التوجيه بالاتصال في نبضات ثيتا المتقطعة مقابل التحفيز المغناطيسي عبر الجمجمة المتكرر لعلاج الاكتئاب المقاوم للعلاج: تجربة عشوائية محكومة Connectivity-guided intermittent theta burst versus repetitive transcranial magnetic stimulation for treatment-resistant depression: a randomized controlled trial
التوجيه بالاتصال في نبضات ثيتا المتقطعة مقابل التحفيز المغناطيسي عبر الجمجمة المتكرر لعلاج الاكتئاب المقاوم للعلاج: تجربة عشوائية محكومة
تاريخ الاستلام: 29 يونيو 2023
تاريخ القبول: 12 ديسمبر 2023
تاريخ النشر على الإنترنت: 16 يناير 2024
(ط) تحقق من التحديثات
تظهر قائمة المؤلفين وانتماءاتهم في نهاية الورقة
الاضطراب في الاتصال المتبادل بين القشرة الحزامية الأمامية اليمنى والقشرة الجبهية الجانبية اليسرى مرتبط بالاكتئاب وقد يكون هدفًا للتعديل العصبي. في تجربة عشوائية محكومة مزدوجة التعمية عبر خمسة مراكز، قمنا بتخصيص التحفيز المغناطيسي المتقطع الموجه بالاتصال (cgiTBS) باستخدام تصوير الرنين المغناطيسي الوظيفي في حالة الراحة في موقع بناءً على الاتصال الفعال من القشرة الحزامية الأمامية اليمنى إلى القشرة الجبهية الجانبية اليسرى. اختبرنا فعاليته في تقليل أعراض الاكتئاب المقاسة بمقياس تقييم الاكتئاب هاملتون GRID المكون من 17 عنصرًا على مدى 8 و16 و26 أسبوعًا، مقارنةً بالتحفيز المغناطيسي المتكرر عبر الجمجمة (rTMS) الموجه بتصوير الرنين المغناطيسي الهيكلي (MRI) المقدم في موقع التحفيز القياسي (F3) لدى المرضى الذين يعانون من ‘الاكتئاب المقاوم للعلاج’. تم تعيين المشاركين عشوائيًا إلى 20 جلسة على مدى أسابيع من إما cgiTBS ( ) أو rTMS ( ) مع تصوير الرنين المغناطيسي الوظيفي في حالة الراحة في البداية و16 أسبوعًا. لوحظت انخفاضات مستمرة في أعراض الاكتئاب على مدى 26 أسبوعًا، دون وجود اختلافات بين المجموعتين في النتيجة الأساسية لمقياس تقييم الاكتئاب هاملتون GRID المكون من 17 عنصرًا (المتوسط المعدل حسب النية للعلاج، -0.31، فترة الثقة 95% (CI) ). كان هناك حدثان سلبيان خطيران قد يكونان مرتبطين بالتحفيز المغناطيسي (الهوس والذهان). كانت فعالية cgiTBS وrTMS متساوية في المرضى الذين يعانون من الاكتئاب المقاوم للعلاج على مدى 26 أسبوعًا (رقم تسجيل التجربة ISRCTN19674644).
تعتبر مضادات الاكتئاب والعلاج النفسي فعالة في علاج اضطراب الاكتئاب الشديد المعتدل إلى الشديد (MDD) . ومع ذلك، فإن نسبة من الأفراد الذين يعانون من MDD لديهم ‘اكتئاب مقاوم للعلاج’ (TRD)، حيث من المرضى في الرعاية المتخصصة و في الرعاية الأولية لم يستجيبوا بشكل كافٍ لتجربتين من مضادات الاكتئاب .
يستخدم التحفيز المغناطيسي المتكرر عبر الجمجمة نبضات مغناطيسية قوية لتغيير النشاط في الدوائر العصبية في الدماغ المرتبطة بـ
فسيولوجيا الاكتئاب. يُعتبر التحفيز المغناطيسي المتكرر عالي التردد إلى القشرة الجبهية الجانبية اليسرى (IDLPFC) أحد البروتوكولات الأكثر استخدامًا في . يستخدم TBS دفعات من النبضات المغناطيسية التي تحاكي إيقاعات ثيتا الذاتية التي قد تحفز اللدونة في مناطق الدماغ الأكثر بعدًا . أكدت دراسة تحليلية شاملة فعالية وسلامة كل من rTMS وTBS لعلاج TRD . أظهرت تجربة THREE-D السريرية متعددة المراكز أن مدة الإدارة الأقصر لـ iTBS لم تكن أقل فعالية
من rTMS طويل المدة المطبق على IDLPFC في تقليل أعراض الاكتئاب حتى 12 أسبوعًا بعد العلاج، ولكن لا توجد بيانات عن المتابعة على المدى الطويل .
وافقت إدارة الغذاء والدواء الأمريكية على rTMS لعلاج الاكتئاب في عام 2008 بعد تأكيد فعاليته في تجربة سريرية عشوائية عالمية شملت 23 موقعًا . وافق المعهد الوطني للصحة والرعاية الممتازة على TMS لعلاج MDD وTRD في خدمة الصحة الوطنية في إنجلترا في عام 2015 (المرجع 8). على الرغم من استخدامه بشكل أوسع في خدمات الصحة النفسية عبر أمريكا الشمالية، إلا أن تطبيقه في الممارسة الروتينية للصحة النفسية في مناطق أخرى من العالم أقل انتظامًا. في إنجلترا، يتوفر TMS في واحدة من كل سبع خدمات للصحة النفسية ولم يُوصى باستخدامه في بعض البلدان مثل فرنسا، على الرغم من استناد ذلك إلى مراجعة مشكوك فيها للأدلة . لذلك، لم تكن قاعدة الأدلة حتى الآن مقنعة بما فيه الكفاية لتؤدي إلى تنفيذ واسع النطاق أو دعم تنظيمي في خدمات الصحة النفسية المتخصصة على مستوى العالم. قد يكون أحد الأسباب لذلك هو أن التأثيرات على TRD تُعتبر قصيرة الأمد بسبب نقص الأدلة من تجارب عشوائية كبيرة وعالية الجودة مع مدة متابعة كافية .
يمكن تقسيم الدماغ إلى شبكات من المناطق التي تؤدي وظائف منفصلة، وتغيرات الاتصال الدماغي كما تم اكتشافها بواسطة تصوير الرنين المغناطيسي الوظيفي في حالة الراحة (rsfMRI) يمكن أن تخصّص العلاج العصبي لـ MDD . قد يؤدي تحفيز TMS لـ IDLPFC (عقدة رئيسية في الشبكة التنفيذية المركزية (CEN)) إلى تعديل العقد الرئيسية داخل شبكة البروز والشبكة الافتراضية (DMN)، مما يؤدي إلى إعادة توازن الاتصال الوظيفي غير الطبيعي (المُحتسب من خلال ارتباط مسارات مستوى الأكسجين في الدم باستخدام rsfMRI من مناطق مختلفة من الدماغ) بين هذه الشبكات وداخلها . ومع ذلك، هناك تباين فردي في الاتصال الوظيفي لـ IDLPFC مع هذه العقد , مما يشير إلى أن نهجًا مخصصًا لاستهداف موقع تقديم TMS قد يحسن إما معدلات الاستجابة أو مدة الاستجابة مقارنةً بموقع تحفيز موحد ومعياري يُستخدم على نطاق واسع في الممارسة السريرية مع TMS لعلاج الاكتئاب. أدت تجربتان عشوائيتان صغيرتان من rTMS أو iTBS المخصصة والمعجلة، بناءً على الاتصال الوظيفي بين القشرة الحزامية الأمامية تحت الجينية وIDLPFC، إلى استجابات أكبر في الاكتئاب على مدى 3-4 أسابيع مقارنةً بـ TBS الموحد أو الوهمي .
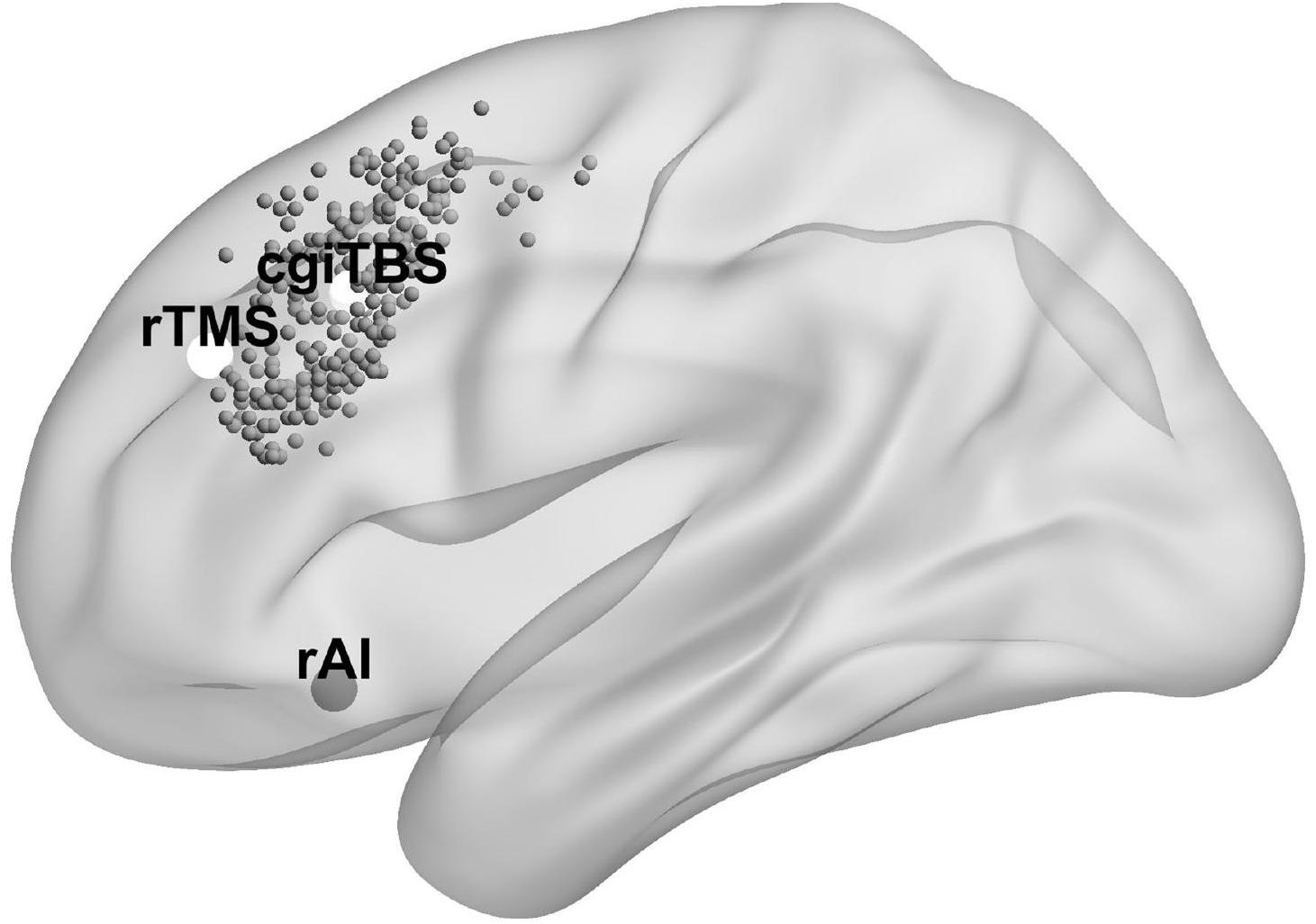
تم العثور على اضطراب في الحلقة المتبادلة بين DLPFC والجزيرة (عقدة رئيسية في شبكة البروز) في الاكتئاب , لذا قد تمثل الجزيرة هدفًا آخر للتعديل العصبي المخصص. وجدت تجربة عشوائية محكومة في 27 متطوعًا صحيًا أن iTBS الموجه إلى هدف قائم على الاتصال في IDLPFC مع أقصى تأثير سلبي من الجزيرة الأمامية اليمنى (rAI) حسّن الاتصال بين الجبهة والجزيرة . في تجربة عشوائية محكومة صغيرة تضم 18 مريضًا يعانون من TRD تقارن بين cgiTBS والتحفيز المتكرر الموجه بالاتصال (cgrTMS)، أظهرت معدل الاستجابة (انخفاض بنسبة 50% في أعراض الاكتئاب) زيادة غير دالة إحصائيًا من 1 إلى 3 أشهر في مجموعة cgiTBS ولكنها انخفضت في مجموعة cgrTMS . في كلا مجموعتي العلاج، حيث تم تخصيص تحفيز TMS/TBS باستخدام الاتصال الفعال (نوع من الاتصال الوظيفي الذي يتم فيه استنتاج الاتجاه من تحليل التوقيت لسلاسل الوقت الإقليمية ), كان توازن التأثير بين rAI وIDLPFC متنبئًا بتحسن بعد دورة من . تشير هذه النتائج إلى أن cgiTBS، المخصصة بناءً على أقصى اتصال فعال من rAI إلى IDLPFC، قد تؤدي إلى فعالية أطول من rTMS في الموقع القياسي، مما يسمح للأشخاص الذين يعانون من TRD بالبقاء بصحة جيدة لفترة أطول. ومع ذلك، هناك حاجة إلى بيانات مع متابعة أطول من تلك التي تم إجراؤها سابقًا.
كانت تجربة BRIGhTMIND تجربة سريرية متعددة المراكز، مجموعة متوازية، مزدوجة التعمية، عشوائية، محكومة. كانت فرضيتنا السريرية الأساسية هي أن cgiTBS الموجه بواسطة rsfMRI، بناءً على الاتصال الفعال من rAI إلى IDLPFC، سيكون أكثر فعالية في تقليل أعراض الاكتئاب على مدى 8 و16 و26 أسبوعًا مقارنةً بـ rTMS الموجه بتصوير الرنين المغناطيسي الهيكلي المقدم في الموقع القياسي
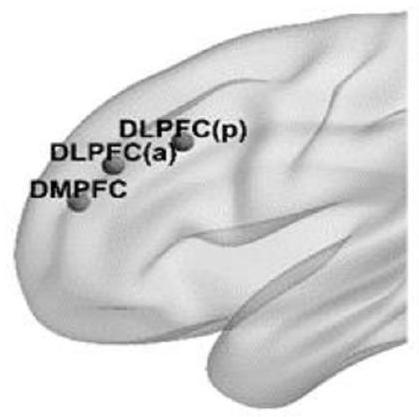
(موقع F3 من تسميات مواقع الأقطاب الكهربائية 10-20) لدى المرضى الذين يعانون من TRD. على الرغم من استخدام موقع قياسي لـ rTMS، تم تخصيص موقع ذلك الموقع F3 باستخدام تصوير الرنين المغناطيسي الهيكلي. كانت الفرضيات الميكانيكية الأساسية التي تستخدم fMRI هي: (1) الاتصال الفعال الأساسي من rAI إلى IDLPFC، أو أن توازن التأثير بين هاتين المنطقتين سيعدل، أو يرتبط، بتحسن في أعراض الاكتئاب على مدى 26 أسبوعًا؛ و(2) سيكون تقليل الاتصال الوظيفي بين IDLPFC والقشرة الجبهية الظهرية اليسرى (IDMPFC) مرتبطًا بتحسن في أعراض الاكتئاب كما وجد في كل من عملنا التجريبي ودراسة أخرى .
النتائج
توزيع المرضى
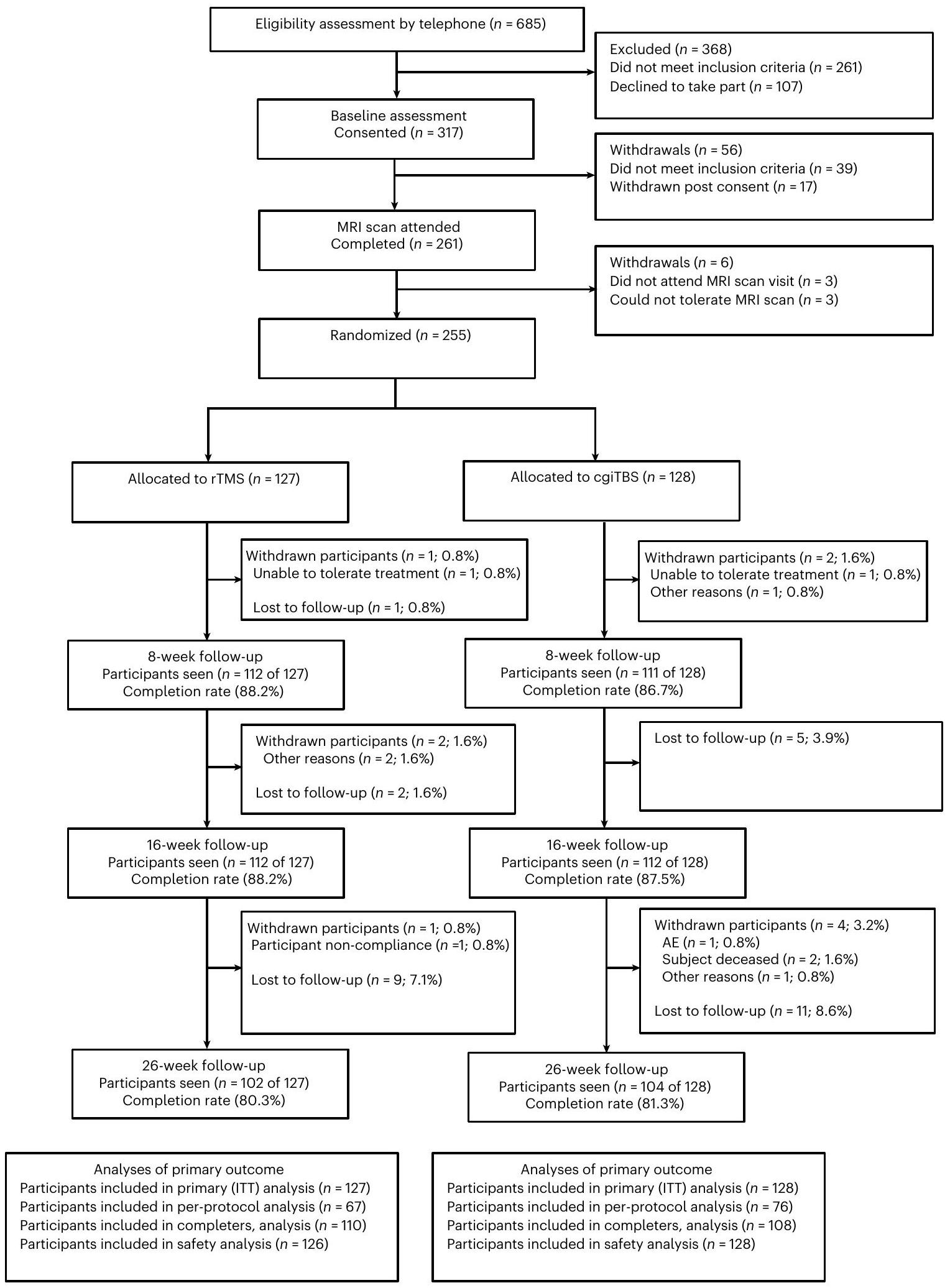
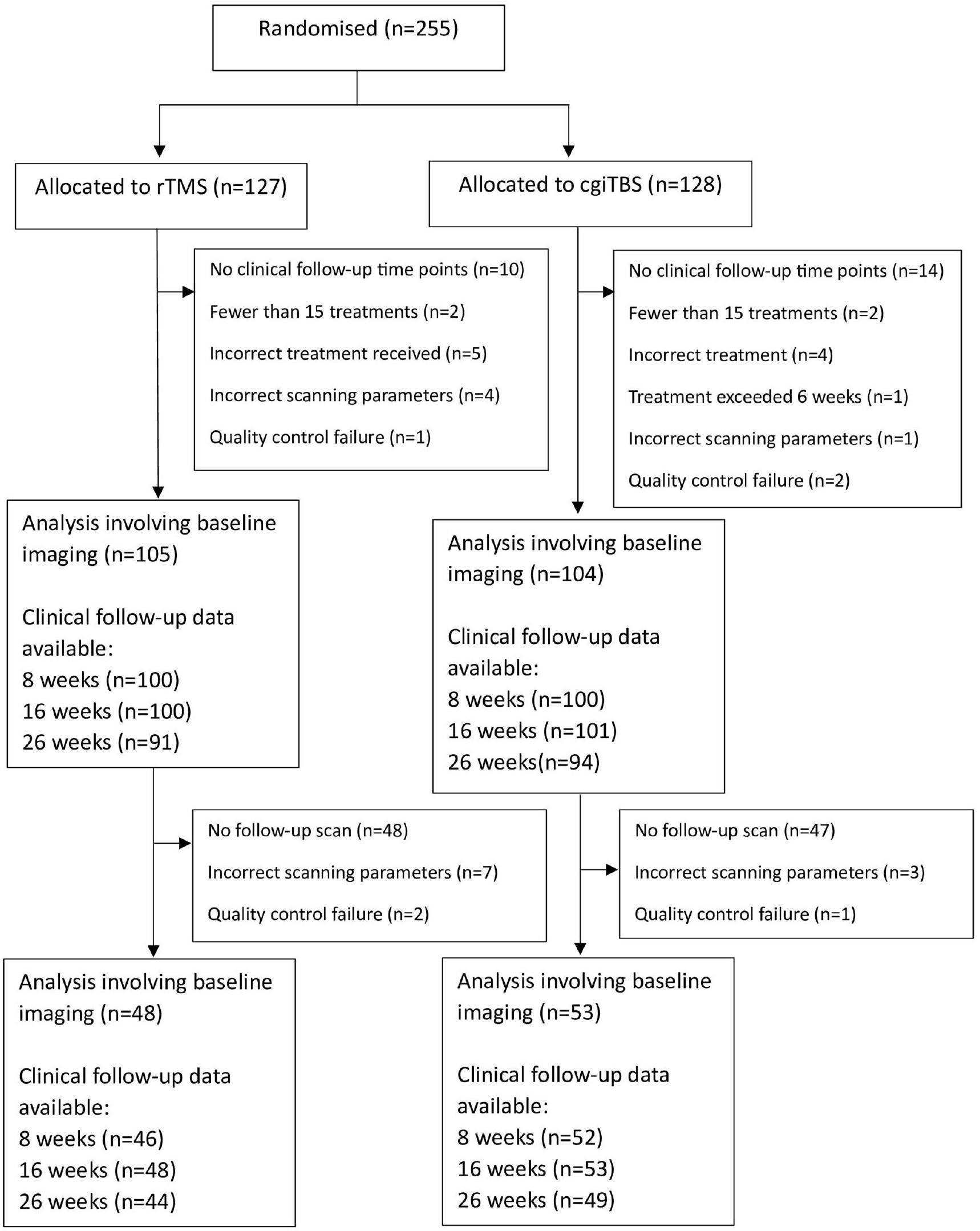
بين 22 يناير 2019 و31 يناير 2022، تم تحديد 685 فردًا وأكملوا الفحص الأولي للهاتف لتحديد الأهلية لتجربة BRIGhTMIND (الشكل 1). تم تعليق التوظيف في الدراسة مؤقتًا بين 30 أبريل و1 أغسطس 2020 بسبب جائحة COVID-19. وافق ما مجموعه 317 مشاركًا على التجربة، حيث لم يستوفِ 39 منهم معايير الإدراج وانسحب 23 بين خط الأساس والتوزيع العشوائي. تم توزيع 255 مشاركًا بشكل عشوائي، 127 إلى rTMS و128 إلى cgiTBS، مع تضمين جميع المشاركين الذين تم توزيعهم عشوائيًا في مجموعة النية للعلاج (ITT). في المجموع، أكمل 235 مشاركًا جميع جلسات TMS الـ 20 (92.8٪؛ حيث انسحب مشاركان من كل من مجموعتي rTMS وcgiTBS من التجربة تمامًا خلال العلاج). كما وُجدت معدلات إكمال مماثلة لـ rTMS مقابل cgiTBS بعد 8 أسابيع (rTMS، 112 منضد cgiTBS، 111 من ، 16 أسبوعًا (rTMS، 112 من ضد cgiTBS، 112 من ) و 26 أسبوعًا (rTMS، 102 من مقابل cgiTBS، 104 من ). تم الانتهاء من التقييم النهائي للمتابعة في 3 أغسطس 2022. وفقًا لخطة التحليل المنشورة مسبقًا بالنسبة لـ 255 مشاركًا أكملوا مسح الهيكل الأساسي ومسح rsfMRI وبدؤوا العلاج بالتحفيز المغناطيسي عبر الجمجمة، كان هناك 209 ( ) تم تضمينها في تحليل الصورة. من بين 114 مشاركًا أكملوا مسح الخط الأساسي ومسح المتابعة بعد 16 أسبوعًا، كان 101 ( تم تحليلها (الشكل البياني الموسع 1).
كان هناك حالتان غير مقصودتين لكشف نتيجة مقيم النتائج وواحدة لمحقق رئيسي عن علاج أحد المشاركين. فيما يتعلق بتخمينات الباحثين، كانت الغالبية العظمى من توقعات تخصيص العلاج هي ‘لا أعرف’، بمعدلات إجمالية تبلغ 84.8 و79.5 وفي 8 و16 و26 أسبوعًا، على التوالي (الجدول البياني الموسع 1).
في البداية، كان متوسط عمر المشاركين 43.7 سنة (الانحراف المعياري 14.0)، معنساء ومن العرق الأبيض (الجدول 1). كانت مدة الحلقة الحالية من الاكتئاب 6.1 سنوات (نطاق الربيع بين الربعين (IQR) 2.1، 12.9) وكان العدد الوسيط للحلقات الاكتئابية اثنتين (IQR 1، 4). تم تصنيف خمسة وتسعين مشاركًا (37.3%) على أنهم مقاومون للعلاج بدرجة عالية (عدم الاستجابة لأكثر من حوالي ستة علاجات) وفقًا لدرجة تصنيف الاكتئاب المقاوم للعلاج المعدلة من مستشفى ماساتشوستس العام (MGH). )، 73 ( ) كمقاومة متوسطة للعلاج (عدم الاستجابة لحوالي أربعة أو خمسة علاجات) و 87 (34.1%) كمقاومة منخفضة للعلاج (عدم الاستجابة لعلاجين أو ثلاثة)، مع 198 مشاركًا (77.6%) يتناولون مضادات الاكتئاب حاليًا. كانت متوسط درجات الأساس على المتغير الأساسي – النسخة GRID من مقياس هاملتون لتقييم الاكتئاب المكون من 17 عنصرًا (GRID-HDRS-17؛ المرجع 24) – 23.9 (الانحراف المعياري 4.7) لمجموعة rTMS و 22.9 (الانحراف المعياري 4.7) لمجموعة cgiTBS (الجدولان 2 و 3). أظهر تقييم موثوقية بين المقيمين لتقييم النتائج، الذي تم إكماله عبر مراكز العلاج، معامل ارتباط داخلي قدره 0.94 بين درجات GRID-HDRS-17، مع فترة مرجعية بنسبة 95% للاختلاف (بين أي زوج من المقيمين) تتراوح بين 0.66-0.99. عبر كلا مجموعتي العلاج، كانت المسافة الوسيطة بين نقطة التحفيز المقصودة على فروة الرأس ونقطة التحفيز الفعلية، أو بين نقطة التحفيز الفعلية في الجلسة الأولى والجلسات اللاحقة، حوالي 0.5 سم، وكان الفرق الوسيط في الزاوية حوالي (الجدول البياني الموسع 2؛ مواقع التحفيز موضحة في الشكل البياني الموسع 2).
الشكل 1| مخطط تدفق المشاركين خلال التجربة. مخطط CONSORT لجميع المشاركين الذين تم تقييمهم من حيث الأهلية للتجربة، وتم توزيعهم عشوائيًا على التحفيز المغناطيسي عبر الجمجمة المتكرر أو التحفيز المتقطع الموجه بالاتصال وتمت متابعتهم لمدة تصل إلى 26 أسبوعًا.
النتيجة الرئيسية
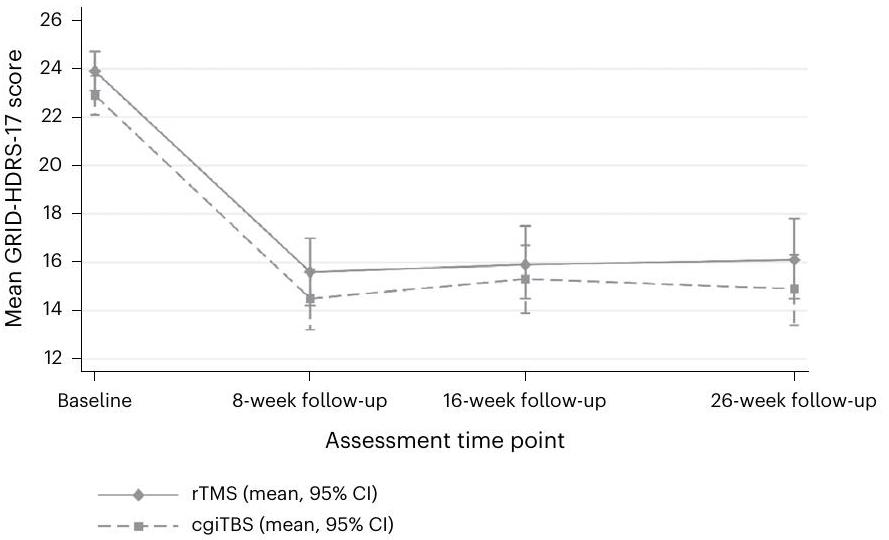
كما هو موضح في الجدولين 2 و 3، لم يكن الفرق المتوسط المعدل لـ GRID-HDRS-17 على مدى 26 أسبوعًا ذا دلالة إحصائية ولم يكن مهمًا سريريًا (فرق أقل من 3 نقاط) ) بين مجموعات علاج rTMS و cgiTBS للتحليل الأساسي ( -0.31 (95% إلى 1.24) ).
بعد 8 أسابيع من التوزيع العشوائي، أظهرت كلا مجموعتي العلاج انخفاضًا سريريًا كبيرًا ( (المرجع 26)، rTMS 8.3، cgiTBS 8.4) في متوسط درجات GRID-HDRS-17 التي تم الحفاظ عليها عند 16 أسبوعًا (rTMS 8.0، cgiTBS 7.6) و 26 أسبوعًا (rTMS 7.8، cgiTBS 8.0؛ الجداول 2 و 3 والشكل 2).
الجدول 1 | الخصائص الأساسية للمشاركين
خصائص
تحفيز الدماغ المتكرر عبر المغناطيسية (rTMS) )
cgiTBS ( )
العمر (سنوات) المتوسط (الانحراف المعياري)
٤٣.٨ (١٣.١)
٤٣.٧ (١٥.٠)
الجنس (%)
رجال
65 (51.2%)
58 (45.3%)
نساء
62 (48.8%)
70 (54.7%)
العرق (ن(%))
بريطاني أبيض
106 (83.5%)
١٠٨ (٨٤.٤٪)
الأيرلندي الأبيض
4 (3.1%)
1 (0.8%)
الأبيض الآخر
6 (4.7%)
7 (5.5%)
الأفريقي الأبيض والأسود
1 (0.8%)
2 (1.6%)
الأبيض والآسيوي
1 (0.8%)
صفر بالمئة (0%)
مختلط آخر
1 (0.8%)
2 (1.6%)
هندي
4 (3.1%)
2 (1.6%)
باكستاني
2 (1.6%)
2 (1.6%)
بنغلاديشي
0 (0%)
1 (0.8%)
آسيوي آخر
0 (0%)
1 (0.8%)
الكاريبي الأسود
1 (0.8%)
0 (0%)
صيني
0 (0%)
1 (0.8%)
مجموعة عرقية أخرى
1 (0.8%)
1 (0.8%)
الحالة الاجتماعية: متزوج/يعيش معاً (نعم، (%)
76 (59.8%)
55 (43.0%)
المعالون (الأطفال/آخرون) (نعم، (%)
42 (33.1%)
٣٦ (٢٨.١٪)
التوظيف/التعليم (%)
دوام كامل
٣٩ (٣٠.٧٪)
37 (28.9%)
وظائف أخرى
٣٦ (٢٨.٣٪)
٢٦ (٢٠.٣٪)
متقاعد
13 (10.2%)
17 (13.3%)
عاطل عن العمل
٣٩ (٣٠.٧٪)
48 (37.5%)
استلام المزايا (نعم، (%)
52 (40.9%)
٤٥ (٣٥.٢٪)
مدة نوبة الاكتئاب الكبرى الحالية (بالشهور)
١١٧
١٢٢
الوسيط (المدى interquartile)
69.7 (27.9, 129.0)
79.3 (24.9, 163.3)
عدد نوبات الاكتئاب
84
91
الوسيط (المدى interquartile)
2.0 (1.0, 4.0)
1.0 (1.0، 4.0)
المؤشرات الأساسية لجودة المنتج (المستجيبين)
١٢٠
١٢٠
المتوسط (الانحراف المعياري)
٤٧.١ (١٧.٤)
٤٥.١ (١٦.٢)
عدد المشاركين الذين لديهم تاريخ علاجي
127
128
فئة درجة الاكتئاب المقاوم للعلاج في خط الأساس MGH (%)
منخفض، 2.0-3.5
42 (33.1%)
٤٥ (٣٥.٢٪)
متوسط، 4-6
٣٦ (٢٨.٣٪)
37 (28.9%)
عالي
49 (38.6%)
46 (35.9%)
استخدام الأدوية الأساسية
مضادات الاكتئاب
94 (74.0%)
104 (81.3%)
مضادات الاكتئاب ثلاثية الحلقات
10 (7.9%)
11 (8.6%)
مثبطات أكسيداز أحادي الأمين
1 (0.8%)
0 (0%)
مثبطات امتصاص السيروتونين الانتقائية
41 (32.3%)
46 (35.9%)
SNRI
31 (24.4%)
٣٩ (٣٠.٥٪)
آخر
34 (26.8%)
٣٦ (٢٨.١٪)
تركيبة مضادات الاكتئاب
22 (17.3%)
19 (14.8%)
الجدول 1 (مستمر) | الخصائص الأساسية للمشاركين
خصائص
تحفيز الدماغ المتكرر عبر المغناطيسية (rTMS) )
cgiTBS ( )
زيادة مضادات الذهان
19 (15.0%)
23 (18.0%)
زيادة الليثيوم
3 (2.4%)
11 (8.6%)
زيادة الميثيلفينيديت
0 (0%)
1 (0.8%)
زيادة المودافينيل
0 (0%)
1 (0.8%)
زيادة التريودوثيرونين
0 (0%)
3 (2.3%)
المهدئات/أقراص النوم
7 (5.5%)
9 (7.0%)
مهدئات القلق
7 (5.5%)
7 (5.5%)
العلاج بالصدمات الكهربائية خلال نوبة الاكتئاب الحالية (%)
6 (4.7%)
4 (3.1%)
مثبطات أكسيداز أحادي الأمين (MAOIs)؛ مثبطات إعادة امتصاص السيروتونين الانتقائية (SSRIs)؛ مثبطات إعادة امتصاص السيروتونين والنورإبينفرين (SNRIs).تشير الأدوية الأساسية الأخرى إلى مضادات الاكتئاب التالية: ترازودون، بوبروبيون، ميرتازابين، ريبوكستين، أغوميلاتين أو فورتيوكستين). تم تعيين عدد نوبات الاكتئاب الكبرى الحالية كغير محدد للمشاركين الذين تم إدخال عددهم كـ 99. تم حساب مدة نوبات الاكتئاب الكبرى الحالية باستخدام تاريخ التوزيع العشوائي وتاريخ بدء النوبة.
