الجروح المزمنة غالبًا ما تكون مصابة ببكتيريا الأغشية الحيوية وتتميز بارتفاع الإجهاد التأكسدي. الضمادات الحالية التي تعزز شفاء الجروح المزمنة إما تتطلب عمليات إضافية مثل الإشعاع الضوئي الحراري أو تترك كميات كبيرة من الرواسب غير المرغوب فيها. نحن نبلغ عن ضمادة هيدروجيل ذات وظيفة مزدوجة تتمتع بخصائص مضادة للأغشية الحيوية ومضادة للأكسدة متكاملة ومنخفضة التسرب. الهيدروجيل هو شبكة متشابكة تحتوي على بوليميدازوليوم كاتيوني مضاد للبكتيريا ومضاد للأكسدة.-أسيتيل سيستين. في نموذج جروح سكري في الفئران، يسرع الهيدروجيل إغلاق الجروح المصابة بسلالة المكورات العنقودية الذهبية المقاومة للميثيسيلين أو بيوفيلم الزائفة الزنجارية المقاومة للكاربينيم. علاوة على ذلك، يظهر نموذج معادل الجلد البشري ثلاثي الأبعاد خارج الجسم أن-أسيتيل سيستين يعزز تمايز الكيراتينوسيت ويسرع عملية إعادة الظهارة. يمكن تصنيع ضمادتنا الهيدروجيل بأشكال مختلفة لعلاج الجروح المزمنة المصابة سواء كانت مسطحة أو عميقة دون تلوث الجرح أو الحاجة إلى وسائل أخرى مثل الإشعاع الضوئي الحراري.
تتقدم الجروح العادية عبر أربع مراحل رئيسية من الشفاء: التجلط، الالتهاب، التكاثر، والنضوج.من ناحية أخرى، غالبًا ما تكون الجروح المزمنة محاصرة في مرحلة الالتهاب، مما يجعلها تفشل في التقدم نحو الشفاء.تشمل الجروح المزمنة أنواعًا مختلفة من القرح، بما في ذلك قرح القدم السكرية، وجروح قرح الساق الوريدية، وقروح الضغط.التكلفة الاقتصادية لجميع الجروح المزمنة غير الشافية في الولايات المتحدة وحدها تقدر بأكثر منمليار في السنة. تمثل قرحات القدم السكري معدل وفيات لمدة 5 سنوات (30.5%) مقارنة بتلك الخاصة بالسرطان (31%)مع تزايد عدد السكان، خاصة في الدول المتقدمة، وشيخوختهم، من المتوقع أن تزداد انتشار وتأثير الجروح المزمنة.
الضمادات التقليدية للجروح ليست مصممة لتعزيز إغلاق الجروح المزمنة التي يصعب شفاؤها. ومن الخصائص الشائعة للجروح المزمنة الالتهاب المطول.تشير دراسات متنوعة إلى أن الجروح غير الشافية محاصرة في حالة التهاب مزمن تعيق التقدم الطبيعي للشفاء.. على وجه التحديد، مؤخرًا
تشير التحقيقات في أنسجة وسوائل الجروح المزمنة إلى وجود تنافس بين الإشارات المؤيدة للالتهاب والإشارات المضادة للالتهاب، مما يؤدي إلى عدم توازن في الأكسدة والاختزال ومنع حدوث الشفاء السليم للجروح.. هذا يقفل الجرح في حالة من الالتهاب المزمن الذي يعيق التقدم نحو إغلاق الجرح. بسبب الالتهاب المستمر، تتواجد الكريات البيضاء المتعادلة والبلعميات في الموقع وتفرز أنواع الأكسجين التفاعلية (ROS) لمكافحة استعمار الكائنات الدقيقة. إن المستويات المرتفعة من ROS في الجروح المزمنة لها تأثيرات سلبية على شفاء الجروح حيث قد تسبب ضررًا للخلايا والأنسجة والمصفوفة خارج الخلوية (ECM)، وتفعيل البروتيازات خارج الخلوية الكامنة (مثل ميتالوبروتيازات المصفوفة (MMPs)) والسيتوكينات الالتهابية.تسبب الحالة المطولة من الالتهاب المرتفع ومستويات الجذور الحرة في عدم قدرة الجرح على الخروج من المرحلة الالتهابية. في الحالات الشديدة، تخضع الخلايا داخل وحول سرير الجرح لموت الخلايا المبرمج (أي الموت المبرمج للخلايا، الموت النخرى، الموت الحديدي) بسبب الإجهاد التأكسدي العالي، مما يؤدي إلى سلسلة من الأحداث في الخلايا المجاورة تؤدي إلى نفس المصير. من المحتمل أن يكون هذا هو السبب في أن العديد من الجروح المزمنة تصبح نخرية، مما يستلزم إجراءات جذرية مثل إزالة الأنسجة الميتة أو الأسوأ، البتر، لحماية حياة المريض.
للتغلب على الإجهاد التأكسدي العالي للجروح المزمنة، استكشف العديد من الباحثين تطبيق مضادات الأكسدة الموضعية.مثل التركيبات التي تستخدم الكركمين و-أسيتيل-ت-سيستين (NAC). ومع ذلك، لوحظ أن التحدي الأكثر شيوعًا في رعاية الجروح المزمنة لم يتم معالجته في مثل هذه التصاميم لغسل الجروح/الضمادات، وهو أن العديد من الجروح مستعمرة ببكتيريا تشكل الأغشية الحيوية. وقد وُجد أن عدوى الأغشية الحيوية تؤخر الشفاء وتقلل من الفعالية السريرية لمحلول مضاد الأكسدة الموضعي.تشكل الأغشية الحيوية، بدلاً من البكتيريا العائمة، الشكل الرئيسي للميكروبات التي تستعمر الجروح المزمنة. وغالبًا ما يكونون متمردين على العلاج تسبب عدوى الأغشية الحيوية في الجروح بشكل شائع بكتيريا المكورات العنقودية الذهبية المقاومة للميثيسيلين (MRSA) وبكتيريا الزائفة الزنجارية (P. aeruginosa).تمتلك الأغشية الحيوية القدرة على امتصاص العناصر الغذائية من المصفوفة خارج الخلوية، مثل الكربون والنيتروجين والفوسفات، لتزويد نموها.تشكل الأغشية الحيوية الناضجة مواد بوليمرية خارج الخلوية (EPS) تحيط بالبكتيريا وتحميها من التدابير المضادة مثل خلايا المناعة في المضيف، البلعميات، الببتيدات المضادة للميكروبات والمضادات الحيوية.تفشل هذه التدابير المضادة في مهاجمة بكتيريا الأغشية الحيوية لأنها لا تستطيع اختراق طبقة EPS الواقية بكميات كافية لتحقيق تأثير علاجي. غالبًا ما تكون الأغشية الحيوية مستقرة بحيث تبقى على أسطح الجروح طالما أنها غير متأثرة بالتدخلات الطبية.
يجب تصميم ضمادات الجروح المزمنة المتقدمة لعلاجات شاملة، تعالج كل من متطلبات مضادات الأكسدة ومضادات البكتيريا/مضادات الأغشية الحيوية. على الرغم من أن الدراسات السابقة قد استكشفت حلولًا محتملة، إلا أن كل نهج واجه قيودًا. حتى الآن، لا توجد علاجات جروح ذات وظيفة مزدوجة مستقلة أو غير ملوثة لأنها تعتمد إما على الاستجابة المناعية الفطرية، أو الإشعاع الضوئي الحراري، أو إطلاق المضادات الحيوية، أو أكاسيد المعادن.تستخدم ضمادة الجروح لدينا الطبيعة المسامية للهيدروجيل، جنبًا إلى جنب مع الخصائص المضادة للبكتيريا والأكسدة الموجودة بشكل طبيعي في البوليمرات الكاتيونية وNAC على التوالي. إنها مستقلة وتتميز بتسرب منخفض للغاية، مما يجعلها مريحة وآمنة للاستخدام.
طور الشيخ وآخرون هلامًا مجمدًا محملاً بالإكسوزومات ومطلقًا للأكسجين، OxOBand، الذي أظهر زيادة في ترسب الكولاجين، وإعادة تكوين الظهارة، وتكوين الأوعية الجديدة، وتقليل الإجهاد التأكسدي في الجروح الناتجة عن السكري.. ومع ذلك، اعتمدت على إطلاق الأكسجين لتحفيز إنتاج الجذور الحرة للأكسجين (مثل و ) بواسطة البلعميات المضيفة لمكافحة العدوى البكتيرية، والتي قد تتأثر سلبًا لدى المرضى الذين يعانون من ضعف المناعة. كما كانت هناك حاجة إلى خلايا جذعية مشتقة من الدهون لإنشاء الإكسوزومات، والتي ترتبط بحدود التصنيع على نطاق واسع ومجموعة من القضايا الأخلاقية والتنظيمية والسلامة. كانت هناك نهج آخر يتضمن مركب نانوي يحتوي على ثنائي كبيديد الموليبدينوم.الأغشية النانوية وثاني أكسيد السيريوم الجسيمات النانوية (NPs) لتوصيل كل من التأثير المضاد للبكتيريا الناتج عن الحرارة الضوئية والوظيفة المضادة للأكسدة لعلاج الجروح المصابةهذه المراهم الموضعية مطلوبةعلاج بالليزر لتنشيط التأثير المضاد للبكتيرياوتركت مكونات معدنية (الموليبدينوم والسيريوم) على الجسم المضيف. كما أظهر هيدروجيل مركب آخر، يتكون من الجيلاتين المعدل بواسطة (البوليمر) الدوبامين المضاد للأكسدة، وأنابيب الكربون النانوية (CNTs)، والمضاد الحيوي دوكسيسيكلين، وعداً في تحقيق خصائص مضادة للبكتيريا ومضادة للأكسدة.. ومع ذلك، كان تأثير CNTs المضاد للبكتيريا الناتج عن الحرارة الضوئية يعتمد على إشعاع NIR، وأثار إطلاق المضاد الحيوي من الضمادة مخاوف بشأن إمكانية تطور مقاومة الأدوية. أظهر هيدروجيل استجابة حرارية قائم على كوبوليمر ثلاثي الكتل من الكابرو لاكتون، والجلايكوليد، والإيثيلين غليكول مع تعديلات من البوليدوبامين وجزيئات الفضة النانوية فعالية ضد بكتيريا S. aureus إيجابية الجرام ولكن ليس ضد بكتيريا P. aeruginosa سالبة الجرام.يجب أن تظهر الضمادات المثالية للجروح المزمنة خصائص مضادة للالتهابات ووظائف مضادة للعدوى واسعة النطاق دون الحاجة إلى تدخلات إضافية مثل الإشعاع، وألا تلوث موقع الجرح. العلاجات الحالية المبلغ عنها لا تلبي جميع هذه المتطلبات.
نقدم هنا هيدروجيل صناعي ذو وظيفتين، PPN، يتمتع بخصائص مضادة للبكتيريا ومضادة للأكسدة تعمل بشكل متكامل لدعم شفاء الجروح المصابة لدى مرضى السكري، كما تم إثباته من خلال نماذج الفئران. يتكون هيدروجيل PPN الصناعي المستقل، الذي لا يتطلب أي وسيلة إضافية أو عملية أخرى، من هيدروجيل بولي إيثيلين جلايكول (PEG) متقاطع الروابط مرتبط مع بوليمر كاتيوني مضاد للبكتيريا شديد الفعالية، بوليميدازوليوم (PIM)، ومضاد للأكسدة.-أسيتيل سيستين (NAC). هذا الهيدروجيل القوي منخفض التسرب تمامًا وخالٍ تمامًا من المضادات الحيوية أو المركبات المعدنية أو الجسيمات النانوية، مما يضمن الحد الأدنى من البقايا في موقع الجرح بعد إزالة الضمادة. تظهر الدراسات على نموذج مكافئ للجلد البشري ثلاثي الأبعاد أن NAC يعزز إعادة تكوين الظهارة وتمايز الكيراتينocytes، بينما لا تعيق إضافة مشتق PIM عملية شفاء الجروح.
النتائج
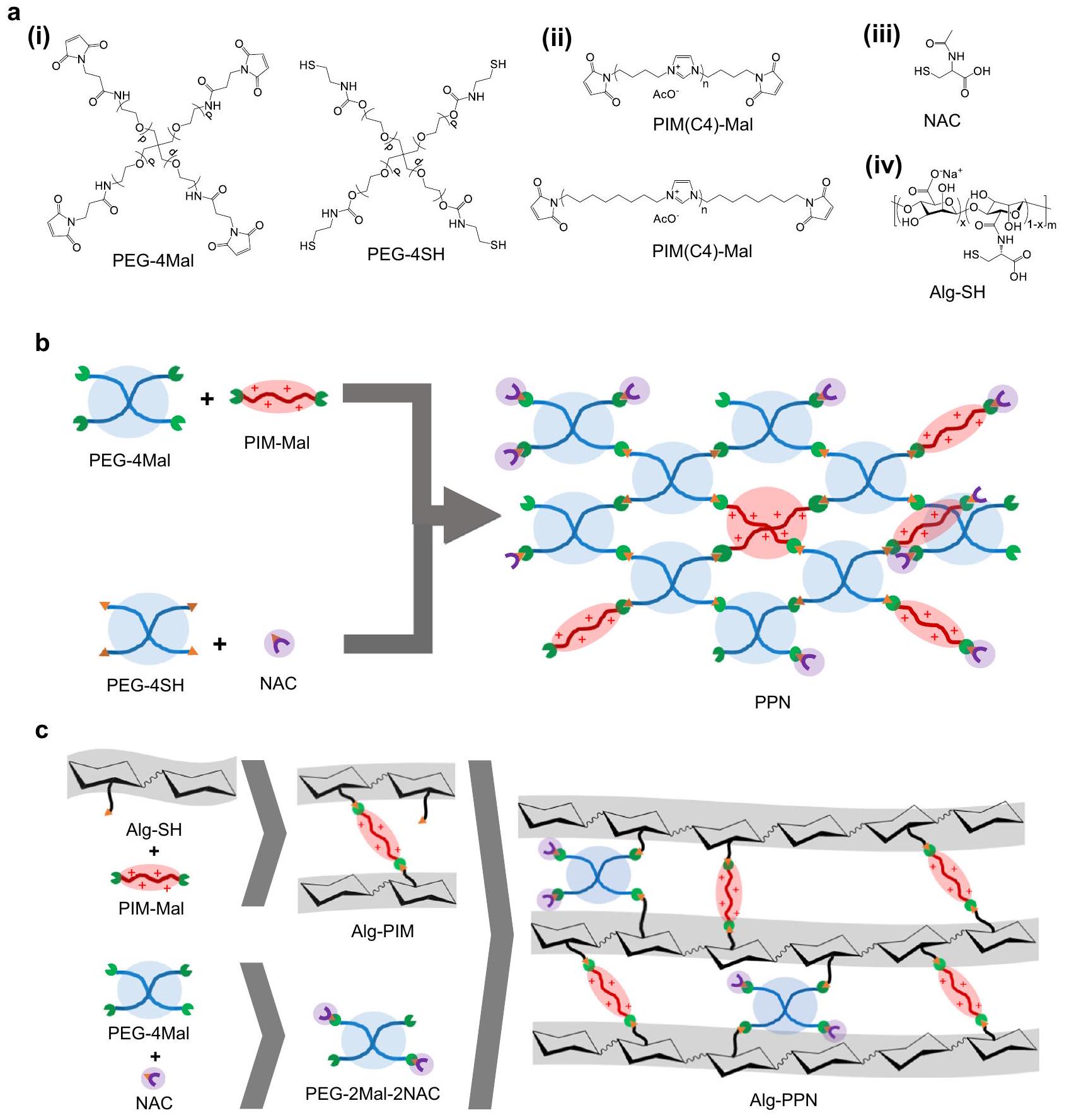
تم تعزيز هيدروجيل مشتق من بولي إيثيلين جلايكول (PEG) بخصائص مضادة للبكتيريا ومضادة للأكسدة من خلال إضافة سلسلة رئيسية كاتيونية من بوليميدازوليوم-ماليميد (PIM-Mal) ومكون ثانٍ من-أسيتيل سيستين (NAC) (الشكل 1a). تم ربط كلا الجزيئين (مشتق PIM-Mal و NAC) بشكل تساهمي في شبكة الهيدروجيل من خلال كيمياء الثيول-ماليميد. تم تحضير PIM-Mal مسبقًا عبر كيمياء بولي-رادزيشيفسكي السهلة لصنع PIM المنتهي بالديامين، تلاها تعديل النهاية مع أنهدريد الماليك. (الشكل التكميلي 1). تم تصنيع الهيدروجيل في شكلين، وهما شكل الفيلم وشكل الألياف. الشكل الأول، وهو شكل هيدروجيل الفيلم المسمى PPN (الشكل 1ب) الذي تم الحصول عليه من تداخل 4 ذراعات من PEG-thiol (PEG-4SH) مع 4 ذراعات من PEG-maleimide (PEG-4Mal)، مع إضافة PIM-Mal و NAC، مناسب للجروح المسطحة نسبياً. الشكل الثاني الذي يستخدم الألجينات (المسمى Alg-PPN (الشكل 1ج)) تم تجميعه من خلال تداخل (i) PEG-2Mal-2NAC المصنوع من PEG-4Mal الذي تم تفاعله مسبقاً مع NAC بحيث تم ربط ذراعين بـ NAC (الشكل التكميلي 2)، و (ii) Alg-SH-PIM الذي تم تفاعله مسبقاً من الألجينات الوظيفية بالثيول (Alg-SH) مع PIM-Mal؛ هذا الشكل مناسب للجروح العميقة.
تظهر صور التنسيقات الاثنين، أي فيلم الأفلام والألياف الجيلاتينية (Alg) في الشكل 2a و 2b. قمنا بإجراء اختبارات أولية باستخدام تنسيق فيلم الهيدروجيل (الأشكال 1b و 2a). تم تحضير PIM(C4)-Mal الكاتيوني، الذي يحتوي على رابط بيوتيلي (C4) بين حلقات الإيميدازوليوم، مسبقًا (الشكل التكميلي 1).تم تقديم توصيف NMR لـ PIM(C4)-Mal في الشكل التكميلي 3a. الوزن الجزيئيتم قياس PIM(C4)-Mal بواسطة كروماتوغرافيا الجل النفاذية وكان 2766 دالتون (الشكل التكميلي 4). تتراوح التركيزات المثبطة الدنيا (MIC) لـ PIM(C4)-Mal من 2 إلى (الجدول التكميلي 1) عند اختباره ضد أنواع مختلفة من بكتيريا ESKAPE (تحديداً. فيسيوم 19434، مقاوم للميثيسيلين. الذهبية (MRSA BAA-40 و
الشكل 1 | مخططات تحضير ضمادات الجروح الهيدروجيلية من الفيلم والألياف. أ هياكل المكونات الرئيسية في ضمادات الفيلم والألياف الهيدروجيلية. تخليق (ب) فيلم هيدروجيل PPN و(ج) ضمادات ألياف هيدروجيل Alg-PPN.
MRSA USA300)، E. cloacae 13047، K. pneumoniae 13883، P. aeruginosa 01 (PAO1)، ومقاومة الكاربابينيم. أيروجينوزا و. باوماني (CR-PA و CR-AB))، مما يشير إلى أن البوليمر هو مثبط قوي للنمو لطيف واسع من البكتيريا إيجابية الجرام وسلبية الجرام.
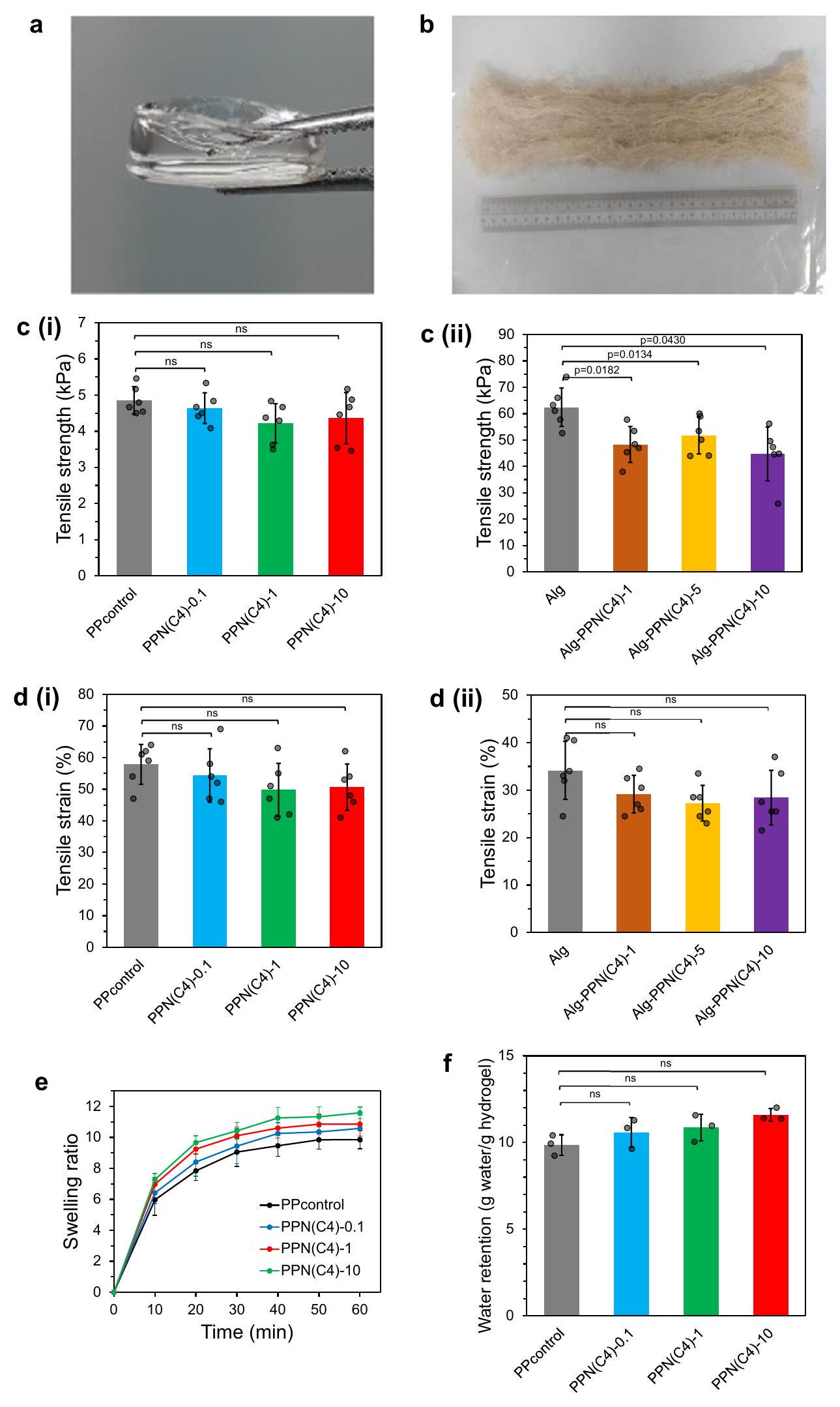
قمنا باختبار تركيبات مختلفة (الجدول 1) من هيدروجيل الأفلام. تُسمى هيدروجيل الأفلام ذات الوظائف المزدوجة (أي التي تحتوي على كل من PIM(C4)-Mal و NAC) بـ PEG-PIM-NAC (PPN(C4)-x)، حيث يشير اللاحقة (x) إلى تركيز PIM(C4)-Mal. (الجدول 1). تم تجميع هيدروجيل التحكم (المشار إليه بـ PPcontrol) عن طريق خلط PEG-4SH مع PEG-4Mal في الماء المنزوع الأيونات (DI) دون المكونات النشطة PIM و NAC. تم أيضًا إعداد هيدروجيلات أحادية الوظيفة تستبعد إما PIM (المعلمة بـ PP-N) أو NAC (PPN-). هيدروجيل الفيلم تم تشكيل الشبكة بشكل رئيسي من خلال تفاعل PEG-4SH مع PEG4Mal؛ تم ربط NAC وجزء من PIM(C4)-Mal بالشبكة كمركبات جانبية (الشكل 1ب). كانت مقدّمات الهيدروجيل قادرة على الربط المتقاطع في الماء المقطر.في أقل من دقيقة واحدةأظهرت أفلام الهيدروجيل قوة شد تتراوح بين 4 إلى 5 كيلو باسكال وانفعال شد (تمدد) بين 50 و 58% (الشكل 2c(i)، d(i))، وهو ما هو أقل قليلاً من قابلية تمدد جلد الإنسان.في بيئة مائية، انتفخت هلاميات الفيلم، مما أدى إلى امتصاصأضعاف كتلتها الأولية من الماء خلال 20 دقيقة؛ وبعد ذلك استقرت حركيات الانتفاخ لتصل إلى 10-12 ضعفًا خلال 60 دقيقة (الشكل 2e، f، الشكل التكميلية 5a، b). كانت الهلاميات المنتفخة مستقرة وأظهرت كتلة ثابتة بعد الحضانة لمدة 7 أيام في مستخلصات بكتيرية (الشكل التكميلية 6a-b) وسوائل جروح مصابة (التكميلية
الشكل 2 | الخصائص الفيزيائية لأغشية وضمادات الجروح الهيدروجيلية. المظهر البصري لضمادات الجروح التي تم التحقيق فيها: (أ) هيدروجيل فيلم PPN(C4)-1 و (ب) هيدروجيل ألياف ألجينات Alg-PPN(C8)-5. قوة الشد لـ (ج(ط)) هيدروجيل الفيلم و (ج(2)) هيدروجيل ألياف ألجينات.تجارب مستقلة، اختبار ستودنت ذو الذيليناختبار). إجهاد الشد (التمدد) لـ ( (i) هيدروجيل الأفلام
الجدول 1 | تركيبات هلاميات فيلم PPN(C4) في 1 مل من الماء المقطر
تركيبة الهيدروجيل
PEG-4SH
PEG-4مال
PIM(C4)-مال
NAC
بي بي كنترول
–
–
PPN(C4)-0.1
PPN(C4)-1
PPN(C4)-10
PP-N
–
PPN-
–
الشكل 6ج). في اختبار النموذج الحي (نموذج الفأر) للجروح المصابة، تحولت الهلاميات الشفافة في البداية إلى لون بني مصفر بعد يومين، على الأرجح بسبب امتصاص سوائل الجروح والبكتيريا الميتة، لكنها ظلت سليمة ومستقرة (الشكل التوضيحي 7). وهذا أثبت أن الهلاميات مقاومة للتحلل بواسطة سوائل الجروح المصابة.
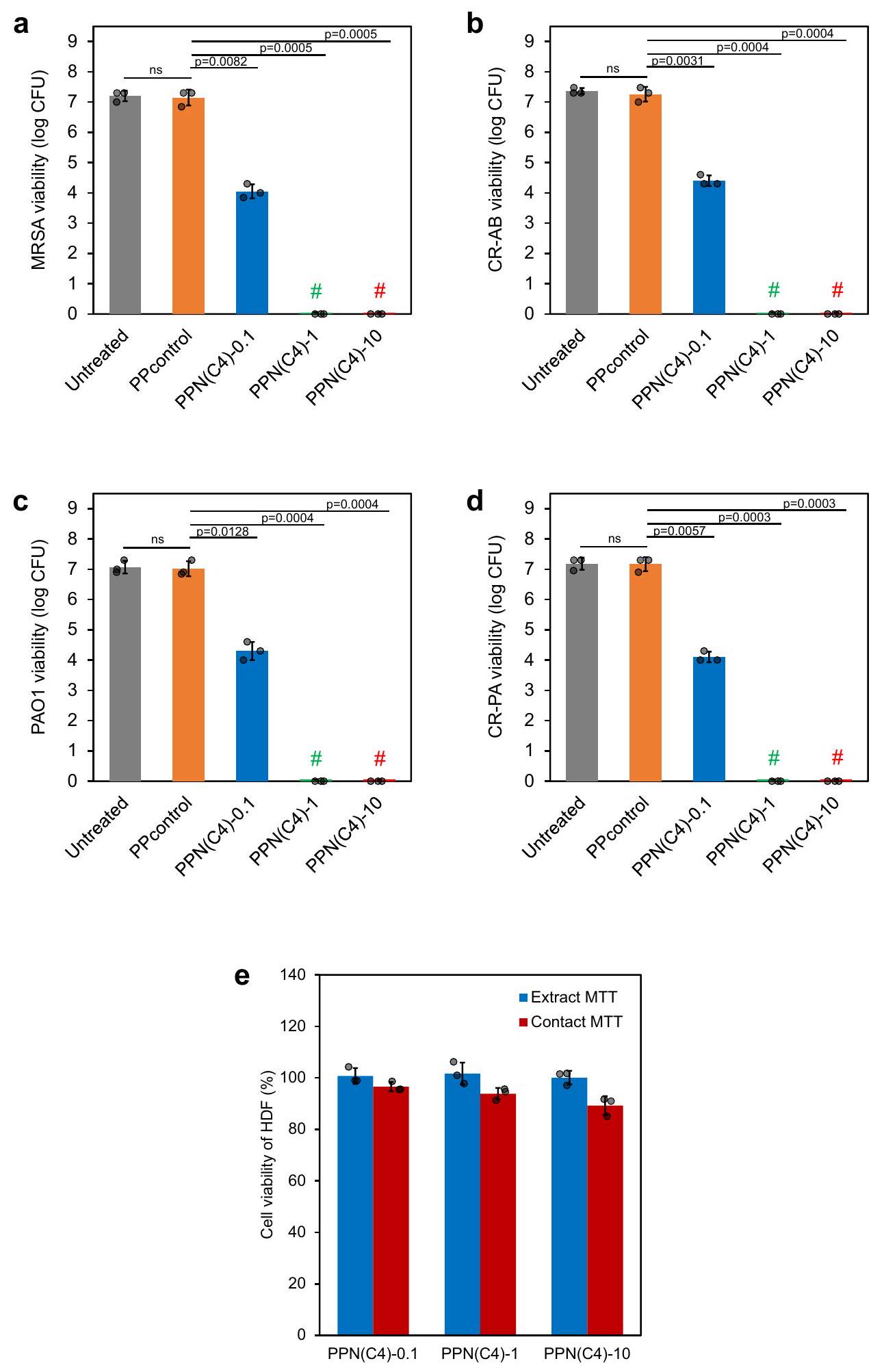
تم قياس فعالية القتل عند الاتصال في المختبر لهلامات PPN(C4) لمجموعة متنوعة من سلالات البكتيريا المقاومة المتعددة للعقاقير (MDR) سالبة وموجبة الجرام التي لها صلة سريرية بالجروح المصابة.، تحديداً MRSA USA300 وCR-AB وPAO1 وCR-PA، وهي مسببات أمراض تثير قلقاً كبيراً على مستوى العالم. لقد قضت PPN(C4)-1 وPPN(C4)-10 تمامًا على سلالات البكتيريا المختلفة المحملة على أقراص الهيدروجيل في ساعة واحدة (الشكل 3أ، د). لم تقض PPN(C4)-0.1 هيدروجيل تمامًا على جميع البكتيريا (الشكل 3أ، د)، ربما بسبب تركيزها المنخفض من مكون PIM-Mal المضاد للبكتيريا النشط حيويًا. لم يظهر PPcontrol خصائص قاتلة للبكتيريا. كما أن الهيدروجيل ومستخلصاته تظهر سمية منخفضة لخلايا الأدمة البشرية (HDFs)، كما تم تقييمه من خلال اختبار 3-(4،5-ثنائي ميثيل ثيازول-2-يل)-2،5-ثنائي فينيل تيترازوليوم بروميد (MTT). كانت نسبة بقاء الخلايا 100% لخلايا HDF المعرضة لجميع مستخلصات الهيدروجيل (الشكل 3هـ). بالنسبة لاختبار الاتصال بالهيدروجيل، كانت نسبة بقاء خلايا HDF و لـ PPN(C4)-0.1 و PPN(C4)-1 و PPN(C4)-10، على التوالي (الشكل 3e)، مما يشير إلى سمية حادة منخفضة وتوافق حيوي جيد لهذه الهلامات.
