DOI: https://doi.org/10.1186/s40729-024-00586-3
PMID: https://pubmed.ncbi.nlm.nih.gov/39751717
تاريخ النشر: 2025-01-03
دقة جراحة زراعة الأسنان بمساعدة الروبوت مقابل الزراعة اليدوية: دراسة سريرية استعادية
الملخص
الغرض من هذه الدراسة هو تقييم دقة وضع الزرعات باستخدام نظام روبوتي (Remebot) مقارنة بالجراحة اليدوية واستكشاف العوامل التي تؤثر على الدقة. الطرق: شملت هذه الدراسة الاستعادية 95 زرعة تم وضعها في 65 مريضًا، مقسمة إلى مجموعتين: مجموعة مساعدة بالروبوت (50 زرعة) ومجموعة يدوية (45 زرعة). تم قياس الانحرافات في المنصة، والقمة، والزوايا من خلال تراكب الخطط قبل العملية وصور CBCT بعد العملية. تم مقارنة الانحرافات المتوسطة بين المجموعتين، وقام تحليل الانحدار بتقييم تأثير أبعاد الزرعة ووضعها على الدقة. النتائج: أظهرت المجموعة المساعدة بالروبوت انحرافات متوسطة أقل بشكل ملحوظ في المنصة.
الخلفية
لقد تم الإشادة بتطبيق التقنيات الرقمية في التشخيص، وتخطيط العلاج، والجراحة، والترميم كخطوة هامة في طب الأسنان المزروع، حيث تقدم أساليب دقيقة وقابلة للتنبؤ وشخصية [3]. لقد قللت جراحة الزرع بمساعدة الكمبيوتر (CAIS) بشكل فعال من خطر النتائج غير المرغوب فيها والمضاعفات الجراحية [4]. كما أنها قدمت درجة أعلى من الدقة والقابلية للتنبؤ في وضع الزرع مقارنة بالطريقة التقليدية اليدوية [5-7].
توجد طريقتان معروفتان ضمن نظام الجراحة بمساعدة الكمبيوتر لزراعة الأسنان (CAIS) وهما الجراحة الثابتة بمساعدة الكمبيوتر (s-CAIS) والجراحة الديناميكية بمساعدة الكمبيوتر (d-CAIS) [8]. يستخدم النظام الثابت دلائل مسبقة الصنع لتقييد حركة المثقاب، مما يوجهه بدقة إلى الموضع وزاوية الزراعة المخطط لها أثناء الجراحة [9، 10]. ومع ذلك، فإن s-CAIS له قيود، بما في ذلك عدم مرونته في التكيف مع التغييرات في خطة العلاج، وعدم القدرة على استخدامه في الحالات التي تعاني من فتح فم محدود، وتقليل الري والرؤية أثناء الجراحة [11-13]. في المقابل، تستخدم d-CAIS تتبعًا بصريًا نشطًا لتوجيه الجراح في ثلاثة أبعاد، باستخدام بيانات CBCT لضبط موضع وزاوية الزرعة [14]. تقدم هذه الطريقة العديد من المزايا، مثل تخطيط العلاج في نفس اليوم، والتعديلات أثناء العملية، والري والرؤية الكافيين، وقابلية التطبيق في الحالات التي تعاني من فتح فم محدود [15]. ومع ذلك، فإن استخدام الملاحة الديناميكية يتطلب منحنى تعليمي ويعتمد بشكل كبير على مهارة وتقنية الجراح [16، 17]. ومع ذلك، فقد أظهرت كل من s-CAIS و d-CAIS دقة محسنة عند مقارنتها بجراحة زراعة الأسنان اليدوية [14، 18-20].
لقد حظيت الظهور الأخير لجراحة زراعة الأسنان بمساعدة الروبوتات (r-CAIS) باهتمام كبير في مجال طب الأسنان. تجمع هذه الطريقة بين مزايا القيود الفيزيائية التي تُرى في s-CAIS مع الرؤية والمرونة التي تقدمها d-CAIS، مما يؤدي إلى إجراء مريح ودقيق للغاية. تم تقديم YOMI (Neocis Inc، ميامي، فلوريدا، الولايات المتحدة الأمريكية) المعتمد من إدارة الغذاء والدواء في عام 2017، كأول روبوت لجراحة زراعة الأسنان، حيث يستخدم نظامًا روبوتيًا سلبياً يوفر إرشادات لمسية وسمعية بصرية أثناء العملية. مع YOMI، يقوم الجراح بتوجيه الذراع الروبوتية يدويًا داخل موقع العظم، حيث يقوم الروبوت بتقييد حركات اليد التي تنحرف عن المسار المخطط.
يمثل ظهور الأنظمة الروبوتية في زراعة الأسنان تقدمًا تكنولوجيًا كبيرًا، يعد بتحسين دقة الجراحة ونتائج المرضى. بينما تم تقييم دقة وضع الزرعات باستخدام الأنظمة الروبوتية في بعض الدراسات، فإن التحليلات السريرية والمقارنة الشاملة مع التقنيات اليدوية نادرة. الدراسات السريرية ضرورية لأنها تأخذ في الاعتبار العوامل المربكة مثل حركة المريض ووجود الدم واللعاب، والتي يمكن أن تؤثر على الدقة. تقيّم هذه الدراسة دقة وضع الزرعات باستخدام نظام روبوتي وتقارنها مع الجراحة اليدوية.
المواد والأساليب
تصميم الدراسة
كانت أهداف الدراسة كما يلي:
- لتقديم نظرة سريرية على استخدام نظام روبوتي في جراحة الزرع بمساعدة الكمبيوتر.
- لتقييم دقة وضع الزرع باستخدام نظام جراحة روبوتي ومقارنتها بتلك الخاصة بالجراحة اليدوية.
- للتحقيق في تأثير منطقة الزرع داخل تجويف الفم على دقة كل من الجراحة بمساعدة الروبوت والجراحة اليدوية.
- المرضى الذين تزيد أعمارهم عن 18 عامًا والذين يتمتعون بصحة عامة جيدة ونظافة فموية.
- فقدان جزئي للأسنان مع وجود ثلاثة أسنان متبقية على الأقل في كل ربع، وحد أقصى من ثلاثة زراعة أسنان في مريض واحد.
- عرض العظم السنخي الكافي
) و الارتفاع كانت متاحة في موقع قطع العظم، مما سهل وضع الزرع باستخدام إجراء قياسي وحافظ على هوامش الأمان مع الهياكل المجاورة. - تم الحصول على موافقة مستنيرة مكتوبة من جميع المشاركين، بما في ذلك الموافقة على استخدام النظام الروبوتي.
- مدخنون بشدة
سجائر في اليوم). - الأفراد الذين يعانون من أمراض نظامية غير مسيطر عليها، مثل السكري، واضطرابات النزيف، أو ارتفاع ضغط الدم.
- المشاركون الذين لديهم موانع نظامية أو محلية لعلاج الزرع، مثل التهاب اللثة غير المنضبط، أو نقص المناعة، أو أمراض عظام الفك.
- المرضى الذين يعانون من عيوب شديدة في العظم السنخي أو الذين يحتاجون إلى إجراءات زيادة العظم السنخي.
- المرضى الذين لديهم خطط جراحية مفقودة أو بيانات CBCT.
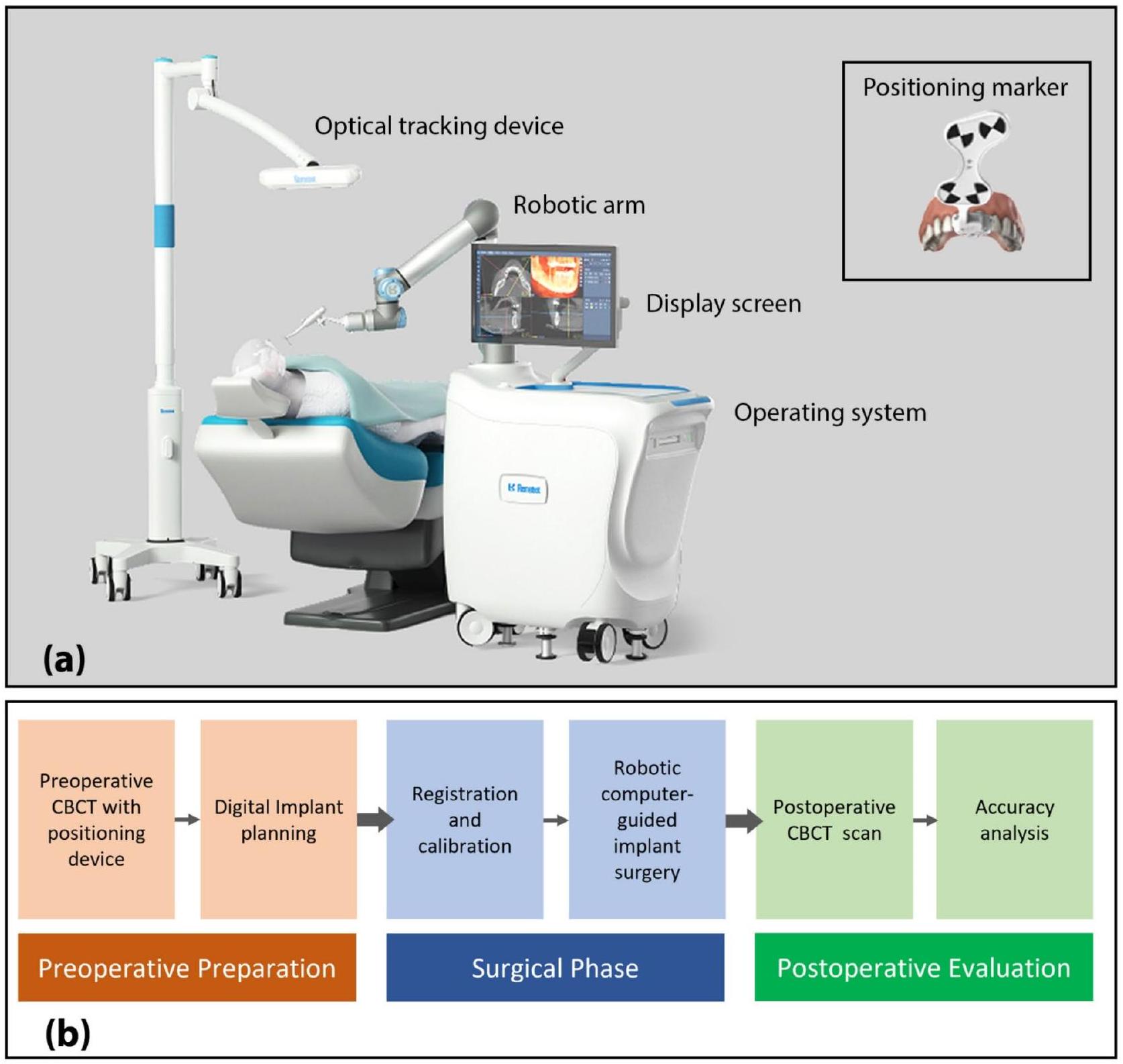
جراحة زراعة الأعضاء بمساعدة الروبوت
(انظر الشكل 1أ). يشمل بروتوكول العلاج، كما هو موضح في الشكل 1ب، التحضير قبل العملية، المرحلة الجراحية، والتقييم بعد العملية.
