النتائج السريرية المرضية، العلاج، والنتيجة في 60 قطة تعاني من التليف الليفي الإيوزينوفيلي المعوي Clinicopathological findings, treatment, and outcome in 60 cats with gastrointestinal eosinophilic sclerosing fibroplasia
النتائج السريرية المرضية، العلاج والنتيجة في 60 قطة تعاني من التليف اليوزيني المعوي في القطط
اقتباس للإصدار المنشور:
تشيرنا، ب، لوبيز-خيمينيز، ج، فوكوشيما، ك، ناكاشيما، ك، ناكاجاوا، ت، آدامز، ف، غروث، أ، دينينغ، أ، إسرائيليانتز غونز، ن & غن-مور، د 2024، ‘النتائج السريرية المرضية، العلاج والنتيجة في 60 قطة تعاني من التليف الوعائي الإيوزينوفيلي المعوي في القطط’، مجلة الطب الداخلي البيطري، المجلد 38، العدد 2، الصفحات 1005-1012.https://doi.org/10.1111/jvim. 16992
معرف الكائن الرقمي (DOI):
10.1111/jvim.16992
رابط:
رابط إلى سجل النشر في مستكشف أبحاث إدنبرة
نسخة الوثيقة:
نسخة الناشر بصيغة PDF، والمعروفة أيضًا باسم النسخة المسجلة
نُشر في:
مجلة الطب الباطني البيطري
الحقوق العامة
حقوق الطبع والنشر للمنشورات المتاحة عبر مستكشف أبحاث إدنبرة يحتفظ بها المؤلف (المؤلفون) و/أو مالكو حقوق الطبع والنشر الآخرين، ومن شروط الوصول إلى هذه المنشورات أن يعترف المستخدمون ويلتزموا بالمتطلبات القانونية المرتبطة بهذه الحقوق.
سياسة الإزالة
لقد بذلت جامعة إدنبرة كل جهد معقول لضمان أن محتوى مستكشف أبحاث إدنبرة يتوافق مع التشريعات البريطانية. إذا كنت تعتقد أن العرض العام لهذا الملف ينتهك حقوق الطبع والنشر، يرجى الاتصال بـopenaccess@ed.ac.ukتوفير التفاصيل، وسنقوم بإزالة الوصول إلى العمل على الفور والتحقيق في ادعائك.
الوصول المفتوح
النتائج السريرية المرضية، العلاج، والنتيجة في 60 قطة تعاني من التليف الليفي الإيوزينوفيلي المعوي
قسم العلوم السريرية، جامعة ولاية كولورادو، فورت كولينز، كولورادو، الولايات المتحدة الأمريكية عيادة الحيوانات الصغيرة، جامعة العلوم البيطرية برنو، برنو، جمهورية التشيك إحالات المتخصصين في نورث داونز، بليتشينغلي، المملكة المتحدة مركز التخصصات البيطرية والطوارئ، كاواغوتشي، سايتاما، اليابان مركز الطب البيطري للحيوانات الصغيرة، سايتاما، اليابان مركز الطب البيطري، جامعة طوكيو، طوكيو، اليابان مدرسة الدراسات البيطرية الملكية (ديك)، جامعة إدنبرة، ميدلوثيان، المملكة المتحدة
المراسلات
بيترًا تشيرنا، قسم العلوم السريرية، جامعة ولاية كولورادو، فورت كولينز، كولورادو، الولايات المتحدة الأمريكية. البريد الإلكتروني: petra.cerna@colostate.edu
الملخص
الخلفية: تتجلى التليف الليفي الإيوزينوفيلي المعوي (GESF) في القطط على شكل كتلة أو كتل مرتبطة بالجهاز الهضمي، المساريقا، والعقد اللمفاوية البطنية. الفرضية/الأهداف: الإبلاغ عن النتائج السريرية والمرضية، والعلاج، والنتيجة للقطط المصابة بـ GESF.
الحيوانات: ستون قطة مملوكة للزبائن تم تشخيصها بمتلازمة التهاب الأنسجة اللمفاوية. الطرق: مراجعة استعادية للسجلات الطبية للقطط التي تم تأكيد تشخيصها بمتلازمة التهاب الأنسجة اللمفاوية بواسطة الفحص النسيجي.
النتائج: كان متوسط العمر 5.4 سنوات (نطاق الربيع بيني [IQR]، 3.3-8.9)؛ كانت 30% من القطط من نوع الشورت هير و12% من نوع اللانغ هير، وكانت السلالات الأكثر شيوعًا هي رagdoll (25%)، والشورت هير الغريبة (10%)، والقطط الفارسية (8%). كان متوسط مدة الأعراض السريرية 90 يومًا (IQR، 17.5-247.0)؛ كانت الأعراض السريرية الأكثر شيوعًا هي فقدان الوزن (60%)، نقص الشهية/فقدان الشهية (55%)، القيء المزمن (37%)، الخمول (35%) والإسهال المزمن (27%). كانت الكتل موجودة في الأمعاء الدقيقة (32%)، والمعدة (27%)، والتقاطع الإيليوكولي (15%)، والقولون (10%)، والعقد اللمفاوية (8%)، والمساريق (8%) و من القطط كان الكتلة. كانت اليوزينوفيلية موجودة فيوانخفاض مستوى الألبومين في الدمالقطط. تم إزالة الكتلة جراحيًا في 37% من الحالات. تم علاج معظم القطط (98%) بالكورتيكوستيرويدات. لم يكن هناك فرق إحصائي في البقاء على قيد الحياة بين القطط التي تم علاجها بالاستئصال الجراحي والقطط التي تم علاجها بالعلاج الطبي فقط،كانت بعض القطط لا تزال على قيد الحياة في وقت كتابة هذا. الاستنتاجات والأهمية السريرية: يعتبر GESF تشخيصًا تفريقيًا مهمًا للكتل البطنية في القطط، وله توقعات أفضل بكثير مما تم الإبلاغ عنه سابقًا.
الكلمات الرئيسية
الحمضات، كتلة معوية، كتلة مساريقية، دمية قماشية
1 | المقدمة
التليف الليفي الحمضي في الجهاز الهضمي (GESF) في القطط هو مرض تم وصفه مؤخرًا يظهر على شكل كتل حمضية في الجهاز الهضمي والعقد اللمفاوية البطنية المرتبطة، وغالبًا ما تكون بالقرب من البواب أو تقاطع الإيليوم والقولون.هناك حالتان موثقتان من GESF موضوعة في المساريقا أو خلف البريتوان في القطط.تقرير حالة يصف نفس نوع الآفة خارج تجويف البطن؛ التهاب العقد اللمفية التصلبي الإيوزينوفيلي في العقد اللمفية الخلفية البلعومية الوسطى كان مرتبطًا بعدوى بكتيريا الزائفة الزنجارية.من المحتمل أن تكون التليف الليفي الإيوزينوفيلي المعوي في القطط غير مشخصة بشكل كافٍ لأن هذه الآفات الكتلية يمكن أن تُفسر بشكل خاطئ على أنها لمفوما، أو غرانولومة، أو ساركوما ليفية، أو أدينوكارسينوما، أو ورم خلايا مAST، كما أن التشخيص النسيجي المرضي يمكن أن يكون تحديًا.تلوين المناعية النسيجية لعامل النمو المحوليمكن أن يساعد في التشخيص.تُرى هذه المرض بشكل شائع في القطط المتوسطة العمر والذكور من جميع السلالات، حيث تكون سلالة رagdoll مفرطة التمثيل، كما تم الإبلاغ عن المرض في قطط Maine Coon وPersian وExotic Shorthair وBengal وScottish Fold.لا تزال آلية حدوث GESF غير مفهومة جيدًا؛ ومع ذلك، مع وجود بعض السلالات، مثل رagdolls، بشكل مفرط، يمكن اعتبار وجود استعداد وراثي.
أكثر العلامات الشائعة التي تظهر على القطط المصابة بمتلازمة التهاب المعدة والأمعاء المزمن هي القيء المزمن، والإسهال، يليه فقدان الوزن، والخمول؛ وأقل شيوعًا تم الإبلاغ عن ظهور حاد للقيء والإسهال.تم الإبلاغ عن كتلة معوية ملحوظة فيإلى من الحالات، حيث أن الألم البطني والحمى أقل شيوعًا.تم إجراء إزالة جراحية للكتلة في معظم الحالات؛ ومع ذلك، تشير عدة دراسات إلى الإدارة الطبية من خلال إعطاء الكورتيكوستيرويدات، والسيكلوسبورين، والميكوفينولات.تتطور كتلة في موقع ثانٍ في بعض الحالات، بعد الإزالة الجراحية للكتلة الأولية.
تختلف التوقعات بين الدراسات؛ ومع ذلك، لم يتم الإبلاغ عن دراسات كبيرة حول التوقعات أو الاستجابة للعلاج.كان الهدف من هذه الدراسة هو تقييم عدد كبير من القطط المصابة بمتلازمة التهاب الأمعاء المزمن (GESF) بشكل رجعي، بما في ذلك عرضها، تشخيصها، علاجها، ونتائجها.
2 | المواد والأساليب
2.1 | تجنيد الحالات
هذه دراسة استعادية متعددة المراكز، لحالات GESF في القطط التي تم جمعها من قبل عدة مستشفيات بيطرية حول العالم (الولايات المتحدة الأمريكية، المملكة المتحدة، واليابان) من خلال الاتصال بأطباء بيطريين سبق لهم رؤية حالات GESF في القطط بين عامي 2010 و2022. كانت معايير الإدراج هي تأكيد تشخيص GESF في القطط بواسطة علم الأنسجة بعد إزالة جراحية أو خزعة من الكتلة؛ تم إجراء علم الأنسجة بواسطة أطباء أنسجة مختلفين من المستشفيات المحالة أو المختبرات المحالة. تم تجميع معلومات القطط، العلامات السريرية، النتائج الفيزيائية، النتائج السريرية المرضية، التقارير الجراحية والإدارة الطبية في جدول بيانات Excel (مايكروسوفت، ريدموند، واشنطن، الولايات المتحدة الأمريكية). تم الحصول على الموافقة الأخلاقية من جامعة إدنبرة (مرجع VERC: 17.22).
2.2 | التحليل الإحصائي
تم قياس أوقات البقاء من تاريخ العرض حتى تاريخ الوفاة أو آخر متابعة. تم استخدام تحليل كابلان-ماير واختبارات الرتبة اللوغاريتمية لتحليل البقاء من أجل تقييم العلاقة بين وقت البقاء والعلاج (GraphPad Prism 9، GraphPad Software، بوسطن، ماساتشوستس، الولايات المتحدة الأمريكية). اعتُبرت النتائج ذات دلالة إحصائية إذا كانت.
