أسباب المرض، وعلم مسبباته، وعلاجه لالتهاب المحيط بالزرعات: منظور أوروبي Etiology, pathogenesis and treatment of peri‐implantitis: A European perspective
أسباب المرض، وعلم مسبباته، وعلاجه لالتهاب المحيط بالزرعات: منظور أوروبي
تورد بيرغلوند | أندريا مومبيلي | فرانك شوارز | جان ديركس¹قسم أمراض اللثة، معهد طب الأسنان، أكاديمية ساهلغرنسكا، جامعة غوتنبرغ، غوتنبرغ، السويدقسم طب الأسنان التجديدي وطب اللثة، العيادات الجامعية لطب الأسنان، جامعة جنيف، جنيف، سويسراقسم جراحة الفم وزراعة الأسنان، جامعة غوته، كارولينيوم، فرانكفورت، ألمانيا
المراسلات
تورد بيرغلوند، قسم أمراض اللثة، معهد طب الأسنان، أكاديمية ساهلغرنسكا في جامعة غوتنبرغ، صندوق 450، SE 40530 غوتنبرغ، السويد. البريد الإلكتروني: tord.berglundh@odontologi.gu.se
الملخص
التهاب الأنسجة المحيطة بالزرع هو حالة مرضية مرتبطة بالبلاك تحدث في الأنسجة المحيطة بزراعة الأسنان. يتميز بالتهاب في الغشاء المخاطي المحيط بالزرع وفقدان تدريجي للعظم الداعم. على مدى الثلاثين عامًا الماضية، أصبح التهاب الأنسجة المحيطة بالزرع عبئًا كبيرًا في طب الأسنان. يجب أن يكون فهم التشخيص والأسباب وعلم الأمراض وعلم الوبائيات وعلاج التهاب الأنسجة المحيطة بالزرع جزءًا مركزيًا في برامج التدريب الجامعي والدراسات العليا في طب الأسنان. نظرًا للدور القوي للبحث الأوروبي في علم اللثة وطب الأسنان الزرعي، كان التركيز في هذه المراجعة على معالجة التهاب الأنسجة المحيطة بالزرع من منظور أوروبي. كان أحد مكونات العمل هو تلخيص بيانات جديدة وموثوقة عن المرضى الذين لديهم زراعة أسنان لدعم أهمية التهاب الأنسجة المحيطة بالزرع من منظور سكاني. تم تقييم طبيعة آفة التهاب الأنسجة المحيطة بالزرع من خلال النتائج المقدمة في نماذج ما قبل السريرية وتقييمات مواد خزعة بشرية مع تقييم الخصائص الميكروبيولوجية. يتم مناقشة نظرة عامة على الاستراتيجيات والنتائج المقدمة في الدراسات السريرية حول العلاج غير الجراحي والجراحي لالتهاب الأنسجة المحيطة بالزرع مع تركيز خاص على نقاط نهاية العلاج والتوصيات المقدمة في إرشادات الممارسة السريرية من المستوى S3 للوقاية والعلاج من أمراض الأنسجة المحيطة بالزرع.
الكلمات الرئيسية
زراعة الأسنان، التهاب المحيط بالزرع، العلاج
1 | المقدمة
تم تقديم مصطلح التهاب المحيط بالزرع في ورشة العمل الأوروبية الأولى لعلم اللثة، التي عقدت في إيتينغن، سويسرا في فبراير 1993.بينما الدراسات المنشورة قبل عام 1993 غالبًا ما استخدمت المصطلحات “عدوى حول الزرع” أو “آفة حول الزرع” لوصف الحالات المرضية في الأنسجة المحيطة بالزرع، قدم التقرير التوافقي من الجلسة الرابعة من ورشة العمل الأوروبية تعريفات لمرض حول الزرع، والتهاب الغشاء المخاطي حول الزرع، والتهاب حول الزرع.تم ذكر أن مرض ما حول الزرع هو مصطلح جماعي لـ
ردود الفعل الالتهابية في الأنسجة المحيطة بالغرسة. بينما كان مصطلح التهاب الغشاء المخاطي المحيط بالغرسة يشير إلى حالة التهابية قابلة للعكس في الأنسجة الرخوة المحيطة بالغرسة، كان التهاب الغرسة يصف ردود الفعل الالتهابية مع فقدان العظام الداعمة في الأنسجة المحيطة بغرسة تعمل. تناولت ورش العمل الأوروبية اللاحقة الأمراض المحيطة بالغرسات كجزء مركزي من البحث السريري في طب الأسنان الغرساتي.ورشة العمل العالمية لعام 2017 حول تصنيف الأمراض والحالات المتعلقة باللثة وزرع الأسنان في شيكاغو، التي نظمتها الاتحاد الأوروبي لطب الأسنان والكلية الأمريكية لطب الأسنان، ميزت بين تعريفات الأمراض وتعريفات الحالات لالتهاب المحيط بالزرع.بينما تهدف تعريفات الحالات إلى أن تكون بمثابة إرشادات للتقييم السريري للحالة، فإن تعريفات الأمراض وصفية وتعرض الخصائص النموذجية للمرض. وبالتالي، فإن التهاب الأنسجة المحيطة بالزرع هو حالة مرضية مرتبطة بالبلاك تحدث في الأنسجة المحيطة بزراعة الأسنان. وتتميز بالتهاب في الغشاء المخاطي المحيط بالزرع وفقدان تدريجي لاحق للعظم الداعم.
على مدى الثلاثين عامًا الماضية، أصبحت التهاب المحيط بالزرع واقعًا مرضيًا رئيسيًا في طب الأسنان. لذلك يجب اعتبار هذه الحالة مرضًا من منظور سكاني بدلاً من كونها مضاعفة بيولوجية في مجال زراعة الأسنان. يجب أن يكون فهم التشخيص، وعلم الأسباب، وعلم الأمراض، وعلم الأوبئة، وعلاج التهاب المحيط بالزرع جزءًا مركزيًا في برامج التدريب الجامعي والدراسات العليا في طب الأسنان. نظرًا للدور القوي للبحث الأوروبي في علم اللثة وزراعة الأسنان، كان التركيز في هذه المراجعة على معالجة التهاب المحيط بالزرع من منظور أوروبي. كان أحد مكونات العمل هو تلخيص بيانات جديدة وموثوقة عن المرضى الذين لديهم زراعة أسنان لدعم أهمية التهاب المحيط بالزرع من منظور سكاني. تم تقييم طبيعة آفة التهاب المحيط بالزرع من خلال النتائج المقدمة في نماذج ما قبل السريرية وتقييمات مواد خزعة بشرية مع تقييم الخصائص الميكروبيولوجية. أخيرًا، تم تقديم نظرة عامة على الاستراتيجيات والنتائج المقدمة في الدراسات السريرية حول العلاج غير الجراحي والجراحي لالتهاب المحيط بالزرع.
2 | أهمية التهاب المحيط بالزرع ككيان مرضي – منظور سكاني
2.1 | انتشار المرضى الذين لديهم زراعة أسنان
يجب أن تؤخذ تقييمات المرضى المعرضين لخطر التهاب المحيط بالزرع من منظور سكاني. غالبًا ما يُستخدم العدد المقدر للزرعات السنية المثبتة سنويًا لتوفير معلومات حول التطبيق العالمي لهذه التقنية في استبدال الأسنان المفقودة. بينما قد تختلف دقة هذه التقديرات، فإن الأرقام الوطنية المستندة إلى الدعم الحكومي لرعاية الأسنان توفر معلومات ذات موثوقية عالية. أظهرت بيانات وكالة الفوائد السنية والصيدلانية (TLV) في السويد أن عدد الزرعات السنية المثبتة كان ضعف العدد في عام 2022 مقارنة بعام 2012. عدد كما زاد عدد المرضى المعالجين خلال نفس الفترة، وظهر أن متوسط عدد الزرعات المثبتة لكل مريض قد انخفض مع مرور الوقت. تدعم بيانات الأبحاث الوبائية حول المرضى الذين لديهم زراعة أسنان في السويد هذه الملاحظة. وبالتالي، كان متوسط عدد الزرعات لكل مريض في عام 1990 و2003 هو 6.2 و4.0 على التوالي.حالياً، متوسط عدد الزرعات لكل مريض في السويد حوالي 2.4.
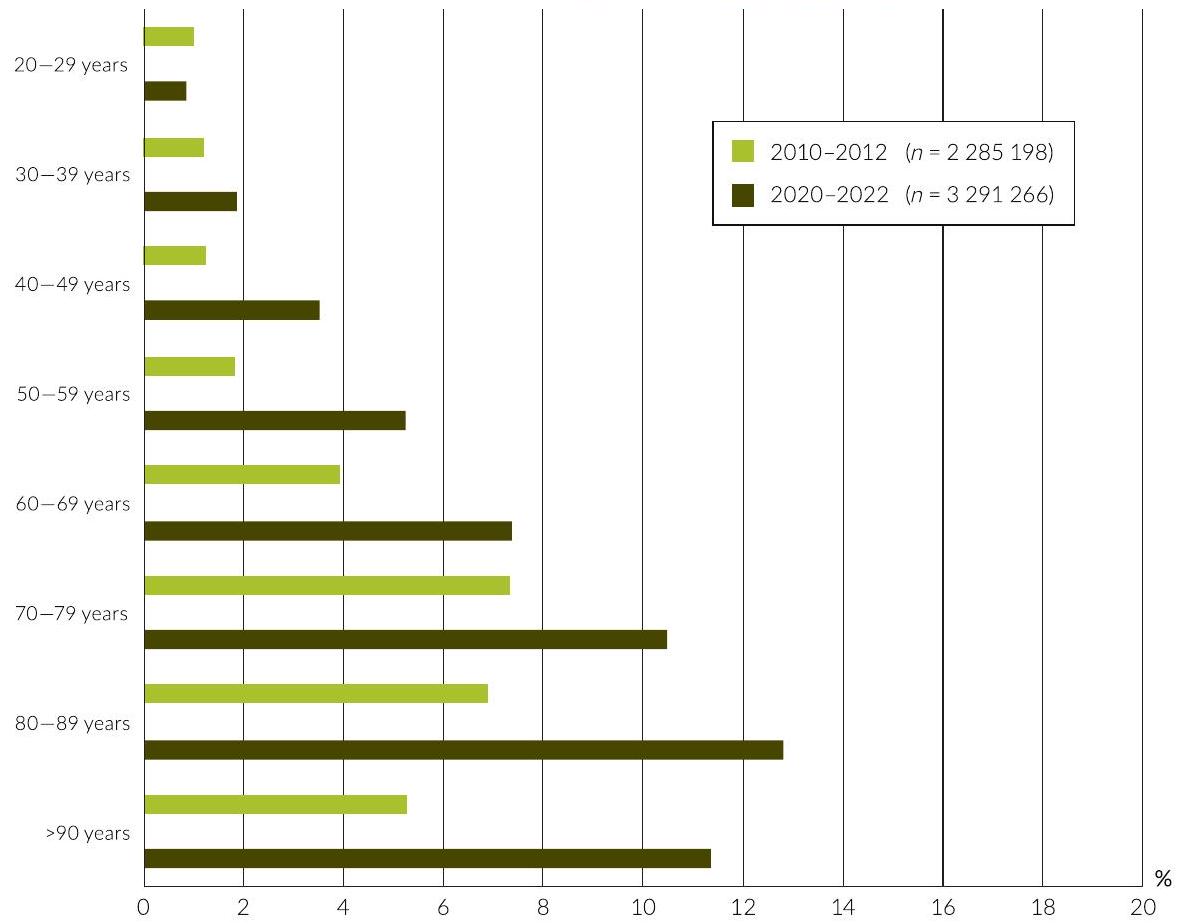
ومع ذلك، فإن العدد الفعلي للزرعات التي تم تركيبها سنويًا ربما يكون له قيمة محدودة لأنه لا يعكس عدد أو نسبة الأفراد الذين لديهم زراعة أسنان من منظور سكاني. في هذا السياق، فإن الوصول إلى بيانات السجل الموثوقة أمر ذو أهمية. سجل الجودة السويدي حول تسوس الأسنان وأمراض اللثة (SKaPa) هو سجل وطني فريد يتمتع بدرجة عالية من الاكتمال. يعتمد السجل على بيانات من سجلات المرضى الإلكترونية التي تمثل حوالي 8 ملايين فرد. توفر التقارير السنوية من سجل SKaPa معلومات حول الحالة السنية بما في ذلك زراعة الأسنان. تقرير عام 2022غطت حوالي 3.3 مليون موضوع سنوات و 155,000 فرد من هؤلاء كان لديهم زراعة الأسنان. بينما بلغت النسبة الإجمالية للأشخاص الذين لديهم زراعة أسنان في السويدكان هناك فرق كبير بين الفئات العمرية (الشكل 1). وبالتالي،من الأشخاص الذين تتراوح أعمارهمكانت نسبة الأشخاص الذين لديهم زراعة أسنان من الفئة العمرية 40-60 عامًا تتراوح بين 3% و5%. على الرغم من أن البيانات مستندة إلى عينة أصغر، إلا أن بيانات الدراسة الخامسة للصحة الفموية في ألمانيا أشارت إلى أن 8% من الأشخاص الذين تتراوح أعمارهم بين 65-74 عامًا في عام 2014 كانوا لديهم زراعة أسنان.
متزامنًا مع زيادة النسبة الإجمالية للأشخاص الذين لديهم زراعة أسنان منإلىعلى مدار السنوات العشر الماضية، أشارت المعلومات المستمدة من SKaPa إلى تحول في العدد المتوسط لزراعة الأسنان لكل فرد. بينما زادت نسبة الأفراد الذين لديهم زراعة واحدة فقط منإلىنسبة الموضوعات التي تحتوي علىانخفضت الزرعات منإلىمن منظور سكاني، يشكل الأفراد الذين لديهم زراعة أسنان مجموعة محددة جيدًا من الأفراد المعرضين لخطر التهاب ما حول الزرعة. استنادًا إلى البيانات السويدية عن الأفراد الذين لديهم زراعة أسنان (حوالي 5% من جميع البالغين)، فإن عدد الأفراد المعرضين لخطر التهاب ما حول الزرعة في الدول الأوروبية وأماكن أخرى كبير ويجب ألا يتم تجاهله.
2.2 | انتشار التهاب المحيط بالزرع
تم تقييم حدوث التهاب المحيط بالزرع في عدة دراسات مقطعية. نظرًا للاختلاف الكبير بين الدراسات فيما يتعلق بعدد ونوع المرضى، ومدة الوظيفة، وتعريفات الحالة المستخدمة لتحديد التهاب المحيط بالزرع، تتراوح أرقام الانتشار منإلىتم الإبلاغ. القيم المتوسطة الموزونة المستخلصة من التحليلات التلوية للدراسات تراوحت بين و لم تُظهر التقارير المختلفة حول انتشار التهاب المحيط بالزرع فقط تباينًا كبيرًا في تعريفات الحالات بما في ذلك عتبات فقدان العظام حول الزرعات، بل كانت التقييمات غالبًا ما تُجرى على عينات صغيرة ومختارة من المرضى تمثل بيئات سريرية في الجامعات/المستشفيات. كانت التقييمات لـ
الشكل 1 نسبة الأفراد الذين لديهم زراعة أسنان في السويد. بيانات من السجل السويدي لجودة تسوس الأسنان وأمراض اللثة.
يجب أن تستند نسبة انتشار التهاب المحيط بالزرع بشكل مثالي إلى عينات سكانية كبيرة وعشوائية مأخوذة من بيئات سريرية مختلفة. في دراسة سريرية على مستوى البلاد في السويد، قام ديركس وآخرون.تم فحص 596 مريضًا يمثلون عينة عشوائية من مجموعة قائمة على السجل. أظهر تحليل البيانات حول الحالة السريرية لأنسجة ما حول الزرع والأشعة السينية بعد 9 سنوات من العلاج الترميمي المدعوم بالزرع وجود التهاب حول الزرع (زراعة الأسنان التي تظهر نزيفًا عند الاستكشاف وفقدان العظام ) في من المرضى. أشكال معتدلة/شديدة من المرض (زراعة الأسنان التي تظهر نزيفًا عند الفحص وفقدان العظام ) تم اكتشافها في للمرضى. يجب أن نلاحظ أن متوسط كمية فقدان العظام في المواقع التي تعاني من التهاب حول الزرع المعتدل/الشديد كان 3.5 مم، مما يتوافق مع حوالي الدعم العظمي الأولي. النتائج التي قدمها ديركس وآخرونعلى انتشار التهاب المحيط بالزرع تدعم البيانات المقدمة في دراسات مقطعية أوروبية أخرى. وبالتالي، عند تطبيق تعريفات الحالة المستخدمة من قبل ديركس وآخرين.إلى مجموعات البيانات التي وصفها كولدسلاند وآخرون،روس-يانساكر وآخرون،مير-ماري وآخرون، ورودريغو وآخرون، تفاوت انتشار التهاب المحيط بالزرع المعتدل/ الشديد بين 16% و 20%. في هذا السياق، من المثير للاهتمام أن البيانات المقدمة حول انتشار التهاب المحيط بالزرع تبدو متسقة مع تلك المبلغ عنها لالتهاب اللثة. كلا المرضين يظهران بحدوث إجمالي يبلغ حوالي 40% في السكان البالغين المختارين عشوائيًا، بينما تؤثر الأشكال الشديدة من الأمراض على نسبة أصغر تبلغ حوالي
تم تقييم عوامل الخطر المحتملة أو مؤشرات الخطر لالتهاب المحيط بالزرع في الدراسات التي تحقق في حدوث المرض. باستخدام نهج استعادي، تم تحديد عدة عوامل خطر خاصة بالمرضى والزراعة. كولدسلاند وآخرون.وديركس وآخرونأفاد أن المرضى الذين لديهم تاريخ من التهاب اللثة كانوا يعانون من زيادة في خطر التهاب المحيط بالزرع. وقد تم تأكيد هذه الملاحظة في مراجعة منهجية حديثة قدمها كاررا. نت وآخرونوأيضًا تم تسليط الضوء عليه في تقرير التوافق من ورشة العمل العالمية لعام 2017والمراجعة المتصلة بواسطة شوارز وآخرون.كان خطر التهاب المحيط بالزرع مرتفعًا بشكل خاص لدى المرضى الذين يعانون من ضعف في السيطرة على اللويحات والذين لم يحضروا برامج الصيانة المنتظمة خلال المتابعة. كما أفاد التقرير التوافقي أن الأدلة الحالية حول مرض السكري والتدخين كعوامل خطر للمرض كانت غير حاسمة. ومع ذلك، يجب الإشارة إلى أنه في التحليل الإحصائي، قد يتم إخفاء التأثير المحتمل للتدخين بواسطة عوامل أخرى وأقوى، مثل تاريخ التهاب اللثة. من بين عوامل الخطر المتعلقة بالزرع أو التعويض المدعوم بالزرع، تم التأكيد على أن الوصول إلى نظافة الفم هو عنصر مهم.وبواسطة رودريغو وآخرونأظهرت الدراسات أن الزرعات التي لا يمكن الوصول إليها لتدابير نظافة الفم كانت لديها مخاطر مرتفعة للإصابة بالتهاب ما حول الزرعة. وقد أظهرت دراسات أخرى أن مدى العلاج، أي عدد الزرعات الموضوعة، كان عامل خطر للإصابة بالتهاب ما حول الزرعة.تظل البيانات حول أهمية عوامل أخرى، مثل نوع التثبيت (مثبت بالأسمنت أو مثبت بالبراغي) أو أبعاد الغشاء المخاطي الكيراتيني غير حاسمة.
3 | آفة التهاب المحيط بالزرع
على الرغم من أن مواقع التهاب المحيط بالزرع تظهر خصائص سريرية مشابهة لتلك الموجودة في التهاب اللثة، مثل علامات الالتهاب المرئية، والنزيف عند الاستكشاف، وفقدان العظام في الأشعة السينية، إلا أن هناك اختلافات واضحة في أنماط تقدم المرض. أظهرت الدراسات أن التهاب المحيط بالزرع غير المعالج يتقدم بنمط غير خطي ومتسارع وبمعدل أسرع من التهاب اللثة.بينما الأسباب وراء الاختلافات في نمط تقدم المرض ليست مفهومة تمامًا، فإن الاختلافات في يجب التأكيد على هيكل وتركيب استجابة المضيف المحلي بين التهاب اللثة والتهاب المحيط بالزرع.
3.1 | نماذج ما قبل السريرية في الجسم الحي
أظهرت الأعمال التجريبية الرائدة باستخدام نماذج حيوانية مسبقة الإعداد المعروفة اختلافات هامة بين آفات التهاب اللثة والتهاب المحيط بالزرع.بينما أدت مجموعة من وضع الرباط تحت اللثة/ تحت الغشاء المخاطي وتراكم البلاك إلى فقدان العظام وتكوين منطقة كبيرة من الأنسجة الضامة المتسللة (ICT) في اللثة/ الغشاء المخاطي المحيط بالزرع عند الأسنان والزراعات، كان فقدان العظام أكثر وضوحًا حول الزرعات. بالإضافة إلى ذلك، امتدت آفات التهاب المحيط بالزرع، على عكس آفات التهاب اللثة، إلى قمة العظم. بعد إزالة الرباطات خلال الإجراء التجريبي، استجابت الأنسجة اللثوية بعملية “تقييد ذاتي” أدت إلى منطقة واقية من الأنسجة الضامة مع بقاء ألياف الرباط اللثوي التي فصلت ICT عن العظم القمي. ومع ذلك، في مواقع التهاب المحيط بالزرع، فشلت مثل هذه العملية التقييدية الذاتية في الحدوث بسبب نقص الألياف اللثوية. تم إجراء ملاحظات مماثلة في دراسات تجريبية بواسطة مارينيلي وآخرين.وشو وآخرونإن ملاحظة عدم وجود عملية ذاتية التقييد في مواقع التهاب المحيط بالزرع فتحت مجالًا لنهج جديد في النماذج التجريبية قبل السريرية. في دراسة أجراها زيتسمان وآخرون،تم إنشاء التهاب المحيط بالزرع التجريبي، وعندما فقد حوالي 40% من دعم العظام، تمت إزالة جميع الرباطات. وقد تم الإبلاغ عن أنه في غياب الرباطات ومع استمرار تكوين اللويحات على مدى عدة أشهر، حدثت “تقدم عفوي” للمرض مع انهيار إضافي لعظام المحيط بالزرع. تم استخدام نموذج “التقدم العفوي” بعد ذلك لفحص الفروق في تقدم المرض بين الزرعات ذات الخصائص السطحية المختلفة. أظهرت بيانات من العديد من هذه الدراسات التجريبية باستمرار أن حجم ICT وفقدان العظام كانا أكثر وضوحًا في المواقع التي تمثل الزرعات ذات الأسطح المعدلة مقارنة بالزرعات ذات الأسطح غير المعدلة والمصقولة.تم تطبيق نموذج “التقدم التلقائي” أيضًا بواسطة كاركواك وآخرون.في مقارنة بين التهاب اللثة التجريبي والتهاب المحيط بالزرعات. تم الإبلاغ عن أن فقدان العظام كان أكبر حول الزرعات مقارنة بالأسنان وأن آفات التهاب المحيط بالزرعات احتلت مناطق أكبر من النسيج الضام وامتدت أقرب إلى العظم القمي مقارنة بآفات التهاب اللثة. كاركواك وآخرون.أخذ النموذج خطوة أخرى من خلال تحليل التقدم التلقائي لالتهاب المحيط بالزرع التجريبي في مرحلة مبكرة دون فترة سابقة من تدهور الأنسجة الواسع. كانت خسارة العظم القمي، مرة أخرى، أكبر حول الزرعات ذات الأسطح المعدلة مقارنة بالزرعات ذات الأسطح المصقولة وغير المعدلة.
لقد ساهمت نتائج الدراسات ما قبل السريرية في فهم طبيعة آفات التهاب المحيط بالزرع والسبب وراء تقدم المرض بشكل أسرع مما هو معتاد في التهاب اللثة. من الواضح أن آفات التهاب المحيط بالزرع غير محاطة بشكل جيد، حيث تفتقر إلى منطقة صحية من الأنسجة الضامة تعمل كحاجز “ذاتي التحديد” تفصل بين التسرب والعظم القمي. الطبيعة المتقدمة والمستمرة لآفات التهاب المحيط بالزرع هي أكثر موضحًا بالأعداد العالية التي تُلاحظ بشكل متكرر من الخلايا العظمية المدمرة على عظم القمة المحيط بالزرع.
3.2 | مادة خزعة بشرية
الميزة في تحليل كل من مكونات الأنسجة الصلبة واللينة في العينات من الدراسات ما قبل السريرية واضحة. بينما تمنع القيود الأخلاقية في معظم الحالات تحليل مكونات الأنسجة الصلبة في المواد الحيوية البشرية المأخوذة من مواقع التهاب حول الزرع، يمكن تطبيق تقنيات متقدمة لاكتشاف الخصائص الظاهرية والوظيفية للخلايا في آفات التهاب حول الزرع. كانت تقييمات المواد الحيوية البشرية مع الحفاظ على توجيه الأنسجة للتحليلات المعتمدة على الأقسام تعتمد بشكل أساسي على التحضيرات المناعية النسيجية، وفي حالات قليلة، تقنيات الشكل. استخدمت تحقيقات أخرى إجراءات، حيث تم تجانس عينات الأنسجة ثم تحليلها باستخدام، على سبيل المثال، RT-PCR، أو الويسترن بلوت، أو تحليل النسخ. يتم تقديم نظرة عامة على الدراسات الأوروبية التي تقدم نتائج من تحليل المواد الحيوية البشرية وتعرض تعريفات واضحة للحالات المتعلقة بالتهاب حول الزرع في الجدول 1.
تم تقديم نتائج تقييمات التركيب الخلوي وخصائص أخرى لآفات التهاب المحيط بالزرع البشري في مراجعات.تمت المقارنات، في معظم الدراسات، بين عينات التهاب المحيط بالزرع وعينات الأنسجة التي تمثل أنواعًا أخرى من الحالات، على سبيل المثال، التهاب اللثة، التهاب الغشاء المخاطي المحيط بالزرع، والأنسجة المحيطة بالزرع أو اللثة الصحية. كانت السمة الأكثر وضوحًا للأنسجة المجمعة من المواقع التي تعاني من التهاب المحيط بالزرع هي ملاحظة تسربات كبيرة من الخلايا الالتهابية التي هيمنت على منطقة العينة.في الدراسات التي تقيم الفروق بين عينات التهاب المحيط بالزرع والتهاب اللثة، كانت الآفة أكبر بشكل متسق في مواقع التهاب المحيط بالزرع وامتدت إلى الأسفل من الظهارة المحيطية. بينما كانت خلايا البلازما هي النوع الخلوي السائد في كلا الآفتين، كانت كثافات خلايا البلازما والبلعميات والعدلات أكبر بشكل ملحوظ في مواقع التهاب المحيط بالزرع مقارنة بمواقع التهاب اللثة.في دراسة حول حالة تنشيط البلعميات في ICT، تم الإبلاغ عن أن عدد البلعميات التي تخضع لقطبية M1 كان أعلى في التهاب المحيط بالزرع مقارنةً بآفات التهاب اللثة.أظهرت النتائج من الدراسات حول الخصائص الوظيفية للخلايا أن آفات التهاب المحيط بالزرع كانت تحمل توقيعات مختلفة من mRNA. ومستويات أعلى من mRNA لبعض السيتوكينات، على سبيل المثال، TNF-a وIL-8 وCCR5 وCXCR3 مقارنةً بآفات التهاب اللثة.
تؤكد الفروق بين آفات التهاب اللثة والتهاب ما حول الزرع التي تم اكتشافها في الدراسات على مواد خزعة بشرية البيانات المقدمة في الأبحاث ما قبل السريرية. معًا، تعكس الفروق في التركيب وكثافات الخلايا الالتهابية الرئيسية في ICT بين نوعي الآفات خصائص استجابة مضيفة محلية غير منظمة في التهاب ما حول الزرع. يتضح ذلك من خلال (i) عدم وجود بطانة ظهارية بين الفيلم الحيوي تحت الهامش وICT في منطقة الجيب، (ii) الانتشار الكبير لـ ICT تحت الظهارة الجيبية نحو العظم القمي، و(iii) الزيادة والتجنيد المستمر لـ
الجدول 1 الدراسات الأوروبية التي تصف الآفات المحيطة بالزرع – مادة خزعة بشرية.
المؤلفون
السكان
تعريف الحالة لالتهاب المحيط بالزرع
طرق
النتائج الرئيسية
سانز وآخرون1991
12 مادة
– ستة مع PI
– ستة ضوابط صحية
بوبا + مبل
خزعات الأنسجة الرخوة
LM و TEM
– أظهرت عينات PI أعدادًا أعلى من الخلايا الالتهابية (بشكل أساسي خلايا البلازما والخلايا الوحيدة النواة) والخلايا المهاجرة في الظهارة الفموية والسُّلقية مقارنةً بالضوابط الصحية.
– PI: تم استبدال خمسة وستين في المئة من النسيج الضام بـ ICT مقابلفي المجموعة الصحية
كورنيلييني وآخرون2001
15 مادة
– 10 زراعة مع PI
– 10 زراعة صحية
أدلة على MBL
PD
بروتوكول العمليات الأساسية/بروتوكول العمليات القياسية+
تورم
خزعات الأنسجة الرخوة
LM، IHC
VEGF، وعامل الثامن
– كانت المواقع الصحية خالية من تكنولوجيا المعلومات والاتصالات، مع توزيع منتظم للسفن
– كانت مواقع PI تحتوي على ICT، معظمها من اللمفاويات وخلايا البلازما. عدد قليل من العدلات.
– تعبير VEGF أقل في المواقع الصحية مقارنة بمواقع التهاب اللثة
غواليني و 2003 بيرغلوند
16 مادة
– ستة مع PI
– 10 مع PiM
أدلة على MBL BOP/SOP+
خزعات الأنسجة الرخوة
LM، IHC
CD3، CD4، CD8، CD19، والإيلاستاز
– في مرض التهاب اللثة المزمن، كان التسلل الالتهابي محددًا جيدًا في المنطقة الجانبية لظهارة الجيب، بينما في مواقع التهاب اللثة، بدت ظهارة الجيب متقرحة، وامتد التسلل الالتهابي بجوارها.
– كان ICT لآفات PI أكبر بثلاث مرات من ذلك الموجود في مواقع PiM
– احتوت PI على نسب أعلى بكثير من خلايا B (CD19+) وخلايا إيجابية للإيلاستاز مقارنة بـ PiM
بيرغلوند وآخرون2004
ستة مواد
– 12 زراعة مع PI
MBL BOP/SOP+ المتقدم
خزعات الأنسجة الرخوة
LM
– الجزء القمي من الظهارة الجيبية رقيق ومصابة بقرحة
– تمتد تكنولوجيا المعلومات والاتصالات (ICT) بشكل قمي من ظهارة الجيب
– كانت معظم الأنسجة الضامة المحتلة بواسطة خلايا البلازما والعدلات.
– كانت هناك وحدات وعائية قليلة ولكن كبيرة تشغل الجزء الهامشي من الآفة، بينما يمكن العثور على العديد من الأوعية الصغيرة في المنطقة الجانبية لظهارة الجيب.
– كانت مستويات CD3 و TIMP-2 مرتفعة في PI مقارنة بـ CP
– مستويات أعلى من IL-1تم العثور على IL-10 و CD3 و CD20 و CD68 في PI أكثر من الضوابط الصحية
– كانت مستويات IL-17 و TIMP-2 و ميتالوبروتيناز المصفوفة-2 و ميتالوبروتيناز المصفوفة-8 و ميتالوبروتيناز المصفوفة-12 و ميتالوبروتيناز المصفوفة-13 مرتفعة في التهاب اللثة المزمن و التهاب اللثة الحاد مقارنةً بالضوابط الصحية.
كاسناك وآخرون2018
37 موضوعًا
– 12 مع PI
– 13 مع الشلل الدماغي
– 13 ضوابط صحية
كال
PD
بروتوكول العمليات الأساسية/بروتوكول العمليات الخاصة+
MBL
خزعات الأنسجة الرخوة
المؤسسة الدولية للحقوق
8-OHdG، PARK7/DJ-1، NFE2L2/NRF2، و KEAP1
– خلايا إيجابية لـ 8-OHdG و PARK7/DJ-1 تنتشر في جميع طبقات الظهارة لعينات PI و CP، ولكن فقط في الطبقة القاعدية من الشواهد الصحية
– خلايا ملونة بـ NFE2L2/NRF2 تنتشر في جميع الطبقات الظهارية في جميع المجموعات
تم العثور على ICT أكثر وضوحًا في عينات PI مقارنة بعينات CP
– كانت نسب الخلايا الإيجابية لـ 8-OHdG في الظهارة أعلى في التهاب اللثة المزمن والتهاب اللثة الحاد مقارنةً بالضوابط الصحية.
– عدد الخلايا الإيجابية لـ PARK7/DJ-1 مرتفع في التهاب البروستاتا المزمن والتهاب البروستاتا مقارنة بالعينات الصحية
لوكاريني وآخرون2019
48 موضوعًا
– 16 مع PI
– 16 مع PiM
– 16 ضوابط صحية
بوب+
أدلة على MBL
خزعات الأنسجة الرخوة
LM، IHC
VEGF، CD34، و CD44
– مواقع PI. ظهارة جيب قرحي و ICT كبير
– أظهرت مجموعة PI مستويات أعلى بشكل ملحوظ من VEGF وCD34 وCD44 مقارنة بالمجموعات الأخرى
– كان PD مرتبطًا إيجابيًا بـ VEGF و CD34 و CD44
الجدول 1 (مستمر)
المؤلفون
السكان
تعريف الحالة لالتهاب المحيط بالزرع
طرق
النتائج الرئيسية
ديونيجي وآخرون2020
80 موضوعًا
– 40 مع PI
– 40 مع CP
بروتوكول العمليات الأساسية/بروتوكول العمليات القياسية+
– كانت كثافات الخلايا الإيجابية لـ CD68 و MPO و iNOS أعلى بشكل ملحوظ في مواقع PI مقارنة بمواقع CP
– كانت كثافات الخلايا لجميع العلامات أعلى بشكل ملحوظ في المنطقة الداخلية من ICT مقارنة بالمنطقة الخارجية من ICT، سواء في PI أو CP.
– أظهرت مستويات أعلى بشكل ملحوظ من خلايا y-H2AX- و iNOS- و NOX2- و MPO- و PAD4/ MPO الإيجابية داخل منطقة NCT مقارنةً بتلك الموجودة في CP
فريتورست وآخرون
٢٠٢٠
14 مادة
– سبعة مع باي
– سبعة مع الشلل الدماغي
بروتوكول العمليات الأساسية/بروتوكول العمليات القياسية+
أدلة على MBL
خزعات الأنسجة الرخوة
LM، IHC، التألق المناعي
CD68، iNOS، وCD206
– تباين استقطاب البلعميات في كل من PI و CP
– أعداد أعلى من الخلايا الإيجابية لـ CD68 في PI مقارنة بـ CP
– مستويات أعلى من البلعميات في شكل M1 في PI مقارنة بـ CP
– مستويات مماثلة من البلعميات في الشكل M2 في المجموعتين
غالاراغا فينويزا
2020 وآخرون
أربعة مواضيع
– خمسة زراعة مع PI
بروتوكول العمليات الأساسية/بروتوكول العمليات الخاصة+
MBL
خزعات الأنسجة الرخوة والعظمية تحت المجهر
– كان متوسط طول العيب 4.7 مم، وكثافة العظام كانتوكان متوسط الاتصال بين العظم والغرسة
– أظهرت عينتان وجود تسلل التهابي مزمن
– أظهرت عينة واحدة علامات على نشاط الخلايا العظمية، بينما أظهرت ثلاث عينات نشاطًا غير نشط في العظم القشري، وأظهرت عينة واحدة تكوين عظم نشط.
