إرشادات الممارسة السريرية من المستوى S3 في طب الأسنان الداخلي: عملية وتوصيات الجمعية الأوروبية لطب الأسنان الداخلي Endodontic S3-level clinical practice guidelines: the European Society of Endodontology process and recommendations
إرشادات الممارسة السريرية من المستوى S3 في طب الأسنان الداخلي: عملية وتوصيات الجمعية الأوروبية لطب الأسنان الداخلي
هنري ف. دنكانوإخلاص الكريم
النقاط الرئيسية
تقدم هذه المراجعة التوصيات السريرية للإرشادات السريرية الأولى لجمعية طب الأسنان الأوروبية لإدارة التهاب اللب والتهاب الأنسجة المحيطة بالذروة.
توفر الإرشادات توصيات قائمة على الأدلة وخبيرة للتشخيص والعلاج في أربعة مجالات موضوعية: علاج التهاب اللب، العلاج غير الجراحي لالتهاب اللثة القمي، الإدارة الجراحية لالتهاب اللثة القمي، والعلاج التجديدي لالتهاب اللثة القمي.
اتبعت العملية نهجًا قويًا من المستوى S3، مع تقييم منهجي للأدبيات، وإرشادات منهجية مستقلة، وتفاعل مع أصحاب المصلحة الخارجيين، بما في ذلك المرضى، وعملية توصية قائمة على التوافق.
الملخص
نشرت الجمعية الأوروبية لطب الأسنان الجذري (ESE) إرشادات جودة في عام 2006؛ ومع ذلك، لم يتم مراجعتها منذ ذلك الحين. تماشيًا مع عملية إرشادية متطورة، تم نشر أول إرشادات سريرية من المستوى S3 في طب الأسنان الجذري من قبل ESE في عام 2023. كان الهدف هو تطوير إرشادات من المستوى S3 لإدارة الأمراض الجذرية باستخدام منهجية صارمة ومثبتة، تركزت على التشخيص والنهج العلاجية المطلوبة للتعامل مع المرضى الذين يعانون من التهاب اللب والتهاب اللثة القمي. تم تطوير هذه الإرشادات السريرية من ESE بمساعدة خبراء من تخصصات طب الأسنان الأخرى وتوجيه منهجي مستقل. شمل عملية تقييم الأدبيات المنهجية تحليل الأبحاث المقارنة في 14 مجالًا محددًا سيتم وصفها في 14 مراجعة منهجية قبل التحقيق في جودة وقوة الأدلة. أخيرًا، تم الاتفاق على سلسلة من التوصيات المستندة إلى الخبراء والأدلة بالتوافق مع أطباء الأسنان الجذريين ومجموعة من أصحاب المصلحة الخارجيين. تتناول التوصيات السريرية الناتجة فعالية تشخيص التهاب اللب والتهاب اللثة القمي قبل تقديم التوصيات بشأن فعالية استراتيجيات إدارة الأسنان الجذرية في علاج هذه الأمراض. استنادًا إلى أدلة قوية، تغطي التوصيات فعالية علاج اللب الحيوي، والإدارة غير الجراحية والجراحية، بالإضافة إلى استراتيجيات التجديد لمعالجة الأمراض الجذرية. ضمن الإرشادات، يتم التأكيد على الأهمية الحاسمة للتاريخ السريري، والتعقيم، والتدريب المناسب، وإعادة التقييم أثناء وبعد العلاج. في الختام، تُعلم هذه الإرشادات السريرية في طب الأسنان الجذري الممارسة، وصانعي السياسات، وأصحاب المصلحة، والمرضى حول أكثر العلاجات فعالية لإدارة المرضى الذين يعانون من التهاب اللب والتهاب اللثة القمي، مع تسليط الضوء على المجالات الحرجة لمزيد من البحث.
خلفية
نشرت الجمعية الأوروبية لطب الأسنان اللبية (ESE) مؤخرًا إرشادات ممارسة سريرية من المستوى S3 للمعالجة السنية للأمراض اللبية والذروية.كانت هذه الإرشادات بشكل أساسي لفائدة الأطباء والمرضى والباحثين وغيرهم من المعنيين. وقد نشرت الجمعية الأوروبية لدراسة السمنة سابقًا معايير الجودة
إرشادات لعلاج قناة الجذر فيومع ذلك، كان من الضروري تحديث هذه، حيث إن عملية التوافق وكتابة الإرشادات قد تغيرت بشكل كبير. في تطوير الإرشادات الحالية من المستوى S3، تم إجراء 14 مراجعة منهجية للأدبيات قبل الاتفاق على التوصيات التي تركز على نتائج المرضى باستخدام إطار عمل تقييم التوصيات والتقييم والتطوير والتقييمات (GRADE).تم استخدام هذه العملية في طب الأسنان من قبل الاتحاد الأوروبي لطب الأسنان اللثوي وفقًا لإرشادات المستوى S3 لعلاج التهاب اللثة من المرحلة I-III.التي تم تلخيصها في مجلة طب الأسنان البريطانية.
تقليديًا، كانت منشورات ESE بما في ذلك الإرشادات وبيانات الموقف على مستوى S1، والذي يتضمن اختيار مجموعة من الخبراء الذين يتفقون على سلسلة من توصيات تستند إلى معرفتهم المشتركة ولكن دون عملية توافق رسمية.لتطوير دليل إرشادي سريري (CPG)، تم الاتفاق على أن تطوير إرشادات علاجية على مستوى أعلى (S3) كان مطلوبًا، والتي استخدمت عملية منظمة ورسمية ومنهجية لضمان قوة وملاءمة النتائج.
تم الانتهاء من مشروع ESE S3 على مدار عامين تحت رعاية مجموعة توجيهية تتكون من عشرة أكاديميين كبار تم تعيينهم لأربعة مجموعات عمل (WGs) مصممة لتغطية الجوانب الرئيسية لإدارة علاج الجذور: WG1 – علاج التهاب اللب؛ WG2 – العلاج غير الجراحي لالتهاب اللثة القمي؛ WG3 – العلاج الجراحي لالتهاب اللثة القمي؛ و WG4 – العلاج التجديدي لالتهاب اللثة القمي. عملت مجموعة التوجيه طوال العملية بمساعدة من دليل مستقل كبير. المنهجية (إينا كوب) التي قدمت المشورة بشأن عدة قضايا، بما في ذلك التدريب المنهجي، مقاييس النتائج المناسبة، اختيار الدراسات، عملية المراجعة وإعلانات المصالح. إذا تم تحديد تضارب في المصالح، تم منع الأفراد من التصويت والمشاركة في المناقشات الجماعية حول الموضوعات ذات الصلة.
كان الغرض من هذه العملية هو تحديد فعالية العلاج اللبّي للأمراض الشائعة مثل التهاب اللب والتهاب الأنسجة المحيطة بالذروة.في بيئة ممارسة واقعية، يفضل أن تكون مدعومة بتجارب مقارنة عملية قائمة على الممارسة. للأسف، مع تطور العملية، أصبح من الواضح أن الجزء الأكبر من الدراسات المؤهلة تم إجراؤه في كليات الأسنان والجامعات على مجموعات فرعية، وبالتالي تم قياس الفعالية بدلاً من الكفاءة.
باختصار، تقدم هذه الإرشادات السريرية لطب الأسنان توصيات لكل طريقة تشخيص وعلاج يمكن أن توجه رعاية الأسنان للسكان بشكل عام. ولهذا الغرض، قمنا في هذه المخطوطة بتلخيص التوصيات باستخدام العبارات: ‘نوصي بـ’، ‘نقترح بـ/نقترح عدم’ و’لا نعرف’ (الجدول 1).
تطوير الإرشادات السريرية
غالبًا ما تعيق وجهات النظر الشخصية، والتحيز في اختيار الزملاء ذوي الآراء المماثلة، وتضارب المصالح، والتفسير الانتقائي للبيانات، تطوير بيانات الموقف والإرشادات السريرية. ونتيجة لذلك، ظهرت في السنوات الأخيرة معايير دولية لأفضل الممارسات حول الطريقة الأكثر ملاءمة لكتابة الإرشادات التي تكون قوية وصحيحة علميًا وتتمتع بأقل قدر من التحيز. هذه الإرشادات تم تطويره باستخدام نظام موثق نهج تحت رعاية المنهجيات التي اتبعت الإرشادات المنشورة من قبل اللجنة الدائمة للإرشادات التابعة لجمعية الجمعيات الطبية العلمية في ألمانيا (AWMF)ومجموعة العمل GRADE (https://www.gradeworkinggroup.org/تم اتخاذ قرار في مرحلة التخطيط لتطوير إطار عمل يُعرف بـ “الإثبات إلى القرار” باستخدام تنسيق توصيات بسيط (الجدول 1)، حيث تم تحليل الأدلة باستخدام GRADE بناءً على جودة الأدلة الداعمة وتم تعديلها (زيادة أو نقصان) بواسطة عوامل أخرى، مثل خطر التحيز، التناسق، الصلة، حجم التأثير السريري، توازن الفوائد والأضرار، الاعتبارات الاقتصادية والقانونية، وأخيرًا، تفضيلات المرضى وقيمهم. دور رئيسي للجنة التوجيه هو تحديد النتائج الأكثر ملاءمة، وأنواع الدراسات، وطول فترة المتابعة، والأدوات المستخدمة لتقييم جودة الدراسات.
الأدلة الداعمة للإرشادات
مجموعة تطوير الإرشادات
اجتمعت مجموعة التوجيه المكونة من عشرة أعضاء بشكل دوري عبر الإنترنت لمناقشة الاستراتيجية، وأيضًا بالتعاون مع مجموعة تطوير الإرشادات، التي تتكون من أكاديميين كبار قادوا المراجعات المنهجية المعتمدة.
