انتشار التهاب المفاصل العظمي الشعاعي في الأطراف والعلامات السريرية المرتبطة به في الكلاب الصغيرة Prevalence of radiographic appendicular osteoarthritis and associated clinical signs in young dogs
هدفت هذه الدراسة إلى تحديد انتشار التهاب المفاصل العظمي (OA) والعلامات السريرية المرتبطة به في الكلاب الصغيرة. تم الاتصال بأصحاب الكلاب الذين تتراوح أعمارهم بين 8 أشهر و4 سنوات من عيادة واحدة، بشكل عشوائي، للمشاركة في فحص صحي عام. تم إجراء الفحوصات السريرية والعظمية. تم تقييم كل مفصل من حيث ردود الفعل للألم (0-4). تم إجراء أشعة سينية عمودية لجميع المفاصل تحت التخدير. تم تقييم كل مفصل من حيث شدة التهاب المفاصل العظمي الإشعاعي (rOA) على مقياس من 11 نقطة. تم تعريف التهاب المفاصل العظمي السريري (cOA) على أنه تداخل بين rOA وألم المفصل فيمشترك. أكمل المالكوناستبيانات. وافق أصحاب 123 كلبًا على المشاركة. بشكل عام، (49/123) من الكلاب كانت تعاني من التهاب المفاصل الروماتويديمشترك، و أو كان لدى الكلاب التهاب المفاصل المزمن، اعتمادًا على قيمة القطع لألم المفاصل؛ معتدل (2) أو خفيف (1)، على التوالي. لاحظ أصحاب الكلاب المصابة بالتهاب المفاصل المزمن علامات ضعف في حوالي من الحالات. كان هناك كلبان فقط يعانيان من التهاب المفاصل التنكسي (cOA) يتلقيان إدارة ألم التهاب المفاصل. كانت المفاصل الأكثر تأثراً بترتيب تنازلي من حيث التكرار هي الكوع، الورك، الكاحل، والركبة. التهاب المفاصل التنكسي المرئي بالأشعة السينية شائع في الكلاب الصغيرة، والكلاب التي تعاني من التهاب المفاصل التنكسي (rOA) كانت تعاني من التهاب المفاصل التنكسي (cOA). ومع ذلك، يبدو أن ألم التهاب المفاصل التنكسي (OA) غير مشخص بشكل كافٍ وغير معالج بشكل كافٍ في الكلاب الصغيرة.
الملخص
لم يتم إجراء دراسات شاملة ومُستقبلية حول انتشار التهاب المفاصل العظمي (OA) في جميع أنحاء الهيكل العظمي، وتقتصر التقديرات الحالية لانتشار التهاب المفاصل العظمي على الكلاب الأكبر سناً. التقدير الأكثر شيوعاً لعدد الكلاب التي تظهر عليها علامات سريرية مرتبطة بالتهاب المفاصل العظمي هو ‘ من السكانالتقدير لـيأتي من منشور عام 1997 الذي أشار إلى بيانات مسح فايزر المتعلقة بالممارسات العامةاستطلاع حول القبول في كليات الطب البيطري الأمريكية على مدى فترة 10 سنوات (1980 إلى 1989)، باستخدام التشخيصات المدخلة في السجلات الطبية، وجد أنمن بين جميع المرضى، تأثر عدد منهم باضطراب في الجهاز العضلي الهيكلي، وبشكل عام تأثرت بمرض المفاصل التنكسي للهيكل العظمي الطرفي. ومع ذلك، قد لا تعكس البيانات من المستشفيات التعليمية البيطرية الممارسة العامة. وقد قدرت الدراسات السابقة أن انتشار التهاب المفاصل التنكسي في المفاصل الطرفية والألم المرتبط به على مدار العام كان في المملكة المتحدة و في الولايات المتحدة في الكلاب من جميع الأعمار التي تتردد على عيادات الرعاية الأولية. في المقابل، مؤخرًا، استخدم الباحثون قائمة فحص في الممارسات العامة، ووجدوا من الكلاب التي تتوجه إلى العيادات الأولى (في الولايات المتحدة) كان لديها تشخيص مؤكد (الأشعة السينية والعلامات السريرية) أو مفترض (العلامات السريرية؛ لم يتم أخذ الأشعة السينية). هذا تقريبًا ضعف التقدير الأكثر استخدامًا من سكان الكلاب. على الرغم من عدم وجود بيانات قوية وشاملة ومباشرة حول الانتشار في الوقت الحالي، فإن التهاب المفاصل التنكسي في الكلاب من المحتمل أن يكون مرضًا شائعًا جدًا.
على الرغم من المعلومات الجديدة الأخيرة، فإن انتشار العلامات السريرية المرتبطة بالتهاب المفاصل التنكسي في الكلاب الصغيرة غير معروف تمامًا. هذه المعلومات ضرورية لأن التهاب المفاصل التنكسي يُعتقد أنه يبدأ بشكل أساسي بسبب التطور.
مرض في الكلاب، وبالتالي يمكن القول إنها مرض يصيب الكلاب الصغيرة، وعلى الرغم من عدم استكشافه، قد يُحسن التدخل المبكر في هذه المرحلة النتائج لاحقًا. ومع ذلك، إذا لم يتم التعرف على التهاب المفاصل (OA) في الكلاب الصغيرة، فإن فرصة التدخل المبكر تضيع. حاليًا، يتم تشخيص معظم حالات التهاب المفاصل في الكلاب في وقت لاحق من حياة الكلب عندما تكون العلامات السريرية أكثر وضوحًا. كان هدف هذه الدراسة هو تحديد انتشار كل من التهاب المفاصل العظمي الإشعاعي، والألم المرتبط بالتهاب المفاصل العظمي (مجموعة التهاب المفاصل العظمي الإشعاعي والألم المفصلي القابل للاكتشاف) في الكلاب التي تقل أعمارها عن 4 سنوات.
النتائج
تم الاتصال بـ 320 مالكًا، ووافق مالكو 123 كلبًا من 40 سلالة مختلفة على المشاركة في الدراسة. كان العدد النهائي للكلاب في كل فئة عمرية هو 25 و26 و30 و42 على التوالي. عبر جميع الكلاب الـ 123، كان المتوسط (العمر، وزن الجسم، ودرجة حالة الجسم كانتأشهر،، و “، على التوالي. كان هناك 16 كلبًا ذكراً غير مختون، و53 كلبًا ذكراً مختونًا؛ 6 كلاب إناث غير مختونة، و48 كلبًا إناثًا مختونة (الملف التكميلي 1). كانت السلالات الأكثر شيوعًا هي المختلطة (لابرادور ريتريفر ) و كلب ستافوردشاير الأمريكي ( (للحصول على القائمة الكاملة للسلالات، انظر الملف التكميلي 2).
تم تصنيف جميع الكلاب باستخدام أداة تصنيف التهاب المفاصل العظمي للكلاب (COAST). تقريبًامن الكلاب كانت في مرحلة ما قبل السريرية/لا ألم في المفاصل (مرحلة COASTالكلاب ومرحلة الساحل ). البقية تم تصنيفها كمرحلة COAST 2 (70/123)، 3 (27/123) أو 4 (3/123) بسبب العلامات السريرية التي كانت مرتبطة بالتهاب المفاصل أو غير مرتبطة به.
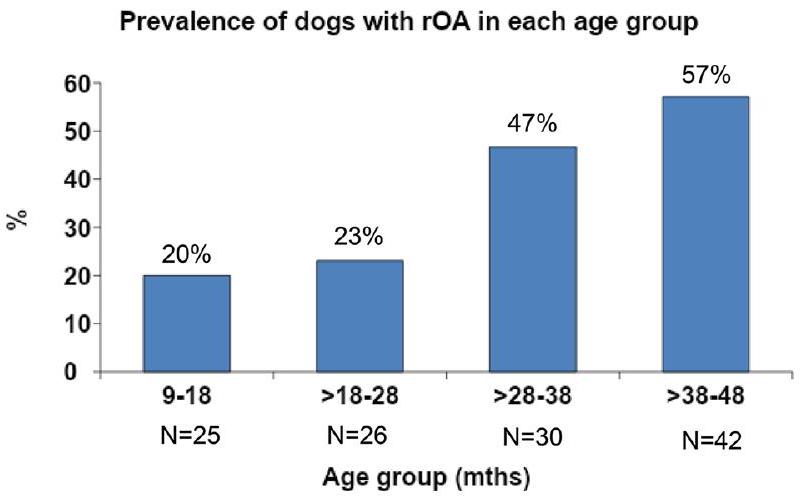
بشكل عام،من الكلاب (49/123) كانت تعاني من التهاب المفاصل الإشعاعي (rOA) في مفصل طرفي واحد على الأقل. يتم عرض انتشار التهاب المفاصل الإشعاعي في كل فئة عمرية في الشكل 1 والملف التكميلي 3. الفروقات في المعلومات الشخصية ودرجات مقاييس النتائج المبلغ عنها من قبل العملاء (CROMs) بين الكلاب المصابة بـ rOA والكلاب غير المصابة بـ rOA موضحة في الجدول 1.
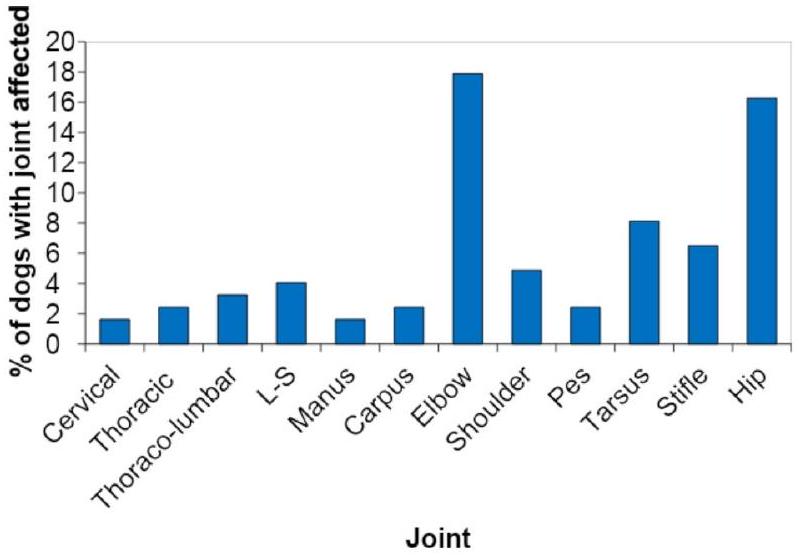
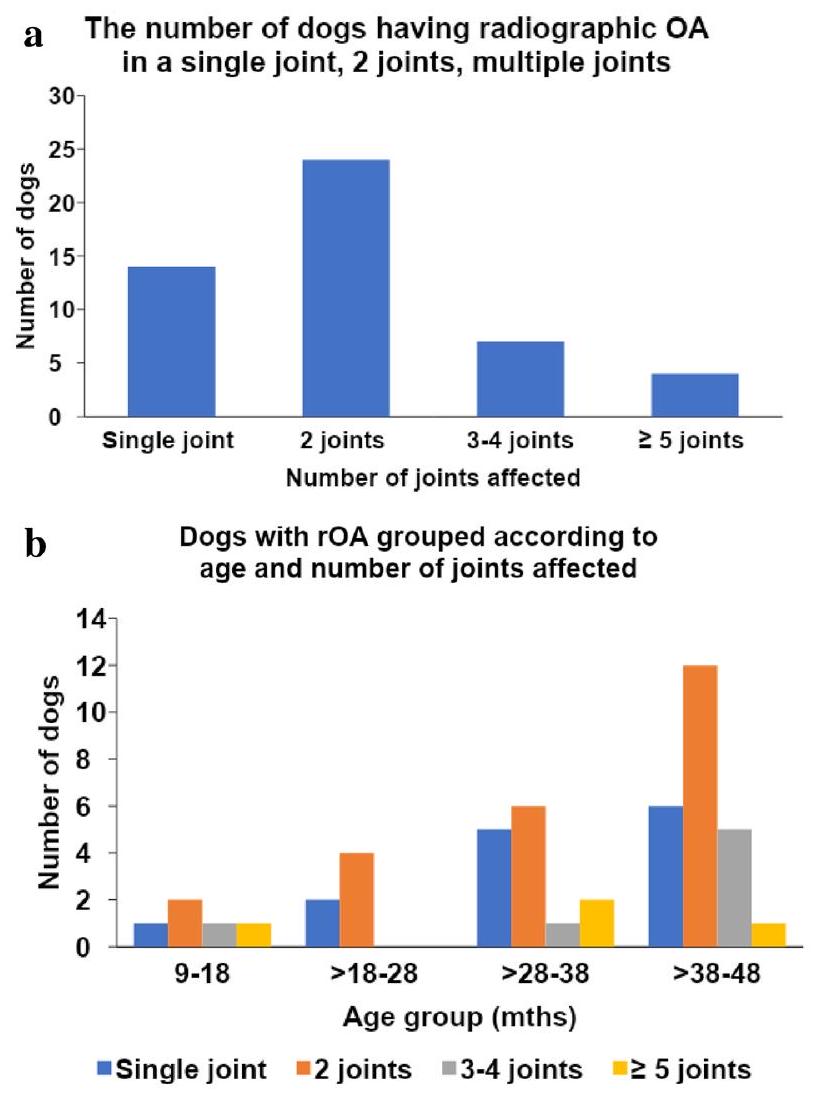
المفاصل المتأثرة شعاعياً بالترتيب التنازلي للتكرار كانت الكوع، الورك، الكاحل، والركبة (الشكل 2). بالإضافة إلى ذلك، يوضح الجدول 2 والشكل 3a عدد المفاصل الطرفية الفردية المتأثرة: تم العثور على التهاب المفاصل التنكسي في مفصل واحد في 14 كلباً؛ ومفصلين في 24 كلباً؛المفاصل في 7 كلاب؛المفاصل في 4 كلاب. الشكل 3ب يوضح انتشار الكلاب في كل فئة عمرية مع أعداد متفاوتة من المفاصل المتأثرة بالتهاب المفاصل.
