آثار التحويلات النقدية المشروطة على حدوث وفيات السل وفقًا للعرق والإثنية والعوامل الاجتماعية الاقتصادية في مجموعة الـ 100 مليون برازيلي Effects of conditional cash transfers on tuberculosis incidence and mortality according to race, ethnicity and socioeconomic factors in the 100 Million Brazilian Cohort
آثار التحويلات النقدية المشروطة على حدوث وفيات السل وفقًا للعرق والإثنية والعوامل الاجتماعية الاقتصادية في مجموعة الـ 100 مليون برازيلي
تاريخ الاستلام: 15 أبريل 2024 تم القبول: 26 أكتوبر 2024 نُشر على الإنترنت: 3 يناير 2025 تحقق من التحديثات
تظهر قائمة بالمؤلفين وانتماءاتهم في نهاية الورقة.
تم تنفيذ برامج التحويلات النقدية المشروطة (CCT) على مستوى العالم لتخفيف الفقر. على الرغم من أن مرض السل (TB) مرتبط ارتباطًا وثيقًا بالفقر، إلا أن آثار برامج CCT على نتائج السل بين السكان الذين يواجهون هشاشة اجتماعية واقتصادية لا تزال غير مؤكدة. هنا قمنا بتقدير العلاقات بين المشاركة في أكبر برنامج CCT في العالم، وهو برنامج بولسا فاميليا البرازيلي (BFP)، وتقليل معدل حدوث السل، والوفيات، ومعدلات الفتك باستخدام مجموعة البرازيل المكونة من 100 مليون شخص على مستوى البلاد بين عامي 2004 و2015. كما قمنا بتقييم هذه العلاقات وفقًا للعرق، والاثنية، ومستويات الثروة، والجنس، والعمر. كانت المشاركة في برنامج BFP مرتبطة بتقليل كبير في معدل حدوث السل (نسبة المعدل المعدلة (aRR): 0.59؛ فترة الثقة (CI) 95%: 0.58-0.60) والوفيات (aRR: 0.69؛ 95% CI: 0.65-0.73). كانت أقوى علاقة مع برنامج BFP ملحوظة في الأفراد من الإثنية الأصلية لكل من معدل حدوث السل (aRR: 0.37؛ 95% CI: 0.32-0.42) والوفيات (aRR: 0.35؛ 95% CI: 0.20-0.62)، وفي الأفراد من الإثنية السوداء والباردو (معدل الحدوث-aRR: 0.58؛ 95% CI: 0.57-0.59؛ معدل الوفيات-aRR: 0.69؛ 95% CI: 0.64-0.73). كانت علاقات برنامج BFP أقوى بكثير بين الأفراد الذين يعيشون في فقر مدقع لكل من معدل حدوث السل (aRR: 0.49؛ 95% CI: 0.49-0.50) والوفيات (aRR: CI: يمكن أن يقلل العلاج المركب بشكل كبير من حدوث السل والوفيات لدى الأفراد الذين يعيشون في فقر مدقع، ومن ذوي الأصول الأصلية، والسود، والأشخاص من عرق باردو، ويمكن أن يسهم بشكل كبير في تحقيق أهداف استراتيجية إنهاء السل وأهداف التنمية المستدامة المتعلقة بالسل.
التحويلات النقدية المشروطة (CCTs) هي أكثر التدخلات التي تم تنفيذها على نطاق واسع في العالم لتخفيف الفقر.تُعترف الحماية الاجتماعية، وتخفيف الفقر، والإجراءات متعددة القطاعات المتعلقة بالعوامل الواسعة للسل (TB) كأعمدة رئيسية لاستراتيجية إنهاء السل بحلول عام 2035، وهي ضرورية لتقليل عبء السل..
لدى برامج CCT القدرة على التأثير الإيجابي على الوقاية من السل، والتشخيص، والعلاج.تحسن التحويلات النقدية المشروطة ظروف المعيشة وتحث على تغييرات سلوكية من خلال تقديم الدعم المالي للأفراد أو الأسر الذين يلتزمون بمعايير صحية محددة. الحالات، المرتبطة غالبًا بصحة الأطفال والأمهاتأظهرت الدراسات السابقة في البلدان ذات الدخل المنخفض والمتوسط أن برامج التحويلات النقدية المشروطة كانت مرتبطة بتحسين نتائج السل، بما في ذلك زيادة الالتزام بالعلاج ومعدلات إكمال العلاج.. علاوة على ذلك، يمكن أن تخفف التحويلات النقدية المشروطة بشكل فعال الأعباء الاقتصادية التي تواجهها الأسر المتأثرة بالسلهذه التكاليف، التي غالبًا ما تنجم عن النفقات الطبية، وفقدان الدخل وعوامل أخرى ذات صلة، يمكن أن تدفع الأسر المتأثرة إلى الفقر وتعيق وصولها إلى الرعاية المناسبة لمرض السل.. وبالتالي، تساعد هذه التحويلات في التخفيف من التكاليف الكارثية المرتبطة
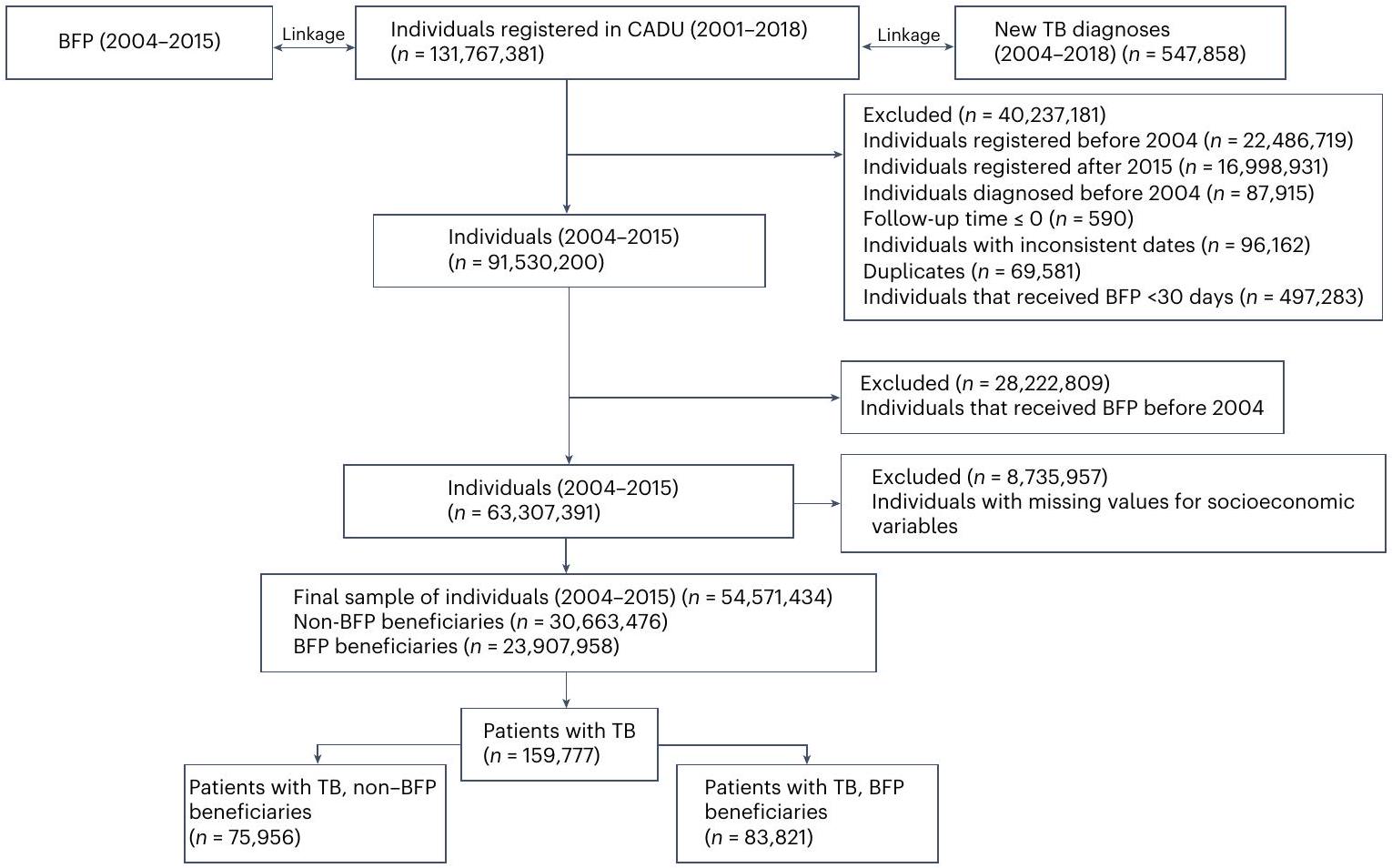
الشكل 1 | مخطط انسيابي لاختيار عينة الدراسة من مجموعة الـ 100 مليون برازيلي، 2004-2015. تم اختيار الأفراد من مجموعة الـ 100 مليون برازيلي أو استبعادهم بناءً على فترة الدراسة (2004-2015) وتوافر المعلومات الكاملة عن الخصائص الديموغرافية والاجتماعية الاقتصادية. تم اختيار ما مجموعه 54,571,434 فردًا: مستفيدو BFPوالمستفيدين غير من برنامج BPFشملت العينة المختارة 159,777 تشخيصًا جديدًا لمرض السل. مع السل، مما يضمن تحسين الوصول إلى العلاج وتقليل الأعباء الاقتصادية على الأسر المتأثرة.
منذ عام 2004، نفذت البرازيل واحدًا من أكبر برامج التحويلات النقدية المشروطة في العالم، وهو برنامج Bolsa Família (BFP).. يوفر البرنامج الحكومي تحويلات نقدية مباشرة للأسر التي تعيش في فقر بدخل أقل من خط الفقر الذي تحدده الحكومة البرازيلية وهو 43.6 دولار أمريكي لكل شخص في الشهر (بسعر صرف 5 ريالات برازيلية مقابل 1 دولار أمريكي). وتبلغ المساعدات النقدية الشهرية على الأقل US; الأطفال في الأسرة الذين تتراوح أعمارهم بين 0 و 6 سنوات يتلقون دعمًا إضافيًا قدره ، والنساء الحوامل، والأطفال والمراهقون حتى سن 18 عامًا يتلقون مبلغًا إضافيًا قدره دولار أمريكي (القيم المصححة في 2023). لمواصلة تلقي الفوائد، يجب على مستفيدي برنامج BFP الوفاء بشروط محددة تتعلق بالرعاية الصحية للنساء الحوامل (تنفيذ الرعاية السابقة للولادة) والأطفال (الامتثال لجدول التطعيم الوطني، ومراقبة الحالة الغذائية) والتعليم (حضور المدرسة) للأطفال والمراهقين.لقد تمكنت BFP من تحسين رفاهية الأسر في حالة الفقر، وتقليل الفوارق الاجتماعية والدخل في المجتمع، مما أدى إلى تحسين الوصول إلى التعليم والغذاء والخدمات الصحية.لقد أظهرت عدة دراسات التأثيرات الإيجابية لبرنامج التغذية الأساسية على نتائج الصحة مثل وفيات الأطفال.أمراض القلب والأوعية الدمويةالانتحارالجذاموبعض جوانب عبء السلمن بين آخرين.
بالإضافة إلى الفجوة في الدخل، تعاني البرازيل من عدم المساواة العرقية والإثنية العميقة. يواجه الأفراد الذين يعلنون عن عرقهم كأفارقة أو باردو أو من السكان الأصليين في البرازيل المزيد من الحواجز في الوصول إلى فرص عمل أفضل، ورواتب أعلى، وإسكان لائق، ونظام غذائي متوازن، وخدمات صحية وتعليمية ذات جودة.. ونتيجة لذلك، فإن هذه الفئات السكانية أكثر عرضة للعنف ومؤشرات الصحة الأسوأ بما في ذلك ارتفاع معدل الإصابة ومعدلات الوفيات من.
نحن غير مدركين للدراسات السابقة التي قامت بتقييم منهجي لتأثيرات برامج CCT في مجموعات كبيرة من الأفراد المعرضين للخطر والذين لديهم مخاطر عالية للإصابة بالسل ولديهم وصول محدود إلى الرعاية الصحية. الخدمات، مثل المجموعات في حالات التهميش الاجتماعي والأفراد الذين يعيشون في فقر مدقع، وتحليل آثارها وفقًا لخصائص الفئات الفرعية وتقييم العلاقة بين المشاركة في برامج التحويلات النقدية المشروطة وعبء مرض السل. كانت هذه الدراسة تهدف إلى تقييم العلاقة الشاملة بين تلقي برنامج المساعدة المالية الحكومية وتقليل معدل الإصابة بالسل ومعدل الوفيات ومعدل الفتك باستخدام مجموعة وطنية تضم 54.5 مليون برازيلي من ذوي الدخل المنخفض على مدى 12 عامًا، مع تقدير فعاليتها المتنوعة عبر طيف العوامل الإثنية والعرقية والظروف الاجتماعية والاقتصادية.
النتائج
تصميم الدراسة والسكان
تمتلك هذه الدراسة تصميم دراسة جماعية، تم الحصول عليها بعد اختيار الأفراد من مجموعة الـ 100 مليون برازيلي.مجموعة موحدة تم إنشاؤها من خلال الربط المعتمدبين السجل الموحد للحكومة الفيدرالية للبرامج الاجتماعية (Cadastro Único) – الذي يجمع بيانات من النصف الأفقر من السكان البرازيليين – ومجموعات البيانات المتعلقة بالصحة من وزارة الصحة البرازيلية. كما هو موضح في مخطط تدفق اختيار السكان للدراسة (الشكل 1)، بعد استبعاد الأفراد الذين كانوا خارج فترة الدراسة 2004-2015 والذين كانت لديهم معلومات مفقودة عن المتغيرات الديموغرافية أو الاجتماعية والاقتصادية، تم اختيار 54,571,434 فردًا، من بينهم 23,907,958 كانوا مستفيدين من برنامج BFP. ) و كانوا مستفيدين غير BFP (، مع إجمالي 159,777 تشخيص جديد لمرض السل و7,993 حالة وفاة بسبب السل.
كانت incidence السل أقل بين المستفيدين من برنامج BFP مقارنة بغير المستفيدين (49.44/100,000 سنة شخص معرضة للخطر (pyr) (فترة الثقة (CI): ) مقابل ( CI: 80.97-82.13))، وكان نفس الشيء مع معدل وفيات السل (2.08/100,000 pyr (كل: ) مقابل : ومعدل الوفيات بسبب السل ( ( ) مقابل 1.37/100 بير (95% CI: 1.25-1.49)) (الجدول 1). أظهر المستفيدون من BFP وغير المستفيدين خصائص ديموغرافية واقتصادية اجتماعية مشابهة
الجدول 1 | التحليلات الوصفية لمستفيدي BFP وغير المستفيدينبرازيل، 2004-2015
مستفيدو BF؛ N-BF، غير المستفيدين؛ Obs، الملاحظات؛ SMD، الفرق المعياري في المتوسط.تم استخدام ما يلي للمقارنة بين المجموعات: (1) ذو طرفين-اختبار المتغيرات المستمرة و (2) اختبار كاي تربيع لبييرسون ( ) للمتغيرات الفئوية. العرق أو الإثنية: أسود أو باردو، مُعلن ذاتياً.نسبي إلى الحد الأدنى للأجور (MW).الإضاءة: غير كهربائية – بدون عداد، مصابيح، شموع وغيرها.نسبة السكان البلديين الذين يعانون من نقص في خدمات الصرف الصحي الأساسية.نسبة السكان البلديين الذين لديهم جمع نفايات أساسي.إمدادات المياه: بئر أخرى، نبع وغيرها.نسبة تغطية الرعاية الصحية الأولية (PHC). الخصائص. بالمقارنة مع غير المستفيدين، فإن المستفيدين من برنامج BFP أصغر سناً (متوسط العمر 25.3 مقابل 24.2 سنة) وكان لديهم نسبة أعلى قليلاً من الأشخاص الذين يعرفون أنفسهم كأشخاص من العرق الأسود أو العرق الباردو. ضد )، أشخاص بلا تعليم ( ضد ) الأسر التي تضم 3 أفراد أو أكثر ( ضد )، الأشخاص ذوو الثروة الأقل ( ضد )، أشخاص بدون مرافق صحية كافية ( ضد ) والأشخاص الذين لا يمتلكون شبكة عامة لمياه الشرب ( ضد ).
التحليلات الرئيسية
بالنسبة للتحليل الإحصائي الرئيسي، استخدمنا نماذج الانحدار بواسون المتعددة المتغيرات مع وزن احتمالية العلاج المعكوس المستقر والمقصور (IPTW) (انظر الطرق للحصول على التفاصيل). كما هو موضح في الجدول 2، كانت التعرض لـ BFP مرتبطًا بانخفاض كبير في حدوث السل (نسبة المعدل المعدلة (aRR): 0.59؛ )، انخفاض معدل وفيات السل (نسبة المخاطر المعدلة: 0.69؛ 95% فترة الثقة: 0.65-0.73) ومعدل وفيات حالات السل المنخفض (نسبة المخاطر المعدلة: سي آي )، على الرغم من عدم دلالته الإحصائية.
التحليلات الطبقية
في التحليلات المصنفة وفقًا لثلاثيات الثروة (الجدول 3)، أظهرت العلاقة بين نسبة الدهون في الجسم وانخفاض حدوث مرض السل تدرج ملحوظ وكان أقوى بكثير بين الأفراد الذين يعيشون في فقر مدقع (aRR: 0.49 ؛ CI: )، تتناقص تدريجياً حتى تبقى فقط ارتباط صغير مع الأفراد الأكثر ثراءً (aRR: 0.95 ؛ CI: ). أيضًا، بالنسبة لوفيات السل، كانت علاقة BFP أقوى بكثير بين الأفراد الذين يعيشون في فقر مدقع (aRR: ) وأظهرت تدرجًا يوضح عدم وجود ارتباط بين BFP في أولئك الأشخاص ذوي الثروة الأعلى (aRR: CI: 0.85-1.17) (الجدول 3).
