DOI: https://doi.org/10.1055/s-0043-1777051
PMID: https://pubmed.ncbi.nlm.nih.gov/38555649
تاريخ النشر: 2024-03-31
أسباب تسوس الأسنان وتدابير الوقاية
الكلمات الرئيسية
- تسوس الأسنان
- أسنان
- لوحة
- معجون الأسنان
- فلوريد
- هيدروكسيباتيت
- الوقاية
- رعاية الفم
الملخص
تسوس الأسنان هو مرض شائع بين الأطفال والبالغين. يحدث تسوس الأسنان نتيجة تحويل الكربوهيدرات القابلة للتخمر بواسطة بكتيريا اللويحات إلى أحماض على سطح الأسنان. لذلك، من المهم التركيز على تقليل السكر والسيطرة على اللويحات. لإزالة اللويحات بشكل فعال، تحتوي معاجين الأسنان الحديثة على مكونات نشطة متنوعة مثل العوامل المضادة للميكروبات (مثل الكلورهيكسيدين، وأملاح القصدير، وأملاح الزنك)، والمواد الكاشطة (مثل كربونات الكالسيوم، والفوسفات الكالسيوم، والسيليكا المائية)، والمواد السطحية (مثل لوريل الصوديوم سلفات وتورات ميثيل كوكويل الصوديوم)، والمركبات الطبيعية (مثل البوليفينولات والزيلتول). العوامل التي تحتوي على خصائص عازلة للرقم الهيدروجيني وإطلاق الكالسيوم (مثل كربونات الكالسيوم والفوسفات الكالسيوم) والمكونات الحيوية المقلدة (مثل هيدروكسيباتيت) تعكس آثار الأحماض. بالإضافة إلى ذلك، تساعد فرش الأسنان الحديثة (أي فرش الأسنان الكهربائية) وكذلك خيط الأسنان وفرش الأسنان بين الأسنان بشكل كبير في إزالة اللويحات من الأسطح السنية بما في ذلك الأسطح بين الأسنان. في الختام، يجب أن تركز المفاهيم الحديثة في الوقاية من تسوس الأسنان ليس فقط على إعادة تمعدن الأسنان وحدها ولكن أيضًا على السيطرة على جميع العوامل الرئيسية المعنية في تطور التسوس.
مقدمة
لها درجة حموضة حرجة تبلغ 5.5. ومع ذلك، فإن درجة الحموضة ليست العامل الحاسم الوحيد في ذوبان بلورات الأسنان، لأن هذه العملية تعتمد أيضًا على تدرجات تركيز أيونات الكالسيوم والفوسفات في اللعاب واللويحات.
مقالة نُشرت على الإنترنت في 31 مارس 2024
© 2024. المؤلف(ون).
هذه مقالة مفتوحة الوصول نشرتها شركة ثييم بموجب شروط رخصة المشاع الإبداعي للاستخدام، والتوزيع، والاستنساخ غير المقيد طالما تم الاقتباس من العمل الأصلي بشكل صحيح.https://creativecommons.org/licenses/by/4.0/شركة ثيم الطبية والناشرين العلميين الخاصة المحدودة، A-12، الطابق الثاني، القطاع 2، نويدا-201301 UP، الهند
يحدث نزع المعادن من الأسنان مع الأحماض غير المشتقة من بكتيريا اللويحات ولكن من الأطعمة والمشروبات الحمضية، وما إلى ذلك.
| فئة العمر (س) |
|
|
||||
| 12 | 0.5 أسنان | 18.7 | ||||
|
|
11.2 سن | 97.5 | ||||
|
|
17.7 سن | 99.9 | ||||
|
|
21.6 سن | 99.7 |
|
|
|
|||||||||
|
|
85.7 | 82.0 | |||||||||
|
|
94.2 | 92.5 | |||||||||
|
|
95.6 | 96.4 |
في السكان الألمان، حيث تم وضع معايير عالية لصحة الفم، تكون النسبة أقل مقارنة بالدول الأخرى؛ ومع ذلك، فقد عانى تقريبًا جميع البالغين من تسوس الأسنان.
- الأطفال والمراهقون: قد تحتوي الحمية على كميات أعلى من السكر، ووقت تنظيف الأسنان محدود، وإزالة اللويحات غير فعالة. ليس فقط كمية السكر ولكن أيضًا التكرار مهم. قد لا تكون تقنية تنظيف الأسنان كافية لإزالة اللويحات بشكل فعال.
- المرضى الذين يخضعون للعلاج التقويمي: تجعل الأجهزة التقويمية، وخاصة الأقواس والدعائم، من الصعب على المرضى إزالة اللويحات بشكل مناسب. تزيد الدعائم من تراكم اللويحات السنية، مما يزيد من خطر التسوس.
- المرضى الذين يعانون من أسنان ناقصة التمعدن: هناك عدة حالات معروفة قد تسبب نقص التمعدن التطوري للأسنان. نقص التمعدن في الأضراس، الذي كان يُطلق عليه حتى وقت قريب نقص التمعدن في الأضراس والقواطع، هو واحد من أكثر العيوب التطورية انتشارًا في مينا الأسنان. ومع ذلك، فإن جميع الأشخاص المتأثرين لديهم شيء مشترك، وهو حساسية الأسنان. وهذا يؤدي إلى تقليل تنظيف الأسنان وتقليل إزالة البلاك. بالإضافة إلى ذلك، فإن هياكل الأسنان الناقصة التمعدن عرضة لتطوير تسوس الأسنان، حيث أن محتوى المعادن غير كاف وسلامة المينا ليست intact. بعد ذلك، يمكن للأحماض أن تذوب المينا الأقل تمعدنًا بشكل أسرع من المينا الصحية.
- المرضى الذين يعانون من انخفاض تدفق اللعاب (نقص اللعاب): يحمي اللعاب الأسنان ويعيد تمعدنها. بينما يساعد اللعاب في تقليل قدرة السكريات على التسبب بالتسوس، فإن انخفاض تدفق اللعاب يؤدي إلى تقليل التأثيرات المضادة للبكتيريا بسبب ضعف تخفيف الأحماض، وانخفاض القدرة على التوازن، وانخفاض القدرة على إعادة التمعدن. يزداد تراكم اللويحات السنية. وبشكل عام، يؤدي ذلك إلى زيادة خطر التسوس لدى الأشخاص المتأثرين.
- كبار السن مع العاج المكشوف: العاج المكشوف أكثر عرضة لتطور تسوس الأسنان حيث أن محتوى المعادن و
كثافة العاج أقل مقارنة بالمينا. أيضًا، فإن الرقم الهيدروجيني الحرج لذوبان العاج هو 6.2 (على عكس المينا، الذي يكون pH 5.5)، لذا فإن العاج يتعرض لإزالة المعادن بسهولة عند التعرض. بالإضافة إلى ذلك، يعاني كبار السن في كثير من الحالات من نقص في إفراز اللعاب وقد لا يكونون قادرين على تنظيف أسنانهم بشكل صحيح، بسبب القيود الجسدية. يُعرف هذا النوع من تسوس الأسنان أيضًا بتسوس الجذور.