كان هناك فرق كبير في العمر ووزن الجسم ودرجة حالة الجسم (BCS) بين الكلاب غير المصابة بـ rOA والكلاب المصابة بـ rOA (الجدول 1). ومع ذلك، زادت نسبة انتشار rOA مع تقدم العمر. ) ووزن الجسم ( )، حيث كانت هذين العاملين مرتبطين بشكل مستقل مع الروماتويد. لم يكن لBCS تأثير كبير على انتشار الروماتويد ( لدرجات 5 و6 و7 على التوالي). تم جدول عدد الكلاب التي تعاني من التهاب المفاصل الروماتويدي وغير الروماتويدي والتي كانت لديها عوامل خطر للإصابة بالتهاب المفاصل في الملف التكميلي 4. كان لدى ثلاثة كلاب عاملان خطر وكان لديها التهاب المفاصل (السلالة ومؤشر كتلة الجسم).الكلب؛ السلالة والتعقيم المبكر، 2 كلب). العلاقة بين الدرجة الشعاعية الإجمالية والعمر موضحة في الملف التكميلي 5.
تم تحديد اثنين وعشرين كلبًا من سلالة الألعاب/السلالات الصغيرة في الدراسة، وكان خمسة منهم يعانون من التهاب المفاصل التنكسي (rOA). ). تم تجميع معلومات أكثر تفصيلاً عن الكلاب من سلالة الألعاب/السلالات الصغيرة المصابة بالتهاب المفاصل في الملف التكميلي 6 . اعتبرنا الكلاب من سلالة الألعاب/السلالات الصغيرة إذا كانت من سلالة مدرجة على موقع نادي الكلاب الأمريكي كـ “كلاب سلالة الألعاب/السلالات الصغيرة” ولكننا شملنا أيضًا الكلاب المختلطة ذات الوزن الجسماني ( 14 كجم ) كـ ‘سلالات صغيرة’ (للحصول على القائمة الكاملة لسلالات الألعاب/السلالات الصغيرة، انظر الملف التكميلي 7).
فيما يتعلق بانتشار الألم المرتبط بالتهاب المفاصل العظمي (‘التهاب المفاصل العظمي السريري’، cOA)،من الكلاب (29/123) كانت تعاني من cOA باستخدام حد قطعلألم المفاصل (ألم خفيف أو أكثر) (المحدد cOA1)؛ ومن الكلاب (20/123) كانت تعاني من cOA باستخدام حد قطعلألم المفاصل (ألم معتدل أو أكبر) في مفصل واحد على الأقل مع التهاب المفاصل التنكسي (انظر الجداول 3 و 4) (المعروف باسم cOA2).
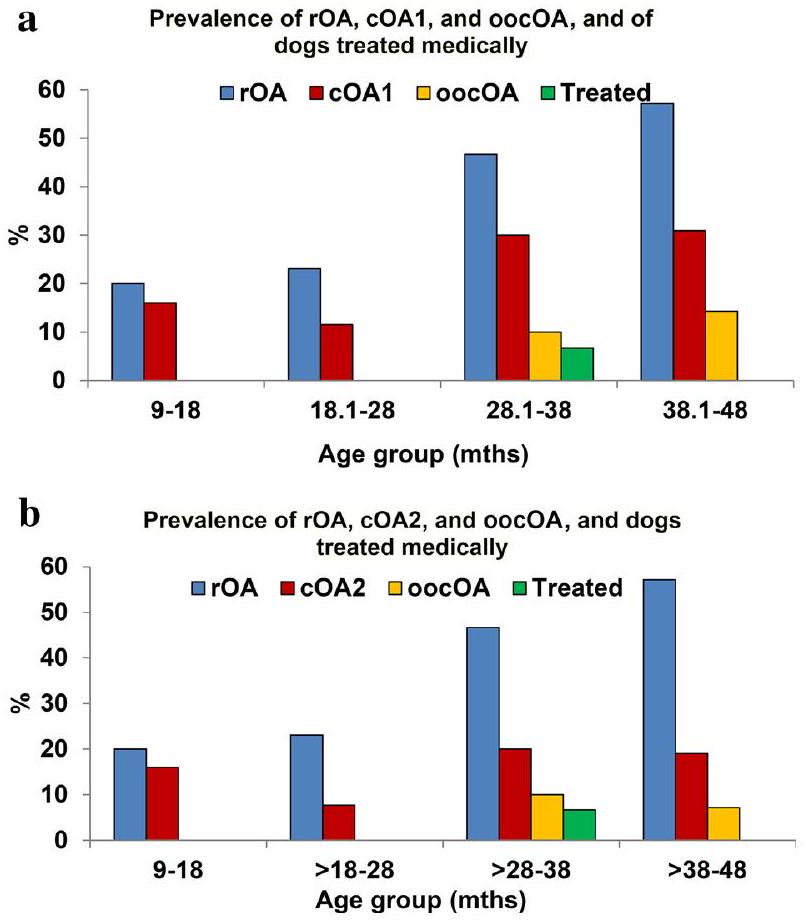
استنادًا إلى درجات مالكي الكلاب في دراسة التهاب المفاصل العظمي في الكلاب (LOAD)، لاحظ مالكو الكلاب المصابة بالتهاب المفاصل المزمن علامات على وجود ضعف فيلـ cOA1، ولـ cOA2، ولكن فقط 2 منهم (أو 2/6) تم علاجهم طبيًا من التهاب المفاصل التنكسي عند وقت تقييم الفحص الصحي (المعروف باسم ‘التهاب المفاصل التنكسي الملاحظ من قبل المالك، oocOA). يتم عرض انتشار rOA و cOA1 و cOA2 و oocOA في كل فئة عمرية في الجداول 3 و 4، ورسمياً في الشكل 4a و 4b.
تم إدراج الأمراض العظمية الأخرى التي تم اكتشافها بالأشعة في الملف التكميلي 8.
الشكل 1. رسم بياني يوضح انتشار الكلاب المصابة بالتهاب المفاصل الإشعاعي (rOA) في كل مجموعة. زاد انتشار rOA مع تقدم العمر. بشكل عام، كان انتشار rOA ( ).
روا (49 كلبًا)
غير rOA (74 كلبًا)
-قيمة
عمر
(37.0، 13.0-49.0)
(24.5، 9.0-49.0)
<0.001
جنس
ذكر: 4، أنثى: 3، متوسط: 22، عائلة: 20
ذكر: 12، أنثى: 3، MC: 31، FS: 28
0.57
سلالة
مختلط، لابرادور
مختلط، لابرادور
0.11
وزن الجسم
(27.4، 4.1-67.0)
(23.3، 3.8-42.9)
0.003
BCS (1-9)
(5, 4-7)
(5, 4-7)
0.017
CBPI PSS
(0، 0-4.75)
(0، 0-2.75)
<0.001
CBPI PIS
(0، 0-4.14)
(0، 0-1.14)
0.002
تحميل
(5، 0-19)
(3، 0-17)
0.011
سنو ر
(2.9، 1-8)
(2.4، 1.4-5.4)
0.054
ساحل
(3، 2-4)
(2، 0-4)
<0.001
إجمالي درجة OA
(4، 1-24)
0
<0.001
الجدول 1. المتوسطقيم SD (الوسيط، النطاق) للسمات وقياسات النتائج المبلغ عنها من قبل العملاء بين الكلاب التي تعاني من التهاب المفاصل الإشعاعي (rOA) وتلك التي لا تعاني منهذكرأنثىمخصي ذكرأنثى مُعقمةالتهاب المفاصل الإشعاعي؛ درجة حالة الجسم BCS؛ قائمة الألم القصيرة للكلاب CBPI؛ درجة شدة الألم PSS؛ درجة تأثير الألم PIS؛ التهاب المفاصل في الكلاب في ليفربول LOAD؛ تقييم النوم والقلق الليلي SNoRE؛ أداة تصنيف التهاب المفاصل في الكلاب COAST. مهم إذا (مُعَزَّز). لم يقم المالك بملء SNoRE لأن الكلب ينام في الخارج (كلب OA).
الشكل 2. يوضح هذا الشكل انتشار التهاب المفاصل الإشعاعي (rOA) عبر المفاصل. كانت المفاصل الأكثر تأثراً بالترتيب هي الكوع، الورك، الكاحل، والركبة.
فئة العمر (بالأشهر)
طبيعي (لا يوجد rOA/DJD)
التهاب المفاصل الروماتويدي المفصلي الأحادي
التهاب المفاصل التنكسي الثنائي
2 مفاصل مع rOA (أنواع مفاصل مختلفة)
3-4 مفاصل مع rOA
المفاصل مع rOA
التنكّس المفصلي في العمود الفقري فقط
9-18
19
1
1
1
1
1
1
> 18-28
١٨
2
٣
1
0
0
٢
>28-38
15
٥
٤
2
1
2
1
>38-48
17
٦
10
2
٥
1
1
إجمالي
69
14
١٨
٦
٧
٤
٥
الجدول 2. عدد الكلاب التي تعاني من التهاب المفاصل العظمي الشعاعي (rOA) في مفصل واحد، مفاصل ثنائية، مفصلين (مختلفين)، مفاصل متعددة، وفقط العمود الفقري. التهاب المفاصل العظمي الشعاعي في مفصل واحد: التهاب المفاصل العظمي الشعاعي في موقع مفصل واحد وفقط على جانب واحد (أحادي الجانب) (مثل التهاب المفاصل العظمي في الكوع الأيسر). ثنائي الجانب: كان لدى الكلب التهاب المفاصل العظمي الشعاعي في نوع مفصل واحد وكان لديه التهاب المفاصل العظمي الشعاعي في كلا المفصلين الأيسر والأيمن (مثل الوركين الثنائيين). التهاب المفاصل العظمي الشعاعي في مفصلين: كان لدى الكلب التهاب المفاصل العظمي الشعاعي في مفصلين مختلفين (بدون مرض ثنائي الجانب؛ مثل الكوع الأيمن والورك الأيمن). التهاب المفاصل العظمي الشعاعي في 3-4 مفاصل: كان لدى الكلب التهاب المفاصل العظمي الشعاعي في 3-4 مفاصل (مثل الأكواع والوركين).التهاب المفاصل الروماتويدي: كان لدى الكلب التهاب المفاصل الروماتويدي في 5 مفاصل أو أكثر (مثل المرفقين، الوركين، والركبتين). فقط التهاب المفاصل التنكسي في العمود الفقري: كان لدى الكلب التهاب المفاصل التنكسي في العمود الفقري، ولكن لا يوجد التهاب مفاصل روماتويدي في المفاصل الطرفية.التهاب المفاصل العظمي الشعاعي؛مرض المفاصل التنكسي.
الشكل 3. (أ) يُظهر هذا الشكل عدد الكلاب التي تعاني من التهاب المفاصل العظمي الشعاعي (rOA) في مفصل واحد، ومفصلين، ومفاصل متعددة. (ب) يُظهر هذا الشكل عدد الكلاب التي تعاني من rOA في مفصل واحد، ومفصلين، ومفاصل متعددة في كل فئة عمرية.
فئة العمر (بالأشهر)
إجمالي عدد الكلاب في المجموعة
عدد الكلاب التي تعاني من التهاب المفاصل وألم المفاصل (cOA1)
الكلاب التي تعاني من التهاب المفاصل السريرية وLOAD(oocOA)
الكلاب التي تعاني من التهاب المفاصل السريرية وLOAD < 10
الانتشار العام لـ oocOA (%) من التهاب المفاصل السريرية وعلامات ألم التهاب المفاصل التي اكتشفها المالك (%)
9-18
٢٥
٤
0
٤
0.0
>18-28
26
٣
0
٣
0.0
>28-
30
9
٣
٦
10.0
>38-48
42
١٣
٦
٧
14.3
إجمالي
123
٢٩
9
20
7.3
الجدول 3. انتشار OA 1 و oocOA في كل فئة عمرية (يتم تعريف oocOA على أنه يوجد تداخل بين OA الشعاعي وألم المفاصل الخفيف أو الأكبر (درجة الألم ) في نفس المفصل، ودرجة التحميل من ). OA التهاب المفاصل العظمي، LOAD التهاب المفاصل العظمي في الكلاب في ليفربول.
