DOI: https://doi.org/10.1038/s41591-023-02702-z
PMID: https://pubmed.ncbi.nlm.nih.gov/38177850
تاريخ النشر: 2024-01-04
نظام تعلم عميق لتوقع وقت تقدم اعتلال الشبكية السكري
تم القبول: 10 نوفمبر 2023
نُشر على الإنترنت: 4 يناير 2024
(د) التحقق من التحديثات
الملخص
لينغ داي
الملخص
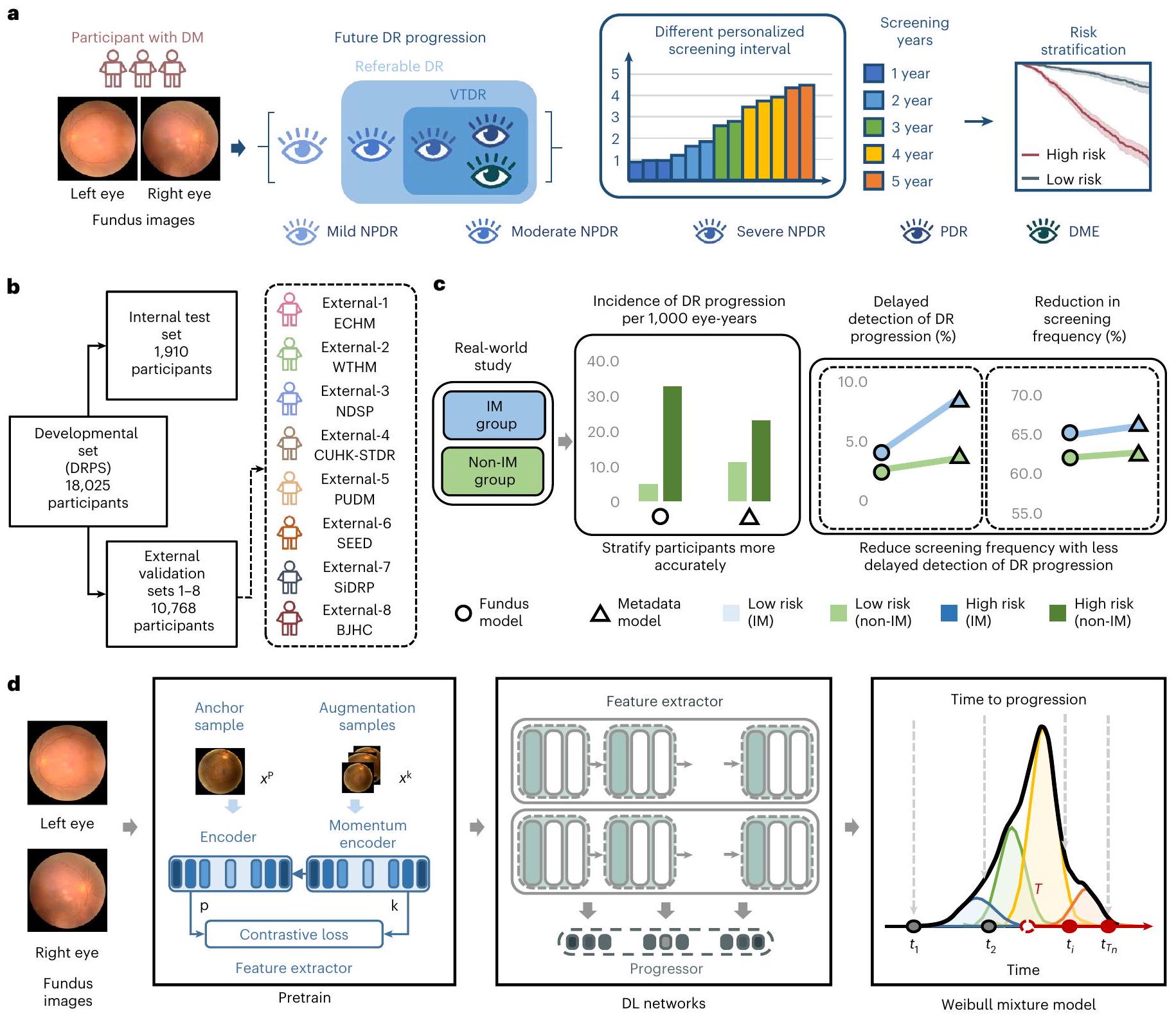
اعتلال الشبكية السكري (DR) هو السبب الرئيسي للعمى الذي يمكن الوقاية منه على مستوى العالم. يختلف خطر تقدم اعتلال الشبكية السكري بشكل كبير بين الأفراد المختلفين، مما يجعل من الصعب التنبؤ بالمخاطر وتخصيص فترات الفحص. قمنا بتطوير والتحقق من نظام تعلم عميق (DeepDR Plus) للتنبؤ بالوقت حتى تقدم اعتلال الشبكية السكري خلال 5 سنوات فقط من خلال صور قاع العين. أولاً، استخدمنا 717,308 صورة لقاع العين من 179,327 مشاركًا مصابًا بالسكري لتدريب النظام مسبقًا. بعد ذلك، قمنا بتدريب والتحقق من النظام باستخدام مجموعة بيانات متعددة الأعراق تضم 118,868 صورة من 29,868 مشاركًا مصابًا بالسكري. للتنبؤ بالوقت حتى تقدم اعتلال الشبكية السكري، حقق النظام مؤشرات توافق تتراوح بين 0.754 و0.846 ودرجات بريير المتكاملة بين 0.153 و0.241 لجميع الأوقات حتى 5 سنوات. علاوة على ذلك، تحققنا من النظام في مجموعات حقيقية من المشاركين المصابين بالسكري. يمكن أن يؤدي دمج النظام مع سير العمل السريري إلى تمديد متوسط فترة الفحص من 12 شهرًا إلى 31.97 شهرًا، وكانت نسبة المشاركين الموصى بفحصهم خلال 1-5 سنوات هي 30.62%، 20.00%، 19.63%، 11.85% و17.89% على التوالي، في حين كان تأخير اكتشاف التقدم إلى اعتلال الشبكية السكري المهدد للبصر 0.18%. مجتمعة، يمكن لنظام DeepDR Plus التنبؤ بالمخاطر الفردية والوقت حتى تقدم اعتلال الشبكية السكري خلال 5 سنوات، مما يتيح إمكانية تخصيص فترات الفحص.
الفحص الروتيني لاعتلال الشبكية السكري على فترات سنوية يُوصى به على نطاق واسع لجميع الأفراد المصابين بالسكري الذين لا يعانون من اعتلال الشبكية السكري أو يعانون من اعتلال شبكية خفيف، وذلك من قبل المنظمات الوطنية والدولية.
النتائج
تصميم الدراسة والمشاركون
ديب دي آر بلس يتنبأ بوقت تقدم اعتلال الشبكية السكري
لوحظ في أداء النموذج لتوقع تقدم اعتلال الشبكية السكري بين المرضى ذوي حالات التحكم في نسبة السكر في الدم المختلفة، بغض النظر عن إضافة مستويات الهيموغلوبين A1c (HbA1c) في المتابعة.
ديب دي آر بلس يتنبأ بوقت التقدم في ثلاث مجموعات فرعية
| المجموعات | مجموعة البيانات المدربة مسبقًا | مجموعة بيانات التطوير | مجموعة الاختبار الداخلية | إي سي إتش إم خارجي-1 | WTHM الخارجي-2 | NDSP الخارجي-3 | CUHK-STDR خارجي-4 | PUDM خارجي-5 | SEED خارجي-6 | SiDRP خارجي-7 | BJHC الخارجي-8 |
| عدد الصور | ٧١٧,٣٠٨ | ٦٨٬٧٦٠ | ٧٬٦٤٠ | ٨٬٥٦٤ | ٣٬٨٨٤ | ٤٬٧٧٦ | ١٬١٨٢ | ١٬٢٢٨ | ٦,٦٧٦ | ١٢٬٨١٨ | ٣٬٣٤٠ |
| عدد المشاركين | ١٧٩٬٣٢٧ | ١٧٬١٩٠ | ١٬٩١٠ | ٢٬١٤١ | ٩٧١ | ١٬١٩٤ | ٣٣٧ | ٣٠٧ | ١٬٦٩٩ | ٣٬٢٨٤ | ٨٣٥ |
| عرق | |||||||||||
| صيني
|
١٧٩٬٣٢٧ (١٠٠٪) | 17,190 (100%) | ١٬٩١٠ (١٠٠٪) | ٢,١٤١ (١٠٠٪) | 971 (100%) | ١٬١٩٤ (١٠٠٪) | 337 (100%) | ٣٠٧ (١٠٠٪) | 411 (24.19%) | ٢٬٤٩٤ (٧٥٫٩٤٪) | 835 (100%) |
| مالاي
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
532 (31.31%) | 518 (15.77%) | غير متوفر
|
| هندي
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
756 (44.50%) | 272 (8.28%) | غير متوفر
|
| الجنس | |||||||||||
| أنثى،
|
96,676 (53.91%) | ٢٬٦٩٢ (١٥٫٦٦٪) | 337 (17.62%) | 826 (38.58%) | 313 (32.23%) | ٧٣٩ (٦١.٨٩٪) | 169 (50.15%) | 131 (42.67%) | 852 (50.15%) | 1,661 (50.58%) | ٤٠٠ (٤٧٫٩٠٪) |
| ذكر،
|
٨٢٬٦٥١ (٤٦٫٠٩٪) | 14,498 (84.34%) | ١,٥٧٣ (٨٢.٣٨٪) | 1,315 (61.42%) | 658 (67.77%) | 455 (38.11%) | 168 (49.85%) | 176 (57.33%) | ٨٤٧ (٤٩.٨٥٪) | 1,623 (49.42%) | 435 (52.10%) |
| العمر (بالسنوات) |
|
|
|
|
|
|
|
|
|
|
|
| مدخن،
|
19,249 (10.73%) | ٤,٢٥٥ (٢٤.٧٥٪) | 470 (24.60%) | 277 (12.94%) | 215 (22.14%) | ٢٠٧ (١٧.٣٤٪) | 83 (24.63%) | 122 (39.74%) | 484 (28.49%) | ٦٣ (١.٩٪) | غير متوفر
|
| مؤشر كتلة الجسم (
|
|
|
|
|
|
|
|
|
|
|
|
| ضغط الدم الانقباضي (مم زئبق) |
|
|
|
|
|
|
|
|
|
|
|
| الهيموغلوبين السكري (%) |
|
|
|
|
|
|
|
|
|
|
غير متوفر
|
| الجلوكوز الصائم في البلازما (
|
|
|
|
|
|
|
|
|
غير متوفر
|
|
|
| مستوى الجلوكوز العشوائي في الدم (
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
غير متوفر
|
|
غير متوفر
|
غير متوفر
|
| الدهون الثلاثية (ممول
|
|
|
|
|
|
|
|
|
|
|
|
| كوليسترول البروتين الدهني منخفض الكثافة (
|
|
|
|
|
|
|
|
|
|
|
|
| كوليسترول البروتين الدهني عالي الكثافة (
|
|
|
|
|
|
|
|
|
|
|
|
| مدة الإصابة بمرض السكري (بالسنوات) | غير متوفر
|
|
|
|
|
|
|
|
|
|
غير متوفر
|
| عيون مع تقدم اعتلال الشبكية السكري،
|
غير متوفر
|
٢,٨١٩ (٨.٢٠٪) | 278 (7.28%) | 321 (7.50%) | 121 (6.23%) | ٤٨ (٢.٠١٪) | 114 (16.91%) | ٢٥ (٤٫٠٧٪) | 184 (5.41%) | 171 (2.60%) | 38 (2.28%) |
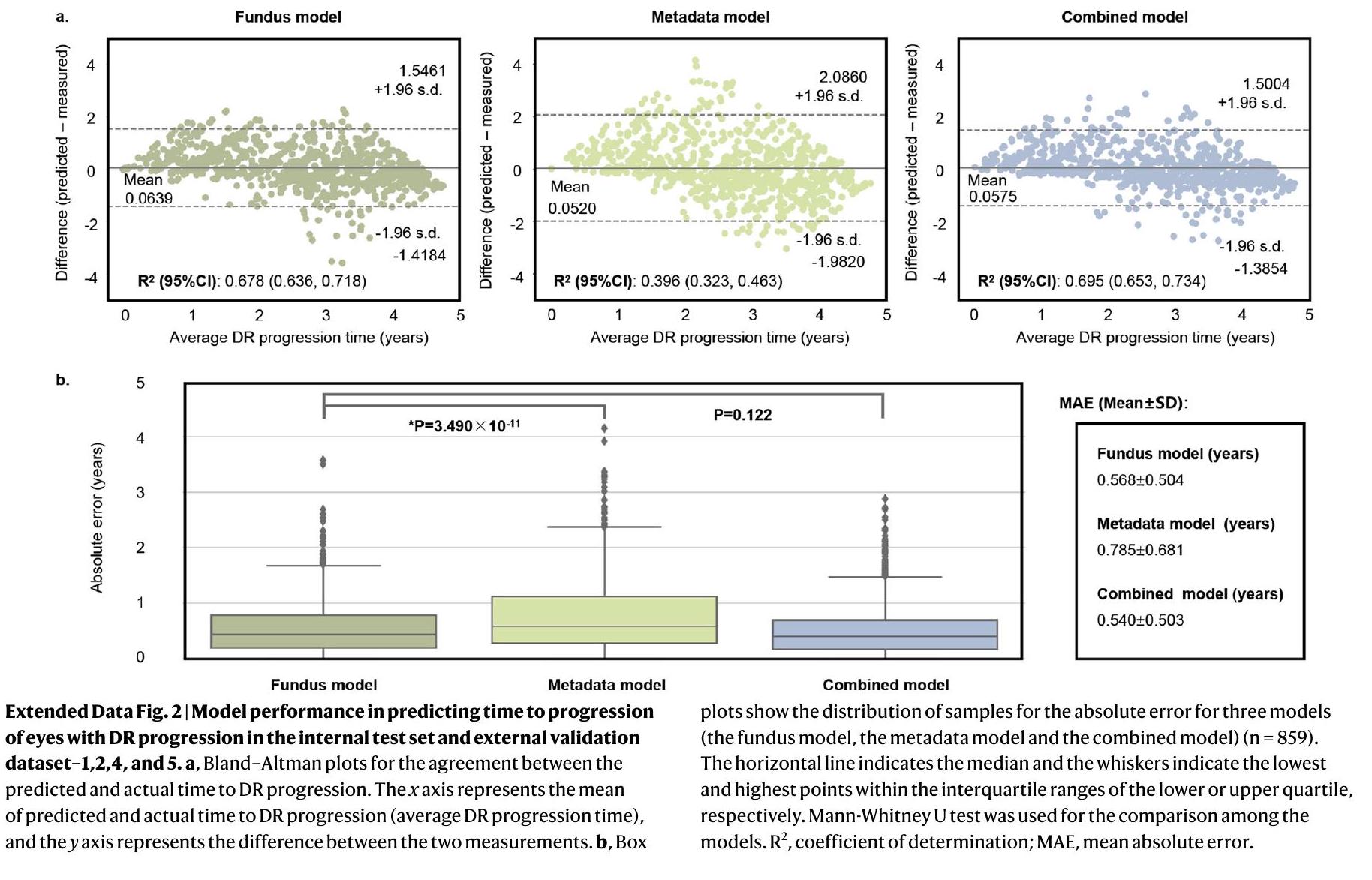
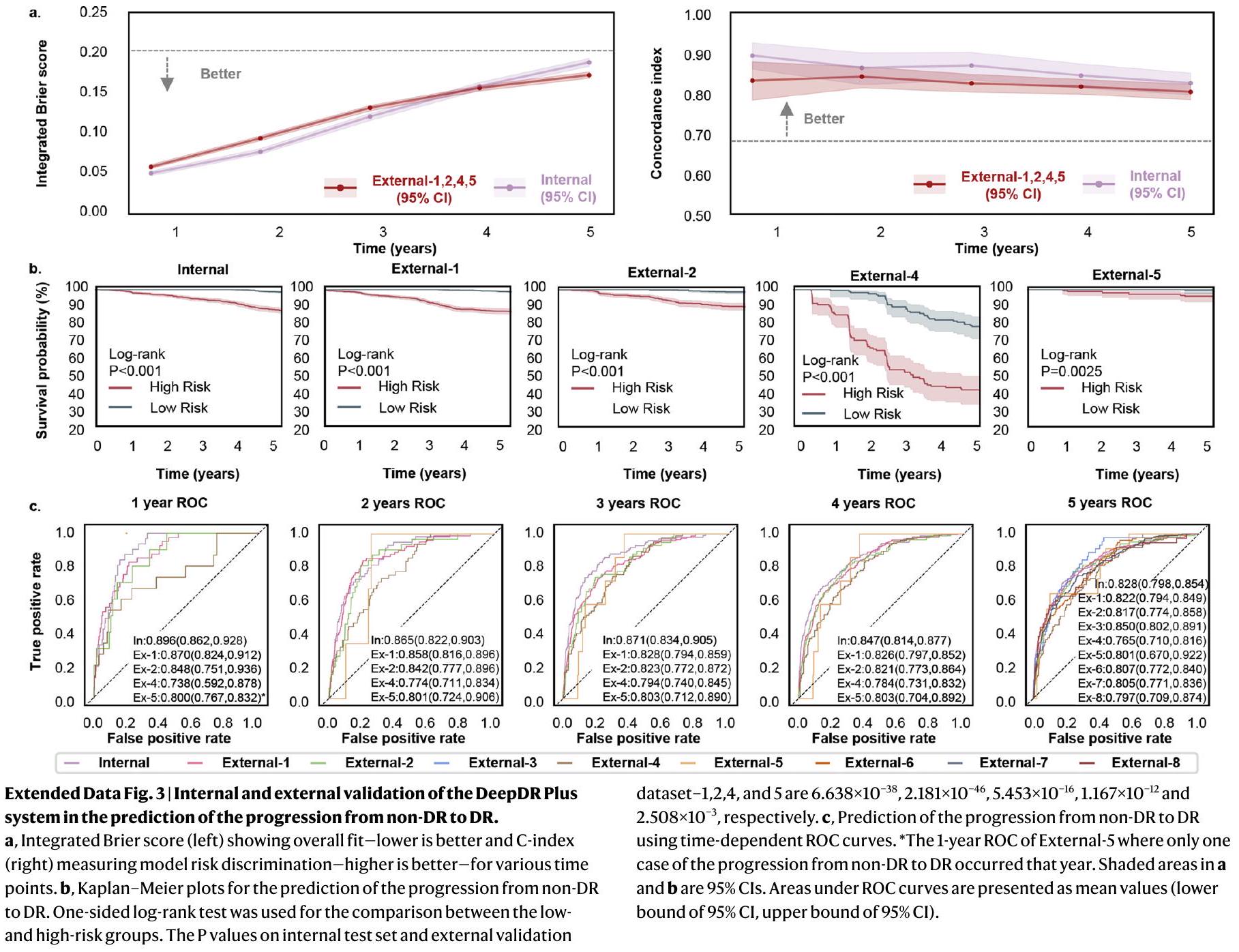
0.797-0.851) لاعتلال الشبكية السكري، 0.820 (فاصل الثقة 95%، 0.785-0.853) لاعتلال الشبكية السكري القابل للإحالة، و0.824 (فاصل الثقة 95%، 0.758-0.880) لاعتلال الشبكية السكري المتقدم، بينما انخفض مؤشر الخطأ المتكامل (IBS) إلى 0.153-0.189 للثلاث مجموعات الفرعية. عند دمج صور قاع العين مع البيانات السريرية، أعطى النموذج المدمج مؤشرات C تتراوح بين 0.835-0.852 وIBS بين 0.145-0.167 للمجموعات الفرعية 1-3 (الجدول الموسع 2). علاوة على ذلك، قمنا بتقييم أداء التنبؤ لنموذج قاع العين في مجموعات البيانات الخارجية وحققنا نتائج مماثلة لمجموعة البيانات الداخلية (الجدول الموسع 2). أشارت النتائج إلى أن صور قاع العين وحدها يمكنها التنبؤ بفعالية بتقدم المرض. وبالمثل لمهمة التنبؤ بالوقت حتى أي تقدم في اعتلال الشبكية السكري، قمنا بتقييم أداء التنبؤ في ثلاث مجموعات فرعية. كما هو موضح في الأشكال الموسعة 3-5، حقق نموذج قاع العين مؤشرات C تتراوح بين 0.820-0.895 وIBS بين 0.045-0.189 في مجموعة البيانات الداخلية للسنوات 1-5. علاوة على ذلك، حققت مجموعات التحقق الخارجية 1، 2، 4 و5 مؤشرات C تتراوح بين 0.794-0.842 وIBS بين 0.058-0.218.
ومجموعات البيانات الخارجية (
لتقييم فعالية نظام DeepDR Plus مع دمج سير العمل السريري، أجرينا دراسة في العالم الحقيقي ضمن دراسة مستقبلية مجتمعية شملت البالغين الصينيين (الطرق). تم تضمين ما مجموعه 2185 مشاركًا في التحليل، مع 538 مشاركًا في مجموعة الإدارة المتكاملة (برنامج إدارة مرض السكري المتكامل بين المستشفى والمجتمع) و1647 مشاركًا في المجموعة غير المتكاملة. تم تزويد المشاركين في مجموعة الإدارة المتكاملة بقياسات سريرية وأيضية منتظمة، بإشراف متخصصين في المستشفيات الشاملة، وتلقوا إرشادات حول نمط الحياة ودعم الأقران في مراكز خدمات الصحة المجتمعية.
| معدل حدوث تقدم اعتلال الشبكية السكري لكل 1000 سنة عين (عدد الحالات/عدد العيون) | ARR
|
|||
| مجموعة IM (
|
ديب دي آر بلس – منخفض المخاطر (الذكاء الاصطناعي – منخفض) | بيانات وصفية – منخفضة المخاطر (ميتا-منخفض) | -33.05 (-67.79، 35.76) | |
| ٥.١١ (١٦/٦٢٦) | ٧.٦٣ (٢٤/٦٢٩) | |||
| ديب دي آر بلس – عالي الخطورة (ذكاء اصطناعي – عالي) | البيانات الوصفية – عالية المخاطر (ميتا-عالية) | 14.54 (-28.26، 74.63) | ||
| 26.67 (60/450) | ٢٣٫٢٧ (٥٢/٤٤٧) | |||
| برنامج متكامل لإدارة داء السكري بين المستشفى والمجتمع | غير IM (
|
ديب دي آر بلس – منخفض المخاطر (الذكاء الاصطناعي – منخفض) | بيانات وصفية – منخفضة المخاطر (ميتا-منخفض) | -91.63 (-93.91، -89.06) |
