DOI: https://doi.org/10.1186/s12889-024-18476-z
PMID: https://pubmed.ncbi.nlm.nih.gov/38566105
تاريخ النشر: 2024-04-02
أثر وساطة متسلسل للدعم الأسري المدرك على الرفاه النفسي
الملخص
للعائلة تأثير كبير على الصحة النفسية للفرد. استنادًا إلى نظرية الدعم الاجتماعي، ونظرية النظام الأسري، ونموذج الصحة النفسية القصير (MHC-SF)، قامت هذه الدراسة ببناء نموذج لمسار الدعم الأسري المدرك على الرفاه النفسي، وأوضحت النتائج تجريبيًا أن الدعم الأسري المدرك له علاقة إيجابية كبيرة مع الرفاه العاطفي، والرفاه الاجتماعي، والرفاه النفسي (
المقدمة
الرفاه الذاتي هو موضوع رئيسي في الدراسة الحالية حول الرفاه. كانت مقالة إد دينر في نشرة علم النفس [8] مساهمة كبيرة في المجال الناشئ للرفاه الذاتي (SWB)، الذي ركز على التقييمات الذاتية للأفراد لحياتهم الخاصة [9]. بالإضافة إلى ذلك، اقترح دينر أن الرفاه الذاتي يتكون من نوعين من المكونات، حكم معرفي على مستوى الرضا عن الحياة بشكل عام وتجارب عاطفية، تعكس ردود الفعل العاطفية الإيجابية
والسلبية للأشخاص تجاه حياتهم [9]. لذلك، شرحت الدراسات الواسعة الرفاه الذاتي من حيث الرضا عن الحياة (LS)، والعاطفة الإيجابية (PA) والعاطفة السلبية (NA). تهدف هذه الدراسة أيضًا إلى التحقيق في الآليات التفاعلية الأساسية في الرفاه. نتيجة لذلك، تم اختيار فرضيات البحث المرتبطة بـ Keyes حول الرفاه لهذه الدراسة. وفقًا للبحث المتعلق بـ Keyes، فإن الرفاه له أولويات مختلفة تحت تيارات مختلفة، وهي التيار الهيدوني والتيار اليوذائمي. يعرف التيار الهيدوني الصحة النفسية على أنها “موقف الناس تجاه الحياة، والحفاظ على المشاعر الإيجابية والصحية في مواجهة تحديات الحياة، والتوازن بين المشاعر السلبية والإيجابية” [10]. على النقيض من ذلك، تعكس تصورات الرفاه النفسي والاجتماعي المنظور اليوذائمي، الذي يركز على كيفية رؤية الناس لوظائفهم في الحياة ويعتبر أن الصحة النفسية هي الإمكانية في الحياة البشرية [11] وإحساس الناس بالانتماء الاجتماعي أو الوظيفة الاجتماعية [12].
النظريات والفرضيات
الأساس النظري
أن الدعم الاجتماعي يمكن أن يأتي من علاقات بين الأفراد وشبكات اجتماعية مختلفة، مثل الأسرة، والأصدقاء، والزملاء، والجيران، ومنظمات المجتمع [15]. بالإضافة إلى ذلك، فإن حجم وهيكل وجودة شبكة الدعم الاجتماعي للفرد سيكون لها أيضًا تأثير على رفاهيته وقدرته على التكيف [16]. يمكن أن تساعد التدخلات والأبحاث المستندة إلى نظرية الدعم الاجتماعي الناس على فهم وتعزيز التأثير الإيجابي للدعم الاجتماعي على صحة الفرد وسعادته، ثم تحسين جودة حياة الفرد ورفاهه.
الدعم الأسري المدرك والرفاه النفسي
الصعوبات [7,22]. من خلال تعزيز التواصل المفتوح، وممارسة الاستماع النشط، وإظهار التعاطف، يمكن للعائلات إنشاء بيئة رعاية يشعر فيها الأفراد بالأمان للتعبير عن مشاعرهم والبحث عن العزاء [23]، مما يؤكد أيضًا المحتوى المحدد لنظرية النظام الأسري. يساعد الدعم الأسري المدرك في تعزيز العلاقات الاجتماعية من خلال تعزيز التفاعلات والعلاقات الإيجابية داخل العائلات. يمكن أن تمتد هذه الروابط إلى ما هو أبعد من العائلات المباشرة ولها تأثير إيجابي على الشبكات الاجتماعية والمجتمعات الأوسع. بشكل عام، يساهم الدعم الأسري المدرك بشكل كبير في الرفاه الاجتماعي من خلال توفير المساعدة العاطفية والمالية والعملية [24].
لدعم الأسرة المدرك علاقة إيجابية كبيرة مع الرفاهية العاطفية.
الصحة النفسية والرفاهية
نتائج صحة نفسية أفضل، بما في ذلك تقليل أعراض الاكتئاب والقلق.
وتعزيز الوعي، يعزز التفاعل الاجتماعي الإيجابي وينشط الوظائف الإدراكية. هذه العوامل معًا تعزز تحسين الرفاه النفسي وتحسين جودة الحياة.
الرفاهية العاطفية لها تأثير إيجابي كبير على الرفاهية النفسية.
