نموذج اللغة الطبية الكبير المعتمد على الأدلة عبر استرجاع الرسوم البيانية: RAG الطبي
الملخص
نقدم MedGraphRAG، إطار عمل جديد قائم على الرسوم البيانية لتعزيز الجيل المعزز بالاسترجاع (RAG) مصمم لتحسين نماذج اللغة الكبيرة في توليد استجابات طبية قائمة على الأدلة، مما يعزز السلامة والموثوقية باستخدام بيانات طبية خاصة. نقدم بناء الرسم البياني الثلاثي واسترجاع U لتعزيز GraphRAG، مما يمكّن من الحصول على رؤى شاملة وتوليد استجابات قائمة على الأدلة للتطبيقات الطبية. على وجه التحديد، نقوم بربط مستندات المستخدم بمصادر طبية موثوقة ودمج الاسترجاع الدقيق من الأعلى مع تحسين الاستجابة من الأسفل لتحقيق وعي متوازن بالسياق وفهرسة دقيقة. تم التحقق من صحة MedGraphRAG على 9 معايير أسئلة وأجوبة طبية، و2 من مجموعات بيانات التحقق من الحقائق الصحية، ومجموعة اختبار لتوليد النصوص الطويلة، حيث يتفوق MedGraphRAG على النماذج الرائدة مع ضمان مصادر موثوقة. كودنا متاح للجمهور.
1 المقدمة
لا تشوه أو تعدل أو تضف عناصر إبداعية إلى البيانات. للأسف، فإن التحقق من دقة الاستجابات في الطب يمثل تحديًا خاصًا للمستخدمين غير الخبراء. لذلك، فإن القدرة على إجراء استدلالات معقدة باستخدام مجموعات بيانات خارجية كبيرة، مع توليد استجابات دقيقة وموثوقة مدعومة بمصادر يمكن التحقق منها، أمر بالغ الأهمية في التطبيقات الطبية لنماذج اللغة الكبيرة.
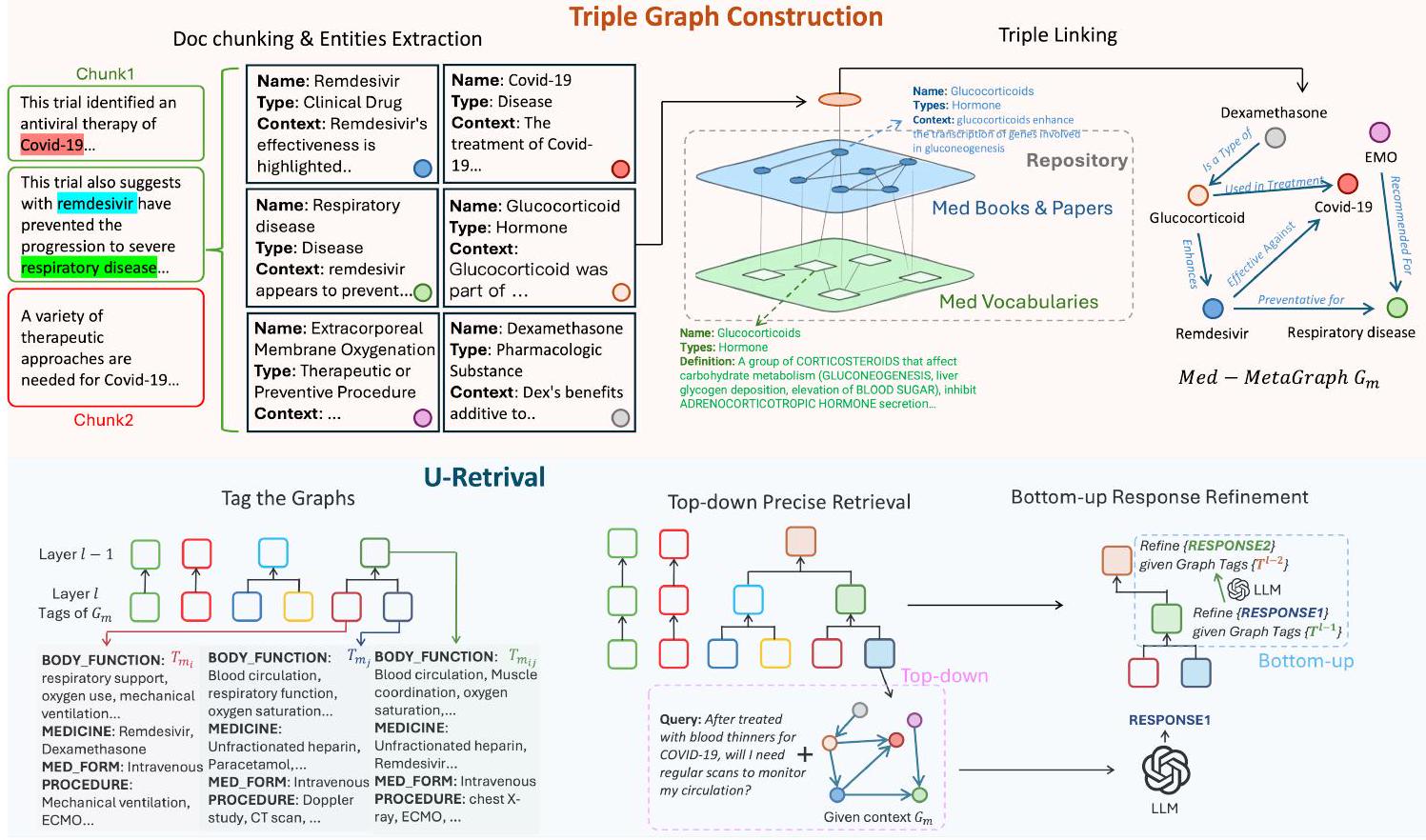
يثبت جودة الاستجابة بتكاليف قليلة. في بناء الرسم البياني الثلاثي، نصمم آلية لربط بيانات RAG الخاصة بالمستخدم بالأوراق الطبية الموثوقة والقواميس الطبية الأساسية. هذه العملية تولد ثلاثيات [بيانات RAG، المصدر، التعريف] لبناء رسم بياني شامل لوثائق المستخدم. يعزز ذلك من تفكير LLM ويضمن أن تكون الاستجابات قابلة للتتبع إلى مصادرها وتعريفاتها، مما يضمن الموثوقية والقدرة على الشرح. كما طورنا استراتيجية فريدة لاسترجاع U-Retrieval للرد على استفسارات المستخدم. بدلاً من بناء مجتمعات رسومية مكلفة، نقوم بتبسيط العملية من خلال تلخيص كل رسم بياني باستخدام علامات طبية محددة مسبقًا، ثم نقوم بتجميع الرسوم البيانية المماثلة بشكل تكراري لتشكيل هيكل علامات هرمي متعدد الطبقات، من علامات عامة إلى علامات تفصيلية. يقوم LLM بإنشاء علامات لاستفسار المستخدم ويقوم بفهرسة الرسم البياني الأكثر صلة بناءً على تشابه العلامات بطريقة من أعلى إلى أسفل، مستخدمًا إياها لصياغة الاستجابة الأولية. ثم يقوم بتحسين الاستجابة من خلال دمج العلامات العليا بشكل تدريجي بطريقة من أسفل إلى أعلى حتى يتم توليد الإجابة النهائية. توازن تقنية U-Retrieval هذه بين الوعي بالسياق العالمي وكفاءة الاسترجاع.
- نحن الأوائل الذين اقترحوا إطارًا متخصصًا لتقديم RAG القائم على الرسوم البيانية في المجال الطبي، والذي أطلقنا عليه اسم MedGraphRAG.
- لقد طورنا طرق بناء الرسوم البيانية الثلاثية الفريدة وطرق استرجاع U التي تمكّن نماذج اللغة الكبيرة من توليد استجابات قائمة على الأدلة بكفاءة باستخدام بيانات RAG الشاملة.
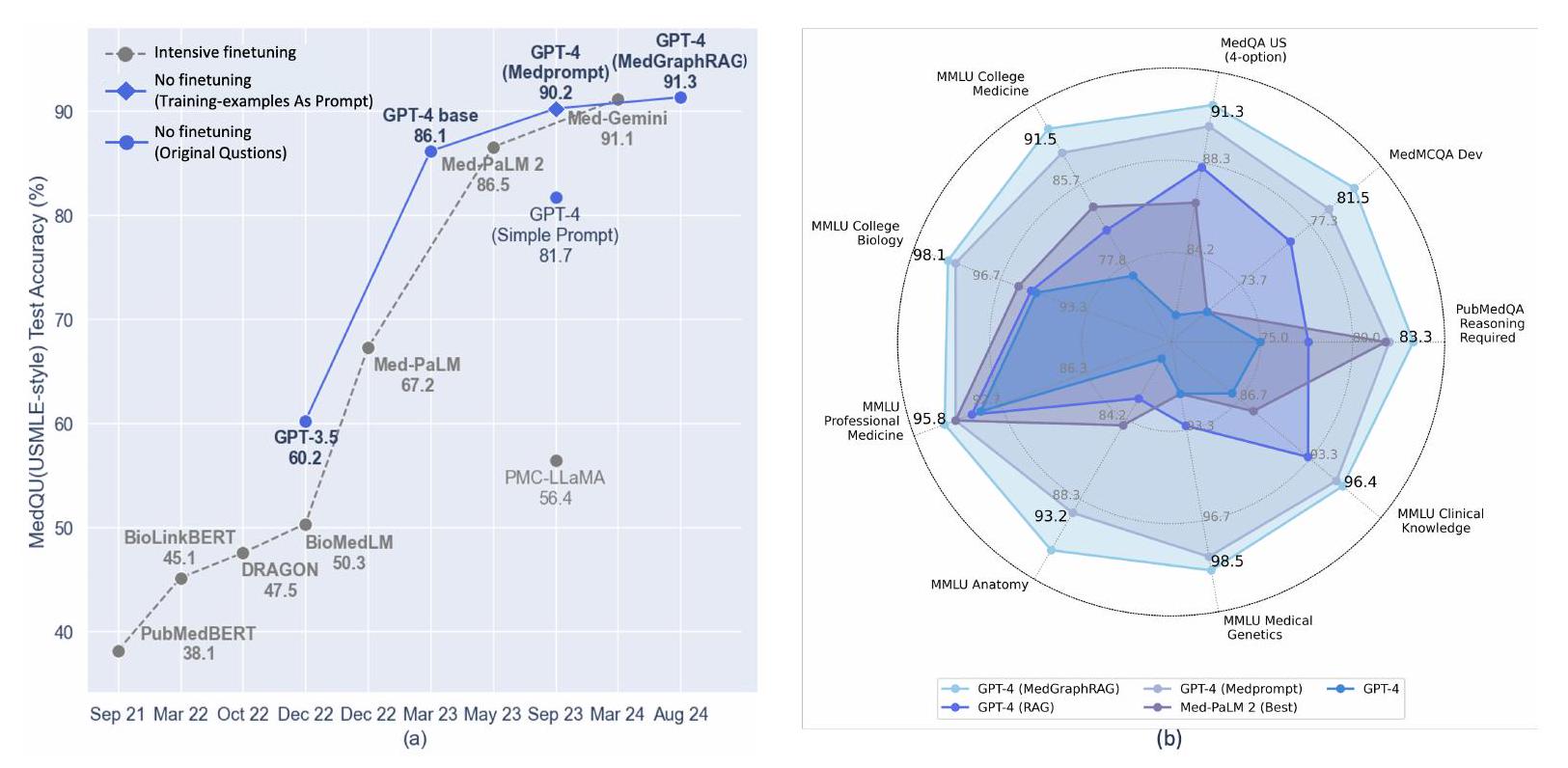
- MedGraphRAG يتفوق على طرق الاسترجاع الأخرى ونماذج اللغة الطبية المدربة بشكل مكثف عبر مجموعة واسعة من معايير الأسئلة والأجوبة الطبية.