3 | النتائج
3.1 | العرض والعلامات السريرية
اجتمع ما مجموعه 60 قطة مع معايير الإدراج للدراسة. كان العمر الوسيط 5.4 سنوات (نطاق الربيع بين الربعين [IQR]، 3.3-8.9). من بين 60 قطة، كانت 18 (30%) من سلالة الشورت هير المحلي، و7 (12%) من سلالة الطويل هير المحلي، و35 (58%) من السلالات النسبية: رagdoll 15/60 (25%)، إكزوتيك شورت هير 6/60 (10%)، فارسي 5/60 (8%)، مين كون 3/60 (5%)، ساكراد بيرمان 2/60 (3%)، أمريكان شورت هير.بنجالبوبتيلو القط البريطاني القصير الشعرمن بين 60 قطة، كانت 34 (57%) من القطط ذكورًا مُعقمة، و25 (42%) إناثًا مُعقمات، و1 (2%) أنثى كاملة.
كانت مدة الأعراض السريرية المتوسطة 90 يومًا (IQR، 17.5-247.0) مع ظهور معظم القطط بمتوسط 3 (IQR، 2-4) أعراض سريرية. الأعراض السريرية الأكثر شيوعًا مذكورة في الجدول 1.
في الفحص البدني، كانت أكثر الشذوذات شيوعًا هي وجود كتلة بطنية ملحوظة في 35 (58%) من أصل 60 قطة، تليها الحمى في 9/60 (15%)، والجفاف في 7/60 (12%)، وألم البطن في. في من بين 60 قطة، تم الإبلاغ عن حالة الجسم بأنها أقل من المثالية (<4/9).
كانت نتائج تعداد خلايا الدم الكامل متاحة لـ 57 (95%) من القطط الـ 60. وكانت أكثر الشذوذات شيوعًا هي اليوزينوفيلية التي كانت موجودة فيمن بين 57 حالة، كانت فترات المرجعية تختلف بين العيادات وكانت الإيوزينوفيلية في الغالب معتدلة إلى شديدة مع نسبة متوسطة فوق RI 243.3 (IQR، 188.7-465.2)؛ ومع ذلك، لم تحتوي جميع السجلات الطبية على أرقام الإيوزينوفيل الفعلية (بعض السجلات ذكرت فقط وجود الإيوزينوفيلية). كانت أكثر الاضطرابات الدموية شيوعًا هي فقر الدم في 16 حالة (28%). وشملت النتائج الأقل شيوعًا زيادة عدد الكريات البيضاء (النيتروفيل) في 10/57 (18%)، وزيادة عدد الوحيدات 7/57 (12%)، وزيادة عدد اللمفاويات 5/57 (9%)، وزيادة عدد القاعديات 3/57 (5%)، ونقص عدد النيتروفيل 1/57 (2%). كانت نتائج الكيمياء الحيوية في المصل متاحة لـ 58 (97%) من 60 قطة. كانت أكثر الاضطرابات شيوعًا هي نقص الألبومين في المصل والتي لوحظت في ( ) من الحالات. كانت فترات المرجعية تختلف بين العيادات وكانت نقص الألبومين في الغالب خفيفة مع النسبة المئوية المتوسطة تحت RI 91.3 (IQR، 83.7-96.2). كانت ثاني أكثر الشذوذات شيوعًا هي فرط الغلوبولين في 8/58 (14%)، تليها نقص الكوليسترول في 6/58 (10%) ونقص الكالسيوم الكلي 6/58 (10%); حيث كان 4/6 (67%) من القطط ناقصة الكالسيوم لديها مستويات ألبومين طبيعية. تم قياس الكوبالامين في المصل في 11 (18%) من القطط الـ 60 وكان طبيعيًا في جميعها، على الرغم من أنه كان في الطرف المنخفض من فترة المرجعية في قطة واحدة (278؛ فترة المرجعية [RI]، كان قياس الفولات متاحًا فيالقطط وكان مرتفعًا بشكل غير طبيعي فيقطط.
3.3 | التصوير التشخيصي
تم إجراء تصوير البطن في جميع القطط؛ ومع ذلك، كانت صور الموجات فوق الصوتية متاحة فقط لـ 30 (50%) من 60 قطة؛ بينما تم إجراء أشعة سينية للبطن للآخرين وكانت تقارير الموجات فوق الصوتية جزءًا من السجلات الطبية، لكن صور الموجات فوق الصوتية لم تكن متاحة للمراجعة. في 25/30 (83%) من القطط، نشأت الكتلة من المعدة أو الأمعاء. من بين الحالات الخمس الأخرى، تأثرت 3 (10%) بالبطن. الغدد اللمفاوية وشملت المساريق (7%). كانت الغالبية العظمى من الكتل المعوية مرتبطة بفقدان طبقات الأمعاء (الشكل 1)، وتثخين دائري متماثل أو غير متماثل، ونمو غير مركزي، وخصائص صدى جدار مختلطة بشكل غير متجانس والتي كانت تحتوي على مناطق ذات صدى مرتفع واحتمالية حدوث تقرحات. في 6 (20%) من الحالات الـ 30، تم الإبلاغ عن أن هذه الكتل كانت مرتبطة بتغير الطبقات بدلاً من فقدانها. لوحظت مناطق ذات صدى مرتفع فيمن حالات المعدة أو الأمعاء، وفي جميع الحالات، بينما لوحظت زيادة سمك طبقة العضلات في الأمعاء الدقيقة في منهم. تم الإبلاغ عن تغييرات في الصفاق في 22 من 30 (73%) من القطط، من بينها كان هناك صفاق هايبر إيكويكان هناك انصباب بريتواني (لم يتم دائمًا الإبلاغ عن كمية الانصباب في السجلات الطبية). لم تظهر أي من الآفات نتائج فوق صوتية تتوافق مع ثقب الجهاز الهضمي. كانت الغدد الليمفاوية المتضخمة موجودة في 27 (90%) من 30 حالة حيث كانت صور الموجات فوق الصوتية متاحة؛ وكانت الغدد الليمفاوية الأكثر تأثرًا هي الإيليوكوليك.، تليها البنكرياس الاثني عشروالم mesenteric،بالنسبة لبقية الحالات (30 قطة)، لم تكن صور الموجات فوق الصوتية للبطن متاحة لتقييم العقد اللمفاوية بشكل أكبر.
3.4 | موقع الكتلة
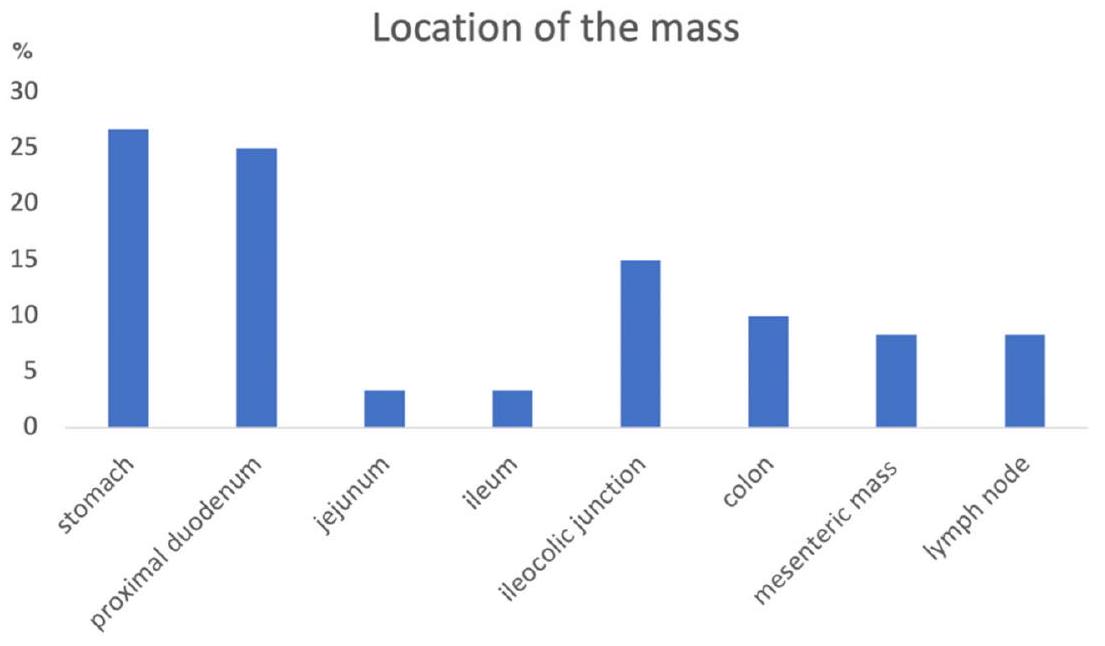
كان الموقع الأكثر شيوعًا للكتل (الشكل 2) هو الأمعاء الدقيقة فيمن بين 60 حالة، بما في ذلك الاثني عشر القريب 15/60 (25٪؛ الشكل التوضيحي 1)، الصائم 2/60 (3٪)، الدقاق 2/60والمعدة في، تليها الوصلة الإيليوكولية 9/60 (15%)، القولون 6/60 (10%)، العقد اللمفاوية 5/60 (8%)، والمساريقا 5/60 (8%; الشكل التوضيحي 2). معظم القطط، 51/60 ( ) كان لديه كتلة واحدة فقط؛ ومع ذلك، في ( ) من القطط كانت هناك كتل موجودة في أكثر من موقع. كانت الكتل الإضافية تتعلق بشكل شائع بالمساريقا والعقد اللمفاوية المحيطة في 4/9 (44%)؛ في 3 قطط، أثرت الكتل الإضافية على المعدة والاثني عشر القريب، وفي 1 قطة على المساريقا واللفائفي، وفي 1 قطة على
الشكل 1 صورة بالموجات فوق الصوتية لكتلة عند مستوى تقاطع الأمعاء الدقيقة والغليظة (السهم الأبيض). تظهر الكتلة فقدان الطبقات، وزيادة سمك محيطي ونمو غير مركزي. جدار الكتلة مختلط بشكل غير متجانس في الصدى بسبب وجود مناطق عالية الصدى. الغشاء البريتوني المحيط عالي الصدى (النجمة).
الشكل 2 المواقع الشائعة للكتل الموجودة في القطط المصابة بالتليف السليفي المعوي في هذه الدراسة. يمثل المحور Y النسبة المئوية للكتل في الموقع.