فئة العمر (بالأشهر)
إجمالي عدد الكلاب في المجموعة
عدد الكلاب التي تعاني من التهاب المفاصل وألم المفاصل (cOA2)
الكلاب التي تعاني من التهاب المفاصل السريرية وLOAD(oocOA)
الكلاب التي تعاني من التهاب المفاصل السريرية وLOAD < 10
الانتشار العام لـ oocOA (%) من التهاب المفاصل السريرية وعلامات ألم التهاب المفاصل التي اكتشفها المالك (%)
9-18
٢٥
٤
0
٤
0.0
>18-28
26
2
0
٢
0.0
>28-38
30
٦
٣
٣
10.0
>38-48
42
٨
٣
٥
7.1
إجمالي
123
20
٦
14
٤.٩
الجدول 4. انتشار cOA2 و oocOA في كل فئة عمرية، والتي تُعرف بوجود تداخل بين التهاب المفاصل الإشعاعي وألم المفاصل المعتدل أو الأكبر (درجة الألم ) في نفس المفصل، ودرجة التحميل المقدرة من قبل المالك OA التهاب المفاصل العظمي، LOAD التهاب المفاصل العظمي في الكلاب في ليفربول.
الشكل 4. (أ) يُظهر هذا الشكل انتشار التهاب المفاصل الإشعاعي (rOA) والتهاب المفاصل السريري (cOA1؛ ألم خفيف في المفاصل أو أكثر) والتهاب المفاصل السريري الملاحظ من قبل المالك (oocOA)، والكلاب التي تم علاجها طبيًا في كل مجموعة عمرية. يشير اللون الأزرق إلى انتشار الكلاب المصابة بـ rOA، واللون الأحمر يشير إلى انتشار cOA1، واللون الأصفر يشير إلى انتشار oocOA، واللون الأخضر يشير إلى انتشار الكلاب التي تتلقى أدوية مسكنة في وقت الفحص. (ب) يُظهر هذا الشكل انتشار التهاب المفاصل الإشعاعيOA السريرية (cOA2؛ ألم مفاصل معتدل أو أكثر)، وOA السريرية الملاحظة من قبل المالك (oocOA)، والكلاب التي تتلقى العلاج الطبي في كل فئة عمرية. الأزرق يشير إلى انتشار الكلاب المصابة بـ rOA، والأحمر يشير إلى انتشار cOA2، والأصفر يشير إلى انتشار oocOA، والأخضر يشير إلى انتشار الكلاب التي تتلقى أدوية مسكنة في وقت الفحص.
نقاش
أظهرت نتائج هذه الدراسة أن التهاب المفاصل التنكسي المرئي بالأشعة السينية شائع جدًا في الكلاب الصغيرة، وحواليمن الكلاب التي تعاني من التهاب المفاصل الروماتويدي كان لديها التهاب المفاصل مع ألم خفيف على الأقل (من الكلاب بشكل عام) في مفصل واحد أو أكثر وكان لديه التهاب المفاصل مع ألم معتدل على الأقل في مفصل واحد أو أكثربالنسبة للكلاب بشكل عام). في الكلاب التي تعاني من التهاب المفاصل المزمن، استنادًا إلى إجابات استبيانات التهاب المفاصل القياسية، حدد المالكون وجود علامات سريرية بشكل نادر نسبيًا (ثلث الكلاب) وكانت هناك قلة من الكلاب تتلقى علاجًا طبيًا.
لم تستكشف أي أعمال أخرى انتشار التهاب المفاصل التنكسي الشعاعي والألم المرتبط به في الكلاب الصغيرة. كما أن هناك عددًا قليلًا نسبيًا من الدراسات التي قيمت انتشار التهاب المفاصل التنكسي في الكلاب من أي عمر. أظهرت دراستان سابقتان أن التقدير السنوي لفترة انتشار التهاب المفاصل التنكسي في المفاصل الطرفية والعلامات السريرية المرتبطة به كان في المملكة المتحدة و في الولايات المتحدة في الكلاب من أي عمر التي تتردد على عيادات الرعاية الأولية. في الدراسة التي أُجريت في تم مراجعة بيانات السجلات الإلكترونية للمرضى من المرضى البيطريين لتحديد حالات التهاب المفاصل التنكسي المحتملة ضمن إطار زمني عينة مدته عام واحد من 1 يناير 2013 إلى 31 ديسمبر 2013. بشكل عام، تم تضمين 455,557 كلبًا (بمتوسط عمر 4.1 سنوات) في الدراسة وتم تحديد 16,437 حالة مرشحة لالتهاب المفاصل التنكسي. من بين هذه الحالات، تم مراجعة 6102 حالة بالتفصيل و4196 كلبًا (تم تأكيد ( ) كحالات التهاب المفاصل العظمي (تم تشخيصها حديثًا كالتهاب مفاصل عظمي أو أظهرت استمرار العلاج لتشخيص موجود مسبقًا خلال فترة الدراسة). على الرغم من عدم وجود وصف تفصيلي في التقرير من أكبر عيادة بيطرية عامة في الولايات المتحدة، تم مراجعة السجلات الطبية لأكثر من 2.5 مليون كلب تم العناية بهم في عام 2018 وتم حساب انتشار التهاب المفاصل العظمي السريري.. في دراسة مشابهة أخرى، تم جمع بيانات السجلات الإلكترونية للمرضى على 148,741 كلبًا حضروا عيادات الرعاية البيطرية الأولية، وتم اختيار 3884 كلبًا (بمتوسط عمر 4.8 سنوات) بشكل عشوائي للتحقيق في انتشار الاضطرابات. كانت فترة أخذ العينات للدراسة من 1 سبتمبر 2009 إلى 31 مارس 2013. أفاد المؤلفون أن انتشار مرض المفاصل التنكسية كانفي الكلاب، ومع ذلك، لم تستخدم الدراسة تعريف حالة صارم كما في دراسة انتشار التهاب المفاصل التنكسي المذكورة أعلاه في المملكة المتحدة. تختلف البيانات في الأدبيات بشكل كبير فيما يتعلق بعدد الكلاب التي تم تشخيصها بالتهاب المفاصل التنكسي السريري، لكنها عمومًا منخفضة بشكل مدهش عندما يؤخذ في الاعتبار أن التهاب المفاصل التنكسي وألم التهاب المفاصل التنكسي يزدادان مع التقدم في العمر، وتsuggest بياناتنا أنمن الكلاب الصغيرة تظهر بالفعل ألمًا معتدلاً أو أكثر في ما لا يقل عن مفصل واحد مع التهاب المفاصل التنكسي.
في هذه الدراسة، زاد إجمالي درجة الأشعة السينية لالتهاب المفاصل مع تقدم العمر. ميل خط الاتجاه ليس حادًا، لكن يبدو أن الدرجة تزداد بشكل رئيسي بسبب تأثر عدة مفاصل بالإضافة إلى تفاقم درجات التهاب المفاصل الفعلية (خلل تنسج الورك/الكوع). على الرغم من اختلاف الأنواع، إلا أن خط الاتجاه ليس مختلفًا كثيرًا عن ذلك الذي يُرى في القطط الأصغر سنًا.. في دراسة القطط، أصبح ميل خط الاتجاه أكثر حدة مع مرور الوقت. نحن نعترف نحن لا نعرف ما ستكون عليه درجات OA الإجمالية في الكلاب الأكبر سناً المصابة بـ OA، ومع ذلك، نتوقع زيادة مماثلة في عبء OA مع مرور الوقت (انظر الملف التكميلي 9).
تشير بياناتنا إلى انتشار مرتفع لالتهاب المفاصل التنكسي في الكلاب الصغيرة، وخاصة في الكوع والورك، مما يدعم assertion أن التهاب المفاصل التنكسي مدفوع أساسًا بمرض تطوري في الكلاب. ومع ذلك، لم نقم بمراجعة السجلات الطبية للتحقق مما إذا كانت المفاصل المتأثرة قد تم تشخيصها بمرض المفاصل التطوري. في دراستنا، كانت المفاصل الأكثر تأثرًا هي الكوع، الورك، الكاحل، والركبة. وهذا مشابه للنتائج السابقة في الكلاب الأكبر سنًا باستثناء الكاحل.ليس من الواضح لماذا لم يتم تحديد الكاحل كموقع لالتهاب المفاصل التنكسي في دراسة جونسون، ولكن السكان الذين تم تقييمهم تم اختيارهم من حالات أُرسلت إلى مستشفى تعليمي، مما قد يكون له تأثير على التحيز في الاختيار.
على الرغم من أن حجم العينة من الكلاب الصغيرة/التي تُستخدم كألعاب كان صغيرًا، يبدو أن التهاب المفاصل التنكسي (rOA) أقل شيوعًا في الكلاب الصغيرة/التي تُستخدم كألعاب، وأيضًا أن مفصل الورك هو الموقع الأكثر تأثرًا في السلالات الصغيرة.
حالياً، يتم تشخيص التهاب المفاصل السريرية (التهاب المفاصل مع ألم المفاصل المصاحب) في الكلاب في وقت لاحق بكثير مع أكثر منالكلاب المشخصة التي تتراوح أعمارها بين 8 إلى 13 عامًا. في الواقع، أفادت الأعمال السابقة أن متوسط عمر التشخيص الأول لالتهاب المفاصل العظمي كان 10.5 سنوات في الكلاب التي تحضر عيادات الطب البيطري الأساسية في المملكة المتحدة (كان متوسط عمر السكان الإجمالي 4.1 سنوات)إن الانتشار العالي للمرض يدعم نهج الفحص النشط للكلاب الأصغر سناً بهدف التدخل مبكراً وتقليل تأثير التهاب المفاصل وألم التهاب المفاصل المرتبط على مدى حياة الكلاب. وقد تم اقتراح مثل هذا النهج الاستباقي.لكن لم يتم تقييمه – أي أنه غير معروف ما إذا كانت التدخلات المبكرة من نوع ما (مثل إدارة الوزن الصارمة، أو النشاط البدني المنتظم منخفض التأثير) تقلل من تأثير التهاب المفاصل العظمي في وقت لاحق من الحياة.
في الدراسة الحالية، أبلغ أصحاب الكلاب الذين يعانون من التهاب المفاصل التنكسي السريري (OA) (استنادًا إلى إجاباتهم التي تم التقاطها عبر أداة LOAD) عن وجود علامات سريرية بشكل نادر نسبيًا – حيث أبلغ ثلث أصحاب الكلاب الذين يعانون من ألم التهاب المفاصل التنكسي القابل للاكتشاف وفقًا لتقييمات المؤلفين. ومن المثير للاهتمام، أنه بغض النظر عن الحدود المحددة، لم يبدو أن أصحاب الكلاب لاحظوا أي علامات لألم التهاب المفاصل التنكسي في الكلاب التي تتراوح أعمارها بين 9 و28 شهرًا (خلال هذه الفئة العمرية، تم اكتشاف 7 كلاب تعاني من ألم التهاب المفاصل التنكسي عند الفحص). هناك عدة تفسيرات محتملة لذلك، والتي ليست متعارضة: أولاً، قد لا تظهر هذه الكلاب الأصغر علامات ألم التهاب المفاصل التنكسي في بيئة المنزل (فهي تعمل بشكل جيد حقًا). ثانيًا، قد لا يتعرف أصحاب الكلاب على علامات ألم التهاب المفاصل التنكسي. تبدو علامات ألم المفاصل في الكلاب الأصغر سريريًا مختلفة عن تلك الموجودة في الكلاب الأكبر سنًا، مع التركيز على التكيفات الوظيفية بدلاً من الوظيفة المعطلة التي تكون أكثر وضوحًا في الكلاب الأكبر سنًا. على سبيل المثال، قد تتمكن الكلاب الصغيرة التي تعاني من التهاب المفاصل التنكسي في الورك والألم من الذهاب في نزهات دون تعب، وما زالت قادرة على الصعود والنزول على السلالم، وما زالت قادرة على اللعب، بينما قد تظهر الكلاب الأكبر سنًا التي تعاني من التهاب المفاصل التنكسي في الورك والألم ضعفًا واضحًا في أداء هذه الأنشطة. بالإضافة إلى ذلك، كانت العديد من الكلاب متأثرة بشكل ثنائي، وقد يكون من المرجح أن يتعرف أصحاب الكلاب على العلامات السريرية إذا كان طرف واحد فقط متأثرًا بدلاً من المفاصل الثنائية. تشير بياناتنا إلى أن المزيد من المفاصل تتأثر مع التقدم في العمر، وإذا تأثرت عدة مفاصل، فقد تكون العلامات السريرية أكثر وضوحًا لأصحاب الكلاب حيث يصبح تأثير ألم التهاب المفاصل التنكسي مرتفعًا. أخيرًا، قد لا تكون الاستبيانات المستخدمة (LOAD) وربما أدوات قياس أخرى (مثل CBPI) مثالية لتقييم علامات ألم التهاب المفاصل التنكسي في الكلاب الأصغر سنًا. قد تكون محاولات قياس ألم التهاب المفاصل التنكسي في الكلاب الصغيرة باستخدام أدوات القياس هذه معيبة بشكل أساسي لأن هذه الأدوات تم تطويرها في مجموعات الكلاب الأكبر سنًا. في الواقع، تم تطوير LOAD باستخدام كلاب بمتوسط أعمار 7.9 سنوات وتم تطوير CBPI باستخدام الكلاب معسنواتومع ذلك، في هذه الدراسة، حدد استخدام LOAD ثلث حالات cOA، مما يشير إلى أن الاستخدام الاستباقي لـ LOAD أو غيرها من CROMs يمكن أن يبرز نسبة جيدة من الكلاب الشابة المصابة بـ cOA، ويعمل كنقطة انطلاق للمحادثة ويسهل تعليم المالكين حول OA. حتى الآن، لم يكن هناك وصف شامل أو تحقيق في العلامات السلوكية لألم OA في الكلاب الشابة، ولم تكن هناك محاولات لتطوير استبيان للمالكين خصيصًا لهذه الفئة العمرية من الكلاب.
