تجربة المرحلة الأولى/الثانية للخلايا العصبية الدوبامينية المشتقة من خلايا iPS لعلاج مرض باركنسون Phase I/II trial of iPS-cell-derived dopaminergic cells for Parkinson’s disease
مرض باركنسون ناتج عن فقدان خلايا الدوبامين العصبية، مما يسبب أعراضًا حركية. أظهرت العلاجات الخلوية الأولية باستخدام الأنسجة الجنينية وعودًا ولكنها واجهت مضاعفات ومخاوف أخلاقية.ظهرت خلايا الجذع متعددة القدرات (PS) كبديل واعد لتطوير علاجات آمنة وفعالة.في هذه التجربة السريرية من المرحلة I/II في مستشفى جامعة كيوتو، تلقى سبعة مرضى (تتراوح أعمارهم بين 50-69) زراعة ثنائية من خلايا سلفية دافعة للدوبامين مستمدة من خلايا جذعية مستحثة (iPS). كانت النتائج الأولية تركز على السلامة والأحداث السلبية، بينما كانت النتائج الثانوية تقيم تغييرات الأعراض الحركية وإنتاج الدوبامين على مدى 24 شهرًا. لم تكن هناك أحداث سلبية خطيرة، مع 73 حدثًا خفيفًا إلى معتدل. تم الحفاظ على جرعات أدوية المرضى المضادة لباركنسون ما لم تكن هناك حاجة لتعديلات علاجية، مما أدى إلى زيادة في خلل الحركة. أظهرت التصوير بالرنين المغناطيسي عدم وجود نمو زائد في الطعوم. من بين ستة مرضى خضعوا لتقييم الفعالية، أظهر أربعة تحسنًا في درجة مقياس تقييم مرض باركنسون الموحد من جمعية اضطرابات الحركة الجزء III OFF، وأظهر خمسة تحسنًا في درجات ON. كانت التغييرات المتوسطة لجميع المرضى الستة هي و 4.3 نقاط ( ) لدرجات OFF و ON، على التوالي. تحسنت مراحل هوهن-يار في أربعة مرضى. فلورين-18-ل-ديهيدروكسي فينيل ألانين ( ثابت معدل تدفق F-DOPA ) زادت القيم في اللوزة مع زيادات أعلى في مجموعة الجرعة العالية. أظهرت مقاييس أخرى تغييرات طفيفة. أظهر هذا التجربة (jRCT2090220384) أن الخلايا الجذعية المستمدة من الخلايا الجذعية المستنسخة (iPS) المولدة للدوبامين نجت، وأنتجت الدوبامين ولم تشكل أورامًا، مما يشير إلى الأمان والفوائد السريرية المحتملة لمرض باركنسون.
مرض باركنسون (PD) يتميز بفقدان خلايا الدوبامين (DA) في المادة السوداء، مما يؤدي إلى متلازمة حركية تتميز بالبطء الحركي، والصلابة، والرعشة أثناء الراحة. العلاج الطبي يخفف بشكل فعال من أعراض مرض باركنسون في المراحل المبكرة، ولكن الاستخدام المزمن يؤدي إلى مضاعفات مثل تقلبات الحركة والخلل الحركي الناتج عن الأدوية. وبالتالي، تم التحقيق في العلاجات الخلوية لاستبدال خلايا الدوبامين المفقودة كعلاج بديل.
أظهرت الدراسات الأولية المفتوحة أن نسيج الدماغ الجانبي الجنيني البشري (hfVM) المزروع في النواة المذنبة للمضيف يمكنه تصنيع الدوبامين وتحسين الأعراض الحركية.ومع ذلك، فشلت التجارب السريرية المزدوجة التعمية التي تستخدم العلاج الوهمي في إثبات فعالية كبيرة وكشفت عن آثار جانبية مثل اضطرابات الحركة الناتجة عن الطعوم (GIDs).علاوة على ذلك، فإن القضايا الأخلاقية والصعوبات في الحفاظ على إمداد مستقر قد أعاقت التطبيق السريري لـ hfVM. يقوم الباحثون الأوروبيون حاليًا بإجراء تجربة سريرية لإعادة تقييم hfVM (NCT01898390).بينما يتم استكشاف خلايا الدوبامين المشتقة من خلايا الجذع كبديل مصدر المتبرعمؤخراً، اقترح حالة واحدة للاستخدام الرحيم لزراعة الخلايا الذاتية إمكانية خلايا iPS.. علاوة على ذلك، فإن التجارب السريرية التي تستخدم خلايا جذعية جنينية بشرية مستمرة أيضًا (NCT04802733 و NCT05635409 ). لقد طورنا سابقًا طريقة لتحفيز خلايا الدوبامين من خلايا iPS البشرية وفرزها للحصول على سلالات الدوبامين.. هذه الخلايا أنتجت الدوبامين في أدمغة نماذج مرض باركنسون لدى الرئيسيات غير البشرية وحسنت من أعراضها الحركية.بعد الدراسات ما قبل السريرية التي تؤكد السلامة من حيث القدرة على تكوين الأورام، السمية وتوزيع المواد الحيويةلقد تلقينا موافقة من الحكومة اليابانية ومجلس المراجعة المؤسسية في جامعة كيوتو. هنا نبلغ عن نتائج تجربتنا السريرية التي أطلقناها في عام 2018.
المشاركون
في البداية، تم تسجيل سبعة مرضى في مستشفى جامعة كيوتو وتم تشخيصهم وفقًا لمعايير الجمعية الدولية لاضطرابات الحركة (MDS) السريرية.
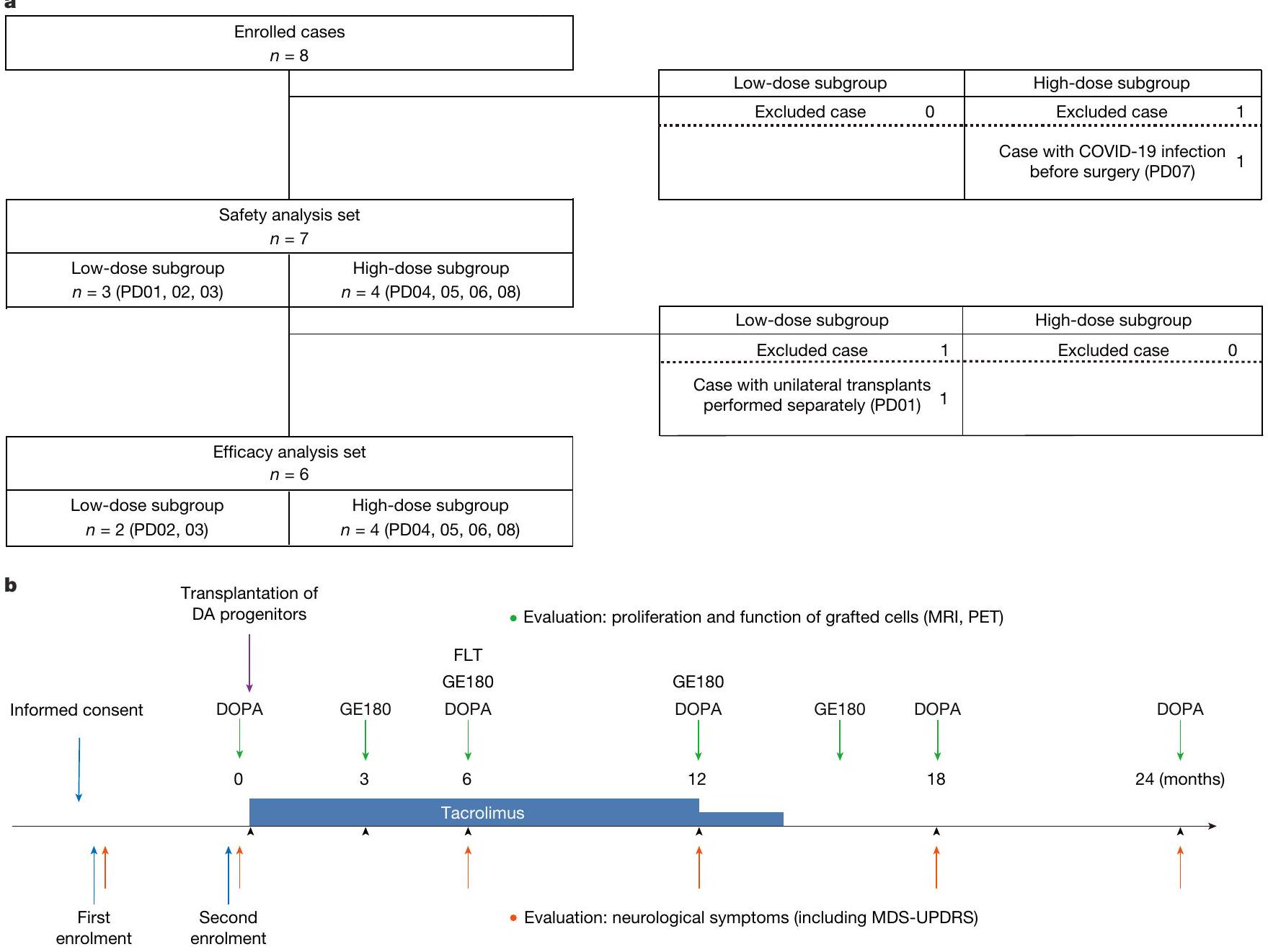
الشكل 1 | التسجيل والمتابعة. أ، تم تجنيد المرضى وتقييمهم في مستشفى جامعة كيوتو بين أغسطس 2018 ويناير 2019. تم تصنيف أول ثلاثة مرضى في مجموعة الجرعة المنخفضة، بينما تم تصنيف الأربعة المتبقية في مجموعة الجرعة العالية. تم استبعاد مريض مسجل قبل الجراحة بسبب إصابته بعدوى COVID-19. تلقى المريض الأول عمليات جراحية أحادية الجانب بفاصل زمني قدره ثمانية أشهر بين الإجراءات وتم تضمينه فقط في تقييم السلامة. تم إجراء تحليل الفعالية على المرضى الستة المتبقين. ب، بعد تقديم الموافقة المستنيرة، تم تسجيل المرضى في هذه التجربة السريرية وخضعوا لتقييم عصبي لأكثر من 6 أشهر. إذا لم يتم ملاحظة تغييرات عرضية ملحوظة خلال هذا خلال هذه الفترة، تم إعادة تسجيل المرضى لإجراء الجراحة وخضعوا لتقييم عصبي إضافي (بما في ذلك MDS-UPDRS) ودراسة PET باستخدام F-DOPA. بعد زراعة الخلايا، تم إجراء تصوير الدماغ (MRI وPET) وتقييمات عصبية (بما في ذلك MDS-UPDRS) فيو 24 شهرًا. شملت دراسات PETF-DOPA (لتقييم تخليق الدوبامين)F-GE180 (للكشف عن الالتهاب) وF-FLT (لتقييم تكاثر الخلايا). بالنسبة لتثبيط المناعة، تم إعطاء التاكروليموس (0.06 ملغ لكل كغ مرتين يومياً)، مع تعديل الجرعة للحفاظ على مستويات القاع المستهدفة منتم تقليل الجرعة إلى النصف بعد 12 شهرًا وتوقفت بعد 15 شهرًا. معايير. ومع ذلك، انسحب مريض واحد بسبب إصابته بفيروس كورونا 2019 (COVID-19)، مما استدعى تسجيل مريض إضافي لاحقًا. لتأكيد سلامة الزرع، تلقى المشارك الأول طعماً من الجسم المخطط الأيسر وتمت مراقبته لمدة 8 أشهر قبل أن يتلقى طعماً من الجسم المخطط الأيمن. تم تضمين هذا المريض فقط في تقييم السلامة. تم تقييم الفعالية في المرضى الستة المتبقين الذين خضعوا لجراحة ثنائية متزامنة (الشكل 1 أ، ب). جميع المرضى استوفوا معايير الأهلية والاستبعاد (طرق إضافية)، وملخص خصائصهم الأساسية موجود في الجدول 1 من البيانات الموسعة.
تصميم التجربة
تم إجراء هذه التجربة السريرية التي بدأها المحقق، وهي تجربة مفتوحة، من المرحلة الأولى/الثانية، في مركز واحد (jRCT2090220384) في مستشفى جامعة كيوتو للتحقيق في سلامة وفعالية زراعة الأنسجة في النواة المذنبة لـ خلايا جذعية مستمدة من خلايا iPS المأخوذة من متبرعين في مرضى باركنسون. خضع المرضى لزراعة ثنائية الجانب لخلايا DA وتمت متابعتهم لمدة 24 شهرًا. تلقى ثلاثة مرضى (PD01-03) زراعة بجرعة منخفضة (2.1-2.6خلايا لكل نصف كرة) وأربعة مرضى (PD04-06 وPD08) تلقوا زراعة جرعة عالية (5.3خلايا لكل نصف كرة) (الشكل 1أ). تم إعطاء التاكروليموس (0.06 ملغ لكل كغ مرتين يوميًا) وتم ضبطه للوصول إلى مستويات القاع المستهدفة ( )، مع تقليل الجرعة إلى النصف عند 12 شهرًا وإيقافها عند 15 شهرًا.
توليد خلايا iPS البشرية
تم إنشاء خط خلايا iPS البشرية من الدرجة السريرية (QHJIO1sO4) من الدم المحيطي من فرد صحي متجانس للنوع الأكثر شيوعًا في السكان اليابانيين (HLA-A 24:02، HLA-B 52:01، HLA-DRB1 15:02، HLA-C 12:02، HLA-DQB1
06:01، HLA-DPB1 09:01)، والذي يتطابق مع 17% من السكان اليابانيين.
تحفيز خلايا DA والزرع
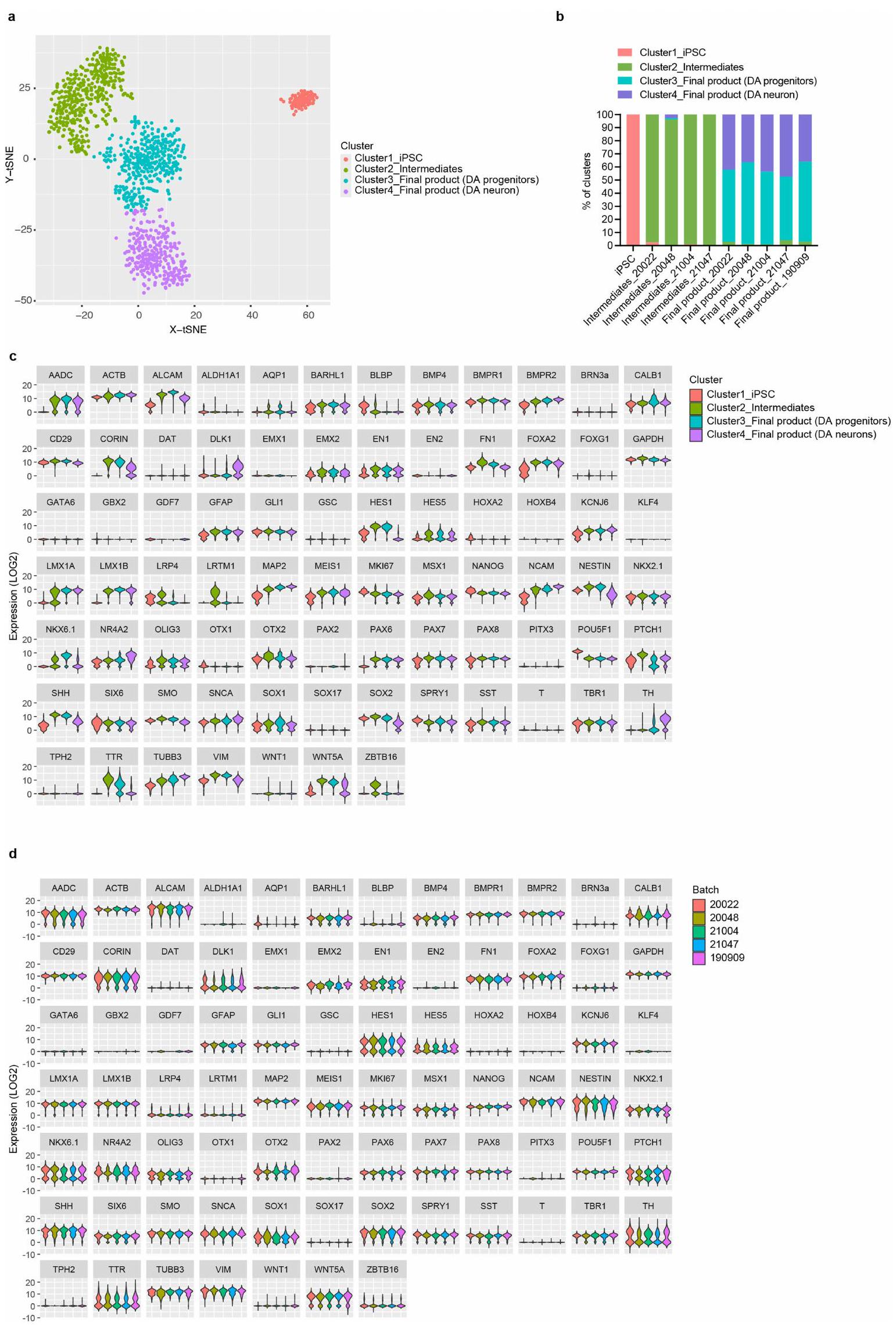
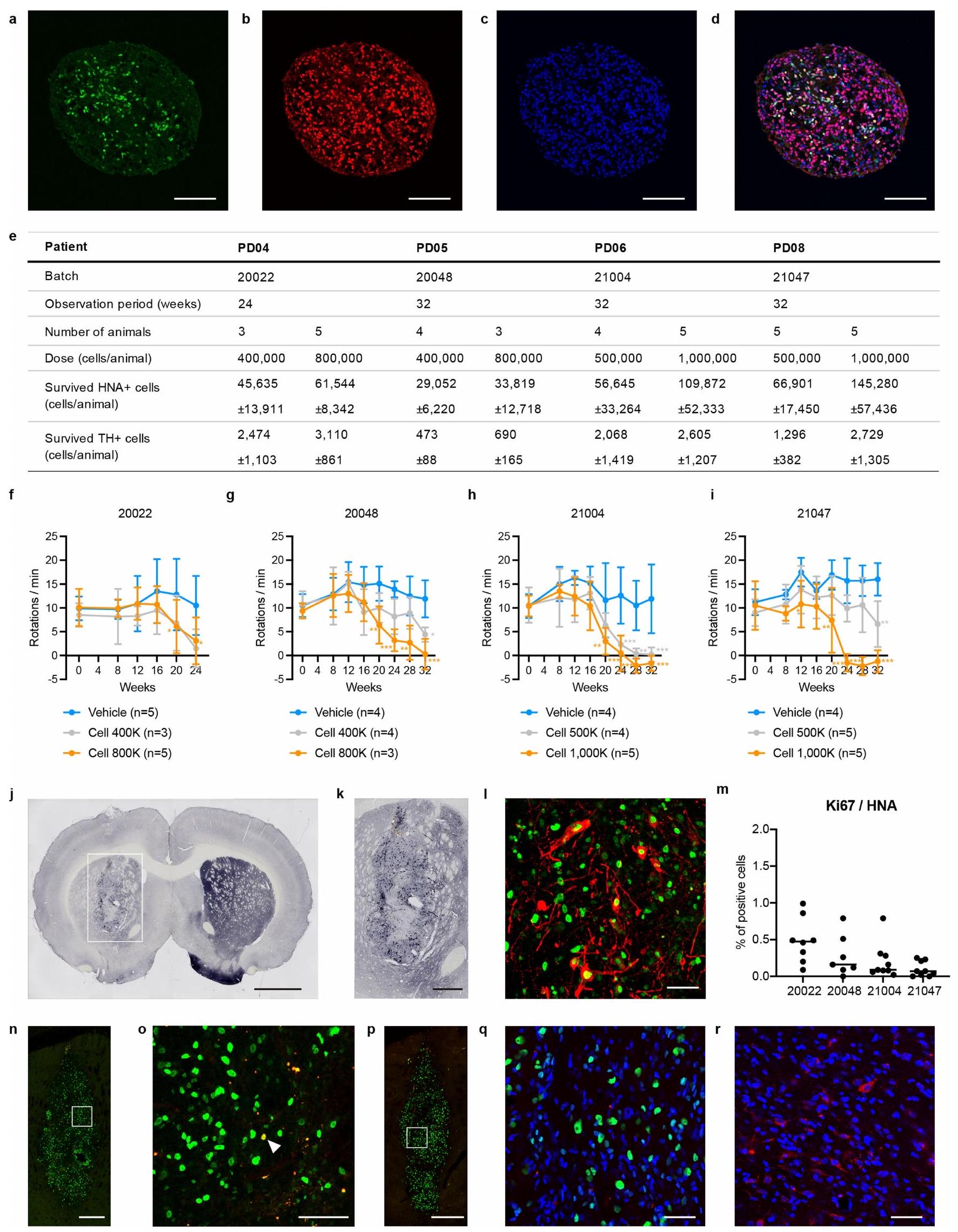
تم تحفيز أسلاف DA كما تم وصفه سابقًالتغذية خلايا DA الأصلية والقضاء على الخلايا غير المستهدفة،(علامة لوحة الأرضية) تم فرز الخلايا في الأيام 11-13، مع زراعة الخلايا المفروزة في وسط تمايز عصبي لتشكيل كرات تجميعية. تم زرع المنتج النهائي الطازج الذي يحتوي على سلالات DA التي تلبي معايير مراقبة الجودة (الجدول التكميلي 1) بشكل ثنائي في البوتامين باستخدام نظام ملاحة جراحية عصبية. أكدت تحليل PCR الكمي للخلايا المفردة مع النسخ العكسي (RT-qPCR) الإنتاج المستقر لسلالات DA. تم تمايز خلايا iPS إلى خلايا عصبية DA، بناءً على الفرز لـ CORIN الخلايا، مما أسفر عن منتج نهائي يتكون من حوالي سلالات DA و خلايا عصبية DA (الشكل البياني الممتد 1). من المهم أنه لم يتم الكشف عن أي خلايا تعبر عن TPH2 (علامة للخلايا العصبية السيروتونية). تم زرع نفس خلايا المتبرعين المستخدمة للمرضى PD04-PD08 في نماذج الفئران PD لتقييم بقاء الخلايا، وتكاثرها وإمكانات تمايزها (الشكل البياني الممتد 2). عبرت خلايا المتبرعين عن NURR1 و FOXA2 وعند زراعتها، تمايزت إلى خلايا عصبية DA إيجابية لـ هيدروكسيل التيروزين ()، مما حسن السلوك الدوراني لفئران نموذج PD. بعد 24 أو 32 أسبوعًا من الزرع، لم يتم ملاحظة أي نمو شبيه بالورم، و(علامة للخلايا المتكاثرة) كانت الخلايا أقل من وموزعة بشكل نادر في الطعوم. علاوة على ذلك، لم يتم الكشف عن أي خلايا إيجابية لـ 5-هيدروكسي تريبتامين (5-HT) (علامة للخلايا العصبية السيروتونية).
النقطة النهائية الأولية: ملف الأحداث السلبية
لم يتم الإبلاغ عن أي أحداث سلبية خطيرة تتطلب دخول المستشفى أو تؤدي إلى الوفاة. عانى جميع المرضى السبعة () من إجمالي 73 حدثًا سلبيًا، يتكون من 72 حدثًا خفيفًا وحالة واحدة متوسطة من خلل الحركة (الجدول التكميلي 2). كان الحدث السلبي الأكثر شيوعًا هو حكة موقع التطبيق، التي لوحظت في أربعة مرضى (57.1%). لم تكن هناك اختلافات واضحة في الطيف، والتكرار وشدة الأحداث السلبية المتعلقة بالعلاج بين مجموعات الجرعة المنخفضة والعالية. كانت هذه الأحداث عابرة، وكان من غير المحتمل أن تكون مرتبطة بزراعة الخلايا أو التاكروليموس. كان الحدث السلبي الوحيد المحتمل المرتبط بزراعة الخلايا هو تصلب الرقبة وخلل الحركة المؤلم في الطرف العلوي الأيمن خلال حالة الدواء. تم تحمل إدارة التاكروليموس بشكل جيد ولكنها مرتبطة بشكل محتمل بأحداث سلبية في ثلاثة مرضى ()، بما في ذلك ضعف الكبد ()، وزيادة مستويات غاما-جلوتاميل ترانسفيراز ()، والتهاب المثانة ()، وفطريات الأظافر () وضعف الكلى ().
النقطة النهائية الثانوية: السلامة
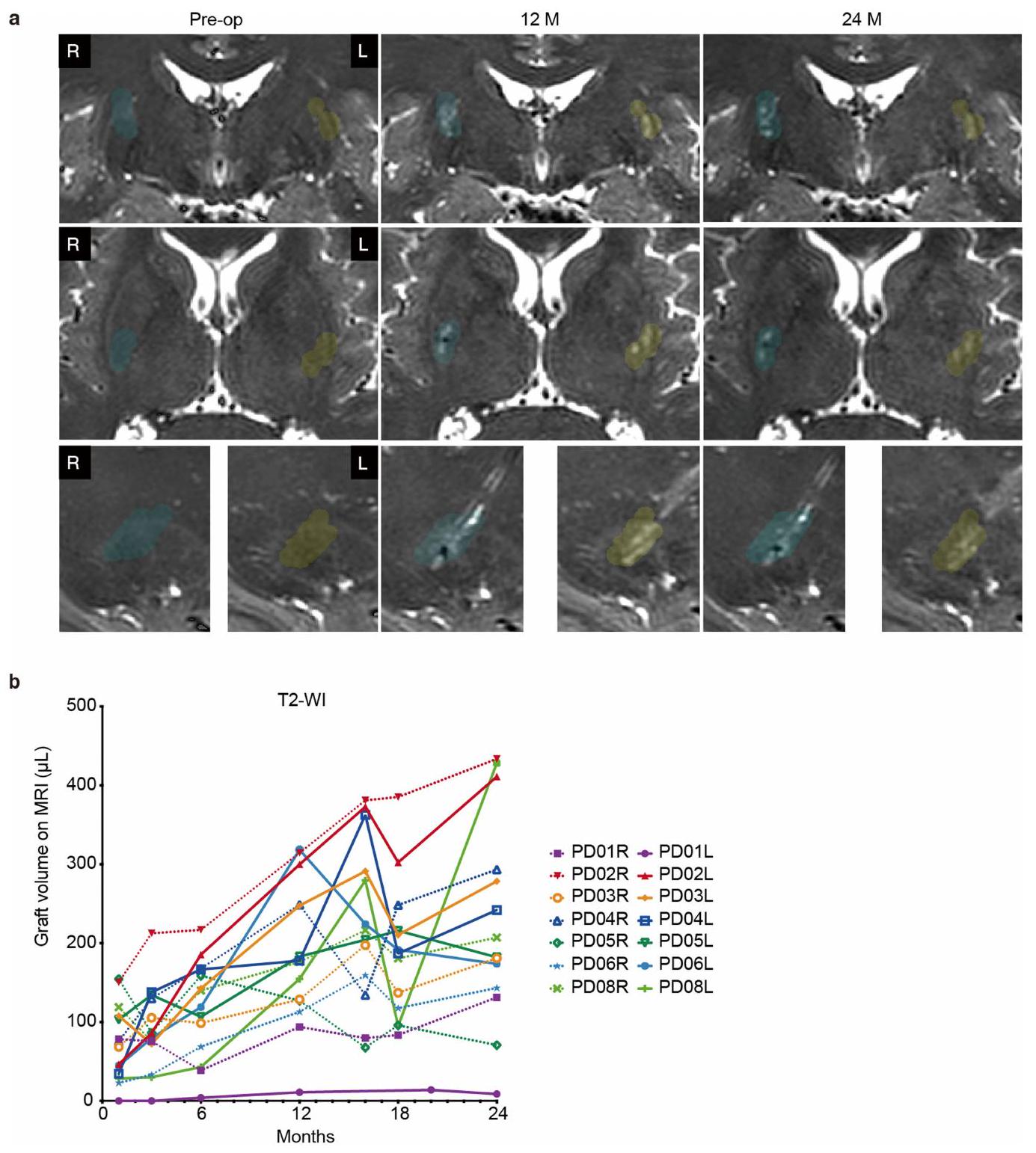
حددت مسحات التصوير بالرنين المغناطيسي (MRI) المتسلسلة خلال فترات المتابعة الطعوم كمناطق شديدة الكثافة في البوتامين على صور T2 الموزونة في جميع المرضى. أظهر التحليل الكمي لحجم الطعوم زيادة تدريجية في الحجم على مدى 24 شهرًا، دون دليل على تضخم غير طبيعي شبيه بالورم (الشكل البياني الممتد 3). لم يظهر أي من المرضى زيادة في تراكم الفلورين-18-فلورثيميدين ( F-FLT) في الشرياني المزروع. علاوة على ذلك، لم يظهر أي مرضى مناطق شديدة الكثافة في T2 واستعادة الانقلاب السائل (FLAIR) أو امتصاص ملحوظ لبروتين الناقل-الليغاند، الفلورين-18-فلوتريسيكلاميد ( F-GE180: علامة على تنشيط الميكروغليا) ، مما يدل على التهاب واضح في البوتامين والمناطق المحيطة.