– كان العظم المتبقي في الغالب قشريًا يظهر مناطق بها أوعية دموية صغيرة ومناطق من العظم اللاميلا.
كانت الأوستيونات الثانوية موجودة بشكل متكرر، بينما كانت الخلايا العظمية متعددة النوى تُرى بشكل متقطع، بالإضافة إلى العظم الإسفنجي الذي كان يقع في الغالب في الأجزاء القمية من العينات.
ميجيرتسكي وآخرون2019
40 موضوعًا
– 20 مع PI
– 20 ضابط صحي
بروتوكول العمليات الأساسية/بروتوكول العمليات القياسية+
تعرض لـخيوط الزرع
فقدان العظام الشعاعي
خزعات الأنسجة الرخوة
LM، IHC، التألق المناعي، TEM، و RT-PCR
– أظهرت عينات PI من تكنولوجيا المعلومات والاتصالات خلايا بلازميةالخلايا اللمفاويةPMNألياف الكولاجين 15%، الخلايا الليفية 8%، والأوعية الدموية 12%
– تم تقليل مستويات جينات ROX وOsterix وb catenin في عينات PI
تم تنظيم إنتاج ROS (NOX4 وأكسيداز NADPH) بشكل متزايد في عينات PI
فريتورست
2021 وآخرون
15 مادة
– سبعة مع PI حول زراعة التيتانيوم
– ثمانية مع PI حول الزرعات الخزفية
بروتوكول العمليات الأساسية/بروتوكول العمليات القياسية+
MBL >2/3 من طول الزرعة
خزعات الأنسجة الرخوة
LM، IHC
CD3، CD20، CD138، وCD68
– لم تكن هناك اختلافات كبيرة في عدد الخلايا الإيجابية في آفات PI بين زراعة السيراميك وزراعة التيتانيوم
– كانت الخلايا البلازمية تشغل بشكل أساسي الـ ICT، تليها الخلايا التائية، والخلايا البائية، والبلعميات.
غالاراغا فينويزا
2021 وآخرون
20 موضوعًا
20 زراعة مع PI
بروتوكول العمليات الأساسية/بروتوكول العمليات القياسية+
PD
MBL
خزعات الأنسجة الرخوة
LM، IHC
CD68 و CD80 و CD206
– كانت كثافة CD68 الإيجابية حواليتكنولوجيا المعلومات والاتصالات في مواقع PI
– كانت الخلايا الإيجابية لـ CD80 و CD206 (البلاعم M1 و M2) تشغل 7.07% و 5.22% من ICT، على التوالي.
– كانت نسبة M1/M2 1.56
تمت ملاحظة وجود ارتباط إيجابي بين مستويات CD68 و M1 و PD.
الاختصارات: AG، التهاب اللثة العدواني؛ BOP، النزيف عند الاستكشاف؛ CAL، مستوى الارتباط السريري؛ CP، التهاب اللثة المزمن؛ ICT، الأنسجة الضامة المتسللة؛ IHC، الكيمياء المناعية النسيجية؛ LM، المجهر الضوئي؛ MBL، مستوى العظم الهامشي؛ PD، عمق الاستكشاف؛ PI، التهاب حول الزرع؛ PiM، التهاب الغشاء المخاطي حول الزرع؛ SOP، القيح عند الاستكشاف؛ TEM، المجهر الإلكتروني الناقل.
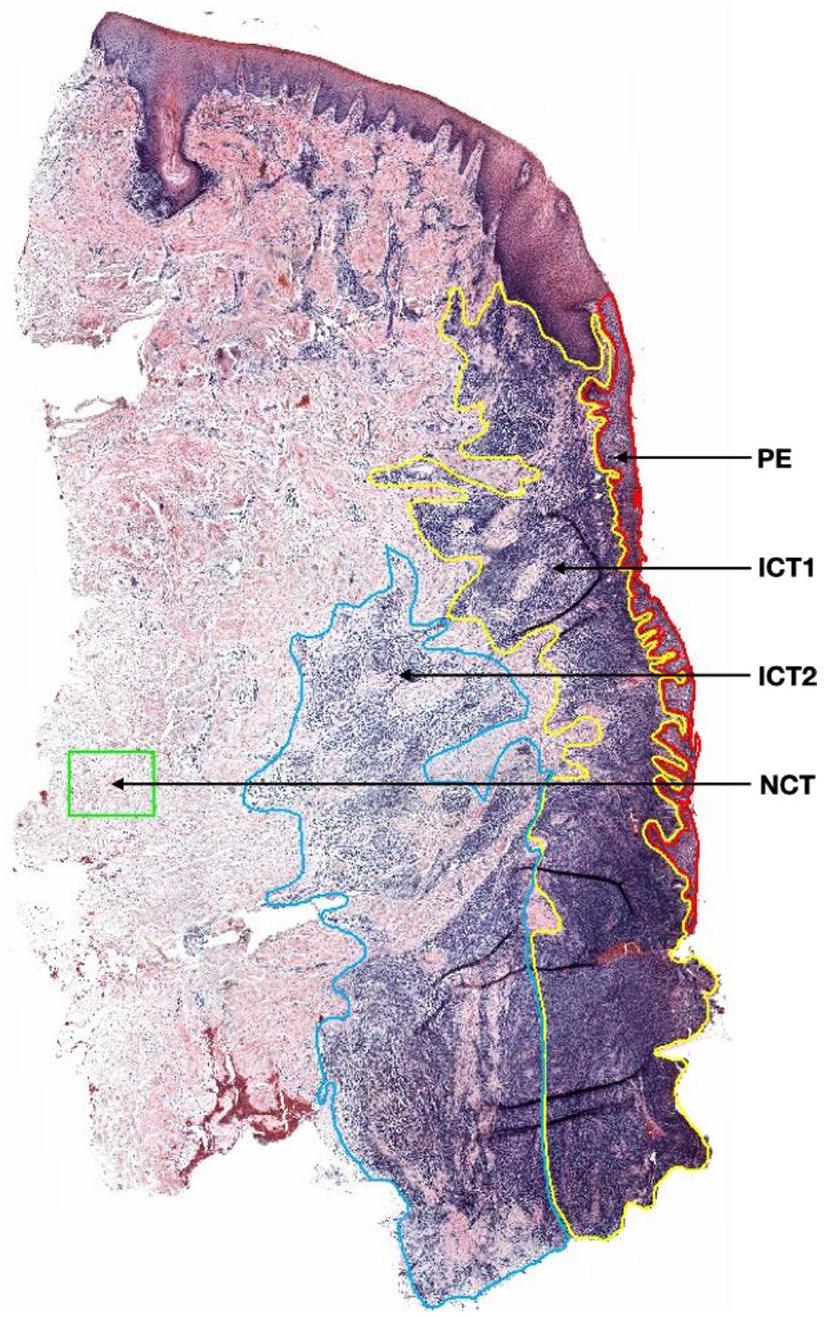
الشكل 2 مقطع تم إعداده من خزعة بشرية تم الحصول عليها من موقع يعاني من التهاب شديد حول الزرع. الظهارة الجيبية (PE)، المناطق الداخلية (ICT-1) والخارجية (ICT-2) من ICT، ومنطقة النسيج الضام غير المت infiltrated (NCT). من ديونيجي وآخرون.
تظهر الخصائص الرئيسية لآفات التهاب المحيط بالزرع عملية التهاب نشطة ومستدامة مع القليل، إن وُجد، من علامات الخمول. يمكن تفسير النمط غير الخطي والمتسارع لتقدم المرض في التهاب المحيط بالزرع، كما تم وصفه أعلاه، إلى حد كبير من خلال هذه الخصائص الآفات.
في تحليل موسع لمواد الخزعة المأخوذة من 80 شخصًا يعانون من التهاب محيط الزرع الشديد أو التهاب اللثة، أفاد ديونيجي وآخرون أن كلا النوعين من الآفات ظهرا بكثافات أعلى من الخلايا الالتهابية في “المنطقة الداخلية” (ICT-1) المجاورة لظهارة الجيب مقارنةً بـ “المنطقة الخارجية” من الآفة (ICT-2). (الشكل 2). كما قام المؤلفون بملاحظات حول الخصائص الخلوية في منطقة الأنسجة الضامة غير المتسللة (NCT) الجانبية للـ ICT. وبالتالي، احتوى قسم NCT في عينات التهاب المحيط بالزرع على كثافات أعلى من الخلايا الإيجابية لـ y-H2AX و iNOS و NOX2 و MPO و PAD4/MPO، أي علامات لتلف الحمض النووي وأكسيد النيتريك المضاد للميكروبات وتكوين NETs، مقارنة بما تم العثور عليه في عينات التهاب اللثة. كانت نتيجة ردود الفعل النسيجية المنتشرة يتجاوز الحد الجانبي للـ ICT الصورة العامة لتفاعل الأنسجة الواسع في المواقع التي تعاني من التهاب حول الزرع. نظرًا لأن الزرع السني هو جهاز معدني مصنوع في الغالب من التيتانيوم، فقد تم اقتراح أن وجود مادة غريبة في مواقع التهاب حول الزرع قد يؤثر على استجابة المضيف المحلية. على الرغم من أن الدراسات قد أفادت بوجود جزيئات معدنية في عينات الأنسجة الرخوة من مواقع التهاب حول الزرع،لا يزال من غير الواضح ما إذا كانت هذه النتائج محددة لأنسجة المحيط بالزرع المريضة، حيث تفتقر المقارنات ذات الصلة إلى عينات مطابقة تمثل أنسجة المحيط بالزرع الصحية. بالإضافة إلى ذلك، تتطلب تقييمات جزيئات المعادن الدقيقة في الأنسجة الرخوة المحيطة بالزرع استخدام تقنيات مناسبة للتحقق من نوع المادة (مثل التيتانيوم) وللكشف عن الجزيئات الصغيرة الحجم.على سبيل المثال،-PIXE (إصدار الأشعة السينية الناتج عن البروتونات الدقيقة)، إشعاع السنكروترون، أو SEM-EDX.
قد تختلف البيانات المستمدة من الدراسات التي تقيم المواد الحيوية البشرية المأخوذة من مواقع التهاب المحيط بالزرع اعتمادًا على شدة الحالة وتعريفات الحالة المستخدمة عند تجنيد المرضى. واحدة من المزايا في التقييم النسيجي لعينات الأنسجة هي الحفاظ على تشريح وهندسة هياكل الأنسجة. وبالتالي، يتم تسهيل اكتشاف الخلايا المستهدفة في مواقع محكومة جيدًا. ومع ذلك، يجب أخذ القيود التقنية لاستخدام علامات الخلايا التي تتميز بشكل أساسي بخصائص فينوتيبية، مثل الكيمياء المناعية، في الاعتبار. من ناحية أخرى، تتطلب تقييمات تعبير mRNA للعناصر الرئيسية في الآفة استخدام عينات أنسجة متجانسة، حيث يتم فقدان اتجاه هيكل الأنسجة. من الناحية المثالية، يجب أن تطبق التحليلات المستقبلية لعينات التهاب المحيط بالزرع البشرية تقنيات “أوميكس” جديدة (مثل البروتيوميات، والترانسكريبتوميات) بالاقتران مع نهج التصور المكاني. على الرغم من أن مثل هذه التقنيات متاحة حاليًا، إلا أن استخدامها يحتاج إلى توازن بين أحجام العينات المعنوية والقابلة للتطبيق والموارد الكبيرة المطلوبة. يجب أن تهدف التقنيات المستقبلية أيضًا إلى الحفاظ على المنطقة التي تشمل الواجهة بين الأنسجة الملتهبة المحيطة بالزرع والبيوفيلم الموجود في الجيب. إن تحليل تفاعلات المضيف والطفيلي لديه القدرة على توفير فهم أعمق لدور الكائنات الدقيقة كعامل سببي رئيسي في التهاب المحيط بالزرع.
4 | الخصائص الميكروبيولوجية لالتهاب المحيط بالزرع
في وقت مبكر من تطوير زراعة الأسنان، لوحظ أن فقدان العظام حول الزرعات يمكن أن يرتبط أحيانًا بعلامات كلاسيكية للعدوى في الأنسجة الرخوة بما في ذلك الاحمرار، والتورم، وتكوين القيح.القيح هو نتيجة استجابة الجهاز المناعي لعدوى، عادة ما تسببها البكتيريا. قد يعتقد المرء أن هذا وحده كان سيقنع المجتمع السني بأن العدوى حول الزرعات يمكن أن تكون تهديدًا خطيرًا وأن نهج مضاد للميكروبات لمنع فشل الزرع سيكون مجديًا. ومع ذلك، فإن مدى مساهمة العدوى في ظاهرة فقدان العظام المحيطة بالزرع بشكل عام لا يزال مثيرًا للجدل منذ ذلك الحين.كما تم الإشارة إليه في الفصول السابقة في Periodontology 2000،تشير عدة خطوط من الأدلة إلى أن البكتيريا التي تستعمر أسطح الزرع تلعب دورًا أساسيًا في مسببات التهاب المحيط بالزرع:
أظهرت التجارب على البشر أن التراكم غير المقيد للبلاك البكتيري على الزرعات على مدى عدة أيام أدى إلى التهاب محلي في الغشاء المخاطي المجاور (يسمى “التهاب الغشاء المخاطي التجريبي حول الزرع”),مشابهًا لتأثير البلاك السني على اللثة (يسمى “التهاب اللثة التجريبي”). في كلتا الحالتين، كانت علامات الالتهاب تتناقص بمجرد إزالة الترسبات البكتيرية.
أظهرت الميكروبيوتا المجمعة من مواقع التهاب المحيط بالزرع اختلافات كمية ونوعية عن الميكروبيوتا في مواقع الزرع ذات الغشاء المخاطي الصحي، كما تم مناقشته بمزيد من التفصيل أدناه.
في الدراسات السريرية السابقة، أدى وضع الرباطات تحت اللثة مع تكوين البلاك إلى تغييرات في تركيب الميكروبيوتا المحلية وفي تدمير أنسجة المحيط بالزرع.
أظهرت بروتوكولات علاج التهاب المحيط بالزرع التي تهدف إلى إزالة الترسبات البكتيرية من الزرعات نتائج سريرية إيجابية، وإن كانت بدرجات متفاوتة، كما تم مراجعتها في القسم التالي.
إن عدم وجود برامج صيانة والامتثال الضعيف (أي، استمرار الترسبات البكتيرية بسبب سوء النظافة الفموية) بعد علاج الزرع يزيد من خطر التهاب المحيط بالزرع.
تشير الأدلة الأولية التي تربط أنواع معينة من الكائنات الدقيقة بالتهاب المحيط بالزرع إلى الفحص المجهري للعينات المجمعة حول الزرعات ذات الجيوب المتقدمة. بينما لم يتم الكشف عن الحلزونات في العينات من مواقع الزرع ذات الأنسجة المحيطة الصحية، تم العثور عليها بأعداد كبيرة في المواقع المريضة.نظرًا لأن المجهر الإلكتروني أظهر أن هذه البكتيريا تغزو الأنسجة اللثوية في التهاب اللثة التقرحي النخري،تساءل المرء عن مدى أهمية ذلك فيما يتعلق بالتهاب المحيط بالزرع. أظهرت دراسة باستخدام طرق زراعة بكتيرية نشرت فيأنمن الكائنات المزروعة من الزرعات ذات أعماق استكشاف المحيط بالزرعوفقدان العظام كانت قضبان سلبية الغرام لاهوائية. من بين هذه الكائنات، تم التعرف على Fusobacterium spp. وPrevotella intermedia بشكل متكرر بمستويات عالية. تم تأكيد وجود الحلزونات وكائنات متحركة أخرى مجهرًا ولكن لم يكن من الممكن دراستها بشكل أكبر باستخدام التقنيات المتاحة في ذلك الوقت. من ناحية أخرى، تم الكشف عن عدد قليل جدًا من البكتيريا، معظمها تم التعرف عليها على أنها كوكيات إيجابية الغرام، في الزرعات بدون أعراض. تشير هذه النتائج إلى أن الحالة التي يشار إليها فيما بعد باسم “التهاب المحيط بالزرع” تبدو كعملية مرضية محددة الموقع تشمل بكتيريا كانت مرتبطة سابقًا بالتهاب اللثة المزمن حول الأسنان.
على مدار ما يقرب من أربعة عقود، أكدت دراسات إضافية باستخدام طرق ميكروبيولوجية كلاسيكية وجديدة النتائج المبكرة ووسعت نطاقها. تم استخدام تقنيات تشمل تفاعل البلمرة المتسلسل DNA-DNA، وqPCR، والهجين الفلوري في الموقع، وPCR المعتمد على جين 16 S rRNA لدراسة
تركيب الميكروبيوتا المحيطة بالزرع في الصحة والمرض. استخدم معظم الباحثين طرقًا تم تطويرها في الأصل لتقييم الميكروبيوتا تحت اللثة في جيوب اللثة حول الأسنان الطبيعية وركزوا بشكل أساسي على ما يسمى بالعوامل المسببة للالتهابات اللثوية. في هذه الدراسات، تم الكشف عن بكتيريا شائعة في التهاب اللثة المزمن، مثل Fusobacterium spp. وP. intermedia بشكل منتظم أيضًا في العينات من التهاب المحيط بالزرع.كانت الكائنات التي تقل شيوعًا في التهاب اللثة المزمن، مثل Aggregatibacter actinomycetemcomitans،تُعرف بشكل أقل تكرارًا.
أظهرت التحليلات باستخدام طرق مختلفة أن الميكروبيوم تحت المخاطي في أمراض المحيط بالزرع هو (ط) مختلط، (2) متغير إلى حد ما، و(3) في معظم الحالات يهيمن عليه أنواع مختلفة من البكتيريا السلبية الغرام اللاهوائية.وفقًا لمراجعة منهجية حديثة،أظهرت التحليلات التلوية للأنواع التي تم تحليلها في دراستين مستقلتين على الأقل أن الأنواع التالية مرتبطة بالتهاب المحيط بالزرع (مقارنة بـ “غير التهاب المحيط بالزرع”): البكتيريا السلبية الغرام اللاهوائية Fusobacterium nucleatum، Porphyromonas gingivalis، Prevotella intermedia، وTannerella forsythia، الحلزون Treponema denticola، والبكتيريا إيجابية الغرام Staphylococcus epidermidis. فيما يتعلق بالأخيرة، تم التكهن منذ فترة طويلة بأن هذه الكائنات قد تكون مسؤولة عن شكل متميز ميكروبيولوجيًا من العدوى المحيطية بالزرع. في الواقع، S.epidermidis، وهو متعايش شائع يعيش على جلد الإنسان والغشاء المخاطي، مرتبط أيضًا بأشكال أخرى من العدوى القيحية للأجهزة المزروعة التي لا تشبه كثيرًا الآفات الشبيهة بالتهاب اللثة التي يتم مواجهتها عادة حول الزرعات الفموية.
أظهرت عدة دراسات أن هناك فرقًا في تركيب الميكروبيوتا المحيطة بالزرع الموجودة في الجيوب العميقة والسطحية،تعكس الاختلافات في الظروف البيئية المعروفة أيضًا من الوضع حول الأسنان الطبيعية.يمكن اعتبار الجيوب ذات عمق الاستكشافموائل محمية للعوامل المسببة المحتملة ويمكن أن تكون مؤشرًا على خطر الإصابة بأمراض المحيط بالزرع.
تستند الميكروبيولوجيا الكلاسيكية إلى حد كبير إلى دراسة خصائص الثقافات النقية من الكائنات الدقيقة التي تنمو في ظروف مختبرية لا تمثل حياتها في الطبيعة. في البرية، تعيش البكتيريا في مجتمعات مختلطة تسمى البيوفيلم التي تلتصق بالأسطح البيئية. ومع ذلك، فإن البيانات التي تم مناقشتها أعلاه، حتى من الدراسات التي تستخدم أحدث التقنيات الجزيئية، تستند إلى عينات تم الحصول عليها باستخدام طرق تدمير البيوفيلم. المعلومات حول التنظيم المكاني للبيوفيلم الذي نما بشكل طبيعي في أمراض المحيط بالزرع البشرية نادرة وقليل ما هو معروف عن سلوكيات العوامل المسببة المشتبه بها، خاصة عند الالتصاق بأسطح الزرع.على نطاق أوسع، فإن عدوى الأغشية الحيوية ليست مجرد مشكلة أسنان. كما تم التعرف عليه في أبحاث زراعة العظام،إنهم يساهمون في مضاعفات شديدة، وزيادة استخدام العلاجات بالمضادات الحيوية، وتطور الكائنات الدقيقة المقاومة للمضادات الحيوية. عند مناقشة النتائج التي قد تكون محبطة أحيانًا لعلاج التهاب اللثة المحيط بالزرعات السنية، يجب أن نأخذ في الاعتبار العدوى المرتبطة بالأغشية الحيوية التي يصعب علاجها في الأجهزة المزروعة، والتي غالبًا ما تسبب القلق، وزيادة المراضة، وتكاليف عالية. هناك حاجة لتحسين تشخيص عدوى الأغشية الحيوية الفموية وغير الفموية لتمكين الكشف المبكر والعلاج لصالح مرضانا.
5 | علاج التهاب المحيط بالزرع
5.1 | المفاهيم
في ورشة العمل العالمية لعام 2017 حول تصنيف الأمراض والحالات المتعلقة باللثة وزرع الأسنان، تم تسليط الضوء على الأسباب البكتيرية لالتهاب الغشاء المخاطي المحيط بالزرع والتهاب الأنسجة المحيطة بالزرع.أظهرت الأبحاث التدخلية العلاقة السببية بين تراكم اللويحات البكتيرية وتطور التهاب ما حول الزرع لاحقًا.أي، التهاب الغشاء المخاطي المحيط بالزرع. الفهم العام لتطور المرض هو نموذج تدريجي، حيث يتطور التهاب الغشاء المخاطي المحيط بالزرع في البداية عند تراكم اللويحات وقد يتقدم بعد ذلك إلى التهاب الأنسجة المحيطة بالزرع.يقترح النموذج أن التهاب الأنسجة المحيطة بالزرع يأتي دائمًا بعد التهاب الغشاء المخاطي المحيط بالزرع. وبالتالي، تمثل اللويحات البكتيرية مكونًا ضروريًا لتطور المرض وفقًا لنموذج “سبب المكون الكافي” الذي وصفه روثمان فيتمامًا كما هو الحال في العلاقة بين اللويحات البكتيرية والتهاب اللثة، فإن صحة مسار مشابه لالتهاب المحيط بالزرع مدعومة ببيانات من الأبحاث الملاحظة والتدخلية. كما تم الإشارة إليه أعلاه، فقد أظهرت مجموعات فرعية من الأفراد الحاملين للزرع الذين لا يحضرون الرعاية الداعمة المنتظمة أنهم يعانون من عبء أعلى بكثير من الأمراض المحيطة بالزرع، بما في ذلك حدوث التهاب المحيط بالزرع.ثانيًا، والأهم من ذلك، أن الأساليب المضادة للعدوى المطبقة في إدارة التهاب المحيط بالزرع المتقدم، أي إنشاء التحكم في اللويحات الذي يقوم به المريض مع إزالة التلوث من أسطح الزرع، قد أظهرت بشكل مفهومي أنها توقف تقدم المرض أيضًا في الدراسات التي تتضمن فترات متابعة طويلة الأمد.
نتيجة لفهم التهاب المحيط بالزرع كاضطراب مدفوع باللويحات البكتيرية، فإن إرشادات الممارسة السريرية من المستوى S3 التي وضعتها الاتحاد الأوروبي لطب الأسنان اللثوي للوقاية من وعلاج أمراض المحيط بالزرع تركز بشكل كبير على هذا العامل.لذا، يجب أن تشمل إدارة التهاب المحيط بالزرع خطوة غير جراحية أولية، يتم خلالها إزالة/تقليل الرواسب البكتيرية من خلال أدوات فوق وتحت الحافة. بعد تقييم استجابة الشفاء لأساليب العلاج غير الجراحية وفي حالة وجود علامات متبقية للمرض، يُوصى بخطوة جراحية. هنا أيضًا، تعتبر إزالة التلوث من أسطح الزرع، بعد رفع الشريحة، هي العنصر العلاجي الرئيسي. يشمل علاج التهاب المحيط بالزرع تدابير نظافة الفم المناسبة التي يتم تنفيذها ذاتيًا وتقديمها بشكل احترافي خلال جميع خطوات العلاج، بما في ذلك الفترة التي تلي الانتهاء من العلاج النشط. تمثل الرعاية الداعمة المنتظمة حول الزرع الخطوة النهائية في النهج المتسلسل.
5.2 | نقاط نهاية العلاج
في الإعداد السريري، يتميز التهاب المحيط بالزرع ويتم تشخيصه من خلال الفحص البصري، وفحص المحيط بالزرع، والتقييم الشعاعي.تماشياً مع التقارير حول نتائج أمراض اللثة العلاج،لقد أبلغت الدراسات حول علاج التهاب المحيط بالزرع عادةً عن تغييرات في المعايير السريرية والأشعة. في الواقع، تم وصف المتغيرات مثل عمق الاستكشاف والنزيف عند الاستكشاف في حوالي 90% من جميع الدراسات حول إدارة أمراض المحيط بالزرع خلال السنوات العشر الماضية، بشكل أساسي كقيم متوسطة للتغييرات التي تحدث قبل العلاج مقابل بعده.
في مجال أمراض اللثة، تم دراسة أهمية النقاط النهائية الملموسة للعلاج النشط على نطاق واسع.بالإضافة إلى النقاط النهائية التي تم تقييمها على المدى الطويل (مثل الحاجة إلى إعادة العلاج وفقدان الأسنان) وجودة الحياة المتعلقة بالصحة الفموية التي أبلغ عنها المرضى، فإن مفهوم إغلاق الجيوب، أي عمق الاستكشاف الضحل وغياب النزيف عند الاستكشاف، مرتبط ارتباطًا وثيقًا بالاستقرار اللثوي. تم تقييم أهمية الجيوب المتبقية في مواقع الزرع بعد العلاج الجراحي للالتهاب المحيط بالزرع بواسطة كاركواك وآخرون.وجد المؤلفون أن عمق الاستكشاف المتبقيعند السنة الواحدة كان مؤشراً قوياً على تكرار المرض (نسبة الأرجحية 7.4) عند مقارنته بعمق الجيوب الأكثر ضحالة.تتحدث هذه النتيجة عن مفهوم الجيب العميق الذي يعمل كموطن محمي لطبقة حيوية ميكروبية كما هو موضح في القسم 4.
تم تقييم القيمة التنبؤية للنزيف عند الفحص في مواقع الزرع أيضًا. وبالتالي، قام كارلسون وآخرون،في دراسة متابعة لمدة 3 سنوات على 70 شخصًا تم تشخيصهم بالتهاب حول الزرع فيزرعاتهم، وجدوا أن تقدم المرض (فقدان العظام الإضافيكان من المرجح أن يحدث في مواقع الزرع التي تظهر بها نقاط نزيف متعددة (نسبة المخاطر 7.1) عند مقارنتها بعدم وجود نزيف أو وجود نزيف معزول فقط. كانت القيمة التنبؤية السلبية للنزيف عند الفحص مرتفعة بشكل خاص (95%). أسفرت التحليلات المقابلة بعد العلاج النشط لالتهاب المحيط بالزرع عن نتائج مماثلة. كانت القيمة التنبؤية السلبية (لغياب النزيف تمامًا عند الفحص) وعودة المرض اللاحقة (فقدان إضافي للعظام)… ) في تقييم مدته عامين بواسطة كاركواك وآخرون.كان. في دراسة أوروبية مبكرة حول التغيرات قصيرة المدى في مستويات ارتباط المحيط بالزرع في مجموعة من المرضى تحت رعاية الصيانة، قام جيبسون وآخرون.أبلغت عن قيمة تنبؤية سلبية شبه متطابقة تبلغ 82%.
بشكل جماعي، تدعم هذه البيانات مفهوم أن النقاط النهائية القصيرة الأجل ذات المعنى لعلاج التهاب المحيط بالزرع النشط يجب أن تتوافق مع ما تم اقتراحه لرعاية اللثة. بعبارة أخرى، يجب أن تهدف الجهود العلاجية إلى تحقيق عمق استكشاف سطحي حول الزرع وتقليل أو القضاء على النزيف عند الاستكشاف. يجب ملاحظة أن البيانات الحديثة قد اقترحت أن المعلمين، أي عمق استكشاف المحيط بالزرع والنزيف المحتمل عند الاستكشاف، مرتبطان ارتباطًا وثيقًا.أيضًا، بعد العلاج الجراحي لالتهاب المحيط بالزرع، وُجد أن احتمال النزيف عند الفحص كان منخفضًا في المواقع ذات الفحص الضحل.; )، بينما الاحتمالية المقابلة في المواقع ذات الجيوب العميقة ( كان مرتفعًا ). وبالتالي، فإن إرشادات الممارسة السريرية من المستوى S3 التي وضعتها الاتحاد الأوروبي لطب الأسنان اللثوي للوقاية من وعلاج الأمراض المحيطة بالزرعاتنقاط النهاية الموصى بها للعلاج الجراحي الناجح تشمل الفحص السطحي (غياب القيح عند الفحص، ونزيف طفيف فقط عند الفحصنقطة).
5.3 | العلاج غير الجراحي لالتهاب المحيط بالزرع
تم تقييم الفعالية السريرية للعلاج غير الجراحي لالتهاب المحيط بالزرع مؤخرًا في ثلاث مراجعات منهجية.تم تضمين إجمالي 15 تجربة عشوائية محكومة، أجريت بشكل رئيسي في دول أوروبية.تم تقييم العديد من الطرق المساعدة والبديلة لإزالة اللويحات و/أو تطهير سطح الزرع، بما في ذلك الطرق الميكانيكية والفيزيائية والفوتوميكانيكية/الحرارية (أي تطبيق الليزر) بالإضافة إلى الأساليب العلاجية الكيميائية. تم تعريف التدخلات الضابطة على أنها طرق تنظيف لا تهدف إلى أي تطهير ميكانيكي أو فيزيائي، باستثناء إزالة الرواسب الصلبة (أي أدوات الكشط أو الأجهزة الصوتية/الموجات فوق الصوتية مع أو بدون ري بالمحلول الملحي).
تم استخدام أجهزة الليزر المختلفة، سواء كعلاج أحادي (مثل ليزر Er:YAG، ليزر Nd:YAG) أو بالاشتراك (ليزر ثنائي، ليزر Er,Cr:YSGG) مع ري الكلورهيكسيدين، وكانت مرتبطة عادةً بتقليصات مماثلة في عمق الاستكشاف ودرجات النزيف كما في مجموعات التحكم المقابلة.تم الإبلاغ عن فوائد كبيرة لمجموعات الاختبار في دراستين فقط تستخدمان ليزر بقطر 3 ميكرون، مع فترات متابعة محدودة تبلغ 6 أشهر.وبناءً عليه، تم اقتراح عدم استخدام تطبيق الليزر، سواء كعلاج مساعد أو كعلاج أحادي، للعلاج غير الجراحي لالتهاب الأنسجة المحيطة بالزرعات في مستوى S3 من إرشادات الممارسة السريرية المقدمة من الاتحاد الأوروبي لطب الأسنان في عام 2023.
تم تقييم فعالية أدوات تحت المخاطية باستخدام تلميع الهواء المعتمد على مسحوق الجليسين في تجربتين عشوائيتين محكمتين.على الرغم من أن دراسة واحدة أفادت بتقليصات كبيرة في درجات النزيف بعد العلاج الأحادي بتقنية تلميع الهواء مقارنة بالعلاج الضابط عند 6 و 12 شهرًا، إلا أن الجودة العامة للأدلة كانت منخفضة. لذلك، اقترحت إرشادات الممارسة السريرية من المستوى S3 عدم استخدام تلميع الهواء في العلاج غير الجراحي لالتهاب المحيط بالزرع.استخدام الأساليب الكيميائية للتطهير السطحي التي تم تقييمها في الأدبيات شمل العلاج الضوئي المضاد للميكروبات (aPDT، الليزر منخفض المستوى:; المواد الحساسة للضوء: التولويدين/الأزرق الميثيليني) بالإضافة إلى هلام مجفف (أي، هيدروكسي بنزين سلفونيك/هيدروكسي ميثوكسي بنزين وحمض الكبريتيك). كانت كلا الإجرائين مرتبطين ببعض التحسينات في تقليل عمق الاستكشاف مقارنة بالمجموعات الضابطة المعنية بعد 6 أشهر.نظرًا لجودة الأدلة المنخفضة جدًا بشكل عام، تم اقتراح عدم استخدام العلاج الضوئي المعتمد على الأدوية أو جل المطهر المجفف في علاج التهاب الأنسجة المحيطة بالزرع غير الجراحي.
تم تقييم إدارة المضادات الميكروبية المحلية والمضادات الحيوية الجهازية وكذلك البروبيوتيك كعلاج مساعد للعلاج التقليدي غير الجراحي لالتهاب المحيط بالزرعات.بشكل أكثر تحديدًا، قامت أربع دراسات بتحليل فعالية المضادات الميكروبية المحلية، مثل كريات المينوسكلين ورقائق الكلورهيكسيدين.ثلاث دراسات تناولت المضادات الحيوية الجهازية، لا سيما الأموكسيسيلين + الميترونيدازول أو الميترونيدازول فقط.قيمت دراستان الفوائد المحتملة لبروبيوتيك لاكتوباسيلس ريوتيري.حسّنت المضادات الميكروبية الموضعية بشكل معتدل من تقليل عمق الاستكشاف، بينما كان للمضادات الحيوية الجهازية تأثير أكثر وضوحًا على تقليل كل من أعماق الاستكشاف ودرجات النزيف، لا سيما في المواقع التي كانت تعاني من جيوب أولية.لا تأثيرات إضافية على تقليل الجيوب لم يتم ملاحظة أي تقليل في درجات النزيف بعد إعطاء البروبيوتيك. في ضوء الأدلة العامة وبعد النظر بعناية في الفوائد والأضرار المحتملة، وخاصة المرتبطة بإعطاء المضادات الحيوية الجهازية، اقترحت إرشادات الممارسة السريرية من المستوى S3 عدم استخدام أي من التدابير المساعدة المذكورة أعلاه في العلاج غير الجراحي لالتهاب المحيط بالزرع.تقدم الجدول 2 نظرة عامة على الدراسات الأوروبية المختارة حول العلاج غير الجراحي لالتهاب المحيط بالزرع.
