DOI: https://doi.org/10.3390/bioengineering11040337
PMID: https://pubmed.ncbi.nlm.nih.gov/38671759
تاريخ النشر: 2024-03-29
دور الذكاء الاصطناعي في المستشفيات والعيادات: تحويل الرعاية الصحية في القرن الحادي والعشرين
تم الاستلام: 28 فبراير 2024
تمت المراجعة: 25 مارس 2024
تم القبول: 26 مارس 2024
تم النشر: 29 مارس 2024
الملخص
بينما تواجه أنظمة الرعاية الصحية حول العالم تحديات مثل ارتفاع التكاليف، والوصول المحدود، والطلب المتزايد على الرعاية الشخصية، يظهر الذكاء الاصطناعي (AI) كقوة رئيسية للتحول. تحفز هذه المراجعة الحاجة الملحة للاستفادة من إمكانيات الذكاء الاصطناعي للتخفيف من هذه القضايا وتهدف إلى تقييم تكامل الذكاء الاصطناعي في مجالات الرعاية الصحية المختلفة بشكل نقدي. نستكشف كيف يمكّن الذكاء الاصطناعي اتخاذ القرارات السريرية، ويعزز كفاءة تشغيل المستشفيات وإدارتها، ويُحسن تحليل الصور الطبية، ويحدث ثورة في رعاية المرضى ومراقبتهم من خلال الأجهزة القابلة للارتداء المدعومة بالذكاء الاصطناعي. من خلال عدة دراسات حالة، نستعرض كيف حول الذكاء الاصطناعي مجالات الرعاية الصحية المحددة ونناقش التحديات المتبقية والحلول الممكنة. بالإضافة إلى ذلك، سنناقش المنهجيات لتقييم حلول الرعاية الصحية المدعومة بالذكاء الاصطناعي، والتحديات الأخلاقية لنشر الذكاء الاصطناعي، وأهمية خصوصية البيانات والتخفيف من التحيز لاستخدام التكنولوجيا بشكل مسؤول. من خلال تقديم تقييم نقدي لإمكانات الذكاء الاصطناعي التحويلية، تزود هذه المراجعة الباحثين بفهم أعمق لتأثير الذكاء الاصطناعي الحالي والمستقبلي على الرعاية الصحية. تشجع على حوار بين التخصصات بين الباحثين، والأطباء، والتقنيين للتنقل في تعقيدات تنفيذ الذكاء الاصطناعي، مما يعزز تطوير حلول مدفوعة بالذكاء الاصطناعي التي تعطي الأولوية للمعايير الأخلاقية، والعدالة، ونهج يركز على المريض.
1. المقدمة
التشخيصات الطبية، يعزز الذكاء الاصطناعي دقة وسرعة تحليل الصور في الأشعة وعلم الأمراض [10]. علاوة على ذلك، يلعب الذكاء الاصطناعي دورًا حاسمًا في رعاية المرضى من خلال المراقبة عن بُعد، والطب عن بُعد، والمساعدة الافتراضية، مما يغير بشكل جذري نموذج التفاعل بين المريض والطبيب [11].
2. الذكاء الاصطناعي في اتخاذ القرار السريري
2.1. خوارزميات الذكاء الاصطناعي للتشخيص والتنبؤ
- التعلم الآلي (ML): تتعلم خوارزميات التعلم الآلي من البيانات لتقديم التنبؤات أو اتخاذ القرارات دون أن يتم برمجتها بشكل صريح لهذه المهمة [18]. في الرعاية الصحية، كانت خوارزميات التعلم تحت الإشراف فعالة في تطوير نماذج تنبؤية لنتائج المرضى بناءً على البيانات التاريخية [19]. من ناحية أخرى، يُستخدم التعلم غير المراقب لتحديد الأنماط أو المجموعات داخل البيانات، وهو مفيد في اكتشاف أنواع فرعية جديدة من الأمراض [20]. التعلم المعزز، حيث تتعلم الخوارزميات اتخاذ تسلسلات من القرارات من خلال التجربة والخطأ، له إمكانيات في تحسين العلاج الشخصي [21].
- التعلم العميق (DL): هو فرع من التعلم الآلي، يستخدم التعلم العميق الشبكات العصبية ذات الطبقات المتعددة (لذا “عميق”) لتحليل هياكل البيانات المعقدة. تعتبر الشبكات العصبية التلافيفية (CNNs) فعالة بشكل خاص في معالجة بيانات التصوير، مما يجعلها لا تقدر بثمن في تشخيص الأمراض من الصور الطبية مثل الأشعة السينية أو التصوير بالرنين المغناطيسي [22]. تشمل بعض الهياكل المتقدمة الأخرى لـ CNN شبكة المتبقي (ResNet)، وInception، ومجموعة الهندسة البصرية (VGG)، والشبكات العصبية التلافيفية البيانية (GCNs)، كل منها له نقاط قوته وتطبيقاته في تحليل الصور، والتصنيف، ومعالجة بيانات الرسوم البيانية [23]. تُستخدم الشبكات العصبية المتكررة (RNNs)، المعروفة بقدرتها على التعامل مع البيانات التسلسلية، لتحليل بيانات السلاسل الزمنية، مثل الإشارات الفسيولوجية المجمعة أثناء مراقبة المرضى، للتنبؤ بتدهور الصحة أو النتائج على مر الزمن [24]. على سبيل المثال، تم استخدام شبكات الذاكرة طويلة وقصيرة المدى (LSTM)، وهي نوع متقدم من RNNs، بشكل واسع في اكتشاف انقطاع النفس أثناء النوم باستخدام بيانات تخطيط النوم [25]. بالإضافة إلى ذلك، تقدم نماذج المحولات، مثل BERT (تمثيلات الترميز ثنائية الاتجاه من المحولات) وGPT (المحول المدرب مسبقًا التوليدي)، طرقًا ثورية لمعالجة اللغة الطبيعية في الملاحظات السريرية، مما يمكّن من استخراج معلومات ورؤى المرضى بدقة أكبر. ظهرت الشبكات التنافسية التوليدية (GANs) [26] ونماذج الانتشار الشرطي [27] كأداة قوية لتوليد صور طبية اصطناعية للتدريب دون مخاوف تتعلق بالخصوصية، بينما تفتح الشبكات العصبية البيانية (GNNs) إمكانيات جديدة في نمذجة الشبكات البيولوجية والصحية المعقدة، من التنبؤ بتفاعلات البروتين إلى فهم مسارات الأمراض.
يوفر الجدول 1 ملخصًا لمختلف نماذج التعلم العميق التي تم مناقشتها، بما في ذلك تطبيقاتها، ونقاط قوتها، والمجالات الصحية التي تقوم بتحويلها.
| نوع الخوارزمية | التطبيق العام | القيود | التعليقات | مثال |
| الشبكات العصبية التلافيفية (CNNs) | التعرف على الصور وتحليلها في التصوير الطبي (مثل الأشعة السينية، التصوير بالرنين المغناطيسي، الأشعة المقطعية) | تتطلب مجموعات بيانات كبيرة مصنفة وموارد حسابية كبيرة؛ يمكن أن تكون “صندوق أسود” مما يجعل التفسير صعبًا | فعالة للغاية للبيانات المكانية؛ تعتبر الأفضل في تحليل الصور الطبية | Deeplab v3+، نوع من CNN لتقسيم سرطان المعدة [28]. النتائج: دقة 95.76%، متفوقة على SegNet/ICNet. |
| الشبكات العصبية المتكررة (RNNs) وشبكات الذاكرة طويلة وقصيرة المدى (LSTM) | تحليل البيانات التسلسلية مثل إشارات ECG، EEG، أو سجلات صحة المرضى | عرضة للتكيف الزائد على مجموعات البيانات الصغيرة؛ أوقات تدريب طويلة؛ صعوبة في تنفيذ المهام بشكل متوازي | مناسبة لبيانات السلاسل الزمنية؛ LSTM تعالج مشكلة تلاشي التدرج في RNNs | LSTM لتصنيف إشارات EEG [29]. النتائج: دقة 71.3%، باستخدام وظائف تنشيط جديدة منحدر أحادي الأبعاد لأداء محسن. |
| نماذج المحولات (مثل BERT، GPT) | مهام معالجة اللغة الطبيعية، بما في ذلك تحليل النصوص السريرية وتلخيص تاريخ المرضى | تتطلب قوة حسابية وذاكرة كبيرة؛ التدريب المسبق على مجموعات بيانات كبيرة يستغرق وقتًا طويلاً | تقدم أداءً متفوقًا في معالجة اللغة الطبيعية؛ تمكّن من فهم السياق في الوثائق السريرية | BERT الخاص بالسريرية (المحول) لتحليل النصوص اليابانية [30]: تم تدريبه مسبقًا على 120 مليون نص، محققًا دقة 0.773 في Masked-LM و0.975 في توقع الجملة التالية، مما يشير إلى إمكانيات لمهام معالجة اللغة الطبيعية الطبية المعقدة. |
| الشبكات التنافسية التوليدية (GANs) | توليد بيانات اصطناعية لتدريب النماذج دون المساس بخصوصية المرضى؛ زيادة مجموعات البيانات | مشكلات استقرار التدريب؛ توليد بيانات عالية الجودة يمثل تحديًا | مفيدة في السيناريوهات المحدودة بالبيانات؛ إمكانيات في إنشاء صور طبية واقعية للتدريب | GAN الخاص بالخصوصية التفاضلية لتوليد البيانات الاصطناعية: يستخدم AEs التلافيفية وGANs لإنتاج بيانات طبية اصطناعية واقعية، مع الحفاظ على خصائص البيانات وتفوقه على النماذج الحالية [31]. |
| الشبكات العصبية البيانية (GNNs) | نمذجة العلاقات والتفاعلات المعقدة بين نقاط بيانات الصحة (مثل توقع تفاعلات الأدوية، نمذجة تقدم المرض) | هياكل نماذج معقدة يصعب تفسيرها؛ قابلية التوسع إلى الرسوم البيانية الكبيرة جدًا | فعالة للبيانات الممثلة كرسوم بيانية؛ تطبيقات ناشئة في الطب الشخصي | Knowledge-GNN لتوقع تفاعلات الأدوية: يستفيد من الرسوم البيانية المعرفية لالتقاط العلاقات المعقدة بين الأدوية ومعلومات الجوار، متفوقًا على النماذج التقليدية [32]. |
- معالجة اللغة الطبيعية (NLP): تتيح خوارزميات معالجة اللغة الطبيعية للكمبيوتر فهم وتفسير اللغة البشرية. في الرعاية الصحية، تُستخدم معالجة اللغة الطبيعية لاستخراج معلومات ذات مغزى من مصادر البيانات غير المنظمة مثل الملاحظات السريرية أو الأدبيات البحثية، مما يساعد في كل من عمليات التشخيص وتجميع المعرفة لتقدير التنبؤ [33]. مثال على مثل هذا النموذج اللغوي هو GatorTron [34]. إنه
نموذج NLP قائم على المحولات على نطاق واسع مصمم خصيصًا لمجال الرعاية الصحية. يستخدم بنية المحولات، المعروفة بكفاءتها في التعامل مع مهام التسلسل إلى التسلسل وقدرتها على معالجة مجموعات بيانات كبيرة، لتفسير وتحليل السجلات الصحية الإلكترونية. مع 8.9 مليار معلمة، تم تدريب GatorTron على أكثر من 90 مليار كلمة من النصوص السريرية، مما يجعله نموذجًا متقدمًا للغاية لاستخراج وفهم المعلومات الطبية المعقدة من مصادر البيانات غير المنظمة.
لا تعتبر خوارزميات الذكاء الاصطناعي مجرد أدوات للتشخيص والتنبؤ الفعالين؛ بل تمثل تحولًا في فهم وإدارة الصحة والمرض. ستوفر الأقسام التالية رؤى أعمق حول دراسات الحالة المحددة ودور الذكاء الاصطناعي في تخصيص الرعاية الطبية، مما يبرز تأثير الذكاء الاصطناعي العميق على اتخاذ القرارات السريرية.
2.2. دراسات حالة للذكاء الاصطناعي في اكتشاف الأمراض
- كشف السرطان: واحدة من أكثر التطبيقات الرائدة للذكاء الاصطناعي هي في الكشف المبكر عن السرطان. تتضمن دراسة حالة ملحوظة استخدام خوارزميات التعلم العميق في تحليل صور الماموجرام للكشف عن سرطان الثدي. أظهرت الأبحاث أن الذكاء الاصطناعي يمكنه تحديد الأنماط في الصور الماموجرامية التي تشير إلى نمو سرطاني، وغالبًا بدقة أكبر من الطرق التقليدية. أفادت دراسة بارزة نُشرت في مجلة Nature بتطوير نموذج ذكاء اصطناعي من قبل Google Health. تم تدريب هذا النموذج على مجموعة بيانات كبيرة من الماموجرامات وأظهر القدرة على الكشف عن سرطان الثدي بدقة أكبر من أطباء الأشعة البشر. أظهر نظام الذكاء الاصطناعي تقليلاً في كل من الإيجابيات الكاذبة والسلبيات الكاذبة، وهما عاملان رئيسيان في تشخيص السرطان. هذا التقدم في تكنولوجيا الذكاء الاصطناعي مهم لأن الكشف المبكر عن سرطان الثدي يمكن أن يحسن بشكل كبير من التوقعات ونتائج العلاج.
- إدارة السكري: دور الذكاء الاصطناعي في إدارة واكتشاف السكري، وخاصة من خلال خوارزميات التعلم الآلي، هو مجال مهم من التحسين في الرعاية الصحية. يمكن لهذه الخوارزميات تحليل بيانات المرضى للتنبؤ بظهور السكري وتطوره ومضاعفاته، كما هو موضح في دراسات مختلفة. في إحدى الدراسات، تم تطبيق عدة خوارزميات تصنيف تحت إشراف للتنبؤ وتصنيف ثمانية مضاعفات للسكري، بما في ذلك متلازمة الأيض، والخلل الدهني، والاعتلال العصبي، والاعتلال الكلوي، وقدم السكري، وارتفاع ضغط الدم، والسمنة، واعتلال الشبكية. تتكون مجموعة البيانات المستخدمة في هذه الدراسة من 79 سمة إدخال، بما في ذلك نتائج الفحوصات الطبية والمعلومات الديموغرافية المجمعة من 884 مريضًا. تم تقييم أداء النماذج باستخدام الدقة ودرجة F1، حيث وصلت إلى أقصى حد من
و ، على التوالي. من بين المصنفات المختلفة، حقق الغابة العشوائية (RF) وAdaboost وXGBoost أفضل أداء. يظهر هذا المستوى العالي من الدقة إمكانيات التعلم الآلي في التنبؤ بفعالية بمضاعفات السكري. تركزت دراسة أخرى على تقييم فعالية خوارزميات التعلم الآلي في التنبؤ بالمضاعفات وسوء التحكم في نسبة السكر في الدم لدى مرضى السكري من النوع 2 غير الملتزمين. استخدمت هذه الدراسة الواقعية بيانات من 800 مريض سكري من النوع 2، من بينهم 165 استوفوا معايير الإدراج. تم استخدام خوارزميات تعلم آلي مختلفة لتطوير نماذج التنبؤ، وتم تقييم الأداء التنبؤي باستخدام المساحة تحت المنحنى. كانت أعلى درجات الأداء في التنبؤ بمضاعفات مختلفة مثل الاعتلال الكلوي السكري، والاعتلال العصبي، والاعتلال الوعائي، وأمراض العين هي و و و - ، مما يبرز فعالية هذه النماذج.
تنبؤ بأمراض القلب: يمثل التنبؤ بأمراض القلب باستخدام الذكاء الاصطناعي تقدمًا كبيرًا في الرعاية الصحية القلبية الوعائية. لا يهدف هذا التطبيق فقط إلى التنبؤ بحدوث أمراض القلب ولكن أيضًا إلى تحديد شدتها، وهو عامل حاسم في العلاج والإدارة الفعالة. ركزت دراسة مبتكرة في هذا المجال على نموذج تنبؤ قائم على التعلم الآلي يقوم بإجراء تصنيفات ثنائية ومتعددة لأمراض القلب. يُعرف النموذج باسم Fuzzy-GBDT، ويجمع بين المنطق الضبابي وشجرة القرار المعززة بالتدرج لتبسيط تعقيد البيانات وتحسين دقة التنبؤ. بالإضافة إلى ذلك، لتجنب الإفراط في التكيف، يتضمن النموذج تقنية التجميع، مما يعزز قدرته على تصنيف شدة أمراض القلب. تظهر نتائج تقييم هذا النموذج دقة واستقرار ممتازين في التنبؤ بأمراض القلب، مما يدل على إمكانيته كأداة قيمة في الرعاية الصحية. تقدم دراسة أخرى مثيرة نظام رعاية صحية متقدم يستخدم التعلم العميق الجماعي مع أساليب دمج الميزات. تم تصميم هذا النظام للتغلب على قيود نماذج التعلم الآلي التقليدية التي تواجه صعوبة مع مجموعات البيانات عالية الأبعاد. يحقق ذلك من خلال دمج بيانات المستشعر مع السجلات الطبية الإلكترونية، مما يخلق مجموعة بيانات أكثر شمولية لتنبؤ بأمراض القلب. يستخدم النظام تقنية كسب المعلومات لتبسيط هذه المجموعة، مع التركيز على الميزات الأكثر صلة وبالتالي تقليل التعقيد الحسابي. جانب رئيسي من هذا النموذج هو تطبيق الاحتمالية الشرطية لوزن الميزات بدقة، مما يعزز الأداء العام للنظام. بشكل مثير للإعجاب، حقق هذا النموذج التعلم العميق الجماعي دقة قدرها، متفوقًا على النماذج الحالية ومظهرًا فعاليته في التنبؤ بأمراض القلب. - الذكاء الاصطناعي في الاضطرابات العصبية: فتح دمج الذكاء الاصطناعي، وخاصة التعلم العميق، في علم الأعصاب آفاقًا جديدة لتشخيص وإدارة الاضطرابات العصبية. تكشف الأدبيات الحديثة عن تقدم كبير في استخدام الذكاء الاصطناعي للكشف المبكر والتشخيص الأكثر دقة لمجموعة متنوعة من الحالات، بما في ذلك مرض الزهايمر. إحدى مجالات التقدم الملحوظة هي استخدام التعلم العميق في دراسات تصوير الأعصاب. قدرة التعلم العميق على معالجة والتعلم من البيانات الخام من خلال تحويلات غير خطية معقدة تجعلها مناسبة تمامًا لتحديد التغيرات الدقيقة والمنتشرة التي تميز العديد من الاضطرابات العصبية والنفسية. أظهرت الأبحاث في هذا المجال أن التعلم العميق يمكن أن يكون أداة قوية في البحث المستمر عن العلامات الحيوية لمثل هذه الحالات، مما يوفر إمكانيات لاكتشافات جديدة في فهم وتشخيص الاضطرابات الدماغية. لتعزيز هذا التقدم، أكدت مراجعة شاملة لتقنيات التعلم العميق في التنبؤ بمجموعة من الاضطرابات النفسية والعصبية، مثل السكتة الدماغية، والزهايمر، وباركنسون، والصرع، والتوحد، والصداع النصفي، والشلل الدماغي، والتصلب المتعدد، على تعددية استخدام التعلم العميق في مواجهة التحديات الحقيقية عبر مجالات مختلفة، بما في ذلك تشخيص الأمراض. في الحالة المحددة لمرض الزهايمر، السبب الأكثر شيوعًا للخرف، أظهر التعلم العميق وعدًا في تعزيز دقة التشخيص. باستخدام الشبكات العصبية التلافيفية، طور الباحثون أطرًا للكشف عن خصائص مرض الزهايمر من بيانات التصوير بالرنين المغناطيسي. من خلال النظر في مراحل مختلفة من الخرف وإنشاء خرائط احتمالية المرض عالية الدقة، توفر هذه النماذج تصورات بصرية بديهية لمخاطر مرض الزهايمر الفردية. لقد حقق هذا النهج، خاصة عند معالجة عدم التوازن في مجموعات البيانات، دقة عالية، متجاوزًا الطرق الحالية. إن تكييف مثل هذه النماذج مع مجموعات بيانات واسعة مثل مبادرة تصوير مرض الزهايمر يعزز من فعاليتها في التنبؤ بفئات مرض الزهايمر.
- رؤى رئيسية: تسلط هذه الدراسات الحالة الضوء على الدور الكبير للذكاء الاصطناعي في تعزيز الكشف عن الأمراض عبر العديد من التخصصات الطبية، مما يوفر تشخيصات دقيقة وفي الوقت المناسب، غالبًا من خلال طرق غير جراحية. ومع ذلك، مع استمرار تطور تكنولوجيا الذكاء الاصطناعي، هناك حاجة ملحة لمعالجة التحديات مثل خصوصية البيانات، وشفافية الخوارزميات، وضمان الوصول العادل إلى هذه التقنيات. يجب أن تركز التطورات المستقبلية على إنشاء أنظمة ذكاء اصطناعي أكثر قوة يمكنها التعامل مع مجموعات بيانات متنوعة، مما يقلل من التحيزات المحتملة في التشخيص. بالإضافة إلى ذلك، سيكون دمج الذكاء الاصطناعي مع الطرق التشخيصية التقليدية وتعزيز التعاون بين التكنولوجيين والأطباء والمرضى أمرًا أساسيًا لاستغلال الإمكانات الكاملة للذكاء الاصطناعي في الكشف عن الأمراض وإدارتها.
2.3. دور الذكاء الاصطناعي في الطب الشخصي
- تخصيص العلاجات وفقًا للملفات الجينية: واحدة من أهم تطبيقات الذكاء الاصطناعي في الطب الشخصي هي في مجال الجينوميات. يمكن لخوارزميات الذكاء الاصطناعي تحليل مجموعات بيانات جينومية ضخمة لتحديد الطفرات والتvariations التي قد تؤثر على استجابة الفرد لعلاجات معينة. على سبيل المثال، في علم الأورام، يساعد الذكاء الاصطناعي في تحديد علامات جينية محددة تكون عرضة للعلاجات المستهدفة للسرطان. تزيد هذه الطريقة من فعالية العلاج وتقلل من خطر ردود الفعل السلبية، مما يضمن خطة علاج أكثر فعالية وأمانًا للمريض. مثال بارز على هذا التطبيق هو دراسة تركز على سرطان الخلايا الانتقالية غير العضلي، وهو نوع من سرطان المثانة المعروف بمخاطر تكراره العالية. في هذه الدراسة، استخدم الباحثون خوارزمية تعلم الآلة لتحليل البيانات الجينومية من المرضى عند تقديمهم الأول. كانوا يهدفون إلى تحديد الجينات الأكثر توقعًا للتكرار خلال خمس سنوات بعد استئصال الورم المثاني عبر الإحليل. شملت الدراسة تحليل الجينوم الكامل لـ 112 عينة من سرطان الخلايا الانتقالية غير العضلي باستخدام شرائح Human WG-6 BeadChips. ثم تم تطبيق خوارزمية برمجة جينية لتطوير نماذج رياضية مصنفة لتوقع النتائج. تضمنت العملية إعادة أخذ العينات بناءً على التحقق المتبادل وتقييم تكرار استخدام الجينات لتحديد الجينات الأكثر توقعًا. تم دمج هذه الجينات لاحقًا في قواعد ضمن خوارزمية تصويت لتوقع احتمال تكرار السرطان. من بين الجينات التي تم تحليلها، تم تحديد 21 كجينات توقعية للتكرار. تم إجراء مزيد من التحقق من خلال تفاعل البوليميراز المتسلسل الكمي على مجموعة فرعية من 100 مريض. كانت النتائج واعدة: أظهرت قاعدة جينية مكونة من خمسة جينات باستخدام خوارزمية التصويت
الحساسية و الخصوصية في توقع التكرار في مجموعة التدريب. بالإضافة إلى ذلك، تم تطوير قاعدة مكونة من ثلاثة جينات، تقدم الحساسية و الخصوصية في مجموعة التدريب لتوقع التكرار. - التحليلات التنبؤية في تطوير الأدوية: يلعب الذكاء الاصطناعي أيضًا دورًا حاسمًا في تطوير الأدوية، خاصة في توقع كيفية استجابة المرضى المختلفين لدواء ما. من خلال تحليل البيانات التاريخية من التجارب السريرية وسجلات المرضى، يمكن لنماذج الذكاء الاصطناعي توقع فعالية الأدوية على مجموعات ديموغرافية مختلفة. هذه القوة التنبؤية لا تقدر بثمن في تصميم التجارب السريرية وفي تطوير أدوية أكثر فعالية لفئات معينة من المرضى. في السنوات الأخيرة، حقق الذكاء الاصطناعي تقدمًا ملحوظًا في تطوير الأدوية. قدمت Exscientia أول جزيء دوائي مصمم بواسطة الذكاء الاصطناعي للتجارب السريرية في أوائل عام 2020. ثم حقق AlphaFold من DeepMind اختراقًا في يوليو 2021 من خلال توقع هياكل لأكثر من 330,000 بروتين، بما في ذلك الجينوم البشري بالكامل. في عام 2022، بدأت Insilico Medicine التجارب من المرحلة الأولى لجزيء اكتشفه الذكاء الاصطناعي، وهي عملية أسرع بكثير وأكثر فعالية من حيث التكلفة من الطرق التقليدية. بحلول عام 2023، ابتكرت AbSci في إنشاء أجسام مضادة باستخدام الذكاء الاصطناعي التوليدي، ورأت Insilico Medicine دواء مصمم بواسطة الذكاء الاصطناعي يحصل على تصنيف دواء يتيم من إدارة الغذاء والدواء، مع خطط للتجارب من المرحلة الثانية بعد ذلك بوقت قصير. تمثل هذه المعالم عصرًا تحويليًا في اكتشاف الأدوية المدفوع بالذكاء الاصطناعي. يمتد تطبيق الذكاء الاصطناعي إلى تحديد بروتينات أو جينات جديدة كأهداف محتملة للأمراض، مع أنظمة قادرة على توقع الهياكل ثلاثية الأبعاد لهذه الأهداف باستخدام التعلم العميق. كما أن الذكاء الاصطناعي يحدث ثورة في المحاكاة الجزيئية وتوقع خصائص الأدوية مثل السمية والنشاط الحيوي، مما يمكّن من إجراء محاكاة عالية الدقة يمكن تنفيذها بالكامل في بيئة حاسوبية. علاوة على ذلك، يقوم الذكاء الاصطناعي بتحويل نموذج اكتشاف الأدوية التقليدي من فحص مكتبات كبيرة من الجزيئات إلى إنشاء جزيئات دوائية جديدة من الصفر. يمكن أن تعزز هذه الطريقة من كفاءة عملية اكتشاف الأدوية وقد تؤدي إلى تطوير علاجات جديدة.
3. تخصيص خطط العلاج: أنظمة الذكاء الاصطناعي بارعة في دمج وتحليل أنواع مختلفة من بيانات الصحة – من السجلات السريرية ونتائج المختبر إلى معلومات نمط الحياة والعوامل البيئية. تتيح هذه القدرة لمقدمي الرعاية الصحية إنشاء خطط علاج أكثر دقة وشمولية. على سبيل المثال، في إدارة الأمراض المزمنة مثل السكري، يمكن للذكاء الاصطناعي تحليل البيانات من الأجهزة القابلة للارتداء، وسجلات النظام الغذائي، وقراءات سكر الدم لتوصية بتعديلات شخصية في نمط الحياة والأدوية من أجل إدارة أفضل للمرض.
4. الذكاء الاصطناعي في الصحة النفسية: في مجال الصحة النفسية، يُستخدم الذكاء الاصطناعي لتخصيص أساليب العلاج. من خلال مراقبة الأنماط في الكلام، والسلوك، ونشاط وسائل التواصل الاجتماعي، يمكن لأدوات الذكاء الاصطناعي المساعدة في تحديد بداية مشكلات الصحة النفسية واقتراح تدخلات مصممة خصيصًا لحالة الفرد الفريدة. هذه الطريقة الشخصية حاسمة في الصحة النفسية، حيث يمكن أن تختلف فعالية العلاج بشكل كبير من شخص لآخر.
في الأبحاث والتطوير المستقبلية في علاج الصحة النفسية، فإن اتجاهًا واعدًا هو دمج أنظمة الذكاء الاصطناعي مع الذكاء العاطفي. يمكن أن تكون هذه الأنظمة حاسمة في الكشف المبكر والتدخل في اضطرابات الصحة النفسية من خلال تحليل أنماط الكلام والسلوك بحثًا عن علامات حالات مثل الاكتئاب أو القلق. يمكن أن يؤدي المزيد من الاستكشاف في تخصيص العلاج باستخدام الذكاء الاصطناعي إلى رعاية أكثر فردية وفعالية.
5. رؤى رئيسية: بينما يقدم دمج الذكاء الاصطناعي في الطب الشخصي إمكانات تحويلية، فإنه يقدم أيضًا مجموعة من التحديات التي يجب معالجتها. بخلاف خصوصية البيانات والتحيز الخوارزمي، تشمل المخاوف الكبيرة التوافقية ودمج البيانات عبر أنظمة الرعاية الصحية المتنوعة، وضمان امتثال أنظمة الذكاء الاصطناعي للمعايير التنظيمية والأخلاقية، وإثبات صلاحيتها السريرية وموثوقيتها.
3. الذكاء الاصطناعي في عمليات وإدارة المستشفيات
يتم الاستفادة منها لإحداث ثورة في عمليات المستشفيات، مما يعزز الكفاءة، ويقلل التكاليف، ويحسن رعاية المرضى. سنستكشف ثلاثة مجالات رئيسية: دور الذكاء الاصطناعي في تحسين اللوجستيات وإدارة الموارد، وتطبيقه في أتمتة المهام الإدارية، ومساهمته في تحسين تدفق المرضى وجدولة المواعيد.
| جانب | التطبيقات | ||
| الذكاء الاصطناعي لإدارة اللوجستيات والموارد في المستشفيات | إدارة المخزون التنبؤية للإمدادات الطبية والأدوية والمعدات؛ إدارة المرافق بكفاءة بما في ذلك أنظمة التدفئة والتهوية وتكييف الهواء والصيانة التنبؤية؛ تحسين تخصيص الموارد للموظفين والمواد؛ وتحسين وإدارة سلسلة الإمداد خلال الطوارئ والأزمات الصحية. | ||
| أتمتة المهام الإدارية باستخدام الذكاء الاصطناعي | إدارة بيانات المرضى بما في ذلك السجلات الطبية الإلكترونية وتحليل البيانات غير المنظمة؛ أتمتة الفوترة ومعالجة المطالبات لضمان الدقة والامتثال؛ أنظمة جدولة مدفوعة بالذكاء الاصطناعي للمواعيد والإجراءات؛ أتمتة إدارة الوثائق والمعالجة؛ التواصل التلقائي والتذكيرات لمشاركة المرضى؛ ومراقبة أمان البيانات والامتثال. | ||
| الذكاء الاصطناعي في تحسين تدفق المرضى وجدولة المواعيد |
|
3.1. الذكاء الاصطناعي لإدارة اللوجستيات والموارد في المستشفيات
- إدارة المخزون: يتم استخدام أنظمة الذكاء الاصطناعي لإدارة المخزون بشكل استباقي في المستشفيات. من خلال تحليل أنماط الاستخدام، وتدفق المرضى، وبيانات أخرى ذات صلة، يمكن للذكاء الاصطناعي التنبؤ بالحاجة إلى المستلزمات الطبية، والأدوية، والمعدات. تضمن هذه القدرة التنبؤية أن تحافظ المستشفيات على مستويات المخزون المثلى، مما يقلل من الفاقد ويضمن توفر المستلزمات الحيوية عند الحاجة.
- إدارة المرافق: تساهم الذكاء الاصطناعي أيضًا في الإدارة الفعالة لمرافق المستشفيات. على سبيل المثال، يمكن للأنظمة المدعومة بالذكاء الاصطناعي التحكم في أنظمة التدفئة والتهوية وتكييف الهواء (HVAC) بشكل أكثر كفاءة، مما يقلل من تكاليف الطاقة مع الحفاظ على بيئة مريحة للمرضى والموظفين. بالإضافة إلى ذلك، يمكن أن يساعد الذكاء الاصطناعي في الصيانة التنبؤية لمعدات المستشفيات، من خلال تحديد المشكلات المحتملة قبل أن تؤدي إلى أعطال، مما يقلل من فترات التوقف وتكاليف الإصلاح.
- تخصيص الموارد: واحدة من أبرز تطبيقات الذكاء الاصطناعي في إدارة المستشفيات هي في تحسين تخصيص الموارد. يمكن لخوارزميات الذكاء الاصطناعي تحليل مجموعات بيانات معقدة، بما في ذلك دخول المرضى، وتوافر الموظفين، والقدرات التشغيلية، لتحسين تخصيص الموارد البشرية والمادية. يشمل ذلك
جدولة العمليات الجراحية والإجراءات الطبية بطريقة تعظم من استخدام غرف العمليات والطاقم الطبي، مع تقليل أوقات انتظار المرضى. - تحسين سلسلة التوريد: تعزز الذكاء الاصطناعي عمليات سلسلة التوريد في المستشفيات من خلال تحليل الاتجاهات وأتمتة عمليات الطلب [66،67]. يمكنه توقع الاضطرابات في سلسلة التوريد واقتراح حلول بديلة، مما يضمن عدم تأثر عمليات المستشفى بالتحديات الخارجية في سلسلة التوريد. في حالات الطوارئ أو خلال الأزمات الصحية، تلعب أنظمة الذكاء الاصطناعي دورًا حاسمًا في إدارة اللوجستيات والموارد [68]. يمكنها تحليل الوضع بسرعة، وتوقع الموارد المطلوبة، والمساعدة في التوزيع الفعال لهذه الموارد حيثما كانت هناك حاجة إليها أكثر.
في الختام، فإن دور الذكاء الاصطناعي في لوجستيات المستشفيات وإدارة الموارد متعدد الأبعاد وله تأثير عميق. من خلال أتمتة وتحسين هذه الجوانب الحيوية، يمكن للذكاء الاصطناعي أن يحقق كفاءات تشغيلية ويعزز الجودة العامة لرعاية المرضى. مع استمرار تقدم تكنولوجيا الذكاء الاصطناعي، فإن إمكانيته في إحداث ثورة أكبر في عمليات وإدارة المستشفيات واسعة، مما يفتح آفاق جديدة للابتكار في تقديم الرعاية الصحية.
3.2. أتمتة المهام الإدارية باستخدام الذكاء الاصطناعي
- إدارة بيانات المرضى: تلعب الذكاء الاصطناعي دورًا مهمًا في إدارة كميات هائلة من بيانات المرضى. يمكن أن تنظم أنظمة الذكاء الاصطناعي وتصنف وتعالج سجلات المرضى والمواعيد وتواريخ العلاج بكفاءة ودقة عالية. يمكن لهذه الأنظمة أيضًا استخراج المعلومات ذات الصلة من البيانات غير المهيكلة، مثل ملاحظات الأطباء، مما يسهل على مقدمي الرعاية الصحية الوصول إلى معلومات المرضى وتحليلها. على سبيل المثال، استخدمت دراسة الذكاء الاصطناعي ومعالجة اللغة الطبيعية (NLP) لتحليل السجلات الطبية الإلكترونية (EMRs)، مع التركيز على ملاحظات الاستشارة غير المشفرة لتوقع الأمراض. تم تطبيق تقنيات مثل حقيبة الكلمات ونمذجة الموضوعات، بالإضافة إلى طريقة لمطابقة الملاحظات مع أنطولوجيا طبية. تم اختبار هذا النهج بشكل خاص لسرطان القولون والمستقيم. وجدت الدراسة أن الطريقة المعتمدة على الأنطولوجيا حسنت بشكل كبير من الأداء التنبؤي، مع AUC قدره 0.870، متجاوزة المعايير التقليدية. يبرز هذا إمكانيات الذكاء الاصطناعي في استخراج معلومات مفيدة من البيانات غير المهيكلة في السجلات الطبية الإلكترونية، مما يحسن دقة توقع الأمراض.