الرفاهية العاطفية والرفاهية الاجتماعية كوسيطين
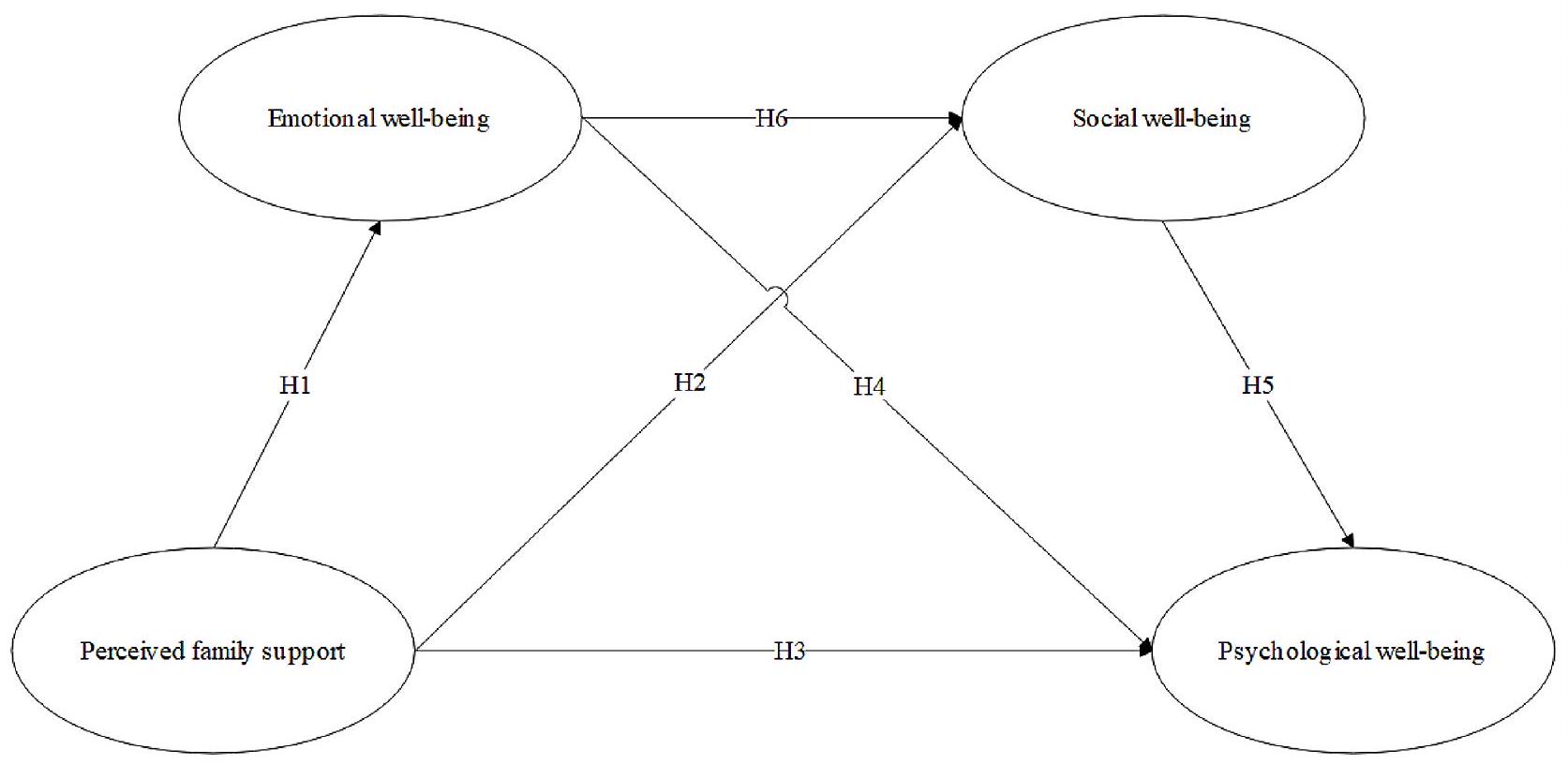
H7 كان هناك تأثيرات وسيطة مباشرة للرفاه العاطفي، وتأثيرات وسيطة مباشرة للرفاه الاجتماعي، وتأثير وسيط تسلسلي بين الدعم الأسري المدرك والرفاه النفسي.
نموذج البحث موضح في الشكل 1.
طريقة
جمع البيانات
قياس
الإجراء
نتائج وتحليل البيانات
تحليل الموثوقية
المتطلبات و
تحليل العوامل التأكيدية واختبار انحياز الطريقة الشائعة
| نموذج | x2/df | RMSEA | SRMR | TLI | CFI | RMSEA |
| النموذج أ | ٤.٠٥٧ | 0.059 | 0.030 | 0.964 | 0.970 | 0.059 |
| النموذج ب | ٣.٥٥٩ | 0.056 | 0.024 | 0.974 | 0.980 | 0.056 |
| النموذج C | 2.973 | 0.047 | 0.022 | 0.981 | 0.985 | 0.047 |
| مسار | تقدير | س.م. | سي آر | P | AVE | سي آر | |
| فام2 <– | PFS | 0.776 | 0.627 | 0.834 | |||
| فام3 <– | PFS | 0.8761 | 0.0474 | ٢٤.١١٢٣ | *** | ||
| فام1 <– | PFS | 0.7159 | 0.٠٤٤٥ | ٢١.٠٠١٧ | *** | ||
| EM1 <– | إي دبليو بي | 0.8621 | 0.775 | 0.912 | |||
| EM2 <– | إي دبليو بي | 0.9048 | 0.0304 | ٣٦.٣٢١ | *** | ||
| EM3 <– | EWB | 0.8729 | 0.0318 | ٣٤.٢٦٦٧ | *** | ||
| PSY1 <– | PWB | 0.8167 | 0.710 | 0.924 | |||
| PSY2 <– | PWB | 0.8502 | 0.033 | 30.3374 | *** | ||
| PSY6 <– | PWB | 0.8604 | 0.0352 | 30.8894 | *** | ||
| PSY4 <– | PWB | 0.8273 | 0.0333 | ٢٩.١٣٧٥ | *** | ||
| PSY5 <– | PWB | 0.8574 | 0.0341 | 30.7279 | *** | ||
| SO3 <– | SWB | 0.8204 | 0.0379 | ٢٨.٠٩٧٣ | *** | 0.707 | 0.879 |
| SO5 <– | SWB | 0.8771 | 0.0356 | 30.648 | *** | ||
| SO4 <– | SWB | 0.8244 |
| PFS | EWB | PWB | SWB | |
| PFS | 0.792 | |||
| إي دبليو بي | 0.5508 | 0.880 | ||
| PWB | 0.5974 | 0.7891 | 0.843 | |
| SWB | 0.5576 | 0.7839 | 0.8093 | 0.841 |
| نموذج | X2/df | RMSEA | SRMR | TLI | CFI |
| النموذج C | 2.973 | 0.047 | 0.022 | 0.981 | 0.985 |
| النموذج C مع التشابه | ٢.٤١٧ | 0.039 | 0.016 | 0.986 | 0.992 |
| تحيز |
خصائص المشاركين
| متغير | تصنيف | تردد | نسبة مئوية (%) | SD |
| جنس | أنثى | ٤٤٣ | ٤٩.٦ | 0.5 |
| ذكر | ٤٥١ | 50.4 | ||
| عمر | من 18 إلى 22 عامًا | 562 | 62.9 | 0.748 |
| من 23 إلى 30 عامًا | 228 | ٢٥.٥ | ||
|
|
87 | 9.7 | ||
| أقل من 45 عامًا | 17 | 1.9 | ||
| مستوى التعليم | المدرسة الإعدادية | ٦ | 0.7 | 0.651 |
| المدرسة الثانوية | ٥٥ | 6.2 | ||
| طالب جامعي | 641 | ٧١.٧ | ||
| سيد | 145 | 16.2 | ||
| دكتوراه | ٤٧ | 5.3 | ||
| مستوى تعليم الوالدين | المدرسة الإعدادية | 371 | ٤١.٥ | 0.919 |
| المدرسة الثانوية | ٣٠٥ | ٣٤.١ | ||
| طالب جامعي | 184 | ٢٠.٦ | ||
| سيد | 19 | 2.1 | ||
| دكتوراه | 15 | 1.7 | ||
| الدخل السنوي للأسرة | أقل من
|
183 | ٢٠.٥ | 1.023 |
|
|
287 | ٣٢.١ | ||
|
|
٢٥١ | ٢٨.١ | ||
| أكثر من 200,000 يوان | 173 | 19.3 | ||
| الوقت اليومي على الإنترنت | أقل من ساعتين | 91 | 10.2 | 0.978 |
|
|
٢٨٢ | 31.5 | ||
|
|
٢٦٥ | ٢٩.٦ | ||
| أكثر من 6 ساعات | 256 | ٢٨.٦ | ||