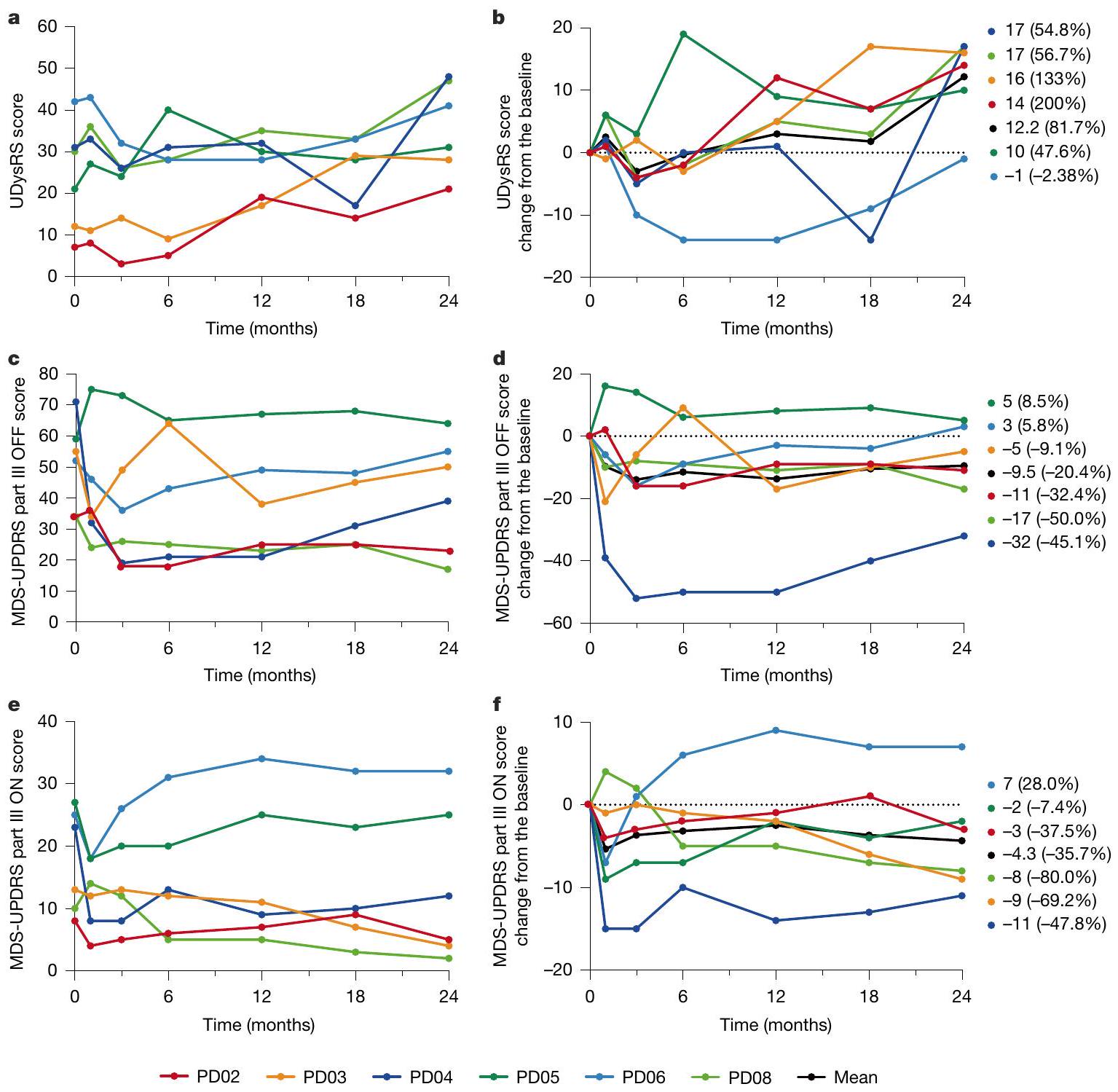
مقياس تقييم خلل الحركة الموحد (UDysRS) الإجمالي زاد عند 24 شهرًا في جميع المرضى، باستثناء PD06، بمتوسط زيادة قدرها 12.3 نقطة () من الخط الأساسي (الجدول التكميلي 2). باستثناء PD01، الذي خضع لعملية جراحية على مرحلتين بفاصل 8 أشهر وتمت ملاحظته لمدة 32 شهرًا، كانت الزيادة المتوسطة 12.2 نقطة (; الشكل 2a,b). في دفاتر الملاحظات الذاتية للحركة، سجل المرضى خلل الحركة خلال فترة الوقت النشط. لم يتم ملاحظة زيادة واضحة في خلل الحركة المزعج خلال فترة الوقت غير النشط.
النقطة النهائية الثانوية: الفعالية
من بين المرضى الستة في مجموعة الفعالية، أظهر أربعة (PD02، PD03، PD04 و PD08) تحسنًا في الوظيفة الحركية خلال فترة الوقت غير النشط (أكثر من 12 ساعة بدون دواء)، كما تم تقييمه بواسطة مقياس تقييم مرض باركنسون الموحد MDS (MDS-UPDRS) الجزء الثالث. كانت التغيرات المتوسطة من الخط الأساسي -9.5 نقاط عند 24 شهرًا، على ما يبدو مستقلة عن جرعة الخلايا المزروعة (الشكل 2c,d والجدول التكميلي 2). فيما يتعلق بـ MDS-UPDRS الجزء الثالث ON (مع الدواء)، تحسن خمسة مرضى (PD02، PD03، PD04، PD05 و PD08)، مع تغير متوسط من الخط الأساسي قدره -4.3 نقاط () عند 24 شهرًا (الشكل 2e,f والجدول التكميلي 2). بينما يعتمد MDS-UPDRS الجزء الثالث على فحص موضوعي من قبل طبيب أعصاب، فإن الأجزاء I و II مشتقة من مقابلات المرضى حول الوظائف الحركية وغير الحركية في الحياة اليومية. عند تقييم MDS-UPDRS الأجزاء I + II + III OFF، لوحظ تحسن طفيف قدره -3.1 نقاط () في المتوسط عند 24 شهرًا (الجدول التكميلي 3).
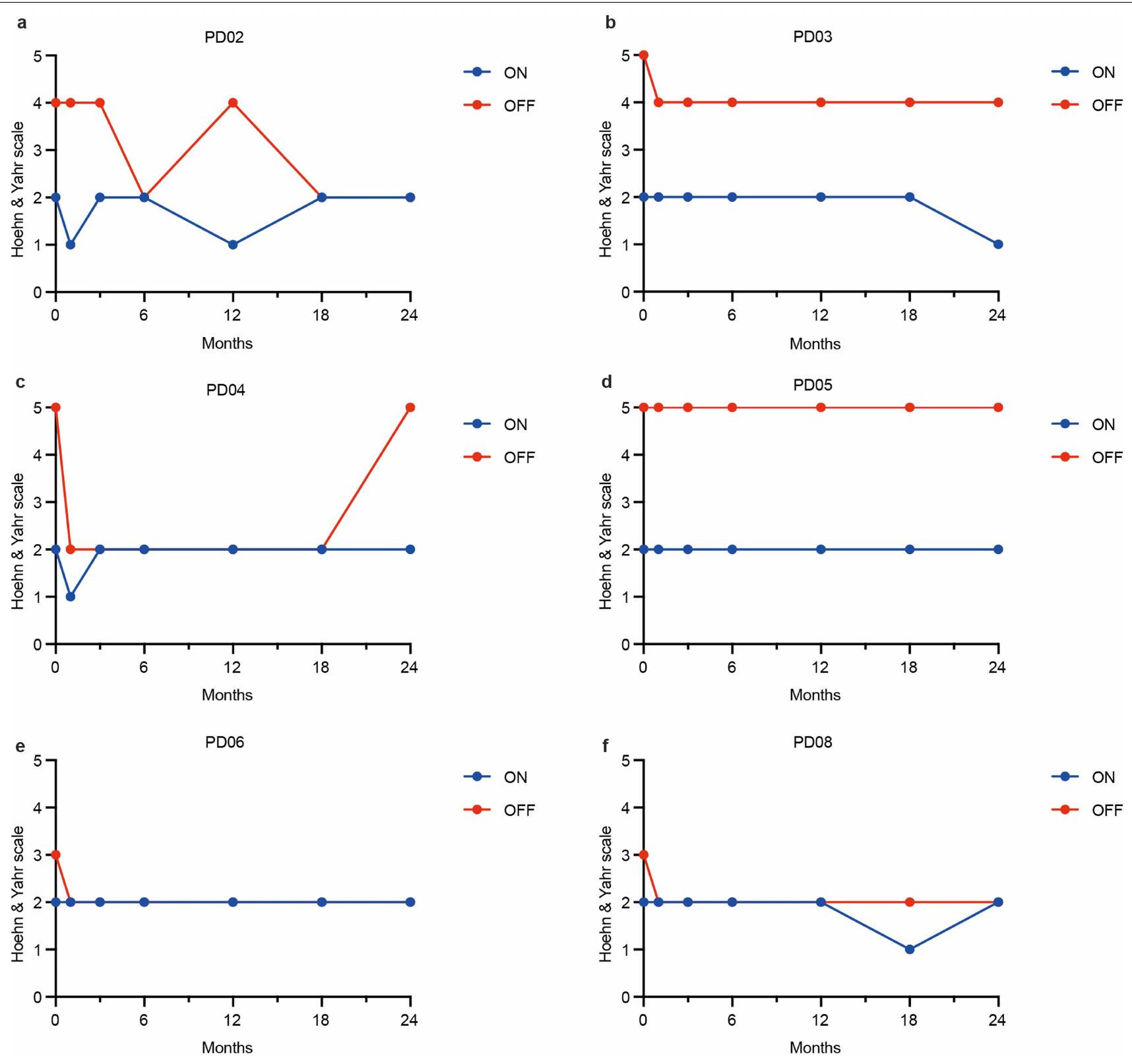
في تقييمنا لمرحلة هوهن-يار خلال فترة الوقت غير النشط، تحسن أربعة مرضى: PD02 بمقدار مرحلتين و PD03 و PD06 و PD08 بمقدار مرحلة واحدة لكل منهم عند 24 شهرًا. تحسن مريض واحد (PDO3) بمقدار مرحلة واحدة خلال الوقت النشط (الشكل البياني الممتد 4 والجدول التكميلي 2).
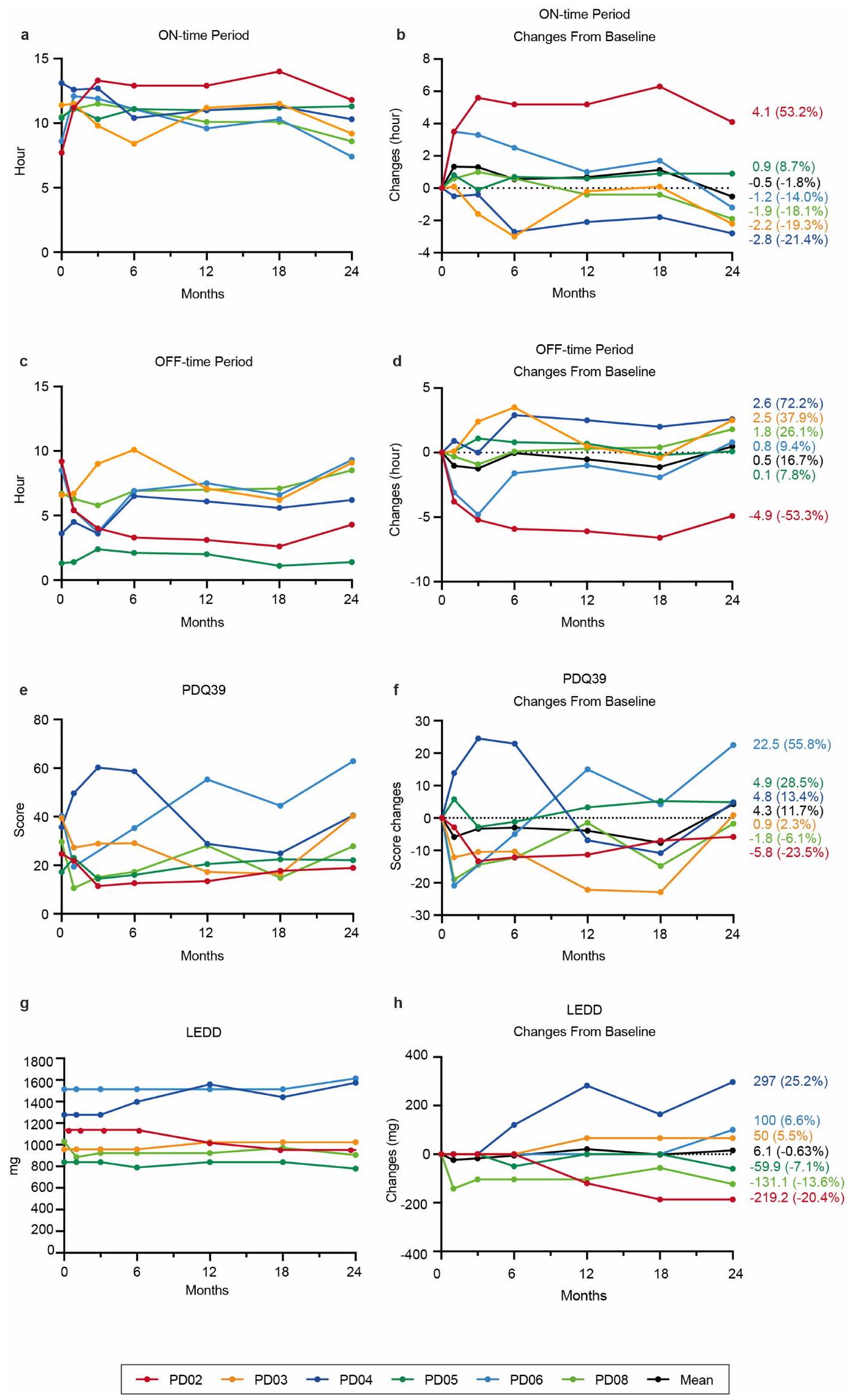
تم تحليل مقاييس ثانوية أخرى، مثل وقت النشاط/عدم النشاط واستبيان مرض باركنسون المكون من 39 عنصرًا (PDQ-39). بينما أظهر بعض المرضى تحسنًا خلال الملاحظات، لم يتم ملاحظة أي تحسن واضح في المتوسط عند 24 شهرًا (الشكل البياني الممتد 5 والجدول التكميلي 2). طوال الدراسة، تم الحفاظ على جرعات أدوية المرضى المضادة لباركنسون ما لم تكن هناك ضرورة علاجية. تم اتخاذ هذا النهج لتجنب تشويش تقييم نتائج الزراعة، حيث يمكن أن تؤثر التغييرات في الأدوية المضادة لباركنسون الفردية على النتائج. وبالتالي، كانت متوسط جرعة الليفودوبا المعادلة اليومية (LEDD) ظلت مستقرة تقريبًا خلال التجربة، مع زيادة متوسطة قدرها 6.15 ملغ يوميًا ( انخفاض) عند 24 شهرًا (الشكل البياني الممتد 5 والجدول التكميلي 2).
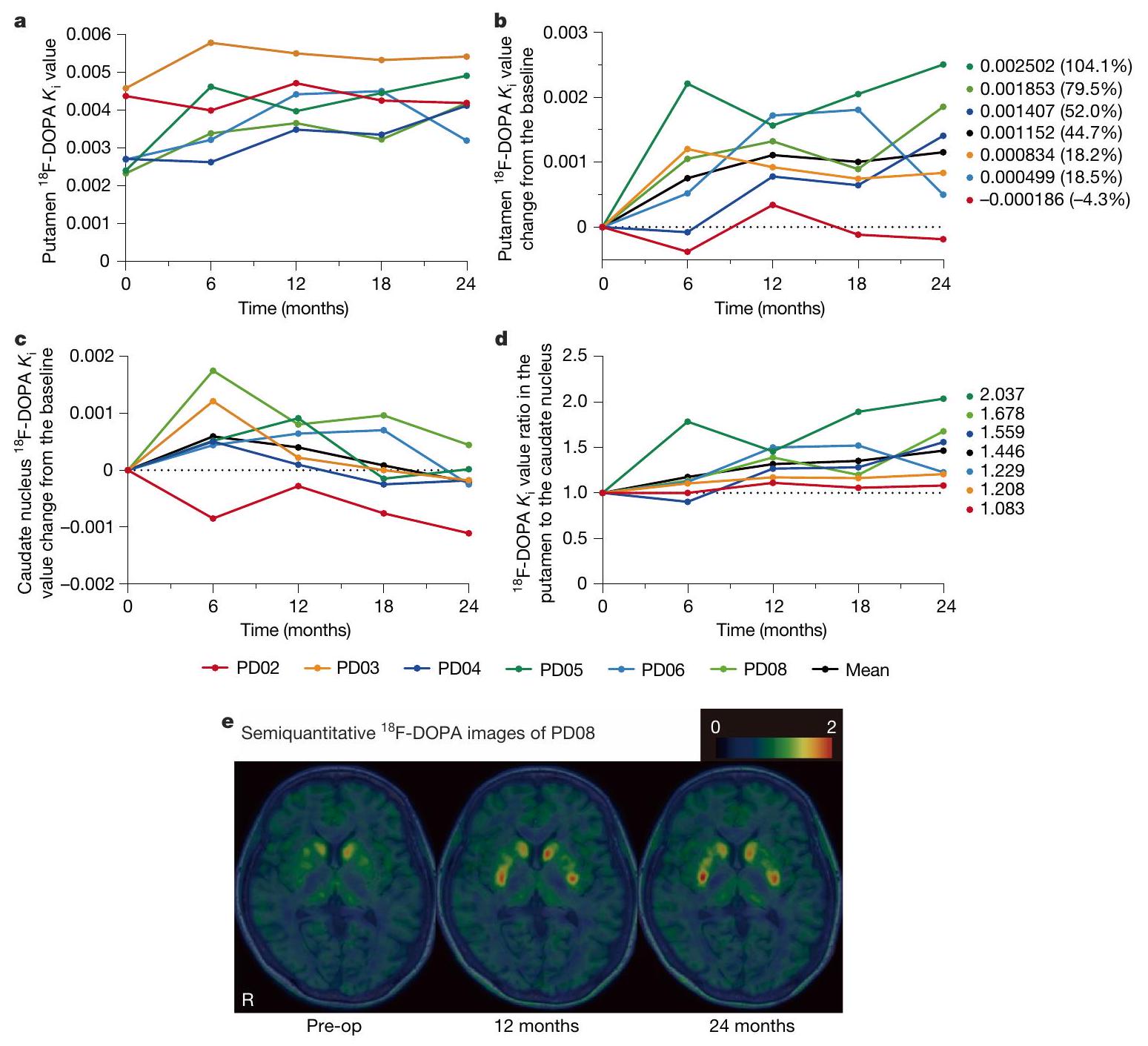
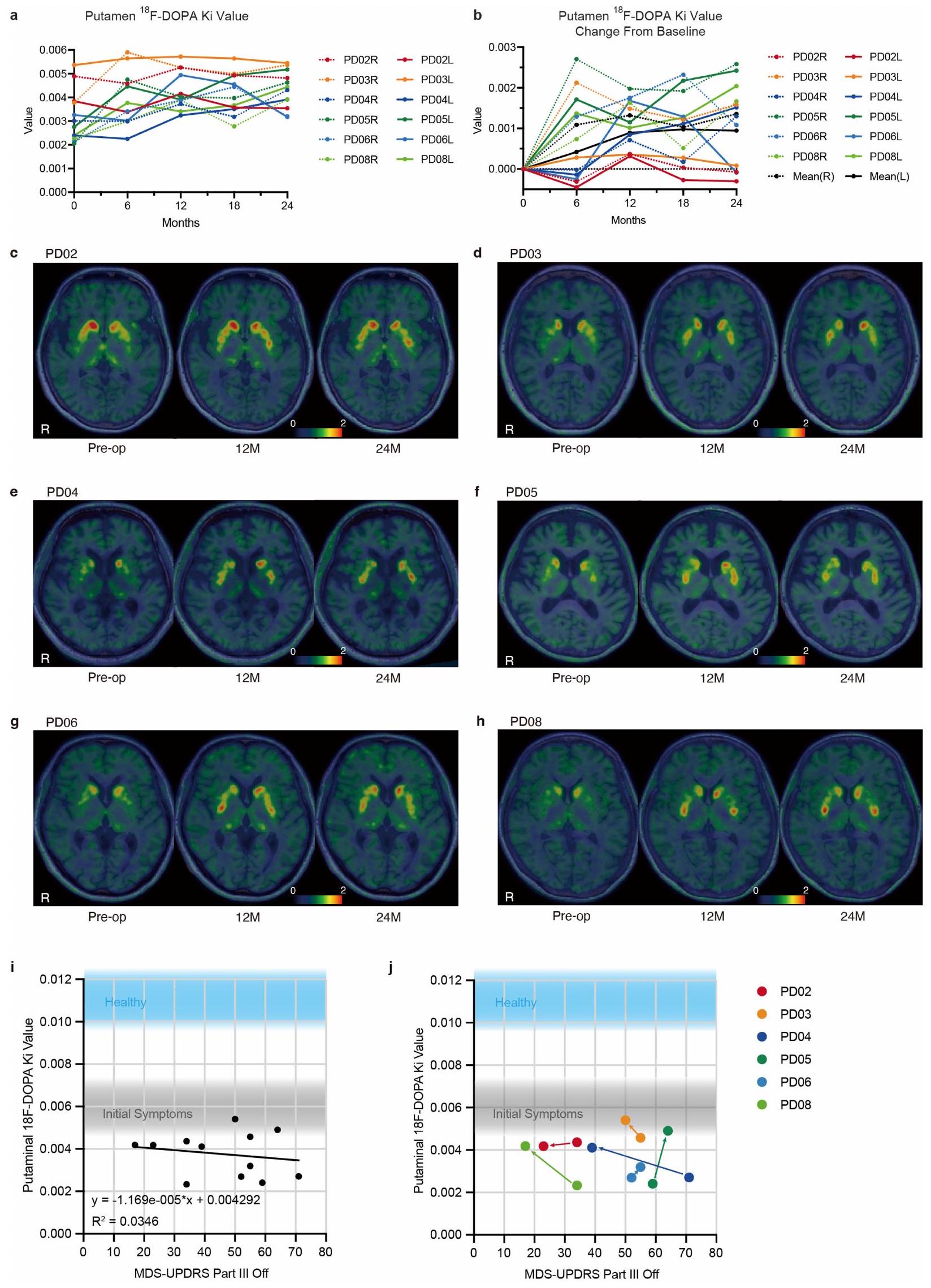
زادت القيم المتوسطة الإجمالية للبوتامين F-DOPA بمقدار (من 0.0032 إلى 0.0043) عند 24 شهرًا. على وجه التحديد، أظهرت مجموعة الجرعة المنخفضة زيادة قدرها ، بينما أظهرت مجموعة الجرعة العالية زيادة قدرها (الجدول التكميلي 2). زادت قيم F-DOPA في اثنين من الأربعة بوتامين المزروعة في مجموعة الجرعة المنخفضة وسبعة من الثمانية بوتامين المزروعة في مجموعة الجرعة العالية (الشكل 3a,b,e والجدول التكميلي 6). بالمقابل، انخفضت القيمة المتوسطة الإجمالية للنواة الذنب F-DOPA (الشكل 3c). وبالتالي، زادت نسبة القيم في البوتامين إلى النواة الذنب عند 24 شهرًا في جميع الحالات، مما يشير إلى زيادة في تخليق DA في البوتامين على الرغم من التدهور المرضي (الشكل 3d).
المناقشة
بدأ استبدال خلايا DA المفقودة بـ hfVM في المرضى الذين يعانون من PD في . على الرغم من أنه من المتوقع أن تكون خلايا PS مصدر خلايا متبرعة بديلة لـ hfVM، إلا أن سلامة وفعالية سلالات DA المستمدة من خلايا iPS لا تزال غير واضحة. أكدت هذه التجربة السريرية الأولى باستخدام خلايا iPS أن سلالات DA المستمدة من خلايا iPS يمكن أن تبقى على قيد الحياة دون تشكيل أورام وتنتج DA في البوتامين للمرضى الذين يعانون من PD. علاوة على ذلك، لم يتم الإبلاغ عن أي أحداث سلبية خطيرة أو GIDs. أظهر أربعة من ستة مرضى تحسنًا في MDS-UPDRS الجزء الثالث OFF عند 24 شهرًا بعد الزرع، مما يشير إلى أن الخلايا المزروعة عملت كخلايا عصبية DA.