| ٥٫٠١ (٥٠/١٬٩٩٦) | 11.34 (113/1,993) | |||
| ديب دي آر بلس – عالي الخطورة (الذكاء الاصطناعي – عالي) | البيانات الوصفية – عالية المخاطر (ميتا-عالية) | 61.36 (25.36، 109.91) | ||
| ٣٣.١٣ (٢١٥/١٬٢٩٨) | 23.37 (152/1,301) | |||
| التدخلات الشاملة: [(AI-مرتفع + AI-منخفض) – (meta-مرتفع + meta-منخفض)] في مجموعة IM – [(Al-مرتفع + Al-منخفض) – (meta-مرتفع + meta-منخفض)] في المجموعة غير IM | 46.80 (12.37، 94.93) | |||
| دراسة سانكارا نيثرالايا لعلم أوبئة اعتلال الشبكية السكري وعلم الوراثة الجزيئي
|
مجموعة IM (
|
ديب دي آر بلس – منخفض المخاطر (الذكاء الاصطناعي – منخفض) | بيانات وصفية – منخفضة المخاطر (ميتا-منخفض) | -9.39 (-79.77، 287.41) |
| ٤.٠٨ (٢/٩٨) | ٤.٤٩ (٢/٨٩) | |||
| ديب دي آر بلس – عالي الخطورة (آل-عالي) | البيانات الوصفية – عالية المخاطر (ميتا-عالية) | 20.48 (-70.93، 400.0) | ||
| ٢٥٫٠ (٦/٤٨) | 21.05 (6/57) | |||
| المجموعة غير التابعة لـ IM (
|
ديب دي آر بلس – منخفض المخاطر (الذكاء الاصطناعي – منخفض) | بيانات وصفية – منخفضة المخاطر (ميتا-منخفض) | -97.32 (-98.28، -96.32) | |
| ٥.٢٤ (٢٨/١٠٦٨) | 13.0 (70/1,077) | |||
| ديب دي آر بلس – عالي الخطورة (آل-عالي) | البيانات الوصفية – عالية المخاطر (ميتا-عالية) | 43.13 (9.1، 87.18) | ||
| ٤٤.١١ (١٦١/٧٣٠) | 33.01 (119/721) | |||
| التدخلات الشاملة: [(AI-مرتفع + AI-منخفض) – (meta-مرتفع + meta-منخفض)] في مجموعة IM – [(AI-مرتفع + AI-منخفض) – (meta-مرتفع + meta-منخفض)] في المجموعة غير IM | 88.74 (10.83، 330.25) | |||
| مجموعة | نموذج | متوسط فترة الفحص (بالأشهر) | انخفاض في تكرار الفحص (%)
|
تأخر اكتشاف أي تقدم في اعتلال الشبكية السكري (%)
|
التأخر في اكتشاف التقدم إلى اعتلال الشبكية السكري المتقدم (%) |
| أنا | البيانات الوصفية | ٣٤٫٠٦ | ٦٤٫٧٧ | 1.86 | 0.93 |
| قاع العين | ٣١٫٥٤ | ٦١٫٩٥ | 0.37 | 0.37 | |
| غير IM | البيانات الوصفية | ٣٥٫٣٢ | ٦٦٫٠٢ | ٦٫٠١ | 0.97 |
| قاع العين | ٣٢٫١١ | ٦٢٫٦٣ | 1.28 | 0.12 | |
| الرسائل الفورية وغير الرسائل الفورية | البيانات الوصفية | ٣٥٫٠١ | ٦٥٫٧٢ | ٤٫٩٩ | 0.96 |
| قاع العين | ٣١٫٩٧ | ٦٢٫٤٦ | 1.05 | 0.18 |
منع
اتبعت المجموعات فترة الفحص الشخصية الموصى بها التي قدمها نموذج قاع العين. بالمقارنة مع نموذج البيانات الوصفية، يمكن لنموذج قاع العين تحقيق تقليل مماثل في تكرار الفحص (
معدل أقل من الكشف المتأخر لأي تقدم في اعتلال الشبكية السكري لدى مرضى مجموعة IM مقارنة بمجموعة غير IM (
التدخلات. يوضح الشكل الموسع 6ب مخطط الشلال للوقت المتوقع لتقدم اعتلال الشبكية السكري للمشاركين في الدراسة الواقعية بواسطة نموذج قاع العين. إذا اتبع جميع المشاركين في مجموعتي IM وغير IM فترة الفحص الشخصية الموصى بها من قبل نموذج قاع العين، فإن نسبة المشاركين الذين تم التوصية لهم بفحص اعتلال الشبكية السكري خلال 1-5 سنوات كانت 30.62%، 20.00%، 19.63%، 11.85% و
تحليل القابلية للتفسير
مناقشة
فقط 0.18%. أظهرت هذه النتائج أن نظام DeepDR Plus الخاص بنا يمكن أن يعزز تقييم المخاطر الخاص بالمريض ورعاية أكثر تخصيصًا لإدارة اعتلال الشبكية السكري، استنادًا إلى فحص شبكية العين لمرة واحدة فقط في المستقبل.
آفاق التعديلات المستقبلية على الإرشادات المتعلقة باستخدام الذكاء الاصطناعي في إدارة اعتلال الشبكية السكري.
المحتوى الإلكتروني
References
- Cheung, N., Mitchell, P. & Wong, T. Y. Diabetic retinopathy. Lancet 376, 124-136 (2010).
- Tan, T. -E. & Wong, T. Y. Diabetic retinopathy: looking forward to 2030. Front Endocrinol. 13, 1077669 (2022).
- Wong, T. Y., Cheung, C. M. G., Larsen, M., Sharma, S. & Simó, R. Diabetic retinopathy. Nat. Rev. Dis. Prim. 2, 16012 (2016).
- Jenkins, A. J. et al. Biomarkers in diabetic retinopathy. Rev. Diabet. Stud. 12, 159-195 (2015).
- Stratton, I. M. et al. UKPDS 50: risk factors for incidence and progression of retinopathy in type II diabetes over 6 years from diagnosis. Diabetologia 44, 156-163 (2001).
- Solomon, S. D. et al. Diabetic Retinopathy: a position statement by the American Diabetes Association. Diabetes Care 40, 412-418 (2017).
- Wong, T. Y. et al. Guidelines on diabetic eye care: the international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology 125, 1608-1622 (2018).
- Flaxel, C. J. et al. Diabetic retinopathy preferred practice pattern. Ophthalmology 127, P66-P145 (2020).
- Wang, L. Z. et al. Availability and variability in guidelines on diabetic retinopathy screening in Asian countries. Br. J. Ophthalmol. 101, 1352-1360 (2017).
- Modjtahedi, B. S. et al. Two-year incidence of retinal intervention in patients with minimal or no diabetic retinopathy on telemedicine screening. JAMA Ophthalmol. 137, 445-448 (2019).
- Gunasekeran, D. V., Ting, D. S. W., Tan, G. S. W. & Wong, T. Y. Artificial intelligence for diabetic retinopathy screening, prediction and management. Curr. Opin. Ophthalmol. 31, 357-365 (2020).
- Fundus photographic risk factors for progression of diabetic retinopathy. ETDRS report number 12. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98, 823-833 (1991).
- Lund, S. H. et al. Individualised risk assessment for diabetic retinopathy and optimisation of screening intervals: a scientific approach to reducing healthcare costs. Br. J. Ophthalmol. 100, 683-687 (2016).
- Broadbent, D. M. et al. Safety and cost-effectiveness of individualised screening for diabetic retinopathy: the ISDR open-label, equivalence RCT. Diabetologia 64, 56-69 (2021).
- Bora, A. et al. Predicting the risk of developing diabetic retinopathy using deep learning. Lancet Digit. Health 3, e10-e19 (2021).
- Guan, Z. et al. Artificial intelligence in diabetes management: advancements, opportunities, and challenges. Cell Rep. Med. 4, 101213 (2023).
- Ting, D. S. W. et al. Artificial intelligence and deep learning in ophthalmology. Br. J. Ophthalmol. 103, 167-175 (2019).
- Ting, D. S. W. et al. Development and validation of a deep learning system for diabetic retinopathy and related eye diseases using retinal images from multiethnic populations with diabetes. JAMA 318, 2211-2223 (2017).
- Gulshan, V. et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 316, 2402-2410 (2016).
- Dai, L. et al. A deep learning system for detecting diabetic retinopathy across the disease spectrum. Nat. Commun. 12, 3242 (2021).
- Arcadu, F. et al. Deep learning algorithm predicts diabetic retinopathy progression in individual patients. NPJ Digit. Med. 2, 92 (2019).
- Cai, C. et al. Effectiveness of quality of care for patients with type 2 diabetes in China: findings from the Shanghai Integration Model (SIM). Front. Med. 16, 126-138 (2022).
- Wilkinson, C. P. et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 110, 1677-1682 (2003).
- Chen, S. et al. A seven-year study on an integrated hospital-community diabetes management program in Chinese patients with diabetes. Prim. Care Diabetes 12, 231-237 (2018).
- Norton, E. C., Miller, M. M. & Kleinman, L. C. Computing adjusted risk ratios and risk differences in Stata. Stata J. 13, 492-509 (2013).