الاثني عشر القريب واللفائفي. من الجدير بالذكر أن قطة واحدة كانت تعاني من كتلة جلدية مكونة من الخلايا الحمضية في نفس الوقت مع GESF. قطة واحدة كانت لديها كتلة في تقاطع الأمعاء الغليظة والصغيرة تمت إزالتها، ثم ظهرت بعد 7 أشهر بكتلة مساريقية. قطة أخرى تمت إزالة كتلة من قولونها، ثم ظهرت بعد عامين بكتلة في البواب، والتي تمت إزالتها أيضًا، ثم ظهرت بعد 3 سنوات مع كتلة أخرى في البواب. في كلتا الحالتين، لم يتم إعطاء القطط العلاج بالكورتيكوستيرويدات حتى بعد الاستئصال الجراحي للكتلة الثانية أو الثالثة، على التوالي، وكانت جميع الكتل في كلا القطتين متوافقة مع GESF في علم الأمراض النسيجي.
3.5 | علم الخلايا
تم إجراء علم الخلايا لعينات الإبرة الدقيقة (FNA) من الكتلة فيمن بين 60 قطة، أظهرت 10 من 22 حالة (45%) التهابًا حمضيًا. في حالات أخرى، كانت الخلايا إما غير تشخيصية، أو أظهرت نخرًا أو التهابًا مختلطًا. تم إجراء تحليل الخلايا على خزعة بالإبرة الدقيقة من العقد اللمفاوية البطنية في 22 من 60 قطة (37%)، ولكنها كانت في الغالب غير تشخيصية أو أظهرت عقد لمفاوية تفاعلية؛ وتم الإبلاغ عن الحمضات فقط في 8 من 22 حالة (36%).
3.6 | جراحة/خزعة
تمت إزالة الكتلة جراحيًا في 22 (37%) من 60 قطة، وتم تحقيق الاستئصال المجهري الكامل في 18/22 (82%) من القطط. في 29 (76%) من الحالات الـ 38 المتبقية، تم إجراء خزعة جراحية، بينما تم تحقيق التشخيص من خلال الخزعات التنظيرية في 9 (24%) من القطط الأخرى. بالنسبة للقطط التي خضعت للخزعات التنظيرية، كانت الكتلة تقع في الاثني عشر القريب في 5/9 (56%) أو في المعدة في 4/9 (44%) من الحالات. تم الإبلاغ عن مضاعفات جراحية في 5/22 ( ) من القطط، مع من القطط التي تطور لديها فقر الدم واحتاجت إلى نقل دم (14% من القطط التي خضعت لعملية جراحية لإزالة أو أخذ خزعة من كتلة GESF)؛ كانت جميع هذه القطط الثلاثة تعاني من فقر الدم عند العرض، حيث كانت نسبة الهيماتوكريت عند العرض 18 و20 وعلى التوالي. تطور لدى قطة التهاب الصفاق الإنتاني مما استدعى إجراء جراحة ثانية، بينما أصبحت قطة واحدة في حالة واحدة، تطور لدى قطة نقص في الوزن الشديد، مما أدى إلى حدوث استسقاء شحمي، وقد تم حل هذه الحالة بالعلاج، وفي حالة أخرى، تطورت لدى قطة سلس براز مستمر بعد استئصال جراحي لكتلة قولونية.
3.7 | علم الأمراض النسيجية وزراعة الأنسجة
في جميع الـ 60 قطة، تم تأكيد الكتلة على أنها GESF من خلال علم الأمراض النسيجي (الأشكال 3 و 4). من بين الـ 22 (من بين 60 حالة تم فيها إزالة الكتلة جراحيًا، تم استئصال الآفة بالكامل في 13 قطة (59%). في 19 من 60 (32%) من القطط، كانت البكتيريا داخل الآفة موجودة في علم الأمراض النسيجي، وتم الكشف عن كائنات فطرية في قطة واحدة (عن طريق صبغة حمض البيريوكسيد الإيجابية [PAS]). تم إجراء تقنية التهجين الموضعي بالفلور (FISH) في 3 قطط وأظهرت بكتيريا حقيقية في قطة واحدة وبكتيريا حقيقية، كامبيلوباكتر جيجوني، أنواع السالمونيلا وإشريكية القولون في القطة الثانية وعدم وجود بكتيريا غازية في القطة الثالثة. تم إجراء زراعة بكتيرية في 18 من 60 (30%) من الحالات؛ 4 من 18كانت النتائج سلبية، بينما في الحالات الأخرى كانت البكتيريا الأكثر شيوعًا هي E. coli (6/12؛ 50%)، وأنواع المكورات العنقودية (6/12؛ 50%)، وأنواع الإنتيروكوكوس (4/12؛ 33%)، وأنواع المكورات العقدية (1/12؛ 8%) وBacteroides fragilis (1/12؛ 8%). لم يكن من الواضح دائمًا ما إذا كانت السوائل أو الكتل أو مسحات الأنسجة قد تم زراعتها في بعض القطط. كانت الخزعة التي كانت إيجابية في صبغة PAS قد زُرعت فيها Candida albicans بالإضافة إلى أنواع الإنتيروكوكوس وE. coli. في 34 (57%) من أصل 60 حالة، تم أيضًا أخذ خزعات من أعضاء إضافية؛ شملت هذه العقد اللمفاوية (28/34؛ 82%)، والمعدة (5/34؛ 15%)، والكبد (4/34؛ 12%)، والاثني عشر (2/34؛ 6%)، والصائم (1/34؛ 3%)، والدهون (1/34؛ 3%). في 12 (42%) من أصل 28 حالة حيث تم إجراء علم الأمراض النسيجي للعقد اللمفاوية، كانت النتائج متوافقة مع GESF، كما كان الحال بالنسبة للدهون في الحالة الوحيدة التي تم أخذ خزعة من هذا الموقع.
3.8 | العلاج
تم علاج معظم القطط 59/60 (98%) بالكورتيكوستيرويدات، على الرغم من أن قطة واحدة تم علاجها بالمضادات الحيوية فقط. جميع القطط باستثناء قطة واحدة التي تم إعطاؤها الكورتيكوستيرويدات تم إعطاؤها
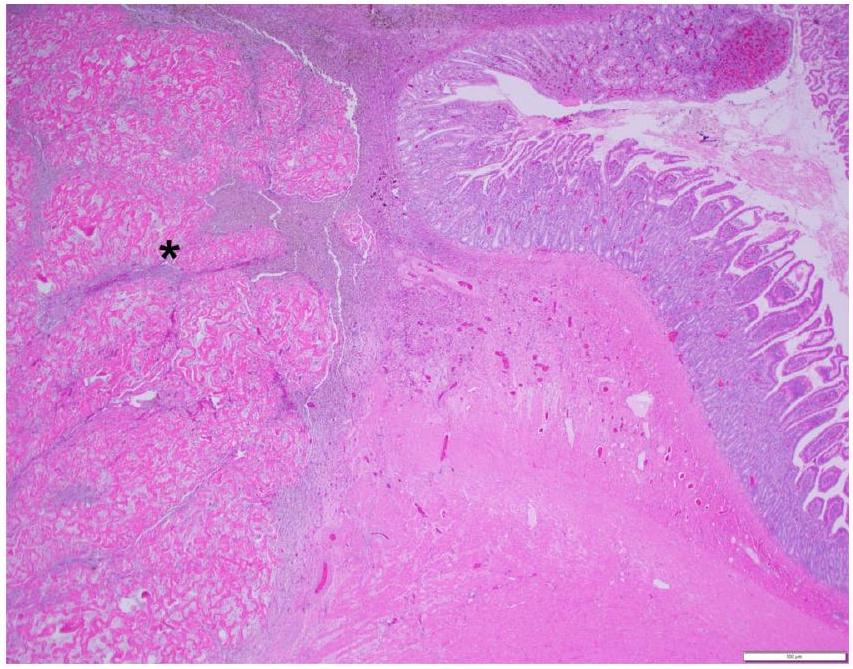
الشكل 3 النتائج النسيجية لكتلة الاثني عشر – يتم توسيع العضلية والطبقة تحت المخاطية بواسطة كتلة منفصلة، ذات خلايا قليلة (*). هيماتوكسيلين وإيوزين،تكبير. شريط المقياسحقوق الصورة: الدكتورة أليسون واتسون من جامعة ولاية كولورادو.
الشكل 4 النتائج النسيجية لكتلة الاثني عشر – الكتلة تتكون من حبال متشابكة من الكولاجين المتصلب مفصولة بالخلايا الليفية، البلعميات، وأعداد صغيرة من الحمضات والخلايا البدينة. صبغة الهيماتوكسيلين واليوزين.تكبير. شريط المقياسحقوق الصورة: الدكتورة أليسون واتسون من جامعة ولاية كولورادو.
بريدنيزولون مرة واحدة يوميًا بجرعة متوسطة مناليوم (IQR، 1.0-2.0). كان الوقت الوسيط لإعطاء الكورتيكوستيرويدات للقطط هو 23 (IQR، 10.5-49.0) يومًا بعد تقديمها لأول مرة. في 49 قطة، تم تغيير جرعة البريدنيزولون بوسيط قدره 32 (IQR، 16.0-60.0) يومًا بعد بدء العلاج بالكورتيكوستيرويدات، وفي 13 قطة، تم إيقاف البريدنيزولون؛ ومع ذلك، في 11 من هذه الـ 13 قطة، كان يجب إعادة بدء البريدنيزولون في وقت وسطي قدره 114 (IQR، 36.0-366.0) يومًا بعد الإيقاف بسبب تكرار العلامات السريرية. كان الوقت الوسيط لأدنى جرعة من البريدنيزولون هو 369 (IQR، 195.0-841.0) يومًا، مع
الشكل 5 مخطط كابلان-ماير لبقاء القطط التي خضعت لاستئصال جراحي للكتلة والقطط التي تم أخذ خزعة منها فقطتمثل علامات التوقف القطط التي تم حذف بياناتها. الخط الأخضر هو للقطط التي تمت إزالة الكتلة جراحيًا، والخط الأزرق هو للقطط التي لم يتم إزالة الكتلة.