| سنوات من ركوب الأمواج | أقل من 3 سنوات | ٤٩ | ٥.٥ | 0.922 |
| 3-6 سنوات | 236 | ٢٦.٤ | ||
| 6-10 سنوات | ٢٨٢ | 31.5 | ||
| أكثر من 10 سنوات | ٣٢٧ | ٣٦.٦ |
توافق النموذج
معيار، مما يدل على أن النموذج يمتلك القدرة على التكيف بفعالية.
اختبار تأثير الوساطة
نقاش
| فرضية | مسار | معامل التوحيد | س.م. | سي.آر. | P |
| H1 | EWB <—PFS | 0.5508 | 0.0334 | ١٤.٥٢٧ | *** |
| H2 | SWB <—-PFS | 0.1807 | 0.0314 | 5.2811 | *** |
| H3 | PWB <—-PFS | 0.1532 | 0.0273 | ٥.١٢٣ | *** |
| H4 | PWB <—-EWB | 0.356 | 0.0446 | 8.2685 | *** |
| H5 | PWB <—-SWB | 0.4448 | 0.045 | 9.8349 | *** |
| H6 | SWB <—-EWB | 0.6844 | 0.0395 | 18.0341 | *** |
العلاقات بين الدعم الأسري المدرك والرفاه النفسي
| معامل | تقدير | أخفض | علوي | P | نسبة مئوية |
| الدعم الأسري المدرك -> الرفاه الاجتماعي -> الرفاه النفسي | 0.0734 | 0.0407 | 0.1195 | 0.0006 | ١٣.٤٥٪ |
| الدعم الأسري المدرك -> الرفاهية العاطفية -> الرفاهية النفسية | 0.179 | 0.1211 | 0.253 | 0.0006 | 32.82% |
| الدعم الأسري المدرك -> الرفاهية العاطفية -> الرفاهية الاجتماعية -> الرفاهية النفسية | 0.153 | 0.1076 | 0.2094 | 0.0007 | ٢٨.٠٧٪ |
| الدعم الأسري المدرك -> الرفاه النفسي | 0.1398 | 0.0751 | 0.2154 | 0.0006 | 25.65% |
| إجمالي | 0.5452 | 0.4716 | 0.6269 | 0.0006 |
أثر الوساطة بين الدعم الأسري المدرك والرفاه النفسي
يؤدي إلى زيادة في الرفاه النفسي. أثر الدعم الأسري المدرك على الرفاه العاطفي والرفاه الاجتماعي، بينما كان للرفاه العاطفي والرفاه الاجتماعي تأثير على الرفاه النفسي. أدت الزيادة في الرفاه العاطفي إلى زيادة في الرفاه الاجتماعي، وهو ما أثبته أيضًا دراسة الذكاء العاطفي. كان للدعم الأسري المدرك تأثير إيجابي على الرفاه العاطفي. عندما كان الناس يدركون مستوى أعلى من الدعم من أسرهم، كانوا أكثر عرضة لتجربة مشاعر إيجابية، ومستويات أقل من الضيق، وحققوا درجة أكبر من السعادة العامة. غطى الرفاه العاطفي السعادة، والرضا، والتجارب العاطفية الإيجابية في الحياة اليومية. لعب الرفاه العاطفي دورًا وسيطًا بين الدعم الأسري المدرك والرفاه الاجتماعي. بالإضافة إلى ذلك، عندما كان لدى الناس مستوى أعلى من الرفاه العاطفي، كانوا أكثر عرضة للمشاركة في تفاعلات اجتماعية إيجابية، وإقامة والحفاظ على علاقات شخصية داعمة، وتجربة شعور بالانتماء والروابط الاجتماعية. علاوة على ذلك، لعب الرفاه الاجتماعي دورًا وسيطًا بين الرفاه العاطفي والرفاه النفسي. عندما كان لدى الناس مستوى أعلى من الرفاه الاجتماعي، كانوا أكثر عرضة للحصول على رفاه نفسي أفضل، والذي شمل مستويات أعلى من تقدير الذات ومستويات أقل من الضيق النفسي. قدم الرفاه الاجتماعي للناس شعورًا بالدعم، والاعتراف، والاندماج الاجتماعي، مما أثر بشكل إيجابي على رفاههم النفسي العام. عزز الدعم الأسري المدرك الرفاه العاطفي، الذي بدوره عزز الرفاه الاجتماعي وأدى في النهاية إلى زيادة في الرفاه النفسي. أكدت عملية الوساطة التسلسلية على أهمية الرفاه العاطفي والرفاه الاجتماعي، كعوامل وسيطة للدعم الأسري المدرك الذي يؤثر على الرفاه النفسي الفردي.
