DOI: https://doi.org/10.1186/s40249-024-01186-4
PMID: https://pubmed.ncbi.nlm.nih.gov/38374211
تاريخ النشر: 2024-02-20
معدل الإصابة وعلامات التحذير من مضاعفات داء البروسيلات البشري: دراسة مراقبة متعددة المراكز من الصين
الملخص
الخلفية: داء البروسيلات هو مرض حيواني المنشأ شديد غالبًا ما يتم تجاهله، خاصة في البلدان الفقيرة. إن التعرف في الوقت المناسب على المضاعفات البؤرية في داء البروسيلات أمر حاسم لتحسين نتائج العلاج. ومع ذلك، لا توجد حاليًا مؤشرات أو علامات حيوية مثبتة لتشخيص هذه المضاعفات. لذلك، كان الهدف من هذه الدراسة هو التحقيق في علامات التحذير المحتملة للمضاعفات البؤرية في داء البروسيلات البشري، بهدف توفير معايير عملية للأطباء للمساعدة في تشخيص وإدارة المرضى. الطرق: تم إجراء دراسة مقطعية متعددة المراكز في الصين من ديسمبر 2019 إلى أغسطس 2021. كانت الدراسة تهدف إلى التحقيق في الخصائص السريرية والمضاعفات لدى المرضى المصابين بداء البروسيلات باستخدام استبيان ونظام السجلات الطبية. تم تقييم وجود علامات التحذير للمضاعفات باستخدام نماذج الانحدار اللوجستي أحادي ومتعدد المتغيرات. تم استخدام منحنيات خصائص التشغيل المستقبلية (ROC) والمساحة تحت المنحنى (AUC) لفرز المتغيرات وتقييم النموذج. النتائج: تم تسجيل ما مجموعه 880 مشاركًا تم تشخيصهم بداء البروسيلات البشري. كان متوسط عمر المرضى 50 عامًا [نطاق الربيع (IQR): 41.5-58.0]، وكان 54.8% منهم يعانون من مضاعفات. كان النظام العضلي الهيكلي هو الأكثر تأثرًا بالمضاعفات (43.1%)، مع التهاب المفاصل المحيطي (30.0%)، والتهاب الفقرات (16.6%)، وخراجات ما حول الفقرات (5.0%)، والتهاب العجز (2.7%) كانت الأكثر انتشارًا. شملت المضاعفات في أنظمة الأعضاء الأخرى الجهاز البولي التناسلي (4.7%)، والجهاز التنفسي (4.7%)، والجهاز الدموي (4.6%). وُجدت عدة عوامل مرتبطة بداء البروسيلات البؤري. شملت هذه العوامل تأخيرًا طويلًا في التشخيص [نسبة الأرجحية
الكلمات المفتاحية: البروسيلا، المضاعفات، الطيف السريري، علامات التحذير
الخلفية
البروسيلا هي عدوى تسببها بكتيريا سالبة الجرام من جنس بروسيلا، والتي لديها القدرة على إقامة عدوى طويلة الأمد في مضيفيها. تتجنب بروسيلا آليات إزالة المناعة في المضيف، وتعتمد مدة العدوى داخل خلايا المضيف على مناعة المضيف والاستخدام المناسب للمضادات الحيوية المحددة. لذلك، فإن التشخيص المبكر والعلاج المناسب أمران حاسمان في تقليل خطر المزمنة والانتكاس. ومع ذلك، يمكن أن تختلف الأعراض السريرية للبروسيلا بشكل كبير وتقلد أمراضًا أخرى، مما يؤدي إلى تشخيص خاطئ أو عدم تشخيص [8]. يتطلب تأكيد البروسيلا مجموعة من تاريخ التعرض والأعراض السريرية والاختبارات المخبرية المحددة. يؤدي عدم تشخيص البروسيلا إلى معدلات أعلى من الحالات المعقدة [9]. يتطلب التورط البؤري في البروسيلا مدة علاج أطول ومواد مضادة للميكروبات إضافية مقارنةً بالحالات غير المعقدة [10]. للأسف، لا توجد حاليًا مؤشرات حيوية محددة تم الإبلاغ عنها لتشخيص المضاعفات. من الصعب تمييز المضاعفات بناءً فقط على الأعراض العامة أو العلامات أو المؤشرات الحيوية الفردية [4]. لذلك، من الضروري استكشاف مؤشرات تحذيرية تشخيصية شاملة للبروسيلا المعقدة لمساعدة الأطباء في تشخيص المرض وعلاجه بسرعة.
فهم الطيف السريري الحقيقي للحمى المالطية ومضاعفاتها أمر بالغ الأهمية لممارسي الطب لاتخاذ قرارات مبكرة. على الرغم من أن بعض الدراسات قد أبلغت عن الطيف السريري لمضاعفات الحمى المالطية والعوامل ذات الصلة، إلا أن هذه الدراسات كانت لها قيود مثل كونها من مركز واحد، ووجود عدد صغير من المشاركين.
حجم العينات، والتركيز فقط على المرضى الداخليين، مما من المحتمل أن يبالغ في تقدير معدلات المضاعفات المبلغ عنها، وقد تكون المؤشرات الكامنة لتحديد المشاركة البؤرية في المرضى الخارجيين قد تم تجاهلها. لمعالجة هذه القيود، أجرينا دراسة رصدية متعددة المراكز لتحديد incidence الحقيقي والطيف السريري لمضاعفات حمى المالطية في كل من المرضى الداخليين والمرضى الخارجيين، ولتحديد المؤشرات السريرية والمخبرية التحذيرية للمضاعفات، والتي يمكن أن تحسن معايير التشخيص وتعزز إدارة المرضى. علاوة على ذلك، من الجدير بالذكر أن النسخة الحالية من الإرشادات حول تشخيص وعلاج حمى المالطية في الصين لا تتضمن مبادئ تشخيصية للمضاعفات. لذلك، فإن دراستنا قيمة في توحيد تشخيص وعلاج مضاعفات حمى المالطية، مما يقلل في النهاية من incidence حمى المالطية المزمنة.
طرق
تصميم الدراسة والمكان
حجم العينة
أخذ العينات والمشاركون
كانت معايير الإدراج للحالات كما يلي: (1) المرضى الذين تم تشخيصهم بالبروسيلا؛ (2) أعمارهم 15 عامًا وما فوق؛ (3) قدموا موافقة مستنيرة وشاركوا طواعية في الدراسة.
كانت معايير استبعاد الحالات هي: (1) مصابون بفيروس نقص المناعة البشرية (HIV)، يخضعون للعلاج الكيميائي، لديهم اضطرابات أخرى في جهاز المناعة، أو يعانون من أمراض خطيرة أخرى؛ (2) يعانون من اضطرابات نفسية، صمم، واضطرابات أخرى تؤدي إلى ضعف التواصل وعدم القدرة على التعاون مع التحقيق؛ (3) امرأة حامل.
جمع البيانات والتعريفات
ظهور الأعراض. بالإضافة إلى ذلك، تم استخراج المتغيرات ذات الصلة من نظام معلومات المستشفى، مثل تاريخ التشخيص، وجود أمراض مصاحبة، تاريخ سابق للبروسيلا، الأعراض والعلامات التي تم تجربتها (مثل الحمى، القشعريرة، التعب، إلخ)، المضاعفات، ونتائج الاختبارات المعملية.