(المراجعات النظامية)، المعنيون الخارجيون ذوو الصلة (الجمعيات والمنظمات السنية ذات الصلة [مثل الجمعيات السنية المتخصصة ذات الصلة، الجمعيات التعليمية والبحثية، الاتحاد الدولي لأخصائيي صحة الأسنان، مجموعات الصحة الفموية الأوروبية]، الطلاب، ممثلو المرضى) وأخصائيي علاج الجذور الكبار. تم تكليف هذه المجموعة بتقييم التوصيات والمشاركة في مؤتمر التوافق. تم تعيين المعنيين لكل من مجموعات العمل الأربعة وعلى مدى عامين، تم تنظيم عدة جلسات عامة واجتماعات لمجموعات العمل لمناقشة مجموعة من القضايا، بما في ذلك العملية، إعلانات المصالح، المنهجية، المراجعات النظامية، التوصيات والتوافق (الشكل 1). على الرغم من أن بعض مجموعات العمل كانت أكبر من غيرها، إلا أن كل مجموعة كانت تتكون من قائدين لمجموعتي العمل، ومؤلفين كبار من كل مراجعة لمجموعة العمل، ومعنيين خارجيين (تم اختيارهم من قبل المجموعة المدعوة) وأخصائيي علاج الجذور (كبار، يعملون في الأكاديمية أو الممارسة السنية، مؤهلين لأكثر من عشر سنوات ولديهم تاريخ من عشرة منشورات على الأقل). كانت مجموعة العمل 1 تضم 19 عضوًا، ومجموعة العمل 2 تضم 20، ومجموعة العمل 3 تضم 18 ومجموعة العمل 4 تضم 15 عضوًا، على التوالي. تم إجراء جميع التصويتات على التوصيات المستندة إلى الخبرة والأدلة في جلسة عامة، والتي، بعد النظر في إعلانات المصالح، أسفرت دائمًا عن مجموعة تصويت تتجاوز النصاب القانوني المكون من 50 عضوًا.
الجدول 1 قوة التوصيات: نظام التقييم. من الجمعية الألمانية AWMF ولجنة الإرشادات الثابتة
درجة التوصية
الصياغة
قوي
نوصي بـ (介 ⇑)
نوصي بعدم ( ⇓ ↓ )
ضعيف
نقترح (↑)
نقترح عدم ( ⇓ )
مفتوح
لا نعرف/ قد يُعتبر ( ⇔ )
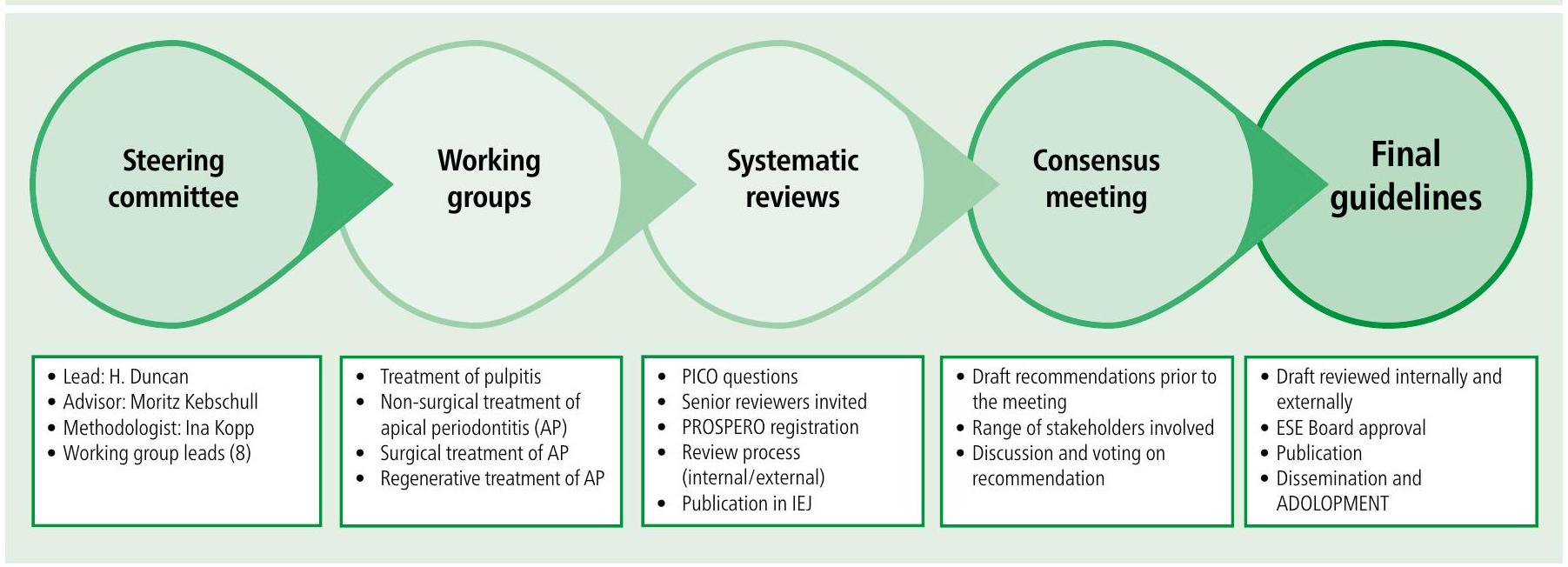
الشكل 1 عملية تطوير الإرشادات
مراجعة منهجية للأدبيات
خلال المناقشات الأولية لمجموعة التوجيه، تم الاتفاق على أنه من أجل تسهيل المقارنة وإعادة الإنتاج بين المراجعات النظامية الفردية، يجب توحيد وترتيب مقاييس النتائج السنية. علاوة على ذلك، تم الاعتراف بأن الجزء الأكبر من نتائج علاج الجذور هي تقارير سريرية تقليدية، بدلاً من تقارير المرضى، مما يتعارض مع روح عملية التوصية المستندة إلى GRADE.لذلك، قبل بدء البحث في الأدبيات، تم تجميع قائمة بجميع نتائج علاج الجذور وترتيبها من قبل 42 عضوًا شاركوا في عملية التطوير المعتمدة لاختيار النتائج باستخدام مقياس ليكرت من تسع نقاط على مدى جولتين.تمت مشاركة ملخص درجات الاستطلاع مع أعضاء المجموعة قبل تأكيد القائمة النهائية لمقاييس النتائج التي تم تقييمها على أنها حاسمة لاتخاذ القرار.بالنسبة للمراجعات النظامية التي تتناول العلاج، تم اختيار مجموعة من مقاييس النتائج التي تم الإبلاغ عنها من قبل المرضى والأطباء، مع كون النتيجة الأكثر أهمية هي ‘بقاء السن’. تضمنت النتائج الحرجة الأخرى ‘الألم، الحساسية، التورم، الحاجة إلى الأدوية (المسكنات)’ و’دليل على الحل/ظهور الشفافية القمية’، بينما تضمنت النتائج الإضافية ‘جودة الحياة المتعلقة بالصحة الفموية.’تم تخصيص نتائج إضافية لبعض مجموعات العمل، على سبيل المثال، التهاب اللب تضمنت ‘الاستجابة لاختبار حساسية اللب’ وعلاج الجراحة لالتهاب اللثة القمي تضمنت ‘وجود مسار الجيب، شفاء الأنسجة الرخوة بشكل مرضٍ’. كانت للمراجعات التشخيصية نتائج مختلفة تمامًا تتعلق بـ ‘الخصوصية’، ‘الحساسية’، ‘نسبة الاحتمالات التشخيصية’، ‘القيمة التنبؤية الإيجابية’ و’القيمة التنبؤية السلبية’ كاحتمالات لاختبار صحيح و’تحليل خصائص التشغيل المستقبلية’.
في الوقت نفسه، تم تحديد فترة المتابعة بعد العلاج المتعلقة بمقياس النتائج المحدد، مع حد أدنى من سنة واحدة لتقييم فعالية العلاجات لالتهاب اللب والتهاب اللثة القمي المختارين. تم تخصيص مقاييس النتائج المتعلقة بالألم، التورم، الأدوية المتناولة، أو التحقيق في دقة التشخيص لفترات متابعة أقصر. تم استخدام مقاييس النتائج وطول المتابعة جنبًا إلى جنب مع الأدوات القياسية لتقييم الجودة المنهجية للتجارب السريرية ثم تم تطبيقها على جميع المراجعات النظامية المفوضة المعنية بإرشادات مستوى ESE S3.
فيما يتعلق بالدراسات التي سيتم تضمينها، تم اعتبار فقط الدراسات المقارنة البشرية ذات المتابعة المناسبة للتضمين.
على وجه التحديد، تم اعتبار التجارب السريرية العشوائية والتجارب السريرية المقارنة غير العشوائية، بالإضافة إلى مجموعة متنوعة من الدراسات الرصدية الطولية، بما في ذلك دراسات المجموعة المقارنة ودراسات الحالة والشاهد. لمنع تقارير الحالة المقارنة، كان يجب أن يكون هناك على الأقل 20 (عشرة في كل ذراع) في نهاية الدراسة.
أخيرًا، تم تكليف 14 مراجعة نظامية من قبل مجموعة توجيه ESE CPG لتقييم الأدلة المتعلقة بأسئلة PICOT المركزة (المريض/السكان؛ التدخل/المؤشر؛ المقارنة/التحكم؛ النتيجة؛ الوقت/النوع). تم توحيد أسئلة PICOT من قبل مجموعة التوجيه في بروتوكول تم تقديمه مسبقًا إلى قاعدة بيانات PROSPERO. لاحقًا، تم نشر جميع المراجعات النظامية الأربعة عشر في المجلة الدولية لعلاج الجذور بعد عملية مراجعة دقيقة من قبل الأقران، بما في ذلك المراجعة الداخلية والخارجية.في جميع المراجعات النظامية، تم تقييم خطر التحيز باستخدام أدوات محددة لكل نوع دراسة (الجدول 2)، مع أداة RoB 2 من Cochrane للتجارب السريرية العشوائية، ومقياس Newcastle-Ottawa للدراسات الرصدية، وQUADAS-2 للدراسات التي تستثمر في الفعالية التشخيصية.
قمة التوافق المنظم
عُقدت قمة التوافق المنظم لعلاج الأمراض اللبية والقمي بمستوى ESE S3 في لشبونة، البرتغال من 29 يناير إلى 1 فبراير 2023. باستخدام المراجعات النظامية الأربعة عشر، تم مناقشة التوصيات المستندة إلى الأدلة المعدة مسبقًا من قبل لجنة تطوير الإرشادات باستخدام تنسيق تطوير توافق منظم تحت قيادة منهجي مستقل. في القمة، تم جدولة مناقشات مجموعات العمل ومناقشات عامة مفتوحة، حيث تم تقديم التوصيات المقترحة، والتصويت عليها واعتمادها بالإجماع.كما تم وصفه سابقًا، امتنع المندوبون الذين أعلنوا عن تضارب محتمل في المصالح عن التصويت أو المناقشة.
تشمل CPG 34 توصية سريرية رئيسية – عشرة مبنية على الخبرة و24 مبنية على الأدلة – لتشخيص وإدارة التهاب اللب والتهاب اللثة القمي. أدناه، تم تلخيص مجموعة من التوصيات الرئيسية. للحصول على وصف تفصيلي للطريقة، العملية والتوصيات، يرجى الرجوع إلى المنشور الأصلي.
