيذ بنية تحتية مستدامة 4 ميسرين و2 حاجزين ( دراسات). من الجدير بالذكر، الإلمام بالتعامل مع أدوات تقنيات الصحة الرقمية ( سهولة تقديم خدمات الصحة عن بُعد بين الأطباء ) وتبادل الخبرات بين المستشفيات المتقدمة والمبتدئة ( تظهر كمسهلين لتنفيذ DHT. وعلى العكس، تشمل الحواجز في هذا الموضوع فجوة التواصل بين أصحاب المصلحة. ) ونهاية جائحة COVID-19 التي تقلل من الطلب على DHTs ( ).
تتكون خصائص موضوع تنظيم الرعاية الصحية من 22 ميسرًا و17 عائقًا لتنفيذ تكنولوجيا الصحة الرقمية.الدراسات). وقد أبرزت الدراسات السابقة توفر التدريب المستمر أثناء العمل ( ) كأكثر الميسرين تكرارًا لتنفيذ DHT في منظمة الرعاية الصحية. على العكس من ذلك، فإن الحواجز مثل نقص التدريب في التقنيات المتقدمة ( ); تأخيرات في تطوير النظام، والتنفيذ، والتحديثات ( معدل دوران الموظفين العالي، عبء العمل الزائد، وتقليل عدد الموظفين ) وكذلك نقص الوقت والطاقة بين مقدمي الرعاية الصحية للمشاركة وتقديم ملاحظات في الوقت المناسب أثناء استخدام تقنيات الصحة الرقمية ( ) منع تنفيذ DHTs.
كانت خصائص المرضى هي الموضوع النهائي الذي يمكن أن يؤثر على نجاح تنفيذ DHT في بيئات المستشفيات في البلدان ذات الدخل المنخفض والمتوسط. وقد شمل ذلك 3 عوامل مساعدة و7 عوائق.الدراسات). ومن الجدير بالذكر أن العامل المساعد الأكثر ذكرًا في هذا الموضوع هو ارتفاع مستوى الوعي الصحي الإلكتروني ومهارات الحاسوب بين المرضى ( ). وليس من المستغرب أن يكون العكس تمامًا، أي المرضى الذين يعانون من ضعف في المهارات والمعرفة الرقمية في التقنيات الصحية الرقمية ( )، يُبلغ عنه كأكثر الحواجز شيوعًا.
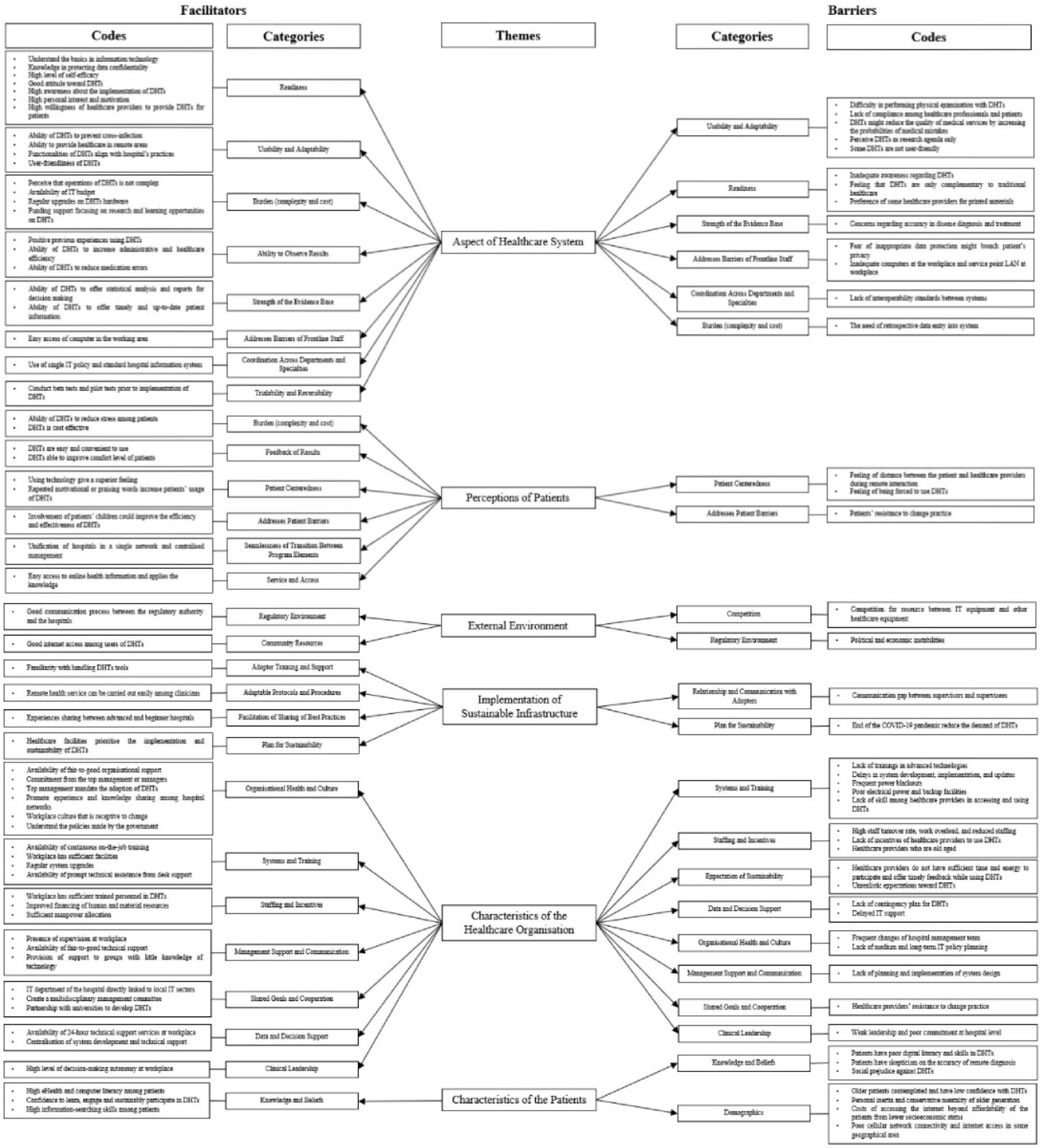
تم تلخيص العلاقة بين الرموز والفئات والمواضيع المتعلقة بالعوامل الميسرة والعوائق لتنفيذ التكنولوجيا الرقمية الصحية في الشكل 2، حيث تم ترتيب الرموز والفئات من الأكثر تكرارًا (الأعلى) إلى الأقل تكرارًا (الأسفل).
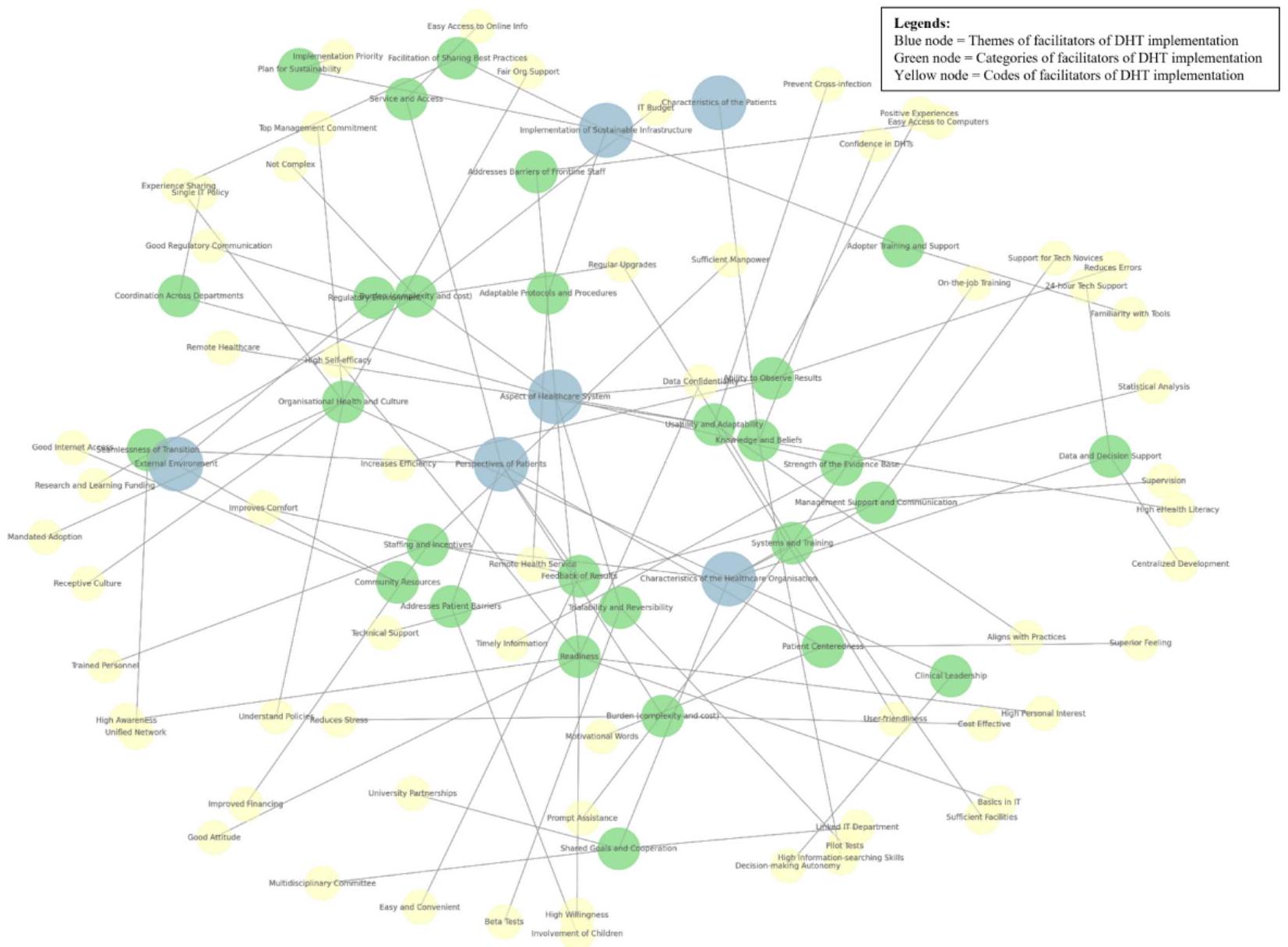
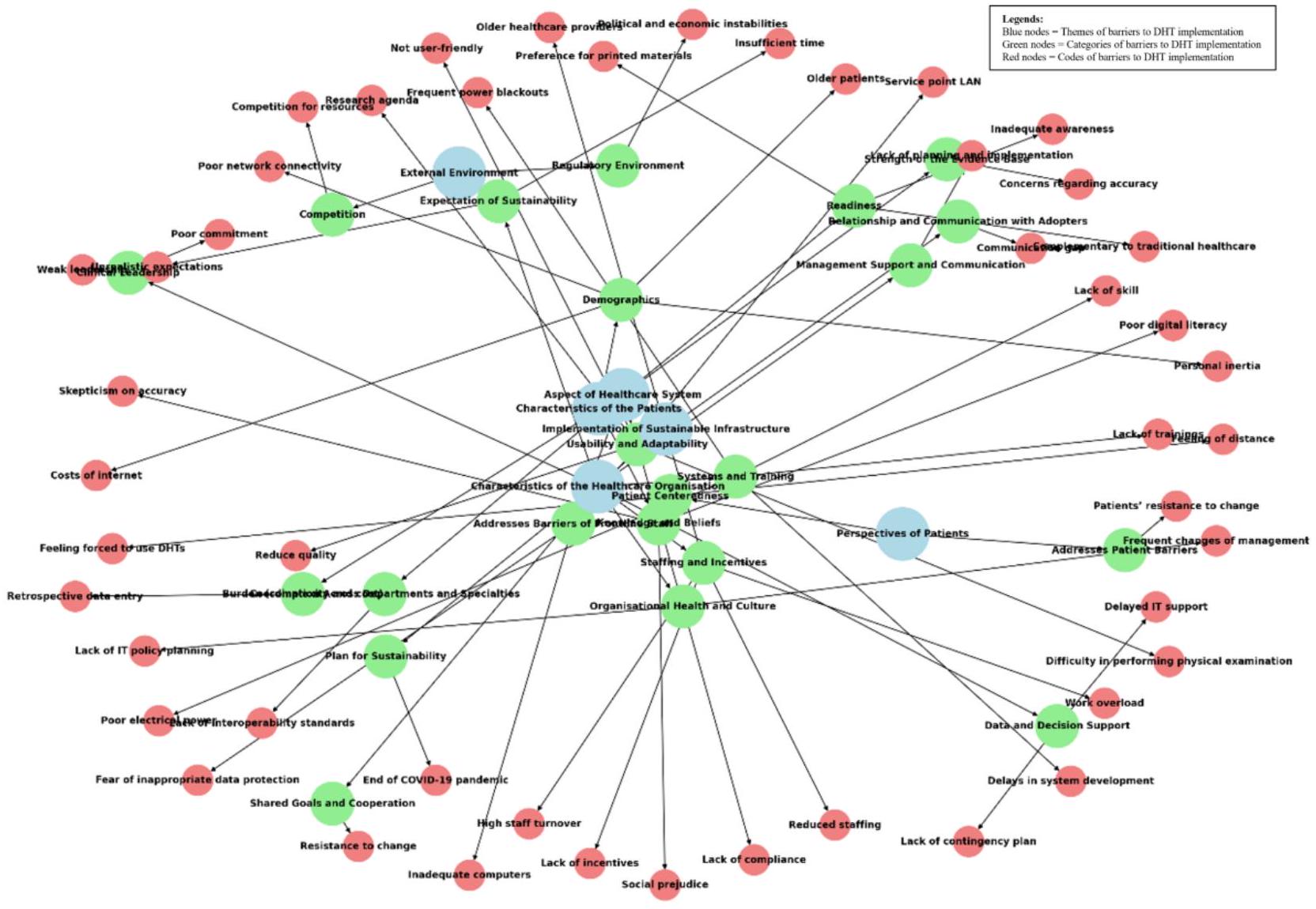
توضح الشكل 3 تحليل الشبكة لميسرات تنفيذ التكنولوجيا الصحية الرقمية. من الجدير بالذكر أن الميسرات مثل “وجهات نظر المرضى” و”جانب نظام الرعاية الصحية” مركزية في الشبكة. وهذا يشير إلى تأثيرها الواسع عبر مجالات متعددة، مما يجعلها نقاط تدخل رئيسية لتنفيذ التكنولوجيا الصحية الرقمية. على الرغم من عدم ملاحظة أي تجمعات واضحة، فإن الترابط يشير إلى أن معالجة بعض الميسرات (مثل “وجهات نظر المرضى” و”جانب نظام الرعاية الصحية” و”خصائص منظمة الرعاية الصحية”) يمكن أن يكون لها تأثيرات متتالية على الآخرين. توضح الشكل 4 تحليل الشبكة للحواجز أمام التكنولوجيا الصحية الرقمية. التنفيذ. لوحظ أن بعض الحواجز أكثر مركزية، مثل “خصائص منظمات الرعاية الصحية” و”جانب من نظام الرعاية الصحية” و”تنفيذ البنية التحتية المستدامة” و”خصائص المرضى”، مما يبرز أدوارها المحورية في الشبكة. تعمل هذه الحواجز المركزية كعوامل مؤثرة رئيسية وتربط بين حواجز متعددة. في حين أن حواجز “البيئة الخارجية” و”وجهات نظر المرضى” تكون أكثر نحو المحيط، وبالتالي، لها تأثير أقل على الشبكة. كان من الممكن ملاحظة تجمع في تحليل الشبكة، يشمل “خصائص منظمة الرعاية الصحية” و”جانب من “حواجز نظام الرعاية الصحية”. العديد من الحواجز مترابطة، مما يشير إلى أن معالجة واحدة (مثل “خصائص منظمات الرعاية الصحية”) قد تخفف من حواجز أخرى. ومع ذلك، يجب ملاحظة أن بعض العقد، مثل “الاستعداد” و”قابلية الاستخدام والتكيف”، يمكن أن تكون عوامل مساعدة وأيضًا حواجز أمام تنفيذ التكنولوجيا الرقمية الصحية، وبالتالي، يمكن أن تظهر في كل من تحليلات الشبكة.