طرق
تم استخدام المنشورات والكتب الدراسية لإعداد المخطوطة. تم استخدام قاعدة بيانات PubMed كمصدر رئيسي للمقالات العلمية. قام جميع المؤلفين بمراجعة الأدبيات التي تم اختيارها لهذه المنشورة وتم تضمين المقالات الأصلية المناسبة.
أسباب تسوس الأسنان
الاعتبارات العامة

اللويحات السنية
- المكورات العقدية المولدة للحمض والستربتوكوكوس الأخرى ذات الرقم الهيدروجيني المنخفض.
- روثيا spp.
- أنواع الأكتينوميسيس
- اللاكتوباسيلس spp.
- بفيدوباكتيريوم spp.
- كانديدا ألبيكانس.
- سيلينوموناس سبوتيجينا.
تطور التسوس على المستوى المجهري
هيكل مسام الآفة
- منطقة السطح.
- جسم الآفة.
- منطقة ثنائية الانكسار الإيجابية (المظلمة).
- المنطقة الشفافة.
فوسفات الكالسيوم ثنائي الهيدرات
كشف التسوس
- الرمز 1: أول تغيير بصري في المينا.
- الرمز 2: تغيير بصري مميز في المينا.
- الرمز 3: تآكل موضعي في المينا بسبب التسوس دون وجود عاج مرئي أو ظل تحت السطح.
- الرمز 4: ظل داكن أساسي من العاج مع أو بدون تدهور موضعي في المينا.
- الرمز 5: تجويف مميز مع عاج مرئي.
- الرمز 6: تجويف واسع مميز مع وجود العاج مرئي.
إجراءات وقائية
الاعتبارات العامة
| هدف | تدخل | ||||
| لوحة |
|
||||
| حمية/سكريات |
|
||||
| أنسجة الأسنان |
|
التحكم الغذائي في تسوس الأسنان
دور الفلورايد
السطح منخفض جداً (فقط بضع ميكروغرامات لكل مليمتر مربع، فقط على السطح الخارجي للسن) ولا يمكن توقع أي “تصلب” للسن.
الإزالة الميكانيكية للبلاك
| مواد كاشطة | الصيغة الكيميائية | الصلابة النسبية |
| بيكربونات الصوديوم |
|
ناعم |
| ثنائي فوسفات الكالسيوم المائي |
|
ناعم |
| كربونات الكالسيوم |
|
ناعم |
| فوسفات الكالسيوم الثنائي |
|
صلابة متوسطة |
| هيدروكسي أباتيت |
|
صلابة متوسطة |
| سيليكا مائية |
|
صلابة متوسطة |
| برلايت | سيليكات معدني | صعب |
| الألومينا |
|
صعب |
| درجة التخفيف (معجون الأسنان: ماء) | ||||
| وقت الفرشاة (ثانية) | 1:1 | 1:2 | 1:4 | 1:8 |
| 10 |
|
|
|
|
| 30 |
|
|
|
|
| 60 |
|
|
|
|
| ١٢٠ |
|
|
|
|
| 180 |
|
|
|
|
| ٣٠٠ |
|
|
|
|
ملاحظة: المبلغ الكامل: 1:1 (الحد الأقصى “الطول الكامل للفرشاة”); مخفض إلى النصف: 1:2 (الحد الأدنى “الطول الكامل للفرشاة”); ربع المبلغ: 1:4 (“حجم حبة البازلاء”); ثمن المبلغ: 1:8 (“حجم حبة الأرز”).
تتميز شعيرات فرشاة الأسنان (مقياس المليمتر) بوجود مواد كاشطة متطورة مثل السيليكا المائية التي تمتلك هيكلًا مجهرًا محددًا (مقياس النانومتر إلى الميكرومتر) يمكن أن يساعد في تنظيف حتى الحفر والشقوق.
التحكم المضاد للميكروبات في اللويحة
| عوامل مضادة للميكروبات | المراجع |
| كلوريد سيتيل بيريدينيوم | مستنقع
|
| كلورهيكسيدين | مستنقع
|
| الزيوت الأساسية (مثل المنثول والثيمول) | مستنقع
|
| فلوريد | ماركيز
|
| سلفات لوريل الصوديوم | مستنقع
|
| أملاح القصدير | مستنقع
|
| أملاح الزنك | مستنقع
|
لها تأثير كبير على تقليل ومنع تكوين اللويحات دون قتل البكتيريا.
تحييد الرقم الهيدروجيني للبلاك
الهيدروكسيباتيت البيوميمتي والوقاية من تسوس الأسنان
- إعادة التمعدن، حتى إلى طبقات أعمق من المينا والعاج.
- تقليل تكوين اللويحات.
- طبقة واقية.
- خزان الكالسيوم والفوسفات.
- تأثير العازل لدرجة الحموضة.
- تنظيف الممتلكات.
توصيات للمرضى
- هناك ثلاثة أسس للوقاية من تسوس الأسنان:
- إعادة التمعدن/تثبيط إزالة التمعدن: زيادة مقاومة الأسنان.
- إزالة اللويحات
- استخدام فرشاة أسنان كهربائية وأجهزة لتنظيف ما بين الأسنان (مثل: خيط الأسنان، فرش الأسنان بين الأسنان).
- استخدام كمية كافية من معجون الأسنان (أي 1 جرام).
- يجب أن تحتوي معجون الأسنان على مواد مضادة للميكروبات (لطيفة). بديل للمبيدات الجرثومية هو استخدام
عوامل محاكاة الطبيعة مثل هيدروكسيباتيت لتقليل تكوين اللويحات. - بالإضافة إلى ذلك، يمكن استخدام غسولات الفم كملحق لإزالة اللويحات الميكانيكية. هناك أدلة تظهر فعالية غسولات الفم التي تحتوي على الزيوت الأساسية أو الهيدروكسيباتيت البيوميمتي في إزالة اللويحات.
- حمية:
- تقليل تناول الأحماض والكربوهيدرات/السكر يوميًا، وخاصة تقليل تكرار تناول السكر.
- تحفيز تدفق اللعاب (على سبيل المثال، باستخدام العلكة الخالية من السكر والتي تحتوي على زيلتول).
- إعادة التمعدن/تثبيط إزالة التمعدن:
- استخدام منتجات العناية الفموية التي تحتوي على عوامل إعادة التمعدن (مثل الفلورايد أو فوسفات الكالسيوم).
- الهيدروكسي أباتيت هو عامل مضاد للتسوس آمن وفعال، يمكن استخدامه من قبل جميع الفئات العمرية بما في ذلك الرضع والأطفال الصغار.
- تعتبر الفحوصات الدورية للأسنان وزيارات طبيب الأسنان مهمة، خاصة للمجموعات ذات المخاطر العالية للتسوس. يجب أن يتم تحديد تكرار الفحوصات بناءً على خطر التسوس الفردي.
الخاتمة
تطور تسوس الأسنان نفسه: تقليل السكر (الكمية الإجمالية والتكرار) وخاصة إزالة البلاك بشكل فعال من أسطح الأسنان خلال العناية الفموية اليومية.