إنشاء SOTAs الجديدة. - تم التحقق منه من خلال تقييمات بشرية، MedGraphRAG قادر على توليد استجابات أكثر قابلية للفهم وقائمة على الأدلة في المجال الطبي.
2 طريقة
2.1 بناء الرسم الثلاثي
2.1.1 تمهيدي: تقسيم الوثائق واستخراج الكيانات
2.1.2 الربط الثلاثي
2.2 استرجاع U
2.2.1 تمهيدي: وسم الرسم البياني
كل ميتا-ميدغراف
2.2.2 الاسترجاع الدقيق من الأعلى إلى الأسفل
في الطبقة
2.2.3 تحسين الاستجابة من الأسفل إلى الأعلى
3 تجربة
3.1 مجموعة البيانات
3.1.1 بيانات RAG
3.1.2 بيانات المستودع
3.1.3 بيانات الاختبار
3.2 إعداد التجربة
3.3 النتائج
3.3.1 تقييم متعدد الخيارات
تحسين متوسط يقارب
3.3.2 تقييم توليد النصوص الطويلة
(CP)، استرجاع الاقتباسات (CR)، وقابلية الفهم (Und.). كما هو موضح في الجدول 2، حصل MedGraphRAG على تقييمات أعلى باستمرار عبر جميع المقاييس. ومن الجدير بالذكر أنه أظهر ميزة كبيرة في CP وCR وUnd.، مما يشير إلى أن ردوده كانت مدعومة في كثير من الأحيان بمصادر دقيقة وكانت أسهل في الفهم، حتى لغير المتخصصين، بفضل الردود المدعومة بالأدلة والتفسيرات الواضحة للمصطلحات الطبية المعقدة.
3.4 الاستئصال والتحليل
3.4.1 دراسة الإزالة الشاملة
| نموذج | صحة مزيفة | الصحة العامة | مدكيو | مد MCQA | باب ميد كيو إيه | MMLU كول-مد | MMLU كول-بايو | إم إم إل يو برو-ميد | تشريح MMLU | جين MMLU | عيادة MMLU |
| الخطوط الأساسية بدون استرجاع | |||||||||||
| لاما 2-13B | 53.8 | ٤٩.٤ | 42.7 | 37.4 | 68.0 | 60.7 | 69.4 | 60.3 | 52.6 | 66.0 | 63.8 |
| لاما 2-70B | ٥٨.٩ | ٥٦.٧ | ٤٣.٧ | ٣٥.٠ | 74.3 | 64.2 | 84.7 | 75.0 | 62.3 | 74.0 | ٧١.٧ |
| لاما 3-8B | ٥١.١ | 53.2 | ٥٩.٨ | 57.3 | 75.2 | ٦١.٩ | 78.5 | 70.2 | 68.9 | ٨٣.٠ | ٧٤.٧ |
| لاما3-70B | 64.2 | 61.0 | 72.1 | 65.5 | 77.5 | 72.3 | 92.5 | ٨٦.٧ | 72.5 | ٨٣.٩ | 82.7 |
| جمني-برو | 60.6 | ٦٣.٧ | ٥٩.٠ | ٥٤.٨ | 69.8 | 69.2 | ٨٨.٠ | 77.7 | 66.7 | 75.8 | ٧٦.٧ |
| جي بي تي-4 | 71.4 | 70.9 | 78.2 | 72.6 | 75.3 | ٧٦.٧ | 95.3 | 93.8 | 81.3 | 90.4 | 86.2 |
| قاعدة
|
|||||||||||
| لاما 2-13B | ٥٦.٢ | 54.3 | ٤٨.١ | 42.0 | 68.6 | 62.5 | 68.3 | ٦٣.٧ | ٥١.٠ | 64.5 | 67.4 |
| لاما 2-70B | 64.6 | 63.2 | ٥٦.٢ | ٤٩.٨ | 75.2 | 69.6 | 85.8 | 77.4 | 63.0 | 75.8 | 73.3 |
| لاما 3-8B | 60.5 | ٥٩.٦ | 64.3 | ٥٨.٢ | 76.0 | 68.6 | 84.9 | 73.2 | 72.1 | 85.2 | 77.8 |
| لاما3-70B | 76.2 | 72.1 | 82.3 | 72.5 | 80.6 | 86.8 | 94.4 | 89.7 | 84.3 | 87.1 | 87.6 |
| جمني-برو | 72.5 | 68.4 | 64.5 | 57.3 | 76.9 | 79.0 | 91.3 | 86.4 | 79.5 | 80.4 | ٨٣.٩ |
| جي بي تي-4 | 78.6 | 77.3 | ٨٨.١ | 76.3 | 77.6 | 81.2 | 95.5 | 94.3 | ٨٣.١ | 92.9 | 93.1 |
| الخطوط الأساسية مع RAG الرسومي | |||||||||||
| لاما2-13B | ٥٨.٧ | ٥٧.٥ | ٥٢.٣ | ٤٤.٦ | 72.8 | 64.1 | 73.0 | 64.6 | ٥٢.١ | 66.2 | 67.9 |
| لاما 2-70B | 65.7 | ٦٣.٨ | ٥٥.١ | ٥٢.٤ | 74.6 | 68.0 | 86.4 | 79.2 | 64.6 | 73.9 | 75.8 |
| لاما3-8B | ٦١.٧ | 61.0 | 64.8 | ٥٨.٧ | 76.6 | 69.2 | 84.3 | 73.9 | 72.8 | 85.5 | 77.4 |
| لاما3-70B | ٧٧.٧ | ٧٤.٥ | 84.1 | 73.2 | 81.2 | ٨٧.٤ | 94.8 | 89.8 | 85.2 | 87.9 | ٨٨.٥ |
| جمني-برو | 73.8 | 70.6 | 65.1 | ٥٩.١ | 75.2 | 79.8 | 90.8 | 85.8 | 80.7 | 81.5 | 84.7 |
| جي بي تي-4 | 78.4 | 77.8 | ٨٨.٩ | 77.2 | ٧٧.٩ | 82.1 | 95.1 | 94.8 | 82.6 | 92.5 | 94.0 |
| الخطوط الأساسية مع MedGraphRAG | |||||||||||
| لاما 2-13B | 64.1 | ٦١.٢ | 65.5 | ٥١.٤ | 73.2 | 68.4 | 76.5 | 67.2 | ٥٦.٠ | 67.3 | 69.5 |
| لاما 2-70B | 69.3 | 68.6 | 69.2 | ٥٨.٧ | 76.0 | 73.3 | ٨٨.٦ | 84.5 | 68.9 | 76.0 | 77.3 |
| لاما 3-8B | 79.9 | 77.6 | 74.2 | ٦١.٦ | ٧٧.٨ | 89.2 | 95.4 | 91.6 | ٨٥.٩ | 89.3 | 89.7 |
| لاما3-70B | 81.2 | 79.2 | ٨٨.٤ | 79.1 | ٨٣.٨ | 91.4 | 96.5 | 93.2 | 89.8 | 91.0 | 94.1 |
| جمني-برو | 79.2 | 76.4 | 71.8 | 62.0 | 76.2 | 86.3 | 92.9 | 89.7 | 85.0 | 87.1 | 89.3 |
| جي بي تي-4 | 86.5 | ٨٣.٤ | 91.3 | 81.5 | ٨٣.٣ | 91.5 | 98.1 | 95.8 | 93.2 | 98.5 | 96.4 |
| بيانات | طرق | مناسب | كور. | سي بي | سي آر | و |
| مالتي ميد كيو إيه | داخل السطر | 91 | ٨٨ | ٨٠ | 74 | 85 |
| ATTR.FIRST | 93 | 91 | 86 | 77 | 93 | |
| سراب | 95 | 90 | 84 | 75 | 91 | |
| مدغراجراغ | 97 | 94 | 92 | 86 | 95 | |
| صحة متنوعة | داخل السطر | 95 | 84 | 78 | 71 | 81 |
| ATTR.FIRST | 96 | 91 | 81 | 78 | 85 | |
| سراب | 97 | 89 | 83 | 76 | 87 | |
| مدغرافراغ | 97 | 96 | 89 | 84 | 93 |
| مدكيو | باب ميد كيو إيه | مدMCQA | |
| GraphRAG | ٨٨.٩ | ٧٧.٩ | 77.2 |
| +بناء الرسم الثلاثي | 91.1 | 81.8 | 80.9 |
| +استرجاع-U |
|
|
|
3.4.2 تحليل مفصل لإزالة الربط الثلاثي
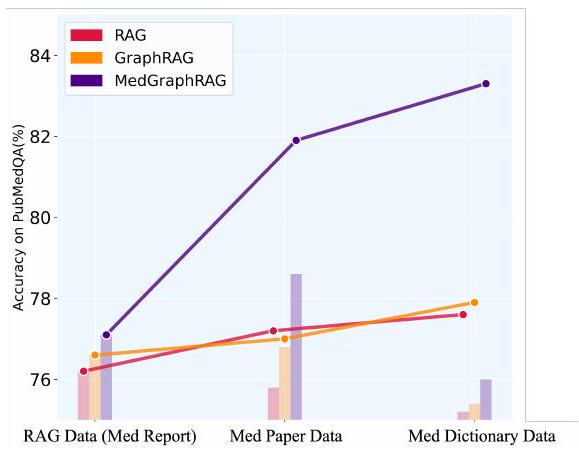
الرسم البياني في الشكل 3)، و(2) إضافة جميع المستويات الثلاثة بشكل تدريجي (الرسم البياني الخطي في الشكل 3). تظهر النتائج أن البيانات وطريقة الاسترجاع الصحيحة يجب أن تعمل معًا لإطلاق العنان للإمكانات الكاملة. عند استرجاع البيانات بواسطة RAG القياسي، فإن بيانات Med-Paper تحسن الأداء بشكل فردي بأقل من
3.5 تحليل تفصيلي على استرجاع U
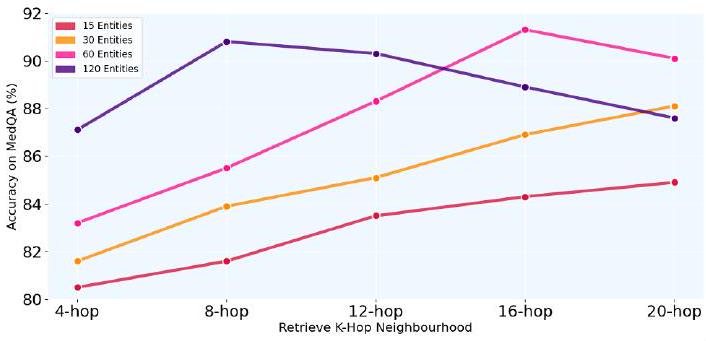
تم تحديده من خلال تجارب شاملة. أولاً، نقوم بفحص تأثير نطاق الاسترجاع، أي عدد الكيانات والجيران، باستخدام GPT-4 مع MedGraphRAG على MedQA، كما هو موضح في الشكل 4. تظهر نتائجنا أن استرجاع المزيد من البيانات لا يؤدي بالضرورة إلى أداء أفضل. في الواقع، يمكن أن تؤدي المزيد من البيانات إلى إدخال ضوضاء وتفاقم مشكلات أداء LLM مع السياقات الطويلة. يحدث الأداء الأقصى عندما يصل حجم الاسترجاع إلى حوالي 120 كيانًا مع 4 جيران أو 60 كيانًا مع 16 جيران. كان إعداد الجيران 16 أداءً أفضل قليلاً، على الأرجح بسبب قوة الربط القائم على الرسوم البيانية مقارنةً بالاسترجاع القائم على تشابه المتجهات.