التخطيط قبل العملية
المرحلة الجراحية
جراحة زراعة الأسنان الحرة
التقييم بعد العملية
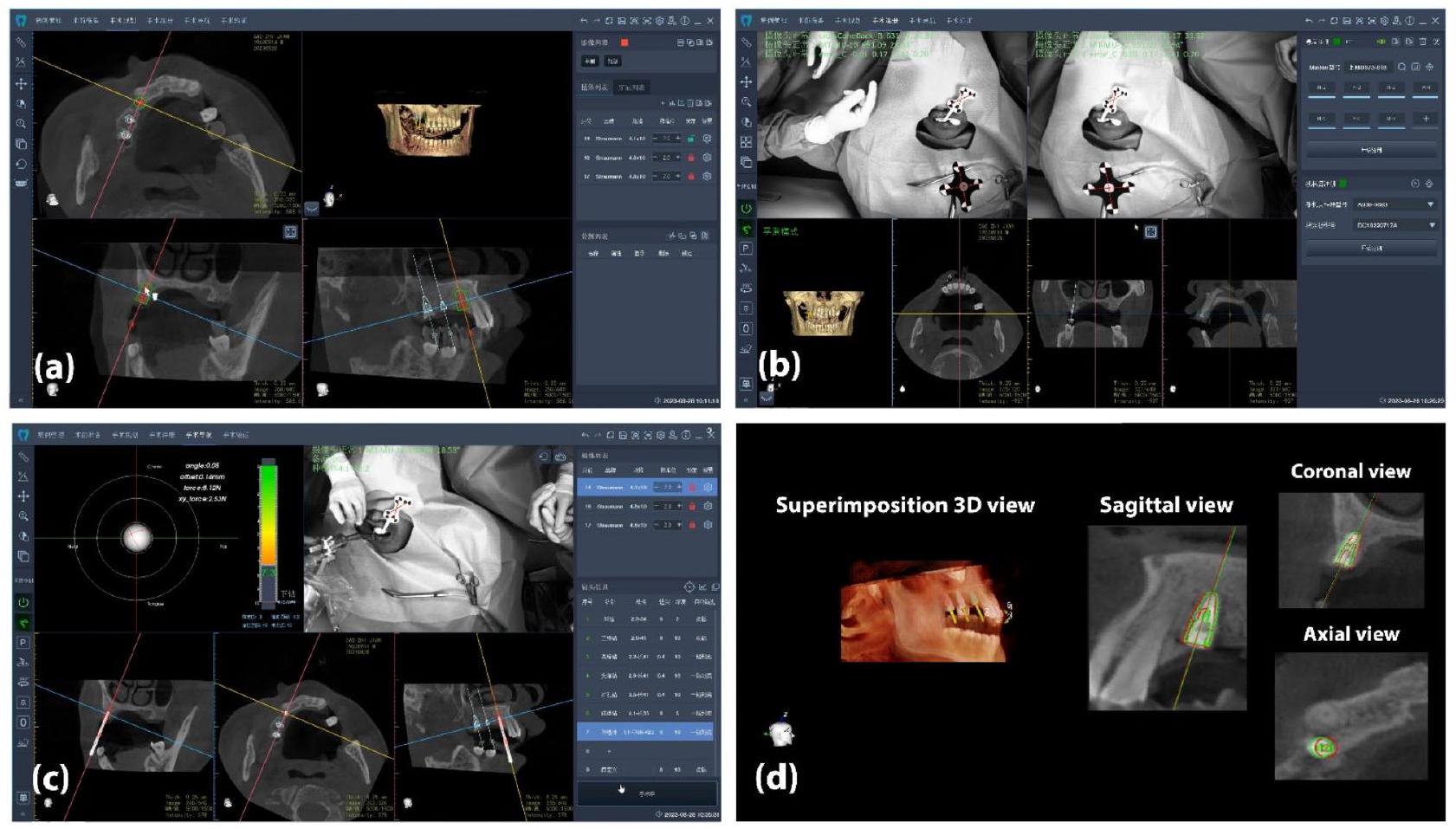
تم تحميل بيانات التخطيط وما بعد الجراحة إلى برنامج RemebotDent. بعد التراكب، قام البرنامج تلقائيًا بتحديد الزرعات وحساب قيم الانحراف بين الزرعات المخطط لها والمزروعة (الشكل 2d). أخيرًا، تم تصدير تقارير الانحراف وحفظها. تم التعبير عن بيانات الدقة من حيث قيم الانحراف بناءً على المحاور المركزية للزرعات المخطط لها والزرعات الفعلية (الشكل 3). كانت المتغيرات الأساسية للنتائج هي الانحرافات العالمية في المنصة، والانحرافات العالمية في القمة والانحرافات الزاوية. كما تم حساب الانحرافات الجانبية والعمق عند المنصة والقمة. بالإضافة إلى ذلك، تم تشكيل عينات فرعية للتحقيق في تباينات الدقة.
لأغراض التحليل الإحصائي، تم تصنيف الزرعات إلى مجموعتين بناءً على قطرها وطولها. تم تصنيف أقطار الزرعات على أنها “قطر ضيق”
التحليل الإحصائي
| مجموعة | المرضى | زراعة | |||||
|
|
نطاق العمر (المتوسط) | ذكر/أنثى |
|
يسار/يمين | الفك العلوي/الفك السفلي | أمامي/خلفي | |
| ر-كيس | ٣٥ | 19-74 (44.49) | 14/21 | 50 | 25/25 | 21/29 | ١٧/٣٣ |
| حر | 30 | ٢٤-٦٨ (٤٧.٦) | 19/11 | ٤٥ | ٢٦/١٩ | ٢٨/١٧ | 17/28 |
| إجمالي | 65 | 19-74 (45.9) | 25/40 | 95 | 51/44 | ٤٩/٤٦ | ٣٤/٦١ |
| معامل الانحراف | مجموعة | المتوسط ± الانحراف المعياري | الوسيط | الحد الأدنى – الحد الأقصى | فترة الثقة 95% | نطاق التداخل الربعي |
|
| المنصة العالمية (مم) | ر-كيس |
|
0.45 | 0.11-0.79 | 0.39 إلى 0.49 | 0.26 | <0.001 |
| حر اليد |
|
1.24 | 0.22-3.76 | 1.15 إلى 1.62 | 1.08 | ||
| القمة العالمية (مم) | ر-كيس |
|
0.46 | 0.10-0.80 | 0.41 إلى 0.51 | 0.26 | <0.001 |
| حر |
|
1.66 | 0.39-3.98 | 1.52 إلى 2.02 | 1.19 | ||
| زاوية (درجات) | ر-كيس |
|
0.78 | 0.08-1.88 | 0.71 إلى 0.98 | 0.75 | <0.001 |
| حر |
|
6.32 | 1.29-18.2 | 5.46 إلى 7.80 | ٥.٧٠٥ | ||
| المنصة الجانبية (مم) | ر-كيس |
|
0.34 | 0.07-0.68 | 0.28 إلى 0.35 | 0.19 | <0.001 |
| حر اليد |
|
0.91 | 0.80-3.68 | 0.87 إلى 1.35 | 1.15 | ||
| الجانبي القمي (مم) | ر-كيس |
|
0.32 | 0.06-0.78 | 0.29 إلى 0.38 | 0.23 | <0.001 |
| حر اليد |
|
1.40 | 0.27-3.93 | 1.28 إلى 1.80 | 1.21 | ||
| عمق المنصة (مم) | ر-كيس |
|
0.28 | 0.01-0.69 | 0.22 إلى 0.32 | 0.34 | <0.001 |
| حر اليد |
|
0.55 | 0.05-1.66 | 0.53 إلى 0.80 | 0.62 | ||
| عمق القمة (مم) | ر-كيس |
|
0.28 | 0.01-0.68 | 0.22 إلى 0.32 | 0.34 | <0.001 |
| حر اليد |
|
0.6 | 0.03-1.74 | 0.55 إلى 0.83 | 0.65 |
مقابل الفك السفلي)، الجانب (الأيسر مقابل الأيمن)، الوضع (الأمامي مقابل الخلفي)، قطر الزرعة، والطول. تم تحديد مستوى الدلالة عند
النتائج
يوفر الجدول 2 ملخصًا لتحليل الانحراف وقيم p لكلا المجموعتين. في مجموعة r-CAIS، كانت الانحرافات المتوسطة للمنصة العالمية، والقمة العالمية، والزوايا هي
تمت ملاحظة الانحرافات في المنصة، والقمية، والزوايا بين زراعة الغرسات بمساعدة الروبوت (r-CAIS) وزراعة الغرسات اليدوية عبر جميع العوامل السريرية التي تم تقييمها، بما في ذلك نوع الفك، وموقع الغرسة، وجانب القوس، وقطر الغرسة، وطول الغرسة. كما هو موضح في الجدول 3، أظهرت مجموعة r-CAIS باستمرار انحرافات أقل بشكل ملحوظ مقارنة بمجموعة الزراعة اليدوية عبر جميع المعايير.
