المجلة: Scientific Reports، المجلد: 14، العدد: 1
DOI: https://doi.org/10.1038/s41598-024-56276-y
PMID: https://pubmed.ncbi.nlm.nih.gov/38448487
تاريخ النشر: 2024-03-06
DOI: https://doi.org/10.1038/s41598-024-56276-y
PMID: https://pubmed.ncbi.nlm.nih.gov/38448487
تاريخ النشر: 2024-03-06
العلاقة بين نسبة الكوليسترول منخفض الكثافة غير المرتبط بالكوليسترول عالي الكثافة (NHHR) وانتشار التهاب اللثة بين البالغين في الولايات المتحدة: دراسة مقطعية من NHANES
نسبة الكوليسترول غير مرتفع الكثافة إلى الكوليسترول مرتفع الكثافة (NHHR) هي معلمة دهنية تم تطويرها مؤخرًا، ولكن هناك نقص حالي في الأبحاث التي تستكشف علاقتها بالتهاب اللثة. تهدف هذه الدراسة إلى تحديد العلاقة المحتملة بين NHHR والتهاب اللثة. تم فحص العلاقة بين NHHR والتهاب اللثة من خلال تحليل الانحدار اللوجستي الأحادي والمتعدد المتغيرات باستخدام بيانات المسح الوطني للصحة والتغذية من 2009 إلى 2014. تم تقسيم المشاركين بناءً على نوع التهاب اللثة. شملت هذه الدراسة ما مجموعه 9023 مشاركًا، مع 1947 فردًا ليس لديهم التهاب لثة، و7076 فردًا يعانون من التهاب اللثة. أظهر المرضى في مجموعة التهاب اللثة زيادة ذات دلالة إحصائية في قيم NHHR 2.82 (2.05-3.80) مقارنةً بأولئك في مجموعة عدم وجود التهاب لثة (
الكلمات الرئيسية: نسبة الكوليسترول غير مرتفع الكثافة إلى الكوليسترول مرتفع الكثافة، التهاب اللثة، NHANES، دراسة مقطعية
التهاب اللثة هو مرض التهابي مزمن متعدد العوامل مرتبط بتراكم اللويحات السنية، ويتميز بتدمير تدريجي للهياكل الداعمة للأسنان، بما في ذلك الرباط اللثوي والعظم السنخي
في السنوات الأخيرة، قدم التقدم التدريجي في علم أسباب التهاب اللثة وعلم الأوبئة أدلة على العلاقة بين التهاب اللثة والأمراض الجهازية، بما في ذلك السكري، وأمراض القلب والأوعية الدموية، والاضطرابات الأيضية، وأمراض الجهاز التنفسي، والتهاب المفاصل الروماتويدي، وبعض أنواع السرطان، والاضطرابات المعرفية
سلطت بعض الدراسات الضوء على أن بداية التهاب اللثة تحفز إطلاق عوامل التهابية في مجرى الدم، مما يؤدي إلى التهاب منخفض المستوى مستمر في جميع أنحاء الجسم، وبالتالي يؤثر على الصحة النظامية
نظرًا لعدم وجود أعراض يمكن التعرف عليها بسهولة في المراحل المبكرة، غالبًا ما يتم تجاهل التهاب اللثة حتى يتقدم إلى مرحلة قد تكون غير قابلة للعكس، حيث قد يحدث تخلخل وفقدان للأسنان
تمت مناقشة العلاقة بين البروتينات الدهنية الشائعة والتهاب اللثة على نطاق واسع في التقارير السابقة. يمكن أن يعدل الكوليسترول مرتفع الكثافة (HDL-C)، وهو دهن له خصائص مضادة للالتهابات ومضادة للأكسدة، الاستجابات المناعية الفطرية والتكيفية
نسبة الكوليسترول غير مرتفع الكثافة (NHDL) إلى HDL-C (NHHR) هي مؤشر شامل ناشئ للدهون الأثريوسكليروسية
على حد علمنا، لا توجد حاليًا تقارير عن العلاقة بين NHHR والتهاب اللثة. نفترض أنه قد تكون هناك علاقة بين NHHR والتهاب اللثة. قد يساهم إدارة NHHR والتحكم فيه في الوقاية من مرض اللثة وإدارته. في هذا الصدد، أجرينا دراسة مقطعية استنادًا إلى مجموعة بيانات NHANES 2009-2014 لاستكشاف العلاقة بين NHHR وانتشار التهاب اللثة بين البالغين في الولايات المتحدة.
المواد والأساليب: عينة الدراسة
البيانات المستخدمة في هذه الدراسة مأخوذة من NHANES 2009-2014، وهو برنامج بحثي يهدف إلى تقييم الرفاهية والحالة الغذائية للبالغين والأطفال في الولايات المتحدة. يتضمن الاستطلاع استفسارات ديموغرافية واجتماعية واقتصادية وغذائية وصحية. تشمل مرحلة الفحص قياسات طبية وسنية وفسيولوجية جنبًا إلى جنب مع اختبارات مختبرية أجراها موظفون طبيون مدربون. ستحدد نتائج الاستطلاع معدلات حدوث الأمراض الكبيرة وانتشار الأمراض المسببة. تتوفر مزيد من التفاصيل عبر الإنترنت (https://www.cdc.gov/nchs/nhanes/index.htm).
شارك ما مجموعه 30,468 فردًا في NHANES بين 2009 و2014. ومع ذلك، بعد تطبيق معايير الاستبعاد، تم تقليل حجم العينة لهذه الدراسة إلى 9,023 مشاركًا. شملت معايير الاستبعاد بيانات ديموغرافية غير مكتملة، وبيانات مفقودة عن المتغيرات (مثل حالة التدخين، ومؤشر كتلة الجسم، واستخدام الكحول، واستخدام خيط الأسنان، وعدد فقدان الأسنان، ومستوى النظام الغذائي، وتاريخ ارتفاع ضغط الدم، وارتفاع سكر الدم)، وغياب فحص اللثة أو بيانات متعلقة بـ NHHR (بيانات الكوليسترول الكلي وبيانات الكوليسترول مرتفع الكثافة). يوضح الشكل 1 مخطط تدفق عملية الفحص.
حساب NHHR
مصدر البيانات لحسابات NHHR مستمد من بيانات المختبر في NHANES المسماة ‘HDL.Doc’ التي توفر بيانات HDL و’TCHOL.Doc’، التي توفر بيانات الكوليسترول الكلي. يتم الحصول على بيانات NHHR باستخدام صيغة الكوليسترول الكلي مطروحًا منه HDL، ثم مقسومًا على HDL.
تقييم التهاب اللثة
تتضمن بيانات فحص NHANES ملفًا يسمى “OHXPER.Doc” الذي يتضمن بيانات عن فحوصات اللثة التي تشمل فقدان الارتباط السريري (CAL) وعمق الاستكشاف (PD). تصنف هذه البيانات المشاركين على أنهم مصابون بالتهاب اللثة أو لا بناءً على المعايير المقدمة من مراكز السيطرة على الأمراض والوقاية منها والأكاديمية الأمريكية لطب اللثة (CDC/AAP)
تم تحديد التهاب اللثة الشديد من خلال وجود منطقتين بين الأسنان على الأقل تظهران مستوى ارتباط سريري (CAL) لا يقل عن 6 مم وليست موجودة على نفس السن، بالإضافة إلى وجود موقع بين الأسنان واحد على الأقل يظهر عمق استكشاف (PD) لا يقل عن 5 مم. تم تعريف التهاب اللثة المعتدل على أنه تحديد منطقتين بين الأسنان أو أكثر بعمق جيوب استكشافية أكبر من أو يساوي 5 مم وليست موجودة على نفس السن، أو منطقتين بين الأسنان أو أكثر بمستويات ارتباط سريري أكبر من أو يساوي 4 مم وليست موجودة على نفس السن. يجب أن يظهر المشاركون الذين تم تشخيصهم بالتهاب اللثة الخفيف على الأقل منطقتين بين الأسنان مع فقدان ارتباط سريري لا يقل عن 3 مم، وعلى الأقل منطقتين بين الأسنان مع عمق استكشاف لا يقل عن 4 مم (ليست على نفس السن) أو موقع واحد بعمق استكشاف لا يقل عن 5 مم. في هذه الدراسة، قمنا بتجميع التهاب اللثة الخفيف والمعتدل والشديد في فئة واحدة (وجود التهاب لثة)، وعدم وجود التهاب لثة في فئة أخرى.