لم يتم الإبلاغ عن أي أحداث سلبية خطيرة لجميع المرضى السبعة الذين خضعوا لتقييم السلامة. تم قياس حجم الطعم باستخدام التصوير بالرنين المغناطيسي
الشكل 2 | التغيرات الزمنية في النقاط النهائية السريرية. أ، ب، التغيرات الزمنية في درجات UDysRS لكل مريض من التسجيل (0 شهر) إلى نهاية فترة الملاحظة (24 شهرًا) لتقييم السلامة. ب، تغييرات الدرجات من الخط الأساسي، مع المتوسط ممثلًا بالخط الأسود. التغيرات المطلقة والنسبية (النسبة المئوية) عند 24 شهرًا موضحة على اليمين. ج-ف، التغيرات الزمنية في درجات MDS-UPDRS الجزء الثالث خلال
فترات الأدوية الموقوفة (c,d) والمستخدمة (e,f) لكل مريض من التسجيل (0 شهر) حتى نهاية الملاحظة (24 شهر) لتقييم الفعالية. d,f, تغييرات الدرجات من الخط الأساسي. المتوسط ممثل بالخط الأسود. التغييرات المطلقة والنسبية (النسبة المئوية) عند 24 شهر موضحة على اليمين.
زادت الصور المعتمدة على T2 تدريجياً على مدار 24 شهرًا. ومع ذلك، لم يتم تحديد أي نمو ورمي، كما يتضح من غياب امتصاص F-FLT، وهو علامة على تكاثر الخلايا، والتي تم دعمها بشكل غير مباشر من خلال نتائج تجربة الزرع باستخدام نفس خلايا المتبرع في نموذج الفأر PD. أظهرت التحليلات النسيجية عند 24 أو 32 أسبوعًا عدم وجود نمو شبيه بالورم، مع أقل من من الخلايا إيجابية Ki-67. بدلاً من التكاثر، أفادت دراسة سابقة على الحيوانات أن الزيادة الظاهرة في حجم الطعوم كانت بسبب انتشار الخلايا المزروعة . بينما قد تنطبق مثل هذه التأثيرات أيضًا على تجربتنا، فإن التأكيد الإضافي من خلال المتابعة طويلة الأمد والفحوصات النسيجية بعد الوفاة ضروري. كان طيف الأحداث السلبية مشابهًا لتلك التي تم مواجهتها مع أدوية استبدال DA المزمنة، وإدارة التاكروليموس وجراحة الدماغ. تم ملاحظة تصلب الرقبة والد dystonia المؤلمة في الطرف العلوي الأيمن في PD01 خلال حالة الدواء، وهو ظاهرة قد تكون مرتبطة بالطعوم. كانت الأحداث السلبية المتعلقة بالتاكروليموس والجراحة قابلة للإدارة وقابلة للعكس.
كانت إحدى القضايا الحرجة بشأن زراعة hfVM هي GIDs . في هذه التجربة، أظهر ستة من أصل سبعة مرضى تفاقمًا طفيفًا في الديسكينيزيا، مما أدى إلى زيادة متوسطة في إجمالي درجة UDysRS بمقدار 12.3 نقطة ( ) من الخط الأساسي عند 24 شهرًا، ربما لأن جرعات الأدوية المضادة للباركنسون تم الحفاظ عليها طوال التجربة، باستثناء عندما كانت التعديلات العلاجية ضرورية. تم تصميم البروتوكول لتقليل تأثير تغييرات الأدوية. بشكل متسق، سجل المرضى الديسكينيزيا في كل من الأطراف العلوية والسفلية خلال فترة الوقت النشط. هذا العرض السريري نموذجي للديسكينيزيا الناتجة عن الأدوية وليس لـ GIDs، التي تحدث خلال الوقت الموقوف وغالبًا ما تُلاحظ بشكل رئيسي في الأطراف السفلية . وهذا يشير إلى أن الخلايا المزروعة تكرر تأثيرات الليفودوبا، بما في ذلك الميل إلى تحفيز الديسكينيزيا في المرضى المعرضين. بدلاً من ذلك، قد يؤدي توزيع التحفيز DA من الطعم بشكل مركزي بدلاً من منتشر إلى تفاقم الديسكينيزيا . في التقارير السابقة، تم نسب GIDs إلى الخلايا العصبية السيروتونينية الموجودة في نسيج hfVM . في تحضيرنا من سلف DA، نحن
الشكل 3 | تم الكشف عن تخليق DA بواسطة F-DOPA PET. أ، ب، التغيرات الزمنية في F-DOPA القيم (متوسط الجانبين) في البوتامين لكل مريض من التسجيل (0 شهر) حتى نهاية فترة الملاحظة (24 شهر).
ب، تغييرات قيمة من الخط الأساسي؛ المتوسط ممثل بالخط الأسود. التغييرات المطلقة والنسبية (النسبة المئوية) عند 24 شهر موضحة على اليمين. ج، تغييرات قيمة F-DOPA (متوسط الجانبين) من الخط الأساسي في النواة الذيلية لكل مريض، مما يشير إلى تدهور مرضي في PD. د، نسبة القيم بين البوتامين و
النواة الذيلية، مما يبرز تأثير زراعة الخلايا على التدهور المرضي. التغييرات النسبية عند 24 شهر موضحة على اليمين. هـ، صور شبه كمية لـ F-DOPA تم إنشاؤها عند بعد الحقن عن طريق طرح إشارة الخلفية القذالية وتطبيع النتيجة على النشاط القذالي في المريض PD08. يشير تغيير اللون من الأخضر الداكن إلى الأحمر في البوتامين الثنائي إلى زيادة امتصاص F-DOPA، مما يعكس تخليق DA بواسطة الخلايا المزروعة. قبل العملية، قبل العملية؛ R، اليمين.
تم تنقية خلايا اللوحة الوسطى وتم القضاء على خلايا اللوحة الجانبية، التي تشمل الخلايا العصبية السيروتونينية. نتيجة لذلك، لم نكتشف أي خلايا 5-HT في الطعوم المشتقة من خلايا المتبرع في نماذج الفأر PD. قد تكون هذه العملية التنقية قد ساهمت في غياب GIDs في تجربتنا.
لا يزال النظام المناسب من مثبطات المناعة في زراعة الأعصاب الألوغينية مثيرًا للجدل. استخدمت التجارب السريرية السابقة مجموعة مختلفة من أدوية مثبطات المناعة، بما في ذلك السيكلوسبورين، الأزايثيوبرين والبريدنيزولون . أظهرت دراساتنا السابقة على الرئيسيات غير البشرية عدم وجود استجابة مناعية حادة بعد زراعة الأنسجة المستمدة من خلايا iPS للقرود دون مثبطات المناعة . علاوة على ذلك، كان التاكروليموس وحده فعالًا في قمع الاستجابات المناعية خلال كل من الزرع الألوغيني (من قرد إلى قرد) وزرع الأنسجة الغريبة (من إنسان إلى قرد) . بناءً على هذه النتائج، استخدمنا التاكروليموس كمثبط المناعة الوحيد في تجربتنا السريرية. أظهرت التحليلات النسيجية من دراسات زراعة خلايا الجنين السابقة أن خلايا DA المزروعة يمكن أن تعيش من 9 إلى 16 عامًا، حتى عند توقف مثبطات المناعة بعد 6 إلى 18 شهرًا من الزراعة . علاوة على ذلك، أظهرت دراستنا باستخدام التصوير المقطعي بالإصدار البوزيتروني (PET) عند 3 و6 و12 شهرًا عدم وجود امتصاص F-GE180، مما يشير إلى غياب التهاب شديد. نتيجة لذلك، أوقفنا علاج التاكروليموس عند 15 شهرًا. بعد إنهاء مثبط المناعة، لم يُلاحظ أي التهاب بسبب الاستجابة المناعية في البوتامين والمناطق المحيطة، كما يتضح من غياب مناطق الزيادة الشديدة على صور T2-weighted وFLAIR MRI أو زيادة امتصاص F-GE180. علاوة على ذلك، لم يكن هناك فرق سريري بين المرضى المتوافقين مع HLA وغير المتوافقين. ومع ذلك، فإن التأكيد الإضافي من خلال المتابعة طويلة الأمد والفحوصات النسيجية بعد الوفاة ضروري للوصول إلى استنتاجات نهائية.
أظهرت نتائجنا تأثيرًا مفيدًا على جزء MDS-UPDRS الثالث خلال كل من فترات الوقت النشط والموقوف. على وجه التحديد، أظهرت PD02 وPD04 وPD08 تحسينات في و خلال الوقت الموقوف عند 24 شهرًا، بينما أظهرت PD03 تحسنًا في . بالنظر إلى الزيادة في امتصاص F-DOPA، تشير هذه النتائج إلى أن
الخلايا المزروعة تعمل كخلايا DA، وبالتالي تحل محل خلايا DA المفقودة وظيفيًا. نظرًا لأن هذه تجربة مفتوحة بدون مجموعة تحكم، من المهم مراعاة التأثير المحتمل لتأثير الدواء الوهمي والتحيز الملاحظ. أبلغت تحليل منهجي لاستجابات الدواء الوهمي (تأثير الدواء الوهمي بالإضافة إلى تحيز الملاحظ) في تسع تجارب مزدوجة التعمية، عشوائية للعلاجات التجديدية لمرض PD عن تحسين متوسط قدره 4.3 نقاط في درجات MDS-UPDRS الجزء الثالث OFF، مع فترة ثقة 95% من 3.1 إلى 5.6، مع متوسط وقت ملاحظة قدره 11.3 شهرًا . علاوة على ذلك، أظهرت دراسة PET أجريت في أربعة من تسع تجارب عدم وجود زيادة كبيرة في امتصاص F-DOPA في المجموعات التي خضعت لعملية وهمية. علاوة على ذلك، يُعتقد أن تأثير الدواء الوهمي في المرضى الذين يعانون من PD يتم وساطته من خلال الإفراج، بدلاً من التخليق، لـ DA الداخلي في النواة المذنبة . بناءً على هذه النتائج، أظهر ثلاثة مرضى على الأقل (PD02 وPD04 وPD08) في هذه التجربة تحسينات في الأعراض الحركية تتجاوز ما يمكن أن يُنسب إلى استجابات الدواء الوهمي، ربما بسبب DA الذي تم تخليقه بواسطة الطعم. يجب التحقق من هذا التفسير بشكل أكبر من خلال الفحوصات النسيجية بعد الوفاة في المستقبل.
من بين المرضى الثلاثة (PD02 وPD04 وPD08) الذين أظهروا تأثيرًا مفيدًا على جزء MDS-UPDRS الثالث، أظهر فقط PD02 تحسنًا في كل من فترة الوقت الموقوف ودرجات PDQ-39. هذه التقييمات ذاتية وتعكس تصورات المريض. من الممكن أن يكون لدى المرضى توقعات عالية جدًا لهذه العلاج الجديد، وأن النتائج لم تلبِ تلك التوقعات العالية على الرغم من التحسينات الموضوعية. في المرضى الآخرين (PD05 وPD06)، استقرت العجز الحركي عند مستوى مشابه من الانخفاض مقارنةً بالذين يتلقون أدوية تقليدية . أظهر هذان المريضان درجة أعلى من التدهور في الأعراض الحركية مقارنةً بالمرضى الآخرين خلال الوقت النشط، مما يشير إلى أن التدهور العصبي الأسرع، خاصة في الأنظمة غير الدوبامينية، قلل من التأثيرات المفيدة التي أنتجها الطعم خلال فترة التجربة. من الجدير بالذكر أن PD05 كان عمره 69 عامًا عند الخط الأساسي، وكما تشير الدراسات السابقة حول زراعة الأنسجة الجنينيةيبدو أن المرضى الأصغر سناً الذين يعانون من أعراض أقل حدة هم مرشحون أكثر ملاءمة لهذا العلاج. بالنظر إلى هذه النتائج، قد يؤدي تحسين معايير أهلية المرضى إلى تعزيز فعالية هذا العلاج.
في بعض الحالات، وخاصة PD03 و PD06، لوحظت تناقضات بين درجات الجزء الثالث من مقياس MDS-UPDRS ومرحلة هوهن-يار. تركز مرحلة هوهن-يار على عدم الاستقرار الوضعي ومشاكل الحركة، في حين يقدم الجزء الثالث من MDS-UPDRS تقييمًا أكثر شمولاً للأعراض الحركية الرئيسية في مرض باركنسون. وبالتالي، قد تفسر تحسينات الاستقرار الوضعي والحركة التحسن الأكبر في مرحلة هوهن-يار مقارنةً بالتغيرات الملحوظة في درجات الجزء الثالث من MDS-UPDRS في هذه الدراسة.
الزيادة الكبيرة في الجسم المخططتشير امتصاص F-DOPA في مجموعة الجرعة العالية مقارنة بمجموعة الجرعة المنخفضة إلى خصائص تعتمد على الجرعة. الرسوم البيانية قبل الزرع وبعد الزرعأظهرت قيم درجات MDS-UPDRS الجزء الثالث في حالة عدم تناول الدواء اتجاهًا عامًا طفيفًا ولكن لم يكن هناك ارتباط واضح على المستوى الفردي (الشكل 6i,j من البيانات الموسعة). قد يكون هذا الافتقار إلى الارتباط بسبب تعقيد علاج استبدال الخلايا:إن امتصاص F-DOPA لا يعكس بالضرورة تنشيط الخلايا العصبية ما بعد المشبك، وتؤثر الأعراض الحركية على كل من الدوائر العصبية الدوبامينية وغير الدوبامينية. من المحتمل أن يتطلب التأثير الوظيفي للخلايا المزروعة أكثر من مجرد توصيل الدوبامين. إن التكامل الناجح للزرع في دماغ المضيف أمر حاسم لتحقيق تعافي سريري ذي مغزى.. احتمال آخر هو أن المطلقالقيمة أكثر أهمية من مستوى الزيادة وأن عدد خلايا الدوبامين العصبية الباقية لا يزال غير كافٍ. وقد أفادت الدراسات السابقة بأنتتراوح قيم الأفراد الأصحاء من 0.010 إلى 0.017 (مع إشارة تجربتنا إلى نطاق من 0.010 إلى 0.015). بينما تظهر أعراض باركنسون عادةً عندماتقل القيم بنسبةإلىمن النطاق الطبيعيحتى أعلىالقيمة الملاحظة عند 24 شهرًا كانت ضمن النطاق المرتبط بظهور الأعراض الأولية. علاوة على ذلك، لم تُظهر 3 من أصل 12 عينة من البوتامين (PDO2R، PD02L، PD06L) زيادة فيامتصاص F-DOPA (الشكل التوضيحي الممتد 6a، b). قد يكون ذلك بسبب إلى القيود التقنية في قياس الامتصاص في كامل البوتامين. ومع ذلك، كشفت صور PET عن امتصاص مميز في مواقع الحقن (الشكل التمديدي 6c-h)، مما قد يكون ساهم في تحسين الأعراض. من المهم أنه لم يكن هناك فرق في الأحداث السلبية بين مجموعات الجرعات المنخفضة والعالية، ولم يتم ملاحظة أي زيادة في نمو الطعوم أو GIDs، حتى في مجموعة الجرعة العالية. بالنظر إلى هذه النتائج، قد يكون من الضروري زراعة المزيد من الخلايا عبر منطقة أوسع لتحقيق تأثيرات علاجية أكثر أهمية. يوفر الملف الأمني الإيجابي الذي لوحظ في هذه التجربة فرصة لاستكشاف ما إذا كانت جرعة أعلى عبر منطقة أوسع يمكن أن تقدم فعالية سريرية أكبر.
أظهرت التجارب السابقة ذات العلامات المفتوحة باستخدام hfVM البشري أن الخلايا المزروعة في الجسم المخطط للمضيف قامت بتخليق الدوبامين وحسنت الأعراض الحركية. في الحالات المواتية، استمرت تحسينات الأعراض لأكثر من 10 سنوات دون حدوث أحداث سلبية خطيرة.“. بينما لم تجد تجربتان مزدوجتا التعمية ومراقبتان بالدواء الوهمي اختلافات كبيرة بين مجموعتي الطعوم والمراقبة، إلا أنهما أظهرتا تحسنًا كبيرًا في الأعراض الحركية في مجموعات فرعية محددة. تشير هذه النتائج إلى أن علاج استبدال الخلايا قد يكون مفيدًا إذا تم اختيار المرضى المناسبين. قد تكون إحدى المجموعات الفرعية المفيدة هي المرضى الذين تبلغ أعمارهم 60 عامًا أو أقل، بينما تضمنت أخرى أولئك الذين في مراحل أقل شدة (أقل من 50 نقطة كما تم تقييمه بواسطة درجة UPDRS الأصلية الجزء الثالث OFF)”.على الرغم من أن نتائجنا لم تتماشى تمامًا مع النتائج المتعلقة بالعمر، إلا أنه من الجدير بالذكر أن أسوأ حالة (PD05) كانت لأكبر مريض سناً، وأفضل حالة (PD08) كانت لأصغر مريض سناً. فيما يتعلق بنتائج الجزء الثالث من مقياس MDS-UPDRS في حالة عدم تناول الدواء، أظهر المرضى PD02 وPD08، وكلاهما لديه درجات أقل من 50، تحسنًا في الأعراض.
كما تم مناقشته أعلاه، فإن هذه التجربة لها بعض القيود. أولاً، للحصول على استنتاجات نهائية بشأن بقاء خلايا الدوبامين الناضجة، فإن التحليلات النسيجية بعد الوفاة مطلوبة حول الالتهاب المحيط بالطعوم، والسرطانية. ثانياً، لم يتم بعد تحديد معايير الأهلية للمرضى المثاليين الذين يعانون من مرض باركنسون والذين يتلقون علاج استبدال الخلايا. ثالثاً، قد تغطي إعادة التوصيل المستمدة من الطعوم بعض المناطق القشرية التي تعاني من نقص الدوبامين فقط.قد تفسر هذه العوامل الأخيرة جزئيًا الاستجابات السريرية المتغيرة التي لوحظت في هذه التجربة. رابعًا، كانت هذه تجربة مفتوحة، عرضة للتأثير من تأثير الدواء الوهمي وتحامل الأطباء. يجب أن تأخذ الدراسات المستقبلية في الاعتبار تصميم مزدوج التعمية، خاضع للرقابة بواسطة دواء وهمي لتقليل هذه التحيزات. أخيرًا، يجب تأكيد نتائج هذه التجربة التي أجريت في مركز واحد وبعينة صغيرة في تجارب متعددة المراكز وبعينة كبيرة مع ضوابط مناسبة.
في الختام، بينما لا تزال سلامة وفعالية منتجات الخلايا المشتقة من خلايا iPS قيد التحقيق، أظهر هذا التجربة ملف السلامة للسلائف DA المشتقة من خلايا iPS. بعد زراعة ثنائية في النواة المذنبة، انخفض متوسط شدة الحركة.تم زيادة امتصاص F-DOPA في المتابعة بعد 24 شهرًا. على الرغم من القيود المذكورة أعلاه، تشير هذه النتائج إلى أن زراعة خلايا جذعية مستمدة من خلايا iPS هي علاج تجديدي آمن وفعال للمرضى الذين يعانون من مرض باركنسون. قد تجمع الاستراتيجيات المستقبلية بين زراعة الخلايا والعلاج الجيني والأدوية وإعادة التأهيل لتعزيز الفعالية.. علاوة على ذلك، كما يتضح في دراسة حالة واحدةقد يكون زراعة الأنسجة الذاتية باستخدام خلايا iPS أيضًا خيارًا واعدًا.
المحتوى عبر الإنترنت
أي طرق، مراجع إضافية، ملخصات تقارير Nature Portfolio، بيانات المصدر، بيانات موسعة، معلومات تكميلية، شكر وتقدير، معلومات مراجعة الأقران؛ تفاصيل مساهمات المؤلفين والمصالح المتنافسة؛ وبيانات توفر البيانات والرموز متاحة علىhttps://doi.org/10.1038/s41586-025-08700-0.
3. باركر، ر. أ.، بارّيت، ج.، ميسون، س. ل. وبيوركلوند، أ. تجارب زراعة الدوبامين في الأجنة ومستقبل زراعة الأعصاب في مرض باركنسون. لانسيت للأعصاب. 12، 84-91 (2013). 4. فريد، سي. آر. وآخرون. زراعة خلايا عصبية دوبا أمينية جنينية لعلاج مرض باركنسون الشديد. نيو إنجلاند جورنال أوف ميديسين 344، 710-719 (2001). 5. أولاونو، سي. دبليو. وآخرون. تجربة مزدوجة التعمية محكومة لزراعة الخلايا الجنينية الثنائية في مرض باركنسون. آن. نيورول. 54، 403-414 (2003). 6. بارمار، م.، غريليش، س. & هينشليف، س. مستقبل علاجات الخلايا الجذعية لمرض باركنسون. نات. ريف. نيوروسايس. 21، 103-115 (2020). 7. باركر، ر. أ. وكونسورتيوم ترانس يورو. تصميم تجارب استبدال خلايا الدوبامين المستندة إلى الخلايا الجذعية لمرض باركنسون. نات. ميد. 25، 1045-1053 (2019). 8. شفايتزر، ج. س. وآخرون. خلايا سلف الدوبامين المستمدة من الخلايا الجذعية المستحثة الشخصية لمرض باركنسون. نيو إنجلاند جورنال أوف ميديسين 382، 1926-1932 (2020). 9. بياو، ج. وآخرون. الفعالية والسلامة قبل السريرية لمنتج خلايا جذعية جنينية بشرية مشتقة من خلايا بروجنitor دوبامين في الدماغ الأوسط، MSK-DAO1. خلية الجذع 28، 217-229 (2021). 10. كيركبي، أ. وآخرون. الجودة والسلامة والفعالية قبل السريرية لمنتج مشتق من خلايا جذعية جنينية بشرية لعلاج مرض باركنسون، STEM-PD. خلية الجذع 30، 1299-1314 (2023). 11. دوي، د. وآخرون. عزل الخلايا الجذعية المستحثة متعددة القدرات المشتقة من الخلايا العصبية الدوبامينية بواسطة فرز الخلايا من أجل زراعة ناجحة. تقارير الخلايا الجذعية. 2، 337-350 (2014). 12. كيكوتشي، ت. وآخرون. خلايا عصبية دوبامينية مشتقة من خلايا iPS البشرية تعمل في نموذج مرض باركنسون في الرئيسيات. ناتشر 548، 592-596 (2017). 13. دوي، د. وآخرون. دراسة قبل السريرية لخلايا السلف العصبية الدوبامينية المستمدة من الخلايا الجذعية متعددة القدرات لعلاج مرض باركنسون. نات. كوميونيك. 11، 3369 (2020). 14. بوستما، ر. ب. وآخرون. معايير التشخيص السريري لمرض باركنسون. اضطرابات الحركة 30، 1591-1601 (2015). 15. أوكيتا، ك. وآخرون. طريقة أكثر كفاءة لتوليد خلايا iPS بشرية خالية من التكامل. نات. ميثودز 8، 409-412 (2011). 16. يوشيدا، س. وآخرون. بنك هابلو من خلايا جذعية متعددة القدرات مستحثة من البشر بدرجة سريرية يتطابق مع حوالي 40% من السكان اليابانيين. ميد 4، 51-66 (2023). 17. فيني، سي. وآخرون. تحليل حركي لمادة التصوير المقطعي بالإصدار البوزيتروني للبروتين الناقل [(18)F]GE-180 في الدماغ البشري. المجلة الأوروبية للطب النووي والتصوير الجزيئي 43، 2201-2210 (2016). 18. غوتز، سي. جي.، نوت، جي. جي. وستيبينز، جي. تي. مقياس تقييم خلل الحركة الموحد: العرض والملف السريري. اضطرابات الحركة 23، 2398-2403 (2008). 19. غوتز، سي. جي. وآخرون. مراجعة مقياس تقييم مرض باركنسون الموحد (MDS-UPDRS) برعاية جمعية اضطرابات الحركة: عرض المقياس ونتائج الاختبارات السريرية. اضطرابات الحركة 23، 2129-2170 (2008). 20. توملينسون، سي. إل. وآخرون. مراجعة منهجية لتقارير تكافؤ جرعة ليفودوبا في مرض باركنسون. اضطرابات الحركة 25، 2649-2653 (2010). 21. جوست، س. ت. وآخرون. معادلة جرعة ليفودوبا في مرض باركنسون: مراجعة منهجية محدثة واقتراحات. اضطرابات الحركة 38، 1236-1252 (2023). 22. ليندفال، أ. وآخرون. خلايا الدوبامين الجنينية البشرية المزروعة في الجسم المخطط لدى مريضين يعانيان من مرض باركنسون الشديد. تقرير مفصل عن المنهجية ومتابعة لمدة 6 أشهر. أرشيف الأعصاب. 46، 615-631 (1989). 23. ليندفال، أ. وآخرون. زراعة خلايا عصبية دوبامينية جنينية تبقى على قيد الحياة وتحسن الوظيفة الحركية في مرض باركنسون. ساينس 247، 574-577 (1990). 24. هاجيل، ب. وآخرون. الحركات غير الطبيعية بعد زراعة الأعصاب في مرض باركنسون. نات. نيوروساينس. 5، 627-628 (2002). 25. بانكيويتز، ك. س. وآخرون. قد يعزز الدوبامين البؤري في العقد القاعدية الحركات غير الطبيعية في القرود المصابة بباركنسون. التجربة العصبية. 197، 363-372 (2006). 26. باركر، ر. أ. و كوان، و. ل. اضطرابات الحركة الناتجة عن الزرع في مرض باركنسون: ما هو كل هذا؟ خلية الجذع 7، 148-149 (2010). 27. بوليتس، م. وآخرون. الخلايا العصبية السيروتونينية تتوسط آثار الديسكينيزيا الجانبية لدى مرضى باركنسون الذين خضعوا لزراعة عصبية. علوم. ترجمة. طب. 2، 38ra46 (2010). 28. بوليتس، م. وآخرون. اضطرابات الحركة الناتجة عن الزرع في مرض باركنسون: نسبة السيروتونين/ الناقل العصبي للدوبامين العالية في العقد القاعدية. اضطرابات الحركة 26، 1997-2003 (2011). 29. مينديز، إ. وآخرون. زراعة خلايا دافعة في الجذع الدماغي وفي النغري في نفس الوقت في مرضى باركنسون: دراسة تجريبية. تقرير عن ثلاث حالات. ج. جراحة الأعصاب. 96، 589-596 (2002). 30. موريزاني، أ. وآخرون. مقارنة مباشرة بين زراعة الخلايا العصبية المشتقة من الخلايا الجذعية المستحثة ذاتياً وزراعة الخلايا العصبية المشتقة من الخلايا الجذعية المستحثة من متبرع في دماغ قرد غير إنساني. تقرير الخلايا الجذعية. 1، 283-292 (2013). 31. موريزاني، أ. وآخرون. تطابق MHC يحسن من زراعة الخلايا العصبية المشتقة من iPSC في الرئيسيات غير البشرية. نات. كوم. 8، 385 (2017). 32. لي، ج. ي. وآخرون. أجسام ليوي في الخلايا العصبية المزروعة لدى الأشخاص المصابين بمرض باركنسون تشير إلى انتشار المرض من المضيف إلى الطعم. نات. ميد. 14، 501-503 (2008). 33. مendez، I. وآخرون. تحليل نوع الخلايا لزراعة خلايا الدوبامين الجنينية الوظيفية في النواة المذنبة والمادة السوداء لدى مرضى باركنسون. الدماغ 128، 1498-1510 (2005). 34. بولغار، س. وآخرون. استجابة الدواء الوهمي في التجارب العشوائية المزدوجة التعمية التي تقيم العلاجات التجديدية لمرض باركنسون: مراجعة منهجية وتحليل تلوي. مجلة أمراض باركنسون 12، 759-771 (2022). 35. دي لا فوانتي-فرناندز، ر. وآخرون. التوقع وإفراز الدوبامين: آلية تأثير الدواء الوهمي في مرض باركنسون. ساينس 293، 1164-1166 (2001). 36. أفيلس-أولموس، إ. وآخرون. إكسيناتيد وعلاج مرضى باركنسون. ج. كلين. إنفست. 123، 2730-2736 (2013). 37. شراج، أ. وآخرون. معدل التقدم السريري في مرض باركنسون. دراسة مستقبلية. اضطرابات الحركة 22، 938-945 (2007). 38. بيشيني، ب. وآخرون. تأخر استعادة وظيفة القشرة المتعلقة بالحركة في مرض باركنسون بعد زراعة الدوبامين في النواة المذنبة. آن. نيورول. 48، 689-695 (2000). 39. بافيسي، ن.، ريفيرو-بوش، م.، لويس، س. ج.، وون، أ. ل. & بروكس، د. ج. تقدم خلل المونوأمين في مرض باركنسون: دراسة طولية باستخدام تصوير PET بـ 18F-دوبا. نيووريميج 56، 1463-1468 (2011). 40. خان، ن. ل. وآخرون. تقدم خلل النيغروستريتال في عائلة باركن: دراسة باستخدام [18F]دوبا PET ودراسة سريرية. الدماغ 125، 2248-2256 (2002). 41. نورمي، إ. وآخرون. معدل التقدم في مرض باركنسون: دراسة باستخدام تصوير PET مع [18F]فلور-ل-دوبا. اضطرابات الحركة 16، 608-615 (2001). 42. كفالوبولو، ز. وآخرون. النتائج السريرية طويلة الأمد لزراعة خلايا الجنين لعلاج مرض باركنسون: حالتان دراسيتان. مجلة الجمعية الطبية الأمريكية للأعصاب. 71، 83-87 (2014). 43. فاهن، س.، إلتون، ر. ل. ولجنة تطوير UPDRS. في التطورات الأخيرة في مرض باركنسون المجلد 2 (تحرير فاهن، س. وآخرون) 153-163 (ماكميلان، 1987). 44. تاكاهashi، ج. الخطوات التالية في الطب التجديدي. خلية الجذع 30، 509-511 (2023).