في التحليلات المتدرجة وفقًا للعرق والإثنية، كان هناك تدرج آخر واضح بين الأفراد من الإثنية الأصلية، والسود أو الباردو، والبيض، سواء بالنسبة لحدوث السل (aRR: 0.37 ( : 0.32-0.42) للسكان الأصليين، aRR: 0.58 ( : 0.57-0.59) للأشخاص السود أو الباردو، aRR: لأجل البيض) ووفيات السل (نسبة الخطر المعدلة: للشعوب الأصلية، aRR:لـ Black أو Pardo، و aRR: 0.83 (CI: 0.73-0.94) للأشخاص البيض)، بينما لم تكن التقديرات لمعدل الوفيات بسبب السل ذات دلالة إحصائية (الجدول 3). من حيث التعليم، كانت العلاقة بين BFP وانخفاض حالات السل أكبر لدى الأشخاص ذوي التعليم الأقل (aRR: مقابل aRR: للأشخاص ذوي التعليم العالي) (الجدول 3). كما ارتبطت BFP بانخفاض أكبر في معدلات وفيات السل لدى الإناث مقارنة بالذكور
الجدول 2 | تقديرات العلاقة بين نسبة الدهون في الجسم (BFP) و incidence السل والوفيات ومعدل الفتك في نموذج بواسون المعدل في البرازيل (مع أخطاء معيارية قوية)، 2004-2015
نموذج معدل
النتائج، aRR (95% CI)
حَدَث
الوفيات
معدل الوفيات
بي إف بي
0.59 (0.58-0.60)
0.69 (0.65-0.73)
0.90 (0.76-1.05)
جنس
ذكر
1 (أساس)
1 (أساس)
1 (أساس)
أنثى
0.58 (0.57-0.59)
0.40 (0.38-0.42)
0.69 (0.59-0.79)
عمر
1.19 (1.19-1.20)
1.63 (1.61-1.65)
1.44 (1.38-1.50)
العرق أو الإثنية
أبيض
1 (أساس)
1 (أساس)
1 (أساس)
أسود أو باردو
1.42 (1.40-1.44)
1.70 (1.60-1.81)
1.02 (0.86-1.21)
محلي
3.63 (3.43-3.84)
4.50 (3.59-5.65)
1.58 (0.92-2.70)
التعليم
أمي، لم يحضر المدرسة أبداً
1 (أساس)
1 (أساس)
1 (أساس)
المدرسة الابتدائية
1.83 (1.80-1.86)
1.05 (0.99-1.11)
0.94 (0.79-1.12)
المدرسة الثانوية
2.21 (2.17-2.25)
0.99 (1.93-1.06)
0.77 (0.62-0.94)
أكثر من المدرسة الثانوية
1.74 (1.70-1.77)
0.60 (0.54-0.67)
0.52 (0.37-0.73)
مواد بناء المنازل
الطوب والأسمنت
1 (أساس)
1 (أساس)
1 (أساس)
الخشب ومواد نباتية أخرى
1.22 (1.20-1.24)
1.21 (1.14-1.29)
1.15 (0.98-1.37)
عدد الأشخاص في العائلة
1 (أساس)
1 (أساس)
1 (أساس)
3 إلى 4
0.97 (0.96-0.99)
0.83 (0.78-0.88)
0.89 (0.89-1.28)
1.20 (1.18-1.21)
0.99 (0.92-1.06)
1.07 (0.76-1.05)
نفقات لكل راتب – % الحد الأدنى للأجور
أقل من الوسيط
1 (أساس)
1 (أساس)
1 (أساس)
فوق الوسيط
0.77 (0.78-0.79)
0.71 (0.66-0.75)
0.89 (0.75-1.05)
الإضاءة
الكهرباء
1 (أساس)
1 (أساسي)
1 (أساس)
غير كهربائي
1.34 (1.32-1.36)
1.54 (1.45-1.65)
1.09 (0.91-1.31)
الصرف الصحي غير الكافي
1.00 (0.99-1.02)
1.08 (1.02-1.15)
0.96 (0.81-1.14)
التخلص من النفايات
0.78 (0.77-0.80)
0.77 (0.71-0.83)
1.03 (0.82-1.30)
إمدادات المياه
شبكة عامة
1 (أساس)
1 (أساس)
1 (أساس)
آخر
0.95 (0.93-0.96)
0.99 (0.92-1.06)
0.95 (0.79-1.15)
مجموعة حدوث السل
1.00 (1.00-1.00)
1.00 (1.00-1.00)
0.99 (0.99-1.00)
الإيدز
–
–
1.93 (1.39-2.68)
السكري
–
–
0.87 (0.68-1.10)
نقطة
–
–
1.54 (1.34-1.77)
السل الرئوي
–
–
0.54 (0.42-0.69)
الرعاية الصحية الأولية
تغطية
1 (أساس)
1 (أساس)
1 (أساس)
لا تغطية
0.99 (0.99-1.00)
1.00 (0.99-1.00)
1.00 (0.99-1.00)
العيادات المتخصصة لكل 1,000 نسمة
0.63 (0.59-0.67)
0.54 (0.39-0.73)
1.15 (0.54-2.42)
الأطباء لكل 1,000 نسمة
1.11 (1.10-1.12)
1.19 (1.00-1.10)
1.08 (0.94-1.25)
الممرضات لكل 1,000 نسمة
0.95 (0.92-0.98)
0.80 (0.70-0.91)
1.11 (0.75-1.66)
معدل البطالة (%)
1.01 (1.01-1.02)
1.03 (1.02-1.04)
1.00 (0.98-1.02)
مؤشر جيني
0.99 (0.99-1.00)
1.00 (0.99-1.00)
0.98 (0.97-1.00)
سنة الدخول إلى المجموعة
نعم
نعم
نعم
ملاحظة
٥٤,٥٦٥,٧٣٥
٥٤,٥٧١,٤٣٤
٤٦٣٤٤
الجدول 3 | تقديرات العلاقة بين نسبة الدهون في الجسم (BFP) و incidence السل والوفيات ومعدل الفتك في البرازيل في نماذج بواسون المعدلة (مع أخطاء معيارية قوية)، 2004-2015
النماذج المعدلة
حَدَث
الوفيات
معدل الوفيات
آر آر
فترة الثقة 95%
أرر
فترة الثقة 95%
آر آر
فترة الثقة 95%
ثروة
ثروة أقل
0.49
(0.49-0.50)
0.60
(0.55-0.65)
0.80
(0.64-1.01)
ملاحظة
18,476,834
18,479,518
٢٠,٧٥٢
ثروة متوسطة
0.55
(0.54-0.57)
0.69
(0.63-0.77)
1.08
(0.82-1.43)
ملاحظة
17,714,018
17,715,984
16,74
ثروة أعلى
0.95
(0.93-0.98)
1.00
(0.85-1.17)
0.92
(0.60-1.42)
ملاحظة
18,596,773
18,597,844
8,979
العرق أو الإثنية
أبيض
0.67
(0.66-0.69)
0.83
(0.73-0.94)
1.26
(0.93-1.71)
ملاحظة
18,612,330
18,613,587
١٢٢٨٨
أسود أو باردو
0.58
(0.57-0.59)
0.69
(0.64-0.73)
0.84
(0.69-1.00)
ملاحظة
٣٥,٦٤١,٣٢١
٣٥٦٤٥٧٠١
٣٣,٣٢٨
محلي
0.37
(0.32-0.42)
0.35
(0.20-0.62)
0.16
(0.007-3.33)
ملاحظة
٣١٢,٠٨٤
٣١٢,١٤٦
717
التعليم
أمي، لم يحضر المدرسة أبداً
0.58
(0.57-0.59)
0.72
(0.68-0.78)
0.90
(0.66-1.23)
ملاحظة
٣٥٨٣٠٢٦٩
٣٥,٨٣٣,٥٣٢
7,741
المدرسة الابتدائية
0.58
(0.57-0.60)
0.63
(0.56-0.71)
0.93
(0.71-1.21)
ملاحظة
11,160,783
11,162,535
١٧١٨٥
التعليم الثانوي والجامعي
0.80
(0.77-0.83)
0.90
(0.71-1.14)
1.06
(0.84-1.35)
ملاحظة
٧,٥٧٧,٧٠٣
7,578,387
٢٥,٢٦٧
جنس
ذكر
0.60
0.59-0.61
0.78
0.72-0.84
0.94
0.78-1.13
ملاحظة
٢٥٤٣٢٦٦١
٢٥,٤٣٥,٩٥٥
٢٥,٦٨١
أنثى
0.61
0.59-0.62
0.63
0.57-0.69
0.90
0.66-1.23
ملاحظة
٢٩١٤٢٣٤٦
٢٩١٤٤٧٥١
٢٠,٦٦٣
السجون في البلدية
نعم
0.62
0.61-0.64
0.74
0.68-0.80
0.92
0.75-1.15
ملاحظة
٢٦٠٧٨٦٥٤
٢٦,٠٨١,٩٦٨
٢٦٧٧٧
لا
0.55
0.54-0.56
0.64
0.59-0.70
0.89
0.71-1.25
ملاحظة
٢٨٤٨٧٠٧٥
٢٨٤٨٩٤٦٠
19,567
المنطقة البرازيلية
شمال
0.48
0.47-0.50
0.47
0.39-0.56
0.97
0.55-1.71
ملاحظة
٦,٢٢٤,٥٢٩
٦,٢٢٥,٢١٨
٥٨٥٩
شمال شرق
0.51
0.49-0.52
0.57
0.52-0.63
0.81
0.63-1.06
مراقبة
18,246,282
18,248,820
١٤٧٠٣
الجنوب الشرقي
0.67
0.66-0.68
0.88
0.80-0.97
1.09
0.82-1.44
ملاحظة
19,438,441
19,439,952
١٧,٩٢٦
جنوب
0.66
0.64-0.69
0.68
0.56-0.82
0.62
0.44-0.87
ملاحظة
٦,٣٠٦,٩٦٣
٦,٣٠٧,٦١٤
٥٧٧٥
الشرق الأوسط
0.58
0.54-0.62
0.68
0.50-0.92
1.37
0.56-3.36
ملاحظة
٤٣٤٩٥١٤
٤,٣٤٩,٨٢٤
2,081
تم تعديل جميع النماذج لنفس المتغيرات الديموغرافية والاجتماعية الاقتصادية الموضحة في الجدول 2. أ تم قياسها من خلال النفقات الفردية النسبية إلى خط الأساس MW في الثلثين 1 و 2 و 3.كل واحد؛ ثروة منخفضة: الثلث 1، ثروة متوسطة: الثلث 2 وثروة أعلى: الثلثالعرق أو الإثنية: أسود أو باردو، مُعلن ذاتياً. (نسبة: 0.63 ( CI: ) مقابل aRR: 0.78 ( )، على التوالي). وفقًا للتحليلات حسب المناطق البرازيلية، كانت أقوى الارتباطات بين برنامج المساعدة الغذائية (BFP) وكل من معدل الإصابة بالسل والوفيات تمت ملاحظة انخفاضات في أفقر المناطق، وبالتحديد في المناطق الشمالية والشمالية الشرقية. عند إجراء تحليل مصنف وفقًا لوجود أو عدم وجود سجون في البلدية، لاحظنا ارتباط أكبر بين BFP وانخفاضات في حدوث السل (aRR 0.55 ( CI: 0.54-0.56) مقابل aRR 0.62 (CI: 0.61-0.64)) والوفيات (aRR 0.64 (95% CI: 0.59-0.70) مقابل aRR 0.74 (CI: 0.68-0.80)) في البلديات التي لا تحتوي على سجون.
تحليلات الحساسية والتثليث
قمنا بتطوير مجموعة واسعة من تحليلات الحساسية (للتفاصيل، انظر الطرق والجداول التكميلية 1-7)، من خلال ملاءمة نماذج بمواصفات مختلفة وضبط المتغيرات. كما أجرينا تحليلين مختلفين للتثليث.تحليل الانحدار المتعدد باستخدام نموذج كوكس ومطابقة درجات الميل (PSM) (الجدول 4 من البيانات الموسعة). أكدت جميع اختبارات الحساسية تقديرات الارتباط، وأظهرت تحليلات التثليث درجة عالية من الثقة في الاستدلال السببي.
نقاش
في هذه الدراسة، قمنا بتحليل تأثير برنامج Bolsa Família (BFP) بشكل منهجي بين الأفراد الذين يعيشون في ظروف التهميش الاجتماعي، مع تقييم الروابط بين المشاركة في برنامج التحويلات النقدية المشروطة (CCT) وعبء مرض السل وفقًا لظروفهم الإثنية والعرقية والاجتماعية والاقتصادية. لاحظنا تأثيرات قوية لبرنامج Bolsa Família في تقليل كل من معدلات الإصابة بالسل ومعدلات الوفيات. ومن الجدير بالذكر أن فعالية برنامج Bolsa Família أظهرت تدرجًا ملحوظًا بناءً على العرق والإثنية والظروف الاجتماعية والاقتصادية، مما يكشف عن تأثيرات أقوى بشكل ملحوظ بين الأفراد من أصل Indigenous أو Black أو Pardo والأفراد الذين يعيشون في فقر مدقع.
تكشف نتائجنا عن وجود تدرج في فعالية برنامج التحويلات النقدية المشروطة بناءً على مستوى الثروة الأساسي للمستفيدين: يظهر البرنامج تأثيرًا كبيرًا على حدوث السل والوفيات في الأفراد الذين يعيشون في فقر مدقع، بينما يظهر تأثيرًا أقل على حدوث السل في الأقل فقرًا، دون وجود تأثيرات ملحوظة على وفيات السل. يمكن تفسير أقوى تأثير للبرنامج في الأفراد الذين يعيشون في فقر مدقع بعاملين. أولاً، لقد ثبت باستمرار أن الفقر المدقع هو عامل خطر كبير للسل، حيث تتناسب مستويات خطر السل بشكل مباشر مع مستويات الفقر.لذلك، يمكن أن يرتبط رفع شخص ما من الفقر المدقع بتقليل كبير في خطر الإصابة بمرض السل وعبءه. بالإضافة إلى ذلك، تزداد فوائد برنامج المساعدة المالية مع مستويات الفقر، مما يوفر تحسينًا أكبر في الوضع الاجتماعي والاقتصادي للأفراد الذين يعيشون في فقر مدقع مقارنةً بأولئك الذين يعيشون في فقر، مما يؤدي إلى تقليل أكثر وضوحًا في خطر الإصابة بمرض السل وعبءه بالنسبة للمجموعة الأولى.
فيما يتعلق بالآليات التي يمكن أن تؤثر بها CCT على السل، يجب أن يؤخذ في الاعتبار أن BFP، من خلال التحويل المباشر للأموال إلى الأسر التي تعيش في فقر مدقع وفي حالات التهميش الاجتماعي في البرازيل، يعزز الوصول الأكبر إلى الغذاء، سواء من حيث الكمية أو الجودة، مما يقلل من انعدام الأمن الغذائي وسوء التغذية، وهو عامل خطر مهم للسل، بالإضافة إلى تحسين دفاعات الجهاز المناعي.علاوة على ذلك، يمكن أن تتحسن ظروف السكن، مما يقلل من الازدحام وسوء التهوية، والتي تُعتبر أيضًا عوامل خطر معترف بها لـيمكن للأسر أيضًا الانتقال من الطهي باستخدام الوقود المحترق مثل الخشب والفحم والفحم الحجري والكيروسين إلى الوقود الأنظف. يمكن أن تساعد هذه التغييرات في تقليل تلوث الهواء الداخلي، الذي تم التعرف عليه كعامل يساهم في زيادة حالات السل. يمكن أن تقلع عادات التدخين وإدمان الكحول، المرتبطة بشدة بالفقر، بين المستفيدين من برنامج دعم الأسر، مما يقلل من خطر الإصابة بالسل. كما يمكن تقليل انتشار مرض السكري وفيروس نقص المناعة البشرية والإيدز، الذي يكون أعلى بين الأفراد الذين يعيشون في ظروف اجتماعية هشة، من خلال تدخلات الحد من الفقر.. وبالتالي، يمكن ربط هذا الانخفاض بتقليل حدوث ووفاة مرض السل. علاوة على ذلك، فإن الأفراد المتأثرين بمرض السل الذين يعيشون في فقر مدقع هم أكثر عرضة لتجنب السعي للحصول على تشخيص في المراكز الصحية أو لقطع علاجهم بسبب التكاليف المباشرة، مثل نفقات النقل، وتكاليف الفرصة، مثل صعوبة التغيب عن يوم عمل بسبب ظروفهم الوظيفية والمعيشية الهشة. يمكن أن تمثل هذه التكاليف عائقًا حتى لو كانت الوقاية والتشخيص والعلاج متاحة مجانًا في النظام الصحي الموحد. النظام الصحي الموحد. بالإضافة إلى تقديم التحويلات المالية، يمكن أن تسهم الشروط المؤهلة لبرنامج BFP أيضًا في تقليل مرض السل. ترتبط هذه الشروط بمتطلبات مثل حضور المدرسة، والتعليم، والوصول إلى خدمات الصحة للنساء الحوامل والأطفال دون سن الخامسة، مما قد يسهل التعرف على المرض والتشخيص المبكر له.باختصار، يعزز برنامج BFP الوصول الأكبر إلى الدخل والغذاء والرعاية الصحية. يمكن ربط ذلك بتقليل حدوث مرض السل، وتسهيل التشخيص المبكر للسل والالتزام بالعلاج، وزيادة معدل الشفاء من السل.وتقليل المضاعفات والوفيات الناتجة عن المرض.
علاوة على ذلك، وجدنا أن برنامج BFP له تأثير قوي في تقليل حدوث السل والوفيات في السكان الأصليين في البرازيل، الذين لديهم خطر أعلى بشكل ملحوظ للإصابة بالسل والوفيات.بينما يمكن تفسير ذلك من خلال نفس الآليات المذكورة أعلاه، لا سيما في سياق السكان الأصليين، فإن تلقي برنامج المساعدة المالية يمكن أن يخفف من الفقر المدقع والهشاشة الاجتماعية والاقتصادية. يمكن أن يقلل ذلك من انعدام الأمن الغذائي وسوء التغذية، اللذين هما مرتفعان بشكل خاص بين السكان الأصليين، ويخفف من الحواجز الجغرافية الكبيرة التي تعيق الوصول حتى إلى خدمات الرعاية الصحية الأساسية..
من الجدير توضيح التأثير الأكبر لبرنامج BFP على معدل الإصابة بمرض السل بين الأشخاص من العرق والإثنية السوداء والباردو، حيث حدث أكثر من 60% من التشخيصات الجديدة لمرض السل الرئوي في البرازيل بين الأشخاص الذين عرّفوا عن أنفسهم كسود وباردو.يمكن تفسير ذلك من خلال الآليات المماثلة التي تم توضيحها سابقًا. خاصة بين الأفراد من العرق الأسود والباردو في البرازيل، يمكن أن يؤثر برنامج BFP على الفوارق الاجتماعية التاريخية والهيكلية.، وزيادة الدخل وتحسين التعليم من خلال شروطها، وتوفير الوصول إلى خدمات الصحة، وبالتالي تقليل عبء السل. يمكن أن تفسر الآليات الموضحة أعلاه أيضًا التأثير الأكبر لبرنامج BFP في المناطق الشمالية والشمالية الشرقية، التي تعد من أفقر وأقل المناطق تطورًا في البلاد، حيث تعاني من أسوأ البنى التحتية وموارد الرعاية الصحية..
لبرنامج المساعدة المالية المباشرة (BFP) تأثير أقوى في تقليل الوفيات الناتجة عن السل لدى النساء. يمكن تفسير ذلك بحقيقة أن المرأة غالبًا ما تكون المسؤولة بشكل أساسي عن الأسرة في تسجيل واستلام المساعدة المالية المباشرة. علاوة على ذلك، فإن النساء الحوامل والمرضعات يتبعن شروط الحصول على المساعدة المالية المباشرة (الرعاية قبل وبعد الولادة، التطعيم، ومراقبة الصحة والتغذية).بهذه الطريقة، تتمتع النساء المستفيدات من برنامج BFP بإمكانية أكبر للوصول إلى خدمات الصحة، مما قد يرتبط بتقليل أكبر في وفيات السل في هذه المجموعة، مقارنة بالرجال.
لقد لاحظنا أيضًا أن التأثيرات الوقائية لبروتوكول BFP وانخفاض معدل الإصابة والوفيات أكبر في البلديات التي لا تحتوي على سجون. عادةً ما تعمل السجون كـ ‘مضخمات مؤسسية’ أو ‘خزانات’ للسل، مما يؤثر على معدل الإصابة بالسل ليس فقط في السجون ولكن أيضًا في السكان غير السجنيين.يمكن أن يُعزى التأثير المنخفض لبرنامج BFP في هذه البلديات إلى عدم وصول البرنامج إلى هذه الفئات السكانية، أو عدم تأثيره على ديناميات العدوى لديهم، مما يؤدي إلى مستوى أعلى وأكثر مرونة من حدوث مرض السل في المجتمع على الرغم من تغطية برنامج BFP..
أصبح الوقاية من السل ورعايته للسكان ذوي الدخل المحدود تحديًا أكبر خلال وبعد جائحة COVID-19 (مرض فيروس كورونا).كل من هذه الفئات السكانية التي تعيش في ظروف اقتصادية هشة لها خصوصيات وتعقيدات عندما يتعلق الأمر بتنفيذ تدخلات الوقاية من السل، والتشخيص، والعلاج. علاوة على ذلك، يمكن أن تتداخل الفجوات المرتبطة بالسياقات المحلية، والمرافق الصحية، والعوامل الاجتماعية والسلوكية والثقافية مع تنظيم خدمات الصحة، مما يؤثر على الرعاية المقدمة لهذه الفئات السكانية.. في هذا السياق، يصبح من الضروري تكثيف إجراءات الوقاية والرعاية الشاملة الموجهة للأشخاص في حالات الضعف الاجتماعي، بالإضافة إلى التنسيق بين القطاعات المختلفة وإدراج مرض السل في أجندات المساعدة الاجتماعية وحقوق الإنسان، من بين أمور أخرى. ولهذا الغرض، تم إنشاء لجنة وزارية مشتركة للقضاء على مرض السل وأمراض أخرى تحددها الظروف الاجتماعية في عام 2023 في البرازيل..
لدراستنا قيود معينة يجب الاعتراف بها. القيد الأول هو أنه، على الرغم من جهودنا للسيطرة على جميع المتغيرات المربكة ذات الصلة واستخدام نماذج قائمة على درجات الميل مع الوزن المعكوس للعلاج، قد لا تأخذ هذه الأساليب في الاعتبار تمامًا المتغيرات المربكة غير القابلة للملاحظة والانحيازات المحتملة في الاختيار. لمعالجة هذه القضايا، قمنا بتطوير نهج متعدد الأبعاد. أولاً، استخدمنا مجموعة واسعة من المتغيرات المعدلة المتعلقة بالعوامل الديموغرافية والاجتماعية والاقتصادية والرعاية الصحية والبيئية على مستوى الفرد والأسرة والبلدية، في كل من الانحدار اللوجستي، لبناء درجة الميل، وفي الانحدار بواسون لتقدير آثار BFP. لقد تم استخدام هذا النهج بنجاح في دراسات سابقة حول تأثير BFP وتدخلات عامة أخرى على عدة نتائج صحية.. ثانياً، قمنا بإدراج معدل البلديات المتوسط لمؤشر السل كمتغير تعديل في نماذج اللوجستية وبواسون على مدار فترة الدراسة لكل نتيجة قيد الدراسة (الحالات، الوفيات ومعدل الفتك). تم تقدير هذه المعدلات بين الأفراد من نفس البلديات في العينة. وهذا سمح لنا بتعديل مستويات الوباء الأساسية للنتيجة المحددة للسل قيد الدراسة في البلديات، وبالتالي، للمتغيرات غير القابلة للملاحظة المرتبطة المحتملة، مع التحكم في انحيازات الاختيار التي تربط مستويات تنفيذ برنامج التحويلات النقدية المشروطة بمستويات السل الوبائية في المجتمع. ثالثاً، تم إجراء تحليلات حساسية شاملة (الجداول التكميلية 1-7 والطرق)، مما أظهر أن تضمين متغيرات مستقلة إضافية أو استبدال المتغيرات الموجودة، بالإضافة إلى العديد من التغييرات الأخرى في مواصفات النماذج، لم يؤثر بشكل كبير على تقديرات تأثير برنامج التحويلات النقدية المشروطة. رابعاً، لزيادة ثقتنا في الاستدلال السببي، وإزالة إمكانية وجود انحيازات اختيارية كبيرة، قمنا بإجراء تحليلين مختلفين للتثليث: تحليل البقاء مع انحدارات كوكس وPSM (البيانات الموسعة الجدول 4)، مما أظهر أنه حتى مع أساليب منهجية مختلفة، كانت تقديرات تأثير برنامج التحويلات النقدية المشروطة لا تزال قوية وذات دلالة إحصائية.
limitation أخرى تتعلق بالصلاحية الخارجية لدراستنا: تتكون مجموعة الـ 100 مليون برازيلي – ومجموعة الدراسة المستمدة منها – من أفراد تم الحصول عليهم من الربط بين السجل الموحد للبرامج الاجتماعية (Cadastro Único (CADU)) وبيانات الصحة. الأفراد المسجلون في CADU يمثلون النصف الأفقر من السكان البرازيليين. ونتيجة لذلك، تشمل مجموعتنا فقط الأفراد ذوي الدخل المنخفض جداً أو المنخفض الذين يحتاجون إلى التسجيل في CADU للوصول إلى برامج المساعدة الحكومية. تؤثر هذه القيود على الصلاحية الخارجية للمجموعة على المستوى الوطني، حيث لا يتم تمثيل الأفراد ذوي الدخل المرتفع.
علاوة على ذلك، على الرغم من أن نظام معلومات الأمراض القابلة للإبلاغ (Sistema de Informação de Agravos de Notificação (SINAN)) يتمتع بحساسية عالية في البرازيل، قد يكون هناك نقص في الإبلاغ عن إشعارات السل.. ومع ذلك، فإن تصميم دراستنا واستراتيجيتنا التحليلية يحدان من إمكانية أن يؤثر التقليل من الإبلاغ على نتائجنا. بالإضافة إلى ذلك، تؤكد النتائج من البلديات التي تم اختيارها لجودة المعلومات الحيوية العالية وانخفاض الإبلاغ الناقص نتائجنا (الجدول التكميلي 6).