تم اختيار PPN(C4)-1 لمزيد من التوصيف لأنه أظهر فعالية مضادة للبكتيريا عند تركيز أقل من PIM(C4)-Mal. قمنا بمزيد من التحقيق في تأثيرات المكونات الحيوية الفردية لـ PIM أو NAC، بالإضافة إلى تأثيراتها المشتركة. قمنا بتشكيل هيدروجيلات مشتقة من PPN(C4)-1 تفتقر إلى PIM أو NAC: تم تصنيع PP-N بدون PIM(C4)-1، بينما تم تصنيع PPN- بدون NAC (الجدول 1). باستخدام نموذج نسيج ثلاثي الأبعاد معاد بناؤه خارج الجسم، تم دراسة تأثيرات هذه الهيدروجيلات المشتقة من PPN(C4)-1 على إغلاق الجروح، وإعادة تكوين البشرة، وتكاثر وتمايز الكيراتينوسيتات البشرية في عملية شفاء الجروح على مدى 7 أيام. على وجه التحديد، استخدمنا نموذج الجلد البشري المعادل (DED-HSE)، وهو بناء نسيجي حي خارج الجسم حيث يتم إعادة توطين هياكل جلدية خلوية من متبرعين بشريين بكيراتينوسيتات متبرعين متجانسين. بالإضافة إلى كونها مشابهة فسيولوجيًا لأنسجة الجلد في الجسم، كما يتضح من دراسة شيا وآخرون.يدعم بناء DEDHSE أيضًا القدرة العالية على التكاثر والتمايز لخلايا الكيراتين المستمدة من المتبرعين الأجنبيين بفضل وجود غشاء قاعدي سليم..
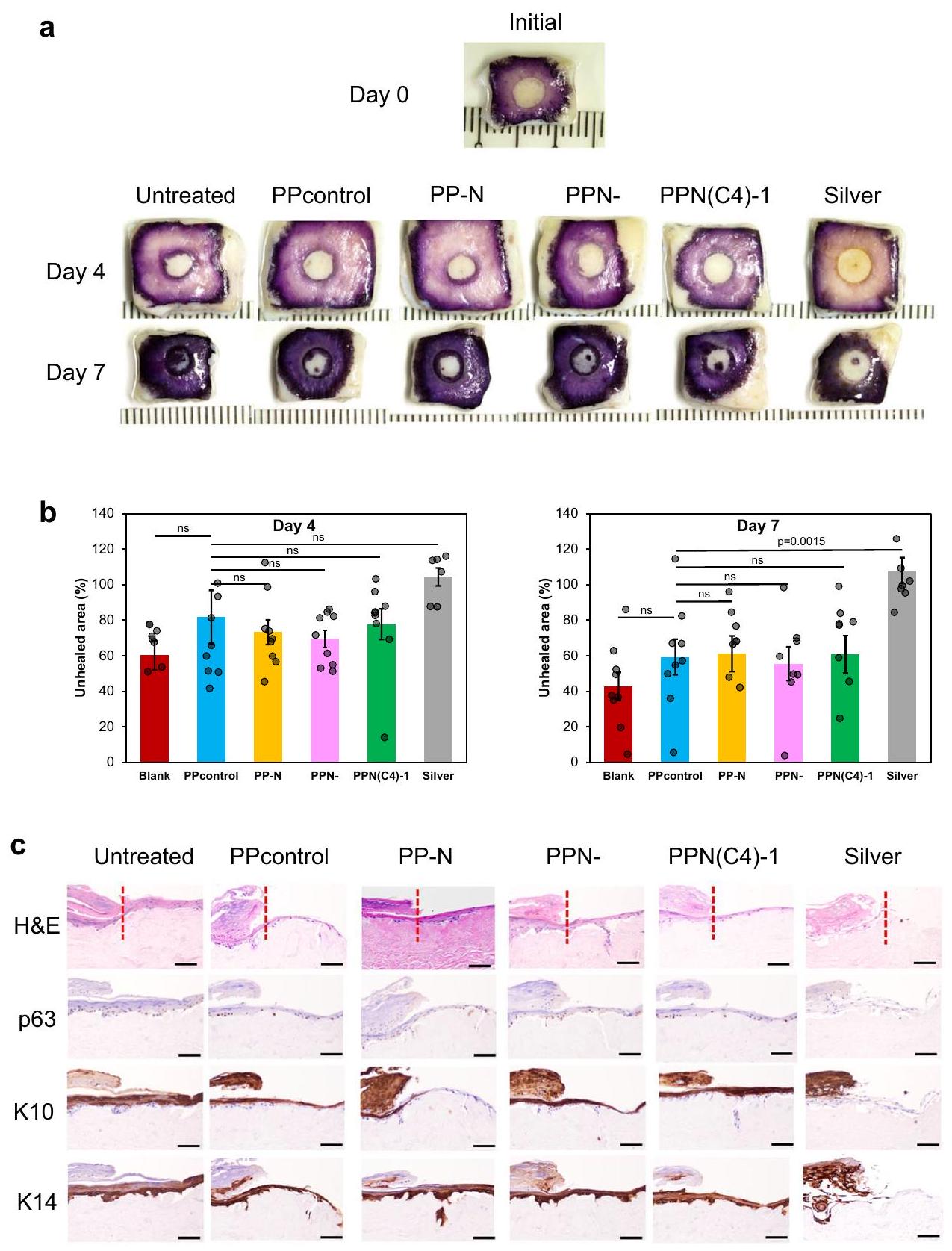
باستخدام اختزال الميتوكوندريا لـ MTT المطبق على نموذج 3D DEDHSE، تم اختبار تأثيرات الهيدروجيلات على الشفاء العام للجروح الاستئصالية (الشكل 4 أ، ب، الشكل التكميلي 8). يتم الإشارة إلى حجم الجرح الأولي (في اليوم 0) على أنهفي الشكل 4 ب. لم يكن هناك أي إغلاق للجروح واضح مع الضمادة الفضية، حيث ظلت منطقة الجرح كبيرة.تمت ملاحظة بعض إغلاقات الجروح في مجموعة التحكم غير المعالجة وجميع مجموعات علاج الهيدروجيل في كل من اليومين 4 و7 بعد الإصابة. على سبيل المثال، مع تركيبات الهيدروجيل المختلفة لدينا في اليوم السابع، كانت المناطق غير الملتئمة المتبقية تقريبًاحجم الجرح الأولي. لم يتم العثور على فرق إحصائي في أحجام الجروح بين مجموعات العلاج المختلفة بالهيدروجيل ومجموعة التحكم PP (جل PEG بدون NAC و PIM) في كل من اليوم الرابع واليوم السابع (الشكل 4 ب). تشير هذه البيانات من نموذج DED-HSE إلى أن الهيدروجيل تمتلك التركيبات (PPcontrol، PP-N، PPN- وPPN(C4)-1) توافقًا حيويًا ممتازًا مقارنةً بضمادة الفضة التجارية الحالية.
قمنا بفحص التشريح الكلي لعينات DED-HSE المعرضة لتركيبات الهيدروجيل (PPcontrol، PP-N، PPN- وPPN(C4)-1). المعمارية الأساسية التي كشفت عنها صبغة الهيماتوكسيلين والإيوزين (H&E) في اليوم السابع تحدد لسانًا ظهاريًا متزايدًا على شكل إسفين وحجمًا أكبر من الظهارة المتعددة الطبقات في جميع مجموعات العلاج، باستثناء عينة الضمادة الفضية. أظهرت عينات DED-HSE المعالجة بـ PPN- وPPN(C4)-1، وكلاهما يحتوي على PIM(C4)-Mal، سماكات جلدية مشابهة إحصائيًا مقارنة بعينة PPcontrol (الشكل 4c، الجدول التكميلي 2)، مما يشير إلى أن دمج PIM(C4) لم يعيق إعادة تكوين الظهارة. ومن الجدير بالذكر أن الجروح المعالجة بـ PP-N أظهرت جلد أسمك من الجروح المعالجة بـ PPcontrol (الجدول التكميلي 2)؛ قد يُعزى ذلك إلى تأثير تعزيز الشفاء لمكون NAC. تؤكد هذه البيانات أن PP-N و PPN و PPN(C4)-1 متوافقة حيوياً، ولا تقلل من عملية إعادة الظهارة، وأن PP-N مع دمج NAC يسرع من إعادة الظهارة للجروح.
تم تأكيد انتشار الخلايا في عينات DED-HSE المعرضة لصيغ الهيدروجيل المختلفة أيضًا من خلال وجود عامل النسخ النووي p63، الذي يتم التعبير عنه بواسطة الكيراتينوسيت غير المتمايز والمتكاثر. النقاط البنية الظاهرة في الشكل 4c (الصف الثاني) هي خلايا تعبر عن p63، مما يشير إلى أن هذه الخلايا الفردية تمر بعملية التكاثر، بينما تشير النقاط الزرقاء إلى نوى كل من الخلايا المتكاثرة وغير المتكاثرة. في اليوم السابع، كانت هناك استجابة مناعية مكثفة واضحة في تجمعات الكيراتينوسيت داخل الطبقات القاعدية من DED-HSEs من جميع مجموعات العلاج (الشكل 4c، الصف الثاني). أظهرت عينات DED-HSE المعرضة لـ PP-N وPPN- وPPN(C4)-1 أعدادًا متقاربة إحصائيًا من الخلايا الإيجابية لـ p63 مقارنةً بـ DED-HSE المعرضة لـ PPcontrol (الجدول التكميلي 2). تشير هذه النتيجة إلى أن الهيدروجيل التي تحتوي على مكونات PIM(C4) أو NAC الفردية أو المجمعة لم تؤثر على تكاثر الكيراتينوسيت. مجتمعة، وجود NAC أو PIM لا يعيق التكاثر، كما هو موضح في اختبارات H&E وp63، ويظهر اختبار MTT أن التركيبة لا تؤثر سلبًا على التكاثر، وهو ما يتناقض مع الضمادات الفضية.
لتقييم التأثير المحتمل لـ PP-N و PPN- و PPN(C4)-1 على نضوج الكيراتينوسيت، قمنا أيضًا بفحص تعبير علامتين محددتين للتمايز الظهاري. بروتين السيتوكيراتين 10 (K10) موجود في جميع طبقات الخلايا فوق القاعدية، بما في ذلك الطبقة القرنية؛ يتم التعبير عنه حصريًا بواسطة الكيراتينوسيت التي تمر بعملية التمايز الحرشفي. بروتين السيتوكيراتين 14 (K14) يتم التعبير عنه حصريًا بواسطة الكيراتينوسيت القاعدية غير المتمايزة. توضح التوزيعات النسبية لـ K10 و K14 دورة حياة الكيراتينوسيت كما تنتقل من حالات التكاثر إلى حالات غير التكاثر والمتمايزة وتعيد ملء أو شفاء الجلد المكشوف. وجدنا أن DED-HSE المعالج بـ PPN- أظهر كثافات إشارة K10 و K14 مقارنة بـ DED-HSE المعالج بـ PPcontrol (الشكل 4c، الجدول التكميلي 2). ومن المثير للاهتمام، أن DED-HSE المعالج بـ PP-N أظهر شدة إشارة أقوى لـ K14 مقارنة بـ PPcontrol )، بينما تظهر كثافة إشارة مماثلة لـ K10 (الجدول التكميلي 2)، مما يشير إلى أن PP-N، الغني بـ NAC، يعزز بشكل أساسي تكاثر الكيراتينوسيت. بالإضافة إلى ذلك، أظهر DED-HSE المعالج بـ PPN(C4)-1 زيادة بنسبة 138% في كثافة الإشارة لـ K10
الشكل 3 | أظهرت هلاميات الأفلام نشاطًا مضادًا للبكتيريا وتوافقًا خلويًا في المختبر. أ-د تم تقييم فعالية PPN(C4) هلاميات الأفلام المضادة للبكتيريا من خلال اختبار الاتصال لمدة ساعة واحدة. # تشير إلى أنه لم يتم ملاحظة مستعمرات بكتيرية على طبق الأجار.عينات مستقلة بيولوجيًا، اختبار ستودنت ذو الذيليناختبار). حيوية خلايا الألياف الجلدية البشرية (HDFs) بعد الحضانة مع المستخلصات (باللون الأزرق) أو الغمر المباشر (باللون الأحمر) لأفلام هيدروجيل PPN(C4) عند لمدة 24 ساعة (تم فحص الخلايا في 3 تجارب مستقلة). تُعرض البيانات كقيم متوسطةSD. مقارنةً بـ PPcontrol ( )، مع ملاحظة شدة إشارة مماثلة لـ K14. تشير هذه النتيجة إلى أن كل من PP-N وPPN(C4)-1، اللذان يحتويان على NAC، يعززان تمايز الكيراتينوسيت، مما قد يرتبط بتحسن إعادة الظهارة بشكل عام كما لوحظ من خلال صبغة H&E. تشير هذه البيانات إلى أن الهيدروجيلات التي تحتوي على PIM(C4) و
NAC متوافقة حيوياً، ولا تعيق عملية التمايز، وأن NAC قد تعزز التمايز الحرشفي للخلايا الكيراتينية.
بعد ذلك، قمنا بتقييم الهيدروجيل في الجسم الحي باستخدام نموذج فئران مصابة بالسكري للجروح المصابة لتقييم فعاليتها في إزالة
الشكل 4 | نموذج معادل الجلد البشري (HSE) خارج الجسم للهيدروجيلات الفيلم. أ صور تمثيلية لصبغة MTT لشفاء الجروح.القياس الكمي لاختبار MTT في نقاط الزمن في اليوم الرابع واليوم السابع (ثلاث نسخ؛عينات مستقلة بيولوجيًا، اختبار ستودنت ذو الطرفيناختبار، البيانات مقدمة على أنها القيم المتوسطةصور التلوين المناعي التمثيلية لـ H&E و p63 و كيراتين 10 (K10) و كيراتين 14 (K14) بعد العلاج بالهيدروجيل PPN(C4)-1 ونسخه (PP-N بدون PIM(C4)-1، و PPN- بدون NAC). مقياس الرسم.
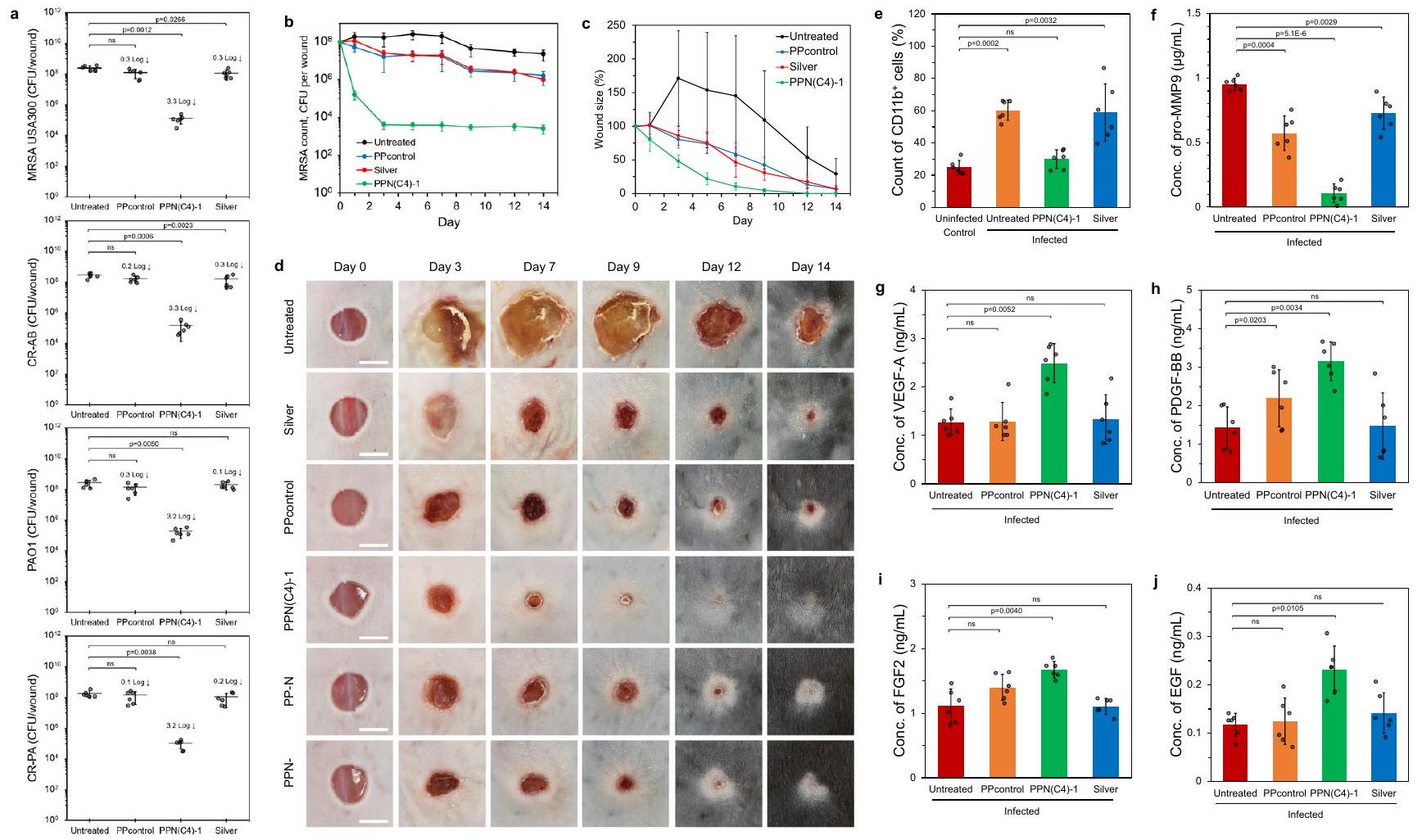
بكتيريا الأغشية الحيوية، باستخدام سلالات متعددة المقاومة للأدوية، وهي MRSA USA300 و PAO1 و CR-AB و CR-PA، مع ضمادة جروح مضادة للميكروبات تعتمد على الفضة كعنصر تحكم. سجلت الجروح المعالجة بهلام PPN(C4)-1 انخفاضًا أكبر من 3 لوغاريتم (>99.9%) في استعمار جميع سلالات البكتيريا المختبرة (الشكل 5أ). تتجاوز هذه الأداء العلاجات غير المثلى عمومًا (0.1-0.3 لوغاريتم) التي لوحظت مع الضمادة الفضية و PPcontrol (الشكل 5أ). لإجراء تحليل أكثر تفصيلًا للأغشية الحيوية داخل الجروح، بدأنا تجربة جروح حية باستخدام بكتيريا موسومة بالفلور، وتحديدًا سلالة MRSA USA300 (AH1263) التي تحمل البلازميد pHC47 الذي يعبر عن جين الفلورسنت الأحمر mCherry . بعد فترة علاج مدتها 24 ساعة، قمنا بفحص آفات الجروح باستخدام المجهر الضوئي المجهري. كشفت النتائج عن أغشية حيوية فلورية بسمك يصل إلى في الجروح (الشكل التكميلي 9أ-د). بناءً على
بيانات عدد البكتيريا (الشكل 5ب) وحجم الأغشية الحيوية، كانت الكثافة البكتيرية المقدرة في الأغشية الحيوية غير المعالجة . من بين جميع مجموعات العينات، أظهرت الجروح المعالجة بهلام PPN(C4)-1 أقل عدد من البكتيريا الفلورية المتبقية في الأغشية الحيوية، مما يؤكد أن علاج PPN(C4)-1 قلل من كثافة بكتيريا الأغشية الحيوية.
درسنا أيضًا ديناميات عدد بكتيريا الأغشية الحيوية (MRSA USA300) وتقليل حجم الجروح في موقع الجروح السكري الفأري على مدى فترة علاج مدتها أسبوعين مع PPN(C4)-1 والمجموعات الضابطة. تم جمع الجروح الموضحة في الشكل 5ب بطريقة مشابهة لتلك الموجودة في الشكل 5أ، حيث تم التضحية بالفئران واستئصال الجروح بالكامل وخلطها كل يوم لتحديد عدد البكتيريا. لوحظ أكبر انخفاض في البكتيريا في الجروح خلال الأيام الثلاثة الأولى من العلاج بهلام PPN(C4)-1، بعد ذلك، كانت أعداد البكتيريا
الشكل 5 | نموذج عدوى جروح السكري الفأري الحي مع علاج أفلام الهلام بعد 24 ساعة من العدوى. أ أعداد البكتيريا من MRSA USA300 و PA01 و CR-AB و CR-PA على جروح مختلفة ضابطة ومعالجة بعد 24 ساعة من العلاج ( الفئران، اختبار ستودنت ذو طرفين ). دراسة شاملة لشفاء الجروح. ب أعداد البكتيريا من MRSA USA300 على الجروح الضابطة غير المعالجة، والضمادة الفضية، و PPcontrol، والجروح المعالجة بهلام PPN(C4)-1 في الأيام و 14 بعد العلاج ( الفئران). ج أحجام الجروح من الجروح الضابطة غير المعالجة، والضمادة الفضية، و PPcontrol، والجروح المعالجة بهلام PPN(C4)-1 في أيام مختلفة كنسبة مئوية من حجم الجرح الأولي ( الفئران). المظهر المرئي للتمثيل
الجروح الضابطة غير المعالجة، والضمادة الفضية، و PPcontrol، والجروح المعالجة بهلام PPN(C4)-1 بين تغييرات الضمادة. مقياس الرسم . هـ-ي توصيف أنسجة الجروح. القياسات في الفئران المصابة بـ MRSA USA300 ( الفئران، اختبار ستودنت ذو طرفين ) في اليوم الثاني بعد العلاج: هـ نسبة خلايا CD11b في الجروح. نسبة الخلايا تتناسب طرديًا مع مدى الالتهاب في الجلد. تركيز البرو- MMP9 في الجروح. تركيزات عوامل شفاء الجروح (ج) VEGF-A، (ح) PDGF-BB، (ط) FGF-2 و (ي) EGF في الجروح. يتم تقديم البيانات كقيم متوسطة SD.
ظلت منخفضة باستمرار (الشكل 5ب). بالمقابل، أدت الضمادة الفضية و PPcontrol إلى عدد أقل بكثير من البكتيريا التي تم القضاء عليها (أقل من 1 لوغاريتم)، وأظهرت الجروح الضابطة غير المعالجة تقريبًا عدم وجود انخفاض في البكتيريا على مدى أسبوعين (الشكل 5ب). علاوة على ذلك، كانت الجروح المعالجة بهلام PPN(C4)-1 أصغر، مع أدلة قليلة على النخر، مقارنة بالجروح الضابطة غير المعالجة، و PPcontrol، والآفات المعالجة بالضمادة الفضية في جميع النقاط الزمنية (الشكل 5ج، د، النسخ البيولوجية موضحة في الشكل التكميلي 10). بشكل ملحوظ، أغلقت الجروح المعالجة بـ PPN(C4)-1 تمامًا في اليوم 12. بالمقابل، فشلت الجروح غير المعالجة و PPcontrol والضمادات الفضية في الإغلاق حتى بعد أسبوعين. كانت هناك علامات على وجود صديد ونخر ملحوظة على الجروح الضابطة غير المعالجة، مما يشير إلى تكوين الأغشية الحيوية والالتهاب المستمر طوال الدراسة (الشكل 5د، الشكل التكميلي 10أ). أظهرت الجروح الضابطة غير المعالجة علامات على التدهور وعرضت أدلة على إعادة العدوى (الشكل التكميلي 10أ).
استخدمنا أيضًا فرز الخلايا المعتمد على الفلورسنت (FACS) لتحديد نسبة الخلايا (أي الكريات البيضاء، التي تشمل وحيدات، العدلات، الخلايا الحبيبية والبلعميات) في الجروح بعد يومين من العلاج. احتوت الجروح غير المعالجة المصابة (التحكم) على تجمعات مرتفعة من الخلايا الحبيبية (الشكل 5هـ، الشكل التكميلي 11). ومع ذلك، لم تظهر الجروح المصابة المعالجة بهلام PPN(C4)-1 زيادة في الخلايا الالتهابية (CD11b ) فوق المستويات التي لوحظت في الجروح غير المصابة الضابطة، مما يشير إلى أن ضمادة الجروح الهلامية PPN(C4)-1 قد تقلل من تدفق الخلايا الالتهابية الناتجة عن العدوى من خلال القضاء على البكتيريا من موقع الجرح. بالمقابل، لم يؤثر العلاج بالضمادة الفضية على عدد الخلايا في الجروح (الشكل 5هـ،
الشكل التكميلي 11)، مما يُعزى على الأرجح إلى عدم فعاليتها في إزالة البكتيريا (الشكل 5أ).
تم استخدام اختبار المناعية المرتبط بالإنزيم (ELISA) لتحديد تركيز عوامل شفاء الجروح ذات الصلة الموجودة في إفرازات الجروح بعد يومين من العلاج. كان تركيز البرو- MMP9 (السابقة لـ MMP9)، الذي يضر بشفاء الجروح , مرتفعًا في الإفرازات من الجروح غير المعالجة المصابة، و PPcontrol، والجروح المعالجة بالضمادة الفضية (الشكل 5و). من المثير للاهتمام، أن الإفرازات من الجروح المعالجة بهلام PPN(C4)-1 احتوت على مستوى منخفض بشكل ملحوظ من البرو- MMP9 (الشكل 5و). علاوة على ذلك، وُجد أن تركيزات عوامل شفاء الجروح المختلفة (VEGF-A، PDGF-BB، FGF-2 و EGF) التي تم قياسها بواسطة ELISA كانت أعلى بشكل ملحوظ في الجروح المعالجة بـ PPN(C4)-1 مقارنة بالجروح الضابطة غير المعالجة المصابة، و PPcontrol، والجروح المعالجة بالضمادة الفضية (الشكل 5ز-ي).
درسنا أيضًا تأثيرات شفاء الجروح المصابة في vivo لهلام PPN و PP-N. مقارنةً بـ PPN(C4)-1، أظهر PPN- (الذي لا يحتوي على NAC في الشبكة) إغلاقًا أبطأ للجروح المصابة بـ MRSA بدءًا من اليوم 7 فصاعدًا (الشكل 5د)، على الرغم من أن كلا الهلامين يحتويان على نفس كمية PIM(C4)-Mal المدمجة. قد يُعزى ذلك إلى عدم وجود NAC في PPN-، مما يؤكد انخفاض التعبير عن عوامل النمو (تحديدًا VEGF-A و PDGF-BB و FGF-2) في إفرازات الجروح مقارنةً بـ PPN(C4)-1 (الشكل التكميلي 12). بالإضافة إلى ذلك، بدون وجود PIM(C4)-Mal في الشبكة، لا يعمل PP-N بشكل جيد مثل PPN(C4)-1 في مساعدة إغلاق الجروح المصابة بـ MRSA بدءًا من اليوم 7 فصاعدًا (الشكل 5د) بسبب عدم وجود وظيفة مضادة للميكروبات. كما أظهرت الجروح المعالجة بـ PP-N انخفاضًا في التعبير عن عوامل النمو VEGF-A و EGF،
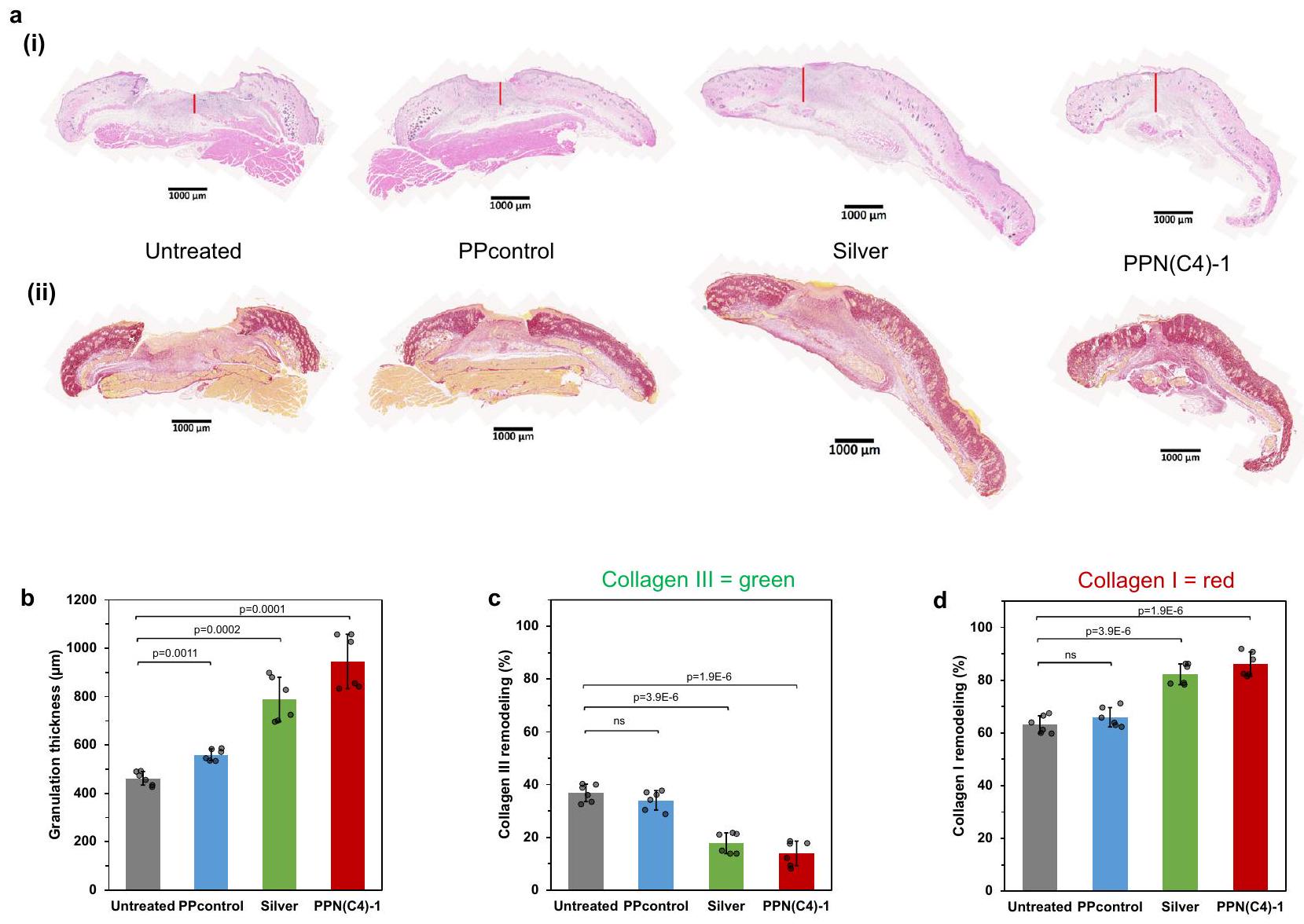
الشكل 6 | علم الأنسجة للجروح في نموذج الفأر السكري المعالج بعد 24 ساعة من العدوى بـ MRSA USA300 باستخدام أفلام الهلام. أ صور تمثيلية توضح (ط) H&E و (ii) أقسام الأنسجة الملونة بالبيكروسيرياس الحمراء للجروح الضابطة غير المعالجة، والضمادة الفضية، و PPcontrol، والجروح المعالجة بهلام PPN(C4)-1 في اليوم 7 بعد العلاج. مقياس الرسم تقدير سمك تشكيل الأنسجة الحبيبية بناءً على
عينات الجروح النسيجية التي تم جمعها في اليوم 7 بعد العلاج. تقدير (ج) الكولاجين III (الكولاجين غير الناضج، الملون بالأخضر) و (د) الكولاجين I (الكولاجين الأصلي، الملون بالأحمر) والترسيب وإعادة تشكيل في عينات الجروح النسيجية التي تم جمعها في اليوم 7 بعد العلاج. ( الفئران، اختبار ستودنت ذو طرفين ، البيانات مقدمة كقيم متوسطة SD).