استبعاد الأسباب الأخرى و/أو مع زراعة إيجابية للبروسيلا في حالات الانصباب التاموري. تم تشخيص المضاعفات الدموية بناءً على مظاهر سريرية غير طبيعية (فقر الدم أو النزيف) ونتائج مختبرية غير طبيعية، مع استبعاد الأسباب الأخرى. تم تشخيص المضاعفات البولية التناسلية مثل التهاب الخصية، التهاب البربخ، والتهاب الحوض بناءً على علامات وأعراض التهاب الجهاز البولي التناسلي (ألم الخصية، تضخم الخصية، وألم أسفل الظهر عند الرجال؛ ألم أسفل البطن عند النساء)، مؤكدة بواسطة الموجات فوق الصوتية. قدمت مضاعفات الجهاز التنفسي على أنها التهاب الشعب الهوائية، الالتهاب الرئوي، أو الانصباب الجنبي، ويمكن تأكيدها من خلال الأشعة السينية للصدر، أو الأشعة المقطعية (CT)، أو مسحات الرنين المغناطيسي (MRI) بمجرد استبعاد الأسباب المحتملة الأخرى. تم تعريف المضاعفات الجلدية على أنها مظاهر سريرية من الطفح الجلدي، الكدمات، الكدمات، التهاب الجلد العقدي، التقرحات، أو الخراجات في حالات البروسيلا المؤكدة، مع استبعاد الأسباب الأخرى.
التحليل الإحصائي
النتائج
الخصائص السكانية والوبائية
| تعقيدات |
|
| الجهاز العظمي المفصلي | ٣٧٩ (٤٣.١) |
| التهاب المفصل العجزي الحرقفي | ٢٤ (٢.٧) |
| التهاب الفقرات | ١٤٦ (١٦.٦) |
| التهاب المفاصل المحيطي | 264 (30.0) |
| خراج حول الفقرات | 44 (5.0) |
| الجهاز البولي التناسلي | 41 (4.7) |
| الجهاز التنفسي | 41 (4.7) |
| الجهاز الدموي | 40 (4.6) |
| الجهاز القلبي الوعائي | 11 (1.3) |
| الجهاز العصبي | 9 (1.0) |
| النظام الجلدي | 1 (0.1) |
| المتغيرات | المجموعات الفرعية | الإجمالي
|
معقد
|
بسيط
|
|
| جنس | ذكر | 642 (73.0) | 354 (73.4) | 288 (72.4) | 0.719 |
| أنثى | 238 (27.0) | 128 (26.6) | 110 (27.6) | ||
| فئة العمر | < 60 سنة | 702 (79.8) | ٣٦٩ (٧٦.٦) | ٣٣٣ (٨٣.٧) | 0.009 |
|
|
178 (20.2) | 113 (23.4) | 65 (16.3) | ||
| الجنسية | القومية الهانية | 614 (69.8) | ٣٥٣ (٧٣.٣) | 261 (65.6) | 0.014 |
| القومية الأقلية | 266 (30.2) | 129 (26.7) | 137 (34.4) | ||
| احتلال | المزارع والرجل الراعي | 754 (85.7) | 418 (86.7) | ٣٣٦ (٨٤.٤) | 0.234 |
| إدارة معالجة الحيوانات ومنتجاتها | 49 (5.6) | 21 (4.4) | ٢٨ (٧.٠) | ||
| مهن أخرى
|
77 (8.8) | ٤٣ (٨.٩) | ٣٤ (٨.٥) | ||
| منطقة | شينجيانغ | ٣٨٥ (٤٣.٨) | 206 (42.7) | 179 (45.0) | 0.426 |
| شاندونغ | 289 (32.8) | 155 (32.2) | 134 (33.7) | ||
| منغوليا الداخلية | 206 (23.4) | 121 (25.0) | 85 (21.4) | ||
| التعليم | الابتدائي أو أقل | ٣٦٤ (٤١.٤) | 216 (44.8) | 148 (37.2) | 0.051 |
| المدرسة الإعدادية | 394 (44.8) | 199 (41.3) | 195 (49.0) | ||
| الثانوية العامة أو أعلى | ١٢٢ (١٣.٩) | 67 (13.9) | 55 (13.8) | ||
| تاريخ التعرض
|
التعرض للحيوانات | 830 (94.3) | 442 (91.7) | 388 (97.5) | < 0.001 |
| الأغنام والماعز | 774 (88.0) | 417 (86.5) | ٣٥٧ (٨٩.٧) | 0.149 | |
| المواشي | ٣٢٨ (٣٧.٣) | 170 (35.3) | 158 (39.7) | 0.176 | |
| حيوانات أخرى
|
225 (27.1) | 145 (32.8) | 80 (20.6) | < 0.001 | |
| طريقة التعرض للحيوانات
|
رفع | 691 (78.5) | 387 (80.3) | 304 (76.4) | 0.160 |
| الرعي | 356 (40.5) | ١٧٦ (٣٦.٥) | 180 (45.2) | 0.009 | |
| ذبح | 222 (25.2) | 132 (27.4) | 90 (22.6) | 0.105 | |
| توليد الحملان | 414 (47.1) | 239 (49.6) | ١٧٥ (٤٤.٠) | 0.097 | |
| طرق أخرى
|
٣٦٩ (٤١.٩) | 195 (40.5) | ١٧٤ (٤٣.٧) | 0.329 | |
| تناول الطعام غير المبستر | نعم | ١٣٠ (١٤.٨) | 97 (20.2) | ٣٣ (٨.٣) | < 0.001 |
| لا | 748 (85.2) | ٣٨٣ (٧٩.٨) | 365 (91.7) | ||
| تاريخ عائلي للحمى المالطية | نعم | 183 (21.1) | 96 (20.2) | 87 (22.1) | 0.489 |
| لا | 685 (78.9) | ٣٧٩ (٧٩.٨) | 306 (77.9) | ||
| تاريخ سابق للإصابة بالبروسيلا | نعم | 77 (8.8) | 42 (8.7) | ٣٥ (٨.٨) | 0.967 |
| لا | ٨٠٣ (٩١.٢) | 440 (91.3) | ٣٦٣ (٩١.٢) | ||
| الأيام من بداية الأعراض إلى التشخيص | 0-7 | 166 (18.9) | 72 (14.9) | 94 (23.8) | < 0.001 |
| 8-30 | 425 (48.5) | ٢١٩ (٤٥.٤) | 206 (52.2) | ||
| ٣١-٩٠ | 207 (23.6) | 132 (27.4) | 75 (19.0) | ||
| >90 | 79 (9.0) | 59 (12.2) | 20 (5.1) | ||
| المرحلة السريرية
|
حادّ | 793 (90.1) | 419 (86.9) | 374 (94.0) | 0.002 |
| تحت الحاد | 50 (5.7) | ٣٨ (٧.٩) | 12 (3.0) | ||
| مزمن | ٣٧ (٤.٢) | 25 (5.2) | 12 (3.0) | ||
| المرض الأساسي | نعم | ٣١١ (٣٥.٣) | 198 (41.1) | 113 (28.4) | < 0.001 |
| لا | 569 (64.7) | 284 (58.9) | ٢٨٥ (٧١.٦) | ||
| مُستشفى | نعم | 614 (71.8) | 395 (84.6) | ٢١٩ (٥٦.٤) | < 0.001 |
| لا | 241 (28.2) | 72 (15.4) | 169 (43.6) |
العرض السريري والنتائج المخبرية
كانت الأعراض والعلامات التي لوحظت في المرضى الذين يعانون من البروسيلات البؤرية مشابهة لتلك التي لا تعاني من مضاعفات بؤرية، باستثناء حدوث أعلى للألم المفصلي، وفقدان الشهية، والغثيان، وألم الخصية، وألم انتفاخ العين.
علامات التحذير المرتبطة بالمضاعفات
قمنا بإجراء تحليل الانحدار اللوجستي المتعدد المتغيرات لتحديد العوامل المستقلة المرتبطة بالمضاعفات. تشير نتائجنا إلى أن عدة عوامل كانت مرتبطة بشكل مستقل بالبروسيلا البؤرية، بما في ذلك عدد الأيام من بداية المرض إلى التشخيص، والأمراض الأساسية، والأعراض مثل ألم المفاصل وآلام العضلات، وألم انتفاخ العين، وCRP.