القيود والدراسات المستقبلية
ضروري. ثالثًا، اعتمدت الدراسة على البيانات المبلغ عنها ذاتيًا من قبل المشاركين، وكان هناك احتمال لوجود تحيز في الإبلاغ الذاتي. قد يتأثر الناس بتحيز الذاكرة، والتوقعات الاجتماعية، وعرض الذات، مما أدى إلى الذاتية والتحيز في الإبلاغ عن الدعم الأسري المدرك، والرفاهية العاطفية، والرفاهية الاجتماعية. أخيرًا، في الدراسة، قد تكون هناك متغيرات لم تؤخذ بعين الاعتبار، والتي قد تؤثر على العلاقة بين الدعم الأسري المدرك، والتحكم الذاتي في الوقت المستغرق على الإنترنت، والسعادة، مثل سمات الشخصية الفردية وشبكات الدعم الاجتماعي.
الخاتمة
مساهمات المؤلفين
تمويل
توفر البيانات
الإعلانات
موافقة الأخلاقيات والموافقة على المشاركة
موافقة على النشر
المصالح المتنافسة
تاريخ الاستلام: 27 ديسمبر 2023 / تاريخ القبول: 28 مارس 2024
نُشر على الإنترنت: 02 أبريل 2024
References
- Praharso N, Tear M, Cruwys T. Stressful life transitions and wellbeing: a comparison of the stress buffering hypothesis and the social identity model of identity change. Psychiatry Res. 2017;247:265-75.
- Lambert SVNEMHLE. Evaluating the impact of loneliness and social isolation on health literacy and health-related factors in young adults. Front Psychol. 2023;14:996611.
- Guite JW, Logan DE, McCue R, Sherry DD, Rose JB. Parental beliefs and worries regarding adolescent chronic pain. Clin J Pain. 2009;25(3):223-32.
- Wan Mohd Azam WMY, Din NC, Ahmad M, Ghazali SE, Ibrahim N, Said Z, Ghazali AR, Shahar S, Razali R, Maniam T. Loneliness and depression among the elderly in an agricultural settlement: mediating effects of social support. Asia Pac Psychiatry. 2013;5(Suppl 1):134-9.
- Wan P, Hu J, Li Q. Impact of Social Support on depressive symptoms among postgraduates during the Coronavirus Disease 2019 pandemic: a moderated mediation analysis. Int J Environ Res Public Health. 2023;20(4):3431.
- Wu S, Wang C, Jiang J, Kelifa MO, Wang X, Zheng C, Wang P. Adverse childhood experiences, Family Support, and Depression: evidence from Internal migrants in China. J Psychosoc Nurs Ment Health Serv. 2023;61(3):19-25.
- LaMontagne L, Diehl D, Doty J, Smith S. The mediation of family Context and Youth depressive symptoms by adolescent emotion regulation. Youth Soc. 2022;55(3):552-80.
- Diener E. Subjective well-being. Psychol Bull. 1984;95(3):542-75.
- Busseri MA, Sadava SW. A review of the tripartite structure of subjective wellbeing: implications for conceptualization, operationalization, analysis, and synthesis. Personality Social Psychol Rev. 2011;15(3):290-314.
- Keyes CLM, Wissing M, Potgieter JP, Temane M, Kruger A, van Rooy S. Evaluation of the Mental Health Continuum-Short form (MHC-SF) in Setswanaspeaking South africans. Clin Psychol Psychother. 2008;15(3):181-92.
- Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J Personal Soc Psychol. 1989;57(6):1069-81.
- Keyes CLM. Social well-being. Social Psychol Q. 1998;61(2):121-40.
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310-57.
- House JS. Work stress and social support: Reading. Mass. [u.a.]: AddisonWesley; 1981.
- Sarason BR, Sarason IG, Pierce GR. Social support: an interactional view. Wiley; 1990.
- Fiori KL, Antonucci TC, Akiyama H. Profiles of social relations among older adults: a cross-cultural approach. Ageing Soc. 2008;28(2):203-31.
- Bowen M. Alcoholism as viewed through family systems theory and family psychotherapy. Ann N Y Acad Sci. 1974;233(1):115-22.
- Erdem G, Safi OA. The cultural lens approach to Bowen family systems theory: contributions of family change theory. J Family Theory Rev. 2018;10(2):469-83.
- Shumaker SA, Brownell A. Toward a theory of social support: closing conceptual gaps. J Soc Issues. 1984;40(4):11-36.
- Smith SM, Landor AM. Toward a better understanding of African American families: development of the Sociocultural family stress model. J Family Theory Rev. 2018;10(2):434-50.
- Stoddard-Bennett N, Coburn J, Dufur M, Jarvis J, Pribesh S. Family structure and child behavior problems in Australia, the United Kingdom, and the United States. Int J Environ Res Public Health. 2023;20(3):1780.
- Eisenberg N, Guthrie IK, Fabes RA, Reiser M, Murphy BC, Holgren R, Maszk P, Losoya S. The relations of regulation and emotionality to resiliency and competent social functioning in elementary school children. Child Dev. 1997;68(2):295-311.
- Harris PL. The child’s understanding of emotion: developmental change and the family environment. Child Psychol Psychiatry Allied Disciplines. 1994;35(1):3-28.
- Addae EA, Kühner S. How socioeconomic status and family social capital matter for the subjective well-being of young people: implications for the child and family welfare policy in Ghana. J Social Policy. 2022;51(4):876-99.
- Lee S-K, Dworkin J. Multiple channels of communication: Association between emerging adults’ communication patterns, Well-Being, and parenting. Emerg Adulthood. 2022;11(1):48-57.