5.4 | العلاج الجراحي للالتهاب المحيط بالزرع
كانت المساهمات الأوروبية في الأدلة العلمية حول تأثير العلاج الجراحي لالتهاب المحيط بالزرع واسعة النطاق. تقريبًا، جميع مجموعات البيانات المذكورة في إرشادات الممارسة السريرية من المستوى S3 المنشورة مؤخرًا للوقاية من الأمراض المحيطة بالزرع وعلاجها.تم توليدها في الدول الأوروبية (الجدول 3). كانت التقارير الأولى من ألمانيا،إيطاليا والسويد، في الغالب على شكل سلسلة حالات بحجم عينة محدود. بدءًا من عام 2010 وما بعده، تم إجراء تجارب عشوائية محكومة.تم نشر تقييم فعالية بروتوكولات جراحية مختلفة بشكل مستمر.
أحد الجوانب الرئيسية التي أبرزتها هذه الدراسات المبكرة هو أهمية خصائص سطح الزرع على نتائج العلاج، كما تم الاقتراح في التقييمات السريرية السابقة.في دراسة سريرية محورية، روكوزو وآخرونوجد أن، بعد 12 شهرًا من العلاج الجراحي، كان تقليل عمق القياس حول الزرعات أكبر في الزرعات التي تم معالجتها بالرمل وحمض الإetching (SLA ) السطح (متوسط الانخفاض 3.4 مم ) عند مقارنته بزراعة الأسنان ذات السطح TPS ( 2.1 مم ). تم ملاحظة نتائج مماثلة للنزيف عند الاستكشاف مع وجود نزيف متبقي أعلى بكثير بعد عام واحد (57% مقابل 15%) في زراعة الأسنان ذات السطح المعالج بمادة البلازمينوجين النسيجي (TPS). تفسر أهمية خصائص سطح الزرع سبب اعتبار الدراسات السريرية في هذا المجال عادةً لفئات/علامات الزرع التي تم تضمينها.هذا الجانب، إلى جانب التفاصيل الفنية مثل إمكانية إزالة الترميم الحامل للزرع خلال الإجراء الجراحي، يميز العلاج الجراحي لالتهاب المحيط بالزرع عن نظيره في مجال أمراض اللثة. ومع ذلك، فإن العديد من الأسئلة السريرية والنهج العلمي العام كانت متشابهة. وبالتالي، تناولت الدراسات التدخلية (i) فعالية بروتوكولات التطهير المختلفة، (ii) الفائدة المحتملة للمطهرات/المضادات الميكروبية، و(iii) أساليب العلاج الترميمية. لقد تم تقييم جميع هذه المجالات بشكل موسع بالفعل ضمن مجال أمراض اللثة.بينما الأدلة المقابلة للإدارة الجراحية لالتهاب المحيط بالزرع لا تزال في مراحلها الأولى.
تم تقييم فعالية العلاج الجراحي لالتهاب المحيط بالزرع، بشكل عام، مؤخرًا في مراجعة نظامية طلبتها EFP. بينما قام كارلسون وآخرون.لم يتمكن من تحديد المقارنات المباشرة للتدخلات الجراحية مع العلاجات القياسية الأخرى (مثل العلاج غير الجراحي)، تم تقدير التأثير العام لجراحة الوصول إلى الفلپ و/أو إزالة الجيب من خلال التحليلات التلوية. استنادًا إلى 18 ذراع دراسة، أسفرت العلاج الجراحي عن تقليل متوسط موحد لعمق الجيب بمقدار 2.2 مم وزيادة في مستوى العظم الهامشي بمقدار 0.2 مم (الشكل 3). هذه البيانات، التي نشأت
الجدول 2 الدراسات الأوروبية المختارة حول العلاج غير الجراحي لالتهاب المحيط بالزرع.
دراسة
مجموعات العلاج
المرضى / الزرعات
معايير الشمول: التهاب المحيط بالزرع
متوسط PD عند خط الأساس
النتائج
تعليقات
ألباسلان يايلي وآخرون2022 RCT 6 أشهر تركيا
كُرَات تيتانيوم AB-AS-
كُرَات التيتانيوم العلاج الضوئي الديناميكي AB-AS-
١٧/١٧
عمق جيب 4-6 مم ونزيف عند المسح/نزيف عند الضغط وفقدان العظام
4.1 مم
PD أحمر: 0.5 مم BOP أحمر: 11.3%
– يُستبعد المدخنون
– تعليمات نظافة الفم
– لم يتم تقديم تفاصيل حول إزالة التعويضات المدعومة بالزرعات (جميعها مثبتة بالأسمنت)
– لم يتم تقديم تفاصيل حول التخدير الموضعي
– تغييرات MBL لم يتم الإبلاغ عنها
كُرَات تيتانيوم ليزر Er,Cr:YSGG AB-AS-
١٧/١٧
بنك الاحتياطي الفيدرالي الأحمر: 48.8%
شوارز وآخرون2005 RCT 6 أشهر ألمانيا
الكوريتات البلاستيكية ABAS+ ليزر Er:YAG AB-AS-
10/16
و BOP و SOP وفقدان العظام
5.5 مم
PD الأحمر: 0.8 مم BOP الأحمر: 52.0% REC: 0.1 مم
– لم يتم تقديم تفاصيل حول إزالة التعويضات المدعومة بالزرعات
– تغييرات MBL لم يتم الإبلاغ عنها
شوارز وآخرون2006 RCT 12 شهر ألمانيا
كُرَات بلاستيكية ABAS+
– يُستبعد المدخنون
– تعليمات نظافة الفم
الجدول 2 (مستمر)
دراسة
مجموعات العلاج
المرضى / الزرعات
معايير الشمول: التهاب المحيط بالزرع
متوسط PD عند خط الأساس
النتائج
تعليقات
روكوزو وآخرون2022 RCT 6 أشهر سويسرا
كُرَات التيتانيوم وكُرَات الفولاذ المقاوم للصدأ
12/12
و BOP/SOP وفقدان العظام
5.3 مم
PD الأحمر: 1.5 مم
بندقية حمراء: 0%
تغيير MBL: 0.0 مم
– تعليمات نظافة الفم
– التخدير الموضعي
– تعويض مدعوم بالزرع لم يتم إزالته
رينفرت وآخرون2009 تجربة عشوائية محكومة لمدة 6 أشهر في السويد
كُرَات التيتانيوم وأكواب المطاط
١٧/١٧
و وفقدان العظام
4.0 مم
PD الأحمر: 0.0 مم
بندقية BOP حمراء (من أربعة مواقع): 0.3
– تعليمات نظافة الفم
– التخدير الموضعي
كارينغ وآخرون2005 تجربة سريرية عشوائية (فم مقسم) 6 أشهر الدنمارك
كُرَات الكربون
11/11
وفقدان العظام و BOP
6.3 مم
PD الأحمر: 0.0 مم
العجز في الميزان التجاري: -9.8% (تدهور)
تغيير MBL: -0.3 (خسارة)
PD الأحمر: -0.1 مم (تدهور)
بنك الاحتياطي الأحمر: 27.2%
تغيير MBL: -0.3 (خسارة)
– تعليمات نظافة الفم
– لم يتم توفير التخدير الموضعي
– لم يتم تقديم تفاصيل حول إزالة التعويضات المدعومة بالزرعات
– رأس فوق صوتي مخصص (فيكتور)
سهم وآخرون2011 RCT 6 أشهر ألمانيا
كُحتات الكربون
ريّ 0.1% من محلول CHX ديغلوكونات + تطبيق جل 0.1% من CHX ديغلوكونات تحت المخاطية
15/22
و وفقدان العظامبعد وضع الزرع
4.0 مم
PD الأحمر: 0.5 مم
بنك الاحتياطي الفيدرالي الأحمر: 11.0%
REC: 0.0 مم
تغيير CAL: 0.5 مم (زيادة)
– تعليمات نظافة الفم
– التخدير الموضعي
– لم يتم تقديم تفاصيل حول إزالة التعويضات المدعومة بالزرعات
جون وآخرون2015
RCT
12 شهر في ألمانيا
تنظيف الكربون 0.1% من محلول الديجلوكونات الكلورهيكسيدين + تطبيق جل 0.1% من محلول الديجلوكونات الكلورهيكسيدين تحت المخاطية
13/18
3.9 مم
PD الأحمر: 0.4 مم
بنك الاحتياطي الفيدرالي الأحمر: 16.6%
REC: 0.1 مم
تغيير CAL: 0.5 مم (زيادة)
– متابعة لمدة 12 شهرًا لدراسة ساهم وآخرون.
– تعليمات نظافة الفم
– التخدير الموضعي
– لم يتم تقديم تفاصيل حول إزالة التعويضات المدعومة بالزرعات
تلميع الهواء (مسحوق الجلايسين)
12/18
3.7 مم
PD الأحمر: 0.5 مم
بنك الاحتياطي الفيدرالي الأحمر: 41.2%
REC: 0.1 مم
تغيير CAL: 0.6 مم (زيادة)
الجدول 2 (مستمر)
دراسة
مجموعات العلاج
المرضى / الزرعات
معايير الشمول: التهاب المحيط بالزرع
متوسط PD عند خط الأساس
النتائج
تعليقات
بوليمري وآخرون
فوق الصوتي
19/19
و BOP/SOP و
8.0 مم
PD الأحمر: 1.5 مم
– تعليمات نظافة الفم
هولندا
كحتات الكربون فوق الصوتية AB+ AS+
18/18
7.4 مم
PD الأحمر: 2.3 مم BOP الأحمر: 15% (تقريباً)
– رأس فوق صوتي مخصص (PEEK)
دي وال وآخرون2021 تجربة عشوائية محكومة 3 أشهر هولندا
PD الأحمر: 1.0 مم BOP الأحمر: لم يتم الإبلاغ عنه تغيير CAL: -1.5 مم (فقدان) REC: 1.4 مم تغيير MBL: -1.0 مم (فقدان)
– لم يتم الإبلاغ عن التعامل مع الأطراف الصناعية المدعومة بالزرع
– شفاء عبر الغشاء المخاطي
لاسير وآخرون
فتحة الوصول وزرع الأسنان
15/20
PD & BOP/SOP & فقدان العظام
6.7 مم
كُرَات
– يُستبعد المدخنون
– السكري ليس استبعادًا
٢٠٢٠
أب-
REC: 0.5 مم
معيار
RCT 6 أشهر
AS+
تغيير CAL: 3.5 مم (زيادة) تغيير MBL: 0.3 مم (زيادة)
– التدخلات قبل الجراحة: ميكانيكية
بلجيكا
فتحة الوصول وتلميع الهواء ABAS+
14/19
5.6 مم
تلميع الهواء باستخدام الكوريت
PD الأحمر: تغيير BOP 3.3 مم. 61.1%
الأدوات، تعليمات نظافة الفم
– إزالة التعويض المدعوم بالزرع للجراحة، إذا كان ذلك ممكنًا
– شفاء عبر الغشاء المخاطي
الجدول 3 (مستمر)
دراسة
مجموعات العلاج
المرضى / الزرعات
معايير الشمول: التهاب المحيط بالزرع
متوسط PD عند خط الأساس
بروتوكول إزالة التلوث
النتائج
تعليقات
ريجيدور وآخرون
فتحة الوصول وزرع العظم و
19/19
و BOP/SOP والعظم
9.4 مم
فرشاة تيتانيوم
PD الأحمر: 4.4 مم
تغيير BOP: 67.3%
– مرض السكري والتدخين ليسا من معايير الاستبعاد
إسبانيا
فتحة الوصول وزرع العظم
AB+
AS+
20/20
8.8 مم
فرشاة تيتانيوم
PD الأحمر: 4.2 مم
تغيير BOP: 66.2%
REC: 0.1 مم
تغيير MBL: 0.9 مم (زيادة)
– التدخلات قبل الجراحة: أدوات ميكانيكية، تعليمات نظافة الفم
– إزالة التعويض المدعوم بالزرع للجراحة، إذا كان ذلك ممكنًا
– شفاء عبر الغشاء المخاطي
مونجي وآخرون
فتحة الوصول وزرع العظم
16/24
و ومستوى العظم
8.7 مم
فرشاة تيتانيوم.
بيروكسيد الهيدروجينمالح
PD الأحمر: 5.0 مم
بند BOP الأحمر: لم يتم الإبلاغ
REC: 2.0 مم
تغيير MBL: 1.7 مم (زيادة)
– كانت السكري والتدخين من معايير الاستبعاد
RCT
AS+
– التدخلات قبل الجراحة: التنظيف الميكانيكي
AB+
AS+
17/24
8.6 مم
فرشاة تيتانيوم.
بيروكسيد الهيدروجين
3% وملح
PD الأحمر: 4.6 مم
بند BOP الأحمر: لم يتم الإبلاغ
REC: 1.8 مم
تغيير MBL: 1.7 مم (زيادة)
– إزالة التعويض المدعوم بالزرع للجراحة، إذا كان ذلك ممكنًا
– زراعة الأسنان في الأسطح المزروعة الموجودة فوق القمة
– شفاء عبر الغشاء المخاطي
بوليمري وآخرون
فتح الوصول وزرع العظم (بقر، BioOss)
11/11
و فقدان العظاموعيب عظمي
7.0 مم
كُرَات التيتانيوم.
بيروكسيد الهيدروجينوالمحلول الملحي
PD الأحمر: 3.6 مم
بنك الاحتياطي الفيدرالي الأحمر: 54.5%
تغيير MBL: 2.2 مم (زيادة)
– التدخين ليس معيار استبعاد. لم يتم تضمين أي أشخاص مصابين بالسكري.
RCT
AS+
١٣/١٣
7.1 مم
كُرَات التيتانيوم.
بيروكسيد الهيدروجين
والمحلول الملحي
PD الأحمر: 3.8 مم
بنك الاحتياطي الفيدرالي الأحمر: 50.5%
تغيير MBL: 2.8 مم (زيادة)
– التدخلات قبل الجراحة: لم يتم وصفها
AB+
AS+
– إزالة التعويض المدعوم بالزرع للجراحة، إذا كان ذلك ممكنًا
– شفاء عبر الغشاء المخاطي
تقليل عمق جيب الفحص
دراسة
متوسط التأثير القياسي مع فترة ثقة 95%
الوزن (%)
1. الباكر 2018
–
–
0.7 (-0.4, 1.8)
3.0
2. الباكر 2018
–
–
0.7 (-0.5, 1.9)
2.8
3. كاركواك 2020
–
-0.2 ( -0.6, 0.2)
٦.٧
4. دي وال 2013
-0.3 (-1.1, 0.5)
٤.٤
5. دي وال 2013
-0.7 ( -1.8, 0.4)
٢.٩
6. دي وال 2015
0.0 ( -0.6, 0.6)
٥.٥
7. دي وال 2015
-0.3 ( -0.9, 0.3)
5.2
8. إنجليزوس 2018
-0.2 ( -0.5, 0.1)
7.3
9. هالستروم 2017
0.3 (0.1، 0.5)
٧.٥
10. هالستروم 2017
–
0.5( 0.3, 0.7)
٧.٧
12. هينتينا 2022
-0.1 ( -0.3, 0.1)
7.8
13. هينتينا 2022
-0.2 (-0.3، -0.1)
٨.٠
14. جيبسون 2016
0.9 (0.4, 1.4)
6.3
15. ديركس 2022
1.1 (0.9، 1.3)
٧.٥
16. رينفرت 2021
1.3 (0.3, 2.3)
3.4
17. رينفرت 2018
–
0.2 ( -0.1, 0.5)
7.4
18. فاغنر 2021
0.6( 0.2, 1.0)
٦.٧
بشكل عام
–
0.2 ( -0.0, 0.5)
-2
-1
0
1
2
نموذج REML ذو التأثيرات العشوائية
تغيير مستوى العظم الهامشي
دراسة
متوسط التأثير القياسي مع فترة ثقة 95%
الوزن (%)
1. الباكر 2018
0.7 ( -0.4, 1.8)
3.0
2. الباكر 2018
0.7 (-0.5, 1.9)
2.8
3. كاركواك 2020
-0.2 (-0.6, 0.2)
٦.٧
4. دي وال 2013
-0.3 (-1.1, 0.5)
٤.٤
5. دي وال 2013
-0.7 (-1.8, 0.4)
2.9
6. دي وال 2015
0.0 ( -0.6, 0.6)
٥.٥
7. دي وال 2015
-0.3 (-0.9, 0.3)
5.2
8. إنجليزوس 2018
-0.2 (-0.5, 0.1)
7.3
9. هالستروم 2017
٧.٥
10. هالستروم 2017
12. هينتينا 2022
-0.1 ( -0.3, 0.1)
7.8
13. هينتينا 2022
-0.2 ( -0.3, -0.1)
8.0
14. جيبسون 2016
0.9 (0.4, 1.4)
6.3
15. ديركس 2022
1.1 (0.9، 1.3)
16. رينفرت 2021
1.3( 0.3, 2.3)
3.4
17. رينفرت 2018
–
0.2 ( -0.1, 0.5)
7.4
18. فاغنر 2021
0.6 (0.2, 1.0)
٦.٧
بشكل عام
0.2 ( -0.0, 0.5)
فقدان العظام
-2
-1 0
01
2
نموذج REML ذو التأثيرات العشوائية
الشكل 3 مقتبس من كارلسون وآخرون.انظر النشر الأصلي للمراجع. متوسط الانخفاض القياسي في عمق جيب الاستكشاف والتغيرات في مستوى العظم الهامشي كما هو موضح في الدراسات الرصدية المستقبلية أو في بعض الأذرع المختارة من التجارب السريرية العشوائية على إجراءات الفتحة الوصول أو القضاء على الجيب. تشير الدراسات الأوروبية بشكل أساسي إلى أن العلاج الجراحي الذي يهدف إلى تطهير سطح الزرع كان فعالًا في تقليل علامات الالتهاب المحيط بالزرع وفي إيقاف تقدم المرض.
5.4.1 | فعالية بروتوكولات التطهير المختلفة
تنظيف وتطهير أسطح الزرع المعرضة هو عنصر حاسم في الإدارة الجراحية لالتهاب المحيط بالزرع.بينما يتم عادةً إزالة الرواسب المعدنية بواسطة الكوريتات أو المكاشط، تم اقتراح العديد من الأدوات والبروتوكولات لتسهيل إزالة الفيلم الحيوي الميكروبي. قامت مراجعة منهجية وتحليل تلوي حديث بتقييم فعالية التدابير المساعدة (أي التدابير المستخدمة بعد تنظيف سطح الزرع التقليدي) أو التدابير البديلة الضوئية/الميكانيكية والفيزيائية لتطهير سطح الزرع بالتزامن مع بروتوكولات جراحية متنوعة.بشكل أكثر تحديدًا، شملت هذه التدابير زراعة الأسنان، وتلميع الهواء، والأجهزة فوق الصوتية، وفرشات التيتانيوم، والليزر، التي استخدمت إما كعلاج أحادي أو كعلاج مركب. تم مقارنة هذه التدخلات مع إما الأدوات القياسية (مثل الكاشطات لإزالة الرواسب الصلبة بالإضافة إلى الشاش المنقوع في محلول ملحي) فقط (المقارنة 1)، أو مع مجموعة من الأدوات القياسية (مثل الكاشطات لإزالة الرواسب الصلبة). بالإضافة إلى الشاش المنقوع في محلول ملحي) وتدابير ميكانيكية/فيزيائية/مضادة للميكروبات إضافية (المقارنة 2).
للمقارنة 1، التحليل التلوي، استنادًا إلى دراستين،كشفت الفروق المتوسطة الموزونة عن تقليصات النزيف وعمق الاستكشافو 0.9 مم، على التوالي، مما يفضل استخدام الطرق المساعدة والبديلة (أي، تلميع الهواء باستخدام مسحوق الجلايسين أو مسحوق الإريثريتول وفرشات التيتانيوم) بدلاً من طرق إزالة التلوث السطحية التقليدية للزرع بين 6 و 12 شهرًا بعد العلاج الجراحي غير الترميمي لالتهاب ما حول الزرع.على مدى فترة من عامين بعد العلاج الجراحي المشترك، ارتبط ليزر Er:YAG بتقليصات مماثلة في عمق الاستكشاف (1.1 مم مقابل 1.5 مم) والنزيف ( مقابل عند مقارنتها بنظام التطهير التقليدي.
للمقارنة 2، تم التحقيق في تجربتين عشوائيتين محكومتين إما فعالية ليزر Er:YAG المستخدم كملحق لجهاز تنظيف بيزو كهربائي، أو التأثير المساعد لفرشاة التيتانيوم بعد إزالة الأنسجة الميكانيكية والتطهير الكيميائي باستخدامالاختلافات المتوسطة الموزونة المبلغ عنها لتقليل النزيف (12%) وعمق الاستكشافلم يُبلغ عن أي فائدة من استخدام أي من بروتوكولي التطهير.
استنادًا إلى هذه الأدلة السريرية المحدودة وللأسباب المقدمة للعلاج غير الجراحي، تم التوصية بعدم استخدام تلميع الهواء وليزر Er:YAG، بينما يمكن اعتبار فرشاة التيتانيوم لتطهير سطح الزرع الجراحي.
5.4.2 | الاستخدام المساعد للمضادات الحيوية الجهازية
تم تقييم استخدام المضادات الحيوية الجهازية كعلاج مساعد للعلاج الجراحي لالتهاب المحيط بالزرع حتى الآن في تجربتين، كلاهما من السويد.في عام 2017، هالستروم وآخروناستخدمت الأزيثرومايسين في 20 شخصًا في مجموعة الاختبار، بينما تم علاج 19 مريضًا في مجموعة التحكم بجراحة الفلپ فقط. بعد 12 شهرًا من العلاج، لاحظ المؤلفون انخفاضات مماثلة في عمق الاستكشاف (مجموعة التحكم 1.5 مم؛ مجموعة الاختبار: 1.3 مم) ومستوى العظم الهامشي (مجموعة التحكم 0.3 مم؛ مجموعة الاختبار: 0.5 مم). وكانت الاستنتاجات اللاحقة أن هذا النظام المحدد من المضادات الحيوية لم يوفر أي فوائد.
في التجربة الثانية ذات الصلة في هذا السياق، كاركواك وآخرونتم تسجيل 100 مريض وتم تخصيص نصفهم عشوائيًا لنظام مضاد حيوي يتكون من 10 أيام من 750 ملغ من الأموكسيسيلين مرتين يوميًا بالتزامن مع العلاج الجراحي. كانت النتائج مختلفة بعض الشيء عن تلك التي لوحظت من قبل هالستروم وآخرين.كخفضات لعمق جيب الاستكشاف مقابل ) ومستوى العظم الهامشي ( مقابل كانت النتائج عند 12 شهرًا أكثر إيجابية في مجموعة الاختبار مقارنة بمجموعة التحكم. تبع المؤلفون عينة المرضى بعد ذلك لمدة تصل إلى 5 سنوات،التقارير عن النتائج طويلة الأمد. لوحظ أن الفوائد التي تم ملاحظتها في البداية للتدخل المضاد للميكروبات لم تستمر بعد السنة الأولى (الشكل 4). وبالتالي، فإن إرشادات الممارسة السريرية من المستوى S3 للوقاية من وعلاج الأمراض المحيطة بالزرع التي نشرتها EFPيوصى بعدم استخدام المضادات الحيوية الجهازية كعلاج مساعد للعلاج الجراحي لالتهاب المحيط بالزرع، مشيرًا إلى جودة الأدلة المنخفضة بشكل عام.
5.4.3 | فعالية الطرق الترميمية
متسق مع الأدبيات المتعلقة بأمراض اللثة،السؤال الأكثر تقييمًا بشكل موسع في مجال الجراحة يتعلق بالتقنيات الترميمية وفوائدها المحتملة.تشمل هذه الطريقة العلاجية استخدام إما طعوم بديلة للعظام، أو أغشية، أو عوامل حيوية، أو تركيبات منها تُطبق داخل أو على سطح العيب العظمي المحيط بالزرع، والذي ينتج عادةً عن عملية المرض.بالإضافة إلى الأهداف العلاجية الأساسية المتعلقة بحل التهاب الأنسجة الرخوة، فإن الطرق الترميمية تهدف بشكل خاص إلى (ط) تجديد العيب العظمي، (2) إعادة الاندماج العظمي، و(3) الحفاظ على ارتفاع الأنسجة الرخوة.عمليًا، جميع الدراسات المنضبطة في هذا تمثل السياق المساهمات من أوروبا.بينما أجرت بعض التجارب مقارنات مباشرة بين تقنيات إعادة البناء المختلفة،في الغالبية العظمى من التقارير، تم تقييم فعالية الطرق الترميمية من خلال مقارنتها بجراحة طية الوصول، أي، استبعاد التقنية الترميمية. في هذا، يتماشى المجال بشكل كبير مع أبحاث أمراض اللثة.
تشمل النقاط النهائية الرئيسية لعلاج التهاب المحيط بالزرع عمق جيب استكشاف ضحل ونزيف محدود عند الاستكشاف، كما هو موضح في الشكل 5 ومفصل في القسم 5.2.
كما تم تلخيصه في مراجعتين منهجيتين، لم تُظهر طرق إعادة البناء، بحد ذاتها، أي فائدة في هذا السياق. يمكن توضيح ذلك من خلال التجربة السريرية العشوائية متعددة المراكز التي قدمها جيبسن وآخرون. شمل المؤلفون 64 موضوعًا يعانون من التهاب حول الزرع ووزعوا هؤلاء إما إلى مجموعة تحكم (جراحة شق الوصول) أو مجموعة اختبار (جراحة شق الوصول وزرع عظم بديل). بعد 12 شهرًا، كان الانخفاض في عمق الاستكشاف 2.6 و2.8 مم، على التوالي. بلغ انخفاض النزيف عند الاستكشاف و . وبالمثل، لم يتمكن رينفرت وآخرون. من ملاحظة أي فائدة لنهج إعادة البناء من حيث النتائج الأولية. جمع المؤلفون بين زرع عظم بديل وغشاء في مجموعة الاختبار ولاحظوا انخفاضًا في عمق الاستكشاف بمقدار 1.9 مم مقارنة بانخفاض قدره 2.3 مم في مجموعة التحكم (جراحة شق الوصول). وأخيرًا، وصف ديركس وآخرون. انخفاضات لمدة 12 شهرًا في كل من عمق الاستكشاف (3.7 مم مقابل 3.7 مم) وفي النزيف عند الاستكشاف ( مقابل ) التي كانت متطابقة تقريبًا في كل من ذراعي التحكم والاختبار. وكانت الأخيرة تتكون من إضافة زرع عظم بديل.
باستثناء دراسة ديركس وآخرون، كانت المعايير الشعاعية، مع ذلك، محسنة باستمرار من خلال التدابير الترميمية. وولفارت وآخرون، جيبسن وآخرون، إيسهيد وآخرون، رينفرت وآخرون، وإيمانويل وآخرون. جميعهم أبلغوا عن فوائد في مجموعات الاختبار تتراوح من 0.5 إلى 2.7 مم من زيادة مستوى العظم الإضافي. يجب ملاحظة، مع ذلك، أن التأثير السريري لهذا التأثير لا يزال بحاجة إلى إثبات. أيضًا، قد يكون التقييم الشعاعي لمستويات العظم الهامشي بعد تطبيق مادة بديلة للعظم صعبًا وقابلًا للتفسير (الشكل 5B).
تم تقييم تأثير التدابير الترميمية على تغييرات مستويات الأنسجة الرخوة، أي، تراجع الأنسجة الرخوة، نادرًا ما تم تقييمه. قيمت تجربتان التراجع في مواقع الزرع البوكالية حتى 12 شهرًا بعد الجراحة ووجدت و انخفاضًا في ارتفاع الأنسجة الرخوة في مجموعات التحكم (جراحة شق الوصول). من المثير للاهتمام، أن كلا الدراستين أبلغتا عن تراجع أقل في مجموعات الاختبار، مع فائدة متسقة
بمقدار 0.4 مم. كما هو موضح أعلاه، لا يزال من الضروري تقييم الأهمية السريرية لهذه الفائدة. كانت رضا المرضى بعد 12 شهرًا عمومًا مرتفعة ولم تختلف عبر مجموعات الدراسة في أي من الدراستين.
تقييمات النتائج على المدى الطويل بعد العلاج الترميمي لالتهاب حول الزرع نادرة. أبلغ روكوزو وآخرون. عن نتائج لمدة 10 سنوات بعد جراحة شق الوصول المدمجة مع زرع عظم
كما هو موضح في الشكل 5C. وجد المؤلفون أن الزرعات الخشنة بشكل معتدل كانت جيدة جدًا بمعدل بقاء وانخفاضات حادة في عمق الاستكشاف (3.9 مم) والنزيف عند الاستكشاف (63%). ومع ذلك، كانت نسبة فقدان الزرع للزرعات ذات السطح المطلي بالبلازما من التيتانيوم مرتفعة تصل إلى . تدعم هذه النتائج الفروق الواضحة في الاستجابة السريرية التي لوحظت بالفعل بعد عام واحد. وهي أيضًا متوافقة مع
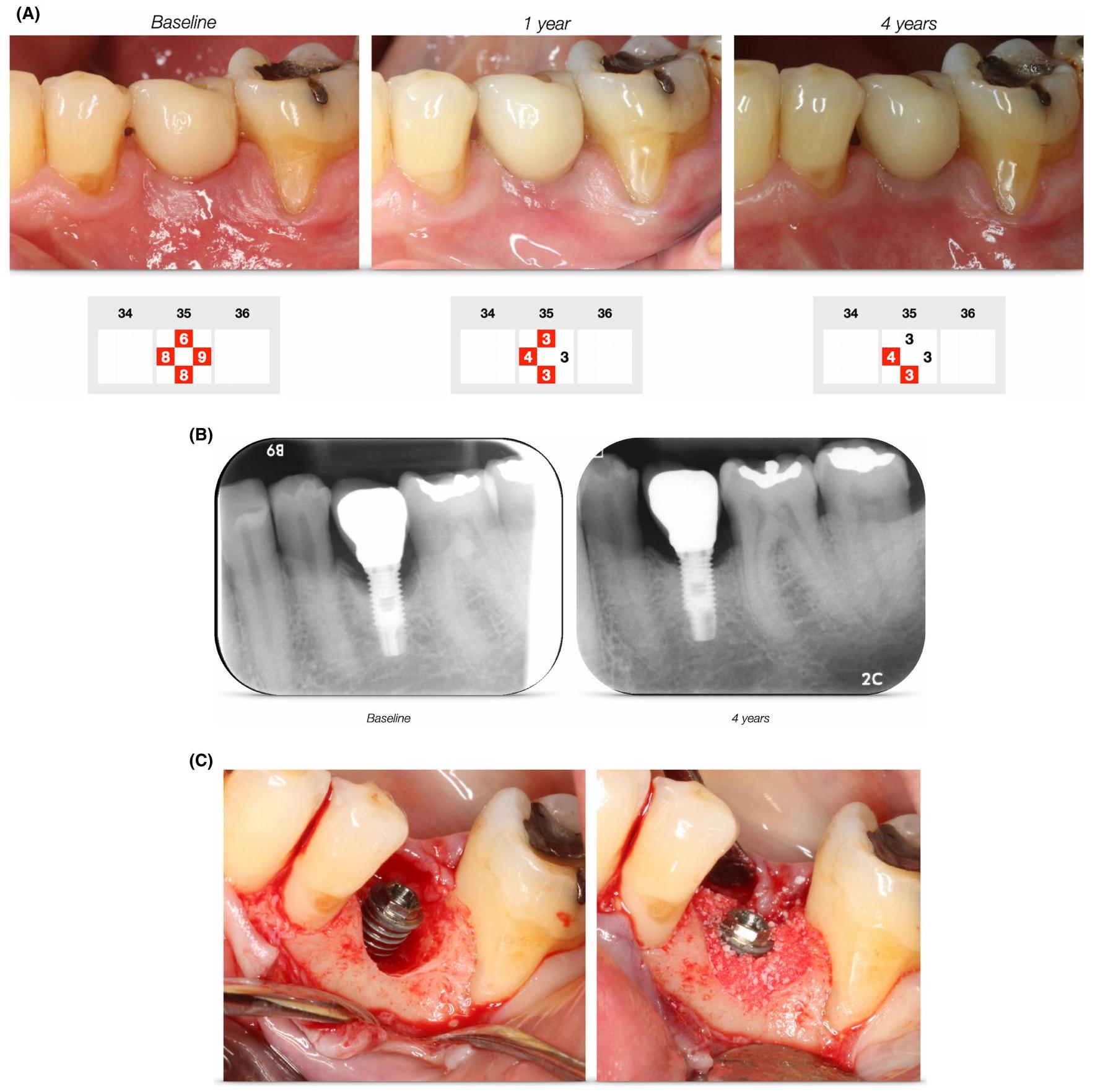
الشكل 5 (A) متابعة سريرية لمدة أربع سنوات بعد العلاج الجراحي لالتهاب حول الزرع. لاحظ الانخفاض في عمق جيب الاستكشاف (المسجل في أربعة مواقع من الزرع) عند 1 و4 سنوات. اللون الأحمر يشير إلى النزيف عند الاستكشاف. (B) متابعة شعاعية لمدة أربع سنوات بعد العلاج الجراحي لالتهاب حول الزرع. تظهر الصور السريرية في (A). (C) صور سريرية توضح التدخل الجراحي. تم إزالة تاج الزرع مؤقتًا لتسهيل الوصول. بعد تطهير سطح الزرع بواسطة أدوات التيتانيوم وفرشاة دوارة من التيتانيوم تحت الري بمحلول ملحي، تم وضع مادة عظمية من الأبقار في العيب العظمي. بعد الخياطة، تم إعادة وضع تاج الزرع (شفاء عبر الغشاء المخاطي). يتم توضيح الحالة قبل وبعد الجراحة والمظهر الشعاعي في (A) و(B) على التوالي.
نتائج من تقييمات قبل السريرية في vivo تشير إلى الصعوبات في إدارة التهاب حول الزرع في الزرعات ذات الخصائص السطحية الخشنة/المعقدة.
5.5 | العوامل المؤثرة على نتائج العلاج
في مجال أمراض اللثة، كان من المفهوم منذ فترة طويلة أن موضع/شكل الأسنان، تكوين العيب، والمعايير المتعلقة بالمريض، مثل مستوى السيطرة على العدوى والتدخين، كلها عوامل حاسمة في نتائج العلاج الجراحي. أيضًا، تم اقتراح أن النهج الجراحي، أي تصميم الشق، له صلة بالنتائج السريرية. لا يزال الفهم المقابل للعوامل المؤثرة على نتائج العلاج الجراحي لالتهاب حول الزرع محدودًا. ومع ذلك، تناولت بعض الدراسات الأوروبية الحديثة هذا السؤال.