4 الأعمال ذات الصلة
5 الخاتمة
6 قيود
استراتيجية تحديث محلية. على وجه التحديد، يمكننا حساب المسافة الدلالية بين المعرفة المدخلة حديثًا وMeta-Graphs الموجودة، وتطبيق التحديثات فقط على الرسوم الفرعية ذات الصلة التي تتجاوز عتبة محددة. هذه الطريقة الانتقائية في التحديث توازن بين الكفاءة والدقة. نحن ندرك هذه كقيود عملية ومهمة، ونخطط لتقديم مناقشة أكثر تفصيلًا حولها كجزء من عملنا المستقبلي في هذا الاتجاه البحثي.
شكر وتقدير
References
langchain. 2024. Enhancing rag-based application accuracy by constructing and leveraging knowledge graphs. https://blog.langchain.dev/enhancing-rag-based-applications-accuracy-by-constructing-and-leveraging-knowledge-graphs/.
microsoft. 2024. Microsoft azure graphrag. https://github.com/Azure-Samples/graphrag-accelerator?tab=readme-ov-file.
use of large language models to provide clinical recommendations in the emergency department. Nature Communications, 15(1):8236.
المحتويات
ب نتائج إضافية وتحليل ….. 13
ب. 1 مقارنة مع نماذج LLM الطبية SOTA ….. 13
ب. 2 دراسة حالة: GPT4 مع وبدون MedGraphRAG ….. 14
ب. 3 دراسة حالة: توليد طويل الشكل لـ MedGraphRAG ….. 14
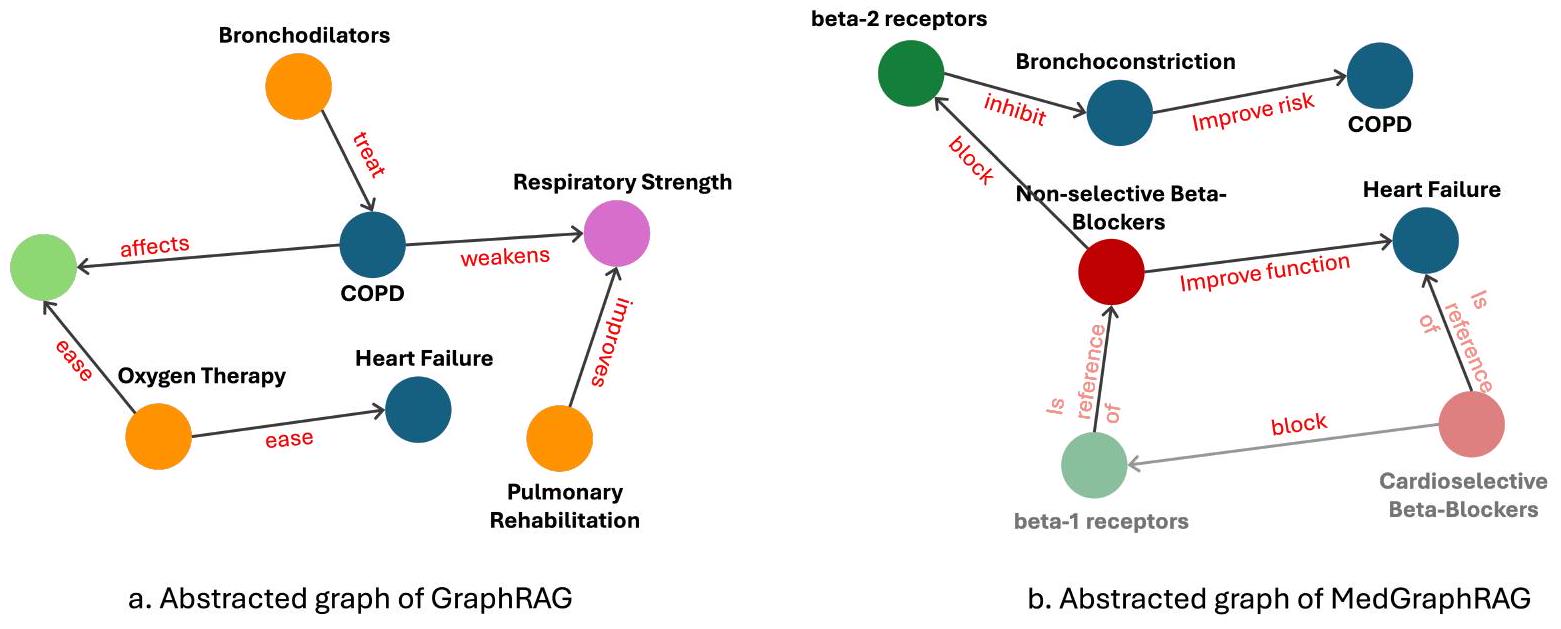
ب. 4 دراسة حالة: مقارنة الرسوم المجردة بين GraphRAG وMedGraphRAG ….. 14
ج تأثير الحدود ….. 15
تنفيذ مفصل
في استخراج الكيانات، ندرج معرفات فريدة لتتبع وثيقتها المصدر. في الممارسة العملية، بالنسبة لبيانات خصوصية المستخدم، نقوم بإنشاء معرف فريد عالميًا (UUID) لكل وثيقة كمعرفاتها. بالنسبة للأوراق الطبية والكتب، نستخدم معرف الكائن الرقمي (DOI) كمعرفاتها، وللقواميس الطبية، نستخدم معرفات المفاهيم الفريدة UMLS (CUI) كمعرفاتها. هذا المعرف ضروري لاسترجاع المعلومات من المصدر، مما يمكّن من إنشاء استجابات قائمة على الأدلة لاحقًا. لتوليد الملخصات المعتمدة على العلامات والدمج، نقوم بإدخال عشرة علامات في المطالبة في وقت واحد لتوليد الاستجابة بشكل تكراري.
ب نتائج إضافية وتحليل
ب. 1 مقارنة مع نماذج LLM الطبية SOTA
| MedQA | MedMCQA | PubMedQA | MMLU-Col-Med | MMLU-Col-Bio | MMLU-Pro-Med | MMLU-Anatomy | MMLU-Gene | MMLU-Clinic | |
| MedCPT | 79.6 | 74.9 | 76.8 | 77.8 | 95.4 | 93.9 | 82.6 | 90.9 | 88.3 |
| MedRAG | 88.5 | 78.1 | 78.9 | 85.5 | 96.8 | 94.8 | 84.5 | 93.6 | 94.5 |
| RAG2 | 85.2 | 76.2 | 79.3 | 83.4 | 96.1 | 94.8 | 83.9 | 91.0 | 93.2 |
| Self-BioRAG | 81.1 | 73.5 | 76.2 | 84.1 | 95.7 | 94.2 | 82.1 | 92.8 | 92.7 |
| نموذجنا | 91.3 | 81.5 | 83.8 | 91.5 | 98.1 | 95.8 | 93.2 | 98.5 | 96.4 |
ب. 2 دراسة حالة: GPT4 مع وبدون MedGraphRAG
استرجاع دقيق وواعي للسياق حتى في مجموعات RAG المعقدة وطويلة المدى.
ب. 3 دراسة حالة: توليد طويل الأمد لـ MedGraphRAG
ب. 4 دراسة حالة: مقارنة الرسوم البيانية المجردة بين GraphRAG وMedGraphRAG
ج. التأثير الأوسع
الشفافية، وقابلية التفسير، وقابلية التحقق. تضمن هذه الأداة أن كل استجابة يتم توليدها بواسطة LLM مصحوبة بمعلومات عن المصدر أو الأصل، مما يوضح بوضوح أن الإجابات مستندة إلى مجموعة البيانات. تتيح توفر المصادر المقتبسة لكل ادعاء للمستخدمين، خاصة في المجال الحرج للطب، تدقيق مخرجات LLM بسرعة ودقة مقابل المواد المصدر الأصلية. هذه الميزة حاسمة حيث (أ) يجب أن توجد علاقة موثوقة – تستند إلى شفافية التفكير، بين الخبراء البشريين ووكلاء LLM و (ب) حيث تكون أمان/خصوصية المعلومات المشتركة مع الوكيل أمرًا حيويًا. من خلال استخدام هذه الطريقة، قمنا بتطوير LLM طبي قائم على الأدلة. يمكن للأطباء التحقق بسهولة من مصدر التفكير وضبط استجابات النموذج، مما يضمن الاستخدام الآمن لنماذج LLM في السيناريوهات السريرية.
سؤال
سؤال:
الخيارات:
ب. الخرف الوعائي
ج. الخرف الجبهي الصدغي
د. خرف أجسام ليوي
الإجابة:
GPT-4
الإجابة:
أ. مرض الزهايمر
التفسير:
2. التصوير العصبي: على الرغم من أن التصوير بالرنين المغناطيسي يظهر تغييرات وعائية، إلا أن المناطق المتقطعة من انخفاض استقلاب الجلوكوز التي لوحظت في أشعة PET يمكن أن تتداخل أحيانًا مع أنماط مرض الزهايمر المبكرة، مما يعكس نشاط الدماغ المضطرب.