النتائج الثانوية
لم تكن هناك اختلافات كبيرة بين rTMS و cgiTBS في أي من مقاييس النتائج السريرية الثانوية (الجدولين 2 و 3). في متابعة الـ 26 أسبوعًا في كلا المجموعتين، كان 67 (32.5%) من 206 مشاركين مستجيبين.انخفاض في درجة GRID-HDRS-17 الأساسية)، 47 (22.8%) من 206 مشاركًا كانوا في حالة شفاء (على درجة GRID-HDRS-17) من 255 مشاركًا كانوا مستجيبين مستمرين ( انخفاض في الخط الأساسي عند 16 و26 أسبوعًا). في 8 و16 و26 أسبوعًا لكلا مجموعتي العلاج، كانت هناك، في المتوسط، تحسينات مهمة سريريًا في الاكتئاب الذاتي التقييم كما تم قياسه بواسطة استبيان صحة المريض (PHQ-9 (مرجع 27)،نقاط ) ومقياس بيك للاكتئاب – النسخة الثانية (BDI-II نقاط )، مع تحسينات أكبر من الحد الأدنى المهم سريرياً في تقييم اضطراب القلق العام (GAD-7) ( نقاطمقياس العمل والتكيف الاجتماعي (WSAS)، نقاط ) ومقياس الفروق البصرية للصحة العامة المدركة (EQ-5D-5L VAS نقاطأظهرت تحليل الإدراك تحسنًا مع مرور الوقت على أداة THINC-it المدمجة لتحويل الصحة مع الرعاية المتكاملة.للاحتفاظ بالتركيز (مهمة استجابة الاختيار) = 11.28، وظائف التنفيذ (مهمة رسم المسار)وذاكرة العمل (مهمة N-back).
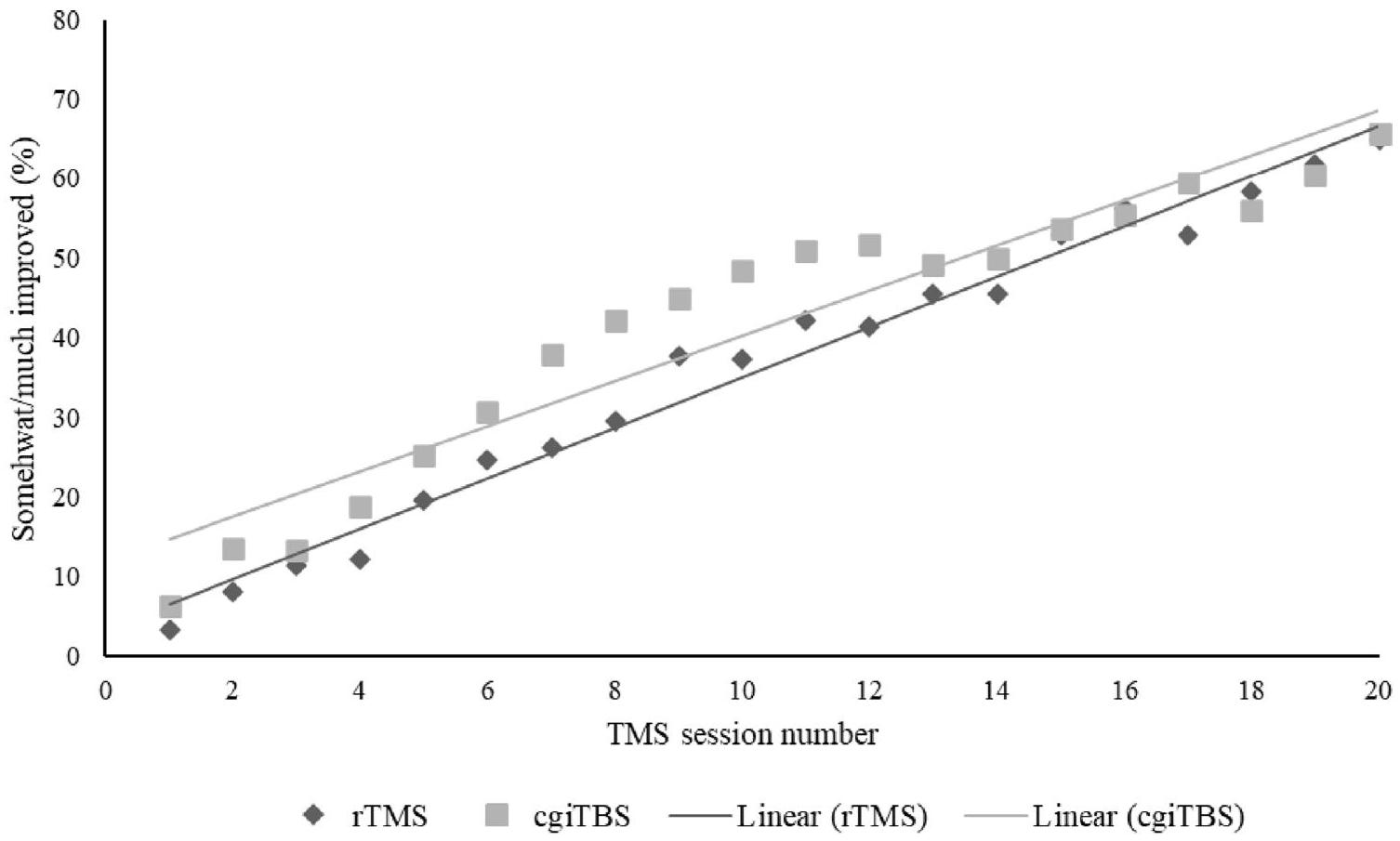
أظهرت انطباعات المشاركين عن تحليل التغيير أنه في الجلسة العاشرة، 105 ( ) من 245 مشاركًا أفادوا بأنهم يشعرون بتحسن ما، أو تحسن كبير. بحلول الجلسة 20، تم الإبلاغ عن ذلك لـ 155 (65.4%) من 237 مشاركًا. كانت العلاقة بين عدد جلسات العلاج والتحسن المدرك تتبع عمومًا اتجاهًا خطيًا لكلا المجموعتين، مع استمرار زيادة النسبة التي تشعر بفائدة حتى في الجلسات 19 و20 (بيانات موسعة الشكل 3).
السلامة
تم استبعاد واحد من كل 255 مشاركًا عشوائيًا من مجموعة السلامة لأنه تعرض لنوبة صرع مشبوهة من النوع الثاني خلال اختبار العتبة الحركية الأول و قبل تقديم أي علاج (الجدول 4). تم الإبلاغ عن سبعة عشر حدثًا ضارًا خطيرًا (SAEs) لـ 12 مشاركًا. كان هناك حالتان وفاة: أحد المشاركين كان يعاني من حالة صحية قلبية أساسية وتوفي بعد إصابته بنوبة قلبية، وشارك آخر توفي بسبب تسمم بالأفيون، حيث خلص تحقيق الطبيب الشرعي إلى أن الوفاة كانت عرضية. كان كلا المشاركين قد أكملوا دورة علاجات التحفيز المغناطيسي عبر الجمجمة (TMS) وتوفيوا بالقرب من تقييم الـ 26 أسبوعًا، مع الإبلاغ عن أن كلا الوفاتين من غير المحتمل أن تكون مرتبطة بعلاجات TMS. تطلبت جميع الأحداث الضارة الخطيرة الأخرى دخول المستشفى. تم الإبلاغ عن حالتين من الأحداث الضارة الخطيرة على أنها قد تكون مرتبطة بعلاج TMS (واحدة في كل ذراع علاج): حلقة نفسية مع قلق شديد واكتئاب.
الجدول 2 | درجات النتائج الأولية والثانوية والاستجابة للعلاج
قياس
خط الأساس
8 أسابيع
16 أسبوع
26 أسبوعًا
cgiTBS مقابل rTMS على مدى 26 أسبوعًا
تحفيز المغناطيسي المتكرر عبر الجمجمةالمتوسط (الانحراف المعياري)
cgiTBSالمتوسط (الانحراف المعياري)
تحفيز المغناطيسي المتكرر عبر الجمجمةالمتوسط (الانحراف المعياري)
cgiTBSالمتوسط (الانحراف المعياري)
تحفيز المغناطيسي المتكرر عبر الجمجمةالمتوسط (الانحراف المعياري)
cgiTBSالمتوسط (الانحراف المعياري)
تحفيز المغناطيسي المتكرر عبر الجمجمةالمتوسط (الانحراف المعياري)
cgiTBSالمتوسط (الانحراف المعياري)
فرق المتوسط المعدل (95% فترة الثقة)
قيمة
تحليل GRID-HDRS-17 الأساسي
127
128
127
128
127
128
127
128
٢٣.٩ (٤.٧)
٢٢.٩ (٤.٧)
15.6 (الخطأ المعياري 0.7؛ 95% فترة الثقة 14.2، 17.0)
14.5 (الخطأ المعياري 0.6؛ 95% فترة الثقة 13.2، 15.7)
15.9 (الخطأ المعياري 0.8؛ 95% فترة الثقة 14.5، 17.5)
15.3 (الخطأ المعياري 0.7؛ 95% فترة الثقة 13.9، 16.7)
14.9 (الخطأ المعياري 0.7؛ 95% فترة الثقة 13.4، 16.3)
-0.31 (-1.87, 1.24)
0.689
BDI-II
127
128
111
١٠٩
١٠٩
١١٠
99
١٠٢
٣٤.٤ (٨.٩)
٣٢.٣ (٨.٨)
٢٣.٥ (١٢.٦)
٢١.٣ (١٠.٧)
٢٤.٧ (١٢.٢)
٢٢.٣ (١٢.٤)
٢٣.٦ (١٢.٦)
٢١.٦ (١٢.٠)
-0.54 (-2.90, 1.82)
0.653
PHQ-9
127
128
111
١٠٩
١٠٩
١٠٩
99
١٠٢
٢٠.٢ (٤.٦)
19.4 (4.4)
١٣.٤ (٧.٥)
١٢.٣ (٦.٣)
١٣.٨ (٧.٢)
١٣.٥ (٧.٣)
١٣.٧ (٧.٦)
١٣.١ (٧.٥)
-0.12 (-1.54, 1.30)
0.871
مقياس القلق العام-7
127
128
111
١٠٩
١٠٩
١٠٨
99
١٠٢
١٣.٣ (٤.٧)
١٣.١ (٤.٦)
9.3 (6.3)
٨.٩ (٤.٩)
9.3 (5.5)
9.1 (5.3)
9.9 (6.1)
8.9 (5.6)
-0.19 (-1.24, 0.86)
0.726
WSAS
127
128
111
١٠٩
١٠٩
١٠٩
99
١٠٢
٢٩.٠ (٦.٨)
٢٧.٦ (٧.٨)
٢٢.١ (١٠.٩)
٢١.٢ (٩.٥)
٢٢.٢ (١٠.٧)
٢٢.٤ (١٠.٢)
٢٢.٢ (١٠.٧)
٢١.٥ (١٠.٨)
0.60 (-1.39, 2.59)
0.554
EQ-5D-5L VAS
127
١٢٨
111
١٠٩
١٠٩
١٠٩
98
١٠٢
٤٣.٠ (١٩.٣)
٤٣.٤ (١٧.١)
٥٢.٨ (٢١.٠)
٥٤.٧ (١٨.٨)
53.2 (20.2)
٥٦.٧ (١٩.٤)
٥٣.٨ (٢١.٢)
٥٥.٨ (٢٠.٥)
1.98 (-1.96, 5.91)
0.325
ثينك-إت
فرق المتوسط المعدل الأساسي بين cgiTBS و rTMS لمدة 16 أسبوعًا (95% CI)
قيمة
وقت استجابة CRT (مللي ثانية)
123
127
غير متوفر
غير متوفر
76
72
غير متوفر
غير متوفر
مفقود
٤
1
717.67 (238.55)
٧٠٨.٠٥ (٢٤٩.٢٥)
606.28 (183.02)
614.12 (210.71)
-1.48 (-55.05, 52.09)
0.957
إجمالي الإجابات الصحيحة في DSST
١٢٢
127
غير متوفر
غير متوفر
76
72
غير متوفر
غير متوفر
مفقود
٥
1
٥١.١٧ (١٨.٢٦)
٤٩.١٥ (٢١.١٨)
٥٥.٧٦ (١٦.٩٣)
٥٢.٣٦ (١٩.٥٩)
-4.25 (-8.56, .062)
0.053
إجمالي صحيح N-back
١٢٢
١٢٦
غير متوفر
غير متوفر
76
72
غير متوفر
غير متوفر
مفقود
٥
2
٢٢.٨٢ (١٠.٨١)
٢١.٥٦ (٩.٦٦)
٢٥.٢٨ (٩.٢٥)
٢٤.٥٦ (٩.٦٣)
-1.27 (-3.51, 0.97)
0.264
وقت استجابة TMT (ثانية)
123
١٢٦
غير متوفر
غير متوفر
76
72
غير متوفر
غير متوفر
مفقود
٤
2
30.08 (15.99)
٣٤.٧٠ (٢٥.٢٦)
27.11 (16.34)
٣١.٠٧ (٢٥.١٠)
21.03 (-3.28, 45.33)
0.090
درجة PDQ-5-D
123
127
غير متوفر
غير متوفر
75
71
غير متوفر
غير متوفر
مفقود
٤
1
12.89 (4.47)
١٣٫٢٩ (٤٫٤٦)
10.55 (5.07)
10.83 (94.79)
0.43 (-0.57, 1.43)
0.394
CRT، استنادًا إلى مهمة رد الفعل الاختياري؛ DSST، استنادًا إلى اختبار استبدال الرموز الرقمية؛ N-back، استنادًا إلى نموذج العودة الواحدة TMT، الذي يستند إلى الجزء B من مهمة صنع المسارات؛ PDQ-5، استبيان العجز المدرك الذاتي، خمسة مجالات. NA، غير متوفر.تم تعديلها لـ: مركز العلاج (متغير التوزيع)، درجة HDRS-17 الأساسية ودرجة الاكتئاب المقاوم للعلاج (متغيرات التخفيف) وذراع العلاج مع معرف المشارك كأثر عشوائي. كما تم تعديل نماذج النتائج السريرية المستمرة الثانوية لقياسها الأساسي المعني. الأخطاء المعيارية مع تم الإبلاغ عن فترات الثقة للمتوسطات المقدرة بواسطة GRID-HDRS-17 في نقاط المتابعة الزمنية، لأن التقدير المتعدد تم استخدامه لإجراء التحليل الأساسي.كانت نتائج الإدراك هي المتغيرات التابعة، بينما كانت المتغيرات المستقلة المعنية هي نقطة زمن THINC-it (الخط الأساسي و16 أسبوعًا)، مجموعة العلاج (rTMS وcgiTBS)، GAD-7 في الخط الأساسي، HDRS-17 في الخط الأساسي والتغير في درجة HDRS-17 بين الخط الأساسي والأسبوع 16. كما شملت النماذج ثلاثة مصطلحات تفاعل: مجموعة العلاجنقطة زمنية، نقطة زمنيةالتغيير في HDRS-17 والتغيير في HDRS-17مجموعة العلاجنقطة زمنية. تضمنت المتغيرات المربكة العمر والجنس والموقع ومجموعة MGH. تم إزالة أي متغير مربك لم يُعتبر ذا دلالة إحصائية في الاختبار الأولي من النماذج وإعادة تحليل البيانات.
الجدول 3 | نسب المستجيبين، المستجيبين المستدامين والمستجيبين المتعافين في مجموعات rTMS و cgiTBS
قياس
النسبة في كل مجموعة علاجية (عدد/إجمالي (%))
cgiTBS مقابل
قيمة P
تحفيز الدماغ المتكرر عبر المغناطيس
cgiTBS
rTMS (نسبة الأرجحية المعدلة (95% فترة الثقة))
المستجيبون
متابعة لمدة 8 أسابيع
35/112 (31.3)
٣٩/١١١ (٣٥.١)
1.13 (0.63, 2.03)
0.682
متابعة لمدة 16 أسبوعًا
٣٨/١١٢ (٣٣.٩)
٣٩/١١٢ (٣٤.٨)
1.03 (0.57، 1.87)
0.916
متابعة لمدة 26 أسبوعًا
31/102 (30.4)
٣٦/١٠٤ (٣٤.٦)
1.18 (0.63, 2.20)
0.615
المستجيبون المستمرون
متابعة لمدة 16 أسبوعًا
23/127 (18.1)
28/128 (21.9)
1.21 (0.64, 2.29)
0.557
متابعة لمدة 26 أسبوعًا
22/127 (17.3)
29/128 (22.7)
1.40 (0.74, 2.66)
0.307
المُرسِلين
متابعة لمدة 8 أسابيع
19/112 (16.9)
23/111 (20.7)
1.09 (0.53, 2.26)
0.818
متابعة لمدة 16 أسبوعًا
23/112 (20.5)
23/112 (20.5)
0.84 (0.42, 1.69)
0.631
متابعة لمدة 26 أسبوعًا
21/102 (20.6)
٢٦/١٠٤ (٢٥.٠)
1.21 (0.61, 2.41)
0.590
تم استخدام نماذج اللوجستية الثنائية لتحليل المستجيبين، والمستجيبين الذين حققوا الشفاء، والمستجيبين المستدامين، مع تقديم تقديرات مقارنة العلاج بطريقة مشابهة لتلك المبلغ عنها في تحليل النتائج الأولية، باستثناء الإبلاغ عن نسب الأرجحية المعدلة. المستجيب (خفض في GRID-HDRS-17 من الخط الأساسي)، المحول (درجة منعلى GRID-HDRS-17) والمستجيب المستمر (استجابة مستمرةخفض في GRID-HDRS-17 بعد الاستجابة في النقطة الزمنية السابقة.
بعد شهر من انتهاء العلاج بالتحفيز المغناطيسي عبر الجمجمة (TMS) ونوبة هوس بعد الجلسة الرابعة عشرة من العلاج. تم إدخال أحد المشاركين إلى المستشفى بسبب الغثيان والقيء بعد إجراء تصوير الرنين المغناطيسي الأساسي، وتم الإبلاغ عن هذا الحدث على أنه مرتبط على الأرجح بالتصوير بسبب وضعية الرقبة أثناء وجوده في جهاز الرنين المغناطيسي. تم الإبلاغ عن جميع الأحداث السلبية الخطيرة الأخرى على أنها غير مرتبطة بالدراسة. كان هناك 17 حدثًا سلبيًا آخر (AEs) من السلوكيات الذاتية الضارة لـ 11 مشاركًا، وحدثان سلبيان يتعلقان بنوبة إغماء خلال العلاجات. أوقف كلا المشاركين العلاج بالتحفيز المغناطيسي في ذلك اليوم ولكن أكملوا بقية دورة العلاج دون أي حادث آخر.
نتائج سريرية استكشافية
أظهرت تحليلات الوسيط أن ارتفاع مستوى GRID-HDRS-17 الأساسي، وارتفاع مستوى القلق العام (GAD-7) وإكمال أقل من 20 جلسة تحفيز تنبأ بتحسن أقل في أعراض الاكتئاب على مدى 26 أسبوعًا من المتابعة (الجدول التكميلي 1). ومع ذلك، لم تكن التفاعلات بين ذراع العلاج وهذه المتغيرات الوسيطة (بالإضافة إلى الجنس) ذات دلالة إحصائية.
نتائج التصوير العصبي
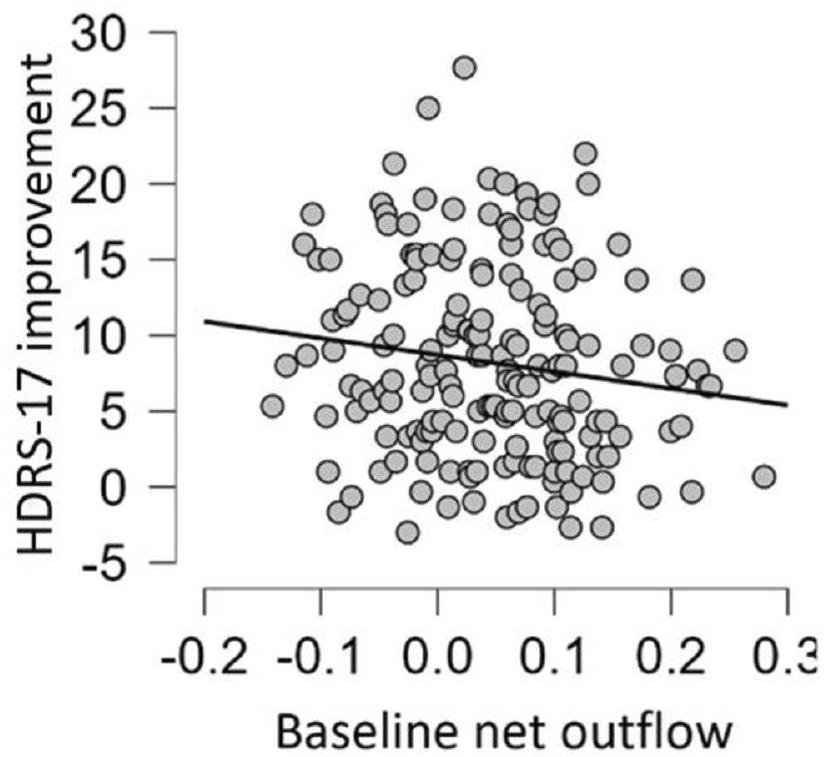
لم يتم دعم الفرضية الأساسية للتصوير العصبي – أن الاتصال الفعال الأساسي من rAI إلى IDLPFC سيتنبأ بتحسن سريري – بالنسبة لدرجات GRID-HDRS-17 أو BDI-II أو PHQ-9.، 185-201 مشاركًا تم تضمينهم عبر نقاط زمنية). ومع ذلك، تم دعم تدفق الصافي الأساسي من rAI (الاتصال الفعال من rAI إلى IDLPFC ناقص ذلك من IDLPFC إلى rAI) لـ GRID-HDRS-17 (التأثير الرئيسي لتدفق الصافي: كان التحسن المعزز مرتبطًا بتأثير إيجابي أكبر من IDLPFC إلى rAI وتأثير إيجابي أقل من rAI إلى IDLPFC (الشكل 4 من البيانات الموسعة). لم يختلف هذا العلاقة بين مجموعات العلاج أو عبر
الشكل 2 | متوسط (الخطأ المعياري) درجات GRID-HDRS-17 على مر الزمن لتحليل العينة الأولية (التحليل المتعدد).
نقاط زمنية بعد العلاج. كانت التدفقات الصافية الأساسية أقل إيجابية لدى المستجيبين في مقياس هاملتون للاكتئاب (HDRS-17) لمدة 16 أسبوعًا مقارنةً بغير المستجيبين عبر كلا مجموعتي العلاج..
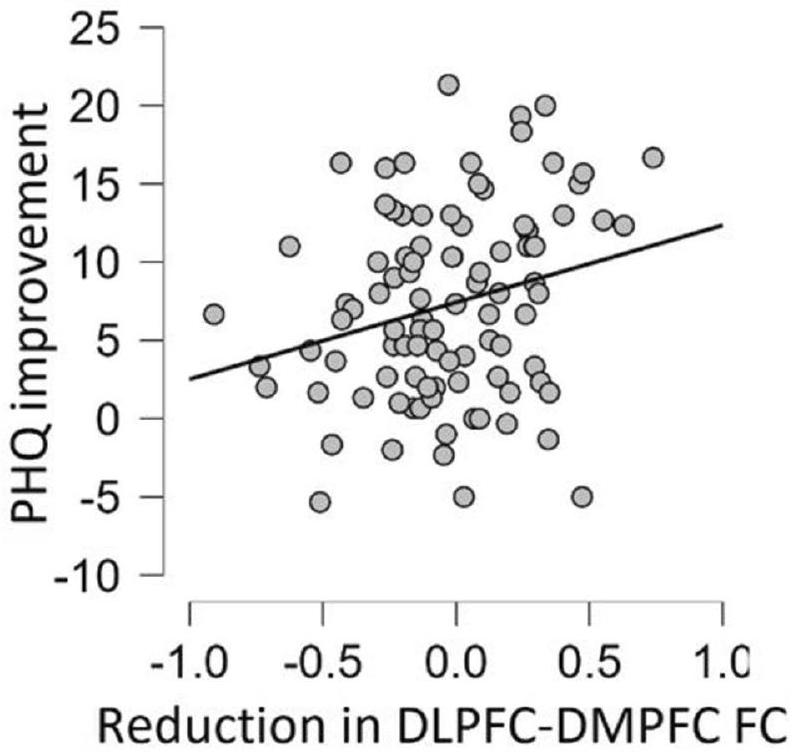
لم يتم دعم الانخفاض في الاتصال الوظيفي بين IDLPFC و IDMPFC من خط الأساس إلى 16 أسبوعًا لتغيير GRID-HDRS-17 سواء لموقع DLPFC الأمامي أو الخلفي المحدد في البروتوكول.شملت المشاركين عبر نقاط زمنية) ولكن كانت ذات دلالة لتحسينات في PHQ-9 (الأثر الرئيسي لتغير الاتصال الوظيفي؛ PHQ-9:; الأشكال البيانية الموسعة 5 و 6) واقتربت من الدلالة لتحسينات في BDI-IIلم تختلف هذه العلاقات عبر المجموعات، مما يشير إلى وجود رابط مباشر بين تغيير الشبكة وتأثير مضادات الاكتئاب.
تحليلات الحساسية
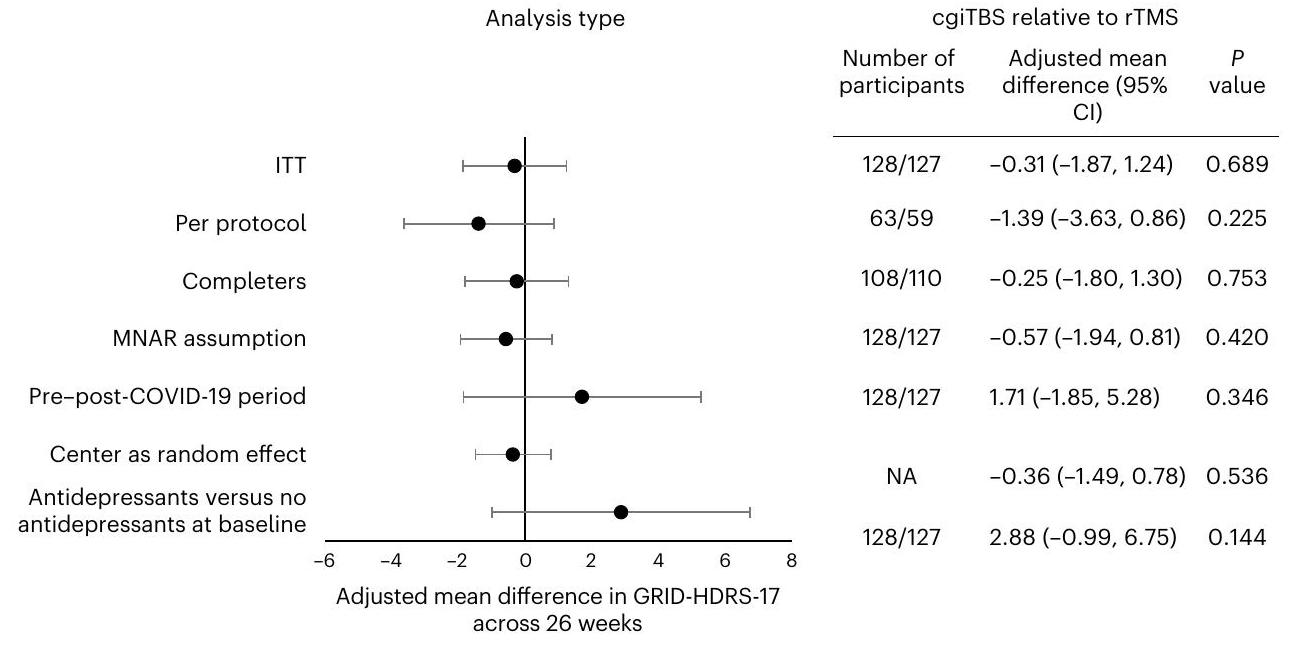
لم تكن الفروق بين مجموعات العلاج ذات دلالة إحصائية لأي من تحليلات الحساسية التي تم إجراؤها؛ لم تُلاحظ أي تأثيرات مركزية ولا تأثيرات لكون المشاركين غير متناولين لمضادات الاكتئاب في البداية (الشكل 3 والجدول الإضافي 3). يتم تقديم الانحرافات التي أدت إلى استبعاد المشاركين في تحليل البروتوكول في الجدول الإضافي 4.
تحليلات ما بعد الحدث
لفهم نتائج التدفق الصافي بشكل أفضل، قمنا بفحص ما إذا كانت الاتصال الفعال الأساسي من IDLPFC إلى rAI وحده يتنبأ بتحسن في أي من درجات GRID-HDRS-17 أو HDRS-6 (مقياس هاملتون لتقييم الاكتئاب المكون من 6 عناصر).. كانت العلاقة غير ذات دلالة بالنسبة لـ GRID-HDRS-17 (لكنها مهمة لـ HDRS-6 (تأثير إيجابي أكبر يتنبأ بتحسن أكبر؛، .
نقاش
دراسة BRIGhTMIND هي تجربة كبيرة ومناسبة في المملكة المتحدة تستخدم التحفيز المغناطيسي عبر الجمجمة (TMS) والتحفيز المغناطيسي عبر الجمجمة المتكرر (iTBS) لعلاج الاكتئاب المقاوم للعلاج (TRD) مع نتائج بعد 26 أسبوعًا. لم تُلاحظ أي اختلافات ذات دلالة إحصائية أو أهمية سريرية بين cgiTBS و rTMS في النتائج السريرية الأولية والثانوية على مدار 26 أسبوعًا، مما يدل على أن cgiTBS لم يظهر فعالية سريرية متفوقة مقارنةً بـ rTMS الموجه بواسطة التصوير بالرنين المغناطيسي الهيكلي. أظهرت كلا مجموعتي العلاج تحسنًا سريريًا كبيرًا في النتيجة الأولية للاكتئاب الملاحظ وقياسات الاكتئاب الذاتية، مع تغييرات فوق الحد الأدنى من الأهمية السريرية في القلق الذاتي، والوظائف، وجودة الحياة. بالنسبة لكلا مجموعتي العلاج، أظهر حوالي ثلث المشاركين استجابة، وحقق خُمسهم الشفاء، وأظهر خُمسهم استجابة مستدامة لمدة 6 أشهر. النتائج مشجعة نظرًا لأن ثلثي المشاركين تم تصنيفهم على أنهم يعانون من اكتئاب مقاوم للعلاج من متوسط إلى مرتفع (حوالي
الجدول 4 | تكرار الأحداث السلبية الخطيرة والأحداث السلبية المتعلقة بالضرر الذاتي والإغماء
نوع الحدث
السكان الآمنون
تحفيز الدماغ المتكرر عبر الجمجمة
cgiTBS،
SAE
الاستشفاء بسبب الغثيان والقيء
1 (1%)
0
الاستشفاء بسبب الانصمام الرئوي
1 (1%)
0
الاستشفاء بسبب COVID-19
0
1 (1%)
وفاة نتيجة تسمم عرضي بالمخدرات الأفيونية
0
1 (1%)
الاستشفاء للتحقيق في التعب
0
1 (1%)
الاستشفاء بسبب إصابة في الرأس
1 (1%)
0
الاستشفاء بسبب الصداع
1 (1%)
0
الموت نتيجة احتشاء عضلة القلب
0
1 (1%)
الاستشفاء بسبب ارتفاع درجة الحرارة
0
1 (1%)
قبول المستشفى بسبب صدمة تحسسية نتيجة لدغات الحشرات
1 (1%)
0
دخول المستشفى بسبب آلام في الصدر وضيق في التنفس
1 (1%)
0
قبول المستشفى بسبب انخفاض ضغط الدم
1 (1%)
0
قبول المستشفى المرتبط بالتهاب الغدد العرقية القيحي الموجود مسبقًا
1 (1%)
0
قبول في المستشفى: نوبة ذهانية مع قلق شديد/اكتئاب
1 (1%)
0
الاستشفاء بسبب نوبة هوس
0
1 (1%)
الاستشفاء بسبب ضيق التنفس
0
1 (1%)
القبول الطوعي في المستشفى للعلاج بالصدمات الكهربائية
1 (1%)
0
نوبة مشتبه بها قبل الجلسة الأولى للعلاج بالتحفيز المغناطيسي عبر الجمجمة
1
0
الإمارات العربية المتحدة
إيذاء النفس
٥؛
12؛
إغماء
2؛
0
تُعرض البيانات على أنهاعدد المشاركين المتأثرين، ونسبة المشاركين المتأثرين لكل حدث ضار خطير أو حدث ضار (لكل مجموعة علاجية) من إجمالي عدد المشاركين الذين تم توزيعهم عشوائيًا. ECT، العلاج بالصدمات الكهربائية.لم يتلقَ المشارك أي علاج بالتحفيز المغناطيسي عبر الجمجمة بسبب تعرضه لنوبة. يعادل الفشل في الاستجابة لأربعة مضادات اكتئاب أو أكثر، مع مدة طويلة من نوبة الاكتئاب الحالية (الوسيط 6 سنوات).
أقرب تجربتين عشوائيتين محكمتين لتصميمنا هما THREE-Dتجارب THETA-DEPكلاهما قارن بين iTBS و rTMS باستخدام الملاحة العصبية بالرنين المغناطيسي الهيكلي، الأول مع متابعة لمدة 12 أسبوعًا والثاني لمدة 26 أسبوعًا. إن معدلات الاستجابة والشفاء للاكتئاب، والتحسينات في القلق وجودة الحياة حتى 26 أسبوعًا في التجربة الحالية، تتماشى مع THETA-DEP، وهي دراسة لموقع واحد تضم 60 مشاركًا فقط مع مدة أقصر من حلقة الاكتئاب الحالية (متوسط 20 شهرًا) ومقاومة علاج أقل.. وبالتالي، بينما تشير الأدلة السابقة إلى أن التأثيرات المفيدة لـ rTMS على المزاج في حالات الاكتئاب المقاوم للعلاج قد تكون قصيرة الأمد نسبيًا، حيث تستمر فقط من 1 إلى 3 أشهركلا بروتوكولي التحفيز المغناطيسي عبر الجمجمة الموجه بواسطة التصوير بالرنين المغناطيسي في دراستنا وTHETA-DEP أديا إلى استجابات مستدامة تم الحفاظ عليها لـشهور بعد العلاج في واحد من كل خمسة مشاركين. تظهر النتائج الحالية هذه النتيجة في عينة ذات قوة كافية، ومع اكتئاب أكثر استمرارية وصعوبة في العلاج مما تم وصفه سابقًا. لا نعرف ما إذا كانت مثل هذه الاستجابات المستدامة ستحدث مع التحفيز المغناطيسي عبر الجمجمة غير الموجه بواسطة التصوير بالرنين المغناطيسي.
قد يكون توجيه الأعصاب المستند إلى التصوير بالرنين المغناطيسي مفيدًا من حيث تقليل انزلاق الملف والتوجيه غير الدقيق مقارنةً باستهداف فروة الرأس التقليدي باستخدام القبعة المرنة.مع دراستنا مبينًا أنه، في الغالبية العظمى من الحالات، كان موقع تحفيز TMS متغيرًا بواسطةوزاوية التحفيز بواسطةمن الموقع المستهدف على مدار 20 جلسة. على الرغم من أن دراسة سابقة عن الاكتئاب الشديد (MDD) أفادت بفعالية سريرية أكبر لتحفيز الدماغ عبر التحفيز المغناطيسي المتكرر الموجه بواسطة التصوير بالرنين المغناطيسي مقارنةً بأساليب الاستهداف القائمة على فروة الرأس.، بينما لم يجد آخرون أي فرق في الفعالية السريرية. كانت هذه الدراسات تركز على الفعالية الفورية بدلاً من الفعالية على المدى الطويل. لأن التجارب السريرية العشوائية السابقة لـ iTBSالاستجابة المقاسة والشفاء فقط بعد العلاج مباشرة، فإن فوائد التحفيز المغناطيسي عبر الجمجمة الموجه بواسطة التصوير بالرنين المغناطيسي مقارنةً بالتحفيز غير الموجه بعد العلاج الأولي غير معروفة. لذلك، قد تقارن الأبحاث المستقبلية الفعالية السريرية والتكلفة الفعالة للتحفيز المغناطيسي عبر الجمجمة الموجه بواسطة التصوير بالرنين المغناطيسي مقابل التحفيز غير الموجه على مدى متابعة طويلة الأمد نظرًا للتكلفة الإضافية لعمليات التصوير بالرنين المغناطيسي.