مساهمة المؤلفين
تمويل
تعارض المصالح
شكر وتقدير
References
2 Dorozhkin SV, Epple M. Biological and medical significance of calcium phosphates. Angew Chem Int Ed 2002;41(17): 3130-3146
3 Fabritius H-O, Enax J, Meyer F. Eine Reise ins Innere unserer Zähne/A Journey into Our Teeth. Bielefeld: Titus Verlag; 2021
4 Dorozhkin SV. Dissolution mechanism of calcium apatites in acids: a review of literature. World J Methodol 2012;2(01):1-17
5 Fejerskov O, Nyvad B, Kidd E. Dental Caries: The Disease and Its Clinical Management. 3rd ed. Oxford: Wiley Blackwell; 2015
6 Cieplik F, Rupp CM, Hirsch S, et al.
7 Dawes C . What is the critical pH and why does a tooth dissolve in acid? J Can Dent Assoc 2003;69(11):722-724
8 Schlueter N, Amaechi BT, Bartlett D, et al. Terminology of erosive tooth wear: Consensus report of a workshop organized by the ORCA and the cariology research group of the IADR. Caries Res 2020;54(01):2-6
9 Lussi A, Ganss C. Erosive Tooth Wear: From Diagnosis to Therapy. Basel: S. Karger AG; 2014
10 Cochrane NJ, Cai F, Huq NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res 2010;89(11):1187-1197
11 O’Reilly MM, Featherstone JD. Demineralization and remineralization around orthodontic appliances: an in vivo study. Am J Orthod Dentofacial Orthop 1987;92(01):33-40
12 Batchelor PA, Sheiham A. Grouping of tooth surfaces by susceptibility to caries: a study in 5-16 year-old children. BMC Oral Health 2004;4(01):2
13 Wyne AH. Early childhood caries: nomenclature and case definition. Community Dent Oral Epidemiol 1999;27(05):313-315
14 Meyer F, Enax J. Early childhood caries: epidemiology, aetiology, and prevention. Int J Dent 2018;2018:1415873
16 Meyer F, Karch A, Schlinkmann KM, et al. Sociodemographic determinants of spatial disparities in early childhood caries: an ecological analysis in Braunschweig, Germany. Community Dent Oral Epidemiol 2017;45(05):442-448
17 Vernazza CR, Birch S, Pitts NB. Reorienting oral health services to prevention: economic perspectives. J Dent Res 2021;100(06): 576-582
18 Jordan AR, Micheelis W. Fünfte Deutsche Mundgesundheitsstudie (DMS V). Köln, Germany: Institut der Deutschen Zahnärzte; 2016
19 National Institute of Dental and Craniofacial Research. Dental caries (tooth decay) in adults (ages 20 to 64 years). Accessed October 15, 2023 at: https://www.nidcr.nih.gov/research/ data-statistics/dental-caries/adults
20 Verma S, Dhinsa K, Tripathi AM, Saha S, Yadav G, Arora D. Molar incisor hypomineralization: prevalence, associated risk factors, its relation with dental caries and various enamel surface defects in 8-16-year-old schoolchildren of Lucknow district. Int J Clin Pediatr Dent 2022;15(01):1-8
21 Gati D, Vieira AR. Elderly at greater risk for root caries: a look at the multifactorial risks with emphasis on genetics susceptibility. Int J Dent 2011;2011:647168
22 Zero DT. Dental caries process. Dent Clin North Am 1999;43(04): 635-664
23 Machiulskiene V, Campus G, Carvalho JC, et al. Terminology of dental caries and dental caries management: consensus report of a workshop organized by ORCA and cariology research group of IADR. Caries Res 2020;54(01):7-14
24 Limeback H. Comprehensive Preventive Dentistry. Hoboken, NY: John Wiley & Sons; 2012
25 ALHumaid J, Bamashmous M. Meta-analysis on the effectiveness of xylitol in caries prevention. J Int Soc Prev Community Dent 2022;12(02):133-138
26 Bernabé E, Vehkalahti MM, Sheiham A, Lundqvist A, Suominen AL. The shape of the dose-response relationship between sugars and caries in adults. J Dent Res 2016;95(02):167-172
27 Meyer F, Enax J, Epple M, Amaechi BT, Simader B. Cariogenic biofilms: development, properties, and biomimetic preventive agents. Dent J 2021;9(08):88
28 Marsh PD. Dental plaque as a biofilm and a microbial community: implications for health and disease. BMC Oral Health 2006;6 (Suppl 1):S14
29 Verma D, Garg PK, Dubey AK. Insights into the human oral microbiome. Arch Microbiol 2018;200(04):525-540
30 Li X, Liu Y, Yang X, Li C, Song Z. The oral microbiota: community composition, influencing factors, pathogenesis, and interventions. Front Microbiol 2022;13:895537
31 Mark Welch JL, Ramírez-Puebla ST, Borisy GG. Oral microbiome geography: micron-scale habitat and niche. Cell Host Microbe 2020;28(02):160-168
32 Anderson AC, Rothballer M, Altenburger MJ, et al. In-vivo shift of the microbiota in oral biofilm in response to frequent sucrose consumption. Sci Rep 2018;8(01):14202
33 Kawada-Matsuo M, Oogai Y, Komatsuzawa H. Sugar allocation to metabolic pathways is tightly regulated and affects the virulence of Streptococcus mutans. Genes (Basel) 2016;8(01):11
34 Torlakovic L, Klepac-Ceraj V, Ogaard B, Cotton SL, Paster BJ, Olsen I. Microbial community succession on developing lesions on human enamel. J Oral Microbiol 2012;4:4
35 Schlafer S, Raarup MK, Meyer RL, et al. pH landscapes in a novel five-species model of early dental biofilm. PLoS One 2011;6(09): e25299
36 Andreadis G, Kalfas S. Correlation of dental plaque acidogenicity and acidurance with caries activity: perspectives of the ecological plaque hypothesis. GSTF J Adv Med Res 2014;1:9
38 Cho H, Ren Z, Divaris K, et al. Selenomonas sputigena acts as a pathobiont mediating spatial structure and biofilm virulence in early childhood caries. Nat Commun 2023;14(01):2919
39 Campbell K. Oral microbiome findings challenge dentistry dogma. Nature 2021. Doi: 10.1038/d41586-021-02920-w
40 Robinson C, Shore RC, Brookes SJ, Strafford S, Wood SR, Kirkham J. The chemistry of enamel caries. Crit Rev Oral Biol Med 2000;11 (04):481-495
42 LeGeros RZ. Chemical and crystallographic events in the caries process. J Dent Res 1990;69(Spec No):567-574, discussion 634-636
43 Ismail AI, Sohn W, Tellez M, et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol 2007;35(03):170-178
44 Paszynska E, Pawinska M, Enax J, et al. Caries-preventing effect of a hydroxyapatite-toothpaste in adults: a 18-month double-blinded randomized clinical trial. Front Public Health 2023;11:1199728
45 Paszynska E, Pawinska M, Gawriolek M, et al. Impact of a toothpaste with microcrystalline hydroxyapatite on the occurrence of early childhood caries: a 1-year randomized clinical trial. Sci Rep 2021;11(01):2650
46 Söchtig F, Hickel R, Kühnisch J. Caries detection and diagnostics with near-infrared light transillumination: clinical experiences. Quintessence Int 2014;45(06):531-538
47 Arends J, ten Bosch JJ. Demineralization and remineralization evaluation techniques. J Dent Res 1992;71(Spec No):924-928
48 Mobley CC. Nutrition and dental caries. Dent Clin North Am 2003; 47(02):319-336
49 Al-Dajani M, Limeback H. Emerging science in the dietary control and prevention of dental caries. J Calif Dent Assoc 2012;40(10): 799-804