الجرعة الدنيا المتوسطة للصيانة 0.65 (نطاق الربيع، ) ملغ/كغ/يوم اللازمة للتحكم في العلامات السريرية. كانت المضاعفات الأكثر شيوعًا من علاج الكورتيكوستيرويد هي فرط ثلاثي الغليسريد في 5 قطط. تم علاج فرط ثلاثي الغليسريد بنظام غذائي منخفض الدهون وزيت السمك في قطة واحدة، وزيت السمك فقط في قطة واحدة، مع نظام غذائي منخفض الدهون وزيت السمك وفينوفيبرات في قطة واحدة، ولم يتم علاج القطتين المتبقيتين، وتطور مرض السكري في 3 قطط (2 منها دخلت في مغفرة السكري تحت علاج الأنسولين، ولا تزال واحدة من هذه القطط على جرعة منخفضة [ يوم البردنيزولون]). تم وصف عوامل مثبطة للمناعة ثانوية (سيكلوسبورين أو كلورامبوسيل) في 14 ( ) من 60 قطة وتم إيقافها في من تلك القطط بعد وسيلة قدرها 80 (IQR، 64.5-236.3) يومًا.
تم وصف المضادات الحيوية لـ 43 (72%) من أصل 60 قطة، وكانت المضادات الحيوية الأكثر شيوعًا هي البنسيلينات. )، الفلوروكينولونات (9/43؛ ميترونيدازول (6/43؛ )، السيفالوسبورينات (5/43؛ ) و كليندامايسين ( كانت المدة المتوسطة للعلاج بالمضادات الحيوية 34 يومًا (النطاق، 7-204).
تمت التوصية بأنظمة غذائية تحتوي على بروتينات مهدرجة أو مختارة في 37% (22/60) من القطط؛ وأفاد 41% (9/22) من المالكين بتحسن العلامات السريرية عند اتباع نظام غذائي يحتوي على بروتينات مهدرجة أو مختارة، على الرغم من أن 3 قطط لم تكن تأكل النظام الغذائي.
3.9 | البقاء
كـمن بين 60 قطة لا تزال على قيد الحياة في وقت كتابة هذا المنشور، لا يمكن تقدير متوسط مدة البقاء. من بين 7 قطط توفيت أو تم euthanized، توفيت 4 قطط بسبب عدم التحكم الجيد في GESF، و2 قطة بسبب ورم البنكرياس، و1 قطة توفيت لأسباب غير معروفة. لم يكن هناك فرق إحصائي بين بقاء القطط التي خضعت لاستئصال جراحي للكتلة والقطط التي تم أخذ خزعة منها فقط.; الشكل 5). لم يكن هناك فرق إحصائي بين بقاء القطط التي خضعت لاستئصال كامل مع تم تأكيد هوامش واضحة بواسطة علم الأمراض النسيجي والقطط التي تم فيها استئصال غير كامل للكتلة والقطط التي تم أخذ خزعة فقط من الكتلة ). لم يكن هناك أيضًا فرق إحصائي بين بقاء القطط التي تم علاجها بالكورتيكوستيرويدات فقط مقابل العوامل المثبطة للمناعة الثانوية ( )، ولا بين القطط التي تم علاجها بالمضادات الحيوية والقطط التي لم يتم علاجها بالمضادات الحيوية ( ).
4 | المناقشة
تقدم هذه الدراسة أكبر دراسة عن GESF في القطط حتى الآن، مع حالات تم جمعها دوليًا على مدى 15 عامًا. كانت الدراسات السابقة قد أفادت بأن كتل GESF في القطط ترتبط بشكل شائع بالمعدة (غالبًا بالقرب من البواب) أو الأمعاء، كما تؤثر أيضًا على العقد اللمفاوية البطنية. المساريقا، والمساحة خلف البريتوان.هذا مشابه للدراسة الحالية، حيث كان الموقع الأكثر شيوعًا لكتل GESF في القطط هو الأمعاء الدقيقة، المعدة، تقاطع الإيليوم والقولون، بينما في 16% من القطط كانت الكتلة مرتبطة بالعقد اللمفاوية أو المساريقا. في 15% من القطط، كانت كتل GESF موجودة في أكثر من موقع واحد؛ في 12 من الحالات كانت العقد اللمفاوية المحلية متأثرة أيضًا، وفي قطة واحدة كانت الصفاق متورطة، مما يظهر أن هذا المرض يمكن أن يؤثر على عدد من المواقع في كل قطة. ومن الجدير بالذكر، أن قطة واحدة كانت لديها أيضًا كتلة جلدية إيوزينوفيلية في نفس الوقت مع GESF – لم يتم الإبلاغ عن ذلك في القطط التي تعاني من GESF؛ ومع ذلك، تم الإبلاغ عن كتل تحت الجلد مع تسلل إيوزينوفيل.وصف تقرير حالة حديث أيضًا مرضًا مشابهًا لمرض GESF خارج تجويف البطن، في العقد اللمفاوية الخلفية البلعومية الوسطى.
عند النظر إلى المعلومات المتعلقة بالحالة، كان متوسط عمر القطط المصابة بـ GESF في هذه الدراسة 5.4 سنوات (النطاق، 1.3-14.5)، وهو مشابه لمتوسط العمر المبلغ عنه وهو 7 سنوات، مع نطاق من 2 إلى 11 سنة.في السابق، تم الإبلاغ عن أن القطط الذكور تتأثر أكثر بـ GESF؛ ومع ذلك، لم يُلاحظ ذلك في هذه الدراسة.أكثر من نصف (58%) القطط في دراستنا كانت قطط سلالة، حيث شكلت قطط الراجدول ربع القطط في الدراسة؛ وهذا مشابه لدراسة أخرى أفادت بأن قطط الراجدول كانت مفرطة التمثيل.السلالات الأخرى التي تم رؤيتها بشكل شائع في الدراسة الحالية كانت القطط الشيرازية القصيرة الشعر (10%) والقطط الفارسية (8%). من غير الواضح لماذا يبدو أن القطط ذات السلالة النقية معرضة لتطوير التهاب الأمعاء اليوزيني (GESF)، وخاصة سلالة رagdoll (25%) والقطط الفارسية/الغريبة (18%)، وهناك حاجة إلى مزيد من الدراسات، بما في ذلك التحليل الجيني، لمعرفة ما إذا كانت هذه السلالات لديها استعداد جيني لتطوير التهاب اليوزينيات استجابةً لمستضدات الأمعاء، والتي يُحتمل أن تكون السبب وراء GESF. من المهم أن نلاحظ أن هذه أيضًا سلالات معرضة لالتهاب الصفاق المعدي الفيروسي في القطط (FIP).GESF و FIP غير الانصهاري هما كلاهما تشخيصات تفريقية ملحوظة للقطط التي تظهر كتلًا في البطن.
في الدراسة الحالية، كانت مدة ظهور العلامات السريرية المتوسطة 90 يومًا، حيث أظهرت معظم القطط متوسط 3 علامات سريرية، وكانت الأكثر شيوعًا هي فقدان الوزن (60%)، نقص الشهية/فقدان الشهية (55%)، القيء المزمن (37%)، الخمول (35%) والإسهال المزمن (27%)، وهو مشابه جدًا لدراسة سابقة تم الإبلاغ عنها؛ ومع ذلك، فقد أبلغوا أيضًا عن الإفراط في العناية بالنفس فيمن الحالات التي كانت تُرى فقط في من القطط في الدراسة الحالية. فحص البطن باللمس
توجد كتلة في من القطط ; ومع ذلك، كان هذا أقل شيوعًا في الدراسة الحالية حيث كانت الكتلة قابلة للإحساس فقط في من القطط. كانت نسبة الحمى مشابهة لدراسات أخرى، 15% مقابل
كانت أكثر شذوذات تحاليل الدم شيوعًا هي اليوزينوفيلية المحيطية، والتي كانت موجودة في من القطط في الدراسة الحالية، وهو مشابه للدراسات السابقة. كانت الأنيميا موجودة في ثلث تقريبًا من القطط في الدراسة الحالية، ولكن لم يتم الإبلاغ عنها. كانت نقص الألبومين وارتفاع الغلوبولينيميا أكثر الشذوذات شيوعًا، حيث حدثت في و من القطط، على التوالي، وهو أقل شيوعًا مما تم الإبلاغ عنه في و ، على التوالي.
تفتقر الدراسات الكبيرة التي تقيم نتائج الموجات فوق الصوتية للبطن للقطط المصابة بـ GESF حتى الآن؛ ومع ذلك، أبلغت دراسة عن 5 قطط كانت لديها كتلة وحيدة مع سماكة جدارية وفقدان الطبقات في المعدة، الاثني عشر، الصائم، والقولون. في الدراسة الحالية، كانت صور الموجات فوق الصوتية للبطن متاحة للمراجعة في 50% من القطط، حيث أظهرت معظم الحالات (83%) أن الغالبية من الكتل نشأت من المعدة أو الأمعاء. كانت هذه الكتل مرتبطة بفقدان الطبقات المعوية وسماكة محيطية في معظم الحالات، على الرغم من أنه في كان هناك تغيير في الطبقات بدلاً من فقدانها. كانت العقد اللمفاوية المحلية المتضخمة موجودة في من الحالات، والتغيرات البطنية في ، من بينها كان لديها انصباب بطني؛ ومع ذلك، لم تظهر أي من الآفات نتائج فوق صوتية متوافقة مع ثقب الجهاز الهضمي.
تم تحديد بكتيريا داخل الآفات في من الحالات بشكل عام (جميع آفات تقاطع الأمعاء الغليظة والقولون) في دراسة واحدة وفي 69% من القطط في دراسة أخرى باستخدام إما الثقافة أو المجهر الضوئي التقليدي، والأصباغ الخاصة وFISH. في الدراسة الحالية، كان فقط من الحالات تحتوي على بكتيريا موجودة في علم الأمراض النسيجي، وتم الكشف عن كائنات فطرية في 1 قطة؛ ومع ذلك، كواحد من قيود هذه الدراسة الاستعادية، قد تكون الكائنات المعدية قد فاتت في بعض القطط حيث تم إجراء FISH فقط في 3 قطط وتم إجراء زراعة بكتيرية في من القطط في هذه الدراسة. على الرغم من أن البكتيريا ترتبط عادةً بـ GESF في القطط، إلا أن الكائنات الفطرية تم الإبلاغ عنها مرة واحدة، في تقرير حالة لـ GESF المرتبط بالفطريات.
تم الإبلاغ عن توقعات القطط المصابة بـ GESF على أنها متغيرة، تتراوح من الحذر، إلى القطط التي تعيش لعدة سنوات. معظم القطط التي نجت من فترة ما حول العملية ظلت بصحة جيدة لعدة سنوات. في الدراسة الحالية، لم يكن من الممكن تقدير متوسط وقت البقاء على قيد الحياة حيث من القطط لا تزال على قيد الحياة في وقت كتابة هذا المنشور. وهذا يظهر أهمية التشخيص الصحيح للقطط المصابة بـ GESF، حيث يمكن أن يتم تشخيص العديد من هذه الكتل بشكل خاطئ على أنها أورام، والتي عادةً ما تحمل توقعات سيئة.