لم تُظهر تحليل الانحدار الخطي المتعدد أي تأثير ذو دلالة إحصائية للمتغيرات المستقلة (نوع الفك، الجانب، الوضع، قطر الزرع، والطول) على الانحرافات في المنصة، القمة، والزوايا.
نقاش
| مؤشر | فئة فرعية | معامل الانحراف |
|
المتوسط الحر ± الانحراف المعياري |
|
| نوع الفك | الفك العلوي | المنصة (مم) |
|
|
< 0.001 |
| القمي (مم) |
|
|
< 0.001 | ||
| زاوية (درجة) |
|
|
<0.001 | ||
| الفك | المنصة (مم) |
|
|
< 0.001 | |
| القمي (مم) |
|
|
< 0.001 | ||
| زاوية (درجة) |
|
|
<0.001 | ||
| جانب القوس | يسار | المنصة (مم) |
|
|
<0.001 |
| القمي (مم) |
|
|
< 0.001 | ||
| زاوية (درجة) |
|
|
< 0.001 | ||
| حق | المنصة (مم) |
|
|
< 0.001 | |
| القمي (مم) |
|
|
<0.001 | ||
| زاوية (درجة) |
|
|
< 0.001 | ||
| موقف | أمامي | المنصة (مم) |
|
|
< 0.001 |
| القمي (مم) |
|
|
< 0.001 | ||
| زاوية (درجة) |
|
|
<0.001 | ||
| خلفي | المنصة (مم) |
|
|
< 0.001 | |
| القمي (مم) |
|
|
< 0.001 | ||
| زاوية (درجة) |
|
|
< 0.001 | ||
| قطر الزرعة | ضيق | المنصة (مم) |
|
|
0.008 |
| القمي (مم) |
|
|
0.001 | ||
| زاوية (درجة) |
|
|
< 0.001 | ||
| معيار | المنصة (مم) |
|
|
< 0.001 | |
| القمي (مم) |
|
|
<0.001 | ||
| زاوية (درجة) |
|
|
< 0.001 | ||
| طول الزرعة | معيار | المنصة (مم) |
|
|
< 0.001 |
| القمي (مم) |
|
|
<0.001 | ||
| زاوية (درجة) |
|
|
<0.001 | ||
| طويل | المنصة (مم) |
|
|
0.048 | |
| القمي (مم) |
|
|
0.023 | ||
| زاوية (درجة) |
|
|
0.007 |
| مؤشر | معامل الانحراف | ر-كيس | حر اليد | ||||||
| ب | SE | فترة الثقة 95% | قيمة p | ب | SE | فترة الثقة 95% | قيمة p | ||
| نوع الفك | منصة | -0.18 | 0.048 | -0.113 إلى 0.076 | 0.701 | -0.112 | 0.269 | -0.656 إلى 0.433 | 0.680 |
| (الفك العلوي مقابل الفك السفلي) | قممي | 0.004 | 0.048 | -0.091 إلى 0.100 | 0.930 | -0.382 | 0.277 | -0.942 إلى 0.178 | 0.176 |
| أنغولار | 0.095 | 0.159 | -0.226 إلى 0.416 | 0.553 | -4.526 | 1.015 | -6.579 إلى -2.473 | <0.001 | |
| جانب القوس (يسار مقابل يمين) | منصة | 0.038 | 0.053 | -0.069 إلى 0.146 | 0.475 | 0.306 | 0.239 | -0.177 إلى 0.788 | 0.208 |
| قممي | 0.094 | 0.050 | -0.007 إلى 0.195 | 0.068 | 0.394 | 0.245 | -0.103 إلى 0.890 | 0.117 | |
| أنغولار | 0.119 | 0.144 | -0.172 إلى 0.409 | 0.415 | 0.174 | 0.899 | -1.993 إلى 1.645 | 0.848 | |
| الموقع (أمامي مقابل خلفي) | منصة | 0.095 | 0.137 | -0.180 إلى 0.370 | 0.491 | -0.136 | 0.341 | -0.825 إلى 0.554 | 0.693 |
| قممي | 0.060 | 0.128 | -0.198 إلى 0.319 | 0.641 | -0.074 | 0.350 | -0.783 إلى 0.635 | 0.834 | |
| أنغولار | -0.489 | 0.368 | -1.231 إلى 0.253 | 0.191 | -3.767 | 1.285 | -6.366 إلى -1.169 | 0.006 | |
| قطر الزرعة (ضيقة مقابل قياسية) | منصة | 0.028 | 0.139 | -0.252 إلى 0.309 | 0.840 | 0.463 | 0.393 | -0.331 إلى 1.257 | 0.246 |
| قممي | 0.045 | 0.131 | -0.218 إلى 0.309 | 0.731 | 0.635 | 0.404 | -0.181 إلى 1.452 | 0.123 | |
| أنغولار | 0.428 | 0.375 | -0.328 إلى 1.184 | 0.260 | 7.121 | 1.480 | 4.128 إلى 10.115 | <0.001 | |
| طول الزرعة (قياسي مقابل طويل) | منصة | 0.217 | 0.125 | -0.035 إلى 0.469 | 0.089 | 0.314 | 0.329 | -0.351 إلى 0.979 | 0.345 |
| قممي | 0.221 | 0.117 | -0.016 إلى 0.457 | 0.067 | 0.120 | 0.338 | -0.563 إلى 0.804 | 0.724 | |
| أنغولار | -0.308 | 0.337 | -0.987 إلى 0.371 | 0.365 | 0.441 | 1.239 | -2.066 إلى 2.947 | 0.724 | |
تحتاج الفم. تقدم جراحة زراعة الأسنان بمساعدة الروبوت نهجًا جديدًا وابتكارًا في جراحة زراعة الأسنان المدعومة بالكمبيوتر، مما يعد بدقة عالية وموثوقية. ومع ذلك، لم تقيم سوى دراسات قليلة دقتها في بيئة سريرية، حيث كانت معظمها تقارير حالات أو سلسلة حالات.
بينما تركز دراستنا بشكل أساسي على مقارنة r-CAIS مع زراعة الغرسات اليدوية، من المهم أن نأخذ في الاعتبار كيف ترتبط هذه النتائج بالأدبيات الموجودة حول s-CAIS و d-CAIS. تستخدم جراحة زراعة الغرسات بمساعدة الكمبيوتر الثابتة (s-CAIS) أدوات جراحية مسبقة الصنع
تقدم الأدلة درجة عالية من الدقة ولكن تفتقر إلى المرونة أثناء العملية. يمكن أن تكون هذه inflexibility قيدًا في الحالات التي تكون فيها التغييرات في خطة الجراحة ضرورية بسبب تحديات تشريحية غير متوقعة. علاوة على ذلك، يمكن أن تؤدي الحاجة إلى دليل جراحي إلى تقييد الرؤية والري أثناء الإجراء، مما قد يؤثر على النتائج السريرية، خاصة في الحالات التي يكون فيها فتح الفم محدودًا. يمكن أن تؤثر عدة عوامل على الدقة ضمن النظام الثابت، بما في ذلك جودة مسح CBCT، ودقة تصنيع الدليل الجراحي، وتحقيق ملاءمة صحيحة. علاوة على ذلك، يمكن أن تؤثر متغيرات مثل مسافة الحفر، وطول المفتاح، وارتفاع الأنبوب أيضًا على الدقة.