التوصيات العامة المبنية على الخبرة
قد يكون التهاب اللب مصحوبًا بألم وحساسية مرتبطة بالسن، بينما قد يكون التهاب اللثة القمي عرضيًا أو غير عرضي، وعادة ما يظهر بأدلة شعاعية على وجود شفاف قمي. تُسبب هذه الأمراض بشكل رئيسي تحديات بكتيرية ويمكن أن تؤثر على جودة حياة المريض وتستدعي علاج الاستخراج إذا لم يتم إجراء علاج جذري مناسب وفي الوقت المناسب. غالبًا ما لا يتم التحقيق في أساسيات الرعاية عالية الجودة في التجارب السريرية (مثل استخدام سد الأسنان)؛ ومع ذلك، فإن هذه العوامل تدعم ممارسة علاج الجذور. لهذا السبب، تم استخدام التوصيات المبنية على الخبرة لتأكيد المكونات الأساسية لإدارة علاج الجذور:
‘لإدارة الأسنان القابلة للإصلاح مع التهاب اللب، يُوصى بأن يكون إما علاج لب حيوي أو علاج قناة جذر، واستعادة مناسبة لوظيفة ورعاية ما بعد الجراحة الداعمة، مفضلًا على الاستخراج’
وبالمثل، ‘لإدارة الأسنان القابلة للإصلاح مع التهاب اللثة القمي، يُوصى بأن يكون علاج قناة الجذر، واستعادة مناسبة ورعاية ما بعد الجراحة الداعمة، بدلاً من الاستخراج، مفضلًا’
للتقليل من وصف المضادات الحيوية في علاج الجذور،أوصي بأنه بالنسبة لـ ‘إدارة الطوارئ لـ
التهاب اللب العرضي أو التهاب اللثة القمي في سن قابل للإصلاح، كان علاج اللب الحيوي أو علاج قناة الجذر، بدلاً من الاستخراج أو وصف المضادات الحيوية النظامية، مناسبًا’
من أجل تشجيع الممارسات الجيدة في طب الأسنان الداخلي وضمان أن الأدلة التي تدعم هذه الإرشاداتتترجم إلى ممارسة الإدارة غير الجراحية لتعرض اللب المكشوف، فضلاً عن الأمراض اللبية والقمي، أوصي بأنه ‘يجب استخدام تقنية معقمة دقيقة ومجال جراحي مثالي، بما في ذلك استخدام سد الأسنان، وإضاءة جيدة وأجهزة تكبير’
فيما يتعلق بالتدريب المناسب بعد التخرج المطلوب لإجراء علاج الأسنان الداخلي، كانت التوصيات الحاليةواحترام مجموعة واسعة من المعايير عالميًا، اقترحنا أنه بالنسبة للتقنيات المتقدمة غير الجراحية بما في ذلك ‘إعادة العلاج المعقد وإدارة التهاب اللثة القمي جراحيًا، سيكون التدريب الإضافي بعد التخرج مفيدًا’. على الرغم من عدم تعريف إعادة العلاج المعقد في CPG، وفقًا لتقييم صعوبة الحالات من قبل الجمعية الأمريكية لطب الأسنان الداخلي، فإن الحالات عالية الصعوبة تتعلق عمومًا بالأسنان متعددة الجذور، أو الأسنان التي تحتوي على انسدادات داخل القناة، مثل الملفات المكسورة، أو الدعامات، أو الحواف، أو الثقوب
أخيرًا، فيما يتعلق بمراقبة نجاح العلاج،بعد علاج اللب الحيوي لإدارة التهاب اللب أو العلاج غير الجراحي أو الجراحي لالتهاب اللثة القمي، أوصي بأن تتم مراقبة الحالات لفترة طويلة مع تمديد فترة المراجعة إذا كان هناك شك حول الشفاء’. لم يتم تحديد الفترة الزمنية الدقيقة بسبب غياب بيانات قوية تشير إلى أن ذكر أي عدد محدد من السنوات كان قائمًا على الأدلة.
التوصيات القائمة على الأدلة المتعلقة بالتشخيص
من أجل إدارة الأمراض اللبية بشكل مناسب، تم تحليل الطرق التشخيصية الحالية في قدرتها على تشخيص وجود أو غياب وشدة المرض. تم التحقيق في تشخيص التهاب اللبو التهاب اللثة القميكلاهما تم التحقيق فيه:
عند تحديد تشخيص التهاب اللب لدى المرضى المشتبه في إصابتهم بالتهاب اللب مع عدم وجود ألم، أو ألم غير تلقائي أو ألم تلقائي، ‘اقترحنا استخدام اختبار البرودة ربما مكملًا بـ
اختبار اللب الكهربائي لتقييم حيوية اللب. علاوة على ذلك، اقترحنا دمج تاريخ الألم (وجود الألم، تاريخ الألم السابق وظهور الألم التلقائي) مع الظروف السريرية (وجود تعرض اللب، حساسية عند الطرق والألم عند تحفيز الحرارة) لتقييم حالة اللب. كما اعترفنا بأننا لا نعرف ما إذا كانت المؤشرات الحيوية الالتهابية يمكن أن تتنبأ بالحالة الالتهابية لللب، مما يبرز مجالًا لنشاط البحث المستقبلي’
‘في المرضى المشتبه في إصابتهم بالتهاب اللثة القمي، أوصينا بشدة باستخدام الأشعة السينية المحيطية بشكل روتيني لتشخيص التهاب اللثة القمي وأن CBCT (التصوير المقطعي المحوسب باستخدام شعاع مخروطي) يمكن اعتباره كإجراء تشخيصي إضافي، في الحالات التي يوجد فيها شك حول التشخيص. من الجدير بالذكر أن وجود مواد غير شفافة في
قناة الجذر والمحيط القمي قد يؤثر على دقة التشخيص لـ CBCT’.
التوصيات القائمة على الأدلة المتعلقة بعلاج التهاب اللب
تم التحقيق في فعالية علاج اللب الحيوي في إدارة التهاب اللب مع عدم وجود ألم أو ألم غير تلقائي،ألم تلقائي،فضلاً عن فعالية علاج قناة الجذر في إدارة الأسنان ذات اللب الحيوي أو النخر،تم التحقيق فيها (الجدول 3):
‘أولاً، في المرضى الذين يعانون من التهاب اللب المرتبط بعدم وجود ألم أو ألم غير تلقائي في الأسنان الدائمة، لا نعرف ما إذا كان التغطية المباشرة لللب أو بضع اللب (جزئي/ كامل) فعالًا مثل إزالة التسوس الانتقائية أو خطوة بخطوة فيما يتعلق بالبقاء على المدى الطويل لللب أو السن’. سلطت هذه التوصية القائمة على الأدلة الضوء على نقص الدراسات التي تركز على هذا السؤال، والذي يمكن أن يُعزى إلى القضايا الأخلاقية، فضلاً عن العملية
الجدول 3 التوصيات الرئيسية – علاج اللب الحيوي وإعادة الحيوية
التدخل
التوصيات القائمة على الأدلة والدرجة
التوصيات المستندة إلى توافق الخبراء
إزالة التسوس الانتقائية مقابل التغطية المباشرة لللب أو بضع اللب لالتهاب اللب غير المؤلم المرتبط بعدم وجود ألم أو ألم غير تلقائي
لم يتم تحديد أي دراسات
يمكن اعتبار إما إزالة التسوس الانتقائية دون تعرض اللب أو بعد تعرض اللب التغطية المباشرة لللب أو بضع اللب
التغطية المباشرة لللب مقابل بضع اللب لالتهاب اللب غير المؤلم المرتبط بعدم وجود ألم أو ألم غير تلقائي
– مفتوح (⇔)
– يمكن اعتبار إما التغطية المباشرة لللب أو بضع اللب (جزئي/ كامل)
– جودة الأدلة:
– منخفضة جدًا ⊕ΘΘΘ
بضع اللب مقابل إزالة اللب لالتهاب اللب غير المؤلم المرتبط بعدم وجود ألم أو ألم غير تلقائي
– مفتوح (⇔)
– يمكن اعتبار إما بضع اللب الكامل أو إزالة اللب
– جودة الأدلة:
– منخفضة جدًا ⊕ΘΘΘ
بضع اللب مقابل إزالة اللب لالتهاب اللب غير المؤلم المرتبط بألم تلقائي
– ضعيف (介)
– نقترح العلاج إما بعلاج قناة الجذر أو بضع اللب الكامل
– جودة الأدلة:
– منخفضة ⊕ ⊕ ΘΘ
علاج نخر اللب مع أو بدون التهاب اللثة القمي في الأسنان الدائمة غير الناضجة
– مفتوح (⇔)
– يمكن اعتبار تقنية السد القمي أو إجراءات إعادة الحيوية
– جودة الأدلة:
– منخفضة ⊕ ⊕ –
علاج نخر اللب مع أو بدون التهاب اللثة القمي في الأسنان الدائمة الناضجة مع إجراءات إعادة الحيوية
– ضعيف (⇓)
– نقترح عدم استخدام إجراءات إعادة الحيوية
– جودة الأدلة:
– منخفضة ⊕ ⊕ ΘΘ
هندسة الأنسجة اللبية في الأسنان الدائمة غير الناضجة
– مفتوح (⇔)
– لا نعرف ما إذا كانت هندسة الأنسجة اللبية تمثل خيار علاج صالح. هناك حاجة إلى مزيد من البحث لمعالجة هذا النقص في الأدلة
لتنظيم مثل هذه الدراسة.نتيجة لغياب الدراسات، تم تقديم توصيات قائمة على الخبرة، بما في ذلك أن استخدام إما إزالة التسوس الانتقائية/ خطوة بخطوة دون تعرض اللب أو بعد تعرض اللب التغطية المباشرة لللب أو بضع اللب (جزئي/ كامل) يمكن اعتباره. علاوة على ذلك، إذا كان اللب مكشوفًا، تم التوصية ببروتوكول معزز لعلاج اللب الحيوي اللاحق، والذي يتكون من استخدام سد الأسنان، وغسل مضاد للميكروبات، والتكبير، واستخدام الأسمنت الهيدروليكي من سيليكات الكالسيوم (HCSC). من منظور قائم على الأدلة، بالنسبة لالتهاب اللب في غياب الأعراض أو الألم غير التلقائي، يمكن اعتبار إما التغطية المباشرة لللب أو بضع اللب (جزئي/ كامل). يمكن أيضًا اعتبار بضع اللب الكامل وإزالة اللب بناءً على الأدلة.
