المجلة: Scientific Reports، المجلد: 14، العدد: 1
DOI: https://doi.org/10.1038/s41598-024-52887-7
PMID: https://pubmed.ncbi.nlm.nih.gov/38282043
تاريخ النشر: 2024-01-28
DOI: https://doi.org/10.1038/s41598-024-52887-7
PMID: https://pubmed.ncbi.nlm.nih.gov/38282043
تاريخ النشر: 2024-01-28
نية المغادرة، إزالة الشخصية ورضا العمل لدى الأطباء والممرضين: دراسة مقطعية في أوروبا
يواجه قطاع الرعاية الصحية الأوروبي نقصًا كبيرًا في العاملين في مجال الرعاية الصحية. إن تقييم انتشار هذه المشكلة وفهم محدداتها المباشرة وغير المباشرة أمران أساسيان لوضع برامج توظيف فعالة وتعزيز استراتيجيات الاحتفاظ بالوظائف للأطباء والممرضين. تم إجراء دراسة مقطعية متعددة المراكز، شملت 381 طبيبًا و1351 ممرضًا تم تجنيدهم من ثمانية مستشفيات أوروبية في بلجيكا وهولندا وإيطاليا وبولندا. ركزت الدراسة على تقييم نوايا التغيير بين العاملين في الرعاية الصحية استنادًا إلى نموذج متطلبات العمل والموارد، باستخدام استبيان عبر الإنترنت. تم استخدام نماذج المعادلات الهيكلية لاختبار صلاحية بناء استبيانات جمع البيانات والاتساق الداخلي. تم تقييم نية التغيير من خلال الاتفاق على نية مغادرة المستشفى أو المهنة. من بين الأطباء،
لقد ظهرت النقص العالمي في العاملين في مجال الرعاية الصحية (HCWs) كقضية حاسمة لها تداعيات واسعة النطاق على أنظمة الرعاية الصحية في جميع أنحاء العالم. يُعزى هذا النقص إلى عوامل مثل شيخوخة السكان، والزيادة في انتشار المرضى الذين يعانون من أمراض مزمنة تتطلب رعاية مستمرة، والطلب المتزايد على خدمات الرعاية الصحية.
ندرة مقدمي الرعاية الصحية لها عواقب بعيدة المدى، بما في ذلك فترات الانتظار الطويلة والوصول المحدود للمرضى إلى خدمات الرعاية الصحية.
يتأثر معدل دوران الممرضين بشكل كبير بعوامل مثل عدم الرضا عن العمل، والضغط النفسي، والإرهاق.
أظهرت نتائج مراجعة منهجية حول العوامل التي تؤثر على احتفاظ الممرضين والأطباء في المستشفيات أن عدم الرضا عن العمل، ونقص فرص تطوير المهنة، وتوازن الحياة العملية، هي العوامل الرئيسية التي تحدد نية المغادرة.
يمكن أن يساعد تحديد العوامل المباشرة وغير المباشرة الهامة لنية الاستقالة في الكشف المبكر عن العاملين في مجال الرعاية الصحية المعرضين لخطر مرتفع، مما يمكّن من تنفيذ تدخلات مستهدفة لتقليل التسرب وتعزيز الاحتفاظ. وقد وُجد أن نية المغادرة هي مؤشر موثوق للتسرب الفعلي للقوى العاملة، مما يبرز أهمية اتخاذ تدابير استباقية لمعالجة هذه القضية.
للتحقيق في نية الدوران فيما يتعلق برضا العمل، والانخراط في العمل، والإرهاق، أجرينا دراسة مقطعية متعددة المراكز شملت ممرضين وأطباء من ثمانية مستشفيات أوروبية. كان الهدف الرئيسي هو تقدير انتشار نية مغادرة المنظمة والمهنة. ثانياً، بعد التحقيق في صلاحية البناء والاتساق الداخلي لاستبيان مخصص تم تطويره لجمع البيانات، كانت هذه الدراسة تهدف إلى تقديم أدلة مستندة إلى البيانات بشأن المحددات المباشرة وغير المباشرة لنية المغادرة، كما اقترح نموذج متطلبات العمل والموارد (JD-R) المعدل لنية الدوران.
النموذج النظري
في إطار المشروع المعنون “الصحة النفسية: التركيز على الاحتفاظ بالعاملين في مجال الرعاية الصحية (METEOR)”، الممول من الوكالة الأوروبية للصحة والرقمنة في عام 2020، هدفنا إلى تقييم رضا الموظفين، والإرهاق، ونوايا ترك العمل، باستخدام الإطار النظري لنموذج JD-R.
نموذج نية الدوران METEOR (MTI)، الذي هو تعديل لنموذج JD-R، يأخذ في الاعتبار متطلبات العمل وموارد العمل كعوامل تؤثر على نوايا الدوران، من خلال وساطة الإرهاق ورضا العمل (الشكل 1). الفرضية الأولى تفترض أن رضا العمل والانخراط في العمل سيزدادان من خلال تقليل متطلبات العمل، كما يتوسطه الإرهاق (H1). تستند هذه الفرضية إلى النتيجة المعروفة أن متطلبات العمل والتحكم في العمل يتم التنبؤ بها من خلال وظيفة أساسية للإرهاق (ارتباط إيجابي) ومن خلال وظيفة انخراط موسعة (ارتباط سلبي).
علاوة على ذلك، لوحظ أن مستويات أعلى من موارد العمل، مثل زيادة فرص التعلم، والدعم من الزملاء، والدعم من المشرفين
تنص الفرضية الثالثة على أن الاحتراق النفسي، وبشكل خاص الإرهاق العاطفي وفقدان الهوية، هو عامل مساهم في نية المغادرة (H3). تتماشى هذه الفرضية مع H1، وبالتالي تركز على الإرهاق العاطفي وفقدان الهوية كالمكونات الأساسية للاحتراق النفسي.
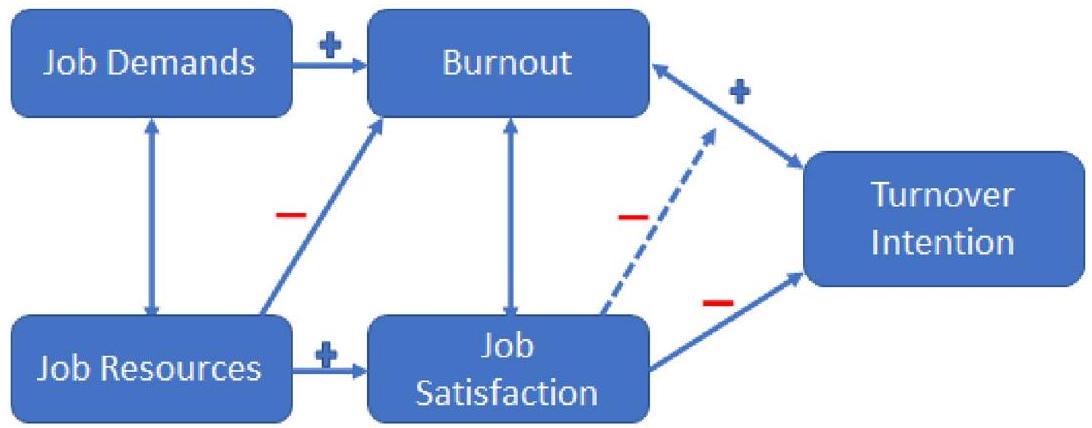
الشكل 1. النية النظرية للت turnover وفقًا لنموذج ميتور (MTI).
تفترض نية الدوران أيضًا وجود تغاير إيجابي بين الإرهاق العاطفي وفقدان الشخصية.
المواد والأساليب تصميم الدراسة
تم اختيار المشاركين في هذه الدراسة متعددة المراكز والمقطعية من مستشفيين، أحدهما أكاديمي والآخر غير أكاديمي، في كل من الدول التالية: بلجيكا، هولندا، إيطاليا، وبولندا. تم إرسال دعوة أولية للمشاركة في الدراسة عبر الإنترنت أو البريد الإلكتروني إلى جميع الأطباء والممرضين العاملين في كل مستشفى مشارك في تاريخ 1 أبريل 2022. كانت تفاصيل الاتصال الفورية للمشاركين مخفية عن مجموعة البحث. بعد أربعة عشر يومًا، تم إرسال بريد إلكتروني تذكيري مرة أخرى إلى جميع المشاركين. في حالة كان عدد المستجيبين أقل من المطلوب، تم إشراك جمعيات الأطباء والممرضين لتحفيز الممرضين والأطباء على المشاركة في البحث من خلال شرح الفوائد المتوقعة من حيث رفاهية مكان العمل. قبل أن يتمكن المستجيبون من المشاركة في الدراسة، كان عليهم قراءة رسالة المعلومات والموافقة على الموافقة المستنيرة عبر الإنترنت. كان يجب أن يحمل المشاركون درجة في التمريض (بكالوريوس أو أعلى) أو الطب (ماجستير) ويمكن أن يعملوا في الرعاية الصحية أو يشغلوا منصبًا إداريًا. كانت المعايير الأخرى للاشتراك هي أن يكونوا بالغين وأن يعملوا حاليًا كممرضين أو أطباء في أحد المستشفيات الثمانية المشاركة. تم استبعاد الممرضين والأطباء المرتبطين بمستشفيات مختلفة عن تلك المدرجة في هذه الدراسة وأولئك الذين يعملون في دول الاتحاد الأوروبي المختلفة عن الدول المشاركة في هذه الدراسة. كما تم استبعاد الخبراء في الرعاية، والقابلات، وعلماء النفس، وفنيي المختبرات، والمسعفين. تم جمع البيانات بين 16 مايو و30 سبتمبر 2022. كان الهدف من حساب حجم العينة هو تقدير نسبة الأفراد الذين أبلغوا عن نيتهم ترك وظائفهم، مع مستوى ثقة
الاستبيان
تم تطوير الاستبيان باللغة الإنجليزية وترجمته إلى الهولندية والإيطالية والبولندية. بعد الترجمة العكسية، تم إجراء الاستبيان من خلال منصة عبر الإنترنت تتوافق مع اللائحة العامة لحماية البيانات (Survey Monkey). تضمن الاستبيان 75 عنصرًا، مع سؤال إضافي حول التعليم تم تضمينه فقط للممرضين. تم تنظيمه في ثمانية أقسام: خصائص الفرد وبيئة العمل، متطلبات العمل (JD)، موارد العمل (JR)، الانخراط في العمل (WE)، رضا العمل (JS)، الإرهاق العاطفي (EE)، نزع الشخصية (DP) ونية المغادرة (IL). تم اشتقاق عناصر JD وJR وWE وJS من استبيان كوبنهاغن النفسي الاجتماعي (COPSOQ).