- Das, S. K. Confidence interval is more informative than p-value in research. Int. J. Eng. Appl. Sci. Technol. 4, 278-282 (2019).
- Raman, R. et al. Incidence and progression of diabetic retinopathy in urban India: Sankara nethralaya-diabetic retinopathy epidemiology and molecular genetics study (SN-DREAMS II), Report 1. Ophthalmic Epidemiol. 24, 294-302 (2017).
- Varadarajan, A. V. et al. Deep learning for predicting refractive error from retinal fundus images. Invest. Ophthalmol. Vis. Sci. 59, 2861-2868 (2018).
- Yang, D. et al. Assessment of parafoveal diabetic macular ischemia on optical coherence tomography angiography images to predict diabetic retinal disease progression and visual acuity deterioration. JAMA Ophthalmol. 141, 641-649 (2023).
- Sun, Z. et al. OCT angiography metrics predict progression of diabetic retinopathy and development of diabetic macular edema: a prospective study. Ophthalmology 126, 1675-1684 (2019).
- Cheung, C. Y. et al. A deep-learning system for the assessment of cardiovascular disease risk via the measurement of retinal-vessel calibre. Nat. Biomed. Eng. 5, 498-508 (2021).
- CHEUNG, C. Y. L. et al. A new method to measure peripheral retinal vascular caliber over an extended area. Microcirculation 17, 495-503 (2010).
- Scanlon, P. H. Screening intervals for diabetic retinopathy and implications for care. Curr. Diab. Rep. 17, 96 (2017).
- Henry, K. E. et al. Human-machine teaming is key to AI adoption: clinicians’ experiences with a deployed machine learning system. NPJ Digit. Med. 5, 97 (2022).
- Dixon, R. F. et al. A virtual type 2 diabetes clinic using continuous glucose monitoring and endocrinology visits. J. Diabetes Sci. Technol. 14, 908-911 (2020).
- Downing, J., Bollyky, J. & Schneider, J. Use of a connected glucose meter and certified diabetes educator coaching to decrease the likelihood of abnormal blood glucose excursions: the livongo for diabetes program. J. Med Internet Res. 19, e234 (2017).
- Poplin, R. et al. Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nat. Biomed. Eng. 2, 158-164 (2018).
- Cheung, C. Y.-L. et al. Retinal vascular geometry and 6 year incidence and progression of diabetic retinopathy. Diabetologia 60, 1770-1781 (2017).
- Lu, Y. et al. Evaluation of automatically quantified foveal avascular zone metrics for diagnosis of diabetic retinopathy using optical coherence tomography angiography. Invest. Ophthalmol. Vis. Sci. 59, 2212-2221 (2018).
- Sawides, L. et al. Alterations to the foveal cone mosaic of diabetic patients. Invest. Ophthalmol. Vis. Sci. 58, 3395-3403 (2017).
- Cheung, C. Y., Ikram, M. K., Klein, R. & Wong, T. Y. The clinical implications of recent studies on the structure and function of the retinal microvasculature in diabetes. Diabetologia 58, 871-885 (2015).
- Klein, R. et al. Retinal vascular abnormalities in persons with type 1 diabetes: the Wisconsin Epidemiologic Study of Diabetic Retinopathy: XVIII. Ophthalmology 110, 2118-2125 (2003).
- Klein, R. et al. The relation of retinal vessel caliber to the incidence and progressionof diabetic retinopathy: Xix: The Wisconsin Epidemiologic Study of Diabetic Retinopathy. Arch. Ophthalmol. 122, 76-83 (2004).
- Oshitari, T. The pathogenesis and therapeutic approaches of diabetic neuropathy in the retina. Int. J. Mol. Sci. 22, 9050 (2021).
- Traversi, C. et al. Fractal analysis of fluoroangiographic patterns in anterior ischaemic optic neuropathy and optic neuritis: a pilot study. Clin. Exp. Ophthalmol. 36, 323-328 (2008).
- Simó, R. & Hernández, C. European Consortium for the Early Treatment of Diabetic Retinopathy (EUROCONDOR) Neurodegeneration in the diabetic eye: new insights and therapeutic perspectives. Trends Endocrinol. Metab. 25, 23-33 (2014).
- Zafar, S., Sachdeva, M., Frankfort, B. J. & Channa, R. Retinal neurodegeneration as an early manifestation of diabetic eye disease and potential neuroprotective therapies. Curr. Diab. Rep. 19, 17 (2019).
- Sohn, E. H. et al. Retinal neurodegeneration may precede microvascular changes characteristic of diabetic retinopathy in diabetes mellitus. Proc. Natl Acad. Sci. USA 113, E2655-E2664 (2016).
- Wong, T. Y. & Sabanayagam, C. The war on diabetic retinopathy: where are we now? Asia Pac. J. Ophthalmol. 8, 448-456 (2019).
- Liu, H. et al. Economic evaluation of combined population-based screening for multiple blindness-causing eye diseases in China: a cost-effectiveness analysis. Lancet Glob. Health 11, e456-e465 (2023).
- Yang, Z., Tan, T.-E., Shao, Y., Wong, T. Y. & Li, X. Classification of diabetic retinopathy: past, present and future. Front. Endocrinol. 13, 1079217 (2022).
- Zhou, Y. et al. A foundation model for generalizable disease detection from retinal images. Nature 622, 156-163 (2023).
© The Author(s) 2024
- e-mail: shengbin@sjtu.edu.cn; huarting99@sjtu.edu.cn; wongtienyin@tsinghua.edu.cn; wpjia@sjtu.edu.cn
الطرق