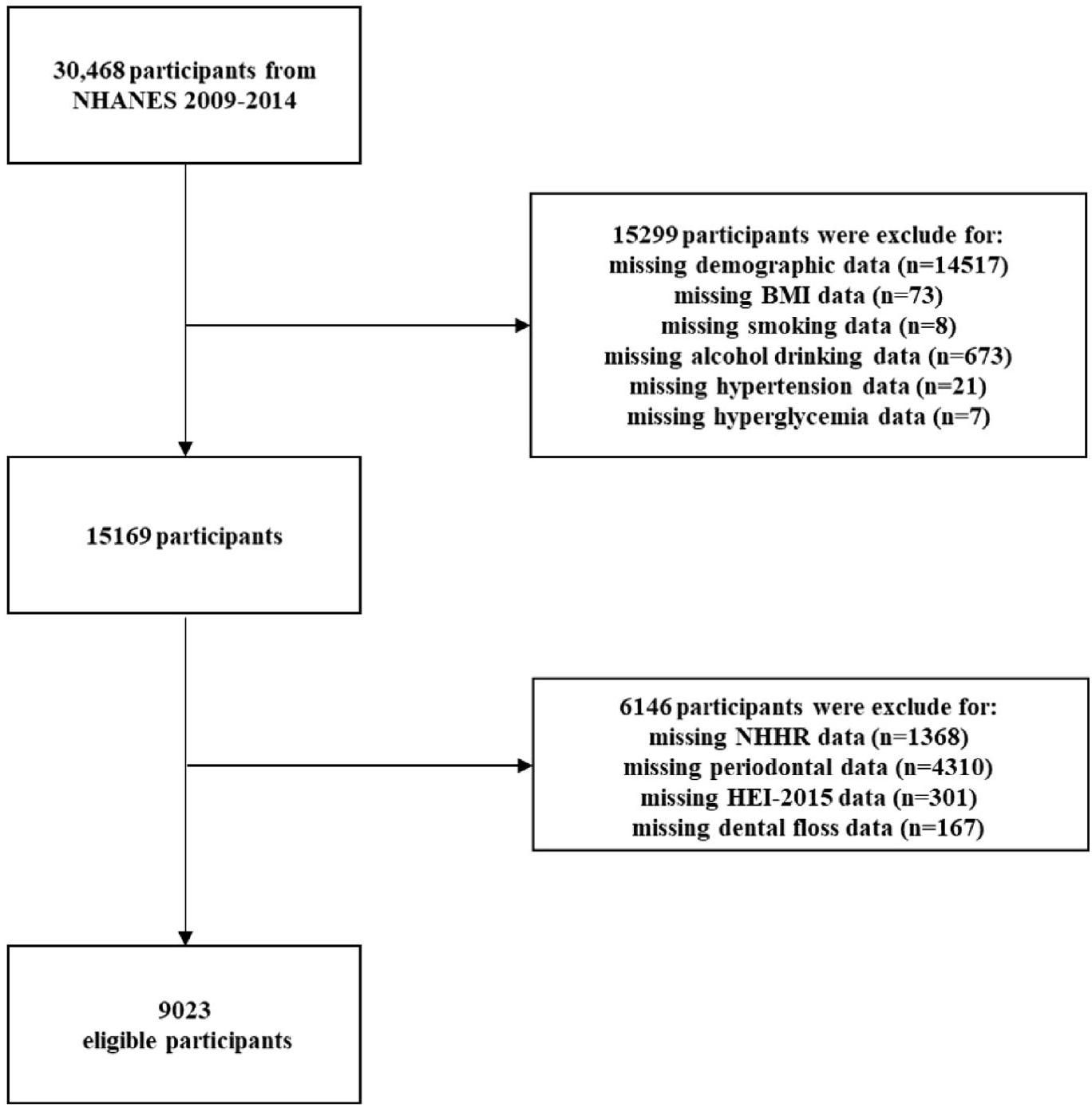
الشكل 1. مخطط انسيابي لاختيار المشاركين في الدراسة.
معالجة المتغيرات المشتركة
لاستكشاف العلاقة بين NHHR والتهاب اللثة، تم اختيار عدة متغيرات للتعديل، تشمل البيانات الديموغرافية، وعادات نمط الحياة، وحالة الصحة.
تضمنت البيانات السكانية العمر، الجنس، العرق، مستوى التعليم، الحالة الاجتماعية، والدخل. شملت سلوكيات نمط الحياة استخدام الكحول، حالة التدخين، استخدام خيط الأسنان ومستويات النظام الغذائي. تم تقييم “استخدام الكحول” من خلال “هل تناولت على الأقل 12 مشروب كحولي/ في سنة؟”. تم تحديد حالة التدخين من خلال “هل تدخنت على الأقل 100 سيجارة في حياتك كلها؟”
تحليل إحصائي
تم إجراء جميع التحليلات الإحصائية باستخدام R (الإصدار 4.2) و SPSS (الإصدار 26.0) و Empowerstats (الإصدار 5.0)، وتم استخدام إرشادات NHANES لوزن جميع البيانات. تم استخدام السبل المكعبة الطبيعية لتحديد العلاقة بين NHHR والتهاب اللثة. ثم قمنا بإجراء تحليلات الانحدار اللوجستي لفحص العلاقة بين NHHR والتهاب اللثة.
موافقة الأخلاقيات والموافقة على المشاركة
NHANES هي قاعدة بيانات عامة. المرضى المشاركون في قاعدة البيانات حصلوا على موافقة أخلاقية. يمكن للمستخدمين تنزيل البيانات ذات الصلة مجانًا لأغراض البحث والنشر.
النتائج
خصائص المشاركين
تظهر خصائص المشاركين في الجدول 1. تشمل الدراسة 9023 فردًا بمتوسط عمر 52.00 عامًا. من بينهم،
العلاقة بين NHHR والتهاب اللثة
تم عرض العلاقة بين NHHR والتهاب اللثة في الجدول 2. بعد إجراء تعديلات متعددة، وُجد أن NHHR مرتبط إيجابيًا بالتهاب اللثة.
تحليلات تحت المجموعة حسب العوامل المؤثرة المحتملة
يمكن العثور على نتائج تحليلات المجموعات الفرعية في الشكل 3. أظهرت نتائج تحليل الانحدار اللوجستي للمجموعات الفرعية نتائج ذات دلالة إحصائية للمشاركين الذين لديهم مستوى تعليم من الصف التاسع إلى الحادي عشر أو غير المدخنين. يعرض الشكل 3 أن نسبة الأرجحية للمشاركين مع
نقاش
وفقًا لهذه الدراسة، يعتبر NHHR علامة بيولوجية تشخيصية مرضية لالتهاب اللثة. تظهر نتائجنا وجود ارتباط إيجابي بين NHHR وزيادة انتشار التهاب اللثة في نموذج معدل. مع كل زيادة وحدة في NHHR، هناك
تعتبر الاضطرابات الأيضية في استقلاب الدهون شائعة لدى المرضى الذين يعانون من التهاب اللثة وترتبط بحدوث وتطور التهاب اللثة.
على مدى السنوات القليلة الماضية، كان هناك اهتمام متزايد بالصلة بين HDL والتهاب اللثة. بينما لم تكشف بعض الدراسات عن اختلافات في مستويات HDL في المصل بين الأفراد الأصحاء والمرضى الذين يعانون من مرض اللثة.
أظهرت دراسات إضافية أن علاج أمراض اللثة زاد بشكل كبير من مستويات HDL-C في مصل الدم لدى المرضى الذين يعانون من التهاب اللثة.
بصرف النظر عن HDL-C، يُعتبر NHDL مكونًا حيويًا آخر من NHHR، قادرًا على قياس كوليسترول البروتين الدهني منخفض الكثافة (LDL-C)، كوليسترول البروتين الدهني منخفض الكثافة جدًا (VLDL-C)، بروتين الشحميات A (apo A)، والبروتين الدهني متوسط الكثافة (IDL). ماكري وآخرون.