إذا كان التهاب اللب مرتبطًا بألم تلقائي في الأسنان الدائمة بناءً على الأدلة،‘اقترحنا أن علاج قناة الجذر أو بضع اللب الكامل يمكن أن يكون فعالًا’
لم يظهر أي فرق بين الأسنان الحيوية وغير الحيوية من حيث مقاييس النتائج؛ ومع ذلك، ‘اقترحنا أن يتم إجراء علاج قناة الجذر على الأسنان ذات اللب غير الحيوي بمجرد تأكيد التشخيص’.
التوصيات القائمة على الأدلة المتعلقة بعلاج الأسنان غير الناضجة مع التهاب اللثة القمي
تختلف إدارة الأسنان غير الناضجة فيما يتعلق بعلاج التهاب اللثة القمي، حيث لا يمكن إجراء التحضير التقليدي لقناة الجذر والتعبئة باستخدام التقنيات التقليدية:
‘بالنسبة للمرضى الذين يعانون من أسنان دائمة غير ناضجة ونخر لب ± التهاب اللثة القمي، يمكن اعتبار تقنية سد HCSC أو إجراءات إعادة الحيوية
‘في الوقت الحالي، لا نعرف ما إذا كانت هندسة الأنسجة اللبية تمثل خيار علاج صالح حيث يتطلب الأمر مزيدًا من الأدلة السريرية والبحث’.
التوصيات القائمة على الأدلة
المتعلقة بالعلاج غير الجراحي للأسنان الناضجة مع التهاب اللثة القمي
عند النظر في العلاج غير الجراحي لالتهاب اللثة القمي في الأسنان الناضجة، تم النظر في جوانب مختلفة من الإدارة، بما في ذلك أدوات قناة الجذر الأدوات،التضميد،الري،التعبئةوالمساعدات المساعدة(الجدول 4):
‘فيما يتعلق بالأدوات، بالنسبة للمرضى الذين يعانون من التهاب اللثة القمي، يمكن اعتبار أي نوع مختبر من أدوات النيكل التيتانيوم (NiTi) المدفوعة بالمحرك للتحضير لقناة الجذر، حيث لم تكن هناك أدلة تشير إلى وجود ميزة لنظام ملف معين على آخر
لري، في المرضى الذين يعانون من التهاب اللثة القمي غير العرضي في الأسنان الدائمة، يُوصى بشكل مفتوح باستخدام هيبوكلوريت الصوديوم يتبعه حمض الإيثيلين ثنائي الأمين رباعي الأسيتيك (EDTA)، و يمكن أن يؤخذ في الاعتبار
فيما يتعلق بالتغليف المؤقت، تم تقديم توصية قوية بأنه حيث تم إجراء إجراءات سريرية كافية، يجب اعتماد نهج الزيارة الواحدة دون استخدام هيدروكسيد الكالسيوم بين المواعيد
‘يمكن اعتبار حشو قناة الجذر باستخدام غوتا بيرشا ومانع التسرب باستخدام أي من التقنيات المدرجة (الضغط الجانبي البارد، الضغط العمودي الدافئ، القائم على الحامل أو المخروط الفردي) بالاشتراك مع
أي من المانعات المدرجة (راتنج الإيبوكسي، ZOE أو سيليكات الكالسيوم)’
‘في المرضى الذين يعانون من التهاب اللثة القمي، نقترح عدم استخدام العلاج المساعد بالإضافة إلى المحاليل التقليدية (المعتمدة على إبرة الحقن). يشمل العلاج المساعد التعقيم بالضوء، الإشعاع بالليزر المباشر، العلاج بالأوزون والتفعيل بالموجات فوق الصوتية السلبية. في الوقت الحالي، لا توجد أدلة مقارنة تشير إلى أن هذه العلاجات أكثر فعالية من التقنيات التقليدية’
أخيرًا، في المرضى الذين يعانون من نخر اللب في الأسنان الدائمة الناضجة، ‘تم اقتراح عدم استخدام تقنيات الإحياء. كان هذا في تناقض مع التوصيات المقدمة للأسنان الدائمة غير الناضجة’.
توصيات قائمة على الأدلة تتعلق بالعلاج الجراحي للأسنان الناضجة التي تعاني من التهاب اللثة القمي
للعلاج الجراحي لالتهاب اللثة القمي في الأسنان الناضجة، تم النظر في جوانب مختلفة، بما في ذلك مقارنة الجراحة مع علاج قناة الجذر غير الجراحي/إعادة العلاج، فعالية استئصال الجذر
الجدول 4 التوصية الرئيسية – العلاج غير الجراحي لالتهاب اللثة القمي
التدخل
التوصيات القائمة على الدرجة والأدلة
الأدوات المستخدمة مع التقنيات المعاصرة مقابل تقنية الأدوات الفولاذية التقليدية
– ضعيف (介)
– نقترح أن يتم إعداد قناة الجذر باستخدام تقنيات معاصرة مدفوعة بالمحرك مع أدوات قناة الجذر من نيتي
– جودة الأدلة:
– البقاء، الألم بعد الجراحة: معتدل
– الشفاء الشعاعي: منخفض
الري باستخدام أي من محاليل الري لقناة الجذر مقابل الري باستخدام NaOCl وEDTA
– مفتوح ( )
– يتبعه EDTA، و يمكن أن يؤخذ في الاعتبار
– جودة الأدلة:
– الألم بعد الجراحة والشفاء الشعاعي: منخفض جدًا ⊕ ΘΘΘ
التغليف داخل القناة باستخدام أي من مواد التغليف لقناة الجذر مقابل هيدروكسيد الكالسيوم مقابل عدم استخدام أي تغليف
– قوي (介 )
– حيث تم إجراء إجراءات سريرية كافية، نوصي باستخدام نهج الزيارة الواحدة دون استخدام هيدروكسيد الكالسيوم بين المواعيد
– جودة الأدلة:
– الشفاء الشعاعي: معتدل
حشو قناة الجذر باستخدام أي نوع آخر من مانعات التسرب مقابل راتنج الإيبوكسي (AH Plus/AH 26) باستخدام غوتا بيرشا
– مفتوح ( ⇔ )
– يمكن اعتبار حشو قناة الجذر باستخدام غوتا بيرشا بالاشتراك مع أي من المانعات المدرجة (راتنج الإيبوكسي، ZOE أو سيليكات الكالسيوم)
حشو قناة الجذر باستخدام أي نوع من تقنيات الضغط غير الجانبي مقابل تقنية الضغط الجانبي البارد باستخدام غوتا بيرشا
– مفتوح ( ⇔ )
– يمكن اعتبار حشو قناة الجذر باستخدام غوتا بيرشا ومانع التسرب باستخدام أي من التقنيات المدرجة (الضغط الجانبي البارد، الضغط العمودي الدافئ، القائم على الحامل أو المخروط الفردي)
العلاج المساعد مقابل توصيل المحاليل التقليدية باستخدام الحقن والإبر
– ضعيف ( ⇓ )
– نقترح عدم استخدام العلاج المساعد بالإضافة إلى المحاليل التقليدية (المعتمدة على إبرة الحقن)
– جودة الأدلة:
– الألم والشفاء الشعاعي منخفض
الجدول 5 التوصيات الرئيسية – العلاج الجراحي لالتهاب اللثة القمي
التدخل
التوصيات القائمة على الدرجة والأدلة
التوصيات المستندة إلى توافق الخبراء
العلاج الجراحي مقابل علاج قناة الجذر غير الجراحي/إعادة العلاج
– مفتوح ( ⇔ )
– عندما يكون علاج قناة الجذر غير الجراحي أو إعادة العلاج غير عملي، يمكن اعتبار الجراحة القمية لإدارة الأسنان الدائمة التي تعاني من التهاب اللثة القمي
– جودة الأدلة:
– بقاء الأسنان: منخفض
استئصال الجذر مقابل إعادة العلاج غير الجراحي لقناة الجذر أو الجراحة القمية
– ضعيف (⇓)
– لا نقترح تقنيات استئصال الجذر كبديل لإعادة العلاج غير الجراحي لقناة الجذر أو الجراحة القمية في إدارة الأسنان الدائمة التي تعاني من التهاب اللثة القمي
– جودة الأدلة:
– بقاء الأسنان: منخفض جدًا ⊕ Θ
إعادة زراعة مقصودة مقابل علاج قناة الجذر غير الجراحي/إعادة العلاج أو الجراحة القمية
– ضعيف ( ⇓ )
– لا نقترح إعادة زراعة الأسنان المقصودة كبديل روتيني لعلاج قناة الجذر غير الجراحي/إعادة العلاج أو الجراحة القمية لإدارة الأسنان الدائمة التي تعاني من التهاب اللثة القمي
– جودة الأدلة:
– لا دراسات مقارنة محددة
أفادت الدراسات السريرية غير المقارنة بمعدلات بقاء عالية بشكل عام على المدى المتوسط إلى الطويل، مع معدلات مضاعفات منخفضة نسبيًا. لذلك، في غياب بدائل علاجية أخرى وبدلاً من الاستخراج، إذا كانت الظروف التشريحية تسمح بالاستخراج غير المؤلم ووقت خارج الفم أقل من 15 دقيقة، يمكن اعتبار إعادة الزراعة المقصودة لإدارة الأسنان الدائمة التي تعاني من التهاب اللثة القمي
وفعالية إعادة الزراعة المقصودة (الجدول 5):
‘لم تقترح الأدلة وجود فرق في فعالية الجراحة القمية، مقارنة بعلاج قناة الجذر غير الجراحي أو إعادة العلاج، من حيث النتائج السريرية، الشعاعية، والمتعلقة بالمرضى، لإدارة الأسنان الدائمة التي تعاني من التهاب اللثة القمي. لذلك، عندما يكون علاج قناة الجذر غير الجراحي أو إعادة العلاج غير عملي، يمكن اعتبار الجراحة القمية لإدارة الأسنان الدائمة التي تعاني من التهاب اللثة القمي
نظرًا لعدم وجود أدلة مقارنة، ‘لم تُقترح تقنيات استئصال الجذر وإعادة الزراعة المقصودة كبديل لإعادة العلاج غير الجراحي لقناة الجذر أو الجراحة القمية في إدارة الأسنان الدائمة التي تعاني من التهاب اللثة القمي. ومع ذلك، نظرًا لوجود بيانات غير مقارنة تدعم استخدامها، يمكن اعتبار إجراءات إعادة الزراعة المقصودة كخيار سريري.’