الموافقة الأخلاقية
اكتساب البيانات
تم تسجيل 3,284 فردًا مصابًا بالسكري من المجموعة للدراسة الخارجية. دراسة BJHC (المجموعة الخارجية 8) هي دراسة مستقبلية قائمة على المجتمع. شملت هذه الدراسة إجمالي 835 مريضًا بالسكري من BJHC. أُجريت الفحوصات الأساسية في الفترة بين 2014 و2016، وأُجريت الفحوصات اللاحقة بين 2019 و2020. في جميع المجموعات الخارجية، تم التقاط صورتين لشبكية العين (مركزهما البقعة الصفراء والقرص البصري) لكل عين في زيارات الأساس والمتابعة.
معايير التشخيص
إجراء مراقبة جودة الصورة وتصنيفها
تطوير النموذج والتدريب
يشمل العمر، الجنس، حالة التدخين، مدة الإصابة بالسكري، مستوى اعتلال الشبكية القاعدي، مؤشر كتلة الجسم، الهيموغلوبين السكري HbA1c، ضغط الدم الانقباضي، ضغط الدم الانبساطي، ثلاثي الغليسريدات، كوليسترول البروتين الدهني منخفض الكثافة وكوليسترول البروتين الدهني عالي الكثافة. كما قمنا بتطوير ومقارنة نموذج البيانات الوصفية، نموذج قاع العين والنموذج المدمج لتوقع تقدم اعتلال الشبكية السكري في ثلاث مجموعات فرعية. شملت المجموعات الفرعية الثلاث السكري من غير اعتلال شبكي إلى اعتلال شبكي (المجموعة الفرعية 1)، من اعتلال شبكي غير قابل للإحالة إلى اعتلال شبكي قابل للإحالة (المجموعة الفرعية 2) ومن اعتلال شبكي غير تهديدي للبصر إلى اعتلال شبكي تهديدي للبصر (المجموعة الفرعية 3).
نموذج تقدم مرض السكري
التدريب المسبق للنموذج
نموذج القاع
من توزيعات ويبول باستخدام الميزات التي تم توليدها بواسطة نموذج ResNet-50 المدرب مسبقًا.
نموذج البيانات الوصفية والنموذج المدمج
تقييم النموذج
تفسير توقعات الذكاء الاصطناعي
ملخص التقرير
توفر البيانات
توفر الشفرة البرمجية
References
- Majithia, S. et al. Cohort profile: The Singapore Epidemiology of Eye Diseases study (SEED). Int. J. Epidemiol. 50, 41-52 (2021).
- Nguyen, H. V. et al. Cost-effectiveness of a National Telemedicine Diabetic Retinopathy Screening Program in Singapore. Ophthalmology 123, 2571-2580 (2016).
- WHO Consultation. Definition, diagnosis and classification of diabetes mellitus and its complications (1999).
- ElSayed, N. A. et al. 2. Classification and diagnosis of diabetes: Standards of Care in Diabetes-2023. Diabetes Care 46, S19-S40 (2023).
- Kaniadakis, G. et al. The
-statistics approach to epidemiology. Sci. Rep. 10, 19949 (2020). - He, K., Fan, H., Wu, Y., Xie, S. & Girshick, R. Momentum contrast for unsupervised visual representation learning. in Proceedings of the IEEE/CVF conference on computer vision and pattern recognition 9729-9738 (2020).
- Chen, X., Fan, H., Girshick, R. & He, K. Improved baselines with momentum contrastive learning. arXiv preprint arXiv:2003.04297 (2020).
- Vaswani, A. et al. Attention is all you need. in Advances in neural information processing systems 5998-6008 (2017).
- Zhao, H., Jia, J. & Koltun, V. Exploring self-attention for image recognition. in Proceedings of the IEEE/CVF conference on computer vision and pattern recognition 10076-10085 (2020).
- Lundberg, S. M. et al. Explainable machine-learning predictions for the prevention of hypoxaemia during surgery. Nat. Biomed. Eng. 2, 749-760 (2018).
- Lundberg, S. M. & Lee, S. -I. A unified approach to interpreting model predictions. in Advances in Neural Information Processing Systems 30 (2017).
الشكر والتقدير
مساهمات المؤلفين
قدم Y.C.T. و C. Y. Cheng تعليقات نقدية وراجعا المخطوطة. ناقش جميع المؤلفين النتائج ووافقوا على النسخة النهائية قبل التقديم.
المصالح المتنافسة
معلومات إضافية
https://doi.org/10.1038/s41591-023-02702-z.
معلومات إضافية النسخة الإلكترونية تحتوي على
المواد التكميلية متاحة على
https://doi.org/10.1038/s41591-023-02702-z.
يجب توجيه المراسلات وطلبات المواد إلى بين شينغ، هوايتينغ لي، تيين يين وونغ أو ويبينغ جيا.
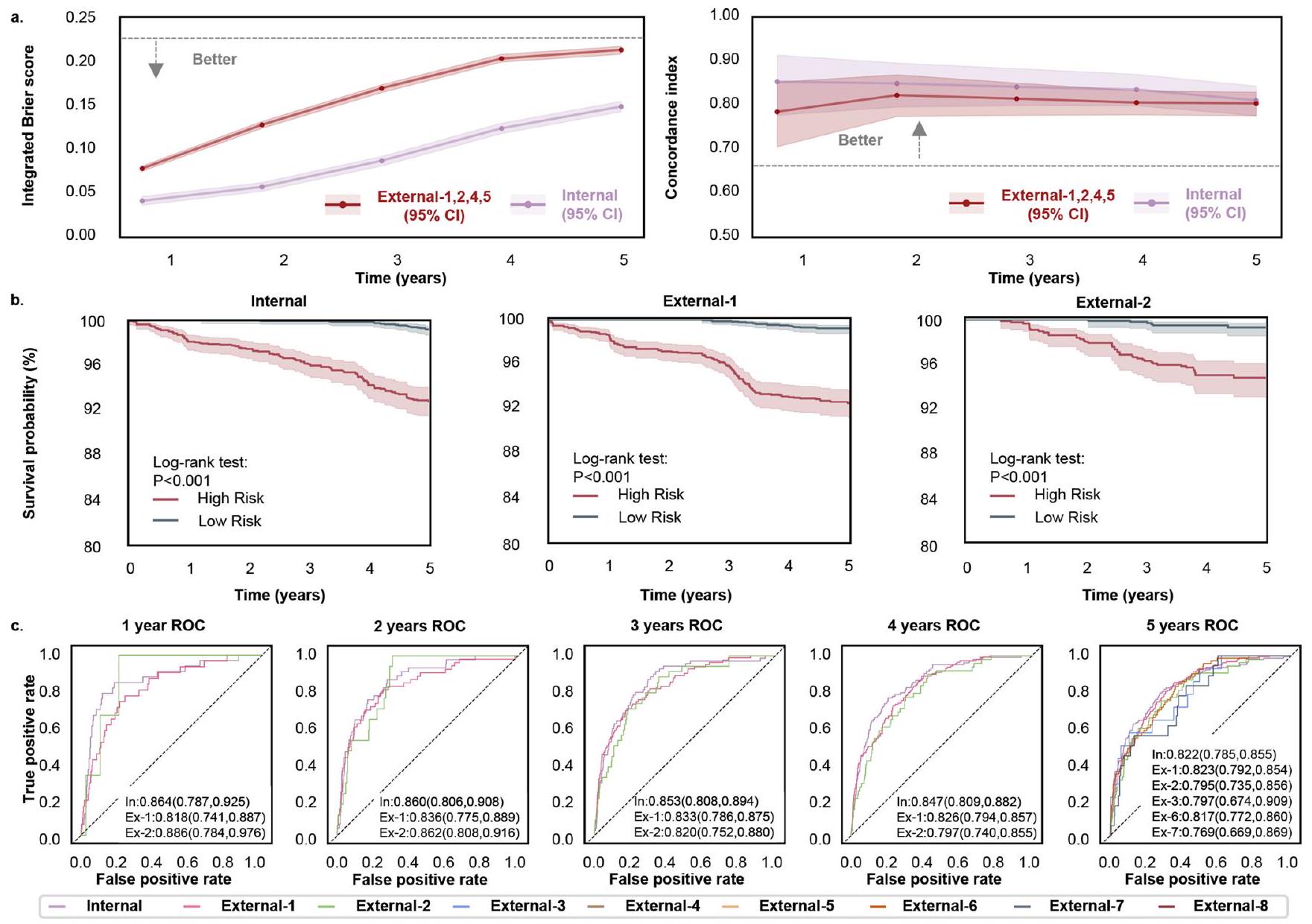
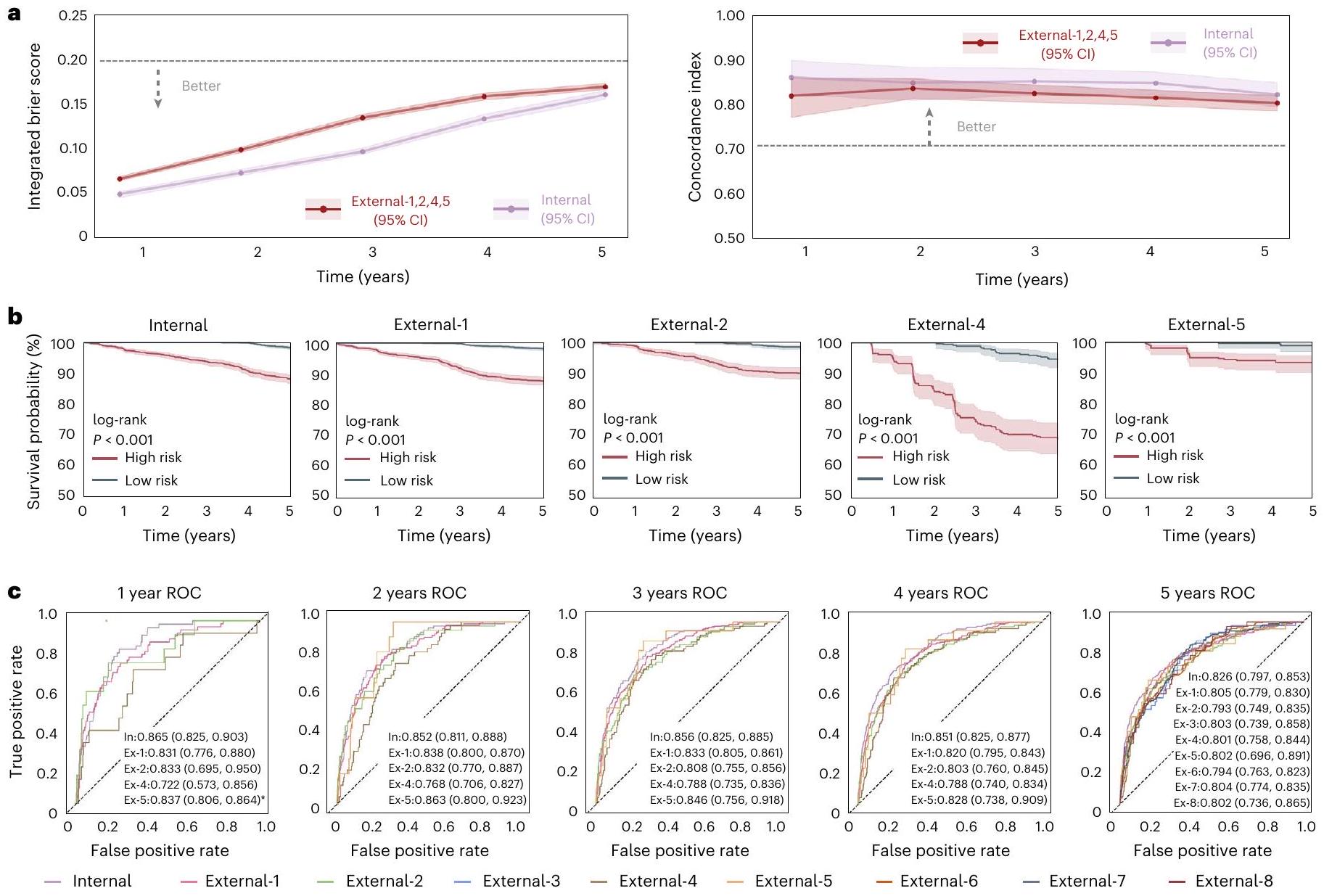
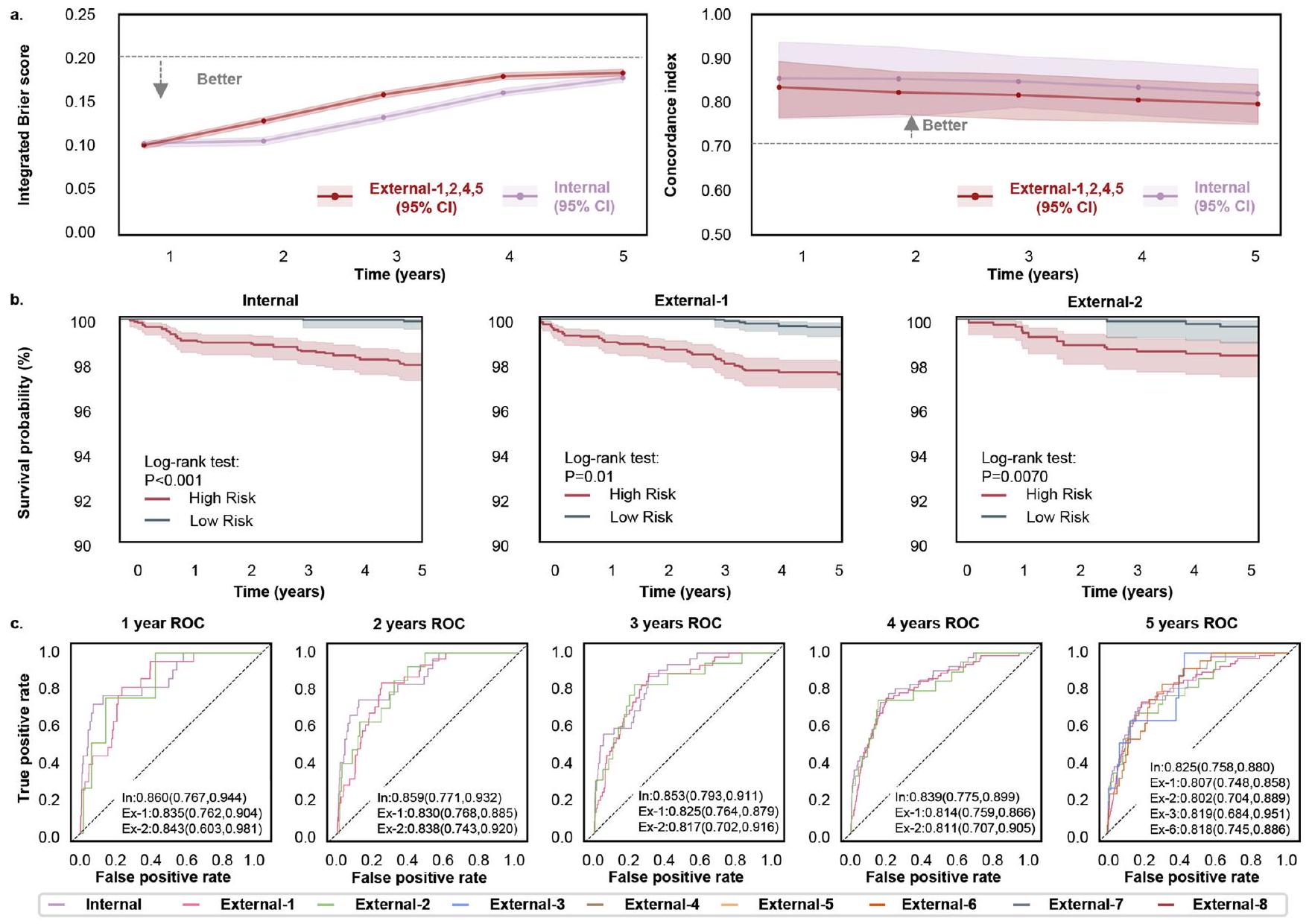
الاعتلال الشبكي القابل للإحالة د. أ، درجة بريير المتكاملة (يسار) تظهر الملاءمة العامة – كلما كانت أقل كان ذلك أفضل، ومؤشر C (يمين) يقيس تمييز مخاطر النموذج – كلما كان أعلى كان ذلك أفضل – لنقاط زمنية مختلفة. ب، مخططات كابلان-ماير لتوقع التقدم من الاعتلال الشبكي غير القابل للإحالة إلى الاعتلال الشبكي القابل للإحالة. تم استخدام اختبار لوغ-رانك أحادي الجانب لـ
المقارنة بين مجموعات المخاطر المنخفضة والعالية. قيم P في مجموعة الاختبار الداخلية ومجموعتي التحقق الخارجي 1 و 2 هي
مجموعات الخطر. الـ
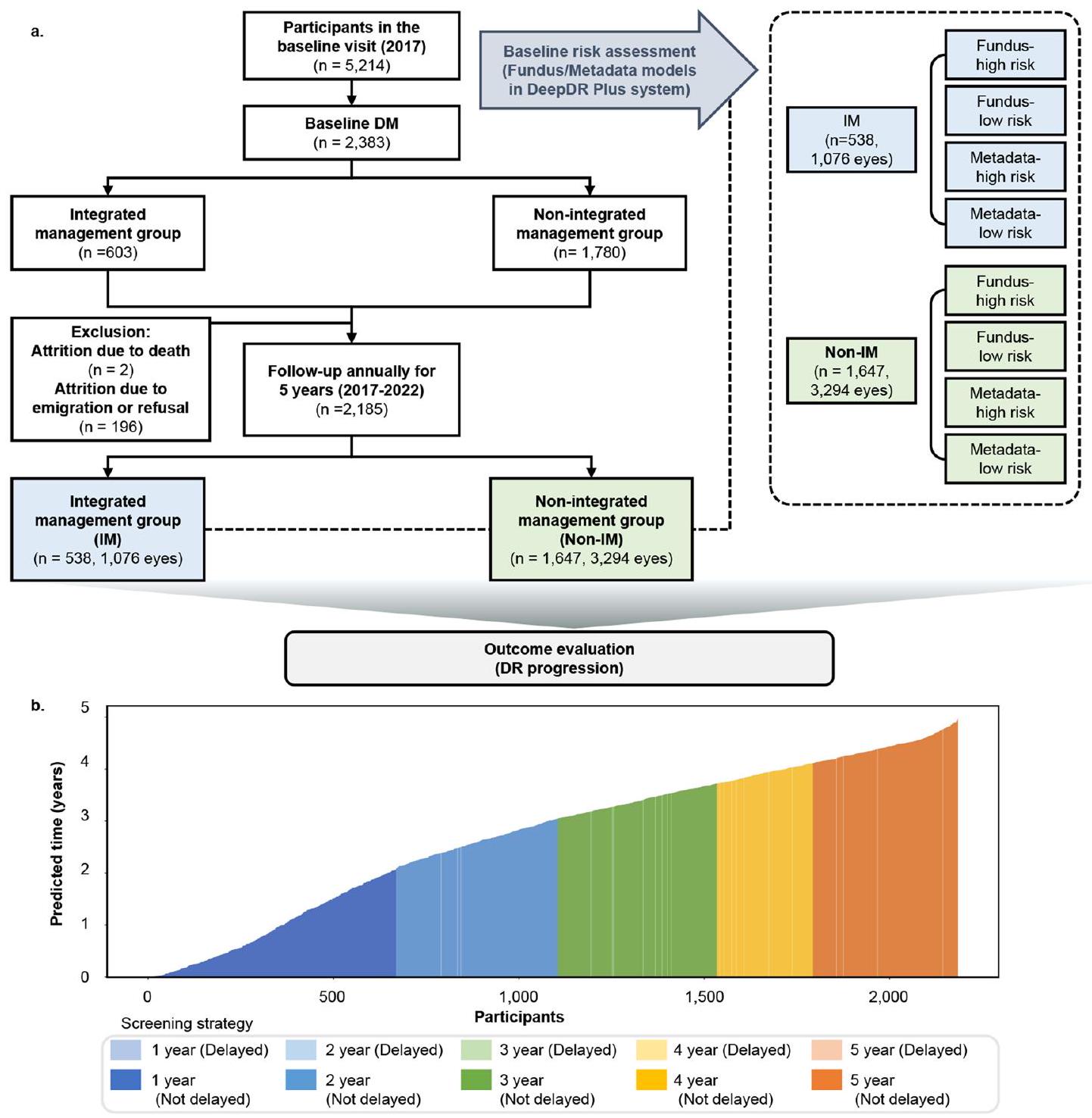
(DeepDR Plus). يعرض مخطط الشلال الوقت المتوقع لتقدم اعتلال الشبكية السكري لجميع المشاركين في الدراسة الواقعية بواسطة نموذج قاع العين. تم تحديد فترة الفحص الفردية عند نقطة زمنية سنوية من الخط الأساسي، والتي كانت فقط بعد عام من الوقت المتوقع لتقدم اعتلال الشبكية السكري الخاص بالمريض حسب نموذج قاع العين.
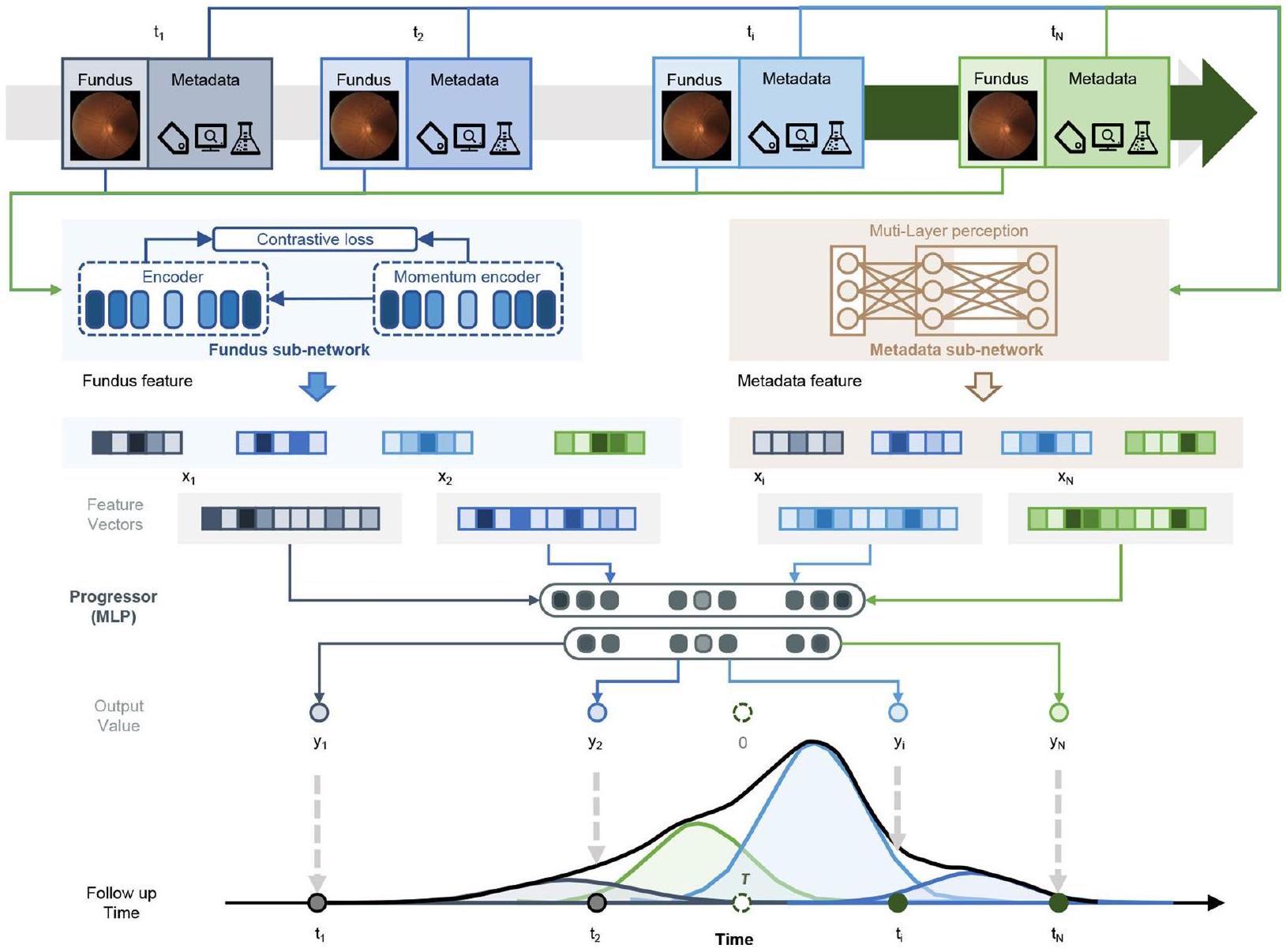
متجهات الميزات عالية المستوى، بينما يقدر المتنبئ وقت البقاء في مزيج بحجم ثابت من توزيعات ويبول بناءً على متجهات ميزات قاع العين لتوليد درجة قاع العين. تشترك نماذج البيانات الوصفية والنماذج المجمعة في نفس الهيكل لكنها تختلف في مدخلاتها مقارنة بنموذج قاع العين. يأخذ نموذج البيانات الوصفية البيانات الوصفية كمدخلات، بينما يأخذ النموذج المدمج كل من البيانات الوصفية ودرجة قاع العين كمدخلات.