تحليل منحنى ROC للعلامات الحيوية السريرية لدى المرضى الذين يعانون من مضاعفات والذين لا يعانون منها
القيمة التي حددها تحليل ROC كانت
نقاش
| الإجمالي
|
معقد
|
بسيط
|
|
|
| الأعراض والعلامات | ||||
| حمى | ٤٦٦ (٥٣.٠) | 256 (53.1) | 210 (52.8) | 0.918 |
| قشعريرة | 193 (21.9) | ١٠٤ (٢١.٦) | 89 (22.4) | 0.779 |
| إرهاق | 626 (71.1) | ٣٢٤ (٦٧.٢) | 302 (75.9) | 0.005 |
| التعرق | ٤٣٧ (٤٩.٧) | 236 (49.0) | 201 (50.5) | 0.649 |
| ألم المفاصل | 732 (83.2) | ٤٣٨ (٩٠.٩) | ٢٩٤ (٧٣.٩) | < 0.001 |
| عجزي | 166 (19.4) | ١٠٤ (٢١.٩) | 62 (16.3) | 0.037 |
| الحرقفي | 162 (19.0) | ١٠٩ (٢٣.٠) | 53 (13.9) | 0.001 |
| كتف | 187 (21.9) | 117 (24.7) | 70 (18.4) | 0.027 |
| ركبة | 319 (37.3) | 181 (38.2) | ١٣٨ (٣٦.٢) | 0.555 |
| كوع | 131 (15.3) | 80 (16.9) | 51 (13.4) | 0.159 |
| معصم | 93 (10.9) | 60 (12.7) | ٣٣ (٨.٧) | 0.062 |
| كاحل | 107 (12.5) | 68 (14.4) | ٣٩ (١٠.٢) | 0.071 |
| العمود الفقري | 295 (34.5) | 202 (42.6) | 93 (24.4) | < 0.001 |
| ألم العضلات | 246 (28.0) | 123 (25.5) | 123 (30.9) | 0.076 |
| سعال | 128 (14.6) | 79 (16.4) | 49 (12.3) | 0.088 |
| فقدان الشهية | ٣٢٢ (٣٦.٦) | 192 (39.8) | ١٣٠ (٣٢.٧) | 0.028 |
| غثيان | 94 (10.7) | 63 (13.1) | 31 (7.8) | 0.012 |
| صداع | ٢٥٤ (٢٨.٩) | 143 (29.7) | 111 (27.9) | 0.562 |
| أوركيالجيا | ٤٥ (٥.١) | ٤٠ (٨.٣) | 5 (1.3) | < 0.001 |
| فقدان الوزن | 273 (31.0) | 162 (33.6) | 111 (27.9) | 0.068 |
| اضطراب النوم | 82 (9.3) | 52 (10.8) | 30 (7.5) | 0.099 |
| قيء | ٣٥ (٤.٠) | ٢٤ (٥.٠) | 11 (2.8) | 0.094 |
| ألم انتفاخ العين | ٣٨ (٤.٣) | 30 (6.2) | 8 (2.0) | 0.002 |
| التبول العاجل والتبول المتكرر | 41 (4.7) | ٢٧ (٥.٦) | 14 (3.5) | 0.144 |
| طفح جلدي | 3 (0.3) | 2 (0.4) | 1 (0.3) | 1.000 |
| هيماتولوجي | ||||
| فقر الدم | 121 (14.1) | 77 (16.4) | 44 (11.3) | 0.033 |
| نقص الكريات البيضاء | 111 (12.9) | 65 (13.8) | ٤٦ (١١.٨) | 0.383 |
| كريات الدم البيضاء | ٤٨ (٥.٦) | 30 (6.4) | 18 (4.6) | 0.265 |
| نقص الصفيحات الدموية | ٢٩ (٣.٤) | 15 (3.2) | 14 (3.6) | 0.747 |
| كيمياء المصل | ||||
| ALT
|
٣٠٣ (٣٤.٩) | 173 (36.5) | ١٣٠ (٣٣.٠) | 0.281 |
| AST
|
200 (23.1) | ١٠٩ (٢٣.٠) | 91 (23.3) | 0.923 |
| البيليروبين
|
148 (17.2) | ٨٨ (١٨.٦) | 60 (15.4) | 0.207 |
| نيتروجين اليوريا
|
86 (10.1) | 51 (10.9) | ٣٥ (٩.٠) | 0.356 |
| كرياتينين
|
2 (0.2) | 2 (0.4) | 0 | 0.504 |
| علامات الالتهاب | ||||
| CRP
|
٣٩٩ (٤٨.٩) | 258 (56.6) | 141 (39.2) | < 0.001 |
| ارتفاع مستوى ESR | 415 (54.3) | 264 (62.0) | 151 (44.5) | <0.001 |
| زراعة البكتيريا واختبار الأجسام المضادة في المصل | ||||
| إيجابي الثقافة | 89 (10.1) | ٣٣ (٦.٩) | 56 (14.1) | <0.001 |
| سات
|
666 (77.0) | ٣٥٩ (٧٦.١) | 307 (78.1) | 0.474 |
| سات
|
387 (44.7) | 193 (40.9) | 194 (49.4) | 0.013 |
| المتغيرات | التحليل الأحادي المتغير | التحليل متعدد المتغيرات
|
||||||
| غابة
|
أو | OR (فواصل الثقة 95%) |
|
غابة
|
أو | OR (فواصل الثقة 95%) |
|
|
| الأيام من بداية الأعراض إلى التشخيص | ٢٩.١٤٢ | – | – | <0.001 | 19.418 | – | – | < 0.001 |
| 0-7 | – | – | 1 (مرجع) | – | – | – | 1 (مرجع) | – |
| 8-30 | 3.166 | 1.388 | 0.967-1.992 | 0.075 | ٤.٢٨٢ | 1.610 | 1.025-2.527 | 0.039 |
| ٣١-٩٠ | 15.233 | 2.298 | 1.513-3.489 | < 0.001 | ١٢.٢١٧ | ٢.٥٥١ | 1.509-4.314 | 0.001 |
| >90 | 10.877 | 3.851 | 2.129-6.967 | < 0.001 | 13.601 | ٣.٩٦٣ | 1.906-8.238 | < 0.001 |
| المرض الأساسي | 15.219 | 1.758 | 1.324-2.335 | <0.001 | 8.180 | 1.675 | 1.176-2.384 | 0.004 |
| ألم المفاصل | 41.655 | ٣.٥٢٠ | 2.402-5.159 | < 0.001 | 22.869 | ٣.١٩٧ | 1.986-5.148 | < 0.001 |
| ألم العضلات | 3.132 | 0.766 | 0.570-1.029 | 0.077 | ٥.٩١٤ | 0.627 | 0.431-0.913 | 0.015 |
| ألم انتفاخ العين | 8.453 | ٣.٢٣٦ | 1.466-7.14 | 0.004 | ٦.٦٤٩ | ٣.٤٨٢ | 1.349-8.988 | 0.001 |