القيود الثالثة هي أن الأفراد الذين لديهم معلومات مفقودة في أي من المتغيرات المعدلة تم استبعادهم. على الرغم من أن هذا الاستبعاد قد يعزز الصلاحية الداخلية للدراسة، حيث تعتبر السجلات ذات القيم المفقودة غالبًا من نوعية أقل، إلا أنه يحد جزئيًا من قابلية تعميم النتائج. ومع ذلك، فإن التحليلات التي شملت الأفراد ذوي القيم المفقودة أسفرت عن تقديرات تأثير BFP مماثلة (الجدول التكميلي 7).
في هذه الدراسة، لم يكن من الممكن إجراء تحليل التكلفة-الفعالية بسبب تعقيدها الإضافي والحاجة إلى بيانات غير متاحة في مجموعات البيانات لدينا.
تقدم دراستنا نقاط قوة تساهم في قيمتها الإجمالية. أولاً، استغللنا مجموعة بيانات طولية كبيرة، والتي، عند دمجها مع طرق تقييم الأثر، سمحت لنا بتقييم آثار التدخلات على نطاق غير مسبوق. هذه الطريقة الفريدة مكنتنا من تضمين عدد كبير من الأفراد. والفئات الفرعية التي غالبًا ما يتم تجاهلها أو تمثيلها بشكل ناقص في الدراسات الوبائية التقليدية والتجارب السريرية العشوائية. إن هذا الشمول الشامل أمر حاسم لتقييم السياسات، حيث يبرز التأثيرات المحتملة المختلفة للتدخلات العامة بناءً على خصائص وظروف المستفيدين من برنامج BFP. بالإضافة إلى ذلك، تكمن قوة دراستنا في النطاق الواسع من تحليلات الحساسية التي تم إجراؤها. وقد قدمت هذه التحليلات مزيدًا من التحقق وتعزيز نتائج الدراسة، مما يضمن قوتها وموثوقيتها. علاوة على ذلك، فإن استخدام تحليلات التثليث المختلفة قد زاد من مستوى الثقة في الاستنتاجات السببية، مما يعزز مصداقية نتائجنا.
نستنتج أن برامج التحويلات النقدية المشروطة يمكن أن تقلل بشكل كبير من حدوث ووفاة مرض السل، لا سيما بين الأفراد الذين يعيشون في فقر مدقع والذين يعلنون عن أنفسهم كأصليين أو من عرق أسود أو باردو، والذين يكونون عادةً في خطر أعلى للإصابة بالسل وآثاره المدمرة. لذلك، يمكن أن يؤدي توسيع برامج التحويلات النقدية المشروطة في البلدان ذات الدخل المنخفض والمتوسط إلى تعزيز الاستجابة العالمية لمرض السل بشكل كبير، مما يقلل من الفوارق الاجتماعية في عبء السل ويساهم في تحقيق استراتيجية إنهاء السل وأهداف التنمية المستدامة المتعلقة بالسل.
المحتوى عبر الإنترنت
أي طرق، مراجع إضافية، ملخصات تقارير Nature Portfolio، بيانات المصدر، بيانات موسعة، معلومات إضافية، شكر وتقدير، معلومات مراجعة الأقران؛ تفاصيل مساهمات المؤلفين والمصالح المتنافسة؛ وبيانات توفر البيانات والرموز متاحة فيhttps://doi.org/10.1038/s41591-024-03381-0.
World Health Organization (WHO). Global Tuberculosis Report 2022; Geneva: World Health organization; 2022 https://www. who.int/teams/global-tuberculosis-programme/tb-reports/ global-tuberculosis-report-2022
Torrens, A. W. et al. Effectiveness of a conditional cash transfer programme on TB cure rate: a retrospective cohort study in Brazil. Trans. R. Soc. Trop. Med. Hyg. 110, 199-206 (2016).
Carter, D. J. et al. The impact of social protection and poverty elimination on global tuberculosis incidence: a statistical modelling analysis of Sustainable Development Goal 1. Lancet Glob. Health 6, e514-e522 (2018).
Boccia, D. et al. Cash transfer and microfinance interventions for tuberculosis control: review of the impact evidence and policy implications. Int. J. Tuberc. Lung Dis. 15, S37-S49 (2011).
Patel, B. H. et al. Cash transfer scheme for people with tuberculosis treated by the National TB Programme in Western India: a mixed methods study. BMJ Open 9, e033158 (2019).
Wingfield, T. et al. A randomized controlled study of socioeconomic support to enhance tuberculosis prevention and treatment, Peru. Bull. World Health Organ. 95, 270-280 (2017).
Sripad, A., Castedo, J., Danford, N., Zaha, R. & Freile, C. Effects of Ecuador’s national monetary incentive program on adherence to treatment for drug-resistant tuberculosis. Int. J. Tuberc. Lung Dis. 18, 44-48 (2014).
Fuady, A., Houweling, T. A. J., Mansyur, M., Burhan, E. & Richardus, J. H. Effect of financial support on reducing the incidence of catastrophic costs among tuberculosis-affected households in Indonesia: eight simulated scenarios. Infect. Dis. Poverty 8, 10 (2019).
Rudgard, W. E. et al. Comparison of two cash transfer strategies to prevent catastrophic costs for poor tuberculosis-affected households in low- and middle-income countries: an economic modelling study. PLoS Med. 14, e1002418 (2017).
Neves, J. A. et al. The Brazilian cash transfer program (Bolsa Família): a tool for reducing inequalities and achieving social rights in Brazil. Glob. Public Health 17, 26-42 (2022).
Rasella, D., Aquino, R., Santos, C. A. T., Paes-Sousa, R. & Barreto, M. L. Effect of a conditional cash transfer programme on childhood mortality: a nationwide analysis of Brazilian municipalities. Lancet 382, 57-64 (2013).
Lindert, K., Linder, A., Hobbs, J., de la Brière, B. The Nuts and Bolts of Brazil’s Bolsa Família Program: Implementing Conditional Cash Transfers in a Decentralized Context (The World Bank, 2007)
Pescarini, J. M. et al. Impact of Brazil’s Bolsa Família Programme on cardiovascular and all-cause mortality: a natural experiment study using the 100 Million Brazilian Cohort. Int. J. Epidemiol. https://doi.org/10.1093/ije/dyac188 (2022).
Machado, D. B. et al. Relationship between the Bolsa Família national cash transfer programme and suicide incidence in Brazil: a quasi-experimental study. PLoS Med. 19, e1004000 (2022).
Pescarini, J. M. et al. Conditional cash transfer program and leprosy incidence: analysis of 12.9 million families from the 100 Million Brazilian Cohort. Am. J. Epidemiol. 189, 1547-1558 (2020).
Oliosi, J. G. N. et al. Effect of the Bolsa Familia Programme on the outcome of tuberculosis treatment: a prospective cohort study. Lancet Glob. Health 7, e219-e226 (2019).
Rebouças, P. et al. Ethnoracial inequalities and child mortality in Brazil: a nationwide longitudinal study of 19 million newborn babies. Lancet Glob. Health 10, e1453-e1462 (2022).
Barbosa, G. C. G. et al. CIDACS-RL: a novel indexing search and scoring-based record linkage system for huge datasets with high accuracy and scalability. BMC Med. Inform. Decis. Mak. 20, 289 (2020).
Lawlor, D. A., Tilling, K. & Davey Smith, G. Triangulation in aetiological epidemiology. Int. J. Epidemiol. 45, 1866-1886 (2016).
Hargreaves, J. R. et al. The social determinants of tuberculosis: from evidence to action. Am. J. Public Health 101, 654-662 (2011).
Hill-Briggs, F. et al. Social determinants of health and diabetes: a scientific review. Diabetes Care 44, 258-279 (2021).
Silva, A. F. et al. Income determines the impact of cash transfers on HIV/AIDS: cohort study of 22.7 million Brazilians. Nat. Commun. 15, 1307 (2024).
de Sampaio Morais, G. A. et al. Effect of a conditional cash transfer programme on AIDS incidence, hospitalisations, and mortality in Brazil: a longitudinal ecological study. Lancet HIV 9, e690-e699 (2022).
Almeida, C. P. B., de Trajman, A., Mitnick, C. D., Kritski, A. L. & Santos-Filho, E. T. D. Beyond goodwill and promises-urgent needs and opportunities to accelerate the fight against tuberculosis in Brazil. Lancet Reg. Health Am. 30, 100663 (2024).
Carter, D. J. et al. The impact of a cash transfer programme on tuberculosis treatment success rate: a quasi-experimental study in Brazil. BMJ Glob. Health 4, e001029 (2019).
Durovni, B. et al. The impact of the Brazilian Family Health Strategy and the conditional cash transfer on tuberculosis treatment outcomes in Rio de Janeiro: an individual-level analysis of secondary data. J. Public Health 40, e359-e366 (2018).
Souza, R. A. D. et al. Family health and conditional cash transfer in Brazil and its effect on tuberculosis mortality. Int. J. Tuberc. Lung Dis. 22, 1300-1306 (2018).
Malacarne, J. et al. Factors associated with TB in an indigenous population in Brazil: the effect of a cash transfer program. Rev. Inst. Med. Trop. São Paulo 60, e63 (2018).
Nogueira, L. M. V., Teixeira, E., Basta, P. C. & da Motta, M. C. S. Therapeutic itineraries and explanations for tuberculosis: an indigenous perspective. Rev. Saúde. Publica 49, 96 (2016).
Lua, I. et al. The effects of social determinants of health on acquired immune deficiency syndrome in a low-income population of Brazil: a retrospective cohort study of 28.3 million individuals. Lancet Reg. Health Am. 24, 100554 (2023).
Ribeiro, L.L., Gomes, J.W.F. Corrupção e pobreza nos municípios brasileiros. Pesqui. Planej. Econôm. 52, 67-86 (2022). https://doi.org/10.38116/ppe52n1art3
Martinez, L. et al. Global, regional, and national estimates of tuberculosis incidence and case detection among incarcerated individuals from 2000 to 2019: a systematic analysis. Lancet Public Health 8, e511-e519 (2023).
Pelissari, D. M. & Diaz-Quijano, F. A. Impact of incarceration on tuberculosis incidence and its interaction with income distribution inequality in Brazil. Trans. R. Soc. Trop. Med. Hyg. 114, 23-30 (2020).
Litvinjenko, S., Magwood, O., Wu, S. & Wei, X. Burden of tuberculosis among vulnerable populations worldwide: an overview of systematic reviews. Lancet Infect. Dis. 23, 1395-1407 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
كلية الطب، الجامعة الفيدرالية في باهيا (UFBA)، سلفادور، البرازيل. معهد الصحة الجماعية، الجامعة الفيدرالية في باهيا (ISC/UFBA)، سلفادور، البرازيل. مركز تكامل البيانات والمعرفة للصحة (CIDACS)، مؤسسة أوزوالدو كروز (FIOCRUZ)، سلفادور، البرازيل. قسم الصحة، الجامعة الحكومية في فييرا دي سانتانا (UEFS)، فييرا دي سانتانا، البرازيل. كلية السكان وسياسة الصحة، مدرسة لندن للصحة والطب الاستوائي (LSHTM)، لندن، المملكة المتحدة. كلية العلوم الصحية، الجامعة الفيدرالية في برازيليا، برازيليا، البرازيل. ISGlobal، برشلونة، إسبانيا. المؤسسة الكتالونية للبحث والدراسات المتقدمة (ICREA)، Pg. لويس كومبانيز 23، برشلونة، إسبانيا. هؤلاء المؤلفون ساهموا بالتساوي: غابرييلا س. جيسوس، بريسيلا ف.ب.س. جيستال. البريد الإلكتروني: davide.rasella@isglobal.org
يستخدم لتحويل التركيبة الخطية من المتنبئين إلى احتمال حدوث الحدث.
حيث هو احتمال النتيجة الثنائية أن تكون 1 بالنظر إلى متغيرات المتنبئين ; هو أساس اللوغاريتم الطبيعي؛ و هي المعاملات المرتبطة بمتغيرات المتنبئين . لقد قدرنا احتمال كل فرد لتلقي BFP (درجة الميل (PS))، بطريقتين. بالنسبة للمعادلة الأولى، حسبنا الاحتمال الهامشي للعلاج ثم قدرنا المتغيرات المتعددة ، المعدلة لجميع المتغيرات ذات الصلة.
استخدمنا PS و PS كأوزان لحساب IPTW المستقر باستخدام الصيغ:
حيث هو الوزن للمستفيدين و هو الوزن لغير المستفيدين. لتصحيح الأوزان المتطرفة المحتملة، وضعنا عتبات، مع تحويل الأوزان التي تتجاوز القيمة المحددة إلى تلك القيمة العتبية . في هذه الدراسة، تم تقليم الأوزان بناءً على توزيع قيمها للـ 1st و 99th percentiles، والتي تمثل هذه العتبات، كما في الدراسات السابقة المماثلة . يستخدم IPTW درجة الميل لموازنة الخصائص الأساسية في المجموعات المعرضة وغير المعرضة من خلال وزن كل فرد بواسطة الاحتمال العكسي لتلقي العلاج .
معادلة بواسون مع IPTW هي إطار يستخدم لتحليل بيانات العد أو حدوث الأحداث، مع الأخذ في الاعتبار التحيز المحتمل الناتج عن تعيين العلاج غير العشوائي في الدراسات الرصدية. في هذا السياق، تقوم معادلة بواسون بنمذجة العلاقة بين نتائج الأحداث والمتغيرات بينما تدمج IPTW لتعديل تحيز اختيار العلاج.
حيث هو اللوغاريتم الطبيعي لمعدل الفرد , هي المتغيرات الفردية هي المعاملات المرتبطة بالمتغيرات؛ و logIPTW يمثل لوغاريتم وزن العلاج العكسي للفرد . أخيرًا، تم تقدير الانحدارات المتعددة لبواسون، المعدلة بواسطة IPTW المستقر والمقصوص، بنفس المتغيرات الاجتماعية والاقتصادية والديموغرافية المعتمدة في النموذج اللوجستي لجميع نتائج السل.
علاوة على ذلك، لفهم تباين ارتباط BFP، قمنا بتكييف نماذج انحدار بواسون IPTW مقسمة حسب العمر والجنس والعرق والإثنية والتعليم وثلاثيات الثروة (النفقات لكل فرد)، ووجود السجون في البلدية والمناطق البرازيلية.
لتأكيد قوة النتائج، قمنا بتطبيق عدة تحليلات حساسية: (1) قمنا بتكييف نفس الانحدارات بدون ومع فقط متغير مستوى انتشار السل (الجداول التكميلية 1 و 2)؛ (2) قمنا بتكييف نماذج مع متغيرات على مستوى الفرد فقط واختبرنا تضمين متغيرات على مستوى التجميع المختلفة (الجدول التكميلية 3)؛ (3) قدرنا وقارننا جميع النماذج بدون IPTW (الجدول التمديد البيانات 5)؛ (4) لتقييم اعتماد النفقات لكل فرد كبديل للثروة، قمنا بإجراء نفس التحليلات مع بدائل أخرى، مثل الدخل لكل فرد (الجدول التكميلية 4)؛ (5) قمنا بتعديل نفس النماذج بمواصفات مختلفة (بما في ذلك مجموعات مختلفة من المتغيرات على مستوى الفرد، تضمين أو استبعاد الأخطاء القياسية القوية (الجدول التكميلية 5)، فقط في البلديات التي تحتوي على معلومات حيوية كافية (الجدول التكميلية 6))؛ و (6) أعدنا تقديراتنا بما في ذلك الأفراد مع فئة مفقودة (الجدول التكميلية 7). أخيرًا، للحصول على درجة أكبر من الثقة
في الاستدلال السببي لتقييم تأثيرنا، قمنا بإجراء تحليلين مختلفين للتثليث ، للتحقق من وجود ارتباطات BFP باستخدام طرق بديلة أيضًا: تحليل البقاء مع انحدار متعدد المتغيرات من كوكس و PSM (الجدول التمديد البيانات 4).
تم إجراء جميع التحليلات الإحصائية في Stata الإصدار MP 15.1.
بيان الشمولية والأخلاقيات
تم تصميم هذا المشروع من خلال شراكة طويلة الأمد بين معهد الصحة الجماعية (Instituto de Saúde Coletiva (ISC)) من الجامعة الفيدرالية في باهيا (Universidade Federal da Bahia (UFBA)) ومركز تكامل البيانات والمعرفة للصحة (CIDACS) من مؤسسة أوزوالدو كروز (Fundação Oswaldo Cruz (FIOCRUZ))، وكلاهما مقره في سلفادور، البرازيل. تم إنشاء مجموعة الـ 100 مليون برازيلي من قبل CIDACS بالتعاون مع باحثي ISC، وتم اختيار وتحليل مجموعة البيانات المستخدمة في هذه الدراسة من قبل مجموعة متعاونة من باحثي ISC وCIDACS. تعاون جميع أعضاء الفريق في ملكية البيانات وحقوق الملكية الفكرية وتأليف المنشورات المتعلقة بالعمل. تم الاتفاق على الأدوار والمسؤوليات بين المتعاونين قبل البحث. تم استخدام الأعمال السابقة والمقالات من تحليلات هذه البيانات، معظمها تم تطويره من قبل المؤلفين المشاركين في هذه المقالة، لتوجيه تصميم هذه الدراسة، وكذلك ربط نتائجنا بأبحاث مماثلة، وقد تم اعتبارها في الاقتباسات لهذه الورقة.
موافقة الأخلاقيات
تمت الموافقة على هذه الدراسة من قبل لجنة الأخلاقيات البحثية لمعهد الصحة الجماعية من الجامعة الفيدرالية في باهيا (ISC، UFBA)، تحت الرقم 41691315.0.0000.5030 (رقم التقييم 3.783.920). في هذه الدراسة، تم التنازل عن موافقة المشاركين بسبب استخدام البيانات الإدارية.
ملخص التقرير
مزيد من المعلومات حول تصميم البحث متاحة في ملخص تقرير Nature Portfolio المرتبط بهذه المقالة.
توفر البيانات
سيتم مشاركة البيانات الأساسية لهذه المقالة عند الطلب من ISC من UFBA، وCIDACS من FIOCRUZ، وبعد الموافقة الأخلاقية. جميع البيانات التي تدعم النتائج المقدمة تم الحصول عليها من مركز تكامل البيانات والمعرفة للصحة (CIDACS). من المهم أن القيود تنطبق على الوصول إلى البيانات، التي تحتوي على معلومات حساسة، وتم ترخيصها للاستخدام الحصري في الدراسة الحالية، وبسبب لوائح الخصوصية من لجنة الأخلاقيات البرازيلية، فهي غير متاحة علنًا. عند الطلب ومع إذن صريح من CIDACS (البريد الإلكتروني: cidacs. curadoria@fiocruz.br) وموافقة من لجنة أخلاقية، يمكن الوصول إلى البيانات بشكل محكم. تم تسجيل مجموعة البيانات تحت معرف DOI التالي: https://hdl.handle.net/20.500.12196/CIDACS/65، والذي يوفر بيانات وصفية وسجل لجميع إصدارات قاعدة البيانات.
توفر الشيفرة
سيتم مشاركة الخوارزميات والشيفرة المستخدمة في هذه المقالة عند الطلب من ISC من UFBA، وCIDACS من FIOCRUZ، وبعد الموافقة الأخلاقية. نظرًا لسرية البيانات ووجود خطوط الشيفرة التي تتعامل مع متغيرات حساسة، فإن خصائصها وقيمها، سيتم منح الوصول إلى الشيفرات عند الطلب ومع إذن صريح من CIDACS (البريد الإلكتروني:cidacs.curadoria@fiocruz.br) وموافقة من لجنة أخلاقية. إذا تمت الموافقة، ستكون الشيفرة متاحة خلال شهر واحد من الطلب الأولي.
References
Austin, P. C. & Stuart, E. A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34, 3661-3679 (2015).
Chesnaye, N. C. et al. An introduction to inverse probability of treatment weighting in observational research. Clin. Kidney J. 15, 14-20 (2022).
Suárez, E., Pérez, C.M., Rivera, R., Martínez, M.N. in Applications of Regression Models in Epidemiology (Wiley & Sons, 2017) Ch. 10 (Wiley & Sons, 2017) https://doi.org/10.1002/9781119212515.ch10
Pescarini, J. M. et al. Effect of a conditional cash transfer programme on leprosy treatment adherence and cure in patients from the nationwide 100 Million Brazilian Cohort: a quasi-experimental study. Lancet Infect. Dis. 20, 618-627 (2020).
Jesus, G. S. et al. The effect of primary health care on tuberculosis in a nationwide cohort of 7.3 million Brazilian people: a quasi-experimental study. Lancet Glob. Health. Mar. 10, e390-e397 (2022).
Khandker, S. R., Koolwal, G. B. & Samad, H. A. Handbook on Impact Evaluation: Quantitative Methods and Practices (The World Bank, 2010); https://openknowledge.worldbank.org/ handle/10986/2693
Lee, B. K., Lessler, J. & Stuart, E. A. Weight trimming and propensity score weighting. PloS ONE 6, e18174 (2011).
الشكر والتقدير
تم دعم هذه الدراسة من قبل مؤسسة ويلكوم، رقم مرجع المنحة: 109949/Z/15/Z؛ ومن قبل المعهد الوطني للحساسية والأمراض المعدية (المعاهد الوطنية للصحة)، رقم مرجع المنحة: 1RO1Al152938؛ ومن قبل وزارة الصحة البرازيلية، رقم مرجع المنحة: VPGDI-003-FIO-19. نحن نعترف بالدعم من المنحة CEX2023-0001290-S الممولة من وزارة العلوم والابتكار والجامعات/الوكالة الحكومية للبحث (MCIN/AEI)/10.13039/501100011033 والدعم من حكومة كاتالونيا من خلال برنامج مراكز البحث في كاتالونيا. يقر د.ر. بالتمويل من CEX2018-000806-S الممولة من MCIN/AEI/10.13039/501100011033. نشكر الباحثين من معهد الصحة الجماعية على المناقشات والاقتراحات القيمة خلال تطوير هذه الدراسة وأعضاء CIDACS المسؤولين عن ربط مجموعة الـ 100 مليون برازيلي.