| المجموعات | عدد المرضى المصابين بالسكري | عدد العيون | في البداية | عند بداية التدهور من الدرجة الأولى لاعتلال الشبكية السكري* | |||||||||
| غير مرتبط بالمرض | اعتلال الشبكية السكري غير التكاثري الخفيف | اعتلال الشبكية السكري غير التكاثري المعتدل | اعتلال الشبكية السكري غير التكاثري الشديد | الانحلال البقعي البؤري | غير مرتبط بالكلى | اعتلال الشبكية السكري غير التكاثري الخفيف | اعتلال الشبكية السكري غير التكاثري المعتدل | اعتلال الشبكية السكري غير التكاثري الشديد | الانحلال البقعي البريتوني | ||||
| مجموعة بيانات التطوير | مجموعة بيانات التدريب | ١٧٬١٩٠ | ٣٤٬٣٨٠ | ٣٠٬٥٥٤ | 1,074 | ١٬٥٩٧ | ٨٥٢ | ٣٠٣ | ٢٨٬٥٨٢ | ١٬٦٤٤ | ٢٬٠٩١ | ١٬٣٨٢ | ٦٨١ |
| مجموعة الاختبار الداخلية | ١٬٩١٠ | ٣٬٨٢٠ | ٣٬٥٥٢ | ٨٤ | ١٢٢ | ٣٨ | ٢٤ | ٣٬٣٢٢ | ١٧٤ | ٢١٦ | ٥٨ | ٥٠ | |
| إي سي إتش إم | ٢٬١٤١ | ٤٬٢٨٢ | ٣٬٩٠٨ | ١٢٨ | ١٦٠ | ٤٤ | ٤٢ | ٣٬٦٥٢ | ٢٢٨ | ٢٥٠ | ٨٢ | ٧٠ | |
| دبليو تي إتش إم | ٩٧١ | ١٬٩٤٢ | ١٬٨٣٠ | ٤٢ | ٥٢ | ١٤ | ٤ | ١٬٧٣٠ | ٩٠ | ٨٣ | ٢٥ | ١٤ | |
| NDSP | ١٬١٩٤ | ٢٬٣٨٨ | ٢٬٢٢٠ | ٨٨ | ٧٤ | ٢ | ٤ | ٢٬١٧٦ | ١١٨ | ٨٠ | ١٠ | ٤ | |
| مجموعات بيانات التحقق الخارجية | جامعة تشونغ كونغ الصينية – قسم الدراسات العليا | ٣٣٧ | ٥٩١ | ٢٩٧ | ١٠٢ | ١٧٩ | ١٣ | 0 | ١٨٣ | ٢١٦ | ١٧٩ | ١٣ | 0 |
| بودم | ٣٠٧ | ٦١٤ | ٥٥٢ | ١٦ | ٣٠ | ١٦ | 0 | ٥٤١ | ١٩ | ٣٤ | ١٢ | ٨ | |
| بذرة | ١٬٦٩٩ | ٣٬٣٩٨ | ٢٬٩١٨ | ٣١٠ | ١٢٣ | ٧ | ٤٠ | ٢٬٨٤٩ | ٣٣٤ | ١٤٨ | ٩ | ٥٨ | |
| SiDRP | ٣٬٢٨٤ | ٦,٥٦٨ | ٦٬٣٤٣ | ١٣٨ | ٦٦ | ١٣ | ٨ | ٦,١٧٧ | ٢٨٦ | ٨٣ | ١٤ | ٨ | |
| بي جي إتش سي | ٨٣٥ | ١٬٦٧٠ | ١٬٦٦٦ | ٤ | 0 | 0 | 0 | ١٬٦٢٩ | ٢٤ | ١٧ | 0 | 0 | |
| الفوج | نموذج | أي تقدم في مرض السكري | المجموعة الفرعية 1 | الفئة الفرعية 2 | الفئة الفرعية 3 | ||||
| مؤشر C
|
متلازمة القولون العصبي
|
مؤشر C (فاصل الثقة 95%) | متلازمة القولون العصبي (فاصل الثقة 95%) | مؤشر C (فاصل الثقة 95%) | متلازمة القولون العصبي (فاصل الثقة 95%) | مؤشر C (فاصل الثقة 95%) | متلازمة القولون العصبي (فاصل الثقة 95%) | ||
| مجموعة البيانات الداخلية | البيانات الوصفية | 0.696 (0.668، 0.725) | 0.340 (0.334، 0.347) | 0.705 (0.672، 0.736) | 0.303 (0.297، 0.310) | 0.700 (0.658، 0.741) | 0.261 (0.255، 0.268) | 0.711 (0.637، 0.778) | 0.328 (0.322، 0.335) |
| قاع العين | 0.823 (0.796، 0.850) | 0.161 (0.156، 0.166) | 0.826 (0.797، 0.851) | 0.189 (0.184، 0.194) | 0.820 (0.785، 0.853) | 0.153 (0.147، 0.159) | 0.824 (0.758، 0.880) | 0.180 (0.175، 0.185) | |
| مُدمج | 0.833 (0.807، 0.857) | 0.152 (0.147، 0.157) | 0.835 (0.810، 0.859) | 0.167 (0.162، 0.172) | 0.838 (0.806، 0.869) | 0.145 (0.141، 0.150) | 0.852 (0.787، 0.909) | 0.164 (0.160، 0.169) | |
| البيانات الوصفية | 0.652 (0.623، 0.680) | 0.301 (0.295، 0.308) | 0.664 (0.634، 0.694) | 0.381 (0.375، 0.387) | 0.679 (0.639، 0.720) | 0.279 (0.273، 0.284) | 0.734 (0.677، 0.791) | 0.270 (0.265، 0.276) | |
| إي سي إتش إم | قاع العين | 0.802 (0.778، 0.827) | 0.158 (0.153، 0.162) | 0.820 (0.793، 0.846) | 0.157 (0.152، 0.162) | 0.821 (0.792، 0.852) | 0.207 (0.202، 0.213) | 0.806 (0.748، 0.857) | 0.188 (0.184، 0.193) |
| مُدمج | 0.811 (0.787، 0.834) | 0.223 (0.218، 0.228) | 0.824 (0.797، 0.848) | 0.212 (0.206، 0.217) | 0.826 (0.794، 0.858) | 0.124 (0.120، 0.128) | 0.830 (0.782، 0.871) | 0.203 (0.199، 0.209) | |
| البيانات الوصفية | 0.652 (0.607، 0.695) | 0.381 (0.373، 0.390) | 0.672 (0.617، 0.726) | 0.286 (0.277، 0.293) | 0.688 (0.613، 0.758) | 0.341 (0.328، 0.354) | 0.671 (0.572، 0.769) | 0.373 (0.364، 0.383) | |
| WTHM” تعني “ما هذا بحق الجحيم؟ | قاع العين | 0.791 (0.748، 0.832) | 0.164 (0.157، 0.170) | 0.814 (0.773، 0.854) | 0.188 (0.181، 0.195) | 0.794 (0.735، 0.854) | 0.240 (0.232، 0.248) | 0.802 (0.705، 0.888) | 0.181 (0.173، 0.190) |
| مُدمج | 0.806 (0.762، 0.844) | 0.154 (0.147، 0.161) | 0.809 (0.764، 0.853) | 0.224 (0.216، 0.232) | 0.801 (0.739، 0.857) | 0.198 (0.188، 0.208) | 0.819 (0.720، 0.907) | 0.141 (0.134، 0.148) | |
| البيانات الوصفية | 0.698 (0.625، 0.768) | 0.339 (0.330، 0.347) | 0.710 (0.629، 0.790) | 0.323 (0.314، 0.332) | 0.748 (0.611، 0.862) | 0.288 (0.280، 0.295) | 0.732 (0.551، 0.897) | 0.241 (0.234، 0.248) | |
| NDSP | قاع العين | 0.800 (0.737، 0.855) | 0.197 (0.190، 0.204) | 0.846 (0.798، 0.886) | 0.191 (0.185، 0.197) | 0.796 (0.674، 0.909) | 0.220 (0.213، 0.227) | 0.818 (0.684، 0.951) | 0.207 (0.200، 0.214) |
| مُدمج | 0.814 (0.752، 0.866) | 0.171 (0.166، 0.178) | 0.852 (0.789، 0.904) | 0.177 (0.171، 0.184) | 0.802 (0.690، 0.904) | 0.198 (0.191، 0.204) | 0.822 (0.653، 0.956) | 0.139 (0.133، 0.145) | |
| CUHKSTDR | البيانات الوصفية | 0.650 (0.602، 0.699) | 0.305 (0.285، 0.326) | 0.621 (0.574، 0.669) | 0.402 (0.366، 0.439) | — | — | — | — |
| قاع العين | 0.789 (0.752، 0.826) | 0.241 (0.227، 0.256) | 0.754 (0.711، 0.793) | 0.197 (0.177، 0.218) | — | — | — | — | |
| مُدمج | 0.793 (0.755، 0.827) | 0.213 (0.200، 0.228) | 0.759 (0.715، 0.800) | 0.207 (0.188، 0.226) | — | — | — | — | |
| البيانات الوصفية | 0.680 (0.568، 0.785) | 0.372 (0.355، 0.389) | 0.668 (0.474، 0.826) | 0.299 (0.284، 0.313) | — | — | — | — | |
| بودم | قاع العين | 0.800 (0.697، 0.887) | 0.211 (0.192، 0.231) | 0.802 (0.672، 0.921) | 0.230 (0.213، 0.248) | — | — | — | — |
| مُدمج | 0.808 (0.708، 0.895) | 0.240 (0.217، 0.263) | 0.802 (0.661، 0.920) | 0.262 (0.247، 0.277) | — | — | — | — | |
| البيانات الوصفية | 0.707 (0.672، 0.742) | 0.277 (0.270، 0.283) | 0.743 (0.702، 0.782) | 0.209 (0.202، 0.215) | 0.708 (0.646، 0.762) | 0.259 (0.253، 0.266) | 0.716 (0.612، 0.814) | 0.298 (0.291، 0.305) | |
| بذرة | قاع العين | 0.786 (0.756، 0.814) | 0.200 (0.195، 0.206) | 0.800 (0.766، 0.833) | 0.210 (0.204، 0.216) | 0.813 (0.769، 0.855) | 0.173 (0.167، 0.178) | 0.817 (0.745، 0.885) | 0.223 (0.217، 0.228) |
| مُدمج | 0.792 (0.760، 0.821) | 0.198 (0.192، 0.203) | 0.804 (0.770، 0.836) | 0.187 (0.181، 0.192) | 0.816 (0.768، 0.861) | 0.208 (0.202، 0.214) | 0.819 (0.737، 0.885) | 0.132 (0.128، 0.138) | |
| البيانات الوصفية | 0.613 (0.572، 0.656) | 0.370 (0.364، 0.376) | 0.585 (0.541، 0.627) | 0.383 (0.376، 0.389) | 0.523 (0.404، 0.642) | 0.473 (0.466، 0.480) | — | — | |
| SiDRP | قاع العين | 0.800 (0.771، 0.831) | 0.172 (0.168، 0.176) | 0.801 (0.769، 0.833) | 0.164 (0.160، 0.168) | 0.769 (0.668، 0.868) | 0.209 (0.205، 0.213) | — | — |
| مُدمج | 0.804 (0.772، 0.834) | 0.219 (0.215، 0.223) | 0.806 (0.774، 0.837) | 0.204 (0.200، 0.208) | 0.783 (0.686، 0.874) | 0.237 (0.233، 0.241) | — | — | |
| البيانات الوصفية | 0.704 (0.607، 0.792) | 0.306 (0.296، 0.316) | 0.712 (0.637، 0.779) | 0.258 (0.249، 0.266) | — | — | — | — | |
| بي جي إتش سي | قاع العين | 0.802 (0.736، 0.865) | 0.197 (0.189، 0.205) | 0.797 (0.709، 0.874) | 0.220 (0.212، 0.228) | — | — | — | — |
| مُدمج | 0.811 (0.753، 0.865) | 0.203 (0.195، 0.211) | 0.803 (0.720، 0.879) | 0.198 (0.190، 0.205) | — | — | — | — | |
نيتشر بورتفوليو
المؤلف المراسل: ويبينغ جيا
ملخص التقرير
الإحصائيات
تم التأكيد
يجب وصف الاختبارات الشائعة فقط بالاسم؛ وصف التقنيات الأكثر تعقيدًا في قسم الطرق.
للتحليل البايزي، معلومات حول اختيار التوزيعات الأولية وإعدادات سلسلة ماركوف مونت كارلو
مجموعتنا على الويب حول الإحصاءات لعلماء الأحياء تحتوي على مقالات حول العديد من النقاط المذكورة أعلاه.
البرمجيات والرموز البرمجية
جمع البيانات
لم يتم استخدام أي برنامج خاص لجمع البيانات.
تحليل البيانات
تم استخدام إصدار بايثون 3.9.0 (مؤسسة برمجيات بايثون، ديلاوير، الولايات المتحدة) لجميع التحليلات الإحصائية في هذه الدراسة. تم استخدام حزم بايثون الخارجية التالية: تم استخدام إصدار Pytorch 2.0.1 (فيسبوك، ماساتشوستس، الولايات المتحدة) للحوسبة باستخدام الشبكات العصبية الالتفافية. تم استخدام إصدار Scikit-learn 1.3.0 (ديفيد كورنوبيو، كاليفورنيا، الولايات المتحدة) لحساب مساحة تحت المنحنى (AUC). تم استخدام إصدار NumPy 1.25.2 (ترافيس أوليفانت، تكساس، الولايات المتحدة) لحساب مؤشر C، ودرجة بريير. تم استخدام إصدار Lifelines 0.27.7 (كاميرون ديفيدسون-بيلون، كندا) لتحليل البقاء. تم استخدام برنامج تقييم الأوعية الدموية في سنغافورة الإصدار 4.0 (الجامعة الوطنية في سنغافورة، سنغافورة) لقياس متغيرات الأوعية الدموية في الشبكية. الكود المستخدم في الدراسة الحالية لتطوير الخوارزمية متوفر على https://github.com/drpredict/DeepDR_Plus.
معلومات السياسة حول توفر البيانات
- رموز الوصول، المعرفات الفريدة، أو روابط الويب لمجموعات البيانات المتاحة للجمهور
- وصف لأي قيود على توفر البيانات
- بالنسبة لمجموعات البيانات السريرية أو بيانات الطرف الثالث، يرجى التأكد من أن البيان يتوافق مع سياستنا
المشاركون في البحوث البشرية
التقارير عن الجنس والنوع الاجتماعي
خصائص السكان
التوظيف
الإشراف على الأخلاقيات
يرجى ملاحظة أنه يجب أيضًا تقديم معلومات كاملة عن الموافقة على بروتوكول الدراسة في المخطوطة.