| CRP
|
٢٤.١٤٤ | 2.024 | 1.528-2.681 | < 0.001 | 11.316 | 1.910 | 1.310-2.784 | 0.001 |
| ارتفاع معدل ترسيب كريات الدم الحمراء | ٢٢.٨٥٤ | 2.029 | 1.518-2.712 | < 0.001 | 7.147 | 1.663 | 1.145-2.415 | 0.008 |
| إيجابي الثقافة | ١٢٫٠٣٧ | 0.449 | 0.285-0.706 | 0.001 | ٥.٠٦٠ | 0.516 | 0.290-0.918 | 0.025 |
| سات
|
٦.٢١٣ | 0.710 | 0.542-0.929 | 0.013 | ١٣.٢٠٩ | 0.529 | 0.376-0.746 | < 0.001 |
| العمر أقل من 60 سنة | 6.772 | 0.637 | 0.454-0.895 | 0.009 | – | – | – | – |
| الجنسية، هان | 6.039 | 1.436 | 1.076-1.917 | 0.014 | – | – | – | – |
| التعليم | 5.959 | – | – | 0.051 | ||||
| الابتدائي أو أقل | – | – | 1 (مرجع) | – | – | – | – | – |
| المدرسة الإعدادية | 5.942 | 0.٦٩٩ | 0.524-0.932 | 0.015 | – | – | – | – |
| الثانوية العامة أو أعلى | 0.975 | 0.806 | 0.525-1.237 | 0.324 | – | – | – | – |
| إرهاق | 7.912 | 0.652 | 0.484-0.878 | 0.005 | – | – | – | – |
| فقدان الشهية | ٤.٨١٩ | 1.365 | 1.034-1.802 | 0.028 | – | – | – | – |
| غثيان | 6.244 | 1.780 | 1.132-2.798 | 0.013 | – | – | – | – |
| أوركيالجيا | ١٦.٧٥٠ | 7.113 | 2.780-18.202 | < 0.001 | – | – | – | – |
| فقر الدم | ٤.٤٧٩ | 1.536 | 1.032-2.286 | 0.034 | – | – | – | – |
| فقدان الوزن | 0.068 | 1.309 | 0.980-1.748 | 0.068 | – | – | – | – |
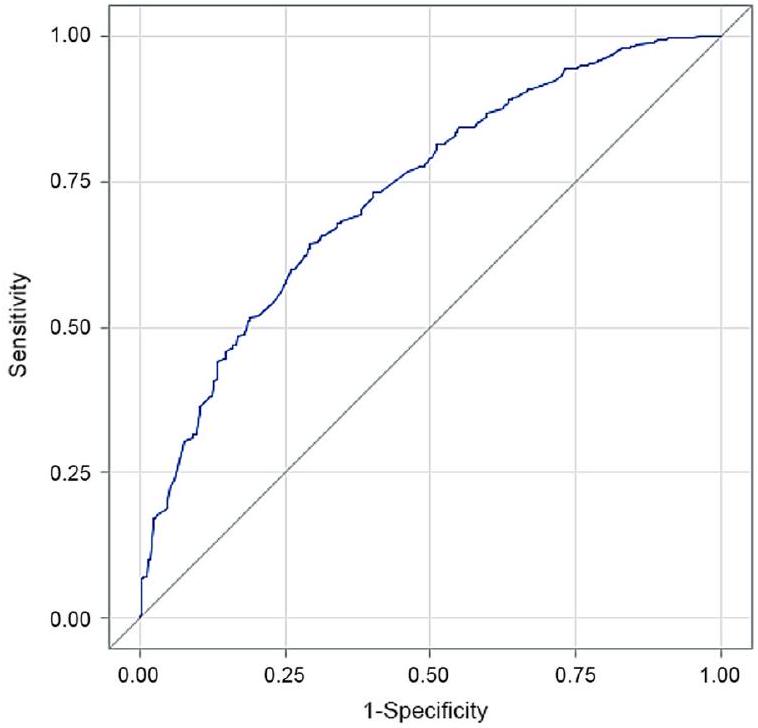
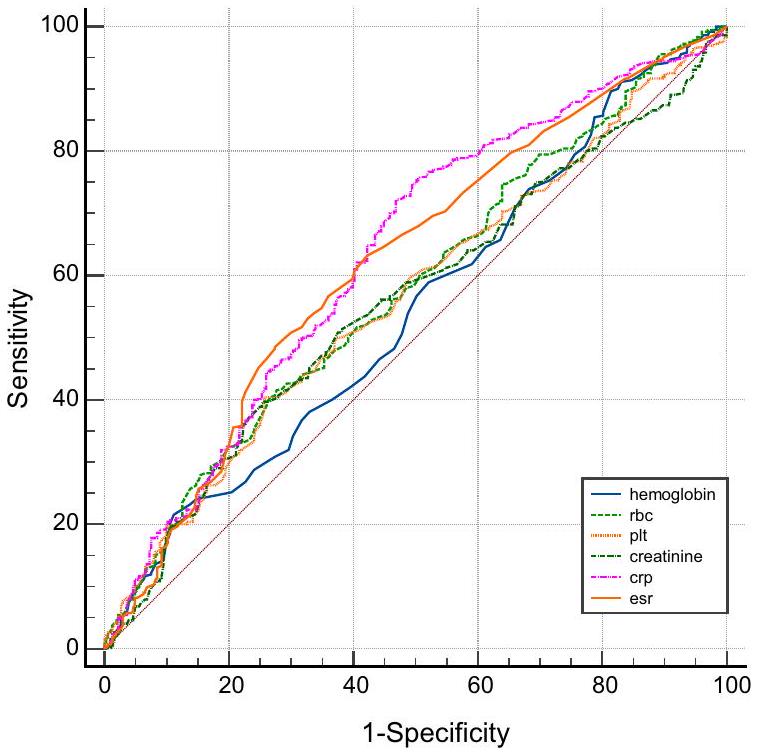
حددت هذه الدراسة بروتين سي التفاعلي ومعدل ترسيب كريات الدم الحمراء كمؤشرات على التورط البؤري في داء البروسيلات، مع قيمة قطع قدرها
تظل فائدة زراعة الدم للتعرف المبكر على المضاعفات في داء البروسيلات مثيرة للجدل، مع توفر أدلة محدودة ومتضاربة. وجد شيو وآخرون [12] أن زراعات الدم الإيجابية كانت تشير إلى داء بروسيلات معقد، بينما أفاد بيركان وآخرون [19] أن زراعات الدم السلبية كانت عوامل ذات دلالة إحصائية للمضاعفات. في دراسات أخرى [20-22]، كانت معدلات إيجابية زراعة الدم واختبار SAT متشابهة في المجموعات التي لديها involvement focal وبدونها. تأثرت دقة نتائج زراعة الدم بشكل كبير بالظروف والتقنيات المستخدمة [8]. في دراستنا، لاحظنا أن زراعات الدم السلبية وعناوين SAT المنخفضة
كانت مرتبطة بمضاعفات حمى البحر الأبيض المتوسط، مما يشير إلى الحاجة إلى مزيد من البحث المتعمق في هذا الموضوع.
الاستنتاجات
الاختصارات
| التبديل | إنزيم الألانين أمينوترانسفيراز |
| AST | أمينوترانسفيراز الأسبارتات |
| الجامعة الأمريكية في القاهرة | المساحة تحت المنحنى |
| كلور | فترات الثقة |
| CRP | بروتين سي التفاعلي |
| سي تي | التصوير المقطعي المحوسب |
| ECG | تخطيط القلب الكهربائي |
| ESR | معدل ترسيب كريات الدم الحمراء |
| هيموغلوبين | الهيموغلوبين |
| نطاق الربيع | نطاق الربيع الربعي |
| الرنين المغناطيسي | التصوير بالرنين المغناطيسي |
| أو | نسبة الأرجحية |
| PLT | صفائح دموية |
| RBC | كريات الدم الحمراء |
| ROC | الخصائص التشغيلية للمستقبل |
| سات | اختبار التكتل القياسي في الأنابيب |
| UCG | تخطيط صدى القلب |
| WBC | كريات الدم البيضاء |
معلومات إضافية
شكر وتقدير
شكرًا لمركز السيطرة على الأمراض في المقاطعات شاندونغ، شينجيانغ ومنغوليا الداخلية على مساعدتهم في اختبار العينات البيولوجية. شكرًا لمركز السيطرة على الأمراض في الصين على دعمهم في عملية البحث.
مساهمات المؤلفين
تمويل
توفر البيانات والمواد
الإعلانات
موافقة الأخلاقيات والموافقة على المشاركة
موافقة على النشر
المصالح المتنافسة
تفاصيل المؤلف
نُشر على الإنترنت: 20 فبراير 2024
References
- Pappas G, Papadimitriou P, Akritidis N, Christou L, Tsianos EV. The new global map of human brucellosis. Lancet Infect Dis. 2006;6:91-9.
- O’Callaghan D. Human brucellosis: recent advances and future challenges. Infect Dis Poverty. 2020;9:101.
- Rossetti CA, Arenas-Gamboa AM, Maurizio E. Caprine brucellosis: a historically neglected disease with significant impact on public health. PLoS Negl Trop Dis. 2017;11: e0005692.