على الرغم من عدم وجود PDGF-BB و FGF-2، والتي قد تُعزى إلى نقطة قياس مبكرة جدًا (يومين من العلاج، الشكل التكميلي 12). تظهر هذه النتائج أن الهلام ثنائي الوظيفة PPN(C4)-1 يسهل إغلاق الجروح بشكل أسرع وزيادة التعبير عن عوامل النمو مقارنةً بالهلام التي تحتوي على أحد المكونات النشطة البيولوجية فقط.
بعد 7 أيام من العلاجات، قمنا بإجراء تقييمات هيستولوجية باستخدام صبغة H&E على أنسجة الجروح. بالمقارنة مع الجروح غير المعالجة والجروح المعالجة بـ PPcontrol، أظهرت الجروح المعالجة بالفضة وPPN(C4)-1 هيدروجيل زيادة ملحوظة في سمك أنسجة التكوين (المعلمة بخط أحمر عمودي في الشكل 6a(i))، مما يشير إلى تعزيز الشفاء مع زيادة تكاثر الكيراتينocytes والأرومات الليفية (الشكل 6b). غالبًا ما يُلاحظ أنسجة التكوين الأكثر سمكًا، التي تتكون من الأرومات الليفية المتكاثرة، والأوعية الدموية، والمصفوفة خارج الخلوية، خلال عملية الشفاء الطبيعية للجروح.يوفر نسيج التجرانولاسيون هيكلاً لهجرة وتكاثر الخلايا الكيراتينية.وجود نسيج حبيبي أكثر سمكًا يشير إلى عملية شفاء جروح نشطة، مما قد يدل على تحسين تكاثر الكيراتينocytes. علاوة على ذلك، أظهرت الجروح المعالجة بهلام PPN(C4)-1 وجود لسانات ظهارية أكثر تطورًا مقارنةً بمجموعات العينات الأخرى (الشكل 6a(i)، الشكل التوضيحي 13)، مما يدل على زيادة تكاثر وهجرة الكيراتينocytes. تؤكد هذه الملاحظة أيضًا التأثير الإيجابي لعلاج هلام PPN(C4)-1 على شفاء الجروح. كما قمنا بتحليل إعادة تشكيل الكولاجين في أنسجة الجروح بعد 7 أيام من العلاجات باستخدام صبغة بيكروسيرياس الحمراء (الشكل 6a(ii)، الشكل التوضيحي
الشكل 14). في الجروح غير المعالجة والجروح المعالجة بهلام PPcontrol، كان الكولاجين من النوع الثالث، الذي يعد غير ناضج ويتشكل خلال عملية الشفاء الأولية لإغلاق الجرح وحمايته من البيئات الخارجية، يشكل حوالي 33-37% من إجمالي الكولاجين (الشكل 6c). على العكس، في الجروح المعالجة بهلام الفضة وPPN(C4)-1، تم استبدال معظم الكولاجين من النوع الثالث بالكولاجين الأكثر نضجًا من النوع الأول، الذي يشكل 82-86% من إجمالي الكولاجين (الشكل 6d). تشير هذه التحولات نحو كولاجين أكثر نضجًا في الجروح المعالجة بهلام PPN(C4)-1 إلى تعزيز إغلاق الجروح وأيضًا النضوج الأساسي لأنسجة الجروح، مما يعزز التجديد العام للبشرة الصحية.
باختصار، أظهر نموذج الجروح الجلدية ثلاثي الأبعاد خارج الجسم توافقًا حيويًا جيدًا للهلاميات المستندة إلى PIM(C4)-Mal في أنسجة الجلد البشرية المعاد بناؤها وتعزيز شفاء الجروح (حتى بدون عدوى) بواسطة NAC. لم يتسبب إضافة PIM(C4) المرتبط تساهميًا إلى الهلاميات في سمية كبيرة ولم يؤثر على التوافق الحيوي للهلاميات المشتقة من PEG. في الجروح المصابة للفئران المصابة بالسكري، قلل الهلام ثنائي المكونات PPN(C4)-1 بشكل كبير (تقليل اللوجاريتم) بكتيريا البيوفيلم متعددة المقاومة إيجابية الجرام وسلبية الجرام. علاوة على ذلك، تسارع PPN(C4)-1 إغلاق الجروح المصابة بـ MRSA في نموذج الفئران السكري وتسبب في زيادة تعبير عوامل شفاء الجروح، مثل VEGFA و PDGF-BB و FGF-2 و EGF، مقارنةً مع الضمادة الفضية و PPcontrol أو ظروف السيطرة المصابة غير المعالجة (الشكل 5b-j). حدث القضاء على البكتيريا في دراسة الفئران السكري الحية في الفترات الزمنية المبكرة (الأيام الثلاثة الأولى) من العلاج مع PPN(C4)-1. وبالتالي،
الجدول 2 | تركيبات ألياف Alg-PPN(C4) في 1 مل من الماء المقطر
تركيبة الألياف
ألج-ش
PIM(C4)-مال
PEG-2Mal-2NAC
PEG-4مال
NAC
الخوارزم
50 ملغ
–
–
–
ألج-PPN(C4)-0.1
50 ملغ
0.1 ملغ
ألج-PPN(C4)-1
50 ملغ
1 ملغ
ألج-PPN(C4)-5
50 ملغ
5 ملغ
ألج-PPN(C4)-10
50 ملغ
10 ملغ
إضافة كل من PIM(C4) و NAC مهمة لإزالة البكتيريا وشفاء الجروح على التوالي.
نظرًا لأن العديد من الجروح المزمنة عميقة إلى حد ما، فإن الضمادات بتنسيق الفيلم ليست مثالية لمثل هذه الجروح، فقد قمنا أيضًا بإنتاج ألياف هيدروجيل الألجينات المرتبطة تساهميًا مع PPN، والتي يمكن أن تملأ الجروح العميقة وتت conform إلى أسطحها. تم إعداد سلسلة من تركيبات الألياف باستخدام Alg-SH و PEG-4Mal و PIM(Cn)-Mal.، أو 10 )، و NAC في ماء DI (الجدول 2). تُسمى هذه الألياف الهلامية Alg-PIM(Cn)-PEG-NAC-x (Alg-PPN(Cn)-x)، حيث يشير اللاحقة (x) إلى تركيز PIM(Cn)-Mal ( ) (الجدول 2). تم تحضير PIM(Cn)-Mal الخطي مع روابط ألكيل (Cn) مختلفة تتراوح من البيوتان (C4) إلى الديكين (C10) مسبقًا وتم فحص حلول PIM(Cn) (الشكل التكميلي 1). تحتوي حلول PIM(Cn) المختلفة على تأثيرات مختلفة ضد الأغشية الحيوية (الشكل التكميلي 15)؛ بالإضافة إلى الأشكال السائلة من PIM(C4) وPIM(C8) وPIM(C10)، تم تحويلها أيضًا إلى ألياف Alg-PPN للاختبار.
باختصار، تم تعديل PEG-4Mal ذو الأربعة أذرع مسبقًا باستخدام 2 مكافئ من NAC لتحويل، في المتوسط، 2 من أذرع PEG لكل سلسلة إلى نهايات NAC لإنتاج PEG-2Mal-2NAC (الشكل 1c، الشكل التوضيحي 2a). تم تفاعل الألجينات المعدلة بالثيول (Alg-SH) مسبقًا مع PIM(Cn)-Mal لإنتاج Alg-SH-PIM(Cn) (الشكل 1c، الشكل التوضيحي 2b). بعض مجموعات الثيول ظلت غير متفاعلة في Alg-SH-PIM(Cn) لتفاعلات النقر اللاحقة، وتم قياسها (الشكل التوضيحي 16). تم تفاعل Alg-SH-PIM و PEG-2Mal-2NAC بشكل إضافي عبر تفاعل الثيول-ماليميد لتشكيل محلول Alg-PPN (الشكل 1c)، والذي تم تجلطه فيحمام للحصول على ألياف Alg-PPN. تم إنتاج تحكم ألياف ألجينات (المعلمة كـ Alg) عن طريق ضغط محلول Alg-SH إلى الحمام (الجدول 2). تم غسل الألياف المحضرة جيدًا في الماء المقطر مع استخدام الموجات فوق الصوتية وتجفيفها في الإيثانول. أظهرت ألياف الهيدروجيل مجموعة من قوى الشد وإجهادات الشد (التمدد) بنسبة 27-34% (الشكل 2c(ii)، d(ii)). وُجد أن كمية مكونات PIM و NAC و PEG القابلة للاستخراج بعد الغسيل كانت أقل من، و من مكونات PIM و NAC و PEG الأولية على التوالي (الأشكال التكميلية 17-18، الجدول التكميلية 3-5). كما استخدمنا ألياف ألجينات تجارية (موسومة كـ Alg-Com) وألياف ألجينات تحتوي على فضة تجارية (Alg-Ag) كعينات تحكم.
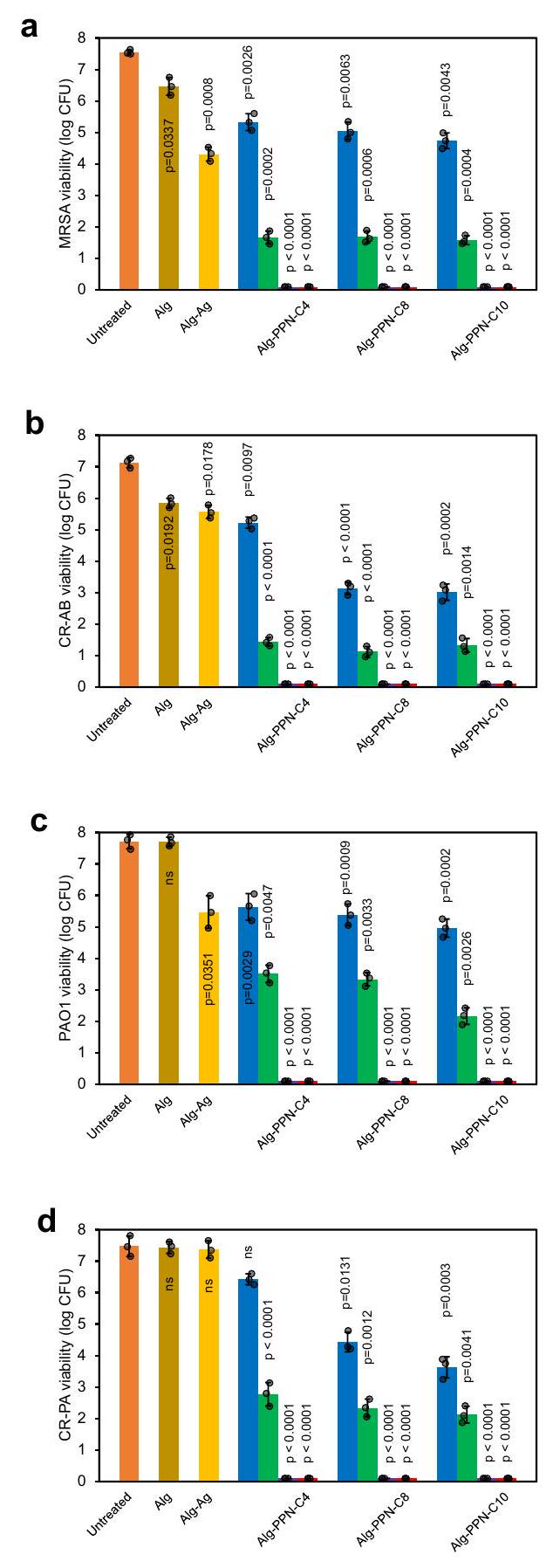
تم قياس فعالية قتل الاتصال للألياف Alg-PPN والألياف الضابطة في المختبر ضد أنواع مختلفة من البكتيريا المقاومة للأدوية المتعددة (MDR) من السلالات سالبة الجرام وإيجابية الجرام، وبالتحديد MRSA USA300 و PAO1 و CR-PA و CR-AB. لم تظهر ألياف Alg-Com والألياف الضابطة Alg خصائص قاتلة للبكتيريا (الشكل 7a-d). قامت ألياف Alg-PPN(Cn)-5 و Alg-PPN(Cn)-10 بالقضاء تمامًا (في ساعة واحدة) على بكتيريا MRSA USA300 و CR-AB إيجابية الجرام، بالإضافة إلى بكتيريا PAO1 و CR-PA سالبة الجرام، التي تم تلقيحها على الألياف (الشكل 7a-d، الجداول التكميلية 6-8). لم تقضِ ألياف Alg-PPN(Cn)-0.1 و Alg-PPN(Cn)-1 على البكتيريا بشكل كامل (الشكل). )، ربما بسبب التركيز المنخفض للمضاد الحيوي النشط PIM(Cn)-Mal المرتبط بالألياف.
تمت دراسة فعالية الألياف المضادة للفيلم الحيوي تجاه الأفلام الحيوية المتكونة مسبقًا. لم تظهر ألياف Alg-Com وألياف Alg التحكم أي نشاط مضاد للفيلم الحيوي تجاه البكتيريا الموجبة والسالبة الجرام المختبرة (الشكل 7e-h). أظهرت ألياف Alg-PPN(C4) نطاقًا من 1.39-3.81 تقليل في اللوج تجاه فيلم MRSA الحيوي (الشكل 7e، الجدول التكميلية 9) بسبب وجود المكون النشط PIM(C4)-Mal في الألياف. ألياف Alg-PPN(C8)، التي تحتوي على المزيد من ذرات الكربون الألكيلية في PIM المكون، أظهر نطاق تقليل لوج أعلى ضد أغشية بيوفيلم MRSA يتراوح بين 1.84-6.80، اعتمادًا على تركيز PIM(C8) (الشكل 7e، الجدول التكميلي 10). أزالت ألياف Alg-PPN(C10)-5 وAlg-PPN(C10)10 أغشية بيوفيلم MRSA تمامًا (الشكل 7e، الجدول التكميلي 11). تم ملاحظة هذه الاتجاه أيضًا في اختبارات مضادات البيوفيلم تجاه بكتيريا CR-AB وPAO1 وCR-PA (الشكل 7f-h، الجداول التكملية 9-11)، مما يوضح فعالية Alg-PPN في مكافحة بكتيريا البيوفيلم المتنوعة.
تمت دراسة التوافق الحيوي في المختبر للألياف ضد خلايا الفيبروبلاست الفأري 3T3 وخلايا الفيبروبلاست الجلدية البشرية (HDFs) باستخدام مستخلصات السائل الفائق والاتصال المباشر مع ألياف Alg-PPN(Cn). كانت نسبة بقاء خلايا HDF و3T3 المعرضة لمستخلصات ألياف Alg-PPN(C4) مرتفعة، في نطاق و على التوالي (الشكل التكميلي 19أ، ب). تشير هذه النتائج إلى أن ألياف Alg-PPN(C4) ذات شحنة موجبة وقليلة التسرب. بعد فترة من الاتصال مع ألياف AlgPPN(C4)، كانت نسبة بقاء الخلايا من خلايا HDF وخلايا 3T3 في نطاق و ، على التوالي (الشكل التكميلي 19أ، ب)، مما يشير إلى انخفاض السمية الخلوية الحادة للألياف. كانت حيوية خلايا 3T3 المتلامسة مع Alg-PPN(C8)-x (لـ ) و Alg-PPN(C10)- (لـ ) كانت (الشكل التوضيحي التكميلي 19c، d).
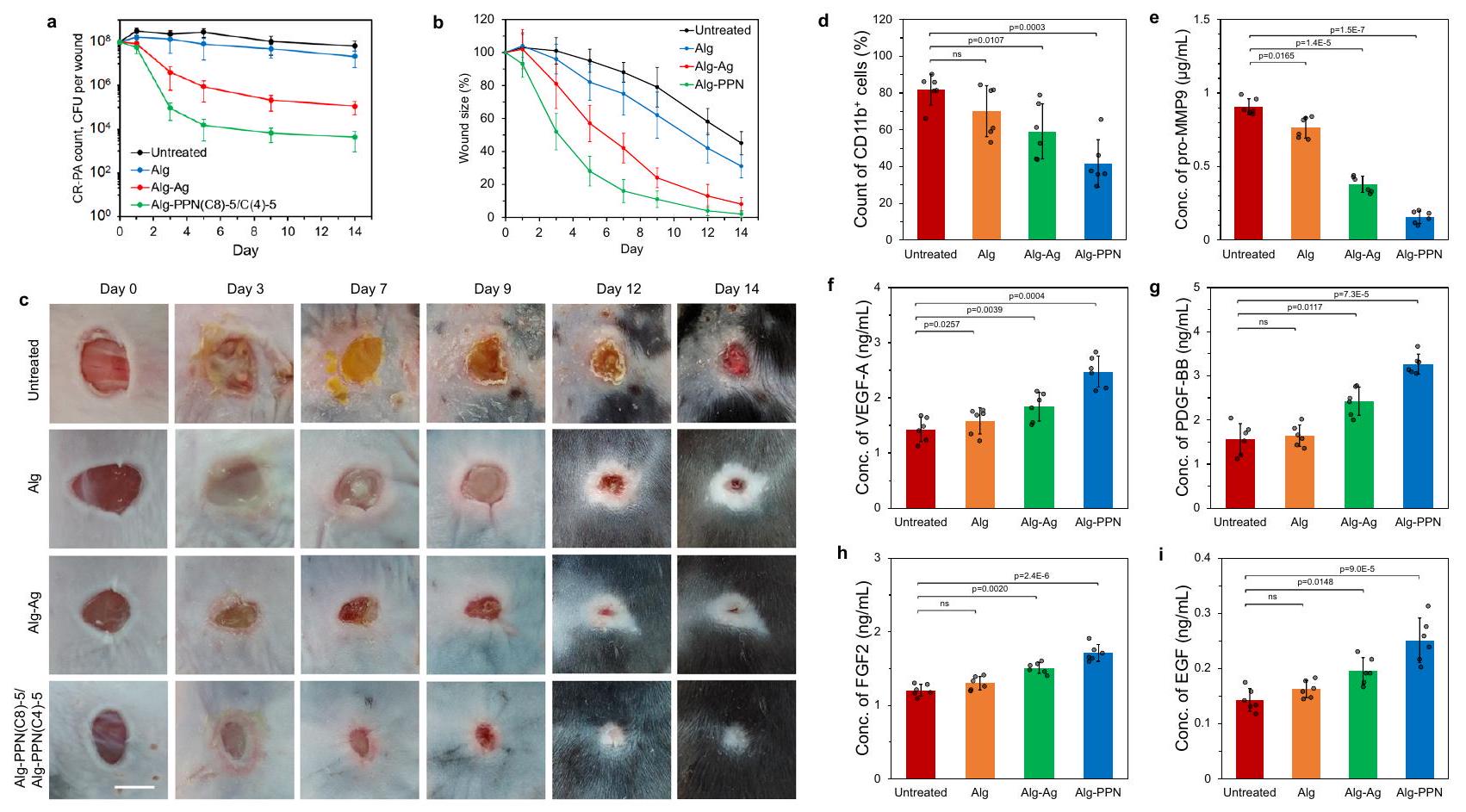
في التحليلات المخبرية المذكورة أعلاه، حقق Alg-PPN(C8)-5 تقليلاً لا يقل عن 4 لوج من البكتيريا الحيوية المقاومة للأدوية من نوع جرام إيجابي وجرام سلبي مع سمية خلوية منخفضة. لذلك اخترنا هذه التركيبة لدراسات التحقق في الجسم الحي باستخدام الفئران. قمنا بدراسة شفاء الجروح المصابة ببكتيريا CR-PA من نوع جرام سلبي في الفئران المصابة بالسكري التي تم علاجها بـ Alg التحكم، والجيلاتين التجاري المحتوي على الفضة (Alg-Ag)، وألياف AlgPPN على مدى فترة أسبوعين. بالنسبة لمجموعة علاج Alg-PPN، تم تطبيق Alg-PPN(C8)-5 (الذي يحتوي على PIM(C8)) على الجرح حتى اليوم الخامس للقضاء على البكتيريا، تلاه استبداله بـ Alg-PPN(C4)-5 (الذي يحتوي على PIM(C4)) من اليوم الخامس إلى اليوم الرابع عشر. لوحظ أكبر انخفاض في عدد بكتيريا CR-PA في الجروح المعالجة بألياف Alg-PPN(C8)-5 خلال الأيام الخمسة الأولى. كانت الجروح المعالجة بألياف Alg-PPN أصغر، مع أدلة قليلة على النخر، مقارنةً بالجروح غير المعالجة، وجروح Alg، وجروح AlgAg في جميع النقاط الزمنية. لوحظ القيح والنخر على الجروح غير المعالجة، مما يدل على تكوين حيوي واستمرار الالتهاب. كما هو الحال في اختبارات هيدروجيل PPN المقابلة، تدهورت الجروح غير المعالجة وأظهرت أدلة على إعادة العدوى. بعد فترة أسبوعين، أغلقت الجروح تمامًا لمجموعة Alg-PPN المعالجة ولكنها لم تغلق للمجموعات الأخرى.
لتقييم تأثير علاجات الضمادات على تسلل خلايا المناعة، قمنا بتوصيف تجمعات خلايا المناعة في أنسجة الجروح بعد يومين من العلاج. أظهرت الجروح المصابة غير المعالجة أعلى نسبة منالخلايا الالتهابية (الشكل 8د). الجروح المصابة التي تم علاجها بألياف Alg-PPN أظهرت أدنى نسبة منالخلايا، تليها الجروح المعالجة بألياف Alg-Ag (الشكل 8d، الشكل التوضيحي 21b-e). النسبة المنخفضة منتشير الخلايا إلى أن عددًا أقل من الكريات البيضاء تسللت إلى الجروح لمحاربة العدوى في الجروح المعالجة بألياف Alg-PPN، مما أدى بالتالي إلى استجابة التهابية أقل في أنسجة الجروح. معظم هذه CD11bالخلايا في مجموعة معالجة ألياف Alg-PPN كانت كريات دم بيضاء من نوع Ly6G (الشكل 8d، الشكل التوضيحي 21a)، مما يشير إلى تقليل الحادة
الشكل 7 | الأنشطة المضادة للبكتيريا والمضادة للأغشية الحيوية لهلام الألياف. قابلية (أ-د) البكتيريا العائمة و(هـ-ح) الأغشية الحيوية لـ (أ، هـ) MRSA، (ب، و) CR-AB، (ج، ز) PAO1، و(CR-PA بعد حضانة الاتصال مع سطح Alg-PPN(Cn)-0.1 (أزرق)، Alg-PPN(Cn)-1 (أخضر)، Alg-PPN(Cn)-5 (برتقالي)، وAlg-PPN(Cn)-10 (أحمر)
e
ف
الألياف في ( عينات مستقلة بيولوجياً، اختبار ستودنت ذو الطرفيناختبار،القيم تشير إلى فرق كبير مقارنةً بالضوابط غير المعالجة، البيانات مقدمة كقيم متوسطةكانت فترات الاتصال ساعة واحدة للبكتيريا العائمة و24 ساعة للأغشية الحيوية.
استجابات التهابية في أنسجة الجروح. (Ly6G هو علامة محددة لعدلات الفئران.) كانت نسبة خلايا Ly6G في الجروح المعالجة بـ Alg-PPN أقل أيضًا من تلك في الجروح المعالجة بـ Alg-Ag (الشكل التوضيحي 21a). تشير هذه النتائج إلى فعالية Alg-PPN مقارنةً بـ Alg-Ag في قتل البكتيريا في موقع الجرح، مما يخفف من الأعباء البيولوجية على الجروح المصابة لتسريع الشفاء. تعتبر العدلات من بين أولى خلايا المناعة التي تصل إلى مواقع الجروح. وبالتالي، بالنسبة للمجموعات غير المعالجة ومجموعة التحكم Alg، كانت النسب العالية من CD11bالخلايا ولكن انخفاض عدد العدلات الإيجابية لـ Ly6G يشير إلى أن الالتهاب قد تقدم إلى ما بعد المرحلة المبكرة.
نتيجة أخرى للاختراق الحاد لخلايا المناعة، وخاصة العدلات، هي إطلاق وتفعيل البروتيازات. قمنا بقياس تركيز البرو-MMP9 (منتج محدد من البلعميات).وسابق لمادة MMP9 ) باستخدام ELISA وتم الكشف عن أعلى التركيزات في الجروح غير المعالجة بسبب الإفراط في إنتاج نظام الاستجابة الفطرية لمكافحة الكمية الكبيرة من البكتيريا. الجروح المعالجة بألياف Alg-PPN أظهرت مستوى منخفضًا بشكل ملحوظ من pro-MMP9 (الشكل 8e)، مما يدل على الفعالية العالية لـ Alg-PPN في قتل البكتيريا. الجروح المعالجة بألياف Alg-Ag أظهرت أيضًا تركيزات منخفضة بشكل ملحوظ من pro-MMP9،
الشكل 8 | دراسة شفاء الجروح الكاملة لجروح مصابة بالسكري في الفئران مع علاج ألياف الهيدروجيل بدءًا من 24 ساعة بعد الإصابة. أعداد البكتيريا من CR-PA في الجروح غير المعالجة، وألياف Alg، وألياف Alg-Ag، وألياف Alg-PPN المعالجة في الأيام و 14 بعد العلاج ( فئران).أحجام الجروح لعلاج التحكم غير المعالج، ألغ، ألغ-فضة، وألغ-PPN على الجروح المعالجة في أيام مختلفة كنسبة مئوية من حجم الجرح الأوليالفئران).المظهر البصري للجروح المعالجة بألياف التحكم غير المعالجة، وألياف الخوارزمية، وألياف الخوارزمية مع الفضة، وألياف الخوارزمية مع PPN بين تغيير الضمادات. شريط القياستوصيف أنسجة الجروح. قياسات في الفئران المصابة بداء السكري والمصابة بـ CR-PAفئران، اختبار ستودنت ذو الذيليناختبار) في اليوم الثاني بعد العلاج:نسبة منالخلايا في الجروح. نسبةتكون خلايا الجلد متناسبة طردياً مع مدى الالتهاب في الجلد. تركيز البرو-MMP9 في الجروح. تركيزات عوامل شفاء الجروح (f) VEGF-A، (g) PDGF-BB، (h) FGF-2 و(i) EGF في الجروح. تُعرض البيانات كقيم متوسطة.SD. على الرغم من أن ذلك كان بدرجة أقل من Alg-PPN. تم قياس تركيزات عدة عوامل رئيسية في شفاء الجروح (VEGF-A، PDGF-BB، FGF-2 وEGF) لتكون الأعلى في الجروح المعالجة بألياف Alg-PPN (الشكل 8f-i)، مما يتوافق مع معدل الشفاء الأسرع في هذه المجموعة مقارنةً بالمجموعة الضابطة غير المعالجة، وAlg، والجروح المعالجة بـ Alg-Ag.
نقاش
تكون الجروح الناتجة عن السكري عادة ملتهبة بشكل مزمن بسبب العدوى البكتيرية، مما يؤدي غالبًا إلى ارتفاع مستويات الأنواع التفاعلية من الأكسجين (ROS).تتضافر هذه العوامل لتقليل نشوء وإصلاح الأوعية الدموية، وتقليل تخليق وتوصيل عوامل شفاء الجروح، وتسبب الفشل في إدارة الحمل البيولوجي على الجروح. هنا، قمنا بتطوير هيدروجيل (يسمى PPN) يحتوي على مكونين حيويين يوفران وظائف تآزرية لتخفيف العدوى وإخماد ROS المفرط مما يؤدي إلى تسريع إغلاق الجروح المصابة لدى مرضى السكري. علاوة على ذلك، فإن مكون N-acetylcysteine (NAC) لدينا (حتى في نموذج الجرح غير المصاب) يعزز مباشرة تكاثر الكيراتينوسيت وتمايز الكيراتينوسيت الحرشفي، مما يؤدي إلى إعادة تكوين الظهارة بشكل أكثر سمكًا.
في عملنا السابق على الهلاميات الهيدروجينية الكاتيونية التي لها خصائص مضادة للبكتيريا ولكنها ليست مخصصة لشفاء الجروحاكتشفنا أن الهلام الكاتيوني يقتل البكتيريا عن طريق (1) امتصاصها في مساحات مسامه (عبر قوة السحب الهيدروديناميكية الناتجة عن تبخر الماء من الهلام وإعادة ترطيبه لاحقًا)، تليها (2) قتل البكتيريا عن طريق الاتصال بواسطة البوليمرات الكاتيونية لجدران المسام. يمتص الهلام الكاتيوني هنا أيضًا البكتيريا في مساحات مسامه ثم يقتلها عن طريق الاتصال عبر جدران مسام الهلام الكاتيوني..
