المجلة: Scientific Reports، المجلد: 15، العدد: 1
DOI: https://doi.org/10.1038/s41598-025-88249-0
PMID: https://pubmed.ncbi.nlm.nih.gov/39994294
تاريخ النشر: 2025-02-24
DOI: https://doi.org/10.1038/s41598-025-88249-0
PMID: https://pubmed.ncbi.nlm.nih.gov/39994294
تاريخ النشر: 2025-02-24
افتح
عبء أمراض اللثة لدى البالغين الشباب
هدفنا هو تقديم نظرة شاملة على العبء العالمي لأمراض اللثة بين البالغين الشباب خلال الفترة من 1990 إلى 2019. اعتبرت التحليل عوامل مختلفة مثل العمر والجنس والدولة ومؤشر السوسيوديموغرافي (SDI). استخدمت هذه الدراسة قاعدة بيانات GBD 2019 لفحص الاتجاهات في كل من معدلات الإصابة وسنوات الحياة المعدلة حسب الإعاقة (DALY) لأمراض اللثة بين البالغين الشباب من 1990 إلى 2019. تم تحليل البيانات بناءً على معدل التوحيد العمري. لتحديد الأنماط الزمنية والجغرافية، قمنا بحساب النسبة المئوية السنوية المقدرة (EAPC) وفترة الثقة المقابلة لها
الكلمات الرئيسية: أمراض اللثة، معدل الإصابة، سنوات الحياة المعدلة حسب الإعاقة (DALYs)، العبء العالمي لدراسة الأمراض، معدل الإصابة، عبء المرض
أمراض اللثة، عدوى شائعة والتهاب، هي استجابة التهابية غير محددة لبكتيريا الفم، تؤثر على الرباط اللثوي، والعظم السنخي، والارتباط اللثوي
تعتبر الفترة بين البلوغ المبكر (15-49 عامًا) مرحلة مهمة ولكنها غير مدروسة بشكل كافٍ، تتميز بظهور عوامل خطر أيضية فردية، مثل السكري، وارتفاع ضغط الدم، وارتفاع الدهون في الدم. هذه العوامل، بدورها، تعمل كعوامل خطر محتملة لأمراض اللثة
تقدم GBD 2019 طريقة وأداة موثوقتين لإجراء أبحاث البيانات والتحليل بطريقة قابلة للمقارنة. غطت GBD 2019 204 دول، وأقاليم، وتفكيك المستوى الإداري الأول لـ 22 دولة، من 1990 إلى 2019. قدمت GBD تقييمًا علميًا منهجيًا للبيانات المنشورة والمتاحة للجمهور والمساهمة حول معدلات الإصابة والانتشار والوفيات للأمراض والإصابات لقائمة شاملة من الأمراض والإصابات. لذلك، توفر GBD أساسًا قويًا لرؤى مفصلة وواسعة حول الاتجاهات الصحية العالمية والتحديات الناشئة. مؤخرًا، أجرت بعض الأبحاث تقييمًا شاملاً للاتجاهات العالمية والإقليمية والوطنية لعبء التهاب اللثة أو التهاب اللثة الشديد من 1990 إلى
طرق
مصادر البيانات
تم الحصول على البيانات المستخدمة في هذا التقييم من دراسة GBD 2019. يمكن العثور على المنهجية التفصيلية لتقدير عبء مرض التهاب اللثة من دراسة GBD 2019 في المنشورات السابقة
تستند هذه الدراسة إلى قاعدة بيانات متاحة للجمهور ولا تتطلب موافقة أخلاقية.
تعريف الحالة
تعتبر أمراض اللثة المزمنة نتيجة لعدوى بكتيرية مزمنة في محيط الأسنان. التهاب اللثة، وهو الشكل الأخف من المرض، يظهر أعراضًا تشمل تورم اللثة، واحمرار، ونزيف عند التحفيز. إذا تُركت دون علاج، ستتقدم العدوى تحت خط اللثة، مما يؤدي إلى حالة التهابية مستمرة داخل الأنسجة اللثوية. كما هو محدد من قبل العبء العالمي للأمراض (GBD)، فإن الإعاقة المرتبطة بأمراض اللثة الشديدة تظهر على شكل رائحة فم كريهة، وطعم غير مستحب في الفم، ونزيف متقطع في اللثة لا يعيق الأنشطة اليومية. الرموز ICD-10 المخصصة لأمراض اللثة هي K05.0 إلى K05.6، بينما الرموز المقابلة في ICD-9 هي 523.0-523.9.
في هذه الدراسة، تم استخدام تعريف عام 2019 للعبء العالمي للأمراض كمعيار للمقارنة. اعتبر الباحثون ثلاثة معايير كتعريفات مرجعية مكافئة: كان مؤشر احتياجات علاج اللثة المجتمعي (CPITN) الذي يبلغ 4 هو الخيار الأول، يليه فقدان الارتباط السريري (AL) الذي يزيد عن 6 مم، وعمق جيب اللثة (PD) الذي يزيد عن 5 مم.
التحليل الإحصائي
تم استخدام معيار العمر استنادًا إلى سكان مرجع GBD لمعالجة التغيرات في حجم السكان وبنية العمر. تم تقييم حدوث أمراض اللثة وDALY باستخدام DisMod-MR 2.1 لضمان الاتساق. تم تقديم تقديرات نقطية مع…
تم الحصول على بيانات الخريطة من ناتشورال إيرث، وهي مجموعة بيانات خرائط عالمية مجانية ومفتوحة المصدر (
تم الحصول على بيانات الخريطة من ناتشورال إيرث، وهي مجموعة بيانات خرائط عالمية مجانية ومفتوحة المصدر (
النتائج
عبء توزيع الأمراض اللثوية عالمياً لدى البالغين الشباب في عام 2019
في عام 2019، كان هناك زيادة ملحوظة في العدد المطلق للحالات وDALYs لأمراض اللثة بين البالغين الشباب في جميع أنحاء العالم، حيث وصلت إلى
على التوالي. كما زادت هذه المعدلات بنسبة
على التوالي. كما زادت هذه المعدلات بنسبة
من منظور الجنس، كان عدد الحالات وسنوات الحياة مع الإعاقة (DALYs) المنسوبة إلى أمراض اللثة أعلى بين الذكور مقارنة بالإناث، على مستوى العالم وفي جميع مناطق SDI الخمس و21 منطقة جغرافية في عام 2019 (الشكل 1، الجدول التكميلي 1). من حيث العمر، تشير مخططات الاتجاه الشريطي إلى أن معدل الإصابة ومعدل DALY لأمراض اللثة كانا الأعلى في الفئة العمرية 45-49، تليها الفئة العمرية 40-44، وكانا الأدنى في الفئة العمرية 15-19. علاوة على ذلك، أظهر معدل الإصابة ومعدل DALY اتجاهًا متزايدًا مع تقدم العمر، حيث بلغ ذروتهما في الفئة العمرية 45-49 وأدنى نقطة في الفئة العمرية 15-19 (الشكل 2، الجداول التكملية 2، 3).
في عام 2019، كانت منطقة SDI المنخفضة لديها أعلى معدل ASIR ومعدل DALY الموحد حسب العمر لأمراض اللثة لكل 100,000 شاب بالغ، كما هو موضح في الجدول 1 والشكل التوضيحي 1. كان معدل ASIR في هذه المنطقة 3469.92، وكان معدل DALY الموحد حسب العمر 259.83. تلتها منطقة SDI المنخفضة المتوسطة بمعدل ASIR قدره 3230.41 و
|
|
|||||||||
| الموقع | 1990 | 2019 | 1990-2019 EAPC (95% CI) | 1990 | 2019 | 1990-2019 EAPC (95% CI) | ||||
| عالمي | 2624.08(2623.18, 2624.98) | 2861.26 (2860.52, 2862.01) | 0.41 (0.32، 0.50) | 164.03 (163.80, 164.26) | 182.88 (182.69, 183.07) | 0.45 (0.36، 0.55) | ||||
| جنس | – | – | – | – | – | – | ||||
| ذكر | 1357.09 (1356.45, 1357.74) | 1457.12 (1456.59, 1457.65) | 0.36 (0.25، 0.46) | ٨٦.٠٢ (٨٥.٨٥، ٨٦.١٨) | ٩٤.٠٢ (٩٣.٨٨، ٩٤.١٥) | 0.38 (0.29، 0.48) | ||||
| أنثى | 1266.99 (1266.36, 1267.61) | 1404.14 (1403.62, 1404.67) | 0.47 (0.38، 0.56) | 78.01 (77.85, 78.17) | ٨٨.٨٦ (٨٨.٧٣، ٨٨.٩٩) | 0.53 (0.45، 0.61) | ||||