التنفيذ، النشر والتحديث
بالإضافة إلى نشر CPG المفتوح الوصول المصحوب بـ 14 SR في عدد خاص من المجلة الدولية لطب الأسنان، تم التصديق على خطة اتصالات متعددة الطبقات من قبل مجلس إدارة ESE وتفويضها إلى لجنة فوائد طب الأسنان في ESE. وشمل ذلك:
برنامج التبني والتكيف من قبل 37 جمعية وطنية تابعة لـ ESE،
بما في ذلك الترجمة إلى لغات مختارة، بما في ذلك الفرنسية، الإيطالية، الإسبانية، الألمانية، الصينية والبولندية
نشر النتائج في جلسات الندوات المحددة في مؤتمرات ESE (هلسنكي 2023 وكراكوف 2024)
نشر مخرجات بسيطة ‘مجزأة’ من الإرشادات من خلال لجنة اتصالات ESE. حيث أن CPG هو وثيقة قائمة على الأدلة ستحتاج إلى تحديث مع ظهور أدلة جديدة، من المخطط أن تكون الإرشادات صالحة لمدة خمس سنوات حتى عام 2028 على الأقل.
وجهات النظر والملخص
تعتبر CPG أول إرشادات شاملة لتشخيص وعلاج التهاب اللب والتهاب اللثة القمي التي تتبع إجراء مستوى S3 المنظم. تغطي المكونات الرئيسية للعلاج اللبي ولكنها لا تغطي جميع جوانب الرعاية اللبي، بما في ذلك الآفات اللثوية اللبية، الكسور الجذرية العمودية، الإصابات السنية الناتجة عن الصدمات والامتصاص، من بين أمور أخرى. يأمل أن يتم تغطية هذه في مشاريع مستقبلية من مستوى S3 أو في صيغة بيان موقف تقليدية.
لا تقتصر التوصيات على سرد المعرفة الحالية القائمة على الأدلة في هذا المجال، بل تسلط الضوء أيضًا على الفجوات في المعرفة والمجالات ذات الأولوية والبحث الإضافي. ستكون الخطوات التالية هي الانخراط في فترة من النشاط لنشر نتائج هذه الإرشادات إلى أطباء الأسنان، وأطباء الأسنان، وأصحاب المصلحة المعنيين، بما في ذلك الطلاب والمرضى.
إعلان الأخلاقيات
يعلن المؤلفون عدم وجود تضارب في المصالح.
مساهمات المؤلفين
قدم كل من HFD وIEK مساهمات كبيرة في المخطوطة ووافقا على النسخة النهائية من النص.
معلومات التمويل
جامعة دبلن، تمويل الوصول المفتوح المقدم من اتحاد IReL.
References
Duncan H F, Kirkevang L L, Peters O A et al. Treatment of pulpal and apical disease: the European Society of Endodontology (ESE) S3-level clinical practice guideline. Int Endod J 2023; DOI: 10.1111/iej.13974.
European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J 2006; 39: 921-930.
Guyatt G H, Oxman A D, Kunz R et al. GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol 2011; 64: 395-400.
Sanz M, Herrera D, Kebschull M etal. Treatment of stage I-III periodontitis – the EFP S3 level clinical practice guideline. J Clin Periodontol 2020; DOI: 10.1111/ јсре. 13290.
Kebschull M, Chapple I. Evidence-based, personalised and minimally invasive treatment for periodontitis patients – the new EFP S3-level clinical treatment guidelines. BrDent J 2020; 229: 443-449.
Duncan H F, Galler K M, Tomson P L et al. European Society of Endodontology position statement: management of deep caries and the exposed pulp. Int Endod J 2019; 52: 923-934.
Nothacker M J, Muche-Borowski C, Kopp I B. Guidelines in the register of the Association of Scientific Medical Societies in Germany – a quality improvement campaign. Geburtshilfe Frauenheilkd 2014; 74: 260-266.
Tibúrcio-Machado C S, Michelon C, Zanatta F B, Gomes M S, Marin J A, Bier C A. The global prevalence of apical periodontitis: a systematic review and meta-analysis. Int Endod J 2021; 54: 712-735.
German Association of the Scientific Medical Societies and Standing Guidelines Commission. AWMF guidance manual and rules for guideline development. 2012. Available at http://www.awmf.org/leitlinien/awmfregelwerk.html (accessed September 2024).
Duncan H F, Nagendrababu V, El-Karim I, Dummer P M H. Outcome measures to assess the effectiveness of endodontic treatment for pulpitis and apical periodontitis for use in the development of European Society of Endodontology S3-level clinical practice guidelines: a consensus-based development. Int Endod J 2021; 54: 2184-2194.
El Karim I A, Duncan H F, Cushley S et al. A protocol for the development of Core Outcome Sets for Endodontic Treatment modalities (COSET): an international consensus process. Trials 2021; 22: 812.
Duncan H F, Nagendrababu V, El-Karim I A, Dummer P M H. Outcome measures to assess the effectiveness of endodontic treatment for pulpitis and apical periodontitis for use in the development of European Society of Endodontology (ESE) S3 level clinical practice guidelines: a protocol. Int Endod J 2021; 54: 646-654.
Doğramacı E J, Rossi-Fedele G. Patient-related outcomes and oral health-related quality of life in endodontics. Int Endod J 2023; DOI: 10.1111/iej.13830.
Bucchi C, Rosen E, Taschieri S. Non-surgical root canal treatment and retreatment versus apical surgery in treating apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13793.
Bürklein , Arias A. Effectiveness of root canal instrumentation for the treatment of apical periodontitis: a systematic review and meta-analysis. Int Endod J 2023; DOI: 10.1111/iej. 13782.
Corbella S, Walter C, Tsesis I. Effectiveness of root resection techniques compared with root canal retreatment or apical surgery for the treatment of apical periodontitis and tooth survival: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13808.
Donnermeyer D, Dammaschke T, Lipski M, Schäfer E. Effectiveness of diagnosing pulpitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13762.
Hilmi A, Patel S, Mirza K, Galicia J C. Efficacy of imaging techniques for the diagnosis of apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/ iej.13921.
Jakovljevic A, Jaćimović J, Aminoshariae A, Fransson H. Effectiveness of vital pulp treatment in managing nontraumatic pulpitis associated with no or nonspontaneous pain: a systematic review. Int Endod J 2023; DOI: 10.1111/iej.13776.
Meire M A, Bronzato J D, Bomfim R A, Gomes B P F A. Effectiveness of adjunct therapy for the treatment of apical periodontitis: a systematic review and metaanalysis. Int Endod J 2023; DOI: 10.1111/iej. 13838.
Meschi N, Palma P J, Cabanillas-Balsera D. Effectiveness of revitalization in treating apical periodontitis: a systematic review and meta-analysis. Int Endod J 2023; DOI: 10.1111/iej.13778.
Pirani C, Camilleri J. Effectiveness of root canal filling materials and techniques for treatment of apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej.13787.
Plotino G, Abella Sans F, Bastos J V, Nagendrababu V. Effectiveness of intentional replantation in managing teeth with apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej.13727.
Rossi-Fedele G, Ng Y-L. Effectiveness of root canal treatment for vital pulps compared with necrotic pulps in the presence or absence of signs of periradicular pathosis: a systematic review and meta-analysis. Int Endod J 2023; DOI: 10.1111/iej. 13833.
Rossi-Fedele G, Rödig T. Effectiveness of root canal irrigation and dressing for the treatment of apical periodontitis: a systematic review and meta-analysis of clinical trials. Int Endod J 2023; DOI: 10.1111/ iej. 13777.
Tomson P L, Vilela Bastos J, Jacimovic J, Jakovljevic A, Pulikkotil S J, Nagendrababu V. Effectiveness of pulpotomy compared with root canal treatment in managing non-traumatic pulpitis associated with spontaneous pain: a systematic review and metaanalysis. Int Endod J 2023; DOI: 10.1111/iej. 13844.
Widbiller M, Knüttel H, Meschi N, Durán-Sindreu Terol F. Effectiveness of endodontic tissue engineering in treatment of apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13784.
Murphy M K, Black N A, Lamping D L et al. Consensus development methods, and their use in clinical guideline development. Health Technol Assess 1998; 2: 1-88
Segura-Egea J J, Gould K, Şen B H et al. European Society of Endodontology position statement: the use of antibiotics in endodontics. Int Endod J 2018; 51: 20-25.
De Moor R, Hülsmann M, Kirkevang L-L, Tanalp J, Whitworth J. Undergraduate curriculum guidelines for endodontology. Int Endod J 2013; 46: 1105-1114.
Gulabivala K, Ahlquist M, Cunnington Setal. Accreditation of postgraduate speciality training programmes in endodontology. Minimum criteria for training specialists in endodontology within Europe. Int Endod J 2010; 43: 725-737.
American Association of Endodontists. AAE endodontic case difficulty assessment form and guidelines. 2022. Available at https://www.aae.org/ specialty/wp-content/uploads/sites/2/2022/01/ CaseDifficultyAssessmentFormFINAL2022.pdf (accessed December 2024).
Duncan H F. Present status and future directions – vital pulp treatment and pulp preservation strategies. Int Endod J 2022; DOI: 10.1111/iej. 13688.
Schunemann H J, Wiercioch W, Brozek J et al. GRADE evidence to decision (EtD) frameworks for adoption, adaptation, and de novo development of trustworthy recommendations: GRADE-ADOLOPMENT. J Clin Epidemiol 2017; 81: 101-110.
الوصول المفتوح.
قسم طب الأسنان الترميمي وأمراض اللثة، كلية ترينيتي دبلن، مستشفى دبلن الجامعي لطب الأسنان، دبلن، أيرلندا؛كلية الطب وطب الأسنان والعلوم الطبية الحيوية، جامعة كوينز بلفاست، بلفاست، المملكة المتحدة.
*المراسلة إلى: هنري ف. دانكان
عنوان البريد الإلكتروني: Hal.Duncan@dental.tcd.ie
ورقة محكمة.
تم التقديم في 10 أكتوبر 2024
تمت المراجعة في 5 ديسمبر 2024
تم القبول في 14 ديسمبر 2024 https://doi.org/10.1038/s41415-025-8335-x
Endodontic S3-level clinical practice guidelines: the European Society of Endodontology process and recommendations
Henry F. Duncan and Ikhlas El-Karim
Key points
This review presents the clinical recommendations of the inaugural European Society of Endodontology clinical practice guideline for the management of pulpitis and apical periodontitis.
The guidelines provide expert and evidenced-based recommendations for diagnosis and treatment in four thematic areas: treatment of pulpitis, non-surgical treatment of apical periodontitis, surgical management of apical periodontitis, and regenerative treatment of apical periodontitis.
The process followed a robust S3-level approach, with systematic assessment of literature, independent methodological guidance, engagement with external stakeholders, including patients, and a consensus-based recommendation process.