كانت هناك عدة قيود على هذه الدراسة: (1) تعتبر الدراسات القائمة على المجموعات أكثر موثوقية للتحقق من نتائج هذه الدراسة. كانت الدراسة تعتمد على بيانات مقطعية، وقد تتأثر النتائج بتحيز الاختيار؛ (2) تم تقييم وتسجيل ملفات الدهون مرة واحدة فقط في هذه الدراسة. قد يكون نقص القياسات المتكررة لملفات الدهون عرضة للتوتر الحاد وآثار عرضية؛ (3) بعض المتغيرات المشتركة لديها قدرة محتملة على التداخل، وتتأثر بقاعدة بيانات NHANES من 2009-2014، وهناك مشاكل تتعلق بالبيانات المفقودة، و هناك
| الإجمالي (
|
لا التهاب دواعم السن
|
التهاب اللثة
|
|
|
| العمر (بالسنوات) | 52.00 (41.00-64.00) | ٤٩.٠٠ (٣٧.٠٠-٦٦.٠٠) | 53.00 (42.00-64.00) | <0.001 |
| جنس | <0.001 | |||
| ذكر | 4569 (50.64%) | 770 (39.55%) | ٣٧٩٩ (٥٣.٦٩٪) | |
| أنثى | 4454 (49.36%) | 1177 (60.45%) | 3277 (46.31%) | |
| سباق | <0.001 | |||
| مكسيكي أمريكي | 1162 (12.88%) | ١٣٣ (٦.٨٣٪) | 1029 (14.54%) | |
| هسبانيون آخرون | 831 (9.21%) | 157 (8.06%) | 674 (9.53%) | |
| الأبيض غير اللاتيني | 4292 (47.57%) | 1126 (57.83%) | 3166 (44.74%) | |
| أسود غير هيسباني | 1827 (20.25%) | 360 (18.49%) | 1467 (20.73%) | |
| عرق آخر | 911 (10.10%) | 171 (8.78%) | 740 (10.46%) | |
| مستوى التعليم | 0.030 | |||
| أقل من الصف التاسع | 810 (8.98%) | 168 (8.63%) | 642 (9.07%) | |
| الصفوف 9-11 | 1249 (13.84%) | 275 (14.12%) | 974 (13.76%) | |
| خريج المدرسة الثانوية | 2022 (22.41%) | 398 (20.44%) | 1624 (22.95%) | |
| بعض الكلية أو درجة AA | 2570 (28.48%) | 546 (28.04%) | 2024 (28.60%) | |
| خريج كلية أو أعلى | 2372 (26.29%) | 560 (28.76%) | 1812 (25.61%) | |
| حالة الزواج | <0.001 | |||
| متزوج | 5206 (57.70%) | 1124 (57.73%) | 4082 (57.69%) | |
| أرملة | 739 (8.19%) | 207 (10.63%) | 532 (7.52%) | |
| مطلق | 1207 (13.38%) | 263 (13.51%) | 944 (13.34%) | |
| مفصول | ٣٢٨ (٣.٦٤٪) | 53 (2.72%) | 275 (3.89%) | |
| لم يتزوج أبداً | 978 (10.84%) | 200 (10.27%) | 778 (10.99%) | |
| العيش مع الشريك | 565 (6.26%) | 100 (5.14%) | 465 (6.57%) | |
| نسبة دخل الأسرة إلى الفقر | 0.005 | |||
| <1.3 | 2715 (30.09%) | 579 (29.74%) | 2136 (30.19%) | |
| 1.3-3.5 | ٣٢٤١ (٣٥.٩٢٪) | 650 (33.38%) | 2591 (36.62%) | |
| > 3.5 | 3067 (33.99%) | 718 (36.88%) | 2349 (33.20%) | |
| مؤشر كتلة الجسم | 28.38 (24.80-32.80) | 28.09 (24.50-32.78) | 28.40 (24.90-32.80) | 0.063 |
| حالة التدخين | 0.842 | |||
| نعم | 4226 (46.84%) | 908 (46.64%) | 3318 (46.89%) | |
| لا | 4797 (53.16%) | ١٠٣٩ (٥٣.٣٦٪) | 3758 (53.11%) | |
| استخدام الكحول | 0.476 | |||
| نعم | 6656 (73.77%) | 1424 (73.14%) | 5232 (73.94%) | |
| لا | 2367 (26.23%) | 523 (26.86%) | 1844 (26.06%) | |
| ارتفاع ضغط الدم | 0.167 | |||
| نعم | 3603 (39.93%) | 751 (38.57%) | 2852 (40.31%) | |
| لا | 5420 (60.07%) | 1196 (61.43%) | 4224 (59.69%) | |
| فرط سكر الدم | 0.789 | |||
| نعم | 1237 (13.71%) | 313 (16.08%) | 1183 (16.72%) | |
| لا | 7786 (86.29%) | 1634 (83.92%) | 5893 (83.28%) | |
| HEI-2015 | 51.61 (42.06-61.58) | 51.12 (41.45-60.39) | 51.77 (42.21-61.94) | 0.007 |
| فقدان الأسنان | 3.00 (0.00-9.00) | 2.00 (0.00-4.00) | 4.00 (1.00-10.00) | <0.001 |
| خيط الأسنان | <0.001 | |||
| نعم | 5803 (64.31%) | 942 (48.38%) | 2278 (32.19%) | |
| لا | 3220 (35.69%) | 1005 (51.62%) | 4798 (67.81%) | |
| HDL-C (ملغ/دل) | 50.00 (41.00-61.00) | 50.00 (41.00-62.00) | 50.00 (41.00-61.00) | 0.101 |
| إجمالي الكوليسترول (ملغ/دل) | 194.00 (168.00-222.00) | 190.00 (165.00-218.00) | 195.00 (169.00-223.00) | <0.001 |
| NHHR | 2.79 (2.03-3.76) | 2.67 (1.96-3.61) | 2.82 (2.05-3.80) | <0.001 |
الجدول 1. خصائص المشاركين. NHHR نسبة الكوليسترول غير مرتفع الكثافة إلى الكوليسترول مرتفع الكثافة، HEI-2015 مؤشر النظام الغذائي الصحي 2015، BMI مؤشر كتلة الجسم، HDL-C كوليسترول مرتفع الكثافة.
| أو |
|
|
|
| النموذج 1 |
|
0.0001 |
|
| النموذج 2 |
|
0.0705 |
|
| موديل 3 |
|
0.0067 |
|
الجدول 2. العلاقة بين NHHR والتهاب اللثة بين المشاركين في NHANES 2009-2014. النموذج 1 لم يعدل لأي عوامل مشوشة محتملة؛ النموذج 2 عدل لـ: الجنس، العمر، العرق؛ النموذج 3 عدل لـ: الجنس، العمر، العرق، مستوى التعليم، PIR، حالة التدخين، ارتفاع ضغط الدم، ارتفاع سكر الدم، HDL-c، الكوليسترول الكلي، مؤشر كتلة الجسم، حالة الزواج، استخدام الكحول، درجة HEI-2015، حالة استخدام خيط الأسنان، عدد فقدان الأسنان. *نتائج ملاءمة النموذج. أظهرت نتائج ملاءمة النموذج أن النموذج
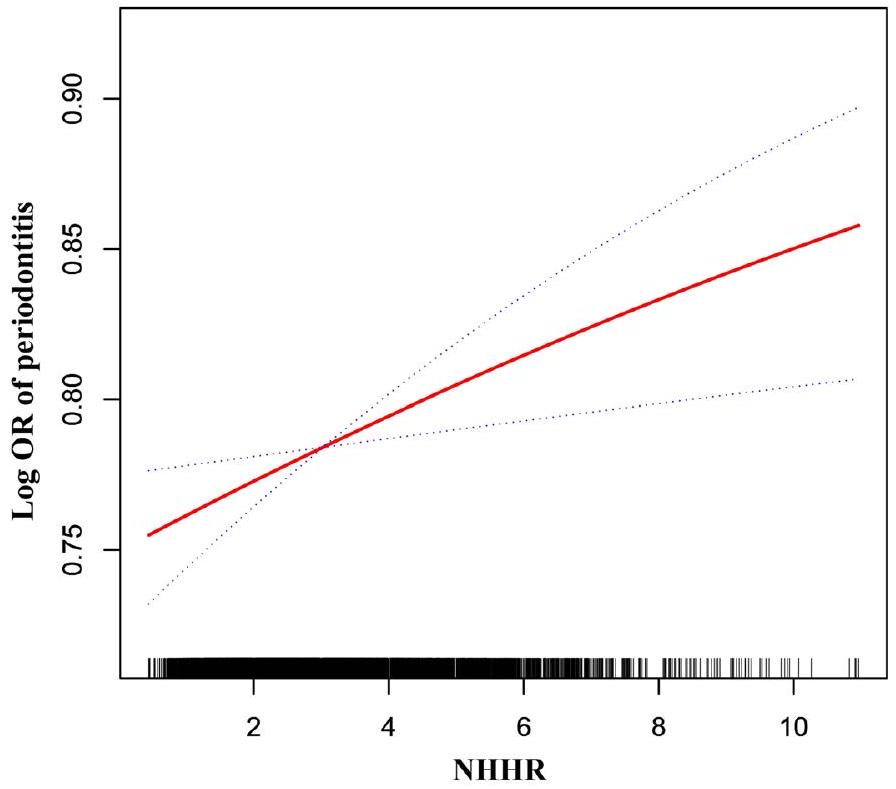
الشكل 2. العلاقة بين NHHR والتهاب اللثة.
قد يكون هناك بعض التحيز في النتائج. في الوقت نفسه، لم يتم التحقيق في معلومات الأدوية التفصيلية للمرضى، بما في ذلك أنواع الأدوية، والتكرار، والمدة، ولم يكن بالإمكان استبعاد تأثير الأدوية على التهاب اللثة.