ملاحظة الناشر: تظل شركة سبرينجر ناتشر محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
الوصول المفتوح هذه المقالة مرخصة بموجب رخصة المشاع الإبداعي النسب-غير التجارية-عدم الاشتقاق 4.0 الدولية، التي تسمح بأي استخدام غير تجاري، ومشاركة، وتوزيع، وإعادة إنتاج في أي وسيلة أو صيغة، طالما أنك تعطي الائتمان المناسب للمؤلفين الأصليين والمصدر، وتوفر رابطًا لرخصة المشاع الإبداعي، وتوضح إذا قمت بتعديل المادة المرخصة. ليس لديك إذن بموجب هذه الرخصة لمشاركة المواد المعدلة المشتقة من هذه المقالة أو أجزاء منها. الصور أو المواد الأخرى من طرف ثالث في هذه المقالة مشمولة في رخصة المشاع الإبداعي الخاصة بالمقالة، ما لم يُشار إلى خلاف ذلك في سطر الائتمان للمادة. إذا لم تكن المادة مشمولة في رخصة المشاع الإبداعي الخاصة بالمقالة وكان استخدامك المقصود غير مسموح به بموجب اللوائح القانونية أو يتجاوز الاستخدام المسموح به، فستحتاج إلى الحصول على إذن مباشرة من صاحب حقوق الطبع والنشر. لعرض نسخة من هذه الرخصة، قم بزيارة http:// creativecommons.org/licenses/by-nc-nd/4.0/. (ج) المؤلف(ون) 2025
طرق
المشاركون
تم تسجيل هذه التجربة في سجل التجارب السريرية في اليابان (jRCT) برقم الدراسة jRCT2090220384 وفي شبكة معلومات المستشفيات الجامعية (UMIN) برقم الدراسة UMINOOOO33564. تم تشخيص المرضى الذين يعانون من مرض باركنسون وفقًا لمعايير MDS السريرية.. بعد التسجيل الأولي، تم مراقبة جميع المرضى باستثناء PD01 لأكثر من 6 أشهر وإعادة تسجيلهم قبل الجراحة. كانت معايير الإدراج تشمل الأعمار من 50 إلى 69 عامًا، ومدة المرض لا تقل عن 5 سنوات، ومرحلة هوهن-يار 3 أو أسوأ خلال فترة عدم الفعالية ومرحلة 3 أو أفضل خلال فترة الفعالية، على الأقلتحسين الحركة مع الأدوية الدوبامينية (MDS-UPDRS) الجزء الثالث) والأعراض غير المستجيبة للأدوية الحالية (الجدول التكميلي 3). شملت معايير الاستبعاد الخرف أو القضايا النفسية (الجدول التكميلي 4). يتم تقديم قائمة كاملة بمعايير الإدراج والاستبعاد، بالإضافة إلى تفاصيل منهجية إضافية، في الطرق التكميلية. قدم جميع المشاركين موافقة خطية مستنيرة وفقًا للإرشادات الأخلاقية لمجلس مراجعة المؤسسات في مستشفى جامعة كيوتو (K044). تلقى ثلاثة مرضى (PD01-03) زراعة بجرعة منخفضة (2.1-2.6خلايا لكل نصف كرة)، وتلقى أربعة مرضى (PD04-06، PD08) زراعة بجرعة عالية (5.3-5.5خلايا لكل نصف كرة) (الشكل 1). تم اختيار الجرعة المنخفضة البالغة 5 ملايين خلية بناءً على دراستنا على القرود، الذي أظهر كل من السلامة والفعالية. بعد تأكيد سلامة هذه الجرعة على مدى عام واحد، تم زيادة عدد الخلايا إلى 10 ملايين. تم تعديل جرعة التاكروليموس للحفاظ على مستويات القاع المستهدفة من، تم تقليصه إلى النصف عند 12 شهرًا، وتم إيقافه عند 15 شهرًا. كانت هذه الخطة المناعية قائمة على دراستنا على الرئيسيات غير البشريةحيث أوقف علاج واحد مع التاكروليموس الاستجابة المناعية بشكل فعال خلال زراعة الأعضاء من نوع آخر. أظهرت الفحوصات النسيجية من حالات زراعة خلايا جنينية سابقة أن الخلايا العصبية DA المزروعة نجت لمدة تتراوح بين 9 إلى 16 عامًا، حتى مع توقف العلاج المناعي بعد 6 إلى 18 شهرًا من الزراعة. وبناءً عليه، تم إيقاف علاج التاكروليموس بعد 15 شهرًا.
نقاط النهاية والتقييم
تشمل النقاط النهائية الأساسية ملف الأحداث السلبية ونمو الطعوم بعد 24 شهرًا بواسطة التصوير بالرنين المغناطيسي) (الجدول التكميلي 5). تضمنت النتائج الثانوية التكاثر الورمي، رفض المناعة المضيفة، خلل الحركة الناتج عن الطعوم، تغييرات في الأعراض الحركية (جزء III من مقياس MDS-UPDRS) وإف-دوباعند 24 شهرًا (طرق إضافية).
تم تقييم السلامة من خلال توثيق الأحداث السلبية من الزرع حتى 24 شهرًا بعد العملية، وتم ترميزها وفقًا لقاموس الطب للأغراض التنظيمية (MedDRA) الإصدار 26.1. تم تقييم شدة خلل الحركة باستخدام مقياس UDysRS.تم تقييم الأعراض الحركية وغير الحركية لمرض باركنسون باستخدام مقياس MDS-UPDRS (الأجزاء I-III)، مراحل هوهن-يار في حالات تناول الدواء وعدم تناوله وLEDD. تم استخدام دفاتر المراقبة الحركية، PDQ-39، يوروكول 5 أبعاد 5 مستويات (EQ-5D-5L)، واستبيان إنتاجية العمل وتأثير النشاط لتقييم نتائج إضافية تم الإبلاغ عنها من قبل المرضى. تم مراقبة النمو الشبيه بالورم ورفض المناعة بواسطة التصوير بالرنين المغناطيسي، ف-فلت بيت و F-GE180تم تقييم بقاء الخلايا العصبية DA وتمايزها من خلال الأعراض الحركية وتصوير PET باستخدام F-DOPA. تم جدولة هذه التقييمات في فترات زمنية مختلفة بعد الزرع (الشكل 1ب).
خلايا iPS البشرية
سلالة خلايا iPS البشرية ذات الجودة السريرية (QHJI01s04) المستخدمة في هذه الدراسة تم إنشاؤها سابقًا من دم محيطي من فرد صحي متجانس الزيجوت لأكثر الأنماط الوراثية شيوعًا في السكان اليابانيين (HLA-A 24:02، HLA-B 52:01، HLA-DRB115:02، HLA-C 12:02، HLA-DQB106:01، HLA-DPB109:01)، والتي تتطابق مع 17% من السكان اليابانيين.تم إنشاء بنك خلايا رئيسي (MCB)، وتم إذابة قارورة واحدة من MCB لتحفيز خلايا سلف DA لكل مريض. إنسان تم الحفاظ على خلايا iPS باستخدام وسائط StemFit AK03N (أجينوموتو) على أطباق ثقافة بستة آبار مغطاة بـ iMatrix (ماتريكسوم).
تحفيز خلايا DA من خلايا iPS البشرية
تم تحفيز أسلاف DA كما تم وصفه سابقًاتم تصنيع الخلايا لـ PD01-PD03 في جامعة كيوتو، بينما تم تصنيع الخلايا لـ PD04-PD08 في شركة سوميتيومو فارما (الاسم غير المملوك دوليًا، راجونيبروسل). باختصار، تم زراعة خلايا iPS البشرية فيخلايا لكلعلى أطباق الثقافة الم coatedة بشظية اللامينين 511-E8 (المعرفة كاليوم 0) وزُرعت من أجل أيام. لإثراء سلفيات DA والقضاء على الخلايا غير المستهدفة، تم عزل خلايا (علامة لوحة الطابق) بواسطة جهاز فرز الخلايا المعتمد على الفلورية (BD Influx من BD Bioscience لـ PD01L، MACSQuant Tyto من Myltenyi Biotec لـ PD01R-PD03، GigaSort من Cytonome لـ PD04-PD08) في الأيام 11-13. تم فرز CORINتم زراعة الخلايا في أطباق 96 بئرًا باستخدام وسط تمايز عصبي لتشكيل كرات تجمعية حتى اليوم 30. تم تحفيز سلالات DA لكل مريض بشكل فردي وتم إعدادها كخلايا طازجة في يوم الجراحة. المنتج النهائي الذي يحتوي على سلالات DA استوفى معايير مراقبة الجودة (الجدول التكميلي 1)، وتم أيضًا تحليل الخلايا بواسطة الصبغة المناعية وRT-qPCR على مستوى الخلية الواحدة (البيانات الموسعة الأشكال 1 و2).
تلوين المناعة
تم تثبيت الكريات المجمعة باستخدام 4% من البارافورمالدهيد، ثم تم تجميدها وقطعها عندسمك م. تم إجراء صبغة المناعة بعد الحضانة مع مادة استرجاع المستضد (LSI Medience) والحجب باستخدام 0.3% Triton X-100 و2% مصل حيوانات اللاما لمدة ساعة واحدة. تم الحصول على صور الفلورسنت باستخدام المجاهر الليزرية الماسحة (Fluoview FV1200، أوليمبوس). الأجسام المضادة المستخدمة موصوفة في قسم ‘تجارب الحيوانات’ أدناه.
تحليل RT-qPCR على مستوى الخلية الواحدة
تم إعداد cDNA من خلية واحدة وفقًا لبروتوكول الشركة المصنعة. باختصار، تم تحضير تعليق خلوي من خلايا iPS (اليوم 0)، والخلايا المتوسطة قبل الفرز (اليوم 13) أو المنتج النهائي (اليوم 30 أو 31) بمعدل 300 خلية لكل.تم استخدامه. تم إضافة تعليق الخلايا إلى كاشف التعليق C 1 (Standard BioTools) بنسبةلخلايا iPS أولخلايا الوسطية وDAPs. ثم،تم تحميل تعليق الخلايا ومزيج مادة التعليق، كما ذُكر أعلاه، على IFC C1 Preamp للخلايا المفردة (“، Standard BioTools)، ثم تمت معالجة الشريحة على جهاز Fluidigm C1 باستخدام برنامج ‘STA: Cell Load (1782×)’. بعد تحميل الخلايا، تم إجراء فحص بصري باستخدام مجهر مقلوب للتحقق مما إذا كان قد تم التقاط خلية حية واحدة فقط في كل موقع التقاط. ثم، تم استخدام ‘STA: Preamp (تم تنفيذ نص (‘)، بما في ذلك تحلل الخلايا، النسخ العكسي، و18 دورة من تفاعل البوليميراز المتسلسل (PCR). بعد الانتهاء،تم خلط cDNA المعزز معمن محلول تخفيف DNA C1 (Standard BioTools). تم استخدام cDNA المعزز في RT-qPCR على مستوى الخلية الواحدة باستخدام نظام Biomark HD (Standard BioTools)، وفقًا لبروتوكول الشركة المصنعة. تم تحليل بيانات التعبير الجيني وتصويرها باستخدام مجموعة أدوات التحليل الفردي v.3.6.2 (Standard BioTools). تم تصوير أنماط التعبير الجيني على-رسم تخطيطي لتضمين الجوار العشوائي الموزع. تم إجراء تجميع غير خاضع للرقابة للخلايا باستخدام-طريقة التجميع باستخدام K-means. تم تصور طيف مستويات التعبير الجيني في كل مجموعة خلوية بواسطة مخططات الكمان. تسلسلات بادئات الحمض النووي مدرجة في الجدول التكميلية 6.
زراعة الخلايا
تم زرع الخلايا بشكل ثنائي في البوتامين باستخدام نظام الملاحة الجراحية العصبية iPlan (BrainLab). تم تصميم المسارات لاستهداف البوتامين الظهري والذيل، مع تجنب الشقوق والأوعية الدموية. تم إجراء الجراحة باستخدام نظام إطار ليكسل G (Elekta) وإبرة حقن مخصصة (TOP). تم تأكيد مواقع الحقن أثناء العملية باستخدام التصوير المقطعي المحوسب بالأشعة المخروطية (CT) باستخدام نظام تصوير الأوعية Artis Zeego (Siemens Healthineers). ثلاثة تم استخدام مسارات لكل نصف كرة، مع أربعة إلى ثمانية حقن لكل مسار، لزراعة 2.1-5.5خلايا لكل من البوتامين (الجدول التكميلي 7 والطرق التكميلية).
تجارب الحيوانات
تمت رعاية جميع الحيوانات والتعامل معها وفقًا لإرشادات تجارب الحيوانات في جامعة كيوتو وشركة سوميتمو فارما. تم اعتماد بروتوكولات الدراسة من قبل اللجان الأخلاقية في جامعة كيوتو (17-87-7) وشركة سوميتمو فارما (2014-20). تم استخدام نفس خلايا المتبرع المستخدمة للمرضى PD04 (دفعة، 20022)، PD05 (دفعة، 20048)، PD06 (دفعة، 21004) وPD08 (دفعة، 21047) في تجارب الزرع. خلايا اليوم-30 الطازجة ( أو الخلايا كجرعة منخفضة، و أو تم حقن الخلايا (مثل الجرعة العالية) في النواة المذنبة لفئران باركنسونية عارية (F344/NJcl-rnu/rnu، CLEA، بعمر 17-21 أسبوعًا) مصابة بـ 6-OHDA. تم إجراء تحليلات الدوران الناتجة عن الميثامفيتامين بعد 8 أسابيع من الزرع وكل 4 أسابيع بعد ذلك. تم حقن محلول ملحي في الفئران الضابطة كمجموعة مركبة في كل تجربة. تم توزيع الفئران عشوائيًا على مجموعة الخلايا ومجموعة المركب. بعد 24 إلى 32 أسبوعًا من المراقبة، تم euthanized الحيوانات باستخدام الإيزوفلوران وتم ضخها بـ-خالي من PBS، و4% بارافورمالدهيد. بعد الغمر في 30% سكروز، شرائح الدماغ المجمدة عندتم إعداد شرائح بسماكة معينة للتلوين المناعي النسيجي. بالنسبة لتلوين 3,3′-ديامينوبنزيدين (DAB)، تم معالجة شرائح الدماغ بمحلول حجب البيروكسيداز (DAKO)، وتم حضنها بالتتابع مع الأجسام المضادة الأولية والثانوية البيوتينية ضد IgG للأرانب (1:1000، مختبرات فيكتور) والبيروكسيداز المرتبط بالأفيدين (مجموعة Vectastain ABC HRP، مختبرات فيكتور). تم إجراء كشف الإشارة باستخدام DAB (مجموعة تلوين DAB، ميتو بيور كيميكالز) مع كلوريد النيكل. الأجسام المضادة الأولية المستخدمة في التلوين المناعي النسيجي هي كما يلي: FOXA2 (ماعز، أنظمة R&D، AF2400، 1:500)، NURR1 (فأر، بيرسيوس بروتيومكس، PP-N1404-00، 1:300)، المستضد النووي البشري (HNA) (فأر، ميلبورو، MAB1281، 1:500)، Ki-67 (أرنب، أبكام، Ab16667، 1:1000)، 5-HT (جرذ، ميلبورو MAB352، 1:100) وTH (أرنب، ميلبورو، AB152، 1:400). الأجسام المضادة الثانوية هي كما يلي: أليكسا فلور 488 مضاد لـ IgG للفأر (حمار، ثيرمو فيشر ساينتيفيك، A21202، 1:400)، أليكسا فلور 594 مضاد لـ IgG للماعز (حمار، ثيرمو فيشر ساينتيفيك، A11058، 1:2000)، أليكسا فلور 594 مضاد لـ IgG للأرنب (حمار، ثيرمو فيشر ساينتيفيك، A21207، 1:400) وأليكسا فلور 594 مضاد لـ IgG للجرذ (حمار، ثيرمو فيشر ساينتيفيك، A21209، 1:400). تم تصور الصور باستخدام ميكروسكوب فلوريسنس.
التحليل الإحصائي
تم جمع البيانات السريرية باستخدام EDMS-Online (الإصدار 3.1، EPS). تم تلخيص نتائج السلامة والفعالية باستخدام القيم المتوسطة، وقيم الانحراف المعياري، والنسب. تم إجراء التحليلات الإحصائية للبيانات السريرية. باستخدام برنامج SAS (الإصدار 9.4، معهد SAS). تم إجراء التحليلات الإحصائية لتجارب الحيوانات باستخدام GraphPad Prism (الإصدار 10.3.1، برنامج GraphPad).
ملخص التقرير
معلومات إضافية حول تصميم البحث متاحة في ملخص تقارير مجموعة نيتشر المرتبط بهذه المقالة.
توفر البيانات
جميع البيانات ذات الصلة من هذه التجربة مدرجة في المقالة والطرق التكميلية. تم توفير بيانات المصدر مع هذه الورقة. 45. باتلاك، سي. إس. وبلسبرغ، ر. ج. التقييم الرسومي لثوابت انتقال الدم إلى الدماغ من بيانات امتصاص متعددة الزمن. التعميمات. مجلة تدفق الدم إلى الدماغ والتمثيل الغذائي 5، 584-590 (1985). 46. شيلدز، أ. ف. وآخرون. تصوير التكاثر في الجسم الحي باستخدام [F-18]FLT والتصوير المقطعي بالإصدار البوزيتروني. نات. ميد. 4، 1334-1336 (1998). 47. أبركرومبي، م. تقدير عدد النوى من مقاطع الميكروتوم. سجلات التشريح. 94، 239-247 (1946).
الشكر والتقدير نشكر جميع المرضى الذين شاركوا في هذه التجربة؛ Y. شيميزو، T. ساغا و K. توغاشي على تصوير الدماغ؛ أعضاء لجنة تقييم الفعالية والسلامة، بما في ذلك S. كينوشيتا، H. ساوادا و H. تودا على نصائحهم؛ الأطباء والمنسقون في معهد تقدم العلوم السريرية والترجمة (iACT)، مستشفى جامعة كيوتو، بما في ذلك A. شيميزو، Y. ناغاي، M. ياماموتو، R. أوزومي، Y. كوسونوكي، A. كورو دا، K. إندو، K. إينوموتو، A. كينوشيتا، C. كيمورا، K. كاواغوتشي، C. إيتشيهارا، N. ماتسوياما، K. توتشغي، Y. ساميشيمَا، M. إيوساكي و C. تويواكا على دعمهم لهذه التجربة السريرية؛ الطاقم الفني في مختبر J.T.، بما في ذلك E. ياماساكي، T. أشييدا، Y. فوجيتا، Y. تانيكاوا، Y. كاتانو، Y. أوزاكي، R. تاكايشي، A. ميهارا، K. فوكوشيما و S. بابا على تصنيع الخلايا؛ أعضاء مشروع PD في سوميتمو فارما، بما في ذلك K. يوشيدا، H. تاكاهاشي، Y. سوغاو، S. سيكيا، M. إيكيدا، Y. ياماموتو، S. أوتا، S. أوكابي، H. أوهارا و T. كارينو على الدعم التنظيمي وتصنيع الخلايا؛ و K. هوي على قراءة هذه المخطوطة. تم دعم هذه الدراسة من خلال منحة من مشروع البحث للتطبيق العملي للطب التجديدي من وكالة اليابان للبحث والتطوير الطبي (AMED) (23bk0104126h0003) إلى J.T.
مساهمات المؤلفين كان J.T. و R.T. المحققين الرئيسيين. كتب N.S. و D.D. و تاكيوكي كيكوتشي المسودة الأولى من الورقة. ساهم N.S. و E.N. و M.S. و H.Y. و Y.T. و A.S. و Y.F. و T.O. و Y.N. و R.T. في جمع البيانات السريرية. ساهم D.D. و تيتسوهيرو كيكوتشي و A.M. و J.T. في توليد خلايا iPS البشرية وخلايا سلف الدوبامين. ساهم S.H. في تجارب الفئران PD. ساهم تاكيوكي كيكوتشي و Y.A. و S. مياamoto في جراحة الأعصاب. ساهم T.A. و T.S. في إدارة العلاج المناعي. قام K.U. و S. موريطا بإجراء التحليلات الإحصائية. ساهم جميع المؤلفين في تحليل أو تفسير البيانات وأجروا مراجعات حاسمة للمخطوطة.
المصالح المتنافسة: حصل N.S. و R.T. و J.T. على منحة للبحث التعاوني من شركة سوميتيومو فارما. حصل R.T. على منحة بحث من نيهون ميدي-فيزيكس. حصل T.O. على منحة بحث من سيمنز للرعاية الصحية. S.H. موظف في شركة سوميتيومو فارما. يعلن المؤلفون الآخرون عدم وجود مصالح متنافسة.
معلومات إضافية
معلومات إضافية النسخة الإلكترونية تحتوي على مواد إضافية متاحة علىhttps://doi.org/10.1038/s41586-025-08700-0. يجب توجيه المراسلات والطلبات للحصول على المواد إلى ريوسوكي تاكاهاشي أو جون تاكاهاشي. تُعرب مجلة Nature عن شكرها لديفيد ديفوس، وهايديوكي أوكانو، والمراجعين الآخرين المجهولين، على مساهمتهم في مراجعة هذا العمل. تقارير مراجعي الأقران متاحة. معلومات إعادة الطباعة والتصاريح متاحة علىhttp://www.nature.com/reprints.
الشكل 1 من البيانات الموسعة | انظر الصفحة التالية للتعليق.
الشكل البياني الممتد 1| تحليل RT-qPCR على مستوى الخلية الواحدة (sc-RT-qPCR) للخلايا خلال تمايز DA. أ. رسم t-SNE لبيانات sc-RT-qPCR للخلايا الجذعية المستحثة (iPSCs) والخلايا المتوسطة (قبل فرز الخلايا الإيجابية لـ CORIN) والمنتجات النهائية. تشكل iPSCs والخلايا المتوسطة كل منهما مجموعة متميزة، بينما تنقسم المنتجات النهائية إلى مجموعتين. ب. النسب النسبية لأنواع الخلايا في كل عينة خلوية، التي تم تحديدها بواسطة تجميع K-means لبيانات sc-RT-qPCR، تشير إلى أن المنتج النهائي يتكون من حوالي 60% من سلالات DA و40% من DA. الخلايا العصبية. كانت دفعة #20022 هي خلايا المتبرع المستخدمة لـ PD04، ودفعة #20048 لـ PD05، ودفعة #21004 لـ PD06، ودفعة #21047 لـ PD08. تم استخدام دفعة #190909 لـ PD02. ج. تُظهر الرسوم البيانية على شكل كمان أنماط التعبير الجيني في مجموعات من خلايا iPSCs، والخلايا المتوسطة، والمنتجات النهائية تغييرات في التعبير الجيني خلال تمايز DA. د. تُظهر الرسوم البيانية على شكل كمان أنماط التعبير الجيني عبر دفعات مختلفة من المنتجات النهائية تعبيرًا مستقرًا بين الدفعات.
الشكل البياني الممتد 2 | انظر الصفحة التالية للتعليق.