50 Loveren CV. Toothpastes. Vol 23;Basel: Karger; 2013
51 Walsh T, Worthington HV, Glenny AM, Marinho VC, Jeroncic A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev 2019;3(03):CD007868
52 Epple M, Enax J, Meyer F. Prevention of caries and dental erosion by fluorides: a critical discussion based on physico-chemical data and principles. Dent J 2022;10(01):6
53 Hausen H, Kärkkäinen S, Seppä L Application of the high-risk strategy to control dental caries. Community Dent Oral Epidemiol 2000;28(01):26-34
54 Ekambaram M, Itthagarun A, King NM. Ingestion of fluoride from dentifrices by young children and fluorosis of the teeth: a literature review. J Clin Pediatr Dent 2011;36(02):111-121
55 Meyer-Lueckel H, Grundmann E, Stang A. Effects of fluoride tablets on caries and fluorosis occurrence among 6- to 9-year olds using fluoridated salt. Community Dent Oral Epidemiol 2010;38(04):315-323
56 Neurath C, Limeback H, Osmunson B, Connett M, Kanter V, Wells CR. Dental fluorosis trends in US oral health surveys: 1986 to 2012. JDR Clin Trans Res 2019;4(04):298-308
58 Marquis RE, Clock SA, Mota-Meira M. Fluoride and organic weak acids as modulators of microbial physiology. FEMS Microbiol Rev 2003;26(05):493-510
59 Valkenburg C, Slot DE, Bakker EW, Van der Weijden FA. Does dentifrice use help to remove plaque? A systematic review. J Clin Periodontol 2016;43(12):1050-1058
61 Zimmer S, Öztürk M, Barthel CR, Bizhang M, Jordan RA. Cleaning efficacy and soft tissue trauma after use of manual toothbrushes with different bristle stiffness. J Periodontol 2011;82(02): 267-271
62 Caporossi LS, Dutra DA, Martins MR, Prochnow EP, Moreira CH, Kantorski KZ. Combined effect of end-rounded versus tapered bristles and a dentifrice on plaque removal and gingival abrasion. Braz Oral Res 2016;30:30
63 Enax J, Epple M. Die charakterisierung von putzkörpern in zahnpasten. Dtsch Zahnarztl Z 2018;73:100-108
64 Enax J, Meyer F, Schulze Zur Wiesche E, Fuhrmann IC, Fabritius HO. Toothpaste abrasion and abrasive particle content: correlating high-resolution profilometric analysis with relative dentin abrasivity (RDA). Dent J 2023;11(03):79
65 Sarembe S, Ufer C, Kiesow A, et al. Influence of the amount of toothpaste on cleaning efficacy: An in vitro study. Eur J Dent 2023; 17(02):497-503
66 Toumba KJ, Twetman S, Splieth C, Parnell C, van Loveren C, Lygidakis NA. Guidelines on the use of fluoride for caries prevention in children: an updated EAPD policy document. Eur Arch Paediatr Dent 2019;20(06):507-516
67 Limeback H, Enax J, Meyer F. Biomimetic hydroxyapatite and caries prevention: a systematic review and meta-analysis. Can J Dent Hyg 2021;55(03):148-159
68 Limeback H, Enax J, Meyer F. Improving oral health with fluoridefree calcium-phosphate-based biomimetic toothpastes: an update of the clinical evidence. Biomimetics (Basel) 2023;8(04):331
69 Wülknitz P. Cleaning power and abrasivity of European toothpastes. Adv Dent Res 1997;11(04):576-579
70 Marsh PD. Contemporary perspective on plaque control. Br Dent J 2012;212(12):601-606
71 Shen Y, Li P, Chen X, et al. Activity of sodium lauryl sulfate, rhamnolipids, and N -acetylcysteine against biofilms of five common pathogens. Microb Drug Resist 2020;26(03):290-299
72 Kensche A, Holder C, Basche S, Tahan N, Hannig C, Hannig M. Efficacy of a mouthrinse based on hydroxyapatite to reduce initial bacterial colonisation in situ. Arch Oral Biol 2017;80:18-26
73 Schlagenhauf U, Kunzelmann K-H, Hannig C, et al. Impact of a nonfluoridated microcrystalline hydroxyapatite dentifrice on enamel caries progression in highly caries-susceptible orthodontic patients: a randomized, controlled 6 -month trial. J Investig Clin Dent 2019;10(02):e12399
74 Kani K, Kani M, Isozaki A, Shintani H, Ohashi T, Tokumoto T. Effect of apatite-containing dentifrices on dental caries in school children. J Dent Health. 1989;19:104-109
75 Flemming J, Meyer-Probst CT, Speer K, Kölling-Speer I, Hannig C, Hannig M. Preventive applications of polyphenols in dentistry: a review. Int J Mol Sci 2021;22(09):22
76 Cieplik F, Kara E, Muehler D, et al. Antimicrobial efficacy of alternative compounds for use in oral care toward biofilms from caries-associated bacteria in vitro. MicrobiologyOpen 2019;8(04):e00695
77 Epple M, Meyer F, Enax J. A critical review of modern concepts for teeth whitening. Dent J 2019;7(03):79
78 Cieplik F, Jakubovics NS, Buchalla W, Maisch T, Hellwig E, AlAhmad A. Resistance toward chlorhexidine in oral bacteria: is there cause for concern? Front Microbiol 2019;10:587
79 Meyer F, Enax J. Hydroxyapatite in oral biofilm management. Eur J Dent 2019;13(02):287-290
80 Enax J, Meyer F, Schulze Zur Wiesche E, Epple M. On the application of calcium phosphate micro- and nanoparticles as food additive. Nanomaterials (Basel) 2022;12(22):4075
83 Tschoppe P, Zandim DL, Martus P, Kielbassa AM. Enamel and dentine remineralization by nano-hydroxyapatite toothpastes. J Dent 2011;39(06):430-437
85 Amaechi BT, AbdulAzees PA, Alshareif DO, et al. Comparative efficacy of a hydroxyapatite and a fluoride toothpaste for prevention and remineralization of dental caries in children. BDJ Open 2019;5:18
DOI: https://doi.org/10.1055/s-0043-1777051
PMID: https://pubmed.ncbi.nlm.nih.gov/38555649
Publication Date: 2024-03-31
Caries Etiology and Preventive Measures
Keywords
- caries
- teeth
- plaque
- toothpaste
- fluoride
- hydroxyapatite
- prevention
- oral care
Abstract
Caries is a widespread disease in both children and adults. Caries is caused by the conversion of fermentable carbohydrates by plaque bacteria into acids on the tooth surface. Thus, it is important to focus on sugar reduction and plaque control. For efficient plaque removal/control, state-of-the-art toothpastes contain various active ingredients such as antimicrobial agents (e.g., chlorhexidine, stannous salts, and zinc salts), abrasives (e.g., calcium carbonate, calcium phosphates, and hydrated silica), surfactants (e.g., sodium lauryl sulfate and sodium methyl cocoyl taurate), and natural compounds (e.g., polyphenols and xylitol). Agents with pH -buffering and calciumreleasing properties (e.g., calcium carbonate and calcium phosphates) and biomimetic actives (e.g., hydroxyapatite) reverse the effects of the acids. Additionally, modern toothbrushes (i.e., electric toothbrushes) as well as dental floss and interdental brushes significantly help remove plaque from dental surfaces including interproximal surfaces. In conclusion, modern concepts in caries prevention should focus not only on tooth remineralization alone but also on the control of all the key factors involved in caries development.