- Shi M, Liu L, Wang ZY, Wang L. The Mediating Role of Resilience in the relationship between big five personality and anxiety among Chinese Medical students: a cross-sectional study. PLOS ONE. 2015;10(3):e0119916.
- Busch H, Hofer J. Self-regulation and milestones of adult development: intimacy and generativity. Dev Psychol. 2012;48(1):282-93.
- Gross JJ. The emerging field of emotion regulation: an integrative review. Rev Gen Psychol. 1998;2(3):271-99.
- Mayer JD, Caruso DR, Salovey P. The ability model of emotional intelligence: principles and updates. Emot Rev. 2016;8(4):290-300.
- Carella M, García-Pereiro T, Pace R. Subjective well-being, transnational families and social integration of married immigrants in Italy. Soc Indic Res. 2020;161(2):785-816.
- Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30-41.
- Lamers SMA, Westerhof GJ, Bohlmeijer ET, ten Klooster PM, Keyes CLM. Evaluating the psychometric properties of the Mental Health Continuum-Short Form (MHC-SF). J Clin Psychol. 2011;67(1):99-110.
- Cavioni V, Grazzani I, Ornaghi V, Agliati A, Pepe A. Adolescents’ Mental Health at School: the mediating role of life satisfaction. Front Psychol. 2021;12:720628.
- Petrillo G, Capone V, Caso D, Keyes CLM. The mental health continuum-short form (MHC-SF) as a measure of well-being in the Italian context. Soc Indic Res. 2015;121(1):291-312.
- Luijten CC, Kuppens S, van de Bongardt D, Nieboer AP. Evaluating the psychometric properties of the mental health continuum-short form (MHC-SF) in Dutch adolescents. Health Qual Life Outcomes. 2019;17(1):157.
- Karaś D, Cieciuch J, Keyes CLM. The Polish adaptation of the mental health continuum-short form (MHC-SF). Pers Indiv Differ. 2014;69:104-9.
- Yeo ZZ, Suárez L. Validation of the mental health continuum-short form: the bifactor model of emotional, social, and psychological well-being. PLOS ONE. 2022;17(5):e0268232.
- Guo C, Tomson G, Guo J-z, Li X, Keller C, Söderqvist F. Psychometric evaluation of the Mental Health Continuum-Short Form (MHC-SF) in Chinese adoles-cents- a methodological study. Health Qual Life Outcomes. 2015;13(1):1-9.
- Weiss LA, Westerhof GJ, Bohlmeijer ET. Can we increase Psychological Well-Being? The effects of interventions on Psychological Well-Being: a Metaanalysis of Randomized controlled trials. PLoS ONE. 2016;11(6):e0158092.
- Giannopoulos VL, Vella-Brodrick DA. Effects of positive interventions and orientations to happiness on subjective well-being. J Posit Psychol. 2011;6(2):95-105.
- Karaś D, Cieciuch J. The relationship between identity processes and wellbeing in various life domains. Pers Indiv Differ. 2018;121:111-9.
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instruments Computers. 2004;36(4):717-31.
- Liu S, Wang M, Fu C. Maternal academic involvement and adolescents’ subjective well-being: the mediating role of adolescents’ academic adjustment in China. Child Youth Serv Rev. 2021;128(9):106154.
- Lam CB, Chung KKH, Li X. Parental warmth and hostility and child executive function problems: a longitudinal study of Chinese families. Front Psychol. 2018,9:1063.
- Snoubar Y, Zengin O. Social Support Effectiveness of the Mental Health of Immigrants Living in Belgium Belçika’da Yaşayan Göçmenlerin Ruh Sağlığının Sosyal Destek Etkinliği. Br J Social Work 2022, 52.
- Zengin O, Erbay E, Yildirim B. Anxiety, coping and Social Support among Parents who have children with chronic kidney disease. Konuralp Tip Dergisi. 2018;10(3):311-7.
- Zengin O, Erbay E, Yıldırım B, Altındağ Ö. Quality of Life, Coping, and Social Support in patients with multiple sclerosis: a pilot study. Turkish J Neurol. 2017;23:211-8.
ملاحظة الناشر
- *المراسلات:
جينغ آن
13776855935@163.com
جينلونغ آن
anjinlongnj@163.com
¹كلية الإدارة، جامعة نانجينغ للبريد و
الاتصالات، 210003 نانجينغ، مقاطعة جيانغسو، الصين
المستشفى الأول لشعب مدينة تشانغشو، المستشفى التابع لجامعة سوتشو
جامعة، تشانغشو، مقاطعة جيانغسو، الصين
DOI: https://doi.org/10.1186/s12889-024-18476-z
PMID: https://pubmed.ncbi.nlm.nih.gov/38566105
Publication Date: 2024-04-02
A serial mediating effect of perceived family support on psychological well-being
Abstract
Family has a significant impact on individual mental health. Based on social support theory, family system theory and the Mental Health Continuum Short Form (MHC-SF), this research constructed a model of the pathway of perceived family support on psychological well-being and the results empirically clarified that perceived family support has a significant positive relationship with emotional well-being, social well-being, and psychological well-being (
Introduction
Subjective well-being is a major topic in the existing study on well-being. Ed Diener’s article in Psychological Bulletin [8] marked a significant contribution to the emerging field of subjective well-being (SWB), which focused on individuals’ subjective assessments of their own lives [9]. Additionally, Diener proposed that subjective well-being consists of two types of components, a cognitive judgment of one’s overall level of life satisfaction and affective experiences, reflecting people’s positive
and negative emotional reactions to their lives [9]. Therefore, widespread studies have explained subjective wellbeing in terms of life satisfaction (LS), positive affect (PA) and negative affect (NA). This study also aims to investigate the underlying interaction mechanisms in wellbeing. As a result, Keyes’s linked research hypotheses on well-being were selected for this research. According to the related research of Keyes, well-being has different priorities under different streams, which are the hedonic stream and the eudaemonic stream. The hedonic stream defines mental health as “people’s attitude toward life, maintaining positive and healthy emotions in the face of life’s challenges, and the balance between negative and positive emotions” [10]. In contrast, the conceptualization of psychological and social well-being reflects the eudaemonic perspective, which focuses on how people view their functions in life and holds that mental health is the potential in human life [11] and people’s sense of social belonging or social function [12].