الشكل البياني الممتد 2 | زراعة نفس خلايا المتبرع المستخدمة للمرضى في نماذج الفئران لمرض باركنسون. أ-د. صور مناعية فلورية لخلايا المتبرع في اليوم 30 (تجارب مستقلة). NURR1 (أ) هو مستقبل نووي معبر عنه في خلايا الدوبامين، بينما FOXA2 (ب) هو عامل نسخ معبر عنه في لوحة القاع. يتم استخدام DAPI (ج) لتلوين النواة. الصورة المدمجة (د) تظهر أن خلايا المتبرع تتكون أساسًا من سلالات الدوبامين وبعض خلايا الدوبامين. قضبان القياس. هـ. ملخص تجارب زراعة الخلايا والنتائج. تم إعطاء حقن خلايا بجرعات منخفضة وعالية لفحص الفروق في بقاء الخلايا وتحسين السلوك. و-ي. سلوك الدوران الناتج عن الميثامفيتامين في الجرذان التي تلقت زراعة يظهر تحسنًا بعد حوالي 24 أسبوعًا. تُعرض البيانات كمتوسط ± انحراف معياري.مقابل مجموعة المركبات من خلال تحليل التباين ثنائي الاتجاه (ANOVA) مع اختبار المقارنات المتعددة لتوكاي. ف. قيمة p المعدلة (20 أسبوعًا) و 0.045 (24 أسبوعًا). ج. قيمة p المعدلة (20 أسبوعًا)، <0.001 (24 أسبوعًا)، 0.002 (28 أسبوعًا)، 0.011 (32 أسبوعًا، المركبة مقابل الخلية 400 ك)، و<0.001 (32 أسبوعًا، المركبة مقابل الخلية 800 ك). قيمة p المعدلة (20 أسبوعًا)، 0.001 (28 أسبوعًا، المركبة مقابل الخلية 500 ك)، والبقية <0.001. i. قيمة p المعدلة (12 أسبوعًا)، 0.001 (20 أسبوعًا)، 0.002 (32 أسبوعًا، المركبة مقابل الخلية 500 ك)، 0.006 (32 أسبوعًا، المركبة مقابل الخلية 1,000 ك)، والبقية <0.001.jk. صبغة DAB لـ TH (هيدروكسيل التيروزين، علامة على خلايا الدوبامين العصبية) في زراعات تمثيلية بعد 32 أسبوعًاتجارب مستقلة). مقياس الرسم. ك. صورة مكبرة للطعم الموضح في اللوحة ج. مقياس الطول. ل . صورة المناعة الفلورية للطعوم مزدوجة الوسم لخلايا إيجابية لـ TH و HNA تشير إلى خلايا عصبية DA المشتقة من المتبرع (تجارب مستقلة). مقياس الرسمنسبة الخلايا الإيجابية لـ KI67 بالنسبة للخلايا الإيجابية لـ HNA لكل طعمة. (دفعة 20022)، 7 (دفعة 20048)، 9 (دفعة 21004)، و9 (دفعة 21047) حيوانات مستقلة بيولوجياً، على التوالي. الخط = الوسيط. ن. صورة مناعية فلورية للطعوم ملونة بـ HNA (أخضر) وKI 67 (أحمر)،تجارب مستقلة. شريط القياسصورة مكبرة للطعم الموضح في اللوحة، مع رأس سهم يشير إلى خلية مزدوجة إيجابية لـ HNA/KI67. ص. صورة المناعة الفلورية للطعوم ملونة بـ HNA (أخضر) و 5-HT (أحمر)،تجارب مستقلة. شريط القياسصورة مكبرة للطعم الموضح في اللوحة (ب)، تظهر غياب الخلايا الموجبة للـ HNA/5HT. تم تلوين DAPI باللون الأزرق. مقياس الرسمصورة التألق المناعي لنواة الرابيه المضيفة كتحكم إيجابي للعصبونات السيروتونية (5-HT، باللون الأحمر) يظهر تلوين DAPI باللون الأزرق.تجارب مستقلة). مقياس الرسم.
الشكل البياني الممتد 3 | بقاء الخلايا من سلالات DA المشتقة من الخلايا الجذعية المستحثة. صور الرنين المغناطيسي بتقنية T2 لمريض PD08، تظهر الطعوم كمناطق ذات كثافة عالية. يتم عرض الصور التاجية والمحورية والسهمية من الأعلى إلى الأسفل. تشير المناطق الزرقاء والصفراء إلى المناطق التي تقع ضمن 3 مم من مواقع حقن الخلايا.
ب. التغيرات في حجم الطعوم كما تم قياسها بواسطة صور الرنين المغناطيسي بتقنية T2 لكل مريض. تم حساب المناطق ذات الكثافة العالية داخل المناطق الزرقاء والصفراء (R: اليمين و L: اليسار).
الشكل البياني الممتد 4 | التغيرات في مقياس هوهن ويار لكل مريض. تم تقييم مقياس هوهن ويار في، و 24 شهرًا. “ON” تشير إلى القياسات التي تم أخذها بينما كان المريض يتناول الدواء، بينما “OFF” تشير إلى القياسات التي تم أخذها بعد أن كان المريض قد توقف عن تناول الدواء لأكثر من 12 ساعة.
الشكل 5 من البيانات الموسعة | انظر الصفحة التالية للتعليق.
الشكل البياني الممتد 5 | التغيرات في وقت التشغيل، وقت الإيقاف، درجات PDQ-39، والتغيرات في جرعة الليفودوبا المعادلة يومياً (LEDD) لكل مريض. أ-و، التغيرات الزمنية في فترة وقت التشغيل، فترة وقت الإيقاف، ودرجات PDQ39 لكل مريض من التسجيل (0 م) حتى نهاية فترة المراقبة.، على التوالي، بناءً على الإدراك الذاتي للمريض. ب، د، ف، تغييرات الدرجات من خط الأساس، مع المتوسط الممثل بالخط الأسود. التغييرات المطلقة والنسبية (النسبة المئوية) بعد 24 شهرًا موضحة على التغييرات في جرعة الليفودوبا المعادلة اليومية (LEDD) لكل مريض. تم جمع بيانات الأدوية لكل مريض من السجلات الطبية، وتم حساب LEDD وفقًا لطريقة تم تحديدها مسبقًا.التغيرات الزمنية في درجة الإعاقة الحركية المرتبطة بالمرض لكل مريض من التسجيل (0 م) حتى نهاية فترة المراقبةتغيرات الدرجات من خط الأساس، مع تمثيل المتوسط بواسطة الخط الأسود. التغيرات المطلقة والنسبية (النسبة المئوية) بعد 24 شهرًا موضحة على اليمين.
الشكل البياني الممتد 6 | انظر الصفحة التالية للتعليق.
الشكل 6 من البيانات الموسعة | تم الكشف عن تخليق الدوبامين بواسطةف-DOPA PET. التغيرات الزمنية في الفلورين-18- L-ديهيدروكسي فينيل ألانينقيم Ki لـ F-DOPA لكل جانب من جوانب اللوزة لكل مريض من التسجيل (0 م) إلى نهاية فترة الملاحظة (24 م)، كملحق للشكل 3.b، التغيرات في قيم Ki من الخط الأساسي، مع تمثيل المتوسط بواسطة الخط الأسود. ج-ح، شبه كميصور F-DOPA التي تم إنشاؤها فيمن بعد الحقن عن طريق طرح إشارة الخلفية القذالية وتطبيع النتيجة على النشاط القذالي لكل مريض (قبل العملية: قبل العملية، 12 م: 12 شهرًا، 24 م: 24 شهرًا). يتغير اللون من الأخضر الداكن إلى الأحمر في الجانبين. يُشير اللوزة إلى زيادةامتصاص F-DOPA، مما يعكس تخليق الدوبامين بواسطة الخلايا المزروعة.العلاقة بينامتصاص F-DOPA وتحسن الأعراض الحركية. (ط) مخططات لقيم Ki قبل وبعد الزرع ودرجات MDS-UPDRS الجزء الثالث OFF لستة مرضى (PD02-08). يتم الإشارة إلى نطاقات الأعراض الصحية والأولية بناءً على دراسات سابقة، حيث تتراوح قيم Ki للأفراد الأصحاء من 0.010 إلى 0.017، وتظهر الأعراض الباركنسونية الأولية بقيم Ki تتراوح بين 0.0045 و 0.0073. (ي) التغيرات في قيم Ki ودرجات MDS-UPDRS الجزء الثالث OFF لكل مريض.
مقالة
البيانات الموسعة الجدول 1 | الخصائص السريرية للمشاركين في البداية
مجموعة الجرعة المنخفضة
مجموعة الجرعة العالية
بي دي 01
بي دي 02
بي دي 03
PD04
بي دي 05
بي دي 06
بي دي 08
العمر (بالسنوات)
50
62
60
61
69
٥٨
٥٦
الجنس (ذكر/أنثى)
M
ف
ف
M
M
M
ف
المدة (بالسنوات)
10.3
٨.٨
9.5
10.3
٨.٧
12.2
9.5
تقلبات الحركة
نعم
نعم
نعم
نعم
نعم
نعم
نعم
هوهن ويار OFF
٣
٤
٥
٥
٥
٣
٣
هوهن ويار ON
2
٢
٢
2
2
٢
٢
استجابة ليفودوبا (%)
69.7
89.7
67.3
٥٧.٤
75.8
68.0
67.0
خلل الحركة
خفيف
لا شيء
خفيف
خفيف
خفيف
خفيف
خفيف
مطابقة HLA (6 أليلات*)
نعم
لا
لا
نعم
لا
نعم
لا
06:01، HLA-DPB1 09:01.
الجدول البياني الموسع 2 | القياسات السريرية الأساسية عند 0 و 24 شهرًا بعد الزرع الثنائي
نقطة النهاية
مجموعة الجرعة المنخفضة )
مجموعة الجرعة العالية )
الإجمالي ( )
0M (SD)
24 م (انحراف معياري)
% التغيير (الانحراف المعياري)
0M (SD)
24 مليون (SD)
% التغيير (الانحراف المعياري)
0M (SD)
24M (SD)
% التغيير (الانحراف المعياري)
UDysRS (الإجمالي)*
7.7 (4.0)
22.0 (5.6)
٢١٩.٤ (٩٧.٣)
31.0 (8.6)
٤١.٨ (٧.٨)
٣٩.٢ (٢٨.٠)
21.0 (14.1)
٣٣.٣ (١٢.٣)
١١٦.٤ (١١٣.٣)
مقياس مرض باركنسون (MDS-UPDRS) الجزء الثالث – بدون علاج
٤٤.٥ (١٤.٨)
٣٦.٥ (١٩.١)
-20.7 (16.4)
٥٤.٠ (١٥.٥)
٤٣.٨ (٢٠.٦)
-20.2 (31.6)
50.8 (14.6)
٤١.٣ (١٨.٥)
-20.4 (25.6)
مقياس MDS-UPDRS III قيد التشغيل
10.5 (3.5)
٤.٥ (٠.٧)
-53.4 (22.4)
٢١.٣ (٧.٧)
17.8 (13.4)
-26.8 (47.1)
17.7 (8.3)
١٣.٣ (١٢.٤)
-35.7 (40.2)
MDS-UPDRS II
14.0 (4.2)
14.0 (5.7)
-1.6 (10.6)
٨.٣ (٤.٣)
١٦.٥ (٧.٢)
127.0 (129.3)
10.2 (4.9)
15.7 (6.3)
٨٤.١ (١٢٠.٢)
MDS-UPDRS I
7.0 (0.0)
7.0 (1.4)
0.0 (20.2)
٤.٥ (٢.٦)
5.8 (4.0)
19.0 (22.3)
٥.٣ (٢.٤)
6.2 (3.3)
12.7 (21.9)
مقياس بطء الحركة
17.0 (4.2)
12.5 (5.0)
-27.9 (11.1)
17.8 (5.0)
١٦.٨ (٧.٤)
-7.0 (33.7)
17.5 (4.3)
15.3 (6.5)
-14.0 (28.7)
هوهن ويار OFF
٤.٥ (٠.٧)
3.0 (1.4)
-35.0 (21.2)
4.0 (1.2)
3.5 (1.7)
-16.7 (19.2)
٤.٢ (١.٠)
3.3 (1.5)
-22.8 (20.0)
هوهن ويار ON
2.0 (0.0)
1.5 (0.7)
-25.0 (35.4)
2.0 (0.0)
2.0 (0.0)
0.0 (0.0)
2.0 (0.0)
1.8 (0.4)
-8.3 (20.4)
وقت OFF بدون خلل حركي (ساعات)
7.93 (1.82)
6.61 (3.38)
-9.4 (63.5)
٤.٦٣ (٣.٤٥)
5.89 (3.83)
٣٤.١ (٦٥.٨)
5.73 (3.27)
6.13 (3.35)
19.6 (62.5)
وقت OFF مع خلل الحركة غير المزعج (ساعات)
0.00 (0.00)
0.07 (0.00)
–
0.30 (0.52)
0.27 (0.54)
-50.0 (70.7)
0.20 (0.43)
0.20 (0.43)
-50.0 (70.7)
وقت OFF مع خلل الحركة المزعج (ساعات)
0.00 (0.00)
0.00 (0.00)
–
0.09 (0.18)
0.20 (0.24)
-20.0 (-)
0.06 (0.15)
0.13 (0.21)
-20.0 (-)
في الوقت المحدد دون خلل حركي (ساعات)
9.57 (2.63)
9.86 (1.31)
9.0 (43.6)
7.86 (0.35)
6.05 (3.56)
-21.7 (48.6)
8.43 (1.50)
7.32 (3.44)
-11.5 (45.3)
في الوقت المحدد مع خلل الحركة غير المزعج (ساعات)
0.00 (0.00)
0.36 (0.10)
–
٢.٣٤ (١.٩٧)
1.48 (1.22)
-30.4 (18.5)
1.56 (1.94)
1.11 (1.11)
-30.4 (18.5)
في الوقت المحدد مع خلل الحركة المزعج (ساعات)
0.00 (0.00)
0.29 (0.40)
–
0.43 (0.43)
1.86 (2.78)
318.3 (338.1)
0.29 (0.40)
1.33 (2.31)
318.3 (338.1)
PDQ-39 (مؤشر ملخص)
٣٢٫٠٨ (١٠٫٣٩)
٢٩.٥٨ (١٥.١٠)
-10.7 (18.2)
30.69 (10.02)
٣٨.٣١ (١٨.٠٢)
٢٣.٠ (٢٦.٠)
٣١.١٥ (٩.٠٧)
٣٥.٤٠ (١٦.١٥)
11.8 (27.9)
LEDD (ملغ/يوم)**
990.00 (115.82)
905.40 (74.53)
-7.47 (18.36)
١١٢٣٫١٠ (٢٩٥٫٧٣)
1174.61 (431.10)
2.76 (17.19)
1078.73 (244.70)
١٠٨٤.٨٨ (٣٦٣.٢٥)
-0.65 (16.51)
F-DOPA بُنية الكُرَة المُخَطَّطَة
0.0045 (0.0001)
0.0048 (0.0009)
7.0 (15.9)
0.0025 (0.0002)
0.0041 (0.0007)
63.5 (36.8)
0.0032 (0.0010)
0.0043 (0.0008)
٤٤.٧ (٤١.٤)
كي ف-دوبا في الرأس المداري
0.0090 (0.0007)
0.0084 (0.0001)
-6.9 (6.8)
0.0068 (0.0004)
0.0068 (0.0001)
0.3 (4.8)
0.0076 (0.0012)
0.0073 (0.0008)
-2.1 (6.0)
المقاييس السريرية الأساسية عند التسجيلونهاية الملاحظة“يتم تقديمها بواسطة المتوسط والانحراف المعياري (SD، بين قوسين). *تم تضمين UDysRS في ملف السلامة، وتُعرض النتائج لسكان السلامة [جرعة منخفضة (جرعة عالية (” )، والإجمالي (تم إجراء زراعة الجانب الأيمن بعد 8 أشهر من الزراعة الأولية للجانب الأيسر في PDO1. لذلك، كانت فترة التقييم من الفترة ما قبل العملية حتى 24 شهرًا بعد الزراعة الثنائية 32 شهرًا. ** تم حساب هذا الـ LEDD باستخدام صيغة محدثة نُشرت بعد بدء التجربة.على الرغم من زيادة الدرجة المتوسطة، إلا أن نسبة التغيير انخفضت. من أجل الشمولية، احتفظنا بالبيانات المحسوبة باستخدام صيغة أقدم في الشكل البياني الممتد.. LEDD، جرعة ليفودوبا المعادلة اليومية؛ MDS-UPDRS، مقياس تقييم مرض باركنسون الموحد لجمعية اضطرابات الحركة؛ OFF، حالة عدم تناول الدواء؛ ON، حالة تناول الدواء؛ PDQ-39، استبيان مرض باركنسون المكون من 39 عنصرًا؛ UDysRS، مقياس تقييم الديسكينيسيا الموحد.
مقالة
الجدول البياني الموسع 3 | مقاييس سريرية إضافية عند 0 و 24 شهرًا بعد الزراعة الثنائية
نقطة النهاية
جرعة منخفضة )
جرعة عالية ( )
الإجمالي ( )
0M (SD)
24 مليون (SD)
% التغيير (الانحراف المعياري)
0M (SD)
24 مليون (SD)
% التغيير (الانحراف المعياري)
0M (SD)
24M (SD)
% التغيير (الانحراف المعياري)
MDS-UPDRS
إجمالي الأجزاء الأول والثاني والثالث
65.5 (19.1)
٥٧.٥ (٢٦.٢)
-14.4 (15.0)
66.8 (17.7)
66.0 (24.9)
-3.6 (22.0)
٦٦.٣ (١٦.٢)
٦٣.٢ (٢٣.٠)
-7.2 (19.1)
إجمالي الأجزاء I و II و III قيد التشغيل
٣١.٥ (٧.٨)
25.5 (6.4)
-19.1 (0.2)
٣٤.٠ (١١.٤)
٤٠.٠ (١٩.٠)
11.9 (25.1)
٣٣.٢ (٩.٦)
٣٥.٢ (١٦.٨)
1.6 (25.2)
EQ-5D-5L
درجة المؤشر
0.66 (0.10)
0.75 (0.20)
١٣.٤ (١٣.٣)
0.61 (0.33)
0.60 (0.29)
13.1 (49.1)
0.62 (0.26)
0.65 (0.26)
١٣.٢ (٣٨.٥)
EQ VAS
75.00 (7.07)
82.50 (10.61)
9.8 (3.8)
55.0 (24.83)
60.00 (26.77)
٣٤.٨ (١١٣.٢)
٦١.٦٧ (٢٢.٠٦)
67.50 (24.24)
٢٦.٥ (٨٨.٧)
WPAI
التغيب
0
0
0
0
0
0
0
0
0
الحضور الفعلي
0
0
0
0
0
0
0
0
0
الضعف العام في العمل
0
0
0
0
0
0
0
0
0
ضعف النشاط
٥٥.٠٠ (٣٥.٣٦)
٥٥.٠٠ (٣٥.٣٦)
0.0 (0.0)
50.00 (39.16)
٥٧.٥٠ (٣٨.٦٢)
11.7 (97.9)
٥١.٦٧ (٣٤.٣٠)
٥٦.٦٧ (٣٣.٨٦)
7.8 (76.1)
محفظة الطبيعة
آخر تحديث من المؤلف(ين): 20 ديسمبر 2024
ملخص التقرير
تسعى Nature Portfolio إلى تحسين إمكانية تكرار العمل الذي ننشره. يوفر هذا النموذج هيكلًا للاتساق والشفافية في الإبلاغ. لمزيد من المعلومات حول سياسات Nature Portfolio، يرجى الاطلاع على سياسات التحرير وقائمة مراجعة سياسة التحرير.
الإحصائيات
لجميع التحليلات الإحصائية، تأكد من أن العناصر التالية موجودة في أسطورة الشكل، أسطورة الجدول، النص الرئيسي، أو قسم الطرق.
غير متوفر
□ □ □ □ X □ □ □ □ □ □ □
مؤكد حجم العينة بالضبطلكل مجموعة/شرط تجريبي، معطاة كرقم منفصل ووحدة قياس بيان حول ما إذا كانت القياسات قد أُخذت من عينات متميزة أو ما إذا كانت نفس العينة قد تم قياسها عدة مرات اختبار(ات) الإحصاء المستخدمة وما إذا كانت أحادية الجانب أو ثنائية الجانب يجب أن تُوصف الاختبارات الشائعة فقط بالاسم؛ واصفًا التقنيات الأكثر تعقيدًا في قسم الطرق. وصف لجميع المتغيرات المشتركة التي تم اختبارها وصف لأي افتراضات أو تصحيحات، مثل اختبارات الطبيعية والتعديل للمقارنات المتعددة وصف كامل للمعلمات الإحصائية بما في ذلك الاتجاه المركزي (مثل المتوسطات) أو تقديرات أساسية أخرى (مثل معامل الانحدار) والتباين (مثل الانحراف المعياري) أو تقديرات عدم اليقين المرتبطة (مثل فترات الثقة)
لاختبار الفرضية الصفرية، إحصائية الاختبار (على سبيل المثال، ) مع فترات الثقة، أحجام التأثير، درجات الحرية وقيمة ملحوظة أعطِالقيم كقيم دقيقة كلما كان ذلك مناسبًا.
لتحليل بايزي، معلومات حول اختيار القيم الأولية وإعدادات سلسلة ماركوف مونت كارلو للتصاميم الهرمية والمعقدة، تحديد المستوى المناسب للاختبارات والتقارير الكاملة عن النتائج تقديرات أحجام التأثير (مثل حجم تأثير كوهين)مؤشر بيرسون (r)، مما يدل على كيفية حسابها تحتوي مجموعتنا على الإنترنت حول الإحصائيات لعلماء الأحياء على مقالات تتناول العديد من النقاط المذكورة أعلاه.
البرمجيات والشيفرة
معلومات السياسة حول توفر كود الكمبيوتر
جمع البيانات تحليل البيانات
EDMS-Online الإصدار 3.1
تم معالجة صور الدماغ باستخدام مكتبة برمجيات التصوير بالرنين المغناطيسي الوظيفي للدماغ (FMRIB) (الإصدار 5.3) وخرائط المعلمات الإحصائية 12 (SPM12، الإصدار 7219). تم إجراء التحليلات الإحصائية للبيانات السريرية باستخدام برنامج SAS (الإصدار 9.4، معهد SAS)، وتم إجراء التحليل الإحصائي لتجارب الحيوانات باستخدام GraphPad Prism (الإصدار 10.3.1، برنامج GraphPad).
بالنسبة للمخطوطات التي تستخدم خوارزميات أو برامج مخصصة تكون مركزية في البحث ولكن لم يتم وصفها بعد في الأدبيات المنشورة، يجب أن تكون البرمجيات متاحة للمحررين والمراجعين. نحن نشجع بشدة على إيداع الشيفرة في مستودع مجتمعي (مثل GitHub). راجع إرشادات مجموعة Nature لتقديم الشيفرة والبرمجيات لمزيد من المعلومات.
بيانات
معلومات السياسة حول توفر البيانات يجب أن تتضمن جميع المخطوطات بيانًا حول توفر البيانات. يجب أن يوفر هذا البيان المعلومات التالية، حيثما ينطبق:
رموز الانضمام، معرفات فريدة، أو روابط ويب لمجموعات البيانات المتاحة للجمهور
وصف لأي قيود على توفر البيانات
بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتماشى مع سياستنا
جميع البيانات ذات الصلة من هذه التجربة مدرجة في المقالة والمواد التكميلية. محفظة الطبيعة | ملخص التقرير أبريل 2023
البحث الذي يتضمن مشاركين بشريين، بياناتهم، أو مواد بيولوجية
معلومات السياسة حول الدراسات التي تشمل مشاركين بشريين أو بيانات بشرية. انظر أيضًا معلومات السياسة حول الجنس، الهوية/التقديم الجنسي، والتوجه الجنسي والعرق، والاثنية والعنصرية.
التقارير عن الجنس والنوع الاجتماعي
تم تسجيل المشاركين بغض النظر عن جنسهم. البيانات متاحة في الجدول الإضافي 1.
التقارير عن العرق أو الإثنية أو غيرها من المجموعات الاجتماعية ذات الصلة
تم تسجيل المشاركين بغض النظر عن عرقهم/أصلهم العرقي.
خصائص السكان
تم توفير البيانات في الجدول 1 للبيانات الموسعة
التوظيف
تم إجراء دعوة عامة من قبل الموقع، مؤتمر صحفي. تم اختيار المرضى من بين الذين رغبوا في المشاركة، بعد استشارة لجنة الاختيار وفقًا لمعايير الاختيار. تم الإشارة إلى التحيزات المحتملة (أثر الدواء الوهمي وتحامل المراقب) في المناقشة.
رقابة الأخلاقيات
تمت مراجعة البروتوكول والموافقة عليه من قبل لجنة المراجعة المؤسسية لمستشفى جامعة كيوتو (K044).
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة حول الموافقة على بروتوكول الدراسة في المخطوطة.
التقارير الخاصة بالمجال
يرجى اختيار الخيار أدناه الذي يناسب بحثك بشكل أفضل. إذا لم تكن متأكدًا، اقرأ الأقسام المناسبة قبل اتخاذ قرارك. علوم الحياة □ العلوم السلوكية والاجتماعية □ العلوم البيئية والتطورية والبيئية لنسخة مرجعية من الوثيقة بجميع الأقسام، انظرnature.com/documents/nr-reporting-summary-flat.pdf
تصميم دراسة العلوم الحياتية
يجب على جميع الدراسات الإفصاح عن هذه النقاط حتى عندما يكون الإفصاح سلبياً.
حجم العينة
استنادًا إلى نتائج دراسة القرود (Kikuchi et al Nature 2017)، قمنا بحساب عدد العينات التي يمكن تقييم سلامتها. التفاصيل موجودة في خطة التحليل الإحصائي الصفحة 3. “حجم العينة المستهدف”.
استثناءات البيانات
لم يتم استبعاد أي بيانات.
التكرار
قمنا بتكرار زراعة الخلايا الجذعية المستمدة من الخلايا الجذعية المستحثة متعددة القدرات (iPSC) المولدة للدوبامين في إجمالي 7 مشاركين. وقد أكدنا أن جميع المحاولات كانت ناجحة.
العشوائية
لم تكن هذه التجربة عشوائية. عند اختيار المرضى، كانت نسبة الذكور إلى الإناث ( ) وتوافق أو عدم توافق HLA ( لم يكن هناك تحيز بين المرضى الذين استوفوا معايير الاختيار.
عمى
كانت هذه التجربة تجربة ذات ذراع واحدة.
التقارير عن مواد وأنظمة وطرق محددة
نحتاج إلى معلومات من المؤلفين حول بعض أنواع المواد والأنظمة التجريبية والأساليب المستخدمة في العديد من الدراسات. هنا، يرجى الإشارة إلى ما إذا كانت كل مادة أو نظام أو طريقة مدرجة ذات صلة بدراستك. إذا لم تكن متأكدًا مما إذا كان عنصر القائمة ينطبق على بحثك، يرجى قراءة القسم المناسب قبل اختيار رد.
المواد والأنظمة التجريبية
طرق
غير متوفر
مشارك في الدراسة
غير متوفر
□
– الأجسام المضادة
□
خطوط خلايا حقيقية النواة
□ علم الحفريات وعلم الآثار
□
أنا
□
【 الحيوانات وغيرها من الكائنات الحية
□
V
□
الأجسام المضادة
الأجسام المضادة المستخدمة
الأجسام المضادة الأولية المستخدمة هي كما يلي: FOXA2 (ماعز، R&D systems، AF2400، 1:500)، NURR1 (فأر، Perseus Proteomics، PP-N1404-00، 1:300)، HNA (فأر، Millipore، MAB1281، 1:500)، KI67 (أرنب، Abcam، Ab16667، 1:1,000)، 5-HT (جرذ، Millipore MAB352، 1:100)، وTH (أرنب، Millipore، AB152، 1:400). الأجسام المضادة الثانوية هي كما يلي: أليكسا فلور 488 مضاد لـ IgG من الفأر (حمار، ThermoFisher، A21202، 1:400)، أليكسا فلور 594 مضاد لـ IgG من الماعز (حمار، ThermoFisher، A11058، 1:2,000)، أليكسا فلور 594 مضاد لـ IgG من الأرنب (حمار، ThermoFisher، A21207، 1:400)، وأليكسا فلور 594 مضاد لـ IgG من الجرذ (حمار، ThermoFisher، A21209، 1:400).