القطط التي تتلقى العلاج بالجراحة فقط لديها وقت بقاء أقصر بشكل ملحوظ من تلك القطط التي تم علاجها بالجراحة والكورتيكوستيرويدات. تم الإبلاغ عن تحسين وقت البقاء عند تضمين البريدنيزولون في النظام العلاجي، بغض النظر عما إذا كانت القطط قد خضعت أيضًا للجراحة أم لا. في الدراسة الحالية، من القطط تم إعطاؤها علاج الكورتيكوستيرويد، لذا لا يمكن تقييم وقت بقاء القطط التي خضعت للجراحة فقط؛ ومع ذلك، لم يكن هناك فرق إحصائي بين بقاء القطط التي تمت إزالة كتلها جراحيًا والقطط التي تم أخذ خزعة فقط من كتلها
بما في ذلك القطط التي تم استئصالها بالكامل مع هوامش واضحة تم تأكيدها بواسطة علم الأمراض النسيجي.
يبدو أن الكورتيكوستيرويدات مهمة في علاج القطط المصابة بـ GESF. تم الإبلاغ عن تكرار الكتل عندما لم تتبع الجراحة بإعطاء الكورتيكوستيرويدات. في الدراسة الحالية، كانت هناك قطة واحدة تم استئصال كتلة من تقاطع الأمعاء الغليظة ولكن لم يتم إعطاؤها علاج الكورتيكوستيرويد، وعادت بعد 7 أشهر مع كتلة مساريقية. قطة أخرى في هذه الدراسة تم تشخيصها بـ GESF في القولون، والتي تم استئصالها، ثم مع كتلة بيلورية بعد عامين، والتي تم استئصالها أيضًا، وكتلة بيلورية أخرى بعد 3 سنوات من ذلك؛ بينما تم استئصال جميع هذه الكتل GESF جراحيًا، لم يتم إعطاء علاج الكورتيكوستيرويد حتى بعد استئصال الكتلة الثالثة. لم يكن هناك تكرار للكتل البطنية في أي من هاتين القطيطتين بعد إعطاء علاج الكورتيكوستيرويد لأكثر من 1.5 سنة. تدعم الإشارة إلى متابعة الجراحة بعلاج الكورتيكوستيرويد أيضًا 13 قطة حيث تم إيقاف البريدنيزولون، من هؤلاء كان عليهم إعادة بدء البريدنيزولون بمتوسط 114 يومًا بعد الإيقاف بسبب تكرار العلامات السريرية. كان متوسط الوقت لأدنى جرعة من البريدنيزولون 369 يومًا، مع أدنى جرعة صيانة متوسطة من يوم للتحكم في العلامات السريرية؛ ومع ذلك، حيث أن هذه دراسة استعادية، فقد فقدت بعض القطط للمتابعة ومن غير الواضح ما إذا كان قد تم تقليل البريدنيزولون أكثر في هذه القطط.
تم الإبلاغ عن استخدام عوامل مثبطة للمناعة الثانوية والمضادات الحيوية في القطط المصابة بـ GESF. في الدراسة الحالية لم يكن هناك فرق إحصائي بين بقاء القطط التي تم علاجها بالكورتيكوستيرويدات فقط مقابل تلك التي تضمنت عوامل مثبطة للمناعة الثانوية، بغض النظر عما إذا كانت المضادات الحيوية قد تم إعطاؤها أم لا.
تم تجربة حميات بروتين مهدر أو مختار في 37% من القطط في الدراسة الحالية، مع من المالكين الذين أبلغوا عن تحسن في العلامات السريرية على هذه الحميات. وهذا يشير إلى تعديل النظام الغذائي كعلاج محتمل للقطط المصابة بـ GESF. ومع ذلك، كانت جميع هذه القطط تتلقى بالفعل علاجًا بالكورتيكوستيرويدات.
شكر وتقدير
لم يتم تلقي أي تمويل لهذه الدراسة. نشكر جميع المالكين على مشاركة السجلات الطبية لقططهم، وجميع الموظفين الذين شاركوا في رعاية القطط في عياداتهم، ومجموعة دعم التصلب الليفي اليوزينوفيلي المعوي للقطط.
إعلان تضارب المصالح
يعلن المؤلفون عدم وجود تضارب في المصالح.
إعلان استخدام مضادات الميكروبات خارج التسمية
يعلن المؤلفون عدم وجود استخدام خارج التسمية للمضادات الميكروبية.
إعلان لجنة رعاية واستخدام الحيوانات المؤسسية (IACUC) أو الموافقة الأخرى
تمت الموافقة عليها من قبل لجنة مراجعة الأخلاقيات بجامعة إدنبرة (مرجع VERC: 17.22).
إعلان موافقة الأخلاقيات البشرية
يعلن المؤلفون أن موافقة الأخلاقيات البشرية لم تكن مطلوبة لهذه الدراسة.
Craig L, Hardam E, Hertzke D, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia. Vet Pathol. 2009;46:63-70.
Linton M, Nimmo JS, Norris JM, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia: 13 cases and review of an emerging clinical entity. J Feline Med Surg. 2015;17:392-404.
Kambe N, Okabe R, Osada H, et al. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia limited to the mesentery. J Small Anim Pract. 2020;61:64-67.
Thieme ME, Olsen AM, Woolcock AD, Miller MA, Simons MC. Diagnosis and management of a case of retroperitoneal eosinophilic sclerosing fibroplasia in a cat. J Feline Med Surg Open Rep. 2019;5: 2055116919867178.
Zampieri B, Church ME, Walsh K, Lennon EM. Feline eosinophilic sclerosing fibroplasia-a characteristic inflammatory response in sites beyond the gastrointestinal tract: case report and proposed nomenclature. J Feline Med Surg Open Rep. 2022;8:2055 1169221117516.
Munday J, Martinez A, Soo M. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia mimicking metastatic neoplasia. N Z Vet J. 2014;62:356-360.
Gamble DA. Letters to the editor and rebuttal regarding the paper recently published in Veterinary and Comparative Oncology, ‘Feline intestinal sclerosing mast cell tumour: 50 cases (1997-2008) 2010; 8: 72-79’ by CHC Halsey, BE Powers and DA Kamstock. Letter to the editor# 2. Vet Comp Oncol. 2010;8:235-242.
Schulman FY, Lipscomb TP. Letters to the editor and rebuttal regarding the paper recently published in Veterinary and Comparative Oncology, ‘Feline intestinal sclerosing mast cell tumour: 50 cases (1997-2008) 2010; 8: 72-79’ by C. H. C. Halsey, B. E. Powers and D. A. Kamstock. Letter to the editor #1. Vet Comp Oncol. 2010;8:234235. author reply 236-242.
Porras N, Rebollada-Merino A, Rodríguez-Franco F, Calvo-Ibbitson A, Rodríguez-Bertos A. Feline gastrointestinal eosinophilic sclerosing fibroplasia-extracellular matrix proteins and TGF- immunoexpression. Vet Sci. 2022;9:291.
Cho M-J, Kim M-C, Seo K-W. Feline gastrointestinal eosinophilic sclerosing fibroplasia in a Bengal cat. J Vet Clin. 2017;34:481-483.
Montenegro NE, Castro DAR, López PAB, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia. Braz J Vet Pathol. 2022;15: 57-61.
Suzuki M, Onchi M, Ozaki M. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia. J Toxicol Pathol. 2013;26:51-53.
Agulla , Díaz-Regañón , García-Sancho , et al. Remission of feline gastrointestinal eosinophilic sclerosing fibroplasia in a cat treated with corticotherapy. Pakistan Vet J. 2021;41:309-312.
Kim M-s, Kim K, Lee G-h, et al. Successful management of feline gastrointestinal eosinophilic sclerosing fibroplasia with mycophenolate mofetil and prednisolone following surgical resection in a cat. Thai Vet Med. 2021;51:773-777.
Takao K, Saitoh S, Nibe K. Surgical treatment of feline gastrointestinal eosinophilic sclerosing fibroplasia in a cat. Jpn J Vet Anesth Surg. 2015;46:81-82.
Weissman A, Penninck D, Webster C, Hecht S, Keating J, Craig LE. Ultrasonographic and clinicopathological features of feline gastrointestinal eosinophilic sclerosing fibroplasia in four cats. J Feline Med Surg. 2013;15:148-154.
Brloznik M, Faraguna S, Goc M, Svara T. Recurrent feline gastrointestinal eosinophilic sclerosing fibroplasia and presumptive eosinophilic
cystitis in a domestic short-haired cat: a case report. Vet Med. 2017; 62:295-300.
Ozaki K, Yamagami T, Nomura K, Haritani M, Tsutsumi Y, Narama I. Abscess-forming inflammatory granulation tissue with Gram-positive cocci and prominent eosinophil infiltration in cats: possible infection of methicillin-resistant Staphylococcus. Vet Pathol. 2003;40:283-287.
Pesteanu-Somogyi LD, Radzai C, Pressler BM. Prevalence of feline infectious peritonitis in specific cat breeds. J Feline Med Surg. 2006;8: 1-5.
Grau-Roma L, Galindo-Cardiel I, Isidoro-Ayza M, Fernández M, Majó N. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia associated with phycomycetes. J Comp Pathol. 2014;151: 318-321.
معلومات داعمة
يمكن العثور على معلومات داعمة إضافية عبر الإنترنت في قسم المعلومات الداعمة في نهاية هذه المقالة.
كيفية اقتباس هذه المقالة: تشيرنا ب، لوبيز-خيمينيز ج، فوكوشيما ك، وآخرون. النتائج السريرية المرضية، العلاج، والنتيجة في 60 قطة مصابة بالتصلب الليفي اليوزينوفيلي المعوي. J Vet Intern Med. 2024;1-8. doi:10. 1111/jvim. 16992
الاختصارات: FGESF، التصلب الليفي اليوزينوفيلي المعوي للقطط؛ FISH، التهجين الفلوري في الموقع؛ FNA، خزعات الإبرة الدقيقة؛ PAS، حمض البيريويد-شيف.