التقارير المتخصصة في المجال
علوم الحياة
العلوم السلوكية والاجتماعية
العلوم البيئية والتطورية والبيئية
للحصول على نسخة مرجعية من الوثيقة مع جميع الأقسام، انظر nature.com/documents/nr-reporting-summary-flat.pdf
تصميم دراسة علوم الحياة
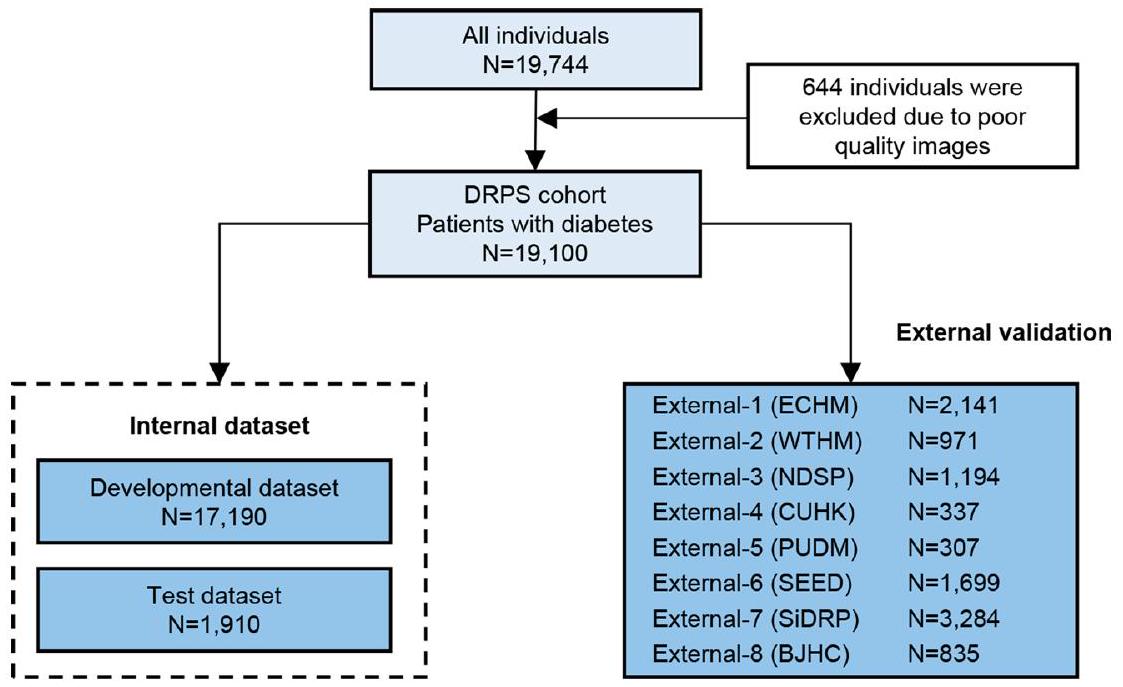
| حجم العينة | قمنا بتطوير نظام DeepDR Plus لتوقع تطور اعتلال الشبكية السكري باستخدام ما مجموعه 76,400 صورة لقاع العين من 19,100 مريض سكري، وقمنا بالتحقق من صحة النظام باستخدام 42,558 صورة لقاع العين من 10,768 مريض سكري. تم تحديد حجم العينة بناءً على توفر البيانات. |
| استثناءات البيانات | تم استبعاد صور الشبكية ذات الجودة الرديئة. |
| التكرار | لم تكن التكرار ذات صلة. استخدمنا ثماني مجموعات تحقق مستقلة لاختبار النماذج، وحققت النماذج أداءً مماثلاً في مجموعات التحقق الخارجية. |
| العشوائية | تم تخصيص العينات عشوائيًا لمجموعات بيانات التطوير والتحقق. |
| مُعمٍ | أثناء معالجة البيانات، تم أولاً إزالة الهوية من جميع البيانات لإزالة أي معلومات متعلقة بالمريض. |
التقارير الخاصة بالمواد والأنظمة والأساليب المحددة
| المواد والأنظمة التجريبية | الطرق | ||
| غير متوفر | مشارك في الدراسة | غير متوفر | مشارك في الدراسة |
| X |  |
|
|
|
|
|
تدفق الخلايا |
|
علم الحفريات والآثار | |
التصوير العصبي القائم على الرنين المغناطيسي |
|
|||
|
|||
|
|
||
البيانات السريرية
يجب أن تتوافق جميع المخطوطات مع إرشادات ICMJE لنشر البحوث السريرية ويجب إرفاق قائمة التحقق المكتملة من CONSORT مع جميع المراسلات.
بروتوكول الدراسة
جمع البيانات
يمكن العثور على بروتوكولات الدراسة فيhttp://www.chictr.org.cn/.
المختبر الدولي المشترك لطريق الحزام في شنغهاي للوقاية الذكية وعلاج اضطرابات الأيض، قسم علوم وهندسة الحاسوب، كلية الهندسة الإلكترونية والمعلومات والكهربائية، جامعة شنغهاي جياو تونغ، قسم الغدد الصماء والأيض، المستشفى السادس الشعبي في شنغهاي التابع لكلية الطب بجامعة شنغهاي جياو تونغ، معهد السكري في شنغهاي، المركز السريري لمرض السكري في شنغهاي، الصين. المختبر الرئيسي لوزارة التعليم للذكاء الاصطناعي، كلية الهندسة الإلكترونية والمعلومات والكهربائية، جامعة شنغهاي جياو تونغ، شنغهاي، الصين. قسم طب العيون، مصحة هوانغدونغ، ووكسي، الصين. قسم طب العيون، المستشفى الشعبي السادس التابع لكلية الطب بجامعة شنغهاي جياو تونغ، شنغهاي، الصين. قسم طب العيون وعلوم البصر، الجامعة الصينية في هونغ كونغ، هونغ كونغ، الصين. معهد أبحاث العين في سنغافورة، المركز الوطني للعين في سنغافورة، سنغافورة، سنغافورة. قسم علوم وهندسة الحاسوب، جامعة هونغ كونغ للعلوم والتكنولوجيا، هونغ كونغ، الصين. قسم الهندسة الكيميائية والبيولوجية، جامعة هونغ كونغ للعلوم والتكنولوجيا، هونغ كونغ، الصين. المختبر الرئيسي للدولة لطب العيون، مركز تشونغشان لطب العيون، جامعة صن يات سين، المختبر الرئيسي الإقليمي لطب العيون وعلوم البصر بمقاطعة قوانغدونغ، قوانغتشو، الصين. قسم طب العيون، مستشفى كلية بكين الطبية المتحدة، كلية بكين الطبية المتحدة، الأكاديمية الصينية للعلوم الطبية، بكين، الصين. مكتب السجلات الطبية والإحصاءات، المستشفى الشعبي السادس في شنغهاي التابع لكلية الطب بجامعة جياو تونغ في شنغهاي، الصين. قسم طب الشيخوخة، مستشفى تونغجي، كلية تونغجي الطبية، جامعة هواجونغ للعلوم والتكنولوجيا، ووهان، الصين. المركز الوطني لأبحاث الهندسة لتقنية ونظام البيانات الضخمة، مختبر تقنية ونظام حوسبة الخدمات، مختبر الحوسبة العنقودية وشبكات الحوسبة، كلية علوم الحاسوب والتكنولوجيا، جامعة هواجونغ للعلوم والتكنولوجيا، ووهان، الصين. خدمات شبكية العين لشري بهاجوان مهافير، مؤسسة البحوث الطبية، سانكارا نيثرالايا، تشيناي، الهند. قسم طب العيون، مستشفى شنغهاي العام، كلية الطب بجامعة شنغهاي جياو تونغ، شنغهاي، الصين. معهد بكين لطب العيون، مركز بكين تونغرن للعيون، مستشفى بكين تونغرن -الفهرس يشير إلى مؤشر التوافق. يشير IBS إلى درجة بريير المتكاملة.
DOI: https://doi.org/10.1038/s41591-023-02702-z
PMID: https://pubmed.ncbi.nlm.nih.gov/38177850
Publication Date: 2024-01-04
A deep learning system for predicting time to progression of diabetic retinopathy
Accepted: 10 November 2023
Published online: 4 January 2024
(D) Check for updates
Abstract
Ling Dai
Abstract
Diabetic retinopathy (DR) is the leading cause of preventable blindness worldwide. The risk of DR progression is highly variable among different individuals, making it difficult to predict risk and personalize screening intervals. We developed and validated a deep learning system (DeepDR Plus) to predict time to DR progression within 5 years solely from fundus images. First, we used 717,308 fundus images from 179,327 participants with diabetes to pretrain the system. Subsequently, we trained and validated the system with a multiethnic dataset comprising 118,868 images from 29,868 participants with diabetes. For predicting time to DR progression, the system achieved concordance indexes of 0.754-0.846 and integrated Brier scores of 0.153-0.241 for all times up to 5 years. Furthermore, we validated the system in real-world cohorts of participants with diabetes. The integration with clinical workflow could potentially extend the mean screening interval from 12 months to 31.97 months, and the percentage of participants recommended to be screened at 1-5 years was 30.62%, 20.00%,19.63%,11.85% and 17.89%, respectively, while delayed detection of progression to vision-threatening DR was 0.18%. Altogether, the DeepDR Plus system could predict individualized risk and time to DR progression over 5 years, potentially allowing personalized screening intervals.
routine screening for DR at yearly intervals is widely recommended for all individuals with diabetes with no DR or mild DR by national and international organizations
Results
Study design and participants
DeepDR Plus predicts time to DR progression
observed in the model performance for predicting DR progression among patients with different glycemic control statuses, regardless of the addition of follow-up hemoglobin A1c (HbA1c) levels.
DeepDR Plus predicts time to progression in three subgroups
| Cohorts | Pretrained dataset | Developmental dataset | Internal test set | ECHM External-1 | WTHM External-2 | NDSP External-3 | CUHK-STDR External-4 | PUDM External-5 | SEED External-6 | SiDRP External-7 | BJHC External-8 |
| Number of images | 717,308 | 68,760 | 7,640 | 8,564 | 3,884 | 4,776 | 1,182 | 1,228 | 6,676 | 12,818 | 3,340 |
| Number of participants | 179,327 | 17,190 | 1,910 | 2,141 | 971 | 1,194 | 337 | 307 | 1,699 | 3,284 | 835 |
| Race | |||||||||||
| Chinese,
|
179,327 (100%) | 17,190 (100%) | 1,910 (100%) | 2,141 (100%) | 971 (100%) | 1,194 (100%) | 337 (100%) | 307 (100%) | 411 (24.19%) | 2,494 (75.94%) | 835 (100%) |
| Malay,
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
532 (31.31%) | 518 (15.77%) | NA
|
| Indian,
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
756 (44.50%) | 272 (8.28%) | NA
|
| Gender | |||||||||||
| Female,
|
96,676 (53.91%) | 2,692 (15.66%) | 337 (17.62%) | 826 (38.58%) | 313 (32.23%) | 739 (61.89%) | 169 (50.15%) | 131 (42.67%) | 852 (50.15%) | 1,661 (50.58%) | 400 (47.90%) |
| Male,
|
82,651 (46.09%) | 14,498 (84.34%) | 1,573 (82.38%) | 1,315 (61.42%) | 658 (67.77%) | 455 (38.11%) | 168 (49.85%) | 176 (57.33%) | 847 (49.85%) | 1,623 (49.42%) | 435 (52.10%) |
| Age (years) |
|
|
|
|
|
|
|
|
|
|
|
| Smoker,
|
19,249 (10.73%) | 4,255 (24.75%) | 470 (24.60%) | 277 (12.94%) | 215 (22.14%) | 207 (17.34%) | 83 (24.63%) | 122 (39.74%) | 484 (28.49%) | 63 (1.9%) | NA
|
| Body mass index (
|
|
|
|
|
|
|
|
|
|
|
|
| Systolic blood pressure (mm Hg) |
|
|
|
|
|
|
|
|
|
|
|
| HbA1c (%) |
|
|
|
|
|
|
|
|
|
|
NA
|
| Fasting plasma glucose (
|
|
|
|
|
|
|
|
|
NA
|
|
|
| Random blood glucose (
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
NA
|
|
NA
|
NA
|
| Triglycerides (mmol
|
|
|
|
|
|
|
|
|
|
|
|
| Low-density lipoprotein cholesterol (
|
|
|
|
|
|
|
|
|
|
|
|
| High-density lipoprotein cholesterol (
|
|
|
|
|
|
|
|
|
|
|
|
| Duration of diabetes mellitus (years) | NA
|
|
|
|
|
|
|
|
|
|
NA
|
| Eyes with DR progression,
|
NA
|
2,819 (8.20%) | 278 (7.28%) | 321 (7.50%) | 121 (6.23%) | 48 (2.01%) | 114 (16.91%) | 25 (4.07%) | 184 (5.41%) | 171 (2.60%) | 38 (2.28%) |
0.797-0.851) for DR, 0.820 (95% CI, 0.785-0.853) for referable DR, and 0.824 (95% CI, 0.758-0.880) for VTDR, while IBS decreased to 0.153-0.189 for three subgroups. When the fundus images were combined with clinical metadata, the combined model gave C -indexes of 0.835-0.852 and IBS of 0.145-0.167 for subgroups 1-3 (Extended Data Table 2). Furthermore, we evaluated the prediction performance of the fundus model in the external datasets and achieved comparable results with the internal dataset (Extended Data Table 2). The results indicated that the fundus images alone could effectively predict the disease progression. Similarly to the task of predicting the time to any DR progression, we evaluated the prediction performance in three subgroups. As shown in Extended Data Figs. 3-5, the fundus model achieved C-indexes of 0.820-0.895 and IBSs of 0.045-0.189 in the internal dataset for years 1-5. Moreover, the external validation datasets1, 2, 4 and 5 achieved C-indexes of 0.794-0.842 and IBSs of 0.058-0.218.
and external datasets (
To evaluate the effectiveness of the DeepDR Plus system with the integration of clinical workflows, we conducted a real-world study within a community-based prospective cohort study of Chinese adults (Methods). A total of 2,185 participants were included in the analysis, with 538 participants in the integrated management (IM) group (integrated hospital-community diabetes management program) and 1,647 participants in the non-IM group. Participants in the IM group were provided regular clinical and metabolic measurements, advised by specialists in comprehensive hospitals and received lifestyle guidance and peer support at community health service centers
| Eyes with DR progression incidence per 1,000 eye-years (number of cases/number of eyes) | ARR
|
|||
| IM group (
|
DeepDR Plus-low risk (AI-low) | Metadata-low risk (meta-low) | -33.05 (-67.79, 35.76) | |
| 5.11 (16/626) | 7.63 (24/629) | |||
| DeepDR Plus-high risk (AI-high) | Metadata-high risk (meta-high) | 14.54 (-28.26, 74.63) | ||
| 26.67 (60/450) | 23.27 (52/447) | |||
| Integrated hospital-community diabetes management program | Non-IM (
|
DeepDR Plus-low risk (AI-low) | Metadata-low risk (meta-low) | -91.63 (-93.91, -89.06) |
| 5.01 (50/1,996) | 11.34 (113/1,993) | |||
| DeepDR Plus-high risk (AI-high) | Metadata-high risk (meta-high) | 61.36 (25.36, 109.91) | ||
| 33.13 (215/1,298) | 23.37 (152/1,301) | |||
| Comprehensive interventions: [(AI-high+AI-low)-(meta-high+meta-low)] in IM group-[(Al-high+Al-low)-(meta-high+meta-low)] in non-IM group | 46.80 (12.37, 94.93) | |||
| Sankara Nethralaya-Diabetic Retinopathy Epidemiology and Molecular Genetics Study
|
IM group (
|
DeepDR Plus-low risk (AI-low) | Metadata-low risk (meta-low) | -9.39 (-79.77, 287.41) |
| 4.08 (2/98) | 4.49 (2/89) | |||
| DeepDR Plus-high risk (Al-high) | Metadata-high risk (meta-high) | 20.48 (-70.93, 400.0) | ||
| 25.0 (6/48) | 21.05 (6/57) | |||
| Non-IM group (
|
DeepDR Plus-low risk (AI-low) | Metadata-low risk (meta-low) | -97.32 (-98.28, -96.32) | |
| 5.24 (28/1,068) | 13.0 (70/1,077) | |||
| DeepDR Plus-high risk (Al-high) | Metadata-high risk (meta-high) | 43.13 (9.1, 87.18) | ||
| 44.11 (161/730) | 33.01 (119/721) | |||
| Comprehensive interventions: [(AI-high+AI-low)-(meta-high+meta-low)] in IM group-[(AI-high+AI-low)-(meta-high+meta-low)] in non-IM group | 88.74 (10.83, 330.25) | |||
| Group | Model | Average screening interval (months) | Reduction in screening frequency (%)
|
Delayed detection of any DR progression (%)
|
Delayed detection of progression to VTDR (%) |
| IM | Metadata | 34.06 | 64.77 | 1.86 | 0.93 |
| Fundus | 31.54 | 61.95 | 0.37 | 0.37 | |
| Non-IM | Metadata | 35.32 | 66.02 | 6.01 | 0.97 |
| Fundus | 32.11 | 62.63 | 1.28 | 0.12 | |
| IM and non-IM | Metadata | 35.01 | 65.72 | 4.99 | 0.96 |
| Fundus | 31.97 | 62.46 | 1.05 | 0.18 |
prevent
groups followed the recommended personalized screening interval given by the fundus model. Compared with the metadata model, the fundus model can achieve a similar reduction in screening frequency (
a lower rate of delayed detection of any DR progression in patients of the IM group compared with the non-IM group (
interventions. Extended Data Fig. 6b shows the waterfall plot of predicted time to DR progression of participants in the real-world study by the fundus model. If all participants in both IM and non-IM groups followed the recommended personalized screening interval given by the fundus model, the percentage of participants who were recommended to screen DR at 1-5 years was 30.62%, 20.00%, 19.63%, 11.85% and
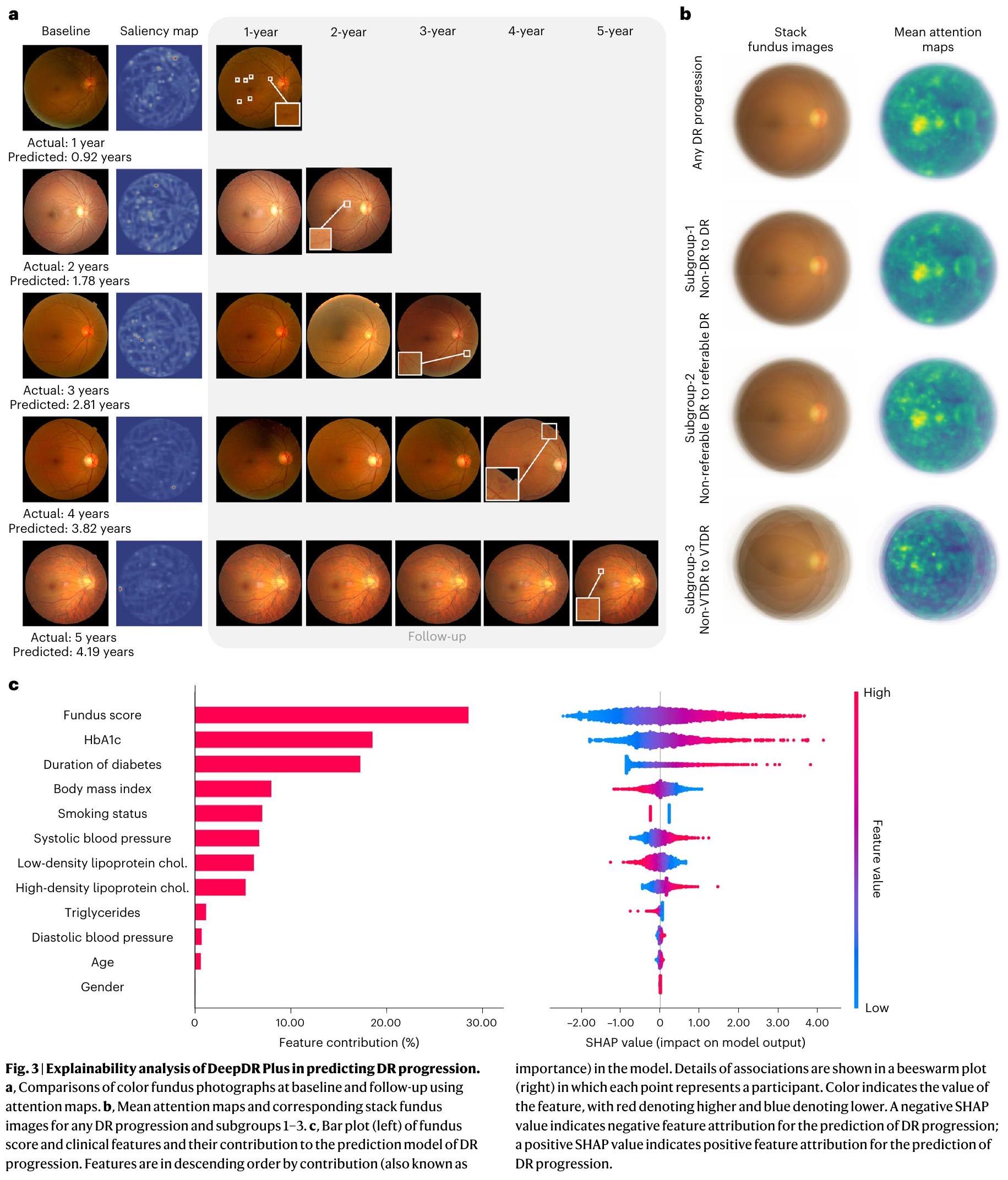
Explainability analysis
Discussion
only 0.18%. These results demonstrated that our DeepDR Plus system could potentially promote patient-specific risk assessment and further personalized care for DR management, based on just one single-time retinal check in the future.