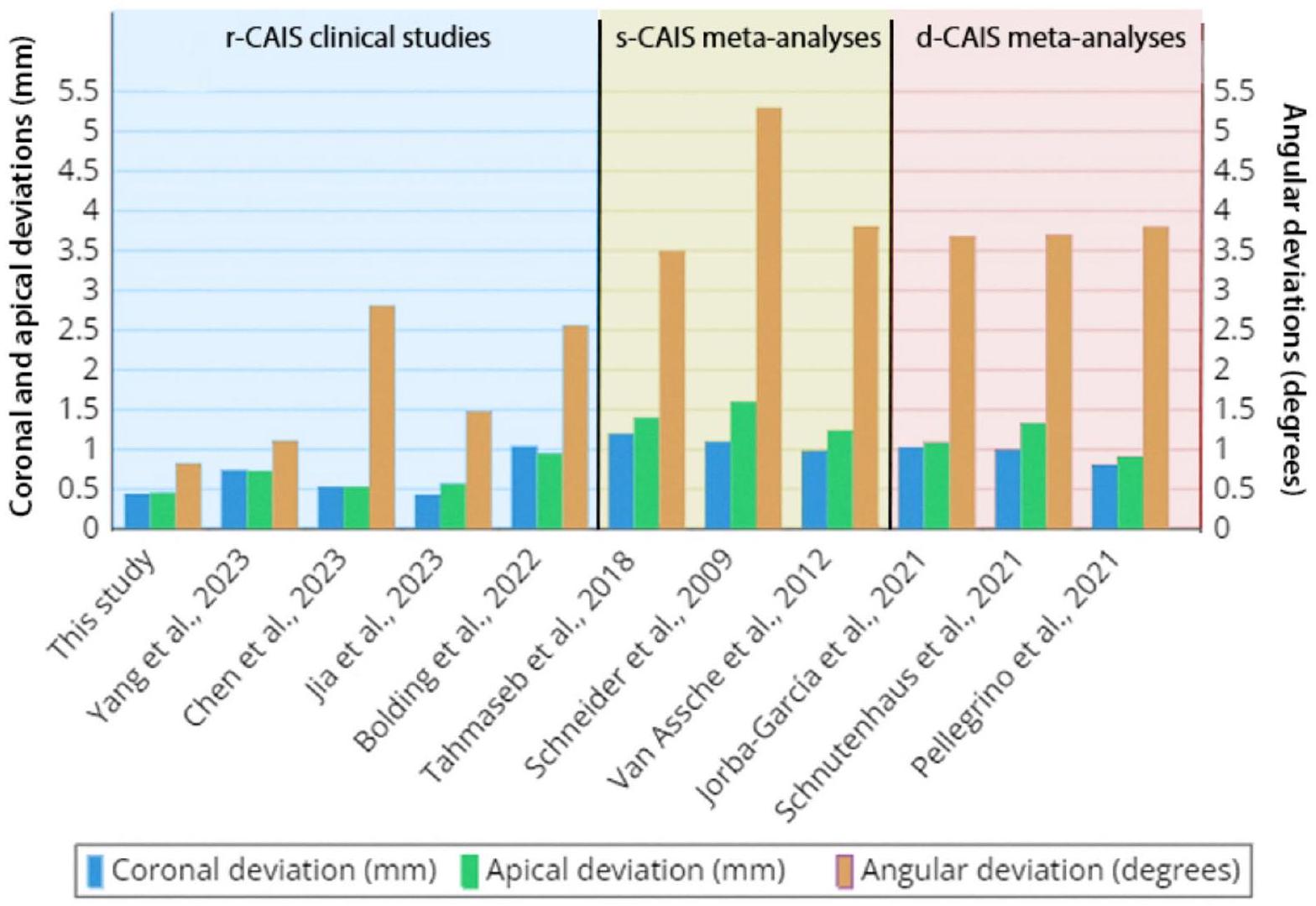
يبدو أن النظام الروبوتي يوفر وضعًا أكثر دقة للزرع مقارنةً بـ s-CAIS و d-CAIS. أظهرت الدراسات السابقة مستويات دقة مماثلة لـ s-CAIS و d-CAIS [2،41]. على الرغم من عدم وجود تجارب عشوائية محكومة رسمية على r-CAIS حاليًا، فإن نتائج هذه الدراسة والأدبيات المتاحة تدعم باستمرار دقة r-CAIS المحسنة. وفقًا للتحليلات التلوية السابقة، تراوحت الانحرافات الزاوية، والتاجية، والذروية المتوسطة لـ s-CAIS بين
تحد من موثوقيتها وإمكانية الوصول إليها وفعاليتها من حيث التكلفة. يتم تمديد مدة الجراحة بسبب الإعدادات اللازمة قبل العملية وعملية المعايرة. يتطلب النظام أيضًا وجود خط رؤية واضح باستمرار بين المتعقب البصري وموقع الجراحة، مع أجهزة وضع غير معاقة. قد يحدث أي انحراف إذا لم يتم ضبط الذراع الروبوتية بسرعة على حركات المريض. بالإضافة إلى ذلك، يمكن أن تكون تنفيذ جراحات الزرع في المنطقة الخلفية مع فتح الفم المحدود تحديًا، حيث تلتزم الذراع الروبوتية بمسار مستقل. من الناحية الأخلاقية والقانونية، على الرغم من أن النظام قد حصل على الموافقة، إلا أن الأطر الأخلاقية والتنظيمية ذات الصلة قد لا تواكب التقدم السريع في تكنولوجيا r-CAIS. ينفذ النظام الروبوتي تخطيطًا وملاحة جراحية تعتمد على CBCT، مما يجعل عوامل مثل الدقة، وحجم الفوكسل، ومجال الرؤية، والفروق بين CBCT وتشريح المريض حاسمة للدقة. لذلك، فإن جودة مسحات CBCT وغياب العيوب أمران أساسيان لتحقيق الدقة.
12. لين سي سي، وو سي زي، هوانغ إم إس، هوانغ سي إف، تشينغ إتش سي، وانغ دي بي. سير العمل الرقمي الكامل لتخطيط جراحة الزرع الموجهة الثابتة: دراسة دقة مستقبلية. مجلة الطب السريري. 2020؛9:1-15.
13. تالاريكو م، كيم ي.ج، كوتشي ف، مارتينولي م، ميلوني س.م. دقة القوالب المصممة على شكل كم التي تم تطويرها حديثًا لزرع الأسنان: تجربة سريرية متعددة المراكز prospective. Clin Implant Dent Relat Res [إنترنت]. 2019 [تم الاستشهاد به في 27 مارس 2023];21:108-13. متاح من:https://onlinelibrary.wiley.com/doi/full/https://doi.org/10.1111/cid. 12704
14. بلوك م، إيمري ر، لانك ك، رايان ج. دقة وضع الزرع باستخدام الملاحة الديناميكية. المجلة الدولية لزراعة الأسنان والفكين. 2017؛32:92-9.
15. بانشال ن، محمود ل، ريتانا أ، إيمري ر. الملاحة الديناميكية لجراحة زراعة الأسنان. عيادات جراحة الفم والوجه والفكين في أمريكا الشمالية [إنترنت]. 2019؛31:53947. متاح من:https://doi.org/10.1016/j.coms.2019.08.001
16. وانغ و، زوانغ م، لي س، شين ي، لان ر، وو ي وآخرون. استكشاف تدريب وضع زراعة الأسنان باستخدام أجهزة ثابتة أو ديناميكية بين طلاب طب الأسنان. المجلة الأوروبية لتعليم طب الأسنان. 2022؛ 438-48.
17. رابين J، بوبوفيتش A، شتراوس M، سبونتراب E، شتاينر A، ستول C. تقييم دقة ثلاثة أنظمة جراحة مدعومة بالحاسوب المختلفة في زراعة الأسنان: أنظمة التتبع البصري مقابل أنظمة القوالب الستيروليثوغرافية. أبحاث زراعة الأسنان السريرية. 2008؛19:709-16.
18. فيركرايسن م، كوكس س، كوك و، نيرت إ، جاكوبس ر، كويرين م. تجربة سريرية عشوائية تقارن جراحة الزرع الموجهة (مدعومة بالعظام أو الغشاء المخاطي) مع الملاحة الذهنية أو استخدام قالب حفر تجريبي. مجلة طب الأسنان السريري. 2014؛41:717-23.
19. تشين سي-كي، يو د-واي، هوانغ ر-واي، فو إي، تسائي سي-إف، تشيانغ سي-واي. دقة وضع الزرع باستخدام نظام الملاحة، ودليل مختبري، والحفر اليدوي. المجلة الدولية لزراعة الأسنان والفكين. 2018؛33:1213-8.
20. شنوتهوس س، فاغنر م، إيدلمان س، لوثاردت ر.ج، رودولف هـ. العوامل المؤثرة على دقة وضع الزرع باليد الحرة: دراسة سريرية مستقبلية. مجلة الأسنان. 2021؛9:1-12.