Introduction
has a critical pH of 5.5. However, the pH is not the only crucial factor for tooth crystal dissolution because this process depends also on the concentration gradients of calcium and phosphate ions in saliva and plaque.
article published online March 31, 2024
© 2024. The Author(s).
This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/) Thieme Medical and Scientific Publishers Pvt. Ltd., A-12, 2nd Floor, Sector 2, Noida-201301 UP, India
tooth demineralization occurs with acids not derived from plaque bacteria but from acidic food, beverages, etc.
| Age group (y) |
|
|
||||
| 12 | 0.5 teeth | 18.7 | ||||
|
|
11.2 teeth | 97.5 | ||||
|
|
17.7 teeth | 99.9 | ||||
|
|
21.6 teeth | 99.7 |
|
|
|
|||||||||
|
|
85.7 | 82.0 | |||||||||
|
|
94.2 | 92.5 | |||||||||
|
|
95.6 | 96.4 |
in the German population, where high oral health standards are established, is lower compared to other countries; however, almost all adults had experienced caries.
- Children and adolescents: Diet might contain higher sugar amounts, tooth brushing time is limited, and plaque removal is inefficient. Not only the amount of sugar but also the frequency is important. Tooth brushing technique might not be sufficient for efficient plaque removal.
- Patients undergoing orthodontic therapy: Orthodontic appliances, especially braces and brackets, make it difficult for patients to remove plaque appropriately. Brackets increase dental plaque buildup, which increases caries risk.
- Patients suffering from hypomineralized teeth: There are several known conditions that may cause developmental hypomineralization of teeth. Molar hypomineralization, until recently often called molar incisor hypomineralization, is one of the most prevalent developmental defects of tooth enamel (DDE). However, all affected persons have one thing in common, which is tooth sensitivity. This leads to diminished brushing of the teeth and reduced plaque removal. Additionally, hypomineralized tooth structures are prone to develop caries, as the mineral content is deficient and enamel integrity is not intact. Following this, acids can dissolve less mineralized enamel faster than healthy enamel.
- Patients with reduced salivary flow (hyposalivation): Saliva protects and remineralizes teeth. While saliva helps reduce the cariogenicity of sugars, a reduced salivary flow results in diminished antibacterial effects because of the inefficient dilution of acids, diminished buffering capacity, and lowered remineralizing potential. Dental plaque buildup is increased. Taken together, this leads to an increased caries risk of the affected persons.
- Elderly with exposed dentin: Exposed dentin is more prone to developing dental caries as the mineral content and
density of dentin is reduced compared to enamel. Also, the critical pH for dentin dissolution is 6.2 (unlike that of enamel, which is pH 5.5 ), so dentin demineralizes easily when exposed. Additionally, elderly people suffer in many cases from hyposalivation and might not be able to brush their teeth properly, due to physical limitations. This type of dental caries is also known as root caries.
Methods
knowledge. Publications and textbooks were used for manuscript preparation. PubMed database was used as the primary source for scientific publications. All the authors reviewed the literature that was chosen for this publication and suitable original articles were included.
Caries Etiology
General Considerations
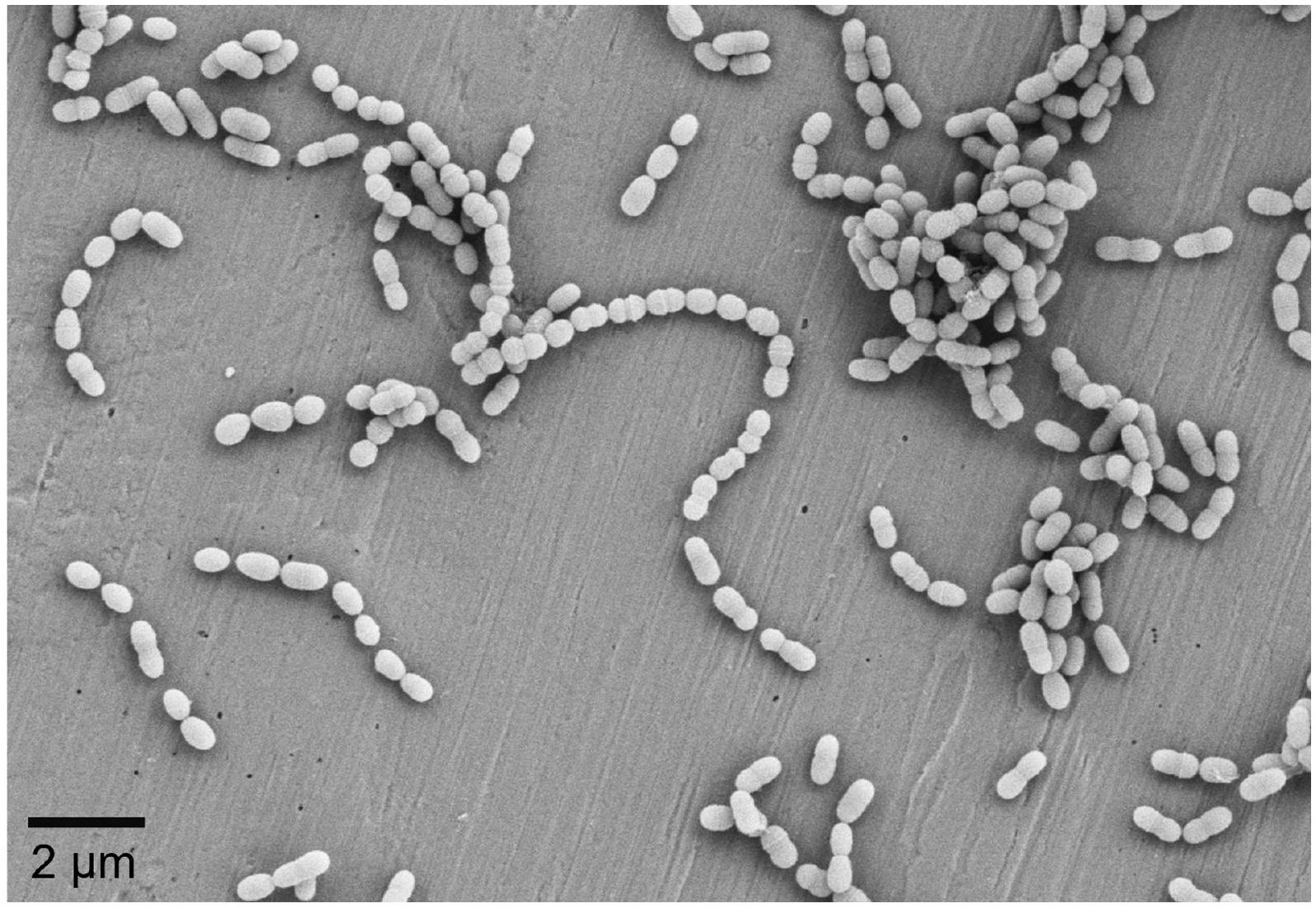
Dental Plaque
- Streptococcus mutans and other low-pH streptococci.