- معالجة الفواتير والمطالبات: يمكن أيضًا استخدام خوارزميات الذكاء الاصطناعي لأتمتة معالجة الفواتير ومطالبات التأمين. يمكنها تحليل ومعالجة بيانات المطالبات بسرعة، وتحديد الأخطاء أو الت inconsistencies، وضمان أن تكون الفواتير دقيقة ومتوافقة مع اللوائح ذات الصلة. لا يسرع هذا فقط من عملية التعويض ولكن أيضًا يقلل من احتمالية حدوث أخطاء في الفواتير، مما يؤدي إلى تحسين العمليات المالية ورضا المرضى. على سبيل المثال، استخدمت دراسة في قطاع التأمين التعلم الآلي لتحسين دقة تقدير احتياطي الخسائر، وهو أمر حاسم للبيانات المالية. بعيدًا عن النماذج التقليدية على المستوى الكلي، استخدمت هذه الطريقة بيانات المطالبات الفردية، مدمجةً تفاصيل حول السياسات، وأصحاب السياسات، والمطالبات. عالجت الطريقة تحدي المتغيرات المقيدة من خلال إنشاء مجموعات بيانات مخصصة لتدريب وتقييم الخوارزميات. مقارنةً بطريقة السلم التقليدية، أظهرت هذه الطريقة المدفوعة بالذكاء الاصطناعي تحسينات ملحوظة في الدقة، كما يتضح من دراسة حالة حقيقية مع محفظة تأمين قروض هولندية.
- جدولة المواعيد: أنظمة الجدولة المدفوعة بالذكاء الاصطناعي تُحدث ثورة في طريقة إدارة المواعيد في بيئات الرعاية الصحية. يمكن لهذه الأنظمة تحليل الأنماط في حجز المواعيد وإلغائها لتحسين جدولة المرضى. من خلال التنبؤ بأوقات الذروة وضبط المواعيد وفقًا لذلك، يساعد الذكاء الاصطناعي في تقليل أوقات الانتظار وتحسين تدفق المرضى. على سبيل المثال، مشروع يهدف إلى تقليل عدم حضور المرضى في مواعيد التصوير بالرنين المغناطيسي الخارجي استخدم بفعالية تحليلات التنبؤ بالذكاء الاصطناعي. في هذه المبادرة لتحسين الجودة، تم تحليل أكثر من 32,000 سجل لمواعيد التصوير بالرنين المغناطيسي الخارجي المجهولة الهوية باستخدام تقنيات التعلم الآلي، وبالتحديد نموذج XGBoost، وهو خوارزمية تجميع قائمة على شجرة القرار. حققت هذه الطريقة
نتائج ملحوظة؛ تم إثبات دقة النموذج التنبؤية من خلال AUC ROC قدره 0.746 ودرجة F1 محسّنة قدرها 0.708. عند تنفيذها جنبًا إلى جنب مع تدخل عملي يتمثل في تذكير المرضى عبر الهاتف الذين تم تحديدهم على أنهم عاليي المخاطر لعدم الحضور، انخفض معدل عدم الحضور منإلى على مدى ستة أشهر. في دراسة أخرى، تم استخدام نهج قائم على البيانات لتحسين جدولة المواعيد وتسلسلها، خاصة في البيئات التي تتميز بمدد خدمة غير مؤكدة وموعد وصول العملاء [75]. من خلال الاستفادة من طريقة جديدة تعتمد على طوابير الخوادم اللانهائية، طورت الدراسة حلولًا قابلة للتوسع مناسبة للأنظمة المعقدة التي تحتوي على العديد من الوظائف والخوادم. تم اختبارها باستخدام مجموعة بيانات شاملة من وحدة تسريب مركز السرطان، وقد حسنت هذه الطريقة بشكل كبير الكفاءة التشغيلية. أظهرت النتائج انخفاضًا مستمرًا في التكاليف – من خلال دمج أوقات الانتظار وساعات العمل الإضافية – بنسبة إلى ، مما يدل على فعالية الاستراتيجيات المعتمدة على الذكاء الاصطناعي في تحسين جدولة المواعيد. - إدارة الوثائق ومعالجتها: تقنيات الذكاء الاصطناعي بارعة في أتمتة معالجة مستندات متنوعة، بما في ذلك نماذج الموافقة، ونماذج القبول، والتقارير الطبية [76]. من خلال استخدام معالجة اللغة الطبيعية (NLP) وتعلم الآلة، يمكن للذكاء الاصطناعي بسرعة تحليل المستندات، واستخراج المعلومات ذات الصلة، وتصنيفها بشكل مناسب. تقلل هذه الأتمتة من العبء الإداري على الموظفين وتسريع معالجة الوثائق.
- التواصل التلقائي والتذكيرات: تطبيق ملحوظ للذكاء الاصطناعي في الرعاية الصحية هو تحسين استخراج المعلومات من السجلات الصحية الإلكترونية (EHRs)، وخاصة من المستندات الممسوحة. أظهرت دراسة ذلك من خلال استخراج مؤشرات انقطاع النفس النومي بنجاح من تقارير دراسة النوم الممسوحة باستخدام مجموعة من تقنيات معالجة الصور ومعالجة اللغة الطبيعية (NLP) [77]. من خلال استخدام طرق مثل تحويل الصورة إلى تدرجات الرمادي وOCR مع Tesseract، تلاها تحليل من خلال نماذج متقدمة مثل ClinicalBERT، حققت الدراسة معدلات دقة عالية (أكثر من
) في تحديد المقاييس الصحية الرئيسية. - التواصل التلقائي والتذكيرات: يتم استخدام الدردشة الآلية والمساعدين الافتراضيين المدعومين بالذكاء الاصطناعي بشكل متزايد للتواصل مع المرضى. يمكنهم التعامل مع الاستفسارات الروتينية، وتقديم معلومات حول الخدمات، وإرسال تذكيرات للمواعيد القادمة أو جداول الأدوية. لا يعزز هذا فقط تفاعل المرضى ولكن أيضًا يحرر الموظفين للتركيز على المهام الأكثر أهمية. مثال على هذا التطبيق يظهر في مشروع ChronologyMD [78]، الذي استخدم الذكاء الاصطناعي لتحسين برامج التواصل الصحي الإلكتروني. عالج المشروع أوجه القصور الرئيسية في استراتيجيات التواصل الصحي الإلكتروني الحالية، التي غالبًا ما فشلت في جذب الجمهور بالكامل وأثرت أحيانًا سلبًا على تقديم المعلومات الصحية الحيوية. من خلال استخدام الذكاء الاصطناعي بشكل استراتيجي، نجح مشروع ChronologyMD في جعل التواصل الصحي أكثر جذبًا وملاءمة وقابلية للتنفيذ. بالإضافة إلى ذلك، أدى ذلك إلى زيادة التعرض للرسائل ذات الصلة، وتقليل عبء العمل على موظفي الرعاية الصحية، وتحسين الكفاءة العامة للبرنامج مع تقليل التكاليف.
- أمان البيانات والامتثال: تساهم أنظمة الذكاء الاصطناعي بشكل كبير في أمان البيانات والامتثال في الرعاية الصحية [79]. يمكنها مراقبة وتحليل أنماط الوصول إلى البيانات لاكتشاف ومنع الوصول غير المصرح به أو الانتهاكات. بالإضافة إلى ذلك، يمكن للذكاء الاصطناعي ضمان أن العمليات الإدارية تتوافق مع اللوائح الصحية، مثل HIPAA، مما يحمي خصوصية المرضى. بناءً على ذلك، استكشفت الأبحاث الحديثة دور الذكاء الاصطناعي في ضمان الامتثال للائحة العامة لحماية البيانات (GDPR)، وهو أمر حاسم لمراقبي البيانات [80]. كانت هذه الدراسة تهدف إلى سد الفجوات في فحص الامتثال من خلال نهج مزدوج: أولاً، من خلال تصور إطار لفحص الامتثال القائم على الوثائق في سلسلة توريد البيانات، وثانيًا، من خلال تطوير طرق لأتمتة فحص الامتثال لسياسات الخصوصية. اختبرت الدراسة نظامًا مكونًا من وحدتين، حيث تستخدم الوحدة الأولى معالجة اللغة الطبيعية (NLP) لاستخراج ممارسات البيانات من سياسات الخصوصية، وتشفّر الوحدة الثانية قواعد GDPR لضمان تضمين جميع المعلومات الإلزامية. أظهرت النتائج أن هذا النهج من النص إلى النص كان أكثر فعالية
من المصنفات المحلية، وقادرًا على استخراج كل من المعلومات العامة والخاصة بنموذج واحد. تم التحقق من فعالية النظام على مجموعة بيانات من 30 سياسة خصوصية، تم التعليق عليها من قبل خبراء قانونيين.
باختصار، فإن أتمتة المهام الإدارية باستخدام الذكاء الاصطناعي تعزز بشكل كبير كفاءة ودقة عمليات المستشفى. يسمح ذلك للمهنيين في الرعاية الصحية بالتركيز أكثر على رعاية المرضى بدلاً من الواجبات الإدارية، مما يؤدي إلى تحسين تقديم الرعاية الصحية. مع استمرار تطور تقنية الذكاء الاصطناعي، يمكن أن تتقدم من أتمتة المهام إلى تخصيص تفاعلات المرضى من خلال الذكاء العاطفي والوعي الثقافي، بهدف تقديم تجربة رعاية أكثر شمولية ودعمًا.
3.3. الذكاء الاصطناعي في تحسين تدفق المرضى وجدولة المواعيد
- تحسين تدفق المرضى: تعتبر خوارزميات الذكاء الاصطناعي بارعة بشكل خاص في تحليل الأنماط في قبول المرضى، والتفريغ، والتحويلات، مما يمكّن من تدفق أكثر كفاءة للمرضى في جميع أنحاء المستشفى [65،81]. من خلال التنبؤ بفترات الطلب العالي، يمكن للذكاء الاصطناعي المساعدة في تخصيص الموارد مسبقًا مثل الأسرة، والموظفين، والمعدات لتلبية احتياجات المرضى. على سبيل المثال، يمكن لأنظمة الذكاء الاصطناعي التنبؤ بالتقلبات اليومية أو الموسمية في قبول المرضى، مما يسمح للمستشفيات بتعديل مستويات التوظيف وتوافر الأسرة وفقًا لذلك [82]. يقلل هذا النهج الاستباقي من الاختناقات، ويقلل من أوقات الانتظار، ويعزز تجربة المرضى بشكل عام.
- أنظمة الجدولة الديناميكية: تحدث أنظمة الجدولة المدفوعة بالذكاء الاصطناعي ثورة في طريقة تنظيم المواعيد والإجراءات. يمكن لهذه الأنظمة تحليل متغيرات متعددة، بما في ذلك توافر مقدمي الرعاية الصحية، وتفضيلات المرضى، وعجلة الرعاية، لإنشاء جداول مثالية. من خلال القيام بذلك، تقلل من عدم حضور المواعيد والإلغاءات في اللحظة الأخيرة، مما يزيد من استخدام وقت المهنيين في الرعاية الصحية. علاوة على ذلك، يمكن لهذه الأنظمة الذكية التكيف في الوقت الفعلي مع التغييرات، مثل الحالات الطارئة، من خلال إعادة جدولة المواعيد غير العاجلة دون حدوث اضطرابات كبيرة [83]. في دراسة تهدف إلى تحسين كفاءة قسم العيادات الخارجية ورضا المرضى، طور الباحثون نظام جدولة مواعيد مبتكر يعتمد على نموذج عملية قرار ماركوف، مع دمج تفضيلات المرضى لتعظيم الرضا [84]. تم استخدام خوارزميات البرمجة الديناميكية التكيفية للتغلب على تعقيد الجدولة، مع التكيف ديناميكيًا مع تفضيلات المرضى وتحسين قرارات المواعيد باستمرار. تم تقييم أداء النظام من خلال تجارب متنوعة، والتي أظهرت سلوك تقارب مثالي ودقة.
- تقليل أوقات الانتظار: واحدة من الفوائد الرئيسية للذكاء الاصطناعي في تدفق المرضى هي تقليل أوقات الانتظار في أقسام الطوارئ والعيادات الخارجية. يمكن للذكاء الاصطناعي التنبؤ بتدفق المرضى وتحديد التأخيرات المحتملة، مما يسمح لموظفي المستشفى باتخاذ تدابير استباقية لإدارة أوقات انتظار المرضى بشكل فعال [85،86]. بالنسبة لأقسام الطوارئ، يعني ذلك تحسين عمليات الفرز وتخصيص المرضى بسرعة للرعاية المناسبة. باستخدام خوارزميات تعلم الآلة، توقعت دراسة حديثة أوقات انتظار المرضى قبل الاستشارة ووقت المرور في عيادة خارجية، بهدف تعزيز رضا المرضى من خلال تقديم معلومات أكثر دقة حول أوقات الانتظار [87]. استخدمت الدراسة خوارزميات الغابة العشوائية وXGBoost، مع تحليل متغيرات الإدخال مثل الجنس، ويوم ووقت الزيارة، وجلسة الاستشارة. حققت الدراسة دقة عالية (
في التنبؤ بأوقات الانتظار والإنتاجية في عيادة خارجية باستخدام نماذج التعلم الآلي مع متغيرات إدخال جديدة. - تعزيز تجربة المريض: يمكن أن تعمل أنظمة الذكاء الاصطناعي أيضًا على تحسين تجربة المريض بشكل عام من خلال توفير معلومات دقيقة حول مواعيد المواعيد، وفترات الانتظار، وجداول العلاج. تساعد هذه الشفافية في إدارة توقعات المرضى وتقلل من القلق المرتبط بالمواعيد والإجراءات الطبية.
في دراسة حديثة، تم تطوير نموذج تعلم آلي للتنبؤ باستجابات المرضى في مجال “اتصالات الأطباء” في استبيان تقييم المستهلكين لمقدمي الرعاية الصحية والأنظمة، باستخدام بيانات من مستشفى رعاية ثالثية (2016-2020) [89]. وقد تنبأ خوارزمية الغابة العشوائية بفعالية باستجابات المرضى حول أدب الأطباء، ووضوح الشرح، والانتباه. حقق النموذج AUC قدرهلهذه الأسئلة المتعلقة باستطلاع رأي التواصل مع الأطباء. - الاندماج مع الرعاية الصحية عن بُعد: في عصر الصحة الرقمية، يمتد استخدام الذكاء الاصطناعي في جدولة المواعيد إلى ما هو أبعد من المواعيد الشخصية ليشمل خدمات الرعاية الصحية عن بُعد. يمكن أن تقوم أنظمة الذكاء الاصطناعي بجدولة وإدارة الاستشارات الافتراضية بفعالية، مما يضمن حصول المرضى على الرعاية في الوقت المناسب دون الحاجة لزيارة المنشأة الصحية فعليًا، وهو ما يكون مفيدًا بشكل خاص للمتابعات الروتينية أو خلال الأزمات الصحية مثل الأوبئة.
في الختام، فإن دور الذكاء الاصطناعي في تحسين تدفق المرضى وجدولة المواعيد في المستشفيات والعيادات هو تحول عميق، حيث يقدم تحسينات كبيرة في الكفاءة التشغيلية، وتقليل أوقات الانتظار، وتحسين تجارب المرضى. كعنصر مهم في تحديث تقديم الرعاية الصحية، فإن استراتيجيات التحسين المدفوعة بالذكاء الاصطناعي أصبحت أكثر أهمية. مع النظر إلى المستقبل، فإن تكنولوجيا الذكاء الاصطناعي مستعدة لمزيد من التطور، مع تقدم محتمل يشمل خوارزميات جدولة تكيفية في الوقت الحقيقي، ودمج أعمق مع السجلات الصحية الإلكترونية لتقديم رعاية أكثر تخصيصًا للمرضى، واستخدام التحليلات التنبؤية لتوقع طلب المرضى وتخصيص الموارد.
4. الذكاء الاصطناعي في التصوير الطبي والتشخيص
4.1. دور الذكاء الاصطناعي في الأشعة وعلم الأمراض
على سبيل المثال، في الهند، تم استخدام برنامج مدعوم بالذكاء الاصطناعي لتحليل العلامات الجزيئية الرئيسية في الصور التنظيرية، مما يتيح تشخيصات أكثر دقة لسرطان المعدة، مما قد يمهد الطريق لأساليب علاج مخصصة.
4.2. تعزيز الدقة والكفاءة في عمليات التشخيص
- تحسين دقة التشخيص: أظهرت خوارزميات الذكاء الاصطناعي، وخاصة تلك المعتمدة على التعلم العميق، دقة ملحوظة في تشخيص الأمراض من الصور الطبية ونتائج الاختبارات. تم تدريب هذه الأنظمة على مجموعات بيانات ضخمة، مما يسمح لها بالتعرف على الأنماط والشذوذات التي قد تكون غير مرئية للعين البشرية. على سبيل المثال، في علم الأمراض الجلدية، أظهرت أنظمة الذكاء الاصطناعي المدربة على صور آفات الجلد القدرة على اكتشاف سرطانات الجلد، مثل الميلانوما، بدقة تعادل تلك التي يتمتع بها أطباء الجلدية ذوو الخبرة.
- تقليل الأخطاء التشخيصية: واحدة من الفوائد الرئيسية للذكاء الاصطناعي في التشخيص هي قدرته على تقليل الأخطاء. التشخيص الخاطئ والتشخيصات المفقودة هما من القضايا المهمة في الطب، وغالبًا ما يؤديان إلى تأخير أو علاج غير مناسب. توفر أنظمة الذكاء الاصطناعي مستوى من الاتساق والانتباه للتفاصيل يصعب على البشر الحفاظ عليه على مدى فترات طويلة، مما يقلل من احتمال حدوث مثل هذه الأخطاء.
- تسريع عمليات التشخيص: الذكاء الاصطناعي يسرع بشكل كبير من عملية التشخيص. تحليل الصور الطبية أو نتائج الاختبارات، وهي مهام قد تستغرق وقتًا طويلاً من قبل متخصصي الرعاية الصحية، يمكن أن يتم بواسطة الذكاء الاصطناعي في جزء من الوقت. هذا التحليل السريع مفيد بشكل خاص في حالات الرعاية العاجلة، حيث يكون اتخاذ القرارات السريعة أمرًا حاسمًا. على سبيل المثال، يمكن لخوارزميات الذكاء الاصطناعي تحليل صور الأشعة المقطعية لمرضى السكتة الدماغية بسرعة لتحديد الانسدادات أو النزيف في الدماغ، مما يتيح بدء العلاجات المنقذة للحياة بشكل أسرع.
- التقارير الآلية والتوثيق: لا تقوم الذكاء الاصطناعي فقط بأتمتة التقارير والتوثيق في العمليات التشخيصية [107] ولكنها تعزز أيضًا جودة هذه العمليات. بينما تولد أنظمة الذكاء الاصطناعي تقارير أولية من تحليل الصور لمراجعة أطباء الأشعة، مما يسهل سير العمل ويقلل من العبء الإداري، فقد زادت دراسة حديثة من هذه الكفاءة من خلال توحيد إرشادات التقارير الحالية الخاصة بالتعلم الآلي [108]. بعد مراجعة شاملة لـ 192 مقالة وتعليقات الخبراء، أنشأت هذه الدراسة قائمة شاملة تضم 37 عنصرًا للتقارير لدراسات التعلم الآلي التنبؤية والتشخيصية. إن هذا الجهد في توحيد تقارير التعلم الآلي يعد محوريًا في تحسين جودة وقابلية تكرار دراسات نمذجة التعلم الآلي، مما يكمل دور الذكاء الاصطناعي في تبسيط التقارير التشخيصية.
- دمج البيانات التشخيصية: يتفوق الذكاء الاصطناعي في دمج وتحليل البيانات من مصادر متنوعة. في حالة الأمراض المعقدة، يمكن للذكاء الاصطناعي دمج المعلومات من التصوير، والاختبارات المعملية، وتاريخ المرضى لتقديم تشخيص أكثر شمولاً.
تقديم رؤى [109]. تعتبر هذه الدمج ذات قيمة خاصة في تشخيص الحالات المعقدة مثل الأمراض المناعية الذاتية أو في الحالات التي تكون فيها الأعراض غامضة. كمثال، استعرضت دراسة شاملة تقنيات الذكاء الاصطناعي لدمج البيانات الطبية متعددة الأنماط، وخاصة السجلات الصحية الإلكترونية مع التصوير الطبي، لتطوير طرق الذكاء الاصطناعي لتطبيقات سريرية متنوعة [110]. قامت المراجعة بتحليل 34 دراسة، ملاحظة سير العمل الذي يجمع البيانات الخام باستخدام خوارزميات التعلم الآلي أو التعلم العميق لتوقع النتائج السريرية. وجدت أن نماذج دمج الأنماط المتعددة تتفوق عمومًا على نماذج النمط الواحد، مع كون الدمج المبكر هو التقنية الأكثر استخدامًا. كانت الاضطرابات العصبية هي الفئة السائدة التي تم دراستها، وكانت نماذج التعلم الآلي التقليدية تستخدم بشكل أكثر تكرارًا من نماذج التعلم العميق. توفر هذه المراجعة رؤى حول الحالة الحالية لدمج البيانات الطبية متعددة الأنماط في أبحاث الرعاية الصحية.
في الختام، يلعب الذكاء الاصطناعي دورًا كبيرًا في تحسين دقة وكفاءة التشخيص، مما يحول الرعاية الصحية، ويقدم تشخيصات أسرع وأكثر دقة. ومع ذلك، فإن القلق الرئيسي هو أن هذه الأنظمة الذكية غالبًا ما تكون مصممة بشكل أساسي لمجموعات معينة، مما قد يؤدي إلى تفاوت في الرعاية الصحية. يجب أن تركز التطورات المستقبلية على تطوير نماذج ذكاء اصطناعي أكثر شمولاً تلبي احتياجات شريحة أوسع من المرضى، مما يضمن تحسينات عادلة في الرعاية الصحية عبر جميع السكان.
4.3. دور تسريع الأجهزة في التشخيص المدعوم بالذكاء الاصطناعي
- وحدات معالجة الرسوميات (GPUs): تم تصميمها في الأصل لتقديم الرسوميات الحاسوبية، تتفوق وحدات معالجة الرسوميات في المعالجة المتوازية، مما يجعلها مثالية للتعامل مع مجموعات البيانات الضخمة والحسابات المعقدة المعنية بخوارزميات الذكاء الاصطناعي. في مجال تحليل الصور الطبية، يمكن استخدام وحدات معالجة الرسوميات لتسريع عمليات معالجة الصور الأساسية مثل التصفية والتداخل. بالإضافة إلى ذلك، يمكن لوحدات معالجة الرسوميات تعزيز تشغيل خوارزميات الذكاء الاصطناعي المختلفة المستخدمة في مهام التصوير الطبي مثل تسجيل الصور، وتقسيم الصور، وإزالة الضوضاء من الصور، وتصنيف الصور [113].
- وحدات معالجة التنسور (TPUs): تعتبر الشرائح المصممة خصيصًا مثل وحدات معالجة التنسور، التي ابتكرتها شركات مثل جوجل، مثالية للتعلم العميق عالي الأداء، وهي تقنية رئيسية مستخدمة في تحليل الصور الطبية. تقدم وحدات معالجة التنسور مزايا سرعة كبيرة مقارنة بوحدات المعالجة المركزية في مهام مثل التعرف على الصور وتصنيفها. على سبيل المثال، نفذ الباحثون نظامًا لتشخيص الزرق باستخدام كل من وحدات معالجة التنسور ووحدات معالجة الرسوميات المدمجة [114]. بينما حقق كلاهما تقسيم وتصنيف سريع للصور لدعم التشخيص في الوقت الحقيقي، وجدت الدراسة أن وحدات معالجة التنسور تستهلك طاقة أقل بكثير مقارنة بوحدات معالجة الرسوميات. وهذا يجعل وحدات معالجة التنسور خيارًا أكثر جاذبية للأجهزة الطبية التي تعمل بالبطارية المستخدمة في سيناريوهات الحوسبة الطرفية.
- المصفوفات القابلة للبرمجة في الميدان (FPGAs): تقدم هذه الشرائح المتعددة الاستخدامات مرونة لتخصيص الأجهزة. على عكس وحدات معالجة الرسوميات ووحدات معالجة التنسور المصممة مسبقًا، يمكن برمجة وحدات FPGA لأداء خوارزميات ذكاء اصطناعي محددة، مما قد يؤدي إلى حلول محسنة للغاية لبعض المهام التشخيصية. ومع ذلك، يتطلب برمجة وحدات FPGA خبرة متخصصة. على سبيل المثال، اقترح الباحثون مسرع MobileNet مصمم خصيصًا لوحدات FPGA يركز على تقليل استخدام الذاكرة على الشريحة
ونقل البيانات، مما يجعله مثاليًا للأجهزة منخفضة الطاقة [115]. يحققون ذلك من خلال استخدام وحدتين قابلتين للتكوين لعمليات الالتفاف المختلفة وطريقة جديدة لاستخدام الذاكرة المؤقتة. توضح تنفيذاتهم معالجة في الوقت الحقيقي مع استخدام منخفض للذاكرة، مما يجعل وحدات FPGA خيارًا قابلاً للتطبيق لتشغيل الشبكات العصبية التلافيفية الفعالة في المهام الطبية المساعدة على الأجهزة المحمولة. - الدوائر المتكاملة الخاصة بالتطبيقات (ASICs): عند التعامل مع خوارزمية ذكاء اصطناعي محددة جيدًا في تطبيق تشخيصي معين، يمكن تصميم ASICs لتقديم الأداء الأمثل [116]. مصممة لمهمة واحدة، توفر ASICs كفاءة وسرعة معالجة لا مثيل لهما لتلك الوظيفة المحددة. ومع ذلك، فإن نقص المرونة يحد من تطبيقها على الخوارزميات المعروفة والثابتة.
من خلال الاستفادة من تسريع الأجهزة، يمكن للتشخيصات المدعومة بالذكاء الاصطناعي تحقيق عدة فوائد: معالجة أسرع لتحليل الصور الطبية في الوقت القريب من الحقيقي، مما يؤدي إلى تدخلات أسرع وقد تكون منقذة للحياة؛ تحسين الدقة من خلال القدرة على إجراء تحليل معقد للصور، مما قد يؤدي إلى درجة أعلى من اكتشاف الأمراض؛ وزيادة الكفاءة من خلال تبسيط عملية التشخيص، مما يسمح لأطباء الأشعة والأطباء بتحليل المزيد من الصور في فترة زمنية أقصر.
4.4. أمثلة على أنظمة الذكاء الاصطناعي المستخدمة في التصوير
| نمط التصوير | التطبيق | مثال على نظام الذكاء الاصطناعي | الأثر |
| التصوير بالرنين المغناطيسي | تشمل تطبيقات الذكاء الاصطناعي في تحليل التصوير بالرنين المغناطيسي اكتشاف الشذوذ في الدماغ، والأورام، والسكتات الدماغية، والأمراض التنكسية العصبية، والمزيد. يمكن للذكاء الاصطناعي تحليل الصور وقياس حجم المناطق المتأثرة. | نظام ذكاء اصطناعي يحلل صور التصوير بالرنين المغناطيسي لاكتشاف الشذوذ في الدماغ، مثل الأورام أو السكتات الدماغية، ويقيس حجمها، مما يساعد في تخطيط العلاج [118]. | تحسين اكتشاف الأورام، والسكتات الدماغية، والأمراض التنكسية العصبية؛ قياس المناطق المتأثرة يساعد في تخطيط العلاج ومراقبة الأمراض. |
| التصوير المقطعي المحوسب | تشمل الذكاء الاصطناعي في تفسير الأشعة المقطعية الكشف عن عقيدات الرئة، وتحديد الكسور والنزيف، وتقييم شدة السكتة الدماغية، وتوصيف تقدم الأورام. يمكن أن تعالج أنظمة الذكاء الاصطناعي الأشعة المقطعية بسرعة ودقة، مما يساعد في التشخيص في الوقت المناسب. | نموذج الذكاء الاصطناعي يشخص سرطان الرئة بدقة عالية وتقليل الإيجابيات الكاذبة، مما يحسن دقة التشخيص [119]. | كشف أسرع للحالات المهددة للحياة؛ دقة محسّنة مقارنة بالطرق التقليدية؛ إمكانية إنقاذ الأرواح في حالات الطوارئ. |
| نمط التصوير | تطبيق | مثال على نظام الذكاء الاصطناعي | أثر |
| أشعة سينية | تطبيقات الذكاء الاصطناعي في الأشعة السينية تعزز تحليل الصور لاكتشاف الأورام، مما يحسن الدقة ويقلل من الإيجابيات الكاذبة والسلبية. تعمل أنظمة الذكاء الاصطناعي كمراجع ثانٍ، مما يعزز حساسية فحص السرطان. | تحسن خوارزميات CAD المعتمدة على الذكاء الاصطناعي بشكل كبير من حساسية أطباء الأشعة في اكتشاف سرطان الثدي، مما يقلل من النتائج السلبية الكاذبة ويزيد من معدلات اكتشاف السرطان [120]. | زيادة الحساسية في اكتشاف آفات سرطان الثدي؛ تقليل النتائج الإيجابية الكاذبة والسلبية الكاذبة؛ تحسين دقة تشخيص أطباء الأشعة. |
| الموجات فوق الصوتية | تساعد الذكاء الاصطناعي في تحليل صور تخطيط صدى القلب لتقييم وظيفة القلب والأوعية الدموية واكتشاف التشوهات الهيكلية في القلب. تقيس أنظمة الذكاء الاصطناعي معايير مثل نسبة الطرد وتساعد في تشخيص وإدارة أمراض القلب. | خوارزمية ذكاء اصطناعي جديدة تحسب بدقة زمن قذف البطين الأيسر في تخطيط صدى القلب، مما يوفر مقاييس موثوقة لتقييم وظيفة القلب [121]. | تقييم دقيق للمعايير القلبية الوعائية؛ تقليل التباين المعتمد على المستخدم؛ تعزيز الفائدة السريرية في تخطيط صدى القلب. |
- الذكاء الاصطناعي في تحليل الرنين المغناطيسي: تطبيقات الذكاء الاصطناعي في تحليل الرنين المغناطيسي متعددة الاستخدامات، تشمل الكشف عن الشذوذات الدماغية، الأورام، السكتات الدماغية، الأمراض التنكسية العصبية، إصابات الجهاز العضلي الهيكلي، الحالات القلبية، وأمراض الكبد وأعضاء البطن، بالإضافة إلى تقييم سرطان الثدي وسرطان البروستاتا، مما يظهر فائدته الواسعة في تشخيص مجموعة متنوعة من الحالات الطبية. بالإضافة إلى ذلك، يلعب التعلم العميق الآن دورًا رئيسيًا في تسريع عملية الحصول على صور الرنين المغناطيسي. مثال على تطبيق الذكاء الاصطناعي في الرنين المغناطيسي هو نظام ذكاء اصطناعي تم تطويره للكشف عن الشذوذات الدماغية. يستخدم هذا النظام شبكة عصبية تلافيفية عميقة لتحليل صور الرنين المغناطيسي ويمكنه تحديد حالات مثل الأورام، السكتات الدماغية، والأمراض التنكسية العصبية. لا يكتفي الذكاء الاصطناعي بالكشف عن هذه الشذوذات، بل يساعد أيضًا في قياس حجم المناطق المتأثرة، وهو أمر حيوي لتخطيط العلاج ومراقبة تقدم المرض. مثال آخر هو تطبيق الذكاء الاصطناعي في تفسير سرطان الثدي. يتم استخدام الشبكات العصبية التلافيفية لاستخراج الميزات من صور الرنين المغناطيسي للثدي، وبالتعاون مع المصنفات، فإنها تكشف بفعالية عن وجود السرطان، مما يظهر إمكانيات الذكاء الاصطناعي في تعزيز دقة التشخيص في الكشف عن سرطان الثدي. تُستخدم أنظمة الذكاء الاصطناعي بشكل متزايد للتقسيم التلقائي للصور في الأشعة. يمكن لهذه الأنظمة التمييز بين الهياكل التشريحية المختلفة في الصور، مثل الأعضاء والأنسجة، مما يساعد أطباء الأشعة في التشخيص وتخطيط العمليات الجراحية أو العلاجات. على سبيل المثال، قدمت دراسة نموذج تعلم عميق ثلاثي الأبعاد، يجمع بين الالتفاف ثلاثي الأبعاد وLSTM، للتقسيم الدقيق لآفات سرطان الكبد الخلوي (HCC) في صور الرنين المغناطيسي المعززة بالتباين الديناميكي. من خلال استخدام المعلومات من الصور متعددة المراحل في كل من المجال المكاني والزمني، حسّن النموذج بشكل كبير من أداء تقسيم أورام الكبد، محققًا مقاييس متفوقة مقارنة بالنماذج الحالية ومقدمًا أداءً مشابهًا لنموذج nnU-Net المتقدم مع تقليل وقت التنبؤ. يتم أيضًا تكييف الذكاء الاصطناعي لتصوير الأطفال، مع معالجة التحديات الفريدة التي تطرحها الأحجام المختلفة ومراحل التطور لدى المرضى الأطفال. تم تصميم أنظمة الذكاء الاصطناعي في هذا المجال للتعرف على الأنماط الخاصة بالأطفال وتفسيرها، مما يساعد في تشخيص الحالات الخلقية والتنموية. على سبيل المثال، في تصوير الأطفال لمرض الصرع البؤري، تم تقديم نموذج شبكة عصبية تلافيفية عميقة، متفوقًا في تصنيف المسارات وتحديد المسارات الحرجة في المادة البيضاء.
الدقة [128]. هذا النموذج توقع بشكل فعال نتائج الجراحة والتغيرات اللغوية بعد العملية، مما يبرز إمكانيته في تعزيز التقييمات قبل الجراحة وتحسين دقة الجراحة لدى الأطفال. - الذكاء الاصطناعي في تفسير الأشعة المقطعية: تشمل تطبيقات الذكاء الاصطناعي في تفسير الأشعة المقطعية اكتشاف العقيدات الرئوية، تحديد الكسور والنزيف، تقييم شدة السكتة الدماغية، و
توصيف تقدم الورم. إحدى التطبيقات المبتكرة للذكاء الاصطناعي في تصوير الأشعة المقطعية هي في التعرف السريع على الانصمام الرئوي. يقوم نظام الذكاء الاصطناعي بمعالجة صور الأشعة المقطعية للأوعية الدموية الرئوية لاكتشاف جلطات الدم في الرئتين بدقة عالية، وغالبًا ما يكون أسرع من الطرق التقليدية. هذه السرعة حاسمة في الحالات الطارئة، حيث يمكن أن يكون التدخل في الوقت المناسب منقذًا للحياة. كمثال آخر، طورت شركة جوجل بالتعاون مع باحثين من جامعة نورث وسترن ومركز NYU-Langone الطبي وستانفورد للطب نموذجًا للأشعة المقطعية يشخص سرطان الرئة بدقة تعادل أو تتجاوز ستة أطباء أشعة. يقوم هذا النموذج بتحليل المسحات ثلاثية الأبعاد للتنبؤ بالسرطانات واكتشاف العقيدات الرئوية الدقيقة، حيث ينظر إلى الرئتين ككائن ثلاثي الأبعاد واحد ويقارن المسحات على مر الزمن لتتبع نمو الآفات. تم اختباره على أكثر من 45,800 فحص للأشعة المقطعية للصدر بدون هوية، واكتشف 5% من حالات السرطان أكثر وقلل من الإيجابيات الكاذبة بأكثر منمقارنةً بتقييمات أطباء الأشعة التقليدية، مما يظهر إمكانيات كبيرة لتحسين تشخيص سرطان الرئة. - الذكاء الاصطناعي في تحليل الأشعة السينية: يقوم الذكاء الاصطناعي بإحداث ثورة في تحليل الأشعة السينية عبر مجالات طبية متنوعة. خذ تصوير الثدي كمثال، حيث يقوم الذكاء الاصطناعي بتحويل فحص سرطان الثدي من خلال تحسين تحليل الصور لاكتشاف الأورام، وزيادة الدقة في تحديد الآفات الحميدة والخبيثة، وتقليل الإيجابيات الكاذبة والسلبية، مما يسهل عملية التشخيص للعلاج المبكر والفعال. تقوم هذه الأنظمة بتحليل صور الأشعة السينية للثدي لتحديد علامات الآفات السرطانية، حيث أظهرت بعض نماذج الذكاء الاصطناعي القدرة على اكتشاف السرطانات التي فاتت في البداية من قبل أطباء الأشعة. من خلال العمل كمراجع ثانٍ، تعزز هذه الأنظمة دقة فحص سرطان الثدي. أظهرت دراسة حديثة أن cm Assist
، خوارزمية CAD المعتمدة على الذكاء الاصطناعي المستندة إلى عدة شبكات عميقة مخصصة، عززت بشكل كبير حساسية أطباء الأشعة في اكتشاف سرطان الثدي [120]. من خلال تحليل 122 صورة شعاعية للثدي مع مزيج من النتائج السلبية الكاذبة وتصنيفات BIRADS 1 و 2، أظهر أطباء الأشعة تحسناً ملحوظاً في معدلات اكتشاف السرطان (CDRs) بمتوسط عند استخدام cmAssist، مع زيادة طفيفة في الإيجابيات الكاذبة. يبرز هذا التحسن الملحوظ إمكانيات برنامج الذكاء الاصطناعي CAD في تحسين الدقة والحساسية في فحص سرطان الثدي. - الذكاء الاصطناعي في الموجات فوق الصوتية: يؤثر الذكاء الاصطناعي بشكل كبير على تطبيقات مختلفة للموجات فوق الصوتية. في تصوير القلب، على سبيل المثال، تُستخدم أنظمة الذكاء الاصطناعي لتحليل الصور من فحوصات تخطيط صدى القلب لتقييم وظيفة القلب والأوعية الدموية. يمكنها قياس معايير مثل الكسر القذفي، الذي يشير إلى مدى كفاءة ضخ القلب للدم، واكتشاف الشذوذات الهيكلية في القلب. هذه المعلومات حاسمة في تشخيص وإدارة أمراض القلب. على سبيل المثال، أظهرت دراسة تقييم ذكاء اصطناعي جديد لحساب زمن قذف البطين الأيسر بشكل آلي في تخطيط صدى القلب دقة عالية، تتوافق بشكل وثيق مع نتائج تصوير القلب بالرنين المغناطيسي. أظهر الذكاء الاصطناعي، الذي أظهر تحيزًا أقل وموثوقية أكبر خاصة في الحالات الصعبة، أداءً أفضل من الطرق التقليدية. يعتمد هذا الخوارزم على شبكة عصبية تلافيفية محمية ببراءة اختراع، على الرغم من أن التفاصيل المحددة لهندسته وعملية تدريبه تظل ملكية خاصة. وهذا يبرز إمكانيات الخوارزم في تقليل التباين المعتمد على المستخدم وتعزيز الفائدة السريرية لتخطيط صدى القلب.