مساهمات المؤلفين
جي. إس. جي.: التحليل الرسمي – الوصول إلى البيانات والتحقق منها، التحقيق، المنهجية، والكتابة – المسودة الأصلية، المراجعة والتحرير. بي. إف. بي. إس. جي.: التحليل الرسمي – الوصول إلى البيانات والتحقق منها، التحقيق، المنهجية، والكتابة – المسودة الأصلية، المراجعة والتحرير. دي. إم. سي.: المنهجية، والكتابة – المسودة الأصلية، المراجعة والتحرير. أي. إف. إس.: التحليل الرسمي – الوصول إلى البيانات والتحقق منها، التحقيق، المنهجية، والكتابة – المسودة الأصلية، المراجعة والتحرير. آي. إل.: التحليل الرسمي – الوصول إلى البيانات والتحقق منها، المنهجية، والكتابة – المسودة الأصلية، المراجعة والتحرير. إم. واي. آي.: تنسيق البيانات، الحصول على التمويل، الموارد والكتابة – المراجعة والتحرير. إم. إل. بي.: تنسيق البيانات، الحصول على التمويل، الموارد، والكتابة – المراجعة والتحرير. إم. إن. إس.: الكتابة – المسودة الأصلية، المراجعة والتحرير. دي. بي.: الكتابة – المراجعة والتحرير. دي. آر.: التصور، إدارة المشروع، الحصول على التمويل، التحقيق، المنهجية، الإشراف – الوصول إلى البيانات والتحقق منها، القرار بتقديم الورقة، والكتابة – المراجعة والتحرير.
يجب توجيه المراسلات والطلبات للحصول على المواد إلى دافيد راسيلا.
معلومات مراجعة الأقران تشكر مجلة ناتشر ميديسين خوليو كرويدا، باسكال جيلدسيتزر، ويمنغ تانغ والمراجعين الآخرين المجهولين على مساهمتهم في مراجعة هذا العمل. المحرر الرئيسي: مينغ يانغ، بالتعاون مع فريق ناتشر ميديسين.
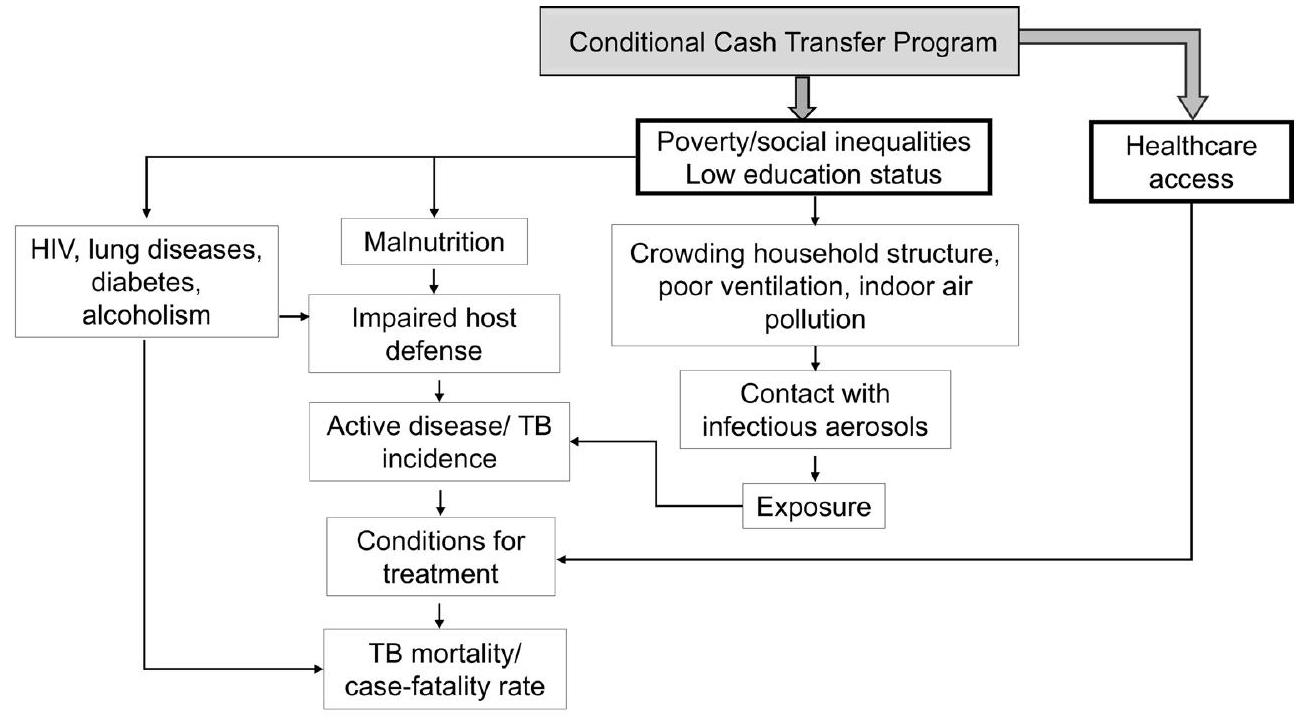
الشكل البياني الممتد 1 | الإطار المفاهيمي حول المحددات والآثار المحتملة للتحويلات النقدية المشروطة (CCT) على نتائج السل (TB). TB=السل. المصدر: المؤلفون.
البيانات الموسعة الجدول 1 | عدد الملاحظات لكل حالة جديدة من السل (TB)، والوفاة بسبب السل، ووفايات السل بين الحالات الجديدة من السل حسب مستفيدي برنامج بولسا فاميليا (BFP) وغير المستفيدين (N-BF)
برنامج Bolsa Familia (BFP) )
إجمالي
N-BF
BF
حالات جديدة من السل
لا
30,584,786
٢٣,٨٢١,١٧٢
٥٤٤٠٥٩٥٨
نعم
75,956
٨٣,٨٢١
١٥٩٧٧٧
إجمالي
30,660,742
٢٣,٩٠٤,٩٩٣
٥٤,٥٦٥,٧٣٥
وفيات السل
لا
30,659,117
٢٣,٩٠٤,٣٢٤
٥٤,٥٦٣,٤٤١
نعم
٤٣٥٩
٣,٦٣٤
٧,٩٩٣
إجمالي
30,663,476
٢٣,٩٠٧,٩٥٨
٥٤,٥٧١,٤٣٤
وفيات السل/حالات السل الجديدة
لا
١٤٤٩٦
30,606
٤٥,١٠٢
نعم
٤٩٥
٧٥١
١٢٤٦
إجمالي
14,991
٣١,٣٥٧
٤٦٣٤٨
ملاحظات: أ) حالات السل الجديدة، تعرف بالحالات الجديدة، حالات الانتكاس من السل والعودة وفقًا لمعايير وزارة الصحة البرازيلية؛ ب) الوفيات الناتجة عن السل، مع اعتبار السبب الأساسي وفقًا للأكواد الدولية للتصنيف الأمراض (ICD-10) A15 إلى A19، J65، 0980 وP370. ج) برنامج بولسا فاميليا
البيانات الموسعة الجدول 2 | نماذج التنبؤ بالانحدار اللوجستي للأفراد المستفيدين أو غير المستفيدين من برنامج بولسا فاميليا (BFP)، لحدوث مرض السل (TB)، والوفيات، ومعدل الفتك، البرازيل، 2004-2015. تقديرات من درجة الميل (PS)
النتائج (aRR – CI 95%)
النموذج المعدل
حدوث ووفيات
معدل الوفيات بسبب الحالة
جنس
ذكر
1 (أساس)
1 (أساس)
أنثى
1.17 (1.17-1.18)
1.73 (1.65-1.81)
العمر (بالسنوات)
0.84 (0.84-0.85)
0.76 (0.75-0.77)
العرق أو الإثنية
أبيض
1 قاعدة
1 (أساس)
أسود وباردو
1.15 (1.15-1.16)
1.25 (1.19-1.32)
محلي
3.09 (3.06-3.12)
3.50 (2.68-4.58)
التعليم
أمي، لم يحضر المدرسة أبداً
1 (أساس)
1 (أساس)
المدرسة الابتدائية
1.07 (1.07-1.08)
1.06 (0.99-1.14)
المدرسة الثانوية
1.08 (1.08-1.09)
0.93 (0.86-0.99)
أكثر من المدرسة الثانوية
0.83 (0.83-0.84
0.65 (0.59-0.70)
مواد البناء المنزلية
طوب/أسمنت
1 (أساس)
1 (أساس)
خشب، مواد نباتية أخرى
0.94 (0.93-0.94)
0.91 (0.86-0.97)
عدد الأشخاص في العائلة
1 (أساس)
1 (أساس)
2
3 إلى 4
1.52(1.51-1.52)
2.03 (1.93-2.14)
>5
2.03 (2.02-2.04)
3.56 (3.33-3.80)
حسب نفقات الرواتب – % الحد الأدنى للأجور
أقل من الوسيط
1 (أساس)
1 (أساس)
فوق الوسيط
0.88 (0.88-0.89)
0.51 (0.48-0.54)
الإضاءة
الكهرباء
1 (أساس)
1 (أساس)
غير كهربائي
1.22 (1.21-1.22)
1.53 (1.43-1.64)
الصرف الصحي غير الكافي
1.02 (1.02-1.03)
1.06 (1.00-1.12)
التخلص من النفايات
1.08 (1.08-1.09)
1.04 (0.96-1.12)
إمدادات المياه
شبكة عامة
1 (أساس)
1 (أساس)
آخر
1.11 (1.11-1.12)
1.17 (1.10-1.25)
مجموعة حدوث السل
1.00 (1.00-1.00)
1.00 (1.00-1.00)
الإيدز
–
0.93 (0.86-1.01)
السكري
–
0.94 (0.86-1.03)
نقطة
–
0.99 (0.94-1.04)
تصنيف السل في الرعاية الصحية الأولية
–
0.91 (0.85-0.97)
تغطية لا تغطية
1 (أساسي) 0.99 (0.99-0.99)
1 (أساسي) 0.99 (0.99-0.99)
العيادات المتخصصة لكل 1,000 نسمة
0.27 (0.26-0.27)
0.27 (0.21-0.34)
الأطباء لكل 1,000 نسمة
1.14 (1.13-1.14)
1.17 (1.11-1.22)
الممرضات لكل 1,000 نسمة
0.99 (0.98-0.99)
0.84 (0.73-0.97)
معدل البطالة (%)
1.01 (1.01-1.01)
1.01 (1.01-1.02)
مؤشر جيني
1.01 (1.01-1.01)
1.01 (1.01-1.02)
سنة الدخول إلى المجموعة
نعم
نعم
ملاحظة:
٥٤,٥٧١,٤٣٤
٤٦٣٤٤
الاختصارات: أ معدل المخاطر المعدلة. ب فترة الثقة. ج العرق أو الإثنية: أسود/باردو مُعلن ذاتيًا. د مادة بناء الأسرة: لا – طين مُغطى، طين غير مُغطى، خشب، وغيرها. هـ متناسب مع الحد الأدنى للأجور (MW) الأساسي. و الإضاءة: غير كهربائية – لا عداد، مصابيح، شموع، وغيرها.من السكان البلديين الذين يعانون من نقص في خدمات الصرف الصحي الأساسية. h إمدادات المياه: بئر أخرى، نبع، وغيرها. i نسبة تغطية الرعاية الصحية الأولية (PHC).
البيانات الموسعة الجدول 3 | تقديرات بواسطة نماذج بواسون المعدلة للعلاقة بين برنامج بولسا فاميليا (BFP) ومعدل الإصابة بالسل، والوفيات ومعدلات الفتك مقسمة حسب ربع الثروة، البرازيل، 2004-2015
ثروة
حَدَث
الوفيات
معدل الوفيات
أرغ
فترة الثقة 95%
أرر
فترة الثقة 95%
آر آر
فترة الثقة 95%
ثروة
الربع
0.49
(0.49-0.50)
0.60
(0.55-0.61)
0.80
(0.64-1.01)
ملاحظات
18,476,834
18,479,518
٢٠,٧٥٢
الربع
0.48
(0.47-0.49)
0.56
(0.50-0.63)
0.86
(0.60-1.22)
ملاحظات
10,565,846
10,567,091
10,350
الربع
0.71
(0.69-0.73)
0.86
(0.76-0.99)
1.20
(0.82-1.75)
ملاحظات
11,599,362
11,600,410
٨,٨٦٥
الربع
0.99
(0.96-1.02)
1.01
(0.83-1.23)
0.86
(0.53-1.40)
ملاحظات
14,145,583
١٤١٤٦٣٢٧
٦٤٦٠
ملاحظات: أ قياساً على النفقات لكل فرد بالنسبة للأجر الأدنى الأساسي (MW). ب الربع الأول:. الربع الثاني: > 0.1% أ الربع الثالث: >أ. الربع. تم حسابها بواسطة سنوات الشخص المعرض للخطر.مخاطر سعر الفائدة المعدلة h فترة الثقة
البيانات الموسعة الجدول 4 | تقديرات العلاقة بين برنامج بولسا فاميليا (BFP) ومرض السل (TB) من حيث الحدوث، والوفيات، ومعدل الفتك باستخدام نماذج تحليل البقاء ومطابقة درجات الميل، 2004-2015
النموذج المعدل
تحليل البقاء
تحليل مطابقة درجات الميل
حَدَث
الوفيات
معدل الوفيات
حَدَث
الوفيات
معدل الوفيات
aHR (CI 95%)
aHR (CI 95%)
aHR (CI 95%)
( 95%)
( 95%)
( 95%)
بي إف بي
0.54 (0.54-0.55)
0.65 (0.61-0.69)
1.04 (0.89-1.22)
0.43 (0.29-0.55)
0.32 (0.30-0.34)
0.53 (0.18-1.50)
جنس
ذكر
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
أنثى
0.58 (0.58-0.59)
0.39 (0.37-0.41)
0.69 (0.60-0.79)
-0.16(-0.17:-0.16)
-0.16 (-0.17:-0.16)
0.69 (0.60-79)
عمر
1.18 (1.18-1.19)
1.62 (1.61-1.64)
1.47 (1.41-1.53)
0.16 (-0.17:-0.16)
0.16 (-0.17:-0.16)
1.47(1.41-1.53)
العرق أو الإثنية
أبيض
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
باردو/أسود
1.42 (1.41-1.45)
1.70 (1.60-1.81)
1.03 (0.86-1.22)
0.14 (0.14-0.15)
0.14 (0.14-0.15)
1.03 (0.87-1.22)
محلي
3.70 (3.49-3.91)
٤.٥٦ (٣.٦٣-٥.٧٢)
1.38 (0.81-2.33)
1.13 (1.12-1.14)
1.13 (1.12-1.14)
1.38 (0.81-2.33)
التعليم
أمي، لم يحضر المدرسة أبداً
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
المدرسة الابتدائية
1.82 (1.79-1.85)
1.04 (0.98-1.10)
0.93(0.78-1.10)
0.07(0.71-0.74)
0.07(0.71-0.74)
0.93 (0.78-1.10)
المدرسة الثانوية
2.20(2.16-2.24)
0.98 (0.92-1.05)
0.78(0.63-0.95)
0.08 (0.08-0.08)
0.08 (0.08-0.08)
0.78 (0.63-0.95)
أكثر من المدرسة الثانوية
1.72 (1.68-1.75)
0.60(0.53-0.67)
0.53(0.38-0.75)
-0.18 (-0.18:-0.17)
-0.18 (-0.18:-0.17)
0.53 (0.38-0.75)
مواد البناء المنزلية (طوب)
نعم
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
لا
1.22 (1.20-1.24)
1.21 (1.13-1.29)
1.14 (0.97-1.34)
-0.06 (-0.06:-0.05)
-0.06 (-0.06:-0.05)
1.14 (0.97-1.34)
عدد الأشخاص في العائلة
2
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
3 إلى 4
0.98 (0.97-0.99)
0.83(0.78-0.88)
0.91 (0.78-1.07)
0.41 (0.41-0.42)
0.41 (0.41-0.42)
0.91 (0.78-1.07)
> 5
1.21 (1.19-1.23)
1.00 (0.93-1.07)
1.05 (0.89-1.25)
0.70 (0.70-0.71)
0.70 (0.70-0.71)
1.05 (0.89-1.25)
حسب نفقات الرواتب – % الحد الأدنى للأجور
أقل من الوسيط
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
فوق الوسيط
0.77 (0.76-0.78)
0.70 (0.65-0.74)
0.89 (0.75-1.05)
-0.12 (-0.12:-0.12)
-0.12 (-0.12:-0.12)
0.89 (0.75-1.05)
الإضاءة
الكهرباء
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
غير كهربائي
1.35 (1.33-1.37)
1.55 (1.45-1.67)
1.19* (1.03-1.38)
0.19 (0.19-0.20)
0.22 (0.22-0.23)
1.10 (0.92-1.31)
الصرف الصحي غير الكافي
1.00 (0.99-1.02)
1.08 (1.02-1.14)
1.00 (0.99-1.01)
0.29 (0.27-0.30)
0.29 (0.27-0.30)
0.98 (0.83-1.15)
التخلص من النفايات
0.78 (0.77-0.80)
0.76(0.70-0.82)
0.08 (0.07-0.08)
0.08 (0.07-0.08)
1.00 (0.80-1.26)
شبكة عامة
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
آخر
0.95 (0.93-0.97)
0.99 (0.92-1.06)
0.11(0.11-0.11)
0.11(0.11-0.11)
0.98 (0.82-1.15)
المتوسط الشهري
السلمعدل الحدوث
1.00 (1.00-1.00)
1.00 (1.00-1.00)
1.00 (0.99-1.00)
0.01 (0.01-0.01)
0.00 (0.00-0.00)
1.00 (0.99-1.00)
أساسي
الرعاية الصحية
تغطية
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
1 (أساس)
لا تغطية
1.00 (0.99-1.00)
0.99 (0.99-0.99)
1.00 (0.99-1.00)
-0.00 (-0.00:-0.00)
-0.00 (-0.00:-0.00)
1.00 (0.99-1.00)
السكان
الأطباء لكل
السكان
الممرضات لكل
١٠٠٠
0.93 (0.90-0.96)
0.78 (0.69-0.89)
1.12 (0.76-1.65)
-0.00 (-0.01:-0.00)
-0.00 (-0.01:-0.00)
1.12 (0.76-1.65)
معدل البطالة (%)
1.01 (1.01-1.02)
1.03(1.02-1.03)
1.01 (0.99-1.02)
0.01 (0.01-0.02)
0.01 (0.01-0.02)
1.01 (0.99-1.02)
مؤشر جيني
0.99 (0.99-1.00)
1.00 (0.99-1.00)
0.99 (0.98-1.00)
0.01 (0.01-0.01)
0.01 (0.01-0.01)
0.99 (0.98-1.00)
سنة دخول الفرد إلى المجموعة
نعم
نعم
نعم
نعم
نعم
نعم
ملاحظات:
٥٤,٥٧١,٤٣٤
٥٤,٥٧١,٤٣٤
٤٦٣٤٤
٥٤,٥٧١,٤٣٤
٥٤,٥٧١,٤٣٤
٤٦٣٤٤
البيانات الموسعة الجدول 5 | تقديرات بواسطة نماذج بواسون المعدلة دون وزن احتمالية العلاج العكسي (IPTW) للعلاقة بين برنامج بولسا فاميليا (BFP) و incidence السل والوفيات ومعدل الفتك، 2004-2015
النتائج ( RR – CI 95%)
نماذج
حَدَث
الوفيات
معدل الوفيات
معدل
غير معدّل
ملاحظة
٤٦٣٤٤
ملاحظاتمخاطر سعر الفائدة المعدلة.فترة الثقة
البيانات الموسعة الجدول 6 | تقديرات بواسطة نماذج بواسون المعدلة للعلاقة بين برنامج بولسا فاميليا (BFP) و incidence السل والوفيات ومعدل الفتك، البرازيل، 2004-2015 – النمذجة مع تضمين مصطلحات التفاعل في الانحدار اللوجستي لتقدير درجة الميل
النتائج (aRR95%)
نماذج
حَدَث
الوفيات
معدل الوفيات
معدل
0.59 (0.58-0.60)
0.69 (0.65-0.73)
0.91 (0.78-1.06)
ملاحظة
٥٤,٥٦٥,٧٢٩
54,571,428
٤٦٣٤٤
ملاحظات: تم إدخال مصطلحات التفاعل في الانحدار اللوجستي لتقدير درجة الميل: الجنس مقابل العرق، الجنس مقابل الثروة، والعرق مقابل الثروة.مخاطر سعر الفائدة المعدلة.فترة الثقة.
البيانات الموسعة الجدول 7 | تقديرات بواسطة نماذج بواسون المعدلة للعلاقة بين برنامج بولسا فاميليا (BFP) و incidence السل (TB) والوفيات ومعدل الفتك، البرازيل، 2004-2015 – تشمل مدة التعرض لبرنامج BFP كإلغاء للكوهر
النتائج
حَدَث
الوفيات
معدل
نموذج
ملاحظة
ملاحظات:مخاطر سعر الفائدة المعدلة.فترة الثقة.
البيانات الموسعة الجدول 8 | تقديرات بواسطة نماذج بواسون المعدلة للعلاقة بين برنامج بولسا فاميليا (BFP) و incidence السل (TB) والوفيات ومعدل الفتك في البرازيل، 2004-2015 – تشمل كمتغير تعديل وجود السجون لكل بلدية
النتائج (aRR95%)
حَدَث
الوفيات
معدل الوفيات
النموذج المعدل
0.59 (0.58-0.60)
0.69 (0.65-0.73)
0.91 (0.78-1.06)
ملاحظة
٥٤,٥٦٥,٧٢٩
54,571,428
٤٦٣٤٤
ملاحظات:مخاطر سعر الفائدة المعدلة.فترة الثقة.
البيانات الموسعة الجدول 9 | تقديرات بواسطة نماذج بواسون المعدلة (مع أخطاء معيارية قوية) للعلاقة بين برنامج بولسا فاميليا (BFP) و incidence السل (TB) والوفيات ومعدل الفتك في البرازيل بما في ذلك incidence السل في بلدية الإقامة و incidence السل المعدل حسب العمر، 2004-2015
النموذج المعدل بواسطة
السلالحوادث في بلدية الإقامة
السلالحوادث المعيارية حسب العمر
النتائج
السلحادثة
السلالوفاة
السلمعدل الوفيات
السلحادثة
السلالوفاة
السلمعدل الوفيات
آر آر ( )
0.58 (0.57-0.59)
0.68 (0.64-0.72)
0.90 (0.77-1.05)
0.58 (0.57-0.59)
0.69 (0.65-0.73)
0.90 (0.77-1.05)
ملاحظات: أ – السل ب – معدل الخطر المعدل. ج – فترة الثقة.