| مؤشر السوسيوديموغرافيا | – | – | – | – | – | – | ||||
| مؤشر التنمية البشرية العالي المتوسط | 2281.98 (2280.23, 2283.73) | 2415.62 (2414.06, 2417.18) | 0.46 (0.28، 0.63) | 130.91 (130.48, 131.33) | 140.45 (140.09, 140.82) | 0.49 (0.32، 0.66) | ||||
| مؤشر التنمية البشرية العالي | 2207.13 (2205.16, 2209.10) | 2244.97 (2243.09, 2246.85) | – 0.22 (- 0.45, 0.02) | 130.56 (130.08, 131.03) | 132.00 (131.56, 132.45) | – 0.28 (- 0.55, – 0.02) | ||||
| مؤشر التنمية البشرية المنخفضة والمتوسطة | ٣٠٥٤.٧٠ (٣٠٥٢.٤٨، ٣٠٥٦.٩٢) | ٣٢٣٠.٤١ (٣٢٢٨.٧٦، ٣٢٣٢.٠٦) | 0.27 (0.23، 0.32) | ٢٠٦.٦٣ (٢٠٦.٠٣، ٢٠٧.٢٢) | 224.01 (223.56, 224.45) | 0.30 (0.25, 0.34) | ||||
| مؤشر التنمية البشرية المنخفض | 3472.40 (3468.87, 3475.94) | 3469.92 (3467.62, 3472.23) | – 0.01 (- 0.02, 0.01) |
|
259.83 (259.17, 260.49) | 0.02 (0.00، 0.04) | ||||
| مؤشر التنمية البشرية المتوسط | 2567.71 (2566.11, 2569.31) | 2688.76 (2687.49, 2690.02) | 0.42 (0.28، 0.56) | 158.50 (158.09, 158.91) | 168.64 (168.32, 168.95) | 0.44 (0.30، 0.58) | ||||
| منطقة | – | – | – | – | – | – | ||||
| أمريكا اللاتينية الأنديزية | ٣٢٥٠.٦٢ (٣٢٣٨.٥٠، ٣٢٦٢.٧٨) | ٣٣٢٨.٤٦ (٣٣١٩.٦٩، ٣٣٣٧.٢٥) | 0.09 (0.08، 0.09) | 214.57 (211.34, 217.85) | 220.72 (218.46, 223.00) | 0.12 (0.11، 0.13) | ||||
| أسترالاسيا | ٢٠٩٠.١٤ (٢٠٧٨.٠٣، ٢١٠٢.٣٠) | 2134.27 (2123.59, 2145.00) | 0.39 (0.24، 0.54) | ١٢٢.٤٢ (١١٩.٥١، ١٢٥.٣٨) | ١٣٠.٤٥ (١٢٧.٨٨، ١٣٣.٠٦) | 0.33 (0.24، 0.43) | ||||
| الكاريبي | 3471.95 (3459.65, 3484.29) | ٣٤٥٦.٦٠ (٣٤٤٦.١٥، ٣٤٦٧.٠٧) | 0.00 (- 0.01, 0.01) | ٢٤٩.٣١ (٢٤٥.٩٠، ٢٥٢.٧٥) |
|
0.02 (0.00، 0.03) | ||||
| آسيا الوسطى | ٢٢١٣.٠٥ (٢٢٠٥.٢٢، ٢٢٢٠.٩١) | 2296.88 (2290.92, 2302.86) | 0.21 (0.12, 0.29) | ١٢٢.٠٧ (١٢٠.١٧، ١٢٤.٠٠) | 127.83 (126.42, 129.25) | 0.26 (0.14، 0.38) | ||||
| أوروبا الوسطى | 2087.63 (2082.56, 2092.71) | 2311.02 (2305.40, 2316.65) | 0.40 (0.35، 0.45) | 120.43 (119.23, 121.65) | ١٣٦.٢٥ (١٣٤.٩٤، ١٣٧.٥٧) | 0.47 (0.42، 0.51) | ||||
| أمريكا الوسطى | ٣٥١٦.٤٢ (٣٥١٠.٤٦، ٣٥٢٢.٣٩) | ٣٥٢٢.١٢ (٣٥١٧.٦٥، ٣٥٢٦.٦٠) | 0.02 (0.00، 0.04) | 252.74 (251.06, 254.43) | ٢٥١.٣٣ (٢٥٠.١٤، ٢٥٢.٥٣) | 0.01 (- 0.02, 0.03) | ||||
| وسط أفريقيا جنوب الصحراء | ٣٨٣٠.٣٢ (٣٨١٩.٠١، ٣٨٤١.٦٧) | ٣٧٦٥.٩٣ (٣٧٥٨.٨٨، ٣٧٧٢.٩٩) | – 0.08 (- 0.10, 0.06) | 287.80 (284.51, 291.12) | 284.71 (282.67, 286.77) | – 0.04 (- 0.08, 0.00) | ||||
| شرق آسيا |
|
2031.77 (2030.39, 2033.15) | 0.48 (0.02, 0.94) | 117.77 (117.37, 118.18) | ١٠٩.٢٩ (١٠٨.٩٨، ١٠٩.٦١) | 0.49 (- 0.01, 0.99) | ||||
| أوروبا الشرقية | 2530.60 (2526.50, 2534.71) | 2549.85 (2545.62, 2554.09) | 0.08 (0.02, 0.13) | 142.81 (141.83, 143.79) | ١٤٤.٦١ (١٤٣.٦٤، ١٤٥.٥٨) | 0.11 (0.04، 0.19) | ||||
| شرق أفريقيا جنوب الصحراء | ٣٤٣٧.٧٦ (٣٤٣١.٨٢، ٣٤٤٣.٧٢) | 3466.72 (3462.90, 3470.55) | 0.05 (0.04، 0.06) | 252.15 (250.44, 253.87) | ٢٥٤.٧٧ (٢٥٣.٦٨، ٢٥٥.٨٧) | 0.08 (0.06، 0.09) | ||||
| آسيا والمحيط الهادئ ذات الدخل المرتفع | 2018.13 (2014.10, 2022.18) | 2176.22 (2171.86, 2180.59) | 0.17 (0.14، 0.21) | 112.33 (111.39, 113.27) | 120.19 (119.21, 121.18) | 0.16 (0.13، 0.19) | ||||
| أمريكا الشمالية ذات الدخل المرتفع | 2142.44 (2139.18, 2145.69) | 1975.81 (1972.88، 1978.74) | – 0.86 (- 1.51, 0.21) | 117.12 (116.36, 117.88) | ١٠٧.٣٨ (١٠٦.٧١، ١٠٨.٠٦) | – 0.84 (- 1.49, – 0.20) | ||||
| شمال أفريقيا والشرق الأوسط | 2580.73 (2576.88, 2584.57) | 2695.95 (2693.39, 2698.51) | 0.19 (0.15، 0.24) | 154.75 (153.78, 155.73) | 164.44 (163.81, 165.08) | 0.27 (0.21، 0.33) | ||||
| أوقيانوسيا | 446.19 (434.60, 458.02) | ٤٤٦.٥٥ (٤٣٩.١٢، ٤٥٤.٠٩) | – 0.02 (- 0.04, 0.01) | ٢٤.٢٤ (٢١.٥٥، ٢٧.١٩) | ٢٤.٢٢ (٢٢.٤٩، ٢٦.٠٤) | – 0.03 (- 0.05, – 0.01) | ||||
| جنوب آسيا | 3445.81 (3443.44, 3448.19) | 3535.03 (3533.32, 3536.73) | 0.09 (0.06، 0.12) | 235.45 (234.81, 236.10) |
|
0.13 (0.08، 0.18) | ||||
| جنوب شرق آسيا | 1807.61 (1805.01, 1810.21) | 1886.63 (1884.65, 1888.62) | 0.19 (0.14، 0.23) | ١٠٥.٨٩ (١٠٥.٢٥، ١٠٦.٥٤) | 112.28 (111.80, 112.77) | 0.21 (0.20، 0.23) | ||||
| أمريكا اللاتينية الجنوبية | 2658.75 (2649.59, 2667.94) | 2799.94 (2792.13, 2807.77) | 0.18 (- 0.01, 0.37) | 170.98 (168.64, 173.33) | ١٨٣.٠١ (١٨١.٠٤، ١٨٥.٠٠) | 0.19 (0.03, 0.35) | ||||
| جنوب الصحراء الكبرى في أفريقيا | 3734.23 (3723.50, 3744.99) | ٣٨٣٥.٧٢ (٣٨٢٧.٤١، ٣٨٤٤.٠٥) | 0.11 (0.08، 0.13) | 267.72 (264.69, 270.79) | 278.69 (276.42, 280.97) | 0.14 (0.08، 0.19) | ||||
| أمريكا اللاتينية الاستوائية | 2544.33 (2539.13, 2549.54) | 2865.74 (2861.54, 2869.94) | 0.55 (0.13، 0.97) | 154.71 (153.40, 156.03) | 180.00 (178.97, 181.05) | 0.63 (0.03, 1.23) | ||||
| أوروبا الغربية | 2189.11 (2186.19, 2192.04) | 2246.49 (2243.52, 2249.45) | – 0.18 (- 0.35, 0.02) | 140.44 (139.70, 141.17) | 140.76 (140.04, 141.47) | – 0.38 (- 0.64, – 0.12) | ||||
| غرب أفريقيا جنوب الصحراء | 4116.29 (4110.00, 4122.59) | 3949.18 (3945.41, 3952.94) | – 0.15 (- 0.16, 0.14) | 355.14 (353.16, 357.13) | ٣٣٦.١٦ (٣٣٥.٠٠، ٣٣٧.٣٣) | – 0.20 (- 0.21, – 0.19) | ||||
الجدول 1. معدل الإصابة الموحد حسب العمر (ASIR) ومعدل DALY الموحد حسب العمر لأمراض اللثة حسب الموقع للبالغين الشباب، من كلا الجنسين، في عام 1990 و2019، والاتجاهات الزمنية من 1990 إلى 2019.
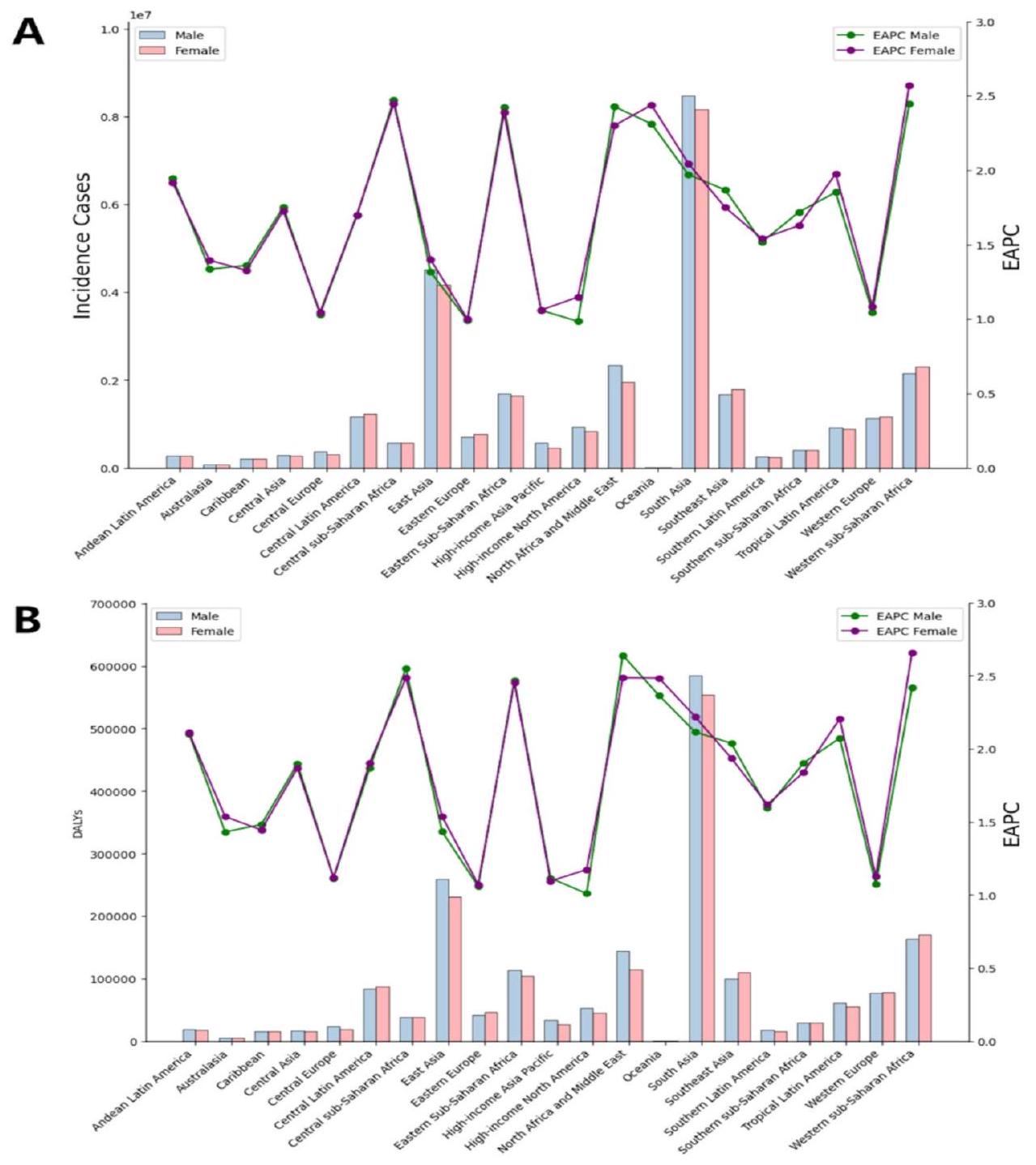
الشكل 1. (أ) حالات الإصابة ومعدل EAPC لأمراض اللثة لدى البالغين الشباب من الذكور والإناث في مناطق مختلفة من العالم في عام 2019؛ (ب) DALYs وEAPC لأمراض اللثة لدى البالغين الشباب من الذكور والإناث في مناطق مختلفة من العالم في عام 2019.