- Zheng R, Xie S, Lu X, Sun L, Zhou Y, Zhang Y, Wang K. A systematic review and meta-analysis of epidemiology and clinical manifestations of human brucellosis in China. Biomed Res Int. 2018;2018:5712920.
- Franco MP, Mulder M, Gilman RH, Smits HL. Human brucellosis. Lancet Infect Dis. 2007;7:775-86.
- Jiao H, Zhou Z, Li B, Xiao Y, Li M, Zeng H, Guo X, Gu G. The mechanism of facultative intracellular parasitism of Brucella. Int J Mol Sci. 2021;22:3673.
- Byndloss MX, Tsolis RM. Brucella spp. virulence factors and immunity. Annu Rev Anim Biosci. 2016;4:111-27.
- Yagupsky P, Morata P, Colmenero JD. Laboratory diagnosis of human brucellosis. Clin Microbiol Rev. 2019;33:10-1128.
- Mohammadbeigi A, Saghafipour A, Hamta A, Khazaei S, Maghsoudi A, Shams S . Epidemiological features of brucellosis and factors affecting its treatment failure and relapse in Qom Province, Iran. Ghana Med J. 2021;55:206-12.
- Bosilkovski M, Keramat F, Arapovic J. The current therapeutical strategies in human brucellosis. Infection. 2021;49:823-32.
- Shi Y, Gao H, Pappas G, Chen Q, Li M, Xu J, Lai S, Liao Q, Yang W, Yi Z, et al. Clinical features of 2041 human brucellosis cases in China. PLoS ONE. 2018;13: e0205500.
- Xu N, Dong X, Yao Y, Guan Y, Chen F, Zheng F, Wang G. Improved early detection of focal brucellosis complications with anti-Brucella IgG. J Clin Microbiol. 2020;58:10-1128.
- Ministry of Health of the People’s Republic of China. Brucellosis Diagnosis and Treatment Guidelines (Trial). Infect Dis Inf. 2012; 25(6):323-324, 359. (in Chinese).
- Buzgan T, Karahocagil MK, Irmak H, Baran AI, Karsen H, Evirgen O, Akdeniz H. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Int J Infect Dis. 2010;14:e469-478.
- Jin M, Fan Z, Gao R, Li X, Gao Z, Wang Z. Research progress on complications of Brucellosis. Front Cell Infect Microbiol. 2023;13:1136674.
- Zhang
, Zhang , Chen , Cui , Cai , Yang , Zhang . Clinical features of human brucellosis and risk factors for focal complications: a retrospective analysis in a tertiary-care hospital in Beijing. China Int J Gen Med. 2022;15:7373-82. - Jiang W, Chen J, Li Q, Jiang L, Huang Y, Lan Y, Li Y. Epidemiological characteristics, clinical manifestations and laboratory findings in 850 patients with brucellosis in Heilongjiang Province, China. BMC Infect Dis. 2019;19:439.
- Jia B, Zhang F, Lu Y, Zhang W, Li J, Zhang Y, Ding J. The clinical features of 590 patients with brucellosis in Xinjiang, China with the emphasis on the treatment of complications. PLoS Negl Trop Dis. 2017;11: e0005577.
- Kayaaslan B, Bastug A, Aydin E, Akinci E, But A, Aslaner H, Yetkin MA, Bodur H. A long-term survey of brucellosis: Is there any marker to predict the complicated cases? Infect Dis (Lond). 2016;48:215-21.
- Demirdal T, Sen P. Risk factors for focal involvement in brucellosis. Diagn Microbiol Infect Dis. 2020;97: 115003.
- Copur B, Sayili U. Laboratory and clinical predictors of focal involvement and bacteremia in brucellosis. Eur J Clin Microbiol Infect Dis. 2022;41:793-801.
- Colmenero JD, Reguera JM, Martos F, Sanchez-De-Mora D, Delgado M, Causse M, Martin-Farfan A, Juarez C. Complications associated with Brucella melitensis infection: a study of 530 cases. Medicine (Baltimore). 1996;75:195-211.
- Eales KM, Norton RE, Ketheesan N. Brucellosis in northern Australia. Am J Trop Med Hyg. 2010;83:876-8.
- Wang Y, Zhang W, Ke Y, Zhen Q, Yuan X, Zou W, Li S, Sun Y, Wang Z, Wang D, et al. Human brucellosis, a heterogeneously distributed, delayed, and misdiagnosed disease in china. Clin Infect Dis. 2013;56:750-1.
- Yousefi-Nooraie R, Mortaz-Hejri S, Mehrani M, Sadeghipour P. Antibiotics for treating human brucellosis. Cochrane Database Syst Rev. 2012;10:CD007179.
- Sen P, Demirdal T, Nemli SA. Predictive value of inflammation markers in brucellosis. Arch Iran Med. 2019;22:640-5.
- Balin SO, Tartar AS, Akbulut A. The predictive role of haematological parameters in the diagnosis of osteoarticular brucellosis. Afr Health Sci. 2018;18:988-94.
- *Correspondence:
Qiu-Lan Chen
chenql@chinacdc.cn
Wen-Wu Yin
yinww@chinacdc.cn
Full list of author information is available at the end of the article - Those with missing values were excluded from analysis. Percentages may not sum to 100 due to rounding
Other occupations include staff, student, teacher, and other non-occupational population with brucellosis
Other animals include pigs, dogs, horses, deer, and camels
Other routes include veterinarian, animal trade, animal product processing and sheep clipping
Patients may have a history of multiple animal contacts or exposure modes. Therefore, the cumulative total may exceed
Inter-group comparison with the method of Bonferroni found that the proportion of complications among the three groups was different
DOI: https://doi.org/10.1186/s40249-024-01186-4
PMID: https://pubmed.ncbi.nlm.nih.gov/38374211
Publication Date: 2024-02-20
Incidence and warning signs for complications of human brucellosis: a multi-center observational study from China
Abstract
Background Brucellosis is a severe zoonotic disease that is often overlooked, particularly in impoverished countries. Timely identification of focal complications in brucellosis is crucial for improving treatment outcomes. However, there is currently a lack of established indicators or biomarkers for diagnosing these complications. Therefore, this study aimed to investigate potential warning signs of focal complications in human brucellosis, with the goal of providing practical parameters for clinicians to aid in the diagnosis and management of patients. Methods A multi-center cross-sectional study was conducted in China from December 2019 to August 2021. The study aimed to investigate the clinical characteristics and complications of patients with brucellosis using a questionnaire survey and medical record system. The presence of warning signs for complications was assessed using univariate and multivariate logistic regression models. Receiver operating characteristic (ROC) curves and the area under the curve (AUC) were used for variable screening and model evaluation. Results A total of 880 participants diagnosed with human brucellosis were enrolled. The median age of the patients was 50 years [interquartile range (IQR): 41.5-58.0], and 54.8% had complications. The most common organ system affected by complications was the osteoarticular system (43.1%), with peripheral arthritis (30.0%), spondylitis (16.6%), paravertebral abscess (5.0%), and sacroiliitis (2.7%) being the most prevalent. Complications in other organ systems included the genitourinary system (4.7%), respiratory system (4.7%), and hematologic system (4.6%). Several factors were found to be associated with focal brucellosis. These factors included a long delay in diagnosis [odds ratio
Keywords Brucellosis, Complications, Clinical spectrum, Warning signs
Background
Brucellosis is caused by Gram-negative bacteria of the genus Brucella, which have the ability to establish longterm infections in their hosts [6, 7]. Brucella evades the host immune system’s clearance mechanisms, and the duration of infection within host cells depends on the host’s immunity and the appropriate use of specific antibiotics. Therefore, early diagnosis and proper treatment are crucial in reducing the risk of chronicity and relapse. However, the clinical manifestations of brucellosis can vary greatly and mimic other diseases, leading to misdiagnosis and missed diagnosis [8]. Confirming brucellosis requires a combination of exposure history, clinical manifestations, and specific laboratory tests. Underdiagnosis of brucellosis leads to higher rates of complicated cases [9]. Focal involvement in brucellosis requires longer treatment duration and additional antimicrobial agents compared to uncomplicated cases [10]. Unfortunately, there are currently no specific biomarkers reported for diagnosing complications. It is challenging to distinguish complications based solely on general symptoms, signs, or single biomarkers [4]. Therefore, it is necessary to explore comprehensive diagnostic warning indicators for complicated brucellosis to aid clinicians in promptly diagnosing and treating the disease.