في الختام، توضح هذه الأمثلة التطبيقات المتنوعة والمؤثرة للذكاء الاصطناعي في تصوير الطب. من خلال تعزيز الدقة والسرعة والكفاءة في تحليل الصور، تثبت أنظمة الذكاء الاصطناعي أنها أصول لا تقدر بثمن في الأشعة التشخيصية، مما يؤدي في النهاية إلى تحسين رعاية المرضى والنتائج. مع استمرار تقدم تكنولوجيا الذكاء الاصطناعي، من المتوقع أن تتوسع تطبيقاتها في تصوير الطب، مما يحول مجال الأشعة بشكل أكبر.
5. الذكاء الاصطناعي في رعاية المرضى والمراقبة
| التطبيقات الرئيسية | التقنيات الرئيسية والتطبيقات | فوائد | التحديات |
| أجهزة قابلة للارتداء مدعومة بالذكاء الاصطناعي | المراقبة الفسيولوجية المستمرة (معدل ضربات القلب، ضغط الدم، إلخ)؛ الكشف المبكر عن المشكلات الصحية؛ توصيات مخصصة لتغييرات نمط الحياة | تحسين مشاركة المرضى؛ إدارة صحية استباقية | جمع البيانات ونشر النموذج؛ تحقيق التوازن بين الدقة وقيود الأجهزة القابلة للارتداء |
| مساعدات التمريض الافتراضية | دعم المرضى على مدار الساعة وطوال أيام الأسبوع وتذكيرات صحية؛ إدارة الأمراض المزمنة؛ تعليم المرضى ومراقبة السلوك | تعزيز مشاركة المرضى والتعليم؛ تحسين الالتزام بخطط العلاج | خصوصية البيانات ودقة المعلومات؛ ضمان تكاملها مع الرعاية الإنسانية |
| الذكاء الاصطناعي في الطب عن بُعد وتفاعل المرضى عن بُعد | تشخيصات متقدمة واستشارات؛ استشارات افتراضية مخصصة؛ مراقبة المرضى عن بُعد وتحليلات تنبؤية | زيادة الوصول إلى الرعاية الصحية؛ رعاية استباقية للحالات المزمنة | خصوصية البيانات، دقة النظام، والتكامل |
5.1. أجهزة قابلة للارتداء مدعومة بالذكاء الاصطناعي للمراقبة المستمرة
البيانات الموثوقة للتدريب، خاصة في مجال الرعاية الصحية، صعبة الحصول عليها بسبب التكاليف العالية وتعقيد ضمان موثوقية البيانات. اختيار الميزات والأطر الأكثر فعالية وتقييم ونشر أفضل نماذج التعلم الآلي يضيف طبقات من التعقيد، بالإضافة إلى ضرورة أن تعمّم النماذج بشكل جيد عبر ميزات شخصية متنوعة. يجب على مطوري الأجهزة القابلة للارتداء أيضًا التنقل بين خيارات النشر، موازنين بين مزايا الحوسبة على الجهاز وقيود استهلاك الطاقة والتخزين والقدرة الحاسوبية. يتطلب معالجة هذه التحديات توازنًا دقيقًا بين دقة النموذج والقيود العملية للتكنولوجيا القابلة للارتداء، مما يتطلب ابتكارات في تصميم النموذج، ومعالجة البيانات، ودمج الأنظمة لتحسين التأثير السريري وقبول المستخدم لتطبيقات التعلم الآلي القابلة للارتداء.
5.2. مساعدات التمريض الافتراضية
5.3. الذكاء الاصطناعي في الطب عن بُعد وتفاعل المرضى عن بُعد
تقلل التكنولوجيا بشكل فعال المسافة بين المرضى ومقدمي الرعاية، بدعم من تنفيذ موجه من الأطباء والالتزام بالممارسات السريرية.
6. منهجيات تقييم حلول الرعاية الصحية القائمة على الذكاء الاصطناعي
6.1. التحقق
- التحقق من الخوارزمية: يعتمد الدمج الناجح لخوارزميات الذكاء الاصطناعي في الرعاية الصحية على دقتها وموثوقيتها وأدائها. يتطلب ذلك اختبارًا شاملاً باستخدام مجموعات بيانات متنوعة [150]. أحد التحديات الرئيسية في هذه العملية هو الإفراط في التكيف، حيث تؤدي الخوارزمية بشكل جيد على بيانات التدريب ولكنها تفشل في التعميم على البيانات غير المرئية. لمعالجة ذلك، يتم استخدام تقنيات مثل التحقق المتقاطع [151]. يتضمن التحقق المتقاطع تقسيم بيانات التدريب إلى عدة طيات وتدريب الخوارزمية بشكل تكراري على مجموعة فرعية من الطيات بينما يتم استخدام الطيات المتبقية للتحقق. تساعد هذه العملية في تقييم مدى جودة تعميم الخوارزمية على بيانات جديدة وتمنع الإفراط في التكيف. بالإضافة إلى القابلية للتعميم، يجب أن يكون الذكاء الاصطناعي في الرعاية الصحية قابلاً للتكيف للاستخدام الشخصي. وهذا يعني أن الخوارزميات يجب أن تتعلم باستمرار من بيانات المرضى الفردية لتمكين أساليب العلاج المخصصة. يساعد التقييم الدقيق في تحديد نقاط القوة والضعف ومجالات التحسين، مما يعزز في النهاية موثوقية حلول الرعاية الصحية القائمة على الذكاء الاصطناعي. علاوة على ذلك، فإن التحقق على مجموعات مرضى مختلفة أمر ضروري لمعالجة التحيزات المحتملة في بيانات التدريب. يمكن أن تؤدي التحيزات إلى نتائج غير عادلة وغير فعالة لبعض الفئات السكانية. من خلال ضمان أداء الخوارزميات بشكل متسق عبر مجموعات سكانية متنوعة، يمكننا ضمان العدالة والفعالية للجميع.
- التحقق السريري: يلعب التحقق السريري دورًا حاسمًا في تقييم فعالية وسلامة تدخلات الذكاء الاصطناعي [152]. يجب إجراء تجارب سريرية صارمة ودراسات لمقارنة تدخلات الذكاء الاصطناعي بالعلاجات القياسية أو الممارسات الحالية. يمكن أن تشمل هذه التقييمات مجموعة من تصاميم الدراسات، بما في ذلك التجارب العشوائية المضبوطة (RCTs)، والدراسات الملاحظة، أو تحليلات الأدلة الواقعية. من خلال هذه الدراسات، يمكن للباحثين تحديد فعالية تقنيات الذكاء الاصطناعي في تحسين نتائج المرضى واتخاذ القرارات السريرية. علاوة على ذلك، فإن تحديد مقاييس النتائج المناسبة أمر ضروري لتقييم تأثير تدخلات الذكاء الاصطناعي على نتائج المرضى. يمكن استخدام مقاييس النتائج مثل معدلات الوفيات، وتقدم المرض، وجودة الحياة، وتكاليف الرعاية الصحية لتقييم فعالية تقنيات الذكاء الاصطناعي في تحسين تقديم الرعاية الصحية.
6.2. القابلية للتفسير وسهولة الاستخدام
(تفسيرات نموذجية قابلة للتفسير) [154]، وقيم SHAP (تفسيرات شابلي الإضافية) [155] رؤى أعمق في منطق النموذج.
- مشاركة أصحاب المصلحة النشطة: من خلال عملية التطوير، فإن المشاركة النشطة للأطباء والمرضى وغيرهم من أصحاب المصلحة توفر رؤى قيمة حول احتياجاتهم وتوقعاتهم. يعزز هذا النهج التعاوني شعورًا بالملكية في الحل، مما يؤدي إلى زيادة المشاركة.
- التطوير التكراري وحلقات التغذية الراجعة: يعد تطوير حلول الذكاء الاصطناعي عملية تكرارية. من خلال دمج ملاحظات المستخدم طوال دورات التطوير، يمكن للباحثين تحسين أداة الذكاء الاصطناعي لتلبية احتياجات المستخدم بشكل أفضل. لا تعمل هذه الحلقة المستمرة من التغذية الراجعة على تحسين سهولة الاستخدام فحسب، بل تعزز أيضًا ثقة المستخدم ومشاركته.
- واجهات سهلة الاستخدام وتصويرات واضحة: يعد تصميم واجهات واضحة وسهلة الاستخدام أمرًا ضروريًا لمشاركة المستخدم. يشمل ذلك تقديم مخرجات الذكاء الاصطناعي بطريقة يسهل فهمها وتفسيرها، حتى بالنسبة للمستخدمين ذوي الخبرة التقنية المحدودة. بالإضافة إلى ذلك، يمكن أن تعزز التصويرات الواضحة لمنطق الذكاء الاصطناعي ثقة المستخدم ومشاركته.
6.3. القابلية للتوسع والتحسين المستمر
- المراقبة بعد السوق: مراقبة أداء حلول الذكاء الاصطناعي عن كثب بعد نشرها في البيئات الواقعية لتحديد أي مشكلات غير متوقعة أو مجالات للتحسين [158].
- مراقبة الأداء: تتبع فعالية أداة الذكاء الاصطناعي باستمرار في تحقيق النتائج المقصودة [159]. يمكن استخدام هذه البيانات لتحديد المجالات التي يمكن تحسين الذكاء الاصطناعي فيها بشكل أكبر.
- تحديث الخوارزميات بناءً على بيانات ورؤى جديدة: خوارزميات الذكاء الاصطناعي ليست ثابتة. مع توفر بيانات جديدة، أو عندما يحصل الباحثون على فهم أعمق للمشكلة الأساسية، يمكن تحديث الخوارزميات لتحسين أدائها ودقتها.
من خلال إعطاء الأولوية للتوسع والتحسين المستمر، يجب على الباحثين والمطورين ضمان النجاح المستدام وطويل الأمد للحلول الصحية المعتمدة على الذكاء الاصطناعي في مواجهة التحديات الصحية المتطورة.
7. الاعتبارات الأخلاقية والتحديات
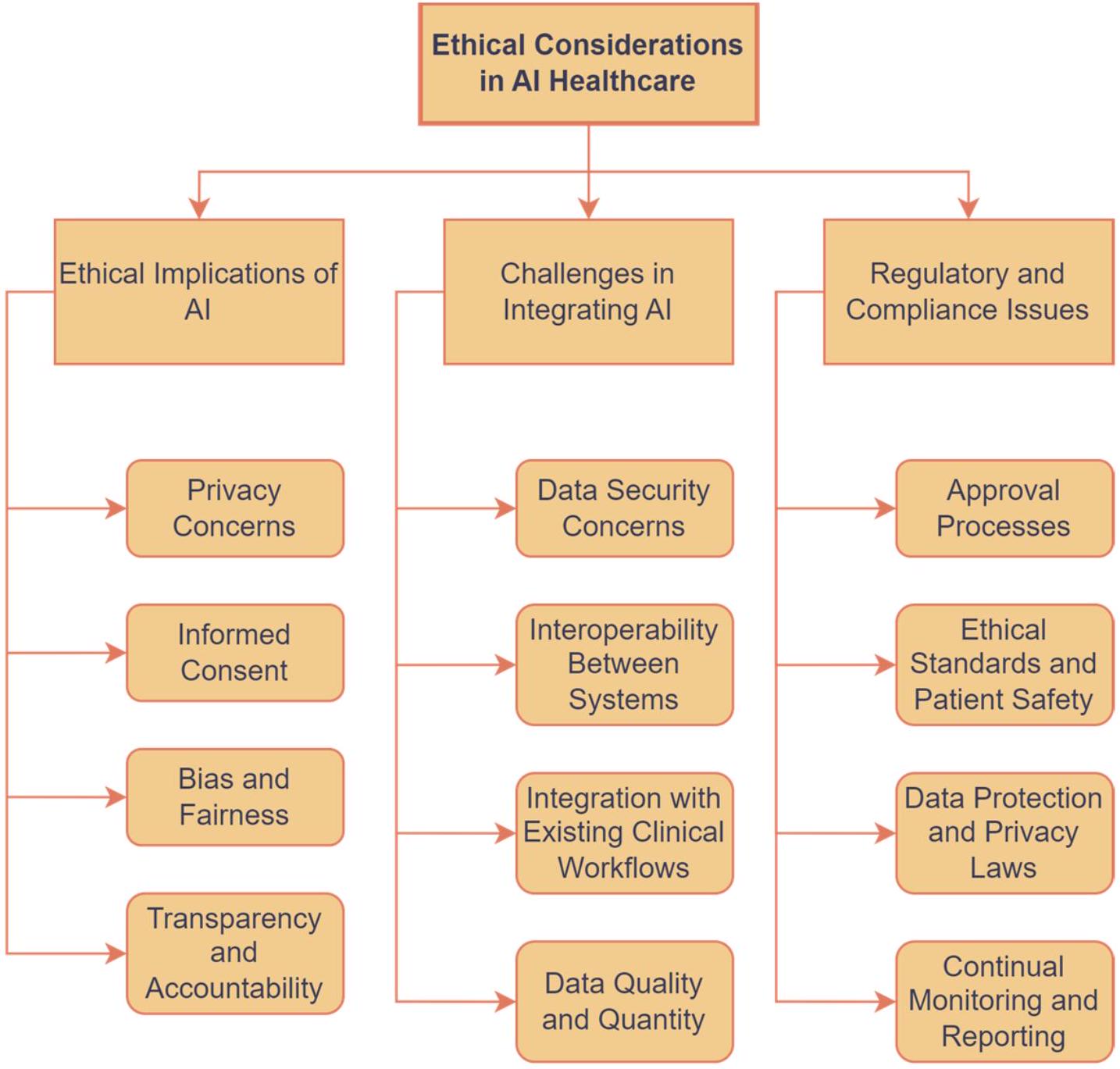
7.1. الآثار الأخلاقية للذكاء الاصطناعي في الرعاية الصحية
- مخاوف الخصوصية: واحدة من أبرز المخاوف الأخلاقية في الرعاية الصحية المعتمدة على الذكاء الاصطناعي هي خصوصية بيانات المرضى. تتطلب أنظمة الذكاء الاصطناعي الوصول إلى مجموعات بيانات كبيرة من معلومات المرضى، مما يثير تساؤلات حول أمان وسرية البيانات الصحية الحساسة. إن ضمان أن تكون بيانات المرضى المستخدمة في تطبيقات الذكاء الاصطناعي مجهولة الهوية ومخزنة بشكل آمن أمر بالغ الأهمية. هناك أيضًا حاجة إلى سياسات شفافة بشأن من لديه حق الوصول إلى هذه البيانات ولأي أغراض.
- الموافقة المستنيرة: قضية الموافقة المستنيرة في الرعاية الصحية المعتمدة على الذكاء الاصطناعي معقدة، مما يتطلب تواصلًا واضحًا مع المرضى حول استخدام بياناتهم، خاصة مع خوارزميات الذكاء الاصطناعي التي قد تكون صعبة الفهم لغير الخبراء. يشمل ذلك توضيح تداعيات مشاركة البيانات، والفوائد والمخاطر المحتملة المرتبطة بالرعاية الصحية المدفوعة بالذكاء الاصطناعي، ومستوى الإشراف البشري في قرارات الذكاء الاصطناعي. يمكن العثور على مزيد من التفاصيل حول استخدام نماذج الموافقة المستنيرة للذكاء الاصطناعي في الطب مع إرشادات شاملة لأطباء الطوارئ في [161].
- التحيز والعدالة: أنظمة الذكاء الاصطناعي ليست محايدة إلا بقدر البيانات التي تم تدريبها عليها. هناك خطر من أن خوارزميات الذكاء الاصطناعي قد تستمر في التحيزات الموجودة في بيانات الرعاية الصحية، مما يؤدي إلى نتائج علاج غير عادلة لبعض المجموعات. على سبيل المثال، إذا تم تدريب نظام ذكاء اصطناعي بشكل أساسي على بيانات من فئة ديموغرافية معينة، فإن
قد تكون الدقة أقل للمرضى خارج تلك الفئة السكانية. من الضروري ضمان تطوير أنظمة الذكاء الاصطناعي وتدريبها على مجموعات بيانات متنوعة للتخفيف من هذه التحيزات. علاوة على ذلك، فإن المراقبة والتدقيق المستمرين لأنظمة الذكاء الاصطناعي من أجل النتائج المتحيزة ضروريان للحفاظ على العدالة في تقديم الرعاية الصحية. - الشفافية والمساءلة: تعتبر الشفافية في عمليات اتخاذ القرار بواسطة الذكاء الاصطناعي قضية أخلاقية رئيسية. من المهم أن يفهم مقدمو الرعاية الصحية والمرضى كيف تتخذ أنظمة الذكاء الاصطناعي توصياتها. هذه الشفافية ضرورية لبناء الثقة في أنظمة الذكاء الاصطناعي وللمساءلة. في الحالات التي تؤثر فيها القرارات المدفوعة بالذكاء الاصطناعي على رعاية المرضى، من الضروري وجود آليات لمراجعة وفهم هذه القرارات، خاصة في حالة حدوث نتائج سلبية. تسلط دراسة حديثة الضوء على الحاجة إلى أنظمة ذكاء اصطناعي شفافة وقابلة للمساءلة في معالجة اللغة الطبيعية لمعالجة قضية “الصندوق الأسود” لنماذج التعلم العميق. تقدم الإطار المعروف باسم “تفسير وتصوير الشبكات العصبية التلافيفية لمعلومات النص” (EVCT)، الذي يقدم حلولًا قابلة للتفسير من قبل البشر لتصنيف النصوص مع الحد الأدنى من فقدان المعلومات، متماشيًا مع المطالبات الأخيرة للعدالة والشفافية في أنظمة دعم القرار المدفوعة بالذكاء الاصطناعي.
في الختام، بينما تقدم الذكاء الاصطناعي فرصًا كبيرة لتعزيز الرعاية الصحية، فإنه يقدم أيضًا تحديات أخلاقية معقدة يجب معالجتها. الخصوصية، والموافقة، والتحيز، والشفافية، والمساءلة هي اعتبارات حاسمة تحتاج إلى إدارة دقيقة لضمان الاستخدام المسؤول والعادل للذكاء الاصطناعي في الرعاية الصحية.
7.2. التحديات في دمج الذكاء الاصطناعي
- مخاوف أمن البيانات: نظرًا لأن أنظمة الذكاء الاصطناعي في الرعاية الصحية تتطلب الوصول إلى كميات كبيرة من بيانات المرضى الحساسة، فإن ضمان أمان هذه البيانات أمر بالغ الأهمية. يشكل خطر خروقات البيانات والهجمات الإلكترونية مصدر قلق كبير. يمكن أن تؤدي هذه الخروقات الأمنية إلى كشف معلومات المرضى السرية، مما يؤدي إلى انتهاكات الخصوصية وقد يضر بالثقة بين المرضى ومقدمي الرعاية الصحية. إن تنفيذ تدابير قوية للأمن السيبراني، بما في ذلك التشفير، وحلول تخزين البيانات الآمنة، والتدقيقات الأمنية المنتظمة، أمر حيوي لحماية بيانات المرضى. بالإضافة إلى ذلك، فإن توعية موظفي الرعاية الصحية بأفضل ممارسات أمان البيانات أمر أساسي للحماية من الخروقات.
- التشغيل البيني بين الأنظمة: تحدٍ رئيسي آخر في دمج الذكاء الاصطناعي في الرعاية الصحية هو مسألة التشغيل البيني – القدرة على تواصل أنظمة تكنولوجيا المعلومات الصحية المختلفة وتطبيقات البرمجيات، وتبادل البيانات، واستخدام المعلومات التي تم تبادلها. تستخدم العديد من أنظمة الرعاية الصحية مجموعة متنوعة من أنظمة السجلات الصحية الإلكترونية (EHR) وأدوات رقمية أخرى قد لا تكون متوافقة مع بعضها البعض أو مع تقنيات الذكاء الاصطناعي الجديدة. يمكن أن تعيق هذه الفجوة في التشغيل البيني تبادل بيانات المرضى بسلاسة، مما يقلل من فعالية أدوات الذكاء الاصطناعي. إن تطوير تنسيقات بيانات موحدة وبروتوكولات اتصال، بالإضافة إلى تشجيع اعتماد أنظمة قابلة للتشغيل البيني، أمر حيوي للتغلب على هذا التحدي.
- الاندماج مع سير العمل السريري الحالي: يمكن أن يكون دمج الذكاء الاصطناعي في سير العمل السريري الحالي تحديًا. قد يحتاج المتخصصون في الرعاية الصحية إلى تعديل سير العمل الخاص بهم لاستيعاب أدوات الذكاء الاصطناعي، وهو ما يمكن أن يكون عملية تستغرق وقتًا طويلاً ومعقدة. من الضروري ضمان أن تكون أنظمة الذكاء الاصطناعي سهلة الاستخدام ومتوافقة مع الممارسات السريرية الحالية لتسهيل اعتمادها. كما أن التدريب والدعم للمتخصصين في الرعاية الصحية في استخدام هذه الأنظمة أمر حاسم لنجاح الاندماج. على سبيل المثال، في دراسة حديثة، تم توضيح نهج تكاملي ثلاثي المستويات لتحليل الصور المعتمد على الذكاء الاصطناعي في سير عمل الأشعة، مع التركيز على تعزيز الأتمتة ودمج ملاحظات أطباء الأشعة لتحسين الذكاء الاصطناعي بشكل مستمر.
تتضمن هذه الطريقة في البداية تصور نتائج الذكاء الاصطناعي دون إنشاء سجلات جديدة للمرضى. إنها تسمح بتخزين النتائج التي تم إنشاؤها بواسطة الذكاء الاصطناعي في الأنظمة المؤسسية وتزود أطباء الأشعة بالأدوات اللازمة لتحسين استنتاجات الذكاء الاصطناعي لإعادة التدريب الدوري. تم توضيح هذه المنهجية في دراسة حالة حول اكتشاف النقائل الدماغية، حيث ساهم إدخال أطباء الأشعة بشكل كبير في تقليل الإيجابيات الكاذبة من خلال إعادة التدريب التكرارية مع مجموعة بيانات موسعة. - جودة البيانات وكميتها: تعتمد فعالية أنظمة الذكاء الاصطناعي بشكل كبير على جودة وكمية البيانات التي تم تدريبها عليها. يمكن أن تؤدي البيانات غير المتسقة أو غير المكتملة أو غير الدقيقة إلى أداء ضعيف للذكاء الاصطناعي. لذلك، فإن ضمان جمع بيانات المرضى عالية الجودة وشاملة يعد تحديًا كبيرًا في دمج الذكاء الاصطناعي. إن توحيد طرق جمع البيانات وضمان عمليات تنسيق البيانات الشاملة هي خطوات أساسية في معالجة هذه القضية.
7.3. القضايا التنظيمية والامتثال
8. مستقبل الذكاء الاصطناعي في الرعاية الصحية
| الاتجاه/التطبيق | التأثير المحتمل | التحديات | الاتجاهات المستقبلية |
| الطب الشخصي | يحدث ثورة في علاج الأمراض ذات المكونات الوراثية، مما يحسن بشكل كبير نتائج المرضى من خلال خطط رعاية مخصصة. | خصوصية البيانات، التكامل في الممارسة السريرية، وضمان الوصول العادل عبر مجموعات المرضى المتنوعة. | توسيع الطب الشخصي ليشمل الصحة النفسية، وأمراض نمط الحياة، ودمج بيانات مراقبة الصحة في الوقت الحقيقي لتعديلات العلاج الديناميكية. |
| أدوات مدعومة بالذكاء الاصطناعي لمراقبة الصحة والنوم | تحسين الكشف والتشخيص لاضطرابات النوم، والتعرف المبكر على القضايا الصحية المحتملة، والعلاج الشخصي، والتدخلات الاستباقية. | خصوصية البيانات، دقة التنبؤات، وقبول المستخدم وراحته مع التقنيات التدخلية. | تصميم تقنيات التحليل والتدخل لمراقبة، وتوقع، وإدارة القضايا الصحية واضطرابات النوم؛ التكامل مع الأجهزة القابلة للارتداء وتقنية المنزل الذكي، مما يوفر تعديلات في الوقت الحقيقي. |
| طول العمر والشيخوخة | يفتح إمكانيات جديدة في أبحاث الشيخوخة، مما يعزز حياة صحية وممتدة من خلال التدخلات الجينومية المدفوعة بالذكاء الاصطناعي والتحليلات التنبؤية للطب الوقائي. | معالجة الآثار الأخلاقية لأبحاث طول العمر، وضمان الوصول والعدالة في علاجات مكافحة الشيخوخة. | استغلال الذكاء الاصطناعي لإنشاء منصات شاملة لصحة طول العمر، ودمج الذكاء الاصطناعي مع الطب التجديدي، وإنشاء خطط علاج شخصية لمكافحة الشيخوخة بناءً على التحليلات الصحية التنبؤية. |
| الذكاء الاصطناعي في اكتشاف الأدوية وتطويرها | يقلل من الوقت والتكاليف في إدخال الأدوية إلى السوق، ويعزز فعالية الأدوية الجديدة من خلال تحديد الجزيئات المرشحة المثلى. | ضمان موثوقية تنبؤات الذكاء الاصطناعي؛ المخاوف الأخلاقية حول اتخاذ القرارات الآلية في تطوير الأدوية. | استغلال الذكاء الاصطناعي لاستكشاف مسارات دوائية جديدة، وتحسين تصميم التجارب السريرية، وتوقع استجابة المرضى للعلاجات بدقة أكبر. |
| الروبوتات المتقدمة في الجراحة وإعادة التأهيل | تحسن الدقة في الجراحة ونتائج المرضى في إعادة التأهيل، مما قد يقلل من أوقات التعافي وتكاليف الرعاية الصحية. | الاعتبارات الأخلاقية حول الاستقلالية؛ الحاجة إلى برامج تدريب قوية للموظفين الطبيين على الأنظمة الروبوتية. | تطوير روبوتات جراحية مستقلة، وتعزيز الأنظمة الروبوتية مع ردود فعل حسية لتحسين نتائج إعادة التأهيل، وتوسيع التطبيقات في الإجراءات الأقل تدخلاً. |
| معجلات الأجهزة المدعومة بالذكاء الاصطناعي | تشخيصات أسرع، تخطيط للعلاج، وتحليل، وتحسين نتائج رعاية المرضى، ومعالجة البيانات الطبية في الوقت الحقيقي. | التكامل مع الأجهزة الطبية؛ تكلفة واستهلاك الطاقة للمعجلات. | تطوير أجهزة ذكاء اصطناعي مخصصة للرعاية الصحية؛ تحسين إمكانية الوصول إلى الرعاية الصحية المدفوعة بالذكاء الاصطناعي. |
| تصوير طبي معزز بالذكاء الاصطناعي | يمكن أن يمكّن من الكشف المبكر والأكثر دقة عن الأمراض، مما قد يحدد حتى المخاطر الصحية قبل ظهور الأعراض، وبالتالي الانتقال نحو نماذج الرعاية الصحية الوقائية. | موازنة الحاجة إلى خصوصية المرضى مع فوائد مشاركة البيانات لتدريب الذكاء الاصطناعي؛ دمج أدوات الذكاء الاصطناعي مع البنى التحتية الحالية للرعاية الصحية. | تطوير أنظمة ذكاء اصطناعي قادرة على التحليل عبر الأنماط، وتحسين تقنيات التصوير ثلاثي الأبعاد، وإنشاء نماذج تنبؤية لتقدم المرض بناءً على بيانات التصوير. |
| الاتجاه/التطبيق | التأثير المحتمل | التحديات | الاتجاهات المستقبلية |
| دمج الذكاء الاصطناعي مع إنترنت الأشياء والأجهزة القابلة للارتداء | يؤدي إلى إدارة صحية استباقية وتوصيات صحية مخصصة، مما قد يقلل من التدخلات الصحية الطارئة. | معالجة أمان البيانات وضمان التوافق بين الأجهزة عبر أنظمة الرعاية الصحية المختلفة. | تعزيز التحليلات التنبؤية للكشف المبكر عن الشذوذات الصحية، وإنشاء نظام بيئي من الأجهزة المتصلة لمراقبة الصحة الشاملة؛ مراقبة صحية غير مزعجة. |
| تحسين نتائج المرضى وكفاءة النظام | يعد بتحسينات كبيرة في رعاية المرضى من خلال الكشف المبكر عن الأمراض، والعلاجات المخصصة، وإدارة موارد الرعاية الصحية بشكل مثالي. | ضمان تحسينات عادلة عبر جميع السكان، ومعالجة الفجوة الرقمية في الوصول إلى الرعاية الصحية. | تنفيذ نصائح صحية مدفوعة بالذكاء الاصطناعي في استراتيجيات الصحة العامة، وتحسين نماذج تقديم الرعاية الصحية مع تخصيص الموارد التنبؤية، وتعزيز أنظمة مراقبة المرضى عن بُعد. |
| أنظمة مراقبة الصحة العالمية | تعزز الأمن الصحي العالمي من خلال تمكين الاستجابة السريعة لتفشي الأمراض وتوجيه التدخلات الصحية العامة برؤى قائمة على البيانات. | دمج تدفقات البيانات المتنوعة في الوقت الحقيقي، وتكييف النماذج بسرعة مع التهديدات الصحية الناشئة. | تطوير أنظمة مراقبة مدفوعة بالذكاء الاصطناعي على مستوى العالم، وتعزيز النماذج التنبؤية لتوقع الأوبئة والجوائح، وإنشاء منصات مدفوعة بالذكاء الاصطناعي لتطوير اللقاحات والعلاجات. |
| معالجة ندرة البيانات | يسهل تطوير الذكاء الاصطناعي في المجالات التي لم يتم البحث فيها بشكل كافٍ، مثل الأمراض النادرة، من خلال الاستخدام الفعال لموارد البيانات المحدودة. | إنشاء نماذج فعالة مع بيانات نادرة، مما يضمن تعميم النتائج من مجموعات بيانات محدودة. | استكشاف تقنيات جديدة لزيادة البيانات، وجمع البيانات من خلال الحشود، ومبادرات تبادل البيانات بين المؤسسات لإثراء مجموعات البيانات. تطوير تقنيات متقدمة تعتمد على التعلم من عدد قليل من الأمثلة. |
| ضمان تنوع النموذج | يسمح بتطبيق أوسع لنماذج الذكاء الاصطناعي عبر بيئات الرعاية الصحية المختلفة وخصائص المرضى، مما يحسن من شمولية وملاءمة حلول الرعاية الصحية المدفوعة بالذكاء الاصطناعي. | تطوير نماذج قابلة للتكيف تحافظ على دقة عالية عبر مجموعات بيانات متنوعة، ومعالجة التحيزات المحتملة في تدريب الذكاء الاصطناعي. | تقدم تقنيات التعلم الانتقالي وتكييف المجال التي يمكن تخصيصها عند نقطة الرعاية. |
| ضمان خصوصية البيانات | يعزز الخصوصية والأمان في تطبيقات الرعاية الصحية، معالجًا واحدة من القضايا الرئيسية في إدارة بيانات الصحة الرقمية. | موازنة فائدة البيانات لتدريب الذكاء الاصطناعي مع متطلبات الخصوصية الصارمة، وتكييف اللوائح لمواكبة التقدم التكنولوجي. | تطوير تقنيات ذكاء اصطناعي أكثر تقدمًا للحفاظ على الخصوصية، مثل الحوسبة متعددة الأطراف الآمنة، والتعلم الفيدرالي، وطرق التشفير المتقدمة لبيانات الصحة. |
| قبول أصحاب المصلحة | الاندماج الناجح للذكاء الاصطناعي في الرعاية الصحية؛ تحسين الثقة والتعاون. | القلق بشأن موثوقية الذكاء الاصطناعي واستقلالية الأطباء. | التواصل الشفاف وبرامج التدريب. |
| بناء الثقة مع الذكاء الاصطناعي القابل للتفسير (XAI) | يعزز من موثوقية أنظمة الذكاء الاصطناعي بين المهنيين الصحيين والمرضى، مما يضمن أن القرارات المدعومة بالذكاء الاصطناعي مستنيرة وأخلاقية. | تبسيط عمليات اتخاذ القرار المعقدة للذكاء الاصطناعي لأصحاب المصلحة غير التقنيين، مما يضمن أن الشروحات ذات مغزى وقابلة للتنفيذ. | دمج XAI في سير العمل السريري، وتطوير معايير لتفسيرات الذكاء الاصطناعي في الرعاية الصحية، وتثقيف المهنيين الصحيين حول تفسير قرارات الذكاء الاصطناعي. |
8.1. تطبيقات الرعاية الصحية الشخصية
- الطب الشخصي: واحدة من أكثر الاتجاهات الواعدة في الرعاية الصحية بالذكاء الاصطناعي هي الانتقال نحو الطب الشخصي [177]. ستتيح قدرة الذكاء الاصطناعي على تحليل كميات هائلة من البيانات الجينية والصحية ومعلومات نمط الحياة تطوير علاجات أكثر دقة وفعالية مصممة لتناسب ملفات تعريف المرضى الفردية. يمكن أن يحسن هذا النهج الشخصي من نتائج العلاج ويقلل من الآثار الجانبية.
- أدوات مدعومة بالذكاء الاصطناعي لمراقبة الصحة والنوم: يجب أن تستكشف الأبحاث المستقبلية تطوير والتحقق من صحة أدوات وخوارزميات مدفوعة بالذكاء الاصطناعي لتشخيص ومراقبة وإدارة القضايا الصحية واضطرابات النوم [178]. يشمل ذلك الاستفادة من التعلم الآلي لتحليل البيانات من الأجهزة القابلة للارتداء مثل أنماط النوم، وتغير معدل ضربات القلب، ومستويات النشاط. يمكن أن تساعد هذه التحليلات، على سبيل المثال، في اكتشاف الشذوذ مثل انقطاع النفس أثناء النوم وتخصيص توصيات العلاج بناءً على ملفات تعريف النوم الفردية.