منذ بداية جائحة كوفيد-19، كانت أكثر تقنيات الصحة الرقمية استخدامًا في مستشفيات البلدان ذات الدخل المنخفض والمتوسط هي الطب عن بُعد، تليها نظم المعلومات الصحية، والسجلات الطبية الإلكترونية، والصحة المتنقلة، كما هو موضح في الشكل 5.
الشكل 2. ملخص الرموز والفئات والمواضيع المتعلقة بالعوامل الميسرة والعوائق لتنفيذ تكنولوجيا الصحة الرقمية (DHT). تكنولوجيا المعلومات: تكنولوجيا المعلومات؛ الشبكة المحلية: الشبكة المحلية.
الشكل 3. تحليل الشبكة لتوضيح العلاقة بين رموز الميسرين لتنفيذ تقنيات الصحة الرقمية (DHTs) في المستشفيات في البلدان ذات الدخل المنخفض والمتوسط (LMICs) منذ بداية جائحة COVID-19.
الشكل 4. تحليل الشبكة لتوضيح العلاقة بين رموز الحواجز لتنفيذ تقنيات الصحة الرقمية (DHTs) في بيئات المستشفيات في البلدان ذات الدخل المنخفض والمتوسط (LMICs) في عصر ما بعد COVID-19. تكنولوجيا المعلومات: تكنولوجيا المعلومات؛ LAN: الشبكة المحلية.
الشكل 5. تقنيات الصحة الرقمية (DHTs) في البلدان ذات الدخل المنخفض والمتوسط (LMICs) منذ بداية جائحة COVID-19.
نقاش
مسهلات وعوائق تنفيذ التكنولوجيا الرقمية الصحية في البلدان ذات الدخل المنخفض والمتوسط
تشمل العوامل الأكثر شيوعًا التي تسهل تنفيذ تقنيات الصحة الرقمية (DHT) سهولة وراحة استخدام هذه التقنيات، وقدرتها على منع العدوى المتبادلة، والتجارب الإيجابية السابقة في استخدام تقنيات الصحة الرقمية، وتوفر التدريب المستمر أثناء العمل، وارتفاع مستوى الوعي الصحي والمهارات الحاسوبية بين المرضى. بالمقابل، حددنا أن الحواجز الأكثر تكرارًا هي الوعي غير الكافي بشأن تقنيات الصحة الرقمية؛ المخاوف المتعلقة بدقة تشخيص الأمراض وعلاجها؛ المنافسة على الموارد بين معدات تكنولوجيا المعلومات ومعدات الرعاية الصحية الأخرى؛ نقص التدريب في التقنيات المتقدمة؛ التأخيرات في تطوير النظام وتنفيذه وتحديثه؛ ارتفاع معدل دوران الموظفين، وزيادة عبء العمل، وتقليل عدد الموظفين؛ عدم كفاية الوقت والطاقة بين مقدمي الرعاية الصحية لاستخدام تقنيات الصحة الرقمية؛ والمرضى الذين يعانون من ضعف في المهارات الرقمية والمعرفة بتقنيات الصحة الرقمية.
حسب علمنا، فإن هذه المراجعة الشاملة هي الأولى التي تفحص العوامل الميسرة والعوائق أمام تنفيذ التقنيات الرقمية الصحية في المستشفيات داخل البلدان ذات الدخل المنخفض والمتوسط منذ بداية جائحة COVID-19. من المهم ملاحظة ندرة الأدبيات المنشورة حول هذا الموضوع في البلدان ذات الدخل المنخفض والمتوسط. حتى المراجعات الموجودة غالبًا ما تركزت على دراسات من دول ذات دخل مرتفع أو تركزت على أمراض معينة [27،48،49]. على سبيل المثال، قامت مراجعة منهجية بواسطة وايتلاو وآخرين [27]، والتي شملت 29 دراسة، بالتحقيق في تنفيذ التقنيات الرقمية الصحية في الأمراض القلبية الوعائية بشكل أساسي في الدول ذات الدخل المرتفع. كما هو متوقع، كانت العوامل الميسرة والعوائق المحددة في هذه المراجعة تختلف بشكل كبير عن نتائجنا. أشار وايتلاو وآخرون إلى عوامل ميسرة مثل تحسين التواصل مع الأطباء، مكونات التقنيات الرقمية الصحية المخصصة، واجهات سهلة الاستخدام، الدعم المؤسسي والتنظيمي، زيادة الكفاءة، والإحساس بفائدة التقنيات الرقمية الصحية. كانت العوائق المبلغ عنها تشمل التكنولوجيا المعقدة، القلق التكنولوجي، زيادة عبء العمل، التكنولوجيا غير الموثوقة، وغياب التكامل مع السجلات الطبية الإلكترونية. هذه التباينات قد تنبع من عوامل مختلفة مثل الاختلافات في بنية الرعاية الصحية [50]، والسياقات الاجتماعية والاقتصادية [51]، وتمويل الرعاية الصحية [52]، فضلاً عن تكاليف تطوير وتنفيذ تقنيات الصحة الرقمية [53] بين البيئات ذات الدخل المرتفع والبلدان ذات الدخل المنخفض والمتوسط. بالإضافة إلى ذلك، قد لا يلتقط التركيز على أمراض معينة في الأدبيات السابقة بشكل كامل الميسرات والعوائق المتنوعة ذات الصلة بتنفيذ تقنيات الصحة الرقمية عبر مختلف سياقات الرعاية الصحية.
أنظمة DHT التي تم تنفيذها
لدهشتنا، كانت الرعاية الصحية عن بُعد هي التقنية الأكثر شيوعًا التي تم الإبلاغ عنها في المستشفيات منذ بداية جائحة COVID-19، متجاوزةً تقنيات الصحة الرقمية الأخرى مثل أنظمة معلومات المستشفيات والسجلات الطبية الإلكترونية والرعاية الصحية المتنقلة. يمكن فهم ذلك من خلال حقيقة أن الرعاية الصحية عن بُعد مناسبة تمامًا لمقدمي الرعاية الصحية والمرضى الذين يعزلون أنفسهم، حيث إنها تقلل بشكل فعال من خطر انتقال COVID-19. إنها تلغي الحاجة إلى الاتصال الجسدي المباشر، وتضمن استمرار الرعاية للمجتمع، وفي النهاية تخفض معدلات المرض والوفاة خلال جائحة COVID-19.
إطار تصنيف لتنفيذ DHT في البلدان ذات الدخل المنخفض والمتوسط
على الرغم من ظهور تقنيات مبتكرة متنوعة مثل التقنيات القابلة للارتداء، الميتافيرس، إنترنت الأشياء الطبية، البلوكشين في الرعاية الصحية، تحليلات البيانات الضخمة، الذكاء الاصطناعي، التعلم الآلي، البرمجيات كأجهزة طبية، الواقع المعزز، والواقع الافتراضي، لا تزال تطبيقات التقنيات الصحية الرقمية في المستشفيات داخل البلدان ذات الدخل المنخفض والمتوسط بدائية مقارنة بالدول ذات الدخل المرتفع. إن الاستخدام الحالي للتقنيات الصحية الرقمية في البلدان ذات الدخل المنخفض والمتوسط، مثل الطب عن بُعد، أنظمة معلومات المستشفيات، السجلات الطبية الإلكترونية، والصحة المتنقلة، قد أبلغت عن المكونات الرئيسية لإطار تصنيف جديد يركز على البلدان ذات الدخل المنخفض والمتوسط. استنادًا إلى الأدبيات الحديثة [13،15،17-23،55] والعوامل الميسرة والعوائق المحددة لاستخدام هذه التقنيات الصحية الرقمية في البلدان ذات الدخل المنخفض والمتوسط، نقترح إطار تصنيف للتقنيات الصحية الرقمية، كما هو موضح في الشكل 6.
الشكل 6. إطار تصنيف التقنيات الصحية الرقمية (DHTs). LMIC: بلد ذو دخل منخفض ومتوسط.
يستند هذا الإطار التصنيفي إلى حقيقة أن التقنيات الصحية الرقمية الأبسط، مثل الطب عن بُعد، أنظمة معلومات المستشفيات، السجلات الطبية الإلكترونية، والصحة المتنقلة، أسهل في التنفيذ في البلدان ذات الدخل المنخفض والمتوسط بسبب انخفاض التكاليف ومتطلبات البنية التحتية، وقابلية التكيف مع الموارد المحدودة، واحتياجات التدريب الدنيا. تعتمد هذه التقنيات بشكل أساسي على الاتصال الأساسي بالإنترنت، والأجهزة المحمولة، وأجهزة الكمبيوتر، مما يجعلها أكثر سهولة وملاءمة نظرًا لتوافر الشبكات المحمولة بشكل أوسع في البلدان ذات الدخل المنخفض والمتوسط. كما أنها تتكامل بسهولة في سير العمل الحالي للرعاية الصحية، مما يتطلب فقط جلسات تدريب قصيرة ومهارات رقمية أساسية. علاوة على ذلك، نظرًا لأن البلدان ذات الدخل المنخفض والمتوسط تعطي الأولوية لمعالجة الاحتياجات الصحية الفورية مثل الأمراض المعدية، فإن هذه التقنيات المتاحة تتلقى دعمًا وتمويلًا أكبر. بالمقابل، تتطلب التقنيات المتقدمة مثل الذكاء الاصطناعي، والواقع الافتراضي، والبلوكشين بنية تحتية متخصصة، وخبرة تقنية، وموارد مالية كبيرة، والتي غالبًا ما تكون نادرة في البلدان ذات الدخل المنخفض والمتوسط.
يتكون هذا الإطار التصنيفي المقترح أيضًا من تقنيات صحية رقمية أخرى تم تنفيذها في البلدان ذات الدخل المرتفع. نأمل أن يساعد ذلك المعنيين في الرعاية الصحية في البلدان ذات الدخل المنخفض والمتوسط على تحديد نطاق التقنيات الصحية الرقمية في البلدان ذات الدخل المنخفض والمتوسط ومساعدتهم على تحديد أولويات التقنيات الصحية الرقمية المناسبة التي يمكن تنفيذها في ظل ندرة الموارد. وبالتالي، يمكن لصانعي السياسات تخصيص تمويل الرعاية الصحية (على سبيل المثال، يمكن لوزارة الصحة تحديد فئات التقنيات الصحية الرقمية المؤهلة للحصول على الدعم)، ويمكن لشركات التأمين تعويض المرضى الذين استخدموا التقنيات الصحية الرقمية (أي تحديد أي فئات من التقنيات الصحية الرقمية يمكن تغطيتها من قبل سياسات التأمين) [56،57]. علاوة على ذلك، يمكن تسهيل التواصل الواضح والفعال بين الجمهور، ومقدمي الرعاية الصحية، وخبراء التكنولوجيا [57،58]. قانونيًا، يتيح إطار التصنيف المحدد للسلطات تنظيم وإدارة استخدام التقنيات الصحية الرقمية [58،59]. أخيرًا، قد يسهل إطار التصنيف المحدد بوضوح للتقنيات الصحية الرقمية التنفيذ، خاصة في البيئات التي تعاني من نقص الموارد، حيث يمكن للمعنيين تحديد أولويات فئات التقنيات الصحية الرقمية التي يجب تنفيذها [56].