- Rothia spp.
- Actinomyces spp.
- Lactobacillus spp.
- Bifidobacterium spp.
- Candida albicans.
- Selenomonas sputigena.
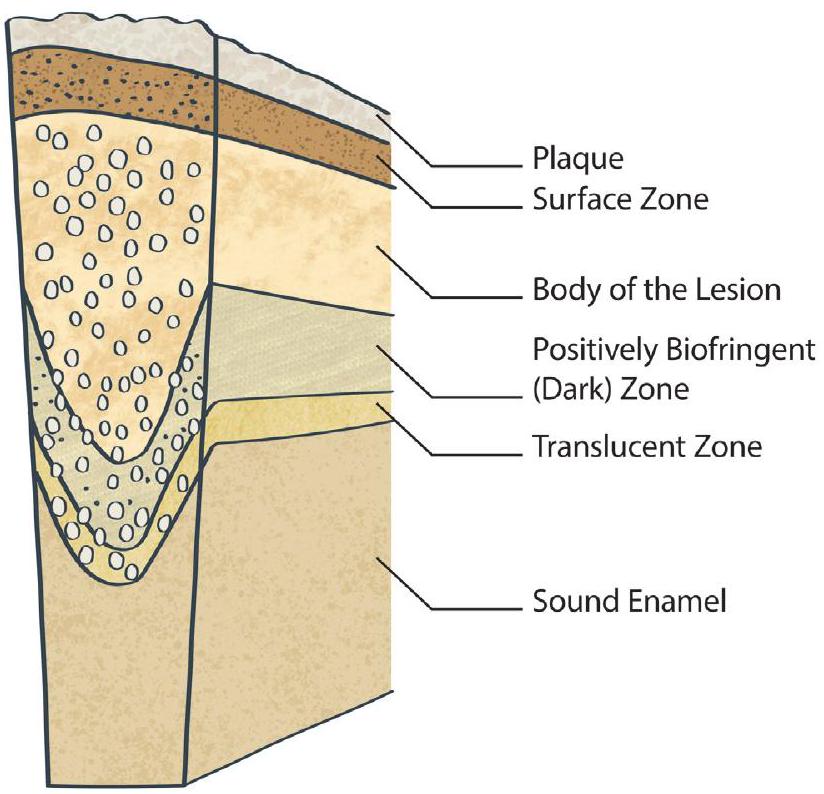
Caries Development on the Microscopic Level
Lesion Pore Structure
- Surface zone.
- Body of the lesion.
- Positively birefringent (dark) zone.
- Translucent zone.
dicalcium phosphate dihydrate,
Caries Detection
- Code 1: First visual change in enamel.
- Code 2: Distinct visual change in enamel.
- Code 3: Localized enamel breakdown because of caries with no visible dentin or underlying shadow.
- Code 4: Underlying dark shadow from dentin with or without localized enamel breakdown.
- Code 5: Distinct cavity with visible dentin.
- Code 6: Extensive distinct cavity with visible dentin.
Preventive Measures
General Considerations
| Target | Intervention | ||||
| Plaque |
|
||||
| Diet/sugars |
|
||||
| Dental tissues |
|
Dietary Control of Caries
The Role of Fluoride
surface is very low (just a few micrograms per square millimeter, only at the outermost tooth surface) and no “hardening” of the tooth can be expected.
Mechanical Removal of the Plaque
| Abrasives | Chemical formula | Relative hardness |
| Sodium bicarbonate |
|
Soft |
| Dicalcium phosphate dihydrate |
|
Soft |
| Calcium carbonate |
|
Soft |
| Calcium pyrophosphate |
|
Medium hardness |
| Hydroxyapatite |
|
Medium hardness |
| Hydrated silica |
|
Medium hardness |
| Perlite | A mineral silicate | Hard |
| Alumina |
|
Hard |
| Dilution degree (toothpaste:water) | ||||
| Brushing time (s) | 1:1 | 1:2 | 1:4 | 1:8 |
| 10 |
|
|
|
|
| 30 |
|
|
|
|
| 60 |
|
|
|
|
| 120 |
|
|
|
|
| 180 |
|
|
|
|
| 300 |
|
|
|
|
Note: Full amount: 1:1 (maximum “full length of brush”); reduced by half: 1:2 (minimum “full length of brush”); one quarter of the amount: 1:4 (“peasize”); one-eighth of the amount: 1:8 (“grain of rice size”).
to the toothbrush filaments (millimeter scale), state-of-theart toothpaste abrasives such as hydrated silica have a specific microscopic structure (nanometer to micrometer scale) that can help clean even pits and fissures.
Antimicrobial Control of the Plaque
| Antimicrobial agents | References |
| Cetylpyridinium chloride | Marsh
|
| Chlorhexidine | Marsh
|
| Essential oils (e.g., menthol and thymol) | Marsh
|
| Fluoride | Marquis
|
| Sodium lauryl sulfate | Marsh
|
| Stannous salts | Marsh
|
| Zinc salts | Marsh
|
have a significant effect on the reduction and inhibition of plaque formation without killing the bacteria.
pH Buffering of Plaque
Biomimetic Hydroxyapatite and Caries Prevention
- Remineralization, even to deeper layers of enamel and dentin.
- Reduction of plaque formation.
- Protective layer.
- Calcium and phosphate reservoir.
- pH-buffering effect.
- Cleaning properties.
Recommendations for Patients
- There are three cornerstones for preventing caries:
- Remineralization/inhibition of demineralization: increasing tooth resistance.
- Plaque removal
- Using an electric toothbrush and devices for interdental cleaning (e.g., dental floss, interdental brushes).
- Using a sufficient amount of toothpaste (i.e., 1 g ).
- The toothpaste should contain (gentle) antimicrobial agents. An alternative to bactericidals is the use of
biomimetic agents such as hydroxyapatite for the reduction of plaque formation. - Additionally, mouthwashes can be used as adjunct to mechanical plaque removal. There is evidence to show the effectiveness of mouthwashes containing essential oils or biomimetic hydroxyapatite in plaque removal.
- Diet:
- Reduction of daily acid and carbohydrate/sugar intake and especially reduction of the frequency of sugar intake.
- Stimulating salivary flow (e.g., by using sugar-free, xylitol-containing chewing gums).
- Remineralization/inhibition of demineralization:
- Using oral care products with remineralizing agents (e.g., fluorides or calcium phosphates).