آلية شفاء الجروح المعجلة في الهيدروجيل ثنائي الوظيفة لدينا تنبع من تآزر إزالة البكتيريا بواسطة الهيدروجيل الكاتيوني المتشابك الذي يؤدي بدوره إلى تقليل الاستجابة الالتهابية، جنبًا إلى جنب مع الخصائص المضادة للأكسدة لـ NAC. أولاً، يقوم ضماد الهيدروجيل PPN بإزالة والقضاء على البكتيريا من موقع الجرح. تؤدي إزالة البكتيريا من الموقع إلى تقليل كبير في تدفق الخلايا الالتهابية المرتبطة عادةً بالعدوى، كما يتضح من المستوى المثبط لـالخلايا في جروح الفئران المصابة المعالجة بهلام PPN(C4)-1 مقارنة بالجروح غير المعالجة (الشكل 5e، الشكل التوضيحي 11). ثانياً، يقلل NAC من مستويات ROS التي تكون مرتفعة في الجروح المزمنة.بينما تنتشر في هيدروجيل PPN وتُخمد. NAC، وهو سلف للجلوتاثيون (GSH)، يمكن أن يحل محل وظيفة GSH في الأنسجة. مضاد الأكسدة NAC يعادل الجذور الحرة، يقلل من الإجهاد التأكسدي والالتهاب، ويعزز الجهاز المناعي.، بحيث يقلل من الالتهاب وتلف الأنسجة بسبب مستويات ROS العالية، ويسمح بالتقدم نحو الشفاء الطبيعي. ثالثًا، يعزز هيدروجيل PPN إمداد عوامل الشفاء الجروح إلى مواقع الجروح، كما يتضح من التركيزات الأعلى بشكل ملحوظ من VEGF-A و PDGF-BB و FGF-2 و EGF في جروح الفئران المعالجة بهيدروجيل PPN(C4)-1 مقارنة بجميع مجموعات العلاج الأخرى (الشكل.يمكن عزو هذا التأثير إلى قمع الوسائط الالتهابية، مثل TNF-alpha و IL-1، الناتج عن انخفاض وجود الخلايا الالتهابية وبكتيريا الأغشية الحيوية.
أخيرًا، فإن دمج مضاد الأكسدة NAC في هيدروجيل PPN يعزز إعادة تكوين الظهارة وتمايز الكيراتينوسيت، كما تم إثباته باستخدام نموذج الجلد البشري المعادل (DED-HSE) الذي تم إزالة البشرة منه ثلاثي الأبعاد (والذي أعيدت فيه زراعة كيراتينوسيت من متبرعين غير متطابقين). أظهرت الجروح غير المصابة المعالجة بـ PP-N (هيدروجيل بدون PIM ولكن مع NAC) زيادة في سمك البشرة عند مقارنتها بالجروح المعالجة بـ
PPcontrol (الجدول التكميلي 2)، يدل على تأثير إعادة الظهارة المعزز الناتج عن دمج NAC. بالإضافة إلى ذلك، عند مقارنتها بمجموعة PPcontrol، أظهرت الجروح غير المصابة المعالجة بهلام PP-N و PPN(C4)-1 كثافة إشارة أقوى بشكل ملحوظ لبروتينات K14 و K10، على التوالي (الشكل 4c والجدول التكميلي 2)، مما يشير إلى أن دمج NAC يعزز التمايز الحرشفي للخلايا الكيراتينية. وبالتالي، فإن الجمع بين NAC والبوليمر المضاد للبكتيريا داخل هلام PPN يعمل بشكل تآزري لتعزيز شفاء الجروح من خلال تقليل مستويات ROS والالتهاب بشكل جماعي.
الهيدروجيل PPN(C4)-1 لدينا أكثر فاعلية في قتل البكتيريا في الأغشية الحيوية مقارنةً بضمادات الجروح التجارية القائمة على الفضة، حتى ضد البكتيريا المقاومة للكاربينيم.. أيروجينوزا و. باوماني (CR-PA و CR-AB)، التي تحتاج بشكل عاجل إلى علاجات مضادة للبكتيريا جديدة. علاوة على ذلك، أظهرت الجروح المعالجة بهلام PPN(C4)-1 احمرارًا طفيفًا، وقمعًا للالتهاب، وتسريعًا في إغلاق الجروح. أكدت نتائج نموذج الفئران السكري أن الهلاميات التي تحتوي على تركيبة PIM و NAC هي الأفضل لإزالة الأغشية الحيوية وتسريع شفاء الجروح، حيث أن العلاج باستخدام PPcontrol (بدون PIM و NAC) لم يقتل البكتيريا بشكل ملحوظ، وشفاء الجروح كان أبطأ (الشكل 5d). أظهرت الهلاميات التي تم تشكيلها بمكون نشط واحد فقط (أي، إما PP-N أو PPN-) شفاءً أبطأ ومستويات منخفضة من عوامل شفاء الجروح (الشكل 5d، الشكل التكميلية 12). تركز العديد من الدراسات حول ضمادات الجروح فقط على جانب واحد من جوانب شفاء الجروح أو نوع واحد من الجروح (مثل الجروح المصابة أو الجروح السكرية).لكن الهيدروجيل لدينا له وظيفتان تؤديان إلى تحسين شفاء الجروح المصابة، مما يلبي الحاجة غير الملباة.
تعتبر الخصائص المضادة للبكتيريا والمضادة للأكسدة ذات الوظيفة المزدوجة الحل الأكثر فعالية الحالي لعلاج الجروح. تم الإبلاغ عن العديد من هذه التركيبات ذات الوظيفة المزدوجة، لكنها تعاني من تسرب كبير، أو ليست فعالة بشكل خاص ضد البكتيريا المقاومة.طور تشو وآخرون شبكة بوليمر شبه متداخلة (sIPN) هيدروجيل بخصائص مضادة للبكتيريا ومضادة للالتهابات يمكن أن تتحلل تمامًا خلال ساعتين بعد تطبيقها على الجروح باستخدام نموذج فئران حية.“. على الرغم من أن الهيدروجيل sIPN كان فعالًا إلى حد ما في قتل الإشريكية القولونية غير المقاومة والمكورات العنقودية الذهبية (أقل من 2 لوج تقليل)، فإن تأثيره المضاد للبكتيريا، الذي يرجع إلى تحلل شبكة حمض الهيالورونيك، يحرر البوليمر الغريب بولي فينيل مع مجموعات إيميدازوليوم كاتيونية متدلية على موقع الجرح. هذا الهيدروجيل القابل للتحلل ليس ضمادة قابلة للاسترجاع، وتبقى كميات كبيرة من البوليمرات المتحللة على الجرح. طور روميرو-مونتيرو وآخرون ألياف نانوية من الهيدروجيل محملة بالمضاد الحيوي كليندامايسين ومضاد الأكسدة بولي (حمض الجاليك)”.. ومع ذلك، فإن إطلاق المضادات الحيوية من هذا المنتج لضمادات الجروح يثير القلق بشأن انتشار مقاومة البكتيريا من خلال نقل الجينات الأفقي. وقد طورت مجموعات أخرى فيلم زيروجيلوغشاء الهيدروجيلالذي يمكن أن يطلق الكيرسيتين بسرعة (خلال 1 أو 2 ساعة)، وهو فلافونويد نباتي تم الإبلاغ عن وجود خصائص مضادة للبكتيريا ومضادة للأكسدة.. ومع ذلك، فقد أظهرت هذه الجل أن لها القدرة على قتل البكتيريا غير المقاومة فقط في المختبر أو معالجة الجروح غير المصابة للفئران غير المصابة بالسكري. بالنظر إلى هذه الدراسات الحديثة، فإن فيلم الألياف الهيدروجيل PPN المستقل ومنخفض التسرب حقق قتل الأغشية الحيوية للبكتيريا متعددة المقاومة (MDR) واسعة الطيف، بالإضافة إلى تسريع إغلاق الجروح المصابة بالأغشية الحيوية لدى مرضى السكري، وهو ما لم يتم إثباته سابقًا.
استخدمنا كيمياء الربط السهل لتفاعل إضافة مايكل بين الثيول والماليميد. لم نجد أي دليل على أن مستخلصات البكتيريا (الشكل التوضيحي التكميلي 6أ، ب) أو سوائل الجروح (الشكل التوضيحي التكميلي 6ج) تقوم بتفكيك هيدروجيل PPN(C4)-1، كما لم نجد دليلًا على تفكيك فيلم هيدروجيل PPN(C4)-1 وألياف هيدروجيل Alg-PPN(C8)-5 على الجروح (الشكل التوضيحي التكميلي 7، الأفلام التكميلية 1-4). تم الحفاظ على السلامة الهيكلية العامة للهيدروجيل بشكل جيد.
يمكن تجميع الهيدروجيل في صيغ متعددة؛ لقد أنشأنا صيغ الأفلام والألياف التي تناسب الاستخدام في العلاج. لجرحى السطحية والعميقة، على التوالي. يُظهر الفيلم الهيدروجيلي المركب فعالية في إزالة الأغشية الحيوية ويسرع شفاء الجروح الجلدية المصابة في الفئران المصابة بالسكري. مع ألياف الألجينات (التي تناسب الجروح العميقة وكذلك السطحية)، احتفظت مكونات PIM و NAC النشطة بيولوجيًا بخصائصها المضادة للبكتيريا والأكسدة في نماذج جروح الفئران. قد تساعد هذه التكنولوجيا في التخفيف من المشكلة المتزايدة للجروح المزمنة والسكري، حيث تقتصر العلاجات الحالية على موانع استخدامها. علاوة على ذلك، يمكن أيضًا تجميع الهيدروجيل عن طريق النسيج الكهربائي أو الطباعة ثلاثية الأبعاد لإنشاء أشكال أو تنسيقات مخصصة تناسب تطبيقات محددة. أخيرًا، يمكن أيضًا استخدام هذا الهيدروجيل في تطبيقات طبية حيوية أخرى، مثل الطلاءات للأجهزة الطبية الحيوية.
باختصار، تقدم دراستنا هيدروجيل متقاطع الربط يحتوي على مكونين حيويين نشطين مرتبطين تساهميًا وبنسبة تسرب منخفضة للغاية: الكاتيون PIM المضاد للبكتيريا ذو الفعالية العالية وNAC المضاد للأكسدة. يظهر الهيدروجيل المركب قدرات فعالة وعريضة النطاق لإزالة الأغشية الحيوية، بينما يسرع أيضًا عملية الشفاء في الجروح المصابة بالسكري. إنه مضاد للبكتيريا ومضاد للأكسدة بشكل جوهري ولا يتطلب عمليات أخرى مثل الإشعاع الضوئي الحراري، مما يجعل هذا الضماد المستقل سهل الاستخدام وآمن. على عكس الضمادات ذات الوظائف المزدوجة السابقة، فإن الهيدروجيل المتقاطع الربط خالٍ تمامًا من المضادات الحيوية القابلة للتسرب، والمركبات المعدنية، وأنابيب الكربون النانوية أو الجسيمات النانوية. تميز هذه الخاصية ذات التسرب المنخفض للغاية عن العديد من ضمادات الجروح التي تطلق الأدوية، مما يعزز بديلاً أكثر أمانًا وتوافقًا حيويًا. يتمتع بسلامة هيكلية جيدة وسهل الإزالة بشكل نظيف من الجروح. علاوة على ذلك، يمكن صنع أشكال مختلفة مثل الأفلام والألياف لتتناسب مع الجروح. تعزز هذه المزايا بشكل كبير راحة المريض وتدعم عملية شفاء غير معقدة.
طرق
المواد
1,4-دايامينوبوتان، 1,6-دايامينوهيكسان، 1,8-دايامينوكتان، 1,10-دايامينوديكين، فورمالديهايد (37%)، جلايكزال (40%)، حمض الأسيتيك، أنهدريد الماليك، بيكربونات الصوديوم،-أسيتيل سيستين (NAC)، ملح الصوديوم لحمض الألجينيك (الألجinate الصوديوم)، إل-سيستين ( ) ، -إيثيل--(3-dيميثيل أمينوبروبيل) كاربودييميد (EDC، 97%)، هيدروكسيد الصوديوم (NaOH)، كلوريد الصوديوم (NaCl)، كلوريد الكالسيوم (حمض الهيدروكلوريك (HCl)، الليسيثين، توين 80، ثيوسلفات الصوديوم، 5,5-ثنائي ثيو-بيس(حمض 2-نيترو بنزويك) (DTNB، 99%)، و3-(4,5-ثنائي ميثيل ثيازول-2-يل)-2,5-ثنائي فينيل تيترازوليوم بروميد (MTT، 98%) تم شراؤها من شركة سيغما-ألدريتش (سانت لويس، ميزوري). بولي(إيثيلين غليكول) رباعي ثيول (PEG-4SH، ) و رباعي ماليميد بولي (إيثيلين جلايكول) (PEG-4mal، تم شراء ( ) من شركة Biochempeg Sci. Inc. (واترتاون، ماساتشوستس). تم شراء الفلورسئين-5-ماليميد (F5M)، محلول ملحي معزز بالفوسفات (PBS)، مرق مولر-هينتون (MHB)، مرق الصويا التربتوكوكسي (TSB)، أجار لوريا-بيرتاني (LB)، مجموعات ELISA لبروتين MMP9 المسبق للفئران (EMMMP9)، VEGF-A (BMS619-2)، PDGF-BB (BMS2071)، FGF-2 (EMFGF2)، وEGF (EMEGF) من شركة Thermo Fisher Sci. Inc. (والثام، ماساتشوستس). CD11b(130-113-231) والأجسام المضادة Ly6G (130-102-296) تم شراؤها من Miltenyi Biotec. الأجسام المضادة أحادية النسيلة الفأرية المضادة لـ K10 (DE-K10) تم شراؤها من Dako (DKO.M7002). الأجسام المضادة أحادية النسيلة الفأرية المضادة لـ K14 (LL001) كانت من السائل الفائق من مختبر E. Birgitte Lane (A*STAR). الأجسام المضادة أحادية النسيلة الفأرية المضادة لـ p63 (4A4) تم شراؤها من Abcam (Ab735). Enterococcus faecium (19434)، Enterobacter cloacae (13047)، Klebsiella pneumonia (13883)، Staphylococcus aureus المقاوم للميثيسيلين (MRSA USA300، BAA-40، و LAC)، Acinetobacter baumannii المقاوم للكاربينيم (CR-AB)، Pseudomonas aeruginosa 01 (PAO1)، المقاوم للكاربينيم. أيروجينوزا (CR-PA)، وخلايا الفيبروبلاست الفأرية القياسية 3T3 تم شراؤها من مجموعة الثقافة الأمريكية (ATCC، ماناساس، فيرجينيا). تم شراء خلايا الفيبروبلاست الجلدية البشرية (HDFs، NHDF-Ad، CC-2511) من لونزا (بازل، سويسرا). كان الإيثانول وثنائي ميثيل سلفوكسيد (DMSO) من الدرجة التحليلية.
تركيب بوليميدازوليوم يحتوي على مجموعات طرفية ماليميد (PIM(Cn)-Mal) تم تخليق PIM(C4)-Mal من خلال الإجراء التالي. تم إذابة 2.974 جرام (33.7 مليمول) من 1,4-ديامينوبوتان في 75 مل من حمض الأسيتيك وتم تبريده في حمام ثلجي. تم استخدام 2.735 جرام (33.7 مليمول) منمحلول الفورمالديهايد و 4.895 جرام (33.7 مليمول) منتم إذابة محلول الجلايوكسال في 37.5 مل من الماء المقطر، وتم إضافة المزيج قطرة قطرة إلى محلول 1،4 -ديامينوبوتان. تم تحريك المزيج الناتج عند 25 درجة.لمدة 24 ساعة، بعد ذلك تم تبخير المذيبات باستخدام جهاز التبخير الدوار. تم إعادة إذابة المنتج المجفف في الماء المقطر، وتمت عملية الغسيل بالماء المقطر لمدة 3 أيام باستخدام غشاء السليلوز المتجدد (MWCO 1 kDa)، وتم تجفيفه بالتجميد للحصول على PIM(C4). تم إذابة 2 جرام (0.7 مليمول) من PIM(C4) في 50 مل من حمض الأسيتيك، ثم أضيفت 0.27 جرام (2.8 مليمول) من أنهدريد المالئيك و0.24 جرام (2.8 مليمول) من بيكربونات الصوديوم. تم تحريك هذا المحلول عندلمدة 24 ساعة، بعد ذلك تم إزالة المذيب باستخدام جهاز التبخر الدوار. تم إعادة إذابة المنتج في الماء المقطر، وتمت عملية الغسيل بالماء المقطر لمدة 3 أيام باستخدام غشاء السليلوز المتجدد (MWCO 2 kDa)، وتم تجفيفه بالتجميد للحصول على PIM(C4)-Mal.الرنين المغناطيسي النووي (NMR) ) ، (الشكل التوضيحي الإضافي 3أ).
PIM(Cn)-مال مع، وتم تخليق 10 باستخدام نفس الطريقة المذكورة أعلاه، مع استبدال الديامينو ألكانات المناسبة بدلاً من 1،4-ديامينوبوتان، أي باستخدام 1،6-ديامينوهكسان لـ PIM(C6)-Mal، و1،8-ديامينوأوكتان لـ PIM(C8)-Mal، و1،10-ديامينوديكين لـ PIM(C10)-Mal.
تحضير أفلام الهيدروجيل (PPN(Cn))
تم تحضير أفلام الهيدروجيل عن طريق صب محاليل مكونات السلف المختلطة باستخدام خلاط دوار. كانت محلول مكون مضاد الأكسدة يحتوي على من PEG-4SH و 2 مللي مول من NAC في الماء المقطر. كانت محلول المكون المضاد للبكتيريا يحتوي على من PEG4 مال و أو من PIM(Cn)-Mal في الماء المقطر. تم خلط هذين المحلولين بحجم متساوي، وتم إيداع كميات من المحلول المختلط بسرعة في آبار لوحة 96 بئر. كانت التركيبة النهائية للهيدروجيل 5% (وزن/حجم) PEG-4SH، 5% (وزن/حجم) PEG-4Mal، 1 مللي مول NAC و أو PIM(Cn)-مال (الجدول 1). تم الاحتفاظ بعينات الهيدروجيل في لمدة 5 دقائق لتشكيل هلام PPN(Cn). ثم أضيفت مياه DI إلى الآبار لتورم الهلام. بعد التورم لمدة 15 دقيقة، تم غسل الهلام ثلاث مرات في الإيثانول وثلاث مرات في مياه DI في حمام بالموجات فوق الصوتية. ) لإزالة جميع المواد الأولية غير المتفاعلة. تم أيضًا صنع هيدروجيلين مشتقين من PPN(Cn) يفتقران إما إلى PIM أو NAC: تم صنع PP-N بدون PIM(Cn)، بينما تم صنع PPN- بدون NAC (الجدول 1). تم أيضًا تحضير هيدروجيل تحكم (PPcontrol) بدون أي وظائف مضادة للأكسدة أو مضادة للبكتيريا، أي فقط 5% (وزن/حجم) PEG-4SH و5% (وزن/حجم) PEG-4Mal.
تركيب الألجينات المفعلة بالثيول (Alg-SH)
تم تخليق Alg-SH باستخدام تفاعل الأميد مع مجموعة الحمض الكربوكسيلي.ألغينات الصوديوموحدات تكرار الألجينات) تم إذابتها في 200 مل من الماء المقطر وتم تنشيطها بإضافة EDC (50 مللي مول). تم تحريك المزيج عندلمدة ساعة واحدة. بعد ذلك، L-سيستين11.4 مللي مول) تم إذابته في 100 مل من الماء المقطر وأضيف إلى خليط التفاعل قطرة قطرة تحت التحريك. خلال الإضافة، تم مراقبة الرقم الهيدروجيني لخليط التفاعل وضبطه على 5 باستخدام محلول هيدروكسيد الصوديوم 2 م. ثم تم تحريك الخليط عندلمدة 24 ساعة. تم غسيل المنتج (MWCO 8 kDa) في ماء منزوع الأيونات يحتوي على 1 مللي مول من حمض الهيدروكلوريك عند. بعد ذلك، تم إجراء دورتين متتاليتين من الغسيل الكلوي في ماء DI يحتوي على و 1 مللي مولار من حمض الهيدروكلوريك. تم تجفيف العينة بالتجميد للحصول على بوليمر Alg-SH. تم تخزين المنتج فيحتى إشعار آخر.
تحضير PEG-2Mal-2NAC
PEG-4مال (تم إذابته في 0.2 مل من الماء المقطر. ثم، 0.1 مل من محلول NAC المائي ) أُضيف قطرة قطرة مع الخلط الدوامي. تم تحريك المزيج للتفاعل لمدة ساعة واحدة لتكوين بوليمر PEG-2Mal-2NAC. مع نسبة مولية تصميم PEG-4Mal:NAC تبلغ 1:2، يؤدي تفاعل النقر الثيولي-ماليميد إلى ارتباط جزيئين من NAC بكل جزيء PEG-4Mal (متوسط إحصائي).
تشكيل ألياف الألجينات المعدلة بـ PIM-Mal و PEG-2Mal-2NAC (Alg-PPN)
ألج-ش ( تم إذابة (مجموعات الثيول) في 0.5 مل من الماء المقطر. ثم، تم تحضير محلول مائي من PIM(Cn)-Mal (، أو 10 ملغ) في 0.2 مل من الماء المقطر تم إضافته بالتنقيط مع التحريك (الجدول 2). تم تحريك المزيج لمدة ساعة واحدة للسماح بالتفاعل بين مجموعة الماليميدومجموعة الثيول من Alg-SH، مما يؤدي إلى بوليمر Alg-SH-PIM(Cn).
لإضافة PEG-2Mal-2NAC إلى Alg-SH-PIM(Cn) بشكل أكبر، تم إضافة 0.3 مل من محلول PEG-2Mal-2NAC بالتنقيط إلى محلول Alg-SH-PIM (الجدول 2) مع التحريك، وتم تحريك المزيج عند 25لمدة ساعة واحدة لتشكيل محلول Alg-PPN(Cn). تم تحميل محلول Alg-PPN(Cn) في حقنة وتم ضغطه من خلال إبرة 25 G إلى حمام سعة 250 مل منمائيالحل. تم تمرير الألياف المتكونة عبرتم غمر الألياف في حمام الإيثانول لإزالة الرطوبة. تم تعريض الألياف للموجات فوق الصوتية في الماء المقطر لمدة ساعة واحدة وغمرها في الماء المقطر لمدة 24 ساعة لغسل المكونات غير المتفاعلة. بعد الغسل، تم إزالة الرطوبة من الألياف في الإيثانول وتجفيفها تحت الهواء المحيط للحصول على ألياف Alg-PPN(Cn).
ديناميات الانتفاخ والخصائص الميكانيكية للهلاميات الفيلم والألياف
قبل اختبار ديناميات الانتفاخ، تم غسل الهيدروجيل بشكل كامل بالماء المقطر ثم تم تجفيفه باستخدام مجفف بالتجميد. تم قياس كتلة الهيدروجيل المجفف بالكامل ككتلة أولية. ثم تم غمر الجل المجفف بالكامل في كمية كبيرة من الماء المقطر ليتورم. كل 5 دقائق، تم إزالة الهيدروجيل من حمام الماء المقطر، وتجفيفه بالتربيت على ورق الترشيح، ووزنه، ثم إعادته إلى حمام الماء المقطر لمتابعة الانتفاخ. تم حساب نسبة الانتفاخ كالتالي:
تم تقييم القوة الميكانيكية للهيدروجيل من خلال إجراء اختبارات الشد أحادية المحور باستخدام نظام اختبار المواد MTS Criterion 43 (إنستران).
اختبار القابلية للتحلل لهلام الفيلم PPN(C4)-1 في مستخلصات بكتيرية
تم تحضير مستخلصات بكتيرية عن طريق هز تركيزات مختلفة من البكتيريا في محلول فوسفات البفر (PBS) عند ودرجة حموضة 7.4 لمدة 24 ساعة، تلتها عملية الطرد المركزي لفصل البكتيريا عن المستخلصات القابلة للذوبان. تم موازنة هلاميات PPN(C4)-1 عن طريق الغمر في PBS لمدة 24 ساعة في طبق 24 بئر، وبعد ذلك تم وزن الكتل الأولية. ثم تم حضن الهلاميات في 1 مل من المستخلص البكتيري عند لمدة 2 أو 7 أيام، بعد ذلك تم وزن الجل.
اختبار القابلية للتحلل لهلام الفيلم PPN(C4)-1 في سوائل الجروح وفي جروح الحيوانات المصابة
لإجراء اختبار الاستقرار في سوائل الجروح، تم هرس نسيج الجرح من الفئران المصابة بسلالة MRSA USA300 أو CR-PA في محلول PBS )، وتم تخفيفه إلى حجم إجمالي قدره 10 مل في PBS. بعد التخفيف، تمت إزالة حطام الأنسجة عن طريق الطرد المركزي. تم موازنة هلام PPN(C4)-1 عن طريق الغمر في PBS لمدة 24 ساعة في طبق 24 بئر، وبعد ذلك تم قياس الكتل الأولية للهلام. ثم تم حضانة الهلام المتوازن في 1 مل من سائل الجرح عند لمدة 2 أو 7 أيام، بعد ذلك تم وزنها. تم تقييم استقرار الهيدروجيل على الجروح المصابة من خلال تصوير هيدروجيل PPN(C4)-1 قبل وبعد التطبيق (لمدة يومين) لعلاج جروح الفئران المصابة بسلالة MRSA USA300.
تحديد محتوى مجموعة الثيول في Alg-SH
تم قياس محتوى مجموعة الثيول في Alg-SH باستخدام التفاعل مع كاشف إيلمان (DTNB). ألج-ش ( تم إذابة Alg-SH (3.52 ملغ) في 0.5 مل من الماء المقطر. بشكل منفصل، تم إذابة DTNB (4 ملغ) في 0.1 مل من PBS عند درجة حموضة محايدة. تم خلط محلول Alg-SH (0.1 مل) ومحلول DTNB (0.1 مل) في 1.8 مل من PBS وتم تحريكه بسرعة 100 دورة في الدقيقة لمدة 20 دقيقة في الظلام. بعد ذلك، تم قياس الامتصاص عند 412 نانومتر باستخدام مطياف الأشعة فوق البنفسجية والمرئية (Shimadzu UV-1800) واستخدم لتحديد تركيز مجموعة الثيول. تم إعداد منحنى المعايرة من خلال تفاعل DTNB مع L-cysteine عند تركيزات محددة مسبقًا. تم التحقق من تحديد محتوى الثيول من خلال تحليل الفلورية عبر تفاعل النقر مع F5M.تم إذابته في 0.5 مل من DMSO. تم خلط محلول Alg-SH ومحلول F5M، وتم تحريكه بسرعة 100 دورة في الدقيقة لمدة 24 ساعة، وتم إجراء عملية الغسيل (MWCO 1 kDa) لمدة 3 أيام في الظلام. بعد التجفيف بالتجميد، تم الحصول على محلول Alg-F5M.تم إعداد ) وتم قياس شدة الفلورية على جهاز قياس الطيف الفلوري شيمادزو RF-6000 تحت طول موجة الإثارة/الإصدارتم إعداد منحنى المعايرة عن طريق قياس شدة الفلورية لـ F5M عند تركيزات محددة مسبقًا.
تحديد معدلات التسرب للمكونات من ألياف Alg-PPN
تم غمر ألياف Alg-PPN(C4) (100 ملغ) في 2 مل من PBS (لاختبار الامتصاص) أو ماء نقي للغاية (لاختبار مطيافية الكتلة) في وتم تحريكها بسرعة 100 دورة في الدقيقة لمدة 24 ساعة. ثم تم جمع 1 مل من السائل الطافي. تم الحصول على كروماتوغرافيا الأيونات المستخرجة (EIC) للسائل الطافي باستخدام جهاز كروماتوغرافيا السائل-مطياف الكتلة (Agilent 6550 iFunnel Q-TOF) مع عمود Acquity UPLC HSS T3 (Waters). تم قياس امتصاص السائل الطافي باستخدام مطياف الأشعة فوق البنفسجية والمرئية (Shimadzu UV-1800). أظهر PEG-4Mal قمة امتصاص عند طول موجي 300 نانومتر. تم إعداد منحنيات المعايرة للمكونات من خلال قياس EIC وامتصاص الطيف لـ PIM(C4) و NAC و PEG-4Mal عند تركيزات محددة مسبقًا.
اختبار التركيز المثبط الأدنى (MIC)
تم زراعة البكتيريا في MHB فيمع اهتزاز مستمر بسرعة 220 دورة في الدقيقة حتى مرحلة منتصف اللوغ. تخفيفات متسلسلة بمعدل الضعف (إلى ) من PIM(C4)-مال في تم تحضير MHB على لوحة 96 بئر. ثم،تعليق بكتيري ) تم إضافته إلى كل بئر يحتوي على محاليل PIM(C4)-Mal. ثم تم حضن اللوحة في لمدة 18 ساعة، وتم قياس الكثافة الضوئية للآبار عند طول موجي 600 نانومتر لتحديد الحد الأدنى من التركيز المثبط (MIC).
اختبار تركيز الحد الأدنى للقضاء على الأغشية الحيوية (MBEC)
تم قياس MBEC باستخدام تقنية قائمة على صفيحة الميكروتيتر. باختصار،تعليق MRSA LAC أو PAO1 (كثافة الخلايا عند ) في TSB تم إضافته إلى لوحة 96 بئر مغطاة بغطاء يحتوي على دبابيس (Innovotech 19111). تم نمو الأغشية الحيوية على غطاء الدبابيس بعد الحضانة في لـبعد إزالة البكتيريا العائمة عن طريق الغسل مرتين بمحلول PBS، تم نقل الغطاء الذي يحتوي على الأغشية الحيوية إلى لوحة تحدي مكونة من 96 بئرًا تحتوي على تخفيفات متسلسلة من محلول البوليمر بحجم إجمالي منفي كل بئر. تم إجراء العلاج فيلمدة 4 ساعات. بعد ذلك، تم غسل غطاء الدبوس بمحلول PBS ونقله إلى لوحة استرداد مكونة من 96 بئرًا تحتوي علىمن المحايد (3% ليثين، 10% توين 80، و0.3% ثيوكبريتات الصوديوم في ماء منزوع الأيونات) في كل بئر. تم إزاحة بكتيريا الأغشية الحيوية من غطاء الدبوس بواسطة الموجات فوق الصوتية ( ) لمدة 30 دقيقة. ثم تم تخفيف البكتيريا المنفصلة بالتسلسل بمعدل 10 أضعاف في PBS ونشرها على أطباق أجار LB. بعد الحضانة في تم عد المستعمرات البكتيرية لمدة 24 ساعة.