لتكون متسقة مع الأدوات المعتمدة من المصدر، تم تقييم العناصر الخاصة بـ JD و JR و WE و JS و IL على مقياس ليكرت من 5 نقاط، مشفرة بين 0 و 4 (بين 4 و 0 للعناصر المعكوسة) بينما تم تقييم العناصر الخاصة بـ EE و DP على مقياس ليكرت من 7 نقاط يتراوح بين 0 و 6. يمكن العثور على الاستبيان الكامل في المواد التكميلية.
طرق إحصائية
تم تحويل كل مجال من مجالات JD و JR و WE و JS و EE و DP و IL إلى
تم إجراء تحليل العوامل التأكيدية (CFA) باستخدام نموذج المعادلات الهيكلية مع مكون قياس لاختبار نموذج MTI. تم اعتبار المجالات السبعة كمتغيرات كامنة، مع متغيرين خارجيين (JD و JR) وخمسة متغيرات داخلية (WE و JS و EE و DP و IL)، تم قياسها من خلال الأقسام المقابلة من الاستبيان.
تم استخدام عدة مؤشرات لملاءمة النموذج لاختيار أفضل نموذج CFA. النماذج الجيدة لديها قيم RMSEA
تم تقييم الاتساق الداخلي للاستبيان العام ولكل من البنى الكامنة السبعة باستخدام معامل ألفا كرونباخ. تشير قيم ألفا الأعلى إلى اتساق داخلي أكبر. يعتبر الاتساق الداخلي ضعيفًا عندما تكون قيم ألفا أقل من 0.60، ومشكوكًا فيه عندما تكون بين 0.60 و 0.70، ومقبولًا بين 0.70 و 0.80، وجيدًا بين 0.80 و 0.90، وممتازًا عندما تكون أعلى من
تم إجراء جميع التحليلات باستخدام برنامج R الإحصائي (الإصدار 4.1.2؛ فريق R 2021) وStata IC/15.1 لنظام Windows.
موافقة الأخلاقيات
تم إجراء هذه الدراسة وفقًا لمبادئ إعلان هلسنكي. تم الموافقة على الدراسة من قبل لجنة الأخلاقيات للبحوث في UZ/KU Leuven في يناير 2022 (S66009).
الموافقة على المشاركة
تم الحصول على موافقة مستنيرة من المشاركين، الذين تلقوا معلومات مفصلة عن الدراسة.
النتائج
من بين 543 طبيبًا قدموا موافقة مستنيرة للمسح، كان هناك 381 (
كانت الاتساق الداخلي للاستبيان ممتازة بشكل عام (ألفا
على
استنادًا إلى مؤشرات ملاءمة CFA (الجدول S2)، كان أفضل نموذج للأطباء يتضمن عاملين مباشرين وعاملين غير مباشرين من عوامل نية الاستقالة (الشكل 2). أظهرت التأثيرات المباشرة علاقة إيجابية بين DP ونية الاستقالة (معامل
من بين 1680 ممرضة شاركت في الدراسة واستجابت للاستبيان، كانت 1351 (
كانت الاتساق الداخلي للاستبيان للممرضات ممتازة بشكل عام (ألفا=0.934). تراوحت قيم ألفا للمجالات السبعة بين القيم المقبولة (ألفا لـ IL)
استنادًا إلى مؤشرات ملاءمة CFA (الجدول S5)، كان أفضل نموذج للممرضين يتضمن عاملين مباشرين وعاملين غير مباشرين من عوامل نية الاستقالة (الشكل 3). أظهرت التأثيرات المباشرة علاقة إيجابية بين DP ونية الاستقالة (معامل
| البناء الكامن* | الأطباء
|
الممرضات
|
||
| المتوسط (الانحراف المعياري) | ألفا | المتوسط (الانحراف المعياري) | ألفا | |
| JD (
|
٥٧.٦٢ (١٢.١١) | 0.882 | ٥٤.٩٣ (١١.١٦) | 0.873 |
| جي آر (
|
62.94 (12.73) | 0.840 | 61.95 (11.64) | 0.816 |
| نحن (
|
66.89 (16.23) | 0.732 | 67.6 (15.77) | 0.787 |
| EE (
|
٣٢.٩٣ (٢٠.٩٨) | 0.908 | 31.04 (19.9) | 0.914 |
| دي بي (
|
13.88 (14.9) | 0.751 | 13.12 (15.93) | 0.786 |
| جي إس (
|
٥٩.٣٨ (١٨.٩٤) | 0.844 | ٥٦.٥٣ (١٦.٣٢) | 0.802 |
| IL (
|
٢٩.٢٧ (٢٣.٧٧) | 0.598 | ٢٩.٦١ (٢٣.٨٣) | 0.725 |
| بشكل عام
|
٤٨.٧٧ (٧.٠٧) | 0.939 | ٤٧.٠٦ (٧.٠٧) | 0.934 |
الجدول 1. المتوسطات، والانحرافات المعيارية، والاتساق الداخلي (ألفا كرونباخ) لاستبيان MTI للأطباء. نية التحول في MTI وفقًا لمؤشر ميتور، ومتطلبات العمل JD، وموارد العمل JR، والانخراط في العمل WE.
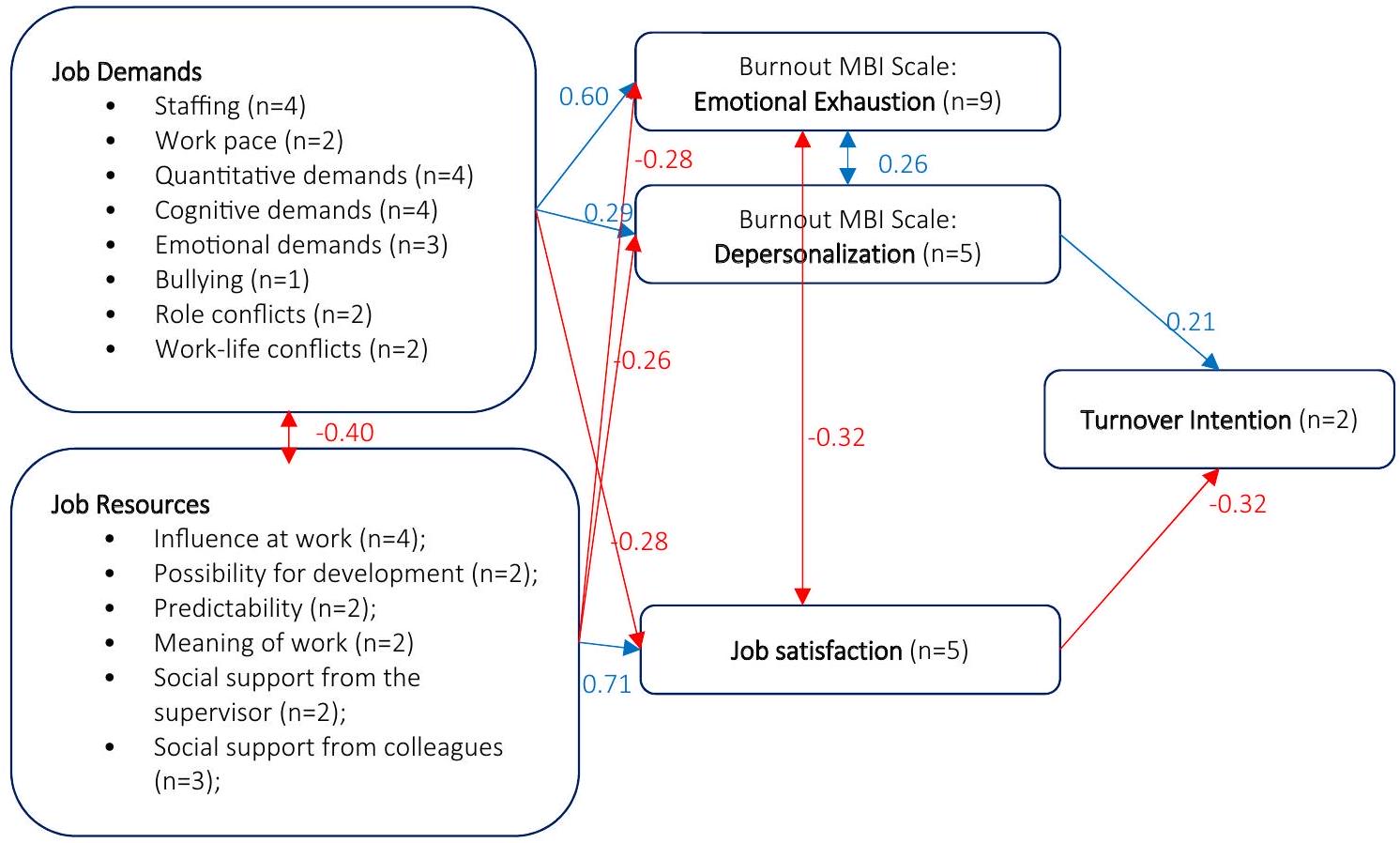
الشكل 2. صلاحية البناء لاستبيان MTI في عينة من 381 طبيبًا من ثمانية مستشفيات أوروبية. في الصورة، يتم عرض معاملات المسار للمكون الكامن لنموذج SEM الخاص بـ MTI للأطباء. التأثيرات والتغايرات الإيجابية موضحة باللون الأزرق، بينما التأثيرات والتغايرات السلبية موضحة باللون الأحمر. نية مغادرة MTI وفقًا لمؤشر Meteor.
| المتغيرات الداخلية | المتغيرات الخارجية | معامل المسار | فترة الثقة 95% |
|
|
| رضا الوظيفة | مطالب العمل | -0.28 | -0.37 | -0.19 | <0.001 |
| موارد العمل | 0.71 | 0.64 | 0.79 | <0.001 | |
| الإرهاق العاطفي | مطالب العمل | 0.60 | 0.52 | 0.68 | <0.001 |
| موارد العمل | -0.28 | -0.37 | -0.19 | <0.001 | |
| فقدان الهوية | مطالب العمل | 0.29 | 0.20 | 0.39 | <0.001 |
| موارد العمل | -0.26 | -0.36 | -0.16 | <0.001 | |
| نية_المغادرة | رضا الوظيفة | -0.61 | -0.73 | -0.49 | <0.001 |
| فقدان الهوية | 0.21 | 0.07 | 0.34 | 0.002 | |
| التغاير بين أزواج المتغيرات الكامنة | التغاير | فترة الثقة 95% |
|
||
| (الإرهاق العاطفي، رضا العمل) | -0.32 | -0.45 | -0.19 | <0.001 | |
| (الإرهاق العاطفي، فقدان الهوية) | 0.26 | 0.16 | 0.35 | <0.001 | |
| (مطالب العمل، موارد العمل) | -0.40 | -0.51 | -0.29 | <0.001 | |
الجدول 2. نتائج تحليل العوامل التأكيدية: معاملات المسار للمكون الكامن لنموذج MTI للأطباء. نية دوران MTI وفقًا لمؤشر Meteor.
نقاش
كان هدف الدراسة هو تحديد انتشار نية الممرضين والأطباء في مغادرة منظماتهم الصحية أو مهنتهم الحالية وتحديد العوامل المرتبطة بهذه الظاهرة.