دراسة THREE-D قدمت ما يصل إلى 30 جلسة تحفيز مغناطيسي عبر الجمجمة لعدد من المشاركين وأظهرت معدلات استجابة أعلى قليلاً. ) وشفاء ( ) من دراستنا بالنظر إلى ذلك، مع نسبة المشاركين في تجربتنا الذين يشعرون بتحسن ما (أو، بشكل كبير) ولا يزالون في زيادة خلال الجلسات العلاجية التاسعة عشرة والعشرون، قد يتم تعزيز النتائج بشكل أكبر لدى هؤلاء المشاركين الذين لا يزالون يتحسنون مع ما يصل إلى 30 علاجًا بالتحفيز المغناطيسي عبر الجمجمة. كانت كلا العلاجات مرتبطة بتحسينات مع مرور الوقت في الانتباه المستدام، والوظائف التنفيذية، والذاكرة العاملة، بما يتماشى مع استنتاج تحليل تلوي حديث يشير إلى أن التحفيز المغناطيسي المتكرر عبر الجمجمة له تأثيرات معتدلة في تعزيز القدرات المعرفية في الاكتئاب الشديد..
تدعم نتائج تصوير الرنين المغناطيسي الوظيفي لدينا الفوائد طويلة الأمد لكل من cgiTBS و rTMS، مع بعض الأدلة المحتملة على تأثير تطبيع عدم الاتصال في الدماغ. يظهر الأشخاص الذين يعانون من الاكتئاب الشديد زيادة في الاتصال الإيجابي بين الشبكة التنفيذية المركزية (CEN) والشبكة الافتراضية (DMN) في تصوير الرنين المغناطيسي الوظيفي أثناء الراحة، بينما في الأفراد الأصحاء تكون هذه الشبكات متضادة أو غير مرتبطة.تشير تحليلاتنا لتصوير الرنين المغناطيسي الوظيفي أثناء الراحة إلى انخفاض في الاتصال الوظيفي بين خط الأساس و16 أسبوعًا بين القشرة الجبهية السفلية الجانبية الخلفية (جزء من الشبكة التنفيذية المركزية) والقشرة الجبهية السفلية المتوسطة (جزء من الشبكة الافتراضية)، مما يتماشى مع الفرضية القائلة بأن استعادة التباين الطبيعي قد تكون مرتبطة بتحسينات في الاكتئاب. على الرغم من القرب المختلف للأهداف من القشرة الجبهية السفلية الجانبية الخلفية (قريب بالنسبة لـ cgiTBS، بعيد بالنسبة لـ rTMS)، كانت النتائج مشابهة بين ذراعي العلاج، مما يكرر عملنا التجريبي غير المنشور ودراسة سابقة.-على الرغم من أنه فقط في مقاييس الاكتئاب التي يتم تقييمها ذاتيًا. إذا تم تأكيد ذلك بشكل مستقل، فإن استعادة نمط التداخل العكسي الطبيعي بين الشبكة التنفيذية المركزية (CEN) والشبكة الافتراضية (DMN) الناتجة عن التحفيز المغناطيسي عبر الجمجمة (TMS) قد تكون آلية محتملة (مباشرة أو غير مباشرة) لفعاليتها المضادة للاكتئاب على الأقل لبعض مجالات الاستجابة. قد تشير التحسينات مع TMS إلى تقليل تدخل معالجة العالم الداخلي المرتبطة بـ DMN والتفكير المتكرر في معالجة العالم الخارجي المرتبطة بـ CEN وأداء المهام، وقد تكون متسقة مع اكتشاف فترات الانتباه المفقودة لدى الأشخاص الذين يعانون منقد يتم التقاط مثل هذه التغييرات بشكل أفضل من خلال مقاييس BDI-II و PHQ-9 الذاتية، التي تقيس ضعف التركيز والمعالجة الذاتية، بدلاً من مقياس GRID-HDRS-17، الذي لا يقيس هذه العمليات بشكل مباشر..
وجدنا أن عدم التوازن في التأثير بين rAI و IDLPFC (‘صافي التدفق الخارجي’) توقع تحسنًا في أعراض الاكتئاب على مدى 26 أسبوعًا عبر كلا مجموعتي العلاج. كان انخفاض صافي التدفق الخارجي من rAI إلى IDLPFC مرتبطًا بالاستجابة على GRID-HDRS-17 بعد 16 أسبوعًا في كلا مجموعتي العلاج. أشارت التحليلات اللاحقة إلى أن التحسن في الأعراض الأساسية للاكتئاب كان مرتبطًا بالاتصال الفعال السائد من IDLPFC إلى rAI في الأساس. تفسير ميكانيكي محتمل يتطلب مزيدًا من البحث هو أن التأثير الأكبر لـ IDLPFC على rAI قد يمكّن تأثيرات TMS من الانتشار بشكل أكثر فعالية من IDLPFC إلى rAI، مما يعزز تأثيره العصبي على الأنسجة.
تتمثل إحدى نقاط القوة في التجربة السريرية العشوائية في تصميمها متعدد المراكز. كانت العينة كبيرة، مع تنوع في العمر والعرق وميزات ديموغرافية أخرى. بالمقارنة مع السكان السريريين الذين يعانون من مقاومة العلاج حيث توجد نسبة أكبر من الإناث، كان هناك تمثيل متساوٍ للرجال والنساء. بخلاف ذلك، يمكن تعميم العينة على السكان السريريين في المملكة المتحدة الذين يعانون من مقاومة العلاج.
الشكل 3| تحليل النتائج الإجمالية وتحليل الحساسية لمقياس النتيجة الأساسية بعد cgiTBS بالنسبة لـنظام إدارة النقل.
تم التحقق من ذلك من حسابات المرضى والسجلات السريرية، على الرغم من أنه قد يكون قد تم التقليل من ذلك إذا كانت ذاكرة المرضى والسجلات غير مكتملة. كما أن قياس مقاومة العلاج لم يشمل العلاجات النفسية، التي تكون غالبًا متاحة في إنجلترا. كان هناك معدل مرتفع (93%) لإكمال العلاج لجميع جلسات TMS العشرين والمتابعة (متوسط 85%). من بيانات التنقل العصبي، تم تقديم علاج TMS بدقة عالية بالنسبة للإحداثيات المستمدة من التصوير بالرنين المغناطيسي وتنوعت قليلاً في الموقع أو غيرها من معلمات TMS عبر 20 جلسة، باستثناء التعديلات الطفيفة في الوضع أو عتبة الحركة وفقًا لمعايير محددة مسبقًا. أشارت فحوصات موثوقية المقيمين إلى أن قياس النتيجة الأساسية كان قابلاً للمقارنة بين المراكز. كانت عملية إخفاء التدخل ناجحة للمراقبين للنتيجة. كان جانب رئيسي من التجربة هو المدخلات النشطة للأشخاص الذين لديهم تجارب حية مع الاكتئاب والتحفيز المغناطيسي عبر الجمجمة (مجموعة استشارية لتجربة BRIGhTMIND)، الذين أبلغوا عن جميع جوانب التصميم والتنفيذ وتفسير التجربة.
ومع ذلك، تم تعطيل الدراسة بشكل كبير وتعليقها لمدة 6 أشهر بسبب التدابير الصحية العامة التي تم اتخاذها للسيطرة على جائحة COVID-19. مع مدخلات مجموعة استشارات تجربة الحياة لدينا ومراجعة خارجية من اللجنة المستقلة لتوجيه التجارب ومراقبة البيانات والأخلاقيات، قمنا بإجراء عدد من التغييرات الجوهرية على البروتوكول بما في ذلك (1) تغيير النتيجة الأساسية من الاستجابة عند 16 أسبوعًا إلى التغيير المتوسط على مدى 8 و16 و26 أسبوعًا، (2) حساب قوة معدل معدل جديد و(3) الانتقال من التقييم وجهًا لوجه إلى التقييم عن بُعد للنتائج حيثما كان ذلك ممكنًا.في ضوء حالة الطوارئ الصحية العامة، لم يكن من الممكن إكمال الدراسة دون هذه التغييرات نظرًا للموارد المتاحة لها. لم تُظهر التحليلات قبل وبعد COVID أي تأثير سريري مهم أو ذو دلالة إحصائية للجائحة. تُظهر معدلات الاستجابة بعد 16 أسبوعًا، وهو النتيجة الأساسية الأصلية، اختلافًا طفيفًا جدًا بين مجموعات العلاج. من غير المحتمل جدًا أن التغييرات التي أُجريت على التجربة بدافع الضرورة بسبب جائحة COVID-19 قد أحدثت أي فرق مادي في أي نتيجة أو استنتاج من التجربة.
تضمنت القيود أنه، على الرغم من أن علاجات TMS كانت متطابقة بشكل جيد من حيث عدد النبضات لكل جلسة علاج، ومدة الجلسة وعدد الجلسات، إلا أنها اختلفت في تردد التحفيز (iTBS أو rTMS)، وشدة التحفيز (80% من عتبة الحركة الساكنة (RMT) أو 120% RMT) وطريقة اختيار موقع العلاج (الاتصال الفعال في حالة الراحة مقابل التصوير بالرنين المغناطيسي الهيكلي). تشير التجارب السريرية العشوائية السابقة إلى أن iTBS و rTMS قد يكون لهما فعالية متساوية في علاج الاكتئاب المقاوم للعلاج (TRD).هناك بعض عدم اليقين بشأن أهمية شدة التحفيز، ولكن في التجربة الحالية،لم يتم تحمل RMT بشكل جيد من قبل أقلية من المشاركين في التجربة، مما استدعى تقليل الشدة في مثل هؤلاء المشاركين في ذراع التحفيز المغناطيسي عبر الجمجمة (rTMS) للحد من الانسحاب من العلاج. كانت تقليل شدة التحفيز أمرًا مهمًا لأن عدد جلسات العلاج أثر على متوسط تقليل أعراض الاكتئاب على مدى 8 و16 و26 أسبوعًا في كل من التجربة السريرية العشوائية الحالية (RCT) وثلاثة-D.أهمية النهج في اختيار موقع العلاج غير معروفة. لمطابقة أذرع العلاج لعدد النبضات لكل جلسة علاج، قدمنا شكلًا متسارعًا من iTBS مع خمسة جولات من 600 نبضة على مدار 37 دقيقة في كل جلسة علاج مع فترات غير تحفيزية تقريبًا مدتها 5 دقائق بين الجولات. يمكن أن تؤثر الجرعة والفترات الزمنية بين بروتوكولات TBS على الميتا-بلاستيكية، إما عن طريق تقليل أو عكس تأثير البلاستيكية المشبكية أو عن طريق زيادة تأثير البلاستيكية المشبكية.في بعض الأفراد، قد تؤدي الفترات الزمنية التي تبلغ 5 دقائق بين جولات iTBS إلى زيادة تثبيط القشرة الدماغية على المدى القصير، مما يقلل من فعالية جلسة iTBS بأكملها.وبذلك يصبح من الصعب إثبات الفرق الجماعي بين cgiTBS و rTMS. ومن الجدير بالذكر أن النتائج الحالية قابلة للمقارنة من حيث الاستجابة لتجربة THETA-DEP العشوائية.على مدى أكثر من 26 أسبوعًا لكل من مجموعتي iTBS و rTMS، لذا قد تكون الجولات الإضافية بعد الجولة الأولى من 600 نبضة قد حققت فائدة إضافية قليلة في مجموعة علاج cgiTBS.
نظرًا لهذه القيود، هناك عدة طرق لتفسير نتائج الدراسة الحالية – أن cgiTBS ليس متفوقًا على rTMS. التفسير الأكثر احتمالاً هو أن الاستهداف الدقيق لدائرة IDLPFC-rAI ليس مهمًا من حيث الفعالية السريرية أو الآلية لـ TMS. سيكون هذا متسقًا مع الفكرة القائلة بأن الأهداف المكانية المتميزة قد تعدل نفس الدوائر الدماغية أو دوائر متداخلة. بدلاً من ذلك، يمكن للمرء أن يفترض أن حلقة الجبهة المعزولة وتفاعلها مع الشبكة الافتراضية غير ذات صلة بتأثير العلاج. نعتبر أن هذا أقل احتمالًا لسببين: (1) أن التدفق الصافي من IDLPFC-rAI كان له تأثير معتدل على النتيجة الأساسية في كلا مجموعتي العلاج، مما يشير إلى أن الاتصال الوظيفي لـ IDLPFC-rAI قد يلعب دورًا ما في استجابة TMS؛ و (2) أن الاتصال بين IDLPFC الخلفي، الذي يتطابق بشكل وثيق مع هدف cgiTBS المتوسط، و dmPFC كان مرتبطًا بتقييمات التحسن الذاتية. لا يمكننا استبعاد أن 80 مقابلأظهرت فعالية قوة RMT ميلاً نحو rTMS، لكننا لم نلاحظ مسارات استجابة متأخرة للموضوعات في cgiTBS. معًا، يدعم عدم وجود اختلاف في أي مقياس سريري أو fMRI، مع تأثيرات مماثلة على الاتصال الوظيفي، التفسير القائل بأن الاستهداف الدقيق لعلاجات TMS قد لا يكون مفيدًا على مستوى المجموعة باستخدام rTMS غير المعجل أو بروتوكول iTBS المعجل الحالي. ستستكشف التحليلات الثانوية المستقبلية للبيانات متعددة الأبعاد الغنية التأثيرات السريرية والنيوروبلاستيكية المحتملة الخاصة بالمجموعات الفرعية.
كانت نتيجة سريرية رئيسية هي مدة تأثيرات التحفيز المغناطيسي عبر الجمجمة تصل إلى 26 أسبوعًا مع كلا مجموعتي العلاج. ومع ذلك، فإن التفسير تُعوق هذه النتائج نقص مجموعة العلاج الوهمي ونقص قياس النتيجة الأساسية في نهاية العلاج بعد 6 أسابيع. فيما يتعلق بالأخيرة، كان هناك فجوة مدتها أسبوعان فقط حتى التقييم الأولي، مع تغييرات ضئيلة في العلاجات الأخرى خلال تلك الفترة. نصحت مجموعة استشارات تجربة الحياة (LEAP) بأن قياس النتيجة بعد 6 و8 أسابيع سيكون مرهقًا، لذا اخترنا قياس النتيجة بعد 8 أسابيع بدلاً من 6 أسابيع لقياس التأثيرات التي لوحظت بعد شهر من العلاج بالتحفيز المغناطيسي عبر الجمجمة (TMS) في دراستنا التجريبية. هناك ثلاثة تفسيرات محتملة لطول مدة العلاج بالتحفيز المغناطيسي عبر الجمجمة في هذه التجربة السريرية العشوائية: (1) تأثير دائم للعلاج بالتحفيز المغناطيسي عبر الجمجمة؛ (2) تأثير علاج غير محدد بسبب الانحدار نحو المتوسط، أو التوقع، أو الأمل، أو تنظيم اليوم؛ أو (3) تأثيرات العلاج الدوائي الإضافي للاكتئاب والقلق، خاصة بعد 16 و26 أسبوعًا. أبلغت دراسة تحليلية شاملة عن استجابات الدواء الوهمي في التجارب السريرية العشوائية للعلاج بالتحفيز المغناطيسي عبر الجمجمة في حالات الاكتئاب المقاوم للعلاج عن معدلات الاستجابة والشفاء بنسبة 20 وفي نهاية العلاج مقابل 33 و 19%، على التوالي، في BRIGhTMIND. يرتبط ارتفاع درجة مقاومة العلاج (جميعهم فشلوا في علاجين، وغالبيةهم في أربعة) وطول مدة المرض الحالي (الوسيط 6 سنوات) باستجابات منخفضة للدواء الوهمي مع العلاجات للاكتئاب، بما في ذلك TMS.. في تجربة عشوائية محكومة لعينة مماثلة من المشاركين مع مدة مشابهة للاكتئاب الحالي، تم تجنيدهم بشكل كبير من أعلى موقع تجنيد في BRIGhTMIND، كانت نسبة الشفاء بعد 26 أسبوعًا فقط (مرجع 59).
إن حدوث تغييرات في التصوير بالرنين المغناطيسي الوظيفي المرتبطة بالعلاج في الدراسة لا يستبعد استجابة وهمية، خاصةً بالنظر إلى العثور على تداخل بين نشاط مناطق الدماغ المعدلة بواسطة الدواء الوهمي وTMS للأهداف بما في ذلك IDLPFC.. ومع ذلك، أظهرت دراسة واحدة أن استجابة الدواء الوهمي لم تؤثر على الاتصال مع rAIكما يتضح من rTMS/cgi TBS في الدراسة الحالية. قد تكون بعض التغيرات في النتائج في كلا المجموعتين، خاصة في الأسابيع 16 و26، ناتجة عن تغييرات في الأدوية. لأسباب سريرية وأخلاقية في هذه المجموعة ذات الاكتئاب المقاوم للعلاج الشديد، كانت التغييرات في مضادات الاكتئاب أو الأدوية الأخرى مسموح بها وتمت في 19% من العينة بحلول 16 أسبوعًا. لم تؤدِ استبعاد مثل هؤلاء المشاركين في تحليل البروتوكول، أو كونهم يتناولون مضادًا للاكتئاب أم لا في البداية، إلى اختلافات ذات دلالة إحصائية أو أهمية سريرية في النتيجة الأساسية بين مجموعات العلاج. مجتمعة، من المحتمل أن يكون لـ TMS تأثير كبير على مدة الاستجابة ولكن بعض هذا التغيير ناتج عن تأثيرات غير محددة وتغييرات في الأدوية الموصى بها سريريًا، كما سيكون الحال في الرعاية السريرية العادية. لا يمكن تحديد مقدار التغيير الناتج عن TMS إلا من خلال تجربة عشوائية محكومة ذات قوة كافية تقارن iTBS أو rTMS مقابل التحكم الوهمي على أعراض الاكتئاب على مدى 26 أسبوعًا. اقترحنا مثل هذه التجربة لممولينا عندما طلبنا التمويل لأول مرة لدراسة BRIGhTMIND، ولكن تم رفض مثل هذا التصميم لأسباب سريرية وأخلاقية في مجموعة المرضى الشديدة والضعيفة. لذلك، قد لا يكون من الممكن إجراء مثل هذه التجربة.
في الختام، وجدت هذه الدراسة أن cgiTBS وMRIneuronavigated rTMS فعّالتان وآمنتان بنفس القدر. أظهر المرضى تحسنات سريرية ملحوظة في الاكتئاب استمرت حتى 26 أسبوعًا. تثير هذه النتائج إمكانية أن بعض مرضى الاكتئاب المقاوم للعلاج الذين لا يستجيبون لعلاجات أخرى يمكن أن يحافظوا على صحتهم، بينما سيستفيد العديد من الآخرين بشكل سريري ملحوظ، من دورة واحدة أو اثنتين من جلسات iTBS أو rTMS الموجهة بالرنين المغناطيسي، والتي تتكون من 20 جلسة (أو ربما أكثر) على مدار عام.
المحتوى عبر الإنترنت
أي طرق، مراجع إضافية، ملخصات تقارير Nature Portfolio، بيانات المصدر، بيانات موسعة، معلومات إضافية، شكر وتقدير، معلومات مراجعة الأقران؛ تفاصيل مساهمات المؤلفين والمصالح المتنافسة؛ وبيانات توفر البيانات والرموز متاحة علىhttps://doi.org/10.1038/s41591-023-02764-z.
References
National Institute for Health and Care Excellence. Depression in Adults: Treatment and Management. NICE Guidelines (NG222) (NICE, 2022).
Rush, A. J. et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am. J. Psychiatry 163, 1905-1917 (2006).
Rizvi, S. J. et al. Treatment-resistant depression in primary care across Canada. Can. J. Psychiatry 59, 349-357 (2014).
Brunoni, A. R. et al. Repetitive transcranial magnetic stimulation for the acute treatment of major depressive episodes: a systematic review with network meta-analysis. JAMA Psychiatry 74, 143-152 (2017).
Berlim, M. T. et al. Response, remission and drop-out rates following high-frequency repetitive transcranial magnetic stimulation (rTMS) for treating major depression: a systematic review and meta-analysis of randomized, double-blind and sham-controlled trials. Psychol. Med. 44, 225-239 (2014).
Health Quality Ontario Repetitive transcranial magnetic stimulation for treatment-resistant depression: a systematic review and meta-analysis of randomized controlled trials. Ont. Health Technol. Assess. Ser. 16, 1-66 (2016).
Larson, J. & Munkácsy, E. Theta-burst LTP. Brain Res. 1621, 38-50 (2015).
National Institute of Health and Clinical Excellence. Repetitive Transcranial Magnetic Stimulation for Depression. Guidance (NICE, 2015).
Blumberger, D. M. et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial. Lancet 391, 1683-1692 (2018).
O’Reardon, J. P. et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biol. Psychiatry 62, 1208-1216 (2007).
Batail, J. M. et al. No place in France for repetitive transcranial magnetic stimulation in the therapeutic armamentarium of treatment-resistant depression? Brain Stimul. 16, 927-929 (2023).
Fox, M. D., Liu, H. & Pascual-Leone, A. Identification of reproducible individualized targets for treatment of depression with TMS based on intrinsic connectivity. Neuroimage 66, 151-160 (2013).
Anderson, R. J. et al. Repetitive transcranial magnetic stimulation for treatment resistant depression: re-establishing connections. Clin. Neurophysiol. 127, 3394-3405 (2016).
Mueller, S. et al. Individual variability in functional connectivity architecture of the human brain. Neuron 77, 586-595 (2013).
Cash, R. F. et al. Functional magnetic resonance imaging-guided personalization of transcranial magnetic stimulation treatment for depression. JAMA Psychiatry 78, 337-339 (2021).
Cole, E. et al. Stanford Neuromodulation Therapy (SNT): a double-blind randomized controlled trial. Am. J. Psychiatry 179, 132-141 (2022).
Iwabuchi, S. J. et al. Alterations in effective connectivity anchored on the insula in major depressive disorder. Eur. Neuropsychopharmacol. 24, 1784-1792 (2014).
Iwabuchi, S. J. et al. Targeted transcranial theta burst stimulation alters fronto-insular network and prefrontal GABA. Neuroimage 146, 395-403 (2017).
Iwabuchi, S. J. et al. Baseline effective connectivity predicts response to repetitive transcranial magnetic stimulation in patients with treatment-resistant depression. Eur. Neuropsychopharmacol. 29, 681-690 (2019).
Roebroeck, A. et al. Mapping directed influence over the brain using Granger causality and fMRI. Neuroimage 25, 230-241 (2005).
Liston, C. et al. Default mode network mechanisms of transcranial magnetic stimulation in depression. Biol. Psychiatry 76, 517-526 (2014).
Briley, P. M. et al. BRIGhTMIND trial motivating mechanism action analysis plan: resting state fMRI. https://doi.org/10.17639/ nott. 7251 (2022).
Fava, M. Diagnosis and definition of treatment-resistant depression. Biol. Psychiatry 53, 649-659 (2003).
Williams, J. et al. The GRID-HAMD: standardization of the Hamilton Depression Rating Scale. Int Clin. Psychopharmacol. 23, 120-129 (2008).
National Institute for Clinical Excellence. Depression: Management of Depression in Primary and Secondary Care. Clinical Guideline 23 (CG23) (NICE, 2004).
Rush, A. J. et al. Clinically significant changes in the 17- and 6-item Hamilton Rating Scales for Depression: a STAR*D report. Neuropsychiatr. Dis. Treat. 14, 2333-2345 (2021).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern Med 16, 606-613 (2001).
Turkoz, I. et al. Clinically meaningful changes on depression symptom measures and patient-reported outcomes in patients with treatment resistant depression. Acta Psychiatr. Scand. 143, 253-263 (2021).
Beck, A. et al. Manual for the Beck Depression Inventory-II (Psychological Corporation, 1996).
Hiroe, T. et al. Gradations of clinical severity and sensitivity to change assessed with the Beck Depression Inventory-II in Japanese patients with depression. Psychiatry Res. 135, 229-235 (2005).
Spitzer, R. L. et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166, 1092-1097 (2006).
Bauer-Staeb, C. et al. Effective dose 50 method as the minimal clinically important difference: evidence from depression trials. J. Clin. Epidemiol. 137, 200-208 (2021).
Mundt, J. C. et al. The work and social adjustment scale: a simple measure of impairment in functioning. Br. J. Psychiatry 180, 461-464 (2002).
Everitt, H. A. et al. Assessing telephone-delivered cognitive-behavioural therapy (CBT) and web-delivered CBT versus treatment as usual in irritable bowel syndrome (ACTIB): a multicentre randomised trial. Gut 68, 1613-1623 (2019).
EuroQol Research Foundation. EQ-5D-5L User Guide version 3 (EuroQol, 2019).
Zanini, A. et al. Estimation of minimal clinically important difference in EQ-5D Visual Analog Scale Score after pulmonary rehabilitation in subjects with COPD. Respir. Care 60, 88-95 (2015).
McIntyre, R. S. The THINC-Integrated Tool (THINC-it) screening assessment for cognitive dysfunction: validation in patients with major depressive disorder. J. Clin. Psychiatry 78, 873-881 (2017).
Bech, P. The Hamilton Depression Scale. Evaluation of objectivity using logistic models. Acta Psychiatr. Scand. 63, 290-29 (1981).
Nixon, N. et al. The bi-factor structure of the 17-item Hamilton Depression Rating Scale in persistent major depression; dimensional measurement of outcome. PLoS ONE 15, e0241370 (2020).
Bulteau, S. et al. Intermittent theta burst stimulation (iTBS) versus 10 Hz high-frequency repetitive transcranial magnetic stimulation (rTMS) to alleviate treatment-resistant unipolar depression: a randomized controlled trial (THETA-DEP). Brain Stimul. 15, 870-880 (2022).
Caulfield, K. A. et al. Neuronavigation maximizes accuracy and precision in TMS positioning: evidence from 11,230 distance, angle, and electric field modeling measurements. Brain Stimul. 15, 1192-1205 (2022).
Fitzgerald, P. B. et al. A randomized trial of rTMS targeted with MRI based neuro-navigation in treatment-resistant depression. Neuropsychopharmacology 34, 1255-1262 (2009).
Li, C. T. et al. Antidepressant efficacy of prolonged intermittent theta burst stimulation monotherapy for recurrent depression and comparison of methods for coil positioning: a randomized, double-blind, sham-controlled study. Biol. Psychiatry 87, 443-450 (2020).
Hebel, T. et al. A direct comparison of neuronavigated and non-neuronavigated intermittent theta burst stimulation in the treatment of depression. Brain Stimul. 14, 335-343 (2021).
Martin, D. M. et al. Cognitive enhancing effects of rTMS administered to the prefrontal cortex in patients with depression: a systematic review and meta-analysis of individual task effects. Depress. Anxiety 34, 1029-1039 (2017).
Kaiser, R. H. et al. Large-scale network dysfunction in major depressive disorder: a meta-analysis of resting-state functional connectivity. JAMA Psychiatry 72, 603-611 (2015).
Gallagher, P. et al. Neurocognitive intra-individual variability in mood disorders: effects on attentional response time distributions. Psychol. Med. 45, 2985-2997 (2015).
Morriss, R. et al. Connectivity guided theta burst transcranial magnetic stimulation versus repetitive transcranial magnetic stimulation for treatment-resistant moderate to severe depression: study protocol for a randomised double-blind controlled trial (BRIGhTMIND). BMJ Open 10, e038430 (2020).
Pszczolkowski, S. et al. Connectivity-guided theta burst transcranial magnetic stimulation versus repetitive transcranial magnetic stimulation for treatment-resistant moderate to severe depression: magnetic resonance imaging protocol and SARS-CoV-2-induced changes for a randomized double-blind controlled trial. JMIR Res. Protoc. 11, e31925 (2022).
Trevizol, A. P. et al. Predictors of remission after repetitive transcranial magnetic stimulation for the treatment of major depressive disorder: an analysis from the randomised non-inferiority THREE-D trial. EClinicalMedicine 22, 100349 (2020).
Tse, N. Y. et al. The effect of stimulation interval on plasticity following repeated blocks of intermittent theta burst stimulation. Sci. Rep. 8, 8526 (2018).
Gamboa, O. L. et al. Impact of repetitive theta burst stimulation on motor cortex excitability. Brain Stimul. 4, 145-151 (2011).
Nettekoven, C. et al. Dose-dependent effects of theta burst rTMS on cortical excitability and resting-state connectivity of the human motor system. J. Neurosci. 34, 6849-6859 (2014).
Jones, B. D. M. et al. Magnitude of the placebo response across treatment modalities used for treatment-resistant depression in adults: a systematic review and meta-analysis. JAMA Netw. Open 4, e2125531 (2021).
Razza, L. B. A systematic review and meta-analysis on placebo response to repetitive transcranial magnetic stimulation for depression trials. Prog. Neuropsychopharmacol. Biol. Psychiatry 81, 105-113 (2018).
Hsu, J. H. et al. Impact of prior treatment on remission with intermittent theta burst versus high-frequency repetitive transcranial magnetic stimulation in treatment resistant depression. Brain Stimul. 12, 553-1555 (2019).
Nelson, J. C. et al. Predictors of remission with placebo using an integrated study database from patients with major depressive disorder. Curr. Med. Res. Opin. 28, 325-334 (2012).
Lisanby, S. H. et al. Daily left prefrontal repetitive transcranial magnetic stimulation in the acute treatment of major depression: clinical predictors of outcome in a multisite, randomized controlled clinical trial. Neuropsychopharmacology 34, 522-534 (2009).
Morriss, R. et al. Efficacy and cost-effectiveness of a specialist depression service versus usual specialist mental health care to manage persistent depression: a randomised controlled trial. Lancet Psychiatry 3, 821-831 (2016).
Burke, M. J. et al. Placebo effects and neuromodulation for depression: a meta-analysis and evaluation of shared mechanisms. Mol. Psychiatry 27, 1658-1666 (2022).
Zhao, K. et al. Individualized fMRI connectivity defines signatures of antidepressant and placebo responses in major depression. Mol. Psychiatry 28, 2490-2499 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
تم تجنيد المشاركين من إعدادات الرعاية الأولية والثانوية في خمسة مراكز علاجية عبر خدمات الصحة الوطنية في المملكة المتحدة (NHS): مؤسسة نوتنغهامشير للرعاية الصحية؛ مؤسسة نورثامبتونشير للرعاية الصحية؛ مؤسسة كمبريا ونورثمبرلاند وتاين ووير للرعاية الصحية؛ مؤسسة كامدن وإيسلينجتون للرعاية الصحية؛ ومؤسسة بينين كير للرعاية الصحية. تم اختيار مراكز العلاج لتعكس التنوع الجغرافي ولأن بعضها كان لديه خبرة سابقة في التحفيز المغناطيسي عبر الجمجمة (TMS). تم توضيح تصميم التجربة وطرقها في بروتوكولين منشورين للتجربة..
تم اعتبار المشارك مستوفياً لمعايير الإدماج إذا كان: في سنسنوات؛ استوفى معايير الاضطراب الاكتئابي الكبير وفقًا لدليل التشخيص والإحصاء للاضطرابات النفسية النسخة الخامسة باستخدام مقابلة سريرية منظمة؛ كان يعاني من اكتئاب معتدل إلى شديد يُعرّف بأنه حصل على درجة 16 أو أكثر في النسخة GRID من GRID-HDRS-17 (المرجع 24)؛ كان يعاني من TRD يُعرّف بأنه حصل على درجة 2 أو أكثر في، الذي تم تكييفه لخيارات العلاج الجديدة (معلومات إضافيةوكان لديهم القدرة على تقديم الموافقة المستنيرة قبل أي أنشطة متعلقة بالتجربة.
تم استبعاد المشاركين إذا كان لديهم: تاريخ من الاضطراب ثنائي القطب أو الاكتئاب الثانوي لاضطراب نفسي آخر؛ حالات عصبية – على سبيل المثال، ورم دماغي، أحداث وعائية دماغية، صرع، اضطرابات تنكس عصبي أو جراحة سابقة في الدماغ؛ موانع قياسية للتصوير بالرنين المغناطيسي (على سبيل المثال، أجسام معدنية غير قابلة للإزالة في وحول الجسم، الحمل، الوشوم الحمراء على الرأس أو الرقبة أو الظهر أو رهاب الأماكن المغلقة)؛ مرض طبي رئيسي غير مستقر يتطلب مزيدًا من التحقيق أو العلاج؛ في الأسبوعين السابقين للتقييم الأساسي، أي تغيير في الأدوية الموصوفة، العلاج باللاموتريجين، الجابابنتين أو البريجابالين، أو البنزوديازيبينات المتقطعة (أو وصف يومي).معادلات الديازيبام) أو المنومات-mg زوبيكلون مكافئ؛ تعاطي المواد الحالية أو الاعتماد (معايير DSM-5) ); علاج TMS السابق؛ خطر مرتفع للانتحار؛ عوامل معقدة محتملة لعلاج TMS (على سبيل المثال، تسريحات الشعر التي تعيق وضع الملف اللولبي عن قرب، والثقوب في الجسم)؛ المشاركة في أي تجربة سريرية أخرى في وقت الموافقة أو قبل 6 أشهر؛ أو غير قادر على قراءة أو فهم اللغة الإنجليزية.
تم تجنيد المشاركين من خلال خدمات الصحة النفسية المتخصصة في خمسة مراكز علاجية وثقة NHS المجاورة بالقرب من مراكز العلاج، بالإضافة إلى الإحالات الذاتية ومن خلال مراكز تحديد المرضى التي تجند من خلال خدمات الرعاية الأولية.
تم استخدام استبيان للاتصال الهاتفي بالمشاركين المهتمين، حيث تم دعوة المشاركين المحتملين المؤهلين لحضور تقييم أساسي مع مقيم النتائج. في التقييم الأساسي، قدم جميع المشاركين موافقة خطية مستنيرة وتم تحديد أهلية الدراسة من قبل مقيمي النتائج باستخدام SCID-5-RV و GRID-HDRS-17 و MGH. علاوة على ذلك، لمساعدة في تحديد أهلية الدراسة، تم الحصول على التاريخ الطبي والنفسي – بما في ذلك تقييم مفصل لمقاومة العلاج – من ملاحظات الرعاية الأولية وملفات خدمات الصحة النفسية الثانوية حيثما كان ذلك متاحًا. كما أكمل المشاركون استبيان صدمة الطفولة (CTQ).تم جمع معلومات السوسيوديموغرافيا من خلال تقرير ذاتي. تم إكمال جميع التقييمات وجهًا لوجه في مواقع المستشفيات قبل جائحة COVID-19، والتي تم تغييرها بعد ذلك إلى طرق مؤتمرات الفيديو أو الهاتف. كما أكمل المشاركون تقييمًا أساسيًا بالرنين المغناطيسي مع استخدام المسح لتحديد أهداف العلاج الشخصية، ولتحليل آلية العمل باستخدام الرنين المغناطيسي في الأساس وبعد 16 أسبوعًا.
موافقة الأخلاقيات
حصلت التجربة السريرية على موافقة لجنة الأخلاقيات البحثية وموافقة هيئة البحث الصحي من لجنة الأخلاقيات البحثية المركزية في ليستر شرق ميدلاندز (رقم 18/EM/0232). شمل تصميم البحث وتنفيذه علماء محليين في كل موقع وتمت مشاركته مع جميع المواقع المحلية.
العشوائية والتعتيم
تم تعيين المشاركين عشوائيًا بنسبة 1:1 إلى rTMS أو cgiTBS. قام موظفو TMS الذين يقدمون العلاج بإجراء العشوائية. عملية عبر نظام عشوائي قائم على الويب (Sealed Envelope، www.sealedenvelope.com) مباشرة قبل بدء جلسة العلاج الأولى للمشارك. تم تقسيم العشوائية حسب موقع الدراسة وتم تقليلها بناءً على شدة الاكتئاب (GRID-HDRS-17: الدرجة 16-23، معتدل أو شديد) ودرجة مقاومة العلاج (منخفضةمتوسطمرتفعتم تقييم ذلك في التقييم الأساسي. تم إبلاغ تخصيص العلاج فقط لموظفي إدارة TMS في كل موقع عبر البريد الإلكتروني.