3. نمط الأعراض: بينما تظهر أعراضه تأثيرات وعائية، فإن النسيان العام وتدهور الإدراك المتزايد على مدار العام الماضي يمكن أن يتماشى أيضًا مع الطبيعة التقدمية لمرض الزهايمر.
MedGraphRAG
الإجابة:
ب. الخرف الوعائي
التفسير:
1. نتائج التصوير العصبي: يظهر التصوير بالرنين المغناطيسي تغييرات وعائية معتدلة وآفات في المادة البيضاء، وهو ما يتسم بأضرار إقفارية مزمنة شائعة في الخرف الوعائي، بدلاً من الأنماط التنكسية العصبية التي تُلاحظ عادةً في مرض الزهايمر أو الخرفات الأخرى [2].
2. النتائج الإضافية: تدعم أعراضه الإدراكية العرضية أيضًا أصلًا وعائيًا بدلاً من مرض عصبي تنكسي مثل مرض الزهايمر، الذي سيظهر عادةً تدهورًا إدراكيًا تدريجيًا ومتسقًا بدلاً من العرضي [3].
تدعم هذه العوامل مجتمعة تشخيص الخرف الوعائي، مما يتماشى أكثر مع تداعيات تاريخه الطبي الوعائي وطبيعة اضطراباته الإدراكية العرضية.
الأعراض العرضية: أعراض تحدث في حلقات منفصلة، بدلاً من أن تكون مستمرة. يمكن أن تختلف في الشدة والطبيعة وتكون عابرة، وعادة ما ترتبط بالأحداث العصبية.
السكتات الدماغية الصغيرة أو النوبات الإقفارية العابرة: السكتات الدماغية الصغيرة هي سكتات غير ملحوظة يمكن أن تسبب أعراضًا عصبية طفيفة مؤقتة. النوبات الإقفارية العابرة هي حلقات قصيرة من الخلل العصبي ناتجة عن فقدان تدفق الدم إلى الدماغ، وعادة ما تستمر أقل من 24 ساعة دون أن تسبب ضررًا دائمًا.
آفات المادة البيضاء: هذه مؤشرات على الأمراض الوعائية في الدماغ، بما في ذلك التغيرات في هيكل الأوعية الدموية ومناطق التلف في المادة البيضاء، وغالبًا ما تكون نتيجة لحالات نقص التروية المزمنة (نقص تدفق الدم). التلف الإقفاري المزمن: تلف طويل الأمد في أنسجة الدماغ ناتج عن تكرار أو استمرار تقليل تدفق الدم، مما يؤدي عادةً إلى فقدان وظيفة وصحة الخلايا العصبية.
أنماط التنكس العصبي: تشير إلى التغيرات الهيكلية والوظيفية في الدماغ المرتبطة بالأمراض العصبية التقدمية مثل مرض الزهايمر، حيث يحدث تدهور تدريجي وموت للخلايا العصبية. الأعراض المعرفية العرضية: ضعف معرفي متقلب يظهر في نوبات، مقابل التدهور المعرفي الثابت الذي يُرى في الأمراض التنكسية.
[1]: أوبراين، ج. ت.، وتوماس، أ. (2015). الخرف الوعائي. لانسيت، 386(10004)، 1698-1706.
[2]: سميث، إ. إ.، وبودين، أ. إ. (2018). رؤى جديدة حول مرض الأوعية الدموية الصغيرة في الدماغ وضعف الإدراك الوعائي من التصوير بالرنين المغناطيسي. الرأي الحالي في علم الأعصاب، 31(1)، 36-43.
[3]: غورليك، ب. ب.، سكتيري، أ.، بلاك، س. إ.، وآخرون. (2011). المساهمات الوعائية في ضعف الإدراك والخرف: بيان للمهنيين الصحيين من جمعية القلب الأمريكية / جمعية السكتة الدماغية الأمريكية. السكتة الدماغية، 42(9)، 2672-2713.
الترافق المرضي
مدغرافراج
تساعد موسعات الشعب الهوائية، مثل المحفزات بيتا-2 طويلة المفعول (LABAs)، على استرخاء عضلات مجرى الهواء، مما يقلل من تضيق الشعب الهوائية ويزيد من تدفق الهواء، وبالتالي يحسن من وظيفة الرئة [3،5]. تعمل مضادات المسكارين، مثل التيتروبيوم، عن طريق حجب تأثير الأستيل كولين على عضلات مجرى الهواء، مما يساعد بشكل أكبر في توسيع الشعب الهوائية وتخفيف أعراض مرض الانسداد الرئوي المزمن (COPD) [5]. يجب الاستمرار في استخدام هذه الأدوية كجزء من نظام العلاج لتعزيز كفاءة التنفس.
تعتبر حاصرات بيتا الانتقائية للقلب، مثل بيسوبرولول وميتوبروLOL، مفيدة بشكل خاص لمرضى COPD لأنها تستهدف بشكل أساسي مستقبلات بيتا-1 في القلب، مما يقلل من الضغط على القلب دون التأثير بشكل كبير على مستقبلات بيتا-2 التي تعتبر حيوية لوظيفة الرئة.
بالنسبة للمرضى الذين يعانون من كل من مرض الانسداد الرئوي المزمن وفشل القلب، يمكن أن يكون استخدام حاصرات بيتا الانتقائية للقلب بالتزامن مع موسعات الشعب الهوائية استراتيجية متوازنة وفعالة لتحسين كل من الصحة القلبية والرئوية. أظهرت الدراسات أن الاستخدام الحذر لحاصرات بيتا الانتقائية للقلب يقلل من خطر الوفاة دون تفاقم الأعراض التنفسية. تساعد هذه المعالجة المركبة في الحفاظ على وظيفة القلب مع تجنب التأثير السلبي على التنفس، مما يسهم في تحسين وظيفة الرئة وتحقيق نتائج أفضل بشكل عام لدى المرضى الذين يعانون من هذه الحالات المشتركة.
References:
2.Du Q, Sun Y, Ding N, Lu L. “Beta-blockers reduced the risk of mortality and exacerbation in patients with COPD: A meta-analysis of observational studies.” PLoS ONE. 2016; 11(11): e0166861.
3.O’Donnell DE, Parker CM. “COPD exacerbations . 3: Pathophysiology.” Thorax. 2006. 4.Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ. “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology.” European Journal of Heart Failure. 2009; 11(2): 130-139.
5.Tashkin DP, Celli B, Senn S, et al. “A 4-year trial of tiotropium in chronic obstructive pulmonary disease.” New England Journal of Medicine. 2008; 359(15): 1543-1554.
6.Rutten FH, Cramer MJ, Lammers JW, Grobbee DE, Hoes AW. “Heart failure and chronic obstructive pulmonary disease: An ignored combination?” European Journal of Heart Failure. 2006; 8(7): 706-711.
توضيح مصطلحي:
فشل القلب: حالة لا يستطيع فيها القلب ضخ الدم بشكل فعال، مما يؤدي إلى أعراض مثل التعب، وضيق التنفس، واحتباس السوائل.
موسعات الشعب الهوائية: أدوية تعمل على استرخاء العضلات المحيطة بالمجاري الهوائية، مما يؤدي إلى توسيع الممرات الهوائية وتحسين تدفق الهواء لتسهيل التنفس لدى مرضى COPD.
-حاصرات بيتا الانتقائية للقلب: نوع من حاصرات بيتا التي تستهدف بشكل أساسي مستقبلات بيتا-1 في القلب، مما يقلل من خطر المضاعفات التنفسية. تُستخدم لإدارة حالات القلب دون التأثير بشكل كبير على وظيفة الرئة.
-حاصرات بيتا: فئة من الأدوية المستخدمة لإدارة الحالات القلبية الوعائية مثل ارتفاع ضغط الدم وفشل القلب. تعمل عن طريق حجب مستقبلات بيتا لتقليل معدل ضربات القلب وضغط الدم. يمكن أن تؤثر حاصرات بيتا غير الانتقائية أيضًا على مستقبلات بيتا-2، مما يؤدي إلى تضيق الشعب الهوائية.
-مستقبلات بيتا-1: مستقبلات توجد بشكل أساسي في القلب، وعند حجبها تؤدي إلى تقليل معدل ضربات القلب وقوة الانقباض، مما يجعلها هدفًا رئيسيًا لعلاج الأمراض القلبية الوعائية.
-مستقبلات بيتا-2: مستقبلات توجد في العضلات الملساء للمجاري الهوائية. يمكن أن يؤدي حجب هذه المستقبلات إلى تضيق الشعب الهوائية، ولهذا السبب يُفضل استخدام حاصرات بيتا الانتقائية للقلب التي لا تؤثر بشكل كبير على هذه المستقبلات لمرضى COPD.
تضيق الشعب الهوائية: هو تضيق الممرات الهوائية في الرئتين نتيجة لتقلص العضلات المحيطة، مما يؤدي إلى صعوبة في التنفس. هذه مشكلة تهم مرضى مرض الانسداد الرئوي المزمن ويمكن أن تتفاقم بسبب حاصرات بيتا غير الانتقائية.
-محفزات بيتا-2: أدوية تحفز مستقبلات بيتا-2 لتهدئة عضلات مجرى الهواء وتعزيز توسع الشعب الهوائية، مما يحسن تدفق الهواء لدى مرضى COPD.
مضادات المسكارين: أدوية تمنع تأثير الأستيل كولين على مستقبلات المسكارين، مما يساعد على استرخاء الممرات الهوائية وتحسين تدفق الهواء، وبالتالي تقليل الأعراض في مرض الانسداد الرئوي المزمن.
مرض نادر
مدغرافراج
يمكن استخدام التهوية غير الغازية (NIV)، مثل BiPAP، لتوفير الدعم التنفسي، خاصة خلال فترات ضعف التنفس بسبب العدوى التنفسية أو النوم. هذا يتجنب الحاجة إلى إجراءات غازية، والتي يمكن أن تحفز HO لدى مرضى FOP [1،2]. يوفر BiPAP بشكل خاص مستويات مختلفة من ضغط الهواء أثناء الشهيق والزفير، مما يجعله خيارًا مريحًا وفعالًا لتحسين وظيفة التنفس.
تلعب العلاج الطبيعي تحت الإشراف دورًا حاسمًا في الحفاظ على سعة الرئة مع تقليل الصدمات. من المهم أن تكون هذه التمارين لطيفة وتُمارس تحت إشراف لتجنب أي إصابة قد تؤدي إلى تطور التكلس غير الطبيعي. الهدف الرئيسي هو الحفاظ على حركة الصدر دون تحفيز نمو العظام غير الطبيعي المميز لمرض FOP. كما أن الدعم الغذائي ضروري أيضًا لتحسين وظيفة التنفس لدى مرضى FOP. يساعد الحفاظ على التغذية الكافية في تحسين الصحة العامة ويدعم العضلات اللازمة للتنفس.
References:
3.Kaplan FS, et al. “Fibrodysplasia ossificans progressiva: Clinical and genetic aspects.” Orphanet Journal of Rare Diseases. 2008.