معدل DALY الموحد حسب العمر يبلغ 224.01. على العكس، المناطق ذات مؤشر التنمية الاجتماعية العالي (SDI) أظهرت أقل عبء لأمراض اللثة، مع ASIR يبلغ 2244.97 ومعدل DALY الموحد حسب العمر يبلغ 132.00.
في عام 2019، تم ملاحظة أعلى ASIR لأمراض اللثة لكل 100,000 بالغ شاب في غرب أفريقيا جنوب الصحراء (ASIR: 3949.18). على العكس، كانت أدنى ASIR لكل 100,000 نسمة في جنوب أفريقيا الصحراوية (ASIR: 3835.72)، ووسط أفريقيا الصحراوية (ASIR: 3765.93)، وأوقيانوسيا (ASIR: 446.55). وبالمثل، من حيث المناطق الجغرافية، كانت جنوب شرق آسيا (ASIR: 1886.63) وأمريكا الشمالية ذات الدخل المرتفع (ASIR: 1975.81) ملحوظة لمعدلات ASIR المرتفعة بشكل معتدل (الجدول 1، الجدول التكميلي 4، الشكل 3B، والشكل التكميلي 2A). من بين 204 دولة تم تحليلها، كانت قطر (ASIR: 7197.30)، والإمارات العربية المتحدة (ASIR: 6152.31)، وعمان (ASIR: 4680.22) لديها أعلى ASIR لكل 100,000 بالغ شاب لأمراض اللثة في عام 2019. على العكس، كانت كيريباتي (ASIR: 388.74)، وجزر سليمان (ASIR: 407.07)، وفانواتو (ASIR: 427.14) تظهر أدنى ASIR (الجدول التكميلي 5، 6، الشكل 3B).
في 21 منطقة جغرافية حول العالم، كان معدل DALY الموحد حسب العمر لأمراض اللثة لكل 100,000 بالغ شاب في عام 2019 هو الأعلى في غرب أفريقيا جنوب الصحراء (336.16)، تليها وسط أفريقيا جنوب الصحراء (284.71)، وجنوب أفريقيا جنوب الصحراء (278.69) (الجدول 1، الجدول التكميلي 4، الشكل التكميلي 2B). من ناحية أخرى، كانت المناطق ذات أدنى معدل DALY الموحد حسب العمر لأمراض اللثة هي أوقيانوسيا (24.22)، وأمريكا الشمالية ذات الدخل المرتفع (107.38)، وشرق آسيا (109.29) (الجدول 1، الجدول التكميلي 4، الشكل التكميلي 2B). عند النظر في السيناريو العالمي عبر 204 دولة، كانت الدول ذات أعلى معدل DALY الموحد حسب العمر لأمراض اللثة لكل 100,000 بالغ شاب في عام 2019 هي قطر (443.44)، وغامبيا (425.36)، والإمارات العربية المتحدة (420.58) وفقًا لبيانات منظمة الصحة العالمية (WHO) (الجدول التكميلي 5، 6، الشكل التكميلي 3B). على العكس،
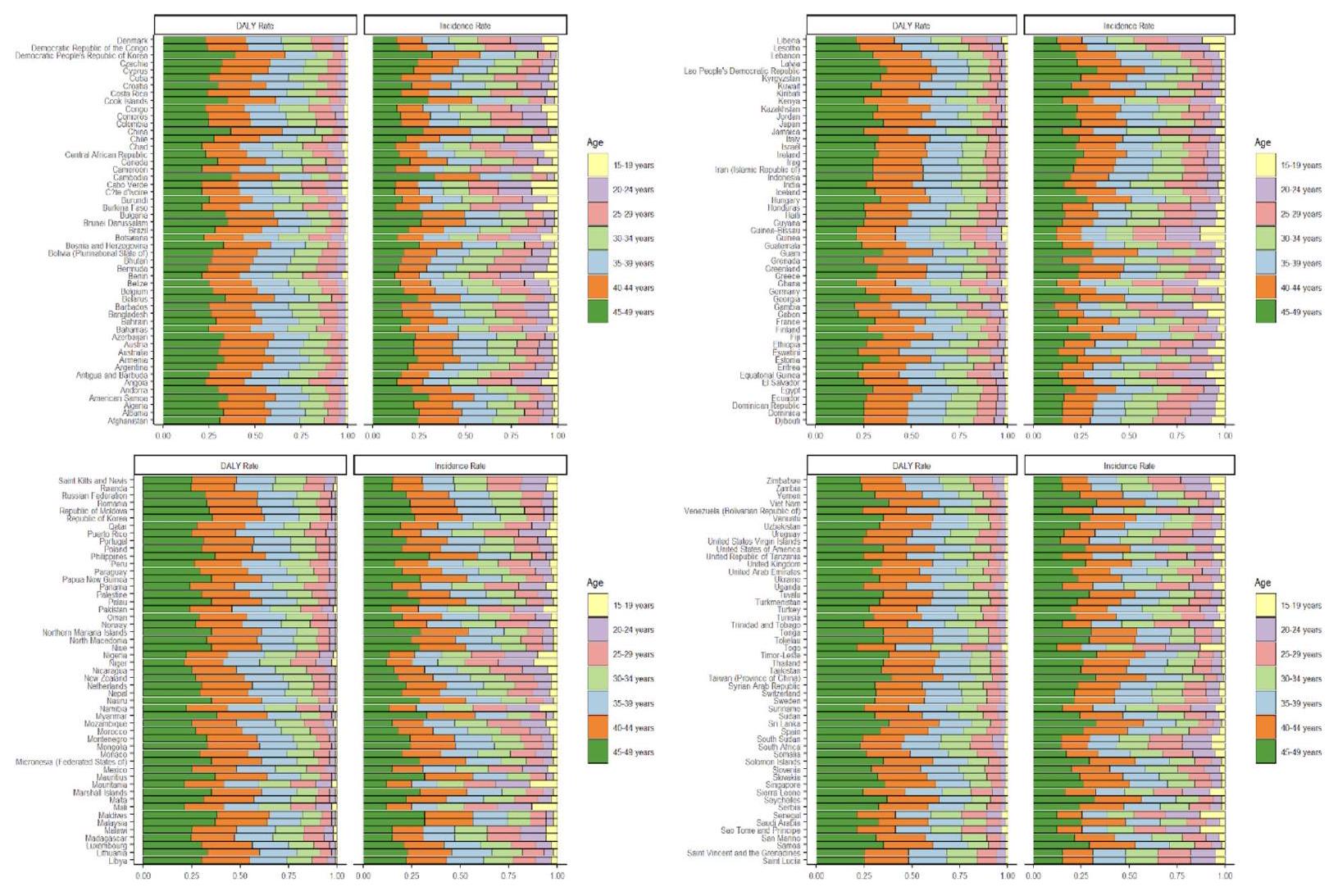
الشكل 2. نسبة معدل DALY ومعدل الإصابة لأمراض اللثة للبالغين الشباب من أعمار 15-49 في الدول حول العالم في عام 2019.
كانت الدول ذات أدنى معدل DALY الموحد حسب العمر لأمراض اللثة هي كيريباتي (21.06)، وجزر سليمان (22.14)، وفانواتو (23.23) (الجدول التكميلي 5، 6، الشكل التكميلي 3B).
اتجاه عبء أمراض اللثة لدى البالغين الشباب من 1990 إلى 2019
بين عامي 1990 و2019، كان هناك ارتفاع ملحوظ في العدد الإجمالي للحالات وDALYs في قطر، والإمارات العربية المتحدة، والمنطقة العربية ككل. أظهر ASIR لأمراض اللثة لكل 100,000 بالغ شاب اتجاهًا تصاعديًا، مع EAPC يبلغ 0.41. وبالمثل، أظهر معدل DALY الموحد حسب العمر لكل 100,000 بالغ شاب نمطًا متزايدًا، مع EAPC يبلغ 0.45. شهد كلا الجنسين زيادة في المعدلات الموحدة حسب العمر، مع اتجاهات متزايدة متشابهة. لمزيد من المعلومات التفصيلية، يرجى الرجوع إلى الجدول 1 والشكل التكميلي 4.