Understanding the true clinical spectrum of brucellosis and its complications is crucial for medical practitioners to make early decisions. Although a few studies have reported on the clinical spectrum of brucellosis complications and related factors [8, 11, 12], these studies had limitations such as being single center, having small
sample sizes, and focusing only on inpatients, which will likely overestimate the reported complication rates, and latent indicators for identifying focal involvement in outpatients might have been missed. To address these limitations, we conducted a multi-center observational study to determine the real incidence and clinical spectrum of brucellosis complications in both inpatients and outpatients and to identify clinical and laboratory warning indicators for complications, which could improve the diagnostic criteria and enhance the management of patients. Furthermore, it is worth noting that the current version of the guideline on the diagnosis and therapy of brucellosis in China does not include diagnostic principles for complications [13]. Therefore, our study is valuable in standardizing the diagnosis and treatment of brucellosis complications, ultimately reducing the incidence of chronic brucellosis.
Methods
Study design and setting
Sample size
Sampling and participants
The inclusion criteria for cases were as follows: (1) patients diagnosed with brucellosis; (2) aged 15 years and above; (3) provided informed consent and willingly participated in the study.
The criteria for case exclusion were: (1) infected with the human immunodeficiency virus (HIV), undergoing chemotherapy, having other immune system disorders, or suffering from other severe illnesses; (2) suffering from mental disorders, deafness and other disorders resulting in poor communication and inability to cooperate with the investigation; (3) pregnant woman.
Data collection and definitions
symptoms onset. Additionally, relevant variables from the Hospital Information System were extracted, such as date of diagnosis, presence of underlying diseases, previous history of brucellosis, symptoms and signs experienced (such as fever, chills, fatigue, etc.), complications, and laboratory test results.
ruling out other causes and/or with positive Brucella culture in cases of pericardial effusion. Hematological complications were diagnosed based on abnormal clinical manifestations (anemia or bleeding) and abnormal laboratory findings, while excluding other causes. Genitourinary complications such as Orchitis, epididymitis, and pelvic inflammation were diagnosed based on signs and symptoms of urogenital system inflammation (orchialgia, testicular enlargement, and lower back pain in men; lower abdominal pain in women), confirmed by ultrasound. Respiratory system complications presented as bronchitis, pneumonia, or pleural effusion, and could be confirmed through chest X-rays, computed tomography (CT) scans, or MRI scans once other possible causes were ruled out. Cutaneous complications were defined as clinical manifestations of skin rash, purpura, ecchymosis, erythema nodosum, ulceration, or abscess in confirmed cases of brucellosis, while excluding other causes.
Statistical analysis
Results
Demographic and epidemiological characteristics
| Complications |
|
| Osteoarticular system | 379 (43.1) |
| Sacroiliitis | 24 (2.7) |
| Spondylitis | 146 (16.6) |
| Peripheral arthritis | 264 (30.0) |
| Paravertebral abscess | 44 (5.0) |
| Genitourinary system | 41 (4.7) |
| Respiratory system | 41 (4.7) |
| Hematologic system | 40 (4.6) |
| Cardiovascular system | 11 (1.3) |
| Neurological system | 9 (1.0) |
| Cutaneous system | 1 (0.1) |
| Variables | Subgroups | Total
|
Complicated
|
Uncomplicated
|
|
| Gender | Male | 642 (73.0) | 354 (73.4) | 288 (72.4) | 0.719 |
| Female | 238 (27.0) | 128 (26.6) | 110 (27.6) | ||
| Age group | < 60 years | 702 (79.8) | 369 (76.6) | 333 (83.7) | 0.009 |
|
|
178 (20.2) | 113 (23.4) | 65 (16.3) | ||
| Nationality | Han nationality | 614 (69.8) | 353 (73.3) | 261 (65.6) | 0.014 |
| Minority nationality | 266 (30.2) | 129 (26.7) | 137 (34.4) | ||
| Occupation | Farmer& Herdman | 754 (85.7) | 418 (86.7) | 336 (84.4) | 0.234 |
| Animal and animal products processing management | 49 (5.6) | 21 (4.4) | 28 (7.0) | ||
| Other occupations
|
77 (8.8) | 43 (8.9) | 34 (8.5) | ||
| Region | Xinjiang | 385 (43.8) | 206 (42.7) | 179 (45.0) | 0.426 |
| Shandong | 289 (32.8) | 155 (32.2) | 134 (33.7) | ||
| Inner Mongolia | 206 (23.4) | 121 (25.0) | 85 (21.4) | ||
| Education | Primary or below | 364 (41.4) | 216 (44.8) | 148 (37.2) | 0.051 |
| Junior high school | 394 (44.8) | 199 (41.3) | 195 (49.0) | ||
| High school or above | 122 (13.9) | 67 (13.9) | 55 (13.8) | ||
| Exposure history
|
Exposure to animals | 830 (94.3) | 442 (91.7) | 388 (97.5) | < 0.001 |
| Sheep & goats | 774 (88.0) | 417 (86.5) | 357 (89.7) | 0.149 | |
| Cattle | 328 (37.3) | 170 (35.3) | 158 (39.7) | 0.176 | |
| Other animals
|
225 (27.1) | 145 (32.8) | 80 (20.6) | < 0.001 | |
| Method of exposures to animals
|
Raising | 691 (78.5) | 387 (80.3) | 304 (76.4) | 0.160 |
| Grazing | 356 (40.5) | 176 (36.5) | 180 (45.2) | 0.009 | |
| Slaughter | 222 (25.2) | 132 (27.4) | 90 (22.6) | 0.105 | |
| Delivering lambs | 414 (47.1) | 239 (49.6) | 175 (44.0) | 0.097 | |
| Other routes
|
369 (41.9) | 195 (40.5) | 174 (43.7) | 0.329 | |
| Ingestion of unpasteurized food | Yes | 130 (14.8) | 97 (20.2) | 33 (8.3) | < 0.001 |
| No | 748 (85.2) | 383 (79.8) | 365 (91.7) | ||
| Family history of brucellosis | Yes | 183 (21.1) | 96 (20.2) | 87 (22.1) | 0.489 |
| No | 685 (78.9) | 379 (79.8) | 306 (77.9) | ||
| Previous history of brucellosis | Yes | 77 (8.8) | 42 (8.7) | 35 (8.8) | 0.967 |
| No | 803 (91.2) | 440 (91.3) | 363 (91.2) | ||
| Days from onset to diagnosis | 0-7 | 166 (18.9) | 72 (14.9) | 94 (23.8) | < 0.001 |
| 8-30 | 425 (48.5) | 219 (45.4) | 206 (52.2) | ||
| 31-90 | 207 (23.6) | 132 (27.4) | 75 (19.0) | ||
| >90 | 79 (9.0) | 59 (12.2) | 20 (5.1) | ||
| Clinical stage
|
Acute | 793 (90.1) | 419 (86.9) | 374 (94.0) | 0.002 |
| Subacute | 50 (5.7) | 38 (7.9) | 12 (3.0) | ||
| Chronic | 37 (4.2) | 25 (5.2) | 12 (3.0) | ||
| Underlying disease | Yes | 311 (35.3) | 198 (41.1) | 113 (28.4) | < 0.001 |
| No | 569 (64.7) | 284 (58.9) | 285 (71.6) | ||
| Hospitalized | Yes | 614 (71.8) | 395 (84.6) | 219 (56.4) | < 0.001 |