مراجعة منهجية حديثة
من المثير للاهتمام أن الاتساق الداخلي للاستبيان ثبت أنه ممتاز بشكل عام، باستثناء نية المغادرة. يمكن أن يُعزى هذا التباين إلى حقيقة أن نية مغادرة المهنة و
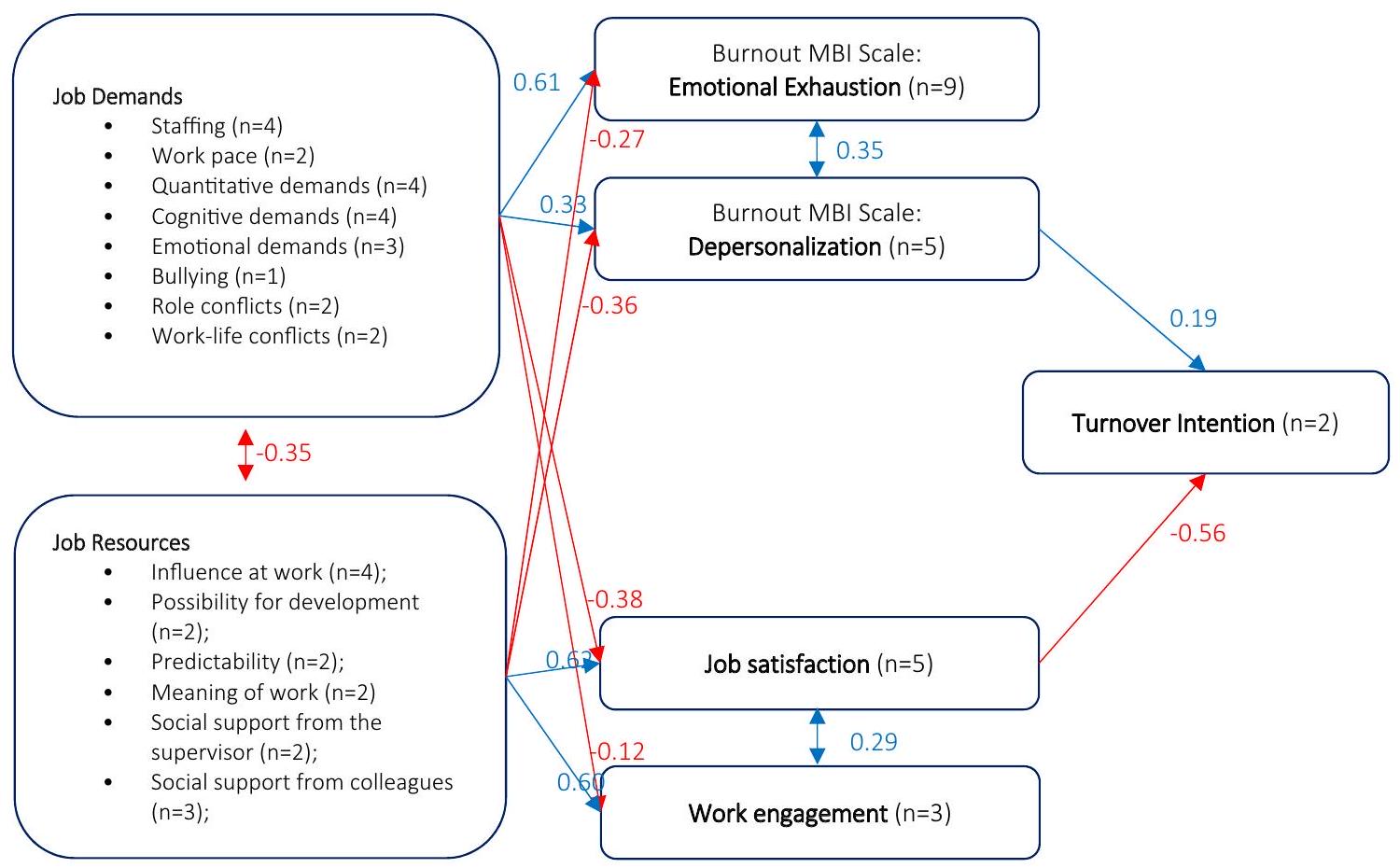
الشكل 3. صلاحية البناء لاستبيان MTI في عينة من 1351 ممرضًا من أربع دول أوروبية. في الصورة، يتم عرض معاملات المسار للمكون الكامن لنموذج SEM الخاص بـ MTI للممرضين. التأثيرات والتغايرات الإيجابية موضحة باللون الأزرق، بينما التأثيرات والتغايرات السلبية موضحة باللون الأحمر. نية مغادرة MTI وفقًا لمؤشر Meteor.
| المتغيرات الداخلية | المتغيرات الخارجية | معامل المسار | فترة الثقة 95% |
|
|
| الانخراط في العمل | مطالب العمل | -0.13 | -0.2 | -0.07 | <0.001 |
| موارد العمل | 0.60 | 0.54 | 0.66 | <0.001 | |
| رضا الوظيفة | متطلبات العمل | -0.38 | -0.43 | -0.33 | <0.001 |
| موارد العمل | 0.62 | 0.57 | 0.67 | <0.001 | |
| الإرهاق العاطفي | مطالب العمل | 0.61 | 0.57 | 0.65 | <0.001 |
| موارد العمل | -0.27 | -0.31 | -0.22 | <0.001 | |
| فقدان الهوية | مطالب العمل | 0.33 | 0.27 | 0.39 | <0.001 |
| موارد العمل | -0.36 | -0.42 | -0.30 | <0.001 | |
| نية_المغادرة | رضا الوظيفة | -0.56 | -0.63 | -0.50 | <0.001 |
| فقدان الهوية | 0.19 | 0.12 | 0.26 | <0.001 | |
| التغاير بين أزواج المتغيرات الكامنة | التغاير | فترة الثقة 95% |
|
||
| (الانخراط في العمل، رضا الوظيفة) | 0.29 | 0.20 | 0.38 | <0.001 | |
| الإرهاق العاطفي، نزع الشخصية | 0.36 | 0.30 | 0.42 | <0.001 | |
| (مطالب العمل، موارد العمل) | -0.35 | -0.41 | -0.28 | <0.001 | |
الجدول 3. نتائج تحليل العوامل التأكيدية: معاملات المسار للمكون الكامن لنموذج MTI للممرضين. نية دوران MTI وفقًا لمؤشر Meteor.
يبدو أن نية مغادرة المستشفى هي ظاهرتان مختلفتان. الأولى تشير إلى مشاعر الاغتراب والرفض مع تأثير سلبي على قطاع الرعاية الصحية (المستوى الكلي)، بينما الثانية تعبر عن رغبة في التغيير تؤثر فقط على المستشفى (المستوى الوسيط) أو القسم (المستوى الدقيق).
وجد استطلاعنا أن الأطباء كانوا أكثر ميلاً لترك مستشفاهم الحالي مقارنة بمهنة الطب، بينما أظهر الممرضون نية أعلى لترك مهنة التمريض نفسها بدلاً من مكان عملهم المحدد. يمكن الافتراض أنه بين الممرضين، لم تعد الممارسة المهنية تثير جاذبية عالية من حيث الإشباع والاعتراف بدورهم الخاص فيما يتعلق بالراتب وظروف العمل أو التنظيم، خاصة عند مقارنتها بالضغوط العاطفية والجسدية العالية التي عانوا منها خلال الجائحة الأخيرة.
تشير البيانات المستمدة من الأدبيات إلى أن خطر فيروس SARS-CoV-2 في بيئات الرعاية الصحية يُعتبر خطرًا عامًا متفاقمًا، بدلاً من كونه خطرًا محددًا، مما يعني أن العمال معرضون بشكل أكبر لفيروس SARS-CoV-2 من حيث شدة وتكرار الاتصال مع أفراد آخرين محتمل إصابتهم أكثر من
غيرها من بيئات العمل الأخرى
غيرها من بيئات العمل الأخرى
هدفت دراستنا إلى فحص العوامل المباشرة وغير المباشرة التي تؤثر على نية المغادرة بين الأطباء والممرضين العاملين في بيئات المستشفيات فيما يتعلق برضاهم الوظيفي، والانخراط في العمل، والإرهاق. تم تأكيد فرضيات الدراسة جزئيًا فقط وتفاوتت بين الأطباء والممرضين.
على وجه التحديد، كانت متطلبات العمل مرتبطة بزيادة الإرهاق العاطفي وفقدان الهوية، فضلاً عن انخفاض الرضا الوظيفي لكل من الأطباء والممرضين (H1 تم تأكيده). وبالمثل، كانت موارد العمل مرتبطة بانخفاض الإرهاق العاطفي وفقدان الهوية، فضلاً عن زيادة الرضا الوظيفي لكل من مجموعتي العاملين في الرعاية الصحية (H2 تم تأكيده).
ومع ذلك، لم تدعم الفرضية التي تقترح أن الإرهاق سيكون دافعًا لنية المغادرة (الفرضية 3) من قبل الأطباء أو الممرضين. في الواقع، وُجد أن فقدان الهوية، وليس الإرهاق العاطفي، هو المحدد المباشر لنية المغادرة، إلى جانب الرضا الوظيفي.
علاوة على ذلك، اقترحت النتائج أن نية المغادرة بين الأطباء لم يتم تفسيرها من خلال الانخراط في العمل (H3 مرفوضة). بدلاً من ذلك، تم تفسير جزء كبير من التباين من خلال العلاقة السلبية بين الرضا الوظيفي والإرهاق العاطفي. من ناحية أخرى، لعب الانخراط في العمل دورًا في تفسير نية المغادرة بين الممرضين، حيث كانت له علاقة إيجابية بالرضا الوظيفي (H4 تم تأكيده).
بالنسبة لكلا فئتي العمال، كان الشعور بفقدان الهوية والإبلاغ عن انخفاض الرضا الوظيفي يمثلان محددين مباشرين لنية المغادرة. بشكل غير مباشر، أثرت متطلبات العمل على نية المغادرة والرضا الوظيفي، بينما عملت موارد العمل كعوامل وقائية. كانت الزيادة في متطلبات العمل مرتبطة بزيادة فقدان الهوية، مما أدى إلى تقليل الرضا الوظيفي. على العكس، أدت زيادة موارد العمل إلى زيادة الرضا الوظيفي وتقليل فقدان الهوية مع تخفيف ضغط العمل والإرهاق.
وفقًا لنموذج JD-R، يتأثر الانخراط في العمل بتوافر موارد العمل، بينما يرتبط الإرهاق بمطالب العمل أكثر من ارتباطه بموارد العمل. من المثير للاهتمام أن غياب تأثير مباشر أو غير مباشر للانخراط في العمل على نوايا مغادرة الأطباء يمكن أن يُعزى إلى العبء غير المتناسب لمتطلبات العمل. عوامل مثل غموض الدور، وصراع الدور، وضغط الدور، والأحداث المجهدة، وحجم العمل، وضغط العمل،
تحدد العملية التحفيزية التي يثيرها إدراك الموارد النتائج الإيجابية مثل الانخراط في العمل والالتزام التنظيمي العالي، حيث تساعد في تحقيق الأهداف، وتقليل متطلبات العمل، وتعزيز النمو والتطور الشخصي.