كما هو موضح في الجدول 1 والشكل التكميلي 1، أظهر ASIR لأمراض اللثة لكل 100,000 بالغ شاب اختلافات ملحوظة بين المجموعات الفرعية الثلاث لمؤشر التنمية الاجتماعية (SDI) من 1990 إلى 2019. كانت المنطقة ذات SDI العالي والمتوسط لديها أعلى زيادة (تغير سنوي تقديري [EAPC
من بين 21 منطقة جغرافية، شهدت أمريكا اللاتينية الاستوائية أكبر زيادة في ASIR لكل 100,000 بالغ شاب من 1990 إلى 2019، مع EAPC يبلغ 0.55. كما شهدت شرق آسيا وأوروبا الوسطى زيادات في ASIR، مع EAPCs تبلغ 0.48 و0.40 على التوالي. على العكس، شهدت أمريكا الشمالية ذات الدخل المرتفع، وأوروبا الغربية، وشرق آسيا أكبر انخفاضات في ASIR لأمراض اللثة، مع EAPCs تبلغ
من بين 21 منطقة جغرافية، شهدت أمريكا اللاتينية الاستوائية أكبر زيادة في معدل DALY الموحد حسب العمر لأمراض اللثة لكل 100,000 بالغ شاب من 1990 إلى 2019، مع تغير سنوي تقديري (EAPC) يبلغ 0.63. تلتها شرق آسيا (EAPC
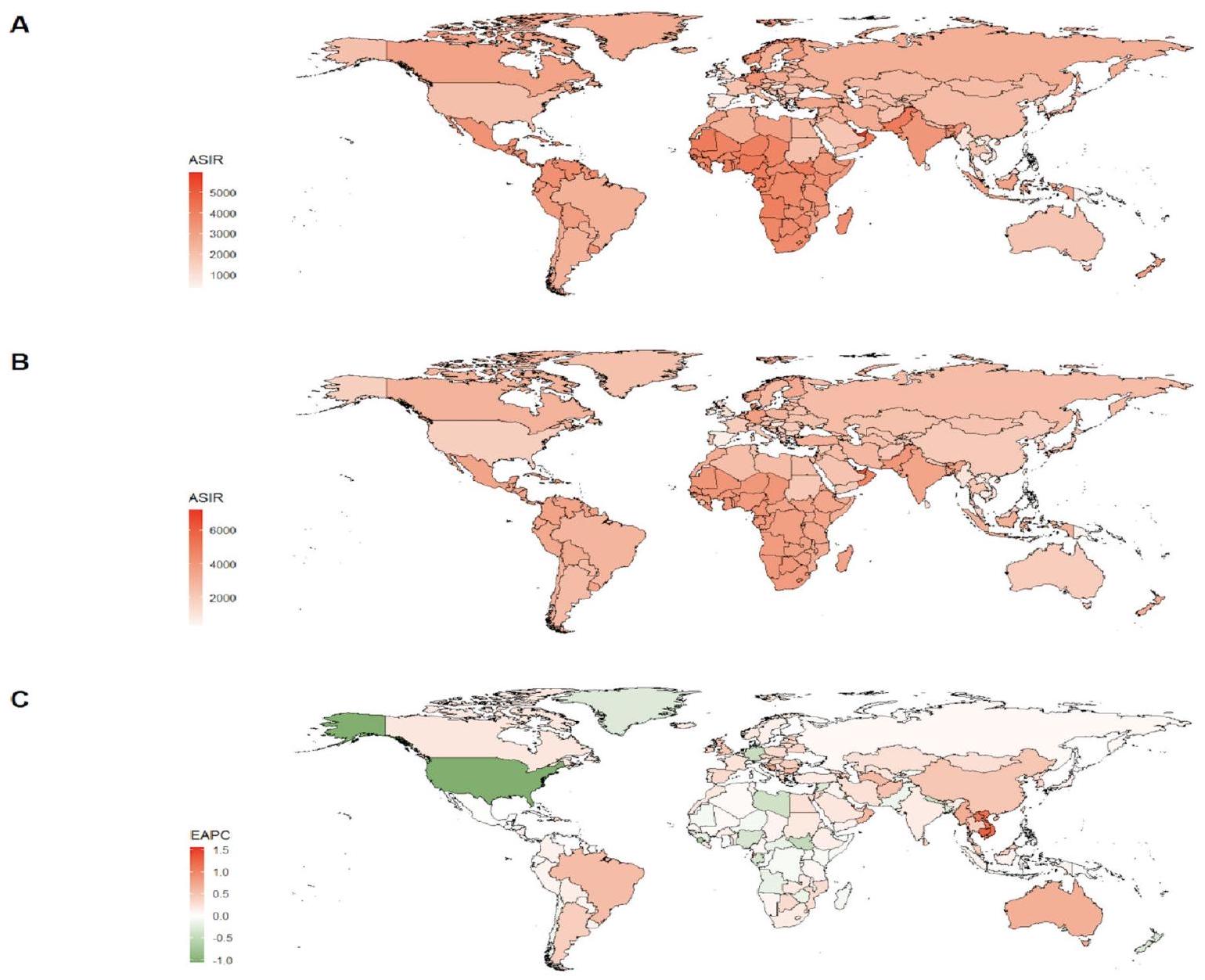
الشكل 3. (أ) ASIR لأمراض اللثة للبالغين الشباب حول العالم في عام 1990؛ (ب) ASIR لأمراض اللثة للبالغين الشباب حول العالم في عام 2019؛ (ج) EAPC لـ ASIR لأمراض اللثة للبالغين الشباب في الدول حول العالم من 1990 إلى 2019.
تم الحصول على بيانات شكل الملف المستخدمة في هذه الدراسة من Natural Earth (http://www.naturalearthdata.com/)، التي توفر حدود الدول والمناطق العالمية. تم استخدام هذه الحدود كطبقة أساسية لعرض معلومات التوزيع الجغرافي ذات الصلة بموضوع الدراسة. بيانات Natural Earth في المجال العام، مما يسمح بالاستخدام والتوزيع المجاني. تم إجراء معالجة البيانات وتصوير بيانات الدراسة في R (الإصدار 4.2.3) باستخدام حزم ggplot2 (الإصدار 3.4.0) وsf (الإصدار 1.0.9).
إلى حد أقل (EAPC=- 0.20) (الجدول 1، الجداول التكملية 4 والشكل التكميلي 2B،3C). عند النظر إلى الدول الفردية، شهدت قطر، وكمبوديا، وجزر المالديف أكبر زيادة في معدل DALY الموحد حسب العمر لأمراض اللثة لكل 100,000 بالغ شاب من 1990 إلى 2019، مع EAPCs تبلغ 1.44، 1.39، و1.44 على التوالي. على العكس، كانت الولايات المتحدة الأمريكية، والكويت، وجزر المالديف لديها أكبر انخفاض في معدل DALY الموحد حسب العمر لأمراض اللثة، مع EAPCs تبلغ
إلى حد أقل (EAPC=- 0.20) (الجدول 1، الجداول التكملية 4 والشكل التكميلي 2B،3C). عند النظر إلى الدول الفردية، شهدت قطر، وكمبوديا، وجزر المالديف أكبر زيادة في معدل DALY الموحد حسب العمر لأمراض اللثة لكل 100,000 بالغ شاب من 1990 إلى 2019، مع EAPCs تبلغ 1.44، 1.39، و1.44 على التوالي. على العكس، كانت الولايات المتحدة الأمريكية، والكويت، وجزر المالديف لديها أكبر انخفاض في معدل DALY الموحد حسب العمر لأمراض اللثة، مع EAPCs تبلغ
نقاش
تشير هذه الدراسة إلى زيادة في انتشار مرض اللثة بين البالغين الشباب بين عامي 1990 و2019. وتظهر هذه الزيادة بشكل رئيسي من خلال الارتفاع الكبير في معدل الإصابة القياسي للعمر (ASIR) ومعدل سنوات الحياة المعدلة حسب الإعاقة (DALY) القياسي للعمر، مما يعكس زيادة التعرض لعوامل الخطر المرتبطة بمرض اللثة. لقد كان لزيادة عدد حالات مرض اللثة تأثير إيجابي على نمو السكان والاتجاه المستمر للشيخوخة. علاوة على ذلك، يُلاحظ أن عبء مرض اللثة أكبر لدى الذكور. كانت المنطقة التي سجلت أعلى معدل إصابة قياسي للعمر (ASIR) ومعدل DALY القياسي للعمر هي غرب أفريقيا جنوب الصحراء الكبرى، وخاصة في المناطق ذات مؤشر التنمية البشرية المنخفض ومؤشر التنمية البشرية المنخفض المتوسط. وعلى العكس، شهدت المناطق ذات مؤشر التنمية البشرية المتوسط العالي والمتوسط اتجاهًا واضحًا نحو الارتفاع. تتشابه هذه النتائج مع الدراسات السابقة.
أظهر معدل حدوث مرض اللثة ومعدل سنوات الحياة المعدلة حسب الإعاقة (DALY) اتجاهًا متزايدًا مع تقدم العمر، حيث بلغ ذروته في الفئة العمرية 45-49 عامًا. تعكس الزيادة في انتشار مرض اللثة زيادة التعرض لعوامل الخطر المرتبطة بمرض اللثة. تشمل عوامل الخطر المحتملة لأمراض اللثة
عوامل قابلة للتعديل مثل التدخين، نظافة الفم، السكري، الأدوية، والضغط النفسي، وعوامل غير قابلة للتعديل مثل العمر، الوراثة، والجنس، والارتباطات مع أمراض أخرى مثل أمراض القلب والأوعية الدموية، الأمراض الأيضية، وجهاز التنفس.
عوامل قابلة للتعديل مثل التدخين، نظافة الفم، السكري، الأدوية، والضغط النفسي، وعوامل غير قابلة للتعديل مثل العمر، الوراثة، والجنس، والارتباطات مع أمراض أخرى مثل أمراض القلب والأوعية الدموية، الأمراض الأيضية، وجهاز التنفس.
يظهر الرجال انتشارًا وشدة أعلى من تدمير اللثة مقارنة بالنساء؛ وهو ما يتماشى مع الأبحاث السابقة.
الحالة الاجتماعية والاقتصادية (SES) هي مؤشر خطر مهم لأمراض اللثة، حيث لوحظت معدلات أعلى من فقدان الارتباط وعمق الاستكشاف.
كانت المنطقة ذات أعلى معدل حدوث موحد بالعمر (ASIR) ومعدل DALY موحد بالعمر هي غرب أفريقيا جنوب الصحراء. تواجه وسط أفريقيا جنوب الصحراء وجنوب أفريقيا جنوب الصحراء، باعتبارها المنطقة ذات أعلى معدل لحدوث الإيدز على مستوى العالم، خطرًا متزايدًا للإصابة بأمراض اللثة بين الأفراد في سن مبكرة بسبب العلاقة بين فيروس نقص المناعة البشرية، ونظافة الفم، وأمراض اللثة.