تم الحفاظ على سرية تخصيص العلاج بالنسبة للمشاركين والفرق السريرية ومقيّمي النتائج حتى بعد التقييم النهائي للمشارك. تم تسجيل أي كشف غير مقصود لمقيّمي النتائج، حيث أكمل مقيّمون آخرون جميع التقييمات اللاحقة لذلك المشارك. في كل تقييم لاحق، طُلب من مقيّم النتائج تخمين تخصيص علاج المشارك.
الإجراءات
تم توصيل ما مجموعه 3000 نبضة في كل جلسة من جلسات rTMS أو cgiTBS، والتي كانت تستغرق حوالي 38 دقيقة لأغراض إخفاء المعلومات عن المشاركين والمقيمين للنتائج.
أتم استخدام ملف لولبي على شكل رقم ثمانية (E-z Cool coil) ومحفز Magstim Horizon Performance مع حزمة StimGuide الموجهة لتحفيز TMS (شركة Magstim) لجميع علاجات rTMS وcgiTBS. تم تقديم عشرين جلسة يومية واحدة لكل مشارك على مدار فترة تتراوح بين 4 إلى 6 أسابيع لكلا ذراعي العلاج.
المشاركون الذين تم تعيينهم إلى cgiTBS تلقوا انفجارات من ثلاث نبضات (عتبة الراحة الحركية)، مع تكرار النبضات كل 200 مللي ثانية (5 هرتز). تم تقديم النبضات في دورات مدتها 10 ثوانٍ تتكون من 2 ثانية من التحفيز و8 ثوانٍ من الراحة؛ كان هناك 20 دورة من هذا القبيل لكل جلسة (600 نبضة لكل جلسة). تم تقديم خمس جلسات لكل جلسة، مع فترات راحة بين الجلسات مدتها 5 دقائق (3,000 نبضة لكل جلسة). تم تحديد هدف الدماغ cgiTBS بناءً على تحليل السببية غرانجر كموقع داخل IDLPFC يتلقى أقصى اتصال فعال من rAI (إحداثيات معهد مونتريال العصبي:، ، تم تحديده باستخدام تصوير الرنين المغناطيسي الوظيفي بالاعتماد على الراحة (rsfMRI) ومسحات التصوير بالرنين المغناطيسي الهيكلي T1حزمة تحفيز TMS الموجهة بواسطة StimGuide حسبت أقرب موقع للتحفيز على فروة الرأس استنادًا إلى نموذج رأس فردي يعتمد على التصوير بالرنين المغناطيسي الهيكلي وثلاث نقاط مرجعية: النقطة الأنفية وموقع الأذن اليسرى وموقع الأذن اليمنى.
تم تعيين المشاركين الذين خضعوا لـ rTMS لاتباع البروتوكول المعتمد من إدارة الغذاء والدواء الأمريكية.. كانت المحفزات عند عتبة الراحة الحركية مع-سلسلة من 10 هرتز متداخلة بفواصل زمنية بين السلاسل تبلغ 26 -ثانية، مع إجمالي 3000 نبضة لكل جلسة. تم تحديد هدف الرTMS في الدماغ باستخدام التصوير بالرنين المغناطيسي الهيكلي للمشاركين لاستهداف إحداثي قياسي لمعهد مونتريال العصبي. (تم اختياره مسبقًا كأقرب فوكسي بارينشيمالي لموقع F 3 في دماغ قياسي). كما هو الحال مع ذراع علاج cgiTBS، تم استخدام حزمة تحفيز TMS الموجهة بواسطة StimGuide لحساب موقع التحفيز من نفس نموذج الرأس الفردي والنقاط الثلاث المرجعية المذكورة أعلاه.
تم تحديد عتبة الحركة (كنسبة مئوية) في جلسة العلاج الأولى وتم تحديدها مرة أخرى في جلسة العلاج السادسة لكلا ذراعي العلاج. تم تطوير خطوات موحدة للمشاركين الذين لم يتمكنوا من تحمل بروتوكولات cgiTBS أو rTMS، والتي تضمنت إما تحريك موقع التحفيز بمقدار 1 سم من الإحداثيات المستمدة من التصوير بالرنين المغناطيسي أو تقليل عتبة الحركة.
بيانات النتائج من مقاييس التقييم (GRID-HDRS-17، BDI-II) )، PHQ-9 (مرجع 27))، GAD-7 (مرجع 31))، WSAS EQ-5D-5L ) و EQ-5D-5L VAS تم جمعها في البداية وفي 8 و16 و26 أسبوعًا بعد التوزيع العشوائي. نسخة معدلة من سجل استلام خدمات العملاءتم جمعها في البداية وفي المتابعات بعد 16 و26 أسبوعًا. أكمل المشاركون فحوصات التصوير بالرنين المغناطيسي في البداية وفي غضون أسبوعين من تقييم المتابعة بعد 16 أسبوعًا. أداة THINC-Itتم جمع بيانات الإدراك في الأصل خلال تقييم الخط الأساسي وفي جميع نقاط المتابعة الثلاث. ومع ذلك، بعد جائحة COVID-19، تم تعديل THINC-It تم جمع الأداة في خط الأساس وعمليات التصوير بالرنين المغناطيسي بعد 16 أسبوعًا فقط. لتقييم معتقدات المشاركين حول فعالية العلاج، واستنادًا إلى نصيحة ممثلينا من المرضى والمشاركة العامة، قمنا بتكييف مقياس الانطباع العام للتغيير لدى المرضى الذي يتكون من سبع نقاط.مقياس ليكرت المختصر المكون من خمسة نقاط (1-5، من أسوأ بكثير إلى أفضل بكثير، مع عدد من نقاط التقييم لكل من الحالة النفسية الأسوأ والمحسنة). تم تقييم قبول المرضى أيضًا باستخدام مقياس ليكرت مصمم خصيصًا يتكون من خمسة نقاط، يتم تقييمه من 1 إلى 5: غير مقبول (الآثار السلبية تفوق الفوائد) إلى مقبول (الآثار المفيدة تفوق الآثار السلبية). تم تقييم هذين المقياسين في كل جلسة TMS وفي كل نقطة متابعة. قبل جائحة COVID-19، تم منح المشاركين خيار إكمال تقييمات المتابعة وجهًا لوجه أو عن بُعد، حيث تم إكمال جميع التقييمات لاحقًا عبر الهاتف أو مؤتمرات الفيديو خلال وبعد جائحة COVID-19. تم تغطية نفقات السفر للمشاركة في الدراسة، جنبًا إلى جنب مع قسيمة تسوق في تقييمات المتابعة بعد 16 و26 أسبوعًا، كعلامة على الاحترام والامتنان لوقت ومساهمة المشاركين في جوانب المتابعة من التجربة. أكمل المشاركون الذين تم تجنيدهم لاحقًا في الدراسة النسخة الذاتية التقييم من الجرد السريع للأعراض الاكتئابية.عند الخط الأساسي و8 و16 و26 أسبوعًا لأغراض دراسة فرعية حول الإدراك والتصوير بالرنين المغناطيسي الوظيفي (معلومات إضافية)لذلك، يجب عدم اعتبار هذا الإجراء نتيجة ثانوية للتجربة وليس مُبلغًا عنه هنا.
النتائج
كان مقياس النتيجة السريرية الأساسي هو متوسط التغير في أعراض الاكتئاب من خط الأساس على مدى 8 و16 و26 أسبوعًا باستخدام GRID-HDRS-17. HDRS-17 هو المقياس الأكثر استخدامًا من قبل المراقبين لتقييم الاكتئاب في التجارب السريرية العشوائية لعلاجات الاكتئاب.، وتم استخدام نموذج GRID نظرًا لوجود أدلة على تحسين موثوقية التقييم بين المقيمين.
كانت النتائج السريرية الثانوية هي التغيرات المتوسطة من خط الأساس على مدى 26 أسبوعًا في BDI-II وPHQ-9 وGAD-7 وWSAS وEQ-5D-5L VAS؛ التغيرات المتوسطة من خط الأساس إلى 16 أسبوعًا للمهام المعرفية الخمس في أداة THINC-It؛ التغيرات المتوسطة من خط الأساس إلى 8 و16 و26 أسبوعًا بشكل منفصل على GRID-HDRS-17؛ نسبة المستجيبين في 8 و16 و26 أسبوعًا (المعرفة بأنها انخفاض في على GRID-HDRS-17 من الخط الأساسي)؛ نسبة المرسلين عند 8 و16 و26 أسبوعًا (مُعرّفة كدرجة منعلى GRID-HDRS-17)؛ نسبة المستجيبين المستمرين عند 16 و 26 أسبوعًا (المعرفة بأنها استجابة مستمرةخفض على GRID-HDRS-17 بعد الاستجابة في النقطة الزمنية السابقة؛ وانطباع المريض العام عن التغيير في كل جلسة TMS وكل نقطة متابعة وقائمة الأحداث السلبية (الآثار الجانبية) بعد كل جلسة TMS.
سيتم الإبلاغ عن الطيف المغناطيسي، ونتائج فعالية التكلفة (EQ-5D-5L ومخزون استلام الخدمة المعدل للعميل)، ونتائج القبول (مقياس ليكرت المصمم خصيصًا من خمس نقاط والمقابلات النوعية) ونتائج السلامة الإضافية (الآثار الجانبية الشائعة وغير الشائعة) بشكل منفصل.
رصد الأحداث السلبية
تم اعتماد وتطبيق التعريفات المتفق عليها دوليًا للأحداث الضائرة العادية والأحداث الضائرة الخطيرة.تم الإبلاغ عن النوبات كأحداث سلبية خطيرة. تم تسجيل الإغماء كحدث سلبي إلا إذا تم إدخال المشارك إلى المستشفى، وفي هذه الحالة تم تعريفه كحدث سلبي خطير. أي مشارك يُكتشف أنه في خطر على نفسه (الانتحار، الإهمال) أو على الآخرين، أو يتطور لديه حدث سلبي خطير، تم إحالته إلى الخدمات السريرية المعنية. تم عرض مراجعة من قبل خبير سريري في الاكتئاب المقاوم للعلاج على أي مشارك أصبح اكتئابه أكثر حدة في المتابعات بعد 16 و26 أسبوعًا، لأسباب تتعلق بالسلامة.
دور LEAP
كان LEAP عبارة عن لجنة من ممثلي المشاركة العامة (PPI) الذين لديهم تجارب حية مع الاكتئاب، بعضهم كان لديه تجارب شخصية إضافية مع TMS، والتي ساهمت في جميع جوانب تصميم وتطوير وإدارة تجربة BRIGhTMIND. ترأس LEAP منظم PPI ذو خبرة (P.B.) وشمل ممثلين من جميع المراكز. تم بذل جهود لضمان الشمولية من حيث الجنس والخلفية العرقية والتجارب الشخصية. تم دفع أجر لأعضاء LEAP مقابل وقتهم. كانت التوصيات المحددة من LEAP هي: إكمال 20 جلسة TMS على مدار 6 أسابيع بدلاً من 4 أسابيع؛ قياس النتائج فقط بعد 8 أسابيع بدلاً من 6 و8 أسابيع بسبب العبء على المشاركين؛ جاء رفاق السفر إلى مواعيد التصوير بالرنين المغناطيسي وTMS؛ تمت إعادة كتابة جميع مواد البحث بلغة بسيطة وشاملة، مما أدى إلى مضاعفة عدد الزيارات لموقع الدراسة؛ الإعلان في مواقع محددة لتعزيز الشمولية – على سبيل المثال، أماكن العبادة لتجنيد الأشخاص من أصل جنوب آسيوي؛ وتكييف الانطباع العام للمريض عن التغيير. تم اقتراح تغييرات إضافية من قبل LEAP لضمان استمرار التجربة خلال جائحة COVID-19، مثل استخدام صور وملفات تعريف الموظفين أثناء ارتداء الأقنعة خلال المواعيد الشخصية والبعيدة.
التغييرات بسبب جائحة COVID-19
تم الإبلاغ عن تعديلات جوهرية على البروتوكول في ضوء جائحة COVID-19 في نشر بروتوكول التجربة.تم إجراء هذه التغييرات استجابةً للتدابير الصحية العامة الوطنية والمحلية المتعلقة بجائحة COVID-19، بموافقة منظمات حوكمة البحث السريري في كل موقع، والراعي (مؤسسة نوتنغهامشير للرعاية الصحية NHS)، وLEAP، ومجموعة إدارة التجارب، واللجنة المستقلة لتوجيه التجارب، ولجنة إدارة البيانات والأخلاقيات، والجهات الممولة. كواحدة من التدابير الصحية العامة في جائحة COVID-19، لم تتطلب هذه التغييرات موافقة الأخلاقيات NHS والسلطة الصحية للبحوث. تم تعليق الدراسة، باستثناء التقييم عن بُعد، من 19 مارس إلى 1 أغسطس 2020. تم إجراء التغييرات الرئيسية التالية من 1 أغسطس 2020 حتى نهاية الدراسة: (1) تم إجراء جميع التقييمات السريرية الأساسية، والحصول على الموافقة المكتوبة والمستنيرة، وجميع التقييمات السريرية اللاحقة عن بُعد عبر مؤتمرات الفيديو المدعومة بالهاتف والبريد الإلكتروني. (2) تم إجراء جميع تقييمات التصوير بالرنين المغناطيسي، وعلاج TMS، وتقييمات THINC-it وجهًا لوجه، مع اتخاذ احتياطات جائحة COVID-19 التي قللت من الحد الأقصى لعدد المشاركين في التجربة. (3) تم إجراء تقييمات THINC-it فقط في الأساس و16 أسبوعًا، جنبًا إلى جنب مع فحوصات التصوير بالرنين المغناطيسي، ولم يتم إجراؤها في 8 و26 أسبوعًا – لم يتم إجراء تغييرات أخرى على التقييمات على الرغم من فقدان فحوصات التصوير بالرنين المغناطيسي في 16 أسبوعًا من 19 مارس إلى 1 أغسطس 2020. (4) تم تغيير النتيجة الأساسية من الاستجابة في 16 أسبوعًا إلى التغيير المتوسط في إجمالي درجة HDRS-17 في 8 و16 و26 أسبوعًا. (5) تم تقليل حجم العينة من 368 إلى 266 مشاركًا نظرًا لمعدل التوظيف الأبطأ بسبب احتياطات الجائحة. (6) لم يتم إعادة فتح أحد المواقع بمجرد إعادة فتح الدراسة بسبب فقدان الموظفين المطلوبين لإجراء تقييم TMS والبحث، وتم استبداله بموقع آخر. (7) تم تغيير خطة التحليل لتعكس تغيير متغير النتيجة الأساسية ولإضافة تحليل حساسية قبل وبعد COVID. (8) تم الحصول على تمويل إضافي لمعالجة فترة تعليق الدراسة ومعدل التوظيف الأبطأ.
حساب حجم العينة
حدد المعهد الوطني للصحة والرعاية الممتازة ثلاث نقاط كفرق مهم سريرياً في النتائج على مقياس هاملتون للاكتئاب – 17 لاضطرابات الاكتئاب.قمنا بمقارنة التغير المتوسط في أعراض الاكتئاب من خط الأساس على مدى 26 أسبوعًا في مجموعة cgiTBS مع تلك في مجموعة rTMS. بافتراض انحراف معياري قدره 8 في الفرق المتوسط بين المجموعتين، كما أبلغتنا أعمالنا التجريبية.ودراسة سابقة عشوائية محكومة في اضطراب الاكتئاب المستمر المزمنحجم عينة مكون من 266 مشاركًا سيوفرالقدرة على اكتشاف فرق متوسط قدره ثلاث نقاط في GRID-HDRS-17 على مدى 26 أسبوعًا بين المجموعات فيمستوى دلالة ذو جانبين، مع افتراض وجود ارتباط بين قياسات المتابعة بنسبة 0.7 وفقدان/انسحاب بيانات بنسبة 20%.
التحليل الإحصائي
تم نشر خطة التحليل الإحصائي قبل إجراء التحليل الأساسي وتوفر مزيدًا من التفاصيل حول التحليل.. الأساسي “تم إجراء تحليل النتيجة الأساسية على مجموعة التحليل حسب النية (جميع المشاركين الذين تم توزيعهم عشوائيًا على العلاجات)، مع تنفيذ تقنية الاستبدال المتعدد للتعامل مع البيانات المفقودة في الحالات التي كانت فيها درجات GRID-HDRS-17 مفقودة. تم استخدام الجنس، والعرق، والعمر، والمركز، ودرجة GRID-HDRS-17 الأساسية ودرجة TRD كمتنبئات للنتيجة الأساسية لاستبدال البيانات المفقودة بالقيم المتوقعة من معادلة الانحدار العادي المتعدد المتغيرات. تم تقدير ما مجموعه 20 استبدالًا. تم استخدام نموذج انحدار خطي مختلط، والذي تم تعديله للمركز (متغير التقسيم)، ودرجة GRID-HDRS-17 الأساسية ودرجة MGH الأساسية (متغيرات التخفيف)، ورقم الزيارة ومتغير فئوي لذراع العلاج (ذراع rTMS كمرجع). تم تضمين معرف المشارك كأثر عشوائي. يتم تقديم تقدير مقارنة العلاج كفرق متوسط معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدل معدلالقيم والأهمية الإحصائية التي تم أخذها في الاعتبار فيتم إجراء تحليل النتائج السريرية الثانوية بطريقة مماثلة، حيث تم ذلك على مجموعة التحليل حسب النية باستخدام نهج البيانات المتاحة. تم استخدام نماذج الانحدار اللوجستي الثنائي لتحليل المستجيبين، والمستجيبين المؤقتين، والمستجيبين المستدامين، مع تقديم تقديرات مقارنة العلاج بطريقة مشابهة لتلك المبلغ عنها في تحليل النتائج الأولية باستثناء الإبلاغ عن نسب الأرجحية المعدلة. تم تضمين المشاركين الذين تم تعيينهم عشوائيًا للعلاج والذين أكملوا جلسة واحدة على الأقل من التحفيز المغناطيسي عبر الجمجمة في مجموعة السلامة.
شملت التحليلات الثانوية للنتيجة الأساسية تحليلًا وفقًا للبروتوكول (باستثناء المشاركين الذين لديهم انتهاكات كبيرة للبروتوكول: إذا لم يتم تنفيذ بروتوكولات العلاج الأصلية؛ تم إكمال 20 جلسة علاج بعد 6 أسابيع؛ مرت أكثر من 4 أيام بين العلاجات؛ تم تغيير العلاج الدوائي أو العلاج النفسي للاكتئاب الشديد قبل المتابعة بعد 16 أسبوعًا) وتحليل المكتملين (أي، المشاركون الذين أكملوا عشر جلسات أو أكثر من rTMS أو cgiTBS المقدمة إلى الإحداثيات الصحيحة للتصوير بالرنين المغناطيسي وتم تقييمهم في البداية وبعد 16 أسبوعًا). شملت تحليلات الحساسية للنتيجة الأساسية تحليل افتراض عدم الغياب العشوائي (MNAR) باستخدام نهج استبدال قائم على التحكم وتحليل فترة ما قبل وما بعد COVID-19.
تم استخدام Stata (الإصدار 16) لجميع تحليلات البيانات باستثناء نتائج الإدراك، التي تم تحليلها في IBM SPSS Statistics (الإصدار 25). فيما يتعلق بتصوير الدماغ، تم نشر بروتوكول قبل استلام أي بيانات سريرية أو تحليل إحصائي.. تم تفصيل خطوات المعالجة المسبقة في ذلك البروتوكول. تم تنفيذ نماذج التأثيرات المختلطة في برنامج SPSS (الإصدار 18) وJASP (الإصدار 0.18) وتم تقديرها باستخدام أقصى احتمال مقيد. كان المشاركون هم التأثير العشوائي مع مصفوفة التباين والتغاير ذات الهوية المقاسة، وكانت المتغيرات التابعة هي التحسن السريري من خط الأساس في GRID-HDRS-17 (مقياس النتيجة الأساسي)، PHQ-9 أو BDI-II (مقاييس النتيجة الاستكشافية المخطط لها). بالإضافة إلى الاتصال الأساسي، أو التغير في الاتصال، ذي الصلة بفرضية معينة، قمنا بتضمين كمتغيرات مستقلة نقطة الوقت بعد العلاج (8، 16 أو 26 أسبوعًا) ومجموعة العلاج (rTMS أو cgiTBS)، وتفاعل الاتصال مع أي من المتغيرين أو كليهما. تم استكشاف العمر، الجنس، مجموعة مقاومة العلاج في MGH، GAD-7، CTQ وموقع مجموعة الدراسة كمتغيرات محتملة للتشويش؛ حيث كانت هذه غير ذات دلالة تم إزالتها من النموذج. كانت مجموعة MGH والموقع ذات دلالة لتحليلات الاتصال الأساسي؛ لم تكن هناك متغيرات مشوشة ذات دلالة لتحليلات فحص التغير في الاتصال. كان الانخفاض في GAD-7 مرتبطًا بشكل كبير بالانخفاض في مقاييس الاكتئاب من خط الأساس إلى المتابعة، لكن هذا لم يغير دلالة النتائج المبلغ عنها. تم تحديد عتبة الدلالة عند مستوى لكل من تحليلاتنا المحددة مسبقًا. نظرًا لاستخدام منطقتين محددتين مسبقًا للاهتمام لـ IDLPFC في التحليلات التي تفحص التغير في الاتصال الوظيفي بين DLPFC و DMPFC، تم تطبيق تصحيح هولم-بونفيروني لاختبارين عبرقيم كل مصطلح (بخلاف متغيرات الارتباك) في هذا النموذج المختلط. في التحليلات الحساسية المخططة مسبقًا التي تستبعد المرضى الذين كان هدف cgiTBS لديهم خارج الجيروس الجبهي الأوسط الأيسر وفقًا لأطلس هارفارد-أكسفورد القشري عند عتبة 10%، تم تحديد حالتين فقط من هذا القبيل و كان هناك تغيير طفيف في المعلمات الإحصائية. تم إجراء تحليل استكشافي غير مخطط له باستخدام HDRS-6 (المرجع 38) الذي، على عكس GRID-HDRS-17، هو مقياس أحادي البعد للاكتئاب على مر الزمن.لفهم المزيد عن تأثيرات صافي rAI الأساسي على نتائج تدفق IDLPFC فيما يتعلق بأعراض الاكتئاب على مدى 26 أسبوعًا.
تم تسجيل تجربة BRIGhTMIND في سجل ISRCTN (رقم ISRCTN19674644) في 2 أكتوبر 2018، وتم تعديلها في 18 سبتمبر 2020 لتأخذ في الاعتبار COVID-19، وهي الآن مسجلة على أنها مكتملة.
ملخص التقرير
معلومات إضافية حول تصميم البحث متاحة في ملخص تقارير مجموعة ناتشر المرتبط بهذه المقالة.
توفر البيانات
سنقوم بتوفير البيانات للمجتمع العلمي مع أقل عدد ممكن من القيود مع الاحتفاظ بالاستخدام الحصري حتى نشر النتائج الرئيسية. سيتم إيداع البيانات المجهولة الهوية، بما في ذلك جميع بيانات التجارب المنشورة في هذه المخطوطة، في مستودع بيانات جامعة نوتنغهام.https://rdmc.nottingham.ac.ukللتشجيع على استخدام أوسع.
توفر الشيفرة
يمكن العثور على كود الكمبيوتر المستخدم لحساب الإحداثيات لتحفيز cgiTBS أو rTMS من مسح fMRI وMRI الهيكلي في دراسة BRIGhTMIND فيhttps://github.com/SPMIC-UoN/خط أنابيب العقل اللامع.
References
Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (American Psychiatric Association, 2013).
First, M. et al. Structured Clinical Interview for DSM-5-Research version (SCID-5 for DSM-5, Research Version; SCID-5-RV) (American Psychiatric Association, 2015).
Bernstein, D. P. et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl. 27, 169-190 (2003).
Beecham, J. & Knapp, M. Costing Psychiatric Interventions (Gaskell, 2001).
Demyttenaere, K. et al. Patient-assessed versus physician-assessed disease severity and outcome in patients with nonspecific pain associated with major depressive disorder. Prim. Care Companion J. Clin. Psychiatry 11, 8-15 (2009).
Rush, A. J. et al. The 16 -item Quick Inventory of Depressive Symptomatology (QIDS) Clinician Rating (QIDS-C) and Self-Report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol. Psychiatry 54, 573-583 (2003).
Salagre, E. et al. Statins for the treatment of depression: a meta-analysis of randomized, double-blind, placebo-controlled trials. J. Affect. Disord. 200, 235-242 (2016).
ICH E2A Clinical Safety Data Management: Definitions and Standards for Expedited Reporting – Scientific Guideline (European Medicines Agency, 1995).
Morriss, R. et al. Statistical analysis plan. Figshare figshare. com/articles/online_resource/SAP_Morriss_BRIGhTMIND_Final_ docx/21271140/1 (2022).
Xia, M. et al. BrainNet Viewer: a network visualization tool for human brain connectomics. PLoS ONE 8, e68910 (2013).
شكر وتقدير
تم تمويل هذا المشروع من قبل برنامج تقييم الفعالية والآلية (رقم المنحة 16/44/02، الممنوحة لـ R.M. وM.A. وC.B. وP.B. وS.L. وP.F.L. وR.H.M.-W. وA.O.-K. وD.P.A.)، وهو شراكة بين MRC والمعهد الوطني للبحوث الصحية والرعاية (NIHR). قامت Magstimplc بتوريد أنظمة توصيل TMS والملاحة العصبية. الآراء والأفكار المعبر عنها من قبل المؤلفين والمقابلين في هذا المنشور إن الآراء المذكورة هي آراء المؤلفين والمشاركين في المقابلات، ولا تعكس بالضرورة آراء هيئة الخدمات الصحية الوطنية، والمعهد الوطني للبحوث الصحية، ومجلس البحوث الطبية، ومركز تمويل الأبحاث، ومركز تقييم الفعالية والآلية، ووزارة الصحة أو شركة ماجستيم. لم يكن للممولين أي دور في تصميم الدراسة، أو جمع البيانات وتحليلها، أو اتخاذ قرار النشر، أو إعداد المخطوطة. نشكر فريق دراسة BRIGhTMIND البحثي: أ. بلماير، ل. بوث، ج. بواتري، و. كوتام، إ. كوكس، ل. دافيسون، ر. دي فاي، د. دوس سانتوس، م. دوغلاس-بايلي، د. هاردينغ، س. إيوابوتشي، م. جيمس، ج. كايلور-هيوز، م. كين، ن. خليفة، هـ. أوه، ج. بارك، إ. ريد، ج. ريفيرا، س. سيمبسون، ج. ستون ول. طومسون. نشكر ممثلينا في لجنة مراقبة البيانات والأمان ولجنة الإشراف: د. بالدوين، ج. داوريك، ر. إيمسلي، ك. كيتس، ج. لانكستر، ب. نوردن، س. ووكر و ب. ويلكنسون. نشكر أعضاء مشاركة المرضى والجمهور: ج. إيستهم، ج. غليدهيل، م. حامي، م. ليدل، ر. مكناوتون، م. ميستري، ج. أوي، أ. ويليس و ت. ويليس.
مساهمات المؤلفين
كان R.M. المحقق الرئيسي للدراسة، وحصل على تمويل للدراسة وتصاريح الدراسة، وصمم الدراسة، وقاد تنفيذها وكتب المسودة الأولى من المخطوطة مع L.W. وهو الضامن للدراسة. كتبت L.W. إرشادات تشغيلية للمشروع، وساعدت في تصميم بروتوكولات التحليل النوعي، وجمعت البيانات السريرية لموقع نوتنغهام، وحللت بيانات التصوير والبيانات النوعية وكتبت المسودة الأولى من المخطوطة مع R.M. كان M.A. المحقق الرئيسي لموقع لندن، بما في ذلك القائد السريري لـ TMS في الموقع، وحصل على تمويل للدراسة كمتقدم للمنحة. ساعد في تصميم تقديم علاج TMS وتفسير تحليل TMS. كانت D.P.A. القائدة في التصوير العصبي للدراسة وحصلت على تمويل للدراسة كمتقدمة للمنحة. صممت إرشادات الاتصال بالرنين المغناطيسي مع P.F.L. ساعدت S.B. في تصميم التجربة السريرية، وأجرت حسابات القوة للدراسة وساهمت في إعادة حساب حجم العينة بعد تغيير النتيجة الأساسية. ساعدت في تصميم خطة التحليل الإحصائي للتجربة السريرية، وقدمت الدعم الإحصائي طوال الدراسة ونصحت في التحليل الإحصائي لبيانات MRS. ساعد P.B. في التصميم وقاد كل من مشاركة المرضى والجمهور في الدراسة طوال الوقت. علق على مسودات التقرير وساعد في تصميم تحليل مساهمة المرضى والجمهور في التقرير. ساعد P.M.B. في التصميم وأجرى تحليل الرنين المغناطيسي للدراسة. نصح في التحليل الإحصائي لبيانات THINC-it. كانت C.B. الإحصائية الرئيسية للتجربة السريرية وحاملة المنحة. قدمت الدعم الإحصائي طوال الدراسة. أشرفت على تصميم خطة التحليل الإحصائي، بالإضافة إلى التحليل الإحصائي وتقرير نتائج التجربة السريرية. أجرت B.H. تحليل THINC-it مع R.H.M.-W. وصاغت تقرير تحليل THINC-it. كانت L.I. مديرة التجربة منذ عام 2021 وحصلت على تصاريح للدراسة. كان M.K. المحقق الرئيسي في موقع أولدهام في الدراسة وكان القائد السريري لـ TMS في الموقع. كان S.L. المحقق الرئيسي في موقع نوتنغهام والقائد السريري لـ TMS في نوتنغهام. ساعد في وضع تدخل TMS للدراسة وكان حامل المنحة. ساعد P.F.L. في وضع تصور التصوير العصبي للدراسة، بما في ذلك طريقة حساب مواقع تحفيز TMS من بيانات MRI. كان حامل منحة. كان R.H.M.-W. الباحث الرئيسي والقائد السريري لموقع نيوكاسل. وضع تحليل THINC-it وقام بتكييف مقياس MGH لمقاومة العلاج للدراسة. كان A.O.-K. الباحث الرئيسي في موقع نورثامبتون وأشرف على تقديم TMS في نورثامبتون. ساعد في وضع تصور علاج TMS في الدراسة وكان حامل منحة. كتب S.P. البرنامج الحاسوبي والطريقة الآلية لحساب موقع تحفيز TMS من بيانات MRI، وحسب دقة تحفيز TMS المقدم بواسطة التنقل العصبي من موقع الهدف المحسوب بواسطة MRI. قدم A.S.D.P. الدعم الإحصائي طوال فترة الدراسة وأجرى التحليل الإحصائي تحت إشراف S.B. وC.B. ساهمت في إعادة حساب حجم العينة بعد تغيير النتيجة الأساسية. كتبت خطة التحليل الإحصائي وأنتجت تقرير نتائج التجربة السريرية بما يتماشى مع خطة التحليل. كانت Y.W. مديرة التجربة منذ بداية التجربة حتى سبتمبر 2021. ثم أشرفت على L.I.، التي تولت الدور.
المصالح المتنافسة
لقد تلقى R.M. تمويلاً للبحث من شركة Electromedical Products, Inc. ورسومًا للمشاركة في لجنة أخلاقيات مراقبة البيانات لاثنين من التجارب في الاكتئاب من شركة Novartis plc. وقد تلقى M.A. رسومًا للاستشارات وإلقاء المحاضرات من شركات Takeda Pharmaceutical وJanssen Pharmaceutical وجمعية Clinical TMS. يعلن R.H.M.-W. عن رسوم للاستشارات وإلقاء المحاضرات من شركات Janssen-Cilag وLivaNova وLundbeck وP1Vital وSage Therapeutics وSothema وTakeda. لم يتم الإبلاغ عن أي تضارب محتمل آخر في المصالح لأي من المؤلفين الآخرين. لم تشارك أي أطراف ثالثة في تصميم الدراسة أو تحليلها أو كتابة المخطوطة.
يجب توجيه المراسلات والطلبات للحصول على المواد إلى ريتشارد موريز.
معلومات مراجعة الأقران تشكر مجلة ناتشر ميديسن تاو تشين، كاثرين سكانغوس والمراجعين الآخرين المجهولين على مساهمتهم في مراجعة هذا العمل. المحرر الرئيسي: مينغ يانغ، بالتعاون مع فريق ناتشر ميديسن.
الشكل البياني الممتد 1 | تدفق المشاركين من خلال بروتوكول fMRI. rTMS، التحفيز المغناطيسي عبر الجمجمة المتكرر cgiTBS، التحفيز المتقطع الموجه بالاتصال باستخدام نبضات ثيتا.
الشكل البياني الممتد 2 | مواقع تحفيز TMS. توضيح لأهداف التحفيز المغناطيسي عبر الجمجمة (TMS) ومناطق الاهتمام (ROIs) لتحليلات الاتصال الدماغي الأساسية. النقاط الصغيرة تشير إلى إحداثيات هدف قشرة الفص الجبهي الجانبي الأيسر (DLPFC) لتحفيز النبضات الثيتا المتقطعة الموجهة بالاتصال (cgiTBS) للمشاركين الأفراد – هذه هي المواقع.
مع أقصى اتصال فعال من القشرة الأمامية اليمنى (rAI) كنقطة رمادية كبيرة. يتم عرض متوسط هدف cgiTBS عبر المشاركين كنقطة بيضاء كبيرة. يتم عرض متوسط هدف التحفيز المغناطيسي عبر الجمجمة المتكرر (rTMS) كنقطة بيضاء كبيرة؛ هذا هو هدف F3 للمجموعة التي تلقت rTMS. تم رسمه باستخدام BrainNet Viewer (شيا وآخرون).على أطلس ICBM152 الملساء.
الشكل البياني الممتد 3 | نسبة المشاركين الذين شعروا بتحسن طفيف أو كبير خلال 20 جلسة من التحفيز المغناطيسي عبر الجمجمة. TMS، التحفيز المغناطيسي عبر الجمجمة. rTMS، التحفيز المغناطيسي المتكرر عبر الجمجمة. cgiTBS، التحفيز المتقطع الموجه بالاتصال باستخدام نبضات ثيتا. قام المشاركون بتقييم أنفسهم على أنهم تحسنوا بشكل طفيف أو كبير وفقًا لمقياس الانطباع السريري العالمي المعدل من 5 نقاط.
الشكل 4 من البيانات الموسعة | انخفاض في التدفق الصافي الأساسي من القشرة الحوفية الأمامية اليمنى إلى القشرة الجبهية الجانبية اليسرى فيما يتعلق بالتحسن المتوسط في درجة GRID-HDRS-17 على مدى 26 أسبوعًا. انخفاض في درجة النسخة GRID من مقياس تقييم الاكتئاب هاملتون المكون من 17 عنصرًا (GRID-HDRS-17) من الأساس إلى المتابعة، مجمعة عبر نقاط المتابعة الزمنية، كدالة للتدفق الصافي الأساسي من منطقة البذور للقشرة الحوفية الأمامية اليمنى (RAI) إلى
منطقة الهدف لتحفيز نبضات ثيتا المتقطعة الموجهة بالاتصال (cgiTBS) داخل القشرة الجبهية الجانبية اليسرى (DLPFC). كل نقطة بيانات تمثل مشاركًا. كان التدفق الصافي المنخفض (أي، تأثير أقل للـ RAI على الـ DLPFC الأيسر وتأثير أكبر للـ DLPFC الأيسر على الـ RAI) مرتبطًا بتحسن أكبر.