21. وو ي، وانغ ف، فان س، تشو جي كيه. الروبوتات في زراعة الأسنان. عيادات جراحة الفم والوجه والفكين في أمريكا الشمالية [إنترنت]. 2019؛31:513-8. متاح من:https://doi.org/10.1016/j.coms.2019.03.013
22. Bolding SL، Reebye UN. دقة التوجيه الروبوتي اللمسي في جراحة زراعة الأسنان للفكين الخاليين تمامًا من الأسنان. J Prosthet Dent [إنترنت]. 2022؛128:639-47. متاح من:https://doi.org/10.1016/j.prosdent.2020.12.0٤٨
23. فنغ ي، فان ج، تاو ب، وانغ س، مو ج، وو ي وآخرون. نظام روبوت هجين موجه بالصورة لجراحة زراعة الأسنان. المجلة الدولية للراديو الجراحي المساعد بالحاسوب [إنترنت]. 2021؛ متاح من:https://doi.org/10.1007/s11548-021-02484-0
24. شو ز، شياو ي، زو ل، لين ي، سو إي، تشن ج وآخرون. دقة وكفاءة جراحة زراعة الأسنان الروبوتية مع تفاعلات إنسان-روبوت مختلفة: دراسة مخبرية. مجلة الأسنان [إنترنت]. 2023؛137:104642. متاح من:https://doi.org /10.1016/j.jdent.2023.104642
25. باي SZ، رين N، فنغ ZH، شياو R، دونغ Y، لي ZW، وآخرون. [تجربة حيوانية حول دقة نظام الروبوتات لزراعة الأسنان المستقلة]. مجلة زونغ هوا كوو تشيانغ للطب=مجلة زونغ هوا كوو تشيانغ للطب=المجلة الصينية لطب الأسنان. 2021؛56:170-4.
26. يانغ إس، تشين جي، لي إيه، دينغ ك، لي بي، شو إس. دقة الجراحة الروبوتية المستقلة لوضع زرع سن واحد: سلسلة حالات. مجلة الأسنان. 2023؛132:1-8.
27. لي ي، هو ج، تاو ب، يو د، شين ي، فان س وآخرون. المعايرة التلقائية للروبوت في نظام الروبوت الجراحي الموجه بصريًا وتطبيقها في زراعة الأسنان. المجلة الدولية للراديو الجراحي المساعد بالحاسوب [إنترنت]. 2020؛ 15:168592. متاح من:https://doi.org/10.1007/s11548-020-02232-w
28. تشين جي، زوانغ إم، تاو بي، وو واي، يي إل، وانغ إف. دقة وضع زرع الأسنان الفوري باستخدام نظام روبوتي مستقل عن المهام ونظام الملاحة: دراسة مخبرية. أبحاث زراعة الأسنان السريرية. 2023؛1-11.
29. تاو ب، فنغ ي، فان إكس، زوانغ م، تشن إكس، وانغ ف وآخرون. دقة جراحة زراعة الأسنان باستخدام أنظمة الملاحة الديناميكية والروبوتية: دراسة مخبرية. مجلة الأسنان [إنترنت]. 2022؛123:104170. متاح من:https://doi.org/10.1016/j.jdent. 2022.104170
30. تشين جي، باي إكس، دينغ واي، شين إل، صن إكس، كاو آر، وآخرون. مقارنة دقة جراحة زراعة الأسنان باستخدام روبوت زراعة جديد ونظام الملاحة الديناميكية: دراسة تجريبية في المختبر. BMC صحة الفم. 2023؛23:1-9.
31. جيا إس، وانغ جي، تشاو واي، وانغ إكس. دقة نظام زراعة الأسنان الروبوتي المستقل مقابل جراحة زراعة الأسنان بمساعدة الدليل الثابت: دراسة سريرية استعادية. مجلة الأسنان الاصطناعية [إنترنت]. 2023؛1-9. متاح من:https://doi. org/10.1016/j.prosdent.2023.04.027
32. تشين و، الطائي كا، تشو تش، شين ي، وو ج، كاي ك وآخرون. دقة وضع زرع الأسنان باستخدام نظام روبوتي في المرضى الذين يعانون من فقدان جزئي للأسنان: تجربة سريرية مستقبلية ذات ذراع واحدة. أبحاث زراعة الأسنان السريرية. 2023؛ 707-18.
33. Sailer I، Karasan D، Todorovic A، Ligoutsikou M، Pjetursson BE. الفشل الصناعي في علاج زراعة الأسنان. Periodontol 2000. 2022;88:130-44.
34. فرانتشينا أ، ستيفانيلي ل. ف، مالتيزي ف، مانديلاريس ج. أ، فانتاجياتو أ، باجليارولو م وآخرون. التحقق من صحة طريقة المسح داخل الفم مقابل تراكب التصوير المقطعي المحوسب باستخدام شعاع مخروطي لتقييم الدقة بين الزرعات السنية المخطط لها والمحققة: دراسة عشوائية في المختبر. المجلة الدولية للبحوث البيئية والصحة العامة [إنترنت]. 2020؛17:1-21. متاح من:https://doi.org/10.1016/j.joms.2017.02.026
35. طهماسبي أ، وو ف، ويسماير د، كوك و، إيفانز ج. دقة جراحة الزرع بمساعدة الكمبيوتر الثابتة: مراجعة منهجية وتحليل تلوي. أبحاث زراعة الأسنان السريرية. 2018؛29:416-35.
36. حجب MS. الدقة باستخدام الملاحة الثابتة أو الديناميكية. جراحة الفم والوجه والفكين. 2016;74:2-3.
37. سيتتيكورنبايبون ب، أرانجارونسووك س، كابوسايا ب، سوببالكها ك، ماثيوس ن، بيمخاوكهام أ. مقارنة دقة وضع الزرعات باستخدام أنظمة حفر مختلفة لجراحة الزرع بمساعدة الكمبيوتر الثابتة: دراسة تجريبية قائمة على المحاكاة. كلين زراعة الأسنان وعلاقات الأبحاث [إنترنت]. 2021؛23:635-43. متاح من:https://onlinelibrary.wiley.com/doi/abs/https ://doi.org/10.1111/cid.13032
38. الكحولي ك، جانر إس إف إم، شيميل م، بوسر د. تأثير ارتفاع الأكمام الموجهة، مسافة الحفر، وطول مفتاح الحفر على دقة جراحة الزرع بمساعدة الكمبيوتر الثابتة. مجلة زراعة الأسنان السريرية والعلاقات البحثية. 2019؛21:101-7.
39. جولوب ديب ج، بنشاريت س، كاريكو سي ك، لوكيك م، هوكينز د، رينر-سيتار ك، وآخرون. استكشاف تدريب وضع زراعة الأسنان باستخدام نظام الملاحة بالكمبيوتر للطلاب قبل التخرج: دراسة تجريبية. المجلة الأوروبية لتعليم طب الأسنان. 2019؛ 23: 415-23.
40. صن ت م، لي هـ، لان ت هـ. تأثير الخبرة السنية على نظام توجيه زراعة الأسنان. بي إم سي صحة الفم. 2019؛ 19: 1-12.
41. سوموجي-غانس إ، هولمز HI، جوكستاد A. دقة نظام جراحة مساعد بالكمبيوتر الديناميكي النموذجي الجديد. أبحاث زراعة الأسنان السريرية. 2015؛ 26: 882-90.
42. شنايدر د، ماركاردت ب، زواهلي م، يونغ ر. مراجعة منهجية حول دقة ونتائج العلاج السريري لزراعة الأسنان المعتمدة على القوالب الموجهة بالكمبيوتر. أبحاث زراعة الأسنان السريرية [إنترنت]. 2009؛20:73-86. متاح من:https://onlinelibrary.wiley.com/doi/abs/https://doi.org/10.1111/j. 160 0-0501.2009.01788.x
43. فان أسيش ن، فيركرويسن م، كوك و، تيغيلز و، جاكوبس ر، كويرين م. دقة وضع الزرع بمساعدة الكمبيوتر. أبحاث الزرع الفموية السريرية [إنترنت]. 2012؛23:112-23. متاح من:https://onlinelibrary.wiley.com/doi /أبس/https://doi.org/10.1111/j.1600-0501.2012.02552.x
44. جوربا-غارسيا أ، غونزاليس-بارناداس أ، كامبس-فونت أ، فيغيريدو ر، فالماثيدا-كاستيلون إ. تقييم دقة وضع الزرع بمساعدة الكمبيوتر الديناميكية: مراجعة منهجية وتحليل تلوي. تحقيقات الفم السريرية. 2021؛ 25: 2479-94.
45. بيليجرينو جي، فيري أ، ديل فابرو م، براتي سي، غاندولفي إم جي، ماركيتي سي. الملاحة الديناميكية في زراعة الأسنان: مراجعة منهجية وتحليل تلوي. المجلة الدولية لزراعة الأسنان الفموية والوجهية. 2021؛36:e121-40.
46. تشنغ ك، كان ت، ليو ي، زو و، زو ف، وانغ و وآخرون. دقة جراحة زراعة الأسنان مع تغذية راجعة موضعية روبوتية وخوارزمية تسجيل: دراسة في المختبر. الحوسبة والطب الحيوي [إنترنت]. 2021؛129:104153. متاح من: https://www.sciencedirect.com/science/article/pii/S0010482520304844
47. يانغ جي-زد، كامبياس جي، كليري ك، دايملر إي، دريك جي، دوبونت بي إي وآخرون. الروبوتات الطبية – الاعتبارات التنظيمية والأخلاقية والقانونية لزيادة مستويات الاستقلالية. ساي روبوت [إنترنت]. 2017؛ 2: eaam8638. متاح من:https://ww w.science.org/doi/abs/https://doi.org/10.1126/scirobotics.aam8638
48. بوترا RH، يودا N، أستوتي ER، ساساكي K. دقة وضع الزرع باستخدام الجراحة الموجهة بالكمبيوتر في المرضى الذين يعانون من فقدان جزئي للأسنان والعوامل المؤثرة المحتملة: مراجعة منهجية وتحليل تلوي. مجلة أبحاث التعويضات السنية. 2022؛66:29-39.