تتأثر العبء العالي لمرض اللثة والاتجاه المتزايد له في قطر بعدة عوامل، بما في ذلك العوامل السلوكية والبيولوجية والاجتماعية الاقتصادية والسياسية والبيئية.
تقدم هذه الدراسة تحليلًا شاملاً للعبء العالمي للأمراض اللثوية لدى البالغين الشباب (الذين تتراوح أعمارهم بين 15-49 عامًا) على مدى العقود الثلاثة الماضية. تفحص توزيع العبء عبر مناطق جغرافية وفترات زمنية مختلفة وتستكشف عوامل الخطر التي تسهم في زيادة حدوث هذه الأمراض. من خلال تحديد الأهداف وتقديم الإرشادات لاستراتيجيات الوقاية والعلاج، تهدف هذه الدراسة إلى تسهيل التوزيع العادل للموارد. ومع ذلك، من المهم الاعتراف بالقيود الجوهرية لنهج GBD المستخدم في هذه الدراسة. أولاً، قد يتم التقليل من عبء الأمراض اللثوية بسبب محدودية توفر البيانات، خاصة من المناطق ذات الوضع الاقتصادي المتدني. ثانيًا، يمكن أن تتأثر دقة تقييم البيانات إلى حد ما بالطرق المستخدمة في معالجة البيانات ونمذجتها.
الاستنتاجات
أظهر معدل ASIR ومعدل DALY الموحد حسب العمر للأمراض اللثوية اتجاهًا تصاعديًا ثابتًا من 1990 إلى 2019، مما يدل على التحدي المستمر الذي تمثله هذه الحالة للصحة العامة العالمية. لوحظت فجوة ملحوظة في عبء الأمراض اللثوية بين الجنسين والمناطق المختلفة. تحمل الرجال عبئًا أكبر، حيث يقع ذروة سن القابلية ضمن نطاق السنوات
توفر البيانات
تم الحصول على البيانات من قاعدة بيانات الصحة العالمية المتاحة للجمهور (GHDx) (https://ghdx.healthdat a.org/gbdالنتائجالأداة).
تاريخ الاستلام: 1 يوليو 2024؛ تاريخ القبول: 28 يناير 2025
تم النشر عبر الإنترنت: 24 فبراير 2025
تم النشر عبر الإنترنت: 24 فبراير 2025
References
- Ge, J. et al. Periodontitis impacts on thrombotic diseases: from clinical aspect to future therapeutic approaches. Int. J. Oral Sci. 16, 58 (2024).
- Nwizu, N., Wactawski-Wende, J. & Genco, R. J. Periodontal disease and cancer: epidemiologic studies and possible mechanisms. Periodontology 83, 213-233 (2020).
- Sanz, M. et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 47, 268-288 (2020).
- Del Pinto, R. et al. Periodontitis and hypertension: is the association causal? High Blood Press. Cardiovasc. Prev. 27, 281-289 (2020).
- Baeza, M. et al. Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta-analysis. J. Appl. Oral Sci. 28, e20190248 (2020).
- Kwon, T., Lamster, I. B. & Levin, L. Current concepts in the management of periodontitis. Int. Dent. J. 71, 462-476 (2021).
- Eke, P. I. et al. Periodontitis in US adults: National Health and Nutrition Examination Survey 2009-2014. J. Am. Dent. Assoc. 149, 576-588 (2018).
- Luo, L. S. et al. Secular trends in severe periodontitis incidence, prevalence and disability-adjusted life years in five Asian countries: a comparative study from 1990 to 2017. J. Clin. Periodontol. 48, 627-637 (2021).
- Genco, R. J. & Borgnakke, W. S. Risk factors for periodontal disease. Periodontology 62, 59-94 (2013).
- AlJehani, Y. A. Risk factors of periodontal disease: review of the literature. Int. J. Dent. 2014, 182513 (2014).
- Kassebaum, N. J. et al. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J. Dent. Res. 93, 1045-1053 (2014).
- Jiao, J. et al. The prevalence and severity of periodontal disease in Mainland China: data from the Fourth National oral health survey (2015-2016). J. Clin. Periodontol. 48, 168-179 (2021).
- Chen, M. X., Zhong, Y. J., Dong, Q. Q., Wong, H. M. & Wen, Y. F. Global, regional, and national burden of severe periodontitis, 1990-2019: an analysis of the global burden of Disease Study 2019. Clin. Periodontol. 48, 1165-1188 (2021).
- Zhang, X. et al. The global burden of periodontal diseases in 204 countries and territories from 1990 to 2019. Oral Dis. 30 (2), 754-768 (2024).
- Collaborators Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of Disease Study 2019. Lancet 396, 1204-1222 (2020).
- Zhang, D., Liu, S., Li, Z. & Wang, R. Global, regional and national burden of gastroesophageal reflux disease, 1990-2019: update from the GBD 2019 study. Ann. Med. 54, 1372-1384 (2022).
- Wu, L., Zhang, S. Q., Zhao, L., Ren, Z. H. & Hu, C. Y. Global, regional, and national burden of periodontitis from 1990 to 2019: results from the Global Burden of Disease study 2019. J. Periodontol. 93 (10), 1445-1454 (2022).
- Nagata, J. M. et al. Food insecurity and chronic disease in US young adults: findings from the National Longitudinal Study of Adolescent to Adult Health. J. Gen. Intern. Med. 34, 2756-2762 (2019).
- Biener, L. & Albers, A. B. Young adults: vulnerable new targets of tobacco marketing. Am. J. Public Health 94, 326-330 (2004).
- Kinane, D. F. & Marshall, G. J. Periodontal manifestations of systemic disease. Aust. Dent. J. 46, 2-12 (2001).
- Charupinijkul, R. A. et al. The effect of obesity on periodontitis progression: the 10-year retrospective cohort study. Clin. Oral Investig. 26, 535-542 (2022).
- Ng, M. et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the global burden of Disease Study 2013. Lancet 384, 766-781 (2014).
- Reners, M. & Brecx, M. Stress and periodontal disease. Int. J. Dent. Hyg. 5, 199-204 (2007).
- Rajabi, F., Drake, L. A., Senna, M. M. & Rezaei, N. Alopecia Areata: a review of disease pathogenesis. Br. J. Dermatol. 179, 10331048 (2018).
- Corbet, E. F., Wong, M. C. & Lin, H. C. Periodontal conditions in adult Southern Chinese. J. Dent. Res. 80, 1480-1485 (2001).
- Gjermo, P., Rösing, C. K., Susin, C. & Oppermann, R. Periodontal diseases in Central and South America. Periodontology 29, 70-78 (2002).
- Hugoson, R. A. & Jordan, T. Frequency distribution of individuals aged
years according to severity of periodontal disease. Community Dent. Oral Epidemiol. 10, 187-192 (1982). - Borrell, L. N., Burt, B. A., Gillespie, B. W., Lynch, J. & Neighbors, H. Periodontitis in the United States: beyond black and white. J. Public Health Dent. 62, 92-101 (2002).
- Borrell, L. N. & Crawford, N. D. Social disparities in periodontitis among United States adults 1999-2004. Community Dent. Oral Epidemiol. 36, 383-391 (2008).
- Nazir, M. et al. Global prevalence of periodontal disease and lack of its surveillance. Sci. World J. 2020, 2146160 (2020).
- Caballero, B. A nutrition paradox-underweight and obesity in developing countries. N. Engl. J. Med. 352, 1514-1516 (2005).
- Morillo, J. M. et al. Nutrition-linked chronic disease and periodontitis: are they the two faces of the same coin? Mediterr. J. Nutr. Metab. 2, 103-109 (2009).
- Doku, D. The tobacco industry tactics-a challenge for tobacco control in low and middle income countries. Afr. Health Sci. 10, 201-203 (2010).
- Alpagot, T., Duzgunes, N., Wolff, L. F. & Lee, A. Risk factors for periodontitis in HIV patients. J. Periodontal Res. 39, 149-157 (2004).
- Tellez, M., Zini, A. & Estupiñan-Day, S. Social determinants and oral health: an update. Curr. Oral Health Rep. 1, 148-152 (2014).
- Awad, S. F., O’Flaherty, M., Critchley, J. & Abu-Raddad, L. J. Forecasting the burden of type 2 diabetes mellitus in Qatar to 2050: a novel modeling approach. Diabetes Res. Clin. Pract. 137, 100-108 (2018).
- Morgano, S. M. et al. Burden of oral disease in the Middle East: opportunities for dental public health. Int. Dent. J. 60, 197-199 (2010).
الشكر والتقدير
نشكر جميع المؤلفين على مساهماتهم في المقال.
مساهمات المؤلفين
Yifeng Wang: التصور؛ Lidan Zhuo: المنهجية؛ Saiyan Yang: تنسيق البيانات؛ Cheng Dong: كتابة – إعداد المسودة الأصلية؛ Peng Shu: التصور، التحليل الرسمي؛ Yifeng Wang: الكتابة – المراجعة والتحرير. قرأ جميع المؤلفين ووافقوا على النسخة النهائية من المخطوطة.
الإعلانات
المصالح المتنافسة
يعلن المؤلفون عدم وجود مصالح متنافسة.
الموافقة الأخلاقية
تستند هذه الدراسة إلى قاعدة بيانات متاحة للجمهور ولا تتطلب موافقة أخلاقية.
معلومات إضافية
المعلومات التكميلية تحتوي النسخة عبر الإنترنت على مواد تكميلية متاحة على https://doi.org/1 0.1038/s41598-025-88249-0.
يجب توجيه المراسلات وطلبات المواد إلى P.S.
معلومات إعادة الطبع والتصاريح متاحة على www.nature.com/reprints.
ملاحظة الناشر تظل Springer Nature محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
معلومات إعادة الطبع والتصاريح متاحة على www.nature.com/reprints.
ملاحظة الناشر تظل Springer Nature محايدة فيما يتعلق بالمطالبات القضائية في الخرائط المنشورة والانتماءات المؤسسية.