4.Additional source not explicitly listed (general reference to supervised physical therapy for maintaining lung capacity in FOP patients).
5.Rocke DM, et al. “Pulmonary function and its management in FOP.” Respiratory Care. 2017.
6.Kaplan FS, Glaser DL, Shore EM, et al. “The medical management of fibrodysplasia ossificans progressiva: current treatment considerations.” Clinical Reviews in Bone and Mineral Metabolism. 2005.
7.Al Mukaddam M, et al. “Nutrition in Fibrodysplasia Ossificans Progressiva: Strategies and Management.” Journal of Clinical Endocrinology & Metabolism. 2020.
توضيح مصطلحي:
-التهوية غير الغازية (NIV): طريقة لدعم التنفس تستخدم قناعًا لتوصيل الهواء إلى الرئتين، مما يساعد على التنفس دون الحاجة إلى إجراءات جراحية. يتم استخدامها عادة لتجنب المضاعفات في مرضى FOP حيث يمكن أن تؤدي الصدمات إلى HO.
-BiPAP (ضغط مجرى الهواء الإيجابي ثنائي المستوى): نوع من NIV يوفر مستويين من ضغط الهواء – ضغط أعلى عند الشهيق وضغط أقل عند الزفير. يساعد في الحفاظ على التهوية الفعالة ويدعم التنفس أثناء النوم أو عندما تكون وظيفة التنفس مهددة.
-التنسج العظمي التقدمي (FOP): اضطراب وراثي نادر يتميز بتشكيل العظام في العضلات والأوتار وغيرها من الأنسجة الضامة، مما يؤدي إلى عدم الحركة التدريجي. حتى الصدمات الطفيفة يمكن أن تحفز نوبات، مما يؤدي إلى نمو غير طبيعي للعظام.
-قصور الصدر: حالة حيث لا يمكن لجدار الصدر دعم التنفس الطبيعي أو نمو الرئة بشكل كافٍ، مما يؤدي إلى تقليل وظيفة الرئة. إنها مضاعفة شائعة في مرضى FOP بسبب تأثير HO على القفص الصدري والعمود الفقري.
-العدوى التنفسية: العدوى التي تؤثر على الجهاز التنفسي، والتي يمكن أن تؤدي بشكل كبير إلى تفاقم التنفس في مرضى FOP. الوقاية والإدارة الفعالة أمران حاسمان لتجنب التحفيز.
-العلاج الطبيعي: تمارين تحت إشراف مصممة للحفاظ على الحركة أو تحسينها. بالنسبة لمرضى FOP، يجب أن يتم ذلك بحذر لتجنب أي ضغط جسدي أو صدمة قد تؤدي إلى HO.
-الدعم الغذائي: التغذية الكافية أمر حاسم للحفاظ على الصحة العامة ودعم وظيفة العضلات التنفسية، خاصة في مرضى FOP حيث يمكن أن تؤدي سعة الرئة المهددة إلى صعوبات في تلبية الاحتياجات الغذائية.
سؤال
صحة الأقلية
MedGraphRAG
المضاعفات التخثرية، بما في ذلك تجلط الأوردة العميقة (DVT) أو الانسداد الرئوي، ممكنة أيضًا ولكن يمكن إدارتها من خلال تصنيف المخاطر بعناية وتدابير وقائية.
References:
2.Nota NM, et al. “Occurrence of Acute Cardiovascular Events in Transgender Individuals Receiving Hormone Therapy.” European Journal of Endocrinology. 2019.
3.Asscheman H, et al. “Venous Thrombosis and Long-Term Use of Estrogens in Transgender Women.” Journal of Sexual Medicine. 2014.
4.Wierckx K, et al. “Long-term evaluation of cross-sex hormone treatment in transsexual persons.” Journal of Clinical Endocrinology & Metabolism. 2012.
5.Hembree WC, et al. “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline.” Journal of Clinical Endocrinology & Metabolism. 2017.
6.Seal LJ, et al. “Health Implications of Gender Affirmation in Transgender Individuals.” Lancet Diabetes Endocrinology. 2016.
توضيح المصطلحات:
-المتحولون من ذكر إلى أنثى: يشير إلى الأفراد الذين تم تعيينهم ذكورًا عند الولادة والذين يحددون ويتحولون إلى أنثى. HRT هو جزء من عملية التحول التي تساعد في تطوير الصفات الجسدية الأنثوية.
-الأحداث القلبية الوعائية: حالات طبية تؤثر على القلب أو الأوعية الدموية، بما في ذلك النوبات القلبية والسكتات الدماغية وغيرها من المضاعفات المتعلقة بالجهاز القلبي الوعائي. يمكن أن تكون هذه الأحداث عامل خطر للأفراد الذين يخضعون لـ HRT على المدى الطويل.
-المضاعفات التخثرية: حالات تتضمن تكوين جلطات دموية في الأوردة، والتي قد تؤدي إلى تجلط الأوردة العميقة (DVT) أو الانسداد الرئوي. هذه هي المخاطر المحتملة المرتبطة بـ HRT في الأفراد المتحولين.
-الإشراف الطبي المناسب: دعم الرعاية الصحية المنتظم الذي يتضمن مراقبة مستويات الهرمونات، وتقييم عوامل الخطر، وتعديل العلاجات حسب الحاجة. يساعد ذلك في تقليل المخاطر المحتملة المرتبطة بـ HRT.
-تقييم المخاطر: عملية تحديد المخاطر الصحية المحتملة، مثل القضايا القلبية الوعائية أو المضاعفات التخثرية، لدى الأفراد الذين يخضعون لـ HRT.
-استراتيجيات الإدارة: تقنيات أو علاجات مصممة لتقليل المخاطر الصحية. بالنسبة للأفراد الذين يخضعون لـ HRT، قد تشمل ذلك تعديلات نمط الحياة، والمراقبة المنتظمة، والرعاية الطبية المخصصة لمعالجة المضاعفات المحتملة.
-تجلط الأوردة العميقة (DVT): حالة تتشكل فيها جلطة دموية في وريد عميق، عادة في الساقين. DVT هو أحد المضاعفات التخثرية المحتملة المرتبطة بـ HRT.
-الانسداد الرئوي: انسداد في أحد الشرايين الرئوية في الرئتين، عادة بسبب جلطة دموية انتقلت من الساقين (DVT). إنها مضاعفة خطيرة يمكن أن تحدث مع HRT على المدى الطويل.
سؤال
إدارة الأمراض المزمنة
MedGraphRAG
مراقبة مستويات الجلوكوز في الدم قبل وأثناء وبعد التمرين تساعد في الحفاظ على مستويات السكر في الدم مستقرة. تناول الكربوهيدرات قبل التمرين إذا كان مستوى الجلوكوز في الدم منخفضًا سيساعد في منع نقص السكر في الدم ويسمح لك بممارسة الرياضة بشكل أكثر راحة [2،3،6]. تعديلات الأنسولين السريع المفعول مهمة، حيث يمكن أن يزيد التمرين بشكل كبير من حساسية الأنسولين، مما يؤدي إلى انخفاض أسرع في مستويات السكر في الدم [2،3،7].
يجب أن تكون الكربوهيدرات سريعة المفعول (مثل أقراص الجلوكوز أو المشروبات السكرية) متاحة بسهولة أثناء التمرين في حالة نقص السكر في الدم. تعمل هذه الأنواع من الكربوهيدرات بسرعة لرفع مستويات السكر في الدم ويمكن أن تساعد في استقرار المستويات إذا انخفضت بشكل كبير أثناء النشاط [1،2،3،5].
References:
2.Riddell MC, et al. “Exercise management in type 1 diabetes: a consensus statement.” The Lancet Diabetes & Endocrinology. 2017.
3.Colberg SR, et al. “Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association.” Diabetes Care. 2016.
4.Yardley JE, et al. “Effects of Exercise on Glucose Levels in Type 1 Diabetes: A Continuous Glucose Monitoring Study.” Diabetes Technology & Therapeutics. 2013.
5.Adolfsson P, et al. “Improvements in Diabetes Control During Physical Activity Intervention for Adolescents with Type 1 Diabetes Mellitus.” Journal of Clinical Endocrinology & Metabolism. 2017.
6.Rabasa-Lhoret R, et al. “Exercise in Type 1 Diabetes: A practical review of its benefits and challenges.” Journal of Diabetes and its Complications. 2009.
7.Heinemann L, et al. “Adjustment of insulin therapy for physical activity in type 1 diabetes mellitus.” Diabetes Obesity and Metabolism. 2014.
توضيح المصطلحات:
-جلوكوز الدم: تركيز الجلوكوز (السكر) في الدم، والذي يُشار إليه عادةً بمستويات السكر في الدم. مراقبة جلوكوز الدم أمر حاسم للأفراد المصابين بداء السكري من النوع 1 لإدارة صحتهم.
-الكربوهيدرات: مغذيات كبيرة توجد في الأطعمة مثل الخبز، والفواكه، والحلويات التي توفر الطاقة. تناول الكربوهيدرات قبل التمرين يمكن أن يساعد في الحفاظ على مستويات جلوكوز الدم، خاصةً لدى الأفراد المصابين بداء السكري.
-الأنسولين السريع المفعول: نوع من الأنسولين يبدأ العمل بسرعة لتقليل مستويات الجلوكوز في الدم، عادةً خلال 15 دقيقة من الحقن. يساعد في إدارة الارتفاعات في مستويات السكر في الدم التي تحدث بعد الوجبات.
-حساسية الأنسولين: استجابة الجسم للأنسولين، مما يعني مدى فعالية الأنسولين في مساعدة الخلايا على امتصاص الجلوكوز. يزيد التمرين من حساسية الأنسولين، مما يعني أن الجسم يحتاج إلى كمية أقل من الأنسولين لخفض مستويات الجلوكوز في الدم.
-مستويات السكر في الدم: كمية الجلوكوز الموجودة في الدم في أي وقت. إدارة مستويات السكر في الدم أمر ضروري للأفراد المصابين بالسكري لمنع كل من نقص السكر في الدم وارتفاع السكر في الدم.
-الكربوهيدرات سريعة المفعول: الكربوهيدرات التي يتم امتصاصها بسرعة في مجرى الدم، مما يؤدي إلى رفع مستويات الجلوكوز في الدم بسرعة. تشمل الأمثلة أقراص الجلوكوز، والمشروبات السكرية، والحلويات. تُستخدم هذه لعلاج نقص السكر في الدم.
-نقص السكر في الدم: حالة تتميز بمستويات جلوكوز الدم المنخفضة بشكل غير طبيعي، والتي يمكن أن تكون ناتجة عن الكثير من الأنسولين، أو تناول طعام غير كافٍ، أو زيادة النشاط البدني دون تعديلات مناسبة.