ملاحظة الناشر
حمزة يونس وبويا شو ساهموا بالتساوي كأول مؤلفين في هذا العمل.
*المراسلة:
شياوفينغ تشانغ
changxf@xjtu.edu.cn
تشينغبينغ ليو
Ivchengpeng@163.com
المختبر الرئيسي لمقاطعة شانشي لأبحاث الطب الدقيق في الوجه والفكين، كلية طب الأسنان، جامعة شيآن جياوتونغ، شيآن، الصين
مركز الأبحاث السريرية في مقاطعة شانشي لأمراض الأسنان والفكين، كلية طب الأسنان، جامعة شيان جياوتونغ، شيان، الصين - © المؤلف(ون) 2024. الوصول المفتوح. هذه المقالة مرخصة بموجب رخصة المشاع الإبداعي للاستخدام والتوزيع والتكيف وإعادة الإنتاج في أي وسيلة أو صيغة، طالما أنك تعطي الائتمان المناسب للمؤلف(ين) الأصليين والمصدر، وتوفر رابطًا لرخصة المشاع الإبداعي، وتوضح ما إذا تم إجراء تغييرات. الصور أو المواد الأخرى من طرف ثالث في هذه المقالة مشمولة في رخصة المشاع الإبداعي للمقالة، ما لم يُذكر خلاف ذلك في سطر الائتمان للمادة. إذا لم تكن المادة مشمولة في رخصة المشاع الإبداعي للمقالة وكان استخدامك المقصود غير مسموح به بموجب اللوائح القانونية أو يتجاوز الاستخدام المسموح به، ستحتاج إلى الحصول على إذن مباشرة من صاحب حقوق الطبع والنشر. لعرض نسخة من هذه الرخصة، قم بزيارة http://creativecommons.org/licenses/by/4.0/.
DOI: https://doi.org/10.1186/s40729-024-00586-3
PMID: https://pubmed.ncbi.nlm.nih.gov/39751717
Publication Date: 2025-01-03
Accuracy of robot-assisted implant surgery versus freehand placement: a retrospective clinical study
Abstract
Purpose This study evaluated the accuracy of implant placement using a robotic system (Remebot) compared to freehand surgery and explored factors influencing accuracy. Methods This retrospective study included 95 implants placed in 65 patients, divided into robot-assisted ( 50 implants) and freehand ( 45 implants) groups. Platform, apical, and angular deviations were measured by superimposing preoperative plans and the postoperative CBCT images. Mean deviations between groups were compared, and regression analysis assessed the impact of implant dimensions and positioning on accuracy. Results The robot-assisted group exhibited significantly lower mean deviations in platform
Background
The application of digital technologies for diagnosis, treatment planning, surgery, and restoration has been lauded as a significant advancement in implant dentistry, offering precise, predictable, and personalized approaches [3]. Computer-assisted implant surgery (CAIS) has effectively reduced the risk of unfavorable outcomes and surgical complications [4]. It has also introduced a higher degree of accuracy and predictability in implant placement when compared to the traditional freehand method [5-7].
Two well-recognized methods within CAIS are static computer-assisted implant surgery (s-CAIS) and dynamic computer-assisted implant surgery (d-CAIS) [8]. The static system employs prefabricated guides to restrict drill movement, directing it precisely to the planned position and angulation during surgery [9, 10]. However, s-CAIS has limitations, including its inflexibility in adapting to changes in the treatment plan, inability to be used in cases with restricted mouth opening, and reduced irrigation and visibility during surgery [11-13]. In contrast, d-CAIS employs active optical tracking to guide the surgeon in three dimensions, using CBCT data to adjust the implant’s position and angulation [14]. This approach offers numerous advantages, such as sameday treatment planning, intraoperative adjustments, adequate irrigation and visibility, and applicability in cases with limited mouth opening [15]. However, using dynamic navigation involves a learning curve and heavily relies on the surgeon’s skill and technique [16, 17]. Nonetheless, both s-CAIS and d-CAIS have demonstrated improved accuracy when compared to freehand implant surgery [14, 18-20].
The recent emergence of robotic computer-assisted implant surgery (r-CAIS) has garnered significant attention in the field of dentistry [21]. This approach combines the advantages of physical constraint seen in s-CAIS with the visibility and flexibility offered by d-CAIS, resulting in a convenient and highly accurate procedure [22]. The FDA-approved YOMI (Neocis Inc, Miami, FL, USA) introduced in 2017, marked the first dental implant surgery robot, employing a passive robotic system that provides haptic and audiovisual guidance during the operation [23]. With YOMI, the surgeon manually guides the robotic arm within the osteotomy site, with the robot constraining hand movements that deviate from the planned path [24].
The advent of robotic systems in implant dentistry represents a significant technological advancement, promising to enhance surgical accuracy and patient outcomes. While the accuracy of implant placement using robotic systems has been evaluated in some studies, clinical and comprehensive comparative analyses with freehand techniques are sparse [22, 26, 29-32]. Clinical studies are imperative as they consider confounding factors such as patient movement and the presence of blood and saliva, which can influence accuracy. This study evaluates the accuracy of implant placement using a robotic system and compares it with freehand surgery.
Materials and methods
Study design
The study objectives were as follows:
- To provide a clinical overview of the utilization of a robotic system in computer-assisted implant surgery.
- To evaluate the accuracy of implant placement using a robotic surgical system and compare it with that of freehand surgery.
- To investigate the impact of implant region within the oral cavity on the accuracy of both robot-assisted and freehand surgery.
- Patients over 18 years of age with good general health and oral hygiene.
- Partially edentulous with at least three remaining teeth in each quadrant, and a maximum of three implants placed in one patient.
- Adequate alveolar bone width (
) and height were available at the osteotomy site, which facilitated implant placement using a standard procedure and maintained safety margins with adjacent structures. - Written informed consent was obtained from all participants, including consent for the use of the robotic system.
- Heavy smokers (
cigarettes a day). - Individuals with uncontrolled systemic diseases, such as diabetes, bleeding disorders, or hypertension.
- Participants with systemic or local contraindications for implant treatment, such as uncontrolled periodontitis, immunodeficiency, or jaw bone pathologies.
- Patients with severe alveolar bone defects or those who required alveolar bone augmentation procedures.
- Patients with missing surgical plans or CBCT data.
Robot-assisted implant surgery
(see Fig. 1a). The treatment protocol, as illustrated in Fig. 1b, encompasses preoperative preparation, the surgical phase, and postoperative assessment.
Preoperative planning
Surgical phase
Freehand implant surgery
Postoperative evaluation
plan and postoperative data were then uploaded to the RemebotDent software. After superimposition, the software automatically located the implants and calculated the deviation values between the planned and placed implants (Fig. 2d). Finally, the deviation reports were exported and saved. Accuracy data were expressed in terms of deviation values based on the central axes of the planned and actual implants (Fig. 3). Primary outcome variables were global platform, global apical and angular deviations. Lateral and depth deviations at the platform and apex were also calculated. Additionally, subsamples were formed to investigate accuracy variations
For the purpose of statistical analysis, implants were classified into two groups based on their diameter and length. Implant diameters were categorized as “Narrow Diameter”
Statistical analysis
| Group | Patients | Implants | |||||
|
|
Age Range (Mean) | Male/Female |
|
Left/Right | Maxilla/Mandible | Anterior/Posterior | |
| r-CAIS | 35 | 19-74 (44.49) | 14/21 | 50 | 25/25 | 21/29 | 17/33 |
| Freehand | 30 | 24-68 (47.6) | 11/19 | 45 | 26/19 | 28/17 | 17/28 |
| Total | 65 | 19-74 (45.9) | 25/40 | 95 | 51/44 | 49/46 | 34/61 |
| Deviation parameter | Group | Mean ± SD | Median | Min – Max | 95% CI | IQR |
|
| Global Platform (mm) | r-CAIS |
|
0.45 | 0.11-0.79 | 0.39 to 0.49 | 0.26 | <0.001 |
| Freehand |
|
1.24 | 0.22-3.76 | 1.15 to 1.62 | 1.08 | ||
| Global Apical (mm) | r-CAIS |
|
0.46 | 0.10-0.80 | 0.41 to 0.51 | 0.26 | <0.001 |
| Freehand |
|
1.66 | 0.39-3.98 | 1.52 to 2.02 | 1.19 | ||
| Angular (degrees) | r-CAIS |
|
0.78 | 0.08-1.88 | 0.71 to 0.98 | 0.75 | <0.001 |
| Freehand |
|
6.32 | 1.29-18.2 | 5.46 to 7.80 | 5.705 | ||
| Platform Lateral (mm) | r-CAIS |
|
0.34 | 0.07-0.68 | 0.28 to 0.35 | 0.19 | <0.001 |
| Freehand |
|
0.91 | 0.80-3.68 | 0.87 to 1.35 | 1.15 | ||
| Apical Lateral (mm) | r-CAIS |
|
0.32 | 0.06-0.78 | 0.29 to 0.38 | 0.23 | <0.001 |
| Freehand |
|
1.40 | 0.27-3.93 | 1.28 to 1.80 | 1.21 | ||
| Platform Depth (mm) | r-CAIS |
|
0.28 | 0.01-0.69 | 0.22 to 0.32 | 0.34 | <0.001 |
| Freehand |
|
0.55 | 0.05-1.66 | 0.53 to 0.80 | 0.62 | ||
| Apical Depth (mm) | r-CAIS |
|
0.28 | 0.01-0.68 | 0.22 to 0.32 | 0.34 | <0.001 |
| Freehand |
|
0.6 | 0.03-1.74 | 0.55 to 0.83 | 0.65 |
vs. mandible), side (left vs. right), position (anterior vs. posterior), implant diameter, and length. The level of significance was set at
Results
Table 2 provides a summary of the deviation analysis and p -values for both groups. In the r-CAIS group, the mean global platform, global apical, and angular deviations were
observed in the platform, apical, and angular deviations between robot-assisted (r-CAIS) and freehand implant placements across all clinical factors evaluated, including jaw type, implant position, side of the arch, implant diameter, and implant length. As shown in Table 3, the r-CAIS group consistently demonstrated significantly lower deviations compared to the freehand group across all parameters.