Theories and hypotheses
Theoretical basis
that social support can come from different interpersonal relationships and social networks, such as family, friends, colleagues, neighbors and community organizations [15]. In addition, the size, structure and quality of an individual’s social support network will also have an impact on their well-being and adaptability [16]. Intervention and research based on social support theory can help people better understand and promote the positive impact of social support on individual health and happiness, and then improve individual quality of life and well-being.
Perceived family support and psychological well-being
difficulties [7,22]. Through fostering open communication, practicing active listening, and displaying empathy, families can establish a nurturing environment where individuals feel safe to express their emotions and seek solace [23], which also confirms the specific content of family system theory. Perceived family support helps to strengthen social relations by promoting positive interactions and relationships within families. These connections can extend beyond immediate families and have a positive impact on wider social networks and communities. Overall, perceived family support contributes significantly to social well-being by providing emotional, financial and practical help [24].
H1 Perceived family support has a significant positive relationship with emotional well-being.
Mental health and well-being
better mental health outcomes, including reduced symptoms of depression and anxiety.
and realization, promotes positive social interaction and stimulates cognitive function. These factors together promote the enhancement of psychological well-being and the improvement of quality of life.
H4 Emotional well-being has a significant positive impact on psychological well-being.
Emotional well-being and social well-being as mediators
H7 There were direct mediating effects of emotional wellbeing, direct mediating effects of social well-being and a serial mediating effect between perceived family support and psychological well-being.
The research model is shown in Fig. 1.
Method
Data collection
Measure
Procedure
Results and data analysis
Reliability analysis
requirements and the
Confirmatory factor analysis and common method bias test
| model | x2/df | RMSEA | SRMR | TLI | CFI | RMSEA |
| Model A | 4.057 | 0.059 | 0.030 | 0.964 | 0.970 | 0.059 |
| Model B | 3.559 | 0.056 | 0.024 | 0.974 | 0.980 | 0.056 |
| Model C | 2.973 | 0.047 | 0.022 | 0.981 | 0.985 | 0.047 |
| path | Estimate | S.E. | CR | P | AVE | CR | |
| FAM2 <– | PFS | 0.776 | 0.627 | 0.834 | |||
| FAM3 <– | PFS | 0.8761 | 0.0474 | 24.1123 | *** | ||
| FAM1 <– | PFS | 0.7159 | 0.0445 | 21.0017 | *** | ||
| EM1 <– | EWB | 0.8621 | 0.775 | 0.912 | |||
| EM2 <– | EWB | 0.9048 | 0.0304 | 36.321 | *** | ||
| EM3 <– | EWB | 0.8729 | 0.0318 | 34.2667 | *** | ||
| PSY1 <– | PWB | 0.8167 | 0.710 | 0.924 | |||
| PSY2 <– | PWB | 0.8502 | 0.033 | 30.3374 | *** | ||
| PSY6 <– | PWB | 0.8604 | 0.0352 | 30.8894 | *** | ||
| PSY4 <– | PWB | 0.8273 | 0.0333 | 29.1375 | *** | ||
| PSY5 <– | PWB | 0.8574 | 0.0341 | 30.7279 | *** | ||
| SO3 <– | SWB | 0.8204 | 0.0379 | 28.0973 | *** | 0.707 | 0.879 |
| SO5 <– | SWB | 0.8771 | 0.0356 | 30.648 | *** | ||
| SO4 <– | SWB | 0.8244 |
| PFS | EWB | PWB | SWB | |
| PFS | 0.792 | |||
| EWB | 0.5508 | 0.880 | ||
| PWB | 0.5974 | 0.7891 | 0.843 | |
| SWB | 0.5576 | 0.7839 | 0.8093 | 0.841 |
| model | X2/df | RMSEA | SRMR | TLI | CFI |
| Model C | 2.973 | 0.047 | 0.022 | 0.981 | 0.985 |
| Model C with homology | 2.417 | 0.039 | 0.016 | 0.986 | 0.992 |
| bias |
Characteristics of participants
| Variable | Classification | Frequency | Percentage (%) | SD |
| Gender | Female | 443 | 49.6 | 0.5 |
| Male | 451 | 50.4 | ||
| Age | 18~22 years old | 562 | 62.9 | 0.748 |
| 23~30 years old | 228 | 25.5 | ||
|
|
87 | 9.7 | ||
| Under 45 years old | 17 | 1.9 | ||
| Education level | Junior high school | 6 | 0.7 | 0.651 |
| High school | 55 | 6.2 | ||
| Undergraduate | 641 | 71.7 | ||
| Master | 145 | 16.2 | ||
| PhD | 47 | 5.3 | ||
| Education level of parents | Junior high school | 371 | 41.5 | 0.919 |
| High school | 305 | 34.1 | ||
| Undergraduate | 184 | 20.6 | ||
| Master | 19 | 2.1 | ||
| PhD | 15 | 1.7 | ||
| Annual family income | Less than
|
183 | 20.5 | 1.023 |
|
|
287 | 32.1 | ||
|
|
251 | 28.1 | ||
| More than 200,000 RMB | 173 | 19.3 | ||
| Daily online time | Less than 2 h | 91 | 10.2 | 0.978 |
|
|
282 | 31.5 | ||
|
|
265 | 29.6 | ||
| More than 6 h | 256 | 28.6 | ||
| Years of surfing | Less than 3 years | 49 | 5.5 | 0.922 |
| 3-6 years | 236 | 26.4 | ||
| 6-10 years | 282 | 31.5 | ||
| More than 10 years | 327 | 36.6 |
Model fitting
standard, indicating that the model possesses the ability to adapt effectively.