على العكس، في حالة الممرضين، وُجد أن الانخراط في العمل مرتبط بالرضا الوظيفي. وهذا يشير إلى أنه بغض النظر عن الموارد الداخلية أو الخارجية المتاحة، فإن درجة الرضا التي يتم تجربتها في مكان العمل تلعب دورًا حاسمًا في تحديد النتائج الإيجابية من حيث الأداء والالتزام. وهذا يبرز أهمية التدخلات المستهدفة والوظيفية التي تهدف إلى تعزيز الرفاهية في مكان العمل، مع التركيز على حاجة معينة عبر عنها الممرضون. تتماشى هذه النتيجة مع الأدبيات الحالية، التي تظهر أن الرضا الوظيفي بين الممرضين مرتبط إيجابيًا بالانخراط في العمل،
بين الأطباء والممرضين، لعب فقدان الهوية وحده، وليس الإرهاق العاطفي، دورًا في تفسير نية المغادرة. يُعتبر الإرهاق العاطفي، في بعض الظروف، حالة عقلية متأصلة في النشاط العملي، بينما يبدو أن فقدان الهوية مرتبط أكثر بمجال علم النفس المرضي، مما يمثل عامل خطر كبير لصحة العاملين في الرعاية الصحية.
تتمثل القوة الرئيسية لهذه الدراسة في تضمين دول قدمت تمثيلًا جغرافيًا متوازنًا لمناطق مختلفة في أوروبا. في الواقع، تمثل الدول المختارة مجموعة واسعة من أنظمة الرعاية الصحية: في بلجيكا، هناك مزيج يجمع بين التأمين الصحي العام الإلزامي والشامل والعالمي مع حرية الاختيار والممارسة الطبية المستقلة؛ في هولندا، يتم تغطية الطلب الصحي من خلال التأمين الأساسي والرعاية التمريضية والرعاية طويلة الأجل، وهما شكلان قانونيان من التأمين؛ في بولندا، يعد التأمين الصحي الإلزامي المصدر الرئيسي للتمويل العام، والذي هو مع ذلك غير كافٍ بالنسبة للاحتياجات المتزايدة للسكان. أخيرًا، يستلهم النظام الصحي الوطني الإيطالي من مبادئ الشمولية والمساواة والعدالة من خلال توفير مستويات أساسية من الرعاية متاحة مجانًا لجميع السكان وبطريقة موحدة. كانت آخر درجة متاحة لمؤشر صحة المستهلك الأوروبي (2018) هي الأعلى في هولندا (883)، بينما أظهرت بلجيكا (849)، وإيطاليا (687)، وبولندا (585) درجات أقل. مقارنة بمتوسط إنفاق الصحة في الاتحاد الأوروبي بالنسبة للناتج المحلي الإجمالي (
قدمت هذه الدراسة أداة موثوقة لتقييم ظاهرة نية المغادرة بين العاملين في الرعاية الصحية في المستشفيات الأوروبية.
تتمثل إحدى قيود الدراسة في عدم التوازن في عدد الأطباء والممرضين، مما قد يكون ساهم في بعض الاختلافات في المحددات المهمة لنية التغيير. ومع ذلك، فإن انخفاض معدل استجابة الأطباء، مقارنة بالممرضين، ليس غير شائع في هذا الموضوع، وقد لاحظت دراسات سابقة أيضًا هذا التفاوت. على سبيل المثال، تم تمثيل فئتي العاملين في الرعاية الصحية في دراسة سابقة بنسبة
نسبة
تتمثل إحدى قيود الدراسة في عدم التوازن في عدد الأطباء والممرضين، مما قد يكون ساهم في بعض الاختلافات في المحددات المهمة لنية التغيير. ومع ذلك، فإن انخفاض معدل استجابة الأطباء، مقارنة بالممرضين، ليس غير شائع في هذا الموضوع، وقد لاحظت دراسات سابقة أيضًا هذا التفاوت. على سبيل المثال، تم تمثيل فئتي العاملين في الرعاية الصحية في دراسة سابقة بنسبة
نسبة
الاستنتاجات
قدمت الدراسة تقديرات حول انتشار نية مغادرة المستشفى والمهنة بين الأطباء والممرضين، مع تسليط الضوء في الوقت نفسه على كيفية تحديد السياق المستشفى لنية تغيير أكبر لدى الأطباء، بينما بدا أن عدم الراحة لدى الممرضين مرتبط بشكل أساسي بالممارسة المهنية نفسها.
علاوة على ذلك، اقترحت نتائجنا الدور المهم لفقدان الهوية في تفسير نية المغادرة في كلا فئتي العاملين في الرعاية الصحية وأكدت الدراسات السابقة التي تشير إلى الانخراط في العمل كمحدد لنية مغادرة الممرضين.
في الختام، استنادًا إلى الأدلة المقدمة من هذه الدراسة المقطعية، يُطلب من الإدارة على المستويات الدقيقة (الجناح)، والمتوسطة (المستشفى) والكبرى (السياسة) تحديد سياسات توظيف واحتفاظ مناسبة، تحديدًا للممرضين والأطباء، مع الأخذ في الاعتبار أن الرضا الوظيفي، والانخراط في العمل، ومناخ العمل الجيد، جميعها تبدو عوامل استراتيجية في تعزيز الاحتفاظ بالوظائف.
توفر البيانات
تتوفر مجموعات البيانات المستخدمة والمحللة خلال الدراسة الحالية من المؤلف المقابل عند الطلب المعقول.
تاريخ الاستلام: 25 يوليو 2023؛ تاريخ القبول: 24 يناير 2024
تم النشر على الإنترنت: 28 يناير 2024
تم النشر على الإنترنت: 28 يناير 2024
References
- Commission of the European Communities. Green paper on the European workforce for health. Hum. Resour. Health 14, 1 (2008).
- Haakenstad, A. et al. Measuring the availability of human resources for health and its relationship to universal health coverage for 204 countries and territories from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 399(10341), 2129-2154 (2022).
- Kroezen, M. et al. Recruitment and retention of health professionals across Europe: A literature review and multiple case study research. Health Policy 119(12), 1517-1528 (2015).
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030 (2016).
- Matranga, D. & Maniscalco, L. Inequality in healthcare utilization in Italy: How important are barriers to access? Int. J. Environ. Res. Public Health 19(3), 1-14 (2022).
- Duffield, C. M., Roche, M. A., Homer, C., Buchan, J. & Dimitrelis, S. A comparative review of nurse turnover rates and costs across countries. J. Adv. Nurs. 70(12), 2703-2712 (2014).
- O’Brien-Pallas, L., Murphy, G. T., Shamian, J., Li, X. & Hayes, L. J. Impact and determinants of nurse turnover: A pan-Canadian study. J. Nurs. Manag. 18(8), 1073-1086 (2010).
- Yang, H., Lv, J., Zhou, X., Liu, H. & Mi, B. Validation of work pressure and associated factors influencing hospital nurse turnover: A cross-sectional investigation in Shaanxi Province. China. BMC Health Serv. Res. 17, 1-11 (2017).
- Windover, A. K. et al. Correlates and outcomes of physician burnout within a large academic medical center. JAMA Intern. Med. 178(6), 856-858 (2018).
- Al Yahyaei, A., Hewison, A., Efstathiou, N. & Carrick-Sen, D. Nurses’ intention to stay in the work environment in acute healthcare: A systematic review. J. Res. Nurs. 27(4), 374-397 (2022).
- Degen, C., Li, J. & Angerer, P. Physicians’ intention to leave direct patient care: An integrative review. Hum. Resour. Health 13, 1-12 (2015).
- de Vries, N. et al. The race to retain healthcare workers: A systematic review on factors that impact retention of nurses and physicians in Hospitals. Inq. J. Health Care Organ. Provision Financ. 60, 00469580231159318 (2023).
- Castle, N. G., Engberg, J., Anderson, R. & Men, A. Job satisfaction of nurse aides in nursing homes: Intent to leave and turnover. Gerontologist 47(2), 193-204 (2007).
- Hann, M., Reeves, D. & Sibbald, B. Relationships between job satisfaction, intentions to leave family practice and actually leaving among family physicians in England. Eur. J. Public Health 21(4), 499-503 (2011).
- Demerouti, E., Bakker, A. B., Nachreiner, F. & Schaufeli, W. B. The job demands-resources model of burnout. J. Appl. Psychol. 86(3), 499 (2001).
- Schaufeli, W. B., Bakker, A. B., Hoogduin, K., Schaap, C. & Kladler, A. On the clinical validity of the maslach burnout inventory and the burnout measure. Psychol. Health 16(5), 565-582 (2001).
17 Demerouti, E., Bakker, A. B., De Jonge, J., Janssen, P. P. M. & Schaufeli, W. B. Burnout and engagement at work as a function of demands and control. Scand. J. Work Environ. Health 1, 279-286 (2001). - Green, D. E., Walkey, F. H. & Taylor, A. J. W. The three-factor structure of the maslach burnout inventory: A multicultural, multinational confirmatory study. J. Soc. Behav. Pers. 6(3), 453 (1991).
- Schaufeli, W. B., Salanova, M., González-Romá, V. & Bakker, A. B. The measurement of engagement and burnout: A two sample confirmatory factor analytic approach. J. Happiness Stud. 3, 71-92 (2002).
- Sarti, D. Job resources as antecedents of engagement at work: Evidence from a long-term care setting. Hum. Resour. Dev. Q. 25(2), 213-237 (2014).
- Hu, Q., Schaufeli, W. B. & Taris, T. W. How are changes in exposure to job demands and job resources related to burnout and engagement? A longitudinal study among Chinese nurses and police officers. Stress Health 33(5), 631-644 (2017).
- Koch, P. et al. How perceived quality of care and job satisfaction are associated with intention to leave the profession in young nurses and physicians. Int. J. Environ. Res. Public Health 17(8), 2714 (2020).
- Burr, H. et al. The third version of the Copenhagen psychosocial questionnaire. Saf. Health Work 10(4), 482-503 (2019).
- Sorra, J. et al. AHRQ Hospital Survey on Patient Safety Culture: User’s Guide (Agency for Healthcare Research and Quality, 2016).
- O’Driscoll, M. P. & Beehr, T. A. Supervisor behaviors, role stressors and uncertainty as predictors of personal outcomes for subordinates. J. Organ Behav. 15(2), 141-155 (1994).
26 Pejtersen, J. H., Kristensen, T. S., Borg, V. & Bjorner, J. B. The second version of the Copenhagen psychosocial questionnaire. Scand. J. Public Health 38, 8-24 (2010). - Bland, J. M. & Altman, D. G. Statistics notes: Cronbach’s alpha. BMJ 314(7080), 572 (1997).