The multiple linear regression analysis did not show any statistically significant influence of the predictors (jaw type, side, position, implant diameter, and length) on the platform, apical, and angular deviations (
Discussion
| Predictor | Subcategory | Deviation Parameter |
|
Freehand Mean ± SD |
|
| Jaw Type | Maxilla | Platform (mm) |
|
|
< 0.001 |
| Apical (mm) |
|
|
< 0.001 | ||
| Angular (deg) |
|
|
<0.001 | ||
| Mandible | Platform (mm) |
|
|
< 0.001 | |
| Apical (mm) |
|
|
< 0.001 | ||
| Angular (deg) |
|
|
<0.001 | ||
| Side of arch | Left | Platform (mm) |
|
|
<0.001 |
| Apical (mm) |
|
|
< 0.001 | ||
| Angular (deg) |
|
|
< 0.001 | ||
| Right | Platform (mm) |
|
|
< 0.001 | |
| Apical (mm) |
|
|
<0.001 | ||
| Angular (deg) |
|
|
< 0.001 | ||
| Position | Anterior | Platform (mm) |
|
|
< 0.001 |
| Apical (mm) |
|
|
< 0.001 | ||
| Angular (deg) |
|
|
<0.001 | ||
| Posterior | Platform (mm) |
|
|
< 0.001 | |
| Apical (mm) |
|
|
< 0.001 | ||
| Angular (deg) |
|
|
< 0.001 | ||
| Implant Diameter | Narrow | Platform (mm) |
|
|
0.008 |
| Apical (mm) |
|
|
0.001 | ||
| Angular (deg) |
|
|
< 0.001 | ||
| Standard | Platform (mm) |
|
|
< 0.001 | |
| Apical (mm) |
|
|
<0.001 | ||
| Angular (deg) |
|
|
< 0.001 | ||
| Implant Length | Standard | Platform (mm) |
|
|
< 0.001 |
| Apical (mm) |
|
|
<0.001 | ||
| Angular (deg) |
|
|
<0.001 | ||
| Long | Platform (mm) |
|
|
0.048 | |
| Apical (mm) |
|
|
0.023 | ||
| Angular (deg) |
|
|
0.007 |
| Predictor | Deviation parameter | r-CAIS | Freehand | ||||||
| B | SE | 95% CI | p-value | B | SE | 95% CI | p-value | ||
| Jaw type | Platform | -0.18 | 0.048 | -0.113 to 0.076 | 0.701 | -0.112 | 0.269 | -0.656 to 0.433 | 0.680 |
| (Maxilla vs. mandible) | Apical | 0.004 | 0.048 | -0.091 to 0.100 | 0.930 | -0.382 | 0.277 | -0.942 to 0.178 | 0.176 |
| Angular | 0.095 | 0.159 | -0.226 to 0.416 | 0.553 | -4.526 | 1.015 | -6.579 to -2.473 | <0.001 | |
| Side of arch (Left vs. right) | Platform | 0.038 | 0.053 | -0.069 to 0.146 | 0.475 | 0.306 | 0.239 | -0.177 to 0.788 | 0.208 |
| Apical | 0.094 | 0.050 | -0.007 to 0.195 | 0.068 | 0.394 | 0.245 | -0.103 to 0.890 | 0.117 | |
| Angular | 0.119 | 0.144 | -0.172 to 0.409 | 0.415 | 0.174 | 0.899 | -1.993 to 1.645 | 0.848 | |
| Position (Anterior vs. posterior) | Platform | 0.095 | 0.137 | -0.180 to 0.370 | 0.491 | -0.136 | 0.341 | -0.825 to 0.554 | 0.693 |
| Apical | 0.060 | 0.128 | -0.198 to 0.319 | 0.641 | -0.074 | 0.350 | -0.783 to 0.635 | 0.834 | |
| Angular | -0.489 | 0.368 | -1.231 to 0.253 | 0.191 | -3.767 | 1.285 | -6.366 to -1.169 | 0.006 | |
| Implant diameter (Narrow vs. standard) | Platform | 0.028 | 0.139 | -0.252 to 0.309 | 0.840 | 0.463 | 0.393 | -0.331 to 1.257 | 0.246 |
| Apical | 0.045 | 0.131 | -0.218 to 0.309 | 0.731 | 0.635 | 0.404 | -0.181 to 1.452 | 0.123 | |
| Angular | 0.428 | 0.375 | -0.328 to 1.184 | 0.260 | 7.121 | 1.480 | 4.128 to 10.115 | <0.001 | |
| Implant length (Standard vs. long) | Platform | 0.217 | 0.125 | -0.035 to 0.469 | 0.089 | 0.314 | 0.329 | -0.351 to 0.979 | 0.345 |
| Apical | 0.221 | 0.117 | -0.016 to 0.457 | 0.067 | 0.120 | 0.338 | -0.563 to 0.804 | 0.724 | |
| Angular | -0.308 | 0.337 | -0.987 to 0.371 | 0.365 | 0.441 | 1.239 | -2.066 to 2.947 | 0.724 | |
mouth is needed. Robot-assisted implant surgery presents a novel approach and breakthrough in computerassisted implant surgery, promising high precision and reliability. However, only a few studies have evaluated its accuracy in a clinical setting, with most of them being case reports or case series.
While our study primarily focuses on comparing r-CAIS with freehand implant placement, it’s important to consider how these findings relate to the existing literature on s-CAIS and d-CAIS. Static Computer-Assisted Implant Surgery (s-CAIS) employs prefabricated surgical
guides, which offer a high degree of accuracy but lack intraoperative flexibility. This inflexibility can be a limitation in cases where changes to the surgical plan are necessary due to unforeseen anatomical challenges. Moreover, the need for a surgical guide can restrict visibility and irrigation during the procedure, which could impact clinical outcomes, especially in cases with limited mouth opening [35]. Several factors can influence accuracy within the static system, including CBCT scan quality, surgical guide fabrication precision, and achieving a proper fit [36, 37]. Moreover, variables like drilling distance, key length, and sleeve height can also affect accuracy [38].
The robotic system appears to provide more accurate implant placement compared to s-CAIS and d-CAIS. Previous studies have shown similar accuracy levels for s-CAIS and d-CAIS [2,41]. Although there are currently no formal randomized controlled trials on r-CAIS, the results of this study and available literature consistently support the enhanced accuracy of r-CAIS. According to previous meta-analyses, the mean angular, coronal, and apical deviations for s-CAIS ranged between
limit its reliability, accessibility, and cost-effectiveness. The surgical duration is extended due to the necessary preoperative setup and calibration process. The system also requires a consistently clear line of sight between the optical tracker and the surgical site, with unobstructed positioning devices. Any deviation may occur if the robotic arm is not promptly adjusted to the patient’s movements [46]. Additionally, executing implant surgeries in the posterior region with limited mouth opening can be challenging, as the robotic arm adheres to an autonomous path. On an ethical and legal front, although the system has received approval, the relevant ethical and regulatory frameworks might not keep pace with the rapid advancements in r-CAIS technology [47]. The robotic system implements a CBCT-based planning and surgical navigation, making factors like resolution, voxel size, field of view, and discrepancies between the CBCT and the patient’s anatomy critical to accuracy [3]. The quality of CBCT scans and the absence of artifacts are therefore paramount to achieving precision.
12. Lin CC, Wu CZ, Huang MS, Huang CF, Cheng HC, Wang DP. Fully digital workflow for planning static guided implant surgery: a prospective accuracy study. J Clin Med. 2020;9:1-15.
13. Tallarico M, Kim YJ, Cocchi F, Martinolli M, Meloni SM. Accuracy of newly developed sleeve-designed templates for insertion of dental implants: A prospective multicenters clinical trial. Clin Implant Dent Relat Res [Internet]. 2019 [cited 2023 Mar 27];21:108-13. Available from: https://onlinelibrary.wiley .com/doi/full/https://doi.org/10.1111/cid. 12704
14. Block M, Emery R, Lank K, Ryan J. Implant Placement Accuracy using dynamic Navigation. Int J Oral Maxillofac Implants. 2017;32:92-9.
15. Panchal N, Mahmood L, Retana A, Emery R. Dynamic Navigation for Dental Implant Surgery. Oral Maxillofac Surg Clin North Am [Internet]. 2019;31:53947. Available from: https://doi.org/10.1016/j.coms.2019.08.001
16. Wang W, Zhuang M, Li S, Shen Y, Lan R, Wu Y et al. Exploring training dental implant placement using static or dynamic devices among dental students. Eur J Dent Educ. 2022;438-48.