Medical Graph RAG: Evidence-based Medical Large Language Model via Graph Retrieval-Augmented Generation
Abstract
We introduce MedGraphRAG, a novel graphbased Retrieval-Augmented Generation (RAG) framework designed to enhance LLMs in generating evidence-based medical responses, improving safety and reliability with private medical data. We introduce Triple Graph Construction and U-Retrieval to enhance GraphRAG, enabling holistic insights and evidence-based response generation for medical applications. Specifically, we connect user documents to credible medical sources and integrate Topdown Precise Retrieval with Bottom-up Response Refinement for balanced context awareness and precise indexing. Validated on 9 medical Q&A benchmarks, 2 health fact-checking datasets, and a long-form generation test set, MedGraphRAG outperforms state-of-the-art models while ensuring credible sourcing. Our code is publicly available.
1 Introduction
not distort, modify, or introduce creative elements into the data. Unfortunately, verifying the accuracy of responses in medicine is particularly challenging for non-expert users. Therefore, the ability to perform complex reasoning using large external datasets, while generating accurate and credible responses backed by verifiable sources, is crucial in medical applications of LLMs.
proves response quality with few costs. In Triple Graph Construction, we design a mechanism to link user RAG data to credible medical papers and foundational medical dictionaries. This process generates triples [RAG data, source, definition] to construct a comprehensive graph of user documents. It enhances LLM reasoning and ensures responses are traceable to their sources and definitions, guaranteeing reliability and explainability. We also developed a unique U-Retrieval strategy to respond to user queries. Instead of building costly graph communities, we streamline the process by summarizing each graph using predefined medical tags, then iteratively clustering similar graphs to form a multi-layer hierarchical tag structure, from broad to detailed tags. The LLM generates tags for the user query and indexes the most relevant graph based on tag similarity in a top-down approach, using it to formulate the initial response. Then it refines the response by progressively integrating back the higher-level tags in a bottom-up manner until the final answer is generated. This U-Retrieval technique strikes a balance between global context awareness and the retrieval efficiency.
- We are the first to propose a specialized framework for introducing graph-based RAG in the medical domain, which we named MedGraphRAG.
- We have developed unique Triple Graph Construction and U-Retrieval methods that enable LLMs to efficiently generate evidence-based responses utilizing holistic RAG data.
- MedGraphRAG outperforms other retrieval methods and extensively fine-tuned Medical LLMs across a wide range of medical Q&A benchmarks,
establishing the new SOTAs. - Validated by human evaluations, MedGraphRAG is able to generate more understandable and evidence-based responses in the medical domain.
2 Method
2.1 Triple Graph Construction
2.1.1 Preliminary: Document Chunking & Entities Extraction
2.1.2 Triple Linking
2.2 U-Retrieval
2.2.1 Preliminary: Graph Tagging
each Meta-MedGraph
2.2.2 Top-down Precise Retrieval
at layer
2.2.3 Bottom-up Response Refinement
3 Experiment
3.1 Dataset
3.1.1 RAG data
3.1.2 Repository data
3.1.3 Test Data
3.2 Experiment Setting
3.3 Results
3.3.1 Multi-Choice Evaluation
an average improvement of nearly
3.3.2 Long-form Generation Evaluation
(CP), citation recall (CR), and understandability (Und.). As shown in Table 2, MedGraphRAG consistently received higher ratings across all metrics. Notably, it showed a significant advantage in CP, CR and Und., indicating that its responses were more often backed by accurate sources and were easier to understand, even for laypersons, thanks to evidence-backed responses and clear explanations of complex medical terms.
3.4 Ablation and Analysis
3.4.1 Overall Ablation Study
| Model | Fake Health | Pub Health | MedQA | Med MCQA | Pub MedQA | MMLU Col-Med | MMLU Col-Bio | MMLU Pro-Med | MMLU Anatomy | MMLU Gene | MMLU Clinic |
| Baselines without retrieval | |||||||||||
| Llama2-13B | 53.8 | 49.4 | 42.7 | 37.4 | 68.0 | 60.7 | 69.4 | 60.3 | 52.6 | 66.0 | 63.8 |
| Llama2-70B | 58.9 | 56.7 | 43.7 | 35.0 | 74.3 | 64.2 | 84.7 | 75.0 | 62.3 | 74.0 | 71.7 |
| Llama3-8B | 51.1 | 53.2 | 59.8 | 57.3 | 75.2 | 61.9 | 78.5 | 70.2 | 68.9 | 83.0 | 74.7 |
| Llama3-70B | 64.2 | 61.0 | 72.1 | 65.5 | 77.5 | 72.3 | 92.5 | 86.7 | 72.5 | 83.9 | 82.7 |
| Gemini-pro | 60.6 | 63.7 | 59.0 | 54.8 | 69.8 | 69.2 | 88.0 | 77.7 | 66.7 | 75.8 | 76.7 |
| GPT-4 | 71.4 | 70.9 | 78.2 | 72.6 | 75.3 | 76.7 | 95.3 | 93.8 | 81.3 | 90.4 | 86.2 |
| Base
|
|||||||||||
| Llama2-13B | 56.2 | 54.3 | 48.1 | 42.0 | 68.6 | 62.5 | 68.3 | 63.7 | 51.0 | 64.5 | 67.4 |
| Llama2-70B | 64.6 | 63.2 | 56.2 | 49.8 | 75.2 | 69.6 | 85.8 | 77.4 | 63.0 | 75.8 | 73.3 |
| Llama3-8B | 60.5 | 59.6 | 64.3 | 58.2 | 76.0 | 68.6 | 84.9 | 73.2 | 72.1 | 85.2 | 77.8 |
| Llama3-70B | 76.2 | 72.1 | 82.3 | 72.5 | 80.6 | 86.8 | 94.4 | 89.7 | 84.3 | 87.1 | 87.6 |
| Gemini-pro | 72.5 | 68.4 | 64.5 | 57.3 | 76.9 | 79.0 | 91.3 | 86.4 | 79.5 | 80.4 | 83.9 |
| GPT-4 | 78.6 | 77.3 | 88.1 | 76.3 | 77.6 | 81.2 | 95.5 | 94.3 | 83.1 | 92.9 | 93.1 |
| Baselines with Graph RAG | |||||||||||
| Llama2-13B | 58.7 | 57.5 | 52.3 | 44.6 | 72.8 | 64.1 | 73.0 | 64.6 | 52.1 | 66.2 | 67.9 |
| Llama2-70B | 65.7 | 63.8 | 55.1 | 52.4 | 74.6 | 68.0 | 86.4 | 79.2 | 64.6 | 73.9 | 75.8 |
| Llama3-8B | 61.7 | 61.0 | 64.8 | 58.7 | 76.6 | 69.2 | 84.3 | 73.9 | 72.8 | 85.5 | 77.4 |
| Llama3-70B | 77.7 | 74.5 | 84.1 | 73.2 | 81.2 | 87.4 | 94.8 | 89.8 | 85.2 | 87.9 | 88.5 |
| Gemini-pro | 73.8 | 70.6 | 65.1 | 59.1 | 75.2 | 79.8 | 90.8 | 85.8 | 80.7 | 81.5 | 84.7 |
| GPT-4 | 78.4 | 77.8 | 88.9 | 77.2 | 77.9 | 82.1 | 95.1 | 94.8 | 82.6 | 92.5 | 94.0 |
| Baselines with MedGraphRAG | |||||||||||
| Llama2-13B | 64.1 | 61.2 | 65.5 | 51.4 | 73.2 | 68.4 | 76.5 | 67.2 | 56.0 | 67.3 | 69.5 |
| Llama2-70B | 69.3 | 68.6 | 69.2 | 58.7 | 76.0 | 73.3 | 88.6 | 84.5 | 68.9 | 76.0 | 77.3 |
| Llama3-8B | 79.9 | 77.6 | 74.2 | 61.6 | 77.8 | 89.2 | 95.4 | 91.6 | 85.9 | 89.3 | 89.7 |
| Llama3-70B | 81.2 | 79.2 | 88.4 | 79.1 | 83.8 | 91.4 | 96.5 | 93.2 | 89.8 | 91.0 | 94.1 |
| Gemini-pro | 79.2 | 76.4 | 71.8 | 62.0 | 76.2 | 86.3 | 92.9 | 89.7 | 85.0 | 87.1 | 89.3 |
| GPT-4 | 86.5 | 83.4 | 91.3 | 81.5 | 83.3 | 91.5 | 98.1 | 95.8 | 93.2 | 98.5 | 96.4 |
| Data | Methods | Pert. | Cor. | CP | CR | Und. |
| MultiMedQA | INLINE | 91 | 88 | 80 | 74 | 85 |
| ATTR.FIRST | 93 | 91 | 86 | 77 | 93 | |
| MIRAGE | 95 | 90 | 84 | 75 | 91 | |
| MedGrapgRAG | 97 | 94 | 92 | 86 | 95 | |
| Diverse Health | INLINE | 95 | 84 | 78 | 71 | 81 |
| ATTR.FIRST | 96 | 91 | 81 | 78 | 85 | |
| MIRAGE | 97 | 89 | 83 | 76 | 87 | |
| MedGrapgRAG | 97 | 96 | 89 | 84 | 93 |
| MedQA | PubMedQA | MedMCQA | |
| GraphRAG | 88.9 | 77.9 | 77.2 |
| +Triple Graph Construction | 91.1 | 81.8 | 80.9 |
| +U-Retrieval |
|
|
|
3.4.2 Detailed Ablation on Triple Linking
chart in Fig. 3), and (2) incrementally adding all three tiers (line chart in Fig. 3). The results show that both the data and the right retrieval method must work together to unlock the full potential. When retrieving data by standard RAG, Med-Paper data individually improves performance by less than
3.5 Detailed Ablation on U-Retrieval
termined through comprehensive trials. First, we examine the impact of the retrieval range, i.e. the number of entities and neighbors, using GPT-4 with MedGraphRAG on MedQA, as shown in Fig. 4. Our findings show that retrieving more data does not necessarily lead to better performance. In fact, more data can introduce noise and exacerbate LLM performance issues with long contexts. The peak performance occurs when the retrieval size reaches approximately 120 entities with 4-hop neighbors or 60 entities with 16 -hop neighbors. The 16 -hop neighbors setting performed slightly better, likely due to the robustness of graph-based linking compared to vector-similarity-based retrieval.
4 Related Work
5 Conclusion
6 Limitation
a local update strategy. Specifically, we can compute the semantic distance between newly inserted knowledge and existing Meta-Graphs, and apply updates only to relevant subgraphs that exceed a defined threshold. This selective updating approach balances both efficiency and accuracy. We recognize these as practical and important limitations, and we plan to supply more detailed discussion on them as part of our future work in this research direction.
Acknowledgments
References
langchain. 2024. Enhancing rag-based application accuracy by constructing and leveraging knowledge graphs. https://blog.langchain.dev/enhancing-rag-based-applications-accuracy-by-constructing-and-leveraging-knowledge-graphs/.
microsoft. 2024. Microsoft azure graphrag. https://github.com/Azure-Samples/graphrag-accelerator?tab=readme-ov-file.
use of large language models to provide clinical recommendations in the emergency department. Nature Communications, 15(1):8236.