- طول العمر والشيخوخة: من خلال استغلال قوة التحليلات التنبؤية، يمكن للذكاء الاصطناعي استكشاف مجموعات بيانات هائلة لكشف العلامات الحيوية للشيخوخة وتقديم استراتيجيات شخصية لإبطاء أو حتى عكس عملية الشيخوخة [179]. يشمل ذلك الاستفادة من الذكاء الاصطناعي للتدخلات الجينومية، حيث يمكن أن يوجه تعديل الجينات المرتبطة بآليات الشيخوخة، مما يعزز من إصلاح الخلايا، والقدرة على التحمل، وطول العمر. يمتد إمكان الذكاء الاصطناعي إلى مجال اكتشاف الأدوية وإعادة استخدامها، حيث يمكن أن يسرع من تحديد المركبات ذات التأثيرات المضادة للشيخوخة [180]. علاوة على ذلك، يعد دمج الذكاء الاصطناعي في الرعاية الصحية بوعد بتحول جذري نحو الطب الوقائي، مع التركيز على الكشف المبكر والتدخل في التدهورات المرتبطة بالعمر.
8.2. تقنيات العلاج المحسنة
- الذكاء الاصطناعي في اكتشاف الأدوية وتطويرها: من المتوقع أن يلعب الذكاء الاصطناعي دورًا كبيرًا في تسريع اكتشاف الأدوية وتطويرها [181]. من خلال تحليل البيانات الجزيئية والسريرية بسرعة، يمتلك الذكاء الاصطناعي القدرة على تحديد مرشحي الأدوية المحتملين بشكل أسرع بكثير من الطرق التقليدية. يمكن أن يقلل هذا التسريع بشكل كبير من الوقت والتكلفة المرتبطة بإدخال أدوية جديدة إلى السوق.
- الروبوتات المتقدمة في الجراحة وإعادة التأهيل: من المتوقع أن يتقدم استخدام الروبوتات المدفوعة بالذكاء الاصطناعي في الجراحة وإعادة التأهيل بشكل أكبر [182]. يمكن أن تؤدي الأنظمة الروبوتية، الموجهة بواسطة خوارزميات الذكاء الاصطناعي، عمليات جراحية معقدة بدقة عالية، مما يقلل من المخاطر ويحسن من نتائج المرضى. في إعادة التأهيل، من المتوقع أن تقدم الهياكل الخارجية والأطراف الصناعية المدعومة بالذكاء الاصطناعي مزيدًا من الحركة والاستقلالية للمرضى.
- معجلات الأجهزة للذكاء الاصطناعي: مع نمو تطبيقات الذكاء الاصطناعي في الرعاية الصحية، تزداد الحاجة إلى قدرات معالجة فعالة. تعمل معجلات الأجهزة للذكاء الاصطناعي مثل وحدات معالجة الرسوميات (GPUs) ووحدات معالجة التوتر (TPUs) والدوائر المبرمجة (FPGAs) على تحسين أداء نماذج الذكاء الاصطناعي، مما يمكّن من معالجة البيانات الطبية في الوقت الحقيقي مع الحد الأدنى من التأخير. يعد دمج هذه المعجلات في الأجهزة الطبية بوعد بتشخيص أسرع، وتخطيط للعلاج، وتحليل، مما يعزز من نتائج رعاية المرضى. يعد تطوير معجلات أجهزة مخصصة للذكاء الاصطناعي مصممة لتلبية احتياجات الرعاية الصحية اتجاهًا مستقبليًا واعدًا لتحسين كفاءة وملاءمة حلول الرعاية الصحية المدفوعة بالذكاء الاصطناعي.
- تصوير طبي معزز بالذكاء الاصطناعي: من المحتمل أن تؤدي التطورات المستقبلية في الذكاء الاصطناعي إلى إنتاج تقنيات تصوير طبي أكثر تقدمًا [183]. يمكن أن توفر هذه التطورات صورًا أوضح وأكثر تفصيلًا وتمكن من الكشف المبكر عن الأمراض، مما قد يساعد في تحديد المخاطر الصحية قبل ظهور الأعراض.
- دمج الذكاء الاصطناعي مع إنترنت الأشياء والأجهزة القابلة للارتداء: يعد دمج الذكاء الاصطناعي مع إنترنت الأشياء (IoT) والتكنولوجيا القابلة للارتداء اتجاهًا ناشئًا [184]. يمكن أن يؤدي هذا المزيج إلى أنظمة مراقبة صحية في الوقت الحقيقي لا تتعقب البيانات الصحية فحسب، بل
تقدم أيضًا توصيات وتنبيهات استباقية. يمكن أيضًا دمج الذكاء الاصطناعي في التقنيات القابلة للارتداء الحالية لتوفير مزيد من المعلومات حول الصحة والأداء [185].
8.3. تحسين نظام الرعاية الصحية
- تحسين نتائج المرضى وكفاءة النظام: يمكن أن يغير الإمكانات التحويلية للذكاء الاصطناعي في الرعاية الصحية رعاية المرضى وكفاءة النظام. تهدف تطبيقات الذكاء الاصطناعي المستقبلية إلى الكشف عن الأمراض في وقت مبكر، وتخصيص العلاجات، وتخصيص رعاية المرضى بشكل كبير، مما يؤدي إلى تحسين أوقات التعافي وتقليل معدلات الوفيات. يمتد دور الذكاء الاصطناعي إلى تحسين موارد الرعاية الصحية، وتقليل التكاليف، وتحسين إمكانية الوصول إلى الرعاية، خاصة للمجتمعات المحرومة [186]. علاوة على ذلك، سيدعم الذكاء الاصطناعي المهنيين الصحيين من خلال تعزيز اتخاذ القرار، مما يعد بتحسينات صحية عادلة ونظام تقديم رعاية صحية أكثر كفاءة.
- أنظمة مراقبة الصحة العالمية: يتم التعرف بشكل متزايد على أهمية الذكاء الاصطناعي في معالجة الأوبئة والطوارئ الصحية العالمية كأمر حاسم [187]. من خلال دمج وتحليل تدفقات البيانات المتنوعة، يتمتع الذكاء الاصطناعي بالقدرة على اكتشاف ظهور تفشي الأمراض بسرعة، وتوقع انتشارها، وتوجيه التدخلات الصحية العامة الفعالة. خلال جائحة COVID-19، تم استخدام نماذج مدعومة بالذكاء الاصطناعي للتنبؤ بمسار المرض، مما يظهر إمكانات الذكاء الاصطناعي في التنقل عبر تعقيدات إدارة الأوبئة [188]. علاوة على ذلك، تمتد قدرات الذكاء الاصطناعي إلى تعزيز استراتيجيات الصحة العامة، مما يمكّن من تطوير وتوزيع اللقاحات والحلول العلاجية بسرعة في أوقات الأزمات.
8.4. إدارة البيانات
- معالجة ندرة البيانات: تشكل ندرة البيانات المصنفة في الرعاية الصحية تحديًا كبيرًا لتطوير الذكاء الاصطناعي، خاصة في مجالات مثل أبحاث الأمراض النادرة حيث تكون البيانات محدودة بطبيعتها. الحل العملي لهذه المشكلة هو تنفيذ تقنيات التعلم شبه المراقب والتعلم المراقب بشكل ضعيف. من خلال الاستفادة من مجموعة صغيرة من البيانات المصنفة وحجم أكبر من البيانات غير المصنفة، تعمل هذه الأساليب على تحسين كفاءة تعلم الذكاء الاصطناعي من معلومات قليلة، مما يوفر استراتيجية قابلة للتطبيق لتقدم البحث والعلاج في المجالات التي تكون فيها مجموعات البيانات المصنفة الشاملة نادرة. ومع ذلك، بالنسبة لبعض التطبيقات في الرعاية الصحية، قد يكون من الصعب حتى الحصول على كمية صغيرة من البيانات المصنفة. في مثل هذه الحالات، تقدم التقنيات الناشئة في مجال التعلم الآلي إمكانيات مثيرة. التعلم القليل: يتطلب التعلم القليل عددًا صغيرًا فقط من الأمثلة المصنفة لمفهوم جديد. قد يكون هذا مفيدًا في الحالات التي يمكن فيها الحصول على حتى كمية صغيرة من البيانات المصنفة لمرض نادر. من خلال التعلم من هذه الأمثلة القليلة، يمكن أن يتمكن النموذج من تعميم النتائج على حالات مشابهة. التعلم بدون أمثلة (ZSL): نظريًا، يمكن أن يسمح ZSL لنماذج الذكاء الاصطناعي بالتعلم عن أمراض جديدة أو حالات طبية حتى بدون بيانات مصنفة لتلك الحالات المحددة. يستفيد ZSL من المعرفة والعلاقات الموجودة بين المفاهيم لإجراء توقعات لفئات غير مرئية. بينما لا يزال ZSL قيد التطوير، فإنه يحمل وعدًا لتطبيقات الرعاية الصحية حيث تكون البيانات محدودة للغاية. التعلم الذاتي: تركز هذه الطريقة على تدريب النماذج على “تعلم كيفية التعلم” بكفاءة. يمكن تدريب نموذج التعلم الذاتي على مهام مختلفة تتعلق بالرعاية الصحية مع مجموعات بيانات محدودة لكل مهمة. يمكن بعد ذلك تطبيق هذه المعرفة المكتسبة حول التعلم نفسه على مشاكل طبية جديدة وغير مرئية مع بيانات قليلة، مما قد يحسن الأداء.
- ضمان تنوع النماذج: تحقيق التنوع في نماذج الذكاء الاصطناعي أمر ضروري لتطبيقها الفعال عبر المشهد المتنوع لإعدادات الرعاية الصحية وخصائص المرضى. تقنيات مثل التكيف مع المجال والتعلم الانتقالي تبرز.
كحلول فعالة، تمكّن نماذج الذكاء الاصطناعي المدربة على مجموعة بيانات واحدة من التكيف والأداء بدقة على مجموعة بيانات أخرى مع القليل من الحاجة لإعادة التدريب. هذه القدرة ذات قيمة خاصة في الرعاية الصحية، حيث يمكن أن تختلف خصائص المرضى، وملفات الأمراض، واستجابات العلاج بشكل كبير. من خلال تعزيز مثل هذه القابلية للتكيف، تضمن هذه التقنيات أن يمكن نشر الذكاء الاصطناعي بشكل أكثر شمولاً، مما يعزز فعاليته وفائدته لمجموعة واسعة من المرضى.
8.5. الاعتبارات الأخلاقية وبناء الثقة
- ضمان خصوصية البيانات: أصبح معالجة مخاوف خصوصية البيانات في الرعاية الصحية أمرًا بالغ الأهمية مع زيادة تطبيقات الذكاء الاصطناعي. إحدى الحلول النموذجية لهذه التحديات هي التعلم الفيدرالي، وهو نهج جديد لتدريب نماذج الذكاء الاصطناعي يتيح للخوارزميات التعلم من البيانات المخزنة على خوادم محلية عبر مؤسسات الرعاية الصحية المختلفة دون الحاجة إلى مشاركة البيانات بشكل مباشر. تعزز هذه الطريقة بشكل كبير الخصوصية والأمان وتوفر ميزة استراتيجية في صناعة الرعاية الصحية حيث تعتبر حساسية وسرية بيانات المرضى في غاية الأهمية.
- قبول أصحاب المصلحة: إن ضمان الثقة والقبول بين أصحاب المصلحة أمر حاسم لنجاح دمج الذكاء الاصطناعي في ممارسات الرعاية الصحية. يشمل ذلك ليس فقط المرضى والأطباء، ولكن أيضًا صانعي السياسات، والهيئات التنظيمية، ومديري الرعاية الصحية، والأطراف المعنية الأخرى. قد يعبر المرضى عن مخاوف بشأن موثوقية ومساءلة عمليات اتخاذ القرار المدفوعة بالذكاء الاصطناعي. لذلك، فإن التواصل الشفاف حول دور الذكاء الاصطناعي في خطط العلاج والفوائد المحتملة التي يقدمها أمر ضروري لتعزيز قبول المرضى. وبالمثل، قد يكون لدى الأطباء تحفظات بشأن إسناد مسؤوليات اتخاذ القرار إلى خوارزميات الذكاء الاصطناعي، خوفًا من فقدان الاستقلالية أو الحكم المهني، بالإضافة إلى الشك في دقة قرارات الذكاء الاصطناعي. يمكن أن تساعد إقامة برامج تدريب شاملة وأطر تعاون تمكّن الأطباء من فهم أدوات الذكاء الاصطناعي والتحقق من صحتها بشكل فعال في التخفيف من هذه المخاوف. علاوة على ذلك، يمتد بناء الثقة إلى إشراك أصحاب المصلحة مثل صانعي السياسات، والهيئات التنظيمية، ومديري الرعاية الصحية. إن الشفافية في تطوير الذكاء الاصطناعي ونشره، إلى جانب التواصل الواضح حول الاعتبارات الأخلاقية والقانونية والتنظيمية، أمر حاسم لكسب ثقة أصحاب المصلحة. يمكن أن تعزز إقامة أطر حوكمة قوية تعالج هذه المخاوف الثقة في أنظمة الذكاء الاصطناعي وتضمن المساءلة.
- بناء الثقة مع الذكاء الاصطناعي القابل للتفسير: يهدف الذكاء الاصطناعي القابل للتفسير (XAI) إلى جعل عمليات اتخاذ القرارات بواسطة الذكاء الاصطناعي شفافة وقابلة للفهم للبشر، وهو جانب حاسم للتطبيقات السريرية. من خلال تقديم رؤى حول كيفية وصول نماذج الذكاء الاصطناعي إلى استنتاجاتها، يعزز XAI الثقة بين المهنيين الصحيين والمرضى، مما يضمن أن القرارات المدعومة بالذكاء الاصطناعي مستندة إلى معلومات جيدة وأخلاقية. هذه الشفافية ضرورية لدمج الذكاء الاصطناعي في القرارات الصحية الحساسة، حيث يمكن أن يؤثر فهم المنطق وراء توصيات الذكاء الاصطناعي بشكل كبير على رعاية المرضى ونتائجهم.
لتلخيص الأمر، فإن مستقبل الذكاء الاصطناعي في الرعاية الصحية مشرق ومليء بالاحتمالات. على الرغم من وجود تحديات، خاصة من حيث الأخلاقيات والتنظيم والتكامل، فإن الفوائد المحتملة هائلة. مع استمرار تطور تكنولوجيا الذكاء الاصطناعي، فإنها تعد بإحداث ثورة في الرعاية الصحية، مما يجعلها أكثر تخصيصًا وكفاءة واستجابة للاحتياجات الصحية العالمية.
9. الاستنتاجات
من خلال تمكين دقة تشخيص محسّنة، وتسهيل العلاجات المخصصة، وتحسين الكفاءة التشغيلية، يحمل الذكاء الاصطناعي وعدًا بإعادة تشكيل مشهد الرعاية الصحية.
بيان توفر البيانات: غير قابل للتطبيق.
تعارض المصالح: يعلن المؤلفون عدم وجود أي تعارض في المصالح.
References
- Rajpurkar, P.; Chen, E.; Banerjee, O.; Topol, E.J. AI in health and medicine. Nat. Med. 2022, 28, 31-38. [CrossRef] [PubMed]
- McCorduck, P.; Cfe, C. Machines Who Think: A Personal Inquiry into the History and Prospects of Artificial Intelligence; CRC Press: Boca Raton, FL, USA, 2004.
- Alpaydin, E. Introduction to Machine Learning; MIT Press: Cambridge, MA, USA, 2020.
- Brynjolfsson, E.; McAfee, A. The Second Machine Age: Work, Progress, and Prosperity in a Time of Brilliant Technologies; WW Norton & Company: New York, NY, USA, 2014.
- Russell, S.J.; Norvig, P. Artificial Intelligence a Modern Approach; Pearson: London, UK, 2010.
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436-444. [CrossRef] [PubMed]
- Wang, F.; Preininger, A. AI in health: State of the art, challenges, and future directions. Yearb. Med. Inform. 2019, 28, 16-26. [CrossRef] [PubMed]
- DuBois, K.N. Deep medicine: How artificial intelligence can make healthcare human again. Perspect. Sci. Christ. Faith 2019, 71, 199-201.
- Davenport, T.H. The AI Advantage: How to Put the Artificial Intelligence Revolution to Work; MIT Press: Cambridge, MA, USA, 2018.
- Kaur, S.; Singla, J.; Nkenyereye, L.; Jha, S.; Prashar, D.; Joshi, G.P.; El-Sappagh, S.; Islam, M.S.; Islam, S.R. Medical diagnostic systems using artificial intelligence (ai) algorithms: Principles and perspectives. IEEE Access 2020, 8, 228049-228069. [CrossRef]
- Cortez, N. Digital Health: Scaling Healthcare to the World; Springer: Cham, Switzerland, 2018; pp. 249-269.
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500-510. [CrossRef] [PubMed]
- Kagiyama, N.; Shrestha, S.; Farjo, P.D.; Sengupta, P.P. Artificial intelligence: Practical primer for clinical research in cardiovascular disease. J. Am. Heart Assoc. 2019, 8, e012788. [CrossRef] [PubMed]
- Bardhan, I.; Chen, H.; Karahanna, E. Connecting systems, data, and people: A multidisciplinary research roadmap for chronic disease management. MIS Q. 2020, 44, 185-200.
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in cancer diagnosis and prognosis: Opportunities and challenges. Cancer Lett. 2020, 471, 61-71. [CrossRef]
- Binhowemel, S.; Alfakhri, M.; AlReshaid, K.; Alyani, A. Role of Artificial Intelligence in Diabetes Research Diagnosis and Prognosis: A Narrative Review. J. Health Inform. Dev. Ctries. 2023, 17, 1-12.
- Guan, Z.; Li, H.; Liu, R.; Cai, C.; Liu, Y.; Li, J.; Wang, X.; Huang, S.; Wu, L.; Liu, D. Artificial intelligence in diabetes management: Advancements, opportunities, and challenges. Cell Rep. Med. 2023, 4, 101213. [CrossRef] [PubMed]
- Waring, J.; Lindvall, C.; Umeton, R. Automated machine learning: Review of the state-of-the-art and opportunities for healthcare. Artif. Intell. Med. 2020, 104, 101822. [CrossRef] [PubMed]
- Eloranta, S.; Boman, M. Predictive models for clinical decision making: Deep dives in practical machine learning. J. Intern. Med. 2022, 292, 278-295. [CrossRef] [PubMed]
- Nezamabadi, K.; Sardaripour, N.; Haghi, B.; Forouzanfar, M. Unsupervised ECG analysis: A review. IEEE Rev. Biomed. Eng. 2022, 16, 208-224. [CrossRef] [PubMed]
- Coronato, A.; Naeem, M.; De Pietro, G.; Paragliola, G. Reinforcement learning for intelligent healthcare applications: A survey. Artif. Intell. Med. 2020, 109, 101964. [CrossRef] [PubMed]
- Sarvamangala, D.; Kulkarni, R.V. Convolutional neural networks in medical image understanding: A survey. Evol. Intell. 2022, 15, 1-22. [CrossRef] [PubMed]
- Yang, Y.; Zhang, L.; Du, M.; Bo, J.; Liu, H.; Ren, L.; Li, X.; Deen, M.J. A comparative analysis of eleven neural networks architectures for small datasets of lung images of COVID-19 patients toward improved clinical decisions. Comput. Biol. Med. 2021, 139, 104887. [CrossRef] [PubMed]
- Rim, B.; Sung, N.-J.; Min, S.; Hong, M. Deep learning in physiological signal data: A survey. Sensors 2020, 20, 969. [CrossRef] [PubMed]
- Bahrami, M.; Forouzanfar, M. Sleep apnea detection from single-lead ECG: A comprehensive analysis of machine learning and deep learning algorithms. IEEE Trans. Instrum. Meas. 2022, 71, 4003011. [CrossRef]
- Yi, X.; Walia, E.; Babyn, P. Generative adversarial network in medical imaging: A review. Med. Image Anal. 2019, 58, 101552. [CrossRef]
- Hu, Y.; Kothapalli, S.V.; Gan, W.; Sukstanskii, A.L.; Wu, G.F.; Goyal, M.; Yablonskiy, D.A.; Kamilov, U.S. DiffGEPCI: 3D MRI Synthesis from mGRE Signals using 2.5 D Diffusion Model. arXiv 2023, arXiv:2311.18073.
- Wang, J.; Liu, X. Medical image recognition and segmentation of pathological slices of gastric cancer based on Deeplab v3+ neural network. Comput. Methods Programs Biomed. 2021, 207, 106210. [CrossRef] [PubMed]
- Nagabushanam, P.; Thomas George, S.; Radha, S. EEG signal classification using LSTM and improved neural network algorithms. Soft Comput. 2020, 24, 9981-10003. [CrossRef]
- Kawazoe, Y.; Shibata, D.; Shinohara, E.; Aramaki, E.; Ohe, K. A clinical specific BERT developed using a huge Japanese clinical text corpus. PLoS ONE 2021, 16, e0259763. [CrossRef] [PubMed]
- Torfi, A.; Fox, E.A.; Reddy, C.K. Differentially private synthetic medical data generation using convolutional GANs. Inf. Sci. 2022, 586, 485-500. [CrossRef]
- Lin, X.; Quan, Z.; Wang, Z.-J.; Ma, T.; Zeng, X. KGNN: Knowledge Graph Neural Network for Drug-Drug Interaction Prediction; IJCAI: Pasadena, CA, USA, 2020; pp. 2739-2745.
- Zhou, B.; Yang, G.; Shi, Z.; Ma, S. Natural language processing for smart healthcare. IEEE Rev. Biomed. Eng. 2022, 17, 4-18. [CrossRef]
- Yang, X.; Chen, A.; PourNejatian, N.; Shin, H.C.; Smith, K.E.; Parisien, C.; Compas, C.; Martin, C.; Costa, A.B.; Flores, M.G. A large language model for electronic health records. NPJ Digit. Med. 2022, 5, 194. [CrossRef] [PubMed]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89-94. [CrossRef]
- Jian, Y.; Pasquier, M.; Sagahyroon, A.; Aloul, F. A machine learning approach to predicting diabetes complications. Healthcare 2021, 9, 1712. [CrossRef]
- Fan, Y.; Long, E.; Cai, L.; Cao, Q.; Wu, X.; Tong, R. Machine learning approaches to predict risks of diabetic complications and poor glycemic control in nonadherent type 2 diabetes. Front. Pharmacol. 2021, 12, 665951. [CrossRef]
- Yuan, X.; Chen, J.; Zhang, K.; Wu, Y.; Yang, T. A stable AI-based binary and multiple class heart disease prediction model for IoMT. IEEE Trans. Ind. Inform. 2021, 18, 2032-2040. [CrossRef]
- Ali, F.; El-Sappagh, S.; Islam, S.R.; Kwak, D.; Ali, A.; Imran, M.; Kwak, K.-S. A smart healthcare monitoring system for heart disease prediction based on ensemble deep learning and feature fusion. Inf. Fusion 2020, 63, 208-222. [CrossRef]
- Vieira, S.; Pinaya, W.H.; Mechelli, A. Using deep learning to investigate the neuroimaging correlates of psychiatric and neurological disorders: Methods and applications. Neurosci. Biobehav. Rev. 2017, 74, 58-75. [CrossRef] [PubMed]
- Gautam, R.; Sharma, M. Prevalence and diagnosis of neurological disorders using different deep learning techniques: A meta-analysis. J. Med. Syst. 2020, 44, 49. [CrossRef] [PubMed]
- Murugan, S.; Venkatesan, C.; Sumithra, M.; Gao, X.-Z.; Elakkiya, B.; Akila, M.; Manoharan, S. DEMNET: A deep learning model for early diagnosis of Alzheimer diseases and dementia from MR images. IEEE Access 2021, 9, 90319-90329. [CrossRef]
- Bartsch, G., Jr.; Mitra, A.P.; Mitra, S.A.; Almal, A.A.; Steven, K.E.; Skinner, D.G.; Fry, D.W.; Lenehan, P.F.; Worzel, W.P.; Cote, R.J. Use of artificial intelligence and machine learning algorithms with gene expression profiling to predict recurrent nonmuscle invasive urothelial carcinoma of the bladder. J. Urol. 2016, 195, 493-498. [CrossRef] [PubMed]
- Paul, D.; Sanap, G.; Shenoy, S.; Kalyane, D.; Kalia, K.; Tekade, R.K. Artificial intelligence in drug discovery and development. Drug Discov. Today 2021, 26, 80. [CrossRef] [PubMed]
- Gupta, R.; Srivastava, D.; Sahu, M.; Tiwari, S.; Ambasta, R.K.; Kumar, P. Artificial intelligence to deep learning: Machine intelligence approach for drug discovery. Mol. Divers. 2021, 25, 1315-1360. [CrossRef] [PubMed]
- Hasselgren, C.; Oprea, T.I. Artificial Intelligence for Drug Discovery: Are We There Yet? Annu. Rev. Pharmacol. Toxicol. 2024, 64, 527-550. [CrossRef]
- Senior, A.W.; Evans, R.; Jumper, J.; Kirkpatrick, J.; Sifre, L.; Green, T.; Qin, C.; Žídek, A.; Nelson, A.W.; Bridgland, A. Improved protein structure prediction using potentials from deep learning. Nature 2020, 577, 706-710. [CrossRef]
- Sadybekov, A.V.; Katritch, V. Computational approaches streamlining drug discovery. Nature 2023, 616, 673-685. [CrossRef] [PubMed]
- Bica, I.; Alaa, A.M.; Lambert, C.; Van Der Schaar, M. From real-world patient data to individualized treatment effects using machine learning: Current and future methods to address underlying challenges. Clin. Pharmacol. Ther. 2021, 109, 87-100. [CrossRef]
- Vettoretti, M.; Cappon, G.; Facchinetti, A.; Sparacino, G. Advanced diabetes management using artificial intelligence and continuous glucose monitoring sensors. Sensors 2020, 20, 3870. [CrossRef] [PubMed]
- Low, D.M.; Bentley, K.H.; Ghosh, S.S. Automated assessment of psychiatric disorders using speech: A systematic review. Laryngoscope Investig. Otolaryngol. 2020, 5, 96-116. [CrossRef] [PubMed]
- Graham, S.; Depp, C.; Lee, E.E.; Nebeker, C.; Tu, X.; Kim, H.-C.; Jeste, D.V. Artificial intelligence for mental health and mental illnesses: An overview. Curr. Psychiatry Rep. 2019, 21, 116. [CrossRef] [PubMed]
- Nasrullah, S.; Jalali, A. Detection of Types of Mental Illness through the Social Network Using Ensembled Deep Learning Model. Comput. Intell. Neurosci. 2022, 2022, 9404242. [CrossRef] [PubMed]
- Guntuku, S.C.; Yaden, D.B.; Kern, M.L.; Ungar, L.H.; Eichstaedt, J.C. Detecting depression and mental illness on social media: An integrative review. Curr. Opin. Behav. Sci. 2017, 18, 43-49. [CrossRef]
- Czerwinski, M.; Hernandez, J.; McDuff, D. Building an AI That Feels: AI systems with emotional intelligence could learn faster and be more helpful. IEEE Spectr. 2021, 58, 32-38. [CrossRef]
- Torab-Miandoab, A.; Samad-Soltani, T.; Jodati, A.; Rezaei-Hachesu, P. Interoperability of heterogeneous health information systems: A systematic literature review. BMC Med. Inform. Decis. Mak. 2023, 23, 18. [CrossRef]
- Díaz-Rodríguez, N.; Del Ser, J.; Coeckelbergh, M.; de Prado, M.L.; Herrera-Viedma, E.; Herrera, F. Connecting the dots in trustworthy Artificial Intelligence: From AI principles, ethics, and key requirements to responsible AI systems and regulation. Inf. Fusion 2023, 99, 101896. [CrossRef]
- Gurevich, E.; El Hassan, B.; El Morr, C. In Equity within AI systems: What can health leaders expect? Healthc. Manag. Forum 2023, 36, 119-124. [CrossRef]
- Dwivedi, Y.K.; Hughes, L.; Ismagilova, E.; Aarts, G.; Coombs, C.; Crick, T.; Duan, Y.; Dwivedi, R.; Edwards, J.; Eirug, A. Artificial Intelligence (AI): Multidisciplinary perspectives on emerging challenges, opportunities, and agenda for research, practice and policy. Int. J. Inf. Manag. 2021, 57, 101994. [CrossRef]
- Jebbor, S.; Raddouane, C.; El Afia, A. A preliminary study for selecting the appropriate AI-based forecasting model for hospital assets demand under disasters. J. Humanit. Logist. Supply Chain Manag. 2022, 12, 1-29. [CrossRef]
- Galli, L.; Levato, T.; Schoen, F.; Tigli, L. Prescriptive analytics for inventory management in health care. J. Oper. Res. Soc. 2021, 72, 2211-2224. [CrossRef]
- Tien, P.W. Deep Learning-Powered Vision-Based Energy Management System for Next-Gen Built Environment; University of Nottingham: Nottingham, UK, 2023.
- Zamzam, A.H.; Hasikin, K.; Wahab, A.K.A. Integrated failure analysis using machine learning predictive system for smart management of medical equipment maintenance. Eng. Appl. Artif. Intell. 2023, 125, 106715. [CrossRef]
- Mizan, T.; Taghipour, S. Medical resource allocation planning by integrating machine learning and optimization models. Artif. Intell. Med. 2022, 134, 102430. [CrossRef]
- Munavalli, J.R.; Boersma, H.J.; Rao, S.V.; Van Merode, G. Real-time capacity management and patient flow optimization in hospitals using AI methods. Artif. Intell. Data Min. Healthc. 2021, 2021, 55-69.
- Adhikari, A.; Joshi, R.; Basu, S. Collaboration and coordination strategies for a multi-level AI-enabled healthcare supply chain under disaster. Int. J. Prod. Res. 2023, 2023, 1-27. [CrossRef]
- Samadhiya, A.; Yadav, S.; Kumar, A.; Majumdar, A.; Luthra, S.; Garza-Reyes, J.A.; Upadhyay, A. The influence of artificial intelligence techniques on disruption management: Does supply chain dynamism matter? Technol. Soc. 2023, 75, 102394. [CrossRef]
- Sun, W.; Bocchini, P.; Davison, B.D. Applications of artificial intelligence for disaster management. Nat. Hazards 2020, 103, 2631-2689. [CrossRef]
- Tang, A.; Tam, R.; Cadrin-Chênevert, A.; Guest, W.; Chong, J.; Barfett, J.; Trump, D.; Noorbakhsh-Sabet, N.; Zand, R.; Zhang, Y. Health information management: Implications of artificial intelligence on healthcare data and information management. Yearb. Med. Inform. 2019, 28, 56-64.
- Hoogendoorn, M.; Szolovits, P.; Moons, L.M.; Numans, M.E. Utilizing uncoded consultation notes from electronic medical records for predictive modeling of colorectal cancer. Artif. Intell. Med. 2016, 69, 53-61. [CrossRef] [PubMed]
- Thesmar, D.; Sraer, D.; Pinheiro, L.; Dadson, N.; Veliche, R.; Greenberg, P. Combining the power of artificial intelligence with the richness of healthcare claims data: Opportunities and challenges. Pharmacoeconomics 2019, 37, 745-752. [CrossRef]
- Baudry, M.; Robert, C.Y. A machine learning approach for individual claims reserving in insurance. Appl. Stoch. Models Bus. Ind. 2019, 35, 1127-1155. [CrossRef]
- Samorani, M.; Blount, L.G. Machine learning and medical appointment scheduling: Creating and perpetuating inequalities in access to health care. Am. Public Health Assoc. 2020, 110, 440-441. [CrossRef]
- Chong, L.R.; Tsai, K.T.; Lee, L.L.; Foo, S.G.; Chang, P.C. Artificial intelligence predictive analytics in the management of outpatient MRI appointment no-shows. Am. J. Roentgenol. 2020, 215, 1155-1162. [CrossRef] [PubMed]
- Mandelbaum, A.; Momčilović, P.; Trichakis, N.; Kadish, S.; Leib, R.; Bunnell, C.A. Data-driven appointment-scheduling under uncertainty: The case of an infusion unit in a cancer center. Manag. Sci. 2020, 66, 243-270. [CrossRef]
- Pandey, M.; Arora, M.; Arora, S.; Goyal, C.; Gera, V.K.; Yadav, H. AI-based Integrated Approach for the Development of Intelligent Document Management System (IDMS). Procedia Comput. Sci. 2023, 230, 725-736. [CrossRef]
- Hsu, E.; Malagaris, I.; Kuo, Y.-F.; Sultana, R.; Roberts, K. Deep learning-based NLP data pipeline for EHR-scanned document information extraction. JAMIA Open 2022, 5, ooac045. [CrossRef]
- Kreps, G.L.; Neuhauser, L. Artificial intelligence and immediacy: Designing health communication to personally engage consumers and providers. Patient Educ. Couns. 2013, 92, 205-210. [CrossRef]
- Kingston, J. Using artificial intelligence to support compliance with the general data protection regulation. Artif. Intell. Law 2017, 25, 429-443. [CrossRef]
- Hamdani, R.E.; Mustapha, M.; Amariles, D.R.; Troussel, A.; Meeùs, S.; Krasnashchok, K. A combined rule-based and machine learning approach for automated GDPR compliance checking. In Proceedings of the Eighteenth International Conference on Artificial Intelligence and Law, São Paulo, Brazil, 21-25 June 2021; pp. 40-49.