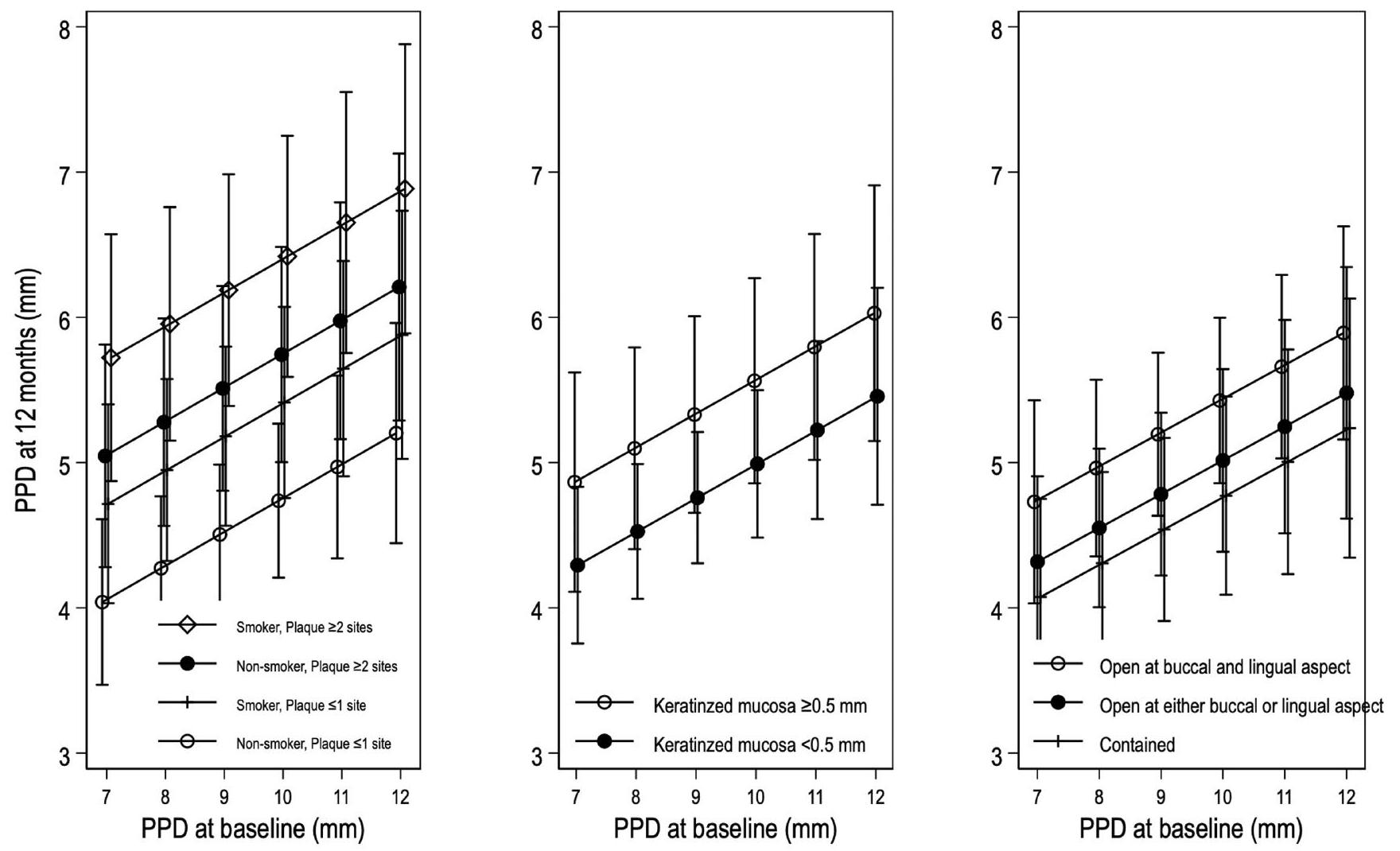
كما تم مناقشته بالفعل أعلاه، أظهرت بيانات المتابعة التي تم جمعها على مدى فترات قصيرة وطويلة الأجل أهمية خصائص سطح الزرع على نتائج العلاج. في تحليل ثانوي لتجربة سريرية عشوائية حول فعالية زرع عظم بديل، قيم إيتشيكا وآخرون. أهمية عوامل خلفية متعددة. لاحظ المؤلفون وجود علاقة قوية بين عمق الاستكشاف الأولي والنهائي (12 شهرًا) (الشكل 6). تتماشى هذه الملاحظة مع التقديرات من مراجعة منهجية قدمها كارلسون وآخرون، حيث كانت شدة انخفاض عمق الاستكشاف مرتبطة مباشرة بالقيم الأولية.
تم تقييم جودة الأنسجة الرخوة، أي، أبعاد الغشاء المخاطي الكيراتيني، كمؤشر لنتائج العلاج في دراستين أوروبيتين على الأقل، حيث أبلغت عن بيانات متناقضة. في سلسلة حالات استعادية مع فترة متابعة متوسطة تبلغ 23 شهرًا، لاحظ مونجي وآخرون. نتائج أقل ملاءمة في مواقع الزرع ذات الأبعاد المخفضة من الغشاء المخاطي الكيراتيني (). ومع ذلك، كانت الفروق واضحة فقط في الزرعات المعالجة بتقنيات ترميمية (). من بين 104 مواقع زرع عولجت بأساليب استئصالية/إزالة الجيب، لم يكن ارتفاع الغشاء المخاطي الكيراتيني مرتبطًا بالنتائج. بشكل عام، أيضًا فشل إيتشيكا وآخرون. في تحديد تأثير متسق للغشاء المخاطي الكيراتيني على نتائج العلاج بعد جراحة شق الوصول سواء بدون (تحكم) أو مع (اختبار) إضافة زرع عظم بديل (الشكل 6). أظهرت التحليلات الإحصائية أن عمق الاستكشاف بعد 12 شهرًا كان، في المتوسط، 0.6 مم أكبر في المواقع التي لا تحتوي على () (الشكل 7A) مقارنة بالمواقع التي تحتوي على () الغشاء المخاطي الكيراتيني (الشكل 7B). لم تكن هذه الفروق ذات دلالة إحصائية. ومع ذلك، كشفت نفس الدراسة عن احتمال أعلى (OR 5.2) للنزيف المتبقي في الزرعات التي لا تحتوي على الغشاء المخاطي الكيراتيني.
الشكل 6 عمق جيب الاستكشاف (PD) بعد 12 شهرًا من العلاج الجراحي لالتهاب حول الزرع مع أو بدون إضافة زرع عظم بديل ( زرعات في 129 مريضًا) كما أبلغ إيتشيكا وآخرون. لاحظ الفروق في الاستكشاف النهائي حسب التدخين واللويحات (بعد 6 أسابيع). لم يكن لأبعاد الغشاء المخاطي الكيراتيني أو تكوين العيب تأثير ذو دلالة إحصائية على النتائج. تم تعديل النماذج الإحصائية للتدخين، اللويحات (بعد 6 أسابيع)، الغشاء المخاطي الكيراتيني في البداية، وتكوين العيب الذي تم تقييمه أثناء الجراحة.
البيانات حول أهمية تكوين العيب العظمي حول الزرع محدودة أيضًا. استنادًا إلى سلسلة حالات مستقبلية مع متابعة لمدة 5 سنوات، لاحظ روكوزو وآخرون. تحسينات ملحوظة في المعايير السريرية، كما يتضح من متوسط انخفاض عمق الاستكشاف بمقدار 3.9 مم. لم يكن حجم التحسين، في هذه البيانات، معتمدًا على نوع العيب، المصنف وفقًا لشوارز وآخرون. تم التوصل إلى استنتاج مشابه من قبل إيتشيكا وآخرون. بينما تم تسجيل أقل عمق استكشاف بعد 12 شهرًا في العيوب المصنفة على أنها محصورة (الشكل 6)، كانت الفروق صغيرة () ولم تكن ذات دلالة إحصائية. في دراسة ثالثة، فشل مونجي وآخرون. أيضًا في تحديد عمق العيب الشعاعي أو زاوية العيب كمتنبئين ذوي دلالة لزوال المرض الذي تم تقييمه سريريًا. ومع ذلك، لاحظ المؤلفون وجود ملء عظمي شعاعي أكثر وضوحًا في المواقع ذات زوايا العيب الأضيق (). تم تقديم نتائج متناقضة بعض الشيء من قبل شوارز وآخرون، الذين أبلغوا عن تحسن سريري أكثر ملاءمة لمدة 6 أشهر (تقليل عمق الاستكشاف ومستوى الارتباط السريري) في العيوب المحتواة بالكامل. ومع ذلك، لم يتم الحفاظ على الفروقات في تقييم 12 شهرًا. أغازاده وآخرون.أبلغوا أن العيوب المحتواة بالكامل كانت مرتبطة بملء عيوب أكبر من أنواع العيوب الأخرى
بعد تطبيق إما عظم ذاتي أو مادة عظمية من الأبقار بعد عام واحد.
بينما يتم تسليط الضوء بقوة على أهمية التزام المريض في إرشادات الممارسة السريرية من المستوى S3 حول الوقاية والعلاج من الأمراض المحيطة بالزرع،فإن الأدلة العلمية ذات الصلة محدودة للغاية.لذا، فإن المنطق يعتمد بقوة على المبادئ المتعلقة بالعلاج اللثوي. في دراسة واحدة، إيتشيكا وآخرونلاحظوا أن ضعف التحكم في اللويحات بعد 6 أسابيع من العلاج الجراحي لالتهاب المحيط بالزرع كان مرتبطًا بنتائج أسوأ بعد 12 شهرًا (الشكل 6). في نفس مجموعة البيانات، كانت وجود اللويحات بعد 12 شهرًا مرتبطة أيضًا بقوة (OR 3.7) بوجود نزيف متبقي. يجب ملاحظة، مع ذلك، أن المشاركين في هذه الدراسة كانوا عمومًا ملتزمين للغاية وتحت صيانة صارمة خلال فترة الملاحظة.
في دراسة استعادية لمدة 5 سنوات شملت 21 مريضًا، طبق كورتيليني وآخرونبروتوكول جراحي طفيف التوغل لمواقع الزرع المتأثرة بالتهاب المحيط بالزرع. في الفحص النهائي، أبلغ المؤلفون عن متوسط تقليل عمق الاستكشاف بمقدار 3.9 مم وزيادة مقابلة في مستويات العظام الشعاعية بمقدار 2.5 مم. نظرًا لعدم وجود دراسات محكومة حول الأساليب الجراحية، فإن تأثير نوع النهج الجراحي في الوصول إلى العيب المحيط بالزرع لا يزال غير واضح.
(أ)
(ب)
الشكل 7 (أ) صور توضح حالة من التهاب المحيط بالزرع مع غياب الغشاء المخاطي الكيراتيني على الجانب الفكي للزرع. (ب) صور توضح حالة من التهاب المحيط بالزرع مع وفرة من الغشاء المخاطي الكيراتيني على الجانب الفكي للزرع.
6 | ملاحظات ختامية
التهاب المحيط بالزرع هو كيان مرضي معترف به يؤثر على نسب كبيرة من المرضى البالغين. عدد السكان المعرضين للخطر كبير.
تدابير مكافحة العدوى التي يقوم بها المريض والمهنيون في مجال الأسنان ضرورية في الوقاية والعلاج من التهاب المحيط بالزرع.
يجب أن يتبع علاج التهاب المحيط بالزرع نهجًا تدريجيًا.
يجب تقديم رعاية داعمة للمحيط بالزرع لجميع المرضى الذين يتلقون علاج الزرع، وخاصة للمرضى الذين تم علاجهم من التهاب المحيط بالزرع.
7 | آفاق المستقبل
نظرًا للاستخدام الواسع والمتزايد لزراعة الأسنان في إعادة تأهيل المرضى، يجب على المهنيين في مجال الأسنان توقع والاستعداد لزيادة الطلب على الرعاية الداعمة للمحيط بالزرع وللتدخلات المتعلقة بأمراض المحيط بالزرع. يجب أن تتناول الأبحاث المستقبلية طرق تقييم المخاطر، وتحسين التشخيصات، بالإضافة إلى بروتوكولات فعالة وآمنة لعلاج التهاب المحيط بالزرع.
معلومات التمويل
هذه الدراسة ممولة ذاتيًا.
بيان تضارب المصالح
يعلن المؤلفون عدم وجود تضارب محتمل في المصالح فيما يتعلق بتأليف و/أو نشر هذه المقالة.
REFERENCES
Lang NP, Karring T. Proceedings of the 1st European Workshop on Periodontology. Quintessence Publishing Co., Ltd; 1993.
Albrektsson T, Isidor F. Consensus Report of Session IV Proceedings of the 1st European Workshop on Periodontology. Switzerland. Quintessence Publishing Co., Ltd.; 1993.
Lang NP, Karring T, Lindhe J. Proceedings of the 3rd European Workshop on Periodontology. Quintessence Publishing Co., Ltd; 1999.
Berglundh T, Persson L, Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 2002;29(Suppl 3):197-212; discussion 232-3.
Lindhe J, Meyle J, Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the sixth European workshop on periodontology. J Clin Periodontol. 2008;35(8 Suppl):282-285.
Lang NP, Berglundh T, Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: where are we now?-Consensus of the seventh European workshop on periodontology. J Clin Periodontol. 2011;38 Suppl 11(s11):178-181.
Sanz M, Chapple IL, Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant
diseases: consensus report of working group 4. J Clin Periodontol. 2012;39(Suppl 12):202-206.
Jepsen S, Berglundh T, Genco R, et al. Primary prevention of periimplantitis: managing peri-implant mucositis. J Clin Periodontol. 2015;42(Suppl 16):S152-S157.
Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Clin Periodontol. 2018;45:S286-S291.
Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Clin Periodontol. 2018;45:S246-S266.
Fransson C, Lekholm U, Jemt T, Berglundh T. Prevalence of subjects with progressive bone loss at implants. Clin Oral Implants Res. 2005;16(4):440-446.
Derks J, Håkansson J, Wennström JL, Tomasi C, Larsson M, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: early and late implant loss. J Dent Res. 2015;94(3 Suppl):44S-51S.
Derks J, Schaller D, Håkansson J, Wennström JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: prevalence of peri-implantitis. J Dent Res. 2016;95(1):43-49.
SKaPa, Swedish Quality Registry for caries and periodontal disease Annual report. Swedish Quality Registry for caries and periodontal disease; 2022.
Jordan RA, Bodechtel C, Hertrampf K, et al. The Fifth German Oral Health Study (Funfte Deutsche Mundgesundheitsstudie, DMS V) – rationale, design, and methods. BMC Oral Health. 2014;14:161.
Jordan AR, Micheelis W. Fünfte Deutsche Mundgesundheitsstudie(DMS V). Vol 35. Deutscher Zahnärzte Verlag DÄV; 2016.
Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015;42(Suppl 16):S158-S171.
Mombelli A, Muller N, Cionca N. The epidemiology of periimplantitis. Clin Oral Implants Res. 2012;23(Suppl 6):67-76.
Koldsland OC, Scheie AA, Aass AM. Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol. 2010;81(2):231-238.
Roos-Jansåker AM, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol. 2006;33(4):290-295.
Mir-Mari J, Mir-Orfila P, Figueiredo R, Valmaseda-Castellón E, Gay-Escoda C. Prevalence of peri-implant diseases. A crosssectional study based on a private practice environment. J Clin Periodontol. 2012;39(5):490-494.
Rodrigo D, Sanz-Sánchez I, Figuero E, et al. Prevalence and risk indicators of peri-implant diseases in Spain. J Clin Periodontol. 2018;45(12):1510-1520.
Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res. 2012;91(10):914-920.
Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJL, Marcenes W. Global burden of severe periodontitis in 19902010: a systematic review and meta-regression. J Dent Res. 2014;93(11):1045-1053.
Koldsland OC, Scheie AA, Aass AM. The association between selected risk indicators and severity of peri-implantitis using mixed model analyses. J Clin Periodontol. 2011;38(3):285-292.
Carra MC, Rangé H, Swerts PJ, Tuand K, Vandamme K, Bouchard P. Effectiveness of implant-supported fixed partial denture in patients with history of periodontitis: a systematic review and metaanalysis. J Clin Periodontol. 2022;49(Suppl 24):208-223.
Serino G, Strom C. Peri-implantitis in partially edentulous patients: association with inadequate plaque control. Clin Oral Implants Res. 2009;20(2):169-174.
Fransson C, Tomasi C, Pikner SS, et al. Severity and pattern of peri-implantitis-associated bone loss. J Clin Periodontol. 2010;37(5):442-448.
Lindhe J, Berglundh T, Ericsson I, Liljenberg B, Marinello C. Experimental breakdown of peri-implant and periodontal tissues. A study in the beagle dog. Clin Oral Implants Res. 1992;3(1):9-16.
Schou S, Holmstrup P, Reibel J, Juhl M, Hjørting-Hansen E, Kornman KS. Ligature-induced marginal inflammation around osseointegrated implants and ankylosed teeth: stereologic and histologic observations in cynomolgus monkeys (Macaca fascicularis). J Periodontol. 1993;64(6):529-537.
Marinello CP, Berglundh T, Ericsson I, Klinge B, Glantz PO, Lindhe J. Resolution of ligature-induced peri-implantitis lesions in the dog. J Clin Periodontol. 1995;22(6):475-479.
Schou S, Holmstrup P, Stoltze K, Hjørting-Hansen E, Fiehn NE, Skovgaard LT. Probing around implants and teeth with healthy or inflamed peri-implant mucosa/gingiva. A histologic comparison in cynomolgus monkeys (Macaca fascicularis). Clin Oral Implants Res. 2002;13(2):113-126.
Zitzmann NU, Berglundh T, Ericsson I, Lindhe J. Spontaneous progression of experimentally induced periimplantitis. J Clin Periodontol. 2004;31(10):845-849.
Berglundh T, Gotfredsen K, Zitzmann NU, Lang NP, Lindhe J. Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: an experimental study in dogs. Clin Oral Implants Res. 2007;18(5):655-661.
Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of peri-implantitis at different types of implants. An experimental study in dogs. I: clinical and radiographic observations. Clin Oral Implants Res. 2008;19(10):997-1002.
Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of ligatured induced peri-implantitis at implants with different surface characteristics. An experimental study in dogs II: histological observations. Clin Oral Implants Res. 2009;20(4):366-371.
Albouy JP, Abrahamsson I, Berglundh T. Spontaneous progression of experimental peri-implantitis at implants with different surface characteristics: an experimental study in dogs. J Clin Periodontol. 2012;39(2):182-187.
Carcuac O, Abrahamsson I, Albouy JP, Linder E, Larsson L, Berglundh T. Experimental periodontitis and peri-implantitis in dogs. Clin Oral Implants Res. 2013;24(4):363-371.
Carcuac O, Abrahamsson I, Derks J, Petzold M, Berglundh T. Spontaneous progression of experimental peri-implantitis in augmented and pristine bone: a pre-clinical in vivo study. Clin Oral Implants Res. 2020;31(2):192-200.
Berglundh T, Zitzmann NU, Donati M. Are peri-implantitis lesions different from periodontitis lesions? J Clin Periodontol. 2011;38(Suppl 11):188-202.
Sanz M, Alandez J, Lazaro P, Calvo JL, Quirynen M, van Steenberghe D. Histo-pathologic characteristics of peri-implant soft tissues in Branemark implants with 2 distinct clinical and radiological patterns. Clin Oral Implants Res. 1991;2(3):128-134.
Gualini F, Berglundh T. Immunohistochemical characteristics of inflammatory lesions at implants. J Clin Periodontol. 2003;30(1):14-18.
Berglundh T, Gislason Ö, Lekholm U, Sennerby L, Lindhe J. Histopathological observations of human periimplantitis lesions. J Clin Periodontol. 2004;31(5):341-347.
Carcuac O, Berglundh T. Composition of human peri-implantitis and periodontitis lesions. J Dent Res. 2014;93(11):1083-1088.
Konermann A, Götz W, le M, Dirk C, Lossdörfer S, Heinemann F. Histopathological verification of osteoimmunological mediators in peri-implantitis and correlation to bone loss and implant functional period. J Oral Implantol. 2016;42(1):61-68.
Galindo-Moreno P, López-Martínez J, Caba-Molina M, et al. Morphological and immunophenotypical differences between
chronic periodontitis and peri-implantitis – a cross-sectional study. Eur J Oral Implantol. 2017;10(4):453-463.
Kasnak G, Firatli E, Könönen E, Olgac V, Zeidán-Chuliá F, Gursoy UK. Elevated levels of 8-OHdG and PARK7/DJ-1 in peri-implantitis mucosa. Clin Implant Dent Relat Res. 2018;20(4):574-582.
Dionigi C, Larsson L, Carcuac O, Berglundh T. Cellular expression of DNA damage/repair and reactive oxygen/nitrogen species in human periodontitis and peri-implantitis lesions. J Clin Periodontol. 2020;47(12):1466-1475.
Fretwurst T, Garaicoa-Pazmino C, Nelson K, et al. Characterization of macrophages infiltrating peri-implantitis lesions. Clin Oral Implants Res. 2020;31(3):274-281.
Becker ST, Beck-Broichsitter BE, Graetz C, Dörfer CE, Wiltfang J, Häsler R. Peri-implantitis versus periodontitis: functional differences indicated by transcriptome profiling. Clin Implant Dent Relat Res. 2014;16(3):401-411.
Venza I, Visalli M, Cucinotta M, de Grazia G, Teti D, Venza M. Proinflammatory gene expression at chronic periodontitis and peri-implantitis sites in patients with or without type 2 diabetes. Periodontol. 2010;81(1):99-108.
Fretwurst T, Buzanich G, Nahles S, Woelber JP, Riesemeier H, Nelson K. Metal elements in tissue with dental peri-implantitis: a pilot study. Clin Oral Implants Res. 2016;27(9):1178-1186.
Pettersson M, Pettersson J, Johansson A, Molin Thorén M. Titanium release in peri-implantitis. J Oral Rehabil. 2019;46(2):179-188.
Nelson K, Hesse B, Addison O, et al. Distribution and chemical speciation of exogenous micro- and nanoparticles in inflamed soft tissue adjacent to titanium and ceramic dental implants. Anal Chem. 2020;92(21):14432-14443.
Albrektsson T, Chrcanovic B, Östman PO, Sennerby L. Initial and long-term crestal bone responses to modern dental implants. Periodontol 2000. 2017;73(1):41-50.
Mombelli A, Lang NP. The diagnosis and treatment of periimplantitis. Periodontol 2000. 1998;17:63-76.
Mombelli A. Maintenance therapy for teeth and implants. Periodontol 2000. 2019;79:190-199.
Pontoriero R, Tonelli MP, Carnevale G, Mombelli A, Nyman SR, Lang NP. Experimentally induced peri-implant mucositis. A clinical study in humans. Clin Oral Implants Res. 1994;5:254-259.
Zitzmann NU, Berglundh T, Marinello CP, Lindhe J. Experimental peri-implant mucositis in man. J Clin Periodontol. 2001;28(6):517-523.
Meyer S, Giannopoulou C, Courvoisier D, Schimmel M, Müller F, Mombelli A. Experimental mucositis and experimental gingivitis in persons aged 70 or over. Clinical and biological responses. Clin Oral Implants Res. 2017;28(8):1005-1012.
Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36:177-187.
Salvi GE, Aglietta M, Eick S, Sculean A, Lang NP, Ramseier CA. Reversibility of experimental peri-implant mucositis compared with experimental gingivitis in humans. Clin Oral Implants Res. 2012;23(2):182-190.
Hickey JS, O’Neal RB, Scheidt MJ, Strong SL, Turgeon D, van Dyke TE. Microbiologic characterization of ligature-induced peri-implantitis in the microswine model. J Periodontol. 1991;62:548-553.
Leonhardt Å, Berglundh T, Ericsson I, Dahlen G. Putative periodontal pathogens on titanium implants and teeth in experimental gingivitis and periodontitis in beagle dogs. Clin Oral Implants Res. 1992;3:112-119.
Tillmanns HW, Hermann JS, Tiffee JC, Burgess AV, Meffert RM. Evaluation of three different dental implants in ligature induced peri implantitis in the beagle dog. Part II. Histology and microbiology. Int J Oral Maxillofac Implants. 1998;13(1):59-68.
Nociti FH Jr, Cesco de Toledo R, Machado MAN, Stefani CM, Line SRP, Gonçalves RB. Clinical and microbiological evaluation of ligature-induced peri-implantitis and periodontitis in dogs. Clin Oral Implants Res. 2001;12(4):295-300.
Lindquist LW, Rockler B, Carlsson GE. Bone resorption around fixtures in edentulous patients treated with mandibular fixed tissueintegrated prostheses. J Prosthet Dent. 1988;59:59-63.
Rinke S, Ohl S, Ziebolz D, Lange K, Eickholz P. Prevalence of periimplant disease in partially edentulous patients: a practice-based cross-sectional study. Clin Oral Implants Res. 2011;22(8):826-833.
Monje A, Aranda L, Diaz KT, et al. Impact of maintenance therapy for the prevention of peri-implant diseases: a systematic review and meta-analysis. J Dent Res. 2016;95(4):372-379.
Rams TE, Link CC. Microbiology of failing dental implants in humans: electron microscopic observations. J Oral Implantol. 1983;11:93-100.
Rams TE, Roberts TW, Tatum H. Subgingival bacteriology of periodontally healthy and diseased human dental implants. J Dent Res. 1984;63(Special issue):200.
Listgarten MA. Electron microscopic observations on the bacterial flora of acute necrotizing ulcerative gingivitis. J Periodontol. 1965;36:328-339.
Mombelli A, van Oosten MAC, Schürch E Jr, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol Immunol. 1987;2:145-151.
Mombelli A, Décaillet F. The characteristics of biofilms in periimplant disease. J Clin Periodontol. 2011;38(Suppl 11):203-213.
Mombelli A, Casagni F, Madianos PN. Can presence or absence of periodontal pathogens distinguish between subjects with chronic and aggressive periodontitis? A systematic review. J Clin Periodontol. 2002;29(Suppl 3):10-21.
Carvalho EBS, Romandini M, Sadilina S, Sant’Ana ACP, Sanz M. Microbiota associated with peri-implantitis-a systematic review with meta-analyses. Clin Oral Implants Res. 2023;34(11):1176-1187.
Kröger A, Hülsmann C, FickI S, et al. The severity of human periimplantitis lesions correlates with the level of submucosal microbial dysbiosis. J Clin Periodontol. 2018;45(12):1498-1509.
Mombelli A, Hashim D, Cionca N. What is the impact of titanium particles and biocorrosion on implant survival and complications? A critical review. Clin Oral Implants Res. 2018;29(Suppl 18):37-53.
Ronin D, Boyer J, Alban N, Natoli RM, Johnson A, Kjellerup BV. Current and novel diagnostics for orthopedic implant biofilm infections: a review. APMIS. 2022;130(2):59-81.
Meyer S, Giannopoulou C, Cancela J, Courvoisier D, Müller F, Mombelli A. Experimental mucositis/gingivitis in persons aged 70 or over: microbiological findings and prediction of clinical outcome. Clin Oral Investig. 2019;23(10):3855-3863.
Tonetti MS, Chapple ILC, Jepsen S, Sanz M. Primary and secondary prevention of periodontal and peri-implant diseases: introduction to, and objectives of the 11th European workshop on periodontology consensus conference. J Clin Periodontol. 2015;42(Suppl 16):S1-S4.
Rothman KJ. Causes. Am J Epidemiol. 1976;104(6):587-592.
Costa FO, Takenaka-Martinez S, Cota LOM, Ferreira SD, Silva GLM, Costa JE. Peri-implant disease in subjects with and without preventive maintenance: a 5-year follow-up. J Clin Periodontol. 2012;39(2):173-181.
Monje A, Wang HL, Nart J. Association of preventive maintenance therapy compliance and peri-implant diseases: a cross-sectional study. J Periodontol. 2017;88(10):1030-1041.
Costa FO, Costa AM, Ferreira SD, et al. Long-term impact of patients’ compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: an 11-year prospective follow-up clinical study. Clin Implant Dent Relat Res. 2023;25(2):303-312.
Schwarz F, John G, Schmucker A, Sahm N, Becker J. Combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination: a 7-year follow-up observation. J Clin Periodontol. 2017;44(3):337-342.
Berglundh T, Wennstrom JL, Lindhe J. Long-term outcome of surgical treatment of peri-implantitis. A 2-11-year retrospective study. Clin Oral Implants Res. 2018;29(4):404-410.
Heitz-Mayfield LJA, Salvi GE, Mombelli A, et al. Supportive periimplant therapy following anti-infective surgical peri-implantitis treatment: 5-year survival and success. Clin Oral Implants Res. 2018;29(1):1-6.
Carcuac O, Derks J, Abrahamsson I, Wennström JL, Berglundh T. Risk for recurrence of disease following surgical therapy of peri-implantitis-a prospective longitudinal study. Clin Oral Implants Res. 2020;31(11):1072-1077.
Roccuzzo M, Fierravanti L, Pittoni D, Dalmasso P, Roccuzzo A. Implant survival after surgical treatment of peri-implantitis lesions by means of deproteinized bovine bone mineral with 10% collagen: 10-year results from a prospective study. Clin Oral Implants Res. 2020;31(8):768-776.
Herrera D, Berglundh T, Schwarz F, et al. Prevention and treatment of peri-implant diseases-the EFP S3 level clinical practice guideline. J Clin Periodontol. 2023;50(Suppl 26):4-76.
Nibali L, Koidou VP, Nieri M, Barbato L, Pagliaro U, Cairo F. Regenerative surgery versus access flap for the treatment of intrabony periodontal defects: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):320-351.
Sanz-Sanchez I, Montero E, Citterio F, Romano F, Molina A, Aimetti M. Efficacy of access flap procedures compared to subgingival debridement in the treatment of periodontitis. A systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):282-302.
Suvan J, Leira Y, Moreno Sancho FM, Graziani F, Derks J, Tomasi C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol. 2020;47(Suppl 22):155-175.
Derks J, Ichioka Y, Dionigi C, et al. Prevention and management of peri-implant mucositis and peri-implantitis: a systematic review of outcome measures used in clinical studies in the last 10 years. J Clin Periodontol. 2023;50(Suppl 25):55-66.
Loos BG, Needleman I. Endpoints of active periodontal therapy. J Clin Periodontol. 2020;47 Suppl 22(Suppl 22):61-71.
Karlsson K, Derks J, Håkansson J, Wennström JL, Petzold M, Berglundh . Interventions for peri-implantitis and their effects on further bone loss: a retrospective analysis of a registry-based cohort. J Clin Periodontol. 2019;46(8):872-879.
Carcuac O, Derks J, Abrahamsson I, Wennström JL, Petzold M, Berglundh T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J Clin Periodontol. 2017;44(12):1294-1303.
Jepsen S, Rühling A, Jepsen K, Ohlenbusch B, Albers HK. Progressive peri-implantitis. Incidence and prediction of periimplant attachment loss. Clin Oral Implants Res. 1996;7(2):133-142.
Farina R, Filippi M, Brazzioli J, Tomasi C, Trombelli L. Bleeding on probing around dental implants: a retrospective study of associated factors. J Clin Periodontol. 2017;44(1):115-122.
Merli M, Bernardelli F, Giulianelli E, Toselli I, Mariotti G, Nieri M. Peri-implant bleeding on probing: a cross-sectional multilevel analysis of associated factors. Clin Oral Implants Res. 2017;28(11):1401-1405.
Ichioka Y , Trullenque-Eriksson A, Ortiz-Vigón A, et al. Factors influencing outcomes of surgical therapy of peri-implantitis: a secondary analysis of 1-year results from a randomized clinical study. J Clin Periodontol. 2023;50(10):1282-1304.
Cosgarea R, Roccuzzo A, Jepsen K, Sculean A, Jepsen S, Salvi GE. Efficacy of mechanical/physical approaches for implant surface decontamination in non-surgical submarginal
instrumentation of peri-implantitis. A systematic review. J Clin Periodontol. 2023;50(Suppl 26):188-211.
de Waal YCM, Winning L, Stavropoulos A, Polyzois I. Efficacy of chemical approaches for implant surface decontamination in conjunction with sub-marginal instrumentation, in the nonsurgical treatment of peri-implantitis: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):212-223.
Linares A, Sanz-Sánchez I, Dopico J, Molina A, Blanco J, Montero E. Efficacy of adjunctive measures in the non-surgical treatment of peri-implantitis: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):224-243.
Karring ES, Stavropoulos A, Ellegaard B, Karring T. Treatment of peri-implantitis by the vector system. Clin Oral Implants Res. 2005;16(3):288-293.
Schwarz F, Sculean A, Rothamel D, Schwenzer K, Georg T, Becker J. Clinical evaluation of an Er:YAG laser for nonsurgical treatment of peri-implantitis: a pilot study. Clin Oral Implants Res. 2005;16(1):44-52.
Schwarz F, Bieling K, Bonsmann M, Latz T, Becker J. Nonsurgical treatment of moderate and advanced periimplantitis lesions: a controlled clinical study. Clin Oral Investig. 2006;10(4):279-288.
Renvert S, Samuelsson E, Lindahl C, Persson GR. Mechanical nonsurgical treatment of peri-implantitis: a double-blind randomized longitudinal clinical study. I: clinical results. J Clin Periodontol. 2009;36(7):604-609.
Sahm N, Becker J, Santel T, Schwarz F. Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: a prospective, randomized, controlled clinical study. J Clin Periodontol. 2011;38(9):872-878.
John G, Sahm N, Becker J, Schwarz F. Nonsurgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine. Twelve-month follow-up of a prospective, randomized, controlled clinical study. Clin Oral Investig. 2015;19(8):1807-1814.
Laleman I, Pauwels M, Quirynen M, Teughels W. The usage of a lactobacilli probiotic in the non-surgical therapy of periimplantitis: a randomized pilot study. Clin Oral Implants Res. 2020;31(1):84-92.
Merli M, Bernardelli F, Giulianelli E, et al. Short-term comparison of two non-surgical treatment modalities of peri-implantitis: clinical and microbiological outcomes in a two-factorial randomized controlled trial. J Clin Periodontol. 2020;47(10):1268-1280.
De Waal YCM, Vangsted TE, Van Winkelhoff AJ. Systemic antibiotic therapy as an adjunct to non-surgical peri-implantitis treatment: a single-blind RCT. J Clin Periodontol. 2021;48(7):996-1006.
Hentenaar DFM, de Waal YCM, Stewart RE, van Winkelhoff AJ, Meijer HJA, Raghoebar GM. Erythritol airpolishing in the nonsurgical treatment of peri-implantitis: a randomized controlled trial. Clin Oral Implants Res. 2021;32:840-852.
Blanco C, Pico A, Dopico J, Gándara P, Blanco J, Liñares A. Adjunctive benefits of systemic metronidazole on non-surgical treatment of peri-implantitis. A randomized placebo-controlled clinical trial. J Clin Periodontol. 2022;49(1):15-27.
Polymeri A, van der Horst J, Anssari Moin D, Wismeijer D, Loos BG, Laine ML. Non-surgical peri-implantitis treatment with or without systemic antibiotics: a randomized controlled clinical trial. Clin Oral Implants Res. 2022;33(5):548-557.
Roccuzzo A, Klossner S, Stähli A, et al. Non-surgical mechanical therapy of peri-implantitis with or without repeated adjunctive diode laser application. A 6-month double-blinded randomized clinical trial. Clin Oral Implants Res. 2022;33(9):900-912.
Yayli NZA, Talmac AC, Keskin Tunc S, Akbal D, Altindal D, Ertugrul AS. Erbium, chromium-doped: yttrium, scandium, gallium, garnet and diode lasers in the treatment of peri-implantitis: clinical and
biochemical outcomes in a randomized-controlled clinical trial. Lasers Med Sci. 2022;37(1):665-674.
Machtei EE, Frankenthal S, Levi G, et al. Treatment of periimplantitis using multiple applications of chlorhexidine chips: a double-blind, randomized multi-centre clinical trial. J Clin Periodontol. 2012;39(12):1198-1205.