الشكل البياني الموسع 5 | مناطق الاهتمام لتحليل التغير في الاتصال الدماغي للقشرة الجبهية الجانبية والقشرة الجبهية المتوسطة. مناطق الاهتمام (ROIs) لتحليلات التغير في الاتصال الدماغي، موضوعة على صورة الدماغ القياسية (خريطة ICBM152 الملساء)، في المستويات السهمية (يسار) والمستعرضة (يمين). DMPFC: القشرة الجبهية الحوفية الظهرية؛ DLPFC(a): موقع DLPFC الأمامي؛ DLPFC(p): موقع DLPFC الخلفي.
الشكل 6 من البيانات الموسعة | انخفاض في الاتصال الوظيفي بين القشرة الجبهية الظهرية الجانبية اليسرى والقشرة الجبهية الظهرية الوسطى اليسرى مع تحسن في درجة PHQ-9 على مدى 26 أسبوعًا. انخفاض في الدرجة الإجمالية لاستبيان الصحة الشخصية المكون من 9 عناصر (PHQ-9) (تحسن) من خط الأساس إلى المتابعة، مجمعة عبر نقطة زمنية بعد العلاج، كدالة لانخفاض في
الاتصال الوظيفي بين منطقة القشرة الجبهية الظهرية الوسطى اليسرى (DMPFC) ومنطقة القشرة الجبهية الظهرية الجانبية اليسرى (DLPFC). كل نقطة بيانات تمثل مشاركًا. كان التحسن السريري الأكبر مرتبطًا بتقليل أكبر في الاتصال الوظيفي بين هذه المناطق.
البيانات الموسعة الجدول 1 | توقعات مقيم النتائج لتوزيع العلاج
تحفيز المغناطيسي المتكرر عبر الجمجمة
cgiTBS
إجمالي
توقع المحلل للنتائج لتوزيع العلاج بعد 8 أسابيع
تنبؤ تخصيص العلاج
لا أعرف
94 (83.9%)
95 (85.6%)
189 (84.8%)
cgiTBS
9 (8.0%)
6 (5.4%)
15 (6.7%)
تحفيز الدماغ المتكرر عبر المغناطيس
9 (8.0%)
10 (9.0%)
19 (8.5%)
توقع تقييم النتائج لتوزيع العلاج بعد 16 أسبوعًا
تنبؤ تخصيص العلاج
لا أعرف
90 (80.4%)
88 (78.6%)
178 (79.5%)
cgiTBS
7 (6.3%)
11 (9.8%)
18 (8.0%)
تحفيز الدماغ المتكرر عبر المغناطيس
15 (13.4%)
12 (10.7%)
27 (12.1%)
غير قابل للتحصيل
0 (0.0%)
1 (0.9%)
1 (0.4%)
توقع مُقيّم النتائج لتوزيع العلاج بعد 26 أسبوعًا
تنبؤ تخصيص العلاج
لا أعرف
77 (75.5%)
76 (73.1%)
153 (74.3%)
cgiTBS
8 (7.8%)
17 (16.3%)
25 (12.1%)
تحفيز الدماغ المتكرر عبر المغناطيس
17 (16.7%)
11 (10.6%)
28 (13.6%)
البيانات الموسعة الجدول 2 | المسافة وزاوية الجلسة المستهدفة والجلسات المتداخلة لـ TMS
الربع الخامس والعشرون
الوسيط
النسب المئوية
تحفيز المغناطيسي عبر الجمجمة المتكرر
cgiTBS
تحفيز الدماغ المتكرر عبر المغناطيس
cgiTBS
تحفيز الدماغ المتكرر عبر المغناطيس
cgiTBS
مسافة الهدف-الجلسة (مم)
٢.٩٩
2.62
٤.٢٠
٤.٦٦
8.66
8.10
زاوية جلسة الهدف (درجات)
5.02
3.89
7.09
6.82
9.69
9.54
المسافة بين الجلسات (مم)
3.88
3.73
5.17
٤.٦٣
8.25
٧.٤٨
زاوية بين الجلسات (درجات)
5.47
5.31
7.51
6.73
10.07
10.22
تحفيز المغناطيسي عبر الجمجمة (TMS)، التحفيز المغناطيسي المتكرر عبر الجمجمة (rTMS)، تحفيز نبضات ثيتا المتقطعة الموجهة بالاتصال (cgiTBS).
البيانات الموسعة الجدول 3 | إحصائيات وصفية لـ GRID-HDRS-17 للتحليلات الثانوية والحساسية للنتيجة الأساسية
GRID-HDRS-17
خط الأساس
8 أسابيع
16 أسبوع
26 أسبوعًا
تحفيز مغناطيسي عبر الجمجمة المتكرر
cgiTBS
تحفيز الدماغ المتكرر عبر المغناطيس
cgiTBS
تحفيز الدماغ المتكرر عبر المغناطيس
cgiTBS
تحفيز الدماغ المتكرر عبر المغناطيس
cgiTBS
المتوسط (الانحراف المعياري)
ن
ن
المتوسط (الانحراف المعياري)
ن
ن
ن
ن
حسب البروتوكول
67
76
٥٨
61
٥٥
63
52
٥٨
٢٤.١ (٤.٨)
٢٣.٢ (٤.٨)
١٧.٢ (٨.٤)
15.0 (6.4)
17.4 (8.3)
15.3 (8.1)
17.6 (9.2)
١٤.٢ (٧.٩)
المكملون
١١٠
١٠٨
١٠٤
١٠٥
١١٠
١٠٨
98
٩٨
٢٤.٠ (٤.٩)
٢٢.٦ (٤.٦)
15.5 (7.5)
14.4 (6.6)
15.8 (7.9)
15.0 (7.7)
١٦.٢ (٨.٦)
14.4 (7.6)
افتراض MNAR
127
128
127
128
127
128
127
128
٢٣.٩ (٤.٧)
٢٢.٩ (٤.٧)
15.8 (7.3)
١٤.٦ (٦.٢)
١٦.١ (٧.٥)
١٥.٢ (٧.٣)
16.5 (7.9)
14.9 (6.9)
فترة ما قبل وما بعد COVID-19
قبل كوفيد 19
٣٥
٣٦
٢٤.٧ (٥.٣)
٢٣.٢ (٥.٣)
ما بعد كوفيد 19
92
92
٢٣.٥ (٤.٤)
٢٢.٩ (٤.٥)
GRID-HDRS-17، النسخة الشبكية من مقياس هاملتون لتقييم الاكتئاب المكون من 17 عنصرًا. rTMS، التحفيز المغناطيسي عبر الجمجمة المتكرر. cgiTBS، التحفيز المتقطع الموجه بالاتصال باستخدام نبضات ثيتا. MNAR، مفقود غير عشوائي.
البيانات الموسعة الجدول 4 | تحليل أسباب الانحرافات الرئيسية عن البروتوكول حسب نوع الانحراف وعدد المشاركين المتأثرين بنوع الانحراف
سبب الانحراف الرئيسي عن البروتوكول
تحفيز المغناطيسي عبر الجمجمة المتكرر
cgiTBS
بشكل عام
ب
ن
ب
ن
ب
ن
عدم الأهلية بعد التوزيع العشوائي، ن(%)
1 (0.9%)
1 (0.8%)
0 (0.0%)
0 (0.0%)
1 (0.4%)
1 (0.4%)
عدم الامتثال للعلاج العشوائي:
المشارك تلقى أقل من 20 جلسة على مدى فترة من 4-6 أسابيع، عدد (%)
11 (9.4%)
11 (8.7%)
9 (7.6%)
9 (7.0%)
20 (8.5%)
20 (7.8%)
تلقي علاج خاطئ وفقًا للتوزيع العشوائي، ن (%)
9 (7.7%)
9 (7.1%)
13 (11.0%)
13 (10.2%)
22 (9.4%)
22 (8.6%)
توقف الجلسة في منتصف العلاج، عدد (%)
5 (4.3%)
5 (3.9%)
3 (2.5%)
3 (2.3%)
8 (3.4%)
8 (3.1%)
الوقت بين الجلسة الأولى والأخيرة يتجاوز 6 أسابيع، عدد (%)
0 (0.0%)
0 (0.0%)
2 (1.7%)
2 (1.6%)
2 (0.9%)
2 (0.8%)
فترة انقطاع بين جلسات العلاج تزيد عن 4 أيام، ن (%)
46 (39.3%)
٣٨ (٢٩.٩٪)
43 (36.4%)
32 (25.0%)
89 (37.9%)
70 (27.5%)
بيانات النتيجة الأساسية المفقودة (بما في ذلك الفقدان للمتابعة)، ن (%)
9 (7.7%)
9 (7.1%)
13 (11.0%)
13 (10.2%)
22 (9.4%)
22 (8.6%)
تلقي أدوية مصاحبة لا ينبغي تناولها أثناء تلقي العلاج (مثل لاموتريجين، بريجابالين أو جابابنتين)، عدد (%)
2 (1.7%)
2 (1.6%)
3 (2.5%)
3 (2.3%)
5 (2.1%)
5 (1.9%)
الأدوية النفسية أو التدخلات النفسية التي لم تُحافظ على استقرارها لمدة 16 أسبوعًا خلال فترة التجربة (باستثناء أولئك المعرضين للخطر على أنفسهم أو الآخرين) (%)
31 (26.5%)
22 (17.3%)
30 (25.4%)
٢٦ (٢٠.٣٪)
61 (25.9%)
48 (18.8%)
الوصفة اليومية لبنزوديازيبين فوق 5 ملغ، ما يعادل ديازيبام، زوبيكلون فوق 7.5 ملغ، زولبيديم فوق 10 ملغ أو زاليبلون فوق 10 ملغ من التقييم الأساسي حتى نهاية علاج التحفيز المغناطيسي عبر الجمجمة، عدد (%)
3 (2.6%)
3 (2.4%)
2 (1.7%)
2 (1.6%)
5 (2.1%)
5 (1.9%)
الإجمالي، ن (%)
117 (100%)
68 (53.5%)
١١٨ (١٠٠٪)
76 (59.4%)
235 (100%)
144 (56.5%)
p : عدد الانحرافات عن البروتوكول حسب نوع الانحراف، n : عدد المشاركين المتأثرين حسب نوع الانحراف. يرجى ملاحظة أن النسبة المئوية المقابلة لنسبة المشاركين المتأثرين حسب نوع الانحراف الرئيسي (بما في ذلك الإجمالي لكل ذراع علاج وإجمالي عام) تم حسابها من إجمالي عدد المشاركين الذين تم توزيعهم عشوائيًا. rTMS، التحفيز المغناطيسي عبر الجمجمة المتكرر. cgiTBS، التحفيز المتقطع الموجه بالاتصال.تم تقديم علاج TMS لجزء من جلسة العلاج أو الدورة عند الإحداثيات غير الصحيحة بالنسبة لبيانات التصوير بالرنين المغناطيسي (MRI) أو عند العتبة الحركية غير الصحيحة في إجراء التشغيل القياسي للتحفيز المغناطيسي عبر الجمجمة. لم تكن هناك حالات لتقديم تخصيص العلاج الخاطئ.تم إضافة انحراف من هذا النوع إلى جدول الملخص أعلاه للمشاركين الذين كانت لديهم فترة انقطاع تزيد عن 4 أيام بين جلسات التحفيز المغناطيسي عبر الجمجمة ولم يكن لديهم انحراف بروتوكول مسجل لذلك في نموذج تقرير حالة انحرافات البروتوكول للدراسة.تعرف على أنها الفشل في تقديم درجة النسخة GRID من مقياس هاملتون لتقييم الاكتئاب (GRID-HDRS-17) في جميع نقاط تقييم المتابعة: 8 و16 و26 أسبوعًا.تم تسجيل التغييرات في الأدوية النفسية تحت فئة ‘انحراف آخر’ وتم تقييمها من قبل الباحث الرئيسي لتحديد ما إذا كانت تُصنف كنوع من هذا الدواء أم لا.
محفظة الطبيعة
المؤلف (المؤلفون) المراسلون: ريتشارد موريز آخر تحديث من المؤلف(ين): 8 ديسمبر 2023
ملخص التقرير
تتمنى Nature Portfolio تحسين قابلية إعادة إنتاج العمل الذي ننشره. يوفر هذا النموذج هيكلًا للاتساق والشفافية في التقرير. لمزيد من المعلومات حول سياسات Nature Portfolio، يرجى الاطلاع على سياسات التحرير وقائمة مراجعة سياسة التحرير.
الإحصائيات
لجميع التحليلات الإحصائية، تأكد من أن العناصر التالية موجودة في أسطورة الشكل، أسطورة الجدول، النص الرئيسي، أو قسم الطرق.
مؤكد
حجم العينة بالضبطلكل مجموعة/شرط تجريبي، معطاة كرقم منفصل ووحدة قياس
بيان حول ما إذا كانت القياسات قد أُخذت من عينات متميزة أو ما إذا كانت نفس العينة قد تم قياسها عدة مرات
اختبار(ات) الإحصاء المستخدمة وما إذا كانت أحادية الجانب أو ثنائية الجانب يجب أن تُوصف الاختبارات الشائعة فقط بالاسم؛ واصفًا التقنيات الأكثر تعقيدًا في قسم الطرق.
وصف لجميع المتغيرات المشتركة التي تم اختبارها
وصف لأي افتراضات أو تصحيحات، مثل اختبارات الطبيعية والتعديل للمقارنات المتعددة
وصف كامل للمعلمات الإحصائية بما في ذلك الاتجاه المركزي (مثل المتوسطات) أو تقديرات أساسية أخرى (مثل معامل الانحدار) و التباين (مثل الانحراف المعياري) أو تقديرات مرتبطة بعدم اليقين (مثل فترات الثقة)
لاختبار الفرضية الصفرية، فإن إحصائية الاختبار (على سبيل المثال ) مع فترات الثقة، أحجام التأثير، درجات الحرية وقيمة ملحوظة أعطِالقيم كقيم دقيقة كلما كان ذلك مناسبًا. لتحليل بايزي، معلومات حول اختيار القيم الأولية وإعدادات سلسلة ماركوف مونت كارلو للتصاميم الهرمية والمعقدة، تحديد المستوى المناسب للاختبارات والتقارير الكاملة عن النتائج تقديرات أحجام التأثير (مثل حجم تأثير كوهين)بيرسون )، مما يشير إلى كيفية حسابها تحتوي مجموعتنا على الإنترنت حول الإحصائيات لعلماء الأحياء على مقالات تتناول العديد من النقاط المذكورة أعلاه.
البرمجيات والشيفرة
معلومات السياسة حول توفر كود الكمبيوتر
جمع البيانات
نقدم الشيفرة البرمجية التي استخدمناها لتحويل مقاييس الاتصال الفعال أو موقع F3 من تصوير الرنين المغناطيسي الوظيفي والصور الهيكلية إلى نقاط تحفيز للتحفيز المغناطيسي عبر الجمجمة فيhttps://github.com/SPMIC-UoN/brightmind_pipeline
تحليل البيانات
تم تحليل النتائج السريرية باستخدام برنامج STATA الإصدار 16 باستثناء الإدراك الذي تم تحليله باستخدام برنامج SPSS الإصدار 25. تم استخدام برنامج SPSS الإصدار 18 وبرنامج JASP 018 في تصوير الأعصاب.
بالنسبة للمخطوطات التي تستخدم خوارزميات أو برامج مخصصة تكون مركزية في البحث ولكن لم يتم وصفها بعد في الأدبيات المنشورة، يجب أن تكون البرمجيات متاحة للمحررين والمراجعين. نحن نشجع بشدة على إيداع الشيفرة في مستودع مجتمعي (مثل GitHub). راجع إرشادات مجموعة Nature لتقديم الشيفرة والبرمجيات لمزيد من المعلومات.
بيانات
معلومات السياسة حول توفر البيانات
يجب أن تتضمن جميع المخطوطات بيانًا عن توفر البيانات. يجب أن يوفر هذا البيان المعلومات التالية، حيثما ينطبق:
رموز الانضمام، معرفات فريدة، أو روابط ويب لمجموعات البيانات المتاحة للجمهور
وصف لأي قيود على توفر البيانات
بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتماشى مع سياستنا
مع دماغ ملس من أطلس ICBM152 لعرض صور الدماغ. قمنا بتحليل البيانات السريرية باستخدام برنامج STATA الإصدار 16 باستثناء بيانات الإدراك التي تم تحليلها باستخدام برنامج SPSS الإصدار 25. تم إجراء تحليل التصوير العصبي باستخدام برنامج SPSS الإصدار 18 وبرنامج JASP018.
البحث الذي يتضمن مشاركين بشريين، بياناتهم، أو مواد بيولوجية
معلومات السياسة حول الدراسات التي تشمل مشاركين بشريين أو بيانات بشرية. انظر أيضًا معلومات السياسة حول الجنس، الهوية/التقديم الجنسي، والتوجه الجنسي والعرق، والعرقية والعنصرية.
التقارير عن الجنس والنوع الاجتماعي
نستخدم مصطلح الجنس طوال النص
التقارير عن العرق أو الإثنية أو غيرها من التجمعات الاجتماعية ذات الصلة
العمر 18 عامًا أو أكثر دون حد أقصى للعمر أو قيود على الجنس أو العرق أو الحالة الاجتماعية أو الطبقة الاجتماعية.
خصائص السكان
معايير الشمول: العمرعمره سنوات؛ استوفى معايير الاضطراب الاكتئابي الكبير وفقًا لدليل التشخيص والإحصاء الخامس باستخدام مقابلة سريرية منظمة؛ كان يعاني من اكتئاب معتدل إلى شديد يُعرف بأنه سجل 16 أو أكثر على النسخة GRID من مقياس هاملتون لتقييم الاكتئاب المكون من 17 عنصرًا؛ كان يعاني من اكتئاب مقاوم للعلاج يُعرف بأنه سجل 2 أو أكثر على مقياس تصنيف الاكتئاب المقاوم للعلاج بمستشفى ماساتشوستس العام؛ وكان لديه القدرة على تقديم موافقة مستنيرة.
معايير الاستبعاد: الاضطراب ثنائي القطب أو الاكتئاب الثانوي لاضطراب نفسي آخر؛ الحالات العصبية مثل ورم الدماغ، الأحداث الوعائية الدماغية، الصرع، الاضطرابات التنكسية العصبية، جراحة الدماغ السابقة؛ موانع الاستخدام القياسية للتصوير بالرنين المغناطيسي (MRI) (مثل الأجسام المعدنية غير القابلة للإزالة في وحول الجسم، الحمل، الوشوم الحمراء على الرأس والرقبة والظهر، رهاب الأماكن المغلقة)؛ مرض طبي رئيسي غير مستقر يتطلب مزيدًا من التحقيق أو العلاج؛ في الأسبوعين السابقين للتقييم الأساسي أي تغيير في الأدوية الموصوفة، العلاج باللاموتريجين، الجابابنتين أو البريجابالين، أو البنزوديازيبينات المتقطعة (أو الوصفة اليومية فوق 5 ملغ من معادلات الديازيبام)، المنومات فوق 7.5 ملغ من معادلات الزوبيكلون؛ تعاطي أو اعتماد المواد الحالية (معايير DSM-5؛ علاج TMS السابق؛ خطر مرتفع للانتحار؛ عوامل معقدة محتملة لعلاج TMS (مثل تسريحات الشعر التي تعيق وضع الملف اللولبي القريب، الثقوب)؛ المشاركة في أي تجربة سريرية أخرى في وقت الموافقة أو 6 أشهر قبل ذلك؛ غير قادر على قراءة أو فهم الإنجليزية.
التوظيف
تم توظيف المشاركين من خلال خدمات الصحة النفسية المتخصصة عبر مراكز العلاج الخمسة في إنجلترا والثقة الصحية المجاورة بالقرب من مراكز العلاج، والإحالات الذاتية، ومن خلال مراكز تحديد المرضى التي تجند من خلال خدمات الرعاية الأولية. نظرًا لأن هذه عينة من الاكتئاب المقاوم للعلاج، فإنه يجب تعريف المشاركين بأنهم يتلقون العلاج الحالي من خدمات الصحة النفسية المتخصصة أو الرعاية الأولية، لذا فإن النتائج لا تنطبق على الأشخاص الذين يعانون من اكتئاب معتدل إلى شديد لا يتلقون العلاج. كان هناك المزيد من الذكور في العينة ولكن بخلاف ذلك كانت العينة تمثل ديموغرافيًا الاكتئاب المقاوم للعلاج في إنجلترا.
الإشراف الأخلاقي
حصلت التجربة السريرية على موافقة لجنة الأخلاقيات البحثية وموافقة هيئة البحث الصحي من لجنة الأخلاقيات البحثية المركزية في ليستر شرق ميدلاندز (المرجع: 18/EM/0232). شمل تصميم البحث وتنفيذه علماء محليين في كل موقع وتمت مشاركته مع جميع المواقع المحلية.
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة حول موافقة بروتوكول الدراسة في المخطوطة.
التقارير الخاصة بالمجال
يرجى اختيار الخيار أدناه الذي يناسب بحثك بشكل أفضل. إذا لم تكن متأكدًا، اقرأ الأقسام المناسبة قبل اتخاذ قرارك.
علوم الحياة العلوم السلوكية والاجتماعية العلوم البيئية والتطورية والبيئية
لنسخة مرجعية من الوثيقة مع جميع الأقسام، انظر nature.com/documents/nr-reporting-summary-flat.pdf
تصميم دراسة علوم الحياة
يجب على جميع الدراسات الإفصاح عن هذه النقاط حتى عندما يكون الإفصاح سلبيًا.
حجم العينة
حدد المعهد الوطني للصحة والرعاية المتميزة (NICE) 3 نقاط كفرق مهم سريريًا في النتيجة على مقياس HDRS-17 لاضطرابات الاكتئاب. 20 قمنا بمقارنة متوسط التغير في أعراض الاكتئاب من خط الأساس على مدى 26 أسبوعًا في مجموعة cgiTBS مع تلك في مجموعة rTMS. بافتراض انحراف معياري قدره 8 في الفرق المتوسط بين المجموعات، كما تم إبلاغنا من خلال عملنا التجريبي19 وتجربة عشوائية محكومة سابقة في اضطراب الاكتئاب المزمن المستمر، 22 فإن حجم عينة قدره 266 مشاركًا سيوفر القدرة على اكتشاف فرق متوسط قدره 3 نقاط في GRID-HDRS-17 على مدى 26 أسبوعًا بين المجموعات عند مستوى الدلالة ذو الجانبين، بافتراض وجود ارتباط بين قياسات المتابعة قدره 0.7 و20% فقدان البيانات/التسرب.
استثناءات البيانات
معايير الإدراج: العمر عامًا؛ استوفى معايير DSM-V لاضطراب الاكتئاب الرئيسي باستخدام مقابلة سريرية منظمة؛ كان لديه اكتئاب معتدل إلى شديد يعرف بأنه درجة 16 أو أكثر على النسخة GRID من مقياس تقييم الاكتئاب هاملتون المكون من 17 عنصرًا؛ كان لديه اكتئاب مقاوم للعلاج يعرف بأنه سجل 2 أو أكثر على مقياس تصنيف الاكتئاب المقاوم للعلاج بمستشفى ماساتشوستس العام؛ وكان لديه القدرة على تقديم موافقة مستنيرة.
معايير الاستبعاد: الاضطراب ثنائي القطب أو الاكتئاب الثانوي لاضطراب نفسي آخر؛ الحالات العصبية مثل ورم الدماغ، الأحداث الوعائية الدماغية، الصرع، الاضطرابات التنكسية العصبية، جراحة الدماغ السابقة؛ موانع الاستخدام القياسية للتصوير بالرنين المغناطيسي (MRI) (مثل الأجسام المعدنية غير القابلة للإزالة في وحول الجسم، الحمل، الوشوم الحمراء على الرأس والرقبة والظهر، رهاب الأماكن المغلقة)؛ مرض طبي رئيسي غير مستقر يتطلب مزيدًا من التحقيق أو العلاج؛ في الأسبوعين السابقين للتقييم الأساسي أي تغيير في الأدوية الموصوفة، العلاج باللاموتريجين، الجابابنتين أو البريجابالين، أو البنزوديازيبينات المتقطعة (أو الوصفة اليومية فوق 5 ملغ
من معادلات الديازيبام)، المنومات فوق 7.5 ملغ من معادلات الزوبيكلون؛ تعاطي أو اعتماد المواد الحالية (معايير DSM-5؛ علاج TMS السابق؛ خطر مرتفع للانتحار؛ عوامل معقدة محتملة لعلاج TMS (مثل تسريحات الشعر التي تعيق وضع الملف اللولبي القريب، الثقوب)؛ المشاركة في أي تجربة سريرية أخرى في وقت الموافقة أو 6 أشهر قبل ذلك؛ غير قادر على قراءة أو فهم الإنجليزية.
التكرار
لم نكرر التجربة لاختبار قابليتها للتكرار لأنها كانت تجربة متعددة المراكز تتطلب موارد كبيرة مع التصوير. لقد وصفنا جميع الإجراءات بحيث يمكن تكرارها.
العشوائية
نحن نصف إجراء العشوائية وكيف تم التواصل بشأن ذلك
التعمية
تمت التعمية وأظهرت
التقارير للمواد والأنظمة والأساليب المحددة
نحن نطلب معلومات من المؤلفين حول بعض أنواع المواد والأنظمة التجريبية والأساليب المستخدمة في العديد من الدراسات. هنا، حدد ما إذا كانت كل مادة أو نظام أو طريقة مدرجة ذات صلة بدراستك. إذا لم تكن متأكدًا مما إذا كان عنصر القائمة ينطبق على بحثك، اقرأ القسم المناسب قبل اختيار رد.
المواد والأنظمة التجريبية
الطرق
غير متاح
المشاركة في الدراسة
غير متاح
المشاركة في الدراسة
علم الحفريات وعلم الآثار
أصل العينة
قدم معلومات عن أصل العينات ووصف التصاريح التي تم الحصول عليها للعمل (بما في ذلك اسم السلطة المصدرة، تاريخ الإصدار، وأي معلومات تعريفية). يجب أن تشمل التصاريح الجمع، وعند الاقتضاء، التصدير.
إيداع العينة
حدد أين تم إيداع العينات للسماح بالوصول الحر من قبل باحثين آخرين.
طرق التأريخ
إذا تم تقديم تواريخ جديدة، وصف كيف تم الحصول عليها (مثل الجمع، التخزين، معالجة العينة والقياس)، أين تم الحصول عليها (أي اسم المختبر)، برنامج المعايرة وبروتوكول ضمان الجودة أو اذكر أنه لم يتم تقديم تواريخ جديدة.
حدد هذا المربع لتأكيد أن التواريخ الخام والمعايرة متاحة في الورقة أو في المعلومات التكميلية.
الإشراف الأخلاقي
حدد المنظمة (المنظمات) التي وافقت أو قدمت إرشادات حول بروتوكول الدراسة، أو اذكر أنه لم تكن هناك حاجة لموافقة أخلاقية أو إرشادات
وشرح لماذا لا.
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة حول موافقة بروتوكول الدراسة في المخطوطة.
البيانات السريرية
معلومات السياسة حول الدراسات السريرية
يجب أن تمتثل جميع المخطوطات لإرشادات ICMJE لنشر الأبحاث السريرية ويجب تضمين قائمة مراجعة CONSORT مكتملة مع جميع التقديمات.
تسجيل التجربة السريرية ISRCTN19674644 مكتمل. قائمة مراجعة CONSORT مرفقة
بروتوكول الدراسة
تم تقديم بروتوكول الدراسة
جمع البيانات
تم وصف هذه في المخطوطة. تم إكمال جميع التقييمات وجهًا لوجه في مواقع المستشفى قبل جائحة COVID-19، والتي تغيرت بعد ذلك إلى طرق مؤتمرات الفيديو أو الهاتف. أكمل المشاركون أيضًا تقييم التصوير بالرنين المغناطيسي (MRI) الأساسي مع المسح المستخدم لاشتقاق أهداف العلاج الشخصية، ولتحليل آلية العمل باستخدام التصوير بالرنين المغناطيسي عند الخط الأساسي و16 أسبوعًا.
النتائج
تم تضمين جميع النتائج الأولية والثانوية باستثناء بيانات الاقتصاد الصحي.
التصوير بالرنين المغناطيسي
تصميم تجريبي
نوع التصميم
حالة الراحة
مواصفات التصميم
موصوفة في الورقة. إنها تجربة سريرية
قياسات الأداء السلوكي
يمكن الحصول على جميع المعلومات التي نحتاجها حول الاتصال الوظيفي أو الفعال من تصوير الرنين المغناطيسي الوظيفي في حالة الراحة، لذا لم تكن مقاييس الأداء السلوكي ضرورية.
استحواذ
نوع (أنواع) التصوير
الرنين المغناطيسي الوظيفي
شدة المجال
3تسلا
معلمات التسلسل والتصوير
تصوير الرنين المغناطيسي متعدد الأوضاع عند 3 تسلا يتكون من مسح هيكلي بتقنية T1-weighted ومسح تصوير الرنين المغناطيسي الوظيفي في حالة الراحة باستخدام تقنية التصوير بالاعتماد على مستوى الأكسجين في الدم (BOLD) مع صور مشفرة بالطور الإيجابي والسلبي إضافية لتمكين تصحيح التشوهات. سيتم الحصول على صور T1-weighted عالية الدقة باستخدام تسلسلات BRAVO (أو ما يعادلها) بتقنية الصدى السريع المفسد مع فوكيلات متساوية الأبعاد بحجم 1 مم³ تغطي الرأس بالكامل من القمة إلى الرقبة. سيتم الحصول على صور rsfMRI مع فتح العينين باستخدام علامة تثبيت. استخدمت جميع المواقع تسلسل EPI بتقنية الصدى المتدرج متماشياً مع خط الوصلة الأمامية والخلفية، مع تغطية الاكتساب من القمة إلى الأسفل (زمن التكرار [TR]/زمن الصدى [TE]=2000/32 مللي ثانية؛ زاوية الانقلاب=77).; 35 شريحة; حجم الفوكسل = 3 مم; فجوة الشريحة = 0.5 مم; مجال الرؤية; متداخلة من الأسفل إلى الأعلى؛ 240 حجمًا؛ اتجاه ترميز الطور = من الخلف إلى الأمام). جميع صور rsfMRI لها صور BO مرتبطة تم ترميزها في الطور للأمام والخلف تم الحصول عليها لتسهيل تصحيح التشوه.
مجال الاستحواذ
الدماغ الكامل
تصوير الرنين المغناطيسي بالانتشارمستعمل
X غير مستخدم
التحضير المسبق
برمجيات المعالجة المسبقة
تم تحميل ملفات جلسات الموضوع المتعلقة بالتصوير الرقمي والاتصالات في الطب (DICOM) على بنية قاعدة بيانات XNAT (جامعة واشنطن في مدرسة الطب) لجميع البيانات باستثناء بيانات MRS باستخدام أرقام موضوعات مجهولة الهوية. بمجرد أرشفة الجلسة داخل XNAT، تم وضعها في حالة الحجر الصحي في انتظار مراقبة الجودة (QC)، وتم تحويل ملفات DICOM تلقائيًا إلى هيكل بيانات تصوير الدماغ NIFTI أو أزواج JSON لكل مسح باستخدام حاوية dcm2bidssession v1.5 XNAT، حيث خضعت الصور الموزونة T1 أيضًا لعملية إزالة التعرف في هذه الخطوة.
التطبيع
التطبيع. تم استخراج الدماغ بشكل خشن من الصور الموزونة T1 باستخدام أداة استخراج الدماغ من FSL (BET). ثم تم تسجيل الصور الأصلية والصور المستخرجة من الدماغ بشكل غير خطي إلى نموذج MNI152 بدقة 1 مم باستخدام أداة التسجيل غير الخطي للصور من FSL FMRIB (FNIRT). تم تحسين استخراج الدماغ الأصلي من FSL BET من خلال تطبيق التحويل غير الخطي الناتج لتشويه قناع دماغ MNI152 على صورة T1 الخاصة بالموضوع. تم تصحيح الصورة المستخرجة من الدماغ أخيرًا من التحيز وتم تقسيمها إلى المادة الرمادية والسائل الدماغي الشوكي (CSF) والمادة البيضاء (WM) باستخدام أداة التقسيم الآلي من FSL FMRIB (FAST). تم تحويل خرائط احتمالية WM وCSF الناتجة إلى ثنائية عند عتبة احتمالية الأنسجةثم تم تآكلها باستخدام نواة كروية بقطر 2 فوكسيلا.
قالب التطبيع
قالب التطبيع. قالب MNI152 بسمك 1 مم باستخدام أداة تسجيل الصور غير الخطية من FSL FMRIB (FNIRT).
إزالة الضوضاء والعيوب
إزالة الضوضاء والعيوب. تم تصحيح الصورة الهيكلية المعتمدة على T1 بعد التحويل غير الخطي. خضعت صور BOLD rsfMRI لتصحيح تشويه EPI من خلال إدخال عمليات الاستحواذ ذات الترميز الإيجابي والسالب في TOPUP. ثم خضعت لتصحيح حركة بين الحجوم (MCFLIRT 6DoF) وتصحيح توقيت الشرائح المتداخلة باستخدام SPM12 (من الأسفل إلى الأعلى). تم بعد ذلك تنعيم صورة BOLD المصححة باستخدام نواة بقطر 5 مم باستخدام تقنية دمج النواة ذات القيمة الدنيا (SUSAN) وتمت إزالة الضوضاء باستخدام ICA-AROMA. تم تصفية صور BOLD بتردد 0.01 هرتز بعد إزالة الضوضاء. تم لاحقًا حساب تحويل بين صورة BOLD الناتجة وصورة T1 المعتمدة باستخدام FSL epi_reg، ثم تم دمجها مع تحويل تصحيح التشويه المكاني TOPUP. تم بعد ذلك عكس التحويل المدمج الناتج لإنشاء تحويل غير خطي من مساحة T1 المعتمدة إلى مساحة BOLD (غير المصححة الأصلية). تم بعد ذلك تشويه الأقنعة الثنائية السابقة للمواد البيضاء (WM) والسائل الدماغي الشوكي (CSF) إلى مساحة BOLD باستخدام تحويل T1 المعتمد إلى BOLD لاستخراج سلسلة الزمن للمواد البيضاء والسائل الدماغي الشوكي من بيانات BOLD. للتحكم في الضوضاء الفسيولوجية أو المتعلقة بالجهاز الإضافية، تم بعد ذلك طرح سلسلة الزمن للمواد البيضاء والسائل الدماغي الشوكي من سلسلة زمن rsfMRI.
تصفية الحجم
تم تقليل مجال الرؤية عن طريق إزالة الجزء السفلي من الرأس والرقبة باستخدام FSL robustfov.
النمذجة الإحصائية والاستدلال
نوع النموذج والإعدادات
نوع النموذج والإعدادات. الاتصال الوظيفي (FC). تم استخراج سلسلة زمنية من منطقتين من الاهتمام (ROIs) باستخدام أداة fslmeants (جزء من مكتبة برامج FSL). تم أخذ المكون الرئيسي الأول من سلسلة الزمن لجميع الفوكيلات داخل ROI كممثل للسلسلة الزمنية العامة لتلك المنطقة. تم التخلص من أول خمس نقاط زمنية للسماح باستقرار المغنطة وتم تصفية السلاسل الزمنية بين 0.01 و 0.1 هرتز. الاتصال بين ROIs بدون تأخير.