محفظة الطبيعة
المؤلف(المؤلفون) المراسلون: دافيد راسيلا آخر تحديث من المؤلف(ين): 18 أكتوبر 2024
ملخص التقرير
تتمنى Nature Portfolio تحسين قابلية تكرار الأعمال التي ننشرها. يوفر هذا النموذج هيكلًا للاتساق والشفافية في التقرير. لمزيد من المعلومات حول سياسات Nature Portfolio، يرجى الاطلاع على سياسات التحرير وقائمة مراجعة سياسة التحرير.
الإحصائيات
لجميع التحليلات الإحصائية، تأكد من أن العناصر التالية موجودة في أسطورة الشكل، أسطورة الجدول، النص الرئيسي، أو قسم الطرق. غير متوفر □ □ □ تم التأكيد
حجم العينة بالضبطلكل مجموعة/شرط تجريبي، معطاة كرقم منفصل ووحدة قياس
بيان حول ما إذا كانت القياسات قد أُخذت من عينات متميزة أو ما إذا كانت نفس العينة قد تم قياسها عدة مرات اختبار(ات) الإحصاء المستخدمة وما إذا كانت أحادية الجانب أو ثنائية الجانب يجب أن تُوصف الاختبارات الشائعة فقط بالاسم؛ واصفًا التقنيات الأكثر تعقيدًا في قسم الطرق. □
وصف لجميع المتغيرات المشتركة التي تم اختبارها □
وصف لأي افتراضات أو تصحيحات، مثل اختبارات الطبيعية والتعديل للمقارنات المتعددة □
وصف كامل للمعلمات الإحصائية بما في ذلك الاتجاه المركزي (مثل المتوسطات) أو تقديرات أساسية أخرى (مثل معامل الانحدار) و التباين (مثل الانحراف المعياري) أو تقديرات مرتبطة بعدم اليقين (مثل فترات الثقة) □
لاختبار الفرضية الصفرية، فإن إحصائية الاختبار (على سبيل المثال ) مع فترات الثقة، أحجام التأثير، درجات الحرية وقيمة ملحوظة أعطِالقيم كقيم دقيقة كلما كان ذلك مناسبًا. □
لتحليل بايزي، معلومات حول اختيار القيم الأولية وإعدادات سلسلة ماركوف مونت كارلو □ لتصميمات هرمية ومعقدة، تحديد المستوى المناسب للاختبارات والتقارير الكاملة عن النتائج □ تقديرات أحجام التأثير (مثل حجم تأثير كوهين)بيرسون )، مما يشير إلى كيفية حسابها تحتوي مجموعتنا على الويب حول الإحصائيات لعلماء الأحياء على مقالات تتناول العديد من النقاط المذكورة أعلاه.
البرمجيات والشيفرة
معلومات السياسة حول توفر كود الكمبيوتر جمع البيانات تم استخدام أداة ربط السجلات (رقم الإصدار 1) من مركز تكامل البيانات والمعرفة للصحة (Centro de Integração de Dados e Conhecimentos para a Saúde – CIDACS) للربط.https://github.com/gcgbarbosa/cidacs-rl-v1
تحليل البيانات تم إجراء جميع التحليلات الإحصائية باستخدام برنامج ستاتا الإصدار MP 15.1 بالنسبة للمخطوطات التي تستخدم خوارزميات أو برامج مخصصة تكون مركزية في البحث ولكن لم يتم وصفها بعد في الأدبيات المنشورة، يجب أن تكون البرمجيات متاحة للمحررين والمراجعين. نحن نشجع بشدة على إيداع الشيفرة في مستودع مجتمعي (مثل GitHub). راجع إرشادات مجموعة Nature لتقديم الشيفرة والبرمجيات لمزيد من المعلومات.
بيانات
معلومات السياسة حول توفر البيانات
يجب أن تتضمن جميع المخطوطات بيانًا حول توفر البيانات. يجب أن يتضمن هذا البيان المعلومات التالية، حيثما ينطبق:
رموز الانضمام، معرفات فريدة، أو روابط ويب لمجموعات البيانات المتاحة للجمهور
وصف لأي قيود على توفر البيانات
بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتماشى مع سياستنا
البيانات الأساسية لهذا المقال ستتم مشاركتها عند الطلب مع ISC/UFBA وCIDACS/Fiocruz وبعد الحصول على الموافقة الأخلاقية. جميع البيانات التي تدعم النتائج المقدمة تم الحصول عليها من مركز تكامل البيانات والمعرفة للصحة (Centro de Integração de Dados e Conhecimentos para a Saúde – CIDACS). من المهم أن نلاحظ أن هناك قيودًا على الوصول إلى البيانات، التي تحتوي على معلومات حساسة، والتي تم ترخيصها للاستخدام الحصري في الدراسة الحالية، وبسبب الخصوصية،
تنظيمات من اللجنة الأخلاقية البرازيلية ليست متاحة بشكل علني. عند الطلب ومع الحصول على إذن صريح من CIDACS (البريد إلىcidacs.curadoria@fiocruz.br) وموافقة من لجنة أخلاقية، يمكن الوصول إلى البيانات بشكل محكوم. مجموعة البيانات مسجلة تحت رقم DOI التالي:https://hdl.handle.net/20.500.12196/CIDACS/65، الذي يوفر بيانات وصفية وسجل لجميع إصدارات قاعدة البيانات.
البحث الذي يشمل المشاركين البشريين، بياناتهم، أو المواد البيولوجية
معلومات السياسة حول الدراسات التي تشمل المشاركين البشريين أو البيانات البشرية. انظر أيضًا معلومات السياسة حول الجنس، الهوية/العرض، والتوجه الجنسي والعرق، الإثنية والعنصرية.
التقارير حول الجنس والهوية
نستخدم فقط مصطلح الجنس، كما في البيانات التالية مصادر البيانات، النتائج، وقسم التدخل: “تم بناء رموز الربط والخوارزميات بناءً على خمسة معرّفات: تاريخ الميلاد، بلدية الإقامة، الجنس، الاسم، واسم الأم للفرد في كل قاعدة بيانات”. قسم التحليلات الإحصائية: “على المستوى الفردي، كانت المتغيرات الديموغرافية والاجتماعية والاقتصادية هي العمر، الجنس، العرق/الإثنية المعرف ذاتيًا (أبيض، أصلي، أسود وباردو – تم تحليل هذه الفئات الأخيرة معًا)، التعليم، الإنفاق للفرد (كبديل للثروة الفردية وحُسب كنسبة مئوية من الحد الأدنى للأجر السنوي، مصنفة حسب الثلثيات)، وسنة الدخول إلى المجموعة” و”علاوة على ذلك، لفهم تباين تأثيرات BFP، قمنا بتطبيق نماذج الانحدار بواسون IPTW المصنفة حسب العمر، الجنس، العرق/الإثنية، التعليم، وثلاثيات الثروة (الإنفاق للفرد).”
التقارير حول العرق، الإثنية، أو مجموعات اجتماعية ذات صلة
نحدد في النص الرئيسي أن المتغيرات تم الحصول عليها من مجموعة 100 مليون برازيلي وأن العرق/الإثنية معرّف ذاتيًا. علاوة على ذلك، نشرح كيف نستخدم متغير ثروة الأسرة (الإنفاق للفرد).
تصميم الدراسة، السكان، والقضايا الأخلاقية: “تم تحقيق مجموعة الدراسة من خلال اختيار مجموعة فرعية من الأفراد من مجموعة 100 مليون برازيلي، وهي مجموعة موحدة تم إنشاؤها من خلال الربط المعتمد بين السجل الموحد للحكومة الفيدرالية للبرامج الاجتماعية (Cadastro Único) – الذي يجمع البيانات من النصف الأفقر من السكان البرازيليين، ويحدد ويصف الأسر ذات الدخل المنخفض لأهلية البرامج الاجتماعية، ويشمل معلومات عن التعرض لـ BFP – ومجموعات البيانات المتعلقة بالصحة من وزارة الصحة البرازيلية.”
قسم التحليلات الإحصائية: “على المستوى الفردي، كانت المتغيرات الديموغرافية والاجتماعية والاقتصادية هي العمر، الجنس، العرق/الإثنية المعرف ذاتيًا (أبيض، أصلي، أسود وباردو – تم تحليل هذه الفئات الأخيرة معًا)، التعليم، الإنفاق للفرد (كبديل للثروة الفردية وحُسب كنسبة مئوية من الحد الأدنى للأجر السنوي، مصنفة حسب الثلثيات)، وسنة الدخول إلى المجموعة” و”علاوة على ذلك، لفهم تباين تأثيرات BFP، قمنا بتطبيق نماذج الانحدار بواسون IPTW المصنفة حسب العمر، الجنس، العرق/الإثنية، التعليم، وثلاثيات الثروة (الإنفاق للفرد).”
مستفيدو BFP وغير المستفيدين أظهروا خصائص ديموغرافية واجتماعية واقتصادية مشابهة. بالمقارنة مع غير المستفيدين، فإن مستفيدي BFP أصغر سناً (متوسط العمر 24.2 مقابل 25.3 سنة)، كان لديهم نسبة أعلى قليلاً من الأشخاص الذين عرّفوا أنفسهم كعرق/إثنية سوداء أو باردة ( مقابل )، أشخاص بلا تعليم ( مقابل ), أسر بها 3 أفراد أو أكثر ( مقابل ), ثروة أقل ( مقابل ), بدون خدمات صحية كافية ( مقابل )، وبدون شبكة عامة لمياه الشرب (70.6% مقابل 76.1%).
في قسم النتائج: “بعد استبعاد الأفراد من مجموعة 100 مليون برازيلي الذين كانوا خارج فترة الدراسة 2004-2015، والذين كانت لديهم معلومات مفقودة عن المتغيرات الديموغرافية أو الاجتماعية والاقتصادية، تم اختيار 54,571,434 فردًا، من بينهم كانوا مستفيدين من BFP (), و غير مستفيدين من BFP (), مع إجمالي 159,777 تشخيص جديد للسل و7,993 حالة وفاة بسبب السل”
تمت الموافقة على هذه الدراسة من قبل لجنة الأخلاقيات البحثية بمعهد الصحة الجماعية بجامعة باهيا الفيدرالية (ISC/UFBA)، تحت الرقم 41691315.0.0000.5030 (تقييم:3.783.920)
الإشراف الأخلاقي
خصائص السكان
التوظيف
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة حول الموافقة على بروتوكول الدراسة في المخطوطة.
محفظة الطبيعة | ملخص التقرير أبريل 2023
التقارير الخاصة بالمجال
يرجى اختيار الخيار أدناه الذي يناسب بحثك بشكل أفضل. إذا لم تكن متأكدًا، اقرأ الأقسام المناسبة قبل اتخاذ قرارك.
□ العلوم السلوكية والاجتماعية
□ العلوم البيئية، التطورية والبيئية
يجب على جميع الدراسات الإفصاح عن هذه النقاط حتى عندما يكون الإفصاح سلبيًا.
حجم العينة
section*{استبعاد البيانات}
تم اعتبار جميع السكان المؤهلين، أي الأفراد المسجلين في Cadastro Único (CADU) بين 2004 و2015، مع أو بدون تشخيص السل، سواء كانوا مستفيدين من BFP أم لا. من هذا الاختيار الأولي، الذي هو مجموعة فرعية من مجموعة 100 مليون برازيلي، تم استبعاد الأفراد الذين لديهم أقل من يوم واحد من المتابعة، الذين تم تشخيصهم بالسل أو الذين تلقوا BFP قبل 2004، الأفراد الذين لديهم تواريخ غير متسقة، التكرارات، الأفراد الذين تلقوا BFP <30 يومًا والأفراد الذين لديهم قيم مفقودة للمتغيرات الاجتماعية والاقتصادية (كما هو موضح في الشكل 1 – مخطط التدفق). بعد هذه الاستبعادات، تم اعتبار جميع السكان النهائيين للتحليل، أي، أفراد، منهم غير مستفيدين من BFP () ومستفيدين من BFP ().
في قسم النتائج: “بعد استبعاد الأفراد من مجموعة 100 مليون برازيلي الذين كانوا خارج فترة الدراسة 2004-2015، والذين كانت لديهم معلومات مفقودة عن المتغيرات الديموغرافية أو الاجتماعية والاقتصادية، تم اختيار أفراد، من بينهم كانوا مستفيدين من BFP (), و غير مستفيدين من BFP (), مع إجمالي 159,777 تشخيص جديد للسل و7,993 حالة وفاة بسبب السل” (كما هو موضح في الشكل 1 – مخطط التدفق).
التكرار
العشوائية
التعتيم
قمنا بإجراء عدة تحليلات حساسية وتحليلات مثلثية. جميع النتائج أكدت النتائج التي تم الحصول عليها في التحليل الرئيسي. قسم التحليلات الحساسية والمثلثية: “قمنا بتطوير مجموعة واسعة من عدة تحليلات حساسية (للتفاصيل انظر قسم الطرق والجداول التكميلية S1-S7) مع نماذج بمواصفات مختلفة وضبط المتغيرات. كما قمنا بإجراء تحليلين مثلثيين مختلفين: الانحدار المتعدد لكوكس ومطابقة درجات الميل (PSM) (الجدول التمديدي 4). جميع اختبارات الحساسية أكدت تقديرات الارتباط، وأظهرت التحليلات المثلثية درجة عالية من الثقة في تقييم تأثير الاستدلال السببي.”
لم يكن التخصيص عشوائيًا. في قسم مصادر البيانات، النتائج، والتدخل:
“تم تعريف مجموعة المستفيدين على أنها الأفراد المؤهلين الذين تلقوا فوائد BFP، وبدأ تعرضهم مع استلام الفائدة، حتى نهاية متابعتهم. تم تعريف مجموعة غير المستفيدين على أنها الأفراد الذين لم يستفيدوا من BFP طوال فترة متابعتهم. في حالة عدم استلام الفوائد، تم تصنيف الأفراد المؤهلين في مجموعة غير المستفيدين”
العمى ليس ذا صلة بهذه الدراسة لأنه ليس دراسة تجريبية. في هذه الدراسة، كانت التعرض الرئيسي هو استلام BFP ولدى الباحث هذه المعلومات من خلال قاعدة بيانات إدارية دون أسماء الأفراد.
التقارير عن مواد وأنظمة وطرق محددة
نحتاج إلى معلومات من المؤلفين حول بعض أنواع المواد والأنظمة التجريبية والطرق المستخدمة في العديد من الدراسات. هنا، حدد ما إذا كانت كل مادة أو نظام أو طريقة مدرجة ذات صلة بدراستك. إذا لم تكن متأكدًا مما إذا كان عنصر القائمة ينطبق على بحثك، اقرأ القسم المناسب قبل اختيار رد.
الفئة العمرية مصنفة كل 10 سنوات.العرق أو الإثنية: أسود أو باردو، مُعلن ذاتيًا.نسبة إلى الحد الأدنى من الأجر الأساسي.الإضاءة: غير كهربائية – لا عداد، مصابيح، شموع وغيرها.نسبة السكان البلديين الذين يعانون من عدم كفاية الصرف الصحي الأساسي.نسبة السكان البلديين الذين لديهم جمع نفايات أساسي.إمدادات المياه: أخرى – بئر، نبع وغيرها.نسبة التغطية.
ملاحظات: أ نسبة الخطر المعدلة ب فترة الثقة. ج نسبة الأرجحية المعدلة د برنامج Bolsa Família هـ الفئة العمرية مصنفة كل 10 سنوات. و العرق أو الإثنية: مُعلن ذاتيًا. ز مادة بناء المنزل: لا – طين مطلي، طين غير مطلي، خشب، وغيرها. ح نسبة إلى الحد الأدنى من الأجر الأساسي (MW). ط الإضاءة: غير كهربائية – لا عداد، مصابيح، شموع، وغيرها.من السكان البلديين الذين يعانون من عدم كفاية الصرف الصحي الأساسي. ك إمدادات المياه: أخرى – بئر، نبع، وغيرها. ل السل م نسبة تغطية الرعاية الصحية الأولية (PHC).
Effects of conditional cash transfers on tuberculosis incidence and mortality according to race, ethnicity and socioeconomic factors in the 100 Million Brazilian Cohort
Received: 15 April 2024
Accepted: 26 October 2024
Published online: 3 January 2025
Check for updates
A list of authors and their affiliations appears at the end of the paper
Conditional cash transfer (CCT) programs have been implemented globally to alleviate poverty. Although tuberculosis (TB) is closely linked to poverty, the effects of CCT on TB outcomes among populations facing social and economic vulnerabilities remain uncertain. Here we estimated the associations between participation in the world’s largest CCT program, the Brazilian Bolsa Família Program (BFP), and the reduction of TB incidence, mortality and case-fatality rates using the nationwide 100 Million Brazilian Cohort between 2004 and 2015. We also evaluated these relationships according to race, ethnicity, wealth levels, sex and age. Exposure to the BFP was associated with a large reduction in TB incidence (adjusted rate ratio (aRR): 0.59; 95% confidence interval (CI): 0.58-0.60) and mortality (aRR:0.69; 95% CI: 0.65-0.73). The strongest BFP association was observed in individuals of Indigenous ethnicity both for TB incidence (aRR: 0.37; 95% CI: 0.32-0.42) and mortality (aRR:0.35; 95% CI: 0.20-0.62), and in individuals of Black and Pardo ethnicity (incidence-aRR: 0.58; 95% CI: 0.57-0.59; mortality-aRR: 0.69; 95% CI: 0.64-0.73). BFP associations were considerably stronger among individuals living in extreme poverty both for TB incidence (aRR: 0.49; 95% CI: 0.49-0.50) and mortality (aRR: CI: ). CCT can strongly reduce TB incidence and mortality in individuals living in extreme poverty, and of Indigenous, Black and Pardo ethnicity, and could significantly contribute to achieving the End TB Strategy targets and TB-related Sustainable Development Goals.
Conditional cash transfers (CCTs) are the world’s most widely implemented interventions for poverty alleviation . Social protection, poverty alleviation and multisectoral actions on broad tuberculosis (TB) determinants are acknowledged as key pillars of the End TB Strategy by 2035, and they are essential to reduce the TB burden .
CCT programs have the potential to positively influence TB prevention, diagnosis and treatment . CCTs improve living conditions and incentivize behavioral changes by providing financial support to individuals or households who adhere to specific health-related
conditions, often associated with child and maternal health . Previous studies in low- and middle-income countries showed that CCT programs were associated with improved TB outcomes, including increased treatment adherence and completion rates . Furthermore, CCTs could effectively alleviate the economic burdens faced by TB-affected households . These costs, which often result from medical expenses, loss of income and other related factors, can push affected households into poverty and hinder their access to proper TB care . Thus, these transfers help mitigate the catastrophic costs associated
Fig.1 | Flowchart of the selection of the study population from the 100 Million Brazilian Cohort, 2004-2015. Individuals from the 100 Million Brazilian Cohort were selected or excluded based on the study period (2004-2015) and availability of complete information of demographic and socioeconomic
variables. A total of 54,571,434 individuals were selected: BFP beneficiaries and non-BPF beneficiaries . The selected population included 159,777 new TB diagnoses.
with TB, ensuring better access to treatment and reducing economic hardships for affected families.
Since 2004, Brazil has implemented one of the world’s largest CCT programs, the Bolsa Família Program (BFP) . The governmental program provides direct cash transfers to households living in poverty with income below the poverty line defined by the Brazilian government as US$43.6 per person per month (at an exchange rate of 5 Brazilian Reais to US$1). The monthly cash benefits are at least US ; children in the family aged between 0 and 6 years old receive an additional US , and pregnant women, children and adolescents up to 18 years old receive an additional of US (values corrected in 2023). To continue receiving the benefits, BFP beneficiaries have to fulfill specific conditionalities related to healthcare for pregnant women (carrying out prenatal care) and children (compliance with the national vaccination schedule, monitoring nutritional status) and education (school attendance) for children and adolescents . The BFP has been able to improve the well-being of families in poverty, and to reduce social and income inequalities in society, improving access to education, food and health services . Several studies have shown the positive effects of the BFP on health outcomes such as child mortality , cardiovascular diseases , suicide , leprosy and some aspects of the TB burden , among others.
In addition to the income disparity, Brazil has a profound ethnic and racial inequality. Individuals with self-declaration of Black, Pardo and Indigenous ethnicity in Brazil face more barriers to accessing better job opportunities, salaries, decent housing, a balanced diet, and quality health and education services . As a consequence, these populations are more subject to violence and worse health indicators , including higher incidence of and mortality rates from .
We are not aware of previous studies that have systematically evaluated the effects of CCT programs in large cohorts of vulnerable individuals at high risk for TB and with limited access to health
services, such as groups in situations of social marginalization and individuals living in extreme poverty, analyzing their effects according to subpopulation characteristics and evaluating the association between the participation in CCT and TB burden indicators. This study aimed to evaluate the comprehensive association between receipt of the BFP and the reduction of TB incidence, mortality and case-fatality rates using a nationwide cohort of 54.5 million low-income Brazilians over 12 years, estimating its heterogeneous effectiveness across the spectrum of ethnoracial factors and socioeconomic conditions.
Results
Study design and population
This study has a cohort study design, obtained after selecting individuals from the 100 Million Brazilian Cohort , a consolidated cohort created through the validated linkage between the Federal Government Unified Registry for Social Programs (Cadastro Único)-which gathers data from the poorest half of the Brazilian population-and health-related datasets from the Brazilian Ministry of Health. As described in the flowchart of the study population selection (Fig. 1), after individuals who were outside the study period 2004-2015 and who had missing information on demographic or socioeconomic variables were excluded, 54,571,434 individuals were selected, of which 23,907,958 were BFP beneficiaries ( ) and were non-BFP beneficiaries ( ), with a total of 159,777 new TB diagnoses and 7,993 TB deaths.