نقاط القوة والقيود
تتمتع هذه المراجعة الشاملة بعدة نقاط قوة ملحوظة. في البداية، جمعنا بيانات شاملة من مجموعة متنوعة من قواعد البيانات، بما في ذلك مصادر الأدبيات الرمادية مثل جوجل
سكولار. تم اتخاذ هذا الخيار المتعمد لضمان شمولية وقوة الدراسات المضمنة. بالإضافة إلى ذلك، خلال مرحلة التخطيط للمراجعة، شاركنا بنشاط المعنيين ذوي الصلة، بما في ذلك تقنيي المعلومات، ساعين إلى دمج ملاحظاتهم في بروتوكول المراجعة. علاوة على ذلك، في هيكلة وتصنيف العوائق والعوامل الميسرة المحددة، استخدمنا نموذجًا مفاهيميًا تم تطويره بواسطة فيلدشتاين وغلاسكو [33]، مما يعزز من دقة التحليل في المراجعة. علاوة على ذلك، تقدم مراجعتنا ثروة من الرؤى النوعية والكمية حول تنفيذ التقنيات الصحية الرقمية، مما يوفر إرشادات شاملة للمعنيين المهتمين بتنفيذ التقنيات الصحية الرقمية ضمن إعداداتهم الخاصة.
على الرغم من نقاط قوتها، فإن مراجعتنا تحتوي على بعض القيود. على وجه التحديد، من خلال التركيز على تحديد العوائق والعوامل الميسرة لتنفيذ التقنيات الصحية الرقمية في بيئات المستشفيات داخل البلدان ذات الدخل المنخفض والمتوسط، قمنا بتقييد معايير الإدراج لدينا للدراسات التي أجريت فقط داخل المستشفيات. وبالتالي، تم استبعاد العديد من الدراسات التي تقدم رؤى من منظور الرعاية الأولية والمجتمع. بالإضافة إلى ذلك، تم حذف الدراسات التي لم تتناول بشكل صريح العوامل الميسرة والعوائق، مما قد يتسبب في تجاهل معلومات قيمة حول تقنيات صحية رقمية أخرى مفيدة لرعاية المرضى. علاوة على ذلك، نظرًا لأن هدفنا الرئيسي كان تقديم نظرة عامة على الأدبيات الموجودة حول التقنيات الصحية الرقمية، لم نطبق أي تدابير لمراقبة الجودة على الدراسات المضمنة. إن التباين في الأساليب التحليلية، وأسئلة المقابلة، وسكان الدراسة عبر الأوراق المضمنة يمثل عدم اتساق محتمل في النتائج ويجعل تقييم الجودة صعبًا. بالإضافة إلى ذلك، مع وجود 128 دولة ذات دخل منخفض ومتوسط في وقت البحث عن الأدبيات، كان من غير العملي إدراج كل دولة بالاسم في سلسلة البحث، مما قد يؤدي إلى عدم التقاط بعض البلدان ذات الدخل المنخفض والمتوسط في نتائج البحث.
الآثار والتوصيات
فهم العوامل الميسرة والعوائق أمام التقنيات الصحية الرقمية في بيئات المستشفيات في البلدان ذات الدخل المنخفض والمتوسط له آثار عميقة على كل من الممارسة السريرية والبحث. إن تحديد العوامل الميسرة لتنفيذ التقنيات الصحية الرقمية يمكّن من التكامل الفعال للتقنيات الصحية الرقمية في المستشفيات، مما يؤدي إلى تحسين دقة التشخيص، وتحسين مراقبة المرضى، وتحسين إدارة سجلات المرضى، وتوافر خدمات الرعاية الصحية عن بُعد. بالمقابل، يمكن أن يؤدي التعرف على العوائق أمام تنفيذ التقنيات الصحية الرقمية إلى دفع مختلف المعنيين في البلدان ذات الدخل المنخفض والمتوسط لوضع استراتيجيات تعالج القضايا المتعلقة بالموارد المالية، والبنية التحتية التكنولوجية، والمعرفة بين مقدمي الرعاية الصحية. من حيث البحث، نأمل أن تعزز هذه المراجعة التعاون الدولي، والدعم الحكومي، والاستثمار في البنية التحتية الرقمية، مما يعزز بدوره القدرة على جمع البيانات، وتحليلها، ومشاركتها. يمكن أن تعزز هذه التطورات من قدرات البحث، مما يسمح بإجراء دراسات وبائية أكثر شمولاً، ومراقبة الأمراض في الوقت الحقيقي، وتطوير تدخلات صحية محددة للسياق.
لزيادة الاستفادة من التقنيات الصحية الرقمية في بيئات المستشفيات في البلدان ذات الدخل المنخفض والمتوسط، يمكن تقديم عدة توصيات للاستفادة من العوامل الميسرة والتخفيف من العوائق. أولاً، يجب التأكيد على الراحة وسهولة استخدام التقنيات الصحية الرقمية من خلال واجهات سهلة الاستخدام وتصاميم بديهية، مما يضمن أن مقدمي الرعاية الصحية يمكنهم اعتماد هذه التقنيات بسرعة وكفاءة في روتينهم اليومي. ثانيًا، يجب تسليط الضوء على دور التقنيات الصحية الرقمية في منع العدوى المتبادلة في برامج التدريب وحملات التوعية، خاصة في المناطق التي تنتشر فيها الأمراض المعدية. يجب مشاركة التجارب الإيجابية السابقة مع التقنيات الصحية الرقمية على نطاق واسع لبناء الثقة وإظهار الفوائد الملموسة لهذه التقنيات. يجب توفير تدريب مستمر أثناء العمل للحفاظ على تحديث العاملين في الرعاية الصحية بأحدث التطورات وأفضل الممارسات، مع تعزيز كفاءتهم التقنية. سيساعد تعزيز مستوى الوعي الصحي الرقمي ومحو الأمية الحاسوبية بين المرضى من خلال برامج التوعية المجتمعية والتعليم على دعم الاستخدام الفعال للتقنيات الصحية الرقمية.
يتطلب معالجة الحواجز نهجًا متعدد الأبعاد. لمواجهة نقص الوعي والمخاوف بشأن دقة التقنيات الصحية الرقمية، من الضروري تنفيذ مبادرات تعليمية شاملة تبرز موثوقية وفعالية هذه التقنيات سريريًا. يجب نشر معلومات واضحة تستند إلى الأدلة لمقدمي الرعاية الصحية والمرضى لبناء الثقة في التقنيات الصحية الرقمية. يمكن التخفيف من المنافسة على الموارد بين معدات تكنولوجيا المعلومات وأدوات الرعاية الصحية الأخرى من خلال الدعوة إلى تخصيص ميزانيات متوازنة والبحث عن تمويل خارجي أو شراكات لدعم الموارد. يجب توسيع برامج التدريب في التقنيات المتقدمة لتزويد مقدمي الرعاية الصحية بالمهارات اللازمة لاستخدام التقنيات الصحية الرقمية بفعالية. لمعالجة التأخيرات في تطوير النظام وتنفيذه، يجب إنشاء عمليات وجداول زمنية مبسطة، مع فرق إدارة مشاريع مخصصة تشرف على هذه المبادرات. يمكن إدارة معدلات دوران الموظفين العالية والضغط في العمل من خلال تحسين ظروف العمل، وتقديم رواتب تنافسية، وتوفير فرص لتطوير المهنة. أخيرًا، سيساهم تعزيز الثقافة الرقمية بين المرضى من خلال برامج تعليمية مستهدفة في ضمان قدرتهم على التفاعل مع التقنيات الصحية الرقمية بفعالية، مما يؤدي في النهاية إلى تحسين النتائج الصحية. من خلال تنفيذ هذه التوصيات، يمكن للدول ذات الدخل المنخفض والمتوسط التغلب على الحواجز واستغلال إمكانيات التقنيات الصحية الرقمية بالكامل لتحسين الممارسة السريرية وتقدم أبحاث الرعاية الصحية.
الاستنتاجات
تسلط المراجعة الشاملة حول تنفيذ التكنولوجيا الرقمية الصحية في البلدان ذات الدخل المنخفض والمتوسط منذ بداية جائحة كوفيد-19 الضوء على تداعيات سياسية وسريرية وبحثية هامة. يمكن لصانعي السياسات الاستفادة من الرؤى لصياغة استراتيجيات مستهدفة لتبني التكنولوجيا الرقمية الصحية، بينما يساعد الإطار التصنيفي المطور في تحديد أولويات التكنولوجيا الرقمية الصحية. في البيئات السريرية، يعزز فهم أنواع التكنولوجيا الرقمية الصحية، والميسرات، والعوائق من اتخاذ القرارات لتحسين رعاية المرضى وتحسين استخدام الموارد. بالإضافة إلى ذلك، فإن الاستثمار في بناء القدرات وبرامج التدريب للمهنيين الصحيين أمر حاسم، مع التركيز على تعزيز المهارات الرقمية والتقنية. علاوة على ذلك، سيساهم تحديد أولويات البحث وتوافق التمويل مع التحديات الرئيسية مثل تحسين المهارات الرقمية ومعالجة المخاوف بشأن دقة التكنولوجيا الرقمية الصحية في دفع التقدم في تنفيذ التكنولوجيا الرقمية الصحية وتقديم الرعاية الصحية في البلدان ذات الدخل المنخفض والمتوسط.
في عصر ما بعد الجائحة، تم استخدام الطب عن بُعد على نطاق واسع في المستشفيات في البلدان ذات الدخل المنخفض والمتوسط، من بين تقنيات الصحة الرقمية الأخرى. تكشف نتائجنا أيضًا عن العديد من العوامل الميسرة والعوائق لتنفيذ تقنيات الصحة الرقمية في بيئات المستشفيات في البلدان ذات الدخل المنخفض والمتوسط. يمكن تنظيم هذه العوامل في 6 مواضيع، وهي: (1) جوانب نظام الرعاية الصحية؛ (2) وجهات نظر المرضى؛ (3) العوامل الخارجية
البيئة؛ (4) تنفيذ البنية التحتية المستدامة؛ (5) خصائص منظمة الرعاية الصحية؛ و (6)
خصائص المرضى.
شكر وتقدير
نحن نُقدّر مساهمات متخصص تكنولوجيا المعلومات في مكتبة جامعة بوترا ماليزيا لتقديمه المساعدة الفنية والفكرية خلال البحث في الأدبيات.
توفر البيانات
جميع البيانات المسترجعة والمحللة مدرجة في هذه المراجعة التمهيدية.
مساهمات المؤلفين
طورت SQY و BHC مفهوم المراجعة الاستكشافية. شارك SQY و DT في تصميم منهجية البحث. قامت NIHA و SQY بإجراء مراجعة أدبية شاملة لتحديد الأطر والأساليب المنهجية ذات الصلة بالمراجعة الاستكشافية. أعدت SQY المسودة الأولية للمراجعة.
World Health Organization (WHO). Tracking universal health coverage: 2023 global monitoring report. WHO. Geneva, Switzerland. WHO; Sep 18, 2023. URL: https://www.who.int/publications/i/item/9789240080379 [accessed 2024-02-10]
Shah SA, Safian N, Ahmad S, Nurumal SR, Mohammad Z, Mansor J, et al. Unmet healthcare needs among elderly Malaysians. JMDH. Oct 2021;Volume 14:2931-2940. [doi: 10.2147/jmdh.s326209]
Njagi P, Arsenijevic J, Groot W. Cost-related unmet need for healthcare services in Kenya. BMC Health Serv Res. Apr 17, 2020;20(1):322. [FREE Full text] [doi: 10.1186/s12913-020-05189-3] [Medline: 32303244]
Sohn M, Che X, Park H-J. Unmet healthcare needs, catastrophic health expenditure, and health in South Korea’s universal healthcare system: progression towards improving equity by NHI type and income level. Healthcare (Basel). Oct 16, 2020;8(4):408. [FREE Full text] [doi: 10.3390/healthcare8040408] [Medline: 33081357]
Baek S, Choi E-H, Lee J. Unmet healthcare needs of children in vulnerable families in South Korea: finding from the Community Child Center Child Panel Survey. Int J Environ Res Public Health. Nov 07, 2020;17(21):8241. [FREE Full text] [doi: 10.3390/ijerph17218241] [Medline: 33171882]
Kim J, You M, Shon C. Impact of the COVID-19 pandemic on unmet healthcare needs in Seoul, South Korea: a cross-sectional study. BMJ Open. Aug 26, 2021;11(8):e045845. [FREE Full text] [doi: 10.1136/bmjopen-2020-045845] [Medline: 34446482]
Harris RB, Cormack DM, Stanley J. Experience of racism and associations with unmet need and healthcare satisfaction: the 2011/12 adult New Zealand Health Survey. Aust N Z J Public Health. Feb 2019;43(1):75-80. [FREE Full text] [doi: 10.1111/1753-6405.12835] [Medline: 30296819]
Rosenthal A, Waitzberg R. The challenges brought by the COVID-19 pandemic to health systems exposed pre-existing gaps. Health Policy Open. Dec 2023;4:100088. [doi: 10.1016/j.hpopen.2022.100088] [Medline: 36536931]
Mitgang EA, Blaya JA, Chopra M. Digital health in response to COVID-19 in low- and middle-income countries: opportunities and challenges. Glob Policy. Jul 2021;12(Suppl 6):107-109. [doi: 10.1111/1758-5899.12880] [Medline: 34230840]
Ronquillo Y, Meyers A, Korvek S. Digital Health. StatPearls. Treasure Island (FL). StatPearls Publishing; Jan 2025.