Abstract
The European Society of Endodontology (ESE) published quality guidelines in 2006; however, they had not been revised since. In line with a state-of the art guideline process, the first S3-level clinical practice guideline (CPG) in endodontics was published by the ESE in 2023. The aim was to systemically develop, using a rigorous validated methodology, an S3-level guideline for the management of endodontic disease which concentrated on diagnosis and the therapeutic approaches required to deal with patients with pulpitis and apical periodontitis. Methodologically, this ESE CPG was developed with the assistance of experts from other dental disciplines and with independent methodological guidance. A systematic literature appraisal process included the analysis of comparative research in 14 specific areas that would be described in 14 systematic reviews prior to investigation of evidence’s quality and strength. Finally, a series of expert and evidence-based recommendations were agreed by consensus with endodontists and a range of external stakeholders. The resulting clinical recommendations address the effectiveness of diagnosing pulpitis and apical periodontitis before recommendations are made on the effectiveness of endodontic management strategies in treatment of these diseases. Based on robust evidence, recommendations cover the effectiveness of vital pulp treatment, non-surgical and surgical management, as well as regenerative strategies to address endodontic disease. Within the guidelines, the critical importance of clinical history, asepsis, appropriate training and re-evaluation during and after treatment are underlined. In conclusion, this clinical endodontic guideline informs practice, policymakers, stakeholders and patients on the most effective treatments to manage patients with pulpitis and apical periodontitis, while highlighting critical areas for further research.
Background
The European Society of Endodontology (ESE) recently published inaugural S3-level clinical practice guidelines (CPG) for the treatment of pulpal and apical disease. These guidelines were principally for the benefit of clinicians, patients, researchers and other stakeholders. The ESE previously published quality
guidelines for endodontic treatment in however, these needed to be updated, as the process of consensus and guideline writing had significantly changed. In the development of the current S3-level guidelines, 14 systematic reviews of the literature were undertaken before recommendations that focus on patientcentred outcomes were agreed using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework. This process has been employed in dentistry by the European Federation of Periodontology S3-level guidelines for treatment of stage I-III periodontitis, which have been summarised in the British Dental Journal.
Traditionally, ESE publications including guidelines and position statements have been at the S1 level, which involves the selection of a group of experts who agree a series of
recommendations based on their shared knowledge but without an official consensus process. For the development of a CPG, it was agreed that the development of higherlevel treatment guidelines (S3) was required, which employed a structured, formalised and systematic process to ensure robustness and relevance of the findings.
The ESE S3-level project was completed over two years under the auspices of a steering group, comprised of ten senior academics assigned to four working groups (WGs) designed to cover the principal facets of endodontic management: WG1 – the treatment of pulpitis; WG2 – the non-surgical treatment of apical periodontitis; WG3 – the surgical treatment of apical periodontitis; and WG4 – the regenerative treatment of apical periodontitis. The steering group worked throughout the process with the assistance of a senior, independent guideline
methodologist (Ina Kopp) who advised on several issues, including methodological training, appropriate outcome measures, study selection, review process and declarations of interest. If conflicts were identified, individuals were prevented from voting and partaking in group discussion on the related subjects.
The purpose of this process was to ascertain the effectiveness of endodontic treatment for the common diseases pulpitis and apical periodontitis in a real-world practice environment, ideally evidenced by pragmatic, practice-based comparative trials. Unfortunately, as the process evolved, it became clear that the bulk of eligible studies were carried out in dental schools and universities on subpopulations and therefore measured efficacy rather than effectiveness.
In summary, this endodontic CPG makes recommendations for each diagnostic and treatment modality which can guide dental care for the general population. To that end, in this manuscript, we have summarised the recommendations using the language, ‘we recommend to, ‘we suggest to/we suggest not to’ and ‘we do not know’ (Table 1).
Development of clinical guidelines
The development of position statements and clinical guidelines is often hampered by personal views, bias in the selection of colleagues with similar views, conflicts of interest, and selective interpretation of data. As a result, over recent years, best-practice international standards have emerged on the most appropriate way in which to write guidelines that are robust, scientifically valid and possess minimal bias. This guideline was developed using a systemic validated
approach under the auspices of methodologists who followed the guidance published by the Standing Guideline Commission of the Association of Scientific Medical Societies in Germany (AWMF) and the GRADE working group (https://www.gradeworkinggroup.org/). A decision was made in the planning stage to develop a so-called ‘evidence-to-decision’ framework using a simple recommendations format (Table 1), with the evidence analysed using GRADE based on the quality of the supporting evidence and modified (up or down) by other factors, such as risk of bias, consistency, relevance and clinical effect size, balance of benefits and harm, economic and legal considerations, and finally, patient preferences and values. A major role of the steering committee is to decide the most appropriate outcomes, study types, length of follow-up and tools used for assessing the quality of studies.
Evidence supporting the guidelines
Guideline development group
The ten-member steering group met periodically online to discuss strategy and also in combination with the guideline development group, who comprised of senior academics who led the commissioned systematic reviews
(SRs), relevant external stakeholders (related dental societies and organisations [i.e. related dental specialist societies, educational and research associations, International Federation of Dental Hygienists, European oral health groups], students, patient representatives) and senior endodontists. This group was tasked with evaluating the recommendations and participating in the consensus conference. Stakeholders were assigned to each of the four WGs and over a two-year period, several online plenaries and WG meetings were organised to discuss a range of issues, including process, declarations of interest, methodology, SRs, recommendations and consensus (Fig. 1). Although some WGs were larger than others, each consisted of two working group leads, two SR senior authors from each WG review, external stakeholders (chosen by invited group) and endodontists (senior, working in endodontic academia or practice, qualified greater than ten years and history of at least ten publications). WG1 had 19, WG2 had 20, WG3 had 18 and WG4 had 15 members, respectively. All votes on expert and evidenced-based recommendations were made in a plenary session, which, after declarations of interest considerations, always resulted in a voting group in excess of the quorum of 50 members voting.
Table 1 Strength of recommendations: grading scheme. From the German AWMF and standing guidelines commission
Grade of recommendation
Syntax
Strong
We recommend to (介 ⇑)
We recommend not to ( ⇓ ↓ )
Weak
We suggest to (↑)
We suggest not to ( ⇓ )
Open
We do not know/ may be considered ( ⇔ )
Fig. 1 Guideline development process
Systematic review of the literature
During initial steering group discussions, it was agreed that in order to aid comparison and reproducibility between the individual SRs, the endodontic outcome measures would have to be standardised and ranked. Furthermore, it was acknowledged that the bulk of endodontic outcomes are classically clinician-reported measures, rather than patient-reported measures, which goes against the spirit of the GRADE-based recommendation process. Therefore, before the literature search began, a list of all endodontic outcomes was compiled and ranked by the 42 members involved in the validated development process for the selecting outcomes using a nine-point Likert-scale over two rounds. A summary of the survey scores was shared with the members of the group before the final list of outcome measures which were rated as critical for decision-making was confirmed. For SRs addressing treatment, a combination of patient- and clinician-reported outcome measures were selected, with the most critical outcome being ‘tooth survival’. Other critical outcomes included ‘pain, tenderness, swelling, need for medication (analgesics)’ and ‘evidence of resolution/emerging apical radiolucency’, while additional outcomes included ‘oral health-related quality of life.’ Additional outcomes were ascribed to some WGs, for example, pulpitis included ‘response to pulp sensibility test’ and surgical treatment of apical periodontitis included ‘presence of sinus tract, satisfactory soft tissue healing’. Diagnostic SRs had completely different outcomes related to ‘specificity’, ‘sensitivity’, ‘diagnostic odds ratio’, ‘positive predictive value’ and the ‘negative predictive value’ as probabilities for a correct test and ‘receiver operating characteristic analysis’.
At the same time, the follow-up period after treatment related to the specific outcome measure was also decided, with a minimum of one-year for assessing the effectiveness of treatments for pulpitis and apical periodontitis selected. Selected outcome measures relating to pain, swelling, medication taken, or investigating diagnostic accuracy were allocated shorter follow-up periods. The outcome measures and length of follow-up were used alongside standard instruments to assess the methodological quality of clinical trials and were then applied to all the commissioned SRs involved in the ESE S3-level guidelines.
In terms of the studies to be included, only human comparative studies with suitable follow-up were considered for inclusion.
Specifically, randomised control trials and nonrandomised comparative clinical trials, as well as various longitudinal observational studies, including comparative cohort and case-control studies. In order to prevent comparative case reports, there had to be at least 20 (ten in each arm) at the end of the study.
Finally, 14 SRs were commissioned by the ESE CPG steering group to evaluate the evidence in relation to focused PICOT (patient/ population; intervention/indicator; compare/ control; outcome; time/type) questions. The PICOT questions were standardised and homogenised by the steering group into a protocol that was submitted a priori to the PROSPERO database. Later, all 14 SRs were published in the International Endodontic Journal after a rigorous peer-review process, including internal and external review. In all the SRs, the risk of bias was evaluated using tools specific to each study type (Table 2), with Cochrane’s RoB 2 for randomised controlled trials, the NewcastleOttawa scale for observational studies, and QUADAS-2 for studies investing diagnostic efficacy.
Structured consensus summit
The structured consensus summit for ESE S3-level treatment of pulpal and apical disease was held in Lisbon, Portugal on 29 January to 1 February 2023. Using the 14 SRs, pre-prepared evidence-based recommendations were debated by the guideline development panel using a structured consensus development format under the leadership of an independent methodologist. At the summit, WG discussions and open plenary discussions were timetabled, where the proposed recommendations were presented, voted upon and adopted by consensus. As described previously, delegates declaring potential conflicts abstained from voting or discussion.
The CPG encompasses 34 key clinical recommendations – ten expert-based and 24 evidenced-based – for the diagnosis and management of pulpitis and apical periodontitis. Below, a selection of the main recommendations are summarised. For a detailed description of the method, process and recommendations, please refer to the original publication.