أشارت الدراسات السابقة إلى أنه بمجرد التعرف على التهاب المفاصل، يُعتبر من قبل الأطباء البيطريين والمالكين مهمًا بما يكفي لتقديم رعاية سريرية كبيرة، غالبًا ما تتضمن وصف مسكنات الألم على المدى الطويل والعديد من التدخلات العلاجية الإضافية، وزيارات متكررة للعيادة ومستويات عالية نسبيًا من الإحالة.. في الواقع، تم الإبلاغ عن إدارة خمسة وثمانين في المئة من حالات التهاب المفاصل العظمي باستخدام ما لا يقل عن نمط علاجي واحد (علاجات طبية أو جراحية) بعد تشخيص التهاب المفاصل العظمي (متوسط العمر 10.5 سنوات) وظل الغالبية منهم تحت الإدارة الطبيةمن المحتمل أن تكون الإدارة الطبية أقل تعقيدًا في وقت مبكر من مسار المرض. قد يؤدي العلاج الفعال المبكر لألم التهاب المفاصل osteoarthritis إلى تحسين السيطرة على ألم المفاصل والتأثيرات السلبية طويلة الأمد لألم المفاصل على أبعاد أخرى مثل الخصائص السلوكية، والحالات العاطفية، وقوة العضلات.. ومع ذلك، أظهرت دراستنا أن عددًا قليلًا جدًا من الكلاب تلقى إدارة طبية حتى بعد تشخيص التهاب المفاصل التنكسي السريري أو في الحالات التي اعترف فيها المالكون بوجود علامات سريرية. من المحتمل أن يبرز هذا الفرق في العلامات السريرية المرتبطة بالتهاب المفاصل التنكسي بين الكلاب الأصغر سنًا والكلاب الأكبر سنًا، وربما الاختلافات في مواقف كل من الأطباء البيطريين ومالكي الحيوانات الأليفة. على سبيل المثال، قد يكون المالكون مترددين في علاج كلابهم إذا لم يكن هناك ضعف واضح في الوظيفة. ومع ذلك، لم نحقق في أسباب ذلك، وهذه منطقة مهمة للبحث في المستقبل.
تمت ملاحظة فرق كبير بين الكلاب التي تعاني من التهاب المفاصل التنكسي والكلاب التي لا تعاني منه من حيث العمر ووزن الجسم ومؤشر حالة الجسم في هذه الدراسة. زادت نسبة التهاب المفاصل التنكسي المتكرر مع تقدم العمر وزيادة وزن الجسم، حيث كانت هذان العاملان مرتبطين بشكل مستقل بالتهاب المفاصل التنكسي المتكرر في هذه الدراسة. وقد تلخصت ورقة مراجعة حديثة عوامل الخطر لالتهاب المفاصل التنكسي في الكلاب في: الوراثة، السلالة، الشكل، العمر، الجنس/حالة التعقيم، ووزن الجسم.كما هو موضح في الجدول 1، لم نجد أي تأثير كبير للجنس أو السلالة على التهاب المفاصل الإشعاعي. قد يكون ذلك بسبب حجم العينة الصغيرة نسبيًا ووجود تنوع واسع من السلالات المختلفة، مما حال دون دراسة تأثير السلالة بالتفصيل. كانت الغالبية العظمى من الكلاب المسجلة في الدراسة مُعقمة، لذا لم يكن من الممكن تقييم تأثير هرمونات الجنس. وقد تم اقتراح أن الإخصاء المبكر يعد عامل خطر لأمراض المفاصل، على الرغم من التأثير المتغير عبر السلالات.لم نتمكن من جمع بيانات دقيقة حول وقت التعقيم لنتمكن من النظر في ذلك كعامل في حالة التهاب المفاصل. كان هناك فرق كبير في معظم مقاييس CROM بين الكلاب التي تعاني من التهاب المفاصل وتلك التي لا تعاني منه. ومع ذلك، كان الفرق صغيرًا وكانت درجات مقاييس CROM منخفضة نسبيًا حتى في الكلاب التي تعاني من التهاب المفاصل. قد يسلط هذا الضوء على البيان أعلاه بأن الملاك قد لا يكونون على دراية أو قد يواجهون صعوبة في التعرف على علامات ألم التهاب المفاصل في هذه الفئة العمرية من الكلاب، و/أو قد لا تكون مقاييس CROM الحالية مثالية لـ تقييم علامات التهاب المفاصل – الألم في الكلاب الأصغر سناً. علاوة على ذلك، فإن ‘قدرة’ مقاييس نطاق الحركة على اكتشاف الألم المرتبط بالتهاب المفاصل لم تتأثر على الأرجح بالعلاجات لألم التهاب المفاصل لأن عددًا قليلاً جدًا من الكلاب كانت تتلقى أي علاج لألم التهاب المفاصل.
أحد القيود المهمة في دراستنا هو أن التهاب المفاصل السريري (cOA) تم تعريفه بناءً على معايير ذاتية (فحص الطبيب البيطري)، وبالتالي قد تكون النتائج مختلفة إذا تم تكرار الدراسة من قبل باحثين مختلفين. لا يوجد حاليًا ‘معيار ذهبي’ لتشخيص أو تقييم شدة ألم التهاب المفاصل في الكلاب، ويجب القيام بعمل للنظر في قابلية تكرار أنواع التقييمات الذاتية التي استخدمناها. بالإضافة إلى ذلك، كانت المعايير لتحديد العلامات التي يلاحظها المالك لالتهاب المفاصل (LOAD) مستندة إلى معايير تم تطويرها في الكلاب الأكبر سنًا التي تعاني من ألم التهاب المفاصل، وبالتالي، قد لا تكون هذه المعايير ذات صلة بعلامات التهاب المفاصل في الكلاب الصغيرة. كانت هناك قيود إضافية في هذه الدراسة، حيث تم إجراؤها في ممارسة واحدة ومنطقة جغرافية واحدة، وبالتالي، قد لا يكون طيف العملاء والسلالات ممثلاً للجمهور العام/سكان الكلاب في الولايات المتحدة. على سبيل المثال، تشكل الكلاب الراعية الألمانيةمن سكان الكلاب في الولايات المتحدة، ولكن تم احتسابه فقطمن مجتمع دراستنا. تم اختيار ممارسة واحدة لهذه الدراسة الأولية لأسباب لوجستية تتعلق بجعل عينة السكان علمية. أردنا أخذ عينة بطريقة غير متحيزة – أي، الوصول إلى قاعدة البيانات الكاملة – واستخدام ممارسة واحدة يمكننا العمل معها بهذه الطريقة كان أفضل قرار متوازن علمياً مع التكاليف والتحديات اللوجستية للدخول إلى ممارسات متعددة.
توفر هذه الدراسة الأساس لزيادة الوعي بالتهاب المفاصل التنكسي (OA) بين الأطباء البيطريين ومالكي الكلاب مع إمكانية أن تؤدي إلى تدخل مبكر وتخفيف آثار التهاب المفاصل التنكسي – الألم في وقت لاحق من الحياة.
المواد والأساليب تصميم الدراسة
كانت الدراسة دراسة انتشار مقطعية لالتهاب المفاصل التنكسي الإشعاعي والسريري في عينة مصنفة من الكلاب الصغيرة التي تتراوح أعمارها بين 8 أشهر إلى 4 سنوات. تمت مراجعة لجنة رعاية واستخدام الحيوانات في جامعة ولاية نورث كارولينا (IACUC) والموافقة على جميع الطرق والإجراءات المستخدمة في الدراسة (IACUC#19-604-O). شملت هذه الموافقة أيضاً الموافقة الأخلاقية. وقع جميع مالكي الكلاب على نموذج موافقة مكتوب بعد شرح شفهي مفصل لبروتوكول الدراسة. تم تنفيذ جميع الطرق وفقاً للإرشادات واللوائح ذات الصلة. تم إجراء جميع الأعمال المتعلقة بالحيوانات وفقاً للإرشادات الموضحة في قانون رفاهية الحيوان لعام 1966 وقانون تمديد البحث الصحي لعام 1985. تم إجراء هذه الدراسة والإبلاغ عنها وفقاً لإرشادات ARRIVE.
التوظيف
تم تجميع الكلاب المسجلة في ممارسة واحدة (خدمة الرعاية الأولية لكلية الطب البيطري بجامعة ولاية نورث كارولينا) في 4 فئات عمرية (، و أشهر). بغض النظر عن الحالة الصحية، تم ترتيب الكلاب في كل فئة عمرية بشكل عشوائي باستخدام برنامج كمبيوتر (https://www.random.org). ثم تم الاتصال بمالكي أول 50 كلباً في كل مجموعة بالترتيب وطلب منهم زيارة المستشفى (مختبر أبحاث الألم بجامعة ولاية نورث كارولينا) لإجراء ‘فحص صحي’. تم تضمين الكلاب في كل مجموعة عمرية التي كان مالكوها مستعدين لمشاركتها في الدراسة. تم الاتصال بالمالكين مرتين عبر البريد الإلكتروني ومرة واحدة عبر مكالمة هاتفية. إذا لم يستجيبوا بعد هذه المحاولات، تم الاتصال بالمالك/الكلب التالي في التسلسل. بدأ التوظيف (والتقييمات – انظر أدناه) في منتصف فبراير 2020 واستمر حتى منتصف أغسطس 2021.
معايير الإدراج
لكي تكون مؤهلة للدراسة، كان يجب أن تتراوح أعمار الكلاب بين 8 أشهر و 4 سنوات في وقت التوظيف ووزن الجسم. بالإضافة إلى ذلك، كان يجب أن يكون المالكون مستعدين لفحص كلابهم وأخذ الأشعة تحت التخدير. لم تكن هناك معايير استبعاد محددة.
الفحص
تم إجراء الفحص البدني والعظام والعصبي، واختبارات الدم، وتحليل البول، وتم التقاط البيانات. بالنسبة لفحص العظام، تم فحص كل مفصل من كل طرف بواسطة طبيب بيطري ذو خبرة في تقييم التهاب المفاصل التنكسي في الكلاب (ME)، وتم تصنيف المفاصل حسب الألم، والقرقرة، والانصباب، والتثخين. تم اعتبار اليد والقدم كمنطقة مفصل واحدة لأغراض التقييم. كانت المفاصل الطرفية الأخرى التي تم تقييمها هي الرسغ، والمرفق، والكتف، والكاحل، والركبة، والورك. تم فحص أجزاء العمود الفقري وتصنيفها حسب الألم. تم تقييم الهيكل العظمي المحوري عن طريق تقسيم العمود الفقري إلى مناطق عنقية، وصدرية (T1-9)، وصدرية قطنية (T10-L6)، وقطنية عجزية. تراوحت درجات الألم من 0 إلى 4؛ تم استخدام هذه الدرجات لإنشاء درجة ألم إجمالية (مجموع درجات الألم الفردية لكل مفصل) مع نطاق منللهيكل العظمي الطرفي. تم تسجيل التقييمات للقرقرة، والانصباب، والتثخين، ومدى الحركة، ولكن لم يتم استخدامها في التحليل. تم تسجيل الدرجات على JESSE (الكلب) (الملف التكميلي 10).
قياسات النتائج المبلغ عنها من قبل العميل (CROMs)
تم استخدام CROMs كما تم وصفه سابقاً. لقد أظهرت مقياس التهاب المفاصل التنكسي في الكلاب (LOAD) ومخزون الألم القصير للكلاب (CBPI) أنهما مقياس صالح لتأثير التهاب المفاصل التنكسي – الألم في الكلاب. تم استخدام استبيان تقييم جودة النوم والقلق الليلي النسخة 2.0 (SnoRE) لجمع البيانات المتعلقة بجودة النوم. تم إكمال CROMs بواسطة مالك الكلب. بالنسبة لـ LOAD، تم حساب مجموع كل عنصر. بالنسبة لـ CBPI (درجات شدة الألم [PSS] ودرجات تداخل الألم [PIS]) وSNoRE، تم حساب متوسط كل عنصر.