Mediating effect test
Discussion
| Hypothesis | Path | Standardization coefficient | S.E. | C.R. | P |
| H1 | EWB <—PFS | 0.5508 | 0.0334 | 14.527 | *** |
| H2 | SWB <—-PFS | 0.1807 | 0.0314 | 5.2811 | *** |
| H3 | PWB <—-PFS | 0.1532 | 0.0273 | 5.123 | *** |
| H4 | PWB <—-EWB | 0.356 | 0.0446 | 8.2685 | *** |
| H5 | PWB <—-SWB | 0.4448 | 0.045 | 9.8349 | *** |
| H6 | SWB <—-EWB | 0.6844 | 0.0395 | 18.0341 | *** |
Associations between perceived family support and psychological well-being
| Parameter | Estimate | Lower | Upper | P | Percentage |
| Perceived Family Support-> Social Well-being-> Psychological Well-being | 0.0734 | 0.0407 | 0.1195 | 0.0006 | 13.45% |
| Perceived family support-> emotional well-being-> psychological well-being | 0.179 | 0.1211 | 0.253 | 0.0006 | 32.82% |
| Perceived family support-> emotional well-being-> social well-being-> psychological well-being | 0.153 | 0.1076 | 0.2094 | 0.0007 | 28.07% |
| Perceived family support-> psychological well-being | 0.1398 | 0.0751 | 0.2154 | 0.0006 | 25.65% |
| Total | 0.5452 | 0.4716 | 0.6269 | 0.0006 |
The mediation effect between perceived family support and psychological well-being
lead to an increase in psychological well-being. Perceived family support affected emotional well-being and social well-being, while emotional well-being and social wellbeing had an impact on psychological well-being. The increase in emotional well-being led to an increase in social well-being, which was also proved by the study of Emotional Intelligence [29]. Perceived family support had a positive impact on emotional well-being. When people perceived a higher level of support from their families, they were more likely to experience positive emotions, lower levels of distress, and achieved a greater degree of overall happiness. Emotional well-being covered happiness, satisfaction and positive emotional experience in daily life. Emotional well-being played a mediating role between perceived family support and social well-being. In addition, when people had a higher level of emotional well-being, they were more likely to participate in positive social interactions, establish and maintain supportive interpersonal relationships, and experience a sense of belonging and social connections. Moreover, social wellbeing played a mediating role between emotional wellbeing and psychological well-being. When people had a higher level of social well-being, they were more likely to have better psychological well-being, which included higher levels of self-esteem and lower levels of psychological distress. Social well-being provided people with a sense of support, recognition and social integration, thus positively affecting their overall psychological well-being. Perceived family support enhanced emotional well-being, which in turn enhanced social well-being and ultimately led to an increase in psychological well-being. The serial mediation process emphasized the importance of emotional well-being and social well-being, as the mediating factors of perceived family support affecting individual psychological well-being.
Limitations and future studies
necessary. Thirdly, the study relied on the self-reported data of the subjects, and there was the possibility of selfreported bias. People might be affected by recall bias, social expectation and self-presentation, which led to subjectivity and bias in reporting perceived family support, emotional well-being and social well-being. Finally, in the study, there might be unconsidered variables, which might have an impact on the relationship between perceived family support, self-control of online time and happiness, such as individual personality traits and social support networks.
Conclusion
Author contributions
Funding
Data availability
Declarations
Ethics approval and consent to participate
Consent for publication
Competing interests
Received: 27 December 2023 / Accepted: 28 March 2024
Published online: 02 April 2024
References
- Praharso N, Tear M, Cruwys T. Stressful life transitions and wellbeing: a comparison of the stress buffering hypothesis and the social identity model of identity change. Psychiatry Res. 2017;247:265-75.
- Lambert SVNEMHLE. Evaluating the impact of loneliness and social isolation on health literacy and health-related factors in young adults. Front Psychol. 2023;14:996611.
- Guite JW, Logan DE, McCue R, Sherry DD, Rose JB. Parental beliefs and worries regarding adolescent chronic pain. Clin J Pain. 2009;25(3):223-32.
- Wan Mohd Azam WMY, Din NC, Ahmad M, Ghazali SE, Ibrahim N, Said Z, Ghazali AR, Shahar S, Razali R, Maniam T. Loneliness and depression among the elderly in an agricultural settlement: mediating effects of social support. Asia Pac Psychiatry. 2013;5(Suppl 1):134-9.
- Wan P, Hu J, Li Q. Impact of Social Support on depressive symptoms among postgraduates during the Coronavirus Disease 2019 pandemic: a moderated mediation analysis. Int J Environ Res Public Health. 2023;20(4):3431.
- Wu S, Wang C, Jiang J, Kelifa MO, Wang X, Zheng C, Wang P. Adverse childhood experiences, Family Support, and Depression: evidence from Internal migrants in China. J Psychosoc Nurs Ment Health Serv. 2023;61(3):19-25.
- LaMontagne L, Diehl D, Doty J, Smith S. The mediation of family Context and Youth depressive symptoms by adolescent emotion regulation. Youth Soc. 2022;55(3):552-80.
- Diener E. Subjective well-being. Psychol Bull. 1984;95(3):542-75.
- Busseri MA, Sadava SW. A review of the tripartite structure of subjective wellbeing: implications for conceptualization, operationalization, analysis, and synthesis. Personality Social Psychol Rev. 2011;15(3):290-314.
- Keyes CLM, Wissing M, Potgieter JP, Temane M, Kruger A, van Rooy S. Evaluation of the Mental Health Continuum-Short form (MHC-SF) in Setswanaspeaking South africans. Clin Psychol Psychother. 2008;15(3):181-92.
- Ryff CD. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J Personal Soc Psychol. 1989;57(6):1069-81.
- Keyes CLM. Social well-being. Social Psychol Q. 1998;61(2):121-40.
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310-57.
- House JS. Work stress and social support: Reading. Mass. [u.a.]: AddisonWesley; 1981.
- Sarason BR, Sarason IG, Pierce GR. Social support: an interactional view. Wiley; 1990.
- Fiori KL, Antonucci TC, Akiyama H. Profiles of social relations among older adults: a cross-cultural approach. Ageing Soc. 2008;28(2):203-31.