نموذج جلد بشري مكافئ للجلد مع إزالة البشرة ثلاثي الأبعاد خارج الجسم (DEDHSE)
زراعة الخلايا. تم الحصول على الكيراتينوسيتات البشرية الأولية من بنك الجلد الآسيوي، A*STAR، بموافقة أخلاقية IRB: B-16-135E. كانت الخلايا مزروعة في وسط نمو كامل (FG) مع ألياف 3T3 المعرضة للإشعاع (i3T3) كخلايا تغذيةباختصار،تم زراعة خلايا التغذية i3T3 مسبقًا في طبق بتري بقطر 10 سم. تم زراعة خلايا التغذية في وسط ديلبيكو المعدل (DMEM، لايف تكنولوجيز، سنغافورة) الذي يحتوي على 10% من مصل العجل الجنيني (FCS، لايف تكنولوجيز، سنغافورة) ومحلول البنسلين/الستربتوميسين عندمعالهواء. بعد تثبيت i3T3، الذي يتطلب حدًا أدنى منمليون خلية كيراتينوسيت بشرية أولية تم زراعتها في كل طبق بتري مع خلايا i3T3، وتم استبدال وسط DMEM بوسط FG جديد. تم الحفاظ على الخلايا في حاضنة عندمعالهواء، وتم استبدال الوسط كلأيام.
تم إنشاء نموذج شفاء الجروح DED-HSE باستخدام الأدمة الخالية من الخلايا المستمدة من جلد الإنسان.باختصار، تم تقليم قطع كبيرة من جلد الإنسان إلىقطع ونقعت في 1 م NaCl طوال الليل، مما أدى إلى الحصول على جلد خالي من الخلايا. ثم تمت إزالة الطبقة الخارجية، وتم وضع حلقات من الفولاذ المقاوم للصدأ المعقمة على الجانب الحليمي من كل جلد خالي من الطبقة الخارجية (DED). الكيراتينوسيتاتتم نقلها إلى كل حلقة موضوعة على DEDs وتم حضنها مع 5%الهواء فيلمدة يومين للسماح بالارتباط. ثم تم نقل العينات المعاد بناؤها إلى واجهة هواء-سائل وتم حضنها لمدة 9 أيام أخرى للسماح بتوسع الطبقة الجلدية.تم إنشاء جرح استئصال سطحي بقطر في DED-HSEs باستخدامتم استخدام أداة أخذ خزعة (إنتيغرا ميلتكس، فيشر ساينتيفيك)، وتم إزالة طبقة البشرة المعاد تشكيلها. ثم تم إجراء علاجات موضعية معقمة عن طريق إضافة الهيدروجيل مباشرة إلى سطح جرح السرير لمدة 4 أيام و 7 أيام.
تلطيخ MTT. تم ملاحظة الهجرة الجانبية للخلايا الكيراتينية القابلة للحياة باستخدام اختبار MTT. تتفاعل الخلايا القابلة للحياة ذات الأيض النشط مع حلقة التترازوليوم لمادة MTT لإنتاج منتج الفورمازان الأرجواني. تم أخذ عينة مجمدة من حجم 10 أضعاف من مخزون MTT. (سيغما M5655) تم تخفيفه في PBS. تم وضع عينات DED-HSE في لوحة تحتوي على 24 بئرًا، وكان يحتوي كل بئر على 1 مل من مادة MTT. تم حضن العينات فيحاضنة هوائية فيلمدة 90 دقيقة للسماح بتكوين منتج الفورمازان. تم التقاط صور لـ DED-HSEs باستخدام ميكروسكوب نيكون SMZ745T. تم إجراء قياس مساحة الجرح غير الملتئم باستخدام برنامج ImageJ.
صبغة الهيماتوكسيلين والإيوزين (H&E). في اليومين 4 و7 بعد الإصابة، تم تثبيت DED-HSEs بعد تحليل MTT في الفورمالين طوال الليل قبل تضمينها في البارافين. مقاطع منتم قطع السمك ونقلها إلى شرائح زجاجية. تم إزالة الشمع من هذه الشرائح باستخدام الزيلين وإعادة ترطيبها في تركيزات متناقصه من الإيثانول قبل صبغها بصبغة هيماتوكسيلين وإيوزين. تم التقاط الصور باستخدام ميكروسكوب أوليمبوس BX43.
التلوين المناعي النسيجي (IHC). تم تثبيت DED-HSEs، وتضمينها، وقطعها إلى شرائح رقيقة، وإزالة الشمع منها وإعادة ترطيبها كما هو موضح أعلاه. ثم تم غمر الشرائح في استرجاع المستضد، محلول سترات بتركيز pH 6.0، وتم إجراء استرجاع المستضد المعتمد على الحرارة فيحمام مائي لمدة 15 دقيقة.تم استخدامه لإخماد البيروكسيداز الداخلي لمدة 30 دقيقة. ثم تم حجب الشرائح وت incubated مع الأجسام المضادة الأولية anti-K10 (1:200)، anti-K14 (1:25)، و anti-p63 (1:50) لمدة ساعتين في درجة حرارة الغرفة. تم غسل الشرائح بمحلول PBS يحتوي علىTween 20 وتم حضنه مع بوليمر مضاد للفأر معلم بالهيدروجين البيروكسايد (HRP) (1:200) وبوليمر مضاد للأرنب معلم بالهيدروجين البيروكسايدالأجسام المضادة الثانوية لمدة ساعة واحدة في درجة حرارة الغرفة. تم تطوير مقاطع IHC باستخدام ركيزة دياامينوبنزيدين (DAB)، وتم صبغ النوى بصبغة الهيماتوكسيلين، وتجفيفها من خلال تركيزات متزايدة من الإيثانول إلى الزيلين، وأخيرًا تم تثبيتها على شرائح زجاجية. تم التقاط الصور باستخدام ميكروسكوب أوليمبوس BX43.
الخصائص المضادة للميكروبات لأفلام وألياف الهيدروجيل في vitro اختبار مضاد للميكروبات تجاه البكتيريا العائمة. تم تلقيح البكتيريا (MRSA USA300، CR-AB، PAO1 أو CR-PA) في MHB (4 مل) وزرعها فيمع الاهتزاز عند 220 دورة في الدقيقة حتى مرحلة منتصف اللوغ. تم جمع البكتيريا المزروعة عن طريق الطرد المركزي وصب السائل الفائق. تم غسل البكتيريا المجمعة ثلاث مرات بمحلول فوسفات البفر (PBS) وتعليقها في محلول PBS بتركيزتم تلقيح عينات من فيلم أو ألياف الهيدروجيل بـمن تعليق بكتيري (يحتوي على ) موزعة بالتساوي على سطح العينة. تم تلقيح طبق بتري بدون فيلم هيدروجيل أو عينة ألياف كعينة تحكم. تم حضن العينات في و الرطوبة النسبية لمدة ساعة واحدة. بعد الحضانة، تم تحرير البكتيريا من العينات عن طريق الغمر في 1 مل من PBS والاهتزاز باستخدام خلاط دوار. تم تخفيف التعليق البكتيري الناتج بالتسلسل بمقدار 10 أضعاف باستخدام PBS في لوحة 96 بئر، وتم زراعتها على أجار LB. تم حضانة أطباق الأجار فيلمدة 16 ساعة، وتم عد المستعمرات البكتيرية. النتائج مُبلغ عنها كالتالي:
اختبار قتل الاتصال بالبيوفيلم. معقمأقسام منتم وضع غشاء بولي كربونات (واتمان، نيو جيرسي) على أطباق أجار LB. تم تحضير تعليق بكتيري في PBS ( ) تحتوي على حوالي تم تلقيح CFU على سطح الغشاء. تم حضن الأغشية فيلمدة 24 ساعة لتشكيل جيل الأغشية الحيوية. ثم تم معالجة الأغشية الحيوية على الغشاء عن طريق الاتصال بعينات الألياف وتم حضنها في لمدة 24 ساعة. تم تحرير البكتيريا عن طريق خلط الغشاء في وسط داي/إنجلي، وتم تخفيفها بالتسلسل بمقدار 10 أضعاف في PBS، ثم تم زراعتها على أطباق أجار LB. تم حضن أطباق أجار LB في لمدة 24 ساعة، وتم عد المستعمرات البكتيرية.
اختبار التوافق الحيوي في المختبر لـ PIM-Mal والهلامات
تم إجراء دراسات التوافق الحيوي على الخلايا الليفية 3T3 من الفئران وخلايا HDF (خلايا الليف البشري المشتقة من الأدمة، NHDF-Ad-Der Fibroblasts، CC2511، لونزا). تم تحضير وسط DMEM مكمل بالكامل بمصل الجنين البقري (FBS،تم استخدام وسط زراعة الخلايا الذي يحتوي على (L-glutamine (1 مليمول) والمضادات الحيوية (بنسلين-ستربتوميسين، 1%).
اختبار MTT لاستخراجات الهيدروجيل. تم وضع عينات من فيلم أو ألياف الهيدروجيل في كل بئر من أطباق 24 بئرًا مع 1 مل من DMEM وتم حضنها فيلمدة 24 ساعة لجمع المستخلصات. تم زراعة خلايا HDF أو 3T3 في 1 مل من DMEM في أطباق 24 بئرًا من كثافة ابتدائية منالخلايا في كل بئر وتم تحضينها فيحاضنة فيلمدة 24 ساعة لالتصاق الخلايا. تم شفط وسط DMEM واستبداله بمستخلصات العينة (أو DMEM جديد للتحكم الإيجابي) لت incubate مع الخلايا فيلمدة 24 ساعة. ثم تم استبدال وسط الثقافة بـ 1 مل من محلول MTT (في DMEM) وتم حضنه فيلـ 4 ساعات لتلوين الخلايا القابلة للحياة. تم شفط محلول MTT برفق، وأضيف 1 مل من ثنائي ميثيل سلفوكسيد (DMSO) إلى كل بئر. بعد 15 دقيقة، تم قياس امتصاص كل بئر عند 570 نانومتر باستخدام جهاز قراءة الميكرو بلايت من نوع Tecan i-control. تم قياس امتصاص DMSO كتحكم فارغ. تم حساب قابلية الخلايا باستخدام المعادلة:
أين، و هي امتصاص العينة، الفراغ، والسيطرة الإيجابية، على التوالي.
اختبار MTT للتلامس المباشر. كانت الإجراءات كما هو موضح أعلاه (اختبار MTT لاستخراج الهيدروجيل)، ولكن بدلاً من غمر الخلايا بمستخلصات السائل الفائق، تم غمر عينات أفلام أو ألياف الهيدروجيل مباشرة في وسط الثقافة في الآبار التي تحتوي على تمت معالجة الخلايا المرفقة لمدة 24 ساعة ثم تمت إزالتها قبل استبدال الوسط بمحلول MTT.
نموذج حي للفئران لعلاج الجروح المصابة في مرضى السكري
تم إجراء جميع دراسات الفئران تحت تنظيم لجنة رعاية واستخدام الحيوانات المؤسسية (IACUC) في جامعة نانيانغ التكنولوجية (NTU) بموجب بروتوكولات معتمدة تحمل الأرقام A18051 و A21023.
تحفيز السكري على الفئران. تم تكييف ذكور الفئران من سلالة C57BL/6 البالغة من العمر ثمانية أسابيع بالصيام لمدة 4 ساعات قبل بدء حقن تحفيز السكري. تم تحفيز السكري باستخدام محلول ستربتوزوتوسين (STZ)، 4 ملغ من STZ مذاب في 1 مل من محلول سترات الصوديوم (50 مليمول) عند درجة حموضة 4، تم حقنه عن طريق البطن بجرعةيوميًا لمدة 5 أيام متتالية. نظام غذائي لتفاقم تقدم مرض الكبد (LIDPAD، المقدم من مختبر N.S. Tan (NTU)) وتم توفير محلول ماء السكروز خلال 5 أيام من الحقن ثم تم تغييره إلى نظام غذائي عادي وماء اعتبارًا من اليوم السادس فصاعدًا. تم قياس مستويات جلوكوز الدم لدى الفئران بعد 3 أسابيع من انتهاء الحقن. تم تقييم الفئران على أنها مصابة بالسكري إذا تجاوز مستوى جلوكوز الدم لديهم.
تعداد الحمل البكتيري على نموذج عدوى جرح الجلد. تم تخدير الفئران وإزالة الشعر منها، وتم إنشاء جرح استئصالي بسمك كامل بقطر على الجلد الظهري والدهون تحت الجلد.. في المجموع، تعليق بكتيري (MRSA USA300، CR-AB، PA01 أو CR-PA عندتم تلقيح CFU في PBS) على الجروح وتركه ليستقر لمدة 10 دقائق قبل تغطية الجروح المصابة بضمادة شفافة من تيغاديرم (3M). تُركت الجروح دون علاج لمدة 24 ساعة للسماح للبكتيريا الملقحة بتكوين الأغشية الحيوية. تم تطبيق فيلم هيدروجيل أو ضمادات ألياف كشرط للعلاج بعد فترة العدوى التي استمرت 24 ساعة. كانت الجروح غير المعالجة بمثابة ضوابط. بعد 24 ساعة، تمت إزالة الضمادات وتم استئصال الجروح (بما في ذلك 5 مم من المنطقة المحيطية). من أجل تصوير الأغشية الحيوية، تم وضع نسيج الجرح المستأصل في PBS (1 مل) وملاحظته باستخدام مجهر LSM 800 المجهري (ZEISS). من أجل عد البكتيريا، تم تجانس نسيج الجرح المستأصل فيمن PBS لإطلاق البكتيريا (تم تخفيف التعليق البكتيري بالتسلسل بمعدل 10 أضعاف باستخدام PBS في لوحة 96 بئر. تم زرع التعليقات المخففة على أجار LB، وتم حضن صفائح الأجار فيلمدة 16 ساعة، بعد ذلك تم عد المستعمرات البكتيرية. اختبار الطالب ذو الذيلينتم استخدام اختبار – للتحليل الإحصائي.
دراسة شفاء الجروح. كما هو موضح أعلاه، تم إنشاء جروح مصابة بسلالات MRSA USA300 أو أغشية CR-PA الحيوية على الفئران. في اليوم 0، تم تأمين الجروح غير المعالجة باستخدام تيغاديرم كتحكم؛ وتم تطبيق فيلم هيدروجيل أو ضمادة ألياف، مؤمنة باستخدام تيغاديرم، على جروح حالة العلاج. تم تصوير الجروح قبل تطبيق الضمادة وفي الأيام و 14 من فترة العلاج، حيث تم استبدال الضمادات بأخرى جديدة. بالنسبة لمجموعة علاج AlgPPN، تم تطبيق Alg-PPN(C8)-5 على الجرح حتى اليوم الخامس للقضاء على البكتيريا، تلاه استبداله بـ Alg-PPN(C4)5 من اليوم الخامس حتى اليوم الرابع عشر. في كل نقطة زمنية، تم قياس حجم الجرح باستخدام برنامج ImageJ ( ) . اختبار ستودنت ذو الذيلين تم استخدام اختبار – لتحليل البيانات الإحصائية. يتم الإبلاغ عن حجم الجرح النسبي كالتالي:
تحليل فرز الخلايا المعتمد على الفلورية (FACS) للخلايا الالتهابية. تم استئصال الجروح (بما في ذلك 5 مم من المنطقة المحيطية) بعد يومين من العلاج في دراسة شفاء جروح الفئران. تم الحصول على تعليقات الخلايا المفردة من عينات الجروح باستخدام جهاز تفكيك gentleMACS (Miltenyi Biotec). تم وسم الخلايا مناعياً بـو Ly6G، وتم إجراء قياس الخلايا باستخدام جهاز قياس التدفق Accuri C6 (BD Biosciences). تم تحليل بيانات السيتومترية باستخدام برنامج FlowJo (الإصدار 7.6.5، Tree Star). تم رسم نتائج التحليل كنسب مئوية متوسطة.خطأ المعيار للمتوسط (SEM، ) . اختبار الطالب ذو الذيلين تم استخدام اختبار – للتحليل الإحصائي.
اختبار الامتصاص المناعي المرتبط بالإنزيم (ELISA) لعوامل الشفاء الجراحي. بعد يومين من علاج دراسة شفاء جروح الفئران، تم استئصال الجروح (بما في ذلك 5 مم من المنطقة المحيطية) وخلطها.من PBS وتم الطرد المركزي لإزالة الأنسجة والبكتيريا. تم اختبار السائل الطافي باستخدام مجموعات ELISA مختلفة (proMMP9، VEGF-A، PDGF-BB، FGF-2 وEGF) وفقًا لبروتوكولات الشركة المصنعة (لونزا). تم رسم النتائج لكل علاج كقيم متوسطة للتركيز.SEM ) . اختبار الطالب ذو الذيلين تم استخدام الاختبار للتحليل الإحصائي.
التحليل النسيجي وصبغ الأنسجة الكيميائية
في اليوم السابع بعد العلاجات، تم التضحية بالحيوانات باستخدامالاختناق. تم استئصال نسيج الجرح، مع النسيج المحيط، بعناية وثبته فيالفورمالين. بعد ذلك، تم تجفيف عينات الأنسجة، وتضمينها في كتل من شمع البارافين، وقطعها إلىأقسام سميكة باستخدام ميكروتوم لايكا (لايكا بيوسيستمز). تم جمع هذه الأقسام على شرائح زجاجية Superfrost Plus (ثيرمو فيشر ساينتيفيك). تم معالجة الأقسام وصبغها بالهيماتوكسيلين والإيوزين (H&E) والبيكروسيرياس الأحمر. تم تصوير الشرائح الملونة باستخدام نظام ميكروسكوب Axio Scan.Z1 (زايس). تم قياس سمك نسيج التئام الجروح ومحتوى الكولاجين باستخدام برنامج ImageJ.
ملخص التقرير
معلومات إضافية حول تصميم البحث متاحة في ملخص تقرير Nature Portfolio المرتبط بهذه المقالة.
توفر البيانات
البيانات التجريبية التي تم توليدها في هذه الدراسة متاحة ضمن المقالة والمعلومات التكميلية. جميع البيانات متاحة من المؤلفين المعنيين عند الطلب.
References
Singer, A. J. & Clark, R. A. F. Cutaneous wound healing. N. Engl. J. Med. 341, 738-746 (1999).
Han, G. & Ceilley, R. Chronic wound healing: A review of current management and treatments. Adv. Ther. 34, 599-610 (2017).
Simoes, D. et al. Recent advances on antimicrobial wound dressing: A review. Eur. J. Pharm. Biopharm. 127, 130-141 (2018).
Eming, S. A., Hammerschmidt, M., Krieg, T. & Roers, A. Interrelation of immunity and tissue repair or regeneration. Semin. Cell Dev. Biol. 20, 517-527 (2009).
Frykberg, R. G. & Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 4, 560-582 (2015).
Fife, C. E., Carter, M. J., Walker, D. & Thomson, B. Wound care outcomes and associated cost among patients treated in US outpatient wound centers: Data From the US Wound Registry. Wounds 24, 10-17 (2012).
Sen, C. K. Human wound and its burden: Updated 2020 compendium of estimates. Adv. Wound Care 10, 281-292 (2021).
Martin, P. & Nunan, R. Cellular and molecular mechanisms of repair in acute and chronic wound healing. Br. J. Dermatol. 173, 370-378 (2015).
Eming, S. A., Martin, P. & Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med. 6, 265sr6 (2014).
Eming, S. A. et al. Differential proteomic analysis distinguishes tissue repair biomarker signatures in wound exudates obtained from normal healing and chronic wounds. J. Proteome Res. 9, 4758-4766 (2010).
Beidler, S. K. et al. Inflammatory cytokine levels in chronic venous insufficiency ulcer tissue before and after compression therapy. J. Vasc. Surg. 49, 1013-1020 (2009).
Dunnill, C. et al. Reactive oxygen species (ROS) and wound healing: the functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int. Wound J. 14, 89-96 (2017).
Ozkaya, H. et al. Successful treatment of non-healing pressure ulcers with topical n-acetyl cysteine. J. Wound Care 24, 608-611 (2015). 606.
Deniz, M., Borman, H., Seyhan, T. & Haberal, M. An effective antioxidant drug on prevention of the necrosis of zone of stasis: N-acetylcysteine. Burns 39, 320-325 (2013).
Castro, B. et al. Development and preclinical evaluation of a new galactomannan-based dressing with antioxidant properties for wound healing. Histol. Histopathol. 30, 1499-1512 (2015).
Comino-Sanz, I. M., López-Franco, M. D., Castro, B. & PancorboHidalgo, P. L. Antioxidant dressing therapy versus standard wound care in chronic wounds (the REOX study): study protocol for a randomized controlled trial. Trials 21, 505 (2020).
Castro, B. et al. The use of an antioxidant dressing on hard-to-heal wounds: a multicentre, prospective case series. J. Wound Care 26, 742-750 (2017).
James, G. A. et al. Biofilms in chronic wounds. Wound Repair Regen 16, 37-44 (2008).
Tomic-Canic, M., Burgess, J. L., O’Neill, K. E., Strbo, N. & Pastar, I. Skin microbiota and its interplay with wound healing. Am. J. Clin. Dermatol. 21, 36-43 (2020).
Edwards, R. & Harding, K. G. Bacteria and wound healing. Curr. Opin. Infect. Dis. 17, 91-96 (2004).
Kirkup, B. C. Jr Bacterial strain diversity within wounds. Adv. Wound Care 4, 12-23 (2015).
Gompelman, M., van Asten, S. A. & Peters, E. J. Update on the role of infection and biofilms in wound healing: Pathophysiology and treatment. Plast. Reconstr. Surg. 138, 61S-70S (2016).
Jayathilake, P. G. et al. Extracellular polymeric substance production and aggregated bacteria colonization influence the competition of microbes in biofilms. Front. Microbiol. 8, 1865 (2017).
Shiekh, P. A., Singh, A. & Kumar, A. Exosome laden oxygen releasing antioxidant and antibacterial cryogel wound dressing OxOBand alleviate diabetic and infectious wound healing. Biomaterials 249, 120020 (2020).
Ma, T. et al. A smart nanoplatform with photothermal antibacterial capability and antioxidant activity for chronic wound healing. Adv. Healthcare Mater. 10, 2100033 (2021).
Liang, Y., Zhao, X., Hu, T., Han, Y. & Guo, B. Mussel-inspired, antibacterial, conductive, antioxidant, injectable composite hydrogel wound dressing to promote the regeneration of infected skin. J. Colloid Interface Sci 556, 514-528 (2019).
Ge, P. et al. An antioxidant and antibacterial polydopaminemodified thermo-sensitive hydrogel dressing for Staphylococcus aureus-infected wound healing. Nanoscale 15, 644-656 (2023).
Lindner, J.-P. Imidazolium-based polymers via the poly-radziszewski reaction. Macromolecules 49, 2046-2053 (2016).
Zhong, W. et al. Designer broad-spectrum polyimidazolium antibiotics. Proc. Natl. Acad. Sci. USA 117, 31376-31385 (2020).
Martinez-Jothar, L. et al. Insights into maleimide-thiol conjugation chemistry: Conditions for efficient surface functionalization of nanoparticles for receptor targeting. J. Control. Release 282, 101-109 (2018).
Nair, D. P. et al. The thiol-michael addition click reaction: A powerful and widely used tool in materials chemistry. Chem. Mater. 26, 724-744 (2013).
Xie, Y. et al. Development of a three-dimensional human skin equivalent wound model for investigating novel wound healing therapies. Tissue Eng. C: Methods 16, 1111-1123 (2010).
Fernandez, T. L., Van Lonkhuyzen, D. R., Dawson, R. A., Kimlin, M. G. & Upton, Z. Characterization of a human skin equivalent model to study the effects of ultraviolet B radiation on keratinocytes. Tissue Eng. C: Methods 20, 588-598 (2014).
Ibberson, C. B. et al. Hyaluronan modulation impacts Staphylococcus aureus biofilm infection. Infect. Immun. 84, 1917-1929 (2016).
Hariono, M., Yuliani, S. H., Istyastono, E. P., Riswanto, F. D. O. & Adhipandito, C. F. Matrix metalloproteinase 9 (MMP9) in wound healing of diabetic foot ulcer: Molecular target and structure-based drug design. Wound Med. 22, 1-13 (2018).
Martin, P. Wound healing-aiming for perfect skin regeneration. Science 276, 75-81 (1997).
Pastar, I. et al. Epithelialization in wound healing: A comprehensive review. Adv. Wound Care 3, 445-464 (2014).
Dreier, R., Grässel, S., Fuchs, S., Schaumburger, J. & Bruckner, P. Pro-MMP-9 is a specific macrophage product and is activated by osteoarthritic chondrocytes via MMP-3 or a MT1-MMP/MMP-13 cascade. Exp. Cell Res. 297, 303-312 (2004).
Noor, S., Zubair, M. & Ahmad, J. Diabetic foot ulcer-A review on pathophysiology, classification and microbial etiology. Diabetes Metab. Syndr. 9, 192-199 (2015).
Yeo, C. K. et al. Hydrogel effects rapid biofilm debridement with ex situ contact-kill to eliminate multidrug resistant bacteria in vivo. ACS Appl. Mater. Interfaces 10, 20356-20367 (2018).
Li, P. et al. A polycationic antimicrobial and biocompatible hydrogel with microbe membrane suctioning ability. Nat. Mater. 10, 149-156 (2011).
Kim, J. H. et al. High levels of oxidative stress and skin microbiome are critical for initiation and development of chronic wounds in diabetic mice. Sci. Rep. 9, 19318 (2019).
Schäfer, M. & Werner, S. Oxidative stress in normal and impaired wound repair. Pharmacol. Res. 58, 165-171 (2008).
Forman, H. J., Zhang, H. & Rinna, A. Glutathione: Overview of its protective roles, measurement, and biosynthesis. Mol. Aspects Med. 30, 1-12 (2009).
Jault, P. et al. Efficacy and tolerability of a cocktail of bacteriophages to treat burn wounds infected by Pseudomonas aeruginosa (PhagoBurn): a randomised, controlled, double-blind phase 1/ 2 trial. Lancet Infect. Dis. 19, 35-45 (2019).
Manzuoerh, R., Farahpour, M. R., Oryan, A. & Sonboli, A. Effectiveness of topical administration of Anethum graveolens essential oil on MRSA-infected wounds. Biomed. Pharmacother. 109, 1650-1658 (2019).
Chen, C. Y. et al. Exosomal DMBT1 from human urine-derived stem cells facilitates diabetic wound repair by promoting angiogenesis. Theranostics 8, 1607-1623 (2018).
Guo, S. C. et al. Exosomes derived from platelet-rich plasma promote the re-epithelization of chronic cutaneous wounds via activation of YAP in a diabetic rat model. Theranostics 7, 81-96 (2017).
Zhou, C. et al. Engineering poly(ionic liquid) semi-IPN hydrogels with fast antibacterial and anti-inflammatory properties for wound healing. Chem. Eng. J. 413, 127429 (2021).
Romero-Montero, A. et al. Development of an antimicrobial and antioxidant hydrogel/nano-electrospun wound dressing. RSC Adv 10, 30508-30518 (2020).
Li, X. et al. Antibacterial, antioxidant and biocompatible nanosized quercetin-PVA xerogel films for wound dressing. Colloids Surfs B: Biointerfaces 209, 112175 (2022).
Hassan, M. A. et al. Antioxidant and antibacterial polyelectrolyte wound dressing based on chitosan/hyaluronan/phosphatidylcholine dihydroquercetin. Int. J. Biol. Macromol. 166, 18-31 (2021).
Chen, C., Zhou, J. & Ji, C. Quercetin: A potential drug to reverse multidrug resistance. Life Sci. 87, 333-338 (2010).
Shtenberg, Y., Goldfeder, M., Schroeder, A. & Bianco-Peled, H. Alginate modified with maleimide-terminated PEG as drug carriers with enhanced mucoadhesion. Carbohydr. Polym. 175, 337-346 (2017).
Bernkop-Schnürch, A., Kast, C. E. & Richter, M. F. Improvement in the mucoadhesive properties of alginate by the covalent attachment of cysteine. J. Control. Release 71, 277-285 (2001).
Davidovich-Pinhas, M. & Bianco-Peled, H. Alginate-PEGAc: A new mucoadhesive polymer. Acta Biomater 7, 625-633 (2011).
Rheinwatd, J. G. & Green, H. Seria cultivation of strains of human epidemal keratinocytes: the formation keratinizin colonies from single cell is. Cell 6, 331-343 (1975).
Hardwick, R., Viergever, C., Chen, A. & Nguyen, D. 3D bioengineered tissues: From advancements in in vitro safety to new horizons in disease modeling. Clin. Pharmacol. Ther. 101, 453-457 (2017).
Tan, N. S. & Wahli, W. Studying wound repair in the mouse. Curr. Protoc. Mouse Biol. 3, 171-185 (2013).
الشكر والتقدير
نشكر الدكتور شي ليو (معهد الميكروبيولوجيا بالأكاديمية الصينية للعلوم) والدكتور كي وانغ (جامعة قوانغشي الطبية) على نصائحهم في دراسة الحيوانات. تم تمويل ودعم هذا العمل من قبل برنامج ASTAR Industry Alignment Fund Pre-Positioning Programme (IAF-PP, HBMS Domain) H17/01/a0/OB9, H17/01/a0/OM9, و H19/01/aO/OY9 كجزء من الابتكار في رعاية الجروح للمناطق الاستوائية (WCIT, HBMS Domain, H17/01/a0/009) ومنحة وزارة التعليم في سنغافورة Tier 3 (MOE2018-T3-1-003). تم دعم هذا البحث أيضًا من قبل مؤسسة البحث الوطنية، مكتب رئيس الوزراء، سنغافورة، في إطار برنامجها Campus for Research Excellence and Technological Enterprise (CREATE)، من خلال SMART AMR IRG. يعترف C.F و P.L.L.K. و D.I.L. بالدعم من ASTAR (IAF-PP, HBMS Domain, H17/01/a0/004). يعترف C.K.Y. بدعم من منحة الدكتوراه NTU IGS-HealthTech ومنحة A*STAR IAF (WCIT, H17/01/a0/009).