الخاتمة
باختصار، تشير الأبحاث الحالية إلى وجود علاقة إيجابية بين NHHR وزيادة انتشار التهاب اللثة، مما قد يكون عاملاً تنبؤياً جديداً للأحداث اللثوية. كما يوفر ذلك دليلاً قيماً للوقاية الأولية لدى الأفراد الذين يعانون من انتشار مرتفع لالتهاب اللثة. يمكن للأطباء استخدام NHHR للمساعدة في تحديد الفئات السكانية عالية المخاطر للإصابة بالتهاب اللثة، مما يحسن من كفاءة الفحص.
| مجموعة فرعية | OR (فاصل الثقة 95%) | مخطط الغابة |
|
تفاعل P | |
| عمر | 0.6214 | ||||
| <40 | 0.98 (0.90، 1.07) |  |
0.6612 | ||
| ٤٠-٦٠ | 1.04 (0.97، 1.12) | 0.2548 | |||
| >60 | 1.01 (0.92, 1.11) | 0.8678 | |||
| جنس | 0.1435 | ||||
| ذكر | 0.99 (0.93، 1.06) | |
0.7871 | ||
| أنثى | 1.06 (0.99، 1.13) | |
0.0706 | ||
| سباق | 0.4041 | ||||
| مكسيكي أمريكي | 0.94 (0.80، 1.10) | |
0.4271 | ||
| هسبانيون آخرون | 1.02 (0.87, 1.20) | |
0.8021 | ||
| الأبيض غير اللاتيني | 1.05 (0.99, 1.12) | 0.1039 | |||
| أسود غير هيسباني | 1.06 (0.95، 1.20) | 0.2880 | |||
| عرق آخر | 1.01 (0.86، 1.20) | |
0.8710 | ||
| مستوى التعليم | 0.4505 | ||||
| أقل من الصف التاسع | 1.04 (0.87, 1.25) | |
0.6547 | ||
| الصفوف 9-11 | 1.14 (1.00, 1.30) | 0.0429 | |||
| خريج المدرسة الثانوية | 1.02 (0.92, 1.12) | 0.7625 | |||
| بعض الكلية أو درجة AA | 0.99 (0.91، 1.07) |
|
0.7310 | ||
| خريج كلية أو أعلى | 1.05 (0.96، 1.16) | 0.2946 | |||
| تمثال ماري | 0.7284 | ||||
| متزوج | 1.03 (0.97, 1.10) | |
0.3524 | ||
| أرملة | 1.15 (0.96, 1.37) | |
0.1397 | ||
| مطلق | 1.04 (0.92, 1.17) | |
0.5413 | ||
| مفصول | 1.02 (0.76, 1.37) | |
0.8924 | ||
| لم يتزوج أبداً | 1.00 (0.87، 1.14) | |
0.9795 | ||
| العيش مع الشريك | 1.14 (0.95, 1.38) | |
0.1643 | ||
| بي آي آر | 0.3992 | ||||
| <1.3 | 1.06 (0.98، 1.16) | |
0.1440 | ||
| 1.3-3.5 | 1.04 (0.96, 1.13) | 0.3231 | |||
| >3.5 | 1.01 (0.94، 1.10) | |
0.7537 | ||
| دخان | 0.2827 | ||||
| نعم | 1.07 (1.00، 1.14) | |
0.0583 | ||
| لا | 1.01 (0.95, 1.08) | |
0.6544 | ||
| استخدام الكحول | 0.0226 | ||||
| نعم | 1.01 (0.96، 1.06) | |
0.6905 | ||
| لا | 1.15 (1.04, 1.26) | |
0.0055 | ||
| ارتفاع ضغط الدم | 0.6121 | ||||
| نعم | 1.01 (0.94, 1.09) | |
0.7290 | ||
| لا | 1.04 (0.98، 1.10) | |
0.2065 | ||
| فرط سكر الدم | 0.4495 | ||||
| نعم | 1.09 (0.94، 1.25) | |
0.2620 | ||
| لا | 1.03 (0.98، 1.09) |
|
0.2013 | ||
| خيط الأسنان | 0.8638 | ||||
| نعم | 1.02 (0.95, 1.09) | |
0.6120 | ||
| لا | 1.03 (0.97, 1.09) | |
0.3907 | ||
الشكل 3. تحليل الفئات الفرعية للعلاقة بين NHHR والتهاب اللثة.
توفر البيانات
البيانات المستخدمة والمفحوصة في هذه الدراسة متاحة عند الطلب المعقول من المؤلف المراسل.
تاريخ الاستلام: 10 يناير 2024؛ تاريخ القبول: 4 مارس 2024
نُشر على الإنترنت: 06 مارس 2024
نُشر على الإنترنت: 06 مارس 2024
References
- Yang, B. et al. Immunomodulation in the treatment of periodontitis: Progress and perspectives. Front. Immunol. 12, 781378 (2021).
- Kwon, T., Lamster, I. B. & Levin, L. Current concepts in the management of periodontitis. Int. Dent. J. 71(6), 462-476 (2021).
- Lin, H. et al. Advances of exosomes in periodontitis treatment. J. Transl. Med. 20(1), 279 (2022).
- Spencer, L. J. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet, 392 (10159), 1789-1858 (2018).
- Kassebaum, N. J. et al. Global burden of severe periodontitis in 1990-2010: A systematic review and meta-regression. J. Dent. Res. 93(11), 1045-1053 (2014).
- Peres, M. A. et al. Oral diseases: A global public health challenge. Lancet 394(10194), 249-260 (2019).
- Eke, P. I., Borgnakke, W. S. & Genco, R. J. Recent epidemiologic trends in periodontitis in the USA. Periodontology 2000 82(1), 257-267 (2020).
- Hajishengallis, G. Interconnection of periodontal disease and comorbidities: Evidence, mechanisms, and implications. Periodontology 2000 89(1), 9-18 (2022).
- Genco, R. J. & Sanz, M. Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontology 2000 83(1), 7-13 (2020).
- Sulijaya, B., Takahashi, N. & Yamazaki, K. Host modulation therapy using anti-inflammatory and antioxidant agents in periodontitis: A review to a clinical translation. Arch. Oral Biol. 105, 72-80 (2019).
- Balta, M. G. et al. Host modulation and treatment of periodontal disease. J. Dent. Res. 100(8), 798-809 (2021).
- Plemmenos, G. et al. Central regulatory role of cytokines in periodontitis and targeting options. Curr. Med. Chem. 28(15), 30323058 (2021).
- Jørgensen, H. L. & Lind, B. S. Blood tests-Too much of a good thing. Scand. J. Prim. Health Care 40(2), 165-166 (2022).
- Buss, L. F., Spitzer, D. & Watson, J. C. Can I have blood tests to check everything is alright?. BMJ 382, e075728 (2023).
- Hu, J. et al. High-density lipoprotein and inflammation and its significance to atherosclerosis. Am. J. Med. Sci. 352(4), 408-415 (2016).
- Ehteshami, A. et al. The association between high-density lipoproteins and periodontitis. Curr. Med. Chem. https://doi.org/10. 2174/0929867331666230726140736 (2023).
- Zhu, H. et al. Association of high-density lipoprotein cholesterol and periodontitis severity in Chinese elderly: A cross-sectional study. Clin. Oral Investig. 26(7), 4753-4759 (2022).
- Koshy, B. S. & Mahendra, J. The association between periodontal status, serum lipid levels, lipoprotein associated phosholipase A2 (Lp-PLA2) in chronic periodontitis subjects and healthy controls. J. Clin. Diagn. Res. 11(9), Zc17-zc21 (2017).
- Hu, G. et al. Causal relationship between circulating lipid traits and periodontitis: Univariable and multivariable Mendelian randomization. Front. Endocrinol. (Lausanne) 14, 1214232 (2023).
- Xu, J. & Duan, X. Association between periodontitis and hyperlipidaemia: A systematic review and meta-analysis. Clin. Exp. Pharmacol. Physiol. 47(11), 1861-1873 (2020).
- Nepomuceno, R. et al. Serum lipid levels in patients with periodontal disease: A meta-analysis and meta-regression. J. Clin. Periodontol. 44(12), 1192-1207 (2017).
- Sheng, G. et al. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. Diabetes Metab. Syndr. Obes. Targets Ther. 15, 1677-1686 (2022).
- Kim, S. W. et al. Non-HDL-cholesterol/HDL-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int. J. Cardiol. 168(3), 2678-2683 (2013).
- Zuo, P. Y. et al. Non-HDL-cholesterol to HDL-cholesterol ratio as an independent risk factor for the development of chronic kidney disease. Nutr. Metab. Cardiovasc. Dis. 25(6), 582-587 (2015).
- Iannuzzi, A. et al. Association between non-HDL-C/HDL-C ratio and carotid intima-media thickness in post-menopausal women. J. Clin. Med. 11(1), 78 (2021).
- Yang, S. et al. Association between the non-HDL-cholesterol to HDL-cholesterol ratio and non-alcoholic fatty liver disease in Chinese children and adolescents: A large single-center cross-sectional study. Lipids Health Dis. 19(1), 242 (2020).