- Andresen, I. H., Hansen, T. & Grov, E. K. Norwegian nurses’ quality of life, job satisfaction, as well as intention to change jobs. Nord. J. Nurs. Res. 37(2), 90-99 (2017).
- Labrague, L. J. & de Los Santos, J. A. A. Fear of Covid-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J. Nurs. Manag. 29(3), 395-403 (2021).
- Ekingen, E., Teleş, M., Yıldız, A. & Yıldırım, M. Mediating effect of work stress in the relationship between fear of COVID-19 and nurses’ organizational and professional turnover intentions. Arch. Psychiatr. Nurs. 42, 97-105 (2023).
- Lavoie-Tremblay, M. et al. Influence of caring for COVID-19 patients on nurse’s turnover, work satisfaction and quality of care. J. Nurs. Manag. 30(1), 33-43 (2022).
- Heinen, M. M. et al. Nurses’ intention to leave their profession: A cross sectional observational study in 10 European countries. Int. J. Nurs. Stud. 50(2), 174-184 (2013).
- Christianson, J., Johnson, N., Nelson, A. & Singh, M. Work-related burnout, compassion fatigue, and nurse intention to leave the profession during COVID-19. Nurse Lead. 21(2), 244-251 (2023).
- Pathman, D. E. et al. Physician job satisfaction, job dissatisfaction, and physician turnover. J. Fam. Pr. 51(7), 593 (2002).
- Far, M. F., Nia, H. S. & Assarroudi, A. Correlation of the job turnover intention of Iranian nurses with job satisfaction and burnout in the COVID-19 pandemic. J. Educ. Health Promot. 11(1), 364 (2022).
- Van den Bulcke, B. et al. Ethical climate and intention to leave among critical care clinicians: An observational study in 68 intensive care units across Europe and the United States. Intens. Care Med. 46, 46-56 (2020).
- Leineweber, C. et al. Nurses’ practice environment and satisfaction with schedule flexibility is related to intention to leave due to dissatisfaction: A multi-country, multilevel study. Int. J. Nurs. Stud. 58, 47-58 (2016).
- Bruyneel, L., Thoelen, T., Adriaenssens, J. & Sermeus, W. Emergency room nurses’ pathway to turnover intention: A moderated serial mediation analysis. J. Adv. Nurs. 73(4), 930-942 (2017).
- Hämmig, O . Explaining burnout and the intention to leave the profession among health professionals-A cross-sectional study in a hospital setting in Switzerland. BMC Health Serv. Res. 18(1), 1-11 (2018).
- Van der Heijden, B., Brown Mahoney, C. & Xu, Y. Impact of job demands and resources on nurses’ burnout and occupational turnover intention towards an age-moderated mediation model for the nursing profession. Int. J. Environ. Res. Public Health 16(11), 2011 (2019).
- Sasso, L. et al. Push and pull factors of nurses’ intention to leave. J. Nurs. Manag. 27(5), 946-954 (2019).
- Cirrincione, L., Rapisarda, V., Mazzucco, W., Provenzano, R. & Cannizzaro, E. SARS-CoV-2 and the risk assessment document in Italian work; specific or generic risk even if aggravated? Int. J. Environ. Res. Public Health 18(7), 3729 (2021).
- Koh, D. & Goh, H. P. Occupational health responses to COVID-19: What lessons can we learn from SARS? J. Occup. Health 62(1), e12128 (2020).
- ÇetinAslan, E., Türkmen, İ & Top, M. The effect of macro-control and organizational support perception on nurses and physicians intention to quit during the COVID-19 pandemic. J. Nurs. Scholarsh. 55, 843 (2022).
- Said, R. M. & El-Shafei, D. A. Occupational stress, job satisfaction, and intent to leave: Nurses working on front lines during COVID-19 pandemic in Zagazig City, Egypt. Environ. Sci. Pollut. Res. 28, 8791-8801 (2021).
46 De los Santos, J. A. A. & Labrague, L. J. The impact of fear of COVID-19 on job stress, and turnover intentions of frontline nurses in the community: A cross-sectional study in the Philippines. Traumatology 27(1), 52 (2021). - Fronda, D. C. & Labrague, L. J. Turnover intention and coronaphobia among frontline nurses during the second surge of COVID19: The mediating role of social support and coping skills. J. Nurs. Manag. 30(3), 612-621 (2022).
- Bakker, A. B., Demerouti, E., Taris, T. W., Schaufeli, W. B. & Schreurs, P. J. G. A multigroup analysis of the job demands-resources model in four home care organizations. Int. J. Stress Manag. 10(1), 16 (2003).
- Maniscalco, L. et al. The long-term effect of job mobility on workers’ mental health: A propensity score analysis. BMC Public Health 22(1), 1145 (2022).
- Bakker, A. B., Demerouti, E. & Sanz-Vergel, A. I. Burnout and work engagement: The JDR approach. Annu. Rev. Organ. Psychol. Organ. Behav. 1, 389-411 (2014).
- De Simone, S., Planta, A. & Cicotto, G. The role of job satisfaction, work engagement, self-efficacy and agentic capacities on nurses’ turnover intention and patient satisfaction. Appl. Nurs. Res. 39, 130-140 (2018).
- De Gieter, S., Hofmans, J. & Pepermans, R. Revisiting the impact of job satisfaction and organizational commitment on nurse turnover intention: An individual differences analysis. Int. J. Nurs. Stud. 48(12), 1562-1569 (2011).
- Hayes, L. J. et al. Nurse turnover: A literature review-An update. Int. J. Nurs. Stud. 49(7), 887-905 (2012).
- Gago-Valiente, F.-J., Mendoza-Sierra, M.-I., Moreno-Sánchez, E., Arbinaga, F. & Segura-Camacho, A. Emotional exhaustion, depersonalization, and mental health in nurses from Huelva: A cross-cutting study during the SARS-CoV-2 pandemic. Int. J. Environ. Res. Public Health 18(15), 7860 (2021).
- Vandenbroeck, S., Van Gerven, E., De Witte, H., Vanhaecht, K. & Godderis, L. Burnout in Belgian physicians and nurses. Occup. Med. 67(7), 546-554 (2017).
- Masum, A. K. M. et al. Job satisfaction and intention to quit: An empirical analysis of nurses in Turkey. PeerJ 4, e1896 (2016).
- ArslanYurumezoglu, H. & Kocaman, G. Predictors of nurses’ intentions to leave the organisation and the profession in Turkey. J. Nurs. Manag. 24(2), 235-243 (2016).
مساهمات المؤلفين
التصور: ل.م، م.إ، د.م؛ المنهجية: ل.م، م.إ، د.م، أ.ب، ن.د.ف، ب.د.و، م.ك، س.س، ل.ج؛ التحليل الرسمي: ل.م، م.إ، د.م؛ التحقيق: أ.ب، أ.ل، ن.د.ف، أ.س، س.ف، ك.ب، م.ك؛ كتابة – إعداد المسودة الأصلية: ل.م، م.إ، س.م، و.م، د.م؛ كتابة – المراجعة والتحرير: ك.ب، س.س، ب.د.و، أ.ب، ن.د.ف، و.م، ل.ج؛ الحصول على التمويل: ل.ج؛ الإشراف: د.م.
التمويل
تم تلقي تمويل خارجي لتطوير هذه الدراسة: الاتحاد الأوروبي، هايديا (اتفاقية المنحة (GA) رقم: 101018310) – البرنامج الصحي الثالث، منحة مشروع متعدد المستفيدين (HP-PJ، HP-JA)، الموضوع: PJ-01-2020-1، نوع العمل: HP-PJ، SEP-210693712: مشروع يسمى METEOR (الصحة النفسية: التركيز على الاحتفاظ بالعاملين في الرعاية الصحية). لم يؤثر مصدر التمويل على تصميم الدراسة، أو جمع البيانات، أو تحليلها، أو تفسيرها، أو كتابة المخطوطة، أو القرار بتقديم المخطوطة للنشر. كل من الآراء المعبر عنها وأي أخطاء أو سهو هي المسؤولية الوحيدة للمؤلفين.
المصالح المتنافسة
يعلن المؤلفون عدم وجود مصالح متنافسة.
معلومات إضافية
المعلومات التكميلية النسخة على الإنترنت تحتوي على مواد تكميلية متاحة على https://doi.org/ 10.1038/s41598-024-52887-7.
يجب توجيه المراسلات والطلبات للحصول على المواد إلى د.م.
معلومات إعادة الطبع والأذونات متاحة على www.nature.com/reprints.
ملاحظة الناشر تظل Springer Nature محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
معلومات إعادة الطبع والأذونات متاحة على www.nature.com/reprints.
ملاحظة الناشر تظل Springer Nature محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
الوصول المفتوح هذه المقالة مرخصة بموجب رخصة المشاع الإبداعي للاستخدام والمشاركة والتكيف والتوزيع وإعادة الإنتاج في أي وسيلة أو صيغة، طالما أنك تعطي الائتمان المناسب للمؤلفين الأصليين والمصدر، وتوفر رابطًا لرخصة المشاع الإبداعي، وتوضح ما إذا كانت هناك تغييرات قد تم إجراؤها. الصور أو المواد الأخرى من طرف ثالث في هذه المقالة مشمولة في رخصة المشاع الإبداعي للمقالة، ما لم يُذكر خلاف ذلك في سطر الائتمان للمادة. إذا لم تكن المادة مشمولة في رخصة المشاع الإبداعي للمقالة واستخدامك المقصود غير مسموح به بموجب اللوائح القانونية أو يتجاوز الاستخدام المسموح به، ستحتاج إلى الحصول على إذن مباشرة من صاحب حقوق الطبع والنشر. لعرض نسخة من هذه الرخصة، قم بزيارة http://creativecommons.org/licenses/by/4.0/.