مساهمات المؤلفين
قام D.P. بأداء العمل التجريبي لهلام الفيلم وهلام الألجينات. قام C.K.Y. بأداء العمل التجريبي لهلام الفيلم. قام D.P. و C.K.Y. بتخليق البوليميدازوليوم وضمادات الهلام، وأجروا التجارب في المختبر وفي الجسم الحي. قام Y.W. و C.F. و P.L.K.L. و D.I.L. بتصميم وتنفيذ وتفسير تجارب نموذج الجرح المعادل للجلد البشري ex vivo. قام X.X. بإجراء اختبار مضاد للفيلم للبوليميدازوليوم. ساعد Y.S.Y. و M.I.G.V. في تجربة الفأر. أسس S.H.M. كيمياء تخليق البوليميدازوليوم وأجرى توصيف NMR. نصح N.S.T. و L.Y. في تصميم وتفسير تجارب نموذج جرح الفأر السكري في الجسم الحي. نصح M.B.C.-P. في تصميم وتفسير جميع التجارب وأدار المشروع بشكل عام. كتب D.P. و C.K.Y. و M.B.C.-P. وحرروا المخطوطة. حرر P.T.H. و D.I.L. و N.S.T. المخطوطة. حصل D.I.L. و M.B.C.-P. على التمويل لدعم هذا المشروع.
المصالح المتنافسة
قام D.P. و C.K.Y. و Y.W. و X.X. و N.S.T. و M.B.C.-P. بتقديم براءات اختراع مؤقتة في سنغافورة لهذا العمل تحت أرقام البراءات 10202250243U و 10202301624S. قدم C.K.Y. و S.H.M. و N.S.T. و M.B.C.-P. براءة اختراع لهذا العمل تحت رقم البراءة US2O210244846A1. يعلن D.P. و C.K.Y. و Y.W. و X.X. و S.H.M. و N.S.T. و M.B.C.-P. عدم وجود مصالح متنافسة أخرى. يعلن C.F. و Y.S.Y. و M.I.G.V. و P.L.K.L. و L.Y. و P.T.H. و D.I.L. عدم وجود مصالح متنافسة.
مركز الهندسة الحيوية لمكافحة الميكروبات، كلية الكيمياء، الهندسة الكيميائية والتكنولوجيا الحيوية، جامعة نانيانغ التكنولوجية، 62 طريق نانيانغ، سنغافورة 637459، سنغافورة.مجموعة البحث بين التخصصات لمقاومة الميكروبات، تحالف سنغافورة-معهد ماساتشوستس للتكنولوجيا للبحث والتكنولوجيا، سنغافورة 138602، سنغافورة.معهد NTU للتكنولوجيا الصحية، المدرسة العليا للدراسات العليا بين التخصصات، جامعة نانيانغ التكنولوجية، سنغافورة 637553، سنغافورة.معهد أبحاث الجلد في سنغافورة، وكالة العلوم والتكنولوجيا والبحث (A*STAR)، 11 طريق مانداي، سنغافورة 308232، سنغافورة.معهد ونتشو، جامعة الأكاديمية الصينية للعلوم، ونتشو، تشجيانغ 325000، الصين.مدرسة لي كونغ تشيان للطب، جامعة نانيانغ التكنولوجية، 59 طريق نانيانغ، سنغافورة 636921، سنغافورة.كلية الطب، جامعة الجنوب للعلوم والتكنولوجيا، شنتشن 518055، الصين.قسم الهندسة الكيميائية، معهد ماساتشوستس للتكنولوجيا، كامبريدج، MA 02142، الولايات المتحدة الأمريكية.كلية العلوم البيولوجية، جامعة نانيانغ التكنولوجية، 60 طريق نانيانغ، سنغافورة 637551، سنغافورة. البريد الإلكتروني:nstan@ntu.edu.sg; mbechan@ntu.edu.sg
Chronic wounds are often infected with biofilm bacteria and characterized by high oxidative stress. Current dressings that promote chronic wound healing either require additional processes such as photothermal irradiation or leave behind gross amounts of undesirable residues. We report a dual-functionality hydrogel dressing with intrinsic antibiofilm and antioxidative properties that are synergistic and low-leaching. The hydrogel is a crosslinked network with tethered antibacterial cationic polyimidazolium and antioxidative -acetylcysteine. In a murine diabetic wound model, the hydrogel accelerates the closure of wounds infected with methicillin-resistant Staphylococcus aureus or carbapenem-resistant Pseudomonas aeruginosa biofilm. Furthermore, a threedimensional ex vivo human skin equivalent model shows that -acetylcysteine promotes the keratinocyte differentiation and accelerates the reepithelialization process. Our hydrogel dressing can be made into different formats for the healing of both flat and deep infected chronic wounds without contamination of the wound or needing other modalities such as photothermal irradiation.
Normal wounds progress through four main stages of healing: coagulation, inflammation, proliferation, and maturation . Chronic wounds, on the other hand, are often trapped in the inflammatory stage so that they fail to progress towards healing . Chronic wounds include various ulcer types, including diabetic foot ulcers, venous leg ulcer wounds and pressure ulcers . The economic cost of all chronic non-healing wounds in the US alone is estimated to be more than billion per year. Diabetic foot ulcers have a 5 -year mortality rate
(30.5%) comparable to that of cancer (31%) . As populations, especially in developed countries, grow and age, the prevalence and impact of chronic wounds is expected to further increase.
Conventional wound dressings are not designed to promote the closure of hard-to-heal chronic wounds. A common characteristic of chronic wounds is prolonged inflammation . Various studies indicate that non-healing wounds are trapped in a chronic inflammatory state that inhibits the normal progress of healing . Specifically, recent
investigations of chronic wound tissues and fluids indicate competition between pro-inflammatory and anti-inflammatory signals that leads to a redox imbalance and prevention of the proper wound healing occurrence . This locks the wound into a state of chronic inflammation that hinders progression to wound closure. Due to the persistent inflammation, infiltrating neutrophils and macrophages dwell in the site and they secrete reactive oxygen species (ROS) to combat colonization by microorganisms. The elevated levels of ROS in chronic wounds have negative effects on wound healing as they may cause damage to cells, tissues, and the extracellular matrix (ECM), and activate latent extracellular proteases (such as matrix metalloproteinases (MMPs)) and inflammatory cytokines . The prolonged state of elevated inflammation and levels of ROS cause the wound to be unable to escape the inflammatory phase. In severe cases, cells within and adjacent to the wound bed undergo programmed cell death (i.e. apoptosis, pyroptosis, ferroptosis) due to the high oxidative stress, triggering a cascade of events in neighboring cells leading to the same fate. This is likely the reason many chronic wounds become necrotic, which necessitates drastic procedures such as tissue debridement or worse, amputation, to protect the patient’s life.
To overcome the high oxidative stress of chronic wounds, many researchers have explored the application of topical antioxidants , such as formulations using curcumin and -acetyl-t-cysteine (NAC) . However, it was noted that the most common challenge in chronic wound care was not addressed in such wound rinse/dressing designs, which is that many wounds are colonized with biofilm-forming bacteria. Biofilm infections have been found to delay healing and reduce the clinical effectiveness of topical antioxidant solution . Biofilms, rather than planktonic bacteria, are the main form of microorganisms colonizing chronic wounds and they are often recalcitrant to treatment . Biofilm infections in wounds are most commonly caused by methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa (P. aeruginosa) . Biofilms have the capability to absorb nutrients from the ECM, such as carbon, nitrogen and phosphate, to supply their growth . Mature biofilms form extracellular polymeric substances (EPS) that surround the bacteria and protect them from countermeasures such as host immune cells, macrophages, antimicrobial peptides and antibiotics . These countermeasures fail to attack the biofilm bacteria because they cannot penetrate the protective EPS layer in sufficient quantity to have therapeutic effect. Biofilms are often stable so that they remain on wound surfaces for as long as they are undisturbed by medical interventions.
Advanced chronic wound dressings should be designed for comprehensive treatments, addressing both antioxidative and antibacterial/antibiofilm requirements. Although previous studies have explored possible solutions, each approach has encountered limitations. Hitherto, no dual-functionality wound treatments is standalone or non-contaminating because they rely on either the innate immune response, photothermal irradiation, antibiotic release or metal oxides . Our wound dressing utilizes the porous nature of the hydrogel, combined with the intrinsic antibacterial and antioxidative properties of cationic polymers and NAC, respectively. It is standalone and features ultra-low leaching, making it both convenient and safe to use.
Shiekh et al. developed an exosome-laden, oxygen-releasing cryogel, OxOBand, which demonstrated enhanced collagen deposition, re-epithelialization, neo-vascularization, and reduced oxidative stress in diabetic wounds . However, it relied on oxygen release to stimulate production of ROS (such as and ) by the host macrophages to combat bacterial infections, which may be dampened in immunocompromised patients. It also needed adipose-derived stem cells for the exosome creation which are associated with large-scale manufacturing limitations and various ethical, regulatory and safety issues. Another approach involved a nanocomposite containing molybdenum disulfide nanosheets and cerium dioxide
nanoparticles (NPs) to deliver both the photothermal antibacterial effect and the antioxidative function for treating infected wounds . This topical ointment required laser treatment to activate the antibacterial effect of and left metal components ( Mo and Ce ) on the host body. Another composite hydrogel, comprising antioxidative (poly)dopamine-modified gelatin, carbon nanotubes (CNTs), and antibiotic doxycycline, also showed promise for effecting antibacterial and antioxidant properties . However, the photothermal antibacterial effect of the CNTs relied on NIR irradiation, and the release of the antibiotic from the dressing raised concerns about the potential drug resistance development. A thermoresponsive hydrogel based on a triblock copolymer of caprolactone, glycolide, and ethylene glycol with polydopamine and silver NPs modifications exhibited efficacy against Gram-positive S. aureus but not against Gram-negative P. aeruginosa bacteria Ideal chronic wound dressings would exhibit both anti-inflammatory and broad-spectrum anti-infection functions without necessitating additional interventions such as irradiation and would not contaminate the wound site. Current reported treatments do not meet all these requirements.
We report herein a dual-functionality synthetic hydrogel, PPN, with intrinsic antibiofilm and antioxidant properties that synergistically act to support healing of infected diabetic wounds, as demonstrated with murine models. The standalone PPN synthetic hydrogel, which does not require any additional modality or further process, comprises a crosslinked polyethylene glycol (PEG) hydrogel tethered with highly potent antibacterial cationic polymer, polyimidazolium (PIM), and the antioxidant -acetylcysteine (NAC). This robust hydrogel is ultralow-leachable and completely devoid from antibiotics, metal compounds, or nanoparticles, ensuring minimal residue at the wound site after dressing removal. Studies on the PPN in a 3D human skin equivalent model shows that NAC promotes re-epithelialization and keratinocyte differentiation, while the incorporation of the PIM derivative does not hinder the wound healing process.
Results
A polyethylene glycol (PEG)-derived hydrogel was supplemented with antibiofilm and antioxidant properties through the addition of a cationic main chain polyimidazolium-maleimide (PIM-Mal) and a second component of -acetylcysteine (NAC) (Fig. 1a). Both molecules (PIM-Mal derivative and NAC) were covalently linked into the hydrogel network through the thiol-maleimide chemistry. PIM-Mal was presynthesized via the facile Poly-Radziszewski chemistry to make the diamine-terminated PIM followed by end modification with maleic anhydride (Supplementary Fig. 1). The hydrogel was made into two formats, specifically the film and fiber formats. The first format, a film hydrogel format labeled as PPN (Fig. 1b) which was obtained from crosslinking a 4 -arm PEG-thiol (PEG-4SH) with a 4 -arm PEG-maleimide (PEG-4Mal), together with the addition of PIM-Mal and NAC, is suitable for relatively flat wounds. The second format utilizing alginate (labeled as Alg-PPN (Fig. 1c)) was assembled by crosslinking (i) PEG-2Mal-2NAC made from PEG-4Mal that was pre-reacted with NAC so that two arms were attached with NAC (Supplementary Fig. 2), and (ii) Alg-SH-PIM that was pre-reacted from thiol-functionalized alginate (Alg-SH) with PIM-Mal; this format is suitable for deep wounds.
Photographs of the two formats, i.e., film and alginate (Alg) fiber, are shown in Fig. 2a, b. We performed initial testing with the hydrogel film format (Figs. 1b, 2a). The cationic PIM(C4)-Mal, which has a butyl (C4) linker between the imidazolium rings, was pre-synthesized (Supplementary Fig. 1). The NMR characterization of PIM(C4)-Mal is presented in Supplementary Fig. 3a. The molecular weight of PIM(C4)-Mal as measured by gel permeation chromatography was 2766 Da (Supplementary Fig. 4). The minimum inhibitory concentration (MIC) of PIM(C4)-Mal varies from 2 to (Supplementary Table 1) when tested against various ESKAPE bacteria (specifically . faecium 19434, methicillin-resistant . aureus (MRSA BAA-40 and
Fig. 1 | Preparation schemes of the film and fiber hydrogel wound dressings. a Structures of the main components in hydrogel film and fiber dressings. Syntheses of (b) PPN hydrogel film and (c) Alg-PPN hydrogel fiber dressings.
MRSA USA300), E. cloacae 13047, K. pneumoniae 13883, P. aeruginosa 01 (PAO1), and carbapenem-resistant . aeruginosa and . baumannii (CR-PA and CR-AB)), indicating that the polymer is a potent growth inhibitor for a wide spectrum of Gram-positive and Gram-negative bacteria.
We tested various compositions (Table 1) of the film hydrogels. The dual-functional film hydrogels (i.e., containing both PIM(C4)-Mal and NAC) are labeled as PEG-PIM-NAC (PPN(C4)-x), where the suffix (x) refers to the PIM(C4)-Mal concentration ( ) (Table 1). A control hydrogel (denoted as PPcontrol) was assembled by mixing PEG-4SH with PEG-4Mal in deionized (DI) water without the active components PIM and NAC. Single-functional hydrogels excluding either PIM (labeled as PP-N) or NAC (PPN-) were also prepared. The film hydrogel
network was formed mainly through the reaction of PEG-4SH with PEG4Mal; NAC and a portion of the PIM(C4)-Mal were tethered to the network as pendant molecules (Fig. 1b). The hydrogel precursors were able to crosslink in DI water at in less than one minute . The hydrogel films showed a tensile strength ranging from 4 to 5 kPa and tensile strain (elongation) between 50 and 58% (Fig. 2c(i), d(i)), which is slightly lower than human skin stretchability ( ). In an aqueous environment, the film hydrogels swelled, absorbing times their initial mass of water within 20 min ; thereafter the swelling kinetics plateaued to reach 10-12 times within 60 min (Fig. 2e, f, Supplementtary Fig. 5a, b). The swollen hydrogels were stable and exhibited constant mass after incubation for 7 days in bacterial extracts (Supplementary Fig. 6a-b) and infected wound fluids (Supplementary
Fig. 2 | Physical characterizations of the film and fiber hydrogel wound dressings. Visual appearance of the wound dressings investigated: (a) PPN(C4)-1 film hydrogel and (b) Alg-PPN(C8)-5 alginate fiber hydrogel. Tensile strength of the (c(i)) film hydrogels and (c(ii)) alginate fiber hydrogels ( independent experiments, two-tailed Student’s test). Tensile strain (elongation) of the ( (i)) film hydrogels
Table 1 | Compositions of the PPN(C4) film hydrogels in 1 mL of DI water
Hydrogel formulation
PEG-4SH
PEG-4Mal
PIM(C4)-Mal
NAC
PPcontrol
–
–
PPN(C4)-0.1
PPN(C4)-1
PPN(C4)-10
PP-N
–
PPN-
–
Fig. 6c). In the in vivo (murine model) test for infected wounds, the initially transparent hydrogels turned yellowish brown after 2 days, presumably due to absorption of wound fluid and dead bacteria, but remained intact and stable (Supplementary Fig. 7). This proved that the hydrogels are resistant to degradation by infected wound fluids.
In vitro contact killing efficacies of the PPN(C4) hydrogels were measured for various multidrug resistant (MDR) Gram-negative and Gram-positive bacterial strains that are clinically relevant to infected wounds , specifically MRSA USA300, CR-AB, PAO1, and CR-PA, which are pathogens of great concern worldwide . PPN(C4)-1 and PPN(C4)-10 completely eradicated the various bacterial strains loaded onto the hydrogel discs in 1 h (Fig. 3a, d). PPN(C4)-0.1 hydrogel did not completely eradicate all bacteria (Fig. 3a, d), probably due to its lower concentration of the bioactive antibacterial PIM-Mal component. PPcontrol did not exhibit bactericidal properties. The hydrogels and their extracts also exhibit low toxicity to human dermal fibroblasts (HDFs), as assessed via 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) testing. Cell viability was 100% for HDF exposed to all the hydrogel extracts (Fig. 3e). For the hydrogel contact assay, the viabilities of HDF were and for PPN(C4)-0.1, PPN(C4)-1 and PPN(C4)-10, respectively (Fig. 3e), indicating low acute toxicity and good biocompatibility of these hydrogels.
PPN(C4)-1 was chosen for further characterization as it exhibited antibacterial efficacy at a lower concentration of PIM(C4)-Mal. We further investigated the effects of the individual bioactive component of PIM or NAC, as well as their combined effects. We formulated PPN(C4)-1-derived hydrogels lacking either PIM or NAC: PP-N was synthesized without PIM(C4)-1, while PPN- was synthesized without NAC (Table 1). Using an ex vivo reconstructed 3D tissue model, the effects of these PPN(C4)-1-derived hydrogels on wound closure, reepithelialization, and proliferation and differentiation of human keratinocytes in the wound healing process were studied over 7 days. Specifically, we utilized the 3D De-Epidermised Dermis Human Skin Equivalent (DED-HSE) model, a living ex vivo tissue construct in which decellularized dermal scaffolds from human donors are repopulated with allogeneic donor keratinocytes. In addition to being physiologically similar to in vivo skin tissues, as evidenced by Xie et al. , the DEDHSE construct also supports the high proliferation and differentiation potential of allogeneic donor keratinocytes owing to the presence of an intact basement membrane .
Using the mitochondrial reduction of MTT applied to the 3D DEDHSE model, the effects of hydrogels on the overall healing of excisional wounds were assayed (Fig. 4a, b, Supplementary Fig. 8). The initial wound size (at day 0 ) is denoted as in Fig. 4 b . No wound closure was evident with the silver dressing, as the wound area remained large . Some wound closures were observed in the untreated control and all hydrogel treatment groups at both 4 and 7 days after wounding. For example, with our various hydrogel formulations at day 7, the remaining unhealed areas were approximately of the size of the initial wound. No statistical difference of wound sizes was found between the various hydrogel treatment groups and the PPcontrol (PEG gel without both NAC and PIM) at both day 4 and day 7 (Fig. 4 b). These data from the DED-HSE model suggest that the hydrogel
formulations (PPcontrol, PP-N, PPN- and PPN(C4)-1) possess excellent biocompatibility compared to the current commercial silver dressing.
We examined the gross anatomy of DED-HSE samples exposed to the hydrogel formulations (PPcontrol, PP-N, PPN- and PPN(C4)-1). The basic architecture revealed by hematoxylin and eosin (H&E) staining on day 7 identifies a growing wedged-shaped epithelial tongue and greater volume of stratified epithelium in all treatment groups, with the exception of the silver dressing sample. The DED-HSE samples treated with PPN- and PPN(C4)-1, both of which contain PIM(C4)-Mal, exhibited statistically similar epidermal thicknesses compared with the PPcontrol sample (Fig. 4c, Supplementary Table 2), indicating that the incorporation of PIM(C4) did not retard re-epithelization. Notably, wounds treated with PP-N exhibited a thicker epidermis than PPcontrol-treated wounds (Supplementary Table 2); this may be attributable to the healing promotion effect of the NAC component. These data confirm that PP-N, PPN- and PPN(C4)-1 are biocompatible, do not attenuate the re-epithelialization process, and that PP-N with NAC incorporation accelerates wound re-epithelialization.
The proliferation of cells in DED-HSE samples exposed to the different hydrogel formulations was also corroborated by the presence of the nuclear transcription factor p63, expressed by undifferentiated proliferating keratinocytes. The brown dots evident in Fig. 4c (second row) are p63-expressing cells, indicating that these individual cells are undergoing proliferation, while the blue dots indicate the nuclei of both proliferative and non-proliferative cells. On day 7, intense immunoreactivity was evident in the keratinocyte populations within the basal layers of DED-HSEs from all treatment groups (Fig. 4c, second row). DED-HSE samples exposed to PP-N, PPN-, and PPN(C4)-1 exhibited statistically comparable numbers of p63-positive cells as compared with DED-HSE exposed to PPcontrol (Supplementary Table 2). This finding suggests that the hydrogels incorporating the individual or combined components of PIM(C4) or NAC did not affect keratinocyte proliferation. Taken together, the presence of NAC or PIM does not retard proliferation, as shown in the H&E and p63 assays, and the MTT assay shows that the combination does not have any negative effect on proliferation, which is in contrast to silver dressing.
To evaluate the potential impact of PP-N, PPN- and PPN(C4)-1 on the maturation of keratinocytes, we also examined the expression of two epithelial-specific differentiation markers. The cytokeratin 10 (K10) protein is present in all suprabasal cell layers, including the stratum corneum; it is exclusively expressed by keratinocytes undergoing squamous differentiation. The cytokeratin 14 (K14) protein is exclusively expressed by the basal undifferentiated keratinocytes. The relative distributions of K10 and K14 illustrate the life-cycle of keratinocytes as they transition from proliferating to non-proliferating, differentiated states and repopulate or heal denuded skin. We found that DED-HSE treated with PPN- expressed comparable K10 and K14 signal intensities to DED-HSE treated with PPcontrol (Fig. 4c, Supplementary Table 2). Interestingly, DED-HSE treated with PP-N exhibited a stronger signal intensity for K14 compared to PPcontrol ( ), while showing comparable signal intensity for K10 (Supplementary Table 2), suggesting that PP-N, enriched with NAC, predominantly fosters keratinocyte proliferation. Additionally, DED-HSE treated with PPN(C4)-1 displayed a 138% increase in signal intensity for K10
Fig. 3 | Film hydrogels exhibited in vitro antibacterial activity and cytocompatibility. a-d Antibacterial efficacy of PPN(C4) film hydrogels assessed via contact testing for 1 h . # denotes that no bacterial colonies were observed on the agar plate ( biologically independent samples, two-tailed Student’s test).
e Cell viability of human dermal fibroblasts (HDFs) after incubation with the extracts (blue) or direct contact immersion (red) of PPN(C4) film hydrogels at for 24 h ( cells examined over 3 independent experiments). Data are presented as mean values SD.
compared to PPcontrol ( ), with a similar signal intensity observed for K14. This finding indicates that both PP-N and PPN(C4)-1, containing NAC, promote keratinocyte differentiation, which may correlate with better overall re-epithelialization as observed by H&E staining. These data suggest that hydrogels incorporating PIM(C4) and
NAC are biocompatible, do not hinder the differentiation process, and that NAC might enhance the squamous differentiation of keratinocytes.
Subsequently, we assessed the hydrogels in vivo using a diabetic murine model of infected wounds to evaluate their efficacy in clearing
Fig. 4 | Ex vivo human skin equivalent (HSE) model of the film hydrogels. a Representative images of MTT staining for wound healing. Quantitative measurement of the MTT assay at the day 4 and day 7 time points (triplicated; biologically independent samples, two-tailed Student’s test, data are presented as
mean values SEM). c Representative immunostaining images of H&E, p63, Keratin 10 (K10), and Keratin 14 (K14) after treatment with the PPN(C4)-1 hydrogel and its variants (PP-N is without PIM(C4)-1, and PPN- is without NAC). Scale bar .
biofilm bacteria, employing various MDR strains, namely MRSA USA300, PAO1, CR-AB, and CR-PA, with a commercial silver-based antimicrobial wound dressing serving as a control. Wounds treated with the PPN(C4)-1 hydrogel recorded greater than 3 log reduction (>99.9%) in the colonization of all bacterial strains tested (Fig. 5a). This performance surpasses the generally suboptimal treatments (0.1-0.3 log reduction) observed with the silver dressing and PPcontrol (Fig. 5a). To conduct a more detailed analysis of the biofilm within the wounds, we initiated an in vivo wound experiment using fluorescent-labeled bacteria, specifically the MRSA USA300 strain (AH1263) carrying the pHC47 plasmid that expresses red fluorescent mCherry gene . After a 24-h treatment period, we examined the wound lesions using confocal microscopy. The results revealed fluorescent biofilms with a thickness of up to in the wounds (Supplementary Fig. 9a-d). Based on the
bacterial count data (Fig. 5b) and biofilm volume, the estimated bacterial density in the untreated biofilm was . Among all sample groups, wounds treated with the PPN(C4)-1 hydrogel showed the lowest number of residual fluorescent bacteria in the biofilms, corroborating that PPN(C4)-1 treatment decreased the density of biofilm bacteria.
We also studied the dynamics of biofilm bacteria (MRSA USA300) count and wound size reduction at the murine diabetic wound site over a 2-week period of treatment with PPN(C4)-1 and controls. The wounds depicted in Fig. 5b were collected similarly to those in Fig. 5a, with mice being sacrificed and the full wounds excised and homogenized each day for bacterial quantification. The largest reduction of bacteria in the wounds was observed during the first 3 days of treatment with PPN(C4)-1 hydrogel, after which the bacterial counts
Fig. 5 | Mouse in vivo diabetic wound infection model with hydrogel films treatment beginning 24 h post-infection. a Bacterial counts of MRSA USA300, PA01, CR-AB, and CR-PA on various control and treated wounds after 24 h of treatment ( mice, two-tailed Student’s test). Full wound healing study. b Bacterial counts of MRSA USA300 on untreated control, silver dressing-, PPcontrol- and PPN(C4)-1 hydrogel-treated wounds on days and 14 post-treatment ( mice). c Wound sizes of untreated control, silver dressing-, PPcontrol- and PPN(C4)-1 hydrogel-treated wounds on various days as a percentage of the initial wound size ( mice). Visual appearance of representative
untreated control-, silver dressing-, PPcontrol- and PPN(C4)-1 hydrogel-treated wounds between dressing changes. Scale bar . e-j Characterization of wound tissues. Measurements in MRSA USA300-infected diabetic mice ( mice, two-tailed Student’s test) on day 2 post-treatment: e Percentage of CD11b cells in wounds. The percentage of cells is directly proportional to the extent of inflammation in the skin. Concentration of pro-MMP9 in wounds. Concentrations of wound healing factors (g) VEGF-A, (h) PDGF-BB, (i) FGF-2 and (j) EGF in wounds. Data are presented as mean values SD.
remained consistently low (Fig. 5b). In contrast, the silver dressing and PPcontrol resulted in significantly fewer bacteria being eliminated (less than 1 log reduction), and the untreated control showed almost no reduction in bacteria over 2 weeks (Fig. 5b). Furthermore, the wounds treated with the PPN(C4)-1 hydrogel were smaller, with minimal evidence of slough, than the untreated control, PPcontrol and silver dressing-treated lesions at all time points (Fig. 5c, d, biological replicates are shown in Supplementary Fig. 10). Significantly, the wounds treated with PPN(C4)-1 fully closed at day 12. In contrast, the untreated, PPcontrol and silver-treated wounds failed to close even after 2 weeks. The presence of pus and slough was noticeable on the untreated control wounds, signaling biofilm formation and persistent inflammation throughout the study (Fig. 5d, Supplementary Fig. 10a). The untreated control wounds showed signs of deterioration and displayed evidence of re-infection (Supplementary Fig. 10a).
We further used fluorescence-activated cell sorting (FACS) to determine the percentage of cells (i.e., leukocytes, which include monocytes, neutrophils, granulocytes and macrophages) in wounds after 2 days of treatment. Infected untreated (control) wounds contained elevated populations of granulocytes (Fig. 5e, Supplementary Fig. 11). However, infected wounds treated with the PPN(C4)-1 hydrogel did not exhibit an increase in inflammatory (CD11b ) cells beyond the levels observed in the control uninfected wounds, indicating that the PPN(C4)-1 hydrogel wound dressing likely attenuates the influx of inflammatory cells resulting from infection by eliminating bacteria from the wound site. In contrast, treatment with silver dressing did not modulate the number of cells in wounds (Fig. 5e,
Supplementary Fig. 11), likely attributable to its inefficacy in bacterial removal (Fig. 5a).
Enzyme-linked immunosorbent assay (ELISA) was used to determine the concentration of relevant wound healing factors present in wound exudates after 2 days of treatment. The concentration of proMMP9 (precursor of MMP9), which is detrimental to wound healing , was high in exudates from the infected untreated control, PPcontrol and silver dressing-treated wounds (Fig. 5f). Interestingly, exudates from wounds treated with the PPN(C4)-1 hydrogel contained a significantly reduced level of pro-MMP9 (Fig. 5f). Furthermore, the concentrations of various wound healing factors (VEGF-A, PDGF-BB, FGF-2 and EGF) measured by ELISA were found to be significantly higher in PPN(C4)-1-treated wounds than in the untreated infected control, PPcontrol and silver dressing-treated wounds (Fig. 5g-j).
We also studied the in vivo infected wound healing effects of PPNand PP-N hydrogels. Compared with PPN(C4)-1, PPN- (which does not contain NAC in the network) exhibited slower closure of MRSAinfected wounds from day 7 onwards (Fig. 5d), although both hydrogels have the same amount of PIM(C4)-Mal incorporated. This might be attributed to the lack of NAC in PPN-, which corroborates the decreased expression of growth factors (specifically VEGF-A, PDGF-BB and FGF-2) in wound exudates compared to PPN(C4)-1 (Supplementary Fig. 12). Additionally, without the presence of PIM(C4)-Mal in the network, PP-N does not perform as well as PPN(C4)-1 in helping the closure of MRSA-infected wounds from day 7 onwards (Fig. 5d) due to the lack of antimicrobial functionality. Wounds treated with PP-N also exhibited reduced expression of VEGF-A and EGF growth factors,
Fig. 6 | Wound histology of diabetic mouse model treated 24 h post-infection of MRSA USA300 with hydrogel films. a Representative images depicting (i) H&E and (ii) picrosirius red stained tissue sections of untreated control, silver dressing, PPcontrol, and PPN(C4)-1 hydrogel-treated wounds on day 7 post-treatment. Scale bar Quantification of granulation tissue formation thickness based on
histological wound samples harvested on day 7 post-treatment. Quantification of (c) collagen III (immature collagen, stained green) and (d) collagen I (native collagen, stained red) deposition and remodeling in the histological wound samples harvested on day 7 post-treatment. ( mice, two-tailed Student’s test, data are presented as mean values SD).
although not PDGF-BB and FGF-2, which may be attributed to a too early time point of measurement (2 days of treatment, Supplementary Fig. 12). These results demonstrate that the dual-function hydrogel PPN(C4)-1 facilitates faster wound closure and increased expression of growth factors compared to hydrogels with only one or the other of the bioactive component.