Bassetti M, Schär D, Wicki B, et al. Anti-infective therapy of periimplantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin Oral Implants Res. 2014;25(3):279-287.
Ahmed P, Bukhari IA, Albaijan R, Sheikh SA, Vohra F. The effectiveness of photodynamic and antibiotic gel therapy as an adjunct to mechanical debridement in the treatment of periimplantitis among diabetic patients. Photodiagnosis Photodyn Ther. 2020;32:102077.
Machtei EE, Romanos G, Kang P, et al. Repeated delivery of chlorhexidine chips for the treatment of peri-implantitis: a multicenter, randomized, comparative clinical trial. J Periodontol. 2021;92(1):11-20.
Shibli JA, Ferrari DS, Siroma RS, Figueiredo LC, Faveri M, Feres M. Microbiological and clinical effects of adjunctive systemic metronidazole and amoxicillin in the non-surgical treatment of periimplantitis: 1 year follow-up. Braz Oral Res. 2019;33(suppl 1):e080.
Almohareb T, Alhamoudi N, al Deeb M, et al. Clinical efficacy of photodynamic therapy as an adjunct to mechanical debridement in the treatment of per-implantitis with abscess. Photodiagnosis Photodyn Ther. 2020;30:101750.
Tada H, Masaki C, Tsuka S, Mukaibo T, Kondo Y, Hosokawa R. The effects of Lactobacillus reuteri probiotics combined with azithromycin on peri-implantitis: a randomized placebo-controlled study. J Prosthodont Res. 2018;62(1):89-96.
Deppe H, Horch HH, Henke J, Donath K. Peri-implant care of ailing implants with the carbon dioxide laser. Int J Oral Maxillofac Implants. 2001;16(5):659-667.
Khoury F, Buchmann R. Surgical therapy of peri-implant disease: a 3-year follow-up study of cases treated with 3 different techniques of bone regeneration. J Periodontol. 2001;72(11):1498-1508.
Deppe H, Horch HH, Neff A. Conventional versus laserassisted treatment of peri-implant defects with the concomitant use of pure-phase beta-tricalcium phosphate: a 5-year clinical report. Int J Oral Maxillofac Implants. 2007;22(1):79-86.
Romeo E, Ghisolfi M, Murgolo N, Chiapasco M, Lops D, Vogel G. Therapy of peri-implantitis with resective surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part I: clinical outcome. Clin Oral Implants Res. 2005;16(1):9-18.
Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces. J Clin Periodontol. 2011;38(8):738-745.
Leonhardt A, Dahlen G, Renvert S. Five-year clinical, microbiological, and radiological outcome following treatment of periimplantitis in man. J Periodontol. 2003;74(10):1415-1422.
Roos-Jansåker AM, Renvert H, Lindahl C, Renvert S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: a prospective cohort study. J Clin Periodontol. 2007;34(7):625-632.
Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. J Clin Periodontol. 2011;38(3):276-284.
Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intrabony defects with autogenous bone or a xenograft: results after 12 months. J Clin Periodontol. 2012;39(7):666-673.
Schwarz F, John G, Mainusch S, Sahm N, Becker J. Combined surgical therapy of peri-implantitis evaluating two methods of surface debridement and decontamination. A two-year clinical follow up report. J Clin Periodontol. 2012;39(8):789-797.
Wohlfahrt JC, Lyngstadaas SP, Rønold HJ, et al. Porous titanium granules in the surgical treatment of peri-implant osseous defects: a randomized clinical trial. Int J Oral Maxillofac Implants. 2012;27(2):401-410.
de Waal YC, Raghoebar GM, Huddleston Slater JJ, Meijer HJ, Winkel EG, van Winkelhoff A. Implant decontamination during surgical peri-implantitis treatment: a randomized, double-blind, placebo-controlled trial. J Clin Periodontol. 2013;40(2):186-195.
Schwarz F, Hegewald A, John G, Sahm N, Becker J. Four-year fol-low-up of combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination. J Clin Periodontol. 2013;40(10):962-967.
Persson LG, Berglundh T, Lindhe J, Sennerby L. Re-osseointegration after treatment of peri-implantitis at different implant surfaces. An experimental study in the dog. Clin Oral Implants Res. 2001;12(6):595-603.
Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Implant surface characteristics influence the outcome of treatment of peri-implantitis: an experimental study in dogs. J Clin Periodontol. 2011;38(1):58-64.
Carcuac O, Derks J, Charalampakis G, Abrahamsson I, Wennström J, Berglundh T. Adjunctive systemic and local antimicrobial therapy in the surgical treatment of peri-implantitis: a randomized controlled clinical trial. J Dent Res. 2016;95(1):50-57.
Donos N, Calciolari E, Brusselaers N, Goldoni M, Bostanci N, Belibasakis GN. The adjunctive use of host modulators in non-surgical periodontal therapy. A systematic review of randomized, placebo-controlled clinical studies. J Clin Periodontol. 2020;47(Suppl 22):199-238.
Herrera D, Matesanz P, Martín C, Oud V, Feres M, Teughels W. Adjunctive effect of locally delivered antimicrobials in periodontitis therapy: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):239-256.
Salvi GE, Stähli A, Schmidt JC, Ramseier CA, Sculean A, Walter C. Adjunctive laser or antimicrobial photodynamic therapy to non-surgical mechanical instrumentation in patients with untreated periodontitis: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):176-198.
Teughels W, Feres M, Oud V, Martín C, Matesanz P, Herrera D. Adjunctive effect of systemic antimicrobials in periodontitis therapy: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):257-281.
Karlsson K, Trullenque-Eriksson A, Tomasi C, Derks J. Efficacy of access flap and pocket elimination procedures in the management of peri-implantitis: a systematic review and meta-analysis. J Clin Periodontol. 2023;50(Suppl 26):244-284.
Ramanauskaite A, Schwarz F, Cafferata EA, Sahrmann P. Photo/ mechanical and physical implant surface decontamination approaches in conjunction with surgical peri-implantitis treatment: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):317-335.
Toma S, Brecx MC, Lasserre JF. Clinical evaluation of three surgical modalities in the treatment of peri-implantitis: a randomized controlled clinical trial. J Clin Med. 2019;8(7):966.
Hentenaar DFM, de Waal YCM, Stewart RE, van Winkelhoff AJ, Meijer HJA, Raghoebar GM. Erythritol air polishing in the surgical treatment of peri-implantitis: a randomized controlled trial. Clin Oral Implants Res. 2022;33(2):184-196.
de Tapia B, Valles C, Ribeiro-Amaral T, et al. The adjunctive effect of a titanium brush in implant surface decontamination at periimplantitis surgical regenerative interventions: a randomized controlled clinical trial. J Clin Periodontol. 2019;46(5):586-596.
Wang CW, Ashnagar S, Gianfilippo RD, Arnett M, Kinney J, Wang HL. Laser-assisted regenerative surgical therapy for periimplantitis: a randomized controlled clinical trial. J Periodontol. 2021;92(3):378-388.
Teughels W, Seyssens L, Christiaens V, Temmerman A, Castro AB, Cosyn J. Adjunctive locally and systemically delivered antimicrobials during surgical treatment of peri-implantitis: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):359-372.
Hallström H, Persson GR, Lindgren S, Renvert S. Open flap debridement of peri-implantitis with or without adjunctive systemic antibiotics: a randomized clinical trial. J Clin Periodontol. 2017;44(12):1285-1293.
Donos N, Calciolari E, Ghuman M, Baccini M, Sousa V, Nibali L. The efficacy of bone reconstructive therapies in the management of peri-implantitis. A systematic review and meta-analysis. J Clin Periodontol. 2023;50(Suppl 26):285-316.
Monje A, Pons R, Insua A, Nart J, Wang HL, Schwarz F. Morphology and severity of peri-implantitis bone defects. Clin Implant Dent Relat Res. 2019;21(4):635-643.
Jepsen S, Schwarz F, Cordaro L, et al. Regeneration of alveolar ridge defects. Consensus report of group 4 of the 15th European workshop on periodontology on bone regeneration. J Clin Periodontol. 2019;46(Suppl 21):277-286.
Isehed C, Holmlund A, Renvert S, Svenson B, Johansson I, Lundberg P. Effectiveness of enamel matrix derivative on the clinical and microbiological outcomes following surgical regenerative treatment of peri-implantitis. A randomized controlled trial. J Clin Periodontol. 2016;43(10):863-873.
Jepsen K, Jepsen S, Laine ML, et al. Reconstruction of peri-implant osseous defects: a multicenter randomized trial. J Dent Res. 2016;95(1):58-66.
Isler SC, Soysal F, Ceyhanlı T, Bakırarar B, Unsal B. Regenerative surgical treatment of peri-implantitis using either a collagen membrane or concentrated growth factor: a 12-month randomized clinical trial. Clin Implant Dent Relat Res. 2018;20(5):703-712.
Renvert S, Roos-Jansåker AM, Persson GR. Surgical treatment of peri-implantitis lesions with or without the use of a bone substitute-a randomized clinical trial. J Clin Periodontol. 2018;45(10):1266-1274.
Polymeri A, Anssari-Moin D, van der Horst J, Wismeijer D, Laine ML, Loos BG. Surgical treatment of peri-implantitis defects with two different xenograft granules: a randomized clinical pilot study. Clin Oral Implants Res. 2020;31(11):1047-1060.
Renvert S, Giovannoli JL, Roos-Jansåker AM, Rinke S. Surgical treatment of peri-implantitis with or without a deproteinized bovine bone mineral and a native bilayer collagen membrane: a randomized clinical trial. J Clin Periodontol. 2021;48(10):1312-1321.
Derks J, Ortiz-Vigón A, Guerrero A, et al. Reconstructive surgical therapy of peri-implantitis: a multicenter randomized controlled clinical trial. Clin Oral Implants Res. 2022;33(9):921-944.
Monje A, Pons R, Vilarrasa J, Nart J, Wang HL. Significance of barrier membrane on the reconstructive therapy of peri-implantitis: a randomized controlled trial. J Periodontol. 2023;94(3):323-335.
Regidor E, Ortiz-Vigón A, Romandini M, Dionigi C, Derks J, Sanz M. The adjunctive effect of a resorbable membrane to a xenogeneic bone replacement graft in the reconstructive surgical therapy of peri-implantitis: a randomized clinical trial. J Clin Periodontol. 2023;50(6):765-783.
Tomasi C, Regidor E, Ortiz-Vigón A, Derks J. Efficacy of reconstructive surgical therapy at peri-implantitis-related bone defects. A systematic review and meta-analysis. J Clin Periodontol. 2019;46(Suppl 21):340-356.
Emanuel N, Machtei EE, Reichart M, Shapira L. D-PLEX500: a local biodegradable prolonged release doxycycline-formulated bone graft for the treatment for peri-implantitis. A randomized controlled clinical study. Quintessence Int. 2020;51(7):546-553.
Mikami R, Mizutani K, Shioyama H, et al. Influence of aging on periodontal regenerative therapy using enamel matrix derivative: a 3-year prospective cohort study. J Clin Periodontol. 2022;49(2):123-133.
Tonetti MS, Pini-Prato G, Cortellini P. Periodontal regeneration of human intrabony defects. IV. Determinants of healing response. J Periodontol. 1993;64(10):934-940.
Tonetti MS, Prato GP, Cortellini P. Factors affecting the healing response of intrabony defects following guided tissue regeneration and access flap surgery. J Clin Periodontol. 1996;23(6):548-556.
Cortellini P, Carnevale G, Sanz M, Tonetti MS. Treatment of deep and shallow intrabony defects. A multicenter randomized controlled clinical trial. J Clin Periodontol. 1998;25(12):981-987.
Cortellini P, Pini-Prato G, Tonetti M. Periodontal regeneration of human infrabony defects (V). Effect of oral hygiene on long-term stability. J Clin Periodontol. 1994;21(9):606-610.
Tonetti MS, Pini-Prato G, Cortellini P. Effect of cigarette smoking on periodontal healing following GTR in infrabony defects. A preliminary retrospective study. J Clin Periodontol. 1995;22(3):229-234.
Cortellini P, Tonetti MS, Lang NP, et al. The simplified papilla preservation flap in the regenerative treatment of deep intrabony defects: clinical outcomes and postoperative morbidity. J Periodontol. 2001;72(12):1702-1712.
Trombelli L, Simonelli A, Schincaglia GP, Cucchi A, Farina R. Single-flap approach for surgical debridement of deep intraosseous defects: a randomized controlled trial. J Periodontol. 2012;83(1):27-35.
Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with collagen. J Clin Periodontol. 2016;43(3):311-318.
Roccuzzo M, Mirra D, Pittoni D, Ramieri G, Roccuzzo A. Reconstructive treatment of peri-implantitis infrabony defects of various configurations: 5-year survival and success. Clin Oral Implants Res. 2021;32(10):1209-1217.
Monje A, Pons R, Amerio E, Wang HL, Nart J. Resolution of periimplantitis by means of implantoplasty as adjunct to surgical therapy: a retrospective study. J Periodontol. 2022;93(1):110-122.
Monje A, Pons R, Sculean A, Nart J, Wang HL. Defect angle as prognostic indicator in the reconstructive therapy of periimplantitis. Clin Implant Dent Relat Res. 2023;25:992-999.
Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J Clin Periodontol. 2010;37(5):449-455.
Aghazadeh A, Persson RG, Renvert S. Impact of bone defect morphology on the outcome of reconstructive treatment of periimplantitis. Int J Implant Dent. 2020;6(1):33.
Stiesch M, Grischke J, Schaefer P, Heitz-Mayfield LJA. Supportive care for the prevention of disease recurrence/progression following peri-implantitis treatment: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):113-134.
Cortellini P, Cortellini S, Bonaccini D, Tonetti MS. Papilla preservation and minimally invasive surgery for the treatment of peri-implant osseous defects. Clinical and radiographic outcomes of a 5-year retrospective study. Clin Oral Implants Res. 2021;32(11):1384-1396.
Cornelini R, Artese L, Rubini C, et al. Vascular endothelial growth factor and microvessel density around healthy and failing dental implants. Int J Oral Maxillofac Implants. 2001;16(3):389-393.
Bullon P, Fioroni M, Goteri G, Rubini C, Battino M. Immunohistochemical analysis of soft tissues in implants with healthy and peri-implantitis condition, and aggressive periodontitis. Clin Oral Implants Res. 2004;15(5):553-559.
Roediger M, Miró X, Geffers R, et al. Profiling of differentially expressed genes in peri-implantitis and periodontitis in vivo by microarray analysis. J Oral Biosci. 2009;51(1):31-45.
Ghighi M, Llorens A, Baroukh B, Chaussain C, Bouchard P, Gosset M . Differences between inflammatory and catabolic mediators of peri-implantitis and periodontitis lesions following initial mechanical therapy: an exploratory study. J Periodontal Res. 2018;53(1):29-39.
Lucarini G, Zizzi A, Rubini C, Ciolino F, Aspriello SD. VEGF, microvessel density, and CD44 as inflammation markers in peri-implant healthy mucosa, peri-implant mucositis, and periimplantitis: impact of age, smoking, PPD, and obesity. Inflammation. 2019;42(2):682-689.
Galárraga-Vinueza ME, Tangl S, Bianchini M, et al. Histological characteristics of advanced peri-implantitis bone defects in humans. Int J Implant Dent. 2020;6(1):12.
Mijiritsky E, Ferroni L, Gardin C, et al. Presence of ROS in inflammatory environment of peri-implantitis tissue in vitro and in vivo human evidence. J Clin Med. 2019;9(1):38.
Fretwurst T, Müller J, Larsson L, et al. Immunohistological composition of peri-implantitis affected tissue around ceramic implants-a pilot study. J Periodontol. 2021;92(4):571-579.
Galarraga-Vinueza ME, Obreja K, Ramanauskaite A, et al. Macrophage polarization in peri-implantitis lesions. Clin Oral Investig. 2021;25(4):2335-2344.
Karring ES, Stavropoulos A, Ellegaard B, Karring T. Treatment of peri-implantitis by the VectorR system. A pilot study. Clin Oral Implants Res. 2005;16(3):288-293.
Schär D, Ramseier CA, Eick S, Arweiler NB, Sculean A, Salvi GE. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: six-month outcomes of a prospective randomized clinical trial. Clin Oral Implants Res. 2013;24(1):104-110.
Andersen H, Aass AM, Wohlfahrt JC. Porous titanium granules in the treatment of peri-implant osseous defects-a 7-year follow-up study. Int J Implant Dent. 2017;3(1):50.
Isehed C, Svenson B, Lundberg P, Holmlund A. Surgical treatment of peri-implantitis using enamel matrix derivative, an RCT: 3- and 5-year follow-up. J Clin Periodontol. 2018;45(6):744-753.
Roos-Jansåker AM , Lindahl C , Persson GR , Renvert S . Longterm stability of surgical bone regenerative procedures of periimplantitis lesions in a prospective case-control study over 3 years. J Clin Periodontol. 2011;38(6):590-597.
Roos-Jansåker AM, Persson GR, Lindahl C, Renvert S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: a 5-year follow-up. J Clin Periodontol. 2014;41(11):1108-1114.
Isler SC, Soysal F, Ceyhanlı T, Bakırarar B, Unsal B. Efficacy of concentrated growth factor versus collagen membrane in reconstructive surgical therapy of peri-implantitis: 3-year results of a randomized clinical trial. Clin Oral Investig. 2022;26(8):5247-5260.
la Monaca G, Pranno N, Annibali S, Cristalli MP, Polimeni A. Clinical and radiographic outcomes of a surgical reconstructive approach in the treatment of peri-implantitis lesions: a 5-year prospective case series. Clin Oral Implants Res. 2018;29(10):1025-1037.
Aghazadeh A, Persson GR, Stavropoulos A, Renvert S. Reconstructive treatment of peri-implant defects-results after three and five years. Clin Oral Implants Res. 2022;33(11):1114-1124.
Regueiro IG, Martínez Rodriguez N, Barona Dorado C, et al. Surgical approach combining implantoplasty and reconstructive therapy with locally delivered antibiotic in the treatment of periimplantitis: a prospective clinical case series. Clin Implant Dent Relat Res. 2021;23(6):864-873.
Toma S, Lasserre JF, Taïeb J, Brecx MC. Evaluation of an air-abrasive device with amino acid glycine-powder during surgical treatment of peri-implantitis. Quintessence Int. 2014;45(3):209-219.
Esposito M, Grusovin MG, de Angelis N, Camurati A, Campailla M, Felice . The adjunctive use of light-activated disinfection (LAD) with FotoSan is ineffective in the treatment of peri-implantitis:
1-year results from a multicentre pragmatic randomised controlled trial. Eur J Oral Implantol. 2013;6(2):109-119.
207. de Waal YC, Raghoebar GM, Meijer HJ, Winkel EG, van Winkelhoff A. Implant decontamination with chlorhexidine during surgical peri-implantitis treatment: a randomized, double-blind, controlled trial. Clin Oral Implants Res. 2015;26(9):1015-1023.
208. Englezos E, Cosyn J, Koole S, Jacquet W, de Bruyn H. Resective treatment of peri-implantitis: clinical and radiographic outcomes after 2 years. Int Periodontics Restorative Dent. 2018;38(5):729-735.
209. Romeo E, Lops D, Chiapasco M, Ghisolfi M, Vogel G. Therapy of peri-implantitis with resective surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part II: radiographic outcome. Clin Oral Implants Res. 2007;18(2):179-187.
210. Lasserre JF, Brecx MC, Toma S. Implantoplasty versus glycine air abrasion for the surgical treatment of peri-implantitis: a randomized clinical trial. Int J Oral Maxillofac Implants. 2020;35(35):197-206.
How to cite this article: Berglundh T, Mombelli A, Schwarz F, Derks J. Etiology, pathogenesis and treatment of periimplantitis: A European perspective. Periodontol 2000. 2024;00:1-36. doi:10.1111/prd. 12549
This is the published version of the publication, made available in accordance with the publisher’s policy.
Etiology, pathogenesis and treatment of peri-implantitis : A European perspective
Berglundh, Tord; Mombelli, Andrea; Schwarz, Frank; Derks, Jan
How to cite
BERGLUNDH, Tord et al. Etiology, pathogenesis and treatment of peri-implantitis : A European perspective. In: Periodontology 2000, 2024, p. prd.12549. doi: 10.1111/prd. 12549
Etiology, pathogenesis and treatment of peri-implantitis: A European perspective
Tord Berglundh | Andrea Mombelli | Frank Schwarz | Jan Derks¹ Department of Periodontology, Institute of Odontology, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden Division of Regenerative Dental Medicine and Periodontology, University Clinics of Dental Medicine, University of Geneva, Geneva, Switzerland Department of Oral Surgery and Implantology, Goethe University, Carolinum, Frankfurt, Germany
Correspondence
Tord Berglundh, Department of Periodontology, Institute of Odontology, The Sahlgrenska Academy at University of Gothenburg, Box 450, SE 40530 Gothenburg, Sweden.
Email: tord.berglundh@odontologi.gu.se
Abstract
Peri-implantitis is a plaque-associated pathological condition occurring in tissues around dental implants. It is characterized by inflammation in the peri-implant mucosa and progressive loss of supporting bone. Over the last 30 years, peri-implantitis has become a major disease burden in dentistry. An understanding of the diagnosis, etiology and pathogenesis, epidemiology, and treatment of peri-implantitis must be a central component in undergraduate and postgraduate training programs in dentistry. In view of the strong role of European research in periodontology and implant dentistry, the focus of this review was to address peri-implantitis from a European perspective. One component of the work was to summarize new and reliable data on patients with dental implants to underpin the relevance of peri-implantitis from a population perspective. The nature of the peri-implantitis lesion was evaluated through results presented in preclinical models and evaluations of human biopsy material together with an appraisal of the microbiological characteristics. An overview of strategies and outcomes presented in clinical studies on nonsurgical and surgical treatment of periimplantitis is discussed with a particular focus on end points of therapy and recommendations presented in the S3 level Clinical Practice Guideline for the prevention and treatment of peri-implant diseases.
KEYWORDS
dental implants, peri-implantitis, treatment
1 | INTRODUCTION
Peri-implantitis was introduced as a term at the first European Workshop on Periodontology, held in Ittingen, Switzerland in February 1993. While studies published prior to 1993 often used
the terms “peri-implant infection” or “peri-implant lesion” to describe pathologic conditions in peri-implant tissues, the consensus report from session IV of the European Workshop presented definitions for peri-implant disease, peri-implant mucositis, and peri-implantitis. It was stated that peri-implant disease was a collective term for
inflammatory reactions in the tissues surrounding an implant. While peri-implant mucositis was a term for a reversible inflammatory condition in the soft tissues surrounding an implant, peri-implantitis described inflammatory reactions with loss of supporting bone in the tissues surrounding a functioning implant. Subsequent European Workshops addressed peri-implant diseases as a central part of clinical research in implant dentistry. The 2017 World Workshop on Classification of Periodontal and Peri-implant diseases and Conditions in Chicago, organized by the European Federation of Periodontology and the American Academy of Periodontology, distinguished between disease definitions and case definitions for peri-implantitis. While case definitions are intended to serve as guidelines for the clinical assessment of the condition, disease definitions are descriptive and present the typical characteristics of the disease. Thus, peri-implantitis is a plaque-associated pathological condition occurring in tissues around dental implants. It is characterized by inflammation in the peri-implant mucosa and subsequent progressive loss of supporting bone.
Over the last 30 years, peri-implantitis has become a major disease reality in dentistry. The condition should therefore be considered a disease from a population perspective rather than a biological complication in the field of implant dentistry. An understanding of the diagnosis, etiology and pathogenesis, epidemiology, and treatment of peri-implantitis must be a central component in undergraduate and postgraduate training programs in dentistry. In view of the strong role of European research in periodontology and implant dentistry, the focus of this review was to address peri-implantitis from a European perspective. One component of the work was to summarize new and reliable data on patients with dental implants to underpin the relevance of peri-implantitis from a population perspective. The nature of the peri-implantitis lesion was evaluated through results presented in preclinical models and evaluations of human biopsy material together with an appraisal of the microbiological characteristics. Finally, an overview of strategies and outcomes presented in clinical studies on nonsurgical and surgical treatment of peri-implantitis was made.
2 | THE RELEVANCE OF PERI-IMPLANTITIS AS A DISEASE ENTITY-A POPULATION PERSPECTIVE
2.1 | Prevalence of patients with dental implants
Assessments of patients at risk for peri-implantitis should be considered from a population perspective. The estimated number of annually installed dental implants is often used to provide information on the global application of the technique in the replacement of lost teeth. While the accuracy of such estimates may vary, national numbers based on state subsidies for dental care provide information of high reliability. Data from the Dental and Pharmaceutical Benefits Agency (TLV) in Sweden revealed that the number of installed dental implants was twice as large in 2022 than in 2012. The number of
treated patients also increased during the same period and the average number of installed implants per patient appeared to have decreased over time. Data from epidemiological research on patients with dental implants in Sweden support this observation. Thus, the mean numbers of implants per patient in 1990 and in 2003 were 6.2 and 4.0 , respectively. Currently, the mean number of implants per patient in Sweden is around 2.4.
The actual number of annually installed implants, however, is probably of limited value as it does not reflect the number or proportion of subjects with dental implants from a population perspective. In this context, the access to reliable registry data is relevant. The Swedish Quality Registry on Caries and Periodontal Diseases (SKaPa) is a unique national registry with a high degree of completeness. The registry is based on data from electronic patient records representing about 8 million subjects. Annual reports from the SKaPa registry provide information on dental status including dental implants. The 2022 report covered about 3.3 million subjects years and 155.000 individuals of these had dental implants. While the overall prevalence of subjects with dental implants in Sweden amounted to , there was a large difference between age groups (Figure 1). Thus, of subjects aged years had dental implants, whereas the corresponding proportion of subjects 40-60years old varied between 3% and 5%. Although based on a smaller subject sample, data from The Fifth German Oral Health Study indicated that 8% of subjects aged 65-74 years in 2014 had dental implants.
Concomitant with an increase in the overall proportion of subjects with dental implants from to over the last 10 years, information derived from SKaPa suggested a shift in the average number of dental implants per individual. While the proportion of subjects with only one implant increased from to , the proportion of subjects with implants decreased from to . From a population perspective, subjects with dental implants constitute a well-defined group of individuals at risk for peri-implantitis. Based on the Swedish data on subjects with dental implants (almost 5% of all adults), the number of individuals at risk for peri-implantitis in European countries and elsewhere is large and should not be overlooked.
2.2 | Prevalence of peri-implantitis
The occurrence of peri-implantitis has been evaluated in several cross-sectional studies. Given the large variation between studies regarding the number and type of patients, function time, and case definitions used for identifying peri-implantitis, prevalence figures ranging from to were reported. Weighted mean values obtained from meta-analyses of studies varied between and Not only did the different reports on the prevalence of peri-implantitis exhibit a large variation in case definitions including thresholds of bone loss around implants, evaluations were also often made on small and selected patient samples representing university/hospital clinical settings. Appraisals of the
FIGURE 1 Proportion of individuals with dental implants in Sweden. Data from the Swedish Quality Registry for Caries and Periodontal Disease.
prevalence of peri-implantitis should ideally be based on large and randomly selected population samples originating from different clinical settings. In a nationwide clinical study in Sweden, Derks et al. examined 596 patients representing a random sample from a registry-based cohort. Analysis of data on the clinical status of periimplant tissues and radiographs at 9 years after implant-supported restorative therapy revealed peri-implantitis ( implants presenting with bleeding on probing and bone loss ) in of the patients. Moderate/severe forms of the disease ( implants presenting with bleeding on probing and bone loss ) were detected in of patients. It should be noted that the average amount of bone loss in sites with moderate/severe peri-implantitis was 3.5 mm , corresponding to about of the initial bone support. The results presented by Derks et al. on the prevalence of peri-implantitis corroborate data presented in other European cross-sectional studies. Thus, when applying the case definitions used by Derks et al. to the datasets described by Koldsland et al., Roos-Jansåker et al., Mir-Mari et al., and Rodrigo et al., the prevalence of moderate/ severe peri-implantitis varied between 16% and 20%. In this context it is interesting to note that the data presented on the prevalence of peri-implantitis appear to be consistent with those reported for periodontitis. Both diseases present with an overall occurrence of about 40% in randomly selected adult populations, while severe forms of the diseases affect a smaller proportion of about
Potential risk factors or risk indicators for peri-implantitis were also assessed in studies investigating the occurrence of disease. Using a retrospective approach, several patient- and implantspecific risk factors were identified. Koldsland et al. and Derks et al. reported that patients with a history of periodontitis presented with an increased risk for peri-implantitis. This observation was confirmed in a recent systematic review presented by Carra
et al. and also highlighted in the consensus report from the 2017 World Workshop and the connected review by Schwarz et al. The risk for peri-implantitis was especially high for patients with poor plaque control and who did not attend regular maintenance programs during follow-up. The consensus report also stated that the current evidence on diabetes and tobacco smoking as risk factors for the disease was inconclusive. It should be pointed out, however, that in a statistical analysis, the potential effect of smoking may be masked by other and stronger factors, such as history of periodontitis. Among risk factors related to the implant or the implantsupported prosthesis, access for oral hygiene has been emphasized to be an important component. Studies by Serino & Ström and by Rodrigo et al. demonstrated that implants not accessible for oral hygiene measures had an elevated risk for peri-implantitis. Other studies have shown that the extent of therapy, that is, the number of placed implants, was a risk factor for peri-implantitis. Data on the importance of other factors, such as type of retention (cemented or screw-retained) or dimensions of the keratinized mucosa remain inconclusive.
3 | THE PERI-IMPLANTITIS LESION
Although peri-implantitis sites exhibit clinical characteristics similar to those of periodontitis, for example, visible signs of inflammation, bleeding on probing, and radiographic bone loss, there are evident differences in the patterns of disease progression. Studies have shown that untreated peri-implantitis progresses in a nonlinear, accelerating pattern and at a rate, which is faster than that of periodontitis. While the reasons for the differences in the pattern of disease progression are not fully understood, differences in the
structure and composition of the local host response between periodontitis and peri-implantitis should be emphasized.
3.1 | Preclinical in vivo models
Pioneer experimental work using well-established preclinical in vivo models showed important differences between periodontitis and peri-implantitis lesions. While the combination of a subgingival/ submucosal placement of ligatures and plaque accumulation resulted in bone loss and the formation of a large area of infiltrated connective tissue (ICT) in the gingiva/peri-implant mucosa at teeth and implants, bone loss was more pronounced around implants. In addition, peri-implantitis lesions, in contrast to periodontitis lesions, extended to the bone crest. Following the removal of ligatures during the experimental procedure, periodontal tissues responded with a “self-limiting” process resulting in a protective zone of connective tissue with remaining periodontal ligament fibers that separated the ICT from the crestal bone. At peri-implantitis sites, however, such a self-limiting process failed to occur due to the lack of periodontal fibers. Similar observations were made in experimental studies by Marinello et al. and Schou et al. The observation of the lack of a self-limiting process in peri-implantitis sites opened for a new approach in experimental preclinical models. In a study by Zitzmann et al., experimental peri-implantitis was established and, when about 40% of the bone support was lost, all ligatures were removed. It was reported that in the absence of ligatures and with an ongoing plaque formation over several months, “spontaneous” progression of disease occurred with additional breakdown of peri-implant bone. The “spontaneous progression” model was subsequently used to examine differences in disease progression between implants with different surface characteristics. Data from numerous such experimental studies consistently demonstrated that size of the ICT and bone loss were more pronounced at sites representing implants with modified surfaces than implants with nonmodified, turned surfaces. The “spontaneous progression” model was also applied by Carcuac et al. in a comparison between experimental periodontitis and peri-implantitis. It was reported that bone loss was greater around implants than around teeth and that peri-implantitis lesions occupied larger areas of the connective tissue and extended closer to the crestal bone when compared to periodontitis lesions. Carcuac et al. took the model a step further by analyzing spontaneous progression of experimental peri-implantitis at an early stage without a preceding period of extensive tissue breakdown. Crestal bone loss was, again, greater around implants with modified surfaces than implants with turned, nonmodified surfaces.
Results from preclinical studies have contributed to the understanding of the nature of peri-implantitis lesions and the reason for a faster disease progression than is typical for periodontitis. It is evident that peri-implantitis lesions are poorly encapsulated since a protective, “self-limiting” zone of healthy connective tissue that separates the infiltrate from the crestal bone is lacking. The advanced and perpetuating nature of peri-implantitis lesions is further
illustrated by the frequently observed high numbers of osteoclasts on the peri-implant crestal bone.
3.2 | Human biopsy material
The advantage of analyzing both hard and soft tissue components in specimens from preclinical studies is obvious. While ethical limitations in most cases prevent analysis of hard tissue components in human biopsy material obtained from sites with peri-implantitis, advanced techniques can still be applied to detect phenotypic and functional characteristics of cells in peri-implantitis lesions. Evaluations of human biopsy material with preserved tissue orientation for section-based analyzes were predominantly based on immunohistochemical preparations and, in few cases, morphologic techniques. Other investigations applied procedures, in which the tissue samples were homogenized and subsequently analyzed using, for example, RT-PCR, western blot, or transcriptome profiling. An overview of European studies reporting on results from analysis of human biopsy material and presenting with clear case definitions for peri-implantitis is presented in Table 1.
Results from assessments of the cellular compositions and other characteristics of human peri-implantitis lesions have been presented in reviews. Comparisons were, in most studies, made between peri-implantitis specimens and tissue samples representing other types of conditions, for example, periodontitis, peri-implant mucositis, and healthy peri-implant mucosa or gingiva. The most conspicuous characteristic of tissues collected from sites with periimplantitis was the observation of large inflammatory cell infiltrates that dominated the specimen area. In studies evaluating differences between peri-implantitis and periodontitis samples, the lesion was consistently larger at peri-implantitis sites and extended apical to the pocket epithelium. While plasma cells were the predominant cell type of both lesions, the densities of plasma cells, macrophages, and neutrophil granulocytes were significantly larger at peri-implantitis than at periodontitis sites. In a study on the activation status of macrophages in the ICT, it was reported that the number of macrophages undergoing M1-polarization was higher in peri-implantitis than in periodontitis lesions. Findings from studies on the functional characteristics of cells demonstrated that periimplantitis lesions presented with different mRNA signatures and higher mRNA levels for specific cytokines, for example, TNF-a, IL-8, CCR5, and CXCR3 than periodontitis lesions.
The differences between periodontitis and peri-implantitis lesions detected in studies on human biopsy material corroborate data presented in preclinical research. Taken together, the differences in structure and in densities of key inflammatory cells of the ICT between the two types of lesions reflect the characteristics of a dysregulated local host response in peri-implantitis. This is evidenced by (i) the lack of an epithelial lining between the submarginal biofilm and the ICT in the pocket area, (ii) the large spread of the ICT apical to the pocket epithelium and toward the crestal bone, and (iii) the increased and continuous recruitment of
TABLE 1 European studies describing the peri-implant lesions-human biopsy material.