17. Ruppin J, Popovic A, Strauss M, Spüntrup E, Steiner A, Stoll C.Evaluation of the accuracy of three different computer-aided surgery systems in dental implantology: optical tracking vs. stereolithographic splint systems. Clin Oral Implants Res. 2008;19:709-16.
18. Vercruyssen M, Cox C, Coucke W, Naert I, Jacobs R, Quirynen M. A randomized clinical trial comparing guided implant surgery (bone- or mucosa-supported) with mental navigation or the use of a pilot-drill template. J Clin Periodontol. 2014;41:717-23.
19. Chen C-K, Yuh D-Y, Huang R-Y, Fu E, Tsai C-F, Chiang C-Y. Accuracy of Implant Placement with a Navigation System, a Laboratory Guide, and Freehand Drilling. Int J Oral Maxillofac Implants. 2018;33:1213-8.
20. Schnutenhaus S, Wagner M, Edelmann C, Luthardt RG, Rudolph H. Factors influencing the accuracy of freehand implant placement: a prospective clinical study. Dent J. 2021;9:1-12.
21. Wu Y, Wang F, Fan S, Chow JKF. Robotics in Dental Implantology. Oral Maxillofac Surg Clin North Am [Internet]. 2019;31:513-8. Available from: https://doi .org/10.1016/j.coms.2019.03.013
22. Bolding SL, Reebye UN. Accuracy of haptic robotic guidance of dental implant surgery for completely edentulous arches. J Prosthet Dent [Internet]. 2022;128:639-47. Available from: https://doi.org/10.1016/j.prosdent.2020.12.0 48
23. Feng Y, Fan J, Tao B, Wang S, Mo J, Wu Y et al. An image – guided hybrid robot system for dental implant surgery. Int J Comput Assist Radiol Surg [Internet]. 2021; Available from: https://doi.org/10.1007/s11548-021-02484-0
24. Xu Z, Xiao Y, Zhou L, Lin Y, Su E, Chen J et al. Accuracy and efficiency of robotic dental implant surgery with different human-robot interactions: An in vitro study. J Dent [Internet]. 2023;137:104642. Available from: https://doi.org /10.1016/j.jdent.2023.104642
25. Bai SZ, Ren N, Feng ZH, Xie R, Dong Y, Li ZW, et al. [Animal experiment on the accuracy of the Autonomous Dental Implant Robotic System]. Zhonghua Kou Qiang Yi Xue Za Zhi=Zhonghua Kouqiang Yixue zazhi=Chinese. J Stomatol. 2021;56:170-4.
26. Yang S, Chen J, Li A, Deng K, Li P, Xu S. Accuracy of autonomous robotic surgery for single-tooth implant placement: a case series. J Dent. 2023;132:1-8.
27. Li Y, Hu J, Tao B, Yu D, Shen Y, Fan S et al. Automatic robot-world calibration in an optical-navigated surgical robot system and its application for oral implant placement. Int J Comput Assist Radiol Surg [Internet]. 2020;15:168592. Available from: https://doi.org/10.1007/s11548-020-02232-w
28. Chen J, Zhuang M, Tao B, Wu Y, Ye L, Wang F. Accuracy of immediate dental implant placement with task-autonomous robotic system and navigation system: an in vitro study. Clin Oral Implants Res. 2023;1-11.
29. Tao B, Feng Y, Fan X, Zhuang M, Chen X, Wang F et al. Accuracy of dental implant surgery using dynamic navigation and robotic systems: An in vitro study. J Dent [Internet]. 2022;123:104170. Available from: https://doi.org/10.1 016/j.jdent. 2022.104170
30. Chen J, Bai X, Ding Y, Shen L, Sun X, Cao R, et al. Comparison the accuracy of a novel implant robot surgery and dynamic navigation system in dental implant surgery: an in vitro pilot study. BMC Oral Health. 2023;23:1-9.
31. Jia S, Wang G, Zhao Y, Wang X. Accuracy of an autonomous dental implant robotic system versus static guide-assisted implant surgery: A retrospective clinical study. J Prosthet Dent [Internet]. 2023;1-9. Available from: https://doi. org/10.1016/j.prosdent.2023.04.027
32. Chen W, Al-Taezi KA, Chu CH, Shen Y, Wu J, Cai K et al. Accuracy of dental implant placement with a robotic system in partially edentulous patients: a prospective, single-arm clinical trial. Clin Oral Implants Res. 2023;707-18.
33. Sailer I, Karasan D, Todorovic A, Ligoutsikou M, Pjetursson BE. Prosthetic failures in dental implant therapy. Periodontol 2000. 2022;88:130-44.
34. Franchina A, Stefanelli LV, Maltese F, Mandelaris GA, Vantaggiato A, Pagliarulo M et al. Validation of an intra-oral scan method versus cone beam computed tomography superimposition to assess the accuracy between planned and achieved dental implants: A randomized in vitro study. Int J Environ Res Public Health [Internet]. 2020;17:1-21. Available from: https://doi.org/10.1016 /j.joms.2017.02.026
35. Tahmaseb A, Wu V, Wismeijer D, Coucke W, Evans C. The accuracy of static computer-aided implant surgery: a systematic review and meta-analysis. Clin Oral Implants Res. 2018;29:416-35.
36. Block MS. Accuracy using static or dynamic navigation. J Oral Maxillofac Surg. 2016;74:2-3.
37. Sittikornpaiboon P, Arunjaroensuk S, Kaboosaya B, Subbalekha K, Mattheos N, Pimkhaokham A. Comparison of the accuracy of implant placement using different drilling systems for static computer-assisted implant surgery: A simulation-based experimental study. Clin Implant Dent Relat Res [Internet]. 2021;23:635-43. Available from: https://onlinelibrary.wiley.com/doi/abs/https ://doi.org/10.1111/cid.13032
38. El Kholy K, Janner SFM, Schimmel M, Buser D. The influence of guided sleeve height, drilling distance, and drilling key length on the accuracy of static computer-assisted Implant surgery. Clin Implant Dent Relat Res. 2019;21:101-7.
39. Golob Deeb J, Bencharit S, Carrico CK, Lukic M, Hawkins D, Rener-Sitar K, et al. Exploring training dental implant placement using computer-guided implant navigation system for predoctoral students: a pilot study. Eur J Dent Educ. 2019;23:415-23.
40. Sun TM, Lee HE, Lan TH. The influence of dental experience on a dental implant navigation system. BMC Oral Health. 2019;19:1-12.
41. Somogyi-Ganss E, Holmes HI, Jokstad A. Accuracy of a novel prototype dynamic computer-assisted surgery system. Clin Oral Implants Res. 2015;26:882-90.
42. Schneider D, Marquardt P, Zwahlen M, Jung RE. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. Clin Oral Implants Res [Internet]. 2009;20:73-86. Available from: https://onlinelibrary.wiley.com/doi/abs/https://doi.org/10.1111/j. 160 0-0501.2009.01788.x
43. Van Assche N, Vercruyssen M, Coucke W, Teughels W, Jacobs R, Quirynen M. Accuracy of computer-aided implant placement. Clin Oral Implants Res [Internet]. 2012;23:112-23. Available from: https://onlinelibrary.wiley.com/doi /abs/https://doi.org/10.1111/j.1600-0501.2012.02552.x
44. Jorba-García A, González-Barnadas A, Camps-Font O, Figueiredo R, Valmaseda-Castellón E. Accuracy assessment of dynamic computer-aided implant placement: a systematic review and meta-analysis. Clin Oral Investig. 2021;25:2479-94.
45. Pellegrino G, Ferri A, Del Fabbro M, Prati C, Gandolfi MG, Marchetti C. Dynamic Navigation in Implant Dentistry: a systematic review and Metaanalysis. Int J Oral Maxillofac Implants. 2021;36:e121-40.
46. Cheng K, Kan T, Liu Y, Zhu W, Zhu F, Wang W et al. Accuracy of dental implant surgery with robotic position feedback and registration algorithm: An in-vitro study. Comput Biol Med [Internet]. 2021;129:104153. Available from: https:// www.sciencedirect.com/science/article/pii/S0010482520304844
47. Yang G-Z, Cambias J, Cleary K, Daimler E, Drake J, Dupont PE et al. Medical robotics-Regulatory, ethical, and legal considerations for increasing levels of autonomy. Sci Robot [Internet]. 2017;2:eaam8638. Available from: https://ww w.science.org/doi/abs/https://doi.org/10.1126/scirobotics.aam8638
48. Putra RH, Yoda N, Astuti ER, Sasaki K. The accuracy of implant placement with computer-guided surgery in partially edentulous patients and possible influencing factors: a systematic review and meta-analysis. J Prosthodont Res. 2022;66:29-39.
Publisher’s note
Hamza Younis and Boya Xu contributed equally as first authors to this work.
*Correspondence:
Xiaofeng Chang
changxf@xjtu.edu.cn
Chengpeng Lv
Ivchengpeng@163.com
Key Laboratory of Shaanxi Province for Craniofacial Precision Medicine Research, College of Stomatology, Xi’an Jiaotong University, Xi’an, China
Clinical Research Center of Shaanxi Province for Dental and Maxillofacial Disease, College of Stomatology, Xi’an Jiaotong University, Xi’an, China - © The Author(s) 2024. Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.