- Lin, W. et al. Association between the non-HDL-cholesterol to HDL-cholesterol ratio and abdominal aortic aneurysm from a Chinese screening program. Lipids Health Dis. 22(1), 187 (2023).
- Sheng, G. et al. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. Diabetes Metab. Syndr. Obes. 15, 1677-1686 (2022).
- Qi, X. et al. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and risk of depression among US adults: A cross-sectional NHANES study. J. Affect. Disord. 344, 451-457 (2024).
- Du, M. et al. Assessing the surveillance use of 2018 EFP/AAP classification of periodontitis: A validation study and clustering analysis. J. Periodontol. 94(10), 1254-1265 (2023).
- Li, X. et al. The association between plain water intake and periodontitis in the population aged over 45: A cross-sectional study based on NHANES 2009-2014. BMC Oral Health 24(1), 27 (2024).
- Chen, X. et al. Association between life’s essential 8 and periodontitis: A population-based study. BMC Oral Health 24(1), 19 (2024).
- Weng, J. et al. Gender differences in the association between healthy eating index-2015 and hypertension in the US population: Evidence from NHANES 1999-2018. BMC Public Health 24(1), 330 (2024).
- Barros, A. J. & Hirakata, V. N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 3, 21 (2003).
- Morita, T. et al. Association between periodontal disease and metabolic syndrome. J. Public Health Dent. 69(4), 248-253 (2009).
- Sun, J. & Guo, G. Association between atherogenic index of plasma and periodontitis among U.S. adults. BMC Oral Health 23(1), 166 (2023).
- von Eckardstein, A. et al. High-density lipoprotein revisited: Biological functions and clinical relevance. Eur. Heart J. 44(16), 1394-1407 (2023).
- Gofman, J. W. et al. Lipoproteins, coronary heart disease, and atherosclerosis. Physiol. Rev. 34(3), 589-607 (1954).
- Pekkanen, J. et al. Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N. Engl. J. Med. 322(24), 1700-1707 (1990).
- Després, J. P. et al. HDL-cholesterol as a marker of coronary heart disease risk: The Québec cardiovascular study. Atherosclerosis 153(2), 263-272 (2000).
- Jeppesen, J. et al. Relation of high TG-low HDL cholesterol and LDL cholesterol to the incidence of ischemic heart disease. An 8-year follow-up in the Copenhagen male study. Arterioscler. Thromb. Vasc. Biol. 17(6), 1114-1120 (1997).
- Ko, D. T. et al. High-density lipoprotein cholesterol and cause-specific mortality in individuals without previous cardiovascular conditions: The CANHEART study. J. Am. Coll. Cardiol. 68(19), 2073-2083 (2016).
- Zvintzou, E. et al. High density lipoprotein in atherosclerosis and coronary heart disease: Where do we stand today?. Vasc. Pharmacol. 141, 106928 (2021).
- Madsen, C. M., Varbo, A. & Nordestgaard, B. G. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: Two prospective cohort studies. Eur. Heart J. 38(32), 2478-2486 (2017).
- Sridhar, R. et al. A study to evaluate the relationship between periodontitis, cardiovascular disease and serum lipid levels. Int. J. Dent. Hyg. 7(2), 144-150 (2009).
- Joseph, R., Nath, S. G. & Joseraj, M. G. Elevated plasma homocysteine levels in chronic periodontitis: A hospital-based case-control study. J. Periodontol. 82(3), 439-444 (2011).
- Taleghani, F., Shamaei, M. & Shamaei, M. Association between chronic periodontitis and serum lipid levels. Acta Med. Iran 48(1), 47-50 (2010).
- Fentoğlu, Ö. et al. Pro-inflammatory cytokine levels in association between periodontal disease and hyperlipidaemia. J. Clin. Periodontol. 38(1), 8-16 (2011).
- Haro, A. et al. Serum lipids modify periodontal infection-Interleukin-6 association. J. Clin. Periodontol. 44(3), 275-282 (2017).
- Macri, E. et al. Atherogenic cholesterol-rich diet and periodontal disease. Arch. Oral Biol. 59(7), 679-686 (2014).
- Penumarthy, S., Penmetsa, G. S. & Mannem, S. Assessment of serum levels of triglycerides, total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol in periodontitis patients. J. Indian Soc. Periodontol. 17(1), 30-35 (2013).
- Fentoğlu, Ö. et al. Is the relationship between periodontitis and hyperlipidemia mediated by lipoprotein-associated inflammatory mediators?. J. Periodontal Implant Sci. 50(3), 135-145 (2020).
- Thomas, B. et al. Comparative evaluation of the lipid profile in the serum of patients with type II diabetes mellitus and healthy individuals with periodontitis. Contemp. Clin. Dent. 8(1), 96-101 (2017).
- Griffiths, R. & Barbour, S. Lipoproteins and lipoprotein metabolism in periodontal disease. Clin. Lipidol. 5(3), 397-411 (2010).
مساهمات المؤلفين
قام ك.هـ. وج.هـ. بتصور الدراسة. ص.م. صمم وأشرف على الدراسة، وراجع وحرر المخطوطة. قام ك.هـ. و و.س. بصياغة المخطوطة. راجع جميع المؤلفين ووافقوا على النسخة النهائية من المخطوطة.
تمويل
تم دعم هذا البحث من قبل برنامج البحث والتطوير في منطقة شوني في بكين، رقم الجائزة: شوني2023Q06.
المصالح المتنافسة
يعلن المؤلفون عدم وجود مصالح متنافسة.
معلومات إضافية
يجب توجيه المراسلات والطلبات للحصول على المواد إلى W.S. أو Z.M.
معلومات إعادة الطباعة والتصاريح متاحة علىwww.nature.com/reprints.
ملاحظة الناشر: تظل شركة سبرينجر ناتشر محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
معلومات إعادة الطباعة والتصاريح متاحة علىwww.nature.com/reprints.
ملاحظة الناشر: تظل شركة سبرينجر ناتشر محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
الوصول المفتوح هذه المقالة مرخصة بموجب رخصة المشاع الإبداعي النسب 4.0 الدولية، التي تسمح بالاستخدام والمشاركة والتكيف والتوزيع وإعادة الإنتاج بأي وسيلة أو صيغة، طالما أنك تعطي الائتمان المناسب للمؤلفين الأصليين والمصدر، وتوفر رابطًا لرخصة المشاع الإبداعي، وتوضح ما إذا تم إجراء تغييرات. الصور أو المواد الأخرى من طرف ثالث في هذه المقالة مشمولة في رخصة المشاع الإبداعي الخاصة بالمقالة، ما لم يُشار إلى خلاف ذلك في سطر الائتمان للمواد. إذا لم تكن المادة مشمولة في رخصة المشاع الإبداعي الخاصة بالمقالة وكان استخدامك المقصود غير مسموح به بموجب اللوائح القانونية أو يتجاوز الاستخدام المسموح به، فستحتاج إلى الحصول على إذن مباشرة من صاحب حقوق الطبع والنشر. لعرض نسخة من هذه الرخصة، قم بزيارةhttp://creativecommons.org/licenses/by/4.0/.
© المؤلف(ون) 2024
© المؤلف(ون) 2024
مستشفى شوني في بكين، بكين 101300، الصين. مستشفى تيانتان، جامعة الطب العاصمة، بكين 100070، الصين. البريد الإلكتروني: 15011482782@163.com; mazhaofeng2022@126.com
Journal: Scientific Reports, Volume: 14, Issue: 1
DOI: https://doi.org/10.1038/s41598-024-56276-y
PMID: https://pubmed.ncbi.nlm.nih.gov/38448487
Publication Date: 2024-03-06
DOI: https://doi.org/10.1038/s41598-024-56276-y
PMID: https://pubmed.ncbi.nlm.nih.gov/38448487
Publication Date: 2024-03-06
The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and prevalence of periodontitis among US adults: a cross-sectional NHANES study
The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) is a recently developed lipid parameter, but there is currently a lack of research exploring its relationship with periodontitis. This study aims to identify the potential association between NHHR and periodontitis. The association between NHHR and periodontitis were examined through univariate and multivariate weighted logistic regression utilizing the National Health and Nutrition Examination Survey data from 2009 to 2014. The participants were grouped based on the type of periodontitis. This study included a total of 9023 participants, with 1947 individuals having no periodontitis, and an additional 7076 individuals suffering from periodontitis. Patients in periodontitis group demonstrated a statistically significant elevation in NHHR values 2.82 (2.05-3.80) compared to those in no periodontitis group (
Keywords The non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio, Periodontitis, NHANES, A cross-sectional study
Periodontitis is a chronic, multifactorial inflammatory disease associated with the accumulation of dental plaque, characterized by progressive destruction of the supporting structures of teeth, including the periodontal ligament and alveolar bone
In recent years, the gradual advancement in the etiology and epidemiology of periodontitis has provided evidence for the association between periodontitis and systemic diseases, including diabetes, cardiovascular diseases, metabolic disorders, respiratory diseases, rheumatoid arthritis, certain cancers, and cognitive disorders
Certain studies have highlighted that the onset of periodontitis triggers the release of inflammatory agents into the bloodstream, leading to persistent low-level inflammation throughout the body, thereby affecting systemic health
Due to the lack of easily identifiable symptoms in the early stages, periodontitis is often overlooked until it progresses to a potentially irreversible stage, where loosening and loss of teeth may occur
The association between common lipoproteins and periodontitis has been widely discussed in previous reports. The high-density lipoprotein cholesterol (HDL-C), a lipid with anti-inflammatory and antioxidant properties, can modulate innate and adaptive immune responses
The non-high-density lipoprotein (NHDL) cholesterol to HDL-C ratio (NHHR) is an emerging comprehensive indicator of atherosclerotic lipid
To the best of our knowledge, there are currently no reports on the relationship between NHHR and periodontitis. We hypothesize that there may be a correlation between NHHR and periodontitis. Managing and controlling NHHR could potentially contribute to the prevention and management of periodontal disease. In this regard, we conducted a cross-sectional study based on the NHANES 2009-2014 dataset to explore the association between NHHR and the prevalence of periodontitis in US adults.