prospects for future guideline modifications pertaining to the use of AI in DR management.
Online content
References
- Cheung, N., Mitchell, P. & Wong, T. Y. Diabetic retinopathy. Lancet 376, 124-136 (2010).
- Tan, T. -E. & Wong, T. Y. Diabetic retinopathy: looking forward to 2030. Front Endocrinol. 13, 1077669 (2022).
- Wong, T. Y., Cheung, C. M. G., Larsen, M., Sharma, S. & Simó, R. Diabetic retinopathy. Nat. Rev. Dis. Prim. 2, 16012 (2016).
- Jenkins, A. J. et al. Biomarkers in diabetic retinopathy. Rev. Diabet. Stud. 12, 159-195 (2015).
- Stratton, I. M. et al. UKPDS 50: risk factors for incidence and progression of retinopathy in type II diabetes over 6 years from diagnosis. Diabetologia 44, 156-163 (2001).
- Solomon, S. D. et al. Diabetic Retinopathy: a position statement by the American Diabetes Association. Diabetes Care 40, 412-418 (2017).
- Wong, T. Y. et al. Guidelines on diabetic eye care: the international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology 125, 1608-1622 (2018).
- Flaxel, C. J. et al. Diabetic retinopathy preferred practice pattern. Ophthalmology 127, P66-P145 (2020).
- Wang, L. Z. et al. Availability and variability in guidelines on diabetic retinopathy screening in Asian countries. Br. J. Ophthalmol. 101, 1352-1360 (2017).
- Modjtahedi, B. S. et al. Two-year incidence of retinal intervention in patients with minimal or no diabetic retinopathy on telemedicine screening. JAMA Ophthalmol. 137, 445-448 (2019).
- Gunasekeran, D. V., Ting, D. S. W., Tan, G. S. W. & Wong, T. Y. Artificial intelligence for diabetic retinopathy screening, prediction and management. Curr. Opin. Ophthalmol. 31, 357-365 (2020).
- Fundus photographic risk factors for progression of diabetic retinopathy. ETDRS report number 12. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology 98, 823-833 (1991).
- Lund, S. H. et al. Individualised risk assessment for diabetic retinopathy and optimisation of screening intervals: a scientific approach to reducing healthcare costs. Br. J. Ophthalmol. 100, 683-687 (2016).
- Broadbent, D. M. et al. Safety and cost-effectiveness of individualised screening for diabetic retinopathy: the ISDR open-label, equivalence RCT. Diabetologia 64, 56-69 (2021).
- Bora, A. et al. Predicting the risk of developing diabetic retinopathy using deep learning. Lancet Digit. Health 3, e10-e19 (2021).
- Guan, Z. et al. Artificial intelligence in diabetes management: advancements, opportunities, and challenges. Cell Rep. Med. 4, 101213 (2023).
- Ting, D. S. W. et al. Artificial intelligence and deep learning in ophthalmology. Br. J. Ophthalmol. 103, 167-175 (2019).
- Ting, D. S. W. et al. Development and validation of a deep learning system for diabetic retinopathy and related eye diseases using retinal images from multiethnic populations with diabetes. JAMA 318, 2211-2223 (2017).
- Gulshan, V. et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 316, 2402-2410 (2016).
- Dai, L. et al. A deep learning system for detecting diabetic retinopathy across the disease spectrum. Nat. Commun. 12, 3242 (2021).
- Arcadu, F. et al. Deep learning algorithm predicts diabetic retinopathy progression in individual patients. NPJ Digit. Med. 2, 92 (2019).
- Cai, C. et al. Effectiveness of quality of care for patients with type 2 diabetes in China: findings from the Shanghai Integration Model (SIM). Front. Med. 16, 126-138 (2022).
- Wilkinson, C. P. et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 110, 1677-1682 (2003).
- Chen, S. et al. A seven-year study on an integrated hospital-community diabetes management program in Chinese patients with diabetes. Prim. Care Diabetes 12, 231-237 (2018).
- Norton, E. C., Miller, M. M. & Kleinman, L. C. Computing adjusted risk ratios and risk differences in Stata. Stata J. 13, 492-509 (2013).
- Das, S. K. Confidence interval is more informative than p-value in research. Int. J. Eng. Appl. Sci. Technol. 4, 278-282 (2019).
- Raman, R. et al. Incidence and progression of diabetic retinopathy in urban India: Sankara nethralaya-diabetic retinopathy epidemiology and molecular genetics study (SN-DREAMS II), Report 1. Ophthalmic Epidemiol. 24, 294-302 (2017).
- Varadarajan, A. V. et al. Deep learning for predicting refractive error from retinal fundus images. Invest. Ophthalmol. Vis. Sci. 59, 2861-2868 (2018).
- Yang, D. et al. Assessment of parafoveal diabetic macular ischemia on optical coherence tomography angiography images to predict diabetic retinal disease progression and visual acuity deterioration. JAMA Ophthalmol. 141, 641-649 (2023).
- Sun, Z. et al. OCT angiography metrics predict progression of diabetic retinopathy and development of diabetic macular edema: a prospective study. Ophthalmology 126, 1675-1684 (2019).
- Cheung, C. Y. et al. A deep-learning system for the assessment of cardiovascular disease risk via the measurement of retinal-vessel calibre. Nat. Biomed. Eng. 5, 498-508 (2021).
- CHEUNG, C. Y. L. et al. A new method to measure peripheral retinal vascular caliber over an extended area. Microcirculation 17, 495-503 (2010).
- Scanlon, P. H. Screening intervals for diabetic retinopathy and implications for care. Curr. Diab. Rep. 17, 96 (2017).
- Henry, K. E. et al. Human-machine teaming is key to AI adoption: clinicians’ experiences with a deployed machine learning system. NPJ Digit. Med. 5, 97 (2022).
- Dixon, R. F. et al. A virtual type 2 diabetes clinic using continuous glucose monitoring and endocrinology visits. J. Diabetes Sci. Technol. 14, 908-911 (2020).
- Downing, J., Bollyky, J. & Schneider, J. Use of a connected glucose meter and certified diabetes educator coaching to decrease the likelihood of abnormal blood glucose excursions: the livongo for diabetes program. J. Med Internet Res. 19, e234 (2017).
- Poplin, R. et al. Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nat. Biomed. Eng. 2, 158-164 (2018).
- Cheung, C. Y.-L. et al. Retinal vascular geometry and 6 year incidence and progression of diabetic retinopathy. Diabetologia 60, 1770-1781 (2017).
- Lu, Y. et al. Evaluation of automatically quantified foveal avascular zone metrics for diagnosis of diabetic retinopathy using optical coherence tomography angiography. Invest. Ophthalmol. Vis. Sci. 59, 2212-2221 (2018).
- Sawides, L. et al. Alterations to the foveal cone mosaic of diabetic patients. Invest. Ophthalmol. Vis. Sci. 58, 3395-3403 (2017).
- Cheung, C. Y., Ikram, M. K., Klein, R. & Wong, T. Y. The clinical implications of recent studies on the structure and function of the retinal microvasculature in diabetes. Diabetologia 58, 871-885 (2015).
- Klein, R. et al. Retinal vascular abnormalities in persons with type 1 diabetes: the Wisconsin Epidemiologic Study of Diabetic Retinopathy: XVIII. Ophthalmology 110, 2118-2125 (2003).
- Klein, R. et al. The relation of retinal vessel caliber to the incidence and progressionof diabetic retinopathy: Xix: The Wisconsin Epidemiologic Study of Diabetic Retinopathy. Arch. Ophthalmol. 122, 76-83 (2004).
- Oshitari, T. The pathogenesis and therapeutic approaches of diabetic neuropathy in the retina. Int. J. Mol. Sci. 22, 9050 (2021).
- Traversi, C. et al. Fractal analysis of fluoroangiographic patterns in anterior ischaemic optic neuropathy and optic neuritis: a pilot study. Clin. Exp. Ophthalmol. 36, 323-328 (2008).
- Simó, R. & Hernández, C. European Consortium for the Early Treatment of Diabetic Retinopathy (EUROCONDOR) Neurodegeneration in the diabetic eye: new insights and therapeutic perspectives. Trends Endocrinol. Metab. 25, 23-33 (2014).
- Zafar, S., Sachdeva, M., Frankfort, B. J. & Channa, R. Retinal neurodegeneration as an early manifestation of diabetic eye disease and potential neuroprotective therapies. Curr. Diab. Rep. 19, 17 (2019).
- Sohn, E. H. et al. Retinal neurodegeneration may precede microvascular changes characteristic of diabetic retinopathy in diabetes mellitus. Proc. Natl Acad. Sci. USA 113, E2655-E2664 (2016).
- Wong, T. Y. & Sabanayagam, C. The war on diabetic retinopathy: where are we now? Asia Pac. J. Ophthalmol. 8, 448-456 (2019).
- Liu, H. et al. Economic evaluation of combined population-based screening for multiple blindness-causing eye diseases in China: a cost-effectiveness analysis. Lancet Glob. Health 11, e456-e465 (2023).
- Yang, Z., Tan, T.-E., Shao, Y., Wong, T. Y. & Li, X. Classification of diabetic retinopathy: past, present and future. Front. Endocrinol. 13, 1079217 (2022).
- Zhou, Y. et al. A foundation model for generalizable disease detection from retinal images. Nature 622, 156-163 (2023).
© The Author(s) 2024
- e-mail: shengbin@sjtu.edu.cn; huarting99@sjtu.edu.cn; wongtienyin@tsinghua.edu.cn; wpjia@sjtu.edu.cn
Methods
Ethical approval
Data acquisition
of 3,284 individuals with diabetes from the cohort were enrolled for external validation. The BJHC (external dataset 8) is a community-based prospective study. In total, 835 patients with diabetes from the BJHC were included in this study. Baseline examinations were performed in the period between 2014 and 2016, and follow-up examinations were conducted between 2019 and 2020. In all external cohorts, two retinal photographs (macular and optic disc-centered) were captured for each eye at baseline and follow-up visits.
Diagnostic criteria
Image quality control and grading procedure
Model development and training
includes age, gender, smoking status, duration of diabetes, baseline DR level, body mass index, glycated HbA1c, systolic blood pressure, diastolic blood pressure, triglycerides, low-density lipoprotein cholesterol and high-density lipoprotein cholesterol. We also developed and compared the metadata model, the fundus model and the combined model for predicting DR progression in three subgroups. The three subgroups included diabetes with non-DR to DR (subgroup 1), non-referable DR to referable DR (subgroup 2) and non-VTDR to VTDR (subgroup3).
DR progression model
Model pretraining
Fundus model
of Weibull distributions taking as input the features generated by the pretrained ResNet-50 model.
Metadata model and combined model
Model evaluation
Interpretation of AI predictions
Reporting summary
Data availability
Code availability
References
- Majithia, S. et al. Cohort profile: The Singapore Epidemiology of Eye Diseases study (SEED). Int. J. Epidemiol. 50, 41-52 (2021).
- Nguyen, H. V. et al. Cost-effectiveness of a National Telemedicine Diabetic Retinopathy Screening Program in Singapore. Ophthalmology 123, 2571-2580 (2016).
- WHO Consultation. Definition, diagnosis and classification of diabetes mellitus and its complications (1999).
- ElSayed, N. A. et al. 2. Classification and diagnosis of diabetes: Standards of Care in Diabetes-2023. Diabetes Care 46, S19-S40 (2023).
- Kaniadakis, G. et al. The
-statistics approach to epidemiology. Sci. Rep. 10, 19949 (2020). - He, K., Fan, H., Wu, Y., Xie, S. & Girshick, R. Momentum contrast for unsupervised visual representation learning. in Proceedings of the IEEE/CVF conference on computer vision and pattern recognition 9729-9738 (2020).
- Chen, X., Fan, H., Girshick, R. & He, K. Improved baselines with momentum contrastive learning. arXiv preprint arXiv:2003.04297 (2020).
- Vaswani, A. et al. Attention is all you need. in Advances in neural information processing systems 5998-6008 (2017).
- Zhao, H., Jia, J. & Koltun, V. Exploring self-attention for image recognition. in Proceedings of the IEEE/CVF conference on computer vision and pattern recognition 10076-10085 (2020).