© المؤلفون 2024
© المؤلفون 2024
قسم تعزيز الصحة، رعاية الأم والطفل، الطب الباطني والتخصصات الطبية، جامعة باليرمو، باليرمو، إيطاليا. قسم الطب الباطني، مستشفى سبارن غاستهاوس، هوفدورب، هولندا. أكاديمية سبارن غاستهاوس، هوفدورب، هولندا. قسم الصحة العامة والرعاية الأولية، مركز البيئة والصحة، جامعة لوفين (جامعة لوفين)، لوفين، بلجيكا. قسم علم الأوبئة، الجامعة الطبية في سيليزيا، كاتوفيتسه، بولندا. قسم علم النفس، العلوم التعليمية والحركة البشرية، جامعة باليرمو، باليرمو، إيطاليا. معهد لوفين للأطفال والصحة، جامعة لوفين، لوفين، بلجيكا. قسم التنمية والتجديد، جامعة لوفين، لوفين، بلجيكا. قسم طب الأطفال، مستشفى سبارن غاستهاوس، هارلم وهوفدورب، هولندا. ساهم هؤلاء المؤلفون بالتساوي: ل. مانيسكالكو وم. إينيا. البريد الإلكتروني: domenica.matranga@unipa.it
Journal: Scientific Reports, Volume: 14, Issue: 1
DOI: https://doi.org/10.1038/s41598-024-52887-7
PMID: https://pubmed.ncbi.nlm.nih.gov/38282043
Publication Date: 2024-01-28
DOI: https://doi.org/10.1038/s41598-024-52887-7
PMID: https://pubmed.ncbi.nlm.nih.gov/38282043
Publication Date: 2024-01-28
Intention to leave, depersonalisation and job satisfaction in physicians and nurses: a cross-sectional study in Europe
The European healthcare sector faces a significant shortage of healthcare workers. Assessing the prevalence of this issue and understanding its direct and indirect determinants are essential for formulating effective recruitment programs and enhancing job retention strategies for physicians and nurses. A multicentric cross-sectional study was conducted, involving 381 physicians and 1351 nurses recruited from eight European hospitals in Belgium, the Netherlands, Italy, and Poland. The study focused on assessing turnover intentions among healthcare workers based on the Job DemandsResources model, using an online questionnaire. Structural equation models were employed to test the data collection questionnaires’ construct validity and internal consistency. The turnover intention was assessed by agreement with the intention to leave either the hospital or the profession. Among physicians,
The global shortage of healthcare workers (HCWs) has emerged as a critical concern with wide-ranging implications for healthcare systems worldwide. This shortage is attributed to factors such as an aging population, the increasing prevalence of patients with chronic diseases requiring continuous care, and the growing demand for healthcare services
The scarcity of healthcare providers has far-reaching consequences, including extended waiting times and limited patient access to healthcare services
Turnover among nurses is highly influenced by factors such as job dissatisfaction, stress and burnout
The findings of a systematic review on factors impacting nurse and physician retention in hospitals highlighted job dissatisfaction, lack of career development and work-life balance, as the main determinants of intention to leave
Identifying significant direct and indirect determinants of turnover intention can aid in the early detection of high-risk healthcare workers, enabling targeted interventions to reduce attrition and promote retention. Intention to leave has been found to be a reliable predictor of actual workforce attrition, emphasizing the importance of proactive measures to address this issue
To investigate turnover intention in relation to job satisfaction, work engagement, and burnout, we conducted a cross-sectional multicentre study involving nurses and physicians from eight European hospitals. The primary objective was to estimate the prevalence of intention to leave the organization and the profession. Secondly, after investigating the construct validity and internal consistency of a dedicated questionnaire developed for data collection, this study aimed to provide data-driven evidence regarding the direct and indirect determinants of intention to leave, as proposed by the adapted Job Demands-Resources (JD-R) model for turnover intention.
Theoretical model
Within the framework of the project entitled “Mental Health: focus on Retention of healthcare workers (METEOR)”, funded by the European Health and Digital Executive Agency in 2020, we aimed to assess job satisfaction, burnout and turnover intentions, using the theoretical framework of the JD-R model
The METEOR Turnover Intention (MTI) model, which is an adaption of the JD-R Model, considers job demands and job resources influencing factors of turnover intentions, through the mediation of burnout and job satisfaction (Fig. 1). The first hypothesis posits that job satisfaction and work engagement will increase by reducing job demands, as mediated by burnout (H1). This assumption is based on the well-known result that job demands and job control are predicted by a core burnout function (positive association) and by an extended engagement function (negative association)
Furthermore, it has been observed that higher levels of job resources, such as increased opportunities for learning, support from co-workers, and support from supervisors
The third hypothesis states that burnout, specifically emotional exhaustion and depersonalisation, is a contributing factor to the intention to leave (H3). This hypothesis aligns with H1 and, hence, focuses on emotional exhaustion and depersonalization as the core components of burnout
Figure 1. The theoretical turnover intention according to Meteor (MTI) model.
turnover intention also assumes a positive covariance between emotional exhaustion and depersonalization
Materials and methods Study design
Participants in this cross-sectional multicentre study were selected from two hospitals, one academic and one non-academic, in each of the following countries: Belgium, the Netherlands, Italy, and Poland. An initial invitation to partake in the study was dispatched via the intranet or email too all physicians and nurses in force at each participating hospital at the date of 1st April 2022. The immediate contact details of the participants were blinded to the research group. Fourteen days later, a reminder email was dispatched once more to all participants. In the case of the number of respondents lower than requested, the medical and nurses’ associations have been involved to solicit nurses and physicians partaking the research by explaining them the expected benefits in terms of workplace well-being. Before respondents could participate in the study, they would have to read the information letter and agree with the online informed consent. Participants had to hold a degree in Nursing (bachelor or higher) or Medicine (master) and could either work in healthcare or hold a managerial position. Other inclusion criteria were adult age and being currently working as a nurse or physician in one of the eight participating hospitals. Nurses and physicians affiliated to hospitals different than the ones included in this study and those working in EU countries different from the ones participating in this study were excluded from the study. Caring experts, midwives, psychologists, lab technicians and paramedics were excluded, too. Data were collected between May 16 and September 30, 2022. The sample size calculation aimed to estimate the proportion of individuals reporting the intention to leave their job, with a confidence level of
The questionnaire
The questionnaire was developed in English and translated into Dutch, Italian and Polish. After back translation, the questionnaire was administered through an online platform compliant with the General Data Protection Regulation (Survey Monkey). The questionnaire consisted of 75 items, with an additional question about education included only for nurses. It was structured into eight sections: individual and work environment characteristics, Job demands (JD), Job resources (JR), Work engagement (WE), Job satisfaction (JS), Emotional Exhaustion (EE), Depersonalization (DP) and intention to leave (IL). Items for JD, JR, WE and JS were derived from the Copenhagen psychosocial questionnaire (COPSOQ)
To be consistent with the source-validated tools, items for JD, JR, WE, JS and IL were scored on a 5-point Likert scale, coded between 0 and 4 (between 4 and 0 for reversed items) while items for EE and DP were scored on a 7-point Likert scale ranging between 0 and 6. The complete questionnaire can be found in the Supplement Materials.
Statistical methods
Each domain of JD, JR, WE, JS, EE, DP and IL, was transformed into a
Confirmatory factor analysis (CFA) was conducted using a structural equation model with measurement component to test the MTI model. The seven domains were treated as latent variables, with two exogenous variables (JD and JR) and five endogenous variables (WE, JS, EE, DP and IL), measured by the corresponding sections of the questionnaire.
Several goodness-of-fit indices were used to select the best CFA model. Good models have RMSEA values
Internal consistency was assessed for the overall questionnaire and for each of the seven latent constructs using Cronbach’s alpha coefficient. Higher alpha values indicate greater internal consistency. Internal consistency is considered poor with alpha values below 0.60 , questionable when between 0.60 and 0.70 , acceptable between 0.70 and 0.80 , good between 0.80 and 0.90 and excellent when higher than
All analyses were performed using R Statistical Software (v4.1.2; R Core Team 2021) and Stata IC/15.1 for Windows.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. The study was approved by the Ethics Committee Research UZ/KU Leuven in January 2022 (S66009).
Consent to participate
Informed consent was obtained from the participants, who received detailed information about the study.
Results
Among the 543 physicians who provided informed consent for the survey, 381 (
The internal consistency of the questionnaire was excellent overall (alpha
On a
Based on CFA fit indices (Table S2), the best model for physicians included two direct and two indirect determinants of turnover intention (Fig. 2). The direct effects showed a positive relation between DP and turnover intention (coeff
Of the 1680 nurses who participated in the study and responded to the survey, 1351 (
The internal consistency of the questionnaire for nurses was excellent overall (alpha=0.934). The alpha values for the seven domains ranged between acceptable values (IL’s alpha
Based on CFA fit indices (Table S5), the best model for nurses included two direct and two indirect determinants of turnover intention (Fig. 3). The direct effects showed a positive relation between DP and turnover intention (coeff
| Latent construct* | Physicians (
|
Nurses (
|
||
| Mean (SD) | Alpha | Mean (SD) | Alpha | |
| JD (
|
57.62 (12.11) | 0.882 | 54.93 (11.16) | 0.873 |
| JR (
|
62.94 (12.73) | 0.840 | 61.95 (11.64) | 0.816 |
| WE (
|
66.89 (16.23) | 0.732 | 67.6 (15.77) | 0.787 |
| EE (
|
32.93 (20.98) | 0.908 | 31.04 (19.9) | 0.914 |
| DP (
|
13.88 (14.9) | 0.751 | 13.12 (15.93) | 0.786 |
| JS (
|
59.38 (18.94) | 0.844 | 56.53 (16.32) | 0.802 |
| IL (
|
29.27 (23.77) | 0.598 | 29.61 (23.83) | 0.725 |
| Overall (
|
48.77 (7.07) | 0.939 | 47.06 (7.07) | 0.934 |
Table 1. Means, standard deviations and internal consistencies (Cronbach’s alpha) of the MTI questionnaire for physicians. MTI turnover intention according to Meteor, JD job demands, JR job resources, WE work engagement,
Figure 2. Construct validity of the MTI questionnaire in a sample of 381 physicians from eight European hospitals. In the picture there are shown the path coefficients of the latent component of the MTI SEM model for physicians. Positive effects and covariances are shown in blue, negative effects and covariances are shown in red. MTI Turnover Intention according to Meteor.
| Endogenous variables | Exogenous variables | Path coefficient | 95% CI |
|
|
| Job satisfaction | Job demands | -0.28 | -0.37 | -0.19 | <0.001 |
| Job resources | 0.71 | 0.64 | 0.79 | <0.001 | |
| Emotional exaustion | Job demands | 0.60 | 0.52 | 0.68 | <0.001 |
| Job resources | -0.28 | -0.37 | -0.19 | <0.001 | |
| Depersonalization | Job demands | 0.29 | 0.20 | 0.39 | <0.001 |
| Job resources | -0.26 | -0.36 | -0.16 | <0.001 | |
| Intention_to_leave | Job satisfaction | -0.61 | -0.73 | -0.49 | <0.001 |
| Depersonalization | 0.21 | 0.07 | 0.34 | 0.002 | |
| Covariance between pairs of latent variables | Covariance | 95% CI |
|
||
| (Emotional Exhaustion, Job satisfaction) | -0.32 | -0.45 | -0.19 | <0.001 | |
| (Emotional Exhaustion, Depersonalization) | 0.26 | 0.16 | 0.35 | <0.001 | |
| (Job demands, Job resources) | -0.40 | -0.51 | -0.29 | <0.001 | |
Table 2. Results of confirmatory factor analysis: path coefficients of the latent component of the MTI model for physicians. MTI turnover intention according to Meteor.
Discussion
The objective of the study was to determine the prevalence of nurses’ and physicians’ intention to leave their respective health organizations or current professions and to identify the determinants associated with this phenomenon.