Clinicopathological Findings, Treatment and Outcome in 60 cats with Feline Gastrointestinal Eosinophilic Sclerosing Fibroplasia
Citation for published version:
Černá, P, Lopez-Jimenez, C, Fukushima, K, Nakashima, K, Nakagawa, T, Adams, F, Groth, A, Denning, A, Israeliantz Gunz, N & Gunn-Moore, D 2024, ‘Clinicopathological Findings, Treatment and Outcome in 60 cats with Feline Gastrointestinal Eosinophilic Sclerosing Fibroplasia’, Journal of Veterinary Internal Medicine, vol. 38, no. 2, pp. 1005-1012. https://doi.org/10.1111/jvim. 16992
Digital Object Identifier (DOI):
10.1111/jvim. 16992
Link:
Link to publication record in Edinburgh Research Explorer
Document Version:
Publisher’s PDF, also known as Version of record
Published In:
Journal of Veterinary Internal Medicine
General rights
Copyright for the publications made accessible via the Edinburgh Research Explorer is retained by the author(s) and / or other copyright owners and it is a condition of accessing these publications that users recognise and abide by the legal requirements associated with these rights.
Take down policy
The University of Edinburgh has made every reasonable effort to ensure that Edinburgh Research Explorer content complies with UK legislation. If you believe that the public display of this file breaches copyright please contact openaccess@ed.ac.uk providing details, and we will remove access to the work immediately and investigate your claim.
Open Access
Clinicopathological findings, treatment, and outcome in 60 cats with gastrointestinal eosinophilic sclerosing fibroplasia
Petra Černá ( ( Cristobal Lopez-Jimenez | Kenjiro Fukushima | Ko Nakashima ( ) Taisuke Nakagawa | Fiona Adam | Anna Groth | Andrew Denning | Nicolas Israeliantz ® | Danièlle A. Gunn-Moore
Department of Clinical Sciences, Colorado State University, Fort Collins, Colorado, USA Small Animal Clinic, The University of Veterinary Sciences Brno, Brno, Czech Republic North Downs Specialist Referrals, Bletchingley, UK Veterinary Specialists & Emergency Center, Kawaguchi-shi, Saitama, Japan Small Animal Medical Center, Saitama, Japan Veterinary Medical Centre, The University of Tokyo, Tokyo, Japan The Royal (Dick) School of Veterinary Studies, University of Edinburgh, Midlothian, UK
Correspondence
Petra Černá, Department of Clinical Sciences, Colorado State University, Fort Collins, CO, USA.
Email: petra.cerna@colostate.edu
Abstract
Background: Gastrointestinal eosinophilic sclerosing fibroplasia (GESF) in cats presents as mass(es) associated with the gastrointestinal tract, mesentery, and abdominal lymph nodes. Hypothesis/Objectives: To report the clinicopathological findings, treatment, and outcome of cats with GESF.
Animals: Sixty client-owned cats diagnosed with GESF. Methods: Retrospective review of medical records of cats with histopathologically confirmed GESF.
Results: The median age was 5.4 years (interquartile range [IQR], 3.3-8.9.); 30% were Domestic Shorthairs and 12% were Domestic Longhair cats, with the most prevalent pedigree breeds being Ragdolls (25%), Exotic Shorthair (10%) and Persian (8%) cats. The median duration of clinical signs was 90 days (IQR, 17.5-247.0); the most common clinical signs were weight loss (60%), hyporexia/anorexia (55%), chronic vomiting (37%), lethargy (35%) and chronic diarrhea (27%). Masses were located in the small intestine (32%), stomach (27%), ileocolic junction (15%), colon (10%), lymph node (8%) and mesentery (8%) and of cats had mass. Eosinophilia was present in and hypoalbuminemia in of cats. The mass was removed surgically in 37% of cases. Most cats (98%) were treated with corticosteroids. Survival was not statistically different between cats treated with surgical resection and cats treated with medical therapy alone, of the cats were still alive at the time of writing. Conclusions and Clinical Importance: GESF is an important differential diagnosis for abdominal masses in cats, and has a much better prognosis than previously reported.
Gastrointestinal eosinophilic sclerosing fibroplasia (GESF) in cats is a recently described disease that presents as eosinophilic mass(es) in the gastrointestinal tract and associated abdominal lymph nodes, most commonly near the pylorus or ileocolic junction. There are 2 case reports of GESF localized to the mesentery or retroperitoneum in cats. A case report describes the same type of lesion outside of the abdominal cavity; eosinophilic sclerosing lymphadenitis in medial retropharyngeal lymph node was associated with Pseudomonas aeruginosa infection. Gastrointestinal eosinophilic sclerosing fibroplasia in cats is likely underdiagnosed because these mass lesions can be misinterpreted as lymphoma, granuloma, fibrosarcoma, adenocarcinoma, and mast cell tumor, and the histopathological diagnosis can be challenging. Immunohistochemical staining for transforming growth factor can aid diagnosis. This disease is most commonly seen in middle aged and male cats of all breeds, with Ragdolls being overrepresented and the disease is also reported in Maine Coons, Persians, Exotic Shorthairs, Bengal, and Scottish fold cats. The pathogenesis of GESF is still poorly understood; however, with some breeds, such as Ragdolls, being overrepresented, a genetic predisposition could be considered.
The most common presenting signs of cats with GESF are chronic vomiting, diarrhea, followed by weight loss, lethargy; less commonly an acute onset of vomiting and diarrhea is been reported. A palpable intestinal mass is reported in to of cases, with abdominal pain and pyrexia being less common. Surgical removal of the mass has been performed in most cases; however, several studies report medical management with administration of corticosteroids, cyclosporine, and mycophenolate. A mass in a second location develops in some of the cases, after surgical removal of the initial mass.
The prognosis varies between studies; however, no large studies on prognosis or response to treatment have been reported. The objective of this study was to retrospectively evaluate a large number of cats with GESF, including their presentation, diagnosis, treatment, and outcome.
2 | MATERIALS AND METHODS
2.1 | Case recruitment
This is a retrospective, multicentric study, of cases of GESF in cats which have been collected by several veterinary hospitals around the world (USA, UK, and Japan) by contacting veterinarians that have previously seen cases of GESF in cats between 2010 and 2022. Inclusion criteria was confirmation of GESF diagnosis in cats by histopathology after surgical removal or biopsy of the mass; histopathology was performed by different pathologist from referral hospitals or referral laboratories. Cat signalment, clinical signs, physical findings, clinicopathological results, surgical reports and medical management were tabulated in an Excel (Microsoft, Redmond, WA, USA) spreadsheet. Ethical approval was gained from University of Edinburgh (VERC Reference: 17.22).
2.2 | Statistical analysis
Survival times were measured from the date of presentation until the date of death or last follow-up. Kaplan-Meier analysis and log rank tests were used for survival analysis in order to evaluate the association of survival time with treatment (GraphPad Prism 9, GraphPad Software, Boston, MA, USA). Results were considered significant if .
3 | RESULTS
3.1 | Presentation and clinical signs
A total of 60 cats met the inclusion criteria for the study. The median age was 5.4 years (interquartile range [IQR], 3.3-8.9). Of the 60 cats, 18 (30%) were Domestic Shorthair, 7 (12%) Domestic Longhair cats, and 35 (58%) were pedigree breeds: Ragdolls 15/60 (25%), Exotic Shorthair 6/60 (10%), Persian 5/60 (8%), Maine Coon 3/60 (5%), Sacred Birman 2/60 (3%), American Shorthair , Bengal , Bobtail , and British Shorthair (2%). Of the 60 cats, 34 (57%) of the cats were neutered males, 25 (42%) were spayed females, and 1 (2%) entire female.
The median duration of clinical signs was 90 days (IQR, 17.5-247.0) with most cats showing median of 3 (IQR, 2-4) clinical signs. The most common clinical signs are reported in Table 1.
On physical examination, the most common abnormality was a palpable abdominal mass in 35 (58%) of the 60 cats, followed by pyrexia, in 9/60 (15%), dehydration, 7/60 (12%), and abdominal pain in . In of the 60 cats, the body condition score was reported as less than ideal (<4/9).
TABLE 1 Presenting clinical signs of cats with gastrointestinal eosinophilic sclerosing fibroplasia.
Clinical sign
Number of cats (%)
Weight loss
36/60 (60)
Hyporexia/anorexia
33/60 (55)
Chronic (>2 weeks) vomiting
22/60 (37)
Lethargy
21/60 (35)
Chronic diarrhea
16/60 (27)
Acute (<2 weeks) vomiting
8/60 (13)
Acute diarrhea
6/60 (10)
Constipation
6/60 (10)
Tenesmus
5/60 (8)
Polyphagia
4/60 (7)
Hematochezia
4/60 (7)
Decreased grooming
3/60 (5)
Melena
1/60 (2)
Excessive grooming
1/60 (2)
3.2 | Clinicopathological findings
Complete blood cell count findings were available for 57 (95%) of the 60 cats. The most common abnormalities were eosinophilia which was present in of the 57 cases-the reference intervals varied between the clinics and the eosinophilia was mostly moderate to severe with the median percentage above RI 243.3 (IQR, 188.7-465.2); however, not all medical records contained actual eosinophil numbers (some records only mentioned eosinophilia being present). Second most common hematological abnormality was anemia in 16 (28%). Less common findings included neutrophilia 10/57 (18%), monocytosis 7/57 (12%), lymphocytosis 5/57 (9%), basophilia 3/57 (5%), and neutropenia 1/57 (2%). Serum biochemistry findings were available for 58 (97%) of the 60 cats. The most common abnormality was hypoalbuminemia which was seen in ( ) of cases. The reference intervals varied between the clinics and the hypoalbuminemia was mostly mild with the median percentage below RI 91.3 (IQR, 83.7-96.2). The second most common abnormality was hyperglobulinemia seen in 8/58 (14%), followed by hypocholesterolemia in 6/58 (10%) and total hypocalcemia 6/58 (10%); with 4/6 (67%) hypocalcemic cats having normal albumin levels. Serum cobalamin was measured in 11 (18%) of the 60 cats and was normal in all of them, although it was at the low end of the reference interval in 1 cat (278; reference interval [RI], ). Folate measurement was available in cats and was abnormally high in cats.