- Lundberg, S. M. et al. Explainable machine-learning predictions for the prevention of hypoxaemia during surgery. Nat. Biomed. Eng. 2, 749-760 (2018).
- Lundberg, S. M. & Lee, S. -I. A unified approach to interpreting model predictions. in Advances in Neural Information Processing Systems 30 (2017).
Acknowledgements
Author contributions
Y.C.T. and C. Y. Cheng provided critical comments and reviewed the manuscript. All authors discussed the results and approved the final version before submission.
Competing interests
Additional information
https://doi.org/10.1038/s41591-023-02702-z.
Supplementary information The online version contains
supplementary material available at
https://doi.org/10.1038/s41591-023-02702-z.
Correspondence and requests for materials should be addressed to Bin Sheng, Huating Li, Tien Yin Wong or Weiping Jia.
referable DR. a, Integrated Brier score (left) showing overall fit-lower is better and C-index (right) measuring model risk discrimination-higher is better-for various time points. b, Kaplan-Meier plots for the prediction of the progression from non-referable DR to referable DR. One-sided log-rank test was used for the
comparison between the low- and high-risk groups. The P values on internal test set and external validation dataset -1 and 2 are
risk groups. The
(DeepDR Plus). The waterfall plot displays the predicted time to DR progression of all participants in the real-world study by the fundus model. The individualized screening interval was set at an annual time point from baseline, which was just the year after the predicted patient-specific time to DR progression by the fundus model.
high-level feature vectors, while the predictor estimates the survival time in a fixed-size mixture of Weibull distributions based on the fundus feature vectors to generate the fundus score. The metadata and combined models share the same structure but differ in their inputs compared to the fundus model. The metadata model takes metadata as inputs, while the combined model takes both metadata and fundus score as inputs.
| Cohorts | Number of patients with diabetes | Number of eyes | At baseline | At the onset of the first DR-grade deterioration* | |||||||||
| non-DR | mild NPDR | moderate NPDR | severe NPDR | PDR | non-DR | mild NPDR | moderate NPDR | severe NPDR | PDR | ||||
| Developmental dataset | Training dataset | 17,190 | 34,380 | 30,554 | 1,074 | 1,597 | 852 | 303 | 28,582 | 1,644 | 2,091 | 1,382 | 681 |
| Internal test set | 1,910 | 3,820 | 3,552 | 84 | 122 | 38 | 24 | 3,322 | 174 | 216 | 58 | 50 | |
| ECHM | 2,141 | 4,282 | 3,908 | 128 | 160 | 44 | 42 | 3,652 | 228 | 250 | 82 | 70 | |
| WTHM | 971 | 1,942 | 1,830 | 42 | 52 | 14 | 4 | 1,730 | 90 | 83 | 25 | 14 | |
| NDSP | 1,194 | 2,388 | 2,220 | 88 | 74 | 2 | 4 | 2,176 | 118 | 80 | 10 | 4 | |
| External validation datasets | CUHK-ST DR | 337 | 591 | 297 | 102 | 179 | 13 | 0 | 183 | 216 | 179 | 13 | 0 |
| PUDM | 307 | 614 | 552 | 16 | 30 | 16 | 0 | 541 | 19 | 34 | 12 | 8 | |
| SEED | 1,699 | 3,398 | 2,918 | 310 | 123 | 7 | 40 | 2,849 | 334 | 148 | 9 | 58 | |
| SiDRP | 3,284 | 6,568 | 6,343 | 138 | 66 | 13 | 8 | 6,177 | 286 | 83 | 14 | 8 | |
| BJHC | 835 | 1,670 | 1,666 | 4 | 0 | 0 | 0 | 1,629 | 24 | 17 | 0 | 0 | |
| Cohort | Model | Any DR progression | Subgroup 1 | Subgroup 2 | Subgroup 3 | ||||
| C-index
|
IBS
|
C-index (95%CI) | IBS (95%CI) | C-index (95%CI) | IBS (95%CI) | C-index (95%CI) | IBS (95%CI) | ||
| Internal dataset | metadata | 0.696 (0.668, 0.725) | 0.340 (0.334, 0.347) | 0.705 (0.672, 0.736) | 0.303 (0.297, 0.310) | 0.700 (0.658, 0.741) | 0.261 (0.255, 0.268) | 0.711 (0.637, 0.778) | 0.328 (0.322, 0.335) |
| fundus | 0.823 (0.796, 0.850) | 0.161 (0.156, 0.166) | 0.826 (0.797, 0.851) | 0.189 (0.184, 0.194) | 0.820 (0.785, 0.853) | 0.153 (0.147, 0.159) | 0.824 (0.758, 0.880) | 0.180 (0.175, 0.185) | |
| combined | 0.833 (0.807, 0.857) | 0.152 (0.147, 0.157) | 0.835 (0.810, 0.859) | 0.167 (0.162, 0.172) | 0.838 (0.806, 0.869) | 0.145 (0.141, 0.150) | 0.852 (0.787, 0.909) | 0.164 (0.160, 0.169) | |
| metadata | 0.652 (0.623, 0.680) | 0.301 (0.295, 0.308) | 0.664 (0.634, 0.694) | 0.381 (0.375, 0.387) | 0.679 (0.639, 0.720) | 0.279 (0.273, 0.284) | 0.734 (0.677, 0.791) | 0.270 (0.265, 0.276) | |
| ECHM | fundus | 0.802 (0.778, 0.827) | 0.158 (0.153, 0.162) | 0.820 (0.793, 0.846) | 0.157 (0.152, 0.162) | 0.821 (0.792, 0.852) | 0.207 (0.202, 0.213) | 0.806 (0.748, 0.857) | 0.188 (0.184, 0.193) |
| combined | 0.811 (0.787, 0.834) | 0.223 (0.218, 0.228) | 0.824 (0.797, 0.848) | 0.212 (0.206, 0.217) | 0.826 (0.794, 0.858) | 0.124 (0.120, 0.128) | 0.830 (0.782, 0.871) | 0.203 (0.199, 0.209) | |
| metadata | 0.652 (0.607, 0.695) | 0.381 (0.373, 0.390) | 0.672 (0.617, 0.726) | 0.286 (0.277, 0.293) | 0.688 (0.613, 0.758) | 0.341 (0.328, 0.354) | 0.671 (0.572, 0.769) | 0.373 (0.364, 0.383) | |
| WTHM | fundus | 0.791 (0.748, 0.832) | 0.164 (0.157, 0.170) | 0.814 (0.773, 0.854) | 0.188 (0.181, 0.195) | 0.794 (0.735, 0.854) | 0.240 (0.232, 0.248) | 0.802 (0.705, 0.888) | 0.181 (0.173, 0.190) |
| combined | 0.806 (0.762, 0.844) | 0.154 (0.147, 0.161) | 0.809 (0.764, 0.853) | 0.224 (0.216, 0.232) | 0.801 (0.739, 0.857) | 0.198 (0.188, 0.208) | 0.819 (0.720, 0.907) | 0.141 (0.134, 0.148) | |
| metadata | 0.698 (0.625, 0.768) | 0.339 (0.330, 0.347) | 0.710 (0.629, 0.790) | 0.323 (0.314, 0.332) | 0.748 (0.611, 0.862) | 0.288 (0.280, 0.295) | 0.732 (0.551, 0.897) | 0.241 (0.234, 0.248) | |
| NDSP | fundus | 0.800 (0.737, 0.855) | 0.197 (0.190, 0.204) | 0.846 (0.798, 0.886) | 0.191 (0.185, 0.197) | 0.796 (0.674, 0.909) | 0.220 (0.213, 0.227) | 0.818 (0.684, 0.951) | 0.207 (0.200, 0.214) |
| combined | 0.814 (0.752, 0.866) | 0.171 (0.166, 0.178) | 0.852 (0.789, 0.904) | 0.177 (0.171, 0.184) | 0.802 (0.690, 0.904) | 0.198 (0.191, 0.204) | 0.822 (0.653, 0.956) | 0.139 (0.133, 0.145) | |
| CUHKSTDR | metadata | 0.650 (0.602, 0.699) | 0.305 (0.285, 0.326) | 0.621 (0.574, 0.669) | 0.402 (0.366, 0.439) | — | — | — | — |
| fundus | 0.789 (0.752, 0.826) | 0.241 (0.227, 0.256) | 0.754 (0.711, 0.793) | 0.197 (0.177, 0.218) | — | — | — | — | |
| combined | 0.793 (0.755, 0.827) | 0.213 (0.200, 0.228) | 0.759 (0.715, 0.800) | 0.207 (0.188, 0.226) | — | — | — | — | |
| metadata | 0.680 (0.568, 0.785) | 0.372 (0.355, 0.389) | 0.668 (0.474, 0.826) | 0.299 (0.284, 0.313) | — | — | — | — | |
| PUDM | fundus | 0.800 (0.697, 0.887) | 0.211 (0.192, 0.231) | 0.802 (0.672, 0.921) | 0.230 (0.213, 0.248) | — | — | — | — |
| combined | 0.808 (0.708, 0.895) | 0.240 (0.217, 0.263) | 0.802 (0.661, 0.920) | 0.262 (0.247, 0.277) | — | — | — | — | |
| metadata | 0.707 (0.672, 0.742) | 0.277 (0.270, 0.283) | 0.743 (0.702, 0.782) | 0.209 (0.202, 0.215) | 0.708 (0.646, 0.762) | 0.259 (0.253, 0.266) | 0.716 (0.612, 0.814) | 0.298 (0.291, 0.305) | |
| SEED | fundus | 0.786 (0.756, 0.814) | 0.200 (0.195, 0.206) | 0.800 (0.766, 0.833) | 0.210 (0.204, 0.216) | 0.813 (0.769, 0.855) | 0.173 (0.167, 0.178) | 0.817 (0.745, 0.885) | 0.223 (0.217, 0.228) |
| combined | 0.792 (0.760, 0.821) | 0.198 (0.192, 0.203) | 0.804 (0.770, 0.836) | 0.187 (0.181, 0.192) | 0.816 (0.768, 0.861) | 0.208 (0.202, 0.214) | 0.819 (0.737, 0.885) | 0.132 (0.128, 0.138) | |
| metadata | 0.613 (0.572, 0.656) | 0.370 (0.364, 0.376) | 0.585 (0.541, 0.627) | 0.383 (0.376, 0.389) | 0.523 (0.404, 0.642) | 0.473 (0.466, 0.480) | — | — | |
| SiDRP | fundus | 0.800 (0.771, 0.831) | 0.172 (0.168, 0.176) | 0.801 (0.769, 0.833) | 0.164 (0.160, 0.168) | 0.769 (0.668, 0.868) | 0.209 (0.205, 0.213) | — | — |
| combined | 0.804 (0.772, 0.834) | 0.219 (0.215, 0.223) | 0.806 (0.774, 0.837) | 0.204 (0.200, 0.208) | 0.783 (0.686, 0.874) | 0.237 (0.233, 0.241) | — | — | |
| metadata | 0.704 (0.607, 0.792) | 0.306 (0.296, 0.316) | 0.712 (0.637, 0.779) | 0.258 (0.249, 0.266) | — | — | — | — | |
| BJHC | fundus | 0.802 (0.736, 0.865) | 0.197 (0.189, 0.205) | 0.797 (0.709, 0.874) | 0.220 (0.212, 0.228) | — | — | — | — |
| combined | 0.811 (0.753, 0.865) | 0.203 (0.195, 0.211) | 0.803 (0.720, 0.879) | 0.198 (0.190, 0.205) | — | — | — | — | |
natureportfolio
Corresponding author(s): Weiping Jia
Reporting Summary
Statistics
Confirmed
Only common tests should be described solely by name; describe more complex techniques in the Methods section.
For Bayesian analysis, information on the choice of priors and Markov chain Monte Carlo settings
Our web collection on statistics for biologists contains articles on many of the points above.
Software and code
Data collection
No special software was used for data collection.
Data analysis
Python version 3.9.0 (Python Software Foundation, Delaware, United States) was used for all statistical analyses in this study. The following third-party python packages were used: Pytorch version 2.0.1 (Facebook, Massachusetts, United States) was used for convolutional neural network computing. Scikit-learn version 1.3.0 (David Cournapeau, California, United States) was used for calculating AUC. NumPy version 1.25.2 (Travis Oliphant, Texas, United States) was used for calculating C-index, Brier score. Lifelines version 0.27.7 (Cameron Davidson-Pilon, Canada) was used for survival analysis. Singapore I vessel assessment software version 4.0 (National University of Singapore, Singapore) was used to quantify retinal vascular variables. The code being used in the current study for developing the algorithm is provided at https:// github.com/drpredict/DeepDR_Plus.
Policy information about availability of data
- Accession codes, unique identifiers, or web links for publicly available datasets
- A description of any restrictions on data availability
- For clinical datasets or third party data, please ensure that the statement adheres to our policy
Human research participants
Reporting on sex and gender
Population characteristics
Recruitment
Ethics oversight
Note that full information on the approval of the study protocol must also be provided in the manuscript.
Field-specific reporting
Life sciences
Behavioural & social sciences
Ecological, evolutionary & environmental sciences
For a reference copy of the document with all sections, see nature.com/documents/nr-reporting-summary-flat.pdf
Life sciences study design
| Sample size | We developed DeepDR Plus system for predicting DR progression using a total of 76,400 retinal fundus images from 19,100 diabetic patients and we validated the system by 42,558 retinal fundus images from 10,768 diabetic patients. The sample size was determined by the data availability. |
| Data exclusions | Retinal images of poor image quality were excluded. |
| Replication | Replication was not relevant. We used eight independent validation cohorts to test the models, and the models achieved similar performances in the external validation sets. |
| Randomization | Samples were randomly allocated to the developing and validation datasets. |
| Blinding | During the data processing, all data was first de-identified to remove any patient related information. |
Reporting for specific materials, systems and methods
| Materials & experimental systems | Methods | ||
| n/a | Involved in the study | n/a | Involved in the study |
| X | |
|
|
|
|
|
Flow cytometry |
|
Palaeontology and archaeology | |
MRI-based neuroimaging |
|
|||
|
|||
|
|
||
Clinical data
All manuscripts should comply with the ICMJE guidelines for publication of clinical research and a completed CONSORT checklist must be included with all submissions.
Study protocol
Data collection
Study protocols can be found in http://www.chictr.org.cn/.
Shanghai Belt and Road International Joint Laboratory for Intelligent Prevention and Treatment of Metabolic Disorders, Department of Computer Science and Engineering, School of Electronic, Information, and Electrical Engineering, Shanghai Jiao Tong University, Department of Endocrinology and Metabolism, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai Diabetes Institute, Shanghai Clinical Center for Diabetes, Shanghai, China. MOE Key Laboratory of AI, School of Electronic, Information, and Electrical Engineering, Shanghai Jiao Tong University, Shanghai, China. Department of Ophthalmology, Huadong Sanatorium, Wuxi, China. Department of Ophthalmology, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China. Department of Ophthalmology and Visual Sciences, The Chinese University of Hong Kong, Hong Kong, China. Singapore Eye Research Institute, Singapore National Eye Centre, Singapore, Singapore. Department of Computer Science and Engineering, The Hong Kong University of Science and Technology, Hong Kong, China. Department of Chemical and Biological Engineering, The Hong Kong University of Science and Technology, Hong Kong, China. State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangdong Provincial Key Laboratory of Ophthalmology and Visual Science, Guangzhou, China. Department of Ophthalmology, Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China. Medical Records and Statistics Office, Shanghai Sixth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, China. Department of Geriatrics, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. National Engineering Research Center for Big Data Technology and System, Services Computing Technology and System Lab, Cluster and Grid Computing Lab, School of Computer Science and Technology, Huazhong University of Science and Technology, Wuhan, China. Shri Bhagwan Mahavir Vitreoretinal Services, Medical Research Foundation, Sankara Nethralaya, Chennai, India. Department of Ophthalmology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China. Beijing Institute of Ophthalmology, Beijing Tongren Eye Center, Beijing Tongren Hospital, -index refers to concordance index. IBS refers to integrated Brier score.