TB incidence was lower among BFP beneficiaries than among non-beneficiaries (49.44/100,000 person-years at risk (pyr) ( confidence interval (CI): ) versus ( CI: 80.97-82.13)), and the same was the case with TB mortality rate (2.08/100,000 pyr ( Cl: ) versus : and TB case-fatality rate ( ( ) versus 1.37/100 pyr (95% CI: 1.25-1.49)) (Table 1). BFP beneficiaries and non-beneficiaries showed similar demographic and socioeconomic
Table 1 | Descriptive analyses of BFP beneficiaries and non-beneficiaries ( ), Brazil, 2004-2015
N-BF (
BF ( )
Total
Rates (95% CI)
Number (%)
Rates (95% CI)
Number (%)
Incidence rate
81.37 (80.97-82.13)
75,956 (47.5)
49.44 (47.84-48.50)
83,821 (52.5)
159,777
Mortality rate
4.68 (4.54-4.81)
4,359 (54.5)
2.08 (2.01-2.15)
3,634 (45.5)
7,993
Case-fatality rate
1.37 (1.25-1.49)
495 (39.7)
0.68 (0.64-0.73)
751 (60.3)
1,246
Social and demographic variables
Number or mean
% or s.d.
Number or mean
% or s.d.
value
SMD
Sex
<0.001
0.0442
Male
14,595,815
47.6
10,854,212
45.4
Female
16,067,661
52.4
13,053,746
54.6
Age
25.32
2.14
24.17
1.60
<0.001
0.3829
Race or ethnicity
<0.001
0.1655
White
11,376,150
37.1
7,244,111
30.3
Black or Pardo
19,195,336
62.6
16,424,767
68.7
Indigenous
91,990
0.3
239,080
1.0
Education
<0.001
0.1986
Illiterate, never attended school
9,965,630
32.5
8,869,852
37.1
Elementary school
9,536,341
31.1
7,459,283
31.2
High school
6,040,705
19.7
5,140,211
21.5
More than high school
5,120,800
16.7
2,438,612
10.2
House construction materials
<0.001
0.0854
Bricks or cement
24,438,790
79.7
18,217,864
76.2
Wood and other vegetal materials
6,224,686
20.3
5,690,094
23.8
Number of people in the family
<0.001
0.3215
10,425,582
34.0
5,044,579
21.1
3 or 4
14,810,459
48.3
12,432,138
52.0
5,427,435
17.7
6,431,241
26.9
Per salary expenses-% MW
<0.001
0.2856
Below median
13,461,266
43.9
13,866,616
58.0
Above median
17,202,210
56.1
10,041,342
42.0
Lighting
<0.001
0.2021
Electricity
27,321,157
89.1
19,604,526
82.0
Non-electric
3,342,319
10.9
4,303,432
18.0
Adequate sanitation
<0.001
0.0795
Yes
19,961,923
65.1
14,655,578
61.3
No
10,701,553
34.9
9,252,380
38.7
Garbage disposal
<0.001
0.1044
Garbage collection
24,745,425
80.7
18,265,680
76.4
Burned or buried
5,918,051
19.3
5,642,2788
23.6
Water supply
<0.001
0.1255
Public network
23,334,905
76.1
16,879,018
70.6
Other
7,328,571
23.9
7,028,940
29.4
Incidence cohort
123.2
90.4
146.0
103.3
<0.001
-0.2361
AIDS
0.060
0.0183
Yes
1,355
8.8
3,009
9.3
No
14,080
91.2
29,331
90.7
Diabetes
<0.001
0.1085
Yes
1,236
8.0
1,716
5.3
No
14,199
92.0
30,624
94.7
Table 1 (continued) | Descriptive analyses of BFP beneficiaries and non-beneficiaries ( ), Brazil, 2004-2015
N-BF (
BF ( )
Total
Rates (95% CI)
Number (%)
Rates (95% CI)
Number (%)
DOT
<0.001
0.0601
Yes
8,445
54.7
16,724
51.7
No
6,990
45.3
15,616
48.3
Pulmonary TB
<0.001
0.3733
Yes
13,373
86.6
28,422
87.9
No
2,062
13.4
3,918
12.1
PHC
69.6
28.1
65.2
29.0
<0.001
0.1486
Specialized clinics per 1,000 inhabitants
0.12
0.14
0.10
0.12
<0.001
0.1535
Doctors per 1,000 inhabitants
1.17
1.01
1,21
0.99
<0.001
-0.0311
Nurses per 1,000 inhabitants
0.58
0.38
0.54
0.35
<0.001
0.3551
Unemployment rate (%)
7.3
5.0
8.98
5.2
<0.001
-0.3674
Gini index
52.3
7.1
54.2
6.9
<0.001
-0.2793
Year of entry into the cohort
<0.001
-0.5093
2004
2,177,107
7.1
2,438,612
10.2
2005
1,318,529
4.3
1,936,545
8.1
2006
5,396,772
17.6
6,072,621
25.4
2007
3,403.646
11.1
2,103,900
8.8
2008
2,269,097
7.4
1,267,122
5.3
2009
1,379,856
4.5
2,175,624
9.1
2010
1,993,126
6.5
1,864,821
7.8
2011
1,655,828
5.4
1,673,557
7.0
2012
3,526,300
11.5
1,601,833
6.7
2013
2,054,453
6.7
1,147,582
4.8
2014
3,035,684
9.9
884,594
3.7
2015
2,422,415
7.9
741,147
3.1
Obs
30,663,476
23,907,958
BF beneficiaries; N-BF, non-beneficiaries; Obs, observations; SMD, standardized mean difference. The following were used for a comparison between the groups: (1) two-tailed -test for continuous variables and (2) Pearson’s chi-squared test ( ) for categorical variables. Race or ethnicity: Black or Pardo, self-declared. Proportional to the baseline minimum wage (MW). Lighting: non-electric-no meter, lamps, candles and others. Percentage of the municipal population with inadequate baseline sanitation. Percentage of the municipal population with baseline garbage collection. Water supply: other-well, spring and others. Primary healthcare (PHC) percentage coverage.
characteristics. Compared with non-beneficiaries, BFP beneficiaries are younger (mean age 25.3 versus 24.2 years) and had a slightly higher percentage of people self-identified as Black or Pardo race or ethnicity ( versus ), people with no education ( versus ), households with 3 or more individuals ( versus ), people with lesser wealth ( versus ), people without adequate sanitation ( versus ) and people without a public network for water supply ( versus ).
Main analyses
For the main statistical analysis, we used stabilized, truncated, inverse probability of treatment weighting (IPTW) multivariable Poisson regression models (see Methods for details). As shown in Table 2, the exposure to the BFP was associated with a significant reduction in TB incidence (adjusted rate ratio (aRR): 0.59 ; ), decreased TB mortality (aRR: 0.69; 95% CI: 0.65-0.73) and lower TB case-fatality rate(aRR: CI ), although not statistically significant.
Stratified analyses
In the stratified analyses according to wealth terciles (Table 3), the association between the BFP and the reduction of TB incidence showed
a marked gradient and was considerably stronger among the individuals living in extreme poverty (aRR: 0.49 ; CI: ), gradually decreasing until having only a small association on the wealthiest individuals (aRR: 0.95 ; CI: ). Also, for TB mortality, the BFP association was considerably stronger among the individuals living in extreme poverty (aRR: ) and showed a gradient demonstrating the lack of association of the BFP in those people with higher wealth (aRR: CI: 0.85-1.17) (Table 3).
In the stratified analyses according to race and ethnicity, another gradient was evident among individuals of Indigenous, Black or Pardo, and White ethnicity, both for TB incidence (aRR: 0.37 ( : 0.32-0.42) for Indigenous, aRR: 0.58 ( : 0.57-0.59) for Black or Pardo, aRR: for White) and TB mortality (aRR: for Indigenous, aRR: for Black or Pardo, and aRR: 0.83 ( CI: 0.73-0.94) for White), while the estimates for TB case-fatality rate was not statistically significant (Table 3). In terms of education, the association between the BFP and reductions in TB incidence was greater in people with less education (aRR: versus aRR: for people with higher education) (Table 3). The BFP was also associated with a higher reduction in TB mortality rates in females than in males
Table 2 | Estimates of the association between the BFP and tuberculosis incidence, mortality and the case-fatality rate in the Brazil adjusted Poisson model (with robust standard errors), 2004-2015
Adjusted model
Outcomes, aRR(95% CI)
Incidence
Mortality
Case-fatality rate
BFP
0.59 (0.58-0.60)
0.69 (0.65-0.73)
0.90 (0.76-1.05)
Sex
Male
1 (base)
1 (base)
1 (base)
Female
0.58 (0.57-0.59)
0.40 (0.38-0.42)
0.69 (0.59-0.79)
Age
1.19 (1.19-1.20)
1.63 (1.61-1.65)
1.44 (1.38-1.50)
Race or ethnicity
White
1 (base)
1 (base)
1 (base)
Black or Pardo
1.42 (1.40-1.44)
1.70 (1.60-1.81)
1.02 (0.86-1.21)
Indigenous
3.63 (3.43-3.84)
4.50 (3.59-5.65)
1.58 (0.92-2.70)
Education
Illiterate, never attended school
1 (base)
1 (base)
1 (base)
Elementary school
1.83 (1.80-1.86)
1.05 (0.99-1.11)
0.94 (0.79-1.12)
High school
2.21 (2.17-2.25)
0.99 (1.93-1.06)
0.77 (0.62-0.94)
More than high school
1.74 (1.70-1.77)
0.60 (0.54-0.67)
0.52 (0.37-0.73)
House construction materials
Bricks and cement
1 (base)
1 (base)
1 (base)
Wood and other vegetal materials
1.22 (1.20-1.24)
1.21 (1.14-1.29)
1.15 (0.98-1.37)
Number of people in the family
1 (base)
1 (base)
1 (base)
3 to 4
0.97 (0.96-0.99)
0.83 (0.78-0.88)
0.89 (0.89-1.28)
1.20 (1.18-1.21)
0.99 (0.92-1.06)
1.07 (0.76-1.05)
Per-salary expenses-% MW
Below the median
1 (base)
1 (base)
1 (base)
Above the median
0.77 (0.78-0.79)
0.71 (0.66-0.75)
0.89 (0.75-1.05)
Lighting
Electricity
1 (base)
1 (base)
1 (base)
Non-electric
1.34 (1.32-1.36)
1.54 (1.45-1.65)
1.09 (0.91-1.31)
Inadequate sanitation
1.00 (0.99-1.02)
1.08 (1.02-1.15)
0.96 (0.81-1.14)
Garbage disposal
0.78 (0.77-0.80)
0.77 (0.71-0.83)
1.03 (0.82-1.30)
Water supply
Public network
1 (base)
1 (base)
1 (base)
Other
0.95 (0.93-0.96)
0.99 (0.92-1.06)
0.95 (0.79-1.15)
TB incidence cohort
1.00 (1.00-1.00)
1.00 (1.00-1.00)
0.99 (0.99-1.00)
AIDS
–
–
1.93 (1.39-2.68)
Diabetes
–
–
0.87 (0.68-1.10)
DOT
–
–
1.54 (1.34-1.77)
Pulmonary TB
–
–
0.54 (0.42-0.69)
PHC
Coverage
1 (base)
1 (base)
1 (base)
No coverage
0.99 (0.99-1.00)
1.00 (0.99-1.00)
1.00 (0.99-1.00)
Specialized clinics per 1,000 inhabitants
0.63 (0.59-0.67)
0.54 (0.39-0.73)
1.15 (0.54-2.42)
Doctors per 1,000 inhabitants
1.11 (1.10-1.12)
1.19 (1.00-1.10)
1.08 (0.94-1.25)
Nurses per 1,000 inhabitants
0.95 (0.92-0.98)
0.80 (0.70-0.91)
1.11 (0.75-1.66)
Unemployment rate (%)
1.01 (1.01-1.02)
1.03 (1.02-1.04)
1.00 (0.98-1.02)
Gini index
0.99 (0.99-1.00)
1.00 (0.99-1.00)
0.98 (0.97-1.00)
Year of entry into the cohort
Yes
Yes
Yes
Obs
54,565,735
54,571,434
46,344
Table 3 | Estimates of the association between the BFP and TB incidence, mortality and case-fatality rate in Brazil in adjusted Poisson models (with robust standard errors), 2004-2015
Adjusted models
Incidence
Mortality
Case-fatality rate
aRR
95% CI
aRR
95% CI
aRR
95% CI
Wealth
Lower wealth
0.49
(0.49-0.50)
0.60
(0.55-0.65)
0.80
(0.64-1.01)
Obs
18,476,834
18,479,518
20,752
Medium wealth
0.55
(0.54-0.57)
0.69
(0.63-0.77)
1.08
(0.82-1.43)
Obs
17,714,018
17,715,984
16,74
Higher wealth
0.95
(0.93-0.98)
1.00
(0.85-1.17)
0.92
(0.60-1.42)
Obs
18,596,773
18,597,844
8,979
Race or ethnicity
White
0.67
(0.66-0.69)
0.83
(0.73-0.94)
1.26
(0.93-1.71)
Obs
18,612,330
18,613,587
12,288
Black or Pardo
0.58
(0.57-0.59)
0.69
(0.64-0.73)
0.84
(0.69-1.00)
Obs
35,641,321
35,645,701
33,328
Indigenous
0.37
(0.32-0.42)
0.35
(0.20-0.62)
0.16
(0.007-3.33)
Obs
312,084
312,146
717
Education
Illiterate, never attended school
0.58
(0.57-0.59)
0.72
(0.68-0.78)
0.90
(0.66-1.23)
Obs
35,830,269
35,833,532
7,741
Elementary school
0.58
(0.57-0.60)
0.63
(0.56-0.71)
0.93
(0.71-1.21)
Obs
11,160,783
11,162,535
17,185
High school and university education
0.80
(0.77-0.83)
0.90
(0.71-1.14)
1.06
(0.84-1.35)
Obs
7,577,703
7,578,387
25,267
Sex
Male
0.60
0.59-0.61
0.78
0.72-0.84
0.94
0.78-1.13
Obs
25,432,661
25,435,955
25,681
Female
0.61
0.59-0.62
0.63
0.57-0.69
0.90
0.66-1.23
Obs
29,142,346
29,144,751
20,663
Prisons in the municipality
Yes
0.62
0.61-0.64
0.74
0.68-0.80
0.92
0.75-1.15
Obs
26,078,654
26,081,968
26,777
No
0.55
0.54-0.56
0.64
0.59-0.70
0.89
0.71-1.25
Obs
28,487,075
28,489,460
19,567
Brazilian region
North
0.48
0.47-0.50
0.47
0.39-0.56
0.97
0.55-1.71
Obs
6,224,529
6,225,218
5,859
Northeast
0.51
0.49-0.52
0.57
0.52-0.63
0.81
0.63-1.06
Obs
18,246,282
18,248,820
14,703
Southeast
0.67
0.66-0.68
0.88
0.80-0.97
1.09
0.82-1.44
Obs
19,438,441
19,439,952
17,926
South
0.66
0.64-0.69
0.68
0.56-0.82
0.62
0.44-0.87
Obs
6,306,963
6,307,614
5,775
Middle-West
0.58
0.54-0.62
0.68
0.50-0.92
1.37
0.56-3.36
Obs
4,349,514
4,349,824
2,081
All models were adjusted for the same demographic and socioeconomic variables described in Table 2. a Measured by per capita expenses proportional to the baseline MW in terciles 1, 2 and 3, each one; lower wealth: tercile 1, medium wealth: tercile 2 and higher wealth: tercile Race or ethnicity: Black or Pardo, self-declared.
(aRR: 0.63 ( CI: ) versus aRR: 0.78 ( ), respectively). According to analyses by Brazilian regions, the strongest associations between the BFP and both TB incidence and mortality
reductions were observed in the poorest areas, specifically the north and northeast regions. When carrying out a stratified analysis according to the existence or not of prisons in the municipality, we observed
a greater association between the BFP and reductions in TB incidence (aRR 0.55 ( CI: 0.54-0.56) versus aRR 0.62 ( CI: 0.61-0.64)) and mortality (aRR 0.64 (95% CI: 0.59-0.70) versus aRR 0.74 ( CI: 0.68-0.80)) in municipalities without prisons.
Sensitivity and triangulation analyses
We developed a wide range of several sensitivity analyses (for details, see Methods and Supplementary Tables 1-7), fitting models with different specifications and adjusting variables. We also performed two different triangulation analyses : Cox multivariate regression and propensity score matching (PSM) (Extended Data Table 4). All sensitivity tests confirmed the association estimates, and the triangulation analyses showed a high degree of confidence in the causal inference.
Discussion
In this study, we systematically analyzed the BFP effect among individuals living in situations of social marginalization, evaluating the associations between participation in a CCT and the burden of TB according to their ethnoracial and socioeconomic conditions. We observed strong effects of the BFP in decreasing both TB incidence and mortality rates. Notably, the effectiveness of the BFP showed a marked gradient based on race, ethnicity and socioeconomic conditions, revealing significantly stronger effects among individuals with Indigenous or Black or Pardo ethnicity and individuals living in extreme poverty.
Our findings reveal a gradient of BFP effectiveness based on the baseline wealth level of its beneficiaries: the BFP shows a significant effect on TB incidence and mortality in individuals living in extreme poverty, while demonstrating a lower effect on TB incidence in the less poor, with no discernible effects on TB mortality. The strongest effect of the BFP in the individuals living in extreme poverty can be explained by two factors. First, extreme poverty has consistently been shown to be a significant risk factor for TB, with TB risk levels correlating directly with poverty levels . Therefore, lifting someone out of extreme poverty can be associated with a substantial reduction in their TB risk and burden. In addition, BFP benefits increase with poverty levels, providing a more significant improvement in socioeconomic position for individuals living in extreme poverty compared with those living in poverty, resulting in a more pronounced reduction in TB risk and burden for the former group.
Regarding the mechanisms by which CCT can affect TB, it has to be considered that the BFP, through the direct transfer of money to the families living in extreme poverty and in situations of social marginalization in Brazil, promotes greater access to food, both in quantity and quality, reducing food insecurity and malnutrition, an important TB risk factor, besides improving immune host defenses . Moreover, housing conditions could improve, reducing crowding and poor ventilation, which are also recognized risk factors for . Households could also transition from cooking with burning fuels such as wood, charcoal, coal and kerosene to cleaner fuels. This change can help reduce indoor air pollution, which has been recognized as a factor contributing to increased TB incidence. Smoking habits and alcoholism, which are strongly associated with poverty, could also decrease among BFP beneficiaries, thereby reducing the risk of contracting TB. The prevalence of diabetes, HIV and AIDS, which is higher in the individuals living in social vulnerability, could also be reduced by poverty-reduction interventions . Consequently, this reduction can be associated with a decrease in the incidence and mortality from TB. Moreover, individuals affected by TB who are living in extreme poverty are more likely to avoid seeking diagnosis at health centers or to interrupt their treatment owing to direct costs, such as transportation expenses, and opportunity costs, such as the difficulty of missing a day of work due to their precarious employment and subsistence conditions. These costs could represent a barrier even if prevention, diagnosis and treatment are available free in the Unified Health System
(Sistema Único de Saúde) . In addition to providing monetary transfers, the conditions that qualify for the BFP could also contribute to reducing TB. These conditions are linked to requirements such as school attendance, education and access to health services for pregnant women and children under 5 years old, which could facilitate the recognition and early diagnosis of . In summary, the BFP promotes a greater access to income, food and healthcare. This can be associated with a reduction on TB incidence, facilitate TB early diagnosis and treatment adherence, increase the TB cure rate and reduce complications and death from the disease .
Moreover, we found that the BFP has a strong reduction effect on TB incidence and mortality in Indigenous populations in Brazil, who have a significantly higher risk of TB infection and mortality . While this could be explained by the same mechanisms listed above, particularly in the context of Indigenous populations, the receipt of the BFP could alleviate extreme poverty and socioeconomic vulnerability. This could reduce food insecurity and malnutrition, which are particularly high among Indigenous populations, and lessen the significant geographic barriers that hinder access to even basic healthcare services .
It is worth elucidating the greater effect of the BFP on TB incidence among people of Black and Pardo race and ethnicity as more than 60% of new diagnoses of pulmonary TB in Brazil occurred among people who self-identified as Black and Pardo . This could potentially be explained by the identical mechanisms detailed earlier. Particularly among individuals of Black and Pardo ethnicity in Brazil, the BFP could act on historical and structural social inequities , increasing income and improving education through its conditionalities, providing access to health services and, in this way, reducing the TB burden. The mechanisms described above can also explain the greater effect of the BFP in the north and northeast regions, which are the poorest and less developed areas of the country, with the worst infrastructures and healthcare resources .
The BFP has also a stronger reduction effect on mortality from TB in women. This can be explained by the fact that a woman is often primarily responsible for the family in registering and receiving the BFP. Furthermore, pregnant and breastfeeding women follow the conditions for receiving the BFP (pre- and postnatal care, vaccination, and health and nutrition surveillance) . In this way, women who benefit from the BFP have greater access to health services, which could be associated with a greater reduction in TB mortality in this group, when compared with men.
We also observed that the protective effects of the BFP and lower incidence and mortality are greater in municipalities that do not have prisons. Prisons usually act as ‘institutional amplifiers’ or ‘reservoirs’ of TB , affecting the TB incidence not only in prison but also in non-prison populations . The lower effect of BFP in these municipalities could be attributed to the program not reaching these populations, or not affecting their infection dynamics, leading to a higher and more resilient level of TB incidence in the community despite the coverage of the BFP .
TB prevention and care for economically vulnerable populations became an even greater challenge during and after the COVID-19 (coronavirus disease) pandemic . Each of these populations living in economic vulnerable conditions has specificities and complexities when it comes to implementing TB prevention, diagnosis and treatment interventions. Furthermore, inequalities linked to local contexts, health facilities, and social, behavioral and cultural factors can superimpose on the organization of health services, influencing the care provided to these populational groups . In this sense, it becomes urgent to intensify the actions of prevention and comprehensive care aimed at people in situations of social vulnerability, as well as intersectoral articulations and the inclusion of TB in the agendas of Social Assistance and Human Rights, among others. For this purpose, an Inter-Ministerial Committee for the Elimination of Tuberculosis and Other Socially Determined Diseases was created in 2023 in Brazil .