General expert-based recommendations
Pulpitis may be accompanied by pain and sensitivity associated with a tooth, while apical periodontitis may be symptomatic or asymptomatic, generally presenting with radiographic evidence of an apical radiolucency. These diseases are principally caused by bacterial challenge and can impact on the patient’s quality of life and necessitate extraction treatment if appropriate and timely endodontic treatment is not carried out. The fundamentals of high-quality care are often not investigated in clinical trials (e.g. dental dam use); however, these factors underpin the practice of endodontics. For that reason, expert-based recommendations were used to stress the essential components of endodontic management:
‘For the management of restorable teeth with pulpitis, it was recommended that either vital pulp treatment or root canal treatment, appropriate restoration to function and supportive postoperative care, were preferable to extraction’
Likewise, ‘for the management of restorable teeth with apical periodontitis, it was recommended that root canal treatment, appropriate restoration and supportive postoperative care, rather than extraction, was preferable’
To limit the prescription of antibiotics in endodontics, it was recommended that for ‘the emergency management of
symptomatic pulpitis or apical periodontitis in a restorable tooth, vital pulp treatment or root canal treatment, rather than extraction or systemic antibiotic prescription, was appropriate’
In order to encourage good practice in endodontics and ensure that the evidence supporting these guidelines translates to practice for the non-surgical management of the exposed pulp exposure, as well as pulpal and apical disease, it was recommended that ‘a meticulous aseptic technique and optimal surgical field, including the use of dental dam, good light and magnifying devices should be used’
With respect to the appropriate postgraduate training required to carry out endodontic treatment, existing recommendations and respecting a broad range of standards globally, we suggested that for advanced non-surgical techniques including ‘complex retreatment and for surgical management of apical periodontitis, further postgraduate training would be beneficial’. Although complex retreatment was not defined in the CPG, according to the American Association of Endodontists’ case difficulty assessment, high-difficulty cases would generally relate to multi-rooted teeth, or teeth with intracanal obstructions, such as fractured files, posts, ledges or perforations
Finally, in term of monitoring the success of treatment, after vital pulp treatment to manage pulpitis or non-surgical or surgical treatment of apical periodontitis, it was recommended that cases are monitored for a prolonged period with the review period extended if there is uncertainty about healing’. The exact time period was not stipulated due to absence of firm data suggesting that stating any specific number of years was evidenced-based.
Evidenced-based recommendations relating to diagnosis
In order to manage endodontic disease appropriately, current diagnostic methods were analysed in their ability to diagnose the presence or absence and severity of disease. The diagnosis of pulpitis and apical periodontitis were both investigated:
When ascertaining a diagnosis of pulpitis in patients suspected of having pulpitis with either no pain, non-spontaneous pain or spontaneous pain, ‘we suggested the use of cold testing possibly supplemented by
electric pulp testing to assess pulp vitality. Furthermore, we suggested a combination of pain history (presence of pain, history of previous pain and occurrence of spontaneous pain) with clinical conditions (presence of pulp exposure, tenderness to percussion and pain on heat stimuli) to assess pulpal condition. We also recognised that we did not know whether inflammatory biomarkers can predict the inflammatory status of the pulp, highlighting an area for future research activity’
‘In patients suspected of having apical periodontitis, we strongly recommended periapical radiography be routinely used to diagnose apical periodontitis and that CBCT (cone beam computed tomography) may be considered as an additional diagnostic measure, in cases where there is doubt about the diagnosis. Notable is the presence of radiopaque materials in
the root canal and periapex may affect the diagnostic accuracy of CBCT’.
Evidenced-based recommendations relating to the treatment of pulpitis
The effectiveness of vital pulp treatment in managing pulpitis with no or nonspontaneous pain, spontaneous pain, as well as the effectiveness of root canal treatment in managing teeth with vital or necrotic pulps, was investigated (Table 3):
‘Firstly, in patients with pulpitis associated with no or non-spontaneous pain in permanent teeth, we do not know whether direct pulp capping or pulpotomy (partial/ full) is as effective as selective or stepwise caries removal regarding the longterm survival of the pulp or the tooth’. This evidence-based recommendation highlighted the lack of studies focused on this question, which could be attributed to ethical issues, as well as the practicality
Table 3 Key recommendations – vital pulp treatment and revitalisation
Intervention
Grade and evidence-based recommendations
Expert consensus-based recommendations
Selective caries removal versus direct pulp capping or pulpotomy for non-traumatic pulpitis associated with no or no spontaneous pain
No studies identified
Either selective caries removal without pulp exposure or after pulp exposure direct pulp capping or pulpotomy may be considered
Direct pulp capping versus pulpotomy for non-traumatic pulpitis associated with no or no spontaneous pain
– Open ( ⇔ )
– Either direct pulp capping or pulpotomy (partial/full) may be considered
– Quality of evidence:
– Very low ⊕ΘΘΘ
Pulpotomy versus pulpectomy for non-traumatic pulpitis associated with no or no spontaneous pain
– Open ( ⇔ )
– Either full pulpotomy or pulpectomy may be considered
– Quality of evidence:
– Very low ⊕ΘΘΘ
Pulpotomy versus pulpectomy for non-traumatic pulpitis associated with spontaneous pain
– Weak (介)
– We suggest treatment with either root canal treatment or full pulpotomy
– Quality of evidence:
– Low ⊕ ⊕ ΘΘ
Treatment of pulp necrosis with or without apical periodontitis in immature permanent teeth
– Open ( ⇔ )
– The apical plug technique or revitalisation procedures may be considered
– Quality of evidence:
– Low ⊕ ⊕ –
Treatment of pulp necrosis with or without apical periodontitis in mature permanent teeth with revitalisation procedures
– Weak ( ⇓ )
– We suggest not to use revitalisation procedures
– Quality of evidence:
– Low ⊕ ⊕ ΘΘ
Endodontic tissue engineering in immature permanent teeth
– Open ( ⇔ )
– We do not know whether endodontic tissue engineering represents a valid treatment option. Further research is necessary to address this lack of evidence
of organising such a study. As a result of an absence of studies, expert-based recommendations were made, including that the use of either selective/stepwise caries removal without pulp exposure or after pulp exposure direct pulp capping or pulpotomy (partial/full) may be considered. Furthermore, if the pulp was exposed, an enhanced protocol was recommended for subsequent vital pulp therapy, which consists of the use of dental dam, antimicrobial lavage, magnification, and use of a hydraulic calcium silicate cement (HCSC). From an evidenced-based perspective, for pulpitis in the absence of symptoms or non-spontaneous pain, either direct pulp capping or pulpotomy (partial/ full) may be considered. Full pulpotomy and pulpectomy based on the evidence may also be considered.
If the pulpitis was associated with spontaneous pain in permanent teeth based on the evidence, ‘we suggested either root canal treatment or full pulpotomy could be effective’
No difference was shown between vital and non-vital teeth in terms of outcome measures; however, ‘we suggested that root canal treatment is performed on teeth with non-vital pulps as soon as the diagnosis is confirmed’.
Evidenced-based recommendations relating to the treatment of immature teeth with apical periodontitis
The management of immature teeth differs in relation to the treatment of apical periodontitis, as conventional root canal preparation and filling is not possible using conventional techniques:
‘For patients with immature permanent teeth and pulp necrosis ± apical periodontitis, the HCSC apical plug technique or revitalisation procedures may be considered
‘At present, we do not know whether endodontic tissue engineering represents a valid treatment option as further clinical evidence and research is required’.
Evidenced-based recommendations
relating to the non-surgical treatment of mature teeth with apical periodontitis
When considering the non-surgical treatment of apical periodontitis in mature teeth, various aspects of management were considered, including root canal
instrumentation, dressing, irrigation, filling and adjunct aids (Table 4):
‘In terms of instrumentation, for patients with apical periodontitis, any tested type of engine-driven nickel titanium (NiTi) instruments may be considered for root canal preparation, as there was no evidence suggestive of an advantage of one particular file system over another
For irrigation, in patients with asymptomatic apical periodontitis in permanent teeth, an open recommendation of sodium hypochlorite followed by ethylenediaminetetraacetic acid (EDTA), and may be considered
With respect to interim dressing, a strong recommendation was made that where adequate clinical procedures had been performed, a single-visit approach without the use of inter appointment calcium hydroxide should be adopted
‘Root canal filling with gutta-percha and sealer using any of the included techniques (cold lateral compaction, warm vertical compaction, carrier-based or single cone) may be considered in combination with
any of the included sealers (epoxy-resin, ZOE or calcium-silicate)’
‘In patients with apical periodontitis, we suggest not to use adjunct therapy in addition to traditionally (syringeneedle based) delivered irrigants. Adjunct therapy would include photoactivated disinfection, direct laser irradiation, ozone therapy and passive ultrasonic activation. At present, there is not comparative outcome evidence to indicate that these are more effective than conventional techniques’
Finally, in patients with pulp necrosis in mature permanent teeth, ‘it was suggested not to use revitalisation techniques. This was in contrast to the recommendations made for immature permanent teeth’.
Evidenced-based recommendations relating to the surgical treatment of mature teeth with apical periodontitis
For surgical treatment of apical periodontitis in mature teeth, various aspects were considered, including comparison of surgery with non-surgical root canal treatment/ retreatment, effectiveness of root resection
Table 4 Key recommendation – non-surgical treatment of apical periodontitis
Intervention
Grade and evidence-based recommendations
Instrumentation performed with contemporary techniques versus ‘traditional’ stainless-steel instruments technique
– Weak (介)
– We suggest root canal preparation should be performed using contemporary engine-driven techniques with NiTi root canal instruments
– Quality of the evidence:
– Survival, postoperative pain: Moderate
– Radiographic healing: Low
Irrigation with any root canal irrigant(s) and sequence versus irrigation with NaOCl and EDTA
– Open ( )
– followed by EDTA, and may be considered
– Quality of evidence:
– Postoperative pain and radiographic healing: Very low ⊕ ΘΘΘ
Intracanal dressing with any root canal dressing(s) versus calcium hydroxide versus no dressing
– Strong (介 )
– Where adequate clinical procedures have been performed, we recommend using a single-visit approach without the use of interappointment calcium hydroxide
– Quality of evidence:
– Radiographic healing: Moderate
Root canal filling with any other type of sealer versus epoxy resin (AH Plus/AH 26) using gutta-percha
– Open ( ⇔ )
– Root canal filling with gutta-percha in combination with any of the included sealers (epoxy resin, ZOE or calcium silicate) may be considered
Root canal filling with any type of non-lateral compaction technique versus cold lateral compaction technique using gutta-percha
– Open ( ⇔ )
– Root canal filling with gutta-percha and sealer using any of the included techniques (cold lateral compaction, warm vertical compaction, carrier based or single cone) may be considered
Adjunct therapy versus traditional syringe and needle irrigants delivery
– Weak ( ⇓ )
– We suggest not to use adjunct therapy in addition to traditionally (syringe-needle-based) delivered irrigants
– Quality of evidence:
– Pain and radiographic healing Low
Table 5 Key recommendations – surgical treatment of apical periodontitis
Intervention
Grade and evidence-based recommendations
Expert consensus-based recommendations
Surgical versus non-surgical root canal treatment/retreatment
– Open ( ⇔ )
– When non-surgical root canal treatment or retreatment is impractical, apical surgery may be considered for the management of permanent teeth with apical periodontitis
– Quality of evidence:
– Tooth survival: Low
Root resection versus non-surgical root canal retreatment or apical surgery
– Weak (⇓)
– We do not suggest root resection techniques as an alternative to non-surgical root canal retreatment or apical surgery in the management of permanent teeth with apical periodontitis
– Quality of evidence:
– Tooth survival: Very low ⊕ Θ
Intentional replantation versus non-surgical root canal treatment/ retreatment or apical surgery
– Weak ( ⇓ )
– We do not suggest intentional tooth replantation as a routine alternative to nonsurgical root canal treatment/retreatment or apical surgery for managing permanent teeth with apical periodontitis
– Quality of evidence:
– No comparative studies identified
Non-comparative clinical studies reported high overall survival rates in the mid- to long-term, with relatively low complication rates. Therefore, in the absence of other treatment alternatives and rather than extraction, if anatomical conditions permit atraumatic extraction and an extra-oral time of less than 15 minutes, then intentional replantation may be considered for the management of permanent teeth with apical periodontitis
and the effectiveness of intentional reimplantation (Table 5):
‘The evidence did not suggest a difference in the effectiveness of apical surgery, compared with non-surgical root canal treatment or retreatment, in terms of clinical, radiological, and patient-related outcomes, for managing permanent teeth with apical periodontitis. Therefore, when non-surgical root canal treatment or retreatment are impractical, apical surgery may be considered for the management of permanent teeth with apical periodontitis
Due to a lack of comparative evidence, ‘root resection and intentional replantation techniques were not suggested as an alternative to non-surgical root canal retreatment or apical surgery in the management of permanent teeth with apical periodontitis. However, due to the presence of non-comparative data supporting its use intentional replantation procedures could be considered as a clinical option.’