After 7 days of treatments, we conducted H&E histological assessments on the wound tissues. Compared to the untreated and PPcontrol-treated wounds, both the silver and PPN(C4)-1 hydrogeltreated wounds demonstrated significantly increased thickness of granulation tissues (marked with a vertical red line in Fig. 6a(i)), indicating enhanced healing with improved keratinocyte and fibroblast proliferation (Fig. 6b). Thicker granulation tissue, which is composed of proliferating fibroblasts, blood vessels, and extracellular matrix, is often observed during the normal wound healing process . The granulation tissue provides a scaffold for keratinocyte migration and proliferation . The presence of a thicker granulation tissue suggests an active wound healing process, which may indicate improved keratinocyte proliferation. Moreover, the PPN(C4)-1 hydrogel-treated wounds displayed more developed epithelial tongues compared to the other sample groups (Fig. 6a(i), Supplementary Fig. 13), indicating heightened proliferation and migration of keratinocytes. This observation further emphasizes the positive impact of PPN(C4)-1 hydrogel treatment on wound healing. We also analysed the collagen remodeling in wound tissues after 7 days of treatments by picrosirius red staining (Fig. 6a(ii), Supplementary
Fig. 14). In the untreated and PPcontrol hydrogel-treated wounds, collagen type III, which is immature and forms during the initial healing process to close and protect the wound from external environments, comprised approximately 33-37% of the total collagen (Fig. 6c). Conversely, in the silver and PPN(C4)-1 hydrogel-treated wounds, most of the collagen type III had been replaced by the more matured collagen type I, comprising 82-86% of the overall collagen (Fig. 6d). This shift towards more mature collagen in the PPN(C4)-1 hydrogel-treated wounds indicates not only enhanced wound closure but also the essential maturation of the wound tissues, promoting overall regeneration of healthy skin.
In summary, the ex vivo 3D skin wound model demonstrated the good biocompatibility of PIM(C4)-Mal-based hydrogels in reconstructed human skin tissue and the promotion of wound healing (even without infection) by NAC. The addition of covalently linked PIM(C4) to the hydrogels did not cause significant toxicity and did not affect the biocompatibility of the PEG-derived hydrogels. In the infected wounds of diabetic mice, the dual-component PPN(C4)-1 hydrogel significantly reduced ( log reduction) Gram-positive and Gramnegative MDR biofilm bacteria. Furthermore, PPN(C4)-1 accelerated the closure of MRSA-infected wounds in the murine diabetic model and caused higher expression of wound healing factors, such as VEGFA, PDGF-BB, FGF-2 and EGF, than with the silver dressing, PPcontrol or the untreated infected control conditions (Fig. 5b-j). The eradication of bacteria in the in vivo diabetic mouse study occurred in the earlier time periods (first 3 days) of treatment with PPN(C4)-1. Thus, the
Table 2 | Compositions of the Alg-PPN(C4) fibers in 1 mL of DI water
Fiber formulation
Alg-SH
PIM(C4)-Mal
PEG-2Mal-2NAC
PEG-4Mal
NAC
Alg
50 mg
–
–
–
Alg-PPN(C4)-0.1
50 mg
0.1 mg
Alg-PPN(C4)-1
50 mg
1 mg
Alg-PPN(C4)-5
50 mg
5 mg
Alg-PPN(C4)-10
50 mg
10 mg
addition of both PIM(C4) and NAC is important for the removal of bacteria and wound healing, respectively.
As many chronic wounds are rather deep and film format dressing is not ideal for such wounds, we also produced alginate hydrogel fibers which are covalently linked with PPN, that can fill deep wounds and conform to their surfaces. A series of fiber formulations were prepared using Alg-SH, PEG-4Mal, PIM(Cn)-Mal ( , or 10 ), and NAC in DI water (Table 2). These hydrogel fibers are labeled as Alg-PIM(Cn)-PEG-NAC-x (Alg-PPN(Cn)-x), where the suffix (x) refers to the PIM(Cn)-Mal concentration ( ) (Table 2). Linear PIM(Cn)-Mal with different alkyl (Cn) linkers ranging from butane (C4) to decane (C10) were presynthesized and the PIM(Cn) solutions were screened (Supplementary Fig. 1). The different PIM(Cn) solutions have different antibiofilm effects (Supplementary Fig. 15); in addition to the solution forms of PIM(C4), PIM(C8) and PIM(C10), they were further made into Alg-PPN fiber for testing.
Briefly, the 4 -arm PEG-4Mal was pre-modified with 2 equivalents of NAC to convert, on average, 2 PEG arms per chain to NAC terminals to produce PEG-2Mal-2NAC (Fig. 1c, Supplementary Fig. 2a). Thiolmodified alginate (Alg-SH) was pre-reacted with PIM(Cn)-Mal to produce Alg-SH-PIM(Cn) (Fig. 1c, Supplementary Fig. 2b). Some thiol groups remained unreacted in Alg-SH-PIM(Cn) for subsequent click reactions, and were quantified (Supplementary Fig. 16). The Alg-SH-PIM and PEG-2Mal-2NAC were further reacted via the thiol-maleimide reaction to form the Alg-PPN solution (Fig. 1c), which was then coagulated in a bath to obtain Alg-PPN fibers. An alginate fiber control (labeled as Alg) was produced by extruding Alg-SH solution into a bath (Table 2). The as-prepared fibers were washed thoroughly in DI water with sonication and dehydrated in ethanol. The hydrogel fibers showed a range of tensile strengths of and tensile strains (elongation) of 27-34% (Fig. 2c(ii), d(ii)). The amount of leachable PIM, NAC, and PEG components after washing was found to be less than , and of the initial PIM, NAC, and PEG components respectively (Supplementary Figs. 17-18, Supplementary Table 3-5). We also used a commercial alginate fiber (labeled as Alg-Com) and commercial silvercontaining alginate fiber (Alg-Ag) as control samples.
Contact killing efficacies of the Alg-PPN and control fibers were measured in vitro against various MDR Gram-negative and Grampositive bacteria, specifically MRSA USA300, PAO1, CR-PA and CR-AB. The Alg-Com and control Alg fibers did not exhibit bactericidal properties (Fig. 7a-d). The Alg-PPN(Cn)-5 and Alg-PPN(Cn)-10 fibers totally eradicated (in 1 h ) Gram-positive MRSA USA300 and CR-AB, as well as Gram-negative PAO1 and CR-PA bacteria, which were inoculated onto the fibers (Fig. 7a-d, Supplementary Tables 6-8). The Alg-PPN(Cn)-0.1 and Alg-PPN(Cn)-1 fibers did not completely eradicate the bacteria (Fig. ), probably due to the lower concentration of the active antibacterial PIM(Cn)-Mal tethered to the fibers.
The antibiofilm efficacies of fibers towards preformed biofilms were also studied. The Alg-Com and control Alg fibers did not exhibit antibiofilm activity towards the tested Gram-positive and Gramnegative bacteria (Fig. 7e-h). Alg-PPN(C4) exhibited a range of 1.39-3.81 log reductions towards MRSA biofilm (Fig. 7e, Supplement tary Table 9) due to the presence of the PIM(C4)-Mal active component in the fibers. Alg-PPN(C8), which has more alkyl carbon atoms in its PIM
component, exhibited a higher log reduction range against MRSA biofilms of 1.84-6.80, depending on the PIM(C8) concentration (Fig. 7e, Supplementary Table 10). Alg-PPN(C10)-5 and Alg-PPN(C10)10 fibers eradicated MRSA biofilms completely (Fig. 7e, Supplementary Table 11). This trend was also observed in the antibiofilm assays towards CR-AB, PAO1, and CR-PA bacteria (Fig. 7f-h, Supplementary Tables 9-11), demonstrating the potency of Alg-PPN in combating various biofilm bacteria.
The in vitro biocompatibility of the fibers against 3T3 mouse fibroblasts and human dermal fibroblasts (HDFs) was studied with supernatant extracts and direct contact with Alg-PPN(Cn) fibers. The viabilities of HDF and 3T3 cells exposed to the extracts of Alg-PPN(C4) fibers were high, in the range of and , respectively (Supplementary Fig. 19a, b). These results suggest that the Alg-PPN(C4) fibers are cationic low-leaching. After contact incubation with the AlgPPN(C4) fibers, the cell viabilities of HDF and 3T3 fibroblasts were in the range of and , respectively (Supplementary Fig. 19a, b), indicating low acute cytotoxicity of the fibers. The viabilities of 3T3 cells in contact with Alg-PPN(C8)-x (for ) and Alg-PPN(C10)- (for ) were (Supplementary Fig. 19c, d).
In the above in vitro analyses, Alg-PPN(C8)-5 achieved at least 4 log reduction of the MDR Gram-positive and Gram-negative biofilm bacteria with low cytotoxicity. We therefore chose this formulation for in vivo validation studies using mice. We investigated the healing of Gram-negative CR-PA-infected wounds on diabetic mice treated with control Alg, silver-containing commercial alginate (Alg-Ag), and AlgPPN fibers over a 2-week period. For the Alg-PPN treatment group, Alg-PPN(C8)-5 (containing PIM(C8)) was applied to the wound until day 5 to eradicate bacteria, followed by replacement with the more biocompatible Alg-PPN(C4)-5 (containing PIM(C4)) from day 5 to day 14. The largest reduction in the CR-PA bacterial count was observed in wounds treated with Alg-PPN(C8)-5 fiber during the initial 5 days (Fig. 8a). Wounds treated with the Alg-PPN fibers were smaller, with minimal evidence of slough, than the untreated control, Alg, and AlgAg fibers-treated wounds at all time points (Fig. 8b, c, Supplementary Fig. 20). Pus and slough were observed on the untreated control wounds, indicative of biofilm formation and sustained inflammation (Fig. 8c, Supplementary Fig. 20a). As in the corresponding PPN hydrogel tests, the untreated control wounds deteriorated and exhibited evidence of re-infection. After a 2-week period, the wounds fully closed for the Alg-PPN-treated group but did not close for the other groups (Fig. 8c, Supplementary Fig. 20).
To evaluate the effect of dressing treatments on immune cell infiltration, we characterized populations of immune cells in wound tissues after 2 days of treatment. The untreated infected wounds exhibited the highest percentage of inflammatory cells (Fig. 8d). Infected wounds treated with Alg-PPN fiber exhibited the lowest percentage of cells, followed by wounds treated with Alg-Ag fiber (Fig. 8d, Supplementary Fig. 21b-e). The low percentage of cells indicates that fewer leukocytes infiltrated wounds to fight infection in wounds treated with Alg-PPN fiber, which thus caused lower inflammatory response in the wound tissues. Most of these CD11b cells in the Alg-PPN fiber treatment group were Ly6G neutrophils (Fig. 8d, Supplementary Fig. 21a), suggesting reduced acute
Fig. 7 | Antibacterial and antibiofilm activities of the fiber hydrogels. Viability of (a-d) planktonic bacteria and (e-h) biofilms of (a, e) MRSA, (b, f) CR-AB, (c, g) PAO1, and ( ) CR-PA after contact incubation with the surface of Alg-PPN(Cn)-0.1 (blue), Alg-PPN(Cn)-1 (green), Alg-PPN(Cn)-5 (orange), and Alg-PPN(Cn)-10 (red)
e
f
fibers at ( biologically independent samples, two-tailed Student’s test, values denote significant difference compared to untreated controls, data are presented as mean values SD). The contact periods were 1 h for planktonic bacteria and 24 h for biofilms.
inflammatory responses in the wound tissues. (Ly6G is a specific marker for mouse neutrophils.) The population of Ly6G cells on the Alg-PPN-treated wounds was also lower than that on the Alg-Ag-treated wounds (Supplementary Fig. 21a). These results suggest the efficacy of Alg-PPN over Alg-Ag in the killing of wound site bacteria, which alleviates the bioburdens on infected wounds for accelerated healing. Neutrophils are among the earliest immune cells to arrive at wound sites. Thus, for the untreated and Alg control groups, high percentages of CD11b cells but low Ly6G-positive neutrophils suggest that the inflammation has advanced beyond the early phase.
Another consequence of the acute infiltration of immune cells, especially neutrophils, is the release and activation of proteases. We assayed the concentration of pro-MMP9 (a specific macrophage product and precursor to MMP9 ) using ELISA and detected the highest concentrations in control untreated wounds due to overproduction of the innate response system to fight the high amount of bacteria. Wounds treated with the Alg-PPN fiber exhibited a significantly reduced level of pro-MMP9 (Fig. 8e), indicating the high efficacy of Alg-PPN in killing bacteria. Wounds treated with the Alg-Ag fiber also exhibited significantly reduced pro-MMP9 concentrations,
Fig. 8 | Full wound healing study of murine infected diabetic wounds with hydrogel fibers treatment beginning 24 h post-infection. a Bacterial counts of CR-PA on untreated control, Alg, Alg-Ag, and Alg-PPN fibers-treated wounds on days and 14 post-treatment ( mice). Wound sizes of untreated control, Alg, Alg-Ag, and Alg-PPN fibers-treated wounds on various days as a percentage of the initial wound size ( mice). Visual appearance of representative untreated control, Alg, Alg-Ag, and Alg-PPN fibers-treated wounds
between dressing changes. Scale bar Characterization of wound tissues. Measurements in CR-PA-infected diabetic mice ( mice, two-tailed Student’s test) on day 2 post-treatment: Percentage of cells in wounds. The percentage of cells is directly proportional to the extent of inflammation in the skin. e Concentration of pro-MMP9 in wounds. Concentrations of wound healing factors (f) VEGF-A, (g) PDGF-BB, (h) FGF-2 and (i) EGF in wounds. Data are presented as mean values SD.
although to a lesser degree than Alg-PPN. The concentrations of several major wound healing factors (VEGF-A, PDGF-BB, FGF-2 and EGF) were assayed to be the highest in Alg-PPN fiber-treated wounds (Fig. 8f-i), correlating with faster healing rate in this group than in untreated control, Alg, and Alg-Ag-treated wounds.
Discussion
Diabetic wounds are commonly chronically inflamed due to bacterial infection which often leads to elevated reactive oxygen species (ROS) levels . These factors conspire to impair the genesis and repair of blood vessels, reduce the biosynthesis and delivery of wound healing factors, and cause failure in the management of the bioburden on wounds. Herein, we have developed a hydrogel (called PPN) that contains 2 bioactive components which provide synergistic functions to alleviate infection and quench the excessive ROS to result in accelerated closure of infected diabetic wounds. Further, our N -acetylcysteine (NAC) component (even in uninfected wound model) directly promote keratinocyte proliferation and the squamous differentiation of keratinocytes, to result in thicker re-epithelialization.
In our previous work on cationic hydrogels that are antibacterial but not wound healing , we discovered that cationic hydrogels kill bacteria by (i) absorbing them into their pore spaces (via the hydrodynamic drag force generated by the evaporation of water from the hydrogel and its subsequent rehydration), followed by (ii) contact killing of bacteria by the cationic polymers of the pore walls. The cationic hydrogel here similarly absorbs bacteria into its pore spaces and then contact kill them via the cationic hydrogel pore walls .
The accelerated wound healing mechanism of our dual functionality hydrogel stems from the synergy of bacteria removal by the
crosslinked cationic hydrogel which itself results in reduced inflammatory response, together with the antioxidative property of NAC. Firstly, our PPN hydrogel dressing eradicates and eliminates bacteria from the wound site. The bacterial removal from the site results in a significant reduction in the influx of inflammatory cells typically associated with infection, as evidenced by the suppressed level of cells in the infected mice wounds treated with PPN(C4)-1 hydrogel as compared to the untreated wounds (Fig. 5e, Supplementary Fig. 11). Secondly, the NAC reduces the levels of ROS which are high in chronic wounds , as they diffuse into the PPN hydrogel and are quenched. NAC, a precursor to glutathione (GSH), can substitute for GSH function in tissues. The NAC antioxidant neutralizes free radicals, reduces oxidative stress and inflammation, and boosts the immune system , so that it reduces inflammation and tissue damage due to high ROS levels, and allow for progression to normal healing. Thirdly, the PPN hydrogel promotes the supply of wound healing factors to the wound sites, as shown by the significantly higher concentrations of VEGF-A, PDGF-BB, FGF-2 and EGF in the PPN(C4)-1 hydrogel-treated mice wounds than in all other treatment groups (Fig. ). This effect can be attributed to the suppression of inflammatory mediators, such as TNF-alpha and IL-1, stemming from the reduced presence of inflammatory cells and biofilm bacteria.
Finally, the incorporation of the antioxidant NAC in the PPN hydrogel promotes re-epithelialization and keratinocyte differentiation, as substantiated using the ex vivo 3D de-epidermised dermis human skin equivalent (DED-HSE) model (that has repopulated allogeneic donor keratinocytes). Uninfected wounds treated with PP-N (hydrogel without PIM but with NAC) exhibited a increase in epidermal thickness when compared to wounds treated with the
PPcontrol (Supplementary Table 2), indicative of the enhanced reepithelialization effect attributed to NAC incorporation. Additionally, when compared to the PPcontrol group, uninfected wounds treated with PP-N and PPN(C4)-1 hydrogels exhibited significantly stronger signal intensity for K14 and K10 proteins, respectively (Fig. 4c and Supplementary Table 2), indicating that NAC incorporation enhances the squamous differentiation of keratinocytes. Consequently, the combination of NAC and the antibacterial polymer within the PPN hydrogel operates synergistically to promote wound healing by collectively diminishing ROS levels and inflammation.
Our PPN(C4)-1 hydrogel is more bactericidal to biofilm bacteria than the commercial silver-based wound dressing, even to carbapenemresistant . aeruginosa and . baumannii (CR-PA and CR-AB), which urgently need new antibacterial therapies . Furthermore, wounds treated with the PPN(C4)-1 hydrogel exhibited minimal erythema, suppressed inflammation, and accelerated wound closure. The diabetic murine model results confirmed that the hydrogels with PIM and NAC combination are the best formulation for the removal of biofilms and acceleration of wound healing, as treatment with PPcontrol (without PIM and NAC) did not significantly kill bacteria, and the wounds healed more slowly (Fig. 5d). The hydrogels formulated with only a single active component (i.e., either PP-N or PPN-) exhibited slower healing and reduced levels of wound healing factors (Fig. 5d, Supplementary Fig. 12). Many studies on wound dressings only focus on one aspect of wound healing or one type of wound (e.g., infected wounds or diabetic wounds) , but our hydrogel has dual functionalities that lead to improved healing of infected wounds, fulfilling the unmet need.
Dual-function antibacterial and antioxidative features are considered to be the most effective current solution for wound treatment. Several such dual-functional formulations have been reported but they suffer from being grossly leaching, or not so effective particularly against resistant bacteria . Zhou et al. developed a semiinterpenetrating polymer network (sIPN) hydrogel with antibacterial and anti-inflammatory activities that could degrade completely within 2 h after being applied to wounds with in vivo murine model . Although the sIPN hydrogel was fairly effective in killing non-resistant E. coli and S. aureus (less than 2 log reduction), its antibacterial effect which is due to degradation of the hyaluronic acid network, releases the foreign polyvinyl with dangling cationic imidazolium moieties onto the wound site. This degradable hydrogel is not a retrievable dressing, and large amounts of degraded polymers are left on the wound. Romero-Montero et al. developed hydrogel nanofibers loaded with the antibiotic clindamycin and the antioxidant poly(gallic acid) . However, the release of antibiotics from this wound dressing product raises concern for the spread of bacterial resistance through horizontal gene transfer. Other groups have developed xerogel film and hydrogel membrane that can rapidly (within 1 or 2 h ) release quercetin, a plant flavonoid that was reported to have antibacterial and antioxidant properties . However, these gels have been demonstrated to kill only non-resistant bacteria in vitro or treat uninfected wounds of nondiabetic mice. Considering these recent studies, our standalone and low-leaching PPN hydrogel film and fiber achieved killing broadspectrum multidrug-resistant (MDR) bacterial biofilms, as well as accelerating the closure of biofilm-infected diabetic wounds, which have not been demonstrated previously.
We employed the facile crosslinking chemistry of thiol-maleimide Michael addition reaction. We found no evidence that bacterial extracts (Supplementary Fig. 6a, b) or wound fluids (Supplementary Fig. 6c) degrade PPN(C4)-1 hydrogel, nor did we find evidence for degradation of PPN(C4)-1 hydrogel film and Alg-PPN(C8)-5 hydrogel fiber on wounds (Supplementary Fig. 7, Supplementary Movies 1-4). The hydrogel’s overall structural integrity is well preserved.
The hydrogels can be assembled into multiple formats; we have created film and fiber formats which are suitable for use in treatment
of shallow and deep wounds, respectively. The composite hydrogel film demonstrates effective biofilm removal and accelerates healing of infected cutaneous wounds in diabetic mice. With the alginate fibers (which are suitable for deep, as well as shallow, wounds), the bioactive PIM and NAC components retained their antibacterial and antioxidative properties in murine wound models. This technology may alleviate the growing problem of chronic and diabetic wounds, as current treatments are limited by their contraindications. Furthermore, hydrogels can also be assembled by electrospinning or 3D printing to easily create custom formats or shapes suited to fit specific applications. Finally, this hydrogel can also be used in other biomedical applications, such as coatings for biomedical devices.
In summary, our study introduces a crosslinked hydrogel with two covalently bound, ultralow-leachable bioactive components: the highly potent antibacterial cationic PIM and the antioxidative NAC. The composite hydrogel exhibits efficient and broad-spectrum biofilm removal capabilities, while also accelerate the healing process in infected diabetic wounds. It is intrinsically antibacterial and antioxidative and does not require other processes such as photothermal irradiation so that this standalone dressing is easy and safe to use. Unlike previous dual functionality dressings, the crosslinked hydrogel is completely devoid of leachable antibiotics, metal compounds, carbon nanotubes or nanoparticles. This ultra-low leaching feature distinguishes it from many other drug-releasing wound dressings, promoting a safer and more biocompatible alternative. It has good structural integrity and is easy to be removed cleanly from the wounds. Furthermore, different formats such as films and fibers can be made to conform to wounds. These advantages greatly enhance patient comfort and support an uncomplicated healing process.
Methods
Materials
1,4-diaminobutane, 1,6-diaminohexane, 1,8-diaminooctane, 1,10-diaminodecane, formaldehyde (37%), glyoxal (40%), acetic acid, maleic anhydride, sodium bicarbonate, -acetylcysteine (NAC), alginic acid sodium salt (sodium alginate), l-cysteine ( ), -ethyl- -(3-dimethylaminopropyl)carbodiimide (EDC, 97%), sodium hydroxide ( NaOH ), sodium chloride ( NaCl ), calcium chloride ( ), hydrochloric acid (HCl), lecithin, Tween 80, sodium thiosulfate, 5,5-dithio-bis(2-nitrobenzoic acid) (DTNB, 99%), and 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT, 98%) were purchased from Sigma-Aldrich Corp. (St. Louis, MO). Poly(ethylene glycol) tetra thiol (PEG-4SH, ) and poly(ethylene glycol) tetra maleimide (PEG-4mal, ) were purchased from Biochempeg Sci. Inc. (Watertown, MA). Fluorescein-5-maleimide (F5M), phosphatebuffered saline (PBS), Mueller-Hinton broth (MHB), tryptic soy broth (TSB), Luria-Bertani (LB) agar, ELISA kits for mouse pro-MMP9 (EMMMP9), VEGF-A (BMS619-2), PDGF-BB (BMS2071), FGF-2 (EMFGF2), and EGF (EMEGF) were purchased from Thermo Fisher Sci. Inc. (Waltham, MA). CD11b (130-113-231) and Ly6G (130-102-296) antibodies were purchased from Miltenyi Biotec. Mouse monoclonal anti-K10 (DE-K10) was purchased from Dako (DKO.M7002). Mouse monoclonal anti-K14 (LL001) was a supernatant from E. Birgitte Lane’s lab (A*STAR). Mouse monoclonal anti-p63 (4A4) was purchased from Abcam (Ab735). Enterococcus faecium (19434), Enterobacter cloacae (13047), Klebsiella pneumonia (13883), methicillin-resistant Staphylococcus aureus (MRSA USA300, BAA-40, and LAC), carbapenemresistant Acinetobacter baumannii (CR-AB), Pseudomonas aeruginosa 01 (PAO1), carbapenem-resistant . aeruginosa (CR-PA), and standard 3T3 mouse fibroblast cells were purchased from American Type Culture Collection (ATCC, Manassas, VA). Human dermal fibroblast cells (HDFs, NHDF-Ad, CC-2511) were purchased from Lonza (Basel, Switzerland). Ethanol and dimethyl sulfoxide (DMSO) were of analytical grade.
Synthesis of polyimidazolium containing maleimide terminal groups (PIM(Cn)-Mal)
PIM(C4)-Mal was synthesized via the following procedure. 2.974 g ( 33.7 mmol ) of 1,4-diaminobutane was dissolved in 75 mL of acetic acid and cooled in an ice bath. 2.735 g ( 33.7 mmol ) of formaldehyde solution and 4.895 g ( 33.7 mmol ) of glyoxal solution were dissolved in 37.5 mL of DI water, and the mixture was added dropwise to the 1,4 -diaminobutane solution. The resulting mixture was stirred at 25 for 24 h , after which the solvents were evaporated with a rotary evaporator. The dried product was re-dissolved in DI water, dialyzed in DI water for 3 days using regenerated cellulose membrane (MWCO 1 kDa ), and lyophilized to obtain PIM(C4). 2 g ( 0.7 mmol ) of PIM(C4) was dissolved in 50 mL of acetic acid, to which 0.27 g ( 2.8 mmol ) of maleic anhydride and 0.24 g ( 2.8 mmol ) of sodium bicarbonate were added. This solution was stirred at for 24 h , after which the solvent was removed with a rotary evaporator. The product was redissolved in DI water, dialyzed in DI water for 3 days using regenerated cellulose membrane (MWCO 2 kDa ), and lyophilized to obtain PIM(C4)-Mal. NMR ( ) , (Supplementary Fig. 3a).
PIM(Cn)-Mal with , and 10 were synthesized following the same method as above, with substitution of the respective diaminoalkanes in place of 1,4-diaminobutane, i.e., using 1,6-diaminohexane for PIM(C6)-Mal, 1,8-diaminooctane for PIM(C8)-Mal, and 1,10-diaminodecane for PIM(C10)-Mal.
Preparation of the hydrogel films (PPN(Cn))
Hydrogels films were prepared by casting of solutions of the precursor components mixed using a vortex mixer. The antioxidant component solution contained of PEG-4SH and 2 mM of NAC in DI water. The antibacterial component solution contained of PEG4 Mal and or of PIM(Cn)-Mal in DI water. These two solutions were mixed at equal volume, and aliquots of the mixed solution were quickly deposited in the wells of a 96 -well plate. The final composition of the hydrogel was 5% (w/v) PEG-4SH, 5% (w/v) PEG-4Mal, 1 mM NAC and or PIM(Cn)-Mal (Table 1). The hydrogel samples were kept at for 5 min to form PPN(Cn) hydrogels. DI water was then added to the wells to swell the hydrogels. After swelling for 15 min , the hydrogels were washed thrice in ethanol and thrice in DI water in an ultrasonic bath ( ) to remove all unreacted precursors. Two PPN(Cn)-derived hydrogels lacking either PIM or NAC were also made: PP-N was made without PIM(Cn), while PPN- was made without NAC (Table 1). A control gel (PPcontrol) with no antioxidant or antibacterial functionalities, i.e. only 5% (w/v) PEG-4SH and 5% (w/v) PEG-4Mal, was also prepared.
Synthesis of thiol-functionalized alginate (Alg-SH)
Alg-SH was synthesized by using amidation of carboxylic acid group . Sodium alginate ( of alginate repeat units) was dissolved in 200 mL of DI water and activated by adding EDC ( 50 mM ). The mixture was stirred at for 1 h . Next, l-cysteine , 11.4 mmol ) was dissolved in 100 mL of DI water and added to the reaction mixture dropwise under stirring. During the addition, the pH of the reaction mixture was monitored and adjusted to 5 using 2 M NaOH solution. The mixture was then stirred at for 24 h . The product was dialyzed (MWCO 8 kDa ) in DI water containing 1 mM HCl at . Next, two consecutive cycles of dialysis were performed in DI water containing and 1 mM HCl . The sample was lyophilized to obtain the Alg-SH polymer. The product was stored at until further use.
Preparation of PEG-2Mal-2NAC
PEG-4Mal ( ) was dissolved in 0.2 mL DI water. Then, 0.1 mL aqueous solution of NAC ( ) was added dropwise
with vortexing. The mixture was agitated to react for 1 h to form the PEG-2Mal-2NAC polymer. With a PEG-4Mal:NAC design molar ratio of 1:2, the thiol-maleimide click reaction leads to the attachment of 2 molecules of NAC on each PEG-4Mal molecule (statistical average).
Formation of fibers of alginate modified with PIM-Mal and PEG-2Mal-2NAC (Alg-PPN)
Alg-SH ( of thiol moieties) was dissolved in 0.5 mL DI water. Then, an aqueous solution of PIM(Cn)-Mal ( , or 10 mg ) in 0.2 mL of DI water was added dropwise with vortexing (Table 2). The mixture was agitated for 1 h to allow reaction between the maleimide group of and the thiol group of Alg-SH, resulting in the Alg-SH-PIM(Cn) polymer.
To further graft PEG-2Mal-2NAC onto Alg-SH-PIM(Cn), 0.3 mL of PEG-2Mal-2NAC solution was added dropwise to the Alg-SH-PIM solution (Table 2) with vortexing, and the mixture was agitated at 25 for 1 h to form the Alg-PPN(Cn) solution. The Alg-PPN(Cn) solution was loaded into a syringe and extruded through a 25 G needle into a 250 mL bath of aqueous solution. The formed fibers were passed along the bath and pulled into an ethanol bath for dehydration. The fibers were sonicated in DI water for 1 h and immersed in DI water for 24 h to wash out unreacted components. After washing, the fibers were dehydrated in ethanol and dried under ambient air to obtain Alg-PPN(Cn) fibers.
Swelling dynamics and mechanical characteristics of the film and fiber hydrogels
Prior to testing of swelling dynamics, hydrogels were thoroughly washed with DI water and then dried with a freeze dryer. The mass of a fully dried hydrogel was measured as the initial mass. The fully dried gel was then immersed in a copious amount of DI water to swell. At 5 min intervals, the hydrogel was removed from the DI water bath, dried by blotting on filter paper, weighed, and then returned to the DI water bath to continue swelling. The swelling ratio was calculated as:
The mechanical strength of the hydrogel was evaluated by performing uniaxial tensile tests using an MTS Criterion 43 (Instron Materials Test system).
Degradability test of the PPN(C4)-1 film hydrogel in bacterial extracts
Bacterial extracts were prepared by shaking various concentrations of bacteria in PBS at and pH 7.4 for 24 h , followed by centrifugation to separate the bacteria from the soluble extracts. PPN(C4)-1 hydrogels were equilibrated by immersion in PBS for 24 h in a 24 -well plate, after which the initial masses were weighed. The hydrogels were then incubated in 1 mL of bacterial extract at for 2 or 7 days, after which the gels were weighed.