- Hydroxyapatite is a safe and efficient anticaries agent, which can be used by all age groups including infants and toddlers.
- Regular dental examinations and dental checkups at the dentists are important, especially for high caries risk groups. Frequency of check-ups needs to be made on individual caries risk.
Conclusion
the caries development themselves: sugar reduction (total amount and frequency) and especially efficient removal of plaque from the tooth surfaces during daily oral care.
Authors’ Contribution
Funding
Conflict of Interest
Acknowledgment
References
2 Dorozhkin SV, Epple M. Biological and medical significance of calcium phosphates. Angew Chem Int Ed 2002;41(17): 3130-3146
3 Fabritius H-O, Enax J, Meyer F. Eine Reise ins Innere unserer Zähne/A Journey into Our Teeth. Bielefeld: Titus Verlag; 2021
4 Dorozhkin SV. Dissolution mechanism of calcium apatites in acids: a review of literature. World J Methodol 2012;2(01):1-17
5 Fejerskov O, Nyvad B, Kidd E. Dental Caries: The Disease and Its Clinical Management. 3rd ed. Oxford: Wiley Blackwell; 2015
6 Cieplik F, Rupp CM, Hirsch S, et al.
7 Dawes C . What is the critical pH and why does a tooth dissolve in acid? J Can Dent Assoc 2003;69(11):722-724
8 Schlueter N, Amaechi BT, Bartlett D, et al. Terminology of erosive tooth wear: Consensus report of a workshop organized by the ORCA and the cariology research group of the IADR. Caries Res 2020;54(01):2-6
9 Lussi A, Ganss C. Erosive Tooth Wear: From Diagnosis to Therapy. Basel: S. Karger AG; 2014
10 Cochrane NJ, Cai F, Huq NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res 2010;89(11):1187-1197
11 O’Reilly MM, Featherstone JD. Demineralization and remineralization around orthodontic appliances: an in vivo study. Am J Orthod Dentofacial Orthop 1987;92(01):33-40
12 Batchelor PA, Sheiham A. Grouping of tooth surfaces by susceptibility to caries: a study in 5-16 year-old children. BMC Oral Health 2004;4(01):2
13 Wyne AH. Early childhood caries: nomenclature and case definition. Community Dent Oral Epidemiol 1999;27(05):313-315
14 Meyer F, Enax J. Early childhood caries: epidemiology, aetiology, and prevention. Int J Dent 2018;2018:1415873
16 Meyer F, Karch A, Schlinkmann KM, et al. Sociodemographic determinants of spatial disparities in early childhood caries: an ecological analysis in Braunschweig, Germany. Community Dent Oral Epidemiol 2017;45(05):442-448
17 Vernazza CR, Birch S, Pitts NB. Reorienting oral health services to prevention: economic perspectives. J Dent Res 2021;100(06): 576-582
18 Jordan AR, Micheelis W. Fünfte Deutsche Mundgesundheitsstudie (DMS V). Köln, Germany: Institut der Deutschen Zahnärzte; 2016
19 National Institute of Dental and Craniofacial Research. Dental caries (tooth decay) in adults (ages 20 to 64 years). Accessed October 15, 2023 at: https://www.nidcr.nih.gov/research/ data-statistics/dental-caries/adults
20 Verma S, Dhinsa K, Tripathi AM, Saha S, Yadav G, Arora D. Molar incisor hypomineralization: prevalence, associated risk factors, its relation with dental caries and various enamel surface defects in 8-16-year-old schoolchildren of Lucknow district. Int J Clin Pediatr Dent 2022;15(01):1-8
21 Gati D, Vieira AR. Elderly at greater risk for root caries: a look at the multifactorial risks with emphasis on genetics susceptibility. Int J Dent 2011;2011:647168
22 Zero DT. Dental caries process. Dent Clin North Am 1999;43(04): 635-664
23 Machiulskiene V, Campus G, Carvalho JC, et al. Terminology of dental caries and dental caries management: consensus report of a workshop organized by ORCA and cariology research group of IADR. Caries Res 2020;54(01):7-14
24 Limeback H. Comprehensive Preventive Dentistry. Hoboken, NY: John Wiley & Sons; 2012
25 ALHumaid J, Bamashmous M. Meta-analysis on the effectiveness of xylitol in caries prevention. J Int Soc Prev Community Dent 2022;12(02):133-138
26 Bernabé E, Vehkalahti MM, Sheiham A, Lundqvist A, Suominen AL. The shape of the dose-response relationship between sugars and caries in adults. J Dent Res 2016;95(02):167-172
27 Meyer F, Enax J, Epple M, Amaechi BT, Simader B. Cariogenic biofilms: development, properties, and biomimetic preventive agents. Dent J 2021;9(08):88
28 Marsh PD. Dental plaque as a biofilm and a microbial community: implications for health and disease. BMC Oral Health 2006;6 (Suppl 1):S14
29 Verma D, Garg PK, Dubey AK. Insights into the human oral microbiome. Arch Microbiol 2018;200(04):525-540
30 Li X, Liu Y, Yang X, Li C, Song Z. The oral microbiota: community composition, influencing factors, pathogenesis, and interventions. Front Microbiol 2022;13:895537
31 Mark Welch JL, Ramírez-Puebla ST, Borisy GG. Oral microbiome geography: micron-scale habitat and niche. Cell Host Microbe 2020;28(02):160-168
32 Anderson AC, Rothballer M, Altenburger MJ, et al. In-vivo shift of the microbiota in oral biofilm in response to frequent sucrose consumption. Sci Rep 2018;8(01):14202
33 Kawada-Matsuo M, Oogai Y, Komatsuzawa H. Sugar allocation to metabolic pathways is tightly regulated and affects the virulence of Streptococcus mutans. Genes (Basel) 2016;8(01):11
34 Torlakovic L, Klepac-Ceraj V, Ogaard B, Cotton SL, Paster BJ, Olsen I. Microbial community succession on developing lesions on human enamel. J Oral Microbiol 2012;4:4
35 Schlafer S, Raarup MK, Meyer RL, et al. pH landscapes in a novel five-species model of early dental biofilm. PLoS One 2011;6(09): e25299
36 Andreadis G, Kalfas S. Correlation of dental plaque acidogenicity and acidurance with caries activity: perspectives of the ecological plaque hypothesis. GSTF J Adv Med Res 2014;1:9
38 Cho H, Ren Z, Divaris K, et al. Selenomonas sputigena acts as a pathobiont mediating spatial structure and biofilm virulence in early childhood caries. Nat Commun 2023;14(01):2919
39 Campbell K. Oral microbiome findings challenge dentistry dogma. Nature 2021. Doi: 10.1038/d41586-021-02920-w
40 Robinson C, Shore RC, Brookes SJ, Strafford S, Wood SR, Kirkham J. The chemistry of enamel caries. Crit Rev Oral Biol Med 2000;11 (04):481-495
42 LeGeros RZ. Chemical and crystallographic events in the caries process. J Dent Res 1990;69(Spec No):567-574, discussion 634-636