الوصول المفتوح هذه المقالة مرخصة بموجب رخصة المشاع الإبداعي للاستخدام غير التجاري، والتي تسمح بأي استخدام غير تجاري، ومشاركة، وتوزيع، وإعادة إنتاج في أي وسيلة أو صيغة، طالما أنك تعطي الائتمان المناسب للمؤلفين الأصليين والمصدر، وتوفر رابطًا لرخصة المشاع الإبداعي، وتوضح إذا قمت بتعديل المادة المرخصة. ليس لديك إذن بموجب هذه الرخصة لمشاركة المواد المعدلة المشتقة من هذه المقالة أو أجزاء منها. الصور أو المواد الأخرى من طرف ثالث في هذه المقالة مشمولة في رخصة المشاع الإبداعي للمقال، ما لم يُشار إلى خلاف ذلك في سطر الائتمان للمادة. إذا لم تكن المادة مشمولة في رخصة المشاع الإبداعي للمقال واستخدامك المقصود غير مسموح به بموجب اللوائح القانونية أو يتجاوز الاستخدام المسموح به، ستحتاج إلى الحصول على إذن مباشرة من صاحب حقوق الطبع والنشر. لعرض نسخة من هذه الرخصة، قم بزيارة http://creativecommo ns.org/licenses/by-nc-nd/4.0/.
© المؤلفون 2025
© المؤلفون 2025
قسم طب الأسنان، مستشفى الشعب في بيلون، نينغبو، تشجيانغ، الصين. مركز أبحاث الطب الدقيق، مستشفى الشعب في بيلون، نينغبو 315800، تشجيانغ، الصين. البريد الإلكتروني: shu_peng0326@163.com
Journal: Scientific Reports, Volume: 15, Issue: 1
DOI: https://doi.org/10.1038/s41598-025-88249-0
PMID: https://pubmed.ncbi.nlm.nih.gov/39994294
Publication Date: 2025-02-24
DOI: https://doi.org/10.1038/s41598-025-88249-0
PMID: https://pubmed.ncbi.nlm.nih.gov/39994294
Publication Date: 2025-02-24
OPEN
Burden of periodontal diseases in young adults
We aimed to provide a comprehensive overview of the global burden of periodontal disease among young adults over the period from 1990 to 2019. The analysis considered various factors such as age, sex, country, and Socio-demographic Index (SDI). This study utilized GBD 2019 database to examine the trends in both incidence and disability-adjusted life years (DALY) rates of periodontal diseases among young adults from 1990 to 2019. The data was analyzed based on age-standardization rate. To quantify the temporal and geographic patterns we calculated the estimated annual percentage change (EAPC) and its corresponding
Keywords Periodontal diseases, Incidence rate, Disability-adjusted life years (DALYs), Global burden of Disease Study, Incidence rate, Disease burden
Periodontal disease, a common infection and inflammation, is a nonspecific inflammatory response to oral biofilm, affecting the periodontal ligament, alveolar bone, and periodontal attachment
The period between young adulthood (15-49 years old) is a significant yet understudied stage characterized by the emergence of individual metabolic risk factors, such as diabetes, hypertension, and hyperlipidemia. These factors, in turn, serve as potential risk factors for periodontal diseases
The GBD 2019 offers a reliable method and tool for conducting data research and analysis in a comparable manner. GBD 2019 covered 204 countries, territories, and first administrative level disaggregation for 22 countries, from 1990 to 2019. GBD provided a systematic scientific assessment of published, publicly available, and contributed data on disease and injury incidence, prevalence, and mortality for a collectively exhaustive list of diseases and injuries. Therefore, GBD provides a powerful basis for detailed and broad insights on global health trends and emerging challenges. Recently, some researches conducted a comprehensive evaluation of the global, regional, and national burden trends of periodontitis or severe periodontitis from 1990 to
Methods
Data sources
The data used for this assessment was obtained from the GBD 2019 study. The detailed methodology for estimating the burden of periodontitis disease from the GBD 2019 study can be found in previous publications
This study is based on a publicly available database and does not require ethical approval.
Case definition
Chronic periodontal disease is a result of chronic bacterial infection in the vicinity of the teeth. Gingivitis, the mildest form of the disease, presents symptoms including gum swelling, redness, and bleeding upon stimulation. If left untreated, the infection will progress beneath the gum line, instigating a persistent inflammatory state within the periodontal tissues. As defined by the Global Burden of Disease (GBD), disability associated with symptomatic severe periodontal disease manifests as halitosis, an unpleasant taste in the mouth, and intermittent gum bleeding that does not impede daily activities. The ICD-10 codes allocated to periodontal disease are K05.0 to K05.6, while the corresponding ICD-9 codes are 523.0-523.9.
In this study, the 2019 GBD was used as the standard definition for comparison. The researchers considered three criteria to be equivalent reference definitions: the Community Periodontal Index of Treatment Needs (CPITN) score of 4 was the first preference, followed by Clinical Attachment Loss (AL) greater than 6 mm , and Gingival Pocket Depth (PD) greater than 5 mm .
Statistical analysis
Age standardization based on the GBD reference population was employed to address changes in population size and age structure. The incidence of periodontal diseases and DALY were evaluated using DisMod-MR 2.1 to ensure consistency. Point estimates along with
“Map data were sourced from Natural Earth, a free and open-source global map dataset (
“Map data were sourced from Natural Earth, a free and open-source global map dataset (
Results
Global distribution burden of periodontal diseases in young adults in 2019
In 2019, there was a significant increase in the absolute number of cases and DALYs of periodontal diseases among young adults worldwide, reaching
respectively. These rates also increased by
respectively. These rates also increased by
From a gender perspective, the number of cases and years lived with disability (DALYs) attributed to periodontal diseases was higher among males than females, globally and in all five SDI regions and 21 geographic regions in 2019 (Fig. 1, Supplementary Table 1). In terms of age, the bar trend chart indicates that the incidence rate and DALY rate of periodontal diseases were highest in the 45-49 age group, followed by the 40-44 age group, and lowest in the 15-19 age group. Furthermore, the incidence rate and DALY rate exhibited an increasing trend with age, reaching their peak in the 45-49 age group and the lowest point in the 15-19 age group (Fig. 2, Supplementary Tables 2, 3).
In 2019, the Low SDI area had the highest ASIR and age-standardized DALY rate of periodontal diseases per 100,000 young adults, as indicated in Table 1 and Supplementary Fig. 1. The ASIR in this area was 3469.92, and the age-standardized DALY rate was 259.83. The Low-middle SDI area followed with an ASIR of 3230.41 and
|
|
|||||||||
| Location | 1990 | 2019 | 1990-2019 EAPC (95% CI) | 1990 | 2019 | 1990-2019 EAPC (95% CI) | ||||
| Global | 2624.08(2623.18, 2624.98) | 2861.26 (2860.52, 2862.01) | 0.41 (0.32, 0.50) | 164.03 (163.80, 164.26) | 182.88 (182.69, 183.07) | 0.45 (0.36, 0.55) | ||||
| Sex | – | – | – | – | – | – | ||||
| Male | 1357.09 (1356.45, 1357.74) | 1457.12 (1456.59, 1457.65) | 0.36 (0.25, 0.46) | 86.02 (85.85, 86.18) | 94.02 (93.88, 94.15) | 0.38 (0.29, 0.48) | ||||
| Female | 1266.99 (1266.36, 1267.61) | 1404.14 (1403.62, 1404.67) | 0.47 (0.38, 0.56) | 78.01 (77.85, 78.17) | 88.86 (88.73, 88.99) | 0.53 (0.45, 0.61) | ||||
| Sociodemographic index | – | – | – | – | – | – | ||||
| High-middle SDI | 2281.98 (2280.23, 2283.73) | 2415.62 (2414.06, 2417.18) | 0.46 (0.28, 0.63) | 130.91 (130.48, 131.33) | 140.45 (140.09, 140.82) | 0.49 (0.32, 0.66) | ||||
| High SDI | 2207.13 (2205.16, 2209.10) | 2244.97 (2243.09, 2246.85) | – 0.22 (- 0.45, 0.02) | 130.56 (130.08, 131.03) | 132.00 (131.56, 132.45) | – 0.28 (- 0.55, – 0.02) | ||||
| Low-middle SDI | 3054.70 (3052.48, 3056.92) | 3230.41 (3228.76, 3232.06) | 0.27 (0.23, 0.32) | 206.63 (206.03, 207.22) | 224.01 (223.56, 224.45) | 0.30 (0.25, 0.34) | ||||
| Low SDI | 3472.40 (3468.87, 3475.94) | 3469.92 (3467.62, 3472.23) | – 0.01 (- 0.02, 0.01) |
|
259.83 (259.17, 260.49) | 0.02 (0.00, 0.04) | ||||
| Middle SDI | 2567.71 (2566.11, 2569.31) | 2688.76 (2687.49, 2690.02) | 0.42 (0.28, 0.56) | 158.50 (158.09, 158.91) | 168.64 (168.32, 168.95) | 0.44 (0.30, 0.58) | ||||
| Region | – | – | – | – | – | – | ||||
| Andean Latin America | 3250.62 (3238.50, 3262.78) | 3328.46 (3319.69, 3337.25) | 0.09 (0.08, 0.09) | 214.57 (211.34, 217.85) | 220.72 (218.46, 223.00) | 0.12 (0.11, 0.13) | ||||
| Australasia | 2090.14 (2078.03, 2102.30) | 2134.27 (2123.59, 2145.00) | 0.39 (0.24, 0.54) | 122.42 (119.51, 125.38) | 130.45 (127.88, 133.06) | 0.33 (0.24, 0.43) | ||||