التحقق
تُستخدم الأجسام المضادة تحت التحقق باستخدام عينات تحكم سلبية وإيجابية كافية. قمنا بتأكيد الصبغة باستخدام عينات حيوانية عند الإمكان، أو نعتمد على العينات الملونة المعروضة في موقع الشركة المصنعة (FOXA2 من R&D، HNA من Millipore، KI67 من Abcam، و5-HT وTH من Millipore).
خطوط خلايا حقيقية النواة
معلومات السياسة حول خطوط الخلايا والجنس والنوع في البحث
مصدر(s) خط الخلايا
تُستخرج الخلايا الجذعية المستحثة متعددة القدرات من خلايا الدم المحيطية البشرية، التي تبرع بها متطوعون أصحاء.
QHJI01s04 مقدمة من مركز أبحاث وتطبيق خلايا iPS (CiRA)، جامعة كيوتو، اليابان. MCBOO3 مقدمة من شركة سوميتيومو للأدوية (طوكيو، اليابان).
المصادقة
نمط STR (التكرار القصير المتتالي) للخلايا الجذعية المستحثة يتطابق مع نمط خلايا المتبرع.
تلوث الميكوبلازما
جميع الخلايا سلبية لوجود تلوث بالميكوبلازما.
الخطوط التي يتم التعرف عليها بشكل خاطئ بشكل شائع (انظر سجل ICLAC)
لا شيء.
الحيوانات وغيرها من الكائنات البحثية
معلومات السياسة حول الدراسات التي تشمل الحيوانات؛ إرشادات ARRIVE الموصى بها للإبلاغ عن أبحاث الحيوانات، والجنس والنوع في البحث
الحيوانات المخبرية
تم استخدام ذكور الفئران العارية البالغة (عمرها 9 أسابيع) (F344/NJcl-rnu/rnu، CLEA، اليابان) في هذه الدراسة.
الحيوانات البرية
لم تتضمن الدراسة حيوانات برية.
التقارير عن الجنس
في هذه الدراسة، تم استخدام الفئران الذكور فقط لفحص تأثير الخلايا المزروعة بدقة من خلال استبعاد تأثيرات دورة الجنس الأنثوي على بقاء أو نضوج الخلايا العصبية الدوبامينية.
عينات تم جمعها من الميدان
لم تتضمن الدراسة عينات تم جمعها من الميدان.
رقابة الأخلاقيات
تمت الموافقة على بروتوكول الدراسة من قبل اللجان الأخلاقية في جامعة كيوتو وشركة سوميتيومو فارما.
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة حول الموافقة على بروتوكول الدراسة في المخطوطة.
البيانات السريرية
معلومات السياسة حول الدراسات السريرية
يجب أن تتوافق جميع المخطوطات مع إرشادات ICMJE لنشر الأبحاث السريرية ويجب أن تتضمن جميع التقديمات قائمة مراجعة CONSORT مكتملة.
تسجيل التجارب السريرية
jRCT2090220384، UMIN000033564
بروتوكول الدراسة
تم توفير بروتوكول الدراسة في المواد التكميلية.
جمع البيانات
تم إجراء هذه التجربة في مستشفى جامعة كيوتو. تم تجنيد المرضى من 1 أغسطس 2018 إلى 19 مايو 2021. تم جمع البيانات من 25 سبتمبر 2018 إلى 18 يناير 2024.
النتائج
شملت النقاط النهائية الأساسية ملف الأحداث السلبية، بينما تضمنت النقاط النهائية الثانوية السلامة والفعالية بعد 24 شهرًا.
محفظة الطبيعة | ملخص التقرير أبريل 2023
النباتات
مخزونات البذور
تقرير عن مصدر جميع مخزونات البذور أو المواد النباتية الأخرى المستخدمة. إذا كان ذلك مناسبًا، يرجى ذكر مركز مخزون البذور ورقم الفهرس. إذا تم جمع عينات نباتية من الحقل، يرجى وصف موقع الجمع، التاريخ وإجراءات أخذ العينات.
أنماط جينية نباتية جديدة
وصف الطرق التي تم من خلالها إنتاج جميع الأنماط الجينية النباتية الجديدة. يشمل ذلك تلك التي تم إنشاؤها من خلال الأساليب الجينية المعدلة، وتحرير الجينات، والطفرات المعتمدة على المواد الكيميائية/الإشعاع، والتهجين. بالنسبة لخطوط الجينات المعدلة، وصف طريقة التحويل، وعدد الخطوط المستقلة التي تم تحليلها، والجيل الذي أجريت عليه التجارب. بالنسبة لخطوط تحرير الجينات، وصف المحرر المستخدم، والتسلسل الداخلي المستهدف للتحرير، وتسلسل RNA الدليل المستهدف (إذا كان ذلك مناسبًا) وكيف تم تطبيق المحرر.
المصادقة
وصف أي إجراءات تحقق لكل مخزون بذور مستخدم أو جينوتيب جديد تم إنشاؤه. وصف أي تجارب تم استخدامها لتقييم تأثير الطفرة، وحيثما ينطبق، كيف تم فحص التأثيرات الثانوية المحتملة (مثل إدخالات T-DNA في موقع ثانٍ، التبقيع، تحرير الجينات خارج الهدف).
التصوير بالرنين المغناطيسي
تصميم تجريبي
نوع التصميم
مواصفات التصميم
مقاييس الأداء السلوكي
لم تكن هذه دراسة تصوير بالرنين المغناطيسي الوظيفي.
لم تكن هذه دراسة تصوير بالرنين المغناطيسي الوظيفي.
لم تكن هذه دراسة تصوير بالرنين المغناطيسي الوظيفي.
حدد ما إذا تم استخدام مسح كامل للدماغ أو عرّف منطقة الاكتساب، موضحًا كيف تم تحديد المنطقة.
التحضير المسبق
التحضير المسبق
برمجيات المعالجة المسبقة
التطبيع
قالب التطبيع
إزالة الضوضاء والعيوب
تصفية الحجم
برنامج التصوير بالرنين المغناطيسي الوظيفي للدماغ (FMRIB)
لم يتم إجراء التطبيع.
غير قابل للتطبيق
غير قابل للتطبيق
غير قابل للتطبيق
النمذجة الإحصائية والاستدلال نوع النموذج والإعدادات غير قابل للتطبيق
التأثيرات المختبرة غير قابل للتطبيق
حدد نوع التحليل: □ الدماغ بالكامل □ قائم على منطقة معينة □ كلاهما نوع الإحصائيات للاستدلال غير قابل للتطبيق (انظر إكلوند وآخرون 2016)
تصحيح
غير قابل للتطبيق محفظة الطبيعة | ملخص التقرير أبريل 2023
النماذج والتحليل
مشارك في الدراسة
الاتصال الوظيفي و/أو الفعال
تحليل الرسوم البيانية
النمذجة متعددة المتغيرات أو التحليل التنبؤي
الاتصال الوظيفي و/أو الفعال
تحليل الرسوم البيانية
قم بالإبلاغ عن مقاييس الاعتماد المستخدمة وتفاصيل النموذج (مثل ارتباط بيرسون، الارتباط الجزئي، المعلومات المتبادلة).
قم بالإبلاغ عن المتغير التابع ومقياس الاتصال، مع تحديد ما إذا كان الرسم البياني موزونًا أو ثنائيًا، على مستوى الموضوع أو المجموعة، والملخصات العالمية و/أو العقد المستخدمة (مثل معامل التجميع، الكفاءة، إلخ).
النمذجة متعددة المتغيرات والتحليل التنبؤي □ حدد المتغيرات المستقلة، استخراج الميزات وتقليل الأبعاد، النموذج، التدريب ومقاييس التقييم.
قسم الأعصاب، كلية الطب بجامعة كيوتو، كيوتو، اليابان.قسم التطبيقات السريرية، مركز أبحاث وتطبيقات خلايا iPS، جامعة كيوتو، كيوتو، اليابان.قسم جراحة الأعصاب، كلية الطب بجامعة كيوتو، كيوتو، اليابان.قسم التصوير التشخيصي والطب النووي، كلية الطب بجامعة كيوتو، كيوتو، اليابان.قسم الجراحة، جامعة كيوتو، كلية الطب العليا، كيوتو، اليابان.قسم أمراض الدم/الأورام، كلية الطب بجامعة كيوتو، كيوتو، اليابان.قسم الإحصاءات الحيوية والمعلوماتية الحيوية، كلية الطب بجامعة كيوتو، كيوتو، اليابان.ساهم هؤلاء المؤلفون بالتساوي: نوبوكاتسو ساواموتو، دايسوكي دوئي، إتسورو ناكانشي، ماسانوري ساوامورا.البريد الإلكتروني: ryosuket@kuhp.kyoto-u.ac.jp; jbtaka@cira.kyoto-u.ac.jp
كوردوفر، ج. هـ. وآخرون. دليل مرضي عصبي على بقاء الطعوم وإعادة ت innervation في النواة المذنبة بعد زراعة نسيج دماغي جنيني في مريض يعاني من مرض باركنسون. نيو إنجلاند جورنال أوف ميديسين 332، 1118-1124 (1995).
بيتشيني، ب. وآخرون. إطلاق الدوبامين من زراعة النغري المرئية في الجسم الحي في مريض باركنسون. نات. نيوروسا. 2، 1137-1140 (1999).
يتم تقسيم المرضى إلى مجموعات الجرعة المنخفضة والجرعة العالية، وتُعرض الخصائص السريرية عند التسجيل. *متبرع HLA-A 24:O2، HLA-B 52:01، HLA-DRB1 15:02، HLA-C 12:02، HLA-DQB1
المقاييس السريرية الأساسية عند التسجيلونهاية الملاحظةيتم تقديمها بواسطة المتوسط والانحراف المعياري (بين قوسين). EQ-5D-5L، يوروكول 5 أبعاد 5 مستويات، [استبيان جودة الحياة الأوروبية – 5 أبعاد (EQ-5D)]; EQ VAS، مقياس يوروكول البصري التمثيلي؛ WPAI، إنتاجية العمل وتأثير النشاط.
Parkinson’s disease is caused by the loss of dopamine neurons, causing motor symptoms. Initial cell therapies using fetal tissues showed promise but had complications and ethical concerns . Pluripotent stem (PS) cells emerged as a promising alternative for developing safe and effective treatments . In this phase I/II trial at Kyoto University Hospital, seven patients (ages 50-69) received bilateral transplantation of dopaminergic progenitors derived from induced PS (iPS) cells. Primary outcomes focused on safety and adverse events, while secondary outcomes assessed motor symptom changes and dopamine production for 24 months. There were no serious adverse events, with 73 mild to moderate events. Patients’ anti-parkinsonian medication doses were maintained unless therapeutic adjustments were required, resulting in increased dyskinesia. Magnetic resonance imaging showed no graft overgrowth. Among six patients subjected to efficacy evaluation, four showed improvements in the Movement Disorder Society Unified Parkinson’s Disease Rating Scale part III OFF score, and five showed improvements in the ON scores. The average changes of all six patients were and 4.3 points ( ) for the OFF and ON scores, respectively. Hoehn-Yahr stages improved in four patients. Fluorine-18-l-dihydroxyphenylalanine ( F-DOPA) influx rate constant ( ) values in the putamen increased by , with higher increases in the high-dose group. Other measures showed minimal changes This trial (jRCT2090220384) demonstrated that allogeneic iPS-cell-derived dopaminergic progenitors survived, produced dopamine and did not form tumours, therefore suggesting safety and potential clinical benefits for Parkinson’s disease.
Parkinson’s disease (PD) is characterized by the loss of dopamine (DA) neurons in the substantia nigra, leading to a motor syndrome characterized by bradykinesia, rigidity and resting tremor. Medical treatment effectively alleviates PD symptoms in the early stages, but chronic use results in complications such as motor fluctuations and drug-induced dyskinesias. Consequently, cell therapies to replace lost DA neurons have been investigated as an alternative treatment.
Initial open-label studies demonstrated that human fetal ventral mesencephalon (hfVM) engrafted to the host striatum can synthesize DA and improve motor symptoms . However, double-blinded placebo-controlled trials failed to demonstrate substantial efficacy and revealed side effects such as graft-induced dyskinesias (GIDs) . Moreover, ethical issues and difficulties in maintaining a stable supply have hindered the clinical application of hfVM. European researchers are currently conducting a clinical trial to re-evaluate hfVM (NCT01898390) , while PS-cell-derived DA neurons are being explored as an alternative
donor source . Recently, a single compassionate use case of autologous transplantation suggested the potential of iPS cells . Moreover, clinical trials using human embryonic stem cells are also ongoing (NCT04802733 and NCT05635409 ).
We previously developed a method to induce DA neurons from human iPS cells and sort for DA progenitors . These cells produced DA in the brains of non-human primate PD models and improved their motor symptoms .After preclinical studies confirming safety in terms of tumorigenicity, toxicity and biodistribution , we received approval from the Japanese government and the institutional review board of Kyoto University. Here we report the results of our clinical trial launched in 2018.
Participants
Initially, seven patients were enrolled at Kyoto University Hospital and diagnosed according to Movement Disorder Society (MDS) clinical
Fig. 1 | Enrolment and follow-up. a, Patients were recruited and evaluated at Kyoto University Hospital between August 2018 and January 2019. The first three patients were categorized into the low-dose subgroup, while the remaining four were classified into the high-dose subgroup. One registered patient was excluded before surgery owing to a COVID-19 infection. The first patient received unilateral surgeries with an eight-month interval between procedures and was included only in the safety assessment. Efficacy analysis was conducted on the remaining six patients.b, After providing informed consent, the patients were enrolled in this clinical trial and underwent neurological evaluation for more than 6 months. If no notable symptomatic changes were observed during this
period, patients were re-enrolled for surgery and underwent further neurological evaluation (including MDS-UPDRS) and an F-DOPA PET study. After cell transplantation, brain imaging (MRI and PET) and neurological assessments (including MDS-UPDRS) were performed at and 24 months. PET studies included F-DOPA (to assess DA synthesis), F-GE180 (to detect inflammation) and F-FLT (to assess cell proliferation). For immunosuppression, tacrolimus ( 0.06 mg per kg twice daily) was administered, with the dosage adjusted to maintain target trough levels of . The dose was reduced by half at 12 months and discontinued at 15 months.
criteria . However, one patient dropped out due to a coronavirus disease 2019 (COVID-19) infection, necessitating the enrolment of an additional patient later. To confirm transplantation safety, the first participant received a left putamen graft and was monitored for 8 months before receiving a right putamen graft. This patient was included only in the safety evaluation. Efficacy was assessed in the remaining six patients who underwent simultaneous bilateral surgery (Fig.1a,b). All of the patients met the eligibility and exclusion criteria (Supplementary Methods), and their baseline characteristics are summarized in Extended Data Table 1.
Trial design
This investigator-initiated, open-label, phase-I/II, single-centre trial (jRCT2090220384) was conducted at Kyoto University Hospital to investigate the safety and efficacy of striatal transplantation of
allogeneic iPS-cell-derived DA progenitors in patients with PD. The patients underwent bilateral transplantation of DA progenitors and were monitored for 24 months. Three patients (PD01-03) received a low-dose transplant (2.1-2.6 cells per hemisphere) and four patients (PD04-06 and PD08) received a high-dose transplant (5.3 cells per hemisphere) (Fig. 1a). Tacrolimus ( 0.06 mg per kg twice daily) was administered and adjusted to target trough levels ( ), with the dosage reduced by half at 12 months and discontinued at 15 months.
Generation of human iPS cells
The clinical-grade human iPS cell line (QHJIO1sO4) was established from peripheral blood from a healthy individual homozygous for the most frequent haplotype in the Japanese population (HLA-A 24:02, HLA-B 52:01, HLA-DRB1 15:02, HLA-C 12:02, HLA-DQB1
06:01, HLA-DPB1 09:01), which matches 17% of the Japanese population .
DA progenitor induction and transplant
DA progenitors were induced as previously described . To enrich DA progenitors and eliminate non-target cells, (a floor plate marker) cells were sorted on days 11-13, with sorted cells cultured in neural differentiation medium to form aggregate spheres. The fresh final product containing DA progenitors meeting quality-control criteria (Supplementary Table 1) was bilaterally transplanted into the putamen using a neurosurgical navigation system. Single-cell quantitative PCR with reverse transcription (RT-qPCR) analysis confirmed the stable production of DA progenitors. iPS cells differentiated into DA neurons, based on sorting for CORIN cells, resulting in a final product comprising approximately DA progenitors and DA neurons (Extended Data Fig. 1). Importantly, no TPH2-expressing (a marker for serotonergic neurons) cells were detected. The same donor cells used for patients PD04-PD08 were transplanted into rat PD models to evaluate cell survival, proliferation and differentiation potential (Extended Data Fig. 2). Donor cells expressed NURR1 and FOXA2 and, when grafted, differentiated into tyrosine hydroxylase-positive ( ) DA neurons, improving the rotational behaviour of PD model rats. At 24 or 32 weeks after transplantation, no tumour-like overgrowth was observed, and (a maker for proliferating cells) cells were less than and sparsely distributed in the grafts. Furthermore, no 5-hydroxytryptamine (5-HT)-positive cells (a marker for serotonergic neurons) were detected.
Primary end point: adverse-event profile
No serious adverse events necessitating hospitalization or resulting in death were reported. All 7 patients ( ) experienced a total of 73 adverse events, comprising 72 mild events and one moderate case of dyskinesia (Supplementary Table 2). The most frequent adverse event was application site pruritus, observed in four patients (57.1%). There were no apparent differences in the spectrum, frequency and severity of treatment-related adverse events between the low-dose and high-dose groups. These events were transient, and most were unlikely related to either cell transplantation or tacrolimus. The single adverse event possibly related to cell transplantation was neck stiffness and painful dystonia in the right upper limb during the drug-on state. Tacrolimus administration was well tolerated but potentially associated with adverse events in three patients ( ), including hepatic impairment ( ), increased gamma-glutamyltransferase levels ( ), cystitis ( ), nail dermatophytosis ( ) and renal impairment ( ).
Secondary end point: safety
Serial magnetic resonance imaging (MRI) scans during follow-up periods identified the grafts as hyperintense areas in the putamen on T2-weighted images in all of the patients. Quantitative analysis of graft size showed a gradual volume increase over 24 months, with no evidence of tumour-like abnormal enlargement (Extended Data Fig. 3). None of the patients exhibited increased accumulation of fluorine-18-fluorothymidine ( F-FLT) in the transplanted striatum. Moreover, no patients displayed T2-weighted and fluid-attenuated inversion recovery (FLAIR) hyperintense regions nor appreciable uptake of the translocator protein-ligand, fluorine-18-flutriciclamide ( F-GE180: a marker of microglial activation) , indicative of apparent inflammation in the putamen and surrounding areas.
The Unified Dyskinesia Rating Scale (UDysRS) total scores increased at 24 months in all patients, except for PD06, with an average increase of 12.3 points ( ) from the baseline (Extended Data Table 2). Excluding PD01, who underwent surgery in two stages with an 8-month interval
and was observed for 32 months, the average increase was 12.2 points ( ; Fig. 2a,b). In the self-report motor diaries, patients recorded dyskinesia during the on-time period. No apparent increase in troublesome dyskinesia was observed during off-time.
Secondary end point: efficacy
Among the six patients in the efficacy group, four (PD02, PD03, PD04 and PD08) showed an improvement in motor function during the offtime period (more than 12 h without medication), as assessed by the MDS Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) part III. The average change from the baseline was -9.5 points at 24 months, apparently independent of the dose of transplanted cells (Fig. 2c,d and Extended Data Table 2). Regarding MDS-UPDRS part III ON (with medication), five patients (PD02, PD03, PD04, PD05 and PD08) improved, with an average change from the baseline of -4.3 points ( ) at 24 months (Fig. 2e,f and Extended Data Table 2). Whereas MDS-UPDRS part III is based on an objective examination by a neurologist, parts I and II are derived from patient interviews about motor and non-motor functions in daily life. When evaluating the combined MDS-UPDRS parts I + II + III OFF, a mild improvement of – 3.1 points ( ) on average was observed at 24 months (Extended Data Table 3).
In our evaluation of the Hoehn-Yahr stage during off-time, four patients improved: PD02 by 2 stages and PD03, PD06 and PD08 by 1 stage each at 24 months. One patient (PDO3) improved by 1 stage during on-time (Extended Data Fig. 4 and Extended Data Table 2).
Other secondary measures, such as on/off time and the 39-item Parkinson’s Disease Questionnaire (PDQ-39), were also analysed. While some patients showed improvement during observations, on average, no apparent improvement was observed at 24 months (Extended Data Fig. 5 and Extended Data Table 2). Throughout the study, patients’ anti-parkinsonian medication doses were maintained unless there was a therapeutic necessity. This approach was taken to avoid confounding the assessment of transplantation outcomes, as changes in individualized anti-parkinsonian medication could affect the results. Consequently, the mean levodopa equivalent daily dose (LEDD) remained nearly stable during the trial, with an average increase of 6.15 mg per day ( decrease) at 24 months (Extended Data Fig. 5 and Extended Data Table 2).
The total mean putaminal F-DOPA values increased by (from 0.0032 to 0.0043 ) at 24 months. Specifically, the low-dose group showed a increase, whereas the high-dose group exhibited a increase (Extended Data Table 2). F-DOPA values increased in two out of the four transplanted putamen in the low-dose group and seven out of the eight transplanted putamen in the high-dose group (Fig. 3a,b,e and Extended Data Fig. 6). By contrast, the total mean caudate nucleus F-DOPA value decreased (Fig.3c). Consequently, the ratio of values in the putamen to the caudate nucleus increased at 24 months in all cases, suggesting an increase of DA synthesis in the putamen despite pathological deterioration (Fig. 3d).
Discussion
The replacement of lost DA neurons with hfVM in patients with PD began in the . Although PS cells are expected to be an alternative donor cell source to hfVM, the safety and efficacy of iPS-cell-derived DA progenitors remains unclear. This first clinical trial using iPS cells confirmed that iPS-cell-derived DA progenitors can survive without forming tumours and produce DA in the putamen of patients with PD. Moreover, there were no serious adverse events or GIDs. Four out of six patients showed improvement in MDS-UPDRS part III OFF at 24 months after transplantation, suggesting that grafted cells functioned as DA neurons.
No serious adverse events were reported for all seven patients subjected to safety assessment. The graft size measured with MRI
Fig. 2 | Chronological changes in clinical end points. a,b, Chronological changes in the UDysRS scores for each patient from registration (0 months) to the end of the observation period (24 months) for safety assessment. b, Score changes from the baseline, with the mean represented by the black line. Absolute and relative (percentage) changes at 24 months are shown on the right. c-f, Chronological changes in MDS-UPDRS part III scores during the
medication-off(c,d) and medication-on (e,f) periods for each patient from registration (0 months) to the end of observation (24 months) for efficacy assessment. d,f, Score changes from the baseline. The mean is represented by the black line. The absolute and relative (percentage) changes at 24 months are shown on the right.
T2-weighted images gradually increased over the 24 months. However, no tumorigenic overgrowth was identified, as evidenced by the absence of F-FLT uptake, a marker of cellular proliferation, which was indirectly supported by results from the transplantation experiment using the same donor cells into PD model rats. Histological analyses at 24 or 32 weeks showed no tumour-like overgrowth, with less than of cells being Ki-67 positive. Rather than proliferation, a previous animal study reported that the apparent increase in graft volume was due to the spread of the grafted cells . While such effects may also apply to our trial, further confirmation through long-term follow-up and post-mortem histological examinations is necessary. The spectrum of adverse events was similar to those encountered with chronic DA replacement medication, tacrolimus administration and brain surgery. Neck stiffness and painful dystonia in the right upper limb were noted in PD01 during the drug-on state, a phenomenon possibly related to the grafts. Tacrolimus- and surgery-related adverse events were manageable and reversible.
One critical concern about hfVM transplantation was GIDs . In this trial, six out of seven patients showed a mild worsening of dyskinesia, resulting in an average increase in the UDysRS total score of 12.3 points ( ) from the baseline at 24 months, probably because anti-parkinsonian medication doses were maintained throughout the trial, except when therapeutic adjustments were necessary. The protocol was designed to minimize the impact of medication changes. Consistently, patients recorded dyskinesia in both upper and lower extremities during the on-time period. This clinical presentation is typical for drug-induced dyskinesia and not for GIDs, which occur during the off-time and are often observed predominantly in the lower extremities . This suggests that grafted cells replicate the effects of levodopa, including the tendency to induce dyskinesias in susceptible patients. Alternatively, a focal rather than diffuse distribution of DA stimulation from the graft may exacerbate dyskinesia . In previous reports, GIDs were attributed to serotonergic neurons contained in hfVM tissue . In our DA progenitor preparation, we
Fig. 3 | DA synthesis detected by F-DOPA PET. a,b, Chronological changes in F-DOPA values (average of both sides) in the putamen for each patient from registration (0 months) to the end of the observation period (24 months).
b, The value changes from the baseline; the mean is represented by the black line. The absolute and relative (percentage) changes at 24 months are shown on the right.c, The F-DOPA value (average of both sides) changes from the baseline in the caudate nucleus for each patient, indicating pathological deterioration in PD. d, The ratio of values between the putamen and the
caudate nucleus, highlighting the impact of cell transplantation on pathological deterioration. The percentage changes at 24 months are shown on the right. e, Semiquantitative F-DOPA images generated at after injection by subtracting the occipital background signal and normalizing the result to the occipital activity in patient PD08. The colour change from dark green to red in the bilateral putamen indicates increased F-DOPA uptake, reflecting DA synthesis by grafted cells. Pre-op, pre-operation; R, right.
purified medial plate cells and eliminated lateral plate cells, which include serotonergic neurons. As a result, we detected no 5-HT cells in donor-cell-derived grafts in rat PD models. This purification process may have contributed to the absence of GIDs in our trial.
The appropriate regimen of immunosuppression in allogeneic neural transplantation remains controversial. Previous clinical trials used a different combination of immunosuppressant drugs, including ciclosporin, azathioprine and prednisolone . Our previous non-human-primate studies demonstrated no acute immune response after allogeneic transplantation of monkey iPS-cell-derived DA progenitors without immunosuppression . Furthermore, tacrolimus alone effectively suppressed immune responses during both allotransplantation (monkey to monkey) and xenotransplantation (human to monkey) . On the basis of these findings, we used tacrolimus as the sole immunosuppressant in our clinical trial. Histological analyses from previous fetal cell transplantation studies have shown that grafted DA neurons can survive for 9 to 16 years, even when immunosuppression
is discontinued 6 to 18 months after transplantation . Moreover, our positron-emission tomography (PET) study at 3,6 and 12 months showed no F-GE180 uptake, suggesting the absence of severe inflammation. As a result, we discontinued tacrolimus treatment at 15 months. After terminating immunosuppression, no inflammation due to immune response was observed in the putamen and surrounding areas, as evident by the absence of hyperintensity regions on T2-weighted and FLAIR MRI or increased F-GE180 uptake. Moreover, there was no clinical difference between HLA-matched and non-matched patients. However, further confirmation through long-term follow-up and post-mortem histological examinations is necessary for definitive conclusions.