الأشعة السينية
تم أخذ الأشعة تحت التخدير باستخدام مزيج من مادة أفيونية مع محفز ألفا-2، على سبيل المثال هيدروكودون وديكسمديتوميدين. ومع ذلك، تم تعديل اختيار الدواء والجرعة وفقاً لحالة صحة الكلب. تم أخذ صور عمودية لجميع المفاصل الطرفية ووجهات جانبية للعمود الفقري. لتقليل التعرض للإشعاع المؤين، حيثما كان ذلك مناسباً، تم تركيز الأشعة على منتصف الطرف أو جزء العمود الفقري لتقليل عدد التعرضات الفردية المستخدمة. تم تعيين مقياس تقييم رقمي إشعاعي لالتهاب المفاصل التنكسي حيثلم يتم تحديد أي شذوذ إشعاعي وأكثر حالات التهاب المفاصل التنكسي الإشعاعي شدة، لكل مفصل بناءً على وجود التغيرات الإشعاعية وشدتها العامة بناءً على المعلومات المبلغ عنها سابقاً. كانت الميزات الإشعاعية التي اعتبرت دالة على وجود التهاب المفاصل التنكسي الطرفي هي العظام الزائدة، والالتهابات العظمية، والتصلب، وتآكل العظام تحت الغضروف والأكياس. تم تقييم التغيرات التنكسية في كل جزء محوري باستخدام نفس المقياس الرقمي الموصوف أعلاه (لم يتم تحديد أي شذوذ إشعاعي، والتحام). كانت الميزات الإشعاعية التي تم تقييمها واعتبرت دالة على التغيرات التنكسية في الهيكل العظمي المحوري هي العظام الزائدة، والتصلب الفقاري، وتدهور القرص المرتبط (تصلب لوحة النهاية، التآكل، تكلس القرص، التضيق)، والانزلاق. تم تقييم الأشعة بشكل مستقل باستخدام عارض DICOM (Horos ver. 3.3.6) من قبل مراقبين، جراح بيطري معتمد من المجلس (BDXL) وطبيب بيطري ذو خبرة في تقييم التهاب المفاصل التنكسي في الكلاب. بمجرد أن قام كلا الشخصين بتقييم جميع الأشعة، تمت مراجعة الدرجات، وتم مناقشة أي درجات تختلف بين المراجعين وتم تعيين درجة توافق. ملاحظة: تم تقييم جميع أجزاء الهيكل العظمي، ولكن التركيز في التقرير الحالي هو لوصف التهاب المفاصل التنكسي الطرفي.
أداة تصنيف التهاب المفاصل التنكسي للكلاب (COAST)
تم استخدام COAST لتصنيف تأثير التهاب المفاصل التنكسي على المرضى. بناءً على الأوراق المنشورة, كانت العناصر التي اعتبرت عوامل خطر لالتهاب المفاصل التنكسي في هذه الدراسة هي الأمراض العظمية دون دليل إشعاعي على التهاب المفاصل التنكسي (مثل الانزلاق الوركي)، إصابة/جراحة المفصل الناتجة عن الصدمة، سلالة معينة، زيادة الوزن (BCS)، والتعقيم المبكر (أشهر من العمر).
تعريفات التهاب المفاصل التنكسي
التهاب المفاصل التنكسي الإشعاعي (rOA)
تم تعريف الكلاب الفردية على أنها ‘التهاب المفاصل التنكسي الإشعاعي (rOA)’ إذا كانت درجة الأشعةلأي مفصل طرفي. ومع ذلك، إذا تم رؤية التغيرات التنكسية فقط في الهيكل العظمي المحوري (لا يوجد التهاب مفاصل تنكسي في المفاصل الطرفية)، اعتبرت الكلبة (ككل) ‘غير مصابة بالتهاب المفاصل التنكسي’ لأغراض هذه الدراسة حول التهاب المفاصل التنكسي الطرفي.
التهاب المفاصل التنكسي السريري (cOA)
تم تعريف الكلاب الفردية على أنها تعاني من ‘التهاب المفاصل التنكسي السريري’ (cOA) باستخدام معيارين: إذا كان هناك تداخل بين التهاب المفاصل التنكسي الإشعاعي (درجة) ودرجة ألم المفصل(ألم خفيف أو أكثر)، تم تعريفها على أنها cOA1؛ وإذا كان هناك تداخل بين التهاب المفاصل التنكسي الإشعاعي (درجة) ودرجة ألم المفصل(ألم معتدل أو أكثر)، تم تعريفها على أنها cOA2.
التهاب المفاصل التنكسي السريري الملاحظ من قبل المالك (oocOA)
تم تعريف الكلاب أيضاً على أنها ‘التهاب المفاصل التنكسي السريري الملاحظ من قبل المالك’ (oocOA) إذا كان هناك تداخل بين التهاب المفاصل التنكسي الإشعاعي وألم المفصل في نفس المفصل، وكانت درجة LOAD(LOAD تعتبر ‘متأثرة بشكل معتدل’). بالإضافة إلى ذلك، اعتبرت الكلاب ‘معالجة’ إذا كانت تتلقى ‘أدوية مسكنة’ معترف بها مثل مضادات الالتهاب غير الستيرويدية، جابابنتين، أمانتادين، ترامادول، والجليكوزامينوجليكانات متعددة الكبريتات القابلة للحقن لإدارة الألم. تم استخدام LOAD لتعريف oocOA لأنه تم التحقق منه بشكل جيد، واستخدامه على نطاق واسع، ويبدو أنه يقيم تأثير ألم المفصل بشكل متعدد الأبعاد مقارنةً بـ CROMs الأخرى.
عوامل خطر rOA
تمت مقارنة الجنس، والعمر، ووزن الجسم، ودرجة حالة الجسم، والسلالة، بين الكلاب المصابة بالتهاب المفاصل التنكسي والكلاب غير المصابة بالتهاب المفاصل التنكسي لفحص أي العوامل كانت مرتبطة بـ rOA.
التحليل الإحصائي
تم استخدام الإحصائيات الوصفية لوصف انتشار التهاب المفاصل OA والألم المرتبط بـ OA. تم تطبيق اختبارات ويلكوكسون لمقارنة الكلاب المصابة بـ rOA وتلك غير المصابة بـ rOA. إذا كان هناك فرق، تم بناء نماذج الانحدار اللوجستي للتحقيق في العلاقة بين وجود OA والفرق (الاختلافات). بالنسبة لمتغير فئوي يحتوي على أكثر من مستويين، تم اعتبار متغير واحد كخط أساسي ومقارنته مع المتغيرات الأخرى. النماذج التي تم النظر فيها تضمنت جميع تركيبات الفروق وعبارات التفاعل الخاصة بها. تم إجراء جميع التحليلات الإحصائية باستخدام الإصدار 4.2.2، كحد أدنى للدلالة الإحصائية.
توفر البيانات
تتوفر مجموعات البيانات المستخدمة و/أو التي تم تحليلها خلال الدراسة الحالية من المؤلف المراسل عند الطلب المعقول.
تاريخ الاستلام: 8 نوفمبر 2023؛ تاريخ القبول: 17 يناير 2024
تم النشر عبر الإنترنت: 03 فبراير 2024
References
Johnston, S. A. Osteoarthritis. Joint anatomy, physiology, and pathobiology. Vet. Clin. North Am. Small Anim. Pract. 27, 699-723. https://doi.org/10.1016/s0195-5616(97)50076-3 (1997).
Johnson, J. A., Austin, C. & Breur, G. J. Incidence of canine appendicular musculoskeletal disorders in 16 veterinary teaching hospitals from 1980 through 1989. Vet. Comp. Orthopaed. 7, 56-69 (1994).
Anderson, K. L. et al. Prevalence, duration and risk factors for appendicular osteoarthritis in a UK dog population under primary veterinary care. Sci. Rep. 8, 5641. https://doi.org/10.1038/s41598-018-23940-z (2018).
Neill, D. G. O., Church, D. B., McGreevy, P. D., Thomson, P. C. & Brodbelt, D. C. Prevalence of disorders recorded in dogs attending primary-care veterinary practices in England. PloS One 9, e90501. https://doi.org/10.1371/journal.pone. 0090501 (2014).
Wright, A. et al. Identification of canine osteoarthritis using an owner-reported questionnaire and treatment monitoring using functional mobility tests. J. Small Anim. Pract. 63, 609-618. https://doi.org/10.1111/jsap. 13500 (2022).
Innes J. F. in Veterinary surgery : Small animal Vol. 1 (ed Johnston AS Tobias KM) Ch. 68, 1078-1112 (Saunders, 2012).
Lascelles, B. D. et al. Cross-sectional study of the prevalence of radiographic degenerative joint disease in domesticated cats. Vet. Surg. 39, 535-544. https://doi.org/10.1111/j.1532-950X.2010.00708.x (2010).
Esteban, M. Epidemiology of osteoarthritis. Vet. Focus 17, 4-10 (2007).
Cachon, T. et al. Face validity of a proposed tool for staging canine osteoarthritis: Canine Osteo Arthritis Staging Tool (COAST). Vet. J. 235, 1-8. https://doi.org/10.1016/j.tvjl.2018.02.017 (2018).
Brown, D. C., Boston, R. C., Coyne, J. C. & Farrar, J. T. Development and psychometric testing of an instrument designed to measure chronic pain in dogs with osteoarthritis. Am. J. Vet. Res. 68, 631-637. https://doi.org/10.2460/ajvr.68.6.631 (2007).
Walton, M. B., Cowderoy, E., Lascelles, D. & Innes, J. F. Evaluation of construct and criterion validity for the ‘Liverpool Osteoarthritis in Dogs’ (LOAD) clinical metrology instrument and comparison to two other instruments. PloS One 8, e58125. https://doi. org/10.1371/journal.pone. 0058125 (2013).
Summers, J. F. et al. Health-related welfare prioritisation of canine disorders using electronic health records in primary care practice in the UK. BMC Vet. Res. 15, 163. https://doi.org/10.1186/s12917-019-1902-0 (2019).
Gruen, M. E. et al. 2022 AAHA pain management guidelines for dogs and cats. J. Am. Vet. Med. Assoc. 58, 55-76. https://doi.org/ 10.5326/JAAHA-MS-7292 (2022).
Anderson, K. L., Zulch, H., O’Neill, D. G., Meeson, R. L. & Collins, L. M. Risk factors for canine osteoarthritis and its predisposing arthropathies: A systematic review. Front. Vet. Sci. 7, 220. https://doi.org/10.3389/fvets.2020.00220 (2020).
Houlihan, K. E. A literature review on the welfare implications of gonadectomy of dogs. J. Am. Vet. Med. Assoc. 250, 1155-1166. https://doi.org/10.2460/javma.250.10.1155 (2017).
Rowlison de Ortiz, A. et al. Initial exploration of the discriminatory ability of the PetPace collar to detect differences in activity and physiological variables between healthy and osteoarthritic dogs. Front. Pain Res. 3, 949877. https://doi.org/10.3389/fpain. 2022.949877 (2022).
Brown, D. C., Boston, R. C., Coyne, J. C. & Farrar, J. T. Ability of the canine brief pain inventory to detect response to treatment in dogs with osteoarthritis. J. Am. Vet. Med. Assoc. 233, 1278-1283. https://doi.org/10.2460/javma.233.8.1278 (2008).
Walton, M. B., Cowderoy, E. C., Wustefeld-Janssens, B., Lascelles, B. D. X. & Innes, J. F. Mavacoxib and meloxicam for canine osteoarthritis: A randomised clinical comparator trial. Vet. Rec. 175, 280. https://doi.org/10.1136/vr. 102435 (2014).
Knazovicky, D., Tomas, A., Motsinger-Reif, A. & Lascelles, B. D. Initial evaluation of nighttime restlessness in a naturally occurring canine model of osteoarthritis pain. PeerJ 3, e772. https://doi.org/10.7717/peerj. 772 (2015).
Brown, D. C., Boston, R. C. & Farrar, J. T. Use of an activity monitor to detect response to treatment in dogs with osteoarthritis. J. Am. Vet. Med. A 237, 66-70. https://doi.org/10.2460/javma.237.1.66 (2010).
Enomoto, M., Baines, E. A., Roe, S. C., Marcellin-Little, D. J. & Lascelles, B. D. X. Defining the rate of, and factors influencing, radiographic progression of osteoarthritis of the canine hip joint. Vet. Rec. 189, e516. https://doi.org/10.1002/vetr.516 (2021).
Smith, G. K. et al. Chronology of hip dysplasia development in a cohort of 48 Labrador retrievers followed for life. Vet. Surg. 41, 20-33. https://doi.org/10.1111/j.1532-950X.2011.00935.x (2012).
van Hagen, M. A., Ducro, B. J., van den Broek, J. & Knol, B. W. Incidence, risk factors, and heritability estimates of hind limb lameness caused by hip dysplasia in a birth cohort of boxers. Am. J. Vet. Res. 66, 307-312. https://doi.org/10.2460/ajvr.2005.66. 307 (2005).