Degradability test of the PPN(C4)-1 film hydrogel in wound fluids and in infected animal wounds
For the test of stability in wound fluids, mouse wound tissue infected with MRSA USA300 or CR-PA was homogenized in PBS ( ), and diluted to a total volume of 10 mL in PBS. After dilution, tissue debris was removed by centrifugation. PPN(C4)-1 hydrogels were equilibrated by immersion in PBS for 24 h in a 24 -well plate, after which initial gel masses were measured. Equilibrated hydrogels were then incubated in 1 mL of wound fluid at for 2 or 7 days, after which they were weighed. Hydrogel stability on infected wounds was assessed by photographing PPN(C4)-1 hydrogels before and after application (for 2 days) to treat mouse wounds infected with MRSA USA300.
Determination of the thiol group content of Alg-SH
The thiol group content of Alg-SH was measured using reaction with Ellman’s reagent (DTNB) . Alg-SH ( ) was dissolved in 0.1 mL of PBS at neutral pH. DTNB ( 4 mg ) was dissolved in 0.1 mL PBS at neutral pH. The Alg-SH solution ( 0.1 mL ) and DTNB solution ( 0.1 mL ) were mixed in 1.8 mL of PBS and agitated at 100 rpm for 20 min in the dark. Then, the absorbance at 412 nm was measured on a UV-Vis spectrophotometer (Shimadzu UV-1800) and used to determine the thiol group concentration. A calibration curve was prepared by reacting DTNB with l-cysteine at predetermined concentrations. The thiol content determination was validated with fluorescence analysis via a click reaction with F5M. The Alg-SH ( 3.52 mg ) was dissolved in 0.5 mL of DI water. Separately, F5M ( ) was dissolved in 0.5 mL of DMSO. The Alg-SH solution and F5M solution were mixed, agitated at 100 rpm for 24 h , and dialyzed (MWCO 1 kDa ) for 3 days in the dark. After lyophilization, a solution of Alg-F5M ( ) was prepared and the fluorescence intensity was measured on a Shimadzu RF-6000 spectrofluorophotometer under an excitation/emission wavelength of . A calibration curve was prepared by measuring the fluorescence intensity of F5M at predetermined concentrations.
Determination of the leaching rates of components from the Alg-PPN fibers
The Alg-PPN(C4) fibers ( 100 mg ) were immersed in 2 mL of PBS (for absorbance test) or ultrapure water (for mass spectroscopy test) at and agitated at 100 rpm for 24 h . Then, 1 mL of the supernatant was collected. The extracted ion chromatogram (EIC) of the supernatant was obtained on a liquid chromatography-mass spectrometer (Agilent 6550 iFunnel Q-TOF) with Acquity UPLC HSS T3 column (Waters). The absorbance of the supernatant was measured on a UV-Vis spectrophotometer (Shimadzu UV-1800). PEG-4Mal exhibited absorbance peak at 300 nm wavelength. Calibration curves of the components were prepared by measuring the EIC and spectral absorbance of PIM(C4), NAC, and PEG-4Mal at predetermined concentrations.
Minimum inhibitory concentration (MIC) assay
Bacteria were cultured in MHB at with continuous shaking at 220 rpm to mid log phase. Two-fold serial dilutions ( to ) of PIM(C4)-Mal in MHB were prepared on a 96 -well plate. Then, bacterial suspension ( ) was added to each well containing PIM(C4)-Mal solutions. The plate was then incubated at for 18 h , and the optical density of the wells was measured at 600 nm wavelength to determine the MIC.
The MBEC was measured using a microtiter plate-based technique. Briefly, of MRSA LAC or PAO1 suspension (cell density at ) in TSB was added to a 96 -well plate covered by a lid containing pegs (Innovotech 19111). Biofilms were grown on the peg lid after incubation at for . After removing planktonic bacteria by washing twice with PBS, the lid with biofilms was transferred into a 96well challenge plate containing two-fold serial dilutions of polymer solutions with a total volume of in each well. The treatment was performed at for 4 h . After that, the peg lid was washed with PBS and transferred to a 96-well recovery plate containing of neutralizer (3% lecithin, 10% tween 80, and 0.3% sodium thiosulfate in DI water) in each well. Biofilm bacteria were dislodged from the peg lid by sonication ( ) for 30 min . The detached bacteria were then serially diluted 10 -fold in PBS and spread on LB agar plates. After incubation at for 24 h , bacterial colonies were counted.
Ex vivo 3D de-epidermised dermis human skin equivalent (DEDHSE) model
Cell culture. Primary human keratinocytes were obtained from Asian Skin Bank, A*STAR, with ethical approval IRB: B-16-135E. Cells were
cultured in full growth (FG) medium with irradiated 3T3 fibroblasts (i3T3) as feeder cells . Briefly, i3T3 feeder cells were preseeded in a Petri dish of 10 cm diameter. The feeder cells were cultured in Dulbecco’s Modified Eagle’s Medium (DMEM, Life Technologies, Singapore) containing 10% fetal calf serum (FCS, Life Technologies, Singapore) and penicillin/streptomycin solution at with air. After the attachment of i3T3, which requires a minimum of million primary human keratinocytes were seeded in each Petri dish with the i3T3, and the DMEM was replaced with fresh FG medium. The cells were maintained in an incubator at with air, and the medium was replaced every days.
Construction of the DED-HSE wound healing model. The DED-HSE wound healing model was established using decellularized dermis derived from human skin . Briefly, large pieces of human skin were trimmed into pieces and soaked in 1 M NaCl overnight, yielding decellularized dermis. The epidermal layer was then removed, and sterile stainless-steel rings were placed onto the papillary side of each de-epidermised dermis (DED). Keratinocytes were transferred into each ring placed on the DEDs and incubated with 5% air at for 2 days to permit attachment. The reconstructed samples were then transferred to an air-liquid interface and incubated for another 9 days to allow expansion of the epidermal layer. A diameter superficial excision wound was created in the DED-HSEs using a biopsy punch (Integra Miltex, Fisher Scientific), and the reformed epidermal layer was removed. Then, sterile topical treatments were performed by adding the hydrogels directly to the wound bed surface for 4 days and 7 days.
MTT staining. The lateral migration of viable keratinocytes was observed using the MTT assay. Viable cells with active metabolism react with the tetrazolium ring of the MTT reagent to produce a purple formazan product. A frozen aliquot of a 10 -fold volume of MTT stock of (Sigma M5655) was diluted in PBS. The DED-HSE samples were placed in a 24 -well plate, and each well contained 1 ml of MTT reagent. The samples were incubated in a air incubator at for 90 min to allow the formation of formazan product. Images of the DED-HSEs were captured using a Nikon SMZ745T microscope. Quantification of the unhealed wound area was performed using ImageJ software.
Hematoxylin and eosin (H&E) staining. On days 4 and 7 after wounding, the DED-HSEs following MTT analysis were fixed in formalin overnight before embedding in paraffin. Sections of thickness were cut and transferred onto glass slides. These sections were dewaxed in xylene and rehydrated in descending concentrations of ethanol before H&E staining. Images were captured using an Olympus BX43 microscope.
Immunohistochemistry (IHC). DED-HSEs were fixed, embedded, cut into thin sections, dewaxed and rehydrated as described above. Sections were then immersed in an antigen retrieval, citrate buffer pH 6.0 , and heat-induced epitope retrieval was performed in a water bath for 15 min . was used to quench endogenous peroxidase for 30 min . Then, the sections were blocked and incubated with antiK10 (1:200), anti-K14 (1:25), and anti-p63 (1:50) primary antibodies for 2 h at room temperature. The slides were washed with PBS containing Tween 20 and incubated with horseradish peroxidase (HRP)labeled anti-mouse polymer (1:200) and HRP-labeled anti-rabbit polymer ( ) secondary antibodies for 1 h at room temperature. IHC sections were developed with diaminobenzidine (DAB) substrate, and nuclei were counterstained with hematoxylin, dehydrated through ascending concentrations of ethanol to xylene, and finally mounted onto coverslips. Images were captured using an Olympus BX43 microscope.
Antimicrobial properties of the hydrogel films and fibers in vitro Antimicrobial assay towards planktonic bacteria. Bacteria (MRSA USA300, CR-AB, PAO1 or CR-PA) were inoculated into MHB ( 4 mL ) and cultured at with shaking at 220 rpm to a mid-log phase. Cultured bacteria were collected by centrifugation and decanting of the supernatant. Collected bacteria were washed thrice with PBS and suspended in PBS at a concentration of . Hydrogel film or fiber samples were inoculated with of bacterial suspension (containing ) spread evenly on the sample surface. A Petri dish without hydrogel film or fiber sample was inoculated as a control. The samples were incubated at and relative humidity for 1 h . After incubation, bacteria were released from the samples by immersion in 1 mL of PBS and agitation with a vortex mixer. The obtained bacterial suspensions were serially diluted 10 -fold with PBS in a 96 -well plate, and plated on LB agar. The agar plates were incubated at for 16 h , and the bacterial colonies were counted. The results are reported as:
Biofilm contact killing assay. Sterile sections of polycarbonate membrane (Whatman, New Jersey) were placed on LB agar plates. A bacterial suspension in PBS ( ) containing approximately CFU was inoculated onto the membrane surface. The membranes were incubated at for 24 h to form biofilm gels. The biofilms on the membrane were then treated by contact with fiber samples and incubated at for 24 h . Bacteria were liberated by vortexing the membrane in Dey/Engley medium, serially diluted 10fold in PBS, and then plated on LB agar. The LB agar plates were incubated at for 24 h , and the bacterial colonies were counted.
In vitro biocompatibility assay of PIM-Mal and hydrogels
Biocompatibility studies were carried out on mouse 3T3 fibroblasts and HDFs (NHDF-Ad-Der Fibroblasts, CC2511, Lonza). DMEM fully supplemented with fetal bovine serum (FBS, ), l-glutamine ( 1 mM ), and antibiotics (penicillin-streptomycin, 1%) was used as cell culture medium.
MTT assay of the hydrogel extracts. Hydrogel film or fiber samples were placed in each well of a 24 -well plate with 1 mL of DMEM and incubated at for 24 h to collect the extracts. HDF or 3T3 cells were cultured in 1 mL DMEM in 24-well plates from an initial density of cells in each well and incubated in a incubator at for 24 h for cell attachment. The DMEM was aspirated and replaced with the sample extracts (or fresh DMEM for positive control) to incubate with the cells at for 24 h . Then, the culture media were replaced with 1 mL MTT solution ( in DMEM) and incubated at for 4 h to stain viable cells. The MTT solution was gently aspirated, and 1 mL dimethyl sulfoxide (DMSO) was added to each well. After 15 min , the absorbance of each well at 570 nm was measured using Tecan i-control microplate reader. The absorbance of DMSO was measured as a blank control. The cell viability was calculated using the equation:
where , and are the absorbance of the sample, blank, and positive control, respectively.
Direct contact MTT assay. The procedures were the same as above (MTT assay of the hydrogel extracts), but instead of immersing the cells with supernatant extracts, the hydrogel film or fiber samples were directly immersed in the culture medium in the wells containing
the attached cells for 24 h and then removed before replacing the medium with MTT solution.
In vivo murine model of infected diabetic wound treatment
All mouse studies were carried out under the regulation of the Institutional Animal Care and Use Committee (IACUC) of Nanyang Technological University (NTU) under the approved protocol numbers A18051 and A21023.
Diabetic induction on mice. Eight-week-old male C57BL/6 mice were conditioned by fasting for 4 h prior to the start of diabetic induction injections. Diabetes was induced with streptozotocin (STZ) solution, 4 mg STZ dissolved in 1 mL of sodium citrate buffer ( 50 mM ) at pH 4 , injected intraperitoneally at dosage daily for 5 consecutive days. Liver Disease Progression Aggravation Diet (LIDPAD, provided by N.S. Tan’s lab (NTU)) and sucrose water solution were supplied during the 5 days of injection and then changed to regular diet and water on day 6 onward. Mouse blood glucose levels were measured 3 weeks after the end of injection. The mice were assessed to be diabetic if their blood glucose level surpassed .
Bacterial load enumeration on skin wound infection model. Mice were anesthetized and depilated, and a diameter full-thickness excisional wound was created on the dorsal skin and the underlying panniculus carnosus . In total, of bacterial suspension (MRSA USA300, CR-AB, PA01 or CR-PA at CFU in PBS) was inoculated onto the wounds and left to settle for 10 min before covering the infected wounds with transparent Tegaderm patch ( 3 M ). The wounds were left untreated for 24 h to allow the inoculated bacteria to form biofilms. Hydrogel film or fiber dressings were applied as treatment condition after the 24 h infection period. Untreated wounds served as controls. After 24 h , the dressings were removed and the wounds (including 5 mm of the peripheral region) were excised. For biofilm imaging, excised wound tissue was placed in PBS ( 1 mL ) and observed with an LSM 800 confocal microscope (ZEISS). For bacterial counting, excised wound tissue was homogenized in of PBS to release the bacteria ( ). The bacterial suspension was serially diluted 10 -fold with PBS in a 96 -well plate. The diluted suspensions were plated on LB agar, and the agar plates were incubated at for 16 h , after which the bacterial colonies were counted. The two-tailed Student’s -test was used for statistical analysis.
Wound healing study. As described above, wounds infected with MRSA USA300 or CR-PA biofilms were created on mice. At day 0, untreated wounds were secured with Tegaderm as control; hydrogel film or fiber dressing, secured with Tegaderm, was applied to treatment condition wounds. The wounds were photographed before dressing application and on days and 14 of the treatment period, at which time points the dressings were replaced with fresh ones. For AlgPPN treatment group, Alg-PPN(C8)-5 was applied to the wound until day 5 to eradicate bacteria, followed by replacement with Alg-PPN(C4)5 from day 5 to day 14 . At each time point, the wound size was measured using ImageJ software ( ). The two-tailed Student’s -test was used for statistical analysis. Relative wound size is reported as:
Fluorescence-activated cell sorting (FACS) analysis of inflammatory cells. Wounds (including 5 mm of the peripheral region) were excised after 2 days of treatment of the mouse wound healing study. Single-cell suspensions were obtained from the wound samples using a gentleMACS Dissociator (Miltenyi Biotec). The cells were immune-labeled with and Ly6G, and cytometry was performed using an Accuri C6 flow cytometer (BD Biosciences). The
cytometry data was analyzed using FlowJo software (version 7.6.5, Tree Star). Analysis results are plotted as mean percentage values standard error of the mean (SEM, ). The two-tailed Student’s -test was used for statistical analysis.
Enzyme-linked immunosorbent assay (ELISA) for wound healingrelated factors. After 2 days of treatment of the mouse wound healing study, wounds (including 5 mm of the peripheral region) were excised, homogenized in of PBS and centrifuged to remove tissue and bacteria. The supernatants were assayed with various ELISA kits (proMMP9, VEGF-A, PDGF-BB, FGF-2 and EGF) according to the manufacturer’s protocols (Lonza). The results for each treatment are plotted as mean concentration values SEM ( ). The two-tailed Student’s test was used for statistical analysis.
Histological analysis and histochemical staining
On day 7 post-treatments, animals were sacrificed using asphyxiation. The wound tissue, along with the surrounding tissue, was carefully excised and fixed in formalin. Subsequently, tissue samples were dehydrated, embedded in paraffin wax blocks, and cut into thick sections using a Leica Microtome (Leica Biosystems). These sections were then collected on Superfrost Plus glass slides (ThermoFisher Scientific). The sections were processed and stained with hematoxylin and eosin (H&E) and picrosirius red. The stained slides were imaged using Axio Scan.Z1 microscope system (ZEISS). Granulation tissue thickness and collagen content were quantified using ImageJ software.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The experimental data generated in this study are provided within the Article and Supplementary Information. All data are available from the corresponding authors upon request.
References
Singer, A. J. & Clark, R. A. F. Cutaneous wound healing. N. Engl. J. Med. 341, 738-746 (1999).
Han, G. & Ceilley, R. Chronic wound healing: A review of current management and treatments. Adv. Ther. 34, 599-610 (2017).
Simoes, D. et al. Recent advances on antimicrobial wound dressing: A review. Eur. J. Pharm. Biopharm. 127, 130-141 (2018).
Eming, S. A., Hammerschmidt, M., Krieg, T. & Roers, A. Interrelation of immunity and tissue repair or regeneration. Semin. Cell Dev. Biol. 20, 517-527 (2009).
Frykberg, R. G. & Banks, J. Challenges in the treatment of chronic wounds. Adv. Wound Care 4, 560-582 (2015).
Fife, C. E., Carter, M. J., Walker, D. & Thomson, B. Wound care outcomes and associated cost among patients treated in US outpatient wound centers: Data From the US Wound Registry. Wounds 24, 10-17 (2012).
Sen, C. K. Human wound and its burden: Updated 2020 compendium of estimates. Adv. Wound Care 10, 281-292 (2021).
Martin, P. & Nunan, R. Cellular and molecular mechanisms of repair in acute and chronic wound healing. Br. J. Dermatol. 173, 370-378 (2015).
Eming, S. A., Martin, P. & Tomic-Canic, M. Wound repair and regeneration: Mechanisms, signaling, and translation. Sci. Transl. Med. 6, 265sr6 (2014).
Eming, S. A. et al. Differential proteomic analysis distinguishes tissue repair biomarker signatures in wound exudates obtained from normal healing and chronic wounds. J. Proteome Res. 9, 4758-4766 (2010).
Beidler, S. K. et al. Inflammatory cytokine levels in chronic venous insufficiency ulcer tissue before and after compression therapy. J. Vasc. Surg. 49, 1013-1020 (2009).
Dunnill, C. et al. Reactive oxygen species (ROS) and wound healing: the functional role of ROS and emerging ROS-modulating technologies for augmentation of the healing process. Int. Wound J. 14, 89-96 (2017).
Ozkaya, H. et al. Successful treatment of non-healing pressure ulcers with topical n-acetyl cysteine. J. Wound Care 24, 608-611 (2015). 606.
Deniz, M., Borman, H., Seyhan, T. & Haberal, M. An effective antioxidant drug on prevention of the necrosis of zone of stasis: N-acetylcysteine. Burns 39, 320-325 (2013).
Castro, B. et al. Development and preclinical evaluation of a new galactomannan-based dressing with antioxidant properties for wound healing. Histol. Histopathol. 30, 1499-1512 (2015).
Comino-Sanz, I. M., López-Franco, M. D., Castro, B. & PancorboHidalgo, P. L. Antioxidant dressing therapy versus standard wound care in chronic wounds (the REOX study): study protocol for a randomized controlled trial. Trials 21, 505 (2020).
Castro, B. et al. The use of an antioxidant dressing on hard-to-heal wounds: a multicentre, prospective case series. J. Wound Care 26, 742-750 (2017).
James, G. A. et al. Biofilms in chronic wounds. Wound Repair Regen 16, 37-44 (2008).
Tomic-Canic, M., Burgess, J. L., O’Neill, K. E., Strbo, N. & Pastar, I. Skin microbiota and its interplay with wound healing. Am. J. Clin. Dermatol. 21, 36-43 (2020).
Edwards, R. & Harding, K. G. Bacteria and wound healing. Curr. Opin. Infect. Dis. 17, 91-96 (2004).
Kirkup, B. C. Jr Bacterial strain diversity within wounds. Adv. Wound Care 4, 12-23 (2015).
Gompelman, M., van Asten, S. A. & Peters, E. J. Update on the role of infection and biofilms in wound healing: Pathophysiology and treatment. Plast. Reconstr. Surg. 138, 61S-70S (2016).
Jayathilake, P. G. et al. Extracellular polymeric substance production and aggregated bacteria colonization influence the competition of microbes in biofilms. Front. Microbiol. 8, 1865 (2017).
Shiekh, P. A., Singh, A. & Kumar, A. Exosome laden oxygen releasing antioxidant and antibacterial cryogel wound dressing OxOBand alleviate diabetic and infectious wound healing. Biomaterials 249, 120020 (2020).
Ma, T. et al. A smart nanoplatform with photothermal antibacterial capability and antioxidant activity for chronic wound healing. Adv. Healthcare Mater. 10, 2100033 (2021).
Liang, Y., Zhao, X., Hu, T., Han, Y. & Guo, B. Mussel-inspired, antibacterial, conductive, antioxidant, injectable composite hydrogel wound dressing to promote the regeneration of infected skin. J. Colloid Interface Sci 556, 514-528 (2019).
Ge, P. et al. An antioxidant and antibacterial polydopaminemodified thermo-sensitive hydrogel dressing for Staphylococcus aureus-infected wound healing. Nanoscale 15, 644-656 (2023).
Lindner, J.-P. Imidazolium-based polymers via the poly-radziszewski reaction. Macromolecules 49, 2046-2053 (2016).
Zhong, W. et al. Designer broad-spectrum polyimidazolium antibiotics. Proc. Natl. Acad. Sci. USA 117, 31376-31385 (2020).
Martinez-Jothar, L. et al. Insights into maleimide-thiol conjugation chemistry: Conditions for efficient surface functionalization of nanoparticles for receptor targeting. J. Control. Release 282, 101-109 (2018).
Nair, D. P. et al. The thiol-michael addition click reaction: A powerful and widely used tool in materials chemistry. Chem. Mater. 26, 724-744 (2013).
Xie, Y. et al. Development of a three-dimensional human skin equivalent wound model for investigating novel wound healing therapies. Tissue Eng. C: Methods 16, 1111-1123 (2010).
Fernandez, T. L., Van Lonkhuyzen, D. R., Dawson, R. A., Kimlin, M. G. & Upton, Z. Characterization of a human skin equivalent model to study the effects of ultraviolet B radiation on keratinocytes. Tissue Eng. C: Methods 20, 588-598 (2014).
Ibberson, C. B. et al. Hyaluronan modulation impacts Staphylococcus aureus biofilm infection. Infect. Immun. 84, 1917-1929 (2016).
Hariono, M., Yuliani, S. H., Istyastono, E. P., Riswanto, F. D. O. & Adhipandito, C. F. Matrix metalloproteinase 9 (MMP9) in wound healing of diabetic foot ulcer: Molecular target and structure-based drug design. Wound Med. 22, 1-13 (2018).
Martin, P. Wound healing-aiming for perfect skin regeneration. Science 276, 75-81 (1997).
Pastar, I. et al. Epithelialization in wound healing: A comprehensive review. Adv. Wound Care 3, 445-464 (2014).
Dreier, R., Grässel, S., Fuchs, S., Schaumburger, J. & Bruckner, P. Pro-MMP-9 is a specific macrophage product and is activated by osteoarthritic chondrocytes via MMP-3 or a MT1-MMP/MMP-13 cascade. Exp. Cell Res. 297, 303-312 (2004).
Noor, S., Zubair, M. & Ahmad, J. Diabetic foot ulcer-A review on pathophysiology, classification and microbial etiology. Diabetes Metab. Syndr. 9, 192-199 (2015).
Yeo, C. K. et al. Hydrogel effects rapid biofilm debridement with ex situ contact-kill to eliminate multidrug resistant bacteria in vivo. ACS Appl. Mater. Interfaces 10, 20356-20367 (2018).
Li, P. et al. A polycationic antimicrobial and biocompatible hydrogel with microbe membrane suctioning ability. Nat. Mater. 10, 149-156 (2011).
Kim, J. H. et al. High levels of oxidative stress and skin microbiome are critical for initiation and development of chronic wounds in diabetic mice. Sci. Rep. 9, 19318 (2019).
Schäfer, M. & Werner, S. Oxidative stress in normal and impaired wound repair. Pharmacol. Res. 58, 165-171 (2008).
Forman, H. J., Zhang, H. & Rinna, A. Glutathione: Overview of its protective roles, measurement, and biosynthesis. Mol. Aspects Med. 30, 1-12 (2009).
Jault, P. et al. Efficacy and tolerability of a cocktail of bacteriophages to treat burn wounds infected by Pseudomonas aeruginosa (PhagoBurn): a randomised, controlled, double-blind phase 1/ 2 trial. Lancet Infect. Dis. 19, 35-45 (2019).
Manzuoerh, R., Farahpour, M. R., Oryan, A. & Sonboli, A. Effectiveness of topical administration of Anethum graveolens essential oil on MRSA-infected wounds. Biomed. Pharmacother. 109, 1650-1658 (2019).
Chen, C. Y. et al. Exosomal DMBT1 from human urine-derived stem cells facilitates diabetic wound repair by promoting angiogenesis. Theranostics 8, 1607-1623 (2018).
Guo, S. C. et al. Exosomes derived from platelet-rich plasma promote the re-epithelization of chronic cutaneous wounds via activation of YAP in a diabetic rat model. Theranostics 7, 81-96 (2017).
Zhou, C. et al. Engineering poly(ionic liquid) semi-IPN hydrogels with fast antibacterial and anti-inflammatory properties for wound healing. Chem. Eng. J. 413, 127429 (2021).
Romero-Montero, A. et al. Development of an antimicrobial and antioxidant hydrogel/nano-electrospun wound dressing. RSC Adv 10, 30508-30518 (2020).
Li, X. et al. Antibacterial, antioxidant and biocompatible nanosized quercetin-PVA xerogel films for wound dressing. Colloids Surfs B: Biointerfaces 209, 112175 (2022).
Hassan, M. A. et al. Antioxidant and antibacterial polyelectrolyte wound dressing based on chitosan/hyaluronan/phosphatidylcholine dihydroquercetin. Int. J. Biol. Macromol. 166, 18-31 (2021).
Chen, C., Zhou, J. & Ji, C. Quercetin: A potential drug to reverse multidrug resistance. Life Sci. 87, 333-338 (2010).
Shtenberg, Y., Goldfeder, M., Schroeder, A. & Bianco-Peled, H. Alginate modified with maleimide-terminated PEG as drug carriers with enhanced mucoadhesion. Carbohydr. Polym. 175, 337-346 (2017).
Bernkop-Schnürch, A., Kast, C. E. & Richter, M. F. Improvement in the mucoadhesive properties of alginate by the covalent attachment of cysteine. J. Control. Release 71, 277-285 (2001).
Davidovich-Pinhas, M. & Bianco-Peled, H. Alginate-PEGAc: A new mucoadhesive polymer. Acta Biomater 7, 625-633 (2011).
Rheinwatd, J. G. & Green, H. Seria cultivation of strains of human epidemal keratinocytes: the formation keratinizin colonies from single cell is. Cell 6, 331-343 (1975).
Hardwick, R., Viergever, C., Chen, A. & Nguyen, D. 3D bioengineered tissues: From advancements in in vitro safety to new horizons in disease modeling. Clin. Pharmacol. Ther. 101, 453-457 (2017).
Tan, N. S. & Wahli, W. Studying wound repair in the mouse. Curr. Protoc. Mouse Biol. 3, 171-185 (2013).
Acknowledgements
We thank Dr. Xi Liu (Institute of Microbiology of the Chinese Academy of Sciences) and Dr. Ke Wang (Guangxi Medical University) for their advice in the animal study. This work was funded and supported by an ASTAR Industry Alignment Fund Pre-Positioning Programme (IAF-PP, HBMS Domain) H17/01/a0/OB9, H17/01/a0/OM9, and H19/01/aO/OY9 as part of the Wound Care Innovation for the Tropics (WCIT, HBMS Domain, H17/ 01/a0/009) and the Singapore MOE Tier 3 grant (MOE2018-T3-1-003). This research was also supported by the National Research Foundation, Prime Minister’s Office, Singapore, under its Campus for Research Excellence and Technological Enterprise (CREATE) programme, through the SMART AMR IRG. C.F, P.L.L.K. and D.I.L. acknowledge infrastructure support from ASTAR (IAF-PP, HBMS Domain, H17/01/a0/004). C.K.Y. acknowledges the support of NTU IGS-HealthTech Ph.D. scholarship and the A*STAR IAF (WCIT, H17/01/a0/009).
Author contributions
D.P. performed the experimental work of film hydrogel and alginate fiber hydrogel. C.K.Y. performed the experimental work of film hydrogel. D.P. and C.K.Y. synthesized the polyimidazolium and hydrogel dressings, and performed the in vitro and in vivo experiments. Y.W., C.F., P.L.K.L., and D.I.L. designed, performed, and interpreted the ex vivo human skin equivalent wound model experiments. X.X. performed the antibiofilm assay of polyimidazolium. Y.S.Y. and M.I.G.V. assisted in the mouse experiment. S.H.M. established the chemistry of polyimidazolium syntheses and performed NMR characterization. N.S.T. and L.Y. advised on the design and interpretation of in vivo diabetic mouse wound model experiments. M.B.C.-P. advised on the design and interpretation of all experiments and directed the overall project. D.P., C.K.Y. and M.B.C.-P. wrote and edited the manuscript. P.T.H., D.I.L. and N.S.T. edited the manuscript. D.I.L. and M.B.C.-P. acquired the funding to support this project.
Competing interests
D.P., C.K.Y., Y.W., X.X., N.S.T., and M.B.C.-P. have filed the Singapore provisional patents for this work under the patent numbers 10202250243U and 10202301624S. C.K.Y., S.H.M., N.S.T., and M.B.C.-P. have filed a patent for this work under the patent number US2O210244846A1. D.P., C.K.Y, Y.W., X.X., S.H.M, N.S.T, and M.B.C.-P. declare no other competing interests. C.F., Y.S.Y., M.I.G.V., P.L.K.L., L.Y., P.T.H., and D.I.L. declare no competing interests.
Correspondence and requests for materials should be addressed to Nguan Soon Tan or Mary B. Chan-Park.
Peer review information : Nature Communications thanks the anonymous reviewers for their contribution to the peer review of this work. A peer review file is available.
Centre for Antimicrobial Bioengineering, School of Chemistry, Chemical Engineering and Biotechnology, Nanyang Technological University, 62 Nanyang Drive, Singapore 637459, Singapore. Antimicrobial Resistance Interdisciplinary Research Group, Singapore-MIT Alliance for Research and Technology, Singapore 138602, Singapore. NTU Institute for Health Technologies, Interdisciplinary Graduate School, Nanyang Technological University, Singapore 637553, Singapore. Skin Research Institute of Singapore, Agency for Science, Technology and Research (A*STAR), 11 Mandalay Road, Singapore 308232, Singapore. Wenzhou Institute, University of Chinese Academy of Sciences, Wenzhou, Zhejiang 325000, China. Lee Kong Chian School of Medicine, Nanyang Technological University, 59 Nanyang Drive, Singapore 636921, Singapore. School of Medicine, Southern University of Science and Technology, Shenzhen 518055, China. Department of Chemical Engineering, Massachusetts Institute of Technology, Cambridge, MA 02142, USA. School of Biological Sciences, Nanyang Technological University, 60 Nanyang Drive, Singapore 637551, Singapore. e-mail: nstan@ntu.edu.sg; mbechan@ntu.edu.sg