3.3 | Diagnostic imaging
Abdominal imaging was performed in all cats; however, ultrasound images were only available for 30 (50%) of the 60 cats; the others had abdominal radiographs performed and ultrasound reports was part of the medical records, but ultrasound images were not available for review. In 25/30 (83%) of the cats the mass originated from the stomach or intestines. Of the other 5 cases, 3 (10%) affected abdominal
lymph nodes and involved the mesentery (7%). The majority of gastrointestinal masses were associated with loss of the intestinal layering (Figure 1), symmetrical or asymmetrical circumferential thickening, eccentric growth and a heterogeneously mixed wall echogenicity which had hyperechoic areas and possible ulceration. In 6 (20%) of the 30 cases, these masses were reported to be associated with altered rather than lost layering. Hyperechoic areas were noted in of the gastric or intestinal cases, and of all cases, whereas thickening of the muscularis layer in the small intestine was seen in of them. Peritoneal changes were reported in 22/30 (73%) of the cats, of which had hyperechoic peritoneum and had a peritoneal effusion (the amount of effusion was not always reported in the medical records). None of the lesions showed ultrasonographic findings compatible with gastrointestinal perforation. Enlarged lymph nodes were present in 27 (90%) of the 30 cases where ultrasound images were available; the most commonly affected lymph nodes were ileocolic in , followed by pancreaticoduodenal , and mesenteric, . For the rest of the cases ( 30 cats), abdominal ultrasound images were not available to assess the lymph nodes further.
3.4 | Location of the mass
The most common location of the masses (Figure 2) was small intestine in of the 60 cases, including the proximal duodenum 15/60 (25%; Supplementary Figure 1), jejunum 2/60 (3%), ileum 2/60 , and the stomach in , followed by the ileocolic junction 9/60 (15%), colon 6/60 (10%), lymph node 5/60 (8%), and mesentery in 5/60 (8%; Supplementary Figure 2). Most of the cats, 51/60 ( ) had only 1 mass; however, in ( ) of cats a mass was present in more than 1 location. The additional masses most commonly involved the mesentery and surrounding lymph nodes in 4/9 (44%); in 3 cats the additional masses affected the stomach and proximal duodenum, in 1 cat the mesentery and jejunum, and in 1 cat the
FIGURE 1 Ultrasonographic image of a mass at the level of the ileocolic junction (white arrow). The mass shows loss of layering, circumferential thickening and eccentric growth. The wall is heterogeneously mixed in echogenicity because of hyperechoic areas. The surrounding peritoneum is hyperechoic (asterisk).
FIGURE 2 Common locations of the masses found in cats with gastrointestinal sclerosing fibroplasia in this study. Y-axis represents the % of masses in the location.
proximal duodenum and jejunum. Of note, 1 cat had an eosinophilic skin mass at the same time as GESF. One cat had a mass in the ileocolic junction removed, then presented 7 months later with a mesenteric mass. Another cat had a mass removed from its colon, then presented 2 years later with a pyloric mass, which was also removed, the represented 3 years after that with another pyloric mass. In both of these cases, the cats were not administered corticosteroid therapy until after surgical resection of the second or third mass, respectively and all of the masses in both cats were consistent with GESF on histopathology.
3.5 | Cytology
Cytology of fine-needle aspirates (FNA) of the mass was performed in of the 60 cats and showed eosinophilic inflammation in 10/22 (45%) of cases. In other cases, the cytology was either non diagnostic, or showed necrosis or mixed inflammation. Cytology on FNA of abdominal lymph nodes was performed 22/60 (37%) of cats but was mostly nondiagnostic or showed reactive lymph nodes; eosinophils were only reported in 8/22 (36%) of cases.
3.6 | Surgery/biopsy
The mass was removed surgically in 22 (37%) of the 60 cats with complete microscopic excision achieved in 18/22 (82%) of the cats. In the remaining 29 (76%) of the 38 cases had a surgical biopsy performed, whereas the diagnosis was achieved on endoscopic biopsies in the other 9 (24%) cats. The cats that had endoscopic biopsies, the mass was located in proximal duodenum in 5/9 (56%) or stomach in 4/9 (44%) of the cases. Surgical complications were reported in 5/22 ( ) of cats, with of the cats developing anemia and requiring transfusion (14% of the cats that had surgery to remove or biopsy a GESF mass); all 3 of these cats were anemic on presentation with HTC on presentation being 18, 20 and respectively. One cat developed septic peritonitis requiring a second surgery, 1 cat became
anorexic, 1 cat developed chyloabdomen, which has resolved with treatment, and 1 cat developed persistent fecal incontinent after surgical resection of a colonic mass.
3.7 | Histopathology and culture
In all 60 cats, the mass was confirmed as GESF on histopathology (Figures 3 and 4). Of the 22 ( ) out of 60 cases in which the mass was surgically removed, the lesion was completely excised in 13 (59%) cats. In 19/60 (32%) of cats, intralesional bacteria were present on histopathology, and fungal organisms were detected in 1 cat (by positive periodic acid-Schiff [PAS] staining). Fluorescence in situ hybridization (FISH) was performed in 3 cats and showed Eubacteria in 1 cat and Eubacteria, Campylobacter jejuni, Salmonella species and Escherichia coli in the second cat and no invasive bacteria in the third cat. Bacterial culture was performed in 18/60 (30%) of cases; 4/18 were negative, whereas in the others the most common bacteria were E. coli (6/12; 50%), Staphylococcus species (6/12; 50%), Enterococcus species (4/12; 33%) and Streptococcus species (1/12; 8%) and Bacteroides fragilis (1/12; 8%;). It was not always clear if effusion or mass or swab of the tissue was cultured in some cats. The biopsy that was positive on PAS staining cultured Candida albicans as well as Enterococcus species and E. coli. In 34 (57%) of the 60 cases, additional organs were also biopsied; these included lymph nodes (28/34; 82%), stomach (5/34; 15%), liver (4/34; 12%), duodenum (2/34; 6%), jejunum (1/34; 3%), and omentum (1/34; 3%). In 12 (42%) of the 28 cases where lymph node histopathology was performed cases, results were consistent with GESF, as was the omentum in the 1 case where this site was biopsied.
3.8 | Treatment
Most cats 59/60 (98%) were treated with corticosteroids, although 1 cat was treated with antibiotics alone. All except for 1 of the cats that were administered corticosteroids were administered
FIGURE 3 Histological findings of the duodenal mass-the muscularis and submucosa are expanded by a discrete, sparsely cellular mass (*). Hematoxylin & eosin, magnification. Scale bar . Photo credit: Dr Allison Watson from Colorado State University.
FIGURE 4 Histological findings of the duodenal mass-the mass is composed of anastomosing trabeculae of sclerotic collagen separated by fibroblasts, macrophages, and small numbers of eosinophils and mast cells. Hematoxylin & eosin, magnification. Scale bar . Photo credit: Dr Allison Watson from Colorado State University.
prednisolone once daily with a median dose of day (IQR, 1.0-2.0). The median time of cats to be administered corticosteroids was 23 (IQR, 10.5-49.0) days after first being presented. In 49 cats, the prednisolone dose was changed on with a median of 32 (IQR, 16.0-60.0) days after starting corticosteroid therapy, and in 13 cats, the prednisolone was discontinued; however, in 11 of these 13 cats, prednisolone had to be restarted at a median time of 114 (IQR, 36.0-366.0) days after discontinuation because of recurrence of clinical signs. The median time to the lowest dose of prednisolone was 369 (IQR, 195.0-841.0) days, with a
FIGURE 5 Kaplan-Meier plot of survival of cats that had a surgical resection of the mass and cats where the mass was biopsied only ( ). Tick marks represent censored cats. Green line is cats where mass was surgically removed, and blue line is cats where mass was not removed.
median lowest maintenance dose of 0.65 (IQR, ) mg/kg/day needed to control the clinical signs. The most common complications from corticosteroid treatment were hypertriglyceridemia in 5 cats. Hypertriglyceridemia was treated with a low-fat diet and fish oil in 1 cat, fish oil alone in 1 cat, with low fat diet, fish oil and fenofibrate in 1 cat, and no treatment in the remaining 2 cats, and the development of diabetes mellitus in 3 cats ( 2 of which went into diabetic remission on insulin therapy1 of these cats still remain on low dose [ day of prednisolone]). Secondary immunosuppressive agents (cyclosporin or chlorambucil) were prescribed in 14 ( ) of the 60 cats and were discontinued in of those cats after a media of 80 (IQR, 64.5-236.3) days.
Antibiotics were prescribed for 43 (72%) of the 60 cats, with the most common antibiotics being penicillins ( ), fluoroquinolones (9/43; ), metronidazole (6/43; ), cephalosporins (5/43; ), and clindamycin ( ). The average duration of treatment with antibiotics was 34 days (range, 7-204).
Hydrolyzed or selected protein diets were advised in 37% (22/60) of cats; 41% (9/22) of the owners reported an improvement of clinical signs on hydrolyzed or selected protein diet, although 3 cats would not eat the diet.
3.9 | Survival
As of the 60 cats still being alive at the time of writing this publication, the median survival time cannot be estimated. Of the 7 cats that died or were euthanized, 4 cats because of poorly controlled GESF, 2 cats of pancreatic neoplasia and 1 cat died of causes unknown. There was no statistical difference between the survival of cats that had a surgical resection of the mass and cats where the mass was biopsied only ( ; Figure 5). There was no statistical difference between the survival of cats that had a complete resection with
clear margins confirmed by histopathology and cats with incomplete resection of the mass and cats where the mass was biopsied only ( ). There was also no statistical difference between the survival of cats that were treated with corticosteroids only vs secondary immunosuppressive agents ( ), nor between cats that were treated with antibiotics and cats that were not treated with antibiotics ( ).
4 | DISCUSSION
This presents the largest study of GESF in cats to date with cases collected internationally over a 15-year period. Previous studies had reported the GESF masses in cats to be associated most commonly with the stomach (often near the pylorus) or the intestines, and also affect the abdominal lymph nodes, the mesentery, and retroperitoneum. This is similar to the current study, where the most common location of the GESF masses in cats were the small intestine, stomach, ileocolic junction or colon, whereas in 16% of the cats the mass was associated with lymph nodes or mesentery. In 15% of the cats, GESF masses were present in more than 1 location; in 12 of the cases the local lymph nodes were also affected, and in 1 cat the omentum was involved, showing that this disease can affect a number of locations in each cat. Of note, 1 cat also had an eosinophilic skin mass at the same time as GESF-this has not been reported in cats with GESF; however, subcutaneous masses with eosinophilic infiltration have been reported, and a recent case report also described possible GESF-like disease outside the abdominal cavity, in medial retropharyngeal lymph node.