| No | 241 (28.2) | 72 (15.4) | 169 (43.6) |
Clinical presentation and laboratory findings
The symptoms and signs observed in patients with focal brucellosis were similar to those without focal complications, except for a higher occurrence of arthralgia, inappetence, nausea, orchialgia, and eye bulging pain (
Warning signs associated with complications
We conducted multivariate logistic regression analysis to identify independent factors associated with complications. Our findings indicate that several factors were independently associated with focal brucellosis, including the number of days from onset to diagnosis, underlying disease, symptoms such as arthralgia and myalgia, eye bulging pain, CRP
ROC curve analysis of clinical biomarkers in patients with and without complications
value determined by the ROC analysis was
Discussion
| Total
|
Complicated
|
Uncomplicated
|
|
|
| Symptoms and signs | ||||
| Fever | 466 (53.0) | 256 (53.1) | 210 (52.8) | 0.918 |
| Chills | 193 (21.9) | 104 (21.6) | 89 (22.4) | 0.779 |
| Fatigue | 626 (71.1) | 324 (67.2) | 302 (75.9) | 0.005 |
| Sweating | 437 (49.7) | 236 (49.0) | 201 (50.5) | 0.649 |
| Arthralgia | 732 (83.2) | 438 (90.9) | 294 (73.9) | < 0.001 |
| Sacral | 166 (19.4) | 104 (21.9) | 62 (16.3) | 0.037 |
| Iliac | 162 (19.0) | 109 (23.0) | 53 (13.9) | 0.001 |
| Shoulder | 187 (21.9) | 117 (24.7) | 70 (18.4) | 0.027 |
| Knee | 319 (37.3) | 181 (38.2) | 138 (36.2) | 0.555 |
| Elbow | 131 (15.3) | 80 (16.9) | 51 (13.4) | 0.159 |
| Wrist | 93 (10.9) | 60 (12.7) | 33 (8.7) | 0.062 |
| Ankle | 107 (12.5) | 68 (14.4) | 39 (10.2) | 0.071 |
| Spine | 295 (34.5) | 202 (42.6) | 93 (24.4) | < 0.001 |
| Myalgia | 246 (28.0) | 123 (25.5) | 123 (30.9) | 0.076 |
| Cough | 128 (14.6) | 79 (16.4) | 49 (12.3) | 0.088 |
| Inappetence | 322 (36.6) | 192 (39.8) | 130 (32.7) | 0.028 |
| Nausea | 94 (10.7) | 63 (13.1) | 31 (7.8) | 0.012 |
| Headache | 254 (28.9) | 143 (29.7) | 111 (27.9) | 0.562 |
| Orchialgia | 45 (5.1) | 40 (8.3) | 5 (1.3) | < 0.001 |
| Weight loss | 273 (31.0) | 162 (33.6) | 111 (27.9) | 0.068 |
| Sleep disturbance | 82 (9.3) | 52 (10.8) | 30 (7.5) | 0.099 |
| Vomit | 35 (4.0) | 24 (5.0) | 11 (2.8) | 0.094 |
| Eye bulging pain | 38 (4.3) | 30 (6.2) | 8 (2.0) | 0.002 |
| Urgent micturition and frequent micturition | 41 (4.7) | 27 (5.6) | 14 (3.5) | 0.144 |
| Rashes | 3 (0.3) | 2 (0.4) | 1 (0.3) | 1.000 |
| Hematologic | ||||
| Anemia | 121 (14.1) | 77 (16.4) | 44 (11.3) | 0.033 |
| Leukopenia | 111 (12.9) | 65 (13.8) | 46 (11.8) | 0.383 |
| Leukocytosis | 48 (5.6) | 30 (6.4) | 18 (4.6) | 0.265 |
| Thrombocytopenia | 29 (3.4) | 15 (3.2) | 14 (3.6) | 0.747 |
| Serum biochemistry | ||||
| ALT
|
303 (34.9) | 173 (36.5) | 130 (33.0) | 0.281 |
| AST
|
200 (23.1) | 109 (23.0) | 91 (23.3) | 0.923 |
| Bilirubin
|
148 (17.2) | 88 (18.6) | 60 (15.4) | 0.207 |
| Urea nitrogen
|
86 (10.1) | 51 (10.9) | 35 (9.0) | 0.356 |
| Creatinine
|
2 (0.2) | 2 (0.4) | 0 | 0.504 |
| Inflammatory markers | ||||
| CRP
|
399 (48.9) | 258 (56.6) | 141 (39.2) | < 0.001 |
| ESR elevation | 415 (54.3) | 264 (62.0) | 151 (44.5) | <0.001 |
| Bacterial culture and serum-antibody-test | ||||
| Culture positive | 89 (10.1) | 33 (6.9) | 56 (14.1) | <0.001 |
| SAT
|
666 (77.0) | 359 (76.1) | 307 (78.1) | 0.474 |
| SAT
|
387 (44.7) | 193 (40.9) | 194 (49.4) | 0.013 |
| Variables | Univariate analysis | Multivariate analysis
|
||||||
| Wald
|
OR | OR(95% Cls) |
|
Wald
|
OR | OR(95% Cls) |
|
|
| Days from onset to diagnosis | 29.142 | – | – | <0.001 | 19.418 | – | – | < 0.001 |
| 0-7 | – | – | 1 (reference) | – | – | – | 1 (reference) | – |
| 8-30 | 3.166 | 1.388 | 0.967-1.992 | 0.075 | 4.282 | 1.610 | 1.025-2.527 | 0.039 |
| 31-90 | 15.233 | 2.298 | 1.513-3.489 | < 0.001 | 12.217 | 2.551 | 1.509-4.314 | 0.001 |
| >90 | 10.877 | 3.851 | 2.129-6.967 | < 0.001 | 13.601 | 3.963 | 1.906-8.238 | < 0.001 |
| Underlying disease | 15.219 | 1.758 | 1.324-2.335 | <0.001 | 8.180 | 1.675 | 1.176-2.384 | 0.004 |
| Arthralgia | 41.655 | 3.520 | 2.402-5.159 | < 0.001 | 22.869 | 3.197 | 1.986-5.148 | < 0.001 |
| Myalgia | 3.132 | 0.766 | 0.570-1.029 | 0.077 | 5.914 | 0.627 | 0.431-0.913 | 0.015 |
| Eye bulging pain | 8.453 | 3.236 | 1.466-7.14 | 0.004 | 6.649 | 3.482 | 1.349-8.988 | 0.001 |
| CRP
|
24.144 | 2.024 | 1.528-2.681 | < 0.001 | 11.316 | 1.910 | 1.310-2.784 | 0.001 |
| ESR elevation | 22.854 | 2.029 | 1.518-2.712 | < 0.001 | 7.147 | 1.663 | 1.145-2.415 | 0.008 |
| Culture positive | 12.037 | 0.449 | 0.285-0.706 | 0.001 | 5.060 | 0.516 | 0.290-0.918 | 0.025 |
| SAT
|
6.213 | 0.710 | 0.542-0.929 | 0.013 | 13.209 | 0.529 | 0.376-0.746 | < 0.001 |
| Age < 60 years | 6.772 | 0.637 | 0.454-0.895 | 0.009 | – | – | – | – |
| Nationality, Han | 6.039 | 1.436 | 1.076-1.917 | 0.014 | – | – | – | – |
| Education | 5.959 | – | – | 0.051 | ||||
| Primary or below | – | – | 1 (reference) | – | – | – | – | – |
| Junior high school | 5.942 | 0.699 | 0.524-0.932 | 0.015 | – | – | – | – |
| High school or above | 0.975 | 0.806 | 0.525-1.237 | 0.324 | – | – | – | – |
| Fatigue | 7.912 | 0.652 | 0.484-0.878 | 0.005 | – | – | – | – |
| Inappetence | 4.819 | 1.365 | 1.034-1.802 | 0.028 | – | – | – | – |
| Nausea | 6.244 | 1.780 | 1.132-2.798 | 0.013 | – | – | – | – |
| Orchialgia | 16.750 | 7.113 | 2.780-18.202 | < 0.001 | – | – | – | – |
| Anemia | 4.479 | 1.536 | 1.032-2.286 | 0.034 | – | – | – | – |
| Weight loss | 0.068 | 1.309 | 0.980-1.748 | 0.068 | – | – | – | – |
This study identified CRP and ESR as indicators of focal involvement in brucellosis, with a cutoff value of
The utility of blood culture for early identification of complications in brucellosis remains controversial, with limited and conflicting evidence available. Xu et al. [12] found that positive blood cultures were indicative of complicated brucellosis, while Bircan et al. [19] reported that negative blood cultures were statistically significant factors for complications. In other studies [20-22], the rates of blood culture and SAT positivity were similar in groups with and without focal involvement. The accuracy of blood culture results was greatly influenced by the conditions and techniques used [8]. In our study, we observed that negative blood cultures and low SAT titers
were associated with brucellosis complications, suggesting the need for further in-depth research on this topic.