Istepanian RSH. Mobile health (m-Health) in retrospect: the known unknowns. Int J Environ Res Public Health. Mar 22, 2022;19(7):3747. [FREE Full text] [doi: 10.3390/ijerph19073747] [Medline: 35409431]
Roy J, Levy DR, Senathirajah Y. Defining telehealth for research, implementation, and equity. J Med Internet Res. Apr 13, 2022;24(4):e35037. [FREE Full text] [doi: 10.2196/35037] [Medline: 35416778]
Huhn S, Axt M, Gunga H-C, Maggioni MA, Munga S, Obor D, et al. The impact of wearable technologies in health research: scoping review. JMIR Mhealth Uhealth. Jan 25, 2022;10(1):e34384. [FREE Full text] [doi: 10.2196/34384] [Medline: 35076409]
Ibrahim AA, Ahmad Zamzuri M’I, Ismail R, Ariffin AH, Ismail A, Muhamad Hasani MH, et al. The role of electronic medical records in improving health care quality: a quasi-experimental study. Medicine (Baltimore). Jul 29, 2022;101(30):e29627. [FREE Full text] [doi: 10.1097/MD.0000000000029627] [Medline: 35905245]
Belle A, Thiagarajan R, Soroushmehr SMR, Navidi F, Beard DA, Najarian K. Big data analytics in healthcare. Biomed Res Int. 2015;2015:370194. [FREE Full text] [doi: 10.1155/2015/370194] [Medline: 26229957]
Dwivedi R, Mehrotra D, Chandra S. Potential of Internet of Medical Things (IoMT) applications in building a smart healthcare system: a systematic review. J Oral Biol Craniofac Res. Mar 2022;12(2):302-318. [FREE Full text] [doi: 10.1016/j.jobcr.2021.11.010] [Medline: 34926140]
Yoon H-J. Blockchain technology and healthcare. Healthc Inform Res. Apr 2019;25(2):59-60. [FREE Full text] [doi: 10.4258/hir.2019.25.2.59] [Medline: 31131139]
Petrigna L, Musumeci G. The metaverse: a new challenge for the healthcare system: a scoping review. J Funct Morphol Kinesiol. Aug 30, 2022;7(3):63. [FREE Full text] [doi: 10.3390/jfmk7030063] [Medline: 36135421]
Yu J, Zhang J, Sengoku S. Innovation process and industrial system of US Food and Drug Administration-approved software as a medical device: review and content analysis. J Med Internet Res. Nov 24, 2023;25:e47505. [FREE Full text] [doi: 10.2196/47505] [Medline: 37999948]
Eckert M, Volmerg JS, Friedrich CM. Augmented reality in medicine: systematic and bibliographic review. JMIR Mhealth Uhealth. Apr 26, 2019;7(4):e10967. [FREE Full text] [doi: 10.2196/10967] [Medline: 31025950]
Halbig A, Babu S, Gatter S, Latoschik M, Brukamp K, von Mammen S. Opportunities and challenges of virtual reality in healthcare – a domain experts inquiry. Front Virtual Real. Mar 23, 2022;3:3. [doi: 10.3389/frvir.2022.837616]
Xu Y, Liu X, Cao X, Huang C, Liu E, Qian S, et al. Artificial intelligence: a powerful paradigm for scientific research. Innovation (Camb). Nov 28, 2021;2(4):100179. [FREE Full text] [doi: 10.1016/j.xinn.2021.100179] [Medline: 34877560]
Sarker IH. Machine learning: algorithms, real-world applications and research directions. SN Comput Sci. Mar 2021;2(3):160. [FREE Full text] [doi: 10.1007/s42979-021-00592-x] [Medline: 33778771]
Mehta N, Pandit A, Shukla S. Transforming healthcare with big data analytics and artificial intelligence: a systematic mapping study. J Biomed Inform. Dec 2019;100:103311. [FREE Full text] [doi: 10.1016/j.jbi.2019.103311] [Medline: 31629922]
Yin J, Ngiam KY, Teo HH. Role of artificial intelligence applications in real-life clinical practice: systematic review. J Med Internet Res. Apr 22, 2021;23(4):e25759. [FREE Full text] [doi: 10.2196/25759] [Medline: 33885365]
Iyamu I, Gómez-Ramírez O, Xu AX, Chang H-J, Watt S, Mckee G, et al. Challenges in the development of digital public health interventions and mapped solutions: findings from a scoping review. Digit Health. 2022;8:20552076221102255. [doi: 10.1177/20552076221102255] [Medline: 35656283]
Whitelaw S, Pellegrini D, Mamas M, Cowie M, Van Spall HGC. Barriers and facilitators of the uptake of digital health technology in cardiovascular care: a systematic scoping review. Eur Heart J Digit Health. Mar 04, 2021;2(1):62-74. [FREE Full text] [doi: 10.1093/ehjdh/ztab005] [Medline: 34048508]
Jacob KS. Public health in low- and middle-income countries and the clash of cultures. J Epidemiol Community Health. Jul 2009;63(7):509. [doi: 10.1136/jech.2009.086934] [Medline: 19525248]
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. Feb 2005;8(1):19-32. [doi: 10.1080/1364557032000119616]
Yew SQ, Trivedi D, Adanan NIH, Chew BH. Facilitators and barriers of digital health technologies implementation in hospital settings in lower-income and middle-income countries since the COVID-19 pandemic: a scoping review protocol. BMJ Open. Jan 31, 2024;14(1):e078508. [FREE Full text] [doi: 10.1136/bmjopen-2023-078508] [Medline: 38296272]
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. Oct 02, 2018;169(7):467-473. [FREE Full text] [doi: 10.7326/M18-0850] [Medline: 30178033]
Feldstein AC, Glasgow RE. A Practical, Robust Implementation and Sustainability Model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf. Apr 2008;34(4):228-243. [doi: 10.1016/s1553-7250(08)34030-6] [Medline: 18468362]
Naeem M, Ozuem W, Howell K, Ranfagni S. A step-by-step process of thematic analysis to develop a conceptual model in qualitative research. International Journal of Qualitative Methods. Nov 08, 2023;22:22. [doi: 10.1177/16094069231205789]
Abdulai M, Aldheleai H, Bokhari M. Health care professionals’ use of health information systems (HIS) in Indian hospitals. IJCA. Apr 19, 2021;174(28):5-12. [doi: 10.5120/ijca2021921185]
Alboraie M, Abdalgaber M, Youssef N, Moaz I, Abdeen N, Abosheaishaa H, et al. Healthcare providers’ perspective about the use of telemedicine in Egypt: a national survey. Int J Telemed Appl. Mar 12, 2022;2022:3811068-3811068. [FREE Full text] [doi: 10.1155/2022/3811068] [Medline: 35313723]
Jiang Y, Sun P, Chen Z, Guo J, Wang S, Liu F, et al. Patients’ and healthcare providers’ perceptions and experiences of telehealth use and online health information use in chronic disease management for older patients with chronic obstructive pulmonary disease: a qualitative study. BMC Geriatr. Jan 03, 2022;22(1):9. [FREE Full text] [doi: 10.1186/s12877-021-02702-z] [Medline: 34979967]
Ning Y, Dong Z, Jia Z, Zhao W, Ding Y, Wang Q, et al. Development of mobile health-based interventions to promote physical activity in patients with head and neck cancer: a qualitative study. Front Public Health. 2023;11:1260804. [doi: 10.3389/fpubh.2023.1260804] [Medline: 38074711]
Shardha H, Kumar G, Sagar N, Kumar R, Qazi M, Munir S, et al. Perceptions of telemedicine among healthcare professionals in rural tertiary care hospitals of rural Sindh, Pakistan: a qualitative study. Ann Med Surg (Lond). Feb 2024;86(2):726-733. [doi: 10.1097/MS9.0000000000001688] [Medline: 38333274]
Yu-Tong T, Yan Z, Zhen L, Bing X, Qing-Yun C. Telehealth readiness and its influencing factors among Chinese clinical nurses: a cross-sectional study. Nurse Educ Pract. Jan 2022;58:103278. [FREE Full text] [doi: 10.1016/j.nepr.2021.103278] [Medline: 34954659]
Mekuria S, Adem HA, Ayele BH, Musa I, Enyew DB. Routine health information system utilization and associated factors among health professionals in public health facilities in Dire Dawa, eastern Ethiopia: a cross-sectional study. Digit Health. 2023;9:20552076231203914. [FREE Full text] [doi: 10.1177/20552076231203914] [Medline: 37808236]
Ngugi PN, Were MC, Babic A. Users’ perception on factors contributing to electronic medical records systems use: a focus group discussion study in healthcare facilities setting in Kenya. BMC Med Inform Decis Mak. Dec 26, 2021;21(1):362. [doi: 10.1186/s12911-021-01737-x] [Medline: 34955098]
Tesfa GA, Kalayou MH, Zemene W. Electronic health-information resource utilization and its associated factors among health professionals in Amhara regional state teaching hospitals, Ethiopia. Adv Med Educ Pract. 2021;12:195-202. [doi: 10.2147/AMEP.S289212] [Medline: 33688292]
Tilahun B, Gashu KD, Mekonnen ZA, Endehabtu BF, Asressie M, Minyihun A, et al. Strengthening the national health information system through a capacity-building and mentorship partnership (CBMP) programme: a health system and university partnership initiative in Ethiopia. Health Res Policy Syst. Dec 09, 2021;19(1):141. [FREE Full text] [doi: 10.1186/s12961-021-00787-x] [Medline: 34886865]
Baradwan S, Al-Hanawi M. Perceived Knowledge, Attitudes, and Barriers Toward the Adoption of Telemedicine Services in the Kingdom of Saudi Arabia: Cross-Sectional Study. JMIR formative research. 2023. :7. [doi: 10.2196/46446]
Mussi CC, Luz R, Damázio DDR, Santos EMD, Sun V, Porto BSDS, et al. The large-scale implementation of a health information system in Brazilian university hospitals: process and outcomes. Int J Environ Res Public Health. Oct 25, 2023;20(21):6971. [doi: 10.3390/ijerph20216971] [Medline: 37947529]
Borges do Nascimento IJ, Abdulazeem H, Vasanthan LT, Martinez EZ, Zucoloto ML, Østengaard L, et al. Barriers and facilitators to utilizing digital health technologies by healthcare professionals. NPJ Digit Med. Sep 18, 2023;6(1):161-128. [FREE Full text] [doi: 10.1038/s41746-023-00899-4] [Medline: 37723240]
Berardi C, Antonini M, Jordan Z, Wechtler H, Paolucci F, Hinwood M. Barriers and facilitators to the implementation of digital technologies in mental health systems: a qualitative systematic review to inform a policy framework. BMC Health Serv Res. Feb 26, 2024;24(1):243. [FREE Full text] [doi: 10.1186/s12913-023-10536-1] [Medline: 38408938]
Mumtaz H, Riaz MH, Wajid H, Saqib M, Zeeshan MH, Khan SE, et al. Current challenges and potential solutions to the use of digital health technologies in evidence generation: a narrative review. Front Digit Health. Sep 28, 2023;5:1203945. [FREE Full text] [doi: 10.3389/fdgth.2023.1203945] [Medline: 37840685]
Chidambaram S, Jain B, Jain U, Mwavu R, Baru R, Thomas B, et al. An introduction to digital determinants of health. PLOS Digit Health. Jan 2024;3(1):e0000346. [FREE Full text] [doi: 10.1371/journal.pdig.0000346] [Medline: 38175828]
Sambo L, Simões J, do Rosario O, Martins M. Firth JD, Conlon CP, Cox TM, Firth J, Conlon C, Cox T, editors. Financing Health Care In Low-Income Developing Countries: A Challenge For Equity In Health. Oxford, UK. Oxford University Press; Jan 2020:168-176.
Sureshkumar K, Bindu M, John S, Kamarul IM. Editorialvidence on low-cost technologies for neurological rehabilitation in low and middle-income countries. Frontiers in Neurology. 2023. :14.
Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health. Aug 01, 2020;20(1):1193. [doi: 10.1186/s12889-020-09301-4] [Medline: 32738884]
Huang C, Wang J, Wang S, Zhang Y. Internet of medical things: A systematic review. Neurocomputing. 2023. :557. [doi: 10.1016/j.neucom.2023.126719]
National Institute for Health and Care Excellence (NICE). Evidence standards framework for digital health technologies. NICE. Mar 2019. URL: https://www.nice.org.uk/about/what-we-do/our-programmes/ evidence-standards-framework-for-digital-health-technologies [accessed 2025-02-11]
Functional classification, according to their intended use, of digital solutions used in the context of medical and paramedical care. Haute Autorité de Santé. 2021. URL: https://www.has-sante.fr/upload/docs/application/pdf/2021-03/ dm eval 270 proposition classification.pdf [accessed 2024-08-04]
World Health Organization (WHO). Classification of digital health interventions v1. WHO. 2018. URL: https://iris.who.int/ bitstream/handle/10665/260480/WHO-RHR-18.06-eng.pdf?sequence [accessed 2024-08-04]
Food and Drug Administration (FDA). Digital Health Center of Excellence. FDA. 2024. URL: https://www.fda.gov/ medical-devices/digital-health-center-excellence [accessed 2024-08-04]
الاختصارات
DHT: تكنولوجيا الصحة الرقمية الدخل القومي الإجمالي تكنولوجيا المعلومات LMIC: دولة ذات دخل منخفض ومتوسط الصحة المتنقلة: الصحة عبر الهاتف المحمول PCC: السكان-المفهوم-السياق PRISM: نموذج التنفيذ العملي والموثوقية والاستدامة PRISMA-ScR: العناصر المفضلة للإبلاغ عن المراجعات المنهجية والتحليلات التلوية – التمديد للمراجعات الاستكشافية منظمة الصحة العالمية
تحرير بواسطةدي أزيفيدو كاردوسو؛ تم تقديمه في 21.06.24؛ تمت مراجعته من قبللينديالخباز؛ تعليقات للمؤلف 29.10.24؛ النسخة المنقحة المستلمة 01.11.24؛ المقبولة 09.12.24؛ المنشورة 06.03.25
Facilitators and Barriers to the Implementation of Digital Health Technologies in Hospital Settings in Lower- and Middle-Income Countries Since the Onset of the COVID-19 Pandemic: Scoping Review
Sheng Qian Yew , MBBS, BMedSci, MSc, MPH, PhD; Daksha Trivedi , BSc, MSc, MPhil, PhD; Nurul Iman Hafizah Adanan , BSc, MSc; Boon How Chew , MD, MMED, PhD Department of Public Health Medicine, Faculty of Medicine, National University of Malaysia, Cheras, Malaysia Centre for Research in Public Health and Community Care, University of Hertfordshire, Hertforshire, United Kingdom Clinical Research Unit, Hospital Sultan Abdul Aziz Shah, Serdang, Malaysia Faculty of Medicine and Health Sciences, Department of Family Medicine, Serdang, MalaysiaCorresponding Author:Daksha Trivedi, BSc, MSc, MPhil, PhDCentre for Research in Public Health and Community CareUniversity of HertfordshireCollege Lane, HatfieldHertforshire, AL10 9ABUnited KingdomPhone: 4401707286389Email: d.trivedi@herts.ac.uk
Abstract
Background: Although the implementation process of digital health technologies (DHTs) has been extensively documented in high-income countries, the factors that facilitate and prevent their implementation in lower- and middle-income countries (LMICs) may differ for various reasons. Objective: To address this gap in research, this scoping review aims to determine the facilitators and barriers to implementing DHTs in LMIC hospital settings following the onset of the COVID-19 pandemic. Additionally, the review outlined the types of DHTs that have been implemented in LMICs’ hospitals during this pandemic and finally developed a classification framework to categorize the landscape of DHTs. Methods: Systematic searches were conducted on PubMed, Scopus, Web of Science, and Google Scholar for studies published from March 2020 to December 2023. We extracted data on authors, publication years, study objectives, study countries, disease conditions, types of DHTs, fields of clinical medicine where the DHTs are applied, study designs, sample sizes, characteristics of the study population, study location, and data collection methods of the included studies. Both quantitative and qualitative data were utilized to conduct a thematic analysis, using a deductive method based on the Practical, Robust Implementation and Sustainability Model (PRISM), to identify facilitators and barriers to DHT implementation. Finally, all accessible DHTs were identified and organized to create a novel classification framework. Results: Twelve studies were included from 292 retrieved articles. Telemedicine was the most commonly used DHT in LMICs’ hospitals, followed by hospital information systems ( ), electronic medical records ( ), and mobile health ( ). These 4 DHTs, among the other existing DHTs, allowed us to develop a novel classification framework for DHTs. The included studies used qualitative methods ( ), which included interviews and focus groups, quantitative methods ( ), or a combination of both ( ). Among the 64 facilitators of DHT implementation, the availability of continuous on-the-job training ( ), the ability of DHTs to prevent cross-infection ( ), and positive previous experiences using DHTs ( ) were the top 3 reported facilitators. However, of the 44 barriers to DHT implementation, patients with poor digital literacy and skills in DHTs ( ), inadequate awareness regarding DHTs among health care professionals and stakeholders ( ), and concerns regarding the accuracy of disease diagnosis and treatment through DHTs ( ) were commonly reported.