Authors
Population
Case definition for peri-implantitis
Methods
Main findings
Sanz et al. 1991
12 subjects
– Six with PI
– Six healthy controls
BOP+ MBL
Soft tissue biopsies
LM and TEM
– PI samples showed higher numbers of inflammatory cells (predominantly plasma cells and mononuclear cells) and transmigrating cells in the oral and sulcular epithelium compared to healthy controls
– PI: Sixty-five percent of the connective tissue was replaced by the ICT versus in the healthy group
Cornelini et al. 2001
15 subjects
– 10 implants with PI
– 10 healthy implants
Evidence of MBL
PD
BOP/SOP+
Swelling
Soft tissue biopsies
LM, IHC
VEGF, and factor VIII
– Healthy sites had no ICT, regular distribution of vessels
– PI sites had ICT, mostly lymphocytes and plasma cells. Few neutrophils
– Expression of VEGF lower in healthy sites than in PI sites
Gualini & 2003 Berglundh
16 subjects
– Six with PI
– 10 with PiM
Evidence of MBL BOP/SOP+
Soft tissue biopsies
LM, IHC
CD3, CD4, CD8, CD19, and elastase
– In PiM, the inflammatory infiltrate was well defined in the area lateral to the pocket epithelium, while in PI sites, the pocket epithelium appeared ulcerated, and the ICT extended adjacent to it
– The ICT of PI lesions was three times larger than the one found in PiM sites
– PI contained significantly higher proportions of B cells (CD19+) and elastase-positive cells compared to PiM
Berglundh et al. 2004
Six subjects
– 12 implants with PI
Advanced MBL BOP/SOP+
Soft tissue biopsies
LM
– The apical portion of pocket epithelium thin and ulcerated
– The ICT extended apically of the pocket epithelium
– Most of the ICT was occupied by plasma cells and PMNs
– Few but large vascular units occupied the marginal portion of the lesion, while numerous small vessels could be found in the area lateral to the pocket epithelium
Bullon et al. 2004
10 subjects
– Five with PI
– Five with AG
PD
Evidence of MBL
BOP+
Soft tissue biopsies
LM and IHC
CD1a, CD3, CD20, CD34, factor VIII, VEGF, and oncoproteins bcl2 and p53
– Multilayered para-keratinized oral epithelium in PI and AG
– Thin nonkeratinized junctional epithelium partly ulcerated in PI
– Oral epithelium: Significantly less CD1a and CD34 but more VEGF and blc2 in PI than in AG sites
– Sulcular and junctional epithelium: Significantly more CD34, Factor-VIII, and VEGF in Pl than in AG sites
Roediger et al. 2009
48 subjects
– 16 with PI
– 16 with CP
– 16 healthy controls
PD
Evidence of MBL
BOP+
Soft tissue biopsies
RT-PCR and gene-ontology
Collagen type IV, integrin b 1, integrin b 4, integrin a 6, and HPRT1
– mRNA expression of collagen type IV was upregulated in PI compared to CP
– No differences in mRNA levels of integrin b 1 and integrin b 4 between PI and CP
– mRNA levels of integrin a 6 were upregulated in PI (5.3-fold more) and in CP (11.6-fold more) compared to healthy controls
– CD3, TIMP-2 levels were increased in PI compared to CP
– Higher levels of IL-1 , IL-10, CD3, CD20, and CD68 were found in PI than in healthy controls
– Levels of IL-17, TIMP-2, Matrix metalloproteinase-2, Matrix metalloproteinase-8, Matrix metalloproteinase-12, and Matrix metalloproteinase-13 were increased in PI and CP compared to healthy controls
Kasnak et al. 2018
37 subjects
– 12 with PI
– 13 with CP
– 13 healthy controls
CAL
PD
BOP/SOP+
MBL
Soft tissue biopsies
IHC
8-OHdG, PARK7/DJ-1, NFE2L2/ NRF2, and KEAP1
– 8-OHdG- and PARK7/DJ-1- positive cells spread in all epithelial layers of PI and CP samples, but only in the basal layer of healthy controls
– NFE2L2/NRF2-stained cells spread in all epithelial layers in all groups
– A more pronounced ICT was found in PI samples compared to CP ones
– Proportions of 8-OHdG- positive cells in the epithelium were higher in PI and CP than in healthy controls
– Number of PARK7/DJ-1-positive cells elevated in PI and CP compared to healthy samples
Lucarini et al. 2019
48 subjects
– 16 with PI
– 16 with PiM
– 16 healthy controls
BOP+
Evidence of MBL
Soft tissue biopsies
LM, IHC
VEGF, CD34, and CD44
– PI sites. Ulcerated pocket epithelium and a large ICT
– PI showed significantly higher levels of VEGF, CD34, and CD44 compared to the other groups
– PD was positively correlated to VEGF, CD34, and CD44
TABLE 1 (Continued)
Authors
Population
Case definition for peri-implantitis
Methods
Main findings
Dionigi et al. 2020
80 subjects
– 40 with PI
– 40 with CP
BOP/SOP+
MBL
Soft tissue biopsies
LM and IHC
y-H2AX, CHK2, 8-OHdG, CD68, MPO, iNOS, NOX2, and PAD4-MPO
– PI had significantly higher densities of CD68-, MPO-, and iNOS-positive cells than CP sites
– Cellular densities for all markers were significantly higher in the inner ICT than in the outer ICT zone, both in PI and CP
– Pl showed significantly higher levels of y-H2AX-, iNOS-, NOX2-, MPO-, and PAD4/ MPO-positive cells within the NCT area than that of CP
Fretwurst et al.
2020
14 subjects
– Seven with PI
– Seven with CP
BOP/SOP+
Evidence of MBL
Soft tissue biopsies
LM, IHC, immunofluorescence
CD68, iNOS, and CD206
– Heterogeneity of macrophage polarization in both PI and CP
– Higher numbers of CD68-positive cells in PI compared to CP
– Higher levels of macrophages in M1 form in PI compared to CP
– Similar levels of macrophages in M2 form in the two groups
GalárragaVinueza
2020 et al.
Four subjects
– Five implants with PI
BOP/SOP+
MBL
Soft and bone tissue biopsies LM
– The mean defect length was 4.7 mm , the bone density was , and the mean bone-to-implant contact was
– Two samples showed a chronic inflammatory infiltrate
– One sample revealed signs of osteoclastic activity, three samples showed inactive crestal bone activity and one site showed active bone formation
– The residual bone was mainly cortical showing areas with small vessels and areas of lamellar bone
– Secondary osteons were frequently present, while osteoclasts were sporadically seen as well as cancellous bone which was located mostly in the apical portions of the specimens
Mijirtsky et al. 2019
40 subjects
– 20 with PI
– 20 healthy controls
BOP/SOP+
Exposure of implant threads
Radiographic bone loss
Soft tissue biopsies
LM, IHC, immunofluorescence, TEM, and RT-PCR
– The ICT of PI samples showed plasma cells , lymphocytes , PMN , collagen fibers 15%, fibroblasts 8%, and blood vessels 12%
– Levels of ROX, Osterix, and b catenin genes were downregulated in PI samples
– ROS production (NOX4 and NADPH oxidase) was upregulated in PI samples
Fretwurst
2021 et al.
15 subjects
– Seven with PI around titanium-implants
– Eight with PI around ceramic implants
BOP/SOP+
MBL >2/3 of the implant length
Soft tissue biopsies
LM, IHC
CD3, CD20, CD138, and CD68
– There were no significant differences in the number of positive cells in PI lesions between ceramic and titanium implants
– The ICT was predominantly occupied by plasma cells, followed by Tlymphocytes, B lymphocytes, and macrophages
GalárragaVinueza
2021 et al.
20 subjects
20 implants with PI
BOP/SOP+
PD
MBL
Soft tissue biopsies
LM, IHC
CD68, CD80, and CD206
– CD68-positive density was about of the ICT in PI sites
– CD80- and CD206-positive cells (M1 and M2 macrophages) occupied 7.07% and 5.22% of the ICT, respectively
– The M1/M2 ratio was 1.56
– A positive correlation between CD68, M1 levels, and PD was observed
Abbreviations: AG, Aggressive periodontitis; BOP, Bleeding on probing; CAL, Clinical attachment level; CP, Chronic periodontitis; ICT, Infiltrated connective tissue; IHC, Immunohistochemistry; LM, Light microscopy; MBL, Marginal bone level; PD, Probing depth; PI, Peri-implantitis; PiM, Peri-implant mucositis; SOP, Suppuration on probing; TEM, Transmission electron microscopy.
FIGURE 2 Section prepared from human biopsy obtained from a site with severe peri-implantitis. Pocket epithelium (PE), inner (ICT1) and outer (ICT-2) zones of ICT, and non-infiltrated connective tissue (NCT) area. From Dionigi et al.
neutrophils and macrophages to the ICT. Thus, the main features of peri-implantitis lesions illustrate an active and perpetuating process of inflammation with few, if any, signs of inactivity. The nonlinear and accelerating pattern of disease progression in periimplantitis described above, may, to a high degree, be explained by these lesion characteristics.
In an extended analysis of biopsy material obtained from 80 subjects with severe peri-implantitis or periodontitis, Dionigi et al. reported that both types of lesions presented with higher densities of inflammatory cells in an “inner zone” (ICT-1) adjacent of the pocket epithelium than in an “outer zone” of the lesion (ICT-2) (Figure 2). The authors also made observations on cellular characteristics in the non-infiltrated connective tissue area (NCT) lateral to the ICT. Thus, the NCT compartment in peri-implantitis specimens contained higher densities of y-H2AX-, iNOS-, NOX2-, MPO-, and PAD4/MPO-positive cells, that is, markers for DNA damage, antimicrobial nitric oxide, and formation of NETs, than found in periodontitis samples. The finding of tissue reactions spreading
beyond the lateral borderline of the ICT adds to the overall picture of an extensive tissue reaction at sites with peri-implantitis. Since the dental implant is a metal device predominantly made of titanium, it has been suggested that the presence of a foreign material at peri-implantitis sites may influence the local host response. Although studies have reported on the presence of metal particles in soft tissue samples from peri-implantitis sites, it remains unclear whether such findings are specific for diseased peri-implant tissues since relevant comparisons to matching specimens representing healthy peri-implant tissues are lacking. In addition, assessments of metal microparticles in peri-implant soft tissues require the use of appropriate techniques to verify the type of material (e.g., titanium) and to detect small-sized particles of , for example, -PIXE (micro proton-induced X-ray emission), synchrotron radiation, or SEM-EDX.
Data from studies evaluating human biopsy material obtained from sites with peri-implantitis may vary depending on the severity of the condition and case definitions used when recruiting patients. One of the upsides of the histological evaluation of tissue samples is the preservation of anatomy and orientation of tissue structures. The detection of target cells in well-controlled locations is thereby facilitated. Technical limitations of using cell markers of primarily phenotypical characteristics with, for example, immunohistochemistry, however, must be considered. On the other hand, assessments of mRNA expression of key elements in the lesion require the use of homogenized tissue samples, in which the orientation of the tissue structure is lost. Ideally, future analysis of human peri-implantitis specimens should apply novel “omics” techniques (e.g., proteomics, transcriptomics) in combination with a spatial visualization approach. Although such techniques are currently available, their use needs to be balanced between meaningful and feasible sample sizes and the extensive resources that are required. Future techniques should also aim at preserving the area that encompasses the interface between the inflamed peri-implant tissues and the biofilm residing in the pocket. The analysis of host-parasite interactions has the potential to provide further understanding of the role of microorganisms as the main etiological factor in peri-implantitis.
4 | MICROBIOLOGICAL CHARACTERISTICS OF PERI-IMPLANTITIS
Early on in the development of oral implantology, it was observed that bone loss around implants could sometimes be associated with classic signs of infection in the soft tissues including redness, swelling, and pus formation. Pus is the result of the immune system responding to an infection, usually caused by bacteria. One might have thought that this alone would have persuaded the dental community that infections around implants could be a serious threat and that an antimicrobial approach to preventing implant failure would be worthwhile. However, the extent to which infection contributes to the phenomenon of peri-implant bone loss in general has remained controversial ever since. As evoked in previous chapters
in Periodontology 2000, several lines of evidence suggest that bacteria colonizing implant surfaces play an essential part in the pathogenesis of peri-implantitis:
Experiments in humans have shown that the unrestrained accumulation of bacterial plaque on implants over several days induced a local inflammation in the adjacent mucosa (called “experimental peri-implant mucositis”), similar to the effect of dental plaque on gingiva (called “experimental gingivitis” ). In both situations, signs of inflammation were diminished once the bacterial deposits were removed.
Microbiota harvested from diseased peri-implant sites showed quantitative and qualitative differences from the microbiota at implant sites with a healthy mucosa, as discussed in more detail below.
In preclinical in vivo studies, subgingival placement of ligatures together with plaque formation resulted in changes in the composition of the local microbiota and in the destruction of peri-implant tissues.
Treatment protocols of peri-implantitis aiming at removing bacterial deposits from implants have shown positive clinical results, albeit to varying degrees, as reviewed in the next section.
The lack of maintenance programs and poor compliance (i.e., persistence of bacterial deposits due to poor oral hygiene) after implant therapy increase the risk for peri-implantitis.
Preliminary evidence implicating certain types of microorganisms in peri-implantitis came from microscopic examination of specimens collected around implants with advanced pocketing. While spirochetes were not detected in specimens from implant sites with healthy peri-implant tissues, they were found in large numbers at diseased sites. Since electron microscopy had shown that these bacteria invaded periodontal tissues in necrotizing ulcerative gingivitis, one wondered what significance this might have with regard to peri-implantitis. A study using bacterial culture methods published in showed that of the organisms cultured from implants with peri-implant probing depths and bone loss were Gram-negative anaerobic rods. Among these organisms, Fusobacterium spp. and Prevotella intermedia were frequently identified at high levels. The presence of spirochetes and other motile organisms was corroborated microscopically but could not be further studied using the techniques available at the time. On the other hand, only very few bacteria, mostly identified as Gram-positive cocci, were detected at implants without symptoms. These results suggested that the condition henceforth referred to as “peri-implantitis” appeared to be a site-specific disease process involving bacteria previously connected to chronic periodontitis around teeth.
Over the course of almost four decades, further studies using classic and newly emerging microbiologic methods have confirmed and extended early findings. Technologies including checkerboard DNA-DNA hybridization, qPCR, fluorescence in situ hybridization, and 16 S rRNA gene-based PCR were used to further study the
composition of the peri-implant microbiota in health and disease. Most investigators used methods originally developed for evaluating the subgingival microbiota in periodontal pockets at natural teeth and primarily looked for so-called putative periodontal pathogens. In these studies, bacteria ubiquitous in chronic periodontitis, such as Fusobacterium spp. and P. intermedia were also regularly detected in specimens from peri-implantitis. Organisms that are less common in chronic periodontitis, such as Aggregatibacter actinomycetemcomitans, were less frequently identified.
Analysis using different methods have shown that the submucosal microbiome in peri-implant diseases is (i) mixed, (ii) rather variable, and (iii) in most cases dominated by various Gram-negative anaerobic bacteria. According to a recent systematic review, meta-analyses for species analyzed in at least two independent studies revealed the following taxa to be associated with peri-implantitis (compared to “non-peri-implantitis”): the Gram-negative anaerobes Fusobacterium nucleatum, Porphyromonas gingivalis, Prevotella intermedia, and Tannerella forsythia, the spirochete Treponema denticola, and the Grampositive bacterium Staphylococcus epidermidis. With regard to the latter, it has long been speculated that this organism might be responsible for a microbiologically distinct form of peri-implant infection. In fact, S.epidermidis, a common symbiont living on the human skin and mucosa, is also linked to other forms of suppurative infections of indwelling devices that have little resemblance to the periodontitis-like lesions commonly encountered around oral implants.
Several studies have shown that there is a difference in the composition of the peri-implant microflora found in deep and shallow pockets, reflecting differences in the ecological conditions that are also known from the situation around natural teeth. Pockets with a probing depth of can be considered as protected habitats for putative pathogens and can be an indicator of risk of peri-implant disease.
Classical microbiology is largely based on the study of the properties of pure cultures of microorganisms grown under laboratory conditions that are not representative of their life in nature. In the wild, bacteria live in mixed communities called biofilms that adhere to environmental surfaces. However, the data discussed above, even from studies using the latest molecular technologies, are based on samples obtained using biofilm-destroying methods. Information on the spatial organization of the naturally grown biofilm in human peri-implant disease is sparse and little is known about the behaviors of suspected pathogens, specifically when adhering to implant surfaces. On a larger scale, biofilm infections are not only a dental problem. As recognized in orthopedic implant research, they contribute to severe complications, increased use of antibiotic treatments, and development of antibiotic-resistant microorganisms. When discussing the sometimes frustrating results of treating oral peri-implantitis, one should keep in mind the difficult-to-treat biofilm-associated infections of indwelling devices, which often cause distress, increased morbidity, and high costs. There is a need to improve the diagnosis of oral and non-oral biofilm infections to enable earlier detection and treatment to the benefit of our patients.
5 | TREATMENT OF PERI-IMPLANTITIS
5.1 | Concepts
At the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions, the bacterial etiology of peri-implant mucositis and peri-implantitis was highlighted. Interventional research has demonstrated the causal link between the accumulation of bacterial plaque and subsequent development of peri-implant inflammation, that is, peri-implant mucositis. The overall understanding of disease development is that of a stepwise model, by which peri-implant mucositis will initially develop upon plaque accumulation and may, subsequently, progress into peri-implantitis. The model proposes that peri-implantitis is always preceded by peri-implant mucositis. Bacterial plaque thereby represents a necessary component of disease development according to the “sufficient component cause” model described by Rothman in Much like the relationship between bacterial plaque and periodontitis, the validity of a similar pathway for peri-implantitis is supported by data from, both, observational and interventional research. As pointed out above, subgroups of implant-carrying individuals not attending regular supportive care have been shown to suffer a significantly higher burden of peri-implant diseases, including the occurrence of peri-implantitis. Secondly, and more importantly, anti-infective approaches applied in the management of established peri-implantitis, that is, establishment of patient-performed plaque control combined with decontamination of implant surfaces, has conceptually been shown to arrest disease progression also in studies with long-term follow-up periods.
As a consequence of the understanding of peri-implantitis as a disorder driven by bacterial plaque, the S3 level Clinical Practice Guideline developed by the European Federation of Periodontology for the prevention and treatment of peri-implant diseases is very much centered on this factor. Thus, management of peri-implantitis should include an initial nonsurgical step, during which bacterial deposits are to be removed/reduced through supra- and submarginal instrumentation. Following an evaluation of the healing response to nonsurgical treatment modalities and in case of residual signs of disease, a surgical step is recommended. Also here, decontamination of the implant surfaces, following flap elevation, is the key therapeutic component. The treatment of peri-implantitis encompasses adequate self-performed and professionally delivered oral hygiene measures during all steps of therapy, including the period upon completion of active treatment. Regular supportive peri-implant care represents the final step of the sequential approach.
5.2 | End points of therapy
In the clinical setting, peri-implantitis is characterized and diagnosed through visual inspection, peri-implant probing, and radiographic evaluation. In line with reports on outcomes of periodontal
therapy, studies on treatment of peri-implantitis have typically reported on changes of clinical and radiographic parameters. In fact, the variables probing depth and bleeding on probing were described in almost 90% of all studies on the management of peri-implant diseases during the last 10 years, primarily as mean values of changes occurring pre- versus post-therapy.
Within the periodontal field, the importance of tangible end points of active therapy has been widely studied. In addition to end points evaluated in the long term (e.g., need for retreatment and tooth loss) and patient-reported oral health-related quality-oflife, the concept of pocket closure, that is, shallow probing depth and the absence of bleeding on probing, is strongly associated with periodontal stability. The relevance of residual pocketing at implant sites following surgical therapy of peri-implantitis was evaluated by Carcuac et al. The authors found that residual probing depth at 1 year was a strong indicator of disease recurrence (odds ratio 7.4) when compared to more shallow pocketing ( ). This finding speaks to the concept of the deepened pocket acting as a protected habitat for a microbial biofilm as outlined in Section 4.
The predictive value of bleeding on probing at implant sites has also been assessed. Thus, Karlsson et al., in a 3-year follow-up study on 70 subjects diagnosed with peri-implantitis at of their implants, found that disease progression (additional bone loss ) was more likely to occur at implant sites presenting with multiple bleeding spots (hazard ratio 7.1) when compared to no or only isolated bleeding. The negative predictive value of bleeding on probing was particularly high (95%). A corresponding analysis following active therapy of peri-implantitis resulted in similar findings. The negative predictive value (for complete absence of bleeding on probing) and subsequent disease recurrence (additional bone loss ) in a 2-year evaluation by Carcuac et al. was . In an early European study on short-term changes of peri-implant attachment levels in a patient population under maintenance care, Jepsen et al. reported an almost identical negative predictive value of 82%.
Collectively, these data support the concept that meaningful short-term end points for the active therapy of peri-implantitis should correspond to what has been proposed for periodontal care. In other words, therapeutic efforts should aim for shallow periimplant probing depths and reduction or elimination of bleeding on probing. It should be noted that recent data has suggested that the two parameters, that is, peri-implant probing depth and possible bleeding upon probing, are closely interlinked. Also, after surgical therapy of peri-implantitis, the probability of bleeding on probing was found to be low at sites with shallow probing ( ; ), while the corresponding likelihood at sites with deep pocketing ( ) was high ( ). Consequently, the S3 level Clinical Practice Guideline by the European Federation of Periodontology for the prevention and treatment of peri-implant diseases recommended end points of successful surgical therapy to include shallow probing ( ), the absence of suppuration on probing, and only minimal bleeding on probing ( point).
5.3 | Nonsurgical therapy of peri-implantitis
The clinical efficacy of nonsurgical treatment of peri-implantitis has recently been evaluated in three systematic reviews. total of 15 RCTs, mainly conducted in European countries, were included. Numerous adjunctive and alternative methods for plaque removal and/or implant surface decontamination were evaluated, including mechanical, physical, photomechanical/-thermal (i.e., laser application) as well as chemical treatment approaches. Control interventions were defined as cleaning approaches that did not aim at any mechanical or physical decontamination, except for the removal of hard deposits (i.e., scalers or sonic/ultrasonic devices with or without saline irrigation).
Various laser devices, used either as monotherapy (i.e., Er:YAG laser, Nd:YAG laser) or in combination (diode laser, Er,Cr:YSGG laser) with chlorhexidine irrigation were commonly associated with similar reductions of probing depth and bleeding scores as respective control groups. Significant benefits for test groups were only reported in two studies employing 3-micron lasers, with limited fol-low-up periods of 6 months. Accordingly, laser application used either as an adjunct or monotherapy was suggested not to be used for nonsurgical treatment of peri-implantitis in the S3 level Clinical Practice Guideline presented by the European Federation of Periodontology in 2023.
The efficacy of submucosal Instrumentation using glycine powder-based air polishing was evaluated in two RCTs. Even though one study reported on significantly greater reductions of bleeding scores following air polishing monotherapy versus control treatment at 6 and 12 months, the overall quality of evidence was low. The S3 level Clinical Practice Guideline therefore suggested not to use air polishing in nonsurgical treatment of peri-implantitis. The adjunctive use of chemical surface decontamination approaches evaluated in the literature encompassed antimicrobial photodynamic therapy (aPDT, low level lasers: ; photosensitizers: toluidine/methylene blue) as well as a desiccant gel (i.e., hydroxybenzenesulphonic/hydroxymethoxybenzene and sulfuric acid). Both procedures were associated with some improvements in reductions of probing depth over respective control groups at 6 months. Due to the very low overall quality of evidence, it was, however, suggested not to use aPDT nor a desiccant antiseptic gel in nonsurgical peri-implantitis therapy.
The administration of local antimicrobials, systemic antibiotics as well as probiotics was evaluated as an adjunct to conventional nonsurgical treatment of peri-implantitis. More specifically, four studies analyzed the efficacy of local antimicrobials, such as minocycline microspheres and chlorhexidine chips. Three studies looked into systemic antibiotics, notably amoxicillin + metronidazole or just metronidazole. Two studies evaluated the potential benefits of Lactobacillus reuteri probiotics. Local antimicrobials moderately improved probing depth reduction, while systemic antibiotics had a more obvious effect on reduction of both probing depths and bleeding scores, particularly at sites with an initial pocketing of . No adjunctive effects on either pocket reduction
or reduction of bleeding scores were noted following the administration of probiotics. In view of the overall evidence and following careful consideration of potential benefits and harms, particularly associated with the administration of systemic antibiotics, the S3 level Clinical Practice Guideline suggested not to use any of the aforementioned adjunctive measures in the nonsurgical treatment of peri-implantitis. Table 2 presents an overview of selected European studies on nonsurgical therapy of peri-implantitis.
5.4 | Surgical therapy of peri-implantitis
European contributions to the scientific evidence on the effect of surgical therapy of peri-implantitis have been extensive. Virtually, all datasets cited by the recently published S3 level Clinical Practice Guideline for the prevention and treatment of peri-implant diseases were generated in European countries (Table 3). The first reports originated from Germany, Italy, and Sweden, mostly in the form of case series with limited sample sizes. From 2010 and onward, randomized controlled trials evaluating efficacy of different surgical protocols have been consistently published.
One key aspect that these early studies highlighted was the importance of implant surface characteristics on the outcomes of therapy, as had been suggested in preclinical in vivo evaluations. In a pivotal such clinical study, Roccuzzo et al. found that, 12 months following surgical treatment, reduction of peri-implant probing depth was greater at implants with a sandblasted and acid-etched (SLA ) surface (mean reduction 3.4 mm ) when compared to TPS-surface implants ( 2.1 mm ). Corresponding results for bleeding on probing were also noted with considerably higher residual bleeding at 1 year (57% vs. 15%) at tissue plasminogen activator (TPS)-surface implants. The importance of implant surface characteristics explains why clinical studies in the field typically account for implant categories/brands that are included. This aspect, along with technical details such as the possibility to remove the implant-borne restoration during the surgical procedure, distinguishes surgical therapy of peri-implantitis with its periodontal counterpart. However, many of the clinical questions and the overall scientific approach, have otherwise been similar. As such, interventional studies addressed (i) the efficacy of different decontamination protocols, (ii) the potential benefit of antiseptics/antimicrobials, and (iii) reconstructive treatment modalities. All these domains have already been extensively evaluated within the periodontal field, while corresponding evidence for the surgical management of peri-implantitis is only emerging.
The effectiveness of surgical therapy of peri-implantitis, in general, was recently evaluated in a systemic review solicited by the EFP. While Karlsson et al. could not identify direct comparisons of surgical interventions with other standard therapies (e.g., nonsurgical treatment), the overall effect of access flap surgery and/or pocket elimination was estimated through meta-analyses. Based on 18 study arms, surgical therapy resulted in a standardized mean reduction of probing pocket depth of 2.2 mm and in a gain of marginal bone level of 0.2 mm (Figure 3). These data, originating
TABLE 2 Selected European studies on nonsurgical therapy of peri-implantitis.
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Outcomes
Comments
Alpaslan Yayli et al. 2022 RCT 6 months Turkey
Titanium curettes AB-AS-
Titanium curettes Photodynamic therapy AB-AS-
17/17
PD 4-6 mm & BOP/SOP and bone loss
4.1 mm
PD red: 0.5 mm BOP red: 11.3%
– Smokers excluded
– Oral hygiene instructions
– No details on removal of implant-supported prosthesis provided (all cemented)
– No details on local anesthesia provided
– MBL changes not reported
Titanium curettes Er,Cr:YSGG laser AB-AS-
17/17
BOP red: 48.8%
Schwarz et al. 2005 RCT 6 months Germany
Plastic curettes ABAS+ Er:YAG laser AB-AS-
10/16
and BOP and SOP and bone loss
5.5 mm
PD red: 0.8 mm BOP red: 52.0% REC: 0.1 mm
– No details on removal of implant-supported prosthesis provided
– MBL changes not reported
Schwarz et al. 2006 RCT 12 months Germany
Plastic curettes ABAS+
– Smokers excluded
– Oral hygiene instructions
TABLE 2 (Continued)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Outcomes
Comments
Roccuzzo et al. 2022 RCT 6 months Switzerland
Titanium curettes and stainless-steel curettes
12/12
and BOP/SOP and bone loss
5.3 mm
PD red: 1.5 mm
BOP red: 0%
MBL change: 0.0 mm
– Oral hygiene instructions
– Local anesthesia
– Implant-supported prosthesis not removed
Renvert et al. 2009 RCT 6 months Sweden
Titanium curettes and rubber cups
17/17
and and bone loss
4.0 mm
PD red: 0.0 mm
BOP red (out of four sites): 0.3
– Oral hygiene instructions
– Local anesthesia
Karring et al. 2005 RCT (split mouth) 6 months Denmark
Carbon curettes
11/11
and BOP and bone loss
6.3 mm
PD red: 0.0 mm
BOP red: -9.8% (worsening)
MBL change: -0.3 (loss)
PD red: -0.1 mm (worsening)
BOP red: 27.2%
MBL change: -0.3 (loss)
– Oral hygiene instructions
– Local anesthesia not provided
– No details on removal of implant-supported prosthesis provided
– Interventions prior to surgery: supramucosal cleaning and oral hygiene instructions
Access flap and bone
AB-
ASrecontouring (if indicated)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Decontamination protocol
Outcomes
Comments
Isehed et al. 2016
AB-
AS-
13/13
and and marginal bone loss
7.6 mm (median)
Titanium curettes, ultrasonics, and gauze with saline
PD red: 4.0 mm
BOP red: 20.0%
MBL change: 0.2 mm (gain)
– Diabetes and smoking not exclusion criteria (uncontrolled diabetes not allowed)
12 months Sweden also reported in: Isehed et al. 2018
Access flap and Emdogain AB-
AS-
12/12
6.5 mm (median)
PD red: 2.5 mm
BOP red: 20.0%
MBL change: 0.7 mm (gain)
– Interventions prior to surgery: not described
– Implant-supported prosthesis removed for surgery
– Transmucosal healing
Emanuel
2020
RCT et al.
12 months
Israel
Access flap and bone graft with local
14/18
and BOP and marginal bone loss
Not
reported
Curettes, sonics, ultrasonics, and saline
PD red: 1.6 mm
BOP red: 14.3%
MBL change: -0.1 mm (loss)
– Diabetes and smoking not exclusion criteria (uncontrolled diabetes not allowed; smoking >5 cigarettes not allowed)
Cohort study
Access flap and bone graft & Membrane
17/29
BOP/SOP and marginal bone loss
5.4 mm
Titanium curettes, Hydrogen peroxide 3%, and saline
PD red: 2.9 mm
BOP red: 57.7%
MBL change: 1.5 mm (gain)
– Interventions prior to surgery: not described
12 months
Sweden also reported in:
Roos-Jansåker et al.
Access flap and bone graft
AB+
AS+
19/36
5.6 mm
PD red: 3.4 mm
BOP red: 67.9%
MBL change: 1.4 mm (gain)
– Implant-supported prosthesis removed for surgery
– Transmucosal healing
2011
Roos-Jansåker
2014 et al.
TABLE 3 (Continued)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Decontamination protocol
Outcomes
Comments
Roccuzzo et al.
Access flap and bone graft AB+
71/71
PD and crater-like lesion
7.2 mm
Titanium curettes, titanium brush. EDTA, CHX, and saline
PD red: 2.9 mm
BOP red: 53.2%
– Diabetes and smoking not exclusion criteria
MBL change: not reported
– Interventions prior to surgery: mechanical cleaning and oral hygiene instructions
Italy also reported in:
– Handling of implantsupported prosthesis not reported
2021
Isler et al. 2018
Access flap and bone graft and Membrane
26/26
and and osseous defect
5.4 mm
Titanium curettes, gauze with saline
PD red: 2.7 mm
BOP red: 67.3%
– Diabetes and smoking not exclusion criteria
RCT
AB+
CAL change: 2.6 mm (gain)
– Interventions prior to
also reported in:
Access flap and bone graft
26/26
5.9 mm
PD red: 2.2 mm
BOP red: 61.5%
– Implant-supported prosthesis removed for surgery
La Monaca et al.
Access flap and bone graft and Membrane
34/34
BOP/SOP and bone loss
5.9 mm
Titanium curettes, titanium brush, ultrasonics, and air polishing.
PD red: 1.3 mm
BOP red: 58.8%
– Diabetes and smoking were exclusion criteria
Aghazadeh et al.
Access flap and bone graft (autologous) and Membrane
22/36
and and bone loss
6.0 mm
Titanium curettes.
Hydrogen peroxide 3%, CHX 0.2%, and saline
PD red: 2.0 mm
BOP red: 44.8%
MBL change: 0.2 mm (gain)
– Diabetes and smoking not exclusion criteria (uncontrolled diabetes not allowed)
AS+
– Interventions prior to
Sweden also reported in:
Access flap and bone graft (bovine) and Membrane
23/39
6.2 mm
PD red: 3.1 mm
BOP red: 50.4%
surgery: mechanical cleaning and oral hygiene instructions
Aghazadeh et al.
AB+
AS+
MBL change: 1.1 mm (gain)
– Handling of implantsupported prosthesis not reported
Aghazadeh et al.
– Transmucosal healing
2022
(Continues)
TABLE 3 (Continued)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Decontamination protocol
Outcomes
Comments
Gonzalez Reguerio et al.
2021 Case series 12 months Spain
Access flap and bone graft
AB-
AS+ and Membrane
43/43
and BOP/SOP and bone loss
6.4 mm
Ultrasonics, implantoplasty.
Orthophosphoric acid 37%, CHX 2.0%, gauze soaked in piperacillin/ tazobactam
PD red: 1.3 mm
BOP red: 58.8%
MBL change: 0.5 mm (gain)
– Diabetes and smoking not exclusion criteria
– Interventions prior to surgery: mechanical cleaning and oral hygiene instructions
– Implant-supported prosthesis removed for surgery, reseated 2 weeks later
– Transmucosal healing
Hentenaar et al.
2022
RCT
12 months
Netherlands
Access flap and bone recontouring (if indicated)
31/40
and and bone loss
4.6 mm
Scaler, gauzes soaked in saline
PD red: 1.1 mm
BOP red: 13.9%
– Diabetes and smoking not exclusion criteria (uncontrolled diabetes not allowed)
Access flap and bone recontouring (if indicated)
27/54
4.9 mm
Scaler, air polishing
PD red: 1.6 mm
BOP red: 18.2%
MBL change: -0.2 mm (loss)
– Interventions prior to surgery: supra and submucosal instrumentation by air polishing or with ultrasonic instrument and oral hygiene instructions
– Implant-supported prosthesis removed for surgery, if possible
Toma et al. 2014 Cohort study 12 months Belgium
Access flap
AB-
AS-
Access flap
AB-
AS-
Air polishing
10/12
and and bone loss
4.9 mm
Plastic curettes, gauzes soaked in saline
PD red: 0.7 mm
MBL change: -0.3 mm (loss)
– Diabetes and smoking not exclusion criteria (uncontrolled diabetes not allowed)
TABLE 3 (Continued)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Decontamination protocol
Outcomes
Comments
De Tapia et al.
Access flap and bone graft and Membrane
15/15
and and bone loss >30%
7.8 mm
Ultrasonics. Hydrogen peroxide
PD red: 2.9 mm
BOP red: 54.0%
– Diabetes and smoking not exclusion criteria (heavy
2019
AB+
of implant length and
3%
REC: 0.2 mm
smoking not allowed)
RCT
AS+
osseous defect
MBL change: 1.1 mm (gain)
– Interventions prior to
12 months
Access flap and bone graft and Membrane
15/15
8.5 mm
surgery: mechanical cleaning and oral hygiene instructions
AB+
AS+
Ultrasonics, titanium brush.