A recent systematic review
Interestingly, the questionnaire’s internal consistency was proven to be overall excellent, except for the intention to leave. This inconsistency can be attributed to the fact that the intention to leave the profession and the
Figure 3. Construct validity of the MTI questionnaire in a sample of 1351 nurses from four European countries. In the picture there are shown the path coefficients of the latent component of the MTI SEM model for nurses. Positive effects and covariances are shown in blue, negative effects and covariances are shown in red. MTI turnover intention according to Meteor.
| Endogenous variables | Exogenous variables | Path coefficient | 95% CI |
|
|
| Work engagement | Job demands | -0.13 | -0.2 | -0.07 | <0.001 |
| Job resources | 0.60 | 0.54 | 0.66 | <0.001 | |
| Job satisfaction | Job demands | -0.38 | -0.43 | -0.33 | <0.001 |
| Job resources | 0.62 | 0.57 | 0.67 | <0.001 | |
| Emotional exaustion | Job demands | 0.61 | 0.57 | 0.65 | <0.001 |
| Job resources | -0.27 | -0.31 | -0.22 | <0.001 | |
| Depersonalization | Job demands | 0.33 | 0.27 | 0.39 | <0.001 |
| Job resources | -0.36 | -0.42 | -0.30 | <0.001 | |
| Intention_to_leave | Job satisfaction | -0.56 | -0.63 | -0.50 | <0.001 |
| Depersonalization | 0.19 | 0.12 | 0.26 | <0.001 | |
| Covariance between pairs of latent variables | Covariance | 95% CI |
|
||
| (Work engagement, job satisfaction) | 0.29 | 0.20 | 0.38 | <0.001 | |
| (Emotional exhaustion, depersonalization) | 0.36 | 0.30 | 0.42 | <0.001 | |
| (Job demands, job resources) | -0.35 | -0.41 | -0.28 | <0.001 | |
Table 3. Results of Confirmatory factor analysis: path coefficients of the latent component of the MTI model for nurses. MTI turnover intention according to Meteor.
intention to leave the hospital seem to be two different phenomena. The former suggests feelings of alienation and rejection with a negative impact on the healthcare sector (macro level), while the latter implies a desire for change that only impacts the hospital (meso level) or the ward (micro level).
Our survey found that physicians were more inclined to leave their current hospital than the medical profession, while nurses exhibited a higher intention to leave the nursing profession itself rather than their specific workplace. It could be hypothesized that among nurses, the professional practice no longer arouses a high attraction in terms of gratification and recognition of their own role concerning salary, working, or organizational conditions, especially if compared to the high emotional and physical pressures suffered in the last pandemic.
Data emerging from the literature suggested how the risk from SARS-CoV-2 in the healthcare settings was considered as an aggravated generic risk, rather than a specific risk, meaning that the workers are more exposed to SARS-CoV-2 in terms of intensity and frequency of contact with other potential infected individuals than the
ones from other working settings
ones from other working settings
Our study aimed to examine the direct and indirect determinants influencing the intention to leave among physicians and nurses working in hospital settings as related to job satisfaction, work engagement and the burnout. The study hypotheses were confirmed only in part and varied between physicians and nurses.
Specifically, job demands were associated with increased emotional exhaustion and depersonalization, as well as with decreased job satisfaction for both physicians and nurses (H1 confirmed). Similarly, job resources were linked to decreased emotional exhaustion and depersonalization, as well as increased job satisfaction for both groups of healthcare workers (H2 confirmed).
However, the hypothesis suggesting that burnout would act as a driving force for the intention to leave (Hypothesis 3) was not supported by either physicians or nurses. In fact, only depersonalization, and not emotional exhaustion, was found to be a direct determinant of the intention to leave, along with job satisfaction.
Furthermore, the results suggested that the intention to leave among physicians was not explained by work engagement (H3 rejected). Rather, a significant portion of the variability was explained by the negative correlation between job satisfaction and emotional exhaustion. On the other hand, work engagement played a role in explaining the intention to leave among nurses, as it was positively correlated with job satisfaction (H4 confirmed).
For both workers’ categories, feeling depersonalized and reporting low job satisfaction represented two direct determinants of the intention to leave. Indirectly, job demands affected the intention to leave and job satisfaction, while job resources acted as protective factors. An increase in job demands was related to increased depersonalization, thereby reducing job satisfaction. On the contrary, increased job resources resulted in increased job satisfaction and reduced depersonalization while mitigating job strain and burnout
According to the JD-R model, work engagement is influenced by the availability of job resources, while burnout is associated with job demands more than job resources. Interestingly, the absence of a direct or indirect impact of work engagement on physicians’ intentions to leave could be attributed to the disproportionate burden of job demands. Factors such as role ambiguity, role conflict, role stress, stressful events, workload, and work pressure
The motivating process triggered by perceived resources determines positive outcomes such as work engagement and high organizational commitment, as they help to achieve goals, reduce job demands, and promote personal growth and development
Conversely, in the case of nurses, work engagement was found to be related to job satisfaction. This suggests that regardless of the internal or external resources available, the degree of satisfaction experienced in the workplace plays a crucial role in determining positive outcomes in terms of performance and commitment. This highlights the importance of targeted and functional interventions aimed at promoting well-being in the workplace, focusing on a particular need expressed by nurses. This finding aligns with the current literature, which shows that among nurses job satisfaction is positively associated with work engagement
In both physicians and nurses, depersonalization alone, and not emotional exhaustion, played a role in explaining the intention to leave. Emotional exhaustion, in some circumstances, is experienced as a mental state inherent in the work activity, while depersonalization appears to be more related to the sphere of psychopathology, representing a significant risk factor for the HCWs’ health
The main strength of this study is including countries that provided a geographically balanced representation of different regions in Europe. In fact, the selected countries represent a wide range of healthcare systems: in Belgium there is a mix combining compulsory, comprehensive and universal public health insurance with freedom of choice and independent medical practice; in the Netherlands, the health demand is covered by basic insurance and long-term nursing and care, that are two statutory forms of insurance; in Poland, the mandatory health insurance is the primary source of public funding, which however is undersized in relation to the increasing population needs. Lastly, the Italian National Health Service is inspired by the principles of universality, equality and equity through the provision of essential levels of care accessible free of charge to the whole population and in a uniform way. The last available Euro Health Consumer Index score (2018) was the highest in the Netherlands (883), while Belgium (849), Italy (687), and Poland (585) showed lower scores. Compared to the EU average health expenditure in proportion to GDP (
This study provided a validated tool to assess the intention to leave phenomenon in European hospital HCWs.
One study limitation is the imbalance in the number of physicians and nurses, which may have contributed to some differences in the significant determinants of turnover intention. However, the lower response rate of physicians, as compared to nurses, is not uncommon on this topic, and previous studies have also observed this imbalance. For example, the two HCWs’ categories have been represented in a
ratio
One study limitation is the imbalance in the number of physicians and nurses, which may have contributed to some differences in the significant determinants of turnover intention. However, the lower response rate of physicians, as compared to nurses, is not uncommon on this topic, and previous studies have also observed this imbalance. For example, the two HCWs’ categories have been represented in a
ratio
Conclusions
The study provided estimates on the prevalence of the intention to leave the hospital and the profession among physicians and nurses, highlighting at the same time how the hospital context determined a greater turnover intention in doctors, while for nurses the discomfort appeared to be prevalently linked to the professional practice itself.
Furthermore, our findings suggested the important role of depersonalization in explaining the intention to leave in both the HCWs’ categories and confirmed previous studies indicating work engagement as a determinant of nurses’ intention to leave.
In conclusion, based on the evidence provided by this cross-sectional study, the management at the micro (ward), meso (hospital) and macro (policy) levels are called to define appropriate recruitment and retention policies, specifically for nurses and physicians, in consideration that job satisfaction, work engagement and a good working climate, they all appear to be strategic factors in promoting the job retention.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Received: 25 July 2023; Accepted: 24 January 2024
Published online: 28 January 2024
Published online: 28 January 2024
References
- Commission of the European Communities. Green paper on the European workforce for health. Hum. Resour. Health 14, 1 (2008).
- Haakenstad, A. et al. Measuring the availability of human resources for health and its relationship to universal health coverage for 204 countries and territories from 1990 to 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 399(10341), 2129-2154 (2022).
- Kroezen, M. et al. Recruitment and retention of health professionals across Europe: A literature review and multiple case study research. Health Policy 119(12), 1517-1528 (2015).
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030 (2016).
- Matranga, D. & Maniscalco, L. Inequality in healthcare utilization in Italy: How important are barriers to access? Int. J. Environ. Res. Public Health 19(3), 1-14 (2022).
- Duffield, C. M., Roche, M. A., Homer, C., Buchan, J. & Dimitrelis, S. A comparative review of nurse turnover rates and costs across countries. J. Adv. Nurs. 70(12), 2703-2712 (2014).
- O’Brien-Pallas, L., Murphy, G. T., Shamian, J., Li, X. & Hayes, L. J. Impact and determinants of nurse turnover: A pan-Canadian study. J. Nurs. Manag. 18(8), 1073-1086 (2010).
- Yang, H., Lv, J., Zhou, X., Liu, H. & Mi, B. Validation of work pressure and associated factors influencing hospital nurse turnover: A cross-sectional investigation in Shaanxi Province. China. BMC Health Serv. Res. 17, 1-11 (2017).
- Windover, A. K. et al. Correlates and outcomes of physician burnout within a large academic medical center. JAMA Intern. Med. 178(6), 856-858 (2018).
- Al Yahyaei, A., Hewison, A., Efstathiou, N. & Carrick-Sen, D. Nurses’ intention to stay in the work environment in acute healthcare: A systematic review. J. Res. Nurs. 27(4), 374-397 (2022).
- Degen, C., Li, J. & Angerer, P. Physicians’ intention to leave direct patient care: An integrative review. Hum. Resour. Health 13, 1-12 (2015).
- de Vries, N. et al. The race to retain healthcare workers: A systematic review on factors that impact retention of nurses and physicians in Hospitals. Inq. J. Health Care Organ. Provision Financ. 60, 00469580231159318 (2023).
- Castle, N. G., Engberg, J., Anderson, R. & Men, A. Job satisfaction of nurse aides in nursing homes: Intent to leave and turnover. Gerontologist 47(2), 193-204 (2007).
- Hann, M., Reeves, D. & Sibbald, B. Relationships between job satisfaction, intentions to leave family practice and actually leaving among family physicians in England. Eur. J. Public Health 21(4), 499-503 (2011).
- Demerouti, E., Bakker, A. B., Nachreiner, F. & Schaufeli, W. B. The job demands-resources model of burnout. J. Appl. Psychol. 86(3), 499 (2001).
- Schaufeli, W. B., Bakker, A. B., Hoogduin, K., Schaap, C. & Kladler, A. On the clinical validity of the maslach burnout inventory and the burnout measure. Psychol. Health 16(5), 565-582 (2001).