تم حساب الارتباطات باستخدام ارتباطات بيرسون بين السلاسل الزمنية، مع استبعاد أربعة وعشرين معلمة لحركة الرأس (ثلاث ترجمات وثلاث دورانات للنقطة الزمنية الحالية ونقطة زمنية سابقة واحدة، ومربعات هذه المعلمات). تم تحويل الارتباطات ذات الاهتمام إلى-الدرجات باستخدام تحويل فيشر من r إلى z. كانت هذه الدرجات z بمثابة مقاييس للتواصل الوظيفي. تم حساب سببية غرانجر للاتصال الفعال (EC) باستخدام أداة REST، التي تعمل تحت MATLAB. وقد وفرت هذه الأداة مقياسًا للاتصال الموجه (الفعال) من منطقة اهتمام واحدة (ROI).، على سبيل المثال، الذكاء الاصطناعي الصحيح ) إلى عائد استثمار آخر (على سبيل المثال، تم ترك DLPFC). توفر مجموعة الأدوات مقاييس لتأثير x على y وكذلك y على x. تم التخلص من أول خمس نقاط زمنية، وتم إدخال أربعة وعشرين من معلمات حركة الرأس كمتغيرات مشتركة. لم يتم تطبيق فلتر تمرير نطاقي، وفقًا لإجراء تحديد الهدف في التجربة. تم تحويل قيم الاتصال الفعال إلى درجات z باستخدام تحويل فيشر من r إلى z، ثم كانت متوسط درجة z الناتجة عبر جميع الفوكسلات في y بمثابة مقياس للاتصال الفعال.
التأثيرات المختبرة
تم حساب خريطة الاتصال الفعال للقشرة الجبهية اليسرى من القشرة الجبهية اليمنى أولاً. يتوافق الحد الأقصى لهذه الخريطة مع هدف cgiTBS. كانت منطقة الاهتمام للقشرة الجبهية اليسرى هيكرة مركزها على إحداثيات هدف cgiTBS نفسها (بغض النظر عن مجموعة العلاج). كانت منطقة الاهتمام للجانب الأيمن من القشرة الحزامية هيكرة مركزها على إحداثيات MNI. قمنا بحساب الاتصال الفعال كدالة للمسافة من هذه القيمة القصوى لفحص ما إذا كانت الأهداف المثلى وفقًا لإجراء تحديد الهدف التجريبي فريدة بوضوح أو ما إذا كانت هناك أهداف محتملة متعددة ومنفصلة داخل القشرة الجبهية الجانبية. لكل مشارك، قمنا بحساب الاتصال الوظيفي بين كل فوكسل صورة ومناطق بذور كروية مركزة على إحداثيات الهدف المراد تحفيزه. قمنا بحساب صور الاتصال الوظيفي لمناطق البذور هذه للخط الأساسي والمتابعة، كما قمنا أيضًا بحساب الفرق بين صور المتابعة وصور الخط الأساسي.
لفحص الاتصال بين DLPFC وDMPFC، تم فحص مركزين لمنطقة DLPFC اليسرى المستقلين عن إحداثيات cgiTBS وrTMS في تحليلات منفصلة: مركز أمامي لـ DLPFC،ومركز دLPFC أكثر خلفية،مركز الثقل لمنطقة DMPFC اليسرى كان.
حدد نوع التحليل:الدماغ الكامل
مبني على العائد على الاستثماركلاهما
الموقع(ات) التشريحية
وصف كيف تم تحديد المواقع التشريحية (على سبيل المثال، تحديد ما إذا كانت خوارزميات التسمية الآلية أو الأطالس الاحتمالية قد تم استخدامها).
نوع الإحصاء للاستدلال
(انظر إكلوند وآخرون 2016)
نوع الإحصاء للاستدلال. تم تنفيذ نماذج التأثيرات المختلطة في برنامج SPSS (الإصدار 18) وبرنامج JASP (0.18) وتم تقديرها باستخدام الاحتمالية القصوى المقيدة. كان المشاركون هم التأثير العشوائي مع مصفوفة تباين-تغاير ذات هوية مقاسة، وكانت المتغير التابع هو التحسن السريري من خط الأساس في GRID-HDRS-17 (مقياس النتيجة الأساسي)، PHQ-9 أو BDI-II (مقاييس النتيجة الاستكشافية المخطط لها). بالإضافة إلى الاتصال الأساسي، أو التغيير في الاتصال، ذي الصلة بفرضية معينة، قمنا بتضمين نقطة الوقت بعد العلاج كمتغيرات مستقلة. (أسابيع) ومجموعة العلاج (rTMS، cgiTBS)، وتفاعل الاتصال مع أي من المتغيرين أو كليهما. تم استكشاف العمر، الجنس، مجموعة مقاومة علاج MGH، GAD-7، CTQ وموقع مجموعة الدراسة كمتغيرات مشوشة محتملة: حيث كانت هذه غير ذات دلالة، تم إزالتها من النموذج.
تصحيح
بونفيروني للاتصال الوظيفي بين القشرة الجبهية الظهرية اليسرى إلى القشرة الجبهية الوسطى اليسرى فقط.
النماذج والتحليل
المشاركة في الدراسة
تحليل الرسم البياني للاتصال الوظيفي و/أو الفعال
X النمذجة متعددة المتغيرات أو التحليل التنبؤي
الاتصال الوظيفي و/أو الفعال
تم استخدام الاتصال الوظيفي والفعال كما هو موضح تحت نوع النموذج والإعدادات.
الصحة النفسية وعلوم الأعصاب السريرية، كلية الطب، جامعة نوتنغهام، نوتنغهام، المملكة المتحدة.معهد الصحة النفسية، مؤسسة خدمات الصحة في نوتنغهامشير، نوتنغهام، المملكة المتحدة.خدمة تعديل الأعصاب السريرية، مؤسسة خدمات الصحة في كامدن وإيسلينغتون، لندن، المملكة المتحدة.وحدة التجارب السريرية في ليستر، جامعة ليستر، ليستر، المملكة المتحدة.كامبريا، نورثمبرلاند، تاين ووير، مؤسسة خدمات الصحة في نيوكاسل أبون تاين، المملكة المتحدة.خدمة TMS لرعاية بنين، مؤسسة خدمات الصحة في بنين، أولدهام، المملكة المتحدة.المركز الشمالي لاضطرابات المزاج، معهد الأبحاث السريرية والترجمة، جامعة نيوكاسل، نيوكاسل أبون تاين، المملكة المتحدة.مركز تعديل الأعصاب، مؤسسة خدمات الصحة في نورثامبتونشاير، نورثامبتون، المملكة المتحدة.البريد الإلكتروني: richard.morriss@nottingham.ac.uk
Connectivity-guided intermittent theta burst versus repetitive transcranial magnetic stimulation for treatment-resistant depression: a randomized controlled trial
Received: 29 June 2023
Accepted: 12 December 2023
Published online: 16 January 2024
(i) Check for updates
A list of authors and their affiliations appears at the end of the paper
Disruption in reciprocal connectivity between the right anterior insula and the left dorsolateral prefrontal cortex is associated with depression and may be a target for neuromodulation. In a five-center, parallel, double-blind, randomized controlled trial we personalized resting-state functional magnetic resonance imaging neuronavigated connectivity-guided intermittent theta burst stimulation (cgiTBS) at a site based on effective connectivity from the right anterior insula to the left dorsolateral prefrontal cortex. We tested its efficacy in reducing the primary outcome depression symptoms measured by the GRID Hamilton Depression Rating Scale 17-item over 8, 16 and 26 weeks, compared with structural magnetic resonance imaging (MRI) neuronavigated repetitive transcranial magnetic stimulation (rTMS) delivered at the standard stimulation site (F3) in patients with ‘treatment-resistant depression’. Participants were randomly assigned to 20 sessions over weeks of either cgiTBS ( ) or rTMS ( ) with resting-state functional MRI at baseline and 16 weeks. Persistent decreases in depressive symptoms were seen over 26 weeks, with no differences between arms on the primary outcome GRID Hamilton Depression Rating Scale 17-item score (intention-to-treat adjusted mean, -0.31, 95% confidence interval (CI) ). Two serious adverse events were possibly related to TMS (mania and psychosis). MRI-neuronavigated cgiTBS and rTMS were equally effective in patients with treatment-resistant depression over 26 weeks (trial registration no. ISRCTN19674644).
Antidepressants and psychotherapies are effective for moderate to severe major depressive disorder (MDD) . However, a proportion of individuals with MDD have ‘treatment-resistant depression’ (TRD), with of patients in specialist care and in primary care failing to respond adequately to two trials of antidepressants .
Repetitive transcranial magnetic stimulation employs strong magnetic pulses to alter activity in neural circuits in the brain implicated in
the pathophysiology of depression. High-frequency rTMS to the left dorsolateral prefrontal cortex (IDLPFC) is one of the protocols most commonly used in . TBS uses bursts of magnetic pulses mimicking endogenous theta rhythms that may induce plasticity in more distal brain areas . A meta-analysis confirmed the effectiveness and safety of both rTMS and TBS for TRD . The multicenter THREE-D clinical trial showed that shorter duration of administration iTBS was noninferior
to longer-duration rTMS applied to the IDLPFC in the reduction of depression symptoms up to 12 weeks after treatment, but there are no data on longer-term follow-up .
The Federal Drug Administration in the United States approved rTMS for depression in 2008 following confirmation of its effectiveness in a worldwide, 23 -site, randomized clinical trial (RCT) . The National Institute for Health and Care Excellence approved TMS for MDD and TRD in the National Health Service in England in 2015(ref.8). Although more widely used in mental health services across North America, there is patchier implementation in routine mental health practice in other areas of the world. In England, TMS is available in only one in seven mental health services and has not been recommended for use in some countries such as France, albeit based on a questionable review of the evidence . Therefore, the evidence base to date has not been sufficiently convincing to result in widespread implementation or regulatory support in specialist mental health services internationally. One reason for this may be that the effects on TRD are seen as short lived because of the paucity of evidence from large, high-quality RCTs with sufficient duration of follow-up .
The brain can be subdivided into networks of regions that serve separable functions, and brain connectivity changes as detected by resting-state functional MRI (rsfMRI) can individualize neurostimulation therapy of MDD . TMS stimulation of the IDLPFC (a key node of the central executive network (CEN)) may modulate key nodes within the salience network and default mode network (DMN), leading to rebalancing of abnormal functional connectivity (calculated by correlation of blood oxygenation level-dependent time courses using rsfMRI from different regions of the brain) between and within these networks . However, there is individual variation in the functional connectivity of the IDLPFC to these nodes , suggesting that a personalized approach to targeting the site of delivery of TMS might improve either response rates or the duration of response compared with a single, standardized site of stimulation that is widely used in clinical practice with TMS for depression. Two small RCTs of personalized and accelerated rTMS or iTBS, based on functional connectivity between the subgenual anterior cingulate cortex and IDLPFC, resulted in greater responses in depression over 3-4 weeks versus standardized or sham TBS .
A disruption of the reciprocal loop between the DLPFC and insula (a key node of the salience network) has been found in depression , so the insula may represent another target for personalized neuromodulation. A RCT in 27 healthy volunteers found that iTBS delivered to a connectivity-guided target in the IDLPFC with maximum negative influence from the right anterior insula (rAI) improved frontal-insula connectivity . In a small pilot RCT of 18 patients with TRD comparing cgiTBS with connectivity-guided repetitive transcranial stimulation (cgrTMS), the response rate (50% decrease in depression symptoms) showed a statistically insignificant increase from 1 to 3 months in the cgiTBS group but decreased in the cgrTMS group . In both treatment groups, where TMS/TBS stimulation was personalized using effective connectivity (a type of functional connectivity in which directionality is inferred from time-shift analysis of the regional time series ), the balance of influence between rAI and IDLPFC was predictive of improvement following a course of . These findings suggested that cgiTBS, personalized based on maximal effective connectivity from rAI to IDLPFC, might lead to longer-lasting efficacy than standard-site rTMS, permitting people with TRD potentially to remain well for longer. However, data are needed with longer follow-up than previously conducted.
The BRIGhTMIND trial was a multicenter, parallel-group, double-blind, randomized, controlled trial. Our primary clinical hypothesis was that rsfMRI-neuronavigated cgiTBS, based on effective connectivity from the rAl to the IDLPFC, would be more efficacious in reducing depression symptoms over 8,16 and 26 weeks compared with structural MRI-neuronavigated rTMS delivered at the standard
stimulation site (F3 of the 10-20-electrode location nomenclature) in patients with TRD. Although a standard site for rTMS was used, the location of that F3 site was personalized using structural MRI. The primary mechanistic hypotheses utilizing fMRI were: (1) baseline effective connectivity from rAI to IDLPFC, or that the balance of influence between these two regions would moderate, or be associated with, improvement in depression symptoms over 26 weeks; and (2) reduction in functional connectivity between the IDLPFC and left dorsomedial prefrontal cortex (IDMPFC) would be associated with improvement in depression symptoms as found in both our pilot work and another study .
Results
Patient disposition
Between 22 January 2019 and 31 January 2022, 685 individuals were identified and completed the initial telephone eligibility screening for the BRIGhTMIND trial (Fig. 1). Recruitment to the study was temporarily suspended between 30 April and 1 August 2020 due to the COVID-19 pandemic. A total of 317 participants consented to the trial, with 39 of these not meeting inclusion criteria and 23 withdrawing between baseline and randomization. A total of 255 participants were randomized, 127 to rTMS and 128 to cgiTBS, with all randomized participants included in the intention-to-treat (ITT) population. In total, 235 participants completed all 20 TMS sessions (92.8%; two participants each in the rTMS and cgiTBS groups discontinued their involvement in the trial altogether during treatment). Comparable completion rates were also found for rTMS versus cgiTBS at 8 weeks (rTMS, 112 out of versus cgiTBS, 111 out of ), 16 weeks (rTMS, 112 out of versus cgiTBS, 112 out of ) and 26 weeks (rTMS, 102 out of versus cgiTBS, 104 out of ). The final follow-up assessment was completed on 3 August 2022. In line with the prepublished analysis plan for the 255 participants who completed baseline structural and rsfMRI scans and started TMS, 209 ( ) were included in the image analysis. Of 114 participants who completed baseline and 16-week follow-up scans, 101 ( ) were analyzed (Extended Data Fig.1).
There were two unintentional unblindings of an outcome assessor and one of a principal investigator to a participant’s treatment. In terms of researchers’ guesses, the majority of treatment allocation predictions were that of ‘don’t know’, with overall rates of 84.8, 79.5 and at 8,16 and 26 weeks, respectively (Extended Data Table 1).
At baseline the mean age of participants was 43.7 years (s.d. 14.0 ), with women and of white ethnicity (Table 1). The median duration of current depression episode was 6.1 years (interquartile range (IQR) 2.1,12.9) and the median number of depressive episodes was two (IQR1,4). Ninety-five participants (37.3%) were categorized as high treatment resistance (nonresponse to more than approximately six treatments) on the modified Massachusetts General Hospital Treatment Resistant Depression staging score (MGH ), 73 ( ) as medium treatment resistance (nonresponse to around four or five treatments) and 87 (34.1%) as low treatment resistance (nonresponse to two or three treatments), with 198 participants (77.6%) currently taking antidepressants. The mean baseline scores on the primary outcome variable-the GRID version of the 17-item Hamilton Depression Rating Scale (GRID-HDRS-17; ref. 24)-were 23.9 (s.d. 4.7) for the rTMS group and 22.9 (s.d. 4.7) for the cgiTBS group (Tables 2 and 3). An inter-rater reliability assessment of outcome assessors, completed across treatment centers, showed an intraclass coefficient of 0.94 between GRID-HDRS-17 scores, with a 95% reference interval for the difference (between any pair of raters) of 0.66-0.99. Across both treatment groups the median distance between the intended stimulation point on the scalp and the actual stimulation point, or between the actual stimulation point on the first, and subsequent, sessions, was about 0.5 cm , and median angle difference was about (Extended Data Table 2; sites of stimulation are shown in Extended Data Fig. 2).
Fig. 1| Flowchart of participants through the trial. CONSORT diagram of all participants who were assessed for eligibility for the trial, randomised to repetitive transcranial magnetic stimulation or connectivity guided intermittent the ta burst stimulation and followed up to 26 weeks.
Primary outcome
As shown in Tables 2 and 3, the adjusted mean difference for GRID-HDRS-17 over 26 weeks was not significant and not clinically important (<3-point difference ) between rTMS and cgiTBS treatment groups for the primary analysis ( -0.31 (95% to 1.24), ).
At 8 weeks following randomization, both treatment groups showed a clinically substantial decrease ( (ref. 26), rTMS 8.3, cgiTBS 8.4) in mean GRID-HDRS-17 scores that were maintained at both 16 weeks (rTMS 8.0, cgiTBS 7.6) and 26 weeks (rTMS 7.8, cgiTBS 8.0; Tables 2 and 3 and Fig. 2).
Table 1 | Baseline characteristics of participants
Characteristics
rTMS ( )
cgiTBS ( )
Age (years) Mean (s.d.)
43.8 (13.1)
43.7 (15.0)
Gender ( (%))
Men
65 (51.2%)
58 (45.3%)
Women
62 (48.8%)
70 (54.7%)
Ethnicity (n(%))
White British
106 (83.5%)
108 (84.4%)
White Irish
4 (3.1%)
1 (0.8%)
Other White
6 (4.7%)
7 (5.5%)
White and black African
1 (0.8%)
2 (1.6%)
White and Asian
1 (0.8%)
O(0%)
Other mixed
1 (0.8%)
2 (1.6%)
Indian
4 (3.1%)
2 (1.6%)
Pakistani
2 (1.6%)
2 (1.6%)
Bangladeshi
0 (0%)
1 (0.8%)
Other Asian
0 (0%)
1 (0.8%)
Black Caribbean
1 (0.8%)
0 (0%)
Chinese
0 (0%)
1 (0.8%)
Other ethnic group
1 (0.8%)
1 (0.8%)
Marital status: married/cohabiting (Yes, (%))
76 (59.8%)
55 (43.0%)
Dependants (children/other) (Yes, (%))
42 (33.1%)
36 (28.1%)
Employment/education ( (%))
Full-time
39 (30.7%)
37 (28.9%)
Other employment
36 (28.3%)
26 (20.3%)
Retired
13 (10.2%)
17 (13.3%)
Unemployed
39 (30.7%)
48 (37.5%)
Receipt of benefits (Yes, (%))
52 (40.9%)
45 (35.2%)
Duration of current major depressive episode (months)
117
122
Median (IQR)
69.7 (27.9, 129.0)
79.3 (24.9, 163.3)
Number of depressive episodes
84
91
Median (IQR)
2.0 (1.0, 4.0)
1.0 (1.0, 4.0)
Baseline CTQ (respondents)
120
120
Mean (s.d.)
47.1 (17.4)
45.1 (16.2)
Number of participants with treatment history
127
128
Category of baseline MGH treatment-resistant depression score ( (%))
Low, 2.0-3.5
42 (33.1%)
45 (35.2%)
Medium, 4-6
36 (28.3%)
37 (28.9%)
High,
49 (38.6%)
46 (35.9%)
Baseline medication use
Antidepressants
94 (74.0%)
104 (81.3%)
Tricyclic antidepressants
10 (7.9%)
11 (8.6%)
MAOIs
1 (0.8%)
0 (0%)
SSRIs
41 (32.3%)
46 (35.9%)
SNRI
31 (24.4%)
39 (30.5%)
Other
34 (26.8%)
36 (28.1%)
Antidepressant combination
22 (17.3%)
19 (14.8%)
Table 1 (continued) | Baseline characteristics of participants
Characteristics
rTMS ( )
cgiTBS ( )
Antipsychotic augmentation
19 (15.0%)
23 (18.0%)
Lithium augmentation
3 (2.4%)
11 (8.6%)
Methylphenidate augmentation
0 (0%)
1 (0.8%)
Modafinil augmentation
0 (0%)
1 (0.8%)
Triiodothyronine augmentation
0 (0%)
3 (2.3%)
Hypnotics/sleeping tablets
7 (5.5%)
9 (7.0%)
Anxiolytics
7 (5.5%)
7 (5.5%)
Electroconvulsive therapy during current episode of depression ( (%))
6 (4.7%)
4 (3.1%)
MAOIs, monoamine oxidase inhibitors; SSRIs, selective serotonin reuptake inhibitors; SNRIs, serotonin and norepinephrine reuptake inhibitors. Other baseline medication refers to the following antidepressants: trazadone, bupropion, mirtazapine, reboxetine, agomelatine or vortioxetine). The number of current major depressive episodes has been set to missing for participants whose number was entered as 99. The duration of current major depressive episodes was calculated using the date of randomization and start date of the episode.
Secondary outcomes
There were no significant differences between rTMS and cgiTBS on any of the secondary clinical outcome measures (Tables 2 and 3). At the 26-week follow-up in both groups, 67 (32.5%) of 206 participants were responders ( drop in baseline GRID-HDRS-17 score), 47 (22.8%) of 206 participants were remitters ( on GRID-HDRS-17 score) and of 255 participants were sustained responders ( drop in baseline at both 16 and 26 weeks). At 8, 16 and 26 weeks for both treatment groups there were, on average, clinically substantial important improvements in self-rated depression as measured by the Patient Health Questionnaire (PHQ-9 (ref. 27), points ) and the Beck Depression Inventory-II (BDI-II points ), with greater than minimum clinically important improvements in Generalized Anxiety Disorder Assessment (GAD-7) ( points ), Work and Social Adjustment Scale (WSAS , points ) and the Euroqol-5D-5L visual analog scale of overall perceived health (EQ-5D-5L VAS points ). The cognition analysis showed improvements over time on the Transforming Health with Integrated Care-integrated tool (THINC-it) cognitive battery for sustained attention (Choice Response Task) ( = 11.28, ), executive functioning (Trail-making Task) and working memory ( N -back task) .
The participants’ impression of change analysis demonstrated that, at the tenth session, 105 ( ) of 245 participants reported feeling somewhat, or much, better. By session 20 this was reported for 155 (65.4%) of 237 participants. The relationship between treatment session number and perceived improvement generally followed a linear trend for both groups, with the proportion experiencing a benefit continuing to increase even at the 19th and 20th sessions (Extended Data Fig.3).
Safety
One out of 255 randomized participants was excluded from the safety population because they had experienced a suspected 2 -s seizure during the first motor threshold testing and before any treatment had been provided (Table 4). Seventeen further serious adverse events (SAEs) were reported for 12 participants. There were two deaths: one participant had an underlying cardiovascular health condition and died following a myocardial infarction and another died from opiate poisoning, with the coroner’s inquest concluding accidental death. Both participants had completed their course of TMS treatments and died close to the 26-week assessment, with both deaths reported as unlikely to be related to TMS treatments. All further SAEs required hospital admission. Two SAEs were reported as possibly related to TMS treatment (one in each treatment arm): a psychotic episode with severe anxiety and depression
Table 2 | Primary and secondary outcome scores and response to treatment
Measure
Baseline
8 weeks
16 weeks
26 weeks
cgiTBS versus rTMS over 26 weeks
rTMS mean (s.d.)
cgiTBS mean (s.d.)
rTMS mean (s.d.)
cgiTBS mean (s.d.)
rTMS mean (s.d.)
cgiTBS mean (s.d.)
rTMS mean (s.d.)
cgiTBS mean (s.d.)
Adjusted mean difference (95% CI)
value
GRID-HDRS-17 primary analysis
127
128
127
128
127
128
127
128
23.9 (4.7)
22.9 (4.7)
15.6 (s.e. 0.7; 95% CI 14.2, 17.0)
14.5 (s.e. 0.6; 95% Cl 13.2, 15.7)
15.9 (s.e. 0.8; 95% CI 14.5, 17.5)
15.3 (s.e 0.7; 95% CI 13.9, 16.7)
16.1 (s.e. 0.8; 95% Cl14.5, 17.8)
14.9 (s.e 0.7; 95% CI 13.4, 16.3)
-0.31 (-1.87, 1.24)
0.689
BDI-II
127
128
111
109
109
110
99
102
34.4 (8.9)
32.3 (8.8)
23.5 (12.6)
21.3 (10.7)
24.7 (12.2)
22.3 (12.4)
23.6 (12.6)
21.6 (12.0)
-0.54 (-2.90, 1.82)
0.653
PHQ-9
127
128
111
109
109
109
99
102
20.2 (4.6)
19.4 (4.4)
13.4 (7.5)
12.3 (6.3)
13.8 (7.2)
13.5 (7.3)
13.7 (7.6)
13.1 (7.5)
-0.12 (-1.54, 1.30)
0.871
GAD-7
127
128
111
109
109
108
99
102
13.3 (4.7)
13.1 (4.6)
9.3 (6.3)
8.9 (4.9)
9.3 (5.5)
9.1 (5.3)
9.9 (6.1)
8.9 (5.6)
-0.19 (-1.24, 0.86)
0.726
WSAS
127
128
111
109
109
109
99
102
29.0 (6.8)
27.6 (7.8)
22.1 (10.9)
21.2 (9.5)
22.2 (10.7)
22.4 (10.2)
22.2 (10.7)
21.5 (10.8)
0.60 (-1.39, 2.59)
0.554
EQ-5D-5L VAS
127
128
111
109
109
109
98
102
43.0 (19.3)
43.4 (17.1)
52.8 (21.0)
54.7 (18.8)
53.2 (20.2)
56.7 (19.4)
53.8 (21.2)
55.8 (20.5)
1.98 (-1.96, 5.91)
0.325
THINC-it
cgiTBS versus rTMS baseline and 16-week adjusted mean difference (95% CI)
value
CRT response time (ms)
123
127
NA
NA
76
72
NA
NA
Missing
4
1
717.67 (238.55)
708.05 (249.25)
606.28 (183.02)
614.12 (210.71)
-1.48 (-55.05, 52.09)
0.957
DSST total correct
122
127
NA
NA
76
72
NA
NA
Missing
5
1
51.17 (18.26)
49.15 (21.18)
55.76 (16.93)
52.36 (19.59)
-4.25 (-8.56, .062)
0.053
N -back total correct
122
126
NA
NA
76
72
NA
NA
Missing
5
2
22.82 (10.81)
21.56 (9.66)
25.28 (9.25)
24.56 (9.63)
-1.27 (-3.51,0.97)
0.264
TMT response time (s)
123
126
NA
NA
76
72
NA
NA
Missing
4
2
30.08 (15.99)
34.70 (25.26)
27.11 (16.34)
31.07 (25.10)
21.03 (-3.28, 45.33)
0.090
PDQ-5-D score
123
127
NA
NA
75
71
NA
NA
Missing
4
1
12.89 (4.47)
13.29 (4.46)
10.55 (5.07)
10.83 (94.79)
0.43 (-0.57, 1.43)
0.394
CRT, based on a choice reaction task; DSST, based on the digit symbol substitution test; N-back, based on the one-back paradigm TMT, which is based on part B of the trails-making task; PDQ-5, subjective perceived deficits questionnaire, five domains. NA, not available. Adjusted for: treatment center (stratification variable), baseline HDRS-17 score and degree of treatment-resistant depression (minimization variables) and treatment arm with participant ID as the random effect. Secondary continuous clinical outcomes models were also adjusted for their respective baseline measure. Standard errors along with CIs are reported for the GRID-HDRS-17-estimated means at follow-up time points, because multiple imputation was used to perform the primary analysis. Cognition outcomes were the dependent variables, with the independent variables of interest being the THINC-it time point (baseline and 16 weeks), treatment group (rTMS and cgiTBS), baseline GAD-7, baseline HDRS-17 and change in HDRS-17 score between baseline and week16. Models also included three interaction terms: treatment group time point, time point change in HDRS-17 and change in HDRS-17 treatment group time point. Confounder variables included age, gender, site and MGH group. Any confounder variable not found to be significant on initial testing was removed from the models and the analysis rerun.
Table 3 | Proportions of responders, sustained responders and remitters in rTMS and cgiTBS groups
Measure
Rate in each treatment arm (n/total (%))
cgiTBS versus
P value
rTMS
cgiTBS
rTMS (adjusted odds ratio (95% CI))
Responders
8-week follow-up
35/112 (31.3)
39/111 (35.1)
1.13 (0.63, 2.03)
0.682
16-week follow-up
38/112 (33.9)
39/112 (34.8)
1.03 (0.57, 1.87)
0.916
26-week follow-up
31/102 (30.4)
36/104 (34.6)
1.18 (0.63, 2.20)
0.615
Sustained responders
16-week follow-up
23/127 (18.1)
28/128 (21.9)
1.21 (0.64, 2.29)
0.557
26-week follow-up
22/127 (17.3)
29/128 (22.7)
1.40 (0.74, 2.66)
0.307
Remitters
8-week follow-up
19/112 (16.9)
23/111 (20.7)
1.09 (0.53, 2.26)
0.818
16-week follow-up
23/112 (20.5)
23/112 (20.5)
0.84 (0.42, 1.69)
0.631
26-week follow-up
21/102 (20.6)
26/104 (25.0)
1.21 (0.61, 2,41)
0.590
Binary logistic models were used for analysis of responders, remitters and sustained responders, with treatment comparison estimates presented similarly to those reported for primary outcome analysis, with the exception of reporting adjusted odd ratios. Responder ( reduction on GRID-HDRS-17 from baseline), remitter (score of on GRID-HDRS-17) and sustained responder (continuing-response reduction on GRID-HDRS-17 following response at the previous timepoint).
1 month following TMS completion and a manic episode following the 14th treatment session. One participant was admitted to hospital for nausea and vomiting following their baseline MRI scan, with this event reported as probably related to the scan due to the position of the neck while in the MRI scanner. All further SAEs were reported as unrelated to the study. There were a further 17 adverse events (AEs) of self-harm for 11 participants, and two AEs regarding an episode of syncope during treatments. Both participants suspended TMS on that day but completed the remainder of their TMS course without further incident.
Exploratory clinical outcomes
Moderator analyses demonstrated that higher baseline GRID-HDRS-17, higher baseline generalized anxiety (GAD-7) and completion of <20 stimulation sessions predicted lesser improvement in depression symptoms over 26-week follow-up (Supplementary Table 1). However, interactions between treatment arm and these moderator variables (as well as gender) were not statistically significant.
Neuroimaging outcomes
The primary neuroimaging hypothesis-that baseline effective connectivity from rAI to IDLPFC would predict clinical improvementwas not supported for GRID-HDRS-17, BDI-II or PHQ-9 scores ( , 185-201 participants included across time points). However, baseline rAI net outflow (effective connectivity from rAI to IDLPFC minus that from IDLPFC to rAI) was supported for GRID-HDRS-17 (main effect of net outflow: ). Enhanced improvement was associated with greater positive influence from IDLPFC to rAI and lesser positive influence from rAI to IDLPFC (Extended Data Fig. 4). This relationship did not differ between treatment groups or across
Fig. 2 | Mean (s.e.) GRID-HDRS-17 scores over time for analysis of primary ITT (multiple imputation).
post-treatment time points. Baseline net outflow was less positive in 16-week HDRS-17 responders than in nonresponders across both treatment groups .
Reduction in functional connectivity between IDLPFC and IDMPFC from baseline to 16 weeks was not supported for change in GRID-HDRS-17 for either the anterior or posterior DLPFC site specified in the protocol ( participants included across time points) but was significant for improvements in PHQ-9 (main effect of change in functional connectivity; PHQ-9: ; Extended Data Figs. 5 and 6) and approached significance for improvements in BDI-II for the posterior IDLPFC site. These relationships did not differ across groups, suggesting a direct link between network change and antidepressant effect.
Sensitivity analyses
Differences between treatment arms were not significant for any of the sensitivity analyses conducted; no center effects and no effects of being on no antidepressants at baseline were observed (Fig. 3 and Extended Data Table 3). Deviations leading to participant exclusion in the per-protocol analysis are given in Extended Data Table 4.
Post hoc analyses
To further understand the net outflow results, we examined whether baseline effective connectivity from IDLPFC to rAI alone predicted improvement on either GRID-HDRS-17 or HDRS-6 (6-item Hamilton Depression Rating Scale) score . The relationship was nonsignificant for GRID-HDRS-17 ( ) but significant for HDRS-6 (greater positive influence predicted greater improvement; , .
Discussion
The BRIGhTMIND study is a large, adequately powered trial in the United Kingdom using TMS and iTBS for TRD with outcomes at 26 weeks. There were no statistically significant or clinically important differences observed between cgiTBS and rTMS on primary and secondary clinical outcomes across 26 weeks, demonstrating that cgiTBS did not show superior clinical efficacy compared with structural MRI-neuronavigated rTMS. Both treatment arms demonstrated clinically substantial improvements in the primary outcome of observed depression and self-rated measures of depression, with above-minimum clinical important changes in self-rated anxiety, functioning and quality of life. For both treatment arms around one-third of participants showed a response, one-fifth achieved remission and one-fifth demonstrated a sustained response for 6 months. The results are encouraging given that two-thirds of participants were classed as medium to high treatment-resistant depression (approximately
Table 4 | Frequency of SAEs and AEs of self-harm and syncope
Event type
Safety population
rTMS,
cgiTBS,
SAE
Hospitalization for nausea and vomiting
1 (1%)
0
Hospitalization for pulmonary embolus
1 (1%)
0
Hospitalization for COVID-19
0
1 (1%)
Death from accidental opiate poisoning
0
1 (1%)
Hospitalization for investigation of fatigue
0
1 (1%)
Hospitalization for head injury
1 (1%)
0
Hospitalization for headache
1 (1%)
0
Death from myocardial infarction
0
1 (1%)
Hospitalization for high temperature
0
1 (1%)
Hospital admission for anaphylaxis due to insect bites
1 (1%)
0
Hospital admission for chest pains and breathlessness
1 (1%)
0
Hospital admission for low blood pressure
1 (1%)
0
Hospital admission related to pre-existing hidradenitis suppurativa
1 (1%)
0
Hospital admission: psychotic episode with severe anxiety/depression
1 (1%)
0
Hospitalization due to mania episode
0
1 (1%)
Hospitalization for shortness of breath
0
1 (1%)
Voluntary hospital admission for ECT
1 (1%)
0
Suspected seizure before first TMS session
1
0
AE
Self-harm
5;
12;
Syncope
2;
0
Data are presented as , number of participants affected, and the percentage of participants affected per SAE or AE (for each treatment arm) from the total number of participants randomized. ECT, electroconvulsive therapy. the participant did not have any TMS treatment delivered due to experiencing a seizure.
equivalent to failure to respond to four or more antidepressants), with a long duration of current depressive episode (median 6 years).
The two RCTs closest in design to ours are the THREE-D and THETA-DEP trials , both of which compared iTBS versus rTMS using structural MRI neuronavigation, the former with follow-up over 12 weeks and the latter for 26 weeks. Response and remission rates for depression, and improvements in anxiety and quality of life up to 26 weeks in the present trial, are consistent with THETA-DEP, a single-site study of only 60 participants with a shorter duration of current depression episode (mean 20 months) and less treatment resistance . Thus, while previous evidence suggests that the beneficial effects of rTMS on mood in TRD may be relatively short lived, lasting only 1-3 months , both MRI-neuronavigated TMS protocols in our study and THETA-DEP led to sustained responses maintained for months post treatment in one in five participants. The current results demonstrate this finding in an adequately powered sample, and with more persistent and difficult-to-treat depression than previously described. We do not know whether such sustained responses would occur with non-MRI-neuronavigated TMS.
Magnetic resonance imaging-guided neuronavigation may be advantageous in terms of reduced coil drift and off-target placement compared with traditional elastic cap scalp targeting , with our study
demonstrating that, in the vast majority of cases, the site of stimulation of TMS varied by and the angle of stimulation by from the target site over the course of 20 sessions. Although one previous MDD study reported greater clinical efficacy for MRI-guided neuronavigated TMS versus scalp-based targeting methods , others found no difference in clinical efficacy . These studies focused on immediate rather than longer-term efficacy. Because previous RCTs of iTBS measured response and remission only immediately following treatment, the benefits of MRI-guided neuronavigated versus non-navigated iTBS following initial treatment are unknown. Therefore, future research might compare the clinical efficacy and cost effectiveness for MRI-neuronavigated TMS versus non-neuronavigated TMS over longer-term follow-up given the additional cost of MRI scans.
The THREE-D study offered up to 30 TMS sessions for a number of participants and demonstrated slightly higher rates of response ( ) and remission ( ) than our study . Taking this into consideration, with the proportion of participants in our trial feeling somewhat (or, much) better and still increasing at the 19th and 20th treatment sessions, outcomes might be further enhanced in those participants who are still improving with up to 30 TMS treatments. Both treatments were associated with improvements over time for sustained attention, executive functioning and working memory, consistent with the conclusion of a recent meta-analysis that rTMS has modest cognitive-enhancing effects in MDD .