| Caribbean | 3471.95 (3459.65, 3484.29) | 3456.60 (3446.15, 3467.07) | 0.00 (- 0.01, 0.01) | 249.31 (245.90, 252.75) |
|
0.02 (0.00, 0.03) | ||||
| Central Asia | 2213.05 (2205.22, 2220.91) | 2296.88 (2290.92, 2302.86) | 0.21 (0.12, 0.29) | 122.07 (120.17, 124.00) | 127.83 (126.42, 129.25) | 0.26 (0.14, 0.38) | ||||
| Central Europe | 2087.63 (2082.56, 2092.71) | 2311.02 (2305.40, 2316.65) | 0.40 (0.35, 0.45) | 120.43 (119.23, 121.65) | 136.25 (134.94, 137.57) | 0.47 (0.42, 0.51) | ||||
| Central Latin America | 3516.42 (3510.46, 3522.39) | 3522.12 (3517.65, 3526.60) | 0.02 (0.00, 0.04) | 252.74 (251.06, 254.43) | 251.33 (250.14, 252.53) | 0.01 (- 0.02, 0.03) | ||||
| Central sub-Saharan Africa | 3830.32 (3819.01, 3841.67) | 3765.93 (3758.88, 3772.99) | – 0.08 (- 0.10, 0.06) | 287.80 (284.51, 291.12) | 284.71 (282.67, 286.77) | – 0.04 (- 0.08, 0.00) | ||||
| East Asia |
|
2031.77 (2030.39, 2033.15) | 0.48 (0.02, 0.94) | 117.77 (117.37, 118.18) | 109.29 (108.98, 109.61) | 0.49 (- 0.01, 0.99) | ||||
| Eastern Europe | 2530.60 (2526.50, 2534.71) | 2549.85 (2545.62, 2554.09) | 0.08 (0.02, 0.13) | 142.81 (141.83, 143.79) | 144.61 (143.64, 145.58) | 0.11 (0.04, 0.19) | ||||
| Eastern sub-Saharan Africa | 3437.76 (3431.82, 3443.72) | 3466.72 (3462.90, 3470.55) | 0.05 (0.04, 0.06) | 252.15 (250.44, 253.87) | 254.77 (253.68, 255.87) | 0.08 (0.06, 0.09) | ||||
| High-income Asia Pacific | 2018.13 (2014.10, 2022.18) | 2176.22 (2171.86, 2180.59) | 0.17 (0.14, 0.21) | 112.33 (111.39, 113.27) | 120.19 (119.21, 121.18) | 0.16 (0.13, 0.19) | ||||
| High-income North America | 2142.44 (2139.18, 2145.69) | 1975.81 (1972.88, 1978.74) | – 0.86 (- 1.51, 0.21) | 117.12 (116.36, 117.88) | 107.38 (106.71, 108.06) | – 0.84 (- 1.49, – 0.20) | ||||
| North Africa and Middle East | 2580.73 (2576.88, 2584.57) | 2695.95 (2693.39, 2698.51) | 0.19 (0.15, 0.24) | 154.75 (153.78, 155.73) | 164.44 (163.81, 165.08) | 0.27 (0.21, 0.33) | ||||
| Oceania | 446.19 (434.60, 458.02) | 446.55 (439.12, 454.09) | – 0.02 (- 0.04, 0.01) | 24.24 (21.55, 27.19) | 24.22 (22.49, 26.04) | – 0.03 (- 0.05, – 0.01) | ||||
| South Asia | 3445.81 (3443.44, 3448.19) | 3535.03 (3533.32, 3536.73) | 0.09 (0.06, 0.12) | 235.45 (234.81, 236.10) |
|
0.13 (0.08, 0.18) | ||||
| Southeast Asia | 1807.61 (1805.01, 1810.21) | 1886.63 (1884.65, 1888.62) | 0.19 (0.14, 0.23) | 105.89 (105.25, 106.54) | 112.28 (111.80, 112.77) | 0.21 (0.20, 0.23) | ||||
| Southern Latin America | 2658.75 (2649.59, 2667.94) | 2799.94 (2792.13, 2807.77) | 0.18 (- 0.01, 0.37) | 170.98 (168.64, 173.33) | 183.01 (181.04, 185.00) | 0.19 (0.03, 0.35) | ||||
| Southern sub-Saharan Africa | 3734.23 (3723.50, 3744.99) | 3835.72 (3827.41, 3844.05) | 0.11 (0.08, 0.13) | 267.72 (264.69, 270.79) | 278.69 (276.42, 280.97) | 0.14 (0.08, 0.19) | ||||
| Tropical Latin America | 2544.33 (2539.13, 2549.54) | 2865.74 (2861.54, 2869.94) | 0.55 (0.13, 0.97) | 154.71 (153.40, 156.03) | 180.00 (178.97, 181.05) | 0.63 (0.03, 1.23) | ||||
| Western Europe | 2189.11 (2186.19, 2192.04) | 2246.49 (2243.52, 2249.45) | – 0.18 (- 0.35, 0.02) | 140.44 (139.70, 141.17) | 140.76 (140.04, 141.47) | – 0.38 (- 0.64, – 0.12) | ||||
| Western sub-Saharan Africa | 4116.29 (4110.00, 4122.59) | 3949.18 (3945.41, 3952.94) | – 0.15 (- 0.16, 0.14) | 355.14 (353.16, 357.13) | 336.16 (335.00, 337.33) | – 0.20 (- 0.21, – 0.19) | ||||
Table 1. The age-standardized incidence rate (ASIR) and age-standardized DALY rate of periodontal disease by location for young adults, both sexes, in 1990 and 2019, and its temporal trends from 1990 to 2019.
Fig. 1. (A) Incidence cases and EAPC of periodontal disease in young male and female adults in different regions of the world in 2019; (B) DALYs and EAPC of periodontal disease in young male and female adults in different regions of the world in 2019.
an age-standardized DALY rate of 224.01. Conversely, the areas with High SDI exhibited the lowest burden of periodontal disease, with an ASIR of 2244.97 and an age-standardized DALY rate of 132.00 .
In 2019, the highest ASIR of periodontal diseases per 100,000 young adults was observed in Western subSaharan Africa (ASIR: 3949.18). Conversely, the lowest ASIRs per 100,000 population were seen in Southern Saharan Africa (ASIR: 3835.72), Central Saharan Africa (ASIR: 3765.93), and Oceania (ASIR: 446.55). Similarly, in terms of geographic regions, Southeast Asia (ASIR: 1886.63) and High-income North America (ASIR: 1975.81) were notable for their moderately high ASIRs (Table 1, Supplementary Table 4, Fig. 3B, and Supplementary Fig. 2A). Among the 204 countries analyzed, Qatar (ASIR: 7197.30), the United Arab Emirates (ASIR: 6152.31), and Oman (ASIR: 4680.22) had the highest ASIRs per 100,000 young adults for periodontal diseases in 2019. Conversely, Kiribati (ASIR: 388.74), Solomon Islands (ASIR: 407.07), and Vanuatu (ASIR: 427.14) showed the lowest ASIRs (Supplementary Tables 5, 6, Fig. 3B).
In 21 geographical regions across the world, the age-standardized DALY rate of periodontal diseases per 100,000 young adults in 2019 was found to be the highest in Western sub-Saharan Africa (336.16), followed closely by Central sub-Saharan Africa (284.71), and Southern sub-Saharan Africa (278.69) (Table 1, Supplementary Table 4, Supplementary Fig. 2B). On the other hand, the regions with the lowest age-standardized DALY rate for periodontal diseases were Oceania (24.22), High-income North America (107.38), and East Asia (109.29) (Table 1, Supplementary Table 4, Supplementary Fig. 2B). When considering the global scenario across 204 countries, the countries with the highest age-standardized DALY rate of periodontal diseases per 100,000 young adults in 2019 were Qatar (443.44), Gambia (425.36), and the United Arab Emirates (420.58) according to data from the World Health Organization (WHO) (Supplementary Tables 5, 6, Supplementary Fig. 3B). Conversely,
Fig. 2. Proportion of DALY rate and incidence rate of periodontal disease for young adults of 15-49 ages in countries around the world in 2019.
countries with the lowest age-standardized DALY rate of periodontal diseases were Kiribati (21.06), Solomon Islands (22.14), and Vanuatu (23.23) (Supplementary Tables 5, 6, Supplementary Fig. 3B).
Trend of periodontal disease burden in young adults from 1990 to 2019
Between 1990 and 2019, there was a notable rise in the total number of cases and DALYs in Qatar, the United Arab Emirates, and the Arab region as a whole. The ASIR of periodontal diseases per 100,000 young adults exhibited an upward trend, with an EAPC of 0.41 . Similarly, the age-standardized DALY rate per 100,000 young adults showed an increasing pattern, with an EAPC of 0.45 . Both genders experienced a rise in age-standardized rates, with comparable increasing trends. For detailed information, refer to Table 1 and Supplementary Fig. 4.
As presented in Table 1 and Supplementary Fig. 1, the ASIR of periodontal diseases per 100,000 young adults exhibited noticeable variations among the three subgroups of Socio-demographic Index (SDI) from 1990 to 2019. The region with high-middle SDI had the highest increase (estimated annual percentage change [EAPC
Among the 21 geographic regions, Tropical Latin America experienced the largest increase in ASIR per 100,000 young adults from 1990 to 2019, with an EAPC of 0.55. East Asia and Central Europe also saw increases in ASIR, with EAPCs of 0.48 and 0.40 , respectively. Conversely, High-income North America, Western Europe, and East Asia witnessed the largest decreases in ASIR for periodontal diseases, with EAPCs of
Among the 21 geographical regions, Tropical Latin America experienced the highest increase in agestandardized DALY rate of periodontal diseases per 100,000 young adults from 1990 to 2019, with an estimated annual percentage change (EAPC) of 0.63 . This was followed by East Asia (EAPC
Fig. 3. (A) ASIR of periodontal disease for young adults around the world in 1990; (B) ASIR of periodontal disease for young adults around the world in 2019; (C) EAPC of ASIR for periodontal disease for young adults in countries worldwide from 1990 to 2019.
The shapefile data used in this study were sourced from Natural Earth (http://www.naturalearthdata.com/), which provides global country and region boundaries. These boundaries were used as a base layer to display geographic distribution information relevant to the study’s theme. Natural Earth data are in the public domain, allowing for free use and distribution. Data processing and visualization of the study’s data were conducted in R (version 4.2.3) using the ggplot2 (version 3.4.0) and sf (version 1.0.9) packages.