- El-Bouri, R.; Taylor, T.; Youssef, A.; Zhu, T.; Clifton, D.A. Machine learning in patient flow: A review. Prog. Biomed. Eng. 2021, 3, 022002. [CrossRef] [PubMed]
- Yang, T.; Asanjan, A.A.; Welles, E.; Gao, X.; Sorooshian, S.; Liu, X. Developing reservoir monthly inflow forecasts using artificial intelligence and climate phenomenon information. Water Resour. Res. 2017, 53, 2786-2812. [CrossRef]
- Knight, D.; Aakre, C.A.; Anstine, C.V.; Munipalli, B.; Biazar, P.; Mitri, G.; Valery, J.R.; Brigham, T.; Niazi, S.K.; Perlman, A.I. Artificial Intelligence for Patient Scheduling in the Real-World Health Care Setting: A Metanarrative Review. Health Policy Technol. 2023, 12, 100824. [CrossRef]
- Wang, J.; Fung, R.Y. Adaptive dynamic programming algorithms for sequential appointment scheduling with patient preferences. Artif. Intell. Med. 2015, 63, 33-40. [CrossRef] [PubMed]
- Li, X.; Tian, D.; Li, W.; Dong, B.; Wang, H.; Yuan, J.; Li, B.; Shi, L.; Lin, X.; Zhao, L. Artificial intelligence-assisted reduction in patients’ waiting time for outpatient process: A retrospective cohort study. BMC Health Serv. Res. 2021, 21, 237. [CrossRef]
- Joshi, I. Waiting for deep medicine. Lancet 2019, 393, 1193-1194. [CrossRef]
- Joseph, J.; Senith, S.; Kirubaraj, A.A.; Ramson, J.S. Machine Learning for Prediction of Wait Times in Outpatient Clinic. Procedia Comput. Sci. 2022, 215, 230-239. [CrossRef]
- Khanbhai, M.; Anyadi, P.; Symons, J.; Flott, K.; Darzi, A.; Mayer, E. Applying natural language processing and machine learning techniques to patient experience feedback: A systematic review. BMJ Health Care Inform. 2021, 28, e100262. [CrossRef]
- Bari, V.; Hirsch, J.S.; Narvaez, J.; Sardinia, R.; Bock, K.R.; Oppenheim, M.I.; Meytlis, M. An approach to predicting patient experience through machine learning and social network analysis. J. Am. Med. Inform. Assoc. 2020, 27, 1834-1843. [CrossRef]
- Darley, S.; Coulson, T.; Peek, N.; Moschogianis, S.; Van Der Veer, S.N.; Wong, D.C.; Brown, B.C. Understanding how the design and implementation of online consultations affect primary care quality: Systematic review of evidence with recommendations for designers, providers, and researchers. J. Med. Internet Res. 2022, 24, e37436. [CrossRef] [PubMed]
- Frid-Adar, M.; Amer, R.; Gozes, O.; Nassar, J.; Greenspan, H. COVID-19 in CXR: From detection and severity scoring to patient disease monitoring. IEEE J. Biomed. Health Inform. 2021, 25, 1892-1903. [CrossRef] [PubMed]
- Chen, Y.; Schönlieb, C.-B.; Lio, P.; Leiner, T.; Dragotti, P.L.; Wang, G.; Rueckert, D.; Firmin, D.; Yang, G. AI-based reconstruction for fast MRI—A systematic review and meta-analysis. Proc. IEEE 2022, 110, 224-245. [CrossRef]
- Fusco, R.; Grassi, R.; Granata, V.; Setola, S.V.; Grassi, F.; Cozzi, D.; Pecori, B.; Izzo, F.; Petrillo, A. Artificial intelligence and COVID-19 using chest CT scan and chest X-ray images: Machine learning and deep learning approaches for diagnosis and treatment. J. Pers. Med. 2021, 11, 993. [CrossRef] [PubMed]
- Panayides, A.S.; Amini, A.; Filipovic, N.D.; Sharma, A.; Tsaftaris, S.A.; Young, A.; Foran, D.; Do, N.; Golemati, S.; Kurc, T. AI in medical imaging informatics: Current challenges and future directions. IEEE J. Biomed. Health Inform. 2020, 24, 1837-1857. [CrossRef] [PubMed]
- Liu, Y.; Zhang, F.; Chen, C.; Wang, S.; Wang, Y.; Yu, Y. Act like a radiologist: Towards reliable multi-view correspondence reasoning for mammogram mass detection. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 5947-5961. [CrossRef] [PubMed]
- Liu, F.; Zhang, Q.; Huang, C.; Shi, C.; Wang, L.; Shi, N.; Fang, C.; Shan, F.; Mei, X.; Shi, J. CT quantification of pneumonia lesions in early days predicts progression to severe illness in a cohort of COVID-19 patients. Theranostics 2020, 10, 5613. [CrossRef] [PubMed]
- Johnson, D.; Goodman, R.; Patrinely, J.; Stone, C.; Zimmerman, E.; Donald, R.; Chang, S.; Berkowitz, S.; Finn, A.; Jahangir, E. Assessing the accuracy and reliability of AI-generated medical responses: An evaluation of the Chat-GPT model. Res. Sq. 2023, Preprint.
- Bera, K.; Braman, N.; Gupta, A.; Velcheti, V.; Madabhushi, A. Predicting cancer outcomes with radiomics and artificial intelligence in radiology. Nat. Rev. Clin. Oncol. 2022, 19, 132-146. [CrossRef]
- Lee, R.Y.; Wu, Y.; Goh, D.; Tan, V.; Ng, C.W.; Lim, J.C.T.; Lau, M.C.; Yeong, J.P.S. Application of Artificial Intelligence to in vitro Tumor Modeling and Characterization of the Tumor Microenvironment. Adv. Healthc. Mater. 2023, 12, 2202457. [CrossRef]
- Acs, B.; Rantalainen, M.; Hartman, J. Artificial intelligence as the next step towards precision pathology. J. Intern. Med. 2020, 288, 62-81. [CrossRef] [PubMed]
- Bera, K.; Schalper, K.A.; Rimm, D.L.; Velcheti, V.; Madabhushi, A. Artificial intelligence in digital pathology-New tools for diagnosis and precision oncology. Nat. Rev. Clin. Oncol. 2019, 16, 703-715. [CrossRef] [PubMed]
- Pandey, I.; Misra, V.; Pandey, A.T.; Ramteke, P.W.; Agrawal, R. Artificial intelligence technologies empowering identification of novel diagnostic molecular markers in gastric cancer. Ind. J. Pathol. Microbiol. 2021, 64 (Suppl. S1), S63-S68.
- Segura, F.; Segura, P.; Segura, F. Measuring Tumor Aggressiveness Through Artificial Intelligence. J. Asoc. Argent. Ortop. Traumatol. 2023, 88, 653-661. [CrossRef]
- Liopyris, K.; Gregoriou, S.; Dias, J.; Stratigos, A.J. Artificial intelligence in dermatology: Challenges and perspectives. Dermatol. Ther. 2022, 12, 2637-2651. [CrossRef] [PubMed]
- Ahmad, S.; Wasim, S. Prevent medical errors through artificial intelligence: A review. Saudi J. Med. Pharm. Sci. 2023, 9, 419-423. [CrossRef]
- Soun, J.; Chow, D.; Nagamine, M.; Takhtawala, R.; Filippi, C.; Yu, W.; Chang, P. Artificial intelligence and acute stroke imaging. Am. J. Neuroradiol. 2021, 42, 2-11. [CrossRef] [PubMed]
- Brereton, T.A.; Malik, M.M.; Lifson, M.; Greenwood, J.D.; Peterson, K.J.; Overgaard, S.M. The Role of Artificial Intelligence Model Documentation in Translational Science: Scoping Review. Interact. J. Med. Res. 2023, 12, e45903. [CrossRef] [PubMed]
- Klement, W.; El Emam, K. Consolidated reporting guidelines for prognostic and diagnostic machine learning modeling studies: Development and validation. J. Med. Internet Res. 2023, 25, e48763. [CrossRef]
- Huang, S.-C.; Pareek, A.; Seyyedi, S.; Banerjee, I.; Lungren, M.P. Fusion of medical imaging and electronic health records using deep learning: A systematic review and implementation guidelines. NPJ Digit. Med. 2020, 3, 136. [CrossRef]
- Mohsen, F.; Ali, H.; El Hajj, N.; Shah, Z. Artificial intelligence-based methods for fusion of electronic health records and imaging data. Sci. Rep. 2022, 12, 17981. [CrossRef] [PubMed]
- Deng, L.; Li, G.; Han, S.; Shi, L.; Xie, Y. Model compression and hardware acceleration for neural networks: A comprehensive survey. Proc. IEEE 2020, 108, 485-532. [CrossRef]
- Alcaín, E.; Fernandez, P.R.; Nieto, R.; Montemayor, A.S.; Vilas, J.; Galiana-Bordera, A.; Martinez-Girones, P.M.; Prieto-de-la-Lastra, C.; Rodriguez-Vila, B.; Bonet, M. Hardware architectures for real-time medical imaging. Electronics 2021, 10, 3118. [CrossRef]
- Eklund, A.; Dufort, P.; Forsberg, D.; LaConte, S.M. Medical image processing on the GPU-Past, present and future. Med. Image Anal. 2013, 17, 1073-1094. [CrossRef] [PubMed]
- Corral, J.M.R.; Civit-Masot, J.; Luna-Perejón, F.; Díaz-Cano, I.; Morgado-Estévez, A.; Domínguez-Morales, M. Energy efficiency in edge TPU vs. embedded GPU for computer-aided medical imaging segmentation and classification. Eng. Appl. Artif. Intell. 2024, 127, 107298. [CrossRef]
- Lin, Y.; Zhang, Y.; Yang, X. A Low Memory Requirement MobileNets Accelerator Based on FPGA for Auxiliary Medical Tasks. Bioengineering 2022, 10, 28. [CrossRef] [PubMed]
- Azghadi, M.R.; Lammie, C.; Eshraghian, J.K.; Payvand, M.; Donati, E.; Linares-Barranco, B.; Indiveri, G. Hardware implementation of deep network accelerators towards healthcare and biomedical applications. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 1138-1159. [CrossRef] [PubMed]
- Jiang, W.; Ye, X.; Chen, R.; Su, F.; Lin, M.; Ma, Y.; Zhu, Y.; Huang, S. Wearable on-device deep learning system for hand gesture recognition based on FPGA accelerator. Math. Biosci. Eng. 2021, 18, 132-153. [CrossRef] [PubMed]
- Nayak, D.R.; Dash, R.; Majhi, B. Automated diagnosis of multi-class brain abnormalities using MRI images: A deep convolutional neural network based method. Pattern Recog. Lett. 2020, 138, 385-391. [CrossRef]
- Soffer, S.; Klang, E.; Shimon, O.; Barash, Y.; Cahan, N.; Greenspana, H.; Konen, E. Deep learning for pulmonary embolism detection on computed tomography pulmonary angiogram: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 15814. [CrossRef]
- Lång, K.; Josefsson, V.; Larsson, A.-M.; Larsson, S.; Högberg, C.; Sartor, H.; Hofvind, S.; Andersson, I.; Rosso, A. Artificial intelligence-supported screen reading versus standard double reading in the Mammography Screening with Artificial Intelligence trial (MASAI): A clinical safety analysis of a randomised, controlled, non-inferiority, single-blinded, screening accuracy study. Lancet Oncol. 2023, 24, 936-944. [PubMed]
- Sveric, K.M.; Ulbrich, S.; Dindane, Z.; Winkler, A.; Botan, R.; Mierke, J.; Trausch, A.; Heidrich, F.; Linke, A. Improved assessment of left ventricular ejection fraction using artificial intelligence in echocardiography: A comparative analysis with cardiac magnetic resonance imaging. Int. J. Cardiol. 2024, 394, 131383. [CrossRef] [PubMed]
- Khan, P.; Kader, M.F.; Islam, S.R.; Rahman, A.B.; Kamal, M.S.; Toha, M.U.; Kwak, K.-S. Machine learning and deep learning approaches for brain disease diagnosis: Principles and recent advances. IEEE Access 2021, 9, 37622-37655. [CrossRef]
- Adam, R.; Dell’Aquila, K.; Hodges, L.; Maldjian, T.; Duong, T.Q. Deep learning applications to breast cancer detection by magnetic resonance imaging: A literature review. Breast Cancer Res. 2023, 25, 87. [CrossRef] [PubMed]
- Sheth, D.; Giger, M.L. Artificial intelligence in the interpretation of breast cancer on MRI. J. Magn. Reson. Imaging 2020, 51, 1310-1324. [CrossRef]
- McCrindle, B.; Zukotynski, K.; Doyle, T.E.; Noseworthy, M.D. A radiology-focused review of predictive uncertainty for AI interpretability in computer-assisted segmentation. Radiol. Artif. Intell. 2021, 3, e210031. [CrossRef] [PubMed]
- Zheng, R.; Wang, Q.; Lv, S.; Li, C.; Wang, C.; Chen, W.; Wang, H. Automatic liver tumor segmentation on dynamic contrast enhanced mri using 4D information: Deep learning model based on 3D convolution and convolutional lstm. IEEE Trans. Med. Imaging 2022, 41, 2965-2976. [CrossRef]
- Schalekamp, S.; Klein, W.M.; van Leeuwen, K.G. Current and emerging artificial intelligence applications in chest imaging: A pediatric perspective. Pediatr. Radiol. 2022, 52, 2120-2130. [CrossRef]
- Lee, M.-H.; O’Hara, N.; Sonoda, M.; Kuroda, N.; Juhasz, C.; Asano, E.; Dong, M.; Jeong, J.-W. Novel deep learning network analysis of electrical stimulation mapping-driven diffusion MRI tractography to improve preoperative evaluation of pediatric epilepsy. IEEE Trans. Biomed. Eng. 2020, 67, 3151-3162. [CrossRef]
- Ardila, D.; Kiraly, A.P.; Bharadwaj, S.; Choi, B.; Reicher, J.J.; Peng, L.; Tse, D.; Etemadi, M.; Ye, W.; Corrado, G. End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography. Nat. Med. 2019, 25, 954-961. [CrossRef]
- Watanabe, A.T.; Lim, V.; Vu, H.X.; Chim, R.; Weise, E.; Liu, J.; Bradley, W.G.; Comstock, C.E. Improved cancer detection using artificial intelligence: A retrospective evaluation of missed cancers on mammography. J. Digit. Imaging 2019, 32, 625-637. [CrossRef] [PubMed]
- Sermesant, M.; Delingette, H.; Cochet, H.; Jais, P.; Ayache, N. Applications of artificial intelligence in cardiovascular imaging. Nat. Rev. Cardiol. 2021, 18, 600-609. [CrossRef]
- Nahavandi, D.; Alizadehsani, R.; Khosravi, A.; Acharya, U.R. Application of artificial intelligence in wearable devices: Opportunities and challenges. Comput. Methods Programs Biomed. 2022, 213, 106541. [CrossRef]
- Stangl, F.J.; Riedl, R. Measurement of heart rate and heart rate variability with wearable devices: A systematic review. Wirtschaftsinformatik 2022, 2022, 15.
- Huang, J.-D.; Wang, J.; Ramsey, E.; Leavey, G.; Chico, T.J.; Condell, J. Applying artificial intelligence to wearable sensor data to diagnose and predict cardiovascular disease: A review. Sensors 2022, 22, 8002. [CrossRef] [PubMed]
- Bahrami, M.; Forouzanfar, M. Deep learning forecasts the occurrence of sleep apnea from single-lead ECG. Cardiovasc. Eng. Technol. 2022, 13, 809-815. [CrossRef]
- Joeris, A.; Zhu, T.Y.; Lambert, S.; Wood, A.; Jayakumar, P. Real-world patient data: Can they support decision making and patient engagement? Injury 2023, 54, S51-S56. [CrossRef]
- Asthana, S.; Megahed, A.; Strong, R. A recommendation system for proactive health monitoring using IoT and wearable technologies. In Proceedings of the 2017 IEEE International Conference on AI & Mobile Services (AIMS), Honolulu, HI, USA, 25-30 June 2017; IEEE: New, York, NY, USA, 2017; pp. 14-21.
- Djanian, S.; Bruun, A.; Nielsen, T.D. Sleep classification using Consumer Sleep Technologies and AI: A review of the current landscape. Sleep Med. 2022, 100, 390-403. [CrossRef] [PubMed]
- Sabry, F.; Eltaras, T.; Labda, W.; Alzoubi, K.; Malluhi, Q. Machine learning for healthcare wearable devices: The big picture. J. Healthc. Eng. 2022, 2022, 1-25. [CrossRef]
- Van Bulck, L.; Couturier, R.; Moons, P. Applications of Artificial Intelligence for Nursing: Has a New Era Arrived? Oxford University Press US: Cary, NC, USA, 2023; Volume 22, pp. e19-e20.
- Jadczyk, T.; Wojakowski, W.; Tendera, M.; Henry, T.D.; Egnaczyk, G.; Shreenivas, S. Artificial intelligence can improve patient management at the time of a pandemic: The role of voice technology. J. Med. Internet Res. 2021, 23, e22959. [CrossRef]
- Adus, S.; Macklin, J.; Pinto, A. Exploring patient perspectives on how they can and should be engaged in the development of artificial intelligence (AI) applications in health care. BMC Health Serv. Res. 2023, 23, 1163. [CrossRef] [PubMed]
- Curtis, R.G.; Bartel, B.; Ferguson, T.; Blake, H.T.; Northcott, C.; Virgara, R.; Maher, C.A. Improving user experience of virtual health assistants: Scoping review. J. Med. Internet Res. 2021, 23, e31737. [CrossRef] [PubMed]
- Ye, J.; He, L.; Beestrum, M. Implications for implementation and adoption of telehealth in developing countries: A systematic review of China’s practices and experiences. NPJ Digit. Med. 2023, 6, 174. [CrossRef] [PubMed]
- Jeddi, Z.; Bohr, A. Remote patient monitoring using artificial intelligence. In Artificial Intelligence in Healthcare; Elsevier: Amsterdam, The Netherlands, 2020; pp. 203-234.
- Shaik, T.; Tao, X.; Higgins, N.; Li, L.; Gururajan, R.; Zhou, X.; Acharya, U.R. Remote patient monitoring using artificial intelligence: Current state, applications, and challenges. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2023, 13, e1485. [CrossRef]
- Khadija, A.; Zahra, F.F.; Naceur, A. AI-powered health chatbots: Toward a general architecture. Procedia Comput. Sci. 2021, 191, 355-360. [CrossRef]
- Görtz, M.; Baumgärtner, K.; Schmid, T.; Muschko, M.; Woessner, P.; Gerlach, A.; Byczkowski, M.; Sültmann, H.; Duensing, S.; Hohenfellner, M. An artificial intelligence-based chatbot for prostate cancer education: Design and patient evaluation study. Digit. Health 2023, 9, 20552076231173304. [CrossRef]
- Sharma, S.; Rawal, R.; Shah, D. Addressing the challenges of AI-based telemedicine: Best practices and lessons learned. J. Educ. Health Promot. 2023, 12, 338. [CrossRef] [PubMed]
- Maleki, F.; Muthukrishnan, N.; Ovens, K.; Reinhold, C.; Forghani, R. Machine learning algorithm validation: From essentials to advanced applications and implications for regulatory certification and deployment. Neuroimaging Clin. 2020, 30, 433-445. [CrossRef] [PubMed]
- Lei, J. Cross-validation with confidence. J. Am. Stat. Assoc. 2020, 115, 1978-1997. [CrossRef]
- Ebrahimian, S.; Kalra, M.K.; Agarwal, S.; Bizzo, B.C.; Elkholy, M.; Wald, C.; Allen, B.; Dreyer, K.J. FDA-regulated AI algorithms: Trends, strengths, and gaps of validation studies. Acad. Radiol. 2022, 29, 559-566. [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable ai: A review of machine learning interpretability methods. Entropy 2020, 23, 18. [CrossRef] [PubMed]
- Davagdorj, K.; Li, M.; Ryu, K.H. Local interpretable model-agnostic explanations of predictive models for hypertension, Advances in Intelligent Information Hiding and Multimedia Signal Processing. In Proceeding of the 16th International Conference on
155. Nohara, Y.; Matsumoto, K.; Soejima, H.; Nakashima, N. Explanation of machine learning models using shapley additive explanation and application for real data in hospital. Comput. Methods Programs Biomed. 2022, 214, 106584. [CrossRef] [PubMed]
156. Puerta-Beldarrain, M.; Gómez-Carmona, O.; Casado-Mansilla, D.; López-de-Ipiña, D. Human-AI collaboration to promote trust, engagement and adaptation in the process of pro-environmental and health behaviour change. In Proceedings of the International Conference on Ubiquitous Computing and Ambient Intelligence, Córdoba, Spain, 29 November-2 December 2022; Springer: Berlin/Heidelberg, Germany, 2022; pp. 381-392.
157. Mishra, A. Scalable AI Governance and Ethics. In Scalable AI and Design Patterns: Design, Develop, and Deploy Scalable AI Solutions; Springer: Berlin/Heidelberg, Germany, 2024; pp. 147-165.
158. Badnjević, A.; Pokvić, L.G.; Deumić, A.; Bećirović, L.S. Post-market surveillance of medical devices: A review. Technol. Health Care 2022, 30, 1315-1329. [CrossRef] [PubMed]
159. Feng, J.; Phillips, R.V.; Malenica, I.; Bishara, A.; Hubbard, A.E.; Celi, L.A.; Pirracchio, R. Clinical artificial intelligence quality improvement: Towards continual monitoring and updating of AI algorithms in healthcare. NPJ Digit. Med. 2022, 5, 66. [CrossRef] [PubMed]
160. Murdoch, B. Privacy and artificial intelligence: Challenges for protecting health information in a new era. BMC Med. Ethics 2021, 22, 122. [CrossRef] [PubMed]
161. Iserson, K.V. Informed consent for artificial intelligence in emergency medicine: A practical guide. Am. J. Emerg. Med. 2024, 76, 225-230. [CrossRef] [PubMed]
162. Fletcher, R.R.; Nakeshimana, A.; Olubeko, O. Addressing fairness, bias, and appropriate use of artificial intelligence and machine learning in global health. Front. Media SA 2021, 3, 561802. [CrossRef] [PubMed]
163. Smith, H. Clinical AI: Opacity, accountability, responsibility and liability. AI Soc. 2021, 36, 535-545. [CrossRef]
164. Moltubakk Kempton, A.; Vassilakopoulou, P. Accountability, Transparency and Explainability in AI for Healthcare. 2021. Available online: https://dl.eusset.eu/items/9c739979-ec3f-4510-a02a-553eadee47e2 (accessed on 28 February 2024).
165. Kim, B.; Park, J.; Suh, J. Transparency and accountability in AI decision support: Explaining and visualizing convolutional neural networks for text information. Decis. Support Syst. 2020, 134, 113302. [CrossRef]
166. Carmody, J.; Shringarpure, S.; Van de Venter, G. AI and privacy concerns: A smart meter case study. J. Inf. Commun. Ethics Soc. 2021, 19, 492-505. [CrossRef]
167. Bandari, V. Enterprise Data Security Measures: A Comparative Review of Effectiveness and Risks Across Different Industries and Organization Types. Int. J. Bus. Intell. Big Data Anal. 2023, 6,1-11.
168. Lehne, M.; Sass, J.; Essenwanger, A.; Schepers, J.; Thun, S. Why digital medicine depends on interoperability. NPJ Digit. Med. 2019, 2, 79. [CrossRef] [PubMed]
169. Perugu, B.; Wadhwa, V.; Kim, J.; Cai, J.; Shin, A.; Gupta, A. Pragmatic Approaches to Interoperability-Surmounting Barriers to Healthcare Data and Information Across Organizations and Political Boundaries. Telehealth Med. Today 2023, 8, 421.
170. Dikici, E.; Bigelow, M.; Prevedello, L.M.; White, R.D.; Erdal, B.S. Integrating AI into radiology workflow: Levels of research, production, and feedback maturity. J. Med. Imaging 2020, 7, 016502. [CrossRef] [PubMed]
171. Balagurunathan, Y.; Mitchell, R.; El Naqa, I. Requirements and reliability of AI in the medical context. Phys. Med. 2021, 83, 72-78. [CrossRef] [PubMed]
172. Schneeberger, D.; Stöger, K.; Holzinger, A. The European Legal Framework for Medical AI, International Cross-Domain Conference for Machine Learning and Knowledge Extraction; Springer: Berlin/Heidelberg, Germany, 2020; pp. 209-226.
173. Larson, D.B.; Harvey, H.; Rubin, D.L.; Irani, N.; Justin, R.T.; Langlotz, C.P. Regulatory frameworks for development and evaluation of artificial intelligence-based diagnostic imaging algorithms: Summary and recommendations. J. Am. Coll. Radiol. 2021, 18, 413-424. [CrossRef]
174. Benjamens, S.; Dhunnoo, P.; Meskó, B. The state of artificial intelligence-based FDA-approved medical devices and algorithms: An online database. NPJ Digit. Med. 2020, 3, 118. [CrossRef] [PubMed]
175. Muehlematter, U.J.; Daniore, P.; Vokinger, K.N. Approval of artificial intelligence and machine learning-based medical devices in the USA and Europe (2015-2020): A comparative analysis. Lancet Digit. Health 2021, 3, e195-e203. [CrossRef]
176. Baric-Parker, J.; Anderson, E.E. Patient data-sharing for AI: Ethical challenges, catholic solutions. Linacre Q. 2020, 87, 471-481. [CrossRef]
177. Johnson, K.B.; Wei, W.Q.; Weeraratne, D.; Frisse, M.E.; Misulis, K.; Rhee, K.; Zhao, J.; Snowdon, J.L. Precision medicine, AI, and the future of personalized health care. Clin. Transl. Sci. 2021, 14, 86-93. [CrossRef]
178. Bandyopadhyay, A.; Goldstein, C. Clinical applications of artificial intelligence in sleep medicine: A sleep clinician’s perspective. Sleep Breath. 2023, 27, 39-55. [CrossRef] [PubMed]
179. Galkin, F.; Zhavoronkov, A. AI in Longevity. In Artificial Intelligence for Healthy Longevity; Springer: Berlin/Heidelberg, Germany, 2023; pp. 3-13.
180. Zhavoronkov, A.; Mamoshina, P.; Vanhaelen, Q.; Scheibye-Knudsen, M.; Moskalev, A.; Aliper, A. Artificial intelligence for aging and longevity research: Recent advances and perspectives. Ageing Res. Rev. 2019, 49, 49-66. [CrossRef] [PubMed]
181. Jiménez-Luna, J.; Grisoni, F.; Weskamp, N.; Schneider, G. Artificial intelligence in drug discovery: Recent advances and future perspectives. Expert Opin. Drug Discov. 2021, 16, 949-959. [CrossRef] [PubMed]
182. Feizi, N.; Tavakoli, M.; Patel, R.V.; Atashzar, S.F. Robotics and ai for teleoperation, tele-assessment, and tele-training for surgery in the era of COVID-19: Existing challenges, and future vision. Front. Robot. AI 2021, 8, 610677. [CrossRef] [PubMed]
183. Bitencourt, A.; Naranjo, I.D.; Gullo, R.L.; Saccarelli, C.R.; Pinker, K. AI-enhanced breast imaging: Where are we and where are we heading? Eur. J. Radiol. 2021, 142, 109882. [CrossRef] [PubMed]
184. Shi, Q.; Dong, B.; He, T.; Sun, Z.; Zhu, J.; Zhang, Z.; Lee, C. Progress in wearable electronics/photonics-Moving toward the era of artificial intelligence and internet of things. InfoMat 2020, 2, 1131-1162. [CrossRef]
185. Forghani, N.; Maghooli, K.; Dabanloo, N.J.; Farahani, A.V.; Forouzanfar, M. Intelligent oscillometric system for automatic detection of peripheral arterial disease. IEEE J. Biomed. Health Inform. 2021, 25, 3209-3218. [CrossRef] [PubMed]
186. Huang, C.-H.; Batarseh, F.A.; Boueiz, A.; Kulkarni, A.; Su, P.-H.; Aman, J. Measuring outcomes in healthcare economics using Artificial Intelligence: With application to resource management. Data Policy 2021, 3, e30. [CrossRef] [PubMed]
187. Giuste, F.; Shi, W.; Zhu, Y.; Naren, T.; Isgut, M.; Sha, Y.; Tong, L.; Gupte, M.; Wang, M.D. Explainable artificial intelligence methods in combating pandemics: A systematic review. IEEE Rev. Biomed. Eng. 2022, 16, 5-21. [CrossRef]
188. Cao, L. AI in Combating the COVID-19 Pandemic. IEEE Intell. Syst. 2022, 37, 3-13. [CrossRef]
189. Gu, X.; Deligianni, F.; Han, J.; Liu, X.; Chen, W.; Yang, G.-Z.; Lo, B. Beyond supervised learning for pervasive healthcare. IEEE Rev. Biomed. Eng. 2023, 17, 42-62. [CrossRef] [PubMed]
190. Fechter, T.; Baltas, D. One-shot learning for deformable medical image registration and periodic motion tracking. IEEE Trans. Med. Imaging 2020, 39, 2506-2517. [CrossRef] [PubMed]
191. Feng, R.; Zheng, X.; Gao, T.; Chen, J.; Wang, W.; Chen, D.Z.; Wu, J. Interactive few-shot learning: Limited supervision, better medical image segmentation. IEEE Trans. Med. Imaging 2021, 40, 2575-2588. [CrossRef] [PubMed]
192. Mahapatra, D.; Bozorgtabar, B.; Ge, Z. Medical image classification using generalized zero shot learning. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Montreal, QC, Canada, 10-17 October 2021; pp. 3344-3353.
193. Hospedales, T.; Antoniou, A.; Micaelli, P.; Storkey, A. Meta-learning in neural networks: A survey. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 5149-5169. [CrossRef] [PubMed]
194. Yang, J.; Soltan, A.A.; Clifton, D.A. Machine learning generalizability across healthcare settings: Insights from multi-site COVID-19 screening. NPJ Digit. Med. 2022, 5, 69. [CrossRef] [PubMed]
195. Khoshnevisan, F.; Chi, M. Unifying domain adaptation and domain generalization for robust prediction across minority racial groups, Machine Learning and Knowledge Discovery in Databases. In Proceedings of the Research Track: European Conference, ECML PKDD 2021, Bilbao, Spain, 13-17 September 2021; Proceedings, Part I 21. Springer: Berlin/Heidelberg, Germany, 2021; pp. 521-537.
196. Rieke, N.; Hancox, J.; Li, W.; Milletari, F.; Roth, H.R.; Albarqouni, S.; Bakas, S.; Galtier, M.N.; Landman, B.A.; Maier-Hein, K. The future of digital health with federated learning. NPJ Digit. Med. 2020, 3, 119. [CrossRef]
197. Hogg, H.D.J.; Al-Zubaidy, M.; Talks, J.; Denniston, A.K.; Kelly, C.J.; Malawana, J.; Papoutsi, C.; Teare, M.D.; A Keane, P.; Beyer, F.R.; et al. Stakeholder perspectives of clinical artificial intelligence implementation: Systematic review of qualitative evidence. J. Med. Internet Res. 2023, 25, e39742. [CrossRef]
198. Gerlings, J.; Jensen, M.S.; Shollo, A. Explainable ai, but explainable to whom? an exploratory case study of xai in healthcare. In Handbook of Artificial Intelligence in Healthcare: Vol 2: Practicalities and Prospects; Springer: Berlin/Heidelberg, Germany, 2022; pp. 169-198.
DOI: https://doi.org/10.3390/bioengineering11040337
PMID: https://pubmed.ncbi.nlm.nih.gov/38671759
Publication Date: 2024-03-29
The Role of AI in Hospitals and Clinics: Transforming Healthcare in the 21st Century
Received: 28 February 2024
Revised: 25 March 2024
Accepted: 26 March 2024
Published: 29 March 2024
Abstract
As healthcare systems around the world face challenges such as escalating costs, limited access, and growing demand for personalized care, artificial intelligence (AI) is emerging as a key force for transformation. This review is motivated by the urgent need to harness AI’s potential to mitigate these issues and aims to critically assess AI’s integration in different healthcare domains. We explore how AI empowers clinical decision-making, optimizes hospital operation and management, refines medical image analysis, and revolutionizes patient care and monitoring through AI-powered wearables. Through several case studies, we review how AI has transformed specific healthcare domains and discuss the remaining challenges and possible solutions. Additionally, we will discuss methodologies for assessing AI healthcare solutions, ethical challenges of AI deployment, and the importance of data privacy and bias mitigation for responsible technology use. By presenting a critical assessment of AI’s transformative potential, this review equips researchers with a deeper understanding of AI’s current and future impact on healthcare. It encourages an interdisciplinary dialogue between researchers, clinicians, and technologists to navigate the complexities of AI implementation, fostering the development of AI-driven solutions that prioritize ethical standards, equity, and a patient-centered approach.
1. Introduction
medical diagnostics, AI enhances the accuracy and speed of image analysis in radiology and pathology [10]. Moreover, AI plays a crucial role in patient care through remote monitoring, telemedicine, and virtual assistance, fundamentally altering the patient-doctor interaction paradigm [11].
2. AI in Clinical Decision-Making
2.1. AI Algorithms for Diagnosis and Prognosis
- Machine learning (ML): ML algorithms learn from data to make predictions or decisions without being explicitly programmed for the task [18]. In healthcare, supervised learning algorithms have been instrumental in developing predictive models for patient outcomes based on historical data [19]. Unsupervised learning, on the other hand, is used to identify patterns or clusters within data, useful in discovering novel disease subtypes [20]. Reinforcement learning, where algorithms learn to make sequences of decisions by trial and error, has potential in personalized treatment optimization [21].
- Deep learning (DL): A subset of ML, deep learning uses neural networks with multiple layers (hence “deep”) to analyze complex data structures. Convolutional Neural Networks (CNNs) are particularly effective in processing imaging data, making them invaluable for diagnosing diseases from medical images like X-rays or MRIs [22]. Some other advanced CNN architectures include Residual Network (ResNet), Inception, Visual Geometry Group (VGG), and Graph Convolutional Networks (GCNs), each with its own strengths and applications in image analysis, classification, and graph data processing [23]. Recurrent Neural Networks (RNNs), known for their ability to handle sequential data, are used for analyzing time-series data, such as physiological signals collected during patient monitoring, to predict health deteriorations or outcomes over time [24]. For instance, Long Short-Term Memory (LSTM) networks, a sophisticated variant of RNNs, have been extensively utilized in the detection of sleep apnea using polysomnography data [25]. Additionally, Transformer models, such as BERT (Bidirectional Encoder Representations from Transformers) and GPT (Generative Pre-trained Transformer), offer revolutionary approaches to processing natural language in clinical notes, enabling more accurate extraction of patient information and insights. Generative Adversarial Networks (GANs) [26] and conditional diffusion models [27] have emerged as a powerful tool for generating synthetic medical images for training without privacy concerns, while Graph Neural Networks (GNNs) are unlocking new possibilities in modeling complex biological and health-related networks, from predicting protein interactions to understanding disease pathways.
Table 1 provides a summary of the various deep learning models discussed, including their applications, strengths, and areas of healthcare they are transforming.
| Algorithm Type | General Application | Limitations | Comments | Example |
| Convolutional Neural Networks (CNNs) | Image recognition and analysis in medical imaging (e.g., X-rays, MRI, CT scans) | Require large labeled datasets and substantial computational resources; can be a “black box” making interpretability difficult | Highly effective for spatial data; state of the art in medical image analysis | Deeplab v3+, a CNN variant for gastric cancer segmentation [28]. Results: 95.76% accuracy, outperforming SegNet/ICNet. |
| Recurrent Neural Networks (RNNs) and Long Short-Term Memory (LSTM) Networks | Analysis of sequential data such as ECG, EEG signals, or patient health records | Prone to overfitting on smaller datasets; long training times; difficulty in parallelizing the tasks | Suited for time-series data; LSTM addresses vanishing gradient problem in RNNs | LSTM for EEG signal classification [29]. Results: 71.3% accuracy, utilizing novel one-dimensional gradient descent activation functions for enhanced performance. |
| Transformer Models (e.g., BERT, GPT) | Natural language processing tasks, including clinical text analysis and patient history summarization | Require significant computational power and memory; pre-training on large datasets is time-consuming | Offer state-of-the-art performance in NLP; enable understanding of context in clinical documentation | Clinical-specific BERT (Transformer) for Japanese text analysis [30]: pre-trained on 120 million texts, achieving 0.773 Masked-LM and 0.975 Next Sentence Prediction accuracy, indicating potential for complex medical NLP tasks. |
| Generative Adversarial Networks (GANs) | Synthetic data generation for training models without compromising patient privacy; augmenting datasets | Training stability issues; generating high-quality data is challenging | Useful in data-limited scenarios; potential in creating realistic medical images for training | Differentially private GAN for synthetic data generation: utilizes convolutional AEs and GANs to produce realistic synthetic medical data, preserving data characteristics and outperforming existing models [31]. |
| Graph Neural Networks (GNNs) | Modeling complex relationships and interactions between health data points (e.g., drug interaction prediction, disease progression modeling) | Complex model architectures that are difficult to interpret; scalability to very large graphs | Effective for data represented as graphs; emerging applications in personalized medicine | Knowledge-GNN for drug-drug interaction prediction: leverages knowledge graphs to capture complex drug relationships and neighborhood information, outperforming conventional models [32]. |
- Natural language processing (NLP): NLP algorithms allow computers to understand and interpret human language. In healthcare, NLP is used to extract meaningful information from unstructured data sources like clinical notes or the research literature, aiding in both diagnostic processes and the aggregation of knowledge for prognosis estimation [33]. An example of such a language model is the GatorTron [34]. It is
a large-scale Transformer-based NLP model tailored for the healthcare domain. It utilizes the Transformer architecture, known for its efficiency in handling sequence-to-sequence tasks and its ability to process large datasets, to interpret and analyze electronic health records. With its 8.9 billion parameters, GatorTron is trained on over 90 billion words of clinical text, making it a highly advanced model for extracting and understanding complex medical information from unstructured data sources.
AI algorithms are not just tools for efficient diagnosis and prognosis; they represent a paradigm shift in understanding and managing health and disease. The next sections will provide deeper insights into specific case studies and the role of AI in personalizing medical care, further highlighting AI’s profound impact on clinical decision-making.