الشكر والتقدير
نشكر الدكاترة آبي تايلور، آمي سنايدر، ماريا روس-إسترادا، كيلي فيريس، ديان ديريسينسكي، وإيرين فري على مساعدتهم في التوظيف. نشكر جيمس روبرتسون على مساعدته في التحليل الإحصائي.
مساهمات المؤلفين
S.R.، J.F.I.، N.A.T. و B.D.X.L.: تصميم الدراسة. M.E.، N.D.C.، J.H.، A.T.، B.D.X.L. و T.C.: توظيف المرضى، جمع البيانات، إدخالها، والتحقق منها (QC). M.E.، A.N.H.، E.P.، S.A.، E.H.: تحليل البيانات. LO: التحليل الإحصائي. M.E. و B.D.X.L.: إعداد المخطوطة. ساهم جميع المؤلفين في المقالة ووافقوا على النسخة المقدمة.
التمويل
تم تمويل هذه الدراسة من قبل إيلانكو لصحة الحيوان (منحة ولاية نورث كارولينا # 2020-0044).
المصالح المتنافسة
NAT هو موظف في إيلانكو لصحة الحيوان. BDXL هو مستشار مدفوع لإيلانكو لصحة الحيوان؛ يتلقى JFI رسوم ترخيص لـ LOAD وقد شارك في محاضرات تعليمية مدفوعة نيابة عن إيلانكو. لا يوجد مؤلفون آخرون لديهم أي تضارب في المصالح للإفصاح عنه.
معلومات إضافية
المعلومات التكميلية النسخة عبر الإنترنت تحتوي على مواد تكميلية متاحة على https://doi.org/ 10.1038/s41598-024-52324-9.
يجب توجيه المراسلات والطلبات للحصول على المواد إلى B.D.X.L.
معلومات إعادة الطبع والتصاريح متاحة على www.nature.com/reprints.
ملاحظة الناشر تظل Springer Nature محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
برنامج البحث الانتقالي في الألم، قسم العلوم السريرية، كلية الطب البيطري، مركز البحث والتعليم في الألم المقارن، جامعة ولاية نورث كارولينا، رالي، NC، الولايات المتحدة الأمريكية. قسم الإحصاء، جامعة ولاية نورث كارولينا، رالي، NC، الولايات المتحدة الأمريكية. إيلانكو لصحة الحيوان، هوك، لندن، المملكة المتحدة. إحالات بيطرية مستقلة للحركة، تشيشاير، إنجلترا، المملكة المتحدة. قسم التخدير، مركز البحث الانتقالي في الألم، جامعة ديوك، دورهام، NC، الولايات المتحدة الأمريكية. مركز التهاب المفاصل ثورستون، UNC، تشابل هيل، NC، الولايات المتحدة الأمريكية. البريد الإلكتروني: dxlascel@ncsu.edu
Prevalence of radiographic appendicular osteoarthritis and associated clinical signs in young dogs
Masataka Enomoto , Nicholas de Castro , Jonathan Hash , Andrea Thomson , Aoi Nakanishi-Hester , Erin Perry , Savannah Aker , Emily Haupt , Logan Opperman , Simon Roe , Tracey Cole , Nichola Archer Thompson , J. F. Innes & B. Duncan X. Lascelles
Abstract
This study aimed to determine the prevalence of osteoarthritis (OA) and associated clinical signs in young dogs. Owners of dogs aged 8 months- 4 years from a single practice, were contacted in random order, to participate in a general health screen. Clinical and orthopedic examinations were performed. Each joint was scored for pain reactions (0-4). Orthogonal radiographs of all joints were made under sedation. Each joint was scored for radiographic OA (rOA) severity on an 11-point scale. Clinical OA (cOA) was defined as an overlap of rOA and joint pain in joint. Owners completed questionnaires. The owners of 123 dogs agreed to participate. Overall, (49/123) of dogs had rOA in joint, and or dogs had cOA, depending on the cut-off value of joint pain; moderate (2), or mild (1), respectively. Owners of dogs with cOA observed signs of impairment in approximately of cases. Only 2 dogs with cOA were receiving OA pain management. The most commonly affected joints in descending order of frequency were elbow, hip, tarsus, and stifle. Radiographically visible OA is common in young dogs, and of dogs with rOA had cOA. However, OA-pain appears underdiagnosed and undertreated in young dogs.
Abstract
No comprehensive, prospective studies of the prevalence of canine osteoarthritis (OA) throughout the skeleton have been performed and current estimates of OA prevalence pertain to older dogs. The most often quoted estimate of the number of dogs with clinical signs associated with OA is ‘ of the population’ . The estimate of comes from a 1997 publication that referenced Pfizer survey data pertaining to general practices . A survey of admissions to US veterinary teaching hospitals over a 10-year period (1980 to 1989), using diagnoses entered into the medical records, found that of all patients had been affected by a disorder of the musculoskeletal system, and overall had been affected by degenerative joint disease of the appendicular skeleton . However, data from veterinary teaching hospitals may not be reflective of general practice. Previous studies have estimated that the annual period prevalence of appendicular joint OA and associated pain was in the UK and in the US in dogs of any age attending primary-care practices . In contrast, recently, employing a screening checklist in general practices, investigators found of dogs presenting to first opinion practices (in the US) had a diagnosis of confirmed (radiographs and clinical signs) or presumed (clinical signs; radiographs not taken) . This is almost double the most commonly used estimate of of the canine population. Although strong, comprehensive, prospective data on prevalence currently do not exist, OA in dogs is likely a very common disease.
Despite recent new information, the prevalence of OA -associated clinical signs in young dogs is completely unknown. This information is crucial to know because OA is thought to be initiated primarily by developmental
disease in dogs , and therefore could be argued to be a young-dog disease, and, although unexplored, early intervention at this stage may improve outcome later. However, if OA is not recognized in young dogs, the opportunity for early intervention is missed. Currently, most diagnoses of OA in dogs are made later in a dog’s life when clinical signs are more evident/overt . The aim of this study was to define the prevalence of both radiographic OA , and of OA -associated pain (combination of radiographic OA and detectable joint pain) in dogs less than 4 years old.
Results
A total of 320 owners were contacted, and owners of 123 dogs across 40 different breeds agreed to participate in the study. The final number of dogs in each age band was 25, 26, 30, and 42 respectively. Across all 123 dogs, mean ( SD) age, body weight, and body condition score were months, , and , respectively. 16 dogs were intact male, and 53 dogs were castrated male; 6 dogs were intact female, and 48 dogs were spayed female (Supplemental file 1). The most common breeds were mixed ( ), Labrador Retriever ( ), and American Staffordshire terrier ( ) (for full list of breeds see Supplemental file 2).
All dogs were COAST (Canine OsteoArthritis Staging Tool) staged. Approximately of the dogs were preclinical/no joint pain (COAST Stage dogs and COAST Stage ). The remainder were classed as COAST Stage 2 (70/123), 3 (27/123) or 4 (3/123) due to clinical signs that were OA or non-OA related.
Overall, of dogs (49/123) had radiographic OA (rOA) in at least one appendicular joint. The prevalence of rOA in each age band is shown in Fig. 1 and supplemental file 3. The differences in signalment and client reported outcome measures (CROMs) scores between rOA dogs and non-rOA dogs are detailed in Table 1.
Radiographically affected joints in descending order of frequency were elbow, hip, tarsus, and stifle (Fig. 2). Additionally, Table 2 and Fig. 3a show how many individual appendicular joints were affected: rOA was found in 1 joint in 14 dogs; 2 joints in 24 dogs; joints in 7 dogs; joints in 4 dogs. Figure 3b shows the prevalence of dogs in each age group with varying numbers of joints affected with OA.
There was a significant difference in age, bodyweight, and body condition score (BCS) between non-rOA and rOA dogs (Table 1). However, prevalence of rOA was increased with age ( ), and bodyweight ( ), with these two factors being independently associated with rOA. BCS did not have significant impact on the prevalence of rOA ( for score of 5,6 , and 7 respectively). The number of dogs with rOA and non-rOA and that had risk factors for OA is tabulated in supplemental file 4. Three dogs had two risk factors and had OA (Breed and BCS dog; breed and early neuter, 2 dogs). The relationship between the total radiographic score and age is shown in supplemental file 5.
Twenty-two toy/small breed dogs were identified in the study, and five of them had rOA ( ). More detailed information of toy/small breed dogs with OA is tabulated in supplemental file 6 . We considered dogs to be toy/small breed if they were a breed listed on the American Kennel Club website as “toy/small breed dogs” but we also included mixed breed dogs with body weight ( 14 kg ) as ‘small breeds’ (for full list of toy/small breeds see supplemental file 7).
With respect to the prevalence of OA-associated pain (‘clinical OA’, cOA), of dogs (29/123) had cOA using a cut-off of for joint pain (mild or greater pain) (designated cOA1); and of dogs (20/123) had cOA using a cut-off of for joint pain (moderate or greater pain) in at least one joint with rOA (see Tables 3 and 4) (designated cOA2).
Based on owner completed Liverpool OsteoArthritis in dogs (LOAD) scores, owners of dogs with cOA observed signs of impairment in for cOA1, and for cOA2, but only 2 of them ( or 2/6) were treated medically for cOA at the time of the health screen evaluation (designated ‘owner observed clinical OA , oocOA). The prevalence of rOA, cOA1, cOA2, and oocOA in each age band is shown in Tables 3 and 4, and graphically Fig. 4a,b.
Other orthopedic diseases that were detected radiographically are listed in supplemental file 8.
Figure 1. Graph depicting the prevalence of dogs with radiographic osteoarthritis (rOA) in each group. The prevalence of rOA increased with age. Overall, the prevalence of rOA was ( ).
rOA (49 dogs)
Non-rOA (74 dogs)
-Value
Age
(37.0, 13.0-49.0)
(24.5, 9.0-49.0)
<0.001
Sex
M: 4, F: 3, MC: 22, FS: 20
M: 12, F: 3, MC: 31, FS: 28
0.57
Breed
Mixed, Labrador
Mixed, Labrador
0.11
Body weight
(27.4, 4.1-67.0)
(23.3, 3.8-42.9)
0.003
BCS (1-9)
(5, 4-7)
(5, 4-7)
0.017
CBPI PSS
(0, 0-4.75)
(0, 0-2.75)
<0.001
CBPI PIS
(0, 0-4.14)
(0, 0-1.14)
0.002
LOAD
(5, 0-19)
(3, 0-17)
0.011
SNoRE *
(2.9, 1-8)
(2.4, 1.4-5.4)
0.054
COAST
(3, 2-4)
(2, 0-4)
<0.001
Total OA score
(4, 1-24)
0
<0.001
Table 1. Mean SD (median, range) values of signalment and client reported outcome measures between dogs with radiographic OA (rOA) and without Male, Female, Male castrated, Female spayed, radiographic osteoarthritis; BCS body condition score; CBPI Canine Brief Pain Inventory; PSS Pain Severity Score; PIS Pain Interference Score; LOAD Liverpool Osteoarthritis in Dogs; SNoRE Sleep and Nighttime Restlessness Evaluation; COAST Canine OsteoArthritis Staging Tool. Significant if (bolded). owner did not fill out SNoRE because the dog sleeps outside (OA dog).
Figure 2. This figure shows the prevalence of radiographic osteoarthritis (rOA) across joints. The most commonly affected joints in order were elbow, hip, tarsus, and stifle.
Age category (months)
Normal (No rOA/DJD)
Single joint rOA
Bilateral joint rOA
2 joints with rOA (different joint types)
3-4 joints with rOA
joints with rOA
Spine DJD only
9-18
19
1
1
1
1
1
1
> 18-28
18
2
3
1
0
0
2
>28-38
15
5
4
2
1
2
1
>38-48
17
6
10
2
5
1
1
Total
69
14
18
6
7
4
5
Table 2. The number of dogs having radiographic osteoarthritis (rOA) in a single joint, bilateral joints, 2 joints (different), multiple joints, and only spine. Single joint rOA: rOA in one joint site and only on one side (unilateral) (e.g. left elbow OA). Bilateral: A dog had rOA in one joint type and had rOA in both left and right joints (e.g. bilateral hips). 2 joints rOA: A dog had rOA in two different joints (no bilateral disease; e.g. right elbow and right hip). 3-4 joints rOA: A dog had rOA in 3-4 joints (e.g. elbows and hips). joints rOA: A dog had rOA in 5 or more joints (e.g. elbows, hips, and stifles). Only spine DJD: A dog had DJD in spine, but no OA in appendicular joint. radiographic osteoarthritis; degenerative joint disease.
Figure 3. (a) This figure shows the number of dogs having radiographic appendicular joint osteoarthritis (rOA) in a single joint, 2 joints, and multiple joints. (b) This figure shows the number of dogs having rOA in a single joint, 2 joints, and multiple joints in each age group.