Conclusions: In the postpandemic era, telemedicine, along with other DHTs, has seen increased implementation in hospitals within LMICs. All facilitators and barriers can be categorized into 6 themes, namely, (1) Aspects of the Health Care System; (2) Perspectives of Patients; (3) External Environment; (4) Implementation of Sustainable Infrastructure; (5) Characteristics of Health Care Organization; and (6) Characteristics of Patients.
(J Med Internet Res 2025;27:e63482) doi: 10.2196/63482
KEYWORDS
digital health implementation; facilitators; barriers; digital health classification framework; lower- and middle-income countries
Introduction
Populations residing in lower- and middle-income countries (LMICs) face numerous unmet health care needs due to various factors [1], including an aging population [2], escalating health care costs [3], widening income disparities [4], increased child morbidity and mortality [5], the emergence of new epidemics and pandemics [6], and growing racial discrimination in health care access [7]. The COVID-19 pandemic has further exacerbated the existing disparities and limitations of health care systems in LMICs, further exposing the issues of understaffing, underfunding, inadequate infrastructure, limited access to testing and treatment, and vulnerability to health emergencies [8]. In response to this unprecedented pandemic, many hospitals in LMICs have attempted to leverage digital health technologies (DHTs) as an innovative approach to curb the spread of the SARS-CoV-2, improve health care provision, and strengthen pandemic response efforts [9].
Generally, DHTs are defined as a set of information and communications technologies utilized in medicine and health care to manage illnesses and promote wellness [10]. These technologies have expanded as a transformative force in health care since the onset of the COVID-19 pandemic era, thereby offering a myriad of benefits that revolutionize health care delivery and improve patient outcomes. These technologies encompass a wide range of digital tools, including mobile health (mHealth) [11], telemedicine [12], wearable technologies [13], electronic medical records [14], big data analytics [15], Internet of Medical Things [16], blockchain in health care [17], metaverse [18], software as a medical device [19], augmented reality [20], and virtual reality [21]. With increasing computing power and appreciation of artificial intelligence [22] and machine learning [23] in health and medicine, many such smart tools are an making appearance in different aspects of hospital care [24,25].
Despite the benefits of DHTs, such as improved access to health care, enhanced patient engagement and empowerment, efficient health care delivery, timely and personalized care, remote monitoring, and data-driven decision-making, the implementation process of DHTs in the hospital settings,
including its facilitators and barriers, is mostly described in the context of high-income countries [26,27]. Given the differences in resources, infrastructure, health care systems, socioeconomic status, level of digital divide, and regulatory frameworks in the LMICs compared with the high-income countries, the evidence on facilitators and barriers to implementing DHTs reported in previous literature may not apply to the LMICs [28]. To address these research gaps, this scoping review aimed to:
Provide an overview of the facilitators and barriers in implementing DHTs within hospital settings in LMICs since the onset of the COVID-19 pandemic.
Identify and describe the types of DHTs that have been put into practice in hospitals within LMICs since the onset of the COVID-19 pandemic.
Develop a classification framework to better define the landscape of DHTs, providing a more comprehensive and practical understanding.
Methods
Design
The scoping review was conducted using the methodological framework developed by Arksey and O’Malley [29]. The protocol has been registered in the Open Science Framework and has been previously published [30]. The PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) [27,31] was used to conduct and report our findings.
Identifying Relevant Literature
To comprehensively identify the literature relevant to DHTs, a broad, sensitive, and specific search strategy was applied to capture all DHT-related literature. With the assistance of an information technologist, a comprehensive list of literature relevant to DHTs was identified according to the criteria below. Textboxes 1 and 2 describe the inclusion and exclusion criteria adopted for this scoping review. The focus was on the period between March 2020 and December 2023, as the World Health Organization (WHO) officially declared COVID-19 as a pandemic in March 2020.
Textbox 1. Inclusion criteria.
Studies that were conducted in lower- and middle-income countries (LMICs). (The World Bank classifies countries by income each year, covering all nations with a population over 30,000 . In 2023, countries are divided into 4 income categories based on their gross national income (GNI) per capita. Low-income countries are defined as those with a GNI per capita of US or less. LMICs have a GNI per capita between US $1146 and US $4515, while upper-middle-income countries fall between US $4516 and US $14,005. High-income countries are those with a GNI per capita exceeding US . Based on this classification, LMICs in the current review are defined as countries with GNI below US $14,005 per capita.)
Studies that reported the implementation of digital health technologies in hospital settings (for both acute and chronic conditions).
Studies that were reported between March 2020 and December 2023.
Studies that were reported in the English language.
Studies that were nondigital-based (ie, studies that did not investigate the effectiveness of digital interventions, such as paper-based studies and postage surveys).
Studies that implemented digital health technologies (DHTs) in primary care or community settings alone. However, studies that concurrently reported on the implementation of DHTs in hospital settings will still be included.
Studies that used DHTs in dentistry and nonclinical medicine area (eg, dentistry, basic sciences, medical education, medical engineering, nutrition, dietetics, veterinary science, laboratory experimentations, and medical anthropology).
Systematic searches were conducted in PubMed, Scopus, and Web of Science databases. Potentially relevant gray literature was searched through targeted searches of Google Scholar. Lateral searching included screening reference lists in identified studies or reviews for relevant publications. Articles published in English between March 2020 and December 2023 were retrieved. Two investigators (SQY and NIHA) independently performed literature searches in the aforementioned electronic databases.
The search strategy was developed based on the “Population-Concept-Context” (PCC) framework as recommended by the Joanna Briggs Institute for Scoping Reviews [32] (Table 1). It aimed to identify the intersection between the “Population,” “Concept,” and “Context.” Based on the PCC framework, the search strategy was “Population combined” AND “Concept” AND “Context.” The details of the search strategy and search terms are tabulated in Multimedia Appendix 1.
Table 1. The PCC framework used to generate search terms.
Framework
Search terms
Population
– Population 1: hospital settings (search terms as in Multimedia Appendix 1).
– Population 2: LMICsb (search terms as in Multimedia Appendix 1).
– Population combined: Population 1 AND Population 2.
Concept
– Digital health technologies (search terms as in Multimedia Appendix 1).
Context
– Facilitators, barriers, and implementation.
PCC: Population-Concept-Context. LMICs: lower- and middle-income countries
Study Selection
Records were downloaded in Rayyan software (an artificial intelligence-assisted article screening software) [24] and after deduplication, all titles and abstracts were screened independently against the inclusion criteria by 2 reviewers (SQY and NIHA). Among all titles and abstracts found, 70 out of 279 were randomly selected and screened to establish interreviewer reliability. The interreviewer reliability ( K ) was 0.63 , indicating good reliability. Full-text articles of potentially
relevant papers identified were screened independently by SQY and NIHA. Disagreements were resolved via discussion, with consultation from a third reviewer (BHC) if needed to reach a consensus. We included studies that met the review criteria and reported on barriers and facilitators of DHT implementation. For this review, DHTs were defined as a set of information and communications technologies used in medicine and health care to manage illnesses and to promote wellness [10].
Charting the Data
Two authors (SQY and NIHA) independently extracted the following data from the included papers: authors, publication years, study objectives, study countries, disease conditions, types of DHTs, fields of clinical medicine where the DHTs are applied, study designs, sample sizes, characteristics of the study population, study location, and data collection methods of the intervention or program. We categorized the DHTs according to the types of equipment and method of operation. Any disagreements were resolved by discussion and consultation with a third author (BHC).
Collating, Summarizing, and Reporting the Results
Descriptions of the included studies, such as study countries, types of DHTs, fields of clinical medicine where the DHTs are applied, and study designs were reported using descriptive statistics (eg, frequency distribution). Facilitators and barriers to DHT implementation, which were in the form of quantitative and qualitative data, were thematically analyzed using a deductive approach. To guide the thematic analysis, facilitators and barriers to DHT implementation were organized using the Practical, Robust Implementation, and Sustainability Model (PRISM) [33].
During the coding process, 2 authors (SQY and NIHA) identified the key components of the PRISM relevant to DHT implementation. They mapped the facilitators and barriers reported in the included studies to the predefined categories and subsequently grouped similar categories under overarching
themes. By organizing the facilitators and barriers into themes and categories, patterns, trends, and relationships among the factors influencing DHT implementation can be identified, providing a structured framework for understanding the complexities of implementing DHTs in LMICs’ hospital settings [34].
Consultation With Stakeholders
Clinicians and information technology (IT) experts from a local teaching hospital were invited to help interpret and contextualize the findings. Through interactive discussions and collaborative sessions, stakeholders provided valuable input on the categorization of facilitators and barriers as well as the implications of implementation of DHTs in their respective contexts. Moving forward, the authors plan to continue engagement with these stakeholders to disseminate the findings of the scoping review through presentations, policy briefs, and peer-reviewed publications.
Results
Literature Search
A systematic search yielded 295 titles and abstracts. After removing 16 duplicates, 279 unique articles remained. Among these, 157 were excluded based on title or abstract review. We thoroughly evaluated 122 full-text articles, and ultimately, 12 met the eligibility criteria. The PRISMA flow diagram was used to illustrate the search decision process of the scoping review [35] (Figure 1 and Multimedia Appendix 2).
Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart. LMIC: lower- and middle-income country.
Characteristics of the Included Studies
Of the 12 articles, were conducted in Asia [36-41], 4 (33%) in Africa [42-45], 1 (8%) in the Middle East [46], and 1 (8%) in South America [47]. Most of the studies (10/12, 83%) [36,37,40-47] did not specify the specific field of clinical medicine where DHTs were applied. However, some reported implementation in respiratory medicine (1/12, 8%) [38] and cancer (1/12, 8%) [39]. Telemedicine (5/12, 42%)
[37,38,40,41,46] was the most commonly reported technology, followed by hospital information systems (4/12, 33%) [36,42,45,47], electronic medical records (2/12, 17%) [43,44], and mHealth (1/12, 8%) [39]. In terms of study design, there were 5 (42%) cross-sectional studies [37,41,42,44,46], 4 (33%) qualitative studies [38-40,43], mixed method studies [45,47], and case study [36]. The participant numbers ranged from 12 to 3386 individuals (Table 2).
Table 2. Overview of the characteristics of the included studies.
Authors and publication years
Study details
Objective(s)
Country
Disease condition
Types of DHTs
Field of clinical medicine
Design
Sample sizes and characteristics of the population
Location
Data collection method
Abdulai et al [36]
To investigate the attitudes, opportunities, and challenges in using health information system.
India
General
Health information system
General
Case study
20 health care providers and managers
Apollo Hospital and Medanta Hospital
Self-administered questionnaire
Alboraie et al [37]
To assess the usefulness of telemedicine and the different barriers hindering its utilization.
Egypt
General
Telemedicine
General medicine, surgery, and radiology
Crosssectional study
642 health care providers
All hospitals across Egypt
Online selfadministered questionnaire
Baradwan and AlHanawi [46]
To gain a holistic understanding of the perceptions and barriers of the end users (participants) toward the utility of telemedicine.
Saudi Arabia
General
Telemedicine
General
Crosssectional study
1024 individuals
Nationwide
Self-administered questionnaire
Jiang et al [38]
To explore the perceptions and experiences of older patients and health care providers in the application of telehealth and online health information to chronic disease management of chronic obstructive pulmonary disease.
China
Chronic obstructive pulmonary disease
Telemedicine
Respiratory medicine
Qualitative
31 older patients with chronic obstructive pulmonary disease and 23 health care providers
A community hospital in Jiangnan, China
In-depth interviews
Mekuria et al [42]
To assess the level of health information system utilization among health professionals in public health facilities.
Ethiopia
General
Health information system
General
Crosssectional study
378 health care providers
Dire Dawa Administration in eastern Ethiopia
Self-administered questionnaire
Authors and publication years
Study details
Objective(s)
Country
Disease condition
Types of DHTs
Field of clinical medicine
Design
Sample sizes and characteristics of the population
Location
Data collection method
Mussi et al [47]
To understand the implementation of a hospital information system in university hospitals.