a lesser extent (EAPC=- 0.20) (Table 1, Supplementary Tables 4 and Supplementary Fig. 2B,3C). Looking at individual countries, Qatar, Cambodia, and the Maldives experienced the largest increase in age-standardized DALY rate of periodontal diseases per 100,000 young adults from 1990 to 2019, with EAPCs of 1.44, 1.39, and 1.44 , respectively. Conversely, the United States of America, Kuwait, and the Maldives had the most significant decrease in age-standardized DALY rate of periodontal diseases, with EAPCs of
a lesser extent (EAPC=- 0.20) (Table 1, Supplementary Tables 4 and Supplementary Fig. 2B,3C). Looking at individual countries, Qatar, Cambodia, and the Maldives experienced the largest increase in age-standardized DALY rate of periodontal diseases per 100,000 young adults from 1990 to 2019, with EAPCs of 1.44, 1.39, and 1.44 , respectively. Conversely, the United States of America, Kuwait, and the Maldives had the most significant decrease in age-standardized DALY rate of periodontal diseases, with EAPCs of
Discussion
This research has indicated a rise in the prevalence of periodontal disease among young adults between 1990 and 2019. This increase is primarily evidenced by the significant rise in ASIR and age-standardized DALY rate, reflecting an increased exposure to risk factors associated with periodontal disease. The growing number of periodontal disease cases has had a positive impact on population growth and the ongoing aging trend. Furthermore, the burden of periodontal disease is observed to be greater in males, The region with the highest age-standardized incidence rate (ASIR) and age-standardized DALY rate was Western sub-Saharan Africa, particularly in regions with low SDI and low-middle SDI. Conversely, high-middle SDI and middle SDI regions have experienced a clear upward trend. These findings are similar with previous studies
The incidence rate and DALY rate of periodontal disease exhibited an increasing trend with age, reaching their peak in the 45-49 age group. The increase prevalence of periodontal disease reflecting an increased exposure to risk factors associated with periodontal disease. Possible risk factors for periodontal diseases include
modifiable factors such as smoking, oral hygiene, diabetes, drugs, and stress, non-modifiable factors such as age, genetics, and gender, and associations with other diseases such as cardiovascular disease, metabolic disease, and respiratory system
modifiable factors such as smoking, oral hygiene, diabetes, drugs, and stress, non-modifiable factors such as age, genetics, and gender, and associations with other diseases such as cardiovascular disease, metabolic disease, and respiratory system
Men exhibit a higher prevalence and severity of periodontal destruction compared to women; a finding consistent with previous research
Socioeconomic status (SES) is a significant risk indicator for periodontal diseases, with higher incidences of attachment loss and probing depth observed
The region with the highest age-standardized incidence rate (ASIR) and age-standardized DALY rate was Western sub-Saharan Africa. Central sub-Saharan Africa, Southern sub-Saharan Africa, as the region with the highest incidence of AIDS globally, faces an increased risk of periodontal diseases among early individuals due to the association between HIV, oral hygiene, and periodontal diseases
The high burden of periodontal disease and its increasing trend in Qatar are influenced by multiple factors, including behavioral, biological, socioeconomic, political, and environmental factors
This study presents a comprehensive analysis of the global burden of periodontal diseases in young adults (aged 15-49) over the past three decades. It examines the distribution of the burden across different geographical regions and time periods and explores the risk factors contributing to the increasing incidence of these diseases. By identifying targets and providing guidance for prevention and treatment strategies, this study aims to facilitate the equitable allocation of resources. However, it is important to acknowledge the inherent limitations of the GBD approach employed in this study. Firstly, the burden of periodontal diseases may be underestimated due to limited data availability, particularly from economically disadvantaged areas. Secondly, data assessment accuracy can be influenced to some extent by the methods used for data processing and modeling.
Conclusions
The ASIR and age-standardized DALY rate of periodontal disease demonstrated a consistent upward trend from 1990 to 2019, indicating the persistent global public health challenge posed by this condition. A notable disparity was observed in the burden of periodontal disease among different genders and regions. Men bore a greater burden, with the peak age of susceptibility falling within the
Data availability
Data were obtained from the publicly accessible Global Health Data Exchange (GHDx) (https://ghdx.healthdat a.org/gbdresultstool).
Received: 1 July 2024; Accepted: 28 January 2025
Published online: 24 February 2025
Published online: 24 February 2025
References
- Ge, J. et al. Periodontitis impacts on thrombotic diseases: from clinical aspect to future therapeutic approaches. Int. J. Oral Sci. 16, 58 (2024).
- Nwizu, N., Wactawski-Wende, J. & Genco, R. J. Periodontal disease and cancer: epidemiologic studies and possible mechanisms. Periodontology 83, 213-233 (2020).
- Sanz, M. et al. Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 47, 268-288 (2020).
- Del Pinto, R. et al. Periodontitis and hypertension: is the association causal? High Blood Press. Cardiovasc. Prev. 27, 281-289 (2020).
- Baeza, M. et al. Effect of periodontal treatment in patients with periodontitis and diabetes: systematic review and meta-analysis. J. Appl. Oral Sci. 28, e20190248 (2020).
- Kwon, T., Lamster, I. B. & Levin, L. Current concepts in the management of periodontitis. Int. Dent. J. 71, 462-476 (2021).
- Eke, P. I. et al. Periodontitis in US adults: National Health and Nutrition Examination Survey 2009-2014. J. Am. Dent. Assoc. 149, 576-588 (2018).
- Luo, L. S. et al. Secular trends in severe periodontitis incidence, prevalence and disability-adjusted life years in five Asian countries: a comparative study from 1990 to 2017. J. Clin. Periodontol. 48, 627-637 (2021).
- Genco, R. J. & Borgnakke, W. S. Risk factors for periodontal disease. Periodontology 62, 59-94 (2013).
- AlJehani, Y. A. Risk factors of periodontal disease: review of the literature. Int. J. Dent. 2014, 182513 (2014).
- Kassebaum, N. J. et al. Global burden of severe periodontitis in 1990-2010: a systematic review and meta-regression. J. Dent. Res. 93, 1045-1053 (2014).
- Jiao, J. et al. The prevalence and severity of periodontal disease in Mainland China: data from the Fourth National oral health survey (2015-2016). J. Clin. Periodontol. 48, 168-179 (2021).
- Chen, M. X., Zhong, Y. J., Dong, Q. Q., Wong, H. M. & Wen, Y. F. Global, regional, and national burden of severe periodontitis, 1990-2019: an analysis of the global burden of Disease Study 2019. Clin. Periodontol. 48, 1165-1188 (2021).
- Zhang, X. et al. The global burden of periodontal diseases in 204 countries and territories from 1990 to 2019. Oral Dis. 30 (2), 754-768 (2024).
- Collaborators Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of Disease Study 2019. Lancet 396, 1204-1222 (2020).
- Zhang, D., Liu, S., Li, Z. & Wang, R. Global, regional and national burden of gastroesophageal reflux disease, 1990-2019: update from the GBD 2019 study. Ann. Med. 54, 1372-1384 (2022).
- Wu, L., Zhang, S. Q., Zhao, L., Ren, Z. H. & Hu, C. Y. Global, regional, and national burden of periodontitis from 1990 to 2019: results from the Global Burden of Disease study 2019. J. Periodontol. 93 (10), 1445-1454 (2022).
- Nagata, J. M. et al. Food insecurity and chronic disease in US young adults: findings from the National Longitudinal Study of Adolescent to Adult Health. J. Gen. Intern. Med. 34, 2756-2762 (2019).
- Biener, L. & Albers, A. B. Young adults: vulnerable new targets of tobacco marketing. Am. J. Public Health 94, 326-330 (2004).
- Kinane, D. F. & Marshall, G. J. Periodontal manifestations of systemic disease. Aust. Dent. J. 46, 2-12 (2001).
- Charupinijkul, R. A. et al. The effect of obesity on periodontitis progression: the 10-year retrospective cohort study. Clin. Oral Investig. 26, 535-542 (2022).
- Ng, M. et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the global burden of Disease Study 2013. Lancet 384, 766-781 (2014).
- Reners, M. & Brecx, M. Stress and periodontal disease. Int. J. Dent. Hyg. 5, 199-204 (2007).
- Rajabi, F., Drake, L. A., Senna, M. M. & Rezaei, N. Alopecia Areata: a review of disease pathogenesis. Br. J. Dermatol. 179, 10331048 (2018).
- Corbet, E. F., Wong, M. C. & Lin, H. C. Periodontal conditions in adult Southern Chinese. J. Dent. Res. 80, 1480-1485 (2001).
- Gjermo, P., Rösing, C. K., Susin, C. & Oppermann, R. Periodontal diseases in Central and South America. Periodontology 29, 70-78 (2002).
- Hugoson, R. A. & Jordan, T. Frequency distribution of individuals aged
years according to severity of periodontal disease. Community Dent. Oral Epidemiol. 10, 187-192 (1982). - Borrell, L. N., Burt, B. A., Gillespie, B. W., Lynch, J. & Neighbors, H. Periodontitis in the United States: beyond black and white. J. Public Health Dent. 62, 92-101 (2002).
- Borrell, L. N. & Crawford, N. D. Social disparities in periodontitis among United States adults 1999-2004. Community Dent. Oral Epidemiol. 36, 383-391 (2008).
- Nazir, M. et al. Global prevalence of periodontal disease and lack of its surveillance. Sci. World J. 2020, 2146160 (2020).
- Caballero, B. A nutrition paradox-underweight and obesity in developing countries. N. Engl. J. Med. 352, 1514-1516 (2005).
- Morillo, J. M. et al. Nutrition-linked chronic disease and periodontitis: are they the two faces of the same coin? Mediterr. J. Nutr. Metab. 2, 103-109 (2009).
- Doku, D. The tobacco industry tactics-a challenge for tobacco control in low and middle income countries. Afr. Health Sci. 10, 201-203 (2010).
- Alpagot, T., Duzgunes, N., Wolff, L. F. & Lee, A. Risk factors for periodontitis in HIV patients. J. Periodontal Res. 39, 149-157 (2004).
- Tellez, M., Zini, A. & Estupiñan-Day, S. Social determinants and oral health: an update. Curr. Oral Health Rep. 1, 148-152 (2014).
- Awad, S. F., O’Flaherty, M., Critchley, J. & Abu-Raddad, L. J. Forecasting the burden of type 2 diabetes mellitus in Qatar to 2050: a novel modeling approach. Diabetes Res. Clin. Pract. 137, 100-108 (2018).
- Morgano, S. M. et al. Burden of oral disease in the Middle East: opportunities for dental public health. Int. Dent. J. 60, 197-199 (2010).
Acknowledgements
We thank all authors for their contributions to the article.
Author contributions
Yifeng Wang: Conceptualization; Lidan Zhuo: Methodology; Saiyan Yang: Data curation; Cheng Dong: Writ-ing-Original draft preparation; Peng Shu: Visualization, Formal analysis; Yifeng Wang: Writing-Reviewing and Editing. All authors read and approved the final manuscript.
Declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study is based on a publicly available database and does not require ethical approval.
Additional information
Supplementary Information The online version contains supplementary material available at https://doi.org/1 0.1038/s41598-025-88249-0.
Correspondence and requests for materials should be addressed to P.S.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommo ns.org/licenses/by-nc-nd/4.0/.
© The Author(s) 2025
© The Author(s) 2025
Department of Stomatology, Beilun People’s Hospital, Ningbo, Zhejiang, China. Precision Medicine Research Center, Beilun People’s Hospital, Ningbo 315800, Zhejiang, China. email: shu_peng0326@163.com