Our results demonstrated a beneficial effect on MDS-UPDRS part III during both on- and off-time periods. Specifically, PD02, PD04 and PD08 showed improvements of and during off-time at 24 months, respectively, while PD03 showed a improvement. Considering the increase in F-DOPA uptake, these results suggest that
grafted cells function as DA neurons, therefore functionally replacing lost DA neurons. As this is an open-label trial without a control group, it is important to consider the potential influence of the placebo effect and observer bias. A systematic analysis of placebo responses (placebo effect plus observer bias) in nine double-blind, randomized trials of regenerative therapies for PD reported an average improvement of 4.3 points in MDS-UPDRS part III OFF scores, with a 95% confidence interval of 3.1 to 5.6 , with a mean observation time of 11.3 months . Moreover, a PET study conducted in four out of nine trials showed no significant increase in F-DOPA uptake in sham-operated groups. Furthermore, the placebo effect in patients with PD is thought to be mediated by the release, rather than synthesis, of endogenous DA in the striatum . On the basis of these findings, at least three patients (PD02, PD04, PD08) in this trial exhibited motor symptom improvements exceeding what could be attributed to placebo responses, potentially due to DA synthesized by the graft. This interpretation should be further validated through post-mortem histological examinations in the future.
Among the three patients (PD02, PD04 and PD08) who exhibited a beneficial effect on MDS-UPDRS part III, only PD02 showed improvement in both the off-time period and PDQ-39 scores. These evaluations are subjective and reflect the patient’s perceptions. It is possible that patients had very high expectations for this new treatment, and the results did not meet such high expectations despite objective improvements. In the remaining two patients (PD05 and PD06), motor deficits stabilized at a similar level of decline to those receiving conventional medication . These two patients exhibited a higher degree of deterioration in motor symptoms compared with the other patients during the on-time, suggesting that faster neurodegeneration, especially in the non-dopaminergic systems, diminished the beneficial effects produced by the graft during the trial period. Notably, PD05 was 69 years old at the baseline, and as previous studies on fetal transplants suggest , younger patients with less severe symptoms appear to be more suitable candidates for this treatment. Considering these results, refining patient eligibility criteria may enhance the efficacy of this treatment.
In some cases, especially PD03 and PD06, discrepancies were noted between the MDS-UPDRS part III scores and the Hoehn-Yahr stage. The Hoehn-Yahr stage emphasizes postural instability and mobility issues, whereas the MDS-UPDRS part III offers a more comprehensive evaluation of major motor symptoms in PD. Consequently, improved postural stability and mobility may account for the greater improvement in the Hoehn-Yahr stage compared with changes observed in MDS-UPDRS part III scores of this study.
The substantial increase in putaminal F-DOPA uptake in the high-dose group compared with the low-dose group suggests dosedependent characteristics. Plots of pre-transplant and post-transplant values and MDS-UPDRS part III OFF scores revealed a mild overall trend but no clear correlation at the individual level (Extended Data Fig. 6i,j). This lack of correlation may be due to the complexity of cell replacement therapy: F-DOPA uptake does not necessarily reflect the activation of postsynaptic neurons, and motor symptoms are influenced by both dopaminergic and non-dopaminergic neural circuits. The functional impact of grafted cells probably requires more than just DA delivery. Successful integration of the graft into the host brain is crucial for achieving meaningful clinical recovery in . Another possibility is that the absolute value is more important than its level of increase and that the number of surviving DA neurons is still insufficient. Previous studies have reported that values of healthy individuals range from 0.010 to 0.017 (with our experience indicating a range of 0.010 to 0.015 ). While Parkinsonian symptoms typically emerge when values decrease by to from the normal range , even the highest value observed at 24 months fell within the range associated with the onset of initial symptoms. Furthermore, 3 out of 12 putamen samples (PDO2R, PD02L, PD06L) did not show an increase in F-DOPA uptake (Extended Data Fig. 6a,b). This may be due
to the technical limitation of measuring uptake in the whole putamen. However, PET images revealed distinct uptake at the injection sites (Extended Data Fig. 6c-h), which may have contributed to symptom improvement. Importantly, there was no difference in adverse events between low- and high-dose groups, and neither graft overgrowth nor GIDs were observed, even in the high-dose group. Considering these results, implanting more cells across a broader area may be necessary to achieve more substantial therapeutic effects. The favourable safety profile observed in this trial provides an opportunity to explore whether a higher dose across a wider region can offer greater clinical efficacy.
Previous open-label trials using human hfVM demonstrated that cells engrafted into the host striatum synthesized DA and improved motor symptoms. In favourable cases, symptom improvement persisted for over 10 years without severe adverse events . While two double-blind, placebo-controlled trials did not find significant differences between the graft and control groups, they did show significant motor symptom improvement in specific subgroups. These findings suggest that cell replacement therapy may be beneficial if appropriate patients are selected. One beneficial subgroup may be patients 60 years old or younger, while another included those with less severe stages (below 50 points as evaluated by the original UPDRS part III OFF score ). Although our results did not fully align with age-related findings, it is notable that the worst case (PD05) was the oldest patient, and the best case (PD08) was the youngest. In terms of MDS-UPDRS part III OFF scores, patients PD02 and PD08, both with scores under 50, demonstrated symptom improvement.
As discussed above, this trial has certain limitations. First, for definitive conclusions regarding the survival of mature DA neurons, inflammation around the graft, and tumorigenicity, post-mortem histological analyses are required. Second, eligibility criteria for optimal patients with PD receiving cell replacement therapy have yet to be defined. Third, graft-derived reinnervation may cover only some DA-depleted striatal regions . These latter factors may partially explain the variable clinical responses observed in this trial. Fourth, this was an open-label trial, susceptible to influence from the placebo effect and physician bias. Future studies should consider a double-blind, placebo-controlled design to minimize these biases. Lastly, the findings of this single-centre, small-sample trial should be confirmed in multi-centre, large-sample trials with appropriate controls.
In conclusion, while the safety and efficacy of iPS-cell-derived cell products continue to be investigated, this trial demonstrated the safety profile of iPS-cell-derived DA progenitors. After bilateral putaminal transplantation, the average motor severity was decreased and the mean F-DOPA uptake was increased at the 24 -month follow-up. Despite the abovementioned limitations, these findings suggest that allogeneic transplantation of iPS-cell-derived DA progenitors is a safe and effective regenerative therapy for patients with PD. Future strategies may combine cell transplantation with gene therapy, medication and rehabilitation to enhance efficacy . Moreover, as demonstrated in a single case study , autologous transplantation using iPS cells may also be a promising option.
Online content
Any methods, additional references, Nature Portfolio reporting summaries, source data, extended data, supplementary information, acknowledgements, peer review information; details of author contributions and competing interests; and statements of data and code availability are available at https://doi.org/10.1038/s41586-025-08700-0.
3. Barker, R. A., Barrett, J., Mason, S. L. & Bjorklund, A. Fetal dopaminergic transplantation trials and the future of neural grafting in Parkinson’s disease. Lancet Neurol. 12, 84-91 (2013).
4. Freed, C. R. et al. Transplantation of embryonic dopamine neurons for severe Parkinson’s disease. N. Engl. J. Med. 344, 710-719 (2001).
5. Olanow, C. W. et al. A double-blind controlled trial of bilateral fetal nigral transplantation in Parkinson’s disease. Ann. Neurol. 54, 403-414 (2003).
6. Parmar, M., Grealish, S. & Henchcliffe, C. The future of stem cell therapies for Parkinson disease. Nat. Rev. Neurosci. 21, 103-115 (2020).
7. Barker, R. A. & TRANSEURO Consortium. Designing stem-cell-based dopamine cell replacement trials for Parkinson’s disease. Nat. Med. 25, 1045-1053 (2019).
8. Schweitzer, J. S. et al. Personalized iPSC-derived dopamine progenitor cells for Parkinson’s disease. N. Engl. J. Med. 382, 1926-1932 (2020).
9. Piao, J. et al. Preclinical efficacy and safety of a human embryonic stem cell-derived midbrain dopamine progenitor product, MSK-DAO1. Cell Stem Cell 28, 217-229 (2021).
10. Kirkeby, A. et al. Preclinical quality, safety, and efficacy of a human embryonic stem cell-derived product for the treatment of Parkinson’s disease, STEM-PD. Cell Stem Cell 30, 1299-1314 (2023).
11. Doi, D. et al. Isolation of human induced pluripotent stem cell-derived dopaminergic progenitors by cell sorting for successful transplantation. Stem Cell Rep. 2, 337-350 (2014).
12. Kikuchi, T. et al. Human iPS cell-derived dopaminergic neurons function in a primate Parkinson’s disease model. Nature 548, 592-596 (2017).
13. Doi, D. et al. Pre-clinical study of induced pluripotent stem cell-derived dopaminergic progenitor cells for Parkinson’s disease. Nat. Commun. 11, 3369 (2020).
14. Postuma, R. B. et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 30, 1591-1601 (2015).
15. Okita, K. et al. A more efficient method to generate integration-free human iPS cells. Nat. Methods 8, 409-412 (2011).
16. Yoshida, S. et al. A clinical-grade HLA haplobank of human induced pluripotent stem cells matching approximately 40% of the Japanese population. Med 4, 51-66 (2023).
17. Feeney, C. et al. Kinetic analysis of the translocator protein positron emission tomography ligand [(18)F]GE-180 in the human brain. Eur. J. Nucl. Med. Mol. Imaging 43, 2201-2210 (2016).
18. Goetz, C. G., Nutt, J. G. & Stebbins, G. T. The unified dyskinesia rating scale: presentation and clinimetric profile. Mov. Disord. 23, 2398-2403 (2008).
19. Goetz, C. G. et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s disease rating scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov. Disord. 23, 2129-2170 (2008).
20. Tomlinson, C. L. et al. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 25, 2649-2653 (2010).
21. Jost, S. T. et al. Levodopa dose equivalency in Parkinson’s disease: updated systematic review and proposals. Mov. Disord. 38, 1236-1252 (2023).
22. Lindvall, O. et al. Human fetal dopamine neurons grafted into the striatum in two patients with severe Parkinson’s disease. A detailed account of methodology and a 6-month follow-up. Arch. Neurol. 46, 615-631 (1989).
23. Lindvall, O. et al. Grafts of fetal dopamine neurons survive and improve motor function in Parkinson’s disease. Science 247, 574-577 (1990).
24. Hagell, P. et al. Dyskinesias following neural transplantation in Parkinson’s disease. Nat. Neurosci. 5, 627-628 (2002).
25. Bankiewicz, K. S. et al. Focal striatal dopamine may potentiate dyskinesias in parkinsonian monkeys. Exp. Neurol. 197, 363-372(2006).
26. Barker, R. A. & Kuan, W. L. Graft-induced dyskinesias in Parkinson’s disease: what is it all about? Cell Stem Cell 7, 148-149 (2010).
27. Politis, M. et al. Serotonergic neurons mediate dyskinesia side effects in Parkinson’s patients with neural transplants. Sci. Transl. Med. 2, 38ra46 (2010).
28. Politis, M. et al. Graft-induced dyskinesias in Parkinson’s disease: High striatal serotonin/ dopamine transporter ratio. Mov. Disord. 26, 1997-2003 (2011).
29. Mendez, I. et al. Simultaneous intrastriatal and intranigral fetal dopaminergic grafts in patients with Parkinson disease: a pilot study. Report of three cases. J. Neurosurg. 96, 589-596 (2002).
30. Morizane, A. et al. Direct comparison of autologous and allogeneic transplantation of iPSC-derived neural cells in the brain of a non-human primate. Stem Cell Rep. 1, 283-292 (2013).
31. Morizane, A. et al. MHC matching improves engraftment of iPSC-derived neurons in non-human primates. Nat. Commun. 8, 385 (2017).
32. Li, J. Y. et al. Lewy bodies in grafted neurons in subjects with Parkinson’s disease suggest host-to-graft disease propagation. Nat. Med. 14, 501-503 (2008).
33. Mendez, I. et al. Cell type analysis of functional fetal dopamine cell suspension transplants in the striatum and substantia nigra of patients with Parkinson’s disease. Brain 128, 1498-1510 (2005).
34. Polgar, S. et al. The placebo response in double-blind randomised trials evaluating regenerative therapies for Parkinson’s disease: a systematic review and meta-analysis. J. Parkinsons Dis. 12, 759-771 (2022).
35. de la Fuente-Fernandez, R. et al. Expectation and dopamine release: mechanism of the placebo effect in Parkinson’s disease. Science 293, 1164-1166 (2001).
36. Aviles-Olmos, I. et al. Exenatide and the treatment of patients with Parkinson’s disease. J. Clin. Invest. 123, 2730-2736 (2013).
37. Schrag, A. et al. Rate of clinical progression in Parkinson’s disease. A prospective study. Mov. Disord. 22, 938-945 (2007).
38. Piccini, P. et al. Delayed recovery of movement-related cortical function in Parkinson’s disease after striatal dopaminergic grafts. Ann. Neurol. 48, 689-695 (2000).
39. Pavese, N., Rivero-Bosch, M., Lewis, S. J., Whone, A. L. & Brooks, D. J. Progression of monoaminergic dysfunction in Parkinson’s disease: a longitudinal 18F-dopa PET study. Neuroimage 56, 1463-1468 (2011).
40. Khan, N. L. et al. Progression of nigrostriatal dysfunction in a parkin kindred: an [18F]dopa PET and clinical study. Brain 125, 2248-2256 (2002).
41. Nurmi, E. et al. Rate of progression in Parkinson’s disease: a 6-[18F]fluoro-L-dopa PET study. Mov. Disord. 16, 608-615 (2001).
42. Kefalopoulou, Z. et al. Long-term clinical outcome of fetal cell transplantation for Parkinson disease: two case reports. JAMA Neurol. 71, 83-87 (2014).
43. Fahn, S., Elton, R. L. & UPDRS Development Committee. in Recent Developments in Parkinson’s Disease Vol. 2 (eds Fahn, S. et al.) 153-163 (Macmillan, 1987).
44. Takahashi, J. Next steps in regenerative medicine. Cell Stem Cell 30, 509-511(2023).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creativecommons.org/licenses/by-nc-nd/4.0/.
(c) The Author(s) 2025
Methods
Participants
This trial is registered in Japan Registry of Clinical Trials (jRCT) as study number jRCT2090220384 and in University Hospital Medical Information Network (UMIN) as study number UMINOOOO33564. Patients with PD were diagnosed according to MDS clinical criteria . After initial enrolment, all of the patients except for PD01 were observed for more than 6 months and re-enrolled just before surgery. Inclusion criteria included ages 50-69, a disease duration of at least 5 years, Hoehn-Yahr stage 3 or worse during off-time and stage 3 or better during on-time, at least motor improvement with dopaminergic medication (MDS-UPDRS part III) and symptoms unresponsive to current medications (Supplementary Table 3). Exclusion criteria included dementia or psychiatric issues (Supplementary Table 4). A complete list of inclusion and exclusion criteria, along with additional methodological details, is provided in the Supplementary Methods. All of the participants provided written informed consent according to the ethical guidelines of the Kyoto University Hospital Institutional Review Board (K044). Three patients (PD01-03) received a low-dose transplant (2.1-2.6 cells per hemisphere), and four patients (PD04-06, PD08) received a high-dose transplant (5.3-5.5 cells per hemisphere) (Fig. 1). The low dose of 5 million cells was selected based on our monkey study , which demonstrated both safety and efficacy. After confirming the safety of this dose over one year, the cell count was increased to 10 million. Tacrolimus dosing was adjusted to maintain target trough levels of , reduced by half at 12 months, and discontinued at 15 months. This immunosuppression regimen was based on our non-human primate study , in which a single treatment with tacrolimus effectively suppressed immune response during xenotransplantation. Histological examinations from previous fetal cell transplantation cases have shown that grafted DA neurons survived for 9 to 16 years, even with immunosuppression discontinued 6 to 18 months after transplantation. Accordingly, tacrolimus treatment was discontinued at 15 months.
End points and evaluation
Primary end points included the adverse-event profile and graft overgrowth at 24 months ( by MRI) (Supplementary Table 5). Secondary outcomes included tumorigenic proliferation, host immune rejection, graft-induced dyskinesia, motor symptom changes (MDS-UPDRS part III) and F-DOPA at 24 months (Supplementary Methods).
Safety was evaluated by documenting adverse events from transplantation to 24 months after operation, coded according to the Medical Dictionary for Regulatory Activities (MedDRA) version 26.1. Dyskinesia severity was assessed using the UDysRS . Parkinsonian motor and non-motor symptoms were evaluated using the MDS-UPDRS (parts I-III), the Hoehn-Yahr stages in drug-on and drug-off states and LEDD. Motor diaries, PDQ-39, EuroQol 5-dimension 5-level (EQ-5D-5L), and the Work Productivity and Activity Impairment questionnaire were used for additional patient-reported outcomes. Tumour-like overgrowth and immune rejection were monitored by MRI, F-FLT PET and F-GE180 . DA neuron survival and differentiation were assessed through motor symptoms and F-DOPA PET. These evaluations were scheduled at various intervals after transplantation (Fig.1b).
Human iPS cells
The clinical-grade human iPS cell line (QHJI01s04) used in this study was previously established from peripheral blood from a healthy individual homozygous for the most frequent haplotype in the Japanese population (HLA-A 24:02, HLA-B 52:01, HLA-DRB115:02, HLA-C 12:02, HLA-DQB106:01, HLA-DPB109:01), which matches17% of the Japanese population . A master cell bank (MCB) was created, and a single MCB vial was thawed to induce DA progenitors for each patient. Human
iPS cells were maintained with StemFit AK03N media (Ajinomoto) on iMatrix-coated (Matrixome) six-well culture dishes.
DA progenitor induction from human iPS cells
DA progenitors were induced as previously described . Cells for PD01-PD03 were manufactured at Kyoto University, while cells for PD04-PD08 were manufactured at Sumitomo Pharma (international non-proprietary name, raguneprocel). In brief, human iPS cells were seeded at cells per onto culture plates coated with laminin 511-E8 fragment (defined as day 0 ) and cultivated for days. To enrich DA progenitors and eliminate non-target cells, (a floor plate marker) cells were isolated by a fluorescence-activated cell sorter (BD Influx by BD Bioscience for PD01L, MACSQuant Tyto by Myltenyi Biotec for PD01R-PD03, GigaSort by Cytonome for PD04-PD08) on days 11-13. Sorted CORIN cells were cultured in 96-well plates with neural differentiation medium to form aggregate spheres until day 30. DA progenitors were induced for each patient individually and prepared as fresh cells on the day of surgery. The final product containing DA progenitors met the quality control criteria (Supplementary Table 1), with cells also analysed by immunostaining and single-cell RT-qPCR (Extended Data Figs. 1 and 2).
Immunostaining
Aggregate spheres were fixed with 4% paraformaldehyde, frozen and sliced at a m thickness. Immunostaining was performed after incubation with an antigen retrieval reagent (LSI Medience) and blocking with 0.3% Triton X-100 and 2% donkey serum for 1 h . Fluorescence images were obtained by using confocal laser microscopes (Fluoview FV1200, Olympus). The antibodies used are described in the ‘Animal experiments’ section below.
Single-cell RT-qPCR analysis
Single-cell cDNA preparation was performed according to the manufacturer’s protocol. In brief, a cell suspension of iPS cells (day 0 ), intermediate cells before sorting (day 13) or the final product (day 30 or 31 ) at 300 cells per were used. The cell suspension was added to C 1 suspension reagent (Standard BioTools) at a ratio of for iPS cells or for intermediate cells and DAPs. Then, of cell suspension and suspension reagent mix, as mentioned above, were loaded onto the C1 Single-Cell Preamp IFC ( , Standard BioTools), and the chip was then processed on a Fluidigm C1 instrument using the ‘STA: Cell Load (1782×)’ script. After cell loading, visual inspection on an inverted microscope observation was performed to check whether only one living cell was captured in each capture site. Then, the ‘STA: Preamp ( )’ script, including cell lysis, reverse transcription, and 18 cycle of PCR, was executed. After completion, of amplified cDNA was mixed with of C1 DNA dilution reagent (Standard BioTools). Amplified cDNA was used for single-cell RT-qPCR using the Biomark HD System (Standard BioTools), according to the manufacturer’s protocol. Gene expression data were analysed and visualized using the Singular Analysis Toolset v.3.6.2 (Standard BioTools). Gene expression patterns were visualized on a -distributed stochastic neighbour embedding plot. Unsupervised clustering of the cells was performed using the -means clustering method. The spectrum of gene expression levels in each cell population was visualized by violin plots. DNA primer sequences are listed in Supplementary Table 6.
Cell transplantation
Cells were bilaterally transplanted into the putamen using the iPlan neurosurgical navigation system (BrainLab). Trajectories were designed to target the dorsal and caudal putamen, avoiding sulci and blood vessels. The surgery was performed using the Leksell G frame system (Elekta) and a custom injection needle (TOP). Injection sites were confirmed intraoperatively by cone-beam computed tomography (CT) using the Artis Zeego angiography system (Siemens Healthineers). Three
trajectories per hemisphere were used, with four to eight injections per trajectory, to transplant 2.1-5.5 cells per putamen (Supplementary Table 7 and Supplementary Methods).
Animal experiments
All of the animals were cared for and handled in accordance with the Guidelines for Animal Experiments of Kyoto University and Sumitomo Pharma. Study protocols were approved by the ethical committees of Kyoto University (17-87-7) and Sumitomo Pharma (2014-20). The same donor cells used for patients PD04 (batch, 20022), PD05 (batch, 20048), PD06 (batch, 21004) and PD08 (batch, 21047) were used for transplantation experiments. Fresh day- 30 cells ( or cells as the low dose, and or cells as the high dose) were injected into the striatum of 6-OHDA-lesioned Parkinsonian nude rats (F344/ NJcl-rnu/rnu, CLEA, aged 17-21 weeks). Methamphetamine-induced rotation analyses were conducted at 8 weeks after transplantation and every 4 weeks subsequently. Saline was injected into control rats as a vehicle group in each experiment. Rats are randomly assigned to cell and vehicle group. After 24 to 32 weeks of observation, animals were euthanized with isoflurane and perfused with -free PBS, and 4% paraformaldehyde. After immersion in 30% sucrose, the frozen brain slices at thickness were prepared for immunohistochemistry. For 3,3′-diaminobenzidine (DAB) staining, brain slices were treated with peroxidase blocking solution (DAKO), incubated sequentially with primary, biotinylated secondary antibodies against rabbit IgG (1:1,000, Vector Laboratories) and avidin-conjugated peroxidase (Vectastain ABC HRP Kit, Vector Laboratories). Signal detection was performed using DAB (DAB Staining Kit, Muto Pure Chemicals) with nickel chloride. Primary antibodies used for immunohistochemistry are as follows: FOXA2 (goat, R&D systems, AF2400, 1:500), NURR1 (mouse, Perseus Proteomics, PP-N1404-00, 1:300), human nucleic antigen (HNA) (mouse, Millipore, MAB1281,1:500, Ki-67 (rabbit, Abcam, Ab16667, 1:1,000), 5-HT (rat, Millipore MAB352, 1:100) and TH (rabbit, Millipore, AB152, 1:400). Secondary antibodies are as follows: Alexa Fluor 488 anti-Mouse IgG, (donkey, Thermo Fisher Scientific, A21202, 1:400), Alexa Fluor 594 anti-Goat IgG (donkey, Thermo Fisher Scientific, A11058, 1:2,000), Alexa Fluor 594 anti-rabbit IgG (donkey, Thermo Fisher Scientific, A21207, 1:400) and Alexa Fluor 594 anti-rat IgG (donkey, Thermo Fisher Scientific, A21209, 1:400). Images were visualized using a fluorescence microscope (BZ-X710, Keyence) and confocal laser microscopes (LSM880 and LSM800, Zeiss). The number of immunoreactive cells for TH and HNA was quantified in every sixth section throughout the grafts for stereological measurements of the total number of cells per animal .
Statistical analysis
Clinical data were collected by using EDMS-Online (v.3.1, EPS). Safety and efficacy outcomes were summarized using mean values, s.d. values and proportions. Statistical analyses of the clinical data were conducted
using SAS software (v.9.4, SAS Institute). Statistical analyses of animal experiments were performed using GraphPad Prism (v.10.3.1, GraphPad Software).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All relevant data from this trial are included in the Article and Supplementary Methods. Source data are provided with this paper.
45. Patlak, C. S. & Blasberg, R. G. Graphical evaluation of blood-to-brain transfer constants from multiple-time uptake data. Generalizations. J Cereb. Blood Flow Metab. 5, 584-590 (1985).
46. Shields, A. F. et al. Imaging proliferation in vivo with [F-18]FLT and positron emission tomography. Nat. Med. 4, 1334-1336 (1998).
47. Abercrombie, M. Estimation of nuclear population from microtome sections. Anat. Rec. 94, 239-247 (1946).
Acknowledgements We thank all of the patients who participated in this trial; Y. Shimizu, T. Saga and K. Togashi for brain imaging; members of the Efficacy and Safety Evaluation Committee, including S. Kinoshita, H. Sawada and H. Toda for their advice; doctors and coordinators at the Institute for Advancement of Clinical and Translational Science (iACT), Kyoto University Hospital, including A. Shimizu, Y. Nagai, M. Yamamoto, R. Uozumi, Y. Kusunoki, A. Kuroda, K. Endo, K. Enomoto, A. Kinoshita, C. Kimura, K. Kawaguchi, C. Ichihara, N. Matsuyama, K. Tochigi, Y. Sameshima, M. Iwasaki and C. Toyooka for supporting this clinical trial; the technical staff of J.T.’s laboratory, including E. Yamasaki, T. Ashida, Y. Fujita, Y. Tanikawa, Y. Katano, Y. Ozaki, R. Takaichi, A. Mihara, K. Fukushima and S. Baba for cell manufacturing; PD project members of Sumitomo Pharma, including K. Yoshida, H. Takahashi, Y. Sugao, S. Sekiya, M. Ikeda, Y. Yamamoto, S. Ota, S. Okabe, H. Ohara and T. Karino for regulatory support and cell manufacturing; and K. Hui for reading this manuscript. This study was supported by a grant from the Research Project for Practical Application of Regenerative Medicine of the Japan Agency for Medical Research and Development (AMED) (23bk0104126h0003) to J.T.