Materials and methods Study population
The data utilized in this study are sourced from the NHANES 2009-2014, a research program aimed at evaluating the wellbeing and nutritional condition of adults and children in the United States. The survey comprises demographic, socio-economic, dietary, and health-related inquiries. The screening segment encompasses medical, dental, and physiological measurements alongside laboratory tests conducted by trained medical personnel. The survey results will establish the occurrence rates of significant diseases and disease-causing prevalences. Further details are available online (https://www.cdc.gov/nchs/nhanes/index.htm).
A total of 30,468 individuals participated in NHANES between 2009 and 2014. However, after applying exclusion criteria, the sample size for this study was reduced to 9,023 participants. The exclusion criteria included incomplete demographics data, missing data on covariates (such as smoking status, BMI, alcohol use, the use of dental floss, the number of tooth loss, diet level, history of hypertension, and hyperglycemia), and lack of periodontal examination or NHHR-related data (total cholesterol and high-density lipoprotein data). Figure 1 shows the screening process flowchart.
The calculation of NHHR
The data source for the NHHR calculations is derived from laboratory data in NHANES called ‘HDL.Doc’ which provides HDL data and ‘TCHOL.Doc’, which provides total cholesterol data. The NHHR data is obtained using the formula for total cholesterol minus HDL, then divided by HDL.
Assessment of periodontitis
The NHANES examination data includes a file named “OHXPER.Doc” that encompasses data on periodontal examinations involving clinical attachment loss (CAL) and probing depth (PD). This data classified participants as periodontitis or not based on criteria provided by the Centers for Disease Control and Prevention and the American Academy of Periodontology (CDC/AAP)
Severe periodontitis was determined by the presence of at least two interproximal regions exhibiting a clinical attachment level (CAL) of no less than 6 mm and not located on the same tooth, alongside at least one interproximal site exhibiting a probing depth (PD) of no less than 5 mm . Moderate periodontitis was defined as the identification of two or more interproximal regions with probing pocket depths that are greater than or equal to 5 mm and not situated on the same tooth, or two or more interproximal areas with clinical attachment levels that are greater than or equal to 4 mm and not found on the same tooth. Participants diagnosed with mild periodontitis must exhibit at least two interproximal sites with a clinical attachment loss of at least 3 mm , and at least two interproximal sites with a probing depth of at least 4 mm (not on the same tooth) or one site with a probing depth of at least 5 mm . In this study, we grouped mild, moderate, and severe periodontitis into one category (having periodontitis), and no periodontitis in another
Figure 1. Flowchart of study participants selection.
Treatment of covariates
To explore the relationship between NHHR and periodontitis, several covariates were selected for adjustment, encompassing demographic data, lifestyle habits, and health status.
Demographic data comprised age, gender, race, education level, marital status, and income. Lifestyle behaviors encompassed the use of alcohol, smoking status, the use of dental floss and dietary levels. “Alcohol use” was judged by “Had at least 12 alcohol drinks/ 1 year?”. Smoking status was determined by “Have you smoked at least 100 cigarettes in your entire life?”
Statistical analyze
All statistical analyses were conducted using R (version 4.2), SPSS (version 26.0) and Empowerstats (version 5.0), and the NHANES guidelines were used to weight all data. Natural cubic spline was used to identify the relationship of NHHR with periodontitis. Then, we performed logistic regression analyses to examine the correlation between NHHR and periodontitis
Ethics approval and consent to participate
The NHANES are public database. The patients involved in the database received ethical approval. Users can download relevant data for free for research and publication purposes.
Results
Characteristics of participants
The characteristics of participants are shown in Table 1. The study includes 9023 individuals with an average age of 52.00 years. Among them,
Association between NHHR and periodontitis
The association between NHHR and periodontitis were displayed in Table 2. Following multiple adjustments, NHHR was found to be positively correlated with periodontitis [
Subgroup analyses by potential effect modifiers
The findings of the subgroup analyses can be found in Fig. 3. The logistic regression analysis results for the subgroups showed statistically significant findings for participants with 9-11 grade education level or non-drinkers. Figure 3 displays that the OR of participants with
Discussion
According to this study, NHHR serves as a satisfactory diagnostic biomarker for periodontitis. Our findings show a positive association between NHHR and an increased prevalence of periodontitis in an adjusted model. For each unit increase in NHHR, there is a
Metabolic abnormalities in lipid metabolism are common in patients with periodontitis and are associated with the occurrence and development of periodontitis
Over the past few years, there has been a growing interest in the connection between HDL and periodontitis. While certain studies have not detected disparities in serum HDL levels between healthy individuals and patients with periodontal disease
Further studies found that periodontal treatment significantly increased serum HDL-C levels in patients with periodontitis
Apart from HDL-C, NHDL is another crucial component of NHHR, capable of measuring low-density lipoprotein cholesterol (LDL-C), very-low-density lipoprotein cholesterol (VLDL-C), apolipoprotein A (apo A), and intermediate-density lipoprotein (IDL). Macri et al.
There were several limitations to this study: (1) Cohort studies are more reliable for validating the results of this study. The study was based on cross-sectional data, and the results may be influenced by selection bias; (2) Lipid profiles were assessed and recorded only once in this study. The lack of repeated measurements of lipid profiles may be subject to acute stress and incidental effects; (3) Some of the covariates have potential confounding power, are affected by the 2009-2014 NHANES database, there are problems with missing data, and there
| Total (
|
None periodontitis (
|
Periodontitis (
|
|
|
| Age (years) | 52.00 (41.00-64.00) | 49.00 (37.00-66.00) | 53.00 (42.00-64.00) | <0.001 |
| Gender | <0.001 | |||
| Male | 4569 (50.64%) | 770 (39.55%) | 3799 (53.69%) | |
| Female | 4454 (49.36%) | 1177 (60.45%) | 3277 (46.31%) | |
| Race | <0.001 | |||
| Mexican American | 1162 (12.88%) | 133 (6.83%) | 1029 (14.54%) | |
| Other Hispanic | 831 (9.21%) | 157 (8.06%) | 674 (9.53%) | |
| Non-Hispanic white | 4292 (47.57%) | 1126 (57.83%) | 3166 (44.74%) | |
| Non-Hispanic black | 1827 (20.25%) | 360 (18.49%) | 1467 (20.73%) | |
| Other race | 911 (10.10%) | 171 (8.78%) | 740 (10.46%) | |
| Education level | 0.030 | |||
| Less than 9th grade | 810 (8.98%) | 168 (8.63%) | 642 (9.07%) | |
| 9-11th grade | 1249 (13.84%) | 275 (14.12%) | 974 (13.76%) | |
| High school grad | 2022 (22.41%) | 398 (20.44%) | 1624 (22.95%) | |
| Some college or AA degree | 2570 (28.48%) | 546 (28.04%) | 2024 (28.60%) | |
| College graduate or above | 2372 (26.29%) | 560 (28.76%) | 1812 (25.61%) | |
| Marry status | <0.001 | |||
| Married | 5206 (57.70%) | 1124 (57.73%) | 4082 (57.69%) | |
| Widowed | 739 (8.19%) | 207 (10.63%) | 532 (7.52%) | |
| Divorced | 1207 (13.38%) | 263 (13.51%) | 944 (13.34%) | |
| Separated | 328 (3.64%) | 53 (2.72%) | 275 (3.89%) | |
| Never married | 978 (10.84%) | 200 (10.27%) | 778 (10.99%) | |
| Living with partner | 565 (6.26%) | 100 (5.14%) | 465 (6.57%) | |
| Ratio of family income to poverty | 0.005 | |||
| <1.3 | 2715 (30.09%) | 579 (29.74%) | 2136 (30.19%) | |
| 1.3-3.5 | 3241 (35.92%) | 650 (33.38%) | 2591 (36.62%) | |
| > 3.5 | 3067 (33.99%) | 718 (36.88%) | 2349 (33.20%) | |
| BMI | 28.38 (24.80-32.80) | 28.09 (24.50-32.78) | 28.40 (24.90-32.80) | 0.063 |
| Smoking status | 0.842 | |||
| Yes | 4226 (46.84%) | 908 (46.64%) | 3318 (46.89%) | |
| No | 4797 (53.16%) | 1039 (53.36%) | 3758 (53.11%) | |
| Alcohol use | 0.476 | |||
| Yes | 6656 (73.77%) | 1424 (73.14%) | 5232 (73.94%) | |
| No | 2367 (26.23%) | 523 (26.86%) | 1844 (26.06%) | |
| Hypertension | 0.167 | |||
| Yes | 3603 (39.93%) | 751 (38.57%) | 2852 (40.31%) | |
| No | 5420 (60.07%) | 1196 (61.43%) | 4224 (59.69%) | |
| Hyperglycemia | 0.789 | |||
| Yes | 1237 (13.71%) | 313 (16.08%) | 1183 (16.72%) | |
| No | 7786 (86.29%) | 1634 (83.92%) | 5893 (83.28%) | |
| HEI-2015 | 51.61 (42.06-61.58) | 51.12 (41.45-60.39) | 51.77 (42.21-61.94) | 0.007 |
| Tooth loss | 3.00 (0.00-9.00) | 2.00 (0.00-4.00) | 4.00 (1.00-10.00) | <0.001 |
| Dental floss | <0.001 | |||
| Yes | 5803 (64.31%) | 942 (48.38%) | 2278 (32.19%) | |
| No | 3220 (35.69%) | 1005 (51.62%) | 4798 (67.81%) | |
| HDL-C(mg/dL) | 50.00 (41.00-61.00) | 50.00 (41.00-62.00) | 50.00 (41.00-61.00) | 0.101 |
| Total Cholesterol (mg/dL) | 194.00 (168.00-222.00) | 190.00 (165.00-218.00) | 195.00 (169.00-223.00) | <0.001 |
| NHHR | 2.79 (2.03-3.76) | 2.67 (1.96-3.61) | 2.82 (2.05-3.80) | <0.001 |
Table 1. Characteristics of participants. NHHR non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio, HEI-2015 The Healthy Eating Index 2015, BMI body mass index, HDL-C high density lipoprotein cholesterol.