- Bowen M. Alcoholism as viewed through family systems theory and family psychotherapy. Ann N Y Acad Sci. 1974;233(1):115-22.
- Erdem G, Safi OA. The cultural lens approach to Bowen family systems theory: contributions of family change theory. J Family Theory Rev. 2018;10(2):469-83.
- Shumaker SA, Brownell A. Toward a theory of social support: closing conceptual gaps. J Soc Issues. 1984;40(4):11-36.
- Smith SM, Landor AM. Toward a better understanding of African American families: development of the Sociocultural family stress model. J Family Theory Rev. 2018;10(2):434-50.
- Stoddard-Bennett N, Coburn J, Dufur M, Jarvis J, Pribesh S. Family structure and child behavior problems in Australia, the United Kingdom, and the United States. Int J Environ Res Public Health. 2023;20(3):1780.
- Eisenberg N, Guthrie IK, Fabes RA, Reiser M, Murphy BC, Holgren R, Maszk P, Losoya S. The relations of regulation and emotionality to resiliency and competent social functioning in elementary school children. Child Dev. 1997;68(2):295-311.
- Harris PL. The child’s understanding of emotion: developmental change and the family environment. Child Psychol Psychiatry Allied Disciplines. 1994;35(1):3-28.
- Addae EA, Kühner S. How socioeconomic status and family social capital matter for the subjective well-being of young people: implications for the child and family welfare policy in Ghana. J Social Policy. 2022;51(4):876-99.
- Lee S-K, Dworkin J. Multiple channels of communication: Association between emerging adults’ communication patterns, Well-Being, and parenting. Emerg Adulthood. 2022;11(1):48-57.
- Shi M, Liu L, Wang ZY, Wang L. The Mediating Role of Resilience in the relationship between big five personality and anxiety among Chinese Medical students: a cross-sectional study. PLOS ONE. 2015;10(3):e0119916.
- Busch H, Hofer J. Self-regulation and milestones of adult development: intimacy and generativity. Dev Psychol. 2012;48(1):282-93.
- Gross JJ. The emerging field of emotion regulation: an integrative review. Rev Gen Psychol. 1998;2(3):271-99.
- Mayer JD, Caruso DR, Salovey P. The ability model of emotional intelligence: principles and updates. Emot Rev. 2016;8(4):290-300.
- Carella M, García-Pereiro T, Pace R. Subjective well-being, transnational families and social integration of married immigrants in Italy. Soc Indic Res. 2020;161(2):785-816.
- Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30-41.
- Lamers SMA, Westerhof GJ, Bohlmeijer ET, ten Klooster PM, Keyes CLM. Evaluating the psychometric properties of the Mental Health Continuum-Short Form (MHC-SF). J Clin Psychol. 2011;67(1):99-110.
- Cavioni V, Grazzani I, Ornaghi V, Agliati A, Pepe A. Adolescents’ Mental Health at School: the mediating role of life satisfaction. Front Psychol. 2021;12:720628.
- Petrillo G, Capone V, Caso D, Keyes CLM. The mental health continuum-short form (MHC-SF) as a measure of well-being in the Italian context. Soc Indic Res. 2015;121(1):291-312.
- Luijten CC, Kuppens S, van de Bongardt D, Nieboer AP. Evaluating the psychometric properties of the mental health continuum-short form (MHC-SF) in Dutch adolescents. Health Qual Life Outcomes. 2019;17(1):157.
- Karaś D, Cieciuch J, Keyes CLM. The Polish adaptation of the mental health continuum-short form (MHC-SF). Pers Indiv Differ. 2014;69:104-9.
- Yeo ZZ, Suárez L. Validation of the mental health continuum-short form: the bifactor model of emotional, social, and psychological well-being. PLOS ONE. 2022;17(5):e0268232.
- Guo C, Tomson G, Guo J-z, Li X, Keller C, Söderqvist F. Psychometric evaluation of the Mental Health Continuum-Short Form (MHC-SF) in Chinese adoles-cents- a methodological study. Health Qual Life Outcomes. 2015;13(1):1-9.
- Weiss LA, Westerhof GJ, Bohlmeijer ET. Can we increase Psychological Well-Being? The effects of interventions on Psychological Well-Being: a Metaanalysis of Randomized controlled trials. PLoS ONE. 2016;11(6):e0158092.
- Giannopoulos VL, Vella-Brodrick DA. Effects of positive interventions and orientations to happiness on subjective well-being. J Posit Psychol. 2011;6(2):95-105.
- Karaś D, Cieciuch J. The relationship between identity processes and wellbeing in various life domains. Pers Indiv Differ. 2018;121:111-9.
- Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instruments Computers. 2004;36(4):717-31.
- Liu S, Wang M, Fu C. Maternal academic involvement and adolescents’ subjective well-being: the mediating role of adolescents’ academic adjustment in China. Child Youth Serv Rev. 2021;128(9):106154.
- Lam CB, Chung KKH, Li X. Parental warmth and hostility and child executive function problems: a longitudinal study of Chinese families. Front Psychol. 2018,9:1063.
- Snoubar Y, Zengin O. Social Support Effectiveness of the Mental Health of Immigrants Living in Belgium Belçika’da Yaşayan Göçmenlerin Ruh Sağlığının Sosyal Destek Etkinliği. Br J Social Work 2022, 52.
- Zengin O, Erbay E, Yildirim B. Anxiety, coping and Social Support among Parents who have children with chronic kidney disease. Konuralp Tip Dergisi. 2018;10(3):311-7.
- Zengin O, Erbay E, Yıldırım B, Altındağ Ö. Quality of Life, Coping, and Social Support in patients with multiple sclerosis: a pilot study. Turkish J Neurol. 2017;23:211-8.
Publisher’s Note
- *Correspondence:
Jing An
13776855935@163.com
Jinlong An
anjinlongnj@163.com
¹School of Management, Nanjing University of Posts and
Telecommunications, 210003 Nanjing, Jiangsu Province, China
First People’s Hospital of Changshu City, Hospital Affiliated to Soochow
University, Changshu, Jiangsu Province, China