Author contributions J.T. and R.T. were the lead investigators. N.S., D.D. and Takayuki Kikuchi wrote the first draft of the paper. N.S., E.N., M.S., H.Y., Y.T., A.S., Y.F., T.O., Y.N. and R.T. contributed to the acquisition of clinical data. D.D., Tetsuhiro Kikuchi, A.M. and J.T. contributed to the generation of human iPS cells and DA progenitor cells. S.H. contributed to the PD rat experiments. Takayuki Kikuchi, Y.A. and S. Miyamoto contributed to neurosurgery. T.A. and T.S. contributed to immunosuppressive therapy management. K.U. and S. Morita performed statistical analyses. All of the authors contributed to the analysis or interpretation of data and performed critical revisions of the manuscript.
Competing interests N.S., R.T. and J.T. received a grant for collaborative research from Sumitomo Pharma. R.T. received a research grant from Nihon Medi-Physics. T.O. received a research grant from Siemens Healthcare. S.H. is an employee of Sumitomo Pharma. The other authors declare no competing interests.
Additional information
Supplementary information The online version contains supplementary material available at https://doi.org/10.1038/s41586-025-08700-0.
Correspondence and requests for materials should be addressed to Ryosuke Takahashi or Jun Takahashi.
Peer review information Nature thanks David Devos, Hideyuki Okano and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Reprints and permissions information is available at http://www.nature.com/reprints.
Extended Data Fig.1|See next page for caption.
Extended Data Fig. 1| Single-cell RT-qPCR (sc-RT-qPCR) analysis of cells during DA differentiation. a. t-SNE plot of sc-RT-qPCR data for iPSCs, intermediate cells (before CORIN-positive cell sorting), and final products. iPSCs and intermediate cells each form a distinct cluster, while final products are divided into two clusters. b. Relative proportions of cell types in each cell sample, determined by K-means clustering of sc-RT-qPCR data, indicate the final product consists of approximately 60% DA progenitors and 40% DA
neurons. Batch #20022 was the donor cells used for PD04, Batch #20048 for PD05, Batch #21004 for PD06, and Batch #21047 for PD08. Batch #190909 was used for PD02. c. Violin plots of gene expression patterns in clusters of iPSCs, intermediate cells, and final products show gene expression changes during DA differentiation.d.Violin plots of gene expression patterns across different batches of final products indicate stable expression among batches.
Extended Data Fig. 2 | See next page for caption.
Extended Data Fig. 2 | Transplantation of the same donor cells used for patients into rat PD models. a-d. Immunofluorescence images of donor cells on day 30 ( independent experiments). NURR1(a) is a nuclear receptor expressed in DA neurons, while FOXA2 (b) is a transcription factor expressed in the floor plate. DAPI (c) is used for nuclear staining. The merged image (d) shows that donor cells consist mainly of DA progenitors and some DA neurons. Scale bars . e. Summary of cell transplantation experiments and results. Low- and high-dose cell injections were administered to examine differences in cell survival and behavioural improvement. f-i. Methamphetamine-induced rotation behaviour in rats with grafts shows improvement at approximately 24 weeks. Data are presented as mean ± s.d. versus vehicle group by a two-way analysis of variance (ANOVA) with Tukey’s multiple comparisons test.f. Adjusted p value (20 weeks) and 0.045 (24 weeks). g. Adjusted p value ( 20 weeks), <0.001 (24 weeks), 0.002 (28 weeks), 0.011 ( 32 weeks, Vehicle vs. Cell 400 K ), and <0.001 ( 32 weeks, Vehicle vs. Cell 800 K ).h. Adjusted p value (20 weeks), 0.001 (28 weeks, Vehicle vs. Cell 500 K ), and the others <0.001. i. Adjusted p value (12 weeks), 0.001 (20 weeks), 0.002 (32 weeks, Vehicle vs. Cell 500 K ), 0.006 (32 weeks, Vehicle vs. Cell 1,000 K), and the others <0.001.jk. DAB staining for TH
(tyrosine hydroxylase, a marker for DA neurons) in representative grafts at 32 weeks independent experiments). Scale bar . k. Magnified image of the graft shown in panel j. Scale bar . l . Immunofluorescence image of the graft double-labelled for TH and HNA-positive cells indicating donorderived DA neurons ( independent experiments). Scale bar . m. Percentage of KI67-positive cells relative to HNA-positive cells for each graft. (batch 20022), 7 (batch 20048), 9 (batch 21004), and 9 (batch 21047) biologically independent animals, respectively. Line = median. n. Immunofluorescence image of the graft stained for HNA (green) and KI 67 (red), independent experiments. Scale bar . Magnified image of the graft shown in panel , with an arrowhead indicating an HNA/KI67 doublepositive cell. p. Immunofluorescence image of the graft stained for HNA (green) and 5-HT (red), independent experiments. Scale bar . q. Magnified image of the graft shown in panel p, showing the absence of HNA/5HT double-positive cells. DAPI staining is shown in blue. Scale bar . r. Immunofluorescence image of the host Raphe nucleus as a positive control for serotonergic neurons (5-HT, red) DAPI staining is shown in blue ( independent experiments). Scale bar .
Extended Data Fig. 3 | Cell survival of iPSC-derived DA progenitors.
a. T2-weighted MR images of patient PD08, showing grafts as hyperintense areas. Coronal, axial, and sagittal images are displayed from top to bottom. Blue and yellow regions indicate areas within 3 mm of cell injection sites.
b. Changes in graft volume as measured by T2-weighted MR images of each patient. Hyperintense areas within the blue and yellow regions were calculated (R:right and L: left).
Extended Data Fig. 4 | Changes in the Hoehn and Yahr scale for each patient.
The Hoehn and Yahr scale was evaluated at , and 24 months. “ON” indicates measurements taken while the patient was on medication, while
“OFF” indicates measurements taken after the patient had been off medication for more than 12 h .
Extended Data Fig.5|See next page for caption.
Extended Data Fig. 5 | Changes in ON-time, OFF-time, PDQ-39 scores, and changes in levodopa equivalent daily dose (LEDD) for each patient. a-f, Chronological changes in ON-time period, OFF-time period, and PDQ39 scores for each patient from registration ( 0 M ) to the end of the observation period , respectively, based on the patient’s subjective perception. b,d,f, Score changes from baseline, with the mean represented by the black line. Absolute and relative (percentage) changes at 24 months are shown on
the right.g,h, Changes in levodopa equivalent daily dose (LEDD) for each patient. Medication data for each patient was collected from medical charts, and LEDD was calculated according to a previously established method , Chronological changes in LEDD for each patient from registration ( 0 M ) to the end of the observation period , Score changes from baseline, with the mean represented by the black line. Absolute and relative (percentage) changes at 24 months are shown on the right.
Extended Data Fig. 6 | See next page for caption.
Extended Data Fig. 6 | Dopamine synthesis detected by F-DOPA PET.
a, Chronological changes in the fluorine-18-L-dihydroxyphenylalanine ( F-DOPA) Ki values for each side of the putamen for each patient from registration (0 M) to the end of the observation period ( 24 M ), as a supplement to Fig. 3.b, Changes in Ki values from baseline, with the mean represented by the black line. c-h, semiquantitative F-DOPA images generated at min post-injection by subtracting the occipital background signal and normalizing the result to the occipital activity for each patient (Pre-Op: pre-operation, 12 M: 12 months, 24 M : 24 months). The colour change from dark green to red in the bilateral
putamen indicates increased F-DOPA uptake, reflecting dopamine synthesis by grafted cells. , Relationship between F-DOPA uptake and motor symptom improvement. (i) Plots of pre- and post-transplant Ki values and MDS-UPDRS part III OFF scores for six (PD02-08) patients. Healthy and initial symptom ranges are indicated based on previous studies, where Ki values for healthy individuals range from 0.010 to 0.017 , and initial Parkinsonian symptoms emerge with Ki values between 0.0045 and 0.0073. (j) Changes in Ki values and MDS-UPDRS part III OFF scores for each patient.
Article
Extended Data Table 1 | Clinical characteristics of the participants at baseline
Low-dose subgroup
High-dose subgroup
PD01
PD02
PD03
PD04
PD05
PD06
PD08
Age (years)
50
62
60
61
69
58
56
Sex (F/M)
M
F
F
M
M
M
F
Duration (years)
10.3
8.8
9.5
10.3
8.7
12.2
9.5
Motor fluctuations
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Hoehn & Yahr OFF
3
4
5
5
5
3
3
Hoehn & Yahr ON
2
2
2
2
2
2
2
Levodopa response (%)
69.7
89.7
67.3
57.4
75.8
68.0
67.0
Dyskinesia
Mild
None
Mild
Mild
Mild
Mild
Mild
HLA-matched (6 alleles*)
Yes
No
No
Yes
No
Yes
No
06:01, HLA-DPB1 09:01.
Extended Data Table 2 | Core clinical measures at 0 and 24 months after bilateral transplantation
End Point
Low-dose subgroup ( )
High-dose subgroup ( )
Total ( )
0M (SD)
24 M (SD)
% change (SD)
0M (SD)
24M (SD)
% change (SD)
0M (SD)
24M (SD)
% change (SD)
UDysRS (total)*
7.7 (4.0)
22.0 (5.6)
219.4 (97.3)
31.0 (8.6)
41.8 (7.8)
39.2 (28.0)
21.0 (14.1)
33.3 (12.3)
116.4 (113.3)
MDS-UPDRS III OFF
44.5 (14.8)
36.5 (19.1)
-20.7 (16.4)
54.0 (15.5)
43.8 (20.6)
-20.2 (31.6)
50.8 (14.6)
41.3 (18.5)
-20.4 (25.6)
MDS-UPDRS III ON
10.5 (3.5)
4.5 (0.7)
-53.4 (22.4)
21.3 (7.7)
17.8 (13.4)
-26.8 (47.1)
17.7 (8.3)
13.3 (12.4)
-35.7 (40.2)
MDS-UPDRS II
14.0 (4.2)
14.0 (5.7)
-1.6 (10.6)
8.3 (4.3)
16.5 (7.2)
127.0 (129.3)
10.2 (4.9)
15.7 (6.3)
84.1 (120.2)
MDS-UPDRS I
7.0 (0.0)
7.0 (1.4)
0.0 (20.2)
4.5 (2.6)
5.8 (4.0)
19.0 (22.3)
5.3 (2.4)
6.2 (3.3)
12.7 (21.9)
Bradykinesia subscale
17.0 (4.2)
12.5 (5.0)
-27.9 (11.1)
17.8 (5.0)
16.8 (7.4)
-7.0 (33.7)
17.5 (4.3)
15.3 (6.5)
-14.0 (28.7)
Hoehn & Yahr OFF
4.5 (0.7)
3.0 (1.4)
-35.0 (21.2)
4.0 (1.2)
3.5 (1.7)
-16.7 (19.2)
4.2 (1.0)
3.3 (1.5)
-22.8 (20.0)
Hoehn & Yahr ON
2.0 (0.0)
1.5 (0.7)
-25.0 (35.4)
2.0 (0.0)
2.0 (0.0)
0.0 (0.0)
2.0 (0.0)
1.8 (0.4)
-8.3 (20.4)
OFF time without dyskinesia (hrs.)
7.93 (1.82)
6.61 (3.38)
-9.4 (63.5)
4.63 (3.45)
5.89 (3.83)
34.1 (65.8)
5.73 (3.27)
6.13 (3.35)
19.6 (62.5)
OFF time with nontroublesome dyskinesia (hrs.)
0.00 (0.00)
0.07 (0.00)
–
0.30 (0.52)
0.27 (0.54)
-50.0 (70.7)
0.20 (0.43)
0.20 (0.43)
-50.0 (70.7)
OFF time with troublesome dyskinesia (hrs.)
0.00 (0.00)
0.00 (0.00)
–
0.09 (0.18)
0.20 (0.24)
-20.0 (-)
0.06 (0.15)
0.13 (0.21)
-20.0 (-)
ON time without dyskinesia (hrs.)
9.57 (2.63)
9.86 (1.31)
9.0 (43.6)
7.86 (0.35)
6.05 (3.56)
-21.7 (48.6)
8.43 (1.50)
7.32 (3.44)
-11.5 (45.3)
ON time with nontroublesome dyskinesia (hrs.)
0.00 (0.00)
0.36 (0.10)
–
2.34 (1.97)
1.48 (1.22)
-30.4 (18.5)
1.56 (1.94)
1.11 (1.11)
-30.4 (18.5)
ON time with troublesome dyskinesia (hrs.)
0.00 (0.00)
0.29 (0.40)
–
0.43 (0.43)
1.86 (2.78)
318.3 (338.1)
0.29 (0.40)
1.33 (2.31)
318.3 (338.1)
PDQ-39 (Summary Index)
32.08 (10.39)
29.58 (15.10)
-10.7 (18.2)
30.69 (10.02)
38.31 (18.02)
23.0 (26.0)
31.15 (9.07)
35.40 (16.15)
11.8 (27.9)
LEDD (mg/day)**
990.00 (115.82)
905.40 (74.53)
-7.47 (18.36)
1123.10 (295.73)
1174.61 (431.10)
2.76 (17.19)
1078.73 (244.70)
1084.88 (363.25)
-0.65 (16.51)
F-DOPA putamen Ki
0.0045 (0.0001)
0.0048 (0.0009)
7.0 (15.9)
0.0025 (0.0002)
0.0041 (0.0007)
63.5 (36.8)
0.0032 (0.0010)
0.0043 (0.0008)
44.7 (41.4)
F-DOPA caudate Ki
0.0090 (0.0007)
0.0084 (0.0001)
-6.9 (6.8)
0.0068 (0.0004)
0.0068 (0.0001)
0.3 (4.8)
0.0076 (0.0012)
0.0073 (0.0008)
-2.1 (6.0)
Core clinical measures at registration and the end of observation are presented by mean and standard deviation (SD, in parentheses). *The UDysRS is included in the safety profile, and results are presented for the safety population [Low-dose ( ), High-dose ( ), and total ( )]. In PDO1, the right-side transplantation was performed 8 months after the initial left-side transplantation. Therefore, the assessment interval from the preoperative period to 24 months post-bilateral transplantation was 32 months. ** This LEDD was calculated using an updated formula published after the trial’s initiation . Although the average score increased, the percentage change decreased. For completeness, we have retained the data calculated using an older formula in Extended Data Fig. . LEDD, Levodopa equivalent daily dose; MDS-UPDRS, Movement Disorder Society Unified Parkinson’s disease Rating Scale; OFF, drug-off state; ON, drug-on state; PDQ-39, 39-item Parkinson’s Disease Questionnaire; UDysRS, Unified Dyskinesia Rating Scale.
Article
Extended Data Table 3 | Additional clinical measures at 0 and 24 months after bilateral transplantation
End Point
Low dose ( )
High dose ( )
Total ( )
0M (SD)
24M (SD)
% change (SD)
0M (SD)
24M (SD)
% change (SD)
0M (SD)
24M (SD)
% change (SD)
MDS-UPDRS
Total of parts I, II, and III
65.5 (19.1)
57.5 (26.2)
-14.4 (15.0)
66.8 (17.7)
66.0 (24.9)
-3.6 (22.0)
66.3 (16.2)
63.2 (23.0)
-7.2 (19.1)
Total of parts I, II, and III ON
31.5 (7.8)
25.5 (6.4)
-19.1 (0.2)
34.0 (11.4)
40.0 (19.0)
11.9 (25.1)
33.2 (9.6)
35.2 (16.8)
1.6 (25.2)
EQ-5D-5L
Index score
0.66 (0.10)
0.75 (0.20)
13.4 (13.3)
0.61 (0.33)
0.60 (0.29)
13.1 (49.1)
0.62 (0.26)
0.65 (0.26)
13.2 (38.5)
EQ VAS
75.00 (7.07)
82.50 (10.61)
9.8 (3.8)
55.0 (24.83)
60.00 (26.77)
34.8 (113.2)
61.67 (22.06)
67.50 (24.24)
26.5 (88.7)
WPAI
Absenteeism
0
0
0
0
0
0
0
0
0
Presenteeism
0
0
0
0
0
0
0
0
0
Overall work impairment
0
0
0
0
0
0
0
0
0
Activity impairment
55.00 (35.36)
55.00 (35.36)
0.0 (0.0)
50.00 (39.16)
57.50 (38.62)
11.7 (97.9)
51.67 (34.30)
56.67 (33.86)
7.8 (76.1)
natureportfolio
Last updated by author(s): Dec 20, 2024
Reporting Summary
Nature Portfolio wishes to improve the reproducibility of the work that we publish. This form provides structure for consistency and transparency in reporting. For further information on Nature Portfolio policies, see our Editorial Policies and the Editorial Policy Checklist.
Statistics
For all statistical analyses, confirm that the following items are present in the figure legend, table legend, main text, or Methods section.
n/a
□
□
□
□ X
□
□
□
□
□
□
□
Confirmed
The exact sample size for each experimental group/condition, given as a discrete number and unit of measurement
A statement on whether measurements were taken from distinct samples or whether the same sample was measured repeatedly
The statistical test(s) used AND whether they are one- or two-sided
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
A description of all covariates tested
A description of any assumptions or corrections, such as tests of normality and adjustment for multiple comparisons
A full description of the statistical parameters including central tendency (e.g. means) or other basic estimates (e.g. regression coefficient) AND variation (e.g. standard deviation) or associated estimates of uncertainty (e.g. confidence intervals)
For null hypothesis testing, the test statistic (e.g. ) with confidence intervals, effect sizes, degrees of freedom and value noted Give values as exact values whenever suitable.
For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
For hierarchical and complex designs, identification of the appropriate level for tests and full reporting of outcomes
Estimates of effect sizes (e.g. Cohen’s , Pearson’s r), indicating how they were calculated
Our web collection on statistics for biologists contains articles on many of the points above.
Software and code
Policy information about availability of computer code
Data collection
Data analysis
EDMS-Online ver.3.1
Brain images were processed using Functional Magnetic Resonance Imaging of the Brain (FMRIB) Sofrware Library (FSL 5.3) and Statistical Parametric Mapping 12 (SPM12, Release 7219). Statistical analyses of clinical data were conducted using SAS software (version 9.4, SAS Institute), and statistical analysis of animal experiments were performed using GraphPad Prism (version 10.3.1, GraphPad Software).
For manuscripts utilizing custom algorithms or software that are central to the research but not yet described in published literature, software must be made available to editors and reviewers. We strongly encourage code deposition in a community repository (e.g. GitHub). See the Nature Portfolio guidelines for submitting code & software for further information.
Data
Policy information about availability of data
All manuscripts must include a data availability statement. This statement should provide the following information, where applicable:
Accession codes, unique identifiers, or web links for publicly available datasets
A description of any restrictions on data availability
For clinical datasets or third party data, please ensure that the statement adheres to our policy
All relevant data from this trial are included in the article and Supplementary Material.
nature portfolio | reporting summary
April 2023
Research involving human participants, their data, or biological material
Policy information about studies with human participants or human data. See also policy information about sex, gender (identity/presentation), and sexual orientation and race, ethnicity and racism.
Reporting on sex and gender
Participants were enrolled irrespective of their sex. Data are provided in Extended Data Table 1.
Reporting on race, ethnicity, or other socially relevant groupings
Participants were enrolled irrespective of their race/ethnicity.
Population characteristics
Data are provided in Extended Data Table 1
Recruitment
A public call was made by website, press conference. Patients were selected from among those who wished to participate, after consultation by a selection committee in accordance with the selection criteria. Potential biases (placebo effect and observer bias) are noted in the discussion.
Ethics oversight
The protocol was reviewed and approved by Kyoto University Hospital Institutional Review Board (K044).
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Field-specific reporting
Please select the one below that is the best fit for your research. If you are not sure, read the appropriate sections before making your selection.
Life sciences □ Behavioural & social sciences □ Ecological, evolutionary & environmental sciences
For a reference copy of the document with all sections, see nature.com/documents/nr-reporting-summary-flat.pdf
Life sciences study design
All studies must disclose on these points even when the disclosure is negative.
Sample size
Based on the results of the monkey study (Kikuchi et al Nature 2017), we calculated number of samples for which safety could be assessed. Details are given in the Statistic Analysis Plan p 3. “Target sample size”.
Data exclusions
No data were excluded.
Replication
We replicated the transplantation of iPSC-derived dopaminergic progenitors in a total of 7 participants. We confirmed all attempts were successful.
Randomization
This trial was not randomized. When selecting patients, the male/female ratio ( ) and HLA match or incompatibility ( ) were not biased among patients who met the selection criteria.
Blinding
This trial was a single-arm trial.
Reporting for specific materials, systems and methods
We require information from authors about some types of materials, experimental systems and methods used in many studies. Here, indicate whether each material, system or method listed is relevant to your study. If you are not sure if a list item applies to your research, read the appropriate section before selecting a response.
Antibodies are used under validation using adequate negative and positive control samples. We confirmed the staining by using animal samples when possible, or we rely on the stained samples presented in manufacturer’s website (FOXA2 from R&D, HNA from Millipore, KI67 from Abcam, and 5-HT and TH from Millipore).
Eukaryotic cell lines
Policy information about cell lines and Sex and Gender in Research
Cell line source(s)
iPSCs are derived from human peripheral blood cells, donated by healthy volunteer.
QHJI01s04 is provided by Center for iPS cell Research and Application (CiRA), Kyoto University, Japan. MCBOO3 is provided by Sumitomo Pharma (Tokyo, Japan).
Authentication
The STR (short tandem repeat) pattern of iPSCs coincide with that of donor cells.
Mycoplasma contamination
All cells are negative for mycoplasma contamination.
Commonly misidentified lines (See ICLAC register)
Nothing.
Animals and other research organisms
Policy information about studies involving animals; ARRIVE guidelines recommended for reporting animal research, and Sex and Gender in Research
Laboratory animals
Adult ( 9 -week-old) male nude rats (F344/NJcl-rnu/rnu, CLEA, Japan) were used for this study.
Wild animals
The study did not involve wild animals.
Reporting on sex
In this study, only male rats were used to precisely examine the effect of transplanted cells by excluding effects of the female’s sexual cycle on the survival or maturation of dopaminergic neurons.
Field-collected samples
The study did not involve samples collected from the field.
Ethics oversight
The study protocol is approved by the ethical committees of Kyoto University and Sumitomo Pharma.
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Clinical data
Policy information about clinical studies
All manuscripts should comply with the ICMJE guidelines for publication of clinical research and a completed CONSORT checklist must be included with all submissions.
Clinical trial registration
jRCT2090220384, UMIN000033564
Study protocol
The study protocol was provided in the supplementary material.
Data collection
This trial was conducted at Kyoto University Hospital. Patients are recruited from Aug. 1, 2018 to May 19, 2021. Data are collected from Sep. 25, 2018 to Jan. 18, 2024.
Outcomes
Primary end points included the adverse-event profile and secondary end points involved the safety and efficacy at 24 months
nature portfolio | reporting summary April2023
Plants
Seed stocks
Report on the source of all seed stocks or other plant material used. If applicable, state the seed stock centre and catalogue number. If plant specimens were collected from the field, describe the collection location, date and sampling procedures.
Novel plant genotypes
Describe the methods by which all novel plant genotypes were produced. This includes those generated by transgenic approaches, gene editing, chemical/radiation-based mutagenesis and hybridization. For transgenic lines, describe the transformation method, the number of independent lines analyzed and the generation upon which experiments were performed. For gene-edited lines, describe the editor used, the endogenous sequence targeted for editing, the targeting guide RNA sequence (if applicable) and how the editor was applied.
Authentication
Describe any authentication procedures for each seed stock used or novel genotype generated. Describe any experiments used to assess the effect of a mutation and, where applicable, how potential secondary effects (e.g. second site T-DNA insertions, mosiacism, off-target gene editing) were examined.
Magnetic resonance imaging
Experimental design
Design type
Design specifications
Behavioral performance measures
This was not an fMRI study.
This was not an fMRI study.
This was not an fMRI study.
Acquisition
Imaging type(s)
Field strength
Sequence & imaging parameters
Area of acquisition
Diffusion MRI □ Used
T1-weighted, T2-weighted, fluid-attenuated inversion recovery (FLAIR), and T2*-weighted images
□
3 Tesla scannar
Whole brain
State whether a whole brain scan was used OR define the area of acquisition, describing how the region was determined.
Preprocessing
Preprocessing
Preprocessing software
Normalization
Normalization template
Noise and artifact removal
Volume censoring
Functional Magnetic Resonance Imaging of the Brain (FMRIB) software
Normalization was not conducted.
Not applicable
Not applicable
Not applicable
Statistical modeling & inference
Model type and settings
Not applicable
Effect(s) tested
Not applicable
Specify type of analysis: □ Whole brain □ ROI-based □ Both
Statistic type for inference
Not applicable
(See Eklund et al. 2016)
Correction
Not applicable
nature portfolio | reporting summary
April 2023
Models & analysis
Involved in the study
Functional and/or effective connectivity
Graph analysis
Multivariate modeling or predictive analysis
Functional and/or effective connectivity
Graph analysis
Report the measures of dependence used and the model details (e.g. Pearson correlation, partial correlation, mutual information).
Report the dependent variable and connectivity measure, specifying weighted graph or binarized graph, subject- or group-level, and the global and/or node summaries used (e.g. clustering coefficient, efficiency, etc.).
Multivariate modeling and predictive analysis □
Specify independent variables, features extraction and dimension reduction, model, training and evaluation metrics.
Department of Neurology, Kyoto University Graduate School of Medicine, Kyoto, Japan. Department of Clinical Application, Center for iPS Cell Research and Application, Kyoto University, Kyoto, Japan. Department of Neurosurgery, Kyoto University Graduate School of Medicine, Kyoto, Japan. Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan. Department of Surgery, Kyoto University Graduate School of Medicine, Kyoto, Japan. Department of Hematology/Oncology, Kyoto University Graduate School of Medicine, Kyoto, Japan. Department of Biomedical Statistics and Bioinformatics, Kyoto University Graduate School of Medicine, Kyoto, Japan. These authors contributed equally: Nobukatsu Sawamoto, Daisuke Doi, Etsuro Nakanishi, Masanori Sawamura. e-mail: ryosuket@kuhp.kyoto-u.ac.jp; jbtaka@cira.kyoto-u.ac.jp
Kordower, J. H. et al. Neuropathological evidence of graft survival and striatal reinnervation after the transplantation of fetal mesencephalic tissue in a patient with Parkinson’s disease. N. Engl. J. Med. 332, 1118-1124 (1995).
Piccini, P. et al. Dopamine release from nigral transplants visualized in vivo in a Parkinson’s patient. Nat. Neurosci. 2, 1137-1140 (1999).
Patients are subdivided into Low- and High-dose groups, and clinical characteristics at registration are presented. *Donor HLA-A 24:O2, HLA-B 52:01, HLA-DRB1 15:02, HLA-C 12:02, HLA-DQB1
Core clinical measures at registration and the end of observation are presented by mean and SD (in parentheses). EQ-5D-5L, EuroQol 5-dimension 5-level, [European Quality of life-5 dimensions questionnaire (EQ-5D)]; EQ VAS, EuroQol Visual Analogue Scale; WPAI, Work Productivity and Activity Impairment.