2.2. Case Studies of AI in Detecting Diseases
- Cancer detection: One of the most groundbreaking applications of AI is in the early detection of cancer. A notable case study involves the use of deep learning algorithms in the analysis of mammograms for breast cancer detection. Research has shown that AI can identify patterns in mammographic images that are indicative of cancerous growths, often with greater accuracy than traditional methods. A notable study published in the journal Nature reported the development of an AI model by Google Health [35]. This model was trained on a large dataset of mammograms and demonstrated the ability to detect breast cancer more accurately than human radiologists. The AI system showed a reduction in both false positives and false negatives, key factors in cancer diagnostics. This progress in AI technology is significant because early detection of breast cancer can dramatically improve prognosis and treatment outcomes.
- Diabetes management: AI’s role in managing and detecting diabetes, particularly through machine learning algorithms, is a significant area of improvement in healthcare. These algorithms can analyze patient data to predict the onset and progression of diabetes and its complications, as demonstrated in different studies. In one study, several supervised classification algorithms were applied to predict and classify eight diabetes complications, including metabolic syndrome, dyslipidemia, neuropathy, nephropathy, diabetic foot, hypertension, obesity, and retinopathy [36]. The dataset utilized in this study comprises 79 input attributes, including results of medical tests and demographic information collected from 884 patients. The performance of the models was evaluated using the accuracy and F1 score, reaching a maximum of
and , respectively. Among different classifiers, random forest (RF), Adaboost, and XGBoost achieved the best performance. This high level of accuracy demonstrates the potential of machine learning in effectively predicting diabetes complications. Another study focused on evaluating the efficacy of machine learning algorithms in predicting complications and poor glycemic control in nonadherent type 2 diabetes patients [37]. This real-world study used data from 800 type 2 diabetes patients, of which 165 met the inclusion criteria. Different machine learning algorithms were used to develop prediction models, with the predictive performance assessed using the area under the curve. The highest performance scores for predicting various complications such as diabetic nephropathy, neuropathy, angiopathy, and eye disease were , , and , showcasing the effectiveness of these models. - Heart disease prediction: The prediction of heart disease using AI represents a significant advancement in cardiovascular healthcare. This application not only aims to predict the occurrence of heart disease but also attempts to determine its severity, a crucial factor in effective treatment and management. One innovative study in this area focused on a machine learning-based prediction model that performs both binary
and multiple classifications of heart disease [38]. The model, known as Fuzzy-GBDT, integrates fuzzy logic with a gradient boosting decision tree to streamline data complexity and improve prediction accuracy. Additionally, to avoid overfitting, the model incorporates a bagging technique, enhancing its capability to classify the severity of heart disease. The evaluation results of this model show excellent accuracy and stability in predicting heart disease, demonstrating its potential as a valuable tool in healthcare. Another interesting study introduces a cutting-edge healthcare system that employs ensemble deep learning coupled with feature fusion approaches [39]. This system is designed to overcome the limitations of traditional machine learning models that struggle with high-dimensional datasets. It achieves this by integrating sensor data with electronic medical records, creating a more holistic dataset for heart disease prediction. The system uses the information gain technique to streamline this dataset, focusing on the most relevant features and thereby reducing computational complexity. A key aspect of this model is the application of conditional probability for precise feature weighting, enhancing the overall performance of the system. Impressively, this ensemble deep learning model achieved an accuracy of, outperforming existing models and illustrating its efficacy in heart disease prediction. - AI in neurological disorders: The integration of AI, particularly deep learning (DL), in neurology has opened new avenues for the diagnosis and management of neurological disorders. The recent literature reveals significant progress in employing AI for the early detection and more accurate diagnosis of various conditions, including AD. One area of notable advancement is the use of deep learning in neuroimaging studies. DL’s ability to process and learn from raw data through complex, nonlinear transformations makes it well suited for identifying the subtle and diffuse alterations characteristic of many neurological and psychiatric disorders. Research in this domain has shown that DL can be a powerful tool in the ongoing search for biomarkers of such conditions, offering potential breakthroughs in understanding and diagnosing brain-based disorders [40]. Furthering this progress, a comprehensive review of deep learning techniques in the prognosis of a range of neuropsychiatric and neurological disorders, such as stroke, Alzheimer’s, Parkinson’s, epilepsy, autism, migraine, cerebral palsy, and multiple sclerosis, has underscored deep learning’s versatility in addressing real-life challenges across various domains, including disease diagnosis [41]. In the specific case of Alzheimer’s Disease (AD), the most common cause of dementia, deep learning has shown promise in enhancing diagnosis accuracy. Utilizing Convolutional Neural Networks (CNNs), researchers have developed frameworks for detecting AD characteristics from Magnetic Resonance Imaging (MRI) data [42]. By considering different stages of dementia and creating high-resolution disease probability maps, these models provide intuitive visualizations of individual AD risk. This approach, especially when addressing class imbalance in datasets, has achieved high accuracy, surpassing existing methods. The adaptation of such models to extensive datasets like the Alzheimer’s Disease Neuroimaging Initiative (ADNI) further validates their effectiveness in predicting AD classes.
- Key insights: These case studies highlight AI’s significant role in advancing disease detection across multiple medical disciplines, offering accurate and timely diagnoses, often through non-invasive methods. However, as AI technology continues to evolve, there is a critical need for addressing challenges such as data privacy, algorithmic transparency, and ensuring equitable access to these technologies. Future developments should focus on creating more robust AI systems that can handle diverse datasets, thereby reducing potential biases in diagnosis. Additionally, integrating AI with traditional diagnostic methods and enhancing interdisciplinary collaboration among technologists, clinicians, and patients will be key to harnessing AI’s full potential in disease detection and management.
2.3. The Role of AI in Personalized Medicine
- Tailoring treatments to genetic profiles: One of the most significant applications of AI in personalized medicine is in the field of genomics. AI algorithms can analyze vast genomic datasets to identify mutations and variations that might influence an individual’s response to certain treatments. For example, in oncology, AI helps in identifying specific genetic markers that are susceptible to targeted cancer therapies. This approach increases the efficacy of the treatment and minimizes the risk of adverse reactions, ensuring a more effective and safer treatment plan for the patient. A prime example of this application is a study focusing on nonmuscle invasive urothelial carcinoma, a type of bladder cancer known for its high recurrence risk [43]. In this study, researchers employed a machine learning algorithm to analyze genomic data from patients at their initial presentation. They aimed to identify genes most predictive of recurrence within five years following transurethral resection of the bladder tumor. The study involved whole-genome profiling of 112 frozen nonmuscle invasive urothelial carcinoma specimens using Human WG-6 BeadChips. A genetic programming algorithm was then applied to evolve classifier mathematical models for outcome prediction. The process involved cross-validation-based resampling and assessing gene use frequencies to pinpoint the most prognostic genes. These genes were subsequently combined into rules within a voting algorithm to predict the likelihood of cancer recurrence. Of the genes analyzed, 21 were identified as predictive of recurrence. Further validation through the quantitative polymerase chain reaction was conducted on a subset of 100 patients. The results were promising: a five-gene combined rule using the voting algorithm showed
sensitivity and specificity in predicting recurrence in the training set. Additionally, a three-gene rule was developed, offering sensitivity and specificity in the training set for recurrence prediction. - Predictive analytics in drug development: AI also plays a crucial role in drug development, particularly in predicting how different patients will respond to a drug. By analyzing historical data from clinical trials and patient records, AI models can predict the effectiveness of drugs on various demographic groups [44,45]. This predictive power is invaluable in designing clinical trials and in developing drugs that are more effective for specific patient populations In recent years, AI has made remarkable strides in drug development. Exscientia introduced the first AI-designed drug molecule for clinical trials in early 2020 [46]. DeepMind’s AlphaFold then achieved a breakthrough in July 2021 by predicting structures for over 330,000 proteins, including the entire human genome. In 2022, Insilico Medicine started Phase I trials for an AI-discovered molecule, a process significantly faster and more cost-effective than traditional methods. By 2023, AbSci had innovated in creating antibodies using generative AI, and Insilico Medicine saw an AI-designed drug receive FDA Orphan Drug Designation, with Phase II trials planned shortly thereafter. These milestones mark a transformative era in AI-driven drug discovery. AI’s application extends to the identification of novel proteins or genes as potential disease targets, with systems capable of predicting the 3D structures of these targets using deep learning [47]. AI is also revolutionizing molecular simulations and the prediction of drug properties such as toxicity and bioactivity, enabling high-fidelity simulations that can be run entirely in silico [44]. Moreover, AI is shifting the paradigm of traditional drug discovery from screening large libraries of molecules to generating novel drug molecules from scratch [48]. This approach can enhance the efficiency of the drug discovery process and can lead to the development of novel therapies.
3. Customizing treatment plans: AI systems are adept at integrating and analyzing various types of health data-from clinical records and lab results to lifestyle information and environmental factors. This capability allows healthcare providers to create more refined and comprehensive treatment plans [49]. For instance, in managing chronic diseases like diabetes, AI can analyze data from wearable devices, diet logs, and blood sugar readings to recommend personalized lifestyle and medication adjustments for better disease management [50].
4. AI in mental health: In the field of mental health, AI is used to personalize treatment approaches. By monitoring patterns in speech [51], behavior [52], and social media activity [53,54], AI tools can help in identifying the onset of mental health issues and suggest interventions tailored to the individual’s unique situation. This personalized approach is crucial in mental health, where treatment efficacy can vary significantly from person to person.
In future research and development within mental health treatment, a promising direction is the integration of AI systems with emotional intelligence [55]. Such systems could be crucial in early detection and intervention of mental health disorders by analyzing speech and behavior patterns for signs of conditions like depression or anxiety. Further exploration into personalizing therapy using AI could lead to more individualized and effective care.
5. Key insights: While the integration of AI into personalized medicine offers transformative potential, it also presents a spectrum of challenges that must be addressed. Beyond data privacy and algorithmic bias, significant concerns include interoperability and data integration across diverse healthcare systems [56], ensuring AI systems are compliant with regulatory and ethical standards, and establishing their clinical validity and reliability [57].
3. AI in Hospital Operations and Management
being leveraged to revolutionize hospital operations, enhancing efficiency, reducing costs, and improving patient care. We will explore three primary areas: AI’s role in optimizing logistics and resource management, its application in automating administrative tasks, and its contribution to improving patient flow and scheduling.
| Aspect | Applications | ||
| AI for hospital logistics and resource management | Predictive inventory management for medical supplies, medications, and equipment; efficient facility management including HVAC systems and predictive maintenance; optimization of resource allocation for staff and materials; and supply chain optimization and management during emergencies and health crises. | ||
| Automating administrative tasks with AI | Patient data management including EMRs and unstructured data analysis; billing and claims processing automation for accuracy and compliance; AI-driven scheduling systems for appointments and procedures; document management and processing automation; automated communication and reminders for patient engagement; and data security and compliance monitoring. | ||
| AI in patient flow and scheduling optimization |
|
3.1. AI for Hospital Logistics and Resource Management
- Inventory management: AI systems are being used to predictively manage inventory in hospitals [60,61]. By analyzing usage patterns, patient inflow, and other relevant data, AI can forecast the need for medical supplies, medications, and equipment. This predictive capability ensures that hospitals maintain optimal stock levels, reducing wastage and ensuring the availability of critical supplies when needed.
- Facility management: AI also contributes to the efficient management of hospital facilities. For example, AI-powered systems can control heating, ventilation, and air conditioning (HVAC) systems more efficiently, reducing energy costs while maintaining a comfortable environment for patients and staff [62]. Additionally, AI can help in the predictive maintenance of hospital equipment, identifying potential issues before they lead to breakdowns, thus minimizing downtime and repair costs [63].
- Resource allocation: One of the most substantial applications of AI in hospital management is in the optimization of resource allocation [64]. AI algorithms can analyze complex datasets, including patient admissions, staff availability, and operational capacities, to optimize the allocation of human and material resources. This includes
scheduling surgeries and medical procedures in a manner that maximizes the utilization of operating rooms and medical staff, while minimizing patient wait times [65]. - Supply chain optimization: AI enhances supply chain operations in hospitals by analyzing trends and automating ordering processes [66,67]. It can anticipate supply chain disruptions and suggest alternative solutions, ensuring that the hospital’s operations are not affected by external supply chain challenges. In emergency situations or during health crises, AI systems play a crucial role in managing logistics and resources [68]. They can quickly analyze the situation, predict the resources required, and assist in the efficient distribution of these resources where they are needed most.
In conclusion, AI’s role in hospital logistics and resource management is multifaceted and profoundly impactful. By automating and optimizing these critical aspects, AI can bring about operational efficiencies and enhance the overall quality of patient care. As AI technology continues to advance, its potential to further revolutionize hospital operations and management is vast, opening new avenues for innovation in healthcare delivery.
3.2. Automating Administrative Tasks with AI
- Patient data management: AI plays an important role in managing vast amounts of patient data [69]. AI systems can organize, categorize, and process patient records, appointments, and treatment histories with high efficiency and accuracy. These systems can also extract relevant information from unstructured data, such as doctor’s notes, making it easier for healthcare providers to access and analyze patient information. For example, a study utilized AI and natural language processing (NLP) to analyze electronic medical records (EMRs), focusing on uncoded consultation notes for disease prediction [70]. Techniques like bag of words and topic modeling were applied, along with a method to match notes with a medical ontology. This approach was particularly tested for colorectal cancer. The study found that the ontology-based method significantly enhanced predictive performance, with an AUC of 0.870 , surpassing traditional benchmarks. This highlights AI’s potential in extracting useful information from EMR’s unstructured data, improving disease prediction accuracy.
- Billing and claims processing: AI algorithms can also be used to automate billing and insurance claims processing. They can quickly analyze and process claims data, identify errors or inconsistencies, and ensure that billing is accurate and compliant with relevant regulations [71]. This not only speeds up the reimbursement process but also reduces the likelihood of billing errors, leading to improved financial operations and patient satisfaction. For example, a study in the insurance sector utilized machine learning to improve loss reserve estimation accuracy, crucial for financial statements [72]. Moving away from traditional macro-level models, this approach used individual claims data, integrating details about policies, policyholders, and claims. The method addressed the challenge of right-censored variables by creating tailored datasets for training and evaluating the algorithms. Compared to the conventional chain ladder method, this AI-driven approach showed notable improvements in accuracy, evidenced by a real case study with a Dutch loan insurance portfolio.
- Scheduling appointments: AI-driven scheduling systems are revolutionizing the way appointments are managed in healthcare settings [73]. These systems can analyze patterns in appointment bookings and cancellations to optimize the scheduling of patients. By predicting peak times and adjusting appointments accordingly, AI helps in reducing wait times and improving patient flow. For example, a project aimed at reducing outpatient MRI no-shows effectively utilized AI predictive analytics [74]. In this quality improvement initiative, over 32,000 anonymized outpatient MRI appointment records were analyzed using machine learning techniques, specifically an XGBoost model, a decision tree-based ensemble algorithm. This approach achieved
notable results; the model’s predictive accuracy was demonstrated by an ROC AUC of 0.746 and an optimized F1 score of 0.708 . When implemented alongside a practical intervention of telephone call reminders for patients identified as high-risk for noshows, the no-show rate decreased fromto over six months. In another study, a data-driven approach was used to optimize appointment scheduling and sequencing, especially in environments with uncertain service durations and customer punctuality [75]. Leveraging a novel method based on infinite-server queues, the study developed scalable solutions suitable for complex systems with numerous jobs and servers. Tested using a comprehensive dataset from a cancer center’s infusion unit, this approach significantly improved operational efficiency. The results showed a consistent reduction in costs-combining waiting times and overtime-by to , demonstrating the effectiveness of AI-based strategies in optimizing appointment scheduling. - Document management and processing: AI technologies are adept at automating the processing of various documents, including consent forms, admission forms, and medical reports [76]. By using natural language processing (NLP) and machine learning, AI can quickly parse through documents, extract relevant information, and categorize them appropriately. This automation reduces the administrative burden on staff and speeds up document processing.
- Automated communication and reminders: A notable application of AI in healthcare is the optimization of information extraction from electronic health records (EHRs), particularly from scanned documents. A study demonstrated this by successfully extracting sleep apnea indicators from scanned sleep study reports using a combination of image preprocessing techniques and natural language processing (NLP) [77]. By employing methods like gray-scaling and OCR with Tesseract, followed by analysis through advanced models like ClinicalBERT, the study achieved high accuracy rates (over
) in identifying key health metrics. - Automated communication and reminders: AI-powered chatbots and virtual assistants are increasingly used for patient communication. They can handle routine inquiries, provide information about services, and send reminders for upcoming appointments or medication schedules. This not only enhances patient engagement but also frees up staff to focus on more critical tasks. An example of this application is seen in the ChronologyMD project [78], which utilized AI to improve eHealth communication programs. The project addressed major deficiencies in existing eHealth communication strategies, which often failed to fully engage audiences and sometimes even negatively impacted the delivery of crucial health information. By strategically employing AI, the ChronologyMD project succeeded in making health communication more engaging, relevant, and actionable. Additionally, it led to increased exposure to relevant messages, reduced the workload of healthcare staff, and improved the overall efficiency of the program while minimizing costs.
- Data security and compliance: AI systems contribute significantly to data security and compliance in healthcare [79]. They can monitor and analyze data access patterns to detect and prevent unauthorized access or breaches. Additionally, AI can ensure that administrative processes are compliant with healthcare regulations, such as HIPAA, thereby safeguarding patient privacy. Building on this, recent research has explored the role of AI in ensuring compliance with the General Data Protection Regulation (GDPR), crucial for data controllers [80]. This study aimed to bridge gaps in compliance checking through a two-pronged approach: firstly, by conceptualizing a framework for document-centric compliance checking in the data supply chain, and secondly, by developing methods to automate the compliance checking of privacy policies. The study tested a two-module system, where the first module uses natural language processing (NLP) to extract data practices from privacy policies, and the second module encodes GDPR rules to ensure the inclusion of all mandatory information. The results demonstrated that this text-to-text approach was more effective
than local classifiers, capable of extracting both broad and specific information with a single model. The system’s effectiveness was validated on a dataset of 30 privacy policies, annotated by legal experts.
In summary, automating administrative tasks with AI significantly enhances the efficiency and accuracy of hospital operations. It allows healthcare professionals to focus more on patient care rather than administrative duties, leading to improved healthcare delivery. As AI technology continues to evolve, it could progress from automating tasks to personalizing patient interactions through emotional intelligence and cultural awareness, ultimately aiming to provide a more holistic and supportive care experience.
3.3. AI in Patient Flow and Scheduling Optimization
- Optimizing patient flow: AI algorithms are particularly adept at analyzing patterns in patient admissions, discharges, and transfers, enabling more efficient patient flow throughout the hospital [65,81]. By predicting high-demand periods, AI can assist in preemptively allocating resources such as beds, staff, and equipment to meet patient needs. For instance, AI systems can forecast daily or seasonal fluctuations in patient admissions, allowing hospitals to adjust staffing levels and bed availability accordingly [82]. This proactive approach reduces bottlenecks, minimizes wait times, and enhances the overall patient experience.
- Dynamic scheduling systems: AI-driven scheduling systems revolutionize the way appointments and procedures are organized. These systems can analyze multiple variables, including healthcare provider availability, patient preferences, and urgency of care, to create optimal schedules. By doing so, they reduce appointment no-shows and last-minute cancellations, maximizing the utilization of healthcare professionals’ time. Moreover, these AI systems can adapt in real time to changes, such as emergency cases, by rescheduling non-urgent appointments without significant disruptions [83]. In a study aimed at improving outpatient department efficiency and patient satisfaction, researchers developed an innovative appointment scheduling system based on a Markov decision process model, incorporating patient preferences to maximize satisfaction [84]. Adaptive dynamic programming algorithms were utilized to overcome the complexity of scheduling, dynamically adjusting to patient preferences and continuously improving appointment decisions. The system’s performance was evaluated through various experiments, which demonstrated optimal convergence behavior and accuracy.
- Reducing waiting times: One of the critical benefits of AI in patient flow is the reduction in waiting times in emergency departments and outpatient clinics. AI can predict patient inflow and identify potential delays, allowing hospital staff to take proactive measures to manage patient wait times effectively [85,86]. For emergency departments, this means better triage processes and quicker allocation of patients to the appropriate care. Utilizing machine learning algorithms, a recent study predicted patient waiting times before consultation and throughput time in an outpatient clinic, aiming to enhance patient satisfaction by providing more accurate wait time information [87]. The study employed random forest and XGBoost algorithms, analyzing input variables such as gender, day and time of visit, and consultation session. The study achieved high accuracy (
) in predicting wait and throughput times in an outpatient clinic using machine learning models with novel input variables. - Enhancing patient experience: AI systems can also improve the overall patient experience by providing accurate information about appointment times, wait periods, and treatment schedules [88]. This transparency helps in managing patient expectations and reduces anxiety associated with medical appointments and procedures. In a
recent study, a machine learning model was developed to predict patient responses to the “Doctor Communications” domain of the Hospital Consumer Assessment of Healthcare Providers and Systems survey, using data from a tertiary care hospital (2016-2020) [89]. The random forest algorithm effectively predicted patient responses about doctors’ courtesy, explanation clarity, and attentiveness. The model achieved an AUC offor these doctor communication survey questions. - Integrating with telehealth: In the era of digital health, AI in scheduling extends beyond in-person appointments to include telehealth services. AI systems can effectively schedule and manage virtual consultations, ensuring that patients receive timely care without the need to physically visit the healthcare facility, which is particularly beneficial for routine follow-ups or during health crises like pandemics [90].
In conclusion, AI’s role in optimizing patient flow and scheduling in hospitals and clinics is profoundly transformative, offering significant enhancements in operational efficiency, reduced waiting times, and improved patient experiences. As an important element in modernizing healthcare delivery, AI-driven optimization strategies are increasingly crucial. Looking to the future, AI technology is poised for further evolution, with potential advances including real-time adaptive scheduling algorithms, deeper integration with electronic health records for more personalized patient care, and the use of predictive analytics for anticipating patient demand and resource allocation.
4. AI in Medical Imaging and Diagnostics
4.1. AI’s Role in Radiology and Pathology
example, in India, an AI-powered software has been used to analyze key molecular markers in endoscopic images, enabling more precise diagnoses of gastric cancer, potentially paving the way for personalized treatment approaches [102].
4.2. Enhancing Accuracy and Efficiency in Diagnostic Processes
- Improving diagnostic accuracy: AI algorithms, particularly those based on deep learning, have demonstrated remarkable accuracy in diagnosing diseases from medical images and test results. These systems are trained on vast datasets, allowing them to recognize patterns and anomalies that might be imperceptible to the human eye. For example, in dermatology, AI systems trained on images of skin lesions have shown the ability to detect skin cancers, such as melanoma, with a level of precision comparable to that of experienced dermatologists [104].
- Reducing diagnostic errors: One of the key benefits of AI in diagnostics is its potential to reduce errors [105]. Misdiagnosis and missed diagnoses are significant concerns in medicine, often leading to delayed or inappropriate treatment. AI systems provide a level of consistency and attention to detail that is challenging for humans to maintain over long periods, thus reducing the likelihood of such errors.
- Speeding up diagnostic processes: AI significantly speeds up the diagnostic process. Analyzing medical images or test results, tasks that would take a healthcare professional considerable time, can be performed by AI in a fraction of the time. This rapid analysis is particularly beneficial in urgent care situations, where quick decisionmaking is critical. For instance, AI algorithms can quickly analyze CT scans of stroke patients to identify blockages or bleeding in the brain, enabling faster initiation of life-saving treatments [106].
- Automated reporting and documentation: AI not only automates reporting and documentation in diagnostic processes [107] but also enhances the quality of these processes. While AI systems generate preliminary reports from image analysis for radiologist review, streamlining workflow and reducing administrative burden, a recent study has furthered this efficiency by consolidating existing ML reporting guidelines [108]. This study, after an extensive review of 192 articles and expert feedback, created a comprehensive checklist encompassing 37 reporting items for prognostic and diagnostic ML studies. This effort in standardizing ML reporting is pivotal in improving the quality and reproducibility of ML modeling studies, complementing AI’s role in simplifying diagnostic reporting.
- Integrating diagnostic data: AI excels in integrating and analyzing data from various sources. In the case of complex diseases, AI can combine information from imaging, laboratory tests, and patient histories to provide a more comprehensive diagnostic
insight [109]. This integration is particularly valuable in diagnosing complex conditions like autoimmune diseases or in cases where symptoms are ambiguous. As an example, a scoping review focused on AI techniques for fusing multimodal medical data, particularly EHR with medical imaging, to develop AI methods for various clinical applications [110]. The review analyzed 34 studies, observing a workflow of combining raw data using ML or DL algorithms for clinical outcome predictions. It found that multimodality fusion models generally outperform single-modality models, with early fusion being the most commonly used technique. Neurological disorders were the dominant category studied, and conventional ML models were more frequently used than DL models. This review provides insights into the current state of multimodal medical data fusion in healthcare research.
In conclusion, AI’s significant role in improving diagnostic accuracy and efficiency is transforming healthcare, delivering faster and more precise diagnoses. However, a critical concern is that these AI systems are often primarily designed for specific groups, which can lead to disparities in healthcare. Future advancements should emphasize the development of more inclusive AI models that cater to a broader patient demographic, ensuring equitable healthcare improvements across all populations.
4.3. The Role of Hardware Acceleration in AI-Powered Diagnostics
- Graphics Processing Units (GPUs): Originally designed for computer graphics rendering, GPUs excel at parallel processing, making them ideal for handling the massive datasets and complex calculations involved in AI algorithms. In the medical image analysis domain, GPUs can be used to accelerate basic image processing operations such as filtering and interpolation. Additionally, GPUs can enhance the operation of different AI algorithms used in medical imaging tasks like image registration, image segmentation, image denoising, and image classification [113].
- Tensor Processing Units (TPUs): Custom-designed chips like TPUs, pioneered by companies like Google, are specifically optimized for high-performance deep learning inference, a key technique used in medical image analysis. TPUs offer significant speed advantages over CPUs for tasks like image recognition and classification. For example, researchers implemented a system for glaucoma diagnosis using both edge TPUs and embedded GPUs [114]. While both achieved fast image segmentation and classification for real-time diagnosis support, the study found that TPUs consumed significantly less energy compared to GPUs. This makes TPUs a more attractive option for battery-powered medical devices used in edge computing scenarios.
- Field-Programmable Gate Arrays (FPGAs): These versatile chips offer flexibility for hardware customization. Unlike pre-designed GPUs and TPUs, FPGAs can be programmed to perform specific AI algorithms, potentially leading to highly optimized solutions for certain diagnostic tasks. However, programming FPGAs requires specialized expertise. For instance, researchers have proposed a MobileNet accelerator designed specifically for FPGAs that focuses on minimizing on-chip memory usage
and data transfer, making it ideal for low-power devices [115]. They achieve this by using two configurable modules for different convolution operations and a new cache usage method. Their implementation demonstrates real-time processing with low memory usage, making FPGAs a viable option for running efficient CNNs in auxiliary medical tasks on portable devices. - Application-Specific Integrated Circuits (ASICs): When dealing with a well-defined AI algorithm in a specific diagnostic application, ASICs can be designed to offer the ultimate performance [116]. Engineered for a single task, ASICs provide unparalleled efficiency and processing speed for that specific function. However, the lack of flexibility limits their application to well-established and unchanging algorithms.
By leveraging hardware acceleration, AI-powered diagnostics can achieve several benefits: faster processing for near-real-time analysis of medical images, leading to quicker and potentially life-saving interventions; improved accuracy through the ability to perform intricate image analysis, potentially leading to a higher degree of disease detection; and enhanced efficiency by streamlining the diagnostic process, allowing radiologists and clinicians to analyze more images in a shorter timeframe.
4.4. Examples of AI Systems Used in Imaging
| Imaging Modality | Application | Example of AI System | Impact |
| MRI | AI applications in MRI analysis encompass detection of brain abnormalities, tumors, strokes, neurodegenerative diseases, and more. AI can analyze images and quantify the volume of affected areas. | An AI system analyzes MRI images to detect brain abnormalities, such as tumors or strokes, and quantifies their volume, aiding in treatment planning [118]. | Improved detection of tumors, strokes, and neurodegenerative diseases; quantification of affected areas aids in treatment planning and disease monitoring. |
| CT | AI in CT scan interpretation includes detecting lung nodules, identifying fractures and hemorrhages, assessing stroke severity, and characterizing tumor progression. AI systems can process CT scans rapidly and accurately, aiding in timely diagnosis. | An AI model diagnoses lung cancer with high accuracy and reduced false positives, improving diagnostic precision [119]. | Faster detection of life-threatening conditions; enhanced accuracy compared to traditional methods; potential to save lives in emergency situations. |
| Imaging Modality | Application | Example of AI System | Impact |
| X-ray | AI applications in X-ray enhance image analysis for tumor detection, improving accuracy and reducing false positives and negatives. AI systems serve as a second reviewer, enhancing the sensitivity of cancer screening. | AI-based CAD algorithms significantly improve radiologists’ sensitivity in breast cancer detection, reducing false negatives and improving cancer detection rates [120]. | Increased sensitivity in detecting breast cancer lesions; reduction in false positives and negatives; enhancement of radiologists’ diagnostic accuracy. |
| Ultrasound | AI aids in analyzing echocardiography scans to assess cardiovascular function and detect structural abnormalities of the heart. AI systems measure parameters such as ejection fraction and aid in diagnosing and managing heart diseases. | A novel AI algorithm accurately calculates left ventricular ejection time in echocardiography, providing reliable metrics for cardiac function assessment [121]. | Accurate assessment of cardiovascular parameters; reduction in user-dependent variability; enhancement of clinical utility in echocardiography. |
- AI in MRI analysis: AI applications in MRI analysis are versatile, encompassing the detection of brain abnormalities, tumors, strokes, neurodegenerative diseases, musculoskeletal injuries, cardiac conditions, and liver and abdominal organ pathologies, as well as evaluating breast and prostate cancers, demonstrating its broad utility in diagnosing a wide range of medical conditions [122,123]. In addition, deep learning is now playing a key role in accelerating the MRI acquisition process [92]. An example of AI application in MRI is an AI system developed for detecting brain abnormalities [118]. This system uses a deep CNN to analyze MRI images and can identify conditions such as tumors, strokes, and neurodegenerative diseases. The AI not only detects these abnormalities but also helps in quantifying the volume of affected areas, which is vital for treatment planning and monitoring disease progression. Another example is the application of AI in the interpretation of breast cancer. CNNs are employed to extract features from MRI breast scans, and alongside classifiers, they effectively detect the presence of cancer, showcasing the potential of AI in enhancing diagnostic accuracy in breast cancer detection [124]. AI systems are increasingly used for the automated segmentation of images in radiology [125]. These systems can differentiate and label various anatomical structures in the images, such as organs and tissues, aiding radiologists in diagnosis and in planning surgeries or treatments. For example, a study introduced a 4D deep learning model, combining 3D convolution and LSTM, for the precise segmentation of hepatocellular carcinoma (HCC) lesions in dynamic contrast-enhanced MRI images [126]. Utilizing both spatial and temporal domain information from multi-phase images, the model significantly improved liver tumor segmentation performance, achieving superior metrics compared to existing models and offering a comparable performance to the state-of-the-art nnU-Net model with reduced prediction time. AI is also being adapted for pediatric imaging, addressing the unique challenges presented by the varying sizes and developmental stages of pediatric patients [127]. AI systems in this domain are tailored to recognize and interpret patterns specific to children, aiding in the diagnosis of congenital and developmental conditions. For instance, in pediatric imaging for focal epilepsy, a deep CNN model was introduced, excelling in tract classification and identifying critical white matter pathways with
accuracy [128]. This model effectively predicted surgical outcomes and postoperative language changes, showcasing its potential to enhance preoperative evaluations and improve surgical precision in children. - AI for CT scan interpretation: AI applications in CT scan interpretation span detecting lung nodules, identifying fractures and hemorrhages, assessing stroke severity, and
characterizing tumor progression. One innovative AI application in CT imaging is in the rapid identification of pulmonary embolisms [119]. The AI system processes CT pulmonary angiograms to detect blood clots in the lungs with high accuracy, often faster than traditional methods. This speed is critical in emergency situations, where timely intervention can be life-saving. As another example, Google’s AI, in collaboration with researchers from Northwestern University, NYU-Langone Medical Center, and Stanford Medicine, has developed a CT scan model that diagnoses lung cancer with accuracy equal to or surpassing six radiologists [129]. This model analyzes 3D volumetric scans to predict malignancy and detect subtle lung nodules, viewing the lungs as a single 3D object and comparing scans over time to track lesion growth. Tested on over 45,800 de-identified chest CT screenings, it detected 5% more cancer cases and reduced false positives by overcompared to traditional radiologist evaluations, demonstrating significant potential for enhancing lung cancer diagnosis. - AI in X-ray analysis: AI is revolutionizing X-ray analysis across various medical fields. Take mammography, for instance, AI is transforming breast cancer screening by enhancing image analysis for tumor detection, improving accuracy in identifying benign and malignant lesions, and reducing false positives and negatives, thereby streamlining the diagnostic process for early and effective treatment [130]. These systems analyze mammograms to identify signs of cancerous lesions, with some AI models demonstrating the ability to detect cancers that were initially missed by radiologists. By serving as a second reviewer, these AI systems enhance the accuracy of breast cancer screening. A recent study demonstrated that cm Assist
, an AI-based CAD algorithm based on multiple custom deep learning-based networks, significantly enhanced radiologists’ sensitivity in breast cancer detection [120]. Analyzing 122 mammograms with a blend of false negatives and BIRADS 1 and 2 ratings, radiologists showed a notable improvement in cancer detection rates (CDRs) by an average of when using cmAssist, with a minimal increase in false positives. This marked improvement underscores the potential of AI-CAD software in improving accuracy and sensitivity in breast cancer screening. - AI in ultrasound: AI is significantly impacting various applications of ultrasound. In cardiac imaging, for example, AI systems are used to analyze images from echocardiography scans to assess cardiovascular function [131]. They can measure parameters such as the ejection fraction, which indicates how well the heart is pumping blood, and detect structural abnormalities of the heart. This information is crucial in diagnosing and managing heart diseases. For example, a study evaluating a novel AI for automated left ventricular ejection time calculation in echocardiography showed high accuracy, closely correlating with cardiac MRI results [121]. The AI, which demonstrated lower bias and greater reliability especially in challenging cases, outperformed conventional methods. This algorithm is based on a patented CNN, though specific details of its architecture and training process remain proprietary. This underscores the algorithm’s potential in reducing user-dependent variability and enhancing the clinical utility of echocardiography.
In conclusion, these examples illustrate the diverse and impactful applications of AI in medical imaging. By enhancing the accuracy, speed, and efficiency of image analysis, AI systems are proving to be invaluable assets in diagnostic radiology, ultimately leading to better patient care and outcomes. As AI technology continues to advance, its applications in medical imaging are expected to broaden, further transforming the field of radiology.
5. AI in Patient Care and Monitoring
| Main Applications | Key Technologies and Applications | Benefits | Challenges |
| AI-powered wearable devices | Continuous physiological monitoring (heart rate, blood pressure, etc.); early detection of health issues; personalized recommendations for lifestyle changes | Improved patient engagement; proactive health management | Data collection and model deployment; balancing accuracy with wearable device limitations |
| Virtual nursing assistants | 24/7 patient support and health reminders; chronic disease management; patient education and behavior monitoring | Enhanced patient engagement and education; improved treatment plan compliance | Data privacy and information accuracy; ensuring they complement human care |
| AI in telemedicine and remote patient engagement | Advanced diagnostics and consultations; personalized virtual consultations; remote patient monitoring and predictive analytics | Increased healthcare accessibility; proactive chronic condition care | Data privacy, system accuracy, and integration |
5.1. AI-Powered Wearable Devices for Continuous Monitoring
reliable data for training, especially in healthcare, is difficult due to high costs and the complexity of ensuring data reliability. Selecting the most effective features and frameworks and evaluating and deploying the best ML models add layers of complexity, compounded by the necessity for models to generalize well across diverse personal features. Wearable device developers must also navigate the selection of deployment options, balancing the advantages of on-device computing against the limitations of power consumption, storage, and computational power. Addressing these challenges involves a careful trade-off between model accuracy and the practical constraints of wearable technology, requiring innovations in model design, data processing, and system integration to optimize the clinical impact and user acceptance of wearable ML applications.