Contents
B Additional Results and Analysis ….. 13
B. 1 Compare to SOTA Medical LLM Models ….. 13
B. 2 Case study: GPT4 with and with- out MedGraphRAG ….. 14
B. 3 Case study: Long-form generation of MedGraphRAG ….. 14
B. 4 Case study: Abstracted Graph comparison between GraphRAG and MedGraphRAG ….. 14
C Boarder Impact ….. 15
A Detailed Implementation
In the entity extraction, we include unique IDs to trace their source document. In practice, for the user privacy data, we generate a universally unique identifier (UUID) for each document as their IDs. For the medical papers and books, we use their Digital object identifier (DOI) as their IDs, and for the medical dictionaries, we use their UMLS Concept Unique Identifiers (CUI) as their IDs. This identifier is crucial for retrieving information from the source, enabling the generation of evidence-based responses later. For tag-based summary generation and merging, we insert ten tags into the prompt at a time to iteratively generate the response.
B Additional Results and Analysis
B. 1 Compare to SOTA Medical LLM Models
| MedQA | MedMCQA | PubMedQA | MMLU-Col-Med | MMLU-Col-Bio | MMLU-Pro-Med | MMLU-Anatomy | MMLU-Gene | MMLU-Clinic | |
| MedCPT | 79.6 | 74.9 | 76.8 | 77.8 | 95.4 | 93.9 | 82.6 | 90.9 | 88.3 |
| MedRAG | 88.5 | 78.1 | 78.9 | 85.5 | 96.8 | 94.8 | 84.5 | 93.6 | 94.5 |
| RAG2 | 85.2 | 76.2 | 79.3 | 83.4 | 96.1 | 94.8 | 83.9 | 91.0 | 93.2 |
| Self-BioRAG | 81.1 | 73.5 | 76.2 | 84.1 | 95.7 | 94.2 | 82.1 | 92.8 | 92.7 |
| Ours | 91.3 | 81.5 | 83.8 | 91.5 | 98.1 | 95.8 | 93.2 | 98.5 | 96.4 |
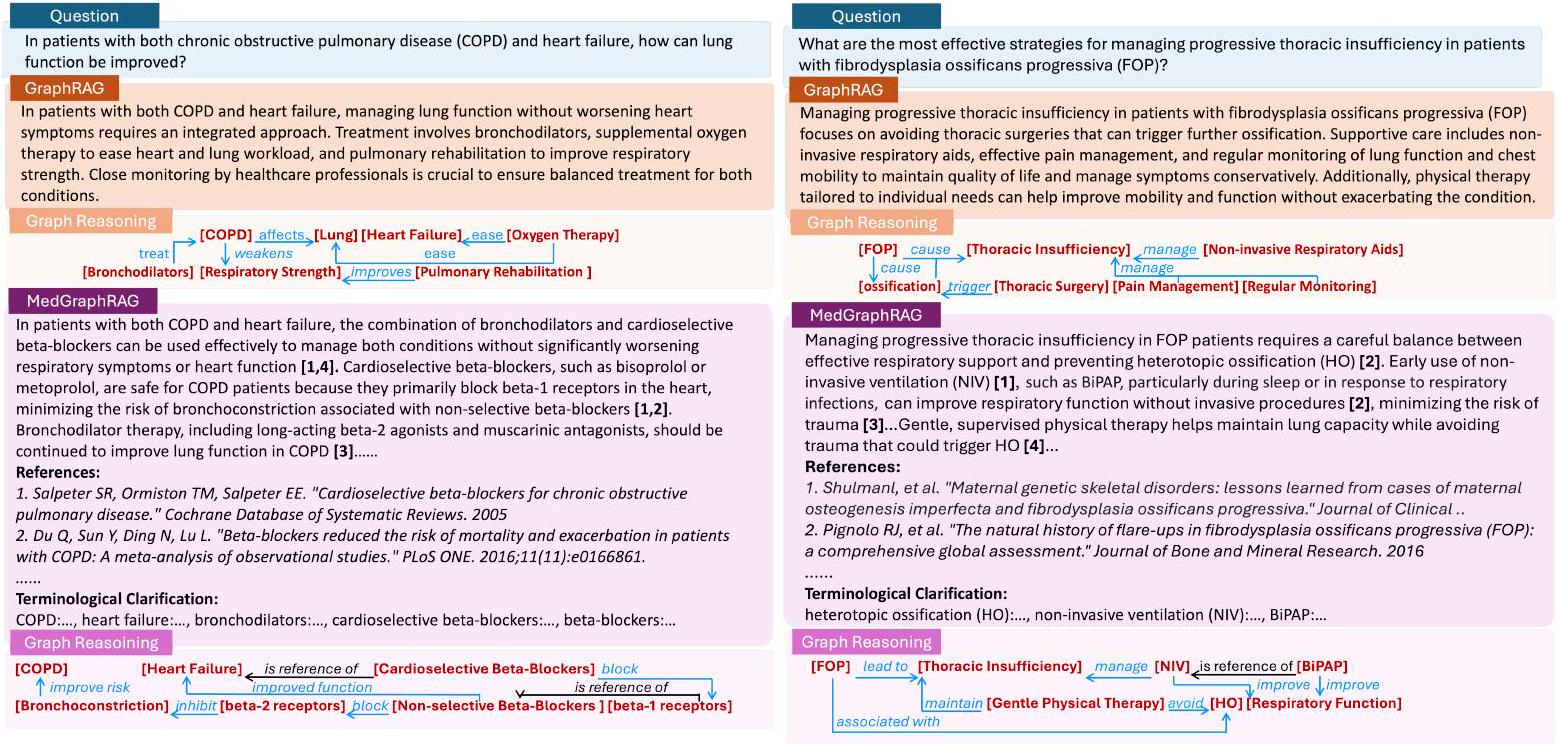
B. 2 Case study: GPT4 with and without MedGraphRAG
cise and context-aware retrieval even in complex and long-range RAG corpora.
B. 3 Case study: Long-form generation of MedGraphRAG
B. 4 Case study: Abstracted Graph comparison between GraphRAG and MedGraphRAG
C Boarder Impact
ing transparency, interpretability, and verifiability. This tool ensures that each response generated by the LLM is accompanied by provenance or source grounding information, clearly demonstrating that answers are rooted in the dataset. The availability of cited sources for each assertion allows users, especially in the critical field of medicine, to swiftly and accurately audit the LLM’s output against the original source material. This feature is crucial where (a) a trustworthy relationship -based on transparency of reasoning, needs to exist between human experts and LLM agents and (b) where the security/privacy of the information shared with the agent is mission critical. By employing this method, we have developed an Evidence-based Medical LLM. Clinicians can easily verify the source of the reasoning and adjust the model’s responses, ensuring the safe use of LLMs in clinical scenarios.
Question
Question:
Options:
B. Vascular Dementia
C. Frontotemporal Dementia
D. Lewy Body Dementia
Answer:
GPT-4
Answer:
A. Alzheimer’s Disease
Explanation:
2.Neuroimaging: Although the MRI shows vascular changes, the patchy areas of decreased glucose metabolism observed in the PET scan can sometimes overlap with early Alzheimer’s patterns, reflecting disrupted brain activity.
3.Symptom Pattern: While his symptoms show vascular influences, the general forgetfulness and worsening cognitive decline over the past year could also align with the progressive nature of Alzheimer’s disease.
MedGraphRAG
Answer:
B. Vascular Dementia
Explanation:
1.Neuroimaging Results: The MRI showing moderate vascular changes and white matter lesions is characteristic of chronic ischemic damage prevalent in vascular dementia, rather than the neurodegenerative patterns typically observed in Alzheimer’s or other dementias [2].
2.Additional Findings: His episodic cognitive symptoms also support a vascular origin rather than a degenerative neurological disease like Alzheimer’s, which would generally present a gradual, consistent cognitive decline rather than episodic [3].
These factors collectively support the diagnosis of vascular dementia, aligning more with the implications of his vascular medical history and the episodic nature of his cognitive disturbances.
Episodic symptoms: Symptoms that occur in discrete episodes, rather than being continuous. These can vary in severity and nature and are transient, typically related to neurological events.
Micro-strokes or TIAs: Micro-strokes are small, unnoticed strokes that can cause temporary, minor neurological symptoms. TIAs are brief episodes of neurological dysfunction caused by loss of blood flow to the brain, typically lasting less than 24 hours without causing permanent damage.
White matter lesions: These are indicators of vascular pathology in the brain, including changes in blood vessel structure and areas of damage in the white matter, often due to chronic ischemic (lack of blood flow) conditions. Chronic ischemic damage: Long-standing damage to brain tissue caused by repeated or persistent reduction in blood supply, typically resulting in loss of neuronal function and health.
Neurodegenerative patterns: Refers to the structural and functional changes in the brain associated with progressive neurological diseases like Alzheimer’s, where there is gradual degradation and death of neurons. Episodic cognitive symptoms: Fluctuating cognitive impairments that appear in episodes, contrasted with steady cognitive decline seen in degenerative diseases.
[1]: O’Brien, J. T., & Thomas, A. (2015). Vascular dementia. Lancet, 386(10004), 1698-1706.
[2]: Smith, E. E., & Beaudin, A. E. (2018). New insights into cerebral small vessel disease and vascular cognitive impairment from MRI. Current Opinion in Neurology, 31(1), 36-43.
[3]: Gorelick, P. B., Scuteri, A., Black, S. E., et al. (2011). Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke, 42(9), 2672-2713.
Comorbidity
MedGraphRAG
Bronchodilators, such as long-acting beta- 2 agonists (LABAs), help relax the airway muscles, which reduces bronchoconstriction and increases airflow, thereby improving lung function [3,5]. Muscarinic antagonists, like tiotropium, work by blocking the action of acetylcholine on airway muscles, further aiding in bronchodilation and easing the symptoms of COPD [5]. These medications should be continued as part of the treatment regimen to enhance respiratory efficiency.
Cardioselective beta-blockers, such as bisoprolol and metoprolol, are particularly beneficial for COPD patients as they predominantly target beta-1 receptors in the heart, reducing cardiovascular strain without significantly affecting the beta-2 receptors that are crucial for lung function
For patients managing both COPD and heart failure, the use of cardioselective beta-blockers in combination with bronchodilators can be a balanced and effective strategy to optimize both cardiovascular and respiratory health. Studies have shown that the careful use of cardioselective beta-blockers reduces mortality risk without exacerbating respiratory symptoms [2]. This combination treatment helps maintain heart function while avoiding respiratory compromise, ultimately contributing to improved lung function and better overall outcomes in patients with these comorbid conditions.