Implementation, dissemination and update
Further to the publication of the open-access CPG accompanied by 14 SRs in a special issue of the International Endodontic Journal, a layered communication plan was ratified by the ESE Executive Board and delegated to the ESE Benefits of Endodontics Committee. This included:
A programme of adoption and adaptation by 37 ESE national member societies,
including translation into selected languages, including French, Italian, Spanish, German, Chinese and Polish
Dissemination of the findings in designated symposia sessions at ESE conferences (Helsinki 2023 and Krakow 2024)
Publication of simple ‘bite-sized’ outputs from the guidelines through the ESE communications committee. As the CPG is an evidenced-based document that will need to be updated as new evidence emerges, it is planned that the guideline is valid for five years until at least 2028.
Perspectives and summary
The CPG is the first comprehensive guideline for the diagnosis and treatment of pulpitis and apical periodontitis that follows the structured S3-level procedure. It covers the principal components of endodontic treatment but does not cover all aspects of endodontic care, including periodontal endodontic lesions, vertical root fractures, dental traumatic injuries and resorption, among others. It is hoped that these will be covered in future S3-level projects or in traditional position statement format.
The recommendations not only list current evidenced-based knowledge in the discipline but also highlights gaps in knowledge and areas for further priority and research. The next steps will be to engage in a period of activity to disseminate the findings of these guidelines to endodontists, dentists, and relevant stakeholders, including students and patients.
Ethics declaration
The authors declare no conflicts of interest.
Author contributions
HFD and IEK both made substantial contributions to the manuscript and approved the final version of the text.
Funding information
University of Dublin, Trinity College Open Access funding provided by the IReL Consortium.
References
Duncan H F, Kirkevang L L, Peters O A et al. Treatment of pulpal and apical disease: the European Society of Endodontology (ESE) S3-level clinical practice guideline. Int Endod J 2023; DOI: 10.1111/iej.13974.
European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J 2006; 39: 921-930.
Guyatt G H, Oxman A D, Kunz R et al. GRADE guidelines: 2. Framing the question and deciding on important outcomes. J Clin Epidemiol 2011; 64: 395-400.
Sanz M, Herrera D, Kebschull M etal. Treatment of stage I-III periodontitis – the EFP S3 level clinical practice guideline. J Clin Periodontol 2020; DOI: 10.1111/ јсре. 13290.
Kebschull M, Chapple I. Evidence-based, personalised and minimally invasive treatment for periodontitis patients – the new EFP S3-level clinical treatment guidelines. BrDent J 2020; 229: 443-449.
Duncan H F, Galler K M, Tomson P L et al. European Society of Endodontology position statement: management of deep caries and the exposed pulp. Int Endod J 2019; 52: 923-934.
Nothacker M J, Muche-Borowski C, Kopp I B. Guidelines in the register of the Association of Scientific Medical Societies in Germany – a quality improvement campaign. Geburtshilfe Frauenheilkd 2014; 74: 260-266.
Tibúrcio-Machado C S, Michelon C, Zanatta F B, Gomes M S, Marin J A, Bier C A. The global prevalence of apical periodontitis: a systematic review and meta-analysis. Int Endod J 2021; 54: 712-735.
German Association of the Scientific Medical Societies and Standing Guidelines Commission. AWMF guidance manual and rules for guideline development. 2012. Available at http://www.awmf.org/leitlinien/awmfregelwerk.html (accessed September 2024).
Duncan H F, Nagendrababu V, El-Karim I, Dummer P M H. Outcome measures to assess the effectiveness of endodontic treatment for pulpitis and apical periodontitis for use in the development of European Society of Endodontology S3-level clinical practice guidelines: a consensus-based development. Int Endod J 2021; 54: 2184-2194.
El Karim I A, Duncan H F, Cushley S et al. A protocol for the development of Core Outcome Sets for Endodontic Treatment modalities (COSET): an international consensus process. Trials 2021; 22: 812.
Duncan H F, Nagendrababu V, El-Karim I A, Dummer P M H. Outcome measures to assess the effectiveness of endodontic treatment for pulpitis and apical periodontitis for use in the development of European Society of Endodontology (ESE) S3 level clinical practice guidelines: a protocol. Int Endod J 2021; 54: 646-654.
Doğramacı E J, Rossi-Fedele G. Patient-related outcomes and oral health-related quality of life in endodontics. Int Endod J 2023; DOI: 10.1111/iej.13830.
Bucchi C, Rosen E, Taschieri S. Non-surgical root canal treatment and retreatment versus apical surgery in treating apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13793.
Bürklein , Arias A. Effectiveness of root canal instrumentation for the treatment of apical periodontitis: a systematic review and meta-analysis. Int Endod J 2023; DOI: 10.1111/iej. 13782.
Corbella S, Walter C, Tsesis I. Effectiveness of root resection techniques compared with root canal retreatment or apical surgery for the treatment of apical periodontitis and tooth survival: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13808.
Donnermeyer D, Dammaschke T, Lipski M, Schäfer E. Effectiveness of diagnosing pulpitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13762.
Hilmi A, Patel S, Mirza K, Galicia J C. Efficacy of imaging techniques for the diagnosis of apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/ iej.13921.
Jakovljevic A, Jaćimović J, Aminoshariae A, Fransson H. Effectiveness of vital pulp treatment in managing nontraumatic pulpitis associated with no or nonspontaneous pain: a systematic review. Int Endod J 2023; DOI: 10.1111/iej.13776.
Meire M A, Bronzato J D, Bomfim R A, Gomes B P F A. Effectiveness of adjunct therapy for the treatment of apical periodontitis: a systematic review and metaanalysis. Int Endod J 2023; DOI: 10.1111/iej. 13838.
Meschi N, Palma P J, Cabanillas-Balsera D. Effectiveness of revitalization in treating apical periodontitis: a systematic review and meta-analysis. Int Endod J 2023; DOI: 10.1111/iej.13778.
Pirani C, Camilleri J. Effectiveness of root canal filling materials and techniques for treatment of apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej.13787.
Plotino G, Abella Sans F, Bastos J V, Nagendrababu V. Effectiveness of intentional replantation in managing teeth with apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej.13727.
Rossi-Fedele G, Ng Y-L. Effectiveness of root canal treatment for vital pulps compared with necrotic pulps in the presence or absence of signs of periradicular pathosis: a systematic review and meta-analysis. Int Endod J 2023; DOI: 10.1111/iej. 13833.
Rossi-Fedele G, Rödig T. Effectiveness of root canal irrigation and dressing for the treatment of apical periodontitis: a systematic review and meta-analysis of clinical trials. Int Endod J 2023; DOI: 10.1111/ iej. 13777.
Tomson P L, Vilela Bastos J, Jacimovic J, Jakovljevic A, Pulikkotil S J, Nagendrababu V. Effectiveness of pulpotomy compared with root canal treatment in managing non-traumatic pulpitis associated with spontaneous pain: a systematic review and metaanalysis. Int Endod J 2023; DOI: 10.1111/iej. 13844.
Widbiller M, Knüttel H, Meschi N, Durán-Sindreu Terol F. Effectiveness of endodontic tissue engineering in treatment of apical periodontitis: a systematic review. Int Endod J 2023; DOI: 10.1111/iej. 13784.
Murphy M K, Black N A, Lamping D L et al. Consensus development methods, and their use in clinical guideline development. Health Technol Assess 1998; 2: 1-88
Segura-Egea J J, Gould K, Şen B H et al. European Society of Endodontology position statement: the use of antibiotics in endodontics. Int Endod J 2018; 51: 20-25.
De Moor R, Hülsmann M, Kirkevang L-L, Tanalp J, Whitworth J. Undergraduate curriculum guidelines for endodontology. Int Endod J 2013; 46: 1105-1114.
Gulabivala K, Ahlquist M, Cunnington Setal. Accreditation of postgraduate speciality training programmes in endodontology. Minimum criteria for training specialists in endodontology within Europe. Int Endod J 2010; 43: 725-737.
American Association of Endodontists. AAE endodontic case difficulty assessment form and guidelines. 2022. Available at https://www.aae.org/ specialty/wp-content/uploads/sites/2/2022/01/ CaseDifficultyAssessmentFormFINAL2022.pdf (accessed December 2024).
Duncan H F. Present status and future directions – vital pulp treatment and pulp preservation strategies. Int Endod J 2022; DOI: 10.1111/iej. 13688.
Schunemann H J, Wiercioch W, Brozek J et al. GRADE evidence to decision (EtD) frameworks for adoption, adaptation, and de novo development of trustworthy recommendations: GRADE-ADOLOPMENT. J Clin Epidemiol 2017; 81: 101-110.
Open Access.
Division of Restorative Dentistry and Periodontology, Trinity College Dublin, Dublin Dental University Hospital, Dublin, Ireland; School of Medicine Dentistry and Biomedical Sciences, Queen’s University Belfast, Belfast, UK.
*Correspondence to: Henry F. Duncan
Email address: Hal.Duncan@dental.tcd.ie
Refereed Paper.
Submitted 10 October 2024
Revised 5 December 2024
Accepted 14 December 2024 https://doi.org/10.1038/s41415-025-8335-x