When looking at signalment, the median age of cats with GESF in this study was 5.4 years (range, 1.3-14.5), which is similar to the reported median age of 7 years, with a range of 2 to 11 years. Previously, male cats are reported to be more affected by GESF; however, this was not seen in this study. More than half (58%) of the cats in our study were pedigree cats, with Ragdolls comprising a quarter of the study cats; this is similar to another study that reported Ragdolls to be overrepresented. Other breeds commonly seen in the current study were Exotic Shorthair (10%) and Persian (8%) cats. It is unclear why pedigree cats appear to be predisposed to develop GESF, notably Ragdolls (25%) and Persian/Exotic cats (18%), and further studies, including genetic analysis, are needed to see if these breeds have a genetic predisposition to develop eosinophilic inflammation as a response to enteric antigens which is the likely cause of GESF. It is important to note that these are also breeds predisposed to feline infectious peritonitis (FIP) ; GESF and noneffusive FIP are both differential diagnoses of note for cats presenting with abdominal masses.
In the current study, the median duration of clinical signs was 90 days with most cats showing median of 3 clinical signs, with the most common being weight loss (60%), hyporexia/anorexia (55%), chronic vomiting (37%), lethargy (35%) and chronic diarrhea (27%), which is very similar to a previously reported study; however, they also reported excessive grooming in of cases which was only seen in of the cats in the current study. Palpation of an abdominal
mass is present in of the cats ; however, this was less common in the current study where a mass was only palpable in of the cats. The prevalence of pyrexia was similar to other studies, 15% vs
The most common bloodwork abnormality was peripheral eosinophilia, which was present in of the cats in the current study, which is similar to previous studies. Anemia was present in almost third of the cats in the current study, but is not reported. Hypoalbuminemia and hyperglobulinemia were the most common abnormalities, occurring in and of cats, respectively, which is less common than reported in and , respectively.
Large studies evaluating abdominal ultrasonography findings of cats with GESF are lacking to date; however, a study did report 5 cats that had solitary mass with mural thickening and loss of layering in the stomach, duodenum, jejunum, and colon. In the current study, abdominal ultrasound images were available for review in 50% of the cats, with most cases (83%) showing that the majority of the masses originated from the stomach or intestines. These masses were associated with loss of the intestinal layering and circumferential thickening in most cases, although in there was alteration of the layering rather than loss of it. Enlarged local lymph nodes were present in of the cases, and peritoneal changes in , of which had a peritoneal effusion; however, none of the lesions showed ultrasonographic findings compatible with gastrointestinal perforation.
Intralesional bacteria were identified in of the cases overall (all of the ileocecocolic junction and colon lesions) in 1 study and in 69% of cats in another study using either culture or conventional light microscopy, special stains and FISH. In the current study, only of the cases had bacteria present on histopathology, and fungal organisms were detected in 1 cat; however, as 1 limitation of this retrospective study, infectious organisms might have been missed in some cats as FISH was only performed in 3 cats and bacterial culture was performed in only of the cats in this study. Even though bacteria are commonly associated with GESF in cats, fungal organisms are reported once, in a case report of GESF associated with phycomycetes.
The prognosis for cats with GESF is reported as variable, varying from guarded, to cats living for several years. Most cats surviving the perioperative period remained well for several years. In the current study, the median survival time could not be estimated as of the cats still alive at the time of writing this publication. This shows the importance of the correct diagnosis for cats with GESF, as many of these masses can be misdiagnosed as neoplasia, which usually carries a poor prognosis.
Cats being treated with surgery alone have a significantly shorter survival time than those cats treated with surgery and corticosteroids. Improved survival time is reported when prednisolone was included in the therapeutic regimen, regardless of whether or not cats also had surgery. In the current study, of the cats were administered corticosteroid therapy, so it is not possible to assess the survival time of the cats with surgery alone; however, there was no statistical difference between the survival of the cats that had their masses surgically resected and cats where their mass were only biopsied
including cats with complete resection with clear margins confirmed by histopathology.
Corticosteroids appear to be important in the treatment of cats with GESF. Reoccurrence of masses is reported when surgery was not followed by administration of corticosteroids. In the current study, 1 cat had a mass resected from the ileocolic junction but was not administered corticosteroid therapy, and re-presented 7 months later with a mesenteric mass. Another cat in this study was diagnosed with GESF in the colon, which was resected, then with a pyloric mass 2 years later, which was also resected, and another pyloric mass 3 years after that; whereas all of these GESF masses were surgically resected, corticosteroid therapy was not administered until after the resection of the third mass. There was no recurrence of abdominal masses in either of these cats after administering corticosteroid therapy for over 1.5 years. The indication to follow surgery with corticosteroid therapy is further supported by 13 cats where prednisolone was discontinued, of these had to have prednisolone restarted a median of 114 days after discontinuation because of recurrence of clinical signs. The median time to the lowest dose of prednisolone was 369 days, with a median lowest maintenance dose of day to control the clinical signs; however, as this is a retrospective study, some cats were lost to follow up and it is therefore unclear if prednisolone was tapered further in these cats.
The use of secondary immunosuppressive agents and antibiotics in cats with GESF is reported. In the current study there was no statistical difference between the survival of cats that were treated with corticosteroids only versus including secondary immunosuppressive agents, regardless of whether or not antibiotics were given.
Hydrolyzed or selected protein diets were tried in 37% of the cats in the current study, with of the owners reporting an improvement of clinical signs on these diets. This suggests diet modification as a possible treatment of cats with GESF. However, all of these cats were already being treated with corticosteroids.
ACKNOWLEDGMENT
No funding was received for this study. We thank all the owners for sharing the medical records of their cats, to all of the staff who were involved with the care of the cats in their clinics, and the Feline Gastrointestinal Eosinophilic Sclerosing Fibroplasia Support Group.
CONFLICT OF INTEREST DECLARATION
Authors declare no conflict of interest.
OFF-LABEL ANTIMICROBIAL DECLARATION
Authors declare no off-label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
Approved by the University of Edinburgh Ethics Review Committee (VERC Reference: 17.22).
HUMAN ETHICS APPROVAL DECLARATION
Authors declare human ethics approval was not needed for this study.
Craig L, Hardam E, Hertzke D, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia. Vet Pathol. 2009;46:63-70.
Linton M, Nimmo JS, Norris JM, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia: 13 cases and review of an emerging clinical entity. J Feline Med Surg. 2015;17:392-404.
Kambe N, Okabe R, Osada H, et al. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia limited to the mesentery. J Small Anim Pract. 2020;61:64-67.
Thieme ME, Olsen AM, Woolcock AD, Miller MA, Simons MC. Diagnosis and management of a case of retroperitoneal eosinophilic sclerosing fibroplasia in a cat. J Feline Med Surg Open Rep. 2019;5: 2055116919867178.
Zampieri B, Church ME, Walsh K, Lennon EM. Feline eosinophilic sclerosing fibroplasia-a characteristic inflammatory response in sites beyond the gastrointestinal tract: case report and proposed nomenclature. J Feline Med Surg Open Rep. 2022;8:2055 1169221117516.
Munday J, Martinez A, Soo M. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia mimicking metastatic neoplasia. N Z Vet J. 2014;62:356-360.
Gamble DA. Letters to the editor and rebuttal regarding the paper recently published in Veterinary and Comparative Oncology, ‘Feline intestinal sclerosing mast cell tumour: 50 cases (1997-2008) 2010; 8: 72-79’ by CHC Halsey, BE Powers and DA Kamstock. Letter to the editor# 2. Vet Comp Oncol. 2010;8:235-242.
Schulman FY, Lipscomb TP. Letters to the editor and rebuttal regarding the paper recently published in Veterinary and Comparative Oncology, ‘Feline intestinal sclerosing mast cell tumour: 50 cases (1997-2008) 2010; 8: 72-79’ by C. H. C. Halsey, B. E. Powers and D. A. Kamstock. Letter to the editor #1. Vet Comp Oncol. 2010;8:234235. author reply 236-242.
Porras N, Rebollada-Merino A, Rodríguez-Franco F, Calvo-Ibbitson A, Rodríguez-Bertos A. Feline gastrointestinal eosinophilic sclerosing fibroplasia-extracellular matrix proteins and TGF- immunoexpression. Vet Sci. 2022;9:291.
Cho M-J, Kim M-C, Seo K-W. Feline gastrointestinal eosinophilic sclerosing fibroplasia in a Bengal cat. J Vet Clin. 2017;34:481-483.
Montenegro NE, Castro DAR, López PAB, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia. Braz J Vet Pathol. 2022;15: 57-61.
Suzuki M, Onchi M, Ozaki M. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia. J Toxicol Pathol. 2013;26:51-53.
Agulla , Díaz-Regañón , García-Sancho , et al. Remission of feline gastrointestinal eosinophilic sclerosing fibroplasia in a cat treated with corticotherapy. Pakistan Vet J. 2021;41:309-312.
Kim M-s, Kim K, Lee G-h, et al. Successful management of feline gastrointestinal eosinophilic sclerosing fibroplasia with mycophenolate mofetil and prednisolone following surgical resection in a cat. Thai Vet Med. 2021;51:773-777.
Takao K, Saitoh S, Nibe K. Surgical treatment of feline gastrointestinal eosinophilic sclerosing fibroplasia in a cat. Jpn J Vet Anesth Surg. 2015;46:81-82.
Weissman A, Penninck D, Webster C, Hecht S, Keating J, Craig LE. Ultrasonographic and clinicopathological features of feline gastrointestinal eosinophilic sclerosing fibroplasia in four cats. J Feline Med Surg. 2013;15:148-154.
Brloznik M, Faraguna S, Goc M, Svara T. Recurrent feline gastrointestinal eosinophilic sclerosing fibroplasia and presumptive eosinophilic
cystitis in a domestic short-haired cat: a case report. Vet Med. 2017; 62:295-300.
Ozaki K, Yamagami T, Nomura K, Haritani M, Tsutsumi Y, Narama I. Abscess-forming inflammatory granulation tissue with Gram-positive cocci and prominent eosinophil infiltration in cats: possible infection of methicillin-resistant Staphylococcus. Vet Pathol. 2003;40:283-287.
Pesteanu-Somogyi LD, Radzai C, Pressler BM. Prevalence of feline infectious peritonitis in specific cat breeds. J Feline Med Surg. 2006;8: 1-5.
Grau-Roma L, Galindo-Cardiel I, Isidoro-Ayza M, Fernández M, Majó N. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia associated with phycomycetes. J Comp Pathol. 2014;151: 318-321.
SUPPORTING INFORMATION
Additional supporting information can be found online in the Supporting Information section at the end of this article.
How to cite this article: Černá P, Lopez-Jimenez C, Fukushima K, et al. Clinicopathological findings, treatment, and outcome in 60 cats with gastrointestinal eosinophilic sclerosing fibroplasia. J Vet Intern Med. 2024;1-8. doi:10. 1111/jvim. 16992