Conclusions
Abbreviations
| ALT | Alanine aminotransferase |
| AST | Aspartate aminotransferase |
| AUC | Area under the curve |
| Cl | Confidence intervals |
| CRP | C-reactive protein |
| CT | Computed tomography |
| ECG | Electrocardiogram |
| ESR | Erythrocyte sedimentation rate |
| Hb | Hemoglobin |
| IQR | Interquartile range |
| MRI | Magnetic resonance imaging |
| OR | Odds ratio |
| PLT | Platelets |
| RBC | Red blood cells |
| ROC | Receiver operating characteristic |
| SAT | Standard tube agglutination test |
| UCG | Ultrasound cardiogram |
| WBC | White blood cells |
Supplementary Information
Acknowledgements
the provincial CDC of Shandong, Xinjiang and Inner Mongolia for their assistance in biological sample testing. Thanks to the China CDC for their support in the research process.
Author contributions
Funding
Availability of data and materials
Declarations
Ethics approval and consent to participate
Consent for publication
Competing interests
Author details
Published online: 20 February 2024
References
- Pappas G, Papadimitriou P, Akritidis N, Christou L, Tsianos EV. The new global map of human brucellosis. Lancet Infect Dis. 2006;6:91-9.
- O’Callaghan D. Human brucellosis: recent advances and future challenges. Infect Dis Poverty. 2020;9:101.
- Rossetti CA, Arenas-Gamboa AM, Maurizio E. Caprine brucellosis: a historically neglected disease with significant impact on public health. PLoS Negl Trop Dis. 2017;11: e0005692.
- Zheng R, Xie S, Lu X, Sun L, Zhou Y, Zhang Y, Wang K. A systematic review and meta-analysis of epidemiology and clinical manifestations of human brucellosis in China. Biomed Res Int. 2018;2018:5712920.
- Franco MP, Mulder M, Gilman RH, Smits HL. Human brucellosis. Lancet Infect Dis. 2007;7:775-86.
- Jiao H, Zhou Z, Li B, Xiao Y, Li M, Zeng H, Guo X, Gu G. The mechanism of facultative intracellular parasitism of Brucella. Int J Mol Sci. 2021;22:3673.
- Byndloss MX, Tsolis RM. Brucella spp. virulence factors and immunity. Annu Rev Anim Biosci. 2016;4:111-27.
- Yagupsky P, Morata P, Colmenero JD. Laboratory diagnosis of human brucellosis. Clin Microbiol Rev. 2019;33:10-1128.
- Mohammadbeigi A, Saghafipour A, Hamta A, Khazaei S, Maghsoudi A, Shams S . Epidemiological features of brucellosis and factors affecting its treatment failure and relapse in Qom Province, Iran. Ghana Med J. 2021;55:206-12.
- Bosilkovski M, Keramat F, Arapovic J. The current therapeutical strategies in human brucellosis. Infection. 2021;49:823-32.
- Shi Y, Gao H, Pappas G, Chen Q, Li M, Xu J, Lai S, Liao Q, Yang W, Yi Z, et al. Clinical features of 2041 human brucellosis cases in China. PLoS ONE. 2018;13: e0205500.
- Xu N, Dong X, Yao Y, Guan Y, Chen F, Zheng F, Wang G. Improved early detection of focal brucellosis complications with anti-Brucella IgG. J Clin Microbiol. 2020;58:10-1128.
- Ministry of Health of the People’s Republic of China. Brucellosis Diagnosis and Treatment Guidelines (Trial). Infect Dis Inf. 2012; 25(6):323-324, 359. (in Chinese).
- Buzgan T, Karahocagil MK, Irmak H, Baran AI, Karsen H, Evirgen O, Akdeniz H. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature. Int J Infect Dis. 2010;14:e469-478.
- Jin M, Fan Z, Gao R, Li X, Gao Z, Wang Z. Research progress on complications of Brucellosis. Front Cell Infect Microbiol. 2023;13:1136674.
- Zhang
, Zhang , Chen , Cui , Cai , Yang , Zhang . Clinical features of human brucellosis and risk factors for focal complications: a retrospective analysis in a tertiary-care hospital in Beijing. China Int J Gen Med. 2022;15:7373-82. - Jiang W, Chen J, Li Q, Jiang L, Huang Y, Lan Y, Li Y. Epidemiological characteristics, clinical manifestations and laboratory findings in 850 patients with brucellosis in Heilongjiang Province, China. BMC Infect Dis. 2019;19:439.
- Jia B, Zhang F, Lu Y, Zhang W, Li J, Zhang Y, Ding J. The clinical features of 590 patients with brucellosis in Xinjiang, China with the emphasis on the treatment of complications. PLoS Negl Trop Dis. 2017;11: e0005577.
- Kayaaslan B, Bastug A, Aydin E, Akinci E, But A, Aslaner H, Yetkin MA, Bodur H. A long-term survey of brucellosis: Is there any marker to predict the complicated cases? Infect Dis (Lond). 2016;48:215-21.
- Demirdal T, Sen P. Risk factors for focal involvement in brucellosis. Diagn Microbiol Infect Dis. 2020;97: 115003.
- Copur B, Sayili U. Laboratory and clinical predictors of focal involvement and bacteremia in brucellosis. Eur J Clin Microbiol Infect Dis. 2022;41:793-801.
- Colmenero JD, Reguera JM, Martos F, Sanchez-De-Mora D, Delgado M, Causse M, Martin-Farfan A, Juarez C. Complications associated with Brucella melitensis infection: a study of 530 cases. Medicine (Baltimore). 1996;75:195-211.
- Eales KM, Norton RE, Ketheesan N. Brucellosis in northern Australia. Am J Trop Med Hyg. 2010;83:876-8.
- Wang Y, Zhang W, Ke Y, Zhen Q, Yuan X, Zou W, Li S, Sun Y, Wang Z, Wang D, et al. Human brucellosis, a heterogeneously distributed, delayed, and misdiagnosed disease in china. Clin Infect Dis. 2013;56:750-1.
- Yousefi-Nooraie R, Mortaz-Hejri S, Mehrani M, Sadeghipour P. Antibiotics for treating human brucellosis. Cochrane Database Syst Rev. 2012;10:CD007179.
- Sen P, Demirdal T, Nemli SA. Predictive value of inflammation markers in brucellosis. Arch Iran Med. 2019;22:640-5.
- Balin SO, Tartar AS, Akbulut A. The predictive role of haematological parameters in the diagnosis of osteoarticular brucellosis. Afr Health Sci. 2018;18:988-94.
- *Correspondence:
Qiu-Lan Chen
chenql@chinacdc.cn
Wen-Wu Yin
yinww@chinacdc.cn
Full list of author information is available at the end of the article - Those with missing values were excluded from analysis. Percentages may not sum to 100 due to rounding
Other occupations include staff, student, teacher, and other non-occupational population with brucellosis
Other animals include pigs, dogs, horses, deer, and camels
Other routes include veterinarian, animal trade, animal product processing and sheep clipping
Patients may have a history of multiple animal contacts or exposure modes. Therefore, the cumulative total may exceed
Inter-group comparison with the method of Bonferroni found that the proportion of complications among the three groups was different