5.2. Virtual Nursing Assistants
5.3. AI in Telemedicine and Remote Patient Engagement
technology effectively narrows the distance between patients and providers, supported by physician-guided implementation and adherence to clinical practices.
6. Methodologies for Assessing AI Healthcare Solutions
6.1. Validation
- Algorithm validation: The successful integration of AI algorithms into healthcare hinges on their accuracy, reliability, and performance. This necessitates comprehensive testing using diverse datasets [150]. A critical challenge in this process is overfitting, where the algorithm performs well on the training data but fails to generalize to unseen data. To address this, techniques like cross-validation are employed [151]. Cross-validation involves splitting the training data into multiple folds and iteratively training the algorithm on a subset of folds while using the remaining folds for validation. This process helps assess how well the algorithm generalizes to new data and prevents overfitting. Beyond generalizability, AI in healthcare should be adaptable for personalized use. This means the algorithms should continuously learn from individual patient data to enable tailored treatment approaches. Rigorous assessment helps identify strengths, weaknesses, and areas for improvement, ultimately enhancing the reliability of AI-based healthcare solutions. Furthermore, validation on different patient groups is essential to address potential biases in the training data. Biases can lead to unfair and ineffective outcomes for certain demographics. By ensuring the algorithms perform consistently across diverse populations, we can ensure fairness and effectiveness for all.
- Clinical validation: Clinical validation plays a crucial role in assessing the efficacy and safety of AI interventions [152]. Rigorous clinical trials and studies should be conducted to compare AI-based interventions with standard treatments or existing practices. These evaluations can encompass a range of study designs, including randomized controlled trials (RCTs), observational studies, or real-world evidence analyses. Through these studies, researchers can determine the effectiveness of AI technologies in improving patient outcomes and clinical decision-making. Furthermore, defining appropriate outcome measures is essential for assessing the impact of AI interventions on patient outcomes. Outcome measures such as mortality rates, disease progression, quality of life, and healthcare costs can be used to evaluate the effectiveness of AI technologies in improving healthcare delivery.
6.2. Interpretability and Usability
(Local Interpretable Model-agnostic Explanations) [154], and SHAP (SHapley Additive exPlanations) [155] values can provide deeper insights into the model’s reasoning.
- Active stakeholder involvement: Throughout the development process, actively involving clinicians, patients, and other stakeholders provides valuable insights into their needs and expectations. This collaborative approach fosters a sense of ownership in the solution, leading to higher engagement.
- Iterative development and feedback loops: Developing AI solutions is an iterative process. By incorporating user feedback throughout development cycles, researchers can refine the AI tool to better address user needs. This ongoing feedback loop not only improves usability but also strengthens user confidence and engagement.
- User-friendly interfaces and clear visualizations: Designing clear and user-friendly interfaces is essential for user engagement. This includes presenting AI outputs in a way that is easy to understand and interpret, even for users with limited technical expertise. Additionally, providing clear visualizations of the AI’s reasoning can further enhance user trust and engagement.
6.3. Scalability and Continuous Improvement
- Post-market surveillance: Closely monitoring the performance of AI solutions after deployment in real-world settings to identify any unforeseen issues or areas for improvement [158].
- Performance monitoring: Continuously tracking the effectiveness of the AI tool in achieving its intended outcomes [159]. These data can be used to identify areas where the AI can be further optimized.
- Updating algorithms based on new data and insights: AI algorithms are not static. As new data become available, or as researchers gain a deeper understanding of the underlying problem, the algorithms can be updated to improve their performance and accuracy.
By prioritizing scalability and continuous improvement, researchers and developers should ensure the long-term success and sustainability of AI-based healthcare solutions in addressing evolving healthcare challenges.
7. Ethical Considerations and Challenges
7.1. Ethical Implications of AI in Healthcare
- Privacy concerns: One of the foremost ethical concerns in AI healthcare is the privacy of patient data. AI systems require access to large datasets of patient information, which raises questions about the security and confidentiality of sensitive health data [160]. Ensuring that patient data used for AI applications are anonymized and securely stored is paramount. There is also a need for transparent policies regarding who has access to these data and for what purposes.
- Informed consent: The issue of informed consent in AI healthcare is complex, necessitating clear communication with patients about the use of their data, especially with AI algorithms that may be challenging for non-experts to grasp. This includes detailing data sharing implications, potential benefits and risks associated with AI-driven healthcare, and the level of human oversight in AI decisions. More details on the use of informed consent forms for AI in medicine with a comprehensive guideline for emergency physicians can be found in [161].
- Bias and fairness: AI systems are only as unbiased as the data they are trained on. There is a risk that AI algorithms may perpetuate existing biases present in healthcare data, leading to unfair treatment outcomes for certain groups [162]. For example, if an AI system is trained predominantly on data from a specific demographic, its
accuracy might be lower for patients outside of that demographic. Ensuring that AI systems are developed and trained on diverse datasets is crucial to mitigate these biases. Moreover, the continuous monitoring and auditing of AI systems for biased outcomes are necessary to uphold fairness in healthcare delivery. - Transparency and accountability: Transparency in AI decision-making processes is a key ethical concern [163]. It is important for healthcare providers and patients to understand how AI systems make their recommendations. This transparency is essential for building trust in AI systems and for accountability [164]. In cases where AI-driven decisions impact patient care, it is crucial to have mechanisms in place to review and understand these decisions, particularly in the event of adverse outcomes. A recent study highlights the need for transparent and accountable AI systems in natural NLP to address the “black box” issue of deep learning models [165]. It introduces the Explaining and Visualizing CNNs for Text Information (EVCT) framework, which offers human-interpretable solutions for text classification with minimal information loss, aligning with recent demands for fairness and transparency in AI-driven decision support systems.
In conclusion, while AI presents significant opportunities for enhancing healthcare, it also introduces complex ethical challenges that must be addressed. Privacy, consent, bias, transparency, and accountability are critical considerations that need to be carefully managed to ensure the responsible and equitable use of AI in healthcare.
7.2. Challenges in Integrating AI
- Data security concerns: As healthcare AI systems require access to large volumes of sensitive patient data, ensuring the security of these data is paramount [166]. The risk of data breaches and cyberattacks poses a significant concern. These security breaches can lead to the exposure of confidential patient information, resulting in privacy violations and potentially harming the trust between patients and healthcare providers. Implementing robust cybersecurity measures, including encryption, secure data storage solutions, and regular security audits, is crucial to protect patient data [167]. Additionally, educating healthcare staff about data security best practices is essential in safeguarding against breaches.
- Interoperability between systems: Another major challenge in integrating AI into healthcare is the issue of interoperability-the ability of different healthcare IT systems and software applications to communicate, exchange data, and use the information that has been exchanged [168]. Many healthcare systems use a variety of electronic health record (EHR) systems and other digital tools that may not be compatible with one another or with new AI technologies. This lack of interoperability can hinder the seamless exchange of patient data, reducing the effectiveness of AI tools. Developing standardized data formats and communication protocols, as well as encouraging the adoption of interoperable systems, is vital to overcome this challenge [169].
- Integration with existing clinical workflows: Integrating AI into existing clinical workflows can be challenging. Healthcare professionals may need to adjust their workflows to accommodate AI tools, which can be a time-consuming and complex process. Ensuring that AI systems are user-friendly and align with current clinical practices is essential to facilitate their adoption. Training and support for healthcare professionals in using these AI systems are also crucial for successful integration. For example, in a recent study, a three-tiered integration approach of AI-based image analysis into radiology workflows is outlined, focusing on enhancing automation and incorporating radiologist feedback for continuous AI improvement [170]. This
approach entails initially visualizing AI outcomes without generating new patient records. It allows for the storage of AI-generated results in institutional systems and equips radiologists with tools to refine AI inferences for periodic retraining. This methodology was exemplified in a case study on brain metastases detection, where radiologist input substantially decreased false positives via iterative retraining with an expanded dataset. - Data quality and quantity: The effectiveness of AI systems depends heavily on the quality and quantity of the data they are trained on. Inconsistent, incomplete, or inaccurate data can lead to poor AI performance. Ensuring the collection of high-quality, comprehensive patient data is therefore a significant challenge in AI integration [171]. Standardizing data collection methods and ensuring thorough data curation processes are essential steps in addressing this issue.
7.3. Regulatory and Compliance Issues
8. The Future of AI in Healthcare
| Trend/Application | Potential Impact | Challenges | Future Directions |
| Personalized medicine | Revolutionizes treatment for diseases with genetic components, significantly improving patient outcomes through customized care plans. | Data privacy, integration into clinical practice, and ensuring equitable access across diverse patient populations. | Expanding personalized medicine to encompass mental health, lifestyle diseases, and integrating real-time health monitoring data for dynamic treatment adjustments. |
| AI-powered tools for health and sleep monitoring | Improved detection and diagnosis of sleep disorders, early identification of potential health issues, personalized treatment, and proactive interventions. | Data privacy, accuracy of predictions, and user acceptance and comfort with interventional technologies. | Designing analysis and intervention technologies to monitor, predict, and manage health issues and sleep disorders; integration with wearable devices and smart home technology, providing real-time adjustments. |
| Longevity and aging | Unlocks new possibilities in aging research, promoting healthier, extended lifespans through AI-driven genomic interventions and predictive analytics for preventive medicine. | Addressing ethical implications of longevity research, ensuring accessibility and fairness in anti-aging treatments. | Leveraging AI for comprehensive health longevity platforms, integrating AI with regenerative medicine, and creating personalized anti-aging treatment plans based on predictive health analytics. |
| AI in drug discovery and development | Reduces time and costs in drug market introduction, enhances the efficacy of new drugs by identifying optimal candidate molecules. | Ensuring the reliability of AI predictions; ethical concerns around automated decision-making in drug development. | Leveraging AI to explore novel drug pathways, improve clinical trial design, and predict patient responses to treatments more accurately. |
| Advanced robotics in surgery and rehabilitation | Improves precision in surgeries and patient outcomes in rehabilitation, potentially reducing recovery times and healthcare costs. | Ethical considerations around autonomy; the need for robust training programs for medical staff on robotic systems. | Developing autonomous surgical robots, enhancing robotic systems with sensory feedback for improved rehabilitation outcomes, and expanding applications in minimally invasive procedures. |
| AI hardware accelerators | Faster diagnoses, treatment planning, and analysis, improved patient care outcomes, and real-time medical data processing. | Integration with medical devices; cost and power consumption of accelerators. | Develop healthcare-specific AI hardware; improve accessibility of AI-driven healthcare. |
| AI-enhanced medical imaging | Enables earlier and more accurate disease detection, potentially even identifying health risks before symptoms appear, thus shifting towards preventive healthcare models. | Balancing the need for patient privacy with the benefits of data sharing for AI training; integrating AI tools with existing healthcare infrastructures. | Developing AI systems capable of cross-modality analysis, improving 3D imaging techniques, and creating predictive models for disease progression based on imaging data. |
| Trend/Application | Potential Impact | Challenges | Future Directions |
| Integrating AI with IoT and wearables | Leads to proactive health management and personalized health recommendations, potentially reducing emergency healthcare interventions. | Addressing data security and ensuring device interoperability across different healthcare systems. | Enhancing predictive analytics for early detection of health anomalies, creating an ecosystem of interconnected devices for holistic health monitoring; unobtrusive health monitoring. |
| Enhancing patient outcomes and system efficiency | Promises significant improvements in patient care through earlier disease detection, customized treatments, and optimized healthcare resource management. | Ensuring equitable improvements across all populations, addressing the digital divide in healthcare access. | Implementing AI-driven health advisories in public health strategies, optimizing healthcare delivery models with predictive resource allocation, and enhancing remote patient monitoring systems. |
| Global health monitoring systems | Strengthens global health security by enabling rapid response to disease outbreaks and guiding public health interventions with data-driven insights. | Integrating diverse data streams in real time, adapting models quickly to emerging health threats. | Developing global AI-powered surveillance systems, enhancing predictive models for epidemic and pandemic forecasting, and creating AI-driven platforms for vaccine and therapeutic development. |
| Addressing data scarcity | Facilitates AI development in under-researched areas, such as rare diseases, by making efficient use of limited data resources. | Creating effective models with sparse data, ensuring the generalizability of findings from limited datasets. | Exploring novel data augmentation techniques, crowdsourcing for data collection, and cross-institutional data sharing initiatives to enrich datasets. Developing advanced techniques based on few-shot leaning. |
| Ensuring model versatility | Allows for the broader application of AI models across varying healthcare settings and patient demographics, improving the universality and accessibility of AI-driven healthcare solutions. | Developing adaptable models that maintain high accuracy across diverse datasets, addressing potential biases in AI training. | Advancing transfer learning and domain adaptation techniques that can be personalized at the point of care. |
| Ensuring data privacy | Enhances privacy and security in healthcare applications, addressing one of the major concerns of digital health data management. | Balancing the utility of data for AI training with stringent privacy requirements, adapting regulations to keep pace with technological advancements. | Developing more advanced privacy-preserving AI techniques, such as secure multi-party computation, federated learning, and advanced encryption methods for health data. |
| Stakeholder acceptance | Successful AI integration in healthcare; improved trust and collaboration. | Concerns about AI reliability and clinician autonomy. | Transparent communication and training programs. |
| Building trust with Explainable AI (XAI) | Enhances the trustworthiness of AI systems among healthcare professionals and patients, ensuring that AI-supported decisions are well informed and ethically sound. | Simplifying complex AI decision-making processes for non-technical stakeholders, ensuring explanations are meaningful and actionable. | Integrating XAI into clinical workflows, developing standards for AI explanations in healthcare, and educating healthcare professionals on interpreting AI decisions. |
8.1. Personalized Healthcare Applications
- Personalized medicine: One of the most promising trends in AI healthcare is the move towards more personalized medicine [177]. AI’s ability to analyze vast amounts of genetic, health data, and lifestyle information will enable the development of more precise and effective treatments tailored to individual patient profiles. This personalized approach can improve treatment outcomes and reduce side effects.
- AI-powered tools for health and sleep monitoring: Future research should explore the development and validation of AI-driven tools and algorithms for the diagnosis, monitoring, and management of health issues and sleep disorders [178]. This includes leveraging machine learning to analyze data from wearable devices such as sleep patterns, heart rate variability, and activity levels. These analyses can, for example, help detect abnormalities such as sleep apnea and personalize treatment recommendations based on individual sleep profiles.
- Longevity and aging: By harnessing the power of predictive analytics, AI can explore vast datasets to uncover biomarkers of aging and offer personalized strategies to slow or even reverse the aging process [179]. This includes leveraging AI for genomic interventions, where it could guide the editing of genes associated with aging mechanisms, enhancing cellular repair, resilience, and longevity. The potential of AI extends to the field of drug discovery and repurposing, where it can expedite the identification of compounds with anti-aging effects [180]. Moreover, AI’s integration into healthcare promises a paradigm shift towards preventive medicine, emphasizing early detection and intervention in age-related declines.
8.2. Enhanced Treatment Technologies
- AI in drug discovery and development: AI is poised to play a significant role in accelerating drug discovery and development [181]. By rapidly analyzing molecular and clinical data, AI has the potential to identify potential drug candidates much faster than traditional methods. This acceleration could significantly reduce the time and cost associated with bringing new drugs to market.
- Advanced robotics in surgery and rehabilitation: The use of AI-driven robotics in surgery and rehabilitation is expected to advance further [182]. Robotic systems, guided by AI algorithms, could potentially perform complex surgeries with high precision, reducing risks and improving patient outcomes. In rehabilitation, AIpowered exoskeletons and prosthetics are anticipated to offer greater mobility and independence to patients.
- AI hardware accelerators: As AI applications in healthcare grow, the demand for efficient processing capabilities rises. AI hardware accelerators like GPUs, TPUs, and FPGAs optimize AI model performance, enabling real-time medical data processing with minimal latency. Integrating these accelerators into medical devices promises faster diagnosis, treatment planning, and analysis, thereby enhancing patient care outcomes. Developing dedicated AI hardware accelerators tailored to healthcare needs is a promising future direction for improving the efficiency and accessibility of AI-driven healthcare solutions.
- AI-enhanced medical imaging: Future developments in AI are likely to produce even more advanced medical imaging techniques [183]. These advancements could provide clearer, more detailed images and enable the earlier detection of diseases, potentially even identifying health risks before symptoms appear.
- Integrating AI with IoT and wearables: The integration of AI with the Internet of Things (IoT) and wearable technology is an emerging trend [184]. This combination could lead to real-time health monitoring systems that not only track health data but
also provide proactive recommendations and alerts. AI can also be integrated into existing wearable technologies to provide further information regarding health and performance [185].
8.3. Healthcare System Optimization
- Enhancing patient outcomes and system efficiency: The transformative potential of AI in healthcare can revolutionize patient care and system efficiency. Future AI applications aim to detect diseases earlier, customize treatments, and significantly personalize patient care, leading to improved recovery times and reduced mortality rates. AI’s role extends to optimizing healthcare resources, reducing costs, and improving care accessibility, especially for underserved communities [186]. Moreover, AI will support healthcare professionals by augmenting decision-making, promising equitable health improvements and a more efficient healthcare delivery system.
- Global health monitoring systems: The significance of AI in addressing pandemics and global health emergencies is increasingly recognized as crucial [187]. By integrating and analyzing diverse data streams, AI is adept at quickly detecting the emergence of disease outbreaks, projecting their spread, and guiding effective public health interventions. During the COVID-19 pandemic, AI-powered models were used to predict the disease’s trajectory, showcasing the potential of AI in navigating the complexities of pandemic management [188]. Moreover, AI’s capabilities extend to enhancing public health strategies, enabling the expedited development and dissemination of vaccines and therapeutic solutions in times of crisis.
8.4. Data Management
- Addressing data scarcity: The scarcity of labeled data in healthcare poses a significant challenge for AI development, especially in areas like rare disease research where data are inherently limited. A practical solution to this problem is the implementation of semi-supervised and weakly supervised learning techniques [189]. By utilizing a combination of a small set of labeled data and a larger volume of unlabeled data, these methods improve AI’s learning efficiency from minimal information, offering a viable strategy for advancing research and treatment in fields where comprehensive labeled datasets are scarce. However, for certain applications in healthcare, even obtaining a small amount of labeled data can be difficult. In such cases, emerging techniques in the field of machine learning offer intriguing possibilities. Few-shot learning: Few-shot learning requires only a small number of labeled examples for a new concept. This could be beneficial for situations where obtaining even a small amount of labeled data for a rare disease is possible. By learning from these few examples, the model could potentially generalize to similar cases [190,191]. Zero-shot learning (ZSL): In theory, ZSL could allow AI models to learn about new diseases or medical conditions even with no labeled data for those specific cases. ZSL leverages existing knowledge and relationships between concepts to make predictions for unseen categories. While ZSL is still under development, it holds promise for healthcare applications where data are extremely limited [192]. Meta-learning: This approach focuses on training models to “learn how to learn” efficiently. A meta-learning model could be trained on various healthcare-related tasks with limited datasets for each task. This acquired knowledge about learning itself could then be applied to new, unseen medical problems with minimal data, potentially improving performance [193].
- Ensuring model versatility: Achieving versatility in AI models is essential for their effective application across the diverse landscape of healthcare settings and patient demographics. Techniques such as domain adaptation and transfer learning stand
out as effective solutions, enabling AI models trained on one dataset to adjust and perform accurately on another with little need for retraining [194]. This capability is particularly valuable in healthcare, where patient characteristics, disease profiles, and treatment responses can vary widely [195]. By fostering such adaptability, these techniques ensure that AI can be deployed more universally, enhancing its effectiveness and utility for a broad spectrum of patients.
8.5. Ethical Considerations and Trust Building
- Ensuring data privacy: Addressing data privacy concerns in healthcare has become increasingly crucial with the rise in AI applications. An exemplary solution to this challenge is federated learning, a novel AI model training approach that enables algorithms to learn from data stored on local servers across different healthcare institutions without the need for direct data sharing [196]. This method significantly enhances privacy and security and offers a strategic advantage in the healthcare industry where the sensitivity and confidentiality of patient data are of utmost importance.
- Stakeholder acceptance: Ensuring trust and acceptance among stakeholders is critical for the successful integration of AI into healthcare practices [197]. This encompasses not only patients and clinicians but also policymakers, regulatory bodies, healthcare administrators, and other relevant parties. Patients may express concerns regarding the reliability and accountability of AI-driven decision-making processes. Therefore, transparent communication about the role of AI in treatment plans and the potential benefits it offers is essential to foster patient acceptance. Similarly, clinicians may have reservations about entrusting AI algorithms with decision-making responsibilities, fearing loss of autonomy or professional judgment, as well as doubting the accuracy of AI decisions. Establishing comprehensive training programs and collaborative frameworks that empower clinicians to understand and validate AI tools effectively can mitigate these concerns. Furthermore, building trust extends to engaging stakeholders such as policymakers, regulatory bodies, and healthcare administrators. Transparency in AI development and deployment, coupled with clear communication about ethical, legal, and regulatory considerations, is crucial for gaining stakeholder trust. Establishing robust governance frameworks that address these concerns can enhance confidence in AI systems and ensure accountability.
- Building trust with Explainable AI: Explainable AI (XAI) aims to make AI decisionmaking processes transparent and understandable to humans, a crucial aspect for clinical applications [198]. By providing insights into how AI models arrive at their conclusions, XAI fosters trust among healthcare professionals and patients, ensuring that AI-supported decisions are well informed and ethically sound. This transparency is vital for integrating AI into sensitive healthcare decisions, where understanding the rationale behind AI recommendations can significantly impact patient care and outcomes.
To sum up, the future of AI in healthcare is bright and filled with possibilities. While challenges remain, particularly in terms of ethics, regulation, and integration, the potential benefits are immense. As AI technology continues to evolve, it promises to revolutionize healthcare, making it more personalized, efficient, and responsive to global health needs.
9. Conclusions
abling enhanced diagnostic accuracy, facilitating personalized treatments, and optimizing operational efficiency, AI holds promise for reshaping the healthcare landscape.
Data Availability Statement: Not applicable.
Conflicts of Interest: The authors declare no conflict of interest.
References
- Rajpurkar, P.; Chen, E.; Banerjee, O.; Topol, E.J. AI in health and medicine. Nat. Med. 2022, 28, 31-38. [CrossRef] [PubMed]
- McCorduck, P.; Cfe, C. Machines Who Think: A Personal Inquiry into the History and Prospects of Artificial Intelligence; CRC Press: Boca Raton, FL, USA, 2004.
- Alpaydin, E. Introduction to Machine Learning; MIT Press: Cambridge, MA, USA, 2020.
- Brynjolfsson, E.; McAfee, A. The Second Machine Age: Work, Progress, and Prosperity in a Time of Brilliant Technologies; WW Norton & Company: New York, NY, USA, 2014.
- Russell, S.J.; Norvig, P. Artificial Intelligence a Modern Approach; Pearson: London, UK, 2010.
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436-444. [CrossRef] [PubMed]
- Wang, F.; Preininger, A. AI in health: State of the art, challenges, and future directions. Yearb. Med. Inform. 2019, 28, 16-26. [CrossRef] [PubMed]
- DuBois, K.N. Deep medicine: How artificial intelligence can make healthcare human again. Perspect. Sci. Christ. Faith 2019, 71, 199-201.
- Davenport, T.H. The AI Advantage: How to Put the Artificial Intelligence Revolution to Work; MIT Press: Cambridge, MA, USA, 2018.
- Kaur, S.; Singla, J.; Nkenyereye, L.; Jha, S.; Prashar, D.; Joshi, G.P.; El-Sappagh, S.; Islam, M.S.; Islam, S.R. Medical diagnostic systems using artificial intelligence (ai) algorithms: Principles and perspectives. IEEE Access 2020, 8, 228049-228069. [CrossRef]
- Cortez, N. Digital Health: Scaling Healthcare to the World; Springer: Cham, Switzerland, 2018; pp. 249-269.
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500-510. [CrossRef] [PubMed]
- Kagiyama, N.; Shrestha, S.; Farjo, P.D.; Sengupta, P.P. Artificial intelligence: Practical primer for clinical research in cardiovascular disease. J. Am. Heart Assoc. 2019, 8, e012788. [CrossRef] [PubMed]
- Bardhan, I.; Chen, H.; Karahanna, E. Connecting systems, data, and people: A multidisciplinary research roadmap for chronic disease management. MIS Q. 2020, 44, 185-200.
- Huang, S.; Yang, J.; Fong, S.; Zhao, Q. Artificial intelligence in cancer diagnosis and prognosis: Opportunities and challenges. Cancer Lett. 2020, 471, 61-71. [CrossRef]
- Binhowemel, S.; Alfakhri, M.; AlReshaid, K.; Alyani, A. Role of Artificial Intelligence in Diabetes Research Diagnosis and Prognosis: A Narrative Review. J. Health Inform. Dev. Ctries. 2023, 17, 1-12.
- Guan, Z.; Li, H.; Liu, R.; Cai, C.; Liu, Y.; Li, J.; Wang, X.; Huang, S.; Wu, L.; Liu, D. Artificial intelligence in diabetes management: Advancements, opportunities, and challenges. Cell Rep. Med. 2023, 4, 101213. [CrossRef] [PubMed]
- Waring, J.; Lindvall, C.; Umeton, R. Automated machine learning: Review of the state-of-the-art and opportunities for healthcare. Artif. Intell. Med. 2020, 104, 101822. [CrossRef] [PubMed]
- Eloranta, S.; Boman, M. Predictive models for clinical decision making: Deep dives in practical machine learning. J. Intern. Med. 2022, 292, 278-295. [CrossRef] [PubMed]
- Nezamabadi, K.; Sardaripour, N.; Haghi, B.; Forouzanfar, M. Unsupervised ECG analysis: A review. IEEE Rev. Biomed. Eng. 2022, 16, 208-224. [CrossRef] [PubMed]
- Coronato, A.; Naeem, M.; De Pietro, G.; Paragliola, G. Reinforcement learning for intelligent healthcare applications: A survey. Artif. Intell. Med. 2020, 109, 101964. [CrossRef] [PubMed]
- Sarvamangala, D.; Kulkarni, R.V. Convolutional neural networks in medical image understanding: A survey. Evol. Intell. 2022, 15, 1-22. [CrossRef] [PubMed]
- Yang, Y.; Zhang, L.; Du, M.; Bo, J.; Liu, H.; Ren, L.; Li, X.; Deen, M.J. A comparative analysis of eleven neural networks architectures for small datasets of lung images of COVID-19 patients toward improved clinical decisions. Comput. Biol. Med. 2021, 139, 104887. [CrossRef] [PubMed]
- Rim, B.; Sung, N.-J.; Min, S.; Hong, M. Deep learning in physiological signal data: A survey. Sensors 2020, 20, 969. [CrossRef] [PubMed]
- Bahrami, M.; Forouzanfar, M. Sleep apnea detection from single-lead ECG: A comprehensive analysis of machine learning and deep learning algorithms. IEEE Trans. Instrum. Meas. 2022, 71, 4003011. [CrossRef]
- Yi, X.; Walia, E.; Babyn, P. Generative adversarial network in medical imaging: A review. Med. Image Anal. 2019, 58, 101552. [CrossRef]
- Hu, Y.; Kothapalli, S.V.; Gan, W.; Sukstanskii, A.L.; Wu, G.F.; Goyal, M.; Yablonskiy, D.A.; Kamilov, U.S. DiffGEPCI: 3D MRI Synthesis from mGRE Signals using 2.5 D Diffusion Model. arXiv 2023, arXiv:2311.18073.
- Wang, J.; Liu, X. Medical image recognition and segmentation of pathological slices of gastric cancer based on Deeplab v3+ neural network. Comput. Methods Programs Biomed. 2021, 207, 106210. [CrossRef] [PubMed]
- Nagabushanam, P.; Thomas George, S.; Radha, S. EEG signal classification using LSTM and improved neural network algorithms. Soft Comput. 2020, 24, 9981-10003. [CrossRef]
- Kawazoe, Y.; Shibata, D.; Shinohara, E.; Aramaki, E.; Ohe, K. A clinical specific BERT developed using a huge Japanese clinical text corpus. PLoS ONE 2021, 16, e0259763. [CrossRef] [PubMed]
- Torfi, A.; Fox, E.A.; Reddy, C.K. Differentially private synthetic medical data generation using convolutional GANs. Inf. Sci. 2022, 586, 485-500. [CrossRef]
- Lin, X.; Quan, Z.; Wang, Z.-J.; Ma, T.; Zeng, X. KGNN: Knowledge Graph Neural Network for Drug-Drug Interaction Prediction; IJCAI: Pasadena, CA, USA, 2020; pp. 2739-2745.
- Zhou, B.; Yang, G.; Shi, Z.; Ma, S. Natural language processing for smart healthcare. IEEE Rev. Biomed. Eng. 2022, 17, 4-18. [CrossRef]
- Yang, X.; Chen, A.; PourNejatian, N.; Shin, H.C.; Smith, K.E.; Parisien, C.; Compas, C.; Martin, C.; Costa, A.B.; Flores, M.G. A large language model for electronic health records. NPJ Digit. Med. 2022, 5, 194. [CrossRef] [PubMed]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A. International evaluation of an AI system for breast cancer screening. Nature 2020, 577, 89-94. [CrossRef]
- Jian, Y.; Pasquier, M.; Sagahyroon, A.; Aloul, F. A machine learning approach to predicting diabetes complications. Healthcare 2021, 9, 1712. [CrossRef]
- Fan, Y.; Long, E.; Cai, L.; Cao, Q.; Wu, X.; Tong, R. Machine learning approaches to predict risks of diabetic complications and poor glycemic control in nonadherent type 2 diabetes. Front. Pharmacol. 2021, 12, 665951. [CrossRef]
- Yuan, X.; Chen, J.; Zhang, K.; Wu, Y.; Yang, T. A stable AI-based binary and multiple class heart disease prediction model for IoMT. IEEE Trans. Ind. Inform. 2021, 18, 2032-2040. [CrossRef]
- Ali, F.; El-Sappagh, S.; Islam, S.R.; Kwak, D.; Ali, A.; Imran, M.; Kwak, K.-S. A smart healthcare monitoring system for heart disease prediction based on ensemble deep learning and feature fusion. Inf. Fusion 2020, 63, 208-222. [CrossRef]
- Vieira, S.; Pinaya, W.H.; Mechelli, A. Using deep learning to investigate the neuroimaging correlates of psychiatric and neurological disorders: Methods and applications. Neurosci. Biobehav. Rev. 2017, 74, 58-75. [CrossRef] [PubMed]
- Gautam, R.; Sharma, M. Prevalence and diagnosis of neurological disorders using different deep learning techniques: A meta-analysis. J. Med. Syst. 2020, 44, 49. [CrossRef] [PubMed]
- Murugan, S.; Venkatesan, C.; Sumithra, M.; Gao, X.-Z.; Elakkiya, B.; Akila, M.; Manoharan, S. DEMNET: A deep learning model for early diagnosis of Alzheimer diseases and dementia from MR images. IEEE Access 2021, 9, 90319-90329. [CrossRef]
- Bartsch, G., Jr.; Mitra, A.P.; Mitra, S.A.; Almal, A.A.; Steven, K.E.; Skinner, D.G.; Fry, D.W.; Lenehan, P.F.; Worzel, W.P.; Cote, R.J. Use of artificial intelligence and machine learning algorithms with gene expression profiling to predict recurrent nonmuscle invasive urothelial carcinoma of the bladder. J. Urol. 2016, 195, 493-498. [CrossRef] [PubMed]
- Paul, D.; Sanap, G.; Shenoy, S.; Kalyane, D.; Kalia, K.; Tekade, R.K. Artificial intelligence in drug discovery and development. Drug Discov. Today 2021, 26, 80. [CrossRef] [PubMed]
- Gupta, R.; Srivastava, D.; Sahu, M.; Tiwari, S.; Ambasta, R.K.; Kumar, P. Artificial intelligence to deep learning: Machine intelligence approach for drug discovery. Mol. Divers. 2021, 25, 1315-1360. [CrossRef] [PubMed]
- Hasselgren, C.; Oprea, T.I. Artificial Intelligence for Drug Discovery: Are We There Yet? Annu. Rev. Pharmacol. Toxicol. 2024, 64, 527-550. [CrossRef]
- Senior, A.W.; Evans, R.; Jumper, J.; Kirkpatrick, J.; Sifre, L.; Green, T.; Qin, C.; Žídek, A.; Nelson, A.W.; Bridgland, A. Improved protein structure prediction using potentials from deep learning. Nature 2020, 577, 706-710. [CrossRef]
- Sadybekov, A.V.; Katritch, V. Computational approaches streamlining drug discovery. Nature 2023, 616, 673-685. [CrossRef] [PubMed]
- Bica, I.; Alaa, A.M.; Lambert, C.; Van Der Schaar, M. From real-world patient data to individualized treatment effects using machine learning: Current and future methods to address underlying challenges. Clin. Pharmacol. Ther. 2021, 109, 87-100. [CrossRef]
- Vettoretti, M.; Cappon, G.; Facchinetti, A.; Sparacino, G. Advanced diabetes management using artificial intelligence and continuous glucose monitoring sensors. Sensors 2020, 20, 3870. [CrossRef] [PubMed]
- Low, D.M.; Bentley, K.H.; Ghosh, S.S. Automated assessment of psychiatric disorders using speech: A systematic review. Laryngoscope Investig. Otolaryngol. 2020, 5, 96-116. [CrossRef] [PubMed]
- Graham, S.; Depp, C.; Lee, E.E.; Nebeker, C.; Tu, X.; Kim, H.-C.; Jeste, D.V. Artificial intelligence for mental health and mental illnesses: An overview. Curr. Psychiatry Rep. 2019, 21, 116. [CrossRef] [PubMed]
- Nasrullah, S.; Jalali, A. Detection of Types of Mental Illness through the Social Network Using Ensembled Deep Learning Model. Comput. Intell. Neurosci. 2022, 2022, 9404242. [CrossRef] [PubMed]
- Guntuku, S.C.; Yaden, D.B.; Kern, M.L.; Ungar, L.H.; Eichstaedt, J.C. Detecting depression and mental illness on social media: An integrative review. Curr. Opin. Behav. Sci. 2017, 18, 43-49. [CrossRef]
- Czerwinski, M.; Hernandez, J.; McDuff, D. Building an AI That Feels: AI systems with emotional intelligence could learn faster and be more helpful. IEEE Spectr. 2021, 58, 32-38. [CrossRef]
- Torab-Miandoab, A.; Samad-Soltani, T.; Jodati, A.; Rezaei-Hachesu, P. Interoperability of heterogeneous health information systems: A systematic literature review. BMC Med. Inform. Decis. Mak. 2023, 23, 18. [CrossRef]
- Díaz-Rodríguez, N.; Del Ser, J.; Coeckelbergh, M.; de Prado, M.L.; Herrera-Viedma, E.; Herrera, F. Connecting the dots in trustworthy Artificial Intelligence: From AI principles, ethics, and key requirements to responsible AI systems and regulation. Inf. Fusion 2023, 99, 101896. [CrossRef]
- Gurevich, E.; El Hassan, B.; El Morr, C. In Equity within AI systems: What can health leaders expect? Healthc. Manag. Forum 2023, 36, 119-124. [CrossRef]
- Dwivedi, Y.K.; Hughes, L.; Ismagilova, E.; Aarts, G.; Coombs, C.; Crick, T.; Duan, Y.; Dwivedi, R.; Edwards, J.; Eirug, A. Artificial Intelligence (AI): Multidisciplinary perspectives on emerging challenges, opportunities, and agenda for research, practice and policy. Int. J. Inf. Manag. 2021, 57, 101994. [CrossRef]
- Jebbor, S.; Raddouane, C.; El Afia, A. A preliminary study for selecting the appropriate AI-based forecasting model for hospital assets demand under disasters. J. Humanit. Logist. Supply Chain Manag. 2022, 12, 1-29. [CrossRef]
- Galli, L.; Levato, T.; Schoen, F.; Tigli, L. Prescriptive analytics for inventory management in health care. J. Oper. Res. Soc. 2021, 72, 2211-2224. [CrossRef]
- Tien, P.W. Deep Learning-Powered Vision-Based Energy Management System for Next-Gen Built Environment; University of Nottingham: Nottingham, UK, 2023.