Age category (months)
Total number of dogs in group
Number of dogs with OA and joint pain (cOA1)
Dogs with clinical OA and LOAD (oocOA)
Dogs with clinical OA and LOAD < 10
Overall prevalence of oocOA (%) of clinical OA and owner detected signs of OA pain (%)
9-18
25
4
0
4
0.0
>18-28
26
3
0
3
0.0
>28-
30
9
3
6
10.0
>38-48
42
13
6
7
14.3
Total
123
29
9
20
7.3
Table 3. The prevalence of cOA 1 and oocOA in each age group (oocOA is defined as there is overlap of radiographic OA and mild or greater joint pain (pain score ) in the same joint, and LOAD score of ). OA osteoarthritis, LOAD Liverpool OsteoArthritis in Dogs.
Age category (months)
Total number of dogs in group
Number of dogs with OA and joint pain (cOA2)
Dogs with clinical OA and LOAD (oocOA)
Dogs with clinical OA and LOAD < 10
Overall prevalence of oocOA (%) of clinical OA and owner detected signs of OA pain (%)
9-18
25
4
0
4
0.0
>18-28
26
2
0
2
0.0
>28-38
30
6
3
3
10.0
>38-48
42
8
3
5
7.1
Total
123
20
6
14
4.9
Table 4. The prevalence of cOA2 and oocOA in each age group, which is defined as there is overlap of radiographic OA and moderate or greater joint pain (pain score ) in the same joint, and owner-assessed LOAD score of . OA osteoarthritis, LOAD Liverpool OsteoArthritis in Dogs.
Figure 4. (a) This figure shows the prevalence of radiographic OA (rOA), clinical OA (cOA1; mild joint pain or greater), and owner-observed clinical OA (oocOA), and dogs treated medically in each age group. Blue indicates the prevalence of rOA dogs, red indicates the prevalence of cOA1, yellow indicates the prevalence of oocOA, and green indicates the prevalence of dogs being treated with pain medications at the time of screening. (b) This figure shows the prevalence of radiographic , clinical OA (cOA2; moderate joint pain or greater), and owner-observed clinical OA (oocOA), and dogs being treated medically in each age group. Blue indicates the prevalence of rOA dogs, red indicates the prevalence of cOA2, yellow indicates the prevalence of oocOA, and green indicates the prevalence of dogs treated with pain medications at the time of screening.
Discussion
The results of this study have demonstrated that radiographically visible OA is very common in young dogs, and approximately of dogs with rOA had cOA with at least mild pain ( of dogs overall) in one or more joints and had cOA with at least moderate pain in one or more joints ( of dogs overall). In dogs with cOA, based on answers to standard OA questionnaires, owners identified the presence of clinical signs relatively infrequently (one third of dogs) and few dogs were medically treated.
No other work has explored the prevalence of radiographic OA and associated pain in young dogs. There are also relatively few studies that have evaluated the prevalence of OA in dogs of any age. Two previous studies showed that the estimated annual period prevalence of appendicular joint OA and associated clinical signs was in the UK and in the US in dogs of any age attending primary-care practices . In the study performed in , electronic patient record data from veterinary patients were reviewed to identify potential OA cases within a one-year sampling time frame from Jan 1st 2013 to Dec 31st 2013. Overall, 455,557 dogs (median age of 4.1 years) were included in the study and 16,437 candidate OA cases were identified. Of these, 6102 were reviewed in detail and 4196 dogs ( ) were confirmed as OA cases (newly diagnosed as OA or showed continuation of treatment for pre-existing diagnosis during the study period). Although there is no detailed description in the report from the largest general veterinary practice in the US, medical records from the more than 2.5 million dogs they cared for in 2018 were reviewed and the prevalence of clinical OA was calculated . In another similar study, electronic patient record data were collected on 148,741 dogs attending primary attending primary care veterinary practices, and 3884 dogs (median age of 4.8 years) were randomly selected to investigate the prevalence of disorders. The study sampling frame was from Sep 1st 2009 to Mar 31st 2013. The authors reported that the prevalence of degenerative joint disease was in dogs, however, the study did not use as tight a case definition as the aforementioned OA prevalence study in UK. The data in the literature vary greatly with respect to how many dogs are diagnosed with clinical OA but are generally surprisingly low when one considers that OA and OA-pain increase with age, and our data suggest that of young dogs are already displaying moderate pain or greater in at least 1 joint with rOA.
In this study, the total radiographic OA score increased with age. The slope of the trendline is not steep, but the score appears to increase mainly due to the presence of multiple joints being affected in addition to worsening of the actual OA scores (hip/elbow dysplasia). Although species are different, the trendline is not dissimilar to that seen in younger cats . In the cat study, the slope of the trendline became steeper over time. We acknowledge
that we do not know what the total OA scores would be in older dogs with OA, however, we anticipate a similar increase in OA burden over time (see supplemental file 9).
Our data indicate a high prevalence of rOA in young dogs, and particularly in the elbow and hip, supporting the assertion that OA is primarily driven by developmental disease in dogs. However, we did not review medical records to ascertain whether the affected joints had been diagnosed with developmental joint disease. In our study, the most commonly affected joints were elbow, hip, tarsus, and stifle. This is similar to previous findings in older dogs except for the tarsus . It is unclear why the tarsus was not identified as a site of OA in Johnson’s study, but the population they evaluated was selected from cases sent to a teaching hospital, which might have had some selection bias.
Although the sample size of toy/small breed dogs was small, it appears that rOA is less common in toy/small dogs and also that the hip joint is the most commonly affected site in smaller breeds.
Currently, clinical OA (OA with associated joint pain) in dogs is diagnosed at a much later timepoint with more than of diagnosed dogs aged from 8 to 13 years . Indeed, previous work has reported that median age at first diagnosis of OA was 10.5 years in dogs attending UK primary care veterinary practices (the median age of the overall denominator population was 4.1 years) . The high prevalence of disease supports the approach of actively screening younger dogs with the goal to intervene earlier and decrease the impact of OA and OA -associated pain over the dogs’ lifespan. Such a proactive approach has been suggested , but has not been assessed-that is, it is not known if early intervention of some sort (e.g. strict weight management, regular low impact activity) decreases the impact of OA later in life.
In the present study, in dogs with clinical OA, owners reported (based on their answers captured via the LOAD instrument) the presence of clinical signs relatively infrequently-only one third of owners of dogs with detectable OA-pain according to the authors’ evaluations. Interestingly, regardless of cut-offs, owners did not appear to notice any signs of OA pain in dogs between 9 and 28 months (across this age range, 7 dogs had OA-pain detected on examination). There are several potential explanations for this, that are not mutually exclusive: Firstly, these younger dogs may not be displaying signs of OA -pain in the home environment (they are truly functioning well). Secondly, owners may not be recognizing the signs of OA -pain. The signs of joint pain in younger dogs do appear, clinically, to be different to that of older dogs, with an emphasis on adaptations of function rather than impaired function which is more obvious in older dogs. For example, young dogs with hip OA and pain may still be able to go on walks without tiring, still able to go up and down stairs, and still able to play, while older dogs with hip OA and pain may show obvious impairment in performing these activities. Additionally, many of the dogs were bilaterally affected, and it may be that owners are more likely to recognize clinical signs if only a single limb is affected rather than bilateral joints. Our data suggest that more joints become affected with age, and if multiple joints are affected, clinical signs may be more noticeable for owners as the impact of OA-pain becomes high. Lastly, the questionnaires used, (LOAD) and potentially other CROMs (e.g., CBPI) may not be ideal for the assessment of signs of OA-pain in younger dogs. Attempts to measure OA-pain in young dogs using CROMs may be fundamentally flawed because these instruments were developed in older dog populations. Indeed, the LOAD was developed using dogs of mean ages 7.9 years and the CBPI was developed using the dogs with years . That said, in this study the use of LOAD identified one third of the cOA cases, suggesting that the proactive use of LOAD or other CROMs can still flag a good proportion of young dogs with cOA , and act as a starting point for conversation and facilitate the education of owners about OA . To date, there has been no comprehensive description or investigation of the behavioral signs of OA-pain in young dogs, and no attempts to develop an owner questionnaire specifically for this younger population of dogs.
Previous studies have suggested that once OA is recognized, it is perceived by both veterinarians and owners as important enough for significant clinical care, often involving long term prescription analgesics and multiple additional treatment interventions, frequent clinic visits and relatively high levels of referral . Indeed, eightyfive percent of OA cases were reported to be managed with at least one clinical modality (medical or surgical treatments) following osteoarthritis diagnosis (median age of 10.5 years) and the majority of them remained on medical management . Medical management is likely to be less complex earlier in the course of the disease. Earlier, effective treatment of OA-pain may better control joint pain and the longer-term negative impacts of joint pain on other dimensions such as behavioral characteristics, affective states and muscle strength . However, our study showed that only a very few dogs received medical management even after clinical OA was diagnosed or in cases where owners recognized the presence of clinical signs. This likely highlights the difference in clinical signs associated with OA between younger dogs and older dogs, and possibly differences in attitudes of both veterinarians and pet owners. For example, owners may be reluctant to treat their dogs if function is not obviously impaired. However, we did not investigate the reasons for this, and this is an important area for future research.
A significant difference was observed between dogs with OA and without OA in age, body weight, and BCS in the present study. The prevalence of rOA was increased with age and bodyweight with these two factors being independently associated with rOA in this study. A recent review paper summarized the risk factors for canine appendicular OA as: genetics, breed, conformation, age, sex/neuter status, and body weight . As shown in Table 1, we did not find any significant impact of sex or breed on the radiographic OA . This may be because we had a relatively small sample size and with a large wide variety of different breeds represented, the effect of breed could not be looked at in detail. The majority of dogs enrolled in the study were neutered and so the effect of sex hormones could not be evaluated. Early de-sexing has been suggested to be a risk factor for joint disease, albeit with variable influence across breeds . We were not able to collect accurate data on the time of de-sexing to be able to look at that as a factor in OA status. There was a significant difference in most CROMs between dogs with OA and without OA. However, the difference was small and the score of CROMs was relatively low even in dogs with OA. This may highlight the statement above that owners may be unaware of or may have difficulty recognizing the signs of OA pain in this age group of dogs, and/or the current CROMs may not be ideal for the
assessment of signs of OA -pain in younger dogs. Further, the ‘ability’ of the CROMs to detect OA-associated pain was not likely affected by treatments for OA pain because very few dogs were receiving any treatment for OA-pain.
An important limitation of our study is that clinical OA (cOA) was defined based on subjective criteria (veterinarian examination), and therefore the results may be different if the study was repeated by different investigators. There is currently no ‘gold standard’ for diagnosing or scoring severity of OA-pain in dogs, and work needs to be performed to look at the reproducibility of the sorts of subjective assessments we used. Additionally, the criteria for determining owner-observed signs of OA (LOAD) were based on criteria developed in older dogs with OA pain, thus, this may not be relevant to signs of OA in young dogs. Additional limitations of this study were that it was performed in a single practice and single geographic area, and therefore, the client and breed spectrum may not be representative of the general public/dog population in the US. For example, German shepherds make up of the US dog population , but only accounted for of our study population. A single practice was chosen for this initial study primarily for logistical reasons around making the sample population scientifically sound. We wanted to sample in an unbiased manner-that is, have access to the full database-and using a single practice that we could work with in this manner was the best decision scientifically balanced with the cost and logistical challenges of going into multiple practices.
This study provides the foundation for increasing awareness of OA among veterinarians and dog owners with the potential to lead to earlier intervention and mitigation of the impacts of OA -pain later in life.
Materials and methods Study design
The study was a cross-sectional prevalence study of radiographic and clinical OA in a stratified sample of young dogs aged 8 months to 4 years old. NC State University Institutional Animal Care and Use Committee (IACUC) reviewed and approved all methods and procedure used in the study (IACUC#19-604-O). This approval also included ethical approval. All dog owners signed a written consent form following a detailed verbal explanation of the study protocol. All methods were performed in accordance with relevant guidelines and regulations. All animal work was conducted according to the guidelines outlined in the Animal Welfare Act of 1966 and the Health Research Extension Act of 1985. This study was carried out and reported in compliance with the ARRIVE guidelines.
Recruitment
The dogs registered in a single practice (NC State College of Veterinary Medicine Primary Care service) were grouped into 4 age bands ( , and months). Regardless of health status, the dogs in each age band were randomly ordered by using a computer software program (https://www.random.org). Then, the owners of the first 50 dogs in each group were contacted in order and asked to visit the hospital (NC State University Pain Research lab) for a ‘health screen’. The dogs in each age group whose owners were willing for them to participate in the study were included. Owners were contacted twice by email and once by phone call. If they had not responded following these attempts, the next owner/dog in sequence was contacted. Recruitment (and evaluations-see below) began mid Feb 2020 and continued through mid Aug 2021.