Brazil
General
Health information system
General
Exploratory mixed methods
770 health managers (24 in indepth interviews, 10 in focus group discussions, and 736 in cross-sectional study)
5 university hospitals in Brazil
Interviews, focus group discussions, questionnaires, and documentary research
Ngugi et al [43]
To explore end users’ perceptions and experiences on factors facilitating and hindering electronic medical record use in health care facilities.
Kenya
General
Electronic medical record
General
Qualitative
20 health care providers
20 health care facilities in Kenya
Focus group discussion
Ning et al [39]
To explore the needs and perceptions of patients with head and neck cancer regarding mobile health-based physical activity programs.
China
Head and neck cancer
Mobile health
ENT
Qualitative
17 patients diagnosed with head and neck cancer
First Hospital of Shanxi Medical University, Taiyuan, China
In-depth interviews
Shardha et al [40]
To explore the view of health care professionals regarding the benefits, challenges, and prospects of telemedicine to address the gap that hinders its effective use in the rural areas.
Pakistan
General
Telemedicine
Nonsurgical disciplines
Qualitative (narrative)
12 health care providers
Two tertiary hospitals in Sindh, Pakistan
In-depth interviews
Tesfa et al [44]
To assess the level of electronic health record utilization and associated factors among health care professionals at teaching hospitals.
Ethiopia
General
Electronic medical record
General
Crosssectional study
383 health care providers
University of Gondar Specialized Teaching Hospital and Tibebe Ghion Specialized Teaching Hospital
Self-administered questionnaire
Authors and publication years
Study details
Objective(s)
Country
Disease condition
Types of DHTs
Field of clinical medicine
Design
Sample sizes and characteristics of the population
Location
Data collection method
Tilahun et al [45]
To evaluate the outcomes and share experiences of working with universities to strengthen the national health information system.
Ethiopia
General
Health information system
General
Mixed methods study
23 health care providers
47 health care organizations in Ethiopia
In-depth interviews
Yu-Tong et al [41]
To assess telehealth readiness among clinical nurses and explore the factors that affect their telehealth readiness.
China
General
Telemedicine
General
Crosssectional study
3386 nurses
19 hospitals in China
Self-administered questionnaire
DHT: digital health technology. ENT: ear, nose, and throat.
Facilitators and Barriers to DHT Implementation
Among the 12 studies, 9 explored both the facilitators and barriers to implementing DHTs in hospital settings in LMICs since the onset of COVID-19 [36-40,43-45,47]. Two studies focused solely on facilitators [41,42], while 1 solely addressed barriers [46]. A total of 63 facilitators and 44 barriers were
identified. Subsequently, these facilitators and barriers were systematically organized into 6 themes according to the PRISM, which include the following: (1) Aspects of the Health Care System; (2) Perspectives of Patients; (3) External Environment; (4) Implementation of Sustainable Infrastructure; (5) Characteristics of Health Care Organization; and (6) Characteristics of Patients. These are outlined in Table 3.
Table 3. Facilitators and barriers to DHT implementation in hospital settings in lower- and middle-income countries after the COVID-19 pandemic.
Themes and categories
Codes for facilitators
Codes for barriers
Aspects of the Health Care System ( )
Readiness (
– Understand the basics of information technology [37]
– Knowledge in protecting data confidentiality [37]
– High level of self-efficacy [42]
– Good attitude toward DHTs [42]
– High awareness about the implementation of DHTs [47]
– High personal interest and motivation [47]
– The high willingness of health care providers to provide DHTs for patients [41]
– Inadequate awareness regarding DHTs [40,44]
– Feeling that DHTs are only complementary to traditional health care [38]
– Preference of some health care providers for printed materials [44]
Strength of the evidence base ; )
– The ability of DHTs to offer statistical analysis and reports for decision-making [36]
– The ability of DHTs to offer timely and up-todate patient information [36]
– Concerns regarding accuracy in disease diagnosis and treatment [40,46]
Addresses barriers to frontline staff ( )
– Easy access to computers in the working area [44]
– Fear of inappropriate data protection might breach patient’s privacy [37]
– Inadequate computers at the workplace and service point local area network at the workplace [43]
Coordination across departments and specialties ( )
– Use of single information technology policy and standard hospital information system [47]
– Lack of interoperability standards between systems [47]
Burden (complexity and cost; ; )
– Perceive that operations of DHTs are not complex [42]
– The availability of information technology budget [47]
– Regular upgrades on DHT hardware [43]
– Funding support focusing on research and learning opportunities on DHTs [45]
– The need for retrospective data entry into systems [43]
Usability and adaptability ( ; )
– The ability of DHTs to prevent cross-infection [38,40]
– Ability to provide health care in remote areas [40]
– The functionalities of DHTs align with hospital’s practices [47]
– User-friendliness of DHTs [43]
– Difficulty in performing physical examination with DHTs [40]
– Lack of compliance among health care professionals and patients [40]
– DHTs might reduce the quality of medical services by increasing the probability of medical mistakes [37]
– Perceive DHTs as research agenda only [45]
– Some DHTs are not user-friendly [36]
Trialability and reversibility ( ; )
– Conduct beta tests and pilot tests before implementation of DHTs [47]
– N/Ae
Ability to observe results ( ; )
– Positive previous experiences using DHTs [41,47]
– The ability of DHTs to increase administrative and health care efficiency [36]
– The ability of DHTs to reduce medication errors [36]
– N/A
Perspectives of Patients ( )
Themes and categories
Codes for facilitators
Codes for barriers
Patient centeredness ( )
– Using technology gives a superior feeling [38]
– Repeated motivational or praising words increase patients’ usage of DHTs [38]
– The feeling of the distance between the patient and health care providers during remote interaction [38]
– The feeling of being forced to use DHTs [38]
Addresses patient barriers ( ; )
– Involvement of patients’ children could improve the efficiency and effectiveness of DHTs [38]
– Patients’ resistance to change practice [46]
Seamlessness of transition between program elements ( )
– Unification of hospitals in a single network and centralized management [47]
– N/A
Service and access ( )
– Easy access to online health information and applying the knowledge [38]
– N/A
Burden (complexity and cost; ; )
– The ability of DHTs to reduce stress among patients [40]
– DHTs are cost-effective [38]
– N/A
Feedback of results (
– DHTs are easy and convenient to use
– DHTs are able to improve the comfort level of patients [39]
– N/A
External Environment ( )
Competition
– N/A
– Competition for resources between information technology equipment and other health care equipment [45,47]
Regulatory environment ( ; )
– Good communication process between the regulatory authority and the hospitals [47]
– Political and economic instabilities [45,47]
Community resources ( )
– Good internet access among users of DHTs [44]
– N/A
Implementation of Sustainable Infrastructure ( )
Adopter training and support ( ; )
– Familiarity with handling DHT tools [40]
– N/A
Relationship and communication with adopters ( )
– N/A
– The communication gap between supervisors and supervisees [45]
Adaptable protocols and procedures ( )
– Remote health service can be carried out easily among clinicians [37]
– N/A
Facilitation of sharing of best practices ( )
– Experience sharing between advanced and beginner hospitals [47]
– N/A
Plan for sustainability ( )
– Health care facilities prioritize the implementation and sustainability of DHTs [47]
– The end of the COVID-19 pandemic reduced the demand for DHTs [46]
Characteristics of the Health Care Organization ( )
Themes and categories
Codes for facilitators
Codes for barriers
Organizational health and culture ( )
– The availability of fair-to-good organizational support [42]
– Commitment from the top management or managers [47]
– Top management mandates the adoption of DHTs [47]
– Promote experience and knowledge sharing among hospital networks [47]
– A workplace culture that is receptive to change [47]
– Understand the policies made by the government [41]
– Frequent changes in the hospital management team [47]
– Lack of medium- and long-term information technology policy planning [47]
Management support and communication ( )
– Presence of supervision at the workplace [42]
– The availability of fair-to-good technical support [42]
– Provision of support to groups with little knowledge of technology [47]
– Lack of planning and implementation of system design [47]
Shared goals and cooperation ( ; )
– The information technology department of the hospital is directly linked to local information technology sectors [47]
– Create a multidisciplinary management committee [47]
– Partnership with universities to develop DHTs [45]
– Health care providers’ resistance to change practice [46]
Clinical leadership ( )
– High level of decision-making autonomy in the workplace [42]
– Weak leadership and poor commitment at the hospital level [45]
Systems and training ( )
– The workplace has sufficient facilities [37]
– The availability of continuous on-the-job training [37,43,47]
– Regular system upgrades [43]
– The availability of prompt technical assistance from desk support [43]
– Lack of training in advanced technologies [36,40]
– Delays in system development, implementation, and updates [43,47]
– Frequent power blackouts [43]
– Poor electrical power and backup facilities [36]
– Lack of skill among health care providers in accessing and using DHTs [44]
Data and decision support ( ; )
– The availability of 24-hour technical support services at the workplace [37]
– Centralization of system development and technical support [47]
– Lack of contingency plan for DHTs [47]
– Delayed information technology support [43]
Staffing and incentives (
– Workplace has sufficient trained personnel in DHTs [37]
– Improved financing of human and material resources [47]
– Sufficient human resource allocation [41]
– Lack of incentives for health care providers to use DHTs [38]
– High staff turnover rate, work overload, and reduced staffing [43,47]
– Health care providers who are old aged [43]
Expectation of sustainability ; )
– N/A
– Health care providers do not have sufficient time and energy to participate and offer timely feedback while using DHTs [38,44]
– Unrealistic expectations toward DHTs [47]
Characteristics of patients ( )
Themes and categories
Codes for facilitators
Codes for barriers
Demographics ( )
– N/A
– Older patients contemplated using and have low confidence in DHTs [38]
– Personal inertia and the conservative mentality of the older generation [38]
– Costs of accessing the internet beyond affordability for patients from lower socioeconomic status [39]
– Poor cellular network connectivity and internet access in some geographical areas [39]
Knowledge and beliefs (
– Confidence to learn, engage, and sustainably participate in DHTs [38]
– High eHealth and computer literacy among patients [38,44]
– High information-searching skills among patients [44]
– Patients have poor digital literacy and skills in DHTs [36,38,39]
– Patients have skepticism about the accuracy of remote diagnosis [38]
– Social prejudice against DHTs [38]
DHT: digital health technology. : number of studies in general. : number of studies that reported on facilitators. : number of studies that reported on barriers. N/A: not applicable.
Specifically, the theme of Aspects of the Health Care System included 23 facilitators and 13 barriers ( studies). Among the prominent facilitators were the ability of DHTs to prevent cross-infection ( ) and positive previous experiences using DHTs ( ). By contrast, inadequate awareness regarding DHTs ( ) and concerns regarding accuracy in disease diagnosis and treatment ( ) were the leading barriers highlighted.
Regarding the theme of Perspectives of Patients, 9 facilitators and 3 barriers were reported ( studies). Among these, the convenience and easiness of using DHTs ( ) were noted as the primary facilitator. However, the feeling of distance between the patient and health care providers during remote interaction , the feeling of being forced to use DHTs ( ), and patients’ resistance to change practice could pose challenges to the implementation of DHTs in hospital settings within LMICs.
The successfulness of implementing DHTs also relies on the theme of External Environment ( studies). Within this context, 2 facilitators are aiding the implementation, which include a good communication process between the regulatory authority and the hospitals ( ) and good internet access among users of DHTs ( ). Among the 2 barriers identified in this context, competition for resources between IT equipment and other health care equipment ( ) stands out as the more prevalent barrier.
The theme of Implementation of Sustainable Infrastructure comprises 4 facilitators and 2 barriers ( studies). Notably, familiarity with handling DHTs tools ( ), the ease of conducting remote health service among clinicians ( ), and experience sharing between advanced and beginner hospitals ( ) emerge as facilitators for DHT implementation. Conversely, barriers in this theme include the communication gap between stakeholders ( ) and the end of the COVID-19 pandemic reducing the demand for DHTs ( ).
The Characteristics of Health Care Organization theme consists of 22 facilitators and 17 barriers to DHT implementation ( studies). Previous studies have highlighted the availability of continuous on-the-job training ( ) as the most frequent facilitator of DHT implementation in the health care organization. Conversely, barriers such as lack of trainings in advanced technologies ( ); delays in system development, implementation, and updates ( ); high staff turnover rate, work overload, and reduced staffing ( ); as well as insufficient time and energy among health care providers to participate and offer timely feedback while using DHTs ( ) prevent the implementation of DHTs.
The Characteristics of Patients was the final theme that could influence the successfulness of DHT implementation in LMICs’ hospital settings. It comprised 3 facilitators and 7 barriers ( studies). Notably, the most frequently mentioned facilitator in this theme is the high eHealth and computer literacy among patients ( ). Not surprisingly, the exact opposite, that is, patients with poor digital literacy and skills in DHTs ( ), is reported as the commonest barrier.
The relationship between codes, categories, and themes of facilitators and barriers to DHT implementation is summarized in Figure 2, in which the codes and categories are arranged from the most frequent (top) to the least frequent (bottom).
Figure 3 illustrates the network analysis of the facilitators of DHT implementation. Of note, facilitators such as “Perspectives of Patients” and “Aspect of the Health Care System” are central to the network. This suggests their broad impact across multiple domains, making them key intervention points for DHT implementation. Although no obvious clusters were observed, the interconnectedness suggests that addressing certain facilitators (eg, “Perspectives of Patients,” “Aspect of the Health Care System,” and “Characteristics of the Health Care Organization”) can have ripple effects on others. Figure 4 illustrates the network analysis of the barriers to DHT
implementation. It was noted that some barriers are more central, such as the “Characteristics of Health Care Organizations,” “Aspect of the Health Care System,” “Implementation of Sustainable Infrastructure,” and “Characteristics of Patients” barriers, highlighting their pivotal roles in the network. These central barriers act as key influencers and bridge multiple barriers. Meanwhile, the “External Environment” and “Perspectives of Patients” barriers are more toward the periphery and, hence, have less impact on the network. A cluster was observable in the network analysis, involving the “Characteristics of Health Care Organization” and “Aspect of
the Health Care System” barriers. Many barriers are interconnected, which indicate that addressing one (eg, “Characteristics of Health Care Organizations”) may alleviate others. However, it should be noted that some nodes, such as “Readiness” and “Usability and Adaptability,” can be both facilitators of and barriers to DHT implementation, and hence, can appear in both network analyses.