43 Ismail AI, Sohn W, Tellez M, et al. The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol 2007;35(03):170-178
44 Paszynska E, Pawinska M, Enax J, et al. Caries-preventing effect of a hydroxyapatite-toothpaste in adults: a 18-month double-blinded randomized clinical trial. Front Public Health 2023;11:1199728
45 Paszynska E, Pawinska M, Gawriolek M, et al. Impact of a toothpaste with microcrystalline hydroxyapatite on the occurrence of early childhood caries: a 1-year randomized clinical trial. Sci Rep 2021;11(01):2650
46 Söchtig F, Hickel R, Kühnisch J. Caries detection and diagnostics with near-infrared light transillumination: clinical experiences. Quintessence Int 2014;45(06):531-538
47 Arends J, ten Bosch JJ. Demineralization and remineralization evaluation techniques. J Dent Res 1992;71(Spec No):924-928
48 Mobley CC. Nutrition and dental caries. Dent Clin North Am 2003; 47(02):319-336
49 Al-Dajani M, Limeback H. Emerging science in the dietary control and prevention of dental caries. J Calif Dent Assoc 2012;40(10): 799-804
50 Loveren CV. Toothpastes. Vol 23;Basel: Karger; 2013
51 Walsh T, Worthington HV, Glenny AM, Marinho VC, Jeroncic A. Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev 2019;3(03):CD007868
52 Epple M, Enax J, Meyer F. Prevention of caries and dental erosion by fluorides: a critical discussion based on physico-chemical data and principles. Dent J 2022;10(01):6
53 Hausen H, Kärkkäinen S, Seppä L Application of the high-risk strategy to control dental caries. Community Dent Oral Epidemiol 2000;28(01):26-34
54 Ekambaram M, Itthagarun A, King NM. Ingestion of fluoride from dentifrices by young children and fluorosis of the teeth: a literature review. J Clin Pediatr Dent 2011;36(02):111-121
55 Meyer-Lueckel H, Grundmann E, Stang A. Effects of fluoride tablets on caries and fluorosis occurrence among 6- to 9-year olds using fluoridated salt. Community Dent Oral Epidemiol 2010;38(04):315-323
56 Neurath C, Limeback H, Osmunson B, Connett M, Kanter V, Wells CR. Dental fluorosis trends in US oral health surveys: 1986 to 2012. JDR Clin Trans Res 2019;4(04):298-308
58 Marquis RE, Clock SA, Mota-Meira M. Fluoride and organic weak acids as modulators of microbial physiology. FEMS Microbiol Rev 2003;26(05):493-510
59 Valkenburg C, Slot DE, Bakker EW, Van der Weijden FA. Does dentifrice use help to remove plaque? A systematic review. J Clin Periodontol 2016;43(12):1050-1058
61 Zimmer S, Öztürk M, Barthel CR, Bizhang M, Jordan RA. Cleaning efficacy and soft tissue trauma after use of manual toothbrushes with different bristle stiffness. J Periodontol 2011;82(02): 267-271
62 Caporossi LS, Dutra DA, Martins MR, Prochnow EP, Moreira CH, Kantorski KZ. Combined effect of end-rounded versus tapered bristles and a dentifrice on plaque removal and gingival abrasion. Braz Oral Res 2016;30:30
63 Enax J, Epple M. Die charakterisierung von putzkörpern in zahnpasten. Dtsch Zahnarztl Z 2018;73:100-108
64 Enax J, Meyer F, Schulze Zur Wiesche E, Fuhrmann IC, Fabritius HO. Toothpaste abrasion and abrasive particle content: correlating high-resolution profilometric analysis with relative dentin abrasivity (RDA). Dent J 2023;11(03):79
65 Sarembe S, Ufer C, Kiesow A, et al. Influence of the amount of toothpaste on cleaning efficacy: An in vitro study. Eur J Dent 2023; 17(02):497-503
66 Toumba KJ, Twetman S, Splieth C, Parnell C, van Loveren C, Lygidakis NA. Guidelines on the use of fluoride for caries prevention in children: an updated EAPD policy document. Eur Arch Paediatr Dent 2019;20(06):507-516
67 Limeback H, Enax J, Meyer F. Biomimetic hydroxyapatite and caries prevention: a systematic review and meta-analysis. Can J Dent Hyg 2021;55(03):148-159
68 Limeback H, Enax J, Meyer F. Improving oral health with fluoridefree calcium-phosphate-based biomimetic toothpastes: an update of the clinical evidence. Biomimetics (Basel) 2023;8(04):331
69 Wülknitz P. Cleaning power and abrasivity of European toothpastes. Adv Dent Res 1997;11(04):576-579
70 Marsh PD. Contemporary perspective on plaque control. Br Dent J 2012;212(12):601-606
71 Shen Y, Li P, Chen X, et al. Activity of sodium lauryl sulfate, rhamnolipids, and N -acetylcysteine against biofilms of five common pathogens. Microb Drug Resist 2020;26(03):290-299
72 Kensche A, Holder C, Basche S, Tahan N, Hannig C, Hannig M. Efficacy of a mouthrinse based on hydroxyapatite to reduce initial bacterial colonisation in situ. Arch Oral Biol 2017;80:18-26
73 Schlagenhauf U, Kunzelmann K-H, Hannig C, et al. Impact of a nonfluoridated microcrystalline hydroxyapatite dentifrice on enamel caries progression in highly caries-susceptible orthodontic patients: a randomized, controlled 6 -month trial. J Investig Clin Dent 2019;10(02):e12399
74 Kani K, Kani M, Isozaki A, Shintani H, Ohashi T, Tokumoto T. Effect of apatite-containing dentifrices on dental caries in school children. J Dent Health. 1989;19:104-109
75 Flemming J, Meyer-Probst CT, Speer K, Kölling-Speer I, Hannig C, Hannig M. Preventive applications of polyphenols in dentistry: a review. Int J Mol Sci 2021;22(09):22
76 Cieplik F, Kara E, Muehler D, et al. Antimicrobial efficacy of alternative compounds for use in oral care toward biofilms from caries-associated bacteria in vitro. MicrobiologyOpen 2019;8(04):e00695
77 Epple M, Meyer F, Enax J. A critical review of modern concepts for teeth whitening. Dent J 2019;7(03):79
78 Cieplik F, Jakubovics NS, Buchalla W, Maisch T, Hellwig E, AlAhmad A. Resistance toward chlorhexidine in oral bacteria: is there cause for concern? Front Microbiol 2019;10:587
79 Meyer F, Enax J. Hydroxyapatite in oral biofilm management. Eur J Dent 2019;13(02):287-290
80 Enax J, Meyer F, Schulze Zur Wiesche E, Epple M. On the application of calcium phosphate micro- and nanoparticles as food additive. Nanomaterials (Basel) 2022;12(22):4075
83 Tschoppe P, Zandim DL, Martus P, Kielbassa AM. Enamel and dentine remineralization by nano-hydroxyapatite toothpastes. J Dent 2011;39(06):430-437
85 Amaechi BT, AbdulAzees PA, Alshareif DO, et al. Comparative efficacy of a hydroxyapatite and a fluoride toothpaste for prevention and remineralization of dental caries in children. BDJ Open 2019;5:18