| OR |
|
|
|
| Model 1 |
|
0.0001 |
|
| Model 2 |
|
0.0705 |
|
| Model 3 |
|
0.0067 |
|
Table 2. Association between NHHR and periodontitis among participants in NHANES 2009-2014. Model 1 did not adjust for any potential confounders; Model 2 adjusted for: gender, age, race; Model 3 adjusted for: gender, age, race, education level, pir, smoking status, hypertension, hyperglycemia, HDL-c, total cholesterol, BMI, marry status, Alcohol use, HEI-2015 score, dental floss use status, tooth loss number. *Goodness-of-fit results. The goodness of fit results showed that Model
Figure 2. The association between NHHR and periodontitis.
may be some bias in the results. Meanwhile, detailed medication information for patients, including types of medications, frequency, and duration, was not investigated in this study, and the impact of medication on periodontitis could not be ruled out.
Conclusion
In summary, current research suggests a positive correlation between NHHR and the increased prevalence of periodontitis, potentially serving as a novel predictive factor for periodontal events. This also provides valuable evidence for primary prevention in individuals at high prevalence of periodontitis. Clinicians can use NHHR to assist in identifying high-risk populations for periodontitis, thereby improving screening efficiency.
| Subgroup | OR(95% CI) | Forest plot |
|
P interaction | |
| Age | 0.6214 | ||||
| <40 | 0.98 (0.90, 1.07) | |
0.6612 | ||
| 40-60 | 1.04 (0.97, 1.12) | 0.2548 | |||
| >60 | 1.01 (0.92, 1.11) | 0.8678 | |||
| Gender | 0.1435 | ||||
| male | 0.99 (0.93, 1.06) | |
0.7871 | ||
| Female | 1.06 (0.99, 1.13) | |
0.0706 | ||
| Race | 0.4041 | ||||
| Mexican American | 0.94 (0.80, 1.10) | |
0.4271 | ||
| Other Hispanic | 1.02 (0.87, 1.20) | |
0.8021 | ||
| Non-Hispanic White | 1.05 (0.99, 1.12) | 0.1039 | |||
| Non-Hispanic Black | 1.06 (0.95, 1.20) | 0.2880 | |||
| Other Race | 1.01 (0.86, 1.20) | |
0.8710 | ||
| Education level | 0.4505 | ||||
| Less Than 9th Grade | 1.04 (0.87, 1.25) | |
0.6547 | ||
| 9-11th Grade | 1.14 (1.00, 1.30) | 0.0429 | |||
| High School Grad | 1.02 (0.92, 1.12) | 0.7625 | |||
| Some College or AA degree | 0.99 (0.91, 1.07) |
|
0.7310 | ||
| College Graduate or above | 1.05 (0.96, 1.16) | 0.2946 | |||
| Marry statue | 0.7284 | ||||
| Married | 1.03 (0.97, 1.10) | |
0.3524 | ||
| Widowed | 1.15 (0.96, 1.37) | |
0.1397 | ||
| Divorced | 1.04 (0.92, 1.17) | |
0.5413 | ||
| Separated | 1.02 (0.76, 1.37) | |
0.8924 | ||
| Never married | 1.00 (0.87, 1.14) | |
0.9795 | ||
| Living with partner | 1.14 (0.95, 1.38) | |
0.1643 | ||
| PIR | 0.3992 | ||||
| <1.3 | 1.06 (0.98, 1.16) | |
0.1440 | ||
| 1.3-3.5 | 1.04 (0.96, 1.13) | 0.3231 | |||
| >3.5 | 1.01 (0.94, 1.10) | |
0.7537 | ||
| Smoke | 0.2827 | ||||
| Yes | 1.07 (1.00, 1.14) | |
0.0583 | ||
| No | 1.01 (0.95, 1.08) | |
0.6544 | ||
| Alcohol use | 0.0226 | ||||
| Yes | 1.01 (0.96, 1.06) | |
0.6905 | ||
| No | 1.15 (1.04, 1.26) | |
0.0055 | ||
| Hypertension | 0.6121 | ||||
| Yes | 1.01 (0.94, 1.09) | |
0.7290 | ||
| No | 1.04 (0.98, 1.10) | |
0.2065 | ||
| Hyperglycemia | 0.4495 | ||||
| Yes | 1.09 (0.94, 1.25) | |
0.2620 | ||
| No | 1.03 (0.98, 1.09) |
|
0.2013 | ||
| Dental floss | 0.8638 | ||||
| Yes | 1.02 (0.95, 1.09) | |
0.6120 | ||
| No | 1.03 (0.97, 1.09) | |
0.3907 | ||
Figure 3. Subgroup analysis of the association between NHHR and periodontitis.
Data availability
The data utilized and examined in this study are available upon reasonable request from the corresponding author.
Received: 10 January 2024; Accepted: 4 March 2024
Published online: 06 March 2024
Published online: 06 March 2024
References
- Yang, B. et al. Immunomodulation in the treatment of periodontitis: Progress and perspectives. Front. Immunol. 12, 781378 (2021).
- Kwon, T., Lamster, I. B. & Levin, L. Current concepts in the management of periodontitis. Int. Dent. J. 71(6), 462-476 (2021).
- Lin, H. et al. Advances of exosomes in periodontitis treatment. J. Transl. Med. 20(1), 279 (2022).
- Spencer, L. J. et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet, 392 (10159), 1789-1858 (2018).
- Kassebaum, N. J. et al. Global burden of severe periodontitis in 1990-2010: A systematic review and meta-regression. J. Dent. Res. 93(11), 1045-1053 (2014).
- Peres, M. A. et al. Oral diseases: A global public health challenge. Lancet 394(10194), 249-260 (2019).
- Eke, P. I., Borgnakke, W. S. & Genco, R. J. Recent epidemiologic trends in periodontitis in the USA. Periodontology 2000 82(1), 257-267 (2020).
- Hajishengallis, G. Interconnection of periodontal disease and comorbidities: Evidence, mechanisms, and implications. Periodontology 2000 89(1), 9-18 (2022).
- Genco, R. J. & Sanz, M. Clinical and public health implications of periodontal and systemic diseases: An overview. Periodontology 2000 83(1), 7-13 (2020).