Hydrogen peroxide 3%
PD red: 4.9 mm
BOP red: 80.0%
REC: 0.6 mm
MBL change: 2.8 mm (gain)
– Implant-supported prosthesis removed for surgery, if possible
– Implantoplasty at supracrestally located implant surfaces
Schwarz et al.
Access flap and bone graft and Membrane
14/16
PD and osseous defect
5.5 mm
Plastic curettes, gauzes soaked in
PD red: 2.0 mm
BOP red: 60.1%
CAL changes: 1.5 mm (gain)
REC: 0.5 mm
– Diabetes and smoking not exclusion criteria (uncontrolled diabetes and heavy smoking not allowed)
Access flap and bone graft and Membrane
10/19
5.1 mm
Er:YAG laser
PD red: 1.7 mm
BOP red: 55.0%
CAL changes: 1.3 mm (gain)
REC: 0.4 mm
– Interventions prior to surgery: mechanical cleaning and oral hygiene instructions
Schwarz et al.
2012
Schwarz et al.
AB-
AS-
– Handling of implantsupported prosthesis not reported
– Implantoplasty at supracrestally located
2013
implant surfaces
Schwarz et al.
– Transmucosal healing
– MBL changes not reported
2017
Esposito et al.
Access flap
AB-
40/40
Signs of soft tissue
inflammation and
6.5 mm
Various curettes, ultrasonics
PD red: 1.0 mm
BOP red (sites out of 4): 1.3
– Diabetes and smoking not exclusion criteria
2013
AS-
marginal bone loss
MBL change: -0.1 mm (loss)
– Interventions prior to
RCT
AB-
AS-
40/40
6.2 mm
Various curettes, ultrasonics, LAD
PD red: 1.1 mm
BOP red (sites out of 4): 1.4
MBL change: 0.0 mm
surgery: Oral hygiene instructions, modification of prostheses when indicated
TABLE 3 (Continued)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Decontamination protocol
Outcomes
Comments
De Waal et al.
Pocket elimination AB-
15 / 48
and and marginal bone loss
5.5 mm
Gauze soaked in saline
PD red: 1.8 mm
BOP red: 22.5%
– Diabetes and smoking not exclusion criteria (insulin-
RCT
AS- (placebo)
and implant function time years
Rinsing of implant surface with placebo solution
MBL change: -0.3 mm (loss)
– Interventions prior to
Netherlands
Pocket elimination ABAS+
15 / 31
6.6 mm
Gauze soaked in saline
Rinsing of implant surface with 0.12% CHX and 0.05% CPC
PD red: 2.3 mm
BOP red: 19.9%
MBL change: -0.7 mm (loss)
surgery: mechanical instrumentation and oral hygiene instructions
De Waal et al.
Pocket elimination AB-
22 / 59
and and marginal bone loss
5.0 mm
Gauze soaked in saline
PD red: 2.1 mm
BOP red: 37.2%
– Diabetes and smoking not exclusion criteria (insulin-
RCT
AS+
and implant function time years
Rinsing of implant surface with
MBL change: 0 mm
dependent diabetes not allowed)
12 months
0.12% CHX and
– Interventions prior to
Netherlands
0.05% CPC
surgery: mechanical
Pocket elimination
AB-
AS+
22 / 49
4.7 mm
PD red: 1.7 mm
BOP red: 39.4%
MBL change: -0.3 mm (loss)
– Implant-supported prosthesis removed for surgery, if possible (in all but 16 patients)
– Transmucosal healing
Englezos et al.
Pocket elimination AB+
25 / 40
and BOP and bone level
9.5 mm
Carbon curettes, PEAK ultrasonic
PD red: 5.6 mm
BOP: 75% no BOP at 2 years
– Smoking not exclusion criterion. No subjects with
2018
AS+
CHX
MBL change: -0.2 mm (loss)
diabetes included
Case series 2 years
– Interventions prior to surgery: supra and submucosal instrumentation with ultrasonic and hand instruments and oral hygiene instructions
TABLE 3 (Continued)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Decontamination protocol
Outcomes
Comments
Hallström et al.
AS-
19/19
and BOP/SOP and bone loss or bone level
5.8 mm
Curettes, gauzes soaked in saline
PD red: 1.5 mm
BOP red: not reported MBL change: 0.3 mm (gain)
– Diabetes and smoking not exclusion criteria (uncontrolled diabetes not allowed)
Romeo et al. 131,209
Access flap and bone recontouring and
9/18
9/18
and BOP/SOP and
5.8 mm
6.5 mm
6.5 mm
.8 mm
Metronidazole gel, gauzes soaked
hydro
Metronidazole gel, gauzes soaked in tetracycline hydrochloride
hydrochloride
PD red: 2.2 mm BOP red: not reported
– Diabetes and smoking not exclusion criteria
2005 & 2007 RCT
AB+
radiolucency
MBL change: -0.0 mm
– Interventions prior to surgery: mechanical
Italy
Access flap and bone recontouring AB+ AS+
PD red: 1.0 mm BOP red: not reported CAL change: -1.5 mm (loss) REC: 1.4 mm MBL change: -1.0 mm (loss)
– Handling of implantsupported prosthesis not reported
– Transmucosal healing
Lasserre et al.
Access flap and Implantoplasty
15/20
PD & BOP/SOP & bone loss
6.7 mm
Curettes
– Smokers excluded
– Diabetes not exclusion
2020
AB-
REC: 0.5 mm
criterion
RCT 6 months
AS+
CAL change: 3.5 mm (gain) MBL change: 0.3 mm (gain)
– Interventions prior to surgery: mechanical
Belgium
Access flap and Air polishing ABAS+
14/19
5.6 mm
Curettes Air polishing
PD red: 3.3 mm BOP change. 61.1%
instrumentation, oral hygiene instructions
– Implant-supported prosthesis removed for surgery, if possible
– Transmucosal healing
TABLE 3 (Continued)
Study
Treatment groups
Patients/ implants
Inclusion criteria: peri-implantitis
Mean PD at baseline
Decontamination protocol
Outcomes
Comments
Regidor et al.
Access flap and Bone graft and
19/19
and BOP/SOP and bone
9.4 mm
Titanium brush
PD red: 4.4 mm
BOP change: 67.3%
– Diabetes and smoking not exclusion criteria
Spain
Access flap and Bone graft
AB+
AS+
20/20
8.8 mm
Titanium brush
PD red: 4.2 mm
BOP change: 66.2%
REC: 0.1 mm
MBL change: 0.9 mm (gain)
– Interventions prior to surgery: mechanical instrumentation, oral hygiene instructions
– Implant-supported prosthesis removed for surgery, if possible
– Transmucosal healing
Monje et al.
Access flap and Bone graft
16/24
and and bone level
8.7 mm
Titanium brush.
Hydrogen peroxide , saline
PD red: 5.0 mm
BOP red: not reported
REC: 2.0 mm
MBL change: 1.7 mm (gain)
– Diabetes and smoking were exclusion criteria
RCT
AS+
– Interventions prior to surgery: mechanical cleaning
AB+
AS+
17/24
8.6 mm
Titanium brush.
Hydrogen peroxide
3% and saline
PD red: 4.6 mm
BOP red: not reported
REC: 1.8 mm
MBL change: 1.7 mm (gain)
– Implant-supported prosthesis removed for surgery, if possible
– Implantoplasty at supracrestally located implant surfaces
– Transmucosal healing
Polymeri et al.
Access flap and bone graft (bovine, BioOss)
11/11
and , bone loss and osseous defect
7.0 mm
Titanium curettes.
Hydrogen peroxide and saline
PD red: 3.6 mm
BOP red: 54.5%
MBL change: 2.2 mm (gain)
– Smoking not exclusion criterion. No subjects with diabetes included
RCT
AS+
13/13
7.1 mm
Titanium curettes.
Hydrogen peroxide
and saline
PD red: 3.8 mm
BOP red: 50.5%
MBL change: 2.8 mm (gain)
– Interventions prior to surgery: not described
AB+
AS+
– Implant-supported prosthesis removed for surgery, if possible
– Transmucosal healing
Probing pocket depth reduction
Study
Std. mean effect with 95% CI
Weight (%)
1. Albaker 2018
–
–
0.7 (-0.4, 1.8)
3.0
2. Albaker 2018
–
–
0.7 (-0.5, 1.9)
2.8
3. Carcuac 2020
–
-0.2 ( -0.6, 0.2)
6.7
4. de Waal 2013
-0.3 (-1.1, 0.5)
4.4
5. de Waal 2013
-0.7 ( -1.8, 0.4)
2.9
6. de Waal 2015
0.0 ( -0.6, 0.6)
5.5
7. de Waal 2015
-0.3 ( -0.9, 0.3)
5.2
8. Englezos 2018
-0.2 ( -0.5, 0.1)
7.3
9. Hallström 2017
0.3 ( 0.1, 0.5)
7.5
10. Hallström 2017
–
0.5( 0.3, 0.7)
7.7
12. Hentenaar 2022
-0.1 ( -0.3, 0.1)
7.8
13. Hentenaar 2022
-0.2 (-0.3, -0.1)
8.0
14. Jepsen 2016
0.9 ( 0.4, 1.4)
6.3
15. Derks 2022
1.1 ( 0.9, 1.3)
7.5
16. Renvert 2021
1.3 ( 0.3, 2.3)
3.4
17. Renvert 2018
–
0.2 ( -0.1, 0.5)
7.4
18. Wagner 2021
0.6( 0.2, 1.0)
6.7
Overall
–
0.2 ( -0.0, 0.5)
-2
-1
0
1
2
Random-effects REML model
Marginal bone level change
Study
Std. mean effect with 95% CI
Weight (%)
1. Albaker 2018
0.7 ( -0.4, 1.8)
3.0
2. Albaker 2018
0.7 (-0.5, 1.9)
2.8
3. Carcuac 2020
-0.2 (-0.6, 0.2)
6.7
4. de Waal 2013
-0.3 (-1.1, 0.5)
4.4
5. de Waal 2013
-0.7 (-1.8, 0.4)
2.9
6. de Waal 2015
0.0 ( -0.6, 0.6)
5.5
7. de Waal 2015
-0.3 (-0.9, 0.3)
5.2
8. Englezos 2018
-0.2 (-0.5, 0.1)
7.3
9. Hallström 2017
7.5
10. Hallström 2017
12. Hentenaar 2022
-0.1 ( -0.3, 0.1)
7.8
13. Hentenaar 2022
-0.2 ( -0.3, -0.1)
8.0
14. Jepsen 2016
0.9 ( 0.4, 1.4)
6.3
15. Derks 2022
1.1 ( 0.9, 1.3)
16. Renvert 2021
1.3( 0.3, 2.3)
3.4
17. Renvert 2018
–
0.2 ( -0.1, 0.5)
7.4
18. Wagner 2021
0.6 ( 0.2, 1.0)
6.7
Overall
0.2 ( -0.0, 0.5)
Bone Loss
-2
-1 0
01
2
Random-effects REML model
FIGURE 3 Adapted from Karlsson et al. See original publication for references. Standardized mean reduction of probing pocket depth and changes in marginal bone level as reported in prospective observational studies or in select arms of randomized controlled trials on access flap or pocket elimination procedures.
predominantly from European studies, suggested that surgical therapy aimed at decontamination of the implant surface was effective in reducing signs of peri-implant inflammation and in arresting disease progression.
5.4.1 | Efficacy of different decontamination protocols
The cleaning and decontamination of exposed implant surfaces is a crucial component of the surgical management of peri-implantitis. While the removal of mineralized deposits is commonly accomplished by means of curettes or scalers, numerous instruments and protocols were proposed to facilitate the removal of the microbial biofilm. A recent systematic review and meta-analysis evaluated the efficacy of either adjunctive (i.e., measures used subsequent to conventional implant surface debridement) or alternative photo-/mechanical and physical measures for implant surface decontamination in conjunction with various surgical protocols. More specifically, these measures included implantoplasty, air polishing, ultrasonic devices, titanium brushes, and lasers, used either as mono- or combination therapies. These interventions were compared with either standard instrumentation (e.g., scalers to remove hard deposits plus gauze soaked in saline) alone (Comparison 1), or with a combination of standard instrumentation (e.g., scalers to remove hard deposits
plus gauze soaked in saline) and additional mechanical/physical/antimicrobial measures (Comparison 2).
For Comparison 1, the meta-analysis, based on two studies, revealed weighted mean differences for reductions of bleeding and probing depth of and 0.9 mm , respectively, favoring the use of adjunctive and alternative (i.e., air polishing with glycine powdered or erythritol-based powder and titanium brushes) over conventional implant surface decontamination methods between 6 and 12 months following non-reconstructive surgical therapy of peri-implantitis. Over a period of 2 years following combined surgical therapy, an Er:YAG laser was associated with similar reductions of probing depth ( 1.1 mm vs. 1.5 mm ) and bleeding ( vs. ) when compared to the conventional decontamination regimen.
For Comparison 2, two RCTs investigated either the efficacy of an Er:YAG laser used as an adjunct to a piezoelectric scaler, or the adjunctive effect of titanium brushes following mechanical debridement and chemical decontamination using The reported weighted mean differences for reductions of bleeding (12%) and probing depth did not report benefit from the use of either of the two decontamination protocols.
Based on this limited clinical evidence and for reasons presented for nonsurgical therapy, air polishing and an Er:YAG laser were recommended not to be used, while titanium brushes may be considered for surgical implant surface decontamination.
5.4.2 | Adjunctive use of systemic antibiotics
The use of systemic antibiotics as an adjunct to surgical therapy of peri-implantitis has so far been evaluated in two trials, both of them originating from Sweden. In 2017, Hallström et al. used azithromycin in 20 subjects in the test group, while the 19 control patients were treated with access flap surgery alone. At 12 months after therapy, the authors noted similar reductions in probing depth (control 1.5 mm ; test: 1.3 mm ) and marginal bone level (control 0.3 mm ; test: 0.5 mm ). Subsequent conclusions were that this specific antibiotic regime did not provide any benefits.
In the second trial relevant in this context, Carcuac et al. enrolled 100 patients and randomly allocated half of these to an antibiotic regime consisting of 10 days of twice daily 750 mg amoxicillin in conjunction with surgical therapy. Results were somewhat different from those observed by Hallström et al. as reductions of probing pocket depth ( vs. ) and marginal bone level ( vs. ) at 12 months were more favorable in the test than in the control group. The authors subsequently followed the patient sample for up to 5 years, reporting on more long-term outcomes. It was noted that the initially observed benefits of the antimicrobial intervention did not persist beyond year 1 (Figure 4). Consequently, the S3 level Clinical Practice Guideline for the prevention and treatment of peri-implant diseases published by the EFP recommended not to use systemic antibiotics as an adjunct to surgical therapy of peri-implantitis, citing an overall low quality of evidence.
5.4.3 | Efficacy of reconstructive methods
Consistent with the periodontal literature, the most extensively evaluated question within the surgical domain relates to reconstructive techniques and their potential benefits. This treatment modality includes the use of either bone replacement grafts, membranes, bioactive agents, or combinations thereof that are applied into or on top of the peri-implant bony defect typically resulting from the disease process. In addition to the basic treatment goals related to resolution of soft tissue inflammation, reconstructive methods are specifically aimed at (i) regeneration of the bony defect, (ii) re-osseointegration, and (iii) the preservation of soft tissue height. Virtually, all controlled studies in this
context represent contributions from Europe. While some trials have performed head-to-head comparisons of different reconstructive techniques, in the majority of reports the efficacy of reconstructive methods was evaluated through comparisons to access flap surgery, that is, omission of the reconstructive technique. In this, the field is very much in line with periodontal research.
The primary end points of peri-implantitis therapy include shallow probing pocket depth and limited bleeding on probing, as illustrated in Figure 5 and outlined in Section 5.2.
As summarized in two systematic reviews, reconstructive methods, per se, have not been shown to provide any benefit in this context. This may be exemplified by the multicenter randomized controlled trial presented by Jepsen et al. The authors included 64 subjects with peri-implantitis and allocated these to either a control (access flap surgery) or a test group (access flap surgery and bone replacement graft). At 12 months, the reduction in probing depth was 2.6 and 2.8 mm , respectively. Reduction of bleeding on probing amounted to and . Similarly, Renvert et al. could not observe any benefit for a reconstructive approach in terms of primary outcomes. The authors combined a bone replacement graft and membrane in the test group and noted a reduction in probing depth of 1.9 mm compared to a reduction of 2.3 mm in controls (access flap surgery). And finally, Derks et al. described 12 -month reductions in both probing depth ( 3.7 mm vs. 3.7 mm ) and in bleeding on probing ( vs. ) that were almost identical in both the control and test arms. The latter consisted of the addition of a bone replacement graft.
With the exception of the study by Derks et al., radiographic parameters, however, were consistently improved by reconstructive measures. Wohlfahrt et al., Jepsen et al., Isehed et al., Renvert et al., and Emanuel et al. all reported benefits in test groups ranging from 0.5 to 2.7 mm of additional bone level gain. It must be noted, however, that the clinical impact of this effect remains to be demonstrated. Also, radiographic evaluation of marginal bone levels following the application of a bone substitute material may be difficult and subject to interpretation (Figure 5B).
The effect of reconstructive measures on changes of soft tissue levels, that is, soft tissue recession, has only rarely been evaluated. Two trials assessed recession at buccal implant sites up to 12 months after surgery and found a and reduction of soft tissue height in control groups (access flap surgery). Interestingly, both studies reported less recession in test groups, with a consistent
benefit of 0.4 mm . As outlined above, the clinical relevance of this benefit remains to be evaluated. Patient satisfaction at 12 months was generally high and not different across study groups in either of the two studies.
Long-term evaluations of outcomes following reconstructive treatment of peri-implantitis are rare. Roccuzzo et al. reported 10-year results following access flap surgery combined with a bone
replacement graft, as illustrated in Figure 5C. The authors found that moderately rough implants fared rather well with a survival rate of and critical reductions in probing depth ( 3.9 mm ) and bleeding on probing (63%). For implants with a titanium plasma-sprayed surface, however, the proportion of implant loss was as high as . These findings are underpinned by the obvious differences in clinical response observed already at 1 year. They are also in line with
FIGURE 5 (A) Four-year clinical follow-up after surgical therapy of peri-implantitis. Note the reduction in probing pocket depth (scored at four sites of the implant) at 1 and 4 years. Red color indicates bleeding on probing. (B) Four-year radiographic follow-up after surgical therapy of peri-implantitis. The clinical images are shown in (A). (C) Clinical images illustrating the surgical intervention. The implant crown was temporarily removed to facilitate access. Following decontamination of the implant surface by means of titanium curettes and a rotating titanium brush under irrigation with saline, a bovine bone material was placed in the bony defect. After suturing, the implant crown was reseated (transmucosal healing). Pre- and postsurgical status and radiographic appearance are illustrated in (A) and (B), respectively.
findings from preclinical in vivo evaluations indicating the difficulties in managing peri-implantitis at implants with rough/complex surfaces characteristics.
5.5 | Factors influencing treatment outcomes
Within the periodontal field, it has long been understood that tooth position/morphology, defect configuration, and patientrelated parameters, such as level of infection control and tobacco smoking, are all critical determinants of outcomes of surgical therapy. Also, the surgical approach, that is, the flap design, has been suggested to be relevant for clinical outcomes. The corresponding understanding of factors influencing outcomes of surgical therapy of peri-implantitis is still limited. Some recent European studies, however, have addressed the question.
As already discussed above, follow-up data gathered over shortand long-term periods demonstrated the importance of implant surface characteristics on treatment outcomes. In a secondary analysis of a randomized controlled trial on the efficacy of a bone replacement graft, Ichioka et al. evaluated the relevance of multiple background factors. The authors observed a strong correlation between initial and final (12 months) probing
depths (Figure 6). This observation is in line with estimates from a systematic review presented by Karlsson et al., in which the magnitude of probing depth reduction was directly related to initial values.
The quality of soft tissues, that is, the dimensions of keratinized mucosa, as an indicator of treatment outcomes have been evaluated in at least two European studies, reporting contradicting data. In a retrospective case series with a mean follow-up period of 23 months, Monje et al. observed less favorable outcomes at implant sites with reduced dimensions of keratinized mucosa ( ). The difference, however, was only apparent at implants treated by reconstructive techniques ( ). Among the 104 implant sites treated by resective/pocket elimination approaches, the height of keratinized mucosa was not associated with outcomes. In general, also Ichioka et al. failed to identify a consistent effect of keratinized mucosa on treatment outcomes following access-flap surgery either without (control) or with (test) the addition of a bone replacement graft (Figure 6). The statistical analysis revealed that probing depth at 12 months was, on average, 0.6 mm greater at sites with no ( ) (Figure 7A) when compared to sites with ( ) keratinized mucosa (Figure 7B). This difference was not statistically significant. The same study did, however, reveal a higher likelihood (OR 5.2) of residual bleeding at implants without keratinized mucosa.
FIGURE 6 Probing pocket depth (PD) at 12 months following surgical therapy of peri-implantitis therapy with or without the adjunctive placement of a bone replacement graft ( implants in 129 patients) as reported by Ichioka et al. Note the differences in final probing by smoking and plaque (at 6 weeks). Neither dimensions of keratinized mucosa nor defect configuration had a statistically significant effect on outcomes. The statistical models are adjusted for smoking, plaque (at 6 weeks), keratinized mucosa at baseline, and defect configuration assessed during surgery.
Data on the relevance of the configuration of the peri-implant bony defect are equally limited. Based on a prospective case series with a 5 -year follow-up, Roccuzzo et al. noted pronounced improvements in clinical parameters, as illustrated by a mean reduction in probing depth of 3.9 mm . The magnitude of improvement, in this dataset, was not dependent on the defect type, classified according to Schwarz et al. A similar conclusion was drawn by Ichioka et al. While the most shallow probing at 12 months was recorded at defects classified as contained (Figure 6), differences were small ( ) and not statistically significant. In a third study, Monje et al. also failed to identify radiographic defect depth or the defect angle to be significant predictors of clinically assessed disease resolution. The authors did, however, observe more pronounced radiographic bone fill at sites with narrower defect angles ( ). Somewhat contradicting findings were presented by Schwarz et al., who reported more favorable 6-month clinical improvements (reductions of probing depth and clinical attachment level) at fully contained defects. Differences, however, were not maintained at the 12-month evaluation. Agazadeh et al. reported that fully contained defects were associated with greater defect fill than other defect types
following application of either autogenous bone or a bovine bone material at 1 year.
While the importance of patient adherence is strongly highlighted in the S3 level Clinical Practice Guideline on the prevention and treatment of peri-implant diseases, relevant scientific evidence is extremely limited. Hence, the reasoning strongly relies on the principles related to periodontal therapy. In one study, Ichioka et al. observed that poor plaque control at 6 weeks subsequent to surgical therapy of peri-implantitis was associated with poorer outcomes at 12 months (Figure 6). In the same dataset, the presence of plaque at 12 months was also strongly related (OR 3.7) to the presence of residual bleeding. It must be noted, however, that participants in this study were generally highly compliant and under strict maintenance during the observation period.
In a retrospective 5-year study including 21 patients, Cortellini et al. applied a minimally invasive surgical protocol to implant sites affected by peri-implantitis. At the final examination, the authors reported an average reduction of probing depth of 3.9 mm and a corresponding gain of radiographic bone levels of 2.5 mm . Due to the lack of controlled studies on surgical approaches, the effect of the type of surgical approach in accessing the peri-implant defect remains unclear.
(A)
(B)
FIGURE 7 (A) Images illustrating a case of peri-implantitis with absence of keratinized mucosa on the buccal aspect of the implant. (B) Images illustrating a case of peri-implantitis with abundant keratinized mucosa on the buccal aspect of the implant.
6 | CONCLUDING REMARKS
Peri-implantitis is a recognized disease entity affecting significant proportions of adult patients. The population at risk is large.
The bacterial etiology and the aggressive nature of peri-implantitis require early diagnosis and intervention.
Anti-infective measures performed by the patient and by dental professionals are imperative in the prevention and treatment of peri-implantitis.
Treatment of peri-implantitis should follow a stepwise approach.
Supportive peri-implant care should be provided to all patients provided with implant therapy, particularly to patients treated for peri-implantitis.
7 | FUTURE PERSPECTIVES
Due to the widespread and increasing use of dental implants in the rehabilitation of patients, dental professionals should expect and be prepared for an increased demand for supportive peri-implant care and for interventions related to peri-implant diseases. Future research should address methods for risk assessment, improved diagnostics as well as effective and safe protocols for treatment of peri-implantitis.
FUNDING INFORMATION
This study is self-funded.
CONFLICT OF INTEREST STATEMENT
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
REFERENCES
Lang NP, Karring T. Proceedings of the 1st European Workshop on Periodontology. Quintessence Publishing Co., Ltd; 1993.
Albrektsson T, Isidor F. Consensus Report of Session IV Proceedings of the 1st European Workshop on Periodontology. Switzerland. Quintessence Publishing Co., Ltd.; 1993.
Lang NP, Karring T, Lindhe J. Proceedings of the 3rd European Workshop on Periodontology. Quintessence Publishing Co., Ltd; 1999.
Berglundh T, Persson L, Klinge B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J Clin Periodontol. 2002;29(Suppl 3):197-212; discussion 232-3.
Lindhe J, Meyle J, Group D of European Workshop on Periodontology. Peri-implant diseases: consensus report of the sixth European workshop on periodontology. J Clin Periodontol. 2008;35(8 Suppl):282-285.
Lang NP, Berglundh T, Working Group 4 of Seventh European Workshop on Periodontology. Periimplant diseases: where are we now?-Consensus of the seventh European workshop on periodontology. J Clin Periodontol. 2011;38 Suppl 11(s11):178-181.
Sanz M, Chapple IL, Working Group 4 of the VIII European Workshop on Periodontology. Clinical research on peri-implant
diseases: consensus report of working group 4. J Clin Periodontol. 2012;39(Suppl 12):202-206.
Jepsen S, Berglundh T, Genco R, et al. Primary prevention of periimplantitis: managing peri-implant mucositis. J Clin Periodontol. 2015;42(Suppl 16):S152-S157.
Berglundh T, Armitage G, Araujo MG, et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Clin Periodontol. 2018;45:S286-S291.
Schwarz F, Derks J, Monje A, Wang HL. Peri-implantitis. J Clin Periodontol. 2018;45:S246-S266.
Fransson C, Lekholm U, Jemt T, Berglundh T. Prevalence of subjects with progressive bone loss at implants. Clin Oral Implants Res. 2005;16(4):440-446.
Derks J, Håkansson J, Wennström JL, Tomasi C, Larsson M, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: early and late implant loss. J Dent Res. 2015;94(3 Suppl):44S-51S.
Derks J, Schaller D, Håkansson J, Wennström JL, Tomasi C, Berglundh T. Effectiveness of implant therapy analyzed in a Swedish population: prevalence of peri-implantitis. J Dent Res. 2016;95(1):43-49.
SKaPa, Swedish Quality Registry for caries and periodontal disease Annual report. Swedish Quality Registry for caries and periodontal disease; 2022.
Jordan RA, Bodechtel C, Hertrampf K, et al. The Fifth German Oral Health Study (Funfte Deutsche Mundgesundheitsstudie, DMS V) – rationale, design, and methods. BMC Oral Health. 2014;14:161.
Jordan AR, Micheelis W. Fünfte Deutsche Mundgesundheitsstudie(DMS V). Vol 35. Deutscher Zahnärzte Verlag DÄV; 2016.
Derks J, Tomasi C. Peri-implant health and disease. A systematic review of current epidemiology. J Clin Periodontol. 2015;42(Suppl 16):S158-S171.
Mombelli A, Muller N, Cionca N. The epidemiology of periimplantitis. Clin Oral Implants Res. 2012;23(Suppl 6):67-76.
Koldsland OC, Scheie AA, Aass AM. Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J Periodontol. 2010;81(2):231-238.
Roos-Jansåker AM, Lindahl C, Renvert H, Renvert S. Nine- to fourteen-year follow-up of implant treatment. Part II: presence of peri-implant lesions. J Clin Periodontol. 2006;33(4):290-295.
Mir-Mari J, Mir-Orfila P, Figueiredo R, Valmaseda-Castellón E, Gay-Escoda C. Prevalence of peri-implant diseases. A crosssectional study based on a private practice environment. J Clin Periodontol. 2012;39(5):490-494.
Rodrigo D, Sanz-Sánchez I, Figuero E, et al. Prevalence and risk indicators of peri-implant diseases in Spain. J Clin Periodontol. 2018;45(12):1510-1520.
Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ. Prevalence of periodontitis in adults in the United States: 2009 and 2010. J Dent Res. 2012;91(10):914-920.
Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJL, Marcenes W. Global burden of severe periodontitis in 19902010: a systematic review and meta-regression. J Dent Res. 2014;93(11):1045-1053.
Koldsland OC, Scheie AA, Aass AM. The association between selected risk indicators and severity of peri-implantitis using mixed model analyses. J Clin Periodontol. 2011;38(3):285-292.
Carra MC, Rangé H, Swerts PJ, Tuand K, Vandamme K, Bouchard P. Effectiveness of implant-supported fixed partial denture in patients with history of periodontitis: a systematic review and metaanalysis. J Clin Periodontol. 2022;49(Suppl 24):208-223.
Serino G, Strom C. Peri-implantitis in partially edentulous patients: association with inadequate plaque control. Clin Oral Implants Res. 2009;20(2):169-174.
Fransson C, Tomasi C, Pikner SS, et al. Severity and pattern of peri-implantitis-associated bone loss. J Clin Periodontol. 2010;37(5):442-448.
Lindhe J, Berglundh T, Ericsson I, Liljenberg B, Marinello C. Experimental breakdown of peri-implant and periodontal tissues. A study in the beagle dog. Clin Oral Implants Res. 1992;3(1):9-16.
Schou S, Holmstrup P, Reibel J, Juhl M, Hjørting-Hansen E, Kornman KS. Ligature-induced marginal inflammation around osseointegrated implants and ankylosed teeth: stereologic and histologic observations in cynomolgus monkeys (Macaca fascicularis). J Periodontol. 1993;64(6):529-537.
Marinello CP, Berglundh T, Ericsson I, Klinge B, Glantz PO, Lindhe J. Resolution of ligature-induced peri-implantitis lesions in the dog. J Clin Periodontol. 1995;22(6):475-479.
Schou S, Holmstrup P, Stoltze K, Hjørting-Hansen E, Fiehn NE, Skovgaard LT. Probing around implants and teeth with healthy or inflamed peri-implant mucosa/gingiva. A histologic comparison in cynomolgus monkeys (Macaca fascicularis). Clin Oral Implants Res. 2002;13(2):113-126.
Zitzmann NU, Berglundh T, Ericsson I, Lindhe J. Spontaneous progression of experimentally induced periimplantitis. J Clin Periodontol. 2004;31(10):845-849.
Berglundh T, Gotfredsen K, Zitzmann NU, Lang NP, Lindhe J. Spontaneous progression of ligature induced peri-implantitis at implants with different surface roughness: an experimental study in dogs. Clin Oral Implants Res. 2007;18(5):655-661.
Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of peri-implantitis at different types of implants. An experimental study in dogs. I: clinical and radiographic observations. Clin Oral Implants Res. 2008;19(10):997-1002.
Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Spontaneous progression of ligatured induced peri-implantitis at implants with different surface characteristics. An experimental study in dogs II: histological observations. Clin Oral Implants Res. 2009;20(4):366-371.
Albouy JP, Abrahamsson I, Berglundh T. Spontaneous progression of experimental peri-implantitis at implants with different surface characteristics: an experimental study in dogs. J Clin Periodontol. 2012;39(2):182-187.
Carcuac O, Abrahamsson I, Albouy JP, Linder E, Larsson L, Berglundh T. Experimental periodontitis and peri-implantitis in dogs. Clin Oral Implants Res. 2013;24(4):363-371.
Carcuac O, Abrahamsson I, Derks J, Petzold M, Berglundh T. Spontaneous progression of experimental peri-implantitis in augmented and pristine bone: a pre-clinical in vivo study. Clin Oral Implants Res. 2020;31(2):192-200.
Berglundh T, Zitzmann NU, Donati M. Are peri-implantitis lesions different from periodontitis lesions? J Clin Periodontol. 2011;38(Suppl 11):188-202.
Sanz M, Alandez J, Lazaro P, Calvo JL, Quirynen M, van Steenberghe D. Histo-pathologic characteristics of peri-implant soft tissues in Branemark implants with 2 distinct clinical and radiological patterns. Clin Oral Implants Res. 1991;2(3):128-134.
Gualini F, Berglundh T. Immunohistochemical characteristics of inflammatory lesions at implants. J Clin Periodontol. 2003;30(1):14-18.
Berglundh T, Gislason Ö, Lekholm U, Sennerby L, Lindhe J. Histopathological observations of human periimplantitis lesions. J Clin Periodontol. 2004;31(5):341-347.
Carcuac O, Berglundh T. Composition of human peri-implantitis and periodontitis lesions. J Dent Res. 2014;93(11):1083-1088.
Konermann A, Götz W, le M, Dirk C, Lossdörfer S, Heinemann F. Histopathological verification of osteoimmunological mediators in peri-implantitis and correlation to bone loss and implant functional period. J Oral Implantol. 2016;42(1):61-68.
Galindo-Moreno P, López-Martínez J, Caba-Molina M, et al. Morphological and immunophenotypical differences between
chronic periodontitis and peri-implantitis – a cross-sectional study. Eur J Oral Implantol. 2017;10(4):453-463.
Kasnak G, Firatli E, Könönen E, Olgac V, Zeidán-Chuliá F, Gursoy UK. Elevated levels of 8-OHdG and PARK7/DJ-1 in peri-implantitis mucosa. Clin Implant Dent Relat Res. 2018;20(4):574-582.
Dionigi C, Larsson L, Carcuac O, Berglundh T. Cellular expression of DNA damage/repair and reactive oxygen/nitrogen species in human periodontitis and peri-implantitis lesions. J Clin Periodontol. 2020;47(12):1466-1475.
Fretwurst T, Garaicoa-Pazmino C, Nelson K, et al. Characterization of macrophages infiltrating peri-implantitis lesions. Clin Oral Implants Res. 2020;31(3):274-281.
Becker ST, Beck-Broichsitter BE, Graetz C, Dörfer CE, Wiltfang J, Häsler R. Peri-implantitis versus periodontitis: functional differences indicated by transcriptome profiling. Clin Implant Dent Relat Res. 2014;16(3):401-411.
Venza I, Visalli M, Cucinotta M, de Grazia G, Teti D, Venza M. Proinflammatory gene expression at chronic periodontitis and peri-implantitis sites in patients with or without type 2 diabetes. Periodontol. 2010;81(1):99-108.
Fretwurst T, Buzanich G, Nahles S, Woelber JP, Riesemeier H, Nelson K. Metal elements in tissue with dental peri-implantitis: a pilot study. Clin Oral Implants Res. 2016;27(9):1178-1186.
Pettersson M, Pettersson J, Johansson A, Molin Thorén M. Titanium release in peri-implantitis. J Oral Rehabil. 2019;46(2):179-188.