Our study has certain limitations that should be acknowledged. The first limitation is that, despite our efforts to control for all relevant confounding variables and use propensity-score-based models with IPTW, these approaches may not fully account for unobservable confounding variables and for potential selection biases. To address this concern, we have developed a multifaceted approach. First, we used a wide range of adjusting variables related to demographic, socioeconomic, healthcare and environmental determinants at the individual, household and municipal level, in both the logistic regression, for the construction of the propensity score, and in the Poisson regression for the estimation of BFP effects. This approach has been successfully used in previous studies on the impact of BFP and other public interventions on several health outcomes . Second, we incorporated as adjusting variable-in the logistic and Poisson models-the average municipal rate of the TB indicator over the study period for each outcome under study (incidence, mortality and case-fatality rate). These rates were estimated among individuals from the same municipalities in the cohort. This allowed us to adjust for baseline endemic levels of the specific TB outcome under study in the municipalities and, consequently, for potentially associated unobservable variablescontrolling for selection biases correlating BFP implementation levels with endemic TB levels in the community. Third, extensive sensitivity analyses were conducted (Supplementary Tables 1-7 and Methods), showing that the inclusion of additional independent variables or the substitution of existing ones, besides many other changes in the models’ specifications, did not significantly affect the BFP effect estimates. Fourth, to increase our confidence in the causal inference, and eliminate the possibility of significant selection biases, we performed two different triangulation analyses: survival analysis with Cox regressions and PSM (Extended Data Table 4), showing that even with different methodological approaches, BFP effect estimates were still strong and statistically significant.
Another limitation is related to the external validity of our study: the 100 Million Brazilian Cohort-and our derived study cohortconsist of individuals obtained from the linkage between the Unified Registry for Social Programs (Cadastro Único (CADU)) and health data. Individuals registered in the CADU represent the poorest half of the Brazilian population. As a consequence, our cohort includes only individuals with extremely low-income or low-income who need to be registered in the CADU to access governmental assistance programs. This limitation affects the external validity of the cohort at the national level, as high-income individuals are not represented.
Moreover, although the Notifiable Diseases Information System (Sistema de Informação de Agravos de Notificação (SINAN)) has high sensitivity in Brazil, there may be underreporting of TB notifications . However, our study design and analytic strategy limit the possibility that underreporting could bias our results. Additionally, results from municipalities selected for the high quality of vital information and low under-notifications confirm our findings (Supplementary Table 6).
A third limitation is that individuals with missing information in any of the adjusting variables were excluded. Although this exclusion may enhance the internal validity of the study, as records with missing values are often considered of lower quality, it also partially limits the generalizability of the results. However, analyses that included individuals with missing values yielded similar BFP effect estimates (Supplementary Table 7).
In this study, it was not possible to perform a cost-effectiveness analysis owing to its additional complexity and to the need for data not available in our datasets.
Our study presents strengths that contribute to its overall value. Firstly, we leveraged a large longitudinal dataset, which, when combined with effect evaluation methods, allowed us to assess the effects of interventions on an unprecedented scale. This unique approach enabled us to include a significant number of individuals
and subpopulations that are often overlooked or underrepresented in traditional epidemiological studies and randomized controlled trials. This comprehensive inclusion is crucial for policy evaluations, as it highlights the potential differential impacts of public interventions based on the characteristics and baseline conditions of the BFP beneficiaries. In addition, our study’s strength lies in the extensive range of sensitivity analyses conducted. These analyses provided further validation and reinforcement of the study’s findings, ensuring their robustness and reliability. Furthermore, using various triangulation analyses instilled a high level of confidence in the causal inference, further bolstering the credibility of our findings.
We conclude that CCT programs can greatly reduce the incidence of and mortality from tuberculosis, particularly among individuals living in extreme poverty and self-declared as Indigenous and Black or Pardo ethnicity, who are usually at higher risk for TB and its devastating impacts. Therefore, the expansion of CCT programs in lowand middle-income countries can significantly strengthen the global response to TB, reducing social inequalities in the TB burden and contributing to the achievement of the End TB Strategy and the TB-related Sustainable Development Goals.
Online content
Any methods, additional references, Nature Portfolio reporting summaries, source data, extended data, supplementary information, acknowledgements, peer review information; details of author contributions and competing interests; and statements of data and code availability are available at https://doi.org/10.1038/s41591-024-03381-0.
World Health Organization (WHO). Global Tuberculosis Report 2022; Geneva: World Health organization; 2022 https://www. who.int/teams/global-tuberculosis-programme/tb-reports/ global-tuberculosis-report-2022
Torrens, A. W. et al. Effectiveness of a conditional cash transfer programme on TB cure rate: a retrospective cohort study in Brazil. Trans. R. Soc. Trop. Med. Hyg. 110, 199-206 (2016).
Carter, D. J. et al. The impact of social protection and poverty elimination on global tuberculosis incidence: a statistical modelling analysis of Sustainable Development Goal 1. Lancet Glob. Health 6, e514-e522 (2018).
Boccia, D. et al. Cash transfer and microfinance interventions for tuberculosis control: review of the impact evidence and policy implications. Int. J. Tuberc. Lung Dis. 15, S37-S49 (2011).
Patel, B. H. et al. Cash transfer scheme for people with tuberculosis treated by the National TB Programme in Western India: a mixed methods study. BMJ Open 9, e033158 (2019).
Wingfield, T. et al. A randomized controlled study of socioeconomic support to enhance tuberculosis prevention and treatment, Peru. Bull. World Health Organ. 95, 270-280 (2017).
Sripad, A., Castedo, J., Danford, N., Zaha, R. & Freile, C. Effects of Ecuador’s national monetary incentive program on adherence to treatment for drug-resistant tuberculosis. Int. J. Tuberc. Lung Dis. 18, 44-48 (2014).
Fuady, A., Houweling, T. A. J., Mansyur, M., Burhan, E. & Richardus, J. H. Effect of financial support on reducing the incidence of catastrophic costs among tuberculosis-affected households in Indonesia: eight simulated scenarios. Infect. Dis. Poverty 8, 10 (2019).
Rudgard, W. E. et al. Comparison of two cash transfer strategies to prevent catastrophic costs for poor tuberculosis-affected households in low- and middle-income countries: an economic modelling study. PLoS Med. 14, e1002418 (2017).
Neves, J. A. et al. The Brazilian cash transfer program (Bolsa Família): a tool for reducing inequalities and achieving social rights in Brazil. Glob. Public Health 17, 26-42 (2022).
Rasella, D., Aquino, R., Santos, C. A. T., Paes-Sousa, R. & Barreto, M. L. Effect of a conditional cash transfer programme on childhood mortality: a nationwide analysis of Brazilian municipalities. Lancet 382, 57-64 (2013).
Lindert, K., Linder, A., Hobbs, J., de la Brière, B. The Nuts and Bolts of Brazil’s Bolsa Família Program: Implementing Conditional Cash Transfers in a Decentralized Context (The World Bank, 2007)
Pescarini, J. M. et al. Impact of Brazil’s Bolsa Família Programme on cardiovascular and all-cause mortality: a natural experiment study using the 100 Million Brazilian Cohort. Int. J. Epidemiol. https://doi.org/10.1093/ije/dyac188 (2022).
Machado, D. B. et al. Relationship between the Bolsa Família national cash transfer programme and suicide incidence in Brazil: a quasi-experimental study. PLoS Med. 19, e1004000 (2022).
Pescarini, J. M. et al. Conditional cash transfer program and leprosy incidence: analysis of 12.9 million families from the 100 Million Brazilian Cohort. Am. J. Epidemiol. 189, 1547-1558 (2020).
Oliosi, J. G. N. et al. Effect of the Bolsa Familia Programme on the outcome of tuberculosis treatment: a prospective cohort study. Lancet Glob. Health 7, e219-e226 (2019).
Rebouças, P. et al. Ethnoracial inequalities and child mortality in Brazil: a nationwide longitudinal study of 19 million newborn babies. Lancet Glob. Health 10, e1453-e1462 (2022).
Barbosa, G. C. G. et al. CIDACS-RL: a novel indexing search and scoring-based record linkage system for huge datasets with high accuracy and scalability. BMC Med. Inform. Decis. Mak. 20, 289 (2020).
Lawlor, D. A., Tilling, K. & Davey Smith, G. Triangulation in aetiological epidemiology. Int. J. Epidemiol. 45, 1866-1886 (2016).
Hargreaves, J. R. et al. The social determinants of tuberculosis: from evidence to action. Am. J. Public Health 101, 654-662 (2011).
Hill-Briggs, F. et al. Social determinants of health and diabetes: a scientific review. Diabetes Care 44, 258-279 (2021).
Silva, A. F. et al. Income determines the impact of cash transfers on HIV/AIDS: cohort study of 22.7 million Brazilians. Nat. Commun. 15, 1307 (2024).
de Sampaio Morais, G. A. et al. Effect of a conditional cash transfer programme on AIDS incidence, hospitalisations, and mortality in Brazil: a longitudinal ecological study. Lancet HIV 9, e690-e699 (2022).
Almeida, C. P. B., de Trajman, A., Mitnick, C. D., Kritski, A. L. & Santos-Filho, E. T. D. Beyond goodwill and promises-urgent needs and opportunities to accelerate the fight against tuberculosis in Brazil. Lancet Reg. Health Am. 30, 100663 (2024).
Carter, D. J. et al. The impact of a cash transfer programme on tuberculosis treatment success rate: a quasi-experimental study in Brazil. BMJ Glob. Health 4, e001029 (2019).
Durovni, B. et al. The impact of the Brazilian Family Health Strategy and the conditional cash transfer on tuberculosis treatment outcomes in Rio de Janeiro: an individual-level analysis of secondary data. J. Public Health 40, e359-e366 (2018).
Souza, R. A. D. et al. Family health and conditional cash transfer in Brazil and its effect on tuberculosis mortality. Int. J. Tuberc. Lung Dis. 22, 1300-1306 (2018).
Malacarne, J. et al. Factors associated with TB in an indigenous population in Brazil: the effect of a cash transfer program. Rev. Inst. Med. Trop. São Paulo 60, e63 (2018).
Nogueira, L. M. V., Teixeira, E., Basta, P. C. & da Motta, M. C. S. Therapeutic itineraries and explanations for tuberculosis: an indigenous perspective. Rev. Saúde. Publica 49, 96 (2016).
Lua, I. et al. The effects of social determinants of health on acquired immune deficiency syndrome in a low-income population of Brazil: a retrospective cohort study of 28.3 million individuals. Lancet Reg. Health Am. 24, 100554 (2023).
Ribeiro, L.L., Gomes, J.W.F. Corrupção e pobreza nos municípios brasileiros. Pesqui. Planej. Econôm. 52, 67-86 (2022). https://doi.org/10.38116/ppe52n1art3
Martinez, L. et al. Global, regional, and national estimates of tuberculosis incidence and case detection among incarcerated individuals from 2000 to 2019: a systematic analysis. Lancet Public Health 8, e511-e519 (2023).
Pelissari, D. M. & Diaz-Quijano, F. A. Impact of incarceration on tuberculosis incidence and its interaction with income distribution inequality in Brazil. Trans. R. Soc. Trop. Med. Hyg. 114, 23-30 (2020).
Litvinjenko, S., Magwood, O., Wu, S. & Wei, X. Burden of tuberculosis among vulnerable populations worldwide: an overview of systematic reviews. Lancet Infect. Dis. 23, 1395-1407 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
Gabriela S. Jesus , Priscila F.P.S. Gesta , Andrea F. Silva , Daniella M. Cavalcanti , Iracema Lua , Maria Yury Ichihara , Mauricio L. Barreto , Delia Boccia , Mauro N. Sanchez & Davide Rasella
Faculty of Medicine, Federal University of Bahia (UFBA), Salvador, Brazil. Institute of Collective Health, Federal University of Bahia (ISC/UFBA), Salvador, Brazil. The Center for Data and Knowledge Integration for Health (CIDACS), Oswaldo Cruz Foundation (FIOCRUZ), Salvador, Brazil. Department of Health, State University of Feira de Santana (UEFS), Feira de Santana, Brazil. Faculty of Population and Health Policy, London School of Hygiene and Tropical Medicine (LSHTM), London, UK. Faculty of Health Sciences, Federal University of Brasília, Brasília, Brazil. ISGlobal, Barcelona, Spain. Institución Catalana de Investigación y Estudios Avanzados (ICREA), Pg. Lluis Companys 23, Barcelona, Spain. These authors contributed equally: Gabriela S. Jesus, Priscila F.P.S. Gestal. e-mail: davide.rasella@isglobal.org
is used to transform the linear combination of predictors into the probability of the event occurring.
where is the probability of the binary outcome being 1 given the predictor variables ; is the base of the natural logarithm; and are the coefficients corresponding to the predictor variables . We estimated the probability of each individual to receive the BFP (propensity score (PS)), in two ways. For the first equation, we calculated the marginal probability of treatment and then we estimated the multivariable , adjusted for all relevant covariates.
We used PS and PS as weights to calculate the stabilized IPTW using the formulas:
where is the weight for the beneficiaries and is the weight for the non-beneficiaries. To correct for possible extreme weights, we set thresholds, with weights exceeding the set value converted to that threshold value . In this study, the weights were truncated based on the distribution of their values for the 1st and 99th percentiles, which represented these thresholds, as in previous similar studies . IPTW uses the propensity score to balance baseline characteristics in the exposed and unexposed groups by weighting each individual by the inverse probability of receiving treatment .
The Poisson equation with IPTW is a framework used to analyze count data or event occurrences, while accounting for the potential bias introduced by non-random treatment assignment in observational studies. In this context, the Poisson equation models the relationship between the event outcomes and covariates while incorporating IPTW to adjust for treatment selection bias.
where is the natural logarithm of the rate for individual , are the covariates for individual are the coefficients associated with the covariates; and logIPTW represents the logarithm of the inverse probability treatment weight for individual . Finally, multivariable Poisson regressions, adjusted by stabilized, truncated IPTW, were estimated with the same socioeconomic and demographic variables adopted in the logistic model for all TB outcomes.
Moreover, to understand BFP association heterogeneity, we fitted these IPTW Poisson regression models stratified by age, sex, race and ethnicity, education, wealth terciles (per capita expenditure), existence of prisons in the municipality and Brazilian regions.
To confirm the robustness of the findings, we applied several sensitivity analyses: (1) we fitted the same regressions without and only with the TB endemicity level variable (Supplementary Tables 1 and 2); (2) we fitted models with only individual-level variables and tested the inclusion of different aggregate-level variables (Supplementary Table 3); (3) we estimated and compared all models without IPTW (Extended Data Table 5); (4) to evaluate the adoption of per capita expenses as a proxy for wealth, we carried out the same analyses with other proxies, such as per capita income (Supplementary Table 4); (5) we adjusted the same models with different specifications (including different sets of individual-level covariates, inclusion or exclusion of robust standard errors (Supplementary Table 5), only in municipalities with adequate vital information (Supplementary Table 6)); and (6) we redid the estimates including individuals with missing category (Supplementary Table 7). Finally, to have a greater degree of confidence
in the causal inference of our impact evaluation, we performed two different triangulation analyses , verifying the existence of BFP associations also using alternative methods: survival analysis with Cox multivariate regression and PSM (Extended Data Table 4).
All statistical analyses were performed in Stata Version MP 15.1.
Inclusion and ethics statement
This project was designed through a longstanding partnership among the Institute of Collective Health (Instituto de Saúde Coletiva (ISC)) of the Federal University of Bahia (Universidade Federal da Bahia (UFBA)) and The Center for Data and Knowledge Integration for Health (CIDACS) of the Oswaldo Cruz Foundation (Fundação Oswaldo Cruz (FIOCRUZ)), both based in Salvador, Brazil. The 100 Million Brazilian Cohort was created by CIDACS in collaboration with ISC researchers, and the subset of data used for this study was selected and analyzed by a collaborating group of ISC and CIDACS researchers. All team members collaborated on data ownership, intellectual property and authorship of publications related to the work. Roles and responsibilities were agreed upon among collaborators ahead of the research. Previous work and articles from the analyses of these datasets, most of them developed by co-authors of this article, were used to guide the design of this study, as well as connect our findings to similar research, and have been considered in the citations for this paper.
Ethics approval
This study was approved by the Research Ethics Committee of the Institute of Collective Health of the Federal University of Bahia (ISC, UFBA), under number 41691315.0.0000.5030 (assessment number 3.783.920). In this study, participant consent was waived owing to the use of administrative data.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data underlying this article will be shared on request to ISC of UFBA, and CIDACS of FIOCRUZ, and after ethical approval. All data supporting the findings presented were obtained from The Center for Data and Knowledge Integration for Health (CIDACS). Importantly, restrictions apply to access to the data, which contain sensitive information, were licensed for exclusive use in the current study and, due to privacy regulations from the Brazilian Ethics Committee, are not openly available. Upon request and with express permission from CIDACS (email: cidacs. curadoria@fiocruz.br) and approval from an ethical committee, controlled access to the data is possible. The dataset is registered under the following DOI handle: https://hdl.handle.net/20.500.12196/CIDACS/65, which provides metadata and a register of all versions of the database.
Code availability
The algorithms and code used in this Article will be shared on request to ISC of UFBA, and CIDACS of FIOCRUZ, and after ethical approval. Due to the confidentiality of the data and the presence of lines of code that deal with sensitive variables, their characteristics and their values, access to the codes will be granted upon request and with express permission from CIDACS (email:cidacs.curadoria@fiocruz.br) and approval from an ethical committee. If approved, the code will be available within 1 month from the initial application.
References
Austin, P. C. & Stuart, E. A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 34, 3661-3679 (2015).
Chesnaye, N. C. et al. An introduction to inverse probability of treatment weighting in observational research. Clin. Kidney J. 15, 14-20 (2022).
Suárez, E., Pérez, C.M., Rivera, R., Martínez, M.N. in Applications of Regression Models in Epidemiology (Wiley & Sons, 2017) Ch. 10 (Wiley & Sons, 2017) https://doi.org/10.1002/9781119212515.ch10
Pescarini, J. M. et al. Effect of a conditional cash transfer programme on leprosy treatment adherence and cure in patients from the nationwide 100 Million Brazilian Cohort: a quasi-experimental study. Lancet Infect. Dis. 20, 618-627 (2020).
Jesus, G. S. et al. The effect of primary health care on tuberculosis in a nationwide cohort of 7.3 million Brazilian people: a quasi-experimental study. Lancet Glob. Health. Mar. 10, e390-e397 (2022).
Khandker, S. R., Koolwal, G. B. & Samad, H. A. Handbook on Impact Evaluation: Quantitative Methods and Practices (The World Bank, 2010); https://openknowledge.worldbank.org/ handle/10986/2693
Lee, B. K., Lessler, J. & Stuart, E. A. Weight trimming and propensity score weighting. PloS ONE 6, e18174 (2011).
Acknowledgements
This study was supported by the Wellcome Trust, grant reference number: 109949/ Z/15/Z; by the National Institute of Allergy and Infectious Diseases (National Institutes of Health), grant reference number: 1RO1Al152938; and by the Brazilian Ministry of Health, grant reference number: VPGDI-003-FIO-19. We acknowledge support from grant CEX2023-0001290-S funded by Ministerio de Ciencia, Innovación y Universidades/Agencia Estatal de Investigación (MCIN/AEI)/10.13039/501100011033 and support from Generalitat de Catalunya through the Centres de Recerca de Catalunya Program. D.R. acknowledges funding from CEX2018-000806-S funded by MCIN/AEI/10.13039/501100011033. We thank researchers from the Institute of Collective Health for the invaluable discussions and suggestions during the development of this study and the CIDACS members responsible for linkage of the 100 Million Brazilian Cohort.
Author contributions
G.S.J.: formal analysis-accessed and verified the data, investigation, methodology, and writing—original draft, review and editing. P.F.P.S.G.: formal analysis-accessed and verified the data, investigation, methodology, and writing—original draft, review and editing. D.M.C.: methodology, and writing—original draft, review and editing. A.F.S.: formal analysis-accessed and verified the data, investigation, methodology, and writing—original draft, review and editing. I.L.: formal analysis-accessed and verified the data, methodology, and writing—original draft, review and editing. M.Y.I.: data curation, funding acquisition, resources and writing—review and editing. M.L.B.: data curation, funding acquisition, resources, and writingreview and editing. M.N.S.: writing—original draft, review and editing. D.B.: writing—review and editing. D.R.: conceptualization, project administration, funding acquisition, investigation, methodology, supervision-accessed and verified the data, decision to submit the paper, and writing—review and editing.
Correspondence and requests for materials should be addressed to Davide Rasella.
Peer review information Nature Medicine thanks Julio Croda, Pascal Geldsetzer, Weiming Tang and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Ming Yang, in collaboration with the Nature Medicine team.
Extended Data Fig. 1 | Conceptual framework about determinants and possible effects of the conditional cash transfers (CCT) on tuberculosis (TB) outcomes. TB=Tuberculosis. Source: the authors.