Since the onset of the COVID-19 pandemic, the most commonly utilized DHTs in LMICs’ hospitals were telemedicine, followed by health information systems, electronic medical records, and mHealth, as depicted in Figure 5.
Figure 2. Summary of the codes, categories, and themes of facilitators and barriers of digital health technology (DHT) implementation. IT: information technology; LAN: local area network.
Figure 3. Network analysis to illustrate the relationship between the codes of facilitators of digital health technologies (DHTs) implementation in lower- and middle-income countries’ (LMICs) hospital settings since the onset of the COVID-19 pandemic.
Figure 4. Network analysis to illustrate the relationship between the codes of barriers of digital health technologies (DHTs) implementation in lowerand middle-income countries’ (LMICs’) hospital settings in the post-COVID-19 era. IT: information technology; LAN: local area network.
Figure 5. Digital health technologies (DHTs) in the lower- and middle-income countries (LMICs) since the onset of the COVID-19 pandemic.
Discussion
Facilitators of and Barriers to DHT Implementation in LMICs
The most common facilitators of DHT implementation include the convenience and easiness of using DHTs, the ability of DHTs to prevent cross-infection, positive previous experiences using DHTs, the availability of continuous on-the-job training, and high eHealth and computer literacy among patients. By contrast, we identified that the most frequently reported barriers are inadequate awareness regarding DHTs; concerns regarding accuracy in disease diagnosis and treatment; competition for resources between IT equipment and other health care equipment; lack of trainings in advanced technologies; delays in system development, implementation, and updates; high staff turnover rate, work overload, and reduced staffing; insufficient time and energy among health care providers to use DHTs; and patients with poor digital literacy and skills in DHTs.
To our knowledge, this scoping review is the first to examine the facilitators and barriers to implementing DHTs in hospitals within LMICs since the onset of the COVID-19 pandemic. It is important to note the scarcity of published literature on this topic in LMICs. Even existing reviews often focused on studies from high-income countries or concentrated on specific diseases [27,48,49]. For example, a systematic review by Whitelaw et al [27], comprising 29 studies, investigated DHT implementation in cardiovascular diseases predominantly in high-income countries. As expected, the facilitators and barriers identified in this review significantly differed from our findings. Whitelaw et al highlighted facilitators such as enhanced communication with clinicians, personalized DHT components, user-friendly interfaces, institutional and organizational support, increased efficiency, and perceived usefulness of DHTs. The reported barriers were complex technology, technological apprehension, increased workload, unreliable technology, and lack of integration with electronic medical records. These discrepancies
may stem from various factors such as differences in health care infrastructure [50], socioeconomic contexts [51], health care financing [52], as well as costs of DHT development and implementation [53] between high-income and LMIC settings. Additionally, the focus on specific diseases in previous literature might not fully capture the diverse facilitators and barriers relevant to DHT implementation across various health care contexts.
DHTs That Have Been Implemented
To our surprise, telemedicine was the most commonly reported technology implemented in hospital settings since the onset of the COVID-19 pandemic, exceeding other DHTs such as hospital information systems, electronic medical records, and mHealth . This can be understood by the fact that telemedicine is well-suited for health care providers and patients who are self-isolating, as it effectively reduces the risk of COVID-19 transmission. It eliminates the need for direct physical contact, ensures ongoing care for the community, and ultimately lowers the rates of illness and death during the COVID-19 pandemic [54].
Classification Framework for DHT Implementation in LMICs
Despite the emergence of various innovative technologies such as wearable technologies, metaverse, Internet of Medical Things, blockchain in health care, big data analytics, artificial intelligence, machine learning, software as medical devices, augmented reality, and virtual reality, the implementation of DHTs in hospitals within LMICs remains rudimentary compared with high-income countries. The current utilization of DHTs in LMICs, such as telemedicine, hospital information systems, electronic medical records, and mHealth, has informed the key components of a new classification framework that emphasizes LMICs. Based on recent literature [13,15,17-23,55] and the specific facilitators and barriers to utilizing these DHTs in LMICs, we propose a classification framework of DHTs, as illustrated in Figure 6.
Figure 6. Classification framework of digital health technologies (DHTs). LMIC: lower- and middle-income country.
This classification framework is justified by the fact that simpler DHTs, such as telemedicine, hospital information systems, electronic medical records, and mHealth, are easier to implement in LMICs due to lower costs and infrastructure requirements, adaptability to limited resources, and minimal training needs. These technologies rely mainly on basic internet connectivity, mobile devices, and computers, making them more accessible and feasible given the broader availability of mobile networks in LMICs. They also integrate easily into existing health care workflows, requiring only short training sessions and basic digital literacy. Furthermore, because LMICs prioritize addressing immediate health care needs such as infectious diseases, these accessible technologies receive more support and funding. By contrast, advanced technologies such as artificial intelligence, virtual reality, and blockchain demand specialized infrastructure, technical expertise, and substantial financial resources, which are often scarce in LMICs.
This proposed classification framework also consists of other DHTs that were implemented in high-income countries. This, hopefully, will aid health care stakeholders in LMICs to
delineate the scope of DHTs in LMICs and help them to prioritize the right DHTs that could be implemented in the scarcity of resources. Consequently, policy makers can allocate health care funding (eg, the Ministry of Health can determine the DHT classes that are eligible for subsidies), and insurers can reimburse patients who utilized DHTs (ie, identifying which DHT classes can be covered by insurance policies) [56,57]. Moreover, clear and effective communication among the public, health care providers, and technology experts can be facilitated [57,58]. Legally, a defined classification framework enables authorities to regulate and govern DHT usage [58,59]. Finally, a clearly outlined classification framework for DHTs may streamline implementation, especially in resource-scarce environments, as stakeholders can prioritize which DHT classes should be implemented [56].
Strengths and Limitations
This scoping review possesses several notable strengths. Initially, we comprehensively gathered data from a diverse array of databases, including gray literature sources such as Google
Scholar. This deliberate choice was made to ensure the inclusivity and robustness of the studies included. Additionally, during the planning phase of the review, we actively engaged relevant stakeholders, including information technologists, seeking and incorporating their feedback into the review protocol. Furthermore, in structuring and categorizing the identified barriers and facilitators, we utilized a conceptual model developed by Feldstein and Glasgow [33], thereby enhancing the analytical rigor of the review. Moreover, our review offers a wealth of qualitative and quantitative insights into the implementation of DHTs, providing comprehensive guidance for stakeholders interested in implementing DHTs within their respective settings.
Despite its strengths, our review does have certain limitations. Specifically, in focusing on identifying barriers and facilitators of DHT implementation in hospital settings within LMICs, we restricted our inclusion criteria to studies conducted solely within hospitals. Consequently, many studies providing insights from primary care and community perspectives were excluded. Additionally, studies that did not explicitly address facilitators and barriers were omitted, potentially overlooking valuable information on other beneficial DHTs for patient care. Furthermore, as our primary aim was to offer an overview of existing literature on DHTs, we did not apply any quality control measures to the included studies. The variation in analytical methods, interview questions, and study populations across the included papers presents a potential inconsistency in the findings and makes quality assessment difficult. Additionally, with 128 LMICs at the time of the literature search, listing each country by name in the search string was impractical, which could result in some LMICs not being captured in the search results.
Implications and Recommendations
Understanding the facilitators and barriers to DHTs in hospital settings of LMICs has profound implications for both clinical practice and research. Identifying facilitators of DHT implementation enables the effective integration of DHTs in hospitals, leading to improved diagnostic accuracy, better patient monitoring, improved patient records management, and the availability of remote health care services. Conversely, recognizing the barriers to DHT implementation can prompt various stakeholders in LMICs to devise strategies that address issues in terms of financial resources, technological infrastructure, and knowledge among health care providers. In terms of research, this review is hoped to promote international collaborations, governmental support, and investment in digital infrastructure, which in turn boost the capacity for data collection, analysis, and sharing. These advancements can enhance research capabilities, allowing for more comprehensive epidemiological studies, real-time disease monitoring, and the development of context-specific health interventions.
To maximize the benefits of DHTs in hospital settings in LMICs, several recommendations can be made to leverage facilitators and mitigate barriers. First, the convenience and ease of using DHTs should be emphasized through user-friendly interfaces and intuitive designs, ensuring that health care providers can quickly and efficiently adopt these technologies in their daily routines. Second, the role of DHTs in preventing cross-infection
should be highlighted in training programs and awareness campaigns, particularly in regions where infectious diseases are prevalent. Positive previous experiences with DHTs should be shared widely to build trust and demonstrate the tangible benefits of these technologies. Continuous on-the-job training must be provided to keep health care workers up-to-date with the latest advancements and best practices, while also enhancing their technical proficiency. Promoting high eHealth and computer literacy among patients through community outreach and education programs will further support the effective use of DHTs.
Addressing barriers requires a multifaceted approach. To tackle inadequate awareness and concerns regarding the accuracy of DHTs, it is crucial to implement comprehensive educational initiatives that highlight the reliability and clinical efficacy of these technologies. Clear, evidence-based information should be disseminated to health care providers and patients to build confidence in DHTs. Competition for resources between IT equipment and other health care tools can be mitigated by advocating for balanced budget allocations and seeking external funding or partnerships to supplement resources. Training programs in advanced technologies must be expanded to equip health care providers with the necessary skills to use DHTs effectively. To address delays in system development and implementation, streamlined processes and timelines should be established, with dedicated project management teams overseeing these initiatives. High staff turnover rates and work overload can be managed by improving working conditions, offering competitive salaries, and providing career development opportunities. Finally, enhancing digital literacy among patients through targeted educational programs will ensure that they can engage with DHTs effectively, ultimately leading to better health outcomes. By implementing these recommendations, LMICs can overcome barriers and fully harness the potential of DHTs to improve clinical practice and advance health care research.
Conclusions
The scoping review on DHT implementation in LMICs since the onset of the COVID-19 pandemic underscores significant policy, clinical, and research implications. Policy makers can utilize the insights to craft targeted strategies for DHT adoption, while the developed classification framework aids in prioritizing DHTs. In clinical settings, understanding DHT types, facilitators, and barriers enhances decision-making for improved patient care and resource optimization. Additionally, investing in capacity building and training programs for health care professionals is crucial, with a focus on enhancing digital literacy and technical skills. Moreover, identifying research priorities and aligning funding with key challenges such as improving digital literacy and addressing concerns about DHT accuracy will drive advancements in DHT implementation and health care delivery in LMICs.
In the postpandemic era, telemedicine has been widely used in hospital settings in LMICs, among other DHTs. Our findings also reveal numerous facilitators and barriers to DHT implementation in LMIC hospital settings. These factors can be organized into 6 themes, namely, (1) Aspects of the Health Care System; (2) Perspectives of Patients; (3) External
Environment; (4) Implementation of Sustainable Infrastructure; (5) Characteristics of Health Care Organization; and (6)
Characteristics of Patients.
Acknowledgments
We acknowledge the contributions of the information technologist at the library of Universiti Putra Malaysia for the provision of technical and intellectual assistance during the literature search.
Data Availability
All data retrieved and analyzed are included in this scoping review.
Authors’ Contributions
SQY and BHC developed the concept for the scoping review. SQY and DT were involved in designing the research methodology. NIHA and SQY carried out an extensive literature review to identify relevant frameworks and methodological approaches for the scoping review. SQY prepared the initial draft of the review.
The PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews) checklist.
[PDF File (Adobe PDF File), 115 KB-Multimedia Appendix 2]
References
World Health Organization (WHO). Tracking universal health coverage: 2023 global monitoring report. WHO. Geneva, Switzerland. WHO; Sep 18, 2023. URL: https://www.who.int/publications/i/item/9789240080379 [accessed 2024-02-10]
Shah SA, Safian N, Ahmad S, Nurumal SR, Mohammad Z, Mansor J, et al. Unmet healthcare needs among elderly Malaysians. JMDH. Oct 2021;Volume 14:2931-2940. [doi: 10.2147/jmdh.s326209]
Njagi P, Arsenijevic J, Groot W. Cost-related unmet need for healthcare services in Kenya. BMC Health Serv Res. Apr 17, 2020;20(1):322. [FREE Full text] [doi: 10.1186/s12913-020-05189-3] [Medline: 32303244]
Sohn M, Che X, Park H-J. Unmet healthcare needs, catastrophic health expenditure, and health in South Korea’s universal healthcare system: progression towards improving equity by NHI type and income level. Healthcare (Basel). Oct 16, 2020;8(4):408. [FREE Full text] [doi: 10.3390/healthcare8040408] [Medline: 33081357]
Baek S, Choi E-H, Lee J. Unmet healthcare needs of children in vulnerable families in South Korea: finding from the Community Child Center Child Panel Survey. Int J Environ Res Public Health. Nov 07, 2020;17(21):8241. [FREE Full text] [doi: 10.3390/ijerph17218241] [Medline: 33171882]
Kim J, You M, Shon C. Impact of the COVID-19 pandemic on unmet healthcare needs in Seoul, South Korea: a cross-sectional study. BMJ Open. Aug 26, 2021;11(8):e045845. [FREE Full text] [doi: 10.1136/bmjopen-2020-045845] [Medline: 34446482]
Harris RB, Cormack DM, Stanley J. Experience of racism and associations with unmet need and healthcare satisfaction: the 2011/12 adult New Zealand Health Survey. Aust N Z J Public Health. Feb 2019;43(1):75-80. [FREE Full text] [doi: 10.1111/1753-6405.12835] [Medline: 30296819]
Rosenthal A, Waitzberg R. The challenges brought by the COVID-19 pandemic to health systems exposed pre-existing gaps. Health Policy Open. Dec 2023;4:100088. [doi: 10.1016/j.hpopen.2022.100088] [Medline: 36536931]
Mitgang EA, Blaya JA, Chopra M. Digital health in response to COVID-19 in low- and middle-income countries: opportunities and challenges. Glob Policy. Jul 2021;12(Suppl 6):107-109. [doi: 10.1111/1758-5899.12880] [Medline: 34230840]
Ronquillo Y, Meyers A, Korvek S. Digital Health. StatPearls. Treasure Island (FL). StatPearls Publishing; Jan 2025.