- Sulijaya, B., Takahashi, N. & Yamazaki, K. Host modulation therapy using anti-inflammatory and antioxidant agents in periodontitis: A review to a clinical translation. Arch. Oral Biol. 105, 72-80 (2019).
- Balta, M. G. et al. Host modulation and treatment of periodontal disease. J. Dent. Res. 100(8), 798-809 (2021).
- Plemmenos, G. et al. Central regulatory role of cytokines in periodontitis and targeting options. Curr. Med. Chem. 28(15), 30323058 (2021).
- Jørgensen, H. L. & Lind, B. S. Blood tests-Too much of a good thing. Scand. J. Prim. Health Care 40(2), 165-166 (2022).
- Buss, L. F., Spitzer, D. & Watson, J. C. Can I have blood tests to check everything is alright?. BMJ 382, e075728 (2023).
- Hu, J. et al. High-density lipoprotein and inflammation and its significance to atherosclerosis. Am. J. Med. Sci. 352(4), 408-415 (2016).
- Ehteshami, A. et al. The association between high-density lipoproteins and periodontitis. Curr. Med. Chem. https://doi.org/10. 2174/0929867331666230726140736 (2023).
- Zhu, H. et al. Association of high-density lipoprotein cholesterol and periodontitis severity in Chinese elderly: A cross-sectional study. Clin. Oral Investig. 26(7), 4753-4759 (2022).
- Koshy, B. S. & Mahendra, J. The association between periodontal status, serum lipid levels, lipoprotein associated phosholipase A2 (Lp-PLA2) in chronic periodontitis subjects and healthy controls. J. Clin. Diagn. Res. 11(9), Zc17-zc21 (2017).
- Hu, G. et al. Causal relationship between circulating lipid traits and periodontitis: Univariable and multivariable Mendelian randomization. Front. Endocrinol. (Lausanne) 14, 1214232 (2023).
- Xu, J. & Duan, X. Association between periodontitis and hyperlipidaemia: A systematic review and meta-analysis. Clin. Exp. Pharmacol. Physiol. 47(11), 1861-1873 (2020).
- Nepomuceno, R. et al. Serum lipid levels in patients with periodontal disease: A meta-analysis and meta-regression. J. Clin. Periodontol. 44(12), 1192-1207 (2017).
- Sheng, G. et al. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. Diabetes Metab. Syndr. Obes. Targets Ther. 15, 1677-1686 (2022).
- Kim, S. W. et al. Non-HDL-cholesterol/HDL-cholesterol is a better predictor of metabolic syndrome and insulin resistance than apolipoprotein B/apolipoprotein A1. Int. J. Cardiol. 168(3), 2678-2683 (2013).
- Zuo, P. Y. et al. Non-HDL-cholesterol to HDL-cholesterol ratio as an independent risk factor for the development of chronic kidney disease. Nutr. Metab. Cardiovasc. Dis. 25(6), 582-587 (2015).
- Iannuzzi, A. et al. Association between non-HDL-C/HDL-C ratio and carotid intima-media thickness in post-menopausal women. J. Clin. Med. 11(1), 78 (2021).
- Yang, S. et al. Association between the non-HDL-cholesterol to HDL-cholesterol ratio and non-alcoholic fatty liver disease in Chinese children and adolescents: A large single-center cross-sectional study. Lipids Health Dis. 19(1), 242 (2020).
- Lin, W. et al. Association between the non-HDL-cholesterol to HDL-cholesterol ratio and abdominal aortic aneurysm from a Chinese screening program. Lipids Health Dis. 22(1), 187 (2023).
- Sheng, G. et al. Utility of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio in evaluating incident diabetes risk. Diabetes Metab. Syndr. Obes. 15, 1677-1686 (2022).
- Qi, X. et al. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio (NHHR) and risk of depression among US adults: A cross-sectional NHANES study. J. Affect. Disord. 344, 451-457 (2024).
- Du, M. et al. Assessing the surveillance use of 2018 EFP/AAP classification of periodontitis: A validation study and clustering analysis. J. Periodontol. 94(10), 1254-1265 (2023).
- Li, X. et al. The association between plain water intake and periodontitis in the population aged over 45: A cross-sectional study based on NHANES 2009-2014. BMC Oral Health 24(1), 27 (2024).
- Chen, X. et al. Association between life’s essential 8 and periodontitis: A population-based study. BMC Oral Health 24(1), 19 (2024).
- Weng, J. et al. Gender differences in the association between healthy eating index-2015 and hypertension in the US population: Evidence from NHANES 1999-2018. BMC Public Health 24(1), 330 (2024).
- Barros, A. J. & Hirakata, V. N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 3, 21 (2003).
- Morita, T. et al. Association between periodontal disease and metabolic syndrome. J. Public Health Dent. 69(4), 248-253 (2009).
- Sun, J. & Guo, G. Association between atherogenic index of plasma and periodontitis among U.S. adults. BMC Oral Health 23(1), 166 (2023).
- von Eckardstein, A. et al. High-density lipoprotein revisited: Biological functions and clinical relevance. Eur. Heart J. 44(16), 1394-1407 (2023).
- Gofman, J. W. et al. Lipoproteins, coronary heart disease, and atherosclerosis. Physiol. Rev. 34(3), 589-607 (1954).
- Pekkanen, J. et al. Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. N. Engl. J. Med. 322(24), 1700-1707 (1990).
- Després, J. P. et al. HDL-cholesterol as a marker of coronary heart disease risk: The Québec cardiovascular study. Atherosclerosis 153(2), 263-272 (2000).
- Jeppesen, J. et al. Relation of high TG-low HDL cholesterol and LDL cholesterol to the incidence of ischemic heart disease. An 8-year follow-up in the Copenhagen male study. Arterioscler. Thromb. Vasc. Biol. 17(6), 1114-1120 (1997).
- Ko, D. T. et al. High-density lipoprotein cholesterol and cause-specific mortality in individuals without previous cardiovascular conditions: The CANHEART study. J. Am. Coll. Cardiol. 68(19), 2073-2083 (2016).
- Zvintzou, E. et al. High density lipoprotein in atherosclerosis and coronary heart disease: Where do we stand today?. Vasc. Pharmacol. 141, 106928 (2021).
- Madsen, C. M., Varbo, A. & Nordestgaard, B. G. Extreme high high-density lipoprotein cholesterol is paradoxically associated with high mortality in men and women: Two prospective cohort studies. Eur. Heart J. 38(32), 2478-2486 (2017).
- Sridhar, R. et al. A study to evaluate the relationship between periodontitis, cardiovascular disease and serum lipid levels. Int. J. Dent. Hyg. 7(2), 144-150 (2009).
- Joseph, R., Nath, S. G. & Joseraj, M. G. Elevated plasma homocysteine levels in chronic periodontitis: A hospital-based case-control study. J. Periodontol. 82(3), 439-444 (2011).
- Taleghani, F., Shamaei, M. & Shamaei, M. Association between chronic periodontitis and serum lipid levels. Acta Med. Iran 48(1), 47-50 (2010).
- Fentoğlu, Ö. et al. Pro-inflammatory cytokine levels in association between periodontal disease and hyperlipidaemia. J. Clin. Periodontol. 38(1), 8-16 (2011).
- Haro, A. et al. Serum lipids modify periodontal infection-Interleukin-6 association. J. Clin. Periodontol. 44(3), 275-282 (2017).
- Macri, E. et al. Atherogenic cholesterol-rich diet and periodontal disease. Arch. Oral Biol. 59(7), 679-686 (2014).
- Penumarthy, S., Penmetsa, G. S. & Mannem, S. Assessment of serum levels of triglycerides, total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol in periodontitis patients. J. Indian Soc. Periodontol. 17(1), 30-35 (2013).
- Fentoğlu, Ö. et al. Is the relationship between periodontitis and hyperlipidemia mediated by lipoprotein-associated inflammatory mediators?. J. Periodontal Implant Sci. 50(3), 135-145 (2020).
- Thomas, B. et al. Comparative evaluation of the lipid profile in the serum of patients with type II diabetes mellitus and healthy individuals with periodontitis. Contemp. Clin. Dent. 8(1), 96-101 (2017).
- Griffiths, R. & Barbour, S. Lipoproteins and lipoprotein metabolism in periodontal disease. Clin. Lipidol. 5(3), 397-411 (2010).
Author contributions
K.H. and J.H. conceived the study. Z.M. designed and supervised the study, revised and edited the manuscript. K.H. and W.S. drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
This research was supported by the Beijing Shunyi District Research and Development Program, Award Number: Shunyi2023Q06.
Competing interests
The authors declare no competing interests.
Additional information
Correspondence and requests for materials should be addressed to W.S. or Z.M.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
© The Author(s) 2024
© The Author(s) 2024
Beijing Shunyi District Hospital, Beijing 101300, China. Beijing Tiantan Hospital, Capital Medical University, Beijing 100070, China. email: 15011482782@163.com; mazhaofeng2022@126.com