Extended Data Table 1 | Number of observations per Tuberculosis (TB) new case, death from TB and TB deaths among TB new cases by Bolsa Familia Program (BFP) beneficiaries (BF) and non-beneficiaries (N-BF)
Bolsa Familia Program (BFP )
Total
N-BF
BF
New TB cases
No
30,584,786
23,821,172
54,405,958
Yes
75,956
83,821
159,777
Total
30,660,742
23,904,993
54,565,735
TB deaths
No
30,659,117
23,904,324
54,563,441
Yes
4,359
3,634
7,993
Total
30,663,476
23,907,958
54,571,434
TB deaths/new TB cases
No
14,496
30,606
45,102
Yes
495
751
1,246
Total
14,991
31,357
46,348
Notes: a New Tuberculosis cases, defined with new cases, relapse cases of TB and re-entry by adapted by Brazilian Ministry of Health criteria; b Deaths from tuberculosis, considering as underlying cause the International Classification of Diseases (ICD-10) codes A15 to A19, J65, 0980 and P370. c Bolsa Familia Program
Extended Data Table 2 | Logistic regression prediction models for individuals benefiting or not from the Bolsa Familia Program (BFP), for Tuberculosis (TB) incidence, mortality, and case-fatality rate, Brazil, 2004-2015. Estimates from the Propensity Score (PS)
Outcomes (aRR – CI 95%)
Adjusted Model
Incidence and Mortality
Case-Fatality Rate
Sex
Male
1 (base)
1 (base)
Female
1.17 (1.17-1.18)
1.73 (1.65-1.81)
Age (years)
0.84 (0.84-0.85)
0.76 (0.75-0.77)
Race or ethnicity
White
1 base
1 (base)
Black and Pardo
1.15 (1.15-1.16)
1.25 (1.19-1.32)
Indigenous
3.09 (3.06-3.12)
3.50 (2.68-4.58)
Education
Illiterate, never attended school
1 (base)
1 (base)
Elementary school
1.07 (1.07-1.08)
1.06 (0.99-1.14)
High school
1.08 (1.08-1.09)
0.93 (0.86-0.99)
More than high school
0.83 (0.83-0.84
0.65 (0.59-0.70)
Household construction material
Bricks/cement
1 (base)
1 (base)
Wood, other vegetal materials
0.94 (0.93-0.94)
0.91 (0.86-0.97)
Number of people in the family
1 (base)
1 (base)
2
3 a 4
1.52(1.51-1.52)
2.03 (1.93-2.14)
>5
2.03 (2.02-2.04)
3.56 (3.33-3.80)
Per salary expenses – % MW
Below median
1 (base)
1 (base)
Above median
0.88 (0.88-0.89)
0.51 (0.48-0.54)
Lighting
Electricity
1 (base)
1 (base)
Non-electric
1.22 (1.21-1.22)
1.53 (1.43-1.64)
Inadequate sanitation
1.02 (1.02-1.03)
1.06 (1.00-1.12)
Garbage disposal
1.08 (1.08-1.09)
1.04 (0.96-1.12)
Water supply
Public network
1 (base)
1 (base)
Other
1.11 (1.11-1.12)
1.17 (1.10-1.25)
TB Incidence Cohort
1.00 (1.00-1.00)
1.00 (1.00-1.00)
AIDS
–
0.93 (0.86-1.01)
Diabetes
–
0.94 (0.86-1.03)
DOT
–
0.99 (0.94-1.04)
TB Classification Primary Health Care
–
0.91 (0.85-0.97)
Coverage no coverage
1 (base) 0.99 (0.99-0.99)
1 (base) 0.99 (0.99-0.99)
Specialized clinics per 1,000 inhabitants
0.27 (0.26-0.27)
0.27 (0.21-0.34)
Doctors per 1,000 inhabitants
1.14 (1.13-1.14)
1.17 (1.11-1.22)
Nurses per 1,000 inhabitants
0.99 (0.98-0.99)
0.84 (0.73-0.97)
Unemployment rate (%)
1.01 (1.01-1.01)
1.01 (1.01-1.02)
Gini index
1.01 (1.01-1.01)
1.01 (1.01-1.02)
Year of entry into the cohort
yes
yes
Obs.:
54,571,434
46,344
Abbreviations: a Adjusted Rate Risks. b Confidence interval. c Race or ethnicity: Black/Pardo selfdeclared. d Household construction Material: No – Coated clay, uncoated clay, wood, and others. e Proportional to the baseline minimum wage (MW) f Lighting: Non-electric – No meter, lamps, candles, and others. of the municipal population with inadequate baseline sanitation. h Water supply: Other well, spring, and others. i Primary Health Care (PHC) percentage coverage.
Extended Data Table 3 | Estimates by adjusted Poisson models of the association between the Bolsa Familia Program (BFP) and Tuberculosis incidence, mortality and case-fatality rates stratified by wealth quartile, Brazil, 2004-2015)
Wealth
Incidence
Mortality
Case-Fatality
aRRg
95% CI
aRR
95% CI
aRR
95% CI
Wealth
Quartile
0.49
(0.49-0.50)
0.60
(0.55-0.61)
0.80
(0.64-1.01)
Obs.
18,476,834
18,479,518
20,752
Quartile
0.48
(0.47-0.49)
0.56
(0.50-0.63)
0.86
(0.60-1.22)
Obs.
10,565,846
10,567,091
10,350
Quartile
0.71
(0.69-0.73)
0.86
(0.76-0.99)
1.20
(0.82-1.75)
Obs.
11,599,362
11,600,410
8,865
Quartile
0.99
(0.96-1.02)
1.01
(0.83-1.23)
0.86
(0.53-1.40)
Obs.
14,145,583
14,146,327
6,460
Notes: a Measured by per capita expenses proportional to the baseline minimum wage (MW). b Quartile 1: . c Quartile 2: > 0.1% a . d Quartile 3: > a . e Quartile . f Calculated by personyears at risk. Adjusted rate risk h Confidence Interval
Extended Data Table 4 | Estimates of the association between the Bolsa Familia Program (BFP) and Tuberculosis (TB) incidence, mortality, and the case-fatality rate using Survival Analysis and Propensity Score Matching models, 2004-2015
Adjusted Model
Survival Analysis
Propensity Score Matching Analysis
Incidence
Mortality
Case-Fatality
Incidence
Mortality
Case-Fatality
aHR (CI 95%)
aHR (CI 95%)
aHR (CI 95%)
( 95%)
( 95%)
( 95%)
BFP
0.54 (0.54-0.55)
0.65 (0.61-0.69)
1.04 (0.89-1.22)
0.43 (0.29-0.55)
0.32 (0.30-0.34)
0.53 (0.18-1.50)
Sex
Male
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
Female
0.58 (0.58-0.59)
0.39 (0.37-0.41)
0.69 (0.60-0.79)
-0.16(-0.17:-0.16)
-0.16 (-0.17:-0.16)
0.69 (0.60-79)
Age
1.18 (1.18-1.19)
1.62 (1.61-1.64)
1.47 (1.41-1.53)
0.16 (-0.17:-0.16)
0.16 (-0.17:-0.16)
1.47(1.41-1.53)
Race or ethnicity
White
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
Pardo/Black
1.42 (1.41-1.45)
1.70 (1.60-1.81)
1.03 (0.86-1.22)
0.14 (0.14-0.15)
0.14 (0.14-0.15)
1.03 (0.87-1.22)
Indigenous
3.70 (3.49-3.91)
4.56 (3.63-5.72)
1.38 (0.81-2.33)
1.13 (1.12-1.14)
1.13 (1.12-1.14)
1.38 (0.81-2.33)
Education
Illiterate, never attended school
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
Elementary school
1.82 (1.79-1.85)
1.04 (0.98-1.10)
0.93(0.78-1.10)
0.07(0.71-0.74)
0.07(0.71-0.74)
0.93 (0.78-1.10)
High school
2.20(2.16-2.24)
0.98 (0.92-1.05)
0.78(0.63-0.95)
0.08 (0.08-0.08)
0.08 (0.08-0.08)
0.78 (0.63-0.95)
More than high school
1.72 (1.68-1.75)
0.60(0.53-0.67)
0.53(0.38-0.75)
-0.18 (-0.18:-0.17)
-0.18 (-0.18:-0.17)
0.53 (0.38-0.75)
Household construction material (brick)
Yes
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
No
1.22 (1.20-1.24)
1.21 (1.13-1.29)
1.14 (0.97-1.34)
-0.06 (-0.06:-0.05)
-0.06 (-0.06:-0.05)
1.14 (0.97-1.34)
Number of people in the family
2
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
3 a 4
0.98 (0.97-0.99)
0.83(0.78-0.88)
0.91 (0.78-1.07)
0.41 (0.41-0.42)
0.41 (0.41-0.42)
0.91 (0.78-1.07)
> 5
1.21 (1.19-1.23)
1.00 (0.93-1.07)
1.05 (0.89-1.25)
0.70 (0.70-0.71)
0.70 (0.70-0.71)
1.05 (0.89-1.25)
Per salary expenses – % MW
below median
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
above median
0.77 (0.76-0.78)
0.70 (0.65-0.74)
0.89 (0.75-1.05)
-0.12 (-0.12:-0.12)
-0.12 (-0.12:-0.12)
0.89 (0.75-1.05)
Lighting
Electricity
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
Non-electric
1.35 (1.33-1.37)
1.55 (1.45-1.67)
1.19* (1.03-1.38)
0.19 (0.19-0.20)
0.22 (0.22-0.23)
1.10 (0.92-1.31)
Inadequate sanitation
1.00 (0.99-1.02)
1.08 (1.02-1.14)
1.00 (0.99-1.01)
0.29 (0.27-0.30)
0.29 (0.27-0.30)
0.98 (0.83-1.15)
Garbage disposal
0.78 (0.77-0.80)
0.76(0.70-0.82)
0.08 (0.07-0.08)
0.08 (0.07-0.08)
1.00 (0.80-1.26)
Public network
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
Other
0.95 (0.93-0.97)
0.99 (0.92-1.06)
0.11(0.11-0.11)
0.11(0.11-0.11)
0.98 (0.82-1.15)
Mun. average
TB incidence rate
1.00 (1.00-1.00)
1.00 (1.00-1.00)
1.00 (0.99-1.00)
0.01 (0.01-0.01)
0.00 (0.00-0.00)
1.00 (0.99-1.00)
Primary
Health Care
Coverage
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
1 (base)
no coverage
1.00 (0.99-1.00)
0.99 (0.99-0.99)
1.00 (0.99-1.00)
-0.00 (-0.00:-0.00)
-0.00 (-0.00:-0.00)
1.00 (0.99-1.00)
inhabitants
Doctors per
inhabitants
Nurses per
1,000
0.93 (0.90-0.96)
0.78 (0.69-0.89)
1.12 (0.76-1.65)
-0.00 (-0.01:-0.00)
-0.00 (-0.01:-0.00)
1.12 (0.76-1.65)
Unemployment rate (%)
1.01 (1.01-1.02)
1.03(1.02-1.03)
1.01 (0.99-1.02)
0.01 (0.01-0.02)
0.01 (0.01-0.02)
1.01 (0.99-1.02)
Gini index
0.99 (0.99-1.00)
1.00 (0.99-1.00)
0.99 (0.98-1.00)
0.01 (0.01-0.01)
0.01 (0.01-0.01)
0.99 (0.98-1.00)
Individual’s year of entry into the cohort
yes
yes
yes
yes
yes
yes
Obs.:
54,571,434
54,571,434
46,344
54,571,434
54,571,434
46,344
Extended Data Table 5 | Estimates by adjusted Poisson models without inverse probability of treatment weighting (IPTW) of the association between the Bolsa Familia Program (BFP) and Tuberculosis incidence, mortality, and the case-fatality rate, 2004-2015
Outcomes ( RR – CI 95%)
Models
Incidence
Mortality
Case-Fatality
Adjusted
Unadjusted
Obs
46,344
Notes Adjusted Rate Risk. Confidence Interval
Extended Data Table 6 | Estimates by adjusted Poisson models of the association between the Bolsa Familia Program (BFP) and Tuberculosis incidence, mortality and case-fatality rate, Brazil, 2004-2015 – Modelling with interaction terms included in the logistic regression for the estimation of the Propensity Score
Outcomes (aRR 95%)
Models
Incidence
Mortality
Case-Fatality
Adjusted
0.59 (0.58-0.60)
0.69 (0.65-0.73)
0.91 (0.78-1.06)
Obs
54,565,729
54,571,428
46,344
Notes: Interaction terms entered into logistic regression to estimate propensity score: sex vs race, sex vs wealth and race vs wealth. Adjusted Rate Risk. Confidence Interval.
Extended Data Table 7 | Estimates by adjusted Poisson models of the association between the Bolsa Familia Program (BFP) and Tuberculosis (TB) incidence, mortality and case-fatality rate, Brazil, 2004-2015 – includes time of exposure to BFP as cohort censoring
Outcomes
Incidence
Mortality
Adjusted
Model
Obs
Notes: Adjusted Rate Risk. Confidence Interval.
Extended Data Table 8 | Estimates by adjusted Poisson models of the association between the Bolsa Familia Program (BFP) and Tuberculosis (TB) incidence, mortality and case-fatality rate in Brazil, 2004-2015 – includes as adjustment variable the existence of prisons per municipality
Outcomes (aRR 95%)
Incidence
Mortality
Case-Fatality
Adjusted Model
0.59 (0.58-0.60)
0.69 (0.65-0.73)
0.91 (0.78-1.06)
Obs
54,565,729
54,571,428
46,344
Notes: Adjusted Rate Risk. Confidence Interval.
Extended Data Table 9 | Estimates by adjusted Poisson models (with robust standard errors) of the association between the Bolsa Familia Program (BFP), and Tuberculosis (TB) incidence, mortality, and case-fatality rate in Brazil including the TB incidence in the municipality of residence and TB incidence standardized by age, 2004-2015
Model adjusted by
TB incidence in the municipality of residence
TB incidence standardized by age
Outcomes
TB incidence
TB mortality
TB case-fatality rate
TB incidence
TB mortality
TB case-fatality rate
aRR ( )
0.58 (0.57-0.59)
0.68 (0.64-0.72)
0.90 (0.77-1.05)
0.58 (0.57-0.59)
0.69 (0.65-0.73)
0.90 (0.77-1.05)
Notes: a Tuberculosis b Adjusted Rate Risk. c Confidence Interval.
natureportfolio
Corresponding author(s):
Davide Rasella
Last updated by author(s): Oct 18, 2024
Reporting Summary
Nature Portfolio wishes to improve the reproducibility of the work that we publish. This form provides structure for consistency and transparency in reporting. For further information on Nature Portfolio policies, see our Editorial Policies and the Editorial Policy Checklist.
Statistics
For all statistical analyses, confirm that the following items are present in the figure legend, table legend, main text, or Methods section.
n/a
□
□
□
Confirmed
The exact sample size for each experimental group/condition, given as a discrete number and unit of measurement
A statement on whether measurements were taken from distinct samples or whether the same sample was measured repeatedly
The statistical test(s) used AND whether they are one- or two-sided
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
□
A description of all covariates tested
□
A description of any assumptions or corrections, such as tests of normality and adjustment for multiple comparisons
□
A full description of the statistical parameters including central tendency (e.g. means) or other basic estimates (e.g. regression coefficient) AND variation (e.g. standard deviation) or associated estimates of uncertainty (e.g. confidence intervals)
□
For null hypothesis testing, the test statistic (e.g. ) with confidence intervals, effect sizes, degrees of freedom and value noted Give values as exact values whenever suitable.
□
For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
□ For hierarchical and complex designs, identification of the appropriate level for tests and full reporting of outcomes
□ Estimates of effect sizes (e.g. Cohen’s , Pearson’s ), indicating how they were calculated
Our web collection on statistics for biologists contains articles on many of the points above.
Software and code
Policy information about availability of computer code
Data collection
The Centre for Data and Knowledge Integration for Health (Centro de Integração de Dados e Conhecimentos para a Saúde – CIDACS)-Record Linkage tool (verson number 1) was used to linkage. https://github.com/gcgbarbosa/cidacs-rl-v1
Data analysis
All statistical analyzes were performed in Stata Version MP 15.1
For manuscripts utilizing custom algorithms or software that are central to the research but not yet described in published literature, software must be made available to editors and reviewers. We strongly encourage code deposition in a community repository (e.g. GitHub). See the Nature Portfolio guidelines for submitting code & software for further information.
Data
Policy information about availability of data
All manuscripts must include a data availability statement. This statement should provide the following information, where applicable:
Accession codes, unique identifiers, or web links for publicly available datasets
A description of any restrictions on data availability
For clinical datasets or third party data, please ensure that the statement adheres to our policy
The data underlying this article will be shared on request to ISC/UFBA and CIDACS/Fiocruz and after ethical approval. All data supporting the findings presented were obtained from The Center for Data and Knowledge Integration for Health ( (Centro de Integração de Dados e Conhecimentos para a Saúde – CIDACS). Importantly, restrictions apply to access to the data, which contains sensitive information, were licensed for exclusive use in the current study and, due to privacy
regulations from the Brazilian Ethics Committee are not openly available. Upon request and with express permission from CIDACS (mail to cidacs.curadoria@fiocruz.br) and approval from an ethical committee, controlled access to the data is possible. The dataset is registered under the following DOI handle: https://hdl.handle.net/20.500.12196/CIDACS/65, which provides metadata and a register of all versions of the database.
Research involving human participants, their data, or biological material
Policy information about studies with human participants or human data. See also policy information about sex, gender (identity/presentation), and sexual orientation and race, ethnicity and racism.
Reporting on sex and gender
We only use the term sex, as in the following statements Data sources, outcomes, and intervention section: “The linkage codes and algorithms were built based on five identifiers: date of birth, municipality of residence, sex, name, and mother`s name of the individual in each database”. Statistical Analyses section: “At the individual level, the demographic and socioeconomic covariables were age, sex, selfidentified race/ethnicity (white, Indigenous, Black and pardo – these last categories were analysed together), education, per capita expenditure (as a proxy for the per capita wealth and calculated as a percentage of the yearly minimum wage, categorised by tertiles), and year of entry into the cohort” and “Moreover, in order to understand BFP effects heterogeneity, we fitted these IPTW Poisson regression models stratified by age, sex, race/ethnicity, education, and wealth- tertiles (per capita expenditure).”
Reporting on race, ethnicity, or other socially relevant groupings
We specify in the main text that the variables were obtained from The 100 Million Brazilians Cohort and that race/ethnicity is self-identified. Furthermore, we explain how we use the family wealth variable (per capita expenditures).
Study design, population, and ethical issues: “The study population was achieved by selecting a subgroup of individuals of the 100 Million Brazilians Cohort, a consolidated cohort created through the validated linkage between the Federal Government Unified Registry for Social Programs (Cadastro Único) – that gathers data from the poorest half of the Brazilian population, identifying and characterising low-income families for social programs eligibility, and including information on exposure to the BFP – and health-related datasets from the Brazilian Ministry of Health’s.”
Statistical Analyses section: “At the individual level, the demographic and socioeconomic covariables were age, sex, selfidentified race/ethnicity (white, Indigenous, Black and pardo – these last categories were analysed together), education, per capita expenditure (as a proxy for the per capita wealth and calculated as a percentage of the yearly minimum wage, categorised by tertiles), and year of entry into the cohort” and “Moreover, in order to understand BFP effects heterogeneity, we fitted these IPTW Poisson regression models stratified by age, sex, race/ethnicity, education, and wealth- tertiles (per capita expenditure).”
BFP beneficiaries and non-beneficiaries showed similar demographic and socioeconomic characteristics. In comparison with non-beneficiaries, BFP beneficiaries are younger (mean age 24.2 vs 25.3 years), had a slightly higher percentage of people self-identified as Black or Pardo race/ethnicity ( vs ), people with no education ( vs ), households with 3 or more individuals ( vs ), lesser wealth ( vs ), without adequate sanitation ( vs ), and without a public network for water supply (70.6% vs 76.1%).
In the Results section: “After excluding individuals of the 100 Million Brazilians Cohort who were outside the study period 2004-2015, and who had missing information on demographic or socioeconomic variables, 54, 571,434 individuals were selected, of which were BFP beneficiaries ( ), and non-BFP beneficiaries ( ), with a total of 159,777 new TB diagnoses and 7,993 TB deaths”
This study was approved by the Research Ethics Committee of the Institute of Collective Health of the Federal University of Bahia (ISC/UFBA), under number 41691315.0.0000.5030 (Assessment :3.783.920)
Ethics oversight
Population characteristics
Recruitment
Note that full information on the approval of the study protocol must also be provided in the manuscript.
hature portfolio | reporting summary April2023
Field-specific reporting
Please select the one below that is the best fit for your research. If you are not sure, read the appropriate sections before making your selection.
□ Behavioural & social sciences
□ Ecological, evolutionary & environmental sciences
All studies must disclose on these points even when the disclosure is negative.
Sample size
section*{Data exclusions}
The entire eligible population was considered, i.e., individuals registered in the Cadastro Único (CADU) between 2004 and 2015, with or without a diagnosis of tuberculosis, whether or not they were beneficiaries of the BFP. From this initial selection, which is a subgroup of the Cohort of 100 Million Brazilians, individuals with less than 1 day of follow-up, diagnosed with TB or who received the BFP before 2004, Individuals with inconsistent dates, duplicates, Individuals who received BFP <30 days and Individuals with missing values for socioeconomic variables were excluded (as described in Figure 1 – Flowchart). After these exclusions, the entire final population was considered for the analysis, i.e., individuals, being Non-BFP beneficiaries ( ) and BFP beneficiaries ( ).
In the Results section: “After excluding individuals of the 100 Million Brazilians Cohort who were outside the study period 2004-2015, and who had missing information on demographic or socioeconomic variables, individuals were selected, of which were BFP beneficiaries ( ), and non-BFP beneficiaries ( ), with a total of 159,777 new TB diagnoses and 7,993 TB deaths” (as described in Figure 1 – Flowchart).
Replication
Randomization
Blinding
We performed several sensitivity and triangulation analyses. All results confirmed the results obtained in the main analysis. Sensitivity and triangulation analyses section: “We developed a wide range of several sensitivity analyses (for details see the Methods section and Supplementary Tables S1-S7) fitting models with differed specifications and adjusting variables. We also performed two different triangulation analyses: Cox multivariate regression and propensity score matching (PSM) (Extended Data Table 4). All sensitivity tests confirmed the association estimates, and the triangulation analyses showed a high degree of confidence in the effect evaluation causal inference.”
The allocation was not random. In the Data sources, outcomes, and intervention section:
“The beneficiary group was defined as eligible individuals who received BFP benefits, and their exposure started with receipt of the benefit, until the end of their follow-up. The non-beneficiary group was defined as individuals who had never benefited from BFP throughout their follow-up period. In case of non-receipt of the benefits, eligible individuals were classified in the non-beneficiary group”
The blinding is not relevant to this study because it is not an experimental study. In this study the main exposure was the receipt of BFP and the researcher has this information through an administrative database without the names of the individuals.
Reporting for specific materials, systems and methods
We require information from authors about some types of materials, experimental systems and methods used in many studies. Here, indicate whether each material, system or method listed is relevant to your study. If you are not sure if a list item applies to your research, read the appropriate section before selecting a response.
Age categorized every 10 years. Race or ethnicity: Black or Pardo, self-declared. Proportional to the baseline MW. Lighting: non-electric-no meter, lamps, candles and others. Percentage of the municipal population with inadequate baseline sanitation. Percentage of the municipal population with baseline garbage collection. Water supply: other-well, spring and others. Percentage of coverage.
Notes: a Adjusted Hazard Ratio b Confidence interval. c Adjusted Odds Ratio d Bolsa Família Program e Age categorized every 10 years. f Race or ethnicity: self-declared. g Household construction material: No – Coated clay, uncoated clay, wood, and others. h Proportional to the baseline minimum wage (MW). i Lighting: Non-electric – No meter, lamps, candles, and others. of the municipal population with inadequate baseline sanitation. k Water supply: Other – well, spring, and others. I Tuberculosis m Primary Health Care (PHC) percentage coverage.