References:
2.Du Q, Sun Y, Ding N, Lu L. “Beta-blockers reduced the risk of mortality and exacerbation in patients with COPD: A meta-analysis of observational studies.” PLoS ONE. 2016; 11(11): e0166861.
3.O’Donnell DE, Parker CM. “COPD exacerbations . 3: Pathophysiology.” Thorax. 2006. 4.Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ. “Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology.” European Journal of Heart Failure. 2009; 11(2): 130-139.
5.Tashkin DP, Celli B, Senn S, et al. “A 4-year trial of tiotropium in chronic obstructive pulmonary disease.” New England Journal of Medicine. 2008; 359(15): 1543-1554.
6.Rutten FH, Cramer MJ, Lammers JW, Grobbee DE, Hoes AW. “Heart failure and chronic obstructive pulmonary disease: An ignored combination?” European Journal of Heart Failure. 2006; 8(7): 706-711.
Terminological Clarification:
-Heart Failure: A condition in which the heart cannot pump blood effectively, leading to symptoms such as fatigue, shortness of breath, and fluid retention.
-Bronchodilators: Medications that relax the muscles surrounding the airways, leading to widened air passages and improved airflow to ease breathing in COPD patients.
-Cardioselective Beta-Blockers: A type of beta-blocker that primarily targets beta-1 receptors in the heart, which reduces the risk of respiratory complications. They are used to manage heart conditions without significantly affecting lung function.
-Beta-Blockers: A class of medications used to manage cardiovascular conditions like hypertension and heart failure. They work by blocking beta receptors to decrease heart rate and blood pressure. Non-selective beta-blockers can also affect beta-2 receptors, leading to bronchoconstriction.
-Beta-1 Receptors: Receptors primarily found in the heart that, when blocked, lead to reduced heart rate and force of contraction, making them a key target for treating cardiovascular diseases.
-Beta-2 Receptors: Receptors found in the smooth muscles of the airways. Blocking these receptors can lead to bronchoconstriction, which is why cardioselective betablockers that do not significantly impact these receptors are preferred for COPD patients.
-Bronchoconstriction: The narrowing of the airways in the lungs due to the tightening of surrounding muscles, leading to difficulty in breathing. This is a concern for COPD patients and can be exacerbated by non-selective beta-blockers.
-Beta-2 Agonists: Medications that stimulate beta-2 receptors to relax airway muscles and promote bronchodilation, improving airflow in COPD patients.
-Muscarinic Antagonists: Medications that block the action of acetylcholine on muscarinic receptors, which helps to relax the airways and improve airflow, thus reducing symptoms in COPD.
Rare Disease
MedGraphRAG
Non-invasive ventilation (NIV), like BiPAP, can be used to provide respiratory support, especially during periods of compromised breathing due to respiratory infections or sleep. This avoids the need for invasive procedures, which can provoke HO in FOP patients [1,2]. BiPAP specifically offers different levels of air pressure during inhalation and exhalation, making it a comfortable and effective choice for improving respiratory function
Supervised physical therapy plays a crucial role in maintaining lung capacity while minimizing trauma. It is important that such exercises are gentle and performed under supervision to avoid any injury that might lead to the development of heterotopic ossification [4,6]. The main goal is to preserve thoracic movement without stimulating the abnormal bone growth characteristic of FOP. Nutritional support is also essential to optimize respiratory function in FOP patients. Maintaining adequate nutrition helps to improve overall health and supports the muscles needed for breathing [7].
References:
3.Kaplan FS, et al. “Fibrodysplasia ossificans progressiva: Clinical and genetic aspects.” Orphanet Journal of Rare Diseases. 2008.
4.Additional source not explicitly listed (general reference to supervised physical therapy for maintaining lung capacity in FOP patients).
5.Rocke DM, et al. “Pulmonary function and its management in FOP.” Respiratory Care. 2017.
6.Kaplan FS, Glaser DL, Shore EM, et al. “The medical management of fibrodysplasia ossificans progressiva: current treatment considerations.” Clinical Reviews in Bone and Mineral Metabolism. 2005.
7.Al Mukaddam M, et al. “Nutrition in Fibrodysplasia Ossificans Progressiva: Strategies and Management.” Journal of Clinical Endocrinology & Metabolism. 2020.
Terminological Clarification:
-Non-Invasive Ventilation (NIV): A respiratory support method that uses a mask to deliver air to the lungs, assisting breathing without requiring surgical procedures. It is commonly used to avoid complications in FOPpatients where trauma can lead to HO.
-BiPAP (Bilevel Positive Airway Pressure): A type of NIV that provides two levels of air pressure-higher pressure when inhaling and lower pressure when exhaling. It helps maintain effective ventilation and supports breathing during sleep or when respiratory function is compromised.
-Fibrodysplasia Ossificans Progressiva (FOP): A rare genetic disorder characterized by the formation of bone in muscles, tendons, and other connective tissues, leading to progressive immobility. Even minor trauma can trigger flare-ups, resulting in abnormal bone growth.
-Thoracic Insufficiency: A condition where the chest wall cannot adequately support normal breathing or lung growth, leading to reduced lung function. It is a common complication in FOP patients due to HO affecting the ribcage and spine.
-Respiratory Infections: Infections affecting the respiratory tract, which can significantly worsen breathing in FOPpatients. Prevention and effective management are crucial to avoid triggering
-Physical Therapy: Supervised exercises designed to maintain or improve mobility. For FOP patients, it must be done cautiously to avoid any physical stress or trauma that could lead to HO.
-Nutritional Support: Adequate nutrition is crucial for maintaining general health and supporting respiratory muscle function, especially in FOP patients where compromised lung capacity can lead to difficulties in meeting nutritional needs.
Question
Minority Health
MedGraphRAG
Thromboembolic complications, including deep vein thrombosis (DVT) or pulmonary embolism, are also possible but can be managed through careful risk stratification and preventive measures
References:
2.Nota NM, et al. “Occurrence of Acute Cardiovascular Events in Transgender Individuals Receiving Hormone Therapy.” European Journal of Endocrinology. 2019.
3.Asscheman H, et al. “Venous Thrombosis and Long-Term Use of Estrogens in Transgender Women.” Journal of Sexual Medicine. 2014.
4.Wierckx K, et al. “Long-term evaluation of cross-sex hormone treatment in transsexual persons.” Journal of Clinical Endocrinology & Metabolism. 2012.
5.Hembree WC, et al. “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline.” Journal of Clinical Endocrinology & Metabolism. 2017.
6.Seal LJ, et al. “Health Implications of Gender Affirmation in Transgender Individuals.” Lancet Diabetes Endocrinology. 2016.
Terminological Clarification:
-Male-to-Female Transgender: Refers to individuals assigned male at birth who identify and transition to female. HRT is a part of the transition process that helps in developing feminine physical traits.
-Cardiovascular Events: Medical conditions affecting the heart or blood vessels, including heart attacks, strokes, and other complications related to the cardiovascular system. These events can be a risk factor for individuals on long-term HRT.
-Thromboembolic Complications: Conditions that involve blood clots forming in the veins, which may lead to deep vein thrombosis (DVT) or pulmonary embolism. These are possible risks associated with HRT in transgender individuals.
-Proper Medical Supervision: Regular healthcare support that includes monitoring hormone levels, evaluating risk factors, and adjusting treatments as necessary. This helps mitigate potential risks associated with HRT.
-Risk Assessment: The process of identifying potential health risks, such as cardiovascular issues or thromboembolic complications, in individuals undergoing HRT.
-Management Strategies: Techniques or treatments designed to minimize health risks. For individuals on HRT, this may include lifestyle modifications, regular monitoring, and tailored medical care to address potential complications.
-Deep Vein Thrombosis (DVT): A condition where a blood clot forms in a deep vein, usually in the legs. DVT is one of the possible thromboembolic complications associated with HRT.
-Pulmonary Embolism: A blockage in one of the pulmonary arteries in the lungs, usually caused by a blood clot that has traveled from the legs (DVT). It is a serious complication that can occur with long-term HRT.
Question
Chornic Disease Managment
MedGraphRAG
Monitoring blood glucose levels before, during, and after exercise helps maintain stable blood sugar levels. Consuming carbohydrates before exercise if blood glucose is low will help prevent hypoglycemia and allow you to exercise more comfortably [2,3,6]. Rapid-acting insulin adjustments are important, as exercise can significantly increase insulin sensitivity, leading to a faster decline in blood sugar levels [2,3,7].
Fast-acting carbohydrates (such as glucose tablets or sugary drinks) should be easily accessible during exercise in case of hypoglycemia. These types of carbohydrates act quickly to raise blood sugar levels and can help stabilize levels if they drop too low during activity [1,2,3,5].
References:
2.Riddell MC, et al. “Exercise management in type 1 diabetes: a consensus statement.” The Lancet Diabetes & Endocrinology. 2017.
3.Colberg SR, et al. “Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association.” Diabetes Care. 2016.
4.Yardley JE, et al. “Effects of Exercise on Glucose Levels in Type 1 Diabetes: A Continuous Glucose Monitoring Study.” Diabetes Technology & Therapeutics. 2013.
5.Adolfsson P, et al. “Improvements in Diabetes Control During Physical Activity Intervention for Adolescents with Type 1 Diabetes Mellitus.” Journal of Clinical Endocrinology & Metabolism. 2017.
6.Rabasa-Lhoret R, et al. “Exercise in Type 1 Diabetes: A practical review of its benefits and challenges.” Journal of Diabetes and its Complications. 2009.
7.Heinemann L, et al. “Adjustment of insulin therapy for physical activity in type 1 diabetes mellitus.” Diabetes Obesity and Metabolism. 2014.
Terminological Clarification:
-Blood Glucose: The concentration of glucose (sugar) in the blood, commonly referred to as blood sugar levels. Monitoring blood glucose is crucial for individuals with Type 1 Diabetes to manage their health.
-Carbohydrate: A macronutrient found in foods such as bread, fruits, and sweets that provides energy. Consuming carbohydrates before exercise can help maintain blood glucose levels, especially in individuals with diabetes.
-Rapid-Acting Insulin: A type of insulin that starts to work quickly to reduce blood glucose levels, typically within 15 minutes of injection. It helps manage the spikes in blood sugar that occur after meals.
-Insulin Sensitivity: The body’s responsiveness to insulin, meaning how effectively insulin helps cells absorb glucose. Exercise increases insulin sensitivity, which means the body requires less insulin to lower blood glucoselevels.
-Blood Sugar Levels: The amount of glucose present in the blood at any given time. Managing blood sugar levelsis essential for individuals with diabetes to prevent both hypoglycemia and hyperglycemia.
-Fast-Acting Carbohydrates: Carbohydrates that are rapidly absorbed into the bloodstream, quickly raising blood glucose levels. Examples include glucose tablets, sugary drinks, and candies. These are used to treat hypoglycemia.
-Hypoglycemia: A condition characterized by abnormally low blood glucose levels, which can be caused by too much insulin, insufficient food intake, or increased physical activity without proper adjustments.