Nelson K, Hesse B, Addison O, et al. Distribution and chemical speciation of exogenous micro- and nanoparticles in inflamed soft tissue adjacent to titanium and ceramic dental implants. Anal Chem. 2020;92(21):14432-14443.
Albrektsson T, Chrcanovic B, Östman PO, Sennerby L. Initial and long-term crestal bone responses to modern dental implants. Periodontol 2000. 2017;73(1):41-50.
Mombelli A, Lang NP. The diagnosis and treatment of periimplantitis. Periodontol 2000. 1998;17:63-76.
Mombelli A. Maintenance therapy for teeth and implants. Periodontol 2000. 2019;79:190-199.
Pontoriero R, Tonelli MP, Carnevale G, Mombelli A, Nyman SR, Lang NP. Experimentally induced peri-implant mucositis. A clinical study in humans. Clin Oral Implants Res. 1994;5:254-259.
Zitzmann NU, Berglundh T, Marinello CP, Lindhe J. Experimental peri-implant mucositis in man. J Clin Periodontol. 2001;28(6):517-523.
Meyer S, Giannopoulou C, Courvoisier D, Schimmel M, Müller F, Mombelli A. Experimental mucositis and experimental gingivitis in persons aged 70 or over. Clinical and biological responses. Clin Oral Implants Res. 2017;28(8):1005-1012.
Löe H, Theilade E, Jensen SB. Experimental gingivitis in man. J Periodontol. 1965;36:177-187.
Salvi GE, Aglietta M, Eick S, Sculean A, Lang NP, Ramseier CA. Reversibility of experimental peri-implant mucositis compared with experimental gingivitis in humans. Clin Oral Implants Res. 2012;23(2):182-190.
Hickey JS, O’Neal RB, Scheidt MJ, Strong SL, Turgeon D, van Dyke TE. Microbiologic characterization of ligature-induced peri-implantitis in the microswine model. J Periodontol. 1991;62:548-553.
Leonhardt Å, Berglundh T, Ericsson I, Dahlen G. Putative periodontal pathogens on titanium implants and teeth in experimental gingivitis and periodontitis in beagle dogs. Clin Oral Implants Res. 1992;3:112-119.
Tillmanns HW, Hermann JS, Tiffee JC, Burgess AV, Meffert RM. Evaluation of three different dental implants in ligature induced peri implantitis in the beagle dog. Part II. Histology and microbiology. Int J Oral Maxillofac Implants. 1998;13(1):59-68.
Nociti FH Jr, Cesco de Toledo R, Machado MAN, Stefani CM, Line SRP, Gonçalves RB. Clinical and microbiological evaluation of ligature-induced peri-implantitis and periodontitis in dogs. Clin Oral Implants Res. 2001;12(4):295-300.
Lindquist LW, Rockler B, Carlsson GE. Bone resorption around fixtures in edentulous patients treated with mandibular fixed tissueintegrated prostheses. J Prosthet Dent. 1988;59:59-63.
Rinke S, Ohl S, Ziebolz D, Lange K, Eickholz P. Prevalence of periimplant disease in partially edentulous patients: a practice-based cross-sectional study. Clin Oral Implants Res. 2011;22(8):826-833.
Monje A, Aranda L, Diaz KT, et al. Impact of maintenance therapy for the prevention of peri-implant diseases: a systematic review and meta-analysis. J Dent Res. 2016;95(4):372-379.
Rams TE, Link CC. Microbiology of failing dental implants in humans: electron microscopic observations. J Oral Implantol. 1983;11:93-100.
Rams TE, Roberts TW, Tatum H. Subgingival bacteriology of periodontally healthy and diseased human dental implants. J Dent Res. 1984;63(Special issue):200.
Listgarten MA. Electron microscopic observations on the bacterial flora of acute necrotizing ulcerative gingivitis. J Periodontol. 1965;36:328-339.
Mombelli A, van Oosten MAC, Schürch E Jr, Lang NP. The microbiota associated with successful or failing osseointegrated titanium implants. Oral Microbiol Immunol. 1987;2:145-151.
Mombelli A, Décaillet F. The characteristics of biofilms in periimplant disease. J Clin Periodontol. 2011;38(Suppl 11):203-213.
Mombelli A, Casagni F, Madianos PN. Can presence or absence of periodontal pathogens distinguish between subjects with chronic and aggressive periodontitis? A systematic review. J Clin Periodontol. 2002;29(Suppl 3):10-21.
Carvalho EBS, Romandini M, Sadilina S, Sant’Ana ACP, Sanz M. Microbiota associated with peri-implantitis-a systematic review with meta-analyses. Clin Oral Implants Res. 2023;34(11):1176-1187.
Kröger A, Hülsmann C, FickI S, et al. The severity of human periimplantitis lesions correlates with the level of submucosal microbial dysbiosis. J Clin Periodontol. 2018;45(12):1498-1509.
Mombelli A, Hashim D, Cionca N. What is the impact of titanium particles and biocorrosion on implant survival and complications? A critical review. Clin Oral Implants Res. 2018;29(Suppl 18):37-53.
Ronin D, Boyer J, Alban N, Natoli RM, Johnson A, Kjellerup BV. Current and novel diagnostics for orthopedic implant biofilm infections: a review. APMIS. 2022;130(2):59-81.
Meyer S, Giannopoulou C, Cancela J, Courvoisier D, Müller F, Mombelli A. Experimental mucositis/gingivitis in persons aged 70 or over: microbiological findings and prediction of clinical outcome. Clin Oral Investig. 2019;23(10):3855-3863.
Tonetti MS, Chapple ILC, Jepsen S, Sanz M. Primary and secondary prevention of periodontal and peri-implant diseases: introduction to, and objectives of the 11th European workshop on periodontology consensus conference. J Clin Periodontol. 2015;42(Suppl 16):S1-S4.
Rothman KJ. Causes. Am J Epidemiol. 1976;104(6):587-592.
Costa FO, Takenaka-Martinez S, Cota LOM, Ferreira SD, Silva GLM, Costa JE. Peri-implant disease in subjects with and without preventive maintenance: a 5-year follow-up. J Clin Periodontol. 2012;39(2):173-181.
Monje A, Wang HL, Nart J. Association of preventive maintenance therapy compliance and peri-implant diseases: a cross-sectional study. J Periodontol. 2017;88(10):1030-1041.
Costa FO, Costa AM, Ferreira SD, et al. Long-term impact of patients’ compliance to peri-implant maintenance therapy on the incidence of peri-implant diseases: an 11-year prospective follow-up clinical study. Clin Implant Dent Relat Res. 2023;25(2):303-312.
Schwarz F, John G, Schmucker A, Sahm N, Becker J. Combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination: a 7-year follow-up observation. J Clin Periodontol. 2017;44(3):337-342.
Berglundh T, Wennstrom JL, Lindhe J. Long-term outcome of surgical treatment of peri-implantitis. A 2-11-year retrospective study. Clin Oral Implants Res. 2018;29(4):404-410.
Heitz-Mayfield LJA, Salvi GE, Mombelli A, et al. Supportive periimplant therapy following anti-infective surgical peri-implantitis treatment: 5-year survival and success. Clin Oral Implants Res. 2018;29(1):1-6.
Carcuac O, Derks J, Abrahamsson I, Wennström JL, Berglundh T. Risk for recurrence of disease following surgical therapy of peri-implantitis-a prospective longitudinal study. Clin Oral Implants Res. 2020;31(11):1072-1077.
Roccuzzo M, Fierravanti L, Pittoni D, Dalmasso P, Roccuzzo A. Implant survival after surgical treatment of peri-implantitis lesions by means of deproteinized bovine bone mineral with 10% collagen: 10-year results from a prospective study. Clin Oral Implants Res. 2020;31(8):768-776.
Herrera D, Berglundh T, Schwarz F, et al. Prevention and treatment of peri-implant diseases-the EFP S3 level clinical practice guideline. J Clin Periodontol. 2023;50(Suppl 26):4-76.
Nibali L, Koidou VP, Nieri M, Barbato L, Pagliaro U, Cairo F. Regenerative surgery versus access flap for the treatment of intrabony periodontal defects: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):320-351.
Sanz-Sanchez I, Montero E, Citterio F, Romano F, Molina A, Aimetti M. Efficacy of access flap procedures compared to subgingival debridement in the treatment of periodontitis. A systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):282-302.
Suvan J, Leira Y, Moreno Sancho FM, Graziani F, Derks J, Tomasi C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J Clin Periodontol. 2020;47(Suppl 22):155-175.
Derks J, Ichioka Y, Dionigi C, et al. Prevention and management of peri-implant mucositis and peri-implantitis: a systematic review of outcome measures used in clinical studies in the last 10 years. J Clin Periodontol. 2023;50(Suppl 25):55-66.
Loos BG, Needleman I. Endpoints of active periodontal therapy. J Clin Periodontol. 2020;47 Suppl 22(Suppl 22):61-71.
Karlsson K, Derks J, Håkansson J, Wennström JL, Petzold M, Berglundh . Interventions for peri-implantitis and their effects on further bone loss: a retrospective analysis of a registry-based cohort. J Clin Periodontol. 2019;46(8):872-879.
Carcuac O, Derks J, Abrahamsson I, Wennström JL, Petzold M, Berglundh T. Surgical treatment of peri-implantitis: 3-year results from a randomized controlled clinical trial. J Clin Periodontol. 2017;44(12):1294-1303.
Jepsen S, Rühling A, Jepsen K, Ohlenbusch B, Albers HK. Progressive peri-implantitis. Incidence and prediction of periimplant attachment loss. Clin Oral Implants Res. 1996;7(2):133-142.
Farina R, Filippi M, Brazzioli J, Tomasi C, Trombelli L. Bleeding on probing around dental implants: a retrospective study of associated factors. J Clin Periodontol. 2017;44(1):115-122.
Merli M, Bernardelli F, Giulianelli E, Toselli I, Mariotti G, Nieri M. Peri-implant bleeding on probing: a cross-sectional multilevel analysis of associated factors. Clin Oral Implants Res. 2017;28(11):1401-1405.
Ichioka Y , Trullenque-Eriksson A, Ortiz-Vigón A, et al. Factors influencing outcomes of surgical therapy of peri-implantitis: a secondary analysis of 1-year results from a randomized clinical study. J Clin Periodontol. 2023;50(10):1282-1304.
Cosgarea R, Roccuzzo A, Jepsen K, Sculean A, Jepsen S, Salvi GE. Efficacy of mechanical/physical approaches for implant surface decontamination in non-surgical submarginal
instrumentation of peri-implantitis. A systematic review. J Clin Periodontol. 2023;50(Suppl 26):188-211.
de Waal YCM, Winning L, Stavropoulos A, Polyzois I. Efficacy of chemical approaches for implant surface decontamination in conjunction with sub-marginal instrumentation, in the nonsurgical treatment of peri-implantitis: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):212-223.
Linares A, Sanz-Sánchez I, Dopico J, Molina A, Blanco J, Montero E. Efficacy of adjunctive measures in the non-surgical treatment of peri-implantitis: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):224-243.
Karring ES, Stavropoulos A, Ellegaard B, Karring T. Treatment of peri-implantitis by the vector system. Clin Oral Implants Res. 2005;16(3):288-293.
Schwarz F, Sculean A, Rothamel D, Schwenzer K, Georg T, Becker J. Clinical evaluation of an Er:YAG laser for nonsurgical treatment of peri-implantitis: a pilot study. Clin Oral Implants Res. 2005;16(1):44-52.
Schwarz F, Bieling K, Bonsmann M, Latz T, Becker J. Nonsurgical treatment of moderate and advanced periimplantitis lesions: a controlled clinical study. Clin Oral Investig. 2006;10(4):279-288.
Renvert S, Samuelsson E, Lindahl C, Persson GR. Mechanical nonsurgical treatment of peri-implantitis: a double-blind randomized longitudinal clinical study. I: clinical results. J Clin Periodontol. 2009;36(7):604-609.
Sahm N, Becker J, Santel T, Schwarz F. Non-surgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine: a prospective, randomized, controlled clinical study. J Clin Periodontol. 2011;38(9):872-878.
John G, Sahm N, Becker J, Schwarz F. Nonsurgical treatment of peri-implantitis using an air-abrasive device or mechanical debridement and local application of chlorhexidine. Twelve-month follow-up of a prospective, randomized, controlled clinical study. Clin Oral Investig. 2015;19(8):1807-1814.
Laleman I, Pauwels M, Quirynen M, Teughels W. The usage of a lactobacilli probiotic in the non-surgical therapy of periimplantitis: a randomized pilot study. Clin Oral Implants Res. 2020;31(1):84-92.
Merli M, Bernardelli F, Giulianelli E, et al. Short-term comparison of two non-surgical treatment modalities of peri-implantitis: clinical and microbiological outcomes in a two-factorial randomized controlled trial. J Clin Periodontol. 2020;47(10):1268-1280.
De Waal YCM, Vangsted TE, Van Winkelhoff AJ. Systemic antibiotic therapy as an adjunct to non-surgical peri-implantitis treatment: a single-blind RCT. J Clin Periodontol. 2021;48(7):996-1006.
Hentenaar DFM, de Waal YCM, Stewart RE, van Winkelhoff AJ, Meijer HJA, Raghoebar GM. Erythritol airpolishing in the nonsurgical treatment of peri-implantitis: a randomized controlled trial. Clin Oral Implants Res. 2021;32:840-852.
Blanco C, Pico A, Dopico J, Gándara P, Blanco J, Liñares A. Adjunctive benefits of systemic metronidazole on non-surgical treatment of peri-implantitis. A randomized placebo-controlled clinical trial. J Clin Periodontol. 2022;49(1):15-27.
Polymeri A, van der Horst J, Anssari Moin D, Wismeijer D, Loos BG, Laine ML. Non-surgical peri-implantitis treatment with or without systemic antibiotics: a randomized controlled clinical trial. Clin Oral Implants Res. 2022;33(5):548-557.
Roccuzzo A, Klossner S, Stähli A, et al. Non-surgical mechanical therapy of peri-implantitis with or without repeated adjunctive diode laser application. A 6-month double-blinded randomized clinical trial. Clin Oral Implants Res. 2022;33(9):900-912.
Yayli NZA, Talmac AC, Keskin Tunc S, Akbal D, Altindal D, Ertugrul AS. Erbium, chromium-doped: yttrium, scandium, gallium, garnet and diode lasers in the treatment of peri-implantitis: clinical and
biochemical outcomes in a randomized-controlled clinical trial. Lasers Med Sci. 2022;37(1):665-674.
Machtei EE, Frankenthal S, Levi G, et al. Treatment of periimplantitis using multiple applications of chlorhexidine chips: a double-blind, randomized multi-centre clinical trial. J Clin Periodontol. 2012;39(12):1198-1205.
Bassetti M, Schär D, Wicki B, et al. Anti-infective therapy of periimplantitis with adjunctive local drug delivery or photodynamic therapy: 12-month outcomes of a randomized controlled clinical trial. Clin Oral Implants Res. 2014;25(3):279-287.
Ahmed P, Bukhari IA, Albaijan R, Sheikh SA, Vohra F. The effectiveness of photodynamic and antibiotic gel therapy as an adjunct to mechanical debridement in the treatment of periimplantitis among diabetic patients. Photodiagnosis Photodyn Ther. 2020;32:102077.
Machtei EE, Romanos G, Kang P, et al. Repeated delivery of chlorhexidine chips for the treatment of peri-implantitis: a multicenter, randomized, comparative clinical trial. J Periodontol. 2021;92(1):11-20.
Shibli JA, Ferrari DS, Siroma RS, Figueiredo LC, Faveri M, Feres M. Microbiological and clinical effects of adjunctive systemic metronidazole and amoxicillin in the non-surgical treatment of periimplantitis: 1 year follow-up. Braz Oral Res. 2019;33(suppl 1):e080.
Almohareb T, Alhamoudi N, al Deeb M, et al. Clinical efficacy of photodynamic therapy as an adjunct to mechanical debridement in the treatment of per-implantitis with abscess. Photodiagnosis Photodyn Ther. 2020;30:101750.
Tada H, Masaki C, Tsuka S, Mukaibo T, Kondo Y, Hosokawa R. The effects of Lactobacillus reuteri probiotics combined with azithromycin on peri-implantitis: a randomized placebo-controlled study. J Prosthodont Res. 2018;62(1):89-96.
Deppe H, Horch HH, Henke J, Donath K. Peri-implant care of ailing implants with the carbon dioxide laser. Int J Oral Maxillofac Implants. 2001;16(5):659-667.
Khoury F, Buchmann R. Surgical therapy of peri-implant disease: a 3-year follow-up study of cases treated with 3 different techniques of bone regeneration. J Periodontol. 2001;72(11):1498-1508.
Deppe H, Horch HH, Neff A. Conventional versus laserassisted treatment of peri-implant defects with the concomitant use of pure-phase beta-tricalcium phosphate: a 5-year clinical report. Int J Oral Maxillofac Implants. 2007;22(1):79-86.
Romeo E, Ghisolfi M, Murgolo N, Chiapasco M, Lops D, Vogel G. Therapy of peri-implantitis with resective surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part I: clinical outcome. Clin Oral Implants Res. 2005;16(1):9-18.
Roccuzzo M, Bonino F, Bonino L, Dalmasso P. Surgical therapy of peri-implantitis lesions by means of a bovine-derived xenograft: comparative results of a prospective study on two different implant surfaces. J Clin Periodontol. 2011;38(8):738-745.
Leonhardt A, Dahlen G, Renvert S. Five-year clinical, microbiological, and radiological outcome following treatment of periimplantitis in man. J Periodontol. 2003;74(10):1415-1422.
Roos-Jansåker AM, Renvert H, Lindahl C, Renvert S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: a prospective cohort study. J Clin Periodontol. 2007;34(7):625-632.
Schwarz F, Sahm N, Iglhaut G, Becker J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: a randomized controlled clinical study. J Clin Periodontol. 2011;38(3):276-284.
Aghazadeh A, Rutger Persson G, Renvert S. A single-centre randomized controlled clinical trial on the adjunct treatment of intrabony defects with autogenous bone or a xenograft: results after 12 months. J Clin Periodontol. 2012;39(7):666-673.
Schwarz F, John G, Mainusch S, Sahm N, Becker J. Combined surgical therapy of peri-implantitis evaluating two methods of surface debridement and decontamination. A two-year clinical follow up report. J Clin Periodontol. 2012;39(8):789-797.
Wohlfahrt JC, Lyngstadaas SP, Rønold HJ, et al. Porous titanium granules in the surgical treatment of peri-implant osseous defects: a randomized clinical trial. Int J Oral Maxillofac Implants. 2012;27(2):401-410.
de Waal YC, Raghoebar GM, Huddleston Slater JJ, Meijer HJ, Winkel EG, van Winkelhoff A. Implant decontamination during surgical peri-implantitis treatment: a randomized, double-blind, placebo-controlled trial. J Clin Periodontol. 2013;40(2):186-195.
Schwarz F, Hegewald A, John G, Sahm N, Becker J. Four-year fol-low-up of combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination. J Clin Periodontol. 2013;40(10):962-967.
Persson LG, Berglundh T, Lindhe J, Sennerby L. Re-osseointegration after treatment of peri-implantitis at different implant surfaces. An experimental study in the dog. Clin Oral Implants Res. 2001;12(6):595-603.
Albouy JP, Abrahamsson I, Persson LG, Berglundh T. Implant surface characteristics influence the outcome of treatment of peri-implantitis: an experimental study in dogs. J Clin Periodontol. 2011;38(1):58-64.
Carcuac O, Derks J, Charalampakis G, Abrahamsson I, Wennström J, Berglundh T. Adjunctive systemic and local antimicrobial therapy in the surgical treatment of peri-implantitis: a randomized controlled clinical trial. J Dent Res. 2016;95(1):50-57.
Donos N, Calciolari E, Brusselaers N, Goldoni M, Bostanci N, Belibasakis GN. The adjunctive use of host modulators in non-surgical periodontal therapy. A systematic review of randomized, placebo-controlled clinical studies. J Clin Periodontol. 2020;47(Suppl 22):199-238.
Herrera D, Matesanz P, Martín C, Oud V, Feres M, Teughels W. Adjunctive effect of locally delivered antimicrobials in periodontitis therapy: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):239-256.
Salvi GE, Stähli A, Schmidt JC, Ramseier CA, Sculean A, Walter C. Adjunctive laser or antimicrobial photodynamic therapy to non-surgical mechanical instrumentation in patients with untreated periodontitis: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):176-198.
Teughels W, Feres M, Oud V, Martín C, Matesanz P, Herrera D. Adjunctive effect of systemic antimicrobials in periodontitis therapy: a systematic review and meta-analysis. J Clin Periodontol. 2020;47(Suppl 22):257-281.
Karlsson K, Trullenque-Eriksson A, Tomasi C, Derks J. Efficacy of access flap and pocket elimination procedures in the management of peri-implantitis: a systematic review and meta-analysis. J Clin Periodontol. 2023;50(Suppl 26):244-284.
Ramanauskaite A, Schwarz F, Cafferata EA, Sahrmann P. Photo/ mechanical and physical implant surface decontamination approaches in conjunction with surgical peri-implantitis treatment: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):317-335.
Toma S, Brecx MC, Lasserre JF. Clinical evaluation of three surgical modalities in the treatment of peri-implantitis: a randomized controlled clinical trial. J Clin Med. 2019;8(7):966.
Hentenaar DFM, de Waal YCM, Stewart RE, van Winkelhoff AJ, Meijer HJA, Raghoebar GM. Erythritol air polishing in the surgical treatment of peri-implantitis: a randomized controlled trial. Clin Oral Implants Res. 2022;33(2):184-196.
de Tapia B, Valles C, Ribeiro-Amaral T, et al. The adjunctive effect of a titanium brush in implant surface decontamination at periimplantitis surgical regenerative interventions: a randomized controlled clinical trial. J Clin Periodontol. 2019;46(5):586-596.
Wang CW, Ashnagar S, Gianfilippo RD, Arnett M, Kinney J, Wang HL. Laser-assisted regenerative surgical therapy for periimplantitis: a randomized controlled clinical trial. J Periodontol. 2021;92(3):378-388.
Teughels W, Seyssens L, Christiaens V, Temmerman A, Castro AB, Cosyn J. Adjunctive locally and systemically delivered antimicrobials during surgical treatment of peri-implantitis: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):359-372.
Hallström H, Persson GR, Lindgren S, Renvert S. Open flap debridement of peri-implantitis with or without adjunctive systemic antibiotics: a randomized clinical trial. J Clin Periodontol. 2017;44(12):1285-1293.
Donos N, Calciolari E, Ghuman M, Baccini M, Sousa V, Nibali L. The efficacy of bone reconstructive therapies in the management of peri-implantitis. A systematic review and meta-analysis. J Clin Periodontol. 2023;50(Suppl 26):285-316.
Monje A, Pons R, Insua A, Nart J, Wang HL, Schwarz F. Morphology and severity of peri-implantitis bone defects. Clin Implant Dent Relat Res. 2019;21(4):635-643.
Jepsen S, Schwarz F, Cordaro L, et al. Regeneration of alveolar ridge defects. Consensus report of group 4 of the 15th European workshop on periodontology on bone regeneration. J Clin Periodontol. 2019;46(Suppl 21):277-286.
Isehed C, Holmlund A, Renvert S, Svenson B, Johansson I, Lundberg P. Effectiveness of enamel matrix derivative on the clinical and microbiological outcomes following surgical regenerative treatment of peri-implantitis. A randomized controlled trial. J Clin Periodontol. 2016;43(10):863-873.
Jepsen K, Jepsen S, Laine ML, et al. Reconstruction of peri-implant osseous defects: a multicenter randomized trial. J Dent Res. 2016;95(1):58-66.
Isler SC, Soysal F, Ceyhanlı T, Bakırarar B, Unsal B. Regenerative surgical treatment of peri-implantitis using either a collagen membrane or concentrated growth factor: a 12-month randomized clinical trial. Clin Implant Dent Relat Res. 2018;20(5):703-712.
Renvert S, Roos-Jansåker AM, Persson GR. Surgical treatment of peri-implantitis lesions with or without the use of a bone substitute-a randomized clinical trial. J Clin Periodontol. 2018;45(10):1266-1274.
Polymeri A, Anssari-Moin D, van der Horst J, Wismeijer D, Laine ML, Loos BG. Surgical treatment of peri-implantitis defects with two different xenograft granules: a randomized clinical pilot study. Clin Oral Implants Res. 2020;31(11):1047-1060.
Renvert S, Giovannoli JL, Roos-Jansåker AM, Rinke S. Surgical treatment of peri-implantitis with or without a deproteinized bovine bone mineral and a native bilayer collagen membrane: a randomized clinical trial. J Clin Periodontol. 2021;48(10):1312-1321.
Derks J, Ortiz-Vigón A, Guerrero A, et al. Reconstructive surgical therapy of peri-implantitis: a multicenter randomized controlled clinical trial. Clin Oral Implants Res. 2022;33(9):921-944.
Monje A, Pons R, Vilarrasa J, Nart J, Wang HL. Significance of barrier membrane on the reconstructive therapy of peri-implantitis: a randomized controlled trial. J Periodontol. 2023;94(3):323-335.
Regidor E, Ortiz-Vigón A, Romandini M, Dionigi C, Derks J, Sanz M. The adjunctive effect of a resorbable membrane to a xenogeneic bone replacement graft in the reconstructive surgical therapy of peri-implantitis: a randomized clinical trial. J Clin Periodontol. 2023;50(6):765-783.
Tomasi C, Regidor E, Ortiz-Vigón A, Derks J. Efficacy of reconstructive surgical therapy at peri-implantitis-related bone defects. A systematic review and meta-analysis. J Clin Periodontol. 2019;46(Suppl 21):340-356.
Emanuel N, Machtei EE, Reichart M, Shapira L. D-PLEX500: a local biodegradable prolonged release doxycycline-formulated bone graft for the treatment for peri-implantitis. A randomized controlled clinical study. Quintessence Int. 2020;51(7):546-553.
Mikami R, Mizutani K, Shioyama H, et al. Influence of aging on periodontal regenerative therapy using enamel matrix derivative: a 3-year prospective cohort study. J Clin Periodontol. 2022;49(2):123-133.
Tonetti MS, Pini-Prato G, Cortellini P. Periodontal regeneration of human intrabony defects. IV. Determinants of healing response. J Periodontol. 1993;64(10):934-940.
Tonetti MS, Prato GP, Cortellini P. Factors affecting the healing response of intrabony defects following guided tissue regeneration and access flap surgery. J Clin Periodontol. 1996;23(6):548-556.
Cortellini P, Carnevale G, Sanz M, Tonetti MS. Treatment of deep and shallow intrabony defects. A multicenter randomized controlled clinical trial. J Clin Periodontol. 1998;25(12):981-987.
Cortellini P, Pini-Prato G, Tonetti M. Periodontal regeneration of human infrabony defects (V). Effect of oral hygiene on long-term stability. J Clin Periodontol. 1994;21(9):606-610.
Tonetti MS, Pini-Prato G, Cortellini P. Effect of cigarette smoking on periodontal healing following GTR in infrabony defects. A preliminary retrospective study. J Clin Periodontol. 1995;22(3):229-234.
Cortellini P, Tonetti MS, Lang NP, et al. The simplified papilla preservation flap in the regenerative treatment of deep intrabony defects: clinical outcomes and postoperative morbidity. J Periodontol. 2001;72(12):1702-1712.
Trombelli L, Simonelli A, Schincaglia GP, Cucchi A, Farina R. Single-flap approach for surgical debridement of deep intraosseous defects: a randomized controlled trial. J Periodontol. 2012;83(1):27-35.
Roccuzzo M, Gaudioso L, Lungo M, Dalmasso P. Surgical therapy of single peri-implantitis intrabony defects, by means of deproteinized bovine bone mineral with collagen. J Clin Periodontol. 2016;43(3):311-318.
Roccuzzo M, Mirra D, Pittoni D, Ramieri G, Roccuzzo A. Reconstructive treatment of peri-implantitis infrabony defects of various configurations: 5-year survival and success. Clin Oral Implants Res. 2021;32(10):1209-1217.
Monje A, Pons R, Amerio E, Wang HL, Nart J. Resolution of periimplantitis by means of implantoplasty as adjunct to surgical therapy: a retrospective study. J Periodontol. 2022;93(1):110-122.
Monje A, Pons R, Sculean A, Nart J, Wang HL. Defect angle as prognostic indicator in the reconstructive therapy of periimplantitis. Clin Implant Dent Relat Res. 2023;25:992-999.
Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J Clin Periodontol. 2010;37(5):449-455.
Aghazadeh A, Persson RG, Renvert S. Impact of bone defect morphology on the outcome of reconstructive treatment of periimplantitis. Int J Implant Dent. 2020;6(1):33.
Stiesch M, Grischke J, Schaefer P, Heitz-Mayfield LJA. Supportive care for the prevention of disease recurrence/progression following peri-implantitis treatment: a systematic review. J Clin Periodontol. 2023;50(Suppl 26):113-134.
Cortellini P, Cortellini S, Bonaccini D, Tonetti MS. Papilla preservation and minimally invasive surgery for the treatment of peri-implant osseous defects. Clinical and radiographic outcomes of a 5-year retrospective study. Clin Oral Implants Res. 2021;32(11):1384-1396.
Cornelini R, Artese L, Rubini C, et al. Vascular endothelial growth factor and microvessel density around healthy and failing dental implants. Int J Oral Maxillofac Implants. 2001;16(3):389-393.
Bullon P, Fioroni M, Goteri G, Rubini C, Battino M. Immunohistochemical analysis of soft tissues in implants with healthy and peri-implantitis condition, and aggressive periodontitis. Clin Oral Implants Res. 2004;15(5):553-559.
Roediger M, Miró X, Geffers R, et al. Profiling of differentially expressed genes in peri-implantitis and periodontitis in vivo by microarray analysis. J Oral Biosci. 2009;51(1):31-45.
Ghighi M, Llorens A, Baroukh B, Chaussain C, Bouchard P, Gosset M . Differences between inflammatory and catabolic mediators of peri-implantitis and periodontitis lesions following initial mechanical therapy: an exploratory study. J Periodontal Res. 2018;53(1):29-39.
Lucarini G, Zizzi A, Rubini C, Ciolino F, Aspriello SD. VEGF, microvessel density, and CD44 as inflammation markers in peri-implant healthy mucosa, peri-implant mucositis, and periimplantitis: impact of age, smoking, PPD, and obesity. Inflammation. 2019;42(2):682-689.
Galárraga-Vinueza ME, Tangl S, Bianchini M, et al. Histological characteristics of advanced peri-implantitis bone defects in humans. Int J Implant Dent. 2020;6(1):12.
Mijiritsky E, Ferroni L, Gardin C, et al. Presence of ROS in inflammatory environment of peri-implantitis tissue in vitro and in vivo human evidence. J Clin Med. 2019;9(1):38.
Fretwurst T, Müller J, Larsson L, et al. Immunohistological composition of peri-implantitis affected tissue around ceramic implants-a pilot study. J Periodontol. 2021;92(4):571-579.
Galarraga-Vinueza ME, Obreja K, Ramanauskaite A, et al. Macrophage polarization in peri-implantitis lesions. Clin Oral Investig. 2021;25(4):2335-2344.
Karring ES, Stavropoulos A, Ellegaard B, Karring T. Treatment of peri-implantitis by the VectorR system. A pilot study. Clin Oral Implants Res. 2005;16(3):288-293.
Schär D, Ramseier CA, Eick S, Arweiler NB, Sculean A, Salvi GE. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: six-month outcomes of a prospective randomized clinical trial. Clin Oral Implants Res. 2013;24(1):104-110.
Andersen H, Aass AM, Wohlfahrt JC. Porous titanium granules in the treatment of peri-implant osseous defects-a 7-year follow-up study. Int J Implant Dent. 2017;3(1):50.
Isehed C, Svenson B, Lundberg P, Holmlund A. Surgical treatment of peri-implantitis using enamel matrix derivative, an RCT: 3- and 5-year follow-up. J Clin Periodontol. 2018;45(6):744-753.
Roos-Jansåker AM , Lindahl C , Persson GR , Renvert S . Longterm stability of surgical bone regenerative procedures of periimplantitis lesions in a prospective case-control study over 3 years. J Clin Periodontol. 2011;38(6):590-597.
Roos-Jansåker AM, Persson GR, Lindahl C, Renvert S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: a 5-year follow-up. J Clin Periodontol. 2014;41(11):1108-1114.
Isler SC, Soysal F, Ceyhanlı T, Bakırarar B, Unsal B. Efficacy of concentrated growth factor versus collagen membrane in reconstructive surgical therapy of peri-implantitis: 3-year results of a randomized clinical trial. Clin Oral Investig. 2022;26(8):5247-5260.
la Monaca G, Pranno N, Annibali S, Cristalli MP, Polimeni A. Clinical and radiographic outcomes of a surgical reconstructive approach in the treatment of peri-implantitis lesions: a 5-year prospective case series. Clin Oral Implants Res. 2018;29(10):1025-1037.
Aghazadeh A, Persson GR, Stavropoulos A, Renvert S. Reconstructive treatment of peri-implant defects-results after three and five years. Clin Oral Implants Res. 2022;33(11):1114-1124.
Regueiro IG, Martínez Rodriguez N, Barona Dorado C, et al. Surgical approach combining implantoplasty and reconstructive therapy with locally delivered antibiotic in the treatment of periimplantitis: a prospective clinical case series. Clin Implant Dent Relat Res. 2021;23(6):864-873.
Toma S, Lasserre JF, Taïeb J, Brecx MC. Evaluation of an air-abrasive device with amino acid glycine-powder during surgical treatment of peri-implantitis. Quintessence Int. 2014;45(3):209-219.
Esposito M, Grusovin MG, de Angelis N, Camurati A, Campailla M, Felice . The adjunctive use of light-activated disinfection (LAD) with FotoSan is ineffective in the treatment of peri-implantitis:
1-year results from a multicentre pragmatic randomised controlled trial. Eur J Oral Implantol. 2013;6(2):109-119.
207. de Waal YC, Raghoebar GM, Meijer HJ, Winkel EG, van Winkelhoff A. Implant decontamination with chlorhexidine during surgical peri-implantitis treatment: a randomized, double-blind, controlled trial. Clin Oral Implants Res. 2015;26(9):1015-1023.
208. Englezos E, Cosyn J, Koole S, Jacquet W, de Bruyn H. Resective treatment of peri-implantitis: clinical and radiographic outcomes after 2 years. Int Periodontics Restorative Dent. 2018;38(5):729-735.
209. Romeo E, Lops D, Chiapasco M, Ghisolfi M, Vogel G. Therapy of peri-implantitis with resective surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part II: radiographic outcome. Clin Oral Implants Res. 2007;18(2):179-187.
210. Lasserre JF, Brecx MC, Toma S. Implantoplasty versus glycine air abrasion for the surgical treatment of peri-implantitis: a randomized clinical trial. Int J Oral Maxillofac Implants. 2020;35(35):197-206.
How to cite this article: Berglundh T, Mombelli A, Schwarz F, Derks J. Etiology, pathogenesis and treatment of periimplantitis: A European perspective. Periodontol 2000. 2024;00:1-36. doi:10.1111/prd. 12549