- Zamzam, A.H.; Hasikin, K.; Wahab, A.K.A. Integrated failure analysis using machine learning predictive system for smart management of medical equipment maintenance. Eng. Appl. Artif. Intell. 2023, 125, 106715. [CrossRef]
- Mizan, T.; Taghipour, S. Medical resource allocation planning by integrating machine learning and optimization models. Artif. Intell. Med. 2022, 134, 102430. [CrossRef]
- Munavalli, J.R.; Boersma, H.J.; Rao, S.V.; Van Merode, G. Real-time capacity management and patient flow optimization in hospitals using AI methods. Artif. Intell. Data Min. Healthc. 2021, 2021, 55-69.
- Adhikari, A.; Joshi, R.; Basu, S. Collaboration and coordination strategies for a multi-level AI-enabled healthcare supply chain under disaster. Int. J. Prod. Res. 2023, 2023, 1-27. [CrossRef]
- Samadhiya, A.; Yadav, S.; Kumar, A.; Majumdar, A.; Luthra, S.; Garza-Reyes, J.A.; Upadhyay, A. The influence of artificial intelligence techniques on disruption management: Does supply chain dynamism matter? Technol. Soc. 2023, 75, 102394. [CrossRef]
- Sun, W.; Bocchini, P.; Davison, B.D. Applications of artificial intelligence for disaster management. Nat. Hazards 2020, 103, 2631-2689. [CrossRef]
- Tang, A.; Tam, R.; Cadrin-Chênevert, A.; Guest, W.; Chong, J.; Barfett, J.; Trump, D.; Noorbakhsh-Sabet, N.; Zand, R.; Zhang, Y. Health information management: Implications of artificial intelligence on healthcare data and information management. Yearb. Med. Inform. 2019, 28, 56-64.
- Hoogendoorn, M.; Szolovits, P.; Moons, L.M.; Numans, M.E. Utilizing uncoded consultation notes from electronic medical records for predictive modeling of colorectal cancer. Artif. Intell. Med. 2016, 69, 53-61. [CrossRef] [PubMed]
- Thesmar, D.; Sraer, D.; Pinheiro, L.; Dadson, N.; Veliche, R.; Greenberg, P. Combining the power of artificial intelligence with the richness of healthcare claims data: Opportunities and challenges. Pharmacoeconomics 2019, 37, 745-752. [CrossRef]
- Baudry, M.; Robert, C.Y. A machine learning approach for individual claims reserving in insurance. Appl. Stoch. Models Bus. Ind. 2019, 35, 1127-1155. [CrossRef]
- Samorani, M.; Blount, L.G. Machine learning and medical appointment scheduling: Creating and perpetuating inequalities in access to health care. Am. Public Health Assoc. 2020, 110, 440-441. [CrossRef]
- Chong, L.R.; Tsai, K.T.; Lee, L.L.; Foo, S.G.; Chang, P.C. Artificial intelligence predictive analytics in the management of outpatient MRI appointment no-shows. Am. J. Roentgenol. 2020, 215, 1155-1162. [CrossRef] [PubMed]
- Mandelbaum, A.; Momčilović, P.; Trichakis, N.; Kadish, S.; Leib, R.; Bunnell, C.A. Data-driven appointment-scheduling under uncertainty: The case of an infusion unit in a cancer center. Manag. Sci. 2020, 66, 243-270. [CrossRef]
- Pandey, M.; Arora, M.; Arora, S.; Goyal, C.; Gera, V.K.; Yadav, H. AI-based Integrated Approach for the Development of Intelligent Document Management System (IDMS). Procedia Comput. Sci. 2023, 230, 725-736. [CrossRef]
- Hsu, E.; Malagaris, I.; Kuo, Y.-F.; Sultana, R.; Roberts, K. Deep learning-based NLP data pipeline for EHR-scanned document information extraction. JAMIA Open 2022, 5, ooac045. [CrossRef]
- Kreps, G.L.; Neuhauser, L. Artificial intelligence and immediacy: Designing health communication to personally engage consumers and providers. Patient Educ. Couns. 2013, 92, 205-210. [CrossRef]
- Kingston, J. Using artificial intelligence to support compliance with the general data protection regulation. Artif. Intell. Law 2017, 25, 429-443. [CrossRef]
- Hamdani, R.E.; Mustapha, M.; Amariles, D.R.; Troussel, A.; Meeùs, S.; Krasnashchok, K. A combined rule-based and machine learning approach for automated GDPR compliance checking. In Proceedings of the Eighteenth International Conference on Artificial Intelligence and Law, São Paulo, Brazil, 21-25 June 2021; pp. 40-49.
- El-Bouri, R.; Taylor, T.; Youssef, A.; Zhu, T.; Clifton, D.A. Machine learning in patient flow: A review. Prog. Biomed. Eng. 2021, 3, 022002. [CrossRef] [PubMed]
- Yang, T.; Asanjan, A.A.; Welles, E.; Gao, X.; Sorooshian, S.; Liu, X. Developing reservoir monthly inflow forecasts using artificial intelligence and climate phenomenon information. Water Resour. Res. 2017, 53, 2786-2812. [CrossRef]
- Knight, D.; Aakre, C.A.; Anstine, C.V.; Munipalli, B.; Biazar, P.; Mitri, G.; Valery, J.R.; Brigham, T.; Niazi, S.K.; Perlman, A.I. Artificial Intelligence for Patient Scheduling in the Real-World Health Care Setting: A Metanarrative Review. Health Policy Technol. 2023, 12, 100824. [CrossRef]
- Wang, J.; Fung, R.Y. Adaptive dynamic programming algorithms for sequential appointment scheduling with patient preferences. Artif. Intell. Med. 2015, 63, 33-40. [CrossRef] [PubMed]
- Li, X.; Tian, D.; Li, W.; Dong, B.; Wang, H.; Yuan, J.; Li, B.; Shi, L.; Lin, X.; Zhao, L. Artificial intelligence-assisted reduction in patients’ waiting time for outpatient process: A retrospective cohort study. BMC Health Serv. Res. 2021, 21, 237. [CrossRef]
- Joshi, I. Waiting for deep medicine. Lancet 2019, 393, 1193-1194. [CrossRef]
- Joseph, J.; Senith, S.; Kirubaraj, A.A.; Ramson, J.S. Machine Learning for Prediction of Wait Times in Outpatient Clinic. Procedia Comput. Sci. 2022, 215, 230-239. [CrossRef]
- Khanbhai, M.; Anyadi, P.; Symons, J.; Flott, K.; Darzi, A.; Mayer, E. Applying natural language processing and machine learning techniques to patient experience feedback: A systematic review. BMJ Health Care Inform. 2021, 28, e100262. [CrossRef]
- Bari, V.; Hirsch, J.S.; Narvaez, J.; Sardinia, R.; Bock, K.R.; Oppenheim, M.I.; Meytlis, M. An approach to predicting patient experience through machine learning and social network analysis. J. Am. Med. Inform. Assoc. 2020, 27, 1834-1843. [CrossRef]
- Darley, S.; Coulson, T.; Peek, N.; Moschogianis, S.; Van Der Veer, S.N.; Wong, D.C.; Brown, B.C. Understanding how the design and implementation of online consultations affect primary care quality: Systematic review of evidence with recommendations for designers, providers, and researchers. J. Med. Internet Res. 2022, 24, e37436. [CrossRef] [PubMed]
- Frid-Adar, M.; Amer, R.; Gozes, O.; Nassar, J.; Greenspan, H. COVID-19 in CXR: From detection and severity scoring to patient disease monitoring. IEEE J. Biomed. Health Inform. 2021, 25, 1892-1903. [CrossRef] [PubMed]
- Chen, Y.; Schönlieb, C.-B.; Lio, P.; Leiner, T.; Dragotti, P.L.; Wang, G.; Rueckert, D.; Firmin, D.; Yang, G. AI-based reconstruction for fast MRI—A systematic review and meta-analysis. Proc. IEEE 2022, 110, 224-245. [CrossRef]
- Fusco, R.; Grassi, R.; Granata, V.; Setola, S.V.; Grassi, F.; Cozzi, D.; Pecori, B.; Izzo, F.; Petrillo, A. Artificial intelligence and COVID-19 using chest CT scan and chest X-ray images: Machine learning and deep learning approaches for diagnosis and treatment. J. Pers. Med. 2021, 11, 993. [CrossRef] [PubMed]
- Panayides, A.S.; Amini, A.; Filipovic, N.D.; Sharma, A.; Tsaftaris, S.A.; Young, A.; Foran, D.; Do, N.; Golemati, S.; Kurc, T. AI in medical imaging informatics: Current challenges and future directions. IEEE J. Biomed. Health Inform. 2020, 24, 1837-1857. [CrossRef] [PubMed]
- Liu, Y.; Zhang, F.; Chen, C.; Wang, S.; Wang, Y.; Yu, Y. Act like a radiologist: Towards reliable multi-view correspondence reasoning for mammogram mass detection. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 5947-5961. [CrossRef] [PubMed]
- Liu, F.; Zhang, Q.; Huang, C.; Shi, C.; Wang, L.; Shi, N.; Fang, C.; Shan, F.; Mei, X.; Shi, J. CT quantification of pneumonia lesions in early days predicts progression to severe illness in a cohort of COVID-19 patients. Theranostics 2020, 10, 5613. [CrossRef] [PubMed]
- Johnson, D.; Goodman, R.; Patrinely, J.; Stone, C.; Zimmerman, E.; Donald, R.; Chang, S.; Berkowitz, S.; Finn, A.; Jahangir, E. Assessing the accuracy and reliability of AI-generated medical responses: An evaluation of the Chat-GPT model. Res. Sq. 2023, Preprint.
- Bera, K.; Braman, N.; Gupta, A.; Velcheti, V.; Madabhushi, A. Predicting cancer outcomes with radiomics and artificial intelligence in radiology. Nat. Rev. Clin. Oncol. 2022, 19, 132-146. [CrossRef]
- Lee, R.Y.; Wu, Y.; Goh, D.; Tan, V.; Ng, C.W.; Lim, J.C.T.; Lau, M.C.; Yeong, J.P.S. Application of Artificial Intelligence to in vitro Tumor Modeling and Characterization of the Tumor Microenvironment. Adv. Healthc. Mater. 2023, 12, 2202457. [CrossRef]
- Acs, B.; Rantalainen, M.; Hartman, J. Artificial intelligence as the next step towards precision pathology. J. Intern. Med. 2020, 288, 62-81. [CrossRef] [PubMed]
- Bera, K.; Schalper, K.A.; Rimm, D.L.; Velcheti, V.; Madabhushi, A. Artificial intelligence in digital pathology-New tools for diagnosis and precision oncology. Nat. Rev. Clin. Oncol. 2019, 16, 703-715. [CrossRef] [PubMed]
- Pandey, I.; Misra, V.; Pandey, A.T.; Ramteke, P.W.; Agrawal, R. Artificial intelligence technologies empowering identification of novel diagnostic molecular markers in gastric cancer. Ind. J. Pathol. Microbiol. 2021, 64 (Suppl. S1), S63-S68.
- Segura, F.; Segura, P.; Segura, F. Measuring Tumor Aggressiveness Through Artificial Intelligence. J. Asoc. Argent. Ortop. Traumatol. 2023, 88, 653-661. [CrossRef]
- Liopyris, K.; Gregoriou, S.; Dias, J.; Stratigos, A.J. Artificial intelligence in dermatology: Challenges and perspectives. Dermatol. Ther. 2022, 12, 2637-2651. [CrossRef] [PubMed]
- Ahmad, S.; Wasim, S. Prevent medical errors through artificial intelligence: A review. Saudi J. Med. Pharm. Sci. 2023, 9, 419-423. [CrossRef]
- Soun, J.; Chow, D.; Nagamine, M.; Takhtawala, R.; Filippi, C.; Yu, W.; Chang, P. Artificial intelligence and acute stroke imaging. Am. J. Neuroradiol. 2021, 42, 2-11. [CrossRef] [PubMed]
- Brereton, T.A.; Malik, M.M.; Lifson, M.; Greenwood, J.D.; Peterson, K.J.; Overgaard, S.M. The Role of Artificial Intelligence Model Documentation in Translational Science: Scoping Review. Interact. J. Med. Res. 2023, 12, e45903. [CrossRef] [PubMed]
- Klement, W.; El Emam, K. Consolidated reporting guidelines for prognostic and diagnostic machine learning modeling studies: Development and validation. J. Med. Internet Res. 2023, 25, e48763. [CrossRef]
- Huang, S.-C.; Pareek, A.; Seyyedi, S.; Banerjee, I.; Lungren, M.P. Fusion of medical imaging and electronic health records using deep learning: A systematic review and implementation guidelines. NPJ Digit. Med. 2020, 3, 136. [CrossRef]
- Mohsen, F.; Ali, H.; El Hajj, N.; Shah, Z. Artificial intelligence-based methods for fusion of electronic health records and imaging data. Sci. Rep. 2022, 12, 17981. [CrossRef] [PubMed]
- Deng, L.; Li, G.; Han, S.; Shi, L.; Xie, Y. Model compression and hardware acceleration for neural networks: A comprehensive survey. Proc. IEEE 2020, 108, 485-532. [CrossRef]
- Alcaín, E.; Fernandez, P.R.; Nieto, R.; Montemayor, A.S.; Vilas, J.; Galiana-Bordera, A.; Martinez-Girones, P.M.; Prieto-de-la-Lastra, C.; Rodriguez-Vila, B.; Bonet, M. Hardware architectures for real-time medical imaging. Electronics 2021, 10, 3118. [CrossRef]
- Eklund, A.; Dufort, P.; Forsberg, D.; LaConte, S.M. Medical image processing on the GPU-Past, present and future. Med. Image Anal. 2013, 17, 1073-1094. [CrossRef] [PubMed]
- Corral, J.M.R.; Civit-Masot, J.; Luna-Perejón, F.; Díaz-Cano, I.; Morgado-Estévez, A.; Domínguez-Morales, M. Energy efficiency in edge TPU vs. embedded GPU for computer-aided medical imaging segmentation and classification. Eng. Appl. Artif. Intell. 2024, 127, 107298. [CrossRef]
- Lin, Y.; Zhang, Y.; Yang, X. A Low Memory Requirement MobileNets Accelerator Based on FPGA for Auxiliary Medical Tasks. Bioengineering 2022, 10, 28. [CrossRef] [PubMed]
- Azghadi, M.R.; Lammie, C.; Eshraghian, J.K.; Payvand, M.; Donati, E.; Linares-Barranco, B.; Indiveri, G. Hardware implementation of deep network accelerators towards healthcare and biomedical applications. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 1138-1159. [CrossRef] [PubMed]
- Jiang, W.; Ye, X.; Chen, R.; Su, F.; Lin, M.; Ma, Y.; Zhu, Y.; Huang, S. Wearable on-device deep learning system for hand gesture recognition based on FPGA accelerator. Math. Biosci. Eng. 2021, 18, 132-153. [CrossRef] [PubMed]
- Nayak, D.R.; Dash, R.; Majhi, B. Automated diagnosis of multi-class brain abnormalities using MRI images: A deep convolutional neural network based method. Pattern Recog. Lett. 2020, 138, 385-391. [CrossRef]
- Soffer, S.; Klang, E.; Shimon, O.; Barash, Y.; Cahan, N.; Greenspana, H.; Konen, E. Deep learning for pulmonary embolism detection on computed tomography pulmonary angiogram: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 15814. [CrossRef]
- Lång, K.; Josefsson, V.; Larsson, A.-M.; Larsson, S.; Högberg, C.; Sartor, H.; Hofvind, S.; Andersson, I.; Rosso, A. Artificial intelligence-supported screen reading versus standard double reading in the Mammography Screening with Artificial Intelligence trial (MASAI): A clinical safety analysis of a randomised, controlled, non-inferiority, single-blinded, screening accuracy study. Lancet Oncol. 2023, 24, 936-944. [PubMed]
- Sveric, K.M.; Ulbrich, S.; Dindane, Z.; Winkler, A.; Botan, R.; Mierke, J.; Trausch, A.; Heidrich, F.; Linke, A. Improved assessment of left ventricular ejection fraction using artificial intelligence in echocardiography: A comparative analysis with cardiac magnetic resonance imaging. Int. J. Cardiol. 2024, 394, 131383. [CrossRef] [PubMed]
- Khan, P.; Kader, M.F.; Islam, S.R.; Rahman, A.B.; Kamal, M.S.; Toha, M.U.; Kwak, K.-S. Machine learning and deep learning approaches for brain disease diagnosis: Principles and recent advances. IEEE Access 2021, 9, 37622-37655. [CrossRef]
- Adam, R.; Dell’Aquila, K.; Hodges, L.; Maldjian, T.; Duong, T.Q. Deep learning applications to breast cancer detection by magnetic resonance imaging: A literature review. Breast Cancer Res. 2023, 25, 87. [CrossRef] [PubMed]
- Sheth, D.; Giger, M.L. Artificial intelligence in the interpretation of breast cancer on MRI. J. Magn. Reson. Imaging 2020, 51, 1310-1324. [CrossRef]
- McCrindle, B.; Zukotynski, K.; Doyle, T.E.; Noseworthy, M.D. A radiology-focused review of predictive uncertainty for AI interpretability in computer-assisted segmentation. Radiol. Artif. Intell. 2021, 3, e210031. [CrossRef] [PubMed]
- Zheng, R.; Wang, Q.; Lv, S.; Li, C.; Wang, C.; Chen, W.; Wang, H. Automatic liver tumor segmentation on dynamic contrast enhanced mri using 4D information: Deep learning model based on 3D convolution and convolutional lstm. IEEE Trans. Med. Imaging 2022, 41, 2965-2976. [CrossRef]
- Schalekamp, S.; Klein, W.M.; van Leeuwen, K.G. Current and emerging artificial intelligence applications in chest imaging: A pediatric perspective. Pediatr. Radiol. 2022, 52, 2120-2130. [CrossRef]
- Lee, M.-H.; O’Hara, N.; Sonoda, M.; Kuroda, N.; Juhasz, C.; Asano, E.; Dong, M.; Jeong, J.-W. Novel deep learning network analysis of electrical stimulation mapping-driven diffusion MRI tractography to improve preoperative evaluation of pediatric epilepsy. IEEE Trans. Biomed. Eng. 2020, 67, 3151-3162. [CrossRef]
- Ardila, D.; Kiraly, A.P.; Bharadwaj, S.; Choi, B.; Reicher, J.J.; Peng, L.; Tse, D.; Etemadi, M.; Ye, W.; Corrado, G. End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography. Nat. Med. 2019, 25, 954-961. [CrossRef]
- Watanabe, A.T.; Lim, V.; Vu, H.X.; Chim, R.; Weise, E.; Liu, J.; Bradley, W.G.; Comstock, C.E. Improved cancer detection using artificial intelligence: A retrospective evaluation of missed cancers on mammography. J. Digit. Imaging 2019, 32, 625-637. [CrossRef] [PubMed]
- Sermesant, M.; Delingette, H.; Cochet, H.; Jais, P.; Ayache, N. Applications of artificial intelligence in cardiovascular imaging. Nat. Rev. Cardiol. 2021, 18, 600-609. [CrossRef]
- Nahavandi, D.; Alizadehsani, R.; Khosravi, A.; Acharya, U.R. Application of artificial intelligence in wearable devices: Opportunities and challenges. Comput. Methods Programs Biomed. 2022, 213, 106541. [CrossRef]
- Stangl, F.J.; Riedl, R. Measurement of heart rate and heart rate variability with wearable devices: A systematic review. Wirtschaftsinformatik 2022, 2022, 15.
- Huang, J.-D.; Wang, J.; Ramsey, E.; Leavey, G.; Chico, T.J.; Condell, J. Applying artificial intelligence to wearable sensor data to diagnose and predict cardiovascular disease: A review. Sensors 2022, 22, 8002. [CrossRef] [PubMed]
- Bahrami, M.; Forouzanfar, M. Deep learning forecasts the occurrence of sleep apnea from single-lead ECG. Cardiovasc. Eng. Technol. 2022, 13, 809-815. [CrossRef]
- Joeris, A.; Zhu, T.Y.; Lambert, S.; Wood, A.; Jayakumar, P. Real-world patient data: Can they support decision making and patient engagement? Injury 2023, 54, S51-S56. [CrossRef]
- Asthana, S.; Megahed, A.; Strong, R. A recommendation system for proactive health monitoring using IoT and wearable technologies. In Proceedings of the 2017 IEEE International Conference on AI & Mobile Services (AIMS), Honolulu, HI, USA, 25-30 June 2017; IEEE: New, York, NY, USA, 2017; pp. 14-21.
- Djanian, S.; Bruun, A.; Nielsen, T.D. Sleep classification using Consumer Sleep Technologies and AI: A review of the current landscape. Sleep Med. 2022, 100, 390-403. [CrossRef] [PubMed]
- Sabry, F.; Eltaras, T.; Labda, W.; Alzoubi, K.; Malluhi, Q. Machine learning for healthcare wearable devices: The big picture. J. Healthc. Eng. 2022, 2022, 1-25. [CrossRef]
- Van Bulck, L.; Couturier, R.; Moons, P. Applications of Artificial Intelligence for Nursing: Has a New Era Arrived? Oxford University Press US: Cary, NC, USA, 2023; Volume 22, pp. e19-e20.
- Jadczyk, T.; Wojakowski, W.; Tendera, M.; Henry, T.D.; Egnaczyk, G.; Shreenivas, S. Artificial intelligence can improve patient management at the time of a pandemic: The role of voice technology. J. Med. Internet Res. 2021, 23, e22959. [CrossRef]
- Adus, S.; Macklin, J.; Pinto, A. Exploring patient perspectives on how they can and should be engaged in the development of artificial intelligence (AI) applications in health care. BMC Health Serv. Res. 2023, 23, 1163. [CrossRef] [PubMed]
- Curtis, R.G.; Bartel, B.; Ferguson, T.; Blake, H.T.; Northcott, C.; Virgara, R.; Maher, C.A. Improving user experience of virtual health assistants: Scoping review. J. Med. Internet Res. 2021, 23, e31737. [CrossRef] [PubMed]
- Ye, J.; He, L.; Beestrum, M. Implications for implementation and adoption of telehealth in developing countries: A systematic review of China’s practices and experiences. NPJ Digit. Med. 2023, 6, 174. [CrossRef] [PubMed]
- Jeddi, Z.; Bohr, A. Remote patient monitoring using artificial intelligence. In Artificial Intelligence in Healthcare; Elsevier: Amsterdam, The Netherlands, 2020; pp. 203-234.
- Shaik, T.; Tao, X.; Higgins, N.; Li, L.; Gururajan, R.; Zhou, X.; Acharya, U.R. Remote patient monitoring using artificial intelligence: Current state, applications, and challenges. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2023, 13, e1485. [CrossRef]
- Khadija, A.; Zahra, F.F.; Naceur, A. AI-powered health chatbots: Toward a general architecture. Procedia Comput. Sci. 2021, 191, 355-360. [CrossRef]
- Görtz, M.; Baumgärtner, K.; Schmid, T.; Muschko, M.; Woessner, P.; Gerlach, A.; Byczkowski, M.; Sültmann, H.; Duensing, S.; Hohenfellner, M. An artificial intelligence-based chatbot for prostate cancer education: Design and patient evaluation study. Digit. Health 2023, 9, 20552076231173304. [CrossRef]
- Sharma, S.; Rawal, R.; Shah, D. Addressing the challenges of AI-based telemedicine: Best practices and lessons learned. J. Educ. Health Promot. 2023, 12, 338. [CrossRef] [PubMed]
- Maleki, F.; Muthukrishnan, N.; Ovens, K.; Reinhold, C.; Forghani, R. Machine learning algorithm validation: From essentials to advanced applications and implications for regulatory certification and deployment. Neuroimaging Clin. 2020, 30, 433-445. [CrossRef] [PubMed]
- Lei, J. Cross-validation with confidence. J. Am. Stat. Assoc. 2020, 115, 1978-1997. [CrossRef]
- Ebrahimian, S.; Kalra, M.K.; Agarwal, S.; Bizzo, B.C.; Elkholy, M.; Wald, C.; Allen, B.; Dreyer, K.J. FDA-regulated AI algorithms: Trends, strengths, and gaps of validation studies. Acad. Radiol. 2022, 29, 559-566. [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable ai: A review of machine learning interpretability methods. Entropy 2020, 23, 18. [CrossRef] [PubMed]
- Davagdorj, K.; Li, M.; Ryu, K.H. Local interpretable model-agnostic explanations of predictive models for hypertension, Advances in Intelligent Information Hiding and Multimedia Signal Processing. In Proceeding of the 16th International Conference on
155. Nohara, Y.; Matsumoto, K.; Soejima, H.; Nakashima, N. Explanation of machine learning models using shapley additive explanation and application for real data in hospital. Comput. Methods Programs Biomed. 2022, 214, 106584. [CrossRef] [PubMed]
156. Puerta-Beldarrain, M.; Gómez-Carmona, O.; Casado-Mansilla, D.; López-de-Ipiña, D. Human-AI collaboration to promote trust, engagement and adaptation in the process of pro-environmental and health behaviour change. In Proceedings of the International Conference on Ubiquitous Computing and Ambient Intelligence, Córdoba, Spain, 29 November-2 December 2022; Springer: Berlin/Heidelberg, Germany, 2022; pp. 381-392.
157. Mishra, A. Scalable AI Governance and Ethics. In Scalable AI and Design Patterns: Design, Develop, and Deploy Scalable AI Solutions; Springer: Berlin/Heidelberg, Germany, 2024; pp. 147-165.
158. Badnjević, A.; Pokvić, L.G.; Deumić, A.; Bećirović, L.S. Post-market surveillance of medical devices: A review. Technol. Health Care 2022, 30, 1315-1329. [CrossRef] [PubMed]
159. Feng, J.; Phillips, R.V.; Malenica, I.; Bishara, A.; Hubbard, A.E.; Celi, L.A.; Pirracchio, R. Clinical artificial intelligence quality improvement: Towards continual monitoring and updating of AI algorithms in healthcare. NPJ Digit. Med. 2022, 5, 66. [CrossRef] [PubMed]
160. Murdoch, B. Privacy and artificial intelligence: Challenges for protecting health information in a new era. BMC Med. Ethics 2021, 22, 122. [CrossRef] [PubMed]
161. Iserson, K.V. Informed consent for artificial intelligence in emergency medicine: A practical guide. Am. J. Emerg. Med. 2024, 76, 225-230. [CrossRef] [PubMed]
162. Fletcher, R.R.; Nakeshimana, A.; Olubeko, O. Addressing fairness, bias, and appropriate use of artificial intelligence and machine learning in global health. Front. Media SA 2021, 3, 561802. [CrossRef] [PubMed]
163. Smith, H. Clinical AI: Opacity, accountability, responsibility and liability. AI Soc. 2021, 36, 535-545. [CrossRef]
164. Moltubakk Kempton, A.; Vassilakopoulou, P. Accountability, Transparency and Explainability in AI for Healthcare. 2021. Available online: https://dl.eusset.eu/items/9c739979-ec3f-4510-a02a-553eadee47e2 (accessed on 28 February 2024).
165. Kim, B.; Park, J.; Suh, J. Transparency and accountability in AI decision support: Explaining and visualizing convolutional neural networks for text information. Decis. Support Syst. 2020, 134, 113302. [CrossRef]
166. Carmody, J.; Shringarpure, S.; Van de Venter, G. AI and privacy concerns: A smart meter case study. J. Inf. Commun. Ethics Soc. 2021, 19, 492-505. [CrossRef]
167. Bandari, V. Enterprise Data Security Measures: A Comparative Review of Effectiveness and Risks Across Different Industries and Organization Types. Int. J. Bus. Intell. Big Data Anal. 2023, 6,1-11.
168. Lehne, M.; Sass, J.; Essenwanger, A.; Schepers, J.; Thun, S. Why digital medicine depends on interoperability. NPJ Digit. Med. 2019, 2, 79. [CrossRef] [PubMed]
169. Perugu, B.; Wadhwa, V.; Kim, J.; Cai, J.; Shin, A.; Gupta, A. Pragmatic Approaches to Interoperability-Surmounting Barriers to Healthcare Data and Information Across Organizations and Political Boundaries. Telehealth Med. Today 2023, 8, 421.
170. Dikici, E.; Bigelow, M.; Prevedello, L.M.; White, R.D.; Erdal, B.S. Integrating AI into radiology workflow: Levels of research, production, and feedback maturity. J. Med. Imaging 2020, 7, 016502. [CrossRef] [PubMed]
171. Balagurunathan, Y.; Mitchell, R.; El Naqa, I. Requirements and reliability of AI in the medical context. Phys. Med. 2021, 83, 72-78. [CrossRef] [PubMed]
172. Schneeberger, D.; Stöger, K.; Holzinger, A. The European Legal Framework for Medical AI, International Cross-Domain Conference for Machine Learning and Knowledge Extraction; Springer: Berlin/Heidelberg, Germany, 2020; pp. 209-226.
173. Larson, D.B.; Harvey, H.; Rubin, D.L.; Irani, N.; Justin, R.T.; Langlotz, C.P. Regulatory frameworks for development and evaluation of artificial intelligence-based diagnostic imaging algorithms: Summary and recommendations. J. Am. Coll. Radiol. 2021, 18, 413-424. [CrossRef]
174. Benjamens, S.; Dhunnoo, P.; Meskó, B. The state of artificial intelligence-based FDA-approved medical devices and algorithms: An online database. NPJ Digit. Med. 2020, 3, 118. [CrossRef] [PubMed]
175. Muehlematter, U.J.; Daniore, P.; Vokinger, K.N. Approval of artificial intelligence and machine learning-based medical devices in the USA and Europe (2015-2020): A comparative analysis. Lancet Digit. Health 2021, 3, e195-e203. [CrossRef]
176. Baric-Parker, J.; Anderson, E.E. Patient data-sharing for AI: Ethical challenges, catholic solutions. Linacre Q. 2020, 87, 471-481. [CrossRef]
177. Johnson, K.B.; Wei, W.Q.; Weeraratne, D.; Frisse, M.E.; Misulis, K.; Rhee, K.; Zhao, J.; Snowdon, J.L. Precision medicine, AI, and the future of personalized health care. Clin. Transl. Sci. 2021, 14, 86-93. [CrossRef]
178. Bandyopadhyay, A.; Goldstein, C. Clinical applications of artificial intelligence in sleep medicine: A sleep clinician’s perspective. Sleep Breath. 2023, 27, 39-55. [CrossRef] [PubMed]
179. Galkin, F.; Zhavoronkov, A. AI in Longevity. In Artificial Intelligence for Healthy Longevity; Springer: Berlin/Heidelberg, Germany, 2023; pp. 3-13.
180. Zhavoronkov, A.; Mamoshina, P.; Vanhaelen, Q.; Scheibye-Knudsen, M.; Moskalev, A.; Aliper, A. Artificial intelligence for aging and longevity research: Recent advances and perspectives. Ageing Res. Rev. 2019, 49, 49-66. [CrossRef] [PubMed]
181. Jiménez-Luna, J.; Grisoni, F.; Weskamp, N.; Schneider, G. Artificial intelligence in drug discovery: Recent advances and future perspectives. Expert Opin. Drug Discov. 2021, 16, 949-959. [CrossRef] [PubMed]
182. Feizi, N.; Tavakoli, M.; Patel, R.V.; Atashzar, S.F. Robotics and ai for teleoperation, tele-assessment, and tele-training for surgery in the era of COVID-19: Existing challenges, and future vision. Front. Robot. AI 2021, 8, 610677. [CrossRef] [PubMed]
183. Bitencourt, A.; Naranjo, I.D.; Gullo, R.L.; Saccarelli, C.R.; Pinker, K. AI-enhanced breast imaging: Where are we and where are we heading? Eur. J. Radiol. 2021, 142, 109882. [CrossRef] [PubMed]
184. Shi, Q.; Dong, B.; He, T.; Sun, Z.; Zhu, J.; Zhang, Z.; Lee, C. Progress in wearable electronics/photonics-Moving toward the era of artificial intelligence and internet of things. InfoMat 2020, 2, 1131-1162. [CrossRef]
185. Forghani, N.; Maghooli, K.; Dabanloo, N.J.; Farahani, A.V.; Forouzanfar, M. Intelligent oscillometric system for automatic detection of peripheral arterial disease. IEEE J. Biomed. Health Inform. 2021, 25, 3209-3218. [CrossRef] [PubMed]
186. Huang, C.-H.; Batarseh, F.A.; Boueiz, A.; Kulkarni, A.; Su, P.-H.; Aman, J. Measuring outcomes in healthcare economics using Artificial Intelligence: With application to resource management. Data Policy 2021, 3, e30. [CrossRef] [PubMed]
187. Giuste, F.; Shi, W.; Zhu, Y.; Naren, T.; Isgut, M.; Sha, Y.; Tong, L.; Gupte, M.; Wang, M.D. Explainable artificial intelligence methods in combating pandemics: A systematic review. IEEE Rev. Biomed. Eng. 2022, 16, 5-21. [CrossRef]
188. Cao, L. AI in Combating the COVID-19 Pandemic. IEEE Intell. Syst. 2022, 37, 3-13. [CrossRef]
189. Gu, X.; Deligianni, F.; Han, J.; Liu, X.; Chen, W.; Yang, G.-Z.; Lo, B. Beyond supervised learning for pervasive healthcare. IEEE Rev. Biomed. Eng. 2023, 17, 42-62. [CrossRef] [PubMed]
190. Fechter, T.; Baltas, D. One-shot learning for deformable medical image registration and periodic motion tracking. IEEE Trans. Med. Imaging 2020, 39, 2506-2517. [CrossRef] [PubMed]
191. Feng, R.; Zheng, X.; Gao, T.; Chen, J.; Wang, W.; Chen, D.Z.; Wu, J. Interactive few-shot learning: Limited supervision, better medical image segmentation. IEEE Trans. Med. Imaging 2021, 40, 2575-2588. [CrossRef] [PubMed]
192. Mahapatra, D.; Bozorgtabar, B.; Ge, Z. Medical image classification using generalized zero shot learning. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Montreal, QC, Canada, 10-17 October 2021; pp. 3344-3353.
193. Hospedales, T.; Antoniou, A.; Micaelli, P.; Storkey, A. Meta-learning in neural networks: A survey. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 5149-5169. [CrossRef] [PubMed]
194. Yang, J.; Soltan, A.A.; Clifton, D.A. Machine learning generalizability across healthcare settings: Insights from multi-site COVID-19 screening. NPJ Digit. Med. 2022, 5, 69. [CrossRef] [PubMed]
195. Khoshnevisan, F.; Chi, M. Unifying domain adaptation and domain generalization for robust prediction across minority racial groups, Machine Learning and Knowledge Discovery in Databases. In Proceedings of the Research Track: European Conference, ECML PKDD 2021, Bilbao, Spain, 13-17 September 2021; Proceedings, Part I 21. Springer: Berlin/Heidelberg, Germany, 2021; pp. 521-537.
196. Rieke, N.; Hancox, J.; Li, W.; Milletari, F.; Roth, H.R.; Albarqouni, S.; Bakas, S.; Galtier, M.N.; Landman, B.A.; Maier-Hein, K. The future of digital health with federated learning. NPJ Digit. Med. 2020, 3, 119. [CrossRef]
197. Hogg, H.D.J.; Al-Zubaidy, M.; Talks, J.; Denniston, A.K.; Kelly, C.J.; Malawana, J.; Papoutsi, C.; Teare, M.D.; A Keane, P.; Beyer, F.R.; et al. Stakeholder perspectives of clinical artificial intelligence implementation: Systematic review of qualitative evidence. J. Med. Internet Res. 2023, 25, e39742. [CrossRef]
198. Gerlings, J.; Jensen, M.S.; Shollo, A. Explainable ai, but explainable to whom? an exploratory case study of xai in healthcare. In Handbook of Artificial Intelligence in Healthcare: Vol 2: Practicalities and Prospects; Springer: Berlin/Heidelberg, Germany, 2022; pp. 169-198.