Our fMRI findings are supportive of the longer-term benefits of both cgiTBS and rTMS, with some putative evidence of a normalizing effect of brain dysconnectivity. People with MDD show increased positive connectivity between the CEN and DMN on rsfMRI while in healthy controls these networks are anticorrelated or uncorrelated . Our resting fMRI analysis suggests reduction in functional connectivity between baseline and 16 weeks between the posterior IDLPFC (part of CEN) and IDMPFC (part of DMN), consistent with the hypothesis that restoration of normal anticorrelation may be associated with improvements in depression. Despite the different proximities of the targets to the posterior IDLPFC (close for cgiTBS, distant for rTMS), the findings were similar between the two treatment arms, replicating our unpublished pilot work and a previous study -although only in self-rated measures of depression. If independently confirmed, TMS-induced restoration of the normal CEN-DMN anticorrelation pattern may be a putative (direct or indirect) mechanism of its antidepressant efficacyat least for some response domains. Improvement with TMS might indicate a reduction in intrusion of DMN-related, internal-world processing and rumination on CEN-related external-world processing and task performance, and might be consistent with the finding of attentional lapses in people with . Such changes may be better captured by the self-report BDI-II and PHQ-9 measures, which measure poor concentration and subjective processing, rather than the GRID-HDRS-17 measure, which does not directly measure these processes .
We found that the imbalance of influence between rAI and IDLPFC (‘net outflow’) predicted improvement in depression symptoms over 26 weeks across both treatment groups. Reduced baseline net outflow from rAI to IDLPFC was associated with response on GRID-HDRS-17 at 16 weeks in both treatment groups. Post hoc analysis suggested that improvement in core symptoms of depression was associated with dominant baseline effective connectivity from the IDLPFC on the rAI. A putative mechanistic explanation requiring further research is that greater influence of IDLPFC on rAI might enable the effects of TMS to spread more effectively from the IDLPFC to rAI, thereby enhancing its neuromodulatory effect on the insula.
One strength of the RCT is the multicenter design. The sample was large, with diversity in age, ethnicity and other demographic features. In comparison with the clinical population of TRD where there is a greater proportion of females, there was equal representation of men and women. Otherwise, the sample is generalizable to clinical populations in the United Kingdom with TRD. Treatment resistance
Fig. 3| ITT and sensitivity analyses of primary outcome measure following cgiTBS relative to TMS.
was verified from both patient accounts and clinical records, although this might have been underestimated if patient recall and records were incomplete. The measurement of treatment resistance also did not include psychological treatments, which are often accessible in England. There was a high rate (93%) of treatment completion of all 20 TMS sessions and follow-up (average 85%). From the neuronavigation data, TMS treatment was delivered with a high level of precision in relation to the MRI-derived coordinates and varied little in either site or other TMS parameters across 20 sessions, except for slight adjustments in positioning or motor threshold according to predetermined criteria. Inter-rater reliability checks suggested that measurement of the primary outcome was comparable between centers. Blinding of the intervention was successful for observers of outcome. A key aspect of the trial was the active input of people with lived experience of depression and transcranial magnetic stimulation (the BRIGhTMIND Lived Experience Advisory Group), who informed all aspects of the design, conduct and interpretation of the trial.
The study was, however, highly disrupted and suspended for 6 months by public health measures put in place to control the COVID-19 pandemic. With the input of our Lived Experience Advisory Group and external review by the Independent Trial Steering and Data Monitoring and Ethics Committee, we made a number of substantial changes to the protocol including (1) a change in primary outcome from response at 16 weeks to average change over 8,16 and 26 weeks, (2) a revised power calculation and (3) a move from face-to-face to remote assessment of outcome where possible . In light of the public health emergency, the study would not have been completed without these changes given the resources available for it. Pre-post COVID analysis of outcomes did not show any clinically important or statistically significant effect of the pandemic. Response rates at 16 weeks, the original primary outcome, show very little difference between treatment groups. It is very unlikely that the changes made to the trial through necessity on account of the COVID-19 pandemic made any material difference to any outcome or conclusion from the trial.
Limitations included that, although TMS treatments were well matched for number of pulses per treatment session, session duration and number of sessions, they differed in stimulation frequency (iTBS or rTMS), intensity of stimulation (80% resting motor threshold (RMT) or 120% RMT) and approach to selection of treatment location (resting state effective connectivity versus structural MRI). Previous RCTs suggest that iTBS and rTMS may be equivalent in efficacy in TRD . There is some uncertainty about the importance of the intensity of stimulation but, in the current trial, RMT was not tolerated well by a minority of trial participants, with a reduction in intensity required in
such participants in the rTMS arm to limit dropout from treatment. The reduction in intensity of stimulation was important because the number of treatment sessions moderated the mean reduction in depression symptoms over 8,16 and 26 weeks in both the current RCT and THREE-D . The importance of the approach to selection of treatment location is unknown. To match the treatment arms for the number of pulses per treatment session, we introduced an accelerated form of iTBS with five runs of 600 pulses over 37 min in each treatment session with approximately 5-min intervals of nonstimulation between runs. Dosage and time intervals between TBS protocols could affect meta-plasticity, either by reducing or reversing the effect of synaptic plasticity or by increasing the effect of synaptic plasticity . In some individuals, 5 -min intervals between iTBS runs might increase short-term cortical inhibition, reducing the effectiveness of the whole iTBS session and thereby making a group difference between cgiTBS and rTMS more difficult to demonstrate. It is worth noting that the current results are comparable in terms of response to the THETA-DEP RCT over 26 weeks for both the iTBS and rTMS groups, so the additional runs after the first run of 600 pulses may have had little additional efficacy in the cgiTBS treatment group.
Given these limitations, there are several ways of interpreting the results of the current study-that cgiTBS is not superior to rTMS. The most probable explanation is that precise targeting of the IDLPFC-rAI loop is unimportant in terms of the clinical or mechanistic efficacy of TMS. This would be consistent with the notion that spatially distinct targets may modulate the same or overlapping brain circuits. Alternatively, one could posit that the frontoinsular loop and its interaction with the DMN are irrelevant for the treatment effect. We consider this less likely for two reasons: (1) the net outflow from IDLPFC-rAI moderated primary outcome in both treatment groups, suggesting that IDLPFC-rAI functional connectivity might play some role in the TMS response; and (2) connectivity between the posterior IDLPFC, closely matching the average cgiTBS target, and dmPFC was associated with subjective improvement ratings. We cannot rule out that the 80 versus RMT strength biased efficacy somewhat towards rTMS, but we did not see delayed subject response trajectories in cgiTBS. Taken together, the lack of difference on any clinical or fMRI measure, with similar effects on functional connectivity, supports the interpretation that precision targeting of TMS treatments may not be advantageous at the group level using nonaccelerated rTMS or the current accelerated iTBS protocol. Future tertiary analyses of the rich multimodal data will explore possible subgroup-specific clinical and neuroplasticity effects.
A key clinical finding was the duration of TMS effects up to 26 weeks with both treatment groups. However, the interpretation
of these results is hampered by the lack of a sham treatment group and the lack of an end-of-treatment measure of primary outcome at 6 weeks. In relation to the latter, there was only a 2 -week gap to the first follow-up assessment, with negligible changes to other treatment in that period. Our Lived Experience Advisory Panel (LEAP) group advised that measurement of outcome at 6 and 8 weeks would be burdensome, so we chose the 8 -week outcome measurement rather than 6 -week to measure effects seen at 1 month following TMS in our pilot study. There are three possible explanations for the long duration of TMS in this RCT: (1) a lasting effect of TMS; (2) a nonspecific treatment effect due to regression to the mean, expectancy, hope or structure to the day; or (3) the effects of additional drug treatment for depression and anxiety, particularly at 16 and 26 weeks. A meta-analysis of placebo responses in RCTs of rTMS in TRD reported response and remission rates of 20 and at the end of treatment versus 33 and 19%, respectively, in BRIGhTMIND. A high degree of treatment resistance (all failed two treatments, the majority four) and long duration of current illness (median 6 years) are associated with lower placebo responses with treatments for depression, including TMS . In a RCT of a similar sample of participants with a comparable duration of current depression, largely recruited from the highest-recruiting site in BRIGhTMIND, the remission rate at 26 weeks was only (ref. 59).
The occurrence of fMRI changes associated with treatment in the study does not exclude a placebo response, especially given the finding of an overlap between brain regional activity modified by placebo and TMS for targets including IDLPFC . Nevertheless, one study showed that the placebo response did not impact on connectivity with the rAI , as seen with rTMS/cgi TBS in the present study. Some of the changes in outcome in both groups, especially at 16 and 26 weeks, may have been due to alterations in medication. For clinical and ethical reasons in this severe TRD group, changes in antidepressant or other medication were allowed and were made in 19% of the sample by 16 weeks. Exclusion of such participants in the per-protocol analysis, or being on an antidepressant or not at baseline, did not result in statistically significant or clinically important differences in primary outcome between treatment groups. Taken together, TMS is likely to have had a substantial impact on the duration of response but some of that change is due to nonspecific effects and clinically indicated medication changes, as would be the case in regular clinical care. How much of the change was due to TMS could be established only by an adequately powered RCT comparing iTBS or rTMS versus sham control on depression symptoms over 26 weeks. We proposed such a RCT to our funders when we first sought funding for the BRIGhTMIND study, but such a design was rejected for clinical and ethical reasons in such a severe, vulnerable group of patients. Therefore, it may not be possible to carry out such a trial.
In conclusion, this study found that cgiTBS and MRIneuronavigated rTMS are equally effective and safe. Patients showed clinically substantial improvements in depression that were sustained up to 26 weeks. These findings raise the possibility that some TRD patients unresponsive to other treatments could be kept well, while many others would derive clinically significant benefits, from one or two MRI-navigated courses of 20 (or possibly more) iTBS or rTMS sessions over a year.
Online content
Any methods, additional references, Nature Portfolio reporting summaries, source data, extended data, supplementary information, acknowledgements, peer review information; details of author contributions and competing interests; and statements of data and code availability are available at https://doi.org/10.1038/s41591-023-02764-z.
References
National Institute for Health and Care Excellence. Depression in Adults: Treatment and Management. NICE Guidelines (NG222) (NICE, 2022).
Rush, A. J. et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am. J. Psychiatry 163, 1905-1917 (2006).
Rizvi, S. J. et al. Treatment-resistant depression in primary care across Canada. Can. J. Psychiatry 59, 349-357 (2014).
Brunoni, A. R. et al. Repetitive transcranial magnetic stimulation for the acute treatment of major depressive episodes: a systematic review with network meta-analysis. JAMA Psychiatry 74, 143-152 (2017).
Berlim, M. T. et al. Response, remission and drop-out rates following high-frequency repetitive transcranial magnetic stimulation (rTMS) for treating major depression: a systematic review and meta-analysis of randomized, double-blind and sham-controlled trials. Psychol. Med. 44, 225-239 (2014).
Health Quality Ontario Repetitive transcranial magnetic stimulation for treatment-resistant depression: a systematic review and meta-analysis of randomized controlled trials. Ont. Health Technol. Assess. Ser. 16, 1-66 (2016).
Larson, J. & Munkácsy, E. Theta-burst LTP. Brain Res. 1621, 38-50 (2015).
National Institute of Health and Clinical Excellence. Repetitive Transcranial Magnetic Stimulation for Depression. Guidance (NICE, 2015).
Blumberger, D. M. et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial. Lancet 391, 1683-1692 (2018).
O’Reardon, J. P. et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biol. Psychiatry 62, 1208-1216 (2007).
Batail, J. M. et al. No place in France for repetitive transcranial magnetic stimulation in the therapeutic armamentarium of treatment-resistant depression? Brain Stimul. 16, 927-929 (2023).
Fox, M. D., Liu, H. & Pascual-Leone, A. Identification of reproducible individualized targets for treatment of depression with TMS based on intrinsic connectivity. Neuroimage 66, 151-160 (2013).
Anderson, R. J. et al. Repetitive transcranial magnetic stimulation for treatment resistant depression: re-establishing connections. Clin. Neurophysiol. 127, 3394-3405 (2016).
Mueller, S. et al. Individual variability in functional connectivity architecture of the human brain. Neuron 77, 586-595 (2013).
Cash, R. F. et al. Functional magnetic resonance imaging-guided personalization of transcranial magnetic stimulation treatment for depression. JAMA Psychiatry 78, 337-339 (2021).
Cole, E. et al. Stanford Neuromodulation Therapy (SNT): a double-blind randomized controlled trial. Am. J. Psychiatry 179, 132-141 (2022).
Iwabuchi, S. J. et al. Alterations in effective connectivity anchored on the insula in major depressive disorder. Eur. Neuropsychopharmacol. 24, 1784-1792 (2014).
Iwabuchi, S. J. et al. Targeted transcranial theta burst stimulation alters fronto-insular network and prefrontal GABA. Neuroimage 146, 395-403 (2017).
Iwabuchi, S. J. et al. Baseline effective connectivity predicts response to repetitive transcranial magnetic stimulation in patients with treatment-resistant depression. Eur. Neuropsychopharmacol. 29, 681-690 (2019).
Roebroeck, A. et al. Mapping directed influence over the brain using Granger causality and fMRI. Neuroimage 25, 230-241 (2005).
Liston, C. et al. Default mode network mechanisms of transcranial magnetic stimulation in depression. Biol. Psychiatry 76, 517-526 (2014).
Briley, P. M. et al. BRIGhTMIND trial motivating mechanism action analysis plan: resting state fMRI. https://doi.org/10.17639/ nott. 7251 (2022).
Fava, M. Diagnosis and definition of treatment-resistant depression. Biol. Psychiatry 53, 649-659 (2003).
Williams, J. et al. The GRID-HAMD: standardization of the Hamilton Depression Rating Scale. Int Clin. Psychopharmacol. 23, 120-129 (2008).
National Institute for Clinical Excellence. Depression: Management of Depression in Primary and Secondary Care. Clinical Guideline 23 (CG23) (NICE, 2004).
Rush, A. J. et al. Clinically significant changes in the 17- and 6-item Hamilton Rating Scales for Depression: a STAR*D report. Neuropsychiatr. Dis. Treat. 14, 2333-2345 (2021).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern Med 16, 606-613 (2001).
Turkoz, I. et al. Clinically meaningful changes on depression symptom measures and patient-reported outcomes in patients with treatment resistant depression. Acta Psychiatr. Scand. 143, 253-263 (2021).
Beck, A. et al. Manual for the Beck Depression Inventory-II (Psychological Corporation, 1996).
Hiroe, T. et al. Gradations of clinical severity and sensitivity to change assessed with the Beck Depression Inventory-II in Japanese patients with depression. Psychiatry Res. 135, 229-235 (2005).
Spitzer, R. L. et al. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 166, 1092-1097 (2006).
Bauer-Staeb, C. et al. Effective dose 50 method as the minimal clinically important difference: evidence from depression trials. J. Clin. Epidemiol. 137, 200-208 (2021).
Mundt, J. C. et al. The work and social adjustment scale: a simple measure of impairment in functioning. Br. J. Psychiatry 180, 461-464 (2002).
Everitt, H. A. et al. Assessing telephone-delivered cognitive-behavioural therapy (CBT) and web-delivered CBT versus treatment as usual in irritable bowel syndrome (ACTIB): a multicentre randomised trial. Gut 68, 1613-1623 (2019).
EuroQol Research Foundation. EQ-5D-5L User Guide version 3 (EuroQol, 2019).
Zanini, A. et al. Estimation of minimal clinically important difference in EQ-5D Visual Analog Scale Score after pulmonary rehabilitation in subjects with COPD. Respir. Care 60, 88-95 (2015).
McIntyre, R. S. The THINC-Integrated Tool (THINC-it) screening assessment for cognitive dysfunction: validation in patients with major depressive disorder. J. Clin. Psychiatry 78, 873-881 (2017).
Bech, P. The Hamilton Depression Scale. Evaluation of objectivity using logistic models. Acta Psychiatr. Scand. 63, 290-29 (1981).
Nixon, N. et al. The bi-factor structure of the 17-item Hamilton Depression Rating Scale in persistent major depression; dimensional measurement of outcome. PLoS ONE 15, e0241370 (2020).
Bulteau, S. et al. Intermittent theta burst stimulation (iTBS) versus 10 Hz high-frequency repetitive transcranial magnetic stimulation (rTMS) to alleviate treatment-resistant unipolar depression: a randomized controlled trial (THETA-DEP). Brain Stimul. 15, 870-880 (2022).
Caulfield, K. A. et al. Neuronavigation maximizes accuracy and precision in TMS positioning: evidence from 11,230 distance, angle, and electric field modeling measurements. Brain Stimul. 15, 1192-1205 (2022).
Fitzgerald, P. B. et al. A randomized trial of rTMS targeted with MRI based neuro-navigation in treatment-resistant depression. Neuropsychopharmacology 34, 1255-1262 (2009).
Li, C. T. et al. Antidepressant efficacy of prolonged intermittent theta burst stimulation monotherapy for recurrent depression and comparison of methods for coil positioning: a randomized, double-blind, sham-controlled study. Biol. Psychiatry 87, 443-450 (2020).
Hebel, T. et al. A direct comparison of neuronavigated and non-neuronavigated intermittent theta burst stimulation in the treatment of depression. Brain Stimul. 14, 335-343 (2021).
Martin, D. M. et al. Cognitive enhancing effects of rTMS administered to the prefrontal cortex in patients with depression: a systematic review and meta-analysis of individual task effects. Depress. Anxiety 34, 1029-1039 (2017).
Kaiser, R. H. et al. Large-scale network dysfunction in major depressive disorder: a meta-analysis of resting-state functional connectivity. JAMA Psychiatry 72, 603-611 (2015).
Gallagher, P. et al. Neurocognitive intra-individual variability in mood disorders: effects on attentional response time distributions. Psychol. Med. 45, 2985-2997 (2015).
Morriss, R. et al. Connectivity guided theta burst transcranial magnetic stimulation versus repetitive transcranial magnetic stimulation for treatment-resistant moderate to severe depression: study protocol for a randomised double-blind controlled trial (BRIGhTMIND). BMJ Open 10, e038430 (2020).
Pszczolkowski, S. et al. Connectivity-guided theta burst transcranial magnetic stimulation versus repetitive transcranial magnetic stimulation for treatment-resistant moderate to severe depression: magnetic resonance imaging protocol and SARS-CoV-2-induced changes for a randomized double-blind controlled trial. JMIR Res. Protoc. 11, e31925 (2022).
Trevizol, A. P. et al. Predictors of remission after repetitive transcranial magnetic stimulation for the treatment of major depressive disorder: an analysis from the randomised non-inferiority THREE-D trial. EClinicalMedicine 22, 100349 (2020).
Tse, N. Y. et al. The effect of stimulation interval on plasticity following repeated blocks of intermittent theta burst stimulation. Sci. Rep. 8, 8526 (2018).
Gamboa, O. L. et al. Impact of repetitive theta burst stimulation on motor cortex excitability. Brain Stimul. 4, 145-151 (2011).
Nettekoven, C. et al. Dose-dependent effects of theta burst rTMS on cortical excitability and resting-state connectivity of the human motor system. J. Neurosci. 34, 6849-6859 (2014).
Jones, B. D. M. et al. Magnitude of the placebo response across treatment modalities used for treatment-resistant depression in adults: a systematic review and meta-analysis. JAMA Netw. Open 4, e2125531 (2021).
Razza, L. B. A systematic review and meta-analysis on placebo response to repetitive transcranial magnetic stimulation for depression trials. Prog. Neuropsychopharmacol. Biol. Psychiatry 81, 105-113 (2018).
Hsu, J. H. et al. Impact of prior treatment on remission with intermittent theta burst versus high-frequency repetitive transcranial magnetic stimulation in treatment resistant depression. Brain Stimul. 12, 553-1555 (2019).
Nelson, J. C. et al. Predictors of remission with placebo using an integrated study database from patients with major depressive disorder. Curr. Med. Res. Opin. 28, 325-334 (2012).
Lisanby, S. H. et al. Daily left prefrontal repetitive transcranial magnetic stimulation in the acute treatment of major depression: clinical predictors of outcome in a multisite, randomized controlled clinical trial. Neuropsychopharmacology 34, 522-534 (2009).
Morriss, R. et al. Efficacy and cost-effectiveness of a specialist depression service versus usual specialist mental health care to manage persistent depression: a randomised controlled trial. Lancet Psychiatry 3, 821-831 (2016).
Burke, M. J. et al. Placebo effects and neuromodulation for depression: a meta-analysis and evaluation of shared mechanisms. Mol. Psychiatry 27, 1658-1666 (2022).
Zhao, K. et al. Individualized fMRI connectivity defines signatures of antidepressant and placebo responses in major depression. Mol. Psychiatry 28, 2490-2499 (2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Participants were recruited from primary and secondary care settings at five treatment centers across UK National Health Services (NHS): Nottinghamshire Healthcare NHS Foundation Trust; Northamptonshire Healthcare NHS Foundation Trust; Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust; Camden and Islington NHS Foundation Trust; and Pennine Care NHS Foundation Trust. The treatment centers were chosen to reflect geographical diversity and the fact that some had previous experience of TMS. The trial design and methods are outlined in two published trial protocols .
A participant met inclusion criteria if they were: aged years; met criteria for DSM-V major depressive disorder using a structured clinical interview ; had moderate to severe depression defined as a score of 16 or more on the GRID version of GRID-HDRS-17 (ref. 24)); had TRD defined as scoring 2 or more on , which was adapted for new treatment options (Supplementary Information ); and had the capacity to provide informed consent before any trial-related activities.
Participants were excluded if they had: a history of bipolar disorder or depression secondary to other mental disorder; neurological condi-tions-for example, brain neoplasm, cerebrovascular events, epilepsy, neurodegenerative disorders or previous brain surgery; standard contraindications to MRI (for example, irremovable metal objects in and around body, pregnancy, red tattoos on the head, neck and back or claustrophobia); major unstable medical illness requiring further investigation or treatment; in 2 weeks before baseline assessment any change in prescribed medication, treatment with lamotrigine, gabapentin or pregabalin, or intermittent benzodiazepines (or daily prescription diazepam equivalents) or hypnotics -mg zopiclone equivalent; current substance abuse or dependence (DSM-5 criteria ); previous TMS treatment; high risk of suicidality; potential complicating factors for TMS treatment (for example, hairstyles impeding close coil placement, piercings); involved with any other clinical trial at the time of consent or 6 months previously; or unable to read or understand English.
Participants were recruited through specialist mental health services across the five treatment centers and neighboring NHS trusts near the treatment centers, self-referrals and through patient identification centers recruiting through primary care services.
A questionnaire was used to telephone prescreen interested participants, with potentially eligible participants invited to attend a baseline assessment with an outcome assessor. At the baseline assessment all participants gave written informed consent and study eligibility was determined by the outcome assessors using SCID-5-RV, GRID-HDRS-17 and MGH. Furthermore, to assist with determination of study eligibility, medical and psychiatric history-including a detailed assessment of treatment resistance-was obtained from primary care notes and secondary care mental health service case files where available. Participants also completed the childhood trauma questionnaire (CTQ ) and self-report sociodemographic information was collected. All assessments were completed face to face at the hospital sites before the COVID-19 pandemic, which were then changed to video conferencing or telephone methods. Participants also completed a baseline MRI assessment with scans used to derive personalized treatment targets, and for a mechanism-of-action analysis with MRI at baseline and 16 weeks.
Ethics approval
The clinical trial received research ethics committee approval and health research authority approval from the East Midlands Leicester Central Research Ethics Committee (no.18/EM/0232). Research design and execution included local scientists at each site and was shared with all local sites.
Randomization and masking
Participants were randomly assigned in a 1:1 ratio to rTMS or cgiTBS. The TMS staff delivering treatment conducted the randomization
process via a web-based randomization system (Sealed Envelope, www. sealedenvelope.com) immediately before the start of the participant’s first treatment session. Randomization was stratified by study site and minimized on severity of depression (GRID-HDRS-17: score 16-23, moderate or , severe) and degree of treatment resistance (low , medium , high ), as assessed at the baseline assessment. Treatment allocation was conveyed only to TMS administration staff at each site via email.
Participants, referring clinical teams and outcome assessors were kept blinded with respect to treatment allocation until after the participant’s final follow-up assessment. Any unintended unblinding of outcome assessors was recorded, with other assessors completing all further assessments for that participant. At each follow-up assessment the outcomes assessor was asked to guess the participant’s treatment allocation.
Procedures
A total of 3,000 pulses were delivered in each rTMS or cgiTBS session, which was around 38 min in duration for the purposes of blinding participants and assessors of outcome.
A , figure-of-eight coil (E-z Cool coil) and a Magstim Horizon Performance Stimulator with StimGuide Navigated TMS Package (Magstim Co.) was used for all rTMS and cgiTBS treatments. Twenty once-daily sessions were delivered per participant over a 4-6-week period for both treatment arms.
Participants assigned to cgiTBS received bursts of three pulses ( resting motor threshold), with bursts repeated every 200 ms ( 5 Hz ). Bursts were presented in 10 -s cycles consisting of 2 s of stimulation and 8 s of rest; there were 20 such cycles per run ( 600 pulses per run). Five runs were presented per session, with 5-min inter-run intervals (3,000 pulses per session). The cgiTBS brain target was defined based on Granger Causality Analysis as the location within the IDLPFC receiving maximal effective connectivity from the rAI (Montreal Neurological Institute coordinates: , , determined using the participant’s rsfMRI and T1-weighted structural MRI scans) . The StimGuide Navigated TMS Package computed the nearest location for stimulation on the scalp from an individualized head model based on structural MRI and three fiducial points: the nasion and left preauricular and right preauricular sites.
Participants assigned to rTMS followed the standard US Food and Drug Administration-approved protocol . Stimulation was at resting motor threshold with -s trains of 10 Hz interspersed by 26 -s intertrain intervals, with a total of 3,000 pulses per session. The rTMS brain target was determined using the participants’ structural MRI to target a standard Montreal Neurological Institute coordinate (selected a priori as the parenchymal voxel closest to the F 3 site in a standard brain). As with the cgiTBS treatment arm, the StimGuide Navigated TMS Package was used to compute the stimulation site from the same individualized head model and the three fiducial points mentioned above.
Motor threshold (percentage) was determined at the first treatment session and determined again on the sixth treatment session for both treatment arms. Standardized steps were developed for participants who were unable to tolerate the cgiTBS or rTMS protocols, which involved either movement of the site of stimulation by 1 cm from the MRI-derived coordinates or a reduction in motor threshold.
Outcome data from assessment scales (GRID-HDRS-17, BDI-II ), PHQ-9 (ref. 27)), GAD-7 (ref.31)), WSAS ), EQ-5D-5L ) and EQ-5D-5L VAS were collected at baseline and at 8,16 and 26 weeks following randomization. An adapted version of the client service receipt inventory was collected at baseline and at 16- and 26-week follow-ups. Participants completed MRI scans at baseline and within 2 weeks of the 16-week follow-up assessment. The THINC-It tool for cognition was originally collected at baseline assessment and at all three follow-up time points. However, following the COVID-19 pandemic the THINC-It
tool was collected at the baseline and 16-week MRI scans only. To assess participants’ beliefs about the efficacy of treatment, and based on the advice of our patient and public involvement (PPI) representatives, we adapted the seven-point patient global impression of change measure to a shortened, five-point Likert scale (1-5, much worse to much better, with as many rating points for worse and improved mental state). Patient acceptability was also assessed with a purposively designed five-point Likert measure rated from 1 to 5: unacceptable (negative effects outweigh benefits) to acceptable (beneficial effects outweigh negative effects). These two measures were assessed at every TMS session and at each follow-up time point. Before the COVID-19 pandemic, participants were given the option to complete follow-up assessments face to face or remotely, with all subsequently being completed by telephone or video conferencing during and after the COVID-19 pandemic. Travel expenses were covered for participation in the study, along with a shopping voucher at 16 – and 26 -week follow-up assessments, as a mark of respect and gratitude for the time and input of the participants to the follow-up aspects of the trial. Participants recruited later in the study completed the Quick Inventory of Depressive Symptomatology Self-Rated version at baseline and 8, 16 and 26 weeks for the purposes of a substudy on cognition and fMRI (Supplementary Information ). Therefore, this measure should not be regarded as a secondary outcome of the trial and is not reported here.
Outcomes
The primary clinical outcome measure was mean change across 8,16 and 26 weeks in depression symptoms from baseline using GRID-HDRS-17. HDRS-17 is the most frequently used observer-rated measure of depression for RCTs of treatments for depression , and the GRID form was utilized given evidence of improved inter-rater reliability .
Secondary clinical outcomes were mean changes from baseline over 26 weeks on BDI-II, PHQ-9, GAD-7, WSAS and EQ-5D-5L VAS; mean changes from baseline to 16 weeks for the five cognitive tasks in the THINC-It tool; mean changes from baseline to 8,16 and 26 weeks separately on GRID-HDRS-17; proportion of responders at 8,16 and 26 weeks (defined as a reduction of on GRID-HDRS-17 from baseline); proportion of remitters at 8,16 and 26 weeks (defined as a score of on GRID-HDRS-17); proportion of sustained responders at 16 and 26 weeks (defined as a continuing-response reduction on GRID-HDRS-17 following response at the previous timepoint); and patient global impression of change at each TMS session and each follow-up time point and adverse events (side effects) checklist after each TMS session.
Magnetic spectroscopy, cost effectiveness outcomes (EQ-5D-5L and adapted client service receipt inventory), acceptability outcomes (five-point, purposively designed Likert scale and qualitative interviews) and further safety outcomes (common and uncommon side effects) will be reported separately.
Monitoring of adverse events
Internationally agreed definitions for AEs and SAEs were adopted and applied . Seizures were reported as SAEs. Syncope was recorded as an AE unless the participant was admitted to hospital, in which case it was defined as a SAE. Any participant found to be at risk to themselves (suicide, neglect) or others, or developing a SAE, was referred to the relevant clinical services. A review by a clinical expert in TRD was offered to any participant whose depression had become more severe at 16- and 26-week follow-ups, for safety reasons.
Role of the LEAP
The LEAP was a panel of PPI representatives with lived experience of depression, some of whom had additional personal experience of TMS, that informed all aspects of the design, development and running of the BRIGhTMIND trial. The LEAP was chaired by an experienced PPI organizer (P.B.) and included representatives from all centers. Efforts were made to ensure inclusivity by gender, ethnic background and personal
experience. LEAP members were paid for their time. Specific recommendations from the LEAP were: the completion of 20 TMS sessions over 6 weeks from 4 weeks; outcomes measured only at 8 weeks rather than at 6 and 8 weeks because of the burden on participants; travel buddies came to MRI and TMS appointments; all research materials were rewritten with lay and inclusive language, leading to a doubling of study website hits; advertising at specific sites to promote inclusiv-ity-for example, places of worship to recruit people of South Asian origin; and adaptation of the patient global impression of change. Further changes were suggested by the LEAP to ensure continuation of the trial during the COVID-19 pandemic, such as the use of staff photographs and profiles while wearing masks during face-to-face and remote appointments.
Changes due to the COVID-19 pandemic
Substantial amendments to the protocol made in light of the COVID-19 pandemic have been reported in a trial protocol publication . These changes were made in response to national and local public health measures in respect to the COVID-19 pandemic, with the approval of each site’s clinical research governance organizations, the sponsor (Nottinghamshire Healthcare NHS Foundation Trust), the LEAP, the Trial Management Group, the Independent Trial Steering Committee and Data Management and Ethics Committee and the funders. As one of the public health measures in the COVID-19 pandemic, these changes did not require NHS Ethics and Health Research Authority approval. The study was suspended, except for remote follow-up assessment, from 19 March to 1 August 2020. The following key changes were made from 1 August 2020 to the end of the study: (1) all baseline clinical assessments, obtaining written and informed consent and all follow-up clinical assessments, were made remotely by video conferencing supported by telephone and email. (2) All MRI, TMS treatment and THINC-it assessments were conducted face to face, with COVID-19 pandemic precautions reducing the maximum throughput of participants in the trial. (3) THINC-it assessments were conducted only at baseline and 16 weeks, alongside MRI scans, and were not conducted at 8 and 26 weeks-no other changes were made to assessments although there was loss of follow-up MRI scans at 16 weeks from 19 March to 1 August 2020. (4) The primary outcome was changed from response at 16 weeks to average change in total HDRS-17 score at 8,16 and 26 weeks. (5) Sample size was reduced from 368 to 266 participants given the slower recruitment rate, because of the pandemic precautions. (6) One site did not reopen once the study reopened because of the loss of staff required to conduct the TMS and research assessment, and was replaced by another site. (7) The analysis plan was changed to reflect the change of the primary outcome variable and to add a pre-post-COVID sensitivity analysis. (8) Further funding was obtained to address the period of suspension of the study and slower recruitment rate.
Sample size calculation
The National Institute for Health and Care Excellence defined three points as a clinically important difference in outcome on HDRS-17 for depression disorders . We compared the mean change in depression symptoms from baseline over 26 weeks in the cgiTBS group with that in the rTMS group. Assuming a standard deviation of 8 in the mean difference between groups, as informed by our pilot work and a previous randomized controlled trial in chronic persistent depressive disorder , a sample size of 266 participants would provide power to detect a mean difference of three points in GRID-HDRS-17 over 26 weeks between the groups at the two-sided significance level, assuming a correlation between follow-up measures of 0.7 and 20% data loss/dropout.
Statistical analysis
A statistical analysis plan was published before the primary analysis was undertaken and provides further detail on the analysis . The primary
analysis of primary outcome was conducted on the ITT population (all participants randomized to treatments), with the multiple-imputation technique being implemented to deal with missing data in instances where participants were missing GRID-HDRS-17 scores. Gender, ethnicity, age, center, baseline GRID-HDRS-17 score and degree of TRD were used as predictors of primary outcome to substitute the missing data with the predicted values from a multivariate normal regression equation. A total of 20 imputations were estimated. A mixed linear regression model was utilized, which adjusted for center (stratification variable), baseline GRID-HDRS-17 score and baseline MGH score (minimization variables), visit number and a categorical variable for treatment arm (rTMS arm as reference). Participant ID was included as random effect. The treatment comparison estimate is presented as adjusted mean difference between the treatment arms, with two-sided 95% CIs and values and statistical significance considered at . Analysis of secondary clinical outcomes was performed in a similar way, conducted on the ITT population using an available-data approach. Binary logistic models were used for analyses of responders, remitters and sustained responders, with treatment comparison estimates presented similarly to those reported for primary outcome analysis except for reporting of adjusted odds ratios. Participants randomly assigned to treatment and who completed at least one TMS session were included in the safety population.
Secondary analyses of primary outcome included a per-protocol analysis (excluding participants with major protocol violations: if original treatment protocols were not administered; 20 treatment sessions were completed after 6 weeks; more than 4 days had elapsed between treatments; MDD pharmacotherapy or psychotherapy changed before 16-week follow-up) and a completers’ analysis (that is, participants completed ten or more sessions of rTMS or cgiTBS delivered to the correct MRI coordinates and assessed at baseline and 16 weeks). Sensitivity analyses of primary outcome included a missing-not-at-random (MNAR) assumption analysis using a control-based imputation approach and a pre-post-COVID-19 period analysis.