17 Demerouti, E., Bakker, A. B., De Jonge, J., Janssen, P. P. M. & Schaufeli, W. B. Burnout and engagement at work as a function of demands and control. Scand. J. Work Environ. Health 1, 279-286 (2001). - Green, D. E., Walkey, F. H. & Taylor, A. J. W. The three-factor structure of the maslach burnout inventory: A multicultural, multinational confirmatory study. J. Soc. Behav. Pers. 6(3), 453 (1991).
- Schaufeli, W. B., Salanova, M., González-Romá, V. & Bakker, A. B. The measurement of engagement and burnout: A two sample confirmatory factor analytic approach. J. Happiness Stud. 3, 71-92 (2002).
- Sarti, D. Job resources as antecedents of engagement at work: Evidence from a long-term care setting. Hum. Resour. Dev. Q. 25(2), 213-237 (2014).
- Hu, Q., Schaufeli, W. B. & Taris, T. W. How are changes in exposure to job demands and job resources related to burnout and engagement? A longitudinal study among Chinese nurses and police officers. Stress Health 33(5), 631-644 (2017).
- Koch, P. et al. How perceived quality of care and job satisfaction are associated with intention to leave the profession in young nurses and physicians. Int. J. Environ. Res. Public Health 17(8), 2714 (2020).
- Burr, H. et al. The third version of the Copenhagen psychosocial questionnaire. Saf. Health Work 10(4), 482-503 (2019).
- Sorra, J. et al. AHRQ Hospital Survey on Patient Safety Culture: User’s Guide (Agency for Healthcare Research and Quality, 2016).
- O’Driscoll, M. P. & Beehr, T. A. Supervisor behaviors, role stressors and uncertainty as predictors of personal outcomes for subordinates. J. Organ Behav. 15(2), 141-155 (1994).
26 Pejtersen, J. H., Kristensen, T. S., Borg, V. & Bjorner, J. B. The second version of the Copenhagen psychosocial questionnaire. Scand. J. Public Health 38, 8-24 (2010). - Bland, J. M. & Altman, D. G. Statistics notes: Cronbach’s alpha. BMJ 314(7080), 572 (1997).
- Andresen, I. H., Hansen, T. & Grov, E. K. Norwegian nurses’ quality of life, job satisfaction, as well as intention to change jobs. Nord. J. Nurs. Res. 37(2), 90-99 (2017).
- Labrague, L. J. & de Los Santos, J. A. A. Fear of Covid-19, psychological distress, work satisfaction and turnover intention among frontline nurses. J. Nurs. Manag. 29(3), 395-403 (2021).
- Ekingen, E., Teleş, M., Yıldız, A. & Yıldırım, M. Mediating effect of work stress in the relationship between fear of COVID-19 and nurses’ organizational and professional turnover intentions. Arch. Psychiatr. Nurs. 42, 97-105 (2023).
- Lavoie-Tremblay, M. et al. Influence of caring for COVID-19 patients on nurse’s turnover, work satisfaction and quality of care. J. Nurs. Manag. 30(1), 33-43 (2022).
- Heinen, M. M. et al. Nurses’ intention to leave their profession: A cross sectional observational study in 10 European countries. Int. J. Nurs. Stud. 50(2), 174-184 (2013).
- Christianson, J., Johnson, N., Nelson, A. & Singh, M. Work-related burnout, compassion fatigue, and nurse intention to leave the profession during COVID-19. Nurse Lead. 21(2), 244-251 (2023).
- Pathman, D. E. et al. Physician job satisfaction, job dissatisfaction, and physician turnover. J. Fam. Pr. 51(7), 593 (2002).
- Far, M. F., Nia, H. S. & Assarroudi, A. Correlation of the job turnover intention of Iranian nurses with job satisfaction and burnout in the COVID-19 pandemic. J. Educ. Health Promot. 11(1), 364 (2022).
- Van den Bulcke, B. et al. Ethical climate and intention to leave among critical care clinicians: An observational study in 68 intensive care units across Europe and the United States. Intens. Care Med. 46, 46-56 (2020).
- Leineweber, C. et al. Nurses’ practice environment and satisfaction with schedule flexibility is related to intention to leave due to dissatisfaction: A multi-country, multilevel study. Int. J. Nurs. Stud. 58, 47-58 (2016).
- Bruyneel, L., Thoelen, T., Adriaenssens, J. & Sermeus, W. Emergency room nurses’ pathway to turnover intention: A moderated serial mediation analysis. J. Adv. Nurs. 73(4), 930-942 (2017).
- Hämmig, O . Explaining burnout and the intention to leave the profession among health professionals-A cross-sectional study in a hospital setting in Switzerland. BMC Health Serv. Res. 18(1), 1-11 (2018).
- Van der Heijden, B., Brown Mahoney, C. & Xu, Y. Impact of job demands and resources on nurses’ burnout and occupational turnover intention towards an age-moderated mediation model for the nursing profession. Int. J. Environ. Res. Public Health 16(11), 2011 (2019).
- Sasso, L. et al. Push and pull factors of nurses’ intention to leave. J. Nurs. Manag. 27(5), 946-954 (2019).
- Cirrincione, L., Rapisarda, V., Mazzucco, W., Provenzano, R. & Cannizzaro, E. SARS-CoV-2 and the risk assessment document in Italian work; specific or generic risk even if aggravated? Int. J. Environ. Res. Public Health 18(7), 3729 (2021).
- Koh, D. & Goh, H. P. Occupational health responses to COVID-19: What lessons can we learn from SARS? J. Occup. Health 62(1), e12128 (2020).
- ÇetinAslan, E., Türkmen, İ & Top, M. The effect of macro-control and organizational support perception on nurses and physicians intention to quit during the COVID-19 pandemic. J. Nurs. Scholarsh. 55, 843 (2022).
- Said, R. M. & El-Shafei, D. A. Occupational stress, job satisfaction, and intent to leave: Nurses working on front lines during COVID-19 pandemic in Zagazig City, Egypt. Environ. Sci. Pollut. Res. 28, 8791-8801 (2021).
46 De los Santos, J. A. A. & Labrague, L. J. The impact of fear of COVID-19 on job stress, and turnover intentions of frontline nurses in the community: A cross-sectional study in the Philippines. Traumatology 27(1), 52 (2021). - Fronda, D. C. & Labrague, L. J. Turnover intention and coronaphobia among frontline nurses during the second surge of COVID19: The mediating role of social support and coping skills. J. Nurs. Manag. 30(3), 612-621 (2022).
- Bakker, A. B., Demerouti, E., Taris, T. W., Schaufeli, W. B. & Schreurs, P. J. G. A multigroup analysis of the job demands-resources model in four home care organizations. Int. J. Stress Manag. 10(1), 16 (2003).
- Maniscalco, L. et al. The long-term effect of job mobility on workers’ mental health: A propensity score analysis. BMC Public Health 22(1), 1145 (2022).
- Bakker, A. B., Demerouti, E. & Sanz-Vergel, A. I. Burnout and work engagement: The JDR approach. Annu. Rev. Organ. Psychol. Organ. Behav. 1, 389-411 (2014).
- De Simone, S., Planta, A. & Cicotto, G. The role of job satisfaction, work engagement, self-efficacy and agentic capacities on nurses’ turnover intention and patient satisfaction. Appl. Nurs. Res. 39, 130-140 (2018).
- De Gieter, S., Hofmans, J. & Pepermans, R. Revisiting the impact of job satisfaction and organizational commitment on nurse turnover intention: An individual differences analysis. Int. J. Nurs. Stud. 48(12), 1562-1569 (2011).
- Hayes, L. J. et al. Nurse turnover: A literature review-An update. Int. J. Nurs. Stud. 49(7), 887-905 (2012).
- Gago-Valiente, F.-J., Mendoza-Sierra, M.-I., Moreno-Sánchez, E., Arbinaga, F. & Segura-Camacho, A. Emotional exhaustion, depersonalization, and mental health in nurses from Huelva: A cross-cutting study during the SARS-CoV-2 pandemic. Int. J. Environ. Res. Public Health 18(15), 7860 (2021).
- Vandenbroeck, S., Van Gerven, E., De Witte, H., Vanhaecht, K. & Godderis, L. Burnout in Belgian physicians and nurses. Occup. Med. 67(7), 546-554 (2017).
- Masum, A. K. M. et al. Job satisfaction and intention to quit: An empirical analysis of nurses in Turkey. PeerJ 4, e1896 (2016).
- ArslanYurumezoglu, H. & Kocaman, G. Predictors of nurses’ intentions to leave the organisation and the profession in Turkey. J. Nurs. Manag. 24(2), 235-243 (2016).
Author contributions
Conceptualization: L.M., M.E., D.M.; Methodology: L.M., M.E., D.M., A.B., N.D.V., P.D.W., M.K., S.S., L.G.; Formal analysis: L.M., M.E., D.M.; Investigation: A.B., O.L., N.D.V., A.S., S.F., K.B., M.K.; Writing-original draft preparation: L.M., M.E., S.M., W.M., D.M.; Writing-review and editing: K.B., S.S., P.D.W., A.B., N.D.V., W.M., L.G.; Funding acquisition: L.G.; Supervision: D.M.
Funding
External funding was received for the development of this study: European Union, HaDEA (Grant Agreement (GA) No: 101018310)-3rd Health Programme, Multibeneficiary Project Grant (HP-PJ, HP-JA), Topic: PJ-01-2020-1, Type of action: HP-PJ, SEP-210693712: Project called METEOR (MEnTal hEalth: fOcus on Retention of healthcare workers). The funding source did not influence the study design, the collection, analysis and interpretation of the data, the manuscript writing or the decision to submit the manuscript for publication. Both the views that are expressed and any errors or omissions are the sole responsibility of the authors.
Competing interests
The authors declare no competing interests.
Additional information
Supplementary Information The online version contains supplementary material available at https://doi.org/ 10.1038/s41598-024-52887-7.
Correspondence and requests for materials should be addressed to D.M.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
© The Author(s) 2024
© The Author(s) 2024
Department of Health Promotion, Mother and Child Care, Internal Medicine and Medical Specialties, University of Palermo, Palermo, Italy. Department of Internal Medicine, Spaarne Gasthuis, Hoofddorp, The Netherlands. Spaarne Gasthuis Academy, Hoofddorp, The Netherlands. Department of Public Health and Primary Care, Centre for Environment and Health, KU Leuven (University of Leuven), Leuven, Belgium. Department of Epidemiology, Medical University of Silesia, Katowice, Poland. Department of Psychology, Educational Science and Human Movement, University of Palermo, Palermo, Italy. Leuven Child and Health Institute, KU Leuven, Leuven, Belgium. Department of Development and Regeneration, KU Leuven, Leuven, Belgium. Department of Pediatrics, Spaarne Gasthuis, Haarlem and Hoofddorp, The Netherlands. These authors contributed equally: L. Maniscalco and M. Enea. email: domenica.matranga@unipa.it