Istepanian RSH. Mobile health (m-Health) in retrospect: the known unknowns. Int J Environ Res Public Health. Mar 22, 2022;19(7):3747. [FREE Full text] [doi: 10.3390/ijerph19073747] [Medline: 35409431]
Roy J, Levy DR, Senathirajah Y. Defining telehealth for research, implementation, and equity. J Med Internet Res. Apr 13, 2022;24(4):e35037. [FREE Full text] [doi: 10.2196/35037] [Medline: 35416778]
Huhn S, Axt M, Gunga H-C, Maggioni MA, Munga S, Obor D, et al. The impact of wearable technologies in health research: scoping review. JMIR Mhealth Uhealth. Jan 25, 2022;10(1):e34384. [FREE Full text] [doi: 10.2196/34384] [Medline: 35076409]
Ibrahim AA, Ahmad Zamzuri M’I, Ismail R, Ariffin AH, Ismail A, Muhamad Hasani MH, et al. The role of electronic medical records in improving health care quality: a quasi-experimental study. Medicine (Baltimore). Jul 29, 2022;101(30):e29627. [FREE Full text] [doi: 10.1097/MD.0000000000029627] [Medline: 35905245]
Belle A, Thiagarajan R, Soroushmehr SMR, Navidi F, Beard DA, Najarian K. Big data analytics in healthcare. Biomed Res Int. 2015;2015:370194. [FREE Full text] [doi: 10.1155/2015/370194] [Medline: 26229957]
Dwivedi R, Mehrotra D, Chandra S. Potential of Internet of Medical Things (IoMT) applications in building a smart healthcare system: a systematic review. J Oral Biol Craniofac Res. Mar 2022;12(2):302-318. [FREE Full text] [doi: 10.1016/j.jobcr.2021.11.010] [Medline: 34926140]
Yoon H-J. Blockchain technology and healthcare. Healthc Inform Res. Apr 2019;25(2):59-60. [FREE Full text] [doi: 10.4258/hir.2019.25.2.59] [Medline: 31131139]
Petrigna L, Musumeci G. The metaverse: a new challenge for the healthcare system: a scoping review. J Funct Morphol Kinesiol. Aug 30, 2022;7(3):63. [FREE Full text] [doi: 10.3390/jfmk7030063] [Medline: 36135421]
Yu J, Zhang J, Sengoku S. Innovation process and industrial system of US Food and Drug Administration-approved software as a medical device: review and content analysis. J Med Internet Res. Nov 24, 2023;25:e47505. [FREE Full text] [doi: 10.2196/47505] [Medline: 37999948]
Eckert M, Volmerg JS, Friedrich CM. Augmented reality in medicine: systematic and bibliographic review. JMIR Mhealth Uhealth. Apr 26, 2019;7(4):e10967. [FREE Full text] [doi: 10.2196/10967] [Medline: 31025950]
Halbig A, Babu S, Gatter S, Latoschik M, Brukamp K, von Mammen S. Opportunities and challenges of virtual reality in healthcare – a domain experts inquiry. Front Virtual Real. Mar 23, 2022;3:3. [doi: 10.3389/frvir.2022.837616]
Xu Y, Liu X, Cao X, Huang C, Liu E, Qian S, et al. Artificial intelligence: a powerful paradigm for scientific research. Innovation (Camb). Nov 28, 2021;2(4):100179. [FREE Full text] [doi: 10.1016/j.xinn.2021.100179] [Medline: 34877560]
Sarker IH. Machine learning: algorithms, real-world applications and research directions. SN Comput Sci. Mar 2021;2(3):160. [FREE Full text] [doi: 10.1007/s42979-021-00592-x] [Medline: 33778771]
Mehta N, Pandit A, Shukla S. Transforming healthcare with big data analytics and artificial intelligence: a systematic mapping study. J Biomed Inform. Dec 2019;100:103311. [FREE Full text] [doi: 10.1016/j.jbi.2019.103311] [Medline: 31629922]
Yin J, Ngiam KY, Teo HH. Role of artificial intelligence applications in real-life clinical practice: systematic review. J Med Internet Res. Apr 22, 2021;23(4):e25759. [FREE Full text] [doi: 10.2196/25759] [Medline: 33885365]
Iyamu I, Gómez-Ramírez O, Xu AX, Chang H-J, Watt S, Mckee G, et al. Challenges in the development of digital public health interventions and mapped solutions: findings from a scoping review. Digit Health. 2022;8:20552076221102255. [doi: 10.1177/20552076221102255] [Medline: 35656283]
Whitelaw S, Pellegrini D, Mamas M, Cowie M, Van Spall HGC. Barriers and facilitators of the uptake of digital health technology in cardiovascular care: a systematic scoping review. Eur Heart J Digit Health. Mar 04, 2021;2(1):62-74. [FREE Full text] [doi: 10.1093/ehjdh/ztab005] [Medline: 34048508]
Jacob KS. Public health in low- and middle-income countries and the clash of cultures. J Epidemiol Community Health. Jul 2009;63(7):509. [doi: 10.1136/jech.2009.086934] [Medline: 19525248]
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. International Journal of Social Research Methodology. Feb 2005;8(1):19-32. [doi: 10.1080/1364557032000119616]
Yew SQ, Trivedi D, Adanan NIH, Chew BH. Facilitators and barriers of digital health technologies implementation in hospital settings in lower-income and middle-income countries since the COVID-19 pandemic: a scoping review protocol. BMJ Open. Jan 31, 2024;14(1):e078508. [FREE Full text] [doi: 10.1136/bmjopen-2023-078508] [Medline: 38296272]
Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. Oct 02, 2018;169(7):467-473. [FREE Full text] [doi: 10.7326/M18-0850] [Medline: 30178033]
Feldstein AC, Glasgow RE. A Practical, Robust Implementation and Sustainability Model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf. Apr 2008;34(4):228-243. [doi: 10.1016/s1553-7250(08)34030-6] [Medline: 18468362]
Naeem M, Ozuem W, Howell K, Ranfagni S. A step-by-step process of thematic analysis to develop a conceptual model in qualitative research. International Journal of Qualitative Methods. Nov 08, 2023;22:22. [doi: 10.1177/16094069231205789]
Abdulai M, Aldheleai H, Bokhari M. Health care professionals’ use of health information systems (HIS) in Indian hospitals. IJCA. Apr 19, 2021;174(28):5-12. [doi: 10.5120/ijca2021921185]
Alboraie M, Abdalgaber M, Youssef N, Moaz I, Abdeen N, Abosheaishaa H, et al. Healthcare providers’ perspective about the use of telemedicine in Egypt: a national survey. Int J Telemed Appl. Mar 12, 2022;2022:3811068-3811068. [FREE Full text] [doi: 10.1155/2022/3811068] [Medline: 35313723]
Jiang Y, Sun P, Chen Z, Guo J, Wang S, Liu F, et al. Patients’ and healthcare providers’ perceptions and experiences of telehealth use and online health information use in chronic disease management for older patients with chronic obstructive pulmonary disease: a qualitative study. BMC Geriatr. Jan 03, 2022;22(1):9. [FREE Full text] [doi: 10.1186/s12877-021-02702-z] [Medline: 34979967]
Ning Y, Dong Z, Jia Z, Zhao W, Ding Y, Wang Q, et al. Development of mobile health-based interventions to promote physical activity in patients with head and neck cancer: a qualitative study. Front Public Health. 2023;11:1260804. [doi: 10.3389/fpubh.2023.1260804] [Medline: 38074711]
Shardha H, Kumar G, Sagar N, Kumar R, Qazi M, Munir S, et al. Perceptions of telemedicine among healthcare professionals in rural tertiary care hospitals of rural Sindh, Pakistan: a qualitative study. Ann Med Surg (Lond). Feb 2024;86(2):726-733. [doi: 10.1097/MS9.0000000000001688] [Medline: 38333274]
Yu-Tong T, Yan Z, Zhen L, Bing X, Qing-Yun C. Telehealth readiness and its influencing factors among Chinese clinical nurses: a cross-sectional study. Nurse Educ Pract. Jan 2022;58:103278. [FREE Full text] [doi: 10.1016/j.nepr.2021.103278] [Medline: 34954659]
Mekuria S, Adem HA, Ayele BH, Musa I, Enyew DB. Routine health information system utilization and associated factors among health professionals in public health facilities in Dire Dawa, eastern Ethiopia: a cross-sectional study. Digit Health. 2023;9:20552076231203914. [FREE Full text] [doi: 10.1177/20552076231203914] [Medline: 37808236]
Ngugi PN, Were MC, Babic A. Users’ perception on factors contributing to electronic medical records systems use: a focus group discussion study in healthcare facilities setting in Kenya. BMC Med Inform Decis Mak. Dec 26, 2021;21(1):362. [doi: 10.1186/s12911-021-01737-x] [Medline: 34955098]
Tesfa GA, Kalayou MH, Zemene W. Electronic health-information resource utilization and its associated factors among health professionals in Amhara regional state teaching hospitals, Ethiopia. Adv Med Educ Pract. 2021;12:195-202. [doi: 10.2147/AMEP.S289212] [Medline: 33688292]
Tilahun B, Gashu KD, Mekonnen ZA, Endehabtu BF, Asressie M, Minyihun A, et al. Strengthening the national health information system through a capacity-building and mentorship partnership (CBMP) programme: a health system and university partnership initiative in Ethiopia. Health Res Policy Syst. Dec 09, 2021;19(1):141. [FREE Full text] [doi: 10.1186/s12961-021-00787-x] [Medline: 34886865]
Baradwan S, Al-Hanawi M. Perceived Knowledge, Attitudes, and Barriers Toward the Adoption of Telemedicine Services in the Kingdom of Saudi Arabia: Cross-Sectional Study. JMIR formative research. 2023. :7. [doi: 10.2196/46446]
Mussi CC, Luz R, Damázio DDR, Santos EMD, Sun V, Porto BSDS, et al. The large-scale implementation of a health information system in Brazilian university hospitals: process and outcomes. Int J Environ Res Public Health. Oct 25, 2023;20(21):6971. [doi: 10.3390/ijerph20216971] [Medline: 37947529]
Borges do Nascimento IJ, Abdulazeem H, Vasanthan LT, Martinez EZ, Zucoloto ML, Østengaard L, et al. Barriers and facilitators to utilizing digital health technologies by healthcare professionals. NPJ Digit Med. Sep 18, 2023;6(1):161-128. [FREE Full text] [doi: 10.1038/s41746-023-00899-4] [Medline: 37723240]
Berardi C, Antonini M, Jordan Z, Wechtler H, Paolucci F, Hinwood M. Barriers and facilitators to the implementation of digital technologies in mental health systems: a qualitative systematic review to inform a policy framework. BMC Health Serv Res. Feb 26, 2024;24(1):243. [FREE Full text] [doi: 10.1186/s12913-023-10536-1] [Medline: 38408938]
Mumtaz H, Riaz MH, Wajid H, Saqib M, Zeeshan MH, Khan SE, et al. Current challenges and potential solutions to the use of digital health technologies in evidence generation: a narrative review. Front Digit Health. Sep 28, 2023;5:1203945. [FREE Full text] [doi: 10.3389/fdgth.2023.1203945] [Medline: 37840685]
Chidambaram S, Jain B, Jain U, Mwavu R, Baru R, Thomas B, et al. An introduction to digital determinants of health. PLOS Digit Health. Jan 2024;3(1):e0000346. [FREE Full text] [doi: 10.1371/journal.pdig.0000346] [Medline: 38175828]
Sambo L, Simões J, do Rosario O, Martins M. Firth JD, Conlon CP, Cox TM, Firth J, Conlon C, Cox T, editors. Financing Health Care In Low-Income Developing Countries: A Challenge For Equity In Health. Oxford, UK. Oxford University Press; Jan 2020:168-176.
Sureshkumar K, Bindu M, John S, Kamarul IM. Editorialvidence on low-cost technologies for neurological rehabilitation in low and middle-income countries. Frontiers in Neurology. 2023. :14.
Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health. Aug 01, 2020;20(1):1193. [doi: 10.1186/s12889-020-09301-4] [Medline: 32738884]
Huang C, Wang J, Wang S, Zhang Y. Internet of medical things: A systematic review. Neurocomputing. 2023. :557. [doi: 10.1016/j.neucom.2023.126719]
National Institute for Health and Care Excellence (NICE). Evidence standards framework for digital health technologies. NICE. Mar 2019. URL: https://www.nice.org.uk/about/what-we-do/our-programmes/ evidence-standards-framework-for-digital-health-technologies [accessed 2025-02-11]
Functional classification, according to their intended use, of digital solutions used in the context of medical and paramedical care. Haute Autorité de Santé. 2021. URL: https://www.has-sante.fr/upload/docs/application/pdf/2021-03/ dm eval 270 proposition classification.pdf [accessed 2024-08-04]
World Health Organization (WHO). Classification of digital health interventions v1. WHO. 2018. URL: https://iris.who.int/ bitstream/handle/10665/260480/WHO-RHR-18.06-eng.pdf?sequence [accessed 2024-08-04]
Food and Drug Administration (FDA). Digital Health Center of Excellence. FDA. 2024. URL: https://www.fda.gov/ medical-devices/digital-health-center-excellence [accessed 2024-08-04]
Abbreviations
DHT: digital health technology
GNI: gross national income
IT: information technology
LMIC: lower- and middle-income country
mHealth: mobile health
PCC: Population-Concept-Context
PRISM: Practical, Robust Implementation and Sustainability Model
PRISMA-ScR: Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews
WHO: World Health Organization
Edited by de Azevedo Cardoso; submitted 21.06.24; peer-reviewed by Linde, Baker; comments to author 29.10.24; revised version received 01.11.24; accepted 09.12.24; published 06.03.25