Inclusion criteria
To be eligible for the study, dogs were required to be between the ages of 8 months and 4 years at the time of recruitment and body weight. Additionally, the owners were required to be willing to have their dogs examined and to have radiographs taken under sedation. There were no specific exclusion criteria.
Examination
Physical, orthopedic, and neurologic examination, blood work, and urinalysis were performed, and data were captured. For the orthopedic examination, every joint of each limb was examined by a veterinarian experienced in evaluating canine OA (ME), and joints were graded for pain, crepitus, effusion, and thickening . The manus and pes were considered as one joint region for evaluation purposes. Other appendicular joints evaluated were carpus, elbow, shoulder, tarsus, stifle, and hip. Spinal column segments were examined and graded for pain. The axial skeleton was evaluated by dividing the spine into cervical, thoracic (T1-9), thoraco-lumbar (T10-L6), and lumbosacral regions. Scores for pain ranged from 0 to 4 ; these scores were used to create a Total Pain Score (sum of individual pain scores for each joint) with a range of for the appendicular skeleton. Assessments for crepitus, effusion, thickening, and range of motion were recorded, but not used in analysis. Scores were recorded on the JESSE (canine) (Supplemental file 10).
Client reported outcome measures (CROMs)
CROMs were used as previously described . The Liverpool Osteoarthritis in Dogs (LOAD) and Canine Brief Pain Inventory (CBPI) have been shown to be a valid measure of the impact of OA- pain in dogs . Sleep and Nighttime Restlessness Evaluation Score Questionnaire version 2.0 (SnoRE) was used to collect the data regarding sleep quality . The CROMs were completed by the dog owner. For the LOAD, the sum of each item was calculated. For CBPI (pain severity scores [PSS] and pain interference scores [PIS]) and the SNoRE, the average of each item was calculated.
Radiography
Radiographs were taken under sedation with a mu-opiate combined with alpha-2 adrenergic agonist, for example hydromorphone and dexmedetomidine . However, the choice of drug and dose was adapted according to the dog’s health condition. Orthogonal views of all appendicular joints and the lateral views of the spine were taken. To minimize ionizing radiation exposure, where appropriate, radiographs were centered on the midpoint of the limb or spinal segment to reduce the number of individual exposures used. A subjective radiographic OA numerical rating scale where no radiographic abnormalities identified and most severe radiographic OA , was assigned to each joint based on presence of radiographic changes and their overall severity based on previously reported information . Radiologic features considered indicative of presence of appendicular OA were osteophytes, enthesophytes, sclerosis, subchondral bone erosions and cysts. Degenerative changes on each axial segment were assessed using the same numerical scale described above ( no radiographic abnormalities identified, and ankylosis). Radiographic features evaluated and considered indicative of degenerative changes in the axial skeleton were osteophytes, spondylosis, disc-associated degeneration (end plate sclerosis, erosion, disc mineralization, narrowing), and subluxation. Radiographs were assessed independently using a DICOM viewer (Horos ver. 3.3.6) by two observers, a board-certified small animal veterinary surgeon (BDXL) and a veterinarian experienced in evaluating canine . Once both individuals had scored all radiographs, scores were reviewed, and any scores that differed between reviewers were discussed a consensus score was assigned. Note: all parts of the skeleton were assessed, but the focus of the current report is to describe appendicular .
The Canine OsteoArthritis Staging tool (COAST)
COAST was used for staging the impact of OA on patients . Based on the published papers , the items considered as the risk factors for OA in this study were orthopedic disease without radiographic evidence of OA (e.g. hip subluxation), traumatic joint injury/surgery, certain breed, overweight (BCS ), and early neuter ( months of age).
Definitions of OA
Radiographic OA (rOA)
Individual dogs were defined as ‘radiographic OA (rOA)’ if the radiographic score was for any appendicular joint. However, if degenerative changes were seen only in the axial skeleton (no OA in appendicular joints), the dog (as a whole) was considered as ‘non-OA’ for the purposes of this study of appendicular OA.
Clinical OA (cOA)
Individual dogs were defined as having ‘Clinical OA’ (cOA) using two criteria: if there was overlap of radiographic OA (score of ) and joint pain score of (mild or greater pain), they were defined at cOA1; and if there was overlap of radiographic OA (score of ) and joint pain score of (moderate or greater pain), they were defined at cOA2.
Owner observed clinical OA (oocOA)
Dogs were also defined as ‘Owner observed clinical OA’ (oocOA) if there was overlap of radiographic OA and joint pain in the same joint, and LOAD score was (LOAD is considered as ‘moderately affected’). Additionally, dogs were considered as ‘treated’ if they were receiving recognized ‘pain medication(s)’ such as non-steroid anti-inflammatories, gabapentin, amantadine, tramadol, injectable polysulfated glycosaminoglycans for the management of pain. LOAD was used to define oocOA because it has been well validated, widely used, and appears to assess the impact of joint pain multidimensionally compared to other CROMs.
Risk factors of rOA
Sex, age, body weight, body condition score, and breed, were compared between OA dogs and non-OA dogs to examine which factors were associated with rOA.
Statistical analysis
Descriptive statistics were used to describe prevalence of OA and OA -associated pain. Wilcoxon rank sum tests were applied to compare the dogs with rOA and without rOA. If there was a difference, logistic regression models were built to investigate the association between the presence of OA and the difference(s). For a categorical variable with more than two levels, one variable was treated as baseline and compared with the other variables. The models considered included all combinations of the differences and their interaction terms. All statistical analyses were performed using version 4.2.2, as our cutoff for statistical significance.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Received: 8 November 2023; Accepted: 17 January 2024
Published online: 03 February 2024
References
Johnston, S. A. Osteoarthritis. Joint anatomy, physiology, and pathobiology. Vet. Clin. North Am. Small Anim. Pract. 27, 699-723. https://doi.org/10.1016/s0195-5616(97)50076-3 (1997).
Johnson, J. A., Austin, C. & Breur, G. J. Incidence of canine appendicular musculoskeletal disorders in 16 veterinary teaching hospitals from 1980 through 1989. Vet. Comp. Orthopaed. 7, 56-69 (1994).
Anderson, K. L. et al. Prevalence, duration and risk factors for appendicular osteoarthritis in a UK dog population under primary veterinary care. Sci. Rep. 8, 5641. https://doi.org/10.1038/s41598-018-23940-z (2018).
Neill, D. G. O., Church, D. B., McGreevy, P. D., Thomson, P. C. & Brodbelt, D. C. Prevalence of disorders recorded in dogs attending primary-care veterinary practices in England. PloS One 9, e90501. https://doi.org/10.1371/journal.pone. 0090501 (2014).
Wright, A. et al. Identification of canine osteoarthritis using an owner-reported questionnaire and treatment monitoring using functional mobility tests. J. Small Anim. Pract. 63, 609-618. https://doi.org/10.1111/jsap. 13500 (2022).
Innes J. F. in Veterinary surgery : Small animal Vol. 1 (ed Johnston AS Tobias KM) Ch. 68, 1078-1112 (Saunders, 2012).
Lascelles, B. D. et al. Cross-sectional study of the prevalence of radiographic degenerative joint disease in domesticated cats. Vet. Surg. 39, 535-544. https://doi.org/10.1111/j.1532-950X.2010.00708.x (2010).
Esteban, M. Epidemiology of osteoarthritis. Vet. Focus 17, 4-10 (2007).
Cachon, T. et al. Face validity of a proposed tool for staging canine osteoarthritis: Canine Osteo Arthritis Staging Tool (COAST). Vet. J. 235, 1-8. https://doi.org/10.1016/j.tvjl.2018.02.017 (2018).
Brown, D. C., Boston, R. C., Coyne, J. C. & Farrar, J. T. Development and psychometric testing of an instrument designed to measure chronic pain in dogs with osteoarthritis. Am. J. Vet. Res. 68, 631-637. https://doi.org/10.2460/ajvr.68.6.631 (2007).
Walton, M. B., Cowderoy, E., Lascelles, D. & Innes, J. F. Evaluation of construct and criterion validity for the ‘Liverpool Osteoarthritis in Dogs’ (LOAD) clinical metrology instrument and comparison to two other instruments. PloS One 8, e58125. https://doi. org/10.1371/journal.pone. 0058125 (2013).
Summers, J. F. et al. Health-related welfare prioritisation of canine disorders using electronic health records in primary care practice in the UK. BMC Vet. Res. 15, 163. https://doi.org/10.1186/s12917-019-1902-0 (2019).
Gruen, M. E. et al. 2022 AAHA pain management guidelines for dogs and cats. J. Am. Vet. Med. Assoc. 58, 55-76. https://doi.org/ 10.5326/JAAHA-MS-7292 (2022).
Anderson, K. L., Zulch, H., O’Neill, D. G., Meeson, R. L. & Collins, L. M. Risk factors for canine osteoarthritis and its predisposing arthropathies: A systematic review. Front. Vet. Sci. 7, 220. https://doi.org/10.3389/fvets.2020.00220 (2020).
Houlihan, K. E. A literature review on the welfare implications of gonadectomy of dogs. J. Am. Vet. Med. Assoc. 250, 1155-1166. https://doi.org/10.2460/javma.250.10.1155 (2017).
Rowlison de Ortiz, A. et al. Initial exploration of the discriminatory ability of the PetPace collar to detect differences in activity and physiological variables between healthy and osteoarthritic dogs. Front. Pain Res. 3, 949877. https://doi.org/10.3389/fpain. 2022.949877 (2022).
Brown, D. C., Boston, R. C., Coyne, J. C. & Farrar, J. T. Ability of the canine brief pain inventory to detect response to treatment in dogs with osteoarthritis. J. Am. Vet. Med. Assoc. 233, 1278-1283. https://doi.org/10.2460/javma.233.8.1278 (2008).
Walton, M. B., Cowderoy, E. C., Wustefeld-Janssens, B., Lascelles, B. D. X. & Innes, J. F. Mavacoxib and meloxicam for canine osteoarthritis: A randomised clinical comparator trial. Vet. Rec. 175, 280. https://doi.org/10.1136/vr. 102435 (2014).
Knazovicky, D., Tomas, A., Motsinger-Reif, A. & Lascelles, B. D. Initial evaluation of nighttime restlessness in a naturally occurring canine model of osteoarthritis pain. PeerJ 3, e772. https://doi.org/10.7717/peerj. 772 (2015).
Brown, D. C., Boston, R. C. & Farrar, J. T. Use of an activity monitor to detect response to treatment in dogs with osteoarthritis. J. Am. Vet. Med. A 237, 66-70. https://doi.org/10.2460/javma.237.1.66 (2010).
Enomoto, M., Baines, E. A., Roe, S. C., Marcellin-Little, D. J. & Lascelles, B. D. X. Defining the rate of, and factors influencing, radiographic progression of osteoarthritis of the canine hip joint. Vet. Rec. 189, e516. https://doi.org/10.1002/vetr.516 (2021).
Smith, G. K. et al. Chronology of hip dysplasia development in a cohort of 48 Labrador retrievers followed for life. Vet. Surg. 41, 20-33. https://doi.org/10.1111/j.1532-950X.2011.00935.x (2012).
van Hagen, M. A., Ducro, B. J., van den Broek, J. & Knol, B. W. Incidence, risk factors, and heritability estimates of hind limb lameness caused by hip dysplasia in a birth cohort of boxers. Am. J. Vet. Res. 66, 307-312. https://doi.org/10.2460/ajvr.2005.66. 307 (2005).
Acknowledgements
We acknowledge Drs. Abi Taylor, Amy Snyder, Mariea Ross-Estrada, Kelli Ferris, Diane Deresienski, and Erin Frey for helping with the recruitment. We thank James Robertson for assisting with the statistical analysis.
Author contributions
S.R., J.F.I., N.A.T. and B.D.X.L.: study design. M.E., N.D.C., J.H., A.T., B.D.X.L. and T.C.: patient recruitment, data collection, entry, and verification (QC). M.E., A.N.H., E.P., S.A., E.H.: data analysis. LO: statistical analysis. M.E. and B.D.X.L.: manuscript preparation. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by Elanco Animal Health (NC State Grant # 2020-0044).
Competing interests
NAT is an employee of Elanco Animal Health. BDXL is a paid consultant for Elanco Animal Health; JFI receives license fees for the LOAD and has engaged in paid continuing education lectures on behalf of Elanco. No other authors have any conflicts to disclose.
Additional information
Supplementary Information The online version contains supplementary material available at https://doi.org/ 10.1038/s41598-024-52324-9.
Correspondence and requests for materials should be addressed to B.D.X.L.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Translational Research in Pain Program, Department of Clinical Sciences, College of Veterinary Medicine, Comparative Pain Research and Education Centre, North Carolina State University, Raleigh, NC, USA. Department of Statistics, North Carolina State University, Raleigh, NC, USA. Elanco Animal Health, Hook, London, UK. Movement Independent Veterinary Referrals, Cheshire, England, UK. Department of Anesthesiology, Center for Translational Pain Research, Duke University, Durham, NC, USA. Thurston Arthritis Center, UNC, Chapel Hill, NC, USA. email: dxlascel@ncsu.edu