Stata (v.16) was used for all data analyses except for cognition outcomes, which were analyzed in IBM SPSS statistics (v.25). With regard to neuroimaging, a protocol was published before receipt of any clinical data or statistical analysis . Preprocessing steps were as detailed in that protocol. Mixed-effects models were implemented in SPSS (v.18) and JASP (0.18) software and estimated with restricted maximum likelihood. Participant served as the random effect with a scaled identity variance-covariance matrix, with the dependent variable being clinical improvement from baseline in GRID-HDRS-17 (primary outcome measure), PHQ-9 or BDI-II (planned exploratory outcome measures). In addition to baseline connectivity, or change in connectivity, relevant to a given hypothesis we included as independent variables the post-treatment time point ( 8,16 or 26 weeks) and treatment group (rTMS or cgiTBS), and the interaction of connectivity with either or both variables. Age, gender, MGH treatment-resistance group, GAD-7, CTQ and study group site were explored as potential confounding variables; where these were nonsignificant they were removed from the model. MGH group and site were significant for baseline connectivity analyses; no confounders were significant for analyses examining change in connectivity. Reduction in GAD-7 was significantly associated with reduction in measures of depression from baseline to follow-up, but this did not change the significance of reported findings. The threshold of significance was set at the level for each of our prespecified analyses. Due to the use of two prespecified regions of interest for IDLPFC in analyses examining change in functional connectivity between DLPFC and DMPFC, Holm-Bonferroni correction was applied for two tests across values for each term (apart from the confounder variables) of that mixed model. In preplanned sensitivity analyses excluding patients for whom the cgiTBS target lay outside the left middle frontal gyrus according to the Harvard-Oxford cortical atlas at 10% threshold, only two such cases were identified and
there was minimal change in statistical parameters. A nonpreplanned exploratory analysis was performed with HDRS-6 (ref.38) which, unlike GRID-HDRS-17, is a unidimensional measure of depression over time , to further understand the effects of baseline net rAI to IDLPFC outflow results in relation to depression symptoms over 26 weeks.
The BRIGhTMIND trial was registered with the ISRCTN registry (no. ISRCTN19674644) on 2 October 2018, amended on 18 September 2020 to account for COVID-19, and is now registered as complete.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
We shall make data available to the scientific community with as few restrictions as feasible while retaining exclusive use until the publication of major outputs. Anonymized data, including all the trial data published in this manuscript, will be deposited at the University of Nottingham data repository (https://rdmc.nottingham.ac.uk) to encourage wider use.
Code availability
The computer code used to calculate the coordinates for cgiTBS or rTMS stimulation from fMRI and structural MRI scans in the BRIGhTMIND study can be found at https://github.com/SPMIC-UoN/ brightmind_pipeline.
References
Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (American Psychiatric Association, 2013).
First, M. et al. Structured Clinical Interview for DSM-5-Research version (SCID-5 for DSM-5, Research Version; SCID-5-RV) (American Psychiatric Association, 2015).
Bernstein, D. P. et al. Development and validation of a brief screening version of the Childhood Trauma Questionnaire. Child Abuse Negl. 27, 169-190 (2003).
Beecham, J. & Knapp, M. Costing Psychiatric Interventions (Gaskell, 2001).
Demyttenaere, K. et al. Patient-assessed versus physician-assessed disease severity and outcome in patients with nonspecific pain associated with major depressive disorder. Prim. Care Companion J. Clin. Psychiatry 11, 8-15 (2009).
Rush, A. J. et al. The 16 -item Quick Inventory of Depressive Symptomatology (QIDS) Clinician Rating (QIDS-C) and Self-Report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol. Psychiatry 54, 573-583 (2003).
Salagre, E. et al. Statins for the treatment of depression: a meta-analysis of randomized, double-blind, placebo-controlled trials. J. Affect. Disord. 200, 235-242 (2016).
ICH E2A Clinical Safety Data Management: Definitions and Standards for Expedited Reporting – Scientific Guideline (European Medicines Agency, 1995).
Morriss, R. et al. Statistical analysis plan. Figshare figshare. com/articles/online_resource/SAP_Morriss_BRIGhTMIND_Final_ docx/21271140/1 (2022).
Xia, M. et al. BrainNet Viewer: a network visualization tool for human brain connectomics. PLoS ONE 8, e68910 (2013).
Acknowledgements
This project was funded by the Efficacy and Mechanism Evaluation program (grant no. 16/44/02, awarded to R.M., M.A., C.B., P.B., S.L., P.F.L., R.H.M.-W., A.O.-K. and D.P.A.), a MRC and National Institute for Health and Care Research (NIHR) partnership. Magstimplc supplied the TMS delivery and neuronavigation systems. The views and opinions expressed by the authors and interviewees in this publication
are those of the authors and interviewees, respectively, and do not necessarily reflect those of the NHS, NIHR, MRC, CCF, NETSCC, the Efficacy and Mechanism Evaluation program, the Department of Health or the Magstim company. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript. We thank our BRIGhTMIND research study team: A. Blamire, L. Booth, C. Boutry, W. Cottam, E. Cox, L. Davison, R. De Vai, D. Dos Santos, M. Douglas-Bailey, D. Harding, S. Iwabuchi, M. James, C. Kaylor-Hughes, M. Keane, N. Khalifa, H. Oh, J. Parikh, I. Reid, J. Rivera, S. Simpson, J. Stone and L. Thomson. We thank our DMEC and TSC representatives: D. Baldwin, C. Dowrick, R. Emsley, K. Keates, G. Lancaster, B. Norden, S. Walker and P. Wilkinson. We thank our patient and public involvement members: J. Eastham, J. Gledhill, M. Hamie, M. Liddell, R. McNaughton, M. Mistry, J. Ooi, A. Willis and T. Willis.
Author contributions
R.M. was the chief investigator of the study, obtained funding for the study and study permissions, designed the study, led its conduct and wrote the first draft of the manuscript with L.W. He is the guarantor of the study. L.W. wrote operational guidelines for the project, helped to design qualitative analysis protocols, collected the clinical data for the Nottingham site, analyzed the imaging and qualitative data and wrote the first draft of the manuscript with R.M. M.A. was the principal investigator for the London site, including the clinical lead for TMS at the site, and obtained funding for the study as a grant applicant. He helped to design TMS treatment delivery and interpret TMS analysis. D.P.A. was the neuroimaging lead for the study and obtained funding for the study as a grant applicant. She designed the MRI connectivity guidance with P.F.L. S.B. helped to design the clinical trial, carried out power calculations for the study and contributed to the recalculation of sample size following the change of primary outcome. He helped to design the statistical analysis plan for the clinical trial, provided statistical support throughout the study and advised on the statistical analysis of the MRS data. P.B. helped to design and led both patient and public involvement in the study throughout. He commented on drafts of the report and helped to design the analysis of the patient and public involvement contribution to the report. P.M.B. helped to design and carried out the MRI analysis of the study. He advised on the statistical analysis of the THINC-it data. C.B. was the lead statistician for the clinical trial and grant holder. She provided statistical support throughout the study. She supervised the design of the statistical analysis plan, as well as the statistical analysis and report of the clinical trial results. B.H. carried out the THINC-it analysis with R.H.M.-W. and drafted the THINC-it analysis report. L.I. was the trial manager from 2021 and obtained permissions for the study. M.K. was the Principal Investigator at the Oldham site in the study and was the clinical lead for TMS at the site. S.L. was the Principal Investigator at the Nottingham site and the TMS clinical lead at Nottingham. He helped to devise the TMS intervention for the study and was a
grant holder. P.F.L. helped to devise the neuroimaging for the study, including the method of computation of the TMS stimulation sites from MRI data. He was a grant holder. R.H.M.-W. was the Principal Investigator and clinical lead for the Newcastle site. He devised the THINC-it analysis and adapted the MGH measure of treatment resistance for the study. A.O.-K. was the Principal Investigator at the Northampton site and supervised TMS delivery at Northampton. He helped to devise the TMS treatment in the study and was a grant holder. S.P. wrote the computer program and automated method for calculating the site of TMS stimulation from MRI data, and calculated the precision of TMS stimulation delivered by neuronavigation from the MRI-calculated target site. A.S.D.P. provided statistical support throughout the study and carried out statistical analysis under the supervision of S.B. and C.B. She contributed to recalculation of sample size following the change of primary outcome. She wrote the statistical analysis plan and produced the report of the clinical trial results in line with the analysis plan. Y.W. was the trial manager from the inception of the trial until September 2021. She then supervised L.I., who took over the role.
Competing interests
R.M. has received funding for research from Electromedical Products, Inc. and fees for participation in a Data Monitoring Ethics Committee for two trials in depression from Novartis plc. M.A. has received fees for consulting and giving lectures by Takeda Pharmaceutical, Janssen Pharmaceutical and the Clinical TMS Society. R.H.M.-W. declares fees for consulting and giving lectures from Janssen-Cilag, LivaNova, Lundbeck, P1Vital, Sage Therapeutics, Sothema and Takeda. No other potential conflicts of interest are reported for any of the other authors. No third parties have been involved in the study design, analysis and writing of the manuscript.
Correspondence and requests for materials should be addressed to Richard Morriss.
Peer review information Nature Medicine thanks Tao Chen, Katherine Scangos and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Ming Yang, in collaboration with the Nature Medicine team.
Extended Data Fig. 1 | Flow of participants through fMRI protocol. rTMS, repetitive transcranial magnetic stimulation cgiTBS, connectivity guided intermittent theta burst stimulation.
Extended Data Fig. 2 | Sites of TMS stimulation. Illustration of transcranial magnetic stimulation (TMS) targets, and regions of interest (ROIs) for the baseline brain connectivity analyses. Small dots indicate the connectivity guided intermittent theta burst stimulation (cgiTBS) left dorsolateral prefrontal cortex (DLPFC) target co-ordinates for individual participants – these are the locations
with maximal effective connectivity from the right anterior insula (rAI) as a large grey dot. The mean cgiTBS target across participants is shown as a large white dot. The mean repetitive transcranial magnetic stimulation (rTMS) target is shown as a large white dot; this is the F3 target for the group that received rTMS. Plotted with BrainNet Viewer (Xia et al. ) on the smoothed ICBM152 atlas.
Extended Data Fig. 3 | Percentage of participants who felt somewhat or much better over the 20 TMS sessions. TMS, transcranial magnetic stimulation. rTMS, repetitive transcranial magnetic stimulation. cgiTBS, connectivity guided intermittent theta burst stimulation. Participant self-rated as somewhat or much improved on modified 5-point clinical global impression scale.
Extended Data Fig. 4 | Reduction in baseline net outflow from right anterior insula to left dorsolateral prefrontal cortex in relation to mean improvement in GRID-HDRS-17 score over 26 weeks. Reduction in GRID version of the 17=item Hamilton Depression Rating Scale (GRID-HDRS-17) total score (improvement) from baseline to follow-up, collapsed across follow-up time points, as a function of baseline net outflow from the right anterior insula (RAI) seed region to
the connectivity guided intermittent theta burst stimulation (cgiTBS) target region within the left dorsolateral prefrontal cortex (DLPFC). Each data point is a participant. Lower net outflow (that is, lesser influence of the RAI on the left DLPFC and greater influence of the left DLPFC on the RAI) was associated with greater improvement.
Extended Data Fig. 5 | Regions of interest for change in brain connectivity analysis for dorsolateral and dorsomedial prefrontal cortex. Regions of interest (ROIs) for the change in brain connectivity analyses, plotted on a
standard brain image (smoothed ICBM152 atlas), in the sagittal (left) and coronal (right) planes. DMPFC: dorsomedial prefrontal cortex; DLPFC(a): anterior DLPFC site; DLPFC(p): posterior DLPFC site.
Extended Data Fig. 6 | Reduction in left dorsolateral prefrontal cortex to left dosrsomedial prefrontal cortex functional connectivity with improvement in PHQ-9 score over 26 weeks. Reduction in 9-item Personal Health Questionnaire (PHQ-9) total score (improvement) from baseline to follow-up, collapsed across post-treatment time point, as a function of reduction in
functional connectivity between the left dorsomedial prefrontal cortex (DMPFC) region and the posterior left dorsolateral prefrontal cortex (DLPFC) region. Each data point is a participant. Greater clinical improvement was associated with greater reduction in functional connectivity between these regions.
Extended Data Table 1 | Outcome assessor predictions of treatment allocation
rTMS
cgiTBS
Total
Outcome Assessor Prediction of treatment allocation at 8 weeks
Prediction of treatment allocation
Don’t know
94 (83.9%)
95 (85.6%)
189 (84.8%)
cgiTBS
9 (8.0%)
6 (5.4%)
15 (6.7%)
rTMS
9 (8.0%)
10 (9.0%)
19 (8.5%)
Outcome Assessor Prediction of treatment allocation at 16 weeks
Prediction of treatment allocation
Don’t know
90 (80.4%)
88 (78.6%)
178 (79.5%)
cgiTBS
7 (6.3%)
11 (9.8%)
18 (8.0%)
rTMS
15 (13.4%)
12 (10.7%)
27 (12.1%)
Unobtainable
0 (0.0%)
1 (0.9%)
1 (0.4%)
Outcome Assessor Prediction of treatment allocation at 26 weeks
Prediction of treatment allocation
Don’t know
77 (75.5%)
76 (73.1%)
153 (74.3%)
cgiTBS
8 (7.8%)
17 (16.3%)
25 (12.1%)
rTMS
17 (16.7%)
11 (10.6%)
28 (13.6%)
Extended Data Table 2 | Target-session and inter-session distance and angle of TMS
25th percentiles
Median
percentiles
rTMS
cgiTBS
rTMS
cgiTBS
rTMS
cgiTBS
target-session distance (mm)
2.99
2.62
4.20
4.66
8.66
8.10
target-session angle (degrees)
5.02
3.89
7.09
6.82
9.69
9.54
inter-session distance (mm)
3.88
3.73
5.17
4.63
8.25
7.48
inter-session angle (degrees)
5.47
5.31
7.51
6.73
10.07
10.22
TMS, transcranial magnetic stimulation. rTMS, repetitive transcranial magnetic stimulation cgiTBS, connectivity guided intermittent theta burst stimulation.
Extended Data Table 3 | GRID-HDRS-17 descriptive statistics for the secondary and sensitivity analyses of the primary outcome
GRID-HDRS-17
Baseline
8 Weeks
16 Weeks
26 Weeks
rTMS
cgiTBS
rTMS
cgiTBS
rTMS
cgiTBS
rTMS
cgiTBS
Mean (SD)
n
n
Mean (SD)
n
n
n
n
Per Protocol
67
76
58
61
55
63
52
58
24.1 (4.8)
23.2 (4.8)
17.2 (8.4)
15.0 (6.4)
17.4 (8.3)
15.3 (8.1)
17.6 (9.2)
14.2 (7.9)
Completers
110
108
104
105
110
108
98
98
24.0 (4.9)
22.6 (4.6)
15.5 (7.5)
14.4 (6.6)
15.8 (7.9)
15.0 (7.7)
16.2 (8.6)
14.4 (7.6)
MNAR assumption
127
128
127
128
127
128
127
128
23.9 (4.7)
22.9 (4.7)
15.8 (7.3)
14.6 (6.2)
16.1 (7.5)
15.2 (7.3)
16.5 (7.9)
14.9 (6.9)
Pre-Post COVID-19 period
Pre-COVID 19
35
36
24.7 (5.3)
23.2 (5.3)
Post-COVID 19
92
92
23.5 (4.4)
22.9 (4.5)
GRID-HDRS-17, GRID version of 17-item Hamilton Depression Rating Scale. rTMS, repetitive transcranial magnetic stimulation. cgiTBS, connectivity guided intermittent theta burst stimulation. MNAR, missing not at random.
Extended Data Table 4 | Breakdown of major protocol deviation reasons by deviation type and number of participants affected by deviation type
Major Protocol Deviation Reason
rTMS
cgiTBS
Overall
p
n
p
n
p
n
Ineligibility post-randomisation, n(%)
1 (0.9%)
1 (0.8%)
0 (0.0%)
0 (0.0%)
1 (0.4%)
1 (0.4%)
Non-compliance with randomised treatment:
Participant received less than 20 sessions over a period of 4-6 weeks, n (%)
11 (9.4%)
11 (8.7%)
9 (7.6%)
9 (7.0%)
20 (8.5%)
20 (7.8%)
Receiving wrong treatment as per randomized allocation , n (%)
9 (7.7%)
9 (7.1%)
13 (11.0%)
13 (10.2%)
22 (9.4%)
22 (8.6%)
Session stopped part way through treatment, n (%)
5 (4.3%)
5 (3.9%)
3 (2.5%)
3 (2.3%)
8 (3.4%)
8 (3.1%)
Time between the first and last session exceeds 6 weeks, n (%)
0 (0.0%)
0 (0.0%)
2 (1.7%)
2 (1.6%)
2 (0.9%)
2 (0.8%)
Break between treatment sessions of more than 4 days , n (%)
46 (39.3%)
38 (29.9%)
43 (36.4%)
32 (25.0%)
89 (37.9%)
70 (27.5%)
Missing Primary Outcome data (including loss to follow-up) , n (%)
9 (7.7%)
9 (7.1%)
13 (11.0%)
13 (10.2%)
22 (9.4%)
22 (8.6%)
Receiving concomitant medications that should not be taken while receiving treatment (i.e., Lamotrigine, Pregabalin or Gabapentin), n (%)
2 (1.7%)
2 (1.6%)
3 (2.5%)
3 (2.3%)
5 (2.1%)
5 (1.9%)
Psychotropic medications or psychological interventions not kept stable for 16 weeks for the duration of the Trial (except for those at risk to themselves or others) (%)
31 (26.5%)
22 (17.3%)
30 (25.4%)
26 (20.3%)
61 (25.9%)
48 (18.8%)
Daily prescription of Benzodiazepine above 5 mg , Diazepam equivalents, Zopiclone above 7.5 mg , Zolpidem above 10 mg or Zaleplon above 10 mg from baseline assessment to the end of Transcranial Magnetic Stimulation treatment, n (%)
3 (2.6%)
3 (2.4%)
2 (1.7%)
2 (1.6%)
5 (2.1%)
5 (1.9%)
Overall, n (%)
117 (100%)
68 (53.5%)
118 (100%)
76 (59.4%)
235 (100%)
144 (56.5%)
p : number of protocol deviations by deviation type, n : number participants affected per deviation type Please note the percentage corresponding to the proportion of participants affected per major deviation type (including the total for each treatment arm and overall) was calculated out of the total number of participants randomised. rTMS, repetitive transcranial magnetic stimulation. cgiTBS, connectivity guided intermittent theta burst stimulation. TMS treatment was delivered for part of a treatment session or course at the incorrect coordinates in relation to the magnetic resonance imaging (MRI) data or at the incorrect motor threshold in the transcranial magnetic stimulation standardized operating procedure. There were no instances of the wrong treatment allocation being delivered. A deviation of this type was added to the summary table above for participants that had a break of more than 4 days between TMS sessions and did not have a protocol deviation recorded for this on the Protocol Deviations Case Report Form of the study. Defined as the failure to provide the GRID version of the 17-item Hamilton Depression Rating Scale (GRID-HDRS-17) score at all the follow-up assessment time points: 8,16 and 26 weeks. Changes in psychotropic medications were captured under the category of ‘Other Deviation’ and they were adjudicated by the Chief Investigator as to determine whether or not they were classed as this type of medication.
natureportfolio
Corresponding author(s): Richard Morriss
Last updated by author(s): Dec 8, 2023
Reporting Summary
Nature Portfolio wishes to improve the reproducibility of the work that we publish. This form provides structure for consistency and transparency in reporting. For further information on Nature Portfolio policies, see our Editorial Policies and the Editorial Policy Checklist.
Statistics
For all statistical analyses, confirm that the following items are present in the figure legend, table legend, main text, or Methods section.
Confirmed
The exact sample size for each experimental group/condition, given as a discrete number and unit of measurement
A statement on whether measurements were taken from distinct samples or whether the same sample was measured repeatedly
The statistical test(s) used AND whether they are one- or two-sided
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
A description of all covariates tested
A description of any assumptions or corrections, such as tests of normality and adjustment for multiple comparisons
A full description of the statistical parameters including central tendency (e.g. means) or other basic estimates (e.g. regression coefficient) AND variation (e.g. standard deviation) or associated estimates of uncertainty (e.g. confidence intervals)
For null hypothesis testing, the test statistic (e.g. ) with confidence intervals, effect sizes, degrees of freedom and value noted Give values as exact values whenever suitable.
For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
For hierarchical and complex designs, identification of the appropriate level for tests and full reporting of outcomes
Estimates of effect sizes (e.g. Cohen’s , Pearson’s ), indicating how they were calculated
Our web collection on statistics for biologists contains articles on many of the points above.
Software and code
Policy information about availability of computer code
Data collection
We provide the computer code we used to turn measures of effective connectivity or F3 site from fMRI and structural images into stimulation points for transcranial magnetic stimulation at https://github.com/SPMIC-UoN/brightmind_pipeline
Data analysis
Clinical outcomes were analyzed with STATA version 16 except cognition which was analyzed using SPSS version 25 . Neuroimaging employed SPSS version 18 and JASP 018 software.
For manuscripts utilizing custom algorithms or software that are central to the research but not yet described in published literature, software must be made available to editors and reviewers. We strongly encourage code deposition in a community repository (e.g. GitHub). See the Nature Portfolio guidelines for submitting code & software for further information.
Data
Policy information about availability of data
All manuscripts must include a data availability statement. This statement should provide the following information, where applicable:
Accession codes, unique identifiers, or web links for publicly available datasets
A description of any restrictions on data availability
For clinical datasets or third party data, please ensure that the statement adheres to our policy
with a smoothed brain from the ICBM152 atlas for presentation of brain images. We analysed clinical data with STATA version 16 except for cognition data analyzed with SPSS version 25. Neuroimaging analysis was performed with SPSS version 18 and JASP018 software.
Research involving human participants, their data, or biological material
Policy information about studies with human participants or human data. See also policy information about sex, gender (identity/presentation), and sexual orientation and race, ethnicity and racism.
Reporting on sex and gender
We use the term gender throughout
Reporting on race, ethnicity, or other socially relevant groupings
Age 18 years or over with no upper age limit or limited on gender, ethnicity, marital status or social class.
Population characteristics
Inclusion criteria: Aged years old; met criteria for DSM-V major depressive disorder using a structured clinical interview; had moderate to severe depression defined as a score of 16 or more on the GRID version of the 17-Item Hamilton Depression Rating Scale ; had treatment resistant depression defined as scoring 2 or more on the Massachusetts General Hospital Treatment Resistant Depression staging score; and had the capacity to provide informed consent.
Exclusion criteria: bipolar disorder or depression secondary to other mental disorder; neurological conditions e.g. brain neoplasm, cerebrovascular events, epilepsy, neurodegenerative disorders, prior brain surgery; standard contraindications to magnetic resonance imaging (MRI) (e.g. irremovable metal objects in and around body, pregnancy, red tattoos on the head, neck and back, claustrophobia); major unstable medical illness requiring further investigation or treatment; in two weeks before baseline assessment any change in prescribed medication, treatment with lamotrigine, gabapentin or pregabalin, or intermittent benzodiazepines (or daily prescription above 5 mg diazepam equivalents), hypnotics above 7.5 mg zopiclone equivalent; current substance abuse or dependence (DSM-5 criteria; prior TMS treatment; high risk of suicidality; potential complicating factors for TMS treatment (e.g. hairstyles impeding close coil placement, piercings); involved with any other clinical trial at the time of consent or 6 months prior; unable to read or understand English.
Recruitment
Participants were recruited through specialist mental health services across the five treatment centres In England and neighbouring NHS trusts near the treatment centres, self-referrals, and through patient identification centres recruiting through primary care services. Since this is a sample of treatment resistan depression, then by definition participants must be receiving current treatment form psciliast mental health services or primary care so the results are not applicable to people with moderate to severe depression not receiving treatment. There were more males in the sample but otherwise the sample was demographically representative of treatment resistant depression in England.
Ethics oversight
The clinical trial received research ethics committee approval and health research authority approval from the East Midlands Leicester Central Research Ethics Committee (ref: 18/EM/0232). The research design and execution included local scientists at each site and was shared with all local sites.
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Field-specific reporting
Please select the one below that is the best fit for your research. If you are not sure, read the appropriate sections before making your selection.
Life sciences Behavioural & social sciences Ecological, evolutionary & environmental sciences
For a reference copy of the document with all sections, see nature.com/documents/nr-reporting-summary-flat.pdf
Life sciences study design
All studies must disclose on these points even when the disclosure is negative.
Sample size
The National Institute for Health and Care Excellence (NICE) defined 3 points as a clinically important difference in outcome on the HDRS-17 for depression disorders. 20 We compared the mean change in depression symptoms from baseline over 26 weeks in the cgiTBS group with that in the rTMS group. Assuming a standard deviation of 8 in the mean difference between groups, as informed by our pilot work19 and a prior randomised controlled trial in chronic persistent depressive disorder, 22 a sample size of 266 participants would provide power to detect a mean difference of 3 points in the GRID-HDRS-17 over 26 weeks between the groups at the two-sided significance level, assuming a correlation between follow-up measures of 0.7 and 20% data loss/drop-out.
Data exclusions
nclusion criteria: Aged years old; met criteria for DSM-V major depressive disorder using a structured clinical interview; had moderate to severe depression defined as a score of 16 or more on the GRID version of the 17-Item Hamilton Depression Rating Scale ; had treatment resistant depression defined as scoring 2 or more on the Massachusetts General Hospital Treatment Resistant Depression staging score; and had the capacity to provide informed consent.
Exclusion criteria: bipolar disorder or depression secondary to other mental disorder; neurological conditions e.g. brain neoplasm, cerebrovascular events, epilepsy, neurodegenerative disorders, prior brain surgery; standard contraindications to magnetic resonance imaging (MRI) (e.g. irremovable metal objects in and around body, pregnancy, red tattoos on the head, neck and back, claustrophobia); major unstable medical illness requiring further investigation or treatment; in two weeks before baseline assessment any change in prescribed medication, treatment with lamotrigine, gabapentin or pregabalin, or intermittent benzodiazepines (or daily prescription above 5 mg
diazepam equivalents), hypnotics above 7.5 mg zopiclone equivalent; current substance abuse or dependence (DSM-5 criteria; prior TMS treatment; high risk of suicidality; potential complicating factors for TMS treatment (e.g. hairstyles impeding close coil placement, piercings); involved with any other clinical trial at the time of consent or 6 months prior; unable to read or understand English.
Replication
We did not repeat the experiment to test its reproducibility because it was a large resource intensive multicentre trial with imaging. We have described all procedures so it could be reproduced.
Randomization
We describe the randomisation procedure and how this was communicated
Blinding
Blinding was undertaken and demonstrated
Reporting for specific materials, systems and methods
We require information from authors about some types of materials, experimental systems and methods used in many studies. Here, indicate whether each material, system or method listed is relevant to your study. If you are not sure if a list item applies to your research, read the appropriate section before selecting a response.
Materials & experimental systems
Methods
n/a
Involved in the study
n/a
Involved in the study
Palaeontology and Archaeology
Specimen provenance
Provide provenance information for specimens and describe permits that were obtained for the work (including the name of the issuing authority, the date of issue, and any identifying information). Permits should encompass collection and, where applicable, export.
Specimen deposition
Indicate where the specimens have been deposited to permit free access by other researchers.
Dating methods
If new dates are provided, describe how they were obtained (e.g. collection, storage, sample pretreatment and measurement), where they were obtained (i.e. lab name), the calibration program and the protocol for quality assurance OR state that no new dates are provided.
Tick this box to confirm that the raw and calibrated dates are available in the paper or in Supplementary Information.
Ethics oversight
Identify the organization(s) that approved or provided guidance on the study protocol, OR state that no ethical approval or guidance
was required and explain why not.
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Clinical data
Policy information about clinical studies
All manuscripts should comply with the ICMJE guidelines for publication of clinical research and a completed CONSORT checklist must be included with all submissions.
Clinical trial registration ISRCTN19674644 complete. CONSORT checklist included
Study protocol
The study protocol has been submitted
Data collection
These are described in the manuscript. All assessments were completed face-to-face at the hospital sites prior to the COVID-19 pandemic, which then changed to video conferencing or telephone methods. Participants also completed a baseline magnetic resonance imaging (MRI) assessment with scans used to derive personalized treatment targets, and for a mechanism of action analysis with MRI at baseline and 16 weeks.
Outcomes
All primary and secondary outcomes are included except health economics data.
Magnetic resonance imaging
Experimental design
Design type
Resting state
Design specifications
Described in the paper. It is a clinical trial
Behavioral performance measures
All the information we required on functional or effective connectivity can be obtained from resting stste fMRI so behavioral performance measures were not necessary.
Acquisition
Imaging type(s)
functional MRI
Field strength
3Tesla
Sequence & imaging parameters
Multimodal MRI at 3T consisting of a structural T1-weighted scan and an eyes-open blood oxygenation level dependent (BOLD) echo-planar imaging (EPI) resting state fMRI scan with additional positive and negative phase-encoded images to enable distortion correction.High-resolution T1-weighted images will be acquired using sagittal fast-spoiled gradient echo BRAVO (or equivalent) sequences with 1 mm 3 isotropic voxels covering the whole head from the vertex to the neck. rsfMRI images will be acquired with the eyes open using a fixation cross. All sites used a gradient echo EPI sequence aligned with the anterior commissure-posterior commissure line, with acquisition covering from the vertex downward (repetition time [TR]/echo time [TE]=2000/32 ms; flip angle=77 ; 35 slices; voxel size= 3 mm ; slice gap=0.5 mm ; field of view ; interleaved bottom/up; 240 volumes; phase encoding direction=posterior>anterior). All rsfMRI images have associated forward- and reverse-phase-encoded BO images acquired to facilitate distortion correction.
Area of acquisition
Whole brain
Diffusion MRI Used
X Not used
Preprocessing
Preprocessing software
Subject digital imaging and communications in medicine (DICOM) session files were uploaded onto an XNAT (Washington University School of Medicine) database infrastructure for all data other than MRS data using anonymized subject numbers. Once the session was archived within XNAT, it was put into a quarantined state awaiting quality control (QC), and DICOM files were automatically converted into Brain Imaging Data Structure NIFTI or JSON pairs for each scan using the dcm2bidssession v1.5 XNAT container, with T1-weighted images also undergoing defacing within this step.
Normalization
Normalization.Structural T1-weighted images were first coarsely brain extracted using the FSL brain extraction tool (BET). The original and brain extracted images are then nonlinearly registered to the MNI152 1-mm template using FSL FMRIB’s nonlinear image registration tool (FNIRT). The original FSL BET brain extraction was then refined by applying the produced nonlinear transformation to warp the MNI152 brain mask onto the subject’s T1 image. The resulting brain extracted image was finally bias-corrected and segmented into gray matter, cerebrospinal fluid (CSF), and white matter (WM) using FSL FMRIB Automated Segmentation Tool (FAST). The resulting WM and CSF probability maps were binarized at a tissue-probability threshold of and then eroded using a spherical kernel with a radius of 2 voxels.
Normalization template
Normalization template. The MNI152 1-mm template using FSL FMRIB’s nonlinear image registration tool (FNIRT).
Noise and artifact removal
Noise and artifact removal.The structural T1-weighted image was bias-corrected after nonlinear transformation. BOLD rsfMRI images underwent EPI distortion correction by inputting the positive and negative phase-encoded acquisitions into TOPUP. Then, they underwent between-volume motion correction (MCFLIRT 6DoF) and SPM12 interleaved slice-timing correction (bottom-up). The corrected BOLD image was subsequently smoothed with a 5 mm full-width half-maximum kernel using Smallest Univalue Segment Assimilating Nucleus (SUSAN) and denoised with ICA-AROMA. BOLD images were high-pass filtered at a frequency of 0.01 Hz after denoising. A transformation between the resulting BOLD image and the T1-weighted image was later computed using FSL epi_reg, and then combined with the TOPUP spatial distortion correction transformation. The resulting combined transformation was then inverted to create a nonlinear transformation from the T1weighted to (original uncorrected) BOLD space. The previously computed binary WM and CSF masks were later warped into BOLD space using the T1-weighted to BOLD transformation to extract the WM and CSF time series from the BOLD data. To control for additional physiological or scanner-related noise, the WM and CSF time series were then regressed out of the rsfMRI time series.
Volume censoring
The field of view was reduced by removing the lower head and neck using FSL robustfov.
Statistical modeling & inference
Model type and settings
Model type and settings.Functional connectivity (FC). Time series was extracted from two regions of interest (ROIs) using the fslmeants tool (part of the FSL software library). The first principal component of the time series of all voxels within an ROI was taken as a representation of the overall time series for that ROI. The first five time points were discarded to allow magnetisation stabilisation and time series were band-pass filtered between 0.01 and 0.1 Hz . Zero-lag ROI-to-ROI
correlations were calculated using Pearson correlations between the times series, partialling out twenty-four head motion parameters (three translations and three rotations for current time point and one time point prior, and squares of these parameters). Correlations of interest were converted to -scores using Fisher’s r-to-z conversion. These z-scores served as the measures of FC.
Effective connectivity (EC) Granger causality was computed using the REST toolbox, which runs under MATLAB. This provided a measure of directed (effective) connectivity, from one ROI ( , for example, right AI ) to another ROI ( , for example, left DLPFC). The toolbox provides measures of the influence of x on y as well as y on x . The first five time points were discarded, and the twenty-four head motion parameters were entered as covariates. No band-pass filter was applied, as per the trial target-identification procedure. Effective connectivity values we converted to z-scores using Fisher’s r-to-z conversion, then the mean z-score output across all voxels in y served as the measure of EC.
Effect(s) tested
A map of left DLPFC effective connectivity from rAI was first calculated. The maximum of this map corresponds to the cgiTBS target. The ROI for left DLPFC was a sphere centred on the cgiTBS target co-ordinates themselves (regardless of treatment group). the ROI for right AI was a sphere centred on MNI co-ordinates . We calculated effective connectivity as a function of distance from this maximum to examine whether optimal targets according to the trial target identification procedure were clearly unique or whether there are multiple, separate, potential targets within DLPFC. For each participant, we computed functional connectivity between each image voxel and spherical seed regions centred on the intended stimulation target co-ordinates. We computed these seed-region functional connectivity images for baseline and follow-up, and also computed the difference between the follow-up and baseline images.
To examine DLPFC-DMPFC connectivity, two centroids for the left DLPFC ROI that are independent from the cgiTBS and rTMS co-ordinates were examined in separate analyses: an anterior DLPFC centroid, , and a more posterior DLPFC centroid, . The centroid for the left DMPFC ROI was .
Specify type of analysis: Whole brain
ROI-based Both
Anatomical location(s)
Describe how anatomical locations were determined (e.g. specify whether automated labeling algorithms or probabilistic atlases were used).
Statistic type for inference
(See Eklund et al. 2016)
Statistic type for inference. Mixed effects models were implemented in SPSS (version 18) and JASP (0.18) software and estimated with restricted maximum likelihood. Participant served as the random effect with a scaled identity variancecovariance matrix, and the dependent variable was clinical improvement from baseline in GRID-HDRS-17 (primary outcome measure), PHQ-9 or BDI-II (planned exploratory outcome measures). As well as the baseline connectivity, or change in connectivity, relevant to a given hypothesis, we included as independent variables the post-treatment time point ( weeks) and treatment group (rTMS, cgiTBS), and the interaction of connectivity with either or both variables. Age, gender, MGH treatment resistance group, GAD-7, CTQ and study group site were explored as potential confounding variables: where these were non-significant, they were removed from the model.
Correction
Bonferroni for functional connectivity between left dorsolateral prefrontal cortex to left dorsomedial prefrontal cortex only.
Functional and effective connectivity were used as outlined under model type and settings.
Mental Health and Clinical Neurosciences, School of Medicine, University of Nottingham, Nottingham, UK. Institute of Mental Health, Nottinghamshire Healthcare NHS Foundation Trust, Nottingham, UK. Clinical Neuromodulation Service, Camden and Islington NHS Foundation Trust, London, UK. Leicester Clinical Trials Unit, University of Leicester, Leicester, UK. Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust, Newcastle upon Tyne, UK. Pennine Care TMS Service, Pennine Care NHS Foundation Trust, Oldham, UK. Northern Centre for Mood Disorders, Translational and Clinical Research Institute, Newcastle University, Newcastle upon Tyne, UK. Centre for Neuromodulation, Northamptonshire Healthcare NHS Foundation Trust, Northampton, UK. e-mail: richard.morriss@nottingham.ac.uk
This is a clinical dataset that will be anonymised and made available as outlined in the manuscript. We used the BrainNet Viewer at www.nitrc.org/projects/bnv/)